User login
Diagnostic Testing for Patients With Suspected Ocular Manifestations of Lyme Disease
Diagnostic Testing for Patients With Suspected Ocular Manifestations of Lyme Disease
Since Lyme disease (LD) was first identified in 1975, there has been uncertainty regarding the proper diagnostic testing for suspected cases.1 Challenges involved with ordering Lyme serology testing include navigating tests with an array of false negatives and false positives.2 Confounding these challenges is the wide variety of ocular manifestations of LD, ranging from nonspecific conjunctivitis, cranial palsies, and anterior and posterior segment inflammation.2,3 This article provides diagnostic testing guidelines for eye care clinicians who encounter patients with suspected LD.
BACKGROUND
LD is a bacterial infection caused by the spirochete Borrelia burgdorferi sensu lato complex transmitted by the Ixodes tick genus. There are 4 species of Ixodes ticks that can infect humans, and only 2 have been identified as principal vectors in North America: Ixodes scapularis and Ixodes pacificus. The incidence of LD is on the rise due to increasing global temperatures and expanding geographic borders for the organism. Cases in endemic areas range from 10 per 100,000 people to 50 per 100,000 people.4
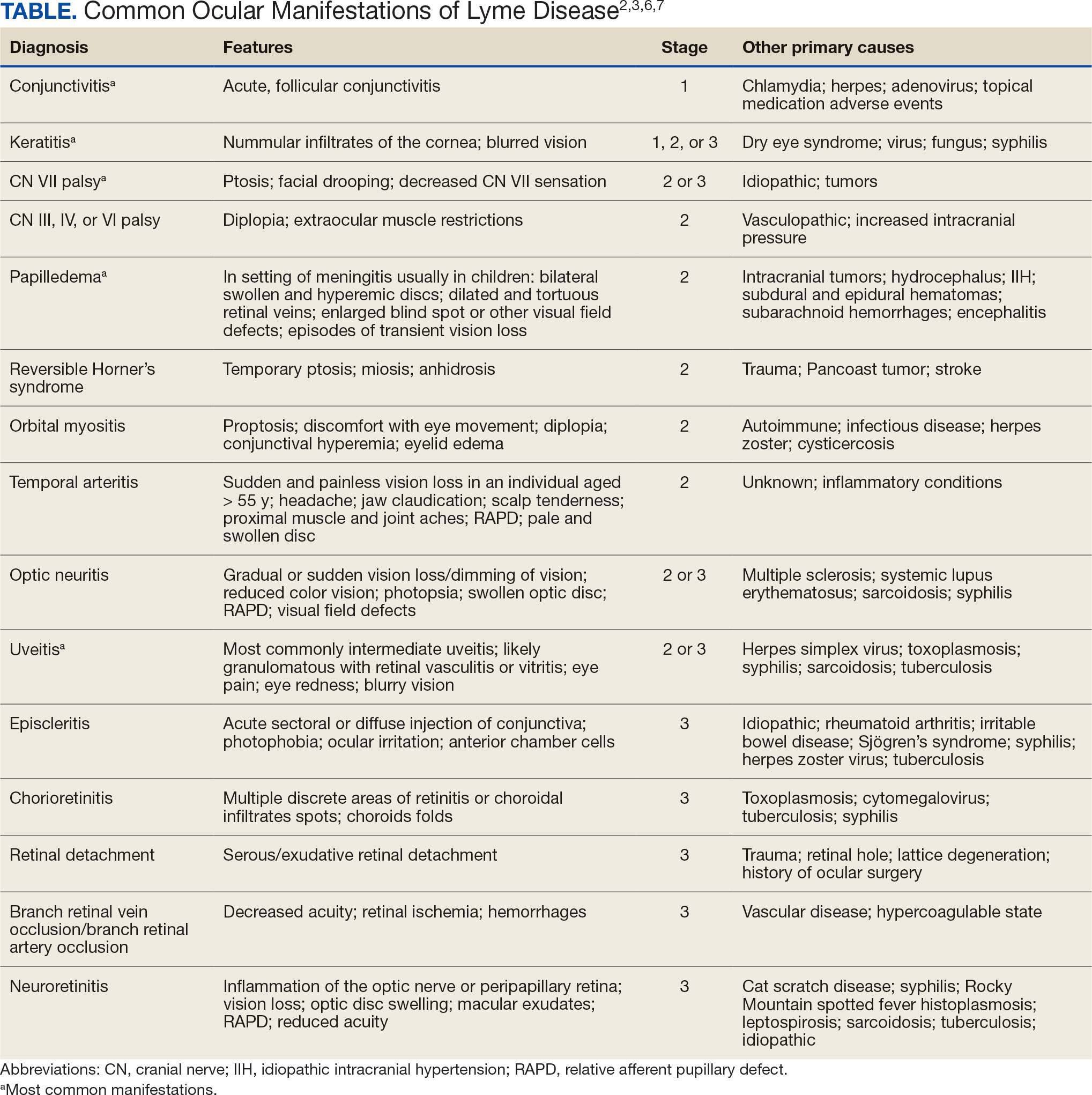
LD occurs in 3 stages: early localized (stage 1), early disseminated (stage 2), and late disseminated (stage 3). In stage 1, patients typically present with erythema migrans (EM) rash (bull’s-eye cutaneous rash) and other nonspecific flu-like symptoms of fever, fatigue, and arthralgia. Stage 2 occurs several weeks to months after the initial infection and the infection has invaded other systemic organs, causing conditions like carditis, meningitis, and arthritis. A small subset of patients may progress to stage 3, which is characterized by chronic arthritis and chronic neurological LD.2,4,5 Ocular manifestations have been well-documented in all stages of LD but are more prevalent in early disseminated disease (Table).2,3,6,7
Indications
Recognizing common ocular manifestations associated with LD will allow eye care practitioners to make a timely diagnosis and initiate treatment. The most common ocular findings from LD include conjunctivitis, keratitis, cranial nerve VII palsy, optic neuritis, granulomatous iridocyclitis, and pars planitis.2,6 While retrospective studies suggest that up to 10% of patients with early localized LD have a nonspecific follicular conjunctivitis, those patients are unlikely to present for ocular evaluation. If a patient does present with an acute conjunctivitis, many clinicians do not consider LD in their differential diagnosis.8 In endemic areas, it is important to query patients for additional symptoms that may indicate LD.
Obtaining a complete patient history is vital in aiding a clinician’s decision to order Lyme serology for suspected LD. Epidemiology, history of geography/travel, pet exposure, sexual history (necessary to rule out other conditions [ie, syphilis] to direct appropriate diagnostic testing), and a complete review of systems should be obtained.2,4 LD may mimic other inflammatory autoimmune conditions or infectious diseases such as syphilis.2,5 This can lead to obtaining unnecessary Lyme serologies or failing to diagnose LD.5,7
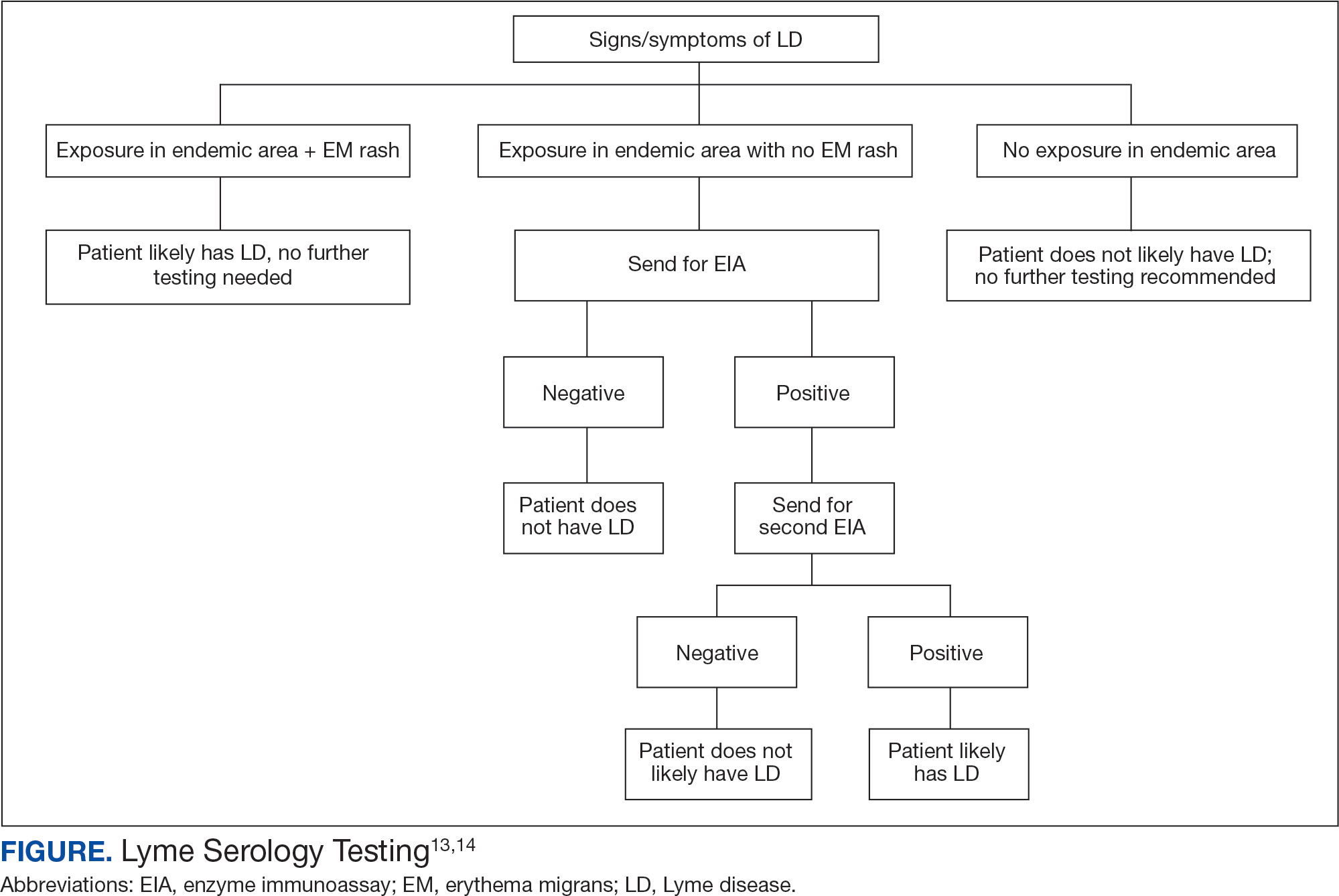
Diagnostic testing is not indicated when a patient presents with an asymptomatic tick bite (ie, has no fever, malaise, or EM rash) or if a patient does not live in or has not recently traveled to an endemic area because it would be highly unlikely the patient has LD.9,10 If the patient reports known contact with a tick and has a rash suspicious for EM, the diagnosis may be made without confirmatory testing because EM is pathognomonic for LD.7,11 Serologic testing is not recommended in these cases, particularly if there is a single EM lesion, since the lesion often presents prior to development of an immune response leading to seronegative results.8
Lyme serology is necessary if a patient presents with ocular manifestations known to be associated with LD and resides in, or has recently traveled to, an area where LD is endemic (ie, New England, Minnesota, or Wisconsin).7,12 These criteria are of particular importance: about 50% of patients do not recall a tick bite and 20% to 40% do not present with an EM.2,9
Diagnostic Testing
In 2019 the Centers for Disease Control and Prevention (CDC) updated their testing guidelines to the modified 2-tier testing (MTTT) method. The MTTT first recommends a Lyme enzyme immunoassay (EIA), with a second EIA recommended only if the first is positive.12-14 The MTTT method has better sensitivity in early localized LD compared to standard 2-tier testing.9,11,12 The CDC advises against the use of any laboratory serology tests not approved by the US Food and Drug Administration.13 The CDC also advises that LD serology testing should not be performed as a “test for cure,” because even after successful treatment, an individual may still test positive.1,9 Follow-up testing in patients treated early in the disease course (ie, in the setting of EM) may never have an antibody response. In these cases, a negative test should not exclude an LD diagnosis. 9 For patients with suspected neuroborreliosis, a lumbar puncture may not be needed if a patient already has a positive peripheral serology via the MTTT method.12 The Figure depicts a flow chart for the process of ordering and interpreting testing.
Most LD testing, if correlated with clinical disease, is positive after 4 to 6 weeks.9 If an eye disease is noted and the patient has positive Lyme serology, the patient should still be screened for Lyme neuroborreliosis of the central nervous system (CNS). Examination of the fundus for papilledema, review of symptoms of aseptic meningitis, and a careful neurologic examination should be performed.15
If CNS disease is suspected, the patient may need additional CNS testing to support treatment decisions. The 2020 Infectious Diseases Society of America Lyme guidelines recommend to: (1) obtain simultaneous samples of cerebrospinal fluid (CSF) and serum for determination of the CSF:serum antibody index; (2) do not obtain CSF serology without measurement of the CSF:serum antibody index; and (3) do not obtain routine polymerase chain reaction or culture of CSF or serum.15 Once an LD diagnosis is confirmed, the CDC recommends a course of 100 mg of oral doxycycline twice daily for 14 to 21 days or an antimicrobial equivalent (eg, amoxicillin) if doxycycline is contraindicated. However, the antimicrobial dosage may vary depending on the stage of LD.11 Patients with confirmed neuroborreliosis should be admitted for 14 days of intravenous ceftriaxone or intravenous penicillin.2
CONCLUSIONS
To ensure timely diagnosis and treatment, eye care clinicians should be familiar with the appropriate diagnostic testing for patients suspected to have ocular manifestations of LD. For patients with suspected LD and a high pretest probability, clinicians should obtain a first-order Lyme EIA.12-14 If testing confirms LD, refer the patient to an infectious disease specialist for antimicrobial treatment and additional management.11
- Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW. Lyme borreliosis: diagnosis and management. BMJ. 2020;369:m1041. doi:10.1136/bmj.m1041
- Zaidman GW. The ocular manifestations of Lyme disease. Int Ophthalmol Clin. 1993;33(1):9-22. doi:10.1097/00004397-199303310-00004
- Lesser RL. Ocular manifestations of Lyme disease. Am J Med. 1995; 98(4A):60S-62S. doi:10.1016/s0002-9343(99)80045-x
- Mead P. Epidemiology of Lyme disease. Infect Dis Clin North Am. 2022;36(3):495-521. doi:10.1016/j.idc.2022.03.004
- Klig JE. Ophthalmologic complications of systemic disease. Emerg Med Clin North Am. 2008;26(1):217-viii. doi:10.1016/j.emc.2007.10.003
- Raja H, Starr MR, Bakri SJ. Ocular manifestations of tickborne diseases. Surv Ophthalmol. 2016;61(6):726-744. doi:10.1016/j.survophthal.2016.03.011
- Mora P, Carta A. Ocular manifestations of Lyme borreliosis in Europe. Int J Med Sci. 2009;6(3):124-125. doi:10.7150/ijms.6.124
- Mikkilä HO, Seppälä IJ, Viljanen MK, Peltomaa MP, Karma A. The expanding clinical spectrum of ocular lyme borreliosis. Ophthalmology. 2000;107(3):581-587. doi:10.1016/s0161-6420(99)00128-1
- Schriefer ME. Lyme disease diagnosis: serology. Clin Lab Med. 2015;35(4):797-814. doi:10.1016/j.cll.2015.08.001
- Beck AR, Marx GE, Hinckley AF. Diagnosis, treatment, and prevention practices for Lyme disease by clinicians, United States, 2013-2015. Public Health Rep. 2021;136(5):609- 617. doi:10.1177/0033354920973235
- Wormser GP, McKenna D, Nowakowski J. Management approaches for suspected and established Lyme disease used at the Lyme disease diagnostic center. Wien Klin Wochenschr. 2018;130(15-16):463-467. doi:10.1007/s00508-015-0936-y
- Kobayashi T, Auwaerter PG. Diagnostic testing for Lyme disease. Infect Dis Clin North Am. 2022;36(3):605-620. doi:10.1016/j.idc.2022.04.001
- Mead P, Petersen J, Hinckley A. Updated CDC recommendation for serologic diagnosis of Lyme disease. MMWR Morb Mortal Wkly Rep. 2019;68(32):703. doi:10.15585/mmwr.mm6832a4
- Association of Public Health Laboratories. Suggested Reporting Language, Interpretation and Guidance Regarding Lyme Disease Serologic Test Results. April 2024. Accessed December 3, 2024. https://www.aphl.org/aboutAPHL/publications/Documents/ID-2024-Lyme-Disease-Serologic-Testing-Reporting.pdf
- Lantos PM, Rumbaugh P, Bockenstedt L, et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1-e48. doi:10.1093/cid/ciaa1215
Since Lyme disease (LD) was first identified in 1975, there has been uncertainty regarding the proper diagnostic testing for suspected cases.1 Challenges involved with ordering Lyme serology testing include navigating tests with an array of false negatives and false positives.2 Confounding these challenges is the wide variety of ocular manifestations of LD, ranging from nonspecific conjunctivitis, cranial palsies, and anterior and posterior segment inflammation.2,3 This article provides diagnostic testing guidelines for eye care clinicians who encounter patients with suspected LD.
BACKGROUND
LD is a bacterial infection caused by the spirochete Borrelia burgdorferi sensu lato complex transmitted by the Ixodes tick genus. There are 4 species of Ixodes ticks that can infect humans, and only 2 have been identified as principal vectors in North America: Ixodes scapularis and Ixodes pacificus. The incidence of LD is on the rise due to increasing global temperatures and expanding geographic borders for the organism. Cases in endemic areas range from 10 per 100,000 people to 50 per 100,000 people.4
LD occurs in 3 stages: early localized (stage 1), early disseminated (stage 2), and late disseminated (stage 3). In stage 1, patients typically present with erythema migrans (EM) rash (bull’s-eye cutaneous rash) and other nonspecific flu-like symptoms of fever, fatigue, and arthralgia. Stage 2 occurs several weeks to months after the initial infection and the infection has invaded other systemic organs, causing conditions like carditis, meningitis, and arthritis. A small subset of patients may progress to stage 3, which is characterized by chronic arthritis and chronic neurological LD.2,4,5 Ocular manifestations have been well-documented in all stages of LD but are more prevalent in early disseminated disease (Table).2,3,6,7
Indications
Recognizing common ocular manifestations associated with LD will allow eye care practitioners to make a timely diagnosis and initiate treatment. The most common ocular findings from LD include conjunctivitis, keratitis, cranial nerve VII palsy, optic neuritis, granulomatous iridocyclitis, and pars planitis.2,6 While retrospective studies suggest that up to 10% of patients with early localized LD have a nonspecific follicular conjunctivitis, those patients are unlikely to present for ocular evaluation. If a patient does present with an acute conjunctivitis, many clinicians do not consider LD in their differential diagnosis.8 In endemic areas, it is important to query patients for additional symptoms that may indicate LD.
Obtaining a complete patient history is vital in aiding a clinician’s decision to order Lyme serology for suspected LD. Epidemiology, history of geography/travel, pet exposure, sexual history (necessary to rule out other conditions [ie, syphilis] to direct appropriate diagnostic testing), and a complete review of systems should be obtained.2,4 LD may mimic other inflammatory autoimmune conditions or infectious diseases such as syphilis.2,5 This can lead to obtaining unnecessary Lyme serologies or failing to diagnose LD.5,7
Diagnostic testing is not indicated when a patient presents with an asymptomatic tick bite (ie, has no fever, malaise, or EM rash) or if a patient does not live in or has not recently traveled to an endemic area because it would be highly unlikely the patient has LD.9,10 If the patient reports known contact with a tick and has a rash suspicious for EM, the diagnosis may be made without confirmatory testing because EM is pathognomonic for LD.7,11 Serologic testing is not recommended in these cases, particularly if there is a single EM lesion, since the lesion often presents prior to development of an immune response leading to seronegative results.8
Lyme serology is necessary if a patient presents with ocular manifestations known to be associated with LD and resides in, or has recently traveled to, an area where LD is endemic (ie, New England, Minnesota, or Wisconsin).7,12 These criteria are of particular importance: about 50% of patients do not recall a tick bite and 20% to 40% do not present with an EM.2,9
Diagnostic Testing
In 2019 the Centers for Disease Control and Prevention (CDC) updated their testing guidelines to the modified 2-tier testing (MTTT) method. The MTTT first recommends a Lyme enzyme immunoassay (EIA), with a second EIA recommended only if the first is positive.12-14 The MTTT method has better sensitivity in early localized LD compared to standard 2-tier testing.9,11,12 The CDC advises against the use of any laboratory serology tests not approved by the US Food and Drug Administration.13 The CDC also advises that LD serology testing should not be performed as a “test for cure,” because even after successful treatment, an individual may still test positive.1,9 Follow-up testing in patients treated early in the disease course (ie, in the setting of EM) may never have an antibody response. In these cases, a negative test should not exclude an LD diagnosis. 9 For patients with suspected neuroborreliosis, a lumbar puncture may not be needed if a patient already has a positive peripheral serology via the MTTT method.12 The Figure depicts a flow chart for the process of ordering and interpreting testing.
Most LD testing, if correlated with clinical disease, is positive after 4 to 6 weeks.9 If an eye disease is noted and the patient has positive Lyme serology, the patient should still be screened for Lyme neuroborreliosis of the central nervous system (CNS). Examination of the fundus for papilledema, review of symptoms of aseptic meningitis, and a careful neurologic examination should be performed.15
If CNS disease is suspected, the patient may need additional CNS testing to support treatment decisions. The 2020 Infectious Diseases Society of America Lyme guidelines recommend to: (1) obtain simultaneous samples of cerebrospinal fluid (CSF) and serum for determination of the CSF:serum antibody index; (2) do not obtain CSF serology without measurement of the CSF:serum antibody index; and (3) do not obtain routine polymerase chain reaction or culture of CSF or serum.15 Once an LD diagnosis is confirmed, the CDC recommends a course of 100 mg of oral doxycycline twice daily for 14 to 21 days or an antimicrobial equivalent (eg, amoxicillin) if doxycycline is contraindicated. However, the antimicrobial dosage may vary depending on the stage of LD.11 Patients with confirmed neuroborreliosis should be admitted for 14 days of intravenous ceftriaxone or intravenous penicillin.2
CONCLUSIONS
To ensure timely diagnosis and treatment, eye care clinicians should be familiar with the appropriate diagnostic testing for patients suspected to have ocular manifestations of LD. For patients with suspected LD and a high pretest probability, clinicians should obtain a first-order Lyme EIA.12-14 If testing confirms LD, refer the patient to an infectious disease specialist for antimicrobial treatment and additional management.11
Since Lyme disease (LD) was first identified in 1975, there has been uncertainty regarding the proper diagnostic testing for suspected cases.1 Challenges involved with ordering Lyme serology testing include navigating tests with an array of false negatives and false positives.2 Confounding these challenges is the wide variety of ocular manifestations of LD, ranging from nonspecific conjunctivitis, cranial palsies, and anterior and posterior segment inflammation.2,3 This article provides diagnostic testing guidelines for eye care clinicians who encounter patients with suspected LD.
BACKGROUND
LD is a bacterial infection caused by the spirochete Borrelia burgdorferi sensu lato complex transmitted by the Ixodes tick genus. There are 4 species of Ixodes ticks that can infect humans, and only 2 have been identified as principal vectors in North America: Ixodes scapularis and Ixodes pacificus. The incidence of LD is on the rise due to increasing global temperatures and expanding geographic borders for the organism. Cases in endemic areas range from 10 per 100,000 people to 50 per 100,000 people.4
LD occurs in 3 stages: early localized (stage 1), early disseminated (stage 2), and late disseminated (stage 3). In stage 1, patients typically present with erythema migrans (EM) rash (bull’s-eye cutaneous rash) and other nonspecific flu-like symptoms of fever, fatigue, and arthralgia. Stage 2 occurs several weeks to months after the initial infection and the infection has invaded other systemic organs, causing conditions like carditis, meningitis, and arthritis. A small subset of patients may progress to stage 3, which is characterized by chronic arthritis and chronic neurological LD.2,4,5 Ocular manifestations have been well-documented in all stages of LD but are more prevalent in early disseminated disease (Table).2,3,6,7
Indications
Recognizing common ocular manifestations associated with LD will allow eye care practitioners to make a timely diagnosis and initiate treatment. The most common ocular findings from LD include conjunctivitis, keratitis, cranial nerve VII palsy, optic neuritis, granulomatous iridocyclitis, and pars planitis.2,6 While retrospective studies suggest that up to 10% of patients with early localized LD have a nonspecific follicular conjunctivitis, those patients are unlikely to present for ocular evaluation. If a patient does present with an acute conjunctivitis, many clinicians do not consider LD in their differential diagnosis.8 In endemic areas, it is important to query patients for additional symptoms that may indicate LD.
Obtaining a complete patient history is vital in aiding a clinician’s decision to order Lyme serology for suspected LD. Epidemiology, history of geography/travel, pet exposure, sexual history (necessary to rule out other conditions [ie, syphilis] to direct appropriate diagnostic testing), and a complete review of systems should be obtained.2,4 LD may mimic other inflammatory autoimmune conditions or infectious diseases such as syphilis.2,5 This can lead to obtaining unnecessary Lyme serologies or failing to diagnose LD.5,7
Diagnostic testing is not indicated when a patient presents with an asymptomatic tick bite (ie, has no fever, malaise, or EM rash) or if a patient does not live in or has not recently traveled to an endemic area because it would be highly unlikely the patient has LD.9,10 If the patient reports known contact with a tick and has a rash suspicious for EM, the diagnosis may be made without confirmatory testing because EM is pathognomonic for LD.7,11 Serologic testing is not recommended in these cases, particularly if there is a single EM lesion, since the lesion often presents prior to development of an immune response leading to seronegative results.8
Lyme serology is necessary if a patient presents with ocular manifestations known to be associated with LD and resides in, or has recently traveled to, an area where LD is endemic (ie, New England, Minnesota, or Wisconsin).7,12 These criteria are of particular importance: about 50% of patients do not recall a tick bite and 20% to 40% do not present with an EM.2,9
Diagnostic Testing
In 2019 the Centers for Disease Control and Prevention (CDC) updated their testing guidelines to the modified 2-tier testing (MTTT) method. The MTTT first recommends a Lyme enzyme immunoassay (EIA), with a second EIA recommended only if the first is positive.12-14 The MTTT method has better sensitivity in early localized LD compared to standard 2-tier testing.9,11,12 The CDC advises against the use of any laboratory serology tests not approved by the US Food and Drug Administration.13 The CDC also advises that LD serology testing should not be performed as a “test for cure,” because even after successful treatment, an individual may still test positive.1,9 Follow-up testing in patients treated early in the disease course (ie, in the setting of EM) may never have an antibody response. In these cases, a negative test should not exclude an LD diagnosis. 9 For patients with suspected neuroborreliosis, a lumbar puncture may not be needed if a patient already has a positive peripheral serology via the MTTT method.12 The Figure depicts a flow chart for the process of ordering and interpreting testing.
