User login
Low rate of occult uterine malignancy with vaginal morcellation
ORLANDO – The Food and Drug Administration’s 2014 warning that laparoscopic power morcellation during hysterectomy or myomectomy could spread unsuspected cancerous tissue had a chilling effect across the specialty, but what about the risks associated with morcellation during vaginal hysterectomy?
“There is only one case of morcellation during vaginal hysterectomy with a leiomyosarcoma recorded in the literature,” Megan N. Wasson, DO, a fellow in minimally invasive gynecologic surgery at the Mayo Clinic in Phoenix said at the meeting sponsored by AAGL. “It is really unclear if vaginal and electromechanical morcellation carry the same inherent risk.”
To find out more, Dr. Wasson and her colleagues identified 2,296 patients who underwent total vaginal hysterectomy at one of three academic medical centers. A total of 611 of these women had uterine removal with uncontained morcellation via cold-knife wedge resection. The investigators assessed this group for incidence of occult malignancy, perioperative outcomes, and long-term survival in a retrospective cohort study.
Of the 611 women who underwent morcellation during the study, five patients had an occult malignancy, for a rate less than one percent, 0.82%. Three patients had a stage IA, grade I endometrial adenocarcinoma, and two patients had a low-grade stromal sarcoma. No patients had a leiomyosarcoma.
This group of five patients had a mean age of 49 years, a mean BMI of 32 kg/m2 and a median parity of two. Abnormal uterine bleeding was the indication for surgery for all five patients with a malignancy. The mean uterine weight was elevated at 231 g. One patient with endometrial adenocarcinoma later underwent pelvic lymphadenectomy and vaginal brachytherapy.
“So far, thankfully, all of these patients show no evidence of disease recurrence,” Dr. Wasson said. All five patients are alive, with a mean disease-free survival of 43 months among those with endometrial adenocarcinoma and 37 months for the low-grade stroma sarcoma patients.
“Overall, the incidence of occult uterine carcinoma at the time of vaginal hysterectomy is less than 1%,” Dr. Wasson said. “Thankfully, it does not appear to have a negative effect on patient outcomes when it occurs.”
More research is needed, however. “The risk is very limited in terms of what we know,” she said. “We investigated cancer in this study, but there is also a risk of dissemination of benign conditions.”
All patients underwent a preoperative evaluation that included sampling of the lining of the uterus and imaging. “Out of the five patients with carcinomas, two of the adenocarcinomas had completely benign preoperative sampling and one had hyperplasia, which unfortunately did develop into occult disease,” Dr. Wasson said. “We wouldn’t recommend morcellating any patient with hyperplasia. In the two patients with low-grade stromal sarcoma, neither had any hyperplasia on preoperative sampling.”
Following the 2014 FDA Safety Communication on power morcellation, the AAGL released its own guidance on morcellation during uterine tissue extraction. The AAGL recommended that clinicians avoid morcellation for any patient who had a premalignant or malignant condition or who was at risk for malignancy, and use caution when considering morcellation. “This was for all types of morcellation, including electromechanical and vaginal morcellation,” Dr. Wasson said.
“This was in response to studies and awareness of increased risk of disease with morcellation – specifically leiomyosarcomas – for dissemination of disease in the abdomen and pelvis, but also for an increased risk of recurrence,” she said. “This means, in turn, that patients can have decreased overall survival and disease-free survival, so this is very important when we are talking to our patients.”
Dr. Wasson reported having no relevant financial disclosures.
ORLANDO – The Food and Drug Administration’s 2014 warning that laparoscopic power morcellation during hysterectomy or myomectomy could spread unsuspected cancerous tissue had a chilling effect across the specialty, but what about the risks associated with morcellation during vaginal hysterectomy?
“There is only one case of morcellation during vaginal hysterectomy with a leiomyosarcoma recorded in the literature,” Megan N. Wasson, DO, a fellow in minimally invasive gynecologic surgery at the Mayo Clinic in Phoenix said at the meeting sponsored by AAGL. “It is really unclear if vaginal and electromechanical morcellation carry the same inherent risk.”
To find out more, Dr. Wasson and her colleagues identified 2,296 patients who underwent total vaginal hysterectomy at one of three academic medical centers. A total of 611 of these women had uterine removal with uncontained morcellation via cold-knife wedge resection. The investigators assessed this group for incidence of occult malignancy, perioperative outcomes, and long-term survival in a retrospective cohort study.
Of the 611 women who underwent morcellation during the study, five patients had an occult malignancy, for a rate less than one percent, 0.82%. Three patients had a stage IA, grade I endometrial adenocarcinoma, and two patients had a low-grade stromal sarcoma. No patients had a leiomyosarcoma.
This group of five patients had a mean age of 49 years, a mean BMI of 32 kg/m2 and a median parity of two. Abnormal uterine bleeding was the indication for surgery for all five patients with a malignancy. The mean uterine weight was elevated at 231 g. One patient with endometrial adenocarcinoma later underwent pelvic lymphadenectomy and vaginal brachytherapy.
“So far, thankfully, all of these patients show no evidence of disease recurrence,” Dr. Wasson said. All five patients are alive, with a mean disease-free survival of 43 months among those with endometrial adenocarcinoma and 37 months for the low-grade stroma sarcoma patients.
“Overall, the incidence of occult uterine carcinoma at the time of vaginal hysterectomy is less than 1%,” Dr. Wasson said. “Thankfully, it does not appear to have a negative effect on patient outcomes when it occurs.”
More research is needed, however. “The risk is very limited in terms of what we know,” she said. “We investigated cancer in this study, but there is also a risk of dissemination of benign conditions.”
All patients underwent a preoperative evaluation that included sampling of the lining of the uterus and imaging. “Out of the five patients with carcinomas, two of the adenocarcinomas had completely benign preoperative sampling and one had hyperplasia, which unfortunately did develop into occult disease,” Dr. Wasson said. “We wouldn’t recommend morcellating any patient with hyperplasia. In the two patients with low-grade stromal sarcoma, neither had any hyperplasia on preoperative sampling.”
Following the 2014 FDA Safety Communication on power morcellation, the AAGL released its own guidance on morcellation during uterine tissue extraction. The AAGL recommended that clinicians avoid morcellation for any patient who had a premalignant or malignant condition or who was at risk for malignancy, and use caution when considering morcellation. “This was for all types of morcellation, including electromechanical and vaginal morcellation,” Dr. Wasson said.
“This was in response to studies and awareness of increased risk of disease with morcellation – specifically leiomyosarcomas – for dissemination of disease in the abdomen and pelvis, but also for an increased risk of recurrence,” she said. “This means, in turn, that patients can have decreased overall survival and disease-free survival, so this is very important when we are talking to our patients.”
Dr. Wasson reported having no relevant financial disclosures.
ORLANDO – The Food and Drug Administration’s 2014 warning that laparoscopic power morcellation during hysterectomy or myomectomy could spread unsuspected cancerous tissue had a chilling effect across the specialty, but what about the risks associated with morcellation during vaginal hysterectomy?
“There is only one case of morcellation during vaginal hysterectomy with a leiomyosarcoma recorded in the literature,” Megan N. Wasson, DO, a fellow in minimally invasive gynecologic surgery at the Mayo Clinic in Phoenix said at the meeting sponsored by AAGL. “It is really unclear if vaginal and electromechanical morcellation carry the same inherent risk.”
To find out more, Dr. Wasson and her colleagues identified 2,296 patients who underwent total vaginal hysterectomy at one of three academic medical centers. A total of 611 of these women had uterine removal with uncontained morcellation via cold-knife wedge resection. The investigators assessed this group for incidence of occult malignancy, perioperative outcomes, and long-term survival in a retrospective cohort study.
Of the 611 women who underwent morcellation during the study, five patients had an occult malignancy, for a rate less than one percent, 0.82%. Three patients had a stage IA, grade I endometrial adenocarcinoma, and two patients had a low-grade stromal sarcoma. No patients had a leiomyosarcoma.
This group of five patients had a mean age of 49 years, a mean BMI of 32 kg/m2 and a median parity of two. Abnormal uterine bleeding was the indication for surgery for all five patients with a malignancy. The mean uterine weight was elevated at 231 g. One patient with endometrial adenocarcinoma later underwent pelvic lymphadenectomy and vaginal brachytherapy.
“So far, thankfully, all of these patients show no evidence of disease recurrence,” Dr. Wasson said. All five patients are alive, with a mean disease-free survival of 43 months among those with endometrial adenocarcinoma and 37 months for the low-grade stroma sarcoma patients.
“Overall, the incidence of occult uterine carcinoma at the time of vaginal hysterectomy is less than 1%,” Dr. Wasson said. “Thankfully, it does not appear to have a negative effect on patient outcomes when it occurs.”
More research is needed, however. “The risk is very limited in terms of what we know,” she said. “We investigated cancer in this study, but there is also a risk of dissemination of benign conditions.”
All patients underwent a preoperative evaluation that included sampling of the lining of the uterus and imaging. “Out of the five patients with carcinomas, two of the adenocarcinomas had completely benign preoperative sampling and one had hyperplasia, which unfortunately did develop into occult disease,” Dr. Wasson said. “We wouldn’t recommend morcellating any patient with hyperplasia. In the two patients with low-grade stromal sarcoma, neither had any hyperplasia on preoperative sampling.”
Following the 2014 FDA Safety Communication on power morcellation, the AAGL released its own guidance on morcellation during uterine tissue extraction. The AAGL recommended that clinicians avoid morcellation for any patient who had a premalignant or malignant condition or who was at risk for malignancy, and use caution when considering morcellation. “This was for all types of morcellation, including electromechanical and vaginal morcellation,” Dr. Wasson said.
