User login
Too Much of a Good Thing: Weakness, Dysphagia, and Stridor After Botulinum Toxin Injections
Case
A 68-year-old woman presented to the ED 5 days after receiving onabotulinumtoxinA cosmetic injections for wrinkles of the face and neck. She stated that she was unable to raise her head while in a supine position and that her head felt heavy when standing. She also experienced spasms and strain of the posterior cervical neck muscles. In addition, the patient described a constant need to swallow forcefully throughout the day, and felt an intermittent heavy sensation over her larynx that was associated with stridor. She noted these symptoms began 5 days after the onabotulinumtoxinA injections and had peaked 2 days prior to presentation. She also complained of dysphagia without odynophagia, but denied any changes in her voice.
The patient first began onabotulinumtoxinA injections 12 years earlier for aesthetic treatment of glabellar and peri-orbital wrinkles. She initially received the injections at a regular interval of 90 to 100 days. During the course of the first 2 years of treatment, the patient was under the care of a plastic surgeon; thereafter, she sought treatment at a physician-owned medical spa because it offered onabotulinumtoxinA at a lower price. The injections at the medical spa were administered by a physician assistant (PA). The patient stated that although the PA had steadily increased the dose of onabotulinumtoxinA to maintain the desired aesthetic effect, this was the first time she had experienced any side effects from the treatment.
The ED staff contacted the medical spa provider, who reviewed the patient’s medical record over the telephone. The PA stated that he had been the only practitioner at the facility to administer the onabotulinumtoxinA injections to the patient over her past 10 years there as a client. He further informed the emergency physician (EP) that 12 days prior to presentation, he had given the patient a total of 50 IU of onabotulinumtoxinA, in five separate injections, into the mid frontalis muscle; a total of 35 IU, in seven separate injections, into the glabellar region (procerus and corrugator muscles bilaterally); 20 IU into the lateral and inferior-lateral orbicularis oculi bilaterally, in four separate injections per side, (40 IU total); and a total of 100 IU in the anterior platysma, in 20 separate injections, for a total 1-day onabotulinumtoxinA dose of 225 IU.
The PA explained to the EP that he mixed the onabotulinumtoxinA in the patient’s room and had shown her the vials and dilution standard as recommended by the manufacturer because she had been requiring increased dosages and had previously questioned whether the onabotulinumtoxinA was diluted. The PA denied any other patients experiencing similar adverse events as those of the patient’s.
Over the last 10 years, the patient had received onabotulinumtoxinA in the nasolabial folds, upper and lower lip wrinkles, mentalis, depressor angular oris, buccal, nasalis, lateral brow, masseter, and calf muscles. The dosage of onabotulinumtoxinA at this most recent injection cycle was unchanged from her previous visit 3 months prior. According to the PA, the practice did not use abobotulinumtoxinA or incobotulinumtoxinA.
Regarding the patient’s medical history, she had no health issues suggestive of myasthenia gravis, multiple sclerosis, or Guillain-Barré syndrome. Examination of the face revealed decreased muscle excursion of the frontalis muscle from mid-brow to mid-brow, and stair-step wrinkle formation bilaterally. The procerus muscle was very weak, and the corrugator muscles were moderately diminished in strength. The lateral orbicularis oculi were very weak at each canthus. The extra-ocular muscles were intact. She had full mandibular excursion, and powerful movement of the tongue. The oropharynx and floor of the mouth were normal. She was noted to purposefully swallow and extend her neck every 90 to 120 seconds to “clear her throat,” though she did not drool and was able to handle her secretions and swallow fluids without aspiration. Her voice was normal and she was able to recite the letters “KKKKK,” “OOOOO,” and “EEEEE” in rapid fashion without breathiness or stridor. The rest of her facial muscles were normal.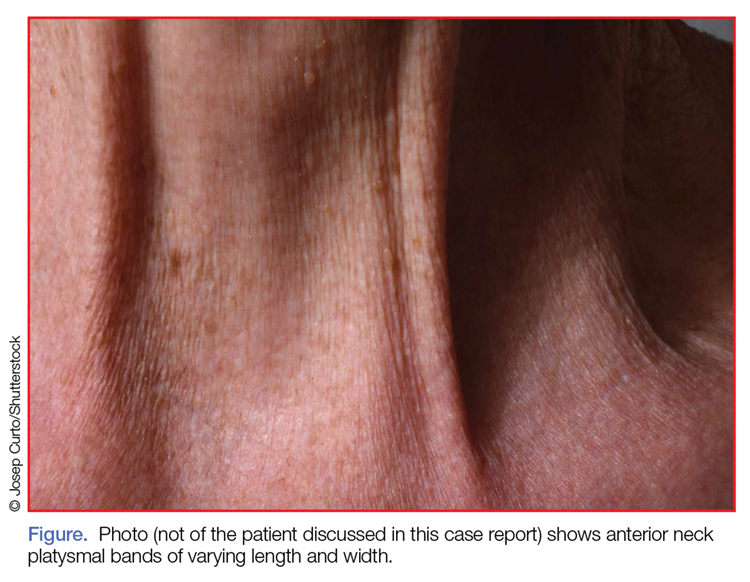
While examining the patient, the EP asked her to refrain from swallowing whenever she extended her neck. Upon complying with this request, her neck extension precipitated swallowing and, by not swallowing, she did not accumulate secretions. Once during the examination, the patient began swallowing and breathing rapidly with stridor. This less than 15-second episode was abated by full-neck extensions, which relieved the patient’s sensation of heaviness over the larynx. Her breathing and voice were normal immediately after this episode.
Examination of the anterior neck revealed four platysmal bands (Figure). One band measured 10 cm in length and extended from the mandible inferiorly; two bands measured 2 cm lateral to the midline bilaterally; and the fourth band extended 4 cm in length from the mandible immediately lateral to the longer platysmal band. The platysma and dermis were flaccid and redundant at rest and with exertion. The sternocleidomastoid muscles were weak with exertion. The larynx moved cephalad with swallowing. The posterior cervical neck and trapezius muscles were of normal tone and strength. No spasms or fasciculations were noted during the examination period.
While supine, the patient strained to lift her head and complained of a suffocating sensation over the larynx. She had no rashes or edema, and the remainder of the physical examination, vital signs, and pulse oximetry were normal. Laboratory evaluation, which included a complete blood count and serum electrolytes, was also normal.
An otolaryngologist consultation for laryngoscopy was obtained. After reviewing the patient’s case, the otolaryngologist concluded that given the patient’s history, intermittent stridor, and an absence of signs or symptoms suggestive of an impending upper airway obstruction (UAO), laryngoscopy was not warranted.
A plastic surgery consultation was then obtained. The patient’s examination was as noted above, and her vital signs and pulse oximetry remained normal throughout her ED stay. Although botulinum and botulinum antibody titers were ordered, the patient refused testing due to cost concerns. She was discharged home by plastic surgery services with a diagnosis of floppy neck and dysphagia secondary to aesthetic botulinum toxin paralysis of the bilateral sternocleidomastoid muscles and platysma. She was given a prescription for metoclopramide hydrochloride to stimulate motility of the upper gastrointestinal tract and to potentially improve swallowing.10
The patient was scheduled for a follow-up evaluation with the plastic surgeon 2 days after discharge. She was instructed to call 911 if she experienced stridor, shortness of breath, drooling, or if any airway issues arose. The patient did not return for her follow-up appointment with the plastic surgeon.
Discussion
Clostridium Botulinum Toxins
Clostridium botulinum is a gram-positive spore-forming anaerobic bacterium that produces extremely potent neuro-exotoxins. C botulinum is found in soil, contaminated foods, and in illicit injectable drugs (eg, heroin). Seven distinct antigenic botulinum toxins (A, B, C1, D, E, F, and G) are produced by several strains of C botulinum. Systemically, each neurotoxin is able to produce severe morbidity and mortality by causing generalized muscle paralysis and death by respiratory failure. The lethal dose of these agents is approximating 10(-9) g/kg body weight. Botulinum toxin type A is the most potent.1,2
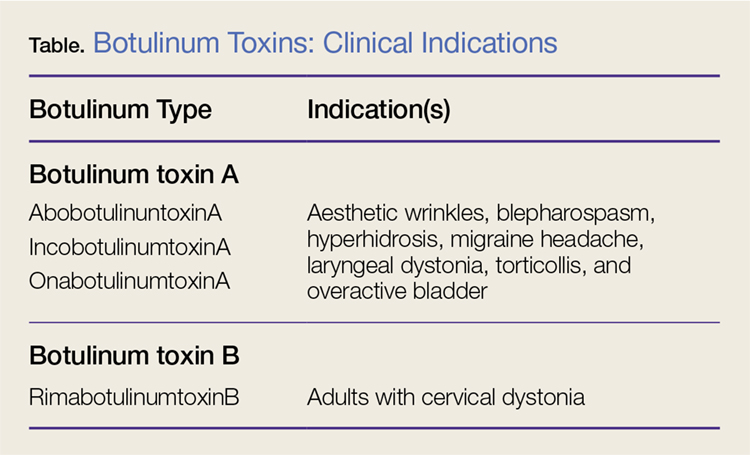
Nonetheless, botulinum toxin has been used clinically since the early 1970s. Currently, there are three FDA-approved botulinum toxin type A agents and one type B formulation (rimabotulinumtoxinB) (Table). Each formulation is unique, proprietary, and differs in molecular weight, toxin-complex size, protein content, and inactive ingredients. The effectiveness and adverse event profile for these four botulinum toxins is individually dependent upon the different dilutions and potency, onset of action, duration of effect, diffusion, and migration potential. Hence, the effective dose of one botulinum toxin does not equate to any other, resulting in a lack of interchangeability between botulinum toxins (eg, 5 IU of incobotulinumtoxinA does not equal 5 IU of onabotulinumtoxinA).
Aesthetic Indications
Historically, the use of botulinum toxin for aesthetic treatment of wrinkles and platysmal bands was first reported by Blitzer3 in 1993.Subsequently, the use of botulinum toxin for the aesthetic treatment of facial wrinkles, hypertrophic platysmal bands and horizontal neck lines gained popularity within the public and medical community.3-5
Anatomically, the platysma is a thin sheet-like muscle that originates in the superior fascia of the pectoralis and deltoid fascia, and extends over the full length of the neck up past the mandible and continuing into the submuscular aponeurotic system. The platysma is innervated by the seventh cranial nerve and functions to pull the jaw downward. The platysma muscle is attached directly to the skin. With normal aging, the anterior neck skin becomes flaccid, the central platysmal bands thicken and contract—forming bands, horizontal wrinkles, and loss of definition of the neck noticed at rest and with contraction of the platysma muscle. These vertical bands are known as platysmal bands. The platysmal bands are benign consequences of aging and as such are targets of correction through surgery or botulinum toxin injection.6,7
Mechanism of Action
Platysmal band and horizontal line injection techniques with botulinum toxin have been reported in the literature with dosages ranging from 15 IU to 200 IU used to block the Soluble N-ethylmaleimide-sensitive factor activating protein receptors. Typical onset of action begins at 3 days, with full paralytic effect at 7 days. Repeat injections every 3 to 4 months are required with prolonged effects seen with each subsequent injection due to chemodenervation-induced muscle atrophy.4,7,8
Adverse Effects
Commercial botulinum toxin type A has been associated with minor and transient side effects. Moderate complications seen in the neck region include transient soft-tissue edema, dermal ecchymoses, intramuscular hematoma, diffuse muscle soreness, neck flexor weakness, and headaches.4,8,9
The use of botulinum toxin for chemodenervation of the platysma can produce significant weakness of other neck muscles, including the sternocleidomastoid, cricothyroid, sternothyroid, and sternohyoid. Floppy neck and dysphagia may be due to diffusion of the toxin into the muscles of deglutition of the larynx; injection directly into the sternocleidomastoid muscle; or a result of the systemic effects of large dosages. Hoarseness, breathiness, and dysphagia may occur 3 to 4 days after injection, especially with doses over 75 IU.10
The recommended concentration of botulinum toxin type A causes a diffusion average of 1 cm in all directions from the injection sites. However, as the dilution increases, so does the zone of diffusion. Typical discharge instructions for platysma treatment include the overuse of the neck muscles for 2 to 4 hours after injection to encourage the botulinum toxin uptake for optimal result. Site manipulation (rubbing or massaging) also increases diffusion. For botulinum toxin type B, the zone of diffusion is greater because its molecular weight is less than the type A toxins, thus making it an undesirable agent for aesthetic facial chemodenervation.4,11
Toxin Resistance
Botulinum toxin resistance is a known complication that occurs normally as a result of the body recognizing the neurotoxin as a foreign substance and producing neutralizing antibodies (NAb). Primary botulinum toxin failure is known in patients who require high doses of the neurotoxin for treatment of neuromuscular disorders.12 Complete secondary therapy failure is known to occur in cosmetic patients after a single dose and those who have been receiving low-dose botulinum toxin regularly. The risk of NAb development increases with long-term treatment and high doses.12-18
Floppy Neck and Dysphagia
As previously noted, floppy neck and dysphagia are adverse clinical findings of botulinum toxin effect on the platysma, sternocleidomastoid, or the paralaryngeal muscles. In this case, the patient was fortunate to have only sustained weakness of the platysma and sternocleidomastoid muscles despite both a large neck and total body dose. Paralaryngeal muscle paralysis is not life-threatening, but the distress may precipitate paradoxical vocal cord motion and stridor.
Stridor
Stridor is typically a symptom of an upper airway obstruction (UAO) process. Typical UAO conditions encountered in the ED are infections (eg, epiglottitis, croup), foreign body, allergy, and laryngeal trauma. The age of the patient, onset of stridor, course of the stridor (ie, intermittent, continuous, worsening), associated symptoms (eg, fever, rash, swelling of oral soft tissues), and bruising must be ascertained.
In differentiating the etiology of stridor, the EP should observe the patient for any associated change in voice, inability to handle secretions, and position of comfort. Patients with stridor require admission and evaluation by an otolaryngologist as expeditiously as possible because impending UAO may quickly progress to complete UAO necessitating emergent intubation.
An atypical presentation of stridor to the ED is sporadic stridor. Sporadic attacks of stridor during activity have been associated with the entity of paradoxical vocal cord motion. Patients usually describe a choking sensation with inability to breathe resulting in an audible inspiratory and/or expiratory sound—ie, stridor. Wheezing may or may not be present. Patients may also describe tightness in the neck and sometimes in the chest. The attacks are usually seconds to minutes in duration. More often, there is a precipitating or an inducing factor such as hyperventilation, cough, panting, phonatory tasks, or the inhalation of irritants or perfume, or an oropharyngeal or laryngeal manipulation prior or postextubation. The feeling of stress alone is commonly reported prior to the attacks. When evaluating patients presenting with floppy neck, dysphagia, and stridor, it is imperative that the clinician conduct a thorough history and physical examination to determine if the symptoms are secondary to a systemic or local effect, and whether the patient will progress to an acute UAO (vocal cord paralysis) necessitating intubation in the ED and subsequent tracheostomy.19,20
Conclusion
The ready availability of botulinum toxins and their low-cost-benefit ratio continue to promote over-utilization for treatment of facial wrinkles, platysmal bands, and horizontal lines; migraine headache; and hyperhidrosis. Complications associated with overuse of botulinum toxins are due to either administration of a large single dose or from regional diffusion. With the increasing number of patients receiving botulinum injections, EPs should be aware of the four available toxin types onset of action, adverse events, and potential life-threatening complications of regional neck injections.
References
1. Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43(2 Pt 1):249-259. doi:10.1067/mjd.2000.105567.
2. Lamanna C. The most poisonous poison. Science. 1959;130(3378):763-772.
3. Blitzer A, Brin MF, Keen MS, Aviv JE. Botulinum toxin for the treatment of hyperfunctional lines of the face. Arch Otolaryngol Head Neck Surg. 1993;119(9):1018-1022.
4. Carruthers A, Carruthers J. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1189-1194.
5. Carruthers J, Carruthers A. Botox use in the mid and lower face and neck. Semin Cutan Med Surg. 2001;20(2):85-92. doi:10.1053/sder.2001.25139
6. Hoefflin SM. Anatomy of the platysma and lip depressor muscles. A simplified mnemonic approach. Dermatol Surg. 1998;24(11):1225-1231.
7. Brandt FS, Bellman B. Cosmetic use of botulinum A exotoxin for the aging neck. Dermatol Surg. 1998;24(11):1232-1234.
8. Klein AW. Complications and adverse reactions with the use of botulinum toxin. Semin Cutan Med Surg. 2001;20(2):109-120. doi:10.1053/sder.2001.25964.
9. Carruthers A, Kiene K, Carruthers J. Botulinum A exotoxin use in clinical dermatology. J Am Acad Dermatol. 1996;34(5 Pt 1):788-797.
10. Howell K, Selber P, Graham HK, Reddihough D. Botulinum neurotoxin A: an unusual systemic effect. J Paediatr Child Health. 2007:43(6):499-501. doi:10.1111/j.1440-1754.2007.01122.x.
11. Carruthers A, Carruthers J. Toxins 99, new information about the botulinum neurotoxins. Dermatol Surg. 2000;26(3):174-176.
12. Dressler D, Adib Saberi F. New formulation of Botox: complete antibody-induced treatment failure in cervical dystonia. J Neurol Neurosurg Psychiatry. 2007;78(1):108-109. doi:10.1136/jnnp.2006.093419.
13. Borodic G. Immunologic resistance after repeated botulinum toxin type a injections for facial rhytides. Ophthal Plast Reconstr Surg. 2006;22:239-240. doi:10.1097/01.iop.0000217703.80859.a3.
14. Goschel H, Wohlfarth K, Frevert J, Dengler R, Bigalke H. Botulinum A toxin therapy: neutralizing and nonneutralizing antibodies—therapeutic consequences. Exp Neurol. 1997;147(1):96-102. doi:10.1006/exnr.1997.6580.
15. Hatheway CL. Toxigenic clostridia. Clin Microbiol Rev. 1990;3(1):66-98.
16. Smith LA. Development of recombinant vaccines for botulinum neurotoxin. Toxicon. 1998;36(11):1539-1548.
17. Houser MK, Sheean GL, Lees AJ. Further studies using higher doses of botulinum toxin type F for torticollis resistant to botulinum toxin type A. J Neurol Neurosurg Psychiatry. 1998;64(5):577-580.
18. Dressler D, Wohlfahrt K, Meyer-Rogge E, Wiest L, Bigalke H. Antibody-induced failure of botulinum toxin a therapy in cosmetic indications. Dermatol Surg. 2010;36 Suppl 4:2182-2187. doi:10.1111/j.1524-4725.2010.01710.x.
19. Maschka DA, Bauman NM, McCray PB Jr, Hoffman HT, Karnell MP, Smith RJ. A classification scheme for paradoxical vocal cord motion. Laryngoscope. 1997;107(11 Pt 1):1429-1435.
20. Altman KW, Simpson CB, Amin MR, Abaza M, Balkissoon R, Casiano RR. Cough and paradoxical vocal fold motion. Otolaryngol Head Neck Surg. 2002;127(6):501-511. doi:10.1067/mhn.2002.127589.
Case
A 68-year-old woman presented to the ED 5 days after receiving onabotulinumtoxinA cosmetic injections for wrinkles of the face and neck. She stated that she was unable to raise her head while in a supine position and that her head felt heavy when standing. She also experienced spasms and strain of the posterior cervical neck muscles. In addition, the patient described a constant need to swallow forcefully throughout the day, and felt an intermittent heavy sensation over her larynx that was associated with stridor. She noted these symptoms began 5 days after the onabotulinumtoxinA injections and had peaked 2 days prior to presentation. She also complained of dysphagia without odynophagia, but denied any changes in her voice.
The patient first began onabotulinumtoxinA injections 12 years earlier for aesthetic treatment of glabellar and peri-orbital wrinkles. She initially received the injections at a regular interval of 90 to 100 days. During the course of the first 2 years of treatment, the patient was under the care of a plastic surgeon; thereafter, she sought treatment at a physician-owned medical spa because it offered onabotulinumtoxinA at a lower price. The injections at the medical spa were administered by a physician assistant (PA). The patient stated that although the PA had steadily increased the dose of onabotulinumtoxinA to maintain the desired aesthetic effect, this was the first time she had experienced any side effects from the treatment.
The ED staff contacted the medical spa provider, who reviewed the patient’s medical record over the telephone. The PA stated that he had been the only practitioner at the facility to administer the onabotulinumtoxinA injections to the patient over her past 10 years there as a client. He further informed the emergency physician (EP) that 12 days prior to presentation, he had given the patient a total of 50 IU of onabotulinumtoxinA, in five separate injections, into the mid frontalis muscle; a total of 35 IU, in seven separate injections, into the glabellar region (procerus and corrugator muscles bilaterally); 20 IU into the lateral and inferior-lateral orbicularis oculi bilaterally, in four separate injections per side, (40 IU total); and a total of 100 IU in the anterior platysma, in 20 separate injections, for a total 1-day onabotulinumtoxinA dose of 225 IU.
The PA explained to the EP that he mixed the onabotulinumtoxinA in the patient’s room and had shown her the vials and dilution standard as recommended by the manufacturer because she had been requiring increased dosages and had previously questioned whether the onabotulinumtoxinA was diluted. The PA denied any other patients experiencing similar adverse events as those of the patient’s.
