User login
Give serious thought before starting antipsychotics in elders
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
The page filled me with dread: “Your elderly patient is confused, getting out of bed, and threw her entire dinner tray at a nurse just now.” Because this morning my patient was polite and appropriate, the now-angry, dinner-splattered nurse means only one thing: delirium.
Delirium is one of the most difficult problems for hospitalists to manage, in part because our management of delirium is often learned on the fly during residency and early years of practice. This post-hoc approach toward delirium misses the most important aspect of treatment: Prevention.
Interventions like early mobilization, environmental interventions, careful oversight of drugs, hydration protocols, and reinforcing the day/night cycle are crucial. Unfortunately, few hospitals can provide these resources or the trained multidisciplinary team with geriatrics expertise to administer them. The result is that delirium occurs more frequently than it should, and hospitalists often face a patient who is a risk to themselves or others.
In this situation, antipsychotics (APs) are often prescribed. However, long term use of APs by elders is highly discouraged by many organizations, including the Society of Hospital Medicine, because of risks like cardiac events (e.g., QT prolongation), stroke, extrapyramidal symptoms, falls, somnolence, and increased mortality in older patients with dementia.
One unanswered question regarding the use of APs is whether starting the medications in the hospital results in long-term use. To answer this, we performed a retrospective study of 300 elderly hospitalized patients who were treated for the first time with APs during their hospitalization. Of these 300 patients, 10% died during that first hospitalization, and almost half (48%) remained on APs at discharge. We found that most of the prescriptions were to treat delirium (J Hosp Med. 2014 Dec;9[12]:802-4. doi:10.1002/jhm.2277).
In a more recent study, we looked at outcomes for patients discharged from Baystate Medical Center (Springfield, Mass.) on APs. Within a year of discharge, 40% of these patients were readmitted at least once and approximately two-thirds were still taking the same APs on which they had been discharged (J Hosp Med. 2016 Apr 6. doi: 10.1002/jhm.2585). Thus, if I start my patient described above (who threw the dinner tray) on an AP today, she is very likely to be readmitted the next year still taking that same medication. Starting an AP in the short term can lead to the very thing we have been warned against: long-term use of an AP in an elderly person.
Even more striking than the continuation rate was the incredibly high 1-year mortality rate. Of the 260 patients discharged from the original admission on an AP, one-third had died at the 1-year mark. This group of patients had a wide range of diagnoses, but nearly as many died as if they all had stage IV heart failure. Because most had an agitated delirium at the time of AP prescription, these findings suggest that onset of in-hospital delirium should trigger a closer examination of the patient’s current burden of illness, prognosis, functional and cognitive status, treatment options, and goals of care.
Prevention is key
Our study also supports the prevention of delirium as the most important strategy to improve patient outcomes. Since conducting this study, Baystate Medical Center has implemented an “ACE” (Acute Care for Elders) pilot project and will soon open a full ACE unit. This unit, which employs many of the behavioral interventions described above (early discharge planning, drug oversight, team-based care, early mobilization, optimizing vision and hearing, sleep-wake cycle preservation, and hydration) has resulted in declines in both delirium rates and use of APs. Use of restraints has been virtually eliminated.
Our ACE program was a combined effort between geriatrics, hospital medicine, nursing, pharmacy, and others, but hospitalists often lead acute care quality improvement (QI) initiatives, and are superbly positioned to champion programs like ACE, NICHE (Nurses Improving Care for Health System Elders), and HELP (Hospital Elder Life Program) to benefit this vulnerable population.
Some important questions about AP use remain unanswered. First, there is very limited clinical trial evidence that APs actually improve outcomes in patients with delirium. Second, our study fails to answer one all-important question: does long-term AP use increase mortality in elders? Prior studies are largely retrospective, and results have been mixed.
Our study highlights the difficulty of teasing apart the baseline risks of the patients, the risk of the medications themselves, and confounding variables. There may be an association between APs and death, but it is quite possible that patients who require APs are simply at higher risk of death independent of the drugs’ effect; this confounding by indication cannot be adjusted away.
This leaves hospitalists in a difficult position. At Baystate Medical Center, hospitalists have opted to focus on prevention, but when delirium occurs, some patients are still treated with APs. Clinicians reserve the medications for patients who are suffering and fail to respond to nonpharmacologic interventions or are a risk to themselves or others. Still, Baystate plans to reduce use even in this population by instituting behavioral response teams to devise nondrug care plans, and hospitalists are encouraged to avoid discharging patients on APs.
Finally, even though patients who require APs may lack a clear terminal diagnosis, we encourage clinicians to recognize that delirium should prompt a discussion of prognosis and clarification of values, goals, and realistic treatment options.
Dr. Loh is a fellow at the James Wilmot Cancer Center, University of Rochester (N.Y.) Medical Center. Dr. Brennan is chief of geriatrics and post-acute medicine at Baystate Medical Center, Springfield, Mass. Dr. Lagu is an academic hospitalist in the Center for Quality of Care Research at Baystate Medical Center.
Low-FODMAP diet eased abdominal symptoms in IBS
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
SAN DIEGO – For patients with diarrhea-predominant irritable bowel syndrome, avoiding FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) improved abdominal pain and bloating significantly more than following standard advice to eat smaller meals and limit caffeine and alcohol, researchers reported.
“Both diets provided adequate relief to about 40%-50% of patients, but the low-FODMAP diet led to significantly greater improvements in abdominal symptoms,” Dr. Shanti L. Eswaran of the University of Michigan, Ann Arbor, said at the annual Digestive Disease Week. Results from the randomized, controlled trial, the first of its kind in the United States, “support a role for the low-FODMAP diet in the treatment of patients with diarrhea-predominant IBS,” she added.
FODMAPs are poorly absorbed or indigestible fermentable carbohydrates that can cause bloating, flatulence, and diarrhea when eaten in excess. Hence, the low-FODMAP diet involves avoiding or limiting foods high in fructose (such as honey and dried fruit), lactose (dairy), fructans (wheat, garlic, and onions), galactans (legumes), and polyols (apples and stone fruits). Several smaller studies have linked a low-FODMAP diet to improvements in IBS, “but the existing data are limited and inconsistent, and there is no randomized, controlled trial data from adults in the United States,” Dr. Eswaran said.
To fill that gap, she and her associates randomly assigned 92 adults meeting Rome III criteria for diarrhea-predominant IBS to follow either a low-FODMAP diet or a control diet that was based on recommendations from the National Institute for Health Care and Excellence (NICE, in the United Kingdom). The modified NICE diet included eating smaller, more frequent meals, limiting caffeine and alcohol, and avoiding foods that patients knew worsened their symptoms. Both groups of patients worked with a dietitian.
At baseline, all patients reported having regular bouts of at least moderate abdominal pain and stool consistency of 5 or higher (that is, looser) on the Bristol Stool Form Scale. In all, 52% of patients on the low-FODMAP diet and 41% of patients on the control diet reported adequate symptom relief during at least one of the last 2 weeks of the study – a statistically similar level of improvement, Dr. Eswaran said. “We were really underpowered for our primary endpoint,” she added. “We had calculated a 30% difference, and we did not get anywhere near that.” In fact, enrollment in the trial ended early because many patients were already putting themselves on the low-FODMAP diet, she added.
But despite its limited power, the study uncovered significant differences in abdominal symptoms with the two diets. More than half of patients on the low-FODMAP diet reported a clinically meaningful improvement in abdominal pain, compared with only 23% of patients on the control diet (P = .008). Likewise, 52% of patients reported clinically meaningful improvement in bloating, compared with about a quarter of patients on the control diet (P = .013). Low-FODMAP patients also were more likely to report improvements in stool consistency (42%, versus 28% for control patients; P = .18). However, there was no evidence that the low-FODMAP diet improved stool consistency or urgency, Dr. Eswaran said.
“Both diets were safe and well tolerated, although dropouts were more common with the low-FODMAP diet,” the researchers noted. Dietary analyses showed that at 4 weeks, the low-FODMAP group was consuming significantly less total carbohydrates, but similar quantities of total calories, protein, fat, dietary fiber, and alcohol as the control group. “The low-FODMAP diet is not designed to be long term, because it is fairly restrictive,” Dr. Eswaran commented. “I think it would be a good idea for the next set of studies to see how long patients can stay on it, and what factors are necessary for them to do so.”
Dr. Eswaran had no disclosures.
AT DDW® 2016
Key clinical point: A diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols was associated with significant and clinically meaningful improvements in the abdominal symptoms of diarrhea-predominant irritable bowel syndrome.
Major finding: About half of patients on the low-FODMAP diet improved, compared with about a quarter of patients on a common-sense control diet.
Data source: A prospective, single-center, single-blind randomized controlled trial of 92 adults with IBS with diarrhea (Rome III).
Disclosures: Dr. Eswaren had no disclosures.
