User login
Targeted therapies predicted to blow out costs for CLL
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
The lifetime cost of treating chronic lymphocytic leukemia is forecast to rise precipitously for patients diagnosed today, as oral targeted therapies take over as the first-line treatment option, according to a study published November 21 in the Journal of Clinical Oncology.
The conclusion is based on economic models that also indicated the annual cost in the United States of managing chronic lymphocytic leukemia (CLL) will increase from its current level of $0.74 billion to $5.13 billion by 2025 (J Clin Oncol. 2016 Nov 21. doi: 10.1200/JCO.2016.68.2856).
While the majority of patients with CLL are covered by Medicare in the United States, they still currently pay $9,200 in out-of-pocket costs for oral agents. This figure is forecast to increase to $57,000 for those who start treatment in 2016 due to the increased costs of oral targeted therapeutics.
“Such an economic impact could result in financial toxicity, limited access, and lower adherence to the oral therapies, which may undermine their clinical effectiveness,” Qiushi Chen, from the Georgia Institute of Technology, Atlanta, and his coauthors wrote. They called for a more sustainable pricing strategy for oral targeted therapies, rather than have clinicians be forced to choose less effective but more affordable management strategies.
The researchers developed a microsimulation model of CLL, simulating the dynamics of the patient population under given management strategies from 2011-2025.
Around 130,000 patients live with CLL in the United States and around 15,000 new cases are diagnosed each year. By 2025, the authors forecast that 199,000 people will be living with the disease; a 55% increase that is both the result of new diagnoses and of improved survival with new oral targeted therapies.
Chemoimmunotherapy regimens – such as fludarabine, cyclophosphamide, and rituximab – have long been the standard first-line approach to CLL. But in recent years, new oral targeted agents such as ibrutinib and idelalisib have significantly improved progression-free survival and overall survival in CLL.
Ibrutinib is approved for first-line management of CLL, idelalisib is approved in combination with rituximab for patients with relapsed/refractory chronic lymphocytic leukemia, and venetoclax is approved for patients with relapsed chronic lymphocytic leukemia with del(17p).
“Both ibrutinib and idelalisib are priced at approximately $130,000 per [CLL patient per] year and are recommended until patients have progressive disease or significant toxicities,” the authors wrote. “In contrast, the costs for chemoimmunotherapy-based treatments range from $60,000 to $100,000 for a finite duration, that is, a typical six-cycle course that lasts for approximately 6 months.”
The higher costs will add up to additional annual spending of $29 billion to 2025, compared with around $1.12 billion annually for chemoimmunotherapy alone.
“Compared with the CIT scenario, the oral targeted therapy scenario resulted in an increase of 107,000 person–quality-adjusted life-years (149,000 person–life years), with additional discounted costs of $20.2 billion,” the authors reported.
The annual cost of cancer care in the United States is increasing across the board, from $143 billion in 2010 to $180 billion in 2020, but the cost of care for CLL is increasing more significantly than for other cancers. For example, breast and prostate cancers are forecast to have a 24%-38% increase in annual cost by 2020, while CLL is predicted to increase by 500%.
Seven authors declared research funding, honoraria and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The high cost of oral therapies for chronic lymphocytic leukemia could result in financial toxicity, limited access, and lower adherence, which may undermine their clinical effectiveness.
Major finding: The cost of treating chronic lymphocytic leukemia is forecast to increase from its current level of $0.74 billion to $5.13 billion by 2025.
Data source: Microsimulation model of chronic lymphocytic leukemia treatment from 2010-2025.
Disclosures: Seven authors declared research funding, honoraria, and consultancy funding from a range of pharmaceutical companies including those involved in the manufacture of therapies for chronic lymphocytic leukemia. Two authors had no conflicts to declare.
ADT not associated with increased risk of dementia in larger study
Treatment with androgen deprivation therapy (ADT) was not associated with an increased risk of dementia in a large, population-based study, according to investigators.
Previous studies have demonstrated that low testosterone levels are associated with cognitive impairment and Alzheimer’s disease, but the association between ADT and cognitive impairment remains controversial, with conflicting results being reported.
In the current large population-based study, compared with nonuse, treatment with ADT did not increase the risk of dementia (incidence, 7.4 vs. 4.4 per 1,000 person years, adjusted hazard ratio, 1.02; 95%CI, 0.87-1.19), reported Farzin Khosrow-Khavar, PhD, of McGill University, Montreal, and colleagues.
“Consistent with our findings, a recent meta-analysis found that although patients treated with ADT performed worse on visuomotor tasks in comparison with control subjects or their own baseline assessments, there were no significant differences in cognitive domains that are pertinent to dementia including performance on attention/working memory, executive function, language, verbal memory, visual memory, and visuospatial ability” they wrote (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2016.69.6203).
In a smaller study of 9,272 patients, recently published in JAMA Oncology, prostate cancer patients treated with ADT were more than twice as likely as were those who were not to develop dementia.
For the current study, investigators identified a cohort of 30,903 men who were newly diagnosed with nonmetastatic prostate cancer between April 1, 1988, and April 30, 2015, using the United Kingdom’s Clinical Practice Research Datalink. The patients were then observed until April 30, 2016.
Within this cohort, 799 patients were newly diagnosed with dementia, which extrapolated to a crude incidence of 6.0 per 1,000 person-years. During the follow-up period, 17,994 patients (58.2%) were treated with ADT, and the median duration of use was 2.3 years.
Men who were using ADT tended to be older and were more likely to have ever used tobacco products, and they were also more likely to have had higher prostate-specific antigen levels and a higher prevalence of comorbidities, compared with nonusers.
In the primary analysis, ADT use was not associated with an overall higher risk of developing dementia (adjusted HR, 1.02; 95% CI, 0.87-1.19).
In secondary analyses, the risk did not vary with cumulative duration of use. Findings were similar when the risk was assessed by the type of ADT used for treatment, and when the association was evaluated with Alzheimer’s disease (adjusted HR, 1.11; 95% CI, 0.85-1.44) versus other types of dementia (adjusted HR, 0.97; 95% CI, 0.80-1.18).
The authors noted that additional studies in different settings are needed to confirm these new findings.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors declared that there were no conflicts of interest.
Treatment with androgen deprivation therapy (ADT) was not associated with an increased risk of dementia in a large, population-based study, according to investigators.
Previous studies have demonstrated that low testosterone levels are associated with cognitive impairment and Alzheimer’s disease, but the association between ADT and cognitive impairment remains controversial, with conflicting results being reported.
In the current large population-based study, compared with nonuse, treatment with ADT did not increase the risk of dementia (incidence, 7.4 vs. 4.4 per 1,000 person years, adjusted hazard ratio, 1.02; 95%CI, 0.87-1.19), reported Farzin Khosrow-Khavar, PhD, of McGill University, Montreal, and colleagues.