Over the last 10 years, the patient had received onabotulinumtoxinA in the nasolabial folds, upper and lower lip wrinkles, mentalis, depressor angular oris, buccal, nasalis, lateral brow, masseter, and calf muscles. The dosage of onabotulinumtoxinA at this most recent injection cycle was unchanged from her previous visit 3 months prior. According to the PA, the practice did not use abobotulinumtoxinA or incobotulinumtoxinA.
Regarding the patient’s medical history, she had no health issues suggestive of myasthenia gravis, multiple sclerosis, or Guillain-Barré syndrome. Examination of the face revealed decreased muscle excursion of the frontalis muscle from mid-brow to mid-brow, and stair-step wrinkle formation bilaterally. The procerus muscle was very weak, and the corrugator muscles were moderately diminished in strength. The lateral orbicularis oculi were very weak at each canthus. The extra-ocular muscles were intact. She had full mandibular excursion, and powerful movement of the tongue. The oropharynx and floor of the mouth were normal. She was noted to purposefully swallow and extend her neck every 90 to 120 seconds to “clear her throat,” though she did not drool and was able to handle her secretions and swallow fluids without aspiration. Her voice was normal and she was able to recite the letters “KKKKK,” “OOOOO,” and “EEEEE” in rapid fashion without breathiness or stridor. The rest of her facial muscles were normal.
While examining the patient, the EP asked her to refrain from swallowing whenever she extended her neck. Upon complying with this request, her neck extension precipitated swallowing and, by not swallowing, she did not accumulate secretions. Once during the examination, the patient began swallowing and breathing rapidly with stridor. This less than 15-second episode was abated by full-neck extensions, which relieved the patient’s sensation of heaviness over the larynx. Her breathing and voice were normal immediately after this episode.
Examination of the anterior neck revealed four platysmal bands (Figure). One band measured 10 cm in length and extended from the mandible inferiorly; two bands measured 2 cm lateral to the midline bilaterally; and the fourth band extended 4 cm in length from the mandible immediately lateral to the longer platysmal band. The platysma and dermis were flaccid and redundant at rest and with exertion. The sternocleidomastoid muscles were weak with exertion. The larynx moved cephalad with swallowing. The posterior cervical neck and trapezius muscles were of normal tone and strength. No spasms or fasciculations were noted during the examination period.
While supine, the patient strained to lift her head and complained of a suffocating sensation over the larynx. She had no rashes or edema, and the remainder of the physical examination, vital signs, and pulse oximetry were normal. Laboratory evaluation, which included a complete blood count and serum electrolytes, was also normal.
An otolaryngologist consultation for laryngoscopy was obtained. After reviewing the patient’s case, the otolaryngologist concluded that given the patient’s history, intermittent stridor, and an absence of signs or symptoms suggestive of an impending upper airway obstruction (UAO), laryngoscopy was not warranted.
A plastic surgery consultation was then obtained. The patient’s examination was as noted above, and her vital signs and pulse oximetry remained normal throughout her ED stay. Although botulinum and botulinum antibody titers were ordered, the patient refused testing due to cost concerns. She was discharged home by plastic surgery services with a diagnosis of floppy neck and dysphagia secondary to aesthetic botulinum toxin paralysis of the bilateral sternocleidomastoid muscles and platysma. She was given a prescription for metoclopramide hydrochloride to stimulate motility of the upper gastrointestinal tract and to potentially improve swallowing.10
The patient was scheduled for a follow-up evaluation with the plastic surgeon 2 days after discharge. She was instructed to call 911 if she experienced stridor, shortness of breath, drooling, or if any airway issues arose. The patient did not return for her follow-up appointment with the plastic surgeon.
Discussion
Clostridium Botulinum Toxins
Clostridium botulinum is a gram-positive spore-forming anaerobic bacterium that produces extremely potent neuro-exotoxins. C botulinum is found in soil, contaminated foods, and in illicit injectable drugs (eg, heroin). Seven distinct antigenic botulinum toxins (A, B, C1, D, E, F, and G) are produced by several strains of C botulinum. Systemically, each neurotoxin is able to produce severe morbidity and mortality by causing generalized muscle paralysis and death by respiratory failure. The lethal dose of these agents is approximating 10(-9) g/kg body weight. Botulinum toxin type A is the most potent.1,2
Nonetheless, botulinum toxin has been used clinically since the early 1970s. Currently, there are three FDA-approved botulinum toxin type A agents and one type B formulation (rimabotulinumtoxinB) (Table). Each formulation is unique, proprietary, and differs in molecular weight, toxin-complex size, protein content, and inactive ingredients. The effectiveness and adverse event profile for these four botulinum toxins is individually dependent upon the different dilutions and potency, onset of action, duration of effect, diffusion, and migration potential. Hence, the effective dose of one botulinum toxin does not equate to any other, resulting in a lack of interchangeability between botulinum toxins (eg, 5 IU of incobotulinumtoxinA does not equal 5 IU of onabotulinumtoxinA).
Aesthetic Indications
Historically, the use of botulinum toxin for aesthetic treatment of wrinkles and platysmal bands was first reported by Blitzer3 in 1993.Subsequently, the use of botulinum toxin for the aesthetic treatment of facial wrinkles, hypertrophic platysmal bands and horizontal neck lines gained popularity within the public and medical community.3-5
Anatomically, the platysma is a thin sheet-like muscle that originates in the superior fascia of the pectoralis and deltoid fascia, and extends over the full length of the neck up past the mandible and continuing into the submuscular aponeurotic system. The platysma is innervated by the seventh cranial nerve and functions to pull the jaw downward. The platysma muscle is attached directly to the skin. With normal aging, the anterior neck skin becomes flaccid, the central platysmal bands thicken and contract—forming bands, horizontal wrinkles, and loss of definition of the neck noticed at rest and with contraction of the platysma muscle. These vertical bands are known as platysmal bands. The platysmal bands are benign consequences of aging and as such are targets of correction through surgery or botulinum toxin injection.6,7
Mechanism of Action
Platysmal band and horizontal line injection techniques with botulinum toxin have been reported in the literature with dosages ranging from 15 IU to 200 IU used to block the Soluble N-ethylmaleimide-sensitive factor activating protein receptors. Typical onset of action begins at 3 days, with full paralytic effect at 7 days. Repeat injections every 3 to 4 months are required with prolonged effects seen with each subsequent injection due to chemodenervation-induced muscle atrophy.4,7,8
Adverse Effects
Commercial botulinum toxin type A has been associated with minor and transient side effects. Moderate complications seen in the neck region include transient soft-tissue edema, dermal ecchymoses, intramuscular hematoma, diffuse muscle soreness, neck flexor weakness, and headaches.4,8,9
The use of botulinum toxin for chemodenervation of the platysma can produce significant weakness of other neck muscles, including the sternocleidomastoid, cricothyroid, sternothyroid, and sternohyoid. Floppy neck and dysphagia may be due to diffusion of the toxin into the muscles of deglutition of the larynx; injection directly into the sternocleidomastoid muscle; or a result of the systemic effects of large dosages. Hoarseness, breathiness, and dysphagia may occur 3 to 4 days after injection, especially with doses over 75 IU.10
The recommended concentration of botulinum toxin type A causes a diffusion average of 1 cm in all directions from the injection sites. However, as the dilution increases, so does the zone of diffusion. Typical discharge instructions for platysma treatment include the overuse of the neck muscles for 2 to 4 hours after injection to encourage the botulinum toxin uptake for optimal result. Site manipulation (rubbing or massaging) also increases diffusion. For botulinum toxin type B, the zone of diffusion is greater because its molecular weight is less than the type A toxins, thus making it an undesirable agent for aesthetic facial chemodenervation.4,11
Toxin Resistance
Botulinum toxin resistance is a known complication that occurs normally as a result of the body recognizing the neurotoxin as a foreign substance and producing neutralizing antibodies (NAb). Primary botulinum toxin failure is known in patients who require high doses of the neurotoxin for treatment of neuromuscular disorders.12 Complete secondary therapy failure is known to occur in cosmetic patients after a single dose and those who have been receiving low-dose botulinum toxin regularly. The risk of NAb development increases with long-term treatment and high doses.12-18
Floppy Neck and Dysphagia
As previously noted, floppy neck and dysphagia are adverse clinical findings of botulinum toxin effect on the platysma, sternocleidomastoid, or the paralaryngeal muscles. In this case, the patient was fortunate to have only sustained weakness of the platysma and sternocleidomastoid muscles despite both a large neck and total body dose. Paralaryngeal muscle paralysis is not life-threatening, but the distress may precipitate paradoxical vocal cord motion and stridor.
Stridor
Stridor is typically a symptom of an upper airway obstruction (UAO) process. Typical UAO conditions encountered in the ED are infections (eg, epiglottitis, croup), foreign body, allergy, and laryngeal trauma. The age of the patient, onset of stridor, course of the stridor (ie, intermittent, continuous, worsening), associated symptoms (eg, fever, rash, swelling of oral soft tissues), and bruising must be ascertained.
In differentiating the etiology of stridor, the EP should observe the patient for any associated change in voice, inability to handle secretions, and position of comfort. Patients with stridor require admission and evaluation by an otolaryngologist as expeditiously as possible because impending UAO may quickly progress to complete UAO necessitating emergent intubation.
An atypical presentation of stridor to the ED is sporadic stridor. Sporadic attacks of stridor during activity have been associated with the entity of paradoxical vocal cord motion. Patients usually describe a choking sensation with inability to breathe resulting in an audible inspiratory and/or expiratory sound—ie, stridor. Wheezing may or may not be present. Patients may also describe tightness in the neck and sometimes in the chest. The attacks are usually seconds to minutes in duration. More often, there is a precipitating or an inducing factor such as hyperventilation, cough, panting, phonatory tasks, or the inhalation of irritants or perfume, or an oropharyngeal or laryngeal manipulation prior or postextubation. The feeling of stress alone is commonly reported prior to the attacks. When evaluating patients presenting with floppy neck, dysphagia, and stridor, it is imperative that the clinician conduct a thorough history and physical examination to determine if the symptoms are secondary to a systemic or local effect, and whether the patient will progress to an acute UAO (vocal cord paralysis) necessitating intubation in the ED and subsequent tracheostomy.19,20
Conclusion
The ready availability of botulinum toxins and their low-cost-benefit ratio continue to promote over-utilization for treatment of facial wrinkles, platysmal bands, and horizontal lines; migraine headache; and hyperhidrosis. Complications associated with overuse of botulinum toxins are due to either administration of a large single dose or from regional diffusion. With the increasing number of patients receiving botulinum injections, EPs should be aware of the four available toxin types onset of action, adverse events, and potential life-threatening complications of regional neck injections.
Case
A 68-year-old woman presented to the ED 5 days after receiving onabotulinumtoxinA cosmetic injections for wrinkles of the face and neck. She stated that she was unable to raise her head while in a supine position and that her head felt heavy when standing. She also experienced spasms and strain of the posterior cervical neck muscles. In addition, the patient described a constant need to swallow forcefully throughout the day, and felt an intermittent heavy sensation over her larynx that was associated with stridor. She noted these symptoms began 5 days after the onabotulinumtoxinA injections and had peaked 2 days prior to presentation. She also complained of dysphagia without odynophagia, but denied any changes in her voice.
The patient first began onabotulinumtoxinA injections 12 years earlier for aesthetic treatment of glabellar and peri-orbital wrinkles. She initially received the injections at a regular interval of 90 to 100 days. During the course of the first 2 years of treatment, the patient was under the care of a plastic surgeon; thereafter, she sought treatment at a physician-owned medical spa because it offered onabotulinumtoxinA at a lower price. The injections at the medical spa were administered by a physician assistant (PA). The patient stated that although the PA had steadily increased the dose of onabotulinumtoxinA to maintain the desired aesthetic effect, this was the first time she had experienced any side effects from the treatment.
The ED staff contacted the medical spa provider, who reviewed the patient’s medical record over the telephone. The PA stated that he had been the only practitioner at the facility to administer the onabotulinumtoxinA injections to the patient over her past 10 years there as a client. He further informed the emergency physician (EP) that 12 days prior to presentation, he had given the patient a total of 50 IU of onabotulinumtoxinA, in five separate injections, into the mid frontalis muscle; a total of 35 IU, in seven separate injections, into the glabellar region (procerus and corrugator muscles bilaterally); 20 IU into the lateral and inferior-lateral orbicularis oculi bilaterally, in four separate injections per side, (40 IU total); and a total of 100 IU in the anterior platysma, in 20 separate injections, for a total 1-day onabotulinumtoxinA dose of 225 IU.
The PA explained to the EP that he mixed the onabotulinumtoxinA in the patient’s room and had shown her the vials and dilution standard as recommended by the manufacturer because she had been requiring increased dosages and had previously questioned whether the onabotulinumtoxinA was diluted. The PA denied any other patients experiencing similar adverse events as those of the patient’s.
Over the last 10 years, the patient had received onabotulinumtoxinA in the nasolabial folds, upper and lower lip wrinkles, mentalis, depressor angular oris, buccal, nasalis, lateral brow, masseter, and calf muscles. The dosage of onabotulinumtoxinA at this most recent injection cycle was unchanged from her previous visit 3 months prior. According to the PA, the practice did not use abobotulinumtoxinA or incobotulinumtoxinA.
Regarding the patient’s medical history, she had no health issues suggestive of myasthenia gravis, multiple sclerosis, or Guillain-Barré syndrome. Examination of the face revealed decreased muscle excursion of the frontalis muscle from mid-brow to mid-brow, and stair-step wrinkle formation bilaterally. The procerus muscle was very weak, and the corrugator muscles were moderately diminished in strength. The lateral orbicularis oculi were very weak at each canthus. The extra-ocular muscles were intact. She had full mandibular excursion, and powerful movement of the tongue. The oropharynx and floor of the mouth were normal. She was noted to purposefully swallow and extend her neck every 90 to 120 seconds to “clear her throat,” though she did not drool and was able to handle her secretions and swallow fluids without aspiration. Her voice was normal and she was able to recite the letters “KKKKK,” “OOOOO,” and “EEEEE” in rapid fashion without breathiness or stridor. The rest of her facial muscles were normal.
While examining the patient, the EP asked her to refrain from swallowing whenever she extended her neck. Upon complying with this request, her neck extension precipitated swallowing and, by not swallowing, she did not accumulate secretions. Once during the examination, the patient began swallowing and breathing rapidly with stridor. This less than 15-second episode was abated by full-neck extensions, which relieved the patient’s sensation of heaviness over the larynx. Her breathing and voice were normal immediately after this episode.
Examination of the anterior neck revealed four platysmal bands (Figure). One band measured 10 cm in length and extended from the mandible inferiorly; two bands measured 2 cm lateral to the midline bilaterally; and the fourth band extended 4 cm in length from the mandible immediately lateral to the longer platysmal band. The platysma and dermis were flaccid and redundant at rest and with exertion. The sternocleidomastoid muscles were weak with exertion. The larynx moved cephalad with swallowing. The posterior cervical neck and trapezius muscles were of normal tone and strength. No spasms or fasciculations were noted during the examination period.
While supine, the patient strained to lift her head and complained of a suffocating sensation over the larynx. She had no rashes or edema, and the remainder of the physical examination, vital signs, and pulse oximetry were normal. Laboratory evaluation, which included a complete blood count and serum electrolytes, was also normal.
An otolaryngologist consultation for laryngoscopy was obtained. After reviewing the patient’s case, the otolaryngologist concluded that given the patient’s history, intermittent stridor, and an absence of signs or symptoms suggestive of an impending upper airway obstruction (UAO), laryngoscopy was not warranted.
A plastic surgery consultation was then obtained. The patient’s examination was as noted above, and her vital signs and pulse oximetry remained normal throughout her ED stay. Although botulinum and botulinum antibody titers were ordered, the patient refused testing due to cost concerns. She was discharged home by plastic surgery services with a diagnosis of floppy neck and dysphagia secondary to aesthetic botulinum toxin paralysis of the bilateral sternocleidomastoid muscles and platysma. She was given a prescription for metoclopramide hydrochloride to stimulate motility of the upper gastrointestinal tract and to potentially improve swallowing.10
The patient was scheduled for a follow-up evaluation with the plastic surgeon 2 days after discharge. She was instructed to call 911 if she experienced stridor, shortness of breath, drooling, or if any airway issues arose. The patient did not return for her follow-up appointment with the plastic surgeon.
Discussion
Clostridium Botulinum Toxins
Clostridium botulinum is a gram-positive spore-forming anaerobic bacterium that produces extremely potent neuro-exotoxins. C botulinum is found in soil, contaminated foods, and in illicit injectable drugs (eg, heroin). Seven distinct antigenic botulinum toxins (A, B, C1, D, E, F, and G) are produced by several strains of C botulinum. Systemically, each neurotoxin is able to produce severe morbidity and mortality by causing generalized muscle paralysis and death by respiratory failure. The lethal dose of these agents is approximating 10(-9) g/kg body weight. Botulinum toxin type A is the most potent.1,2
Nonetheless, botulinum toxin has been used clinically since the early 1970s. Currently, there are three FDA-approved botulinum toxin type A agents and one type B formulation (rimabotulinumtoxinB) (Table). Each formulation is unique, proprietary, and differs in molecular weight, toxin-complex size, protein content, and inactive ingredients. The effectiveness and adverse event profile for these four botulinum toxins is individually dependent upon the different dilutions and potency, onset of action, duration of effect, diffusion, and migration potential. Hence, the effective dose of one botulinum toxin does not equate to any other, resulting in a lack of interchangeability between botulinum toxins (eg, 5 IU of incobotulinumtoxinA does not equal 5 IU of onabotulinumtoxinA).
Aesthetic Indications
Historically, the use of botulinum toxin for aesthetic treatment of wrinkles and platysmal bands was first reported by Blitzer3 in 1993.Subsequently, the use of botulinum toxin for the aesthetic treatment of facial wrinkles, hypertrophic platysmal bands and horizontal neck lines gained popularity within the public and medical community.3-5
Anatomically, the platysma is a thin sheet-like muscle that originates in the superior fascia of the pectoralis and deltoid fascia, and extends over the full length of the neck up past the mandible and continuing into the submuscular aponeurotic system. The platysma is innervated by the seventh cranial nerve and functions to pull the jaw downward. The platysma muscle is attached directly to the skin. With normal aging, the anterior neck skin becomes flaccid, the central platysmal bands thicken and contract—forming bands, horizontal wrinkles, and loss of definition of the neck noticed at rest and with contraction of the platysma muscle. These vertical bands are known as platysmal bands. The platysmal bands are benign consequences of aging and as such are targets of correction through surgery or botulinum toxin injection.6,7
Mechanism of Action
Platysmal band and horizontal line injection techniques with botulinum toxin have been reported in the literature with dosages ranging from 15 IU to 200 IU used to block the Soluble N-ethylmaleimide-sensitive factor activating protein receptors. Typical onset of action begins at 3 days, with full paralytic effect at 7 days. Repeat injections every 3 to 4 months are required with prolonged effects seen with each subsequent injection due to chemodenervation-induced muscle atrophy.4,7,8
Adverse Effects
Commercial botulinum toxin type A has been associated with minor and transient side effects. Moderate complications seen in the neck region include transient soft-tissue edema, dermal ecchymoses, intramuscular hematoma, diffuse muscle soreness, neck flexor weakness, and headaches.4,8,9
The use of botulinum toxin for chemodenervation of the platysma can produce significant weakness of other neck muscles, including the sternocleidomastoid, cricothyroid, sternothyroid, and sternohyoid. Floppy neck and dysphagia may be due to diffusion of the toxin into the muscles of deglutition of the larynx; injection directly into the sternocleidomastoid muscle; or a result of the systemic effects of large dosages. Hoarseness, breathiness, and dysphagia may occur 3 to 4 days after injection, especially with doses over 75 IU.10
The recommended concentration of botulinum toxin type A causes a diffusion average of 1 cm in all directions from the injection sites. However, as the dilution increases, so does the zone of diffusion. Typical discharge instructions for platysma treatment include the overuse of the neck muscles for 2 to 4 hours after injection to encourage the botulinum toxin uptake for optimal result. Site manipulation (rubbing or massaging) also increases diffusion. For botulinum toxin type B, the zone of diffusion is greater because its molecular weight is less than the type A toxins, thus making it an undesirable agent for aesthetic facial chemodenervation.4,11
Toxin Resistance
Botulinum toxin resistance is a known complication that occurs normally as a result of the body recognizing the neurotoxin as a foreign substance and producing neutralizing antibodies (NAb). Primary botulinum toxin failure is known in patients who require high doses of the neurotoxin for treatment of neuromuscular disorders.12 Complete secondary therapy failure is known to occur in cosmetic patients after a single dose and those who have been receiving low-dose botulinum toxin regularly. The risk of NAb development increases with long-term treatment and high doses.12-18
Floppy Neck and Dysphagia
As previously noted, floppy neck and dysphagia are adverse clinical findings of botulinum toxin effect on the platysma, sternocleidomastoid, or the paralaryngeal muscles. In this case, the patient was fortunate to have only sustained weakness of the platysma and sternocleidomastoid muscles despite both a large neck and total body dose. Paralaryngeal muscle paralysis is not life-threatening, but the distress may precipitate paradoxical vocal cord motion and stridor.
Stridor
Stridor is typically a symptom of an upper airway obstruction (UAO) process. Typical UAO conditions encountered in the ED are infections (eg, epiglottitis, croup), foreign body, allergy, and laryngeal trauma. The age of the patient, onset of stridor, course of the stridor (ie, intermittent, continuous, worsening), associated symptoms (eg, fever, rash, swelling of oral soft tissues), and bruising must be ascertained.
