User login
Discharging select diverticulitis patients from the ED found to be acceptable
CORONADO, CALIF. – Among patients diagnosed with diverticulitis via CT scan in the emergency department who were discharged home, only 13% required a return visit to the hospital, results from a long-term retrospective analysis demonstrated.
“In select patients whose assessment includes a CT scan, discharge to home from the emergency department with treatment for diverticulitis is safe,” study author Anne-Marie Sirany, MD, said at the annual meeting of the Western Surgical Association.

A few years ago, researchers conducted a randomized trial to evaluate the treatment of uncomplicated diverticulitis (Ann Surg. 2014;259[1]:38-44). Patients were diagnosed with diverticulitis in the emergency department and randomized to either hospital admission or outpatient management at home. The investigators found no significant differences between the readmission rates of the inpatient and outpatient groups, but the health care costs were three times lower in the outpatient group. Dr. Sirany and her associates set out to compare the outcomes of patients diagnosed with and treated for diverticulitis in the emergency department who were discharged to home, versus those who were admitted to the hospital. They reviewed the medical records of 240 patients with a primary diagnosis of diverticulitis by CT scan who were evaluated in the emergency department at one of four hospitals and one academic medical center from September 2010 to January 2012. The primary outcome was hospital readmission or return to the emergency department within 30 days, while the secondary outcomes were recurrent diverticulitis or surgical resection for diverticulitis.
The mean age of the 240 patients was 59 years, 45% were men, 22% had a Charlson Comorbidity Index (CCI) of greater than 2, and 7.5% were on steroids or immunosuppressant medications. More than half (62%) were admitted to the hospital, while the remaining 38% were discharged home on oral antibiotics. Compared with patients discharged home, those admitted to the hospital were more likely to be older than age 65 (43% vs. 24%, respectively; P = .003), have a CCI of 2 or greater (28% vs. 13%; P = .007), were more likely to be on immunosuppressant or steroid medications (11% vs. 1%; P = .003), show extraluminal air on CT (30% vs. 7%; P less than .0001), or show abscess on CT (19% vs. 1%; P less than .0001). “Of note: We did not have any patients who had CT scan findings of pneumoperitoneum who were discharged home, and 48% of patients admitted to the hospital had uncomplicated diverticulitis,” she said.
After a median follow-up of 37 months, no significant differences were observed between patients discharged to home and those admitted to the hospital in readmission or return to the emergency department (13% vs. 14%), recurrent diverticulitis (23% in each group), or in colon resection at subsequent encounter (16% vs. 19%). “Among patients discharged to home, only one patient required emergency surgery, and this was 20 months after their index admission,” Dr. Sirany said. “We think that the low rate of readmission in patients discharged home demonstrates that this is a safe approach to management of patients with diverticulitis, when using information from the CT scan.”
Closer analysis of patients who were discharged home revealed that six patients had extraluminal air on CT scan, three of whom returned to the emergency department or were admitted to the hospital. In addition, 11% of those with uncomplicated diverticulitis returned to the emergency department or were admitted to the hospital.
Dr. Sirany acknowledged certain limitations of the study, including its retrospective design, a lack of complete follow-up for all patients, and the fact that it included patients with recurrent diverticulitis. “Despite the limitations, we recommend that young, relatively healthy patients, with uncomplicated findings on CT scan, can be discharged to home and managed as an outpatient,” she said. “In an era where there’s increasing attention to health care costs, we need to think more critically about which patients need to be admitted for management of uncomplicated diverticulitis.” She reported having no financial disclosures.
[email protected]
CORONADO, CALIF. – Among patients diagnosed with diverticulitis via CT scan in the emergency department who were discharged home, only 13% required a return visit to the hospital, results from a long-term retrospective analysis demonstrated.
“In select patients whose assessment includes a CT scan, discharge to home from the emergency department with treatment for diverticulitis is safe,” study author Anne-Marie Sirany, MD, said at the annual meeting of the Western Surgical Association.
A few years ago, researchers conducted a randomized trial to evaluate the treatment of uncomplicated diverticulitis (Ann Surg. 2014;259[1]:38-44). Patients were diagnosed with diverticulitis in the emergency department and randomized to either hospital admission or outpatient management at home. The investigators found no significant differences between the readmission rates of the inpatient and outpatient groups, but the health care costs were three times lower in the outpatient group. Dr. Sirany and her associates set out to compare the outcomes of patients diagnosed with and treated for diverticulitis in the emergency department who were discharged to home, versus those who were admitted to the hospital. They reviewed the medical records of 240 patients with a primary diagnosis of diverticulitis by CT scan who were evaluated in the emergency department at one of four hospitals and one academic medical center from September 2010 to January 2012. The primary outcome was hospital readmission or return to the emergency department within 30 days, while the secondary outcomes were recurrent diverticulitis or surgical resection for diverticulitis.
The mean age of the 240 patients was 59 years, 45% were men, 22% had a Charlson Comorbidity Index (CCI) of greater than 2, and 7.5% were on steroids or immunosuppressant medications. More than half (62%) were admitted to the hospital, while the remaining 38% were discharged home on oral antibiotics. Compared with patients discharged home, those admitted to the hospital were more likely to be older than age 65 (43% vs. 24%, respectively; P = .003), have a CCI of 2 or greater (28% vs. 13%; P = .007), were more likely to be on immunosuppressant or steroid medications (11% vs. 1%; P = .003), show extraluminal air on CT (30% vs. 7%; P less than .0001), or show abscess on CT (19% vs. 1%; P less than .0001). “Of note: We did not have any patients who had CT scan findings of pneumoperitoneum who were discharged home, and 48% of patients admitted to the hospital had uncomplicated diverticulitis,” she said.
After a median follow-up of 37 months, no significant differences were observed between patients discharged to home and those admitted to the hospital in readmission or return to the emergency department (13% vs. 14%), recurrent diverticulitis (23% in each group), or in colon resection at subsequent encounter (16% vs. 19%). “Among patients discharged to home, only one patient required emergency surgery, and this was 20 months after their index admission,” Dr. Sirany said. “We think that the low rate of readmission in patients discharged home demonstrates that this is a safe approach to management of patients with diverticulitis, when using information from the CT scan.”
Closer analysis of patients who were discharged home revealed that six patients had extraluminal air on CT scan, three of whom returned to the emergency department or were admitted to the hospital. In addition, 11% of those with uncomplicated diverticulitis returned to the emergency department or were admitted to the hospital.
Dr. Sirany acknowledged certain limitations of the study, including its retrospective design, a lack of complete follow-up for all patients, and the fact that it included patients with recurrent diverticulitis. “Despite the limitations, we recommend that young, relatively healthy patients, with uncomplicated findings on CT scan, can be discharged to home and managed as an outpatient,” she said. “In an era where there’s increasing attention to health care costs, we need to think more critically about which patients need to be admitted for management of uncomplicated diverticulitis.” She reported having no financial disclosures.
[email protected]
CORONADO, CALIF. – Among patients diagnosed with diverticulitis via CT scan in the emergency department who were discharged home, only 13% required a return visit to the hospital, results from a long-term retrospective analysis demonstrated.
“In select patients whose assessment includes a CT scan, discharge to home from the emergency department with treatment for diverticulitis is safe,” study author Anne-Marie Sirany, MD, said at the annual meeting of the Western Surgical Association.
A few years ago, researchers conducted a randomized trial to evaluate the treatment of uncomplicated diverticulitis (Ann Surg. 2014;259[1]:38-44). Patients were diagnosed with diverticulitis in the emergency department and randomized to either hospital admission or outpatient management at home. The investigators found no significant differences between the readmission rates of the inpatient and outpatient groups, but the health care costs were three times lower in the outpatient group. Dr. Sirany and her associates set out to compare the outcomes of patients diagnosed with and treated for diverticulitis in the emergency department who were discharged to home, versus those who were admitted to the hospital. They reviewed the medical records of 240 patients with a primary diagnosis of diverticulitis by CT scan who were evaluated in the emergency department at one of four hospitals and one academic medical center from September 2010 to January 2012. The primary outcome was hospital readmission or return to the emergency department within 30 days, while the secondary outcomes were recurrent diverticulitis or surgical resection for diverticulitis.
The mean age of the 240 patients was 59 years, 45% were men, 22% had a Charlson Comorbidity Index (CCI) of greater than 2, and 7.5% were on steroids or immunosuppressant medications. More than half (62%) were admitted to the hospital, while the remaining 38% were discharged home on oral antibiotics. Compared with patients discharged home, those admitted to the hospital were more likely to be older than age 65 (43% vs. 24%, respectively; P = .003), have a CCI of 2 or greater (28% vs. 13%; P = .007), were more likely to be on immunosuppressant or steroid medications (11% vs. 1%; P = .003), show extraluminal air on CT (30% vs. 7%; P less than .0001), or show abscess on CT (19% vs. 1%; P less than .0001). “Of note: We did not have any patients who had CT scan findings of pneumoperitoneum who were discharged home, and 48% of patients admitted to the hospital had uncomplicated diverticulitis,” she said.
After a median follow-up of 37 months, no significant differences were observed between patients discharged to home and those admitted to the hospital in readmission or return to the emergency department (13% vs. 14%), recurrent diverticulitis (23% in each group), or in colon resection at subsequent encounter (16% vs. 19%). “Among patients discharged to home, only one patient required emergency surgery, and this was 20 months after their index admission,” Dr. Sirany said. “We think that the low rate of readmission in patients discharged home demonstrates that this is a safe approach to management of patients with diverticulitis, when using information from the CT scan.”
Closer analysis of patients who were discharged home revealed that six patients had extraluminal air on CT scan, three of whom returned to the emergency department or were admitted to the hospital. In addition, 11% of those with uncomplicated diverticulitis returned to the emergency department or were admitted to the hospital.
Dr. Sirany acknowledged certain limitations of the study, including its retrospective design, a lack of complete follow-up for all patients, and the fact that it included patients with recurrent diverticulitis. “Despite the limitations, we recommend that young, relatively healthy patients, with uncomplicated findings on CT scan, can be discharged to home and managed as an outpatient,” she said. “In an era where there’s increasing attention to health care costs, we need to think more critically about which patients need to be admitted for management of uncomplicated diverticulitis.” She reported having no financial disclosures.
[email protected]
AT WSA 2016
Key clinical point:
Major finding: After a median follow-up of 37 months, no significant differences were observed between patients discharged to home and those admitted to the hospital in readmission or return to the emergency department (13% vs. 14%, respectively).
Data source: A retrospective review of 240 patients with a primary diagnosis of diverticulitis by CT scan who were evaluated in the emergency department at one of four hospitals and one academic medical center from September 2010 to January 2012.
Disclosures: Dr. Sirany reported having no financial disclosures.

Emergent colon cancer resection does not negatively affect patient outcomes
CORONADO, CALIF. – With the exception of patients that present with perforation, emergent resection of colon cancers does not appear to adversely affect operative outcomes or patient survival, a 3-year analysis of data showed.
At the annual meeting of the Western Surgical Association, Jason W. Smith, MD, said that of the estimated 106,100 new cases of colon cancer each year, 6%-30% of patients have symptoms or late complications related to the disease that require an emergency intervention, often leading to dismal outcomes. “The problem with many existing studies of emergent colon cancer resections is that they tend to throw everybody into one large group, making it difficult to compare some of these patients,” said Dr. Smith, a trauma surgeon in the department of surgery at the University of Louisville (Ky.) School of Medicine. “Our thought was, if we provide an appropriate oncologic resection at the time of our initial management in these patients when they come to the emergency department, can we affect the similar rate of overall outcomes for these patients with regard to their cancer prognosis?”

Of the 117 patients in the emergent group, 35 had a perforation and 82 had an emergent resection. In an unmatched analysis comparing perforation, emergent resection, and elective resection, the patients who presented with a perforation had a much higher Charlson Comorbidity Index (CCI) score and a higher American Society of Anesthesiologists (ASA) class. They tended to be on vasopressors or suffering from inflammatory response related to their perforation, they had lower levels of blood pressure and hemoglobin, and they had much higher rates of 30-day mortality and overall 30-day morbidity, compared with their counterparts in the other two groups. Of the eight deaths that occurred in patients with colon perforation, four were related to sepsis and multiple organ failure, one to respiratory failure/acute respiratory distress syndrome, one to acute MI, one to exacerbation of chronic lung disease, and one to transition to palliative care due to cancer diagnosis. “So the overall predominance of the deaths associated in the first 30 days were related to the inflammatory responses associated with that perforation, not specific to the cancer itself,” Dr. Smith said. At the same time, the ASA and CCI scores were not different between those with morbidity/mortality and those who survived. “So it’s difficult to identify these patients out of the gate,” he said.
When the researchers more closely examined data from patients with a perforation, 27 of 35 (77%) survived at 30 days. Survival at 1, 2, and 3 years was 78%, 57%, and 43%, respectively. “This is a mixture of stage II and stage IV patients, so they’re difficult to compare and difficult to standardize across the board,” Dr. Smith noted. “But what you see is that their survival is not significantly different related to their disease if you discount the inflammatory process. Our initial thought was that for these perforated cancers, what we really need to do is provide the appropriate oncologic resection management [in order to] get the same oncologic outcomes.”
Next, the researchers compared the 82 patients who presented without a perforation but required an emergent operation with 82 of the elective surgery patients, matched for age, gender, the CCI, ASA class, oncology stage, and body mass index. There were no differences between the two groups in terms of R0 resection, the number of lymph nodes sampled, or estimated blood loss. However, compared with patients in the elective resection group, those in the emergent resection group had higher rates of ostomy placement (30% vs. 10%, respectively; P = .01), and a longer hospital length of stay (an average of 18 vs. 12 days; P = .0007). “Most of that difference occurred on the front end of hospital stays,” Dr. Smith said. “Their postoperative days were not significantly different.”
As for long-term outcomes, more than 90% of all patients in both groups received chemotherapy within the first year postprocedure, and overall time to initiation of chemotherapy was not significantly different in the emergent vs. elective groups (6.6 vs. 5.5 weeks, respectively; P = .43). However, patients suffering postsurgical complications had an increased risk of delayed chemotherapy.
In a risk-adjusted analysis, overall survival at 3 years was not different between the emergent and elective operation groups (hazard ratio, 1.1; P = .54). Similarly, disease-free survival was not different at 3 years between the two groups (HR, 1.06; P = .84). Independent predictors of poor long-term outcome included age greater than 70 (HR, 1.45; P less than 0.03); elevated ASA class (HR, 2.99 for class III vs. class I-II; P = .08; and HR, 7.45 for ASA class IV vs. I-II; P = .03); presence of residual disease (HR, 3.08; P less than .001), and advanced cancer stage.
He acknowledged certain limitations of the study, including the fact that it was a blinded retrospective cohort with the potential for unrecognized bias, and that it measured 3-year survival instead of 5-year survival data.
“Emergent resection of nonperforated colon cancers does not appear to adversely affect operative outcomes or patient survival when proper oncologic principles are applied to their initial management,” Dr. Smith concluded. “Outcome differences in patients suffering perforation may correlate with the physiologic derangements associated with the perforation rather than the oncologic disease; thus, every effort should be made to provide an appropriate oncologic operation.” He reported having no financial disclosures.
[email protected]
CORONADO, CALIF. – With the exception of patients that present with perforation, emergent resection of colon cancers does not appear to adversely affect operative outcomes or patient survival, a 3-year analysis of data showed.
At the annual meeting of the Western Surgical Association, Jason W. Smith, MD, said that of the estimated 106,100 new cases of colon cancer each year, 6%-30% of patients have symptoms or late complications related to the disease that require an emergency intervention, often leading to dismal outcomes. “The problem with many existing studies of emergent colon cancer resections is that they tend to throw everybody into one large group, making it difficult to compare some of these patients,” said Dr. Smith, a trauma surgeon in the department of surgery at the University of Louisville (Ky.) School of Medicine. “Our thought was, if we provide an appropriate oncologic resection at the time of our initial management in these patients when they come to the emergency department, can we affect the similar rate of overall outcomes for these patients with regard to their cancer prognosis?”