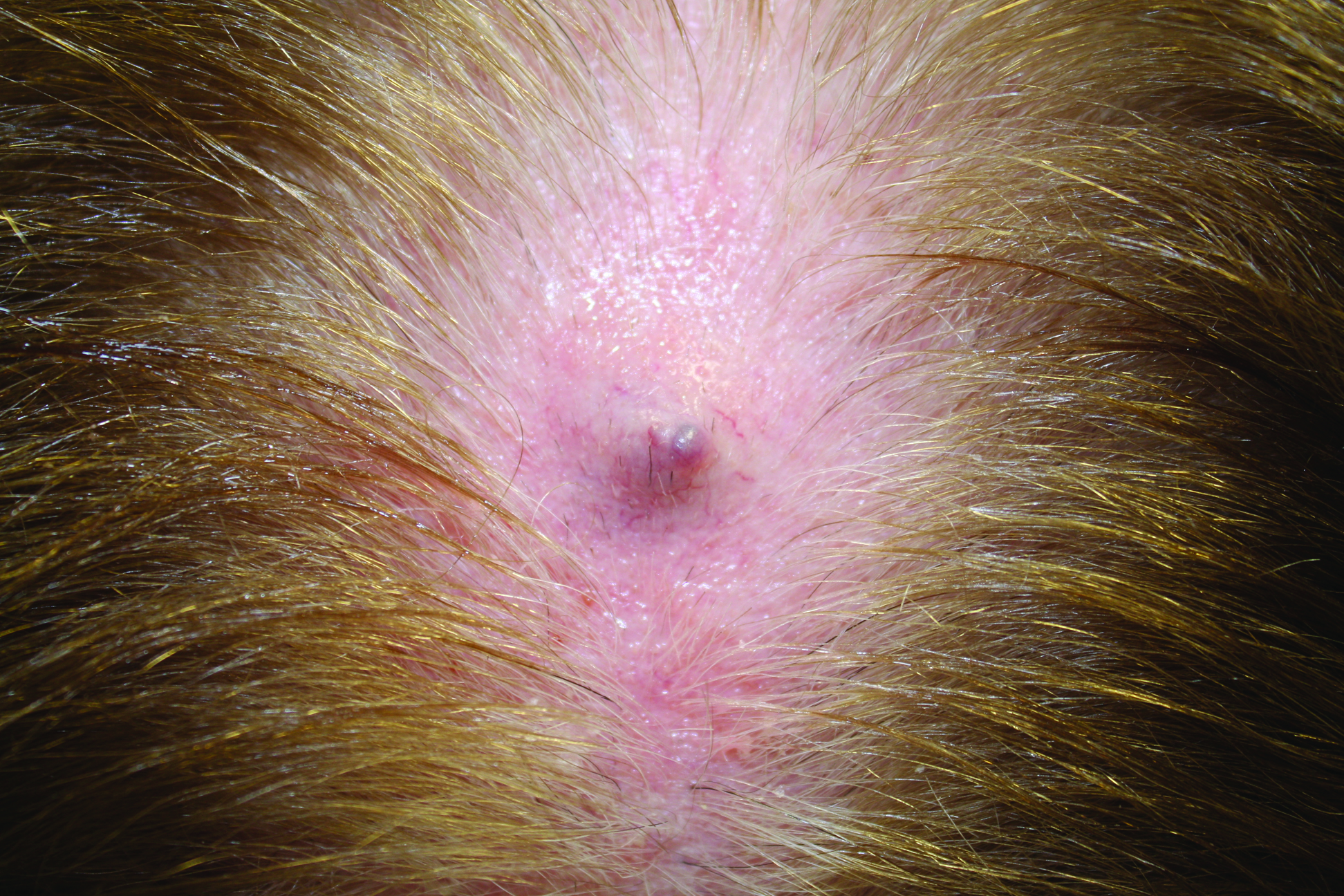
Firm Gray Nodule on the Scalp
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
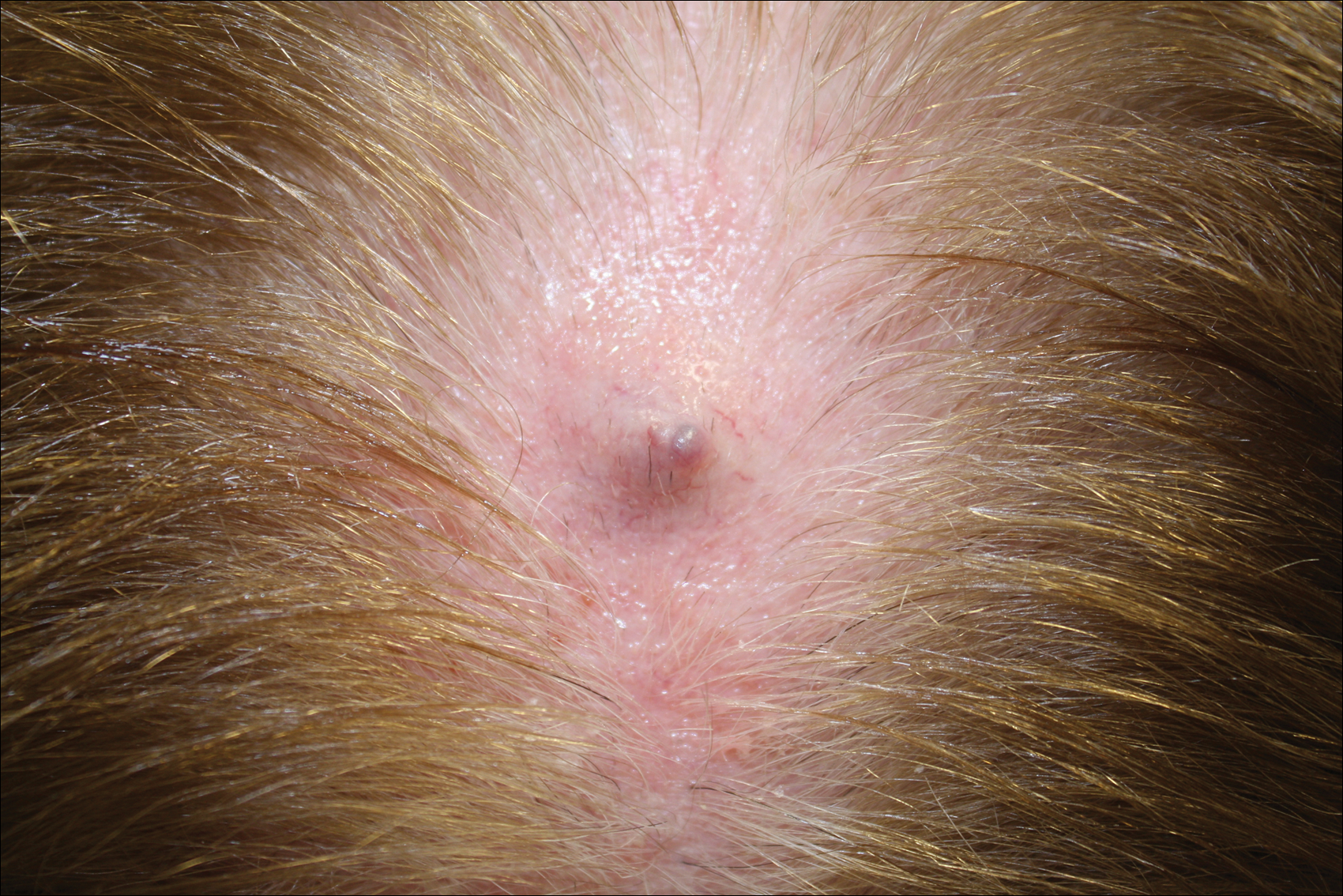
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
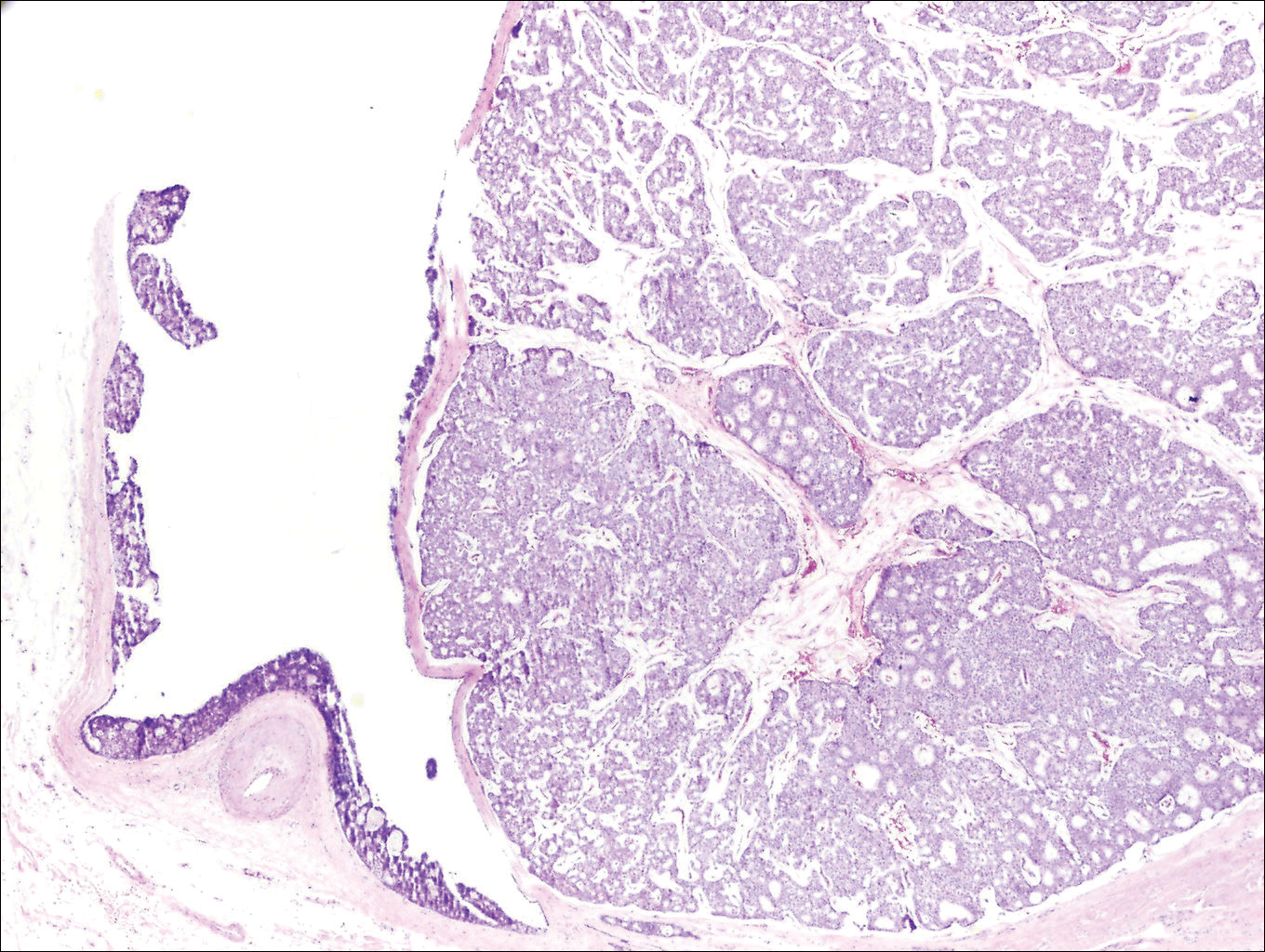
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
The Diagnosis: Primary Cutaneous Mucinous Carcinoma
Primary cutaneous mucinous carcinoma is a rare tumor of the sweat glands that was first reported in 1952 by Lennox et al.1 These tumors are slow growing and have a predilection for the head and neck, with the eyelid being the most commonly reported location.2 In general, they present as erythematous asymptomatic nodules measuring less than 7 cm in diameter.2-4 Primary cutaneous mucinous carcinoma tends to have a good prognosis with complete resection, but cases of metastasis and recurrence have been reported.2 Although there is no standard of care, treatment typically consists of surgical management, as the tumors are nonresponsive to chemotherapy or radiation.4 Kamalpour et al2 compared outcomes for Mohs micrographic surgery versus standard excision, the former showing a lower percentage of poor outcomes. Of note, there were fewer cases treated with Mohs surgery in this study; only more recently reported cases have been treated with Mohs surgery.
Histologically, primary cutaneous mucinous carcinoma is composed of cords, tubules, and lobules of epithelial cells floating in large pools of basophilic mucin, separated by thin fibrovascular septa.5 It can be difficult to distinguish a primary tumor from a mucinous carcinoma metastasis with histology alone, especially on the breasts and in the gastrointestinal tract. Immunohistochemistry can be helpful in determining the origin of the tumor. A homologue of p53, p63 expressed in basal and myoepithelial cells of the skin can aid in the confirmation of a primary tumor when present.6,7 Negative staining for cytokeratin 20 and positive staining for cytokeratin 7 also are helpful in distinguishing a primary cutaneous mucinous carcinoma from a gastrointestinal tract metastasis.4,8
In our patient, no other symptoms were present that raised concern for an internal malignancy. Findings that supported a primary versus metastatic tumor included the clinicopathologic findings (Figure) as well as positive p63, cytokeratin 7, and negative cytokeratin 20 staining. The initial standard excision had tumor cells within 1 mm of the specimen margin; thus, a subsequent wider reexcision was performed. Reexcision was negative for tumor cells. Close follow-up with a primary care physician was recommended, with emphasis on colon and breast cancer screening. A follow-up mammogram was negative for breast cancer.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin: with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Kamalpour L, Brindise RT, Nodzenski M, et al. Primary cutaneous mucinous carcinoma a systematic review and meta-analysis of outcomes after surgery. JAMA Dermatol. 2014;150:380-384.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathological and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Walsh SN, Santa Cruz DJ. Adnexal carcinomas of the skin. In: Rigel DS, Robinson JK, Ross M, et al, eds. Cancer of the Skin. 2nd ed. Beijing, China: Elsevier Saunders; 2011:140-149.
- Jo VY, Fletcher CD. p63 Immunohistochemical staining is limited in soft tissue tumors. Am J Clin Pathol. 2011;136:762-766.
- Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2006;34:478-489.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
Dimethyl Fumarate and Fingolimod May Decrease Relapse Rate More Than Other DMTs
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.

Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.
Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson
NATIONAL HARBOR, MD—In a real-world comparison in patients with multiple sclerosis (MS), dimethyl fumarate and fingolimod were associated with the largest reduction in unadjusted relapse rates after initiation of disease-modifying therapy (DMT), according to data presented at the 2016 CMSC Annual Meeting. In addition, dimethyl fumarate was associated with significantly fewer arrhythmias, compared with glatiramer acetate, interferon beta, and teriflunomide after initiation of DMT.
Real-world data on the comparative effectiveness of DMTs for MS management are limited. The goal of this study, led by Aaron Boster, MD, Systems Medical Chief of Neuroimmunology for OhioHealth in Columbus, Ohio, and his colleagues was to compare the annual relapse rate in patients initiating delayed-release dimethyl fumarate, glatiramer acetate, interferon beta, fingolimod, or teriflunomide.
For this investigation, researchers used data from the Truven MarketScan Claim database, which includes information from 80 million commercially insured people in the United States. Patients with MS between ages 18 and 64 who initiated a DMT of choice in 2013 were included in the study.
Aaron Boster, MD
Dr. Boster and his colleagues calculated arrhythmias based on the number of MS-related relapses within one year after DMT initiation and examined chronic disease burden and MS-related symptoms. Composite scores depended on the presence of 22 chronic conditions, including diabetes, peptic ulcer, liver disease, and cancer. The Poisson regression model was used to estimate adjusted incidence rate ratios of relapse rate. The researchers adjusted the data for demographic and clinical characteristics such as age, sex, region, and place of residence.
