User login
Combo shows early promise in newly diagnosed AML

© Todd Buchanan 2016
SAN DIEGO—A targeted therapy combined with standard chemotherapy can produce rapid, deep remissions in patients with newly diagnosed acute myeloid leukemia (AML), according to research presented at the 2016 ASH Annual Meeting.
In this phase 1b study, investigators tested vadastuximab talirine, an antibody drug conjugate targeting CD33, in combination with 7+3 chemotherapy—a continuous infusion of cytarabine for 7 days plus daunorubicin for 3 days.
The combination produced a high rate of response, which included minimal residual disease (MRD)-negative complete remissions (CRs).
The treatment also resulted in “acceptable” on-target myelosuppression and non-hematologic adverse events (AEs) similar to what would be expected with 7+3 alone, according to study investigator Harry Erba, MD, PhD, of the University of Alabama at Birmingham.
Dr Erba presented these results in abstract 211.* The research was sponsored by Seattle Genetics, Inc.
The study included 42 newly diagnosed AML patients with a median age of 45.5. Half the patients had intermediate-risk karyotypes, 36% had adverse karyotypes, and 17% had secondary AML.
Patients received escalating doses of vadastuximab talirine (10+10 mcg/kg [n=4] and 20+10 mcg/kg [n=38]) in combination with 7+3 induction (cytarabine at 100 mg/m2 and daunorubicin at 60 mg/m2) on days 1 and 4 of a 28-day treatment cycle. Responses were assessed on days 15 and 28.
A second induction regimen and post-remission therapies were prescribed according to investigator choice and did not include vadastuximab talirine.
Results
The maximum tolerated dose of vadastuximab talirine was 20+10 mcg/kg.
Hematologic treatment-related AEs included febrile neutropenia (43%, grade 1-3), thrombocytopenia (38%, grade 3-4), anemia (24%, grade 3), and neutropenia (17%, grade 3-4).
Non-hematologic treatment-related AEs included nausea (17%), fatigue (14%), diarrhea (7%), and decreased appetite (7%). All of these AEs were grade 1-2.
None of the patients experienced infusion-related reactions, veno-occlusive disease, or significant liver damage.
A total of 76% of patients responded to treatment, with 60% percent achieving a CR and 17% achieving a CR with incomplete blood count recovery (CRi).
The 76% response rate is close to what would be expected for a well-chosen population fit for a clinical trial, Dr Erba said.
There was a hint of additional benefit as well, he added.
“The first hint was that 30 out of the 32 patients [who achieved a CR/CRi] required only 1 round of chemotherapy to achieve that remission,” Dr Erba said. “This also suggested that deeper remissions may be possible.”
MRD assessments using a sensitive flow cytometric assay revealed that 25 of the 32 patients (78%) who achieved a CR/CRi were MRD-negative.
Dr Erba said a randomized, phase 2 trial of vadastuximab talirine plus 7+3 versus 7+3 alone is planned for the first quarter of 2017. ![]()
*Information presented at the meeting differs from the abstract.
© Todd Buchanan 2016
SAN DIEGO—A targeted therapy combined with standard chemotherapy can produce rapid, deep remissions in patients with newly diagnosed acute myeloid leukemia (AML), according to research presented at the 2016 ASH Annual Meeting.
In this phase 1b study, investigators tested vadastuximab talirine, an antibody drug conjugate targeting CD33, in combination with 7+3 chemotherapy—a continuous infusion of cytarabine for 7 days plus daunorubicin for 3 days.
The combination produced a high rate of response, which included minimal residual disease (MRD)-negative complete remissions (CRs).
The treatment also resulted in “acceptable” on-target myelosuppression and non-hematologic adverse events (AEs) similar to what would be expected with 7+3 alone, according to study investigator Harry Erba, MD, PhD, of the University of Alabama at Birmingham.
Dr Erba presented these results in abstract 211.* The research was sponsored by Seattle Genetics, Inc.
The study included 42 newly diagnosed AML patients with a median age of 45.5. Half the patients had intermediate-risk karyotypes, 36% had adverse karyotypes, and 17% had secondary AML.
Patients received escalating doses of vadastuximab talirine (10+10 mcg/kg [n=4] and 20+10 mcg/kg [n=38]) in combination with 7+3 induction (cytarabine at 100 mg/m2 and daunorubicin at 60 mg/m2) on days 1 and 4 of a 28-day treatment cycle. Responses were assessed on days 15 and 28.
A second induction regimen and post-remission therapies were prescribed according to investigator choice and did not include vadastuximab talirine.
Results
The maximum tolerated dose of vadastuximab talirine was 20+10 mcg/kg.
Hematologic treatment-related AEs included febrile neutropenia (43%, grade 1-3), thrombocytopenia (38%, grade 3-4), anemia (24%, grade 3), and neutropenia (17%, grade 3-4).
Non-hematologic treatment-related AEs included nausea (17%), fatigue (14%), diarrhea (7%), and decreased appetite (7%). All of these AEs were grade 1-2.
None of the patients experienced infusion-related reactions, veno-occlusive disease, or significant liver damage.
A total of 76% of patients responded to treatment, with 60% percent achieving a CR and 17% achieving a CR with incomplete blood count recovery (CRi).
The 76% response rate is close to what would be expected for a well-chosen population fit for a clinical trial, Dr Erba said.
There was a hint of additional benefit as well, he added.
“The first hint was that 30 out of the 32 patients [who achieved a CR/CRi] required only 1 round of chemotherapy to achieve that remission,” Dr Erba said. “This also suggested that deeper remissions may be possible.”
MRD assessments using a sensitive flow cytometric assay revealed that 25 of the 32 patients (78%) who achieved a CR/CRi were MRD-negative.
Dr Erba said a randomized, phase 2 trial of vadastuximab talirine plus 7+3 versus 7+3 alone is planned for the first quarter of 2017. ![]()
*Information presented at the meeting differs from the abstract.
© Todd Buchanan 2016
SAN DIEGO—A targeted therapy combined with standard chemotherapy can produce rapid, deep remissions in patients with newly diagnosed acute myeloid leukemia (AML), according to research presented at the 2016 ASH Annual Meeting.
In this phase 1b study, investigators tested vadastuximab talirine, an antibody drug conjugate targeting CD33, in combination with 7+3 chemotherapy—a continuous infusion of cytarabine for 7 days plus daunorubicin for 3 days.
The combination produced a high rate of response, which included minimal residual disease (MRD)-negative complete remissions (CRs).
The treatment also resulted in “acceptable” on-target myelosuppression and non-hematologic adverse events (AEs) similar to what would be expected with 7+3 alone, according to study investigator Harry Erba, MD, PhD, of the University of Alabama at Birmingham.
Dr Erba presented these results in abstract 211.* The research was sponsored by Seattle Genetics, Inc.
The study included 42 newly diagnosed AML patients with a median age of 45.5. Half the patients had intermediate-risk karyotypes, 36% had adverse karyotypes, and 17% had secondary AML.
Patients received escalating doses of vadastuximab talirine (10+10 mcg/kg [n=4] and 20+10 mcg/kg [n=38]) in combination with 7+3 induction (cytarabine at 100 mg/m2 and daunorubicin at 60 mg/m2) on days 1 and 4 of a 28-day treatment cycle. Responses were assessed on days 15 and 28.
A second induction regimen and post-remission therapies were prescribed according to investigator choice and did not include vadastuximab talirine.
Results
The maximum tolerated dose of vadastuximab talirine was 20+10 mcg/kg.
Hematologic treatment-related AEs included febrile neutropenia (43%, grade 1-3), thrombocytopenia (38%, grade 3-4), anemia (24%, grade 3), and neutropenia (17%, grade 3-4).
Non-hematologic treatment-related AEs included nausea (17%), fatigue (14%), diarrhea (7%), and decreased appetite (7%). All of these AEs were grade 1-2.
None of the patients experienced infusion-related reactions, veno-occlusive disease, or significant liver damage.
A total of 76% of patients responded to treatment, with 60% percent achieving a CR and 17% achieving a CR with incomplete blood count recovery (CRi).
The 76% response rate is close to what would be expected for a well-chosen population fit for a clinical trial, Dr Erba said.
There was a hint of additional benefit as well, he added.
“The first hint was that 30 out of the 32 patients [who achieved a CR/CRi] required only 1 round of chemotherapy to achieve that remission,” Dr Erba said. “This also suggested that deeper remissions may be possible.”
MRD assessments using a sensitive flow cytometric assay revealed that 25 of the 32 patients (78%) who achieved a CR/CRi were MRD-negative.
Dr Erba said a randomized, phase 2 trial of vadastuximab talirine plus 7+3 versus 7+3 alone is planned for the first quarter of 2017. ![]()
*Information presented at the meeting differs from the abstract.
Negotiating The Professional Contract
For the freshly minted NP or PA, finding the right place to practice and negotiating a reasonable professional contract can be a challenge. The keys to successful negotiation are similar to those for attaining proficiency in your clinical practice—providing insight into your personality, an evaluation of your personal and professional goals, and a commitment of time for preparation. For most NPs and PAs, employment opportunities do not just happen. Preparation, persistence, and personal contacts are basic requirements for finding the right position.
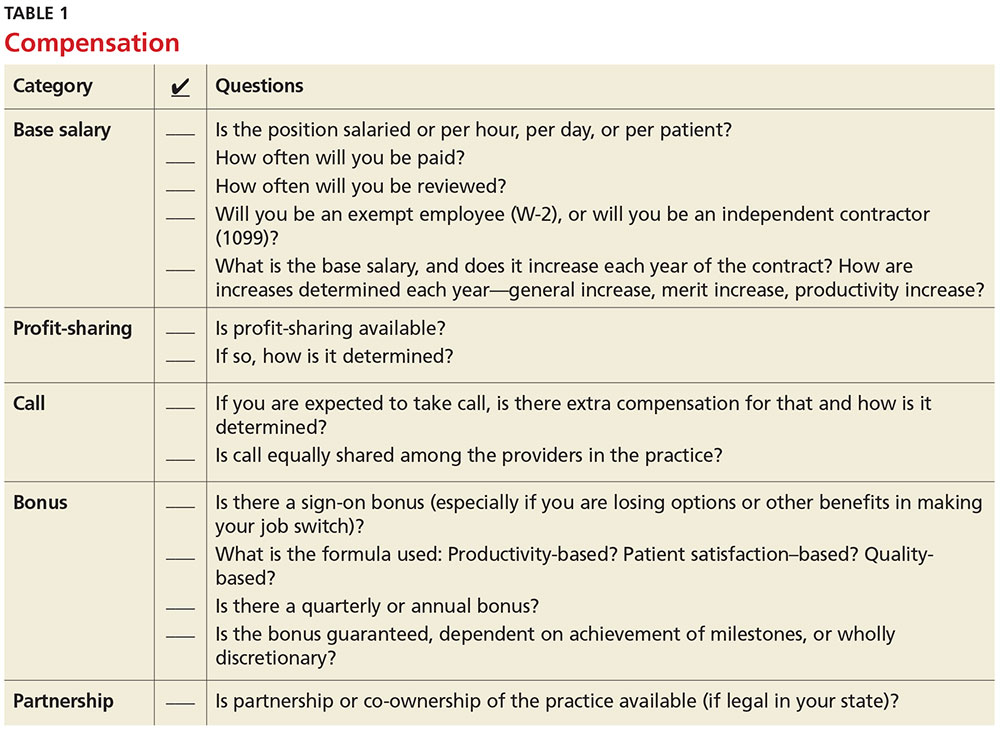
Of great interest to NPs and PAs—especially those with looming loan payments—is the compensation package. There are many important questions and topics to discuss regarding compensation (see Table 1). However, salaries are often determined by the “going rate” for particular services in your geographic region, in addition to your specialty, experience, and credentials. Your professional association (AAPA for PAs, AANP for NPs) has robust data on salaries in your particular specialty, practice setting, and geographic region; the average salary for both professions is currently about $97,000.1,2
Familiarize yourself with the statutes and regulations that govern the scope of practice in your state—this is especially important if there are specific supervision or collaboration rules. Be prepared to present applicable statutes, rules, and regulations to the physician and/or office manager. Know whether any reimbursement restrictions exist. Be sure to review IRS guidelines for employee status versus independent contractor status.
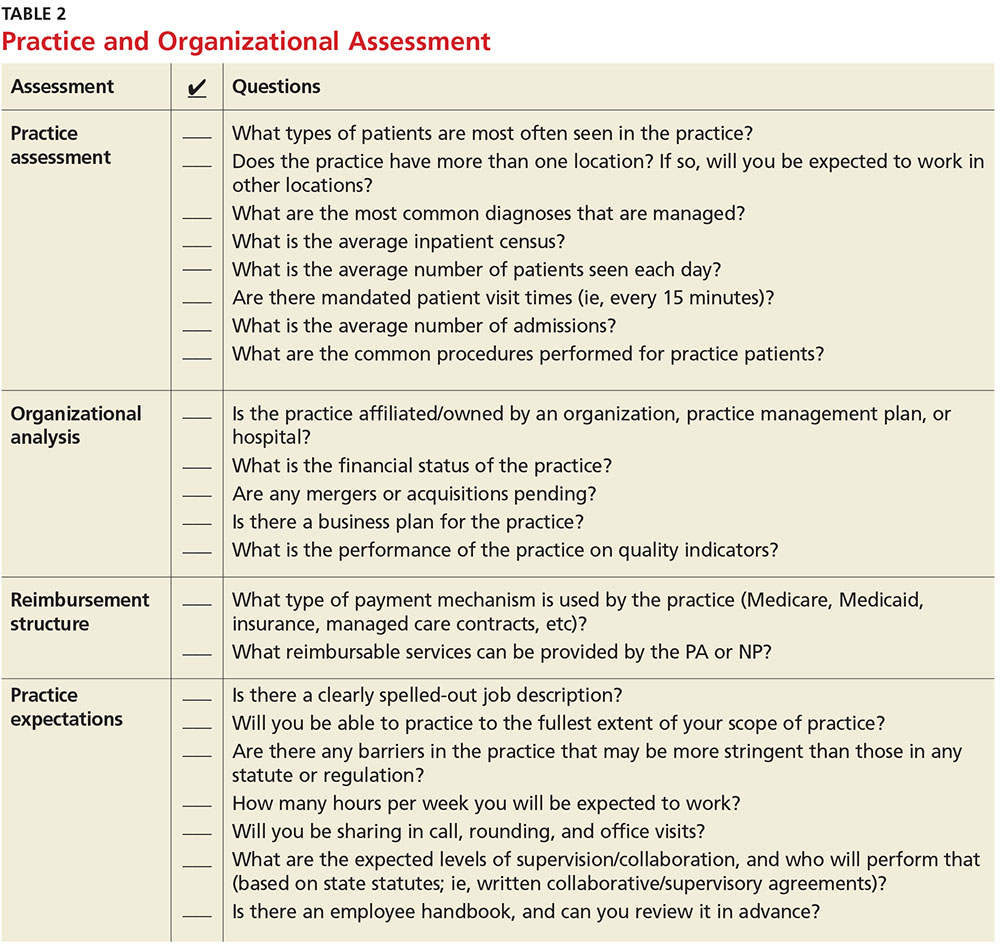
The diversity of NP and PA practices means one size does not fit all, so it is best to identify the practice that complements your own personality. So, before you open negotiations, it is important that you research the practice. (For suggestions on what to inquire about, see Table 2). It is also a good idea to check the Docinfo website (http://docinfo.org/#/search/query), sponsored by the Federation of State Medical Boards, to research disciplinary records of the physician(s). Additional information can be acquired at each state regulatory board site.
NEGOTIATION
When you’ve decided which employment offer to pursue, it’s time to think about how you want to negotiate your contract. Many people feel that negotiation is equivalent to confrontation, inevitably leading to an awkward disagreement with the practice. This is rarely the case; negotiation is simply a professional conversation, best had one-on-one with the key decision maker, rather than a group.
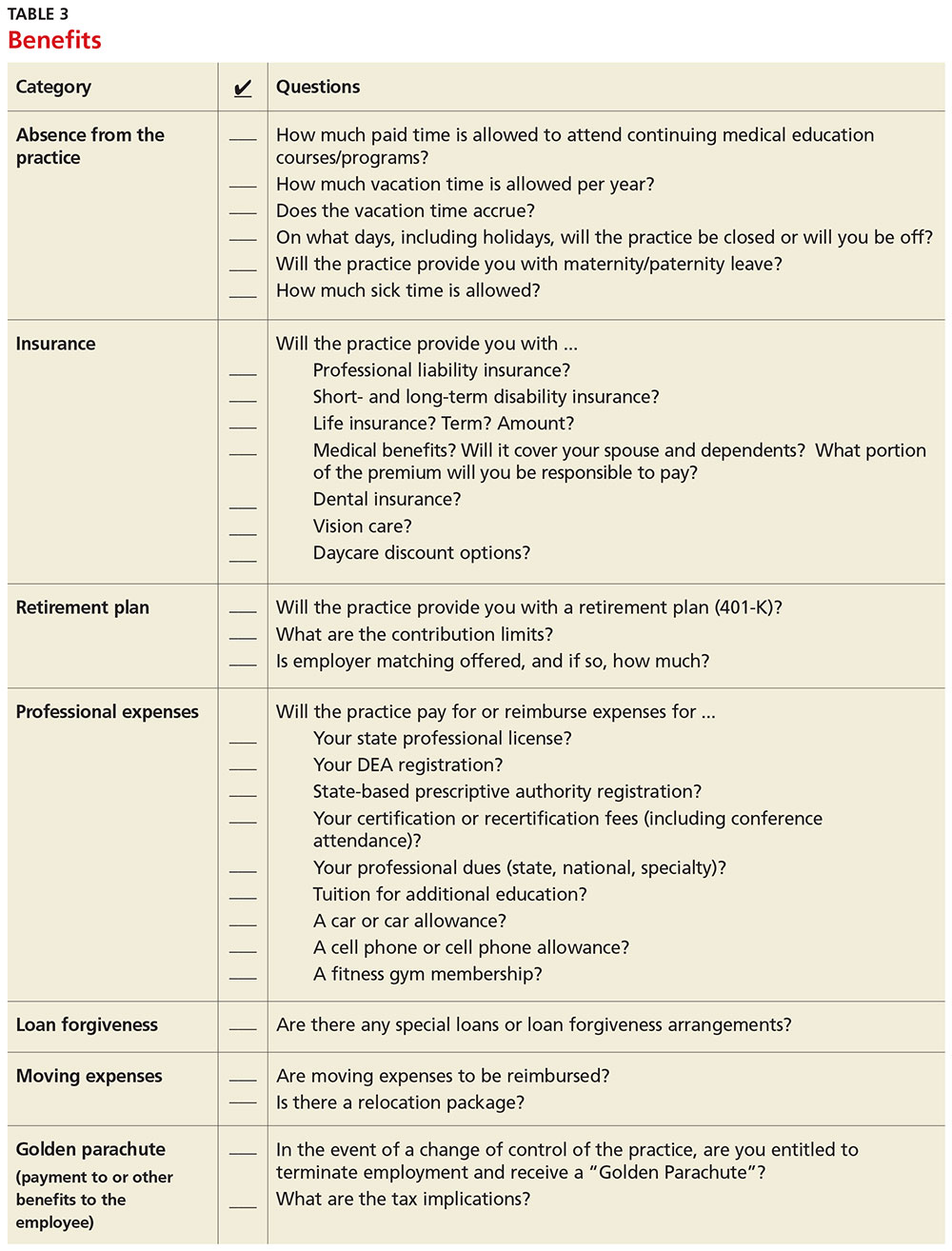
Never assume that your compensation package is predetermined. Whether you are starting a new job or looking to enhance your current situation, you can make a difference by asking for what you need.3 Knowing the local market and data is essential. Research the average salary in the region (for experienced versus new NP or PA). Be sure to think beyond salary and evaluate which benefits you’d like to have as part of your compensation package (see Table 3, as well as our survey results).
Carolyn Buppert, a specialist in legal and reimbursement issues for NPs and PAs, suggests three “P’s” of negotiation: Prepare, probe, and propose.4
Prepare. Learn how to calculate the projected revenue you would bring into a practice. You can determine the profit you generate by asking the practice administrator for data, noting Current Procedural Terminology codes and dates and becoming familiar with the fee schedule. According to Buppert, your salary and benefits should amount to about one-third of your total billings, and the benefits should equate to about 25% of your base salary.4 It is worthwhile to discuss nonmonetary contributions to the practice, such as improvements in patient satisfaction or reduction in no-shows.
Probe. Ask about the practice’s financial health during your interview and determine employer expectations for profits.
Propose. Once your prospective employer proves their value to you and after you have done due diligence researching the practice, do not hesitate to ask for what you deserve. When doing this, it is important to maintain neutral body language, keep an unemotional tone of voice, and convey an understanding of the employer’s point of view.4
Most successful negotiations occur over a couple of meetings. Careful listening is essential to avoid misunderstandings and false assumptions. By listening intently, you can identify the issues most important to the employer (eg, pay may be negotiable, but moonlighting not; or control over shift schedules is a hot button, but pay is not). Evaluating and weighing those against your own requirements may avoid an unnecessary impasse and result in a better outcome for you.
One question lives at the heart of negotiations: Should agreements be in writing? Written agreements carry more weight and prevent misunderstandings, a benefit to both parties involved. Formal, written negotiation of a contract forces the parties to discuss issues and provides a record for future reference.5
CONTRACTS
Because courses in negotiations, contract law, and business principles are rarely taught in educational programs, you should consider consulting an attorney who is familiar with contract and business issues. Avoid attorneys who have to research the laws regarding NP and PA practice—there are many who are well versed in these contracts. It is also usually more acceptable to conduct initial negotiations yourself, rather than through an attorney.
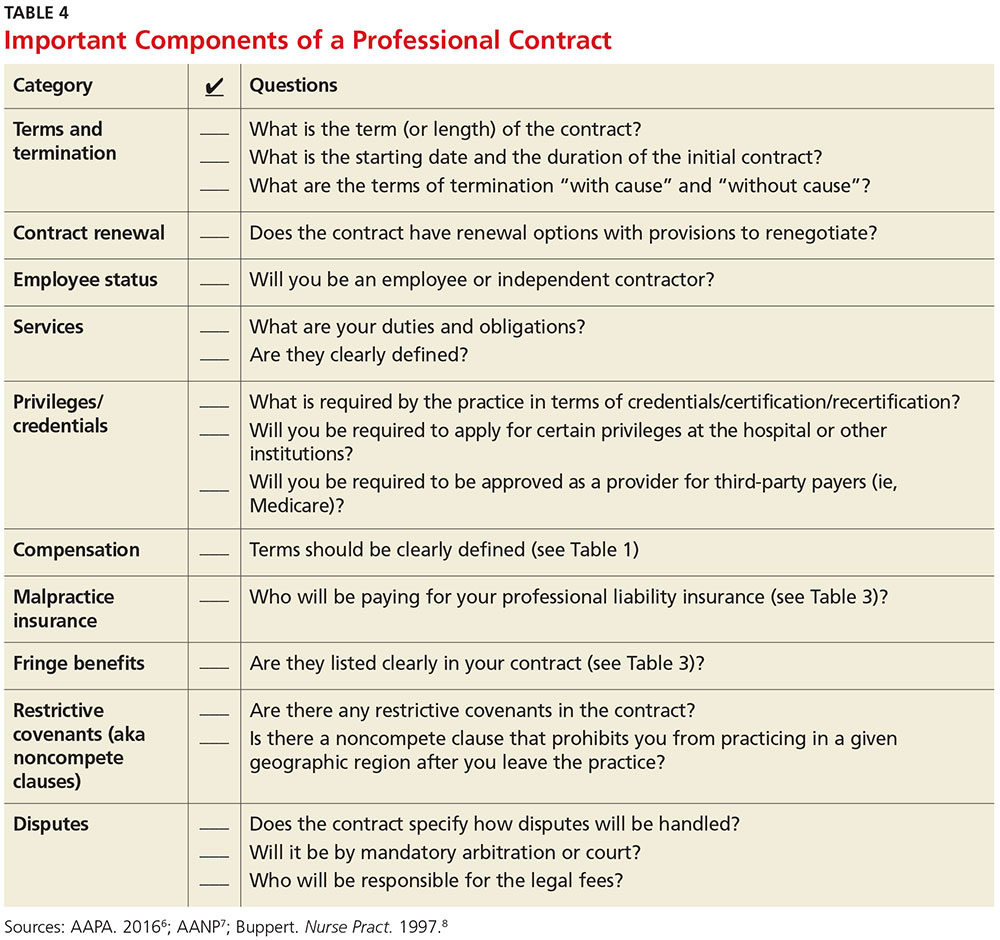
First, ask the attorney to review the contract and advise you of any troublesome provision or obvious omissions (see Table 4; a sample contract is also available on our website).6-8 Many attorneys with experience reviewing and negotiating such contracts will be willing to do an initial read and consultation for a fixed, predetermined fee. Following that consultation, it is best to discuss your concerns and questions directly with your potential employer. If you can come to a general agreement on revisions, either your lawyer or the employer’s can make the necessary changes.
When considering an employment agreement, there are specific issues and potential hurdles to look out for. Following is a brief discussion of some of them.
Liability insurance
Find out which type of liability insurance is offered (occurrence-based or claims-made), as well as the limits of liability. Occurrence-based insurance is usually recommended. However, if the policy is claims-made, it’s important to know if the tail coverage will be paid by the employer, or if there is a rider on the physician’s policy. Determine if your contract will allow for the cost of the tail to be deducted from final amounts that may be owed to you upon termination. Be prepared to acquire the tail, if needed, to ensure coverage.
Restrictive covenants (noncompete clauses)
Unfortunately, not all employment relationships work out in the long term. In recognition of this, many professional contracts contain an agreement known as a restrictive covenant, which impedes the NP’s or PA’s ability to practice in the community following a relationship cessation. Depending on where the practice is located, such restrictions can be devastating and may even require the NP or PA to move in order to pursue a career. The law of restrictive covenants varies greatly from state to state. Your attorney can help you evaluate the enforceability and effect of a restrictive covenant, advise you on what is or isn’t reasonable in the community, and give you suggestions on how to negotiate a more reasonable one.
Moonlighting
Whether or not you can moonlight—and where—is often negotiable. An employer certainly has the right to require that moonlighting not interfere with your regular duties or schedule; endorse competitors of your employer or potentially divert patients; or expose the employer to malpractice liability. If you can assure your employer that these three situations will not transpire, then moonlighting (with advance scheduling notice and permission) should be acceptable.
Training/continuing education
It is typical for the employer to reimburse some or all of the cost of continuing education, up to a maximum annual amount. It is also reasonable for the employer (if paying for the CME) to pre-approve the curriculum, as well as the timing to avoid scheduling problems.
Salary and bonus
Compensation systems can be entirely objective (ie, production based), subjective (entirely up to the discretion of the employer based on internal criteria), or a combination of both. It is important to get a clear understanding of the system so that you know what is expected of you and what the rewards are for meeting performance goals.
Income guarantee/advanced expenses/repayment obligation
It is not uncommon for a local hospital to help a medical practice by guaranteeing the salary for a certain period of time. In this situation, the guarantee can be structured in a number of different ways—but it typically involves an obligation to repay a predetermined amount if you leave the practice area before the expiration of the term. Often, the practice will seek to pass that liability on to you. The same may apply for advanced moving expenses, CME, etc. A practice may require you to be employed for a specified amount of time to “earn” those advanced expenses, or to pay them back if an early termination occurs. In any case, it is important to know what the expectations are, and what circumstances could lead to an early termination and/or repayment obligation.
Terms and termination
Pay particular attention to the terms of your agreement. In one paragraph, it may say that the contract is for one year with annual renewals, but later on it explains that it can be terminated by either party upon 30 days notice. In that case, it is not a one-year contract; it is a 30-day contract. If there is a possibility of early termination and a restrictive covenant, or even a repayment obligation, you could really be at risk. Pay attention to whether early termination is “for cause” or “without cause.” If it is only for cause, inquire what constitutes a cause and whether there are any opportunities to rectify a perceived problem.
CONCLUSION
Constant changes in the health care marketplace will continue to generate opportunities for NPs and PAs. This is especially true for clinicians who demonstrate competence, enthusiasm, and commitment to quality patient care. The same clinical skills you learned in school and practice will help you find a clinical position and negotiate a good professional contract. Attention to detail, evidence-based research, and excellent communication skills will enable you to land a position beneficial to both parties.
1. American Academy of Physician Assistants. 2016 AAPA Salary Report. www.aapa.org/research/salary-report. Accessed November 4, 2016.
2. American Academy of Nurse Practitioners. Annual income for full-time nurse practitioners up 10% since 2011. www.aanp.org/press-room/press-releases/166-press-room/2015-press-releases/1803-annual- income-for-full-time-nurse-practitioners-up-10-since-2011. Accessed November 4, 2016.
3. Bourne H. A Great Deal! Compensation Negotiation for Nurse Practitioners & Physician Assistants. 3rd ed. Arcata, CA: Open Spaces; 1998.
4. Buppert C. Nurse Practitioner’s Business Practice and Legal Guide. 5th ed. Burlington, MA: Jones & Bartlett Learning; 2015.
5. Henley MB. Finding your ideal job and negotiating your contract: where to get the information and numbers you need to know. J Orthop Trauma. 2012;26(1):S9-S13.
6. AAPA. Contacts and contracts: a guide to your PA career. www.aapa.org/WorkArea/DownloadAsset.aspx?id=2147486883. Accessed November 4, 2016.
7. AANP. Employment negotiations. www.aanp.org/practice/reimbursement/68-articles/579-employment-negotiations. Accessed November 4, 2016.
8. Buppert C. Employment agreements: clauses that can change an NP’s life. Nurse Pract. 1997;22(8):108-109.
For the freshly minted NP or PA, finding the right place to practice and negotiating a reasonable professional contract can be a challenge. The keys to successful negotiation are similar to those for attaining proficiency in your clinical practice—providing insight into your personality, an evaluation of your personal and professional goals, and a commitment of time for preparation. For most NPs and PAs, employment opportunities do not just happen. Preparation, persistence, and personal contacts are basic requirements for finding the right position.
Of great interest to NPs and PAs—especially those with looming loan payments—is the compensation package. There are many important questions and topics to discuss regarding compensation (see Table 1). However, salaries are often determined by the “going rate” for particular services in your geographic region, in addition to your specialty, experience, and credentials. Your professional association (AAPA for PAs, AANP for NPs) has robust data on salaries in your particular specialty, practice setting, and geographic region; the average salary for both professions is currently about $97,000.1,2
Familiarize yourself with the statutes and regulations that govern the scope of practice in your state—this is especially important if there are specific supervision or collaboration rules. Be prepared to present applicable statutes, rules, and regulations to the physician and/or office manager. Know whether any reimbursement restrictions exist. Be sure to review IRS guidelines for employee status versus independent contractor status.
The diversity of NP and PA practices means one size does not fit all, so it is best to identify the practice that complements your own personality. So, before you open negotiations, it is important that you research the practice. (For suggestions on what to inquire about, see Table 2). It is also a good idea to check the Docinfo website (http://docinfo.org/#/search/query), sponsored by the Federation of State Medical Boards, to research disciplinary records of the physician(s). Additional information can be acquired at each state regulatory board site.
NEGOTIATION
When you’ve decided which employment offer to pursue, it’s time to think about how you want to negotiate your contract. Many people feel that negotiation is equivalent to confrontation, inevitably leading to an awkward disagreement with the practice. This is rarely the case; negotiation is simply a professional conversation, best had one-on-one with the key decision maker, rather than a group.
Never assume that your compensation package is predetermined. Whether you are starting a new job or looking to enhance your current situation, you can make a difference by asking for what you need.3 Knowing the local market and data is essential. Research the average salary in the region (for experienced versus new NP or PA). Be sure to think beyond salary and evaluate which benefits you’d like to have as part of your compensation package (see Table 3, as well as our survey results).
Carolyn Buppert, a specialist in legal and reimbursement issues for NPs and PAs, suggests three “P’s” of negotiation: Prepare, probe, and propose.4
Prepare. Learn how to calculate the projected revenue you would bring into a practice. You can determine the profit you generate by asking the practice administrator for data, noting Current Procedural Terminology codes and dates and becoming familiar with the fee schedule. According to Buppert, your salary and benefits should amount to about one-third of your total billings, and the benefits should equate to about 25% of your base salary.4 It is worthwhile to discuss nonmonetary contributions to the practice, such as improvements in patient satisfaction or reduction in no-shows.
Probe. Ask about the practice’s financial health during your interview and determine employer expectations for profits.
Propose. Once your prospective employer proves their value to you and after you have done due diligence researching the practice, do not hesitate to ask for what you deserve. When doing this, it is important to maintain neutral body language, keep an unemotional tone of voice, and convey an understanding of the employer’s point of view.4
Most successful negotiations occur over a couple of meetings. Careful listening is essential to avoid misunderstandings and false assumptions. By listening intently, you can identify the issues most important to the employer (eg, pay may be negotiable, but moonlighting not; or control over shift schedules is a hot button, but pay is not). Evaluating and weighing those against your own requirements may avoid an unnecessary impasse and result in a better outcome for you.
One question lives at the heart of negotiations: Should agreements be in writing? Written agreements carry more weight and prevent misunderstandings, a benefit to both parties involved. Formal, written negotiation of a contract forces the parties to discuss issues and provides a record for future reference.5
CONTRACTS
Because courses in negotiations, contract law, and business principles are rarely taught in educational programs, you should consider consulting an attorney who is familiar with contract and business issues. Avoid attorneys who have to research the laws regarding NP and PA practice—there are many who are well versed in these contracts. It is also usually more acceptable to conduct initial negotiations yourself, rather than through an attorney.
First, ask the attorney to review the contract and advise you of any troublesome provision or obvious omissions (see Table 4; a sample contract is also available on our website).6-8 Many attorneys with experience reviewing and negotiating such contracts will be willing to do an initial read and consultation for a fixed, predetermined fee. Following that consultation, it is best to discuss your concerns and questions directly with your potential employer. If you can come to a general agreement on revisions, either your lawyer or the employer’s can make the necessary changes.
When considering an employment agreement, there are specific issues and potential hurdles to look out for. Following is a brief discussion of some of them.
Liability insurance
Find out which type of liability insurance is offered (occurrence-based or claims-made), as well as the limits of liability. Occurrence-based insurance is usually recommended. However, if the policy is claims-made, it’s important to know if the tail coverage will be paid by the employer, or if there is a rider on the physician’s policy. Determine if your contract will allow for the cost of the tail to be deducted from final amounts that may be owed to you upon termination. Be prepared to acquire the tail, if needed, to ensure coverage.
Restrictive covenants (noncompete clauses)
Unfortunately, not all employment relationships work out in the long term. In recognition of this, many professional contracts contain an agreement known as a restrictive covenant, which impedes the NP’s or PA’s ability to practice in the community following a relationship cessation. Depending on where the practice is located, such restrictions can be devastating and may even require the NP or PA to move in order to pursue a career. The law of restrictive covenants varies greatly from state to state. Your attorney can help you evaluate the enforceability and effect of a restrictive covenant, advise you on what is or isn’t reasonable in the community, and give you suggestions on how to negotiate a more reasonable one.
Moonlighting
Whether or not you can moonlight—and where—is often negotiable. An employer certainly has the right to require that moonlighting not interfere with your regular duties or schedule; endorse competitors of your employer or potentially divert patients; or expose the employer to malpractice liability. If you can assure your employer that these three situations will not transpire, then moonlighting (with advance scheduling notice and permission) should be acceptable.
Training/continuing education
It is typical for the employer to reimburse some or all of the cost of continuing education, up to a maximum annual amount. It is also reasonable for the employer (if paying for the CME) to pre-approve the curriculum, as well as the timing to avoid scheduling problems.
Salary and bonus
Compensation systems can be entirely objective (ie, production based), subjective (entirely up to the discretion of the employer based on internal criteria), or a combination of both. It is important to get a clear understanding of the system so that you know what is expected of you and what the rewards are for meeting performance goals.
Income guarantee/advanced expenses/repayment obligation
It is not uncommon for a local hospital to help a medical practice by guaranteeing the salary for a certain period of time. In this situation, the guarantee can be structured in a number of different ways—but it typically involves an obligation to repay a predetermined amount if you leave the practice area before the expiration of the term. Often, the practice will seek to pass that liability on to you. The same may apply for advanced moving expenses, CME, etc. A practice may require you to be employed for a specified amount of time to “earn” those advanced expenses, or to pay them back if an early termination occurs. In any case, it is important to know what the expectations are, and what circumstances could lead to an early termination and/or repayment obligation.
Terms and termination
Pay particular attention to the terms of your agreement. In one paragraph, it may say that the contract is for one year with annual renewals, but later on it explains that it can be terminated by either party upon 30 days notice. In that case, it is not a one-year contract; it is a 30-day contract. If there is a possibility of early termination and a restrictive covenant, or even a repayment obligation, you could really be at risk. Pay attention to whether early termination is “for cause” or “without cause.” If it is only for cause, inquire what constitutes a cause and whether there are any opportunities to rectify a perceived problem.
CONCLUSION
Constant changes in the health care marketplace will continue to generate opportunities for NPs and PAs. This is especially true for clinicians who demonstrate competence, enthusiasm, and commitment to quality patient care. The same clinical skills you learned in school and practice will help you find a clinical position and negotiate a good professional contract. Attention to detail, evidence-based research, and excellent communication skills will enable you to land a position beneficial to both parties.
For the freshly minted NP or PA, finding the right place to practice and negotiating a reasonable professional contract can be a challenge. The keys to successful negotiation are similar to those for attaining proficiency in your clinical practice—providing insight into your personality, an evaluation of your personal and professional goals, and a commitment of time for preparation. For most NPs and PAs, employment opportunities do not just happen. Preparation, persistence, and personal contacts are basic requirements for finding the right position.
Of great interest to NPs and PAs—especially those with looming loan payments—is the compensation package. There are many important questions and topics to discuss regarding compensation (see Table 1). However, salaries are often determined by the “going rate” for particular services in your geographic region, in addition to your specialty, experience, and credentials. Your professional association (AAPA for PAs, AANP for NPs) has robust data on salaries in your particular specialty, practice setting, and geographic region; the average salary for both professions is currently about $97,000.1,2
Familiarize yourself with the statutes and regulations that govern the scope of practice in your state—this is especially important if there are specific supervision or collaboration rules. Be prepared to present applicable statutes, rules, and regulations to the physician and/or office manager. Know whether any reimbursement restrictions exist. Be sure to review IRS guidelines for employee status versus independent contractor status.
The diversity of NP and PA practices means one size does not fit all, so it is best to identify the practice that complements your own personality. So, before you open negotiations, it is important that you research the practice. (For suggestions on what to inquire about, see Table 2). It is also a good idea to check the Docinfo website (http://docinfo.org/#/search/query), sponsored by the Federation of State Medical Boards, to research disciplinary records of the physician(s). Additional information can be acquired at each state regulatory board site.
NEGOTIATION
When you’ve decided which employment offer to pursue, it’s time to think about how you want to negotiate your contract. Many people feel that negotiation is equivalent to confrontation, inevitably leading to an awkward disagreement with the practice. This is rarely the case; negotiation is simply a professional conversation, best had one-on-one with the key decision maker, rather than a group.
Never assume that your compensation package is predetermined. Whether you are starting a new job or looking to enhance your current situation, you can make a difference by asking for what you need.3 Knowing the local market and data is essential. Research the average salary in the region (for experienced versus new NP or PA). Be sure to think beyond salary and evaluate which benefits you’d like to have as part of your compensation package (see Table 3, as well as our survey results).
Carolyn Buppert, a specialist in legal and reimbursement issues for NPs and PAs, suggests three “P’s” of negotiation: Prepare, probe, and propose.4
Prepare. Learn how to calculate the projected revenue you would bring into a practice. You can determine the profit you generate by asking the practice administrator for data, noting Current Procedural Terminology codes and dates and becoming familiar with the fee schedule. According to Buppert, your salary and benefits should amount to about one-third of your total billings, and the benefits should equate to about 25% of your base salary.4 It is worthwhile to discuss nonmonetary contributions to the practice, such as improvements in patient satisfaction or reduction in no-shows.
Probe. Ask about the practice’s financial health during your interview and determine employer expectations for profits.
Propose. Once your prospective employer proves their value to you and after you have done due diligence researching the practice, do not hesitate to ask for what you deserve. When doing this, it is important to maintain neutral body language, keep an unemotional tone of voice, and convey an understanding of the employer’s point of view.4
Most successful negotiations occur over a couple of meetings. Careful listening is essential to avoid misunderstandings and false assumptions. By listening intently, you can identify the issues most important to the employer (eg, pay may be negotiable, but moonlighting not; or control over shift schedules is a hot button, but pay is not). Evaluating and weighing those against your own requirements may avoid an unnecessary impasse and result in a better outcome for you.
One question lives at the heart of negotiations: Should agreements be in writing? Written agreements carry more weight and prevent misunderstandings, a benefit to both parties involved. Formal, written negotiation of a contract forces the parties to discuss issues and provides a record for future reference.5
CONTRACTS
Because courses in negotiations, contract law, and business principles are rarely taught in educational programs, you should consider consulting an attorney who is familiar with contract and business issues. Avoid attorneys who have to research the laws regarding NP and PA practice—there are many who are well versed in these contracts. It is also usually more acceptable to conduct initial negotiations yourself, rather than through an attorney.
First, ask the attorney to review the contract and advise you of any troublesome provision or obvious omissions (see Table 4; a sample contract is also available on our website).6-8 Many attorneys with experience reviewing and negotiating such contracts will be willing to do an initial read and consultation for a fixed, predetermined fee. Following that consultation, it is best to discuss your concerns and questions directly with your potential employer. If you can come to a general agreement on revisions, either your lawyer or the employer’s can make the necessary changes.
When considering an employment agreement, there are specific issues and potential hurdles to look out for. Following is a brief discussion of some of them.
Liability insurance
Find out which type of liability insurance is offered (occurrence-based or claims-made), as well as the limits of liability. Occurrence-based insurance is usually recommended. However, if the policy is claims-made, it’s important to know if the tail coverage will be paid by the employer, or if there is a rider on the physician’s policy. Determine if your contract will allow for the cost of the tail to be deducted from final amounts that may be owed to you upon termination. Be prepared to acquire the tail, if needed, to ensure coverage.
Restrictive covenants (noncompete clauses)
Unfortunately, not all employment relationships work out in the long term. In recognition of this, many professional contracts contain an agreement known as a restrictive covenant, which impedes the NP’s or PA’s ability to practice in the community following a relationship cessation. Depending on where the practice is located, such restrictions can be devastating and may even require the NP or PA to move in order to pursue a career. The law of restrictive covenants varies greatly from state to state. Your attorney can help you evaluate the enforceability and effect of a restrictive covenant, advise you on what is or isn’t reasonable in the community, and give you suggestions on how to negotiate a more reasonable one.
Moonlighting
Whether or not you can moonlight—and where—is often negotiable. An employer certainly has the right to require that moonlighting not interfere with your regular duties or schedule; endorse competitors of your employer or potentially divert patients; or expose the employer to malpractice liability. If you can assure your employer that these three situations will not transpire, then moonlighting (with advance scheduling notice and permission) should be acceptable.
Training/continuing education
It is typical for the employer to reimburse some or all of the cost of continuing education, up to a maximum annual amount. It is also reasonable for the employer (if paying for the CME) to pre-approve the curriculum, as well as the timing to avoid scheduling problems.
Salary and bonus
Compensation systems can be entirely objective (ie, production based), subjective (entirely up to the discretion of the employer based on internal criteria), or a combination of both. It is important to get a clear understanding of the system so that you know what is expected of you and what the rewards are for meeting performance goals.
Income guarantee/advanced expenses/repayment obligation
It is not uncommon for a local hospital to help a medical practice by guaranteeing the salary for a certain period of time. In this situation, the guarantee can be structured in a number of different ways—but it typically involves an obligation to repay a predetermined amount if you leave the practice area before the expiration of the term. Often, the practice will seek to pass that liability on to you. The same may apply for advanced moving expenses, CME, etc. A practice may require you to be employed for a specified amount of time to “earn” those advanced expenses, or to pay them back if an early termination occurs. In any case, it is important to know what the expectations are, and what circumstances could lead to an early termination and/or repayment obligation.
Terms and termination
Pay particular attention to the terms of your agreement. In one paragraph, it may say that the contract is for one year with annual renewals, but later on it explains that it can be terminated by either party upon 30 days notice. In that case, it is not a one-year contract; it is a 30-day contract. If there is a possibility of early termination and a restrictive covenant, or even a repayment obligation, you could really be at risk. Pay attention to whether early termination is “for cause” or “without cause.” If it is only for cause, inquire what constitutes a cause and whether there are any opportunities to rectify a perceived problem.
CONCLUSION
Constant changes in the health care marketplace will continue to generate opportunities for NPs and PAs. This is especially true for clinicians who demonstrate competence, enthusiasm, and commitment to quality patient care. The same clinical skills you learned in school and practice will help you find a clinical position and negotiate a good professional contract. Attention to detail, evidence-based research, and excellent communication skills will enable you to land a position beneficial to both parties.
1. American Academy of Physician Assistants. 2016 AAPA Salary Report. www.aapa.org/research/salary-report. Accessed November 4, 2016.