Most LD testing, if correlated with clinical disease, is positive after 4 to 6 weeks.9 If an eye disease is noted and the patient has positive Lyme serology, the patient should still be screened for Lyme neuroborreliosis of the central nervous system (CNS). Examination of the fundus for papilledema, review of symptoms of aseptic meningitis, and a careful neurologic examination should be performed.15
If CNS disease is suspected, the patient may need additional CNS testing to support treatment decisions. The 2020 Infectious Diseases Society of America Lyme guidelines recommend to: (1) obtain simultaneous samples of cerebrospinal fluid (CSF) and serum for determination of the CSF:serum antibody index; (2) do not obtain CSF serology without measurement of the CSF:serum antibody index; and (3) do not obtain routine polymerase chain reaction or culture of CSF or serum.15 Once an LD diagnosis is confirmed, the CDC recommends a course of 100 mg of oral doxycycline twice daily for 14 to 21 days or an antimicrobial equivalent (eg, amoxicillin) if doxycycline is contraindicated. However, the antimicrobial dosage may vary depending on the stage of LD.11 Patients with confirmed neuroborreliosis should be admitted for 14 days of intravenous ceftriaxone or intravenous penicillin.2
CONCLUSIONS
To ensure timely diagnosis and treatment, eye care clinicians should be familiar with the appropriate diagnostic testing for patients suspected to have ocular manifestations of LD. For patients with suspected LD and a high pretest probability, clinicians should obtain a first-order Lyme EIA.12-14 If testing confirms LD, refer the patient to an infectious disease specialist for antimicrobial treatment and additional management.11
- Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW. Lyme borreliosis: diagnosis and management. BMJ. 2020;369:m1041. doi:10.1136/bmj.m1041
- Zaidman GW. The ocular manifestations of Lyme disease. Int Ophthalmol Clin. 1993;33(1):9-22. doi:10.1097/00004397-199303310-00004
- Lesser RL. Ocular manifestations of Lyme disease. Am J Med. 1995; 98(4A):60S-62S. doi:10.1016/s0002-9343(99)80045-x
- Mead P. Epidemiology of Lyme disease. Infect Dis Clin North Am. 2022;36(3):495-521. doi:10.1016/j.idc.2022.03.004
- Klig JE. Ophthalmologic complications of systemic disease. Emerg Med Clin North Am. 2008;26(1):217-viii. doi:10.1016/j.emc.2007.10.003
- Raja H, Starr MR, Bakri SJ. Ocular manifestations of tickborne diseases. Surv Ophthalmol. 2016;61(6):726-744. doi:10.1016/j.survophthal.2016.03.011
- Mora P, Carta A. Ocular manifestations of Lyme borreliosis in Europe. Int J Med Sci. 2009;6(3):124-125. doi:10.7150/ijms.6.124
- Mikkilä HO, Seppälä IJ, Viljanen MK, Peltomaa MP, Karma A. The expanding clinical spectrum of ocular lyme borreliosis. Ophthalmology. 2000;107(3):581-587. doi:10.1016/s0161-6420(99)00128-1
- Schriefer ME. Lyme disease diagnosis: serology. Clin Lab Med. 2015;35(4):797-814. doi:10.1016/j.cll.2015.08.001
- Beck AR, Marx GE, Hinckley AF. Diagnosis, treatment, and prevention practices for Lyme disease by clinicians, United States, 2013-2015. Public Health Rep. 2021;136(5):609- 617. doi:10.1177/0033354920973235
- Wormser GP, McKenna D, Nowakowski J. Management approaches for suspected and established Lyme disease used at the Lyme disease diagnostic center. Wien Klin Wochenschr. 2018;130(15-16):463-467. doi:10.1007/s00508-015-0936-y
- Kobayashi T, Auwaerter PG. Diagnostic testing for Lyme disease. Infect Dis Clin North Am. 2022;36(3):605-620. doi:10.1016/j.idc.2022.04.001
- Mead P, Petersen J, Hinckley A. Updated CDC recommendation for serologic diagnosis of Lyme disease. MMWR Morb Mortal Wkly Rep. 2019;68(32):703. doi:10.15585/mmwr.mm6832a4
- Association of Public Health Laboratories. Suggested Reporting Language, Interpretation and Guidance Regarding Lyme Disease Serologic Test Results. April 2024. Accessed December 3, 2024. https://www.aphl.org/aboutAPHL/publications/Documents/ID-2024-Lyme-Disease-Serologic-Testing-Reporting.pdf
- Lantos PM, Rumbaugh P, Bockenstedt L, et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1-e48. doi:10.1093/cid/ciaa1215
- Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW. Lyme borreliosis: diagnosis and management. BMJ. 2020;369:m1041. doi:10.1136/bmj.m1041
- Zaidman GW. The ocular manifestations of Lyme disease. Int Ophthalmol Clin. 1993;33(1):9-22. doi:10.1097/00004397-199303310-00004
- Lesser RL. Ocular manifestations of Lyme disease. Am J Med. 1995; 98(4A):60S-62S. doi:10.1016/s0002-9343(99)80045-x
- Mead P. Epidemiology of Lyme disease. Infect Dis Clin North Am. 2022;36(3):495-521. doi:10.1016/j.idc.2022.03.004
- Klig JE. Ophthalmologic complications of systemic disease. Emerg Med Clin North Am. 2008;26(1):217-viii. doi:10.1016/j.emc.2007.10.003
- Raja H, Starr MR, Bakri SJ. Ocular manifestations of tickborne diseases. Surv Ophthalmol. 2016;61(6):726-744. doi:10.1016/j.survophthal.2016.03.011
- Mora P, Carta A. Ocular manifestations of Lyme borreliosis in Europe. Int J Med Sci. 2009;6(3):124-125. doi:10.7150/ijms.6.124
- Mikkilä HO, Seppälä IJ, Viljanen MK, Peltomaa MP, Karma A. The expanding clinical spectrum of ocular lyme borreliosis. Ophthalmology. 2000;107(3):581-587. doi:10.1016/s0161-6420(99)00128-1
- Schriefer ME. Lyme disease diagnosis: serology. Clin Lab Med. 2015;35(4):797-814. doi:10.1016/j.cll.2015.08.001
- Beck AR, Marx GE, Hinckley AF. Diagnosis, treatment, and prevention practices for Lyme disease by clinicians, United States, 2013-2015. Public Health Rep. 2021;136(5):609- 617. doi:10.1177/0033354920973235
- Wormser GP, McKenna D, Nowakowski J. Management approaches for suspected and established Lyme disease used at the Lyme disease diagnostic center. Wien Klin Wochenschr. 2018;130(15-16):463-467. doi:10.1007/s00508-015-0936-y
- Kobayashi T, Auwaerter PG. Diagnostic testing for Lyme disease. Infect Dis Clin North Am. 2022;36(3):605-620. doi:10.1016/j.idc.2022.04.001
- Mead P, Petersen J, Hinckley A. Updated CDC recommendation for serologic diagnosis of Lyme disease. MMWR Morb Mortal Wkly Rep. 2019;68(32):703. doi:10.15585/mmwr.mm6832a4
- Association of Public Health Laboratories. Suggested Reporting Language, Interpretation and Guidance Regarding Lyme Disease Serologic Test Results. April 2024. Accessed December 3, 2024. https://www.aphl.org/aboutAPHL/publications/Documents/ID-2024-Lyme-Disease-Serologic-Testing-Reporting.pdf
- Lantos PM, Rumbaugh P, Bockenstedt L, et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 guidelines for the prevention, diagnosis and treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1-e48. doi:10.1093/cid/ciaa1215
Diagnostic Testing for Patients With Suspected Ocular Manifestations of Lyme Disease
Diagnostic Testing for Patients With Suspected Ocular Manifestations of Lyme Disease

When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
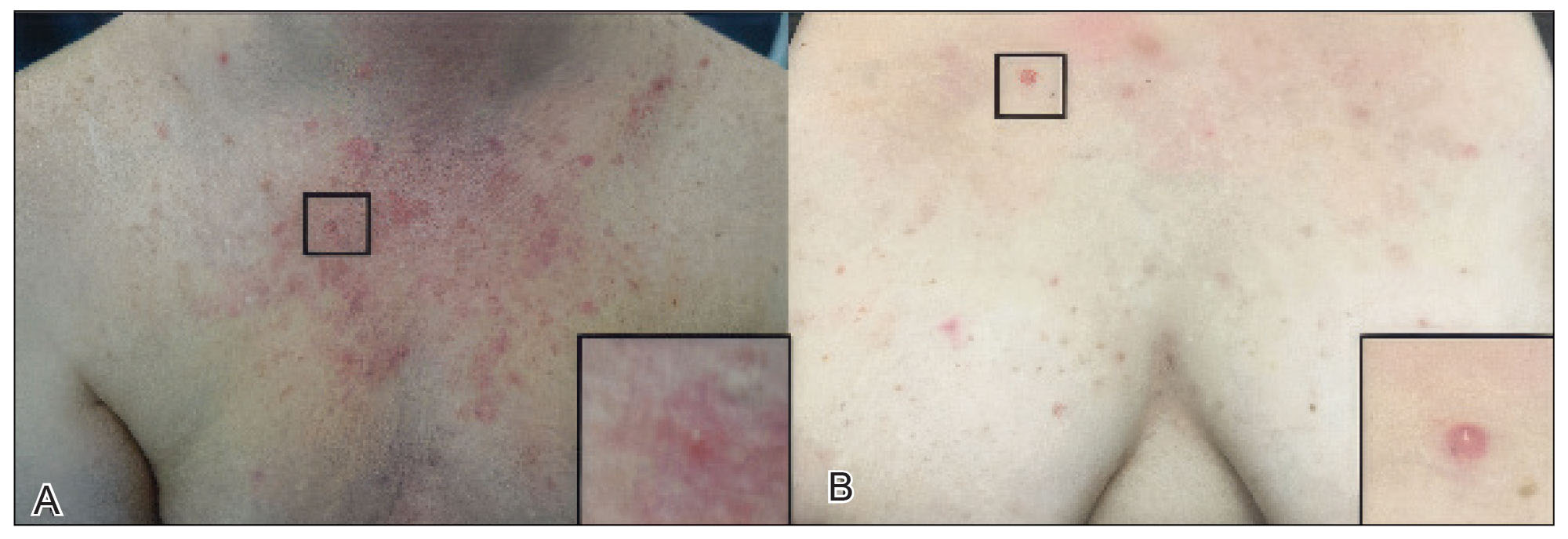
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).

Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
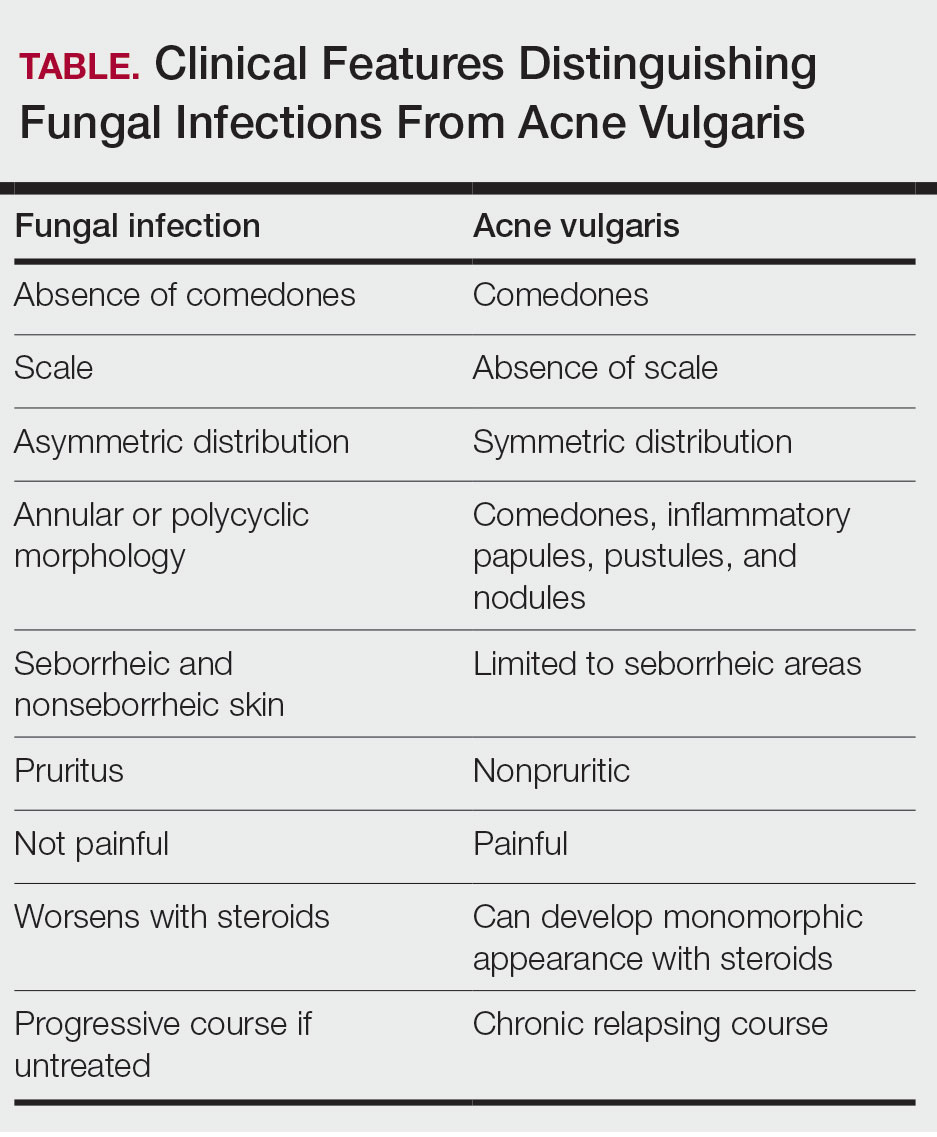
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
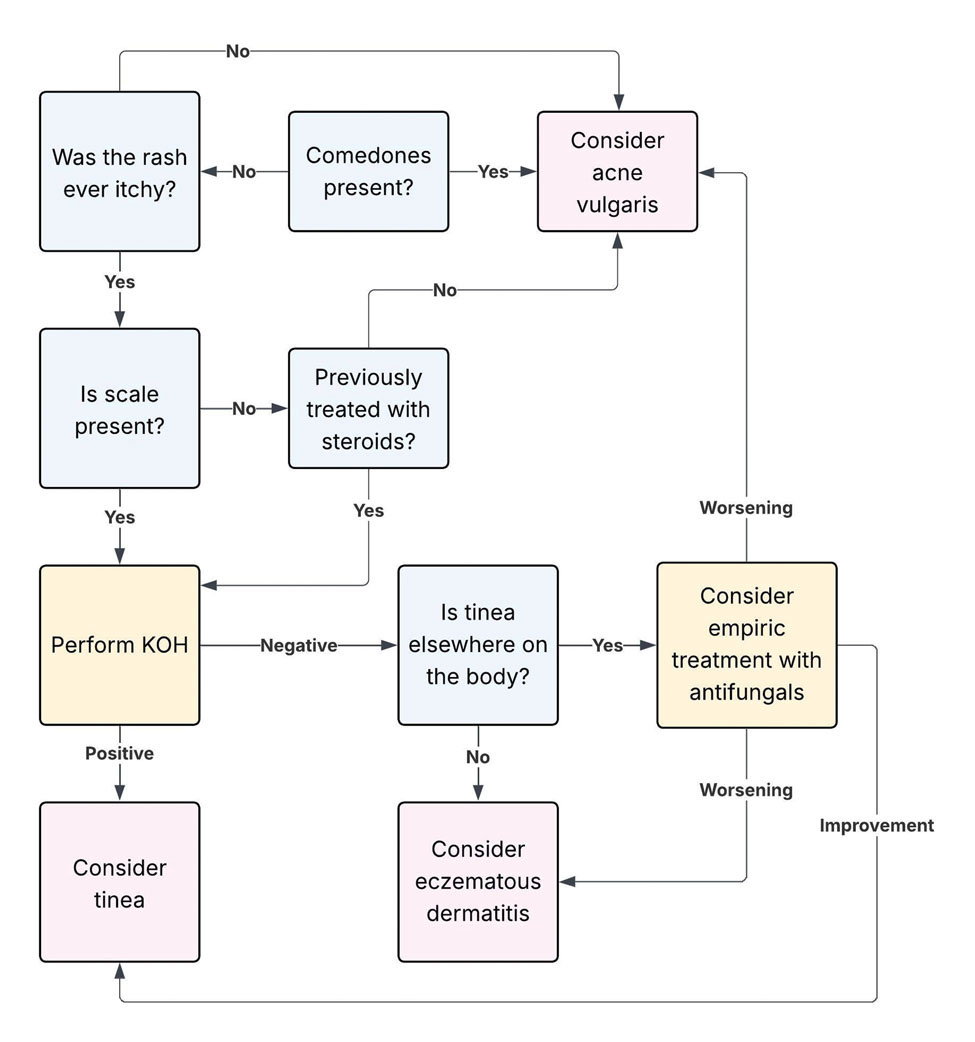
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Practice Points
- Folliculocentric pustules and/or papules from dermatophytes (including tinea incognita and Majocchi granuloma) or Malassezia folliculitis can closely mimic acne, especially following steroid use.
- Key red flags for dermatophyte infection include an absence of comedones, pruritus, and asymmetric or localized lesions in sebum‐rich zones.
- Bedside tools such as dermoscopy, Wood lamp examination, and in-office potassium hydroxide preparation can provide rapid differentiation between dermatophyte infections and acne.
- Prompt antifungal treatment and avoidance of topical steroids can prevent deeper fungal invasion.

Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
PRACTICE POINTS
- Horse flies (Tabanidae) are hematophagous insects that can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers or systemic illness.
- Mild reactions are managed symptomatically; anaphylaxis requires epinephrine, and tularemia requires systemic antibiotics such as gentamicin.
- Patients should be counseled on avoidance strategies, including wearing protective clothing and using topical repellents and environmental traps.

Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?

Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Several newly identified biomarkers can help distinguish invasive aspergillosis from aspergillus colonization in lung transplant recipients, according to data from a new study presented at the annual meeting of the International Society for Heart and Lung Transplantation.
Aspergillus, a common environmental mold, can cause potentially serious infection or asymptomatic colonization in patients who have significant lung disease or are immunosuppressed, said Aaron Mishkin, MD, associate professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, who was not involved in the study.
“Determining if the aspergillus that is present is a colonizing organism vs disease is challenging clinically,” Mishkin said. Clinicians currently rely on criteria including a compatible patient, imaging findings, and a laboratory-based diagnostic such as tissue from a biopsy, cultures, polymerase chain reaction (PCR), or fungal antigen detection, said Mishkin. “Fungal antigen detection has variable specificity and sensitivity,” he noted. New biomarkers that look for an immune response could help differentiate between colonization and infection by assessing an immune-mediated inflammatory response, the hallmark of infection, he said.
To tease out potential biomarkers associated with invasive aspergillosis, Christine Ng, MS, a researcher at the University Health Network, Toronto, Ontario, Canada, and colleagues performed RNA sequencing on samples from 14 control lung transplant patients, 34 with aspergillus colonization, and seven with invasive aspergillosis. They identified potential candidate genes in 15 control samples, 17 aspergillus colonization samples, and 15 invasive aspergillosis samples.
Overall, signaling pathway analysis showed robust immune response, T-cell immunity, and leukocyte immunity in patients with invasive aspergillosis. By contrast, patients with aspergillus colonization showed enriched cellular responses (response to stimuli, epithelium development).
In a real-time quantitative PCR analysis, the researchers validated three biomarkers specific to invasive aspergillosis (IRF7, ZBP1, CYP27B1). Biomarkers AKR1C2, FGF10, and VGLL3 demonstrated specificity for aspergillus colonization. Additionally, biomarkers PTGER3, LPAR3, and COL14A1 were significant when aspergillus colonization was compared to controls but not in comparisons between invasive aspergillosis and aspergillus colonization.
The study findings were limited by the small sample size, and larger studies are needed before they can be implemented in clinical practice, the researchers wrote. However, the results suggest that the new biomarkers reveal distinct host immune patterns and may improve differentiation of aspergillosis from colonization in lung transplant recipients, they concluded.
Clinical Implications and Next Steps
RNA testing can help differentiate colonization vs infection, Mishkin said. “Colonization is not typically treated, whereas infection would be treated with an anti-fungal and, in the case of a transplant recipient, a reduction in immunosuppression,” he said. “In lung transplantation, a delicate equilibrium must be maintained between achieving optimal immunosuppression and minimizing or treating infection. Any tools that can aid in this decision-making have the potential to enhance patient outcomes,” he added.
The current study was limited by the use of data only from a single center, and the broader applicability to additional populations, broader geographic areas, and a larger number of organisms remains unknown, Mishkin said. “This type of assay does have the possibility of applicability to a larger number of fungal and even bacterial species,” he noted.
A version of this article first appeared on Medscape.com.
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Biomarkers Pinpoint Invasive Aspergillosis in Lung Transplant Recipients
Chromoblastomycosis Leading to Squamous Cell Carcinoma: An Overlooked Outcome of a Neglected Tropical Disease
Chromoblastomycosis Leading to Squamous Cell Carcinoma: An Overlooked Outcome of a Neglected Tropical Disease
Chromoblastomycosis is a neglected tropical implantation mycosis caused by dematiaceous fungi that leads to substantial morbidity. This condition is diagnosed microscopically by visualizing the characteristic thick-walled, single, or multicellular clusters of pigmented fungal cells (also known as medlar bodies, muriform cells, or sclerotic bodies).1 The main causative fungi varies by geographic region, but most commonly is caused by Cladophialophora carrionii, Fonsecaea species, Phialophora verrucosa species complex, and Rhinocladiella aquaspersa.2-4 Standardized treatment guidelines have not been established, but itraconazole typically is considered first-line regardless of causative fungi.5 Terbinafine, other azoles, and topical immunomodulators, either as monotherapy or in combination, may be appropriate alternative or adjunctive options for refractory disease, although supporting data are limited.6-9
Complications from chromoblastomycosis are common, particularly in long-standing, severe, or refractory disease. An analysis using billing codes in the United States found 14% (35/255) of hospitalized patients with chromoblastomycosis had lymphedema.10 In Mexico, 63% (32/51) of patients with chromoblastomycosis developed secondary bacterial infections.11 Skin fibrosis and ankylosis also can occur and cause mobility issues and decreased quality of life. An infrequent but potentially life-threatening complication12 is the development of squamous cell carcinoma (SCC) associated with chronic lesions, representing a preventable end-stage complication of delayed diagnosis and treatment (Figure).
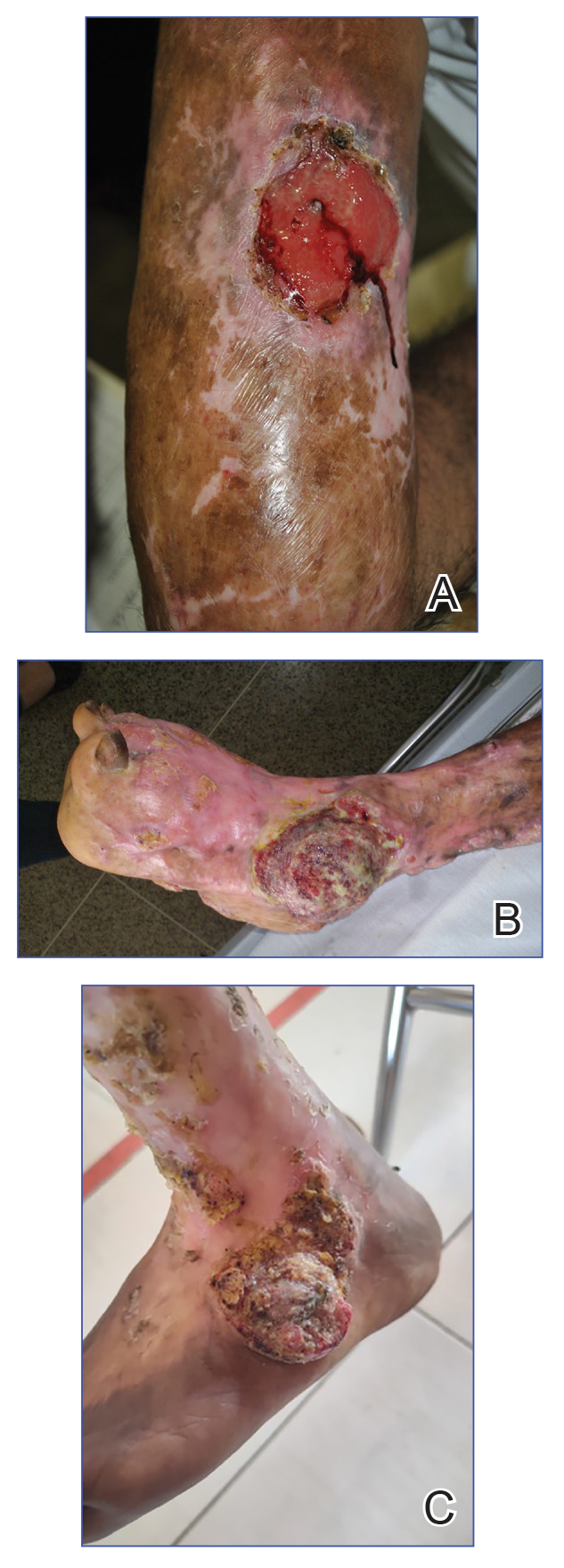
In this review, we summarize reported epidemiology and clinical risk factors for SCC complicating chromoblastomycosis. We also discuss plausible inflammatory mechanisms of malignant transformation and propose pragmatic clinical and public health interventions, including decentralized microscopy-based diagnosis, timely antifungal access, and biopsy-triggered surveillance of chronically inflamed lesions, to reduce preventable morbidity.
Epidemiology and Risk Factors
The epidemiology of SCC developing from chromoblastomycosis is not well understood due to gaps in national and global surveillance. Some studies have found that 2% to 13% of patients with chromoblastomycosis developed SCC.4,11,13-15 Based on case reports and case series, a symptom duration of more than 10 years appears to be the most substantial risk factor for the development of SCC rather than host immune status.16-18 Severity, specifically the size of the injury, and vegetating lesions also have been suggested as risk factors for the development of SCC.16 Additionally, the appearance of new lesions (mainly ulcers not related to secondary infection) that appear during the healing phase should raise the suspicion of SCC and warrant a biopsy for evaluation.16
Pathophysiology
The exact mechanism of malignant transformation has not been elucidated, but histopathologic features suggest substantial epidermal proliferation. In some cases, this leads to pseudoepitheliomatous hyperplasia, a nonmalignant hyperproliferative state that is an important differential HPV to leishmaniasis and lupus vulgaris.19 The chronic inflammation from long-standing chromoblastomycosis likely contributes to the further malignant transformation to SCC.
Polymorphonuclear cells and activated macrophages seen in chronic inflammation can promote the release of enzymes and free radicals that has led to malignant transformation in vitro but has not been investigated specifically in chromoblastomycosis.16 Additionally, chronic inflammation and metabolic products of phagocytosis often are accompanied by excessive production of reactive oxygen and nitrogen species, which can damage DNA, lipoproteins, and cell membranes. Other potential contributors include the expression of cyclooxygenase 2 and release of arachidonic acid metabolites (eg, prostaglandins, leukotrienes), which can damage the cell and promote carcinogenesis. It is not clear whether similar mechanisms account for the development of SCCs in other chronic skin inflammations or infections such as cutaneous tuberculosis or Marjolin ulcers.20
Clinical and Public Health Interventions
Squamous cell carcinoma arising in the setting of chromoblastomycosis warrants prompt oncologic evaluation and definitive surgical management, which may require extensive surgical excision and, in advanced disease, amputation.14,17,18 Advanced malignant tumors can be difficult to manage and can result in death.21,22 Additionally, clinicians should maintain a low threshold for biopsy in long-standing chromoblastomycosis, particularly when lesions demonstrate new ulceration, rapid growth, bleeding, pain, malodor, or failure to improve with appropriate antifungal therapy.16 Recurrent or new lesions after amputation may indicate persistent or recurrent infection and may require continued antifungal management alongside cancer care.16
Squamous cell carcinoma arising from chromoblastomycosis results after substantial diagnostic delays, allowing chronic inflammation to transform infection into malignancy. Separating benign inflammation-associated epidermal proliferation from transformation to SCC requires histopathologic skill. An assay based on increased expression of chromosome 15 open reading frame 48 (C15orf48), an immune regulatory protein, has been developed to aid in this distinction; however, it is not widely available.23
Raising awareness of chromoblastomycosis among clinicians and communities, particularly in rural areas where the disease is more common, is critical to improve health care–seeking behaviors and expedite access to care pathways.2 Furthermore, access and training on microscopy to diagnose chromoblastomycosis in decentralized areas can facilitate earlier diagnosis in primary health care settings rather than waiting for diagnosis in tertiary care settings, at which point disease usually is advanced. Global implementation of existing programs that use microscopy (eg, malaria in rural areas) can be partnered with frontline health worker cross-training on chromoblastomycosis diagnosis to improve appropriate identification of disease.24 Finally, improving access to affordable antifungals, particularly itraconazole, is necessary along with further research into novel therapeutic strategies. Approaches that utilize local manufacturing and pooled procurement could help expand treatment availability in parallel with diagnostic improvement initiatives.25
Final Thoughts
Squamous cell carcinoma resulting from chromoblastomycosis is a devastating complication, often leading to limb amputation. The true prevalence is unknown, but it occurs more commonly in long-standing disease without appropriate therapy. The appearance of new lesions or ulcers after initial improvement should increase suspicion and lead to biopsy and careful pathologic evaluation. Prevention of SCC requires increased clinical awareness, early diagnosis, and timely initiation of antifungal treatment. Enhanced surveillance among individuals with chromoblastomycosis would help to better understand its prevalence, associated risk factors, and impact on quality of life.
- Queiroz-Telles F, de Hoog S, Santos DWCL, et al. Chromoblastomycosis. Clin Microbiol Rev. 2017;30:233-276.
- Smith DJ, Queiroz-Telles F, Rabenja FR, et al. A global chromoblastomycosis strategy and development of the global chromoblastomycosis working group. PLoS Negl Trop Dis. 2024;18:E0012562.
- Yen JS, Shih IH, Chung WH, et al. Chromoblastomycosis in northern Taiwan from 2017 to 2024: unique characteristics. Clin Exp Dermatol. Published online July 18, 2025. doi:10.1093/ced/llaf329
- Santos DWCL, Vicente VA, Weiss VA, et al. Chromoblastomycosis in an endemic area of Brazil: a clinical-epidemiological analysis and a worldwide haplotype network. J Fungi. 2020;6:204.
- Smith DJ, Melhem MSC, Dirven J, et al. Establishment of epidemiological cutoff values for Fonsecaea pedrosoi, the primary etiologic agent of chromoblastomycosis, and eight antifungal medications. J Clin Microbiol. 2025;63:E01903-24.
- Logan C, Singh M, Fox N, et al. Chromoblastomycosis treated with posaconazole and adjunctive imiquimod: lending innate immunity a helping hand. Open Forum Infect Dis. 2023;10:ofad124.
- de Sousa M da GT, Belda W, Spina R, et al. Topical application of imiquimod as a treatment for chromoblastomycosis. Clin Infect Dis. 2014;58:1734-1737.
- Criado PR, Careta MF, Valente NYS, et al. Extensive long-standing chromomycosis due to Fonsecaea pedrosoi: three cases with relevant improvement under voriconazole therapy. J Dermatol Treat. 2011;22:167-174.
- Esterre P, Inzan CK, Ramarcel ER, et al. Treatment of chromomycosis with terbinafine: preliminary results of an open pilot study. Br J Dermatol. 1996;134:33-36.
- Smith DJ, Benedict K, Lockhart SR, et al. Chromoblastomycosis and phaeohyphomycotic abscess-associated hospitalizations, United States, 2016–2021. PLoS Negl Trop Dis. 2025;19:E0013499.
- Bonifaz A, Carrasco‐Gerard E, Saúl A. Chromoblastomycosis: clinical and mycologic experience of 51 cases. Mycoses. 2001;44:1-7.
- Torres E, Beristain JG, Lievanos Z, et al. Chromoblastomycosis associated with a lethal squamous cell carcinoma. An Bras Dermatol. 2010;85:267-270.
- Verma S, Thakur BK, Raphael V, et al. Epidemiology of subcutaneous mycoses in northeast India: a retrospective study. Indian J Dermatol. 2018;63:496-501.
- Siregar GO, Harianja M, Rinonce HT, et al. Chromoblastomycosis: a case series from Sumba, eastern Indonesia. Clin Exp Dermatol. 2025;50:1447-1450.
- Valentin J, Grotta G, Muller T, et al. Chromoblastomycosis in French Guiana: epidemiology and practices, 1955-2023. J Fungi. 2024;10:168.
- Azevedo CMPS, Marques SG, Santos DWCL, et al. Squamous cell carcinoma derived from chronic chromoblastomycosis in Brazil. Clin Infect Dis. 2015;60:1500-1504.
- Belda Jr W, Criado PR, Casteleti P, et al. Chromoblastomycosis evolving to sarcomatoid squamous cell carcinoma: a case report. Dermatol Rep. 2021;13:9009.
