User login
Considering the true costs of clinical trials
This transcript has been edited for clarity.
We need to think about the ways that participating in clinical trials results in increased out-of-pocket costs to our patients and how that limits the ability of marginalized groups to participate. That should be a problem for us.
There are many subtle and some egregious ways that participating in clinical trials can result in increased costs. We may ask patients to come to the clinic more frequently. That may mean costs for transportation, wear and tear on your car, and gas prices. It may also mean that if you work in a job where you don’t have time off, and if you’re not at work, you don’t get paid. That’s a major hit to your take-home pay.
We also need to take a close and more honest look at our study budgets and what we consider standard of care. Now, this becomes a slippery slope because there are clear recommendations that we would all agree, but there are also differences of practice and differences of opinion.
How often should patients with advanced disease, who clinically are doing well, have scans to evaluate their disease status and look for subtle evidence of progression? Are laboratory studies part of the follow-up in patients in the adjuvant setting? Did you really need a urinalysis in somebody who’s going to be starting chemotherapy? Do you need an EKG if you’re going to be giving them a drug that doesn’t have potential cardiac toxicity, for which QTc prolongation is not a problem?
Those are often included in our clinical trials. In some cases, they might be paid for by the trial. In other cases, they’re billed to the insurance provider, which means they’ll contribute to deductibles and copays will apply. It is very likely that they will cost your patient something out of pocket.
Now, this becomes important because many of our consent forms would specifically say that things that are only done for the study are paid for by the study. How we define standard of care becomes vitally important. These issues have not been linked in this way frequently.
Clinical trials are how we make progress. The more patients who are able to participate in clinical trials, the better it is for all of us and all our future patients.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
We need to think about the ways that participating in clinical trials results in increased out-of-pocket costs to our patients and how that limits the ability of marginalized groups to participate. That should be a problem for us.
There are many subtle and some egregious ways that participating in clinical trials can result in increased costs. We may ask patients to come to the clinic more frequently. That may mean costs for transportation, wear and tear on your car, and gas prices. It may also mean that if you work in a job where you don’t have time off, and if you’re not at work, you don’t get paid. That’s a major hit to your take-home pay.
We also need to take a close and more honest look at our study budgets and what we consider standard of care. Now, this becomes a slippery slope because there are clear recommendations that we would all agree, but there are also differences of practice and differences of opinion.
How often should patients with advanced disease, who clinically are doing well, have scans to evaluate their disease status and look for subtle evidence of progression? Are laboratory studies part of the follow-up in patients in the adjuvant setting? Did you really need a urinalysis in somebody who’s going to be starting chemotherapy? Do you need an EKG if you’re going to be giving them a drug that doesn’t have potential cardiac toxicity, for which QTc prolongation is not a problem?
Those are often included in our clinical trials. In some cases, they might be paid for by the trial. In other cases, they’re billed to the insurance provider, which means they’ll contribute to deductibles and copays will apply. It is very likely that they will cost your patient something out of pocket.
Now, this becomes important because many of our consent forms would specifically say that things that are only done for the study are paid for by the study. How we define standard of care becomes vitally important. These issues have not been linked in this way frequently.
Clinical trials are how we make progress. The more patients who are able to participate in clinical trials, the better it is for all of us and all our future patients.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
We need to think about the ways that participating in clinical trials results in increased out-of-pocket costs to our patients and how that limits the ability of marginalized groups to participate. That should be a problem for us.
There are many subtle and some egregious ways that participating in clinical trials can result in increased costs. We may ask patients to come to the clinic more frequently. That may mean costs for transportation, wear and tear on your car, and gas prices. It may also mean that if you work in a job where you don’t have time off, and if you’re not at work, you don’t get paid. That’s a major hit to your take-home pay.
We also need to take a close and more honest look at our study budgets and what we consider standard of care. Now, this becomes a slippery slope because there are clear recommendations that we would all agree, but there are also differences of practice and differences of opinion.
How often should patients with advanced disease, who clinically are doing well, have scans to evaluate their disease status and look for subtle evidence of progression? Are laboratory studies part of the follow-up in patients in the adjuvant setting? Did you really need a urinalysis in somebody who’s going to be starting chemotherapy? Do you need an EKG if you’re going to be giving them a drug that doesn’t have potential cardiac toxicity, for which QTc prolongation is not a problem?
Those are often included in our clinical trials. In some cases, they might be paid for by the trial. In other cases, they’re billed to the insurance provider, which means they’ll contribute to deductibles and copays will apply. It is very likely that they will cost your patient something out of pocket.
Now, this becomes important because many of our consent forms would specifically say that things that are only done for the study are paid for by the study. How we define standard of care becomes vitally important. These issues have not been linked in this way frequently.
Clinical trials are how we make progress. The more patients who are able to participate in clinical trials, the better it is for all of us and all our future patients.
Kathy D. Miller, MD, is associate director of clinical research and codirector of the breast cancer program at the Melvin and Bren Simon Cancer Center at Indiana University, Indianapolis. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Prioritize nutrients, limit ultraprocessed food in diabetes
In a large cohort of older adults with type 2 diabetes in Italy, those with the highest intake of ultraprocessed food and beverages (UPF) were more likely to die of all causes or cardiovascular disease (CVD) within a decade than those with the lowest intake – independent of adherence to a healthy Mediterranean diet.
Adults in the top quartile of UPF intake had a 64% increased risk of all-cause death and a 2.5-fold increased risk of CVD death during follow-up, compared with those in the lowest quartile, after adjusting for variables including Mediterranean diet score.
These findings from the Moli-sani study by Marialaura Bonaccio, PhD, from the Institute for Research, Hospitalization and Healthcare (IRCCS) Neuromed, in Pozzilli, Italy, and colleagues, were published online in the American Journal of Clinical Nutrition.
“Dietary recommendations for prevention and management of type 2 diabetes almost exclusively prioritize consumption of nutritionally balanced foods that are the source of fiber [and] healthy fats and [are] poor in free sugars, and promote dietary patterns – such as the Mediterranean diet and the DASH diet – that place a large emphasis on food groups (for example, whole grains, legumes, nuts, fruits, and vegetables) regardless of food processing,” the researchers note.
The research suggests that “besides prioritizing the adoption of a diet based on nutritional requirements, dietary guidelines for the management of type 2 diabetes should also recommend limiting UPF,” they conclude.
“In addition to the adoption of a diet based on well-known nutritional requirements, dietary recommendations should also suggest limiting the consumption of ultraprocessed foods as much as possible,” Giovanni de Gaetano, MD, PhD, president, IRCCS Neuromed, echoed, in a press release from the institute.
“In this context, and not only for people with diabetes, the front-of-pack nutrition labels should also include information on the degree of food processing,” he observed.
Caroline M. Apovian, MD, who was not involved with the study, agrees that it is wise to limit consumption of UPF.
However, we need more research to better understand which components of UPF are harmful and the biologic mechanisms, Dr. Apovian, who is codirector, Center for Weight Management and Wellness, Brigham and Women’s Hospital, and a professor of medicine at Harvard Medical School, both in Boston, told this news organization in an interview.
She noted that in a randomized crossover trial in 20 patients who were instructed to eat as much or as little as they wanted, people ate more and gained weight during 2 weeks of a diet high in UPF, compared with 2 weeks of an unprocessed diet matched for presented calories, carbohydrate, sugar, fat, sodium, and fiber.
Ultraprocessed foods classed according to Nova system
UPF is “made mostly or entirely from substances derived from foods and additives, using a series of processes and containing minimal whole foods,” and they “are usually nutrient-poor, high in calories, added sugar, sodium, and unhealthy fats,” the Italian researchers write.
High intake of UPF, they add, may exacerbate health risks in people with type 2 diabetes, who are already at higher risk of premature mortality, mainly due to diabetes-related complications.
The researchers analyzed data from a subset of patients in the Moli-sani study of environmental and genetic factors underlying disease, which enrolled 24,325 individuals aged 35 and older who lived in Molise, in central-southern Italy, in 2005-2010.
The current analysis included 1,065 participants in Moli-sani who had type 2 diabetes at baseline and completed a food frequency questionnaire by which participants reported their consumption of 188 foods and beverages in the previous 12 months.
Participants were a mean age of 65 years, and 60% were men.
Most UPF intake was from processed meat (22.4%), crispbread/rusks (16.6%), nonhomemade pizza (11.2%), and cakes, pies, pastries, and puddings (8.8%).
Researchers categorized foods and beverages into four groups with increasing degrees of processing, based on the Nova Food Classification System:
- Group 1: Fresh or minimally processed foods and beverages (for example, fruit, meat, milk).
- Group 2: Processed culinary ingredients (for example, oils, butter).
- Group 3: Processed foods and beverages (for example, canned fish, bread).
- Group 4: UPF (22 foods and beverages including carbonated drinks, processed meats, sweet or savory packaged snacks, margarine, and foods and beverages with artificial sweeteners).
Participants were divided into four quartiles based on UPF consumption.
The mean percentage of UPF consumption out of total food and beverage intake was 2.8%, 5.2%, 7.7%, and 14.4% for quartiles 1, 2, 3, and 4, respectively. By sex, these rates for quartile 1 were < 4.7% for women and < 3.7% for men, and for quartile 4 were ≥ 10.5% for women and ≥ 9% for men.
Participants with the highest UPF intake were younger (mean age, 63 vs. 67 years) but otherwise had similar characteristics as other participants.
During a median follow-up of 11.6 years, 308 participants died from all causes, including 129 who died from CVD.
Compared with participants with the lowest intake of UPF (quartile 1), those with the highest intake (quartile 4) had a higher risk of all-cause mortality (hazard ratio, 1.70) and CVD mortality (HR, 2.64) during follow-up, after multivariable adjustment. The analysis adjusted for sex, age, energy intake, residence, education, housing, smoking, body mass index, leisure-time physical activity, history of cancer or cardiovascular disease, hypertension, hyperlipidemia, aspirin use, years since type 2 diabetes diagnosis, and special diet for blood glucose control.
After further adjusting for Mediterranean diet score, the risk of all-cause and CVD mortality during follow-up for patients with the highest versus lowest intake of UPF remained similar (HR, 1.64 and 2.55, respectively).
There was a linear dose–response relationship between UPF and all-cause and CVD mortality.
Increasing intake of fruit drinks, carbonated drinks, and salty biscuits was associated with higher all-cause and CVD mortality rates, and consumption of stock cubes and margarine was further related to higher CVD death.
The researchers acknowledge that the study was observational, and therefore cannot determine cause and effect, and was not designed to specifically collect dietary data according to the Nova classification. The findings may not be generalizable to other populations.
The analysis was partly funded by grants from the AIRC and Italian Ministry of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large cohort of older adults with type 2 diabetes in Italy, those with the highest intake of ultraprocessed food and beverages (UPF) were more likely to die of all causes or cardiovascular disease (CVD) within a decade than those with the lowest intake – independent of adherence to a healthy Mediterranean diet.
Adults in the top quartile of UPF intake had a 64% increased risk of all-cause death and a 2.5-fold increased risk of CVD death during follow-up, compared with those in the lowest quartile, after adjusting for variables including Mediterranean diet score.
These findings from the Moli-sani study by Marialaura Bonaccio, PhD, from the Institute for Research, Hospitalization and Healthcare (IRCCS) Neuromed, in Pozzilli, Italy, and colleagues, were published online in the American Journal of Clinical Nutrition.
“Dietary recommendations for prevention and management of type 2 diabetes almost exclusively prioritize consumption of nutritionally balanced foods that are the source of fiber [and] healthy fats and [are] poor in free sugars, and promote dietary patterns – such as the Mediterranean diet and the DASH diet – that place a large emphasis on food groups (for example, whole grains, legumes, nuts, fruits, and vegetables) regardless of food processing,” the researchers note.
The research suggests that “besides prioritizing the adoption of a diet based on nutritional requirements, dietary guidelines for the management of type 2 diabetes should also recommend limiting UPF,” they conclude.
“In addition to the adoption of a diet based on well-known nutritional requirements, dietary recommendations should also suggest limiting the consumption of ultraprocessed foods as much as possible,” Giovanni de Gaetano, MD, PhD, president, IRCCS Neuromed, echoed, in a press release from the institute.
“In this context, and not only for people with diabetes, the front-of-pack nutrition labels should also include information on the degree of food processing,” he observed.
Caroline M. Apovian, MD, who was not involved with the study, agrees that it is wise to limit consumption of UPF.
However, we need more research to better understand which components of UPF are harmful and the biologic mechanisms, Dr. Apovian, who is codirector, Center for Weight Management and Wellness, Brigham and Women’s Hospital, and a professor of medicine at Harvard Medical School, both in Boston, told this news organization in an interview.
She noted that in a randomized crossover trial in 20 patients who were instructed to eat as much or as little as they wanted, people ate more and gained weight during 2 weeks of a diet high in UPF, compared with 2 weeks of an unprocessed diet matched for presented calories, carbohydrate, sugar, fat, sodium, and fiber.
Ultraprocessed foods classed according to Nova system
UPF is “made mostly or entirely from substances derived from foods and additives, using a series of processes and containing minimal whole foods,” and they “are usually nutrient-poor, high in calories, added sugar, sodium, and unhealthy fats,” the Italian researchers write.
High intake of UPF, they add, may exacerbate health risks in people with type 2 diabetes, who are already at higher risk of premature mortality, mainly due to diabetes-related complications.
The researchers analyzed data from a subset of patients in the Moli-sani study of environmental and genetic factors underlying disease, which enrolled 24,325 individuals aged 35 and older who lived in Molise, in central-southern Italy, in 2005-2010.
The current analysis included 1,065 participants in Moli-sani who had type 2 diabetes at baseline and completed a food frequency questionnaire by which participants reported their consumption of 188 foods and beverages in the previous 12 months.
Participants were a mean age of 65 years, and 60% were men.
Most UPF intake was from processed meat (22.4%), crispbread/rusks (16.6%), nonhomemade pizza (11.2%), and cakes, pies, pastries, and puddings (8.8%).
Researchers categorized foods and beverages into four groups with increasing degrees of processing, based on the Nova Food Classification System:
- Group 1: Fresh or minimally processed foods and beverages (for example, fruit, meat, milk).
- Group 2: Processed culinary ingredients (for example, oils, butter).
- Group 3: Processed foods and beverages (for example, canned fish, bread).
- Group 4: UPF (22 foods and beverages including carbonated drinks, processed meats, sweet or savory packaged snacks, margarine, and foods and beverages with artificial sweeteners).
Participants were divided into four quartiles based on UPF consumption.
The mean percentage of UPF consumption out of total food and beverage intake was 2.8%, 5.2%, 7.7%, and 14.4% for quartiles 1, 2, 3, and 4, respectively. By sex, these rates for quartile 1 were < 4.7% for women and < 3.7% for men, and for quartile 4 were ≥ 10.5% for women and ≥ 9% for men.
Participants with the highest UPF intake were younger (mean age, 63 vs. 67 years) but otherwise had similar characteristics as other participants.
During a median follow-up of 11.6 years, 308 participants died from all causes, including 129 who died from CVD.
Compared with participants with the lowest intake of UPF (quartile 1), those with the highest intake (quartile 4) had a higher risk of all-cause mortality (hazard ratio, 1.70) and CVD mortality (HR, 2.64) during follow-up, after multivariable adjustment. The analysis adjusted for sex, age, energy intake, residence, education, housing, smoking, body mass index, leisure-time physical activity, history of cancer or cardiovascular disease, hypertension, hyperlipidemia, aspirin use, years since type 2 diabetes diagnosis, and special diet for blood glucose control.