2. American Academy of Nurse Practitioners. Annual income for full-time nurse practitioners up 10% since 2011. www.aanp.org/press-room/press-releases/166-press-room/2015-press-releases/1803-annual- income-for-full-time-nurse-practitioners-up-10-since-2011. Accessed November 4, 2016.
3. Bourne H. A Great Deal! Compensation Negotiation for Nurse Practitioners & Physician Assistants. 3rd ed. Arcata, CA: Open Spaces; 1998.
4. Buppert C. Nurse Practitioner’s Business Practice and Legal Guide. 5th ed. Burlington, MA: Jones & Bartlett Learning; 2015.
5. Henley MB. Finding your ideal job and negotiating your contract: where to get the information and numbers you need to know. J Orthop Trauma. 2012;26(1):S9-S13.
6. AAPA. Contacts and contracts: a guide to your PA career. www.aapa.org/WorkArea/DownloadAsset.aspx?id=2147486883. Accessed November 4, 2016.
7. AANP. Employment negotiations. www.aanp.org/practice/reimbursement/68-articles/579-employment-negotiations. Accessed November 4, 2016.
8. Buppert C. Employment agreements: clauses that can change an NP’s life. Nurse Pract. 1997;22(8):108-109.
1. American Academy of Physician Assistants. 2016 AAPA Salary Report. www.aapa.org/research/salary-report. Accessed November 4, 2016.
2. American Academy of Nurse Practitioners. Annual income for full-time nurse practitioners up 10% since 2011. www.aanp.org/press-room/press-releases/166-press-room/2015-press-releases/1803-annual- income-for-full-time-nurse-practitioners-up-10-since-2011. Accessed November 4, 2016.
3. Bourne H. A Great Deal! Compensation Negotiation for Nurse Practitioners & Physician Assistants. 3rd ed. Arcata, CA: Open Spaces; 1998.
4. Buppert C. Nurse Practitioner’s Business Practice and Legal Guide. 5th ed. Burlington, MA: Jones & Bartlett Learning; 2015.
5. Henley MB. Finding your ideal job and negotiating your contract: where to get the information and numbers you need to know. J Orthop Trauma. 2012;26(1):S9-S13.
6. AAPA. Contacts and contracts: a guide to your PA career. www.aapa.org/WorkArea/DownloadAsset.aspx?id=2147486883. Accessed November 4, 2016.
7. AANP. Employment negotiations. www.aanp.org/practice/reimbursement/68-articles/579-employment-negotiations. Accessed November 4, 2016.
8. Buppert C. Employment agreements: clauses that can change an NP’s life. Nurse Pract. 1997;22(8):108-109.
Antibody face-off in follicular lymphoma gives PFS, but not OS, edge to obinutuzumab
SAN DIEGO – Obinutuzumab, a second-generation anti-CD20 antibody touted as the heir apparent to rituximab, offered a progression-free survival (PFS) edge over rituximab when combined with standard chemotherapy in patients with previously untreated advanced follicular lymphoma.

But other clinicians and investigators who
attended the presentation of the GALLIUM data at a plenary session during the American Society of Hematology annual meeting indicated that despite the data, they weren’t ready to make a switch to the newer, costlier antibody.
“I feel that it is not convincing for practice-changing,” said Kanti R. Rai, MD, professor of medicine and molecular medicine at Hofstra University, Hempstead, N.Y.
“Unless we have evidence of a survival advantage in indolent disease, progression-free survivorship is not an adequate reason to jump to another antibody,” he said in an interview.
In GALLIUM, the primary endpoint of investigator-assessed 3-year PFS at a median follow-up of 34.5 months was 80% for patients with follicular lymphoma treated with obinutuzumab and one of three standard chemotherapy regimens, compared with 73.3% for patients treated with rituximab and chemotherapy. This difference translated into a hazard ratio of 0.68 favoring obinutuzumab (P = .0012).
Respective 3-year overall survival rates were similar, however, at 94% and 92.1% (HR, 0.75; P = .21).
Indolent lymphoma trial
The GALLIUM trial is a phase III study comparing obinutuzumab with rituximab when paired with one of three standard chemotherapy regimens for indolent non-Hodgkin lymphomas, including follicular lymphoma and splenic, nodal, or extranodal marginal zone lymphoma. Dr. Marcus presented data on patients with follicular lymphoma only.
The antibodies were delivered in combination with either CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone; 33.1% of patients), CVP (cyclophosphamide, vincristine, prednisone; 9.8%) or bendamustine alone (B; 57.1%) as the chemotherapy backbone. The choice of regimen was at the discretion of the treating center.
A total of 1,202 patients with follicular lymphoma were enrolled and randomized to treatment and were included in an intention-to-treat analysis.
The treatment arms were well balanced with regard to distribution of patients characteristics, with approximately 21% in each arm having Follicular Lymphoma International Prognostic Index low-risk disease; 37% having intermediate-risk disease; and 34% having high-risk disease.
Roughly half of patients in each arm had bone marrow involvement, and two-thirds had extranodal involvement.
Obinutuzumab was dosed 1,000 mg IV on days 1, 8, and 15 of cycle one, and either on day 1 of cycles two through eight every 3 weeks, or every 4 weeks during cycles two through six.
Overall response rates at the end of induction were 86.9% with rituximab and 88.5% with obinutuzumab, with complete responses of 23.8% and 19.5%, respectively.
As noted before, investigator-assessed PFS favored obinutuzumab, as did PFS assessed by independent reviewer, at 81.9% vs. 77.9% for rituximab (HR, 0.71; P = .0138).
The newer antibody also had a slight edge in time to new treatment, with 87.1% of patients on obinutuzumab not starting on new therapy, compared with 81.2% of patients on rituximab.
More bendamustine deaths
Nearly all patients in each arm had an adverse event, with grade 3 or greater events occurring in 74.6% of patients on obinutuzumab vs. 67.8% on rituximab. Rates of neutropenia, leukopenia, febrile neutropenia, infusion reactions, and thrombocytopenia were all slightly higher with obinutuzumab. Grade 3 or greater infections occurred in 20% with obinutuzumab, compared with 15.6% with rituximab.
“What we did note, however, was a high level of mortality in patients receiving either obinutuzumab-based therapy or rituximab-based therapy, which were no different between the two arms and were somewhat higher than one might expect from patients receiving induction treatment in follicular lymphoma. Hence, we did a more detailed analysis of safety by treatment regimen,” Dr. Marcus said.
There were more deaths among patients treated with bendamustine (5.6% for patients in the B-obinutuzumab cohort, and 4.4% of patients in the B-rituximab cohort) vs. 1.6% and 2.0%, respectively, for patients on CHOP, and 1.6 and 1.8% for patients on CVP.
Dose effect?
John P. Leonard, MD, from Cornell University, New York , who introduced Dr. Marcus, commented that PFS may not be the ideal endpoint for patients with follicular lymphoma.

He pointed out that in trials comparing rituximab with obinutuzumab for other diseases, results have been mixed, with obinutuzumab showing superiority in chronic lymphocytic leukemia, but in data presented elsewhere at ASH 2016, obinutuzumab was not superior to rituximab for treatment of diffuse large B-cell lymphoma.
“One question is whether obinutuzumab, which is generally administered at a higher mg dose to patients, is in fact a better antibody or if it is in fact a dose effect,” he said.
In response to a similar question following his presentation, Dr. Marcus replied that, despite sharing a target, the two antibodies are different, with different mechanisms of action. He also noted that there is no evidence to suggest that rituximab potency would be greater in follicular lymphoma if it were given at higher doses.
The GALLIUM trial is sponsored by Hoffmann-La Roche, Dr, Marcus disclosed consulting with and receiving honoraria from the company, and relationships with other companies.
SAN DIEGO – Obinutuzumab, a second-generation anti-CD20 antibody touted as the heir apparent to rituximab, offered a progression-free survival (PFS) edge over rituximab when combined with standard chemotherapy in patients with previously untreated advanced follicular lymphoma.
But other clinicians and investigators who
attended the presentation of the GALLIUM data at a plenary session during the American Society of Hematology annual meeting indicated that despite the data, they weren’t ready to make a switch to the newer, costlier antibody.
“I feel that it is not convincing for practice-changing,” said Kanti R. Rai, MD, professor of medicine and molecular medicine at Hofstra University, Hempstead, N.Y.
“Unless we have evidence of a survival advantage in indolent disease, progression-free survivorship is not an adequate reason to jump to another antibody,” he said in an interview.
In GALLIUM, the primary endpoint of investigator-assessed 3-year PFS at a median follow-up of 34.5 months was 80% for patients with follicular lymphoma treated with obinutuzumab and one of three standard chemotherapy regimens, compared with 73.3% for patients treated with rituximab and chemotherapy. This difference translated into a hazard ratio of 0.68 favoring obinutuzumab (P = .0012).
Respective 3-year overall survival rates were similar, however, at 94% and 92.1% (HR, 0.75; P = .21).
Indolent lymphoma trial
The GALLIUM trial is a phase III study comparing obinutuzumab with rituximab when paired with one of three standard chemotherapy regimens for indolent non-Hodgkin lymphomas, including follicular lymphoma and splenic, nodal, or extranodal marginal zone lymphoma. Dr. Marcus presented data on patients with follicular lymphoma only.
The antibodies were delivered in combination with either CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone; 33.1% of patients), CVP (cyclophosphamide, vincristine, prednisone; 9.8%) or bendamustine alone (B; 57.1%) as the chemotherapy backbone. The choice of regimen was at the discretion of the treating center.
A total of 1,202 patients with follicular lymphoma were enrolled and randomized to treatment and were included in an intention-to-treat analysis.
The treatment arms were well balanced with regard to distribution of patients characteristics, with approximately 21% in each arm having Follicular Lymphoma International Prognostic Index low-risk disease; 37% having intermediate-risk disease; and 34% having high-risk disease.
Roughly half of patients in each arm had bone marrow involvement, and two-thirds had extranodal involvement.
Obinutuzumab was dosed 1,000 mg IV on days 1, 8, and 15 of cycle one, and either on day 1 of cycles two through eight every 3 weeks, or every 4 weeks during cycles two through six.
Overall response rates at the end of induction were 86.9% with rituximab and 88.5% with obinutuzumab, with complete responses of 23.8% and 19.5%, respectively.
As noted before, investigator-assessed PFS favored obinutuzumab, as did PFS assessed by independent reviewer, at 81.9% vs. 77.9% for rituximab (HR, 0.71; P = .0138).
The newer antibody also had a slight edge in time to new treatment, with 87.1% of patients on obinutuzumab not starting on new therapy, compared with 81.2% of patients on rituximab.
More bendamustine deaths
Nearly all patients in each arm had an adverse event, with grade 3 or greater events occurring in 74.6% of patients on obinutuzumab vs. 67.8% on rituximab. Rates of neutropenia, leukopenia, febrile neutropenia, infusion reactions, and thrombocytopenia were all slightly higher with obinutuzumab. Grade 3 or greater infections occurred in 20% with obinutuzumab, compared with 15.6% with rituximab.
“What we did note, however, was a high level of mortality in patients receiving either obinutuzumab-based therapy or rituximab-based therapy, which were no different between the two arms and were somewhat higher than one might expect from patients receiving induction treatment in follicular lymphoma. Hence, we did a more detailed analysis of safety by treatment regimen,” Dr. Marcus said.
There were more deaths among patients treated with bendamustine (5.6% for patients in the B-obinutuzumab cohort, and 4.4% of patients in the B-rituximab cohort) vs. 1.6% and 2.0%, respectively, for patients on CHOP, and 1.6 and 1.8% for patients on CVP.
Dose effect?
John P. Leonard, MD, from Cornell University, New York , who introduced Dr. Marcus, commented that PFS may not be the ideal endpoint for patients with follicular lymphoma.
He pointed out that in trials comparing rituximab with obinutuzumab for other diseases, results have been mixed, with obinutuzumab showing superiority in chronic lymphocytic leukemia, but in data presented elsewhere at ASH 2016, obinutuzumab was not superior to rituximab for treatment of diffuse large B-cell lymphoma.
“One question is whether obinutuzumab, which is generally administered at a higher mg dose to patients, is in fact a better antibody or if it is in fact a dose effect,” he said.
In response to a similar question following his presentation, Dr. Marcus replied that, despite sharing a target, the two antibodies are different, with different mechanisms of action. He also noted that there is no evidence to suggest that rituximab potency would be greater in follicular lymphoma if it were given at higher doses.
The GALLIUM trial is sponsored by Hoffmann-La Roche, Dr, Marcus disclosed consulting with and receiving honoraria from the company, and relationships with other companies.
SAN DIEGO – Obinutuzumab, a second-generation anti-CD20 antibody touted as the heir apparent to rituximab, offered a progression-free survival (PFS) edge over rituximab when combined with standard chemotherapy in patients with previously untreated advanced follicular lymphoma.
But other clinicians and investigators who
attended the presentation of the GALLIUM data at a plenary session during the American Society of Hematology annual meeting indicated that despite the data, they weren’t ready to make a switch to the newer, costlier antibody.
“I feel that it is not convincing for practice-changing,” said Kanti R. Rai, MD, professor of medicine and molecular medicine at Hofstra University, Hempstead, N.Y.
“Unless we have evidence of a survival advantage in indolent disease, progression-free survivorship is not an adequate reason to jump to another antibody,” he said in an interview.
In GALLIUM, the primary endpoint of investigator-assessed 3-year PFS at a median follow-up of 34.5 months was 80% for patients with follicular lymphoma treated with obinutuzumab and one of three standard chemotherapy regimens, compared with 73.3% for patients treated with rituximab and chemotherapy. This difference translated into a hazard ratio of 0.68 favoring obinutuzumab (P = .0012).
Respective 3-year overall survival rates were similar, however, at 94% and 92.1% (HR, 0.75; P = .21).
Indolent lymphoma trial
The GALLIUM trial is a phase III study comparing obinutuzumab with rituximab when paired with one of three standard chemotherapy regimens for indolent non-Hodgkin lymphomas, including follicular lymphoma and splenic, nodal, or extranodal marginal zone lymphoma. Dr. Marcus presented data on patients with follicular lymphoma only.
The antibodies were delivered in combination with either CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone; 33.1% of patients), CVP (cyclophosphamide, vincristine, prednisone; 9.8%) or bendamustine alone (B; 57.1%) as the chemotherapy backbone. The choice of regimen was at the discretion of the treating center.
A total of 1,202 patients with follicular lymphoma were enrolled and randomized to treatment and were included in an intention-to-treat analysis.
The treatment arms were well balanced with regard to distribution of patients characteristics, with approximately 21% in each arm having Follicular Lymphoma International Prognostic Index low-risk disease; 37% having intermediate-risk disease; and 34% having high-risk disease.
Roughly half of patients in each arm had bone marrow involvement, and two-thirds had extranodal involvement.
Obinutuzumab was dosed 1,000 mg IV on days 1, 8, and 15 of cycle one, and either on day 1 of cycles two through eight every 3 weeks, or every 4 weeks during cycles two through six.
Overall response rates at the end of induction were 86.9% with rituximab and 88.5% with obinutuzumab, with complete responses of 23.8% and 19.5%, respectively.
As noted before, investigator-assessed PFS favored obinutuzumab, as did PFS assessed by independent reviewer, at 81.9% vs. 77.9% for rituximab (HR, 0.71; P = .0138).
The newer antibody also had a slight edge in time to new treatment, with 87.1% of patients on obinutuzumab not starting on new therapy, compared with 81.2% of patients on rituximab.
More bendamustine deaths
Nearly all patients in each arm had an adverse event, with grade 3 or greater events occurring in 74.6% of patients on obinutuzumab vs. 67.8% on rituximab. Rates of neutropenia, leukopenia, febrile neutropenia, infusion reactions, and thrombocytopenia were all slightly higher with obinutuzumab. Grade 3 or greater infections occurred in 20% with obinutuzumab, compared with 15.6% with rituximab.
“What we did note, however, was a high level of mortality in patients receiving either obinutuzumab-based therapy or rituximab-based therapy, which were no different between the two arms and were somewhat higher than one might expect from patients receiving induction treatment in follicular lymphoma. Hence, we did a more detailed analysis of safety by treatment regimen,” Dr. Marcus said.
There were more deaths among patients treated with bendamustine (5.6% for patients in the B-obinutuzumab cohort, and 4.4% of patients in the B-rituximab cohort) vs. 1.6% and 2.0%, respectively, for patients on CHOP, and 1.6 and 1.8% for patients on CVP.
Dose effect?
John P. Leonard, MD, from Cornell University, New York , who introduced Dr. Marcus, commented that PFS may not be the ideal endpoint for patients with follicular lymphoma.
He pointed out that in trials comparing rituximab with obinutuzumab for other diseases, results have been mixed, with obinutuzumab showing superiority in chronic lymphocytic leukemia, but in data presented elsewhere at ASH 2016, obinutuzumab was not superior to rituximab for treatment of diffuse large B-cell lymphoma.
“One question is whether obinutuzumab, which is generally administered at a higher mg dose to patients, is in fact a better antibody or if it is in fact a dose effect,” he said.
In response to a similar question following his presentation, Dr. Marcus replied that, despite sharing a target, the two antibodies are different, with different mechanisms of action. He also noted that there is no evidence to suggest that rituximab potency would be greater in follicular lymphoma if it were given at higher doses.
The GALLIUM trial is sponsored by Hoffmann-La Roche, Dr, Marcus disclosed consulting with and receiving honoraria from the company, and relationships with other companies.
AT ASH 2016
Key clinical point: Obinutuzumab plus chemotherapy was associated with better 3-year progression-free survival in patients with untreated follicular lymphoma.
Major finding: Obinutuzumab/chemo was associated with a hazard ratio for investigator-assessed PFS of 0.68 (P = .0012)
Data source: Randomized phase III trial in 1202 patients with previously untreated follicular lymphoma.
Disclosures: The GALLIUM trial was sponsored by Hoffmann-La Roche. Dr. Marcus disclosed consulting with and receiving honoraria from the company, and relationships with other companies.
Laxative Use with Patient-Controlled Analgesia in the Hospital and Associated Outcomes
From the Division of General Internal Medicine (Dr. Lenz), Division of Biomedical Statistics and Informatics (Mr. Schroeder), and the Division of Hospital Internal Medicine (Ms. Lawson and Dr. Yu), Mayo Clinic, Rochester, MN.
Abstract
- Objective: To describe prophylactic laxative effectiveness and prescribing patterns in patients initiated on intravenous (IV) opioid analgesia.
- Design: Retrospective cohort study.
- Setting and participants: All patients who were on IV narcotics with a patient-controlled pump while admitted to a general medicine service at the Mayo Clinic in Rochester in 2011 and 2012 were identified. Patients were excluded if constipation or diarrhea were diagnosed prior to IV opioid analgesia initiation.
- Measurements: Prophylactic laxatives were defined as laxatives prescribed within 24 hours of IV opioid analgesia initiation to be given even in the absence of constipation. Constipation was recorded when diagnosed during the hospitalization. Severe constipation was defined as constipation resulting in an abdominal CT or X-ray; abdominal distension, pain, or bloating; or if an enema was performed during the hospitalization.
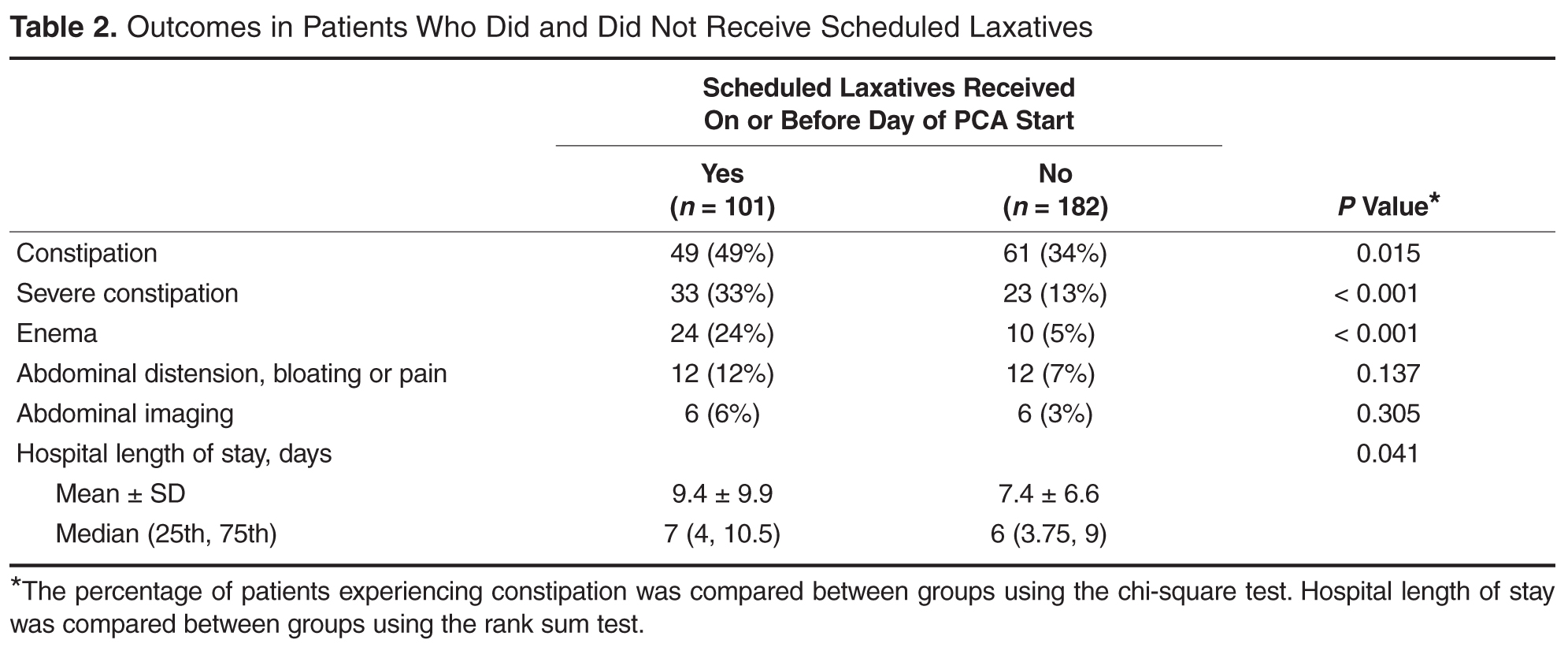
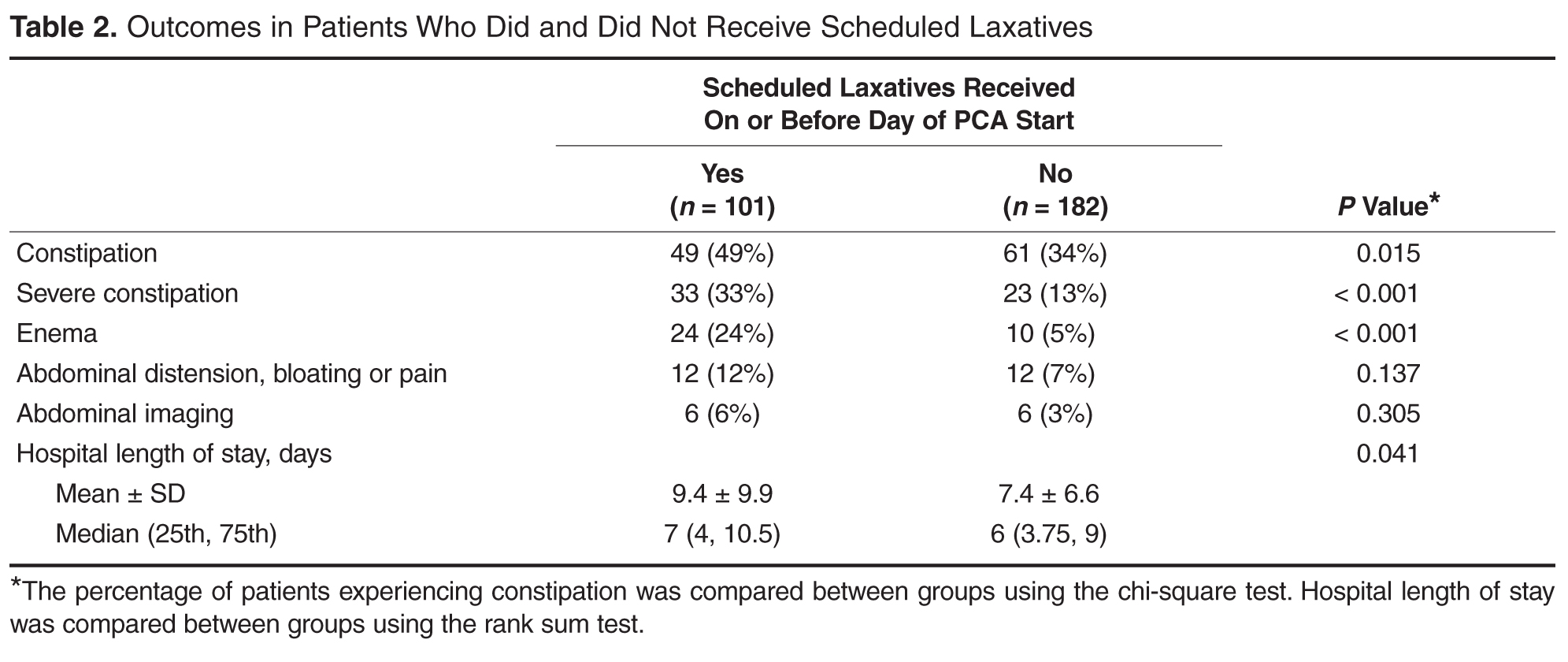
- Results: Of 283 patients, 101 (36%) received prophylactic laxatives and 182 (64%) did not. Constipation occurred in 61 (34%) not on prophylactic laxatives and in 49 (49%) on prophylactic laxatives (P = 0.015). Severe constipation occurred in 23 (13%) not on prophylactic laxatives and in 33 (33%) on prophylactic laxatives (P < 0.001).
- Conclusion: A large percentage of patients are not receiving prophylactic laxatives when receiving IV opioid analgesia in the hospital. Current laxative strategies are not effectively preventing constipation in patients when prescribed.
Key words: constipation; opioids; hospital medicine; patient-controlled analgesia; laxatives.
Opioid-induced constipation (OIC) is defined as a change, when initiating opioid therapy, from baseline bowel habits and defecation patterns that is characterized by any of the following: reduced bowel frequency; development or worsening of straining; a sense of incomplete evacuation; or a patient’s perception of distress related to bowel habits [1]. It is an important side effect to consider when initiating narcotic analgesia. It has been estimated that approximately 3% to 4% of the population is on chronic narcotic pain relievers in the outpatient setting [2,3], and 37% to 81% of these patients will experience constipation [3–9]. Because of the high incidence of constipation, the prophylactic prescription of laxatives with initiation of opioid pain relievers is frequently recommended [10–15]. Furthermore, it has been shown that among patients admitted to the hospital with cancer, there is a lower incidence of constipation amongst those who have received prophylactic laxatives [16]. However, there is no evidence in the literature that prophylactic laxatives improve outcomes in patients on opioid analgesia in the general medicine inpatient setting. Furthermore, studies have illustrated that recommendations for prophylactic laxative use are not reliably followed [3,9].
While the incidence of OIC is well described in the outpatient setting [17,18], there are few studies looking at the incidence of OIC in the hospital setting. It has been shown, however, that occurrence during even a brief hospitalization is possible [4,6]. Acute constipation while hospitalized can theoretically lead to longer hospitalizations, increased pain, and decreased quality of life [6,7,19]. Recent research has focused heavily on the use of novel agents such as peripherally acting mu-opioid receptor antagonists in the treatment of OIC [20–23]. However, the expense of these agents makes them less than ideal in the prophylactic setting. This study will assess the effectiveness and prescribing patterns of prophylactic laxatives in the inpatient general medicine setting over a 2-year period at our institution in patients initiated on patient-controlled analgesia with hydromorphone, morphine, or fentanyl.
Methods
This study was approved by the institutional review board at the Mayo Clinic Rochester. All patients who were initiated on intravenous analgesia with an electronic patient-controlled opioid pump (PCA) while admitted to a general medicine service in 2011 and 2012 were identified. Patients who received PCA therapy were identified through a pharmacy database. Only patients older than 18 years of age were included in the study. PCA therapy was selected for our analysis because PCA therapy is not regularly administered on an outpatient basis. All of these patients, therefore, had a change in their narcotic regimen on admission to the hospital. Patients were excluded from the study if they were on a PCA for less than 24 hours; had a PCA initiated on a service other than a general medicine service; were on a scheduled laxative regimen prior to admission; or carried a diagnosis of bowel obstruction, chronic diarrhea, constipation, or intestinal discontinuity (eg, those with previous diversions or ostomies).
A retrospective review of each patient’s chart was conducted with the assistance of a team of nurse abstractors. Basic demographic data were recorded for each patient. Date of hospital admission and discharge; scheduled laxatives ordered and administered (any dose of sennosides, polyethylene glycol, docusate, bisacodyl, lactulose, or magnesium citrate); abdominal X-rays and abdominal CT scans performed for constipation; and any administration of enemas were recorded. Fiber supplements were not considered laxatives. If a patient was documented to have constipation during their hospitalization this was recorded. Patients were classified as having severe constipation if an abdominal CT or x-ray was performed for the indication of constipation; if abdominal distension, pain, or bloating were documented due to constipation; or if an enema was performed during the hospitalization.
For analysis purposes, patients who started receiving scheduled laxatives (as opposed to laxatives “as needed”)on or before the day of PCA initiation were classified as receiving prophylactic laxatives. Baseline patient characteristics and outcomes were compared using the chi-square test for nominal variables and the rank sum test for continuous variables. In all cases, 2-tailed tests were performed with P values ≤ 0.05 considered statistically significant. A nominal logistic regression model was utilized to assess for independent association of risk factors with the outcome of constipation.
Results
Discussion
Patients initiated on opioid therapy were not prescribed prophylactic laxatives in 64% of our cohort in the inpatient setting. When prescribed, current laxative strategies did not effectively prevent constipation with 49% experiencing OIC. Our data serves as a strong reminder of the magnitude of the problem of OIC in the inpatient setting.
The strength of our paper lies in its role as a magnitude assessment. This retrospective review reveals for that among a diverse group of patients hospitalized within a large academic institution, OIC remains prevalent. Furthermore, the high incidence of severe constipation indicates the potential for increased health care costs and patient discomfort secondary to OIC emphasizing the importance of prevention of OIC. Recent guidelines have made a push toward prophylactic laxative utilization earlier. Specifically, the European Palliative Research Collaborative offers a “strong recommendation to routinely prescribe laxatives for the management or prophylaxis of opioid-induced constipation” [10]. Additionally, the American Society of Interventional Pain Physicians suggests that “a physician should consider the initiation of a bowel regimen even before the development of constipation and definitely after the development of constipation” [11]. Our manuscript serves as a reminder that OIC remains a very prevalent problem and that prophylactic laxatives are still being underutilized.
This is a retrospective study and thus has inherent limitations. Specifically, we are limited to those cases of constipation that were documented in the medical record. The presentation of constipation is varied between patients. This variation in presentation of OIC is inherent to the disease process as is demonstrated in the broad definition for OIC [1]. The cases of constipation that we are reporting clearly were bothersome enough to warrant documentation in the medical record, and while there may have been cases that escaped documentation, we can be confident that the cases of OIC we are reporting are true cases of OIC. The numbers we report can therefore be taken to represent a minimum number of cases of constipation occurring in our study population.
It has been suggested that OIC prevalence varies with type of opioid and duration of opioid therapy [24]. We did not compare dose, type, or duration of opioid therapy in this study. This could certainly account for the seemingly higher rate of constipation within the group treated with prophylactic laxatives as compared with those not treated with prophylactic laxatives. Physicians likely have a higher propensity to prescribe prophylactic laxatives to patients receiving high doses of opioids who are in turn at higher risk for OIC. We cannot say whether differences in efficacy exist between prophylactic laxative regimens or which opioids (dose and duration) cause the most constipation based upon our data. Future studies incorporating dose, duration, and opioid type along with the variables we collected in this study could potentially construct successful logistic regression models with predictive power to identify those at highest risk of OIC.
Our rate of OIC is consistent with previously published figures [3–9]. However, we demonstrate for the first time that prophylactic laxatives are prescribed infrequently and unsuccessfully in the inpatient setting. This is consistent with prescribing rates in the outpatient setting [9,25]. Furthermore, we observed a higher rate of constipation in those treated with prophylactic laxatives compared to those that did not receive prophylactic laxatives. Pottegard et al similarly demonstrated an increased rate of constipation in those utilizing laxative therapy [25]. This is likely secondary to providers recommending prophylactic laxatives to those patients most likely to develop constipation. Despite being able to recognize high-risk patients, providers are unable to prevent OIC as little is known regarding optimal laxative strategies. Previous studies comparing treatment regimens for the relief of constipation in the palliative care population have been largely inconclusive [26]. There have been no studies to date comparing different prophylactic laxatives in the inpatient setting.
Future directions for research in this area would ideally take the form of randomized controlled trials investigating efficacy of different prophylactic laxatives in the inpatient setting. These trials would ideally include well-defined patient groups receiving specific narcotics for specific reasons. These studies would be best if powered to assess the effect of narcotic dosage and duration of therapy as well. Alternatively, larger retrospective chart reviews could be performed including narcotic dosage, type, and duration of therapy with a planned logistic regression model attempting to account for likely independent variables.
Conclusion
Our study demonstrates for the first time that prophylactic laxatives are not being prescribed frequently to patients on opioid analgesia in the inpatient general medicine setting. Additionally, while providers seem to be identifying patients at higher risk of constipation, they are still unable to prevent constipation in a high percentage of patients. Further research into this area would be beneficial to prevent this uncomfortable, costly, and preventable complication of opioid analgesia.
Corresponding author: Roger Yu, MD, Mayo Clinic, 200 First St. SW, Rochester, MN 55905, [email protected].
Funding/support: This research was supported by the Mayo Clinic Return to Work program nurses for data abstraction.
Financial disclosures: None.
1. Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology 2016.
2. Boudreau D, Von Korff M, Rutter CM, et al. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol Drug Saf 2009;18:1166–75.
3. Choung RS, Locke GR 3rd, Zinsmeister AR, et al. Opioid bowel dysfunction and narcotic bowel syndrome: a population-based study. Am J Gastroenterol 2009;104:1199–204.
4. Droney J, Ross J, Gretton S, et al. Constipation in cancer patients on morphine. Support Care Cancer 2008;16:453–9.
5. Sykes NP. The relationship between opioid use and laxative use in terminally ill cancer patients. Palliat Med 1998;12:375–82.
6. Bell TJ, Panchal SJ, Miaskowski C, et al. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European Patient Survey (PROBE 1). Pain Med 2009;10:35–42.
7. Cook SF, Lanza L, Zhou X, et al. Gastrointestinal side effects in chronic opioid users: results from a population-based survey. Aliment Pharmacol Ther 2008;27:1224–32.
8. Moore RA, McQuay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomised trials of oral opioids. Arthritis Res Ther 2005:7:R1046–51.
9. Bouvy ML, Buurma H, Egberts TC. Laxative prescribing in relation to opioid use and the influence of pharmacy-based intervention. J Clin Pharm Ther 2002;27:107–10.
10. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol 2012:13:e58–68.
11. Manchikanti L, Abdi S, Atluri S, et al. American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: Part 2--guidance. Pain Physician 2012;15(3 Suppl):S67–116.
12. Cameron JC. Constipation related to narcotic therapy. A protocol for nurses and patients. Cancer Nurs 1992;15:372–7.
13. Levy MH. Pharmacologic treatment of cancer pain. N Engl J Med 1996;335:1124–32.
14. Swegle JM, Logemann D. Management of common opioid-induced adverse effects. Am Fam Physician 2006;74:1347–54.
15. Donnelly S, Davis MP, Walsh D, Naughton M. Morphine in cancer pain management: a practical guide. Support Care Cancer 2002;10:13–35.
16. Ishihara M, Ikesue H Matsunaga H, et al. A multi-institutional study analyzing effect of prophylactic medication for prevention of opioid-induced gastrointestinal dysfunction. Clin J Pain 2012;28:373–81.
17. Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain 2004;112:372–80.
18. Tuteja AK, Biskupiak J, Stoddard GJ, Lipman AG. Opioid-induced bowel disorders and narcotic bowel syndrome in patients with chronic non-cancer pain. Neurogastroenterol Motil 2010; 22:424–30, e96.
19. Brock C, Olesen SS, Olesen AE, et al. Opioid-induced bowel dysfunction: pathophysiology and management. Drugs 2012;72:1847–65.
20. Camilleri M. Opioid-induced constipation: challenges and therapeutic opportunities. Am J Gastroenterol 2011;106:835–42.
21. Candy B, Jones L, Goodman ML, et al. Laxatives or methylnaltrexone for the management of constipation in palliative care patients. Cochrane Database Syst Rev 2011(1):CD003448.
22. Ford AC, Brenner DM, Schoenfeld PS. Efficacy of pharmacological therapies for the treatment of opioid-induced constipation: systematic review and meta-analysis. Am J Gastroenterol 2013;108:1566–74.
23. Jansen JP, Lorch D, Langan J, et al. A randomized, placebo-controlled phase 3 trial (Study SB-767905/012) of alvimopan for opioid-induced bowel dysfunction in patients with non-cancer pain. J Pain 2011;12:185–93.
24. Camilleri M, Drossman DA, Becker G, et al. Emerging treatments in neurogastroenterology: a multidisciplinary working group consensus statement on opioid-induced constipation. Neurogastroenterol Motil 2014;26:1386–95.
25. Pottegard A, Knudsen TB, van Heesch K, et al. Information on risk of constipation for Danish users of opioids, and their laxative use. Int J Clin Pharm 2014;36:291–4.
26. Candy B, Jones L, Larkin PJ, et al. Laxatives for the management of constipation in people receiving palliative care. Cochrane Database Syst Rev 2015(5):CD003448.
From the Division of General Internal Medicine (Dr. Lenz), Division of Biomedical Statistics and Informatics (Mr. Schroeder), and the Division of Hospital Internal Medicine (Ms. Lawson and Dr. Yu), Mayo Clinic, Rochester, MN.
Abstract
- Objective: To describe prophylactic laxative effectiveness and prescribing patterns in patients initiated on intravenous (IV) opioid analgesia.
- Design: Retrospective cohort study.
- Setting and participants: All patients who were on IV narcotics with a patient-controlled pump while admitted to a general medicine service at the Mayo Clinic in Rochester in 2011 and 2012 were identified. Patients were excluded if constipation or diarrhea were diagnosed prior to IV opioid analgesia initiation.
- Measurements: Prophylactic laxatives were defined as laxatives prescribed within 24 hours of IV opioid analgesia initiation to be given even in the absence of constipation. Constipation was recorded when diagnosed during the hospitalization. Severe constipation was defined as constipation resulting in an abdominal CT or X-ray; abdominal distension, pain, or bloating; or if an enema was performed during the hospitalization.
- Results: Of 283 patients, 101 (36%) received prophylactic laxatives and 182 (64%) did not. Constipation occurred in 61 (34%) not on prophylactic laxatives and in 49 (49%) on prophylactic laxatives (P = 0.015). Severe constipation occurred in 23 (13%) not on prophylactic laxatives and in 33 (33%) on prophylactic laxatives (P < 0.001).
- Conclusion: A large percentage of patients are not receiving prophylactic laxatives when receiving IV opioid analgesia in the hospital. Current laxative strategies are not effectively preventing constipation in patients when prescribed.
Key words: constipation; opioids; hospital medicine; patient-controlled analgesia; laxatives.
Opioid-induced constipation (OIC) is defined as a change, when initiating opioid therapy, from baseline bowel habits and defecation patterns that is characterized by any of the following: reduced bowel frequency; development or worsening of straining; a sense of incomplete evacuation; or a patient’s perception of distress related to bowel habits [1]. It is an important side effect to consider when initiating narcotic analgesia. It has been estimated that approximately 3% to 4% of the population is on chronic narcotic pain relievers in the outpatient setting [2,3], and 37% to 81% of these patients will experience constipation [3–9]. Because of the high incidence of constipation, the prophylactic prescription of laxatives with initiation of opioid pain relievers is frequently recommended [10–15]. Furthermore, it has been shown that among patients admitted to the hospital with cancer, there is a lower incidence of constipation amongst those who have received prophylactic laxatives [16]. However, there is no evidence in the literature that prophylactic laxatives improve outcomes in patients on opioid analgesia in the general medicine inpatient setting. Furthermore, studies have illustrated that recommendations for prophylactic laxative use are not reliably followed [3,9].
While the incidence of OIC is well described in the outpatient setting [17,18], there are few studies looking at the incidence of OIC in the hospital setting. It has been shown, however, that occurrence during even a brief hospitalization is possible [4,6]. Acute constipation while hospitalized can theoretically lead to longer hospitalizations, increased pain, and decreased quality of life [6,7,19]. Recent research has focused heavily on the use of novel agents such as peripherally acting mu-opioid receptor antagonists in the treatment of OIC [20–23]. However, the expense of these agents makes them less than ideal in the prophylactic setting. This study will assess the effectiveness and prescribing patterns of prophylactic laxatives in the inpatient general medicine setting over a 2-year period at our institution in patients initiated on patient-controlled analgesia with hydromorphone, morphine, or fentanyl.
Methods
This study was approved by the institutional review board at the Mayo Clinic Rochester. All patients who were initiated on intravenous analgesia with an electronic patient-controlled opioid pump (PCA) while admitted to a general medicine service in 2011 and 2012 were identified. Patients who received PCA therapy were identified through a pharmacy database. Only patients older than 18 years of age were included in the study. PCA therapy was selected for our analysis because PCA therapy is not regularly administered on an outpatient basis. All of these patients, therefore, had a change in their narcotic regimen on admission to the hospital. Patients were excluded from the study if they were on a PCA for less than 24 hours; had a PCA initiated on a service other than a general medicine service; were on a scheduled laxative regimen prior to admission; or carried a diagnosis of bowel obstruction, chronic diarrhea, constipation, or intestinal discontinuity (eg, those with previous diversions or ostomies).
A retrospective review of each patient’s chart was conducted with the assistance of a team of nurse abstractors. Basic demographic data were recorded for each patient. Date of hospital admission and discharge; scheduled laxatives ordered and administered (any dose of sennosides, polyethylene glycol, docusate, bisacodyl, lactulose, or magnesium citrate); abdominal X-rays and abdominal CT scans performed for constipation; and any administration of enemas were recorded. Fiber supplements were not considered laxatives. If a patient was documented to have constipation during their hospitalization this was recorded. Patients were classified as having severe constipation if an abdominal CT or x-ray was performed for the indication of constipation; if abdominal distension, pain, or bloating were documented due to constipation; or if an enema was performed during the hospitalization.
For analysis purposes, patients who started receiving scheduled laxatives (as opposed to laxatives “as needed”)on or before the day of PCA initiation were classified as receiving prophylactic laxatives. Baseline patient characteristics and outcomes were compared using the chi-square test for nominal variables and the rank sum test for continuous variables. In all cases, 2-tailed tests were performed with P values ≤ 0.05 considered statistically significant. A nominal logistic regression model was utilized to assess for independent association of risk factors with the outcome of constipation.
Results
Discussion
Patients initiated on opioid therapy were not prescribed prophylactic laxatives in 64% of our cohort in the inpatient setting. When prescribed, current laxative strategies did not effectively prevent constipation with 49% experiencing OIC. Our data serves as a strong reminder of the magnitude of the problem of OIC in the inpatient setting.
The strength of our paper lies in its role as a magnitude assessment. This retrospective review reveals for that among a diverse group of patients hospitalized within a large academic institution, OIC remains prevalent. Furthermore, the high incidence of severe constipation indicates the potential for increased health care costs and patient discomfort secondary to OIC emphasizing the importance of prevention of OIC. Recent guidelines have made a push toward prophylactic laxative utilization earlier. Specifically, the European Palliative Research Collaborative offers a “strong recommendation to routinely prescribe laxatives for the management or prophylaxis of opioid-induced constipation” [10]. Additionally, the American Society of Interventional Pain Physicians suggests that “a physician should consider the initiation of a bowel regimen even before the development of constipation and definitely after the development of constipation” [11]. Our manuscript serves as a reminder that OIC remains a very prevalent problem and that prophylactic laxatives are still being underutilized.
This is a retrospective study and thus has inherent limitations. Specifically, we are limited to those cases of constipation that were documented in the medical record. The presentation of constipation is varied between patients. This variation in presentation of OIC is inherent to the disease process as is demonstrated in the broad definition for OIC [1]. The cases of constipation that we are reporting clearly were bothersome enough to warrant documentation in the medical record, and while there may have been cases that escaped documentation, we can be confident that the cases of OIC we are reporting are true cases of OIC. The numbers we report can therefore be taken to represent a minimum number of cases of constipation occurring in our study population.
It has been suggested that OIC prevalence varies with type of opioid and duration of opioid therapy [24]. We did not compare dose, type, or duration of opioid therapy in this study. This could certainly account for the seemingly higher rate of constipation within the group treated with prophylactic laxatives as compared with those not treated with prophylactic laxatives. Physicians likely have a higher propensity to prescribe prophylactic laxatives to patients receiving high doses of opioids who are in turn at higher risk for OIC. We cannot say whether differences in efficacy exist between prophylactic laxative regimens or which opioids (dose and duration) cause the most constipation based upon our data. Future studies incorporating dose, duration, and opioid type along with the variables we collected in this study could potentially construct successful logistic regression models with predictive power to identify those at highest risk of OIC.