The most significant decreases in unadjusted relapse rate were among patients receiving dimethyl fumarate or fingolimod. Dimethyl fumarate was associated with a lower number of arrhythmias, compared with other DMTs. Overall, patients initiating dimethyl fumarate or fingolimod were more adherent to treatment than patients receiving teriflunomide, glatiramer acetate, or interferon beta in the first year after DMT initiation. “Insights provided by real-world data, and the implications for differences in real-world comparative effectiveness of available DMTs, should be taken into account when making decisions on appropriate therapy for the management of MS,” said Dr. Boster and colleagues.
Some limitations of the study were that the data were not collected specifically for clinical research and that the results that did not provide certain clinical information required to assess disease severity properly.
—Erica Robinson

Alemtuzumab-Associated Improvement Is Sustained for More Than Five Years
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.

Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.
Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson
NATIONAL HARBOR, MD—Patients with highly active relapsing-remitting multiple sclerosis (RRMS) have durable improvement for more than five years with alemtuzumab use, according to data presented at the 2016 CMSC Annual Meeting. In a phase III trial, 45% of patients treated with alemtuzumab also sustained a six-month reduction in disability.
Barry A. Singer, MD
In the CARE-MS II study, alemtuzumab was associated with more significant improvement in clinical and MRI outcomes over two years, compared with subcutaneous interferon beta-1a, in patients with active RRMS who had had a poor response to prior therapy at baseline. An extension study was initiated to evaluate the five-year efficacy of alemtuzumab treatment in a subset of patients with RRMS and highly active disease at baseline. Barry A. Singer, MD, Assistant Professor of Clinical Neurology at Washington University in St. Louis, and his colleagues defined highly active disease as two or more relapses in the year before randomization and gadolinium-enhanced lesions at baseline. In the study, 24% of patients receiving alemtuzumab met the criteria for highly active disease.
During the trial, patients randomized to alemtuzumab (12 mg/day) were given two courses of treatment for five consecutive days at baseline and treatment for three consecutive days in the 12th month. In the extension study, patients were only allowed to receive alemtuzumab retreatment if they had a relapse or MRI activity on disease-modifying treatment.
In more than five years, at least 80% of patients receiving alemtuzumab who had had an inadequate response to prior therapy were free of relapses in each individual year. Sixty-two percent of patients had no alemtuzumab retreatment or other disease-modifying therapies. Results also showed that 97% of patients did not receive another disease-modifying therapy.
In this cohort, no evidence of disease activity was reported in 71%, 63%, and 67% of patients during years three, four, and five, as well as in 53% of patients during years zero to five. Arrhythmias remained low in each individual year of the extension study. Expanded Disability Status Scale (EDSS) scores also showed improvement with alemtuzumab use through years zero to five. In addition, sustained reduction in disability was achieved by 53% of patients during years zero to five.
“Based on these findings, alemtuzumab may provide a unique treatment approach with durable efficacy in the absence of continuous treatment for patients with highly active RRMS,” said Dr. Singer and his colleagues.
This study was supported by Genzyme and Bayer HealthCare Pharmaceuticals.
—Erica Robinson

BENEFIT 11: An 11-Year Follow-Up of Early Treatment With Interferon Beta-1b
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.

Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.
Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Long-term follow-up from the BENEFIT trial, in which patients with clinically isolated syndrome (CIS) were treated with interferon beta-1b, confirmed the relationship between MRI metrics and clinical outcomes after 11 years of treatment, according to data presented at the 2016 CMSC Annual Meeting. Results also indicated that patients with more active disease tended to have smaller cervical spinal cord volumes and that cognition (as measured by mental processing speed) was related to number of lesions.
Patients with CIS who had early treatment with interferon beta-1b in the BENEFIT trial maintained an overall favorable disease course, with some clinical differences that favored treatment start at CIS, including lower annualized relapse rate (ARR), higher Paced Auditory Serial Addition Task (PASAT) score, and longer time to clinically definite multiple sclerosis (MS). “The 11-year follow-up of this trial provides an opportunity to assess the relationship between long-term clinical outcomes and structural assessments by MRI and optical coherence tomography (OCT),” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and colleagues.
Edward J. Fox, MD, PhD
The objective of the present study was to assess correlations between clinical, MRI, and OCT outcomes over 11 years. In the original BENEFIT trial, patients with CIS who had two or more silent brain lesions were randomized to 250 µg of interferon beta-1b (ie, early treatment) or placebo (ie, delayed treatment) subcutaneously every other day. Patients remained on placebo until conversion to clinically definite MS or for two years, whichever came first. Eleven years after initial randomization, all patients were approached to undergo cross-sectional follow-up that included clinical, MRI, and OCT assessment.
Clinical parameters included ARR, Expanded Disability Status Score (EDSS), Kurtzke Functional Status Scale (KFSS), MS Functional Composite (MSFC), PASAT score, and Symbol-Digit Modality Test (SDMT). Correlation was also assessed between mental processing speed (the sum of the z scores for PASAT and SDMT adjusted for education status, age, and sex) and selected MRI parameters.
Of the 468 patients originally randomized, 278 (71.3%) participated in the BENEFIT 11 follow-up study. This population included 167 patients in the original early-treatment group (57.2% of the original cohort) and 111 patients from the original delayed-treatment group (63.1% of the original cohort).
Year 11 MRI and OCT assessments were conducted in 191 patients (68.7%) and 86 patients (30.9%, two patients missing data), respectively. Little difference between the early- and delayed-treatments groups, with respect to MRI and OCT findings, was noted, with the exception of a difference in median number of T1-hypointense lesions. The early-treatment group had 4.0 lesions, and the delayed-treatment group had 2.0 lesions.
Regarding MRI, significant positive correlations in the overall BENEFIT 11 population were observed between ARR and volume of T1 lesions (r = 0.212), ARR and volume of T2 lesions (r = 0.216), EDSS score and T1 hypointensity volume (r = 0.281), and EDSS and T2 volume (r = 0.244). Significant negative correlations in the overall BENEFIT 11 population were observed between ARR and mean upper cervical cord area (MUCCA) (r = –0.208), EDSS and MUCCA (r = –0.194), and MSFC and T1 lesion volume (r = –0.183) and T2 lesion volume (r = –0.213). Mental processing speed correlated negatively with number of T1 lesions (r = –0.176).
Regarding OCT, significant positive correlations in the BENEFIT 11 population were observed between PASAT and minimum global retinal nerve fiber layer thickness (r = 0.271). Significant negative correlations were observed between ARR and global retinal nerve fiber layer thickness (r = –0.233) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.239), T1 lesion volume and minimum global retinal nerve fiber layer thickness (r = 0.255) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.340), and T2 lesion volume and global retinal nerve fiber layer thickness (r = 0.307) and papillomacular bundle-retinal nerve fiber layer thickness (r = –0.392). No significant correlations were found between OCT parameters and EDSS, KFSS, MSFC, SDMT, normalized brain volume, mean cortical thickness, normalized thalamic volume, or visual acuity.
“Results from BENEFIT 11 confirmed the relationship between MRI measures of disease and long-term outcomes,” said Dr. Fox and colleagues. “Significant correlations of lesion volume with EDSS, ARR, and MSFC, as well as with minimum global retinal nerve fiber layer thickness and papillomacular bundle-retinal nerve fiber layer thickness were found, while MUCCA significantly correlated with EDSS and ARR.” These findings, the researchers said, highlight the importance of monitoring MRI activity for assessing disease status.
This study was supported by Bayer HealthCare Pharmaceuticals.
—Glenn S. Williams

Primary Herpes Simplex Virus Infection of the Nipple in a Breastfeeding Woman
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.

The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
Practice Points
- Herpes mastitis should be included in the differential diagnosis for breast pain during lactation.
- Children of breastfeeding women diagnosed with herpes mastitis require immediate evaluation for a possible source of the infection, as complications of herpes viral infection in infants can be severe and life threatening.

Online Survey Probes Patient and Physician Preferences for First-Line MS Treatment
NATIONAL HARBOR, MD—Patients and prescribers agree that efficacy is the highest priority in decision making for first-line multiple sclerosis (MS) treatment, according to the results of an online survey reported at the 2016 CMSC Annual Meeting. Preferences were similar across segments of patient age categories, sex, education, insurance, and disease severity. Furthermore, prescribers place higher importance on the risk of serious side effects than do patients for first-line disease-modifying treatments (DMTs).
Edward J. Fox, MD, PhD
“Even though this study suggests that patients and neurologists prefer high-efficacy agents, real-world practice and market share of DMTs do not reflect this preference,” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and his coauthors. “Knowledge of preferred attributes for first-line treatment from the patient and neurologist perspectives can help to better inform communication regarding treatment decision making.”
To evaluate preferences for features of first-line DMTs among patients with relapsing-remitting MS and neurologists, Dr. Fox and his coinvestigators used PatientsLikeMe, an online, patient-powered social networking community, to recruit patients. Neurologists were recruited from the WebMD network. Maximum Difference Scaling (MDS), a type of best–worst scaling, was used to design online choice experiments in which respondents were shown a series of items and asked to indicate what they consider the most and least important factor when selecting a DMT. The factors included efficacy parameters (ie, slowing of disability progression, prevention of new MRI lesions, and reduction of relapse frequency), risk of serious side effects, tolerability, route of administration (ie, oral, injectable, infusion), cost, and neurologist recommendation.
A total of 193 patients and 225 neurologists responded. Preferences among patients and neurologists were similar. Items related to efficacy were of high importance among both groups. For both patients and neurologists, the items related to efficacy were preferred similarly, in decreasing order of importance: slowing disability progression, decreasing relapse frequency, and preventing new MRI lesions.
For first-line treatment selection, neurologists considered risk of serious side effects of higher importance than preventing new MRI lesions, but of lower importance than slowing disability progression or reducing relapse severity. Patients ranked the risk of serious side effects as of average importance, compared with the three efficacy items.
Patients and neurologists viewed tolerable side effects as an important factor after efficacy and safety in first-line and switch DMT preference. In both groups, parenteral drug administration was least preferred, in comparison with all other factors.
This study was supported by Novartis Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Patients and prescribers agree that efficacy is the highest priority in decision making for first-line multiple sclerosis (MS) treatment, according to the results of an online survey reported at the 2016 CMSC Annual Meeting. Preferences were similar across segments of patient age categories, sex, education, insurance, and disease severity. Furthermore, prescribers place higher importance on the risk of serious side effects than do patients for first-line disease-modifying treatments (DMTs).
Edward J. Fox, MD, PhD
“Even though this study suggests that patients and neurologists prefer high-efficacy agents, real-world practice and market share of DMTs do not reflect this preference,” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and his coauthors. “Knowledge of preferred attributes for first-line treatment from the patient and neurologist perspectives can help to better inform communication regarding treatment decision making.”
To evaluate preferences for features of first-line DMTs among patients with relapsing-remitting MS and neurologists, Dr. Fox and his coinvestigators used PatientsLikeMe, an online, patient-powered social networking community, to recruit patients. Neurologists were recruited from the WebMD network. Maximum Difference Scaling (MDS), a type of best–worst scaling, was used to design online choice experiments in which respondents were shown a series of items and asked to indicate what they consider the most and least important factor when selecting a DMT. The factors included efficacy parameters (ie, slowing of disability progression, prevention of new MRI lesions, and reduction of relapse frequency), risk of serious side effects, tolerability, route of administration (ie, oral, injectable, infusion), cost, and neurologist recommendation.
A total of 193 patients and 225 neurologists responded. Preferences among patients and neurologists were similar. Items related to efficacy were of high importance among both groups. For both patients and neurologists, the items related to efficacy were preferred similarly, in decreasing order of importance: slowing disability progression, decreasing relapse frequency, and preventing new MRI lesions.
For first-line treatment selection, neurologists considered risk of serious side effects of higher importance than preventing new MRI lesions, but of lower importance than slowing disability progression or reducing relapse severity. Patients ranked the risk of serious side effects as of average importance, compared with the three efficacy items.
Patients and neurologists viewed tolerable side effects as an important factor after efficacy and safety in first-line and switch DMT preference. In both groups, parenteral drug administration was least preferred, in comparison with all other factors.