“Consistent with our findings, a recent meta-analysis found that although patients treated with ADT performed worse on visuomotor tasks in comparison with control subjects or their own baseline assessments, there were no significant differences in cognitive domains that are pertinent to dementia including performance on attention/working memory, executive function, language, verbal memory, visual memory, and visuospatial ability” they wrote (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2016.69.6203).
In a smaller study of 9,272 patients, recently published in JAMA Oncology, prostate cancer patients treated with ADT were more than twice as likely as were those who were not to develop dementia.
For the current study, investigators identified a cohort of 30,903 men who were newly diagnosed with nonmetastatic prostate cancer between April 1, 1988, and April 30, 2015, using the United Kingdom’s Clinical Practice Research Datalink. The patients were then observed until April 30, 2016.
Within this cohort, 799 patients were newly diagnosed with dementia, which extrapolated to a crude incidence of 6.0 per 1,000 person-years. During the follow-up period, 17,994 patients (58.2%) were treated with ADT, and the median duration of use was 2.3 years.
Men who were using ADT tended to be older and were more likely to have ever used tobacco products, and they were also more likely to have had higher prostate-specific antigen levels and a higher prevalence of comorbidities, compared with nonusers.
In the primary analysis, ADT use was not associated with an overall higher risk of developing dementia (adjusted HR, 1.02; 95% CI, 0.87-1.19).
In secondary analyses, the risk did not vary with cumulative duration of use. Findings were similar when the risk was assessed by the type of ADT used for treatment, and when the association was evaluated with Alzheimer’s disease (adjusted HR, 1.11; 95% CI, 0.85-1.44) versus other types of dementia (adjusted HR, 0.97; 95% CI, 0.80-1.18).
The authors noted that additional studies in different settings are needed to confirm these new findings.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors declared that there were no conflicts of interest.
Treatment with androgen deprivation therapy (ADT) was not associated with an increased risk of dementia in a large, population-based study, according to investigators.
Previous studies have demonstrated that low testosterone levels are associated with cognitive impairment and Alzheimer’s disease, but the association between ADT and cognitive impairment remains controversial, with conflicting results being reported.
In the current large population-based study, compared with nonuse, treatment with ADT did not increase the risk of dementia (incidence, 7.4 vs. 4.4 per 1,000 person years, adjusted hazard ratio, 1.02; 95%CI, 0.87-1.19), reported Farzin Khosrow-Khavar, PhD, of McGill University, Montreal, and colleagues.
“Consistent with our findings, a recent meta-analysis found that although patients treated with ADT performed worse on visuomotor tasks in comparison with control subjects or their own baseline assessments, there were no significant differences in cognitive domains that are pertinent to dementia including performance on attention/working memory, executive function, language, verbal memory, visual memory, and visuospatial ability” they wrote (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2016.69.6203).
In a smaller study of 9,272 patients, recently published in JAMA Oncology, prostate cancer patients treated with ADT were more than twice as likely as were those who were not to develop dementia.
For the current study, investigators identified a cohort of 30,903 men who were newly diagnosed with nonmetastatic prostate cancer between April 1, 1988, and April 30, 2015, using the United Kingdom’s Clinical Practice Research Datalink. The patients were then observed until April 30, 2016.
Within this cohort, 799 patients were newly diagnosed with dementia, which extrapolated to a crude incidence of 6.0 per 1,000 person-years. During the follow-up period, 17,994 patients (58.2%) were treated with ADT, and the median duration of use was 2.3 years.
Men who were using ADT tended to be older and were more likely to have ever used tobacco products, and they were also more likely to have had higher prostate-specific antigen levels and a higher prevalence of comorbidities, compared with nonusers.
In the primary analysis, ADT use was not associated with an overall higher risk of developing dementia (adjusted HR, 1.02; 95% CI, 0.87-1.19).
In secondary analyses, the risk did not vary with cumulative duration of use. Findings were similar when the risk was assessed by the type of ADT used for treatment, and when the association was evaluated with Alzheimer’s disease (adjusted HR, 1.11; 95% CI, 0.85-1.44) versus other types of dementia (adjusted HR, 0.97; 95% CI, 0.80-1.18).
The authors noted that additional studies in different settings are needed to confirm these new findings.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors declared that there were no conflicts of interest.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point:
Major finding: Compared with nonuse of ADT, the use of ADT was not associated with an increased risk of dementia (incidence, 7.4 vs. 4.4 per 1,000 person-years, HR, 1.02; 95% CI, 0.87-1.19).
Data source: Population-based study that included 30,903 men newly diagnosed with nonmetastatic prostate cancer.
Disclosures: The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors declared that there were no conflicts of interest.
DNA methylation markers prognostic for metastatic breast cancer
A novel panel of DNA methylation markers may aid in predicting survival outcomes in metastatic breast cancer (MBC), according to new findings.
Using a new quantitative assay known as cMethDNA, researchers found that a high cumulative methylation index (CMI) level, as measured with a six-gene panel after beginning a new treatment, was consistently associated with both progression-free survival and overall survival, as well as progressive disease.
Even though these results are encouraging, however, its clinical application is still unknown, they noted.

Epigenetic alterations are common in human malignancies, and DNA methylation is a form of epigenetic alteration that is heritable during DNA replication. The authors developed a highly sensitive, high-throughput quantitative multiplex methylation-specific polymerase chain reaction assay known as cMethDNA that was able to detect circulating cell-free methylated DNA.
In this study, 10 genes were tested from 141 women with MBC who were beginning a new systemic therapy and who received treatment at participating academic medical centers.
Among patients with a high CMI, the median progression-free survival and overall survival were significantly shorter (PFS, 2.1 months; OS, 12.3 months), compared with those with a low CMI (PFS, 5.8 months; OS, 21.7 months), Dr. Visvanathan and her associates reported (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2015.66.2080).
Upon multivariable analysis, a high CMI versus low CMI at 4 weeks was independently associated with poorer PFS (hazard ratio, 1.79; 95% CI, 1.23-2.60; P = .002) and OS (hazard ratio, 1.75; 95% CI, 1.21-2.54; P = .003). Rising CMI levels from baseline to week 4 also were associated with worse PFS (P less than .001) as well as a 4.6-fold increase in the risk of progressive disease at first restaging (OR, 4.58; 95% CI, 1.82-11.60; P = .001) when compared with either a drop in CMI or no change at all.
The CMI level at week 4 was observed to be a strong predictor of PFS and improved the prediction of the base model, even in the presence of circulating tumor cells (P = .004).
Dr. Visvanathan and her colleagues concluded that these findings “must be validated to determine the clinical usefulness of the cMethDNA assay for specific treatments and tumor phenotypes in patients with metastatic disease and early-stage breast cancer.”