Our rate of OIC is consistent with previously published figures [3–9]. However, we demonstrate for the first time that prophylactic laxatives are prescribed infrequently and unsuccessfully in the inpatient setting. This is consistent with prescribing rates in the outpatient setting [9,25]. Furthermore, we observed a higher rate of constipation in those treated with prophylactic laxatives compared to those that did not receive prophylactic laxatives. Pottegard et al similarly demonstrated an increased rate of constipation in those utilizing laxative therapy [25]. This is likely secondary to providers recommending prophylactic laxatives to those patients most likely to develop constipation. Despite being able to recognize high-risk patients, providers are unable to prevent OIC as little is known regarding optimal laxative strategies. Previous studies comparing treatment regimens for the relief of constipation in the palliative care population have been largely inconclusive [26]. There have been no studies to date comparing different prophylactic laxatives in the inpatient setting.
Future directions for research in this area would ideally take the form of randomized controlled trials investigating efficacy of different prophylactic laxatives in the inpatient setting. These trials would ideally include well-defined patient groups receiving specific narcotics for specific reasons. These studies would be best if powered to assess the effect of narcotic dosage and duration of therapy as well. Alternatively, larger retrospective chart reviews could be performed including narcotic dosage, type, and duration of therapy with a planned logistic regression model attempting to account for likely independent variables.
Conclusion
Our study demonstrates for the first time that prophylactic laxatives are not being prescribed frequently to patients on opioid analgesia in the inpatient general medicine setting. Additionally, while providers seem to be identifying patients at higher risk of constipation, they are still unable to prevent constipation in a high percentage of patients. Further research into this area would be beneficial to prevent this uncomfortable, costly, and preventable complication of opioid analgesia.
Corresponding author: Roger Yu, MD, Mayo Clinic, 200 First St. SW, Rochester, MN 55905, [email protected].
Funding/support: This research was supported by the Mayo Clinic Return to Work program nurses for data abstraction.
Financial disclosures: None.
From the Division of General Internal Medicine (Dr. Lenz), Division of Biomedical Statistics and Informatics (Mr. Schroeder), and the Division of Hospital Internal Medicine (Ms. Lawson and Dr. Yu), Mayo Clinic, Rochester, MN.
Abstract
- Objective: To describe prophylactic laxative effectiveness and prescribing patterns in patients initiated on intravenous (IV) opioid analgesia.
- Design: Retrospective cohort study.
- Setting and participants: All patients who were on IV narcotics with a patient-controlled pump while admitted to a general medicine service at the Mayo Clinic in Rochester in 2011 and 2012 were identified. Patients were excluded if constipation or diarrhea were diagnosed prior to IV opioid analgesia initiation.
- Measurements: Prophylactic laxatives were defined as laxatives prescribed within 24 hours of IV opioid analgesia initiation to be given even in the absence of constipation. Constipation was recorded when diagnosed during the hospitalization. Severe constipation was defined as constipation resulting in an abdominal CT or X-ray; abdominal distension, pain, or bloating; or if an enema was performed during the hospitalization.
- Results: Of 283 patients, 101 (36%) received prophylactic laxatives and 182 (64%) did not. Constipation occurred in 61 (34%) not on prophylactic laxatives and in 49 (49%) on prophylactic laxatives (P = 0.015). Severe constipation occurred in 23 (13%) not on prophylactic laxatives and in 33 (33%) on prophylactic laxatives (P < 0.001).
- Conclusion: A large percentage of patients are not receiving prophylactic laxatives when receiving IV opioid analgesia in the hospital. Current laxative strategies are not effectively preventing constipation in patients when prescribed.
Key words: constipation; opioids; hospital medicine; patient-controlled analgesia; laxatives.
Opioid-induced constipation (OIC) is defined as a change, when initiating opioid therapy, from baseline bowel habits and defecation patterns that is characterized by any of the following: reduced bowel frequency; development or worsening of straining; a sense of incomplete evacuation; or a patient’s perception of distress related to bowel habits [1]. It is an important side effect to consider when initiating narcotic analgesia. It has been estimated that approximately 3% to 4% of the population is on chronic narcotic pain relievers in the outpatient setting [2,3], and 37% to 81% of these patients will experience constipation [3–9]. Because of the high incidence of constipation, the prophylactic prescription of laxatives with initiation of opioid pain relievers is frequently recommended [10–15]. Furthermore, it has been shown that among patients admitted to the hospital with cancer, there is a lower incidence of constipation amongst those who have received prophylactic laxatives [16]. However, there is no evidence in the literature that prophylactic laxatives improve outcomes in patients on opioid analgesia in the general medicine inpatient setting. Furthermore, studies have illustrated that recommendations for prophylactic laxative use are not reliably followed [3,9].
While the incidence of OIC is well described in the outpatient setting [17,18], there are few studies looking at the incidence of OIC in the hospital setting. It has been shown, however, that occurrence during even a brief hospitalization is possible [4,6]. Acute constipation while hospitalized can theoretically lead to longer hospitalizations, increased pain, and decreased quality of life [6,7,19]. Recent research has focused heavily on the use of novel agents such as peripherally acting mu-opioid receptor antagonists in the treatment of OIC [20–23]. However, the expense of these agents makes them less than ideal in the prophylactic setting. This study will assess the effectiveness and prescribing patterns of prophylactic laxatives in the inpatient general medicine setting over a 2-year period at our institution in patients initiated on patient-controlled analgesia with hydromorphone, morphine, or fentanyl.
Methods
This study was approved by the institutional review board at the Mayo Clinic Rochester. All patients who were initiated on intravenous analgesia with an electronic patient-controlled opioid pump (PCA) while admitted to a general medicine service in 2011 and 2012 were identified. Patients who received PCA therapy were identified through a pharmacy database. Only patients older than 18 years of age were included in the study. PCA therapy was selected for our analysis because PCA therapy is not regularly administered on an outpatient basis. All of these patients, therefore, had a change in their narcotic regimen on admission to the hospital. Patients were excluded from the study if they were on a PCA for less than 24 hours; had a PCA initiated on a service other than a general medicine service; were on a scheduled laxative regimen prior to admission; or carried a diagnosis of bowel obstruction, chronic diarrhea, constipation, or intestinal discontinuity (eg, those with previous diversions or ostomies).
A retrospective review of each patient’s chart was conducted with the assistance of a team of nurse abstractors. Basic demographic data were recorded for each patient. Date of hospital admission and discharge; scheduled laxatives ordered and administered (any dose of sennosides, polyethylene glycol, docusate, bisacodyl, lactulose, or magnesium citrate); abdominal X-rays and abdominal CT scans performed for constipation; and any administration of enemas were recorded. Fiber supplements were not considered laxatives. If a patient was documented to have constipation during their hospitalization this was recorded. Patients were classified as having severe constipation if an abdominal CT or x-ray was performed for the indication of constipation; if abdominal distension, pain, or bloating were documented due to constipation; or if an enema was performed during the hospitalization.
For analysis purposes, patients who started receiving scheduled laxatives (as opposed to laxatives “as needed”)on or before the day of PCA initiation were classified as receiving prophylactic laxatives. Baseline patient characteristics and outcomes were compared using the chi-square test for nominal variables and the rank sum test for continuous variables. In all cases, 2-tailed tests were performed with P values ≤ 0.05 considered statistically significant. A nominal logistic regression model was utilized to assess for independent association of risk factors with the outcome of constipation.
Results
Discussion
Patients initiated on opioid therapy were not prescribed prophylactic laxatives in 64% of our cohort in the inpatient setting. When prescribed, current laxative strategies did not effectively prevent constipation with 49% experiencing OIC. Our data serves as a strong reminder of the magnitude of the problem of OIC in the inpatient setting.
The strength of our paper lies in its role as a magnitude assessment. This retrospective review reveals for that among a diverse group of patients hospitalized within a large academic institution, OIC remains prevalent. Furthermore, the high incidence of severe constipation indicates the potential for increased health care costs and patient discomfort secondary to OIC emphasizing the importance of prevention of OIC. Recent guidelines have made a push toward prophylactic laxative utilization earlier. Specifically, the European Palliative Research Collaborative offers a “strong recommendation to routinely prescribe laxatives for the management or prophylaxis of opioid-induced constipation” [10]. Additionally, the American Society of Interventional Pain Physicians suggests that “a physician should consider the initiation of a bowel regimen even before the development of constipation and definitely after the development of constipation” [11]. Our manuscript serves as a reminder that OIC remains a very prevalent problem and that prophylactic laxatives are still being underutilized.
This is a retrospective study and thus has inherent limitations. Specifically, we are limited to those cases of constipation that were documented in the medical record. The presentation of constipation is varied between patients. This variation in presentation of OIC is inherent to the disease process as is demonstrated in the broad definition for OIC [1]. The cases of constipation that we are reporting clearly were bothersome enough to warrant documentation in the medical record, and while there may have been cases that escaped documentation, we can be confident that the cases of OIC we are reporting are true cases of OIC. The numbers we report can therefore be taken to represent a minimum number of cases of constipation occurring in our study population.
It has been suggested that OIC prevalence varies with type of opioid and duration of opioid therapy [24]. We did not compare dose, type, or duration of opioid therapy in this study. This could certainly account for the seemingly higher rate of constipation within the group treated with prophylactic laxatives as compared with those not treated with prophylactic laxatives. Physicians likely have a higher propensity to prescribe prophylactic laxatives to patients receiving high doses of opioids who are in turn at higher risk for OIC. We cannot say whether differences in efficacy exist between prophylactic laxative regimens or which opioids (dose and duration) cause the most constipation based upon our data. Future studies incorporating dose, duration, and opioid type along with the variables we collected in this study could potentially construct successful logistic regression models with predictive power to identify those at highest risk of OIC.
Our rate of OIC is consistent with previously published figures [3–9]. However, we demonstrate for the first time that prophylactic laxatives are prescribed infrequently and unsuccessfully in the inpatient setting. This is consistent with prescribing rates in the outpatient setting [9,25]. Furthermore, we observed a higher rate of constipation in those treated with prophylactic laxatives compared to those that did not receive prophylactic laxatives. Pottegard et al similarly demonstrated an increased rate of constipation in those utilizing laxative therapy [25]. This is likely secondary to providers recommending prophylactic laxatives to those patients most likely to develop constipation. Despite being able to recognize high-risk patients, providers are unable to prevent OIC as little is known regarding optimal laxative strategies. Previous studies comparing treatment regimens for the relief of constipation in the palliative care population have been largely inconclusive [26]. There have been no studies to date comparing different prophylactic laxatives in the inpatient setting.
Future directions for research in this area would ideally take the form of randomized controlled trials investigating efficacy of different prophylactic laxatives in the inpatient setting. These trials would ideally include well-defined patient groups receiving specific narcotics for specific reasons. These studies would be best if powered to assess the effect of narcotic dosage and duration of therapy as well. Alternatively, larger retrospective chart reviews could be performed including narcotic dosage, type, and duration of therapy with a planned logistic regression model attempting to account for likely independent variables.
Conclusion
Our study demonstrates for the first time that prophylactic laxatives are not being prescribed frequently to patients on opioid analgesia in the inpatient general medicine setting. Additionally, while providers seem to be identifying patients at higher risk of constipation, they are still unable to prevent constipation in a high percentage of patients. Further research into this area would be beneficial to prevent this uncomfortable, costly, and preventable complication of opioid analgesia.
Corresponding author: Roger Yu, MD, Mayo Clinic, 200 First St. SW, Rochester, MN 55905, [email protected].
Funding/support: This research was supported by the Mayo Clinic Return to Work program nurses for data abstraction.
Financial disclosures: None.
1. Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology 2016.
2. Boudreau D, Von Korff M, Rutter CM, et al. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol Drug Saf 2009;18:1166–75.
3. Choung RS, Locke GR 3rd, Zinsmeister AR, et al. Opioid bowel dysfunction and narcotic bowel syndrome: a population-based study. Am J Gastroenterol 2009;104:1199–204.
4. Droney J, Ross J, Gretton S, et al. Constipation in cancer patients on morphine. Support Care Cancer 2008;16:453–9.
5. Sykes NP. The relationship between opioid use and laxative use in terminally ill cancer patients. Palliat Med 1998;12:375–82.
6. Bell TJ, Panchal SJ, Miaskowski C, et al. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European Patient Survey (PROBE 1). Pain Med 2009;10:35–42.
7. Cook SF, Lanza L, Zhou X, et al. Gastrointestinal side effects in chronic opioid users: results from a population-based survey. Aliment Pharmacol Ther 2008;27:1224–32.
8. Moore RA, McQuay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomised trials of oral opioids. Arthritis Res Ther 2005:7:R1046–51.
9. Bouvy ML, Buurma H, Egberts TC. Laxative prescribing in relation to opioid use and the influence of pharmacy-based intervention. J Clin Pharm Ther 2002;27:107–10.
10. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol 2012:13:e58–68.
11. Manchikanti L, Abdi S, Atluri S, et al. American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: Part 2--guidance. Pain Physician 2012;15(3 Suppl):S67–116.
12. Cameron JC. Constipation related to narcotic therapy. A protocol for nurses and patients. Cancer Nurs 1992;15:372–7.
13. Levy MH. Pharmacologic treatment of cancer pain. N Engl J Med 1996;335:1124–32.
14. Swegle JM, Logemann D. Management of common opioid-induced adverse effects. Am Fam Physician 2006;74:1347–54.
15. Donnelly S, Davis MP, Walsh D, Naughton M. Morphine in cancer pain management: a practical guide. Support Care Cancer 2002;10:13–35.
16. Ishihara M, Ikesue H Matsunaga H, et al. A multi-institutional study analyzing effect of prophylactic medication for prevention of opioid-induced gastrointestinal dysfunction. Clin J Pain 2012;28:373–81.
17. Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain 2004;112:372–80.
18. Tuteja AK, Biskupiak J, Stoddard GJ, Lipman AG. Opioid-induced bowel disorders and narcotic bowel syndrome in patients with chronic non-cancer pain. Neurogastroenterol Motil 2010; 22:424–30, e96.
19. Brock C, Olesen SS, Olesen AE, et al. Opioid-induced bowel dysfunction: pathophysiology and management. Drugs 2012;72:1847–65.
20. Camilleri M. Opioid-induced constipation: challenges and therapeutic opportunities. Am J Gastroenterol 2011;106:835–42.
21. Candy B, Jones L, Goodman ML, et al. Laxatives or methylnaltrexone for the management of constipation in palliative care patients. Cochrane Database Syst Rev 2011(1):CD003448.
22. Ford AC, Brenner DM, Schoenfeld PS. Efficacy of pharmacological therapies for the treatment of opioid-induced constipation: systematic review and meta-analysis. Am J Gastroenterol 2013;108:1566–74.
23. Jansen JP, Lorch D, Langan J, et al. A randomized, placebo-controlled phase 3 trial (Study SB-767905/012) of alvimopan for opioid-induced bowel dysfunction in patients with non-cancer pain. J Pain 2011;12:185–93.
24. Camilleri M, Drossman DA, Becker G, et al. Emerging treatments in neurogastroenterology: a multidisciplinary working group consensus statement on opioid-induced constipation. Neurogastroenterol Motil 2014;26:1386–95.
25. Pottegard A, Knudsen TB, van Heesch K, et al. Information on risk of constipation for Danish users of opioids, and their laxative use. Int J Clin Pharm 2014;36:291–4.
26. Candy B, Jones L, Larkin PJ, et al. Laxatives for the management of constipation in people receiving palliative care. Cochrane Database Syst Rev 2015(5):CD003448.
1. Mearin F, Lacy BE, Chang L, et al. Bowel disorders. Gastroenterology 2016.
2. Boudreau D, Von Korff M, Rutter CM, et al. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol Drug Saf 2009;18:1166–75.
3. Choung RS, Locke GR 3rd, Zinsmeister AR, et al. Opioid bowel dysfunction and narcotic bowel syndrome: a population-based study. Am J Gastroenterol 2009;104:1199–204.
4. Droney J, Ross J, Gretton S, et al. Constipation in cancer patients on morphine. Support Care Cancer 2008;16:453–9.
5. Sykes NP. The relationship between opioid use and laxative use in terminally ill cancer patients. Palliat Med 1998;12:375–82.
6. Bell TJ, Panchal SJ, Miaskowski C, et al. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European Patient Survey (PROBE 1). Pain Med 2009;10:35–42.
7. Cook SF, Lanza L, Zhou X, et al. Gastrointestinal side effects in chronic opioid users: results from a population-based survey. Aliment Pharmacol Ther 2008;27:1224–32.
8. Moore RA, McQuay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomised trials of oral opioids. Arthritis Res Ther 2005:7:R1046–51.
9. Bouvy ML, Buurma H, Egberts TC. Laxative prescribing in relation to opioid use and the influence of pharmacy-based intervention. J Clin Pharm Ther 2002;27:107–10.
10. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol 2012:13:e58–68.
11. Manchikanti L, Abdi S, Atluri S, et al. American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: Part 2--guidance. Pain Physician 2012;15(3 Suppl):S67–116.
12. Cameron JC. Constipation related to narcotic therapy. A protocol for nurses and patients. Cancer Nurs 1992;15:372–7.
13. Levy MH. Pharmacologic treatment of cancer pain. N Engl J Med 1996;335:1124–32.
14. Swegle JM, Logemann D. Management of common opioid-induced adverse effects. Am Fam Physician 2006;74:1347–54.
15. Donnelly S, Davis MP, Walsh D, Naughton M. Morphine in cancer pain management: a practical guide. Support Care Cancer 2002;10:13–35.
16. Ishihara M, Ikesue H Matsunaga H, et al. A multi-institutional study analyzing effect of prophylactic medication for prevention of opioid-induced gastrointestinal dysfunction. Clin J Pain 2012;28:373–81.
17. Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain 2004;112:372–80.
18. Tuteja AK, Biskupiak J, Stoddard GJ, Lipman AG. Opioid-induced bowel disorders and narcotic bowel syndrome in patients with chronic non-cancer pain. Neurogastroenterol Motil 2010; 22:424–30, e96.
19. Brock C, Olesen SS, Olesen AE, et al. Opioid-induced bowel dysfunction: pathophysiology and management. Drugs 2012;72:1847–65.
20. Camilleri M. Opioid-induced constipation: challenges and therapeutic opportunities. Am J Gastroenterol 2011;106:835–42.
21. Candy B, Jones L, Goodman ML, et al. Laxatives or methylnaltrexone for the management of constipation in palliative care patients. Cochrane Database Syst Rev 2011(1):CD003448.
22. Ford AC, Brenner DM, Schoenfeld PS. Efficacy of pharmacological therapies for the treatment of opioid-induced constipation: systematic review and meta-analysis. Am J Gastroenterol 2013;108:1566–74.
23. Jansen JP, Lorch D, Langan J, et al. A randomized, placebo-controlled phase 3 trial (Study SB-767905/012) of alvimopan for opioid-induced bowel dysfunction in patients with non-cancer pain. J Pain 2011;12:185–93.
24. Camilleri M, Drossman DA, Becker G, et al. Emerging treatments in neurogastroenterology: a multidisciplinary working group consensus statement on opioid-induced constipation. Neurogastroenterol Motil 2014;26:1386–95.
25. Pottegard A, Knudsen TB, van Heesch K, et al. Information on risk of constipation for Danish users of opioids, and their laxative use. Int J Clin Pharm 2014;36:291–4.
26. Candy B, Jones L, Larkin PJ, et al. Laxatives for the management of constipation in people receiving palliative care. Cochrane Database Syst Rev 2015(5):CD003448.
Preventing Wrong-Patient Electronic Orders in the Emergency Department
From SBH Health System, Bronx, NY.
Abstract
- Objective: To decrease the number of near-miss wrong-patient orders in a computerized physician order entry (CPOE) system.
- Methods: A CPOE alert was built that prompted the ordering clinician to reaffirm the identity of the patient by entering the patient’s initials and year of birth prior to placing an order. We used a retract and reorder tool to measure the frequency of near-miss wrong-patient order errors before and after implementation of the alert.
- Results: The ID reentry function decreased near-miss wrong-patient orders in the ED by 35% during the 8-week pilot period. The system was also successful in helping to decrease the percentage of all CPOE near-miss events by 49%.
- Conclusion: An alert that requires the prescriber to enter the patient’s initials and birth year is effective in decreasing wrong-patient orders in the CPOE system.
Key words: CPOE, near miss, patient safety, medical errors, wrong-patient errors.
Computerized provider order entry (CPOE) systems are commonly used to place orders. CPOE has been shown to reduce errors [1–4]. However, medication errors also can be caused or exacerbated by the CPOE system [5–7]. One type of error that can occur is placing orders on the wrong patient [8]. Wrong-patient CPOE errors can lead to significant morbidity and mortality [8–11]. To reduce wrong-patient CPOE errors in our health system, we developed an alert that required the ordering clinician to verify the identity of the patient. In this paper, we describe our project and outcomes attained.
Methods
Setting
SBH Health System is a not for profit health system located in Bronx, New York. The SBH Health System also has academic affiliations, and AOA and ACGME residency and fellowship programs. St. Barnabas Hospital, SBH Health System’s acute care facility, is a safety net hospital, Level 1 trauma center, primary stroke center, and STEMI receiving center. St. Barnabas Hospital has 422 licensed beds and had a total of 91,476 emergency department visits in 2015. The electronic health record in use at the time of the project was Allscripts 6.1. The Allscripts product, including its CPOE functions, has been in use in the SBH emergency department (ED) since 2011.
Review of Current Process
A team of multidisciplinary stakeholders was assembled comprised of hospital senior leadership, ED leadership, and front-line staff. Representatives from all disciplines involved in the CPOE process were invited, including nursing, pharmacy, radiology, clinical laboratory, and information technology.
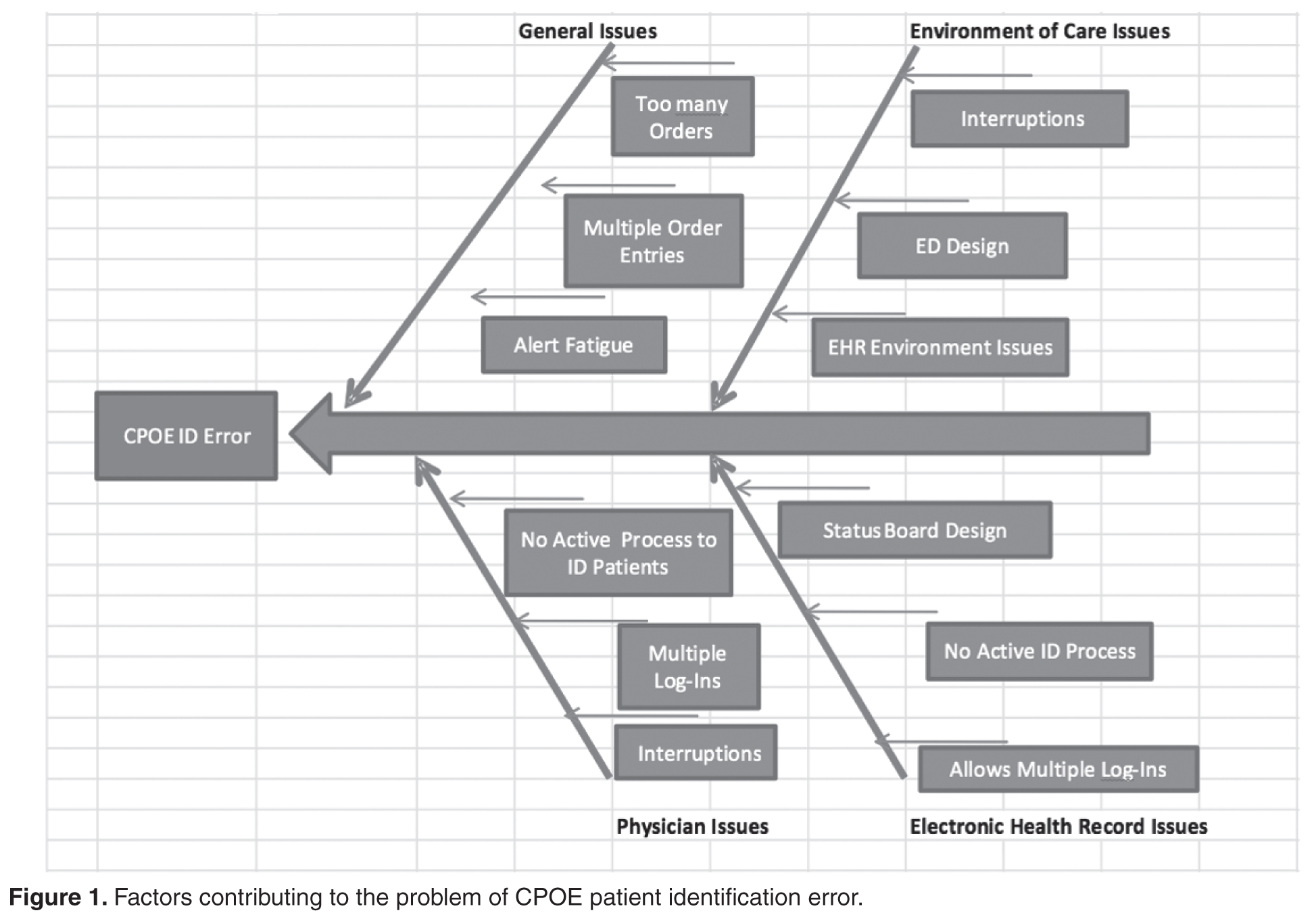
Next, we assessed our current error rate using a “retract and reorder” tool, which flags orders that have been placed for one patient, then erased and added to another patient’s file by the same clinician within a 10-minute time frame [8]. This tool, developed by Adelman et al, picks up near-miss errors, self-caught by the provider before causing harm [8]. Safety research has demonstrated that near-miss errors share the same causal pathway; therefore, measuring and preventing near-miss wrong-patient errors should reduce related errors that reach the patient.
For the period October–December 2014, we tabulated 231 near-miss wrong-patient orders that occured throughout the health system, of which 37% occurred in the ED. This translated to about 1 near-miss event per day in the ED. Given this data, the ED was the location for our quality improvement project.
Intervention
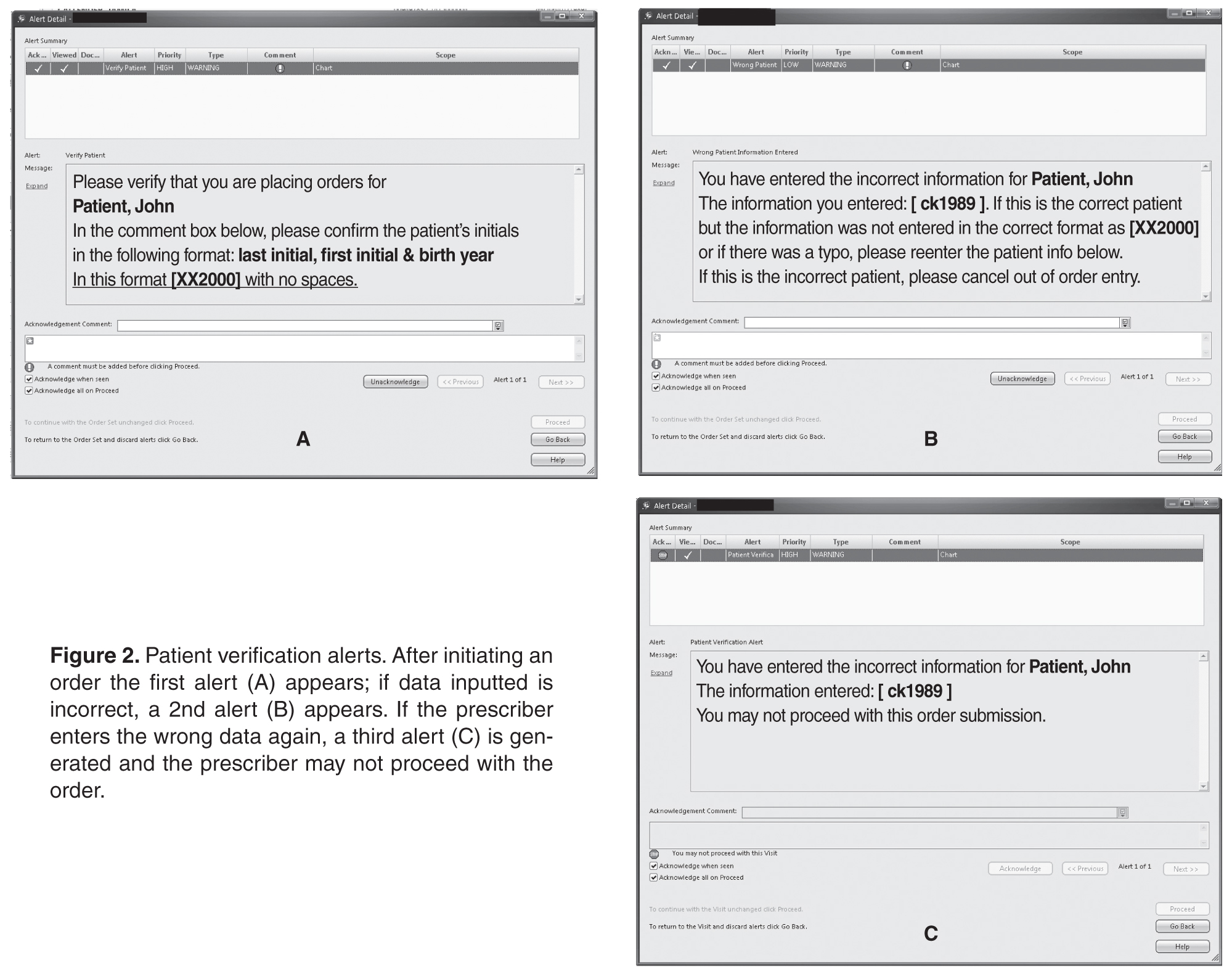
Outcomes
After a beta testing period of 1 week, the system was implemented on 3 November 2015. To assess the effectiveness of the alert system to prevent ordering errors, we used the retract and reorder tool to measure the rate of wrong-patient order entries for the 8-week period November–December 2015 and compared this with the preimplementation rate. Prior to the intervention, the average number of wrong patient order entries in the ED was 6.125 events per week. After implementation, the average number decreased to 4 events per week, a 35% decrease, and the proportion of near-miss ID errors in the ED relative to all such errors within the health system decreased from 37% to 19%.
Discussion
The original aim of the project was to decrease “wrong patient, right order” near-miss events by 30% in 3 months in the ED using an order-based patient ID reentry function. The goal was rapid improvement using a hard-wired EHR process, which is why a 3-month time frame was chosen. During our 8-week project, we surpassed this goal, documenting a 35% decrease in near-miss wrong-patient orders in the ED. This rate was similar to that achieved by Adelman et al [8] and Green et al [10]. Adelman et al found a 41% error reduction, while Green et al found a short-term 30% reduction in CPOE wrong-patient orders utilizing a 2.5-second mandatory delay before continuing the order entry for the purposes of patient verification.
Resident and attending staff conveyed to us anecdotally during both beta testing and implementation that the ID reentry function made them aware of incorrect patient selection even before entering the required initials and birth year. They then cancelled the order session on the wrong patient and chose the correct patient. This is consistent with the findings of Green’s study, which noted that ED practitioners backed out of appropriately 1 in 200 order entry sessions due to wrong patient selection [10].
We also assessed the additional time added to each order entry session. Initially, using observational data, the CPOE ID reentry function added 6.2 seconds to each order entry session. However, providers that were more familiar with the system took an average of 4.0 seconds. While this added time per order entry session does not seem like much of an issue or delay, in a busy 12-hour shift in the ED it could be seen as significant. Adelman reported 6.6 seconds additional time required in for the ID reentry function used in his study [8], while Green’s study was designed using a 2.5-second mandatory delay before users could close the verification dialogue box [10].
The biggest challenges in implementing our project were unforeseen IT issues. The “go-live” date for ICD-10 was the same as the date we were to start the ID reentry requirement. IT personnel were needed to help in the EHR ICD-10 development and support, which delayed our start date. Additionally, other IT issues were identified. For example, the initial implementation of this project was to begin in the ED involving active ED patients only. At the project’s onset, the ID reentry function erroneously became active in all hospital locations. To fix this error, the entire double ID system alert, including the ED location, had to be removed and adjusted.
In addition to the above challenges, the team discovered errors that needed to be addressed during beta testing. For example, some clinicians would enter an order but no alert asking for the identifying data appeared. The order was entered and completed without the use of the double ID. Once discovered, IT was able to identify and correct the error. Beta testing also revealed an error in the system where providers who incorrectly identified a patient were “locking-out” of the CPOE system for that particular patient during the patient’s entire encounter. This issue was also quickly identified and resolved.
Despite the effectiveness of this system in reducing the rate of near-miss wrong-patient orders in the ED, errors still occur. It is possible that providers are entering the patient’s initials and year of birth without carefully verifying the patient’s identity [9].The CPOE double ID system alert is about three-quarters the size of the monitor screen. Thus, the clinician is able to verify the patient’s initials and year of birth using the patient’s header on the screen behind the patient identification alert. If the provider simply types the initials and year of birth on the patient’s header, then an identification error can occur.
More work is needed to decrease CPOE-related patient identification errors. Possible improvements may include single sign-ons and a no-interruption policy when writing orders. During our investigation, it was found that some clinicians would have multiple EHR sign-on sessions open at one computer terminal. These multiple EHR sign-on sessions were sometimes the root cause of a wrong patient error. With multiple sign-on sessions open, clinicians could toggle back and forth between patients on the same computer terminal and mistakenly complete an order on the wrong patient.
No-interruption zones and policies have been proven to be an effective way of decreasing interruptions and enhancing safety during medication preparation [13,14]. Utilization of no-interruption zones for CPOE may also be effective. Potentially, the EHR background color could change when a clinician selects the “enter order” tab within the EHR. The new background color would signify to those around the clinician that he/she is not to be interrupted during that time.
After the success of this initial quality improvement project in the ED, the intensive care unit has been added as a location for the CPOE double identification system. The data and results for this phase of the project are being tabulated and seem promising. In addition, SBH Health System is exploring single sign-on software to both help clinicians provide service and enhance patient safety.
Corresponding author: Daniel Lombardi, DO, 4422 Third Ave., Bronx, NY 10457.
Financial disclosures: None.
1. Bates, DW, Leape L, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA 1998;280:1311–16.
2. Bates, DW, Teich JM, Lee J, et al. The impact of computerized physician order entry on medication error prevention. J Am Med Inform Assoc 1999;6:313–21.
3. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med 2003;163:1409–16.
4. Reckmann, MH, Westbrook JI, Koh Y, et al. Does computeized provider order entry reduce prescribing errors for hospital inpatients? A systematic review. J Am Med Inform Assoc 2009;16:613–23.
5. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA 2005;293:1197–203.
6. Broder C. Study: CPOE can increase risk of medication errors. Health IT News. March 9, 2005.
7. Schiff GD, Amato MG, Eguale T, et al. Computerised physician order entry-related medication errors: analysis of reported errors and vulnerability testing of current systems. BMJ Qual Saf 2015;24:264–71.
8. Adelman, JS, Kalkut GE, Schechter CB, et al. Understanding and preventing wrong-patient electronic orders: a randomized controlled trial. JAM Med Inform Assoc 2013;20:305–10.
9. Yang A, Grissinger M. Pennsylvania Patient Safety Authority. Wrong-patient medication errors: an analysis of event reports in Pennsylvania and strategies for prevention. PA Patient Saf Advis 2013 June;10:41–9.
10. Green RA, Hripcsak G, Salmasian H, et al. Intercepting wrong-patient orders in a computerized provider order entry system. Ann Emerg Med 2015;65:679–86.
11. Institute for Safe Medication Practices. Oops, sorry, wrong patient! A patient verification process is needed everywhere, not just at the bedside. 10 Mar 2011. Accessed at www.ismp.org/Newsletters/acutecare/articles/20110310.asp.
12. Anthony K, Wiencek C, Bauer C, et al. No interruptions please: impact of a No Interruption Zone on medication safety in intensive care units. Crit Care Nurse 2010;30:21–9.
13. Institute for Safe Medication Practices. Side tracks on the safety express. interruptions lead to errors and unfinished…wait, what was i doing? 29 Nov 2012. Accessed at www.ismp.org/Newsletters/acutecare/showarticle.aspx?id=37.
From SBH Health System, Bronx, NY.
Abstract
- Objective: To decrease the number of near-miss wrong-patient orders in a computerized physician order entry (CPOE) system.
- Methods: A CPOE alert was built that prompted the ordering clinician to reaffirm the identity of the patient by entering the patient’s initials and year of birth prior to placing an order. We used a retract and reorder tool to measure the frequency of near-miss wrong-patient order errors before and after implementation of the alert.
- Results: The ID reentry function decreased near-miss wrong-patient orders in the ED by 35% during the 8-week pilot period. The system was also successful in helping to decrease the percentage of all CPOE near-miss events by 49%.
- Conclusion: An alert that requires the prescriber to enter the patient’s initials and birth year is effective in decreasing wrong-patient orders in the CPOE system.
Key words: CPOE, near miss, patient safety, medical errors, wrong-patient errors.
Computerized provider order entry (CPOE) systems are commonly used to place orders. CPOE has been shown to reduce errors [1–4]. However, medication errors also can be caused or exacerbated by the CPOE system [5–7]. One type of error that can occur is placing orders on the wrong patient [8]. Wrong-patient CPOE errors can lead to significant morbidity and mortality [8–11]. To reduce wrong-patient CPOE errors in our health system, we developed an alert that required the ordering clinician to verify the identity of the patient. In this paper, we describe our project and outcomes attained.
Methods
Setting
SBH Health System is a not for profit health system located in Bronx, New York. The SBH Health System also has academic affiliations, and AOA and ACGME residency and fellowship programs. St. Barnabas Hospital, SBH Health System’s acute care facility, is a safety net hospital, Level 1 trauma center, primary stroke center, and STEMI receiving center. St. Barnabas Hospital has 422 licensed beds and had a total of 91,476 emergency department visits in 2015. The electronic health record in use at the time of the project was Allscripts 6.1. The Allscripts product, including its CPOE functions, has been in use in the SBH emergency department (ED) since 2011.
Review of Current Process
A team of multidisciplinary stakeholders was assembled comprised of hospital senior leadership, ED leadership, and front-line staff. Representatives from all disciplines involved in the CPOE process were invited, including nursing, pharmacy, radiology, clinical laboratory, and information technology.
Next, we assessed our current error rate using a “retract and reorder” tool, which flags orders that have been placed for one patient, then erased and added to another patient’s file by the same clinician within a 10-minute time frame [8]. This tool, developed by Adelman et al, picks up near-miss errors, self-caught by the provider before causing harm [8]. Safety research has demonstrated that near-miss errors share the same causal pathway; therefore, measuring and preventing near-miss wrong-patient errors should reduce related errors that reach the patient.
For the period October–December 2014, we tabulated 231 near-miss wrong-patient orders that occured throughout the health system, of which 37% occurred in the ED. This translated to about 1 near-miss event per day in the ED. Given this data, the ED was the location for our quality improvement project.
Intervention
Outcomes
After a beta testing period of 1 week, the system was implemented on 3 November 2015. To assess the effectiveness of the alert system to prevent ordering errors, we used the retract and reorder tool to measure the rate of wrong-patient order entries for the 8-week period November–December 2015 and compared this with the preimplementation rate. Prior to the intervention, the average number of wrong patient order entries in the ED was 6.125 events per week. After implementation, the average number decreased to 4 events per week, a 35% decrease, and the proportion of near-miss ID errors in the ED relative to all such errors within the health system decreased from 37% to 19%.
Discussion
The original aim of the project was to decrease “wrong patient, right order” near-miss events by 30% in 3 months in the ED using an order-based patient ID reentry function. The goal was rapid improvement using a hard-wired EHR process, which is why a 3-month time frame was chosen. During our 8-week project, we surpassed this goal, documenting a 35% decrease in near-miss wrong-patient orders in the ED. This rate was similar to that achieved by Adelman et al [8] and Green et al [10]. Adelman et al found a 41% error reduction, while Green et al found a short-term 30% reduction in CPOE wrong-patient orders utilizing a 2.5-second mandatory delay before continuing the order entry for the purposes of patient verification.
Resident and attending staff conveyed to us anecdotally during both beta testing and implementation that the ID reentry function made them aware of incorrect patient selection even before entering the required initials and birth year. They then cancelled the order session on the wrong patient and chose the correct patient. This is consistent with the findings of Green’s study, which noted that ED practitioners backed out of appropriately 1 in 200 order entry sessions due to wrong patient selection [10].
We also assessed the additional time added to each order entry session. Initially, using observational data, the CPOE ID reentry function added 6.2 seconds to each order entry session. However, providers that were more familiar with the system took an average of 4.0 seconds. While this added time per order entry session does not seem like much of an issue or delay, in a busy 12-hour shift in the ED it could be seen as significant. Adelman reported 6.6 seconds additional time required in for the ID reentry function used in his study [8], while Green’s study was designed using a 2.5-second mandatory delay before users could close the verification dialogue box [10].
The biggest challenges in implementing our project were unforeseen IT issues. The “go-live” date for ICD-10 was the same as the date we were to start the ID reentry requirement. IT personnel were needed to help in the EHR ICD-10 development and support, which delayed our start date. Additionally, other IT issues were identified. For example, the initial implementation of this project was to begin in the ED involving active ED patients only. At the project’s onset, the ID reentry function erroneously became active in all hospital locations. To fix this error, the entire double ID system alert, including the ED location, had to be removed and adjusted.
In addition to the above challenges, the team discovered errors that needed to be addressed during beta testing. For example, some clinicians would enter an order but no alert asking for the identifying data appeared. The order was entered and completed without the use of the double ID. Once discovered, IT was able to identify and correct the error. Beta testing also revealed an error in the system where providers who incorrectly identified a patient were “locking-out” of the CPOE system for that particular patient during the patient’s entire encounter. This issue was also quickly identified and resolved.
Despite the effectiveness of this system in reducing the rate of near-miss wrong-patient orders in the ED, errors still occur. It is possible that providers are entering the patient’s initials and year of birth without carefully verifying the patient’s identity [9].The CPOE double ID system alert is about three-quarters the size of the monitor screen. Thus, the clinician is able to verify the patient’s initials and year of birth using the patient’s header on the screen behind the patient identification alert. If the provider simply types the initials and year of birth on the patient’s header, then an identification error can occur.
More work is needed to decrease CPOE-related patient identification errors. Possible improvements may include single sign-ons and a no-interruption policy when writing orders. During our investigation, it was found that some clinicians would have multiple EHR sign-on sessions open at one computer terminal. These multiple EHR sign-on sessions were sometimes the root cause of a wrong patient error. With multiple sign-on sessions open, clinicians could toggle back and forth between patients on the same computer terminal and mistakenly complete an order on the wrong patient.
No-interruption zones and policies have been proven to be an effective way of decreasing interruptions and enhancing safety during medication preparation [13,14]. Utilization of no-interruption zones for CPOE may also be effective. Potentially, the EHR background color could change when a clinician selects the “enter order” tab within the EHR. The new background color would signify to those around the clinician that he/she is not to be interrupted during that time.
After the success of this initial quality improvement project in the ED, the intensive care unit has been added as a location for the CPOE double identification system. The data and results for this phase of the project are being tabulated and seem promising. In addition, SBH Health System is exploring single sign-on software to both help clinicians provide service and enhance patient safety.
Corresponding author: Daniel Lombardi, DO, 4422 Third Ave., Bronx, NY 10457.
Financial disclosures: None.
From SBH Health System, Bronx, NY.
Abstract
- Objective: To decrease the number of near-miss wrong-patient orders in a computerized physician order entry (CPOE) system.
- Methods: A CPOE alert was built that prompted the ordering clinician to reaffirm the identity of the patient by entering the patient’s initials and year of birth prior to placing an order. We used a retract and reorder tool to measure the frequency of near-miss wrong-patient order errors before and after implementation of the alert.
- Results: The ID reentry function decreased near-miss wrong-patient orders in the ED by 35% during the 8-week pilot period. The system was also successful in helping to decrease the percentage of all CPOE near-miss events by 49%.
- Conclusion: An alert that requires the prescriber to enter the patient’s initials and birth year is effective in decreasing wrong-patient orders in the CPOE system.
Key words: CPOE, near miss, patient safety, medical errors, wrong-patient errors.
Computerized provider order entry (CPOE) systems are commonly used to place orders. CPOE has been shown to reduce errors [1–4]. However, medication errors also can be caused or exacerbated by the CPOE system [5–7]. One type of error that can occur is placing orders on the wrong patient [8]. Wrong-patient CPOE errors can lead to significant morbidity and mortality [8–11]. To reduce wrong-patient CPOE errors in our health system, we developed an alert that required the ordering clinician to verify the identity of the patient. In this paper, we describe our project and outcomes attained.
Methods
Setting
SBH Health System is a not for profit health system located in Bronx, New York. The SBH Health System also has academic affiliations, and AOA and ACGME residency and fellowship programs. St. Barnabas Hospital, SBH Health System’s acute care facility, is a safety net hospital, Level 1 trauma center, primary stroke center, and STEMI receiving center. St. Barnabas Hospital has 422 licensed beds and had a total of 91,476 emergency department visits in 2015. The electronic health record in use at the time of the project was Allscripts 6.1. The Allscripts product, including its CPOE functions, has been in use in the SBH emergency department (ED) since 2011.
