User login
Cystic fibrosis–related diabetes requires unique treatment
SAN DIEGO – according to Katie Larson Ode, MD.
Medical advances have dramatically boosted life expectancy for people with cystic fibrosis, allowing some to survive into middle age. “As more of our patients live longer, [cystic fibrosis–related diabetes (CFRD)] will become a much more common problem for endocrinologists, educators, nurses, and nutritionists to address,” said Dr. Ode, a pediatrician at the University of Iowa in Iowa City. “Proper management of cystic fibrosis-related diabetes is lifesaving for our CF patients.”

“CF is caused by a defect in an important chloride channel that regulates the salt and water content of secretions,” said Antoinette Moran, MD, professor and division chief of pediatric endocrinology and diabetes at the University of Minnesota, Minneapolis, while speaking at the annual meeting of the American Association of Diabetes Educators. “This affects many organs, but death is generally due to chronic obstructive lung disease.”
In the 1950s, few children with CF lived past elementary school age. Now, researchers estimate that the median life span for babies born and diagnosed in 2010 could reach more than 50 years (Ann Intern Med. 2014 Aug 19;161[4]:233-41), according to the Cystic Fibrosis Foundation.
But as they age, CF patients’ risk for CFRD also increases.
A 2009 study led by Dr. Moran (Diabetes Care 2009 Sep;32[9]: 1626-31) tracked 872 CF patients from three periods in the 1990s and 2000s and found CFRD in 2% of children, 19% of adolescents, and 40%-50% of adults. “For a typical CF patient, the chances of developing CFRD by age 40 are roughly 80%,” said Andrew Norris, MD, PhD, of the departments of pediatrics and biochemistry at the University of Iowa.

CF patients aren’t limited to one form of diabetes. “Occasionally a patient may be unlucky enough to have more than one type,” Dr. Moran said, since the diseases have separate pathophysiologies. While rare, type 1 appears to be more common than type 2, which is often linked to obesity; CF patients struggle to put on weight. “It would be highly unusual for a CF patient to develop type 2 diabetes,” Dr. Norris said.
The specialists said patients with CFRD are unique among diabetics for several reasons:
• Microvascular complications are rare. “After many years of diabetes, CFRD patients are at risk for microvascular complications, but they tend to be less common and less severe than in other forms of diabetes, likely because CF patients still make some of their own insulin,” Dr. Moran said.
• Macrovascular complications are not seen. “This is important because recommendations given to people with other forms of the diabetes to reduce risk of macrovascular complications – weight loss, low-fat diet, low-salt diet, etc.– do no apply in CF and can actually be harmful,” Dr. Moran said.
• Insulin is especially crucial. “Maintaining weight and lean body mass is critical for survival in CF, so the chief clinical concern with CFRD is nutrition and the potential impact of insulin insufficiency on mortality,” Dr. Moran said. “Insulin replacement is the only approved therapy for CFRD. Treatment is very similar to that of type 1 diabetic patients in a honeymoon state. Very early on, patients may receive a single dose of basal insulin only or of premeal rapid-acting insulin only. Eventually most CF patients require basal-bolus insulin therapy.”
Doses tend to be lower than in other diabetics, she said, “except for when CF patients are acutely ill. During acute illness, CF patients become insulin resistant and require high insulin doses.”
Still, “once I start insulin, my goal is to deliver as large a dose as the patient can safely tolerate, to maximize anabolic impact,” she said.
The physicians offered these tips about tracking and treating CF patients:
• Screen CF patients via oral glucose tolerance testing on an annual basis, starting no later than age 10. Don’t trust hemoglobin A1c levels or fasting glucose levels, Dr. Norris said, because they are not sensitive enough. In fact, Dr. Moran said, “HbA1cis spuriously low in CF. “Even mild diabetes can be immediately detrimental to a CF patient’s lung health and mortality risk,” Dr. Norris said. “If you wait until the onset of classic diabetes symptoms or until the fasting glucose or hemoglobin A1c is elevated, you will have done a great disservice to the CF patient, as preventable potentially life-threatening lung damage may have already occurred.”
• Check into your center’s testing protocol. “Unfortunately, current screening rates are markedly insufficient at many centers,” Dr. Norris said. “I encourage endocrine teams to reach out to their affiliated CF treatment center to discuss and help implement screening.”
What’s next? The University of Iowa’s Dr. Larson said he is hopeful about advances in medical care. “Currently, patients must follow an extremely complex regimen of airway clearance, inhaled antibiotics, and oral medications, typically with recurrent hospitalization with increasing age and eventual death from lung disease or lung transplant,” she said. “However, in the past few years, we have had a dramatic change for a percentage of our patients with the development of small molecules that can actually fix the chloride-channel defect itself.”
The treatment seems to arrest and even improve lung disease in eligible patients, she said. “So the future seems very bright for CF.”
The Cystic Fibrosis Foundation has developed a 3-year Envision program to train adult and pediatric endocrinologists in the care of CFRD and endocrine issues.
Dr. Moran had no relevant disclosures. Dr. Norris has consulted for Vertex Pharmaceuticals, which makes cystic fibrosis therapeutics, in the past year. Dr. Larson Ode reports that her research is funded by the National Institutes of Health and the Cystic Fibrosis Foundation.
SAN DIEGO – according to Katie Larson Ode, MD.
Medical advances have dramatically boosted life expectancy for people with cystic fibrosis, allowing some to survive into middle age. “As more of our patients live longer, [cystic fibrosis–related diabetes (CFRD)] will become a much more common problem for endocrinologists, educators, nurses, and nutritionists to address,” said Dr. Ode, a pediatrician at the University of Iowa in Iowa City. “Proper management of cystic fibrosis-related diabetes is lifesaving for our CF patients.”
“CF is caused by a defect in an important chloride channel that regulates the salt and water content of secretions,” said Antoinette Moran, MD, professor and division chief of pediatric endocrinology and diabetes at the University of Minnesota, Minneapolis, while speaking at the annual meeting of the American Association of Diabetes Educators. “This affects many organs, but death is generally due to chronic obstructive lung disease.”
In the 1950s, few children with CF lived past elementary school age. Now, researchers estimate that the median life span for babies born and diagnosed in 2010 could reach more than 50 years (Ann Intern Med. 2014 Aug 19;161[4]:233-41), according to the Cystic Fibrosis Foundation.
But as they age, CF patients’ risk for CFRD also increases.
A 2009 study led by Dr. Moran (Diabetes Care 2009 Sep;32[9]: 1626-31) tracked 872 CF patients from three periods in the 1990s and 2000s and found CFRD in 2% of children, 19% of adolescents, and 40%-50% of adults. “For a typical CF patient, the chances of developing CFRD by age 40 are roughly 80%,” said Andrew Norris, MD, PhD, of the departments of pediatrics and biochemistry at the University of Iowa.
CF patients aren’t limited to one form of diabetes. “Occasionally a patient may be unlucky enough to have more than one type,” Dr. Moran said, since the diseases have separate pathophysiologies. While rare, type 1 appears to be more common than type 2, which is often linked to obesity; CF patients struggle to put on weight. “It would be highly unusual for a CF patient to develop type 2 diabetes,” Dr. Norris said.
The specialists said patients with CFRD are unique among diabetics for several reasons:
• Microvascular complications are rare. “After many years of diabetes, CFRD patients are at risk for microvascular complications, but they tend to be less common and less severe than in other forms of diabetes, likely because CF patients still make some of their own insulin,” Dr. Moran said.
• Macrovascular complications are not seen. “This is important because recommendations given to people with other forms of the diabetes to reduce risk of macrovascular complications – weight loss, low-fat diet, low-salt diet, etc.– do no apply in CF and can actually be harmful,” Dr. Moran said.
• Insulin is especially crucial. “Maintaining weight and lean body mass is critical for survival in CF, so the chief clinical concern with CFRD is nutrition and the potential impact of insulin insufficiency on mortality,” Dr. Moran said. “Insulin replacement is the only approved therapy for CFRD. Treatment is very similar to that of type 1 diabetic patients in a honeymoon state. Very early on, patients may receive a single dose of basal insulin only or of premeal rapid-acting insulin only. Eventually most CF patients require basal-bolus insulin therapy.”
Doses tend to be lower than in other diabetics, she said, “except for when CF patients are acutely ill. During acute illness, CF patients become insulin resistant and require high insulin doses.”
Still, “once I start insulin, my goal is to deliver as large a dose as the patient can safely tolerate, to maximize anabolic impact,” she said.
The physicians offered these tips about tracking and treating CF patients:
• Screen CF patients via oral glucose tolerance testing on an annual basis, starting no later than age 10. Don’t trust hemoglobin A1c levels or fasting glucose levels, Dr. Norris said, because they are not sensitive enough. In fact, Dr. Moran said, “HbA1cis spuriously low in CF. “Even mild diabetes can be immediately detrimental to a CF patient’s lung health and mortality risk,” Dr. Norris said. “If you wait until the onset of classic diabetes symptoms or until the fasting glucose or hemoglobin A1c is elevated, you will have done a great disservice to the CF patient, as preventable potentially life-threatening lung damage may have already occurred.”
• Check into your center’s testing protocol. “Unfortunately, current screening rates are markedly insufficient at many centers,” Dr. Norris said. “I encourage endocrine teams to reach out to their affiliated CF treatment center to discuss and help implement screening.”
What’s next? The University of Iowa’s Dr. Larson said he is hopeful about advances in medical care. “Currently, patients must follow an extremely complex regimen of airway clearance, inhaled antibiotics, and oral medications, typically with recurrent hospitalization with increasing age and eventual death from lung disease or lung transplant,” she said. “However, in the past few years, we have had a dramatic change for a percentage of our patients with the development of small molecules that can actually fix the chloride-channel defect itself.”
The treatment seems to arrest and even improve lung disease in eligible patients, she said. “So the future seems very bright for CF.”
The Cystic Fibrosis Foundation has developed a 3-year Envision program to train adult and pediatric endocrinologists in the care of CFRD and endocrine issues.
Dr. Moran had no relevant disclosures. Dr. Norris has consulted for Vertex Pharmaceuticals, which makes cystic fibrosis therapeutics, in the past year. Dr. Larson Ode reports that her research is funded by the National Institutes of Health and the Cystic Fibrosis Foundation.
SAN DIEGO – according to Katie Larson Ode, MD.
Medical advances have dramatically boosted life expectancy for people with cystic fibrosis, allowing some to survive into middle age. “As more of our patients live longer, [cystic fibrosis–related diabetes (CFRD)] will become a much more common problem for endocrinologists, educators, nurses, and nutritionists to address,” said Dr. Ode, a pediatrician at the University of Iowa in Iowa City. “Proper management of cystic fibrosis-related diabetes is lifesaving for our CF patients.”
“CF is caused by a defect in an important chloride channel that regulates the salt and water content of secretions,” said Antoinette Moran, MD, professor and division chief of pediatric endocrinology and diabetes at the University of Minnesota, Minneapolis, while speaking at the annual meeting of the American Association of Diabetes Educators. “This affects many organs, but death is generally due to chronic obstructive lung disease.”
In the 1950s, few children with CF lived past elementary school age. Now, researchers estimate that the median life span for babies born and diagnosed in 2010 could reach more than 50 years (Ann Intern Med. 2014 Aug 19;161[4]:233-41), according to the Cystic Fibrosis Foundation.
But as they age, CF patients’ risk for CFRD also increases.
A 2009 study led by Dr. Moran (Diabetes Care 2009 Sep;32[9]: 1626-31) tracked 872 CF patients from three periods in the 1990s and 2000s and found CFRD in 2% of children, 19% of adolescents, and 40%-50% of adults. “For a typical CF patient, the chances of developing CFRD by age 40 are roughly 80%,” said Andrew Norris, MD, PhD, of the departments of pediatrics and biochemistry at the University of Iowa.
CF patients aren’t limited to one form of diabetes. “Occasionally a patient may be unlucky enough to have more than one type,” Dr. Moran said, since the diseases have separate pathophysiologies. While rare, type 1 appears to be more common than type 2, which is often linked to obesity; CF patients struggle to put on weight. “It would be highly unusual for a CF patient to develop type 2 diabetes,” Dr. Norris said.
The specialists said patients with CFRD are unique among diabetics for several reasons:
• Microvascular complications are rare. “After many years of diabetes, CFRD patients are at risk for microvascular complications, but they tend to be less common and less severe than in other forms of diabetes, likely because CF patients still make some of their own insulin,” Dr. Moran said.
