User login
Weather or not
There was an outdoor equipment designer for a well-known Maine-based outfitter who was fond of saying that there was no such thing as bad weather, just bad or inappropriate clothing. The origin of this pearl is claimed by the Norwegians, the Germans, and the English – all nations that have some experience with inclement weather.
The folks who continue to go about their business regardless of the weather usually place a high value on the benefits of being outdoors. They often claim that they simply feel healthier when they are breathing fresh air. It is likely they have grown up in a place, in a family, and in a culture in which waiting for good weather to get something done means it’s not going to get done.

For example, my daughter-in-law’s visual impairment prevents her from driving a car. As a result, she and my two grandchildren get to almost all of their in-town destinations here in Brunswick, Maine, by bicycle or on foot ... 12 months a year ... rain or shine. They can afford appropriate clothing, but they still get wet and cold from time to time. I have never heard them complain. They accept bad weather as a given just as much as they accept a sunny day as something to enjoy.
While my grandchildren’s attitude toward the weather may not be typical of most 9- and 11-year-olds, they may not be alone in a few decades. Preschools are popping up around the country that not only accept the vagaries in the weather, but embrace the outdoors as an educational tool (“Preschool Without Walls,” by Lillian Mongeau, the New York Times, Dec. 29, 2015). The Natural Start Alliance, founded in 2013, has a membership of 92 preschools whose students spend a significant portion of their school day playing and exploring outdoors rain or shine. While most of these schools emphasize the value of learning from the natural environment, one of my granddaughters attended an outdoors-rain-or-shine preschool in urban San Francisco.
At the other end of the spectrum are the schools that feel obligated to shield their students from the realities of meteorological variability. While excessive sun exposure and tissue-freezing wind chills are to be avoided, a crisp calm sunny day with temperatures in the middle teens can be fun, particularly if there is some dry snow to tromp around in. However, during the months from November 2014 to March 2015, the children who attended Public School 126 in New York City were not given the opportunity to play outside on more than 40 school days. The situation is complicated because their school, which lacks its own playground, must rely on nearby parks (“A Casualty of a Frigid New York Winter: Outdoor School Recess,” by Ginia Bellafante, the New York Times, March 6, 2015). But we aren’t talking Siberia. It was a colder-than-usual winter, but I suspect there must have been more than a few missed opportunities to go outside and enjoy the snow. I wonder how often the decision to stay inside was influenced by teachers and administrators who hadn’t come prepared to spend any more time outside than it took them to walk from the parking lot or bus stop.
The data are accumulating that adding physical activity to the school day improves student behavior and even promotes learning. The evidence that being outside is beneficial is a bit more difficult to find. Early in the last century, when indoor air was saturated with smoke from cooking and open combustion heating sources, many physicians recommended that even for infants, raising a healthy child meant having the child spend a large part of the day outdoors.
It’s time for pediatricians to spread the word to parents that their little darlings won’t catch pneumonia from playing outdoors on a cool damp day. Nor will they shrink if they get a little wet on a rainy day ... but they will run ... and the running will be good for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
There was an outdoor equipment designer for a well-known Maine-based outfitter who was fond of saying that there was no such thing as bad weather, just bad or inappropriate clothing. The origin of this pearl is claimed by the Norwegians, the Germans, and the English – all nations that have some experience with inclement weather.
The folks who continue to go about their business regardless of the weather usually place a high value on the benefits of being outdoors. They often claim that they simply feel healthier when they are breathing fresh air. It is likely they have grown up in a place, in a family, and in a culture in which waiting for good weather to get something done means it’s not going to get done.
For example, my daughter-in-law’s visual impairment prevents her from driving a car. As a result, she and my two grandchildren get to almost all of their in-town destinations here in Brunswick, Maine, by bicycle or on foot ... 12 months a year ... rain or shine. They can afford appropriate clothing, but they still get wet and cold from time to time. I have never heard them complain. They accept bad weather as a given just as much as they accept a sunny day as something to enjoy.
While my grandchildren’s attitude toward the weather may not be typical of most 9- and 11-year-olds, they may not be alone in a few decades. Preschools are popping up around the country that not only accept the vagaries in the weather, but embrace the outdoors as an educational tool (“Preschool Without Walls,” by Lillian Mongeau, the New York Times, Dec. 29, 2015). The Natural Start Alliance, founded in 2013, has a membership of 92 preschools whose students spend a significant portion of their school day playing and exploring outdoors rain or shine. While most of these schools emphasize the value of learning from the natural environment, one of my granddaughters attended an outdoors-rain-or-shine preschool in urban San Francisco.
At the other end of the spectrum are the schools that feel obligated to shield their students from the realities of meteorological variability. While excessive sun exposure and tissue-freezing wind chills are to be avoided, a crisp calm sunny day with temperatures in the middle teens can be fun, particularly if there is some dry snow to tromp around in. However, during the months from November 2014 to March 2015, the children who attended Public School 126 in New York City were not given the opportunity to play outside on more than 40 school days. The situation is complicated because their school, which lacks its own playground, must rely on nearby parks (“A Casualty of a Frigid New York Winter: Outdoor School Recess,” by Ginia Bellafante, the New York Times, March 6, 2015). But we aren’t talking Siberia. It was a colder-than-usual winter, but I suspect there must have been more than a few missed opportunities to go outside and enjoy the snow. I wonder how often the decision to stay inside was influenced by teachers and administrators who hadn’t come prepared to spend any more time outside than it took them to walk from the parking lot or bus stop.
The data are accumulating that adding physical activity to the school day improves student behavior and even promotes learning. The evidence that being outside is beneficial is a bit more difficult to find. Early in the last century, when indoor air was saturated with smoke from cooking and open combustion heating sources, many physicians recommended that even for infants, raising a healthy child meant having the child spend a large part of the day outdoors.
It’s time for pediatricians to spread the word to parents that their little darlings won’t catch pneumonia from playing outdoors on a cool damp day. Nor will they shrink if they get a little wet on a rainy day ... but they will run ... and the running will be good for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
There was an outdoor equipment designer for a well-known Maine-based outfitter who was fond of saying that there was no such thing as bad weather, just bad or inappropriate clothing. The origin of this pearl is claimed by the Norwegians, the Germans, and the English – all nations that have some experience with inclement weather.
The folks who continue to go about their business regardless of the weather usually place a high value on the benefits of being outdoors. They often claim that they simply feel healthier when they are breathing fresh air. It is likely they have grown up in a place, in a family, and in a culture in which waiting for good weather to get something done means it’s not going to get done.
