User login
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Wrist Air Samplers Detect Virus Exposure in Kids With Asthma
Wrist Air Samplers Detect Virus Exposure in Kids With Asthma
A novel wearable wrist device was feasible and effective for identifying exposure to respiratory viruses in children with asthma, based on new data presented at the American Thoracic Society 2026 International Conference.
Upper respiratory infections are the main trigger of asthma exacerbations in children, and documented racial and ethnic disparities in upper respiratory infections likely contribute to similar disparities in asthma exacerbations, noted Darlene Bhavnani, PhD, MPH, of The University of Texas at Austin, et al in their abstract.
“Understanding differences in personal exposure to upper respiratory viruses in children with asthma may help to inform these differences in the risk of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
The researchers hypothesized that the use of a wearable passive air sampler could monitor respiratory virus exposure as a way to identify children at increased risk for asthma exacerbations.
Wrist devices to measure respiratory virus exposure are an emerging technology and have not been tested in children, the researchers noted. In their study, the researchers identified 25 children aged 6 to 17 years with persistent asthma who were enrolled in the TexHALE study. Participants were given a Fresh Air Clip to station in their homes and were asked to wear a wristband with a Fresh Air Clip for about 5 consecutive days. The median age of the participants was 12 years, and 64% were male.
At the end of the study period, families reported the number of days the wristband was worn, and the researchers used droplet digital polymerase chain reaction tests to quantify exposure to rhinovirus, respiratory syncytial virus (RSV), influenza A, and influenza B.
A total of 24 clips and 24 wristbands were distributed; 23 clips and all 24 wristbands were recovered for analysis. A total of 22 participants (92%) wore the wristband over a median of 6 days. Overall, approximately one-third of the wristbands (33%) tested positive for any respiratory virus, defined as > 6 copies of viral RNA, with 5 positive tests for rhinovirus, 5 for influenza B, 2 for RSV, and none for influenza A. None of the stationary home-based clips tested positive for any respiratory virus.
The researchers were not sure what to expect from the study, as personal exposure to upper respiratory viruses has not been well studied in children, said Bhavnani.
“One third of the children in our pilot study were exposed to one or more upper respiratory viruses in their personal environments, which is a substantial portion of the population studied,” she noted. “Given that viral exposure is the first step in the pathway leading to a viral infection and viral-associated asthma exacerbations, understanding differences in viral exposure could help us to learn more about how to prevent viral infection and viral-associated asthma exacerbations in children with asthma,” she said.
The study was limited by the small sample size, and larger studies are needed. However, the finding the one-third of wristbands and zero stationary clips tested positive for upper respiratory viruses suggests that clips stationed in homes may not be optimal to detect household exposures, or and that exposure outside the home may be more important for monitoring exposure to respiratory viruses in this population, and the results support the feasibility of the devices, the researchers wrote.
“Fresh Air Clips in the form of wearables can be used to understand differences in personal viral exposure and to target interventions that ultimately, would reduce the burden of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
New Role for New Technology
“New technology now allows us to quantitate exposure to specific respiratory viruses on wearable and stationary devices,” said Tim Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
The current study findings suggest that the majority of the exposure to respiratory viruses occurs outside the home, said Joos, who was not involved in the study. Consequently, technology that can detect community exposure could be useful, although the role it may play in public health and clinical practice is yet to be determined, Joos said.
The wristbands and clips were easy to deploy and recover, which supports their value, and potential applications include testing the effectiveness of infection control strategies such as social distancing, masking, and isolation in lowering viral exposures, Joos noted.
The study received no outside funding but was supported by core funds from the Dell Medical School at the University of Texas at Austin. The researchers had no financial conflicts to disclose. Joos had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A novel wearable wrist device was feasible and effective for identifying exposure to respiratory viruses in children with asthma, based on new data presented at the American Thoracic Society 2026 International Conference.
Upper respiratory infections are the main trigger of asthma exacerbations in children, and documented racial and ethnic disparities in upper respiratory infections likely contribute to similar disparities in asthma exacerbations, noted Darlene Bhavnani, PhD, MPH, of The University of Texas at Austin, et al in their abstract.
“Understanding differences in personal exposure to upper respiratory viruses in children with asthma may help to inform these differences in the risk of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
The researchers hypothesized that the use of a wearable passive air sampler could monitor respiratory virus exposure as a way to identify children at increased risk for asthma exacerbations.
Wrist devices to measure respiratory virus exposure are an emerging technology and have not been tested in children, the researchers noted. In their study, the researchers identified 25 children aged 6 to 17 years with persistent asthma who were enrolled in the TexHALE study. Participants were given a Fresh Air Clip to station in their homes and were asked to wear a wristband with a Fresh Air Clip for about 5 consecutive days. The median age of the participants was 12 years, and 64% were male.
At the end of the study period, families reported the number of days the wristband was worn, and the researchers used droplet digital polymerase chain reaction tests to quantify exposure to rhinovirus, respiratory syncytial virus (RSV), influenza A, and influenza B.
A total of 24 clips and 24 wristbands were distributed; 23 clips and all 24 wristbands were recovered for analysis. A total of 22 participants (92%) wore the wristband over a median of 6 days. Overall, approximately one-third of the wristbands (33%) tested positive for any respiratory virus, defined as > 6 copies of viral RNA, with 5 positive tests for rhinovirus, 5 for influenza B, 2 for RSV, and none for influenza A. None of the stationary home-based clips tested positive for any respiratory virus.
The researchers were not sure what to expect from the study, as personal exposure to upper respiratory viruses has not been well studied in children, said Bhavnani.
“One third of the children in our pilot study were exposed to one or more upper respiratory viruses in their personal environments, which is a substantial portion of the population studied,” she noted. “Given that viral exposure is the first step in the pathway leading to a viral infection and viral-associated asthma exacerbations, understanding differences in viral exposure could help us to learn more about how to prevent viral infection and viral-associated asthma exacerbations in children with asthma,” she said.
The study was limited by the small sample size, and larger studies are needed. However, the finding the one-third of wristbands and zero stationary clips tested positive for upper respiratory viruses suggests that clips stationed in homes may not be optimal to detect household exposures, or and that exposure outside the home may be more important for monitoring exposure to respiratory viruses in this population, and the results support the feasibility of the devices, the researchers wrote.
“Fresh Air Clips in the form of wearables can be used to understand differences in personal viral exposure and to target interventions that ultimately, would reduce the burden of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
New Role for New Technology
“New technology now allows us to quantitate exposure to specific respiratory viruses on wearable and stationary devices,” said Tim Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
The current study findings suggest that the majority of the exposure to respiratory viruses occurs outside the home, said Joos, who was not involved in the study. Consequently, technology that can detect community exposure could be useful, although the role it may play in public health and clinical practice is yet to be determined, Joos said.
The wristbands and clips were easy to deploy and recover, which supports their value, and potential applications include testing the effectiveness of infection control strategies such as social distancing, masking, and isolation in lowering viral exposures, Joos noted.
The study received no outside funding but was supported by core funds from the Dell Medical School at the University of Texas at Austin. The researchers had no financial conflicts to disclose. Joos had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
A novel wearable wrist device was feasible and effective for identifying exposure to respiratory viruses in children with asthma, based on new data presented at the American Thoracic Society 2026 International Conference.
Upper respiratory infections are the main trigger of asthma exacerbations in children, and documented racial and ethnic disparities in upper respiratory infections likely contribute to similar disparities in asthma exacerbations, noted Darlene Bhavnani, PhD, MPH, of The University of Texas at Austin, et al in their abstract.
“Understanding differences in personal exposure to upper respiratory viruses in children with asthma may help to inform these differences in the risk of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
The researchers hypothesized that the use of a wearable passive air sampler could monitor respiratory virus exposure as a way to identify children at increased risk for asthma exacerbations.
Wrist devices to measure respiratory virus exposure are an emerging technology and have not been tested in children, the researchers noted. In their study, the researchers identified 25 children aged 6 to 17 years with persistent asthma who were enrolled in the TexHALE study. Participants were given a Fresh Air Clip to station in their homes and were asked to wear a wristband with a Fresh Air Clip for about 5 consecutive days. The median age of the participants was 12 years, and 64% were male.
At the end of the study period, families reported the number of days the wristband was worn, and the researchers used droplet digital polymerase chain reaction tests to quantify exposure to rhinovirus, respiratory syncytial virus (RSV), influenza A, and influenza B.
A total of 24 clips and 24 wristbands were distributed; 23 clips and all 24 wristbands were recovered for analysis. A total of 22 participants (92%) wore the wristband over a median of 6 days. Overall, approximately one-third of the wristbands (33%) tested positive for any respiratory virus, defined as > 6 copies of viral RNA, with 5 positive tests for rhinovirus, 5 for influenza B, 2 for RSV, and none for influenza A. None of the stationary home-based clips tested positive for any respiratory virus.
The researchers were not sure what to expect from the study, as personal exposure to upper respiratory viruses has not been well studied in children, said Bhavnani.
“One third of the children in our pilot study were exposed to one or more upper respiratory viruses in their personal environments, which is a substantial portion of the population studied,” she noted. “Given that viral exposure is the first step in the pathway leading to a viral infection and viral-associated asthma exacerbations, understanding differences in viral exposure could help us to learn more about how to prevent viral infection and viral-associated asthma exacerbations in children with asthma,” she said.
The study was limited by the small sample size, and larger studies are needed. However, the finding the one-third of wristbands and zero stationary clips tested positive for upper respiratory viruses suggests that clips stationed in homes may not be optimal to detect household exposures, or and that exposure outside the home may be more important for monitoring exposure to respiratory viruses in this population, and the results support the feasibility of the devices, the researchers wrote.
“Fresh Air Clips in the form of wearables can be used to understand differences in personal viral exposure and to target interventions that ultimately, would reduce the burden of viral infection and viral-associated asthma exacerbations,” Bhavnani said.
New Role for New Technology
“New technology now allows us to quantitate exposure to specific respiratory viruses on wearable and stationary devices,” said Tim Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
The current study findings suggest that the majority of the exposure to respiratory viruses occurs outside the home, said Joos, who was not involved in the study. Consequently, technology that can detect community exposure could be useful, although the role it may play in public health and clinical practice is yet to be determined, Joos said.
The wristbands and clips were easy to deploy and recover, which supports their value, and potential applications include testing the effectiveness of infection control strategies such as social distancing, masking, and isolation in lowering viral exposures, Joos noted.