In differentiating the etiology of stridor, the EP should observe the patient for any associated change in voice, inability to handle secretions, and position of comfort. Patients with stridor require admission and evaluation by an otolaryngologist as expeditiously as possible because impending UAO may quickly progress to complete UAO necessitating emergent intubation.
An atypical presentation of stridor to the ED is sporadic stridor. Sporadic attacks of stridor during activity have been associated with the entity of paradoxical vocal cord motion. Patients usually describe a choking sensation with inability to breathe resulting in an audible inspiratory and/or expiratory sound—ie, stridor. Wheezing may or may not be present. Patients may also describe tightness in the neck and sometimes in the chest. The attacks are usually seconds to minutes in duration. More often, there is a precipitating or an inducing factor such as hyperventilation, cough, panting, phonatory tasks, or the inhalation of irritants or perfume, or an oropharyngeal or laryngeal manipulation prior or postextubation. The feeling of stress alone is commonly reported prior to the attacks. When evaluating patients presenting with floppy neck, dysphagia, and stridor, it is imperative that the clinician conduct a thorough history and physical examination to determine if the symptoms are secondary to a systemic or local effect, and whether the patient will progress to an acute UAO (vocal cord paralysis) necessitating intubation in the ED and subsequent tracheostomy.19,20
Conclusion
The ready availability of botulinum toxins and their low-cost-benefit ratio continue to promote over-utilization for treatment of facial wrinkles, platysmal bands, and horizontal lines; migraine headache; and hyperhidrosis. Complications associated with overuse of botulinum toxins are due to either administration of a large single dose or from regional diffusion. With the increasing number of patients receiving botulinum injections, EPs should be aware of the four available toxin types onset of action, adverse events, and potential life-threatening complications of regional neck injections.
References
1. Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43(2 Pt 1):249-259. doi:10.1067/mjd.2000.105567.
2. Lamanna C. The most poisonous poison. Science. 1959;130(3378):763-772.
3. Blitzer A, Brin MF, Keen MS, Aviv JE. Botulinum toxin for the treatment of hyperfunctional lines of the face. Arch Otolaryngol Head Neck Surg. 1993;119(9):1018-1022.
4. Carruthers A, Carruthers J. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1189-1194.
5. Carruthers J, Carruthers A. Botox use in the mid and lower face and neck. Semin Cutan Med Surg. 2001;20(2):85-92. doi:10.1053/sder.2001.25139
6. Hoefflin SM. Anatomy of the platysma and lip depressor muscles. A simplified mnemonic approach. Dermatol Surg. 1998;24(11):1225-1231.
7. Brandt FS, Bellman B. Cosmetic use of botulinum A exotoxin for the aging neck. Dermatol Surg. 1998;24(11):1232-1234.
8. Klein AW. Complications and adverse reactions with the use of botulinum toxin. Semin Cutan Med Surg. 2001;20(2):109-120. doi:10.1053/sder.2001.25964.
9. Carruthers A, Kiene K, Carruthers J. Botulinum A exotoxin use in clinical dermatology. J Am Acad Dermatol. 1996;34(5 Pt 1):788-797.
10. Howell K, Selber P, Graham HK, Reddihough D. Botulinum neurotoxin A: an unusual systemic effect. J Paediatr Child Health. 2007:43(6):499-501. doi:10.1111/j.1440-1754.2007.01122.x.
11. Carruthers A, Carruthers J. Toxins 99, new information about the botulinum neurotoxins. Dermatol Surg. 2000;26(3):174-176.
12. Dressler D, Adib Saberi F. New formulation of Botox: complete antibody-induced treatment failure in cervical dystonia. J Neurol Neurosurg Psychiatry. 2007;78(1):108-109. doi:10.1136/jnnp.2006.093419.
13. Borodic G. Immunologic resistance after repeated botulinum toxin type a injections for facial rhytides. Ophthal Plast Reconstr Surg. 2006;22:239-240. doi:10.1097/01.iop.0000217703.80859.a3.
14. Goschel H, Wohlfarth K, Frevert J, Dengler R, Bigalke H. Botulinum A toxin therapy: neutralizing and nonneutralizing antibodies—therapeutic consequences. Exp Neurol. 1997;147(1):96-102. doi:10.1006/exnr.1997.6580.
15. Hatheway CL. Toxigenic clostridia. Clin Microbiol Rev. 1990;3(1):66-98.
16. Smith LA. Development of recombinant vaccines for botulinum neurotoxin. Toxicon. 1998;36(11):1539-1548.
17. Houser MK, Sheean GL, Lees AJ. Further studies using higher doses of botulinum toxin type F for torticollis resistant to botulinum toxin type A. J Neurol Neurosurg Psychiatry. 1998;64(5):577-580.
18. Dressler D, Wohlfahrt K, Meyer-Rogge E, Wiest L, Bigalke H. Antibody-induced failure of botulinum toxin a therapy in cosmetic indications. Dermatol Surg. 2010;36 Suppl 4:2182-2187. doi:10.1111/j.1524-4725.2010.01710.x.
19. Maschka DA, Bauman NM, McCray PB Jr, Hoffman HT, Karnell MP, Smith RJ. A classification scheme for paradoxical vocal cord motion. Laryngoscope. 1997;107(11 Pt 1):1429-1435.
20. Altman KW, Simpson CB, Amin MR, Abaza M, Balkissoon R, Casiano RR. Cough and paradoxical vocal fold motion. Otolaryngol Head Neck Surg. 2002;127(6):501-511. doi:10.1067/mhn.2002.127589.
References
1. Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43(2 Pt 1):249-259. doi:10.1067/mjd.2000.105567.
2. Lamanna C. The most poisonous poison. Science. 1959;130(3378):763-772.
3. Blitzer A, Brin MF, Keen MS, Aviv JE. Botulinum toxin for the treatment of hyperfunctional lines of the face. Arch Otolaryngol Head Neck Surg. 1993;119(9):1018-1022.
4. Carruthers A, Carruthers J. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1189-1194.
5. Carruthers J, Carruthers A. Botox use in the mid and lower face and neck. Semin Cutan Med Surg. 2001;20(2):85-92. doi:10.1053/sder.2001.25139
6. Hoefflin SM. Anatomy of the platysma and lip depressor muscles. A simplified mnemonic approach. Dermatol Surg. 1998;24(11):1225-1231.
7. Brandt FS, Bellman B. Cosmetic use of botulinum A exotoxin for the aging neck. Dermatol Surg. 1998;24(11):1232-1234.
8. Klein AW. Complications and adverse reactions with the use of botulinum toxin. Semin Cutan Med Surg. 2001;20(2):109-120. doi:10.1053/sder.2001.25964.
9. Carruthers A, Kiene K, Carruthers J. Botulinum A exotoxin use in clinical dermatology. J Am Acad Dermatol. 1996;34(5 Pt 1):788-797.
10. Howell K, Selber P, Graham HK, Reddihough D. Botulinum neurotoxin A: an unusual systemic effect. J Paediatr Child Health. 2007:43(6):499-501. doi:10.1111/j.1440-1754.2007.01122.x.
11. Carruthers A, Carruthers J. Toxins 99, new information about the botulinum neurotoxins. Dermatol Surg. 2000;26(3):174-176.
12. Dressler D, Adib Saberi F. New formulation of Botox: complete antibody-induced treatment failure in cervical dystonia. J Neurol Neurosurg Psychiatry. 2007;78(1):108-109. doi:10.1136/jnnp.2006.093419.
13. Borodic G. Immunologic resistance after repeated botulinum toxin type a injections for facial rhytides. Ophthal Plast Reconstr Surg. 2006;22:239-240. doi:10.1097/01.iop.0000217703.80859.a3.
14. Goschel H, Wohlfarth K, Frevert J, Dengler R, Bigalke H. Botulinum A toxin therapy: neutralizing and nonneutralizing antibodies—therapeutic consequences. Exp Neurol. 1997;147(1):96-102. doi:10.1006/exnr.1997.6580.
15. Hatheway CL. Toxigenic clostridia. Clin Microbiol Rev. 1990;3(1):66-98.
16. Smith LA. Development of recombinant vaccines for botulinum neurotoxin. Toxicon. 1998;36(11):1539-1548.
17. Houser MK, Sheean GL, Lees AJ. Further studies using higher doses of botulinum toxin type F for torticollis resistant to botulinum toxin type A. J Neurol Neurosurg Psychiatry. 1998;64(5):577-580.
18. Dressler D, Wohlfahrt K, Meyer-Rogge E, Wiest L, Bigalke H. Antibody-induced failure of botulinum toxin a therapy in cosmetic indications. Dermatol Surg. 2010;36 Suppl 4:2182-2187. doi:10.1111/j.1524-4725.2010.01710.x.
19. Maschka DA, Bauman NM, McCray PB Jr, Hoffman HT, Karnell MP, Smith RJ. A classification scheme for paradoxical vocal cord motion. Laryngoscope. 1997;107(11 Pt 1):1429-1435.
20. Altman KW, Simpson CB, Amin MR, Abaza M, Balkissoon R, Casiano RR. Cough and paradoxical vocal fold motion. Otolaryngol Head Neck Surg. 2002;127(6):501-511. doi:10.1067/mhn.2002.127589.

Dung Lung: Reactive Airway Disease Syndrome From Yak-Dung Biomass Fuel Smoke
Case
A 30-year-old man without prior respiratory illness presented with coughing, wheezing, dyspnea on exertion, and decreased exercise tolerance after a 7-hour overnight exposure to yak-dung smoke. This episode took place at 4,240 m elevation in Pheriche village, along the Everest Base Camp trekking route within the Khumbu region of the Nepali Himalayas. Prior to going to bed that evening, the group of five cohabitants had a difficult time igniting the potbelly heating stove filled with yak-dung biomass fuel in the common room. Each time they tried to light it, the fire would smolder and go out within a few minutes, despite the group’s attempts at adjusting the flue and air intake. Eventually, they abandoned further attempts and retired to bed at approximately 9:30
The differential diagnosis included altitude illness, airway mucociliary dysfunction (commonly known as Khumbu cough),1 carbon monoxide (CO) poisoning, acute inhalation injury (AII) resulting in reactive airway disease syndrome (RADS), and high-altitude pulmonary edema (HAPE). Although the group hiked to Kongma La Pass (elevation, 5,545 m), and slept at 5,200 m (960 m higher than their starting point), the patient had not exhibited any symptoms of altitude illness (eg, headache, dizziness, fatigue, sleep disturbances, anorexia, nausea). Auscultation of the patient by the two physicians who accompanied him on the hike noted mild expiratory wheezing without rales or rhonchi, making HAPE unlikely in the differential diagnosis.
Although it is likely the patient had significant CO exposure, he did not display profound symptoms of CO toxicity (eg, light-headedness, headache, vertigo, nausea, or confusion). It is unclear whether the symptoms of decreased exercise tolerance and fatigue were due to CO poisoning as no co-oximeter was available to assess the patient’s CO levels.2,3 Upon return from the trip, pulse oximetry showed the patient to have an oxygen (O2) saturation of 89% on room air, which was within appropriate range for their altitude.
One of the physicians offered the patient an albuterol metered-dose inhaler, which provided profound and immediate relief of his coughing and wheezing. The patient continued to use the albuterol inhaler every 2 to 4 hours over the next 2 days. The dyspnea on exertion and decreased exercise tolerance improved after 24 hours of treatment; the rest of his respiratory symptoms resolved after approximately 5 days at the starting elevation, and he returned to his usual baseline state of health. No follow-up chest X-rays were obtained, and the patient has had no subsequent recurrence of these symptoms despite return to higher altitude in the subsequent year.
Discussion
Nearly one-third to one-half of the world’s population relies on biomass fuels for domestic heating or cooking, with developing countries accounting for 99% of its use.4 These fuels consist of dried dung cakes or patties, agricultural products, coal, and firewood. In the Khumbu region of Nepal above timberline, yak-dung patties are used exclusively for heating and frequently for cooking. Most guesthouses in this region have potbelly-style stoves in the common dining areas, which are fueled by yak dung and ventilated with a chimney.
Pulmonary Pathophysiology of Inhaled Irritants
Biomass fuels are responsible for numerous air pollutants due to incomplete combustion. These fuels suspend particulate matter, CO, nitrogen dioxide, polycyclic aromatic hydrocarbons, and volatile organic compounds, including acetone, methyl ethyl ketone, benzene, formaldehyde, and toluene.5 Compared to other biomass fuel sources, dung-cake combustion results in higher emissions of relatively very small particulate matter with peak concentrations ranging from 0.23 to 0.3 μm in size, which penetrate and affect the distal airway. 6 Their combustion also releases volatile organic compounds and CO.7,8 Aside from indoor air pollution, yak-dung combustion in the Nepali Himalayan valley contributes significantly to the ambient airborne concentrations of lead, copper, aluminum, magnesium, and elemental and organic carbon.9
Emergency physicians (EPs) are often the first-line treating physician for patients exposed not only to biomass fuels, but also home, forest, or occupational fires resulting in smoke inhalation or AII.10 These terms refer to the wide number of substances that may be present in the smoke and collectively affect the patient. Inhaled substances classified as irritants, such as smoke and particulate matter, can harm the epithelium of the respiratory tract, with highly water-soluble or larger particles (>10 μm) mostly affecting the upper airways. These irritants cause symptoms of progressive coughing, and wheezing; or stridor resulting in tracheitis, bronchitis, bronchiolitis, alveolitis, pulmonary edema, and/or airway obstruction. Smaller particles (<2.5 μm) can penetrate further into the lung and affect the distal airway to a greater degree. These particles are able to infiltrate the terminal bronchioles and alveoli, leading to localized inflammatory reaction and bronchospasm.11Smoke may also contain chemical asphyxiants such as CO or hydrogen cyanide, which can be absorbed, leading to systemic toxicity and interfering with O2 delivery or utilization. Importantly, high concentrations of any gas can act as an asphyxiant due to displacement of O2.12 Thermal injuries are also possible from fire and smoke exposure, typically affecting the upper airways. Steam inhalation can even cause irritation and burns below the vocal cords.13
Reactive Airway Disease Syndrome
Reactive airway disease syndrome is a constellation of symptoms presenting similar to asthma with persistent airway reactivity after an AII, and is the most common sequelae of exposure to biomass fuel combustion. This syndrome is not specifically caused by one type of particulate, irritant, or chemical component of the smoke.
Symptoms
Symptoms such as cough, dyspnea, and wheezing may begin minutes after exposure, and can persist for years due to bronchial hyperresponsiveness.14 These chronic symptoms of RADS have been well highlighted by New York Fire Department rescue workers from the World Trade Center collapse, of whom 16% continued to show symptoms of RADS 1 year later.15
Treatment
Bronchodilator therapy is the mainstay of treatment for RADS. Patients who have RADS often respond well to treatment, and show improvement in symptoms and spirometry testing.
Sequelae Associated With Biomass Fuel Exposure
A cross-sectional study showed significant reductions (P < .001) in all pulmonary function testing parameters for cow-dung fuel users compared to those who use modern energy sources: forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and mid-flow rate between the first 25% and 75% of forced expiratory flow. Linear regression showed a 12.4% reduction in FVC of cow-dung users, and 36% (compared to 20% in modern energy-source users) were noted to have pulmonary infections.16
Due to these emissions, biomass fuel exposure causes high levels of morbidity and mortality in developing countries, with nearly 2 million attributable deaths annually.1 Chronic exposure to biomass fuel emissions can lead to increased risk of diseases, including respiratory problems (eg, pneumonia, tuberculosis and chronic obstructive pulmonary disease, lung cancer, asthma), low birthweight, cataracts, and cardiovascular events.2,17 Women are at higher risk compared to other family members, as they typically spend approximately 3 to 4 hours longer daily in tents,5 and perform the majoring of the cooking duties. For pregnant women, the developing fetus may also be exposed, which can lead to increased rates of fetal demise.18
Conclusion
Our report represents the first reported case of “dung lung” or RADS from yak-dung biomass fuel combustion exposure. In the medical literature, there has been one previous case report of dung lung by Osbern and Crapo19 in 1981 in which the authors described three patients who died from aspiration of liquid manure in a storage facility.Our case highlights the prevalence of biomass fuel combustion in the third world, the dangerous air pollutants from their emissions, and the morbidity associated with improper ventilation of biomass fuel combustion.
1. Rodway GW, Windsor JS. Airway mucociliary function at high altitude. Wilderness Environ Med. 2006;17(4):271-275.
2. Leigh-Smith S. Carbon monoxide poisoning in tents—a review. Wilderness Environ Med. 2004;15(3):157-163.
3. Lipman GL. Carbon monoxide toxicity at high altitude [Commentary]. Wilderness Environ Med. 2006;17(2):144-145.
4. Prasad R, Singh A, Garg R, Giridhar GB. Biomass fuel exposure and respiratory diseases in India. Biosci Trends. 2012;6(5):219-228.
5. Kim KH, Jahan SA, Kabir E. A review of diseases associated with household air pollution due to the use of biomass fuels. J Hazard Mater. 2011;192(2):425-431.
6. Park D, Barabad ML, Lee G, et al. Emission characteristics of particulate matter and volatile organic compounds in cow dung combustion. Environ Sci Technol. 2013;47(22):12952-12957.
7. Venkataraman C, Rao GU. Emission factors of carbon monoxide and size-resolved aerosols from biofuel combustion. Environ Sci Technol. 2001;35(10):2100-2107.
8. Chen PF, Li CL, Kang SC, et al. [Indoor air pollution in the Nam Co and Ando Regions in the Tibetan Plateau]. [Article in Chinese]. Huan Jing Ke Xue. 2011;32(5):1231-1236.
9. avidson CI, Grimm TC, Nasta MA. Airborne lead and other elements derived from local fires in the himalayas. Science. 1981;214(4527):1344-1366.
10. Gorguner M, Akgun M. Acute inhalation injury. Eurasian J Med. 2010;42(1):28-35.
11. Ainslie G. Inhalational injuries produced by smoke and nitrogen dioxide. Respir Med. 1993;87(3):169-174.
12. Glazer CS. Acute inhalational injury. In: Hanley ME, Welsh CH, eds. Current Diagnosis & Treatment in Pulmonary Medicine. International Ed. New York, NY: McGraw Hill; 2003:354-360.
13. Gu TL, Liou SH, Hsu CH, Hsu JC, Wu TN. Acute health hazards of firefighters after fighting a department store fire. Indust Health. 1996;34(1):13-23.
14. Alberts WM, do Picco GA. Reactive airways dysfunction syndrome. Chest. 1996;109(6):1618-1626.
15. Banauch GI, Dhala A, Alleyne D, et al. Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Crit Care Med. 2005;33(1 Suppl):S102-S106.
16. Sümer H, Turaçlar UT, Onarlioğlu T, Ozdemir L, Zwahlen M. The association of biomass fuel combustion on pulmonary function tests in the adult population of Mid-Anatolia. Soz Praventivmed. 2004;49(4):247-253.
17. Cesaroni G, Forastiere F, Stafoggia M, et al. Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ. 2014;348:f7412.
18. de Koning HW, Smith KR, Last JM. Biomass fuel combustion and health. Bull World Health Organ. 1985;63(1):11-26.
19. Osbern LN, Crapo RO. Dung lung: a report of toxic exposure to liquid manure. Ann Intern Med. 1981;95(3):312-314.
Case
A 30-year-old man without prior respiratory illness presented with coughing, wheezing, dyspnea on exertion, and decreased exercise tolerance after a 7-hour overnight exposure to yak-dung smoke. This episode took place at 4,240 m elevation in Pheriche village, along the Everest Base Camp trekking route within the Khumbu region of the Nepali Himalayas. Prior to going to bed that evening, the group of five cohabitants had a difficult time igniting the potbelly heating stove filled with yak-dung biomass fuel in the common room. Each time they tried to light it, the fire would smolder and go out within a few minutes, despite the group’s attempts at adjusting the flue and air intake. Eventually, they abandoned further attempts and retired to bed at approximately 9:30
The differential diagnosis included altitude illness, airway mucociliary dysfunction (commonly known as Khumbu cough),1 carbon monoxide (CO) poisoning, acute inhalation injury (AII) resulting in reactive airway disease syndrome (RADS), and high-altitude pulmonary edema (HAPE). Although the group hiked to Kongma La Pass (elevation, 5,545 m), and slept at 5,200 m (960 m higher than their starting point), the patient had not exhibited any symptoms of altitude illness (eg, headache, dizziness, fatigue, sleep disturbances, anorexia, nausea). Auscultation of the patient by the two physicians who accompanied him on the hike noted mild expiratory wheezing without rales or rhonchi, making HAPE unlikely in the differential diagnosis.
Although it is likely the patient had significant CO exposure, he did not display profound symptoms of CO toxicity (eg, light-headedness, headache, vertigo, nausea, or confusion). It is unclear whether the symptoms of decreased exercise tolerance and fatigue were due to CO poisoning as no co-oximeter was available to assess the patient’s CO levels.2,3 Upon return from the trip, pulse oximetry showed the patient to have an oxygen (O2) saturation of 89% on room air, which was within appropriate range for their altitude.
One of the physicians offered the patient an albuterol metered-dose inhaler, which provided profound and immediate relief of his coughing and wheezing. The patient continued to use the albuterol inhaler every 2 to 4 hours over the next 2 days. The dyspnea on exertion and decreased exercise tolerance improved after 24 hours of treatment; the rest of his respiratory symptoms resolved after approximately 5 days at the starting elevation, and he returned to his usual baseline state of health. No follow-up chest X-rays were obtained, and the patient has had no subsequent recurrence of these symptoms despite return to higher altitude in the subsequent year.