Review of Current Process
A team of multidisciplinary stakeholders was assembled comprised of hospital senior leadership, ED leadership, and front-line staff. Representatives from all disciplines involved in the CPOE process were invited, including nursing, pharmacy, radiology, clinical laboratory, and information technology.
Next, we assessed our current error rate using a “retract and reorder” tool, which flags orders that have been placed for one patient, then erased and added to another patient’s file by the same clinician within a 10-minute time frame [8]. This tool, developed by Adelman et al, picks up near-miss errors, self-caught by the provider before causing harm [8]. Safety research has demonstrated that near-miss errors share the same causal pathway; therefore, measuring and preventing near-miss wrong-patient errors should reduce related errors that reach the patient.
For the period October–December 2014, we tabulated 231 near-miss wrong-patient orders that occured throughout the health system, of which 37% occurred in the ED. This translated to about 1 near-miss event per day in the ED. Given this data, the ED was the location for our quality improvement project.
Intervention
Outcomes
After a beta testing period of 1 week, the system was implemented on 3 November 2015. To assess the effectiveness of the alert system to prevent ordering errors, we used the retract and reorder tool to measure the rate of wrong-patient order entries for the 8-week period November–December 2015 and compared this with the preimplementation rate. Prior to the intervention, the average number of wrong patient order entries in the ED was 6.125 events per week. After implementation, the average number decreased to 4 events per week, a 35% decrease, and the proportion of near-miss ID errors in the ED relative to all such errors within the health system decreased from 37% to 19%.
Discussion
The original aim of the project was to decrease “wrong patient, right order” near-miss events by 30% in 3 months in the ED using an order-based patient ID reentry function. The goal was rapid improvement using a hard-wired EHR process, which is why a 3-month time frame was chosen. During our 8-week project, we surpassed this goal, documenting a 35% decrease in near-miss wrong-patient orders in the ED. This rate was similar to that achieved by Adelman et al [8] and Green et al [10]. Adelman et al found a 41% error reduction, while Green et al found a short-term 30% reduction in CPOE wrong-patient orders utilizing a 2.5-second mandatory delay before continuing the order entry for the purposes of patient verification.
Resident and attending staff conveyed to us anecdotally during both beta testing and implementation that the ID reentry function made them aware of incorrect patient selection even before entering the required initials and birth year. They then cancelled the order session on the wrong patient and chose the correct patient. This is consistent with the findings of Green’s study, which noted that ED practitioners backed out of appropriately 1 in 200 order entry sessions due to wrong patient selection [10].
We also assessed the additional time added to each order entry session. Initially, using observational data, the CPOE ID reentry function added 6.2 seconds to each order entry session. However, providers that were more familiar with the system took an average of 4.0 seconds. While this added time per order entry session does not seem like much of an issue or delay, in a busy 12-hour shift in the ED it could be seen as significant. Adelman reported 6.6 seconds additional time required in for the ID reentry function used in his study [8], while Green’s study was designed using a 2.5-second mandatory delay before users could close the verification dialogue box [10].
The biggest challenges in implementing our project were unforeseen IT issues. The “go-live” date for ICD-10 was the same as the date we were to start the ID reentry requirement. IT personnel were needed to help in the EHR ICD-10 development and support, which delayed our start date. Additionally, other IT issues were identified. For example, the initial implementation of this project was to begin in the ED involving active ED patients only. At the project’s onset, the ID reentry function erroneously became active in all hospital locations. To fix this error, the entire double ID system alert, including the ED location, had to be removed and adjusted.
In addition to the above challenges, the team discovered errors that needed to be addressed during beta testing. For example, some clinicians would enter an order but no alert asking for the identifying data appeared. The order was entered and completed without the use of the double ID. Once discovered, IT was able to identify and correct the error. Beta testing also revealed an error in the system where providers who incorrectly identified a patient were “locking-out” of the CPOE system for that particular patient during the patient’s entire encounter. This issue was also quickly identified and resolved.
Despite the effectiveness of this system in reducing the rate of near-miss wrong-patient orders in the ED, errors still occur. It is possible that providers are entering the patient’s initials and year of birth without carefully verifying the patient’s identity [9].The CPOE double ID system alert is about three-quarters the size of the monitor screen. Thus, the clinician is able to verify the patient’s initials and year of birth using the patient’s header on the screen behind the patient identification alert. If the provider simply types the initials and year of birth on the patient’s header, then an identification error can occur.
More work is needed to decrease CPOE-related patient identification errors. Possible improvements may include single sign-ons and a no-interruption policy when writing orders. During our investigation, it was found that some clinicians would have multiple EHR sign-on sessions open at one computer terminal. These multiple EHR sign-on sessions were sometimes the root cause of a wrong patient error. With multiple sign-on sessions open, clinicians could toggle back and forth between patients on the same computer terminal and mistakenly complete an order on the wrong patient.
No-interruption zones and policies have been proven to be an effective way of decreasing interruptions and enhancing safety during medication preparation [13,14]. Utilization of no-interruption zones for CPOE may also be effective. Potentially, the EHR background color could change when a clinician selects the “enter order” tab within the EHR. The new background color would signify to those around the clinician that he/she is not to be interrupted during that time.
After the success of this initial quality improvement project in the ED, the intensive care unit has been added as a location for the CPOE double identification system. The data and results for this phase of the project are being tabulated and seem promising. In addition, SBH Health System is exploring single sign-on software to both help clinicians provide service and enhance patient safety.
Corresponding author: Daniel Lombardi, DO, 4422 Third Ave., Bronx, NY 10457.
Financial disclosures: None.
1. Bates, DW, Leape L, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA 1998;280:1311–16.
2. Bates, DW, Teich JM, Lee J, et al. The impact of computerized physician order entry on medication error prevention. J Am Med Inform Assoc 1999;6:313–21.
3. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med 2003;163:1409–16.
4. Reckmann, MH, Westbrook JI, Koh Y, et al. Does computeized provider order entry reduce prescribing errors for hospital inpatients? A systematic review. J Am Med Inform Assoc 2009;16:613–23.
5. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA 2005;293:1197–203.
6. Broder C. Study: CPOE can increase risk of medication errors. Health IT News. March 9, 2005.
7. Schiff GD, Amato MG, Eguale T, et al. Computerised physician order entry-related medication errors: analysis of reported errors and vulnerability testing of current systems. BMJ Qual Saf 2015;24:264–71.
8. Adelman, JS, Kalkut GE, Schechter CB, et al. Understanding and preventing wrong-patient electronic orders: a randomized controlled trial. JAM Med Inform Assoc 2013;20:305–10.
9. Yang A, Grissinger M. Pennsylvania Patient Safety Authority. Wrong-patient medication errors: an analysis of event reports in Pennsylvania and strategies for prevention. PA Patient Saf Advis 2013 June;10:41–9.
10. Green RA, Hripcsak G, Salmasian H, et al. Intercepting wrong-patient orders in a computerized provider order entry system. Ann Emerg Med 2015;65:679–86.
11. Institute for Safe Medication Practices. Oops, sorry, wrong patient! A patient verification process is needed everywhere, not just at the bedside. 10 Mar 2011. Accessed at www.ismp.org/Newsletters/acutecare/articles/20110310.asp.
12. Anthony K, Wiencek C, Bauer C, et al. No interruptions please: impact of a No Interruption Zone on medication safety in intensive care units. Crit Care Nurse 2010;30:21–9.
13. Institute for Safe Medication Practices. Side tracks on the safety express. interruptions lead to errors and unfinished…wait, what was i doing? 29 Nov 2012. Accessed at www.ismp.org/Newsletters/acutecare/showarticle.aspx?id=37.
1. Bates, DW, Leape L, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA 1998;280:1311–16.
2. Bates, DW, Teich JM, Lee J, et al. The impact of computerized physician order entry on medication error prevention. J Am Med Inform Assoc 1999;6:313–21.
3. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med 2003;163:1409–16.
4. Reckmann, MH, Westbrook JI, Koh Y, et al. Does computeized provider order entry reduce prescribing errors for hospital inpatients? A systematic review. J Am Med Inform Assoc 2009;16:613–23.
5. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA 2005;293:1197–203.
6. Broder C. Study: CPOE can increase risk of medication errors. Health IT News. March 9, 2005.
7. Schiff GD, Amato MG, Eguale T, et al. Computerised physician order entry-related medication errors: analysis of reported errors and vulnerability testing of current systems. BMJ Qual Saf 2015;24:264–71.
8. Adelman, JS, Kalkut GE, Schechter CB, et al. Understanding and preventing wrong-patient electronic orders: a randomized controlled trial. JAM Med Inform Assoc 2013;20:305–10.
9. Yang A, Grissinger M. Pennsylvania Patient Safety Authority. Wrong-patient medication errors: an analysis of event reports in Pennsylvania and strategies for prevention. PA Patient Saf Advis 2013 June;10:41–9.
10. Green RA, Hripcsak G, Salmasian H, et al. Intercepting wrong-patient orders in a computerized provider order entry system. Ann Emerg Med 2015;65:679–86.
11. Institute for Safe Medication Practices. Oops, sorry, wrong patient! A patient verification process is needed everywhere, not just at the bedside. 10 Mar 2011. Accessed at www.ismp.org/Newsletters/acutecare/articles/20110310.asp.
12. Anthony K, Wiencek C, Bauer C, et al. No interruptions please: impact of a No Interruption Zone on medication safety in intensive care units. Crit Care Nurse 2010;30:21–9.
13. Institute for Safe Medication Practices. Side tracks on the safety express. interruptions lead to errors and unfinished…wait, what was i doing? 29 Nov 2012. Accessed at www.ismp.org/Newsletters/acutecare/showarticle.aspx?id=37.
Supporting the Needs of Stroke Caregivers Across the Care Continuum
From the School of Nursing, University of North Carolina-Wilmington, Wilmington, NC (Dr. Lutz), and the Kaiser Foundation Rehabilitation Center, Kaiser Permanente, Vallejo, CA (Ms. Camicia).
Abstract
- Objectives: To describe issues faced by stroke family caregivers, discuss evidence-based interventions to improve caregiver outcomes, and provide recommendations for clinicians caring for stroke survivors and their family caregivers.
- Methods: Literature review.
- Results: Caregiver health is linked to the stroke survivor’s degree of functional recovery; the more severe the level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health. Inadequate caregiver preparation contributes to poorer outcomes. Caregivers describe many unmet needs including skills training; communicating with providers; resource identification and activation; finances; respite; and emotional support. Caregivers need to be assessed for gaps in preparation to provide care. Interventions are recommended that combine skill-building and psycho-educational strategies; are tailored to individual caregiver needs; are face-to-face when feasible; and include 5 to 9 sessions. Family counseling may also be indicated. Intermittent assessment of caregiving outcomes should be conducted so that changing needs can be addressed.
- Conclusions: Stroke caregiving affects the caregiver’s physical, mental, and emotional health, and these effects are sustained over time. Poorly prepared caregivers are more likely to experience negative outcomes and their needs are high during the transition from inpatient care to home. Ongoing support is also important, especially for caregivers who are caring for a stroke survivor with moderate to severe functional limitations. In order to better address unmet needs of stroke caregivers, intermittent assessments should be conducted so that interventions can be tailored to their changing needs over time.
Key words: stroke; family caregivers; care transitions; patient-centered care.
Stroke is a leading cause of major disability in the United States [1] and around the world [2]. Of the estimated 6.6 million stroke survivors living in the US, more than 4.5 million have some level of disability following stroke [1]. In 2009, more than 970,000 persons were hospitalized with stroke in the US with an average length of stay of 5.3 days [3]. Approximately 44% of stroke survivors are discharged home directly from acute care without post-acute care [4]. Only about 25% of stroke survivors receive care in inpatient rehabilitation facilities [4] even though the American Heart Association (AHA) stroke rehabilitation guidelines recommend this level of care for qualified patients [5]. Regardless of the care trajectory, when stroke survivors return home they frequently require assistance with basic and instrumental activities of daily living (BADL/IADL), usually provided by family members who often feel unprepared and overwhelmed by the demands and responsibilities of this caregiving role.
The deleterious effects of caregiving have been identified as a major public health concern [6]. A robust body of literature has established that caregivers are often adversely affected by the demands of their caregiving role. However, much of this literature focuses on caregivers for persons with dementia. Needs of stroke caregivers are categorically different from caregivers of persons with dementia in that stroke is an unpredictable, life-disrupting, crisis event that occurs suddenly leaving family members with insufficient time to prepare for the new roles and caregiving responsibilities. The patient typically transitions from being cared for by multiple providers in an acute care, inpatient rehabilitation facility, or skilled nursing facility (SNF)—24 hours a day, 7 days a week—to relying fully on one person (most often a spouse or adult child) who may not be ready to handle the overwhelming demands and constant vigilance required for adequate care at home. Studies have repeatedly demonstrated the damaging health effects of caregiving. Caregivers describe feeling isolated, abandoned, and alone [7–9], and what frequently follows is a predictable trajectory of depression and deteriorating health and well-being [7,10–13]. The purpose of this article is to describe difficulties and issues faced by family members who are caring for a loved one following stroke, discuss evidence-based interventions designed to improve stroke caregiver outcomes, and provide recommendations for clinicians who care for stroke survivors and their family caregivers post-stroke.
Difficulties and Issues Faced by Caregivers
With an aging population and increasing incidence of stroke, it is imperative that we identify and address the ongoing needs of stroke survivors and their family caregivers in the post-stroke recovery period. Multiple studies acknowledge that stroke is a life-changing event for patients and their family members [9,14] that often results in overwhelming feelings of uncertainty, fear [15], grief, and loss [9]. Stroke also can have long-term effects on the health of stroke survivors and their family caregivers. Studies have identified the effects of caregiving on the health of caregivers and subsequent links between stroke survivor and caregiver outcomes over time [12,16,17]; the ongoing needs of stroke caregivers post-discharge [18,19]; and the importance of assessing caregiver preparedness and subsequent caregiving outcomes [5,20].
Effects of Caregiving on the Health of Caregivers and Stroke Survivors
Research on stroke caregiving consistently indicates that caregiver health is inextricably linked to the stroke survivor’s degree of physical, cognitive, psychological, and emotional recovery. The more severe the patient’s level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health outcomes [21]. Studies also indicate that certain caregiver characteristics, such as being female or having lower educational level, pre-existing health conditions [7,22,23], poor family functioning, lack of social support [22,24], or lack of preparation [25], are all risk factors for poorer caregiver outcomes.
Stroke family caregivers often experience overwhelming physical and emotional strain, depressive symptoms, sleep deprivation, decline in physical and mental health, reduced quality of life, and increased isolation [7,10,11,14,26,27]. Perceived burden has been positively associated with caregiver depressive symptoms [12,14,28,29]. Depressive symptoms in caregivers, with a reported incidence of 14% [30] to 33% [31], may persist for several years post-stroke. In a study of the long-term effects of caregiving with 235 stroke caregivers when compared with non-caregivers, researchers found that caregivers had more depressive symptoms and poorer life satisfaction and mental health quality of life at 9 months post-stroke, and many of these differences continued for 3 years post-discharge [23].
Lower stroke survivor functioning and higher depressive symptoms are correlated with higher caregiver depressive symptoms and burden, and poorer coping skills and mental health [12,21]. A review of stroke caregiving literature by van Heugten et al [32] indicated that long-term caregiver functioning was influenced by stroke survivor physical and cognitive functioning and behavioral issues; caregiver psychological and emotional health; quality of family relationships; social support; and caregiver demographics. Caregivers of stroke survivors with aphasia may have more difficulties providing care, increased burden and strain, higher depressive symptoms, and other negative stroke-related outcomes [33].
Gaugler [34] conducted a systematic review of 117 studies and reported that caring for stroke survivors who were older, in poorer health, and had greater stroke severity increased the likelihood of poorer emotional and psychological family caregiver outcomes. Caregivers who had “negative problem orientation and less social support” were more likely to have depressive symptoms and poorer self-rated health at 1-year post-stroke. One of the best predictors of caregiver stress and poor health in the first year post-stroke was lack of caregiver preparation [25,34].
Research also suggests that stroke survivor outcomes are influenced by the ability of the family caregiver to provide emotional and instrumental support as well as assistance with BADL/IADL [6,35]. As the caregiver’s health decreases, the stroke survivor’s health and recovery will also likely suffer and ultimately may result in re-hospitalization or nursing home placement. For example, Perrin et al found a consistent reciprocal relationship between caregiver health and stroke survivor functioning, such that the quality of caregiving may be affected by caregiver burden and depressive symptoms, which in turn can impair the functional, psychological, and emotional recovery of the stroke survivor [21]. Studies have also linked poorer caregiver well-being to increased depressive symptoms in stroke survivors [36,37].
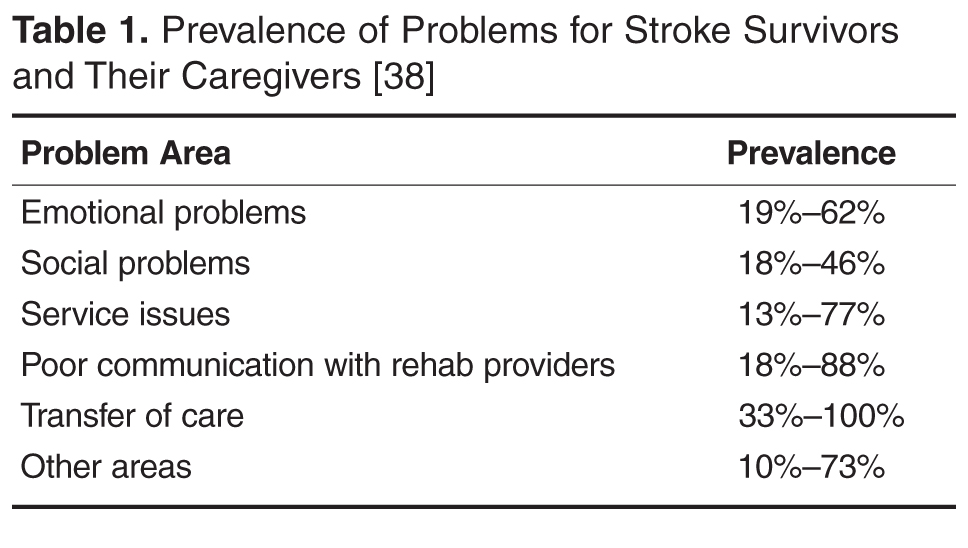
Positive effects of caregiving have also been reported, including a feeling of confidence, satisfaction in providing good quality care [30,39,40], an improved relationship with the care recipient [30,40,41], having greater life appreciation, and feeling needed and appreciated [40]. In a systematic review of 9 studies, improvements in the stroke survivor’s condition was a source of positive caregiving experiences [40]. In 2 studies, two-thirds of caregivers surveyed affirmed all survey items related to positive aspects of caregiving [30,42]. Additionally, studies have demonstrated that caregivers who engaged in emotion- and problem-focused coping strategies had positive caregiving experiences [40]. Haley et al found that by 3 years post-stroke many of the ill effects of caregiving had resolved, suggesting that some caregivers may be successful in adapting to their “new” post-stroke lives [23].
Understanding the difficulties and issues faced by caregivers throughout the trajectory, from immediately following the stroke through the transition home and, ideally, the adaptation of the caregiver to this new life, provides an opportunity for health care professionals to intervene with strategies to support this major life change.
Caregiving Trajectory and Ongoing Needs of Stroke Caregivers
Stroke survivors and their family caregivers rapidly move from intensive therapy and nursing case management while in a facility to little or no assistance following discharge. Despite case management and discharge planning services received while in an institutional setting, the transition from inpatient care to home can be a crisis point for caregivers [9]. They describe having to figure things out for themselves with little or no formal support after discharge [9,43,44], leaving them feeling overwhelmed, exhausted, and abandoned once they return home [9].
These family members rarely make an active choice to become caregivers; rather, they take on the role because they are unable to perceive or access any other suitable alternatives [8,45]. Whatever their circumstances, these devoted family members are particularly vulnerable as they transition into the caregiving role without an adequate support system for assessing and addressing their needs [7–9,46]. Without this assistance, caregivers develop their own solutions and strategies to meet the needs of the care recipient after discharge [47,48]. Unfortunately, these strategies are often ineffective and may result in safety risks for patients (eg, falls, skin breakdown, choking), and care-related injuries (eg, falls, muscle strains, bruises) and increased stress and anxiety for caregivers [48–50].
Caregivers have described unmet needs in many domains including skills training, communicating with providers, resource identification and activation, finances, respite, and emotional support [35,44,48,51,52]. Bakas et al found that in the first 6 months post-discharge, stroke caregivers had needs and concerns related to information, emotions and behaviors, physical care, instrumental care, and personal responses to caregiving [48], and that their information needs change during the course of the patient’s recovery [53]. In a study by Lutz et al [44], caregivers identified multiple areas where they felt they were unprepared to assume the caregiving role post-discharge. These included identifying and activating resources; making home and transportation modifications to improve accessibility; developing skills in providing physical care and therapies; managing medications and behavioral issues; preventing falls; coordinating care across settings; attending to other family responsibilities; and caring for themselves.
In a study of interactions between rehabilitation providers and stroke caregivers, Creasy et al [52] noted that caregivers have needs, which were often not recognized, in the following areas: information; providing emotional support for the stroke survivor and having their own emotional support needs met; being involved in treatment decisions; and being adequately prepared for discharge home. Caregivers’ interaction styles with providers, which ranged from passive to active/directing, affected their abilities to have their needs recognized and addressed. These findings highlight the importance of recognizing the caregiver’s interaction style and tailoring communication strategies accordingly.
Cameron et al [54] noted that caregiver support needs change over time, with needs being highest during the inpatient phase as they prepare for discharge home. Moreover, caregivers who are providing care for stroke survivors with more severe functional limitations need more support over a longer period of time. Recognizing the needs of stroke caregivers, the 2016 Canadian Stroke Best Practice Recommendations on Managing Transitions of Care Following Stroke includes recommendations related to assessing, educating, and supporting stroke family caregivers [55].
Assessing Caregiver Readiness and Related Outcomes
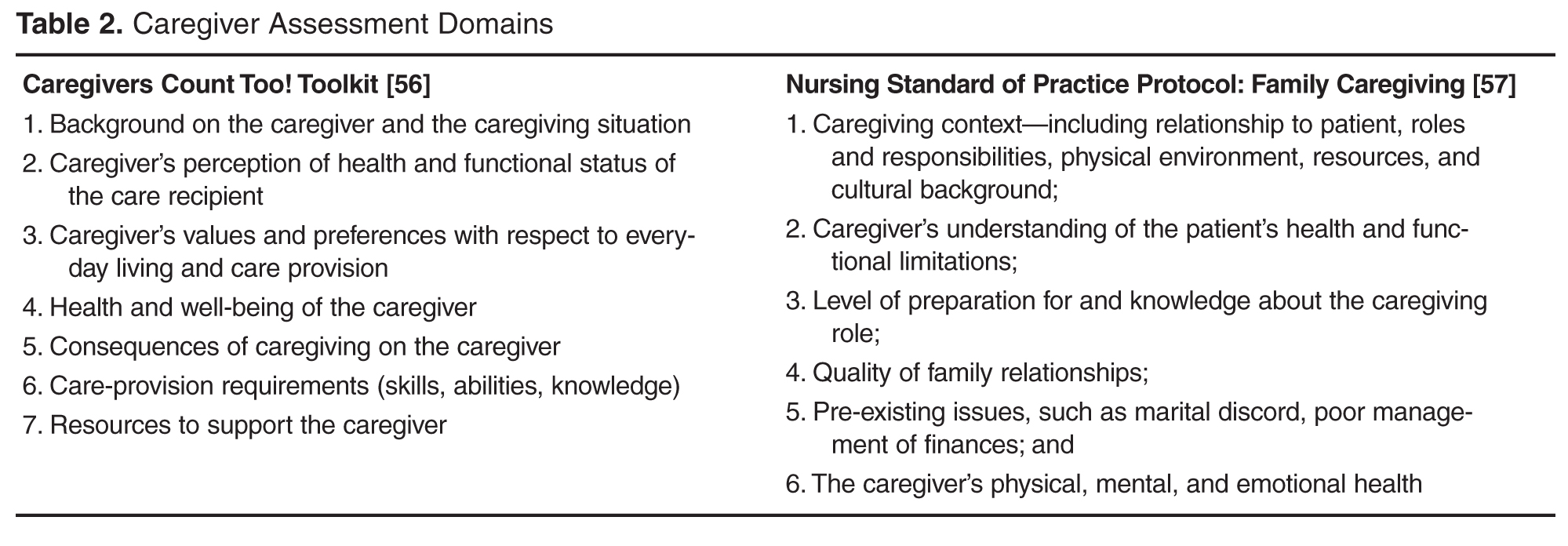
Young et al [58] recommend specific domains for a comprehensive readiness assessment of stroke family caregivers. Caregiver domains include strength of the caregiver/care recipient relationship; caregiver willingness to provide care; pre-existing health conditions, previous responsibilities, caregiving experience, home and transportation accessibility, available resources, emotional response to the stroke, and ability to sustain the caregiving role. This type of readiness assessment should be completed early in the care trajectory, while the stroke survivor is receiving inpatient care, so that care plans can be tailored to address gaps in caregiver preparation prior to discharge. It is especially important for new caregivers and those caring for stroke survivors with significant functional limitations [44]. Currently there are no tools designed to assess a family member’s readiness to assume the caregiver role.
Validated instruments have been developed to assess caregiving outcomes, including preparedness, with caregivers who have been providing care for a period of time. For example, the Mutuality and Preparedness Scales of the Family Caregiver Inventory was developed with caregivers 6 months post-discharge [59] and has been validated with stroke caregivers at 3 months post-discharge [60].
Several validated tools are available to assess the caregiver’s changing needs and the effects of care provision on well-being [8,45,61]. For example, the Caregiver Strain Index [62] has been validated in studies with stroke family caregivers [11,28]. Bakas developed 2 scales to specifically assess stroke caregivers post-discharge. The Bakas Caregiving Outcomes Scale assesses caregiver life changes [63] and the Needs and Concerns Checklist assesses post-discharge caregiver needs [48]. There are many other instruments designed to assess general caregiving outcomes, including depressive symptoms, burden, anxiety, and well-being. For a list relevant tools see Deeken et al [61] and The Selected Caregiver Assessment Measures from the Family Caregiver Alliance [64].
While these scales are helpful for assessing caregivers who are already providing care, they do not capture the gaps in caregiver readiness prior to patient discharge from the institutional setting. Taken together, these studies suggest that assessing readiness and implementing interventions to improve caregiver preparation prior to discharge and assessing and addressing their changing needs over time, from inpatient care to community reintegration, may be important strategies for improving both caregiver and stroke survivor outcomes. These strategies may also facilitate sustainability of the caregiver role over time.
Interventions to Improve Caregiver Outcomes
In a review of 39 articles representing 32 caregiver and dyad intervention studies, researchers from the AHA made 13 evidence-based recommendations. Recommendations with the highest level of evidence indicated that (1) interventions that combined skill-building with psycho-educational programs were better than psycho-educational interventions alone; (2) interventions that are tailored to the individual are preferred over “one-size-fits-all” interventions; (3) face-to-face interventions are preferred, but telephone interventions can be useful when face-to-face is not feasible; and (4) interventions with 5 to 9 sessions are recommended [65]. In a review of 18 studies, Cheng et al confirmed the recommendation that psychoeducational interventions that focused on skill building improved caregiver well-being and reduced stroke survivor heath care utilization [66].
Studies also recommend that families may need family counseling to help them develop positive coping strategies and adjust to their lives after stroke [66]. Stroke survivors and their families experience grief and loss as they begin to realize how the stroke has changed their relationships, roles, responsibilities, and future plans for their lives (eg, work, retirement). While many inpatient rehabilitation facilities may provide services from a neuro-psychologist to discuss post-stroke changes in the brain and possible behavioral and emotional manifestations, referrals for family counseling to address the impact of stroke on the family and community reintegration are seldom provided [9].
Recent interventions have shown promise in improving stroke caregiver outcomes. For example, Bakas et al. completed a randomized controlled trial of an 8-week, nurse-delivered, Telephone Assessment and Skill-Building Kit (TASK) intervention [67]. Caregivers in the intervention group with moderate to severe depressive symptoms at baseline demonstrated significant improvements in depressive symptoms and life changes at 8, 24, and 52 weeks. The TASK shows promise because it can reach caregivers in rural and urban areas at a relatively low cost [67].
Recognizing the need to improve post-acute care for stroke survivors and their family caregivers, several large funded clinical trials are being tested in the US and globally. For example, the ATTEND Trial in India is testing a home-based, caregiver-led rehabilitation intervention [68]. The Comprehensive Post-Acute Stroke Services (COMPASS) study in North Carolina, is a state-wide pragmatic, randomized controlled trial testing a comprehensive community-based patient-centered post-acute care intervention with stroke survivors and their caregivers (www.nccompass-study.org). Results of these and other studies will continue to identify evidence-based strategies to improve care coordination, quality of care, and post-stroke outcomes for stroke survivors and their caregivers
Recommendations for Clinicians
Based on this review we have identified strategies that clinicians can implement across the care continuum that may help reduce caregiver strain and burden, and improve outcomes for family caregivers and the stroke survivors for whom they provide care. The evidence suggests that caregivers need assistance in building skills, not only in providing the care needed by the stroke survivor but also in solving problems as they arise; navigating the multiple systems of care, including understanding options for post-acute care; accessing community resources; communicating effectively with health care and social support providers; and dealing with the emotional effects of stroke [44,52].
Caregivers need help in navigating the multiple providers and systems of care to get the services the stroke survivor needs as well as to secure support services. They need information from trusted sources about stroke prevention and available community resources. Providinga list of resources is often insufficient, especially in the first few weeks or months post-stroke; these caregivers are already overwhelmed with the enormity of the tasks and responsibilities that they have taken on as a caregiver. Instead they need someone who can advocate for them and connect them with the appropriate resources at the right time.
They also need assistance developing and maintaining self-care strategies so they can sustain the caregiving role long-term. Identifying opportunities for respite and helping them activate informal and formal resources, such as other family members, friends, church groups, neighbors, and services from local senior centers, independent living centers, or area agencies on aging can help them identify assistance with the breadth of duties including care of the stroke survivor, meal preparation, transportation, or a supportive listening ear. It is important for the caregiver, in addition to any other close support person as available, to have a facilitated discussion withthe healthcare team to brainstorm activities where assistance may be provided and who might be approached to help.
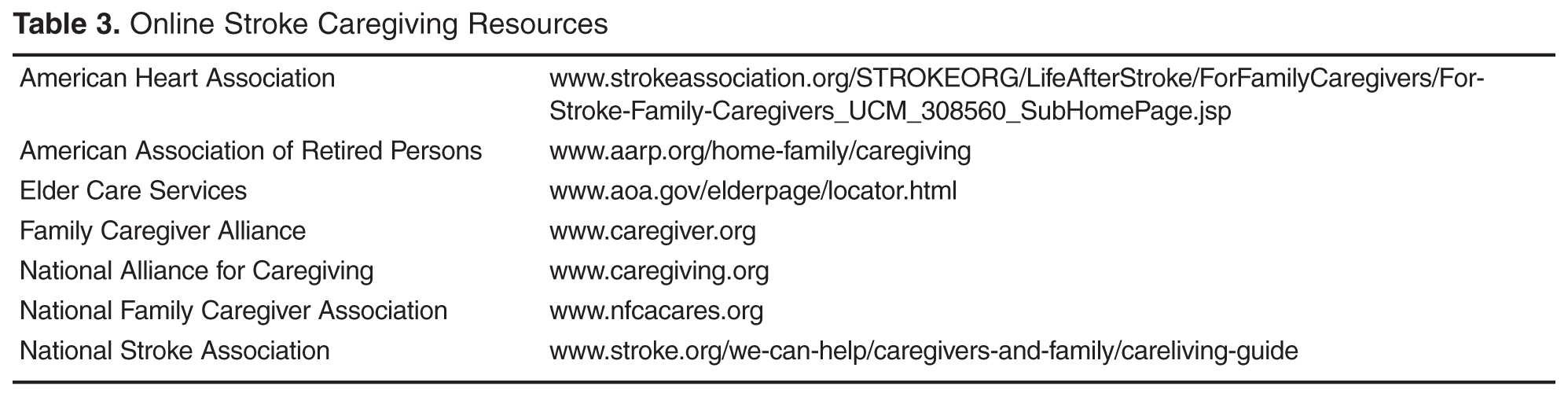
The timing of providing support and resources is also critical. Becoming a caregiver is a process and often family members who are new to the role need more intense direct assistance and support when the stroke survivor first comes home, but many may need ongoing support over time. Research suggests it can take caregivers up to 3 years to figure out how to manage the new responsibilities, learn to navigate the multiple systems for careand services, establish confidence in their abilities, deal with the emotional upheaval, and to adapt to their new lives [23].
Research indicates the 44% of stroke patients receive no post-acute care. Clinicians also need to advocate for patients to get the most appropriate level of organized, coordinated, and inter-professional post-acute care [5]. This requires that they understand the different levels of post-acute care, including the criteria for admission, the scope and intensity of nursing, therapy, physician and other services provided in each setting, and the associated clinical outcomes. This knowledge is also necessary to enable clinicians to educate stroke survivors and their caregivers on post-acute care so that they understand the process and can effectively self-advocate for the provision of appropriate services as needed.
Approximately 45% of stroke survivors in the US are discharged either to an inpatient rehabilitation facility or SNF for rehabilitation [4]. Patients discharged to an inpatient rehabilitation facility receive a minimum of 3 hours of therapy per day and are cared for 24 hours/day by a staff led by registered nurses (RNs) with rehabilitation expertise. SNFs do not have minimum requirements for hours of therapy, 24-hour RN staffing, nor a requirement for nurses with specialty training in rehabilitation. Pressure to reduce the length of stay in acute care often results in providers transitioning stroke survivors to the post-acute care setting that accepts the patient first. Because SNFs have fewer criteria for admission, they are more likely to rapidly accept a patient for care when compared to an inpatient rehabilitation facility. Providers must determine and make recommendations for the most appropriate level of post-acute care to ensure the stroke patients’ rehabilitation needs can be met in the recommended setting [5,69]. It is also essential that family caregivers have the knowledge and skills to advocate for the appropriate level of post-acute care based on the stroke survivor’s expected recovery trajectory. Research has demonstrated that that stroke survivors admitted to an inpatient rehabilitation facility, when compared to similar patients in a SNF, have better outcomes, including improved function [70] and lower re-hospitalization and death rates [71,72]. The Association of Rehabilitation Nurses provides resources for health care professionals and patients regarding rehabilitation. For more information for professionals about levels of post-acute care, see www.rehabnurse.org/uploads/files/healthpolicy/ARN_Care_Transitions_White_Paper_Journal_Copy_FINAL.pdf [73]. For information for patients and caregivers, see www.restartrecovery.org.
Providers must also be knowledgeable about community resources in order to provide connections to services and agencies that are relevant to the changing needs of the caregiver over time. Initially, caregivers may need assistance in meeting the stroke survivor’s BADL/IADL, and later needs may expand to include support groups, respite, and opportunities for a greater community engagement.
Training in time management provides room in the busy caregiving schedule for self-care for the caregiver. Providers must assist with determining routines that meet the needs of both the caregiver and stroke survivor, as the health of each is dependent on the other. Assistance in developing a wellness program that is feasible for the caregiver to maintain will improve adoption of health promoting practices.
As discussed above, the needs of both the stroke survivor and caregiver vary along the post-stroke trajectory. Therefore, both caregivers and stroke survivors should be assessed intermittently over time: caregivers for evidence of effective coping strategies and confidence in the sustaining the caregiving role, and stroke survivors for improvement in their functional abilities and compensatory strategies in BADL/IADL. The opportunity for the stroke survivor to assume household tasks that decrease the caregiver burden, in addition to providing a greater sense of purpose for the stroke survivor, must be explored. For example, the stroke survivor may be able to assist with activities such as meal planning and components of meal preparation or light housekeeping utilizing adaptive devices as needed.
Additional research is necessary to understand how the needs of caregivers change over time, the appropriate timing of reassessment, and the evaluation of interventions to facilitate the transition into this role, while preventing the adverse effects of caregiving on the health of the caregiver and stroke survivor during this transition period.
Conclusion
There is clear evidence that stroke caregiving can have detrimental effects on the physical, mental, and emotional health of caregivers, and that these effects are sustained over time. Evidence also indicates that caregivers who are not well-prepared to assume the caregiving role are more likely to experience negative outcomes. Studies suggest that the time of transition from inpatient care to home is a time of crisis for caregivers and that their support needs are high during this time. However, research also indicates that while needs may change over time, caregivers need ongoing support, especially if they are providing care for a stroke survivor who has moderate to severe physical, cognitive, and/or communication limitations.
In order to better understand the needs of stroke caregivers, a pre-discharge assessment of their readiness to provide care should be conducted so that interventions can be tailored to address their needs to minimize negative effects of a poorly planned transition [69]. Currently, there are assessment tools that can be used with caregivers post-discharge to assess their self-reported needs (after they have an understanding of the role) and caregiving outcomes. Research is needed to develop a valid and reliable tool thatpre-emptively assesses the gaps in caregiver readiness that can be utilized prior to the transition from the institutional setting to home. This will enable the identification and evaluation of primary prevention strategies to improve caregiver preparation so that the adaption to the new caregiving role can be expedited, minimizing the adverse health effects on both the caregiver and stroke survivor.
Providers must be aware of the changing needs of stroke survivors and tailor plans of care accordingly, using evidenced-based interventions. Policy makers must consider research on the long term effects of caregiving and consider legislation to support the health and respite needs of the growing population of caregivers. This will contribute to attaining the 3 aims of the National Quality Strategy: improving quality of care, improving health, and reducing health care system costs [74].
Corresponding author: Barbara J. Lutz, PhD, 601 S. College Rd., Wilmington, NC 28403, [email protected].
Financial disclosures: None.
1. Mozaffarian D, Benjamin EJ, Go AS, et al. on behalf of the American Heart Association Statistics Committee & Stroke Statistics Subcommittee. Heart disease and stroke statistics - 2016 update: A report from the American Heart Association. Circulation 2016;132:e38–e360.
2. Feigin VL, Krishnamurthi RV, Parmar P, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology 2015;45:161–76.
3. Hall MJ, Levant S, DeFrances CJ. Hospitalization for stroke in U.S. hospitals, 1989-2009. Hyattsville, MD: National Center for Heatlh Statistics; 2012.
4. Prvu Bettger J, McCoy L, Smith EE, et al. Contemporary trends and predictors of postacute service use and routine discharge home after stroke. J Am Heart Assoc 2015;4(2).
5. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016;47:e98–e169.
6. Talley RC, Crews JE. Framing the public health of caregiving. Am J Public Health 2007;97:224–8.
7. van Exel NJ, Koopmanschap MA, van den Berg B, et al. Burden of informal caregiving for stroke patients: odentification of caregivers at risk of adverse health effects. Cerebrovasc Dis 2005;19:11–7.
8. van Exel NJ, Scholte op Reimer WJ, Brouwer WB, et al. Instruments for assessing the burden of informal caregiving for stroke patients in clinical practice: a comparison of CSI, CRA, SCQ and self-rated burden. Clin Rehabil 2004;18:203–14.
9. Lutz BJ, Young ME, Cox KJ, et al. The crisis of stroke: experiences of patients and their family caregivers. Top Stroke Rehabil 2011;18:786–97.
10. McCullagh E, Brigstocke G, Donaldson N, Kalra L. Determinants of caregiving burden and quality of life in caregivers of stroke patients. Stroke 2005;36:2181–6.
11. van Exel NJ, Brouwer WB, van den Berg B, et al. What really matters: an inquiry into the relative importance of dimensions of informal caregiver burden. Clin Rehabil 2004;18:683–93.
12. Perrin PB, Heesacker M, Hinojosa MS et al. Identifying at-risk, ethnically diverse stroke caregivers for counseling: a longitudinal study of mental health. Rehabil Psychol 2009;54:138–49.
13. Greenwood N, Mackenzie A, Cloud GC, Wilson N. Informal carers of stroke survivors--factors influencing carers: a systematic review of quantitative studies. Disabil Rehabil 2008;30:1329–49.
14. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs 2015;24:2376–82.
15. White CL, Barrientos R, Dunn K. Dimensions of uncertainty after stroke: perspectives of the stroke survivor and family caregiver. J Neurosci Nurs 2014;46:233–40.
16. Saban KL, Sherwood PR, DeVon HA, Hynes DM. Measures of psychological stress and physical health in family caregivers of stroke survivors: a literature review. J Neurosci Nurs 2010;42:128–38.
17. Kruithof WJ, Post, MWM, van Mierlo M, et al. Caregiver burden and emotional problems in partners of stroke patients at two months and one year post-stroke: determinants and prediction. Patient Educ Couns 2016. Forthcoming.
18. Sarre S, Redlich C, Tinker A, et al. A systematic review of qualitative studies on adjusting after stroke: lessons for the study of resilience. Disabil Rehabil 2014;36:716–26.
19. Cameron JI, Naglie G, Dick T, et al. Are we meeting the changing needs of family caregivers to stroke survivors across the care continuum? A systematic review of the caregiver intervention literature. Stroke 2012;43:E143-E.
20. Miller EL, Murray L, Richards L, et al. Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke ptient: a scientific statement from the American Heart Association. Stroke 2010;41:2402–48.
21. Perrin PB, Heesacker M, Stidham BS, et al. Structural equation modeling of the relationship between caregiver psychosocial variables and functioning of individuals with stroke. Rehabil Psychol 2008;53:54–62.
22. Roth DL, Perkins M, Wadley VG, et al. Family caregiving and emotional strain: associations with quality of life in a large national sample of middle-aged and older adults. Qual Life Res 2009;18:679–88.
23. Haley WE, Roth DL, Hovater M, Clay OJ. Long-term impact of stroke on family caregiver well-being: a population-based case-control study. Neurology 2015;84:1323–9.
24. Greenwood N, Mackenzie A. Informal caring for stroke survivors: meta-ethnographic review of qualitative literature. Maturitas 2010;66:268–76.
25. Ostwald SK, Bernal MP, Cron SG, Godwin KM. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Top Stroke Rehabil 2009;16:93–104.
26. Brereton L, Carroll C, Barnston S. Interventions for adult family carers of people who have had a stroke: a systematic review. Clin Rehabil 2007;21:867–84.
27. Greenwood N, Mackenzie A, Cloud G, Wilson N. Loss of autonomy, control and independence when caring: a qualitative study of informal carers of stroke survivors in the first three months after discharge. Disabil Rehabil 2009:1–9.
28. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses of patients with stroke from initial inpatient rehabilitation to 3 years poststroke: course and relations with coping strategies. Stroke 2009;40:1399–404.
29. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses in the chronic phase after stroke: improvement or deterioration between 1 and 3 years after stroke? Patient Educ Couns 2008;73:153–8.
30. Haley WE, Allen JY, Grant JS, et al. Problems and benefits reported by stroke family caregivers: results from a prospective epidemiological study. Stroke 2009;40:2129–33.
31. Berg A, Palomaki H, Lonnqvist J, et al. Depression among caregivers of stroke survivors. Stroke 2005;36:639–43.
32. van Heugten C, Visser-Meily A, Post M, Lindeman E. Care for carers of stroke patients: evidence-based clinical practice guidelines. J Rehabil Med 2006;38:153–8.
33. Bakas T, Kroenke K, Plue LD, et al. Outcomes among family caregivers of aphasic versus nonaphasic stroke survivors. Rehabil Nurs 2006;31:33–42.
34. Gaugler JE. The longitudinal ramifications of stroke caregiving: a systematic review. Rehabil Psychol 2010;55:108–25.
35. Andrew NE, Kilkenny MF, Naylor R, et al. The relationship between caregiver impacts and the unmet needs of survivors of stroke. Patient Prefer Adher 2015;9:1065–73.
36. Chung ML, Bakas T, Plue LD, Williams LS. Effects of self-esteem, optimism, and perceived control on depressive symptoms in stroke survivor-spouse dyads. J Cardiovasc Nurs 2016;31:E8–E16.
37. Grant JS, Clay OJ, Keltner NL, et al. Does caregiver well-being predict stroke survivor depressive symptoms? a mediation analysis. Top Stroke Rehabil 2013;20:44–51.
38. Murray J, Young J, Forster A, Ashworth R. Developing a primary care-based stroke model: the prevalence of longer-term problems experienced by patients and carers. Br J Gen Pract 2003;53:803–7.
39. Pierce LL, Steiner V, Govoni A, et al. Two sides to the caregiving story. Top Stroke Rehabil 2007;14:13–20.
40. Mackenzie A, Greenwood N. Positive experiences of caregiving in stroke: a systematic review. Disabil Rehabil 2012;34:1413–22.
41. Parag V, Hackett ML, Yapa CM, et al. The impact of stroke on unpaid caregivers: results from The Auckland Regional Community Stroke study, 2002-2003. Cerebrovasc Dis (Basel, Switzerland) 2008;25:548–54.
42. Kruithof WJ, Post MWM, Visser-Meily JMA. Measuring negative and positive caregiving experiences: a psychometric analysis of the Caregiver Strain Index Expanded. Clin Rehabil 2015;29:1224–33.
