User login
This Month in CHEST: Editor’s Picks
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
ABIM Pulmonary Medicine Board urges participation in survey
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
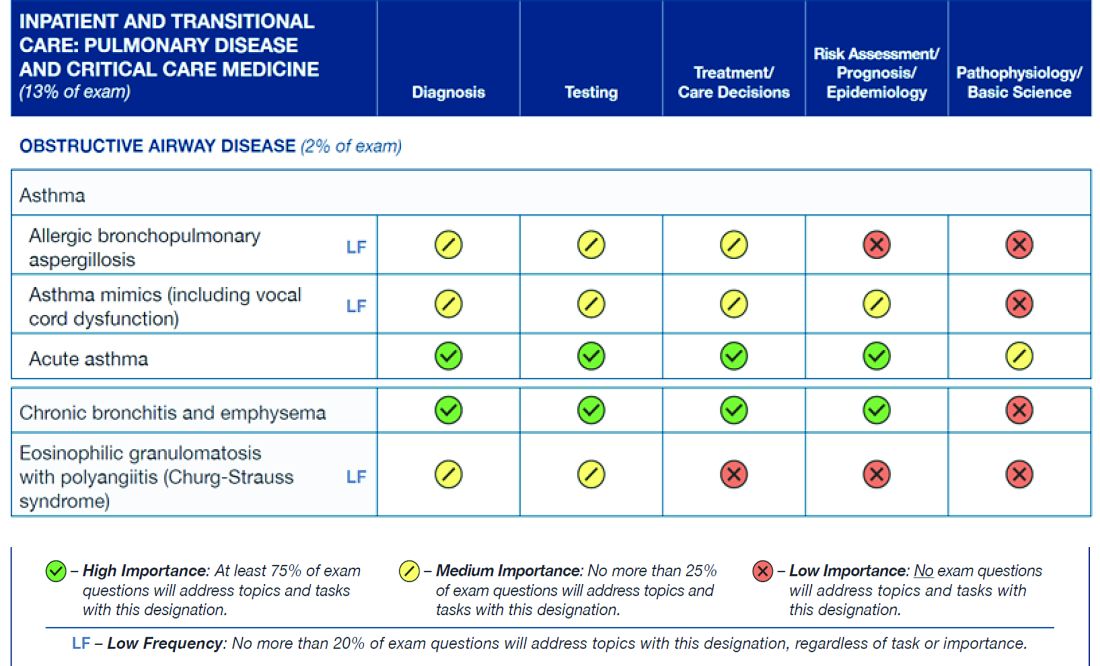
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
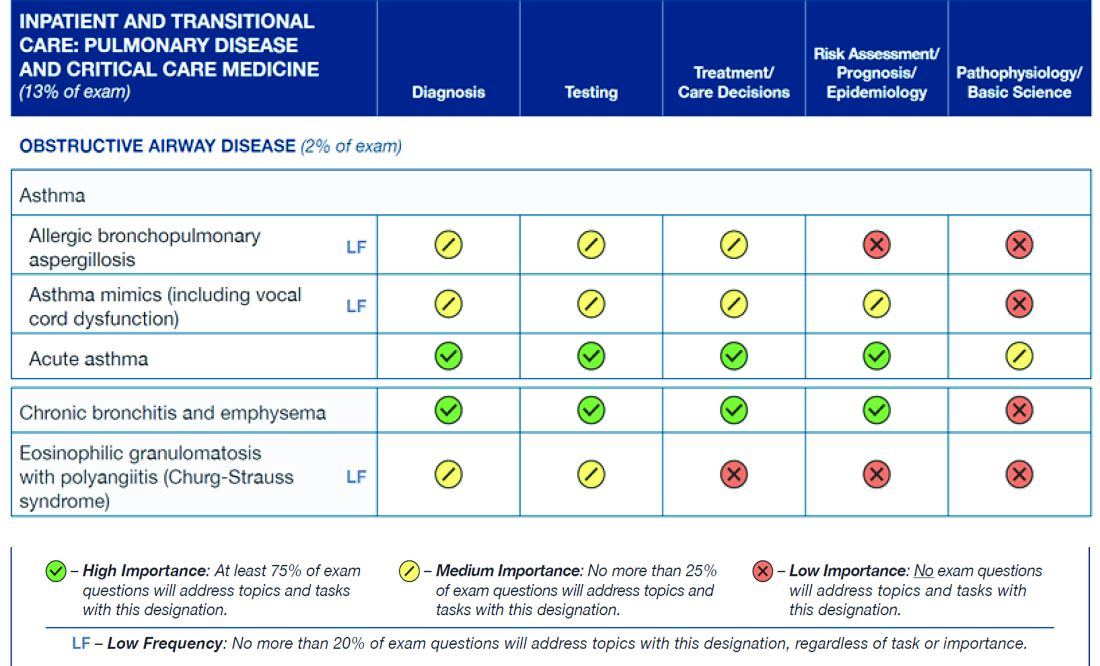
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
Update on NAMDRC Activities
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.

The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.
The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.
The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
Can We Count on You?
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.
VIDEO: Combination venetoclax-LDAC therapy boosts overall survival in AML
SAN DIEGO – Combination therapy with the BCL-2 inhibitor venetoclax and low-dose cytarabine (LDAC) achieved a 61% overall response rate in older patients with treatment-naive acute myeloid leukemia, Andrew Wei, MBBS, PhD, reported at the annual meeting of the American Society of Hematology.
That is about three times higher than historically reported response rates for this deadly blood cancer, said Dr. Wei of Alfred Hospital in Melbourne, Australia. He discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The multicenter phase II study evaluated 28-cycles of venetoclax (600 mg, given orally) and LDAC (20 mg/m2 subcutaneously) in 53 treatment-naive AML patients aged 65 years and older, who were ineligible for intensive chemotherapy but had adequate liver and kidney function and an ECOG performance status between 0 and 2.
A total of 21% of patients had a complete remission, 33% had complete remission with incomplete marrow recovery, and 70% reached one of these endpoints during cycles 1 and 2. Common adverse events included vomiting, diarrhea, hypokalemia, and febrile neutropenia. Grade 3-4 adverse events included febrile neutropenia, hypokalemia, hypophosphatemia, and hypertension.
Researchers are planning larger randomized trials of venetoclax/LDAC combination therapy in AML, Dr. Wei said. Larger sample sizes will yield more data on how to best target this regimen based on prognostic indicators, such as gene mutations, he added.
Abbvie is the maker of venetoclax and sponsored the study. Dr. Wei disclosed a consulting relationship with Abbvie and ties to Novartis, Celgene, and several other pharmaceutical companies.