Discussion
Nearly one-third to one-half of the world’s population relies on biomass fuels for domestic heating or cooking, with developing countries accounting for 99% of its use.4 These fuels consist of dried dung cakes or patties, agricultural products, coal, and firewood. In the Khumbu region of Nepal above timberline, yak-dung patties are used exclusively for heating and frequently for cooking. Most guesthouses in this region have potbelly-style stoves in the common dining areas, which are fueled by yak dung and ventilated with a chimney.
Pulmonary Pathophysiology of Inhaled Irritants
Biomass fuels are responsible for numerous air pollutants due to incomplete combustion. These fuels suspend particulate matter, CO, nitrogen dioxide, polycyclic aromatic hydrocarbons, and volatile organic compounds, including acetone, methyl ethyl ketone, benzene, formaldehyde, and toluene.5 Compared to other biomass fuel sources, dung-cake combustion results in higher emissions of relatively very small particulate matter with peak concentrations ranging from 0.23 to 0.3 μm in size, which penetrate and affect the distal airway. 6 Their combustion also releases volatile organic compounds and CO.7,8 Aside from indoor air pollution, yak-dung combustion in the Nepali Himalayan valley contributes significantly to the ambient airborne concentrations of lead, copper, aluminum, magnesium, and elemental and organic carbon.9
Emergency physicians (EPs) are often the first-line treating physician for patients exposed not only to biomass fuels, but also home, forest, or occupational fires resulting in smoke inhalation or AII.10 These terms refer to the wide number of substances that may be present in the smoke and collectively affect the patient. Inhaled substances classified as irritants, such as smoke and particulate matter, can harm the epithelium of the respiratory tract, with highly water-soluble or larger particles (>10 μm) mostly affecting the upper airways. These irritants cause symptoms of progressive coughing, and wheezing; or stridor resulting in tracheitis, bronchitis, bronchiolitis, alveolitis, pulmonary edema, and/or airway obstruction. Smaller particles (<2.5 μm) can penetrate further into the lung and affect the distal airway to a greater degree. These particles are able to infiltrate the terminal bronchioles and alveoli, leading to localized inflammatory reaction and bronchospasm.11Smoke may also contain chemical asphyxiants such as CO or hydrogen cyanide, which can be absorbed, leading to systemic toxicity and interfering with O2 delivery or utilization. Importantly, high concentrations of any gas can act as an asphyxiant due to displacement of O2.12 Thermal injuries are also possible from fire and smoke exposure, typically affecting the upper airways. Steam inhalation can even cause irritation and burns below the vocal cords.13
Reactive Airway Disease Syndrome
Reactive airway disease syndrome is a constellation of symptoms presenting similar to asthma with persistent airway reactivity after an AII, and is the most common sequelae of exposure to biomass fuel combustion. This syndrome is not specifically caused by one type of particulate, irritant, or chemical component of the smoke.
Symptoms
Symptoms such as cough, dyspnea, and wheezing may begin minutes after exposure, and can persist for years due to bronchial hyperresponsiveness.14 These chronic symptoms of RADS have been well highlighted by New York Fire Department rescue workers from the World Trade Center collapse, of whom 16% continued to show symptoms of RADS 1 year later.15
Treatment
Bronchodilator therapy is the mainstay of treatment for RADS. Patients who have RADS often respond well to treatment, and show improvement in symptoms and spirometry testing.
Sequelae Associated With Biomass Fuel Exposure
A cross-sectional study showed significant reductions (P < .001) in all pulmonary function testing parameters for cow-dung fuel users compared to those who use modern energy sources: forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and mid-flow rate between the first 25% and 75% of forced expiratory flow. Linear regression showed a 12.4% reduction in FVC of cow-dung users, and 36% (compared to 20% in modern energy-source users) were noted to have pulmonary infections.16
Due to these emissions, biomass fuel exposure causes high levels of morbidity and mortality in developing countries, with nearly 2 million attributable deaths annually.1 Chronic exposure to biomass fuel emissions can lead to increased risk of diseases, including respiratory problems (eg, pneumonia, tuberculosis and chronic obstructive pulmonary disease, lung cancer, asthma), low birthweight, cataracts, and cardiovascular events.2,17 Women are at higher risk compared to other family members, as they typically spend approximately 3 to 4 hours longer daily in tents,5 and perform the majoring of the cooking duties. For pregnant women, the developing fetus may also be exposed, which can lead to increased rates of fetal demise.18
Conclusion
Our report represents the first reported case of “dung lung” or RADS from yak-dung biomass fuel combustion exposure. In the medical literature, there has been one previous case report of dung lung by Osbern and Crapo19 in 1981 in which the authors described three patients who died from aspiration of liquid manure in a storage facility.Our case highlights the prevalence of biomass fuel combustion in the third world, the dangerous air pollutants from their emissions, and the morbidity associated with improper ventilation of biomass fuel combustion.
Case
A 30-year-old man without prior respiratory illness presented with coughing, wheezing, dyspnea on exertion, and decreased exercise tolerance after a 7-hour overnight exposure to yak-dung smoke. This episode took place at 4,240 m elevation in Pheriche village, along the Everest Base Camp trekking route within the Khumbu region of the Nepali Himalayas. Prior to going to bed that evening, the group of five cohabitants had a difficult time igniting the potbelly heating stove filled with yak-dung biomass fuel in the common room. Each time they tried to light it, the fire would smolder and go out within a few minutes, despite the group’s attempts at adjusting the flue and air intake. Eventually, they abandoned further attempts and retired to bed at approximately 9:30
The differential diagnosis included altitude illness, airway mucociliary dysfunction (commonly known as Khumbu cough),1 carbon monoxide (CO) poisoning, acute inhalation injury (AII) resulting in reactive airway disease syndrome (RADS), and high-altitude pulmonary edema (HAPE). Although the group hiked to Kongma La Pass (elevation, 5,545 m), and slept at 5,200 m (960 m higher than their starting point), the patient had not exhibited any symptoms of altitude illness (eg, headache, dizziness, fatigue, sleep disturbances, anorexia, nausea). Auscultation of the patient by the two physicians who accompanied him on the hike noted mild expiratory wheezing without rales or rhonchi, making HAPE unlikely in the differential diagnosis.
Although it is likely the patient had significant CO exposure, he did not display profound symptoms of CO toxicity (eg, light-headedness, headache, vertigo, nausea, or confusion). It is unclear whether the symptoms of decreased exercise tolerance and fatigue were due to CO poisoning as no co-oximeter was available to assess the patient’s CO levels.2,3 Upon return from the trip, pulse oximetry showed the patient to have an oxygen (O2) saturation of 89% on room air, which was within appropriate range for their altitude.
One of the physicians offered the patient an albuterol metered-dose inhaler, which provided profound and immediate relief of his coughing and wheezing. The patient continued to use the albuterol inhaler every 2 to 4 hours over the next 2 days. The dyspnea on exertion and decreased exercise tolerance improved after 24 hours of treatment; the rest of his respiratory symptoms resolved after approximately 5 days at the starting elevation, and he returned to his usual baseline state of health. No follow-up chest X-rays were obtained, and the patient has had no subsequent recurrence of these symptoms despite return to higher altitude in the subsequent year.
Discussion
Nearly one-third to one-half of the world’s population relies on biomass fuels for domestic heating or cooking, with developing countries accounting for 99% of its use.4 These fuels consist of dried dung cakes or patties, agricultural products, coal, and firewood. In the Khumbu region of Nepal above timberline, yak-dung patties are used exclusively for heating and frequently for cooking. Most guesthouses in this region have potbelly-style stoves in the common dining areas, which are fueled by yak dung and ventilated with a chimney.
Pulmonary Pathophysiology of Inhaled Irritants
Biomass fuels are responsible for numerous air pollutants due to incomplete combustion. These fuels suspend particulate matter, CO, nitrogen dioxide, polycyclic aromatic hydrocarbons, and volatile organic compounds, including acetone, methyl ethyl ketone, benzene, formaldehyde, and toluene.5 Compared to other biomass fuel sources, dung-cake combustion results in higher emissions of relatively very small particulate matter with peak concentrations ranging from 0.23 to 0.3 μm in size, which penetrate and affect the distal airway. 6 Their combustion also releases volatile organic compounds and CO.7,8 Aside from indoor air pollution, yak-dung combustion in the Nepali Himalayan valley contributes significantly to the ambient airborne concentrations of lead, copper, aluminum, magnesium, and elemental and organic carbon.9
Emergency physicians (EPs) are often the first-line treating physician for patients exposed not only to biomass fuels, but also home, forest, or occupational fires resulting in smoke inhalation or AII.10 These terms refer to the wide number of substances that may be present in the smoke and collectively affect the patient. Inhaled substances classified as irritants, such as smoke and particulate matter, can harm the epithelium of the respiratory tract, with highly water-soluble or larger particles (>10 μm) mostly affecting the upper airways. These irritants cause symptoms of progressive coughing, and wheezing; or stridor resulting in tracheitis, bronchitis, bronchiolitis, alveolitis, pulmonary edema, and/or airway obstruction. Smaller particles (<2.5 μm) can penetrate further into the lung and affect the distal airway to a greater degree. These particles are able to infiltrate the terminal bronchioles and alveoli, leading to localized inflammatory reaction and bronchospasm.11Smoke may also contain chemical asphyxiants such as CO or hydrogen cyanide, which can be absorbed, leading to systemic toxicity and interfering with O2 delivery or utilization. Importantly, high concentrations of any gas can act as an asphyxiant due to displacement of O2.12 Thermal injuries are also possible from fire and smoke exposure, typically affecting the upper airways. Steam inhalation can even cause irritation and burns below the vocal cords.13
Reactive Airway Disease Syndrome
Reactive airway disease syndrome is a constellation of symptoms presenting similar to asthma with persistent airway reactivity after an AII, and is the most common sequelae of exposure to biomass fuel combustion. This syndrome is not specifically caused by one type of particulate, irritant, or chemical component of the smoke.
Symptoms
Symptoms such as cough, dyspnea, and wheezing may begin minutes after exposure, and can persist for years due to bronchial hyperresponsiveness.14 These chronic symptoms of RADS have been well highlighted by New York Fire Department rescue workers from the World Trade Center collapse, of whom 16% continued to show symptoms of RADS 1 year later.15
Treatment
Bronchodilator therapy is the mainstay of treatment for RADS. Patients who have RADS often respond well to treatment, and show improvement in symptoms and spirometry testing.
Sequelae Associated With Biomass Fuel Exposure
A cross-sectional study showed significant reductions (P < .001) in all pulmonary function testing parameters for cow-dung fuel users compared to those who use modern energy sources: forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and mid-flow rate between the first 25% and 75% of forced expiratory flow. Linear regression showed a 12.4% reduction in FVC of cow-dung users, and 36% (compared to 20% in modern energy-source users) were noted to have pulmonary infections.16
Due to these emissions, biomass fuel exposure causes high levels of morbidity and mortality in developing countries, with nearly 2 million attributable deaths annually.1 Chronic exposure to biomass fuel emissions can lead to increased risk of diseases, including respiratory problems (eg, pneumonia, tuberculosis and chronic obstructive pulmonary disease, lung cancer, asthma), low birthweight, cataracts, and cardiovascular events.2,17 Women are at higher risk compared to other family members, as they typically spend approximately 3 to 4 hours longer daily in tents,5 and perform the majoring of the cooking duties. For pregnant women, the developing fetus may also be exposed, which can lead to increased rates of fetal demise.18
Conclusion
Our report represents the first reported case of “dung lung” or RADS from yak-dung biomass fuel combustion exposure. In the medical literature, there has been one previous case report of dung lung by Osbern and Crapo19 in 1981 in which the authors described three patients who died from aspiration of liquid manure in a storage facility.Our case highlights the prevalence of biomass fuel combustion in the third world, the dangerous air pollutants from their emissions, and the morbidity associated with improper ventilation of biomass fuel combustion.
1. Rodway GW, Windsor JS. Airway mucociliary function at high altitude. Wilderness Environ Med. 2006;17(4):271-275.
2. Leigh-Smith S. Carbon monoxide poisoning in tents—a review. Wilderness Environ Med. 2004;15(3):157-163.
3. Lipman GL. Carbon monoxide toxicity at high altitude [Commentary]. Wilderness Environ Med. 2006;17(2):144-145.
4. Prasad R, Singh A, Garg R, Giridhar GB. Biomass fuel exposure and respiratory diseases in India. Biosci Trends. 2012;6(5):219-228.
5. Kim KH, Jahan SA, Kabir E. A review of diseases associated with household air pollution due to the use of biomass fuels. J Hazard Mater. 2011;192(2):425-431.
6. Park D, Barabad ML, Lee G, et al. Emission characteristics of particulate matter and volatile organic compounds in cow dung combustion. Environ Sci Technol. 2013;47(22):12952-12957.
7. Venkataraman C, Rao GU. Emission factors of carbon monoxide and size-resolved aerosols from biofuel combustion. Environ Sci Technol. 2001;35(10):2100-2107.
8. Chen PF, Li CL, Kang SC, et al. [Indoor air pollution in the Nam Co and Ando Regions in the Tibetan Plateau]. [Article in Chinese]. Huan Jing Ke Xue. 2011;32(5):1231-1236.
9. avidson CI, Grimm TC, Nasta MA. Airborne lead and other elements derived from local fires in the himalayas. Science. 1981;214(4527):1344-1366.
10. Gorguner M, Akgun M. Acute inhalation injury. Eurasian J Med. 2010;42(1):28-35.
11. Ainslie G. Inhalational injuries produced by smoke and nitrogen dioxide. Respir Med. 1993;87(3):169-174.
12. Glazer CS. Acute inhalational injury. In: Hanley ME, Welsh CH, eds. Current Diagnosis & Treatment in Pulmonary Medicine. International Ed. New York, NY: McGraw Hill; 2003:354-360.
13. Gu TL, Liou SH, Hsu CH, Hsu JC, Wu TN. Acute health hazards of firefighters after fighting a department store fire. Indust Health. 1996;34(1):13-23.
14. Alberts WM, do Picco GA. Reactive airways dysfunction syndrome. Chest. 1996;109(6):1618-1626.
15. Banauch GI, Dhala A, Alleyne D, et al. Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Crit Care Med. 2005;33(1 Suppl):S102-S106.
16. Sümer H, Turaçlar UT, Onarlioğlu T, Ozdemir L, Zwahlen M. The association of biomass fuel combustion on pulmonary function tests in the adult population of Mid-Anatolia. Soz Praventivmed. 2004;49(4):247-253.
17. Cesaroni G, Forastiere F, Stafoggia M, et al. Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ. 2014;348:f7412.
18. de Koning HW, Smith KR, Last JM. Biomass fuel combustion and health. Bull World Health Organ. 1985;63(1):11-26.
19. Osbern LN, Crapo RO. Dung lung: a report of toxic exposure to liquid manure. Ann Intern Med. 1981;95(3):312-314.
1. Rodway GW, Windsor JS. Airway mucociliary function at high altitude. Wilderness Environ Med. 2006;17(4):271-275.
2. Leigh-Smith S. Carbon monoxide poisoning in tents—a review. Wilderness Environ Med. 2004;15(3):157-163.
3. Lipman GL. Carbon monoxide toxicity at high altitude [Commentary]. Wilderness Environ Med. 2006;17(2):144-145.
4. Prasad R, Singh A, Garg R, Giridhar GB. Biomass fuel exposure and respiratory diseases in India. Biosci Trends. 2012;6(5):219-228.
5. Kim KH, Jahan SA, Kabir E. A review of diseases associated with household air pollution due to the use of biomass fuels. J Hazard Mater. 2011;192(2):425-431.
6. Park D, Barabad ML, Lee G, et al. Emission characteristics of particulate matter and volatile organic compounds in cow dung combustion. Environ Sci Technol. 2013;47(22):12952-12957.
7. Venkataraman C, Rao GU. Emission factors of carbon monoxide and size-resolved aerosols from biofuel combustion. Environ Sci Technol. 2001;35(10):2100-2107.
8. Chen PF, Li CL, Kang SC, et al. [Indoor air pollution in the Nam Co and Ando Regions in the Tibetan Plateau]. [Article in Chinese]. Huan Jing Ke Xue. 2011;32(5):1231-1236.
9. avidson CI, Grimm TC, Nasta MA. Airborne lead and other elements derived from local fires in the himalayas. Science. 1981;214(4527):1344-1366.
10. Gorguner M, Akgun M. Acute inhalation injury. Eurasian J Med. 2010;42(1):28-35.
11. Ainslie G. Inhalational injuries produced by smoke and nitrogen dioxide. Respir Med. 1993;87(3):169-174.
12. Glazer CS. Acute inhalational injury. In: Hanley ME, Welsh CH, eds. Current Diagnosis & Treatment in Pulmonary Medicine. International Ed. New York, NY: McGraw Hill; 2003:354-360.
13. Gu TL, Liou SH, Hsu CH, Hsu JC, Wu TN. Acute health hazards of firefighters after fighting a department store fire. Indust Health. 1996;34(1):13-23.
14. Alberts WM, do Picco GA. Reactive airways dysfunction syndrome. Chest. 1996;109(6):1618-1626.
15. Banauch GI, Dhala A, Alleyne D, et al. Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Crit Care Med. 2005;33(1 Suppl):S102-S106.
16. Sümer H, Turaçlar UT, Onarlioğlu T, Ozdemir L, Zwahlen M. The association of biomass fuel combustion on pulmonary function tests in the adult population of Mid-Anatolia. Soz Praventivmed. 2004;49(4):247-253.
17. Cesaroni G, Forastiere F, Stafoggia M, et al. Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ. 2014;348:f7412.
18. de Koning HW, Smith KR, Last JM. Biomass fuel combustion and health. Bull World Health Organ. 1985;63(1):11-26.
19. Osbern LN, Crapo RO. Dung lung: a report of toxic exposure to liquid manure. Ann Intern Med. 1981;95(3):312-314.

Parents look online for atopic dermatitis advice
Many caregivers of children with atopic dermatitis do not receive clear instructions on how to properly use topical corticosteroids and seek advice on online forums, according to Emma Teasdale, PhD, and her associates.
The investigators analyzed 27 forum discussions involving 95 participants from 2003 to 2015 and found that parents expressed a range of beliefs regarding the use of topical corticosteroids. Some parents expressed positive views, but many were cautious and perceived topical corticosteroids as unnatural or too strong. Notably, parents said they believed that topical corticosteroids thinned or weakened the skin.
Parents also expressed uncertainty over how to use topical corticosteroids. Common questions involved duration of use, where and when to apply, and confusion over the strength of different preparations. Parents also noted that they received conflicting physician instructions regarding duration, dosage, tapering, and safety.
“Given the prevalence of concerns about potential adverse effects of topical-corticosteroids, it would seem prudent to signpost parents/carers towards convenient, consistent, evidence-based information to ensure that the potential negative impacts of seeking (unsubstantiated) medical advice online are minimized. In the absence of such information they are likely to turn to online discussion forums as their sole resource where, although much useful support and advice can be found, some is of questionable validity,” the investigators concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.15130).
Many caregivers of children with atopic dermatitis do not receive clear instructions on how to properly use topical corticosteroids and seek advice on online forums, according to Emma Teasdale, PhD, and her associates.
The investigators analyzed 27 forum discussions involving 95 participants from 2003 to 2015 and found that parents expressed a range of beliefs regarding the use of topical corticosteroids. Some parents expressed positive views, but many were cautious and perceived topical corticosteroids as unnatural or too strong. Notably, parents said they believed that topical corticosteroids thinned or weakened the skin.
Parents also expressed uncertainty over how to use topical corticosteroids. Common questions involved duration of use, where and when to apply, and confusion over the strength of different preparations. Parents also noted that they received conflicting physician instructions regarding duration, dosage, tapering, and safety.
“Given the prevalence of concerns about potential adverse effects of topical-corticosteroids, it would seem prudent to signpost parents/carers towards convenient, consistent, evidence-based information to ensure that the potential negative impacts of seeking (unsubstantiated) medical advice online are minimized. In the absence of such information they are likely to turn to online discussion forums as their sole resource where, although much useful support and advice can be found, some is of questionable validity,” the investigators concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.15130).
Many caregivers of children with atopic dermatitis do not receive clear instructions on how to properly use topical corticosteroids and seek advice on online forums, according to Emma Teasdale, PhD, and her associates.
The investigators analyzed 27 forum discussions involving 95 participants from 2003 to 2015 and found that parents expressed a range of beliefs regarding the use of topical corticosteroids. Some parents expressed positive views, but many were cautious and perceived topical corticosteroids as unnatural or too strong. Notably, parents said they believed that topical corticosteroids thinned or weakened the skin.
Parents also expressed uncertainty over how to use topical corticosteroids. Common questions involved duration of use, where and when to apply, and confusion over the strength of different preparations. Parents also noted that they received conflicting physician instructions regarding duration, dosage, tapering, and safety.
“Given the prevalence of concerns about potential adverse effects of topical-corticosteroids, it would seem prudent to signpost parents/carers towards convenient, consistent, evidence-based information to ensure that the potential negative impacts of seeking (unsubstantiated) medical advice online are minimized. In the absence of such information they are likely to turn to online discussion forums as their sole resource where, although much useful support and advice can be found, some is of questionable validity,” the investigators concluded.
Find the full study in the British Journal of Dermatology (doi: 10.1111/bjd.15130).