“This was in response to studies and awareness of increased risk of disease with morcellation – specifically leiomyosarcomas – for dissemination of disease in the abdomen and pelvis, but also for an increased risk of recurrence,” she said. “This means, in turn, that patients can have decreased overall survival and disease-free survival, so this is very important when we are talking to our patients.”
Dr. Wasson reported having no relevant financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Key clinical point:
Major finding: Of 611 patients who underwent morcellation during total vaginal hysterectomy, five patients (0.82%) had occult uterine carcinoma.
Data source: A retrospective cohort study of 611 women who had uterine removal with uncontained morcellation.
Disclosures: Dr. Wasson reported having no relevant financial disclosures.
Scoring Formula Consolidates Stroke and Bleeding Risk in Patients With Atrial Fibrillation
ROME—A new risk-stratification formula for patients with atrial fibrillation starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin. This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, said Christina L. Fanola, MD, at the 2016 European Society of Cardiology Congress.

“It is a great time to think about this type of score because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto). “Each NOAC may need its own scoring formula,” Dr. Fanola said.
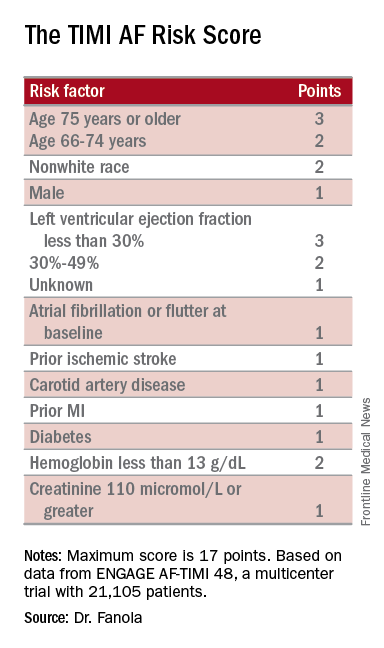
The concept behind the TIMI AF Risk Score is that patients with nonvalvular atrial fibrillation who receive anticoagulant treatment may have fewer disabling ischemic strokes, but also may face the potential risk of life-threatening bleeding events. To create a risk-prediction model that takes into account both of these outcomes, Dr. Fanola and her research associates used data collected in the ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48) trial, a study that randomized more than 21,000 patients with atrial fibrillation, and on no prior oral anticoagulant regimen, to treatment with edoxaban (Savaysa) or warfarin. This was the pivotal trial for edoxaban’s approval for this indication. All patients enrolled in the study had a CHADS2 score of at least 2, identifying a significant ischemic stroke risk.
A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
An analysis that applied the scoring formula to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0 to 6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7 to 9 correlated with a 10% per year incidence of this combined outcome; and a high-risk score of 10 or greater correlated with a 21% annual event rate.
Dr. Fanola and her associates conducted a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. Patients at high risk received a major benefit from edoxaban, with a 30% overall incidence of the combined end point during three years of follow-up, compared with a 51% rate among patients on warfarin. Patients at intermediate risk also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But patients at low risk had identical 10% event rates with either treatment.
These findings suggest that patients with atrial fibrillation with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Patients at low risk seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
—Mitchel L. Zoler
ROME—A new risk-stratification formula for patients with atrial fibrillation starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin. This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, said Christina L. Fanola, MD, at the 2016 European Society of Cardiology Congress.
“It is a great time to think about this type of score because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto). “Each NOAC may need its own scoring formula,” Dr. Fanola said.
The concept behind the TIMI AF Risk Score is that patients with nonvalvular atrial fibrillation who receive anticoagulant treatment may have fewer disabling ischemic strokes, but also may face the potential risk of life-threatening bleeding events. To create a risk-prediction model that takes into account both of these outcomes, Dr. Fanola and her research associates used data collected in the ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48) trial, a study that randomized more than 21,000 patients with atrial fibrillation, and on no prior oral anticoagulant regimen, to treatment with edoxaban (Savaysa) or warfarin. This was the pivotal trial for edoxaban’s approval for this indication. All patients enrolled in the study had a CHADS2 score of at least 2, identifying a significant ischemic stroke risk.
A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
An analysis that applied the scoring formula to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0 to 6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7 to 9 correlated with a 10% per year incidence of this combined outcome; and a high-risk score of 10 or greater correlated with a 21% annual event rate.
Dr. Fanola and her associates conducted a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. Patients at high risk received a major benefit from edoxaban, with a 30% overall incidence of the combined end point during three years of follow-up, compared with a 51% rate among patients on warfarin. Patients at intermediate risk also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But patients at low risk had identical 10% event rates with either treatment.
These findings suggest that patients with atrial fibrillation with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Patients at low risk seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
—Mitchel L. Zoler
ROME—A new risk-stratification formula for patients with atrial fibrillation starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin. This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, said Christina L. Fanola, MD, at the 2016 European Society of Cardiology Congress.
“It is a great time to think about this type of score because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto). “Each NOAC may need its own scoring formula,” Dr. Fanola said.
The concept behind the TIMI AF Risk Score is that patients with nonvalvular atrial fibrillation who receive anticoagulant treatment may have fewer disabling ischemic strokes, but also may face the potential risk of life-threatening bleeding events. To create a risk-prediction model that takes into account both of these outcomes, Dr. Fanola and her research associates used data collected in the ENGAGE AF-TIMI 48 (Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48) trial, a study that randomized more than 21,000 patients with atrial fibrillation, and on no prior oral anticoagulant regimen, to treatment with edoxaban (Savaysa) or warfarin. This was the pivotal trial for edoxaban’s approval for this indication. All patients enrolled in the study had a CHADS2 score of at least 2, identifying a significant ischemic stroke risk.
A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
An analysis that applied the scoring formula to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0 to 6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7 to 9 correlated with a 10% per year incidence of this combined outcome; and a high-risk score of 10 or greater correlated with a 21% annual event rate.
Dr. Fanola and her associates conducted a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. Patients at high risk received a major benefit from edoxaban, with a 30% overall incidence of the combined end point during three years of follow-up, compared with a 51% rate among patients on warfarin. Patients at intermediate risk also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But patients at low risk had identical 10% event rates with either treatment.
These findings suggest that patients with atrial fibrillation with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Patients at low risk seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
—Mitchel L. Zoler

Prognostic Models Fail to Predict Posttraumatic Seizures
Investigators have developed prognostic models that discriminate between patients with and without posttraumatic seizures (PTS) at year 1 and year 2 after traumatic brain injury (TBI), but perform little better than chance at predicting PTS, according to research published in the September issue of Epilepsia. The models do, however, identify potentially important predictors that may help to identify populations at risk for PTS.
“Individuals with characteristics identified in prognostic models as predictors of PTS represent subpopulations that may benefit from tailored seizure prophylaxis guidelines addressing unique premorbid characteristics, pathologies, and procedures,” said Anne Ritter, MPH, PhD, of Uniformed Services University of the Health Sciences in Bethesda, Maryland.
PTS is commonly recognized as a complication of TBI that may be acute or chronic. Although risk factors for PTS have been identified, predicting who will develop PTS remains difficult. Current PTS prognostic models are not widely accepted for clinical use and do not reflect current trends in injury, diagnosis, or care.
“Accurate PTS risk prediction could help define high-risk populations in support of clinical intervention trials. Predictive models could also inform clinical algorithms to identify individuals likely to benefit from tailored seizure prophylaxis or treatment,” said Dr. Ritter.
Dr. Ritter and colleagues conducted a study to develop and internally validate preliminary prognostic regression models that predict PTS during acute care hospitalization and at year 1 and year 2 post injury.
Study Population
Eligible participants had moderate or severe TBI, were admitted to a participating hospital emergency department within 72 hours of injury, were age 16 or older, and received acute care and inpatient rehabilitation within a TBI Model System (TBIMS) designated hospital system. Moderate or severe TBI was defined as posttraumatic amnesia lasting longer than 24 h, loss of consciousness lasting longer than 30 minutes, an emergency department Glasgow Coma Scale score less than 13, or positive neuroimaging findings.
People injured between October 1, 2011, and August 31, 2014, were included in the study. Patients injured during this time period, but not eligible for year 1 follow-up were excluded, however. Data for all participants were selected from the TBIMS National Database.
Researchers limited data to those collected at enrollment, year 1, or year 2 post injury. Enrollment data were collected using chart review and interview and included demographic, social, and injury characteristics, as well as preinjury personal and medical history and acute hospitalization outcome. PTS status, defined as the presence or absence of seizure activity, was the main outcome. It was determined during acute hospitalization, at year 1, and at year 2. In addition, investigators used multivariable logistic regression to generate prognostic models for PTS during acute hospitalization, at year 1, and at year 2. They internally validated models with resampling.
PTS Predictors of Interest
Of 2,136 participants, 2,042 had data available on all predictors identified in simple logistic regression for seizure during acute hospitalization. The sample’s demographic and clinical variables were similar in this investigation to those in previous TBI studies.
The final year 1 prognostic model identified injury severity, subdural hematoma, contusion load, craniotomy, craniectomy, seizure during acute hospitalization, preinjury condition limiting physical activity, preinjury mental health treatment or psychiatric hospitalization, and incarceration as risk factors for PTS. Craniectomy was the most statistically significant predictor in the final model.
At year 2, following validation, predictor variables included subdural hematoma, intraparenchymal fragment, craniotomy, craniectomy, seizure during acute hospitalization, and preinjury incarceration. Acute hospitalization seizure and craniectomy were the most statistically significant predictors of PTS at year 2.