For example, my daughter-in-law’s visual impairment prevents her from driving a car. As a result, she and my two grandchildren get to almost all of their in-town destinations here in Brunswick, Maine, by bicycle or on foot ... 12 months a year ... rain or shine. They can afford appropriate clothing, but they still get wet and cold from time to time. I have never heard them complain. They accept bad weather as a given just as much as they accept a sunny day as something to enjoy.
While my grandchildren’s attitude toward the weather may not be typical of most 9- and 11-year-olds, they may not be alone in a few decades. Preschools are popping up around the country that not only accept the vagaries in the weather, but embrace the outdoors as an educational tool (“Preschool Without Walls,” by Lillian Mongeau, the New York Times, Dec. 29, 2015). The Natural Start Alliance, founded in 2013, has a membership of 92 preschools whose students spend a significant portion of their school day playing and exploring outdoors rain or shine. While most of these schools emphasize the value of learning from the natural environment, one of my granddaughters attended an outdoors-rain-or-shine preschool in urban San Francisco.
At the other end of the spectrum are the schools that feel obligated to shield their students from the realities of meteorological variability. While excessive sun exposure and tissue-freezing wind chills are to be avoided, a crisp calm sunny day with temperatures in the middle teens can be fun, particularly if there is some dry snow to tromp around in. However, during the months from November 2014 to March 2015, the children who attended Public School 126 in New York City were not given the opportunity to play outside on more than 40 school days. The situation is complicated because their school, which lacks its own playground, must rely on nearby parks (“A Casualty of a Frigid New York Winter: Outdoor School Recess,” by Ginia Bellafante, the New York Times, March 6, 2015). But we aren’t talking Siberia. It was a colder-than-usual winter, but I suspect there must have been more than a few missed opportunities to go outside and enjoy the snow. I wonder how often the decision to stay inside was influenced by teachers and administrators who hadn’t come prepared to spend any more time outside than it took them to walk from the parking lot or bus stop.
The data are accumulating that adding physical activity to the school day improves student behavior and even promotes learning. The evidence that being outside is beneficial is a bit more difficult to find. Early in the last century, when indoor air was saturated with smoke from cooking and open combustion heating sources, many physicians recommended that even for infants, raising a healthy child meant having the child spend a large part of the day outdoors.
It’s time for pediatricians to spread the word to parents that their little darlings won’t catch pneumonia from playing outdoors on a cool damp day. Nor will they shrink if they get a little wet on a rainy day ... but they will run ... and the running will be good for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”

Adjuvant temozolomide increases survival in rare anaplastic glioma
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?

Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?
Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?
Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Adjuvant temozolomide post-radiation improves survival in non-1p/19q-deleted anaplastic glioma.
Major finding: Adjuvant temozolomide improved overall survival to 56% from 44%.
Data source: Randomized, 4-arm trial of adjuvant temozolomide or not among 751 patients with non-1p/19q-deleted anaplastic glioma.
Disclosures: Schering Plough/MSD provided an unrestricted grant for the research and supplied temozolomide. Dr. van den Bent has consulting or advisory roles with Merck, Roche, Celldex, Novocure, Abbvie, and Amgen; has received honoraria from Roche, Actelion, Celldex, Bristol-Myers Squibb, Merck, Abbvie, and Novocure; and has research funding from Abbvie and Roche.

Up-front ASCT superior for fit patients with newly diagnosed myeloma
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
Although novel drug combinations have become a standard of care for newly diagnosed multiple myeloma patients, high-dose melphalan and ASCT improve the depth of remission, regardless of the induction regimen. Four trials comparing differing induction and consolidation regimens to one or more ASCTs now have shown significantly improved progression-free survival. Two of the trials have more than 36 months of follow-up.
Dr. William Bensinger is with the Fred Hutchinson Cancer Research Center and the Swedish Cancer Institute in Seattle.
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
CHICAGO – Up-front high-dose melphalan and autologous stem cell transplantation (ASCT) was superior to bortezomib-melphalan-prednisone (VMP) for fit patients younger than age 65 years with newly diagnosed multiple myeloma, based on the interim results from a randomized study of the European Myeloma Network.
With more than 1,200 patients, the study is the largest trial yet to show superior progression-free survival for ASCT. Follow-up has been too short to show significance for overall survival.
“Up-front ASCT was associated with a significant improvement in progression-free survival as compared to bortezomib-melphalan-prednisone in the overall patient population, (and the advantage) was retained across prespecified subgroups of patients at low and high risk … (as well as) in a multivariate analysis” of the overall population, Dr. Michele Cavo of the University of Bologna, Italy, reported at the annual meeting of the American Society of Clinical Oncology. “Up-front high-dose melphalan and ASCT continue to be the reference treatment choice for fit patients with newly diagnosed multiple myeloma, even in the novel agent era.”
ASCT was associated with higher rates of grade 3 or more adverse events in nearly every category, however, with the exception of peripheral nephropathy.
For the study, 1,266 patients, stratified by International Staging System stage and FISH (fluorescence in situ hybridization) analysis, were randomized to either VMP (512 pts) or to high-dose melphalan and ASCT (754 pts). At the meeting, Dr. Cavo reported on the study’s interim outcome results in 695 patients who had ASCT and 497 newly diagnosed patients who received VMP.
At 3 years, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the VMP patients. The median progression-free survival had not yet been reached in the ASCT patients and was 44 months in the bortezomib-melphalan-prednisone patients. (hazard ratio, 95% confidence interval, 0.73 [0.59-0.90]; P = .003).
Stringent complete responses were seen in 18.2% of patients in the VMP group and 17% of the ASCT group; Complete responses occurred in 25.3% of both groups. The main difference observed was in the number of very good partial responses, seen in 30.4% of the VMP group and in 43.2% of the ASCT group. Also, 11.2% of those in the VMP group had less than a partial response while that was the case for only 3.3% of the ASCT group.
Alternatively, the rate of grade 3 or more adverse events was higher in the ASCT group, with 17.5% experiencing febrile neutropenia, 15.6% mucositis, 3.2% sepsis, and 2.6% respiratory infections. The rates of these side effects in the VMP group were 0.2%, 0%, 0%, and 1.7%, respectively. The only grade 3 or more adverse event seen with greater frequency in the VMP group was peripheral neuropathy, seen in 13.8% as compared with 1.6% in the ASCT group.
Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
On Twitter @maryjodales
This story was updated on June 10, 2016.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Up-front high-dose melphalan and autologous stem cell transplantation was superior to bortezomib-melphalan-prednisone for fit patients under age 65 years with newly diagnosed multiple myeloma.
Major finding: At 3 years of follow-up, progression-free survival rates were 66.1% in the ASCT patients and 57.5% in the bortezomib-melphalan-prednisone patients.
Data source: Interim results from a randomized study of over 1200 patients in the European Myeloma Network.
Disclosures: Dr. Cavo receives honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and Takeda. He serves as a consultant or advisor to and is on the speakers bureau for Amgen. Celgene, Janssen.
Improve Quality, Patient Safety with SHM’s Online Toolkits and Implementation Guides
SHM’s implementation toolkits provide hospitalists with the resources they need to lead quality improvement projects on a variety of clinical topics, including a new toolkit on venous thromboembolism (VTE) released in May. The new toolkit features a literature review, an implementation guide, and additional reference materials, such as discharge instructions and checklists. Be on the lookout for information about an upcoming webinar series on the treatment of patients with VTE with free CME.
Don’t miss other online toolkits and implementation guides from SHM, covering:
- COPD
- Acute coronary syndrome
- Pain management
- Glycemic control
Check out all available toolkits at www.hospitalmedicine.org/qi.
Brett Radler is SHM’s communications coordinator.
SHM’s implementation toolkits provide hospitalists with the resources they need to lead quality improvement projects on a variety of clinical topics, including a new toolkit on venous thromboembolism (VTE) released in May. The new toolkit features a literature review, an implementation guide, and additional reference materials, such as discharge instructions and checklists. Be on the lookout for information about an upcoming webinar series on the treatment of patients with VTE with free CME.
Don’t miss other online toolkits and implementation guides from SHM, covering:
- COPD
- Acute coronary syndrome
- Pain management
- Glycemic control
Check out all available toolkits at www.hospitalmedicine.org/qi.
Brett Radler is SHM’s communications coordinator.
SHM’s implementation toolkits provide hospitalists with the resources they need to lead quality improvement projects on a variety of clinical topics, including a new toolkit on venous thromboembolism (VTE) released in May. The new toolkit features a literature review, an implementation guide, and additional reference materials, such as discharge instructions and checklists. Be on the lookout for information about an upcoming webinar series on the treatment of patients with VTE with free CME.
Don’t miss other online toolkits and implementation guides from SHM, covering:
- COPD
- Acute coronary syndrome
- Pain management
- Glycemic control
Check out all available toolkits at www.hospitalmedicine.org/qi.
Brett Radler is SHM’s communications coordinator.
Join SHM, JHM on Twitter for #JHMChat on Monday, July 11

During the chat, we invite you to join the conversation with Robert Mahoney, MD, associate professor of medicine at the Washington University School of Medicine, and Vinny Arora, MD, #JHMChat moderator and JHM deputy editor, to discuss the recent JHM publication “As-Needed Intravenous Antihypertensive Therapy and Blood Pressure Control.”
Participating in a #JHMChat allows you to have a dialogue with experts in the field conducting research with implications for your daily practice, network with fellow hospital medicine professionals, and lend your expertise to help others improve patient care. As you get ready for the chat, follow us and our Twitter partners:
- @JHospMedicine (Journal of Hospital Medicine)
- @SHMLive (Society of Hospital Medicine)
- @mahoneyr (Dr. Mahoney)
- @FutureDocs (Dr. Arora)
- @CostsofCare and @ABIMFoundation (#JHMChat partners)
On chat day, don’t forget to include #JHMChat in each of your tweets related to the chat to make sure all participants see them and are able to respond. To learn more, read the featured paper, and check out transcripts from our first three chats, visit www.hospitalmedicine.org/jhmchat.
See you on Twitter!
Brett Radler is SHM’s communications coordinator.
During the chat, we invite you to join the conversation with Robert Mahoney, MD, associate professor of medicine at the Washington University School of Medicine, and Vinny Arora, MD, #JHMChat moderator and JHM deputy editor, to discuss the recent JHM publication “As-Needed Intravenous Antihypertensive Therapy and Blood Pressure Control.”
Participating in a #JHMChat allows you to have a dialogue with experts in the field conducting research with implications for your daily practice, network with fellow hospital medicine professionals, and lend your expertise to help others improve patient care. As you get ready for the chat, follow us and our Twitter partners:
- @JHospMedicine (Journal of Hospital Medicine)
- @SHMLive (Society of Hospital Medicine)
- @mahoneyr (Dr. Mahoney)
- @FutureDocs (Dr. Arora)
- @CostsofCare and @ABIMFoundation (#JHMChat partners)
On chat day, don’t forget to include #JHMChat in each of your tweets related to the chat to make sure all participants see them and are able to respond. To learn more, read the featured paper, and check out transcripts from our first three chats, visit www.hospitalmedicine.org/jhmchat.
See you on Twitter!
Brett Radler is SHM’s communications coordinator.
During the chat, we invite you to join the conversation with Robert Mahoney, MD, associate professor of medicine at the Washington University School of Medicine, and Vinny Arora, MD, #JHMChat moderator and JHM deputy editor, to discuss the recent JHM publication “As-Needed Intravenous Antihypertensive Therapy and Blood Pressure Control.”
Participating in a #JHMChat allows you to have a dialogue with experts in the field conducting research with implications for your daily practice, network with fellow hospital medicine professionals, and lend your expertise to help others improve patient care. As you get ready for the chat, follow us and our Twitter partners:
- @JHospMedicine (Journal of Hospital Medicine)
- @SHMLive (Society of Hospital Medicine)
- @mahoneyr (Dr. Mahoney)
- @FutureDocs (Dr. Arora)
- @CostsofCare and @ABIMFoundation (#JHMChat partners)
On chat day, don’t forget to include #JHMChat in each of your tweets related to the chat to make sure all participants see them and are able to respond. To learn more, read the featured paper, and check out transcripts from our first three chats, visit www.hospitalmedicine.org/jhmchat.
See you on Twitter!
Brett Radler is SHM’s communications coordinator.

Ingredient in aspirin may help fight leukemia

Photo credit: Jill Watson
Researchers say they may have found a new use for an ancient anti-inflammatory drug, salicylate, which was first described by the Greek physician Hippocrates.
“Salicylic acid is one of the oldest drugs on the planet,” said senior author Eric Verdin, MD, of the Gladstone Institutes/UCSF, “dating back to the Egyptians and the Greeks, but we're still discovering new things about it.”