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Restrict gluten if necessary, but confirm condition first
SAN FRANCISCO – Elimination diet crazes have been around for centuries, and one of today’s biggest targets is gluten, contributing to an industry of gluten-free products with revenue in the billions of dollars.
But does taking gluten off your child’s plate actually improve their health? It will if they have a condition in which gluten actually causes symptoms, explained Michelle M. Pietzak, MD, a pediatrician at the University of Southern California, Los Angeles.
Gluten is a mixture of proteins found in wheat, rye, barley, oats, corn, and rice that gives food its elasticity and helps dough rise. Only the gluten in wheat, rye, and barley causes gluten-related symptoms, but it is found in a variety of derivative products, such as spelt, kamut, triticale, couscous, bulgar, faro, matzo flour, and other grains as well. Oats are also considered cross-contaminated with gluten because they are milled with wheat, and other foods containing gluten may be difficult to identify due to food labeling and preparation practices in the United States.
For those with celiac disease, wheat allergy, irritable bowel syndrome (IBS), or nonceliac gluten sensitivity or intolerance, a gluten-free diet can reduce or eliminate the symptoms causing problems. For others, however, the symptoms likely come from somewhere besides gluten or may be a nocebo effect, where a patient who expects negative symptoms becomes more likely to have them.
Lactose intolerance is one example that can cause symptoms similar to those that respond to restricting gluten. Another is sensitivity to fructans, a wheat carbohydrate and one of the fermentable oligo-di-monosaccharides and polyols (FODMAPs) that can improve IBS when restricted. Imbalance in a person’s gut bacteria, called dysbiosis, also may cause similar symptoms and results from excess yeast, parasites, or an overgrowth of bad bacteria in the absence of beneficial ones.
Understanding celiac disease
This immune-mediated disease causes primarily gastrointestinal symptoms when someone ingests proteins called prolamines, which those with celiac disease are genetically predisposed to have difficulty digesting. Common symptoms include diarrhea, nausea, vomiting, abdominal pain, constipation, appetite changes, and, in unusual cases, excess fat in the feces (steatorrhea).
But celiac disease also may contribute to a short stature, osteoporosis, dermatitis herpetiformis, delayed onset of puberty, infertility, anemia (from iron and/or folic acid deficits), epilepsy, and behavioral changes. Although those with celiac disease are at a higher risk for arthritis, osteoporosis, osteopenia, osteomalacia, and rickets, a gluten-free diet can improve children’s low bone mineral density.
Screening for celiac disease includes testing for antigliadin (AGA) IgG and IgA, antiendomysial IgA, anti-tissue transglutaminase (tTG) IgA, total serum IgA, and genetic testing related to HLA-DQ2 and HLA-DQ8 genes.
Wheat allergy
A wheat allergy, among the eight most common food allergies, involves an IgE-mediated reaction to water- and salt-insoluble gliadins, especially omega-5 gliadin, which can cause anaphylaxis in a wheat-allergic person who exercises after ingesting wheat. Symptoms of wheat allergy include hives; swelling, itching or irritation of the mouth, throat, eyes, and nose; difficulty breathing; and cramps, nausea, vomiting, and diarrhea. Wheat allergy most commonly occurs in infants or toddlers, and typically co-occurs with other food allergies, but children usually outgrow the allergy by ages 3-5 years.
Nonceliac gluten sensitivity or intolerance
Physicians only should consider gluten insensitivity or intolerance after ruling out celiac disease and wheat allergy. Less understood and more controversial, gluten sensitivity or intolerance may be an immune-mediated condition – or instead an intestinal malfunction. Some patients may simply have an intolerance to high fiber foods in general. Patients with this sensitivity or intolerance will have a normal intestinal biopsy, but AGA IgG and/or IgA testing and genetic HLA-DQ2 testing may be positive. The clinical diagnosis is ultimately one of exclusion determined when a gluten-free diet alleviates symptoms.
Although gas, diarrhea, weight loss, and abdominal pain are the most common symptoms, other transient symptoms may include dyspepsia, nausea, vomiting, bloating, constipation, intestinal rumbling, joint or bone pain, muscle cramps or pain, fatigue, numbness, cramps, headaches, rashes, tongue inflammation, anemia, leg numbness, osteoporosis, or unexplained anemia.
Another potential effect of gluten sensitivity is dermatitis herpetiformis, a skin inflammation involving blisters, hives, or other types of erythematous or urticarial papules, usually symmetrically distributed, with severe itching. Although 90% of individuals with dermatitis herpetiformis lack any gastrointestinal symptoms, about 75% have villous atrophy, Dr. Pietzak said.
Even less understood are neurologic symptoms of gluten sensitivity and their potential mechanisms. Reported neurologic findings of gluten sensitivity include ataxia, peripheral neuropathy, depression, schizophrenia, epilepsy, and intracranial calcifications.
Irritable bowel syndrome
The similarity of symptoms between IBS and celiac disease has meant many with celiac disease were misdiagnosed with IBS, particularly women, Dr. Pietzak said. To confuse matters more, restricting gluten has shown improvement in IBS symptoms for some patients: in one study, 60% of those with diarrhea returned to having normal stools after 6 months of a gluten-free diet. Again, AGA IgG and tTG IgG testing was more likely to be positive among these patients. IBS and celiac disease can co-occur in patients, but it’s necessary to rule out celiac disease before diagnosing a patient with IBS.
Importance of differential diagnosis
It’s important to know the difference between celiac disease and other conditions because patients may face different risks even if their treatment is similar. Those with celiac disease, for example, have a greater risk of nutritional deficiencies leading to conditions such as iron-deficiency anemia and osteoporosis, and are more likely to develop gastrointestinal cancers or other autoimmune conditions, such as thyroid disease, type 1 diabetes, joint diseases, and liver diseases.
Those with food allergies and intolerances do not share those increased risks, and their symptoms resolve without long-term organ damage when they remove the gluten or wheat from their diet. Further, only those with celiac disease must restrict all foods with gluten. Those with a wheat allergy may be able to eat rye, barley, and oats, for example, and restricting gluten may improve IBS symptoms for only a subset of patients.
Dr. Pietzak has consulted for Nestle Nutrition and is on the speaker’s bureau for Prometheus Labs, a lab which does business in testing for celiac disease.
SAN FRANCISCO – Elimination diet crazes have been around for centuries, and one of today’s biggest targets is gluten, contributing to an industry of gluten-free products with revenue in the billions of dollars.
But does taking gluten off your child’s plate actually improve their health? It will if they have a condition in which gluten actually causes symptoms, explained Michelle M. Pietzak, MD, a pediatrician at the University of Southern California, Los Angeles.
Gluten is a mixture of proteins found in wheat, rye, barley, oats, corn, and rice that gives food its elasticity and helps dough rise. Only the gluten in wheat, rye, and barley causes gluten-related symptoms, but it is found in a variety of derivative products, such as spelt, kamut, triticale, couscous, bulgar, faro, matzo flour, and other grains as well. Oats are also considered cross-contaminated with gluten because they are milled with wheat, and other foods containing gluten may be difficult to identify due to food labeling and preparation practices in the United States.
For those with celiac disease, wheat allergy, irritable bowel syndrome (IBS), or nonceliac gluten sensitivity or intolerance, a gluten-free diet can reduce or eliminate the symptoms causing problems. For others, however, the symptoms likely come from somewhere besides gluten or may be a nocebo effect, where a patient who expects negative symptoms becomes more likely to have them.
Lactose intolerance is one example that can cause symptoms similar to those that respond to restricting gluten. Another is sensitivity to fructans, a wheat carbohydrate and one of the fermentable oligo-di-monosaccharides and polyols (FODMAPs) that can improve IBS when restricted. Imbalance in a person’s gut bacteria, called dysbiosis, also may cause similar symptoms and results from excess yeast, parasites, or an overgrowth of bad bacteria in the absence of beneficial ones.
Understanding celiac disease
This immune-mediated disease causes primarily gastrointestinal symptoms when someone ingests proteins called prolamines, which those with celiac disease are genetically predisposed to have difficulty digesting. Common symptoms include diarrhea, nausea, vomiting, abdominal pain, constipation, appetite changes, and, in unusual cases, excess fat in the feces (steatorrhea).
But celiac disease also may contribute to a short stature, osteoporosis, dermatitis herpetiformis, delayed onset of puberty, infertility, anemia (from iron and/or folic acid deficits), epilepsy, and behavioral changes. Although those with celiac disease are at a higher risk for arthritis, osteoporosis, osteopenia, osteomalacia, and rickets, a gluten-free diet can improve children’s low bone mineral density.
Screening for celiac disease includes testing for antigliadin (AGA) IgG and IgA, antiendomysial IgA, anti-tissue transglutaminase (tTG) IgA, total serum IgA, and genetic testing related to HLA-DQ2 and HLA-DQ8 genes.
Wheat allergy
A wheat allergy, among the eight most common food allergies, involves an IgE-mediated reaction to water- and salt-insoluble gliadins, especially omega-5 gliadin, which can cause anaphylaxis in a wheat-allergic person who exercises after ingesting wheat. Symptoms of wheat allergy include hives; swelling, itching or irritation of the mouth, throat, eyes, and nose; difficulty breathing; and cramps, nausea, vomiting, and diarrhea. Wheat allergy most commonly occurs in infants or toddlers, and typically co-occurs with other food allergies, but children usually outgrow the allergy by ages 3-5 years.
Nonceliac gluten sensitivity or intolerance
Physicians only should consider gluten insensitivity or intolerance after ruling out celiac disease and wheat allergy. Less understood and more controversial, gluten sensitivity or intolerance may be an immune-mediated condition – or instead an intestinal malfunction. Some patients may simply have an intolerance to high fiber foods in general. Patients with this sensitivity or intolerance will have a normal intestinal biopsy, but AGA IgG and/or IgA testing and genetic HLA-DQ2 testing may be positive. The clinical diagnosis is ultimately one of exclusion determined when a gluten-free diet alleviates symptoms.
Although gas, diarrhea, weight loss, and abdominal pain are the most common symptoms, other transient symptoms may include dyspepsia, nausea, vomiting, bloating, constipation, intestinal rumbling, joint or bone pain, muscle cramps or pain, fatigue, numbness, cramps, headaches, rashes, tongue inflammation, anemia, leg numbness, osteoporosis, or unexplained anemia.
Another potential effect of gluten sensitivity is dermatitis herpetiformis, a skin inflammation involving blisters, hives, or other types of erythematous or urticarial papules, usually symmetrically distributed, with severe itching. Although 90% of individuals with dermatitis herpetiformis lack any gastrointestinal symptoms, about 75% have villous atrophy, Dr. Pietzak said.
Even less understood are neurologic symptoms of gluten sensitivity and their potential mechanisms. Reported neurologic findings of gluten sensitivity include ataxia, peripheral neuropathy, depression, schizophrenia, epilepsy, and intracranial calcifications.
Irritable bowel syndrome
The similarity of symptoms between IBS and celiac disease has meant many with celiac disease were misdiagnosed with IBS, particularly women, Dr. Pietzak said. To confuse matters more, restricting gluten has shown improvement in IBS symptoms for some patients: in one study, 60% of those with diarrhea returned to having normal stools after 6 months of a gluten-free diet. Again, AGA IgG and tTG IgG testing was more likely to be positive among these patients. IBS and celiac disease can co-occur in patients, but it’s necessary to rule out celiac disease before diagnosing a patient with IBS.
Importance of differential diagnosis
It’s important to know the difference between celiac disease and other conditions because patients may face different risks even if their treatment is similar. Those with celiac disease, for example, have a greater risk of nutritional deficiencies leading to conditions such as iron-deficiency anemia and osteoporosis, and are more likely to develop gastrointestinal cancers or other autoimmune conditions, such as thyroid disease, type 1 diabetes, joint diseases, and liver diseases.
Those with food allergies and intolerances do not share those increased risks, and their symptoms resolve without long-term organ damage when they remove the gluten or wheat from their diet. Further, only those with celiac disease must restrict all foods with gluten. Those with a wheat allergy may be able to eat rye, barley, and oats, for example, and restricting gluten may improve IBS symptoms for only a subset of patients.
Dr. Pietzak has consulted for Nestle Nutrition and is on the speaker’s bureau for Prometheus Labs, a lab which does business in testing for celiac disease.
SAN FRANCISCO – Elimination diet crazes have been around for centuries, and one of today’s biggest targets is gluten, contributing to an industry of gluten-free products with revenue in the billions of dollars.
But does taking gluten off your child’s plate actually improve their health? It will if they have a condition in which gluten actually causes symptoms, explained Michelle M. Pietzak, MD, a pediatrician at the University of Southern California, Los Angeles.
Gluten is a mixture of proteins found in wheat, rye, barley, oats, corn, and rice that gives food its elasticity and helps dough rise. Only the gluten in wheat, rye, and barley causes gluten-related symptoms, but it is found in a variety of derivative products, such as spelt, kamut, triticale, couscous, bulgar, faro, matzo flour, and other grains as well. Oats are also considered cross-contaminated with gluten because they are milled with wheat, and other foods containing gluten may be difficult to identify due to food labeling and preparation practices in the United States.
For those with celiac disease, wheat allergy, irritable bowel syndrome (IBS), or nonceliac gluten sensitivity or intolerance, a gluten-free diet can reduce or eliminate the symptoms causing problems. For others, however, the symptoms likely come from somewhere besides gluten or may be a nocebo effect, where a patient who expects negative symptoms becomes more likely to have them.
Lactose intolerance is one example that can cause symptoms similar to those that respond to restricting gluten. Another is sensitivity to fructans, a wheat carbohydrate and one of the fermentable oligo-di-monosaccharides and polyols (FODMAPs) that can improve IBS when restricted. Imbalance in a person’s gut bacteria, called dysbiosis, also may cause similar symptoms and results from excess yeast, parasites, or an overgrowth of bad bacteria in the absence of beneficial ones.
Understanding celiac disease
This immune-mediated disease causes primarily gastrointestinal symptoms when someone ingests proteins called prolamines, which those with celiac disease are genetically predisposed to have difficulty digesting. Common symptoms include diarrhea, nausea, vomiting, abdominal pain, constipation, appetite changes, and, in unusual cases, excess fat in the feces (steatorrhea).
But celiac disease also may contribute to a short stature, osteoporosis, dermatitis herpetiformis, delayed onset of puberty, infertility, anemia (from iron and/or folic acid deficits), epilepsy, and behavioral changes. Although those with celiac disease are at a higher risk for arthritis, osteoporosis, osteopenia, osteomalacia, and rickets, a gluten-free diet can improve children’s low bone mineral density.
Screening for celiac disease includes testing for antigliadin (AGA) IgG and IgA, antiendomysial IgA, anti-tissue transglutaminase (tTG) IgA, total serum IgA, and genetic testing related to HLA-DQ2 and HLA-DQ8 genes.
Wheat allergy
A wheat allergy, among the eight most common food allergies, involves an IgE-mediated reaction to water- and salt-insoluble gliadins, especially omega-5 gliadin, which can cause anaphylaxis in a wheat-allergic person who exercises after ingesting wheat. Symptoms of wheat allergy include hives; swelling, itching or irritation of the mouth, throat, eyes, and nose; difficulty breathing; and cramps, nausea, vomiting, and diarrhea. Wheat allergy most commonly occurs in infants or toddlers, and typically co-occurs with other food allergies, but children usually outgrow the allergy by ages 3-5 years.
Nonceliac gluten sensitivity or intolerance
Physicians only should consider gluten insensitivity or intolerance after ruling out celiac disease and wheat allergy. Less understood and more controversial, gluten sensitivity or intolerance may be an immune-mediated condition – or instead an intestinal malfunction. Some patients may simply have an intolerance to high fiber foods in general. Patients with this sensitivity or intolerance will have a normal intestinal biopsy, but AGA IgG and/or IgA testing and genetic HLA-DQ2 testing may be positive. The clinical diagnosis is ultimately one of exclusion determined when a gluten-free diet alleviates symptoms.
Although gas, diarrhea, weight loss, and abdominal pain are the most common symptoms, other transient symptoms may include dyspepsia, nausea, vomiting, bloating, constipation, intestinal rumbling, joint or bone pain, muscle cramps or pain, fatigue, numbness, cramps, headaches, rashes, tongue inflammation, anemia, leg numbness, osteoporosis, or unexplained anemia.
Another potential effect of gluten sensitivity is dermatitis herpetiformis, a skin inflammation involving blisters, hives, or other types of erythematous or urticarial papules, usually symmetrically distributed, with severe itching. Although 90% of individuals with dermatitis herpetiformis lack any gastrointestinal symptoms, about 75% have villous atrophy, Dr. Pietzak said.
Even less understood are neurologic symptoms of gluten sensitivity and their potential mechanisms. Reported neurologic findings of gluten sensitivity include ataxia, peripheral neuropathy, depression, schizophrenia, epilepsy, and intracranial calcifications.
Irritable bowel syndrome
The similarity of symptoms between IBS and celiac disease has meant many with celiac disease were misdiagnosed with IBS, particularly women, Dr. Pietzak said. To confuse matters more, restricting gluten has shown improvement in IBS symptoms for some patients: in one study, 60% of those with diarrhea returned to having normal stools after 6 months of a gluten-free diet. Again, AGA IgG and tTG IgG testing was more likely to be positive among these patients. IBS and celiac disease can co-occur in patients, but it’s necessary to rule out celiac disease before diagnosing a patient with IBS.
Importance of differential diagnosis
It’s important to know the difference between celiac disease and other conditions because patients may face different risks even if their treatment is similar. Those with celiac disease, for example, have a greater risk of nutritional deficiencies leading to conditions such as iron-deficiency anemia and osteoporosis, and are more likely to develop gastrointestinal cancers or other autoimmune conditions, such as thyroid disease, type 1 diabetes, joint diseases, and liver diseases.
Those with food allergies and intolerances do not share those increased risks, and their symptoms resolve without long-term organ damage when they remove the gluten or wheat from their diet. Further, only those with celiac disease must restrict all foods with gluten. Those with a wheat allergy may be able to eat rye, barley, and oats, for example, and restricting gluten may improve IBS symptoms for only a subset of patients.
Dr. Pietzak has consulted for Nestle Nutrition and is on the speaker’s bureau for Prometheus Labs, a lab which does business in testing for celiac disease.
EXPERT ANALYSIS FROM AAP 16
Rate of resistant P. aeruginosa in children rising steadily
The rate of infection with resistant Pseudomonas aeruginosa among children has risen steadily about 4% per year since 1999, according to a report.
Infections with P aeruginosa in children occur most often associated with pulmonary disease in patients with cystic fibrosis, but healthy children also can experience a variety of P aeruginosa infection types.
They focused on 77,349 P. aeruginosa isolates that were tested for resistance for all five antibiotic classes: cephalosporins, beta-lactam and beta-lactamase inhibitors, carbapenems, fluoroquinolones, and aminoglycosides. The investigators were specifically interested in multidrug- and carbapenem-resistant P. aeruginosa. They described the organism as “arguably the most resistance-prone health care–related pathogen.”
The study samples were obtained from the respiratory tract, urinary tract, ear, sinuses, wounds, skin, and connective tissues of children aged 1-17 years who were treated in 1999-2012; 2012 was the last year for which this information was collected in this database. Patients were treated in ambulatory, inpatient, ICU, and long-term-care settings. The study excluded children with cystic fibrosis and children under 1 year of age, so as to improve the applicability of the results to the general pediatric population.
The proportion of multidrug-resistant P. aeruginosa samples rose from 15% to 26% during the 13-year study period, and the proportion of carbapenem-resistant P. aeruginosa samples rose from 9% to 20%. This represents an average annual increase of approximately 4% for both types of resistance, Dr. Logan and her associates said (J Ped Infect Dis. 2016 Nov 16. doi: 10.1093/jpids/piw064).
These increases were consistent across all but one age group and all but one treatment setting, the exception being inpatients aged 13-17 years. The prevalence of resistant P. aeruginosa was highest among adolescents in ambulatory, ICU, or long-term-care settings; their rates were three times higher than those in children aged 1 year and two times higher than those in children aged 5 years. It is possible that this pattern reflects “an increasing number of older children with a medically complex condition who have frequent exposure to the health care environment,” the investigators noted.
“The results of our study highlight the need for bacterial surveillance, strategies for implementing effective infection prevention, and antimicrobial stewardship programs.” In addition, all health care facilities should consider using rapid molecular diagnostic platforms to guide antibiotic treatment decisions, “to reduce the burden of the persistent and continually evolving global threat of extensively drug-resistant organisms,” Dr. Logan and her associates added.
This study was supported by the National Institute of Allergy and Infectious Diseases; the Global Antibiotic Resistance Partnership, funded by the Bill and Melinda Gates Foundation; and the Health Grand Challenges Program at Princeton University. Dr. Logan and her associates reported having no relevant financial disclosures.
The rate of infection with resistant Pseudomonas aeruginosa among children has risen steadily about 4% per year since 1999, according to a report.
Infections with P aeruginosa in children occur most often associated with pulmonary disease in patients with cystic fibrosis, but healthy children also can experience a variety of P aeruginosa infection types.
They focused on 77,349 P. aeruginosa isolates that were tested for resistance for all five antibiotic classes: cephalosporins, beta-lactam and beta-lactamase inhibitors, carbapenems, fluoroquinolones, and aminoglycosides. The investigators were specifically interested in multidrug- and carbapenem-resistant P. aeruginosa. They described the organism as “arguably the most resistance-prone health care–related pathogen.”