• Macrovascular complications are not seen. “This is important because recommendations given to people with other forms of the diabetes to reduce risk of macrovascular complications – weight loss, low-fat diet, low-salt diet, etc.– do no apply in CF and can actually be harmful,” Dr. Moran said.
• Insulin is especially crucial. “Maintaining weight and lean body mass is critical for survival in CF, so the chief clinical concern with CFRD is nutrition and the potential impact of insulin insufficiency on mortality,” Dr. Moran said. “Insulin replacement is the only approved therapy for CFRD. Treatment is very similar to that of type 1 diabetic patients in a honeymoon state. Very early on, patients may receive a single dose of basal insulin only or of premeal rapid-acting insulin only. Eventually most CF patients require basal-bolus insulin therapy.”
Doses tend to be lower than in other diabetics, she said, “except for when CF patients are acutely ill. During acute illness, CF patients become insulin resistant and require high insulin doses.”
Still, “once I start insulin, my goal is to deliver as large a dose as the patient can safely tolerate, to maximize anabolic impact,” she said.
The physicians offered these tips about tracking and treating CF patients:
• Screen CF patients via oral glucose tolerance testing on an annual basis, starting no later than age 10. Don’t trust hemoglobin A1c levels or fasting glucose levels, Dr. Norris said, because they are not sensitive enough. In fact, Dr. Moran said, “HbA1cis spuriously low in CF. “Even mild diabetes can be immediately detrimental to a CF patient’s lung health and mortality risk,” Dr. Norris said. “If you wait until the onset of classic diabetes symptoms or until the fasting glucose or hemoglobin A1c is elevated, you will have done a great disservice to the CF patient, as preventable potentially life-threatening lung damage may have already occurred.”
• Check into your center’s testing protocol. “Unfortunately, current screening rates are markedly insufficient at many centers,” Dr. Norris said. “I encourage endocrine teams to reach out to their affiliated CF treatment center to discuss and help implement screening.”
What’s next? The University of Iowa’s Dr. Larson said he is hopeful about advances in medical care. “Currently, patients must follow an extremely complex regimen of airway clearance, inhaled antibiotics, and oral medications, typically with recurrent hospitalization with increasing age and eventual death from lung disease or lung transplant,” she said. “However, in the past few years, we have had a dramatic change for a percentage of our patients with the development of small molecules that can actually fix the chloride-channel defect itself.”
The treatment seems to arrest and even improve lung disease in eligible patients, she said. “So the future seems very bright for CF.”
The Cystic Fibrosis Foundation has developed a 3-year Envision program to train adult and pediatric endocrinologists in the care of CFRD and endocrine issues.
Dr. Moran had no relevant disclosures. Dr. Norris has consulted for Vertex Pharmaceuticals, which makes cystic fibrosis therapeutics, in the past year. Dr. Larson Ode reports that her research is funded by the National Institutes of Health and the Cystic Fibrosis Foundation.
EXPERT ANALYSIS FROM AADE 16
Chief resident service increased trainees’ confidence and independence
CORONADO, CALIF. – Creation of a surgical chief resident service meant to increase resident autonomy and provide continuity of patient care with appropriate faculty supervision has been successful, results from a small single-center study showed.
“Providing opportunities for autonomy to bolster the development of independence and confidence during surgery residency remains among the most pronounced challenges of the current training paradigm,” Benjamin T. Jarman, MD, said at the annual meeting of the Western Surgical Association. “Prior to 2011, our graduating surgery residents reported a lack of perceived autonomy during their training and a need to improve practice management skills. To be clear, they consistently felt confident in their surgical abilities, but they did not sense that they were routinely engaged in directing all phases of care.”

In an effort to provide chief surgery residents with increased autonomy and full-spectrum continuity of patient care, Dr. Jarman and his associates initiated a chief resident service (CRS) in January of 2011. It was designed as an independent service with call responsibilities, office hours, operative scheduling, procedural coding, and endoscopy time. “We constructed a weekly schedule to be consistent with the practice of a general surgeon in the first year after residency,” Dr. Jarman explained. “We also added administrative time for research, patient coordination, and completion of records. Each class of chief residents was educated about these responsibilities as a group, and individual sit-down sessions occurred before they started the rotation. Expectations were made clear, and the importance of clear communication was stressed. The service was geared to provide excellent exposure to practice management skills.” Members of teaching faculty were assigned to each episode of patient care to meet all supervision guidelines and patients were educated accordingly. “The primary difference of and key to this service is that of patient continuity with the chief resident from preoperative assessment to postoperative care,” he said. “So our faculty had to adapt to the transient role that our residents are accustomed to.”
Dr. Jarman presented results from a study of nine surgeons who completed the CRS between January 2011 and June 2014. Total operative volume during residency was assessed in addition to select procedures for the chief service experience versus the residents’ first year of clinical practice. Residents who pursued fellowship training submitted their operative logs from their first year postfellowship. Graduates were surveyed to assess their current clinical practice, satisfaction with the chief service, and whether they perceived a correlation of the CRS with their clinical practice. Patient evaluations were reviewed as well. The researchers focused on the following procedures for comparison: laparoscopic appendectomy, laparoscopic cholecystectomy, colectomy, ventral/incisional hernia repair, inguinal hernia repair, upper endoscopy, and lower endoscopy.
All nine chief surgery residents completed the chief service and completed case logs. “The first three residents to graduate after implementation of the service spent 2 months each on the rotation, while subsequent graduates spent between 4 and 6 months, depending on how many chiefs we had in a given year,” Dr. Jarman said. The median total case volume was 1,101 during the 5-year residency, 92 during the CRS, and 299 during the first year of practice. When the researchers evaluated overall median case volumes, lower endoscopy volumes were higher during the first year of practice, compared with during the CRS (a median of 71 vs. 10 cases, respectively); otherwise there were similar case volumes across the other procedures selected for evaluation. Next, they determined the mean case volumes by month for the selected general surgical procedures and found similar case volumes with the exception of colectomy, which was more commonly performed during the CRS, compared with during the first year of practice (a mean of 1 vs. 0.4 cases; P=0.016).
All nine graduates completed an electronic survey relaying details about their current practice and degree of satisfaction with the CRS; 100% reported being “very satisfied” with their CRS, and 100% found it “very beneficial” to their practice. In addition, 56% said that their cases on the CRS were “somewhat similar” to their current practice, while 44% said that their cases were “very similar” to their current practice.
Since the inception of the CRS, Dr. Jarman and his associates have made several adjustments to the CRS, including incorporation of endoscopy time, adjusted office hours, the required presence of surgery assistants in the OR, and requiring fourth-year residents to attend the ACS Leadership Conference in preparation for the CRS role. He acknowledged certain limitations of the study, including its small sample size and the fact that its participants had variable clinical experience. “But we’re on the ground running,” Dr. Jarman said of the CRS. “The chief residents are wide-eyed and very engaged in this process, and the impact on their development and respect for all the caveats of independent practice has been significant. The strengths of the service include exposure to practice management skills, whole-spectrum clinical care for a single resident at a time, and operative experience which correlates to that experience of a first-year surgeon.” He reported having no financial disclosures.
CORONADO, CALIF. – Creation of a surgical chief resident service meant to increase resident autonomy and provide continuity of patient care with appropriate faculty supervision has been successful, results from a small single-center study showed.
“Providing opportunities for autonomy to bolster the development of independence and confidence during surgery residency remains among the most pronounced challenges of the current training paradigm,” Benjamin T. Jarman, MD, said at the annual meeting of the Western Surgical Association. “Prior to 2011, our graduating surgery residents reported a lack of perceived autonomy during their training and a need to improve practice management skills. To be clear, they consistently felt confident in their surgical abilities, but they did not sense that they were routinely engaged in directing all phases of care.”
In an effort to provide chief surgery residents with increased autonomy and full-spectrum continuity of patient care, Dr. Jarman and his associates initiated a chief resident service (CRS) in January of 2011. It was designed as an independent service with call responsibilities, office hours, operative scheduling, procedural coding, and endoscopy time. “We constructed a weekly schedule to be consistent with the practice of a general surgeon in the first year after residency,” Dr. Jarman explained. “We also added administrative time for research, patient coordination, and completion of records. Each class of chief residents was educated about these responsibilities as a group, and individual sit-down sessions occurred before they started the rotation. Expectations were made clear, and the importance of clear communication was stressed. The service was geared to provide excellent exposure to practice management skills.” Members of teaching faculty were assigned to each episode of patient care to meet all supervision guidelines and patients were educated accordingly. “The primary difference of and key to this service is that of patient continuity with the chief resident from preoperative assessment to postoperative care,” he said. “So our faculty had to adapt to the transient role that our residents are accustomed to.”
Dr. Jarman presented results from a study of nine surgeons who completed the CRS between January 2011 and June 2014. Total operative volume during residency was assessed in addition to select procedures for the chief service experience versus the residents’ first year of clinical practice. Residents who pursued fellowship training submitted their operative logs from their first year postfellowship. Graduates were surveyed to assess their current clinical practice, satisfaction with the chief service, and whether they perceived a correlation of the CRS with their clinical practice. Patient evaluations were reviewed as well. The researchers focused on the following procedures for comparison: laparoscopic appendectomy, laparoscopic cholecystectomy, colectomy, ventral/incisional hernia repair, inguinal hernia repair, upper endoscopy, and lower endoscopy.
All nine chief surgery residents completed the chief service and completed case logs. “The first three residents to graduate after implementation of the service spent 2 months each on the rotation, while subsequent graduates spent between 4 and 6 months, depending on how many chiefs we had in a given year,” Dr. Jarman said. The median total case volume was 1,101 during the 5-year residency, 92 during the CRS, and 299 during the first year of practice. When the researchers evaluated overall median case volumes, lower endoscopy volumes were higher during the first year of practice, compared with during the CRS (a median of 71 vs. 10 cases, respectively); otherwise there were similar case volumes across the other procedures selected for evaluation. Next, they determined the mean case volumes by month for the selected general surgical procedures and found similar case volumes with the exception of colectomy, which was more commonly performed during the CRS, compared with during the first year of practice (a mean of 1 vs. 0.4 cases; P=0.016).
All nine graduates completed an electronic survey relaying details about their current practice and degree of satisfaction with the CRS; 100% reported being “very satisfied” with their CRS, and 100% found it “very beneficial” to their practice. In addition, 56% said that their cases on the CRS were “somewhat similar” to their current practice, while 44% said that their cases were “very similar” to their current practice.
Since the inception of the CRS, Dr. Jarman and his associates have made several adjustments to the CRS, including incorporation of endoscopy time, adjusted office hours, the required presence of surgery assistants in the OR, and requiring fourth-year residents to attend the ACS Leadership Conference in preparation for the CRS role. He acknowledged certain limitations of the study, including its small sample size and the fact that its participants had variable clinical experience. “But we’re on the ground running,” Dr. Jarman said of the CRS. “The chief residents are wide-eyed and very engaged in this process, and the impact on their development and respect for all the caveats of independent practice has been significant. The strengths of the service include exposure to practice management skills, whole-spectrum clinical care for a single resident at a time, and operative experience which correlates to that experience of a first-year surgeon.” He reported having no financial disclosures.
CORONADO, CALIF. – Creation of a surgical chief resident service meant to increase resident autonomy and provide continuity of patient care with appropriate faculty supervision has been successful, results from a small single-center study showed.
“Providing opportunities for autonomy to bolster the development of independence and confidence during surgery residency remains among the most pronounced challenges of the current training paradigm,” Benjamin T. Jarman, MD, said at the annual meeting of the Western Surgical Association. “Prior to 2011, our graduating surgery residents reported a lack of perceived autonomy during their training and a need to improve practice management skills. To be clear, they consistently felt confident in their surgical abilities, but they did not sense that they were routinely engaged in directing all phases of care.”
In an effort to provide chief surgery residents with increased autonomy and full-spectrum continuity of patient care, Dr. Jarman and his associates initiated a chief resident service (CRS) in January of 2011. It was designed as an independent service with call responsibilities, office hours, operative scheduling, procedural coding, and endoscopy time. “We constructed a weekly schedule to be consistent with the practice of a general surgeon in the first year after residency,” Dr. Jarman explained. “We also added administrative time for research, patient coordination, and completion of records. Each class of chief residents was educated about these responsibilities as a group, and individual sit-down sessions occurred before they started the rotation. Expectations were made clear, and the importance of clear communication was stressed. The service was geared to provide excellent exposure to practice management skills.” Members of teaching faculty were assigned to each episode of patient care to meet all supervision guidelines and patients were educated accordingly. “The primary difference of and key to this service is that of patient continuity with the chief resident from preoperative assessment to postoperative care,” he said. “So our faculty had to adapt to the transient role that our residents are accustomed to.”