SAN DIEGO – Combination therapy with the BCL-2 inhibitor venetoclax and low-dose cytarabine (LDAC) achieved a 61% overall response rate in older patients with treatment-naive acute myeloid leukemia, Andrew Wei, MBBS, PhD, reported at the annual meeting of the American Society of Hematology.
That is about three times higher than historically reported response rates for this deadly blood cancer, said Dr. Wei of Alfred Hospital in Melbourne, Australia. He discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The multicenter phase II study evaluated 28-cycles of venetoclax (600 mg, given orally) and LDAC (20 mg/m2 subcutaneously) in 53 treatment-naive AML patients aged 65 years and older, who were ineligible for intensive chemotherapy but had adequate liver and kidney function and an ECOG performance status between 0 and 2.
A total of 21% of patients had a complete remission, 33% had complete remission with incomplete marrow recovery, and 70% reached one of these endpoints during cycles 1 and 2. Common adverse events included vomiting, diarrhea, hypokalemia, and febrile neutropenia. Grade 3-4 adverse events included febrile neutropenia, hypokalemia, hypophosphatemia, and hypertension.
Researchers are planning larger randomized trials of venetoclax/LDAC combination therapy in AML, Dr. Wei said. Larger sample sizes will yield more data on how to best target this regimen based on prognostic indicators, such as gene mutations, he added.
Abbvie is the maker of venetoclax and sponsored the study. Dr. Wei disclosed a consulting relationship with Abbvie and ties to Novartis, Celgene, and several other pharmaceutical companies.
SAN DIEGO – Combination therapy with the BCL-2 inhibitor venetoclax and low-dose cytarabine (LDAC) achieved a 61% overall response rate in older patients with treatment-naive acute myeloid leukemia, Andrew Wei, MBBS, PhD, reported at the annual meeting of the American Society of Hematology.
That is about three times higher than historically reported response rates for this deadly blood cancer, said Dr. Wei of Alfred Hospital in Melbourne, Australia. He discussed the findings in a video interview.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The multicenter phase II study evaluated 28-cycles of venetoclax (600 mg, given orally) and LDAC (20 mg/m2 subcutaneously) in 53 treatment-naive AML patients aged 65 years and older, who were ineligible for intensive chemotherapy but had adequate liver and kidney function and an ECOG performance status between 0 and 2.
A total of 21% of patients had a complete remission, 33% had complete remission with incomplete marrow recovery, and 70% reached one of these endpoints during cycles 1 and 2. Common adverse events included vomiting, diarrhea, hypokalemia, and febrile neutropenia. Grade 3-4 adverse events included febrile neutropenia, hypokalemia, hypophosphatemia, and hypertension.
Researchers are planning larger randomized trials of venetoclax/LDAC combination therapy in AML, Dr. Wei said. Larger sample sizes will yield more data on how to best target this regimen based on prognostic indicators, such as gene mutations, he added.
Abbvie is the maker of venetoclax and sponsored the study. Dr. Wei disclosed a consulting relationship with Abbvie and ties to Novartis, Celgene, and several other pharmaceutical companies.
AT ASH 2016
Key clinical point: Combination therapy with venetoclax and low-dose cytarabine (LDAC) achieved a high overall response rate in patients with AML.
Major finding: In all, 61% of patients achieved an overall response. Grade 3-4 adverse events included febrile neutropenia, hypokalemia, hypophosphatemia, and hypertension.
Data source: A multicenter phase II study of venetoclax (600 mg) and LDAC (20 mg/m2) in 53 treatment-naive AML patients aged 65 years and older, who were ineligible for intensive chemotherapy but had adequate liver and kidney function and an ECOG performance status of 0-2.
Disclosures: Abbvie is the maker of venetoclax and sponsored the study. Dr. Wei disclosed a consulting relationship with Abbvie and ties to Novartis, Celgene, and several other pharmaceutical companies.

VIDEO: CPX-351 may allow more high-risk AML patients to have allogeneic transplants
SAN DIEGO – Induction therapy with the investigational drug CPX-351 (Vyxeos), a liposomal formulation of cytarabine and daunorubicin, allowed more older patients with newly diagnosed secondary AML to bridge successfully to transplant than did standard 7+3 cytarabine and daunorubicin, based on data reported by Jeffrey E. Lancet, MD, at the annual meeting of the American Society of Hematology.
The data come from a subgroup analysis of a phase III study in 60- to 75-year-old patients with secondary AML. Initial survival data from that randomized open-label study, reported last June at the annual meeting of the American Society of Clinical Oncology, indicated CPX-351 significantly improved overall survival, event-free survival, and treatment response without an increase in 60-day mortality or in the frequency and severity of adverse events, compared with the standard 7+3 regimen of cytarabine and daunorubicin.
Dr. Lancet of the H. Lee Moffitt Cancer Center and Research Institute, Tampa, Fla., credited the better results to the higher level of complete responses and complete responses with incomplete platelet or neutrophil recovery with the liposomal formulation.
In a video interview, Dr. Lancet discussed how better disease control allowed more patients to be transplanted and next steps for expanded study in this patient population as well as in younger patients with AML.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @maryjodales
SAN DIEGO – Induction therapy with the investigational drug CPX-351 (Vyxeos), a liposomal formulation of cytarabine and daunorubicin, allowed more older patients with newly diagnosed secondary AML to bridge successfully to transplant than did standard 7+3 cytarabine and daunorubicin, based on data reported by Jeffrey E. Lancet, MD, at the annual meeting of the American Society of Hematology.
The data come from a subgroup analysis of a phase III study in 60- to 75-year-old patients with secondary AML. Initial survival data from that randomized open-label study, reported last June at the annual meeting of the American Society of Clinical Oncology, indicated CPX-351 significantly improved overall survival, event-free survival, and treatment response without an increase in 60-day mortality or in the frequency and severity of adverse events, compared with the standard 7+3 regimen of cytarabine and daunorubicin.
Dr. Lancet of the H. Lee Moffitt Cancer Center and Research Institute, Tampa, Fla., credited the better results to the higher level of complete responses and complete responses with incomplete platelet or neutrophil recovery with the liposomal formulation.
In a video interview, Dr. Lancet discussed how better disease control allowed more patients to be transplanted and next steps for expanded study in this patient population as well as in younger patients with AML.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @maryjodales
SAN DIEGO – Induction therapy with the investigational drug CPX-351 (Vyxeos), a liposomal formulation of cytarabine and daunorubicin, allowed more older patients with newly diagnosed secondary AML to bridge successfully to transplant than did standard 7+3 cytarabine and daunorubicin, based on data reported by Jeffrey E. Lancet, MD, at the annual meeting of the American Society of Hematology.