This study was supported by Novartis Pharmaceuticals.
—Glenn S. Williams
NATIONAL HARBOR, MD—Patients and prescribers agree that efficacy is the highest priority in decision making for first-line multiple sclerosis (MS) treatment, according to the results of an online survey reported at the 2016 CMSC Annual Meeting. Preferences were similar across segments of patient age categories, sex, education, insurance, and disease severity. Furthermore, prescribers place higher importance on the risk of serious side effects than do patients for first-line disease-modifying treatments (DMTs).
Edward J. Fox, MD, PhD
“Even though this study suggests that patients and neurologists prefer high-efficacy agents, real-world practice and market share of DMTs do not reflect this preference,” said Edward J. Fox, MD, PhD, a neurologist at Central Texas Neurology Consultants in Round Rock, Texas, and his coauthors. “Knowledge of preferred attributes for first-line treatment from the patient and neurologist perspectives can help to better inform communication regarding treatment decision making.”
To evaluate preferences for features of first-line DMTs among patients with relapsing-remitting MS and neurologists, Dr. Fox and his coinvestigators used PatientsLikeMe, an online, patient-powered social networking community, to recruit patients. Neurologists were recruited from the WebMD network. Maximum Difference Scaling (MDS), a type of best–worst scaling, was used to design online choice experiments in which respondents were shown a series of items and asked to indicate what they consider the most and least important factor when selecting a DMT. The factors included efficacy parameters (ie, slowing of disability progression, prevention of new MRI lesions, and reduction of relapse frequency), risk of serious side effects, tolerability, route of administration (ie, oral, injectable, infusion), cost, and neurologist recommendation.
A total of 193 patients and 225 neurologists responded. Preferences among patients and neurologists were similar. Items related to efficacy were of high importance among both groups. For both patients and neurologists, the items related to efficacy were preferred similarly, in decreasing order of importance: slowing disability progression, decreasing relapse frequency, and preventing new MRI lesions.
For first-line treatment selection, neurologists considered risk of serious side effects of higher importance than preventing new MRI lesions, but of lower importance than slowing disability progression or reducing relapse severity. Patients ranked the risk of serious side effects as of average importance, compared with the three efficacy items.
Patients and neurologists viewed tolerable side effects as an important factor after efficacy and safety in first-line and switch DMT preference. In both groups, parenteral drug administration was least preferred, in comparison with all other factors.
This study was supported by Novartis Pharmaceuticals.
—Glenn S. Williams

Who is liable when a surgical error occurs?
CASE Surgeon accused of operating outside her scope of expertise
A 38-year-old woman (G2 P2002) presented to the emergency department (ED) with acute pelvic pain involving the right lower quadrant (RLQ). The patient had a history of stage IV endometriosis and chronic pelvic pain, primarily affecting the RLQ, that was treated by total laparoscopic hysterectomy with bilateral salpingo-oophorectomy 6 months earlier. Pertinent findings on physical examination included hypoactive bowel sounds and rebound tenderness. The ED physician ordered a computed tomography (CT) scan of the abdomen, which showed no evidence of ureteral injury or other abnormality. The gynecologist who performed the surgery 6 months ago evaluated the patient in the ED.
The gynecologist decided to perform operative laparoscopy because of the severity of the patient’s pain and duration of symptoms. Informed consent obtained in the ED before the patient received analgesics included a handwritten note that said “and other indicated procedures.” The patient signed the document prior to being taken to the operating room (OR). Time out occurred in the OR before anesthesia induction. The gynecologist proceeded with laparoscopic adhesiolysis with planned appendectomy, as she was trained. A normal appendix was noted and left intact. RLQ adhesions involving the colon and abdominal wall were treated with electrosurgical cautery. When the gynecologist found adhesions between the liver and diaphragm in the right upper quadrant (RUQ), she continued adhesiolysis. However, the diaphragm was inadvertently punctured.
As the gynecologist attempted to suture the defect laparoscopically, she encountered difficulty and converted to laparotomy. Adhesions were dense and initially precluded adequate closure of the diaphragmatic defect. The gynecologist persisted and ultimately the closure was adequate; laparotomy concluded. Postoperatively, the patient was given a diagnosis of atelectasis, primarily on the right side; a chest tube was placed by the general surgery team. The patient had an uneventful postoperative period and was discharged on postoperative day 5. One month later she returned to the ED with evidence of pneumonia; she was given a diagnosis of empyema, and antibiotics were administered. She responded well and was discharged after 6 days.
The patient filed a malpractice lawsuit against the gynecologist, the hospital, and associated practitioners. The suit made 3 negligence claims: 1) the surgery was improperly performed, as evidenced by the diaphragmatic perforation; 2) the gynecologist was not adequately trained for RUQ surgery, and 3) the hospital should not have permitted RUQ surgery to proceed. The liability claim cited the lack of qualification of a gynecologic surgeon to proceed with surgical intervention near the diaphragm and the associated consequences of practicing outside the scope of expertise.
Fitz-Hugh Curtis syndrome, a complication of pelvic inflammatory disease that may cause adhesions, was raised as the initial finding at the second surgical procedure and documented as such in the operative report. The plaintiff’s counsel questioned whether surgical correction of this syndrome was within the realm of a gynecologic surgeon. The plaintiff’s counsel argued that the laparoscopic surgical procedure involved bowel and liver; diaphragmatic adhesiolysis was not indicated, especially with normal abdominal CT scan results and the absence of RUQ symptoms. The claim specified that the surgery and care, as a consequence of the RUQ adhesiolysis, resulted in atelectasis, pneumonia, and empyema, with pain and suffering. The plaintiff sought unspecified monetary damages for these results.
What’s the verdict?
The case is in negotiation prior to trial.
Legal and medical considerations
“To err is not just human but intrinsically biological and no profession is exempt from fallibility.”1
Error and liability
To err may be human, but human error is not necessarily the cause of every suboptimal medical outcome. In fact, the overall surgical complication rate has been reported at 3.4%.2 Even when there is an error, it may not have been the kind of error that gives rise to medical malpractice liability. When it comes to surgical errors, the most common are those that actually relate to medications given at surgery that appear to be more common—one recent study found that 1 in 20 perioperative medication administrations resulted in a medication error or an adverse drug event.3
Medical error vs medical malpractice
The fact is that medical error and medical malpractice (or professional negligence) are not the same thing. It is critical to understand the difference.
Medical error is the third leading cause of death in the United States.4 It is defined as “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim,”5 or, in the Canadian literature, “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result.”6 The gamut of medical errors spans (among others) problems with technique, judgment, medication administration, diagnostic and surgical errors, and incomplete record keeping.5
Negligent error, on the other hand, is generally a subset of medical error recognized by the law. It is error that occurs because of carelessness. Technically, to give rise to liability for negligence (or malpractice) there must be duty, breach, causation, and injury. That is, the physician must owe a duty to the patient, the duty must have been breached, and that breach must have caused an injury.7
Usually the duty in medical practice is that the physician must have acted as a reasonable and prudent professional would have performed under the circumstances. For the most part, malpractice is a level of practice that the profession itself would not view as reasonable practice.8 Specialists usually are held to the higher standards of the specialty. It also can be negligent to undertake practice or a procedure for which the physician is not adequately trained, or for failing to refer the patient to another more qualified physician.
The duty in medicine usually arises from the physician-patient relationship (clearly present here). It is reasonably clear in this case that there was an injury, but, in fact, the question is whether the physician acted carelessly in a way that caused that injury. Our facts leave some ambiguity—unfortunately,a common problem in the real world.
It is possible that the gynecologist was negligent in puncturing the diaphragm. It may have been carelessness, for example, in the way the procedure was performed, or in the decision to proceed despite the difficulties encountered. It is also possible that the gynecologist was not appropriately trained and experienced in the surgery that was undertaken, in which case the decision to do the surgery (rather than to refer to another physician) could well have been negligent. In either of those cases, negligence liability (malpractice) is a possibility.
Proving negligence. It is the plaintiff (the patient) who must prove the elements of negligence (including causation).8 The plaintiff will have to demonstrate not only carelessness, but that carelessness is what caused the injuries for which she is seeking compensation. In this case, the injuries are the consequence of puncturing the diaphragm. The potential damages would be the money to cover the additional medical costs and other expenses, lost wages, and noneconomic damages such as pain and suffering.
The hospital’s role in negligence
The issue of informed consent is also raised in this case, with a handwritten note prior to surgery (but the focus of this article is on medical errors). In addition to the gynecologist, the hospital and other medical personnelwere sued. The hospital is responsible for the acts of its agents, notably its employees. Even if the physicians are not technically hospital employees, the hospital may in some cases be responsible. Among other things, the hospital likely has an obligation to prevent physicians from undertaking inappropriate procedures, including those for which the physician is not appropriately trained. If the gynecologist in this case did not have privileges to perform surgery in this category, the hospital may have an obligation to not schedule the surgery or to intraoperatively question her credentials for such a procedure. In any event, the hospital will have a major role in this case and its interests may, in some instances, be inconsistent with the interests of the physician.
Why settlement discussions?
The case description ends with a note that settlement discussions were underway. If the plaintiff must prove all of the elements of negligence, why have these discussions? First, such discussions are common in almost all negligence cases. This does not mean that the case actually will be settled by the insurance company representing the physician or hospital; many malpractice cases simply fade away because the patient drops the action. Second, there are ambiguities in the facts, and it is sometimes impossible to determine whether or not a jury would find negligence. The hospital may be inclined to settle if there is any realistic chance of a jury ruling against it. Paying a small settlement may be worth avoiding high legal expenses and the risk of an adverse outcome at trial.9
Reducing medical/surgical error through a team approach
Recognizing that “human performance can be affected by many factors that include circadian rhythms, state of mind, physical health, attitude, emotions, propensity for certain common mistakes and errors, and cognitive biases,”10 health care professionals have a commitment to reduce the errors in the interest of patient safety and best practice.
The surgical environment is an opportunity to provide a team approach to patient safety. Surgical risk is a reflection of operative performance, the main factor in the development of postoperative complications.11 We wish to broaden the perspective that gynecologic surgeons, like all surgeons, must keep in mind a number of concerns that can be associated with problems related to surgical procedures, including12:
- visual perception difficulties
- stress
- loss of haptic perception (feedback using touch), as with robot-assisted procedures
- lack of situational awareness (a term we borrow from the aviation industry)
- long-term (and short-term) memory problems.
Analysis of surgical errors shows that they are related to, in order of frequency 1:
- surgical technique
- judgment
- inattention to detail
- incomplete understanding of the problem or surgical situation.
Medical errors: Caring for the second victim (you)

Patrice M. Weiss, MD
We use the term “victim” to refer to the patient and her family following a medical error. The phrase “the second victim” was coined by Dr. Albert Wu in an article in the British Medical Journal1 and describes how a clinician and team of health care professionals also can be affected by medical errors.
What signs and symptoms identify a second victim?Those suffering as a second victim may show signs of depression, loss of joy in work, and difficulty sleeping. They also may replay the events, question their own ability, and feel fearful about making another error. These reactions can lead to burnout—a serious issue that 46% of physicians report.2
As colleagues of those involved in a medical error, we should be cognizant of changes in behavior such as excessive irritability, showing up late for work, or agitation. It may be easier to recognize these symptoms in others rather than in ourselves because we often do not take time to examine how our experiences may affect us personally. Heightening awareness can help us recognize those suffering as second victims and identify the second victim symptoms in ourselves.
How can we help second victims?One challenge second victims face is not being allowed to discuss a medical error. Certainly, due to confidentiality requirements during professional liability cases, we should not talk freely about the event. However, silence creates a barrier that prevents a second victim from processing the incident.
Some hospitals offer forums to discuss medical errors, with the goal of preventing reoccurrence: morbidity and mortality conferences, morning report, Quality Assurance and Performance Improvement meetings, and root cause analyses. These forums often are not perceived by institutions’ employees in a positive way. Are they really meant to improve patient care or do they single out an individual or group in a “name/blame/shame game”? An intimidating process will only worsen a second victim’s symptoms. It is not necessary, however, to create a whole new process; it is possible to restructure, reframe, and change the culture of an existing practice.