The study was supported by the Avon Foundation for Women, the Breast Cancer Research Foundation, Janssen Diagnostics, the Rubenstein Family Fund, the Susan G. Komen Foundation, and National Institutes of Health Grants. Dr. Visvanathan has declared holding patents, royalties, and other intellectual property, and several coauthors also have declared relationships with industry.
A novel panel of DNA methylation markers may aid in predicting survival outcomes in metastatic breast cancer (MBC), according to new findings.
Using a new quantitative assay known as cMethDNA, researchers found that a high cumulative methylation index (CMI) level, as measured with a six-gene panel after beginning a new treatment, was consistently associated with both progression-free survival and overall survival, as well as progressive disease.
Even though these results are encouraging, however, its clinical application is still unknown, they noted.
Epigenetic alterations are common in human malignancies, and DNA methylation is a form of epigenetic alteration that is heritable during DNA replication. The authors developed a highly sensitive, high-throughput quantitative multiplex methylation-specific polymerase chain reaction assay known as cMethDNA that was able to detect circulating cell-free methylated DNA.
In this study, 10 genes were tested from 141 women with MBC who were beginning a new systemic therapy and who received treatment at participating academic medical centers.
Among patients with a high CMI, the median progression-free survival and overall survival were significantly shorter (PFS, 2.1 months; OS, 12.3 months), compared with those with a low CMI (PFS, 5.8 months; OS, 21.7 months), Dr. Visvanathan and her associates reported (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2015.66.2080).
Upon multivariable analysis, a high CMI versus low CMI at 4 weeks was independently associated with poorer PFS (hazard ratio, 1.79; 95% CI, 1.23-2.60; P = .002) and OS (hazard ratio, 1.75; 95% CI, 1.21-2.54; P = .003). Rising CMI levels from baseline to week 4 also were associated with worse PFS (P less than .001) as well as a 4.6-fold increase in the risk of progressive disease at first restaging (OR, 4.58; 95% CI, 1.82-11.60; P = .001) when compared with either a drop in CMI or no change at all.
The CMI level at week 4 was observed to be a strong predictor of PFS and improved the prediction of the base model, even in the presence of circulating tumor cells (P = .004).
Dr. Visvanathan and her colleagues concluded that these findings “must be validated to determine the clinical usefulness of the cMethDNA assay for specific treatments and tumor phenotypes in patients with metastatic disease and early-stage breast cancer.”
The study was supported by the Avon Foundation for Women, the Breast Cancer Research Foundation, Janssen Diagnostics, the Rubenstein Family Fund, the Susan G. Komen Foundation, and National Institutes of Health Grants. Dr. Visvanathan has declared holding patents, royalties, and other intellectual property, and several coauthors also have declared relationships with industry.
A novel panel of DNA methylation markers may aid in predicting survival outcomes in metastatic breast cancer (MBC), according to new findings.
Using a new quantitative assay known as cMethDNA, researchers found that a high cumulative methylation index (CMI) level, as measured with a six-gene panel after beginning a new treatment, was consistently associated with both progression-free survival and overall survival, as well as progressive disease.
Even though these results are encouraging, however, its clinical application is still unknown, they noted.
Epigenetic alterations are common in human malignancies, and DNA methylation is a form of epigenetic alteration that is heritable during DNA replication. The authors developed a highly sensitive, high-throughput quantitative multiplex methylation-specific polymerase chain reaction assay known as cMethDNA that was able to detect circulating cell-free methylated DNA.
In this study, 10 genes were tested from 141 women with MBC who were beginning a new systemic therapy and who received treatment at participating academic medical centers.
Among patients with a high CMI, the median progression-free survival and overall survival were significantly shorter (PFS, 2.1 months; OS, 12.3 months), compared with those with a low CMI (PFS, 5.8 months; OS, 21.7 months), Dr. Visvanathan and her associates reported (J Clin Oncol. 2016 Nov. 21 doi: 10.1200/JCO.2015.66.2080).
Upon multivariable analysis, a high CMI versus low CMI at 4 weeks was independently associated with poorer PFS (hazard ratio, 1.79; 95% CI, 1.23-2.60; P = .002) and OS (hazard ratio, 1.75; 95% CI, 1.21-2.54; P = .003). Rising CMI levels from baseline to week 4 also were associated with worse PFS (P less than .001) as well as a 4.6-fold increase in the risk of progressive disease at first restaging (OR, 4.58; 95% CI, 1.82-11.60; P = .001) when compared with either a drop in CMI or no change at all.
The CMI level at week 4 was observed to be a strong predictor of PFS and improved the prediction of the base model, even in the presence of circulating tumor cells (P = .004).
Dr. Visvanathan and her colleagues concluded that these findings “must be validated to determine the clinical usefulness of the cMethDNA assay for specific treatments and tumor phenotypes in patients with metastatic disease and early-stage breast cancer.”
The study was supported by the Avon Foundation for Women, the Breast Cancer Research Foundation, Janssen Diagnostics, the Rubenstein Family Fund, the Susan G. Komen Foundation, and National Institutes of Health Grants. Dr. Visvanathan has declared holding patents, royalties, and other intellectual property, and several coauthors also have declared relationships with industry.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point:
Major finding: Among patients with a high cumulative methylation index, the median PFS and OS were significantly shorter (PFS, 2.1 months; OS, 12.3 months), compared with those with a low CMI (PFS, 5.8 months; OS, 21.7 months).
Data source: An experimental study that evaluated 10 genes from samples obtained from 141 metastatic breast cancer patients at varying intervals.
Disclosures: The study was supported by the Avon Foundation for Women, the Breast Cancer Research Foundation, Janssen Diagnostics, the Rubenstein Family Fund, the Susan G. Komen Foundation, and National Institutes of Health Grants. Dr. Visvanathan has declared holding patents, royalties, and other intellectual property, and several coauthors also have declared relationships with industry.
Pediatric psoriasis linked to multiple psychiatric comorbidities
VIENNA – Psoriasis in children and adolescents is associated with significantly increased risk of a variety of psychiatric comorbidities, according to a large Danish national study.
This finding has important public health implications. Psoriasis is a common skin disease, and 30% of cases have their onset in childhood or adolescence, Tanja Todberg, MD, observed at the annual congress of the European Academy of Dermatology and Venereology.

Diagnosis of psoriasis was based upon medical records and documentation that at least a second prescription for a topical vitamin D derivative had been filled. Those agents are the overwhelming choice as first-line therapy in the pediatric population, explained Dr. Todberg of the University of Copenhagen.