The data come from a subgroup analysis of a phase III study in 60- to 75-year-old patients with secondary AML. Initial survival data from that randomized open-label study, reported last June at the annual meeting of the American Society of Clinical Oncology, indicated CPX-351 significantly improved overall survival, event-free survival, and treatment response without an increase in 60-day mortality or in the frequency and severity of adverse events, compared with the standard 7+3 regimen of cytarabine and daunorubicin.
Dr. Lancet of the H. Lee Moffitt Cancer Center and Research Institute, Tampa, Fla., credited the better results to the higher level of complete responses and complete responses with incomplete platelet or neutrophil recovery with the liposomal formulation.
In a video interview, Dr. Lancet discussed how better disease control allowed more patients to be transplanted and next steps for expanded study in this patient population as well as in younger patients with AML.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @maryjodales
AT ASH 2016

Non-TNF-Targeted Therapy in Unresponsive RA More Effective than a Second Anti-TNF Drug
Study Overview
Objective. To determine whether a non–tumor necrosis factor (TNF)-targeted drug is more effective than a second anti-TNF drug in rheumatoid arthritis (RA) patients who have had an inadequate response to a first anti-TNF drug.
Design. 52-week pragmatic, multicenter, open-label, parallel-group, randomized clinical trial (the “Rotation or Change” trial).
Setting and participants. 300 patients who were at least 18 years old were recruited from December 2009 to August 2012 from 47 French clinical centers. These patients had to have a diagnosis of RA according to the 1987 American College of Rheumatology criteria, presence of erosions, a DAS28-ESR (a measure of disease burden using patient global health, tender and swollen joint counts, and the erythrocyte sedimentation rate) of 3.2 or more, and insufficient response to an anti-TNF according to the physician (based on 1 or more of: persistent tender and swollen joints, persistent disease activity according to patient global assessment, elevated levels of acute-phase reactants, and dependence on analgesics, nonsteroidal anti-inflammatory drugs, or corticosteroids). In addition, patients had to have a stable dose of oral corticosteroids of 15 mg/d or less of equivalent prednisone within 4 weeks before enrollment, a stable dose of synthetic disease-modifying antirheumatic drugs (DMARDs) within 4 weeks of enrollment, and informed written consent. Exclusion criteria included cessation of the first anti-TNF agent due only to an adverse event, previous treatment with 2 or more anti-TNF agents, previous treatment with abatacept, rituximab, or tocilizumab, a contraindication to all anti-TNF agents and other biologics such as an infection or cancer, pregnancy and breastfeeding.
Intervention. Patients were randomly assigned in equal proportions to receive either a non-TNF biologic (abatacept, rituximab, or tocilizumab) or a second anti-TNF agent (adalimumab, certolizumab, etanercept, infliximab, or golimumab); the choice of agent after randomization was decided by the physician. The starting dose and frequency of treatment was predetermined. Golimumab was not available for use at the time of this study. The choice of future dosing and frequency of the treatment was left up to the treating physician in both groups. The assigned drug treatments continued for 12 months but were allowed to be discontinued for adverse events, patient choice, or inefficacy. Treatment and dose adjustments for oral corticosteroids and glucocorticoid intra-articular injections were allowed for both treatment groups.
Main outcome measures. The primary outcome was the proportion of patients at week 24 with a good or moderate European League Against Rheumatism (EULAR) response. A good EULAR response is defined as a decrease in DAS28-ESR of more than 1.2 points leading to a score of 3.2 or lower while a moderate EULAR response is defined as a decrease of more than 0.6 and resulting in a score of 5.1 points or lower. Secondary end points were EULAR response at weeks 12 and 52, DAS28-ESR at weeks 12, 24, and 52, low disease activity (DAS28-ESR < 3.2) and remission (DAS28-ESR < 2.6) at weeks 12, 24, and 52, mean oral corticosteroid use at weeks 24 and 52, therapeutic maintenance (defined as the proportion of patients who did not discontinue the assigned biologic treatment) at weeks 24 and 52, and health assessment questionnaire (HAQ) score (range, 0–3 with 0 representing the best and 3 the worst outcomes) at weeks 12, 24, and 52. Safety including serious adverse events as well as serious infections was also evaluated throughout the study.
Main results. 300 patients were randomized. The 2 groups were not different with regard to demographic and disease characteristics. In the non-TNF group of 150 patients, 33 of 146 patients (23%) received abatacept, 41 (28%) rituximab, and 70 (48%) tocilizumab; 2 patients (1%) did not receive the intervention as planned, 1 patient received adalimumab and 1 patient received no treatment. For the anti-TNF group, 57 of 146 patients (39%) received adalimumab, 23 (16%) certolizumab, 53 (36%) etanercept, and 8 (5%) infliximab. Five patients (3%) did not receive the intervention assigned as 2 patients received rituximab, 1 patient received tocilizumab, and 2 patients received no treatment. About two-thirds of patients in each group received concomitant methotrexate and about half in each group received oral corticosteroids.
With regard to the primary outcome, at week 24 101 of 146 patients (69%) in the non-TNF group and 76 (52%) in the second anti-TNF group achieved a good or moderate EULAR response, with 39% with a good response and 30% with a moderate response in the non-TNF group and 21% with a good response and 31% with a moderate response in the second anti-TNF group (odds ratio [OR], 2.06; 95% confidence interval [CI], 1.27 to 3.37; P = 0.004, with imputation of missing data; absolute difference, 17.2%; 95% CI, 6.2% to 28.2%). The DAS28-ESR was lower in the non-TNF group (mean difference adjusted for baseline differences, −0.43; 95% CI, −0.72 to −0.14; P = 0.004). More patients in the non-TNF group vs the second anti-TNF group showed low disease activity at week 24 (45% vs 28%; OR, 2.09; 95% CI, 1.27 to 3.43; P = 0.004) and at week 52 (41% vs 23%; OR, 2.26; 95% CI, 1.33 to 3.86; P = 0.003).
The mean DAS28-ESR change from baseline was greater for patients in the non-TNF group than for patients in the second anti-TNF group with a 24-week mean difference of −0.43 (95% CI,−0.72 to −0.14; P = 0.004) and 52-week mean difference of −0.38 (95% CI, −0.69 to −0.08; P = 0.01).
The proportion of EULAR good and moderate responders at week 24 did not significantly differ with abatacept, rituximab, and tocilizumab treatment. The therapeutic maintenance rate, defined as the proportion of patients who continued the biologic treatment, was found to be significantly higher at weeks 24 and 52 in the non-TNF group than in the second anti-TNF group. The mean change from baseline to weeks 24 and 52 in the level of prednisone doses was not significantly different between patients between treatment groups.