Dr. Jarman presented results from a study of nine surgeons who completed the CRS between January 2011 and June 2014. Total operative volume during residency was assessed in addition to select procedures for the chief service experience versus the residents’ first year of clinical practice. Residents who pursued fellowship training submitted their operative logs from their first year postfellowship. Graduates were surveyed to assess their current clinical practice, satisfaction with the chief service, and whether they perceived a correlation of the CRS with their clinical practice. Patient evaluations were reviewed as well. The researchers focused on the following procedures for comparison: laparoscopic appendectomy, laparoscopic cholecystectomy, colectomy, ventral/incisional hernia repair, inguinal hernia repair, upper endoscopy, and lower endoscopy.
All nine chief surgery residents completed the chief service and completed case logs. “The first three residents to graduate after implementation of the service spent 2 months each on the rotation, while subsequent graduates spent between 4 and 6 months, depending on how many chiefs we had in a given year,” Dr. Jarman said. The median total case volume was 1,101 during the 5-year residency, 92 during the CRS, and 299 during the first year of practice. When the researchers evaluated overall median case volumes, lower endoscopy volumes were higher during the first year of practice, compared with during the CRS (a median of 71 vs. 10 cases, respectively); otherwise there were similar case volumes across the other procedures selected for evaluation. Next, they determined the mean case volumes by month for the selected general surgical procedures and found similar case volumes with the exception of colectomy, which was more commonly performed during the CRS, compared with during the first year of practice (a mean of 1 vs. 0.4 cases; P=0.016).
All nine graduates completed an electronic survey relaying details about their current practice and degree of satisfaction with the CRS; 100% reported being “very satisfied” with their CRS, and 100% found it “very beneficial” to their practice. In addition, 56% said that their cases on the CRS were “somewhat similar” to their current practice, while 44% said that their cases were “very similar” to their current practice.
Since the inception of the CRS, Dr. Jarman and his associates have made several adjustments to the CRS, including incorporation of endoscopy time, adjusted office hours, the required presence of surgery assistants in the OR, and requiring fourth-year residents to attend the ACS Leadership Conference in preparation for the CRS role. He acknowledged certain limitations of the study, including its small sample size and the fact that its participants had variable clinical experience. “But we’re on the ground running,” Dr. Jarman said of the CRS. “The chief residents are wide-eyed and very engaged in this process, and the impact on their development and respect for all the caveats of independent practice has been significant. The strengths of the service include exposure to practice management skills, whole-spectrum clinical care for a single resident at a time, and operative experience which correlates to that experience of a first-year surgeon.” He reported having no financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: More than half of general surgery residency graduates (56%) said that their cases on the chief resident service were “somewhat similar” to their current practice, while 44% said that their cases were “very similar” to their current practice.
Data source: An study of nine surgeons who completed the chief resident service between January 2011 and June 2014.
Disclosures: Dr. Jarman reported having no financial disclosures.
Idelalisib held unlikely to become frontline therapy for CLL
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
NEW YORK – Safety issues with idelalisib, a first-in-class PI3K delta inhibitor, are an important concern in patients with chronic lymphocytic leukemia – particularly those aged 65 years and younger, according to Steven Coutre, MD.
Findings from the second interim analysis of the pivotal trial for idelalisib as reported at the 2014 annual meeting of the American Society of Hematology (Sharman J., et al. Abstract 330) and a recent update from an open-label extension represent the longest reported follow-up of idelalisib-treated patients to date. Those analyses showed substantial progression-free and overall survival advantages with idelalisib plus rituximab vs. placebo plus rituximab (progression-free survival in the latest update was 19.4 vs. 7.3 months, respectively; hazard ratio 0.25), said Dr. Coutre, professor of medicine at Stanford (Calif.) University.
“Still, even with that report, the follow-up on that initial study was relatively short, and I think it really underreports some of the safety issues of the toxicities that we see,” he said at an international congress on hematologic malignancies.
To further investigate those safety issues, Dr. Coutre and his colleagues performed an integrated analysis of eight clinical trials, including the pivotal trial. That analysis found idelalisib to be efficacious, but significant toxicities were noted, “particularly in younger less heavily-pretreated patients. [Idelalisib] should not be used as frontline therapy ... and I don’t think it will be developed in the future as frontline therapy,” Dr. Coutre said.
“At least in the relapse setting, idelalisib plus rituximab is a choice for all of our patients, but it has to be a considered choice; you have to put it in the context of other therapies that the patients have available to them and make a decision based on your individual patient.”
In the analysis, Dr. Coutre and his colleagues found numerous adverse events occurring in 15% or more of idelalisib-treated patients. These included diarrhea/colitis – with median onset at 7.1 months – in 37% who received monotherapy and 40% who received combination therapy (grade 3 or greater diarrhea/colitis in 11% and 17%, respectively), and pneumonia in 13% and 18% of patients (grade 3 or greater in 11% and 14%, respectively), Dr. Coutre said.
Transaminitis – which was observed early in the studies, usually within the first 8 weeks of treatment – also was common, occurring in 50% and 47% of those with monotherapy and combination therapy, respectively (grade 3 or greater, 16% and 13%, respectively).
Pneumonitis occurred in about 3% of patients, and usually within the first 6 months of therapy.
“So that’s sort of where things were until earlier this year when we learned from several ongoing studies, very important studies in both previously treated patients with low-grade lymphomas and previously untreated patients, that there was a further problem – and that is a difference in mortality,” he said.
Patients in many of these studies, including all of those where it was being used for previously untreated patients, were taken off the drug because of this finding.
“As a result of further analysis of these studies, there’s a new safety label indication,” he said.
Of note, in another idelalisib study reported at ASH 2015 an age-related toxicity concern emerged.
“Idelalisib was used for previously untreated patients. But the distinction here is that for the first time it was being used in younger patients – patients under the age of 65,” he said, noting that severe transaminitis occurred in a significant number of the younger patients.
More than half (52%) of patients had grade 3 or greater hepatotoxicity and all 7 subjects aged 65 years and younger required systemic steroids for toxicities.
Age was found in the study to be a significant risk factor for early hepatotoxicity.
“We’re finally starting to understand the mechanisms behind this, or at least the likely mechanisms, and this seems to be immune mediated,” he said, adding, “you see a lymphocytic infiltrate on liver biopsies, you see a lymphocytic colitis in patients who receive idelalisib.”
Typically, toxicities in these patients can be managed with corticosteroids, but in some cases of severe toxicity even steroids seem to be insufficient, he said.
Further, rapid recurrence is often seen upon re-exposure to the drug, especially with respect to hepatotoxicity, he added.
Preclinical data from mouse models supports this mechanism.
“And importantly [those models] demonstrated a decrease in regulatory T cells in patients treated with idelalisib,” he said.
Dr. Coutre reported consulting for Abbvie, Celgene, Gilead, Janssen, and Pharmacyclics.
EXPERT ANALYSIS FROM LYMPHOMA & MYELOMA
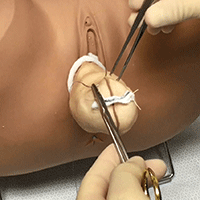
Complete colpectomy & colpocleisis: Model for simulation

Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
Related articles:
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
This video is brought to you by![]()
View more videos from SGS here
The eyelids have it: bug bites 101
NEWPORT BEACH, CA. – Bed bugs rise when night falls. Drawn by the carbon dioxide of sleeping humans, they gather to feast, leaving bites galore.
But other insects dine on people, too. Telling their bites apart is an important – and sometimes difficult – job for dermatologists who treat children. Fortunately, there are clinical signs to look for, a pediatric dermatologist told an audience of colleagues, including one that she herself helped introduce.
It’s called the “Eyelid Sign,” a clinical clue, Andrea Zaenglein, MD, said at Skin Diseases Education Foundation’s Women & Pediatric Dermatology Seminar.

Dr. Zaenglein, professor of dermatology and pediatric dermatology at Penn State University, Hershey, has often seen children with bites on their eyelids since they’re being bitten by bed bugs while they’re asleep. “You don’t get a lot of eyelid bites with other things,” she said. “Think about bed bugs whenever you see eyelid bites.”
She and a colleague reported on the “Eyelid Sign” in a study published in 2014, describing papules on the upper eyelid or eyelids associated with erythema and edema in six patients (Pediatr Dermatol. 2014 May-Jun;31[3]:353-5).
During her presentation, Dr. Zaenglein offered more tips on detecting bed bugs:
• Keep in mind that they’re probably not going to be sitting there under the pillow, waiting for your patients to find them. “They like to hide in nooks and crannies,” she said. “They don’t really stay in your bed.” Common hiding places include mattresses, floorboards, and wallpaper.
• Bed bugs are about the size of an apple seed. Stains and dark spots on bed sheets and mattresses can be signs of crushed bed bugs and bed bug excrement.
• They’re more common in urban areas, but “bed bugs are a problem in probably all of our communities,” Dr. Zaenglein noted.
• Some children can develop a reaction to bed bugs and other insects known as papular urticaria. “I have to explain to parents that this is a hypersensitivity response that’s abnormal,” Dr. Zaenglein said.
She noted that papular urticaria tends to be worse in summer and rarely involves the face. Treatments include antihistamines, strong topical steroids, and prevention of insect bites.
As for bed bug bites in general, the Centers for Disease Control and Prevention recommends antiseptic creams or lotions and antihistamine use.
How can bed bugs be killed off for good? The CDC suggests insecticide spraying to eliminate bed bugs, and states that “the best way to prevent bed bugs is regular inspection for the signs of an infestation.”
During the presentation, Dr. Zaenglein also spoke about scabies, focusing on the unique traits of the condition in babies.
“They always present with a lot of rash,” she said. “They won’t have a few papules on their hands and feet like older kids.” The rash will be “dirty-looking,” she continued, and more asymmetric than symmetric. Also, “you’ll almost always get a lot of mites burden if you scrape a baby,” she said. “It’s much harder to find a mite in older kids and young adults.”
Affected babies may be referred from an emergency department or primary care doctor with an incorrect diagnosis of eczema, she said, adding that scabies is extremely contagious. “If a baby has scabies,” she said, “you inevitably have to get your prescription pad. Treat all the household members.”
Babies may be itchy, but itchiness is much more common in older kids and young adults, keeping them up at night, she said. “College students come home over the break with a couple of papules on the belly, and they say it’s driving them crazy. They say it’s crazy, crazy itchy. If you hear that, think scabies.”
Another scabies clue in older kids: hand involvement. “Always look at the wrist, between the fingers. You get these generalized eruptions there.”
Scabies bites can be treated with a topical corticosteroid and, in children aged 2 months and older, permethrin 5% cream. Dr. Zaenglein said there’s concern about a leukemia risk associated with permethrin, but that applies to industrial use and overuse. Ivermectin is an alternative for stubborn and institutional cases.
As for prevention, she said pesticide sprays and fogs are generally discouraged. She advises families to wash recently used clothing and bedding in hot water. Clothing and bedding, including pillows, can also be stored in a closed plastic bag for up to a week.
“You could dry clean it all too,” she said, “but I’ll bet your dry cleaner won’t be too happy about it.”
Dr. Zaenglein disclosed serving as a consultant and researcher for Ranbaxy Laboratories Limited.
SDEF and this news organization are owned by the same parent company.
NEWPORT BEACH, CA. – Bed bugs rise when night falls. Drawn by the carbon dioxide of sleeping humans, they gather to feast, leaving bites galore.
But other insects dine on people, too. Telling their bites apart is an important – and sometimes difficult – job for dermatologists who treat children. Fortunately, there are clinical signs to look for, a pediatric dermatologist told an audience of colleagues, including one that she herself helped introduce.
It’s called the “Eyelid Sign,” a clinical clue, Andrea Zaenglein, MD, said at Skin Diseases Education Foundation’s Women & Pediatric Dermatology Seminar.
Dr. Zaenglein, professor of dermatology and pediatric dermatology at Penn State University, Hershey, has often seen children with bites on their eyelids since they’re being bitten by bed bugs while they’re asleep. “You don’t get a lot of eyelid bites with other things,” she said. “Think about bed bugs whenever you see eyelid bites.”
She and a colleague reported on the “Eyelid Sign” in a study published in 2014, describing papules on the upper eyelid or eyelids associated with erythema and edema in six patients (Pediatr Dermatol. 2014 May-Jun;31[3]:353-5).