After further adjusting for Mediterranean diet score, the risk of all-cause and CVD mortality during follow-up for patients with the highest versus lowest intake of UPF remained similar (HR, 1.64 and 2.55, respectively).
There was a linear dose–response relationship between UPF and all-cause and CVD mortality.
Increasing intake of fruit drinks, carbonated drinks, and salty biscuits was associated with higher all-cause and CVD mortality rates, and consumption of stock cubes and margarine was further related to higher CVD death.
The researchers acknowledge that the study was observational, and therefore cannot determine cause and effect, and was not designed to specifically collect dietary data according to the Nova classification. The findings may not be generalizable to other populations.
The analysis was partly funded by grants from the AIRC and Italian Ministry of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large cohort of older adults with type 2 diabetes in Italy, those with the highest intake of ultraprocessed food and beverages (UPF) were more likely to die of all causes or cardiovascular disease (CVD) within a decade than those with the lowest intake – independent of adherence to a healthy Mediterranean diet.
Adults in the top quartile of UPF intake had a 64% increased risk of all-cause death and a 2.5-fold increased risk of CVD death during follow-up, compared with those in the lowest quartile, after adjusting for variables including Mediterranean diet score.
These findings from the Moli-sani study by Marialaura Bonaccio, PhD, from the Institute for Research, Hospitalization and Healthcare (IRCCS) Neuromed, in Pozzilli, Italy, and colleagues, were published online in the American Journal of Clinical Nutrition.
“Dietary recommendations for prevention and management of type 2 diabetes almost exclusively prioritize consumption of nutritionally balanced foods that are the source of fiber [and] healthy fats and [are] poor in free sugars, and promote dietary patterns – such as the Mediterranean diet and the DASH diet – that place a large emphasis on food groups (for example, whole grains, legumes, nuts, fruits, and vegetables) regardless of food processing,” the researchers note.
The research suggests that “besides prioritizing the adoption of a diet based on nutritional requirements, dietary guidelines for the management of type 2 diabetes should also recommend limiting UPF,” they conclude.
“In addition to the adoption of a diet based on well-known nutritional requirements, dietary recommendations should also suggest limiting the consumption of ultraprocessed foods as much as possible,” Giovanni de Gaetano, MD, PhD, president, IRCCS Neuromed, echoed, in a press release from the institute.
“In this context, and not only for people with diabetes, the front-of-pack nutrition labels should also include information on the degree of food processing,” he observed.
Caroline M. Apovian, MD, who was not involved with the study, agrees that it is wise to limit consumption of UPF.
However, we need more research to better understand which components of UPF are harmful and the biologic mechanisms, Dr. Apovian, who is codirector, Center for Weight Management and Wellness, Brigham and Women’s Hospital, and a professor of medicine at Harvard Medical School, both in Boston, told this news organization in an interview.
She noted that in a randomized crossover trial in 20 patients who were instructed to eat as much or as little as they wanted, people ate more and gained weight during 2 weeks of a diet high in UPF, compared with 2 weeks of an unprocessed diet matched for presented calories, carbohydrate, sugar, fat, sodium, and fiber.
Ultraprocessed foods classed according to Nova system
UPF is “made mostly or entirely from substances derived from foods and additives, using a series of processes and containing minimal whole foods,” and they “are usually nutrient-poor, high in calories, added sugar, sodium, and unhealthy fats,” the Italian researchers write.
High intake of UPF, they add, may exacerbate health risks in people with type 2 diabetes, who are already at higher risk of premature mortality, mainly due to diabetes-related complications.
The researchers analyzed data from a subset of patients in the Moli-sani study of environmental and genetic factors underlying disease, which enrolled 24,325 individuals aged 35 and older who lived in Molise, in central-southern Italy, in 2005-2010.
The current analysis included 1,065 participants in Moli-sani who had type 2 diabetes at baseline and completed a food frequency questionnaire by which participants reported their consumption of 188 foods and beverages in the previous 12 months.
Participants were a mean age of 65 years, and 60% were men.
Most UPF intake was from processed meat (22.4%), crispbread/rusks (16.6%), nonhomemade pizza (11.2%), and cakes, pies, pastries, and puddings (8.8%).
Researchers categorized foods and beverages into four groups with increasing degrees of processing, based on the Nova Food Classification System:
- Group 1: Fresh or minimally processed foods and beverages (for example, fruit, meat, milk).
- Group 2: Processed culinary ingredients (for example, oils, butter).
- Group 3: Processed foods and beverages (for example, canned fish, bread).
- Group 4: UPF (22 foods and beverages including carbonated drinks, processed meats, sweet or savory packaged snacks, margarine, and foods and beverages with artificial sweeteners).
Participants were divided into four quartiles based on UPF consumption.
The mean percentage of UPF consumption out of total food and beverage intake was 2.8%, 5.2%, 7.7%, and 14.4% for quartiles 1, 2, 3, and 4, respectively. By sex, these rates for quartile 1 were < 4.7% for women and < 3.7% for men, and for quartile 4 were ≥ 10.5% for women and ≥ 9% for men.
Participants with the highest UPF intake were younger (mean age, 63 vs. 67 years) but otherwise had similar characteristics as other participants.
During a median follow-up of 11.6 years, 308 participants died from all causes, including 129 who died from CVD.
Compared with participants with the lowest intake of UPF (quartile 1), those with the highest intake (quartile 4) had a higher risk of all-cause mortality (hazard ratio, 1.70) and CVD mortality (HR, 2.64) during follow-up, after multivariable adjustment. The analysis adjusted for sex, age, energy intake, residence, education, housing, smoking, body mass index, leisure-time physical activity, history of cancer or cardiovascular disease, hypertension, hyperlipidemia, aspirin use, years since type 2 diabetes diagnosis, and special diet for blood glucose control.
After further adjusting for Mediterranean diet score, the risk of all-cause and CVD mortality during follow-up for patients with the highest versus lowest intake of UPF remained similar (HR, 1.64 and 2.55, respectively).
There was a linear dose–response relationship between UPF and all-cause and CVD mortality.
Increasing intake of fruit drinks, carbonated drinks, and salty biscuits was associated with higher all-cause and CVD mortality rates, and consumption of stock cubes and margarine was further related to higher CVD death.
The researchers acknowledge that the study was observational, and therefore cannot determine cause and effect, and was not designed to specifically collect dietary data according to the Nova classification. The findings may not be generalizable to other populations.
The analysis was partly funded by grants from the AIRC and Italian Ministry of Health. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Does tamoxifen use increase the risk of endometrial cancer in premenopausal patients?
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
- Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
- Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
- Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
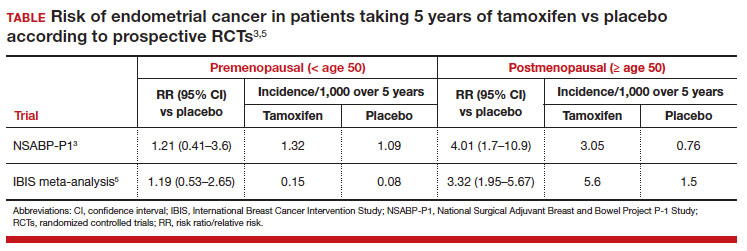
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
- Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
- Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
- Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
- Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
- Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
- Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
- Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
- Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
- Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
- American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
- Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
- Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
- Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
- Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
- Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
- Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
- Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
- Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
- Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
- Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
- Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
- Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
- Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
- Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
- Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
- American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
- Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
- Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
- Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
- Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
- Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
- Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
- Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
- Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
- Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
- American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.

How newly discovered genes might fit into obesity
Identifying specific genes adds to growing evidence that biology, in part, drives obesity. Researchers hope the findings will lead to effective treatments, and in the meantime add to the understanding that there are many types of obesity that come from a mix of genes and environmental factors.
Although the study is not the first to point to specific genes, “we were quite surprised by the proposed function of some of the genes we identified,” Lena R. Kaisinger, lead study investigator and a PhD student in the MRC Epidemiology Unit at the University of Cambridge (England), wrote in an email. For example, the genes also manage cell death and influence how cells respond to DNA damage.
The investigators are not sure why genes involved in body size perform this kind of double duty, which opens avenues for future research.
The gene sequencing study was published online in the journal Cell Genomics.
Differences between women and men
The researchers found five new genes in females and two new genes in males linked to greater body mass index (BMI): DIDO1, KIAA1109, MC4R, PTPRG and SLC12A5 in women and MC4R and SLTM in men. People who recall having obesity as a child were more likely to have rare genetic changes in two other genes, OBSCN and MADD.
“The key thing is that when you see real genes with real gene names, it really makes real the notion that genetics underlie obesity,” said Lee Kaplan, MD, PhD, director of the Obesity and Metabolism Institute in Boston, who was not affiliated with the research.
Ms. Kaisinger and colleagues found these significant genetic differences by studying genomes of about 420,000 people stored in the UK Biobank, a huge biomedical database. The researchers decided to look at genes by sex and age because these are “two areas that we still know very little about,” Ms. Kaisinger said.
“We know that different types of obesity connect to different ages,” said Dr. Kaplan, who is also past president of the Obesity Society. “But what they’ve done now is find genes that are associated with particular subtypes of obesity ... some more common in one sex and some more common in different phases of life, including early onset obesity.”
The future is already here
Treatment for obesity based on a person’s genes already exists. For example, in June 2022, the Food and Drug Administration approved setmelanotide (Imcivree) for weight management in adults and children aged over 6 years with specific genetic markers.
Even as encouraging as setmelanotide is to Ms. Kaisinger and colleagues, these are still early days for translating the current research findings into clinical obesity tests and potential treatment, she said.
The “holy grail,” Dr. Kaplan said, is a future where people get screened for a particular genetic profile and their provider can say something like, “You’re probably most susceptible to this type, so we’ll treat you with this particular drug that’s been developed for people with this phenotype.”
Dr. Kaplan added: “That’s exactly what we are trying to do.”
Moving forward, Ms. Kaisinger and colleagues plan to repeat the study in larger and more diverse populations. They also plan to reverse the usual road map for studies, which typically start in animals and then progress to humans.
“We plan to take the most promising gene candidates forward into mouse models to learn more about their function and how exactly their dysfunction results in obesity,” Ms. Kaisinger said.
Three study coauthors are employees and shareholders of Adrestia Therapeutics. No other conflicts of interest were reported.
A version of this article appeared on WebMD.com.
Identifying specific genes adds to growing evidence that biology, in part, drives obesity. Researchers hope the findings will lead to effective treatments, and in the meantime add to the understanding that there are many types of obesity that come from a mix of genes and environmental factors.
Although the study is not the first to point to specific genes, “we were quite surprised by the proposed function of some of the genes we identified,” Lena R. Kaisinger, lead study investigator and a PhD student in the MRC Epidemiology Unit at the University of Cambridge (England), wrote in an email. For example, the genes also manage cell death and influence how cells respond to DNA damage.
The investigators are not sure why genes involved in body size perform this kind of double duty, which opens avenues for future research.
The gene sequencing study was published online in the journal Cell Genomics.
Differences between women and men
The researchers found five new genes in females and two new genes in males linked to greater body mass index (BMI): DIDO1, KIAA1109, MC4R, PTPRG and SLC12A5 in women and MC4R and SLTM in men. People who recall having obesity as a child were more likely to have rare genetic changes in two other genes, OBSCN and MADD.
“The key thing is that when you see real genes with real gene names, it really makes real the notion that genetics underlie obesity,” said Lee Kaplan, MD, PhD, director of the Obesity and Metabolism Institute in Boston, who was not affiliated with the research.
Ms. Kaisinger and colleagues found these significant genetic differences by studying genomes of about 420,000 people stored in the UK Biobank, a huge biomedical database. The researchers decided to look at genes by sex and age because these are “two areas that we still know very little about,” Ms. Kaisinger said.
“We know that different types of obesity connect to different ages,” said Dr. Kaplan, who is also past president of the Obesity Society. “But what they’ve done now is find genes that are associated with particular subtypes of obesity ... some more common in one sex and some more common in different phases of life, including early onset obesity.”
The future is already here
Treatment for obesity based on a person’s genes already exists. For example, in June 2022, the Food and Drug Administration approved setmelanotide (Imcivree) for weight management in adults and children aged over 6 years with specific genetic markers.
Even as encouraging as setmelanotide is to Ms. Kaisinger and colleagues, these are still early days for translating the current research findings into clinical obesity tests and potential treatment, she said.
The “holy grail,” Dr. Kaplan said, is a future where people get screened for a particular genetic profile and their provider can say something like, “You’re probably most susceptible to this type, so we’ll treat you with this particular drug that’s been developed for people with this phenotype.”
Dr. Kaplan added: “That’s exactly what we are trying to do.”
Moving forward, Ms. Kaisinger and colleagues plan to repeat the study in larger and more diverse populations. They also plan to reverse the usual road map for studies, which typically start in animals and then progress to humans.
“We plan to take the most promising gene candidates forward into mouse models to learn more about their function and how exactly their dysfunction results in obesity,” Ms. Kaisinger said.
Three study coauthors are employees and shareholders of Adrestia Therapeutics. No other conflicts of interest were reported.
A version of this article appeared on WebMD.com.
Identifying specific genes adds to growing evidence that biology, in part, drives obesity. Researchers hope the findings will lead to effective treatments, and in the meantime add to the understanding that there are many types of obesity that come from a mix of genes and environmental factors.
Although the study is not the first to point to specific genes, “we were quite surprised by the proposed function of some of the genes we identified,” Lena R. Kaisinger, lead study investigator and a PhD student in the MRC Epidemiology Unit at the University of Cambridge (England), wrote in an email. For example, the genes also manage cell death and influence how cells respond to DNA damage.
The investigators are not sure why genes involved in body size perform this kind of double duty, which opens avenues for future research.
The gene sequencing study was published online in the journal Cell Genomics.
Differences between women and men
The researchers found five new genes in females and two new genes in males linked to greater body mass index (BMI): DIDO1, KIAA1109, MC4R, PTPRG and SLC12A5 in women and MC4R and SLTM in men. People who recall having obesity as a child were more likely to have rare genetic changes in two other genes, OBSCN and MADD.
“The key thing is that when you see real genes with real gene names, it really makes real the notion that genetics underlie obesity,” said Lee Kaplan, MD, PhD, director of the Obesity and Metabolism Institute in Boston, who was not affiliated with the research.
Ms. Kaisinger and colleagues found these significant genetic differences by studying genomes of about 420,000 people stored in the UK Biobank, a huge biomedical database. The researchers decided to look at genes by sex and age because these are “two areas that we still know very little about,” Ms. Kaisinger said.
“We know that different types of obesity connect to different ages,” said Dr. Kaplan, who is also past president of the Obesity Society. “But what they’ve done now is find genes that are associated with particular subtypes of obesity ... some more common in one sex and some more common in different phases of life, including early onset obesity.”
The future is already here
Treatment for obesity based on a person’s genes already exists. For example, in June 2022, the Food and Drug Administration approved setmelanotide (Imcivree) for weight management in adults and children aged over 6 years with specific genetic markers.
Even as encouraging as setmelanotide is to Ms. Kaisinger and colleagues, these are still early days for translating the current research findings into clinical obesity tests and potential treatment, she said.
The “holy grail,” Dr. Kaplan said, is a future where people get screened for a particular genetic profile and their provider can say something like, “You’re probably most susceptible to this type, so we’ll treat you with this particular drug that’s been developed for people with this phenotype.”
Dr. Kaplan added: “That’s exactly what we are trying to do.”