With respect to safety, 16 patients (11%) in the non-TNF group experienced 18 serious adverse events and 8 patients (5%) in the second anti-TNF group experienced 13 events (P = 0.10) with 7 patients (5%) in each group developing serious infections.
Conclusion. In patients with RA previously treated with an anti-TNF drug with an inadequate response, the use of a non-TNF biologic agent was found to be more effective in achieving a good or moderate disease activity response at 24 weeks compared with a second anti-TNF medication.
Commentary
In patients with RA who have shown an inadequate response to methotrexate, TNF-α inhibitors have been shown to improve quality of life. However, it has been shown that almost one-third of patients have an insufficient and inadequate response to anti-TNF agents and continue to have persistent disease activity [1–3].Alternative treatments are therefore needed, but there is currently little guidance available for choosing the next treatment.
There are 3 placebo-controlled trials that have shown that switching to a non–TNF-targeted therapy may be appropriate [4–6]. The most commonly used non-TNF agents are abatacept, rituximab, and tocilizumab. However, there is evidence that switching to another anti-TNF agent after failure of a first can also be a good choice, as the molecular structure of TNF-inhibitors and their affinity for membrane and TNF-α vary. There were 2 randomized placebo-controlled trials that reported that approximately half of patients with RA with insufficient response to a TNF-α inhibitor responded to a second anti-TNF drug [7,8].
Although there have been observational studies addressing this question, this is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic compared to a second anti-TNF drug to treat RA in patients with an insufficient response to a first anti-TNF drug. Data showed that at week 24, 69% in the non-TNF group and 52% in the anti-TNF group achieved a good or moderate EULAR response. The non-TNF treatment was also associated with a better EULAR response than a second anti-TNF drug at weeks 12 and 52. The DAS28-ESR and the number of patients achieving low disease activity status were found to be greater at months 6 and 12 in the non-TNF group than in the second anti-TNF group. One strength of the study is its pragmatic design—the study evaluated the effectiveness of interventions under real-life, routine practice conditions where physicians often choose one drug over another for reasons based on the habits or characteristics of the patient. The comparison of strategies and not individual drugs more appropriately addresses the questions that physicians face in daily practice. However, there were some limitations including the lack of blinding by participants, the exclusion of some biologic agents such as golimunab, the lack of assessment of individual drug efficacy, and the fact that approximately 40% of patients in each group did not have concomitant treatment with methotrexate, an agent known to improve the efficacy of most biologic agents.
Applications for Clinical Practice
This is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic vs. a second anti-TNF in patients with RA who have an insufficient response to a first anti-TNF drug. Further studies addressing the limitations identified in this study are needed before physicians can employ these findings in clinical practice.
—Anita Laloo, MD
1. Hyrich KL, Lunt M, Watson KD, et al; British Society for Rheumatology Biologics Register. Outcomes after switching from one antitumor necrosis factor alpha agent to a second anti-tumor necrosis factor alpha agent in patients with rheumatoid arthritis: results from a large UK national cohort study. Arthritis Rheum 2007;56:13–20.
2. Hetland ML, Christensen IJ, Tarp U, et al; All Departments of Rheumatology in Denmark. Direct comparison of treatment responses, remission rates, and drug adherence in patients with rheumatoid arthritis treated with adalimumab, etanercept, or infliximab: results from eight years of surveillance of clinical practice in the nationwide Danish DANBIO registry. Arthritis Rheum 2010;62:22–32.
3. Smolen JS, Landewé R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis 2010;69:964–75.
4. Cohen SB, Emery P, Greenwald MW, et al; REFLEX Trial Group. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase 3 trial evaluating primary efficacy and safety at twenty-four weeks. Arthritis Rheum 2006;54:2793–806.
5. Emery P, Keystone E, Tony HP, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial. Ann Rheum Dis 2008;67:1516–23.
6. Genovese MC, Becker JC, Schiff M, et al. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor alpha inhibition. N Engl J Med 2005;353:1114–23.
7. Smolen JS, Kay J, Doyle MK, et al; GO-AFTER study investigators. Golimumab in patients with active rheumatoid arthritis after treatment with tumour necrosis factor alpha inhibitors (GO-AFTER study): a multicentre, randomised, double-blind, placebo-controlled, phase III trial. Lancet 2009;374:210–21.
8. Schiff MH, von Kempis J, Goldblum R, et al. Rheumatoid arthritis secondary non-responders to TNF can attain an efficacious and safe response by switching to certolizumab pegol: a phase IV, randomised, multicentre, double-blind, 12-week study, followed by a 12-week open-label phase. Ann Rheum Dis 2014;73:2174–7.
Study Overview
Objective. To determine whether a non–tumor necrosis factor (TNF)-targeted drug is more effective than a second anti-TNF drug in rheumatoid arthritis (RA) patients who have had an inadequate response to a first anti-TNF drug.
Design. 52-week pragmatic, multicenter, open-label, parallel-group, randomized clinical trial (the “Rotation or Change” trial).
Setting and participants. 300 patients who were at least 18 years old were recruited from December 2009 to August 2012 from 47 French clinical centers. These patients had to have a diagnosis of RA according to the 1987 American College of Rheumatology criteria, presence of erosions, a DAS28-ESR (a measure of disease burden using patient global health, tender and swollen joint counts, and the erythrocyte sedimentation rate) of 3.2 or more, and insufficient response to an anti-TNF according to the physician (based on 1 or more of: persistent tender and swollen joints, persistent disease activity according to patient global assessment, elevated levels of acute-phase reactants, and dependence on analgesics, nonsteroidal anti-inflammatory drugs, or corticosteroids). In addition, patients had to have a stable dose of oral corticosteroids of 15 mg/d or less of equivalent prednisone within 4 weeks before enrollment, a stable dose of synthetic disease-modifying antirheumatic drugs (DMARDs) within 4 weeks of enrollment, and informed written consent. Exclusion criteria included cessation of the first anti-TNF agent due only to an adverse event, previous treatment with 2 or more anti-TNF agents, previous treatment with abatacept, rituximab, or tocilizumab, a contraindication to all anti-TNF agents and other biologics such as an infection or cancer, pregnancy and breastfeeding.