Of the 117 patients in the emergent group, 35 had a perforation and 82 had an emergent resection. In an unmatched analysis comparing perforation, emergent resection, and elective resection, the patients who presented with a perforation had a much higher Charlson Comorbidity Index (CCI) score and a higher American Society of Anesthesiologists (ASA) class. They tended to be on vasopressors or suffering from inflammatory response related to their perforation, they had lower levels of blood pressure and hemoglobin, and they had much higher rates of 30-day mortality and overall 30-day morbidity, compared with their counterparts in the other two groups. Of the eight deaths that occurred in patients with colon perforation, four were related to sepsis and multiple organ failure, one to respiratory failure/acute respiratory distress syndrome, one to acute MI, one to exacerbation of chronic lung disease, and one to transition to palliative care due to cancer diagnosis. “So the overall predominance of the deaths associated in the first 30 days were related to the inflammatory responses associated with that perforation, not specific to the cancer itself,” Dr. Smith said. At the same time, the ASA and CCI scores were not different between those with morbidity/mortality and those who survived. “So it’s difficult to identify these patients out of the gate,” he said.
When the researchers more closely examined data from patients with a perforation, 27 of 35 (77%) survived at 30 days. Survival at 1, 2, and 3 years was 78%, 57%, and 43%, respectively. “This is a mixture of stage II and stage IV patients, so they’re difficult to compare and difficult to standardize across the board,” Dr. Smith noted. “But what you see is that their survival is not significantly different related to their disease if you discount the inflammatory process. Our initial thought was that for these perforated cancers, what we really need to do is provide the appropriate oncologic resection management [in order to] get the same oncologic outcomes.”
Next, the researchers compared the 82 patients who presented without a perforation but required an emergent operation with 82 of the elective surgery patients, matched for age, gender, the CCI, ASA class, oncology stage, and body mass index. There were no differences between the two groups in terms of R0 resection, the number of lymph nodes sampled, or estimated blood loss. However, compared with patients in the elective resection group, those in the emergent resection group had higher rates of ostomy placement (30% vs. 10%, respectively; P = .01), and a longer hospital length of stay (an average of 18 vs. 12 days; P = .0007). “Most of that difference occurred on the front end of hospital stays,” Dr. Smith said. “Their postoperative days were not significantly different.”
As for long-term outcomes, more than 90% of all patients in both groups received chemotherapy within the first year postprocedure, and overall time to initiation of chemotherapy was not significantly different in the emergent vs. elective groups (6.6 vs. 5.5 weeks, respectively; P = .43). However, patients suffering postsurgical complications had an increased risk of delayed chemotherapy.
In a risk-adjusted analysis, overall survival at 3 years was not different between the emergent and elective operation groups (hazard ratio, 1.1; P = .54). Similarly, disease-free survival was not different at 3 years between the two groups (HR, 1.06; P = .84). Independent predictors of poor long-term outcome included age greater than 70 (HR, 1.45; P less than 0.03); elevated ASA class (HR, 2.99 for class III vs. class I-II; P = .08; and HR, 7.45 for ASA class IV vs. I-II; P = .03); presence of residual disease (HR, 3.08; P less than .001), and advanced cancer stage.
He acknowledged certain limitations of the study, including the fact that it was a blinded retrospective cohort with the potential for unrecognized bias, and that it measured 3-year survival instead of 5-year survival data.
“Emergent resection of nonperforated colon cancers does not appear to adversely affect operative outcomes or patient survival when proper oncologic principles are applied to their initial management,” Dr. Smith concluded. “Outcome differences in patients suffering perforation may correlate with the physiologic derangements associated with the perforation rather than the oncologic disease; thus, every effort should be made to provide an appropriate oncologic operation.” He reported having no financial disclosures.
[email protected]
CORONADO, CALIF. – With the exception of patients that present with perforation, emergent resection of colon cancers does not appear to adversely affect operative outcomes or patient survival, a 3-year analysis of data showed.
At the annual meeting of the Western Surgical Association, Jason W. Smith, MD, said that of the estimated 106,100 new cases of colon cancer each year, 6%-30% of patients have symptoms or late complications related to the disease that require an emergency intervention, often leading to dismal outcomes. “The problem with many existing studies of emergent colon cancer resections is that they tend to throw everybody into one large group, making it difficult to compare some of these patients,” said Dr. Smith, a trauma surgeon in the department of surgery at the University of Louisville (Ky.) School of Medicine. “Our thought was, if we provide an appropriate oncologic resection at the time of our initial management in these patients when they come to the emergency department, can we affect the similar rate of overall outcomes for these patients with regard to their cancer prognosis?”
Of the 117 patients in the emergent group, 35 had a perforation and 82 had an emergent resection. In an unmatched analysis comparing perforation, emergent resection, and elective resection, the patients who presented with a perforation had a much higher Charlson Comorbidity Index (CCI) score and a higher American Society of Anesthesiologists (ASA) class. They tended to be on vasopressors or suffering from inflammatory response related to their perforation, they had lower levels of blood pressure and hemoglobin, and they had much higher rates of 30-day mortality and overall 30-day morbidity, compared with their counterparts in the other two groups. Of the eight deaths that occurred in patients with colon perforation, four were related to sepsis and multiple organ failure, one to respiratory failure/acute respiratory distress syndrome, one to acute MI, one to exacerbation of chronic lung disease, and one to transition to palliative care due to cancer diagnosis. “So the overall predominance of the deaths associated in the first 30 days were related to the inflammatory responses associated with that perforation, not specific to the cancer itself,” Dr. Smith said. At the same time, the ASA and CCI scores were not different between those with morbidity/mortality and those who survived. “So it’s difficult to identify these patients out of the gate,” he said.
When the researchers more closely examined data from patients with a perforation, 27 of 35 (77%) survived at 30 days. Survival at 1, 2, and 3 years was 78%, 57%, and 43%, respectively. “This is a mixture of stage II and stage IV patients, so they’re difficult to compare and difficult to standardize across the board,” Dr. Smith noted. “But what you see is that their survival is not significantly different related to their disease if you discount the inflammatory process. Our initial thought was that for these perforated cancers, what we really need to do is provide the appropriate oncologic resection management [in order to] get the same oncologic outcomes.”
Next, the researchers compared the 82 patients who presented without a perforation but required an emergent operation with 82 of the elective surgery patients, matched for age, gender, the CCI, ASA class, oncology stage, and body mass index. There were no differences between the two groups in terms of R0 resection, the number of lymph nodes sampled, or estimated blood loss. However, compared with patients in the elective resection group, those in the emergent resection group had higher rates of ostomy placement (30% vs. 10%, respectively; P = .01), and a longer hospital length of stay (an average of 18 vs. 12 days; P = .0007). “Most of that difference occurred on the front end of hospital stays,” Dr. Smith said. “Their postoperative days were not significantly different.”
As for long-term outcomes, more than 90% of all patients in both groups received chemotherapy within the first year postprocedure, and overall time to initiation of chemotherapy was not significantly different in the emergent vs. elective groups (6.6 vs. 5.5 weeks, respectively; P = .43). However, patients suffering postsurgical complications had an increased risk of delayed chemotherapy.
In a risk-adjusted analysis, overall survival at 3 years was not different between the emergent and elective operation groups (hazard ratio, 1.1; P = .54). Similarly, disease-free survival was not different at 3 years between the two groups (HR, 1.06; P = .84). Independent predictors of poor long-term outcome included age greater than 70 (HR, 1.45; P less than 0.03); elevated ASA class (HR, 2.99 for class III vs. class I-II; P = .08; and HR, 7.45 for ASA class IV vs. I-II; P = .03); presence of residual disease (HR, 3.08; P less than .001), and advanced cancer stage.
He acknowledged certain limitations of the study, including the fact that it was a blinded retrospective cohort with the potential for unrecognized bias, and that it measured 3-year survival instead of 5-year survival data.
“Emergent resection of nonperforated colon cancers does not appear to adversely affect operative outcomes or patient survival when proper oncologic principles are applied to their initial management,” Dr. Smith concluded. “Outcome differences in patients suffering perforation may correlate with the physiologic derangements associated with the perforation rather than the oncologic disease; thus, every effort should be made to provide an appropriate oncologic operation.” He reported having no financial disclosures.
[email protected]
AT WSA 2016
Key clinical point:
Major finding: In a risk-adjusted analysis, overall survival at 3 years was not different between the emergent and elective operation groups (HR, 1.1; P = .54).
Data source: A retrospective review of 548 elective and emergent colectomies for colon cancer performed at the University of Louisville (Ky.) from 2011 to 2015.
Disclosures: Dr. Smith reported having no financial disclosures.
Kaiser experience: A helping hand reduces COPD readmissions
LOS ANGELES – With a handful of common-sense steps, the Kaiser Permanente Los Angeles Medical Center reduced 30-day hospital readmissions for chronic obstructive pulmonary disease (COPD) from 17.4/1,000 in Dec. 2013 to 11.9/1,000 in Dec. 2015.
The 57 readmissions avoided in 2015 saved the medical center $700,359, according to a report at the annual meeting of the American College of Chest Physicians.

The quality improvement project – dubbed KP Breath – started in 2013 after staff realized their COPD readmission rates were significantly higher than other area hospitals, and likely to increase. “We knew we had a problem, and that if we did not address it, it was going to be out of control,” Mr. Cam said. There was also the risk of Centers for Medicare & Medicaid Services penalties for COPD readmissions.
Mr. Cam and his colleagues discovered several problems. “Leaving the hospital, [COPD patients] didn’t know what medication was for what, or their medication schedule. They didn’t know how to use their inhalers, and didn’t understand what the disease process was all about, and what it was doing to them,” he said.
There was little continuity of care after discharge; many patients didn’t even have a pulmonologist. Essentially, COPD patients were lost to follow-up until they returned to the emergency department with another exacerbation.
A rapid Plan, Do, Study, Act cycle was the first step; it identified solutions that would work based on COPD management guidelines and published studies. “They were all things that have been shown to reduce rehospitalizations,” said pulmonologist Luis Moreta-Sainz, MD, another key project member.
The team staggered their changes over 2 years. Pulmonary consults for acute exacerbation admissions shot up, and respiratory therapists started to stop by to educate almost every COPD patient about medication use, trigger avoidance, and other matters. Patients began watching educational videos from their bed.
Changes were made after discharge, too. “We felt strongly that pulmonary rehabilitation needed to be an integral part of care, and that patients had to be connected to the pulmonary clinic,” Dr. Moreta-Sainz said.
Patients were booked for a pulmonologist at the clinic soon after they left the hospital, and greeted there by their COPD navigator – a respiratory therapist operating at the top of their license – who bridged the gap between inpatient and outpatient care and oversaw their case, helping with medical, psychosocial, and palliative needs.
Patients were also channeled into pulmonary rehab, three sessions per week for 6-8 weeks, with additional sessions as needed. The outpatient education emphasized and expanded the inpatient lessons, and patients exercised on treadmills and other equipment. They learned how to use resistance bands at home to increase upper body strength and decrease disability. Kaiser increased the number of weekly pulmonary rehab slots from 8 to 64 to make it happen.
After rehab, patients were offered a pedometer to measure how many steps they walked, and a phone number to report it each day. Those who participated got a call from the navigator when they fell below targets.
It has all made a huge difference. Dr. Moreta-Sainz said he’d like to add in-home visits and family support groups, so caregivers know what to do if things head south.
The work was funded by Kaiser; Dr. Moreta-Sainz and Mr. Cam have no disclosures.
[email protected]
On a recent morning, two of my scheduled clinic patients were “no-shows.” Both of them were patients with COPD that I had recently cared for in-hospital for an exacerbation. While I know that snow may have played a role, there are other barriers to care, including lack of access to transportation, poor health literacy, and no effective health insurance.
On a recent morning, two of my scheduled clinic patients were “no-shows.” Both of them were patients with COPD that I had recently cared for in-hospital for an exacerbation. While I know that snow may have played a role, there are other barriers to care, including lack of access to transportation, poor health literacy, and no effective health insurance.
On a recent morning, two of my scheduled clinic patients were “no-shows.” Both of them were patients with COPD that I had recently cared for in-hospital for an exacerbation. While I know that snow may have played a role, there are other barriers to care, including lack of access to transportation, poor health literacy, and no effective health insurance.
LOS ANGELES – With a handful of common-sense steps, the Kaiser Permanente Los Angeles Medical Center reduced 30-day hospital readmissions for chronic obstructive pulmonary disease (COPD) from 17.4/1,000 in Dec. 2013 to 11.9/1,000 in Dec. 2015.
The 57 readmissions avoided in 2015 saved the medical center $700,359, according to a report at the annual meeting of the American College of Chest Physicians.
The quality improvement project – dubbed KP Breath – started in 2013 after staff realized their COPD readmission rates were significantly higher than other area hospitals, and likely to increase. “We knew we had a problem, and that if we did not address it, it was going to be out of control,” Mr. Cam said. There was also the risk of Centers for Medicare & Medicaid Services penalties for COPD readmissions.
Mr. Cam and his colleagues discovered several problems. “Leaving the hospital, [COPD patients] didn’t know what medication was for what, or their medication schedule. They didn’t know how to use their inhalers, and didn’t understand what the disease process was all about, and what it was doing to them,” he said.
There was little continuity of care after discharge; many patients didn’t even have a pulmonologist. Essentially, COPD patients were lost to follow-up until they returned to the emergency department with another exacerbation.
A rapid Plan, Do, Study, Act cycle was the first step; it identified solutions that would work based on COPD management guidelines and published studies. “They were all things that have been shown to reduce rehospitalizations,” said pulmonologist Luis Moreta-Sainz, MD, another key project member.
The team staggered their changes over 2 years. Pulmonary consults for acute exacerbation admissions shot up, and respiratory therapists started to stop by to educate almost every COPD patient about medication use, trigger avoidance, and other matters. Patients began watching educational videos from their bed.
Changes were made after discharge, too. “We felt strongly that pulmonary rehabilitation needed to be an integral part of care, and that patients had to be connected to the pulmonary clinic,” Dr. Moreta-Sainz said.
Patients were booked for a pulmonologist at the clinic soon after they left the hospital, and greeted there by their COPD navigator – a respiratory therapist operating at the top of their license – who bridged the gap between inpatient and outpatient care and oversaw their case, helping with medical, psychosocial, and palliative needs.
Patients were also channeled into pulmonary rehab, three sessions per week for 6-8 weeks, with additional sessions as needed. The outpatient education emphasized and expanded the inpatient lessons, and patients exercised on treadmills and other equipment. They learned how to use resistance bands at home to increase upper body strength and decrease disability. Kaiser increased the number of weekly pulmonary rehab slots from 8 to 64 to make it happen.
After rehab, patients were offered a pedometer to measure how many steps they walked, and a phone number to report it each day. Those who participated got a call from the navigator when they fell below targets.
It has all made a huge difference. Dr. Moreta-Sainz said he’d like to add in-home visits and family support groups, so caregivers know what to do if things head south.
The work was funded by Kaiser; Dr. Moreta-Sainz and Mr. Cam have no disclosures.
[email protected]
LOS ANGELES – With a handful of common-sense steps, the Kaiser Permanente Los Angeles Medical Center reduced 30-day hospital readmissions for chronic obstructive pulmonary disease (COPD) from 17.4/1,000 in Dec. 2013 to 11.9/1,000 in Dec. 2015.
The 57 readmissions avoided in 2015 saved the medical center $700,359, according to a report at the annual meeting of the American College of Chest Physicians.