The study samples were obtained from the respiratory tract, urinary tract, ear, sinuses, wounds, skin, and connective tissues of children aged 1-17 years who were treated in 1999-2012; 2012 was the last year for which this information was collected in this database. Patients were treated in ambulatory, inpatient, ICU, and long-term-care settings. The study excluded children with cystic fibrosis and children under 1 year of age, so as to improve the applicability of the results to the general pediatric population.
The proportion of multidrug-resistant P. aeruginosa samples rose from 15% to 26% during the 13-year study period, and the proportion of carbapenem-resistant P. aeruginosa samples rose from 9% to 20%. This represents an average annual increase of approximately 4% for both types of resistance, Dr. Logan and her associates said (J Ped Infect Dis. 2016 Nov 16. doi: 10.1093/jpids/piw064).
These increases were consistent across all but one age group and all but one treatment setting, the exception being inpatients aged 13-17 years. The prevalence of resistant P. aeruginosa was highest among adolescents in ambulatory, ICU, or long-term-care settings; their rates were three times higher than those in children aged 1 year and two times higher than those in children aged 5 years. It is possible that this pattern reflects “an increasing number of older children with a medically complex condition who have frequent exposure to the health care environment,” the investigators noted.
“The results of our study highlight the need for bacterial surveillance, strategies for implementing effective infection prevention, and antimicrobial stewardship programs.” In addition, all health care facilities should consider using rapid molecular diagnostic platforms to guide antibiotic treatment decisions, “to reduce the burden of the persistent and continually evolving global threat of extensively drug-resistant organisms,” Dr. Logan and her associates added.
This study was supported by the National Institute of Allergy and Infectious Diseases; the Global Antibiotic Resistance Partnership, funded by the Bill and Melinda Gates Foundation; and the Health Grand Challenges Program at Princeton University. Dr. Logan and her associates reported having no relevant financial disclosures.
The rate of infection with resistant Pseudomonas aeruginosa among children has risen steadily about 4% per year since 1999, according to a report.
Infections with P aeruginosa in children occur most often associated with pulmonary disease in patients with cystic fibrosis, but healthy children also can experience a variety of P aeruginosa infection types.
They focused on 77,349 P. aeruginosa isolates that were tested for resistance for all five antibiotic classes: cephalosporins, beta-lactam and beta-lactamase inhibitors, carbapenems, fluoroquinolones, and aminoglycosides. The investigators were specifically interested in multidrug- and carbapenem-resistant P. aeruginosa. They described the organism as “arguably the most resistance-prone health care–related pathogen.”
The study samples were obtained from the respiratory tract, urinary tract, ear, sinuses, wounds, skin, and connective tissues of children aged 1-17 years who were treated in 1999-2012; 2012 was the last year for which this information was collected in this database. Patients were treated in ambulatory, inpatient, ICU, and long-term-care settings. The study excluded children with cystic fibrosis and children under 1 year of age, so as to improve the applicability of the results to the general pediatric population.
The proportion of multidrug-resistant P. aeruginosa samples rose from 15% to 26% during the 13-year study period, and the proportion of carbapenem-resistant P. aeruginosa samples rose from 9% to 20%. This represents an average annual increase of approximately 4% for both types of resistance, Dr. Logan and her associates said (J Ped Infect Dis. 2016 Nov 16. doi: 10.1093/jpids/piw064).
These increases were consistent across all but one age group and all but one treatment setting, the exception being inpatients aged 13-17 years. The prevalence of resistant P. aeruginosa was highest among adolescents in ambulatory, ICU, or long-term-care settings; their rates were three times higher than those in children aged 1 year and two times higher than those in children aged 5 years. It is possible that this pattern reflects “an increasing number of older children with a medically complex condition who have frequent exposure to the health care environment,” the investigators noted.
“The results of our study highlight the need for bacterial surveillance, strategies for implementing effective infection prevention, and antimicrobial stewardship programs.” In addition, all health care facilities should consider using rapid molecular diagnostic platforms to guide antibiotic treatment decisions, “to reduce the burden of the persistent and continually evolving global threat of extensively drug-resistant organisms,” Dr. Logan and her associates added.
This study was supported by the National Institute of Allergy and Infectious Diseases; the Global Antibiotic Resistance Partnership, funded by the Bill and Melinda Gates Foundation; and the Health Grand Challenges Program at Princeton University. Dr. Logan and her associates reported having no relevant financial disclosures.
FROM THE JOURNAL OF PEDIATRIC INFECTIOUS DISEASES
Key clinical point:
Major finding: The proportion of multidrug-resistant P. aeruginosa samples rose from 15% to 26% during the 13-year study period, and the proportion of carbapenem-resistant P. aeruginosa samples rose from 9% to 20%.
Data source: A longitudinal analysis of information in a nationally representative database of microbiology laboratories serving approximately 300 U.S. hospitals.
Disclosures: This study was supported by the National Institute of Allergy and Infectious Diseases; the Global Antibiotic Resistance Partnership, funded by the Bill and Melinda Gates Foundation; and the Health Grand Challenges Program at Princeton University. Dr. Logan and her associates reported having no relevant financial disclosures.
How social media solved a skin outbreak
Several teens who came home from a trip abroad with ugly ulcerated skin lesions in 2014 got vague and unhelpful diagnoses: Physicians thought they had bug bites. True, but that was only part of the story. It took an alert dermatologist and Facebook to identify the true cause, spread the word, and stop the outbreak.
“Social media facilitated communication between patients, crowd sourcing a diagnosis,” said Kanokporn Mongkolrattanothai, MD, who treated three of the teens at Children’s Hospital Los Angeles.
What did the kids have? Read on and see if you can make the diagnosis yourself.

Upon their return, pruritic red papules appeared on a 16-year-old girl’s ankle and thigh. They transformed into ulcers with raised edges and a central crater, according to a report that published online in Pediatric Dermatology (2016 Sep;33[5]:e276-7. doi: 10.1111/pde.12910). At least 12 teens from the trip had similar ulcerated lesions, mostly in exposed areas like arms and legs, said Dr. Mongkolrattanothai, an infectious disease specialist at Children’s Hospital Los Angeles and a coauthor of the report.
Six patients received a diagnosis of insect bites, and one was diagnosed with a bacterial skin infection, noted Dr. Mongkolrattanothai of the University of Southern California, Los Angeles. But these diagnoses were incorrect.

“The light bulb really came on when she mentioned that the lesions were still present several months after the trip to Israel,” said Dr. Krakowski, who was at Rady Children’s Hospital–San Diego at the time. “On physical exam, the lesions were ulcerated and eroded and did not look to be typical bug bite reactions.” The Centers for Disease Control and Prevention confirmed the diagnosis.
On Facebook, the teenager posted a picture of a T-shirt with the words “I went to Israel, and all I got was leishmaniasis.” At the same time, another traveler on the same trip posted pictures of lesions. This set off a wave of awareness that sent affected teens to seek care at Children’s Hospital Los Angeles, Mattel Children’s Hospital UCLA, Cedars-Sinai Medical Center, Kaiser Permanente Woodland Hills Medical Center, and Rady Children’s Hospital–San Diego.
“It is likely that our patients became infected with leishmaniasis while camping in the Negev Desert, sleeping on sand dunes at night without use of mosquito netting or tents,” Dr. Mongkolrattanothai said in an interview. “Most of the affected teens did not take precautions against insect bites, which would have included appropriate clothing to minimize areas of exposed skin and the use of repellent products. This placed them at risk for sand fly bites, as sand flies are most active in twilight, evening, and nighttime hours.”

Cutaneous leishmaniasis can lead to permanent scarring, and another form, visceral leishmaniasis, can be fatal.
What helped Dr. Krakowski crack the case? “Training at the University of California at San Diego, in such close proximity to the Navy’s Balboa Medical Center, we are taught from day 1 to think outside of the box because ‘there are zebras in Africa,’ ” he said. “With so much international travel in and out of the region, including to locations where leishmaniasis is endemic, it is warranted to consider that specific diagnosis on the differential. Normally, I do not have to biopsy ‘bug bites,’ but considering the patient’s entire presentation, you almost have to do a biopsy to make sure the lesions were not leishmaniasis.”
Dr. Krakowski praised the CDC. “They have a tremendous amount of resources dedicated to helping investigators work through diagnostic dilemmas such as this, and they helped us – free of charge – to confirm the diagnosis, type the leishmaniasis, and plot a treatment course to resolution,” he said. “They also were instrumental in helping us identify and educate other potentially exposed patients from the camping trip.”
In November, the Infectious Diseases Society of America and the American Society of Tropical Medicine and Hygiene published new guidelines about leishmaniasis in Clinical Infectious Diseases (doi: 10.1093/cid/ciw670). The societies warn that leishmaniasis is becoming more common in the United States, in part because of ecotourists infected in Central and South America and returning soldiers infected in Afghanistan and Iraq.
Dr. Mongkolrattanothai and Dr. Krakowski reported no relevant financial disclosures.
Several teens who came home from a trip abroad with ugly ulcerated skin lesions in 2014 got vague and unhelpful diagnoses: Physicians thought they had bug bites. True, but that was only part of the story. It took an alert dermatologist and Facebook to identify the true cause, spread the word, and stop the outbreak.
“Social media facilitated communication between patients, crowd sourcing a diagnosis,” said Kanokporn Mongkolrattanothai, MD, who treated three of the teens at Children’s Hospital Los Angeles.
What did the kids have? Read on and see if you can make the diagnosis yourself.
Upon their return, pruritic red papules appeared on a 16-year-old girl’s ankle and thigh. They transformed into ulcers with raised edges and a central crater, according to a report that published online in Pediatric Dermatology (2016 Sep;33[5]:e276-7. doi: 10.1111/pde.12910). At least 12 teens from the trip had similar ulcerated lesions, mostly in exposed areas like arms and legs, said Dr. Mongkolrattanothai, an infectious disease specialist at Children’s Hospital Los Angeles and a coauthor of the report.
Six patients received a diagnosis of insect bites, and one was diagnosed with a bacterial skin infection, noted Dr. Mongkolrattanothai of the University of Southern California, Los Angeles. But these diagnoses were incorrect.
“The light bulb really came on when she mentioned that the lesions were still present several months after the trip to Israel,” said Dr. Krakowski, who was at Rady Children’s Hospital–San Diego at the time. “On physical exam, the lesions were ulcerated and eroded and did not look to be typical bug bite reactions.” The Centers for Disease Control and Prevention confirmed the diagnosis.
On Facebook, the teenager posted a picture of a T-shirt with the words “I went to Israel, and all I got was leishmaniasis.” At the same time, another traveler on the same trip posted pictures of lesions. This set off a wave of awareness that sent affected teens to seek care at Children’s Hospital Los Angeles, Mattel Children’s Hospital UCLA, Cedars-Sinai Medical Center, Kaiser Permanente Woodland Hills Medical Center, and Rady Children’s Hospital–San Diego.
“It is likely that our patients became infected with leishmaniasis while camping in the Negev Desert, sleeping on sand dunes at night without use of mosquito netting or tents,” Dr. Mongkolrattanothai said in an interview. “Most of the affected teens did not take precautions against insect bites, which would have included appropriate clothing to minimize areas of exposed skin and the use of repellent products. This placed them at risk for sand fly bites, as sand flies are most active in twilight, evening, and nighttime hours.”
Cutaneous leishmaniasis can lead to permanent scarring, and another form, visceral leishmaniasis, can be fatal.
What helped Dr. Krakowski crack the case? “Training at the University of California at San Diego, in such close proximity to the Navy’s Balboa Medical Center, we are taught from day 1 to think outside of the box because ‘there are zebras in Africa,’ ” he said. “With so much international travel in and out of the region, including to locations where leishmaniasis is endemic, it is warranted to consider that specific diagnosis on the differential. Normally, I do not have to biopsy ‘bug bites,’ but considering the patient’s entire presentation, you almost have to do a biopsy to make sure the lesions were not leishmaniasis.”
Dr. Krakowski praised the CDC. “They have a tremendous amount of resources dedicated to helping investigators work through diagnostic dilemmas such as this, and they helped us – free of charge – to confirm the diagnosis, type the leishmaniasis, and plot a treatment course to resolution,” he said. “They also were instrumental in helping us identify and educate other potentially exposed patients from the camping trip.”
In November, the Infectious Diseases Society of America and the American Society of Tropical Medicine and Hygiene published new guidelines about leishmaniasis in Clinical Infectious Diseases (doi: 10.1093/cid/ciw670). The societies warn that leishmaniasis is becoming more common in the United States, in part because of ecotourists infected in Central and South America and returning soldiers infected in Afghanistan and Iraq.
Dr. Mongkolrattanothai and Dr. Krakowski reported no relevant financial disclosures.
Several teens who came home from a trip abroad with ugly ulcerated skin lesions in 2014 got vague and unhelpful diagnoses: Physicians thought they had bug bites. True, but that was only part of the story. It took an alert dermatologist and Facebook to identify the true cause, spread the word, and stop the outbreak.
“Social media facilitated communication between patients, crowd sourcing a diagnosis,” said Kanokporn Mongkolrattanothai, MD, who treated three of the teens at Children’s Hospital Los Angeles.
What did the kids have? Read on and see if you can make the diagnosis yourself.
Upon their return, pruritic red papules appeared on a 16-year-old girl’s ankle and thigh. They transformed into ulcers with raised edges and a central crater, according to a report that published online in Pediatric Dermatology (2016 Sep;33[5]:e276-7. doi: 10.1111/pde.12910). At least 12 teens from the trip had similar ulcerated lesions, mostly in exposed areas like arms and legs, said Dr. Mongkolrattanothai, an infectious disease specialist at Children’s Hospital Los Angeles and a coauthor of the report.
Six patients received a diagnosis of insect bites, and one was diagnosed with a bacterial skin infection, noted Dr. Mongkolrattanothai of the University of Southern California, Los Angeles. But these diagnoses were incorrect.
“The light bulb really came on when she mentioned that the lesions were still present several months after the trip to Israel,” said Dr. Krakowski, who was at Rady Children’s Hospital–San Diego at the time. “On physical exam, the lesions were ulcerated and eroded and did not look to be typical bug bite reactions.” The Centers for Disease Control and Prevention confirmed the diagnosis.
On Facebook, the teenager posted a picture of a T-shirt with the words “I went to Israel, and all I got was leishmaniasis.” At the same time, another traveler on the same trip posted pictures of lesions. This set off a wave of awareness that sent affected teens to seek care at Children’s Hospital Los Angeles, Mattel Children’s Hospital UCLA, Cedars-Sinai Medical Center, Kaiser Permanente Woodland Hills Medical Center, and Rady Children’s Hospital–San Diego.
“It is likely that our patients became infected with leishmaniasis while camping in the Negev Desert, sleeping on sand dunes at night without use of mosquito netting or tents,” Dr. Mongkolrattanothai said in an interview. “Most of the affected teens did not take precautions against insect bites, which would have included appropriate clothing to minimize areas of exposed skin and the use of repellent products. This placed them at risk for sand fly bites, as sand flies are most active in twilight, evening, and nighttime hours.”
Cutaneous leishmaniasis can lead to permanent scarring, and another form, visceral leishmaniasis, can be fatal.
What helped Dr. Krakowski crack the case? “Training at the University of California at San Diego, in such close proximity to the Navy’s Balboa Medical Center, we are taught from day 1 to think outside of the box because ‘there are zebras in Africa,’ ” he said. “With so much international travel in and out of the region, including to locations where leishmaniasis is endemic, it is warranted to consider that specific diagnosis on the differential. Normally, I do not have to biopsy ‘bug bites,’ but considering the patient’s entire presentation, you almost have to do a biopsy to make sure the lesions were not leishmaniasis.”
Dr. Krakowski praised the CDC. “They have a tremendous amount of resources dedicated to helping investigators work through diagnostic dilemmas such as this, and they helped us – free of charge – to confirm the diagnosis, type the leishmaniasis, and plot a treatment course to resolution,” he said. “They also were instrumental in helping us identify and educate other potentially exposed patients from the camping trip.”
In November, the Infectious Diseases Society of America and the American Society of Tropical Medicine and Hygiene published new guidelines about leishmaniasis in Clinical Infectious Diseases (doi: 10.1093/cid/ciw670). The societies warn that leishmaniasis is becoming more common in the United States, in part because of ecotourists infected in Central and South America and returning soldiers infected in Afghanistan and Iraq.
Dr. Mongkolrattanothai and Dr. Krakowski reported no relevant financial disclosures.
Influences and beliefs on vaccine hesitancy remain complex
ATLANTA – Before clinicians can learn new and effective strategies on addressing vaccine hesitancy in their practices, they need to understand both the “forest” and the “trees.” That is, it helps to understand the big picture in terms of national trends, and it’s equally important to understand the motivations and psychology of parents who refuse or remain hesitant about vaccines.
Paula Frew, PhD, MPH, of Emory University in Atlanta, pointed out that vaccination coverage of children under 3 years old in the United States remains consistently high. An estimated 93% of children have received at least three doses of the polio vaccine, 92% have received at least one dose of the MMR vaccine, 92% have received at least three doses of the hepatitis B vaccine, and 91% have received at least one dose of the varicella vaccine.
In fact, less than 1% of parents selectively or completely refuse all vaccines – but an estimated 13%-22% of parents intentionally delay vaccines, Dr. Frew said at a conference sponsored by the Centers for Disease Control and Prevention..
She described findings from a study she and colleagues conducted to assess the influence of vaccination decisions among parents of children under age 7 years. They categorized the parents as nonhesitant acceptors of vaccines, hesitant acceptors, delayers, or refusers. Surveys of 2,603 parents in 2012 and 2,518 parents in 2014 revealed that parents overwhelmingly cite their health care provider as their most trusted source of information on vaccines, including 99% of acceptors and 71% of refusers. Among hesitant acceptors, 49% of parents in 2012 and 48% of parents in 2014 said their doctor positively influenced their vaccination decision.
Qualitative findings from focus groups
Still, hesitancy is common enough that qualitative research is seeking to understand parents’ vaccine concerns. One such study involved focus groups with vaccine-hesitant mothers because mothers or other female guardians are the caregivers most often involved in their children’s health care decisions, according to Judith Mendel, MPH, of the U.S. Department of Health and Human Services.
Ms. Mendel’s study aimed to understand what drives vaccine-related confidence, how to overcome hesitancy over vaccines, and what messaging approaches might work most effectively. She and her colleagues recruited 61 women who participated in one of four groups in the Philadelphia area or one of four in the San Francisco area during April and May 2016. The women all were responsible for the health decisions of at least one child age 5 years or younger and had previously delayed or declined a recommended vaccine for their child.
Each group included six to nine women and involved a 2-hour semistructured discussion about health concerns; what vaccine confidence is; the mothers’ knowledge, attitudes, and beliefs about vaccines and immunization; and feedback on videos and info-graphics designed to educate others about immunization. The focus groups defined having confidence about vaccines as feeling trust, feeling good about a decision, having many years of research or practice, and being informed and knowledgeable.
“Three themes bubbled up together from the groups,” Ms. Mendel said. “Women had concerns about vaccine ingredients and their effects on physiology, about the recommended schedule, and about the medical system.”
Their concerns about vaccine ingredients and physiology would be familiar to pediatric providers:
• A persistent belief that autism is caused by vaccines.
• Concerns about vaccines made from weakened pathogens.
• Belief that vaccines replace a function that the body is equipped to handle on its own.
• Fears about short-term and long-term side effects.
• Little tolerance for established minor reactions to vaccines.
The mothers were accepting of the vaccines that had been on the schedule when they were children, such as polio, but they did not understand why vaccination starts so young and preferred “alternative” or catch-up schedules.
“They believed that when they were younger, the schedule started later,” Ms. Mendel said. “Some women felt there were too many injections given, while other women preferred not to use combination vaccines.”
Their concerns about the medical system, meanwhile, involved a general lack of trust for mainstream medicine and anyone involved in the immunization system. They believed that interactions with doctors today differ significantly from the way it was when they were children.
“They did not like feeling pressured by health care providers to vaccinate their kid,” Ms. Mendel said. “If they thought the provider was providing a somewhat authoritative or paternalistic stance with their recommendation, some of these women really shied from that and were dissuaded by that.”
What messages work?
The researchers then tested several messaging approaches with the women that included videos and printouts about vaccine safety, herd immunity, and how vaccines work. The materials received high ratings for being informative, coalescing around 4 on a Likert scale of 1-5, but “in terms of really swaying the needle on confidence, it was barely middle ground,” Ms. Mendel said, referring to scores ranging from 3.1 to 3.4.
“Despite someone thinking something was informative, it doesn’t necessarily change their attitudes or perceptions,” she said.
What the women liked about the materials were clear messaging with a respectful tone that was not patronizing, as well as statistics.
“They wanted information on both the pros and cons, the risks as well as the benefits,” Ms. Mendel said. “They also wanted to believe the information they were interacting with was coming from a reliable source,” although she added that “what we may consider a reliable source may not necessarily be what they consider a reliable source.”
Ultimately, no single message or approach worked well for all the mothers, but they all wanted “balanced messages,” although it wasn’t clear if giving more attention to possible risks would positively influence their beliefs about immunization.
“It’s clear that many sources really shape these views and perceptions around vaccines and immunization for these women,” Ms. Mendel said. “It’s really clear that these women are doing the best they can, or believe they can, to make the best health and wellness decisions for their children. However, as health communicators, I think there remains a lot of opportunities for us to help them do a better job.”