43. Lutz BJ. Determinants of discharge destination for stroke patients. Rehabil Nurs 2004;29:154–63.
44. Lutz BJ, Young ME, Creasy KR, et al. Improving stroke caregiver readiness for transition from inpatinet rehabilitation to home. Gerontologist 2016. Forthcoming.
45. Visser-Meily JM, Post MW, Riphagen II, Lindeman E. Measures used to assess burden among caregivers of stroke patients: a review. Clin Rehabil 2004;18:601–23.
46. Moon M. The unprepared caregiver. Gerontologist 2016 Apr 21.
47. Pierce LL, Steiner V, Govoni AL, et al. Internet-based support for rural caregivers of persons with stroke shows promise. Rehabil Nurs 2004;29:95–9,103.
48. Bakas T, Austin JK, Okonkwo KF, et al. Needs, concerns, strategies, and advice of stroke caregivers the first 6 months after discharge. J Neurosci Nurs 2002;34:242–51.
49. Lutz BJ, Chumbler NR, Lyles T, et al. Testing a home-telehealth programme for US veterans recovering from stroke and their family caregivers. Disabil Rehabil 2009;31:402–9.
50. Hayes J, Chapman P, Young LJ, Rittman M. The prevalence of injury for stroke caregivers and associated risk factors. Top Stroke Rehabil 2009;16:300–7.
51. Cameron JI, Gignac MA. “Timing It Right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns 2008;70:305–14.
52. Creasy KR, Lutz BJ, Young ME, et al. The impact of interactions with providers on stroke caregivers’ needs. Rehabil Nurs 2013;38:88–98.
53. Bakas T, Farran CJ, Austin JK, et al. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building Kit (TASK). Top Stroke Rehabil 2009;16:105–21.
54. Cameron JI, Naglie G, Silver FL, Gignac MA. Stroke family caregivers’ support needs change across the care continuum: a qualitative study using the timing it right framework. Disabil Rehabil 2013;35:315–24.
55. Cameron JI, O’Connell C, Foley N, et al. Canadian Stroke Best Practice Recommendations: Managing transitions of care following Stroke. Guidelines Update 2016. Int J Stroke. 2016.
56. Family Caregiver Alliance. Caregivers Count Too! A toolkit to help practitioners assess the needs of family caregivers. San Francisco: 2006. Accessed 16 Aug 2016 at www.caregiver.org/caregivers-count-too-toolkit.
57. Messecar DC. Nursing standard of practice protocol: family caregiving [Internet]. Accessed at www.consultgeri.org/geriatric-topics/family-caregiving.
58. Young ME, Lutz BJ, Creasy KR et al. A comprehensive assessment of family caregivers of stroke survivors during inpatient rehabilitation. Disabil Rehabil 2014;36:1892–902.
59. Archbold PG, Stewart BJ, Greenlick MR, Harvath T. Mutuality and preparedness as predictors of caregiver role strain. Res Nurs Health 1990;13:375–84.
60. Pucciarelli G, Savini S, Byun E, et al. Psychometric properties of the Caregiver Preparedness Scale in caregivers of stroke survivors. Heart & Lung 2014;43:555–60.
61. Deeken JF, Taylor KL, Mangan P et al. Care for the caregivers: a review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J Pain Symptom Manage 2003;26:922–53.
62. Haley WE, Roth DL, Howard G, Safford MM. Caregiving strain and estimated risk for stroke and coronary heart disease among spouse caregivers: differential effects by race and sex. Stroke 2010;41:331–6.
63. Bakas T, Champion V, Perkins SM, et al. Psychometric testing of the revised 15-item Bakas Caregiving Outcomes Scale. Nurs Res 2006;55:346–55.
64. Family Caregiver Alliance. Selected caregiver assessment measures: A resource inventory for practitioners. 2d ed. Accessed at www.caregiver.org/selected-caregiver-assessment-measures-resource-inventory-practitioners-2012.
65. Bakas T, Clark PC, Kelly-Hayes M, et al. Evidence for stroke family caregiver and dyad interventions: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:2836–52.
66. Cheng HY, Chair SY, Chau JPC. The effectiveness of psychosocial interventions for stroke family caregivers and stroke survivors: a systematic review and meta-analysis. Patient Educ Couns 2014;95:30–44.
67. Bakas T, Austin JK, Habermann B, et al. Telephone assessment and skill-building kit for stroke caregivers a randomized controlled clinical trial. Stroke 2015;46:3478–87.
68. Alim M, Lindley R, Felix C, et al. Family-led rehabilitation after stroke in India: the ATTEND trial, study protocol for a randomized controlled trial. Trials 2016;17:13.
69. Camicia M, Lutz B. Nursing’s role in successful transitions across settings. Stroke 2016. Forthcoming.
70. Chan L, Sandel ME, Jette AM, et al. Does postacute care site matter? A longitudinal study assessing functional recovery after a stroke. Arch Phys Med Rehabil 2013;94:622–9.
71. Kind AJ, Smith MA, Pandhi N, et al. Bouncing-back: rehospitalization in patients with complicated transitions in the first thirty days after hospital discharge for acute stroke. Home Health Care Serv Q 2007;26:37–55.
72. Bettger JP, Liang L, Xian Y, et al. Inpatient rehabilitation facility care reduces the likelihood of death and rehospitalization after stroke compared with skilled nursing facility care [abstract]. Stroke 2015; A146.
73. Camicia M, Black T, Farrell J, et al. The essential role of the rehabilitation nurse in facilitating care transitions: a white paper by the Association of Rehabilitation Nurses. Rehabil Nurs 2014;39:3–15.
74. Centers for Medicare and Medicaid. CMS quality strategy 2016. Accessed at www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualityinitiativesgeninfo/downloads/cms-quality-strategy.pdf.
From the School of Nursing, University of North Carolina-Wilmington, Wilmington, NC (Dr. Lutz), and the Kaiser Foundation Rehabilitation Center, Kaiser Permanente, Vallejo, CA (Ms. Camicia).
Abstract
- Objectives: To describe issues faced by stroke family caregivers, discuss evidence-based interventions to improve caregiver outcomes, and provide recommendations for clinicians caring for stroke survivors and their family caregivers.
- Methods: Literature review.
- Results: Caregiver health is linked to the stroke survivor’s degree of functional recovery; the more severe the level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health. Inadequate caregiver preparation contributes to poorer outcomes. Caregivers describe many unmet needs including skills training; communicating with providers; resource identification and activation; finances; respite; and emotional support. Caregivers need to be assessed for gaps in preparation to provide care. Interventions are recommended that combine skill-building and psycho-educational strategies; are tailored to individual caregiver needs; are face-to-face when feasible; and include 5 to 9 sessions. Family counseling may also be indicated. Intermittent assessment of caregiving outcomes should be conducted so that changing needs can be addressed.
- Conclusions: Stroke caregiving affects the caregiver’s physical, mental, and emotional health, and these effects are sustained over time. Poorly prepared caregivers are more likely to experience negative outcomes and their needs are high during the transition from inpatient care to home. Ongoing support is also important, especially for caregivers who are caring for a stroke survivor with moderate to severe functional limitations. In order to better address unmet needs of stroke caregivers, intermittent assessments should be conducted so that interventions can be tailored to their changing needs over time.
Key words: stroke; family caregivers; care transitions; patient-centered care.
Stroke is a leading cause of major disability in the United States [1] and around the world [2]. Of the estimated 6.6 million stroke survivors living in the US, more than 4.5 million have some level of disability following stroke [1]. In 2009, more than 970,000 persons were hospitalized with stroke in the US with an average length of stay of 5.3 days [3]. Approximately 44% of stroke survivors are discharged home directly from acute care without post-acute care [4]. Only about 25% of stroke survivors receive care in inpatient rehabilitation facilities [4] even though the American Heart Association (AHA) stroke rehabilitation guidelines recommend this level of care for qualified patients [5]. Regardless of the care trajectory, when stroke survivors return home they frequently require assistance with basic and instrumental activities of daily living (BADL/IADL), usually provided by family members who often feel unprepared and overwhelmed by the demands and responsibilities of this caregiving role.
The deleterious effects of caregiving have been identified as a major public health concern [6]. A robust body of literature has established that caregivers are often adversely affected by the demands of their caregiving role. However, much of this literature focuses on caregivers for persons with dementia. Needs of stroke caregivers are categorically different from caregivers of persons with dementia in that stroke is an unpredictable, life-disrupting, crisis event that occurs suddenly leaving family members with insufficient time to prepare for the new roles and caregiving responsibilities. The patient typically transitions from being cared for by multiple providers in an acute care, inpatient rehabilitation facility, or skilled nursing facility (SNF)—24 hours a day, 7 days a week—to relying fully on one person (most often a spouse or adult child) who may not be ready to handle the overwhelming demands and constant vigilance required for adequate care at home. Studies have repeatedly demonstrated the damaging health effects of caregiving. Caregivers describe feeling isolated, abandoned, and alone [7–9], and what frequently follows is a predictable trajectory of depression and deteriorating health and well-being [7,10–13]. The purpose of this article is to describe difficulties and issues faced by family members who are caring for a loved one following stroke, discuss evidence-based interventions designed to improve stroke caregiver outcomes, and provide recommendations for clinicians who care for stroke survivors and their family caregivers post-stroke.
Difficulties and Issues Faced by Caregivers
With an aging population and increasing incidence of stroke, it is imperative that we identify and address the ongoing needs of stroke survivors and their family caregivers in the post-stroke recovery period. Multiple studies acknowledge that stroke is a life-changing event for patients and their family members [9,14] that often results in overwhelming feelings of uncertainty, fear [15], grief, and loss [9]. Stroke also can have long-term effects on the health of stroke survivors and their family caregivers. Studies have identified the effects of caregiving on the health of caregivers and subsequent links between stroke survivor and caregiver outcomes over time [12,16,17]; the ongoing needs of stroke caregivers post-discharge [18,19]; and the importance of assessing caregiver preparedness and subsequent caregiving outcomes [5,20].
Effects of Caregiving on the Health of Caregivers and Stroke Survivors
Research on stroke caregiving consistently indicates that caregiver health is inextricably linked to the stroke survivor’s degree of physical, cognitive, psychological, and emotional recovery. The more severe the patient’s level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health outcomes [21]. Studies also indicate that certain caregiver characteristics, such as being female or having lower educational level, pre-existing health conditions [7,22,23], poor family functioning, lack of social support [22,24], or lack of preparation [25], are all risk factors for poorer caregiver outcomes.
Stroke family caregivers often experience overwhelming physical and emotional strain, depressive symptoms, sleep deprivation, decline in physical and mental health, reduced quality of life, and increased isolation [7,10,11,14,26,27]. Perceived burden has been positively associated with caregiver depressive symptoms [12,14,28,29]. Depressive symptoms in caregivers, with a reported incidence of 14% [30] to 33% [31], may persist for several years post-stroke. In a study of the long-term effects of caregiving with 235 stroke caregivers when compared with non-caregivers, researchers found that caregivers had more depressive symptoms and poorer life satisfaction and mental health quality of life at 9 months post-stroke, and many of these differences continued for 3 years post-discharge [23].
Lower stroke survivor functioning and higher depressive symptoms are correlated with higher caregiver depressive symptoms and burden, and poorer coping skills and mental health [12,21]. A review of stroke caregiving literature by van Heugten et al [32] indicated that long-term caregiver functioning was influenced by stroke survivor physical and cognitive functioning and behavioral issues; caregiver psychological and emotional health; quality of family relationships; social support; and caregiver demographics. Caregivers of stroke survivors with aphasia may have more difficulties providing care, increased burden and strain, higher depressive symptoms, and other negative stroke-related outcomes [33].
Gaugler [34] conducted a systematic review of 117 studies and reported that caring for stroke survivors who were older, in poorer health, and had greater stroke severity increased the likelihood of poorer emotional and psychological family caregiver outcomes. Caregivers who had “negative problem orientation and less social support” were more likely to have depressive symptoms and poorer self-rated health at 1-year post-stroke. One of the best predictors of caregiver stress and poor health in the first year post-stroke was lack of caregiver preparation [25,34].
Research also suggests that stroke survivor outcomes are influenced by the ability of the family caregiver to provide emotional and instrumental support as well as assistance with BADL/IADL [6,35]. As the caregiver’s health decreases, the stroke survivor’s health and recovery will also likely suffer and ultimately may result in re-hospitalization or nursing home placement. For example, Perrin et al found a consistent reciprocal relationship between caregiver health and stroke survivor functioning, such that the quality of caregiving may be affected by caregiver burden and depressive symptoms, which in turn can impair the functional, psychological, and emotional recovery of the stroke survivor [21]. Studies have also linked poorer caregiver well-being to increased depressive symptoms in stroke survivors [36,37].
Positive effects of caregiving have also been reported, including a feeling of confidence, satisfaction in providing good quality care [30,39,40], an improved relationship with the care recipient [30,40,41], having greater life appreciation, and feeling needed and appreciated [40]. In a systematic review of 9 studies, improvements in the stroke survivor’s condition was a source of positive caregiving experiences [40]. In 2 studies, two-thirds of caregivers surveyed affirmed all survey items related to positive aspects of caregiving [30,42]. Additionally, studies have demonstrated that caregivers who engaged in emotion- and problem-focused coping strategies had positive caregiving experiences [40]. Haley et al found that by 3 years post-stroke many of the ill effects of caregiving had resolved, suggesting that some caregivers may be successful in adapting to their “new” post-stroke lives [23].
Understanding the difficulties and issues faced by caregivers throughout the trajectory, from immediately following the stroke through the transition home and, ideally, the adaptation of the caregiver to this new life, provides an opportunity for health care professionals to intervene with strategies to support this major life change.
Caregiving Trajectory and Ongoing Needs of Stroke Caregivers
Stroke survivors and their family caregivers rapidly move from intensive therapy and nursing case management while in a facility to little or no assistance following discharge. Despite case management and discharge planning services received while in an institutional setting, the transition from inpatient care to home can be a crisis point for caregivers [9]. They describe having to figure things out for themselves with little or no formal support after discharge [9,43,44], leaving them feeling overwhelmed, exhausted, and abandoned once they return home [9].
These family members rarely make an active choice to become caregivers; rather, they take on the role because they are unable to perceive or access any other suitable alternatives [8,45]. Whatever their circumstances, these devoted family members are particularly vulnerable as they transition into the caregiving role without an adequate support system for assessing and addressing their needs [7–9,46]. Without this assistance, caregivers develop their own solutions and strategies to meet the needs of the care recipient after discharge [47,48]. Unfortunately, these strategies are often ineffective and may result in safety risks for patients (eg, falls, skin breakdown, choking), and care-related injuries (eg, falls, muscle strains, bruises) and increased stress and anxiety for caregivers [48–50].
Caregivers have described unmet needs in many domains including skills training, communicating with providers, resource identification and activation, finances, respite, and emotional support [35,44,48,51,52]. Bakas et al found that in the first 6 months post-discharge, stroke caregivers had needs and concerns related to information, emotions and behaviors, physical care, instrumental care, and personal responses to caregiving [48], and that their information needs change during the course of the patient’s recovery [53]. In a study by Lutz et al [44], caregivers identified multiple areas where they felt they were unprepared to assume the caregiving role post-discharge. These included identifying and activating resources; making home and transportation modifications to improve accessibility; developing skills in providing physical care and therapies; managing medications and behavioral issues; preventing falls; coordinating care across settings; attending to other family responsibilities; and caring for themselves.
In a study of interactions between rehabilitation providers and stroke caregivers, Creasy et al [52] noted that caregivers have needs, which were often not recognized, in the following areas: information; providing emotional support for the stroke survivor and having their own emotional support needs met; being involved in treatment decisions; and being adequately prepared for discharge home. Caregivers’ interaction styles with providers, which ranged from passive to active/directing, affected their abilities to have their needs recognized and addressed. These findings highlight the importance of recognizing the caregiver’s interaction style and tailoring communication strategies accordingly.
Cameron et al [54] noted that caregiver support needs change over time, with needs being highest during the inpatient phase as they prepare for discharge home. Moreover, caregivers who are providing care for stroke survivors with more severe functional limitations need more support over a longer period of time. Recognizing the needs of stroke caregivers, the 2016 Canadian Stroke Best Practice Recommendations on Managing Transitions of Care Following Stroke includes recommendations related to assessing, educating, and supporting stroke family caregivers [55].
Assessing Caregiver Readiness and Related Outcomes
Young et al [58] recommend specific domains for a comprehensive readiness assessment of stroke family caregivers. Caregiver domains include strength of the caregiver/care recipient relationship; caregiver willingness to provide care; pre-existing health conditions, previous responsibilities, caregiving experience, home and transportation accessibility, available resources, emotional response to the stroke, and ability to sustain the caregiving role. This type of readiness assessment should be completed early in the care trajectory, while the stroke survivor is receiving inpatient care, so that care plans can be tailored to address gaps in caregiver preparation prior to discharge. It is especially important for new caregivers and those caring for stroke survivors with significant functional limitations [44]. Currently there are no tools designed to assess a family member’s readiness to assume the caregiver role.
Validated instruments have been developed to assess caregiving outcomes, including preparedness, with caregivers who have been providing care for a period of time. For example, the Mutuality and Preparedness Scales of the Family Caregiver Inventory was developed with caregivers 6 months post-discharge [59] and has been validated with stroke caregivers at 3 months post-discharge [60].
Several validated tools are available to assess the caregiver’s changing needs and the effects of care provision on well-being [8,45,61]. For example, the Caregiver Strain Index [62] has been validated in studies with stroke family caregivers [11,28]. Bakas developed 2 scales to specifically assess stroke caregivers post-discharge. The Bakas Caregiving Outcomes Scale assesses caregiver life changes [63] and the Needs and Concerns Checklist assesses post-discharge caregiver needs [48]. There are many other instruments designed to assess general caregiving outcomes, including depressive symptoms, burden, anxiety, and well-being. For a list relevant tools see Deeken et al [61] and The Selected Caregiver Assessment Measures from the Family Caregiver Alliance [64].
While these scales are helpful for assessing caregivers who are already providing care, they do not capture the gaps in caregiver readiness prior to patient discharge from the institutional setting. Taken together, these studies suggest that assessing readiness and implementing interventions to improve caregiver preparation prior to discharge and assessing and addressing their changing needs over time, from inpatient care to community reintegration, may be important strategies for improving both caregiver and stroke survivor outcomes. These strategies may also facilitate sustainability of the caregiver role over time.
Interventions to Improve Caregiver Outcomes
In a review of 39 articles representing 32 caregiver and dyad intervention studies, researchers from the AHA made 13 evidence-based recommendations. Recommendations with the highest level of evidence indicated that (1) interventions that combined skill-building with psycho-educational programs were better than psycho-educational interventions alone; (2) interventions that are tailored to the individual are preferred over “one-size-fits-all” interventions; (3) face-to-face interventions are preferred, but telephone interventions can be useful when face-to-face is not feasible; and (4) interventions with 5 to 9 sessions are recommended [65]. In a review of 18 studies, Cheng et al confirmed the recommendation that psychoeducational interventions that focused on skill building improved caregiver well-being and reduced stroke survivor heath care utilization [66].
Studies also recommend that families may need family counseling to help them develop positive coping strategies and adjust to their lives after stroke [66]. Stroke survivors and their families experience grief and loss as they begin to realize how the stroke has changed their relationships, roles, responsibilities, and future plans for their lives (eg, work, retirement). While many inpatient rehabilitation facilities may provide services from a neuro-psychologist to discuss post-stroke changes in the brain and possible behavioral and emotional manifestations, referrals for family counseling to address the impact of stroke on the family and community reintegration are seldom provided [9].
Recent interventions have shown promise in improving stroke caregiver outcomes. For example, Bakas et al. completed a randomized controlled trial of an 8-week, nurse-delivered, Telephone Assessment and Skill-Building Kit (TASK) intervention [67]. Caregivers in the intervention group with moderate to severe depressive symptoms at baseline demonstrated significant improvements in depressive symptoms and life changes at 8, 24, and 52 weeks. The TASK shows promise because it can reach caregivers in rural and urban areas at a relatively low cost [67].
Recognizing the need to improve post-acute care for stroke survivors and their family caregivers, several large funded clinical trials are being tested in the US and globally. For example, the ATTEND Trial in India is testing a home-based, caregiver-led rehabilitation intervention [68]. The Comprehensive Post-Acute Stroke Services (COMPASS) study in North Carolina, is a state-wide pragmatic, randomized controlled trial testing a comprehensive community-based patient-centered post-acute care intervention with stroke survivors and their caregivers (www.nccompass-study.org). Results of these and other studies will continue to identify evidence-based strategies to improve care coordination, quality of care, and post-stroke outcomes for stroke survivors and their caregivers
Recommendations for Clinicians
Based on this review we have identified strategies that clinicians can implement across the care continuum that may help reduce caregiver strain and burden, and improve outcomes for family caregivers and the stroke survivors for whom they provide care. The evidence suggests that caregivers need assistance in building skills, not only in providing the care needed by the stroke survivor but also in solving problems as they arise; navigating the multiple systems of care, including understanding options for post-acute care; accessing community resources; communicating effectively with health care and social support providers; and dealing with the emotional effects of stroke [44,52].
Caregivers need help in navigating the multiple providers and systems of care to get the services the stroke survivor needs as well as to secure support services. They need information from trusted sources about stroke prevention and available community resources. Providinga list of resources is often insufficient, especially in the first few weeks or months post-stroke; these caregivers are already overwhelmed with the enormity of the tasks and responsibilities that they have taken on as a caregiver. Instead they need someone who can advocate for them and connect them with the appropriate resources at the right time.
They also need assistance developing and maintaining self-care strategies so they can sustain the caregiving role long-term. Identifying opportunities for respite and helping them activate informal and formal resources, such as other family members, friends, church groups, neighbors, and services from local senior centers, independent living centers, or area agencies on aging can help them identify assistance with the breadth of duties including care of the stroke survivor, meal preparation, transportation, or a supportive listening ear. It is important for the caregiver, in addition to any other close support person as available, to have a facilitated discussion withthe healthcare team to brainstorm activities where assistance may be provided and who might be approached to help.
The timing of providing support and resources is also critical. Becoming a caregiver is a process and often family members who are new to the role need more intense direct assistance and support when the stroke survivor first comes home, but many may need ongoing support over time. Research suggests it can take caregivers up to 3 years to figure out how to manage the new responsibilities, learn to navigate the multiple systems for careand services, establish confidence in their abilities, deal with the emotional upheaval, and to adapt to their new lives [23].
Research indicates the 44% of stroke patients receive no post-acute care. Clinicians also need to advocate for patients to get the most appropriate level of organized, coordinated, and inter-professional post-acute care [5]. This requires that they understand the different levels of post-acute care, including the criteria for admission, the scope and intensity of nursing, therapy, physician and other services provided in each setting, and the associated clinical outcomes. This knowledge is also necessary to enable clinicians to educate stroke survivors and their caregivers on post-acute care so that they understand the process and can effectively self-advocate for the provision of appropriate services as needed.
Approximately 45% of stroke survivors in the US are discharged either to an inpatient rehabilitation facility or SNF for rehabilitation [4]. Patients discharged to an inpatient rehabilitation facility receive a minimum of 3 hours of therapy per day and are cared for 24 hours/day by a staff led by registered nurses (RNs) with rehabilitation expertise. SNFs do not have minimum requirements for hours of therapy, 24-hour RN staffing, nor a requirement for nurses with specialty training in rehabilitation. Pressure to reduce the length of stay in acute care often results in providers transitioning stroke survivors to the post-acute care setting that accepts the patient first. Because SNFs have fewer criteria for admission, they are more likely to rapidly accept a patient for care when compared to an inpatient rehabilitation facility. Providers must determine and make recommendations for the most appropriate level of post-acute care to ensure the stroke patients’ rehabilitation needs can be met in the recommended setting [5,69]. It is also essential that family caregivers have the knowledge and skills to advocate for the appropriate level of post-acute care based on the stroke survivor’s expected recovery trajectory. Research has demonstrated that that stroke survivors admitted to an inpatient rehabilitation facility, when compared to similar patients in a SNF, have better outcomes, including improved function [70] and lower re-hospitalization and death rates [71,72]. The Association of Rehabilitation Nurses provides resources for health care professionals and patients regarding rehabilitation. For more information for professionals about levels of post-acute care, see www.rehabnurse.org/uploads/files/healthpolicy/ARN_Care_Transitions_White_Paper_Journal_Copy_FINAL.pdf [73]. For information for patients and caregivers, see www.restartrecovery.org.
Providers must also be knowledgeable about community resources in order to provide connections to services and agencies that are relevant to the changing needs of the caregiver over time. Initially, caregivers may need assistance in meeting the stroke survivor’s BADL/IADL, and later needs may expand to include support groups, respite, and opportunities for a greater community engagement.
Training in time management provides room in the busy caregiving schedule for self-care for the caregiver. Providers must assist with determining routines that meet the needs of both the caregiver and stroke survivor, as the health of each is dependent on the other. Assistance in developing a wellness program that is feasible for the caregiver to maintain will improve adoption of health promoting practices.
As discussed above, the needs of both the stroke survivor and caregiver vary along the post-stroke trajectory. Therefore, both caregivers and stroke survivors should be assessed intermittently over time: caregivers for evidence of effective coping strategies and confidence in the sustaining the caregiving role, and stroke survivors for improvement in their functional abilities and compensatory strategies in BADL/IADL. The opportunity for the stroke survivor to assume household tasks that decrease the caregiver burden, in addition to providing a greater sense of purpose for the stroke survivor, must be explored. For example, the stroke survivor may be able to assist with activities such as meal planning and components of meal preparation or light housekeeping utilizing adaptive devices as needed.
Additional research is necessary to understand how the needs of caregivers change over time, the appropriate timing of reassessment, and the evaluation of interventions to facilitate the transition into this role, while preventing the adverse effects of caregiving on the health of the caregiver and stroke survivor during this transition period.
Conclusion
There is clear evidence that stroke caregiving can have detrimental effects on the physical, mental, and emotional health of caregivers, and that these effects are sustained over time. Evidence also indicates that caregivers who are not well-prepared to assume the caregiving role are more likely to experience negative outcomes. Studies suggest that the time of transition from inpatient care to home is a time of crisis for caregivers and that their support needs are high during this time. However, research also indicates that while needs may change over time, caregivers need ongoing support, especially if they are providing care for a stroke survivor who has moderate to severe physical, cognitive, and/or communication limitations.
In order to better understand the needs of stroke caregivers, a pre-discharge assessment of their readiness to provide care should be conducted so that interventions can be tailored to address their needs to minimize negative effects of a poorly planned transition [69]. Currently, there are assessment tools that can be used with caregivers post-discharge to assess their self-reported needs (after they have an understanding of the role) and caregiving outcomes. Research is needed to develop a valid and reliable tool thatpre-emptively assesses the gaps in caregiver readiness that can be utilized prior to the transition from the institutional setting to home. This will enable the identification and evaluation of primary prevention strategies to improve caregiver preparation so that the adaption to the new caregiving role can be expedited, minimizing the adverse health effects on both the caregiver and stroke survivor.
Providers must be aware of the changing needs of stroke survivors and tailor plans of care accordingly, using evidenced-based interventions. Policy makers must consider research on the long term effects of caregiving and consider legislation to support the health and respite needs of the growing population of caregivers. This will contribute to attaining the 3 aims of the National Quality Strategy: improving quality of care, improving health, and reducing health care system costs [74].
Corresponding author: Barbara J. Lutz, PhD, 601 S. College Rd., Wilmington, NC 28403, [email protected].
Financial disclosures: None.
From the School of Nursing, University of North Carolina-Wilmington, Wilmington, NC (Dr. Lutz), and the Kaiser Foundation Rehabilitation Center, Kaiser Permanente, Vallejo, CA (Ms. Camicia).
Abstract
- Objectives: To describe issues faced by stroke family caregivers, discuss evidence-based interventions to improve caregiver outcomes, and provide recommendations for clinicians caring for stroke survivors and their family caregivers.
- Methods: Literature review.
- Results: Caregiver health is linked to the stroke survivor’s degree of functional recovery; the more severe the level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health. Inadequate caregiver preparation contributes to poorer outcomes. Caregivers describe many unmet needs including skills training; communicating with providers; resource identification and activation; finances; respite; and emotional support. Caregivers need to be assessed for gaps in preparation to provide care. Interventions are recommended that combine skill-building and psycho-educational strategies; are tailored to individual caregiver needs; are face-to-face when feasible; and include 5 to 9 sessions. Family counseling may also be indicated. Intermittent assessment of caregiving outcomes should be conducted so that changing needs can be addressed.
- Conclusions: Stroke caregiving affects the caregiver’s physical, mental, and emotional health, and these effects are sustained over time. Poorly prepared caregivers are more likely to experience negative outcomes and their needs are high during the transition from inpatient care to home. Ongoing support is also important, especially for caregivers who are caring for a stroke survivor with moderate to severe functional limitations. In order to better address unmet needs of stroke caregivers, intermittent assessments should be conducted so that interventions can be tailored to their changing needs over time.
Key words: stroke; family caregivers; care transitions; patient-centered care.
Stroke is a leading cause of major disability in the United States [1] and around the world [2]. Of the estimated 6.6 million stroke survivors living in the US, more than 4.5 million have some level of disability following stroke [1]. In 2009, more than 970,000 persons were hospitalized with stroke in the US with an average length of stay of 5.3 days [3]. Approximately 44% of stroke survivors are discharged home directly from acute care without post-acute care [4]. Only about 25% of stroke survivors receive care in inpatient rehabilitation facilities [4] even though the American Heart Association (AHA) stroke rehabilitation guidelines recommend this level of care for qualified patients [5]. Regardless of the care trajectory, when stroke survivors return home they frequently require assistance with basic and instrumental activities of daily living (BADL/IADL), usually provided by family members who often feel unprepared and overwhelmed by the demands and responsibilities of this caregiving role.
The deleterious effects of caregiving have been identified as a major public health concern [6]. A robust body of literature has established that caregivers are often adversely affected by the demands of their caregiving role. However, much of this literature focuses on caregivers for persons with dementia. Needs of stroke caregivers are categorically different from caregivers of persons with dementia in that stroke is an unpredictable, life-disrupting, crisis event that occurs suddenly leaving family members with insufficient time to prepare for the new roles and caregiving responsibilities. The patient typically transitions from being cared for by multiple providers in an acute care, inpatient rehabilitation facility, or skilled nursing facility (SNF)—24 hours a day, 7 days a week—to relying fully on one person (most often a spouse or adult child) who may not be ready to handle the overwhelming demands and constant vigilance required for adequate care at home. Studies have repeatedly demonstrated the damaging health effects of caregiving. Caregivers describe feeling isolated, abandoned, and alone [7–9], and what frequently follows is a predictable trajectory of depression and deteriorating health and well-being [7,10–13]. The purpose of this article is to describe difficulties and issues faced by family members who are caring for a loved one following stroke, discuss evidence-based interventions designed to improve stroke caregiver outcomes, and provide recommendations for clinicians who care for stroke survivors and their family caregivers post-stroke.
Difficulties and Issues Faced by Caregivers
With an aging population and increasing incidence of stroke, it is imperative that we identify and address the ongoing needs of stroke survivors and their family caregivers in the post-stroke recovery period. Multiple studies acknowledge that stroke is a life-changing event for patients and their family members [9,14] that often results in overwhelming feelings of uncertainty, fear [15], grief, and loss [9]. Stroke also can have long-term effects on the health of stroke survivors and their family caregivers. Studies have identified the effects of caregiving on the health of caregivers and subsequent links between stroke survivor and caregiver outcomes over time [12,16,17]; the ongoing needs of stroke caregivers post-discharge [18,19]; and the importance of assessing caregiver preparedness and subsequent caregiving outcomes [5,20].
Effects of Caregiving on the Health of Caregivers and Stroke Survivors
Research on stroke caregiving consistently indicates that caregiver health is inextricably linked to the stroke survivor’s degree of physical, cognitive, psychological, and emotional recovery. The more severe the patient’s level of disability, the more likely the caregiver will experience higher levels of strain, increased depression, and poor health outcomes [21]. Studies also indicate that certain caregiver characteristics, such as being female or having lower educational level, pre-existing health conditions [7,22,23], poor family functioning, lack of social support [22,24], or lack of preparation [25], are all risk factors for poorer caregiver outcomes.
Stroke family caregivers often experience overwhelming physical and emotional strain, depressive symptoms, sleep deprivation, decline in physical and mental health, reduced quality of life, and increased isolation [7,10,11,14,26,27]. Perceived burden has been positively associated with caregiver depressive symptoms [12,14,28,29]. Depressive symptoms in caregivers, with a reported incidence of 14% [30] to 33% [31], may persist for several years post-stroke. In a study of the long-term effects of caregiving with 235 stroke caregivers when compared with non-caregivers, researchers found that caregivers had more depressive symptoms and poorer life satisfaction and mental health quality of life at 9 months post-stroke, and many of these differences continued for 3 years post-discharge [23].
Lower stroke survivor functioning and higher depressive symptoms are correlated with higher caregiver depressive symptoms and burden, and poorer coping skills and mental health [12,21]. A review of stroke caregiving literature by van Heugten et al [32] indicated that long-term caregiver functioning was influenced by stroke survivor physical and cognitive functioning and behavioral issues; caregiver psychological and emotional health; quality of family relationships; social support; and caregiver demographics. Caregivers of stroke survivors with aphasia may have more difficulties providing care, increased burden and strain, higher depressive symptoms, and other negative stroke-related outcomes [33].
Gaugler [34] conducted a systematic review of 117 studies and reported that caring for stroke survivors who were older, in poorer health, and had greater stroke severity increased the likelihood of poorer emotional and psychological family caregiver outcomes. Caregivers who had “negative problem orientation and less social support” were more likely to have depressive symptoms and poorer self-rated health at 1-year post-stroke. One of the best predictors of caregiver stress and poor health in the first year post-stroke was lack of caregiver preparation [25,34].
Research also suggests that stroke survivor outcomes are influenced by the ability of the family caregiver to provide emotional and instrumental support as well as assistance with BADL/IADL [6,35]. As the caregiver’s health decreases, the stroke survivor’s health and recovery will also likely suffer and ultimately may result in re-hospitalization or nursing home placement. For example, Perrin et al found a consistent reciprocal relationship between caregiver health and stroke survivor functioning, such that the quality of caregiving may be affected by caregiver burden and depressive symptoms, which in turn can impair the functional, psychological, and emotional recovery of the stroke survivor [21]. Studies have also linked poorer caregiver well-being to increased depressive symptoms in stroke survivors [36,37].
Positive effects of caregiving have also been reported, including a feeling of confidence, satisfaction in providing good quality care [30,39,40], an improved relationship with the care recipient [30,40,41], having greater life appreciation, and feeling needed and appreciated [40]. In a systematic review of 9 studies, improvements in the stroke survivor’s condition was a source of positive caregiving experiences [40]. In 2 studies, two-thirds of caregivers surveyed affirmed all survey items related to positive aspects of caregiving [30,42]. Additionally, studies have demonstrated that caregivers who engaged in emotion- and problem-focused coping strategies had positive caregiving experiences [40]. Haley et al found that by 3 years post-stroke many of the ill effects of caregiving had resolved, suggesting that some caregivers may be successful in adapting to their “new” post-stroke lives [23].
Understanding the difficulties and issues faced by caregivers throughout the trajectory, from immediately following the stroke through the transition home and, ideally, the adaptation of the caregiver to this new life, provides an opportunity for health care professionals to intervene with strategies to support this major life change.
Caregiving Trajectory and Ongoing Needs of Stroke Caregivers
Stroke survivors and their family caregivers rapidly move from intensive therapy and nursing case management while in a facility to little or no assistance following discharge. Despite case management and discharge planning services received while in an institutional setting, the transition from inpatient care to home can be a crisis point for caregivers [9]. They describe having to figure things out for themselves with little or no formal support after discharge [9,43,44], leaving them feeling overwhelmed, exhausted, and abandoned once they return home [9].
These family members rarely make an active choice to become caregivers; rather, they take on the role because they are unable to perceive or access any other suitable alternatives [8,45]. Whatever their circumstances, these devoted family members are particularly vulnerable as they transition into the caregiving role without an adequate support system for assessing and addressing their needs [7–9,46]. Without this assistance, caregivers develop their own solutions and strategies to meet the needs of the care recipient after discharge [47,48]. Unfortunately, these strategies are often ineffective and may result in safety risks for patients (eg, falls, skin breakdown, choking), and care-related injuries (eg, falls, muscle strains, bruises) and increased stress and anxiety for caregivers [48–50].
Caregivers have described unmet needs in many domains including skills training, communicating with providers, resource identification and activation, finances, respite, and emotional support [35,44,48,51,52]. Bakas et al found that in the first 6 months post-discharge, stroke caregivers had needs and concerns related to information, emotions and behaviors, physical care, instrumental care, and personal responses to caregiving [48], and that their information needs change during the course of the patient’s recovery [53]. In a study by Lutz et al [44], caregivers identified multiple areas where they felt they were unprepared to assume the caregiving role post-discharge. These included identifying and activating resources; making home and transportation modifications to improve accessibility; developing skills in providing physical care and therapies; managing medications and behavioral issues; preventing falls; coordinating care across settings; attending to other family responsibilities; and caring for themselves.
In a study of interactions between rehabilitation providers and stroke caregivers, Creasy et al [52] noted that caregivers have needs, which were often not recognized, in the following areas: information; providing emotional support for the stroke survivor and having their own emotional support needs met; being involved in treatment decisions; and being adequately prepared for discharge home. Caregivers’ interaction styles with providers, which ranged from passive to active/directing, affected their abilities to have their needs recognized and addressed. These findings highlight the importance of recognizing the caregiver’s interaction style and tailoring communication strategies accordingly.
Cameron et al [54] noted that caregiver support needs change over time, with needs being highest during the inpatient phase as they prepare for discharge home. Moreover, caregivers who are providing care for stroke survivors with more severe functional limitations need more support over a longer period of time. Recognizing the needs of stroke caregivers, the 2016 Canadian Stroke Best Practice Recommendations on Managing Transitions of Care Following Stroke includes recommendations related to assessing, educating, and supporting stroke family caregivers [55].
Assessing Caregiver Readiness and Related Outcomes
Young et al [58] recommend specific domains for a comprehensive readiness assessment of stroke family caregivers. Caregiver domains include strength of the caregiver/care recipient relationship; caregiver willingness to provide care; pre-existing health conditions, previous responsibilities, caregiving experience, home and transportation accessibility, available resources, emotional response to the stroke, and ability to sustain the caregiving role. This type of readiness assessment should be completed early in the care trajectory, while the stroke survivor is receiving inpatient care, so that care plans can be tailored to address gaps in caregiver preparation prior to discharge. It is especially important for new caregivers and those caring for stroke survivors with significant functional limitations [44]. Currently there are no tools designed to assess a family member’s readiness to assume the caregiver role.
Validated instruments have been developed to assess caregiving outcomes, including preparedness, with caregivers who have been providing care for a period of time. For example, the Mutuality and Preparedness Scales of the Family Caregiver Inventory was developed with caregivers 6 months post-discharge [59] and has been validated with stroke caregivers at 3 months post-discharge [60].
Several validated tools are available to assess the caregiver’s changing needs and the effects of care provision on well-being [8,45,61]. For example, the Caregiver Strain Index [62] has been validated in studies with stroke family caregivers [11,28]. Bakas developed 2 scales to specifically assess stroke caregivers post-discharge. The Bakas Caregiving Outcomes Scale assesses caregiver life changes [63] and the Needs and Concerns Checklist assesses post-discharge caregiver needs [48]. There are many other instruments designed to assess general caregiving outcomes, including depressive symptoms, burden, anxiety, and well-being. For a list relevant tools see Deeken et al [61] and The Selected Caregiver Assessment Measures from the Family Caregiver Alliance [64].
While these scales are helpful for assessing caregivers who are already providing care, they do not capture the gaps in caregiver readiness prior to patient discharge from the institutional setting. Taken together, these studies suggest that assessing readiness and implementing interventions to improve caregiver preparation prior to discharge and assessing and addressing their changing needs over time, from inpatient care to community reintegration, may be important strategies for improving both caregiver and stroke survivor outcomes. These strategies may also facilitate sustainability of the caregiver role over time.
Interventions to Improve Caregiver Outcomes
In a review of 39 articles representing 32 caregiver and dyad intervention studies, researchers from the AHA made 13 evidence-based recommendations. Recommendations with the highest level of evidence indicated that (1) interventions that combined skill-building with psycho-educational programs were better than psycho-educational interventions alone; (2) interventions that are tailored to the individual are preferred over “one-size-fits-all” interventions; (3) face-to-face interventions are preferred, but telephone interventions can be useful when face-to-face is not feasible; and (4) interventions with 5 to 9 sessions are recommended [65]. In a review of 18 studies, Cheng et al confirmed the recommendation that psychoeducational interventions that focused on skill building improved caregiver well-being and reduced stroke survivor heath care utilization [66].
Studies also recommend that families may need family counseling to help them develop positive coping strategies and adjust to their lives after stroke [66]. Stroke survivors and their families experience grief and loss as they begin to realize how the stroke has changed their relationships, roles, responsibilities, and future plans for their lives (eg, work, retirement). While many inpatient rehabilitation facilities may provide services from a neuro-psychologist to discuss post-stroke changes in the brain and possible behavioral and emotional manifestations, referrals for family counseling to address the impact of stroke on the family and community reintegration are seldom provided [9].
Recent interventions have shown promise in improving stroke caregiver outcomes. For example, Bakas et al. completed a randomized controlled trial of an 8-week, nurse-delivered, Telephone Assessment and Skill-Building Kit (TASK) intervention [67]. Caregivers in the intervention group with moderate to severe depressive symptoms at baseline demonstrated significant improvements in depressive symptoms and life changes at 8, 24, and 52 weeks. The TASK shows promise because it can reach caregivers in rural and urban areas at a relatively low cost [67].
Recognizing the need to improve post-acute care for stroke survivors and their family caregivers, several large funded clinical trials are being tested in the US and globally. For example, the ATTEND Trial in India is testing a home-based, caregiver-led rehabilitation intervention [68]. The Comprehensive Post-Acute Stroke Services (COMPASS) study in North Carolina, is a state-wide pragmatic, randomized controlled trial testing a comprehensive community-based patient-centered post-acute care intervention with stroke survivors and their caregivers (www.nccompass-study.org). Results of these and other studies will continue to identify evidence-based strategies to improve care coordination, quality of care, and post-stroke outcomes for stroke survivors and their caregivers
Recommendations for Clinicians
Based on this review we have identified strategies that clinicians can implement across the care continuum that may help reduce caregiver strain and burden, and improve outcomes for family caregivers and the stroke survivors for whom they provide care. The evidence suggests that caregivers need assistance in building skills, not only in providing the care needed by the stroke survivor but also in solving problems as they arise; navigating the multiple systems of care, including understanding options for post-acute care; accessing community resources; communicating effectively with health care and social support providers; and dealing with the emotional effects of stroke [44,52].
Caregivers need help in navigating the multiple providers and systems of care to get the services the stroke survivor needs as well as to secure support services. They need information from trusted sources about stroke prevention and available community resources. Providinga list of resources is often insufficient, especially in the first few weeks or months post-stroke; these caregivers are already overwhelmed with the enormity of the tasks and responsibilities that they have taken on as a caregiver. Instead they need someone who can advocate for them and connect them with the appropriate resources at the right time.
They also need assistance developing and maintaining self-care strategies so they can sustain the caregiving role long-term. Identifying opportunities for respite and helping them activate informal and formal resources, such as other family members, friends, church groups, neighbors, and services from local senior centers, independent living centers, or area agencies on aging can help them identify assistance with the breadth of duties including care of the stroke survivor, meal preparation, transportation, or a supportive listening ear. It is important for the caregiver, in addition to any other close support person as available, to have a facilitated discussion withthe healthcare team to brainstorm activities where assistance may be provided and who might be approached to help.
The timing of providing support and resources is also critical. Becoming a caregiver is a process and often family members who are new to the role need more intense direct assistance and support when the stroke survivor first comes home, but many may need ongoing support over time. Research suggests it can take caregivers up to 3 years to figure out how to manage the new responsibilities, learn to navigate the multiple systems for careand services, establish confidence in their abilities, deal with the emotional upheaval, and to adapt to their new lives [23].
Research indicates the 44% of stroke patients receive no post-acute care. Clinicians also need to advocate for patients to get the most appropriate level of organized, coordinated, and inter-professional post-acute care [5]. This requires that they understand the different levels of post-acute care, including the criteria for admission, the scope and intensity of nursing, therapy, physician and other services provided in each setting, and the associated clinical outcomes. This knowledge is also necessary to enable clinicians to educate stroke survivors and their caregivers on post-acute care so that they understand the process and can effectively self-advocate for the provision of appropriate services as needed.