The study received no outside funding but was supported by core funds from the Dell Medical School at the University of Texas at Austin. The researchers had no financial conflicts to disclose. Joos had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Wrist Air Samplers Detect Virus Exposure in Kids With Asthma
Wrist Air Samplers Detect Virus Exposure in Kids With Asthma
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
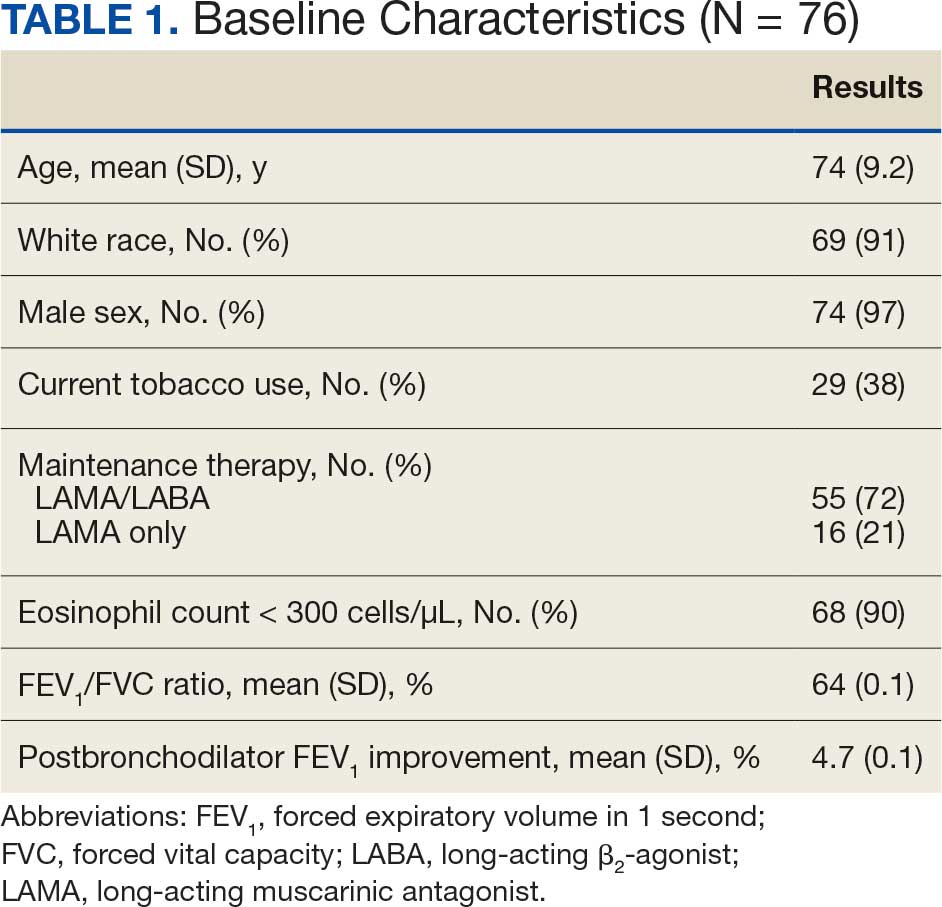
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
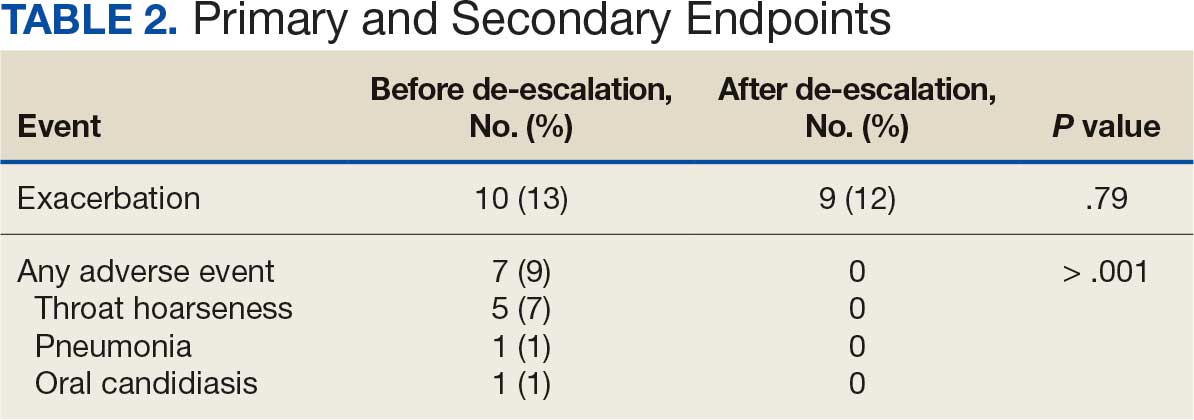
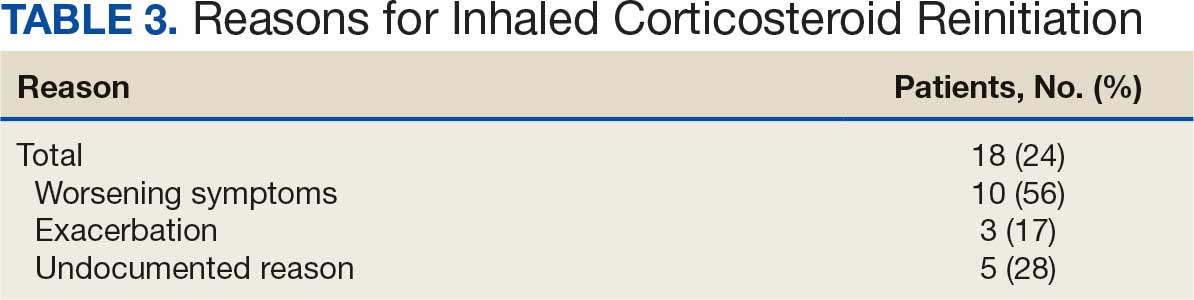
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
Chronic obstructive pulmonary disease (COPD) affects about 25% of the veteran population and is the third-leading cause of death globally.1,2 In patients with COPD, cigarette smoking leads to increased respiratory symptoms, a greater annual rate of decline in forced expiratory volume in 1 second (FEV1), and an increase in COPD mortality rate vs nonsmokers.3 Veterans are at a higher risk of COPD due to increased prevalence of smoking within this population as well as military activities leading to environmental and occupational exposure.4
According to the 2024 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, the primary treatment goals of COPD therapy are to reduce symptoms and future risk of exacerbations.3 Bronchodilators are recommended for initial COPD pharmacotherapy, including long-acting muscarinic antagonists (LAMAs) and/or long-acting Β2-agonists (LABAs). In some cases, treatment may include inhaled corticosteroids (ICS). Evidence supports ICS therapy in patients with COPD experiencing hospitalizations for exacerbations, ≥ 2 moderate exacerbations per year, blood eosinophil count ≥ 300 cells/μL or concomitant asthma.3
While the 2024 GOLD guidelines caution against the use of ICS outside of certain patient groups, previous GOLD guidelines recommended the use of ICS more broadly.5 Due to these changes, many patients may be using ICS therapy unnecessarily. At the Sioux Falls Veterans Affairs Health Care System (SFVAHCS), ICS overuse was identified as a driver of increased medication burden and potential adverse effects (AEs). To help reduce unnecessary ICS use, a data dashboard was created to identify potential candidates for ICS deprescribing. SFVAHCS clinical pharmacy practitioners are licensed pharmacists who work as independent practitioners with a scope of practice that allows them to initiate, modify, or discontinue medication therapy within medication management clinics. Pharmacists contacted dashboard patients to de-escalate ICS therapy when appropriate.
The SUNSET trial directly compared the continuation of triple therapy (tiotropium + salmeterol/fluticasone propionate) vs deprescribing to LABA/LAMA (indacaterol/ glycopyrronium) in patients with COPD.6 It evaluated whether LABA/LAMA was noninferior to LABA/LAMA/ICS therapy when comparing COPD exacerbations in patients whose COPD exacerbations were infrequent. Participants were randomized to triple therapy continuation or indacaterol/glycopyrronium and followed for 26 weeks. Patients on indacaterol/glycopyrronium did not have a significant difference in exacerbations than patients utilizing triple therapy.
The Implementation of a Targeted ICS De-Escalation in Patients with COPD in the Primary Care Setting trial evaluated the success of pharmacist-led ICS deprescribing in appropriate patients with COPD.7 Pharmacists followed GOLD guidelines to recommend ICS deprescribing and have risk vs benefit discussions with certain patients. Patients were considered for ICS deprescribing if they had a history of recurrent pneumonia or had no exacerbations within the previous year and eosinophils < 300 cells/μL (risk-benefit discussion if no eosinophil count available). This study found that 19.6% of patients were unable to tolerate ICS withdrawal and resumed either a standard or reduced dose of ICS therapy.7
Current guidelines and evidence recommend deprescribing ICS for appropriate patients. There is no current literature defining the impact of pharmacists on ICS deprescribing within the US Department of Veterans Affairs (VA) system. This study will allow for a quantifiable measure of pharmacists’ impact on reducing AEs associated with unnecessary ICS use.
Methods
This retrospective, single-center study was conducted at the SFVAHCS. Data were collected through manual chart review of SFVAHCS electronic health records. Veterans aged ≥ 18 years with a COPD diagnosis who underwent ICS deprescribing by a SFVAHCS pharmacist between February 2022 and December 2023 were included. Records were examined for 52 weeks prior to ICS withdrawal (baseline) and 52 weeks following withdrawal. Patients were excluded from the study if they had a history of asthma or ICS was used for < 52 weeks before deprescribing. Baseline characteristics were collected, including age, race, sex, current tobacco use, eosinophil count, COPD maintenance therapy, FEV1/forced vital capacity (FVC) ratio, and mean postbronchodilator FEV1 improvement.
The primary endpoint was number of COPD exacerbations at 52 weeks before vs after deprescribing. Secondary endpoints included the number of patients restarted on an ICS within 52 weeks of deprescribing, as well as ICS AEs, including pneumonia, oral candidiasis, and throat hoarseness.
Statistical Analysis
The primary endpoint was analyzed using the Wilcoxon signed rank test and secondary endpoints were analyzed using the McNemar exact test. Results with P < .05 were considered statistically significant for both tests.
Results
Seventy-six patients were included. Patients had a mean age of 75 years and 91% identified as White, which is representative of the SFVAHCS patient population (Table 1). Twenty-nine (38%) patients were current tobacco users and 55 patients (72%) used LAMA/LABA therapy (after ICS deprescribing) with an eosinophil count < 300 cells/μL. There was no significant difference in exacerbations before vs after ICS deprescribing (P = .78) (Table 2). There were 7 AEs reported before ICS deprescribing vs 0 following ICS deprescribing (P < .001). Five patients (7%) reported throat hoarseness, 1 (1%) reported pneumonia, and 1 (1%) reported oral candidiasis. Eighteen patients were reinitiated on ICS (24%). ICS reinitiation was most commonly due to patients reporting worsening symptoms (56%) (Table 3).
Discussion
This study sought to determine the impact of pharmacist-led ICS deprescribing on AEs and exacerbations experienced by patients with COPD. COPD exacerbations were not significantly different before vs after ICS deprescribing. The pharmacist-led ICS deprescribing program did not lead to increased COPD exacerbations. Similar to the SUNSET trial, the results of this study showed exacerbations did not significantly increase upon ICS deprescribing; however, this study differed by specifying pharmacist- led intervention.6
There was a decrease in ICS-related AEs following ICS deprescribing. Several patients were reinitiated on an ICS. As expected with deprescribing, some patients were not able to tolerate ICS withdrawal or had clinical indications to resume therapy (ie, an exacerbation). Similar results were found in another study where 8.9% of patients were restarted on ICS and 10.9% were de-escalated to a lower dose but were unable to stop completely.7 A 2024 systematic review by Georgiou et al found a wide range of patients resumed ICS therapy following withdrawal (21%-74%). Of note, only 2 of the randomized controlled trials and 3 observational studies included this meta-analysis included data on ICS reinitiation. Georgiou et al concluded there was insufficient evidence to determine the proportion of patients reinitiated on ICS but patients were commonly resumed on ICS therapy due to worsening symptoms, experiencing an exacerbation or decline in FEV1.8 Although the rate of ICS reinitiation was unclear in the Georgiou et al meta-analysis, reasons for re-initiation were similar to what was found in our study.8
Strengths and Limitations
The retrospective nature of this study and its small sample size of 76 patients limit its findings. The retrospective nature of the study required researchers to rely on proper chart documentation, which is not always accurate or up to date. Lack of documentation of COPD exacerbations or patients who received care outside the VA following initial deprescribing could have biased study results. This patient population is representative of the veteran population in South Dakota but is not representative of the female or non-White patient population which may be more prevalent at other VA Health Care Systems as well as nonveteran patient populations. Additionally, this study was limited to a review of 52 weeks pre- and post-ICS deprescribing which may have impacted results. Patients may have had a COPD exacerbation or were restarted on ICS therapy beyond 52 weeks. Finally, the retrospective nature and small sample size limited the findings for the primary endpoint which could have been improved with a larger sample size and a randomized controlled design.
The comparison of patients with themselves before and after ICS deprescribing reduced the potential for bias seen in retrospective studies. This method did not require a second control group which would potentially introduce confounding factors.
Conclusions
This study found that in a small population of veterans with COPD, pharmacist-led ICS deprescribing did not lead to an increase in COPD exacerbations and decreased the risk of AEs related to ICS therapy. Some patients were reinitiated on ICS therapy; however, reinitiation was rarely attributable to a COPD exacerbation. This study suggests that pharmacists were able to appropriately identify candidates for ICS deprescribing without increasing their risk of exacerbations. By de-escalating ICS therapy, pharmacists decreased medication burden and potential AEs caused by ICS therapy. These findings support expanding the role of clinical pharmacists in COPD management, particularly in identifying candidates for safe ICS deprescribing.
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
- Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28:29-36. doi:10.1111/resp.14349/
- Anderson E, Wiener RS, Resnick K, et al. Care coordination for veterans with COPD: a positive deviance study. Am J Manag Care. 2020;26:63-68. doi:10.37765/ajmc.2020.42394
- Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report. November 12, 2023. Accessed April 1, 2026. https://goldcopd.org/2023-gold-report-2/
- US Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for the management of chronic obstructive pulmonary disease. April 2021. Accessed April 1, 2026. https://www.healthquality.va.gov /guidelines/cd/copd/
- Gruffydd-Jones K. GOLD guidelines 2011: what are the implications for primary care? Prim Care Respir J. 2012;21:437-441. doi:10.4104/pcrj.2012.00058
- Chapman KR, Hurst JR, Frent SM, et al. Long-term triple therapy de-escalation to indacaterol/glycopyrronium in patients with chronic obstructive pulmonary disease (SUNSET): a randomized, double-blind, triple-dummy clinical trial. Am J Respir Crit Care Med. 2018;198:329-339. doi:10.1164/rccm.201803-0405OC
- Hahn NM, Nagy MW. Implementation of a targeted inhaled corticosteroid de-escalation process in patients with chronic obstructive pulmonary disease in the primary care setting. Innov Pharm. 2022;13:10.24926/iip.v13i1.4349. doi:10.24926/iip.v13i1.4349
- Georgiou A, Ramesh R, Schofield P, et al. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. Int J Chron Obstruct Pulmon Dis. 2024;19:1403- 1419. doi:10.2147/COPD.S436525
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Impact of a Pharmacist ICS Deprescribing Intervention on COPD Exacerbations and Adverse Events
Mycobacteria May Predict Graft Failure After Lung Transplant
Mycobacteria May Predict Graft Failure After Lung Transplant
Rapid-growing nontuberculous mycobacteria (NTM) were strongly associated with death or retransplantation in adult lung transplant patients, based on data from a new study of about 1000 individuals.