Intervention. Patients were randomly assigned in equal proportions to receive either a non-TNF biologic (abatacept, rituximab, or tocilizumab) or a second anti-TNF agent (adalimumab, certolizumab, etanercept, infliximab, or golimumab); the choice of agent after randomization was decided by the physician. The starting dose and frequency of treatment was predetermined. Golimumab was not available for use at the time of this study. The choice of future dosing and frequency of the treatment was left up to the treating physician in both groups. The assigned drug treatments continued for 12 months but were allowed to be discontinued for adverse events, patient choice, or inefficacy. Treatment and dose adjustments for oral corticosteroids and glucocorticoid intra-articular injections were allowed for both treatment groups.
Main outcome measures. The primary outcome was the proportion of patients at week 24 with a good or moderate European League Against Rheumatism (EULAR) response. A good EULAR response is defined as a decrease in DAS28-ESR of more than 1.2 points leading to a score of 3.2 or lower while a moderate EULAR response is defined as a decrease of more than 0.6 and resulting in a score of 5.1 points or lower. Secondary end points were EULAR response at weeks 12 and 52, DAS28-ESR at weeks 12, 24, and 52, low disease activity (DAS28-ESR < 3.2) and remission (DAS28-ESR < 2.6) at weeks 12, 24, and 52, mean oral corticosteroid use at weeks 24 and 52, therapeutic maintenance (defined as the proportion of patients who did not discontinue the assigned biologic treatment) at weeks 24 and 52, and health assessment questionnaire (HAQ) score (range, 0–3 with 0 representing the best and 3 the worst outcomes) at weeks 12, 24, and 52. Safety including serious adverse events as well as serious infections was also evaluated throughout the study.
Main results. 300 patients were randomized. The 2 groups were not different with regard to demographic and disease characteristics. In the non-TNF group of 150 patients, 33 of 146 patients (23%) received abatacept, 41 (28%) rituximab, and 70 (48%) tocilizumab; 2 patients (1%) did not receive the intervention as planned, 1 patient received adalimumab and 1 patient received no treatment. For the anti-TNF group, 57 of 146 patients (39%) received adalimumab, 23 (16%) certolizumab, 53 (36%) etanercept, and 8 (5%) infliximab. Five patients (3%) did not receive the intervention assigned as 2 patients received rituximab, 1 patient received tocilizumab, and 2 patients received no treatment. About two-thirds of patients in each group received concomitant methotrexate and about half in each group received oral corticosteroids.
With regard to the primary outcome, at week 24 101 of 146 patients (69%) in the non-TNF group and 76 (52%) in the second anti-TNF group achieved a good or moderate EULAR response, with 39% with a good response and 30% with a moderate response in the non-TNF group and 21% with a good response and 31% with a moderate response in the second anti-TNF group (odds ratio [OR], 2.06; 95% confidence interval [CI], 1.27 to 3.37; P = 0.004, with imputation of missing data; absolute difference, 17.2%; 95% CI, 6.2% to 28.2%). The DAS28-ESR was lower in the non-TNF group (mean difference adjusted for baseline differences, −0.43; 95% CI, −0.72 to −0.14; P = 0.004). More patients in the non-TNF group vs the second anti-TNF group showed low disease activity at week 24 (45% vs 28%; OR, 2.09; 95% CI, 1.27 to 3.43; P = 0.004) and at week 52 (41% vs 23%; OR, 2.26; 95% CI, 1.33 to 3.86; P = 0.003).
The mean DAS28-ESR change from baseline was greater for patients in the non-TNF group than for patients in the second anti-TNF group with a 24-week mean difference of −0.43 (95% CI,−0.72 to −0.14; P = 0.004) and 52-week mean difference of −0.38 (95% CI, −0.69 to −0.08; P = 0.01).
The proportion of EULAR good and moderate responders at week 24 did not significantly differ with abatacept, rituximab, and tocilizumab treatment. The therapeutic maintenance rate, defined as the proportion of patients who continued the biologic treatment, was found to be significantly higher at weeks 24 and 52 in the non-TNF group than in the second anti-TNF group. The mean change from baseline to weeks 24 and 52 in the level of prednisone doses was not significantly different between patients between treatment groups.
With respect to safety, 16 patients (11%) in the non-TNF group experienced 18 serious adverse events and 8 patients (5%) in the second anti-TNF group experienced 13 events (P = 0.10) with 7 patients (5%) in each group developing serious infections.
Conclusion. In patients with RA previously treated with an anti-TNF drug with an inadequate response, the use of a non-TNF biologic agent was found to be more effective in achieving a good or moderate disease activity response at 24 weeks compared with a second anti-TNF medication.
Commentary
In patients with RA who have shown an inadequate response to methotrexate, TNF-α inhibitors have been shown to improve quality of life. However, it has been shown that almost one-third of patients have an insufficient and inadequate response to anti-TNF agents and continue to have persistent disease activity [1–3].Alternative treatments are therefore needed, but there is currently little guidance available for choosing the next treatment.
There are 3 placebo-controlled trials that have shown that switching to a non–TNF-targeted therapy may be appropriate [4–6]. The most commonly used non-TNF agents are abatacept, rituximab, and tocilizumab. However, there is evidence that switching to another anti-TNF agent after failure of a first can also be a good choice, as the molecular structure of TNF-inhibitors and their affinity for membrane and TNF-α vary. There were 2 randomized placebo-controlled trials that reported that approximately half of patients with RA with insufficient response to a TNF-α inhibitor responded to a second anti-TNF drug [7,8].
Although there have been observational studies addressing this question, this is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic compared to a second anti-TNF drug to treat RA in patients with an insufficient response to a first anti-TNF drug. Data showed that at week 24, 69% in the non-TNF group and 52% in the anti-TNF group achieved a good or moderate EULAR response. The non-TNF treatment was also associated with a better EULAR response than a second anti-TNF drug at weeks 12 and 52. The DAS28-ESR and the number of patients achieving low disease activity status were found to be greater at months 6 and 12 in the non-TNF group than in the second anti-TNF group. One strength of the study is its pragmatic design—the study evaluated the effectiveness of interventions under real-life, routine practice conditions where physicians often choose one drug over another for reasons based on the habits or characteristics of the patient. The comparison of strategies and not individual drugs more appropriately addresses the questions that physicians face in daily practice. However, there were some limitations including the lack of blinding by participants, the exclusion of some biologic agents such as golimunab, the lack of assessment of individual drug efficacy, and the fact that approximately 40% of patients in each group did not have concomitant treatment with methotrexate, an agent known to improve the efficacy of most biologic agents.
Applications for Clinical Practice
This is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic vs. a second anti-TNF in patients with RA who have an insufficient response to a first anti-TNF drug. Further studies addressing the limitations identified in this study are needed before physicians can employ these findings in clinical practice.