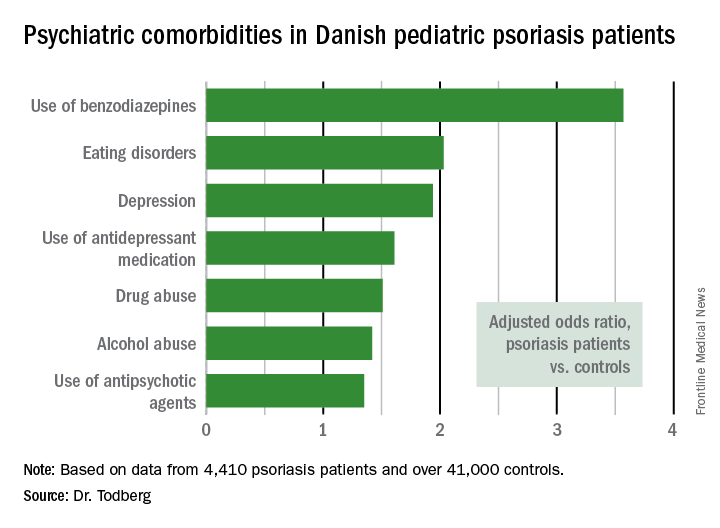
The pediatric psoriasis patients proved to be at significantly increased risk of being diagnosed with depression, eating disorders, drug abuse, and alcohol abuse. They were also more likely than controls to be prescribed antidepressants, antipsychotic agents, and benzodiazepines. That was every prespecified psychiatric outcome that Dr. Todberg and her coinvestigators included in the study except for one: anxiety disorders occurred at a similar rate in the pediatric psoriasis patients and controls.
Dr. Todberg reported having no financial conflicts of interest regarding this study, which was supported by Danish medical research funding.
[email protected]
VIENNA – Psoriasis in children and adolescents is associated with significantly increased risk of a variety of psychiatric comorbidities, according to a large Danish national study.
This finding has important public health implications. Psoriasis is a common skin disease, and 30% of cases have their onset in childhood or adolescence, Tanja Todberg, MD, observed at the annual congress of the European Academy of Dermatology and Venereology.
Diagnosis of psoriasis was based upon medical records and documentation that at least a second prescription for a topical vitamin D derivative had been filled. Those agents are the overwhelming choice as first-line therapy in the pediatric population, explained Dr. Todberg of the University of Copenhagen.
The pediatric psoriasis patients proved to be at significantly increased risk of being diagnosed with depression, eating disorders, drug abuse, and alcohol abuse. They were also more likely than controls to be prescribed antidepressants, antipsychotic agents, and benzodiazepines. That was every prespecified psychiatric outcome that Dr. Todberg and her coinvestigators included in the study except for one: anxiety disorders occurred at a similar rate in the pediatric psoriasis patients and controls.
Dr. Todberg reported having no financial conflicts of interest regarding this study, which was supported by Danish medical research funding.
[email protected]
VIENNA – Psoriasis in children and adolescents is associated with significantly increased risk of a variety of psychiatric comorbidities, according to a large Danish national study.
This finding has important public health implications. Psoriasis is a common skin disease, and 30% of cases have their onset in childhood or adolescence, Tanja Todberg, MD, observed at the annual congress of the European Academy of Dermatology and Venereology.
Diagnosis of psoriasis was based upon medical records and documentation that at least a second prescription for a topical vitamin D derivative had been filled. Those agents are the overwhelming choice as first-line therapy in the pediatric population, explained Dr. Todberg of the University of Copenhagen.
The pediatric psoriasis patients proved to be at significantly increased risk of being diagnosed with depression, eating disorders, drug abuse, and alcohol abuse. They were also more likely than controls to be prescribed antidepressants, antipsychotic agents, and benzodiazepines. That was every prespecified psychiatric outcome that Dr. Todberg and her coinvestigators included in the study except for one: anxiety disorders occurred at a similar rate in the pediatric psoriasis patients and controls.
Dr. Todberg reported having no financial conflicts of interest regarding this study, which was supported by Danish medical research funding.
[email protected]
AT THE EADV CONGRESS
Key clinical point:
Major finding: Danish pediatric patients with psoriasis were significantly more at risk of developing a range of psychiatric disorders than were control subjects.
Data source: This was a retrospective study of prospectively collected registry data on all 4,410 Danish children and adolescents diagnosed with psoriasis during 1997-2012 and more than 41,000 Danish controls matched for age, sex, and calendar year.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study, which was supported by Danish medical research funds.
AGA members take center stage at UEG Week 2016
AGA leaders in their respective fields attended the recent UEG Week in Vienna, Austria. There was a record attendance of 13,300 with delegates from around the world. AGA members were highlighted in the “Best of Digestive Disease Week® (DDW)” session, which saw more than 1,000 attendees.
AGA President Timothy Wang, MD, AGAF, co-chaired the session along with UEG President Michael P. Manns, MD. Other AGA speakers included:
• C. Richard Boland, MD, AGAF: GI Oncology
• Robert J. Fontana, MD: Liver
• Stuart J. Spechler, MD, AGAF: Esophagus and Upper GI
• Santhi Swaroop Vege, MD, AGAF: Pancreatic Disorders
AGA Education and Training Councillor Deborah D. Proctor, MD: IBD
Additionally, in the “Rising Stars from Europe and the USA” session – co-chaired by Dr. Proctor and UEG Representative Luigi Riccardiello, MD – AGA Research Scholar Award holder Kyle Staller, MD, and UEG Rising Star 2016 Mira Wouters, MD, of Belgium discussed their latest research into the epidemiology and pathogenesis of irritable bowel syndrome (IBS).
Dr. Staller spoke about his ongoing research identifying adolescent dietary and lifestyle risk factors that play a role in the development of IBS in adulthood, potentially identifying adolescents at risk for IBS to be targeted for lifestyle interventions.
AGA leaders in their respective fields attended the recent UEG Week in Vienna, Austria. There was a record attendance of 13,300 with delegates from around the world. AGA members were highlighted in the “Best of Digestive Disease Week® (DDW)” session, which saw more than 1,000 attendees.
AGA President Timothy Wang, MD, AGAF, co-chaired the session along with UEG President Michael P. Manns, MD. Other AGA speakers included:
• C. Richard Boland, MD, AGAF: GI Oncology
• Robert J. Fontana, MD: Liver
• Stuart J. Spechler, MD, AGAF: Esophagus and Upper GI
• Santhi Swaroop Vege, MD, AGAF: Pancreatic Disorders
AGA Education and Training Councillor Deborah D. Proctor, MD: IBD
Additionally, in the “Rising Stars from Europe and the USA” session – co-chaired by Dr. Proctor and UEG Representative Luigi Riccardiello, MD – AGA Research Scholar Award holder Kyle Staller, MD, and UEG Rising Star 2016 Mira Wouters, MD, of Belgium discussed their latest research into the epidemiology and pathogenesis of irritable bowel syndrome (IBS).