NTM are ubiquitous environmental organisms, but the clinical significance of isolating NTM posttransplant remains poorly defined, and previous studies have been mainly small and single center, said lead author Gabrielle Mezochow, MD, a pulmonology and critical care fellow at the University of Pennsylvania in Philadelphia.
“This is important because treatment is particularly challenging in lung transplant recipients, requiring prolonged multidrug regimens that can be toxic and interact with immunosuppression,” Mezochow said. “We conducted this study to better understand how often NTM is isolated after lung transplant, and whether isolation is associated with important outcomes such as chronic lung allograft dysfunction (CLAD) and death or retransplantation in a large multicenter cohort,” she said.
In the study, presented at the annual meeting of the International Society for Heart and Lung Transplantation (ISHLT), Mezochow et al reviewed data from 1044 adult lung transplant recipients in the Lung Transplant Outcomes Group cohort who underwent transplant between 2007 and 2022 at 3 centers.
The researchers evaluated the time from transplantation to graft failure (defined as death or retransplantation) and CLAD (as defined by the ISHLT). They used a proportional hazards model adjusted for age, diagnosis, BMI, primary graft dysfunction, postoperative extracorporeal membrane oxygenation, and transplant type.
A total of 136 patients (13%) had pulmonary growth of NTM within a year of their transplants; the most common types were Mycobacterium avium (88 patients) and Mycobacterium abscessus (16 patients).
Overall, the association between early growth of any NTM and the risk for graft failure did not reach statistical significance (adjusted hazard ratio [HR], 1.27). However, patients who had early growth of rapid-growing NTM (including M abscessus, Mycobacterium chelonae, Mycobacterium fortuitum, Mycobacterium immunogenum, Mycobacterium mageritense, and Mycobacterium mucogenicum) had an increased risk for graft failure compared to those with early growth of slow-growing NTM such as M avium (unadjusted HR, 2.36; adjusted HR, 2.49). The associations were consistent when patients with cystic fibrosis were excluded, and no significant association was observed between early NTM growth by slow or rapid types and increased risk for CLAD (adjusted HR, 1.09).
“One of the most interesting findings was that associations differed by NTM species,” Mezochow said. “Rapid-growing NTM were most strongly associated with death or retransplantation, whereas slow-growing NTM appeared to have a stronger association with CLAD,” she said. “We were also intrigued by the stronger associations with negative outcomes observed among recipients with ILD [interstitial lung disease], particularly those undergoing single lung transplantation,” Mezochow noted. “This raises the possibility that characteristics of the native lung or underlying lung disease may influence susceptibility and outcomes,” she said.
“Importantly, our study evaluated NTM isolation rather than NTM pulmonary disease, which is often difficult to define in lung transplant recipients,” said Mezochow. The results suggest that NTM isolation should not be dismissed as a benign microbiologic finding and could serve as an early marker of lung transplant recipients at increased risk for poor outcomes, even before disease can be definitively established, she noted. “Certain subgroups of recipients, including those with specific NTM species or underlying diagnoses, may be at a particularly elevated risk for poor outcomes, while not all patients with NTM isolation are likely to require treatment,” she added.
Limitations and Next Steps
The findings were limited by several factors including the observational design and lack of detailed patient-level medication data including longitudinal immunosuppression, antibiotic exposures, and azithromycin use for bronchiolitis obliterans syndrome prevention, any of which could influence both NTM isolation and downstream outcomes, Mezochow said.
The researchers also were unable to adjudicate NTM pulmonary disease according to current guideline-based definitions because of the lack of longitudinal radiographic and symptom data, she added. “That said, these diagnostic criteria were developed outside the transplant setting and have not been validated in lung transplant recipients, so their applicability here is uncertain,” she added. “Although we focused on the first posttransplant year, when surveillance bronchoscopy is relatively routine, some residual ascertainment bias is still likely,” she noted.
“Future research should focus on identifying which recipients with NTM isolation are most likely to progress to CLAD or death, understanding the biologic mechanisms linking NTM and allograft injury, and determining whether treatment strategies or immunosuppression modifications can improve outcomes,” said Mezochow. “Ultimately, the goal is to develop a framework that helps clinicians distinguish who may benefit from treatment from those who can be safely observed,” she said.
Added Value for Patient Assessment
The current study addresses major questions in lung transplantation, namely, whether isolation of NTM species in the first year after a lung transplant is a marker of airway vulnerability, structural airway defects, patient frailty, or a true contributor to allograft function and failure, said Jacqueline Burnell, MD, an associate professor of clinical medicine at the Lewis Katz School of Medicine at Temple University in Philadelphia, and a specialist in infections in transplant and immunocompromised patients. “This study separated rapidly growing NTM from slow growers to attempt to identify species associated with poor outcomes and provide prognostication,” said Burnell, who was not involved in the study. The association of rapidly growing NTM and poorer outcomes was not surprising, she noted. “Mycobacterium abscessus species, which accounted for the majority of rapidly growing isolates, are thought to be more aggressive and are certainly more challenging to treat,” she said. “The absence of association with CLAD is interesting, as this has been found in other studies looking at NTM infections post-lung transplant,” she added.
The results suggest that rapidly growing NTM should be risk-stratified separately from slow-growing NTM, said Burnell. “Early growth of rapid-growing NTM should prompt careful evaluation and assessment in a multidisciplinary fashion and not be deemed colonization without thorough evaluation,” she said. Routine posttransplant cultures also may have prognostic value in graft failure, she noted.
However, additional research with more granular detail regarding patient characteristics would be useful for risk stratification, said Burnell. “For example, information about pretransplant colonization, type of transplant (single vs double), immunosuppressive regimens, co-infections, and other factors would be useful,” she said. The current study did not address delineation between colonization, transient isolation, and infection, and data on treatment regimens and timing were lacking; therefore, collaborative studies are needed to assess these factors and their relationship to patient outcomes, Burnell noted.
The study was funded by institutional grants from the National Heart, Lung, and Blood Institute. Mezochow and Burnell had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Rapid-growing nontuberculous mycobacteria (NTM) were strongly associated with death or retransplantation in adult lung transplant patients, based on data from a new study of about 1000 individuals.
NTM are ubiquitous environmental organisms, but the clinical significance of isolating NTM posttransplant remains poorly defined, and previous studies have been mainly small and single center, said lead author Gabrielle Mezochow, MD, a pulmonology and critical care fellow at the University of Pennsylvania in Philadelphia.
“This is important because treatment is particularly challenging in lung transplant recipients, requiring prolonged multidrug regimens that can be toxic and interact with immunosuppression,” Mezochow said. “We conducted this study to better understand how often NTM is isolated after lung transplant, and whether isolation is associated with important outcomes such as chronic lung allograft dysfunction (CLAD) and death or retransplantation in a large multicenter cohort,” she said.
In the study, presented at the annual meeting of the International Society for Heart and Lung Transplantation (ISHLT), Mezochow et al reviewed data from 1044 adult lung transplant recipients in the Lung Transplant Outcomes Group cohort who underwent transplant between 2007 and 2022 at 3 centers.
The researchers evaluated the time from transplantation to graft failure (defined as death or retransplantation) and CLAD (as defined by the ISHLT). They used a proportional hazards model adjusted for age, diagnosis, BMI, primary graft dysfunction, postoperative extracorporeal membrane oxygenation, and transplant type.
A total of 136 patients (13%) had pulmonary growth of NTM within a year of their transplants; the most common types were Mycobacterium avium (88 patients) and Mycobacterium abscessus (16 patients).
Overall, the association between early growth of any NTM and the risk for graft failure did not reach statistical significance (adjusted hazard ratio [HR], 1.27). However, patients who had early growth of rapid-growing NTM (including M abscessus, Mycobacterium chelonae, Mycobacterium fortuitum, Mycobacterium immunogenum, Mycobacterium mageritense, and Mycobacterium mucogenicum) had an increased risk for graft failure compared to those with early growth of slow-growing NTM such as M avium (unadjusted HR, 2.36; adjusted HR, 2.49). The associations were consistent when patients with cystic fibrosis were excluded, and no significant association was observed between early NTM growth by slow or rapid types and increased risk for CLAD (adjusted HR, 1.09).
“One of the most interesting findings was that associations differed by NTM species,” Mezochow said. “Rapid-growing NTM were most strongly associated with death or retransplantation, whereas slow-growing NTM appeared to have a stronger association with CLAD,” she said. “We were also intrigued by the stronger associations with negative outcomes observed among recipients with ILD [interstitial lung disease], particularly those undergoing single lung transplantation,” Mezochow noted. “This raises the possibility that characteristics of the native lung or underlying lung disease may influence susceptibility and outcomes,” she said.
“Importantly, our study evaluated NTM isolation rather than NTM pulmonary disease, which is often difficult to define in lung transplant recipients,” said Mezochow. The results suggest that NTM isolation should not be dismissed as a benign microbiologic finding and could serve as an early marker of lung transplant recipients at increased risk for poor outcomes, even before disease can be definitively established, she noted. “Certain subgroups of recipients, including those with specific NTM species or underlying diagnoses, may be at a particularly elevated risk for poor outcomes, while not all patients with NTM isolation are likely to require treatment,” she added.
Limitations and Next Steps
The findings were limited by several factors including the observational design and lack of detailed patient-level medication data including longitudinal immunosuppression, antibiotic exposures, and azithromycin use for bronchiolitis obliterans syndrome prevention, any of which could influence both NTM isolation and downstream outcomes, Mezochow said.
The researchers also were unable to adjudicate NTM pulmonary disease according to current guideline-based definitions because of the lack of longitudinal radiographic and symptom data, she added. “That said, these diagnostic criteria were developed outside the transplant setting and have not been validated in lung transplant recipients, so their applicability here is uncertain,” she added. “Although we focused on the first posttransplant year, when surveillance bronchoscopy is relatively routine, some residual ascertainment bias is still likely,” she noted.
“Future research should focus on identifying which recipients with NTM isolation are most likely to progress to CLAD or death, understanding the biologic mechanisms linking NTM and allograft injury, and determining whether treatment strategies or immunosuppression modifications can improve outcomes,” said Mezochow. “Ultimately, the goal is to develop a framework that helps clinicians distinguish who may benefit from treatment from those who can be safely observed,” she said.
Added Value for Patient Assessment
The current study addresses major questions in lung transplantation, namely, whether isolation of NTM species in the first year after a lung transplant is a marker of airway vulnerability, structural airway defects, patient frailty, or a true contributor to allograft function and failure, said Jacqueline Burnell, MD, an associate professor of clinical medicine at the Lewis Katz School of Medicine at Temple University in Philadelphia, and a specialist in infections in transplant and immunocompromised patients. “This study separated rapidly growing NTM from slow growers to attempt to identify species associated with poor outcomes and provide prognostication,” said Burnell, who was not involved in the study. The association of rapidly growing NTM and poorer outcomes was not surprising, she noted. “Mycobacterium abscessus species, which accounted for the majority of rapidly growing isolates, are thought to be more aggressive and are certainly more challenging to treat,” she said. “The absence of association with CLAD is interesting, as this has been found in other studies looking at NTM infections post-lung transplant,” she added.
The results suggest that rapidly growing NTM should be risk-stratified separately from slow-growing NTM, said Burnell. “Early growth of rapid-growing NTM should prompt careful evaluation and assessment in a multidisciplinary fashion and not be deemed colonization without thorough evaluation,” she said. Routine posttransplant cultures also may have prognostic value in graft failure, she noted.
However, additional research with more granular detail regarding patient characteristics would be useful for risk stratification, said Burnell. “For example, information about pretransplant colonization, type of transplant (single vs double), immunosuppressive regimens, co-infections, and other factors would be useful,” she said. The current study did not address delineation between colonization, transient isolation, and infection, and data on treatment regimens and timing were lacking; therefore, collaborative studies are needed to assess these factors and their relationship to patient outcomes, Burnell noted.
The study was funded by institutional grants from the National Heart, Lung, and Blood Institute. Mezochow and Burnell had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Rapid-growing nontuberculous mycobacteria (NTM) were strongly associated with death or retransplantation in adult lung transplant patients, based on data from a new study of about 1000 individuals.