The quality improvement project – dubbed KP Breath – started in 2013 after staff realized their COPD readmission rates were significantly higher than other area hospitals, and likely to increase. “We knew we had a problem, and that if we did not address it, it was going to be out of control,” Mr. Cam said. There was also the risk of Centers for Medicare & Medicaid Services penalties for COPD readmissions.
Mr. Cam and his colleagues discovered several problems. “Leaving the hospital, [COPD patients] didn’t know what medication was for what, or their medication schedule. They didn’t know how to use their inhalers, and didn’t understand what the disease process was all about, and what it was doing to them,” he said.
There was little continuity of care after discharge; many patients didn’t even have a pulmonologist. Essentially, COPD patients were lost to follow-up until they returned to the emergency department with another exacerbation.
A rapid Plan, Do, Study, Act cycle was the first step; it identified solutions that would work based on COPD management guidelines and published studies. “They were all things that have been shown to reduce rehospitalizations,” said pulmonologist Luis Moreta-Sainz, MD, another key project member.
The team staggered their changes over 2 years. Pulmonary consults for acute exacerbation admissions shot up, and respiratory therapists started to stop by to educate almost every COPD patient about medication use, trigger avoidance, and other matters. Patients began watching educational videos from their bed.
Changes were made after discharge, too. “We felt strongly that pulmonary rehabilitation needed to be an integral part of care, and that patients had to be connected to the pulmonary clinic,” Dr. Moreta-Sainz said.
Patients were booked for a pulmonologist at the clinic soon after they left the hospital, and greeted there by their COPD navigator – a respiratory therapist operating at the top of their license – who bridged the gap between inpatient and outpatient care and oversaw their case, helping with medical, psychosocial, and palliative needs.
Patients were also channeled into pulmonary rehab, three sessions per week for 6-8 weeks, with additional sessions as needed. The outpatient education emphasized and expanded the inpatient lessons, and patients exercised on treadmills and other equipment. They learned how to use resistance bands at home to increase upper body strength and decrease disability. Kaiser increased the number of weekly pulmonary rehab slots from 8 to 64 to make it happen.
After rehab, patients were offered a pedometer to measure how many steps they walked, and a phone number to report it each day. Those who participated got a call from the navigator when they fell below targets.
It has all made a huge difference. Dr. Moreta-Sainz said he’d like to add in-home visits and family support groups, so caregivers know what to do if things head south.
The work was funded by Kaiser; Dr. Moreta-Sainz and Mr. Cam have no disclosures.
[email protected]
AT CHEST 2016

California bucks trend of rising U.S. maternal mortality
While the United States as a whole is seeing an unsettling rise in maternal mortality, California is on a divergent path.
Maternal mortality in the Golden State was tracking at a similar rate with national figures from 1999-2008 when the trend started to change. By 2013, the U.S. maternal mortality rate had grown to 22.0 deaths per 100,000 live births, while California’s rate had dropped to 7.3 per 100,000, according to data from the California Department of Public Health and the U.S. Centers for Disease Control and Prevention.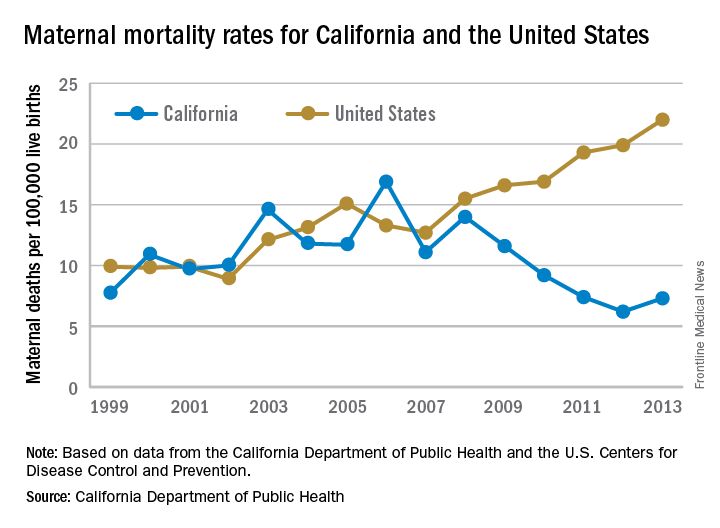
“We reviewed every maternal death for almost 10 years and through that process, we learned a lot about practices of care and the opportunities to really have intervened,” Elliott Main, MD, medical director of the Collaborative, said in an interview. “There were certain causes of death that had a pretty high chance of preventability and those were hemorrhage and preeclampsia.”
Identifying risk factors
The Collaborative’s research identified a number of risk factors that were significant contributors to maternal morbidity.

Dr. Main noted that obesity and older maternal age are both associated with an increased likelihood of having a cesarean delivery, which is associated with an increased risk of hemorrhage.
“So there are pathways that can get you into more trouble, but again if you are on top of those, you can be proactive and not necessarily have this high rate of complications,” he added.
With data in hand about what was contributing to the risks of maternal mortality, the Collaborative set out to build a series of toolkits or “bundles” to help guide hospitals in limiting complications and responding to emergencies. These toolkits are based on the state’s own data, as well as best practices identified in the medical literature and national guidelines from organizations such as the American College of Obstetricians and Gynecologists.
For example, the hypertension bundle includes information aimed at readiness, recognition and prevention, response, and reporting/system learning. Other bundles, which the Collaborative helped to develop and which are distributed through the Council on Patient Safety in Women’s Health Care, cover areas such as mental health, thromboembolism, hemorrhage, and safe reduction in primary cesarean births.
“It’s all about the implementation of those and that’s where we spent a lot of time in California with what are called quality collaboratives,” he said. “These are generally state-based [efforts], where you put together a consortium of providers, hospitals, and public health and patient advocates, and you work on improving the care for these certain conditions.”
The bundles are not meant to be cookbook medicine, Dr. Main noted, but rather are designed so that they can be customized based on the resources of an individual hospital, whether the facility handles 300 births a year or 5,000.
“There is no such thing as a national protocol for this,” Dr. Main said. “You have to have some flexibility and differences in the protocols but what we really are striving for is that for emergencies, people have standard protocols for the treatment of that emergency.”
Disparities remain
While California is a success story in terms of its overall drop in maternal mortality, racial disparities remain, particularly for African American women.
Maternal mortality among African Americans has dropped 50% in the state, mirroring the overall decline in the state during the 2008-2013 time period, but it is still three to four times higher than for other racial/ethnic groups.
“African American women do have more risk factors. There is more obesity. There is more hypertension and they have more social stresses and so forth, but none of those are reasons that they should die,” Dr. Main said. “They are reasons that they should have more intensive attention and care. If you have an older African American woman with hypertension, you’ve got to be on your toes when you are taking care of her and be a lot more responsive to warning signs than in a 25-year-old white woman that is perfectly healthy.”

“Minorities represent half of all U.S. persons, yet racial and ethnic minorities suffer higher rates of maternal mortality than whites in this country,” said Dr. Howell, who also chairs ACOG’s work group on reduction of peripartum racial disparities. “In fact, black and African Americans are three to four times more likely to die than whites. This is the largest disparity among population perinatal health measures.”
Native Americans, Asians, and some Latinas also have elevated rates of maternal mortality, compared with white women, she noted.
Depending on the city, those rates could be even higher, she said.
“In New York City, a recent publication by our Department of Health reviewed deaths from 2006 to 2010 and they found that black women were 10 times more likely to die than white women,” Dr. Howell said. “It’s also important to remember that for every maternal death, over 100 women experience severe obstetric morbidity or a life-threatening diagnosis or undergo a lifesaving procedure during their delivery hospitalization.”
But there are care tools available to help address this issue, too. The Alliance for Innovation on Maternal Health, which includes the California collaborative and ACOG, has developed a safety bundle that focuses on themes of shared decision making, implicit bias, continuity of care, provider and patient education, and care fragmentation. It also recommends implementation of a disparity dashboard, meaning that hospitals and health systems would stratify their quality results by race and ethnicity to identify and address gaps in care, Dr. Howell said.
[email protected]
While the United States as a whole is seeing an unsettling rise in maternal mortality, California is on a divergent path.
Maternal mortality in the Golden State was tracking at a similar rate with national figures from 1999-2008 when the trend started to change. By 2013, the U.S. maternal mortality rate had grown to 22.0 deaths per 100,000 live births, while California’s rate had dropped to 7.3 per 100,000, according to data from the California Department of Public Health and the U.S. Centers for Disease Control and Prevention.
“We reviewed every maternal death for almost 10 years and through that process, we learned a lot about practices of care and the opportunities to really have intervened,” Elliott Main, MD, medical director of the Collaborative, said in an interview. “There were certain causes of death that had a pretty high chance of preventability and those were hemorrhage and preeclampsia.”
Identifying risk factors
The Collaborative’s research identified a number of risk factors that were significant contributors to maternal morbidity.
Dr. Main noted that obesity and older maternal age are both associated with an increased likelihood of having a cesarean delivery, which is associated with an increased risk of hemorrhage.
“So there are pathways that can get you into more trouble, but again if you are on top of those, you can be proactive and not necessarily have this high rate of complications,” he added.
With data in hand about what was contributing to the risks of maternal mortality, the Collaborative set out to build a series of toolkits or “bundles” to help guide hospitals in limiting complications and responding to emergencies. These toolkits are based on the state’s own data, as well as best practices identified in the medical literature and national guidelines from organizations such as the American College of Obstetricians and Gynecologists.
For example, the hypertension bundle includes information aimed at readiness, recognition and prevention, response, and reporting/system learning. Other bundles, which the Collaborative helped to develop and which are distributed through the Council on Patient Safety in Women’s Health Care, cover areas such as mental health, thromboembolism, hemorrhage, and safe reduction in primary cesarean births.
“It’s all about the implementation of those and that’s where we spent a lot of time in California with what are called quality collaboratives,” he said. “These are generally state-based [efforts], where you put together a consortium of providers, hospitals, and public health and patient advocates, and you work on improving the care for these certain conditions.”
The bundles are not meant to be cookbook medicine, Dr. Main noted, but rather are designed so that they can be customized based on the resources of an individual hospital, whether the facility handles 300 births a year or 5,000.
“There is no such thing as a national protocol for this,” Dr. Main said. “You have to have some flexibility and differences in the protocols but what we really are striving for is that for emergencies, people have standard protocols for the treatment of that emergency.”
Disparities remain
While California is a success story in terms of its overall drop in maternal mortality, racial disparities remain, particularly for African American women.
Maternal mortality among African Americans has dropped 50% in the state, mirroring the overall decline in the state during the 2008-2013 time period, but it is still three to four times higher than for other racial/ethnic groups.
“African American women do have more risk factors. There is more obesity. There is more hypertension and they have more social stresses and so forth, but none of those are reasons that they should die,” Dr. Main said. “They are reasons that they should have more intensive attention and care. If you have an older African American woman with hypertension, you’ve got to be on your toes when you are taking care of her and be a lot more responsive to warning signs than in a 25-year-old white woman that is perfectly healthy.”
“Minorities represent half of all U.S. persons, yet racial and ethnic minorities suffer higher rates of maternal mortality than whites in this country,” said Dr. Howell, who also chairs ACOG’s work group on reduction of peripartum racial disparities. “In fact, black and African Americans are three to four times more likely to die than whites. This is the largest disparity among population perinatal health measures.”
Native Americans, Asians, and some Latinas also have elevated rates of maternal mortality, compared with white women, she noted.
Depending on the city, those rates could be even higher, she said.
“In New York City, a recent publication by our Department of Health reviewed deaths from 2006 to 2010 and they found that black women were 10 times more likely to die than white women,” Dr. Howell said. “It’s also important to remember that for every maternal death, over 100 women experience severe obstetric morbidity or a life-threatening diagnosis or undergo a lifesaving procedure during their delivery hospitalization.”
But there are care tools available to help address this issue, too. The Alliance for Innovation on Maternal Health, which includes the California collaborative and ACOG, has developed a safety bundle that focuses on themes of shared decision making, implicit bias, continuity of care, provider and patient education, and care fragmentation. It also recommends implementation of a disparity dashboard, meaning that hospitals and health systems would stratify their quality results by race and ethnicity to identify and address gaps in care, Dr. Howell said.
[email protected]
While the United States as a whole is seeing an unsettling rise in maternal mortality, California is on a divergent path.
Maternal mortality in the Golden State was tracking at a similar rate with national figures from 1999-2008 when the trend started to change. By 2013, the U.S. maternal mortality rate had grown to 22.0 deaths per 100,000 live births, while California’s rate had dropped to 7.3 per 100,000, according to data from the California Department of Public Health and the U.S. Centers for Disease Control and Prevention.
“We reviewed every maternal death for almost 10 years and through that process, we learned a lot about practices of care and the opportunities to really have intervened,” Elliott Main, MD, medical director of the Collaborative, said in an interview. “There were certain causes of death that had a pretty high chance of preventability and those were hemorrhage and preeclampsia.”
Identifying risk factors
The Collaborative’s research identified a number of risk factors that were significant contributors to maternal morbidity.
Dr. Main noted that obesity and older maternal age are both associated with an increased likelihood of having a cesarean delivery, which is associated with an increased risk of hemorrhage.
“So there are pathways that can get you into more trouble, but again if you are on top of those, you can be proactive and not necessarily have this high rate of complications,” he added.
With data in hand about what was contributing to the risks of maternal mortality, the Collaborative set out to build a series of toolkits or “bundles” to help guide hospitals in limiting complications and responding to emergencies. These toolkits are based on the state’s own data, as well as best practices identified in the medical literature and national guidelines from organizations such as the American College of Obstetricians and Gynecologists.
For example, the hypertension bundle includes information aimed at readiness, recognition and prevention, response, and reporting/system learning. Other bundles, which the Collaborative helped to develop and which are distributed through the Council on Patient Safety in Women’s Health Care, cover areas such as mental health, thromboembolism, hemorrhage, and safe reduction in primary cesarean births.
“It’s all about the implementation of those and that’s where we spent a lot of time in California with what are called quality collaboratives,” he said. “These are generally state-based [efforts], where you put together a consortium of providers, hospitals, and public health and patient advocates, and you work on improving the care for these certain conditions.”
The bundles are not meant to be cookbook medicine, Dr. Main noted, but rather are designed so that they can be customized based on the resources of an individual hospital, whether the facility handles 300 births a year or 5,000.
“There is no such thing as a national protocol for this,” Dr. Main said. “You have to have some flexibility and differences in the protocols but what we really are striving for is that for emergencies, people have standard protocols for the treatment of that emergency.”
Disparities remain
While California is a success story in terms of its overall drop in maternal mortality, racial disparities remain, particularly for African American women.
Maternal mortality among African Americans has dropped 50% in the state, mirroring the overall decline in the state during the 2008-2013 time period, but it is still three to four times higher than for other racial/ethnic groups.
“African American women do have more risk factors. There is more obesity. There is more hypertension and they have more social stresses and so forth, but none of those are reasons that they should die,” Dr. Main said. “They are reasons that they should have more intensive attention and care. If you have an older African American woman with hypertension, you’ve got to be on your toes when you are taking care of her and be a lot more responsive to warning signs than in a 25-year-old white woman that is perfectly healthy.”
“Minorities represent half of all U.S. persons, yet racial and ethnic minorities suffer higher rates of maternal mortality than whites in this country,” said Dr. Howell, who also chairs ACOG’s work group on reduction of peripartum racial disparities. “In fact, black and African Americans are three to four times more likely to die than whites. This is the largest disparity among population perinatal health measures.”
Native Americans, Asians, and some Latinas also have elevated rates of maternal mortality, compared with white women, she noted.
Depending on the city, those rates could be even higher, she said.
“In New York City, a recent publication by our Department of Health reviewed deaths from 2006 to 2010 and they found that black women were 10 times more likely to die than white women,” Dr. Howell said. “It’s also important to remember that for every maternal death, over 100 women experience severe obstetric morbidity or a life-threatening diagnosis or undergo a lifesaving procedure during their delivery hospitalization.”