- Jamil A, Lee YY, Thevarajah S. Invasive squamous cell carcinoma arising from chromoblastomycosis. Med Mycol. 2012;50:99-102.
- Delahaye T, Orduz-Robledo M, Beltran A M, et al. Pseudo-epitheliomatous hyperplasia and skin infections. Open Dermatol J. 2024;18:E18743722304513.
- Fania L, Didona D, Di Pietro FR, et al. Cutaneous squamous cell carcinoma: from pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9:171.
- Torres E, Beristain JG, Lievanos Z, et al. Carcinoma epidermoide como complicação letal de lesões crônicas de cromoblastomicose. An Bras Dermatol. 2010;85:267-270.
- Rojas OC, González GM, Moreno-Treviño M, et al. Chromoblastomycosis by Cladophialophora carrionii associated with squamous cell carcinoma and review of published reports. Mycopathologia. 2015;179:153-157.
- Su A, Ra S, Li X, et al. Differentiating cutaneous squamous cell carcinoma and pseudoepitheliomatous hyperplasia by multiplex qRT-PCR. Mod Pathol. 2013;26:1433-1437.
- Siregar GO, Harianja M, Smith DJ, et al. Leveraging malaria microscopy infrastructure to diagnose common and neglected skin diseases using direct microscopy in Sumba, Indonesia. Lancet Reg Health - West Pac. 2025;64:101739.
- Smith DJ, Soebono H, Parajuli N, et al. South-East Asia regional neglected tropical disease framework: improving control of mycetoma, chromoblastomycosis, and sporotrichosis. Lancet Reg Health Southeast Asia. 2025;35:100561.
Chromoblastomycosis is a neglected tropical implantation mycosis caused by dematiaceous fungi that leads to substantial morbidity. This condition is diagnosed microscopically by visualizing the characteristic thick-walled, single, or multicellular clusters of pigmented fungal cells (also known as medlar bodies, muriform cells, or sclerotic bodies).1 The main causative fungi varies by geographic region, but most commonly is caused by Cladophialophora carrionii, Fonsecaea species, Phialophora verrucosa species complex, and Rhinocladiella aquaspersa.2-4 Standardized treatment guidelines have not been established, but itraconazole typically is considered first-line regardless of causative fungi.5 Terbinafine, other azoles, and topical immunomodulators, either as monotherapy or in combination, may be appropriate alternative or adjunctive options for refractory disease, although supporting data are limited.6-9
Complications from chromoblastomycosis are common, particularly in long-standing, severe, or refractory disease. An analysis using billing codes in the United States found 14% (35/255) of hospitalized patients with chromoblastomycosis had lymphedema.10 In Mexico, 63% (32/51) of patients with chromoblastomycosis developed secondary bacterial infections.11 Skin fibrosis and ankylosis also can occur and cause mobility issues and decreased quality of life. An infrequent but potentially life-threatening complication12 is the development of squamous cell carcinoma (SCC) associated with chronic lesions, representing a preventable end-stage complication of delayed diagnosis and treatment (Figure).
In this review, we summarize reported epidemiology and clinical risk factors for SCC complicating chromoblastomycosis. We also discuss plausible inflammatory mechanisms of malignant transformation and propose pragmatic clinical and public health interventions, including decentralized microscopy-based diagnosis, timely antifungal access, and biopsy-triggered surveillance of chronically inflamed lesions, to reduce preventable morbidity.
Epidemiology and Risk Factors
The epidemiology of SCC developing from chromoblastomycosis is not well understood due to gaps in national and global surveillance. Some studies have found that 2% to 13% of patients with chromoblastomycosis developed SCC.4,11,13-15 Based on case reports and case series, a symptom duration of more than 10 years appears to be the most substantial risk factor for the development of SCC rather than host immune status.16-18 Severity, specifically the size of the injury, and vegetating lesions also have been suggested as risk factors for the development of SCC.16 Additionally, the appearance of new lesions (mainly ulcers not related to secondary infection) that appear during the healing phase should raise the suspicion of SCC and warrant a biopsy for evaluation.16
Pathophysiology
The exact mechanism of malignant transformation has not been elucidated, but histopathologic features suggest substantial epidermal proliferation. In some cases, this leads to pseudoepitheliomatous hyperplasia, a nonmalignant hyperproliferative state that is an important differential HPV to leishmaniasis and lupus vulgaris.19 The chronic inflammation from long-standing chromoblastomycosis likely contributes to the further malignant transformation to SCC.
Polymorphonuclear cells and activated macrophages seen in chronic inflammation can promote the release of enzymes and free radicals that has led to malignant transformation in vitro but has not been investigated specifically in chromoblastomycosis.16 Additionally, chronic inflammation and metabolic products of phagocytosis often are accompanied by excessive production of reactive oxygen and nitrogen species, which can damage DNA, lipoproteins, and cell membranes. Other potential contributors include the expression of cyclooxygenase 2 and release of arachidonic acid metabolites (eg, prostaglandins, leukotrienes), which can damage the cell and promote carcinogenesis. It is not clear whether similar mechanisms account for the development of SCCs in other chronic skin inflammations or infections such as cutaneous tuberculosis or Marjolin ulcers.20
Clinical and Public Health Interventions
Squamous cell carcinoma arising in the setting of chromoblastomycosis warrants prompt oncologic evaluation and definitive surgical management, which may require extensive surgical excision and, in advanced disease, amputation.14,17,18 Advanced malignant tumors can be difficult to manage and can result in death.21,22 Additionally, clinicians should maintain a low threshold for biopsy in long-standing chromoblastomycosis, particularly when lesions demonstrate new ulceration, rapid growth, bleeding, pain, malodor, or failure to improve with appropriate antifungal therapy.16 Recurrent or new lesions after amputation may indicate persistent or recurrent infection and may require continued antifungal management alongside cancer care.16
Squamous cell carcinoma arising from chromoblastomycosis results after substantial diagnostic delays, allowing chronic inflammation to transform infection into malignancy. Separating benign inflammation-associated epidermal proliferation from transformation to SCC requires histopathologic skill. An assay based on increased expression of chromosome 15 open reading frame 48 (C15orf48), an immune regulatory protein, has been developed to aid in this distinction; however, it is not widely available.23
Raising awareness of chromoblastomycosis among clinicians and communities, particularly in rural areas where the disease is more common, is critical to improve health care–seeking behaviors and expedite access to care pathways.2 Furthermore, access and training on microscopy to diagnose chromoblastomycosis in decentralized areas can facilitate earlier diagnosis in primary health care settings rather than waiting for diagnosis in tertiary care settings, at which point disease usually is advanced. Global implementation of existing programs that use microscopy (eg, malaria in rural areas) can be partnered with frontline health worker cross-training on chromoblastomycosis diagnosis to improve appropriate identification of disease.24 Finally, improving access to affordable antifungals, particularly itraconazole, is necessary along with further research into novel therapeutic strategies. Approaches that utilize local manufacturing and pooled procurement could help expand treatment availability in parallel with diagnostic improvement initiatives.25
Final Thoughts
Squamous cell carcinoma resulting from chromoblastomycosis is a devastating complication, often leading to limb amputation. The true prevalence is unknown, but it occurs more commonly in long-standing disease without appropriate therapy. The appearance of new lesions or ulcers after initial improvement should increase suspicion and lead to biopsy and careful pathologic evaluation. Prevention of SCC requires increased clinical awareness, early diagnosis, and timely initiation of antifungal treatment. Enhanced surveillance among individuals with chromoblastomycosis would help to better understand its prevalence, associated risk factors, and impact on quality of life.
Chromoblastomycosis is a neglected tropical implantation mycosis caused by dematiaceous fungi that leads to substantial morbidity. This condition is diagnosed microscopically by visualizing the characteristic thick-walled, single, or multicellular clusters of pigmented fungal cells (also known as medlar bodies, muriform cells, or sclerotic bodies).1 The main causative fungi varies by geographic region, but most commonly is caused by Cladophialophora carrionii, Fonsecaea species, Phialophora verrucosa species complex, and Rhinocladiella aquaspersa.2-4 Standardized treatment guidelines have not been established, but itraconazole typically is considered first-line regardless of causative fungi.5 Terbinafine, other azoles, and topical immunomodulators, either as monotherapy or in combination, may be appropriate alternative or adjunctive options for refractory disease, although supporting data are limited.6-9
Complications from chromoblastomycosis are common, particularly in long-standing, severe, or refractory disease. An analysis using billing codes in the United States found 14% (35/255) of hospitalized patients with chromoblastomycosis had lymphedema.10 In Mexico, 63% (32/51) of patients with chromoblastomycosis developed secondary bacterial infections.11 Skin fibrosis and ankylosis also can occur and cause mobility issues and decreased quality of life. An infrequent but potentially life-threatening complication12 is the development of squamous cell carcinoma (SCC) associated with chronic lesions, representing a preventable end-stage complication of delayed diagnosis and treatment (Figure).
In this review, we summarize reported epidemiology and clinical risk factors for SCC complicating chromoblastomycosis. We also discuss plausible inflammatory mechanisms of malignant transformation and propose pragmatic clinical and public health interventions, including decentralized microscopy-based diagnosis, timely antifungal access, and biopsy-triggered surveillance of chronically inflamed lesions, to reduce preventable morbidity.
Epidemiology and Risk Factors
The epidemiology of SCC developing from chromoblastomycosis is not well understood due to gaps in national and global surveillance. Some studies have found that 2% to 13% of patients with chromoblastomycosis developed SCC.4,11,13-15 Based on case reports and case series, a symptom duration of more than 10 years appears to be the most substantial risk factor for the development of SCC rather than host immune status.16-18 Severity, specifically the size of the injury, and vegetating lesions also have been suggested as risk factors for the development of SCC.16 Additionally, the appearance of new lesions (mainly ulcers not related to secondary infection) that appear during the healing phase should raise the suspicion of SCC and warrant a biopsy for evaluation.16
Pathophysiology
The exact mechanism of malignant transformation has not been elucidated, but histopathologic features suggest substantial epidermal proliferation. In some cases, this leads to pseudoepitheliomatous hyperplasia, a nonmalignant hyperproliferative state that is an important differential HPV to leishmaniasis and lupus vulgaris.19 The chronic inflammation from long-standing chromoblastomycosis likely contributes to the further malignant transformation to SCC.
Polymorphonuclear cells and activated macrophages seen in chronic inflammation can promote the release of enzymes and free radicals that has led to malignant transformation in vitro but has not been investigated specifically in chromoblastomycosis.16 Additionally, chronic inflammation and metabolic products of phagocytosis often are accompanied by excessive production of reactive oxygen and nitrogen species, which can damage DNA, lipoproteins, and cell membranes. Other potential contributors include the expression of cyclooxygenase 2 and release of arachidonic acid metabolites (eg, prostaglandins, leukotrienes), which can damage the cell and promote carcinogenesis. It is not clear whether similar mechanisms account for the development of SCCs in other chronic skin inflammations or infections such as cutaneous tuberculosis or Marjolin ulcers.20
Clinical and Public Health Interventions
Squamous cell carcinoma arising in the setting of chromoblastomycosis warrants prompt oncologic evaluation and definitive surgical management, which may require extensive surgical excision and, in advanced disease, amputation.14,17,18 Advanced malignant tumors can be difficult to manage and can result in death.21,22 Additionally, clinicians should maintain a low threshold for biopsy in long-standing chromoblastomycosis, particularly when lesions demonstrate new ulceration, rapid growth, bleeding, pain, malodor, or failure to improve with appropriate antifungal therapy.16 Recurrent or new lesions after amputation may indicate persistent or recurrent infection and may require continued antifungal management alongside cancer care.16
Squamous cell carcinoma arising from chromoblastomycosis results after substantial diagnostic delays, allowing chronic inflammation to transform infection into malignancy. Separating benign inflammation-associated epidermal proliferation from transformation to SCC requires histopathologic skill. An assay based on increased expression of chromosome 15 open reading frame 48 (C15orf48), an immune regulatory protein, has been developed to aid in this distinction; however, it is not widely available.23
Raising awareness of chromoblastomycosis among clinicians and communities, particularly in rural areas where the disease is more common, is critical to improve health care–seeking behaviors and expedite access to care pathways.2 Furthermore, access and training on microscopy to diagnose chromoblastomycosis in decentralized areas can facilitate earlier diagnosis in primary health care settings rather than waiting for diagnosis in tertiary care settings, at which point disease usually is advanced. Global implementation of existing programs that use microscopy (eg, malaria in rural areas) can be partnered with frontline health worker cross-training on chromoblastomycosis diagnosis to improve appropriate identification of disease.24 Finally, improving access to affordable antifungals, particularly itraconazole, is necessary along with further research into novel therapeutic strategies. Approaches that utilize local manufacturing and pooled procurement could help expand treatment availability in parallel with diagnostic improvement initiatives.25
Final Thoughts
Squamous cell carcinoma resulting from chromoblastomycosis is a devastating complication, often leading to limb amputation. The true prevalence is unknown, but it occurs more commonly in long-standing disease without appropriate therapy. The appearance of new lesions or ulcers after initial improvement should increase suspicion and lead to biopsy and careful pathologic evaluation. Prevention of SCC requires increased clinical awareness, early diagnosis, and timely initiation of antifungal treatment. Enhanced surveillance among individuals with chromoblastomycosis would help to better understand its prevalence, associated risk factors, and impact on quality of life.
- Queiroz-Telles F, de Hoog S, Santos DWCL, et al. Chromoblastomycosis. Clin Microbiol Rev. 2017;30:233-276.
- Smith DJ, Queiroz-Telles F, Rabenja FR, et al. A global chromoblastomycosis strategy and development of the global chromoblastomycosis working group. PLoS Negl Trop Dis. 2024;18:E0012562.
- Yen JS, Shih IH, Chung WH, et al. Chromoblastomycosis in northern Taiwan from 2017 to 2024: unique characteristics. Clin Exp Dermatol. Published online July 18, 2025. doi:10.1093/ced/llaf329
- Santos DWCL, Vicente VA, Weiss VA, et al. Chromoblastomycosis in an endemic area of Brazil: a clinical-epidemiological analysis and a worldwide haplotype network. J Fungi. 2020;6:204.
- Smith DJ, Melhem MSC, Dirven J, et al. Establishment of epidemiological cutoff values for Fonsecaea pedrosoi, the primary etiologic agent of chromoblastomycosis, and eight antifungal medications. J Clin Microbiol. 2025;63:E01903-24.
- Logan C, Singh M, Fox N, et al. Chromoblastomycosis treated with posaconazole and adjunctive imiquimod: lending innate immunity a helping hand. Open Forum Infect Dis. 2023;10:ofad124.
- de Sousa M da GT, Belda W, Spina R, et al. Topical application of imiquimod as a treatment for chromoblastomycosis. Clin Infect Dis. 2014;58:1734-1737.
- Criado PR, Careta MF, Valente NYS, et al. Extensive long-standing chromomycosis due to Fonsecaea pedrosoi: three cases with relevant improvement under voriconazole therapy. J Dermatol Treat. 2011;22:167-174.
- Esterre P, Inzan CK, Ramarcel ER, et al. Treatment of chromomycosis with terbinafine: preliminary results of an open pilot study. Br J Dermatol. 1996;134:33-36.
- Smith DJ, Benedict K, Lockhart SR, et al. Chromoblastomycosis and phaeohyphomycotic abscess-associated hospitalizations, United States, 2016–2021. PLoS Negl Trop Dis. 2025;19:E0013499.
- Bonifaz A, Carrasco‐Gerard E, Saúl A. Chromoblastomycosis: clinical and mycologic experience of 51 cases. Mycoses. 2001;44:1-7.
- Torres E, Beristain JG, Lievanos Z, et al. Chromoblastomycosis associated with a lethal squamous cell carcinoma. An Bras Dermatol. 2010;85:267-270.
- Verma S, Thakur BK, Raphael V, et al. Epidemiology of subcutaneous mycoses in northeast India: a retrospective study. Indian J Dermatol. 2018;63:496-501.
- Siregar GO, Harianja M, Rinonce HT, et al. Chromoblastomycosis: a case series from Sumba, eastern Indonesia. Clin Exp Dermatol. 2025;50:1447-1450.
- Valentin J, Grotta G, Muller T, et al. Chromoblastomycosis in French Guiana: epidemiology and practices, 1955-2023. J Fungi. 2024;10:168.
- Azevedo CMPS, Marques SG, Santos DWCL, et al. Squamous cell carcinoma derived from chronic chromoblastomycosis in Brazil. Clin Infect Dis. 2015;60:1500-1504.
- Belda Jr W, Criado PR, Casteleti P, et al. Chromoblastomycosis evolving to sarcomatoid squamous cell carcinoma: a case report. Dermatol Rep. 2021;13:9009.
- Jamil A, Lee YY, Thevarajah S. Invasive squamous cell carcinoma arising from chromoblastomycosis. Med Mycol. 2012;50:99-102.
- Delahaye T, Orduz-Robledo M, Beltran A M, et al. Pseudo-epitheliomatous hyperplasia and skin infections. Open Dermatol J. 2024;18:E18743722304513.
- Fania L, Didona D, Di Pietro FR, et al. Cutaneous squamous cell carcinoma: from pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9:171.
- Torres E, Beristain JG, Lievanos Z, et al. Carcinoma epidermoide como complicação letal de lesões crônicas de cromoblastomicose. An Bras Dermatol. 2010;85:267-270.
- Rojas OC, González GM, Moreno-Treviño M, et al. Chromoblastomycosis by Cladophialophora carrionii associated with squamous cell carcinoma and review of published reports. Mycopathologia. 2015;179:153-157.
- Su A, Ra S, Li X, et al. Differentiating cutaneous squamous cell carcinoma and pseudoepitheliomatous hyperplasia by multiplex qRT-PCR. Mod Pathol. 2013;26:1433-1437.
- Siregar GO, Harianja M, Smith DJ, et al. Leveraging malaria microscopy infrastructure to diagnose common and neglected skin diseases using direct microscopy in Sumba, Indonesia. Lancet Reg Health - West Pac. 2025;64:101739.
- Smith DJ, Soebono H, Parajuli N, et al. South-East Asia regional neglected tropical disease framework: improving control of mycetoma, chromoblastomycosis, and sporotrichosis. Lancet Reg Health Southeast Asia. 2025;35:100561.
- Queiroz-Telles F, de Hoog S, Santos DWCL, et al. Chromoblastomycosis. Clin Microbiol Rev. 2017;30:233-276.
- Smith DJ, Queiroz-Telles F, Rabenja FR, et al. A global chromoblastomycosis strategy and development of the global chromoblastomycosis working group. PLoS Negl Trop Dis. 2024;18:E0012562.
- Yen JS, Shih IH, Chung WH, et al. Chromoblastomycosis in northern Taiwan from 2017 to 2024: unique characteristics. Clin Exp Dermatol. Published online July 18, 2025. doi:10.1093/ced/llaf329
- Santos DWCL, Vicente VA, Weiss VA, et al. Chromoblastomycosis in an endemic area of Brazil: a clinical-epidemiological analysis and a worldwide haplotype network. J Fungi. 2020;6:204.
- Smith DJ, Melhem MSC, Dirven J, et al. Establishment of epidemiological cutoff values for Fonsecaea pedrosoi, the primary etiologic agent of chromoblastomycosis, and eight antifungal medications. J Clin Microbiol. 2025;63:E01903-24.
- Logan C, Singh M, Fox N, et al. Chromoblastomycosis treated with posaconazole and adjunctive imiquimod: lending innate immunity a helping hand. Open Forum Infect Dis. 2023;10:ofad124.
- de Sousa M da GT, Belda W, Spina R, et al. Topical application of imiquimod as a treatment for chromoblastomycosis. Clin Infect Dis. 2014;58:1734-1737.
- Criado PR, Careta MF, Valente NYS, et al. Extensive long-standing chromomycosis due to Fonsecaea pedrosoi: three cases with relevant improvement under voriconazole therapy. J Dermatol Treat. 2011;22:167-174.
- Esterre P, Inzan CK, Ramarcel ER, et al. Treatment of chromomycosis with terbinafine: preliminary results of an open pilot study. Br J Dermatol. 1996;134:33-36.
- Smith DJ, Benedict K, Lockhart SR, et al. Chromoblastomycosis and phaeohyphomycotic abscess-associated hospitalizations, United States, 2016–2021. PLoS Negl Trop Dis. 2025;19:E0013499.
- Bonifaz A, Carrasco‐Gerard E, Saúl A. Chromoblastomycosis: clinical and mycologic experience of 51 cases. Mycoses. 2001;44:1-7.
- Torres E, Beristain JG, Lievanos Z, et al. Chromoblastomycosis associated with a lethal squamous cell carcinoma. An Bras Dermatol. 2010;85:267-270.
- Verma S, Thakur BK, Raphael V, et al. Epidemiology of subcutaneous mycoses in northeast India: a retrospective study. Indian J Dermatol. 2018;63:496-501.
- Siregar GO, Harianja M, Rinonce HT, et al. Chromoblastomycosis: a case series from Sumba, eastern Indonesia. Clin Exp Dermatol. 2025;50:1447-1450.
- Valentin J, Grotta G, Muller T, et al. Chromoblastomycosis in French Guiana: epidemiology and practices, 1955-2023. J Fungi. 2024;10:168.
- Azevedo CMPS, Marques SG, Santos DWCL, et al. Squamous cell carcinoma derived from chronic chromoblastomycosis in Brazil. Clin Infect Dis. 2015;60:1500-1504.
- Belda Jr W, Criado PR, Casteleti P, et al. Chromoblastomycosis evolving to sarcomatoid squamous cell carcinoma: a case report. Dermatol Rep. 2021;13:9009.
- Jamil A, Lee YY, Thevarajah S. Invasive squamous cell carcinoma arising from chromoblastomycosis. Med Mycol. 2012;50:99-102.
- Delahaye T, Orduz-Robledo M, Beltran A M, et al. Pseudo-epitheliomatous hyperplasia and skin infections. Open Dermatol J. 2024;18:E18743722304513.
- Fania L, Didona D, Di Pietro FR, et al. Cutaneous squamous cell carcinoma: from pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9:171.
- Torres E, Beristain JG, Lievanos Z, et al. Carcinoma epidermoide como complicação letal de lesões crônicas de cromoblastomicose. An Bras Dermatol. 2010;85:267-270.
- Rojas OC, González GM, Moreno-Treviño M, et al. Chromoblastomycosis by Cladophialophora carrionii associated with squamous cell carcinoma and review of published reports. Mycopathologia. 2015;179:153-157.
- Su A, Ra S, Li X, et al. Differentiating cutaneous squamous cell carcinoma and pseudoepitheliomatous hyperplasia by multiplex qRT-PCR. Mod Pathol. 2013;26:1433-1437.
- Siregar GO, Harianja M, Smith DJ, et al. Leveraging malaria microscopy infrastructure to diagnose common and neglected skin diseases using direct microscopy in Sumba, Indonesia. Lancet Reg Health - West Pac. 2025;64:101739.
- Smith DJ, Soebono H, Parajuli N, et al. South-East Asia regional neglected tropical disease framework: improving control of mycetoma, chromoblastomycosis, and sporotrichosis. Lancet Reg Health Southeast Asia. 2025;35:100561.
Chromoblastomycosis Leading to Squamous Cell Carcinoma: An Overlooked Outcome of a Neglected Tropical Disease
Chromoblastomycosis Leading to Squamous Cell Carcinoma: An Overlooked Outcome of a Neglected Tropical Disease
Practice Points
- Chromoblastomycosis is recognized by the World Health Organization as a neglected tropical disease and principally affects agricultural workers in tropical and subtropical regions.
- Long-standing or refractory chromoblastomycosis can lead to substantial morbidity, including lymphedema, secondary bacterial infections, extensive scarring, functional impairment, and squamous cell carcinoma (SCC).
- The development of SCC is thought to be related to chronic inflammation and prolonged disease duration (Mathematical Pi LT Std>10 years). Advanced cases may require extensive surgical excision or amputation.
- Early recognition with support of direct microscopy or histopathology, timely antifungal treatment (often with itraconazole), and a low threshold for repeat biopsy of new ulceration or rapidly changing lesions may prevent malignant transformation and disability.

High VA Telehealth Use Linked to Reduced Vaccination Rates
Quality measures for primary care in the US Department of Veterans Affairs (VA) remained stable when telehealth was mixed with in-person visits, but influenza vaccination fell among patients who relied on online visits the most, a retrospective cohort study finds.
Analysis of the medical records for 744,599 veterans from federal fiscal years 2022 and 2023 revealed that patients aged 19-65 years who relied on telehealth for at least half of their primary care visits were less likely to receive an influenza vaccine (37.9%) compared with those seen only in person (50.0%, P < .001). The study was lead by researchers at VA Puget Sound and published in JAMA Network Open.
There was also an influenza vaccination gap in patients aged ≥ 66 years: 62.8% in patients who received some care via telehealth telehealth vs 71.5% seen only in person, respectively (P < .001).
“Our study showed that primary care quality at the VA is quite high,” Jonathan Staloff, MD, MSc, a family medicine physician with VA Puget Sound told Federal Practitioner. “And we found that for almost all quality measures, having a low proportion of care via telehealth was associated with the same quality as in-person care.”
As Staloff explained, “telehealth in primary care, as well as in general, has emerged as an additional means of preserving access to care for veterans. Evidence suggests that veterans have a high degree of satisfaction with telehealth but it’s mixed as it relates to quality outcome differences between those who receive any via telehealth vs none.”
For the study, Staloff said, “we wanted to see if there was a dose-response relationship between telehealth utilization and care quality and if certain hybrid models could help optimize quality of care. To our knowledge, this study was the first national evaluation to investigate primary care telehealth and care quality in this way.”
Reassuring Findings About Low Telehealth Use
For the study, researchers tracked a national sample of patient data from the Veterans Health Administration (VHA) Support Service Center Capital Assets Databases, Primary Care Management Module, and VHA Corporate Data Warehouse (mean age, 65 years; 86% male; 63% White, 22% Black, 10% Hispanic).
The study defined categories of primary-care telehealth use as no telehealth, low telehealth (> 0.0% to < 28.6%), intermediate telehealth (28.6% to < 50.0%), and high telehealth (> 50.0%).
Highest Telehealth Use Raises Red Flags
The differences in influenza vaccine rates between the no-telehealth and high-telehealth groups held up in an adjusted analysis.
The study found small but statistically significant worsening of several quality measures in the high-telehealth use vs no-telehealth use cohorts: hypertension control, statin therapy and adherence, and annual screening for depression, alcohol use, and tobacco use.
The study cites limitations such as reliance on patients with ≥ 3 or more evaluation-and- management visits and lack of information about influenza vaccines delivered outside the VA.
In a statement, VA Telehealth Services said it is “encouraged” the study demonstrates “equivalence in many clinical measures among veterans using telehealth. This study reinforces the potential of telehealth to provide high-quality health care to veterans.”
The organization added that it’s “committed to better understanding potential gaps highlighted in this study,” and “it is critical that research databases capture care rendered outside VA … and whether care was offered during a telehealth visit.”
Batching In-Person Services May Be Helpful
As for messages from the study for clinicians, Staloff said there are some preventive care measures that may be more difficult to deliver through telehealth.
“Clinicians should consider batching these in-person services for patients that have a high reliance on telehealth when they have an opportunity to see these patients in-person,” Staloff said. “Health systems may need new workflows to optimize hybrid care, particularly for those that receive most of their care via telehealth.”
Outside Perspective: ‘Access is Not the Same as Quality’
After reviewing the study findings, Ilana Graetz, PhD, a professor who studies health policy at the Emory University Rollins School of Public Health, praised the research design and said the results overall are “more reassuring than alarming.” However, she did caution that there could potentially be ways these patients differ that could not be categorized by the data.
“Patients with higher telehealth use may differ from those with lower telehealth use in important ways not fully captured in the data — barriers to in-person care, the complexity of the visit, patient preferences, or care received outside the system,” Graetz said.
As for the influenza vaccine, Graetz said patients need to be physically present: “Patients seen mostly by telehealth will have fewer opportunities to receive any preventive care that can only be delivered in person.”
Graetz said the study is timely given ongoing debates over COVID-19 pandemic-era telehealth flexibilities.
“The findings suggest that telehealth can function well as part of a hybrid primary care model,” she said, “but health systems still need to ensure that preventive services, chronic disease management, and follow-up care are not lost in the shift to virtual care.”
VHA Primary Care Analytics Team supported the study with funding from the VHA Office of Primary Care. Staloff has no disclosures. One coauthor disclosed a relationship with the US Department of Veterans Affairs.
Graetz disclosed relationships the Donaghue Foundation, Pfizer, PRIME Education, and the National Institutes of Health.
Quality measures for primary care in the US Department of Veterans Affairs (VA) remained stable when telehealth was mixed with in-person visits, but influenza vaccination fell among patients who relied on online visits the most, a retrospective cohort study finds.
Analysis of the medical records for 744,599 veterans from federal fiscal years 2022 and 2023 revealed that patients aged 19-65 years who relied on telehealth for at least half of their primary care visits were less likely to receive an influenza vaccine (37.9%) compared with those seen only in person (50.0%, P < .001). The study was lead by researchers at VA Puget Sound and published in JAMA Network Open.
There was also an influenza vaccination gap in patients aged ≥ 66 years: 62.8% in patients who received some care via telehealth telehealth vs 71.5% seen only in person, respectively (P < .001).
“Our study showed that primary care quality at the VA is quite high,” Jonathan Staloff, MD, MSc, a family medicine physician with VA Puget Sound told Federal Practitioner. “And we found that for almost all quality measures, having a low proportion of care via telehealth was associated with the same quality as in-person care.”
As Staloff explained, “telehealth in primary care, as well as in general, has emerged as an additional means of preserving access to care for veterans. Evidence suggests that veterans have a high degree of satisfaction with telehealth but it’s mixed as it relates to quality outcome differences between those who receive any via telehealth vs none.”
For the study, Staloff said, “we wanted to see if there was a dose-response relationship between telehealth utilization and care quality and if certain hybrid models could help optimize quality of care. To our knowledge, this study was the first national evaluation to investigate primary care telehealth and care quality in this way.”