NTM are ubiquitous environmental organisms, but the clinical significance of isolating NTM posttransplant remains poorly defined, and previous studies have been mainly small and single center, said lead author Gabrielle Mezochow, MD, a pulmonology and critical care fellow at the University of Pennsylvania in Philadelphia.
“This is important because treatment is particularly challenging in lung transplant recipients, requiring prolonged multidrug regimens that can be toxic and interact with immunosuppression,” Mezochow said. “We conducted this study to better understand how often NTM is isolated after lung transplant, and whether isolation is associated with important outcomes such as chronic lung allograft dysfunction (CLAD) and death or retransplantation in a large multicenter cohort,” she said.
In the study, presented at the annual meeting of the International Society for Heart and Lung Transplantation (ISHLT), Mezochow et al reviewed data from 1044 adult lung transplant recipients in the Lung Transplant Outcomes Group cohort who underwent transplant between 2007 and 2022 at 3 centers.
The researchers evaluated the time from transplantation to graft failure (defined as death or retransplantation) and CLAD (as defined by the ISHLT). They used a proportional hazards model adjusted for age, diagnosis, BMI, primary graft dysfunction, postoperative extracorporeal membrane oxygenation, and transplant type.
A total of 136 patients (13%) had pulmonary growth of NTM within a year of their transplants; the most common types were Mycobacterium avium (88 patients) and Mycobacterium abscessus (16 patients).
Overall, the association between early growth of any NTM and the risk for graft failure did not reach statistical significance (adjusted hazard ratio [HR], 1.27). However, patients who had early growth of rapid-growing NTM (including M abscessus, Mycobacterium chelonae, Mycobacterium fortuitum, Mycobacterium immunogenum, Mycobacterium mageritense, and Mycobacterium mucogenicum) had an increased risk for graft failure compared to those with early growth of slow-growing NTM such as M avium (unadjusted HR, 2.36; adjusted HR, 2.49). The associations were consistent when patients with cystic fibrosis were excluded, and no significant association was observed between early NTM growth by slow or rapid types and increased risk for CLAD (adjusted HR, 1.09).
“One of the most interesting findings was that associations differed by NTM species,” Mezochow said. “Rapid-growing NTM were most strongly associated with death or retransplantation, whereas slow-growing NTM appeared to have a stronger association with CLAD,” she said. “We were also intrigued by the stronger associations with negative outcomes observed among recipients with ILD [interstitial lung disease], particularly those undergoing single lung transplantation,” Mezochow noted. “This raises the possibility that characteristics of the native lung or underlying lung disease may influence susceptibility and outcomes,” she said.
“Importantly, our study evaluated NTM isolation rather than NTM pulmonary disease, which is often difficult to define in lung transplant recipients,” said Mezochow. The results suggest that NTM isolation should not be dismissed as a benign microbiologic finding and could serve as an early marker of lung transplant recipients at increased risk for poor outcomes, even before disease can be definitively established, she noted. “Certain subgroups of recipients, including those with specific NTM species or underlying diagnoses, may be at a particularly elevated risk for poor outcomes, while not all patients with NTM isolation are likely to require treatment,” she added.
Limitations and Next Steps
The findings were limited by several factors including the observational design and lack of detailed patient-level medication data including longitudinal immunosuppression, antibiotic exposures, and azithromycin use for bronchiolitis obliterans syndrome prevention, any of which could influence both NTM isolation and downstream outcomes, Mezochow said.
The researchers also were unable to adjudicate NTM pulmonary disease according to current guideline-based definitions because of the lack of longitudinal radiographic and symptom data, she added. “That said, these diagnostic criteria were developed outside the transplant setting and have not been validated in lung transplant recipients, so their applicability here is uncertain,” she added. “Although we focused on the first posttransplant year, when surveillance bronchoscopy is relatively routine, some residual ascertainment bias is still likely,” she noted.
“Future research should focus on identifying which recipients with NTM isolation are most likely to progress to CLAD or death, understanding the biologic mechanisms linking NTM and allograft injury, and determining whether treatment strategies or immunosuppression modifications can improve outcomes,” said Mezochow. “Ultimately, the goal is to develop a framework that helps clinicians distinguish who may benefit from treatment from those who can be safely observed,” she said.
Added Value for Patient Assessment
The current study addresses major questions in lung transplantation, namely, whether isolation of NTM species in the first year after a lung transplant is a marker of airway vulnerability, structural airway defects, patient frailty, or a true contributor to allograft function and failure, said Jacqueline Burnell, MD, an associate professor of clinical medicine at the Lewis Katz School of Medicine at Temple University in Philadelphia, and a specialist in infections in transplant and immunocompromised patients. “This study separated rapidly growing NTM from slow growers to attempt to identify species associated with poor outcomes and provide prognostication,” said Burnell, who was not involved in the study. The association of rapidly growing NTM and poorer outcomes was not surprising, she noted. “Mycobacterium abscessus species, which accounted for the majority of rapidly growing isolates, are thought to be more aggressive and are certainly more challenging to treat,” she said. “The absence of association with CLAD is interesting, as this has been found in other studies looking at NTM infections post-lung transplant,” she added.
The results suggest that rapidly growing NTM should be risk-stratified separately from slow-growing NTM, said Burnell. “Early growth of rapid-growing NTM should prompt careful evaluation and assessment in a multidisciplinary fashion and not be deemed colonization without thorough evaluation,” she said. Routine posttransplant cultures also may have prognostic value in graft failure, she noted.
However, additional research with more granular detail regarding patient characteristics would be useful for risk stratification, said Burnell. “For example, information about pretransplant colonization, type of transplant (single vs double), immunosuppressive regimens, co-infections, and other factors would be useful,” she said. The current study did not address delineation between colonization, transient isolation, and infection, and data on treatment regimens and timing were lacking; therefore, collaborative studies are needed to assess these factors and their relationship to patient outcomes, Burnell noted.
The study was funded by institutional grants from the National Heart, Lung, and Blood Institute. Mezochow and Burnell had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Mycobacteria May Predict Graft Failure After Lung Transplant
Mycobacteria May Predict Graft Failure After Lung Transplant
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Offering lung cancer screening to everyone with a 20-year smoking history could expand access to screening, identify more cancers, and reduce disparities, new research suggests.
In an analysis of nearly 1 million US veterans, researchers estimated that a simplified approach to lung cancer screening — based on smoking duration rather than pack-years — would expand screening eligibility by nearly 30% and reduce potentially missed lung cancers by over 70%.
Those shifts would be especially pronounced among women and Black individuals — 2 groups that are underserved by current screening criteria.
The results, presented at the American Society of Clinical Oncology (ASCO) 2026, come at a time when some groups are revisiting their lung cancer screening guidelines.
And they support smoking duration as a “simpler, more sensitive, and more equitable metric for screening eligibility,” researcher Brendan T. Heiden, MD, MPHS, Washington University School of Medicine in St. Louis, St. Louis, told meeting attendees.
Toward a Better Metric
Current guidelines from the US Preventive Services Task Force (USPSTF) recommend annual lung cancer screening with low-dose CT for adults aged 50-80 years who have at least a 20 pack-year smoking history and either currently smoke or quit within the past 15 years.
The 20 pack-year metric is equivalent to smoking a pack of cigarettes per day for 20 years. Because it requires patients to remember their smoking intensity over decades, it can be challenging to calculate and translate into care, Heiden said.
As it stands, few Americans who are eligible under current USPSTF guidelines actually undergo lung cancer screening, at about 15%-20%, Heiden noted. Meanwhile, mounting evidence suggests that many lung cancers occur in individuals who never meet those eligibility criteria.
Boosting screening uptake, Heiden said, is not enough: There’s a need to revisit eligibility itself to reach more high-risk individuals.
Some groups are already taking steps in that direction. Recently updated guidelines from the National Comprehensive Cancer Network (NCCN) added a category 2B recommendation supporting screening for individuals with at least a 20-year smoking history, regardless of pack-years. (The guidelines also say former smokers are eligible no matter how long ago they quit.)
For their study, Heiden’s team sought to estimate the performance of that smoking-duration metric against current USPSTF pack-year criteria. They used Veterans Health Administration data on over 980,000 veterans whose smoking histories were prospectively collected; lung cancer diagnoses were identified through the Veterans Affairs Central Cancer Registry.
Most of the included veterans (67%) had a smoking history; their mean age was 64 years, and 21% were Black.
Overall, the researchers found that basing eligibility on 20-year smoking duration would substantially expand access to screening: Among veterans with a smoking history, 68% qualified for screening under current USPSTF criteria compared with 87% using the smoking-duration approach.
The gains were especially pronounced among women and Black individuals (who, based on prior research, typically smoke less intensely than White males). Under USPSTF criteria, only about 55% of female and Black veterans qualified for screening compared with 83% for both groups under the smoking-duration criterion.
Importantly, Heiden said, people meeting the smoking-duration threshold remained at substantially elevated risk for lung cancer, suggesting the broader screening criteria were not merely capturing low-risk smokers.
The 5-year lung cancer incidence among veterans eligible under the smoking-duration approach was 1.59% — 11 times the rate of 0.14% among never smokers.
Perhaps most striking, Heiden said, the proportion of potentially missed cancers dropped from 13% with the pack-year metric to just 4% using the smoking-duration metric — a relative reduction of more than 70%.
Again, women and Black individuals would see the largest gains: Among Black veterans, potentially missed cancers fell from 25% to 6%, whereas among female veterans they declined from 22% to 7%.
Optimal Approach Still Unclear
The analysis had limitations, including a predominantly male veteran population whose smoking exposure was far greater than that of the general US population, indicating high inherent lung cancer risk.
But the results support what the NCCN has already done, according to Mary Reid, PhD, MSPH, BSN, a member of the group’s lung cancer screening guideline panel and chief of cancer screening, survivorship and mentorship at Roswell Park Comprehensive Cancer Center in Buffalo, New York.
“Doing the calculation for pack-years can be difficult,” Reid told Medscape Medical News. “Smoking duration is easier to calculate and really the way to go.”
The USPSTF does not comment on individual studies outside of its recommendation development process.
At the meeting, study discussant Katharine A. Rendle, PhD, called the work “impressive,” citing the size of the cohort and strength of the data.
It’s particularly noteworthy that the simpler screening criteria improved sensitivity for all veterans, while largely eliminating disparities, according to Rendle, of the Abramson Cancer Center at the University of Pennsylvania in Philadelphia.
Still, she said, further research could better define the optimal screening strategy.
“Smoking duration is a promising approach, but in my opinion, guidelines likely need to account for the underlying risk in the population,” Rendle said, noting that current smoking prevalence in the US population is about 10%.
She suggested future studies consider other smoking-duration thresholds, such as 30 or 40 years, and look at other outcomes, including life-years gained.
“It’s critical that we prioritize strategies that maximize potential benefit from screening — not just identify those at lung cancer risk — given downstream costs and burden on populations and health care systems,” Rendle said.
The study had no commercial funding. Heiden, Rendle, and Reid had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Simpler Screening Criteria Could Catch More Lung Cancers
Simpler Screening Criteria Could Catch More Lung Cancers
Pharmacist Interventions Pay Off in Veterans' COPD Care
A pharmacist-driven Veterans Health Administration (VHA) care program for veterans recovering from hospital visits for chronic obstructive pulmonary disease (COPD) is helping reduce symptom burden, a new retrospective cohort study finds.
Of 286 patients with COPD who participated in the program and reported outcomes, 62.6% said their symptoms improved, 28.7% said they had no change, and 8.7% reported worsening symptoms, according to Edward Portillo, PharmD, and colleagues in Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation. Patients whose medications were changed by VHA pharmacists with prescribing authority were more likely to experience clinically meaningful improvement in symptoms compared to those without this medication change (66.3% vs. 46.6%, respectively, P < .001).
“If you had a debilitating lung disease that was affecting your ability to breathe all day, affected your ability to go to the grocery store, made it hard for you to see your grandkids, and all of a sudden you had this visit and a month to 2 months later reported feeling a heck of a lot better—that’s a really big deal,” Portillo said in an interview with Federal Practitioner.
COPD, a progressive and irreversible lung disease that encompasses emphysema and chronic bronchitis, is the fifth-leading cause of death in the US according to the most recently available data. Research has suggested that many patients do not receive guidance-concordant care.
“The prevalence of COPD among our veteran population is threefold greater than in the civilian population, and 1 in 4 veterans have a COPD diagnosis,” noted Portillo a pharmacist at the William S. Middleton Veterans Affairs (VA) Hospital and an associate professor at the University of Wisconsin, Madison School of Pharmacy.
In 2015, Portillo developed a program called COPD Coordinated Access to Reduce Exacerbations (COPD CARE). The program, now operating at 50 VA medical centers, allows pharmacists to optimize medication, order spirometry, assess symptoms, place referrals for pulmonary rehabilitation, and support inhaler adherence and tobacco cessation. The pharmacists work with other members of the patient care teams such as primary care physicians and nurses.