Approximately 45% of stroke survivors in the US are discharged either to an inpatient rehabilitation facility or SNF for rehabilitation [4]. Patients discharged to an inpatient rehabilitation facility receive a minimum of 3 hours of therapy per day and are cared for 24 hours/day by a staff led by registered nurses (RNs) with rehabilitation expertise. SNFs do not have minimum requirements for hours of therapy, 24-hour RN staffing, nor a requirement for nurses with specialty training in rehabilitation. Pressure to reduce the length of stay in acute care often results in providers transitioning stroke survivors to the post-acute care setting that accepts the patient first. Because SNFs have fewer criteria for admission, they are more likely to rapidly accept a patient for care when compared to an inpatient rehabilitation facility. Providers must determine and make recommendations for the most appropriate level of post-acute care to ensure the stroke patients’ rehabilitation needs can be met in the recommended setting [5,69]. It is also essential that family caregivers have the knowledge and skills to advocate for the appropriate level of post-acute care based on the stroke survivor’s expected recovery trajectory. Research has demonstrated that that stroke survivors admitted to an inpatient rehabilitation facility, when compared to similar patients in a SNF, have better outcomes, including improved function [70] and lower re-hospitalization and death rates [71,72]. The Association of Rehabilitation Nurses provides resources for health care professionals and patients regarding rehabilitation. For more information for professionals about levels of post-acute care, see www.rehabnurse.org/uploads/files/healthpolicy/ARN_Care_Transitions_White_Paper_Journal_Copy_FINAL.pdf [73]. For information for patients and caregivers, see www.restartrecovery.org.
Providers must also be knowledgeable about community resources in order to provide connections to services and agencies that are relevant to the changing needs of the caregiver over time. Initially, caregivers may need assistance in meeting the stroke survivor’s BADL/IADL, and later needs may expand to include support groups, respite, and opportunities for a greater community engagement.
Training in time management provides room in the busy caregiving schedule for self-care for the caregiver. Providers must assist with determining routines that meet the needs of both the caregiver and stroke survivor, as the health of each is dependent on the other. Assistance in developing a wellness program that is feasible for the caregiver to maintain will improve adoption of health promoting practices.
As discussed above, the needs of both the stroke survivor and caregiver vary along the post-stroke trajectory. Therefore, both caregivers and stroke survivors should be assessed intermittently over time: caregivers for evidence of effective coping strategies and confidence in the sustaining the caregiving role, and stroke survivors for improvement in their functional abilities and compensatory strategies in BADL/IADL. The opportunity for the stroke survivor to assume household tasks that decrease the caregiver burden, in addition to providing a greater sense of purpose for the stroke survivor, must be explored. For example, the stroke survivor may be able to assist with activities such as meal planning and components of meal preparation or light housekeeping utilizing adaptive devices as needed.
Additional research is necessary to understand how the needs of caregivers change over time, the appropriate timing of reassessment, and the evaluation of interventions to facilitate the transition into this role, while preventing the adverse effects of caregiving on the health of the caregiver and stroke survivor during this transition period.
Conclusion
There is clear evidence that stroke caregiving can have detrimental effects on the physical, mental, and emotional health of caregivers, and that these effects are sustained over time. Evidence also indicates that caregivers who are not well-prepared to assume the caregiving role are more likely to experience negative outcomes. Studies suggest that the time of transition from inpatient care to home is a time of crisis for caregivers and that their support needs are high during this time. However, research also indicates that while needs may change over time, caregivers need ongoing support, especially if they are providing care for a stroke survivor who has moderate to severe physical, cognitive, and/or communication limitations.
In order to better understand the needs of stroke caregivers, a pre-discharge assessment of their readiness to provide care should be conducted so that interventions can be tailored to address their needs to minimize negative effects of a poorly planned transition [69]. Currently, there are assessment tools that can be used with caregivers post-discharge to assess their self-reported needs (after they have an understanding of the role) and caregiving outcomes. Research is needed to develop a valid and reliable tool thatpre-emptively assesses the gaps in caregiver readiness that can be utilized prior to the transition from the institutional setting to home. This will enable the identification and evaluation of primary prevention strategies to improve caregiver preparation so that the adaption to the new caregiving role can be expedited, minimizing the adverse health effects on both the caregiver and stroke survivor.
Providers must be aware of the changing needs of stroke survivors and tailor plans of care accordingly, using evidenced-based interventions. Policy makers must consider research on the long term effects of caregiving and consider legislation to support the health and respite needs of the growing population of caregivers. This will contribute to attaining the 3 aims of the National Quality Strategy: improving quality of care, improving health, and reducing health care system costs [74].
Corresponding author: Barbara J. Lutz, PhD, 601 S. College Rd., Wilmington, NC 28403, [email protected].
Financial disclosures: None.
1. Mozaffarian D, Benjamin EJ, Go AS, et al. on behalf of the American Heart Association Statistics Committee & Stroke Statistics Subcommittee. Heart disease and stroke statistics - 2016 update: A report from the American Heart Association. Circulation 2016;132:e38–e360.
2. Feigin VL, Krishnamurthi RV, Parmar P, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology 2015;45:161–76.
3. Hall MJ, Levant S, DeFrances CJ. Hospitalization for stroke in U.S. hospitals, 1989-2009. Hyattsville, MD: National Center for Heatlh Statistics; 2012.
4. Prvu Bettger J, McCoy L, Smith EE, et al. Contemporary trends and predictors of postacute service use and routine discharge home after stroke. J Am Heart Assoc 2015;4(2).
5. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016;47:e98–e169.
6. Talley RC, Crews JE. Framing the public health of caregiving. Am J Public Health 2007;97:224–8.
7. van Exel NJ, Koopmanschap MA, van den Berg B, et al. Burden of informal caregiving for stroke patients: odentification of caregivers at risk of adverse health effects. Cerebrovasc Dis 2005;19:11–7.
8. van Exel NJ, Scholte op Reimer WJ, Brouwer WB, et al. Instruments for assessing the burden of informal caregiving for stroke patients in clinical practice: a comparison of CSI, CRA, SCQ and self-rated burden. Clin Rehabil 2004;18:203–14.
9. Lutz BJ, Young ME, Cox KJ, et al. The crisis of stroke: experiences of patients and their family caregivers. Top Stroke Rehabil 2011;18:786–97.
10. McCullagh E, Brigstocke G, Donaldson N, Kalra L. Determinants of caregiving burden and quality of life in caregivers of stroke patients. Stroke 2005;36:2181–6.
11. van Exel NJ, Brouwer WB, van den Berg B, et al. What really matters: an inquiry into the relative importance of dimensions of informal caregiver burden. Clin Rehabil 2004;18:683–93.
12. Perrin PB, Heesacker M, Hinojosa MS et al. Identifying at-risk, ethnically diverse stroke caregivers for counseling: a longitudinal study of mental health. Rehabil Psychol 2009;54:138–49.
13. Greenwood N, Mackenzie A, Cloud GC, Wilson N. Informal carers of stroke survivors--factors influencing carers: a systematic review of quantitative studies. Disabil Rehabil 2008;30:1329–49.
14. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs 2015;24:2376–82.
15. White CL, Barrientos R, Dunn K. Dimensions of uncertainty after stroke: perspectives of the stroke survivor and family caregiver. J Neurosci Nurs 2014;46:233–40.
16. Saban KL, Sherwood PR, DeVon HA, Hynes DM. Measures of psychological stress and physical health in family caregivers of stroke survivors: a literature review. J Neurosci Nurs 2010;42:128–38.
17. Kruithof WJ, Post, MWM, van Mierlo M, et al. Caregiver burden and emotional problems in partners of stroke patients at two months and one year post-stroke: determinants and prediction. Patient Educ Couns 2016. Forthcoming.
18. Sarre S, Redlich C, Tinker A, et al. A systematic review of qualitative studies on adjusting after stroke: lessons for the study of resilience. Disabil Rehabil 2014;36:716–26.
19. Cameron JI, Naglie G, Dick T, et al. Are we meeting the changing needs of family caregivers to stroke survivors across the care continuum? A systematic review of the caregiver intervention literature. Stroke 2012;43:E143-E.
20. Miller EL, Murray L, Richards L, et al. Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke ptient: a scientific statement from the American Heart Association. Stroke 2010;41:2402–48.
21. Perrin PB, Heesacker M, Stidham BS, et al. Structural equation modeling of the relationship between caregiver psychosocial variables and functioning of individuals with stroke. Rehabil Psychol 2008;53:54–62.
22. Roth DL, Perkins M, Wadley VG, et al. Family caregiving and emotional strain: associations with quality of life in a large national sample of middle-aged and older adults. Qual Life Res 2009;18:679–88.
23. Haley WE, Roth DL, Hovater M, Clay OJ. Long-term impact of stroke on family caregiver well-being: a population-based case-control study. Neurology 2015;84:1323–9.
24. Greenwood N, Mackenzie A. Informal caring for stroke survivors: meta-ethnographic review of qualitative literature. Maturitas 2010;66:268–76.
25. Ostwald SK, Bernal MP, Cron SG, Godwin KM. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Top Stroke Rehabil 2009;16:93–104.
26. Brereton L, Carroll C, Barnston S. Interventions for adult family carers of people who have had a stroke: a systematic review. Clin Rehabil 2007;21:867–84.
27. Greenwood N, Mackenzie A, Cloud G, Wilson N. Loss of autonomy, control and independence when caring: a qualitative study of informal carers of stroke survivors in the first three months after discharge. Disabil Rehabil 2009:1–9.
28. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses of patients with stroke from initial inpatient rehabilitation to 3 years poststroke: course and relations with coping strategies. Stroke 2009;40:1399–404.
29. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses in the chronic phase after stroke: improvement or deterioration between 1 and 3 years after stroke? Patient Educ Couns 2008;73:153–8.
30. Haley WE, Allen JY, Grant JS, et al. Problems and benefits reported by stroke family caregivers: results from a prospective epidemiological study. Stroke 2009;40:2129–33.
31. Berg A, Palomaki H, Lonnqvist J, et al. Depression among caregivers of stroke survivors. Stroke 2005;36:639–43.
32. van Heugten C, Visser-Meily A, Post M, Lindeman E. Care for carers of stroke patients: evidence-based clinical practice guidelines. J Rehabil Med 2006;38:153–8.
33. Bakas T, Kroenke K, Plue LD, et al. Outcomes among family caregivers of aphasic versus nonaphasic stroke survivors. Rehabil Nurs 2006;31:33–42.
34. Gaugler JE. The longitudinal ramifications of stroke caregiving: a systematic review. Rehabil Psychol 2010;55:108–25.
35. Andrew NE, Kilkenny MF, Naylor R, et al. The relationship between caregiver impacts and the unmet needs of survivors of stroke. Patient Prefer Adher 2015;9:1065–73.
36. Chung ML, Bakas T, Plue LD, Williams LS. Effects of self-esteem, optimism, and perceived control on depressive symptoms in stroke survivor-spouse dyads. J Cardiovasc Nurs 2016;31:E8–E16.
37. Grant JS, Clay OJ, Keltner NL, et al. Does caregiver well-being predict stroke survivor depressive symptoms? a mediation analysis. Top Stroke Rehabil 2013;20:44–51.
38. Murray J, Young J, Forster A, Ashworth R. Developing a primary care-based stroke model: the prevalence of longer-term problems experienced by patients and carers. Br J Gen Pract 2003;53:803–7.
39. Pierce LL, Steiner V, Govoni A, et al. Two sides to the caregiving story. Top Stroke Rehabil 2007;14:13–20.
40. Mackenzie A, Greenwood N. Positive experiences of caregiving in stroke: a systematic review. Disabil Rehabil 2012;34:1413–22.
41. Parag V, Hackett ML, Yapa CM, et al. The impact of stroke on unpaid caregivers: results from The Auckland Regional Community Stroke study, 2002-2003. Cerebrovasc Dis (Basel, Switzerland) 2008;25:548–54.
42. Kruithof WJ, Post MWM, Visser-Meily JMA. Measuring negative and positive caregiving experiences: a psychometric analysis of the Caregiver Strain Index Expanded. Clin Rehabil 2015;29:1224–33.
43. Lutz BJ. Determinants of discharge destination for stroke patients. Rehabil Nurs 2004;29:154–63.
44. Lutz BJ, Young ME, Creasy KR, et al. Improving stroke caregiver readiness for transition from inpatinet rehabilitation to home. Gerontologist 2016. Forthcoming.
45. Visser-Meily JM, Post MW, Riphagen II, Lindeman E. Measures used to assess burden among caregivers of stroke patients: a review. Clin Rehabil 2004;18:601–23.
46. Moon M. The unprepared caregiver. Gerontologist 2016 Apr 21.
47. Pierce LL, Steiner V, Govoni AL, et al. Internet-based support for rural caregivers of persons with stroke shows promise. Rehabil Nurs 2004;29:95–9,103.
48. Bakas T, Austin JK, Okonkwo KF, et al. Needs, concerns, strategies, and advice of stroke caregivers the first 6 months after discharge. J Neurosci Nurs 2002;34:242–51.
49. Lutz BJ, Chumbler NR, Lyles T, et al. Testing a home-telehealth programme for US veterans recovering from stroke and their family caregivers. Disabil Rehabil 2009;31:402–9.
50. Hayes J, Chapman P, Young LJ, Rittman M. The prevalence of injury for stroke caregivers and associated risk factors. Top Stroke Rehabil 2009;16:300–7.
51. Cameron JI, Gignac MA. “Timing It Right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns 2008;70:305–14.
52. Creasy KR, Lutz BJ, Young ME, et al. The impact of interactions with providers on stroke caregivers’ needs. Rehabil Nurs 2013;38:88–98.
53. Bakas T, Farran CJ, Austin JK, et al. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building Kit (TASK). Top Stroke Rehabil 2009;16:105–21.
54. Cameron JI, Naglie G, Silver FL, Gignac MA. Stroke family caregivers’ support needs change across the care continuum: a qualitative study using the timing it right framework. Disabil Rehabil 2013;35:315–24.
55. Cameron JI, O’Connell C, Foley N, et al. Canadian Stroke Best Practice Recommendations: Managing transitions of care following Stroke. Guidelines Update 2016. Int J Stroke. 2016.
56. Family Caregiver Alliance. Caregivers Count Too! A toolkit to help practitioners assess the needs of family caregivers. San Francisco: 2006. Accessed 16 Aug 2016 at www.caregiver.org/caregivers-count-too-toolkit.
57. Messecar DC. Nursing standard of practice protocol: family caregiving [Internet]. Accessed at www.consultgeri.org/geriatric-topics/family-caregiving.
58. Young ME, Lutz BJ, Creasy KR et al. A comprehensive assessment of family caregivers of stroke survivors during inpatient rehabilitation. Disabil Rehabil 2014;36:1892–902.
59. Archbold PG, Stewart BJ, Greenlick MR, Harvath T. Mutuality and preparedness as predictors of caregiver role strain. Res Nurs Health 1990;13:375–84.
60. Pucciarelli G, Savini S, Byun E, et al. Psychometric properties of the Caregiver Preparedness Scale in caregivers of stroke survivors. Heart & Lung 2014;43:555–60.
61. Deeken JF, Taylor KL, Mangan P et al. Care for the caregivers: a review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J Pain Symptom Manage 2003;26:922–53.
62. Haley WE, Roth DL, Howard G, Safford MM. Caregiving strain and estimated risk for stroke and coronary heart disease among spouse caregivers: differential effects by race and sex. Stroke 2010;41:331–6.
63. Bakas T, Champion V, Perkins SM, et al. Psychometric testing of the revised 15-item Bakas Caregiving Outcomes Scale. Nurs Res 2006;55:346–55.
64. Family Caregiver Alliance. Selected caregiver assessment measures: A resource inventory for practitioners. 2d ed. Accessed at www.caregiver.org/selected-caregiver-assessment-measures-resource-inventory-practitioners-2012.
65. Bakas T, Clark PC, Kelly-Hayes M, et al. Evidence for stroke family caregiver and dyad interventions: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:2836–52.
66. Cheng HY, Chair SY, Chau JPC. The effectiveness of psychosocial interventions for stroke family caregivers and stroke survivors: a systematic review and meta-analysis. Patient Educ Couns 2014;95:30–44.
67. Bakas T, Austin JK, Habermann B, et al. Telephone assessment and skill-building kit for stroke caregivers a randomized controlled clinical trial. Stroke 2015;46:3478–87.
68. Alim M, Lindley R, Felix C, et al. Family-led rehabilitation after stroke in India: the ATTEND trial, study protocol for a randomized controlled trial. Trials 2016;17:13.
69. Camicia M, Lutz B. Nursing’s role in successful transitions across settings. Stroke 2016. Forthcoming.
70. Chan L, Sandel ME, Jette AM, et al. Does postacute care site matter? A longitudinal study assessing functional recovery after a stroke. Arch Phys Med Rehabil 2013;94:622–9.
71. Kind AJ, Smith MA, Pandhi N, et al. Bouncing-back: rehospitalization in patients with complicated transitions in the first thirty days after hospital discharge for acute stroke. Home Health Care Serv Q 2007;26:37–55.
72. Bettger JP, Liang L, Xian Y, et al. Inpatient rehabilitation facility care reduces the likelihood of death and rehospitalization after stroke compared with skilled nursing facility care [abstract]. Stroke 2015; A146.
73. Camicia M, Black T, Farrell J, et al. The essential role of the rehabilitation nurse in facilitating care transitions: a white paper by the Association of Rehabilitation Nurses. Rehabil Nurs 2014;39:3–15.
74. Centers for Medicare and Medicaid. CMS quality strategy 2016. Accessed at www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualityinitiativesgeninfo/downloads/cms-quality-strategy.pdf.
1. Mozaffarian D, Benjamin EJ, Go AS, et al. on behalf of the American Heart Association Statistics Committee & Stroke Statistics Subcommittee. Heart disease and stroke statistics - 2016 update: A report from the American Heart Association. Circulation 2016;132:e38–e360.
2. Feigin VL, Krishnamurthi RV, Parmar P, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology 2015;45:161–76.
3. Hall MJ, Levant S, DeFrances CJ. Hospitalization for stroke in U.S. hospitals, 1989-2009. Hyattsville, MD: National Center for Heatlh Statistics; 2012.
4. Prvu Bettger J, McCoy L, Smith EE, et al. Contemporary trends and predictors of postacute service use and routine discharge home after stroke. J Am Heart Assoc 2015;4(2).
5. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016;47:e98–e169.
6. Talley RC, Crews JE. Framing the public health of caregiving. Am J Public Health 2007;97:224–8.
7. van Exel NJ, Koopmanschap MA, van den Berg B, et al. Burden of informal caregiving for stroke patients: odentification of caregivers at risk of adverse health effects. Cerebrovasc Dis 2005;19:11–7.
8. van Exel NJ, Scholte op Reimer WJ, Brouwer WB, et al. Instruments for assessing the burden of informal caregiving for stroke patients in clinical practice: a comparison of CSI, CRA, SCQ and self-rated burden. Clin Rehabil 2004;18:203–14.
9. Lutz BJ, Young ME, Cox KJ, et al. The crisis of stroke: experiences of patients and their family caregivers. Top Stroke Rehabil 2011;18:786–97.
10. McCullagh E, Brigstocke G, Donaldson N, Kalra L. Determinants of caregiving burden and quality of life in caregivers of stroke patients. Stroke 2005;36:2181–6.
11. van Exel NJ, Brouwer WB, van den Berg B, et al. What really matters: an inquiry into the relative importance of dimensions of informal caregiver burden. Clin Rehabil 2004;18:683–93.
12. Perrin PB, Heesacker M, Hinojosa MS et al. Identifying at-risk, ethnically diverse stroke caregivers for counseling: a longitudinal study of mental health. Rehabil Psychol 2009;54:138–49.
13. Greenwood N, Mackenzie A, Cloud GC, Wilson N. Informal carers of stroke survivors--factors influencing carers: a systematic review of quantitative studies. Disabil Rehabil 2008;30:1329–49.
14. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs 2015;24:2376–82.
15. White CL, Barrientos R, Dunn K. Dimensions of uncertainty after stroke: perspectives of the stroke survivor and family caregiver. J Neurosci Nurs 2014;46:233–40.
16. Saban KL, Sherwood PR, DeVon HA, Hynes DM. Measures of psychological stress and physical health in family caregivers of stroke survivors: a literature review. J Neurosci Nurs 2010;42:128–38.
17. Kruithof WJ, Post, MWM, van Mierlo M, et al. Caregiver burden and emotional problems in partners of stroke patients at two months and one year post-stroke: determinants and prediction. Patient Educ Couns 2016. Forthcoming.
18. Sarre S, Redlich C, Tinker A, et al. A systematic review of qualitative studies on adjusting after stroke: lessons for the study of resilience. Disabil Rehabil 2014;36:716–26.
19. Cameron JI, Naglie G, Dick T, et al. Are we meeting the changing needs of family caregivers to stroke survivors across the care continuum? A systematic review of the caregiver intervention literature. Stroke 2012;43:E143-E.
20. Miller EL, Murray L, Richards L, et al. Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke ptient: a scientific statement from the American Heart Association. Stroke 2010;41:2402–48.
21. Perrin PB, Heesacker M, Stidham BS, et al. Structural equation modeling of the relationship between caregiver psychosocial variables and functioning of individuals with stroke. Rehabil Psychol 2008;53:54–62.
22. Roth DL, Perkins M, Wadley VG, et al. Family caregiving and emotional strain: associations with quality of life in a large national sample of middle-aged and older adults. Qual Life Res 2009;18:679–88.
23. Haley WE, Roth DL, Hovater M, Clay OJ. Long-term impact of stroke on family caregiver well-being: a population-based case-control study. Neurology 2015;84:1323–9.
24. Greenwood N, Mackenzie A. Informal caring for stroke survivors: meta-ethnographic review of qualitative literature. Maturitas 2010;66:268–76.
25. Ostwald SK, Bernal MP, Cron SG, Godwin KM. Stress experienced by stroke survivors and spousal caregivers during the first year after discharge from inpatient rehabilitation. Top Stroke Rehabil 2009;16:93–104.
26. Brereton L, Carroll C, Barnston S. Interventions for adult family carers of people who have had a stroke: a systematic review. Clin Rehabil 2007;21:867–84.
27. Greenwood N, Mackenzie A, Cloud G, Wilson N. Loss of autonomy, control and independence when caring: a qualitative study of informal carers of stroke survivors in the first three months after discharge. Disabil Rehabil 2009:1–9.
28. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses of patients with stroke from initial inpatient rehabilitation to 3 years poststroke: course and relations with coping strategies. Stroke 2009;40:1399–404.
29. Visser-Meily A, Post M, van de Port I, et al. Psychosocial functioning of spouses in the chronic phase after stroke: improvement or deterioration between 1 and 3 years after stroke? Patient Educ Couns 2008;73:153–8.
30. Haley WE, Allen JY, Grant JS, et al. Problems and benefits reported by stroke family caregivers: results from a prospective epidemiological study. Stroke 2009;40:2129–33.
31. Berg A, Palomaki H, Lonnqvist J, et al. Depression among caregivers of stroke survivors. Stroke 2005;36:639–43.
32. van Heugten C, Visser-Meily A, Post M, Lindeman E. Care for carers of stroke patients: evidence-based clinical practice guidelines. J Rehabil Med 2006;38:153–8.
33. Bakas T, Kroenke K, Plue LD, et al. Outcomes among family caregivers of aphasic versus nonaphasic stroke survivors. Rehabil Nurs 2006;31:33–42.
34. Gaugler JE. The longitudinal ramifications of stroke caregiving: a systematic review. Rehabil Psychol 2010;55:108–25.
35. Andrew NE, Kilkenny MF, Naylor R, et al. The relationship between caregiver impacts and the unmet needs of survivors of stroke. Patient Prefer Adher 2015;9:1065–73.
36. Chung ML, Bakas T, Plue LD, Williams LS. Effects of self-esteem, optimism, and perceived control on depressive symptoms in stroke survivor-spouse dyads. J Cardiovasc Nurs 2016;31:E8–E16.
37. Grant JS, Clay OJ, Keltner NL, et al. Does caregiver well-being predict stroke survivor depressive symptoms? a mediation analysis. Top Stroke Rehabil 2013;20:44–51.
38. Murray J, Young J, Forster A, Ashworth R. Developing a primary care-based stroke model: the prevalence of longer-term problems experienced by patients and carers. Br J Gen Pract 2003;53:803–7.
39. Pierce LL, Steiner V, Govoni A, et al. Two sides to the caregiving story. Top Stroke Rehabil 2007;14:13–20.
40. Mackenzie A, Greenwood N. Positive experiences of caregiving in stroke: a systematic review. Disabil Rehabil 2012;34:1413–22.
41. Parag V, Hackett ML, Yapa CM, et al. The impact of stroke on unpaid caregivers: results from The Auckland Regional Community Stroke study, 2002-2003. Cerebrovasc Dis (Basel, Switzerland) 2008;25:548–54.
42. Kruithof WJ, Post MWM, Visser-Meily JMA. Measuring negative and positive caregiving experiences: a psychometric analysis of the Caregiver Strain Index Expanded. Clin Rehabil 2015;29:1224–33.
43. Lutz BJ. Determinants of discharge destination for stroke patients. Rehabil Nurs 2004;29:154–63.
44. Lutz BJ, Young ME, Creasy KR, et al. Improving stroke caregiver readiness for transition from inpatinet rehabilitation to home. Gerontologist 2016. Forthcoming.
45. Visser-Meily JM, Post MW, Riphagen II, Lindeman E. Measures used to assess burden among caregivers of stroke patients: a review. Clin Rehabil 2004;18:601–23.
46. Moon M. The unprepared caregiver. Gerontologist 2016 Apr 21.
47. Pierce LL, Steiner V, Govoni AL, et al. Internet-based support for rural caregivers of persons with stroke shows promise. Rehabil Nurs 2004;29:95–9,103.
48. Bakas T, Austin JK, Okonkwo KF, et al. Needs, concerns, strategies, and advice of stroke caregivers the first 6 months after discharge. J Neurosci Nurs 2002;34:242–51.
49. Lutz BJ, Chumbler NR, Lyles T, et al. Testing a home-telehealth programme for US veterans recovering from stroke and their family caregivers. Disabil Rehabil 2009;31:402–9.
50. Hayes J, Chapman P, Young LJ, Rittman M. The prevalence of injury for stroke caregivers and associated risk factors. Top Stroke Rehabil 2009;16:300–7.
51. Cameron JI, Gignac MA. “Timing It Right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns 2008;70:305–14.
52. Creasy KR, Lutz BJ, Young ME, et al. The impact of interactions with providers on stroke caregivers’ needs. Rehabil Nurs 2013;38:88–98.
53. Bakas T, Farran CJ, Austin JK, et al. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building Kit (TASK). Top Stroke Rehabil 2009;16:105–21.
54. Cameron JI, Naglie G, Silver FL, Gignac MA. Stroke family caregivers’ support needs change across the care continuum: a qualitative study using the timing it right framework. Disabil Rehabil 2013;35:315–24.
55. Cameron JI, O’Connell C, Foley N, et al. Canadian Stroke Best Practice Recommendations: Managing transitions of care following Stroke. Guidelines Update 2016. Int J Stroke. 2016.
56. Family Caregiver Alliance. Caregivers Count Too! A toolkit to help practitioners assess the needs of family caregivers. San Francisco: 2006. Accessed 16 Aug 2016 at www.caregiver.org/caregivers-count-too-toolkit.
57. Messecar DC. Nursing standard of practice protocol: family caregiving [Internet]. Accessed at www.consultgeri.org/geriatric-topics/family-caregiving.
58. Young ME, Lutz BJ, Creasy KR et al. A comprehensive assessment of family caregivers of stroke survivors during inpatient rehabilitation. Disabil Rehabil 2014;36:1892–902.
59. Archbold PG, Stewart BJ, Greenlick MR, Harvath T. Mutuality and preparedness as predictors of caregiver role strain. Res Nurs Health 1990;13:375–84.
60. Pucciarelli G, Savini S, Byun E, et al. Psychometric properties of the Caregiver Preparedness Scale in caregivers of stroke survivors. Heart & Lung 2014;43:555–60.
61. Deeken JF, Taylor KL, Mangan P et al. Care for the caregivers: a review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J Pain Symptom Manage 2003;26:922–53.
62. Haley WE, Roth DL, Howard G, Safford MM. Caregiving strain and estimated risk for stroke and coronary heart disease among spouse caregivers: differential effects by race and sex. Stroke 2010;41:331–6.
63. Bakas T, Champion V, Perkins SM, et al. Psychometric testing of the revised 15-item Bakas Caregiving Outcomes Scale. Nurs Res 2006;55:346–55.
64. Family Caregiver Alliance. Selected caregiver assessment measures: A resource inventory for practitioners. 2d ed. Accessed at www.caregiver.org/selected-caregiver-assessment-measures-resource-inventory-practitioners-2012.
65. Bakas T, Clark PC, Kelly-Hayes M, et al. Evidence for stroke family caregiver and dyad interventions: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:2836–52.
66. Cheng HY, Chair SY, Chau JPC. The effectiveness of psychosocial interventions for stroke family caregivers and stroke survivors: a systematic review and meta-analysis. Patient Educ Couns 2014;95:30–44.
67. Bakas T, Austin JK, Habermann B, et al. Telephone assessment and skill-building kit for stroke caregivers a randomized controlled clinical trial. Stroke 2015;46:3478–87.
68. Alim M, Lindley R, Felix C, et al. Family-led rehabilitation after stroke in India: the ATTEND trial, study protocol for a randomized controlled trial. Trials 2016;17:13.
69. Camicia M, Lutz B. Nursing’s role in successful transitions across settings. Stroke 2016. Forthcoming.
70. Chan L, Sandel ME, Jette AM, et al. Does postacute care site matter? A longitudinal study assessing functional recovery after a stroke. Arch Phys Med Rehabil 2013;94:622–9.
71. Kind AJ, Smith MA, Pandhi N, et al. Bouncing-back: rehospitalization in patients with complicated transitions in the first thirty days after hospital discharge for acute stroke. Home Health Care Serv Q 2007;26:37–55.
72. Bettger JP, Liang L, Xian Y, et al. Inpatient rehabilitation facility care reduces the likelihood of death and rehospitalization after stroke compared with skilled nursing facility care [abstract]. Stroke 2015; A146.
73. Camicia M, Black T, Farrell J, et al. The essential role of the rehabilitation nurse in facilitating care transitions: a white paper by the Association of Rehabilitation Nurses. Rehabil Nurs 2014;39:3–15.
74. Centers for Medicare and Medicaid. CMS quality strategy 2016. Accessed at www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualityinitiativesgeninfo/downloads/cms-quality-strategy.pdf.
First-in-kind study parsed risks of central lines in children
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.

Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.
Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
SAN DIEGO – Rising rates of pediatric venous thromboembolism in the United States underscore the need to carefully weigh the risks and benefits of placing central lines, Julie Jaffray, MD, said at the annual meeting of the American Society of Hematology.
Peripherally inserted central catheters (PICCs) are especially likely to lead to deep vein thrombosis in children, said Dr. Jaffray of Children’s Hospital Los Angeles, University of Southern California. Children and adolescents who received PICCs had about fourfold the rate of this outcome in the next 6 months as did those who received tunneled lines, based on interim results from her first-in-kind, prospective multicenter observational study.
Earlier research has shown that the placement of PICCs approximately doubled at Children’s Hospital Los Angeles between 2005 and 2012, while the use of tunneled lines remained constant at a much-lower rate, Dr. Jaffray noted.
To better understand how central lines contribute to pediatric thrombotic events, she and her associates at the Children’s Hospital of Philadelphia and Texas Children’s Hospital in Houston are studying patients aged 6 months to 18 years who had these devices placed at their centers starting in 2013. To parse out risk factors, the investigators are analyzing numerous relevant keywords from nursing notes and other parts of electronic health records.
As of October 2016, the study included 1,096 patients who received a total of 1,233 central lines related to the treatment of cancer, infection, and other serious conditions. Among 827 PICC recipients, the 6-month cumulative rate of venous thromboembolism was 7.5%. In contrast, only 406 patients received tunneled lines, and only 2% developed venous thromboembolism (P = .004).
But tunneled lines had their own risks. About 16% of recipients developed CLABSI within 6 months, compared with 9% of children who received PICCs (P = .005). The overall rate of CLABSI was 12%, Dr. Jaffray noted.
Thromboses were identified a median of 15 days after PICC placement and 40 days after tunneled line placement, she said. Children with leukemia, other cancers, and congenital heart disease were at significantly increased risk of venous thromboembolism, as were children who received multilumen catheters, she noted.
Ongoing analyses should lead to new guidelines on pediatric catheter selection, insertion techniques, and the prophylactic use of anticoagulation or antiseptics, Dr. Jaffray said. She also is planning a separate study of children younger than 6 months, to examine their unique coagulation systems, she added.
The conclusion at this point is that two-thirds of this cohort received PICCs instead of tunneled lines, and 85% of venous thromboembolism episodes occurred in PICC recipients, Dr. Jaffray emphasized. “Due to their ease of insertion, PICCs are being placed at increasing rates in some pediatric centers, [and] this may be the leading factor for the increasing incidence of pediatric venous thromboembolism,” she commented. “A lot of us pediatric treaters aren’t necessarily giving anticoagulation for an incidental clot, but I think this is something we certainly need to look at. And maybe if we can choose the patients who are at highest risk of VTE, we can consider prophylactic anticoagulation in those kids.”
Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
AT ASH 2016
Key clinical point: Children who received peripherally inserted central catheters were at greatest risk of venous thromboembolism, while those who received tunneled lines were more likely to develop bloodstream infections.
Major finding: Venous thromboembolism occurred in 7.5% of PICC recipients and 2% of tunneled line recipients (P = .004) within 6 months after placement. CLABSI occurred in 16% of tunneled line recipients and 9% of PICC recipients (P = .005).
Data source: An observational study of 1,096 children and adolescents who received central venous catheters at three nationally recognized pediatric hospitals.
Disclosures: Dr. Jaffray did not report funding sources and had no relevant financial disclosures.
Nivolumab plus ipilimumab shines as first-line in advanced NSCLC
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.

CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.

“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.
CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.
“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
VIENNA – The combination of nivolumab and ipilimumab as first-line therapy in patients with advanced non–small cell lung cancer (NSCLC) doubled median progression-free survival time compared with nivolumab monotherapy in updated results from the CheckMate 012 trial, Scott N. Gettinger, MD, reported at the World Congress on Lung Cancer.
This doubling of progression-free survival (PFS) applied to all comers regardless of whether or not their tumor expressed programmed death-ligand 1 (PD-L1). In those patients with any degree of PD-L1 expression – even if just 1% of tumor cells stained positive – combination therapy didn’t just double median PFS, it tripled it, compared with nivolumab alone, added Dr. Gettinger of the Yale Cancer Center in New Haven, Conn.
CheckMate 012 is a phase I study of nivolumab as first-line therapy for advanced NSCLC with numerous treatment arms. Dr. Gettinger presented updated results for 52 patients who received intravenous nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks, 36 patients on nivolumab plus intravenous ipilimumab at 1 mg/kg every 12 weeks, and 39 who received nivolumab plus ipilimumab every 6 weeks. None of the participants had prior chemotherapy for their advanced stage IIIb or IV NSCLC.
Median PFS in the overall study population was 3.6 months with nivolumab monotherapy and 8.0 months with combination therapy. In the roughly 70% of participants who had any degree of tumor PD-L1 expression, median PFS was 3.5 months with monotherapy, compared with 12.7 months in the combined dual therapy arms. And, in the roughly one-quarter of patients whose tumor showed at least 50% PD-L1 expression, median PFS rose to 8.3 months with nivolumab monotherapy and hasn’t yet been reached in patients on combination therapy.
The 1-year overall survival rate in patients on nivolumab monotherapy was 73% in all treated patients, 69% in those with any detectable tumor PD-L1 expression, and 83% in patients with at least 50% PD-L1 expression. In patients on combination therapy, the corresponding figures were higher at 76%, 87%, and 100%.
The clearly enhanced efficacy achieved with the combination of nivolumab plus ipilimumab was accomplished with only a modest increase in toxicity compared with nivolumab alone. At a median follow-up of 22 months in the nivolumab monotherapy group and 16 months for combination therapy, the rate of any treatment-related adverse event leading to study withdrawal was 12% with monotherapy and 18% with combination therapy.
The combination of nivolumab (Opdivo), a PD-L1 immune checkpoint inhibitor, and ipilimumab (Yervoy), a cytotoxic T-lymphocyte–associated protein 4 immune checkpoint inhibitor, is biologically attractive: “The ipilimumab primes the immune system by inducing tumor infiltration of effector T cells while depleting the number of myeloid-derived suppressor cells and suppressive regulatory T cells within the tumor microenvironment,” Dr. Gettinger explained.
Nivolumab is approved for treatment of advanced NSCLC that has progressed despite platinum-based chemotherapy. Of the various toxicities associated with the drug, only dermatologic and GI adverse events occurred more frequently with combination therapy than nivolumab alone.
There were five complete responses in the nivolumab monotherapy group and six with combination therapy. Of note, four of these complete responses occurred in patients without any measurable tumor PD-L1 expression.
Based upon these encouraging results from CheckMate 012, a phase III randomized clinical trial of nivolumab as first-line therapy in patients with advanced NSCLC is underway. In the CheckMate 227 trial, patients with any detectable PD-L1 expression are randomized to nivolumab at 3mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks, nivolumab monotherapy at 240 mg every 2 weeks, or standard platinum-based chemotherapy. Patients with no PD-L1 expression in their tumor are assigned to the nivolumab/ipilimumab combination, or nivolumab at 360 mg every 3 weeks plus chemotherapy, or chemotherapy alone.
“I think we should be cautious despite the excitement about the combination,” argued Dr. Garon, director of thoracic oncology at the University of California, Los Angeles.
He noted that various iterations of the large CheckMate 012 phase I program have been presented repeatedly at major meetings, and the shifting data have raised concerns in his mind about possible patient selection bias stemming from the study design.
“From my perspective, until we see randomized data that can control for these biases, I will remain hopeful but not yet extremely confident that this combination will be the new frontline therapy for metastatic non–small cell lung cancer,” Dr. Garon said.
Dr. Gettinger reported serving as a consultant to Bristol-Myers Squibb, which markets nivolumab.
Dr. Garon reported that his institution receives funding from Bristol-Myers Squibb as well as AstraZeneca, Boehringer Ingelheim, Eli Lilly, Genentech, Mirati, Merck, Pfizer, and Novartis.
AT WCLC 2016
Key clinical point: A combination of two immunotherapy agents with different mechanisms of action produced impressive efficacy and acceptable toxicities as first-line therapy in patients with chemotherapy-naive advanced non–small cell lung cancer.
Major finding: in patients with any detectable tumor PD-L1 expression.
Data source: This analysis from a larger phase I study included 127 patients with no prior chemotherapy for advanced NSCLC.
Disclosures: The study presenter is a consultant to Bristol-Myers Squibb, which sponsored the CheckMate 012 trial.
Using a Medical Interpreter with Persons of Limited English Proficiency
From the Department of Medicine, Mayo Clinic, Rochester, MN.
Abstract
- Objective: To provide an overview of important aspects of interpreting for medical visits for persons with limited English proficiency (LEP).
- Methods: Literature review.
- Results: When working with persons of LEP, providing a professional medical interpreter will facilitate optimal communication. Interpreters may work in different roles including as a conduit, cultural broker, clarifier, and advocate. In-person and remote (videoconferencing or telephonic) interpreting are available and one may be preferred depending on the medical visit. Clinicians should recognize that patients may have a preference for the interpreter’s gender and dialect and accommodations should be made if possible. Prior to the visit, the provider may want to clarify the goals of the medical encounter with the interpreter as some topics may be viewed differently in certain cultures. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient rather than to the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately to allow interpretation. Additionally, providers should assess patient understanding of what has been discussed. After the medical visit, providers should consider discussing with the interpreter any issues with communication or cultural factors noted to have affected the visit.
- Conclusion: Providers should utilize a professional medical interpreter for visits with persons with LEP. Appropriate communication techniques, including talking in first and second tenses and maintaining eye contact with the patient rather than the interpreter, are important for a successful visit. Realizing patients may have interpreter preferences is also important to facilitate patient-centered-care.
Key words: language barriers; quality of care; physician-patient communication; interpreter services.
The United States is a diverse country that includes many persons whose first language is not English. According to the U.S. Census Bureau, more than 63 million persons age 5 and above (about 51 million adults) reported speaking a language other than English at home. Also, about 25.7 million of the population age 5 and up (around 10.6 million adults) noted speaking English less than “very well” [1]. Protecting people from discrimination based on the language they speak is highlighted in Title VI of the Civil Rights Act of 1964 (which focuses on those receiving federal funding). President Clinton, furthermore, in 2000 signed Executive Order 13166, which encouraged federal agencies to provide appropriate access of their services to those with limited English proficiency (LEP) [2,3].
The benefits of using professional interpreters is well-documented. In addition to increased satisfaction with communication when professional medical interpreters are used [4], they also make fewer clinically significant interpretation errors compared to ad hoc interpreters (ie, untrained individuals such as bilingual staff member, family member, or friend who are asked to interpret) [5–7]. LEP patients who do not have a professional interpreter have less understanding of their medical issues, have less satisfaction of their medical care, and may have more tests ordered and be hospitalized more often compared to those who do utilize professional medical interpreters [8]. In addition to improved satisfaction and understanding of medical diagnoses, hospitalized persons requiring interpreters who utilized a professional medical interpreter on admission and discharge were noted to have a shorter length of stay than persons who required an interpreter and did not receive one [9].
Despite the documented benefits of using professional interpreters, they are underutilized. Reasons include underfunded medical interpreting services [10,11], lack of awareness of the risks involved with using an ad hoc interpreter [2,12], providers using their own or another worker’s limited second language skills to communicate rather than using a professional medical interpreter [13,14], perceived delay in obtaining a professional medical interpreter, and judging a medical situation as minor rather than complex [13]. In this article, the roles, importance, and considerations of using a professional medical interpreter are explored.
Case Study
Initial Presentation
A 23-year-old married Somali-speaking female who moved to the United States recently called a local primary care provider’s office to schedule an appointment. When asked the reason for the visit, she said the reason was private. The clinical assistant scheduled her with the next available provider.
When the patient arrived for her clinic appointment, a clinical assistant roomed her and her mother and asked the patient the reason for the visit. The patient remained quiet and her mother replied that she needed to speak with the doctor. When the female medical provider entered, she observed that the patient appeared anxious. When the doctor initiated conversation with the patient, she noted that her English was limited. Her mother tried to explain the reason for the visit saying her daughter was having severe pain. She then pointed towards her daughter’s lower abdomen. The clinician noted the limited English abilities of the patient and mother and used the interpreter line to request a Somali interpreter and placed the first available interpreter available on speaker.
How can patients who need an interpreter be identified?
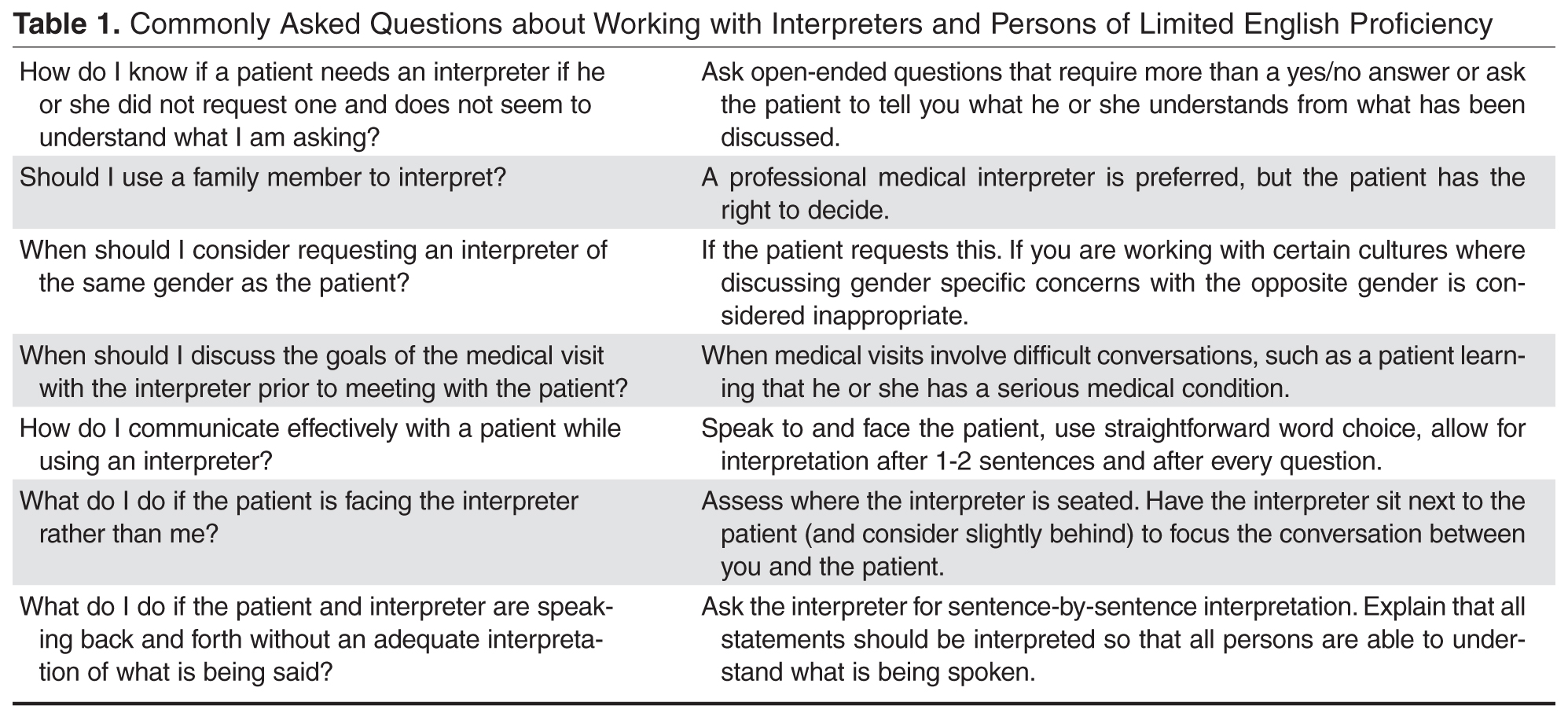
Health care systems can facilitate identifying patients in need of an interpreter by routinely collecting information on LEP status. The patient should be asked during registration if her or she speaks English and has a preferred language, and the answers should be recorded in the medical record [3]. If an interpreter is used during the hospital stay, it should be recorded to alert future providers to the need of an interpreter [15]. Patients may speak a dialect of a common language and this also should be noted, as an interpreter with a similar dialect to the patient should ideally be requested when necessary [16]. Furthermore, health care systems can measure rate of screening for language need at registration and rate of interpreter use during hospital stay to assess language need and adequacy of provision of interpreters to LEP patients [15].