—Anita Laloo, MD
Study Overview
Objective. To determine whether a non–tumor necrosis factor (TNF)-targeted drug is more effective than a second anti-TNF drug in rheumatoid arthritis (RA) patients who have had an inadequate response to a first anti-TNF drug.
Design. 52-week pragmatic, multicenter, open-label, parallel-group, randomized clinical trial (the “Rotation or Change” trial).
Setting and participants. 300 patients who were at least 18 years old were recruited from December 2009 to August 2012 from 47 French clinical centers. These patients had to have a diagnosis of RA according to the 1987 American College of Rheumatology criteria, presence of erosions, a DAS28-ESR (a measure of disease burden using patient global health, tender and swollen joint counts, and the erythrocyte sedimentation rate) of 3.2 or more, and insufficient response to an anti-TNF according to the physician (based on 1 or more of: persistent tender and swollen joints, persistent disease activity according to patient global assessment, elevated levels of acute-phase reactants, and dependence on analgesics, nonsteroidal anti-inflammatory drugs, or corticosteroids). In addition, patients had to have a stable dose of oral corticosteroids of 15 mg/d or less of equivalent prednisone within 4 weeks before enrollment, a stable dose of synthetic disease-modifying antirheumatic drugs (DMARDs) within 4 weeks of enrollment, and informed written consent. Exclusion criteria included cessation of the first anti-TNF agent due only to an adverse event, previous treatment with 2 or more anti-TNF agents, previous treatment with abatacept, rituximab, or tocilizumab, a contraindication to all anti-TNF agents and other biologics such as an infection or cancer, pregnancy and breastfeeding.
Intervention. Patients were randomly assigned in equal proportions to receive either a non-TNF biologic (abatacept, rituximab, or tocilizumab) or a second anti-TNF agent (adalimumab, certolizumab, etanercept, infliximab, or golimumab); the choice of agent after randomization was decided by the physician. The starting dose and frequency of treatment was predetermined. Golimumab was not available for use at the time of this study. The choice of future dosing and frequency of the treatment was left up to the treating physician in both groups. The assigned drug treatments continued for 12 months but were allowed to be discontinued for adverse events, patient choice, or inefficacy. Treatment and dose adjustments for oral corticosteroids and glucocorticoid intra-articular injections were allowed for both treatment groups.
Main outcome measures. The primary outcome was the proportion of patients at week 24 with a good or moderate European League Against Rheumatism (EULAR) response. A good EULAR response is defined as a decrease in DAS28-ESR of more than 1.2 points leading to a score of 3.2 or lower while a moderate EULAR response is defined as a decrease of more than 0.6 and resulting in a score of 5.1 points or lower. Secondary end points were EULAR response at weeks 12 and 52, DAS28-ESR at weeks 12, 24, and 52, low disease activity (DAS28-ESR < 3.2) and remission (DAS28-ESR < 2.6) at weeks 12, 24, and 52, mean oral corticosteroid use at weeks 24 and 52, therapeutic maintenance (defined as the proportion of patients who did not discontinue the assigned biologic treatment) at weeks 24 and 52, and health assessment questionnaire (HAQ) score (range, 0–3 with 0 representing the best and 3 the worst outcomes) at weeks 12, 24, and 52. Safety including serious adverse events as well as serious infections was also evaluated throughout the study.
Main results. 300 patients were randomized. The 2 groups were not different with regard to demographic and disease characteristics. In the non-TNF group of 150 patients, 33 of 146 patients (23%) received abatacept, 41 (28%) rituximab, and 70 (48%) tocilizumab; 2 patients (1%) did not receive the intervention as planned, 1 patient received adalimumab and 1 patient received no treatment. For the anti-TNF group, 57 of 146 patients (39%) received adalimumab, 23 (16%) certolizumab, 53 (36%) etanercept, and 8 (5%) infliximab. Five patients (3%) did not receive the intervention assigned as 2 patients received rituximab, 1 patient received tocilizumab, and 2 patients received no treatment. About two-thirds of patients in each group received concomitant methotrexate and about half in each group received oral corticosteroids.
With regard to the primary outcome, at week 24 101 of 146 patients (69%) in the non-TNF group and 76 (52%) in the second anti-TNF group achieved a good or moderate EULAR response, with 39% with a good response and 30% with a moderate response in the non-TNF group and 21% with a good response and 31% with a moderate response in the second anti-TNF group (odds ratio [OR], 2.06; 95% confidence interval [CI], 1.27 to 3.37; P = 0.004, with imputation of missing data; absolute difference, 17.2%; 95% CI, 6.2% to 28.2%). The DAS28-ESR was lower in the non-TNF group (mean difference adjusted for baseline differences, −0.43; 95% CI, −0.72 to −0.14; P = 0.004). More patients in the non-TNF group vs the second anti-TNF group showed low disease activity at week 24 (45% vs 28%; OR, 2.09; 95% CI, 1.27 to 3.43; P = 0.004) and at week 52 (41% vs 23%; OR, 2.26; 95% CI, 1.33 to 3.86; P = 0.003).
The mean DAS28-ESR change from baseline was greater for patients in the non-TNF group than for patients in the second anti-TNF group with a 24-week mean difference of −0.43 (95% CI,−0.72 to −0.14; P = 0.004) and 52-week mean difference of −0.38 (95% CI, −0.69 to −0.08; P = 0.01).
The proportion of EULAR good and moderate responders at week 24 did not significantly differ with abatacept, rituximab, and tocilizumab treatment. The therapeutic maintenance rate, defined as the proportion of patients who continued the biologic treatment, was found to be significantly higher at weeks 24 and 52 in the non-TNF group than in the second anti-TNF group. The mean change from baseline to weeks 24 and 52 in the level of prednisone doses was not significantly different between patients between treatment groups.
With respect to safety, 16 patients (11%) in the non-TNF group experienced 18 serious adverse events and 8 patients (5%) in the second anti-TNF group experienced 13 events (P = 0.10) with 7 patients (5%) in each group developing serious infections.
Conclusion. In patients with RA previously treated with an anti-TNF drug with an inadequate response, the use of a non-TNF biologic agent was found to be more effective in achieving a good or moderate disease activity response at 24 weeks compared with a second anti-TNF medication.
Commentary
In patients with RA who have shown an inadequate response to methotrexate, TNF-α inhibitors have been shown to improve quality of life. However, it has been shown that almost one-third of patients have an insufficient and inadequate response to anti-TNF agents and continue to have persistent disease activity [1–3].Alternative treatments are therefore needed, but there is currently little guidance available for choosing the next treatment.