Moving forward, Ms. Kaisinger and colleagues plan to repeat the study in larger and more diverse populations. They also plan to reverse the usual road map for studies, which typically start in animals and then progress to humans.
“We plan to take the most promising gene candidates forward into mouse models to learn more about their function and how exactly their dysfunction results in obesity,” Ms. Kaisinger said.
Three study coauthors are employees and shareholders of Adrestia Therapeutics. No other conflicts of interest were reported.
A version of this article appeared on WebMD.com.
FROM CELL GENOMICS
New consensus on managing acetaminophen poisoning
TOPLINE:
An expert panel has updated recommendations for emergency department assessment, management, and treatment of acetaminophen poisoning.
METHODOLOGY:
The United States and Canada have no formal guidelines for managing acetaminophen poisoning, which is characterized by hepatocellular damage and potential liver failure, which can be life-threatening.
The past 25 years has seen the introduction of products that contain greater amounts of acetaminophen, extended-release preparations, and new drugs that combine acetaminophen with opioids or other ingredients.
From the medical literature and current poison control guidelines, the panel used a modified Delphi method to create a decision framework and determine appropriate management, including triage and laboratory evaluation, for acetaminophen poisoning, addressing scenarios such as extended-release and high-risk ingestion, co-ingestion of anticholinergics or opioids, pregnancy, weight greater than 100 kg, and criteria for consultation with a toxicologist.
TAKEAWAY:
The panel emphasized the role of the patient’s history; an inaccurate estimate of the time of ingestion, for example, can lead to the erroneous conclusion that acetylcysteine, a medication used to treat overdose, is not needed or can be discontinued prematurely – a potentially fatal mistake.
The initial dose of acetylcysteine should be administered as soon as the need becomes evident, with the panel recommending at least 300 mg/kg orally or intravenously during the first 20 or 24 hours of treatment.
Management of ingestion of extended-release preparations is the same, with the exception of obtaining a second acetaminophen blood concentration in some cases.
When acetaminophen is co-ingested with anticholinergic or opioid agonist medications, management is the same, except if the first acetaminophen concentration measured at 4-24 hours after ingestion is 10 mcg/mL or less, another measurement and acetylcysteine treatment are not needed.
IN PRACTICE:
“A guideline that provides management guidance could optimize patient outcomes, reduce disruption for patients and caregivers, and reduce costs by shortening the length of hospitalization,” write the authors.
SOURCE:
The study was conducted by Richard C. Dart, MD, PhD, Rocky Mountain Poison and Drug Safety, University of Colorado, Denver, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
The work lacked high-quality data that address clinical decisions needed for managing acetaminophen poisoning. There were only a few well-controlled comparative studies, which focused on specific issues and not on patient management.
DISCLOSURES:
The work was supported by a grant from Johnson & Johnson Consumer Inc. Dr. Dart has reported receiving grants from Johnson & Johnson outside the submitted work. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
An expert panel has updated recommendations for emergency department assessment, management, and treatment of acetaminophen poisoning.
METHODOLOGY:
The United States and Canada have no formal guidelines for managing acetaminophen poisoning, which is characterized by hepatocellular damage and potential liver failure, which can be life-threatening.
The past 25 years has seen the introduction of products that contain greater amounts of acetaminophen, extended-release preparations, and new drugs that combine acetaminophen with opioids or other ingredients.
From the medical literature and current poison control guidelines, the panel used a modified Delphi method to create a decision framework and determine appropriate management, including triage and laboratory evaluation, for acetaminophen poisoning, addressing scenarios such as extended-release and high-risk ingestion, co-ingestion of anticholinergics or opioids, pregnancy, weight greater than 100 kg, and criteria for consultation with a toxicologist.
TAKEAWAY:
The panel emphasized the role of the patient’s history; an inaccurate estimate of the time of ingestion, for example, can lead to the erroneous conclusion that acetylcysteine, a medication used to treat overdose, is not needed or can be discontinued prematurely – a potentially fatal mistake.
The initial dose of acetylcysteine should be administered as soon as the need becomes evident, with the panel recommending at least 300 mg/kg orally or intravenously during the first 20 or 24 hours of treatment.
Management of ingestion of extended-release preparations is the same, with the exception of obtaining a second acetaminophen blood concentration in some cases.
When acetaminophen is co-ingested with anticholinergic or opioid agonist medications, management is the same, except if the first acetaminophen concentration measured at 4-24 hours after ingestion is 10 mcg/mL or less, another measurement and acetylcysteine treatment are not needed.
IN PRACTICE:
“A guideline that provides management guidance could optimize patient outcomes, reduce disruption for patients and caregivers, and reduce costs by shortening the length of hospitalization,” write the authors.
SOURCE:
The study was conducted by Richard C. Dart, MD, PhD, Rocky Mountain Poison and Drug Safety, University of Colorado, Denver, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
The work lacked high-quality data that address clinical decisions needed for managing acetaminophen poisoning. There were only a few well-controlled comparative studies, which focused on specific issues and not on patient management.
DISCLOSURES:
The work was supported by a grant from Johnson & Johnson Consumer Inc. Dr. Dart has reported receiving grants from Johnson & Johnson outside the submitted work. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
An expert panel has updated recommendations for emergency department assessment, management, and treatment of acetaminophen poisoning.
METHODOLOGY:
The United States and Canada have no formal guidelines for managing acetaminophen poisoning, which is characterized by hepatocellular damage and potential liver failure, which can be life-threatening.
The past 25 years has seen the introduction of products that contain greater amounts of acetaminophen, extended-release preparations, and new drugs that combine acetaminophen with opioids or other ingredients.
From the medical literature and current poison control guidelines, the panel used a modified Delphi method to create a decision framework and determine appropriate management, including triage and laboratory evaluation, for acetaminophen poisoning, addressing scenarios such as extended-release and high-risk ingestion, co-ingestion of anticholinergics or opioids, pregnancy, weight greater than 100 kg, and criteria for consultation with a toxicologist.
TAKEAWAY:
The panel emphasized the role of the patient’s history; an inaccurate estimate of the time of ingestion, for example, can lead to the erroneous conclusion that acetylcysteine, a medication used to treat overdose, is not needed or can be discontinued prematurely – a potentially fatal mistake.
The initial dose of acetylcysteine should be administered as soon as the need becomes evident, with the panel recommending at least 300 mg/kg orally or intravenously during the first 20 or 24 hours of treatment.
Management of ingestion of extended-release preparations is the same, with the exception of obtaining a second acetaminophen blood concentration in some cases.
When acetaminophen is co-ingested with anticholinergic or opioid agonist medications, management is the same, except if the first acetaminophen concentration measured at 4-24 hours after ingestion is 10 mcg/mL or less, another measurement and acetylcysteine treatment are not needed.
IN PRACTICE:
“A guideline that provides management guidance could optimize patient outcomes, reduce disruption for patients and caregivers, and reduce costs by shortening the length of hospitalization,” write the authors.
SOURCE:
The study was conducted by Richard C. Dart, MD, PhD, Rocky Mountain Poison and Drug Safety, University of Colorado, Denver, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
The work lacked high-quality data that address clinical decisions needed for managing acetaminophen poisoning. There were only a few well-controlled comparative studies, which focused on specific issues and not on patient management.
DISCLOSURES:
The work was supported by a grant from Johnson & Johnson Consumer Inc. Dr. Dart has reported receiving grants from Johnson & Johnson outside the submitted work. See paper for disclosures of other authors.
A version of this article appeared on Medscape.com.
What's the diagnosis?
Given the characteristic clinical presentation, the most likely diagnosis is pilomatrixoma.
Pilomatrixomas are benign adnexal tumors that arise from immature matrix cells of the hair follicles located on dermal or subcutaneous tissue.
The cause of pilomatrixoma remains unclear. Recent studies have suggested that the development of pilomatrixoma are related to mutations in the Wnt signaling pathway, where beta-catenin gene (CTNNB1) mutation is the most frequently reported.1-4
Pilomatrixomas are more common in children and often present before 10 years of age.1,2,5 They commonly appear in head and neck, as well as upper extremities, trunk, and lower extremities.2,6
The clinical manifestations of pilomatrixomas are diverse and according to their appearance five classic clinical types are described: mass, pigmented, mixed, ulcerated, and keloid-like.2,3 The mass type is the predominant form, where it generally presents as a hard and freely mobile nodule covered by skin that may present a firm calcified protruding nodule. Other less common types include: lymphangiectasic, anetodermic, perforating, and bullous.2,6,7

Pilomatrixomas are mostly solitary, whereas multiple forms are reported to be associated with familial inheritance or syndromic conditions, such as myotonic dystrophy, Gardner syndrome, Turner’s syndrome, and Rubinstein-Taybi syndrome.2-4 However, children and adolescents occasionally present with multiple pilomatricomas with no associated syndrome.
On physical exam a helpful features for the diagnosis is the “teeter-totter sign,” which can be illustrated by pressing on one edge of the lesion that will cause the opposite edge to protrude from the skin. Another helpful tool is to use a light to transilluminate and the calcification produces a bluish opaque hue,8 as light cannot transmit through the calcification, often differentiating it from epidermal inclusion cysts or other noncalcified lesions.
What is the differential diagnosis?
Because of the diverse clinical presentations, pilomatrixomas are frequently misdiagnosed. The percentage of correct preoperative diagnosis reported is low, varying from 16% to 43% in different series.1,9-11 They most frequently are misdiagnosed as other types of cysts such as epidermal, dermoid, or sebaceous.2,3,5,12,13 Rapidly growing pilomatrixomas can be also be misdiagnosed as malignant soft-tissue tumors, cutaneous lymphoma, or sarcomas.5,13

When presenting with a classic history and physical features, diagnosis is clinical, and no further studies are recommended.14 To improve diagnostic accuracy when encountering unusual subtypes, imaging is recommended, including ultrasound. Ultrasound adds a high positive predictive value (95.56%).2 Generally, on ultrasound a pilomatrixoma is described as an oval, well-defined, heterogeneous, hyperechoic subcutaneous mass with or without posterior shadowing.2 The definitive diagnosis is, however, made by histopathologic examination.
Pilomatrixomas do not spontaneously regress, therefore complete surgical resection is the standard treatment. During the follow-up period, very low recurrence rates have been reported, varying from 1.5% to 2% which generally occurs because of incomplete resection.2,3

Plexiform neurofibromas are usually congenital tumors of peripheral nerve sheath associated with neurofibromatosis type 1, often with a “bag of worms” feel on palpation. Epidermoid cysts generally present as dermal nodules often with a visible puncture, mobile on soft and mobile on palpation. Dermatofibromas present as firm, usually hyperpigmented papule or nodules that are fixed to subcutaneous tissue, thus often “dimpling” when pitched. Dermatofibrosarcoma protuberans is a rare soft-tissue sarcoma which presents as a firm, slow growing indurated plaques growing over months to years.
Conclusion
Pilomatrixomas are a benign adnexal tumor that sometimes can present as atypical forms such as this case. Diagnosis is usually based on clinical diagnosis, and transillumination can be a bedside clue. When the clinical diagnosis remains obscure an ultrasound can be helpful. The main aim of this case is to improve awareness of the variable presentations of pilomatrixomas and the importance of high level of suspicion supported by careful clinical evaluation.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Al-Nabti is a clinical fellow in the division of pediatric and adolescent dermatology, University of California, San Diego. Dr. Guelfand is a visiting dermatology resident in the division of pediaric and adolescent dermatology, University of Califonia, San Diego.
References
1. Jones CD et al. Am J Dermatopathol. 2018;40:631-41.
2. Hu JL et al. Arch Craniofac Surg. 2020;21(5):288-93.
3. Adhikari G and Jadhav GS. Cureus. 2022;14(2):22228.
4. Cóbar JP et al. J Surg Case Rep. 2023;2023(4):rjad182.
5. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
6. Kose D et al. J Cancer Res Ther. 2014;10(3):549-51.
7. Sabater-Abad J et al. Dermatol Online J. 2020;26(8):13030/qt4h16s45w.
8. Alkatan HM et al. Int J Surg Case Rep. 2021;84:106068.
9. Pant I et al. Indian J Dermatol. 2010;55:390-2.
10. Kaddu S et al. Am J Dermatopathol. 1996;18(4):333-8
11. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
12. Wang YN et al. Chin Med J (Engl). 2021;134(16):2011-2.
13. Yannoutsos A et al. Am J Dermatopathol. 2018;40(9):690-3.
14. Zhao A et al. Ear Nose Throat J. 2021;1455613211044778.
Given the characteristic clinical presentation, the most likely diagnosis is pilomatrixoma.
Pilomatrixomas are benign adnexal tumors that arise from immature matrix cells of the hair follicles located on dermal or subcutaneous tissue.
The cause of pilomatrixoma remains unclear. Recent studies have suggested that the development of pilomatrixoma are related to mutations in the Wnt signaling pathway, where beta-catenin gene (CTNNB1) mutation is the most frequently reported.1-4
Pilomatrixomas are more common in children and often present before 10 years of age.1,2,5 They commonly appear in head and neck, as well as upper extremities, trunk, and lower extremities.2,6
The clinical manifestations of pilomatrixomas are diverse and according to their appearance five classic clinical types are described: mass, pigmented, mixed, ulcerated, and keloid-like.2,3 The mass type is the predominant form, where it generally presents as a hard and freely mobile nodule covered by skin that may present a firm calcified protruding nodule. Other less common types include: lymphangiectasic, anetodermic, perforating, and bullous.2,6,7
Pilomatrixomas are mostly solitary, whereas multiple forms are reported to be associated with familial inheritance or syndromic conditions, such as myotonic dystrophy, Gardner syndrome, Turner’s syndrome, and Rubinstein-Taybi syndrome.2-4 However, children and adolescents occasionally present with multiple pilomatricomas with no associated syndrome.
On physical exam a helpful features for the diagnosis is the “teeter-totter sign,” which can be illustrated by pressing on one edge of the lesion that will cause the opposite edge to protrude from the skin. Another helpful tool is to use a light to transilluminate and the calcification produces a bluish opaque hue,8 as light cannot transmit through the calcification, often differentiating it from epidermal inclusion cysts or other noncalcified lesions.
What is the differential diagnosis?
Because of the diverse clinical presentations, pilomatrixomas are frequently misdiagnosed. The percentage of correct preoperative diagnosis reported is low, varying from 16% to 43% in different series.1,9-11 They most frequently are misdiagnosed as other types of cysts such as epidermal, dermoid, or sebaceous.2,3,5,12,13 Rapidly growing pilomatrixomas can be also be misdiagnosed as malignant soft-tissue tumors, cutaneous lymphoma, or sarcomas.5,13
When presenting with a classic history and physical features, diagnosis is clinical, and no further studies are recommended.14 To improve diagnostic accuracy when encountering unusual subtypes, imaging is recommended, including ultrasound. Ultrasound adds a high positive predictive value (95.56%).2 Generally, on ultrasound a pilomatrixoma is described as an oval, well-defined, heterogeneous, hyperechoic subcutaneous mass with or without posterior shadowing.2 The definitive diagnosis is, however, made by histopathologic examination.
Pilomatrixomas do not spontaneously regress, therefore complete surgical resection is the standard treatment. During the follow-up period, very low recurrence rates have been reported, varying from 1.5% to 2% which generally occurs because of incomplete resection.2,3
Plexiform neurofibromas are usually congenital tumors of peripheral nerve sheath associated with neurofibromatosis type 1, often with a “bag of worms” feel on palpation. Epidermoid cysts generally present as dermal nodules often with a visible puncture, mobile on soft and mobile on palpation. Dermatofibromas present as firm, usually hyperpigmented papule or nodules that are fixed to subcutaneous tissue, thus often “dimpling” when pitched. Dermatofibrosarcoma protuberans is a rare soft-tissue sarcoma which presents as a firm, slow growing indurated plaques growing over months to years.