Reassuring Findings About Low Telehealth Use
For the study, researchers tracked a national sample of patient data from the Veterans Health Administration (VHA) Support Service Center Capital Assets Databases, Primary Care Management Module, and VHA Corporate Data Warehouse (mean age, 65 years; 86% male; 63% White, 22% Black, 10% Hispanic).
The study defined categories of primary-care telehealth use as no telehealth, low telehealth (> 0.0% to < 28.6%), intermediate telehealth (28.6% to < 50.0%), and high telehealth (> 50.0%).
Highest Telehealth Use Raises Red Flags
The differences in influenza vaccine rates between the no-telehealth and high-telehealth groups held up in an adjusted analysis.
The study found small but statistically significant worsening of several quality measures in the high-telehealth use vs no-telehealth use cohorts: hypertension control, statin therapy and adherence, and annual screening for depression, alcohol use, and tobacco use.
The study cites limitations such as reliance on patients with ≥ 3 or more evaluation-and- management visits and lack of information about influenza vaccines delivered outside the VA.
In a statement, VA Telehealth Services said it is “encouraged” the study demonstrates “equivalence in many clinical measures among veterans using telehealth. This study reinforces the potential of telehealth to provide high-quality health care to veterans.”
The organization added that it’s “committed to better understanding potential gaps highlighted in this study,” and “it is critical that research databases capture care rendered outside VA … and whether care was offered during a telehealth visit.”
Batching In-Person Services May Be Helpful
As for messages from the study for clinicians, Staloff said there are some preventive care measures that may be more difficult to deliver through telehealth.
“Clinicians should consider batching these in-person services for patients that have a high reliance on telehealth when they have an opportunity to see these patients in-person,” Staloff said. “Health systems may need new workflows to optimize hybrid care, particularly for those that receive most of their care via telehealth.”
Outside Perspective: ‘Access is Not the Same as Quality’
After reviewing the study findings, Ilana Graetz, PhD, a professor who studies health policy at the Emory University Rollins School of Public Health, praised the research design and said the results overall are “more reassuring than alarming.” However, she did caution that there could potentially be ways these patients differ that could not be categorized by the data.
“Patients with higher telehealth use may differ from those with lower telehealth use in important ways not fully captured in the data — barriers to in-person care, the complexity of the visit, patient preferences, or care received outside the system,” Graetz said.
As for the influenza vaccine, Graetz said patients need to be physically present: “Patients seen mostly by telehealth will have fewer opportunities to receive any preventive care that can only be delivered in person.”
Graetz said the study is timely given ongoing debates over COVID-19 pandemic-era telehealth flexibilities.
“The findings suggest that telehealth can function well as part of a hybrid primary care model,” she said, “but health systems still need to ensure that preventive services, chronic disease management, and follow-up care are not lost in the shift to virtual care.”
VHA Primary Care Analytics Team supported the study with funding from the VHA Office of Primary Care. Staloff has no disclosures. One coauthor disclosed a relationship with the US Department of Veterans Affairs.
Graetz disclosed relationships the Donaghue Foundation, Pfizer, PRIME Education, and the National Institutes of Health.
Quality measures for primary care in the US Department of Veterans Affairs (VA) remained stable when telehealth was mixed with in-person visits, but influenza vaccination fell among patients who relied on online visits the most, a retrospective cohort study finds.
Analysis of the medical records for 744,599 veterans from federal fiscal years 2022 and 2023 revealed that patients aged 19-65 years who relied on telehealth for at least half of their primary care visits were less likely to receive an influenza vaccine (37.9%) compared with those seen only in person (50.0%, P < .001). The study was lead by researchers at VA Puget Sound and published in JAMA Network Open.
There was also an influenza vaccination gap in patients aged ≥ 66 years: 62.8% in patients who received some care via telehealth telehealth vs 71.5% seen only in person, respectively (P < .001).
“Our study showed that primary care quality at the VA is quite high,” Jonathan Staloff, MD, MSc, a family medicine physician with VA Puget Sound told Federal Practitioner. “And we found that for almost all quality measures, having a low proportion of care via telehealth was associated with the same quality as in-person care.”
As Staloff explained, “telehealth in primary care, as well as in general, has emerged as an additional means of preserving access to care for veterans. Evidence suggests that veterans have a high degree of satisfaction with telehealth but it’s mixed as it relates to quality outcome differences between those who receive any via telehealth vs none.”
For the study, Staloff said, “we wanted to see if there was a dose-response relationship between telehealth utilization and care quality and if certain hybrid models could help optimize quality of care. To our knowledge, this study was the first national evaluation to investigate primary care telehealth and care quality in this way.”
Reassuring Findings About Low Telehealth Use
For the study, researchers tracked a national sample of patient data from the Veterans Health Administration (VHA) Support Service Center Capital Assets Databases, Primary Care Management Module, and VHA Corporate Data Warehouse (mean age, 65 years; 86% male; 63% White, 22% Black, 10% Hispanic).
The study defined categories of primary-care telehealth use as no telehealth, low telehealth (> 0.0% to < 28.6%), intermediate telehealth (28.6% to < 50.0%), and high telehealth (> 50.0%).
Highest Telehealth Use Raises Red Flags
The differences in influenza vaccine rates between the no-telehealth and high-telehealth groups held up in an adjusted analysis.
The study found small but statistically significant worsening of several quality measures in the high-telehealth use vs no-telehealth use cohorts: hypertension control, statin therapy and adherence, and annual screening for depression, alcohol use, and tobacco use.
The study cites limitations such as reliance on patients with ≥ 3 or more evaluation-and- management visits and lack of information about influenza vaccines delivered outside the VA.
In a statement, VA Telehealth Services said it is “encouraged” the study demonstrates “equivalence in many clinical measures among veterans using telehealth. This study reinforces the potential of telehealth to provide high-quality health care to veterans.”
The organization added that it’s “committed to better understanding potential gaps highlighted in this study,” and “it is critical that research databases capture care rendered outside VA … and whether care was offered during a telehealth visit.”
Batching In-Person Services May Be Helpful
As for messages from the study for clinicians, Staloff said there are some preventive care measures that may be more difficult to deliver through telehealth.
“Clinicians should consider batching these in-person services for patients that have a high reliance on telehealth when they have an opportunity to see these patients in-person,” Staloff said. “Health systems may need new workflows to optimize hybrid care, particularly for those that receive most of their care via telehealth.”
Outside Perspective: ‘Access is Not the Same as Quality’
After reviewing the study findings, Ilana Graetz, PhD, a professor who studies health policy at the Emory University Rollins School of Public Health, praised the research design and said the results overall are “more reassuring than alarming.” However, she did caution that there could potentially be ways these patients differ that could not be categorized by the data.
“Patients with higher telehealth use may differ from those with lower telehealth use in important ways not fully captured in the data — barriers to in-person care, the complexity of the visit, patient preferences, or care received outside the system,” Graetz said.
As for the influenza vaccine, Graetz said patients need to be physically present: “Patients seen mostly by telehealth will have fewer opportunities to receive any preventive care that can only be delivered in person.”
Graetz said the study is timely given ongoing debates over COVID-19 pandemic-era telehealth flexibilities.
“The findings suggest that telehealth can function well as part of a hybrid primary care model,” she said, “but health systems still need to ensure that preventive services, chronic disease management, and follow-up care are not lost in the shift to virtual care.”
VHA Primary Care Analytics Team supported the study with funding from the VHA Office of Primary Care. Staloff has no disclosures. One coauthor disclosed a relationship with the US Department of Veterans Affairs.
Graetz disclosed relationships the Donaghue Foundation, Pfizer, PRIME Education, and the National Institutes of Health.
Cutaneous Manifestations of Neglected Infectious Diseases in US Military Personnel
Cutaneous Manifestations of Neglected Infectious Diseases in US Military Personnel
Infectious diseases historically have posed major challenges to the operations and health of military forces. In recent conflicts, nonbattle injuries including infections have caused more evacuations than combat trauma.1 Deployment to endemic regions, poor sanitation, and trauma increase susceptibility to both common and rare infections, many of which have cutaneous manifestations.
Surveillance programs such as the Armed Forces Health Surveillance Division serve a critical role in monitoring outbreaks among deployed personnel.2 Cutaneous manifestations of systemic disease often serve as early clinical indicators, especially in settings with limited diagnostic resources. This review describes rarely encountered infectious agents for which US military personnel are at increased risk and outlines management strategies for clinicians practicing in austere environments.
EPIDEMIOLOGIC RISK FACTORS IN MILITARY POPULATIONS
United States military personnel face an elevated risk for infectious diseases when deployed in tropical and subtropical regions where endemic pathogens are prevalent. Exposure to soil, water, and insect vectors facilitates transmission. Direct exposure during combat or training combined with high-density housing, combat-related trauma, and constraints on hygiene access during operations increases infection risk.3
REGION-SPECIFIC PATHOGENS
Middle East
Leishmania species—Leishmania, a protozoa transmitted via sand fly bites, has caused multiple documented outbreaks among US troops in Iraq and Afghanistan, with a reported incidence of 14%.4 Leishmaniasis can present as 3 main clinical variants: cutaneous, visceral, and mucocutaneous. Cutaneous leishmaniasis typically manifests as painless ulcers covered with hemorrhagic crusts on exposed regions of the body. While typically self-limited, lesions frequently result in irreversible scarring. Many Leishmania species respond well to antimonials such as sodium stibogluconate. Preventive measures include wearing protective clothing and sleeping inside insecticide-treated bed nets.5
Coxiella burnetii—Coxiella burnetii transmits through inhalation of aerosolized particles originating from the urine, feces, birth products, or milk of infected bovine. In 2003, a small number of cases were identified in US service members exposed to livestock while serving in Iraq.6 Outbreaks also occurred during World War II, but it is unclear whether they were caused by naturally occurring C burnetii or biowarfare.7 Though primarily a systemic illness with severe pneumonia, Q fever may manifest with an associated purpuric or morbilliform rash.8 Doxycycline is recommended both for treatment and empiric coverage.6
Acinetobacter baumannii—This multidrug-resistant organism is known to infect combat wounds and is associated with nosocomial outbreaks in military hospitals. Studies suggest environmental contamination and health care transmission contribute substantially to outbreaks in military hospitals.9 Cutaneous manifestations can include cellulitis with a peau d’orange appearance or necrotizing fasciitis; however, pneumonia and bacteremia have been reported. Prompt culture and antibiotic initiation with debridement are essential for treatment.10 Antibiotic stewardship and strict infection control are critical to prevent outbreaks and limit resistance.9
Africa
Plasmodium species—Malaria remains a life-threatening disease found in tropical and subtropical areas around the world. Despite preventive measures, 30 cases among US service members were reported in 2024.11 Cutaneous findings include purpura fulminans, petechiae, acral necrosis, or reticulated erythema.12 Service members stationed in endemic areas should take prophylactic antimalarials. Symptoms include fevers, headaches, and malaise, with possible rapid deterioration.13
Mycobacterium ulcerans—Mycobacterium ulcerans causes extensive necrotic ulcers—commonly known as Buruli ulcers—which generally begin as a nodule, plaque, papule, or edematous lesion, eventually progressing to extensive ulceration. Despite no documented cases of US personnel contracting Buruli ulcers, those stationed in endemic regions remain at risk. Environmental reservoirs of M ulcerans are unknown, but its DNA has been isolated from water sources.14,15 These ulcers take months to heal, making wound management and antimycobacterial therapy essential. Primary preventive measures include avoidance of swimming in rivers or agricultural work in endemic areas.14
Mpox Virus—During the 2022 mpox outbreak, male service members who engaged in sexual activity with other men were at the highest risk, with 88.8% of infected service members reporting this practice.16 While the virus is endemic to Africa, 89.0% of cases were reported from service members stationed in the United States.17 Typical infection results in fever, headache, lymphadenopathy, and myalgias, followed by a facial rash that spreads over the body, palms, and soles. Safe-sex practices help prevent transmission, and there is a vaccine available for high-risk patients.16
Southeast Asia
Leptospira species—Leptospira is an aerobic spirochete found in tropical regions worldwide. Transmission occurs when water contaminated with urine from infected animals exposes humans to the organism. Infection manifests as a mild febrile illness, though approximately 10% of patients develop Weil syndrome, consisting of conjunctival suffusion, jaundice, and acute kidney injury. Treatment and prophylaxis include doxycycline, but severe disease warrants intravenous antibiotics.17,18 A 2014 outbreak among Marines in Japan highlighted poor prophylactic compliance as a key risk factor.19 Proper education for those at risk is essential to prevent future outbreaks.
Mycobacterium leprae—Leprosy is an acid-fast mycobacterium that remains endemic in the Pacific Islands and Southeast Asia. Case reports of US service members diagnosed with leprosy exist, though only in patients who emigrated from endemic areas.20 This disease has a spectrum of manifestations depending on the immune response, with tuberculoid leprosy showing a cell-mediated (T helper 1) response and lepromatous leprosy having more of a humoral (T helper 2) response.21 It manifests with hypopigmented anesthetic macules and peripheral neuropathy. Diagnosis is made by skin biopsy, which shows perineural lymphohistiocytic inflammation and non-necrotizing granulomas.20 The infection typically is curable with a multidrug regimen.21
Strongyloides stercoralis—This nematode causes infection by transdermal penetration of bare feet. They then migrate to the lungs where the patient coughs and swallows the nematode into the gastrointestinal tract. Strongyloides stercoralis autoinfect by penetrating the intestinal wall, resulting in chronic digestive, respiratory, and cutaneous symptoms. Worldwide prevalence of S stercoralis infection is estimated to be 10% to 40%, with foreign-born US military members at increased risk compared to the general military population.22,23 Larva currens may manifest with a pruritic erythematous plaque at the site of penetration that progresses to an intensely pruritic, creeping dermatitis as the nematode migrates under the skin. Avoidance of barefoot soil exposure and treatment with ivermectin are effective preventive and therapeutic measures.23
South America
Ancylostoma braziliense—Found throughout the subtropical world, this hookworm primarily infects dogs and cats and is found in their stool. Larva currens has a similar manifestation and life cycle to cutaneous larva migrans, but autoinfection does not occur. Transmission occurs similarly to S stercoralis and responds well to oral albendazole or ivermectin; however, the infection is self-limited.24 Military cases have been reported,25 though overall morbidity remains poorly characterized.
Dengue Virus—An arbovirus transmitted by Aedes mosquitoes, dengue remains a major military threat. Service members in the Vietnam War experienced an attack rate as high as 80%.26,27 Infection often manifests with retro-orbital pain and a morbilliform rash that occurs 2 to 5 days after fever, though severe cases may progress to hemorrhagic dengue with skin petechiae or ecchymosis.28 Immediate intervention is essential in symptomatic patients to prevent life-threatening progression. There are no dengue vaccines approved by the US Food and Drug Administration for adults, thus military personnel in endemic areas remain at risk.27
Trypanosoma cruzi—Chagas disease is transmitted when a reduviid infected with T cruzi bites and defecates on the patient’s skin. A skin nodule (chagoma) or painless eyelid edema (Romaña sign) may appear at the site of parasite entry. Chronic disease may result in dilated cardiomyopathy.29 Several cases of Chagas disease have been reported in South American military operations, including an outbreak in 9 Columbian military personnel.30 Cases in the southwestern United States have recently emerged, emphasizing the need for increased awareness.31 Proper insect repellent helps to ward off reduviid bugs. Nifurtimox and benznidazole are the only drugs with proven efficacy against T cruzi.29
Continental United States of America
Coccidioides immitis—The first reported case of coccidiomycosis was described in 1892 in a service member with debilitating masses and ulcers.32 Endemic to arid regions of the western United States, coccidioidomycosis affects military trainees at rates up to 32% annually in high-risk settings.33 Primary infection occurs in the lungs and may spread hematologically. The fungi prefer dry desert soils, which may aerosolize during military maneuvers. Coccidioidomycosis occasionally causes erythema nodosum, and diffuse infection shows verrucous plaques, ulcers, or abscesses. Dust avoidance and mask wearing are advised for those in endemic regions. Ketoconazole and amphotericin B are the only treatments approved by the US Food and Drug Administration.32 When starting immunosuppressive drugs, clinicians should inquire if patients have previously been stationed in Coccidioides-endemic areas, such as Fort Irwin, California, to avoid reactivation of the fungi.33
Francisella tularensis—Acquired via ticks or contact with wild animals, tularemia causes an ulceroglandular disease with regional lymphadenopathy. Inoculation requires as few as 10 to 25 organisms; thus it is considered a Category A agent for bioterror.34 Natural outbreaks have occurred during war times, most recently during the civil wars in Bosnia and Kosovo.35 Patients may present with a painful ulcer that enlarges to form a plaque with raised borders. Personnel in wooded areas should use tick precautions and handle wild animals cautiously. Treatment includes gentamicin for severe disease, with tetracyclines effective in mild cases.34
PREVENTION AND MANAGEMENT STRATEGIES IN AUSTERE SETTINGS
For health care professionals practicing in military settings, austere environments can provide a challenge for diagnosis of neglected diseases. Despite a lack of advanced diagnostic tools, practical options can be applied to the diagnostic process; for example, teledermatology is utilized for treatment of service members deployed to remote environments.36
Management of uncommon infectious diseases in military personnel often requires treatments outside those practiced in domestic clinics. Field management may indicate prompt empiric therapy while balancing the risks of overtreatment against those of missed diagnoses37; however, medical evacuation to a higher level of care may be indicated in patients with severe presentations to expedite diagnosis and treatment.38
Prevention remains the primary goal to avoid local outbreaks. Long-sleeved uniforms, DEET (N, N-diethyl-meta-toluamide)–based repellents, permethrin-impregnated clothing, and bed nets are effective for vector protection. Prophylactic medications and vaccinations often are provided when personnel are deployed to endemic locations.39
Onsite entomology teams also can provide surveillance of the local insect populations. They may contribute to vector control through insecticide application and environmental modification. The Armed Forces Health Surveillance Division and the Global Emerging Infections Surveillance Program monitor infectious threats in real time to locate any potential outbreaks, guiding operational responses.40
FINAL THOUGHTS
Dermatologic signs often provide early evidence of infection in military personnel. With increasing antimicrobial resistance and the emergence of new pathogens, it is imperative for clinicians treating members of the military to recognize cutaneous signs, employ efficient diagnostic strategies, and encourage proactive prevention. A collaborative approach spanning dermatology, infectious disease, and public health is essential to protect the modern service member.
- Murray CK. Infectious disease complications of combat-related injuries. Crit Care Med. 2008;36(7 suppl):S358-S364. doi:10.1097/CCM.0b013e31817e2ffc
- Armed Forces Health Surveillance Division. AFHSD Annual Report. Defense Health Agency; 2023. Accessed March 5, 2026. https://www.health.mil/Reference-Center/Reports/2024/09/19/AFHSD-Annual-Report-2023
- Murray CK, Yun HC, Markelz AE, et al. Operation United Assistance: infectious disease threats to deployed military personnel. Military Medicine. 2015;180:626-651. doi:10.7205/MILMED-D-14-00691
- Niba Rawlings N, Bailey M, Courtenay O. Leishmaniasis in deployed military populations: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2025;19:E0012680. doi:10.1371/journal.pntd.0012680
- de Vries HJC, Schallig HD. Cutaneous leishmaniasis: a 2022 updated narrative review into diagnosis and management developments. Am J Clin Dermatol. 2022;23:823-840. doi:10.1007/s40257-022-00726-8
- Anderson AD, Smoak B, Shuping E, et al. Q fever and the US military. Emerg Infect Dis. 2005;11:1320-1322. doi:10.3201/eid1108.050314
- Madariaga MG, Rezai K, Trenholme GM, et al. Q fever: a biological weapon in your backyard. Lancet Infect Dis. 2003;3:709-721. doi:10.1016/S1473-3099(03)00804-1
- Uribe Pulido N, Escorcia García C, Cabrera Orrego R, et al. Acute Q fever with dermatologic manifestations, molecular diagnosis, and no seroconversion. Open Forum Infect Dis. 2021;8:ofab458. doi:10.1093/ofid/ofab458
- Scott P, Deye G, Srinivasan A, et al. An outbreak of multidrug-resistant acinetobacter baumannii-calcoaceticus complex infection in the US Military Health Care System associated with military operations in Iraq. Clin Infect Dis. 2007;44:1577-1584. doi:10.1086/518170
- Guerrero DM, Perez F, Conger NG, et al. Acinetobacter baumannii-associated skin and soft tissue infections: recognizing a broadening spectrum of disease. Surg Infect (Larchmt). 2010;11:49-57. doi:10.1089/sur.2009.022
- Armed Forces Health Surveillance Division. Malaria among members of the US Armed Forces, 2024. MSMR. 2025;32:22-28.
- Farkouh CS, Abdi P, Amatul-Hadi F, et al. Cutaneous manifestations of malaria and their prognostic windows: a narrative review. Cureus. 2023;15:E41706. doi:10.7759/cureus.41706
- Shahbodaghi SD, Rathjen NA. Malaria: prevention, diagnosis, and treatment. Am Fam Physician. 2022;106:270-278.
- Yotsu RR, Suzuki K, Simmonds RE, et al. Buruli ulcer: a review of the current knowledge. Curr Trop Med Rep. 2018;5:247-256. doi:10.1007/s40475-018-0166-2
- Portaels F, Meyers WM, Ablordey A, et al. First cultivation and characterization of Mycobacterium ulcerans from the environment. PLoS Negl Trop Dis. 2008;2:E178. doi:10.1371/journal.pntd.0000178
- Metcalf-Kelly M, Garrison M, Stidham R. Characteristics of mpox cases diagnosed in Military Health System beneficiaries, May 2022-April 2024. MSMR. 2024;31:7-11.
- Rajapakse S. Leptospirosis: clinical aspects. Clin Med (Lond). 2022;22:14-17. doi:10.7861/clinmed.2021-0784
- Heath CW, Alexander AD, Galton MM. Leptospirosis in the United States: a of 483 cases in man, 1949–1961. N Engl J Med. 1965;273:857-864. doi:10.1056/NEJM196510142731606
- Mason V. Mystery outbreak investigation 2014—Leptospirosis licerasiae. November 17, 2017. Accessed March 5, 2026. https://usupulse.blogspot.com/2017/11/mystery-outbreak-investigation-2014.html
- Berjohn CM, DuPlessis CA, Tieu K, et al. Multibacillary leprosy in an active duty military member. Emerg Infect Dis. 2015;21:1077-1078. doi:10.3201/eid2106.141666
- Scollard DM, Adams LB, Gillis TP, et al. The continuing challenges of leprosy. Clin Microbiol Rev. 2006;19:338-381. doi:10.1128/CMR.19.2.338-381.2006
- Schär F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis. 2013;7:E2288. doi:10.1371/journal.pntd.0002288
- Taheri B, Kuo HC, Hockenbury N, et al. Strongyloides stercoralis in the US Military Health System. Open Forum Infect Dis. 2023;10:ofad127. doi:10.1093/ofid/ofad127
- Bowman DD, Montgomery SP, Zajac AM, et al. Hookworms of dogs and cats as agents of cutaneous larva migrans. Trends Parasitol. 2010;26:162-167. doi:10.1016/j.pt.2010.01.005
- Inglis DM, Bailey MS. Unusual presentations of cutaneous larva migrans in British military personnel. BMJ Mil Health. 2023;169:E78-E81. doi:10.1136/bmjmilitary-2020-001677
- Halstead SB, Udomsakdi S, Singharaj P, et al. Dengue and chikungunya virus infection in man in Thailand, 1962–1964. 3. clinical, epidemiologic, and virologic observations on disease in non-indigenous white persons. Am J Trop Med Hyg. 1969;18:984-996. doi:10.4269/ajtmh.1969.18.984
- Gibbons RV, Streitz M, Babina T, et al. Dengue and US military operations from the Spanish-American War through today. Emerg Infect Dis. 2012;18:623-630. doi:10.3201/eid1804.110134
- Guzman MG, Harris E. Dengue. Lancet. 2015;385:453-465. doi:10.1016/S0140-6736(14)60572-9
- Bern C. Chagas’ disease. N Engl J Med. 2015;373:456-466. doi:10.1056/NEJMra1410150
- Vergara HD, Gómez CH, Faccini-Martínez ÁA, et al. Acute Chagas disease outbreak among military personnel, Colombia, 2021. Emerg Infect Dis. 2023;29:1882-1885. doi:10.3201/eid2909.230886
- Harris N, Woc-Colburn L, Gunter SM, et al. Autochthonous Chagas disease in the southern United States: a case report of suspected residential and military exposures. Zoonoses Public Health. 2017;64:491-493. doi:10.1111/zph.12360
- Crum NF. Coccidioidomycosis: a contemporary review. Infect Dis Ther. 2022;11:713-742. doi:10.1007/s40121-022-00606-y
- Crum NF, Potter M, Pappagianis D. Seroincidence of coccidioidomycosis during military desert training exercises. J Clin Microbiol. 2004;42:4552-4555. doi:10.1128/JCM.42.10.4552-4555.2004
- Antonello RM, Giacomelli A, Riccardi N. Tularemia for clinicians: an up-to-date review on epidemiology, diagnosis, prevention and treatment. Eur J Intern Med. 2025;135:25-32. doi:10.1016/j.ejim.2025.03.013
- Nelson CA, Sjöstedt A. Tularemia: a storied history, an ongoing threat. Clin Infect Dis. 2024;78(supplement_1):S1-S3. doi:10.1093/cid/ciad681
- Pendlebury GA, Roman J, Shrivastava V, et al. A call to action: evidence for the military integration of teledermoscopy in a pandemic era. Dermatopathology (Basel). 2022;9:327-342. doi:10.3390/dermatopathology9040039
- Bhagchandani R, Singhi S, Peter JV, et al. Tropical fevers: management guidelines. Indian J Crit Care Med. 2014;18:62-69. doi:10.4103/0972-5229.126074
- Joint Chiefs of Staff. Joint Publication 4-02: Joint Health Services. December 11, 2017. Accessed March 5, 2026. https://cdmrp.health.mil/pubs/pdf/Joint%20Health%20Services%20Publication%20JP%204-02.pdf
- Armed Services Pest Management Board. Technical Guide No. 36: Personal Protective Measures Against Insects and Other Arthropods of Military Significance. Updated November 2015. Accessed March 5, 2026. https://www.acq.osd.mil/eie/afpmb/docs/techguides/tg36.pdf
- Global Emerging Infections Surveillance. Armed Forces Health Surveillance Division Annual Report 2024. Defense Health Agency; 2024:15-28. Accessed March 17, 2026. https://www.health.mil/Reference-Center/Reports/2026/01/05/AFHSD-Annual-Report-2024
Infectious diseases historically have posed major challenges to the operations and health of military forces. In recent conflicts, nonbattle injuries including infections have caused more evacuations than combat trauma.1 Deployment to endemic regions, poor sanitation, and trauma increase susceptibility to both common and rare infections, many of which have cutaneous manifestations.
Surveillance programs such as the Armed Forces Health Surveillance Division serve a critical role in monitoring outbreaks among deployed personnel.2 Cutaneous manifestations of systemic disease often serve as early clinical indicators, especially in settings with limited diagnostic resources. This review describes rarely encountered infectious agents for which US military personnel are at increased risk and outlines management strategies for clinicians practicing in austere environments.
EPIDEMIOLOGIC RISK FACTORS IN MILITARY POPULATIONS
United States military personnel face an elevated risk for infectious diseases when deployed in tropical and subtropical regions where endemic pathogens are prevalent. Exposure to soil, water, and insect vectors facilitates transmission. Direct exposure during combat or training combined with high-density housing, combat-related trauma, and constraints on hygiene access during operations increases infection risk.3
REGION-SPECIFIC PATHOGENS
Middle East
Leishmania species—Leishmania, a protozoa transmitted via sand fly bites, has caused multiple documented outbreaks among US troops in Iraq and Afghanistan, with a reported incidence of 14%.4 Leishmaniasis can present as 3 main clinical variants: cutaneous, visceral, and mucocutaneous. Cutaneous leishmaniasis typically manifests as painless ulcers covered with hemorrhagic crusts on exposed regions of the body. While typically self-limited, lesions frequently result in irreversible scarring. Many Leishmania species respond well to antimonials such as sodium stibogluconate. Preventive measures include wearing protective clothing and sleeping inside insecticide-treated bed nets.5
Coxiella burnetii—Coxiella burnetii transmits through inhalation of aerosolized particles originating from the urine, feces, birth products, or milk of infected bovine. In 2003, a small number of cases were identified in US service members exposed to livestock while serving in Iraq.6 Outbreaks also occurred during World War II, but it is unclear whether they were caused by naturally occurring C burnetii or biowarfare.7 Though primarily a systemic illness with severe pneumonia, Q fever may manifest with an associated purpuric or morbilliform rash.8 Doxycycline is recommended both for treatment and empiric coverage.6
Acinetobacter baumannii—This multidrug-resistant organism is known to infect combat wounds and is associated with nosocomial outbreaks in military hospitals. Studies suggest environmental contamination and health care transmission contribute substantially to outbreaks in military hospitals.9 Cutaneous manifestations can include cellulitis with a peau d’orange appearance or necrotizing fasciitis; however, pneumonia and bacteremia have been reported. Prompt culture and antibiotic initiation with debridement are essential for treatment.10 Antibiotic stewardship and strict infection control are critical to prevent outbreaks and limit resistance.9
Africa
Plasmodium species—Malaria remains a life-threatening disease found in tropical and subtropical areas around the world. Despite preventive measures, 30 cases among US service members were reported in 2024.11 Cutaneous findings include purpura fulminans, petechiae, acral necrosis, or reticulated erythema.12 Service members stationed in endemic areas should take prophylactic antimalarials. Symptoms include fevers, headaches, and malaise, with possible rapid deterioration.13
Mycobacterium ulcerans—Mycobacterium ulcerans causes extensive necrotic ulcers—commonly known as Buruli ulcers—which generally begin as a nodule, plaque, papule, or edematous lesion, eventually progressing to extensive ulceration. Despite no documented cases of US personnel contracting Buruli ulcers, those stationed in endemic regions remain at risk. Environmental reservoirs of M ulcerans are unknown, but its DNA has been isolated from water sources.14,15 These ulcers take months to heal, making wound management and antimycobacterial therapy essential. Primary preventive measures include avoidance of swimming in rivers or agricultural work in endemic areas.14
Mpox Virus—During the 2022 mpox outbreak, male service members who engaged in sexual activity with other men were at the highest risk, with 88.8% of infected service members reporting this practice.16 While the virus is endemic to Africa, 89.0% of cases were reported from service members stationed in the United States.17 Typical infection results in fever, headache, lymphadenopathy, and myalgias, followed by a facial rash that spreads over the body, palms, and soles. Safe-sex practices help prevent transmission, and there is a vaccine available for high-risk patients.16
Southeast Asia
Leptospira species—Leptospira is an aerobic spirochete found in tropical regions worldwide. Transmission occurs when water contaminated with urine from infected animals exposes humans to the organism. Infection manifests as a mild febrile illness, though approximately 10% of patients develop Weil syndrome, consisting of conjunctival suffusion, jaundice, and acute kidney injury. Treatment and prophylaxis include doxycycline, but severe disease warrants intravenous antibiotics.17,18 A 2014 outbreak among Marines in Japan highlighted poor prophylactic compliance as a key risk factor.19 Proper education for those at risk is essential to prevent future outbreaks.