During her presentation, Dr. Zaenglein offered more tips on detecting bed bugs:
• Keep in mind that they’re probably not going to be sitting there under the pillow, waiting for your patients to find them. “They like to hide in nooks and crannies,” she said. “They don’t really stay in your bed.” Common hiding places include mattresses, floorboards, and wallpaper.
• Bed bugs are about the size of an apple seed. Stains and dark spots on bed sheets and mattresses can be signs of crushed bed bugs and bed bug excrement.
• They’re more common in urban areas, but “bed bugs are a problem in probably all of our communities,” Dr. Zaenglein noted.
• Some children can develop a reaction to bed bugs and other insects known as papular urticaria. “I have to explain to parents that this is a hypersensitivity response that’s abnormal,” Dr. Zaenglein said.
She noted that papular urticaria tends to be worse in summer and rarely involves the face. Treatments include antihistamines, strong topical steroids, and prevention of insect bites.
As for bed bug bites in general, the Centers for Disease Control and Prevention recommends antiseptic creams or lotions and antihistamine use.
How can bed bugs be killed off for good? The CDC suggests insecticide spraying to eliminate bed bugs, and states that “the best way to prevent bed bugs is regular inspection for the signs of an infestation.”
During the presentation, Dr. Zaenglein also spoke about scabies, focusing on the unique traits of the condition in babies.
“They always present with a lot of rash,” she said. “They won’t have a few papules on their hands and feet like older kids.” The rash will be “dirty-looking,” she continued, and more asymmetric than symmetric. Also, “you’ll almost always get a lot of mites burden if you scrape a baby,” she said. “It’s much harder to find a mite in older kids and young adults.”
Affected babies may be referred from an emergency department or primary care doctor with an incorrect diagnosis of eczema, she said, adding that scabies is extremely contagious. “If a baby has scabies,” she said, “you inevitably have to get your prescription pad. Treat all the household members.”
Babies may be itchy, but itchiness is much more common in older kids and young adults, keeping them up at night, she said. “College students come home over the break with a couple of papules on the belly, and they say it’s driving them crazy. They say it’s crazy, crazy itchy. If you hear that, think scabies.”
Another scabies clue in older kids: hand involvement. “Always look at the wrist, between the fingers. You get these generalized eruptions there.”
Scabies bites can be treated with a topical corticosteroid and, in children aged 2 months and older, permethrin 5% cream. Dr. Zaenglein said there’s concern about a leukemia risk associated with permethrin, but that applies to industrial use and overuse. Ivermectin is an alternative for stubborn and institutional cases.
As for prevention, she said pesticide sprays and fogs are generally discouraged. She advises families to wash recently used clothing and bedding in hot water. Clothing and bedding, including pillows, can also be stored in a closed plastic bag for up to a week.
“You could dry clean it all too,” she said, “but I’ll bet your dry cleaner won’t be too happy about it.”
Dr. Zaenglein disclosed serving as a consultant and researcher for Ranbaxy Laboratories Limited.
SDEF and this news organization are owned by the same parent company.
NEWPORT BEACH, CA. – Bed bugs rise when night falls. Drawn by the carbon dioxide of sleeping humans, they gather to feast, leaving bites galore.
But other insects dine on people, too. Telling their bites apart is an important – and sometimes difficult – job for dermatologists who treat children. Fortunately, there are clinical signs to look for, a pediatric dermatologist told an audience of colleagues, including one that she herself helped introduce.
It’s called the “Eyelid Sign,” a clinical clue, Andrea Zaenglein, MD, said at Skin Diseases Education Foundation’s Women & Pediatric Dermatology Seminar.
Dr. Zaenglein, professor of dermatology and pediatric dermatology at Penn State University, Hershey, has often seen children with bites on their eyelids since they’re being bitten by bed bugs while they’re asleep. “You don’t get a lot of eyelid bites with other things,” she said. “Think about bed bugs whenever you see eyelid bites.”
She and a colleague reported on the “Eyelid Sign” in a study published in 2014, describing papules on the upper eyelid or eyelids associated with erythema and edema in six patients (Pediatr Dermatol. 2014 May-Jun;31[3]:353-5).
During her presentation, Dr. Zaenglein offered more tips on detecting bed bugs:
• Keep in mind that they’re probably not going to be sitting there under the pillow, waiting for your patients to find them. “They like to hide in nooks and crannies,” she said. “They don’t really stay in your bed.” Common hiding places include mattresses, floorboards, and wallpaper.
• Bed bugs are about the size of an apple seed. Stains and dark spots on bed sheets and mattresses can be signs of crushed bed bugs and bed bug excrement.
• They’re more common in urban areas, but “bed bugs are a problem in probably all of our communities,” Dr. Zaenglein noted.
• Some children can develop a reaction to bed bugs and other insects known as papular urticaria. “I have to explain to parents that this is a hypersensitivity response that’s abnormal,” Dr. Zaenglein said.
She noted that papular urticaria tends to be worse in summer and rarely involves the face. Treatments include antihistamines, strong topical steroids, and prevention of insect bites.
As for bed bug bites in general, the Centers for Disease Control and Prevention recommends antiseptic creams or lotions and antihistamine use.
How can bed bugs be killed off for good? The CDC suggests insecticide spraying to eliminate bed bugs, and states that “the best way to prevent bed bugs is regular inspection for the signs of an infestation.”
During the presentation, Dr. Zaenglein also spoke about scabies, focusing on the unique traits of the condition in babies.
“They always present with a lot of rash,” she said. “They won’t have a few papules on their hands and feet like older kids.” The rash will be “dirty-looking,” she continued, and more asymmetric than symmetric. Also, “you’ll almost always get a lot of mites burden if you scrape a baby,” she said. “It’s much harder to find a mite in older kids and young adults.”
Affected babies may be referred from an emergency department or primary care doctor with an incorrect diagnosis of eczema, she said, adding that scabies is extremely contagious. “If a baby has scabies,” she said, “you inevitably have to get your prescription pad. Treat all the household members.”
Babies may be itchy, but itchiness is much more common in older kids and young adults, keeping them up at night, she said. “College students come home over the break with a couple of papules on the belly, and they say it’s driving them crazy. They say it’s crazy, crazy itchy. If you hear that, think scabies.”
Another scabies clue in older kids: hand involvement. “Always look at the wrist, between the fingers. You get these generalized eruptions there.”
Scabies bites can be treated with a topical corticosteroid and, in children aged 2 months and older, permethrin 5% cream. Dr. Zaenglein said there’s concern about a leukemia risk associated with permethrin, but that applies to industrial use and overuse. Ivermectin is an alternative for stubborn and institutional cases.
As for prevention, she said pesticide sprays and fogs are generally discouraged. She advises families to wash recently used clothing and bedding in hot water. Clothing and bedding, including pillows, can also be stored in a closed plastic bag for up to a week.
“You could dry clean it all too,” she said, “but I’ll bet your dry cleaner won’t be too happy about it.”
Dr. Zaenglein disclosed serving as a consultant and researcher for Ranbaxy Laboratories Limited.
SDEF and this news organization are owned by the same parent company.
AT SDEF WOMEN'S & PEDIATRIC DERMATOLOGY SEMINAR
My Fitness Journey
One month into my doctoral program, I was stressed out, anxious, not sleeping well, and gaining weight. I expressed these concerns to my daughter, who is a professional bodybuilder and fitness coach; she offered to help me get healthy and fit while earning my doctorate from Rocky Mountain University of Health Professions in Provo, Utah. Over the next two years, I lost 35 pounds and 12 inches of fat from my belly and became more muscular than ever before! I even decided to participate in my first bodybuilding show, “Debut at 62,” on November 19th in Providence, Rhode Island.
I was honored to be the student commencement speaker and recipient of the Student Service Award for my contributions to the NP profession—but what I’m most proud of is adopting a healthy and fit lifestyle in the midst of the most stressful two years of my life. In fact, I believe learning to cope with extreme stress helped me perform more effectively in my doctoral program. I had more energy and concentration, better sleep, and very few physical complaints.

Certainly, I realize that it can be difficult for us to walk our talk and be role models for our patients. When faced with extreme stress we often “crash and burn.” We gain weight, get depressed, sleep poorly, stop having sex, drink excessively, you name it! We know what we should do but lack the energy, time, and motivation to implement and maintain healthy habits. In order to effectively deal with the stress in our lives, we must practice self-care. This approach may seem counterintuitive, as our natural reaction to stress is usually to abandon healthy habits and resort to eating junk food, drinking alcohol, watching TV, and not exercising. It requires conscious effort, development of new habits (and breaking of old ones!), practice, consistency, and a lot of support to cope with stress in a positive way. Mind control, meditation, and paced breathing are other cognitive-based techniques that can be used to help combat the negative effects of stress and anxiety.
As a result of my experience and transformation, my daughter and I decided to team up to help other NPs and PAs make positive changes in their lives. Under the names Coach Kat and Doctor Mimi, we developed The Secor Initiative—an intensive, one-year, online program for NPs or PAs who are seriously committed to becoming healthy, happy, and fit. Upon completion of the program, participants achieve the esteemed title of “Top NP” or “Top PA,” enabling them to be role models for their peers and patients.
The Secor Initiative helps NPs and PAs gain insight into all the sources of stress in their lives and then go on to learn how to cope with these stressors. Our program includes five (10-week) courses, with topics such as nutrition, exercise, money/wealth, stress management, and advanced women’s health; for more information, visit www.MimiSecor.com and click on The Secor Initiative or check out our Facebook page, Coach Kat and Dr. Mimi.
Let’s step up to the plate and become healthy (and happy) role models for our patients.

One month into my doctoral program, I was stressed out, anxious, not sleeping well, and gaining weight. I expressed these concerns to my daughter, who is a professional bodybuilder and fitness coach; she offered to help me get healthy and fit while earning my doctorate from Rocky Mountain University of Health Professions in Provo, Utah. Over the next two years, I lost 35 pounds and 12 inches of fat from my belly and became more muscular than ever before! I even decided to participate in my first bodybuilding show, “Debut at 62,” on November 19th in Providence, Rhode Island.
I was honored to be the student commencement speaker and recipient of the Student Service Award for my contributions to the NP profession—but what I’m most proud of is adopting a healthy and fit lifestyle in the midst of the most stressful two years of my life. In fact, I believe learning to cope with extreme stress helped me perform more effectively in my doctoral program. I had more energy and concentration, better sleep, and very few physical complaints.
Certainly, I realize that it can be difficult for us to walk our talk and be role models for our patients. When faced with extreme stress we often “crash and burn.” We gain weight, get depressed, sleep poorly, stop having sex, drink excessively, you name it! We know what we should do but lack the energy, time, and motivation to implement and maintain healthy habits. In order to effectively deal with the stress in our lives, we must practice self-care. This approach may seem counterintuitive, as our natural reaction to stress is usually to abandon healthy habits and resort to eating junk food, drinking alcohol, watching TV, and not exercising. It requires conscious effort, development of new habits (and breaking of old ones!), practice, consistency, and a lot of support to cope with stress in a positive way. Mind control, meditation, and paced breathing are other cognitive-based techniques that can be used to help combat the negative effects of stress and anxiety.
As a result of my experience and transformation, my daughter and I decided to team up to help other NPs and PAs make positive changes in their lives. Under the names Coach Kat and Doctor Mimi, we developed The Secor Initiative—an intensive, one-year, online program for NPs or PAs who are seriously committed to becoming healthy, happy, and fit. Upon completion of the program, participants achieve the esteemed title of “Top NP” or “Top PA,” enabling them to be role models for their peers and patients.
The Secor Initiative helps NPs and PAs gain insight into all the sources of stress in their lives and then go on to learn how to cope with these stressors. Our program includes five (10-week) courses, with topics such as nutrition, exercise, money/wealth, stress management, and advanced women’s health; for more information, visit www.MimiSecor.com and click on The Secor Initiative or check out our Facebook page, Coach Kat and Dr. Mimi.
Let’s step up to the plate and become healthy (and happy) role models for our patients.
One month into my doctoral program, I was stressed out, anxious, not sleeping well, and gaining weight. I expressed these concerns to my daughter, who is a professional bodybuilder and fitness coach; she offered to help me get healthy and fit while earning my doctorate from Rocky Mountain University of Health Professions in Provo, Utah. Over the next two years, I lost 35 pounds and 12 inches of fat from my belly and became more muscular than ever before! I even decided to participate in my first bodybuilding show, “Debut at 62,” on November 19th in Providence, Rhode Island.