Some institutions have developed a formalized program to help second victims. The University of Missouri has a “forYOU team,” an internal, rapid response group that provides emotional first aid to the entire team involved in a medical error case. These responders are not from human resources and do not need to be sought out; they are peers who have been educated about the struggles of the second victim. They will not discuss the case or how care was rendered; they naturally and instinctively provide emotional support to their colleagues.
At my institution, the Carilion Clinic at the Virginia Tech Carilion School of Medicine, “The Trust Program” encourages truth, respectfulness, understanding, support, and transparency. All health care clinicians receive basic training, but many have volunteered for additional instruction to become mentors because they have experienced second-victim symptoms themselves.
Clinicians want assistance when dealing with a medical error. One poll reports that 90% of physicians felt that health care organizations did not adequately help them cope with the stresses associated with a medical error.3 The goal is to have all institutions recognize that clinicians can be affected by a medical error and offer support.
To hear an expanded audiocast from Dr. Weiss on “the second victim” click here.
Dr. Weiss is Professor, Department of Obstetrics & Gynecology, Virginia Tech Carilion School of Medicine, and Chief Medical Officer and Executive Vice President, Carilion Clinic, Roanoke, Virginia.
The author reports no financial relationships relevant to this article.
References
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726–727.
- Peckham C. Medscape Physician Lifestyle Report 2015. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2015/public/overview#1. Published January 26, 2015. Accessed May 24, 2016.
- White AA, Waterman AD, McCotter P, Boyle DJ, Gallagher TH. Supporting health care workers after medical error: considerations for health care leaders. JCOM. 2008;15(5):240–247.
“Inadequacy” with regard to surgical proceduresIndication for surgery is intrinsic to provision of appropriate care. Surgery inherently poses the possibility of unexpected problems. Adequate training and skill, therefore, must include the ability to deal with a range of problems that arise in the course of surgery. The spectrum related to inadequacy as related to surgical problems includes “failed surgery,” defined as “if despite the utmost care of everyone involved and with the responsible consideration of all knowledge, the designed aim is not achieved, surgery by itself has failed.”5 Of paramount importance is the surgeon’s knowledge of technology and the ability to troubleshoot, as well as the OR team’s responsibility for proper maintenance of equipment to ensure optimal functionality.1
Aviation industry studies indicate that “high performing cockpit crews have been shown to devote one third of their communications to discuss threats and mistakes in their environment, while poor performing teams devoted much less, about 5%, of their time to such.”1,13 A well-trained and well-motivated OR nursing team has been equated with reduction in operative time and rate of conversion to laparotomy.14 Outdated instruments may also contribute to surgical errors.1
Moving the “learning curve” out of the OR and into the simulation lab remains valuable, which is also confirmed by the aviation industry.15 The significance of loss of haptic perception continues to be debated between laparoscopic (straight-stick) surgeons and those performing robotic approaches. Does haptic perception play a major role in surgical intervention? Most surgeons do not view loss of haptic perception, as with minimally invasive procedures, as a major impediment to successful surgery. From the legal perspective, loss of haptic perception has not been well addressed.
The American College of Obstetricians and Gynecologists has focused on patient safety in the surgical environment including concerns for wrong-patient surgery, wrong-side surgery, wrong-level surgery, and wrong-part surgery.16 The Joint Commission has identified factors that may enhance the risk of wrong-site surgery: multiple surgeons involved in the case, multiple procedures during a single surgical visit, unusual time pressures to start or complete the surgery, and unusual physical characteristics including morbid obesity or physical deformity.16
10 starting points for medical error preventionSo what are we to do? Consider:
- Using a preprocedure verification checklist.
- Marking the operative site.
- Completing a time out process prior to starting the procedure, according to the Joint Commission protocol. [For more information on Joint Commission-recommended time out protocols and ways to prevent medical errors, click here.]
- Involving the patient in the identification and procedure definition process. (This is an important part of informed consent.)
- Providing appropriate proctoring and sign-off for new procedures and technology.
- Avoiding sleep deprivation situations, especially with regard to emergency procedures.
- Using only radiopaque-labeled materials placed into the operating cavity.
- Considering medication effect on a fetus, if applicable.
- Reducing distractions from pagers, telephone calls, etc.
- Maintaining a “sterile cockpit” (or distraction free) environment for everyone in the OR.
Set the stage for best outcomesA true team approach is an excellent modus operandi before, during, and after surgery,setting the stage for best outcomes for patients.
“As human beings, surgeons will commit errors and for this reason they have to adopt and utilize stringent defense systems to minimize the incidence of these adverse events … Transparency is the first step on the way to a new safety culture with the acknowledgement of errors when they occur with adoption of systems destined to establish their cause and future prevention.”1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Galleano R, Franceschi A, Ciciliot M, Falchero F, Cuschieri A. Errors in laparoscopic surgery: what surgeons should know. Mineva Chir. 2011;66(2):107−117.
- Fabri P, Zyas-Castro J. Human error, not communication and systems, underlies surgical complications. Surgery. 2008;144(4):557−565.
- Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124(1):25−34.
- Makary MA, Daniel M. Medical error−the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139. Balogun J, Bramall A, Berstein M. How surgical trainees handle catastrophic errors: a qualitative study. J Surg Educ. 2015;72(6):1179−1184.
- Grober E, Bohnen J. Defining medical error. Can J Surg. 2005;48(1):39−44.
- Anderson RE, ed. Medical Malpractice: A Physician's Sourcebook. Totowa, NJ: Humana Press, Inc; 2004.
- Mehlman MJ. Professional power and the standard of care in medicine. 44 Arizona State Law J. 2012;44:1165−1777. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2205485. Revised February 13, 2013.
- Hyman DA, Silver C. On the table: an examination of medical malpractice, litigation, and methods of reform: healthcare quality, patient safety, and the culture of medicine: "Denial Ain't Just a River in Egypt." New Eng Law Rev. 2012;46:417−931.
- Landers R. Reducing surgical errors: implementing a three-hinge approach to success. AORN J. 2015;101(6):657−665.
- Pettigrew R, Burns H, Carter D. Evaluating surgical risk: the importance of technical factors in determining outcome. Br J Surg. 1987;74(9):791−794.
- Parker W. Understanding errors during laparoscopic surgery. Obstet Gynecol Clin North Am. 2010;37(3):437−449.
- Sexton JB, Helmreich RL. Analyzing cockpit communications: the links between language, performance, error, and workload. Hum Perf Extrem Environ. 2000;5(1):63−68.
- Kenyon T, Lenker M, Bax R, Swanstrom L. Cost and benefit of the trained laparoscopic team: a comparative study of a designated nursing team vs. a non-trained team. Surg Endosc. 1997;11(8):812−814.
- Woodman R. Surgeons should train like pilots. BMJ. 1999;319:1321.
- American College of Obstetrics and Gynecology. ACOG Committee Opinion No. 464: Patient safety in the surgical environment. Obstet Gynecol. 2010;116(3):786−790.
In this quarterly column, these medical and legal experts and educators present a case-based* discussion and provide clear teaching points and takeaways for your practice.

Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology and Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.

Mr. Smith is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California.
The authors report no financial relationships relevant to this article.
*The "facts" of this case are based on actual cases and are a compilation of several cases. The "Verdict" regarding negotiation is for discussion only. The legal discussion that follows is based on the general legal rules in the United States. Medical malpractice liability law varies from state to state; the following discussion does not include individual state law.
In this quarterly column, these medical and legal experts and educators present a case-based* discussion and provide clear teaching points and takeaways for your practice.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology and Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.
Mr. Smith is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California.
The authors report no financial relationships relevant to this article.
*The "facts" of this case are based on actual cases and are a compilation of several cases. The "Verdict" regarding negotiation is for discussion only. The legal discussion that follows is based on the general legal rules in the United States. Medical malpractice liability law varies from state to state; the following discussion does not include individual state law.
In this quarterly column, these medical and legal experts and educators present a case-based* discussion and provide clear teaching points and takeaways for your practice.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology and Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.
Mr. Smith is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California.
The authors report no financial relationships relevant to this article.
*The "facts" of this case are based on actual cases and are a compilation of several cases. The "Verdict" regarding negotiation is for discussion only. The legal discussion that follows is based on the general legal rules in the United States. Medical malpractice liability law varies from state to state; the following discussion does not include individual state law.
CASE Surgeon accused of operating outside her scope of expertise
A 38-year-old woman (G2 P2002) presented to the emergency department (ED) with acute pelvic pain involving the right lower quadrant (RLQ). The patient had a history of stage IV endometriosis and chronic pelvic pain, primarily affecting the RLQ, that was treated by total laparoscopic hysterectomy with bilateral salpingo-oophorectomy 6 months earlier. Pertinent findings on physical examination included hypoactive bowel sounds and rebound tenderness. The ED physician ordered a computed tomography (CT) scan of the abdomen, which showed no evidence of ureteral injury or other abnormality. The gynecologist who performed the surgery 6 months ago evaluated the patient in the ED.
The gynecologist decided to perform operative laparoscopy because of the severity of the patient’s pain and duration of symptoms. Informed consent obtained in the ED before the patient received analgesics included a handwritten note that said “and other indicated procedures.” The patient signed the document prior to being taken to the operating room (OR). Time out occurred in the OR before anesthesia induction. The gynecologist proceeded with laparoscopic adhesiolysis with planned appendectomy, as she was trained. A normal appendix was noted and left intact. RLQ adhesions involving the colon and abdominal wall were treated with electrosurgical cautery. When the gynecologist found adhesions between the liver and diaphragm in the right upper quadrant (RUQ), she continued adhesiolysis. However, the diaphragm was inadvertently punctured.
As the gynecologist attempted to suture the defect laparoscopically, she encountered difficulty and converted to laparotomy. Adhesions were dense and initially precluded adequate closure of the diaphragmatic defect. The gynecologist persisted and ultimately the closure was adequate; laparotomy concluded. Postoperatively, the patient was given a diagnosis of atelectasis, primarily on the right side; a chest tube was placed by the general surgery team. The patient had an uneventful postoperative period and was discharged on postoperative day 5. One month later she returned to the ED with evidence of pneumonia; she was given a diagnosis of empyema, and antibiotics were administered. She responded well and was discharged after 6 days.
The patient filed a malpractice lawsuit against the gynecologist, the hospital, and associated practitioners. The suit made 3 negligence claims: 1) the surgery was improperly performed, as evidenced by the diaphragmatic perforation; 2) the gynecologist was not adequately trained for RUQ surgery, and 3) the hospital should not have permitted RUQ surgery to proceed. The liability claim cited the lack of qualification of a gynecologic surgeon to proceed with surgical intervention near the diaphragm and the associated consequences of practicing outside the scope of expertise.
Fitz-Hugh Curtis syndrome, a complication of pelvic inflammatory disease that may cause adhesions, was raised as the initial finding at the second surgical procedure and documented as such in the operative report. The plaintiff’s counsel questioned whether surgical correction of this syndrome was within the realm of a gynecologic surgeon. The plaintiff’s counsel argued that the laparoscopic surgical procedure involved bowel and liver; diaphragmatic adhesiolysis was not indicated, especially with normal abdominal CT scan results and the absence of RUQ symptoms. The claim specified that the surgery and care, as a consequence of the RUQ adhesiolysis, resulted in atelectasis, pneumonia, and empyema, with pain and suffering. The plaintiff sought unspecified monetary damages for these results.
What’s the verdict?
The case is in negotiation prior to trial.
Legal and medical considerations
“To err is not just human but intrinsically biological and no profession is exempt from fallibility.”1
Error and liability
To err may be human, but human error is not necessarily the cause of every suboptimal medical outcome. In fact, the overall surgical complication rate has been reported at 3.4%.2 Even when there is an error, it may not have been the kind of error that gives rise to medical malpractice liability. When it comes to surgical errors, the most common are those that actually relate to medications given at surgery that appear to be more common—one recent study found that 1 in 20 perioperative medication administrations resulted in a medication error or an adverse drug event.3
Medical error vs medical malpractice
The fact is that medical error and medical malpractice (or professional negligence) are not the same thing. It is critical to understand the difference.