Dr. Staller spoke about his ongoing research identifying adolescent dietary and lifestyle risk factors that play a role in the development of IBS in adulthood, potentially identifying adolescents at risk for IBS to be targeted for lifestyle interventions.
AGA leaders in their respective fields attended the recent UEG Week in Vienna, Austria. There was a record attendance of 13,300 with delegates from around the world. AGA members were highlighted in the “Best of Digestive Disease Week® (DDW)” session, which saw more than 1,000 attendees.
AGA President Timothy Wang, MD, AGAF, co-chaired the session along with UEG President Michael P. Manns, MD. Other AGA speakers included:
• C. Richard Boland, MD, AGAF: GI Oncology
• Robert J. Fontana, MD: Liver
• Stuart J. Spechler, MD, AGAF: Esophagus and Upper GI
• Santhi Swaroop Vege, MD, AGAF: Pancreatic Disorders
AGA Education and Training Councillor Deborah D. Proctor, MD: IBD
Additionally, in the “Rising Stars from Europe and the USA” session – co-chaired by Dr. Proctor and UEG Representative Luigi Riccardiello, MD – AGA Research Scholar Award holder Kyle Staller, MD, and UEG Rising Star 2016 Mira Wouters, MD, of Belgium discussed their latest research into the epidemiology and pathogenesis of irritable bowel syndrome (IBS).
Dr. Staller spoke about his ongoing research identifying adolescent dietary and lifestyle risk factors that play a role in the development of IBS in adulthood, potentially identifying adolescents at risk for IBS to be targeted for lifestyle interventions.
Expanding treatment options and ongoing challenges for urologic cancers
Urologic cancers are those that form in organs of the urinary and male reproductive systems, the most significant among them being cancers of the bladder, kidney, prostate, and testicles. Collectively, they are diagnosed in close to 400,000 Americans each year and are responsible for almost 60,000 deaths annually.1 Here, we describe the most recent developments in treating these malignancies.
Update/related article
Atezolizumab approval marks first new treatment option for bladder cancer in more than 3 decades
Click on the PDF icon at the top of this introduction to read the full article.
Urologic cancers are those that form in organs of the urinary and male reproductive systems, the most significant among them being cancers of the bladder, kidney, prostate, and testicles. Collectively, they are diagnosed in close to 400,000 Americans each year and are responsible for almost 60,000 deaths annually.1 Here, we describe the most recent developments in treating these malignancies.
Update/related article
Atezolizumab approval marks first new treatment option for bladder cancer in more than 3 decades
Click on the PDF icon at the top of this introduction to read the full article.
Urologic cancers are those that form in organs of the urinary and male reproductive systems, the most significant among them being cancers of the bladder, kidney, prostate, and testicles. Collectively, they are diagnosed in close to 400,000 Americans each year and are responsible for almost 60,000 deaths annually.1 Here, we describe the most recent developments in treating these malignancies.
Update/related article
Atezolizumab approval marks first new treatment option for bladder cancer in more than 3 decades
Click on the PDF icon at the top of this introduction to read the full article.
Join me in supporting GI research
A letter from Dr. Robert S. Sandler, MPH, AGAF, Chair of the AGA Research Foundation
At a time when we are on the brink of major scientific breakthroughs, there is a growing gap in federal funding for research. Without gastroenterology and hepatology research, there would be no discoveries to improve our understanding of the pathogenesis of digestive diseases and to develop new diagnostic and therapeutic approaches.
As a member of the AGA, you understand the physical, emotional, and financial costs of digestive diseases. And you understand the tremendous value of research to advance patient care.

Gifts to the Foundation this past year directly supported 66 bright investigators. Despite this success, close to 300 other innovative and promising research ideas went unfunded. We must continue to foster the careers of talented scientists and protect the GI research pipeline.
A financial contribution to the AGA Research Foundation is the opportunity for you to give back to the field in a lasting way. All contributions to the Foundation go to support the Foundation’s research endowment. Please make your tax-deductible donation of $250, $500, $1,000, or any amount you can give.
Thank you in advance for your support and best wishes for a happy, healthy holiday season and successful New Year.
Three easy ways to give
Online: www.gastro.org/donateonline
Through the mail:
AGA Research Foundation
4930 Del Ray Avenue
Bethesda, MD 20814
By phone: 301-222-4002
All gifts are tax deductible to the fullest extent of U.S. law.
A letter from Dr. Robert S. Sandler, MPH, AGAF, Chair of the AGA Research Foundation
At a time when we are on the brink of major scientific breakthroughs, there is a growing gap in federal funding for research. Without gastroenterology and hepatology research, there would be no discoveries to improve our understanding of the pathogenesis of digestive diseases and to develop new diagnostic and therapeutic approaches.
As a member of the AGA, you understand the physical, emotional, and financial costs of digestive diseases. And you understand the tremendous value of research to advance patient care.
Gifts to the Foundation this past year directly supported 66 bright investigators. Despite this success, close to 300 other innovative and promising research ideas went unfunded. We must continue to foster the careers of talented scientists and protect the GI research pipeline.
A financial contribution to the AGA Research Foundation is the opportunity for you to give back to the field in a lasting way. All contributions to the Foundation go to support the Foundation’s research endowment. Please make your tax-deductible donation of $250, $500, $1,000, or any amount you can give.
Thank you in advance for your support and best wishes for a happy, healthy holiday season and successful New Year.
Three easy ways to give
Online: www.gastro.org/donateonline
Through the mail:
AGA Research Foundation
4930 Del Ray Avenue
Bethesda, MD 20814
By phone: 301-222-4002
All gifts are tax deductible to the fullest extent of U.S. law.
A letter from Dr. Robert S. Sandler, MPH, AGAF, Chair of the AGA Research Foundation
At a time when we are on the brink of major scientific breakthroughs, there is a growing gap in federal funding for research. Without gastroenterology and hepatology research, there would be no discoveries to improve our understanding of the pathogenesis of digestive diseases and to develop new diagnostic and therapeutic approaches.
As a member of the AGA, you understand the physical, emotional, and financial costs of digestive diseases. And you understand the tremendous value of research to advance patient care.
Gifts to the Foundation this past year directly supported 66 bright investigators. Despite this success, close to 300 other innovative and promising research ideas went unfunded. We must continue to foster the careers of talented scientists and protect the GI research pipeline.
A financial contribution to the AGA Research Foundation is the opportunity for you to give back to the field in a lasting way. All contributions to the Foundation go to support the Foundation’s research endowment. Please make your tax-deductible donation of $250, $500, $1,000, or any amount you can give.
Thank you in advance for your support and best wishes for a happy, healthy holiday season and successful New Year.