I was honored to be the student commencement speaker and recipient of the Student Service Award for my contributions to the NP profession—but what I’m most proud of is adopting a healthy and fit lifestyle in the midst of the most stressful two years of my life. In fact, I believe learning to cope with extreme stress helped me perform more effectively in my doctoral program. I had more energy and concentration, better sleep, and very few physical complaints.
Certainly, I realize that it can be difficult for us to walk our talk and be role models for our patients. When faced with extreme stress we often “crash and burn.” We gain weight, get depressed, sleep poorly, stop having sex, drink excessively, you name it! We know what we should do but lack the energy, time, and motivation to implement and maintain healthy habits. In order to effectively deal with the stress in our lives, we must practice self-care. This approach may seem counterintuitive, as our natural reaction to stress is usually to abandon healthy habits and resort to eating junk food, drinking alcohol, watching TV, and not exercising. It requires conscious effort, development of new habits (and breaking of old ones!), practice, consistency, and a lot of support to cope with stress in a positive way. Mind control, meditation, and paced breathing are other cognitive-based techniques that can be used to help combat the negative effects of stress and anxiety.
As a result of my experience and transformation, my daughter and I decided to team up to help other NPs and PAs make positive changes in their lives. Under the names Coach Kat and Doctor Mimi, we developed The Secor Initiative—an intensive, one-year, online program for NPs or PAs who are seriously committed to becoming healthy, happy, and fit. Upon completion of the program, participants achieve the esteemed title of “Top NP” or “Top PA,” enabling them to be role models for their peers and patients.
The Secor Initiative helps NPs and PAs gain insight into all the sources of stress in their lives and then go on to learn how to cope with these stressors. Our program includes five (10-week) courses, with topics such as nutrition, exercise, money/wealth, stress management, and advanced women’s health; for more information, visit www.MimiSecor.com and click on The Secor Initiative or check out our Facebook page, Coach Kat and Dr. Mimi.
Let’s step up to the plate and become healthy (and happy) role models for our patients.
Threats in school: Is there a role for you?
Do you remember that kid in your class threatening to beat up a peer (or maybe you) after school? Mean children are not unique to current times. But actual threat to life while in school is a more recent problem, mainly due to the availability of firearms in American homes. Although rates of victimization have actually dropped 86% from 1992 to 2014, stories about school shootings are instantly broadcast across the country, making everyone feel that it could happen to them. Such public awareness also models threatening violence as a potent attention getter.

Often the threatening child lacks not only the skills to manage the frustrating situation, but also the language ability to choose less incendiary words. Saying, “I don’t think the way you handled that was fair to me,” might always be difficult, but is certainly impossible under the high emotions of the moment. Instead, “I’m going to kill you” pops out of their mouths. As for asking for help, school-aged children can only apologize or confess to being unsure a limited number of times before their need to save face takes precedence. This is especially true if they are confronted and humiliated in front of their peers.
Children who have oppositional or aggressive behavior diagnoses are by definition already in a pattern of reacting with hostility when demands are placed on them. In some cases, these negative reactions successfully get their parent(s) to back off the demand, resulting in what is called the “coercive cycle of interaction,” a prodrome to conduct disorder. Then, when a teacher issues a command, their reflexive response is more likely to be a defiant or aggressive one.
When threatening behavior is met by the supervising adults with confrontation, things may further accelerate, again especially in front of peers before whom the student does not want to look weak. Instead, a methodical approach to threat assessment in schools has been shown to be more effective. The main features of effective threat assessment involve identifying student threats, determining their seriousness, and developing intervention plans that both protect potential victims and address the underlying problem or conflict that sparked the threat.
A model program, Virginia Model for Student Threat Assessment by Dewey G. Cornell, PhD, of the University of Virginia, has been shown to help sort out transient (70%) from substantive (30%) threats and resulted in fewer long-term suspensions or expulsions and no cases in which the threats were carried out. (Send a copy to your local school superintendent.) While children receiving special education made three times more threats and more severe threats, they did not require more suspensions. With this threat assessment program, the number of disciplinary office referrals for these students declined by about 55% for the rest of that school year. Students in schools using this method reported less bullying, a greater willingness to seek help for bullying and threats, and more positive perceptions of the school climate as having fairer discipline and less aggression. Resulting plans to help the students involved in threats included modifications to special education plans, academic and behavioral support services, and referrals to mental health services. All these interventions are intended to address gaps in skills. In addition, ways to give even struggling students a meaningful connection to their school – for example, through sports, art, music, clubs, or volunteering – are essential components of both prevention and management.
There are several ways you, as a pediatrician, may be involved in the issue of threats at school. If one of your patients has been accused of threatening behavior, your knowledge of the child and family puts you in the best position to sort out the seriousness of the threat and appropriate next steps. Recently, one of my patients with mild autism was suspended for threatening to “kill the teacher.” He had never been aggressive at home or at school. This 8-year-old usually has a one-on-one aide, but the aide had been pulled to help other students. After an unannounced fire drill, the child called the teacher “evil” and was given his “third strike” for behavior, resulting in him making this threat.
Threat assessment in schools needs to follow the method of functional behavioral assessment, which should actually be standard for all school behavior problems. The method should consider the A (antecedent), B (behavior), C (consequence), and G (gaps) of the behavior. The antecedent here included the “setting” event of the fire drill. The behavior (sometimes also the belief) was the child’s negative reaction to the teacher (who had failed to protect him from being frightened). The consequence was a punishment (third strike) that the child felt was unfair. The gaps in skills included the facts that this is an anxious child who depends on support and routine because of his autism and who is also hypersensitive to loud noise such as a fire drill. In this case, I was able to explain these things to the school, but, in any case, you can, and should, request that the school perform a functional behavioral assessment when dealing with threats.
When you have a child with learning or emotional problems under your care, you need to include asking if they feel safe at school and if anything scary or bad has happened to them there. The parents may need to be directed to meet with school personnel about threats or fears the child reports. School violence prevention programs often include education of the children to be alert for and report threatening peers. This gives students an active role, but also may cause increased anxiety. Parents may need your support in requesting exemption from the school’s “violence prevention training” for anxious children. Anxious parents also may need extra coaching to avoid exposing their children to discussions about school threats.
In caring for all school-aged children (girls are as likely to be involved in school violence as boys), I ask about whether their teachers are nice or mean. I also ask if they have been bullied at school or have bullied others. I also sometimes ask struggling children, “If you had the choice, would you rather go to school or stay home?” The normal, almost universal preference is to go to school. School is the child’s job and social home, and, even when the work is hard, the need for mastery drives children to keep trying. Children preferring to be home are likely in pain and deserve careful assessment of their skills, their emotions, and the school and family environments.
While the percentage of students who reported being afraid of attack or harm at school decreased from 12% in 1995 to 3% in 2013, twice as many African American and Hispanic students feared being attacked than white students. It is clear that feeling anxious interferes with learning. Actual past experience with violence further lowers the threshold for feeling upset. The risk to learning of being fearful at school for children in stressed neighborhoods is multiplied by violence they may experience around them at home, causing even greater impact. Even when actual violence is rare, the media have put all kids and parents on edge about whether they are safe at school. This is a tragedy for everyone involved.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
Do you remember that kid in your class threatening to beat up a peer (or maybe you) after school? Mean children are not unique to current times. But actual threat to life while in school is a more recent problem, mainly due to the availability of firearms in American homes. Although rates of victimization have actually dropped 86% from 1992 to 2014, stories about school shootings are instantly broadcast across the country, making everyone feel that it could happen to them. Such public awareness also models threatening violence as a potent attention getter.
Often the threatening child lacks not only the skills to manage the frustrating situation, but also the language ability to choose less incendiary words. Saying, “I don’t think the way you handled that was fair to me,” might always be difficult, but is certainly impossible under the high emotions of the moment. Instead, “I’m going to kill you” pops out of their mouths. As for asking for help, school-aged children can only apologize or confess to being unsure a limited number of times before their need to save face takes precedence. This is especially true if they are confronted and humiliated in front of their peers.
Children who have oppositional or aggressive behavior diagnoses are by definition already in a pattern of reacting with hostility when demands are placed on them. In some cases, these negative reactions successfully get their parent(s) to back off the demand, resulting in what is called the “coercive cycle of interaction,” a prodrome to conduct disorder. Then, when a teacher issues a command, their reflexive response is more likely to be a defiant or aggressive one.
When threatening behavior is met by the supervising adults with confrontation, things may further accelerate, again especially in front of peers before whom the student does not want to look weak. Instead, a methodical approach to threat assessment in schools has been shown to be more effective. The main features of effective threat assessment involve identifying student threats, determining their seriousness, and developing intervention plans that both protect potential victims and address the underlying problem or conflict that sparked the threat.
A model program, Virginia Model for Student Threat Assessment by Dewey G. Cornell, PhD, of the University of Virginia, has been shown to help sort out transient (70%) from substantive (30%) threats and resulted in fewer long-term suspensions or expulsions and no cases in which the threats were carried out. (Send a copy to your local school superintendent.) While children receiving special education made three times more threats and more severe threats, they did not require more suspensions. With this threat assessment program, the number of disciplinary office referrals for these students declined by about 55% for the rest of that school year. Students in schools using this method reported less bullying, a greater willingness to seek help for bullying and threats, and more positive perceptions of the school climate as having fairer discipline and less aggression. Resulting plans to help the students involved in threats included modifications to special education plans, academic and behavioral support services, and referrals to mental health services. All these interventions are intended to address gaps in skills. In addition, ways to give even struggling students a meaningful connection to their school – for example, through sports, art, music, clubs, or volunteering – are essential components of both prevention and management.
There are several ways you, as a pediatrician, may be involved in the issue of threats at school. If one of your patients has been accused of threatening behavior, your knowledge of the child and family puts you in the best position to sort out the seriousness of the threat and appropriate next steps. Recently, one of my patients with mild autism was suspended for threatening to “kill the teacher.” He had never been aggressive at home or at school. This 8-year-old usually has a one-on-one aide, but the aide had been pulled to help other students. After an unannounced fire drill, the child called the teacher “evil” and was given his “third strike” for behavior, resulting in him making this threat.
Threat assessment in schools needs to follow the method of functional behavioral assessment, which should actually be standard for all school behavior problems. The method should consider the A (antecedent), B (behavior), C (consequence), and G (gaps) of the behavior. The antecedent here included the “setting” event of the fire drill. The behavior (sometimes also the belief) was the child’s negative reaction to the teacher (who had failed to protect him from being frightened). The consequence was a punishment (third strike) that the child felt was unfair. The gaps in skills included the facts that this is an anxious child who depends on support and routine because of his autism and who is also hypersensitive to loud noise such as a fire drill. In this case, I was able to explain these things to the school, but, in any case, you can, and should, request that the school perform a functional behavioral assessment when dealing with threats.
When you have a child with learning or emotional problems under your care, you need to include asking if they feel safe at school and if anything scary or bad has happened to them there. The parents may need to be directed to meet with school personnel about threats or fears the child reports. School violence prevention programs often include education of the children to be alert for and report threatening peers. This gives students an active role, but also may cause increased anxiety. Parents may need your support in requesting exemption from the school’s “violence prevention training” for anxious children. Anxious parents also may need extra coaching to avoid exposing their children to discussions about school threats.
In caring for all school-aged children (girls are as likely to be involved in school violence as boys), I ask about whether their teachers are nice or mean. I also ask if they have been bullied at school or have bullied others. I also sometimes ask struggling children, “If you had the choice, would you rather go to school or stay home?” The normal, almost universal preference is to go to school. School is the child’s job and social home, and, even when the work is hard, the need for mastery drives children to keep trying. Children preferring to be home are likely in pain and deserve careful assessment of their skills, their emotions, and the school and family environments.
While the percentage of students who reported being afraid of attack or harm at school decreased from 12% in 1995 to 3% in 2013, twice as many African American and Hispanic students feared being attacked than white students. It is clear that feeling anxious interferes with learning. Actual past experience with violence further lowers the threshold for feeling upset. The risk to learning of being fearful at school for children in stressed neighborhoods is multiplied by violence they may experience around them at home, causing even greater impact. Even when actual violence is rare, the media have put all kids and parents on edge about whether they are safe at school. This is a tragedy for everyone involved.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
Do you remember that kid in your class threatening to beat up a peer (or maybe you) after school? Mean children are not unique to current times. But actual threat to life while in school is a more recent problem, mainly due to the availability of firearms in American homes. Although rates of victimization have actually dropped 86% from 1992 to 2014, stories about school shootings are instantly broadcast across the country, making everyone feel that it could happen to them. Such public awareness also models threatening violence as a potent attention getter.