“It's integrated within the teams themselves that serve our veterans, which is very unique for a service like this,” Portillo said.
The program is especially beneficial for patients within their first 30 to 90 days posthospitalization when they may not normally be seen in the clinic, Portillo said.
“We use a national dashboard to identify patients who left the [emergency department] or hospital, and then we assess if they’d be appropriate candidates for the program,” he said. “Our goal is to see patients as fast as 30 days and as late as 90 days, but ideally within 30 to 60 days of discharge.”
An initial in-person visit of ≤ 30 minutes is followed by a 15-minute follow-up phone call in 30 days to see if interventions have been continued, he said.
The study analyzed data from September 2020 to February 2024 from 28 VA medical centers that administer the COPD CARE program. All patients had an initial wellness visit within 90 days of hospitalization and 2 COPD Assessment Test (CAT) scores. Among 326 patients, the average age was 73.2 years; 95.7% were male; 77.9% were White, 15.6% were Black, and 2.1% had Hispanic ethnicity.
At the time of the wellness visit, patients mean CAT score was 18.4. It improved to 15.2 by follow-up, with especially large improvements in limitations (2.5 to 2.0), tightness (1.7 to 1.2), cough (2.5 to 2.1), energy (2.9 to 2.5), phlegm (2.4 to 2.0), and sleep (1.9 to 1.5).
Pharmacists created 236 COPD action plans, changed 208 medications, provided 151 service referrals, identified 117 nonadherent patients, and identified 62 incorrect techniques.
But only 1 intervention – medication change – was linked to clinically meaningful improvements in symptoms.
“This is not a disease that's easy to change symptomatically,” Portillo said. “My hope is that over time, and with multiple visits, those patients shift into a mode of ‘I am actually feeling much better now.’”
Suzanne Bollmeier, PharmD, professor of Pharmacy Practice at the University of Health Sciences and Pharmacy in St. Louis, who is familiar with the study but did not take part in it, told Federal Practitioner that the results align with previous research.
Bollmeier mentioned several studies that link pharmacist interventions to better health outcomes, including inhalation technique and medication adherence.
“Pharmacists are well-positioned within the health care team to help care for patients with COPD,” she said. “Pharmacists can help with patient adherence, inhaler education, and reduction in disease risk but also identify drug-related problems and modify respiratory regimens to better optimize patient outcomes.”
Moving forward, she said, “it would be interesting to see what specific medication regimen changes were made in this present study that led to improvement in symptoms.”
The study was funded by the VA Office of Rural Health and the University of Wisconsin Institute for Clinical and Translational Research, which is supported by the National Center for Advancing Translational Sciences. The study authors and Bollmeier had no disclosures.
A pharmacist-driven Veterans Health Administration (VHA) care program for veterans recovering from hospital visits for chronic obstructive pulmonary disease (COPD) is helping reduce symptom burden, a new retrospective cohort study finds.
Of 286 patients with COPD who participated in the program and reported outcomes, 62.6% said their symptoms improved, 28.7% said they had no change, and 8.7% reported worsening symptoms, according to Edward Portillo, PharmD, and colleagues in Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation. Patients whose medications were changed by VHA pharmacists with prescribing authority were more likely to experience clinically meaningful improvement in symptoms compared to those without this medication change (66.3% vs. 46.6%, respectively, P < .001).
“If you had a debilitating lung disease that was affecting your ability to breathe all day, affected your ability to go to the grocery store, made it hard for you to see your grandkids, and all of a sudden you had this visit and a month to 2 months later reported feeling a heck of a lot better—that’s a really big deal,” Portillo said in an interview with Federal Practitioner.
COPD, a progressive and irreversible lung disease that encompasses emphysema and chronic bronchitis, is the fifth-leading cause of death in the US according to the most recently available data. Research has suggested that many patients do not receive guidance-concordant care.
“The prevalence of COPD among our veteran population is threefold greater than in the civilian population, and 1 in 4 veterans have a COPD diagnosis,” noted Portillo a pharmacist at the William S. Middleton Veterans Affairs (VA) Hospital and an associate professor at the University of Wisconsin, Madison School of Pharmacy.
In 2015, Portillo developed a program called COPD Coordinated Access to Reduce Exacerbations (COPD CARE). The program, now operating at 50 VA medical centers, allows pharmacists to optimize medication, order spirometry, assess symptoms, place referrals for pulmonary rehabilitation, and support inhaler adherence and tobacco cessation. The pharmacists work with other members of the patient care teams such as primary care physicians and nurses.
“It's integrated within the teams themselves that serve our veterans, which is very unique for a service like this,” Portillo said.
The program is especially beneficial for patients within their first 30 to 90 days posthospitalization when they may not normally be seen in the clinic, Portillo said.
“We use a national dashboard to identify patients who left the [emergency department] or hospital, and then we assess if they’d be appropriate candidates for the program,” he said. “Our goal is to see patients as fast as 30 days and as late as 90 days, but ideally within 30 to 60 days of discharge.”
An initial in-person visit of ≤ 30 minutes is followed by a 15-minute follow-up phone call in 30 days to see if interventions have been continued, he said.
The study analyzed data from September 2020 to February 2024 from 28 VA medical centers that administer the COPD CARE program. All patients had an initial wellness visit within 90 days of hospitalization and 2 COPD Assessment Test (CAT) scores. Among 326 patients, the average age was 73.2 years; 95.7% were male; 77.9% were White, 15.6% were Black, and 2.1% had Hispanic ethnicity.
At the time of the wellness visit, patients mean CAT score was 18.4. It improved to 15.2 by follow-up, with especially large improvements in limitations (2.5 to 2.0), tightness (1.7 to 1.2), cough (2.5 to 2.1), energy (2.9 to 2.5), phlegm (2.4 to 2.0), and sleep (1.9 to 1.5).
Pharmacists created 236 COPD action plans, changed 208 medications, provided 151 service referrals, identified 117 nonadherent patients, and identified 62 incorrect techniques.
But only 1 intervention – medication change – was linked to clinically meaningful improvements in symptoms.
“This is not a disease that's easy to change symptomatically,” Portillo said. “My hope is that over time, and with multiple visits, those patients shift into a mode of ‘I am actually feeling much better now.’”
Suzanne Bollmeier, PharmD, professor of Pharmacy Practice at the University of Health Sciences and Pharmacy in St. Louis, who is familiar with the study but did not take part in it, told Federal Practitioner that the results align with previous research.
Bollmeier mentioned several studies that link pharmacist interventions to better health outcomes, including inhalation technique and medication adherence.
“Pharmacists are well-positioned within the health care team to help care for patients with COPD,” she said. “Pharmacists can help with patient adherence, inhaler education, and reduction in disease risk but also identify drug-related problems and modify respiratory regimens to better optimize patient outcomes.”
Moving forward, she said, “it would be interesting to see what specific medication regimen changes were made in this present study that led to improvement in symptoms.”
The study was funded by the VA Office of Rural Health and the University of Wisconsin Institute for Clinical and Translational Research, which is supported by the National Center for Advancing Translational Sciences. The study authors and Bollmeier had no disclosures.
A pharmacist-driven Veterans Health Administration (VHA) care program for veterans recovering from hospital visits for chronic obstructive pulmonary disease (COPD) is helping reduce symptom burden, a new retrospective cohort study finds.
Of 286 patients with COPD who participated in the program and reported outcomes, 62.6% said their symptoms improved, 28.7% said they had no change, and 8.7% reported worsening symptoms, according to Edward Portillo, PharmD, and colleagues in Chronic Obstructive Pulmonary Diseases: Journal of the COPD Foundation. Patients whose medications were changed by VHA pharmacists with prescribing authority were more likely to experience clinically meaningful improvement in symptoms compared to those without this medication change (66.3% vs. 46.6%, respectively, P < .001).
“If you had a debilitating lung disease that was affecting your ability to breathe all day, affected your ability to go to the grocery store, made it hard for you to see your grandkids, and all of a sudden you had this visit and a month to 2 months later reported feeling a heck of a lot better—that’s a really big deal,” Portillo said in an interview with Federal Practitioner.
COPD, a progressive and irreversible lung disease that encompasses emphysema and chronic bronchitis, is the fifth-leading cause of death in the US according to the most recently available data. Research has suggested that many patients do not receive guidance-concordant care.
“The prevalence of COPD among our veteran population is threefold greater than in the civilian population, and 1 in 4 veterans have a COPD diagnosis,” noted Portillo a pharmacist at the William S. Middleton Veterans Affairs (VA) Hospital and an associate professor at the University of Wisconsin, Madison School of Pharmacy.
In 2015, Portillo developed a program called COPD Coordinated Access to Reduce Exacerbations (COPD CARE). The program, now operating at 50 VA medical centers, allows pharmacists to optimize medication, order spirometry, assess symptoms, place referrals for pulmonary rehabilitation, and support inhaler adherence and tobacco cessation. The pharmacists work with other members of the patient care teams such as primary care physicians and nurses.
“It's integrated within the teams themselves that serve our veterans, which is very unique for a service like this,” Portillo said.
The program is especially beneficial for patients within their first 30 to 90 days posthospitalization when they may not normally be seen in the clinic, Portillo said.
“We use a national dashboard to identify patients who left the [emergency department] or hospital, and then we assess if they’d be appropriate candidates for the program,” he said. “Our goal is to see patients as fast as 30 days and as late as 90 days, but ideally within 30 to 60 days of discharge.”
An initial in-person visit of ≤ 30 minutes is followed by a 15-minute follow-up phone call in 30 days to see if interventions have been continued, he said.
The study analyzed data from September 2020 to February 2024 from 28 VA medical centers that administer the COPD CARE program. All patients had an initial wellness visit within 90 days of hospitalization and 2 COPD Assessment Test (CAT) scores. Among 326 patients, the average age was 73.2 years; 95.7% were male; 77.9% were White, 15.6% were Black, and 2.1% had Hispanic ethnicity.
At the time of the wellness visit, patients mean CAT score was 18.4. It improved to 15.2 by follow-up, with especially large improvements in limitations (2.5 to 2.0), tightness (1.7 to 1.2), cough (2.5 to 2.1), energy (2.9 to 2.5), phlegm (2.4 to 2.0), and sleep (1.9 to 1.5).
Pharmacists created 236 COPD action plans, changed 208 medications, provided 151 service referrals, identified 117 nonadherent patients, and identified 62 incorrect techniques.
But only 1 intervention – medication change – was linked to clinically meaningful improvements in symptoms.
“This is not a disease that's easy to change symptomatically,” Portillo said. “My hope is that over time, and with multiple visits, those patients shift into a mode of ‘I am actually feeling much better now.’”
Suzanne Bollmeier, PharmD, professor of Pharmacy Practice at the University of Health Sciences and Pharmacy in St. Louis, who is familiar with the study but did not take part in it, told Federal Practitioner that the results align with previous research.
Bollmeier mentioned several studies that link pharmacist interventions to better health outcomes, including inhalation technique and medication adherence.
“Pharmacists are well-positioned within the health care team to help care for patients with COPD,” she said. “Pharmacists can help with patient adherence, inhaler education, and reduction in disease risk but also identify drug-related problems and modify respiratory regimens to better optimize patient outcomes.”
Moving forward, she said, “it would be interesting to see what specific medication regimen changes were made in this present study that led to improvement in symptoms.”
The study was funded by the VA Office of Rural Health and the University of Wisconsin Institute for Clinical and Translational Research, which is supported by the National Center for Advancing Translational Sciences. The study authors and Bollmeier had no disclosures.
CMS CPAP Rule Could Deny Coverage for Some Who Benefit Long Term
CMS CPAP Rule Could Deny Coverage for Some Who Benefit Long Term
ORLANDO, Fla. — The Centers for Medicare & Medicaid Services (CMS) will not cover continuous positive airway pressure (CPAP) treatment for people who are nonadherent by 90 days. However, that requirement is too stringent, said researchers who found more than one third of adults who struggled with adherence initially still used the therapy 1 year later at levels associated with clinical benefit.
To test the requirement, investigators assessed 132,492 patients in the Kaiser Permanente Southern California system. The patients were issued CPAP devices to treat obstructive sleep apnea from 2015 to 2023. At 1 year, 36% who would have failed the CMS requirement were still using their CPAP.
The results counter CMS’ assumption that poor early CPAP use always leads to long-term abandonment, said Dennis Hwang, MD, co-chair of Sleep Medicine and medical director of the Sleep Disorders Center at Kaiser Permanente Southern California in Fontana, California.
"We should transition away from a one-size-fits-all definition of success," Hwang added at the American Thoracic Society (ATS) 2026 International Conference.