Conclusion
Pilomatrixomas are a benign adnexal tumor that sometimes can present as atypical forms such as this case. Diagnosis is usually based on clinical diagnosis, and transillumination can be a bedside clue. When the clinical diagnosis remains obscure an ultrasound can be helpful. The main aim of this case is to improve awareness of the variable presentations of pilomatrixomas and the importance of high level of suspicion supported by careful clinical evaluation.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Al-Nabti is a clinical fellow in the division of pediatric and adolescent dermatology, University of California, San Diego. Dr. Guelfand is a visiting dermatology resident in the division of pediaric and adolescent dermatology, University of Califonia, San Diego.
References
1. Jones CD et al. Am J Dermatopathol. 2018;40:631-41.
2. Hu JL et al. Arch Craniofac Surg. 2020;21(5):288-93.
3. Adhikari G and Jadhav GS. Cureus. 2022;14(2):22228.
4. Cóbar JP et al. J Surg Case Rep. 2023;2023(4):rjad182.
5. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
6. Kose D et al. J Cancer Res Ther. 2014;10(3):549-51.
7. Sabater-Abad J et al. Dermatol Online J. 2020;26(8):13030/qt4h16s45w.
8. Alkatan HM et al. Int J Surg Case Rep. 2021;84:106068.
9. Pant I et al. Indian J Dermatol. 2010;55:390-2.
10. Kaddu S et al. Am J Dermatopathol. 1996;18(4):333-8
11. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
12. Wang YN et al. Chin Med J (Engl). 2021;134(16):2011-2.
13. Yannoutsos A et al. Am J Dermatopathol. 2018;40(9):690-3.
14. Zhao A et al. Ear Nose Throat J. 2021;1455613211044778.
Given the characteristic clinical presentation, the most likely diagnosis is pilomatrixoma.
Pilomatrixomas are benign adnexal tumors that arise from immature matrix cells of the hair follicles located on dermal or subcutaneous tissue.
The cause of pilomatrixoma remains unclear. Recent studies have suggested that the development of pilomatrixoma are related to mutations in the Wnt signaling pathway, where beta-catenin gene (CTNNB1) mutation is the most frequently reported.1-4
Pilomatrixomas are more common in children and often present before 10 years of age.1,2,5 They commonly appear in head and neck, as well as upper extremities, trunk, and lower extremities.2,6
The clinical manifestations of pilomatrixomas are diverse and according to their appearance five classic clinical types are described: mass, pigmented, mixed, ulcerated, and keloid-like.2,3 The mass type is the predominant form, where it generally presents as a hard and freely mobile nodule covered by skin that may present a firm calcified protruding nodule. Other less common types include: lymphangiectasic, anetodermic, perforating, and bullous.2,6,7
Pilomatrixomas are mostly solitary, whereas multiple forms are reported to be associated with familial inheritance or syndromic conditions, such as myotonic dystrophy, Gardner syndrome, Turner’s syndrome, and Rubinstein-Taybi syndrome.2-4 However, children and adolescents occasionally present with multiple pilomatricomas with no associated syndrome.
On physical exam a helpful features for the diagnosis is the “teeter-totter sign,” which can be illustrated by pressing on one edge of the lesion that will cause the opposite edge to protrude from the skin. Another helpful tool is to use a light to transilluminate and the calcification produces a bluish opaque hue,8 as light cannot transmit through the calcification, often differentiating it from epidermal inclusion cysts or other noncalcified lesions.
What is the differential diagnosis?
Because of the diverse clinical presentations, pilomatrixomas are frequently misdiagnosed. The percentage of correct preoperative diagnosis reported is low, varying from 16% to 43% in different series.1,9-11 They most frequently are misdiagnosed as other types of cysts such as epidermal, dermoid, or sebaceous.2,3,5,12,13 Rapidly growing pilomatrixomas can be also be misdiagnosed as malignant soft-tissue tumors, cutaneous lymphoma, or sarcomas.5,13
When presenting with a classic history and physical features, diagnosis is clinical, and no further studies are recommended.14 To improve diagnostic accuracy when encountering unusual subtypes, imaging is recommended, including ultrasound. Ultrasound adds a high positive predictive value (95.56%).2 Generally, on ultrasound a pilomatrixoma is described as an oval, well-defined, heterogeneous, hyperechoic subcutaneous mass with or without posterior shadowing.2 The definitive diagnosis is, however, made by histopathologic examination.
Pilomatrixomas do not spontaneously regress, therefore complete surgical resection is the standard treatment. During the follow-up period, very low recurrence rates have been reported, varying from 1.5% to 2% which generally occurs because of incomplete resection.2,3
Plexiform neurofibromas are usually congenital tumors of peripheral nerve sheath associated with neurofibromatosis type 1, often with a “bag of worms” feel on palpation. Epidermoid cysts generally present as dermal nodules often with a visible puncture, mobile on soft and mobile on palpation. Dermatofibromas present as firm, usually hyperpigmented papule or nodules that are fixed to subcutaneous tissue, thus often “dimpling” when pitched. Dermatofibrosarcoma protuberans is a rare soft-tissue sarcoma which presents as a firm, slow growing indurated plaques growing over months to years.
Conclusion
Pilomatrixomas are a benign adnexal tumor that sometimes can present as atypical forms such as this case. Diagnosis is usually based on clinical diagnosis, and transillumination can be a bedside clue. When the clinical diagnosis remains obscure an ultrasound can be helpful. The main aim of this case is to improve awareness of the variable presentations of pilomatrixomas and the importance of high level of suspicion supported by careful clinical evaluation.
Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Dr. Al-Nabti is a clinical fellow in the division of pediatric and adolescent dermatology, University of California, San Diego. Dr. Guelfand is a visiting dermatology resident in the division of pediaric and adolescent dermatology, University of Califonia, San Diego.
References
1. Jones CD et al. Am J Dermatopathol. 2018;40:631-41.
2. Hu JL et al. Arch Craniofac Surg. 2020;21(5):288-93.
3. Adhikari G and Jadhav GS. Cureus. 2022;14(2):22228.
4. Cóbar JP et al. J Surg Case Rep. 2023;2023(4):rjad182.
5. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
6. Kose D et al. J Cancer Res Ther. 2014;10(3):549-51.
7. Sabater-Abad J et al. Dermatol Online J. 2020;26(8):13030/qt4h16s45w.
8. Alkatan HM et al. Int J Surg Case Rep. 2021;84:106068.
9. Pant I et al. Indian J Dermatol. 2010;55:390-2.
10. Kaddu S et al. Am J Dermatopathol. 1996;18(4):333-8
11. Schwarz Y et al. Int J Pediatr Otorhinolaryngol. 2016;85:148-53.
12. Wang YN et al. Chin Med J (Engl). 2021;134(16):2011-2.
13. Yannoutsos A et al. Am J Dermatopathol. 2018;40(9):690-3.
14. Zhao A et al. Ear Nose Throat J. 2021;1455613211044778.

On physical exam there was a well-circumscribed skin-colored nodule measuring 3.1 x 3 cm that was tender on palpation. The nodule was mobile, with a firm, stony feel, and no punctum was visualized. Transillumination revealed a subtle bluish hue within the nodule.
Gout: Suboptimal management a continuing problem
The prevalence of gout is skyrocketing worldwide, and while drugs in the pipeline hold promise for improving the efficacy and safety of treatment, experts warn that “gout remains suboptimally managed.”
“For a really well-understood disease, gout is remarkably undertreated,” said Robert A. Terkeltaub, MD, professor of medicine emeritus at the University of California, San Diego. “This is amazing and depressing because allopurinol has been around for about 60 years or so.”
Randomized, controlled trials show that 80%-90% of patients with gout can be effectively treated to target with existing gout therapies. “Over a year or two, gout flares improve and patients do well,” Dr. Terkeltaub said.
By lowering excessive levels of serum urate, current therapies slow the formation of monosodium urate crystals that precipitate within joints and soft tissues, inducing a highly inflammatory local response with superimposed systemic inflammation. These therapies reduce the frequency of excruciatingly painful gout flares.
“Many patients with gout are not taking urate-lowering therapy at all,” Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, Boston, and head of crystal-induced arthritis diseases at Brigham and Women’s Hospital, also in Boston, said in an interview.
“Unfortunately, a common problem in gout is treatment inertia,” said Tuhina Neogi, MD, PhD, chief of rheumatology at Boston Medical Center.
On a global scale, only one-third of patients with gout are started on urate-lowering therapy, and more than 50% abandon treatment after 1 year. As a result, the effectiveness of urate-lowering therapies in reality is well below 50%, Dr. Terkeltaub said.
“I think gout has been taken less seriously than it should be for quite some time,” he explained in an interview. Gout’s impact on health and well-being is no trivial matter. A recent study showed that a diagnosis of gout was associated with an increased risk of anxiety and depression, and there is new evidence suggesting that gout flares are associated with an increased risk of cardiovascular events, including fatal myocardial infarction and stroke.
“We need drugs that are not just effective but also safe, and we need to incorporate real-world data into our assessment of treatment effectiveness, especially in the presence of comorbidities,” Dr. Terkeltaub said.
The prevalence of what used to be thought of as the “disease of kings” has increased 100% over the last 30 years, outstripping world population growth and life expectancy. In the United States, an estimated 5% of adults, or 12 million, have gout. Globally, the number affected exceeds 50 million.
The patient demographics associated with gout have also expanded. Once seen primarily in fleshy, middle-aged men of privilege, gout affects more women, more adults at either end of the age spectrum, and more people in Third World countries than ever before.
Management
In the United States, the optimal management of gout remains the subject of debate, with differences in expert opinion reflected in evidence-based clinical guidelines. “We know that the perception of gout is different between primary care physicians, patients, and rheumatologists,” Dr. Terkeltaub said.
The 2017 American College of Physicians guidelines for the management of gout recommend a treat-to-symptom approach to urate-lowering therapy. However, the 2020 American College of Rheumatology guidelines reinforce a standard treat-to-target strategy to a serum urate target of < 6.0 mg/dL.
In their report, the ACR guidelines’ authors stated that the use of urate-lowering therapy for gout has not increased in the last decade. Research shows that adherence to treatment for gout continues to be the lowest among seven common chronic medical conditions, including hypertension and seizure disorders, they said.
Some physicians don’t recommend urate-lowering medication to their patients with gout, and others don’t up-titrate it sufficiently to meet the recommended serum urate target, said Dr. Tedeschi. The latter “can require increasing the dose of allopurinol well beyond the 300 mg that often seems the landing point for many patients with gout,” she pointed out.
In fact, it can take up to 800 mg a day of allopurinol – less in patients with moderate to severe kidney disease – to reduce the symptom burden in gout. And it can take a year or longer of drug testing and titration to reach the optimal serum urate target. Paradoxically, gout flares usually get worse during this time.
“We need to reduce the time it takes to get the patient to the serum urate target, and simplify regimens with once-a-day dosing,” Dr. Terkeltaub said. “We also need greater precision so that we can get a home run, hitting the serum urate target the first or second visit, with minimal dose titration.”
Clinician education is important, but education alone is not enough, Dr. Neogi emphasized. “Just as clinicians treat-to-target in other conditions such as hypertension and diabetes, or titrate warfarin to maintain a certain level of anticoagulation, gout must be monitored and treatments adjusted accordingly,” she said.
Practice changes, such as partnering with nursing or pharmacy, may help facilitate in-clinic dose titration, “much like a warfarin clinic,” Dr. Neogi suggested.
That’s exactly what Dr. Terkeltaub has done. Overwhelmed by the number of gout consults, Dr. Terkeltaub and his team set up a pharmacist-managed, rheumatology-supervised clinic to care for gout patients remotely. The model has been very successful, he said. Nurses and clinical pharmacists educate the patients and manage their lab testing and prescriptions, all according to ACR guidelines.
The treatment of gout has become more complex, with a greater risk of drug complications and interactions, particularly in older patients with comorbid diabetes, chronic kidney disease, and heart disease. Many of the patients he sees are already on “10, 15, or 20 other medications,” Dr. Terkeltaub noted.
The steps involved in the titration of urate-lowering therapy also complicate the treatment of gout, making it impractical for many patients and impossible for others whose access to primary care is limited to one or two visits a year. The process of drug titration, with steadily increasing doses, can make patients anxious about the possibility of being overmedicated. Taking a drug every day, even when joints feel “normal,” can also increase the risk of nonadherence.
“In our conversations with patients with gout, it’s extremely important that we counsel them about the need to take urate-lowering therapy on an ongoing basis to reduce the risk of a gout flare,” said Dr. Tedeschi. “Patients need to have prescription refills available and know to contact the doctor before they run out, so that the chances of having a gout flare are reduced.”
Current drugs
Although urate-lowering drugs form the cornerstone of gout therapy, there are only three oral medications available in the United States currently, and all have significant limitations. “We need more drugs, basically,” Dr. Terkeltaub said.
- Allopurinol (Zyloprim, Aloprim), an inexpensive xanthine oxidase inhibitor (XOI), is still considered a first-line treatment, but is associated with allopurinol hypersensitivity syndrome. In select patients of Asian, African, and Arab descent, this adverse drug reaction can be life-threatening, and is associated with a mortality rate of 20%-25%.
- Febuxostat (Uloric), another XOI, is considered a second-line drug in the treatment of gout, but has carried a boxed warning from the Food and Drug Administration since 2019. It is associated with a significantly increased risk of cardiovascular death.
- Probenecid (Probalan), a uricosuric agent that increases renal uric acid excretion, is associated with an increased risk of drug interactions and kidney stones, and is rarely used.
Drugs in the pipeline
New drugs in the pipeline offer treatment options that are not only effective but also safe. “This will be important in clinical practice, especially for patients in whom existing medications are contraindicated or there is an increased risk of side effects,” Dr. Neogi said.
Most of these investigational drugs are uricosuric agents that increase the renal excretion of uric acid, reducing serum levels. “The pipeline of new drugs is rich,” Dr. Terkeltaub said. “These drugs are very selective and really work well and they appear to be safe.”
AR882, an inhibitor of selective uric acid transporter 1 (URAT1), is shaping up to be one of them. In July, results from a phase 2b study of AR882 were presented at the annual European Congress of Rheumatology in Milan. They showed that in the intent-to-treat population, 73% of patients had serum uric acid levels < 5 mg/dL and 55% had < 4 mg/dL by week 12 of therapy. In the per-protocol analysis, 82% had serum uric acid levels < 5 mg/dL and 63% < 4 mg/dL.
“These efficacy results are not typically what you see with a once-daily oral medication, so it is really exciting,” said Robert Keenan, MD, chief medical officer of Arthrosi Therapeutics, San Diego, who presented the results.
“More efficacious URAT1 inhibitors that are safe and have a reduced pill burden will be useful additions to current urate lowering options,” Dr. Neogi said.
The recent phase 3 DISSOLVE I and II trials of the investigational uricase-based infusion therapy SEL-212 in refractory gout have also demonstrated encouraging results, particularly in older patients. In DISSOLVE I, a response rate of 65% was observed in patients 50 years of age and older at least 80% of the time during month 6 of treatment. In DISSOLVE II, a response rate of 47% was reported in older patients.
SEL-212, which is made up of PEGylated uricase (pegadricase) coadministered with sirolimus (Rapamycin), will be submitted for U.S. regulatory approval in the first half of 2024.