Mycobacterium leprae—Leprosy is an acid-fast mycobacterium that remains endemic in the Pacific Islands and Southeast Asia. Case reports of US service members diagnosed with leprosy exist, though only in patients who emigrated from endemic areas.20 This disease has a spectrum of manifestations depending on the immune response, with tuberculoid leprosy showing a cell-mediated (T helper 1) response and lepromatous leprosy having more of a humoral (T helper 2) response.21 It manifests with hypopigmented anesthetic macules and peripheral neuropathy. Diagnosis is made by skin biopsy, which shows perineural lymphohistiocytic inflammation and non-necrotizing granulomas.20 The infection typically is curable with a multidrug regimen.21
Strongyloides stercoralis—This nematode causes infection by transdermal penetration of bare feet. They then migrate to the lungs where the patient coughs and swallows the nematode into the gastrointestinal tract. Strongyloides stercoralis autoinfect by penetrating the intestinal wall, resulting in chronic digestive, respiratory, and cutaneous symptoms. Worldwide prevalence of S stercoralis infection is estimated to be 10% to 40%, with foreign-born US military members at increased risk compared to the general military population.22,23 Larva currens may manifest with a pruritic erythematous plaque at the site of penetration that progresses to an intensely pruritic, creeping dermatitis as the nematode migrates under the skin. Avoidance of barefoot soil exposure and treatment with ivermectin are effective preventive and therapeutic measures.23
South America
Ancylostoma braziliense—Found throughout the subtropical world, this hookworm primarily infects dogs and cats and is found in their stool. Larva currens has a similar manifestation and life cycle to cutaneous larva migrans, but autoinfection does not occur. Transmission occurs similarly to S stercoralis and responds well to oral albendazole or ivermectin; however, the infection is self-limited.24 Military cases have been reported,25 though overall morbidity remains poorly characterized.
Dengue Virus—An arbovirus transmitted by Aedes mosquitoes, dengue remains a major military threat. Service members in the Vietnam War experienced an attack rate as high as 80%.26,27 Infection often manifests with retro-orbital pain and a morbilliform rash that occurs 2 to 5 days after fever, though severe cases may progress to hemorrhagic dengue with skin petechiae or ecchymosis.28 Immediate intervention is essential in symptomatic patients to prevent life-threatening progression. There are no dengue vaccines approved by the US Food and Drug Administration for adults, thus military personnel in endemic areas remain at risk.27
Trypanosoma cruzi—Chagas disease is transmitted when a reduviid infected with T cruzi bites and defecates on the patient’s skin. A skin nodule (chagoma) or painless eyelid edema (Romaña sign) may appear at the site of parasite entry. Chronic disease may result in dilated cardiomyopathy.29 Several cases of Chagas disease have been reported in South American military operations, including an outbreak in 9 Columbian military personnel.30 Cases in the southwestern United States have recently emerged, emphasizing the need for increased awareness.31 Proper insect repellent helps to ward off reduviid bugs. Nifurtimox and benznidazole are the only drugs with proven efficacy against T cruzi.29
Continental United States of America
Coccidioides immitis—The first reported case of coccidiomycosis was described in 1892 in a service member with debilitating masses and ulcers.32 Endemic to arid regions of the western United States, coccidioidomycosis affects military trainees at rates up to 32% annually in high-risk settings.33 Primary infection occurs in the lungs and may spread hematologically. The fungi prefer dry desert soils, which may aerosolize during military maneuvers. Coccidioidomycosis occasionally causes erythema nodosum, and diffuse infection shows verrucous plaques, ulcers, or abscesses. Dust avoidance and mask wearing are advised for those in endemic regions. Ketoconazole and amphotericin B are the only treatments approved by the US Food and Drug Administration.32 When starting immunosuppressive drugs, clinicians should inquire if patients have previously been stationed in Coccidioides-endemic areas, such as Fort Irwin, California, to avoid reactivation of the fungi.33
Francisella tularensis—Acquired via ticks or contact with wild animals, tularemia causes an ulceroglandular disease with regional lymphadenopathy. Inoculation requires as few as 10 to 25 organisms; thus it is considered a Category A agent for bioterror.34 Natural outbreaks have occurred during war times, most recently during the civil wars in Bosnia and Kosovo.35 Patients may present with a painful ulcer that enlarges to form a plaque with raised borders. Personnel in wooded areas should use tick precautions and handle wild animals cautiously. Treatment includes gentamicin for severe disease, with tetracyclines effective in mild cases.34
PREVENTION AND MANAGEMENT STRATEGIES IN AUSTERE SETTINGS
For health care professionals practicing in military settings, austere environments can provide a challenge for diagnosis of neglected diseases. Despite a lack of advanced diagnostic tools, practical options can be applied to the diagnostic process; for example, teledermatology is utilized for treatment of service members deployed to remote environments.36
Management of uncommon infectious diseases in military personnel often requires treatments outside those practiced in domestic clinics. Field management may indicate prompt empiric therapy while balancing the risks of overtreatment against those of missed diagnoses37; however, medical evacuation to a higher level of care may be indicated in patients with severe presentations to expedite diagnosis and treatment.38
Prevention remains the primary goal to avoid local outbreaks. Long-sleeved uniforms, DEET (N, N-diethyl-meta-toluamide)–based repellents, permethrin-impregnated clothing, and bed nets are effective for vector protection. Prophylactic medications and vaccinations often are provided when personnel are deployed to endemic locations.39
Onsite entomology teams also can provide surveillance of the local insect populations. They may contribute to vector control through insecticide application and environmental modification. The Armed Forces Health Surveillance Division and the Global Emerging Infections Surveillance Program monitor infectious threats in real time to locate any potential outbreaks, guiding operational responses.40
FINAL THOUGHTS
Dermatologic signs often provide early evidence of infection in military personnel. With increasing antimicrobial resistance and the emergence of new pathogens, it is imperative for clinicians treating members of the military to recognize cutaneous signs, employ efficient diagnostic strategies, and encourage proactive prevention. A collaborative approach spanning dermatology, infectious disease, and public health is essential to protect the modern service member.
Infectious diseases historically have posed major challenges to the operations and health of military forces. In recent conflicts, nonbattle injuries including infections have caused more evacuations than combat trauma.1 Deployment to endemic regions, poor sanitation, and trauma increase susceptibility to both common and rare infections, many of which have cutaneous manifestations.
Surveillance programs such as the Armed Forces Health Surveillance Division serve a critical role in monitoring outbreaks among deployed personnel.2 Cutaneous manifestations of systemic disease often serve as early clinical indicators, especially in settings with limited diagnostic resources. This review describes rarely encountered infectious agents for which US military personnel are at increased risk and outlines management strategies for clinicians practicing in austere environments.
EPIDEMIOLOGIC RISK FACTORS IN MILITARY POPULATIONS
United States military personnel face an elevated risk for infectious diseases when deployed in tropical and subtropical regions where endemic pathogens are prevalent. Exposure to soil, water, and insect vectors facilitates transmission. Direct exposure during combat or training combined with high-density housing, combat-related trauma, and constraints on hygiene access during operations increases infection risk.3
REGION-SPECIFIC PATHOGENS
Middle East
Leishmania species—Leishmania, a protozoa transmitted via sand fly bites, has caused multiple documented outbreaks among US troops in Iraq and Afghanistan, with a reported incidence of 14%.4 Leishmaniasis can present as 3 main clinical variants: cutaneous, visceral, and mucocutaneous. Cutaneous leishmaniasis typically manifests as painless ulcers covered with hemorrhagic crusts on exposed regions of the body. While typically self-limited, lesions frequently result in irreversible scarring. Many Leishmania species respond well to antimonials such as sodium stibogluconate. Preventive measures include wearing protective clothing and sleeping inside insecticide-treated bed nets.5
Coxiella burnetii—Coxiella burnetii transmits through inhalation of aerosolized particles originating from the urine, feces, birth products, or milk of infected bovine. In 2003, a small number of cases were identified in US service members exposed to livestock while serving in Iraq.6 Outbreaks also occurred during World War II, but it is unclear whether they were caused by naturally occurring C burnetii or biowarfare.7 Though primarily a systemic illness with severe pneumonia, Q fever may manifest with an associated purpuric or morbilliform rash.8 Doxycycline is recommended both for treatment and empiric coverage.6
Acinetobacter baumannii—This multidrug-resistant organism is known to infect combat wounds and is associated with nosocomial outbreaks in military hospitals. Studies suggest environmental contamination and health care transmission contribute substantially to outbreaks in military hospitals.9 Cutaneous manifestations can include cellulitis with a peau d’orange appearance or necrotizing fasciitis; however, pneumonia and bacteremia have been reported. Prompt culture and antibiotic initiation with debridement are essential for treatment.10 Antibiotic stewardship and strict infection control are critical to prevent outbreaks and limit resistance.9
Africa
Plasmodium species—Malaria remains a life-threatening disease found in tropical and subtropical areas around the world. Despite preventive measures, 30 cases among US service members were reported in 2024.11 Cutaneous findings include purpura fulminans, petechiae, acral necrosis, or reticulated erythema.12 Service members stationed in endemic areas should take prophylactic antimalarials. Symptoms include fevers, headaches, and malaise, with possible rapid deterioration.13
Mycobacterium ulcerans—Mycobacterium ulcerans causes extensive necrotic ulcers—commonly known as Buruli ulcers—which generally begin as a nodule, plaque, papule, or edematous lesion, eventually progressing to extensive ulceration. Despite no documented cases of US personnel contracting Buruli ulcers, those stationed in endemic regions remain at risk. Environmental reservoirs of M ulcerans are unknown, but its DNA has been isolated from water sources.14,15 These ulcers take months to heal, making wound management and antimycobacterial therapy essential. Primary preventive measures include avoidance of swimming in rivers or agricultural work in endemic areas.14
Mpox Virus—During the 2022 mpox outbreak, male service members who engaged in sexual activity with other men were at the highest risk, with 88.8% of infected service members reporting this practice.16 While the virus is endemic to Africa, 89.0% of cases were reported from service members stationed in the United States.17 Typical infection results in fever, headache, lymphadenopathy, and myalgias, followed by a facial rash that spreads over the body, palms, and soles. Safe-sex practices help prevent transmission, and there is a vaccine available for high-risk patients.16
Southeast Asia
Leptospira species—Leptospira is an aerobic spirochete found in tropical regions worldwide. Transmission occurs when water contaminated with urine from infected animals exposes humans to the organism. Infection manifests as a mild febrile illness, though approximately 10% of patients develop Weil syndrome, consisting of conjunctival suffusion, jaundice, and acute kidney injury. Treatment and prophylaxis include doxycycline, but severe disease warrants intravenous antibiotics.17,18 A 2014 outbreak among Marines in Japan highlighted poor prophylactic compliance as a key risk factor.19 Proper education for those at risk is essential to prevent future outbreaks.
Mycobacterium leprae—Leprosy is an acid-fast mycobacterium that remains endemic in the Pacific Islands and Southeast Asia. Case reports of US service members diagnosed with leprosy exist, though only in patients who emigrated from endemic areas.20 This disease has a spectrum of manifestations depending on the immune response, with tuberculoid leprosy showing a cell-mediated (T helper 1) response and lepromatous leprosy having more of a humoral (T helper 2) response.21 It manifests with hypopigmented anesthetic macules and peripheral neuropathy. Diagnosis is made by skin biopsy, which shows perineural lymphohistiocytic inflammation and non-necrotizing granulomas.20 The infection typically is curable with a multidrug regimen.21
Strongyloides stercoralis—This nematode causes infection by transdermal penetration of bare feet. They then migrate to the lungs where the patient coughs and swallows the nematode into the gastrointestinal tract. Strongyloides stercoralis autoinfect by penetrating the intestinal wall, resulting in chronic digestive, respiratory, and cutaneous symptoms. Worldwide prevalence of S stercoralis infection is estimated to be 10% to 40%, with foreign-born US military members at increased risk compared to the general military population.22,23 Larva currens may manifest with a pruritic erythematous plaque at the site of penetration that progresses to an intensely pruritic, creeping dermatitis as the nematode migrates under the skin. Avoidance of barefoot soil exposure and treatment with ivermectin are effective preventive and therapeutic measures.23
South America
Ancylostoma braziliense—Found throughout the subtropical world, this hookworm primarily infects dogs and cats and is found in their stool. Larva currens has a similar manifestation and life cycle to cutaneous larva migrans, but autoinfection does not occur. Transmission occurs similarly to S stercoralis and responds well to oral albendazole or ivermectin; however, the infection is self-limited.24 Military cases have been reported,25 though overall morbidity remains poorly characterized.
Dengue Virus—An arbovirus transmitted by Aedes mosquitoes, dengue remains a major military threat. Service members in the Vietnam War experienced an attack rate as high as 80%.26,27 Infection often manifests with retro-orbital pain and a morbilliform rash that occurs 2 to 5 days after fever, though severe cases may progress to hemorrhagic dengue with skin petechiae or ecchymosis.28 Immediate intervention is essential in symptomatic patients to prevent life-threatening progression. There are no dengue vaccines approved by the US Food and Drug Administration for adults, thus military personnel in endemic areas remain at risk.27
Trypanosoma cruzi—Chagas disease is transmitted when a reduviid infected with T cruzi bites and defecates on the patient’s skin. A skin nodule (chagoma) or painless eyelid edema (Romaña sign) may appear at the site of parasite entry. Chronic disease may result in dilated cardiomyopathy.29 Several cases of Chagas disease have been reported in South American military operations, including an outbreak in 9 Columbian military personnel.30 Cases in the southwestern United States have recently emerged, emphasizing the need for increased awareness.31 Proper insect repellent helps to ward off reduviid bugs. Nifurtimox and benznidazole are the only drugs with proven efficacy against T cruzi.29
Continental United States of America
Coccidioides immitis—The first reported case of coccidiomycosis was described in 1892 in a service member with debilitating masses and ulcers.32 Endemic to arid regions of the western United States, coccidioidomycosis affects military trainees at rates up to 32% annually in high-risk settings.33 Primary infection occurs in the lungs and may spread hematologically. The fungi prefer dry desert soils, which may aerosolize during military maneuvers. Coccidioidomycosis occasionally causes erythema nodosum, and diffuse infection shows verrucous plaques, ulcers, or abscesses. Dust avoidance and mask wearing are advised for those in endemic regions. Ketoconazole and amphotericin B are the only treatments approved by the US Food and Drug Administration.32 When starting immunosuppressive drugs, clinicians should inquire if patients have previously been stationed in Coccidioides-endemic areas, such as Fort Irwin, California, to avoid reactivation of the fungi.33
Francisella tularensis—Acquired via ticks or contact with wild animals, tularemia causes an ulceroglandular disease with regional lymphadenopathy. Inoculation requires as few as 10 to 25 organisms; thus it is considered a Category A agent for bioterror.34 Natural outbreaks have occurred during war times, most recently during the civil wars in Bosnia and Kosovo.35 Patients may present with a painful ulcer that enlarges to form a plaque with raised borders. Personnel in wooded areas should use tick precautions and handle wild animals cautiously. Treatment includes gentamicin for severe disease, with tetracyclines effective in mild cases.34
PREVENTION AND MANAGEMENT STRATEGIES IN AUSTERE SETTINGS
For health care professionals practicing in military settings, austere environments can provide a challenge for diagnosis of neglected diseases. Despite a lack of advanced diagnostic tools, practical options can be applied to the diagnostic process; for example, teledermatology is utilized for treatment of service members deployed to remote environments.36
Management of uncommon infectious diseases in military personnel often requires treatments outside those practiced in domestic clinics. Field management may indicate prompt empiric therapy while balancing the risks of overtreatment against those of missed diagnoses37; however, medical evacuation to a higher level of care may be indicated in patients with severe presentations to expedite diagnosis and treatment.38
Prevention remains the primary goal to avoid local outbreaks. Long-sleeved uniforms, DEET (N, N-diethyl-meta-toluamide)–based repellents, permethrin-impregnated clothing, and bed nets are effective for vector protection. Prophylactic medications and vaccinations often are provided when personnel are deployed to endemic locations.39
Onsite entomology teams also can provide surveillance of the local insect populations. They may contribute to vector control through insecticide application and environmental modification. The Armed Forces Health Surveillance Division and the Global Emerging Infections Surveillance Program monitor infectious threats in real time to locate any potential outbreaks, guiding operational responses.40
FINAL THOUGHTS
Dermatologic signs often provide early evidence of infection in military personnel. With increasing antimicrobial resistance and the emergence of new pathogens, it is imperative for clinicians treating members of the military to recognize cutaneous signs, employ efficient diagnostic strategies, and encourage proactive prevention. A collaborative approach spanning dermatology, infectious disease, and public health is essential to protect the modern service member.
- Murray CK. Infectious disease complications of combat-related injuries. Crit Care Med. 2008;36(7 suppl):S358-S364. doi:10.1097/CCM.0b013e31817e2ffc
- Armed Forces Health Surveillance Division. AFHSD Annual Report. Defense Health Agency; 2023. Accessed March 5, 2026. https://www.health.mil/Reference-Center/Reports/2024/09/19/AFHSD-Annual-Report-2023
- Murray CK, Yun HC, Markelz AE, et al. Operation United Assistance: infectious disease threats to deployed military personnel. Military Medicine. 2015;180:626-651. doi:10.7205/MILMED-D-14-00691
- Niba Rawlings N, Bailey M, Courtenay O. Leishmaniasis in deployed military populations: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2025;19:E0012680. doi:10.1371/journal.pntd.0012680
- de Vries HJC, Schallig HD. Cutaneous leishmaniasis: a 2022 updated narrative review into diagnosis and management developments. Am J Clin Dermatol. 2022;23:823-840. doi:10.1007/s40257-022-00726-8
- Anderson AD, Smoak B, Shuping E, et al. Q fever and the US military. Emerg Infect Dis. 2005;11:1320-1322. doi:10.3201/eid1108.050314
- Madariaga MG, Rezai K, Trenholme GM, et al. Q fever: a biological weapon in your backyard. Lancet Infect Dis. 2003;3:709-721. doi:10.1016/S1473-3099(03)00804-1
- Uribe Pulido N, Escorcia García C, Cabrera Orrego R, et al. Acute Q fever with dermatologic manifestations, molecular diagnosis, and no seroconversion. Open Forum Infect Dis. 2021;8:ofab458. doi:10.1093/ofid/ofab458
- Scott P, Deye G, Srinivasan A, et al. An outbreak of multidrug-resistant acinetobacter baumannii-calcoaceticus complex infection in the US Military Health Care System associated with military operations in Iraq. Clin Infect Dis. 2007;44:1577-1584. doi:10.1086/518170
- Guerrero DM, Perez F, Conger NG, et al. Acinetobacter baumannii-associated skin and soft tissue infections: recognizing a broadening spectrum of disease. Surg Infect (Larchmt). 2010;11:49-57. doi:10.1089/sur.2009.022
- Armed Forces Health Surveillance Division. Malaria among members of the US Armed Forces, 2024. MSMR. 2025;32:22-28.
- Farkouh CS, Abdi P, Amatul-Hadi F, et al. Cutaneous manifestations of malaria and their prognostic windows: a narrative review. Cureus. 2023;15:E41706. doi:10.7759/cureus.41706
- Shahbodaghi SD, Rathjen NA. Malaria: prevention, diagnosis, and treatment. Am Fam Physician. 2022;106:270-278.
- Yotsu RR, Suzuki K, Simmonds RE, et al. Buruli ulcer: a review of the current knowledge. Curr Trop Med Rep. 2018;5:247-256. doi:10.1007/s40475-018-0166-2
- Portaels F, Meyers WM, Ablordey A, et al. First cultivation and characterization of Mycobacterium ulcerans from the environment. PLoS Negl Trop Dis. 2008;2:E178. doi:10.1371/journal.pntd.0000178
- Metcalf-Kelly M, Garrison M, Stidham R. Characteristics of mpox cases diagnosed in Military Health System beneficiaries, May 2022-April 2024. MSMR. 2024;31:7-11.
- Rajapakse S. Leptospirosis: clinical aspects. Clin Med (Lond). 2022;22:14-17. doi:10.7861/clinmed.2021-0784
- Heath CW, Alexander AD, Galton MM. Leptospirosis in the United States: a of 483 cases in man, 1949–1961. N Engl J Med. 1965;273:857-864. doi:10.1056/NEJM196510142731606
- Mason V. Mystery outbreak investigation 2014—Leptospirosis licerasiae. November 17, 2017. Accessed March 5, 2026. https://usupulse.blogspot.com/2017/11/mystery-outbreak-investigation-2014.html
- Berjohn CM, DuPlessis CA, Tieu K, et al. Multibacillary leprosy in an active duty military member. Emerg Infect Dis. 2015;21:1077-1078. doi:10.3201/eid2106.141666
- Scollard DM, Adams LB, Gillis TP, et al. The continuing challenges of leprosy. Clin Microbiol Rev. 2006;19:338-381. doi:10.1128/CMR.19.2.338-381.2006
- Schär F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis. 2013;7:E2288. doi:10.1371/journal.pntd.0002288
- Taheri B, Kuo HC, Hockenbury N, et al. Strongyloides stercoralis in the US Military Health System. Open Forum Infect Dis. 2023;10:ofad127. doi:10.1093/ofid/ofad127
- Bowman DD, Montgomery SP, Zajac AM, et al. Hookworms of dogs and cats as agents of cutaneous larva migrans. Trends Parasitol. 2010;26:162-167. doi:10.1016/j.pt.2010.01.005
- Inglis DM, Bailey MS. Unusual presentations of cutaneous larva migrans in British military personnel. BMJ Mil Health. 2023;169:E78-E81. doi:10.1136/bmjmilitary-2020-001677
- Halstead SB, Udomsakdi S, Singharaj P, et al. Dengue and chikungunya virus infection in man in Thailand, 1962–1964. 3. clinical, epidemiologic, and virologic observations on disease in non-indigenous white persons. Am J Trop Med Hyg. 1969;18:984-996. doi:10.4269/ajtmh.1969.18.984
- Gibbons RV, Streitz M, Babina T, et al. Dengue and US military operations from the Spanish-American War through today. Emerg Infect Dis. 2012;18:623-630. doi:10.3201/eid1804.110134
- Guzman MG, Harris E. Dengue. Lancet. 2015;385:453-465. doi:10.1016/S0140-6736(14)60572-9
- Bern C. Chagas’ disease. N Engl J Med. 2015;373:456-466. doi:10.1056/NEJMra1410150
- Vergara HD, Gómez CH, Faccini-Martínez ÁA, et al. Acute Chagas disease outbreak among military personnel, Colombia, 2021. Emerg Infect Dis. 2023;29:1882-1885. doi:10.3201/eid2909.230886
- Harris N, Woc-Colburn L, Gunter SM, et al. Autochthonous Chagas disease in the southern United States: a case report of suspected residential and military exposures. Zoonoses Public Health. 2017;64:491-493. doi:10.1111/zph.12360
- Crum NF. Coccidioidomycosis: a contemporary review. Infect Dis Ther. 2022;11:713-742. doi:10.1007/s40121-022-00606-y
- Crum NF, Potter M, Pappagianis D. Seroincidence of coccidioidomycosis during military desert training exercises. J Clin Microbiol. 2004;42:4552-4555. doi:10.1128/JCM.42.10.4552-4555.2004
- Antonello RM, Giacomelli A, Riccardi N. Tularemia for clinicians: an up-to-date review on epidemiology, diagnosis, prevention and treatment. Eur J Intern Med. 2025;135:25-32. doi:10.1016/j.ejim.2025.03.013
- Nelson CA, Sjöstedt A. Tularemia: a storied history, an ongoing threat. Clin Infect Dis. 2024;78(supplement_1):S1-S3. doi:10.1093/cid/ciad681
- Pendlebury GA, Roman J, Shrivastava V, et al. A call to action: evidence for the military integration of teledermoscopy in a pandemic era. Dermatopathology (Basel). 2022;9:327-342. doi:10.3390/dermatopathology9040039
- Bhagchandani R, Singhi S, Peter JV, et al. Tropical fevers: management guidelines. Indian J Crit Care Med. 2014;18:62-69. doi:10.4103/0972-5229.126074
- Joint Chiefs of Staff. Joint Publication 4-02: Joint Health Services. December 11, 2017. Accessed March 5, 2026. https://cdmrp.health.mil/pubs/pdf/Joint%20Health%20Services%20Publication%20JP%204-02.pdf
- Armed Services Pest Management Board. Technical Guide No. 36: Personal Protective Measures Against Insects and Other Arthropods of Military Significance. Updated November 2015. Accessed March 5, 2026. https://www.acq.osd.mil/eie/afpmb/docs/techguides/tg36.pdf
- Global Emerging Infections Surveillance. Armed Forces Health Surveillance Division Annual Report 2024. Defense Health Agency; 2024:15-28. Accessed March 17, 2026. https://www.health.mil/Reference-Center/Reports/2026/01/05/AFHSD-Annual-Report-2024
- Murray CK. Infectious disease complications of combat-related injuries. Crit Care Med. 2008;36(7 suppl):S358-S364. doi:10.1097/CCM.0b013e31817e2ffc
- Armed Forces Health Surveillance Division. AFHSD Annual Report. Defense Health Agency; 2023. Accessed March 5, 2026. https://www.health.mil/Reference-Center/Reports/2024/09/19/AFHSD-Annual-Report-2023
- Murray CK, Yun HC, Markelz AE, et al. Operation United Assistance: infectious disease threats to deployed military personnel. Military Medicine. 2015;180:626-651. doi:10.7205/MILMED-D-14-00691
- Niba Rawlings N, Bailey M, Courtenay O. Leishmaniasis in deployed military populations: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2025;19:E0012680. doi:10.1371/journal.pntd.0012680
- de Vries HJC, Schallig HD. Cutaneous leishmaniasis: a 2022 updated narrative review into diagnosis and management developments. Am J Clin Dermatol. 2022;23:823-840. doi:10.1007/s40257-022-00726-8
- Anderson AD, Smoak B, Shuping E, et al. Q fever and the US military. Emerg Infect Dis. 2005;11:1320-1322. doi:10.3201/eid1108.050314
- Madariaga MG, Rezai K, Trenholme GM, et al. Q fever: a biological weapon in your backyard. Lancet Infect Dis. 2003;3:709-721. doi:10.1016/S1473-3099(03)00804-1
- Uribe Pulido N, Escorcia García C, Cabrera Orrego R, et al. Acute Q fever with dermatologic manifestations, molecular diagnosis, and no seroconversion. Open Forum Infect Dis. 2021;8:ofab458. doi:10.1093/ofid/ofab458
- Scott P, Deye G, Srinivasan A, et al. An outbreak of multidrug-resistant acinetobacter baumannii-calcoaceticus complex infection in the US Military Health Care System associated with military operations in Iraq. Clin Infect Dis. 2007;44:1577-1584. doi:10.1086/518170
- Guerrero DM, Perez F, Conger NG, et al. Acinetobacter baumannii-associated skin and soft tissue infections: recognizing a broadening spectrum of disease. Surg Infect (Larchmt). 2010;11:49-57. doi:10.1089/sur.2009.022
- Armed Forces Health Surveillance Division. Malaria among members of the US Armed Forces, 2024. MSMR. 2025;32:22-28.
- Farkouh CS, Abdi P, Amatul-Hadi F, et al. Cutaneous manifestations of malaria and their prognostic windows: a narrative review. Cureus. 2023;15:E41706. doi:10.7759/cureus.41706
- Shahbodaghi SD, Rathjen NA. Malaria: prevention, diagnosis, and treatment. Am Fam Physician. 2022;106:270-278.
- Yotsu RR, Suzuki K, Simmonds RE, et al. Buruli ulcer: a review of the current knowledge. Curr Trop Med Rep. 2018;5:247-256. doi:10.1007/s40475-018-0166-2
- Portaels F, Meyers WM, Ablordey A, et al. First cultivation and characterization of Mycobacterium ulcerans from the environment. PLoS Negl Trop Dis. 2008;2:E178. doi:10.1371/journal.pntd.0000178
- Metcalf-Kelly M, Garrison M, Stidham R. Characteristics of mpox cases diagnosed in Military Health System beneficiaries, May 2022-April 2024. MSMR. 2024;31:7-11.