Its derivatives, acetylsalicylic acid, or aspirin, and diflunisal suppress 2 key proteins, CREB-binding protein (CBP) and p300, which control levels of proteins that cause inflammation or are involved in cell growth.
By inhibiting p300 and CBP, salicylic acid and diflunisal block the activation of these proteins and prevent cellular damage caused by inflammation. The research team believes that both p300 and CBP can be targeted by drugs, which would have important clinical implications.
Earlier research conducted by coauthor Stephen D. Nimer, MD, of the University of Miami Miller School of Medicine in Florida, and colleagues found a link between p300 and the leukemia-promoting protein AML1-ETO.
In the current study, published in eLife, researchers tested whether suppressing p300 with diflunisal would suppress leukemia growth in mice.
The research team inoculated SCID mice with Kasumi-1 cells, an AML cell line with the t(8;21) translocation, which represents one of the subtypes of CBF leukemia.
Three weeks later, they started treating the mice with diflunisal. Diflunisal reduced tumor size in a dose-dependent manner, and after 3 weeks of treatment, the tumors were significantly smaller than in the vehicle-treated control mice.
In fact, the researchers noted most tumors disappeared in mice treated with higher doses of diflunisal. The researchers also pointed out that diflunisal, an FDA-approved drug containing a salicylic acid substructure, inhibited CBP/p300 more potently than salicylate.
The researchers concluded that diflunisal and salicylate have promise as an oral therapy for AML patients with a t(8;21) translocation, and called it “an exciting potential application” for this new characterization of older drugs.
“Uncovering this pathway of inflammation that salicylic acid acts upon opens up a host of new clinical possibilities for these drugs,” Dr Verdin added.
The scientists are now pursuing a clinical trial to test whether salicylic acid can treat patients with leukemia as part of novel combination therapies. ![]()
Photo credit: Jill Watson
Researchers say they may have found a new use for an ancient anti-inflammatory drug, salicylate, which was first described by the Greek physician Hippocrates.
“Salicylic acid is one of the oldest drugs on the planet,” said senior author Eric Verdin, MD, of the Gladstone Institutes/UCSF, “dating back to the Egyptians and the Greeks, but we're still discovering new things about it.”
Its derivatives, acetylsalicylic acid, or aspirin, and diflunisal suppress 2 key proteins, CREB-binding protein (CBP) and p300, which control levels of proteins that cause inflammation or are involved in cell growth.
By inhibiting p300 and CBP, salicylic acid and diflunisal block the activation of these proteins and prevent cellular damage caused by inflammation. The research team believes that both p300 and CBP can be targeted by drugs, which would have important clinical implications.
Earlier research conducted by coauthor Stephen D. Nimer, MD, of the University of Miami Miller School of Medicine in Florida, and colleagues found a link between p300 and the leukemia-promoting protein AML1-ETO.
In the current study, published in eLife, researchers tested whether suppressing p300 with diflunisal would suppress leukemia growth in mice.
The research team inoculated SCID mice with Kasumi-1 cells, an AML cell line with the t(8;21) translocation, which represents one of the subtypes of CBF leukemia.
Three weeks later, they started treating the mice with diflunisal. Diflunisal reduced tumor size in a dose-dependent manner, and after 3 weeks of treatment, the tumors were significantly smaller than in the vehicle-treated control mice.
In fact, the researchers noted most tumors disappeared in mice treated with higher doses of diflunisal. The researchers also pointed out that diflunisal, an FDA-approved drug containing a salicylic acid substructure, inhibited CBP/p300 more potently than salicylate.
The researchers concluded that diflunisal and salicylate have promise as an oral therapy for AML patients with a t(8;21) translocation, and called it “an exciting potential application” for this new characterization of older drugs.
“Uncovering this pathway of inflammation that salicylic acid acts upon opens up a host of new clinical possibilities for these drugs,” Dr Verdin added.
The scientists are now pursuing a clinical trial to test whether salicylic acid can treat patients with leukemia as part of novel combination therapies. ![]()
Photo credit: Jill Watson
Researchers say they may have found a new use for an ancient anti-inflammatory drug, salicylate, which was first described by the Greek physician Hippocrates.
“Salicylic acid is one of the oldest drugs on the planet,” said senior author Eric Verdin, MD, of the Gladstone Institutes/UCSF, “dating back to the Egyptians and the Greeks, but we're still discovering new things about it.”
Its derivatives, acetylsalicylic acid, or aspirin, and diflunisal suppress 2 key proteins, CREB-binding protein (CBP) and p300, which control levels of proteins that cause inflammation or are involved in cell growth.
By inhibiting p300 and CBP, salicylic acid and diflunisal block the activation of these proteins and prevent cellular damage caused by inflammation. The research team believes that both p300 and CBP can be targeted by drugs, which would have important clinical implications.
Earlier research conducted by coauthor Stephen D. Nimer, MD, of the University of Miami Miller School of Medicine in Florida, and colleagues found a link between p300 and the leukemia-promoting protein AML1-ETO.
In the current study, published in eLife, researchers tested whether suppressing p300 with diflunisal would suppress leukemia growth in mice.
The research team inoculated SCID mice with Kasumi-1 cells, an AML cell line with the t(8;21) translocation, which represents one of the subtypes of CBF leukemia.
Three weeks later, they started treating the mice with diflunisal. Diflunisal reduced tumor size in a dose-dependent manner, and after 3 weeks of treatment, the tumors were significantly smaller than in the vehicle-treated control mice.
In fact, the researchers noted most tumors disappeared in mice treated with higher doses of diflunisal. The researchers also pointed out that diflunisal, an FDA-approved drug containing a salicylic acid substructure, inhibited CBP/p300 more potently than salicylate.
The researchers concluded that diflunisal and salicylate have promise as an oral therapy for AML patients with a t(8;21) translocation, and called it “an exciting potential application” for this new characterization of older drugs.
“Uncovering this pathway of inflammation that salicylic acid acts upon opens up a host of new clinical possibilities for these drugs,” Dr Verdin added.
The scientists are now pursuing a clinical trial to test whether salicylic acid can treat patients with leukemia as part of novel combination therapies. ![]()
Long-Term Mortality Benefits With Coronary Artery Bypass Grafting for Ischemic Cardiomyopathy
Clinical question: Does coronary artery bypass grafting added to medical therapy decrease mortality in patients with coronary artery disease and systolic heart failure?