It should be noted that patients may be wary about the presence of an interpreter. In one study involving pediatric oncologists and Spanish-speaking parents, the former reported concern regarding the accuracy of interpretation and the latter were concerned about missing out on important information even with the use of professional medical interpreters [17]. The concern for accuracy of interpreting was shared in a study by Chinese and Vietnamese Americans with LEP [18] as well as in a Swedish study involving Arabic-speaking persons. In the latter study, Arabic-speaking patients also felt uncomfortable speaking about bodily issues in the presence of interpreters [19]. In a study of Latina patients, there were concerns about confidentiality with interpreters [20].
What is the role of the interpreter? Should they offer emotional support to the patient?
Interpreter-as-conduit reflects a neutral, more literal information exchange and is preferred by certain medical providers who prioritize a more exact interpretation of the medical conversation. In this role, the interpreter assumes a more passive role and the emphasis is on the interpreter’s linguistic ability [21]. Providers need to be aware that word-for-word interpretation may not align with what is regarded as culturally sensitive care—such as when the term “cancer” is to be used. Also, word-for-word interpretation does not necessarily mean the patient will understand what is being interpreted if the terminology does not reflect the literacy level or dialect of the person with LEP [22].
Interpreters may also assume an active role, sometimes referred to as clarifier and cultural broker. Clarifying may be utilized, for example, when a medical provider is discussing complicated treatment options. This requires an interpreter to step out of a conduit role (if that is the preferred role) and confirm or clarify information to ensure accurate information exchange [21,23]. As a cultural broker, communication between provider and patient is exchanged in a manner that reflects consideration of the patient’s cultural background. Interpreters may explain, to the provider, the cultural reason for the patient’s perspective of what is causing or contributing to the illness. Cultural brokering may as well include communicating the medical terminology and disease explanation, given by the medical provider, in a way that the patient would understand. This role, additionally, can involve educating the provider about aspects of the culture that may influence the patient’s communication with him or her [22].
Furthermore, interpreters may fulfill an advocate role for patients by helping them understand the health care system and increasing patient empowerment by seeking information and services that the patient may not know to ask about [23].
The interpreter may offer emotional support during a medical visit, for example, where the diagnosis of cancer is conveyed. In such a case, an interpreter’s emotional support may be considered by providers to be appropriate. In contrast, with visits related to mental health evaluations, having the interpreter remain neutral, rather than being a more active participant by offering emotional support, may be preferred [24]. In addition to interpreters remaining more neutral during mental health visits, providers may prefer that interpreters not speak with the patient prior to the visit, depending on the mental health condition, as negative therapeutic consequences may occur [21]. Trust is an important element of the provider-patient relationship and, as such, there is concern on the part of some providers that if the trust of patients falls to the interpreter rather than to the provider, then therapeutic progress may be compromised [24]. In general, clarifying with interpreters the goals of the visit and expectations regarding speaking to the patient outside of the visit may ensure the provider-patient relationship is not diminished [21].
What are the disadvantages and caveats of using family members or bilingual staff as interpreters?
Although family members and other ad hoc interpreters may be present and willing to interpret, the risk of miscommunication is greater than with professional medical interpreters [5,6]. This risk of miscommunication extends to partially bilingual medical providers who do not utilize appropriate interpreter services [10,25]. Ad hoc interpreters may try to answer on behalf the patient [6,26] and may not have the appropriate medical terminology to correctly interpret what the provider is trying to communicate to the patient [6].
Professional medical interpreters are trained to facilitate communication of a spoken language in a medical setting [2,10]. Certification is offered by the National Board of Certification for Medical Interpreters and the Certification Commission for Healthcare Interpreters. In order to be certified certain requirements must be met which include a minimum of 40 hours of health care interpreter training (which includes medical terminology as well as roles and ethics involved in medical interpreting) as well as demonstrated oral proficiency in English as well as another chosen language (such as Spanish) [10].
In certain circumstances, patients may feel more comfortable disclosing personal details with a professional medical interpreter rather than in the presence of an ad hoc interpreter. For example, more details of traumatic events and psychological symptoms were spoken of in the presence of a professional, rather than an ad hoc, interpreter in medical interviews of asylum seekers requiring an interpreter in Switzerland. In the presence of ad hoc interpreters, more physical symptoms were disclosed rather than psychological [6].
Furthermore, in visits concerning sexuality or abuse issues, using family members as interpreters may violate privacy concerns of the patient [2,27]. Additionally, in certain cultures where respect for elders is very important, parents who use children as interpreters may feel that the structure of the family changes when he or she interprets on behalf of the parent [18]. Also, what children consider as embarrassing may not be interpreted to either the parent or to the care provider [8]. Furthermore, one should note there are ethical issues of using non-adult children as interpreters in situations involving confidentiality and privacy—by doing so, there may be resulting harmful effects on non-adult children [27,28].
Patients may at times decline the use of a professional medical interpreter and prefer to have a family member interpret; this preference should be documented in the patient’s medical chart [10]. Caution should be had using an ad hoc interpreter when obtaining informed consent [12].
What professional interpreting services are available to the clinician?
For the most part, access to interpreters via a telephone service is widely available [10]. The cost of providing interpreters in-person and/or remotely varies depending on the health care site [29–31] In general, considerations of using professional medical interpreters, whether remotely or in-person, involves accessibility and cost. There are certain sites that have explored having a shared network of interpreters available via the telephone and videoconference to reduce the cost of providing interpreters for individual hospitals [32]. While the costs of providing a person with LEP with interpretation varies depending on the health care site, the costs of not providing a professional medical interpreter should be considered as well, which include greater malpractice risk and potential medical errors [32]. In addition, the use of employees as interpreters takes time away from their respective jobs, which results in staff time lost [31].
In-person interpreting may be preferred for certain medical visits, as an in-person interpreter can interpret both verbal and nonverbal communication [16]. When emotional support is anticipated, in-person interpreting is usually preferred by providers [24]. There may be improved cultural competence when using an in-person interpreter, which may be important for certain visits such as those involving end-of life care discussions [4]. One concern may involve the comfort level of the patient if he or she personally knows the interpreter; this can occur in smaller ethnic communities [12]. Telephonic interpreting may be preferred in certain medical situations where confidentiality is desired [16].
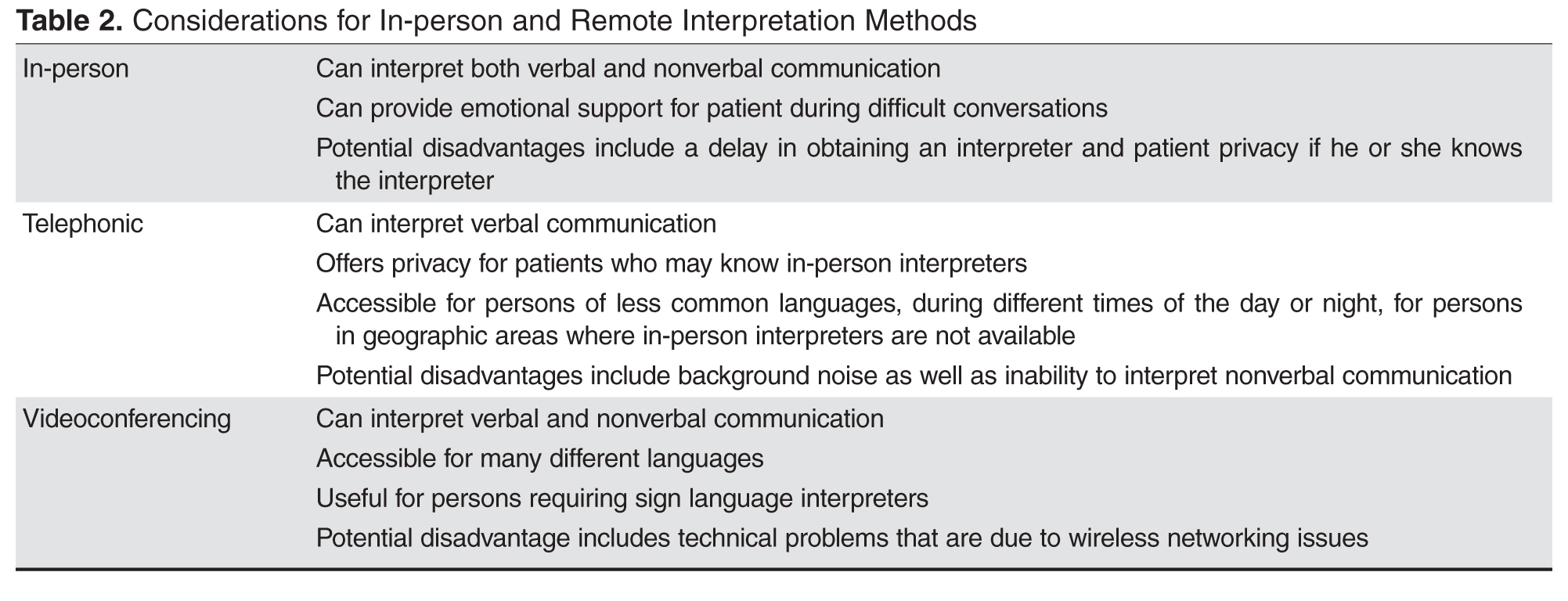
For providers working with persons who are deaf, options for interpreting include in-person sign language interpreters as well as remote videoconference interpretation [10].
- Are in-person interpreting and remote interpreting comparable?
In general, using in-person or remote interpreters does not significantly change patient satisfaction. In a study involving Spanish-speaking patients in a clinic setting, persons requiring an interpreter rated satisfaction of interpreting between in-person, videoconferencing, and telephonic methods highly with no significant differences. Of note, though, medical providers and interpreters preferred in-person rather than the 2 remote interpreting options [33]. In a different study involving Spanish, Chinese, Russian, or Vietnamese interpreters, satisfaction of information exchange was considered equal among the 3 interpreting modalities, although in-person interpreting was felt to establish rapport between clinician and patient with LEP better than telephonic and videoconferencing interpreting [35]. Additionally, in a study of providers in a clinic setting who worked with persons with LEP, no significant differences were noted in provider satisfaction of the medical visit, or in the quality of interpretation or communication, when using in-person versus remote videoconferencing interpretation. Providers, though, noted improved knowledge of the patient’s cultural beliefs when using in-person interpreting [4].
Regarding the question of a difference in understanding when using in-person versus remote interpreters, a study was done in a pediatric emergency department (ED) that compared in-person and telephonic interpretation. Family understanding of the discharge diagnosis was high (about 95%) regardless of whether an in-person or telephonic interpreter was utilized [36]. In a different study comparing telephone and video interpretation in a pediatric ED, while quality of communication and interpretation were rated similarly, the parents who used video interpretation were more likely to name their child’s diagnosis correctly [29].
Case Continued
The physician proceeded with introductions and explained that all conversations would be interpreted. She further stated that if there were any questions, the patient and mother should feel free to ask them. Via the interpreter, who was male, the provider began by asking about the nature of the abdominal pain. The patient looked to her mother and then down without answering. The mother nodded, but did not say more. The provider wondered if their reticence might be due to discomfort with discussing the issue through a male interpreter. The physician asked the patient if she would prefer a female interpreter and, once that was confirmed, she asked if she wanted an in-person or telephonic interpreter. The mother requested a female in-person interpreter.
How might gender-specific issues impact working with an interpreter?
As gender concordance of patient and physician [37] at times is desired, gender concordance of patient and interpreter [16,18] may also be important to optimize communication of gender-specific issues [16,18,37]. For example, an Arabic-speaking man from the Middle East may prefer to discuss sexuality-related concerns in the presence of a male rather than female interpreter [16]. An Arabic-speaking female who has a preference for female providers may prefer a female interpreter when discussing sexuality and undergoing a physical examination [19]. In one study, the majority of Somali females preferred female interpreters as well as female providers for breast, pelvic, and abdominal examinations [38]. If a same-gender interpreter cannot be present, an option is to have the interpreter either leave the room or step behind a curtain or turn away from the patient during a sensitive part of the physical examination [39].
What are recommended strategies for using a medical interpreter?
It is often helpful to have a brief discussion with the interpreter prior to the medical visit with the patient to speak about the general topics that will be discussed (especially if the topics involve sensitive issues or news that could be upsetting to the patient) and the goal of the visit [2, 11]. Certain topics may be viewed dissimilarly in different cultures, thus approaching the interpreter from the view point of cultural broker or liaison [10] may bring to light cultural factors that may influence the medical visit [40,41]. the name of the interpreter should be noted for documentation purposes [10].
To start the visit, introductions of everyone involved should take place with a brief disclosure about the role of the interpreter and assurance of confidentiality on the part of the interpreter [2,11]. Also, the provider should set the expectation that all statements said in the room will be interpreted so that all persons can understand what it being spoken [10].
There are several options for where each person should be positioned. In some medical visits, a triangle is pursued where the interpreter sits lateral to the provider, but this may lead to challenges in maintaining eye contact between the patient and provider. Another option is have the interpreter sit next to [10] and slightly behind the patient to improve eye contact between provider-patient and to maintain the patient-provider relationship [2,41]. When seated, the medical provider should try to sit at the same level as the patient [16]. Seating is different with persons requiring the use of sign language interpreters as the interpreter needs to be visible to the patient for communications purposes. One possibility is having the interpreter sit beside and slightly behind the provider; this positioning allows the patient to understand what is being communicated and also allows the patient to understand what is being communicated and allows him or her to see the provider during the conversation [40].
There are 2 main communication styles used by interpreters: consecutive interpreting, where the interpreter exchanges what has been said by the clinician or patient after each one has finished speaking, and simultaneous interpreting, where the interpreter translates as the person is speaking. Interpreters and medical providers may have a preference and it is important to clarify, if needed, which method is preferred [21].
The provider should face the patient and direct conversation to him or her rather than to the interpreter. Third-person statements should not be used, such as “tell her,” as this directs the conversation to the interpreter rather than to the patient [10]. By using the first and second person (when addressing the patient) and making eye contact, the relationship between the provider and patient is emphasized [14,40].
Choosing the right word is important to have meaningful communication. Interpreters advise that providers should understand that medical concepts may be unfamiliar to patients with LEP. Providers should use simpler words rather than medical terminology to discuss medical issues [42]. In general, straightforward word choice is recommended [16]. Providers are advised to not use acronyms or idioms. It is important to note that humor may be difficult to convey as well [10].
Clinicians are advised to speak clearly and not quickly and to use shorter sentences with appropriate pauses to allow time for the interpreter to interpret (if consecutive rather than simultaneous interpreting style is being used) [2,41,43,44]. In addition to limiting speech to one to two sentences at a time, asking one question at a time is important for optimal communication [43]. To improve information gathering, patients may respond better to open-ended questions [42], which is an aspect of patient-centered communication, as directive questioning often leads to shorter answers [43].
Furthermore, the provider should be aware that persons with LEP may know some English, so statements that one would not say to an English-speaking patient should not be said in the room with a person with LEP [10].
Encouraging the interpreter to clarify certain concepts, if necessary, may provide for improved information exchange [21] as well as encouraging the patient to ask questions during the medical visit may help elucidate potential areas of confusion [22,40,44]. Summarizing important concepts [40] and limiting the number of concepts discussed may increase patient understanding [10]. Additionally, asking the patient to repeat what was discussed in his or her words [10], rather than directly asking if he or she understands, will allow for more meaningful assessment of patient understanding [43].
Finally, recognition that interpreters may experience distress after certain visits, such as an oncologic medical encounters, is important and debriefing may be desired by the interpreter [22,45]. Also, discussing any communication concerns may be helpful [40,42] in addition to discussing certain cultural beliefs that impacted the visit may be educational for the provider [45].
Case Continued
After the female translator arrived, the physician asked the patient if she felt comfortable with her mother in the room for this medical visit. After the patient confirmed that she wanted her mother present, the physician tried to further clarify the reason for the medical visit. Her mother, appearing very concerned, began speaking quickly to the interpreter without stopping for interpretation. When the mother did stop speaking, the interpreter, rather than informing the provider what was spoken of by the mother, dialoged with the mother and the back and forth conversation continued.
What are strategies to optimize the medical visit when the provider is not satisfied with the flow of conversation?
If there are conversations occurring between the patient and interpreter with the exclusion of the provider, the provider should request sentence-by-sentence interpretation by the interpreter. If the interpreter is answering on behalf of the patient, providers should redirect communication to the patient [10]. At times, patients may speak for longer periods without stopping for the interpreter to provide accurate information exchange. The provider in this case may need to interrupt conversation to allow the interpreter time to convey what is being said [14].
If there are family members who know English, but the patient and/or others do not know English, there may be a risk of miscommunication if the exchange of medical information is done by a combination of family members and the interpreter, as the medical information may not accurately reflect what the clinician is trying to convey. The provider may need to redirect the conversation flow through the interpreter to make sure there is consistent information being communicated [22].
Case Continued
Finally, the provider interrupted. She emphasized with the patient, mother, and the interpreter that all that was being said should be interpreted. She asked the interpreter to sit next to the patient and mother (rather than lateral to the physician) so that eye contact between the patient and mother and the provider could be maintained thus supporting the patient-provider relationship. She then asked one question at a time to the patient. She needed to interrupt the conversation again when the mother started to speak to the interpreter without waiting for interpretation. The doctor reemphasized the need to allow time for the interpreter to adequately convey the information. After this the medical visit progressed successfully. Soon the provider found out that the mother was concerned that something serious could be happening to her daughter, as her daughter previously had a miscarriage. After hearing the mother’s concern, the provider was able to clarify with the daughter that the pain was suprapubic and she was having burning when she urinated. After further evaluation, the provider diagnosed a urinary tract infection. She told the patient about the diagnosis and provided her with appropriate medication and instructions on how to take it and for how long. The provider then asked the patient to tell her what she understood about the diagnosis and how to take the medication. The doctor then asked if either had any further questions. After the medical visit, the provider made sure that the patient’s chart reflected the need for a Somali interpreter with the notation that a female interpreter was preferred.
Conclusion
When working with persons with LEP, providing a professional medical interpreter will facilitate optimal communication. In-person and remote (videoconferencing or telephonic) interpreting are options. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient not the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately. Clinicians should remember that patients may have a preference in the gender and dialect of the interpreter and accommodations should be made if available. Finally, asking the patient to repeat back in his or her own words what has been discussed is important to make sure the patient understood what was communicated during the medical visit [10,16].
Corresponding author: Kimberly Schoonover, MD, 200 First Street SW, Rochester, MN 55905, [email protected].
Financial disclosures: None.
1. U.S. Census Bureau. American community survey. Accessed 11 Jul 2016 at www.census.gov/acs/www.
2. Wiener ESR, Ivonne M. Bridging language barriers: how to work with an interpreter. Clin Pediatr Emerg Med 2004;5:93–101.
3. Perez-Stable EJ, Karliner LS. What do we know about patient-clinician interactions with interpreters? J Gen Intern Med 2013;28:339–41.
4. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Clinician ratings of interpreter mediated visits in underserved primary care settings with ad hoc, in-person professional, and video conferencing modes. J Health Care Poor Underserved 2010;21:301–17.
5. Flores G, Abreu M, Barone CP, et al. Errors of medical interpretation and their potential clinical consequences: a comparison of professional versus ad hoc versus no interpreters. Ann Emerg Med 2012;60:545–53.
6. Bauer AM, Alegria M. Impact of patient language proficiency and interpreter service use on the quality of psychiatric care: a systematic review. Psychiatr Serv 2010;61:765–73.
7. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
8. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev 2005;62:255–99.
9. Lindholm M, Hargraves JL, Ferguson WJ, Reed G. Professional language interpretation and inpatient length of stay and readmission rates. J Gen Intern Med 2012;27:1294–9.
10. Juckett G, Unger K. Appropriate use of medical interpreters. Am Fam Physician 2014;90:476–80.
11. Schapira L, Vargas E, Hidalgo R, et al. Lost in translation: integrating medical interpreters into the multidisciplinary team. Oncologist 2008;13:586–92.
12. Gray B, Hilder J, Stubbe M. How to use interpreters in general practice: the development of a New Zealand toolkit. J Prim Health Care 2012;4:52–61, A1-8.
13. Hsieh E. Not just “getting by”: factors influencing providers’ choice of interpreters. J Gen Intern Med 2015;30:75–82.
14. Philips C. Using interpreters--a guide for GPs. Austr Fam Physician 2010;39:188–95.
15. Boscolo-Hightower A, Rafton SA, Tolman M, et al. Identifying families with limited English proficiency using a capture-recapture approach. Hosp Pediatr 2014;4:16–22.
16. Hadziabdic E, Hjelm K. Working with interpreters: practical advice for use of an interpreter in healthcare. Int J Evid Based Healthc 2013;11:69–76.
17. Abbe M, Simon C, Angiolillo A, et al. A survey of language barriers from the perspective of pediatric oncologists, interpreters, and parents. Pediatr Blood Cancer 2006;47:819–24.
18. Ngo-Metzger Q, Massagli MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med 2003;18:44–52.
19. Hadziabdic E, Hjelm K. Arabic-speaking migrants’ experiences of the use of interpreters in healthcare: a qualitative explorative study. Int J Equity Health 2014;13:49.
20. Julliard K, Vivar J, Delgado C, et al. What Latina patients don’t tell their doctors: a qualitative study. Ann Family Med 2008;6:543–9.
21. Hsieh E, Ju H, Kong H. Dimensions of trust: the tensions and challenges in provider--interpreter trust. Qual Health Res 2010;20:170–81.
22. Butow PN, Lobb E, Jefford M, et al. A bridge between cultures: interpreters’ perspectives of consultations with migrant oncology patients. Support Care Cancer 2012;20:235-44.
23. Hsieh E. “I am not a robot!” Interpreters’ views of their roles in health care settings. Qual Health Res 2008;18:1367–83.
24. Hsieh E, Hong SJ. Not all are desired: providers’ views on interpreters’ emotional support for patients. Patient Educ Couns 2010;81:192–7.
25. Elderkin-Thompson V, Silver RC, Waitzkin H. When nurses double as interpreters: a study of Spanish-speaking patients in a US primary care setting. Soc Sci Med 2001;52:1343–58.
26. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Inaccurate language interpretation and its clinical significance in the medical encounters of Spanish-speaking Latinos. Med Care 2015;53:940–7.
27. Gray B, Hilder J, Donaldson H. Why do we not use trained interpreters for all patients with limited English proficiency? Is there a place for using family members? Austr J Prim Health 2011;17:240–9.
28. Jacobs B, Kroll L, Green J, David TJ. The hazards of using a child as an interpreter. J Royal Soc Med 1995;88:474P–5P.
29. Lion KC, Brown JC, Ebel BE, et al. Effect of telephone vs video interpretation on parent comprehension, communication, and utilization in the pediatric emergency department: a randomized clinical trial. JAMA Pediatr 2015;169:1117–25.
30. Wofford JL CC, Johnson DA, Brown MT. Providing a Spanish interpreter using low-cost videoconferencing in a community health centre: a pilot study using tablet computers. Inform Prim Care 2012;20:141–6.
31. Jacobs EA SL, Rathouz PJ. The impact of an enhanced interpreter service intervention on hospital costs and patient satisfaction. J Gen Intern Med 2007;22(Suppl 2):306–11.
32. Jacobs EA LG, Rathouz PJ, Fu P Jr. Shared networks of interpreter services, at relatively low cost, can help providers serve patients with limited english skills. Health Aff (Millwood) 2011;30:1930–8.
33. Locatis C, Williamson D, Gould-Kabler C, et al. Comparing in-person, video, and telephonic medical interpretation. J Gen Intern Med 2010;25:345–50.
34. Jones D, Gill P, Harrison R, et al. An exploratory study of language interpretation services provided by videoconferencing. J Telemed Telecare 2003;9:51–6.
35. Price EL, Perez-Stable EJ, Nickleach D, et al. Interpreter perspectives of in-person, telephonic, and videoconferencing medical interpretation in clinical encounters. Patient Educ Couns 2012;87:226–32.
36. Crossman KL, Wiener E, Roosevelt G, et al. Interpreters: telephonic, in-person interpretation and bilingual providers. Pediatrics 2010;125:e631–8.
37. Degni F, Suominen S, Essen B, et al. Communication and cultural issues in providing reproductive health care to immigrant women: health care providers’ experiences in meeting the needs of [corrected] Somali women living in Finland. J Immigr Minor Health 2012;14:330–43.
38. Odunukan OW, Abdulai RM, Hagi Salaad MF, et al. Provider and interpreter preferences among Somali women in a primary care setting. J Prim Care Comm Health 2015;6:105–10.
39. Poss JE, Beeman T. Effective use of interpreters in health care: guidelines for nurse managers and clinicians. Semin Nurse Manag 1999;7:166–71.
40. Phelan M, Parkman S. How to work with an interpreter. BMJ 1995;311:555–7.
41. Lubrano di Ciccone B, Brown RF, Gueguen JA, et al. Interviewing patients using interpreters in an oncology setting: initial evaluation of a communication skills module. Ann Oncol 2010;21:27–32.
42. Hudelson P. Improving patient-provider communication: insights from interpreters. Fam Pract 2005;22:311–6.
43. Hudelson P, Dao MD, Perron NJ, Bischoff A. Interpreter-mediated diabetes consultations: a qualitative analysis of physician communication practices. BMC Fam Pract 2013;14:163.
44. Green AR, Ngo-Metzger Q, Legedza AT, et al. Interpreter services, language concordance, and health care quality. Experiences of Asian Americans with limited English proficiency. J Gen Intern Med 2005;20:1050–6.
45. Schenker Y, Smith AK, Arnold RM, Fernandez A. “Her husband doesn’t speak much English”: conducting a family meeting with an interpreter. J Palliat Med 2012;15:494–8.
From the Department of Medicine, Mayo Clinic, Rochester, MN.
Abstract
- Objective: To provide an overview of important aspects of interpreting for medical visits for persons with limited English proficiency (LEP).
- Methods: Literature review.
- Results: When working with persons of LEP, providing a professional medical interpreter will facilitate optimal communication. Interpreters may work in different roles including as a conduit, cultural broker, clarifier, and advocate. In-person and remote (videoconferencing or telephonic) interpreting are available and one may be preferred depending on the medical visit. Clinicians should recognize that patients may have a preference for the interpreter’s gender and dialect and accommodations should be made if possible. Prior to the visit, the provider may want to clarify the goals of the medical encounter with the interpreter as some topics may be viewed differently in certain cultures. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient rather than to the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately to allow interpretation. Additionally, providers should assess patient understanding of what has been discussed. After the medical visit, providers should consider discussing with the interpreter any issues with communication or cultural factors noted to have affected the visit.
- Conclusion: Providers should utilize a professional medical interpreter for visits with persons with LEP. Appropriate communication techniques, including talking in first and second tenses and maintaining eye contact with the patient rather than the interpreter, are important for a successful visit. Realizing patients may have interpreter preferences is also important to facilitate patient-centered-care.
Key words: language barriers; quality of care; physician-patient communication; interpreter services.
The United States is a diverse country that includes many persons whose first language is not English. According to the U.S. Census Bureau, more than 63 million persons age 5 and above (about 51 million adults) reported speaking a language other than English at home. Also, about 25.7 million of the population age 5 and up (around 10.6 million adults) noted speaking English less than “very well” [1]. Protecting people from discrimination based on the language they speak is highlighted in Title VI of the Civil Rights Act of 1964 (which focuses on those receiving federal funding). President Clinton, furthermore, in 2000 signed Executive Order 13166, which encouraged federal agencies to provide appropriate access of their services to those with limited English proficiency (LEP) [2,3].
The benefits of using professional interpreters is well-documented. In addition to increased satisfaction with communication when professional medical interpreters are used [4], they also make fewer clinically significant interpretation errors compared to ad hoc interpreters (ie, untrained individuals such as bilingual staff member, family member, or friend who are asked to interpret) [5–7]. LEP patients who do not have a professional interpreter have less understanding of their medical issues, have less satisfaction of their medical care, and may have more tests ordered and be hospitalized more often compared to those who do utilize professional medical interpreters [8]. In addition to improved satisfaction and understanding of medical diagnoses, hospitalized persons requiring interpreters who utilized a professional medical interpreter on admission and discharge were noted to have a shorter length of stay than persons who required an interpreter and did not receive one [9].
Despite the documented benefits of using professional interpreters, they are underutilized. Reasons include underfunded medical interpreting services [10,11], lack of awareness of the risks involved with using an ad hoc interpreter [2,12], providers using their own or another worker’s limited second language skills to communicate rather than using a professional medical interpreter [13,14], perceived delay in obtaining a professional medical interpreter, and judging a medical situation as minor rather than complex [13]. In this article, the roles, importance, and considerations of using a professional medical interpreter are explored.
Case Study
Initial Presentation
A 23-year-old married Somali-speaking female who moved to the United States recently called a local primary care provider’s office to schedule an appointment. When asked the reason for the visit, she said the reason was private. The clinical assistant scheduled her with the next available provider.
When the patient arrived for her clinic appointment, a clinical assistant roomed her and her mother and asked the patient the reason for the visit. The patient remained quiet and her mother replied that she needed to speak with the doctor. When the female medical provider entered, she observed that the patient appeared anxious. When the doctor initiated conversation with the patient, she noted that her English was limited. Her mother tried to explain the reason for the visit saying her daughter was having severe pain. She then pointed towards her daughter’s lower abdomen. The clinician noted the limited English abilities of the patient and mother and used the interpreter line to request a Somali interpreter and placed the first available interpreter available on speaker.
How can patients who need an interpreter be identified?
Health care systems can facilitate identifying patients in need of an interpreter by routinely collecting information on LEP status. The patient should be asked during registration if her or she speaks English and has a preferred language, and the answers should be recorded in the medical record [3]. If an interpreter is used during the hospital stay, it should be recorded to alert future providers to the need of an interpreter [15]. Patients may speak a dialect of a common language and this also should be noted, as an interpreter with a similar dialect to the patient should ideally be requested when necessary [16]. Furthermore, health care systems can measure rate of screening for language need at registration and rate of interpreter use during hospital stay to assess language need and adequacy of provision of interpreters to LEP patients [15].
It should be noted that patients may be wary about the presence of an interpreter. In one study involving pediatric oncologists and Spanish-speaking parents, the former reported concern regarding the accuracy of interpretation and the latter were concerned about missing out on important information even with the use of professional medical interpreters [17]. The concern for accuracy of interpreting was shared in a study by Chinese and Vietnamese Americans with LEP [18] as well as in a Swedish study involving Arabic-speaking persons. In the latter study, Arabic-speaking patients also felt uncomfortable speaking about bodily issues in the presence of interpreters [19]. In a study of Latina patients, there were concerns about confidentiality with interpreters [20].
What is the role of the interpreter? Should they offer emotional support to the patient?
Interpreter-as-conduit reflects a neutral, more literal information exchange and is preferred by certain medical providers who prioritize a more exact interpretation of the medical conversation. In this role, the interpreter assumes a more passive role and the emphasis is on the interpreter’s linguistic ability [21]. Providers need to be aware that word-for-word interpretation may not align with what is regarded as culturally sensitive care—such as when the term “cancer” is to be used. Also, word-for-word interpretation does not necessarily mean the patient will understand what is being interpreted if the terminology does not reflect the literacy level or dialect of the person with LEP [22].
Interpreters may also assume an active role, sometimes referred to as clarifier and cultural broker. Clarifying may be utilized, for example, when a medical provider is discussing complicated treatment options. This requires an interpreter to step out of a conduit role (if that is the preferred role) and confirm or clarify information to ensure accurate information exchange [21,23]. As a cultural broker, communication between provider and patient is exchanged in a manner that reflects consideration of the patient’s cultural background. Interpreters may explain, to the provider, the cultural reason for the patient’s perspective of what is causing or contributing to the illness. Cultural brokering may as well include communicating the medical terminology and disease explanation, given by the medical provider, in a way that the patient would understand. This role, additionally, can involve educating the provider about aspects of the culture that may influence the patient’s communication with him or her [22].
Furthermore, interpreters may fulfill an advocate role for patients by helping them understand the health care system and increasing patient empowerment by seeking information and services that the patient may not know to ask about [23].
The interpreter may offer emotional support during a medical visit, for example, where the diagnosis of cancer is conveyed. In such a case, an interpreter’s emotional support may be considered by providers to be appropriate. In contrast, with visits related to mental health evaluations, having the interpreter remain neutral, rather than being a more active participant by offering emotional support, may be preferred [24]. In addition to interpreters remaining more neutral during mental health visits, providers may prefer that interpreters not speak with the patient prior to the visit, depending on the mental health condition, as negative therapeutic consequences may occur [21]. Trust is an important element of the provider-patient relationship and, as such, there is concern on the part of some providers that if the trust of patients falls to the interpreter rather than to the provider, then therapeutic progress may be compromised [24]. In general, clarifying with interpreters the goals of the visit and expectations regarding speaking to the patient outside of the visit may ensure the provider-patient relationship is not diminished [21].
What are the disadvantages and caveats of using family members or bilingual staff as interpreters?
Although family members and other ad hoc interpreters may be present and willing to interpret, the risk of miscommunication is greater than with professional medical interpreters [5,6]. This risk of miscommunication extends to partially bilingual medical providers who do not utilize appropriate interpreter services [10,25]. Ad hoc interpreters may try to answer on behalf the patient [6,26] and may not have the appropriate medical terminology to correctly interpret what the provider is trying to communicate to the patient [6].
Professional medical interpreters are trained to facilitate communication of a spoken language in a medical setting [2,10]. Certification is offered by the National Board of Certification for Medical Interpreters and the Certification Commission for Healthcare Interpreters. In order to be certified certain requirements must be met which include a minimum of 40 hours of health care interpreter training (which includes medical terminology as well as roles and ethics involved in medical interpreting) as well as demonstrated oral proficiency in English as well as another chosen language (such as Spanish) [10].
In certain circumstances, patients may feel more comfortable disclosing personal details with a professional medical interpreter rather than in the presence of an ad hoc interpreter. For example, more details of traumatic events and psychological symptoms were spoken of in the presence of a professional, rather than an ad hoc, interpreter in medical interviews of asylum seekers requiring an interpreter in Switzerland. In the presence of ad hoc interpreters, more physical symptoms were disclosed rather than psychological [6].
Furthermore, in visits concerning sexuality or abuse issues, using family members as interpreters may violate privacy concerns of the patient [2,27]. Additionally, in certain cultures where respect for elders is very important, parents who use children as interpreters may feel that the structure of the family changes when he or she interprets on behalf of the parent [18]. Also, what children consider as embarrassing may not be interpreted to either the parent or to the care provider [8]. Furthermore, one should note there are ethical issues of using non-adult children as interpreters in situations involving confidentiality and privacy—by doing so, there may be resulting harmful effects on non-adult children [27,28].
Patients may at times decline the use of a professional medical interpreter and prefer to have a family member interpret; this preference should be documented in the patient’s medical chart [10]. Caution should be had using an ad hoc interpreter when obtaining informed consent [12].
What professional interpreting services are available to the clinician?
For the most part, access to interpreters via a telephone service is widely available [10]. The cost of providing interpreters in-person and/or remotely varies depending on the health care site [29–31] In general, considerations of using professional medical interpreters, whether remotely or in-person, involves accessibility and cost. There are certain sites that have explored having a shared network of interpreters available via the telephone and videoconference to reduce the cost of providing interpreters for individual hospitals [32]. While the costs of providing a person with LEP with interpretation varies depending on the health care site, the costs of not providing a professional medical interpreter should be considered as well, which include greater malpractice risk and potential medical errors [32]. In addition, the use of employees as interpreters takes time away from their respective jobs, which results in staff time lost [31].
In-person interpreting may be preferred for certain medical visits, as an in-person interpreter can interpret both verbal and nonverbal communication [16]. When emotional support is anticipated, in-person interpreting is usually preferred by providers [24]. There may be improved cultural competence when using an in-person interpreter, which may be important for certain visits such as those involving end-of life care discussions [4]. One concern may involve the comfort level of the patient if he or she personally knows the interpreter; this can occur in smaller ethnic communities [12]. Telephonic interpreting may be preferred in certain medical situations where confidentiality is desired [16].
For providers working with persons who are deaf, options for interpreting include in-person sign language interpreters as well as remote videoconference interpretation [10].
- Are in-person interpreting and remote interpreting comparable?
In general, using in-person or remote interpreters does not significantly change patient satisfaction. In a study involving Spanish-speaking patients in a clinic setting, persons requiring an interpreter rated satisfaction of interpreting between in-person, videoconferencing, and telephonic methods highly with no significant differences. Of note, though, medical providers and interpreters preferred in-person rather than the 2 remote interpreting options [33]. In a different study involving Spanish, Chinese, Russian, or Vietnamese interpreters, satisfaction of information exchange was considered equal among the 3 interpreting modalities, although in-person interpreting was felt to establish rapport between clinician and patient with LEP better than telephonic and videoconferencing interpreting [35]. Additionally, in a study of providers in a clinic setting who worked with persons with LEP, no significant differences were noted in provider satisfaction of the medical visit, or in the quality of interpretation or communication, when using in-person versus remote videoconferencing interpretation. Providers, though, noted improved knowledge of the patient’s cultural beliefs when using in-person interpreting [4].
Regarding the question of a difference in understanding when using in-person versus remote interpreters, a study was done in a pediatric emergency department (ED) that compared in-person and telephonic interpretation. Family understanding of the discharge diagnosis was high (about 95%) regardless of whether an in-person or telephonic interpreter was utilized [36]. In a different study comparing telephone and video interpretation in a pediatric ED, while quality of communication and interpretation were rated similarly, the parents who used video interpretation were more likely to name their child’s diagnosis correctly [29].
Case Continued
The physician proceeded with introductions and explained that all conversations would be interpreted. She further stated that if there were any questions, the patient and mother should feel free to ask them. Via the interpreter, who was male, the provider began by asking about the nature of the abdominal pain. The patient looked to her mother and then down without answering. The mother nodded, but did not say more. The provider wondered if their reticence might be due to discomfort with discussing the issue through a male interpreter. The physician asked the patient if she would prefer a female interpreter and, once that was confirmed, she asked if she wanted an in-person or telephonic interpreter. The mother requested a female in-person interpreter.
How might gender-specific issues impact working with an interpreter?
As gender concordance of patient and physician [37] at times is desired, gender concordance of patient and interpreter [16,18] may also be important to optimize communication of gender-specific issues [16,18,37]. For example, an Arabic-speaking man from the Middle East may prefer to discuss sexuality-related concerns in the presence of a male rather than female interpreter [16]. An Arabic-speaking female who has a preference for female providers may prefer a female interpreter when discussing sexuality and undergoing a physical examination [19]. In one study, the majority of Somali females preferred female interpreters as well as female providers for breast, pelvic, and abdominal examinations [38]. If a same-gender interpreter cannot be present, an option is to have the interpreter either leave the room or step behind a curtain or turn away from the patient during a sensitive part of the physical examination [39].
What are recommended strategies for using a medical interpreter?
It is often helpful to have a brief discussion with the interpreter prior to the medical visit with the patient to speak about the general topics that will be discussed (especially if the topics involve sensitive issues or news that could be upsetting to the patient) and the goal of the visit [2, 11]. Certain topics may be viewed dissimilarly in different cultures, thus approaching the interpreter from the view point of cultural broker or liaison [10] may bring to light cultural factors that may influence the medical visit [40,41]. the name of the interpreter should be noted for documentation purposes [10].
To start the visit, introductions of everyone involved should take place with a brief disclosure about the role of the interpreter and assurance of confidentiality on the part of the interpreter [2,11]. Also, the provider should set the expectation that all statements said in the room will be interpreted so that all persons can understand what it being spoken [10].
There are several options for where each person should be positioned. In some medical visits, a triangle is pursued where the interpreter sits lateral to the provider, but this may lead to challenges in maintaining eye contact between the patient and provider. Another option is have the interpreter sit next to [10] and slightly behind the patient to improve eye contact between provider-patient and to maintain the patient-provider relationship [2,41]. When seated, the medical provider should try to sit at the same level as the patient [16]. Seating is different with persons requiring the use of sign language interpreters as the interpreter needs to be visible to the patient for communications purposes. One possibility is having the interpreter sit beside and slightly behind the provider; this positioning allows the patient to understand what is being communicated and also allows the patient to understand what is being communicated and allows him or her to see the provider during the conversation [40].
There are 2 main communication styles used by interpreters: consecutive interpreting, where the interpreter exchanges what has been said by the clinician or patient after each one has finished speaking, and simultaneous interpreting, where the interpreter translates as the person is speaking. Interpreters and medical providers may have a preference and it is important to clarify, if needed, which method is preferred [21].
The provider should face the patient and direct conversation to him or her rather than to the interpreter. Third-person statements should not be used, such as “tell her,” as this directs the conversation to the interpreter rather than to the patient [10]. By using the first and second person (when addressing the patient) and making eye contact, the relationship between the provider and patient is emphasized [14,40].
Choosing the right word is important to have meaningful communication. Interpreters advise that providers should understand that medical concepts may be unfamiliar to patients with LEP. Providers should use simpler words rather than medical terminology to discuss medical issues [42]. In general, straightforward word choice is recommended [16]. Providers are advised to not use acronyms or idioms. It is important to note that humor may be difficult to convey as well [10].
Clinicians are advised to speak clearly and not quickly and to use shorter sentences with appropriate pauses to allow time for the interpreter to interpret (if consecutive rather than simultaneous interpreting style is being used) [2,41,43,44]. In addition to limiting speech to one to two sentences at a time, asking one question at a time is important for optimal communication [43]. To improve information gathering, patients may respond better to open-ended questions [42], which is an aspect of patient-centered communication, as directive questioning often leads to shorter answers [43].
Furthermore, the provider should be aware that persons with LEP may know some English, so statements that one would not say to an English-speaking patient should not be said in the room with a person with LEP [10].
Encouraging the interpreter to clarify certain concepts, if necessary, may provide for improved information exchange [21] as well as encouraging the patient to ask questions during the medical visit may help elucidate potential areas of confusion [22,40,44]. Summarizing important concepts [40] and limiting the number of concepts discussed may increase patient understanding [10]. Additionally, asking the patient to repeat what was discussed in his or her words [10], rather than directly asking if he or she understands, will allow for more meaningful assessment of patient understanding [43].
Finally, recognition that interpreters may experience distress after certain visits, such as an oncologic medical encounters, is important and debriefing may be desired by the interpreter [22,45]. Also, discussing any communication concerns may be helpful [40,42] in addition to discussing certain cultural beliefs that impacted the visit may be educational for the provider [45].
Case Continued
After the female translator arrived, the physician asked the patient if she felt comfortable with her mother in the room for this medical visit. After the patient confirmed that she wanted her mother present, the physician tried to further clarify the reason for the medical visit. Her mother, appearing very concerned, began speaking quickly to the interpreter without stopping for interpretation. When the mother did stop speaking, the interpreter, rather than informing the provider what was spoken of by the mother, dialoged with the mother and the back and forth conversation continued.
What are strategies to optimize the medical visit when the provider is not satisfied with the flow of conversation?
If there are conversations occurring between the patient and interpreter with the exclusion of the provider, the provider should request sentence-by-sentence interpretation by the interpreter. If the interpreter is answering on behalf of the patient, providers should redirect communication to the patient [10]. At times, patients may speak for longer periods without stopping for the interpreter to provide accurate information exchange. The provider in this case may need to interrupt conversation to allow the interpreter time to convey what is being said [14].
If there are family members who know English, but the patient and/or others do not know English, there may be a risk of miscommunication if the exchange of medical information is done by a combination of family members and the interpreter, as the medical information may not accurately reflect what the clinician is trying to convey. The provider may need to redirect the conversation flow through the interpreter to make sure there is consistent information being communicated [22].
Case Continued
Finally, the provider interrupted. She emphasized with the patient, mother, and the interpreter that all that was being said should be interpreted. She asked the interpreter to sit next to the patient and mother (rather than lateral to the physician) so that eye contact between the patient and mother and the provider could be maintained thus supporting the patient-provider relationship. She then asked one question at a time to the patient. She needed to interrupt the conversation again when the mother started to speak to the interpreter without waiting for interpretation. The doctor reemphasized the need to allow time for the interpreter to adequately convey the information. After this the medical visit progressed successfully. Soon the provider found out that the mother was concerned that something serious could be happening to her daughter, as her daughter previously had a miscarriage. After hearing the mother’s concern, the provider was able to clarify with the daughter that the pain was suprapubic and she was having burning when she urinated. After further evaluation, the provider diagnosed a urinary tract infection. She told the patient about the diagnosis and provided her with appropriate medication and instructions on how to take it and for how long. The provider then asked the patient to tell her what she understood about the diagnosis and how to take the medication. The doctor then asked if either had any further questions. After the medical visit, the provider made sure that the patient’s chart reflected the need for a Somali interpreter with the notation that a female interpreter was preferred.