Overall, the models displayed poor discrimination ability for PTS; however, these models may have added benefit, compared with prior models that were not being used clinically, said Dr. Ritter.
“These models must be examined in independent study populations to determine discriminability and validity outside the TBIMS population,” she added.
—Erica Tricarico
Suggested Reading
Ritter AC, Wagner AK, Szaflarski, et al. Prognostic models for predicting posttraumatic seizures during acute hospitalization, and 1 and 2 years following traumatic brain injury. Epilepsia. 2016;57(9):1503-1514.
Investigators have developed prognostic models that discriminate between patients with and without posttraumatic seizures (PTS) at year 1 and year 2 after traumatic brain injury (TBI), but perform little better than chance at predicting PTS, according to research published in the September issue of Epilepsia. The models do, however, identify potentially important predictors that may help to identify populations at risk for PTS.
“Individuals with characteristics identified in prognostic models as predictors of PTS represent subpopulations that may benefit from tailored seizure prophylaxis guidelines addressing unique premorbid characteristics, pathologies, and procedures,” said Anne Ritter, MPH, PhD, of Uniformed Services University of the Health Sciences in Bethesda, Maryland.
PTS is commonly recognized as a complication of TBI that may be acute or chronic. Although risk factors for PTS have been identified, predicting who will develop PTS remains difficult. Current PTS prognostic models are not widely accepted for clinical use and do not reflect current trends in injury, diagnosis, or care.
“Accurate PTS risk prediction could help define high-risk populations in support of clinical intervention trials. Predictive models could also inform clinical algorithms to identify individuals likely to benefit from tailored seizure prophylaxis or treatment,” said Dr. Ritter.
Dr. Ritter and colleagues conducted a study to develop and internally validate preliminary prognostic regression models that predict PTS during acute care hospitalization and at year 1 and year 2 post injury.
Study Population
Eligible participants had moderate or severe TBI, were admitted to a participating hospital emergency department within 72 hours of injury, were age 16 or older, and received acute care and inpatient rehabilitation within a TBI Model System (TBIMS) designated hospital system. Moderate or severe TBI was defined as posttraumatic amnesia lasting longer than 24 h, loss of consciousness lasting longer than 30 minutes, an emergency department Glasgow Coma Scale score less than 13, or positive neuroimaging findings.
People injured between October 1, 2011, and August 31, 2014, were included in the study. Patients injured during this time period, but not eligible for year 1 follow-up were excluded, however. Data for all participants were selected from the TBIMS National Database.
Researchers limited data to those collected at enrollment, year 1, or year 2 post injury. Enrollment data were collected using chart review and interview and included demographic, social, and injury characteristics, as well as preinjury personal and medical history and acute hospitalization outcome. PTS status, defined as the presence or absence of seizure activity, was the main outcome. It was determined during acute hospitalization, at year 1, and at year 2. In addition, investigators used multivariable logistic regression to generate prognostic models for PTS during acute hospitalization, at year 1, and at year 2. They internally validated models with resampling.
PTS Predictors of Interest
Of 2,136 participants, 2,042 had data available on all predictors identified in simple logistic regression for seizure during acute hospitalization. The sample’s demographic and clinical variables were similar in this investigation to those in previous TBI studies.
The final year 1 prognostic model identified injury severity, subdural hematoma, contusion load, craniotomy, craniectomy, seizure during acute hospitalization, preinjury condition limiting physical activity, preinjury mental health treatment or psychiatric hospitalization, and incarceration as risk factors for PTS. Craniectomy was the most statistically significant predictor in the final model.
At year 2, following validation, predictor variables included subdural hematoma, intraparenchymal fragment, craniotomy, craniectomy, seizure during acute hospitalization, and preinjury incarceration. Acute hospitalization seizure and craniectomy were the most statistically significant predictors of PTS at year 2.
Overall, the models displayed poor discrimination ability for PTS; however, these models may have added benefit, compared with prior models that were not being used clinically, said Dr. Ritter.
“These models must be examined in independent study populations to determine discriminability and validity outside the TBIMS population,” she added.
—Erica Tricarico
Suggested Reading
Ritter AC, Wagner AK, Szaflarski, et al. Prognostic models for predicting posttraumatic seizures during acute hospitalization, and 1 and 2 years following traumatic brain injury. Epilepsia. 2016;57(9):1503-1514.
Investigators have developed prognostic models that discriminate between patients with and without posttraumatic seizures (PTS) at year 1 and year 2 after traumatic brain injury (TBI), but perform little better than chance at predicting PTS, according to research published in the September issue of Epilepsia. The models do, however, identify potentially important predictors that may help to identify populations at risk for PTS.
“Individuals with characteristics identified in prognostic models as predictors of PTS represent subpopulations that may benefit from tailored seizure prophylaxis guidelines addressing unique premorbid characteristics, pathologies, and procedures,” said Anne Ritter, MPH, PhD, of Uniformed Services University of the Health Sciences in Bethesda, Maryland.
PTS is commonly recognized as a complication of TBI that may be acute or chronic. Although risk factors for PTS have been identified, predicting who will develop PTS remains difficult. Current PTS prognostic models are not widely accepted for clinical use and do not reflect current trends in injury, diagnosis, or care.
“Accurate PTS risk prediction could help define high-risk populations in support of clinical intervention trials. Predictive models could also inform clinical algorithms to identify individuals likely to benefit from tailored seizure prophylaxis or treatment,” said Dr. Ritter.
Dr. Ritter and colleagues conducted a study to develop and internally validate preliminary prognostic regression models that predict PTS during acute care hospitalization and at year 1 and year 2 post injury.
Study Population
Eligible participants had moderate or severe TBI, were admitted to a participating hospital emergency department within 72 hours of injury, were age 16 or older, and received acute care and inpatient rehabilitation within a TBI Model System (TBIMS) designated hospital system. Moderate or severe TBI was defined as posttraumatic amnesia lasting longer than 24 h, loss of consciousness lasting longer than 30 minutes, an emergency department Glasgow Coma Scale score less than 13, or positive neuroimaging findings.
People injured between October 1, 2011, and August 31, 2014, were included in the study. Patients injured during this time period, but not eligible for year 1 follow-up were excluded, however. Data for all participants were selected from the TBIMS National Database.
Researchers limited data to those collected at enrollment, year 1, or year 2 post injury. Enrollment data were collected using chart review and interview and included demographic, social, and injury characteristics, as well as preinjury personal and medical history and acute hospitalization outcome. PTS status, defined as the presence or absence of seizure activity, was the main outcome. It was determined during acute hospitalization, at year 1, and at year 2. In addition, investigators used multivariable logistic regression to generate prognostic models for PTS during acute hospitalization, at year 1, and at year 2. They internally validated models with resampling.
PTS Predictors of Interest
Of 2,136 participants, 2,042 had data available on all predictors identified in simple logistic regression for seizure during acute hospitalization. The sample’s demographic and clinical variables were similar in this investigation to those in previous TBI studies.
The final year 1 prognostic model identified injury severity, subdural hematoma, contusion load, craniotomy, craniectomy, seizure during acute hospitalization, preinjury condition limiting physical activity, preinjury mental health treatment or psychiatric hospitalization, and incarceration as risk factors for PTS. Craniectomy was the most statistically significant predictor in the final model.
At year 2, following validation, predictor variables included subdural hematoma, intraparenchymal fragment, craniotomy, craniectomy, seizure during acute hospitalization, and preinjury incarceration. Acute hospitalization seizure and craniectomy were the most statistically significant predictors of PTS at year 2.
Overall, the models displayed poor discrimination ability for PTS; however, these models may have added benefit, compared with prior models that were not being used clinically, said Dr. Ritter.
“These models must be examined in independent study populations to determine discriminability and validity outside the TBIMS population,” she added.
—Erica Tricarico
Suggested Reading
Ritter AC, Wagner AK, Szaflarski, et al. Prognostic models for predicting posttraumatic seizures during acute hospitalization, and 1 and 2 years following traumatic brain injury. Epilepsia. 2016;57(9):1503-1514.
HCT survivors experience high rates of late respiratory and infectious complications
Cancer survivors who underwent hematopoietic cell transplantation (HCT) face a greater risk for hospitalizations and mortality, compared with survivors who did not have HCT.
New findings show that disparities in infectious and respiratory complications were marked between the two groups, but differences in circulatory disease, mental health diagnoses, and second cancers were insignificant.
“Clinicians who care for long-term survivors of HCT should be aware of comprehensive surveillance guidelines available for this high-risk population,” wrote Eric J. Chow, MD, of the Fred Hutchinson Cancer Research Center, Seattle, and his colleagues (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.8457).
There have only been a few comprehensive analyses that have compared HCT with non-HCT cancer survivors. Thus, the authors noted that it is unclear if HCT survivors are at a greater risk of late complications, compared with other cancer survivors.
To address this issue, Dr. Chow and his team matched 2-year cancer survivors who had undergone HCT (n = 1,792; 52% allogeneic and 90% hematologic malignancies) to non-HCT 2-year cancer survivors, using a state cancer registry (n = 5,455), and the general population (n = 16,340), using driver’s license files.
The investigators found that the 10-year cumulative incidence of any hospitalization or death related to all major organ-system outcomes was significantly different (P less than .05) between the HCT survivors and general population.
Patients with a history of HCT had a 30.6% cumulative incidence of infectious complications (difference vs. non-HCT: 8.7%) and a 26.8% incidence of any respiratory complications (difference vs. non-HCT: 6.9%), the investigators reported.
In contrast, the 10-year cumulative incidences of nervous system, circulatory, and genitourinary complications; mental health outcomes; and the development of new cancers did not differ between the HCT and non-HCT groups.