Bottom line: Coronary artery bypass grafting (CABG) plus medical therapy decreases mortality as compared with medical therapy alone in patients with ischemic cardiomyopathy. You would need to treat 14 patients with CABG to prevent one death. (LOE = 1b)
Reference: Velazquez EJ, Lee KL, Jones RH, et al, for the STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med 2016;374(16):1511-1520.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using concealed allocation, these investigators randomized patients with heart failure with ejection fraction of 35% or less and coronary artery disease amenable to CABG to receive either guideline-directed medical therapy plus CABG (n = 610) or guideline-directed medical therapy alone (n = 602). The 2 groups were similar at baseline and the majority was categorized as New York Heart Failure Association class II. Overall, 91% of the CABG group underwent the procedure within the first year following randomization. Notably, 20% of the medical therapy group also underwent CABG during the long-term follow-up period (11% crossed over to CABG within the first year). The medial duration for follow-up was 9.8 years and analysis was by intention to treat. CABG plus medical therapy resulted in fewer deaths over 10 years as compared with medical therapy alone (59% vs 66%; hazard ratio [HR] = 0.84; 95% CI 0.73 - 0.97; P = .02). The CABG group also had fewer deaths specifically from cardiovascular causes (40% vs 49%; P = .006). A per-protocol analysis showed an even greater benefit with CABG (HR = 0.77; 0.67 - 0.90; P = .001) suggesting that the crossovers in this trial may have diluted the observed effect of CABG.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does coronary artery bypass grafting added to medical therapy decrease mortality in patients with coronary artery disease and systolic heart failure?
Bottom line: Coronary artery bypass grafting (CABG) plus medical therapy decreases mortality as compared with medical therapy alone in patients with ischemic cardiomyopathy. You would need to treat 14 patients with CABG to prevent one death. (LOE = 1b)
Reference: Velazquez EJ, Lee KL, Jones RH, et al, for the STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med 2016;374(16):1511-1520.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using concealed allocation, these investigators randomized patients with heart failure with ejection fraction of 35% or less and coronary artery disease amenable to CABG to receive either guideline-directed medical therapy plus CABG (n = 610) or guideline-directed medical therapy alone (n = 602). The 2 groups were similar at baseline and the majority was categorized as New York Heart Failure Association class II. Overall, 91% of the CABG group underwent the procedure within the first year following randomization. Notably, 20% of the medical therapy group also underwent CABG during the long-term follow-up period (11% crossed over to CABG within the first year). The medial duration for follow-up was 9.8 years and analysis was by intention to treat. CABG plus medical therapy resulted in fewer deaths over 10 years as compared with medical therapy alone (59% vs 66%; hazard ratio [HR] = 0.84; 95% CI 0.73 - 0.97; P = .02). The CABG group also had fewer deaths specifically from cardiovascular causes (40% vs 49%; P = .006). A per-protocol analysis showed an even greater benefit with CABG (HR = 0.77; 0.67 - 0.90; P = .001) suggesting that the crossovers in this trial may have diluted the observed effect of CABG.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does coronary artery bypass grafting added to medical therapy decrease mortality in patients with coronary artery disease and systolic heart failure?
Bottom line: Coronary artery bypass grafting (CABG) plus medical therapy decreases mortality as compared with medical therapy alone in patients with ischemic cardiomyopathy. You would need to treat 14 patients with CABG to prevent one death. (LOE = 1b)
Reference: Velazquez EJ, Lee KL, Jones RH, et al, for the STICHES Investigators. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med 2016;374(16):1511-1520.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Using concealed allocation, these investigators randomized patients with heart failure with ejection fraction of 35% or less and coronary artery disease amenable to CABG to receive either guideline-directed medical therapy plus CABG (n = 610) or guideline-directed medical therapy alone (n = 602). The 2 groups were similar at baseline and the majority was categorized as New York Heart Failure Association class II. Overall, 91% of the CABG group underwent the procedure within the first year following randomization. Notably, 20% of the medical therapy group also underwent CABG during the long-term follow-up period (11% crossed over to CABG within the first year). The medial duration for follow-up was 9.8 years and analysis was by intention to treat. CABG plus medical therapy resulted in fewer deaths over 10 years as compared with medical therapy alone (59% vs 66%; hazard ratio [HR] = 0.84; 95% CI 0.73 - 0.97; P = .02). The CABG group also had fewer deaths specifically from cardiovascular causes (40% vs 49%; P = .006). A per-protocol analysis showed an even greater benefit with CABG (HR = 0.77; 0.67 - 0.90; P = .001) suggesting that the crossovers in this trial may have diluted the observed effect of CABG.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Stent Retriever Therapy Added to tPA Effective for Treating Acute Ischemic Stroke
Clinical question: Does the use of stent retrievers in conjunction with tissue plasminogen activator improve outcomes in patients with acute ischemic stroke?
Bottom line: The use of stent retriever devices in addition to tissue plasminogen activator (tPA) in patients with anterior circulation acute ischemic stroke results in more patients with functional independence at 90 days. Based on data from the studies included in this review, the American Heart Association/American Stroke Association guidelines now strongly recommend the use of stent retrievers with class 1a level of evidence. (LOE = 1a)
Reference: Touma L, Filion KB, Sterling LH, Atallah R, Windle SB, Eisenberg MJ. Stent retrievers for the treatment of acute ischemic stroke. JAMA Neurol 2016;73(3):275-281.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Intra-arterial therapy using stent retriever devices for thrombectomy added to standard therapy with tPA is a promising treatment for acute ischemic stroke. Four recent randomized controlled trials examining the effectiveness of stent retrievers have been terminated early because of the strong benefit seen with this therapy.
In this study, investigators searched MEDLINE, EMBASE, and the Cochrane Library, as well as trial registries and references of included studies, to find randomized controlled trials that compared stent retrievers plus tPA with tPA alone. Two authors independently extracted data from the 5 included studies (N = 1287) and assessed study quality using the Cochrane Collaboration Risk of Bias Tool.
All studies included patients with imaging-confirmed anterior circulation strokes and used the modified Rankin Scale (mRS) to assess for improvement in functional status at 90 days. Four of the 5 studies only included patients with excellent pre-stroke functional independence. Additionally, 4 of the 5 studies restricted stent retriever therapy to patients who presented within 6 hours of onset of stroke symptoms. The studies had a low risk of bias overall.