Background and Methodology
The 90-day adherence requirement does not only apply to Medicare or Medicaid recipients, Hwang said; many private insurers have adopted the same policy. In contrast, Kaiser Permanente Southern California does not restrict usage based on early adherence.
Hwang et al considered any Kaiser Permanente member with any CPAP usage during the 12 months after being issued a device an active user. They tracked mean nightly minutes of use and the percentage of nights with ≥ 2 and ≥ 4 hours of average use.
Overall, 49% would have met the CMS criteria and used the therapy ≥ 4 hours on average each night for 70% of nights during the first 90 days. Kaiser Permanente members aged ≥ 65 years were more compliant, with 54% meeting the CMS benchmarks. ATS guidelines recognize that even ≥ 2 hours of CPAP per night on average can confer some benefits.
The average age in the study was 55 years, and the mean apnea-hypopnea index was 32-33 events per hour, suggesting severe obstructive sleep apnea at baseline. The cohort was diverse, with 42% White, 35% Hispanic, 10% Black, 9% Asian, and 4% other race or ethnicity.
Key Findings
A total of 64,568 adults would have been CMS adherent at 90 days; investigators compared outcomes at 12 months with another 67,867 nonadherent adults.
There were some significant differences between groups. The mean age was 56.4 years vs 53.7 years in the adherent group vs the nonadherent group; men made up a greater proportion of the adherent group, 68.5% vs 62.6%; and the mean number of events per hour was 35 vs 30 (P < .001 for all).
Among the 90-day nonadherent group, about 21% met the 2-hour or greater adherence benchmark, and approximately 14% used CPAP an average of ≥ 4 hours.
“Still a substantial number of [non-CMS adherent] patients are using CPAP,” Hwang said.
Failure to meet CMS adherence was associated with younger age, female sex, non-White race or ethnicity, lower socioeconomic status, and lower severity of obstructive sleep apnea.
“There is also an equity dimension. Whites had better adherence rates during the first 90 days, so there is already a disparity here in terms of outcomes,” Hwang said. Policy changes could improve access to long-term therapy on a more equitable basis, he added. For example, a 2023 ATS policy statement calls for a more patient-centric approach and a focus on reducing inequities.
An Arbitrary Requirement
The 90-day requirement seems a little short, said session co-moderator Oren Cohen, MD, assistant professor in the Department of Medicine, Division of Pulmonary, Critical Care and Sleep Medicine at Icahn School of Medicine at Mount Sinai in New York City, when asked to comment. “It can take longer to get a patient back into the clinic and go through a lot of the trial and error that it takes to do a mask fitting and adjust the pressures.”
If a patient is using their CPAP device for fewer than 4 hours a night in the early period, it doesn’t mean things are failing, Cohen said. “It’s just that you’ve got to keep trying and pushing forward.”
Nonetheless, there are some long-term noncompliant patients, Cohen said. “I certainly don’t think that somebody who’s not using the device for years should continue to hold on to it. That resource can be reallocated to somebody who would get more benefit from it. But I think setting a 90-day and 4-hour rule seems arbitrary…and there should be more leeway there.”
The study was independently supported.
Hwang and Cohen reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
ORLANDO, Fla. — The Centers for Medicare & Medicaid Services (CMS) will not cover continuous positive airway pressure (CPAP) treatment for people who are nonadherent by 90 days. However, that requirement is too stringent, said researchers who found more than one third of adults who struggled with adherence initially still used the therapy 1 year later at levels associated with clinical benefit.
To test the requirement, investigators assessed 132,492 patients in the Kaiser Permanente Southern California system. The patients were issued CPAP devices to treat obstructive sleep apnea from 2015 to 2023. At 1 year, 36% who would have failed the CMS requirement were still using their CPAP.
The results counter CMS’ assumption that poor early CPAP use always leads to long-term abandonment, said Dennis Hwang, MD, co-chair of Sleep Medicine and medical director of the Sleep Disorders Center at Kaiser Permanente Southern California in Fontana, California.
"We should transition away from a one-size-fits-all definition of success," Hwang added at the American Thoracic Society (ATS) 2026 International Conference.
Background and Methodology
The 90-day adherence requirement does not only apply to Medicare or Medicaid recipients, Hwang said; many private insurers have adopted the same policy. In contrast, Kaiser Permanente Southern California does not restrict usage based on early adherence.
Hwang et al considered any Kaiser Permanente member with any CPAP usage during the 12 months after being issued a device an active user. They tracked mean nightly minutes of use and the percentage of nights with ≥ 2 and ≥ 4 hours of average use.
Overall, 49% would have met the CMS criteria and used the therapy ≥ 4 hours on average each night for 70% of nights during the first 90 days. Kaiser Permanente members aged ≥ 65 years were more compliant, with 54% meeting the CMS benchmarks. ATS guidelines recognize that even ≥ 2 hours of CPAP per night on average can confer some benefits.
The average age in the study was 55 years, and the mean apnea-hypopnea index was 32-33 events per hour, suggesting severe obstructive sleep apnea at baseline. The cohort was diverse, with 42% White, 35% Hispanic, 10% Black, 9% Asian, and 4% other race or ethnicity.
Key Findings
A total of 64,568 adults would have been CMS adherent at 90 days; investigators compared outcomes at 12 months with another 67,867 nonadherent adults.
There were some significant differences between groups. The mean age was 56.4 years vs 53.7 years in the adherent group vs the nonadherent group; men made up a greater proportion of the adherent group, 68.5% vs 62.6%; and the mean number of events per hour was 35 vs 30 (P < .001 for all).
Among the 90-day nonadherent group, about 21% met the 2-hour or greater adherence benchmark, and approximately 14% used CPAP an average of ≥ 4 hours.
“Still a substantial number of [non-CMS adherent] patients are using CPAP,” Hwang said.
Failure to meet CMS adherence was associated with younger age, female sex, non-White race or ethnicity, lower socioeconomic status, and lower severity of obstructive sleep apnea.
“There is also an equity dimension. Whites had better adherence rates during the first 90 days, so there is already a disparity here in terms of outcomes,” Hwang said. Policy changes could improve access to long-term therapy on a more equitable basis, he added. For example, a 2023 ATS policy statement calls for a more patient-centric approach and a focus on reducing inequities.
An Arbitrary Requirement
The 90-day requirement seems a little short, said session co-moderator Oren Cohen, MD, assistant professor in the Department of Medicine, Division of Pulmonary, Critical Care and Sleep Medicine at Icahn School of Medicine at Mount Sinai in New York City, when asked to comment. “It can take longer to get a patient back into the clinic and go through a lot of the trial and error that it takes to do a mask fitting and adjust the pressures.”
If a patient is using their CPAP device for fewer than 4 hours a night in the early period, it doesn’t mean things are failing, Cohen said. “It’s just that you’ve got to keep trying and pushing forward.”
Nonetheless, there are some long-term noncompliant patients, Cohen said. “I certainly don’t think that somebody who’s not using the device for years should continue to hold on to it. That resource can be reallocated to somebody who would get more benefit from it. But I think setting a 90-day and 4-hour rule seems arbitrary…and there should be more leeway there.”
The study was independently supported.
Hwang and Cohen reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
ORLANDO, Fla. — The Centers for Medicare & Medicaid Services (CMS) will not cover continuous positive airway pressure (CPAP) treatment for people who are nonadherent by 90 days. However, that requirement is too stringent, said researchers who found more than one third of adults who struggled with adherence initially still used the therapy 1 year later at levels associated with clinical benefit.
To test the requirement, investigators assessed 132,492 patients in the Kaiser Permanente Southern California system. The patients were issued CPAP devices to treat obstructive sleep apnea from 2015 to 2023. At 1 year, 36% who would have failed the CMS requirement were still using their CPAP.
The results counter CMS’ assumption that poor early CPAP use always leads to long-term abandonment, said Dennis Hwang, MD, co-chair of Sleep Medicine and medical director of the Sleep Disorders Center at Kaiser Permanente Southern California in Fontana, California.
"We should transition away from a one-size-fits-all definition of success," Hwang added at the American Thoracic Society (ATS) 2026 International Conference.
Background and Methodology
The 90-day adherence requirement does not only apply to Medicare or Medicaid recipients, Hwang said; many private insurers have adopted the same policy. In contrast, Kaiser Permanente Southern California does not restrict usage based on early adherence.
Hwang et al considered any Kaiser Permanente member with any CPAP usage during the 12 months after being issued a device an active user. They tracked mean nightly minutes of use and the percentage of nights with ≥ 2 and ≥ 4 hours of average use.
Overall, 49% would have met the CMS criteria and used the therapy ≥ 4 hours on average each night for 70% of nights during the first 90 days. Kaiser Permanente members aged ≥ 65 years were more compliant, with 54% meeting the CMS benchmarks. ATS guidelines recognize that even ≥ 2 hours of CPAP per night on average can confer some benefits.
The average age in the study was 55 years, and the mean apnea-hypopnea index was 32-33 events per hour, suggesting severe obstructive sleep apnea at baseline. The cohort was diverse, with 42% White, 35% Hispanic, 10% Black, 9% Asian, and 4% other race or ethnicity.
Key Findings
A total of 64,568 adults would have been CMS adherent at 90 days; investigators compared outcomes at 12 months with another 67,867 nonadherent adults.
There were some significant differences between groups. The mean age was 56.4 years vs 53.7 years in the adherent group vs the nonadherent group; men made up a greater proportion of the adherent group, 68.5% vs 62.6%; and the mean number of events per hour was 35 vs 30 (P < .001 for all).
Among the 90-day nonadherent group, about 21% met the 2-hour or greater adherence benchmark, and approximately 14% used CPAP an average of ≥ 4 hours.
“Still a substantial number of [non-CMS adherent] patients are using CPAP,” Hwang said.
Failure to meet CMS adherence was associated with younger age, female sex, non-White race or ethnicity, lower socioeconomic status, and lower severity of obstructive sleep apnea.
“There is also an equity dimension. Whites had better adherence rates during the first 90 days, so there is already a disparity here in terms of outcomes,” Hwang said. Policy changes could improve access to long-term therapy on a more equitable basis, he added. For example, a 2023 ATS policy statement calls for a more patient-centric approach and a focus on reducing inequities.
An Arbitrary Requirement
The 90-day requirement seems a little short, said session co-moderator Oren Cohen, MD, assistant professor in the Department of Medicine, Division of Pulmonary, Critical Care and Sleep Medicine at Icahn School of Medicine at Mount Sinai in New York City, when asked to comment. “It can take longer to get a patient back into the clinic and go through a lot of the trial and error that it takes to do a mask fitting and adjust the pressures.”
If a patient is using their CPAP device for fewer than 4 hours a night in the early period, it doesn’t mean things are failing, Cohen said. “It’s just that you’ve got to keep trying and pushing forward.”
Nonetheless, there are some long-term noncompliant patients, Cohen said. “I certainly don’t think that somebody who’s not using the device for years should continue to hold on to it. That resource can be reallocated to somebody who would get more benefit from it. But I think setting a 90-day and 4-hour rule seems arbitrary…and there should be more leeway there.”
The study was independently supported.
Hwang and Cohen reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
CMS CPAP Rule Could Deny Coverage for Some Who Benefit Long Term
CMS CPAP Rule Could Deny Coverage for Some Who Benefit Long Term
Can PAK6 Transform Small Cell Lung Cancer Diagnosis?
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Serum P21 Activated Kinase 6 (PAK6) demonstrated diagnostic accuracy comparable to pro-gastrin-releasing peptide (ProGRP) for small cell lung cancer (SCLC), with area under the curve (AUC) values of 0.892 and 0.935, respectively, in a study of 109 patients with SCLC. Combining PAK6, ProGRP, and neuron-specific enolase (NSE) achieved diagnostic efficiency of 0.98. Elevated baseline PAK6 levels correlated with shorter progression-free survival and increased risk for disease progression.
METHODOLOGY:
Participants included 380 people in China: 109 with SCLC, 92 with non–small cell lung cancer (NSCLC), 85 with benign pulmonary nodules, and 94 healthy controls who received routine physical examinations.
Laboratory testing measured serum PAK6 by ELISA, while NSE, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and ProGRP were quantified by chemiluminescence.
Pretreatment and posttreatment serum samples from 56 patients with SCLC were analyzed to evaluate changes in biomarker levels following 3 months of treatment.
Progression-free survival data were collected through case review and follow-up, defined as time from treatment initiation to radiographic disease progression per RECIST 1.1 criteria or death from any cause.
TAKEAWAY:
Median serum PAK6 is reported as 56.44 ng/L in SCLC vs 41.06 ng/L in NSCLC, 37.82 ng/L in pulmonary nodules, and 34.75 ng/L in healthy controls (P < .01).