But there are care tools available to help address this issue, too. The Alliance for Innovation on Maternal Health, which includes the California collaborative and ACOG, has developed a safety bundle that focuses on themes of shared decision making, implicit bias, continuity of care, provider and patient education, and care fragmentation. It also recommends implementation of a disparity dashboard, meaning that hospitals and health systems would stratify their quality results by race and ethnicity to identify and address gaps in care, Dr. Howell said.
[email protected]
Improving cryopreservation of RBCs
![]()
Photo from UAB Hospital
A class of small-molecule ice recrystallization inhibitors could improve the cryopreservation of red blood cells (RBCs) intended for transfusion, according to researchers.
The team said these molecules can decrease the time needed to thaw cryopreserved RBCs, thereby reducing transfusion wait times.
But the molecules also protect RBCs from injury during cryopreservation and reduce the risk of post-thaw hemolysis.
Robert N. Ben, PhD, of the University of Ottawa in Ontario, Canada, and his colleagues conducted this research and detailed the results in the journal ACS Omega.
The researchers began with a class of glucose-based molecules they had previously found to be cryoprotective.
The team set out to determine whether these molecules, known as O-aryl-glycosides, could potentially reduce the time needed to process frozen RBCs.
They found that changes in the structure of O-aryl-glycosides affect their ability to inhibit ice recrystallization and protect against cryoinjury. But 3 O-aryl-glycosides—β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal—proved particularly effective in these areas.
The researchers said low concentrations of β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal provided “high post-thaw RBC integrity” and reduced the needed concentration of glycerol from 40% to between 10% and 15%.
The highest post-thaw integrity observed in slow freezing conditions was with β-pBrPh-Glc and β-pBrPh-Gal. The post-thaw integrity was 65% with 55 mM of β-pBrPh-Gal and 67% with 30 mM of β-pBrPh-Glc.
The researchers noted that these molecules were “very effective” in rapid freezing conditions as well. And the addition of glycerol improved post-thaw RBC integrity.
Combining 30 mM of either molecule with 15% glycerol resulted in almost 95% post-thaw RBC integrity, whereas 15% glycerol alone provides 75% post-thaw integrity.
The researchers said 30 mM of β-pBrPh-Glc was even “highly effective” in preventing post-thaw hemolysis with a glycerol concentration of 10%. In this case, the post-thaw integrity was 67%, whereas 10% glycerol alone provides 23% post-thaw integrity.
The researchers noted that lowering the amount of glycerol needed during the cryopreservation process could help minimize the time required to prepare thawed RBCs for transfusion and provide patients with faster access to cryopreserved RBCs.
The team added that O-aryl-glycosides are structurally simple and amenable to large-scale preparation for use in cryopreservation. ![]()
![]()
Photo from UAB Hospital
A class of small-molecule ice recrystallization inhibitors could improve the cryopreservation of red blood cells (RBCs) intended for transfusion, according to researchers.
The team said these molecules can decrease the time needed to thaw cryopreserved RBCs, thereby reducing transfusion wait times.
But the molecules also protect RBCs from injury during cryopreservation and reduce the risk of post-thaw hemolysis.
Robert N. Ben, PhD, of the University of Ottawa in Ontario, Canada, and his colleagues conducted this research and detailed the results in the journal ACS Omega.
The researchers began with a class of glucose-based molecules they had previously found to be cryoprotective.
The team set out to determine whether these molecules, known as O-aryl-glycosides, could potentially reduce the time needed to process frozen RBCs.
They found that changes in the structure of O-aryl-glycosides affect their ability to inhibit ice recrystallization and protect against cryoinjury. But 3 O-aryl-glycosides—β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal—proved particularly effective in these areas.
The researchers said low concentrations of β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal provided “high post-thaw RBC integrity” and reduced the needed concentration of glycerol from 40% to between 10% and 15%.
The highest post-thaw integrity observed in slow freezing conditions was with β-pBrPh-Glc and β-pBrPh-Gal. The post-thaw integrity was 65% with 55 mM of β-pBrPh-Gal and 67% with 30 mM of β-pBrPh-Glc.
The researchers noted that these molecules were “very effective” in rapid freezing conditions as well. And the addition of glycerol improved post-thaw RBC integrity.
Combining 30 mM of either molecule with 15% glycerol resulted in almost 95% post-thaw RBC integrity, whereas 15% glycerol alone provides 75% post-thaw integrity.
The researchers said 30 mM of β-pBrPh-Glc was even “highly effective” in preventing post-thaw hemolysis with a glycerol concentration of 10%. In this case, the post-thaw integrity was 67%, whereas 10% glycerol alone provides 23% post-thaw integrity.
The researchers noted that lowering the amount of glycerol needed during the cryopreservation process could help minimize the time required to prepare thawed RBCs for transfusion and provide patients with faster access to cryopreserved RBCs.
The team added that O-aryl-glycosides are structurally simple and amenable to large-scale preparation for use in cryopreservation. ![]()
![]()
Photo from UAB Hospital
A class of small-molecule ice recrystallization inhibitors could improve the cryopreservation of red blood cells (RBCs) intended for transfusion, according to researchers.
The team said these molecules can decrease the time needed to thaw cryopreserved RBCs, thereby reducing transfusion wait times.
But the molecules also protect RBCs from injury during cryopreservation and reduce the risk of post-thaw hemolysis.
Robert N. Ben, PhD, of the University of Ottawa in Ontario, Canada, and his colleagues conducted this research and detailed the results in the journal ACS Omega.
The researchers began with a class of glucose-based molecules they had previously found to be cryoprotective.
The team set out to determine whether these molecules, known as O-aryl-glycosides, could potentially reduce the time needed to process frozen RBCs.
They found that changes in the structure of O-aryl-glycosides affect their ability to inhibit ice recrystallization and protect against cryoinjury. But 3 O-aryl-glycosides—β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal—proved particularly effective in these areas.
The researchers said low concentrations of β-PMP-Glc, β-pBrPh-Glc, and β-pBrPh-Gal provided “high post-thaw RBC integrity” and reduced the needed concentration of glycerol from 40% to between 10% and 15%.
The highest post-thaw integrity observed in slow freezing conditions was with β-pBrPh-Glc and β-pBrPh-Gal. The post-thaw integrity was 65% with 55 mM of β-pBrPh-Gal and 67% with 30 mM of β-pBrPh-Glc.
The researchers noted that these molecules were “very effective” in rapid freezing conditions as well. And the addition of glycerol improved post-thaw RBC integrity.
Combining 30 mM of either molecule with 15% glycerol resulted in almost 95% post-thaw RBC integrity, whereas 15% glycerol alone provides 75% post-thaw integrity.
The researchers said 30 mM of β-pBrPh-Glc was even “highly effective” in preventing post-thaw hemolysis with a glycerol concentration of 10%. In this case, the post-thaw integrity was 67%, whereas 10% glycerol alone provides 23% post-thaw integrity.
The researchers noted that lowering the amount of glycerol needed during the cryopreservation process could help minimize the time required to prepare thawed RBCs for transfusion and provide patients with faster access to cryopreserved RBCs.
The team added that O-aryl-glycosides are structurally simple and amenable to large-scale preparation for use in cryopreservation. ![]()
Tofacitinib effective after TNFi failure
WASHINGTON – The oral Janus kinase inhibitor tofacitinib is safe and effective in patients with active psoriatic arthritis and an inadequate response to tumor necrosis factor inhibitors, according to findings from the phase III OPAL Beyond trial.
Both the American College of Rheumatology 20% improvement criteria (ACR20) response rate and change from baseline in Health Assessment Questionnaire Disability Index (HAQ-DI) scores at month 3 – the primary endpoints of the study – were superior with tofacitinib (Xeljanz) versus placebo in the 6-month, double-blind, randomized, multicenter trial, Dafna D. Gladman, MD, reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.

The superiority of tofacitinib over placebo in achieving an ACR20 response was evident as early as 2 weeks when the response rates were 13% in 131 patients who received placebo, 26.7% in 131 patients who received 5 mg of tofacitinib twice daily, and 28.8% in 132 patients who received 10 mg of tofacitinib twice daily, Dr. Gladman said. Later on at 3 months, the ACR20 response rates were 23.7% for placebo, 49.6% for 5 mg of tofacitinib twice daily, and 47% for 10 mg of tofacitinib twice daily.
The change from baseline in HAQ-DI scores was –0.14 with placebo, –0.39 with 5 mg tofacitinib, and –0.35 with 10 mg tofacitinib.
Study subjects had a 6-month or greater psoriatic arthritis diagnosis, fulfilled classification criteria for psoriatic arthritis, had active arthritis at screening and baseline and active plaque psoriasis at screening, and inadequate response to TNF inhibitors, which was defined as discontinuation for inadequate efficacy or due to an adverse event. All had ongoing treatment with a conventional synthetic disease-modifying antirheumatic agent, and those in the placebo group were advanced after 3 months to receive either 5 mg or 10 mg of tofacitinib twice daily (66 and 65 patients, respectively).
The effects of treatment on secondary efficacy endpoints were generally consistent with the findings with respect to the primary endpoints, Dr. Gladman said.
As for safety endpoints, serious adverse events and drug discontinuations due to adverse events were rare. Serious adverse event rates at 6 months were 3% in the placebo group who advanced to 5 mg tofacitinib, 1.5% in those who advanced to 10 mg tofacitinib, 3.8% in the original 5 mg tofacitinib group, and 6.1% in the original 10 mg tofacitinib group. Corresponding rates for all adverse events were 60.6%, 58.5%, 71%, and 72.7%. The most common adverse events were upper respiratory tract infections, nasopharyngitis, and headache.
OPAL Beyond was sponsored by Pfizer. Dr. Gladman disclosed financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Novartis, Pfizer, and UCB. Several other authors disclosed financial relationships with pharmaceutical companies, including Pfizer. Five of the 11 authors were employees of Pfizer.
[email protected]
WASHINGTON – The oral Janus kinase inhibitor tofacitinib is safe and effective in patients with active psoriatic arthritis and an inadequate response to tumor necrosis factor inhibitors, according to findings from the phase III OPAL Beyond trial.
Both the American College of Rheumatology 20% improvement criteria (ACR20) response rate and change from baseline in Health Assessment Questionnaire Disability Index (HAQ-DI) scores at month 3 – the primary endpoints of the study – were superior with tofacitinib (Xeljanz) versus placebo in the 6-month, double-blind, randomized, multicenter trial, Dafna D. Gladman, MD, reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.
The superiority of tofacitinib over placebo in achieving an ACR20 response was evident as early as 2 weeks when the response rates were 13% in 131 patients who received placebo, 26.7% in 131 patients who received 5 mg of tofacitinib twice daily, and 28.8% in 132 patients who received 10 mg of tofacitinib twice daily, Dr. Gladman said. Later on at 3 months, the ACR20 response rates were 23.7% for placebo, 49.6% for 5 mg of tofacitinib twice daily, and 47% for 10 mg of tofacitinib twice daily.
The change from baseline in HAQ-DI scores was –0.14 with placebo, –0.39 with 5 mg tofacitinib, and –0.35 with 10 mg tofacitinib.
Study subjects had a 6-month or greater psoriatic arthritis diagnosis, fulfilled classification criteria for psoriatic arthritis, had active arthritis at screening and baseline and active plaque psoriasis at screening, and inadequate response to TNF inhibitors, which was defined as discontinuation for inadequate efficacy or due to an adverse event. All had ongoing treatment with a conventional synthetic disease-modifying antirheumatic agent, and those in the placebo group were advanced after 3 months to receive either 5 mg or 10 mg of tofacitinib twice daily (66 and 65 patients, respectively).
The effects of treatment on secondary efficacy endpoints were generally consistent with the findings with respect to the primary endpoints, Dr. Gladman said.
As for safety endpoints, serious adverse events and drug discontinuations due to adverse events were rare. Serious adverse event rates at 6 months were 3% in the placebo group who advanced to 5 mg tofacitinib, 1.5% in those who advanced to 10 mg tofacitinib, 3.8% in the original 5 mg tofacitinib group, and 6.1% in the original 10 mg tofacitinib group. Corresponding rates for all adverse events were 60.6%, 58.5%, 71%, and 72.7%. The most common adverse events were upper respiratory tract infections, nasopharyngitis, and headache.
OPAL Beyond was sponsored by Pfizer. Dr. Gladman disclosed financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Novartis, Pfizer, and UCB. Several other authors disclosed financial relationships with pharmaceutical companies, including Pfizer. Five of the 11 authors were employees of Pfizer.
[email protected]
WASHINGTON – The oral Janus kinase inhibitor tofacitinib is safe and effective in patients with active psoriatic arthritis and an inadequate response to tumor necrosis factor inhibitors, according to findings from the phase III OPAL Beyond trial.
Both the American College of Rheumatology 20% improvement criteria (ACR20) response rate and change from baseline in Health Assessment Questionnaire Disability Index (HAQ-DI) scores at month 3 – the primary endpoints of the study – were superior with tofacitinib (Xeljanz) versus placebo in the 6-month, double-blind, randomized, multicenter trial, Dafna D. Gladman, MD, reported in a late-breaking poster at the annual meeting of the American College of Rheumatology.
The superiority of tofacitinib over placebo in achieving an ACR20 response was evident as early as 2 weeks when the response rates were 13% in 131 patients who received placebo, 26.7% in 131 patients who received 5 mg of tofacitinib twice daily, and 28.8% in 132 patients who received 10 mg of tofacitinib twice daily, Dr. Gladman said. Later on at 3 months, the ACR20 response rates were 23.7% for placebo, 49.6% for 5 mg of tofacitinib twice daily, and 47% for 10 mg of tofacitinib twice daily.
The change from baseline in HAQ-DI scores was –0.14 with placebo, –0.39 with 5 mg tofacitinib, and –0.35 with 10 mg tofacitinib.
Study subjects had a 6-month or greater psoriatic arthritis diagnosis, fulfilled classification criteria for psoriatic arthritis, had active arthritis at screening and baseline and active plaque psoriasis at screening, and inadequate response to TNF inhibitors, which was defined as discontinuation for inadequate efficacy or due to an adverse event. All had ongoing treatment with a conventional synthetic disease-modifying antirheumatic agent, and those in the placebo group were advanced after 3 months to receive either 5 mg or 10 mg of tofacitinib twice daily (66 and 65 patients, respectively).
The effects of treatment on secondary efficacy endpoints were generally consistent with the findings with respect to the primary endpoints, Dr. Gladman said.
As for safety endpoints, serious adverse events and drug discontinuations due to adverse events were rare. Serious adverse event rates at 6 months were 3% in the placebo group who advanced to 5 mg tofacitinib, 1.5% in those who advanced to 10 mg tofacitinib, 3.8% in the original 5 mg tofacitinib group, and 6.1% in the original 10 mg tofacitinib group. Corresponding rates for all adverse events were 60.6%, 58.5%, 71%, and 72.7%. The most common adverse events were upper respiratory tract infections, nasopharyngitis, and headache.
OPAL Beyond was sponsored by Pfizer. Dr. Gladman disclosed financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Novartis, Pfizer, and UCB. Several other authors disclosed financial relationships with pharmaceutical companies, including Pfizer. Five of the 11 authors were employees of Pfizer.
[email protected]
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: ACR20 response rates at 3 months were 23.7%, 49.6%, and 47% with placebo, 5 mg, and 10 mg of tofacitinib twice daily, respectively.
Data source: The phase III, double-blind, randomized, placebo-controlled OPAL Beyond trial.
Disclosures: OPAL Beyond was sponsored by Pfizer. Dr. Gladman disclosed financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Novartis, Pfizer, and UCB. Several other authors disclosed financial relationships with pharmaceutical companies, including Pfizer. Five of the 11 authors were employees of Pfizer.