The pooled 90-day outcomes showed that patients who received stent retriever therapy plus tPA were more likely to achieve greater functional independence, defined as an mRS score of 0 to 2, than patients who received tPA alone (relative risk 1.72; 95% CI 1.38 - 1.99). You would need to treat 6 patients with stent retriever therapy to have one patient achieve functional independence. There were no significant differences detected in mortality or in the rates of intracranial bleeds or parenchymal hematomas.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of stent retrievers in conjunction with tissue plasminogen activator improve outcomes in patients with acute ischemic stroke?
Bottom line: The use of stent retriever devices in addition to tissue plasminogen activator (tPA) in patients with anterior circulation acute ischemic stroke results in more patients with functional independence at 90 days. Based on data from the studies included in this review, the American Heart Association/American Stroke Association guidelines now strongly recommend the use of stent retrievers with class 1a level of evidence. (LOE = 1a)
Reference: Touma L, Filion KB, Sterling LH, Atallah R, Windle SB, Eisenberg MJ. Stent retrievers for the treatment of acute ischemic stroke. JAMA Neurol 2016;73(3):275-281.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Intra-arterial therapy using stent retriever devices for thrombectomy added to standard therapy with tPA is a promising treatment for acute ischemic stroke. Four recent randomized controlled trials examining the effectiveness of stent retrievers have been terminated early because of the strong benefit seen with this therapy.
In this study, investigators searched MEDLINE, EMBASE, and the Cochrane Library, as well as trial registries and references of included studies, to find randomized controlled trials that compared stent retrievers plus tPA with tPA alone. Two authors independently extracted data from the 5 included studies (N = 1287) and assessed study quality using the Cochrane Collaboration Risk of Bias Tool.
All studies included patients with imaging-confirmed anterior circulation strokes and used the modified Rankin Scale (mRS) to assess for improvement in functional status at 90 days. Four of the 5 studies only included patients with excellent pre-stroke functional independence. Additionally, 4 of the 5 studies restricted stent retriever therapy to patients who presented within 6 hours of onset of stroke symptoms. The studies had a low risk of bias overall.
The pooled 90-day outcomes showed that patients who received stent retriever therapy plus tPA were more likely to achieve greater functional independence, defined as an mRS score of 0 to 2, than patients who received tPA alone (relative risk 1.72; 95% CI 1.38 - 1.99). You would need to treat 6 patients with stent retriever therapy to have one patient achieve functional independence. There were no significant differences detected in mortality or in the rates of intracranial bleeds or parenchymal hematomas.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of stent retrievers in conjunction with tissue plasminogen activator improve outcomes in patients with acute ischemic stroke?
Bottom line: The use of stent retriever devices in addition to tissue plasminogen activator (tPA) in patients with anterior circulation acute ischemic stroke results in more patients with functional independence at 90 days. Based on data from the studies included in this review, the American Heart Association/American Stroke Association guidelines now strongly recommend the use of stent retrievers with class 1a level of evidence. (LOE = 1a)
Reference: Touma L, Filion KB, Sterling LH, Atallah R, Windle SB, Eisenberg MJ. Stent retrievers for the treatment of acute ischemic stroke. JAMA Neurol 2016;73(3):275-281.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (any location) with outpatient follow-up
Synopsis: Intra-arterial therapy using stent retriever devices for thrombectomy added to standard therapy with tPA is a promising treatment for acute ischemic stroke. Four recent randomized controlled trials examining the effectiveness of stent retrievers have been terminated early because of the strong benefit seen with this therapy.
In this study, investigators searched MEDLINE, EMBASE, and the Cochrane Library, as well as trial registries and references of included studies, to find randomized controlled trials that compared stent retrievers plus tPA with tPA alone. Two authors independently extracted data from the 5 included studies (N = 1287) and assessed study quality using the Cochrane Collaboration Risk of Bias Tool.
All studies included patients with imaging-confirmed anterior circulation strokes and used the modified Rankin Scale (mRS) to assess for improvement in functional status at 90 days. Four of the 5 studies only included patients with excellent pre-stroke functional independence. Additionally, 4 of the 5 studies restricted stent retriever therapy to patients who presented within 6 hours of onset of stroke symptoms. The studies had a low risk of bias overall.
The pooled 90-day outcomes showed that patients who received stent retriever therapy plus tPA were more likely to achieve greater functional independence, defined as an mRS score of 0 to 2, than patients who received tPA alone (relative risk 1.72; 95% CI 1.38 - 1.99). You would need to treat 6 patients with stent retriever therapy to have one patient achieve functional independence. There were no significant differences detected in mortality or in the rates of intracranial bleeds or parenchymal hematomas.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
VIDEO: Accelerated infliximab dosing halved colectomy rate in severe ulcerative colitis
SAN DIEGO – Inpatient infliximab rescue for severe, steroid-refractory ulcerative colitis is more likely to work if patients receive a second infusion 3 days after the first, according to a review of 55 University of Michigan, Ann Arbor, patients.
The traditional approach is one inpatient 5-mg/kg infusion, followed by either colectomy or subsequent outpatient infusions, depending on response. In 2013, physicians at the university began offering a second infusion at 72 hours to patients whose C-reactive protein (CRP) levels did not drop below 0.7 mg/dL after their first infusion, and they also began opting more often for 10-mg/kg dosing.
The review found that 90-day colectomy-free survival was 50% in the 16 accelerated-dosing patients, up from 10.2% in the 36 patients treated with the traditional approach (P less than .001). The finding has led to a new, more aggressive infliximab protocol for inpatient ulcerative colitis.
Among patients who did undergo colectomies, postoperative complications were similar between the two groups. But for reasons that are not clear, 30-day postoperative readmission rates were higher in accelerated patients (58% vs. 25%).
In an interview at the annual Digestive Disease Week, lead investigator Dr. Shail Govani of the University of Michigan explained the thinking behind the new approach, how CRP/albumin ratios come into play, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Inpatient infliximab rescue for severe, steroid-refractory ulcerative colitis is more likely to work if patients receive a second infusion 3 days after the first, according to a review of 55 University of Michigan, Ann Arbor, patients.
The traditional approach is one inpatient 5-mg/kg infusion, followed by either colectomy or subsequent outpatient infusions, depending on response. In 2013, physicians at the university began offering a second infusion at 72 hours to patients whose C-reactive protein (CRP) levels did not drop below 0.7 mg/dL after their first infusion, and they also began opting more often for 10-mg/kg dosing.
The review found that 90-day colectomy-free survival was 50% in the 16 accelerated-dosing patients, up from 10.2% in the 36 patients treated with the traditional approach (P less than .001). The finding has led to a new, more aggressive infliximab protocol for inpatient ulcerative colitis.