- Rajapakse S. Leptospirosis: clinical aspects. Clin Med (Lond). 2022;22:14-17. doi:10.7861/clinmed.2021-0784
- Heath CW, Alexander AD, Galton MM. Leptospirosis in the United States: a of 483 cases in man, 1949–1961. N Engl J Med. 1965;273:857-864. doi:10.1056/NEJM196510142731606
- Mason V. Mystery outbreak investigation 2014—Leptospirosis licerasiae. November 17, 2017. Accessed March 5, 2026. https://usupulse.blogspot.com/2017/11/mystery-outbreak-investigation-2014.html
- Berjohn CM, DuPlessis CA, Tieu K, et al. Multibacillary leprosy in an active duty military member. Emerg Infect Dis. 2015;21:1077-1078. doi:10.3201/eid2106.141666
- Scollard DM, Adams LB, Gillis TP, et al. The continuing challenges of leprosy. Clin Microbiol Rev. 2006;19:338-381. doi:10.1128/CMR.19.2.338-381.2006
- Schär F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis. 2013;7:E2288. doi:10.1371/journal.pntd.0002288
- Taheri B, Kuo HC, Hockenbury N, et al. Strongyloides stercoralis in the US Military Health System. Open Forum Infect Dis. 2023;10:ofad127. doi:10.1093/ofid/ofad127
- Bowman DD, Montgomery SP, Zajac AM, et al. Hookworms of dogs and cats as agents of cutaneous larva migrans. Trends Parasitol. 2010;26:162-167. doi:10.1016/j.pt.2010.01.005
- Inglis DM, Bailey MS. Unusual presentations of cutaneous larva migrans in British military personnel. BMJ Mil Health. 2023;169:E78-E81. doi:10.1136/bmjmilitary-2020-001677
- Halstead SB, Udomsakdi S, Singharaj P, et al. Dengue and chikungunya virus infection in man in Thailand, 1962–1964. 3. clinical, epidemiologic, and virologic observations on disease in non-indigenous white persons. Am J Trop Med Hyg. 1969;18:984-996. doi:10.4269/ajtmh.1969.18.984
- Gibbons RV, Streitz M, Babina T, et al. Dengue and US military operations from the Spanish-American War through today. Emerg Infect Dis. 2012;18:623-630. doi:10.3201/eid1804.110134
- Guzman MG, Harris E. Dengue. Lancet. 2015;385:453-465. doi:10.1016/S0140-6736(14)60572-9
- Bern C. Chagas’ disease. N Engl J Med. 2015;373:456-466. doi:10.1056/NEJMra1410150
- Vergara HD, Gómez CH, Faccini-Martínez ÁA, et al. Acute Chagas disease outbreak among military personnel, Colombia, 2021. Emerg Infect Dis. 2023;29:1882-1885. doi:10.3201/eid2909.230886
- Harris N, Woc-Colburn L, Gunter SM, et al. Autochthonous Chagas disease in the southern United States: a case report of suspected residential and military exposures. Zoonoses Public Health. 2017;64:491-493. doi:10.1111/zph.12360
- Crum NF. Coccidioidomycosis: a contemporary review. Infect Dis Ther. 2022;11:713-742. doi:10.1007/s40121-022-00606-y
- Crum NF, Potter M, Pappagianis D. Seroincidence of coccidioidomycosis during military desert training exercises. J Clin Microbiol. 2004;42:4552-4555. doi:10.1128/JCM.42.10.4552-4555.2004
- Antonello RM, Giacomelli A, Riccardi N. Tularemia for clinicians: an up-to-date review on epidemiology, diagnosis, prevention and treatment. Eur J Intern Med. 2025;135:25-32. doi:10.1016/j.ejim.2025.03.013
- Nelson CA, Sjöstedt A. Tularemia: a storied history, an ongoing threat. Clin Infect Dis. 2024;78(supplement_1):S1-S3. doi:10.1093/cid/ciad681
- Pendlebury GA, Roman J, Shrivastava V, et al. A call to action: evidence for the military integration of teledermoscopy in a pandemic era. Dermatopathology (Basel). 2022;9:327-342. doi:10.3390/dermatopathology9040039
- Bhagchandani R, Singhi S, Peter JV, et al. Tropical fevers: management guidelines. Indian J Crit Care Med. 2014;18:62-69. doi:10.4103/0972-5229.126074
- Joint Chiefs of Staff. Joint Publication 4-02: Joint Health Services. December 11, 2017. Accessed March 5, 2026. https://cdmrp.health.mil/pubs/pdf/Joint%20Health%20Services%20Publication%20JP%204-02.pdf
- Armed Services Pest Management Board. Technical Guide No. 36: Personal Protective Measures Against Insects and Other Arthropods of Military Significance. Updated November 2015. Accessed March 5, 2026. https://www.acq.osd.mil/eie/afpmb/docs/techguides/tg36.pdf
- Global Emerging Infections Surveillance. Armed Forces Health Surveillance Division Annual Report 2024. Defense Health Agency; 2024:15-28. Accessed March 17, 2026. https://www.health.mil/Reference-Center/Reports/2026/01/05/AFHSD-Annual-Report-2024
Cutaneous Manifestations of Neglected Infectious Diseases in US Military Personnel
Cutaneous Manifestations of Neglected Infectious Diseases in US Military Personnel
Practice Points
- Military personnel stationed overseas are at risk for encountering infectious organisms that are not regularly observed domestically—many of which have cutaneous manifestations.
- Health care professionals treating military personnel should consider uncommonly encountered infections in the differential diagnosis for certain dermatologic presentations.
- Clinicians should inquire if patients have been stationed in Coccidioides immitis–endemic areas prior to the initiation of immunosuppression.

Implementation of a Pharmacist-Led Penicillin Allergy Interview at a Veterans Care Facility
Implementation of a Pharmacist-Led Penicillin Allergy Interview at a Veterans Care Facility
Self-reported penicillin allergies are common, with a prevalence of about 10% of patients, according to the Centers for Disease Control and Prevention (CDC).1 However, only about 1% of patients have a true immunoglobulin E (IgE)-mediated allergy. This issue is often further complicated by inaccurate classification of nonallergic adverse effects as an allergy, resulting in incomplete allergy documentation in the electronic health record (EHR). The cross-reactivity rate with cephalosporins (Β-lactam antibiotics) in patients reporting a penicillin allergy is < 1%, which suggests that many patients with reported penicillin allergies can safely receive them.2 Despite this, patients with self-reported penicillin allergies often receive non–Β-lactam antibiotic agents, which may be associated with an increased risk of adverse drug reactions (ADRs), increased health care costs, and inferior clinical outcomes.3
Several strategies are recommended to assess patients with self-reported penicillin allergies. According to the CDC, evaluating a patient who reports a penicillin or other Β-lactam antibiotic allergy involves 3 steps: (1) obtaining a thorough medical history, including previous exposures to penicillin or other Β-lactam antibiotic; (2) performing a skin test using the penicillin major and minor determinants; and (3) among those who have a negative penicillin skin test, performing an observed oral challenge with 250 mg amoxicillin before proceeding directly to treatment with the indicated Β-lactam therapy.4
Most existing clinical guidance for assessing patients with self-reported penicillin allergies stems from site-specific policies and primarily focuses on oral amoxicillin challenges or penicillin skin testing (PST). However, performing these tests may not be feasible at all facilities due to time constraints and lack of allergists. Therefore, alternative strategies are necessary, such as conducting detailed patient interviews. Few studies have evaluated switching to Β-lactam agents following a penicillin allergy interview alone. However, with thorough patient histories and detailed interviews, patients with reported penicillin allergies can safely use Β-lactam antibiotics.5 Implementing this procedure provides a cost-savings opportunity by not having to administer additional antibiotics for testing in addition to improving antibiotic stewardship.
The Memphis Veterans Affairs Medical Center (MVAMC) created the Allergy to Β-Lactam Evaluation (ABLE) process to clarify and remove penicillin allergies. The process involves conducting a thorough chart review and patient interview followed by completion of a note template that provides recommendations about patient allergies and Β-lactam prescribing. Mitchell et al found that the pharmacist-led process to be beneficial for addressing Β-lactam allergy clearance.6 As a result, the ABLE process was implemented at several other US Department of Veterans Affairs (VA) medical centers (VAMCs). Using the ABLE template, the purpose of this study was to evaluate the impact of a pharmacist-led penicillin allergy initiative on penicillin allergy delabeling with an interview process alone.
Methods
Prior to ABLE process implementation, there were no standardized procedures for documenting allergy histories. ABLE was implemented at the Robley Rex VAMC (RRVAMC) in November 2022. During the interview phase, patients were initially identified during admission via TheraDoc as having either a penicillin allergy or ADR. The infectious disease pharmacist or pharmacy resident interviewed patients with documented penicillin allergies or ADRs using a standardized questionnaire (eAppendix 1). Not all identified patients could be interviewed. Patients currently receiving an antibiotic were prioritized for interviews. Patients were excluded if they declined or were unable to be interviewed, although a patient’s caregiver(s) could be interviewed in person or via telephone, if the patient was not available.
Following the interview, pharmacists used guidance from the ABLE process in addition to a detailed EHR review to determine whether the patient was eligible for an allergy update or removal and/or switch to a Β-lactam antibiotic (Figure). If eligible for modification, the interviewing pharmacist made the necessary changes. A templated process note with patient-specific recommendations was entered into the Computerized Patient Record System (CPRS) and the primary care team attending physician was added as an additional signer to be alerted in the system note (eAppendix 2).
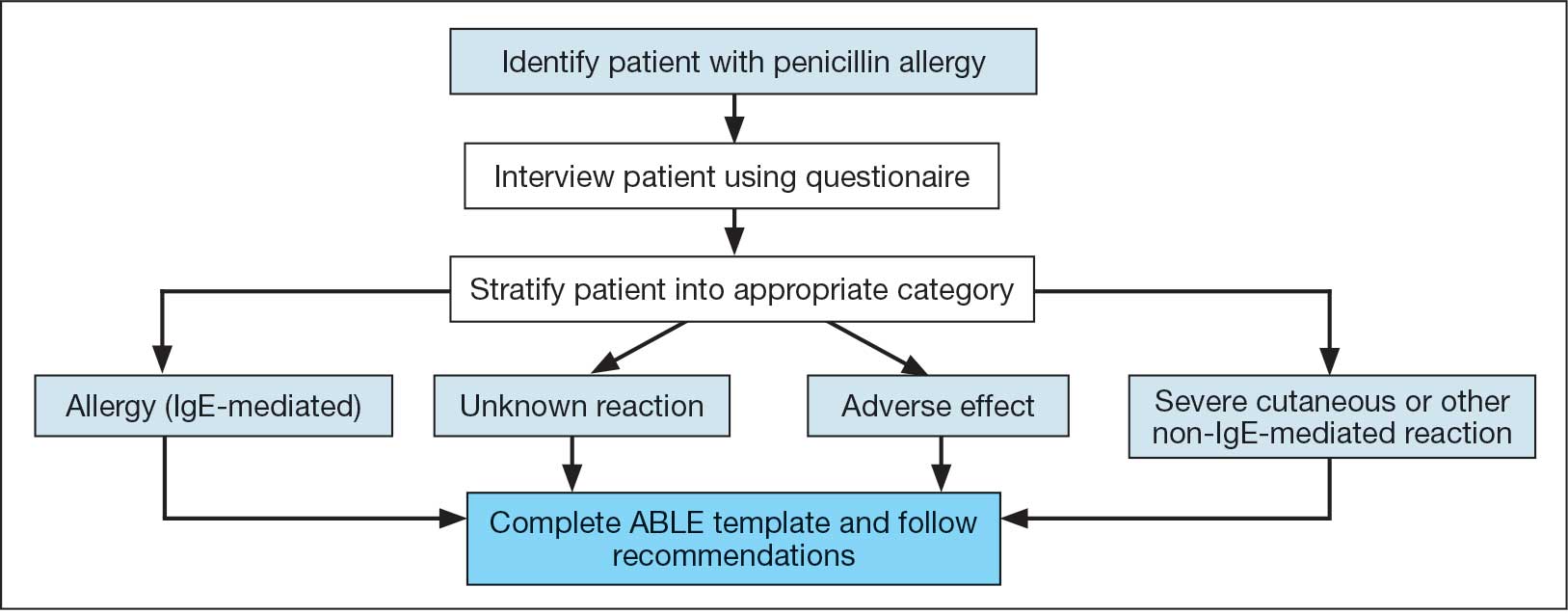
This single-center, retrospective cohort study involved review of CPRS notes and clinical interviews in the interviewed group. Hospitalized patients at the RRVAMC aged ≥ 18 years with a documented penicillin allergy or ADR were included. The historical control group consisted of patients admitted between October 31, 2019, and October 31, 2022, and the intervention group consisted of patients admitted between November 1, 2022, and March 1, 2023. Patients in the historical control group were matched 1:1 to the intervention group for penicillin allergy severity (allergy [IgE-mediated], unknown, adverse effect, severe cutaneous or other non–IgE-mediated reaction) and whether they received a noncarbapenem non–Β-lactam antibiotic.
The primary outcome was the number of patient allergies/ADRs removed or changed on patient profiles regardless of whether their antibiotic regimen was changed. This outcome was further assessed by evaluating the number of patient allergies or ADRs removed or changed on patient profiles with or without a change in antibiotic regimen. Primary outcomes were analyzed using χ2 and/ or Fisher exact tests, as appropriate to determine statistically significant differences between the interviewed group and the historical control.
Results
Seventy patients were included: 35 patients in the interviewed group and 35 patients in the historical control group, respectively. Both groups had a mean age of 72 years and predominantly included White male patients (Table 1). Following the interview, the allergy profile was modified for 6 patients (17%) in the interview group vs 0 patients in the control group (P = .03) (Table 2). The primary outcome was analyzed separately regardless of an antibiotic regimen change. There was not a statistically significant difference between groups when assessing patients for change in therapy (P > .99). All 6 patients with an allergy profile modification had no change in antibiotic regimen.
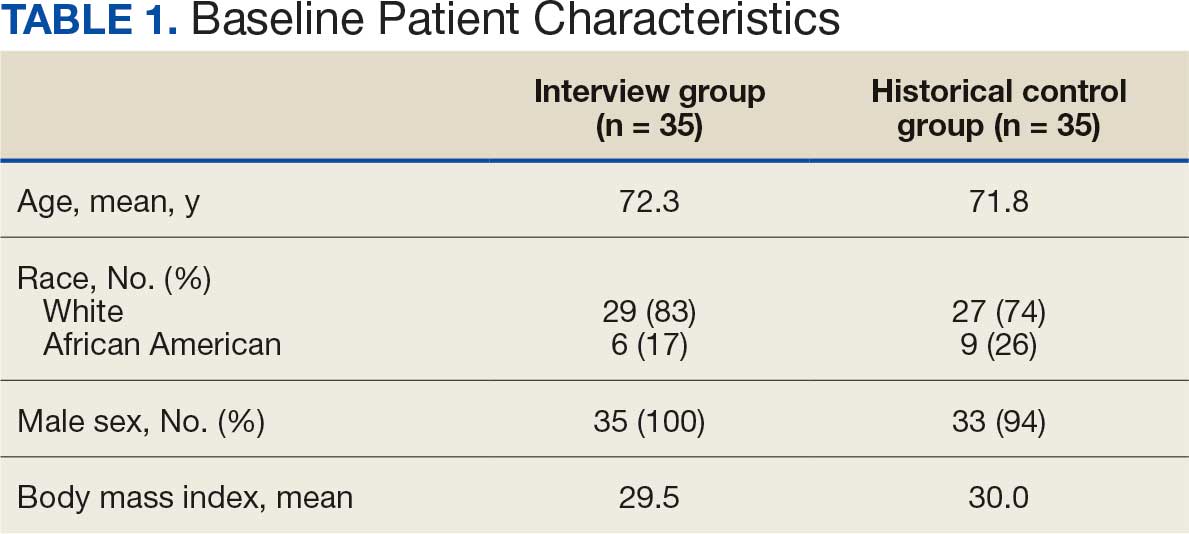
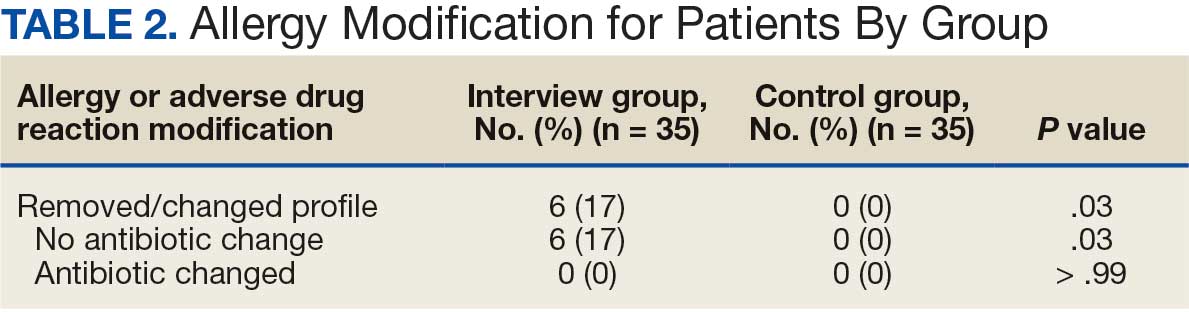
Discussion
This study suggests the ABLE process may be a valuable tool for adjusting penicillin allergies or ADRs within patient EHRs. In the interview group, allergies were modified in 6 (17%) patients while no patients in the control group had allergy modifications. Of the 6 allergy profile modifications, 4 allergy labels were changed from an allergy to an ADR. These patients were cleared to receive future Β-lactam antibiotics after clinicians recognized the lack of a true IgE-mediated allergic reaction. In addition, 2 of the modified allergy profiles removed the allergy designation. Although this represents a small subset of interviewed patients, it illustrates the clinical effectiveness of an interview process alone to remove penicillin allergy designations.
Previous research has assessed the impact of pharmacist intervention on penicillin allergy clarification. Mitchell et al implemented a pharmacist-driven Β-lactam allergy assessment and penicillin allergy clinic (PAC) at the MVAMC with the goal of evaluating its impact on allergy clearance. In their study, clinical pharmacy specialists evaluated patients with Β-lactam allergies, and those deemed eligible were later seen in the PAC. Among the 246 patients evaluated using the Β-lactam allergy assessment alone and who were not seen in the PAC, 25% had their penicillin allergy removed following a detailed assessment.6
Song et al evaluated the effectiveness and feasibility of a pharmacist-driven penicillin allergy delabeling pilot program without skin testing or oral challenges. Patients with penicillin allergies were interviewed by a pharmacy resident using a standardized checklist. Among the 66 patients interviewed, 12 (18%) met the criteria for delabeling and consented to removal of their allergy.7 The delabeling rates in these 2 studies are similar to the 17% rate of allergy modification in our study, although this study is the only one to compare results to a historical control group.
Harper et al evaluated the impact of a penicillin allergy assessment, including penicillin skin testing and oral amoxicillin challenges, on delabeling penicillin allergies. Pharmacists completed a penicillin allergy assessment and performed penicillin skin testing and/or oral amoxicillin challenges for eligible patients. Of 35 patients, 31 (89%) had their penicillin allergies delabeled in the EHR.8 The rate of penicillin allergy delabeling in Harper et al was likely higher than that seen in our study due to the use of oral challenge and skin testing. Regardless, a detailed penicillin allergy interview alone was effective at RRVAMC, resulting in a significant rate of allergy removal or change. This supports the use of detailed penicillin allergy assessments in settings where penicillin skin testing or oral challenges may not be feasible.
Mann et al demonstrated the effectiveness of penicillin allergy assessments in switching eligible patients to Β-lactam antibiotics. Their single-center, prospective study assessed the impact of a pharmacist-driven detailed penicillin allergy interview initiative. Interviews that evaluated potential changes to allergy profiles were conducted with 175 patients. Of these patients, 135 (77.1%) were on antimicrobial therapy and 42 (31.1%) patients receiving therapy met criteria to switch to a noncarbapenem Β-lactam antibiotic. Thirty-one patients (73.8%) switched with no signs or symptoms of intolerance demonstrating that an interview can be a valuable tool for antibiotic optimization, specifically in patients with penicillin allergy.9 No patients in our study switched antibiotic therapy, likely because only a small number of patients were eligible for transition to a noncarbapenem Β-lactam antibiotic. In the Mann et al study, non–Β-lactam antibiotics, such as fluoroquinolones and carbapenems, accounted for > 75% of the antibiotics used.
Limitations
The sample size of this study was small and its duration was short. There is a risk for selection bias as not all identified patients were able to be interviewed while admitted, but patients on antibiotics were prioritized as they were most likely to directly benefit during their current admission from a modification of their allergy. Most patients in the study were White and male, which may limit the generalizability of the results. Additionally, recommendations regarding antibiotic changes were primarily communicated to the treatment team based on a templated note in CPRS alone. Therefore, implementation of these recommendations largely relied upon nonverbal communication. Direct pharmacist-physician communication could have led to a larger impact on antimicrobial therapy changes. The interviewer’s participation in daily rounds with time allotted to discuss this topic can be considered in the future to improve these processes.
Conclusions
This study found that the ABLE process identified patients for penicillin allergy delabeling. With the high prevalence of inaccurate penicillin allergy documentation, this tool offers VA health care systems a way to empower pharmacists in allergy clarification, leading to improvements in antibiotic stewardship. Although the sample size was small, the ABLE process may provide a framework for VA clinicians. Future research has the potential to demonstrate the practicality and effectiveness this pharmacist-led penicillin allergy interview process can offer clinicians.
- Health care providers. Clinical features of penicillin allergy. Centers for Disease Control and Prevention. August 25, 2025. Accessed February 4, 2026. https://www.cdc.gov /antibiotic-use/hcp/clinical-signs/index.html
- Wrynn AF. Penicillin allergies: A guide for NPs. Nurse Pract. 2022;47:30-36. doi:10.1097/01.NPR.0000855312.11145.78
- Mohsen S, Dickinson JA, Somayaji R. Update on the adverse effects of antimicrobial therapies in community practice. Can Fam Physician. 2020;66:651-659.
- Sexually Transmitted Infections Treatment Guidelines, 2021. Managing persons who have a history of penicillin allergy. Centers for Disease Control and Prevention. September 21, 2022. Accessed February 4, 2026. https:// www.cdc.gov/std/treatment-guidelines/penicillin-allergy .htm
- Holmes AK, Bennett NT, Berry TP. Pharmacy driven assessment of appropriate antibiotic selection in patients with reported beta-lactam allergy. J Am Coll Clin Pharm. 2019;2:509-514. doi:10.1002/jac5.1135
- Mitchell AB, Ness RA, Bennett JG, et al. Implementation and impact of a Β-lactam allergy assessment protocol in a veteran population. Fed Pract. 2021;38:420-425. doi:10.12788/fp.0172
- Song YC, Nelson ZJ, Wankum MA, et al. Effectiveness and feasibility of pharmacist-driven penicillin allergy de-labeling pilot program without skin testing or oral challenges. Pharmacy (Basel). 2021;9:127. doi:10.3390/pharmacy9030127
- Harper HM, Sanchez M. Review of pharmacist driven penicillin allergy assessments and skin testing: a multicenter case-series. Hosp Pharm. 2022;57:469-473. doi:10.1177/00185787211046862
- Mann KL, Wu JY, Shah SS. Implementation of a pharmacist- driven detailed penicillin allergy interview. Ann Pharmacother. 2020;54:364-370. doi:10.1177/1060028019884874
Self-reported penicillin allergies are common, with a prevalence of about 10% of patients, according to the Centers for Disease Control and Prevention (CDC).1 However, only about 1% of patients have a true immunoglobulin E (IgE)-mediated allergy. This issue is often further complicated by inaccurate classification of nonallergic adverse effects as an allergy, resulting in incomplete allergy documentation in the electronic health record (EHR). The cross-reactivity rate with cephalosporins (Β-lactam antibiotics) in patients reporting a penicillin allergy is < 1%, which suggests that many patients with reported penicillin allergies can safely receive them.2 Despite this, patients with self-reported penicillin allergies often receive non–Β-lactam antibiotic agents, which may be associated with an increased risk of adverse drug reactions (ADRs), increased health care costs, and inferior clinical outcomes.3
Several strategies are recommended to assess patients with self-reported penicillin allergies. According to the CDC, evaluating a patient who reports a penicillin or other Β-lactam antibiotic allergy involves 3 steps: (1) obtaining a thorough medical history, including previous exposures to penicillin or other Β-lactam antibiotic; (2) performing a skin test using the penicillin major and minor determinants; and (3) among those who have a negative penicillin skin test, performing an observed oral challenge with 250 mg amoxicillin before proceeding directly to treatment with the indicated Β-lactam therapy.4
Most existing clinical guidance for assessing patients with self-reported penicillin allergies stems from site-specific policies and primarily focuses on oral amoxicillin challenges or penicillin skin testing (PST). However, performing these tests may not be feasible at all facilities due to time constraints and lack of allergists. Therefore, alternative strategies are necessary, such as conducting detailed patient interviews. Few studies have evaluated switching to Β-lactam agents following a penicillin allergy interview alone. However, with thorough patient histories and detailed interviews, patients with reported penicillin allergies can safely use Β-lactam antibiotics.5 Implementing this procedure provides a cost-savings opportunity by not having to administer additional antibiotics for testing in addition to improving antibiotic stewardship.
The Memphis Veterans Affairs Medical Center (MVAMC) created the Allergy to Β-Lactam Evaluation (ABLE) process to clarify and remove penicillin allergies. The process involves conducting a thorough chart review and patient interview followed by completion of a note template that provides recommendations about patient allergies and Β-lactam prescribing. Mitchell et al found that the pharmacist-led process to be beneficial for addressing Β-lactam allergy clearance.6 As a result, the ABLE process was implemented at several other US Department of Veterans Affairs (VA) medical centers (VAMCs). Using the ABLE template, the purpose of this study was to evaluate the impact of a pharmacist-led penicillin allergy initiative on penicillin allergy delabeling with an interview process alone.
Methods
Prior to ABLE process implementation, there were no standardized procedures for documenting allergy histories. ABLE was implemented at the Robley Rex VAMC (RRVAMC) in November 2022. During the interview phase, patients were initially identified during admission via TheraDoc as having either a penicillin allergy or ADR. The infectious disease pharmacist or pharmacy resident interviewed patients with documented penicillin allergies or ADRs using a standardized questionnaire (eAppendix 1). Not all identified patients could be interviewed. Patients currently receiving an antibiotic were prioritized for interviews. Patients were excluded if they declined or were unable to be interviewed, although a patient’s caregiver(s) could be interviewed in person or via telephone, if the patient was not available.
Following the interview, pharmacists used guidance from the ABLE process in addition to a detailed EHR review to determine whether the patient was eligible for an allergy update or removal and/or switch to a Β-lactam antibiotic (Figure). If eligible for modification, the interviewing pharmacist made the necessary changes. A templated process note with patient-specific recommendations was entered into the Computerized Patient Record System (CPRS) and the primary care team attending physician was added as an additional signer to be alerted in the system note (eAppendix 2).
This single-center, retrospective cohort study involved review of CPRS notes and clinical interviews in the interviewed group. Hospitalized patients at the RRVAMC aged ≥ 18 years with a documented penicillin allergy or ADR were included. The historical control group consisted of patients admitted between October 31, 2019, and October 31, 2022, and the intervention group consisted of patients admitted between November 1, 2022, and March 1, 2023. Patients in the historical control group were matched 1:1 to the intervention group for penicillin allergy severity (allergy [IgE-mediated], unknown, adverse effect, severe cutaneous or other non–IgE-mediated reaction) and whether they received a noncarbapenem non–Β-lactam antibiotic.
The primary outcome was the number of patient allergies/ADRs removed or changed on patient profiles regardless of whether their antibiotic regimen was changed. This outcome was further assessed by evaluating the number of patient allergies or ADRs removed or changed on patient profiles with or without a change in antibiotic regimen. Primary outcomes were analyzed using χ2 and/ or Fisher exact tests, as appropriate to determine statistically significant differences between the interviewed group and the historical control.
Results
Seventy patients were included: 35 patients in the interviewed group and 35 patients in the historical control group, respectively. Both groups had a mean age of 72 years and predominantly included White male patients (Table 1). Following the interview, the allergy profile was modified for 6 patients (17%) in the interview group vs 0 patients in the control group (P = .03) (Table 2). The primary outcome was analyzed separately regardless of an antibiotic regimen change. There was not a statistically significant difference between groups when assessing patients for change in therapy (P > .99). All 6 patients with an allergy profile modification had no change in antibiotic regimen.
Discussion
This study suggests the ABLE process may be a valuable tool for adjusting penicillin allergies or ADRs within patient EHRs. In the interview group, allergies were modified in 6 (17%) patients while no patients in the control group had allergy modifications. Of the 6 allergy profile modifications, 4 allergy labels were changed from an allergy to an ADR. These patients were cleared to receive future Β-lactam antibiotics after clinicians recognized the lack of a true IgE-mediated allergic reaction. In addition, 2 of the modified allergy profiles removed the allergy designation. Although this represents a small subset of interviewed patients, it illustrates the clinical effectiveness of an interview process alone to remove penicillin allergy designations.
Previous research has assessed the impact of pharmacist intervention on penicillin allergy clarification. Mitchell et al implemented a pharmacist-driven Β-lactam allergy assessment and penicillin allergy clinic (PAC) at the MVAMC with the goal of evaluating its impact on allergy clearance. In their study, clinical pharmacy specialists evaluated patients with Β-lactam allergies, and those deemed eligible were later seen in the PAC. Among the 246 patients evaluated using the Β-lactam allergy assessment alone and who were not seen in the PAC, 25% had their penicillin allergy removed following a detailed assessment.6
Song et al evaluated the effectiveness and feasibility of a pharmacist-driven penicillin allergy delabeling pilot program without skin testing or oral challenges. Patients with penicillin allergies were interviewed by a pharmacy resident using a standardized checklist. Among the 66 patients interviewed, 12 (18%) met the criteria for delabeling and consented to removal of their allergy.7 The delabeling rates in these 2 studies are similar to the 17% rate of allergy modification in our study, although this study is the only one to compare results to a historical control group.
Harper et al evaluated the impact of a penicillin allergy assessment, including penicillin skin testing and oral amoxicillin challenges, on delabeling penicillin allergies. Pharmacists completed a penicillin allergy assessment and performed penicillin skin testing and/or oral amoxicillin challenges for eligible patients. Of 35 patients, 31 (89%) had their penicillin allergies delabeled in the EHR.8 The rate of penicillin allergy delabeling in Harper et al was likely higher than that seen in our study due to the use of oral challenge and skin testing. Regardless, a detailed penicillin allergy interview alone was effective at RRVAMC, resulting in a significant rate of allergy removal or change. This supports the use of detailed penicillin allergy assessments in settings where penicillin skin testing or oral challenges may not be feasible.