In the management of gout flares, interleukin (IL)-1beta and inflammasome inhibitors, both of which target specific inflammatory pathways, could also provide attractive additions to urate-lowering therapies. Other agents commonly used in the treatment of flares, such as NSAIDs, steroids, and colchicine (Colcrys), are not as specific, and have side effects that often limit their usability, Dr. Neogi said.
In the meantime, new research indicates that an inflammasome inhibitor that has already been approved for use in diabetes may provide distinct benefits for the management of gout. An analysis of data from 15,067 adults with both gout and type 2 diabetes showed that when a sodium-glucose cotransporter 2 (SGLT-2) inhibitor was added to urate-lowering therapy, the symptoms of gout, including flares, were significantly reduced, resulting in fewer emergency department visits and hospitalizations.
“SGLT-2 inhibitors have anti-inflammatory activity that limits the progression of kidney failure, heart failure, and will also lower the serum uric acid,” said Dr. Terkeltaub. “That’s a major development.”
Dr. Neogi disclosed relationships with Novartis, Pfizer/Lilly, and Regeneron, Dr. Terkeltaub reported relationships with Dyve, Fortress, and Atom, and Dr. Tedeschi reported a relationship with Novartis.
This story was updated on August 14, 2023.
The prevalence of gout is skyrocketing worldwide, and while drugs in the pipeline hold promise for improving the efficacy and safety of treatment, experts warn that “gout remains suboptimally managed.”
“For a really well-understood disease, gout is remarkably undertreated,” said Robert A. Terkeltaub, MD, professor of medicine emeritus at the University of California, San Diego. “This is amazing and depressing because allopurinol has been around for about 60 years or so.”
Randomized, controlled trials show that 80%-90% of patients with gout can be effectively treated to target with existing gout therapies. “Over a year or two, gout flares improve and patients do well,” Dr. Terkeltaub said.
By lowering excessive levels of serum urate, current therapies slow the formation of monosodium urate crystals that precipitate within joints and soft tissues, inducing a highly inflammatory local response with superimposed systemic inflammation. These therapies reduce the frequency of excruciatingly painful gout flares.
“Many patients with gout are not taking urate-lowering therapy at all,” Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, Boston, and head of crystal-induced arthritis diseases at Brigham and Women’s Hospital, also in Boston, said in an interview.
“Unfortunately, a common problem in gout is treatment inertia,” said Tuhina Neogi, MD, PhD, chief of rheumatology at Boston Medical Center.
On a global scale, only one-third of patients with gout are started on urate-lowering therapy, and more than 50% abandon treatment after 1 year. As a result, the effectiveness of urate-lowering therapies in reality is well below 50%, Dr. Terkeltaub said.
“I think gout has been taken less seriously than it should be for quite some time,” he explained in an interview. Gout’s impact on health and well-being is no trivial matter. A recent study showed that a diagnosis of gout was associated with an increased risk of anxiety and depression, and there is new evidence suggesting that gout flares are associated with an increased risk of cardiovascular events, including fatal myocardial infarction and stroke.
“We need drugs that are not just effective but also safe, and we need to incorporate real-world data into our assessment of treatment effectiveness, especially in the presence of comorbidities,” Dr. Terkeltaub said.
The prevalence of what used to be thought of as the “disease of kings” has increased 100% over the last 30 years, outstripping world population growth and life expectancy. In the United States, an estimated 5% of adults, or 12 million, have gout. Globally, the number affected exceeds 50 million.
The patient demographics associated with gout have also expanded. Once seen primarily in fleshy, middle-aged men of privilege, gout affects more women, more adults at either end of the age spectrum, and more people in Third World countries than ever before.
Management
In the United States, the optimal management of gout remains the subject of debate, with differences in expert opinion reflected in evidence-based clinical guidelines. “We know that the perception of gout is different between primary care physicians, patients, and rheumatologists,” Dr. Terkeltaub said.
The 2017 American College of Physicians guidelines for the management of gout recommend a treat-to-symptom approach to urate-lowering therapy. However, the 2020 American College of Rheumatology guidelines reinforce a standard treat-to-target strategy to a serum urate target of < 6.0 mg/dL.
In their report, the ACR guidelines’ authors stated that the use of urate-lowering therapy for gout has not increased in the last decade. Research shows that adherence to treatment for gout continues to be the lowest among seven common chronic medical conditions, including hypertension and seizure disorders, they said.
Some physicians don’t recommend urate-lowering medication to their patients with gout, and others don’t up-titrate it sufficiently to meet the recommended serum urate target, said Dr. Tedeschi. The latter “can require increasing the dose of allopurinol well beyond the 300 mg that often seems the landing point for many patients with gout,” she pointed out.
In fact, it can take up to 800 mg a day of allopurinol – less in patients with moderate to severe kidney disease – to reduce the symptom burden in gout. And it can take a year or longer of drug testing and titration to reach the optimal serum urate target. Paradoxically, gout flares usually get worse during this time.
“We need to reduce the time it takes to get the patient to the serum urate target, and simplify regimens with once-a-day dosing,” Dr. Terkeltaub said. “We also need greater precision so that we can get a home run, hitting the serum urate target the first or second visit, with minimal dose titration.”
Clinician education is important, but education alone is not enough, Dr. Neogi emphasized. “Just as clinicians treat-to-target in other conditions such as hypertension and diabetes, or titrate warfarin to maintain a certain level of anticoagulation, gout must be monitored and treatments adjusted accordingly,” she said.
Practice changes, such as partnering with nursing or pharmacy, may help facilitate in-clinic dose titration, “much like a warfarin clinic,” Dr. Neogi suggested.
That’s exactly what Dr. Terkeltaub has done. Overwhelmed by the number of gout consults, Dr. Terkeltaub and his team set up a pharmacist-managed, rheumatology-supervised clinic to care for gout patients remotely. The model has been very successful, he said. Nurses and clinical pharmacists educate the patients and manage their lab testing and prescriptions, all according to ACR guidelines.
The treatment of gout has become more complex, with a greater risk of drug complications and interactions, particularly in older patients with comorbid diabetes, chronic kidney disease, and heart disease. Many of the patients he sees are already on “10, 15, or 20 other medications,” Dr. Terkeltaub noted.
The steps involved in the titration of urate-lowering therapy also complicate the treatment of gout, making it impractical for many patients and impossible for others whose access to primary care is limited to one or two visits a year. The process of drug titration, with steadily increasing doses, can make patients anxious about the possibility of being overmedicated. Taking a drug every day, even when joints feel “normal,” can also increase the risk of nonadherence.
“In our conversations with patients with gout, it’s extremely important that we counsel them about the need to take urate-lowering therapy on an ongoing basis to reduce the risk of a gout flare,” said Dr. Tedeschi. “Patients need to have prescription refills available and know to contact the doctor before they run out, so that the chances of having a gout flare are reduced.”
Current drugs
Although urate-lowering drugs form the cornerstone of gout therapy, there are only three oral medications available in the United States currently, and all have significant limitations. “We need more drugs, basically,” Dr. Terkeltaub said.
- Allopurinol (Zyloprim, Aloprim), an inexpensive xanthine oxidase inhibitor (XOI), is still considered a first-line treatment, but is associated with allopurinol hypersensitivity syndrome. In select patients of Asian, African, and Arab descent, this adverse drug reaction can be life-threatening, and is associated with a mortality rate of 20%-25%.
- Febuxostat (Uloric), another XOI, is considered a second-line drug in the treatment of gout, but has carried a boxed warning from the Food and Drug Administration since 2019. It is associated with a significantly increased risk of cardiovascular death.
- Probenecid (Probalan), a uricosuric agent that increases renal uric acid excretion, is associated with an increased risk of drug interactions and kidney stones, and is rarely used.
Drugs in the pipeline
New drugs in the pipeline offer treatment options that are not only effective but also safe. “This will be important in clinical practice, especially for patients in whom existing medications are contraindicated or there is an increased risk of side effects,” Dr. Neogi said.
Most of these investigational drugs are uricosuric agents that increase the renal excretion of uric acid, reducing serum levels. “The pipeline of new drugs is rich,” Dr. Terkeltaub said. “These drugs are very selective and really work well and they appear to be safe.”
AR882, an inhibitor of selective uric acid transporter 1 (URAT1), is shaping up to be one of them. In July, results from a phase 2b study of AR882 were presented at the annual European Congress of Rheumatology in Milan. They showed that in the intent-to-treat population, 73% of patients had serum uric acid levels < 5 mg/dL and 55% had < 4 mg/dL by week 12 of therapy. In the per-protocol analysis, 82% had serum uric acid levels < 5 mg/dL and 63% < 4 mg/dL.
“These efficacy results are not typically what you see with a once-daily oral medication, so it is really exciting,” said Robert Keenan, MD, chief medical officer of Arthrosi Therapeutics, San Diego, who presented the results.
“More efficacious URAT1 inhibitors that are safe and have a reduced pill burden will be useful additions to current urate lowering options,” Dr. Neogi said.
The recent phase 3 DISSOLVE I and II trials of the investigational uricase-based infusion therapy SEL-212 in refractory gout have also demonstrated encouraging results, particularly in older patients. In DISSOLVE I, a response rate of 65% was observed in patients 50 years of age and older at least 80% of the time during month 6 of treatment. In DISSOLVE II, a response rate of 47% was reported in older patients.
SEL-212, which is made up of PEGylated uricase (pegadricase) coadministered with sirolimus (Rapamycin), will be submitted for U.S. regulatory approval in the first half of 2024.
In the management of gout flares, interleukin (IL)-1beta and inflammasome inhibitors, both of which target specific inflammatory pathways, could also provide attractive additions to urate-lowering therapies. Other agents commonly used in the treatment of flares, such as NSAIDs, steroids, and colchicine (Colcrys), are not as specific, and have side effects that often limit their usability, Dr. Neogi said.
In the meantime, new research indicates that an inflammasome inhibitor that has already been approved for use in diabetes may provide distinct benefits for the management of gout. An analysis of data from 15,067 adults with both gout and type 2 diabetes showed that when a sodium-glucose cotransporter 2 (SGLT-2) inhibitor was added to urate-lowering therapy, the symptoms of gout, including flares, were significantly reduced, resulting in fewer emergency department visits and hospitalizations.
“SGLT-2 inhibitors have anti-inflammatory activity that limits the progression of kidney failure, heart failure, and will also lower the serum uric acid,” said Dr. Terkeltaub. “That’s a major development.”
Dr. Neogi disclosed relationships with Novartis, Pfizer/Lilly, and Regeneron, Dr. Terkeltaub reported relationships with Dyve, Fortress, and Atom, and Dr. Tedeschi reported a relationship with Novartis.
This story was updated on August 14, 2023.
The prevalence of gout is skyrocketing worldwide, and while drugs in the pipeline hold promise for improving the efficacy and safety of treatment, experts warn that “gout remains suboptimally managed.”
“For a really well-understood disease, gout is remarkably undertreated,” said Robert A. Terkeltaub, MD, professor of medicine emeritus at the University of California, San Diego. “This is amazing and depressing because allopurinol has been around for about 60 years or so.”
Randomized, controlled trials show that 80%-90% of patients with gout can be effectively treated to target with existing gout therapies. “Over a year or two, gout flares improve and patients do well,” Dr. Terkeltaub said.
By lowering excessive levels of serum urate, current therapies slow the formation of monosodium urate crystals that precipitate within joints and soft tissues, inducing a highly inflammatory local response with superimposed systemic inflammation. These therapies reduce the frequency of excruciatingly painful gout flares.
“Many patients with gout are not taking urate-lowering therapy at all,” Sara K. Tedeschi, MD, MPH, assistant professor of medicine at Harvard Medical School, Boston, and head of crystal-induced arthritis diseases at Brigham and Women’s Hospital, also in Boston, said in an interview.
“Unfortunately, a common problem in gout is treatment inertia,” said Tuhina Neogi, MD, PhD, chief of rheumatology at Boston Medical Center.
On a global scale, only one-third of patients with gout are started on urate-lowering therapy, and more than 50% abandon treatment after 1 year. As a result, the effectiveness of urate-lowering therapies in reality is well below 50%, Dr. Terkeltaub said.
“I think gout has been taken less seriously than it should be for quite some time,” he explained in an interview. Gout’s impact on health and well-being is no trivial matter. A recent study showed that a diagnosis of gout was associated with an increased risk of anxiety and depression, and there is new evidence suggesting that gout flares are associated with an increased risk of cardiovascular events, including fatal myocardial infarction and stroke.
“We need drugs that are not just effective but also safe, and we need to incorporate real-world data into our assessment of treatment effectiveness, especially in the presence of comorbidities,” Dr. Terkeltaub said.
The prevalence of what used to be thought of as the “disease of kings” has increased 100% over the last 30 years, outstripping world population growth and life expectancy. In the United States, an estimated 5% of adults, or 12 million, have gout. Globally, the number affected exceeds 50 million.
The patient demographics associated with gout have also expanded. Once seen primarily in fleshy, middle-aged men of privilege, gout affects more women, more adults at either end of the age spectrum, and more people in Third World countries than ever before.
Management
In the United States, the optimal management of gout remains the subject of debate, with differences in expert opinion reflected in evidence-based clinical guidelines. “We know that the perception of gout is different between primary care physicians, patients, and rheumatologists,” Dr. Terkeltaub said.
The 2017 American College of Physicians guidelines for the management of gout recommend a treat-to-symptom approach to urate-lowering therapy. However, the 2020 American College of Rheumatology guidelines reinforce a standard treat-to-target strategy to a serum urate target of < 6.0 mg/dL.
In their report, the ACR guidelines’ authors stated that the use of urate-lowering therapy for gout has not increased in the last decade. Research shows that adherence to treatment for gout continues to be the lowest among seven common chronic medical conditions, including hypertension and seizure disorders, they said.
Some physicians don’t recommend urate-lowering medication to their patients with gout, and others don’t up-titrate it sufficiently to meet the recommended serum urate target, said Dr. Tedeschi. The latter “can require increasing the dose of allopurinol well beyond the 300 mg that often seems the landing point for many patients with gout,” she pointed out.
In fact, it can take up to 800 mg a day of allopurinol – less in patients with moderate to severe kidney disease – to reduce the symptom burden in gout. And it can take a year or longer of drug testing and titration to reach the optimal serum urate target. Paradoxically, gout flares usually get worse during this time.
“We need to reduce the time it takes to get the patient to the serum urate target, and simplify regimens with once-a-day dosing,” Dr. Terkeltaub said. “We also need greater precision so that we can get a home run, hitting the serum urate target the first or second visit, with minimal dose titration.”
Clinician education is important, but education alone is not enough, Dr. Neogi emphasized. “Just as clinicians treat-to-target in other conditions such as hypertension and diabetes, or titrate warfarin to maintain a certain level of anticoagulation, gout must be monitored and treatments adjusted accordingly,” she said.
Practice changes, such as partnering with nursing or pharmacy, may help facilitate in-clinic dose titration, “much like a warfarin clinic,” Dr. Neogi suggested.
That’s exactly what Dr. Terkeltaub has done. Overwhelmed by the number of gout consults, Dr. Terkeltaub and his team set up a pharmacist-managed, rheumatology-supervised clinic to care for gout patients remotely. The model has been very successful, he said. Nurses and clinical pharmacists educate the patients and manage their lab testing and prescriptions, all according to ACR guidelines.
The treatment of gout has become more complex, with a greater risk of drug complications and interactions, particularly in older patients with comorbid diabetes, chronic kidney disease, and heart disease. Many of the patients he sees are already on “10, 15, or 20 other medications,” Dr. Terkeltaub noted.