Conclusion
When working with persons with LEP, providing a professional medical interpreter will facilitate optimal communication. In-person and remote (videoconferencing or telephonic) interpreting are options. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient not the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately. Clinicians should remember that patients may have a preference in the gender and dialect of the interpreter and accommodations should be made if available. Finally, asking the patient to repeat back in his or her own words what has been discussed is important to make sure the patient understood what was communicated during the medical visit [10,16].
Corresponding author: Kimberly Schoonover, MD, 200 First Street SW, Rochester, MN 55905, [email protected].
Financial disclosures: None.
From the Department of Medicine, Mayo Clinic, Rochester, MN.
Abstract
- Objective: To provide an overview of important aspects of interpreting for medical visits for persons with limited English proficiency (LEP).
- Methods: Literature review.
- Results: When working with persons of LEP, providing a professional medical interpreter will facilitate optimal communication. Interpreters may work in different roles including as a conduit, cultural broker, clarifier, and advocate. In-person and remote (videoconferencing or telephonic) interpreting are available and one may be preferred depending on the medical visit. Clinicians should recognize that patients may have a preference for the interpreter’s gender and dialect and accommodations should be made if possible. Prior to the visit, the provider may want to clarify the goals of the medical encounter with the interpreter as some topics may be viewed differently in certain cultures. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient rather than to the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately to allow interpretation. Additionally, providers should assess patient understanding of what has been discussed. After the medical visit, providers should consider discussing with the interpreter any issues with communication or cultural factors noted to have affected the visit.
- Conclusion: Providers should utilize a professional medical interpreter for visits with persons with LEP. Appropriate communication techniques, including talking in first and second tenses and maintaining eye contact with the patient rather than the interpreter, are important for a successful visit. Realizing patients may have interpreter preferences is also important to facilitate patient-centered-care.
Key words: language barriers; quality of care; physician-patient communication; interpreter services.
The United States is a diverse country that includes many persons whose first language is not English. According to the U.S. Census Bureau, more than 63 million persons age 5 and above (about 51 million adults) reported speaking a language other than English at home. Also, about 25.7 million of the population age 5 and up (around 10.6 million adults) noted speaking English less than “very well” [1]. Protecting people from discrimination based on the language they speak is highlighted in Title VI of the Civil Rights Act of 1964 (which focuses on those receiving federal funding). President Clinton, furthermore, in 2000 signed Executive Order 13166, which encouraged federal agencies to provide appropriate access of their services to those with limited English proficiency (LEP) [2,3].
The benefits of using professional interpreters is well-documented. In addition to increased satisfaction with communication when professional medical interpreters are used [4], they also make fewer clinically significant interpretation errors compared to ad hoc interpreters (ie, untrained individuals such as bilingual staff member, family member, or friend who are asked to interpret) [5–7]. LEP patients who do not have a professional interpreter have less understanding of their medical issues, have less satisfaction of their medical care, and may have more tests ordered and be hospitalized more often compared to those who do utilize professional medical interpreters [8]. In addition to improved satisfaction and understanding of medical diagnoses, hospitalized persons requiring interpreters who utilized a professional medical interpreter on admission and discharge were noted to have a shorter length of stay than persons who required an interpreter and did not receive one [9].
Despite the documented benefits of using professional interpreters, they are underutilized. Reasons include underfunded medical interpreting services [10,11], lack of awareness of the risks involved with using an ad hoc interpreter [2,12], providers using their own or another worker’s limited second language skills to communicate rather than using a professional medical interpreter [13,14], perceived delay in obtaining a professional medical interpreter, and judging a medical situation as minor rather than complex [13]. In this article, the roles, importance, and considerations of using a professional medical interpreter are explored.
Case Study
Initial Presentation
A 23-year-old married Somali-speaking female who moved to the United States recently called a local primary care provider’s office to schedule an appointment. When asked the reason for the visit, she said the reason was private. The clinical assistant scheduled her with the next available provider.
When the patient arrived for her clinic appointment, a clinical assistant roomed her and her mother and asked the patient the reason for the visit. The patient remained quiet and her mother replied that she needed to speak with the doctor. When the female medical provider entered, she observed that the patient appeared anxious. When the doctor initiated conversation with the patient, she noted that her English was limited. Her mother tried to explain the reason for the visit saying her daughter was having severe pain. She then pointed towards her daughter’s lower abdomen. The clinician noted the limited English abilities of the patient and mother and used the interpreter line to request a Somali interpreter and placed the first available interpreter available on speaker.
How can patients who need an interpreter be identified?
Health care systems can facilitate identifying patients in need of an interpreter by routinely collecting information on LEP status. The patient should be asked during registration if her or she speaks English and has a preferred language, and the answers should be recorded in the medical record [3]. If an interpreter is used during the hospital stay, it should be recorded to alert future providers to the need of an interpreter [15]. Patients may speak a dialect of a common language and this also should be noted, as an interpreter with a similar dialect to the patient should ideally be requested when necessary [16]. Furthermore, health care systems can measure rate of screening for language need at registration and rate of interpreter use during hospital stay to assess language need and adequacy of provision of interpreters to LEP patients [15].
It should be noted that patients may be wary about the presence of an interpreter. In one study involving pediatric oncologists and Spanish-speaking parents, the former reported concern regarding the accuracy of interpretation and the latter were concerned about missing out on important information even with the use of professional medical interpreters [17]. The concern for accuracy of interpreting was shared in a study by Chinese and Vietnamese Americans with LEP [18] as well as in a Swedish study involving Arabic-speaking persons. In the latter study, Arabic-speaking patients also felt uncomfortable speaking about bodily issues in the presence of interpreters [19]. In a study of Latina patients, there were concerns about confidentiality with interpreters [20].
What is the role of the interpreter? Should they offer emotional support to the patient?
Interpreter-as-conduit reflects a neutral, more literal information exchange and is preferred by certain medical providers who prioritize a more exact interpretation of the medical conversation. In this role, the interpreter assumes a more passive role and the emphasis is on the interpreter’s linguistic ability [21]. Providers need to be aware that word-for-word interpretation may not align with what is regarded as culturally sensitive care—such as when the term “cancer” is to be used. Also, word-for-word interpretation does not necessarily mean the patient will understand what is being interpreted if the terminology does not reflect the literacy level or dialect of the person with LEP [22].
Interpreters may also assume an active role, sometimes referred to as clarifier and cultural broker. Clarifying may be utilized, for example, when a medical provider is discussing complicated treatment options. This requires an interpreter to step out of a conduit role (if that is the preferred role) and confirm or clarify information to ensure accurate information exchange [21,23]. As a cultural broker, communication between provider and patient is exchanged in a manner that reflects consideration of the patient’s cultural background. Interpreters may explain, to the provider, the cultural reason for the patient’s perspective of what is causing or contributing to the illness. Cultural brokering may as well include communicating the medical terminology and disease explanation, given by the medical provider, in a way that the patient would understand. This role, additionally, can involve educating the provider about aspects of the culture that may influence the patient’s communication with him or her [22].
Furthermore, interpreters may fulfill an advocate role for patients by helping them understand the health care system and increasing patient empowerment by seeking information and services that the patient may not know to ask about [23].
The interpreter may offer emotional support during a medical visit, for example, where the diagnosis of cancer is conveyed. In such a case, an interpreter’s emotional support may be considered by providers to be appropriate. In contrast, with visits related to mental health evaluations, having the interpreter remain neutral, rather than being a more active participant by offering emotional support, may be preferred [24]. In addition to interpreters remaining more neutral during mental health visits, providers may prefer that interpreters not speak with the patient prior to the visit, depending on the mental health condition, as negative therapeutic consequences may occur [21]. Trust is an important element of the provider-patient relationship and, as such, there is concern on the part of some providers that if the trust of patients falls to the interpreter rather than to the provider, then therapeutic progress may be compromised [24]. In general, clarifying with interpreters the goals of the visit and expectations regarding speaking to the patient outside of the visit may ensure the provider-patient relationship is not diminished [21].
What are the disadvantages and caveats of using family members or bilingual staff as interpreters?
Although family members and other ad hoc interpreters may be present and willing to interpret, the risk of miscommunication is greater than with professional medical interpreters [5,6]. This risk of miscommunication extends to partially bilingual medical providers who do not utilize appropriate interpreter services [10,25]. Ad hoc interpreters may try to answer on behalf the patient [6,26] and may not have the appropriate medical terminology to correctly interpret what the provider is trying to communicate to the patient [6].
Professional medical interpreters are trained to facilitate communication of a spoken language in a medical setting [2,10]. Certification is offered by the National Board of Certification for Medical Interpreters and the Certification Commission for Healthcare Interpreters. In order to be certified certain requirements must be met which include a minimum of 40 hours of health care interpreter training (which includes medical terminology as well as roles and ethics involved in medical interpreting) as well as demonstrated oral proficiency in English as well as another chosen language (such as Spanish) [10].
In certain circumstances, patients may feel more comfortable disclosing personal details with a professional medical interpreter rather than in the presence of an ad hoc interpreter. For example, more details of traumatic events and psychological symptoms were spoken of in the presence of a professional, rather than an ad hoc, interpreter in medical interviews of asylum seekers requiring an interpreter in Switzerland. In the presence of ad hoc interpreters, more physical symptoms were disclosed rather than psychological [6].
Furthermore, in visits concerning sexuality or abuse issues, using family members as interpreters may violate privacy concerns of the patient [2,27]. Additionally, in certain cultures where respect for elders is very important, parents who use children as interpreters may feel that the structure of the family changes when he or she interprets on behalf of the parent [18]. Also, what children consider as embarrassing may not be interpreted to either the parent or to the care provider [8]. Furthermore, one should note there are ethical issues of using non-adult children as interpreters in situations involving confidentiality and privacy—by doing so, there may be resulting harmful effects on non-adult children [27,28].
Patients may at times decline the use of a professional medical interpreter and prefer to have a family member interpret; this preference should be documented in the patient’s medical chart [10]. Caution should be had using an ad hoc interpreter when obtaining informed consent [12].
What professional interpreting services are available to the clinician?
For the most part, access to interpreters via a telephone service is widely available [10]. The cost of providing interpreters in-person and/or remotely varies depending on the health care site [29–31] In general, considerations of using professional medical interpreters, whether remotely or in-person, involves accessibility and cost. There are certain sites that have explored having a shared network of interpreters available via the telephone and videoconference to reduce the cost of providing interpreters for individual hospitals [32]. While the costs of providing a person with LEP with interpretation varies depending on the health care site, the costs of not providing a professional medical interpreter should be considered as well, which include greater malpractice risk and potential medical errors [32]. In addition, the use of employees as interpreters takes time away from their respective jobs, which results in staff time lost [31].
In-person interpreting may be preferred for certain medical visits, as an in-person interpreter can interpret both verbal and nonverbal communication [16]. When emotional support is anticipated, in-person interpreting is usually preferred by providers [24]. There may be improved cultural competence when using an in-person interpreter, which may be important for certain visits such as those involving end-of life care discussions [4]. One concern may involve the comfort level of the patient if he or she personally knows the interpreter; this can occur in smaller ethnic communities [12]. Telephonic interpreting may be preferred in certain medical situations where confidentiality is desired [16].
For providers working with persons who are deaf, options for interpreting include in-person sign language interpreters as well as remote videoconference interpretation [10].
- Are in-person interpreting and remote interpreting comparable?
In general, using in-person or remote interpreters does not significantly change patient satisfaction. In a study involving Spanish-speaking patients in a clinic setting, persons requiring an interpreter rated satisfaction of interpreting between in-person, videoconferencing, and telephonic methods highly with no significant differences. Of note, though, medical providers and interpreters preferred in-person rather than the 2 remote interpreting options [33]. In a different study involving Spanish, Chinese, Russian, or Vietnamese interpreters, satisfaction of information exchange was considered equal among the 3 interpreting modalities, although in-person interpreting was felt to establish rapport between clinician and patient with LEP better than telephonic and videoconferencing interpreting [35]. Additionally, in a study of providers in a clinic setting who worked with persons with LEP, no significant differences were noted in provider satisfaction of the medical visit, or in the quality of interpretation or communication, when using in-person versus remote videoconferencing interpretation. Providers, though, noted improved knowledge of the patient’s cultural beliefs when using in-person interpreting [4].
Regarding the question of a difference in understanding when using in-person versus remote interpreters, a study was done in a pediatric emergency department (ED) that compared in-person and telephonic interpretation. Family understanding of the discharge diagnosis was high (about 95%) regardless of whether an in-person or telephonic interpreter was utilized [36]. In a different study comparing telephone and video interpretation in a pediatric ED, while quality of communication and interpretation were rated similarly, the parents who used video interpretation were more likely to name their child’s diagnosis correctly [29].
Case Continued
The physician proceeded with introductions and explained that all conversations would be interpreted. She further stated that if there were any questions, the patient and mother should feel free to ask them. Via the interpreter, who was male, the provider began by asking about the nature of the abdominal pain. The patient looked to her mother and then down without answering. The mother nodded, but did not say more. The provider wondered if their reticence might be due to discomfort with discussing the issue through a male interpreter. The physician asked the patient if she would prefer a female interpreter and, once that was confirmed, she asked if she wanted an in-person or telephonic interpreter. The mother requested a female in-person interpreter.
How might gender-specific issues impact working with an interpreter?
As gender concordance of patient and physician [37] at times is desired, gender concordance of patient and interpreter [16,18] may also be important to optimize communication of gender-specific issues [16,18,37]. For example, an Arabic-speaking man from the Middle East may prefer to discuss sexuality-related concerns in the presence of a male rather than female interpreter [16]. An Arabic-speaking female who has a preference for female providers may prefer a female interpreter when discussing sexuality and undergoing a physical examination [19]. In one study, the majority of Somali females preferred female interpreters as well as female providers for breast, pelvic, and abdominal examinations [38]. If a same-gender interpreter cannot be present, an option is to have the interpreter either leave the room or step behind a curtain or turn away from the patient during a sensitive part of the physical examination [39].
What are recommended strategies for using a medical interpreter?
It is often helpful to have a brief discussion with the interpreter prior to the medical visit with the patient to speak about the general topics that will be discussed (especially if the topics involve sensitive issues or news that could be upsetting to the patient) and the goal of the visit [2, 11]. Certain topics may be viewed dissimilarly in different cultures, thus approaching the interpreter from the view point of cultural broker or liaison [10] may bring to light cultural factors that may influence the medical visit [40,41]. the name of the interpreter should be noted for documentation purposes [10].
To start the visit, introductions of everyone involved should take place with a brief disclosure about the role of the interpreter and assurance of confidentiality on the part of the interpreter [2,11]. Also, the provider should set the expectation that all statements said in the room will be interpreted so that all persons can understand what it being spoken [10].
There are several options for where each person should be positioned. In some medical visits, a triangle is pursued where the interpreter sits lateral to the provider, but this may lead to challenges in maintaining eye contact between the patient and provider. Another option is have the interpreter sit next to [10] and slightly behind the patient to improve eye contact between provider-patient and to maintain the patient-provider relationship [2,41]. When seated, the medical provider should try to sit at the same level as the patient [16]. Seating is different with persons requiring the use of sign language interpreters as the interpreter needs to be visible to the patient for communications purposes. One possibility is having the interpreter sit beside and slightly behind the provider; this positioning allows the patient to understand what is being communicated and also allows the patient to understand what is being communicated and allows him or her to see the provider during the conversation [40].
There are 2 main communication styles used by interpreters: consecutive interpreting, where the interpreter exchanges what has been said by the clinician or patient after each one has finished speaking, and simultaneous interpreting, where the interpreter translates as the person is speaking. Interpreters and medical providers may have a preference and it is important to clarify, if needed, which method is preferred [21].
The provider should face the patient and direct conversation to him or her rather than to the interpreter. Third-person statements should not be used, such as “tell her,” as this directs the conversation to the interpreter rather than to the patient [10]. By using the first and second person (when addressing the patient) and making eye contact, the relationship between the provider and patient is emphasized [14,40].
Choosing the right word is important to have meaningful communication. Interpreters advise that providers should understand that medical concepts may be unfamiliar to patients with LEP. Providers should use simpler words rather than medical terminology to discuss medical issues [42]. In general, straightforward word choice is recommended [16]. Providers are advised to not use acronyms or idioms. It is important to note that humor may be difficult to convey as well [10].
Clinicians are advised to speak clearly and not quickly and to use shorter sentences with appropriate pauses to allow time for the interpreter to interpret (if consecutive rather than simultaneous interpreting style is being used) [2,41,43,44]. In addition to limiting speech to one to two sentences at a time, asking one question at a time is important for optimal communication [43]. To improve information gathering, patients may respond better to open-ended questions [42], which is an aspect of patient-centered communication, as directive questioning often leads to shorter answers [43].
Furthermore, the provider should be aware that persons with LEP may know some English, so statements that one would not say to an English-speaking patient should not be said in the room with a person with LEP [10].
Encouraging the interpreter to clarify certain concepts, if necessary, may provide for improved information exchange [21] as well as encouraging the patient to ask questions during the medical visit may help elucidate potential areas of confusion [22,40,44]. Summarizing important concepts [40] and limiting the number of concepts discussed may increase patient understanding [10]. Additionally, asking the patient to repeat what was discussed in his or her words [10], rather than directly asking if he or she understands, will allow for more meaningful assessment of patient understanding [43].
Finally, recognition that interpreters may experience distress after certain visits, such as an oncologic medical encounters, is important and debriefing may be desired by the interpreter [22,45]. Also, discussing any communication concerns may be helpful [40,42] in addition to discussing certain cultural beliefs that impacted the visit may be educational for the provider [45].
Case Continued
After the female translator arrived, the physician asked the patient if she felt comfortable with her mother in the room for this medical visit. After the patient confirmed that she wanted her mother present, the physician tried to further clarify the reason for the medical visit. Her mother, appearing very concerned, began speaking quickly to the interpreter without stopping for interpretation. When the mother did stop speaking, the interpreter, rather than informing the provider what was spoken of by the mother, dialoged with the mother and the back and forth conversation continued.
What are strategies to optimize the medical visit when the provider is not satisfied with the flow of conversation?
If there are conversations occurring between the patient and interpreter with the exclusion of the provider, the provider should request sentence-by-sentence interpretation by the interpreter. If the interpreter is answering on behalf of the patient, providers should redirect communication to the patient [10]. At times, patients may speak for longer periods without stopping for the interpreter to provide accurate information exchange. The provider in this case may need to interrupt conversation to allow the interpreter time to convey what is being said [14].
If there are family members who know English, but the patient and/or others do not know English, there may be a risk of miscommunication if the exchange of medical information is done by a combination of family members and the interpreter, as the medical information may not accurately reflect what the clinician is trying to convey. The provider may need to redirect the conversation flow through the interpreter to make sure there is consistent information being communicated [22].
Case Continued
Finally, the provider interrupted. She emphasized with the patient, mother, and the interpreter that all that was being said should be interpreted. She asked the interpreter to sit next to the patient and mother (rather than lateral to the physician) so that eye contact between the patient and mother and the provider could be maintained thus supporting the patient-provider relationship. She then asked one question at a time to the patient. She needed to interrupt the conversation again when the mother started to speak to the interpreter without waiting for interpretation. The doctor reemphasized the need to allow time for the interpreter to adequately convey the information. After this the medical visit progressed successfully. Soon the provider found out that the mother was concerned that something serious could be happening to her daughter, as her daughter previously had a miscarriage. After hearing the mother’s concern, the provider was able to clarify with the daughter that the pain was suprapubic and she was having burning when she urinated. After further evaluation, the provider diagnosed a urinary tract infection. She told the patient about the diagnosis and provided her with appropriate medication and instructions on how to take it and for how long. The provider then asked the patient to tell her what she understood about the diagnosis and how to take the medication. The doctor then asked if either had any further questions. After the medical visit, the provider made sure that the patient’s chart reflected the need for a Somali interpreter with the notation that a female interpreter was preferred.
Conclusion
When working with persons with LEP, providing a professional medical interpreter will facilitate optimal communication. In-person and remote (videoconferencing or telephonic) interpreting are options. When using an interpreter, the provider should maintain eye contact with and direct speech to the patient not the interpreter. The provider should speak clearly, avoid complex terminology, and pause appropriately. Clinicians should remember that patients may have a preference in the gender and dialect of the interpreter and accommodations should be made if available. Finally, asking the patient to repeat back in his or her own words what has been discussed is important to make sure the patient understood what was communicated during the medical visit [10,16].
Corresponding author: Kimberly Schoonover, MD, 200 First Street SW, Rochester, MN 55905, [email protected].
Financial disclosures: None.
1. U.S. Census Bureau. American community survey. Accessed 11 Jul 2016 at www.census.gov/acs/www.
2. Wiener ESR, Ivonne M. Bridging language barriers: how to work with an interpreter. Clin Pediatr Emerg Med 2004;5:93–101.
3. Perez-Stable EJ, Karliner LS. What do we know about patient-clinician interactions with interpreters? J Gen Intern Med 2013;28:339–41.
4. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Clinician ratings of interpreter mediated visits in underserved primary care settings with ad hoc, in-person professional, and video conferencing modes. J Health Care Poor Underserved 2010;21:301–17.
5. Flores G, Abreu M, Barone CP, et al. Errors of medical interpretation and their potential clinical consequences: a comparison of professional versus ad hoc versus no interpreters. Ann Emerg Med 2012;60:545–53.
6. Bauer AM, Alegria M. Impact of patient language proficiency and interpreter service use on the quality of psychiatric care: a systematic review. Psychiatr Serv 2010;61:765–73.
7. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
8. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev 2005;62:255–99.
9. Lindholm M, Hargraves JL, Ferguson WJ, Reed G. Professional language interpretation and inpatient length of stay and readmission rates. J Gen Intern Med 2012;27:1294–9.
10. Juckett G, Unger K. Appropriate use of medical interpreters. Am Fam Physician 2014;90:476–80.
11. Schapira L, Vargas E, Hidalgo R, et al. Lost in translation: integrating medical interpreters into the multidisciplinary team. Oncologist 2008;13:586–92.
12. Gray B, Hilder J, Stubbe M. How to use interpreters in general practice: the development of a New Zealand toolkit. J Prim Health Care 2012;4:52–61, A1-8.
13. Hsieh E. Not just “getting by”: factors influencing providers’ choice of interpreters. J Gen Intern Med 2015;30:75–82.
14. Philips C. Using interpreters--a guide for GPs. Austr Fam Physician 2010;39:188–95.
15. Boscolo-Hightower A, Rafton SA, Tolman M, et al. Identifying families with limited English proficiency using a capture-recapture approach. Hosp Pediatr 2014;4:16–22.
16. Hadziabdic E, Hjelm K. Working with interpreters: practical advice for use of an interpreter in healthcare. Int J Evid Based Healthc 2013;11:69–76.
17. Abbe M, Simon C, Angiolillo A, et al. A survey of language barriers from the perspective of pediatric oncologists, interpreters, and parents. Pediatr Blood Cancer 2006;47:819–24.
18. Ngo-Metzger Q, Massagli MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med 2003;18:44–52.
19. Hadziabdic E, Hjelm K. Arabic-speaking migrants’ experiences of the use of interpreters in healthcare: a qualitative explorative study. Int J Equity Health 2014;13:49.
20. Julliard K, Vivar J, Delgado C, et al. What Latina patients don’t tell their doctors: a qualitative study. Ann Family Med 2008;6:543–9.
21. Hsieh E, Ju H, Kong H. Dimensions of trust: the tensions and challenges in provider--interpreter trust. Qual Health Res 2010;20:170–81.
22. Butow PN, Lobb E, Jefford M, et al. A bridge between cultures: interpreters’ perspectives of consultations with migrant oncology patients. Support Care Cancer 2012;20:235-44.
23. Hsieh E. “I am not a robot!” Interpreters’ views of their roles in health care settings. Qual Health Res 2008;18:1367–83.
24. Hsieh E, Hong SJ. Not all are desired: providers’ views on interpreters’ emotional support for patients. Patient Educ Couns 2010;81:192–7.
25. Elderkin-Thompson V, Silver RC, Waitzkin H. When nurses double as interpreters: a study of Spanish-speaking patients in a US primary care setting. Soc Sci Med 2001;52:1343–58.
26. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Inaccurate language interpretation and its clinical significance in the medical encounters of Spanish-speaking Latinos. Med Care 2015;53:940–7.
27. Gray B, Hilder J, Donaldson H. Why do we not use trained interpreters for all patients with limited English proficiency? Is there a place for using family members? Austr J Prim Health 2011;17:240–9.
28. Jacobs B, Kroll L, Green J, David TJ. The hazards of using a child as an interpreter. J Royal Soc Med 1995;88:474P–5P.
29. Lion KC, Brown JC, Ebel BE, et al. Effect of telephone vs video interpretation on parent comprehension, communication, and utilization in the pediatric emergency department: a randomized clinical trial. JAMA Pediatr 2015;169:1117–25.
30. Wofford JL CC, Johnson DA, Brown MT. Providing a Spanish interpreter using low-cost videoconferencing in a community health centre: a pilot study using tablet computers. Inform Prim Care 2012;20:141–6.
31. Jacobs EA SL, Rathouz PJ. The impact of an enhanced interpreter service intervention on hospital costs and patient satisfaction. J Gen Intern Med 2007;22(Suppl 2):306–11.
32. Jacobs EA LG, Rathouz PJ, Fu P Jr. Shared networks of interpreter services, at relatively low cost, can help providers serve patients with limited english skills. Health Aff (Millwood) 2011;30:1930–8.
33. Locatis C, Williamson D, Gould-Kabler C, et al. Comparing in-person, video, and telephonic medical interpretation. J Gen Intern Med 2010;25:345–50.
34. Jones D, Gill P, Harrison R, et al. An exploratory study of language interpretation services provided by videoconferencing. J Telemed Telecare 2003;9:51–6.
35. Price EL, Perez-Stable EJ, Nickleach D, et al. Interpreter perspectives of in-person, telephonic, and videoconferencing medical interpretation in clinical encounters. Patient Educ Couns 2012;87:226–32.
36. Crossman KL, Wiener E, Roosevelt G, et al. Interpreters: telephonic, in-person interpretation and bilingual providers. Pediatrics 2010;125:e631–8.
37. Degni F, Suominen S, Essen B, et al. Communication and cultural issues in providing reproductive health care to immigrant women: health care providers’ experiences in meeting the needs of [corrected] Somali women living in Finland. J Immigr Minor Health 2012;14:330–43.
38. Odunukan OW, Abdulai RM, Hagi Salaad MF, et al. Provider and interpreter preferences among Somali women in a primary care setting. J Prim Care Comm Health 2015;6:105–10.
39. Poss JE, Beeman T. Effective use of interpreters in health care: guidelines for nurse managers and clinicians. Semin Nurse Manag 1999;7:166–71.
40. Phelan M, Parkman S. How to work with an interpreter. BMJ 1995;311:555–7.
41. Lubrano di Ciccone B, Brown RF, Gueguen JA, et al. Interviewing patients using interpreters in an oncology setting: initial evaluation of a communication skills module. Ann Oncol 2010;21:27–32.
42. Hudelson P. Improving patient-provider communication: insights from interpreters. Fam Pract 2005;22:311–6.
43. Hudelson P, Dao MD, Perron NJ, Bischoff A. Interpreter-mediated diabetes consultations: a qualitative analysis of physician communication practices. BMC Fam Pract 2013;14:163.
44. Green AR, Ngo-Metzger Q, Legedza AT, et al. Interpreter services, language concordance, and health care quality. Experiences of Asian Americans with limited English proficiency. J Gen Intern Med 2005;20:1050–6.
45. Schenker Y, Smith AK, Arnold RM, Fernandez A. “Her husband doesn’t speak much English”: conducting a family meeting with an interpreter. J Palliat Med 2012;15:494–8.
1. U.S. Census Bureau. American community survey. Accessed 11 Jul 2016 at www.census.gov/acs/www.
2. Wiener ESR, Ivonne M. Bridging language barriers: how to work with an interpreter. Clin Pediatr Emerg Med 2004;5:93–101.
3. Perez-Stable EJ, Karliner LS. What do we know about patient-clinician interactions with interpreters? J Gen Intern Med 2013;28:339–41.
4. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Clinician ratings of interpreter mediated visits in underserved primary care settings with ad hoc, in-person professional, and video conferencing modes. J Health Care Poor Underserved 2010;21:301–17.
5. Flores G, Abreu M, Barone CP, et al. Errors of medical interpretation and their potential clinical consequences: a comparison of professional versus ad hoc versus no interpreters. Ann Emerg Med 2012;60:545–53.
6. Bauer AM, Alegria M. Impact of patient language proficiency and interpreter service use on the quality of psychiatric care: a systematic review. Psychiatr Serv 2010;61:765–73.
7. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res 2007;42:727–54.
8. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev 2005;62:255–99.
9. Lindholm M, Hargraves JL, Ferguson WJ, Reed G. Professional language interpretation and inpatient length of stay and readmission rates. J Gen Intern Med 2012;27:1294–9.
10. Juckett G, Unger K. Appropriate use of medical interpreters. Am Fam Physician 2014;90:476–80.
11. Schapira L, Vargas E, Hidalgo R, et al. Lost in translation: integrating medical interpreters into the multidisciplinary team. Oncologist 2008;13:586–92.
12. Gray B, Hilder J, Stubbe M. How to use interpreters in general practice: the development of a New Zealand toolkit. J Prim Health Care 2012;4:52–61, A1-8.
13. Hsieh E. Not just “getting by”: factors influencing providers’ choice of interpreters. J Gen Intern Med 2015;30:75–82.
14. Philips C. Using interpreters--a guide for GPs. Austr Fam Physician 2010;39:188–95.
15. Boscolo-Hightower A, Rafton SA, Tolman M, et al. Identifying families with limited English proficiency using a capture-recapture approach. Hosp Pediatr 2014;4:16–22.
16. Hadziabdic E, Hjelm K. Working with interpreters: practical advice for use of an interpreter in healthcare. Int J Evid Based Healthc 2013;11:69–76.
17. Abbe M, Simon C, Angiolillo A, et al. A survey of language barriers from the perspective of pediatric oncologists, interpreters, and parents. Pediatr Blood Cancer 2006;47:819–24.
18. Ngo-Metzger Q, Massagli MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med 2003;18:44–52.
19. Hadziabdic E, Hjelm K. Arabic-speaking migrants’ experiences of the use of interpreters in healthcare: a qualitative explorative study. Int J Equity Health 2014;13:49.
20. Julliard K, Vivar J, Delgado C, et al. What Latina patients don’t tell their doctors: a qualitative study. Ann Family Med 2008;6:543–9.
21. Hsieh E, Ju H, Kong H. Dimensions of trust: the tensions and challenges in provider--interpreter trust. Qual Health Res 2010;20:170–81.
22. Butow PN, Lobb E, Jefford M, et al. A bridge between cultures: interpreters’ perspectives of consultations with migrant oncology patients. Support Care Cancer 2012;20:235-44.
23. Hsieh E. “I am not a robot!” Interpreters’ views of their roles in health care settings. Qual Health Res 2008;18:1367–83.
24. Hsieh E, Hong SJ. Not all are desired: providers’ views on interpreters’ emotional support for patients. Patient Educ Couns 2010;81:192–7.
25. Elderkin-Thompson V, Silver RC, Waitzkin H. When nurses double as interpreters: a study of Spanish-speaking patients in a US primary care setting. Soc Sci Med 2001;52:1343–58.
26. Napoles AM, Santoyo-Olsson J, Karliner LS, et al. Inaccurate language interpretation and its clinical significance in the medical encounters of Spanish-speaking Latinos. Med Care 2015;53:940–7.
27. Gray B, Hilder J, Donaldson H. Why do we not use trained interpreters for all patients with limited English proficiency? Is there a place for using family members? Austr J Prim Health 2011;17:240–9.
28. Jacobs B, Kroll L, Green J, David TJ. The hazards of using a child as an interpreter. J Royal Soc Med 1995;88:474P–5P.
29. Lion KC, Brown JC, Ebel BE, et al. Effect of telephone vs video interpretation on parent comprehension, communication, and utilization in the pediatric emergency department: a randomized clinical trial. JAMA Pediatr 2015;169:1117–25.
30. Wofford JL CC, Johnson DA, Brown MT. Providing a Spanish interpreter using low-cost videoconferencing in a community health centre: a pilot study using tablet computers. Inform Prim Care 2012;20:141–6.
31. Jacobs EA SL, Rathouz PJ. The impact of an enhanced interpreter service intervention on hospital costs and patient satisfaction. J Gen Intern Med 2007;22(Suppl 2):306–11.
32. Jacobs EA LG, Rathouz PJ, Fu P Jr. Shared networks of interpreter services, at relatively low cost, can help providers serve patients with limited english skills. Health Aff (Millwood) 2011;30:1930–8.
33. Locatis C, Williamson D, Gould-Kabler C, et al. Comparing in-person, video, and telephonic medical interpretation. J Gen Intern Med 2010;25:345–50.
34. Jones D, Gill P, Harrison R, et al. An exploratory study of language interpretation services provided by videoconferencing. J Telemed Telecare 2003;9:51–6.
35. Price EL, Perez-Stable EJ, Nickleach D, et al. Interpreter perspectives of in-person, telephonic, and videoconferencing medical interpretation in clinical encounters. Patient Educ Couns 2012;87:226–32.
36. Crossman KL, Wiener E, Roosevelt G, et al. Interpreters: telephonic, in-person interpretation and bilingual providers. Pediatrics 2010;125:e631–8.
37. Degni F, Suominen S, Essen B, et al. Communication and cultural issues in providing reproductive health care to immigrant women: health care providers’ experiences in meeting the needs of [corrected] Somali women living in Finland. J Immigr Minor Health 2012;14:330–43.
38. Odunukan OW, Abdulai RM, Hagi Salaad MF, et al. Provider and interpreter preferences among Somali women in a primary care setting. J Prim Care Comm Health 2015;6:105–10.
39. Poss JE, Beeman T. Effective use of interpreters in health care: guidelines for nurse managers and clinicians. Semin Nurse Manag 1999;7:166–71.
40. Phelan M, Parkman S. How to work with an interpreter. BMJ 1995;311:555–7.
41. Lubrano di Ciccone B, Brown RF, Gueguen JA, et al. Interviewing patients using interpreters in an oncology setting: initial evaluation of a communication skills module. Ann Oncol 2010;21:27–32.
42. Hudelson P. Improving patient-provider communication: insights from interpreters. Fam Pract 2005;22:311–6.
43. Hudelson P, Dao MD, Perron NJ, Bischoff A. Interpreter-mediated diabetes consultations: a qualitative analysis of physician communication practices. BMC Fam Pract 2013;14:163.
44. Green AR, Ngo-Metzger Q, Legedza AT, et al. Interpreter services, language concordance, and health care quality. Experiences of Asian Americans with limited English proficiency. J Gen Intern Med 2005;20:1050–6.
45. Schenker Y, Smith AK, Arnold RM, Fernandez A. “Her husband doesn’t speak much English”: conducting a family meeting with an interpreter. J Palliat Med 2012;15:494–8.
Younger age, greater anxiety, affect pain after breast reconstruction
Younger age, bilateral procedure, and presurgery depression and anxiety are among the significant contributors to pain after breast reconstruction surgery, according to findings from a prospective study of 2,207 women who underwent several types of breast reconstruction procedures.
Although breast reconstruction is an important element of breast cancer treatment, and most acute postoperative pain resolves with time and pain management intervention, some patients suffer from persistent, severe postoperative pain that increases their risk for long-term pain and clinical morbidity, wrote Anita R. Kulkarni, MD, of Memorial Sloan-Kettering Cancer Center, New York, and her colleagues.
Overall, greater acute postoperative pain was significantly associated with younger age, bilateral procedures, higher levels of preoperative pain, and higher levels of preoperative anxiety and depression, the researchers said.
“Moreover, the degree of patients’ self-reported preoperative anxiety and depressive symptoms both appeared to bear a linear relationship with the magnitude of increased postoperative pain at 1 week” on the MPQ sensory pain rating, they noted.
Similarly, lower scores of physical well-being based on the BREAST-Q physical well-being scale were significantly associated with younger age, bilateral procedures, immediate reconstruction, and higher levels of preoperative pain, anxiety, and depression.
The average age of the women was 50 years, and 87% were white. Most patients (69%) had tissue expander (TE)/implant reconstruction procedures; 93% were immediate reconstruction; and 53% were bilateral reconstruction. The majority (90%) underwent surgery as part of breast cancer treatment.
“The comparative effect of procedure type on postoperative pain showed variable results across our multiple pain scales,” the researchers said.
The patients who underwent autologous flap reconstruction procedures – pedicled transverse rectus abdominis myocutaneous flap (PTRAMS), deep inferior epigastric perforator (DIEP), or superficial inferior epigastric artery (SIEA) – reported less-severe postoperative pain than did those who had TE/Implant procedures. Specifically, patients with SIEA and DIEP procedures reported significantly less pain 1 week after surgery than did those who had TE/Implant procedures, based on the MPQ sensory scale. In addition, patients with PTRAMS reported significantly less postoperative pain 1 week after surgery than did those who had TE/Implant procedures based on the NPRS scale. All three flap procedures were significantly associated with less-severe postoperative pain, compared with TE/Implant procedures.
The findings support data from previous studies that identified preoperative pain, mood disturbance, and age as factors for increased risk of acute postoperative pain, the researchers noted. In addition, “the findings have important implications for the identification of women who might be at risk for significant early postoperative pain following breast reconstruction, as acute postoperative pain is associated with poor functional outcomes, diminished quality of life, and the risk for development of persistent postsurgical pain,” they wrote.
The study results were limited by several factors, including the lack of standardization for postoperative pain treatment regimens, variability in the timing of preoperative assessment, and nonresponder bias, the researchers said.
However, “Once high-risk patients are identified, appropriate referrals can be considered to facilitate careful monitoring of postsurgical pain for selected patients,” they said. “Early intervention can give clinicians the opportunity to reduce postoperative morbidity and improve patients’ surgical experience and satisfaction with breast reconstruction outcome,” they added.
The researchers had no financial conflicts to disclose. The study was supported in part by a grant from the National Institutes of Health/National Cancer Institute.
Younger age, bilateral procedure, and presurgery depression and anxiety are among the significant contributors to pain after breast reconstruction surgery, according to findings from a prospective study of 2,207 women who underwent several types of breast reconstruction procedures.
Although breast reconstruction is an important element of breast cancer treatment, and most acute postoperative pain resolves with time and pain management intervention, some patients suffer from persistent, severe postoperative pain that increases their risk for long-term pain and clinical morbidity, wrote Anita R. Kulkarni, MD, of Memorial Sloan-Kettering Cancer Center, New York, and her colleagues.
Overall, greater acute postoperative pain was significantly associated with younger age, bilateral procedures, higher levels of preoperative pain, and higher levels of preoperative anxiety and depression, the researchers said.
“Moreover, the degree of patients’ self-reported preoperative anxiety and depressive symptoms both appeared to bear a linear relationship with the magnitude of increased postoperative pain at 1 week” on the MPQ sensory pain rating, they noted.
Similarly, lower scores of physical well-being based on the BREAST-Q physical well-being scale were significantly associated with younger age, bilateral procedures, immediate reconstruction, and higher levels of preoperative pain, anxiety, and depression.
The average age of the women was 50 years, and 87% were white. Most patients (69%) had tissue expander (TE)/implant reconstruction procedures; 93% were immediate reconstruction; and 53% were bilateral reconstruction. The majority (90%) underwent surgery as part of breast cancer treatment.
“The comparative effect of procedure type on postoperative pain showed variable results across our multiple pain scales,” the researchers said.
The patients who underwent autologous flap reconstruction procedures – pedicled transverse rectus abdominis myocutaneous flap (PTRAMS), deep inferior epigastric perforator (DIEP), or superficial inferior epigastric artery (SIEA) – reported less-severe postoperative pain than did those who had TE/Implant procedures. Specifically, patients with SIEA and DIEP procedures reported significantly less pain 1 week after surgery than did those who had TE/Implant procedures, based on the MPQ sensory scale. In addition, patients with PTRAMS reported significantly less postoperative pain 1 week after surgery than did those who had TE/Implant procedures based on the NPRS scale. All three flap procedures were significantly associated with less-severe postoperative pain, compared with TE/Implant procedures.
The findings support data from previous studies that identified preoperative pain, mood disturbance, and age as factors for increased risk of acute postoperative pain, the researchers noted. In addition, “the findings have important implications for the identification of women who might be at risk for significant early postoperative pain following breast reconstruction, as acute postoperative pain is associated with poor functional outcomes, diminished quality of life, and the risk for development of persistent postsurgical pain,” they wrote.
The study results were limited by several factors, including the lack of standardization for postoperative pain treatment regimens, variability in the timing of preoperative assessment, and nonresponder bias, the researchers said.
However, “Once high-risk patients are identified, appropriate referrals can be considered to facilitate careful monitoring of postsurgical pain for selected patients,” they said. “Early intervention can give clinicians the opportunity to reduce postoperative morbidity and improve patients’ surgical experience and satisfaction with breast reconstruction outcome,” they added.
The researchers had no financial conflicts to disclose. The study was supported in part by a grant from the National Institutes of Health/National Cancer Institute.
Younger age, bilateral procedure, and presurgery depression and anxiety are among the significant contributors to pain after breast reconstruction surgery, according to findings from a prospective study of 2,207 women who underwent several types of breast reconstruction procedures.
Although breast reconstruction is an important element of breast cancer treatment, and most acute postoperative pain resolves with time and pain management intervention, some patients suffer from persistent, severe postoperative pain that increases their risk for long-term pain and clinical morbidity, wrote Anita R. Kulkarni, MD, of Memorial Sloan-Kettering Cancer Center, New York, and her colleagues.
Overall, greater acute postoperative pain was significantly associated with younger age, bilateral procedures, higher levels of preoperative pain, and higher levels of preoperative anxiety and depression, the researchers said.
“Moreover, the degree of patients’ self-reported preoperative anxiety and depressive symptoms both appeared to bear a linear relationship with the magnitude of increased postoperative pain at 1 week” on the MPQ sensory pain rating, they noted.
Similarly, lower scores of physical well-being based on the BREAST-Q physical well-being scale were significantly associated with younger age, bilateral procedures, immediate reconstruction, and higher levels of preoperative pain, anxiety, and depression.
The average age of the women was 50 years, and 87% were white. Most patients (69%) had tissue expander (TE)/implant reconstruction procedures; 93% were immediate reconstruction; and 53% were bilateral reconstruction. The majority (90%) underwent surgery as part of breast cancer treatment.
“The comparative effect of procedure type on postoperative pain showed variable results across our multiple pain scales,” the researchers said.
The patients who underwent autologous flap reconstruction procedures – pedicled transverse rectus abdominis myocutaneous flap (PTRAMS), deep inferior epigastric perforator (DIEP), or superficial inferior epigastric artery (SIEA) – reported less-severe postoperative pain than did those who had TE/Implant procedures. Specifically, patients with SIEA and DIEP procedures reported significantly less pain 1 week after surgery than did those who had TE/Implant procedures, based on the MPQ sensory scale. In addition, patients with PTRAMS reported significantly less postoperative pain 1 week after surgery than did those who had TE/Implant procedures based on the NPRS scale. All three flap procedures were significantly associated with less-severe postoperative pain, compared with TE/Implant procedures.
The findings support data from previous studies that identified preoperative pain, mood disturbance, and age as factors for increased risk of acute postoperative pain, the researchers noted. In addition, “the findings have important implications for the identification of women who might be at risk for significant early postoperative pain following breast reconstruction, as acute postoperative pain is associated with poor functional outcomes, diminished quality of life, and the risk for development of persistent postsurgical pain,” they wrote.
The study results were limited by several factors, including the lack of standardization for postoperative pain treatment regimens, variability in the timing of preoperative assessment, and nonresponder bias, the researchers said.
However, “Once high-risk patients are identified, appropriate referrals can be considered to facilitate careful monitoring of postsurgical pain for selected patients,” they said. “Early intervention can give clinicians the opportunity to reduce postoperative morbidity and improve patients’ surgical experience and satisfaction with breast reconstruction outcome,” they added.
The researchers had no financial conflicts to disclose. The study was supported in part by a grant from the National Institutes of Health/National Cancer Institute.
FROM THE JOURNAL OF PLASTIC, RECONSTRUCTIVE & AESTHETIC SURGERY OPEN
Key clinical point: Identifying women at increased risk for severe acute postoperative pain allows clinicians the opportunity to reduce postoperative morbidity and improve patients’ surgical experience.
Major finding: Younger age (P = .002), bilateral procedures (P less than .0001), higher levels of preoperative pain (P less than .0001), and higher levels of preoperative anxiety (P less than .01) were among the strongest factors significantly associated with acute postoperative pain.
Data source: A prospective study of 2,207 women who underwent several types of breast reconstruction procedures.
Disclosures: The researchers had no financial conflicts to disclose. The study was supported in part by a grant from the National Institutes of Health/National Cancer Institute.