The researchers reported no disclosures and did not report external funding sources.
ATLANTA – Before clinicians can learn new and effective strategies on addressing vaccine hesitancy in their practices, they need to understand both the “forest” and the “trees.” That is, it helps to understand the big picture in terms of national trends, and it’s equally important to understand the motivations and psychology of parents who refuse or remain hesitant about vaccines.
Paula Frew, PhD, MPH, of Emory University in Atlanta, pointed out that vaccination coverage of children under 3 years old in the United States remains consistently high. An estimated 93% of children have received at least three doses of the polio vaccine, 92% have received at least one dose of the MMR vaccine, 92% have received at least three doses of the hepatitis B vaccine, and 91% have received at least one dose of the varicella vaccine.
In fact, less than 1% of parents selectively or completely refuse all vaccines – but an estimated 13%-22% of parents intentionally delay vaccines, Dr. Frew said at a conference sponsored by the Centers for Disease Control and Prevention..
She described findings from a study she and colleagues conducted to assess the influence of vaccination decisions among parents of children under age 7 years. They categorized the parents as nonhesitant acceptors of vaccines, hesitant acceptors, delayers, or refusers. Surveys of 2,603 parents in 2012 and 2,518 parents in 2014 revealed that parents overwhelmingly cite their health care provider as their most trusted source of information on vaccines, including 99% of acceptors and 71% of refusers. Among hesitant acceptors, 49% of parents in 2012 and 48% of parents in 2014 said their doctor positively influenced their vaccination decision.
Qualitative findings from focus groups
Still, hesitancy is common enough that qualitative research is seeking to understand parents’ vaccine concerns. One such study involved focus groups with vaccine-hesitant mothers because mothers or other female guardians are the caregivers most often involved in their children’s health care decisions, according to Judith Mendel, MPH, of the U.S. Department of Health and Human Services.
Ms. Mendel’s study aimed to understand what drives vaccine-related confidence, how to overcome hesitancy over vaccines, and what messaging approaches might work most effectively. She and her colleagues recruited 61 women who participated in one of four groups in the Philadelphia area or one of four in the San Francisco area during April and May 2016. The women all were responsible for the health decisions of at least one child age 5 years or younger and had previously delayed or declined a recommended vaccine for their child.
Each group included six to nine women and involved a 2-hour semistructured discussion about health concerns; what vaccine confidence is; the mothers’ knowledge, attitudes, and beliefs about vaccines and immunization; and feedback on videos and info-graphics designed to educate others about immunization. The focus groups defined having confidence about vaccines as feeling trust, feeling good about a decision, having many years of research or practice, and being informed and knowledgeable.
“Three themes bubbled up together from the groups,” Ms. Mendel said. “Women had concerns about vaccine ingredients and their effects on physiology, about the recommended schedule, and about the medical system.”
Their concerns about vaccine ingredients and physiology would be familiar to pediatric providers:
• A persistent belief that autism is caused by vaccines.
• Concerns about vaccines made from weakened pathogens.
• Belief that vaccines replace a function that the body is equipped to handle on its own.
• Fears about short-term and long-term side effects.
• Little tolerance for established minor reactions to vaccines.
The mothers were accepting of the vaccines that had been on the schedule when they were children, such as polio, but they did not understand why vaccination starts so young and preferred “alternative” or catch-up schedules.
“They believed that when they were younger, the schedule started later,” Ms. Mendel said. “Some women felt there were too many injections given, while other women preferred not to use combination vaccines.”
Their concerns about the medical system, meanwhile, involved a general lack of trust for mainstream medicine and anyone involved in the immunization system. They believed that interactions with doctors today differ significantly from the way it was when they were children.
“They did not like feeling pressured by health care providers to vaccinate their kid,” Ms. Mendel said. “If they thought the provider was providing a somewhat authoritative or paternalistic stance with their recommendation, some of these women really shied from that and were dissuaded by that.”
What messages work?
The researchers then tested several messaging approaches with the women that included videos and printouts about vaccine safety, herd immunity, and how vaccines work. The materials received high ratings for being informative, coalescing around 4 on a Likert scale of 1-5, but “in terms of really swaying the needle on confidence, it was barely middle ground,” Ms. Mendel said, referring to scores ranging from 3.1 to 3.4.
“Despite someone thinking something was informative, it doesn’t necessarily change their attitudes or perceptions,” she said.
What the women liked about the materials were clear messaging with a respectful tone that was not patronizing, as well as statistics.
“They wanted information on both the pros and cons, the risks as well as the benefits,” Ms. Mendel said. “They also wanted to believe the information they were interacting with was coming from a reliable source,” although she added that “what we may consider a reliable source may not necessarily be what they consider a reliable source.”
Ultimately, no single message or approach worked well for all the mothers, but they all wanted “balanced messages,” although it wasn’t clear if giving more attention to possible risks would positively influence their beliefs about immunization.
“It’s clear that many sources really shape these views and perceptions around vaccines and immunization for these women,” Ms. Mendel said. “It’s really clear that these women are doing the best they can, or believe they can, to make the best health and wellness decisions for their children. However, as health communicators, I think there remains a lot of opportunities for us to help them do a better job.”
The researchers reported no disclosures and did not report external funding sources.
ATLANTA – Before clinicians can learn new and effective strategies on addressing vaccine hesitancy in their practices, they need to understand both the “forest” and the “trees.” That is, it helps to understand the big picture in terms of national trends, and it’s equally important to understand the motivations and psychology of parents who refuse or remain hesitant about vaccines.
Paula Frew, PhD, MPH, of Emory University in Atlanta, pointed out that vaccination coverage of children under 3 years old in the United States remains consistently high. An estimated 93% of children have received at least three doses of the polio vaccine, 92% have received at least one dose of the MMR vaccine, 92% have received at least three doses of the hepatitis B vaccine, and 91% have received at least one dose of the varicella vaccine.
In fact, less than 1% of parents selectively or completely refuse all vaccines – but an estimated 13%-22% of parents intentionally delay vaccines, Dr. Frew said at a conference sponsored by the Centers for Disease Control and Prevention..
She described findings from a study she and colleagues conducted to assess the influence of vaccination decisions among parents of children under age 7 years. They categorized the parents as nonhesitant acceptors of vaccines, hesitant acceptors, delayers, or refusers. Surveys of 2,603 parents in 2012 and 2,518 parents in 2014 revealed that parents overwhelmingly cite their health care provider as their most trusted source of information on vaccines, including 99% of acceptors and 71% of refusers. Among hesitant acceptors, 49% of parents in 2012 and 48% of parents in 2014 said their doctor positively influenced their vaccination decision.
Qualitative findings from focus groups
Still, hesitancy is common enough that qualitative research is seeking to understand parents’ vaccine concerns. One such study involved focus groups with vaccine-hesitant mothers because mothers or other female guardians are the caregivers most often involved in their children’s health care decisions, according to Judith Mendel, MPH, of the U.S. Department of Health and Human Services.
Ms. Mendel’s study aimed to understand what drives vaccine-related confidence, how to overcome hesitancy over vaccines, and what messaging approaches might work most effectively. She and her colleagues recruited 61 women who participated in one of four groups in the Philadelphia area or one of four in the San Francisco area during April and May 2016. The women all were responsible for the health decisions of at least one child age 5 years or younger and had previously delayed or declined a recommended vaccine for their child.
Each group included six to nine women and involved a 2-hour semistructured discussion about health concerns; what vaccine confidence is; the mothers’ knowledge, attitudes, and beliefs about vaccines and immunization; and feedback on videos and info-graphics designed to educate others about immunization. The focus groups defined having confidence about vaccines as feeling trust, feeling good about a decision, having many years of research or practice, and being informed and knowledgeable.
“Three themes bubbled up together from the groups,” Ms. Mendel said. “Women had concerns about vaccine ingredients and their effects on physiology, about the recommended schedule, and about the medical system.”
Their concerns about vaccine ingredients and physiology would be familiar to pediatric providers:
• A persistent belief that autism is caused by vaccines.
• Concerns about vaccines made from weakened pathogens.
• Belief that vaccines replace a function that the body is equipped to handle on its own.
• Fears about short-term and long-term side effects.
• Little tolerance for established minor reactions to vaccines.
The mothers were accepting of the vaccines that had been on the schedule when they were children, such as polio, but they did not understand why vaccination starts so young and preferred “alternative” or catch-up schedules.
“They believed that when they were younger, the schedule started later,” Ms. Mendel said. “Some women felt there were too many injections given, while other women preferred not to use combination vaccines.”
Their concerns about the medical system, meanwhile, involved a general lack of trust for mainstream medicine and anyone involved in the immunization system. They believed that interactions with doctors today differ significantly from the way it was when they were children.
“They did not like feeling pressured by health care providers to vaccinate their kid,” Ms. Mendel said. “If they thought the provider was providing a somewhat authoritative or paternalistic stance with their recommendation, some of these women really shied from that and were dissuaded by that.”
What messages work?
The researchers then tested several messaging approaches with the women that included videos and printouts about vaccine safety, herd immunity, and how vaccines work. The materials received high ratings for being informative, coalescing around 4 on a Likert scale of 1-5, but “in terms of really swaying the needle on confidence, it was barely middle ground,” Ms. Mendel said, referring to scores ranging from 3.1 to 3.4.
“Despite someone thinking something was informative, it doesn’t necessarily change their attitudes or perceptions,” she said.
What the women liked about the materials were clear messaging with a respectful tone that was not patronizing, as well as statistics.
“They wanted information on both the pros and cons, the risks as well as the benefits,” Ms. Mendel said. “They also wanted to believe the information they were interacting with was coming from a reliable source,” although she added that “what we may consider a reliable source may not necessarily be what they consider a reliable source.”
Ultimately, no single message or approach worked well for all the mothers, but they all wanted “balanced messages,” although it wasn’t clear if giving more attention to possible risks would positively influence their beliefs about immunization.
“It’s clear that many sources really shape these views and perceptions around vaccines and immunization for these women,” Ms. Mendel said. “It’s really clear that these women are doing the best they can, or believe they can, to make the best health and wellness decisions for their children. However, as health communicators, I think there remains a lot of opportunities for us to help them do a better job.”
The researchers reported no disclosures and did not report external funding sources.

Targeted interventions aid in HPV vaccination uptake
ATLANTA – Holly Groom, MPH, of the Center for Health Research at Kaiser Permanente Northwest, described the intervention to improve HPV vaccination rates within the Kaiser Permanente NW health care system involving two hospitals and 31 medical offices, which serves 44,000 adolescents aged 11-17 years. About a quarter of patients reside in Washington, with the remainder in Oregon.
In addition to two in-person provider education and feedback sessions, the intervention included quarterly vaccine coverage, missed vaccination opportunity assessment reports, and a mailed parent survey. The staff education sessions covered six different cancers caused by HPV – cervical, anal, oropharyngeal, penile, vaginal, and vulvar – and their annual incidence, such as an estimated 10,000 oropharyngeal cancer cases in males and more than 11,000 cervical cancer cases in females each year.
One of the tip sheets distributed during provider and staff education offered specific language that providers could use to recommend the vaccine to parents and educate them about what HPV disease is and what cancers it can cause. For parents who are confused or concerned about why the vaccine is recommended at ages 11-12 years, for example, providers can respond, “We’re vaccinating today so your child will have the best protection possible long before the start of any kind of sexual activity. We vaccinate people well before they are exposed to an infection, as is the case with measles and the other recommended childhood vaccines.”
For those providers uneasy about mentioning sexual activity, Ms. Groom said, they can stick with telling parents the vaccine should be administered “long before the risk of infection” without mentioning the mechanism of infection.
Ms. Groom provided three other recommended statements as well:
• “I strongly believe in the importance of this cancer-preventing vaccine.”
• “I have given HPV vaccine to my son/daughter (or grandchild/niece/nephew/friend’s children).”
• “Experts, such as the American Academy of Pediatrics, cancer doctors, and the Centers for Disease Control and Prevention, also agree that getting the HPV vaccine is very important for your child.”
Feedback from the training sessions was “overwhelmingly positive,” with 87% of the respondents stating that they planned to implement the strategies and tools discussed and an additional 12% said they were already using those strategies and tools.
The parental survey, although it had only a 12% response rate, initially revealed that just over a third (36%) of parents weren’t sure if they were going to vaccinate their child when they went in for a well visit, but more than 90% of these parents did vaccinate their children.
Ms. Groom reported no disclosures. No external funding was reported.
Communication strategies to improve HPV immunization
Several communication strategies have been developed by the Centers for Disease Control and Prevention to help providers overcome barriers to improving HPV immunization coverage, Yvonne Garcia said at the National Immunization Conference.
Among providers’ barriers are hesitancy to make a recommendation for the HPV vaccine, and the need to understand the burden of the disease and the need for the vaccine, said Ms. Garcia, a health communications specialist for the CDC.
“Also, they overestimate parents’ concerns about the vaccine when what we have learned from parents is that they value the HPV vaccine, but they’re not hearing their child’s doctor recommend it,” she said.
Overcoming these barriers requires patient outreach and awareness of HPV coverage rates at the city and state levels, as well as their individual and practice rates. Providers should bundle their recommendation with the other vaccines recommended by the CDC at the ages of 11 and 12 years: “Your child is due for three vaccines today that offer protection against meningitis, HPV cancers, and whooping cough,” is one example of language to use, Ms. Garcia said.
“Effective patient outreach for HPV vaccination includes the reminder/recall system, scheduling remaining doses at the time of receiving the first doses, and creating parental expectation that HPV vaccination is a very normal part of the immunization process, and that it occurs at ages 11 and 12,” she said.
She also reviewed the barriers among parents for HPV vaccination that providers can address. To respond to parents’ lack of knowledge about the vaccine or the need for it, providers “need to stress that it’s needed for cancer prevention,” Ms. Garcia said.
Providers also can reassure parents with concerns about safety and side effects that extensive safety research exists regarding HPV immunization from the past 10 years.
For those worried that HPV vaccination gives “permission for sexual activity” or that kids are too young, providers can reassure parents that the shot is not linked with increased sexual activity, and that it’s recommended at ages 11 and 12 years because the vaccine induces a better immune response at those ages than later on, she said.
Ms. Garcia reported no disclosures. No external funding was reported.
This article was updated Dec. 2, 2016.
ATLANTA – Holly Groom, MPH, of the Center for Health Research at Kaiser Permanente Northwest, described the intervention to improve HPV vaccination rates within the Kaiser Permanente NW health care system involving two hospitals and 31 medical offices, which serves 44,000 adolescents aged 11-17 years. About a quarter of patients reside in Washington, with the remainder in Oregon.
In addition to two in-person provider education and feedback sessions, the intervention included quarterly vaccine coverage, missed vaccination opportunity assessment reports, and a mailed parent survey. The staff education sessions covered six different cancers caused by HPV – cervical, anal, oropharyngeal, penile, vaginal, and vulvar – and their annual incidence, such as an estimated 10,000 oropharyngeal cancer cases in males and more than 11,000 cervical cancer cases in females each year.
One of the tip sheets distributed during provider and staff education offered specific language that providers could use to recommend the vaccine to parents and educate them about what HPV disease is and what cancers it can cause. For parents who are confused or concerned about why the vaccine is recommended at ages 11-12 years, for example, providers can respond, “We’re vaccinating today so your child will have the best protection possible long before the start of any kind of sexual activity. We vaccinate people well before they are exposed to an infection, as is the case with measles and the other recommended childhood vaccines.”
For those providers uneasy about mentioning sexual activity, Ms. Groom said, they can stick with telling parents the vaccine should be administered “long before the risk of infection” without mentioning the mechanism of infection.
Ms. Groom provided three other recommended statements as well:
• “I strongly believe in the importance of this cancer-preventing vaccine.”
• “I have given HPV vaccine to my son/daughter (or grandchild/niece/nephew/friend’s children).”
• “Experts, such as the American Academy of Pediatrics, cancer doctors, and the Centers for Disease Control and Prevention, also agree that getting the HPV vaccine is very important for your child.”
Feedback from the training sessions was “overwhelmingly positive,” with 87% of the respondents stating that they planned to implement the strategies and tools discussed and an additional 12% said they were already using those strategies and tools.
The parental survey, although it had only a 12% response rate, initially revealed that just over a third (36%) of parents weren’t sure if they were going to vaccinate their child when they went in for a well visit, but more than 90% of these parents did vaccinate their children.
Ms. Groom reported no disclosures. No external funding was reported.
Communication strategies to improve HPV immunization
Several communication strategies have been developed by the Centers for Disease Control and Prevention to help providers overcome barriers to improving HPV immunization coverage, Yvonne Garcia said at the National Immunization Conference.
Among providers’ barriers are hesitancy to make a recommendation for the HPV vaccine, and the need to understand the burden of the disease and the need for the vaccine, said Ms. Garcia, a health communications specialist for the CDC.
“Also, they overestimate parents’ concerns about the vaccine when what we have learned from parents is that they value the HPV vaccine, but they’re not hearing their child’s doctor recommend it,” she said.
Overcoming these barriers requires patient outreach and awareness of HPV coverage rates at the city and state levels, as well as their individual and practice rates. Providers should bundle their recommendation with the other vaccines recommended by the CDC at the ages of 11 and 12 years: “Your child is due for three vaccines today that offer protection against meningitis, HPV cancers, and whooping cough,” is one example of language to use, Ms. Garcia said.
“Effective patient outreach for HPV vaccination includes the reminder/recall system, scheduling remaining doses at the time of receiving the first doses, and creating parental expectation that HPV vaccination is a very normal part of the immunization process, and that it occurs at ages 11 and 12,” she said.
She also reviewed the barriers among parents for HPV vaccination that providers can address. To respond to parents’ lack of knowledge about the vaccine or the need for it, providers “need to stress that it’s needed for cancer prevention,” Ms. Garcia said.
Providers also can reassure parents with concerns about safety and side effects that extensive safety research exists regarding HPV immunization from the past 10 years.
For those worried that HPV vaccination gives “permission for sexual activity” or that kids are too young, providers can reassure parents that the shot is not linked with increased sexual activity, and that it’s recommended at ages 11 and 12 years because the vaccine induces a better immune response at those ages than later on, she said.
Ms. Garcia reported no disclosures. No external funding was reported.
This article was updated Dec. 2, 2016.
ATLANTA – Holly Groom, MPH, of the Center for Health Research at Kaiser Permanente Northwest, described the intervention to improve HPV vaccination rates within the Kaiser Permanente NW health care system involving two hospitals and 31 medical offices, which serves 44,000 adolescents aged 11-17 years. About a quarter of patients reside in Washington, with the remainder in Oregon.
In addition to two in-person provider education and feedback sessions, the intervention included quarterly vaccine coverage, missed vaccination opportunity assessment reports, and a mailed parent survey. The staff education sessions covered six different cancers caused by HPV – cervical, anal, oropharyngeal, penile, vaginal, and vulvar – and their annual incidence, such as an estimated 10,000 oropharyngeal cancer cases in males and more than 11,000 cervical cancer cases in females each year.
One of the tip sheets distributed during provider and staff education offered specific language that providers could use to recommend the vaccine to parents and educate them about what HPV disease is and what cancers it can cause. For parents who are confused or concerned about why the vaccine is recommended at ages 11-12 years, for example, providers can respond, “We’re vaccinating today so your child will have the best protection possible long before the start of any kind of sexual activity. We vaccinate people well before they are exposed to an infection, as is the case with measles and the other recommended childhood vaccines.”
For those providers uneasy about mentioning sexual activity, Ms. Groom said, they can stick with telling parents the vaccine should be administered “long before the risk of infection” without mentioning the mechanism of infection.
Ms. Groom provided three other recommended statements as well:
• “I strongly believe in the importance of this cancer-preventing vaccine.”
• “I have given HPV vaccine to my son/daughter (or grandchild/niece/nephew/friend’s children).”
• “Experts, such as the American Academy of Pediatrics, cancer doctors, and the Centers for Disease Control and Prevention, also agree that getting the HPV vaccine is very important for your child.”
Feedback from the training sessions was “overwhelmingly positive,” with 87% of the respondents stating that they planned to implement the strategies and tools discussed and an additional 12% said they were already using those strategies and tools.
The parental survey, although it had only a 12% response rate, initially revealed that just over a third (36%) of parents weren’t sure if they were going to vaccinate their child when they went in for a well visit, but more than 90% of these parents did vaccinate their children.
Ms. Groom reported no disclosures. No external funding was reported.
Communication strategies to improve HPV immunization
Several communication strategies have been developed by the Centers for Disease Control and Prevention to help providers overcome barriers to improving HPV immunization coverage, Yvonne Garcia said at the National Immunization Conference.
Among providers’ barriers are hesitancy to make a recommendation for the HPV vaccine, and the need to understand the burden of the disease and the need for the vaccine, said Ms. Garcia, a health communications specialist for the CDC.
“Also, they overestimate parents’ concerns about the vaccine when what we have learned from parents is that they value the HPV vaccine, but they’re not hearing their child’s doctor recommend it,” she said.
Overcoming these barriers requires patient outreach and awareness of HPV coverage rates at the city and state levels, as well as their individual and practice rates. Providers should bundle their recommendation with the other vaccines recommended by the CDC at the ages of 11 and 12 years: “Your child is due for three vaccines today that offer protection against meningitis, HPV cancers, and whooping cough,” is one example of language to use, Ms. Garcia said.
“Effective patient outreach for HPV vaccination includes the reminder/recall system, scheduling remaining doses at the time of receiving the first doses, and creating parental expectation that HPV vaccination is a very normal part of the immunization process, and that it occurs at ages 11 and 12,” she said.