The incidence of pregnancy-related hospitalization among women of childbearing age was lower in the HCT group, compared with non-HCT patients (group difference, 24.4%).
At the 2-year endpoint, Dr. Chow and his associates noted that certain risks were “notably higher” in patients who had undergone HCT, including primary infections (hazard ratio, 1.4), respiratory complications (HR, 1.3), and death from any cause (HR, 1.1).
A significantly greater hospitalization rate also was observed in the HCT group versus the non-HCT group (280 episodes per 1,000 person-years vs. 173 episodes per 1,000 person years; P less than .001).
“Future work to identify more specific risk factors associated with late infections and respiratory complications may help to further refine these guidelines and identify new prevention strategies,” the authors concluded.
The study was funded by grants from the National Institutes of Health. Dr. Chow had no disclosures and several coauthors report relationships with industry.
Cancer survivors who underwent hematopoietic cell transplantation (HCT) face a greater risk for hospitalizations and mortality, compared with survivors who did not have HCT.
New findings show that disparities in infectious and respiratory complications were marked between the two groups, but differences in circulatory disease, mental health diagnoses, and second cancers were insignificant.
“Clinicians who care for long-term survivors of HCT should be aware of comprehensive surveillance guidelines available for this high-risk population,” wrote Eric J. Chow, MD, of the Fred Hutchinson Cancer Research Center, Seattle, and his colleagues (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.8457).
There have only been a few comprehensive analyses that have compared HCT with non-HCT cancer survivors. Thus, the authors noted that it is unclear if HCT survivors are at a greater risk of late complications, compared with other cancer survivors.
To address this issue, Dr. Chow and his team matched 2-year cancer survivors who had undergone HCT (n = 1,792; 52% allogeneic and 90% hematologic malignancies) to non-HCT 2-year cancer survivors, using a state cancer registry (n = 5,455), and the general population (n = 16,340), using driver’s license files.
The investigators found that the 10-year cumulative incidence of any hospitalization or death related to all major organ-system outcomes was significantly different (P less than .05) between the HCT survivors and general population.
Patients with a history of HCT had a 30.6% cumulative incidence of infectious complications (difference vs. non-HCT: 8.7%) and a 26.8% incidence of any respiratory complications (difference vs. non-HCT: 6.9%), the investigators reported.
In contrast, the 10-year cumulative incidences of nervous system, circulatory, and genitourinary complications; mental health outcomes; and the development of new cancers did not differ between the HCT and non-HCT groups.
The incidence of pregnancy-related hospitalization among women of childbearing age was lower in the HCT group, compared with non-HCT patients (group difference, 24.4%).
At the 2-year endpoint, Dr. Chow and his associates noted that certain risks were “notably higher” in patients who had undergone HCT, including primary infections (hazard ratio, 1.4), respiratory complications (HR, 1.3), and death from any cause (HR, 1.1).
A significantly greater hospitalization rate also was observed in the HCT group versus the non-HCT group (280 episodes per 1,000 person-years vs. 173 episodes per 1,000 person years; P less than .001).
“Future work to identify more specific risk factors associated with late infections and respiratory complications may help to further refine these guidelines and identify new prevention strategies,” the authors concluded.
The study was funded by grants from the National Institutes of Health. Dr. Chow had no disclosures and several coauthors report relationships with industry.
Cancer survivors who underwent hematopoietic cell transplantation (HCT) face a greater risk for hospitalizations and mortality, compared with survivors who did not have HCT.
New findings show that disparities in infectious and respiratory complications were marked between the two groups, but differences in circulatory disease, mental health diagnoses, and second cancers were insignificant.
“Clinicians who care for long-term survivors of HCT should be aware of comprehensive surveillance guidelines available for this high-risk population,” wrote Eric J. Chow, MD, of the Fred Hutchinson Cancer Research Center, Seattle, and his colleagues (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.8457).
There have only been a few comprehensive analyses that have compared HCT with non-HCT cancer survivors. Thus, the authors noted that it is unclear if HCT survivors are at a greater risk of late complications, compared with other cancer survivors.
To address this issue, Dr. Chow and his team matched 2-year cancer survivors who had undergone HCT (n = 1,792; 52% allogeneic and 90% hematologic malignancies) to non-HCT 2-year cancer survivors, using a state cancer registry (n = 5,455), and the general population (n = 16,340), using driver’s license files.
The investigators found that the 10-year cumulative incidence of any hospitalization or death related to all major organ-system outcomes was significantly different (P less than .05) between the HCT survivors and general population.
Patients with a history of HCT had a 30.6% cumulative incidence of infectious complications (difference vs. non-HCT: 8.7%) and a 26.8% incidence of any respiratory complications (difference vs. non-HCT: 6.9%), the investigators reported.
In contrast, the 10-year cumulative incidences of nervous system, circulatory, and genitourinary complications; mental health outcomes; and the development of new cancers did not differ between the HCT and non-HCT groups.
The incidence of pregnancy-related hospitalization among women of childbearing age was lower in the HCT group, compared with non-HCT patients (group difference, 24.4%).
At the 2-year endpoint, Dr. Chow and his associates noted that certain risks were “notably higher” in patients who had undergone HCT, including primary infections (hazard ratio, 1.4), respiratory complications (HR, 1.3), and death from any cause (HR, 1.1).
A significantly greater hospitalization rate also was observed in the HCT group versus the non-HCT group (280 episodes per 1,000 person-years vs. 173 episodes per 1,000 person years; P less than .001).
“Future work to identify more specific risk factors associated with late infections and respiratory complications may help to further refine these guidelines and identify new prevention strategies,” the authors concluded.
The study was funded by grants from the National Institutes of Health. Dr. Chow had no disclosures and several coauthors report relationships with industry.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Clinicians who care for HCT survivors should be aware of their high rates of late respiratory and infectious complications.
Major finding: Patients with a history of HCT had a 30.6% cumulative incidence of infectious complications (difference vs. non-HCT: 8.7%) and a 26.8% incidence of any respiratory complications (difference vs. non-HCT: 6.9%).
Data source: Retrospective population study using databases to match outcomes between two patient groups and the general population.
Disclosures: The study was funded by grants from the National Institutes of Health. Dr. Chow has no disclosures and several coauthors report relationships with industry.
VIDEO: Tune in to psoriasis patients’ quality of life
LAS VEGAS – Physicians often fail to predict the impact of disease on quality of life in their psoriasis patients, which can help guide treatment, Joel Gelfand, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“This is true across all medical conditions,” said Dr. Gelfand, professor of dermatology, at the University of Pennsylvania, Philadelphia. For example, some patients with psoriasis may have extensive disease, but it doesn’t bother them, and therefore they may need less treatment, he pointed out.
In his practice, patients with psoriasis are asked to rate physical symptoms (including flaking and itching) and emotional symptoms (including anxiety and depression) related to their disease on a scale of 0 to 10, with 10 being the worst. “The higher those scores are, the more aggressive I’ll be in treating them,” he said. Patient scores can be tracked over time, to review progress with their chosen treatment, he noted.
Dr. Gelfand disclosed relationships with multiple companies including AbbVie, Janssen, Lilly, Novartis, Celgene, Merck, Sanofi, Pfizer, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Physicians often fail to predict the impact of disease on quality of life in their psoriasis patients, which can help guide treatment, Joel Gelfand, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“This is true across all medical conditions,” said Dr. Gelfand, professor of dermatology, at the University of Pennsylvania, Philadelphia. For example, some patients with psoriasis may have extensive disease, but it doesn’t bother them, and therefore they may need less treatment, he pointed out.
In his practice, patients with psoriasis are asked to rate physical symptoms (including flaking and itching) and emotional symptoms (including anxiety and depression) related to their disease on a scale of 0 to 10, with 10 being the worst. “The higher those scores are, the more aggressive I’ll be in treating them,” he said. Patient scores can be tracked over time, to review progress with their chosen treatment, he noted.
Dr. Gelfand disclosed relationships with multiple companies including AbbVie, Janssen, Lilly, Novartis, Celgene, Merck, Sanofi, Pfizer, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Physicians often fail to predict the impact of disease on quality of life in their psoriasis patients, which can help guide treatment, Joel Gelfand, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“This is true across all medical conditions,” said Dr. Gelfand, professor of dermatology, at the University of Pennsylvania, Philadelphia. For example, some patients with psoriasis may have extensive disease, but it doesn’t bother them, and therefore they may need less treatment, he pointed out.
In his practice, patients with psoriasis are asked to rate physical symptoms (including flaking and itching) and emotional symptoms (including anxiety and depression) related to their disease on a scale of 0 to 10, with 10 being the worst. “The higher those scores are, the more aggressive I’ll be in treating them,” he said. Patient scores can be tracked over time, to review progress with their chosen treatment, he noted.
Dr. Gelfand disclosed relationships with multiple companies including AbbVie, Janssen, Lilly, Novartis, Celgene, Merck, Sanofi, Pfizer, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
At SDEF LAS VEGAS DERMATOLOGY SEMINAR

Which Treatments Effectively Prevent Pediatric Migraine?
Amitriptyline and topiramate, the most commonly used medications for preventing pediatric migraine, are no more effective than placebo, according to trial results published online ahead of print October 27 in the New England Journal of Medicine. The drugs are, however, associated with higher rates of adverse events.
While the researchers were conducting this study, the FDA approved topiramate for the treatment of episodic migraine in adolescents between ages 12 and 17. “Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” said Scott W. Powers, PhD, Codirector of the Headache Center at Cincinnati Children’s, and colleagues.