Acute kidney injury common in children, young adults in ICU
Acute kidney injury is common in children and young adults admitted to ICUs, and cannot always be identified by plasma creatinine level alone, according to the authors of a study presented at the meeting sponsored by the American Society of Nephrology.
The Assessment of Worldwide Acute Kidney Injury, Renal Angina, and Epidemiology (AWARE) study was a prospective, international, observational study in 4,683 patients aged 3 months to 25 years, recruited from 32 pediatric ICUs over the course of 3 months.
Ahmad Kaddourah, MD, from the Center for Acute Care Nephrology at the Cincinnati Children’s Hospital Medical Center, and his coauthors found that 27% of the participants developed acute kidney injury and 12% developed severe acute kidney injury – defined as stage 2 or 3 acute kidney injury – within the first 7 days after admission.
The risk of death within 28 days was 77% higher among individuals with severe acute kidney injury, even after accounting for their original diagnosis when they were admitted to the ICU. Mortality among these individuals was 11%, compared with 2.5% among patients without severe acute kidney injury. These patients also had an increased use of renal replacement therapy and mechanical ventilation, and were more likely to have longer stays in hospital.
Researchers also saw a stepwise increase in 28-day mortality associated with maximum stage of acute kidney injury.
“The common and early occurrence of acute kidney injury reinforces the need for systematic surveillance for acute kidney injury at the time of admission to the ICU,” Dr. Kaddourah and his associates wrote. “Early identification of modifiable risk factors for acute kidney injury (e.g., nephrotoxic medications) or adverse sequelae (e.g., fluid overload) has the potential to decrease morbidity and mortality.”
Of particular note was the observation that 67% of the patients who met the urine-output criteria for acute kidney injury would not have been diagnosed using the plasma creatinine criteria alone. Furthermore, “mortality was higher among patients diagnosed with stage 3 acute kidney injury according to urine output than among those diagnosed according to plasma creatinine levels,” the authors reported.
There was a steady increase in the daily prevalence of acute kidney disease, from 15% on day 1 after admission to 20% by day 7. Patients with stage 1 acute kidney injury on day 1 also were more likely to progress to stage 2 or 3 by day 7, compared with patients who did not have acute kidney injury on admission.
However, around three-quarters of this increase in stage occurred within the first 4 days after admission, which the authors suggested would support a 4-day time frame for future studies on acute kidney injury in children. They also stressed that as their assessments for acute kidney injury stopped at day 7 after admission, there may have been incidents that were missed.
Dr. Kaddourah and his associates noted that although the rates of severe and acute kidney injury seen in the study were slightly lower than those observed in studies in adults, the associations with morbidity and mortality were similar.
“The presence of chronic systemic diseases contributes to residual confounding in studies of acute kidney injury in adults,” they wrote. “Children have a low prevalence of such chronic diseases; thus, although the incremental association between acute kidney injury and risk of death mirrors that seen in adults, our study suggests that acute kidney injury itself may be key to the associated morbidity and mortality.”
The study was supported by the Pediatric Nephrology Center for Excellence at Cincinnati Children’s Hospital Medical Center. The authors declared grants, consultancies, speaking engagements, and other support from private industry, some related to and some outside of the submitted work.
A strength of this study is the definition of acute kidney injury, with the use of precise and validated criteria. Limitations of the study, beyond its observational nature, include the lack of data about diuretic and other treatment that may have influenced urine output, and the requirement for just a single baseline plasma creatinine level for study entry.
However, the study results indicate that acute injury is not only common among critically ill children and young adults, but is associated with adverse outcomes, implying that we should look more carefully for markers of acute kidney injury. Given the link between acute kidney injury and subsequent chronic kidney disease, it possible that identifying and treating acute kidney injury promptly might reduce the prevalence of chronic kidney disease, now estimated as roughly one in eight adults in the United States.
Julie R. Ingelfinger, MD, is a pediatric nephrologist at Massachusetts General Hospital and deputy editor of the New England Journal of Medicine. These comments are excerpted from an accompanying editorial (N Eng J Med. 2016 Nov 18. doi: 10.1056/NEJMe613456). No conflicts of interest were declared.
A strength of this study is the definition of acute kidney injury, with the use of precise and validated criteria. Limitations of the study, beyond its observational nature, include the lack of data about diuretic and other treatment that may have influenced urine output, and the requirement for just a single baseline plasma creatinine level for study entry.
However, the study results indicate that acute injury is not only common among critically ill children and young adults, but is associated with adverse outcomes, implying that we should look more carefully for markers of acute kidney injury. Given the link between acute kidney injury and subsequent chronic kidney disease, it possible that identifying and treating acute kidney injury promptly might reduce the prevalence of chronic kidney disease, now estimated as roughly one in eight adults in the United States.
Julie R. Ingelfinger, MD, is a pediatric nephrologist at Massachusetts General Hospital and deputy editor of the New England Journal of Medicine. These comments are excerpted from an accompanying editorial (N Eng J Med. 2016 Nov 18. doi: 10.1056/NEJMe613456). No conflicts of interest were declared.
A strength of this study is the definition of acute kidney injury, with the use of precise and validated criteria. Limitations of the study, beyond its observational nature, include the lack of data about diuretic and other treatment that may have influenced urine output, and the requirement for just a single baseline plasma creatinine level for study entry.
However, the study results indicate that acute injury is not only common among critically ill children and young adults, but is associated with adverse outcomes, implying that we should look more carefully for markers of acute kidney injury. Given the link between acute kidney injury and subsequent chronic kidney disease, it possible that identifying and treating acute kidney injury promptly might reduce the prevalence of chronic kidney disease, now estimated as roughly one in eight adults in the United States.
Julie R. Ingelfinger, MD, is a pediatric nephrologist at Massachusetts General Hospital and deputy editor of the New England Journal of Medicine. These comments are excerpted from an accompanying editorial (N Eng J Med. 2016 Nov 18. doi: 10.1056/NEJMe613456). No conflicts of interest were declared.
Acute kidney injury is common in children and young adults admitted to ICUs, and cannot always be identified by plasma creatinine level alone, according to the authors of a study presented at the meeting sponsored by the American Society of Nephrology.
The Assessment of Worldwide Acute Kidney Injury, Renal Angina, and Epidemiology (AWARE) study was a prospective, international, observational study in 4,683 patients aged 3 months to 25 years, recruited from 32 pediatric ICUs over the course of 3 months.
Ahmad Kaddourah, MD, from the Center for Acute Care Nephrology at the Cincinnati Children’s Hospital Medical Center, and his coauthors found that 27% of the participants developed acute kidney injury and 12% developed severe acute kidney injury – defined as stage 2 or 3 acute kidney injury – within the first 7 days after admission.
The risk of death within 28 days was 77% higher among individuals with severe acute kidney injury, even after accounting for their original diagnosis when they were admitted to the ICU. Mortality among these individuals was 11%, compared with 2.5% among patients without severe acute kidney injury. These patients also had an increased use of renal replacement therapy and mechanical ventilation, and were more likely to have longer stays in hospital.
Researchers also saw a stepwise increase in 28-day mortality associated with maximum stage of acute kidney injury.
“The common and early occurrence of acute kidney injury reinforces the need for systematic surveillance for acute kidney injury at the time of admission to the ICU,” Dr. Kaddourah and his associates wrote. “Early identification of modifiable risk factors for acute kidney injury (e.g., nephrotoxic medications) or adverse sequelae (e.g., fluid overload) has the potential to decrease morbidity and mortality.”
Of particular note was the observation that 67% of the patients who met the urine-output criteria for acute kidney injury would not have been diagnosed using the plasma creatinine criteria alone. Furthermore, “mortality was higher among patients diagnosed with stage 3 acute kidney injury according to urine output than among those diagnosed according to plasma creatinine levels,” the authors reported.
There was a steady increase in the daily prevalence of acute kidney disease, from 15% on day 1 after admission to 20% by day 7. Patients with stage 1 acute kidney injury on day 1 also were more likely to progress to stage 2 or 3 by day 7, compared with patients who did not have acute kidney injury on admission.
However, around three-quarters of this increase in stage occurred within the first 4 days after admission, which the authors suggested would support a 4-day time frame for future studies on acute kidney injury in children. They also stressed that as their assessments for acute kidney injury stopped at day 7 after admission, there may have been incidents that were missed.
Dr. Kaddourah and his associates noted that although the rates of severe and acute kidney injury seen in the study were slightly lower than those observed in studies in adults, the associations with morbidity and mortality were similar.
“The presence of chronic systemic diseases contributes to residual confounding in studies of acute kidney injury in adults,” they wrote. “Children have a low prevalence of such chronic diseases; thus, although the incremental association between acute kidney injury and risk of death mirrors that seen in adults, our study suggests that acute kidney injury itself may be key to the associated morbidity and mortality.”
The study was supported by the Pediatric Nephrology Center for Excellence at Cincinnati Children’s Hospital Medical Center. The authors declared grants, consultancies, speaking engagements, and other support from private industry, some related to and some outside of the submitted work.
Acute kidney injury is common in children and young adults admitted to ICUs, and cannot always be identified by plasma creatinine level alone, according to the authors of a study presented at the meeting sponsored by the American Society of Nephrology.
The Assessment of Worldwide Acute Kidney Injury, Renal Angina, and Epidemiology (AWARE) study was a prospective, international, observational study in 4,683 patients aged 3 months to 25 years, recruited from 32 pediatric ICUs over the course of 3 months.
Ahmad Kaddourah, MD, from the Center for Acute Care Nephrology at the Cincinnati Children’s Hospital Medical Center, and his coauthors found that 27% of the participants developed acute kidney injury and 12% developed severe acute kidney injury – defined as stage 2 or 3 acute kidney injury – within the first 7 days after admission.
The risk of death within 28 days was 77% higher among individuals with severe acute kidney injury, even after accounting for their original diagnosis when they were admitted to the ICU. Mortality among these individuals was 11%, compared with 2.5% among patients without severe acute kidney injury. These patients also had an increased use of renal replacement therapy and mechanical ventilation, and were more likely to have longer stays in hospital.
Researchers also saw a stepwise increase in 28-day mortality associated with maximum stage of acute kidney injury.
“The common and early occurrence of acute kidney injury reinforces the need for systematic surveillance for acute kidney injury at the time of admission to the ICU,” Dr. Kaddourah and his associates wrote. “Early identification of modifiable risk factors for acute kidney injury (e.g., nephrotoxic medications) or adverse sequelae (e.g., fluid overload) has the potential to decrease morbidity and mortality.”
Of particular note was the observation that 67% of the patients who met the urine-output criteria for acute kidney injury would not have been diagnosed using the plasma creatinine criteria alone. Furthermore, “mortality was higher among patients diagnosed with stage 3 acute kidney injury according to urine output than among those diagnosed according to plasma creatinine levels,” the authors reported.
There was a steady increase in the daily prevalence of acute kidney disease, from 15% on day 1 after admission to 20% by day 7. Patients with stage 1 acute kidney injury on day 1 also were more likely to progress to stage 2 or 3 by day 7, compared with patients who did not have acute kidney injury on admission.
However, around three-quarters of this increase in stage occurred within the first 4 days after admission, which the authors suggested would support a 4-day time frame for future studies on acute kidney injury in children. They also stressed that as their assessments for acute kidney injury stopped at day 7 after admission, there may have been incidents that were missed.
Dr. Kaddourah and his associates noted that although the rates of severe and acute kidney injury seen in the study were slightly lower than those observed in studies in adults, the associations with morbidity and mortality were similar.
“The presence of chronic systemic diseases contributes to residual confounding in studies of acute kidney injury in adults,” they wrote. “Children have a low prevalence of such chronic diseases; thus, although the incremental association between acute kidney injury and risk of death mirrors that seen in adults, our study suggests that acute kidney injury itself may be key to the associated morbidity and mortality.”
The study was supported by the Pediatric Nephrology Center for Excellence at Cincinnati Children’s Hospital Medical Center. The authors declared grants, consultancies, speaking engagements, and other support from private industry, some related to and some outside of the submitted work.
FROM KIDNEY WEEK 2016
Key clinical point: Acute kidney injury is common in children and young adults admitted to ICU, but many cases may be missed using plasma creatinine criteria alone.
Major finding: Among children and young adults admitted to intensive care, as many as 1 in 4 may have acute kidney injury and 1 in 10 may have severe acute kidney injury.
Data source: Prospective observational study in 4,683 patients aged 3 months to 25 years admitted to pediatric intensive care.
Disclosures: The study was supported by the Pediatric Nephrology Center for Excellence at Cincinnati Children’s Hospital Medical Center. The authors declared grants, consultancies, speaking engagements and other support from private industry, some related to and some outside of the submitted work.
Risk stratification important for aortic valve disease in pregnancy
CHICAGO – Pregnancy-associated hemodynamic and physiologic changes can challenge hearts with diseased aortic valves. Understanding pregnancy’s toll on the body can help physicians take better care of pregnant women with aortic stenosis or aortic regurgitation, said Patrick T. O’Gara, MD. “This is a relatively infrequent condition, and it causes all of us a great deal of apprehension,” he said.
Dr. O’Gara, director of clinical cardiology at Brigham and Women’s Hospital, Boston, walked attendees through current recommendations for caring for pregnant women with aortic valve disease in a presentation at the annual Heart Valve Summit.
When talking to women with aortic valve disease, it’s important to let them know that a pregnancy during which they experience an adverse maternal cardiac event appears to increase their risk for later events as well, said Dr. O’Gara. One study of pregnancy in women with aortic valve disease, said Dr. O’Gara, found that the risk of later events for women who had had a cardiac event in pregnancy was 27% plus or minus 9 percentage points in the 5 years following pregnancy, while the risk was just 15% plus or minus 3 percentage points for women whose pregnancies were not complicated by cardiac adverse events (P = .02) (Heart. 2010 Oct;96(20):1656-61).
The World Health Organization classification of pregnancy risk, said Dr. O’Gara, provides some guidance. Patients who are WHO class III are considered to be high risk; pregnancy in these individuals calls for counseling and a multidisciplinary care team. Patients who fall into this class are those with mechanical heart valves, those with Marfan syndrome and aortic involvement with a valve diameter of 40-45 mm, and those with bicuspid aortic valve disease with a valve diameter of 45-50 mm.
WHO class IV patients, according to the guidelines, are at prohibitive risk. These patients should consider terminating a pregnancy if one occurs. Conditions that place women into WHO class IV include symptomatic severe aortic stenosis (AS), severe left ventricular dysfunction with an ejection fraction less than 40%, and severe coarctation of the aorta. Women with Marfan syndrome with aortic valve diameters greater than 45 mm and women with bicuspid aortic valves and a diameter over 50 mm also fall into this category of prohibitive risk.
If a physician is lucky enough to have a pre-conception relationship with a patient, then a host of considerations can come into play. In addition to cardiac risk stratification, obstetric and intrapartum risk to the mother as well as neonatal risk should be considered. Some factors to take into account are maternal life expectancy and potential long-term complications to the mother from pregnancy and childbirth.
Plasma volume increases rapidly through the first trimester, plateauing about halfway through pregnancy. With this normal dilutional anemia, “Most normal pregnancies are accompanied by a grade II systolic murmur, best heard at the upper left sternal border,” said Dr. O’Gara. Since stroke volume and heart rate both also increase through pregnancy, cardiac output goes up as well.
“Importantly, systemic vascular resistance is reduced throughout pregnancy,” said Dr. O’Gara. Consequently, “regurgitant heart valve problems are generally much better tolerated than stenotic lesions in pregnancy. That’s physiologic principle number one.”
In labor, abrupt hemodynamic changes include increases in cardiac output, heart rate, blood pressure, and venous return. “Labor and delivery are very stressful hemodynamic times for women,” said Dr. O’Gara.