Often the threatening child lacks not only the skills to manage the frustrating situation, but also the language ability to choose less incendiary words. Saying, “I don’t think the way you handled that was fair to me,” might always be difficult, but is certainly impossible under the high emotions of the moment. Instead, “I’m going to kill you” pops out of their mouths. As for asking for help, school-aged children can only apologize or confess to being unsure a limited number of times before their need to save face takes precedence. This is especially true if they are confronted and humiliated in front of their peers.
Children who have oppositional or aggressive behavior diagnoses are by definition already in a pattern of reacting with hostility when demands are placed on them. In some cases, these negative reactions successfully get their parent(s) to back off the demand, resulting in what is called the “coercive cycle of interaction,” a prodrome to conduct disorder. Then, when a teacher issues a command, their reflexive response is more likely to be a defiant or aggressive one.
When threatening behavior is met by the supervising adults with confrontation, things may further accelerate, again especially in front of peers before whom the student does not want to look weak. Instead, a methodical approach to threat assessment in schools has been shown to be more effective. The main features of effective threat assessment involve identifying student threats, determining their seriousness, and developing intervention plans that both protect potential victims and address the underlying problem or conflict that sparked the threat.
A model program, Virginia Model for Student Threat Assessment by Dewey G. Cornell, PhD, of the University of Virginia, has been shown to help sort out transient (70%) from substantive (30%) threats and resulted in fewer long-term suspensions or expulsions and no cases in which the threats were carried out. (Send a copy to your local school superintendent.) While children receiving special education made three times more threats and more severe threats, they did not require more suspensions. With this threat assessment program, the number of disciplinary office referrals for these students declined by about 55% for the rest of that school year. Students in schools using this method reported less bullying, a greater willingness to seek help for bullying and threats, and more positive perceptions of the school climate as having fairer discipline and less aggression. Resulting plans to help the students involved in threats included modifications to special education plans, academic and behavioral support services, and referrals to mental health services. All these interventions are intended to address gaps in skills. In addition, ways to give even struggling students a meaningful connection to their school – for example, through sports, art, music, clubs, or volunteering – are essential components of both prevention and management.
There are several ways you, as a pediatrician, may be involved in the issue of threats at school. If one of your patients has been accused of threatening behavior, your knowledge of the child and family puts you in the best position to sort out the seriousness of the threat and appropriate next steps. Recently, one of my patients with mild autism was suspended for threatening to “kill the teacher.” He had never been aggressive at home or at school. This 8-year-old usually has a one-on-one aide, but the aide had been pulled to help other students. After an unannounced fire drill, the child called the teacher “evil” and was given his “third strike” for behavior, resulting in him making this threat.
Threat assessment in schools needs to follow the method of functional behavioral assessment, which should actually be standard for all school behavior problems. The method should consider the A (antecedent), B (behavior), C (consequence), and G (gaps) of the behavior. The antecedent here included the “setting” event of the fire drill. The behavior (sometimes also the belief) was the child’s negative reaction to the teacher (who had failed to protect him from being frightened). The consequence was a punishment (third strike) that the child felt was unfair. The gaps in skills included the facts that this is an anxious child who depends on support and routine because of his autism and who is also hypersensitive to loud noise such as a fire drill. In this case, I was able to explain these things to the school, but, in any case, you can, and should, request that the school perform a functional behavioral assessment when dealing with threats.
When you have a child with learning or emotional problems under your care, you need to include asking if they feel safe at school and if anything scary or bad has happened to them there. The parents may need to be directed to meet with school personnel about threats or fears the child reports. School violence prevention programs often include education of the children to be alert for and report threatening peers. This gives students an active role, but also may cause increased anxiety. Parents may need your support in requesting exemption from the school’s “violence prevention training” for anxious children. Anxious parents also may need extra coaching to avoid exposing their children to discussions about school threats.
In caring for all school-aged children (girls are as likely to be involved in school violence as boys), I ask about whether their teachers are nice or mean. I also ask if they have been bullied at school or have bullied others. I also sometimes ask struggling children, “If you had the choice, would you rather go to school or stay home?” The normal, almost universal preference is to go to school. School is the child’s job and social home, and, even when the work is hard, the need for mastery drives children to keep trying. Children preferring to be home are likely in pain and deserve careful assessment of their skills, their emotions, and the school and family environments.
While the percentage of students who reported being afraid of attack or harm at school decreased from 12% in 1995 to 3% in 2013, twice as many African American and Hispanic students feared being attacked than white students. It is clear that feeling anxious interferes with learning. Actual past experience with violence further lowers the threshold for feeling upset. The risk to learning of being fearful at school for children in stressed neighborhoods is multiplied by violence they may experience around them at home, causing even greater impact. Even when actual violence is rare, the media have put all kids and parents on edge about whether they are safe at school. This is a tragedy for everyone involved.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
Ph-like ALL is highly prevalent in adults
Philadelphia chromosome–like acute lymphoblastic leukemia, a high-risk subtype of childhood ALL, accounts for more than 24% of ALL in adults and is associated with poor outcome, according to gene-expression profiling in nearly 800 adults with B-cell ALL.
In the 798 subjects aged 21-86 years, Philadelphia chromosome–like (Ph-like) ALL accounted for 27.9% of ALL cases in those aged 21-39 years, 20.4% of cases in those aged 40-59 years, and 24% of cases in those aged 60-86 years. The overall 5-year event-free survival rate was inferior in those with Ph-like ALL vs. non–Ph-like ALL (22.5% vs. 49.3%), as was the 5-year overall survival (23.8% vs. 52.4%). Increasing age also was associated with inferior outcomes: 5-year event-free survival was 40.4%, 29.8%, and 18.9% in the age groups, respectively, and 5-year overall survival was 45.2%, 35.1%, and 28.4% in the groups, respectively, Kathryn G. Roberts, Ph.D., of St. Jude Children’s Research Hospital in Memphis and her colleagues reported online ahead of print (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.69.0073).

Ph-like ALL in children is characterized by kinase-activating alterations amenable to treatment with tyrosine kinase inhibitors, but the prevalence in adults was unclear.
“These findings warrant the development of clinical trials in adults that assess the efficacy of TKIs, similar to those that are being established for pediatric ALL,” Dr. Roberts and her associates wrote.
This study was supported by grants and other awards, some to individual authors, from the American Lebanese Syrian Associated Charities of St. Jude Children’s Research Hospital; Stand Up to Cancer, St. Baldrick’s Foundation, the American Society of Hematology, the Lady Tata Memorial Trust, the Leukemia Research Foundation, the National Cancer Institute, and the National Institutes of Health. Dr. Roberts reported that she is the inventor on a pending patent application related to gene-expression signatures for detection of underlying Philadelphia chromosome-live events and therapeutic targeting in leukemia.
Philadelphia chromosome–like acute lymphoblastic leukemia, a high-risk subtype of childhood ALL, accounts for more than 24% of ALL in adults and is associated with poor outcome, according to gene-expression profiling in nearly 800 adults with B-cell ALL.
In the 798 subjects aged 21-86 years, Philadelphia chromosome–like (Ph-like) ALL accounted for 27.9% of ALL cases in those aged 21-39 years, 20.4% of cases in those aged 40-59 years, and 24% of cases in those aged 60-86 years. The overall 5-year event-free survival rate was inferior in those with Ph-like ALL vs. non–Ph-like ALL (22.5% vs. 49.3%), as was the 5-year overall survival (23.8% vs. 52.4%). Increasing age also was associated with inferior outcomes: 5-year event-free survival was 40.4%, 29.8%, and 18.9% in the age groups, respectively, and 5-year overall survival was 45.2%, 35.1%, and 28.4% in the groups, respectively, Kathryn G. Roberts, Ph.D., of St. Jude Children’s Research Hospital in Memphis and her colleagues reported online ahead of print (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.69.0073).
Ph-like ALL in children is characterized by kinase-activating alterations amenable to treatment with tyrosine kinase inhibitors, but the prevalence in adults was unclear.
“These findings warrant the development of clinical trials in adults that assess the efficacy of TKIs, similar to those that are being established for pediatric ALL,” Dr. Roberts and her associates wrote.
This study was supported by grants and other awards, some to individual authors, from the American Lebanese Syrian Associated Charities of St. Jude Children’s Research Hospital; Stand Up to Cancer, St. Baldrick’s Foundation, the American Society of Hematology, the Lady Tata Memorial Trust, the Leukemia Research Foundation, the National Cancer Institute, and the National Institutes of Health. Dr. Roberts reported that she is the inventor on a pending patent application related to gene-expression signatures for detection of underlying Philadelphia chromosome-live events and therapeutic targeting in leukemia.
Philadelphia chromosome–like acute lymphoblastic leukemia, a high-risk subtype of childhood ALL, accounts for more than 24% of ALL in adults and is associated with poor outcome, according to gene-expression profiling in nearly 800 adults with B-cell ALL.
In the 798 subjects aged 21-86 years, Philadelphia chromosome–like (Ph-like) ALL accounted for 27.9% of ALL cases in those aged 21-39 years, 20.4% of cases in those aged 40-59 years, and 24% of cases in those aged 60-86 years. The overall 5-year event-free survival rate was inferior in those with Ph-like ALL vs. non–Ph-like ALL (22.5% vs. 49.3%), as was the 5-year overall survival (23.8% vs. 52.4%). Increasing age also was associated with inferior outcomes: 5-year event-free survival was 40.4%, 29.8%, and 18.9% in the age groups, respectively, and 5-year overall survival was 45.2%, 35.1%, and 28.4% in the groups, respectively, Kathryn G. Roberts, Ph.D., of St. Jude Children’s Research Hospital in Memphis and her colleagues reported online ahead of print (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.69.0073).
Ph-like ALL in children is characterized by kinase-activating alterations amenable to treatment with tyrosine kinase inhibitors, but the prevalence in adults was unclear.
“These findings warrant the development of clinical trials in adults that assess the efficacy of TKIs, similar to those that are being established for pediatric ALL,” Dr. Roberts and her associates wrote.
This study was supported by grants and other awards, some to individual authors, from the American Lebanese Syrian Associated Charities of St. Jude Children’s Research Hospital; Stand Up to Cancer, St. Baldrick’s Foundation, the American Society of Hematology, the Lady Tata Memorial Trust, the Leukemia Research Foundation, the National Cancer Institute, and the National Institutes of Health. Dr. Roberts reported that she is the inventor on a pending patent application related to gene-expression signatures for detection of underlying Philadelphia chromosome-live events and therapeutic targeting in leukemia.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point:
Major finding: Ph-like ALL accounted for 27.9% of ALL cases in adults aged 21-39 years, 20.4% of cases in those aged 40-59 years, and 24% of cases in those aged 60-86 years.
Data source: Gene-expression profiling of 798 patients.
Disclosures: This study was supported by grants and other awards, some to individual authors, from the American Lebanese Syrian Associated Charities of St. Jude Children’s Research Hospital; Stand Up to Cancer, St. Baldrick’s Foundation, the American Society of Hematology, the Lady Tata Memorial Trust, the Leukemia Research Foundation, the National Cancer Institute, and the National Institutes of Health. Dr. Roberts reported that she is the inventor on a pending patent application related to gene-expression signatures for detection of underlying Philadelphia chromosome–like events and therapeutic targeting in leukemia.
Blood Pressure Changes and Persistent Hypertension Increase Dementia Risk
BALTIMORE—The impact of blood pressure on the risk of dementia in late life follows a U-shaped curve in which elevated mid-life and late-life blood pressure, as well as late-life decline in blood pressure, all independently increase the risk of dementia, according to findings from a longitudinal study of the Framingham Offspring cohort of the Framingham Heart Study.
The findings highlight the benefits of establishing and maintaining lower blood pressure in mid-life for preventing or decreasing the risk of dementia, said Emer McGrath, MD, a neurology resident at Massachusetts General Hospital in Boston, at the 141st Annual Meeting of the American Neurological Association.
Hypertension has been linked to stroke and dementia and is the most important modifiable risk factor for both outcomes. Likewise, elevated blood pressure in mid-life (ie, ages 40 to 64) and late life (ie, age 65 or older) has been linked with a heightened risk of cognitive decline, as has low blood pressure in late life, but “the relationship between blood pressure in mid and late life and dementia [is] less clear, and the relationship of blood pressure changes from mid to late life is unknown,” said Dr. McGrath.