Three easy ways to give
Online: www.gastro.org/donateonline
Through the mail:
AGA Research Foundation
4930 Del Ray Avenue
Bethesda, MD 20814
By phone: 301-222-4002
All gifts are tax deductible to the fullest extent of U.S. law.
Sofosbuvir/velpatasvir improved patient-reported outcomes, knocked out HCV genotypes 1-6
BOSTON – When given with ribavirin, a fixed-dose combination of sofosbuvir/velpatasvir (Epclusa) achieved a sustained viral response at 12 weeks (SVR-12) in 94% of decompensated cirrhotic patients with hepatitis C virus (HCV) genotypes 1-6 infection, according to Zobair M. Younossi, MD.
Patients with and without cirrhosis also reported meaningful improvements across a variety of outcome measures after successfully completing treatment with Epclusa or sofosbuvir (Harvoni), said Dr. Younossi of Inova Fairfax Hospital in Falls Church, Va. “Although on-treatment patient-reported outcomes improved more with ribavirin-free regimens, post-SVR improvements were similar,” regardless of whether patients had received ribavirin, he reported at the annual meeting of the American Association for the Study of Liver Diseases.

Epclusa without ribavirin led to SVR-12 in 85% of decompensated cirrhotic patients and nearly 99% of noncirrhotic patients of all HCV genotypes, Dr. Younossi reported. For sofosbuvir with ribavirin, rates of SVR-12 were 66% in genotype 3 cirrhotic patients and 95% in cirrhotic patients of other HCV genotypes.
At baseline, cirrhotic patients scored up to 33.5 points worse than noncirrhotics on a universal 100-point scale covering 26 patient-reported domains (P less than .05 for all but 3 domains). Decompensated cirrhotics reported more baseline depression and fatigue than other patients (P less than .002 for each comparison), while patients without cirrhosis were more likely to be treatment naive and employed (both P less than .0001). But after the investigators controlled for these differences, decompensated cirrhotics who received Epclusa reported an additional 5.5-9 points of improvement in treatment-emergent outcomes than those who received sofosbuvir plus ribavirin (P less than .002). Patients with compensated cirrhosis reported 2.3-5 points more improvement in treatment-emergent outcomes on Epclusa than on sofosbuvir plus ribavirin (P less than .05). “Decompensated cirrhotics experienced the best and greatest improvement of patient-reported outcome scores during treatment with sofosbuvir/velpatasvir,” Dr. Younossi said.
Patients who received ribavirin reported similar changes across domains at the end of treatment, regardless of cirrhosis status. Among patients who achieved SVR-12, decompensated cirrhotics reported significantly more improvement 12 weeks later than did patients with less severe liver disease, although both groups showed long-term improvements (5.8 points vs. 4.1 points, P less than .05). Clearly, patients continue to report improvements in various domains as time goes on, “suggesting that all the benefit of cure is not achieved by 12 weeks of follow-up,” said Dr. Younossi.
Gilead Sciences makes Epclusa and Harvoni and funded the study. Dr. Younossi reported having no relevant financial conflicts.
BOSTON – When given with ribavirin, a fixed-dose combination of sofosbuvir/velpatasvir (Epclusa) achieved a sustained viral response at 12 weeks (SVR-12) in 94% of decompensated cirrhotic patients with hepatitis C virus (HCV) genotypes 1-6 infection, according to Zobair M. Younossi, MD.
Patients with and without cirrhosis also reported meaningful improvements across a variety of outcome measures after successfully completing treatment with Epclusa or sofosbuvir (Harvoni), said Dr. Younossi of Inova Fairfax Hospital in Falls Church, Va. “Although on-treatment patient-reported outcomes improved more with ribavirin-free regimens, post-SVR improvements were similar,” regardless of whether patients had received ribavirin, he reported at the annual meeting of the American Association for the Study of Liver Diseases.
Epclusa without ribavirin led to SVR-12 in 85% of decompensated cirrhotic patients and nearly 99% of noncirrhotic patients of all HCV genotypes, Dr. Younossi reported. For sofosbuvir with ribavirin, rates of SVR-12 were 66% in genotype 3 cirrhotic patients and 95% in cirrhotic patients of other HCV genotypes.
At baseline, cirrhotic patients scored up to 33.5 points worse than noncirrhotics on a universal 100-point scale covering 26 patient-reported domains (P less than .05 for all but 3 domains). Decompensated cirrhotics reported more baseline depression and fatigue than other patients (P less than .002 for each comparison), while patients without cirrhosis were more likely to be treatment naive and employed (both P less than .0001). But after the investigators controlled for these differences, decompensated cirrhotics who received Epclusa reported an additional 5.5-9 points of improvement in treatment-emergent outcomes than those who received sofosbuvir plus ribavirin (P less than .002). Patients with compensated cirrhosis reported 2.3-5 points more improvement in treatment-emergent outcomes on Epclusa than on sofosbuvir plus ribavirin (P less than .05). “Decompensated cirrhotics experienced the best and greatest improvement of patient-reported outcome scores during treatment with sofosbuvir/velpatasvir,” Dr. Younossi said.
Patients who received ribavirin reported similar changes across domains at the end of treatment, regardless of cirrhosis status. Among patients who achieved SVR-12, decompensated cirrhotics reported significantly more improvement 12 weeks later than did patients with less severe liver disease, although both groups showed long-term improvements (5.8 points vs. 4.1 points, P less than .05). Clearly, patients continue to report improvements in various domains as time goes on, “suggesting that all the benefit of cure is not achieved by 12 weeks of follow-up,” said Dr. Younossi.
Gilead Sciences makes Epclusa and Harvoni and funded the study. Dr. Younossi reported having no relevant financial conflicts.
BOSTON – When given with ribavirin, a fixed-dose combination of sofosbuvir/velpatasvir (Epclusa) achieved a sustained viral response at 12 weeks (SVR-12) in 94% of decompensated cirrhotic patients with hepatitis C virus (HCV) genotypes 1-6 infection, according to Zobair M. Younossi, MD.
Patients with and without cirrhosis also reported meaningful improvements across a variety of outcome measures after successfully completing treatment with Epclusa or sofosbuvir (Harvoni), said Dr. Younossi of Inova Fairfax Hospital in Falls Church, Va. “Although on-treatment patient-reported outcomes improved more with ribavirin-free regimens, post-SVR improvements were similar,” regardless of whether patients had received ribavirin, he reported at the annual meeting of the American Association for the Study of Liver Diseases.
Epclusa without ribavirin led to SVR-12 in 85% of decompensated cirrhotic patients and nearly 99% of noncirrhotic patients of all HCV genotypes, Dr. Younossi reported. For sofosbuvir with ribavirin, rates of SVR-12 were 66% in genotype 3 cirrhotic patients and 95% in cirrhotic patients of other HCV genotypes.