Medical error is the third leading cause of death in the United States.4 It is defined as “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim,”5 or, in the Canadian literature, “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result.”6 The gamut of medical errors spans (among others) problems with technique, judgment, medication administration, diagnostic and surgical errors, and incomplete record keeping.5
Negligent error, on the other hand, is generally a subset of medical error recognized by the law. It is error that occurs because of carelessness. Technically, to give rise to liability for negligence (or malpractice) there must be duty, breach, causation, and injury. That is, the physician must owe a duty to the patient, the duty must have been breached, and that breach must have caused an injury.7
Usually the duty in medical practice is that the physician must have acted as a reasonable and prudent professional would have performed under the circumstances. For the most part, malpractice is a level of practice that the profession itself would not view as reasonable practice.8 Specialists usually are held to the higher standards of the specialty. It also can be negligent to undertake practice or a procedure for which the physician is not adequately trained, or for failing to refer the patient to another more qualified physician.
The duty in medicine usually arises from the physician-patient relationship (clearly present here). It is reasonably clear in this case that there was an injury, but, in fact, the question is whether the physician acted carelessly in a way that caused that injury. Our facts leave some ambiguity—unfortunately,a common problem in the real world.
It is possible that the gynecologist was negligent in puncturing the diaphragm. It may have been carelessness, for example, in the way the procedure was performed, or in the decision to proceed despite the difficulties encountered. It is also possible that the gynecologist was not appropriately trained and experienced in the surgery that was undertaken, in which case the decision to do the surgery (rather than to refer to another physician) could well have been negligent. In either of those cases, negligence liability (malpractice) is a possibility.
Proving negligence. It is the plaintiff (the patient) who must prove the elements of negligence (including causation).8 The plaintiff will have to demonstrate not only carelessness, but that carelessness is what caused the injuries for which she is seeking compensation. In this case, the injuries are the consequence of puncturing the diaphragm. The potential damages would be the money to cover the additional medical costs and other expenses, lost wages, and noneconomic damages such as pain and suffering.
The hospital’s role in negligence
The issue of informed consent is also raised in this case, with a handwritten note prior to surgery (but the focus of this article is on medical errors). In addition to the gynecologist, the hospital and other medical personnelwere sued. The hospital is responsible for the acts of its agents, notably its employees. Even if the physicians are not technically hospital employees, the hospital may in some cases be responsible. Among other things, the hospital likely has an obligation to prevent physicians from undertaking inappropriate procedures, including those for which the physician is not appropriately trained. If the gynecologist in this case did not have privileges to perform surgery in this category, the hospital may have an obligation to not schedule the surgery or to intraoperatively question her credentials for such a procedure. In any event, the hospital will have a major role in this case and its interests may, in some instances, be inconsistent with the interests of the physician.
Why settlement discussions?
The case description ends with a note that settlement discussions were underway. If the plaintiff must prove all of the elements of negligence, why have these discussions? First, such discussions are common in almost all negligence cases. This does not mean that the case actually will be settled by the insurance company representing the physician or hospital; many malpractice cases simply fade away because the patient drops the action. Second, there are ambiguities in the facts, and it is sometimes impossible to determine whether or not a jury would find negligence. The hospital may be inclined to settle if there is any realistic chance of a jury ruling against it. Paying a small settlement may be worth avoiding high legal expenses and the risk of an adverse outcome at trial.9
Reducing medical/surgical error through a team approach
Recognizing that “human performance can be affected by many factors that include circadian rhythms, state of mind, physical health, attitude, emotions, propensity for certain common mistakes and errors, and cognitive biases,”10 health care professionals have a commitment to reduce the errors in the interest of patient safety and best practice.
The surgical environment is an opportunity to provide a team approach to patient safety. Surgical risk is a reflection of operative performance, the main factor in the development of postoperative complications.11 We wish to broaden the perspective that gynecologic surgeons, like all surgeons, must keep in mind a number of concerns that can be associated with problems related to surgical procedures, including12:
- visual perception difficulties
- stress
- loss of haptic perception (feedback using touch), as with robot-assisted procedures
- lack of situational awareness (a term we borrow from the aviation industry)
- long-term (and short-term) memory problems.
Analysis of surgical errors shows that they are related to, in order of frequency 1:
- surgical technique
- judgment
- inattention to detail
- incomplete understanding of the problem or surgical situation.
Medical errors: Caring for the second victim (you)
Patrice M. Weiss, MD
We use the term “victim” to refer to the patient and her family following a medical error. The phrase “the second victim” was coined by Dr. Albert Wu in an article in the British Medical Journal1 and describes how a clinician and team of health care professionals also can be affected by medical errors.
What signs and symptoms identify a second victim?Those suffering as a second victim may show signs of depression, loss of joy in work, and difficulty sleeping. They also may replay the events, question their own ability, and feel fearful about making another error. These reactions can lead to burnout—a serious issue that 46% of physicians report.2
As colleagues of those involved in a medical error, we should be cognizant of changes in behavior such as excessive irritability, showing up late for work, or agitation. It may be easier to recognize these symptoms in others rather than in ourselves because we often do not take time to examine how our experiences may affect us personally. Heightening awareness can help us recognize those suffering as second victims and identify the second victim symptoms in ourselves.
How can we help second victims?One challenge second victims face is not being allowed to discuss a medical error. Certainly, due to confidentiality requirements during professional liability cases, we should not talk freely about the event. However, silence creates a barrier that prevents a second victim from processing the incident.
Some hospitals offer forums to discuss medical errors, with the goal of preventing reoccurrence: morbidity and mortality conferences, morning report, Quality Assurance and Performance Improvement meetings, and root cause analyses. These forums often are not perceived by institutions’ employees in a positive way. Are they really meant to improve patient care or do they single out an individual or group in a “name/blame/shame game”? An intimidating process will only worsen a second victim’s symptoms. It is not necessary, however, to create a whole new process; it is possible to restructure, reframe, and change the culture of an existing practice.
Some institutions have developed a formalized program to help second victims. The University of Missouri has a “forYOU team,” an internal, rapid response group that provides emotional first aid to the entire team involved in a medical error case. These responders are not from human resources and do not need to be sought out; they are peers who have been educated about the struggles of the second victim. They will not discuss the case or how care was rendered; they naturally and instinctively provide emotional support to their colleagues.
At my institution, the Carilion Clinic at the Virginia Tech Carilion School of Medicine, “The Trust Program” encourages truth, respectfulness, understanding, support, and transparency. All health care clinicians receive basic training, but many have volunteered for additional instruction to become mentors because they have experienced second-victim symptoms themselves.
Clinicians want assistance when dealing with a medical error. One poll reports that 90% of physicians felt that health care organizations did not adequately help them cope with the stresses associated with a medical error.3 The goal is to have all institutions recognize that clinicians can be affected by a medical error and offer support.
To hear an expanded audiocast from Dr. Weiss on “the second victim” click here.
Dr. Weiss is Professor, Department of Obstetrics & Gynecology, Virginia Tech Carilion School of Medicine, and Chief Medical Officer and Executive Vice President, Carilion Clinic, Roanoke, Virginia.
The author reports no financial relationships relevant to this article.
References
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726–727.
- Peckham C. Medscape Physician Lifestyle Report 2015. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2015/public/overview#1. Published January 26, 2015. Accessed May 24, 2016.
- White AA, Waterman AD, McCotter P, Boyle DJ, Gallagher TH. Supporting health care workers after medical error: considerations for health care leaders. JCOM. 2008;15(5):240–247.
“Inadequacy” with regard to surgical proceduresIndication for surgery is intrinsic to provision of appropriate care. Surgery inherently poses the possibility of unexpected problems. Adequate training and skill, therefore, must include the ability to deal with a range of problems that arise in the course of surgery. The spectrum related to inadequacy as related to surgical problems includes “failed surgery,” defined as “if despite the utmost care of everyone involved and with the responsible consideration of all knowledge, the designed aim is not achieved, surgery by itself has failed.”5 Of paramount importance is the surgeon’s knowledge of technology and the ability to troubleshoot, as well as the OR team’s responsibility for proper maintenance of equipment to ensure optimal functionality.1
Aviation industry studies indicate that “high performing cockpit crews have been shown to devote one third of their communications to discuss threats and mistakes in their environment, while poor performing teams devoted much less, about 5%, of their time to such.”1,13 A well-trained and well-motivated OR nursing team has been equated with reduction in operative time and rate of conversion to laparotomy.14 Outdated instruments may also contribute to surgical errors.1
Moving the “learning curve” out of the OR and into the simulation lab remains valuable, which is also confirmed by the aviation industry.15 The significance of loss of haptic perception continues to be debated between laparoscopic (straight-stick) surgeons and those performing robotic approaches. Does haptic perception play a major role in surgical intervention? Most surgeons do not view loss of haptic perception, as with minimally invasive procedures, as a major impediment to successful surgery. From the legal perspective, loss of haptic perception has not been well addressed.
The American College of Obstetricians and Gynecologists has focused on patient safety in the surgical environment including concerns for wrong-patient surgery, wrong-side surgery, wrong-level surgery, and wrong-part surgery.16 The Joint Commission has identified factors that may enhance the risk of wrong-site surgery: multiple surgeons involved in the case, multiple procedures during a single surgical visit, unusual time pressures to start or complete the surgery, and unusual physical characteristics including morbid obesity or physical deformity.16
10 starting points for medical error preventionSo what are we to do? Consider:
- Using a preprocedure verification checklist.
- Marking the operative site.
- Completing a time out process prior to starting the procedure, according to the Joint Commission protocol. [For more information on Joint Commission-recommended time out protocols and ways to prevent medical errors, click here.]
- Involving the patient in the identification and procedure definition process. (This is an important part of informed consent.)
- Providing appropriate proctoring and sign-off for new procedures and technology.
- Avoiding sleep deprivation situations, especially with regard to emergency procedures.
- Using only radiopaque-labeled materials placed into the operating cavity.
- Considering medication effect on a fetus, if applicable.
- Reducing distractions from pagers, telephone calls, etc.
- Maintaining a “sterile cockpit” (or distraction free) environment for everyone in the OR.
Set the stage for best outcomesA true team approach is an excellent modus operandi before, during, and after surgery,setting the stage for best outcomes for patients.
“As human beings, surgeons will commit errors and for this reason they have to adopt and utilize stringent defense systems to minimize the incidence of these adverse events … Transparency is the first step on the way to a new safety culture with the acknowledgement of errors when they occur with adoption of systems destined to establish their cause and future prevention.”1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE Surgeon accused of operating outside her scope of expertise
A 38-year-old woman (G2 P2002) presented to the emergency department (ED) with acute pelvic pain involving the right lower quadrant (RLQ). The patient had a history of stage IV endometriosis and chronic pelvic pain, primarily affecting the RLQ, that was treated by total laparoscopic hysterectomy with bilateral salpingo-oophorectomy 6 months earlier. Pertinent findings on physical examination included hypoactive bowel sounds and rebound tenderness. The ED physician ordered a computed tomography (CT) scan of the abdomen, which showed no evidence of ureteral injury or other abnormality. The gynecologist who performed the surgery 6 months ago evaluated the patient in the ED.
The gynecologist decided to perform operative laparoscopy because of the severity of the patient’s pain and duration of symptoms. Informed consent obtained in the ED before the patient received analgesics included a handwritten note that said “and other indicated procedures.” The patient signed the document prior to being taken to the operating room (OR). Time out occurred in the OR before anesthesia induction. The gynecologist proceeded with laparoscopic adhesiolysis with planned appendectomy, as she was trained. A normal appendix was noted and left intact. RLQ adhesions involving the colon and abdominal wall were treated with electrosurgical cautery. When the gynecologist found adhesions between the liver and diaphragm in the right upper quadrant (RUQ), she continued adhesiolysis. However, the diaphragm was inadvertently punctured.
As the gynecologist attempted to suture the defect laparoscopically, she encountered difficulty and converted to laparotomy. Adhesions were dense and initially precluded adequate closure of the diaphragmatic defect. The gynecologist persisted and ultimately the closure was adequate; laparotomy concluded. Postoperatively, the patient was given a diagnosis of atelectasis, primarily on the right side; a chest tube was placed by the general surgery team. The patient had an uneventful postoperative period and was discharged on postoperative day 5. One month later she returned to the ED with evidence of pneumonia; she was given a diagnosis of empyema, and antibiotics were administered. She responded well and was discharged after 6 days.