PAK6 demonstrated diagnostic efficacy with and AUC of 0.892 (95% CI, 0.857-0.927), sensitivity of 0.82, and specificity of 0.86 at optimal cut-off value of 47.30 ng/L, comparable to ProGRP (AUC, 0.935) and superior to CEA (AUC, 0.676) and CA19-9 (AUC, 0.611).
In 56 paired SCLC samples, PAK6, NSE, and ProGRP decrease after 3 months of treatment (P < .001), while CEA and CA19-9 display no meaningful change.
Elevated baseline PAK6 expression correlated with shorter progression-free survival, with high-expression patients demonstrating median survival of 92 days vs 194 days in low-expression patients (HR, 2.02; 95% CI, 1.33-3.07; P = .001).
IN PRACTICE: “We identify PAK6 as a multi-faceted biomarker for SCLC with diagnostic, prognostic, and therapeutic monitoring value. Its cost-effective ELISA quantification facilitates clinical translation,” wrote the authors of the study. “Integrating PAK6 with emerging technologies could further refine SCLC management paradigms.”
SOURCE:The study was led by Simei Chen, Department of Blood Transfusion, the Second Affiliated Hospital, Jiangxi Medical College, Nanchang University in Nanchang, China. It was published online in PeerJ.
LIMITATIONS: A single-center design and modest sample size may limit generalizability of the diagnostic and prognostic estimates. The authors also note the absence of immunohistochemical validation, leaving tissue-level correlation of PAK6 unaddressed. Finally, insufficient overall survival data were reported, which constrains interpretation beyond PFS and supports the need for prospective follow-up and larger multi-center validation.
DISCLOSURES: Grant support came from the Science and Technology Program Project of Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant 2024B1433). The authors stated the funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. No competing interests were disclosed.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Race-Neutral Data Show Biologics’ Benefits for Kids’ Asthma
Race-Neutral Data Show Biologics’ Benefits for Kids’ Asthma
Asthma biologics significantly improved lung function in children with asthma using race-based reference points, based on new data from 115 individuals.
Data on the effect of biologics on lung function in pediatric asthma are limited, and the main previous study of this relationship, the VOYAGE trial, was limited by its reliance on older, race-specific spirometry equations, according to Ken Wu, medical student at Indiana University School of Medicine in Indianapolis.
Newer, race-neutral reference equations prevent the systematic underestimation of asthma severity in Black patients and consequently provide a more accurate assessment of therapeutic benefits, said Wu. “Our study offers a novel contribution to the literature as the first known to utilize race-neutral equations to evaluate lung function following biologic therapy in a pediatric asthma population,” he said.
In a new study, presented at the American Thoracic Society (ATS) 2026 International Conference, the researchers conducted a real-world analysis with race-neutral reference equations developed by the Global Lung Function Initiative to assess the effect of biologics on lung function. They reviewed data from 115 pediatric patients with asthma who started biologics for the first time between 2015 and 2025. Their analysis included height, weight, forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratios. The mean age of the patients was 11.4 years, 52% were male, and 62% were Black. A majority (97 patients) received dupilumab; 13 received omalizumab, and 5 received mepolizumab.
The analysis included an average of three spirometry measures 1 year before starting biologics and an average of four measures during the year after starting biologics.
Treatment with dupilumab was associated with a significant improvement in lung function, with an increase in the average FEV1 from 86.4 percent-predicted prior to biologics to 91.7 after biologics (mean difference, 5.31; P = .044). No significant differences appeared among omalizumab or mepolizumab patients, likely because of the small numbers, the researchers noted.
Overall, in a linear mixed model adjusting for biologic type, FEV1 remained significantly higher after use of biologics than in the period prior to use (97.9 vs. 92.5), with a mean difference of 5.37 (P = .039).
The primary finding that dupilumab improved the percent-predicted FEV1 by 5.31 is considered a modest effect size and mainly aligns with previous research, said Wu. “We are currently in the process of conducting additional analysis of whether there is a difference in lung function when we use the older race-specific equations versus our current findings with the newer race-neutral equations,” he said.
The findings were limited by several factors, including the relatively small study population and inclusion of only 3 types of biologics, with samples of omalizumab and mepolizumab that were underpowered to detect differences in lung function, said Wu. Additional studies with larger sample sizes, more biologics (including benralizumab and tezepelumab), and longer follow-up periods are needed to compare benefits across agents, he said.
Promising Implications for Practice
The ATS has recommended abandoning the previous race-adjusted pulmonary function test norms, said Timothy Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
These norms assigned smaller lung volumes to Black and Asian individuals and tended to underestimate lung disease in these populations, said Joos, who was not involved in the new study.
The current study, though small, showed with race-neutral reference equations that biologic agents significantly improved FEV1 values in children with severe asthma, said Joos. The association was especially strong with dupilumab, used by 85% of the patients, he noted. However, additional studies are needed with larger patient populations and other biologic agents to confirm the results, he said.
The study was supported by the Indiana Clinical and Translational Sciences Institute. The previous VOYAGE trial received funding from Sanofi and Regeneron Pharmaceuticals. The researchers reported having no financial conflicts to disclose. Joos reported having no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Asthma biologics significantly improved lung function in children with asthma using race-based reference points, based on new data from 115 individuals.
Data on the effect of biologics on lung function in pediatric asthma are limited, and the main previous study of this relationship, the VOYAGE trial, was limited by its reliance on older, race-specific spirometry equations, according to Ken Wu, medical student at Indiana University School of Medicine in Indianapolis.
Newer, race-neutral reference equations prevent the systematic underestimation of asthma severity in Black patients and consequently provide a more accurate assessment of therapeutic benefits, said Wu. “Our study offers a novel contribution to the literature as the first known to utilize race-neutral equations to evaluate lung function following biologic therapy in a pediatric asthma population,” he said.
In a new study, presented at the American Thoracic Society (ATS) 2026 International Conference, the researchers conducted a real-world analysis with race-neutral reference equations developed by the Global Lung Function Initiative to assess the effect of biologics on lung function. They reviewed data from 115 pediatric patients with asthma who started biologics for the first time between 2015 and 2025. Their analysis included height, weight, forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratios. The mean age of the patients was 11.4 years, 52% were male, and 62% were Black. A majority (97 patients) received dupilumab; 13 received omalizumab, and 5 received mepolizumab.
The analysis included an average of three spirometry measures 1 year before starting biologics and an average of four measures during the year after starting biologics.
Treatment with dupilumab was associated with a significant improvement in lung function, with an increase in the average FEV1 from 86.4 percent-predicted prior to biologics to 91.7 after biologics (mean difference, 5.31; P = .044). No significant differences appeared among omalizumab or mepolizumab patients, likely because of the small numbers, the researchers noted.
Overall, in a linear mixed model adjusting for biologic type, FEV1 remained significantly higher after use of biologics than in the period prior to use (97.9 vs. 92.5), with a mean difference of 5.37 (P = .039).
The primary finding that dupilumab improved the percent-predicted FEV1 by 5.31 is considered a modest effect size and mainly aligns with previous research, said Wu. “We are currently in the process of conducting additional analysis of whether there is a difference in lung function when we use the older race-specific equations versus our current findings with the newer race-neutral equations,” he said.
The findings were limited by several factors, including the relatively small study population and inclusion of only 3 types of biologics, with samples of omalizumab and mepolizumab that were underpowered to detect differences in lung function, said Wu. Additional studies with larger sample sizes, more biologics (including benralizumab and tezepelumab), and longer follow-up periods are needed to compare benefits across agents, he said.
Promising Implications for Practice
The ATS has recommended abandoning the previous race-adjusted pulmonary function test norms, said Timothy Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
These norms assigned smaller lung volumes to Black and Asian individuals and tended to underestimate lung disease in these populations, said Joos, who was not involved in the new study.
The current study, though small, showed with race-neutral reference equations that biologic agents significantly improved FEV1 values in children with severe asthma, said Joos. The association was especially strong with dupilumab, used by 85% of the patients, he noted. However, additional studies are needed with larger patient populations and other biologic agents to confirm the results, he said.
The study was supported by the Indiana Clinical and Translational Sciences Institute. The previous VOYAGE trial received funding from Sanofi and Regeneron Pharmaceuticals. The researchers reported having no financial conflicts to disclose. Joos reported having no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Asthma biologics significantly improved lung function in children with asthma using race-based reference points, based on new data from 115 individuals.
Data on the effect of biologics on lung function in pediatric asthma are limited, and the main previous study of this relationship, the VOYAGE trial, was limited by its reliance on older, race-specific spirometry equations, according to Ken Wu, medical student at Indiana University School of Medicine in Indianapolis.
Newer, race-neutral reference equations prevent the systematic underestimation of asthma severity in Black patients and consequently provide a more accurate assessment of therapeutic benefits, said Wu. “Our study offers a novel contribution to the literature as the first known to utilize race-neutral equations to evaluate lung function following biologic therapy in a pediatric asthma population,” he said.
In a new study, presented at the American Thoracic Society (ATS) 2026 International Conference, the researchers conducted a real-world analysis with race-neutral reference equations developed by the Global Lung Function Initiative to assess the effect of biologics on lung function. They reviewed data from 115 pediatric patients with asthma who started biologics for the first time between 2015 and 2025. Their analysis included height, weight, forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratios. The mean age of the patients was 11.4 years, 52% were male, and 62% were Black. A majority (97 patients) received dupilumab; 13 received omalizumab, and 5 received mepolizumab.
The analysis included an average of three spirometry measures 1 year before starting biologics and an average of four measures during the year after starting biologics.
Treatment with dupilumab was associated with a significant improvement in lung function, with an increase in the average FEV1 from 86.4 percent-predicted prior to biologics to 91.7 after biologics (mean difference, 5.31; P = .044). No significant differences appeared among omalizumab or mepolizumab patients, likely because of the small numbers, the researchers noted.
Overall, in a linear mixed model adjusting for biologic type, FEV1 remained significantly higher after use of biologics than in the period prior to use (97.9 vs. 92.5), with a mean difference of 5.37 (P = .039).
The primary finding that dupilumab improved the percent-predicted FEV1 by 5.31 is considered a modest effect size and mainly aligns with previous research, said Wu. “We are currently in the process of conducting additional analysis of whether there is a difference in lung function when we use the older race-specific equations versus our current findings with the newer race-neutral equations,” he said.
The findings were limited by several factors, including the relatively small study population and inclusion of only 3 types of biologics, with samples of omalizumab and mepolizumab that were underpowered to detect differences in lung function, said Wu. Additional studies with larger sample sizes, more biologics (including benralizumab and tezepelumab), and longer follow-up periods are needed to compare benefits across agents, he said.
Promising Implications for Practice
The ATS has recommended abandoning the previous race-adjusted pulmonary function test norms, said Timothy Joos, MD, who practices internal medicine and pediatrics at a community health center in Seattle.
These norms assigned smaller lung volumes to Black and Asian individuals and tended to underestimate lung disease in these populations, said Joos, who was not involved in the new study.
The current study, though small, showed with race-neutral reference equations that biologic agents significantly improved FEV1 values in children with severe asthma, said Joos. The association was especially strong with dupilumab, used by 85% of the patients, he noted. However, additional studies are needed with larger patient populations and other biologic agents to confirm the results, he said.
The study was supported by the Indiana Clinical and Translational Sciences Institute. The previous VOYAGE trial received funding from Sanofi and Regeneron Pharmaceuticals. The researchers reported having no financial conflicts to disclose. Joos reported having no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Race-Neutral Data Show Biologics’ Benefits for Kids’ Asthma
Race-Neutral Data Show Biologics’ Benefits for Kids’ Asthma
COPD Surfaces During Lung Cancer Screening
COPD Surfaces During Lung Cancer Screening
Approximately 20% of adults screened for early lung cancer met criteria undiagnosed chronic obstructive pulmonary disease (COPD), based on new data from approximately 300 individuals presented at the American Thoracic Society (ATS) 2026 International Conference.
“Patients undergoing lung cancer screening with low-dose CT scans represent a high-risk population for smoking-related lung disease, including COPD,” said lead author Stephen Dachert, MD, assistant professor of clinical thoracic medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“While lung cancer screening programs are well established, COPD remains frequently underrecognized despite many patients having respiratory symptoms, airflow obstruction, and structural lung abnormalities detectable during screening,” Dachert told Medscape Medical News. Currently, the US Preventive Services Task Force does not recommend routine COPD screening, he noted.
To evaluate how often COPD was being missed and whether patients were receiving appropriate therapy, a particular concern in underserved populations, Dachert and colleagues reviewed data from electronic medical record, and pre-bronchodilator spirometry data were collected for 305 adults enrolled in the Temple Healthy Chest Initiative. Symptom burden was assessed using questionnaires about prior inhaler use and the COPD Airway Assessment Test (CAAT). The median age of the participants was 63 years; 182 were women, and 187 were active smokers. Most of the participants (228) self-identified as Black/African American, 42 as non-Caucasian Hispanic, and 31 as White/Caucasian.