At baseline, cirrhotic patients scored up to 33.5 points worse than noncirrhotics on a universal 100-point scale covering 26 patient-reported domains (P less than .05 for all but 3 domains). Decompensated cirrhotics reported more baseline depression and fatigue than other patients (P less than .002 for each comparison), while patients without cirrhosis were more likely to be treatment naive and employed (both P less than .0001). But after the investigators controlled for these differences, decompensated cirrhotics who received Epclusa reported an additional 5.5-9 points of improvement in treatment-emergent outcomes than those who received sofosbuvir plus ribavirin (P less than .002). Patients with compensated cirrhosis reported 2.3-5 points more improvement in treatment-emergent outcomes on Epclusa than on sofosbuvir plus ribavirin (P less than .05). “Decompensated cirrhotics experienced the best and greatest improvement of patient-reported outcome scores during treatment with sofosbuvir/velpatasvir,” Dr. Younossi said.
Patients who received ribavirin reported similar changes across domains at the end of treatment, regardless of cirrhosis status. Among patients who achieved SVR-12, decompensated cirrhotics reported significantly more improvement 12 weeks later than did patients with less severe liver disease, although both groups showed long-term improvements (5.8 points vs. 4.1 points, P less than .05). Clearly, patients continue to report improvements in various domains as time goes on, “suggesting that all the benefit of cure is not achieved by 12 weeks of follow-up,” said Dr. Younossi.
Gilead Sciences makes Epclusa and Harvoni and funded the study. Dr. Younossi reported having no relevant financial conflicts.
AT THE LIVER MEETING 2016
Key clinical point: Sofosbuvir/velpatasvir with ribavirin effectively cured most hepatitis C virus–infected patients with decompensated cirrhosis.
Major finding: In all, 94% of patients achieved a sustained viral response at 12 weeks, regardless of HCV genotype.
Data source: The phase III ASTRAL trials involving 1,701 patients with pangenotypic hepatitis C virus infections.
Disclosures: Gilead Sciences makes Epclusa and Harvoni and funded the study. Dr. Younossi reported having no relevant financial conflicts.
Primary chest-wall leiomyosarcoma: a rare mimic of a malignant rib lesion
Primary chest-wall leiomyosarcoma (LMS) is an uncommon, malignant, soft-tissue tumor that most often affects the extremities. Malignant LMS originates from mesenchymal cells with smooth muscle differentiation. It is rare in adults, forming only 7% of all soft-tissue sarcomas (STS), but it is the most common STS. In adults, this type of tumor is usually found in the retroperitoneum and extremities.1 Chest-wall LMS is rare and most often occurs in men aged 50-70 years.2 When LMS is associated with rib destruction, it may mimic a primary bone tumor or metastasis. We present here the case of histologically proven chest-wall sarcoma with associated rib destruction that was initially mistaken on imaging for either a metastasis or primary bone tumor.
Case presentation and summary
A 69-year-old man presented to the emergency department complaining of pain over the right side of the chest. The pain, which was pleuritic in nature, had worsened over the previous 6 months and was severe at presentation. The patient had no fever, shortness of breath, or loss of weight. He had no history of chest trauma or chest wall radiation, and nothing noteworthy was discovered in his medical history. Subsequent test results for hemoglobin, white blood cell count, lymphocyte count, and cardiac enzymes were normal.
A frontal chest radiograph showed an osteolytic destructive lesion involving the posterior right 6th rib (Figure 1). A contrast-enhanced computedtomography (CE-CT) scan of the chest showed a heterogeneously enhancing, ovoid, soft-tissue mass of 5.6 x 3.6 cm (2.2 x 1.2 in) centered on the postero- lateral right 6th rib, with associated rib erosion. There was another 2.0-cm (0.8-in) subpleural nodule in the left upper lobe (Figure 2).
Click on the PDF icon below to read the full article.
Primary chest-wall leiomyosarcoma (LMS) is an uncommon, malignant, soft-tissue tumor that most often affects the extremities. Malignant LMS originates from mesenchymal cells with smooth muscle differentiation. It is rare in adults, forming only 7% of all soft-tissue sarcomas (STS), but it is the most common STS. In adults, this type of tumor is usually found in the retroperitoneum and extremities.1 Chest-wall LMS is rare and most often occurs in men aged 50-70 years.2 When LMS is associated with rib destruction, it may mimic a primary bone tumor or metastasis. We present here the case of histologically proven chest-wall sarcoma with associated rib destruction that was initially mistaken on imaging for either a metastasis or primary bone tumor.
Case presentation and summary
A 69-year-old man presented to the emergency department complaining of pain over the right side of the chest. The pain, which was pleuritic in nature, had worsened over the previous 6 months and was severe at presentation. The patient had no fever, shortness of breath, or loss of weight. He had no history of chest trauma or chest wall radiation, and nothing noteworthy was discovered in his medical history. Subsequent test results for hemoglobin, white blood cell count, lymphocyte count, and cardiac enzymes were normal.
A frontal chest radiograph showed an osteolytic destructive lesion involving the posterior right 6th rib (Figure 1). A contrast-enhanced computedtomography (CE-CT) scan of the chest showed a heterogeneously enhancing, ovoid, soft-tissue mass of 5.6 x 3.6 cm (2.2 x 1.2 in) centered on the postero- lateral right 6th rib, with associated rib erosion. There was another 2.0-cm (0.8-in) subpleural nodule in the left upper lobe (Figure 2).
Click on the PDF icon below to read the full article.
Primary chest-wall leiomyosarcoma (LMS) is an uncommon, malignant, soft-tissue tumor that most often affects the extremities. Malignant LMS originates from mesenchymal cells with smooth muscle differentiation. It is rare in adults, forming only 7% of all soft-tissue sarcomas (STS), but it is the most common STS. In adults, this type of tumor is usually found in the retroperitoneum and extremities.1 Chest-wall LMS is rare and most often occurs in men aged 50-70 years.2 When LMS is associated with rib destruction, it may mimic a primary bone tumor or metastasis. We present here the case of histologically proven chest-wall sarcoma with associated rib destruction that was initially mistaken on imaging for either a metastasis or primary bone tumor.
Case presentation and summary
A 69-year-old man presented to the emergency department complaining of pain over the right side of the chest. The pain, which was pleuritic in nature, had worsened over the previous 6 months and was severe at presentation. The patient had no fever, shortness of breath, or loss of weight. He had no history of chest trauma or chest wall radiation, and nothing noteworthy was discovered in his medical history. Subsequent test results for hemoglobin, white blood cell count, lymphocyte count, and cardiac enzymes were normal.