The FDA has not approved any migraine-prevention medication for children younger than 12, and clinical practice guidelines for this indication are based on consensus, rather than evidence. Dr. Powers and colleagues conducted the Childhood and Adolescent Migraine Prevention (CHAMP) trial to compare the efficacy of common medications in children and adolescents between ages 8 and 17 with migraine. They randomized 361 patients to amitriptyline (1 mg/kg/day), topiramate (2 mg/kg/day), or placebo in a 2:2:1 ratio.
The trial included a 28-day baseline period, an eight-week dose-escalation period, and a 16-week maintenance phase. The primary outcome was a reduction of 50% or more in the number of headache days during the last 28 days of the trial, compared with baseline. Secondary outcomes included headache-related disability, headache days, number of trial completers, and serious adverse events.
The baseline characteristics of the three treatment groups were similar. The population’s mean age was 14. About 68% of the population was female, and 70% was white.
After a planned interim analysis, the investigators ended the trial early for futility. They found no significant between-group differences in the primary outcome. Approximately 52% of patients receiving amitriptyline, 55% of those receiving topiramate, and 61% of controls had a reduction in headache days of at least 50%. Headache-related disability, headache days, and the rate of trial completion also did not differ between groups.
Patients who received amitriptyline or topiramate had higher rates of several adverse events than those receiving placebo, including fatigue (30% vs 14%) and dry mouth (25% vs 12%) in the amitriptyline group and paresthesia (31% vs 8%) and weight loss (8% vs 0%) in the topiramate group. Three patients receiving amitriptyline had serious adverse events of altered mood, and one patient receiving topiramate attempted suicide.
“We see this [study] as an important opportunity for health care providers, scientists, children, and families because our findings suggest a paradigm shift,” said Dr. Powers. “First-line prevention treatment will involve a multidisciplinary team approach and focus on nonpharmacologic aspects of care. The good news is we can help children with migraines get better.”
—Erik Greb
Suggested Reading
Powers SW, Coffey CS, Chamberlin LA, et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2016 Oct 27 [Epub ahead of print].
Amitriptyline and topiramate, the most commonly used medications for preventing pediatric migraine, are no more effective than placebo, according to trial results published online ahead of print October 27 in the New England Journal of Medicine. The drugs are, however, associated with higher rates of adverse events.
While the researchers were conducting this study, the FDA approved topiramate for the treatment of episodic migraine in adolescents between ages 12 and 17. “Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” said Scott W. Powers, PhD, Codirector of the Headache Center at Cincinnati Children’s, and colleagues.
The FDA has not approved any migraine-prevention medication for children younger than 12, and clinical practice guidelines for this indication are based on consensus, rather than evidence. Dr. Powers and colleagues conducted the Childhood and Adolescent Migraine Prevention (CHAMP) trial to compare the efficacy of common medications in children and adolescents between ages 8 and 17 with migraine. They randomized 361 patients to amitriptyline (1 mg/kg/day), topiramate (2 mg/kg/day), or placebo in a 2:2:1 ratio.
The trial included a 28-day baseline period, an eight-week dose-escalation period, and a 16-week maintenance phase. The primary outcome was a reduction of 50% or more in the number of headache days during the last 28 days of the trial, compared with baseline. Secondary outcomes included headache-related disability, headache days, number of trial completers, and serious adverse events.
The baseline characteristics of the three treatment groups were similar. The population’s mean age was 14. About 68% of the population was female, and 70% was white.
After a planned interim analysis, the investigators ended the trial early for futility. They found no significant between-group differences in the primary outcome. Approximately 52% of patients receiving amitriptyline, 55% of those receiving topiramate, and 61% of controls had a reduction in headache days of at least 50%. Headache-related disability, headache days, and the rate of trial completion also did not differ between groups.
Patients who received amitriptyline or topiramate had higher rates of several adverse events than those receiving placebo, including fatigue (30% vs 14%) and dry mouth (25% vs 12%) in the amitriptyline group and paresthesia (31% vs 8%) and weight loss (8% vs 0%) in the topiramate group. Three patients receiving amitriptyline had serious adverse events of altered mood, and one patient receiving topiramate attempted suicide.
“We see this [study] as an important opportunity for health care providers, scientists, children, and families because our findings suggest a paradigm shift,” said Dr. Powers. “First-line prevention treatment will involve a multidisciplinary team approach and focus on nonpharmacologic aspects of care. The good news is we can help children with migraines get better.”
—Erik Greb
Suggested Reading
Powers SW, Coffey CS, Chamberlin LA, et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2016 Oct 27 [Epub ahead of print].
Amitriptyline and topiramate, the most commonly used medications for preventing pediatric migraine, are no more effective than placebo, according to trial results published online ahead of print October 27 in the New England Journal of Medicine. The drugs are, however, associated with higher rates of adverse events.
While the researchers were conducting this study, the FDA approved topiramate for the treatment of episodic migraine in adolescents between ages 12 and 17. “Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” said Scott W. Powers, PhD, Codirector of the Headache Center at Cincinnati Children’s, and colleagues.
The FDA has not approved any migraine-prevention medication for children younger than 12, and clinical practice guidelines for this indication are based on consensus, rather than evidence. Dr. Powers and colleagues conducted the Childhood and Adolescent Migraine Prevention (CHAMP) trial to compare the efficacy of common medications in children and adolescents between ages 8 and 17 with migraine. They randomized 361 patients to amitriptyline (1 mg/kg/day), topiramate (2 mg/kg/day), or placebo in a 2:2:1 ratio.
The trial included a 28-day baseline period, an eight-week dose-escalation period, and a 16-week maintenance phase. The primary outcome was a reduction of 50% or more in the number of headache days during the last 28 days of the trial, compared with baseline. Secondary outcomes included headache-related disability, headache days, number of trial completers, and serious adverse events.
The baseline characteristics of the three treatment groups were similar. The population’s mean age was 14. About 68% of the population was female, and 70% was white.
After a planned interim analysis, the investigators ended the trial early for futility. They found no significant between-group differences in the primary outcome. Approximately 52% of patients receiving amitriptyline, 55% of those receiving topiramate, and 61% of controls had a reduction in headache days of at least 50%. Headache-related disability, headache days, and the rate of trial completion also did not differ between groups.
Patients who received amitriptyline or topiramate had higher rates of several adverse events than those receiving placebo, including fatigue (30% vs 14%) and dry mouth (25% vs 12%) in the amitriptyline group and paresthesia (31% vs 8%) and weight loss (8% vs 0%) in the topiramate group. Three patients receiving amitriptyline had serious adverse events of altered mood, and one patient receiving topiramate attempted suicide.
“We see this [study] as an important opportunity for health care providers, scientists, children, and families because our findings suggest a paradigm shift,” said Dr. Powers. “First-line prevention treatment will involve a multidisciplinary team approach and focus on nonpharmacologic aspects of care. The good news is we can help children with migraines get better.”
—Erik Greb
Suggested Reading
Powers SW, Coffey CS, Chamberlin LA, et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2016 Oct 27 [Epub ahead of print].

Infants with congenital Zika born without microcephaly still can still develop it
Infants born with laboratory-confirmed congenital Zika virus but who show no signs of microcephaly at birth may still experience a reduction in cranial size as they grow older, according to the Centers for Disease Control and Prevention’s latest Morbidity and Mortality Weekly Report.
“These findings demonstrate the importance of early neuroimaging for infants exposed to Zika virus prenatally and the need for comprehensive medical and developmental follow-up,” wrote Vanessa van der Linden, MD, of the Association for Assistance of Disabled Children in Recife, Brazil, and her coauthors.
Dr. van der Linden and her coinvestigators examined 13 infants, all of whom were born in Brazil between October 2015 and January 2016, who had confirmed brain abnormalities at birth despite having a normal head size. These abnormalities included ventriculomegaly, subcortical calcifications, cortical malformations, and decreased brain volume. Investigators defined microcephaly as being “head circumference (HC) [that’s] more than 2 [standard deviations] below the mean for gestational age and sex.”
Nine of the infants were male, four were female. Eleven of the infants were born within 37-41 weeks’ of gestation. The remaining two were born at 35-36 weeks’ of gestation, considered “preterm” by the investigators. All infants tested positive for Zika via immunoglobulin M testing of cerebrospinal fluid, serum, or both. Only six of the mothers reported having a rash while pregnant; four reported experiencing it during the first trimester, while the other two said it occurred in the second.
All 13 infants showed a decrease in HC to what was defined as microcephaly within 1 year of birth (October 2016). Neuroimaging showed that all but one had decreased brain volume, all had malformations of cortical development, four had cerebellum or brain-stem hypoplasia, ten had ventriculomegaly, and three had increased extra-axial CSF space.
“More than 60% of infants in this series had epilepsy (likely related to the cortical malformations), and all had significant motor disabilities consistent with mixed cerebral palsy,” the authors noted, adding that the “pathogenesis of postnatal microcephaly from congenital Zika virus infections is [still] not known.”
Infants born with laboratory-confirmed congenital Zika virus but who show no signs of microcephaly at birth may still experience a reduction in cranial size as they grow older, according to the Centers for Disease Control and Prevention’s latest Morbidity and Mortality Weekly Report.
“These findings demonstrate the importance of early neuroimaging for infants exposed to Zika virus prenatally and the need for comprehensive medical and developmental follow-up,” wrote Vanessa van der Linden, MD, of the Association for Assistance of Disabled Children in Recife, Brazil, and her coauthors.