The patient filed a malpractice lawsuit against the gynecologist, the hospital, and associated practitioners. The suit made 3 negligence claims: 1) the surgery was improperly performed, as evidenced by the diaphragmatic perforation; 2) the gynecologist was not adequately trained for RUQ surgery, and 3) the hospital should not have permitted RUQ surgery to proceed. The liability claim cited the lack of qualification of a gynecologic surgeon to proceed with surgical intervention near the diaphragm and the associated consequences of practicing outside the scope of expertise.
Fitz-Hugh Curtis syndrome, a complication of pelvic inflammatory disease that may cause adhesions, was raised as the initial finding at the second surgical procedure and documented as such in the operative report. The plaintiff’s counsel questioned whether surgical correction of this syndrome was within the realm of a gynecologic surgeon. The plaintiff’s counsel argued that the laparoscopic surgical procedure involved bowel and liver; diaphragmatic adhesiolysis was not indicated, especially with normal abdominal CT scan results and the absence of RUQ symptoms. The claim specified that the surgery and care, as a consequence of the RUQ adhesiolysis, resulted in atelectasis, pneumonia, and empyema, with pain and suffering. The plaintiff sought unspecified monetary damages for these results.
What’s the verdict?
The case is in negotiation prior to trial.
Legal and medical considerations
“To err is not just human but intrinsically biological and no profession is exempt from fallibility.”1
Error and liability
To err may be human, but human error is not necessarily the cause of every suboptimal medical outcome. In fact, the overall surgical complication rate has been reported at 3.4%.2 Even when there is an error, it may not have been the kind of error that gives rise to medical malpractice liability. When it comes to surgical errors, the most common are those that actually relate to medications given at surgery that appear to be more common—one recent study found that 1 in 20 perioperative medication administrations resulted in a medication error or an adverse drug event.3
Medical error vs medical malpractice
The fact is that medical error and medical malpractice (or professional negligence) are not the same thing. It is critical to understand the difference.
Medical error is the third leading cause of death in the United States.4 It is defined as “the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim,”5 or, in the Canadian literature, “an act of omission or commission in planning or execution that contributes or could contribute to an unintended result.”6 The gamut of medical errors spans (among others) problems with technique, judgment, medication administration, diagnostic and surgical errors, and incomplete record keeping.5
Negligent error, on the other hand, is generally a subset of medical error recognized by the law. It is error that occurs because of carelessness. Technically, to give rise to liability for negligence (or malpractice) there must be duty, breach, causation, and injury. That is, the physician must owe a duty to the patient, the duty must have been breached, and that breach must have caused an injury.7
Usually the duty in medical practice is that the physician must have acted as a reasonable and prudent professional would have performed under the circumstances. For the most part, malpractice is a level of practice that the profession itself would not view as reasonable practice.8 Specialists usually are held to the higher standards of the specialty. It also can be negligent to undertake practice or a procedure for which the physician is not adequately trained, or for failing to refer the patient to another more qualified physician.
The duty in medicine usually arises from the physician-patient relationship (clearly present here). It is reasonably clear in this case that there was an injury, but, in fact, the question is whether the physician acted carelessly in a way that caused that injury. Our facts leave some ambiguity—unfortunately,a common problem in the real world.
It is possible that the gynecologist was negligent in puncturing the diaphragm. It may have been carelessness, for example, in the way the procedure was performed, or in the decision to proceed despite the difficulties encountered. It is also possible that the gynecologist was not appropriately trained and experienced in the surgery that was undertaken, in which case the decision to do the surgery (rather than to refer to another physician) could well have been negligent. In either of those cases, negligence liability (malpractice) is a possibility.
Proving negligence. It is the plaintiff (the patient) who must prove the elements of negligence (including causation).8 The plaintiff will have to demonstrate not only carelessness, but that carelessness is what caused the injuries for which she is seeking compensation. In this case, the injuries are the consequence of puncturing the diaphragm. The potential damages would be the money to cover the additional medical costs and other expenses, lost wages, and noneconomic damages such as pain and suffering.
The hospital’s role in negligence
The issue of informed consent is also raised in this case, with a handwritten note prior to surgery (but the focus of this article is on medical errors). In addition to the gynecologist, the hospital and other medical personnelwere sued. The hospital is responsible for the acts of its agents, notably its employees. Even if the physicians are not technically hospital employees, the hospital may in some cases be responsible. Among other things, the hospital likely has an obligation to prevent physicians from undertaking inappropriate procedures, including those for which the physician is not appropriately trained. If the gynecologist in this case did not have privileges to perform surgery in this category, the hospital may have an obligation to not schedule the surgery or to intraoperatively question her credentials for such a procedure. In any event, the hospital will have a major role in this case and its interests may, in some instances, be inconsistent with the interests of the physician.
Why settlement discussions?
The case description ends with a note that settlement discussions were underway. If the plaintiff must prove all of the elements of negligence, why have these discussions? First, such discussions are common in almost all negligence cases. This does not mean that the case actually will be settled by the insurance company representing the physician or hospital; many malpractice cases simply fade away because the patient drops the action. Second, there are ambiguities in the facts, and it is sometimes impossible to determine whether or not a jury would find negligence. The hospital may be inclined to settle if there is any realistic chance of a jury ruling against it. Paying a small settlement may be worth avoiding high legal expenses and the risk of an adverse outcome at trial.9
Reducing medical/surgical error through a team approach
Recognizing that “human performance can be affected by many factors that include circadian rhythms, state of mind, physical health, attitude, emotions, propensity for certain common mistakes and errors, and cognitive biases,”10 health care professionals have a commitment to reduce the errors in the interest of patient safety and best practice.
The surgical environment is an opportunity to provide a team approach to patient safety. Surgical risk is a reflection of operative performance, the main factor in the development of postoperative complications.11 We wish to broaden the perspective that gynecologic surgeons, like all surgeons, must keep in mind a number of concerns that can be associated with problems related to surgical procedures, including12:
- visual perception difficulties
- stress
- loss of haptic perception (feedback using touch), as with robot-assisted procedures
- lack of situational awareness (a term we borrow from the aviation industry)
- long-term (and short-term) memory problems.
Analysis of surgical errors shows that they are related to, in order of frequency 1:
- surgical technique
- judgment
- inattention to detail
- incomplete understanding of the problem or surgical situation.
Medical errors: Caring for the second victim (you)
Patrice M. Weiss, MD
We use the term “victim” to refer to the patient and her family following a medical error. The phrase “the second victim” was coined by Dr. Albert Wu in an article in the British Medical Journal1 and describes how a clinician and team of health care professionals also can be affected by medical errors.
What signs and symptoms identify a second victim?Those suffering as a second victim may show signs of depression, loss of joy in work, and difficulty sleeping. They also may replay the events, question their own ability, and feel fearful about making another error. These reactions can lead to burnout—a serious issue that 46% of physicians report.2
As colleagues of those involved in a medical error, we should be cognizant of changes in behavior such as excessive irritability, showing up late for work, or agitation. It may be easier to recognize these symptoms in others rather than in ourselves because we often do not take time to examine how our experiences may affect us personally. Heightening awareness can help us recognize those suffering as second victims and identify the second victim symptoms in ourselves.
How can we help second victims?One challenge second victims face is not being allowed to discuss a medical error. Certainly, due to confidentiality requirements during professional liability cases, we should not talk freely about the event. However, silence creates a barrier that prevents a second victim from processing the incident.
Some hospitals offer forums to discuss medical errors, with the goal of preventing reoccurrence: morbidity and mortality conferences, morning report, Quality Assurance and Performance Improvement meetings, and root cause analyses. These forums often are not perceived by institutions’ employees in a positive way. Are they really meant to improve patient care or do they single out an individual or group in a “name/blame/shame game”? An intimidating process will only worsen a second victim’s symptoms. It is not necessary, however, to create a whole new process; it is possible to restructure, reframe, and change the culture of an existing practice.
Some institutions have developed a formalized program to help second victims. The University of Missouri has a “forYOU team,” an internal, rapid response group that provides emotional first aid to the entire team involved in a medical error case. These responders are not from human resources and do not need to be sought out; they are peers who have been educated about the struggles of the second victim. They will not discuss the case or how care was rendered; they naturally and instinctively provide emotional support to their colleagues.
At my institution, the Carilion Clinic at the Virginia Tech Carilion School of Medicine, “The Trust Program” encourages truth, respectfulness, understanding, support, and transparency. All health care clinicians receive basic training, but many have volunteered for additional instruction to become mentors because they have experienced second-victim symptoms themselves.
Clinicians want assistance when dealing with a medical error. One poll reports that 90% of physicians felt that health care organizations did not adequately help them cope with the stresses associated with a medical error.3 The goal is to have all institutions recognize that clinicians can be affected by a medical error and offer support.
To hear an expanded audiocast from Dr. Weiss on “the second victim” click here.
Dr. Weiss is Professor, Department of Obstetrics & Gynecology, Virginia Tech Carilion School of Medicine, and Chief Medical Officer and Executive Vice President, Carilion Clinic, Roanoke, Virginia.
The author reports no financial relationships relevant to this article.
References
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726–727.
- Peckham C. Medscape Physician Lifestyle Report 2015. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2015/public/overview#1. Published January 26, 2015. Accessed May 24, 2016.
- White AA, Waterman AD, McCotter P, Boyle DJ, Gallagher TH. Supporting health care workers after medical error: considerations for health care leaders. JCOM. 2008;15(5):240–247.
“Inadequacy” with regard to surgical proceduresIndication for surgery is intrinsic to provision of appropriate care. Surgery inherently poses the possibility of unexpected problems. Adequate training and skill, therefore, must include the ability to deal with a range of problems that arise in the course of surgery. The spectrum related to inadequacy as related to surgical problems includes “failed surgery,” defined as “if despite the utmost care of everyone involved and with the responsible consideration of all knowledge, the designed aim is not achieved, surgery by itself has failed.”5 Of paramount importance is the surgeon’s knowledge of technology and the ability to troubleshoot, as well as the OR team’s responsibility for proper maintenance of equipment to ensure optimal functionality.1
Aviation industry studies indicate that “high performing cockpit crews have been shown to devote one third of their communications to discuss threats and mistakes in their environment, while poor performing teams devoted much less, about 5%, of their time to such.”1,13 A well-trained and well-motivated OR nursing team has been equated with reduction in operative time and rate of conversion to laparotomy.14 Outdated instruments may also contribute to surgical errors.1
Moving the “learning curve” out of the OR and into the simulation lab remains valuable, which is also confirmed by the aviation industry.15 The significance of loss of haptic perception continues to be debated between laparoscopic (straight-stick) surgeons and those performing robotic approaches. Does haptic perception play a major role in surgical intervention? Most surgeons do not view loss of haptic perception, as with minimally invasive procedures, as a major impediment to successful surgery. From the legal perspective, loss of haptic perception has not been well addressed.
The American College of Obstetricians and Gynecologists has focused on patient safety in the surgical environment including concerns for wrong-patient surgery, wrong-side surgery, wrong-level surgery, and wrong-part surgery.16 The Joint Commission has identified factors that may enhance the risk of wrong-site surgery: multiple surgeons involved in the case, multiple procedures during a single surgical visit, unusual time pressures to start or complete the surgery, and unusual physical characteristics including morbid obesity or physical deformity.16
10 starting points for medical error preventionSo what are we to do? Consider:
- Using a preprocedure verification checklist.
- Marking the operative site.
- Completing a time out process prior to starting the procedure, according to the Joint Commission protocol. [For more information on Joint Commission-recommended time out protocols and ways to prevent medical errors, click here.]
- Involving the patient in the identification and procedure definition process. (This is an important part of informed consent.)
- Providing appropriate proctoring and sign-off for new procedures and technology.
- Avoiding sleep deprivation situations, especially with regard to emergency procedures.
- Using only radiopaque-labeled materials placed into the operating cavity.
- Considering medication effect on a fetus, if applicable.
- Reducing distractions from pagers, telephone calls, etc.
- Maintaining a “sterile cockpit” (or distraction free) environment for everyone in the OR.
Set the stage for best outcomesA true team approach is an excellent modus operandi before, during, and after surgery,setting the stage for best outcomes for patients.
“As human beings, surgeons will commit errors and for this reason they have to adopt and utilize stringent defense systems to minimize the incidence of these adverse events … Transparency is the first step on the way to a new safety culture with the acknowledgement of errors when they occur with adoption of systems destined to establish their cause and future prevention.”1
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Galleano R, Franceschi A, Ciciliot M, Falchero F, Cuschieri A. Errors in laparoscopic surgery: what surgeons should know. Mineva Chir. 2011;66(2):107−117.