The researchers explored the issue using data from the Framingham Offspring cohort of the Framingham Heart Study. The cohort comprises 5,124 children and spouses of children of the original Framingham cohort. They have been examined clinically at regular intervals since 1971. The present study focused on 1,440 individuals who had five consecutive examinations during a 15-year period anytime between 1983 and 2001 and who had not been diagnosed with dementia at the time of the final blood pressure determination.
The 1,440 participants had a mean age of 69 at their fifth examination. Slightly more than half were female, 20% had been diagnosed with cardiovascular disease, and slightly less than 20% had been diagnosed with diabetes. Half were using antihypertensive medications.
During a mean eight-year follow-up period, 107 individuals developed dementia. Dementia was independently associated with mid-life hypertension (ie, blood pressure of 140/90 mm Hg or higher), with a stronger association for systolic hypertension (hazard ratio [HR], 1.57). Persistence of hypertension into late life, particularly systolic hypertension (HR, 1.96), was another independent risk factor for dementia.
Among individuals who did not have hypertension at mid-life, a decline in systolic blood pressure to less than 100/70 mm Hg in the ensuing years increased the risk of dementia (HR, 1.63).
The findings support the hypothesis of the U-shaped relationship between blood pressure and dementia, according to the researchers. “Our data also highlight the potential sustained cognitive benefits of lower mid-life blood pressure,” said Dr. McGrath.
The study was funded by the Framingham Heart Study, the National Institute on Aging, and the National Institute for Neurological Diseases and Stroke.
—Brian Hoyle
Suggested Reading
McDonald C, Pearce MS, Kerr SR, Newton JL. Blood pressure variability and cognitive decline in older people: a 5-year longitudinal study. J Hypertens. 2016 Sep 17 [Epub ahead of print].
BALTIMORE—The impact of blood pressure on the risk of dementia in late life follows a U-shaped curve in which elevated mid-life and late-life blood pressure, as well as late-life decline in blood pressure, all independently increase the risk of dementia, according to findings from a longitudinal study of the Framingham Offspring cohort of the Framingham Heart Study.
The findings highlight the benefits of establishing and maintaining lower blood pressure in mid-life for preventing or decreasing the risk of dementia, said Emer McGrath, MD, a neurology resident at Massachusetts General Hospital in Boston, at the 141st Annual Meeting of the American Neurological Association.
Hypertension has been linked to stroke and dementia and is the most important modifiable risk factor for both outcomes. Likewise, elevated blood pressure in mid-life (ie, ages 40 to 64) and late life (ie, age 65 or older) has been linked with a heightened risk of cognitive decline, as has low blood pressure in late life, but “the relationship between blood pressure in mid and late life and dementia [is] less clear, and the relationship of blood pressure changes from mid to late life is unknown,” said Dr. McGrath.
The researchers explored the issue using data from the Framingham Offspring cohort of the Framingham Heart Study. The cohort comprises 5,124 children and spouses of children of the original Framingham cohort. They have been examined clinically at regular intervals since 1971. The present study focused on 1,440 individuals who had five consecutive examinations during a 15-year period anytime between 1983 and 2001 and who had not been diagnosed with dementia at the time of the final blood pressure determination.
The 1,440 participants had a mean age of 69 at their fifth examination. Slightly more than half were female, 20% had been diagnosed with cardiovascular disease, and slightly less than 20% had been diagnosed with diabetes. Half were using antihypertensive medications.
During a mean eight-year follow-up period, 107 individuals developed dementia. Dementia was independently associated with mid-life hypertension (ie, blood pressure of 140/90 mm Hg or higher), with a stronger association for systolic hypertension (hazard ratio [HR], 1.57). Persistence of hypertension into late life, particularly systolic hypertension (HR, 1.96), was another independent risk factor for dementia.
Among individuals who did not have hypertension at mid-life, a decline in systolic blood pressure to less than 100/70 mm Hg in the ensuing years increased the risk of dementia (HR, 1.63).
The findings support the hypothesis of the U-shaped relationship between blood pressure and dementia, according to the researchers. “Our data also highlight the potential sustained cognitive benefits of lower mid-life blood pressure,” said Dr. McGrath.
The study was funded by the Framingham Heart Study, the National Institute on Aging, and the National Institute for Neurological Diseases and Stroke.
—Brian Hoyle
Suggested Reading
McDonald C, Pearce MS, Kerr SR, Newton JL. Blood pressure variability and cognitive decline in older people: a 5-year longitudinal study. J Hypertens. 2016 Sep 17 [Epub ahead of print].
BALTIMORE—The impact of blood pressure on the risk of dementia in late life follows a U-shaped curve in which elevated mid-life and late-life blood pressure, as well as late-life decline in blood pressure, all independently increase the risk of dementia, according to findings from a longitudinal study of the Framingham Offspring cohort of the Framingham Heart Study.
The findings highlight the benefits of establishing and maintaining lower blood pressure in mid-life for preventing or decreasing the risk of dementia, said Emer McGrath, MD, a neurology resident at Massachusetts General Hospital in Boston, at the 141st Annual Meeting of the American Neurological Association.
Hypertension has been linked to stroke and dementia and is the most important modifiable risk factor for both outcomes. Likewise, elevated blood pressure in mid-life (ie, ages 40 to 64) and late life (ie, age 65 or older) has been linked with a heightened risk of cognitive decline, as has low blood pressure in late life, but “the relationship between blood pressure in mid and late life and dementia [is] less clear, and the relationship of blood pressure changes from mid to late life is unknown,” said Dr. McGrath.
The researchers explored the issue using data from the Framingham Offspring cohort of the Framingham Heart Study. The cohort comprises 5,124 children and spouses of children of the original Framingham cohort. They have been examined clinically at regular intervals since 1971. The present study focused on 1,440 individuals who had five consecutive examinations during a 15-year period anytime between 1983 and 2001 and who had not been diagnosed with dementia at the time of the final blood pressure determination.
The 1,440 participants had a mean age of 69 at their fifth examination. Slightly more than half were female, 20% had been diagnosed with cardiovascular disease, and slightly less than 20% had been diagnosed with diabetes. Half were using antihypertensive medications.
During a mean eight-year follow-up period, 107 individuals developed dementia. Dementia was independently associated with mid-life hypertension (ie, blood pressure of 140/90 mm Hg or higher), with a stronger association for systolic hypertension (hazard ratio [HR], 1.57). Persistence of hypertension into late life, particularly systolic hypertension (HR, 1.96), was another independent risk factor for dementia.
Among individuals who did not have hypertension at mid-life, a decline in systolic blood pressure to less than 100/70 mm Hg in the ensuing years increased the risk of dementia (HR, 1.63).
The findings support the hypothesis of the U-shaped relationship between blood pressure and dementia, according to the researchers. “Our data also highlight the potential sustained cognitive benefits of lower mid-life blood pressure,” said Dr. McGrath.
The study was funded by the Framingham Heart Study, the National Institute on Aging, and the National Institute for Neurological Diseases and Stroke.
—Brian Hoyle
Suggested Reading
McDonald C, Pearce MS, Kerr SR, Newton JL. Blood pressure variability and cognitive decline in older people: a 5-year longitudinal study. J Hypertens. 2016 Sep 17 [Epub ahead of print].
Fear and hope: Helping LGBT youth cope with the 2016 election results
The day after the election, Time magazine reported an increased call volume to the Trevor Project, an organization that provides suicide counseling for LGBT youth.1 A colleague of mine who works closely with the Trevor Project told me that this was the second-highest call volume the organization has received since its inception.
Regardless of your political affiliation, we all can agree that this year’s election was divisive. Many minority groups, including the LGBT community, felt singled out. Although many of us have seen contentious elections in our lifetimes, teenagers, especially LGBT youth, are sensitive to this divisiveness.

Many LGBT youth who called the Trevor Project had expressed fear about the future. Whenever someone becomes suicidal, they have an overwhelming sense of hopelessness.2 Many perceive that the upcoming administration may be hostile to the LGBT community, and because many fear that this new administration may undo all the progress made in LGBT rights in the last 8 years, they have little hope for the future. Numerous reports of increased hate-crime incidents since the start of the election season last year may have exacerbated this feeling of hopelessness.3 This hopelessness may cause many to feel that the best way out is through suicide. Others feel that their sexual orientation or gender identity may be an additional burden to their family during this new era, and so to relieve them of this burden, they consider ending their own lives.4
For adults who have seen many administrations come and go, this may seem like hyperbole. But we have the advantage of living through various elections and administrations, knowing that they were not as catastrophic as others claimed. However, for many LGBT teens or young adults, this is probably their first election after reaching adolescence since Obama was elected in 2008. The Obama administration has been friendly to the LGBT community,5 and for LGBT youth, the upcoming Trump administration may be a substantial departure from this friendliness. In addition, people across the political spectrum have stoked fears among LGBT youth that the new administration will be devastating for the LGBT community. Adolescents, compared with adults, respond more strongly to the limbic system of the brain – the part of the brain involved in emotional processing, which includes fear.6 This fear will override any attempt by the prefrontal cortex – the part of the brain involved in cognitive processing6 – to put the results of this election within context and within perspective. In other words, it is easier for the adolescent brain to become much more despondent over a disappointing outcome.
What can providers do for LGBT youth who feel distressed over the outcome of the election? The approach is twofold. First, address the emotions emanating from the limbic system. Once this influence is dampened, engage the prefrontal cortex to process the emotions and address these fears in a more constructive way.
For LGBT youth who are actively suicidal, providers should first determine the risk for suicide (for example, determine the level of family support, access to lethal means of suicide, etc.) Then, depending on the risk, create a suicide safety plan that will help the teen or young adult cope with the distress. For more information on how to address suicidality among LGBT youth, please see my previous column (“It does get better... with your help: Preventing suicide,” October 2016, page 30).
Recognize and validate the fears of LGBT youth. Do not dismiss their fears as an overreaction. Because of the adolescent brain’s responsiveness to the limbic system, their fears and emotions are much more intense than are those of adults. Allow them to express how worried they are about the future. Remind them that you are their advocate and that your goal is to keep them safe. Remind your LGBT patients that people who have advocated for them did not disappear overnight because of the election. Some parents of my LGBT patients have pointed out that many LGBT youth feel safer when a nonfamily member advocates for them; therefore, it is essential to remind your LGBT patients about your role as their physician and their advocate.
Another way to support your LGBT patients during this stressful time is to help create a safe environment for them, especially at school. There are some concerns about an increase in antigay and antitrans harassment and bullying since the election.7 Schools are doing their best to respond appropriately to these incidents.8 Fortunately, many schools are responsive to physicians’ recommendations for preventing and addressing school bullying.9 For more information on how providers can address bullying of LGBT youth in school, please refer to my column on bullying (“Bullying,” May 2016, p.1).
Once you reduce the responsiveness of the adolescent brain to the limbic system, you then can focus on the prefrontal cortex to help adolescents engage and cope with their distress. Have them recall from their civics classes that the United States government has checks and balances and that one person does not have unilateral power. Remind the adolescent that administrations and governments do not last forever and that there is an opportunity to change administrations every 4 years.
One of the most powerful ways to engage the prefrontal cortex of the distressed adolescent is to provide the individual with opportunities to be an active member of the community. They can volunteer in many organizations that share their values and beliefs. These organizations do not need to be political, but they should provide some service to the community. This will remind the adolescents that they can have an impact on their own lives and in the lives of others. Volunteering in these organizations will give them a sense of purpose and create a stronger connection to their communities10 – both are antidotes to the intense feeling of despair and hopelessness.
The fear and concerns that LGBT youth have over the election results are intense and deserve attention. Their neurobiology and lack of experience make these fears much more powerful. Providers, parents, and advocates have the responsibility to address these fears, remind LGBT youth that they are their advocates, and remind LGBT youth of the ability to influence the outcomes of their own lives. Providing skills to cope with disappointing outcomes also will prepare LGBT youth for the challenges of adulthood and for the many elections to come.
Resources
AAP: Talking to your children about the election
HealthyChildren.org: How to support your child’s resilience in a time of crisis
Suicide Prevention Lifeline: Patient safety plan template
References
1. “Donald Trump Win Causes Spike in Crisis Support Line Calls,” Time magazine, Nov. 9, 2016.
2. Int Rev Psychiatry. 1992;4(2):177-84.
3. “U.S. Hate Crimes Surge 6%, Fueled by Attacks on Muslims,” the New York Times, Nov. 14, 2016.
4. Arch Suicide Res. 2015;19(3):385-400.
5. “The president of the United States shifted the mainstream in one interview,” Newsweek, May 13, 2012.