In the immediate postpartum period, uterine contraction results in a return of a significant amount of blood to the maternal circulation. This effectively creates an autotransfusion, with resulting increased preload and cardiac output. The inferior vena cava is also freed from the pressure of a gravid uterus, increasing venous return further. Finally, there’s also a marked increase in systemic vascular resistance.
Aside from the risk of adverse cardiac events, other adverse outcomes for women can include an increased risk of premature rupture of membranes and postpartum hemorrhage. For the neonate, preterm birth and respiratory distress are more likely. Newborns are more likely to be small for gestational age, to suffer intraventricular hemorrhage, and to die. Depending on the parental genetic status, the infant may be at risk of congenital heart disease as well.
Neonatal risk may also be increased, said Dr. O’Gara. Some maternal conditions that can increase risk for the infant include a baseline New York Heart Association (NYHA) class of greater than II or having cyanosis; having a left heart obstruction; being a smoker; having a multiple gestation; having a mechanical heart valve; and taking an oral anticoagulant.
Ideally, a full discussion would include a genetic referral if indicated, as well as coordination with a gynecologist or primary care provider to provide contraception and to assist with planning for and optimizing outcomes of a pregnancy.
The American College of Cardiology and the American Heart Association have issued guidelines that include a class I recommendation regarding valve intervention before pregnancy for symptomatic patients with severe AS (those with aortic velocity of at least 4.0 m/sec, or mean pressure gradient greater than 41 mm Hg; stage D). For patients who meet the same hemodynamic criteria for severe AS but who are asymptomatic (stage C), the guidelines have a class IIa recommendation that pre-pregnancy valve intervention is “reasonable.” These recommendations have level C evidence supporting them.
However, another class IIa recommendation for patients with severe AS who are already pregnant advises valve intervention only in the case of hemodynamic deterioration, or the development of NYHA class III to IV heart failure symptoms. This is backed by grade B evidence, according to the associations.
For aortic regurgitation (AR), a level I recommendation advises valve repair or replacement before pregnancy if patients are symptomatic and have severe (stage D) regurgitation. Pregnant patients with severe regurgitation should only be considered for a valve operation if they have refractory NYHA class IV heart failure symptoms. These recommendations have level C evidence supporting them.
Since AR is better tolerated in pregnancy than AS, the nature of the valve disease is one of many factors to consider when deciding whether to perform intervention before the patient becomes pregnant. Plans for future pregnancy may also affect the choice of prosthesis, as anticoagulation management during pregnancy can be extremely tricky.
The recommendations overall make clear that, based on available evidence, “there should be a high threshold for intervention during pregnancy,” said Dr. O’Gara. And no one should go it alone when taking care of these complicated patients. “Care of pregnant women with heart disease requires coordination with a multidisciplinary team,” he said.
Dr. O’Gara reported no relevant disclosures.
[email protected]
On Twitter @karioakes
CHICAGO – Pregnancy-associated hemodynamic and physiologic changes can challenge hearts with diseased aortic valves. Understanding pregnancy’s toll on the body can help physicians take better care of pregnant women with aortic stenosis or aortic regurgitation, said Patrick T. O’Gara, MD. “This is a relatively infrequent condition, and it causes all of us a great deal of apprehension,” he said.
Dr. O’Gara, director of clinical cardiology at Brigham and Women’s Hospital, Boston, walked attendees through current recommendations for caring for pregnant women with aortic valve disease in a presentation at the annual Heart Valve Summit.
When talking to women with aortic valve disease, it’s important to let them know that a pregnancy during which they experience an adverse maternal cardiac event appears to increase their risk for later events as well, said Dr. O’Gara. One study of pregnancy in women with aortic valve disease, said Dr. O’Gara, found that the risk of later events for women who had had a cardiac event in pregnancy was 27% plus or minus 9 percentage points in the 5 years following pregnancy, while the risk was just 15% plus or minus 3 percentage points for women whose pregnancies were not complicated by cardiac adverse events (P = .02) (Heart. 2010 Oct;96(20):1656-61).
The World Health Organization classification of pregnancy risk, said Dr. O’Gara, provides some guidance. Patients who are WHO class III are considered to be high risk; pregnancy in these individuals calls for counseling and a multidisciplinary care team. Patients who fall into this class are those with mechanical heart valves, those with Marfan syndrome and aortic involvement with a valve diameter of 40-45 mm, and those with bicuspid aortic valve disease with a valve diameter of 45-50 mm.
WHO class IV patients, according to the guidelines, are at prohibitive risk. These patients should consider terminating a pregnancy if one occurs. Conditions that place women into WHO class IV include symptomatic severe aortic stenosis (AS), severe left ventricular dysfunction with an ejection fraction less than 40%, and severe coarctation of the aorta. Women with Marfan syndrome with aortic valve diameters greater than 45 mm and women with bicuspid aortic valves and a diameter over 50 mm also fall into this category of prohibitive risk.
If a physician is lucky enough to have a pre-conception relationship with a patient, then a host of considerations can come into play. In addition to cardiac risk stratification, obstetric and intrapartum risk to the mother as well as neonatal risk should be considered. Some factors to take into account are maternal life expectancy and potential long-term complications to the mother from pregnancy and childbirth.
Plasma volume increases rapidly through the first trimester, plateauing about halfway through pregnancy. With this normal dilutional anemia, “Most normal pregnancies are accompanied by a grade II systolic murmur, best heard at the upper left sternal border,” said Dr. O’Gara. Since stroke volume and heart rate both also increase through pregnancy, cardiac output goes up as well.
“Importantly, systemic vascular resistance is reduced throughout pregnancy,” said Dr. O’Gara. Consequently, “regurgitant heart valve problems are generally much better tolerated than stenotic lesions in pregnancy. That’s physiologic principle number one.”
In labor, abrupt hemodynamic changes include increases in cardiac output, heart rate, blood pressure, and venous return. “Labor and delivery are very stressful hemodynamic times for women,” said Dr. O’Gara.
In the immediate postpartum period, uterine contraction results in a return of a significant amount of blood to the maternal circulation. This effectively creates an autotransfusion, with resulting increased preload and cardiac output. The inferior vena cava is also freed from the pressure of a gravid uterus, increasing venous return further. Finally, there’s also a marked increase in systemic vascular resistance.
Aside from the risk of adverse cardiac events, other adverse outcomes for women can include an increased risk of premature rupture of membranes and postpartum hemorrhage. For the neonate, preterm birth and respiratory distress are more likely. Newborns are more likely to be small for gestational age, to suffer intraventricular hemorrhage, and to die. Depending on the parental genetic status, the infant may be at risk of congenital heart disease as well.
Neonatal risk may also be increased, said Dr. O’Gara. Some maternal conditions that can increase risk for the infant include a baseline New York Heart Association (NYHA) class of greater than II or having cyanosis; having a left heart obstruction; being a smoker; having a multiple gestation; having a mechanical heart valve; and taking an oral anticoagulant.
Ideally, a full discussion would include a genetic referral if indicated, as well as coordination with a gynecologist or primary care provider to provide contraception and to assist with planning for and optimizing outcomes of a pregnancy.
The American College of Cardiology and the American Heart Association have issued guidelines that include a class I recommendation regarding valve intervention before pregnancy for symptomatic patients with severe AS (those with aortic velocity of at least 4.0 m/sec, or mean pressure gradient greater than 41 mm Hg; stage D). For patients who meet the same hemodynamic criteria for severe AS but who are asymptomatic (stage C), the guidelines have a class IIa recommendation that pre-pregnancy valve intervention is “reasonable.” These recommendations have level C evidence supporting them.
However, another class IIa recommendation for patients with severe AS who are already pregnant advises valve intervention only in the case of hemodynamic deterioration, or the development of NYHA class III to IV heart failure symptoms. This is backed by grade B evidence, according to the associations.
For aortic regurgitation (AR), a level I recommendation advises valve repair or replacement before pregnancy if patients are symptomatic and have severe (stage D) regurgitation. Pregnant patients with severe regurgitation should only be considered for a valve operation if they have refractory NYHA class IV heart failure symptoms. These recommendations have level C evidence supporting them.
Since AR is better tolerated in pregnancy than AS, the nature of the valve disease is one of many factors to consider when deciding whether to perform intervention before the patient becomes pregnant. Plans for future pregnancy may also affect the choice of prosthesis, as anticoagulation management during pregnancy can be extremely tricky.
The recommendations overall make clear that, based on available evidence, “there should be a high threshold for intervention during pregnancy,” said Dr. O’Gara. And no one should go it alone when taking care of these complicated patients. “Care of pregnant women with heart disease requires coordination with a multidisciplinary team,” he said.
Dr. O’Gara reported no relevant disclosures.
[email protected]
On Twitter @karioakes
CHICAGO – Pregnancy-associated hemodynamic and physiologic changes can challenge hearts with diseased aortic valves. Understanding pregnancy’s toll on the body can help physicians take better care of pregnant women with aortic stenosis or aortic regurgitation, said Patrick T. O’Gara, MD. “This is a relatively infrequent condition, and it causes all of us a great deal of apprehension,” he said.
Dr. O’Gara, director of clinical cardiology at Brigham and Women’s Hospital, Boston, walked attendees through current recommendations for caring for pregnant women with aortic valve disease in a presentation at the annual Heart Valve Summit.
When talking to women with aortic valve disease, it’s important to let them know that a pregnancy during which they experience an adverse maternal cardiac event appears to increase their risk for later events as well, said Dr. O’Gara. One study of pregnancy in women with aortic valve disease, said Dr. O’Gara, found that the risk of later events for women who had had a cardiac event in pregnancy was 27% plus or minus 9 percentage points in the 5 years following pregnancy, while the risk was just 15% plus or minus 3 percentage points for women whose pregnancies were not complicated by cardiac adverse events (P = .02) (Heart. 2010 Oct;96(20):1656-61).
The World Health Organization classification of pregnancy risk, said Dr. O’Gara, provides some guidance. Patients who are WHO class III are considered to be high risk; pregnancy in these individuals calls for counseling and a multidisciplinary care team. Patients who fall into this class are those with mechanical heart valves, those with Marfan syndrome and aortic involvement with a valve diameter of 40-45 mm, and those with bicuspid aortic valve disease with a valve diameter of 45-50 mm.
WHO class IV patients, according to the guidelines, are at prohibitive risk. These patients should consider terminating a pregnancy if one occurs. Conditions that place women into WHO class IV include symptomatic severe aortic stenosis (AS), severe left ventricular dysfunction with an ejection fraction less than 40%, and severe coarctation of the aorta. Women with Marfan syndrome with aortic valve diameters greater than 45 mm and women with bicuspid aortic valves and a diameter over 50 mm also fall into this category of prohibitive risk.
If a physician is lucky enough to have a pre-conception relationship with a patient, then a host of considerations can come into play. In addition to cardiac risk stratification, obstetric and intrapartum risk to the mother as well as neonatal risk should be considered. Some factors to take into account are maternal life expectancy and potential long-term complications to the mother from pregnancy and childbirth.
Plasma volume increases rapidly through the first trimester, plateauing about halfway through pregnancy. With this normal dilutional anemia, “Most normal pregnancies are accompanied by a grade II systolic murmur, best heard at the upper left sternal border,” said Dr. O’Gara. Since stroke volume and heart rate both also increase through pregnancy, cardiac output goes up as well.
“Importantly, systemic vascular resistance is reduced throughout pregnancy,” said Dr. O’Gara. Consequently, “regurgitant heart valve problems are generally much better tolerated than stenotic lesions in pregnancy. That’s physiologic principle number one.”
In labor, abrupt hemodynamic changes include increases in cardiac output, heart rate, blood pressure, and venous return. “Labor and delivery are very stressful hemodynamic times for women,” said Dr. O’Gara.
In the immediate postpartum period, uterine contraction results in a return of a significant amount of blood to the maternal circulation. This effectively creates an autotransfusion, with resulting increased preload and cardiac output. The inferior vena cava is also freed from the pressure of a gravid uterus, increasing venous return further. Finally, there’s also a marked increase in systemic vascular resistance.
Aside from the risk of adverse cardiac events, other adverse outcomes for women can include an increased risk of premature rupture of membranes and postpartum hemorrhage. For the neonate, preterm birth and respiratory distress are more likely. Newborns are more likely to be small for gestational age, to suffer intraventricular hemorrhage, and to die. Depending on the parental genetic status, the infant may be at risk of congenital heart disease as well.
Neonatal risk may also be increased, said Dr. O’Gara. Some maternal conditions that can increase risk for the infant include a baseline New York Heart Association (NYHA) class of greater than II or having cyanosis; having a left heart obstruction; being a smoker; having a multiple gestation; having a mechanical heart valve; and taking an oral anticoagulant.
Ideally, a full discussion would include a genetic referral if indicated, as well as coordination with a gynecologist or primary care provider to provide contraception and to assist with planning for and optimizing outcomes of a pregnancy.
The American College of Cardiology and the American Heart Association have issued guidelines that include a class I recommendation regarding valve intervention before pregnancy for symptomatic patients with severe AS (those with aortic velocity of at least 4.0 m/sec, or mean pressure gradient greater than 41 mm Hg; stage D). For patients who meet the same hemodynamic criteria for severe AS but who are asymptomatic (stage C), the guidelines have a class IIa recommendation that pre-pregnancy valve intervention is “reasonable.” These recommendations have level C evidence supporting them.
However, another class IIa recommendation for patients with severe AS who are already pregnant advises valve intervention only in the case of hemodynamic deterioration, or the development of NYHA class III to IV heart failure symptoms. This is backed by grade B evidence, according to the associations.
For aortic regurgitation (AR), a level I recommendation advises valve repair or replacement before pregnancy if patients are symptomatic and have severe (stage D) regurgitation. Pregnant patients with severe regurgitation should only be considered for a valve operation if they have refractory NYHA class IV heart failure symptoms. These recommendations have level C evidence supporting them.
Since AR is better tolerated in pregnancy than AS, the nature of the valve disease is one of many factors to consider when deciding whether to perform intervention before the patient becomes pregnant. Plans for future pregnancy may also affect the choice of prosthesis, as anticoagulation management during pregnancy can be extremely tricky.
The recommendations overall make clear that, based on available evidence, “there should be a high threshold for intervention during pregnancy,” said Dr. O’Gara. And no one should go it alone when taking care of these complicated patients. “Care of pregnant women with heart disease requires coordination with a multidisciplinary team,” he said.
Dr. O’Gara reported no relevant disclosures.
[email protected]
On Twitter @karioakes
EXPERT ANALYSIS FROM THE HEART VALVE SUMMIT
ASTRO guidelines lower age thresholds for APBI
The American Society for Radiation Oncology has issued new guidelines recommending accelerated partial breast irradiation brachytherapy (APBI) as an alternative to whole breast irradiation (WBI) after surgery in early-stage breast cancer patients, and lowering the age range of patients considered suitable for the procedure to people 50 and older, from 60.
With APBI, localized radiation is delivered to the region around the excised tissue, reducing treatment time and sparing healthy tissue. APBI may also be considered for patients 40 and older, according to ASTRO, if they meet all of the pathologic criteria for suitability listed in the guidelines for patients 50 and above.
The guidelines represent the first ASTRO update on APBI since 2009. In addition to expanding the age range for APBI treatment, the guidelines add low-risk ductal carcinoma in situ as an indication. The guidelines also address intraoperative radiation therapy, or IORT, in which patients receive low-energy photon or electron radiation during surgery (Pract Rad Oncol. 2016 Nov. 17 doi: 10.1016/j.prro.2016.09.007).
While IORT is suitable for patients with invasive cancer eligible for APBI, the guidelines say, patients considering this option should be counseled about the risk of recurrence compared with standard treatment, and, with photon IORT, about potential toxicity risk requiring follow-up. Though more than 40 studies were considered by the ASTRO committee, including large randomized trials comparing APBI with WBI, the new recommendations represent “more of a tweak than a revolution,” said Jay Harris, MD, of Brigham and Women’s Hospital and Dana-Farber Cancer Institute, Boston, one of the guideline authors.