About half of the participants (52%) had no previous COPD diagnosis. Of these, 49 (31.2%) had evidence of airflow obstruction, and almost all (97%) had symptoms defined as CAAT scores of > 1 for mucus, cough, or breathlessness.
Overall, “Twenty-one percent met criteria for undiagnosed COPD based on airflow obstruction and positive CAAT symptoms, and many had moderate disease severity by GOLD COPD classification,” Dachert said.
The high prevalence of previously undiagnosed COPD, despite a substantial symptom burden, was a striking finding, Dachert told Medscape Medical News. “We were also struck by the degree of undertreatment, with more than 60% of these patients not receiving any inhaler therapy,” he added. Among the 48 undiagnosed COPD patients in the total cohort, approximately 10% had received short-acting beta 2-agonist-only therapy.
“While prior studies have suggested underdiagnosis in lung cancer screening populations, the magnitude seen in this predominantly minority cohort reinforces how common missed opportunities for diagnosis remain in clinical practice,” Dachert said.
The findings were limited by the use of data from a single region and may not be generalized to other areas. However, the results suggest that lung cancer screening (LCS) programs are an opportunity to identify and treat chronic smoking-related lung disease, Dachert said. “Incorporating spirometry, symptom assessment, and review of respiratory therapies into LCS programs may help identify patients with clinically significant but previously unrecognized COPD, and earlier diagnosis could allow for smoking cessation reinforcement, initiation of evidence-based inhaler therapy, symptom improvement, and potentially reduction in exacerbations and health care utilization,” he said.
“Future studies should evaluate whether systematic COPD screening embedded within lung cancer screening programs improves clinical outcomes such as quality of life, exacerbations, hospitalizations, and healthcare utilization,” Dachert said. Additional work is needed to determine the best combination of screening tools to efficiently identify high-risk patients, which may include spirometry, quantitative CT imaging, symptom questionnaires, and biomarkers, he noted. “Longitudinal studies may help clarify whether earlier identification during lung cancer screening changes disease trajectory over time,” Dachert added.
Value Added for Underserved Populations
The new study’s results suggest that incorporating routine symptom assessment and spirometry into LCS pathways may improve earlier diagnosis and optimization of COPD management, said Jesse R. Sherratt, DO, a pulmonologist and critical care specialist at the University of Texas Health Science Center at San Antonio.
“Individuals undergoing lung cancer screening are at particularly high risk for smoking-related lung disease, yet COPD frequently remains unrecognized and untreated in this population,” said Sherratt, who was not involved in the study. The current study highlights the potential value, particularly among underserved populations, of incorporating spirometry and symptom assessment into LCS programs for earlier identification of patients with clinically significant COPD, he said.
The high rates of undiagnosed COPD and undertreatment were not unexpected, given the substantial smoking exposure and high-risk characteristics of patients undergoing LCS, said Sherratt. “However, the degree of symptom burden and the disproportionate impact on minority populations were especially notable and emphasize ongoing disparities in respiratory healthcare access and diagnosis,” he said.
“Additional studies are needed to determine whether integrating spirometry and structured COPD screening into lung cancer screening programs improves long-term clinical outcomes, healthcare utilization, and quality of life,” Sherratt noted. Further research also should evaluate strategies to reduce disparities in COPD diagnosis and treatment among minority populations, he said.
The study was supported by grants from AstraZeneca and the Temple Lung Center. AstraZeneca collaborators participated in the study as coauthors. Sherratt had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately 20% of adults screened for early lung cancer met criteria undiagnosed chronic obstructive pulmonary disease (COPD), based on new data from approximately 300 individuals presented at the American Thoracic Society (ATS) 2026 International Conference.
“Patients undergoing lung cancer screening with low-dose CT scans represent a high-risk population for smoking-related lung disease, including COPD,” said lead author Stephen Dachert, MD, assistant professor of clinical thoracic medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“While lung cancer screening programs are well established, COPD remains frequently underrecognized despite many patients having respiratory symptoms, airflow obstruction, and structural lung abnormalities detectable during screening,” Dachert told Medscape Medical News. Currently, the US Preventive Services Task Force does not recommend routine COPD screening, he noted.
To evaluate how often COPD was being missed and whether patients were receiving appropriate therapy, a particular concern in underserved populations, Dachert and colleagues reviewed data from electronic medical record, and pre-bronchodilator spirometry data were collected for 305 adults enrolled in the Temple Healthy Chest Initiative. Symptom burden was assessed using questionnaires about prior inhaler use and the COPD Airway Assessment Test (CAAT). The median age of the participants was 63 years; 182 were women, and 187 were active smokers. Most of the participants (228) self-identified as Black/African American, 42 as non-Caucasian Hispanic, and 31 as White/Caucasian.
About half of the participants (52%) had no previous COPD diagnosis. Of these, 49 (31.2%) had evidence of airflow obstruction, and almost all (97%) had symptoms defined as CAAT scores of > 1 for mucus, cough, or breathlessness.
Overall, “Twenty-one percent met criteria for undiagnosed COPD based on airflow obstruction and positive CAAT symptoms, and many had moderate disease severity by GOLD COPD classification,” Dachert said.
The high prevalence of previously undiagnosed COPD, despite a substantial symptom burden, was a striking finding, Dachert told Medscape Medical News. “We were also struck by the degree of undertreatment, with more than 60% of these patients not receiving any inhaler therapy,” he added. Among the 48 undiagnosed COPD patients in the total cohort, approximately 10% had received short-acting beta 2-agonist-only therapy.
“While prior studies have suggested underdiagnosis in lung cancer screening populations, the magnitude seen in this predominantly minority cohort reinforces how common missed opportunities for diagnosis remain in clinical practice,” Dachert said.
The findings were limited by the use of data from a single region and may not be generalized to other areas. However, the results suggest that lung cancer screening (LCS) programs are an opportunity to identify and treat chronic smoking-related lung disease, Dachert said. “Incorporating spirometry, symptom assessment, and review of respiratory therapies into LCS programs may help identify patients with clinically significant but previously unrecognized COPD, and earlier diagnosis could allow for smoking cessation reinforcement, initiation of evidence-based inhaler therapy, symptom improvement, and potentially reduction in exacerbations and health care utilization,” he said.
“Future studies should evaluate whether systematic COPD screening embedded within lung cancer screening programs improves clinical outcomes such as quality of life, exacerbations, hospitalizations, and healthcare utilization,” Dachert said. Additional work is needed to determine the best combination of screening tools to efficiently identify high-risk patients, which may include spirometry, quantitative CT imaging, symptom questionnaires, and biomarkers, he noted. “Longitudinal studies may help clarify whether earlier identification during lung cancer screening changes disease trajectory over time,” Dachert added.
Value Added for Underserved Populations
The new study’s results suggest that incorporating routine symptom assessment and spirometry into LCS pathways may improve earlier diagnosis and optimization of COPD management, said Jesse R. Sherratt, DO, a pulmonologist and critical care specialist at the University of Texas Health Science Center at San Antonio.
“Individuals undergoing lung cancer screening are at particularly high risk for smoking-related lung disease, yet COPD frequently remains unrecognized and untreated in this population,” said Sherratt, who was not involved in the study. The current study highlights the potential value, particularly among underserved populations, of incorporating spirometry and symptom assessment into LCS programs for earlier identification of patients with clinically significant COPD, he said.
The high rates of undiagnosed COPD and undertreatment were not unexpected, given the substantial smoking exposure and high-risk characteristics of patients undergoing LCS, said Sherratt. “However, the degree of symptom burden and the disproportionate impact on minority populations were especially notable and emphasize ongoing disparities in respiratory healthcare access and diagnosis,” he said.
“Additional studies are needed to determine whether integrating spirometry and structured COPD screening into lung cancer screening programs improves long-term clinical outcomes, healthcare utilization, and quality of life,” Sherratt noted. Further research also should evaluate strategies to reduce disparities in COPD diagnosis and treatment among minority populations, he said.
The study was supported by grants from AstraZeneca and the Temple Lung Center. AstraZeneca collaborators participated in the study as coauthors. Sherratt had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately 20% of adults screened for early lung cancer met criteria undiagnosed chronic obstructive pulmonary disease (COPD), based on new data from approximately 300 individuals presented at the American Thoracic Society (ATS) 2026 International Conference.
“Patients undergoing lung cancer screening with low-dose CT scans represent a high-risk population for smoking-related lung disease, including COPD,” said lead author Stephen Dachert, MD, assistant professor of clinical thoracic medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia.
“While lung cancer screening programs are well established, COPD remains frequently underrecognized despite many patients having respiratory symptoms, airflow obstruction, and structural lung abnormalities detectable during screening,” Dachert told Medscape Medical News. Currently, the US Preventive Services Task Force does not recommend routine COPD screening, he noted.
To evaluate how often COPD was being missed and whether patients were receiving appropriate therapy, a particular concern in underserved populations, Dachert and colleagues reviewed data from electronic medical record, and pre-bronchodilator spirometry data were collected for 305 adults enrolled in the Temple Healthy Chest Initiative. Symptom burden was assessed using questionnaires about prior inhaler use and the COPD Airway Assessment Test (CAAT). The median age of the participants was 63 years; 182 were women, and 187 were active smokers. Most of the participants (228) self-identified as Black/African American, 42 as non-Caucasian Hispanic, and 31 as White/Caucasian.
About half of the participants (52%) had no previous COPD diagnosis. Of these, 49 (31.2%) had evidence of airflow obstruction, and almost all (97%) had symptoms defined as CAAT scores of > 1 for mucus, cough, or breathlessness.
Overall, “Twenty-one percent met criteria for undiagnosed COPD based on airflow obstruction and positive CAAT symptoms, and many had moderate disease severity by GOLD COPD classification,” Dachert said.
The high prevalence of previously undiagnosed COPD, despite a substantial symptom burden, was a striking finding, Dachert told Medscape Medical News. “We were also struck by the degree of undertreatment, with more than 60% of these patients not receiving any inhaler therapy,” he added. Among the 48 undiagnosed COPD patients in the total cohort, approximately 10% had received short-acting beta 2-agonist-only therapy.
“While prior studies have suggested underdiagnosis in lung cancer screening populations, the magnitude seen in this predominantly minority cohort reinforces how common missed opportunities for diagnosis remain in clinical practice,” Dachert said.
The findings were limited by the use of data from a single region and may not be generalized to other areas. However, the results suggest that lung cancer screening (LCS) programs are an opportunity to identify and treat chronic smoking-related lung disease, Dachert said. “Incorporating spirometry, symptom assessment, and review of respiratory therapies into LCS programs may help identify patients with clinically significant but previously unrecognized COPD, and earlier diagnosis could allow for smoking cessation reinforcement, initiation of evidence-based inhaler therapy, symptom improvement, and potentially reduction in exacerbations and health care utilization,” he said.
“Future studies should evaluate whether systematic COPD screening embedded within lung cancer screening programs improves clinical outcomes such as quality of life, exacerbations, hospitalizations, and healthcare utilization,” Dachert said. Additional work is needed to determine the best combination of screening tools to efficiently identify high-risk patients, which may include spirometry, quantitative CT imaging, symptom questionnaires, and biomarkers, he noted. “Longitudinal studies may help clarify whether earlier identification during lung cancer screening changes disease trajectory over time,” Dachert added.
Value Added for Underserved Populations
The new study’s results suggest that incorporating routine symptom assessment and spirometry into LCS pathways may improve earlier diagnosis and optimization of COPD management, said Jesse R. Sherratt, DO, a pulmonologist and critical care specialist at the University of Texas Health Science Center at San Antonio.
“Individuals undergoing lung cancer screening are at particularly high risk for smoking-related lung disease, yet COPD frequently remains unrecognized and untreated in this population,” said Sherratt, who was not involved in the study. The current study highlights the potential value, particularly among underserved populations, of incorporating spirometry and symptom assessment into LCS programs for earlier identification of patients with clinically significant COPD, he said.
The high rates of undiagnosed COPD and undertreatment were not unexpected, given the substantial smoking exposure and high-risk characteristics of patients undergoing LCS, said Sherratt. “However, the degree of symptom burden and the disproportionate impact on minority populations were especially notable and emphasize ongoing disparities in respiratory healthcare access and diagnosis,” he said.
“Additional studies are needed to determine whether integrating spirometry and structured COPD screening into lung cancer screening programs improves long-term clinical outcomes, healthcare utilization, and quality of life,” Sherratt noted. Further research also should evaluate strategies to reduce disparities in COPD diagnosis and treatment among minority populations, he said.
The study was supported by grants from AstraZeneca and the Temple Lung Center. AstraZeneca collaborators participated in the study as coauthors. Sherratt had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
COPD Surfaces During Lung Cancer Screening
COPD Surfaces During Lung Cancer Screening