The steps involved in the titration of urate-lowering therapy also complicate the treatment of gout, making it impractical for many patients and impossible for others whose access to primary care is limited to one or two visits a year. The process of drug titration, with steadily increasing doses, can make patients anxious about the possibility of being overmedicated. Taking a drug every day, even when joints feel “normal,” can also increase the risk of nonadherence.
“In our conversations with patients with gout, it’s extremely important that we counsel them about the need to take urate-lowering therapy on an ongoing basis to reduce the risk of a gout flare,” said Dr. Tedeschi. “Patients need to have prescription refills available and know to contact the doctor before they run out, so that the chances of having a gout flare are reduced.”
Current drugs
Although urate-lowering drugs form the cornerstone of gout therapy, there are only three oral medications available in the United States currently, and all have significant limitations. “We need more drugs, basically,” Dr. Terkeltaub said.
- Allopurinol (Zyloprim, Aloprim), an inexpensive xanthine oxidase inhibitor (XOI), is still considered a first-line treatment, but is associated with allopurinol hypersensitivity syndrome. In select patients of Asian, African, and Arab descent, this adverse drug reaction can be life-threatening, and is associated with a mortality rate of 20%-25%.
- Febuxostat (Uloric), another XOI, is considered a second-line drug in the treatment of gout, but has carried a boxed warning from the Food and Drug Administration since 2019. It is associated with a significantly increased risk of cardiovascular death.
- Probenecid (Probalan), a uricosuric agent that increases renal uric acid excretion, is associated with an increased risk of drug interactions and kidney stones, and is rarely used.
Drugs in the pipeline
New drugs in the pipeline offer treatment options that are not only effective but also safe. “This will be important in clinical practice, especially for patients in whom existing medications are contraindicated or there is an increased risk of side effects,” Dr. Neogi said.
Most of these investigational drugs are uricosuric agents that increase the renal excretion of uric acid, reducing serum levels. “The pipeline of new drugs is rich,” Dr. Terkeltaub said. “These drugs are very selective and really work well and they appear to be safe.”
AR882, an inhibitor of selective uric acid transporter 1 (URAT1), is shaping up to be one of them. In July, results from a phase 2b study of AR882 were presented at the annual European Congress of Rheumatology in Milan. They showed that in the intent-to-treat population, 73% of patients had serum uric acid levels < 5 mg/dL and 55% had < 4 mg/dL by week 12 of therapy. In the per-protocol analysis, 82% had serum uric acid levels < 5 mg/dL and 63% < 4 mg/dL.
“These efficacy results are not typically what you see with a once-daily oral medication, so it is really exciting,” said Robert Keenan, MD, chief medical officer of Arthrosi Therapeutics, San Diego, who presented the results.
“More efficacious URAT1 inhibitors that are safe and have a reduced pill burden will be useful additions to current urate lowering options,” Dr. Neogi said.
The recent phase 3 DISSOLVE I and II trials of the investigational uricase-based infusion therapy SEL-212 in refractory gout have also demonstrated encouraging results, particularly in older patients. In DISSOLVE I, a response rate of 65% was observed in patients 50 years of age and older at least 80% of the time during month 6 of treatment. In DISSOLVE II, a response rate of 47% was reported in older patients.
SEL-212, which is made up of PEGylated uricase (pegadricase) coadministered with sirolimus (Rapamycin), will be submitted for U.S. regulatory approval in the first half of 2024.
In the management of gout flares, interleukin (IL)-1beta and inflammasome inhibitors, both of which target specific inflammatory pathways, could also provide attractive additions to urate-lowering therapies. Other agents commonly used in the treatment of flares, such as NSAIDs, steroids, and colchicine (Colcrys), are not as specific, and have side effects that often limit their usability, Dr. Neogi said.
In the meantime, new research indicates that an inflammasome inhibitor that has already been approved for use in diabetes may provide distinct benefits for the management of gout. An analysis of data from 15,067 adults with both gout and type 2 diabetes showed that when a sodium-glucose cotransporter 2 (SGLT-2) inhibitor was added to urate-lowering therapy, the symptoms of gout, including flares, were significantly reduced, resulting in fewer emergency department visits and hospitalizations.
“SGLT-2 inhibitors have anti-inflammatory activity that limits the progression of kidney failure, heart failure, and will also lower the serum uric acid,” said Dr. Terkeltaub. “That’s a major development.”
Dr. Neogi disclosed relationships with Novartis, Pfizer/Lilly, and Regeneron, Dr. Terkeltaub reported relationships with Dyve, Fortress, and Atom, and Dr. Tedeschi reported a relationship with Novartis.
This story was updated on August 14, 2023.
We asked doctors using AI scribes: Just how good are they?
Andrea Partida, DO, an obstetrician and gynecologist in Enid, Okla., loves her new assistant.
The 15 or 20 minutes she used to spend on documentation for each patient visit is now 3. The 2-3 hours she’d spend charting outside clinic hours is maybe 1.
All that time saved allows her to see two to five more patients a day, provide better care to each patient, and get more involved in hospital leadership at Integris Health, where she works.
“I have a better work-life balance with my family,” Dr. Partida said. “I leave work at work and get home earlier.”
You’ve probably figured out the plot twist: Dr. Partida’s assistant is not a person – it’s artificial intelligence (AI).
Dr. Partida uses IRIS, a tool from OnPoint Healthcare Partners, part of a fast-growing niche of AI medical scribes designed to automate onerous data entry. The evolution of generative AI – specifically, large language models, such as ChatGPT – has led to a rapid explosion of these tools. Other companies in the space include Abridge, Ambience Healthcare, Augmedix, DeepScribe, Nuance (part of Microsoft), and Suki. The newest kid on the block, Amazon Web Services, announced the launch of HealthScribe in July.
These tools – some of which are already on the market, with more on the way – record patient visits and generate notes for treatment and billing. Earlier iterations combine AI with offsite human scribes who provide quality control. But more and more are fully automated, no human required. Some also offer video recording and foreign language translation.
The promise is alluring: Ease your workload and reclaim hours in your day so you can spend more time with patients or try that “work-life balance” thing you’ve heard so much about.
But do these tools fulfill that promise?
According to Dr. Partida and other doctors who spoke with this news organization, the answer is a resounding yes.
A tech solution for a tech problem
“I believe a lot of doctors see patients for free. They get paid to do paperwork,” said Anthony J. Mazzarelli, MD, JD, MBE, co-president and CEO of Cooper University Health Care, in Camden, N.J.
Indeed, for every hour U.S. clinicians spend with their patients, they may spend 2 more hours documenting in electronic health records (EHRs), estimates show. About half of doctors, especially those in primary care, report feeling burned out, and some 42% say they want to quit clinical practice.
Enter AI scribes.
“The holy grail in medicine right now is improving burnout while also maintaining or improving productivity and quality,” said Patricia Garcia, MD, associate clinical information officer for ambulatory care at Stanford (Calif.) Health Care. “These ambient digital scribes have the potential to do just that.”
While anyone can buy these products, their use has been mostly limited to pilot programs and early adopters so far, said Dr. Garcia, who has been helping to pilot Nuance’s digital scribe, DAX, at Stanford.
But that’s expected to change quickly. “I don’t think the time horizon is a decade,” Dr. Garcia said. “I think within a matter of 2 or 3 years, these tools will be pervasive throughout health care.”
Since introducing these tools at Cooper, “our doctors’ paperwork burden is significantly lighter,” said Dr. Mazzarelli, who decides which technologies Cooper should invest in and who monitors their results. In Cooper studies, physicians who used DAX more than half the time spent 43% less time working on notes.
“They spend more time connecting with their patients, talking with them, and looking them in the eye,” Dr. Mazzarelli said. That, in turn, seems to improve patient outcomes, reduce doctor burnout and turnover, and lower costs.
The AI scribes, by virtue of eliminating the distraction of note taking, also allow doctors to give their full attention to the patient. “The patient relationship is the most important aspect of medicine,” said Raul Ayala, MD, MHCM, a family medicine physician at Adventist Health, in Hanford, Calif., who uses Augmedix. The digital scribe “helps us strengthen that relationship.”
What’s it like to use an AI medical scribe?
The scribes feature hardware (typically a smartphone or tablet) and software built on automatic speech recognition, natural language processing, and machine learning. Download an app to your device, and you’re ready to go. Use it to record in-person or telehealth visits.
In the first week, a company may help train you to use the hardware and software. You’ll likely start by using it for a few patient visits per day, ramping up gradually. Dr. Partida said she was comfortable using the system for all her patients in 6 weeks.
Each day, Dr. Partida logs in to a dedicated smartphone or tablet, opens the app, and reviews her schedule, including details she needs to prepare for each patient.
At the start of each patient visit, Dr. Partida taps the app icon to begin recording and lays the device nearby. She can pause as needed. At the end of the visit, she taps the icon again to stop recording.
The AI listens, creates the note, and updates relevant data in the EHR. The note includes patient problems, assessment, treatment plan, patient history, orders, and tasks for staff, along with medications, referrals, and preauthorizations. A human scribe, who is also a physician, reviews the information for accuracy and edits it as needed. By the next morning, the data are ready for Dr. Partida to review.
Fully automated versions can generate notes much faster. Jack Shilling, MD, MBA, an orthopedic surgeon at Cooper University Health Care, in Voorhees, N.J., uses DAX. A new feature called DAX Express – which uses OpenAI’s GPT-4 but no humans – provides him with a draft of his clinical notes in just seconds.
How accurate are AI notes?
The accuracy of those notes remains an open question, Dr. Garcia said – mostly because accuracy can be hard to define.
“If you asked five docs to write a note based on the same patient encounter, you’d get five different notes,” Dr. Garcia said. “That makes it hard to assess these technologies in a scientifically rigorous way.”
Still, the onus is on the physician to review the notes and edit them as needed, Dr. Garcia said. How light or heavy those edits are can depend on your unique preferences.
Dr. Shilling said he may need to lightly edit transcripts of his conversations with patients. “When someone tells me how long their knee hurts, slight variability in their transcribed words is tolerable,” he said. But for some things – such as physical exam notes and x-ray readings – he dictates directly into the device, speaking at a closer range and being less conversational, more exact in his speech.
Should you let patients know they’re being recorded?
The federal Health Insurance Portability and Accountability Act (HIPAA) does not require providers to inform patients that their face-to-face conversations are being recorded, said Daniel Lebovic, JD, corporate legal counsel at Compliancy Group, in Greenlawn, N.Y., a company that helps providers adhere to HIPAA rules.
But make sure you know the laws in your state and the policies at your health care practice. State laws may require providers to inform patients and to get patients’ consent in advance of being recorded.
All the doctors who spoke to this news organization said their patients are informed that they’ll be recorded and that they can opt out if they wish.
How much do AI scribes cost?
As the marketplace for these tools expands, companies are offering more products and services at different price points that target a range of organizations, from large health care systems to small private practices.
Price models vary, said Dr. Garcia. Some are based on the number of users, others on the number of notes, and still others on minutes.
Amazon’s HealthScribe is priced at 10 cents per minute. For 1,000 consultation transcripts per month, with each call averaging 15 minutes, it would take 15,000 minutes at a total cost of $1,500 for the month.
In general, the rapidly growing competition in this space could mean prices become more affordable, Dr. Garcia said. “It’s good that so many are getting into this game, because that means the price will come down and it will be a lot more accessible to everybody.”
A version of this article appeared on Medscape.com.
Andrea Partida, DO, an obstetrician and gynecologist in Enid, Okla., loves her new assistant.
The 15 or 20 minutes she used to spend on documentation for each patient visit is now 3. The 2-3 hours she’d spend charting outside clinic hours is maybe 1.
All that time saved allows her to see two to five more patients a day, provide better care to each patient, and get more involved in hospital leadership at Integris Health, where she works.
“I have a better work-life balance with my family,” Dr. Partida said. “I leave work at work and get home earlier.”
You’ve probably figured out the plot twist: Dr. Partida’s assistant is not a person – it’s artificial intelligence (AI).
Dr. Partida uses IRIS, a tool from OnPoint Healthcare Partners, part of a fast-growing niche of AI medical scribes designed to automate onerous data entry. The evolution of generative AI – specifically, large language models, such as ChatGPT – has led to a rapid explosion of these tools. Other companies in the space include Abridge, Ambience Healthcare, Augmedix, DeepScribe, Nuance (part of Microsoft), and Suki. The newest kid on the block, Amazon Web Services, announced the launch of HealthScribe in July.
These tools – some of which are already on the market, with more on the way – record patient visits and generate notes for treatment and billing. Earlier iterations combine AI with offsite human scribes who provide quality control. But more and more are fully automated, no human required. Some also offer video recording and foreign language translation.
The promise is alluring: Ease your workload and reclaim hours in your day so you can spend more time with patients or try that “work-life balance” thing you’ve heard so much about.
But do these tools fulfill that promise?
According to Dr. Partida and other doctors who spoke with this news organization, the answer is a resounding yes.
A tech solution for a tech problem
“I believe a lot of doctors see patients for free. They get paid to do paperwork,” said Anthony J. Mazzarelli, MD, JD, MBE, co-president and CEO of Cooper University Health Care, in Camden, N.J.
Indeed, for every hour U.S. clinicians spend with their patients, they may spend 2 more hours documenting in electronic health records (EHRs), estimates show. About half of doctors, especially those in primary care, report feeling burned out, and some 42% say they want to quit clinical practice.
Enter AI scribes.
“The holy grail in medicine right now is improving burnout while also maintaining or improving productivity and quality,” said Patricia Garcia, MD, associate clinical information officer for ambulatory care at Stanford (Calif.) Health Care. “These ambient digital scribes have the potential to do just that.”
While anyone can buy these products, their use has been mostly limited to pilot programs and early adopters so far, said Dr. Garcia, who has been helping to pilot Nuance’s digital scribe, DAX, at Stanford.
But that’s expected to change quickly. “I don’t think the time horizon is a decade,” Dr. Garcia said. “I think within a matter of 2 or 3 years, these tools will be pervasive throughout health care.”
Since introducing these tools at Cooper, “our doctors’ paperwork burden is significantly lighter,” said Dr. Mazzarelli, who decides which technologies Cooper should invest in and who monitors their results. In Cooper studies, physicians who used DAX more than half the time spent 43% less time working on notes.
“They spend more time connecting with their patients, talking with them, and looking them in the eye,” Dr. Mazzarelli said. That, in turn, seems to improve patient outcomes, reduce doctor burnout and turnover, and lower costs.
The AI scribes, by virtue of eliminating the distraction of note taking, also allow doctors to give their full attention to the patient. “The patient relationship is the most important aspect of medicine,” said Raul Ayala, MD, MHCM, a family medicine physician at Adventist Health, in Hanford, Calif., who uses Augmedix. The digital scribe “helps us strengthen that relationship.”
What’s it like to use an AI medical scribe?
The scribes feature hardware (typically a smartphone or tablet) and software built on automatic speech recognition, natural language processing, and machine learning. Download an app to your device, and you’re ready to go. Use it to record in-person or telehealth visits.
In the first week, a company may help train you to use the hardware and software. You’ll likely start by using it for a few patient visits per day, ramping up gradually. Dr. Partida said she was comfortable using the system for all her patients in 6 weeks.
Each day, Dr. Partida logs in to a dedicated smartphone or tablet, opens the app, and reviews her schedule, including details she needs to prepare for each patient.
At the start of each patient visit, Dr. Partida taps the app icon to begin recording and lays the device nearby. She can pause as needed. At the end of the visit, she taps the icon again to stop recording.