Mann et al demonstrated the effectiveness of penicillin allergy assessments in switching eligible patients to Β-lactam antibiotics. Their single-center, prospective study assessed the impact of a pharmacist-driven detailed penicillin allergy interview initiative. Interviews that evaluated potential changes to allergy profiles were conducted with 175 patients. Of these patients, 135 (77.1%) were on antimicrobial therapy and 42 (31.1%) patients receiving therapy met criteria to switch to a noncarbapenem Β-lactam antibiotic. Thirty-one patients (73.8%) switched with no signs or symptoms of intolerance demonstrating that an interview can be a valuable tool for antibiotic optimization, specifically in patients with penicillin allergy.9 No patients in our study switched antibiotic therapy, likely because only a small number of patients were eligible for transition to a noncarbapenem Β-lactam antibiotic. In the Mann et al study, non–Β-lactam antibiotics, such as fluoroquinolones and carbapenems, accounted for > 75% of the antibiotics used.
Limitations
The sample size of this study was small and its duration was short. There is a risk for selection bias as not all identified patients were able to be interviewed while admitted, but patients on antibiotics were prioritized as they were most likely to directly benefit during their current admission from a modification of their allergy. Most patients in the study were White and male, which may limit the generalizability of the results. Additionally, recommendations regarding antibiotic changes were primarily communicated to the treatment team based on a templated note in CPRS alone. Therefore, implementation of these recommendations largely relied upon nonverbal communication. Direct pharmacist-physician communication could have led to a larger impact on antimicrobial therapy changes. The interviewer’s participation in daily rounds with time allotted to discuss this topic can be considered in the future to improve these processes.
Conclusions
This study found that the ABLE process identified patients for penicillin allergy delabeling. With the high prevalence of inaccurate penicillin allergy documentation, this tool offers VA health care systems a way to empower pharmacists in allergy clarification, leading to improvements in antibiotic stewardship. Although the sample size was small, the ABLE process may provide a framework for VA clinicians. Future research has the potential to demonstrate the practicality and effectiveness this pharmacist-led penicillin allergy interview process can offer clinicians.
Self-reported penicillin allergies are common, with a prevalence of about 10% of patients, according to the Centers for Disease Control and Prevention (CDC).1 However, only about 1% of patients have a true immunoglobulin E (IgE)-mediated allergy. This issue is often further complicated by inaccurate classification of nonallergic adverse effects as an allergy, resulting in incomplete allergy documentation in the electronic health record (EHR). The cross-reactivity rate with cephalosporins (Β-lactam antibiotics) in patients reporting a penicillin allergy is < 1%, which suggests that many patients with reported penicillin allergies can safely receive them.2 Despite this, patients with self-reported penicillin allergies often receive non–Β-lactam antibiotic agents, which may be associated with an increased risk of adverse drug reactions (ADRs), increased health care costs, and inferior clinical outcomes.3
Several strategies are recommended to assess patients with self-reported penicillin allergies. According to the CDC, evaluating a patient who reports a penicillin or other Β-lactam antibiotic allergy involves 3 steps: (1) obtaining a thorough medical history, including previous exposures to penicillin or other Β-lactam antibiotic; (2) performing a skin test using the penicillin major and minor determinants; and (3) among those who have a negative penicillin skin test, performing an observed oral challenge with 250 mg amoxicillin before proceeding directly to treatment with the indicated Β-lactam therapy.4
Most existing clinical guidance for assessing patients with self-reported penicillin allergies stems from site-specific policies and primarily focuses on oral amoxicillin challenges or penicillin skin testing (PST). However, performing these tests may not be feasible at all facilities due to time constraints and lack of allergists. Therefore, alternative strategies are necessary, such as conducting detailed patient interviews. Few studies have evaluated switching to Β-lactam agents following a penicillin allergy interview alone. However, with thorough patient histories and detailed interviews, patients with reported penicillin allergies can safely use Β-lactam antibiotics.5 Implementing this procedure provides a cost-savings opportunity by not having to administer additional antibiotics for testing in addition to improving antibiotic stewardship.
The Memphis Veterans Affairs Medical Center (MVAMC) created the Allergy to Β-Lactam Evaluation (ABLE) process to clarify and remove penicillin allergies. The process involves conducting a thorough chart review and patient interview followed by completion of a note template that provides recommendations about patient allergies and Β-lactam prescribing. Mitchell et al found that the pharmacist-led process to be beneficial for addressing Β-lactam allergy clearance.6 As a result, the ABLE process was implemented at several other US Department of Veterans Affairs (VA) medical centers (VAMCs). Using the ABLE template, the purpose of this study was to evaluate the impact of a pharmacist-led penicillin allergy initiative on penicillin allergy delabeling with an interview process alone.
Methods
Prior to ABLE process implementation, there were no standardized procedures for documenting allergy histories. ABLE was implemented at the Robley Rex VAMC (RRVAMC) in November 2022. During the interview phase, patients were initially identified during admission via TheraDoc as having either a penicillin allergy or ADR. The infectious disease pharmacist or pharmacy resident interviewed patients with documented penicillin allergies or ADRs using a standardized questionnaire (eAppendix 1). Not all identified patients could be interviewed. Patients currently receiving an antibiotic were prioritized for interviews. Patients were excluded if they declined or were unable to be interviewed, although a patient’s caregiver(s) could be interviewed in person or via telephone, if the patient was not available.
Following the interview, pharmacists used guidance from the ABLE process in addition to a detailed EHR review to determine whether the patient was eligible for an allergy update or removal and/or switch to a Β-lactam antibiotic (Figure). If eligible for modification, the interviewing pharmacist made the necessary changes. A templated process note with patient-specific recommendations was entered into the Computerized Patient Record System (CPRS) and the primary care team attending physician was added as an additional signer to be alerted in the system note (eAppendix 2).
This single-center, retrospective cohort study involved review of CPRS notes and clinical interviews in the interviewed group. Hospitalized patients at the RRVAMC aged ≥ 18 years with a documented penicillin allergy or ADR were included. The historical control group consisted of patients admitted between October 31, 2019, and October 31, 2022, and the intervention group consisted of patients admitted between November 1, 2022, and March 1, 2023. Patients in the historical control group were matched 1:1 to the intervention group for penicillin allergy severity (allergy [IgE-mediated], unknown, adverse effect, severe cutaneous or other non–IgE-mediated reaction) and whether they received a noncarbapenem non–Β-lactam antibiotic.
The primary outcome was the number of patient allergies/ADRs removed or changed on patient profiles regardless of whether their antibiotic regimen was changed. This outcome was further assessed by evaluating the number of patient allergies or ADRs removed or changed on patient profiles with or without a change in antibiotic regimen. Primary outcomes were analyzed using χ2 and/ or Fisher exact tests, as appropriate to determine statistically significant differences between the interviewed group and the historical control.
Results
Seventy patients were included: 35 patients in the interviewed group and 35 patients in the historical control group, respectively. Both groups had a mean age of 72 years and predominantly included White male patients (Table 1). Following the interview, the allergy profile was modified for 6 patients (17%) in the interview group vs 0 patients in the control group (P = .03) (Table 2). The primary outcome was analyzed separately regardless of an antibiotic regimen change. There was not a statistically significant difference between groups when assessing patients for change in therapy (P > .99). All 6 patients with an allergy profile modification had no change in antibiotic regimen.
Discussion
This study suggests the ABLE process may be a valuable tool for adjusting penicillin allergies or ADRs within patient EHRs. In the interview group, allergies were modified in 6 (17%) patients while no patients in the control group had allergy modifications. Of the 6 allergy profile modifications, 4 allergy labels were changed from an allergy to an ADR. These patients were cleared to receive future Β-lactam antibiotics after clinicians recognized the lack of a true IgE-mediated allergic reaction. In addition, 2 of the modified allergy profiles removed the allergy designation. Although this represents a small subset of interviewed patients, it illustrates the clinical effectiveness of an interview process alone to remove penicillin allergy designations.
Previous research has assessed the impact of pharmacist intervention on penicillin allergy clarification. Mitchell et al implemented a pharmacist-driven Β-lactam allergy assessment and penicillin allergy clinic (PAC) at the MVAMC with the goal of evaluating its impact on allergy clearance. In their study, clinical pharmacy specialists evaluated patients with Β-lactam allergies, and those deemed eligible were later seen in the PAC. Among the 246 patients evaluated using the Β-lactam allergy assessment alone and who were not seen in the PAC, 25% had their penicillin allergy removed following a detailed assessment.6
Song et al evaluated the effectiveness and feasibility of a pharmacist-driven penicillin allergy delabeling pilot program without skin testing or oral challenges. Patients with penicillin allergies were interviewed by a pharmacy resident using a standardized checklist. Among the 66 patients interviewed, 12 (18%) met the criteria for delabeling and consented to removal of their allergy.7 The delabeling rates in these 2 studies are similar to the 17% rate of allergy modification in our study, although this study is the only one to compare results to a historical control group.
Harper et al evaluated the impact of a penicillin allergy assessment, including penicillin skin testing and oral amoxicillin challenges, on delabeling penicillin allergies. Pharmacists completed a penicillin allergy assessment and performed penicillin skin testing and/or oral amoxicillin challenges for eligible patients. Of 35 patients, 31 (89%) had their penicillin allergies delabeled in the EHR.8 The rate of penicillin allergy delabeling in Harper et al was likely higher than that seen in our study due to the use of oral challenge and skin testing. Regardless, a detailed penicillin allergy interview alone was effective at RRVAMC, resulting in a significant rate of allergy removal or change. This supports the use of detailed penicillin allergy assessments in settings where penicillin skin testing or oral challenges may not be feasible.
Mann et al demonstrated the effectiveness of penicillin allergy assessments in switching eligible patients to Β-lactam antibiotics. Their single-center, prospective study assessed the impact of a pharmacist-driven detailed penicillin allergy interview initiative. Interviews that evaluated potential changes to allergy profiles were conducted with 175 patients. Of these patients, 135 (77.1%) were on antimicrobial therapy and 42 (31.1%) patients receiving therapy met criteria to switch to a noncarbapenem Β-lactam antibiotic. Thirty-one patients (73.8%) switched with no signs or symptoms of intolerance demonstrating that an interview can be a valuable tool for antibiotic optimization, specifically in patients with penicillin allergy.9 No patients in our study switched antibiotic therapy, likely because only a small number of patients were eligible for transition to a noncarbapenem Β-lactam antibiotic. In the Mann et al study, non–Β-lactam antibiotics, such as fluoroquinolones and carbapenems, accounted for > 75% of the antibiotics used.
Limitations
The sample size of this study was small and its duration was short. There is a risk for selection bias as not all identified patients were able to be interviewed while admitted, but patients on antibiotics were prioritized as they were most likely to directly benefit during their current admission from a modification of their allergy. Most patients in the study were White and male, which may limit the generalizability of the results. Additionally, recommendations regarding antibiotic changes were primarily communicated to the treatment team based on a templated note in CPRS alone. Therefore, implementation of these recommendations largely relied upon nonverbal communication. Direct pharmacist-physician communication could have led to a larger impact on antimicrobial therapy changes. The interviewer’s participation in daily rounds with time allotted to discuss this topic can be considered in the future to improve these processes.
Conclusions
This study found that the ABLE process identified patients for penicillin allergy delabeling. With the high prevalence of inaccurate penicillin allergy documentation, this tool offers VA health care systems a way to empower pharmacists in allergy clarification, leading to improvements in antibiotic stewardship. Although the sample size was small, the ABLE process may provide a framework for VA clinicians. Future research has the potential to demonstrate the practicality and effectiveness this pharmacist-led penicillin allergy interview process can offer clinicians.
- Health care providers. Clinical features of penicillin allergy. Centers for Disease Control and Prevention. August 25, 2025. Accessed February 4, 2026. https://www.cdc.gov /antibiotic-use/hcp/clinical-signs/index.html
- Wrynn AF. Penicillin allergies: A guide for NPs. Nurse Pract. 2022;47:30-36. doi:10.1097/01.NPR.0000855312.11145.78
- Mohsen S, Dickinson JA, Somayaji R. Update on the adverse effects of antimicrobial therapies in community practice. Can Fam Physician. 2020;66:651-659.
- Sexually Transmitted Infections Treatment Guidelines, 2021. Managing persons who have a history of penicillin allergy. Centers for Disease Control and Prevention. September 21, 2022. Accessed February 4, 2026. https:// www.cdc.gov/std/treatment-guidelines/penicillin-allergy .htm
- Holmes AK, Bennett NT, Berry TP. Pharmacy driven assessment of appropriate antibiotic selection in patients with reported beta-lactam allergy. J Am Coll Clin Pharm. 2019;2:509-514. doi:10.1002/jac5.1135
- Mitchell AB, Ness RA, Bennett JG, et al. Implementation and impact of a Β-lactam allergy assessment protocol in a veteran population. Fed Pract. 2021;38:420-425. doi:10.12788/fp.0172
- Song YC, Nelson ZJ, Wankum MA, et al. Effectiveness and feasibility of pharmacist-driven penicillin allergy de-labeling pilot program without skin testing or oral challenges. Pharmacy (Basel). 2021;9:127. doi:10.3390/pharmacy9030127
- Harper HM, Sanchez M. Review of pharmacist driven penicillin allergy assessments and skin testing: a multicenter case-series. Hosp Pharm. 2022;57:469-473. doi:10.1177/00185787211046862
- Mann KL, Wu JY, Shah SS. Implementation of a pharmacist- driven detailed penicillin allergy interview. Ann Pharmacother. 2020;54:364-370. doi:10.1177/1060028019884874
- Health care providers. Clinical features of penicillin allergy. Centers for Disease Control and Prevention. August 25, 2025. Accessed February 4, 2026. https://www.cdc.gov /antibiotic-use/hcp/clinical-signs/index.html
- Wrynn AF. Penicillin allergies: A guide for NPs. Nurse Pract. 2022;47:30-36. doi:10.1097/01.NPR.0000855312.11145.78
- Mohsen S, Dickinson JA, Somayaji R. Update on the adverse effects of antimicrobial therapies in community practice. Can Fam Physician. 2020;66:651-659.
- Sexually Transmitted Infections Treatment Guidelines, 2021. Managing persons who have a history of penicillin allergy. Centers for Disease Control and Prevention. September 21, 2022. Accessed February 4, 2026. https:// www.cdc.gov/std/treatment-guidelines/penicillin-allergy .htm
- Holmes AK, Bennett NT, Berry TP. Pharmacy driven assessment of appropriate antibiotic selection in patients with reported beta-lactam allergy. J Am Coll Clin Pharm. 2019;2:509-514. doi:10.1002/jac5.1135
- Mitchell AB, Ness RA, Bennett JG, et al. Implementation and impact of a Β-lactam allergy assessment protocol in a veteran population. Fed Pract. 2021;38:420-425. doi:10.12788/fp.0172
- Song YC, Nelson ZJ, Wankum MA, et al. Effectiveness and feasibility of pharmacist-driven penicillin allergy de-labeling pilot program without skin testing or oral challenges. Pharmacy (Basel). 2021;9:127. doi:10.3390/pharmacy9030127
- Harper HM, Sanchez M. Review of pharmacist driven penicillin allergy assessments and skin testing: a multicenter case-series. Hosp Pharm. 2022;57:469-473. doi:10.1177/00185787211046862
- Mann KL, Wu JY, Shah SS. Implementation of a pharmacist- driven detailed penicillin allergy interview. Ann Pharmacother. 2020;54:364-370. doi:10.1177/1060028019884874
Implementation of a Pharmacist-Led Penicillin Allergy Interview at a Veterans Care Facility
Implementation of a Pharmacist-Led Penicillin Allergy Interview at a Veterans Care Facility
Outcomes From the Use of Cefazolin for Surgical Prophylaxis in Patients Allergic to Penicillin
Outcomes From the Use of Cefazolin for Surgical Prophylaxis in Patients Allergic to Penicillin
Given its safety profile and bactericidal activity against the predominant organisms causing surgical site infections (SSIs), cefazolin remains the most popular choice for surgical prophylaxis.1 Cefazolin offers protection against the pathogens most likely to contaminate the surgical site while minimizing inappropriate methicillin- resistant Staphylococcus aureus coverage that occurs with alternatives such as vancomycin and clindamycin. Documented allergies to Β-lactam antibiotics have historically forced clinicians to avoid the use of cephalosporins due to the potential risk of cross-reactivity. True type 1 (immunoglobin E [IgE]-mediated) cross-allergic reactions between penicillin and cephalosporins are rare, and previously reported data indicate cross-reactivity as a result of antibody recognition is more closely related to the side-chain identity rather than the Β-lactam ring.2,3
About 10% of US patients report having a penicillin allergy; however, < 1% of the population has a true IgE-mediated allergic reaction.4 Previous research that has challenged penicillin allergies with cefazolin for surgical prophylaxis has reported minimal rates of allergic reactions.2-5
In previous trials, patients with a history of delayed skin reactions, such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS), were excluded. Additionally, patients with an allergy to cefazolin including those with urticaria, angioedema, bronchospasm, or anaphylaxis, were excluded from perioperative retrial of cefazolin. Grant et al found that cefazolin can be safely given to patients with IgE-mediated reactions to penicillin and other cephalosporins due to a structurally different side chain.3
In January 2023, the Veteran Health Indiana (VHI) pharmacy team in conjunction with surgery, infectious disease, and anesthesiology, implemented a screening tool as an amendment to perioperative antibiotic guidance to help determine which patients with a documented penicillin allergy could be candidates for perioperative cefazolin. The implemented screening tool (Allergy Clarification for Cefazolin Evidence-Based Prescribing Tool) has been described by Lam et al, who reported that an increased proportion of patients with documented penicillin allergy received cefazolin without more adverse drug reactions (ADRs).5 Patients with a Β-lactam allergy were eligible to receive cefazolin unless the ADR was SJS, TEN, or DRESS, or the offending agent was cefazolin and the patient experienced urticaria, angioedema, bronchospasm, or anaphylaxis. If the reaction was not from cefazolin or was unknown, patients were eligible to receive cefazolin (Figure).
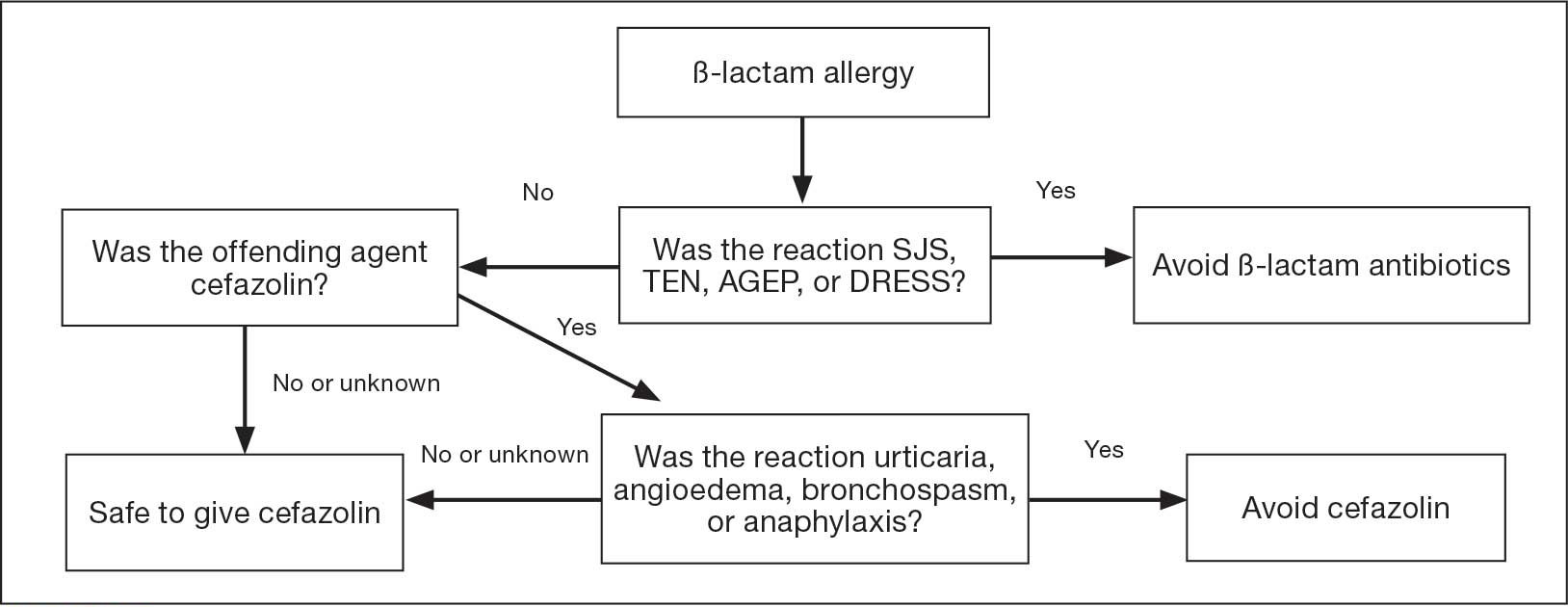
To date, minimal data exist to evaluate the incidence of ADRs when cefazolin is given perioperatively to patients with a previously documented penicillin allergy. The purpose of this study was to evaluate the incidence of allergic ADRs in patients who had a documented penicillin allergy and received periprocedural antibiotics.
Methods
This single-center, retrospective chart review used the US Department of Veterans Affairs (VA) Computerized Patient Record System (CPRS) to identify patients with a documented penicillin allergy who underwent an operation and received periprocedural antibiotics between February 1, 2023, and January 31, 2024. This study was reviewed and approved by the Indiana University Health Institutional Review Board and the VHI Research and Development Committee.
Patients were enrolled if they were aged ≥ 18 years, had a documented penicillin allergy, underwent a surgical intervention, and received perioperative antibiotics during the study period. Patients were excluded if they had a documented penicillin allergy resulting in severe delayed skin reactions (ie, SJS, TEN, or DRESS). These criteria produced 197 surgical procedures. Data were collected for each surgical procedure, so patients could be included more than once. Patient history of allergic reaction to penicillin was obtained through CPRS.
The primary endpoint was the percentage of allergic ADRs in patients with penicillin allergies receiving cefazolin perioperatively. Secondary outcomes included the appropriateness of the antibiotic regimen in congruence with American System of Health Pharmacists (ASHP) recommendations, incidence of SSIs within 30 days of the procedure, incidence of ADRs in those with a history of anaphylaxis vs nonanaphylaxis allergy, incidence of allergic reaction requiring pharmacologic and nonpharmacologic interventions, and incidence of acute kidney injury (AKI). AKI was defined as an increase in serum creatinine by ≥ 0.3 mg/dL within 48 hours or an increase in serum creatinine to ≥ 1.5 times baseline.
Demographic data included sex, age, race, preoperative serum creatinine, and postoperative serum creatinine. Anaphylaxis was defined as an acute onset of illness (within minutes to several hours) with involvement of skin, mucosal tissue, or both involving either respiratory compromise or reduced blood pressures. Allergic reactions were defined as facial, tongue, throat, airway, lip, mouth, periorbital, or eye swelling, urticaria, angioedema, dyspnea, anaphylaxis, or a positive penicillin skin test. Additionally, data collected included the description and severity of postprophylactic antibiotic reaction, antibiotic choice, interventions required for the allergic reaction, SSI occurrence, date of SSI, operating specialty, and postoperative change in renal function.
Descriptive statistics, including mean, SD, and percentages were reported for baseline characteristics of the study population. Percentages were used to demonstrate the differences in primary and secondary outcomes for each study group. Fisher exact tests were used for incidence of ADRs in patients with penicillin allergy who received cefazolin and reported incidence of SSIs.
Results
A total of 197 surgical procedures in patients with a documented penicillin allergy were included; 127 procedures used cefazolin perioperatively, 3 procedures used cefazolin plus gentamicin, and 67 procedures used other antibiotics. Most patients were White (n = 160; 81.2%), male (n = 158; 80.2%), and had a mean age of 64.9 years. Urology was the most common surgical specialty (n = 59; 29.9%) (Table 1). Of the 16 patients with documented penicillin anaphylaxis reaction, 8 received cefazolin and 8 received a different antibiotic. A total of 181 patients reported a nonanaphylaxis allergy. One hundred fifty-one patients (68.6%) reported a reaction history of hives, rash, or swelling (Table 2). Patients could report ≥ 1 reaction. The most prevalent antibiotics used were cefazolin, which was used by 130 patients (61.3%), and clindamycin which was used by 33 patients (15.6%) (Table 3). Patients could receive ≥ 1 antibiotic.
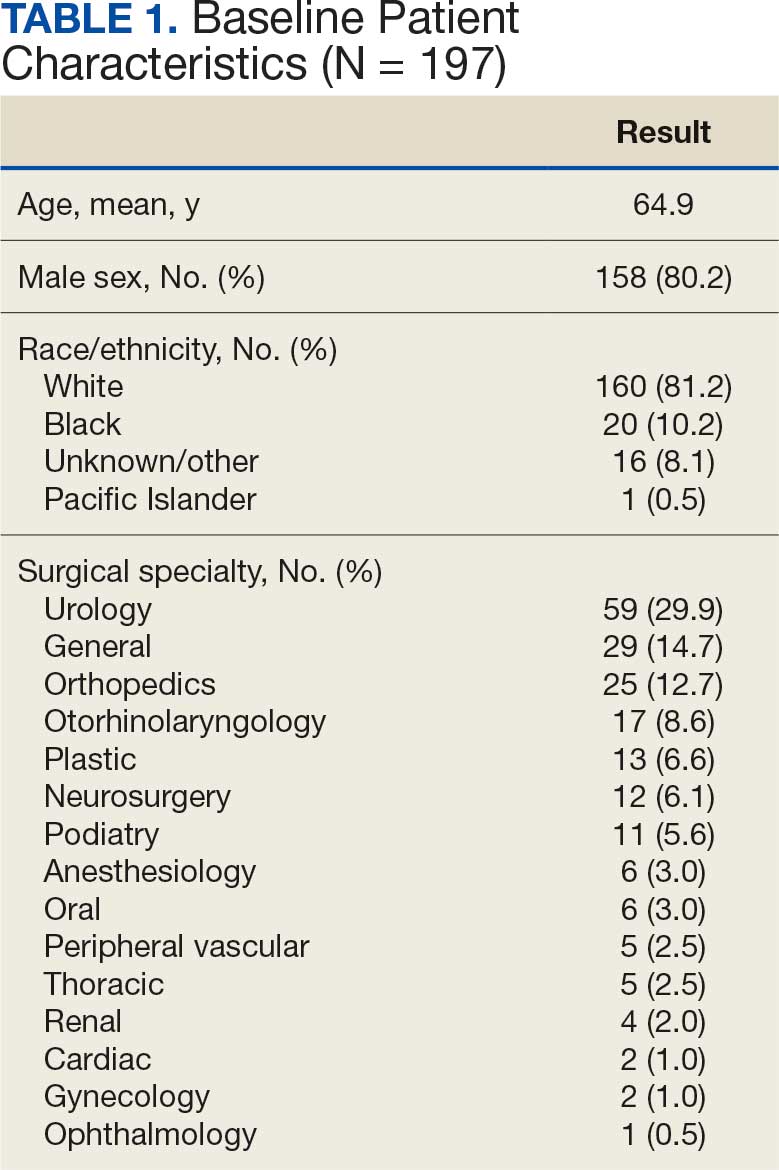
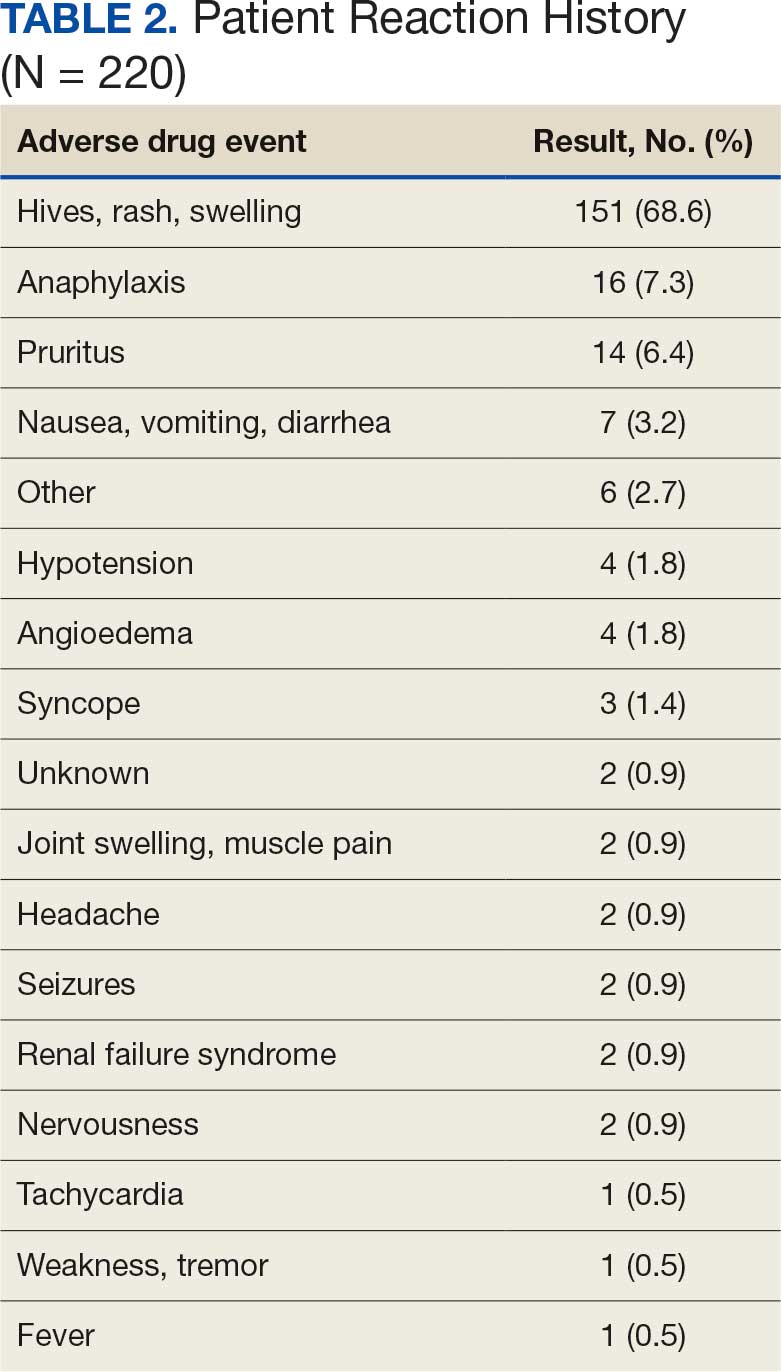
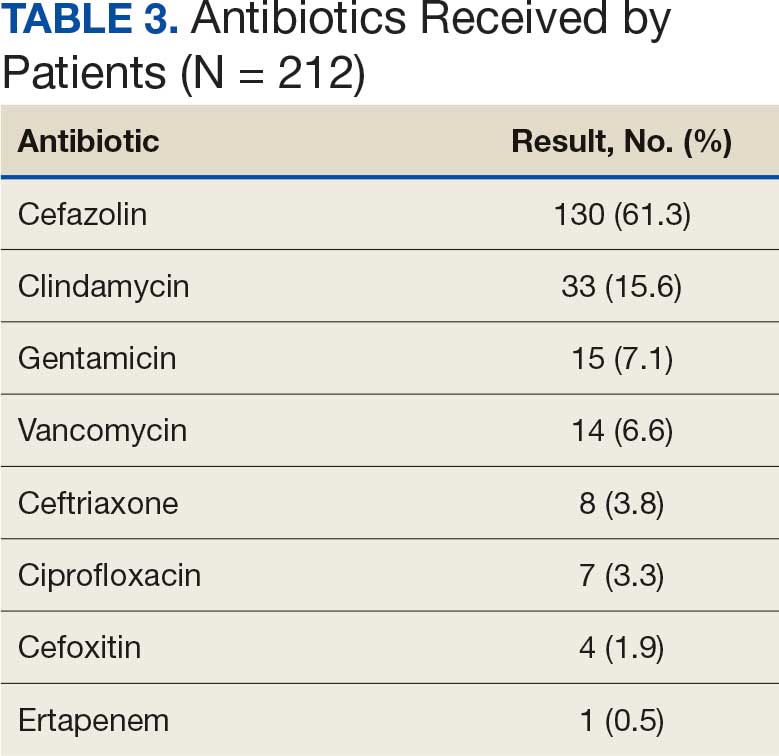
For the primary outcome, the incidence of allergic reactions in patients allergic to penicillin, there was no incidence of allergic reactions in either the cefazolin or other group. Given the absence of reactions, no interventions were required.