6. Neuropsychiatric Disease and Treatment. 2013;9:449-61.
7. “This is Trump’s America: LGBT community fears surge in hate crimes following reports of homophobic attacks,” Salon magazine, Nov. 13, 2016.
8. “School officials grapple with bullying, harassment after election,” Lansing State Journal, Nov. 13, 2016.
9. “Roles for pediatricians in bullying prevention and intervention,” StopBullying.gov, 2016.
10. Adv Psych Treatment. 2014;20(3):217-24.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics the University of Pittsburgh. Email him at [email protected].
The day after the election, Time magazine reported an increased call volume to the Trevor Project, an organization that provides suicide counseling for LGBT youth.1 A colleague of mine who works closely with the Trevor Project told me that this was the second-highest call volume the organization has received since its inception.
Regardless of your political affiliation, we all can agree that this year’s election was divisive. Many minority groups, including the LGBT community, felt singled out. Although many of us have seen contentious elections in our lifetimes, teenagers, especially LGBT youth, are sensitive to this divisiveness.
Many LGBT youth who called the Trevor Project had expressed fear about the future. Whenever someone becomes suicidal, they have an overwhelming sense of hopelessness.2 Many perceive that the upcoming administration may be hostile to the LGBT community, and because many fear that this new administration may undo all the progress made in LGBT rights in the last 8 years, they have little hope for the future. Numerous reports of increased hate-crime incidents since the start of the election season last year may have exacerbated this feeling of hopelessness.3 This hopelessness may cause many to feel that the best way out is through suicide. Others feel that their sexual orientation or gender identity may be an additional burden to their family during this new era, and so to relieve them of this burden, they consider ending their own lives.4
For adults who have seen many administrations come and go, this may seem like hyperbole. But we have the advantage of living through various elections and administrations, knowing that they were not as catastrophic as others claimed. However, for many LGBT teens or young adults, this is probably their first election after reaching adolescence since Obama was elected in 2008. The Obama administration has been friendly to the LGBT community,5 and for LGBT youth, the upcoming Trump administration may be a substantial departure from this friendliness. In addition, people across the political spectrum have stoked fears among LGBT youth that the new administration will be devastating for the LGBT community. Adolescents, compared with adults, respond more strongly to the limbic system of the brain – the part of the brain involved in emotional processing, which includes fear.6 This fear will override any attempt by the prefrontal cortex – the part of the brain involved in cognitive processing6 – to put the results of this election within context and within perspective. In other words, it is easier for the adolescent brain to become much more despondent over a disappointing outcome.
What can providers do for LGBT youth who feel distressed over the outcome of the election? The approach is twofold. First, address the emotions emanating from the limbic system. Once this influence is dampened, engage the prefrontal cortex to process the emotions and address these fears in a more constructive way.
For LGBT youth who are actively suicidal, providers should first determine the risk for suicide (for example, determine the level of family support, access to lethal means of suicide, etc.) Then, depending on the risk, create a suicide safety plan that will help the teen or young adult cope with the distress. For more information on how to address suicidality among LGBT youth, please see my previous column (“It does get better... with your help: Preventing suicide,” October 2016, page 30).
Recognize and validate the fears of LGBT youth. Do not dismiss their fears as an overreaction. Because of the adolescent brain’s responsiveness to the limbic system, their fears and emotions are much more intense than are those of adults. Allow them to express how worried they are about the future. Remind them that you are their advocate and that your goal is to keep them safe. Remind your LGBT patients that people who have advocated for them did not disappear overnight because of the election. Some parents of my LGBT patients have pointed out that many LGBT youth feel safer when a nonfamily member advocates for them; therefore, it is essential to remind your LGBT patients about your role as their physician and their advocate.
Another way to support your LGBT patients during this stressful time is to help create a safe environment for them, especially at school. There are some concerns about an increase in antigay and antitrans harassment and bullying since the election.7 Schools are doing their best to respond appropriately to these incidents.8 Fortunately, many schools are responsive to physicians’ recommendations for preventing and addressing school bullying.9 For more information on how providers can address bullying of LGBT youth in school, please refer to my column on bullying (“Bullying,” May 2016, p.1).
Once you reduce the responsiveness of the adolescent brain to the limbic system, you then can focus on the prefrontal cortex to help adolescents engage and cope with their distress. Have them recall from their civics classes that the United States government has checks and balances and that one person does not have unilateral power. Remind the adolescent that administrations and governments do not last forever and that there is an opportunity to change administrations every 4 years.
One of the most powerful ways to engage the prefrontal cortex of the distressed adolescent is to provide the individual with opportunities to be an active member of the community. They can volunteer in many organizations that share their values and beliefs. These organizations do not need to be political, but they should provide some service to the community. This will remind the adolescents that they can have an impact on their own lives and in the lives of others. Volunteering in these organizations will give them a sense of purpose and create a stronger connection to their communities10 – both are antidotes to the intense feeling of despair and hopelessness.
The fear and concerns that LGBT youth have over the election results are intense and deserve attention. Their neurobiology and lack of experience make these fears much more powerful. Providers, parents, and advocates have the responsibility to address these fears, remind LGBT youth that they are their advocates, and remind LGBT youth of the ability to influence the outcomes of their own lives. Providing skills to cope with disappointing outcomes also will prepare LGBT youth for the challenges of adulthood and for the many elections to come.
Resources
AAP: Talking to your children about the election
HealthyChildren.org: How to support your child’s resilience in a time of crisis
Suicide Prevention Lifeline: Patient safety plan template
References
1. “Donald Trump Win Causes Spike in Crisis Support Line Calls,” Time magazine, Nov. 9, 2016.
2. Int Rev Psychiatry. 1992;4(2):177-84.
3. “U.S. Hate Crimes Surge 6%, Fueled by Attacks on Muslims,” the New York Times, Nov. 14, 2016.
4. Arch Suicide Res. 2015;19(3):385-400.
5. “The president of the United States shifted the mainstream in one interview,” Newsweek, May 13, 2012.
6. Neuropsychiatric Disease and Treatment. 2013;9:449-61.
7. “This is Trump’s America: LGBT community fears surge in hate crimes following reports of homophobic attacks,” Salon magazine, Nov. 13, 2016.
8. “School officials grapple with bullying, harassment after election,” Lansing State Journal, Nov. 13, 2016.
9. “Roles for pediatricians in bullying prevention and intervention,” StopBullying.gov, 2016.
10. Adv Psych Treatment. 2014;20(3):217-24.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics the University of Pittsburgh. Email him at [email protected].
The day after the election, Time magazine reported an increased call volume to the Trevor Project, an organization that provides suicide counseling for LGBT youth.1 A colleague of mine who works closely with the Trevor Project told me that this was the second-highest call volume the organization has received since its inception.
Regardless of your political affiliation, we all can agree that this year’s election was divisive. Many minority groups, including the LGBT community, felt singled out. Although many of us have seen contentious elections in our lifetimes, teenagers, especially LGBT youth, are sensitive to this divisiveness.
Many LGBT youth who called the Trevor Project had expressed fear about the future. Whenever someone becomes suicidal, they have an overwhelming sense of hopelessness.2 Many perceive that the upcoming administration may be hostile to the LGBT community, and because many fear that this new administration may undo all the progress made in LGBT rights in the last 8 years, they have little hope for the future. Numerous reports of increased hate-crime incidents since the start of the election season last year may have exacerbated this feeling of hopelessness.3 This hopelessness may cause many to feel that the best way out is through suicide. Others feel that their sexual orientation or gender identity may be an additional burden to their family during this new era, and so to relieve them of this burden, they consider ending their own lives.4
For adults who have seen many administrations come and go, this may seem like hyperbole. But we have the advantage of living through various elections and administrations, knowing that they were not as catastrophic as others claimed. However, for many LGBT teens or young adults, this is probably their first election after reaching adolescence since Obama was elected in 2008. The Obama administration has been friendly to the LGBT community,5 and for LGBT youth, the upcoming Trump administration may be a substantial departure from this friendliness. In addition, people across the political spectrum have stoked fears among LGBT youth that the new administration will be devastating for the LGBT community. Adolescents, compared with adults, respond more strongly to the limbic system of the brain – the part of the brain involved in emotional processing, which includes fear.6 This fear will override any attempt by the prefrontal cortex – the part of the brain involved in cognitive processing6 – to put the results of this election within context and within perspective. In other words, it is easier for the adolescent brain to become much more despondent over a disappointing outcome.
What can providers do for LGBT youth who feel distressed over the outcome of the election? The approach is twofold. First, address the emotions emanating from the limbic system. Once this influence is dampened, engage the prefrontal cortex to process the emotions and address these fears in a more constructive way.
For LGBT youth who are actively suicidal, providers should first determine the risk for suicide (for example, determine the level of family support, access to lethal means of suicide, etc.) Then, depending on the risk, create a suicide safety plan that will help the teen or young adult cope with the distress. For more information on how to address suicidality among LGBT youth, please see my previous column (“It does get better... with your help: Preventing suicide,” October 2016, page 30).
Recognize and validate the fears of LGBT youth. Do not dismiss their fears as an overreaction. Because of the adolescent brain’s responsiveness to the limbic system, their fears and emotions are much more intense than are those of adults. Allow them to express how worried they are about the future. Remind them that you are their advocate and that your goal is to keep them safe. Remind your LGBT patients that people who have advocated for them did not disappear overnight because of the election. Some parents of my LGBT patients have pointed out that many LGBT youth feel safer when a nonfamily member advocates for them; therefore, it is essential to remind your LGBT patients about your role as their physician and their advocate.
Another way to support your LGBT patients during this stressful time is to help create a safe environment for them, especially at school. There are some concerns about an increase in antigay and antitrans harassment and bullying since the election.7 Schools are doing their best to respond appropriately to these incidents.8 Fortunately, many schools are responsive to physicians’ recommendations for preventing and addressing school bullying.9 For more information on how providers can address bullying of LGBT youth in school, please refer to my column on bullying (“Bullying,” May 2016, p.1).
Once you reduce the responsiveness of the adolescent brain to the limbic system, you then can focus on the prefrontal cortex to help adolescents engage and cope with their distress. Have them recall from their civics classes that the United States government has checks and balances and that one person does not have unilateral power. Remind the adolescent that administrations and governments do not last forever and that there is an opportunity to change administrations every 4 years.
One of the most powerful ways to engage the prefrontal cortex of the distressed adolescent is to provide the individual with opportunities to be an active member of the community. They can volunteer in many organizations that share their values and beliefs. These organizations do not need to be political, but they should provide some service to the community. This will remind the adolescents that they can have an impact on their own lives and in the lives of others. Volunteering in these organizations will give them a sense of purpose and create a stronger connection to their communities10 – both are antidotes to the intense feeling of despair and hopelessness.
The fear and concerns that LGBT youth have over the election results are intense and deserve attention. Their neurobiology and lack of experience make these fears much more powerful. Providers, parents, and advocates have the responsibility to address these fears, remind LGBT youth that they are their advocates, and remind LGBT youth of the ability to influence the outcomes of their own lives. Providing skills to cope with disappointing outcomes also will prepare LGBT youth for the challenges of adulthood and for the many elections to come.
Resources
AAP: Talking to your children about the election
HealthyChildren.org: How to support your child’s resilience in a time of crisis
Suicide Prevention Lifeline: Patient safety plan template
References
1. “Donald Trump Win Causes Spike in Crisis Support Line Calls,” Time magazine, Nov. 9, 2016.
2. Int Rev Psychiatry. 1992;4(2):177-84.
3. “U.S. Hate Crimes Surge 6%, Fueled by Attacks on Muslims,” the New York Times, Nov. 14, 2016.
4. Arch Suicide Res. 2015;19(3):385-400.
5. “The president of the United States shifted the mainstream in one interview,” Newsweek, May 13, 2012.
6. Neuropsychiatric Disease and Treatment. 2013;9:449-61.
7. “This is Trump’s America: LGBT community fears surge in hate crimes following reports of homophobic attacks,” Salon magazine, Nov. 13, 2016.
8. “School officials grapple with bullying, harassment after election,” Lansing State Journal, Nov. 13, 2016.
9. “Roles for pediatricians in bullying prevention and intervention,” StopBullying.gov, 2016.
10. Adv Psych Treatment. 2014;20(3):217-24.
Dr. Montano is an adolescent medicine fellow at Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center and a postdoctoral fellow in the department of pediatrics the University of Pittsburgh. Email him at [email protected].