Dr. van der Linden and her coinvestigators examined 13 infants, all of whom were born in Brazil between October 2015 and January 2016, who had confirmed brain abnormalities at birth despite having a normal head size. These abnormalities included ventriculomegaly, subcortical calcifications, cortical malformations, and decreased brain volume. Investigators defined microcephaly as being “head circumference (HC) [that’s] more than 2 [standard deviations] below the mean for gestational age and sex.”
Nine of the infants were male, four were female. Eleven of the infants were born within 37-41 weeks’ of gestation. The remaining two were born at 35-36 weeks’ of gestation, considered “preterm” by the investigators. All infants tested positive for Zika via immunoglobulin M testing of cerebrospinal fluid, serum, or both. Only six of the mothers reported having a rash while pregnant; four reported experiencing it during the first trimester, while the other two said it occurred in the second.
All 13 infants showed a decrease in HC to what was defined as microcephaly within 1 year of birth (October 2016). Neuroimaging showed that all but one had decreased brain volume, all had malformations of cortical development, four had cerebellum or brain-stem hypoplasia, ten had ventriculomegaly, and three had increased extra-axial CSF space.
“More than 60% of infants in this series had epilepsy (likely related to the cortical malformations), and all had significant motor disabilities consistent with mixed cerebral palsy,” the authors noted, adding that the “pathogenesis of postnatal microcephaly from congenital Zika virus infections is [still] not known.”
Infants born with laboratory-confirmed congenital Zika virus but who show no signs of microcephaly at birth may still experience a reduction in cranial size as they grow older, according to the Centers for Disease Control and Prevention’s latest Morbidity and Mortality Weekly Report.
“These findings demonstrate the importance of early neuroimaging for infants exposed to Zika virus prenatally and the need for comprehensive medical and developmental follow-up,” wrote Vanessa van der Linden, MD, of the Association for Assistance of Disabled Children in Recife, Brazil, and her coauthors.
Dr. van der Linden and her coinvestigators examined 13 infants, all of whom were born in Brazil between October 2015 and January 2016, who had confirmed brain abnormalities at birth despite having a normal head size. These abnormalities included ventriculomegaly, subcortical calcifications, cortical malformations, and decreased brain volume. Investigators defined microcephaly as being “head circumference (HC) [that’s] more than 2 [standard deviations] below the mean for gestational age and sex.”
Nine of the infants were male, four were female. Eleven of the infants were born within 37-41 weeks’ of gestation. The remaining two were born at 35-36 weeks’ of gestation, considered “preterm” by the investigators. All infants tested positive for Zika via immunoglobulin M testing of cerebrospinal fluid, serum, or both. Only six of the mothers reported having a rash while pregnant; four reported experiencing it during the first trimester, while the other two said it occurred in the second.
All 13 infants showed a decrease in HC to what was defined as microcephaly within 1 year of birth (October 2016). Neuroimaging showed that all but one had decreased brain volume, all had malformations of cortical development, four had cerebellum or brain-stem hypoplasia, ten had ventriculomegaly, and three had increased extra-axial CSF space.
“More than 60% of infants in this series had epilepsy (likely related to the cortical malformations), and all had significant motor disabilities consistent with mixed cerebral palsy,” the authors noted, adding that the “pathogenesis of postnatal microcephaly from congenital Zika virus infections is [still] not known.”
FROM THE MMWR
Update on New Drugs in Dermatology
CenterWatch (http://www.centerwatch.com/) is an online resource that provides directories, analysis, and market research of medications that are either under clinical evaluation or available for use in patients. A list of currently approved drugs by the US Food and Drug Administration (FDA) also is available by specialty. It is important for dermatologists in-training to know about recently approved drugs and those that are in the pipeline, as these treatments may benefit patients who are unresponsive to other previously used medications. New drugs also may be useful for physicians who have a difficult time getting insurance to cover prescriptions for their patients, as most new medications have built-in patient assistance.
New Drugs in Dermatology
Actinic Keratosis
Ameluz (aminolevulinic acid hydrochloride)(Biofrontera AG) is a new drug that was approved in May 2016 for treatment of mild to moderate actinic keratosis on the face and scalp.1 It is only intended for in-office use on patients who may not be candidates for other treatment options for actinic keratosis. The product is a gel formulation that should be applied to cover the lesions and approximately 5 mm of the surrounding area with a film of approximately 1-mm thickness. The entire treatment area is then illuminated with a red light source, either with a narrow spectrum around 630 nm with a light dose of approximately 37 J/cm2 or a broader and continuous spectrum in the range of 570 to 670 nm with a light dose between 75 and 200 J/cm2.1 Similar to the previously used aminolevulinic acid treatment method for actinic keratosis, the patient may experience a burning stinging sensation throughout the treatment and the skin will then proceed to peel.
Psoriasis and Psoriatic Arthritis
Taltz (ixekizumab)(Eli Lilly and Company) was approved by the FDA in March 2016 for the treatment of moderate to severe plaque psoriasis.2 It is a humanized IL-17A antagonist that works when IgG4 monoclonal antibodies selectively bind with IL-17A cytokines and inhibit their interaction with the IL-17 receptor. Although this injectable medication is approved for the treatment of psoriasis, it also can potentially be used off label for the treatment of psoriatic arthritis and rheumatoid arthritis. The approved dosage is 160 mg (two 80-mg injections) at week 0, followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12, then 80 mg every 4 weeks.2 Injectable immunomodulatory medications such as ixekizumab are ideal for patients in whom topical treatments and light therapy failed and they continue to have serious psoriatic discomfort as well as for those who have substantial body surface area coverage.
In January 2015, Cosentyx (secukinumab)(Novartis Corporation) was approved by the FDA.3 Similar to ixekizumab, this injectable is an IgG1 monoclonal antibody that selectively binds to the IL-17A cytokine and inhibits its interaction with the IL-17 receptor. It is approved for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis. The approved dosage for plaque psoriasis is 300 mg (two 150-mg subcutaneous injections) at weeks 0 through 4 followed by 300 mg every 4 weeks as needed until clearance.3 Similar to ixekizumab, secukinumab may be used for the treatment of recalcitrant psoriasis or psoriasis with substantial body surface area involvement.
Melanoma
Cotellic (cobimetinib)(Genentech USA, Inc) was FDA approved in November 2015.4 Cobimetinib is a reversible inhibitor of mitogen-activated protein kinase (MAPK)/extracellular signal regulated kinase 1. Mitogen-activated protein kinase MEK1 and MEK2 are regulators of the extracellular signal-related kinase pathway, which promotes cellular proliferation. This pathway is key, as melanomas that have a BRAF V600E and kinase mutation continue to proliferate due to the constitutive activation of MEK1 and MEK2, further promoting cellular proliferation. Cobimetinib is approved for the treatment of melanoma in patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, in conjunction with vemurafenib. Zelboraf (vemurafenib)(Genentech USA, Inc), another inhibitor of BRAF V600E, also is used for the treatment of unresectable melanomas and was initially approved in 2011.5
BRAF is a serine/threonine protein kinase. When unregulated, it results in the deregulation of cell proliferation. According to Ascierto et al,6 50% of melanomas have a BRAF mutation, with nearly 90% of them with a V600E mutation. Hence, since the advent of direct chemotherapeutic agents such as BRAF inhibitors, clinical trials have shown notable reduction in mortality and morbidity of melanoma patients with BRAF mutations.6
Imlygic (talimogene laherparepvec)(Amgen, Inc) is a modified oncolytic viral therapy.7 This treatment was approved by the FDA in 2015 and replicates within tumors to produce granulocyte-macrophage colony-stimulating factor protein, which promotes an antitumor immune response within unresectable cutaneous, subcutaneous, and nodal melanoma lesions. Although it is not a gene-directed therapy, the melanoma does not require a specific mutation for treatment. Again, this medication is better served in conjunction with other melanoma chemotherapeutic and surgical interventions.
Submental Fat
Kybella (deoxycholic acid)(Allergan) is a nonhuman, nonanimal, synthetically created compound that is naturally found within the human body for the breakdown and absorption of dietary fat.8 This drug was FDA approved in 2015 for the improvement of the appearance of moderate subcutaneous fat under the chin. Patients are evaluated in clinic to determine if the submental fat would be responsive to an injectable or require more radical surgical intervention based on desired outcomes. The treatment is administered as 0.2-mL injections (up to a total of 10 mL) spaced 1-cm apart and ideally is repeated at regular intervals to evaluate for efficacy.
Basal Cell Carcinoma
Odomzo (sonidegib)(Novartis Corporation) was FDA approved in 2015 for locally advanced basal cell carcinoma.9 Odomzo is a smoothened antagonist that inhibits the hedgehog signaling pathway. Smoothened is a transmembrane protein that allows for signal transduction of hedgehog proteins.10 Protein patched homolog 1 binds to smoothened protein and prevents the signal transduction through the cell for Gli family zinc factor 1 to continue protein translation; however, when PTCH is mutated and can no longer bind to smoothened, tumor formation results, specifically basal cell carcinoma. Hence, sonidegib is for the treatment of basal cell carcinomas that have persisted despite radiation treatment and/or surgery as well as for patients who have multiple basal cell carcinomas that can no longer be treated with surgery or radiation.
Final Thoughts
Overall, although there are several medications that can be used in conjunction for treatment of dermatological conditions, it always is recommended to know what is in the pipeline as FDA-approved medications for dermatology.
- Ameluz [package insert]. Leverkusen, Germany: Biofrontera Bioscience GmbH; 2016.
- Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2016.
- Cosentyx [package insert]. East Hanover, NJ: Novartis Corporation; 2015.
- Cotellic [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Zelboraf [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Ascierto PA, Kirkwood JM, Grob JJ, et al. The role of BRAF V600 mutation in melanoma. J Transl Med. 2012;10:85.