The AI listens, creates the note, and updates relevant data in the EHR. The note includes patient problems, assessment, treatment plan, patient history, orders, and tasks for staff, along with medications, referrals, and preauthorizations. A human scribe, who is also a physician, reviews the information for accuracy and edits it as needed. By the next morning, the data are ready for Dr. Partida to review.
Fully automated versions can generate notes much faster. Jack Shilling, MD, MBA, an orthopedic surgeon at Cooper University Health Care, in Voorhees, N.J., uses DAX. A new feature called DAX Express – which uses OpenAI’s GPT-4 but no humans – provides him with a draft of his clinical notes in just seconds.
How accurate are AI notes?
The accuracy of those notes remains an open question, Dr. Garcia said – mostly because accuracy can be hard to define.
“If you asked five docs to write a note based on the same patient encounter, you’d get five different notes,” Dr. Garcia said. “That makes it hard to assess these technologies in a scientifically rigorous way.”
Still, the onus is on the physician to review the notes and edit them as needed, Dr. Garcia said. How light or heavy those edits are can depend on your unique preferences.
Dr. Shilling said he may need to lightly edit transcripts of his conversations with patients. “When someone tells me how long their knee hurts, slight variability in their transcribed words is tolerable,” he said. But for some things – such as physical exam notes and x-ray readings – he dictates directly into the device, speaking at a closer range and being less conversational, more exact in his speech.
Should you let patients know they’re being recorded?
The federal Health Insurance Portability and Accountability Act (HIPAA) does not require providers to inform patients that their face-to-face conversations are being recorded, said Daniel Lebovic, JD, corporate legal counsel at Compliancy Group, in Greenlawn, N.Y., a company that helps providers adhere to HIPAA rules.
But make sure you know the laws in your state and the policies at your health care practice. State laws may require providers to inform patients and to get patients’ consent in advance of being recorded.
All the doctors who spoke to this news organization said their patients are informed that they’ll be recorded and that they can opt out if they wish.
How much do AI scribes cost?
As the marketplace for these tools expands, companies are offering more products and services at different price points that target a range of organizations, from large health care systems to small private practices.
Price models vary, said Dr. Garcia. Some are based on the number of users, others on the number of notes, and still others on minutes.
Amazon’s HealthScribe is priced at 10 cents per minute. For 1,000 consultation transcripts per month, with each call averaging 15 minutes, it would take 15,000 minutes at a total cost of $1,500 for the month.
In general, the rapidly growing competition in this space could mean prices become more affordable, Dr. Garcia said. “It’s good that so many are getting into this game, because that means the price will come down and it will be a lot more accessible to everybody.”
A version of this article appeared on Medscape.com.
Andrea Partida, DO, an obstetrician and gynecologist in Enid, Okla., loves her new assistant.
The 15 or 20 minutes she used to spend on documentation for each patient visit is now 3. The 2-3 hours she’d spend charting outside clinic hours is maybe 1.
All that time saved allows her to see two to five more patients a day, provide better care to each patient, and get more involved in hospital leadership at Integris Health, where she works.
“I have a better work-life balance with my family,” Dr. Partida said. “I leave work at work and get home earlier.”
You’ve probably figured out the plot twist: Dr. Partida’s assistant is not a person – it’s artificial intelligence (AI).
Dr. Partida uses IRIS, a tool from OnPoint Healthcare Partners, part of a fast-growing niche of AI medical scribes designed to automate onerous data entry. The evolution of generative AI – specifically, large language models, such as ChatGPT – has led to a rapid explosion of these tools. Other companies in the space include Abridge, Ambience Healthcare, Augmedix, DeepScribe, Nuance (part of Microsoft), and Suki. The newest kid on the block, Amazon Web Services, announced the launch of HealthScribe in July.
These tools – some of which are already on the market, with more on the way – record patient visits and generate notes for treatment and billing. Earlier iterations combine AI with offsite human scribes who provide quality control. But more and more are fully automated, no human required. Some also offer video recording and foreign language translation.
The promise is alluring: Ease your workload and reclaim hours in your day so you can spend more time with patients or try that “work-life balance” thing you’ve heard so much about.
But do these tools fulfill that promise?
According to Dr. Partida and other doctors who spoke with this news organization, the answer is a resounding yes.
A tech solution for a tech problem
“I believe a lot of doctors see patients for free. They get paid to do paperwork,” said Anthony J. Mazzarelli, MD, JD, MBE, co-president and CEO of Cooper University Health Care, in Camden, N.J.
Indeed, for every hour U.S. clinicians spend with their patients, they may spend 2 more hours documenting in electronic health records (EHRs), estimates show. About half of doctors, especially those in primary care, report feeling burned out, and some 42% say they want to quit clinical practice.
Enter AI scribes.
“The holy grail in medicine right now is improving burnout while also maintaining or improving productivity and quality,” said Patricia Garcia, MD, associate clinical information officer for ambulatory care at Stanford (Calif.) Health Care. “These ambient digital scribes have the potential to do just that.”
While anyone can buy these products, their use has been mostly limited to pilot programs and early adopters so far, said Dr. Garcia, who has been helping to pilot Nuance’s digital scribe, DAX, at Stanford.
But that’s expected to change quickly. “I don’t think the time horizon is a decade,” Dr. Garcia said. “I think within a matter of 2 or 3 years, these tools will be pervasive throughout health care.”
Since introducing these tools at Cooper, “our doctors’ paperwork burden is significantly lighter,” said Dr. Mazzarelli, who decides which technologies Cooper should invest in and who monitors their results. In Cooper studies, physicians who used DAX more than half the time spent 43% less time working on notes.
“They spend more time connecting with their patients, talking with them, and looking them in the eye,” Dr. Mazzarelli said. That, in turn, seems to improve patient outcomes, reduce doctor burnout and turnover, and lower costs.
The AI scribes, by virtue of eliminating the distraction of note taking, also allow doctors to give their full attention to the patient. “The patient relationship is the most important aspect of medicine,” said Raul Ayala, MD, MHCM, a family medicine physician at Adventist Health, in Hanford, Calif., who uses Augmedix. The digital scribe “helps us strengthen that relationship.”
What’s it like to use an AI medical scribe?
The scribes feature hardware (typically a smartphone or tablet) and software built on automatic speech recognition, natural language processing, and machine learning. Download an app to your device, and you’re ready to go. Use it to record in-person or telehealth visits.
In the first week, a company may help train you to use the hardware and software. You’ll likely start by using it for a few patient visits per day, ramping up gradually. Dr. Partida said she was comfortable using the system for all her patients in 6 weeks.
Each day, Dr. Partida logs in to a dedicated smartphone or tablet, opens the app, and reviews her schedule, including details she needs to prepare for each patient.
At the start of each patient visit, Dr. Partida taps the app icon to begin recording and lays the device nearby. She can pause as needed. At the end of the visit, she taps the icon again to stop recording.
The AI listens, creates the note, and updates relevant data in the EHR. The note includes patient problems, assessment, treatment plan, patient history, orders, and tasks for staff, along with medications, referrals, and preauthorizations. A human scribe, who is also a physician, reviews the information for accuracy and edits it as needed. By the next morning, the data are ready for Dr. Partida to review.
Fully automated versions can generate notes much faster. Jack Shilling, MD, MBA, an orthopedic surgeon at Cooper University Health Care, in Voorhees, N.J., uses DAX. A new feature called DAX Express – which uses OpenAI’s GPT-4 but no humans – provides him with a draft of his clinical notes in just seconds.
How accurate are AI notes?
The accuracy of those notes remains an open question, Dr. Garcia said – mostly because accuracy can be hard to define.
“If you asked five docs to write a note based on the same patient encounter, you’d get five different notes,” Dr. Garcia said. “That makes it hard to assess these technologies in a scientifically rigorous way.”
Still, the onus is on the physician to review the notes and edit them as needed, Dr. Garcia said. How light or heavy those edits are can depend on your unique preferences.
Dr. Shilling said he may need to lightly edit transcripts of his conversations with patients. “When someone tells me how long their knee hurts, slight variability in their transcribed words is tolerable,” he said. But for some things – such as physical exam notes and x-ray readings – he dictates directly into the device, speaking at a closer range and being less conversational, more exact in his speech.
Should you let patients know they’re being recorded?
The federal Health Insurance Portability and Accountability Act (HIPAA) does not require providers to inform patients that their face-to-face conversations are being recorded, said Daniel Lebovic, JD, corporate legal counsel at Compliancy Group, in Greenlawn, N.Y., a company that helps providers adhere to HIPAA rules.
But make sure you know the laws in your state and the policies at your health care practice. State laws may require providers to inform patients and to get patients’ consent in advance of being recorded.
All the doctors who spoke to this news organization said their patients are informed that they’ll be recorded and that they can opt out if they wish.
How much do AI scribes cost?
As the marketplace for these tools expands, companies are offering more products and services at different price points that target a range of organizations, from large health care systems to small private practices.
Price models vary, said Dr. Garcia. Some are based on the number of users, others on the number of notes, and still others on minutes.
Amazon’s HealthScribe is priced at 10 cents per minute. For 1,000 consultation transcripts per month, with each call averaging 15 minutes, it would take 15,000 minutes at a total cost of $1,500 for the month.
In general, the rapidly growing competition in this space could mean prices become more affordable, Dr. Garcia said. “It’s good that so many are getting into this game, because that means the price will come down and it will be a lot more accessible to everybody.”
A version of this article appeared on Medscape.com.
Generic inhalers for COPD support hold their own
Sometimes we get what we pay for. Other times we pay too much.
That’s the message of a study published in Annals of Internal Medicine, which finds that a generic maintenance inhaler is as effective at managing symptoms of chronic obstructive pulmonary disorder (COPD) as a pricier branded alternative.
In 2019, the Food and Drug Administration approved Wixela Inhub (the combination corticosteroid/long-acting beta2 adrenergic agonist fluticasone-salmeterol; Viatris) as a generic dry powder inhaler for managing symptoms of COPD. This approval was based on evidence of the generic’s effectiveness against asthma, although COPD also was on the product label. The study authors compared Wixela’s effectiveness in controlling symptoms of COPD with that of the brand name inhaler Advair Diskus (fluticasone-salmeterol; GlaxoSmithKline), which uses the same active ingredients.
The result: “The generic looks to be as safe and effective as the brand name. I don’t see a clinical reason why one would ever need to get the brand name over the generic version,” said study author William Feldman, MD, DPhil, MPH, a health services researcher and pulmonologist at Harvard Medical School and Brigham and Women’s Hospital, both in Boston.
Same types of patients, different inhalers, same outcomes
Dr. Feldman and colleagues compared the medical records of 10,000 patients with COPD who began using the branded inhaler to the records of another 10,000 patients with COPD who opted for the generic alternative. Participants in the two groups were evenly matched by age, sex, race, and ethnicity, region, severity of COPD, and presence of other comorbidities, according to the researchers. Participants were all older than age 40, and the average age in both groups was 72 years.
The researchers looked for a difference in a first episode of a moderate exacerbation of COPD, defined as requiring a course of prednisone for 5-14 days. They also looked for cases of severe COPD exacerbation requiring hospitalization in the year after people began using either the generic or brand name inhaler. And they looked for differences across 1 year in rates of hospitalization for pneumonia.
For none of those outcomes, however, did the type of inhaler appear to matter. Compared with the brand-name drug, using the generic was associated with nearly identical rates of moderate or severe COPD exacerbation (hazard ratio, 0.97; 95% confidence interval, 0.90-1.04. The same was true for the proportion of people who went to the hospital for pneumonia at least once (HR, 0.99; 95% CI, 0.86-1.15).
“To get through the FDA as an interchangeable generic, the generic firms have to show that their product can be used in just the same way as the brand-name version,” Dr. Feldman said, which may explain why the generic and brand-name versions of the inhaler performed so similarly.
Dr. Feldman cautioned that the price savings for patients who opt for the generic over the branded product are hard to determine, given the vagaries of different insurance plans and potential rebates when using the branded project. As a general matter, having a single generic competitor will not lower costs much, Dr. Feldman noted, pointing to 2017 research from Harvard that found a profusion of generic competitors is needed to significantly lower health care costs.
“I don’t want to in any way underestimate the importance of getting that first generic onto the market, because it sets the stage for future generics,” Dr. Feldman said.
“There are very few generic options for patients with COPD,” said Surya Bhatt, MD, director of the Pulmonary Function and Exercise Physiology Lab at the University of Alabama at Birmingham. Even the rescue inhalers that people with COPD use to manage acute episodes of the condition are usually branded at this time, Dr. Bhatt noted, with few generic options.*
“The results are quite compelling,” said Dr. Bhatt, who was not involved in the research. Although the trial was not randomized, he commended the researchers for stratifying participants in the two groups to be as comparable as possible.
Dr. Bhatt noted that the FDA’s 2019 approval – given that the agency requires bioequivalence studies between branded and generic products – was enough to cause him to begin prescribing the generic inhaler. The fact that this approval was based on asthma but not also COPD is not a concern.
“There are so many similarities between asthma, COPD, and some obstructive lung diseases,” Dr. Bhatt noted.
In his experience, the only time someone with COPD continues using the branded inhaler – now that a potentially cheaper generic is available – is when their insurance plan makes their out-of-pocket cost minimal. Otherwise, brand loyalty does not exist.
“Patients are generally okay with being on a generic for inhalers, just because of the high cost,” Dr. Bhatt said.
The study was primarily supported by the National Heart, Lung, and Blood Institute. Dr. Feldman reported funding from Arnold Ventures, the Commonwealth Fund, and the FDA, and consulting relationships with Alosa Health and Aetion. Dr. Bhatt reported no relevant financial relationships.
*Correction, 8/16/23: An earlier version of this article mischaracterized Dr. Bhatt's comments on the availability of generic options.
A version of this article first appeared on Medscape.com.
Sometimes we get what we pay for. Other times we pay too much.
That’s the message of a study published in Annals of Internal Medicine, which finds that a generic maintenance inhaler is as effective at managing symptoms of chronic obstructive pulmonary disorder (COPD) as a pricier branded alternative.
In 2019, the Food and Drug Administration approved Wixela Inhub (the combination corticosteroid/long-acting beta2 adrenergic agonist fluticasone-salmeterol; Viatris) as a generic dry powder inhaler for managing symptoms of COPD. This approval was based on evidence of the generic’s effectiveness against asthma, although COPD also was on the product label. The study authors compared Wixela’s effectiveness in controlling symptoms of COPD with that of the brand name inhaler Advair Diskus (fluticasone-salmeterol; GlaxoSmithKline), which uses the same active ingredients.
The result: “The generic looks to be as safe and effective as the brand name. I don’t see a clinical reason why one would ever need to get the brand name over the generic version,” said study author William Feldman, MD, DPhil, MPH, a health services researcher and pulmonologist at Harvard Medical School and Brigham and Women’s Hospital, both in Boston.
Same types of patients, different inhalers, same outcomes
Dr. Feldman and colleagues compared the medical records of 10,000 patients with COPD who began using the branded inhaler to the records of another 10,000 patients with COPD who opted for the generic alternative. Participants in the two groups were evenly matched by age, sex, race, and ethnicity, region, severity of COPD, and presence of other comorbidities, according to the researchers. Participants were all older than age 40, and the average age in both groups was 72 years.
The researchers looked for a difference in a first episode of a moderate exacerbation of COPD, defined as requiring a course of prednisone for 5-14 days. They also looked for cases of severe COPD exacerbation requiring hospitalization in the year after people began using either the generic or brand name inhaler. And they looked for differences across 1 year in rates of hospitalization for pneumonia.