She also reviewed the barriers among parents for HPV vaccination that providers can address. To respond to parents’ lack of knowledge about the vaccine or the need for it, providers “need to stress that it’s needed for cancer prevention,” Ms. Garcia said.
Providers also can reassure parents with concerns about safety and side effects that extensive safety research exists regarding HPV immunization from the past 10 years.
For those worried that HPV vaccination gives “permission for sexual activity” or that kids are too young, providers can reassure parents that the shot is not linked with increased sexual activity, and that it’s recommended at ages 11 and 12 years because the vaccine induces a better immune response at those ages than later on, she said.
Ms. Garcia reported no disclosures. No external funding was reported.
This article was updated Dec. 2, 2016.
AT THE NATIONAL IMMUNIZATION CONFERENCE
Key clinical point: Targeted interventions to improve HPV vaccination can be effective.
Major finding: In one health care system’s intervention, 87% of providers found the tools and strategies for increasing HPV vaccination uptake helpful and worth using.
Data source: A study within the Kaiser Permanente NW health care system involving two hospitals and 31 medical offices, which serves 44,000 adolescents aged 11-17 years.
Disclosures: Dr. Groom reported no disclosures. No external funding was reported.
Checkpoint inhibitors for lung cancer figure prominently at WCLC 2016
Oncology Practice will be on-site this coming week at the 17th World Conference on Lung Cancer in Vienna with the latest on checkpoint inhibitors and other treatments for lung cancer. Look for coverage of the best clinical presentations at the conference, hosted by the International Association for the Study of Lung Cancer, including the following and more, beginning Sunday, Dec. 4.
OA03.01 - First-Line Nivolumab Monotherapy and Nivolumab Plus Ipilimumab in Patients With Advanced NSCLC: Long-Term Outcomes from CheckMate 012.
OA03.02 - Atezolizumab as 1L Therapy for Advanced NSCLC in PD-L1–Selected Patients: Updated ORR, PFS, and OS Data From the BIRCH Study.
OA03.03 - JAVELIN Solid Tumor: Safety and Clinical Activity of Avelumab (Anti–PD-L1) as First-Line Treatment in Patients With Advanced NSCLC.
OA03.05 - Analysis of Early Survival in Patients With Advanced Nonsquamous NSCLC Treated With Nivolumab vs. Docetaxel in CheckMate 057.
OA03.07 - KEYNOTE-010: Durable Clinical Benefit in Patients With Previously Treated, PD-L1–Expressing NSCLC Who Completed Pembrolizumab.
OA05.01 - Pembrolizumab in Patients With Extensive-Stage Small Cell Lung Cancer: Updated Survival Results from KEYNOTE-028.
OA13.03 - Long-Term Overall Survival for Patients With Malignant Pleural Mesothelioma on Pembrolizumab Enrolled in KEYNOTE-028.
PL03.03 - Randomised Phase III Study of Osimertinib vs. Platinum-Pemetrexed for EGFR T790M-Positive Advanced NSCLC (AURA3).
PL03.05 - BRAIN: A Phase III Trial Comparing WBI and Chemotherapy With Icotinib in NSCLC With Brain Metastases Harboring EGFR Mutations (CTONG 1201).
PL03.07 - First-line Ceritinib Versus Chemotherapy in Patients With ALK-Rearranged (ALK+) NSCLC: A Randomized, Phase III Study (ASCEND-4).
PL03.09 - Phase III Study of Ganetespib, a Heat Shock Protein 90 Inhibitor, With Docetaxel versus Docetaxel in Advanced Non–Small Cell Lung Cancer (GALAXY-2).
PL04a.01 - Health-Related Quality of Life for Pembrolizumab vs. Chemotherapy in Advanced NSCLC With PD-L1 TPS Greater Than or Equal to 50%: Data From KEYNOTE-024.
PL04a.02 - OAK, a Randomized Phase III Study of Atezolizumab vs. Docetaxel in Patients With Advanced NSCLC: Results From Subgroup Analyses.
PL04a.03 - Durvalumab in 3rd-Line Locally Advanced or Metastatic, EGFR/ALK Wild-Type NSCLC: Results from the Phase II ATLANTIC Study.
MA09.02 - Pembrolizumab + Carboplatin and Pemetrexed as 1st-Line Therapy for Advanced Non–Small Cell Lung Cancer: KEYNOTE-021.
MA09.11 - Efficacy and Safety of Necitumumab and Pembrolizumab Combination Therapy in Stage IV Nonsquamous Non–Small Cell Lung Cancer.
Oncology Practice will be on-site this coming week at the 17th World Conference on Lung Cancer in Vienna with the latest on checkpoint inhibitors and other treatments for lung cancer. Look for coverage of the best clinical presentations at the conference, hosted by the International Association for the Study of Lung Cancer, including the following and more, beginning Sunday, Dec. 4.
OA03.01 - First-Line Nivolumab Monotherapy and Nivolumab Plus Ipilimumab in Patients With Advanced NSCLC: Long-Term Outcomes from CheckMate 012.
OA03.02 - Atezolizumab as 1L Therapy for Advanced NSCLC in PD-L1–Selected Patients: Updated ORR, PFS, and OS Data From the BIRCH Study.
OA03.03 - JAVELIN Solid Tumor: Safety and Clinical Activity of Avelumab (Anti–PD-L1) as First-Line Treatment in Patients With Advanced NSCLC.
OA03.05 - Analysis of Early Survival in Patients With Advanced Nonsquamous NSCLC Treated With Nivolumab vs. Docetaxel in CheckMate 057.
OA03.07 - KEYNOTE-010: Durable Clinical Benefit in Patients With Previously Treated, PD-L1–Expressing NSCLC Who Completed Pembrolizumab.
OA05.01 - Pembrolizumab in Patients With Extensive-Stage Small Cell Lung Cancer: Updated Survival Results from KEYNOTE-028.
OA13.03 - Long-Term Overall Survival for Patients With Malignant Pleural Mesothelioma on Pembrolizumab Enrolled in KEYNOTE-028.
PL03.03 - Randomised Phase III Study of Osimertinib vs. Platinum-Pemetrexed for EGFR T790M-Positive Advanced NSCLC (AURA3).
PL03.05 - BRAIN: A Phase III Trial Comparing WBI and Chemotherapy With Icotinib in NSCLC With Brain Metastases Harboring EGFR Mutations (CTONG 1201).
PL03.07 - First-line Ceritinib Versus Chemotherapy in Patients With ALK-Rearranged (ALK+) NSCLC: A Randomized, Phase III Study (ASCEND-4).
PL03.09 - Phase III Study of Ganetespib, a Heat Shock Protein 90 Inhibitor, With Docetaxel versus Docetaxel in Advanced Non–Small Cell Lung Cancer (GALAXY-2).
PL04a.01 - Health-Related Quality of Life for Pembrolizumab vs. Chemotherapy in Advanced NSCLC With PD-L1 TPS Greater Than or Equal to 50%: Data From KEYNOTE-024.
PL04a.02 - OAK, a Randomized Phase III Study of Atezolizumab vs. Docetaxel in Patients With Advanced NSCLC: Results From Subgroup Analyses.
PL04a.03 - Durvalumab in 3rd-Line Locally Advanced or Metastatic, EGFR/ALK Wild-Type NSCLC: Results from the Phase II ATLANTIC Study.
MA09.02 - Pembrolizumab + Carboplatin and Pemetrexed as 1st-Line Therapy for Advanced Non–Small Cell Lung Cancer: KEYNOTE-021.
MA09.11 - Efficacy and Safety of Necitumumab and Pembrolizumab Combination Therapy in Stage IV Nonsquamous Non–Small Cell Lung Cancer.
Oncology Practice will be on-site this coming week at the 17th World Conference on Lung Cancer in Vienna with the latest on checkpoint inhibitors and other treatments for lung cancer. Look for coverage of the best clinical presentations at the conference, hosted by the International Association for the Study of Lung Cancer, including the following and more, beginning Sunday, Dec. 4.
OA03.01 - First-Line Nivolumab Monotherapy and Nivolumab Plus Ipilimumab in Patients With Advanced NSCLC: Long-Term Outcomes from CheckMate 012.
OA03.02 - Atezolizumab as 1L Therapy for Advanced NSCLC in PD-L1–Selected Patients: Updated ORR, PFS, and OS Data From the BIRCH Study.
OA03.03 - JAVELIN Solid Tumor: Safety and Clinical Activity of Avelumab (Anti–PD-L1) as First-Line Treatment in Patients With Advanced NSCLC.
OA03.05 - Analysis of Early Survival in Patients With Advanced Nonsquamous NSCLC Treated With Nivolumab vs. Docetaxel in CheckMate 057.
OA03.07 - KEYNOTE-010: Durable Clinical Benefit in Patients With Previously Treated, PD-L1–Expressing NSCLC Who Completed Pembrolizumab.
OA05.01 - Pembrolizumab in Patients With Extensive-Stage Small Cell Lung Cancer: Updated Survival Results from KEYNOTE-028.
OA13.03 - Long-Term Overall Survival for Patients With Malignant Pleural Mesothelioma on Pembrolizumab Enrolled in KEYNOTE-028.
PL03.03 - Randomised Phase III Study of Osimertinib vs. Platinum-Pemetrexed for EGFR T790M-Positive Advanced NSCLC (AURA3).
PL03.05 - BRAIN: A Phase III Trial Comparing WBI and Chemotherapy With Icotinib in NSCLC With Brain Metastases Harboring EGFR Mutations (CTONG 1201).
PL03.07 - First-line Ceritinib Versus Chemotherapy in Patients With ALK-Rearranged (ALK+) NSCLC: A Randomized, Phase III Study (ASCEND-4).
PL03.09 - Phase III Study of Ganetespib, a Heat Shock Protein 90 Inhibitor, With Docetaxel versus Docetaxel in Advanced Non–Small Cell Lung Cancer (GALAXY-2).
PL04a.01 - Health-Related Quality of Life for Pembrolizumab vs. Chemotherapy in Advanced NSCLC With PD-L1 TPS Greater Than or Equal to 50%: Data From KEYNOTE-024.
PL04a.02 - OAK, a Randomized Phase III Study of Atezolizumab vs. Docetaxel in Patients With Advanced NSCLC: Results From Subgroup Analyses.
PL04a.03 - Durvalumab in 3rd-Line Locally Advanced or Metastatic, EGFR/ALK Wild-Type NSCLC: Results from the Phase II ATLANTIC Study.
MA09.02 - Pembrolizumab + Carboplatin and Pemetrexed as 1st-Line Therapy for Advanced Non–Small Cell Lung Cancer: KEYNOTE-021.
MA09.11 - Efficacy and Safety of Necitumumab and Pembrolizumab Combination Therapy in Stage IV Nonsquamous Non–Small Cell Lung Cancer.
FROM WCLC 2016
Prenatal exposure to hydroxychloroquine cuts risk of neonatal cutaneous lupus
WASHINGTON – Prenatal hydroxychloroquine reduces the risk of cutaneous neonatal lupus by 60% among the infants of women with a systemic autoimmune rheumatic disease.
The medication easily passes the placental barrier and confers significant protection to neonates born to women who have anti-Ro and anti-La antibodies, Julie Barsalou, MD, said at the annual meeting of the American College of Rheumatology.

Toll-like receptors 7 and 9 have been implicated in the initiation and maintenance of interface dermatitis, and hydroxychloroquine inhibits these receptors. In mouse studies, the drug has led to improvement of this type of dermatitis. Hydroxychloroquine also works well in treating subacute cutaneous lupus, she said, and because it can travel across the placenta, it could be an effective means of preventing this disorder in at-risk neonates.
To examine any potential benefit, Dr. Barsalou looked at three pediatric lupus databases: the SickKids NLE database from Toronto, the U.S. Research Registry for Neonatal Lupus, and the French Registry for Neonatal Lupus.
These registries include infants born to mothers with anti-Ro and/or anti-La antibodies, and a diagnosis of lupus, dermatomyositis, Sjögren’s syndrome, juvenile idiopathic arthritis, or rheumatic arthritis. No infants with cardiac neonatal lupus were included in the study.
In addition to hydroxychloroquine, Dr. Barsalou examined the use of prenatal azathioprine, nonfluorinated and fluorinated steroids, and intravenous immunoglobulin.
The cohort comprised 545 neonates born to 535 mothers. Among these, 112 developed cNLE. The remaining 433 infants were used as controls.
Mothers of both cases and controls were a mean age of 31 years. Among cases, the most common diagnosis was Sjögren’s syndrome (53%), followed by systemic lupus erythematosus (46%). Among controls, the most common maternal diagnosis was SLE (62%), followed by Sjögren’s (31%).
All mothers of cases were positive for anti-Ro antibodies; 72% were positive for anti-La antibodies. Among mothers of controls, 99% had anti-Ro antibodies and 48% had anti-La antibodies.
Mothers of cases took hydroxychloroquine (17%), fluorinated steroids (6%), and nonfluorinated steroids with or without azathioprine (28%). Mothers of controls took hydroxychloroquine (34%), fluorinated steroids (4%), and nonfluorinated steroids with or without azathioprine (44%),
There were significantly more female than male infants in the case group (65%). The median age at rash onset was 6 weeks.
Dr. Barsalou performed several multivariate analyses on the entire cohort, as well as two subgroup analyses: one on infants who developed the cNLE rash within the first 4 weeks of life and one on only the infants of mothers with SLE.
In the primary analysis, maternal anti-Ro and anti-La antibodies more than doubled the risk of an infant developing cNLE (odds ratio, 2.5). The use of hydroxychloroquine decreased this risk by 60% (OR, 0.4). Being a female infant increased the risk by 70% (OR, 1.7).
In the group of infants with early-onset rash, maternal anti-La antibodies more than tripled the risk (OR, 3.5), while the use of hydroxychloroquine decreased the risk by 80% (OR, 0.2).
Among the infants born to women with SLE, concomitant secondary Sjögren’s syndrome increased the risk of cNLE by more than threefold (OR, 3.5). Anti-La antibodies more than doubled the risk (OR, 2.5), and the use of hydroxychloroquine decreased it by 60% (OR, 0.4).
“This is the first study to address the prevention of cutaneous neonatal lupus,” Dr. Barsalou said. “We found that prenatal exposure to hydroxychloroquine is likely protective.”
She had no financial disclosures.
[email protected]
On Twitter @alz_gal
WASHINGTON – Prenatal hydroxychloroquine reduces the risk of cutaneous neonatal lupus by 60% among the infants of women with a systemic autoimmune rheumatic disease.
The medication easily passes the placental barrier and confers significant protection to neonates born to women who have anti-Ro and anti-La antibodies, Julie Barsalou, MD, said at the annual meeting of the American College of Rheumatology.
Toll-like receptors 7 and 9 have been implicated in the initiation and maintenance of interface dermatitis, and hydroxychloroquine inhibits these receptors. In mouse studies, the drug has led to improvement of this type of dermatitis. Hydroxychloroquine also works well in treating subacute cutaneous lupus, she said, and because it can travel across the placenta, it could be an effective means of preventing this disorder in at-risk neonates.
To examine any potential benefit, Dr. Barsalou looked at three pediatric lupus databases: the SickKids NLE database from Toronto, the U.S. Research Registry for Neonatal Lupus, and the French Registry for Neonatal Lupus.
These registries include infants born to mothers with anti-Ro and/or anti-La antibodies, and a diagnosis of lupus, dermatomyositis, Sjögren’s syndrome, juvenile idiopathic arthritis, or rheumatic arthritis. No infants with cardiac neonatal lupus were included in the study.
In addition to hydroxychloroquine, Dr. Barsalou examined the use of prenatal azathioprine, nonfluorinated and fluorinated steroids, and intravenous immunoglobulin.
The cohort comprised 545 neonates born to 535 mothers. Among these, 112 developed cNLE. The remaining 433 infants were used as controls.
Mothers of both cases and controls were a mean age of 31 years. Among cases, the most common diagnosis was Sjögren’s syndrome (53%), followed by systemic lupus erythematosus (46%). Among controls, the most common maternal diagnosis was SLE (62%), followed by Sjögren’s (31%).
All mothers of cases were positive for anti-Ro antibodies; 72% were positive for anti-La antibodies. Among mothers of controls, 99% had anti-Ro antibodies and 48% had anti-La antibodies.
Mothers of cases took hydroxychloroquine (17%), fluorinated steroids (6%), and nonfluorinated steroids with or without azathioprine (28%). Mothers of controls took hydroxychloroquine (34%), fluorinated steroids (4%), and nonfluorinated steroids with or without azathioprine (44%),
There were significantly more female than male infants in the case group (65%). The median age at rash onset was 6 weeks.
Dr. Barsalou performed several multivariate analyses on the entire cohort, as well as two subgroup analyses: one on infants who developed the cNLE rash within the first 4 weeks of life and one on only the infants of mothers with SLE.
In the primary analysis, maternal anti-Ro and anti-La antibodies more than doubled the risk of an infant developing cNLE (odds ratio, 2.5). The use of hydroxychloroquine decreased this risk by 60% (OR, 0.4). Being a female infant increased the risk by 70% (OR, 1.7).
In the group of infants with early-onset rash, maternal anti-La antibodies more than tripled the risk (OR, 3.5), while the use of hydroxychloroquine decreased the risk by 80% (OR, 0.2).
Among the infants born to women with SLE, concomitant secondary Sjögren’s syndrome increased the risk of cNLE by more than threefold (OR, 3.5). Anti-La antibodies more than doubled the risk (OR, 2.5), and the use of hydroxychloroquine decreased it by 60% (OR, 0.4).
“This is the first study to address the prevention of cutaneous neonatal lupus,” Dr. Barsalou said. “We found that prenatal exposure to hydroxychloroquine is likely protective.”
She had no financial disclosures.
[email protected]
On Twitter @alz_gal
WASHINGTON – Prenatal hydroxychloroquine reduces the risk of cutaneous neonatal lupus by 60% among the infants of women with a systemic autoimmune rheumatic disease.
The medication easily passes the placental barrier and confers significant protection to neonates born to women who have anti-Ro and anti-La antibodies, Julie Barsalou, MD, said at the annual meeting of the American College of Rheumatology.
Toll-like receptors 7 and 9 have been implicated in the initiation and maintenance of interface dermatitis, and hydroxychloroquine inhibits these receptors. In mouse studies, the drug has led to improvement of this type of dermatitis. Hydroxychloroquine also works well in treating subacute cutaneous lupus, she said, and because it can travel across the placenta, it could be an effective means of preventing this disorder in at-risk neonates.
To examine any potential benefit, Dr. Barsalou looked at three pediatric lupus databases: the SickKids NLE database from Toronto, the U.S. Research Registry for Neonatal Lupus, and the French Registry for Neonatal Lupus.
These registries include infants born to mothers with anti-Ro and/or anti-La antibodies, and a diagnosis of lupus, dermatomyositis, Sjögren’s syndrome, juvenile idiopathic arthritis, or rheumatic arthritis. No infants with cardiac neonatal lupus were included in the study.
In addition to hydroxychloroquine, Dr. Barsalou examined the use of prenatal azathioprine, nonfluorinated and fluorinated steroids, and intravenous immunoglobulin.
The cohort comprised 545 neonates born to 535 mothers. Among these, 112 developed cNLE. The remaining 433 infants were used as controls.
Mothers of both cases and controls were a mean age of 31 years. Among cases, the most common diagnosis was Sjögren’s syndrome (53%), followed by systemic lupus erythematosus (46%). Among controls, the most common maternal diagnosis was SLE (62%), followed by Sjögren’s (31%).
All mothers of cases were positive for anti-Ro antibodies; 72% were positive for anti-La antibodies. Among mothers of controls, 99% had anti-Ro antibodies and 48% had anti-La antibodies.
Mothers of cases took hydroxychloroquine (17%), fluorinated steroids (6%), and nonfluorinated steroids with or without azathioprine (28%). Mothers of controls took hydroxychloroquine (34%), fluorinated steroids (4%), and nonfluorinated steroids with or without azathioprine (44%),
There were significantly more female than male infants in the case group (65%). The median age at rash onset was 6 weeks.
Dr. Barsalou performed several multivariate analyses on the entire cohort, as well as two subgroup analyses: one on infants who developed the cNLE rash within the first 4 weeks of life and one on only the infants of mothers with SLE.
In the primary analysis, maternal anti-Ro and anti-La antibodies more than doubled the risk of an infant developing cNLE (odds ratio, 2.5). The use of hydroxychloroquine decreased this risk by 60% (OR, 0.4). Being a female infant increased the risk by 70% (OR, 1.7).
In the group of infants with early-onset rash, maternal anti-La antibodies more than tripled the risk (OR, 3.5), while the use of hydroxychloroquine decreased the risk by 80% (OR, 0.2).
Among the infants born to women with SLE, concomitant secondary Sjögren’s syndrome increased the risk of cNLE by more than threefold (OR, 3.5). Anti-La antibodies more than doubled the risk (OR, 2.5), and the use of hydroxychloroquine decreased it by 60% (OR, 0.4).
“This is the first study to address the prevention of cutaneous neonatal lupus,” Dr. Barsalou said. “We found that prenatal exposure to hydroxychloroquine is likely protective.”
She had no financial disclosures.
[email protected]
On Twitter @alz_gal
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: The drug was associated with a 60% decreased risk of developing the disorder.
Data source: The case-control study involved 545 infants.
Disclosures: Dr. Barsalou had no financial disclosures.