There were no ADRs in those with history of anaphylaxis or nonanaphylaxis allergy. In the cefazolin group, 126 of 127 surgical procedure regimens (99.2%) were congruent with ASHP recommendations, all 3 surgical procedures regimens in the cefazolin plus gentamicin group were congruent with ASHP recommendations, and 58 of 67 surgical procedure regimens (86.6%) in the other antibiotic group were congruent with ASHP recommendations. None of the 127 patients in the cefazolin group or of the 3 patients in the cefazolin plus gentamicin group reported an SSI, and 3 of 67 patients (4.5%) had an SSI in the other antibiotic group. One procedure that resulted in SSI was not congruent with ASHP recommendations. Twenty-four patients had 2 serum creatinine levels drawn within 48 hours of surgery. One of 12 patients (8.3%) and 0 of 12 patients had an AKI in the cefazolin and other antibiotic group, respectively (Table 4).
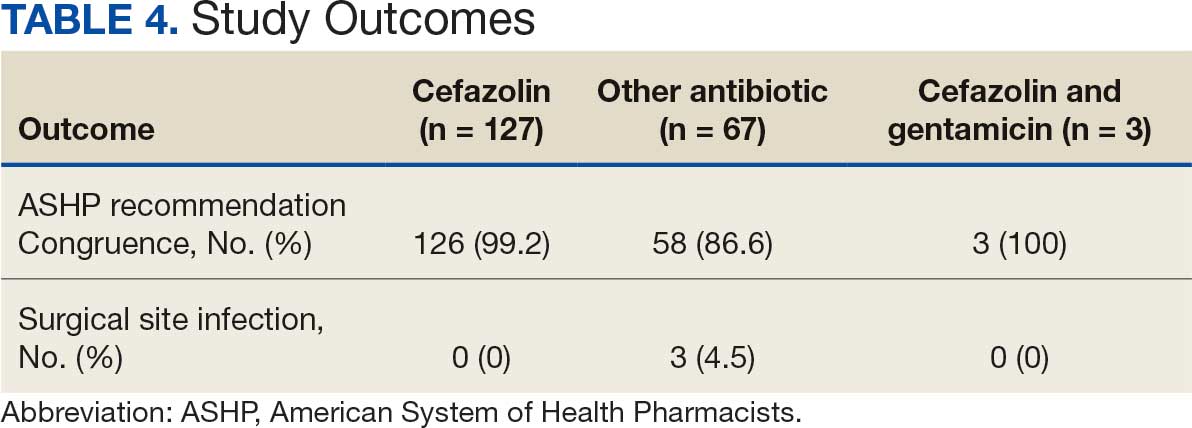
Discussion
Implementation of a screening tool at VHI allowed patients with documented penicillin allergy, including anaphylaxis, to receive cefazolin perioperatively. Broad spectrum antibiotics such as vancomycin, clindamycin, and fluoroquinolones are frequently used in patients allergic to penicillin, which can increase health care costs, risk of toxicity, and antimicrobial resistance.4 There was no incidence of allergic reactions noted in patients allergic to penicillin who received cefazolin. When comparing the incidence of observed allergic reactions to received perioperative antibiotics in the cefazolin group to previously published literature, no difference in allergy rates (P = .09) was found.3 Most antibiotics administered were congruent with ASHP guideline recommendations, and most patients eligible for cefazolin received it perioperatively.
Similar to this study, Goodman et al concluded that cefazolin appears to be a safe regimen in patients with documented penicillin anaphylactic reaction for surgical prophylaxis with only 1 (0.2%) potential allergic reaction.6 Patients who received cefazolin perioperatively had a statistically significant decrease in SSI rates. There were no clinically or statistically significant differences found between the proportion of allergic reactions or ADRs when compared to alternative antibiotics. Lessard et al concluded that a pharmacist-led interdisciplinary collaborative practice agreement increased cefazolin use in patients allergic to penicillin, including those with urticaria and anaphylaxis, with no reported ADRs.7 This study further demonstrated the safety of cefazolin use in patients with anaphylaxis to penicillin.
Limitations
This study’s single-center, retrospective design, patient population, and small sample size limit the generalizability of its results. The data collected are dependent on documentation in the chart. No ADRs were reported from the antibiotics patients received perioperatively. When considering safety data, information such as serum creatinine were available only in CPRS and some patients did not receive a postprocedure serum creatinine level. Additionally, this study did not investigate whether there was an increase in preferred preoperative antimicrobial prophylaxis after implementation of this protocol.
Conclusions
The results of this study support the use of cefazolin perioperatively in patients allergic to penicillin, including those with a history of anaphylaxis. Additional research should be conducted to validate data given the low incidence of ADRs. The primary outcome did not reach statistical significance, but the results may be clinically significant from a stewardship and safety perspective. VHI continues to use the screening tool described in this article.
- Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70:195-283. doi:10.2146/ajhp120568
- Romano A, Valluzzi RL, Caruso C, et al. Tolerability of cefazolin and ceftibuten in patients with IgE-mediated aminopenicillin allergy. J Allergy Clin Immunol Pract. 2020;8:1989-1993.e2. doi:10.1016/j.jaip.2020.02.025
- Grant JM, Song WHC, Shajari S, et al. Safety of administering cefazolin versus other antibiotics in penicillin- allergic patients for surgical prophylaxis at a major Canadian teaching hospital. Surgery. 2021;170:783-789. doi:10.1016/j.surg.2021.03.022
- Centers for Disease Control and Prevention. Clinical Features of Penicillin Allergy. August 25, 2025. Accessed January 6, 2026. https://www.cdc.gov/antibiotic-use/hcp/clinical-signs/index.html
- Lam PW, Tarighi P, Elligsen M, et al. Impact of the allergy clarification for cefazolin evidence-based prescribing tool on receipt of preferred perioperative prophylaxis: an interrupted time series study. Clin Infect Dis. 2020;71:2955- 2957. doi:10.1093/cid/ciaa516
- Goodman EJ, Morgan MJ, Johnson Pa, et al. Cephalosporins can be given to penicillin-allergic patients who do not exhibit an anaphylactic response. J Clin Anesth. 2001;13:561-564. doi:10.1016/s0952-8180(01)00329-4
- Lessard S, Huiras C, Dababneh A, et al. Pharmacist adjustment of preoperative antibiotic orders to the preferred preoperative antibiotic cefazolin for patients with penicillin allergy labeling. Am J Health Syst Pharm. 2023;80:532- 536. doi:10.1093/ajhp/zxac385
Given its safety profile and bactericidal activity against the predominant organisms causing surgical site infections (SSIs), cefazolin remains the most popular choice for surgical prophylaxis.1 Cefazolin offers protection against the pathogens most likely to contaminate the surgical site while minimizing inappropriate methicillin- resistant Staphylococcus aureus coverage that occurs with alternatives such as vancomycin and clindamycin. Documented allergies to Β-lactam antibiotics have historically forced clinicians to avoid the use of cephalosporins due to the potential risk of cross-reactivity. True type 1 (immunoglobin E [IgE]-mediated) cross-allergic reactions between penicillin and cephalosporins are rare, and previously reported data indicate cross-reactivity as a result of antibody recognition is more closely related to the side-chain identity rather than the Β-lactam ring.2,3
About 10% of US patients report having a penicillin allergy; however, < 1% of the population has a true IgE-mediated allergic reaction.4 Previous research that has challenged penicillin allergies with cefazolin for surgical prophylaxis has reported minimal rates of allergic reactions.2-5
In previous trials, patients with a history of delayed skin reactions, such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS), were excluded. Additionally, patients with an allergy to cefazolin including those with urticaria, angioedema, bronchospasm, or anaphylaxis, were excluded from perioperative retrial of cefazolin. Grant et al found that cefazolin can be safely given to patients with IgE-mediated reactions to penicillin and other cephalosporins due to a structurally different side chain.3
In January 2023, the Veteran Health Indiana (VHI) pharmacy team in conjunction with surgery, infectious disease, and anesthesiology, implemented a screening tool as an amendment to perioperative antibiotic guidance to help determine which patients with a documented penicillin allergy could be candidates for perioperative cefazolin. The implemented screening tool (Allergy Clarification for Cefazolin Evidence-Based Prescribing Tool) has been described by Lam et al, who reported that an increased proportion of patients with documented penicillin allergy received cefazolin without more adverse drug reactions (ADRs).5 Patients with a Β-lactam allergy were eligible to receive cefazolin unless the ADR was SJS, TEN, or DRESS, or the offending agent was cefazolin and the patient experienced urticaria, angioedema, bronchospasm, or anaphylaxis. If the reaction was not from cefazolin or was unknown, patients were eligible to receive cefazolin (Figure).
To date, minimal data exist to evaluate the incidence of ADRs when cefazolin is given perioperatively to patients with a previously documented penicillin allergy. The purpose of this study was to evaluate the incidence of allergic ADRs in patients who had a documented penicillin allergy and received periprocedural antibiotics.
Methods
This single-center, retrospective chart review used the US Department of Veterans Affairs (VA) Computerized Patient Record System (CPRS) to identify patients with a documented penicillin allergy who underwent an operation and received periprocedural antibiotics between February 1, 2023, and January 31, 2024. This study was reviewed and approved by the Indiana University Health Institutional Review Board and the VHI Research and Development Committee.
Patients were enrolled if they were aged ≥ 18 years, had a documented penicillin allergy, underwent a surgical intervention, and received perioperative antibiotics during the study period. Patients were excluded if they had a documented penicillin allergy resulting in severe delayed skin reactions (ie, SJS, TEN, or DRESS). These criteria produced 197 surgical procedures. Data were collected for each surgical procedure, so patients could be included more than once. Patient history of allergic reaction to penicillin was obtained through CPRS.
The primary endpoint was the percentage of allergic ADRs in patients with penicillin allergies receiving cefazolin perioperatively. Secondary outcomes included the appropriateness of the antibiotic regimen in congruence with American System of Health Pharmacists (ASHP) recommendations, incidence of SSIs within 30 days of the procedure, incidence of ADRs in those with a history of anaphylaxis vs nonanaphylaxis allergy, incidence of allergic reaction requiring pharmacologic and nonpharmacologic interventions, and incidence of acute kidney injury (AKI). AKI was defined as an increase in serum creatinine by ≥ 0.3 mg/dL within 48 hours or an increase in serum creatinine to ≥ 1.5 times baseline.
Demographic data included sex, age, race, preoperative serum creatinine, and postoperative serum creatinine. Anaphylaxis was defined as an acute onset of illness (within minutes to several hours) with involvement of skin, mucosal tissue, or both involving either respiratory compromise or reduced blood pressures. Allergic reactions were defined as facial, tongue, throat, airway, lip, mouth, periorbital, or eye swelling, urticaria, angioedema, dyspnea, anaphylaxis, or a positive penicillin skin test. Additionally, data collected included the description and severity of postprophylactic antibiotic reaction, antibiotic choice, interventions required for the allergic reaction, SSI occurrence, date of SSI, operating specialty, and postoperative change in renal function.
Descriptive statistics, including mean, SD, and percentages were reported for baseline characteristics of the study population. Percentages were used to demonstrate the differences in primary and secondary outcomes for each study group. Fisher exact tests were used for incidence of ADRs in patients with penicillin allergy who received cefazolin and reported incidence of SSIs.
Results
A total of 197 surgical procedures in patients with a documented penicillin allergy were included; 127 procedures used cefazolin perioperatively, 3 procedures used cefazolin plus gentamicin, and 67 procedures used other antibiotics. Most patients were White (n = 160; 81.2%), male (n = 158; 80.2%), and had a mean age of 64.9 years. Urology was the most common surgical specialty (n = 59; 29.9%) (Table 1). Of the 16 patients with documented penicillin anaphylaxis reaction, 8 received cefazolin and 8 received a different antibiotic. A total of 181 patients reported a nonanaphylaxis allergy. One hundred fifty-one patients (68.6%) reported a reaction history of hives, rash, or swelling (Table 2). Patients could report ≥ 1 reaction. The most prevalent antibiotics used were cefazolin, which was used by 130 patients (61.3%), and clindamycin which was used by 33 patients (15.6%) (Table 3). Patients could receive ≥ 1 antibiotic.
For the primary outcome, the incidence of allergic reactions in patients allergic to penicillin, there was no incidence of allergic reactions in either the cefazolin or other group. Given the absence of reactions, no interventions were required.
There were no ADRs in those with history of anaphylaxis or nonanaphylaxis allergy. In the cefazolin group, 126 of 127 surgical procedure regimens (99.2%) were congruent with ASHP recommendations, all 3 surgical procedures regimens in the cefazolin plus gentamicin group were congruent with ASHP recommendations, and 58 of 67 surgical procedure regimens (86.6%) in the other antibiotic group were congruent with ASHP recommendations. None of the 127 patients in the cefazolin group or of the 3 patients in the cefazolin plus gentamicin group reported an SSI, and 3 of 67 patients (4.5%) had an SSI in the other antibiotic group. One procedure that resulted in SSI was not congruent with ASHP recommendations. Twenty-four patients had 2 serum creatinine levels drawn within 48 hours of surgery. One of 12 patients (8.3%) and 0 of 12 patients had an AKI in the cefazolin and other antibiotic group, respectively (Table 4).
Discussion
Implementation of a screening tool at VHI allowed patients with documented penicillin allergy, including anaphylaxis, to receive cefazolin perioperatively. Broad spectrum antibiotics such as vancomycin, clindamycin, and fluoroquinolones are frequently used in patients allergic to penicillin, which can increase health care costs, risk of toxicity, and antimicrobial resistance.4 There was no incidence of allergic reactions noted in patients allergic to penicillin who received cefazolin. When comparing the incidence of observed allergic reactions to received perioperative antibiotics in the cefazolin group to previously published literature, no difference in allergy rates (P = .09) was found.3 Most antibiotics administered were congruent with ASHP guideline recommendations, and most patients eligible for cefazolin received it perioperatively.
Similar to this study, Goodman et al concluded that cefazolin appears to be a safe regimen in patients with documented penicillin anaphylactic reaction for surgical prophylaxis with only 1 (0.2%) potential allergic reaction.6 Patients who received cefazolin perioperatively had a statistically significant decrease in SSI rates. There were no clinically or statistically significant differences found between the proportion of allergic reactions or ADRs when compared to alternative antibiotics. Lessard et al concluded that a pharmacist-led interdisciplinary collaborative practice agreement increased cefazolin use in patients allergic to penicillin, including those with urticaria and anaphylaxis, with no reported ADRs.7 This study further demonstrated the safety of cefazolin use in patients with anaphylaxis to penicillin.
Limitations
This study’s single-center, retrospective design, patient population, and small sample size limit the generalizability of its results. The data collected are dependent on documentation in the chart. No ADRs were reported from the antibiotics patients received perioperatively. When considering safety data, information such as serum creatinine were available only in CPRS and some patients did not receive a postprocedure serum creatinine level. Additionally, this study did not investigate whether there was an increase in preferred preoperative antimicrobial prophylaxis after implementation of this protocol.
Conclusions
The results of this study support the use of cefazolin perioperatively in patients allergic to penicillin, including those with a history of anaphylaxis. Additional research should be conducted to validate data given the low incidence of ADRs. The primary outcome did not reach statistical significance, but the results may be clinically significant from a stewardship and safety perspective. VHI continues to use the screening tool described in this article.
Given its safety profile and bactericidal activity against the predominant organisms causing surgical site infections (SSIs), cefazolin remains the most popular choice for surgical prophylaxis.1 Cefazolin offers protection against the pathogens most likely to contaminate the surgical site while minimizing inappropriate methicillin- resistant Staphylococcus aureus coverage that occurs with alternatives such as vancomycin and clindamycin. Documented allergies to Β-lactam antibiotics have historically forced clinicians to avoid the use of cephalosporins due to the potential risk of cross-reactivity. True type 1 (immunoglobin E [IgE]-mediated) cross-allergic reactions between penicillin and cephalosporins are rare, and previously reported data indicate cross-reactivity as a result of antibody recognition is more closely related to the side-chain identity rather than the Β-lactam ring.2,3
About 10% of US patients report having a penicillin allergy; however, < 1% of the population has a true IgE-mediated allergic reaction.4 Previous research that has challenged penicillin allergies with cefazolin for surgical prophylaxis has reported minimal rates of allergic reactions.2-5
In previous trials, patients with a history of delayed skin reactions, such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS), were excluded. Additionally, patients with an allergy to cefazolin including those with urticaria, angioedema, bronchospasm, or anaphylaxis, were excluded from perioperative retrial of cefazolin. Grant et al found that cefazolin can be safely given to patients with IgE-mediated reactions to penicillin and other cephalosporins due to a structurally different side chain.3
In January 2023, the Veteran Health Indiana (VHI) pharmacy team in conjunction with surgery, infectious disease, and anesthesiology, implemented a screening tool as an amendment to perioperative antibiotic guidance to help determine which patients with a documented penicillin allergy could be candidates for perioperative cefazolin. The implemented screening tool (Allergy Clarification for Cefazolin Evidence-Based Prescribing Tool) has been described by Lam et al, who reported that an increased proportion of patients with documented penicillin allergy received cefazolin without more adverse drug reactions (ADRs).5 Patients with a Β-lactam allergy were eligible to receive cefazolin unless the ADR was SJS, TEN, or DRESS, or the offending agent was cefazolin and the patient experienced urticaria, angioedema, bronchospasm, or anaphylaxis. If the reaction was not from cefazolin or was unknown, patients were eligible to receive cefazolin (Figure).
To date, minimal data exist to evaluate the incidence of ADRs when cefazolin is given perioperatively to patients with a previously documented penicillin allergy. The purpose of this study was to evaluate the incidence of allergic ADRs in patients who had a documented penicillin allergy and received periprocedural antibiotics.
Methods
This single-center, retrospective chart review used the US Department of Veterans Affairs (VA) Computerized Patient Record System (CPRS) to identify patients with a documented penicillin allergy who underwent an operation and received periprocedural antibiotics between February 1, 2023, and January 31, 2024. This study was reviewed and approved by the Indiana University Health Institutional Review Board and the VHI Research and Development Committee.
Patients were enrolled if they were aged ≥ 18 years, had a documented penicillin allergy, underwent a surgical intervention, and received perioperative antibiotics during the study period. Patients were excluded if they had a documented penicillin allergy resulting in severe delayed skin reactions (ie, SJS, TEN, or DRESS). These criteria produced 197 surgical procedures. Data were collected for each surgical procedure, so patients could be included more than once. Patient history of allergic reaction to penicillin was obtained through CPRS.
The primary endpoint was the percentage of allergic ADRs in patients with penicillin allergies receiving cefazolin perioperatively. Secondary outcomes included the appropriateness of the antibiotic regimen in congruence with American System of Health Pharmacists (ASHP) recommendations, incidence of SSIs within 30 days of the procedure, incidence of ADRs in those with a history of anaphylaxis vs nonanaphylaxis allergy, incidence of allergic reaction requiring pharmacologic and nonpharmacologic interventions, and incidence of acute kidney injury (AKI). AKI was defined as an increase in serum creatinine by ≥ 0.3 mg/dL within 48 hours or an increase in serum creatinine to ≥ 1.5 times baseline.
Demographic data included sex, age, race, preoperative serum creatinine, and postoperative serum creatinine. Anaphylaxis was defined as an acute onset of illness (within minutes to several hours) with involvement of skin, mucosal tissue, or both involving either respiratory compromise or reduced blood pressures. Allergic reactions were defined as facial, tongue, throat, airway, lip, mouth, periorbital, or eye swelling, urticaria, angioedema, dyspnea, anaphylaxis, or a positive penicillin skin test. Additionally, data collected included the description and severity of postprophylactic antibiotic reaction, antibiotic choice, interventions required for the allergic reaction, SSI occurrence, date of SSI, operating specialty, and postoperative change in renal function.
Descriptive statistics, including mean, SD, and percentages were reported for baseline characteristics of the study population. Percentages were used to demonstrate the differences in primary and secondary outcomes for each study group. Fisher exact tests were used for incidence of ADRs in patients with penicillin allergy who received cefazolin and reported incidence of SSIs.
Results
A total of 197 surgical procedures in patients with a documented penicillin allergy were included; 127 procedures used cefazolin perioperatively, 3 procedures used cefazolin plus gentamicin, and 67 procedures used other antibiotics. Most patients were White (n = 160; 81.2%), male (n = 158; 80.2%), and had a mean age of 64.9 years. Urology was the most common surgical specialty (n = 59; 29.9%) (Table 1). Of the 16 patients with documented penicillin anaphylaxis reaction, 8 received cefazolin and 8 received a different antibiotic. A total of 181 patients reported a nonanaphylaxis allergy. One hundred fifty-one patients (68.6%) reported a reaction history of hives, rash, or swelling (Table 2). Patients could report ≥ 1 reaction. The most prevalent antibiotics used were cefazolin, which was used by 130 patients (61.3%), and clindamycin which was used by 33 patients (15.6%) (Table 3). Patients could receive ≥ 1 antibiotic.
For the primary outcome, the incidence of allergic reactions in patients allergic to penicillin, there was no incidence of allergic reactions in either the cefazolin or other group. Given the absence of reactions, no interventions were required.
There were no ADRs in those with history of anaphylaxis or nonanaphylaxis allergy. In the cefazolin group, 126 of 127 surgical procedure regimens (99.2%) were congruent with ASHP recommendations, all 3 surgical procedures regimens in the cefazolin plus gentamicin group were congruent with ASHP recommendations, and 58 of 67 surgical procedure regimens (86.6%) in the other antibiotic group were congruent with ASHP recommendations. None of the 127 patients in the cefazolin group or of the 3 patients in the cefazolin plus gentamicin group reported an SSI, and 3 of 67 patients (4.5%) had an SSI in the other antibiotic group. One procedure that resulted in SSI was not congruent with ASHP recommendations. Twenty-four patients had 2 serum creatinine levels drawn within 48 hours of surgery. One of 12 patients (8.3%) and 0 of 12 patients had an AKI in the cefazolin and other antibiotic group, respectively (Table 4).
Discussion
Implementation of a screening tool at VHI allowed patients with documented penicillin allergy, including anaphylaxis, to receive cefazolin perioperatively. Broad spectrum antibiotics such as vancomycin, clindamycin, and fluoroquinolones are frequently used in patients allergic to penicillin, which can increase health care costs, risk of toxicity, and antimicrobial resistance.4 There was no incidence of allergic reactions noted in patients allergic to penicillin who received cefazolin. When comparing the incidence of observed allergic reactions to received perioperative antibiotics in the cefazolin group to previously published literature, no difference in allergy rates (P = .09) was found.3 Most antibiotics administered were congruent with ASHP guideline recommendations, and most patients eligible for cefazolin received it perioperatively.
Similar to this study, Goodman et al concluded that cefazolin appears to be a safe regimen in patients with documented penicillin anaphylactic reaction for surgical prophylaxis with only 1 (0.2%) potential allergic reaction.6 Patients who received cefazolin perioperatively had a statistically significant decrease in SSI rates. There were no clinically or statistically significant differences found between the proportion of allergic reactions or ADRs when compared to alternative antibiotics. Lessard et al concluded that a pharmacist-led interdisciplinary collaborative practice agreement increased cefazolin use in patients allergic to penicillin, including those with urticaria and anaphylaxis, with no reported ADRs.7 This study further demonstrated the safety of cefazolin use in patients with anaphylaxis to penicillin.
Limitations
This study’s single-center, retrospective design, patient population, and small sample size limit the generalizability of its results. The data collected are dependent on documentation in the chart. No ADRs were reported from the antibiotics patients received perioperatively. When considering safety data, information such as serum creatinine were available only in CPRS and some patients did not receive a postprocedure serum creatinine level. Additionally, this study did not investigate whether there was an increase in preferred preoperative antimicrobial prophylaxis after implementation of this protocol.
Conclusions
The results of this study support the use of cefazolin perioperatively in patients allergic to penicillin, including those with a history of anaphylaxis. Additional research should be conducted to validate data given the low incidence of ADRs. The primary outcome did not reach statistical significance, but the results may be clinically significant from a stewardship and safety perspective. VHI continues to use the screening tool described in this article.
- Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70:195-283. doi:10.2146/ajhp120568
- Romano A, Valluzzi RL, Caruso C, et al. Tolerability of cefazolin and ceftibuten in patients with IgE-mediated aminopenicillin allergy. J Allergy Clin Immunol Pract. 2020;8:1989-1993.e2. doi:10.1016/j.jaip.2020.02.025
- Grant JM, Song WHC, Shajari S, et al. Safety of administering cefazolin versus other antibiotics in penicillin- allergic patients for surgical prophylaxis at a major Canadian teaching hospital. Surgery. 2021;170:783-789. doi:10.1016/j.surg.2021.03.022
- Centers for Disease Control and Prevention. Clinical Features of Penicillin Allergy. August 25, 2025. Accessed January 6, 2026. https://www.cdc.gov/antibiotic-use/hcp/clinical-signs/index.html
- Lam PW, Tarighi P, Elligsen M, et al. Impact of the allergy clarification for cefazolin evidence-based prescribing tool on receipt of preferred perioperative prophylaxis: an interrupted time series study. Clin Infect Dis. 2020;71:2955- 2957. doi:10.1093/cid/ciaa516
- Goodman EJ, Morgan MJ, Johnson Pa, et al. Cephalosporins can be given to penicillin-allergic patients who do not exhibit an anaphylactic response. J Clin Anesth. 2001;13:561-564. doi:10.1016/s0952-8180(01)00329-4
- Lessard S, Huiras C, Dababneh A, et al. Pharmacist adjustment of preoperative antibiotic orders to the preferred preoperative antibiotic cefazolin for patients with penicillin allergy labeling. Am J Health Syst Pharm. 2023;80:532- 536. doi:10.1093/ajhp/zxac385
- Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70:195-283. doi:10.2146/ajhp120568
- Romano A, Valluzzi RL, Caruso C, et al. Tolerability of cefazolin and ceftibuten in patients with IgE-mediated aminopenicillin allergy. J Allergy Clin Immunol Pract. 2020;8:1989-1993.e2. doi:10.1016/j.jaip.2020.02.025
- Grant JM, Song WHC, Shajari S, et al. Safety of administering cefazolin versus other antibiotics in penicillin- allergic patients for surgical prophylaxis at a major Canadian teaching hospital. Surgery. 2021;170:783-789. doi:10.1016/j.surg.2021.03.022
- Centers for Disease Control and Prevention. Clinical Features of Penicillin Allergy. August 25, 2025. Accessed January 6, 2026. https://www.cdc.gov/antibiotic-use/hcp/clinical-signs/index.html
- Lam PW, Tarighi P, Elligsen M, et al. Impact of the allergy clarification for cefazolin evidence-based prescribing tool on receipt of preferred perioperative prophylaxis: an interrupted time series study. Clin Infect Dis. 2020;71:2955- 2957. doi:10.1093/cid/ciaa516
- Goodman EJ, Morgan MJ, Johnson Pa, et al. Cephalosporins can be given to penicillin-allergic patients who do not exhibit an anaphylactic response. J Clin Anesth. 2001;13:561-564. doi:10.1016/s0952-8180(01)00329-4
- Lessard S, Huiras C, Dababneh A, et al. Pharmacist adjustment of preoperative antibiotic orders to the preferred preoperative antibiotic cefazolin for patients with penicillin allergy labeling. Am J Health Syst Pharm. 2023;80:532- 536. doi:10.1093/ajhp/zxac385
Outcomes From the Use of Cefazolin for Surgical Prophylaxis in Patients Allergic to Penicillin
Outcomes From the Use of Cefazolin for Surgical Prophylaxis in Patients Allergic to Penicillin