There are 3 placebo-controlled trials that have shown that switching to a non–TNF-targeted therapy may be appropriate [4–6]. The most commonly used non-TNF agents are abatacept, rituximab, and tocilizumab. However, there is evidence that switching to another anti-TNF agent after failure of a first can also be a good choice, as the molecular structure of TNF-inhibitors and their affinity for membrane and TNF-α vary. There were 2 randomized placebo-controlled trials that reported that approximately half of patients with RA with insufficient response to a TNF-α inhibitor responded to a second anti-TNF drug [7,8].
Although there have been observational studies addressing this question, this is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic compared to a second anti-TNF drug to treat RA in patients with an insufficient response to a first anti-TNF drug. Data showed that at week 24, 69% in the non-TNF group and 52% in the anti-TNF group achieved a good or moderate EULAR response. The non-TNF treatment was also associated with a better EULAR response than a second anti-TNF drug at weeks 12 and 52. The DAS28-ESR and the number of patients achieving low disease activity status were found to be greater at months 6 and 12 in the non-TNF group than in the second anti-TNF group. One strength of the study is its pragmatic design—the study evaluated the effectiveness of interventions under real-life, routine practice conditions where physicians often choose one drug over another for reasons based on the habits or characteristics of the patient. The comparison of strategies and not individual drugs more appropriately addresses the questions that physicians face in daily practice. However, there were some limitations including the lack of blinding by participants, the exclusion of some biologic agents such as golimunab, the lack of assessment of individual drug efficacy, and the fact that approximately 40% of patients in each group did not have concomitant treatment with methotrexate, an agent known to improve the efficacy of most biologic agents.
Applications for Clinical Practice
This is the first randomized controlled trial to evaluate the efficacy of a non-TNF-targeted biologic vs. a second anti-TNF in patients with RA who have an insufficient response to a first anti-TNF drug. Further studies addressing the limitations identified in this study are needed before physicians can employ these findings in clinical practice.
—Anita Laloo, MD
1. Hyrich KL, Lunt M, Watson KD, et al; British Society for Rheumatology Biologics Register. Outcomes after switching from one antitumor necrosis factor alpha agent to a second anti-tumor necrosis factor alpha agent in patients with rheumatoid arthritis: results from a large UK national cohort study. Arthritis Rheum 2007;56:13–20.
2. Hetland ML, Christensen IJ, Tarp U, et al; All Departments of Rheumatology in Denmark. Direct comparison of treatment responses, remission rates, and drug adherence in patients with rheumatoid arthritis treated with adalimumab, etanercept, or infliximab: results from eight years of surveillance of clinical practice in the nationwide Danish DANBIO registry. Arthritis Rheum 2010;62:22–32.
3. Smolen JS, Landewé R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis 2010;69:964–75.
4. Cohen SB, Emery P, Greenwald MW, et al; REFLEX Trial Group. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase 3 trial evaluating primary efficacy and safety at twenty-four weeks. Arthritis Rheum 2006;54:2793–806.
5. Emery P, Keystone E, Tony HP, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial. Ann Rheum Dis 2008;67:1516–23.
6. Genovese MC, Becker JC, Schiff M, et al. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor alpha inhibition. N Engl J Med 2005;353:1114–23.
7. Smolen JS, Kay J, Doyle MK, et al; GO-AFTER study investigators. Golimumab in patients with active rheumatoid arthritis after treatment with tumour necrosis factor alpha inhibitors (GO-AFTER study): a multicentre, randomised, double-blind, placebo-controlled, phase III trial. Lancet 2009;374:210–21.
8. Schiff MH, von Kempis J, Goldblum R, et al. Rheumatoid arthritis secondary non-responders to TNF can attain an efficacious and safe response by switching to certolizumab pegol: a phase IV, randomised, multicentre, double-blind, 12-week study, followed by a 12-week open-label phase. Ann Rheum Dis 2014;73:2174–7.
1. Hyrich KL, Lunt M, Watson KD, et al; British Society for Rheumatology Biologics Register. Outcomes after switching from one antitumor necrosis factor alpha agent to a second anti-tumor necrosis factor alpha agent in patients with rheumatoid arthritis: results from a large UK national cohort study. Arthritis Rheum 2007;56:13–20.
2. Hetland ML, Christensen IJ, Tarp U, et al; All Departments of Rheumatology in Denmark. Direct comparison of treatment responses, remission rates, and drug adherence in patients with rheumatoid arthritis treated with adalimumab, etanercept, or infliximab: results from eight years of surveillance of clinical practice in the nationwide Danish DANBIO registry. Arthritis Rheum 2010;62:22–32.
3. Smolen JS, Landewé R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis 2010;69:964–75.
4. Cohen SB, Emery P, Greenwald MW, et al; REFLEX Trial Group. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase 3 trial evaluating primary efficacy and safety at twenty-four weeks. Arthritis Rheum 2006;54:2793–806.
5. Emery P, Keystone E, Tony HP, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial. Ann Rheum Dis 2008;67:1516–23.
6. Genovese MC, Becker JC, Schiff M, et al. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor alpha inhibition. N Engl J Med 2005;353:1114–23.
7. Smolen JS, Kay J, Doyle MK, et al; GO-AFTER study investigators. Golimumab in patients with active rheumatoid arthritis after treatment with tumour necrosis factor alpha inhibitors (GO-AFTER study): a multicentre, randomised, double-blind, placebo-controlled, phase III trial. Lancet 2009;374:210–21.
8. Schiff MH, von Kempis J, Goldblum R, et al. Rheumatoid arthritis secondary non-responders to TNF can attain an efficacious and safe response by switching to certolizumab pegol: a phase IV, randomised, multicentre, double-blind, 12-week study, followed by a 12-week open-label phase. Ann Rheum Dis 2014;73:2174–7.
VIDEO: Half-dose TKI safe, cost-effective in CML in stable remission
SAN DIEGO – Tyrosine kinase inhibitors have dramatically improved survival for patients with chronic myeloid leukemia, but for some patients with solid stable remissions, halving the TKI dose or even stopping therapy altogether, at least temporarily, appears to be safe and to offer both health and financial benefits,
In the British Destiny [De-escalation and Stopping Treatment of Imatinib, Nilotinib, or Sprycel (dasatinib)], there were 12 molecular relapses occurring between the second and twelfth month of dose reduction among 174 patients with either an MR3 or MR4 molecular response, and all patients had restoration of molecular remissions after resumption of full dose TKIs.