For none of those outcomes, however, did the type of inhaler appear to matter. Compared with the brand-name drug, using the generic was associated with nearly identical rates of moderate or severe COPD exacerbation (hazard ratio, 0.97; 95% confidence interval, 0.90-1.04. The same was true for the proportion of people who went to the hospital for pneumonia at least once (HR, 0.99; 95% CI, 0.86-1.15).
“To get through the FDA as an interchangeable generic, the generic firms have to show that their product can be used in just the same way as the brand-name version,” Dr. Feldman said, which may explain why the generic and brand-name versions of the inhaler performed so similarly.
Dr. Feldman cautioned that the price savings for patients who opt for the generic over the branded product are hard to determine, given the vagaries of different insurance plans and potential rebates when using the branded project. As a general matter, having a single generic competitor will not lower costs much, Dr. Feldman noted, pointing to 2017 research from Harvard that found a profusion of generic competitors is needed to significantly lower health care costs.
“I don’t want to in any way underestimate the importance of getting that first generic onto the market, because it sets the stage for future generics,” Dr. Feldman said.
“There are very few generic options for patients with COPD,” said Surya Bhatt, MD, director of the Pulmonary Function and Exercise Physiology Lab at the University of Alabama at Birmingham. Even the rescue inhalers that people with COPD use to manage acute episodes of the condition are usually branded at this time, Dr. Bhatt noted, with few generic options.*
“The results are quite compelling,” said Dr. Bhatt, who was not involved in the research. Although the trial was not randomized, he commended the researchers for stratifying participants in the two groups to be as comparable as possible.
Dr. Bhatt noted that the FDA’s 2019 approval – given that the agency requires bioequivalence studies between branded and generic products – was enough to cause him to begin prescribing the generic inhaler. The fact that this approval was based on asthma but not also COPD is not a concern.
“There are so many similarities between asthma, COPD, and some obstructive lung diseases,” Dr. Bhatt noted.
In his experience, the only time someone with COPD continues using the branded inhaler – now that a potentially cheaper generic is available – is when their insurance plan makes their out-of-pocket cost minimal. Otherwise, brand loyalty does not exist.
“Patients are generally okay with being on a generic for inhalers, just because of the high cost,” Dr. Bhatt said.
The study was primarily supported by the National Heart, Lung, and Blood Institute. Dr. Feldman reported funding from Arnold Ventures, the Commonwealth Fund, and the FDA, and consulting relationships with Alosa Health and Aetion. Dr. Bhatt reported no relevant financial relationships.
*Correction, 8/16/23: An earlier version of this article mischaracterized Dr. Bhatt's comments on the availability of generic options.
A version of this article first appeared on Medscape.com.
Sometimes we get what we pay for. Other times we pay too much.
That’s the message of a study published in Annals of Internal Medicine, which finds that a generic maintenance inhaler is as effective at managing symptoms of chronic obstructive pulmonary disorder (COPD) as a pricier branded alternative.
In 2019, the Food and Drug Administration approved Wixela Inhub (the combination corticosteroid/long-acting beta2 adrenergic agonist fluticasone-salmeterol; Viatris) as a generic dry powder inhaler for managing symptoms of COPD. This approval was based on evidence of the generic’s effectiveness against asthma, although COPD also was on the product label. The study authors compared Wixela’s effectiveness in controlling symptoms of COPD with that of the brand name inhaler Advair Diskus (fluticasone-salmeterol; GlaxoSmithKline), which uses the same active ingredients.
The result: “The generic looks to be as safe and effective as the brand name. I don’t see a clinical reason why one would ever need to get the brand name over the generic version,” said study author William Feldman, MD, DPhil, MPH, a health services researcher and pulmonologist at Harvard Medical School and Brigham and Women’s Hospital, both in Boston.
Same types of patients, different inhalers, same outcomes
Dr. Feldman and colleagues compared the medical records of 10,000 patients with COPD who began using the branded inhaler to the records of another 10,000 patients with COPD who opted for the generic alternative. Participants in the two groups were evenly matched by age, sex, race, and ethnicity, region, severity of COPD, and presence of other comorbidities, according to the researchers. Participants were all older than age 40, and the average age in both groups was 72 years.
The researchers looked for a difference in a first episode of a moderate exacerbation of COPD, defined as requiring a course of prednisone for 5-14 days. They also looked for cases of severe COPD exacerbation requiring hospitalization in the year after people began using either the generic or brand name inhaler. And they looked for differences across 1 year in rates of hospitalization for pneumonia.
For none of those outcomes, however, did the type of inhaler appear to matter. Compared with the brand-name drug, using the generic was associated with nearly identical rates of moderate or severe COPD exacerbation (hazard ratio, 0.97; 95% confidence interval, 0.90-1.04. The same was true for the proportion of people who went to the hospital for pneumonia at least once (HR, 0.99; 95% CI, 0.86-1.15).
“To get through the FDA as an interchangeable generic, the generic firms have to show that their product can be used in just the same way as the brand-name version,” Dr. Feldman said, which may explain why the generic and brand-name versions of the inhaler performed so similarly.
Dr. Feldman cautioned that the price savings for patients who opt for the generic over the branded product are hard to determine, given the vagaries of different insurance plans and potential rebates when using the branded project. As a general matter, having a single generic competitor will not lower costs much, Dr. Feldman noted, pointing to 2017 research from Harvard that found a profusion of generic competitors is needed to significantly lower health care costs.
“I don’t want to in any way underestimate the importance of getting that first generic onto the market, because it sets the stage for future generics,” Dr. Feldman said.
“There are very few generic options for patients with COPD,” said Surya Bhatt, MD, director of the Pulmonary Function and Exercise Physiology Lab at the University of Alabama at Birmingham. Even the rescue inhalers that people with COPD use to manage acute episodes of the condition are usually branded at this time, Dr. Bhatt noted, with few generic options.*
“The results are quite compelling,” said Dr. Bhatt, who was not involved in the research. Although the trial was not randomized, he commended the researchers for stratifying participants in the two groups to be as comparable as possible.
Dr. Bhatt noted that the FDA’s 2019 approval – given that the agency requires bioequivalence studies between branded and generic products – was enough to cause him to begin prescribing the generic inhaler. The fact that this approval was based on asthma but not also COPD is not a concern.
“There are so many similarities between asthma, COPD, and some obstructive lung diseases,” Dr. Bhatt noted.
In his experience, the only time someone with COPD continues using the branded inhaler – now that a potentially cheaper generic is available – is when their insurance plan makes their out-of-pocket cost minimal. Otherwise, brand loyalty does not exist.
“Patients are generally okay with being on a generic for inhalers, just because of the high cost,” Dr. Bhatt said.
The study was primarily supported by the National Heart, Lung, and Blood Institute. Dr. Feldman reported funding from Arnold Ventures, the Commonwealth Fund, and the FDA, and consulting relationships with Alosa Health and Aetion. Dr. Bhatt reported no relevant financial relationships.
*Correction, 8/16/23: An earlier version of this article mischaracterized Dr. Bhatt's comments on the availability of generic options.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
COPD plus PRISm may promote frailty progression
Chronic obstructive pulmonary disease and a new phenotype of lung function impairment predicted progression of frailty in older adults, based on data from more than 5,000 individuals.
COPD has been associated with frailty, but longitudinal data on the association of COPD with progression of frailty are limited, as are data on the potential association of preserved ratio impaired spirometry (PRISm) with frailty progression, wrote Di He, BS, of Zhejiang University, China, and colleagues.
PRISm has been defined in recent studies as “proportional impairments in FEV1 and FVC, resulting in the normal ratio of FEV1 and FVC.” Individuals with PRISm may transition to normal spirometry or COPD over time, the researchers wrote.
In a study published in the journal Chest, the researchers reviewed data from 5,901 adults aged 50 years and older who were participating on the English Longitudinal Study of Ageing (ELSA), a prospective cohort study. Of these, 3,765 were included in an additional analysis of the association between transitions from normal spirometry to PRISm and the progression of frailty. The mean age of the participants was 65.5 years; 54.9% were women.
The median follow-up period for analysis with frailty progression was 9.5 years for PRISm and COPD and 5.8 years for PRISm transitions. Lung function data were collected at baseline. Based on spirometry data, participants were divided into three lung function groups – normal spirometry, PRISm, and COPD – and each of these was classified based on severity. Frailty was assessed using the frailty index (FI) during the follow-up period.
with additional annual increases of 0.301 and 0.172, respectively (P < .001 for both).
When stratified by severity, individuals with more severe PRISm and with more COPD had higher baseline FI and faster FI progression, compared with those with mild PRISm and COPD.
PRISm transitions were assessed over a 4-year interval at the start of the ELSA. Individuals with normal spirometry who transitioned to PRISm during the study had accelerated progression of frailty, as did those with COPD who transitioned to PRISm. However, no significant frailty progression occurred in those who changed from PRISm to normal spirometry.
The mechanisms behind the associations of PRISm and COPD with frailty remain unclear, but the results were consistent after controlling for multiple confounders, “suggesting PRISm and COPD had independent pathophysiological mechanisms for frailty,” the researchers write in their discussion. Other recent studies have identified sarcopenia as a complication for individuals with lung function impairment, they noted. “Therefore, another plausible explanation could be that PRISm and COPD caused sarcopenia, which accelerated frailty progression,” they say.
The findings were limited by several factors, including the observational design and the potential underestimation of lung function in participants with reversible airflow obstruction because of the use of prebronchodilator spirometry in the cohort study, the researchers noted.
However, the results were strengthened by the large sample size and high-quality data from the ELSA, as well as by the repeat measures of FI and lung function. The results were consistent after controlling for multiple confounders, and support the need for more research to explore the causality behind the association of PRISm and COPD with frailty, the researchers concluded.
The study was supported by the Zhejiang Provincial Basic Public Welfare Research Project, the Zhoushan Science and Technology Project, and the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province. The researchers report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Chronic obstructive pulmonary disease and a new phenotype of lung function impairment predicted progression of frailty in older adults, based on data from more than 5,000 individuals.
COPD has been associated with frailty, but longitudinal data on the association of COPD with progression of frailty are limited, as are data on the potential association of preserved ratio impaired spirometry (PRISm) with frailty progression, wrote Di He, BS, of Zhejiang University, China, and colleagues.
PRISm has been defined in recent studies as “proportional impairments in FEV1 and FVC, resulting in the normal ratio of FEV1 and FVC.” Individuals with PRISm may transition to normal spirometry or COPD over time, the researchers wrote.
In a study published in the journal Chest, the researchers reviewed data from 5,901 adults aged 50 years and older who were participating on the English Longitudinal Study of Ageing (ELSA), a prospective cohort study. Of these, 3,765 were included in an additional analysis of the association between transitions from normal spirometry to PRISm and the progression of frailty. The mean age of the participants was 65.5 years; 54.9% were women.
The median follow-up period for analysis with frailty progression was 9.5 years for PRISm and COPD and 5.8 years for PRISm transitions. Lung function data were collected at baseline. Based on spirometry data, participants were divided into three lung function groups – normal spirometry, PRISm, and COPD – and each of these was classified based on severity. Frailty was assessed using the frailty index (FI) during the follow-up period.
with additional annual increases of 0.301 and 0.172, respectively (P < .001 for both).
When stratified by severity, individuals with more severe PRISm and with more COPD had higher baseline FI and faster FI progression, compared with those with mild PRISm and COPD.
PRISm transitions were assessed over a 4-year interval at the start of the ELSA. Individuals with normal spirometry who transitioned to PRISm during the study had accelerated progression of frailty, as did those with COPD who transitioned to PRISm. However, no significant frailty progression occurred in those who changed from PRISm to normal spirometry.
The mechanisms behind the associations of PRISm and COPD with frailty remain unclear, but the results were consistent after controlling for multiple confounders, “suggesting PRISm and COPD had independent pathophysiological mechanisms for frailty,” the researchers write in their discussion. Other recent studies have identified sarcopenia as a complication for individuals with lung function impairment, they noted. “Therefore, another plausible explanation could be that PRISm and COPD caused sarcopenia, which accelerated frailty progression,” they say.
The findings were limited by several factors, including the observational design and the potential underestimation of lung function in participants with reversible airflow obstruction because of the use of prebronchodilator spirometry in the cohort study, the researchers noted.
However, the results were strengthened by the large sample size and high-quality data from the ELSA, as well as by the repeat measures of FI and lung function. The results were consistent after controlling for multiple confounders, and support the need for more research to explore the causality behind the association of PRISm and COPD with frailty, the researchers concluded.
The study was supported by the Zhejiang Provincial Basic Public Welfare Research Project, the Zhoushan Science and Technology Project, and the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province. The researchers report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Chronic obstructive pulmonary disease and a new phenotype of lung function impairment predicted progression of frailty in older adults, based on data from more than 5,000 individuals.
COPD has been associated with frailty, but longitudinal data on the association of COPD with progression of frailty are limited, as are data on the potential association of preserved ratio impaired spirometry (PRISm) with frailty progression, wrote Di He, BS, of Zhejiang University, China, and colleagues.
PRISm has been defined in recent studies as “proportional impairments in FEV1 and FVC, resulting in the normal ratio of FEV1 and FVC.” Individuals with PRISm may transition to normal spirometry or COPD over time, the researchers wrote.
In a study published in the journal Chest, the researchers reviewed data from 5,901 adults aged 50 years and older who were participating on the English Longitudinal Study of Ageing (ELSA), a prospective cohort study. Of these, 3,765 were included in an additional analysis of the association between transitions from normal spirometry to PRISm and the progression of frailty. The mean age of the participants was 65.5 years; 54.9% were women.
The median follow-up period for analysis with frailty progression was 9.5 years for PRISm and COPD and 5.8 years for PRISm transitions. Lung function data were collected at baseline. Based on spirometry data, participants were divided into three lung function groups – normal spirometry, PRISm, and COPD – and each of these was classified based on severity. Frailty was assessed using the frailty index (FI) during the follow-up period.
with additional annual increases of 0.301 and 0.172, respectively (P < .001 for both).
When stratified by severity, individuals with more severe PRISm and with more COPD had higher baseline FI and faster FI progression, compared with those with mild PRISm and COPD.
PRISm transitions were assessed over a 4-year interval at the start of the ELSA. Individuals with normal spirometry who transitioned to PRISm during the study had accelerated progression of frailty, as did those with COPD who transitioned to PRISm. However, no significant frailty progression occurred in those who changed from PRISm to normal spirometry.
The mechanisms behind the associations of PRISm and COPD with frailty remain unclear, but the results were consistent after controlling for multiple confounders, “suggesting PRISm and COPD had independent pathophysiological mechanisms for frailty,” the researchers write in their discussion. Other recent studies have identified sarcopenia as a complication for individuals with lung function impairment, they noted. “Therefore, another plausible explanation could be that PRISm and COPD caused sarcopenia, which accelerated frailty progression,” they say.
The findings were limited by several factors, including the observational design and the potential underestimation of lung function in participants with reversible airflow obstruction because of the use of prebronchodilator spirometry in the cohort study, the researchers noted.
However, the results were strengthened by the large sample size and high-quality data from the ELSA, as well as by the repeat measures of FI and lung function. The results were consistent after controlling for multiple confounders, and support the need for more research to explore the causality behind the association of PRISm and COPD with frailty, the researchers concluded.
The study was supported by the Zhejiang Provincial Basic Public Welfare Research Project, the Zhoushan Science and Technology Project, and the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province. The researchers report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL CHEST