- Fabri P, Zyas-Castro J. Human error, not communication and systems, underlies surgical complications. Surgery. 2008;144(4):557−565.
- Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124(1):25−34.
- Makary MA, Daniel M. Medical error−the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139. Balogun J, Bramall A, Berstein M. How surgical trainees handle catastrophic errors: a qualitative study. J Surg Educ. 2015;72(6):1179−1184.
- Grober E, Bohnen J. Defining medical error. Can J Surg. 2005;48(1):39−44.
- Anderson RE, ed. Medical Malpractice: A Physician's Sourcebook. Totowa, NJ: Humana Press, Inc; 2004.
- Mehlman MJ. Professional power and the standard of care in medicine. 44 Arizona State Law J. 2012;44:1165−1777. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2205485. Revised February 13, 2013.
- Hyman DA, Silver C. On the table: an examination of medical malpractice, litigation, and methods of reform: healthcare quality, patient safety, and the culture of medicine: "Denial Ain't Just a River in Egypt." New Eng Law Rev. 2012;46:417−931.
- Landers R. Reducing surgical errors: implementing a three-hinge approach to success. AORN J. 2015;101(6):657−665.
- Pettigrew R, Burns H, Carter D. Evaluating surgical risk: the importance of technical factors in determining outcome. Br J Surg. 1987;74(9):791−794.
- Parker W. Understanding errors during laparoscopic surgery. Obstet Gynecol Clin North Am. 2010;37(3):437−449.
- Sexton JB, Helmreich RL. Analyzing cockpit communications: the links between language, performance, error, and workload. Hum Perf Extrem Environ. 2000;5(1):63−68.
- Kenyon T, Lenker M, Bax R, Swanstrom L. Cost and benefit of the trained laparoscopic team: a comparative study of a designated nursing team vs. a non-trained team. Surg Endosc. 1997;11(8):812−814.
- Woodman R. Surgeons should train like pilots. BMJ. 1999;319:1321.
- American College of Obstetrics and Gynecology. ACOG Committee Opinion No. 464: Patient safety in the surgical environment. Obstet Gynecol. 2010;116(3):786−790.
- Galleano R, Franceschi A, Ciciliot M, Falchero F, Cuschieri A. Errors in laparoscopic surgery: what surgeons should know. Mineva Chir. 2011;66(2):107−117.
- Fabri P, Zyas-Castro J. Human error, not communication and systems, underlies surgical complications. Surgery. 2008;144(4):557−565.
- Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124(1):25−34.
- Makary MA, Daniel M. Medical error−the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139. Balogun J, Bramall A, Berstein M. How surgical trainees handle catastrophic errors: a qualitative study. J Surg Educ. 2015;72(6):1179−1184.
- Grober E, Bohnen J. Defining medical error. Can J Surg. 2005;48(1):39−44.
- Anderson RE, ed. Medical Malpractice: A Physician's Sourcebook. Totowa, NJ: Humana Press, Inc; 2004.
- Mehlman MJ. Professional power and the standard of care in medicine. 44 Arizona State Law J. 2012;44:1165−1777. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2205485. Revised February 13, 2013.
- Hyman DA, Silver C. On the table: an examination of medical malpractice, litigation, and methods of reform: healthcare quality, patient safety, and the culture of medicine: "Denial Ain't Just a River in Egypt." New Eng Law Rev. 2012;46:417−931.
- Landers R. Reducing surgical errors: implementing a three-hinge approach to success. AORN J. 2015;101(6):657−665.
- Pettigrew R, Burns H, Carter D. Evaluating surgical risk: the importance of technical factors in determining outcome. Br J Surg. 1987;74(9):791−794.
- Parker W. Understanding errors during laparoscopic surgery. Obstet Gynecol Clin North Am. 2010;37(3):437−449.
- Sexton JB, Helmreich RL. Analyzing cockpit communications: the links between language, performance, error, and workload. Hum Perf Extrem Environ. 2000;5(1):63−68.
- Kenyon T, Lenker M, Bax R, Swanstrom L. Cost and benefit of the trained laparoscopic team: a comparative study of a designated nursing team vs. a non-trained team. Surg Endosc. 1997;11(8):812−814.
- Woodman R. Surgeons should train like pilots. BMJ. 1999;319:1321.
- American College of Obstetrics and Gynecology. ACOG Committee Opinion No. 464: Patient safety in the surgical environment. Obstet Gynecol. 2010;116(3):786−790.
In this Article
- Medical error vs negligence
- Caring for the second victim
- 10 starting points for reducing medical errors

VIDEO: Daily fecal transplants put refractory ulcerative colitis into remission
SAN DIEGO – When fecal transplants don’t work for ulcerative colitis, it’s probably because they aren’t used often enough, according to investigators from the University of New South Wales, Sydney.
The researchers made sure that wasn’t the case in their own double-blind trial, the largest to date of fecal microbiota transplantation (FMT) for ulcerative colitis. Forty-one patients with active, mild to moderate disease (Mayo score 4-10) that was resistant to standard medications were randomized to 150-mL, self-administered fecal enemas 5 days a week for 8 weeks, and 40 others to placebo enemas. Patients were tapered off steroids at study entrance, and each FMT patient received stool from 3-7 unrelated donors.
Steroid-free clinical remission and endoscopic remission or response were achieved in 11 FMT patients (27%), compared with 3 (8%) placebo patients (P = .02). A total of 18 treated patients (44%) and 8 placebo patients (20%) had steroid-free clinical remissions, while 22 treated patients (54%) and 9 patients in the placebo group (23%) had some type of positive clinical response (P less than .01).
Patients were in their mid-30s, on average, with disease durations of about 6 years. More than half were men. About one-quarter were on oral steroids, and more than half were on oral 5-aminosalicylic acid medications, which were allowed during the study. Almost half were on methotrexate or other oral immunomodulators, which were also allowed. Patients were excluded if they had been on a biologic in the previous 12 weeks.
Afterward, 37 patients in the placebo arm opted for open-label FMT. Results were similar, with steroid-free clinical remission and endoscopic remission or response in 10 patients (27%), clinical remission in 17 (46%), and endoscopic remission in 9 (24%).
The anatomical extent of disease did not affect outcome, but patients with more severe endoscopic disease and those on steroids at study entrance didn’t do as well. Three patients flared during the trial, one in the placebo arm and two in the FMT arm, one of whom required colectomy.
The investigators were surprised by the magnitude of the benefit, given the mixed results in previous investigations with less frequent dosing. But they were not surprised that FMT worked.
“In ulcerative colitis, the microbiota appear to be the antigenic driver, so it makes sense that correcting the disturbance” helps, said lead investigator Dr. Sudarshan Paramsothy, a gastroenterologist at the University of New South Wales.
Dr. Paramsothy and his colleagues have a hunch they can do even better. They are looking into the microbiologic factors of donors and patients that influence response, with the ultimate goal of matching the best donor to the best patient. They’re examining maintenance therapy, too; “it’s one thing to induce remission, it’s another thing to maintain remission,” Dr. Paramsothy said.
In an interview at the annual Digestive Disease Week, he explained the technique, the thinking behind it, future directions, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – When fecal transplants don’t work for ulcerative colitis, it’s probably because they aren’t used often enough, according to investigators from the University of New South Wales, Sydney.
The researchers made sure that wasn’t the case in their own double-blind trial, the largest to date of fecal microbiota transplantation (FMT) for ulcerative colitis. Forty-one patients with active, mild to moderate disease (Mayo score 4-10) that was resistant to standard medications were randomized to 150-mL, self-administered fecal enemas 5 days a week for 8 weeks, and 40 others to placebo enemas. Patients were tapered off steroids at study entrance, and each FMT patient received stool from 3-7 unrelated donors.
Steroid-free clinical remission and endoscopic remission or response were achieved in 11 FMT patients (27%), compared with 3 (8%) placebo patients (P = .02). A total of 18 treated patients (44%) and 8 placebo patients (20%) had steroid-free clinical remissions, while 22 treated patients (54%) and 9 patients in the placebo group (23%) had some type of positive clinical response (P less than .01).
Patients were in their mid-30s, on average, with disease durations of about 6 years. More than half were men. About one-quarter were on oral steroids, and more than half were on oral 5-aminosalicylic acid medications, which were allowed during the study. Almost half were on methotrexate or other oral immunomodulators, which were also allowed. Patients were excluded if they had been on a biologic in the previous 12 weeks.
Afterward, 37 patients in the placebo arm opted for open-label FMT. Results were similar, with steroid-free clinical remission and endoscopic remission or response in 10 patients (27%), clinical remission in 17 (46%), and endoscopic remission in 9 (24%).
The anatomical extent of disease did not affect outcome, but patients with more severe endoscopic disease and those on steroids at study entrance didn’t do as well. Three patients flared during the trial, one in the placebo arm and two in the FMT arm, one of whom required colectomy.
The investigators were surprised by the magnitude of the benefit, given the mixed results in previous investigations with less frequent dosing. But they were not surprised that FMT worked.
“In ulcerative colitis, the microbiota appear to be the antigenic driver, so it makes sense that correcting the disturbance” helps, said lead investigator Dr. Sudarshan Paramsothy, a gastroenterologist at the University of New South Wales.
Dr. Paramsothy and his colleagues have a hunch they can do even better. They are looking into the microbiologic factors of donors and patients that influence response, with the ultimate goal of matching the best donor to the best patient. They’re examining maintenance therapy, too; “it’s one thing to induce remission, it’s another thing to maintain remission,” Dr. Paramsothy said.
In an interview at the annual Digestive Disease Week, he explained the technique, the thinking behind it, future directions, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – When fecal transplants don’t work for ulcerative colitis, it’s probably because they aren’t used often enough, according to investigators from the University of New South Wales, Sydney.
The researchers made sure that wasn’t the case in their own double-blind trial, the largest to date of fecal microbiota transplantation (FMT) for ulcerative colitis. Forty-one patients with active, mild to moderate disease (Mayo score 4-10) that was resistant to standard medications were randomized to 150-mL, self-administered fecal enemas 5 days a week for 8 weeks, and 40 others to placebo enemas. Patients were tapered off steroids at study entrance, and each FMT patient received stool from 3-7 unrelated donors.
Steroid-free clinical remission and endoscopic remission or response were achieved in 11 FMT patients (27%), compared with 3 (8%) placebo patients (P = .02). A total of 18 treated patients (44%) and 8 placebo patients (20%) had steroid-free clinical remissions, while 22 treated patients (54%) and 9 patients in the placebo group (23%) had some type of positive clinical response (P less than .01).
Patients were in their mid-30s, on average, with disease durations of about 6 years. More than half were men. About one-quarter were on oral steroids, and more than half were on oral 5-aminosalicylic acid medications, which were allowed during the study. Almost half were on methotrexate or other oral immunomodulators, which were also allowed. Patients were excluded if they had been on a biologic in the previous 12 weeks.
Afterward, 37 patients in the placebo arm opted for open-label FMT. Results were similar, with steroid-free clinical remission and endoscopic remission or response in 10 patients (27%), clinical remission in 17 (46%), and endoscopic remission in 9 (24%).
The anatomical extent of disease did not affect outcome, but patients with more severe endoscopic disease and those on steroids at study entrance didn’t do as well. Three patients flared during the trial, one in the placebo arm and two in the FMT arm, one of whom required colectomy.
The investigators were surprised by the magnitude of the benefit, given the mixed results in previous investigations with less frequent dosing. But they were not surprised that FMT worked.
“In ulcerative colitis, the microbiota appear to be the antigenic driver, so it makes sense that correcting the disturbance” helps, said lead investigator Dr. Sudarshan Paramsothy, a gastroenterologist at the University of New South Wales.
Dr. Paramsothy and his colleagues have a hunch they can do even better. They are looking into the microbiologic factors of donors and patients that influence response, with the ultimate goal of matching the best donor to the best patient. They’re examining maintenance therapy, too; “it’s one thing to induce remission, it’s another thing to maintain remission,” Dr. Paramsothy said.
In an interview at the annual Digestive Disease Week, he explained the technique, the thinking behind it, future directions, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT DDW 2016