Coinvestigator Mhairi Copland, MD, PhD, of the University of Glasgow, Scotland, discussed in a video interview the potential clinical benefits of lower-dose therapy in patients in stable CML remissions, and notes that de-escalation strategy is associated with a nearly 50% saving in costs compared with full-dose TKI therapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Tyrosine kinase inhibitors have dramatically improved survival for patients with chronic myeloid leukemia, but for some patients with solid stable remissions, halving the TKI dose or even stopping therapy altogether, at least temporarily, appears to be safe and to offer both health and financial benefits,
In the British Destiny [De-escalation and Stopping Treatment of Imatinib, Nilotinib, or Sprycel (dasatinib)], there were 12 molecular relapses occurring between the second and twelfth month of dose reduction among 174 patients with either an MR3 or MR4 molecular response, and all patients had restoration of molecular remissions after resumption of full dose TKIs.
Coinvestigator Mhairi Copland, MD, PhD, of the University of Glasgow, Scotland, discussed in a video interview the potential clinical benefits of lower-dose therapy in patients in stable CML remissions, and notes that de-escalation strategy is associated with a nearly 50% saving in costs compared with full-dose TKI therapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Tyrosine kinase inhibitors have dramatically improved survival for patients with chronic myeloid leukemia, but for some patients with solid stable remissions, halving the TKI dose or even stopping therapy altogether, at least temporarily, appears to be safe and to offer both health and financial benefits,
In the British Destiny [De-escalation and Stopping Treatment of Imatinib, Nilotinib, or Sprycel (dasatinib)], there were 12 molecular relapses occurring between the second and twelfth month of dose reduction among 174 patients with either an MR3 or MR4 molecular response, and all patients had restoration of molecular remissions after resumption of full dose TKIs.
Coinvestigator Mhairi Copland, MD, PhD, of the University of Glasgow, Scotland, discussed in a video interview the potential clinical benefits of lower-dose therapy in patients in stable CML remissions, and notes that de-escalation strategy is associated with a nearly 50% saving in costs compared with full-dose TKI therapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ASH 2016

VIDEO: Venetoclax shows early good results in multiple myeloma
SAN DIEGO – Venetoclax has shown preliminary good results as an investigational monotherapy in patients with relapsed/refractory multiple myeloma, based on phase I data reported at the annual meeting of the American Society of Hematology.
Shaji Kumar, MD, of the Mayo Clinic, Rochester, Minn., reported that venetoclax monotherapy had anti-myeloma activity in a dose-finding study among patients treated with a median of five previous therapies. As would be expected, the best responses to the small-molecule BCL-2 inhibitor were seen primarily in patients with t(11;14) chromosomal aberrations and high BCL-2, low BCL-XL and low MCL-1 expression levels.
In a video interview, Dr. Kumar discussed the results of this early-stage research as well as ongoing studies that are beginning to examine venetoclax in combination regimens for multiple myeloma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Venetoclax is approved for the treatment of patients with chronic lymphocytic leukemia with 17p deletion who have received at least one prior treatment. Dr. Kumar receives research funding from Abbvie, the maker of venetoclax (Venclexta), and is a consultant to and receives research funding from several other drug companies.
[email protected]
On Twitter @maryjodales
SAN DIEGO – Venetoclax has shown preliminary good results as an investigational monotherapy in patients with relapsed/refractory multiple myeloma, based on phase I data reported at the annual meeting of the American Society of Hematology.
Shaji Kumar, MD, of the Mayo Clinic, Rochester, Minn., reported that venetoclax monotherapy had anti-myeloma activity in a dose-finding study among patients treated with a median of five previous therapies. As would be expected, the best responses to the small-molecule BCL-2 inhibitor were seen primarily in patients with t(11;14) chromosomal aberrations and high BCL-2, low BCL-XL and low MCL-1 expression levels.
In a video interview, Dr. Kumar discussed the results of this early-stage research as well as ongoing studies that are beginning to examine venetoclax in combination regimens for multiple myeloma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Venetoclax is approved for the treatment of patients with chronic lymphocytic leukemia with 17p deletion who have received at least one prior treatment. Dr. Kumar receives research funding from Abbvie, the maker of venetoclax (Venclexta), and is a consultant to and receives research funding from several other drug companies.
[email protected]
On Twitter @maryjodales
SAN DIEGO – Venetoclax has shown preliminary good results as an investigational monotherapy in patients with relapsed/refractory multiple myeloma, based on phase I data reported at the annual meeting of the American Society of Hematology.
Shaji Kumar, MD, of the Mayo Clinic, Rochester, Minn., reported that venetoclax monotherapy had anti-myeloma activity in a dose-finding study among patients treated with a median of five previous therapies. As would be expected, the best responses to the small-molecule BCL-2 inhibitor were seen primarily in patients with t(11;14) chromosomal aberrations and high BCL-2, low BCL-XL and low MCL-1 expression levels.
In a video interview, Dr. Kumar discussed the results of this early-stage research as well as ongoing studies that are beginning to examine venetoclax in combination regimens for multiple myeloma.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Venetoclax is approved for the treatment of patients with chronic lymphocytic leukemia with 17p deletion who have received at least one prior treatment. Dr. Kumar receives research funding from Abbvie, the maker of venetoclax (Venclexta), and is a consultant to and receives research funding from several other drug companies.
[email protected]
On Twitter @maryjodales
AT ASH 2016

VIDEO: Decision aids can relay relative risks to lung cancer patients
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.

[email protected]
On Twitter @mitchelzoler
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.
[email protected]
On Twitter @mitchelzoler
VIENNA – Many lung cancer patients would like to work with their physicians to reach a shared decision about their care, but often feel inadequately informed to comfortably participate in the decision process.
Patient decision aids offer a way to address this knowledge and participation gap, Laurie E. Gaspar, MD, said in a video interview at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
She and her associates have run an online survey that so far has received responses from 196 lung cancer patients, caregivers of patients, or significant others of patients. One hundred seventeen (60%) said that they faced a difficult management decision, but more than half these patients said they felt they had inadequate information to make their decision. The most popular form of decision making was a shared decision with their physician, favored by 73% of the respondents, but only about half the patients believed they had actually participated in a shared-decision process with their physician, reported Dr. Gaspar, professor of radiation oncology at the University of Colorado in Aurora.
“A majority of the patients felt there was a problem in not having sufficient information, and a majority want to make decisions in a shared way,” she explained.
[email protected]
On Twitter @mitchelzoler
At WCLC 2016
Key clinical point:
Major finding: A shared-decision process received support from 73% of patients, but just half believed they participated in shared decision making.
Data source: Online survey completed by 196 lung cancer patients, caregivers or significant others.
Disclosures: Dr. Gaspar had no disclosures.