Dr. Harris noted in an interview that two important randomized controlled trials comparing APBI and WBI are still underway, with full follow-up results expected in 2-3 years, after which more definitive recommendations can be made. For the intraoperative radiation advice contained in the guidelines, “we had evidence from two trials looking at different approaches,” Dr. Harris said. “One has long-term data using an electron beam in the operating room – this group showed that that approach seems reasonable in patients that we at ASTRO considered suitable in general for APBI. The other approach is low-dose photon radiation, for which we have only short-term follow-up, making us more hesitant to endorse it.” As for the new recommendation sanctioning APBI for ductal carcinoma, “There’s a lot of variation [in protocols] across the country, compared with invasive cancer,” Dr. Harris said. “We’re kind of all over the map with DCIS. This guideline presents another option.”
The guidelines were sponsored by ASTRO; two authors disclosed financial relationships with firms that make radiologic technology.
The American Society for Radiation Oncology has issued new guidelines recommending accelerated partial breast irradiation brachytherapy (APBI) as an alternative to whole breast irradiation (WBI) after surgery in early-stage breast cancer patients, and lowering the age range of patients considered suitable for the procedure to people 50 and older, from 60.
With APBI, localized radiation is delivered to the region around the excised tissue, reducing treatment time and sparing healthy tissue. APBI may also be considered for patients 40 and older, according to ASTRO, if they meet all of the pathologic criteria for suitability listed in the guidelines for patients 50 and above.
The guidelines represent the first ASTRO update on APBI since 2009. In addition to expanding the age range for APBI treatment, the guidelines add low-risk ductal carcinoma in situ as an indication. The guidelines also address intraoperative radiation therapy, or IORT, in which patients receive low-energy photon or electron radiation during surgery (Pract Rad Oncol. 2016 Nov. 17 doi: 10.1016/j.prro.2016.09.007).
While IORT is suitable for patients with invasive cancer eligible for APBI, the guidelines say, patients considering this option should be counseled about the risk of recurrence compared with standard treatment, and, with photon IORT, about potential toxicity risk requiring follow-up. Though more than 40 studies were considered by the ASTRO committee, including large randomized trials comparing APBI with WBI, the new recommendations represent “more of a tweak than a revolution,” said Jay Harris, MD, of Brigham and Women’s Hospital and Dana-Farber Cancer Institute, Boston, one of the guideline authors.
Dr. Harris noted in an interview that two important randomized controlled trials comparing APBI and WBI are still underway, with full follow-up results expected in 2-3 years, after which more definitive recommendations can be made. For the intraoperative radiation advice contained in the guidelines, “we had evidence from two trials looking at different approaches,” Dr. Harris said. “One has long-term data using an electron beam in the operating room – this group showed that that approach seems reasonable in patients that we at ASTRO considered suitable in general for APBI. The other approach is low-dose photon radiation, for which we have only short-term follow-up, making us more hesitant to endorse it.” As for the new recommendation sanctioning APBI for ductal carcinoma, “There’s a lot of variation [in protocols] across the country, compared with invasive cancer,” Dr. Harris said. “We’re kind of all over the map with DCIS. This guideline presents another option.”
The guidelines were sponsored by ASTRO; two authors disclosed financial relationships with firms that make radiologic technology.
The American Society for Radiation Oncology has issued new guidelines recommending accelerated partial breast irradiation brachytherapy (APBI) as an alternative to whole breast irradiation (WBI) after surgery in early-stage breast cancer patients, and lowering the age range of patients considered suitable for the procedure to people 50 and older, from 60.
With APBI, localized radiation is delivered to the region around the excised tissue, reducing treatment time and sparing healthy tissue. APBI may also be considered for patients 40 and older, according to ASTRO, if they meet all of the pathologic criteria for suitability listed in the guidelines for patients 50 and above.
The guidelines represent the first ASTRO update on APBI since 2009. In addition to expanding the age range for APBI treatment, the guidelines add low-risk ductal carcinoma in situ as an indication. The guidelines also address intraoperative radiation therapy, or IORT, in which patients receive low-energy photon or electron radiation during surgery (Pract Rad Oncol. 2016 Nov. 17 doi: 10.1016/j.prro.2016.09.007).
While IORT is suitable for patients with invasive cancer eligible for APBI, the guidelines say, patients considering this option should be counseled about the risk of recurrence compared with standard treatment, and, with photon IORT, about potential toxicity risk requiring follow-up. Though more than 40 studies were considered by the ASTRO committee, including large randomized trials comparing APBI with WBI, the new recommendations represent “more of a tweak than a revolution,” said Jay Harris, MD, of Brigham and Women’s Hospital and Dana-Farber Cancer Institute, Boston, one of the guideline authors.
Dr. Harris noted in an interview that two important randomized controlled trials comparing APBI and WBI are still underway, with full follow-up results expected in 2-3 years, after which more definitive recommendations can be made. For the intraoperative radiation advice contained in the guidelines, “we had evidence from two trials looking at different approaches,” Dr. Harris said. “One has long-term data using an electron beam in the operating room – this group showed that that approach seems reasonable in patients that we at ASTRO considered suitable in general for APBI. The other approach is low-dose photon radiation, for which we have only short-term follow-up, making us more hesitant to endorse it.” As for the new recommendation sanctioning APBI for ductal carcinoma, “There’s a lot of variation [in protocols] across the country, compared with invasive cancer,” Dr. Harris said. “We’re kind of all over the map with DCIS. This guideline presents another option.”
The guidelines were sponsored by ASTRO; two authors disclosed financial relationships with firms that make radiologic technology.
FROM PRACTICAL RADIATION ONCOLOGY
Newly available tissue containment system brings back power morcellation to advanced MIG surgeons
In the 11 studies that have examined the incidence of leiomyosarcoma (LMS) since the 2014 communications by the US Food and Drug Administration (FDA),1 Dr. Matthew Siedhoff and colleagues found that the cumulative LMS incidence in 318,006 women was 0.0017%, or approximately 1 in 600. This is according to data Dr. Seidhoff presented November 16, 2016, at the 45th annual AAGL Global Congress on MIGS.2 This reported risk is smaller than the 1 in 350 cited by the FDA in its 2014 notice.1 Dr. Seidhoff concluded that, particularly in women aged younger than 50 years, minimally invasive hysterectomy remains a safe option for the informed patient to consider.
Regardless of the incidence of unsuspected LMS found in the studies published since 2014, what have been the practice changes among gynecologic surgeons as a result of the FDA’s 2014 actions? Kerac N. Falk, MD, explored this question with his colleagues at the Icahn School of Medicine in New York, New York. He presented these findings to AAGL congress attendees on November 16 in Orlando, Florida.3 Notably, of 197 responders to a survey sent to members of the Society of Gynecologic Oncologists, 12.5% reported decreasing their use of power morcellation. A full 38.8% reported discontinuing altogether the use of a power morcellator.
One in 5 (20%) of gyn oncologists previously using power morcellation reported switching to laparotomy. Importantly, the drive for the switch was “driven by media, patient request, and the FDA rather than physician choice,” Falk said.
What if physicians, and patients, have another choice?
Here at the AAGL meeting, Olympus announced the FDA clearance, marketing, and initial training on its contained tissue extraction system—the PneumoLiner containment device and its accompanying laparoscopic PK Morcellator (FIGURE).

Both tools, FDA cleared in April and October 2016, respectively, provide low-risk, appropriate women with “an improved safety device,” said Jubilee Brown, MD, AAGL representative on power morcellation to the FDA and Associate Director of Gynecologic Oncology at the Levine Cancer Institute of the Carolinas HealthCare System in Charlotte, North Carolina.
“We have found at our institution that we have had to do more opens and minilaps on patients without the option for power morcellation, and this new device offers a way for us not to have to do that. Minimally invasive surgery stays truly minimally invasive surgery,” said Dr. Brown.
“Although I have a handful of patients who have chosen open surgery over minimally invasive surgery when MIS was appropriate, by and large most patients prefer the minimally invasive approach to surgery—especially when they learn that they have reduced risk for complications, blood loss, and pain; will be back to normal life faster; and will have less cosmetic incisions,” said Dr. Brown. “We all have tried workarounds, but for low-risk, appropriate patients under FDA guidelines, this new device by Olympus brings us back to minimally invasive options, and that is a good thing.”
How does the Olympus containment system work?
The PneumoLiner is the first containment device to receive FDA market clearance that is designed for use with certain laparoscopic morcellators to isolate uterine tissue that is not suspected to contain cancer.4
The containment bag and morcellator are not indicated for use in women with tissue that is known or suspected to contain malignancy; and should not be used for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or candidates for en bloc tissue removal vaginally or via mini-laparotomy.4
When insufflated, the PneumoLiner bag allows for space and surgeon visibility throughout the power morcellation procedure while maintaining a barrier to the escape of fluids, cells, and tissue fragments. The bag creates a barrier between the targeted tissue and nontargeted abdominal contents, minimizing the risk of inadvertent damage to adjacent structures, says Olympus.4 See this video, which demonstrates the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Filtration, immersion, and stress testing were conducted to demonstrate the PneumoLiner as impermeable to human cells, that it maintains its integrity following morcellation, and that its mechanical strength withholds forces in excess of those demonstrated during actual use.5 To support FDA 510 clearance of the PK Morcellator, Olympus performed additional testing with both devices used together, demonstrating compatibility.4
Surgeon training on new device use is rigid, comprehensive, and not to be overlooked
“This is one of the rare times in my career when, right out of the gate, we have a very rigid and comprehensive way of educating and training physicians on the proper utilization of a new technology (avoiding the cart-before-the-horse phenomenon, in which a clinician is given the tools without the proper education),” said AAGL immediate past president Arnold Advincula, MD, “and it is important to underscore that.” Dr. Advincula is the Levine Family Professor, Vice-Chair of Women’s Health, and Chief of Gynecology at Sloane Women’s Hospital, Columbia University Medical Center/New York-Presbyterian Hospital, New York, New York.
Training plans
Instead of its sales force, Olympus is having surgeons train other surgeons. Clinical Education Specialists, a small, select group of individuals within the company, also will be able to train. The required training follows a rigid protocol that was validated and submitted to the FDA as part of the approval process, said Jerilyn Hitchings, Director of Procedure Marketing at Olympus. After training up to 40 surgeons in the past 3 weeks, Olympus expects to train another 100 at AAGL.
“We have strict criteria for training, including that they are advanced laparoscopists,” fulfilling a minimum number of surgeries within a 90-day period, said Hitchings.
The 1-hour training requires surgeons to perform a 4-step protocol and demonstrate unaided proficiency at training conclusion. Olympus will not sell its product to a facility until an advanced surgeon has been trained there, according to Hitchings. And many physicians are approaching their institutions inquiring about training now, she reports.
Applications for training will be submitted to the Olympus Professional Education Team for approval. “We want this to go well. We know that there are many physicians who are hoping that this becomes a good reality, and we want to make sure that it is done properly. The training process adheres to that agenda.”
Having the technology is step 1
OBG Management Board of Editors member Dr. Advincula struck an optimistic tone in his June 2016 Guest Editorial for the journal,6 indicating his belief that the “tissue morcellation pendulum,” which has swung toward non−minimally invasive approaches since 2014, can change direction. At the Olympus containment system official introduction event at AAGL, he expressed the same optimism:
“We now have technology that has the promise of being able to deliver to women a safe way to undergo tissue extraction, to undergo a minimally invasive surgical procedure. …When you combine innovation and education together, you ultimately are going to advance MIS worldwide. With all the things going on around the world today, I think it is important that women be able to have a choice, an autonomous choice with her physician. Having the technology that allows physicians to extract tissue safely, to give women the option of undergoing a minimally invasive surgery, is critically important. I look forward to seeing how we can continue to advance surgery. Partnership with clinicians and with industry, such as Olympus, is going to be key to the success of how we advance women’s health care in general.”
What do AAGL attendees have to say about it?
“It’s a good thing for the minimally invasive market,” said John B. Gebhart, MD, MS, vaginal hysterectomy representative at the star-studded Operating with the Stars event on Thursday, November 17, and Professor of Obstetrics and Gynecology at the Mayo Clinic in Rochester, Minnesota.
May Thomassee, MD, who practices in Lafayette, Louisiana, said that, for the past 3 years, she has been performing extracorporeal morcellation at her institution. “I think the new containment bag and morcellator devices that are attempting to be safer are a very good thing; however, my concern of introducing this new technology, such as bags, is that it may increase the cost within our health care system. We have had great success, and patients feel that they have options when we offer them—after informed consent and appropriate preoperative workup—an abdominal, vaginal, or extracorporeal morcellation approach.”
As a developer and proponent of the Extracorporeal Tissue Extraction (ExCITE) technique, Mireille Truong, MD, who demonstrated the ExCITE surgical approach with Dr. Advincula as part of the Research and Science Plenary here at AAGL, said, “I think the PneumoLiner is a great example of creativity and innovation. It’s good that we now have an FDA-approved device to offer and counsel patients as one of many options.” She added that, overall, the morcellation controversy has been “a positive experience. We have learned better as a community about how to approach new technology.”
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Updated November 24, 2014. Accessed November 17, 2016.
- Siedhoff MT, Doll KM, Rutstein SE, et al. Laparoscopic hysterectomy with morcellation versus abdominal hysterectomy for presumed uterine leiomyomata: an updated decision analysis. J Minim Invasiv Gynecol. 2016;23(7):S4-S5.
- Mandelberger AH, Mathews S, Chuang L. Practice changes in power morcellation among gynecologic-oncologists since 2014. J Minim Invasiv Gynecol. 2016;23(7):S3.
Olympus introduces first-of-its-kind contained tissue extraction system, restoring healthcare option for gynecologists and women [press release]. November 16, 2016. Olympus website. http://www.olympusamerica.com/corporate/corp_presscenter_headline.asp?pressNo=2079. Accessed November 16, 2016.
- FDA allows marketing of first-of-kind tissue containment system for use with certain laparoscopic power morcellators in select patients. FDA website. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm494650.htm. Updated April 7, 2016. Accessed November 16, 2016.
- Advincula AP. Tissue extraction: can the pendulum change direction? OBG Manag. 2016;28(6):8, 10, 12.
In the 11 studies that have examined the incidence of leiomyosarcoma (LMS) since the 2014 communications by the US Food and Drug Administration (FDA),1 Dr. Matthew Siedhoff and colleagues found that the cumulative LMS incidence in 318,006 women was 0.0017%, or approximately 1 in 600. This is according to data Dr. Seidhoff presented November 16, 2016, at the 45th annual AAGL Global Congress on MIGS.2 This reported risk is smaller than the 1 in 350 cited by the FDA in its 2014 notice.1 Dr. Seidhoff concluded that, particularly in women aged younger than 50 years, minimally invasive hysterectomy remains a safe option for the informed patient to consider.
Regardless of the incidence of unsuspected LMS found in the studies published since 2014, what have been the practice changes among gynecologic surgeons as a result of the FDA’s 2014 actions? Kerac N. Falk, MD, explored this question with his colleagues at the Icahn School of Medicine in New York, New York. He presented these findings to AAGL congress attendees on November 16 in Orlando, Florida.3 Notably, of 197 responders to a survey sent to members of the Society of Gynecologic Oncologists, 12.5% reported decreasing their use of power morcellation. A full 38.8% reported discontinuing altogether the use of a power morcellator.
One in 5 (20%) of gyn oncologists previously using power morcellation reported switching to laparotomy. Importantly, the drive for the switch was “driven by media, patient request, and the FDA rather than physician choice,” Falk said.
What if physicians, and patients, have another choice?