- Imlygic (talimogene laherparepvec). Thousand Oaks, CA: Amgen Inc; 2015.
- Kybella [package insert]. West Lake Village, CA: Kythera Biopharmaceuticals, Inc; 2015.
- Odomzo [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
- Villavicencio EH, Walterhouse DO, Iannaccone PM. The sonic hedgehog-patched-gli pathway in human development and disease. Am J Hum Genet. 2000;67:1047-1054.
CenterWatch (http://www.centerwatch.com/) is an online resource that provides directories, analysis, and market research of medications that are either under clinical evaluation or available for use in patients. A list of currently approved drugs by the US Food and Drug Administration (FDA) also is available by specialty. It is important for dermatologists in-training to know about recently approved drugs and those that are in the pipeline, as these treatments may benefit patients who are unresponsive to other previously used medications. New drugs also may be useful for physicians who have a difficult time getting insurance to cover prescriptions for their patients, as most new medications have built-in patient assistance.
New Drugs in Dermatology
Actinic Keratosis
Ameluz (aminolevulinic acid hydrochloride)(Biofrontera AG) is a new drug that was approved in May 2016 for treatment of mild to moderate actinic keratosis on the face and scalp.1 It is only intended for in-office use on patients who may not be candidates for other treatment options for actinic keratosis. The product is a gel formulation that should be applied to cover the lesions and approximately 5 mm of the surrounding area with a film of approximately 1-mm thickness. The entire treatment area is then illuminated with a red light source, either with a narrow spectrum around 630 nm with a light dose of approximately 37 J/cm2 or a broader and continuous spectrum in the range of 570 to 670 nm with a light dose between 75 and 200 J/cm2.1 Similar to the previously used aminolevulinic acid treatment method for actinic keratosis, the patient may experience a burning stinging sensation throughout the treatment and the skin will then proceed to peel.
Psoriasis and Psoriatic Arthritis
Taltz (ixekizumab)(Eli Lilly and Company) was approved by the FDA in March 2016 for the treatment of moderate to severe plaque psoriasis.2 It is a humanized IL-17A antagonist that works when IgG4 monoclonal antibodies selectively bind with IL-17A cytokines and inhibit their interaction with the IL-17 receptor. Although this injectable medication is approved for the treatment of psoriasis, it also can potentially be used off label for the treatment of psoriatic arthritis and rheumatoid arthritis. The approved dosage is 160 mg (two 80-mg injections) at week 0, followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12, then 80 mg every 4 weeks.2 Injectable immunomodulatory medications such as ixekizumab are ideal for patients in whom topical treatments and light therapy failed and they continue to have serious psoriatic discomfort as well as for those who have substantial body surface area coverage.
In January 2015, Cosentyx (secukinumab)(Novartis Corporation) was approved by the FDA.3 Similar to ixekizumab, this injectable is an IgG1 monoclonal antibody that selectively binds to the IL-17A cytokine and inhibits its interaction with the IL-17 receptor. It is approved for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis. The approved dosage for plaque psoriasis is 300 mg (two 150-mg subcutaneous injections) at weeks 0 through 4 followed by 300 mg every 4 weeks as needed until clearance.3 Similar to ixekizumab, secukinumab may be used for the treatment of recalcitrant psoriasis or psoriasis with substantial body surface area involvement.
Melanoma
Cotellic (cobimetinib)(Genentech USA, Inc) was FDA approved in November 2015.4 Cobimetinib is a reversible inhibitor of mitogen-activated protein kinase (MAPK)/extracellular signal regulated kinase 1. Mitogen-activated protein kinase MEK1 and MEK2 are regulators of the extracellular signal-related kinase pathway, which promotes cellular proliferation. This pathway is key, as melanomas that have a BRAF V600E and kinase mutation continue to proliferate due to the constitutive activation of MEK1 and MEK2, further promoting cellular proliferation. Cobimetinib is approved for the treatment of melanoma in patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, in conjunction with vemurafenib. Zelboraf (vemurafenib)(Genentech USA, Inc), another inhibitor of BRAF V600E, also is used for the treatment of unresectable melanomas and was initially approved in 2011.5
BRAF is a serine/threonine protein kinase. When unregulated, it results in the deregulation of cell proliferation. According to Ascierto et al,6 50% of melanomas have a BRAF mutation, with nearly 90% of them with a V600E mutation. Hence, since the advent of direct chemotherapeutic agents such as BRAF inhibitors, clinical trials have shown notable reduction in mortality and morbidity of melanoma patients with BRAF mutations.6
Imlygic (talimogene laherparepvec)(Amgen, Inc) is a modified oncolytic viral therapy.7 This treatment was approved by the FDA in 2015 and replicates within tumors to produce granulocyte-macrophage colony-stimulating factor protein, which promotes an antitumor immune response within unresectable cutaneous, subcutaneous, and nodal melanoma lesions. Although it is not a gene-directed therapy, the melanoma does not require a specific mutation for treatment. Again, this medication is better served in conjunction with other melanoma chemotherapeutic and surgical interventions.
Submental Fat
Kybella (deoxycholic acid)(Allergan) is a nonhuman, nonanimal, synthetically created compound that is naturally found within the human body for the breakdown and absorption of dietary fat.8 This drug was FDA approved in 2015 for the improvement of the appearance of moderate subcutaneous fat under the chin. Patients are evaluated in clinic to determine if the submental fat would be responsive to an injectable or require more radical surgical intervention based on desired outcomes. The treatment is administered as 0.2-mL injections (up to a total of 10 mL) spaced 1-cm apart and ideally is repeated at regular intervals to evaluate for efficacy.
Basal Cell Carcinoma
Odomzo (sonidegib)(Novartis Corporation) was FDA approved in 2015 for locally advanced basal cell carcinoma.9 Odomzo is a smoothened antagonist that inhibits the hedgehog signaling pathway. Smoothened is a transmembrane protein that allows for signal transduction of hedgehog proteins.10 Protein patched homolog 1 binds to smoothened protein and prevents the signal transduction through the cell for Gli family zinc factor 1 to continue protein translation; however, when PTCH is mutated and can no longer bind to smoothened, tumor formation results, specifically basal cell carcinoma. Hence, sonidegib is for the treatment of basal cell carcinomas that have persisted despite radiation treatment and/or surgery as well as for patients who have multiple basal cell carcinomas that can no longer be treated with surgery or radiation.
Final Thoughts
Overall, although there are several medications that can be used in conjunction for treatment of dermatological conditions, it always is recommended to know what is in the pipeline as FDA-approved medications for dermatology.
CenterWatch (http://www.centerwatch.com/) is an online resource that provides directories, analysis, and market research of medications that are either under clinical evaluation or available for use in patients. A list of currently approved drugs by the US Food and Drug Administration (FDA) also is available by specialty. It is important for dermatologists in-training to know about recently approved drugs and those that are in the pipeline, as these treatments may benefit patients who are unresponsive to other previously used medications. New drugs also may be useful for physicians who have a difficult time getting insurance to cover prescriptions for their patients, as most new medications have built-in patient assistance.
New Drugs in Dermatology
Actinic Keratosis
Ameluz (aminolevulinic acid hydrochloride)(Biofrontera AG) is a new drug that was approved in May 2016 for treatment of mild to moderate actinic keratosis on the face and scalp.1 It is only intended for in-office use on patients who may not be candidates for other treatment options for actinic keratosis. The product is a gel formulation that should be applied to cover the lesions and approximately 5 mm of the surrounding area with a film of approximately 1-mm thickness. The entire treatment area is then illuminated with a red light source, either with a narrow spectrum around 630 nm with a light dose of approximately 37 J/cm2 or a broader and continuous spectrum in the range of 570 to 670 nm with a light dose between 75 and 200 J/cm2.1 Similar to the previously used aminolevulinic acid treatment method for actinic keratosis, the patient may experience a burning stinging sensation throughout the treatment and the skin will then proceed to peel.
Psoriasis and Psoriatic Arthritis
Taltz (ixekizumab)(Eli Lilly and Company) was approved by the FDA in March 2016 for the treatment of moderate to severe plaque psoriasis.2 It is a humanized IL-17A antagonist that works when IgG4 monoclonal antibodies selectively bind with IL-17A cytokines and inhibit their interaction with the IL-17 receptor. Although this injectable medication is approved for the treatment of psoriasis, it also can potentially be used off label for the treatment of psoriatic arthritis and rheumatoid arthritis. The approved dosage is 160 mg (two 80-mg injections) at week 0, followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12, then 80 mg every 4 weeks.2 Injectable immunomodulatory medications such as ixekizumab are ideal for patients in whom topical treatments and light therapy failed and they continue to have serious psoriatic discomfort as well as for those who have substantial body surface area coverage.
In January 2015, Cosentyx (secukinumab)(Novartis Corporation) was approved by the FDA.3 Similar to ixekizumab, this injectable is an IgG1 monoclonal antibody that selectively binds to the IL-17A cytokine and inhibits its interaction with the IL-17 receptor. It is approved for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis. The approved dosage for plaque psoriasis is 300 mg (two 150-mg subcutaneous injections) at weeks 0 through 4 followed by 300 mg every 4 weeks as needed until clearance.3 Similar to ixekizumab, secukinumab may be used for the treatment of recalcitrant psoriasis or psoriasis with substantial body surface area involvement.