Among patients who did undergo colectomies, postoperative complications were similar between the two groups. But for reasons that are not clear, 30-day postoperative readmission rates were higher in accelerated patients (58% vs. 25%).
In an interview at the annual Digestive Disease Week, lead investigator Dr. Shail Govani of the University of Michigan explained the thinking behind the new approach, how CRP/albumin ratios come into play, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – Inpatient infliximab rescue for severe, steroid-refractory ulcerative colitis is more likely to work if patients receive a second infusion 3 days after the first, according to a review of 55 University of Michigan, Ann Arbor, patients.
The traditional approach is one inpatient 5-mg/kg infusion, followed by either colectomy or subsequent outpatient infusions, depending on response. In 2013, physicians at the university began offering a second infusion at 72 hours to patients whose C-reactive protein (CRP) levels did not drop below 0.7 mg/dL after their first infusion, and they also began opting more often for 10-mg/kg dosing.
The review found that 90-day colectomy-free survival was 50% in the 16 accelerated-dosing patients, up from 10.2% in the 36 patients treated with the traditional approach (P less than .001). The finding has led to a new, more aggressive infliximab protocol for inpatient ulcerative colitis.
Among patients who did undergo colectomies, postoperative complications were similar between the two groups. But for reasons that are not clear, 30-day postoperative readmission rates were higher in accelerated patients (58% vs. 25%).
In an interview at the annual Digestive Disease Week, lead investigator Dr. Shail Govani of the University of Michigan explained the thinking behind the new approach, how CRP/albumin ratios come into play, and how to counsel patients in light of the findings.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT DDW 2016

2016 Update on infectious disease

Chlorhexidine-alcohol is superior to iodine-alcohol for reducing SSIs after cesarean deliveryTuuli Mg, Liu J, Stout Mj, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647-655.
In the United States, cesarean delivery is the most commonly performed major surgical procedure, with 32.7% of births--or 1.3 million--occurring in this fashion in 2013.1,2 In general, for all surgical procedures, the SSI rate is 2% to 5%, with the rate rising to 5% to 12% for cesarean delivery, especially in obese patients.3-6 Not only do SSIs increase morbidity for the patient but they also contribute to high medical costs, with an estimated additional expense of $3,529 per cesarean-associated infection.7
Skin pathogens are a major source of SSIs. Choosing the proper antiseptic has the potential to decrease infection risk. While current guidelines recommend use of an antiseptic containing alcohol, it is unclear which disinfectant is the most effective agent to combine with the alcohol.3
Most trials evaluating preoperative antiseptic skin preparation have studied patients undergoing general surgery procedures. A well-designed trial by Darouiche and coauthors demonstrated that chlorhexidine was superior to iodine when used as an antiseptic for skin preparation.8 Interestingly, however, this trial, like most others, compared chlorhexidine-alcohol to iodine without alcohol. It is therefore unclear whether the chlorhexidine or the alcohol is responsible for the enhanced antiseptic effect.
Details of the studyIn the single-center randomized trial conducted by Tuuli and colleagues, patients were assigned to preoperative skin antisepsis with either chlorhexidine-alcohol (2% chlorhexidine gluconate with 70% isopropyl alcohol) or iodine-alcohol (8.3% povidone-iodine with 72.5% isopropyl alcohol). Antiseptic was applied according to the manufacturer's instructions, with a standard wait time of 3 minutes between application and skin incision. However, wait time was eliminated for patients undergoing emergency cesarean delivery. Additionally, patients received standard, weight-based preoperative antibiotic prophylaxis (agent not specified).
The authors estimated the necessary sample size for the trial by assuming an 8% baseline SSI rate and an anticipated 50% reduction of infection in the chlorhexidine-alcohol group. Exclusion criteria included a known allergy to chlorhexidine, alcohol, iodine, or shellfish or a preexisting skin infection adjacent to the operative site.
In addition to assessing the primary outcome of SSI with the 2 preparations, the authors conducted 4 prespecified subgroup analyses. These subgroups were based on: type of cesarean delivery (scheduled vs unscheduled), body weight (obese vs nonobese), type of skin closure (subcuticular suture vs staples), and presence or absence of chronic medical conditions (diabetes, hypertension, renal disease). Additionally, a post hoc analysis was performed, comparing women with diabetes (gestational and pregestational) to those without diabetes.
A total of 1,636 pregnant women were screened for eligibility. Of these, 489 women were excluded because they did not meet inclusion criteria or declined to participate or because informed consent could not be obtained. Baseline characteristics were similar across both groups.
Patients were followed for 30 days after surgery. A total of 1,082 women (94.3% of sample size) completed the follow-up. Among these patients, the rate of SSI was significantly lower in the chlorhexidine-alcohol group (4.3%) compared with the iodine-alcohol group (7.7%, P = .02).
In the subgroup analyses, the frequency of SSI remained lower for the chlorhexidine-alcohol group than for the iodine-alcohol group. These reductions were not affected by whether the cesarean was scheduled or unscheduled, the presence or absence of obesity, the type of skin closure, the presence of chronic disease, or diabetes status.
Several secondary outcomes also were examined in this study. There were no significant differences between the 2 antiseptic groups with respect to rates of endometritis, hospital readmission for infection-related complications, length of hospital stay, use of other health care services (such as emergency department visits, additional wound surgery, and home health services), and rates of other wound complications (seroma, hematoma, and cellulitis). Patients in the chlorhexidine-alcohol group were significantly less likely than those in the iodine-alcohol group to have physician office visits for concerns about possible wound complications (P = .009).
The authors concluded that the use of chlorhexidine-alcohol was superior to iodine-alcohol in preventing SSI after cesarean delivery.
Study strengths and limitations The authors acknowledged that their study had some minor limitations. First, the trial was conducted at a single site, which may limit the generalizability of the findings. However, the study population was racially and economically diverse. Second, the lack of blinding among providers and participants may have introduced bias, although, as the authors explain, we would expect this bias to be largely nondirectional.
A major strength of this study is its randomized design. Another strength is that the authors included emergency cesarean deliveries in their analysis. Emergency procedures represent a substantial proportion of cesarean deliveries, and they place the patient at increased risk for SSIs because of limited time available to prepare the skin before surgery begins. Thus, it is of great interest that chlorhexidine-alcohol was so effective even in the highest-risk patients.