Here at the AAGL meeting, Olympus announced the FDA clearance, marketing, and initial training on its contained tissue extraction system—the PneumoLiner containment device and its accompanying laparoscopic PK Morcellator (FIGURE).
Both tools, FDA cleared in April and October 2016, respectively, provide low-risk, appropriate women with “an improved safety device,” said Jubilee Brown, MD, AAGL representative on power morcellation to the FDA and Associate Director of Gynecologic Oncology at the Levine Cancer Institute of the Carolinas HealthCare System in Charlotte, North Carolina.
“We have found at our institution that we have had to do more opens and minilaps on patients without the option for power morcellation, and this new device offers a way for us not to have to do that. Minimally invasive surgery stays truly minimally invasive surgery,” said Dr. Brown.
“Although I have a handful of patients who have chosen open surgery over minimally invasive surgery when MIS was appropriate, by and large most patients prefer the minimally invasive approach to surgery—especially when they learn that they have reduced risk for complications, blood loss, and pain; will be back to normal life faster; and will have less cosmetic incisions,” said Dr. Brown. “We all have tried workarounds, but for low-risk, appropriate patients under FDA guidelines, this new device by Olympus brings us back to minimally invasive options, and that is a good thing.”
How does the Olympus containment system work?
The PneumoLiner is the first containment device to receive FDA market clearance that is designed for use with certain laparoscopic morcellators to isolate uterine tissue that is not suspected to contain cancer.4
The containment bag and morcellator are not indicated for use in women with tissue that is known or suspected to contain malignancy; and should not be used for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or candidates for en bloc tissue removal vaginally or via mini-laparotomy.4
When insufflated, the PneumoLiner bag allows for space and surgeon visibility throughout the power morcellation procedure while maintaining a barrier to the escape of fluids, cells, and tissue fragments. The bag creates a barrier between the targeted tissue and nontargeted abdominal contents, minimizing the risk of inadvertent damage to adjacent structures, says Olympus.4 See this video, which demonstrates the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Filtration, immersion, and stress testing were conducted to demonstrate the PneumoLiner as impermeable to human cells, that it maintains its integrity following morcellation, and that its mechanical strength withholds forces in excess of those demonstrated during actual use.5 To support FDA 510 clearance of the PK Morcellator, Olympus performed additional testing with both devices used together, demonstrating compatibility.4
Surgeon training on new device use is rigid, comprehensive, and not to be overlooked
“This is one of the rare times in my career when, right out of the gate, we have a very rigid and comprehensive way of educating and training physicians on the proper utilization of a new technology (avoiding the cart-before-the-horse phenomenon, in which a clinician is given the tools without the proper education),” said AAGL immediate past president Arnold Advincula, MD, “and it is important to underscore that.” Dr. Advincula is the Levine Family Professor, Vice-Chair of Women’s Health, and Chief of Gynecology at Sloane Women’s Hospital, Columbia University Medical Center/New York-Presbyterian Hospital, New York, New York.
Training plans
Instead of its sales force, Olympus is having surgeons train other surgeons. Clinical Education Specialists, a small, select group of individuals within the company, also will be able to train. The required training follows a rigid protocol that was validated and submitted to the FDA as part of the approval process, said Jerilyn Hitchings, Director of Procedure Marketing at Olympus. After training up to 40 surgeons in the past 3 weeks, Olympus expects to train another 100 at AAGL.
“We have strict criteria for training, including that they are advanced laparoscopists,” fulfilling a minimum number of surgeries within a 90-day period, said Hitchings.
The 1-hour training requires surgeons to perform a 4-step protocol and demonstrate unaided proficiency at training conclusion. Olympus will not sell its product to a facility until an advanced surgeon has been trained there, according to Hitchings. And many physicians are approaching their institutions inquiring about training now, she reports.
Applications for training will be submitted to the Olympus Professional Education Team for approval. “We want this to go well. We know that there are many physicians who are hoping that this becomes a good reality, and we want to make sure that it is done properly. The training process adheres to that agenda.”
Having the technology is step 1
OBG Management Board of Editors member Dr. Advincula struck an optimistic tone in his June 2016 Guest Editorial for the journal,6 indicating his belief that the “tissue morcellation pendulum,” which has swung toward non−minimally invasive approaches since 2014, can change direction. At the Olympus containment system official introduction event at AAGL, he expressed the same optimism:
“We now have technology that has the promise of being able to deliver to women a safe way to undergo tissue extraction, to undergo a minimally invasive surgical procedure. …When you combine innovation and education together, you ultimately are going to advance MIS worldwide. With all the things going on around the world today, I think it is important that women be able to have a choice, an autonomous choice with her physician. Having the technology that allows physicians to extract tissue safely, to give women the option of undergoing a minimally invasive surgery, is critically important. I look forward to seeing how we can continue to advance surgery. Partnership with clinicians and with industry, such as Olympus, is going to be key to the success of how we advance women’s health care in general.”
What do AAGL attendees have to say about it?
“It’s a good thing for the minimally invasive market,” said John B. Gebhart, MD, MS, vaginal hysterectomy representative at the star-studded Operating with the Stars event on Thursday, November 17, and Professor of Obstetrics and Gynecology at the Mayo Clinic in Rochester, Minnesota.
May Thomassee, MD, who practices in Lafayette, Louisiana, said that, for the past 3 years, she has been performing extracorporeal morcellation at her institution. “I think the new containment bag and morcellator devices that are attempting to be safer are a very good thing; however, my concern of introducing this new technology, such as bags, is that it may increase the cost within our health care system. We have had great success, and patients feel that they have options when we offer them—after informed consent and appropriate preoperative workup—an abdominal, vaginal, or extracorporeal morcellation approach.”
As a developer and proponent of the Extracorporeal Tissue Extraction (ExCITE) technique, Mireille Truong, MD, who demonstrated the ExCITE surgical approach with Dr. Advincula as part of the Research and Science Plenary here at AAGL, said, “I think the PneumoLiner is a great example of creativity and innovation. It’s good that we now have an FDA-approved device to offer and counsel patients as one of many options.” She added that, overall, the morcellation controversy has been “a positive experience. We have learned better as a community about how to approach new technology.”
In the 11 studies that have examined the incidence of leiomyosarcoma (LMS) since the 2014 communications by the US Food and Drug Administration (FDA),1 Dr. Matthew Siedhoff and colleagues found that the cumulative LMS incidence in 318,006 women was 0.0017%, or approximately 1 in 600. This is according to data Dr. Seidhoff presented November 16, 2016, at the 45th annual AAGL Global Congress on MIGS.2 This reported risk is smaller than the 1 in 350 cited by the FDA in its 2014 notice.1 Dr. Seidhoff concluded that, particularly in women aged younger than 50 years, minimally invasive hysterectomy remains a safe option for the informed patient to consider.
Regardless of the incidence of unsuspected LMS found in the studies published since 2014, what have been the practice changes among gynecologic surgeons as a result of the FDA’s 2014 actions? Kerac N. Falk, MD, explored this question with his colleagues at the Icahn School of Medicine in New York, New York. He presented these findings to AAGL congress attendees on November 16 in Orlando, Florida.3 Notably, of 197 responders to a survey sent to members of the Society of Gynecologic Oncologists, 12.5% reported decreasing their use of power morcellation. A full 38.8% reported discontinuing altogether the use of a power morcellator.
One in 5 (20%) of gyn oncologists previously using power morcellation reported switching to laparotomy. Importantly, the drive for the switch was “driven by media, patient request, and the FDA rather than physician choice,” Falk said.
What if physicians, and patients, have another choice?
Here at the AAGL meeting, Olympus announced the FDA clearance, marketing, and initial training on its contained tissue extraction system—the PneumoLiner containment device and its accompanying laparoscopic PK Morcellator (FIGURE).
Both tools, FDA cleared in April and October 2016, respectively, provide low-risk, appropriate women with “an improved safety device,” said Jubilee Brown, MD, AAGL representative on power morcellation to the FDA and Associate Director of Gynecologic Oncology at the Levine Cancer Institute of the Carolinas HealthCare System in Charlotte, North Carolina.
“We have found at our institution that we have had to do more opens and minilaps on patients without the option for power morcellation, and this new device offers a way for us not to have to do that. Minimally invasive surgery stays truly minimally invasive surgery,” said Dr. Brown.
“Although I have a handful of patients who have chosen open surgery over minimally invasive surgery when MIS was appropriate, by and large most patients prefer the minimally invasive approach to surgery—especially when they learn that they have reduced risk for complications, blood loss, and pain; will be back to normal life faster; and will have less cosmetic incisions,” said Dr. Brown. “We all have tried workarounds, but for low-risk, appropriate patients under FDA guidelines, this new device by Olympus brings us back to minimally invasive options, and that is a good thing.”
How does the Olympus containment system work?
The PneumoLiner is the first containment device to receive FDA market clearance that is designed for use with certain laparoscopic morcellators to isolate uterine tissue that is not suspected to contain cancer.4
The containment bag and morcellator are not indicated for use in women with tissue that is known or suspected to contain malignancy; and should not be used for removal of uterine tissue containing suspected fibroids in patients who are peri- or post-menopausal, or candidates for en bloc tissue removal vaginally or via mini-laparotomy.4
When insufflated, the PneumoLiner bag allows for space and surgeon visibility throughout the power morcellation procedure while maintaining a barrier to the escape of fluids, cells, and tissue fragments. The bag creates a barrier between the targeted tissue and nontargeted abdominal contents, minimizing the risk of inadvertent damage to adjacent structures, says Olympus.4 See this video, which demonstrates the procedure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Filtration, immersion, and stress testing were conducted to demonstrate the PneumoLiner as impermeable to human cells, that it maintains its integrity following morcellation, and that its mechanical strength withholds forces in excess of those demonstrated during actual use.5 To support FDA 510 clearance of the PK Morcellator, Olympus performed additional testing with both devices used together, demonstrating compatibility.4
Surgeon training on new device use is rigid, comprehensive, and not to be overlooked
“This is one of the rare times in my career when, right out of the gate, we have a very rigid and comprehensive way of educating and training physicians on the proper utilization of a new technology (avoiding the cart-before-the-horse phenomenon, in which a clinician is given the tools without the proper education),” said AAGL immediate past president Arnold Advincula, MD, “and it is important to underscore that.” Dr. Advincula is the Levine Family Professor, Vice-Chair of Women’s Health, and Chief of Gynecology at Sloane Women’s Hospital, Columbia University Medical Center/New York-Presbyterian Hospital, New York, New York.
Training plans
Instead of its sales force, Olympus is having surgeons train other surgeons. Clinical Education Specialists, a small, select group of individuals within the company, also will be able to train. The required training follows a rigid protocol that was validated and submitted to the FDA as part of the approval process, said Jerilyn Hitchings, Director of Procedure Marketing at Olympus. After training up to 40 surgeons in the past 3 weeks, Olympus expects to train another 100 at AAGL.
“We have strict criteria for training, including that they are advanced laparoscopists,” fulfilling a minimum number of surgeries within a 90-day period, said Hitchings.
The 1-hour training requires surgeons to perform a 4-step protocol and demonstrate unaided proficiency at training conclusion. Olympus will not sell its product to a facility until an advanced surgeon has been trained there, according to Hitchings. And many physicians are approaching their institutions inquiring about training now, she reports.
Applications for training will be submitted to the Olympus Professional Education Team for approval. “We want this to go well. We know that there are many physicians who are hoping that this becomes a good reality, and we want to make sure that it is done properly. The training process adheres to that agenda.”
Having the technology is step 1
OBG Management Board of Editors member Dr. Advincula struck an optimistic tone in his June 2016 Guest Editorial for the journal,6 indicating his belief that the “tissue morcellation pendulum,” which has swung toward non−minimally invasive approaches since 2014, can change direction. At the Olympus containment system official introduction event at AAGL, he expressed the same optimism:
“We now have technology that has the promise of being able to deliver to women a safe way to undergo tissue extraction, to undergo a minimally invasive surgical procedure. …When you combine innovation and education together, you ultimately are going to advance MIS worldwide. With all the things going on around the world today, I think it is important that women be able to have a choice, an autonomous choice with her physician. Having the technology that allows physicians to extract tissue safely, to give women the option of undergoing a minimally invasive surgery, is critically important. I look forward to seeing how we can continue to advance surgery. Partnership with clinicians and with industry, such as Olympus, is going to be key to the success of how we advance women’s health care in general.”
What do AAGL attendees have to say about it?
“It’s a good thing for the minimally invasive market,” said John B. Gebhart, MD, MS, vaginal hysterectomy representative at the star-studded Operating with the Stars event on Thursday, November 17, and Professor of Obstetrics and Gynecology at the Mayo Clinic in Rochester, Minnesota.
May Thomassee, MD, who practices in Lafayette, Louisiana, said that, for the past 3 years, she has been performing extracorporeal morcellation at her institution. “I think the new containment bag and morcellator devices that are attempting to be safer are a very good thing; however, my concern of introducing this new technology, such as bags, is that it may increase the cost within our health care system. We have had great success, and patients feel that they have options when we offer them—after informed consent and appropriate preoperative workup—an abdominal, vaginal, or extracorporeal morcellation approach.”
As a developer and proponent of the Extracorporeal Tissue Extraction (ExCITE) technique, Mireille Truong, MD, who demonstrated the ExCITE surgical approach with Dr. Advincula as part of the Research and Science Plenary here at AAGL, said, “I think the PneumoLiner is a great example of creativity and innovation. It’s good that we now have an FDA-approved device to offer and counsel patients as one of many options.” She added that, overall, the morcellation controversy has been “a positive experience. We have learned better as a community about how to approach new technology.”
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Updated November 24, 2014. Accessed November 17, 2016.
- Siedhoff MT, Doll KM, Rutstein SE, et al. Laparoscopic hysterectomy with morcellation versus abdominal hysterectomy for presumed uterine leiomyomata: an updated decision analysis. J Minim Invasiv Gynecol. 2016;23(7):S4-S5.
- Mandelberger AH, Mathews S, Chuang L. Practice changes in power morcellation among gynecologic-oncologists since 2014. J Minim Invasiv Gynecol. 2016;23(7):S3.
Olympus introduces first-of-its-kind contained tissue extraction system, restoring healthcare option for gynecologists and women [press release]. November 16, 2016. Olympus website. http://www.olympusamerica.com/corporate/corp_presscenter_headline.asp?pressNo=2079. Accessed November 16, 2016.
- FDA allows marketing of first-of-kind tissue containment system for use with certain laparoscopic power morcellators in select patients. FDA website. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm494650.htm. Updated April 7, 2016. Accessed November 16, 2016.
- Advincula AP. Tissue extraction: can the pendulum change direction? OBG Manag. 2016;28(6):8, 10, 12.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Updated November 24, 2014. Accessed November 17, 2016.
- Siedhoff MT, Doll KM, Rutstein SE, et al. Laparoscopic hysterectomy with morcellation versus abdominal hysterectomy for presumed uterine leiomyomata: an updated decision analysis. J Minim Invasiv Gynecol. 2016;23(7):S4-S5.
- Mandelberger AH, Mathews S, Chuang L. Practice changes in power morcellation among gynecologic-oncologists since 2014. J Minim Invasiv Gynecol. 2016;23(7):S3.
Olympus introduces first-of-its-kind contained tissue extraction system, restoring healthcare option for gynecologists and women [press release]. November 16, 2016. Olympus website. http://www.olympusamerica.com/corporate/corp_presscenter_headline.asp?pressNo=2079. Accessed November 16, 2016.
- FDA allows marketing of first-of-kind tissue containment system for use with certain laparoscopic power morcellators in select patients. FDA website. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm494650.htm. Updated April 7, 2016. Accessed November 16, 2016.
- Advincula AP. Tissue extraction: can the pendulum change direction? OBG Manag. 2016;28(6):8, 10, 12.