Melanoma
Cotellic (cobimetinib)(Genentech USA, Inc) was FDA approved in November 2015.4 Cobimetinib is a reversible inhibitor of mitogen-activated protein kinase (MAPK)/extracellular signal regulated kinase 1. Mitogen-activated protein kinase MEK1 and MEK2 are regulators of the extracellular signal-related kinase pathway, which promotes cellular proliferation. This pathway is key, as melanomas that have a BRAF V600E and kinase mutation continue to proliferate due to the constitutive activation of MEK1 and MEK2, further promoting cellular proliferation. Cobimetinib is approved for the treatment of melanoma in patients with unresectable or metastatic melanoma with a BRAF V600E or V600K mutation, in conjunction with vemurafenib. Zelboraf (vemurafenib)(Genentech USA, Inc), another inhibitor of BRAF V600E, also is used for the treatment of unresectable melanomas and was initially approved in 2011.5
BRAF is a serine/threonine protein kinase. When unregulated, it results in the deregulation of cell proliferation. According to Ascierto et al,6 50% of melanomas have a BRAF mutation, with nearly 90% of them with a V600E mutation. Hence, since the advent of direct chemotherapeutic agents such as BRAF inhibitors, clinical trials have shown notable reduction in mortality and morbidity of melanoma patients with BRAF mutations.6
Imlygic (talimogene laherparepvec)(Amgen, Inc) is a modified oncolytic viral therapy.7 This treatment was approved by the FDA in 2015 and replicates within tumors to produce granulocyte-macrophage colony-stimulating factor protein, which promotes an antitumor immune response within unresectable cutaneous, subcutaneous, and nodal melanoma lesions. Although it is not a gene-directed therapy, the melanoma does not require a specific mutation for treatment. Again, this medication is better served in conjunction with other melanoma chemotherapeutic and surgical interventions.
Submental Fat
Kybella (deoxycholic acid)(Allergan) is a nonhuman, nonanimal, synthetically created compound that is naturally found within the human body for the breakdown and absorption of dietary fat.8 This drug was FDA approved in 2015 for the improvement of the appearance of moderate subcutaneous fat under the chin. Patients are evaluated in clinic to determine if the submental fat would be responsive to an injectable or require more radical surgical intervention based on desired outcomes. The treatment is administered as 0.2-mL injections (up to a total of 10 mL) spaced 1-cm apart and ideally is repeated at regular intervals to evaluate for efficacy.
Basal Cell Carcinoma
Odomzo (sonidegib)(Novartis Corporation) was FDA approved in 2015 for locally advanced basal cell carcinoma.9 Odomzo is a smoothened antagonist that inhibits the hedgehog signaling pathway. Smoothened is a transmembrane protein that allows for signal transduction of hedgehog proteins.10 Protein patched homolog 1 binds to smoothened protein and prevents the signal transduction through the cell for Gli family zinc factor 1 to continue protein translation; however, when PTCH is mutated and can no longer bind to smoothened, tumor formation results, specifically basal cell carcinoma. Hence, sonidegib is for the treatment of basal cell carcinomas that have persisted despite radiation treatment and/or surgery as well as for patients who have multiple basal cell carcinomas that can no longer be treated with surgery or radiation.
Final Thoughts
Overall, although there are several medications that can be used in conjunction for treatment of dermatological conditions, it always is recommended to know what is in the pipeline as FDA-approved medications for dermatology.
- Ameluz [package insert]. Leverkusen, Germany: Biofrontera Bioscience GmbH; 2016.
- Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2016.
- Cosentyx [package insert]. East Hanover, NJ: Novartis Corporation; 2015.
- Cotellic [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Zelboraf [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Ascierto PA, Kirkwood JM, Grob JJ, et al. The role of BRAF V600 mutation in melanoma. J Transl Med. 2012;10:85.
- Imlygic (talimogene laherparepvec). Thousand Oaks, CA: Amgen Inc; 2015.
- Kybella [package insert]. West Lake Village, CA: Kythera Biopharmaceuticals, Inc; 2015.
- Odomzo [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
- Villavicencio EH, Walterhouse DO, Iannaccone PM. The sonic hedgehog-patched-gli pathway in human development and disease. Am J Hum Genet. 2000;67:1047-1054.
- Ameluz [package insert]. Leverkusen, Germany: Biofrontera Bioscience GmbH; 2016.
- Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2016.
- Cosentyx [package insert]. East Hanover, NJ: Novartis Corporation; 2015.
- Cotellic [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Zelboraf [package insert]. San Francisco, CA: Genentech, Inc; 2016.
- Ascierto PA, Kirkwood JM, Grob JJ, et al. The role of BRAF V600 mutation in melanoma. J Transl Med. 2012;10:85.
- Imlygic (talimogene laherparepvec). Thousand Oaks, CA: Amgen Inc; 2015.
- Kybella [package insert]. West Lake Village, CA: Kythera Biopharmaceuticals, Inc; 2015.
- Odomzo [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.
- Villavicencio EH, Walterhouse DO, Iannaccone PM. The sonic hedgehog-patched-gli pathway in human development and disease. Am J Hum Genet. 2000;67:1047-1054.

VIDEO: Challenging case – consider HSV with erythema multiforme
LAS VEGAS – In a presentation at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Miriam S. Bettencourt, MD, shared a challenging diagnostic case of erythema multiforme associated with herpes simplex, in a patient who presented with blisters all over his body.
“We know that 90% of cases of erythema multiforme are related to herpetic infections,” but this patient had no recent history of herpes simplex outbreaks, Dr. Bettencourt, of the University of Nevada, Las Vegas, said in a video interview.
‘“Let’s remember that HSV [herpes simplex virus] ... can be associated with erythema multiforme even if a patient does not have any flares,” Dr. Bettencourt said. A consult with a rheumatologist can be helpful, as in this case, if a patient has a positive antinuclear antibody test, which could not be explained, she added, noting that the patient is doing well after 6 months of therapy.
Dr. Bettencourt disclosed relationships with AbbVie, Allergan, Aqua, Celgene, Janssen, IntraDerm, Leo, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – In a presentation at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Miriam S. Bettencourt, MD, shared a challenging diagnostic case of erythema multiforme associated with herpes simplex, in a patient who presented with blisters all over his body.
“We know that 90% of cases of erythema multiforme are related to herpetic infections,” but this patient had no recent history of herpes simplex outbreaks, Dr. Bettencourt, of the University of Nevada, Las Vegas, said in a video interview.
‘“Let’s remember that HSV [herpes simplex virus] ... can be associated with erythema multiforme even if a patient does not have any flares,” Dr. Bettencourt said. A consult with a rheumatologist can be helpful, as in this case, if a patient has a positive antinuclear antibody test, which could not be explained, she added, noting that the patient is doing well after 6 months of therapy.
Dr. Bettencourt disclosed relationships with AbbVie, Allergan, Aqua, Celgene, Janssen, IntraDerm, Leo, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – In a presentation at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Miriam S. Bettencourt, MD, shared a challenging diagnostic case of erythema multiforme associated with herpes simplex, in a patient who presented with blisters all over his body.
“We know that 90% of cases of erythema multiforme are related to herpetic infections,” but this patient had no recent history of herpes simplex outbreaks, Dr. Bettencourt, of the University of Nevada, Las Vegas, said in a video interview.
‘“Let’s remember that HSV [herpes simplex virus] ... can be associated with erythema multiforme even if a patient does not have any flares,” Dr. Bettencourt said. A consult with a rheumatologist can be helpful, as in this case, if a patient has a positive antinuclear antibody test, which could not be explained, she added, noting that the patient is doing well after 6 months of therapy.
Dr. Bettencourt disclosed relationships with AbbVie, Allergan, Aqua, Celgene, Janssen, IntraDerm, Leo, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR

VIDEO: For facial resurfacing, revisit CO2 lasers
LAS VEGAS – Patients can enjoy positive results from facial resurfacing with fractionated lasers, but they don’t always yield the same benefits as the traditional CO2 laser, Christopher Zachary, M.D., said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“A lot of us are going back to using traditional laser resurfacing” for the patients who need it, such as those with many wrinkles, crepey skin, and extensive sun damage, Dr. Zachary, professor and chair of the department of dermatology at the University of California, Irvine, said in a video interview.
“Those patients are not going to have an optimal result, even with the most aggressive of fractionated ablative lasers, as compared to the traditional laser resurfacing,” he added.
Dr. Zachary disclosed relationships with multiple companies, including Solta, Zeltiq, Scion, Amway, and Candela. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Patients can enjoy positive results from facial resurfacing with fractionated lasers, but they don’t always yield the same benefits as the traditional CO2 laser, Christopher Zachary, M.D., said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“A lot of us are going back to using traditional laser resurfacing” for the patients who need it, such as those with many wrinkles, crepey skin, and extensive sun damage, Dr. Zachary, professor and chair of the department of dermatology at the University of California, Irvine, said in a video interview.
“Those patients are not going to have an optimal result, even with the most aggressive of fractionated ablative lasers, as compared to the traditional laser resurfacing,” he added.
Dr. Zachary disclosed relationships with multiple companies, including Solta, Zeltiq, Scion, Amway, and Candela. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Patients can enjoy positive results from facial resurfacing with fractionated lasers, but they don’t always yield the same benefits as the traditional CO2 laser, Christopher Zachary, M.D., said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
“A lot of us are going back to using traditional laser resurfacing” for the patients who need it, such as those with many wrinkles, crepey skin, and extensive sun damage, Dr. Zachary, professor and chair of the department of dermatology at the University of California, Irvine, said in a video interview.
“Those patients are not going to have an optimal result, even with the most aggressive of fractionated ablative lasers, as compared to the traditional laser resurfacing,” he added.
Dr. Zachary disclosed relationships with multiple companies, including Solta, Zeltiq, Scion, Amway, and Candela. SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR
