User login
He Huffed and He Puffed and He Got Frostbite
Case
A 27-year-old man presented to an ED after experiencing a syncopal episode. His vital signs at presentation were normal. Physical examination was generally normal except that there were blisters on the patient’s abdomen, left hand, and right arm, as well as a hypertrophic nodule on the right elbow (Figure) and hard growths on the digits of the right hand. The patient stated the growths started 5 months ago and had been increasing in size. On further questioning, the patient admitted to “huffing” (ie, inhaling) at least six cans of pressurized dust-removal keyboard cleaning spray daily for the past 11 months.

Why do patients abuse keyboard cleaning spray?
The propellant used in certain liquefied compressed gas products is 1,1-difluoroethane (1,1-DFE), a fluorinated hydrocarbon. It is a member of a broad class of related compounds that are present in spray paints, glues, nail polish removers, fuels, hair sprays, and air-freshening products. These 1,1-DFE-containing products are abused for their rapid and short-acting central nervous system (CNS) depressant effects—not unlike that of ethanol. Typically, the vapor of a volatile hydrocarbon is inhaled directly from the open container (“sniffing”), from a bag (“bagging”), or from a soaked rag (huffing). Not only are such hydrocarbon-containing products easy to conceal, they are also highly accessible and inexpensive. Moreover, there are generally no direct legal consequences resulting from abuse of these substances.
All of the aforementioned factors make hydrocarbons a popular drug of abuse among adolescents. Approximately 75% of the population abusing hydrocarbons is younger than age 18 years, half of whom reported first use prior to age 13 years.1,2 Though inhalant abuse rarely continues into adulthood, 0.1% of individuals between the ages of 18 and 30 years report having an inhalant-use disorder.
Hydrocarbons and their halogenated derivatives are lipophilic compounds that are rapidly absorbed after inhalation and rapidly distributed to CNS and cardiac tissue. The brain concentration of 1,1-DFE likely peaks higher than concentrations in other organs and is cleared more rapidly.3 Hydrocarbons produce CNS depression secondary to multiple mechanisms, including gamma-aminobutyric acid agonism, dopamine modulation, and N-methyl-D-aspartate-receptor antagonism.4,5
What causes skin lesions on the abdomen and arms?
The lesions on the patient’s abdomen and extremities were consistent with frostbite. The liquefied compressed gas in computer-cleaning and related products is housed in a pressurized canister. The pressure is released when the spray nozzle is depressed; this causes the liquid to rapidly expand to a gas as it is released, resulting in a quick decrease in the temperature of the metal canister. This process, referred to as adiabatic cooling, demonstrates the first law of thermodynamics. The cold temperature of both the liquid and the canister can cause frostbite in the digits and other parts of the body with which the canister or liquid comes into contact.6
Why did the patient have syncope?
Halogenated hydrocarbons inhibit the cardiac delayed rectifier potassium channels involved in the repolarization of cardiac myocytes, causing a delay in repolarization that is manifested as prolongation of the QT interval on an electrocardiogram. This condition places patients at an increased risk of developing torsades de pointes (TdP).7 In most cases, TdP is self-terminating; however, if TdP persists, degeneration to ventricular fibrillation will result. Deaths caused in this fashion have been referred to as “sudden sniffing death syndrome,” and account for half of all hydrocarbon-related deaths.6,8 In addition to the cardiac effects, hydrocarbons are simple asphyxiants that act by displacing oxygen from inspired air, which also contributes to syncope.
It is important to note that epinephrine and other catecholamines increase the risk for dysrhythmias such as TdP in the setting of hydrocarbon abuse.9 For this reason, epinephrine should be used with caution in the setting of a hydrocarbon-induced arrhythmia. Beta-adrenergic antagonists such as esmolol and propranolol are preferable because they reduce the incidence of ectopia that may trigger TdP.10
What is the significance of the masses noted on the examination and radiograph?
Fluorosis is associated with abnormalities of skeletal and dental tissue. Skeletal fluorosis causes osteosclerosis of the axial skeleton, periosteal new bone formation, ligamentous and tendinous ossification, and osteophyte formation. Dental fluorosis causes a yellow/brown discoloration of the teeth with horizontal streaking (mottling), pitting, and chipping.11 Fluorosis is well-described in regions where water fluoride concentrations are high due to industrial exposure; from consumption of fluorinated wine or chronic overconsumption of tea (especially green or black tea); or from fluoridated toothpaste.12-14 More recently, fluorosis has been described in patients treated for an extended duration of time with voriconazole, a fluorinated antifungal agent.15 Unlike other hydrocarbon products, fluorinated hydrocarbons such as 1,1-DFE can significantly increase systemic fluoride concentrations with excessive use. Rapid skeletal fluorosis is not well described, but has been reported after chronic abuse of fluorinated hydrocarbons.16
How is fluorosis diagnosed and managed?
The lack of rapid laboratory testing available for serum, urine, and bone fluoride concentrations makes the initial diagnosis of fluorosis a clinical one. Imaging studies are generally highly suggestive of fluorosis and can be used to support the diagnosis. A dual energy X-ray absorptiometry scan of the spine, hip, femur, and distal portions of the radii can reveal elevated T-scores consistent with osteosclerosis.14 These findings, in conjunction with bone or joint pain, reduced range of motion, or kyphosis, should prompt clinicians to conduct further testing—even without a confirmed fluoride source. A serum fluoride (reference range, 0.2-3.2 mg/L) and 24-hour urine fluoride (reference range, 0.2-3.2 mg/dL) and creatinine evaluation can be used to diagnose fluorosis. However, a bone biopsy with quantitative bone ash fluoride analysis remains the gold standard for the diagnosis of skeletal fluorosis.16 Laboratory evaluation should also include an assessment of electrolytes, specifically calcium, 25-hydroxyvitamin D, and alkaline phosphatase. The differential diagnosis should include hemoglobinopathies, renal osteodystrophy, Paget disease, hypothyroidism, and skeletal metastases.16
Treatment of fluorosis is largely symptomatic and supportive, with identification and discontinuation of the fluoride source. Patients should be referred to an orthopedist for evaluation and management as needed. Evaluation by an endocrinologist should also be considered because patients may have chronic vitamin D and calcium deficiencies as a result of systemic fluorosis.
Case Conclusion
The patient’s laboratory assessment was notable for the following: alkaline phosphatase, 624 U/L (reference range, 44-147 IU/L); vitamin D, 10 ng/mL (reference range, 20-40 ng/mL); serum fluoride, 0.3 mg/L (reference range, 0.2-3.2 mg/L); urine fluoride, 52 mg/dL (0.2-3.2 mg/dL); and urine creatinine, 1 g/L (reference range, 0.3-3 g/L). Imaging studies noted periosteal bone formation on the lateral epicondyle of the distal right humerus, as well as similar osseous abnormalities in other locations. A bone biopsy was scheduled. The patient was treated with oral vitamin D and educated about the importance of discontinuing the huffing of all hydrocarbons.
1. Williams JF, Storck M; American Academy of Pediatrics Committee on Substance Abuse; American Academy of Pediatrics Committee on Native American Child Health. Inhalant abuse. Pediatrics. 2007;119(5):1009-1017.
2. Wu LT, Pilowsky DJ, Schlenger WE. Inhalant abuse and dependence among adolescents in the United States. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1206-1214.
3. Avella J, Kunaparaju N, Kumar S, Lehrer M, Zito SW, Barletta M. Uptake and distribution of the abused inhalant 1,1-difluoroethane in the rat. J Anal Toxicol. 2010;34(7):381-388.
4. Tormoehlen LM, Tekulve KJ, Nañagas KA. Hydrocarbon toxicity: A review. Clin Toxicol (Phila). 2014;52(5):479-489.
5. Duncan JR, Lawrence AJ. Conventional concepts and new perspectives for understanding the addictive properties of inhalants. J Pharmacol Sci. 2013;122(4):237-243.
6. Sakai K, Maruyama-Maebashi K, Takatsu A, et al. Sudden death involving inhalation of 1,1-difluoroethane (HFC-152a) with spray cleaner: three case reports. Forensic Sci Int. 2011;206(1-3):e58-e61.
7. Himmel HM. Mechanisms involved in cardiac sensitization by volatile anesthetics: general applicability to halogenated hydrocarbons? Crit Rev Toxicol. 2008;38(9):773-803.
8. Avella J, Wilson JC, Lehrer M. Fatal cardiac arrhythmia after repeated exposure to 1,1-difluoroethane (DFE). Am J Forensic Med Pathol. 2006;27(1):58-60.
9. Nelson LS. Toxicologic myocardial sensitization. J Toxicol Clin Toxicol. 2002;40(7):867-879.
10. Mortiz F, de La Chapelle A, Bauer F, Leroy JP, Goullé JP, Bonmarchand G. Esmolol in the treatment of severe arrhythmia after acute trichloroethylene poisoning. Intensive Care Med. 2000;26(2):256.
11. Majumdar KK. Health impact of supplying safe drinking water containing fluoride below permissible level on flourosis patients in a fluoride-endemic rural area of West Bengal. Indian J Public Health. 2011;55(4):303-308.
12. Kakumanu N, Rao SD. Images in clinical medicine. Skeletal fluorosis due to excessive tea drinking. N Engl J Med 2013;368(12):1140.
13. Soriano M, Manchón F. Radiological aspects of a new type of bone fluorosis, periostitis deformans. Radiology 1966;87(6):1089-1094.
14. Tamer MN, Kale Köroğlu B, Arslan C, et al. Osteosclerosis due to endemic fluorosis. Sci Total Environ. 2007;373(1):43-48.
15. Bucknor MD, Gross AJ, Link TM. Voriconazole-induced periostitis in two post-transplant patients. J Radiol Case Rep. 2013;7(8):10-17.
16. Cohen E, Hsu RY, Evangelista P, Aaron R, Rubin LE. Rapid-onset diffuse skeletal fluorosis from inhalant abuse: a case report. JBJS Case Connector. 2014;4(4):e108.
Case
A 27-year-old man presented to an ED after experiencing a syncopal episode. His vital signs at presentation were normal. Physical examination was generally normal except that there were blisters on the patient’s abdomen, left hand, and right arm, as well as a hypertrophic nodule on the right elbow (Figure) and hard growths on the digits of the right hand. The patient stated the growths started 5 months ago and had been increasing in size. On further questioning, the patient admitted to “huffing” (ie, inhaling) at least six cans of pressurized dust-removal keyboard cleaning spray daily for the past 11 months.
Why do patients abuse keyboard cleaning spray?
The propellant used in certain liquefied compressed gas products is 1,1-difluoroethane (1,1-DFE), a fluorinated hydrocarbon. It is a member of a broad class of related compounds that are present in spray paints, glues, nail polish removers, fuels, hair sprays, and air-freshening products. These 1,1-DFE-containing products are abused for their rapid and short-acting central nervous system (CNS) depressant effects—not unlike that of ethanol. Typically, the vapor of a volatile hydrocarbon is inhaled directly from the open container (“sniffing”), from a bag (“bagging”), or from a soaked rag (huffing). Not only are such hydrocarbon-containing products easy to conceal, they are also highly accessible and inexpensive. Moreover, there are generally no direct legal consequences resulting from abuse of these substances.
All of the aforementioned factors make hydrocarbons a popular drug of abuse among adolescents. Approximately 75% of the population abusing hydrocarbons is younger than age 18 years, half of whom reported first use prior to age 13 years.1,2 Though inhalant abuse rarely continues into adulthood, 0.1% of individuals between the ages of 18 and 30 years report having an inhalant-use disorder.
Hydrocarbons and their halogenated derivatives are lipophilic compounds that are rapidly absorbed after inhalation and rapidly distributed to CNS and cardiac tissue. The brain concentration of 1,1-DFE likely peaks higher than concentrations in other organs and is cleared more rapidly.3 Hydrocarbons produce CNS depression secondary to multiple mechanisms, including gamma-aminobutyric acid agonism, dopamine modulation, and N-methyl-D-aspartate-receptor antagonism.4,5
What causes skin lesions on the abdomen and arms?
The lesions on the patient’s abdomen and extremities were consistent with frostbite. The liquefied compressed gas in computer-cleaning and related products is housed in a pressurized canister. The pressure is released when the spray nozzle is depressed; this causes the liquid to rapidly expand to a gas as it is released, resulting in a quick decrease in the temperature of the metal canister. This process, referred to as adiabatic cooling, demonstrates the first law of thermodynamics. The cold temperature of both the liquid and the canister can cause frostbite in the digits and other parts of the body with which the canister or liquid comes into contact.6
Why did the patient have syncope?
Halogenated hydrocarbons inhibit the cardiac delayed rectifier potassium channels involved in the repolarization of cardiac myocytes, causing a delay in repolarization that is manifested as prolongation of the QT interval on an electrocardiogram. This condition places patients at an increased risk of developing torsades de pointes (TdP).7 In most cases, TdP is self-terminating; however, if TdP persists, degeneration to ventricular fibrillation will result. Deaths caused in this fashion have been referred to as “sudden sniffing death syndrome,” and account for half of all hydrocarbon-related deaths.6,8 In addition to the cardiac effects, hydrocarbons are simple asphyxiants that act by displacing oxygen from inspired air, which also contributes to syncope.
It is important to note that epinephrine and other catecholamines increase the risk for dysrhythmias such as TdP in the setting of hydrocarbon abuse.9 For this reason, epinephrine should be used with caution in the setting of a hydrocarbon-induced arrhythmia. Beta-adrenergic antagonists such as esmolol and propranolol are preferable because they reduce the incidence of ectopia that may trigger TdP.10
What is the significance of the masses noted on the examination and radiograph?
Fluorosis is associated with abnormalities of skeletal and dental tissue. Skeletal fluorosis causes osteosclerosis of the axial skeleton, periosteal new bone formation, ligamentous and tendinous ossification, and osteophyte formation. Dental fluorosis causes a yellow/brown discoloration of the teeth with horizontal streaking (mottling), pitting, and chipping.11 Fluorosis is well-described in regions where water fluoride concentrations are high due to industrial exposure; from consumption of fluorinated wine or chronic overconsumption of tea (especially green or black tea); or from fluoridated toothpaste.12-14 More recently, fluorosis has been described in patients treated for an extended duration of time with voriconazole, a fluorinated antifungal agent.15 Unlike other hydrocarbon products, fluorinated hydrocarbons such as 1,1-DFE can significantly increase systemic fluoride concentrations with excessive use. Rapid skeletal fluorosis is not well described, but has been reported after chronic abuse of fluorinated hydrocarbons.16
How is fluorosis diagnosed and managed?
The lack of rapid laboratory testing available for serum, urine, and bone fluoride concentrations makes the initial diagnosis of fluorosis a clinical one. Imaging studies are generally highly suggestive of fluorosis and can be used to support the diagnosis. A dual energy X-ray absorptiometry scan of the spine, hip, femur, and distal portions of the radii can reveal elevated T-scores consistent with osteosclerosis.14 These findings, in conjunction with bone or joint pain, reduced range of motion, or kyphosis, should prompt clinicians to conduct further testing—even without a confirmed fluoride source. A serum fluoride (reference range, 0.2-3.2 mg/L) and 24-hour urine fluoride (reference range, 0.2-3.2 mg/dL) and creatinine evaluation can be used to diagnose fluorosis. However, a bone biopsy with quantitative bone ash fluoride analysis remains the gold standard for the diagnosis of skeletal fluorosis.16 Laboratory evaluation should also include an assessment of electrolytes, specifically calcium, 25-hydroxyvitamin D, and alkaline phosphatase. The differential diagnosis should include hemoglobinopathies, renal osteodystrophy, Paget disease, hypothyroidism, and skeletal metastases.16
Treatment of fluorosis is largely symptomatic and supportive, with identification and discontinuation of the fluoride source. Patients should be referred to an orthopedist for evaluation and management as needed. Evaluation by an endocrinologist should also be considered because patients may have chronic vitamin D and calcium deficiencies as a result of systemic fluorosis.
Case Conclusion
The patient’s laboratory assessment was notable for the following: alkaline phosphatase, 624 U/L (reference range, 44-147 IU/L); vitamin D, 10 ng/mL (reference range, 20-40 ng/mL); serum fluoride, 0.3 mg/L (reference range, 0.2-3.2 mg/L); urine fluoride, 52 mg/dL (0.2-3.2 mg/dL); and urine creatinine, 1 g/L (reference range, 0.3-3 g/L). Imaging studies noted periosteal bone formation on the lateral epicondyle of the distal right humerus, as well as similar osseous abnormalities in other locations. A bone biopsy was scheduled. The patient was treated with oral vitamin D and educated about the importance of discontinuing the huffing of all hydrocarbons.
Case
A 27-year-old man presented to an ED after experiencing a syncopal episode. His vital signs at presentation were normal. Physical examination was generally normal except that there were blisters on the patient’s abdomen, left hand, and right arm, as well as a hypertrophic nodule on the right elbow (Figure) and hard growths on the digits of the right hand. The patient stated the growths started 5 months ago and had been increasing in size. On further questioning, the patient admitted to “huffing” (ie, inhaling) at least six cans of pressurized dust-removal keyboard cleaning spray daily for the past 11 months.
Why do patients abuse keyboard cleaning spray?
The propellant used in certain liquefied compressed gas products is 1,1-difluoroethane (1,1-DFE), a fluorinated hydrocarbon. It is a member of a broad class of related compounds that are present in spray paints, glues, nail polish removers, fuels, hair sprays, and air-freshening products. These 1,1-DFE-containing products are abused for their rapid and short-acting central nervous system (CNS) depressant effects—not unlike that of ethanol. Typically, the vapor of a volatile hydrocarbon is inhaled directly from the open container (“sniffing”), from a bag (“bagging”), or from a soaked rag (huffing). Not only are such hydrocarbon-containing products easy to conceal, they are also highly accessible and inexpensive. Moreover, there are generally no direct legal consequences resulting from abuse of these substances.
All of the aforementioned factors make hydrocarbons a popular drug of abuse among adolescents. Approximately 75% of the population abusing hydrocarbons is younger than age 18 years, half of whom reported first use prior to age 13 years.1,2 Though inhalant abuse rarely continues into adulthood, 0.1% of individuals between the ages of 18 and 30 years report having an inhalant-use disorder.
Hydrocarbons and their halogenated derivatives are lipophilic compounds that are rapidly absorbed after inhalation and rapidly distributed to CNS and cardiac tissue. The brain concentration of 1,1-DFE likely peaks higher than concentrations in other organs and is cleared more rapidly.3 Hydrocarbons produce CNS depression secondary to multiple mechanisms, including gamma-aminobutyric acid agonism, dopamine modulation, and N-methyl-D-aspartate-receptor antagonism.4,5
What causes skin lesions on the abdomen and arms?
The lesions on the patient’s abdomen and extremities were consistent with frostbite. The liquefied compressed gas in computer-cleaning and related products is housed in a pressurized canister. The pressure is released when the spray nozzle is depressed; this causes the liquid to rapidly expand to a gas as it is released, resulting in a quick decrease in the temperature of the metal canister. This process, referred to as adiabatic cooling, demonstrates the first law of thermodynamics. The cold temperature of both the liquid and the canister can cause frostbite in the digits and other parts of the body with which the canister or liquid comes into contact.6
Why did the patient have syncope?
Halogenated hydrocarbons inhibit the cardiac delayed rectifier potassium channels involved in the repolarization of cardiac myocytes, causing a delay in repolarization that is manifested as prolongation of the QT interval on an electrocardiogram. This condition places patients at an increased risk of developing torsades de pointes (TdP).7 In most cases, TdP is self-terminating; however, if TdP persists, degeneration to ventricular fibrillation will result. Deaths caused in this fashion have been referred to as “sudden sniffing death syndrome,” and account for half of all hydrocarbon-related deaths.6,8 In addition to the cardiac effects, hydrocarbons are simple asphyxiants that act by displacing oxygen from inspired air, which also contributes to syncope.
It is important to note that epinephrine and other catecholamines increase the risk for dysrhythmias such as TdP in the setting of hydrocarbon abuse.9 For this reason, epinephrine should be used with caution in the setting of a hydrocarbon-induced arrhythmia. Beta-adrenergic antagonists such as esmolol and propranolol are preferable because they reduce the incidence of ectopia that may trigger TdP.10
What is the significance of the masses noted on the examination and radiograph?
Fluorosis is associated with abnormalities of skeletal and dental tissue. Skeletal fluorosis causes osteosclerosis of the axial skeleton, periosteal new bone formation, ligamentous and tendinous ossification, and osteophyte formation. Dental fluorosis causes a yellow/brown discoloration of the teeth with horizontal streaking (mottling), pitting, and chipping.11 Fluorosis is well-described in regions where water fluoride concentrations are high due to industrial exposure; from consumption of fluorinated wine or chronic overconsumption of tea (especially green or black tea); or from fluoridated toothpaste.12-14 More recently, fluorosis has been described in patients treated for an extended duration of time with voriconazole, a fluorinated antifungal agent.15 Unlike other hydrocarbon products, fluorinated hydrocarbons such as 1,1-DFE can significantly increase systemic fluoride concentrations with excessive use. Rapid skeletal fluorosis is not well described, but has been reported after chronic abuse of fluorinated hydrocarbons.16
How is fluorosis diagnosed and managed?
The lack of rapid laboratory testing available for serum, urine, and bone fluoride concentrations makes the initial diagnosis of fluorosis a clinical one. Imaging studies are generally highly suggestive of fluorosis and can be used to support the diagnosis. A dual energy X-ray absorptiometry scan of the spine, hip, femur, and distal portions of the radii can reveal elevated T-scores consistent with osteosclerosis.14 These findings, in conjunction with bone or joint pain, reduced range of motion, or kyphosis, should prompt clinicians to conduct further testing—even without a confirmed fluoride source. A serum fluoride (reference range, 0.2-3.2 mg/L) and 24-hour urine fluoride (reference range, 0.2-3.2 mg/dL) and creatinine evaluation can be used to diagnose fluorosis. However, a bone biopsy with quantitative bone ash fluoride analysis remains the gold standard for the diagnosis of skeletal fluorosis.16 Laboratory evaluation should also include an assessment of electrolytes, specifically calcium, 25-hydroxyvitamin D, and alkaline phosphatase. The differential diagnosis should include hemoglobinopathies, renal osteodystrophy, Paget disease, hypothyroidism, and skeletal metastases.16
Treatment of fluorosis is largely symptomatic and supportive, with identification and discontinuation of the fluoride source. Patients should be referred to an orthopedist for evaluation and management as needed. Evaluation by an endocrinologist should also be considered because patients may have chronic vitamin D and calcium deficiencies as a result of systemic fluorosis.
Case Conclusion
The patient’s laboratory assessment was notable for the following: alkaline phosphatase, 624 U/L (reference range, 44-147 IU/L); vitamin D, 10 ng/mL (reference range, 20-40 ng/mL); serum fluoride, 0.3 mg/L (reference range, 0.2-3.2 mg/L); urine fluoride, 52 mg/dL (0.2-3.2 mg/dL); and urine creatinine, 1 g/L (reference range, 0.3-3 g/L). Imaging studies noted periosteal bone formation on the lateral epicondyle of the distal right humerus, as well as similar osseous abnormalities in other locations. A bone biopsy was scheduled. The patient was treated with oral vitamin D and educated about the importance of discontinuing the huffing of all hydrocarbons.
1. Williams JF, Storck M; American Academy of Pediatrics Committee on Substance Abuse; American Academy of Pediatrics Committee on Native American Child Health. Inhalant abuse. Pediatrics. 2007;119(5):1009-1017.
2. Wu LT, Pilowsky DJ, Schlenger WE. Inhalant abuse and dependence among adolescents in the United States. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1206-1214.
3. Avella J, Kunaparaju N, Kumar S, Lehrer M, Zito SW, Barletta M. Uptake and distribution of the abused inhalant 1,1-difluoroethane in the rat. J Anal Toxicol. 2010;34(7):381-388.
4. Tormoehlen LM, Tekulve KJ, Nañagas KA. Hydrocarbon toxicity: A review. Clin Toxicol (Phila). 2014;52(5):479-489.
5. Duncan JR, Lawrence AJ. Conventional concepts and new perspectives for understanding the addictive properties of inhalants. J Pharmacol Sci. 2013;122(4):237-243.
6. Sakai K, Maruyama-Maebashi K, Takatsu A, et al. Sudden death involving inhalation of 1,1-difluoroethane (HFC-152a) with spray cleaner: three case reports. Forensic Sci Int. 2011;206(1-3):e58-e61.
7. Himmel HM. Mechanisms involved in cardiac sensitization by volatile anesthetics: general applicability to halogenated hydrocarbons? Crit Rev Toxicol. 2008;38(9):773-803.
8. Avella J, Wilson JC, Lehrer M. Fatal cardiac arrhythmia after repeated exposure to 1,1-difluoroethane (DFE). Am J Forensic Med Pathol. 2006;27(1):58-60.
9. Nelson LS. Toxicologic myocardial sensitization. J Toxicol Clin Toxicol. 2002;40(7):867-879.
10. Mortiz F, de La Chapelle A, Bauer F, Leroy JP, Goullé JP, Bonmarchand G. Esmolol in the treatment of severe arrhythmia after acute trichloroethylene poisoning. Intensive Care Med. 2000;26(2):256.
11. Majumdar KK. Health impact of supplying safe drinking water containing fluoride below permissible level on flourosis patients in a fluoride-endemic rural area of West Bengal. Indian J Public Health. 2011;55(4):303-308.
12. Kakumanu N, Rao SD. Images in clinical medicine. Skeletal fluorosis due to excessive tea drinking. N Engl J Med 2013;368(12):1140.
13. Soriano M, Manchón F. Radiological aspects of a new type of bone fluorosis, periostitis deformans. Radiology 1966;87(6):1089-1094.
14. Tamer MN, Kale Köroğlu B, Arslan C, et al. Osteosclerosis due to endemic fluorosis. Sci Total Environ. 2007;373(1):43-48.
15. Bucknor MD, Gross AJ, Link TM. Voriconazole-induced periostitis in two post-transplant patients. J Radiol Case Rep. 2013;7(8):10-17.
16. Cohen E, Hsu RY, Evangelista P, Aaron R, Rubin LE. Rapid-onset diffuse skeletal fluorosis from inhalant abuse: a case report. JBJS Case Connector. 2014;4(4):e108.
1. Williams JF, Storck M; American Academy of Pediatrics Committee on Substance Abuse; American Academy of Pediatrics Committee on Native American Child Health. Inhalant abuse. Pediatrics. 2007;119(5):1009-1017.
2. Wu LT, Pilowsky DJ, Schlenger WE. Inhalant abuse and dependence among adolescents in the United States. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1206-1214.
3. Avella J, Kunaparaju N, Kumar S, Lehrer M, Zito SW, Barletta M. Uptake and distribution of the abused inhalant 1,1-difluoroethane in the rat. J Anal Toxicol. 2010;34(7):381-388.
4. Tormoehlen LM, Tekulve KJ, Nañagas KA. Hydrocarbon toxicity: A review. Clin Toxicol (Phila). 2014;52(5):479-489.
5. Duncan JR, Lawrence AJ. Conventional concepts and new perspectives for understanding the addictive properties of inhalants. J Pharmacol Sci. 2013;122(4):237-243.
6. Sakai K, Maruyama-Maebashi K, Takatsu A, et al. Sudden death involving inhalation of 1,1-difluoroethane (HFC-152a) with spray cleaner: three case reports. Forensic Sci Int. 2011;206(1-3):e58-e61.
7. Himmel HM. Mechanisms involved in cardiac sensitization by volatile anesthetics: general applicability to halogenated hydrocarbons? Crit Rev Toxicol. 2008;38(9):773-803.
8. Avella J, Wilson JC, Lehrer M. Fatal cardiac arrhythmia after repeated exposure to 1,1-difluoroethane (DFE). Am J Forensic Med Pathol. 2006;27(1):58-60.
9. Nelson LS. Toxicologic myocardial sensitization. J Toxicol Clin Toxicol. 2002;40(7):867-879.
10. Mortiz F, de La Chapelle A, Bauer F, Leroy JP, Goullé JP, Bonmarchand G. Esmolol in the treatment of severe arrhythmia after acute trichloroethylene poisoning. Intensive Care Med. 2000;26(2):256.
11. Majumdar KK. Health impact of supplying safe drinking water containing fluoride below permissible level on flourosis patients in a fluoride-endemic rural area of West Bengal. Indian J Public Health. 2011;55(4):303-308.
12. Kakumanu N, Rao SD. Images in clinical medicine. Skeletal fluorosis due to excessive tea drinking. N Engl J Med 2013;368(12):1140.
13. Soriano M, Manchón F. Radiological aspects of a new type of bone fluorosis, periostitis deformans. Radiology 1966;87(6):1089-1094.
14. Tamer MN, Kale Köroğlu B, Arslan C, et al. Osteosclerosis due to endemic fluorosis. Sci Total Environ. 2007;373(1):43-48.
15. Bucknor MD, Gross AJ, Link TM. Voriconazole-induced periostitis in two post-transplant patients. J Radiol Case Rep. 2013;7(8):10-17.
16. Cohen E, Hsu RY, Evangelista P, Aaron R, Rubin LE. Rapid-onset diffuse skeletal fluorosis from inhalant abuse: a case report. JBJS Case Connector. 2014;4(4):e108.

Medical Mimics of Psychiatric Conditions, Part 2
Although the emergency physician (EP) typically encounters common conditions such as chest pain, urinary tract infection, and gastroenteritis, many other clinical presentations can confound diagnosis of the true underlying condition. This may be the case with a patient who presents with apparent psychiatric symptoms that are actually masking an acute medical condition. For example, a patient who appears to be depressed may actually be exhibiting early signs of dementia. Likewise, a manic patient may not have a true underlying psychiatric disorder but rather rhabdomyolysis and hyperthermia from ingesting an illicit substance such as synthetic cathinones (“bath salts”).
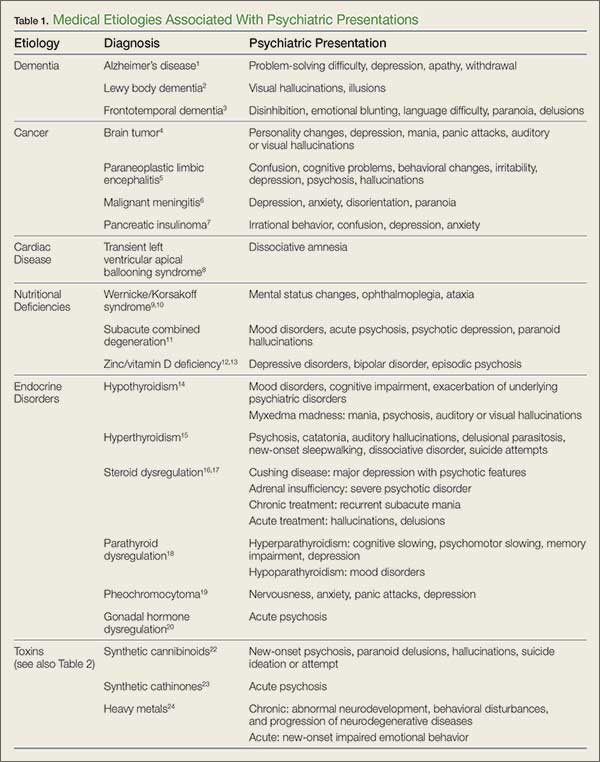
Part 1 of this series reviewed psychiatric presentations caused by underlying infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, and central nervous system etiologies (Emerg Med. 2016;48[5]:202-211). Part 2 covers psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, or toxins (Table 1).
Case Scenarios
Case 1
A 62-year-old man with a history of hypertension, hyperlipidemia, and past alcohol abuse presented to the ED with reported mental status changes after he was pulled over by police for driving the wrong way down the highway. On presentation, the patient’s vital signs were normal. When questioned, the patient was alert and fully oriented and believed the officers were mistaken about what was reported. He denied any recent illness and had a normal physical examination, including neurological examination.
A brief work-up was ordered and the patient passed the time by politely flirting with the nurses. When his wife arrived at the ED, she was relieved that her husband seemed to be all right. She confirmed that the patient had not consumed any alcohol in years. The patient, meanwhile, playfully minimized his wife’s concern at his presence in the ED. A full toxicology screen, laboratory evaluation, and head computed tomography (CT) scan were ordered.
Case 2
A 48-year-old woman with a history of anxiety disorder, depression, and diabetes mellitus presented to the ED with a 2-hour history of chest pain. She stated that the pain had started toward the end of a heated argument with her son. The patient was escorted into the examination room by hospital security because she was still agitated and kept yelling at her son. On examination the patient was tachycardic (110 beats/minute), diaphoretic, and crying. During the examination, she asked the EP for a “Xanax”; her son further noted that this would help his mother’s condition.
The patient repeatedly claimed she could not breathe and could not lie flat on the stretcher. After verbal de-escalation, she cooperated with the electrocardiography (ECG) technician and phlebotomist. Her ECG showed nonspecific ST changes with no prior study for comparison. While glaring at her son, she maintained that she had constant chest pain.
Dementia
Alzheimer’s Disease
Alzheimer’s disease (AD), the most common cause of dementia, is a chronic neurodegenerative disease characterized by an insidiously progressive cognitive decline and loss of function. There is considerable apparent variability in the early signs of the disease, and recent literature has suggested that the manifestation of initial symptoms may be age-dependent. Younger patients tend to present with non-memory cognitive changes such as problem-solving difficulties, as well as personality changes and behavioral symptoms of depression, apathy, and withdrawal.1
Lewy Body Dementia
Lewy body dementia (LBD) is a chronic neurodegenerative disease with a presentation that overlaps substantially with AD. However, LBD is associated with a significantly more rapid course than AD and presents more frequently with visual hallucinations or illusions due to specific visuospatial dysfunction.2
Frontotemporal Dementia
Frontotemporal dementia is a comparatively rare chronic neurodegenerative disease characterized by early-onset memory impairment with cognitive decline, as well as behavioral changes such as disinhibition, emotional blunting, and language difficulty. Initial presentations can also include atypical features such as paranoia or delusion, and misdiagnosis as a primary psychiatric problem is common.3
Cancer
Brain Tumor
Primary and metastatic brain tumors classically present with either focal neurological signs or less specific symptoms such as headaches, seizures, or syncope. Additionally, central nervous system (CNS) tumors can also initially present with primary psychiatric complaints (eg, personality changes, depression, mania, panic attacks, auditory or visual hallucinations). Patients with a brain neoplasm who are initially misdiagnosed with a primary psychiatric disorder face significant delays in proper diagnosis and treatment, leading to increased morbidity. To correctly diagnose the true cause as soon as possible, early imaging is recommended for patients who present with psychiatric symptoms that are abrupt in onset, atypical in presentation, resistant to conventional treatments, or associated with a change in headache pattern.4
Paraneoplastic Limbic Encephalitis
Paraneoplastic limbic encephalitis (PLE) is a rare neurological consequence of certain cancers. Although PLE most commonly occurs in patients with small cell lung cancer, the condition has also been reported (though less frequently) in cases of esophageal adenocarcinoma, ovarian teratoma, metastatic breast cancer, and germ cell testicular cancer.5 This disease overlaps substantially with anti-N-methyl-D-aspartate (anti-NMDA) receptor encephalitis. Moreover, PLE can present initially with prominent neuropsychiatric symptoms such as confusion, cognitive problems, behavioral changes, irritability, depression, or frank psychosis with hallucinations. Paraneoplastic limbic encephalitis can occur early in the course of cancer—often before other systemic signs appear—and its significance is often only recognized in retrospect or postmortem. A higher index of suspicion for the disorder may lead to earlier detection of treatable cancers.
Malignant Meningitis
Malignant meningitis is the metastatic spread of a primary solid tumor to the leptomeninges. It can present as a wide variety of neuropsychiatric complaints, including depression, anxiety, disorientation, and paranoia. Diagnosis can often be made through lumbar puncture. Malignant meningitis should be considered in the differential diagnosis of new psychiatric symptoms in a patient with a history of cancer—even in the absence of focal neurological deficits or meningeal signs.6
Pancreatic Insulinoma
Pancreatic insulinoma is a rare, potentially curable endocrine tumor that can present initially with vague psychiatric complaints such as irrational behavior, confusion, depression, or anxiety. In up to 64% of patients, insulinomas are misdiagnosed as primary neurological or psychiatric disease, which can delay potentially curative surgery—sometimes for years.7 The EP should suspect pancreatic insulinoma in any patient who presents with psychiatric symptoms and unexplained episodes of hypoglycemia.7
Cardiac Disease
Transient Left Ventricular Apical Ballooning Syndrome
Transient left ventricular apical ballooning syndrome (TLVABS), first identified in Japan as Takotsubo syndrome, has more recently been recognized worldwide as overlapping with the classic broken heart syndrome. In postmenopausal women, TLVABS appears to follow a catecholamine surge triggered by extreme emotional stress, resulting in an acute coronary artery spasm. Researchers have hypothesized that there may be a link between TLVABS and dissociative amnesia, which is also thought to result from a catecholamine surge in response to emotional stress.8
Nutritional Deficiencies
Wernicke/Korsakoff Syndrome and Thiamine Deficiency
Wernicke encephalopathy and Korsakoff syndrome (WKS) represent a spectrum of neurodegenerative disorders caused by thiamine deficiency. The condition typically occurs in malnourished alcoholic patients, manifesting as a triad of mental status changes, ophthalmoplegia, and ataxia. Recent research has suggested that WKS is more common than previously thought, is not confined exclusively to alcoholic patients, is unlikely to present with the full classic triad, and is typically only diagnosed postmortem.9
Nonalcoholic WKS tends to occur in younger female patients with a wide array of conditions that affect nutrition (eg, gastrointestinal malignancy, bariatric surgery, hyperemesis gravidarum, anorexia nervosa).9 In a patient with chronic alcoholism, application of the Caine criteria (any two of the following findings: ophthalmoplegia, ataxia, even mild memory impairment or confusion without another cause, evidence of malnutrition) has been shown to be more sensitive and specific than the classic triad.10
Subacute Combined Degeneration
Patients with subacute combined degeneration and extrapyramidal symptoms due to B12 (cobalamin) deficiency are well documented. However, patients with B12 deficiency can also present with mood disorders, acute psychosis, psychotic depression, or paranoid hallucinations. The EP should always consider vitamin B12 deficiency as an important, reversible cause of altered mental status—even in the absence of megaloblastic anemia—especially in patients with celiac disease or anorexia nervosa, and in teenagers and those who are vegans/vegetarians.11
Zinc/Vitamin D Deficiency
Zinc and vitamin D deficiency are both highly prevalent in geriatric patients and have been associated with a range of psychiatric complaints, including depressive disorders, bipolar disorder, and psychotic episodes. Though the neurodevelopmental effects of long-term deficiency of these nutrients are well documented in pediatric patients, the role and relationship to acute psychiatric complaints in elderly patients remain unclear.12,13
Endocrine Disorders
Hypothyroidism
Hypothyroidism is a commonly encountered endocrine disruption that classically presents with fatigue, cold insensitivity, weight gain, and thinning hair. Thyroid dysfunction can result in various neuropsychiatric presentations, including mood disorders, cognitive impairment, and exacerbation of underlying psychiatric disorders. Though rare, primary hypothyroidism can present as mania, psychosis, and auditory or visual hallucinations, a phenomenon termed “myxedema madness.” Myxedema madness typically occurs in older women, but has also been described in adolescents and as a postoperative complication of thyroidectomy.14
Hyperthyroidism
Hyperthyroidism classically presents with tachycardia, nervousness or anxiety, heat insensitivity, and weight loss despite increased appetite. Involvement of the CNS in thyrotoxicosis is rare, but when present, it is a significant predictor of mortality. Neuropsychiatric presentations of hyperthyroidism or thyroid storm vary widely, and have been reported to include psychosis, catatonia, auditory hallucinations, delusional parasitosis, new-onset sleepwalking, dissociative disorder, and suicide attempts.15
Steroid Dysregulation
Steroid dysregulation, either endogenous or iatrogenic in nature, has been reported to cause neuropsychiatric symptoms. Major depression with psychotic features can be an initial presentation of Cushing disease, especially in the presence of other systemic signs.16 Adrenal insufficiency has also been shown to cause severe psychotic disorder.17
Chronic treatment with exogenous corticosteroids can cause a recurrent steroid psychosis, primarily manifesting as subacute mania with psychotic features. Treatment of acute adrenal crisis can also cause an acute steroid psychosis with hallucinations, delusions, and dangerous behavior.17
Parathyroid Dysregulation
Elevated calcium levels caused by primary hyperparathyroidism can present as cognitive slowing, reductions in psychomotor speed, memory impairment, and depression. While the disorder is most prevalent in older women, it has been reported in adolescents, and often remains undiagnosed in younger patients until end-organ damage occurs.18 Hypoparathyroidism has also been reported to cause mood disorders, which can occur with or without the classic symptoms of hypocalcemia (eg, tetany, seizures, dementia, and parkinsonism).18
Pheochromocytoma
Pheochromocytoma is a neuroendocrine tumor of the adrenal medulla that causes sympathetic hyperactivity by the release of large amounts of catecholamines. Pheochromocytoma is well-reported to present with nervousness, anxiety, panic attacks, or depression.19
Gonadal Hormone Dysregulation
Gonadal hormone dysregulation can be either congenital or acquired and is typically caused by a pituitary tumor or traumatic brain injury. Thought to be a result of dopaminergic hyperactivity, acute psychosis can develop in cases of hypogonadotropic hypogonadism, hypopituitarism, and/or hyperprolactinemia.20 There is a high incidence of psychotic manifestations in hypogonadal disorders such as Klinefelter syndrome and Prader-Willi syndrome.
Toxins
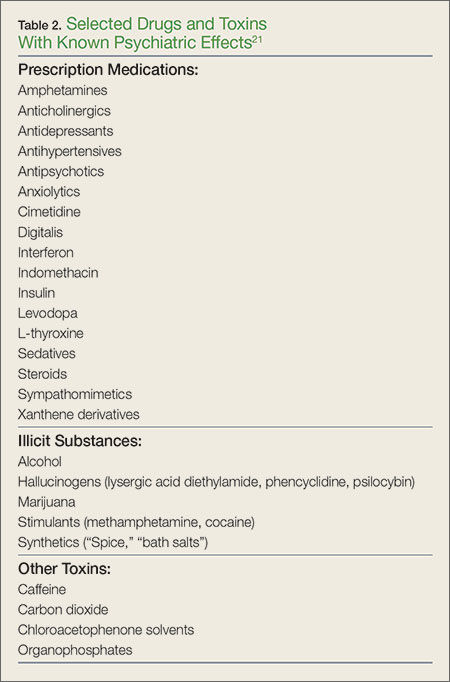
Many toxins can cause altered mental status and psychiatric manifestations. The administration of these toxins can be iatrogenic, related to prescribed use, or overdose—whether accidental, recreational, or intentional (eg, suicide attempt). Table 2 lists common drugs and toxins associated with psychiatric symptoms.21
Synthetic Drugs
The use of numerous unregulated, synthetic analogues of popular recreational drugs has greatly increased over the last several years. Synthetic cannabinoids are available under a variety of names (eg, “Spice,” “K2”) and can cause prominent psychiatric symptoms, including new-onset psychosis, paranoid delusions, hallucinations, and suicide ideation or attempt. While most clinical symptoms are self-limited and require only supportive care, more serious complications have been reported, including myocardial infarction, ischemic stroke, and acute kidney injury.22 Synthetic cathinones (bath salts) can also cause autonomic instability and prominent acute psychosis, sometimes creating a clinical picture indistinguishable from excited delirium syndrome.23
Heavy Metals
Chronic toxicity of many heavy metals is implicated in abnormal neurodevelopment, behavioral disturbances, and progression of neurodegenerative diseases. Recent literature has also implicated acute metal overload in new-onset impaired emotional behavior, though the mechanism is not currently well understood.24
Case Scenarios Continued
Case 1
[The 62-year-old man with altered mental status.]
The patient’s laboratory evaluation and toxicology screen were negative, including a screen for alcohol. He remained jovial but otherwise in no distress. Since the noncontrast head CT scan showed a subtle asymmetry in the frontal lobes, a magnetic resonance imaging (MRI) study was recommended. The brain MRI showed a 5-cm mass in the right frontal lobe with surrounding edema, findings consistent with glioblastoma multiforme. A neurosurgeon was consulted, and the patient was admitted to the intensive care unit.
Case Scenarios Continued
Case 2
[The 48-year-old woman with chest pain.]
The patient received a dose of oral lorazepam, after which she began to feel less anxious, and her chest pain and shortness of breath also improved slightly. The repeat ECG showed worsening of the ST segment changes. The laboratory evaluation was negative. The patient’s son asked if he could take his mother home for what he felt was much needed rest. The EP, however, ordered a stat two-dimensional echocardiogram (ECHO) and repeat troponin level test. The repeat troponin test was positive, and the ECHO was remarkable for a decreased left ventricular ejection fraction of 15%, with apical ballooning. These findings were consistent with stress cardiomyopathy (Takotsubo syndrome). The patient was admitted to the cardiology service and given a beta blocker and an angiotensin-converting enzyme inhibitor.
After a normal coronary angiogram, the patient developed cardiogenic shock and was intubated. Seven days later, she was extubated and transferred to inpatient rehabilitation services where she also received an assessment and treatment for her underlying depression. Eight weeks postdiagnosis, the patient’s ejection fraction had returned to 50%, and she was close to her baseline exercise tolerance.
1. Barnes J, Dickerson BC, Frost C, Jiskoot LC, Wolk D, van der Flier WM. Alzheimer’s disease first symptoms are age dependent: Evidence from the NACC dataset. Alzheimers Dement. 2015;11(11):1349-1357.
2. Yoshizawa H, Vonsattel JP, Honig LS. Early neuropsychological discriminants for Lewy body disease: an autopsy series. J Neurol Neurosurg Psychiatry. 2013;84(12):1326-1330.
3. Iroka N, Jehangir W, Ii JL, Pattan V, Yousif A, Mishra AK. Paranoid personality masking an atypical case of frontotemporal dementia. J Clin Med Res. 2015;7(5):364-366.
4. Filley CM, Kleinschmidt-DeMasters BK. Neurobehavioral presentations of brain neoplasms. West J Med. 1995;163(1):19-25.
5. Said S, Cooper CJ, Reyna E, Alkhateeb H, Diaz J, Nahleh Z. Paraneoplastic limbic encephalitis, an uncommon presentation of a common cancer: Case report and discussion. Am J Case Rep. 2013;14:391-394.
6. Weitzner MA, Olofsson SM, Forman AD. Patients with malignant meningitis presenting with neuropsychiatric manifestations. Cancer. 1995;76(10):1804-1808.
7. Ding Y, Wang S, Liu J. Neuropsychiatric profiles of patients with insulinomas. Eur Neurol. 2010;63(1):48-51.
8. Toussi A, Bryk J, Alam A. Forgetting heart break: a fascinating case of transient left ventricular apical ballooning syndrome associated with dissociative amnesia. Gen Hosp Psychiatry. 2014;36(2):225-227.
9. Scalzo SJ, Bowden SC, Ambrose ML, Whelan G, Cook MJ. Wernicke-Korsakoff syndrome not related to alcohol use: a systematic review. J Neurol Neurosurg Psychiatry. 2015;86(12):1362-1368.
10. Isenberg-Grzeda E, Kutner HE, Nicolson SE. Wernicke-Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics. 2012;53(6):507-516.
11. Issac TG, Soundarya S, Christopher R, Chandra SR. Vitamin B12 deficiency: an important reversible co-morbidity in neuropsychiatric manifestations. Indian J Psychol Med. 2015;37(1):26-29.
12. Grønli O, Kvamme JM, Friborg O, Wynn R. Zinc deficiency is common in several psychiatric disorders. PLoS One. 2013;8(12):e82793.
13. Grønli O, Kvamme JM, Jorde R, Wynn R. Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry. 2014;14:134.
14. Heinrich TW, Grahm G. Hypothyroidism presenting as psychosis: myxedema madness revisited. Prim Care Companion J Clin Psychiatry. 2003;5(6):260-266.
15. Swee du S, Chng CL, Lim A. Clinical characteristics and outcome of thyroid storm: a case series and review of neuropsychiatric derangements in thyrotoxicosis. Endocr Pract. 2015;21(2):182-189.
16. Tang A, O’Sullivan AJ, Diamond T, Gerard A, Campbell P. Psychiatric symptoms as a clinical presentation of Cushing’s syndrome. Ann Gen Psychiatry. 2013;12(1):23.
17. Farah Jde L, Lauand CV, Chequi L, et al. Severe psychotic disorder as the main manifestation of adrenal insufficiency. Case Rep Psychiatry. 2015;2015:512430.
18. Rice T, Azova S, Coffey BJ. Negative symptoms in a depressed teen? Primary hyperparathyroidism and its psychiatric manifestations. J Child Adolesc Psychopharmacol. 2015;25(8):653-655.
19. Zardawi IM. Phaeochromocytoma masquerading as anxiety and depression. Am J Case Rep. 2013;14:161-163.
20. Kate S, Dhanwal DK, Kumar S, Bharti P. Acute psychosis as a presentation of hypopituitarism. BMJ Case Rep. 2013;2013.
21. Abramowicz M. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther. 2008;50(1301-1302):100-103.
22. Tait RJ, Caldicott D, Mountain D, Hill SL, Lenton S. A systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin Toxicol (Phila). 2016;54(1):1-13.
23. Karch SB. Cathinone neurotoxicity (“The “3Ms”). Curr Neuropharmacol. 2015;13(1): 21-25.
24. Menon AV, Chang J, Kim J. Mechanisms of divalent metal toxicity in affective disorders. Toxicology. 2016;339:58-72.
Although the emergency physician (EP) typically encounters common conditions such as chest pain, urinary tract infection, and gastroenteritis, many other clinical presentations can confound diagnosis of the true underlying condition. This may be the case with a patient who presents with apparent psychiatric symptoms that are actually masking an acute medical condition. For example, a patient who appears to be depressed may actually be exhibiting early signs of dementia. Likewise, a manic patient may not have a true underlying psychiatric disorder but rather rhabdomyolysis and hyperthermia from ingesting an illicit substance such as synthetic cathinones (“bath salts”).
Part 1 of this series reviewed psychiatric presentations caused by underlying infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, and central nervous system etiologies (Emerg Med. 2016;48[5]:202-211). Part 2 covers psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, or toxins (Table 1).
Case Scenarios
Case 1
A 62-year-old man with a history of hypertension, hyperlipidemia, and past alcohol abuse presented to the ED with reported mental status changes after he was pulled over by police for driving the wrong way down the highway. On presentation, the patient’s vital signs were normal. When questioned, the patient was alert and fully oriented and believed the officers were mistaken about what was reported. He denied any recent illness and had a normal physical examination, including neurological examination.
A brief work-up was ordered and the patient passed the time by politely flirting with the nurses. When his wife arrived at the ED, she was relieved that her husband seemed to be all right. She confirmed that the patient had not consumed any alcohol in years. The patient, meanwhile, playfully minimized his wife’s concern at his presence in the ED. A full toxicology screen, laboratory evaluation, and head computed tomography (CT) scan were ordered.
Case 2
A 48-year-old woman with a history of anxiety disorder, depression, and diabetes mellitus presented to the ED with a 2-hour history of chest pain. She stated that the pain had started toward the end of a heated argument with her son. The patient was escorted into the examination room by hospital security because she was still agitated and kept yelling at her son. On examination the patient was tachycardic (110 beats/minute), diaphoretic, and crying. During the examination, she asked the EP for a “Xanax”; her son further noted that this would help his mother’s condition.
The patient repeatedly claimed she could not breathe and could not lie flat on the stretcher. After verbal de-escalation, she cooperated with the electrocardiography (ECG) technician and phlebotomist. Her ECG showed nonspecific ST changes with no prior study for comparison. While glaring at her son, she maintained that she had constant chest pain.
Dementia
Alzheimer’s Disease
Alzheimer’s disease (AD), the most common cause of dementia, is a chronic neurodegenerative disease characterized by an insidiously progressive cognitive decline and loss of function. There is considerable apparent variability in the early signs of the disease, and recent literature has suggested that the manifestation of initial symptoms may be age-dependent. Younger patients tend to present with non-memory cognitive changes such as problem-solving difficulties, as well as personality changes and behavioral symptoms of depression, apathy, and withdrawal.1
Lewy Body Dementia
Lewy body dementia (LBD) is a chronic neurodegenerative disease with a presentation that overlaps substantially with AD. However, LBD is associated with a significantly more rapid course than AD and presents more frequently with visual hallucinations or illusions due to specific visuospatial dysfunction.2
Frontotemporal Dementia
Frontotemporal dementia is a comparatively rare chronic neurodegenerative disease characterized by early-onset memory impairment with cognitive decline, as well as behavioral changes such as disinhibition, emotional blunting, and language difficulty. Initial presentations can also include atypical features such as paranoia or delusion, and misdiagnosis as a primary psychiatric problem is common.3
Cancer
Brain Tumor
Primary and metastatic brain tumors classically present with either focal neurological signs or less specific symptoms such as headaches, seizures, or syncope. Additionally, central nervous system (CNS) tumors can also initially present with primary psychiatric complaints (eg, personality changes, depression, mania, panic attacks, auditory or visual hallucinations). Patients with a brain neoplasm who are initially misdiagnosed with a primary psychiatric disorder face significant delays in proper diagnosis and treatment, leading to increased morbidity. To correctly diagnose the true cause as soon as possible, early imaging is recommended for patients who present with psychiatric symptoms that are abrupt in onset, atypical in presentation, resistant to conventional treatments, or associated with a change in headache pattern.4
Paraneoplastic Limbic Encephalitis
Paraneoplastic limbic encephalitis (PLE) is a rare neurological consequence of certain cancers. Although PLE most commonly occurs in patients with small cell lung cancer, the condition has also been reported (though less frequently) in cases of esophageal adenocarcinoma, ovarian teratoma, metastatic breast cancer, and germ cell testicular cancer.5 This disease overlaps substantially with anti-N-methyl-D-aspartate (anti-NMDA) receptor encephalitis. Moreover, PLE can present initially with prominent neuropsychiatric symptoms such as confusion, cognitive problems, behavioral changes, irritability, depression, or frank psychosis with hallucinations. Paraneoplastic limbic encephalitis can occur early in the course of cancer—often before other systemic signs appear—and its significance is often only recognized in retrospect or postmortem. A higher index of suspicion for the disorder may lead to earlier detection of treatable cancers.
Malignant Meningitis
Malignant meningitis is the metastatic spread of a primary solid tumor to the leptomeninges. It can present as a wide variety of neuropsychiatric complaints, including depression, anxiety, disorientation, and paranoia. Diagnosis can often be made through lumbar puncture. Malignant meningitis should be considered in the differential diagnosis of new psychiatric symptoms in a patient with a history of cancer—even in the absence of focal neurological deficits or meningeal signs.6
Pancreatic Insulinoma
Pancreatic insulinoma is a rare, potentially curable endocrine tumor that can present initially with vague psychiatric complaints such as irrational behavior, confusion, depression, or anxiety. In up to 64% of patients, insulinomas are misdiagnosed as primary neurological or psychiatric disease, which can delay potentially curative surgery—sometimes for years.7 The EP should suspect pancreatic insulinoma in any patient who presents with psychiatric symptoms and unexplained episodes of hypoglycemia.7
Cardiac Disease
Transient Left Ventricular Apical Ballooning Syndrome
Transient left ventricular apical ballooning syndrome (TLVABS), first identified in Japan as Takotsubo syndrome, has more recently been recognized worldwide as overlapping with the classic broken heart syndrome. In postmenopausal women, TLVABS appears to follow a catecholamine surge triggered by extreme emotional stress, resulting in an acute coronary artery spasm. Researchers have hypothesized that there may be a link between TLVABS and dissociative amnesia, which is also thought to result from a catecholamine surge in response to emotional stress.8
Nutritional Deficiencies
Wernicke/Korsakoff Syndrome and Thiamine Deficiency
Wernicke encephalopathy and Korsakoff syndrome (WKS) represent a spectrum of neurodegenerative disorders caused by thiamine deficiency. The condition typically occurs in malnourished alcoholic patients, manifesting as a triad of mental status changes, ophthalmoplegia, and ataxia. Recent research has suggested that WKS is more common than previously thought, is not confined exclusively to alcoholic patients, is unlikely to present with the full classic triad, and is typically only diagnosed postmortem.9
Nonalcoholic WKS tends to occur in younger female patients with a wide array of conditions that affect nutrition (eg, gastrointestinal malignancy, bariatric surgery, hyperemesis gravidarum, anorexia nervosa).9 In a patient with chronic alcoholism, application of the Caine criteria (any two of the following findings: ophthalmoplegia, ataxia, even mild memory impairment or confusion without another cause, evidence of malnutrition) has been shown to be more sensitive and specific than the classic triad.10
Subacute Combined Degeneration
Patients with subacute combined degeneration and extrapyramidal symptoms due to B12 (cobalamin) deficiency are well documented. However, patients with B12 deficiency can also present with mood disorders, acute psychosis, psychotic depression, or paranoid hallucinations. The EP should always consider vitamin B12 deficiency as an important, reversible cause of altered mental status—even in the absence of megaloblastic anemia—especially in patients with celiac disease or anorexia nervosa, and in teenagers and those who are vegans/vegetarians.11
Zinc/Vitamin D Deficiency
Zinc and vitamin D deficiency are both highly prevalent in geriatric patients and have been associated with a range of psychiatric complaints, including depressive disorders, bipolar disorder, and psychotic episodes. Though the neurodevelopmental effects of long-term deficiency of these nutrients are well documented in pediatric patients, the role and relationship to acute psychiatric complaints in elderly patients remain unclear.12,13
Endocrine Disorders
Hypothyroidism
Hypothyroidism is a commonly encountered endocrine disruption that classically presents with fatigue, cold insensitivity, weight gain, and thinning hair. Thyroid dysfunction can result in various neuropsychiatric presentations, including mood disorders, cognitive impairment, and exacerbation of underlying psychiatric disorders. Though rare, primary hypothyroidism can present as mania, psychosis, and auditory or visual hallucinations, a phenomenon termed “myxedema madness.” Myxedema madness typically occurs in older women, but has also been described in adolescents and as a postoperative complication of thyroidectomy.14
Hyperthyroidism
Hyperthyroidism classically presents with tachycardia, nervousness or anxiety, heat insensitivity, and weight loss despite increased appetite. Involvement of the CNS in thyrotoxicosis is rare, but when present, it is a significant predictor of mortality. Neuropsychiatric presentations of hyperthyroidism or thyroid storm vary widely, and have been reported to include psychosis, catatonia, auditory hallucinations, delusional parasitosis, new-onset sleepwalking, dissociative disorder, and suicide attempts.15
Steroid Dysregulation
Steroid dysregulation, either endogenous or iatrogenic in nature, has been reported to cause neuropsychiatric symptoms. Major depression with psychotic features can be an initial presentation of Cushing disease, especially in the presence of other systemic signs.16 Adrenal insufficiency has also been shown to cause severe psychotic disorder.17
Chronic treatment with exogenous corticosteroids can cause a recurrent steroid psychosis, primarily manifesting as subacute mania with psychotic features. Treatment of acute adrenal crisis can also cause an acute steroid psychosis with hallucinations, delusions, and dangerous behavior.17
Parathyroid Dysregulation
Elevated calcium levels caused by primary hyperparathyroidism can present as cognitive slowing, reductions in psychomotor speed, memory impairment, and depression. While the disorder is most prevalent in older women, it has been reported in adolescents, and often remains undiagnosed in younger patients until end-organ damage occurs.18 Hypoparathyroidism has also been reported to cause mood disorders, which can occur with or without the classic symptoms of hypocalcemia (eg, tetany, seizures, dementia, and parkinsonism).18
Pheochromocytoma
Pheochromocytoma is a neuroendocrine tumor of the adrenal medulla that causes sympathetic hyperactivity by the release of large amounts of catecholamines. Pheochromocytoma is well-reported to present with nervousness, anxiety, panic attacks, or depression.19
Gonadal Hormone Dysregulation
Gonadal hormone dysregulation can be either congenital or acquired and is typically caused by a pituitary tumor or traumatic brain injury. Thought to be a result of dopaminergic hyperactivity, acute psychosis can develop in cases of hypogonadotropic hypogonadism, hypopituitarism, and/or hyperprolactinemia.20 There is a high incidence of psychotic manifestations in hypogonadal disorders such as Klinefelter syndrome and Prader-Willi syndrome.
Toxins
Many toxins can cause altered mental status and psychiatric manifestations. The administration of these toxins can be iatrogenic, related to prescribed use, or overdose—whether accidental, recreational, or intentional (eg, suicide attempt). Table 2 lists common drugs and toxins associated with psychiatric symptoms.21
Synthetic Drugs
The use of numerous unregulated, synthetic analogues of popular recreational drugs has greatly increased over the last several years. Synthetic cannabinoids are available under a variety of names (eg, “Spice,” “K2”) and can cause prominent psychiatric symptoms, including new-onset psychosis, paranoid delusions, hallucinations, and suicide ideation or attempt. While most clinical symptoms are self-limited and require only supportive care, more serious complications have been reported, including myocardial infarction, ischemic stroke, and acute kidney injury.22 Synthetic cathinones (bath salts) can also cause autonomic instability and prominent acute psychosis, sometimes creating a clinical picture indistinguishable from excited delirium syndrome.23
Heavy Metals
Chronic toxicity of many heavy metals is implicated in abnormal neurodevelopment, behavioral disturbances, and progression of neurodegenerative diseases. Recent literature has also implicated acute metal overload in new-onset impaired emotional behavior, though the mechanism is not currently well understood.24
Case Scenarios Continued
Case 1
[The 62-year-old man with altered mental status.]
The patient’s laboratory evaluation and toxicology screen were negative, including a screen for alcohol. He remained jovial but otherwise in no distress. Since the noncontrast head CT scan showed a subtle asymmetry in the frontal lobes, a magnetic resonance imaging (MRI) study was recommended. The brain MRI showed a 5-cm mass in the right frontal lobe with surrounding edema, findings consistent with glioblastoma multiforme. A neurosurgeon was consulted, and the patient was admitted to the intensive care unit.
Case Scenarios Continued
Case 2
[The 48-year-old woman with chest pain.]
The patient received a dose of oral lorazepam, after which she began to feel less anxious, and her chest pain and shortness of breath also improved slightly. The repeat ECG showed worsening of the ST segment changes. The laboratory evaluation was negative. The patient’s son asked if he could take his mother home for what he felt was much needed rest. The EP, however, ordered a stat two-dimensional echocardiogram (ECHO) and repeat troponin level test. The repeat troponin test was positive, and the ECHO was remarkable for a decreased left ventricular ejection fraction of 15%, with apical ballooning. These findings were consistent with stress cardiomyopathy (Takotsubo syndrome). The patient was admitted to the cardiology service and given a beta blocker and an angiotensin-converting enzyme inhibitor.
After a normal coronary angiogram, the patient developed cardiogenic shock and was intubated. Seven days later, she was extubated and transferred to inpatient rehabilitation services where she also received an assessment and treatment for her underlying depression. Eight weeks postdiagnosis, the patient’s ejection fraction had returned to 50%, and she was close to her baseline exercise tolerance.
Although the emergency physician (EP) typically encounters common conditions such as chest pain, urinary tract infection, and gastroenteritis, many other clinical presentations can confound diagnosis of the true underlying condition. This may be the case with a patient who presents with apparent psychiatric symptoms that are actually masking an acute medical condition. For example, a patient who appears to be depressed may actually be exhibiting early signs of dementia. Likewise, a manic patient may not have a true underlying psychiatric disorder but rather rhabdomyolysis and hyperthermia from ingesting an illicit substance such as synthetic cathinones (“bath salts”).
Part 1 of this series reviewed psychiatric presentations caused by underlying infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, and central nervous system etiologies (Emerg Med. 2016;48[5]:202-211). Part 2 covers psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, or toxins (Table 1).
Case Scenarios
Case 1
A 62-year-old man with a history of hypertension, hyperlipidemia, and past alcohol abuse presented to the ED with reported mental status changes after he was pulled over by police for driving the wrong way down the highway. On presentation, the patient’s vital signs were normal. When questioned, the patient was alert and fully oriented and believed the officers were mistaken about what was reported. He denied any recent illness and had a normal physical examination, including neurological examination.
A brief work-up was ordered and the patient passed the time by politely flirting with the nurses. When his wife arrived at the ED, she was relieved that her husband seemed to be all right. She confirmed that the patient had not consumed any alcohol in years. The patient, meanwhile, playfully minimized his wife’s concern at his presence in the ED. A full toxicology screen, laboratory evaluation, and head computed tomography (CT) scan were ordered.
Case 2
A 48-year-old woman with a history of anxiety disorder, depression, and diabetes mellitus presented to the ED with a 2-hour history of chest pain. She stated that the pain had started toward the end of a heated argument with her son. The patient was escorted into the examination room by hospital security because she was still agitated and kept yelling at her son. On examination the patient was tachycardic (110 beats/minute), diaphoretic, and crying. During the examination, she asked the EP for a “Xanax”; her son further noted that this would help his mother’s condition.
The patient repeatedly claimed she could not breathe and could not lie flat on the stretcher. After verbal de-escalation, she cooperated with the electrocardiography (ECG) technician and phlebotomist. Her ECG showed nonspecific ST changes with no prior study for comparison. While glaring at her son, she maintained that she had constant chest pain.
Dementia
Alzheimer’s Disease
Alzheimer’s disease (AD), the most common cause of dementia, is a chronic neurodegenerative disease characterized by an insidiously progressive cognitive decline and loss of function. There is considerable apparent variability in the early signs of the disease, and recent literature has suggested that the manifestation of initial symptoms may be age-dependent. Younger patients tend to present with non-memory cognitive changes such as problem-solving difficulties, as well as personality changes and behavioral symptoms of depression, apathy, and withdrawal.1
Lewy Body Dementia
Lewy body dementia (LBD) is a chronic neurodegenerative disease with a presentation that overlaps substantially with AD. However, LBD is associated with a significantly more rapid course than AD and presents more frequently with visual hallucinations or illusions due to specific visuospatial dysfunction.2
Frontotemporal Dementia
Frontotemporal dementia is a comparatively rare chronic neurodegenerative disease characterized by early-onset memory impairment with cognitive decline, as well as behavioral changes such as disinhibition, emotional blunting, and language difficulty. Initial presentations can also include atypical features such as paranoia or delusion, and misdiagnosis as a primary psychiatric problem is common.3
Cancer
Brain Tumor
Primary and metastatic brain tumors classically present with either focal neurological signs or less specific symptoms such as headaches, seizures, or syncope. Additionally, central nervous system (CNS) tumors can also initially present with primary psychiatric complaints (eg, personality changes, depression, mania, panic attacks, auditory or visual hallucinations). Patients with a brain neoplasm who are initially misdiagnosed with a primary psychiatric disorder face significant delays in proper diagnosis and treatment, leading to increased morbidity. To correctly diagnose the true cause as soon as possible, early imaging is recommended for patients who present with psychiatric symptoms that are abrupt in onset, atypical in presentation, resistant to conventional treatments, or associated with a change in headache pattern.4
Paraneoplastic Limbic Encephalitis
Paraneoplastic limbic encephalitis (PLE) is a rare neurological consequence of certain cancers. Although PLE most commonly occurs in patients with small cell lung cancer, the condition has also been reported (though less frequently) in cases of esophageal adenocarcinoma, ovarian teratoma, metastatic breast cancer, and germ cell testicular cancer.5 This disease overlaps substantially with anti-N-methyl-D-aspartate (anti-NMDA) receptor encephalitis. Moreover, PLE can present initially with prominent neuropsychiatric symptoms such as confusion, cognitive problems, behavioral changes, irritability, depression, or frank psychosis with hallucinations. Paraneoplastic limbic encephalitis can occur early in the course of cancer—often before other systemic signs appear—and its significance is often only recognized in retrospect or postmortem. A higher index of suspicion for the disorder may lead to earlier detection of treatable cancers.
Malignant Meningitis
Malignant meningitis is the metastatic spread of a primary solid tumor to the leptomeninges. It can present as a wide variety of neuropsychiatric complaints, including depression, anxiety, disorientation, and paranoia. Diagnosis can often be made through lumbar puncture. Malignant meningitis should be considered in the differential diagnosis of new psychiatric symptoms in a patient with a history of cancer—even in the absence of focal neurological deficits or meningeal signs.6
Pancreatic Insulinoma
Pancreatic insulinoma is a rare, potentially curable endocrine tumor that can present initially with vague psychiatric complaints such as irrational behavior, confusion, depression, or anxiety. In up to 64% of patients, insulinomas are misdiagnosed as primary neurological or psychiatric disease, which can delay potentially curative surgery—sometimes for years.7 The EP should suspect pancreatic insulinoma in any patient who presents with psychiatric symptoms and unexplained episodes of hypoglycemia.7
Cardiac Disease
Transient Left Ventricular Apical Ballooning Syndrome
Transient left ventricular apical ballooning syndrome (TLVABS), first identified in Japan as Takotsubo syndrome, has more recently been recognized worldwide as overlapping with the classic broken heart syndrome. In postmenopausal women, TLVABS appears to follow a catecholamine surge triggered by extreme emotional stress, resulting in an acute coronary artery spasm. Researchers have hypothesized that there may be a link between TLVABS and dissociative amnesia, which is also thought to result from a catecholamine surge in response to emotional stress.8
Nutritional Deficiencies
Wernicke/Korsakoff Syndrome and Thiamine Deficiency
Wernicke encephalopathy and Korsakoff syndrome (WKS) represent a spectrum of neurodegenerative disorders caused by thiamine deficiency. The condition typically occurs in malnourished alcoholic patients, manifesting as a triad of mental status changes, ophthalmoplegia, and ataxia. Recent research has suggested that WKS is more common than previously thought, is not confined exclusively to alcoholic patients, is unlikely to present with the full classic triad, and is typically only diagnosed postmortem.9
Nonalcoholic WKS tends to occur in younger female patients with a wide array of conditions that affect nutrition (eg, gastrointestinal malignancy, bariatric surgery, hyperemesis gravidarum, anorexia nervosa).9 In a patient with chronic alcoholism, application of the Caine criteria (any two of the following findings: ophthalmoplegia, ataxia, even mild memory impairment or confusion without another cause, evidence of malnutrition) has been shown to be more sensitive and specific than the classic triad.10
Subacute Combined Degeneration
Patients with subacute combined degeneration and extrapyramidal symptoms due to B12 (cobalamin) deficiency are well documented. However, patients with B12 deficiency can also present with mood disorders, acute psychosis, psychotic depression, or paranoid hallucinations. The EP should always consider vitamin B12 deficiency as an important, reversible cause of altered mental status—even in the absence of megaloblastic anemia—especially in patients with celiac disease or anorexia nervosa, and in teenagers and those who are vegans/vegetarians.11
Zinc/Vitamin D Deficiency
Zinc and vitamin D deficiency are both highly prevalent in geriatric patients and have been associated with a range of psychiatric complaints, including depressive disorders, bipolar disorder, and psychotic episodes. Though the neurodevelopmental effects of long-term deficiency of these nutrients are well documented in pediatric patients, the role and relationship to acute psychiatric complaints in elderly patients remain unclear.12,13
Endocrine Disorders
Hypothyroidism
Hypothyroidism is a commonly encountered endocrine disruption that classically presents with fatigue, cold insensitivity, weight gain, and thinning hair. Thyroid dysfunction can result in various neuropsychiatric presentations, including mood disorders, cognitive impairment, and exacerbation of underlying psychiatric disorders. Though rare, primary hypothyroidism can present as mania, psychosis, and auditory or visual hallucinations, a phenomenon termed “myxedema madness.” Myxedema madness typically occurs in older women, but has also been described in adolescents and as a postoperative complication of thyroidectomy.14
Hyperthyroidism
Hyperthyroidism classically presents with tachycardia, nervousness or anxiety, heat insensitivity, and weight loss despite increased appetite. Involvement of the CNS in thyrotoxicosis is rare, but when present, it is a significant predictor of mortality. Neuropsychiatric presentations of hyperthyroidism or thyroid storm vary widely, and have been reported to include psychosis, catatonia, auditory hallucinations, delusional parasitosis, new-onset sleepwalking, dissociative disorder, and suicide attempts.15
Steroid Dysregulation
Steroid dysregulation, either endogenous or iatrogenic in nature, has been reported to cause neuropsychiatric symptoms. Major depression with psychotic features can be an initial presentation of Cushing disease, especially in the presence of other systemic signs.16 Adrenal insufficiency has also been shown to cause severe psychotic disorder.17
Chronic treatment with exogenous corticosteroids can cause a recurrent steroid psychosis, primarily manifesting as subacute mania with psychotic features. Treatment of acute adrenal crisis can also cause an acute steroid psychosis with hallucinations, delusions, and dangerous behavior.17
Parathyroid Dysregulation
Elevated calcium levels caused by primary hyperparathyroidism can present as cognitive slowing, reductions in psychomotor speed, memory impairment, and depression. While the disorder is most prevalent in older women, it has been reported in adolescents, and often remains undiagnosed in younger patients until end-organ damage occurs.18 Hypoparathyroidism has also been reported to cause mood disorders, which can occur with or without the classic symptoms of hypocalcemia (eg, tetany, seizures, dementia, and parkinsonism).18
Pheochromocytoma
Pheochromocytoma is a neuroendocrine tumor of the adrenal medulla that causes sympathetic hyperactivity by the release of large amounts of catecholamines. Pheochromocytoma is well-reported to present with nervousness, anxiety, panic attacks, or depression.19
Gonadal Hormone Dysregulation
Gonadal hormone dysregulation can be either congenital or acquired and is typically caused by a pituitary tumor or traumatic brain injury. Thought to be a result of dopaminergic hyperactivity, acute psychosis can develop in cases of hypogonadotropic hypogonadism, hypopituitarism, and/or hyperprolactinemia.20 There is a high incidence of psychotic manifestations in hypogonadal disorders such as Klinefelter syndrome and Prader-Willi syndrome.
Toxins
Many toxins can cause altered mental status and psychiatric manifestations. The administration of these toxins can be iatrogenic, related to prescribed use, or overdose—whether accidental, recreational, or intentional (eg, suicide attempt). Table 2 lists common drugs and toxins associated with psychiatric symptoms.21
Synthetic Drugs
The use of numerous unregulated, synthetic analogues of popular recreational drugs has greatly increased over the last several years. Synthetic cannabinoids are available under a variety of names (eg, “Spice,” “K2”) and can cause prominent psychiatric symptoms, including new-onset psychosis, paranoid delusions, hallucinations, and suicide ideation or attempt. While most clinical symptoms are self-limited and require only supportive care, more serious complications have been reported, including myocardial infarction, ischemic stroke, and acute kidney injury.22 Synthetic cathinones (bath salts) can also cause autonomic instability and prominent acute psychosis, sometimes creating a clinical picture indistinguishable from excited delirium syndrome.23
Heavy Metals
Chronic toxicity of many heavy metals is implicated in abnormal neurodevelopment, behavioral disturbances, and progression of neurodegenerative diseases. Recent literature has also implicated acute metal overload in new-onset impaired emotional behavior, though the mechanism is not currently well understood.24
Case Scenarios Continued
Case 1
[The 62-year-old man with altered mental status.]
The patient’s laboratory evaluation and toxicology screen were negative, including a screen for alcohol. He remained jovial but otherwise in no distress. Since the noncontrast head CT scan showed a subtle asymmetry in the frontal lobes, a magnetic resonance imaging (MRI) study was recommended. The brain MRI showed a 5-cm mass in the right frontal lobe with surrounding edema, findings consistent with glioblastoma multiforme. A neurosurgeon was consulted, and the patient was admitted to the intensive care unit.
Case Scenarios Continued
Case 2
[The 48-year-old woman with chest pain.]
The patient received a dose of oral lorazepam, after which she began to feel less anxious, and her chest pain and shortness of breath also improved slightly. The repeat ECG showed worsening of the ST segment changes. The laboratory evaluation was negative. The patient’s son asked if he could take his mother home for what he felt was much needed rest. The EP, however, ordered a stat two-dimensional echocardiogram (ECHO) and repeat troponin level test. The repeat troponin test was positive, and the ECHO was remarkable for a decreased left ventricular ejection fraction of 15%, with apical ballooning. These findings were consistent with stress cardiomyopathy (Takotsubo syndrome). The patient was admitted to the cardiology service and given a beta blocker and an angiotensin-converting enzyme inhibitor.
After a normal coronary angiogram, the patient developed cardiogenic shock and was intubated. Seven days later, she was extubated and transferred to inpatient rehabilitation services where she also received an assessment and treatment for her underlying depression. Eight weeks postdiagnosis, the patient’s ejection fraction had returned to 50%, and she was close to her baseline exercise tolerance.
1. Barnes J, Dickerson BC, Frost C, Jiskoot LC, Wolk D, van der Flier WM. Alzheimer’s disease first symptoms are age dependent: Evidence from the NACC dataset. Alzheimers Dement. 2015;11(11):1349-1357.
2. Yoshizawa H, Vonsattel JP, Honig LS. Early neuropsychological discriminants for Lewy body disease: an autopsy series. J Neurol Neurosurg Psychiatry. 2013;84(12):1326-1330.
3. Iroka N, Jehangir W, Ii JL, Pattan V, Yousif A, Mishra AK. Paranoid personality masking an atypical case of frontotemporal dementia. J Clin Med Res. 2015;7(5):364-366.
4. Filley CM, Kleinschmidt-DeMasters BK. Neurobehavioral presentations of brain neoplasms. West J Med. 1995;163(1):19-25.
5. Said S, Cooper CJ, Reyna E, Alkhateeb H, Diaz J, Nahleh Z. Paraneoplastic limbic encephalitis, an uncommon presentation of a common cancer: Case report and discussion. Am J Case Rep. 2013;14:391-394.
6. Weitzner MA, Olofsson SM, Forman AD. Patients with malignant meningitis presenting with neuropsychiatric manifestations. Cancer. 1995;76(10):1804-1808.
7. Ding Y, Wang S, Liu J. Neuropsychiatric profiles of patients with insulinomas. Eur Neurol. 2010;63(1):48-51.
8. Toussi A, Bryk J, Alam A. Forgetting heart break: a fascinating case of transient left ventricular apical ballooning syndrome associated with dissociative amnesia. Gen Hosp Psychiatry. 2014;36(2):225-227.
9. Scalzo SJ, Bowden SC, Ambrose ML, Whelan G, Cook MJ. Wernicke-Korsakoff syndrome not related to alcohol use: a systematic review. J Neurol Neurosurg Psychiatry. 2015;86(12):1362-1368.
10. Isenberg-Grzeda E, Kutner HE, Nicolson SE. Wernicke-Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics. 2012;53(6):507-516.
11. Issac TG, Soundarya S, Christopher R, Chandra SR. Vitamin B12 deficiency: an important reversible co-morbidity in neuropsychiatric manifestations. Indian J Psychol Med. 2015;37(1):26-29.
12. Grønli O, Kvamme JM, Friborg O, Wynn R. Zinc deficiency is common in several psychiatric disorders. PLoS One. 2013;8(12):e82793.
13. Grønli O, Kvamme JM, Jorde R, Wynn R. Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry. 2014;14:134.
14. Heinrich TW, Grahm G. Hypothyroidism presenting as psychosis: myxedema madness revisited. Prim Care Companion J Clin Psychiatry. 2003;5(6):260-266.
15. Swee du S, Chng CL, Lim A. Clinical characteristics and outcome of thyroid storm: a case series and review of neuropsychiatric derangements in thyrotoxicosis. Endocr Pract. 2015;21(2):182-189.
16. Tang A, O’Sullivan AJ, Diamond T, Gerard A, Campbell P. Psychiatric symptoms as a clinical presentation of Cushing’s syndrome. Ann Gen Psychiatry. 2013;12(1):23.
17. Farah Jde L, Lauand CV, Chequi L, et al. Severe psychotic disorder as the main manifestation of adrenal insufficiency. Case Rep Psychiatry. 2015;2015:512430.
18. Rice T, Azova S, Coffey BJ. Negative symptoms in a depressed teen? Primary hyperparathyroidism and its psychiatric manifestations. J Child Adolesc Psychopharmacol. 2015;25(8):653-655.
19. Zardawi IM. Phaeochromocytoma masquerading as anxiety and depression. Am J Case Rep. 2013;14:161-163.
20. Kate S, Dhanwal DK, Kumar S, Bharti P. Acute psychosis as a presentation of hypopituitarism. BMJ Case Rep. 2013;2013.
21. Abramowicz M. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther. 2008;50(1301-1302):100-103.
22. Tait RJ, Caldicott D, Mountain D, Hill SL, Lenton S. A systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin Toxicol (Phila). 2016;54(1):1-13.
23. Karch SB. Cathinone neurotoxicity (“The “3Ms”). Curr Neuropharmacol. 2015;13(1): 21-25.
24. Menon AV, Chang J, Kim J. Mechanisms of divalent metal toxicity in affective disorders. Toxicology. 2016;339:58-72.
1. Barnes J, Dickerson BC, Frost C, Jiskoot LC, Wolk D, van der Flier WM. Alzheimer’s disease first symptoms are age dependent: Evidence from the NACC dataset. Alzheimers Dement. 2015;11(11):1349-1357.
2. Yoshizawa H, Vonsattel JP, Honig LS. Early neuropsychological discriminants for Lewy body disease: an autopsy series. J Neurol Neurosurg Psychiatry. 2013;84(12):1326-1330.
3. Iroka N, Jehangir W, Ii JL, Pattan V, Yousif A, Mishra AK. Paranoid personality masking an atypical case of frontotemporal dementia. J Clin Med Res. 2015;7(5):364-366.
4. Filley CM, Kleinschmidt-DeMasters BK. Neurobehavioral presentations of brain neoplasms. West J Med. 1995;163(1):19-25.
5. Said S, Cooper CJ, Reyna E, Alkhateeb H, Diaz J, Nahleh Z. Paraneoplastic limbic encephalitis, an uncommon presentation of a common cancer: Case report and discussion. Am J Case Rep. 2013;14:391-394.
6. Weitzner MA, Olofsson SM, Forman AD. Patients with malignant meningitis presenting with neuropsychiatric manifestations. Cancer. 1995;76(10):1804-1808.
7. Ding Y, Wang S, Liu J. Neuropsychiatric profiles of patients with insulinomas. Eur Neurol. 2010;63(1):48-51.
8. Toussi A, Bryk J, Alam A. Forgetting heart break: a fascinating case of transient left ventricular apical ballooning syndrome associated with dissociative amnesia. Gen Hosp Psychiatry. 2014;36(2):225-227.
9. Scalzo SJ, Bowden SC, Ambrose ML, Whelan G, Cook MJ. Wernicke-Korsakoff syndrome not related to alcohol use: a systematic review. J Neurol Neurosurg Psychiatry. 2015;86(12):1362-1368.
10. Isenberg-Grzeda E, Kutner HE, Nicolson SE. Wernicke-Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics. 2012;53(6):507-516.
11. Issac TG, Soundarya S, Christopher R, Chandra SR. Vitamin B12 deficiency: an important reversible co-morbidity in neuropsychiatric manifestations. Indian J Psychol Med. 2015;37(1):26-29.
12. Grønli O, Kvamme JM, Friborg O, Wynn R. Zinc deficiency is common in several psychiatric disorders. PLoS One. 2013;8(12):e82793.
13. Grønli O, Kvamme JM, Jorde R, Wynn R. Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry. 2014;14:134.
14. Heinrich TW, Grahm G. Hypothyroidism presenting as psychosis: myxedema madness revisited. Prim Care Companion J Clin Psychiatry. 2003;5(6):260-266.
15. Swee du S, Chng CL, Lim A. Clinical characteristics and outcome of thyroid storm: a case series and review of neuropsychiatric derangements in thyrotoxicosis. Endocr Pract. 2015;21(2):182-189.
16. Tang A, O’Sullivan AJ, Diamond T, Gerard A, Campbell P. Psychiatric symptoms as a clinical presentation of Cushing’s syndrome. Ann Gen Psychiatry. 2013;12(1):23.
17. Farah Jde L, Lauand CV, Chequi L, et al. Severe psychotic disorder as the main manifestation of adrenal insufficiency. Case Rep Psychiatry. 2015;2015:512430.
18. Rice T, Azova S, Coffey BJ. Negative symptoms in a depressed teen? Primary hyperparathyroidism and its psychiatric manifestations. J Child Adolesc Psychopharmacol. 2015;25(8):653-655.
19. Zardawi IM. Phaeochromocytoma masquerading as anxiety and depression. Am J Case Rep. 2013;14:161-163.
20. Kate S, Dhanwal DK, Kumar S, Bharti P. Acute psychosis as a presentation of hypopituitarism. BMJ Case Rep. 2013;2013.
21. Abramowicz M. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther. 2008;50(1301-1302):100-103.
22. Tait RJ, Caldicott D, Mountain D, Hill SL, Lenton S. A systematic review of adverse events arising from the use of synthetic cannabinoids and their associated treatment. Clin Toxicol (Phila). 2016;54(1):1-13.
23. Karch SB. Cathinone neurotoxicity (“The “3Ms”). Curr Neuropharmacol. 2015;13(1): 21-25.
24. Menon AV, Chang J, Kim J. Mechanisms of divalent metal toxicity in affective disorders. Toxicology. 2016;339:58-72.

Pediatric Heat-Related Illnesses
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
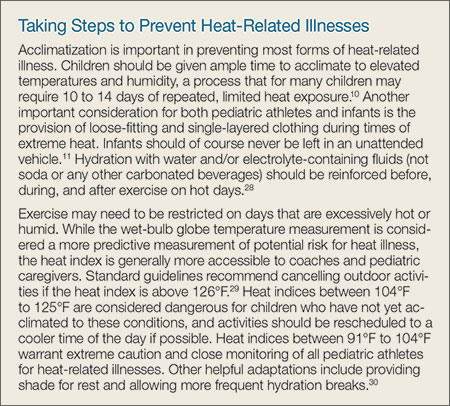
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
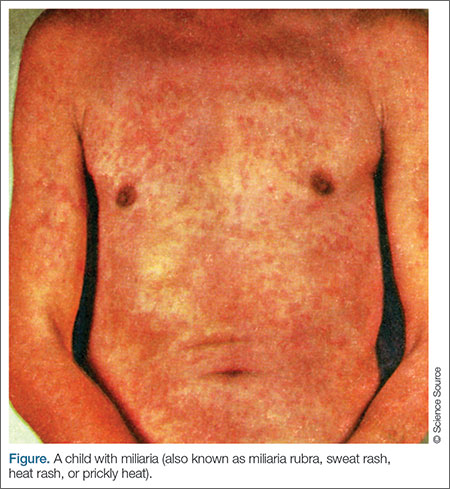
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
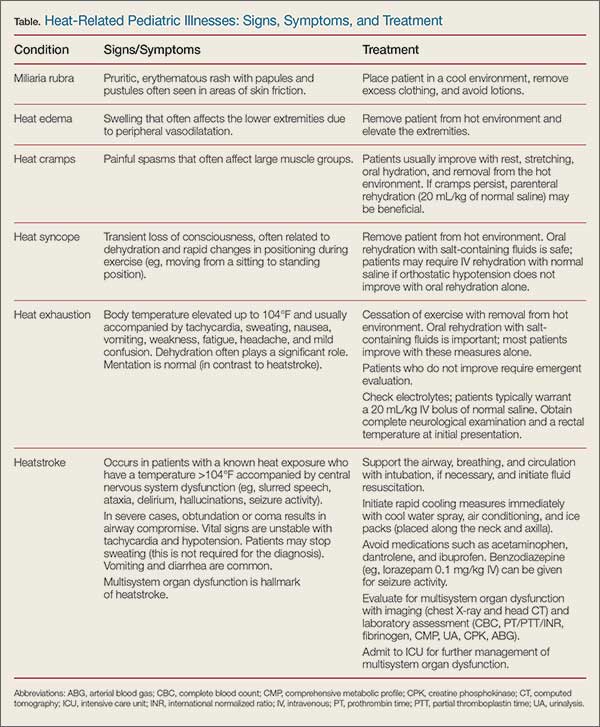
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.

First EDition: News for and about the practice of emergency medicine
Medication for Out-of-Hospital Cardiac Arrest: For Which Patients Is It Effective?
BY JEFF BAUER
FROM N ENGL J MED
A recent double-blind, randomized trial that compared parenteral amiodarone, lidocaine, and saline placebo for patients who experienced out-of-hospital cardiac arrest found that overall, neither medication resulted in a significantly higher survival rate nor better neurological outcomes.1 However, among a subgroup of patients whose cardiac arrest was witnessed by a bystander, the rate of survival to hospital discharge was significantly higher with amiodarone or lidocaine than with placebo.
Researchers studied 3,026 adults who had nontraumatic out-of-hospital cardiac arrest and shock-refractory ventricular fibrillation or pulseless ventricular tachycardia. These patients were treated in accordance with local emergency medical service (EMS) protocols that complied with American Heart Association (AHA) guidelines for advanced life support. After one or more shocks failed to end ventricular fibrillation or pulseless ventricular tachycardia, patients were randomly treated with one of three parenteral preparations: lidocaine (993 patients), a recently approved cyclodextrin-based formulation of amiodarone that is designed to reduce hypotensive effects (974 patients), or a normal saline placebo (1,059 patients). The initial treatment consisted of two syringes that were administered by rapid bolus. If the ventricular fibrillation or pulseless ventricular tachycardia persisted after this initial dose, a supplemental dose (one syringe) of the same drug was administered. The average time to treatment with these drugs was 19 minutes from the initial call to EMS. On arrival at the hospital, patients were treated with usual postcardiac arrest care in accordance with AHA guidelines.
The primary outcome was survival to hospital discharge. The secondary outcome was survival with favorable neurological status at discharge, which was defined as a score of ≤3 on the modified Rankin scale, indicating the ability to conduct daily activities independently or with minimal assistance.
The hospital survival rates were 23.7% for patients who received lidocaine, 24.4% for those who received amiodarone, and 21.0% for those who received placebo. The differences in survival rates for each drug compared to placebo, and one drug compared to the other drug, were not statistically significant. Rates of survival with favorable neurological status were similar among all three groups.
However, among 1,934 patients who experienced a witnessed out-of-hospital cardiac arrest, each drug was associated with a significantly higher rate of survival (5 percentage points) compared to placebo. In these patients, the survival rate was 27.8% with lidocaine, 27.7% with amiodarone, and 22.7% with placebo. This absolute risk difference was significant for lidocaine versus placebo and for amiodarone versus placebo, but not for lidocaine versus amiodarone.
Researchers said patients who have a witnessed out-of-hospital cardiac arrest presumably have “early recognition of cardiac arrest, a short interval between the patient’s collapse from cardiac arrest and the initiation of treatment, and a greater likelihood of therapeutic responsiveness.” In an accompanying editorial, Joglar and Page2 said EMS personnel should consider using lidocaine or amiodarone when a patient’s cardiac arrest is witnessed.
1. Kudenchuk PJ, Brown SP, Daya M, et al; Resuscitation Outcomes Consortium Investigators. Amiodarone, lidocaine, or placebo in out-of-hospital cardiac arrest. N Engl J Med. 2016;374(18):1711-1722.
2. Joglar JA, Page RL. Out-of-hospital cardiac arrest--are drugs ever the answer? N Engl J Med. 2016;374(18):1781-1782.
Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, Is Honored at Two Medical School Graduations on the Same Day

On Wednesday, May 25, 2016, Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, emergency physician-in-chief (1996-2016) and emergency medical services (EMS) medical director (1996- ) at New York Presbyterian Hospital, professor of clinical medicine at Weill Cornell Medical College, was honored at two New York City medical school graduations.
First, at the midday Weill Cornell Medical College commencement exercises in Carnegie Hall, Dr Flomenbaum helped present the second annual “Neal Flomenbaum, MD, Prize for Excellence in Emergency Medicine,” a $50,000 award endowed by a generous gift named for Dr Flomenbaum by Jeanne and Herbert Seigel. A few hours later, at the Lincoln Center commencement exercises of his alma mater, Dr Flomenbaum received the “Albert Einstein College of Medicine 2016 Lifetime Achievement Award,” for, according to Einstein Dean Allen M. Spiegel, MD, his “extraordinary career in emergency medicine and...many contributions to the health and welfare of underserved communities and all populations in New York City.”
Dr Flomenbaum has dedicated his life to ensuring the highest quality emergency care for patients; to educating and training students, residents, and attending physicians; and to helping establish and support the specialty of emergency medicine. Dr Flomenbaum’s accomplishments include coauthoring and coediting eight editions of the leading medical toxicology textbook, two editions of a text on diagnostic testing, and more than 150 research and review papers, book chapters, and editorials. He has served as a senior examiner for the American Board of Emergency Medicine, senior consultant to the NYC Poison Control Center, a fellow and the founding chair of the New York Academy of Medicine Section on Emergency Medicine, and chair of the Medical Advisory Committee to NYC EMS. Prior to joining the Weill Cornell faculty in 1996, Dr Flomenbaum held academic appointments at Einstein, New York University, and SUNY/Downstate Schools of Medicine.
He received his bachelor’s degree from Columbia College in 1969, and his MD from Albert Einstein as an alpha omega alpha member of the class of 1973. Dr Flomenbaum completed an internal medicine residency at Einstein/Jacobi Medical Center in the Bronx. In 1996, Dr Flomenbaum arrived at what was then New York Hospital-Cornell University Medical Center after serving as associate director of emergency medicine at Jacobi/Einstein and NYU/Bellevue Hospitals, and then as chairman of emergency medicine at SUNY/Long Island College Hospital.
According to the Dean of Weill Cornell Medical College, its Division of Emergency Medicine “has grown significantly in the last 20 years under the leadership of Dr Neal Flomenbaum and is operating at a scale and scope [of] an academic department.” At Weill Cornell, Dr Flomenbaum created the nation’s first fellowship and division of geriatric emergency medicine (GEM) in 2005, a decade before GEM fellowships were offered at other academic centers around the country; he also created divisions of medical toxicology, EM/critical care, and other traditional EM subspecialties. Dr Flomenbaum most recently embarked on creating a new fellowship and division of Women’s Health Emergencies.
Since 2006, Dr Flomenbaum has also been editor-in-chief of Emergency Medicine, the oldest and one of the most widely read journals for the specialty. His incisive monthly editorials on current concerns in emergency medicine and emergency departments are available at www.emed-journal.com and at www.NYMeDED.org.
Medication for Out-of-Hospital Cardiac Arrest: For Which Patients Is It Effective?
BY JEFF BAUER
FROM N ENGL J MED
A recent double-blind, randomized trial that compared parenteral amiodarone, lidocaine, and saline placebo for patients who experienced out-of-hospital cardiac arrest found that overall, neither medication resulted in a significantly higher survival rate nor better neurological outcomes.1 However, among a subgroup of patients whose cardiac arrest was witnessed by a bystander, the rate of survival to hospital discharge was significantly higher with amiodarone or lidocaine than with placebo.
Researchers studied 3,026 adults who had nontraumatic out-of-hospital cardiac arrest and shock-refractory ventricular fibrillation or pulseless ventricular tachycardia. These patients were treated in accordance with local emergency medical service (EMS) protocols that complied with American Heart Association (AHA) guidelines for advanced life support. After one or more shocks failed to end ventricular fibrillation or pulseless ventricular tachycardia, patients were randomly treated with one of three parenteral preparations: lidocaine (993 patients), a recently approved cyclodextrin-based formulation of amiodarone that is designed to reduce hypotensive effects (974 patients), or a normal saline placebo (1,059 patients). The initial treatment consisted of two syringes that were administered by rapid bolus. If the ventricular fibrillation or pulseless ventricular tachycardia persisted after this initial dose, a supplemental dose (one syringe) of the same drug was administered. The average time to treatment with these drugs was 19 minutes from the initial call to EMS. On arrival at the hospital, patients were treated with usual postcardiac arrest care in accordance with AHA guidelines.
The primary outcome was survival to hospital discharge. The secondary outcome was survival with favorable neurological status at discharge, which was defined as a score of ≤3 on the modified Rankin scale, indicating the ability to conduct daily activities independently or with minimal assistance.
The hospital survival rates were 23.7% for patients who received lidocaine, 24.4% for those who received amiodarone, and 21.0% for those who received placebo. The differences in survival rates for each drug compared to placebo, and one drug compared to the other drug, were not statistically significant. Rates of survival with favorable neurological status were similar among all three groups.
However, among 1,934 patients who experienced a witnessed out-of-hospital cardiac arrest, each drug was associated with a significantly higher rate of survival (5 percentage points) compared to placebo. In these patients, the survival rate was 27.8% with lidocaine, 27.7% with amiodarone, and 22.7% with placebo. This absolute risk difference was significant for lidocaine versus placebo and for amiodarone versus placebo, but not for lidocaine versus amiodarone.
Researchers said patients who have a witnessed out-of-hospital cardiac arrest presumably have “early recognition of cardiac arrest, a short interval between the patient’s collapse from cardiac arrest and the initiation of treatment, and a greater likelihood of therapeutic responsiveness.” In an accompanying editorial, Joglar and Page2 said EMS personnel should consider using lidocaine or amiodarone when a patient’s cardiac arrest is witnessed.
1. Kudenchuk PJ, Brown SP, Daya M, et al; Resuscitation Outcomes Consortium Investigators. Amiodarone, lidocaine, or placebo in out-of-hospital cardiac arrest. N Engl J Med. 2016;374(18):1711-1722.
2. Joglar JA, Page RL. Out-of-hospital cardiac arrest--are drugs ever the answer? N Engl J Med. 2016;374(18):1781-1782.
Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, Is Honored at Two Medical School Graduations on the Same Day
On Wednesday, May 25, 2016, Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, emergency physician-in-chief (1996-2016) and emergency medical services (EMS) medical director (1996- ) at New York Presbyterian Hospital, professor of clinical medicine at Weill Cornell Medical College, was honored at two New York City medical school graduations.
First, at the midday Weill Cornell Medical College commencement exercises in Carnegie Hall, Dr Flomenbaum helped present the second annual “Neal Flomenbaum, MD, Prize for Excellence in Emergency Medicine,” a $50,000 award endowed by a generous gift named for Dr Flomenbaum by Jeanne and Herbert Seigel. A few hours later, at the Lincoln Center commencement exercises of his alma mater, Dr Flomenbaum received the “Albert Einstein College of Medicine 2016 Lifetime Achievement Award,” for, according to Einstein Dean Allen M. Spiegel, MD, his “extraordinary career in emergency medicine and...many contributions to the health and welfare of underserved communities and all populations in New York City.”
Dr Flomenbaum has dedicated his life to ensuring the highest quality emergency care for patients; to educating and training students, residents, and attending physicians; and to helping establish and support the specialty of emergency medicine. Dr Flomenbaum’s accomplishments include coauthoring and coediting eight editions of the leading medical toxicology textbook, two editions of a text on diagnostic testing, and more than 150 research and review papers, book chapters, and editorials. He has served as a senior examiner for the American Board of Emergency Medicine, senior consultant to the NYC Poison Control Center, a fellow and the founding chair of the New York Academy of Medicine Section on Emergency Medicine, and chair of the Medical Advisory Committee to NYC EMS. Prior to joining the Weill Cornell faculty in 1996, Dr Flomenbaum held academic appointments at Einstein, New York University, and SUNY/Downstate Schools of Medicine.
He received his bachelor’s degree from Columbia College in 1969, and his MD from Albert Einstein as an alpha omega alpha member of the class of 1973. Dr Flomenbaum completed an internal medicine residency at Einstein/Jacobi Medical Center in the Bronx. In 1996, Dr Flomenbaum arrived at what was then New York Hospital-Cornell University Medical Center after serving as associate director of emergency medicine at Jacobi/Einstein and NYU/Bellevue Hospitals, and then as chairman of emergency medicine at SUNY/Long Island College Hospital.
According to the Dean of Weill Cornell Medical College, its Division of Emergency Medicine “has grown significantly in the last 20 years under the leadership of Dr Neal Flomenbaum and is operating at a scale and scope [of] an academic department.” At Weill Cornell, Dr Flomenbaum created the nation’s first fellowship and division of geriatric emergency medicine (GEM) in 2005, a decade before GEM fellowships were offered at other academic centers around the country; he also created divisions of medical toxicology, EM/critical care, and other traditional EM subspecialties. Dr Flomenbaum most recently embarked on creating a new fellowship and division of Women’s Health Emergencies.
Since 2006, Dr Flomenbaum has also been editor-in-chief of Emergency Medicine, the oldest and one of the most widely read journals for the specialty. His incisive monthly editorials on current concerns in emergency medicine and emergency departments are available at www.emed-journal.com and at www.NYMeDED.org.
Medication for Out-of-Hospital Cardiac Arrest: For Which Patients Is It Effective?
BY JEFF BAUER
FROM N ENGL J MED
A recent double-blind, randomized trial that compared parenteral amiodarone, lidocaine, and saline placebo for patients who experienced out-of-hospital cardiac arrest found that overall, neither medication resulted in a significantly higher survival rate nor better neurological outcomes.1 However, among a subgroup of patients whose cardiac arrest was witnessed by a bystander, the rate of survival to hospital discharge was significantly higher with amiodarone or lidocaine than with placebo.
Researchers studied 3,026 adults who had nontraumatic out-of-hospital cardiac arrest and shock-refractory ventricular fibrillation or pulseless ventricular tachycardia. These patients were treated in accordance with local emergency medical service (EMS) protocols that complied with American Heart Association (AHA) guidelines for advanced life support. After one or more shocks failed to end ventricular fibrillation or pulseless ventricular tachycardia, patients were randomly treated with one of three parenteral preparations: lidocaine (993 patients), a recently approved cyclodextrin-based formulation of amiodarone that is designed to reduce hypotensive effects (974 patients), or a normal saline placebo (1,059 patients). The initial treatment consisted of two syringes that were administered by rapid bolus. If the ventricular fibrillation or pulseless ventricular tachycardia persisted after this initial dose, a supplemental dose (one syringe) of the same drug was administered. The average time to treatment with these drugs was 19 minutes from the initial call to EMS. On arrival at the hospital, patients were treated with usual postcardiac arrest care in accordance with AHA guidelines.
The primary outcome was survival to hospital discharge. The secondary outcome was survival with favorable neurological status at discharge, which was defined as a score of ≤3 on the modified Rankin scale, indicating the ability to conduct daily activities independently or with minimal assistance.
The hospital survival rates were 23.7% for patients who received lidocaine, 24.4% for those who received amiodarone, and 21.0% for those who received placebo. The differences in survival rates for each drug compared to placebo, and one drug compared to the other drug, were not statistically significant. Rates of survival with favorable neurological status were similar among all three groups.
However, among 1,934 patients who experienced a witnessed out-of-hospital cardiac arrest, each drug was associated with a significantly higher rate of survival (5 percentage points) compared to placebo. In these patients, the survival rate was 27.8% with lidocaine, 27.7% with amiodarone, and 22.7% with placebo. This absolute risk difference was significant for lidocaine versus placebo and for amiodarone versus placebo, but not for lidocaine versus amiodarone.
Researchers said patients who have a witnessed out-of-hospital cardiac arrest presumably have “early recognition of cardiac arrest, a short interval between the patient’s collapse from cardiac arrest and the initiation of treatment, and a greater likelihood of therapeutic responsiveness.” In an accompanying editorial, Joglar and Page2 said EMS personnel should consider using lidocaine or amiodarone when a patient’s cardiac arrest is witnessed.
1. Kudenchuk PJ, Brown SP, Daya M, et al; Resuscitation Outcomes Consortium Investigators. Amiodarone, lidocaine, or placebo in out-of-hospital cardiac arrest. N Engl J Med. 2016;374(18):1711-1722.
2. Joglar JA, Page RL. Out-of-hospital cardiac arrest--are drugs ever the answer? N Engl J Med. 2016;374(18):1781-1782.
Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, Is Honored at Two Medical School Graduations on the Same Day
On Wednesday, May 25, 2016, Emergency Medicine Editor-in-Chief Neal Flomenbaum, MD, emergency physician-in-chief (1996-2016) and emergency medical services (EMS) medical director (1996- ) at New York Presbyterian Hospital, professor of clinical medicine at Weill Cornell Medical College, was honored at two New York City medical school graduations.
First, at the midday Weill Cornell Medical College commencement exercises in Carnegie Hall, Dr Flomenbaum helped present the second annual “Neal Flomenbaum, MD, Prize for Excellence in Emergency Medicine,” a $50,000 award endowed by a generous gift named for Dr Flomenbaum by Jeanne and Herbert Seigel. A few hours later, at the Lincoln Center commencement exercises of his alma mater, Dr Flomenbaum received the “Albert Einstein College of Medicine 2016 Lifetime Achievement Award,” for, according to Einstein Dean Allen M. Spiegel, MD, his “extraordinary career in emergency medicine and...many contributions to the health and welfare of underserved communities and all populations in New York City.”
Dr Flomenbaum has dedicated his life to ensuring the highest quality emergency care for patients; to educating and training students, residents, and attending physicians; and to helping establish and support the specialty of emergency medicine. Dr Flomenbaum’s accomplishments include coauthoring and coediting eight editions of the leading medical toxicology textbook, two editions of a text on diagnostic testing, and more than 150 research and review papers, book chapters, and editorials. He has served as a senior examiner for the American Board of Emergency Medicine, senior consultant to the NYC Poison Control Center, a fellow and the founding chair of the New York Academy of Medicine Section on Emergency Medicine, and chair of the Medical Advisory Committee to NYC EMS. Prior to joining the Weill Cornell faculty in 1996, Dr Flomenbaum held academic appointments at Einstein, New York University, and SUNY/Downstate Schools of Medicine.
He received his bachelor’s degree from Columbia College in 1969, and his MD from Albert Einstein as an alpha omega alpha member of the class of 1973. Dr Flomenbaum completed an internal medicine residency at Einstein/Jacobi Medical Center in the Bronx. In 1996, Dr Flomenbaum arrived at what was then New York Hospital-Cornell University Medical Center after serving as associate director of emergency medicine at Jacobi/Einstein and NYU/Bellevue Hospitals, and then as chairman of emergency medicine at SUNY/Long Island College Hospital.
According to the Dean of Weill Cornell Medical College, its Division of Emergency Medicine “has grown significantly in the last 20 years under the leadership of Dr Neal Flomenbaum and is operating at a scale and scope [of] an academic department.” At Weill Cornell, Dr Flomenbaum created the nation’s first fellowship and division of geriatric emergency medicine (GEM) in 2005, a decade before GEM fellowships were offered at other academic centers around the country; he also created divisions of medical toxicology, EM/critical care, and other traditional EM subspecialties. Dr Flomenbaum most recently embarked on creating a new fellowship and division of Women’s Health Emergencies.
Since 2006, Dr Flomenbaum has also been editor-in-chief of Emergency Medicine, the oldest and one of the most widely read journals for the specialty. His incisive monthly editorials on current concerns in emergency medicine and emergency departments are available at www.emed-journal.com and at www.NYMeDED.org.
More Hospitals to Be Replaced by FSEDs
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.

Optical Imaging to Detect Lentigo Maligna

In an article published online on January 26 in the Journal of the American Academy of Dermatology, my colleagues and I (Menge et al) reported on the use of reflectance confocal microscopy (RCM) for challenging facial lesions. We studied the diagnosis of lentigo maligna (LM) based on RCM versus the histopathologic diagnosis after biopsy.
In this study 17 patients were seen for evaluation of known or suspected LM at Memorial Sloan Kettering Cancer Center (New York, New York). Among these patients, a total of 63 sites on the skin were evaluated using RCM and a presumptive diagnosis was made. These sites were then biopsied to compare the diagnosis using RCM with that made by histopathology. When LM was present as determined by biopsy, RCM also was able to detect it 100% of the time (sensitivity). When LM was absent as determined by biopsy, RCM also indicated it was absent 71% of the time (specificity).
What’s the issue?
Lentigo maligna is a form of melanoma in situ occurring on sun-damaged skin. It can be quite subtle to detect clinically and therefore may go undiagnosed for a while. Lentigo maligna also has been shown to have notable subclinical extension with which traditional surgical margins for truncal melanoma may be too narrow to clear LM on the head and neck. Therefore, presurgical consultation may be difficult due to the amorphous borders. Random blind biopsies also are discouraged because of sampling error.
Additionally, repetitive biopsies over time, which may be frequently needed in individuals with heavy sun exposure, can be costly and cause adverse effects.
This study showed the usefulness and reliability of using RCM for challenging facial lesions that are suspicious for LM. The sensitivity and specificity of RCM in this study indicated that this technology performs well in detecting LM when present; however, false-positives were noted in this study. False-positives included pigmented actinic keratosis and melanocytosis. Dermatologists who are advanced in RCM technology and interpretation also were utilized in this study. More research is needed to understand how to best utilize this technology, but overall the ability of RCM to accurately identify LM without biopsy represents an exciting new development in how dermatologists can better diagnose, manage, and treat melanoma.
How will you adopt advances in cutaneous noninvasive imaging?
In an article published online on January 26 in the Journal of the American Academy of Dermatology, my colleagues and I (Menge et al) reported on the use of reflectance confocal microscopy (RCM) for challenging facial lesions. We studied the diagnosis of lentigo maligna (LM) based on RCM versus the histopathologic diagnosis after biopsy.
In this study 17 patients were seen for evaluation of known or suspected LM at Memorial Sloan Kettering Cancer Center (New York, New York). Among these patients, a total of 63 sites on the skin were evaluated using RCM and a presumptive diagnosis was made. These sites were then biopsied to compare the diagnosis using RCM with that made by histopathology. When LM was present as determined by biopsy, RCM also was able to detect it 100% of the time (sensitivity). When LM was absent as determined by biopsy, RCM also indicated it was absent 71% of the time (specificity).
What’s the issue?
Lentigo maligna is a form of melanoma in situ occurring on sun-damaged skin. It can be quite subtle to detect clinically and therefore may go undiagnosed for a while. Lentigo maligna also has been shown to have notable subclinical extension with which traditional surgical margins for truncal melanoma may be too narrow to clear LM on the head and neck. Therefore, presurgical consultation may be difficult due to the amorphous borders. Random blind biopsies also are discouraged because of sampling error.
Additionally, repetitive biopsies over time, which may be frequently needed in individuals with heavy sun exposure, can be costly and cause adverse effects.
This study showed the usefulness and reliability of using RCM for challenging facial lesions that are suspicious for LM. The sensitivity and specificity of RCM in this study indicated that this technology performs well in detecting LM when present; however, false-positives were noted in this study. False-positives included pigmented actinic keratosis and melanocytosis. Dermatologists who are advanced in RCM technology and interpretation also were utilized in this study. More research is needed to understand how to best utilize this technology, but overall the ability of RCM to accurately identify LM without biopsy represents an exciting new development in how dermatologists can better diagnose, manage, and treat melanoma.
How will you adopt advances in cutaneous noninvasive imaging?
In an article published online on January 26 in the Journal of the American Academy of Dermatology, my colleagues and I (Menge et al) reported on the use of reflectance confocal microscopy (RCM) for challenging facial lesions. We studied the diagnosis of lentigo maligna (LM) based on RCM versus the histopathologic diagnosis after biopsy.
In this study 17 patients were seen for evaluation of known or suspected LM at Memorial Sloan Kettering Cancer Center (New York, New York). Among these patients, a total of 63 sites on the skin were evaluated using RCM and a presumptive diagnosis was made. These sites were then biopsied to compare the diagnosis using RCM with that made by histopathology. When LM was present as determined by biopsy, RCM also was able to detect it 100% of the time (sensitivity). When LM was absent as determined by biopsy, RCM also indicated it was absent 71% of the time (specificity).
What’s the issue?
Lentigo maligna is a form of melanoma in situ occurring on sun-damaged skin. It can be quite subtle to detect clinically and therefore may go undiagnosed for a while. Lentigo maligna also has been shown to have notable subclinical extension with which traditional surgical margins for truncal melanoma may be too narrow to clear LM on the head and neck. Therefore, presurgical consultation may be difficult due to the amorphous borders. Random blind biopsies also are discouraged because of sampling error.
Additionally, repetitive biopsies over time, which may be frequently needed in individuals with heavy sun exposure, can be costly and cause adverse effects.
This study showed the usefulness and reliability of using RCM for challenging facial lesions that are suspicious for LM. The sensitivity and specificity of RCM in this study indicated that this technology performs well in detecting LM when present; however, false-positives were noted in this study. False-positives included pigmented actinic keratosis and melanocytosis. Dermatologists who are advanced in RCM technology and interpretation also were utilized in this study. More research is needed to understand how to best utilize this technology, but overall the ability of RCM to accurately identify LM without biopsy represents an exciting new development in how dermatologists can better diagnose, manage, and treat melanoma.
How will you adopt advances in cutaneous noninvasive imaging?

Spontaneous Repigmentation of Silvery Hair in an Infant With Congenital Hydrops Fetalis and Hypoproteinemia
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.

Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
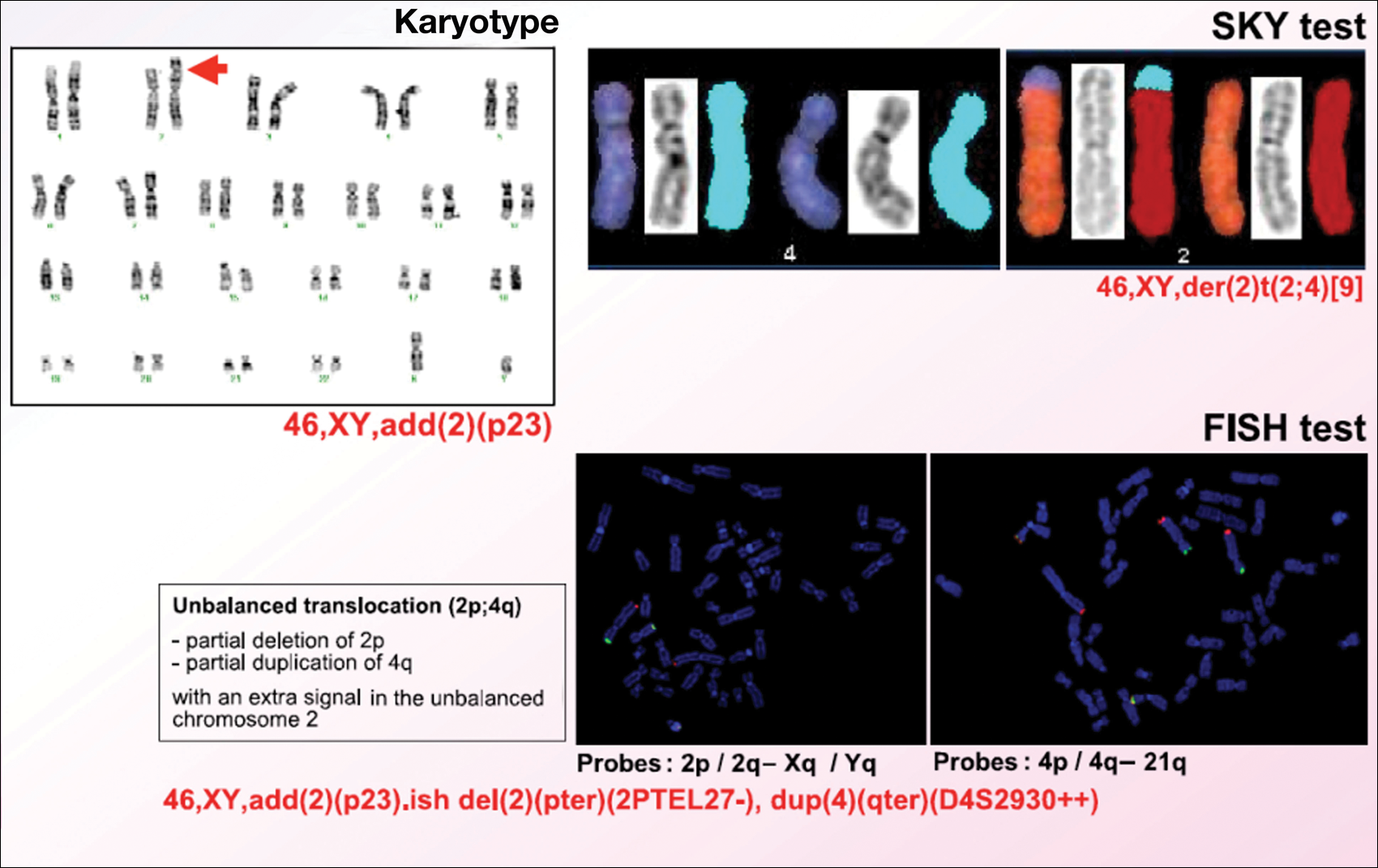
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.


Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
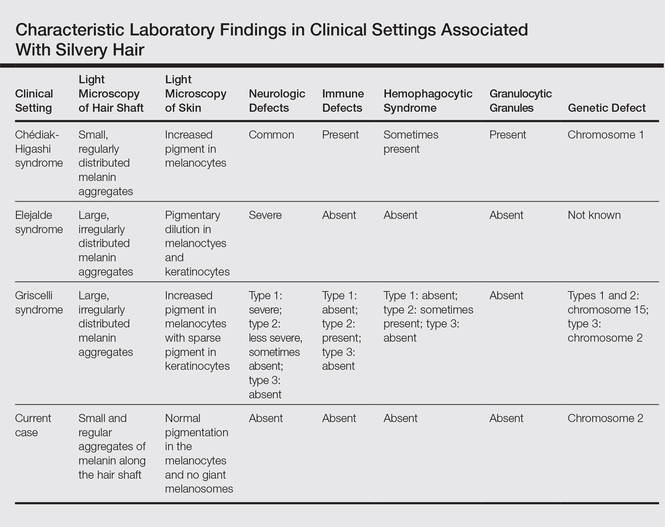
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
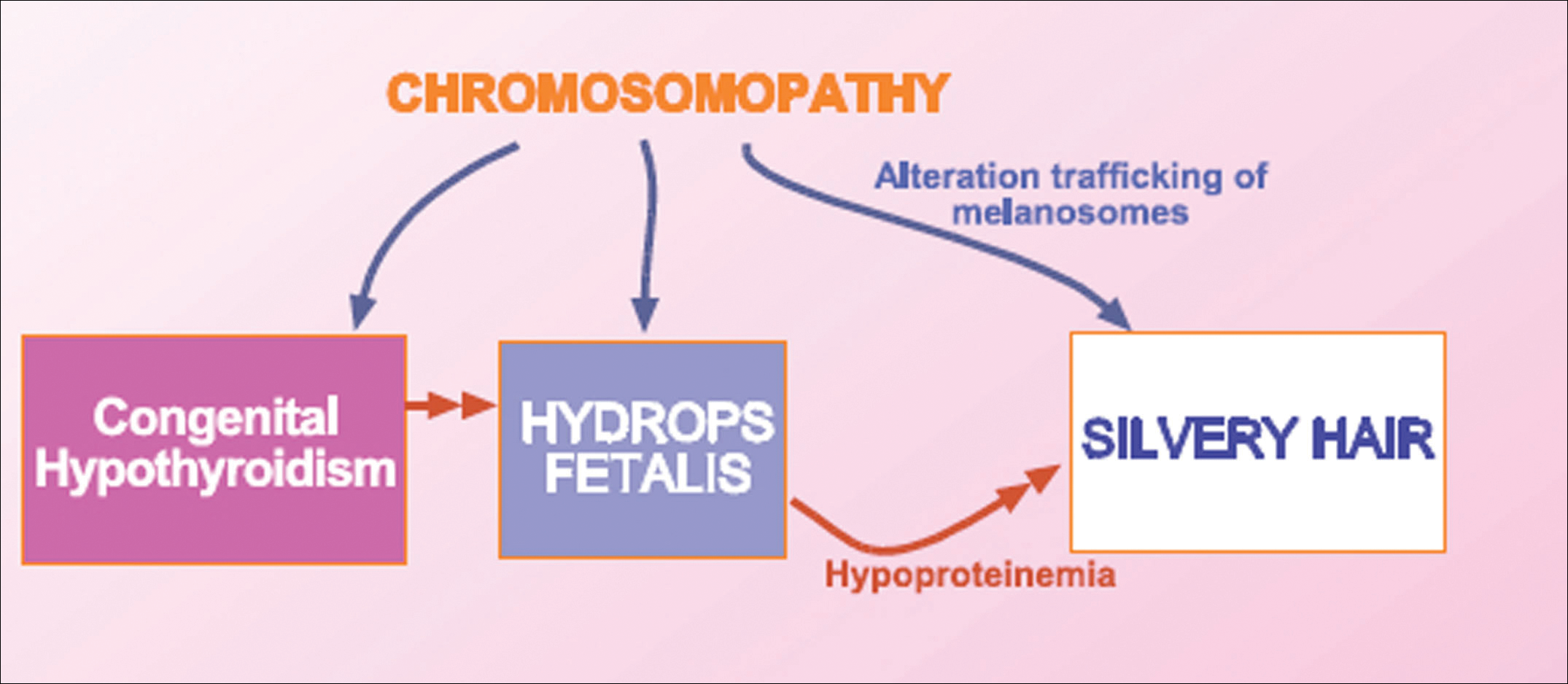
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.
Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.
Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.
Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.
Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
Practice Points
- Silvery hair is characteristic of 3 rare autosomal-recessive disorders: Chédiak-Higashi syndrome, Elejalde syndrome, and Griscelli syndrome.
- Hypopigmentation is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes.
- Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.

Coldiron Truth: Beware the state pharmacy board
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.

But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.
But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].
What does the pharmacy board have to do with me? I’m a physician, regulated by the state medical board. Well heads up. If regulations coming your way are adopted, you will have the additional privilege of being licensed, inspected by, and financially supporting your state pharmacy board.
How did all this happen? In 2012, a compounding pharmacy inadequately sterilized multiple lots of methylprednisolone, which were sold around the country and used for intrathecal injections. As a result, 753 patients developed fungal infections, including 386 cases of meningitis, and 64 of them died. The owner of the pharmacy and the head pharmacist are up on second degree murder charges.
But what does this have to do with you?
After a media bonfire, a congressional hearing complete with the taking of the fifth amendment, and a major rewrite of pharmacy regulations with increased scrutiny and oversight, the State of Ohio Board of Pharmacy rushed to adopt rules before reasonable regulations could be worked out by the Food and Drug Administration, the American Medical Association, and the Federation of State Medical Boards. The Ohio board of pharmacy adopted the U.S. Pharmacopeial Convention (USP) regulations, written for compounding pharmacies, and applied them to physicians’ offices.
In an overreaching bureaucratic coup de grace, any practitioners who reconstitute any drug in their offices is considered to be a compounding pharmacy, ordered to pay compounding pharmacy registration fees ($112 yearly), and to undergo the same inspections as compounding pharmacies. You can’t be too safe, you know, and all those registration fees (totaling about $2 million per year in Ohio alone) will decrease what would have been an onerous registration and inspection expense for true compounding pharmacies.
This is the reality we are facing in Ohio, and this situation may soon be “coming to a theater near you.” I understand that several pharmacy boards in other states are preparing to roll out similar regulations.
As a kicker, if the product you reconstitute is preservative free (botulinum toxin anyone?), you must use it or dispose of it within one hour. Yes, one hour. If you dilute bleomycin or 5-fluorouracil (5-FU), you must install an outside vented laminar flow hood, and wear level 5 hazmat gear while drawing it up.
Is this situation insane or what? As the result of a pharmacy in Massachusetts that skirted existing regulations and sold contaminated drugs that killed patients, doctors now need more regulations, licensing, inspections, and fees?
The real problem here, of course, is not the $112 fee. It will be the loss of many drugs and therapies that can be used inexpensively in the office, but will now either be unavailable to patients or available at a greatly increased cost. I pointed this situation out at a pharmacy board meeting, and they helpfully responded that I can have my friendly local pharmacist compound any drug I need in a specific strength and unit dose. Who is going to pay for this? I can make diclofenac or 5-FU cream in my office for less than $20. Instead, it will cost over $700 at the pharmacy! Further, making something fiscally impossible, like installing a laminar flow hood, is not different that denying it outright. I consider this to be restraint of trade.
Don’t allow yourselves to be compromised as Ohio physicians have been. You must be vigilant. Attend the public hearings and testify. In Ohio, the hearings were held over the Christmas holidays. Guess what? No one came to the hearings! You must show up and complain. Loudly. You must point out how patients are going to be hurt, not helped, by these rules. You must point out the superb safety record of physicians when using in-office pharmaceuticals. You must alert your neurology, ophthalmology, gynecology, and urology colleagues to the problem since they all use neurotoxins, too. The primary care doctors all reconstitute drugs (think antibiotics) for office use, too.
These efforts are also part of a larger campaign to give pharmacists a larger clinical role in patient care. If pharmacists license you, if they inspect your office, how can you oppose them when they want clinical privileges?
The fix is to enact a moratorium on regulations until the FDA rules come out. These will be more reasonable than the rules issued by the USP. Another fix is a legislative change that instructs that physicians, not pharmacists, will define what is considered to be a dangerous drug.
It is time to be alert, vigilant, and outspoken. You must do this to preserve your ability to do what is best for patients, to be able to deliver care in an expeditious, efficient, and cost-effective manner. This is what being physician is all about! Keep your state board of pharmacy off your license and out of your office.
Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. Reach him at [email protected].

Experts present first recommendations for treating acne fulminans
SCOTTSDALE, ARIZ. – Patients with acne fulminans should first begin corticosteroid monotherapy before adding isotretinoin, according to the first evidence-based consensus recommendations on this disease.
Antibiotics should not be used as first line treatment or monotherapy for acne fulminans, according to the experts who drafted the recommendations. Acne fulminans is an uncommon, understudied, and severe disorder that “typically manifests as an explosive worsening and ulceration of skin lesions, and can be associated with fever, bone pain, and other systemic symptoms,” noted panel co-chairs Dr. Andrea Zaenglein, professor of dermatology and pediatric dermatology, Pennsylvania State University, Hershey, and Dr. Sheila Friedlander, professor of medicine and pediatrics, University of California, San Diego, together with their associates.
The recommendations – based on a full literature review, a 5-hour audioconference, and two rounds of surveys to achieve consensus on these topics – were summarized in a poster presented at the annual meeting of the Society for Investigative Dermatology.
Until now, there have been no clear guidelines on the pathogenesis, treatment, and prevention of acne fulminans, according to the panelists.
Consensus definitions
“Acne fulminans is not just an extreme form of acne, but rather, a distinct, likely auto-inflammatory disorder,” the experts stated. Affected patients typically have an “abrupt, dramatic flare of inflammatory acne, with erosions, and with or without crusts, hemorrhagic nodules/plaques, and systemic findings.”
Systemic involvement is uncommon, but when present, includes fever, malaise, bone pain, arthralgias, erythema nodosum, and leukocytosis, they noted. Some patients also have anemia, an elevated erythrocyte sedimentation rate, and an increased C-reactive protein level. Radiography typically reveals osteolytic lesions of the sternum, clavicles, sacroiliac joints, and hips.
Acne fulminans is most often triggered by isotretinoin therapy, but can occur without it, the panel said. Isotretinoin-induced acne fulminans can have systemic involvement, but usually does not.
Corticosteroids
Patients should start corticosteroid monotherapy at a dose of 0.5 to 1.0 mg per kg per day, according to the recommendations. Patients with systemic involvement should receive steroids for at least 4 weeks, and other patients should continue steroids for at least 2 weeks and until all lesions have healed.
Oral corticosteroids should be tapered slowly over about 4 to 8 weeks, first by halving the dose to a physiologic dose each week, and then by dosing every other day for 2 weeks. Topical corticosteroids also can be used for eroded sites with granulation tissue, they noted.
Isotretinoin
Ironically, isotretinoin is both a treatment and a potential trigger of acne fulminans, and the recommendations included detailed guidance on its use.
Patients should wait at least 2 weeks after crusting resolves before starting isotretinoin, and should overlap isotretinoin with corticosteroids for at least 4 weeks, the experts emphasized. They recommended starting isotretinoin at 0.1 mg per kg per day, and waiting at least 2 months to increase this dose. Because patients clear at different rates, there is no universal optimal cumulative dose of isotretinoin, they noted.
If patients on isotretinoin develop flare, crusts, and erosions, they should halt treatment and either start corticosteroids, or increase the steroid dose to 1.0 mg per kg. If crusts and erosions persist, the panelists recommended considering cyclosporine, biologics, or dapsone.
If hemorrhagic crusts or erosions resolve after stopping isotretinoin, it can be restarted at the initial dose of 0.1 mg per kg and overlapped with steroids for 4 weeks.
If flares, crusts, and erosions begin when patients on isotretinoin are tapering corticosteroids, then steroids should be continued without tapering, isotretinoin should be stopped temporarily, and it should be restarted at 0.1 mg per kg after crusts and erosions have healed. This dose should be continued for 4 weeks, and then slowly increased as tolerated.
Antibiotics
Antibiotics are not useful as monotherapy for first-line therapy for acne fulminans, according to the recommendations. But to avoid isotretinoin-induced acne fulminans, the experts often pretreat patients with oral antibiotics before starting isotretinoin, and may continue oral antibiotics during the initial phase of isotretinoin treatment. However, there have been no prospective studies supporting this approach, they noted.
Other treatment considerations
Acne fulminans lesions should not be debrided, the experts emphasized. Acne fulminans associated with SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis), PAPA (pyogenic arthritis, pyoderma gangrenosum, and acne), and PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, and hidradenitis suppurativa) has responded successfully to tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists, they noted. Pulsed dye laser also has been used to successfully treat acne fulminans, particularly when there is associated granulation tissue, they stated.
Reducing the risk of pseudotumor cerebri syndrome
Several drugs used to treat acne fulminans have been linked to pseudotumor cerebri syndrome, the experts cautioned. “Among the tetracyclines, minocycline carries the highest risk,” they noted. Both isotretinoin and corticosteroids have been linked to pseudotumor cerebri syndrome, but clinicians can reduce this risk by avoiding an abrupt steroid taper, they emphasized.
The panel included physicians from the University of California, San Diego; Pennsylvania State University, Hershey; State University of New York, Brooklyn; Cornell University, New York; Touro University California, Vallejo; the University of California, San Francisco; the University of Pennsylvania, Philadelphia; and Jefferson Medical College, Philadelphia. They did not disclose conflicts of interest.
SCOTTSDALE, ARIZ. – Patients with acne fulminans should first begin corticosteroid monotherapy before adding isotretinoin, according to the first evidence-based consensus recommendations on this disease.
Antibiotics should not be used as first line treatment or monotherapy for acne fulminans, according to the experts who drafted the recommendations. Acne fulminans is an uncommon, understudied, and severe disorder that “typically manifests as an explosive worsening and ulceration of skin lesions, and can be associated with fever, bone pain, and other systemic symptoms,” noted panel co-chairs Dr. Andrea Zaenglein, professor of dermatology and pediatric dermatology, Pennsylvania State University, Hershey, and Dr. Sheila Friedlander, professor of medicine and pediatrics, University of California, San Diego, together with their associates.
The recommendations – based on a full literature review, a 5-hour audioconference, and two rounds of surveys to achieve consensus on these topics – were summarized in a poster presented at the annual meeting of the Society for Investigative Dermatology.
Until now, there have been no clear guidelines on the pathogenesis, treatment, and prevention of acne fulminans, according to the panelists.
Consensus definitions
“Acne fulminans is not just an extreme form of acne, but rather, a distinct, likely auto-inflammatory disorder,” the experts stated. Affected patients typically have an “abrupt, dramatic flare of inflammatory acne, with erosions, and with or without crusts, hemorrhagic nodules/plaques, and systemic findings.”
Systemic involvement is uncommon, but when present, includes fever, malaise, bone pain, arthralgias, erythema nodosum, and leukocytosis, they noted. Some patients also have anemia, an elevated erythrocyte sedimentation rate, and an increased C-reactive protein level. Radiography typically reveals osteolytic lesions of the sternum, clavicles, sacroiliac joints, and hips.
Acne fulminans is most often triggered by isotretinoin therapy, but can occur without it, the panel said. Isotretinoin-induced acne fulminans can have systemic involvement, but usually does not.
Corticosteroids
Patients should start corticosteroid monotherapy at a dose of 0.5 to 1.0 mg per kg per day, according to the recommendations. Patients with systemic involvement should receive steroids for at least 4 weeks, and other patients should continue steroids for at least 2 weeks and until all lesions have healed.
Oral corticosteroids should be tapered slowly over about 4 to 8 weeks, first by halving the dose to a physiologic dose each week, and then by dosing every other day for 2 weeks. Topical corticosteroids also can be used for eroded sites with granulation tissue, they noted.
Isotretinoin
Ironically, isotretinoin is both a treatment and a potential trigger of acne fulminans, and the recommendations included detailed guidance on its use.
Patients should wait at least 2 weeks after crusting resolves before starting isotretinoin, and should overlap isotretinoin with corticosteroids for at least 4 weeks, the experts emphasized. They recommended starting isotretinoin at 0.1 mg per kg per day, and waiting at least 2 months to increase this dose. Because patients clear at different rates, there is no universal optimal cumulative dose of isotretinoin, they noted.
If patients on isotretinoin develop flare, crusts, and erosions, they should halt treatment and either start corticosteroids, or increase the steroid dose to 1.0 mg per kg. If crusts and erosions persist, the panelists recommended considering cyclosporine, biologics, or dapsone.
If hemorrhagic crusts or erosions resolve after stopping isotretinoin, it can be restarted at the initial dose of 0.1 mg per kg and overlapped with steroids for 4 weeks.
If flares, crusts, and erosions begin when patients on isotretinoin are tapering corticosteroids, then steroids should be continued without tapering, isotretinoin should be stopped temporarily, and it should be restarted at 0.1 mg per kg after crusts and erosions have healed. This dose should be continued for 4 weeks, and then slowly increased as tolerated.
Antibiotics
Antibiotics are not useful as monotherapy for first-line therapy for acne fulminans, according to the recommendations. But to avoid isotretinoin-induced acne fulminans, the experts often pretreat patients with oral antibiotics before starting isotretinoin, and may continue oral antibiotics during the initial phase of isotretinoin treatment. However, there have been no prospective studies supporting this approach, they noted.
Other treatment considerations
Acne fulminans lesions should not be debrided, the experts emphasized. Acne fulminans associated with SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis), PAPA (pyogenic arthritis, pyoderma gangrenosum, and acne), and PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, and hidradenitis suppurativa) has responded successfully to tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists, they noted. Pulsed dye laser also has been used to successfully treat acne fulminans, particularly when there is associated granulation tissue, they stated.
Reducing the risk of pseudotumor cerebri syndrome
Several drugs used to treat acne fulminans have been linked to pseudotumor cerebri syndrome, the experts cautioned. “Among the tetracyclines, minocycline carries the highest risk,” they noted. Both isotretinoin and corticosteroids have been linked to pseudotumor cerebri syndrome, but clinicians can reduce this risk by avoiding an abrupt steroid taper, they emphasized.
The panel included physicians from the University of California, San Diego; Pennsylvania State University, Hershey; State University of New York, Brooklyn; Cornell University, New York; Touro University California, Vallejo; the University of California, San Francisco; the University of Pennsylvania, Philadelphia; and Jefferson Medical College, Philadelphia. They did not disclose conflicts of interest.
SCOTTSDALE, ARIZ. – Patients with acne fulminans should first begin corticosteroid monotherapy before adding isotretinoin, according to the first evidence-based consensus recommendations on this disease.
Antibiotics should not be used as first line treatment or monotherapy for acne fulminans, according to the experts who drafted the recommendations. Acne fulminans is an uncommon, understudied, and severe disorder that “typically manifests as an explosive worsening and ulceration of skin lesions, and can be associated with fever, bone pain, and other systemic symptoms,” noted panel co-chairs Dr. Andrea Zaenglein, professor of dermatology and pediatric dermatology, Pennsylvania State University, Hershey, and Dr. Sheila Friedlander, professor of medicine and pediatrics, University of California, San Diego, together with their associates.
The recommendations – based on a full literature review, a 5-hour audioconference, and two rounds of surveys to achieve consensus on these topics – were summarized in a poster presented at the annual meeting of the Society for Investigative Dermatology.
Until now, there have been no clear guidelines on the pathogenesis, treatment, and prevention of acne fulminans, according to the panelists.
Consensus definitions
“Acne fulminans is not just an extreme form of acne, but rather, a distinct, likely auto-inflammatory disorder,” the experts stated. Affected patients typically have an “abrupt, dramatic flare of inflammatory acne, with erosions, and with or without crusts, hemorrhagic nodules/plaques, and systemic findings.”
Systemic involvement is uncommon, but when present, includes fever, malaise, bone pain, arthralgias, erythema nodosum, and leukocytosis, they noted. Some patients also have anemia, an elevated erythrocyte sedimentation rate, and an increased C-reactive protein level. Radiography typically reveals osteolytic lesions of the sternum, clavicles, sacroiliac joints, and hips.
Acne fulminans is most often triggered by isotretinoin therapy, but can occur without it, the panel said. Isotretinoin-induced acne fulminans can have systemic involvement, but usually does not.
Corticosteroids
Patients should start corticosteroid monotherapy at a dose of 0.5 to 1.0 mg per kg per day, according to the recommendations. Patients with systemic involvement should receive steroids for at least 4 weeks, and other patients should continue steroids for at least 2 weeks and until all lesions have healed.
Oral corticosteroids should be tapered slowly over about 4 to 8 weeks, first by halving the dose to a physiologic dose each week, and then by dosing every other day for 2 weeks. Topical corticosteroids also can be used for eroded sites with granulation tissue, they noted.
Isotretinoin
Ironically, isotretinoin is both a treatment and a potential trigger of acne fulminans, and the recommendations included detailed guidance on its use.
Patients should wait at least 2 weeks after crusting resolves before starting isotretinoin, and should overlap isotretinoin with corticosteroids for at least 4 weeks, the experts emphasized. They recommended starting isotretinoin at 0.1 mg per kg per day, and waiting at least 2 months to increase this dose. Because patients clear at different rates, there is no universal optimal cumulative dose of isotretinoin, they noted.
If patients on isotretinoin develop flare, crusts, and erosions, they should halt treatment and either start corticosteroids, or increase the steroid dose to 1.0 mg per kg. If crusts and erosions persist, the panelists recommended considering cyclosporine, biologics, or dapsone.
If hemorrhagic crusts or erosions resolve after stopping isotretinoin, it can be restarted at the initial dose of 0.1 mg per kg and overlapped with steroids for 4 weeks.
If flares, crusts, and erosions begin when patients on isotretinoin are tapering corticosteroids, then steroids should be continued without tapering, isotretinoin should be stopped temporarily, and it should be restarted at 0.1 mg per kg after crusts and erosions have healed. This dose should be continued for 4 weeks, and then slowly increased as tolerated.
Antibiotics
Antibiotics are not useful as monotherapy for first-line therapy for acne fulminans, according to the recommendations. But to avoid isotretinoin-induced acne fulminans, the experts often pretreat patients with oral antibiotics before starting isotretinoin, and may continue oral antibiotics during the initial phase of isotretinoin treatment. However, there have been no prospective studies supporting this approach, they noted.
Other treatment considerations
Acne fulminans lesions should not be debrided, the experts emphasized. Acne fulminans associated with SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis), PAPA (pyogenic arthritis, pyoderma gangrenosum, and acne), and PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, and hidradenitis suppurativa) has responded successfully to tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists, they noted. Pulsed dye laser also has been used to successfully treat acne fulminans, particularly when there is associated granulation tissue, they stated.
Reducing the risk of pseudotumor cerebri syndrome
Several drugs used to treat acne fulminans have been linked to pseudotumor cerebri syndrome, the experts cautioned. “Among the tetracyclines, minocycline carries the highest risk,” they noted. Both isotretinoin and corticosteroids have been linked to pseudotumor cerebri syndrome, but clinicians can reduce this risk by avoiding an abrupt steroid taper, they emphasized.
The panel included physicians from the University of California, San Diego; Pennsylvania State University, Hershey; State University of New York, Brooklyn; Cornell University, New York; Touro University California, Vallejo; the University of California, San Francisco; the University of Pennsylvania, Philadelphia; and Jefferson Medical College, Philadelphia. They did not disclose conflicts of interest.
AT THE 2016 SID ANNUAL MEETING
Mobile App: VAM Info at Your Fingertips
At the Vascular Annual Meeting, there’s no need to cart around a lot of paper. Instead, the Mobile App puts all the information you need – abstracts, exhibitor map, schedules and more – within fingertip reach, to keep you more organized than ever.
Quick tips for using the Mobile App:

Create a personal schedule. Bookmark potential sessions in the program tab by clinking the small calendar icon the right for each session of interest. Reminders will pop up 10 minutes before the start time, including session details. The information will be pinned to the top of your activity feed to help you stay organized.
Review abstracts and take notes. The index contains all abstracts with author names and affiliations, presentation time, location, and a link to view the full abstract online. All index information is searchable. Take notes on each abstract within the app and export those notes to an email. Create a list of favorite abstracts by bookmarking those you want to refer to again.
Share. Share your thoughts in the app’s activity feed. Let all your friends know what you’re up to by linking your social media accounts to the app so you can post in the app and your social media feed at the same time!
The VAM Meeting App Is ...
Comprehensive: It includes all meeting content, including abstracts.
Searchable: Quickly locate sessions, abstracts, speakers and more.
Interactive: Network with colleagues, share photos and rate programs.
Visit vsweb.org/mobileapp to download the app.
At the Vascular Annual Meeting, there’s no need to cart around a lot of paper. Instead, the Mobile App puts all the information you need – abstracts, exhibitor map, schedules and more – within fingertip reach, to keep you more organized than ever.
Quick tips for using the Mobile App:
Create a personal schedule. Bookmark potential sessions in the program tab by clinking the small calendar icon the right for each session of interest. Reminders will pop up 10 minutes before the start time, including session details. The information will be pinned to the top of your activity feed to help you stay organized.
Review abstracts and take notes. The index contains all abstracts with author names and affiliations, presentation time, location, and a link to view the full abstract online. All index information is searchable. Take notes on each abstract within the app and export those notes to an email. Create a list of favorite abstracts by bookmarking those you want to refer to again.
Share. Share your thoughts in the app’s activity feed. Let all your friends know what you’re up to by linking your social media accounts to the app so you can post in the app and your social media feed at the same time!
The VAM Meeting App Is ...
Comprehensive: It includes all meeting content, including abstracts.
Searchable: Quickly locate sessions, abstracts, speakers and more.
Interactive: Network with colleagues, share photos and rate programs.
Visit vsweb.org/mobileapp to download the app.
At the Vascular Annual Meeting, there’s no need to cart around a lot of paper. Instead, the Mobile App puts all the information you need – abstracts, exhibitor map, schedules and more – within fingertip reach, to keep you more organized than ever.
Quick tips for using the Mobile App:
Create a personal schedule. Bookmark potential sessions in the program tab by clinking the small calendar icon the right for each session of interest. Reminders will pop up 10 minutes before the start time, including session details. The information will be pinned to the top of your activity feed to help you stay organized.
Review abstracts and take notes. The index contains all abstracts with author names and affiliations, presentation time, location, and a link to view the full abstract online. All index information is searchable. Take notes on each abstract within the app and export those notes to an email. Create a list of favorite abstracts by bookmarking those you want to refer to again.
Share. Share your thoughts in the app’s activity feed. Let all your friends know what you’re up to by linking your social media accounts to the app so you can post in the app and your social media feed at the same time!
The VAM Meeting App Is ...
Comprehensive: It includes all meeting content, including abstracts.
Searchable: Quickly locate sessions, abstracts, speakers and more.
Interactive: Network with colleagues, share photos and rate programs.
Visit vsweb.org/mobileapp to download the app.