A frontal chest radiograph showed an osteolytic destructive lesion involving the posterior right 6th rib (Figure 1). A contrast-enhanced computedtomography (CE-CT) scan of the chest showed a heterogeneously enhancing, ovoid, soft-tissue mass of 5.6 x 3.6 cm (2.2 x 1.2 in) centered on the postero- lateral right 6th rib, with associated rib erosion. There was another 2.0-cm (0.8-in) subpleural nodule in the left upper lobe (Figure 2).
Click on the PDF icon below to read the full article.
Flare risk lower in early-gout patients treated with urate-lowering therapy
WASHINGTON – Putting patients on urate-lowering therapy after their first flare of gout and treating urate levels to target appeared to reduce risk for additional disease flares over a 2-year period, based on results from 314 patients in a randomized, double-blind, placebo-controlled trial.
Among patients with early gout – those experiencing their first gout flare or a second flare that occurred more than 1 year after their first flare – the risk for one or more gout flares during the course of the study was 41% in the placebo group and 29% in the group of patients given febuxostat, a statistically significant difference (P = .033).
The significant advantage for active therapy to prevent flares was seen at 6-12 months, 12-18 months, and 18-24 months.
“The reduction in flares with febuxostat is clinically important and statistically significant,” said lead author Nicola Dalbeth, MD, of the University of Auckland (New Zealand). “This is the first clinical trial of [urate-lowering therapy] in patients with early gout. These are patients who would not be treated under current [American College of Rheumatology] guidelines,” which call for urate-lowering therapy if patients are symptomatic and have experienced two or more flares per year.
Dr. Dalbeth presented the study results at a late-breaker session during the annual meeting of the American College of Rheumatology.
The 314 patients were initially randomized to febuxostat 40 mg or placebo. The febuxostat dosage was increased to 80 mg if serum uric acid levels were above target on day 14, and 60 patients had their febuxostat doses increased.
The study was completed by 57% of placebo patients and 59% of febuxostat patients. Baseline characteristics were similar across treatment arms. Mean baseline serum uric acid was about 8.7 mg/dL, mean age was around 50 years, and more than three-quarters of study participants were white. Mean body-mass index was about 32.5, and mild renal impairment was present in 73% of placebo patients and 67% of febuxostat-treated patients.
Based on imaging studies, febuxostat had no significant effect on joint erosion during the observation period, but it reduced synovitis, compared with placebo, she said.
Dr. Dalbeth disclosed relationships with a variety of drug companies, including serving as a consultant for Takeda, the maker of febuxostat (Uloric).
WASHINGTON – Putting patients on urate-lowering therapy after their first flare of gout and treating urate levels to target appeared to reduce risk for additional disease flares over a 2-year period, based on results from 314 patients in a randomized, double-blind, placebo-controlled trial.
Among patients with early gout – those experiencing their first gout flare or a second flare that occurred more than 1 year after their first flare – the risk for one or more gout flares during the course of the study was 41% in the placebo group and 29% in the group of patients given febuxostat, a statistically significant difference (P = .033).
The significant advantage for active therapy to prevent flares was seen at 6-12 months, 12-18 months, and 18-24 months.
“The reduction in flares with febuxostat is clinically important and statistically significant,” said lead author Nicola Dalbeth, MD, of the University of Auckland (New Zealand). “This is the first clinical trial of [urate-lowering therapy] in patients with early gout. These are patients who would not be treated under current [American College of Rheumatology] guidelines,” which call for urate-lowering therapy if patients are symptomatic and have experienced two or more flares per year.
Dr. Dalbeth presented the study results at a late-breaker session during the annual meeting of the American College of Rheumatology.
The 314 patients were initially randomized to febuxostat 40 mg or placebo. The febuxostat dosage was increased to 80 mg if serum uric acid levels were above target on day 14, and 60 patients had their febuxostat doses increased.
The study was completed by 57% of placebo patients and 59% of febuxostat patients. Baseline characteristics were similar across treatment arms. Mean baseline serum uric acid was about 8.7 mg/dL, mean age was around 50 years, and more than three-quarters of study participants were white. Mean body-mass index was about 32.5, and mild renal impairment was present in 73% of placebo patients and 67% of febuxostat-treated patients.
Based on imaging studies, febuxostat had no significant effect on joint erosion during the observation period, but it reduced synovitis, compared with placebo, she said.
Dr. Dalbeth disclosed relationships with a variety of drug companies, including serving as a consultant for Takeda, the maker of febuxostat (Uloric).
WASHINGTON – Putting patients on urate-lowering therapy after their first flare of gout and treating urate levels to target appeared to reduce risk for additional disease flares over a 2-year period, based on results from 314 patients in a randomized, double-blind, placebo-controlled trial.
Among patients with early gout – those experiencing their first gout flare or a second flare that occurred more than 1 year after their first flare – the risk for one or more gout flares during the course of the study was 41% in the placebo group and 29% in the group of patients given febuxostat, a statistically significant difference (P = .033).
The significant advantage for active therapy to prevent flares was seen at 6-12 months, 12-18 months, and 18-24 months.
“The reduction in flares with febuxostat is clinically important and statistically significant,” said lead author Nicola Dalbeth, MD, of the University of Auckland (New Zealand). “This is the first clinical trial of [urate-lowering therapy] in patients with early gout. These are patients who would not be treated under current [American College of Rheumatology] guidelines,” which call for urate-lowering therapy if patients are symptomatic and have experienced two or more flares per year.
Dr. Dalbeth presented the study results at a late-breaker session during the annual meeting of the American College of Rheumatology.
The 314 patients were initially randomized to febuxostat 40 mg or placebo. The febuxostat dosage was increased to 80 mg if serum uric acid levels were above target on day 14, and 60 patients had their febuxostat doses increased.
The study was completed by 57% of placebo patients and 59% of febuxostat patients. Baseline characteristics were similar across treatment arms. Mean baseline serum uric acid was about 8.7 mg/dL, mean age was around 50 years, and more than three-quarters of study participants were white. Mean body-mass index was about 32.5, and mild renal impairment was present in 73% of placebo patients and 67% of febuxostat-treated patients.
Based on imaging studies, febuxostat had no significant effect on joint erosion during the observation period, but it reduced synovitis, compared with placebo, she said.
Dr. Dalbeth disclosed relationships with a variety of drug companies, including serving as a consultant for Takeda, the maker of febuxostat (Uloric).
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: Early-gout patients given febuxostat had a 29% risk of a flare and placebo-treated patients had a 41% risk of a flare over 2 years, a significant difference.
Data source: Randomized, double-blind, placebo-controlled, phase II study of 314 patients with early gout.
Disclosures: Dr. Dalbeth disclosed relationships with a variety of drug companies, including serving as a consultant for Takeda, the maker of febuxostat (Uloric).