Several properties may make chlorhexidine superior to iodine as an antiseptic: high binding affinity for the skin, high antibacterial activity against both gram-positive and gram-negative bacteria, and longer residual effects than iodine. Additionally, iodine is inactivated by organic matter, such as body fluids, whereas chlorhexidine is not.
A recent study by Ngai and colleagues9 compared chlorhexidine-alcohol with iodine-alcohol for skin preparation before cesarean delivery. These authors found no difference in SSI when comparing the 2 solutions used separately or sequentially, except in morbidly obese women. In these women, sequential application of both solutions reduced the infection rate. However, this study specifically excluded emergency cesarean deliveries, making the generalizability of the results questionable.9
What this evidence means for practiceThis large, randomized study found chlorhexidine-alcohol to be superior to iodine-alchol in reducing the risk of SSIs after cesarean delivery. These results confirm those of previous studies from both the obstetric and general surgery literature. Although chlorhexidine-alcohol is more expensive than iodine-alcohol, we strongly recommend its use in patients having cesarean delivery.
Five effective oral and intramuscular antibiotic regimens for treating postpartum endometritisMeaney-Delman D, Bartlett LA, Gravett MG, Jamieson DJ. Oral and intramuscular treatment options for early postpartum endometritis in low-resource settings: a systematic review. Obstet Gynecol. 2015;125(4):789-800.
The authors of this excellent systematic review on antibiotic treatments for early postpartum endometritis conducted their study in 3 phases. Initially, Meaney-Delman and colleagues searched the literature for reports of prospective studies that evaluated the use of oral and intramuscular (IM) antibiotics for treatment of patients who developed endometritis following either cesarean or vaginal delivery. When they discovered that these initial trials were few in number and of relatively poor quality, they reviewed more rigorous trials of intravenous (IV) antibiotics. Finally, they evaluated clinical trials that specifically identified microorganisms isolated from the uterus in patients with endometritis and used this information to help inform their recommendations for treatment options.
Details of the studyIn evaluating the trials of oral and IM antibiotics, the authors set as a standard for effectiveness a cure rate of 85%, a figure comparable to that generally achieved with IV antibiotics. They identified 2 oral antibiotic regimens that met this standard of effectiveness: amoxicillin-clavulanate (100% cure in 36 patients; 95% confidence interval [CI], 90-100) and ampicillin plus metronidazole (97% cure in 37 patients; 95% CI, 86-100).
Two studies demonstrated acceptable levels of cure with single-agent IM antibiotics: aztreonam (100% cure in 16 patients; 95% CI, 81-100) and imipenem (91% cure in 23 patients; 95% CI, 73-98). One additional trial demonstrated an acceptable clinical response rate when IV clindamycin was combined with IM gentamicin (100% cure in 54 patients; 95% CI, 94-100). By contrast, the authors noted, many different IV regimens--either as a single agent or as a drug combination--provided cure rates that equaled or exceeded 85%.
In the study's final phase, the authors provided an excellent overview of the polymicrobial nature of puerperal endometritis. As documented in multiple prior reports, the most common pathogens are the gram-negative anaerobic bacilli, such as Bacteroides and Prevotella species; the anaerobic gram-positive organisms, including Peptococcus and Peptostreptococcus species; aerobic gram-negative bacilli, such as Escherichia coli, Klebsiella pneumoniae, and Proteus species; and aerobic gram-positive cocci, such as group B streptococci, enterococci, and staphylococci.
Recommended regimens. Based on their review of clinical and microbiological studies, the authors proposed 5 oral or combined oral-IM treatment regimens that could be used in low-resource settings:
- oral clindamycin (600 mg every 6 hours)
- plus IM gentamicin (4.5 g every 24 hours)
- oral amoxicillin-clavulanic acid (875 mg every 12 hours)
- IM cefotetan (2 g every 8 hours)
- IM meropenem or imipenem-cilastatin (500 mg every 8 hours)
- oral amoxicillin (500 mg every 8 hours) plus oral metronidazole (500 mg every 8 hours).
Typical endometritis treamentEndometritis is the single most common complication following cesarean delivery. The frequency of its occurrence depends on several factors, including: the socioeconomic characteristics of the patient population, length of labor, length of ruptured membranes, number of internal vaginal examinations, presence of preexisting lower genital tract infection, type of anesthesia, surgical technique, and use of prophylactic antibiotics. Endometritis is much less common after vaginal delivery but still may occur in 3% to 5% of patients.10
Endometritis is clearly a polymicrobial infection that includes multiple aerobic and anaerobic organisms. Accordingly, antibiotic therapy must target all the major groups of pathogens. The usual standard of care for treatment of early-onset endometritis is IV antibiotics, and patients typically are treated until they have been afebrile and asymptomatic for a minimum of 24 hours. Several different IV regimens provide acceptable treatment10:
- clindamycin plus gentamicin
- metronidazole plus ampicillin plus gentamicin
- extended-spectrum cephalosporins, such as cefepime, cefotetan, and cefoxitin
- extended-spectrum penicillins, such as ampicillin-sulbactam, piperacillin- tazobactam, and ticarcillin-clavulanic acid
- carbapenems, such as imipenem-cilastatin and meropenem.
What this evidence means for practiceClearly, IV antibiotics, even generic drugs, are more expensive than oral agents. They also are more difficult to administer than oral or IM drugs. The systematic review by Meaney-Delman and co-workers is therefore a very important contribution to the literature and should reassure clinicians practicing in low-resource settings that oral and oral-IM regimens can provide safe and effective treatment for endometritis. Until more rigorous comparative trials are conducted, however, we agree with the authors' caveat that, for now, such treatment should be limited to individuals whose infection occurred after vaginal delivery or who have evidence of only mild postcesarean endometritis.
Treatment options for chlamydia infection: How does azithromycin compare with doxycycline?Geisler WM, Uniyal A, Lee JY, et al. Azithromycin versus doxycycline for urogenital Chlamydia trachomatis infection. N Engl J Med. 2015;373(26):2512-2521.
The Centers for Disease Control and Prevention recommendations for treatment of chlamydia genital tract infection are either oral doxycycline, 100 mg twice daily for 7 days, or azithromycin, 1,000 mg in a single dose.11 Recent reports have raised questions about the relative effectiveness of single-dose azithromycin compared with the multiple-day doxycycline regimen. Accordingly, Geisler and colleagues conducted an interesting randomized controlled trial to determine if azithromycin is noninferior to doxycycline.
Details of the studyThe study took place in a unique institutional setting--the Los Angeles County youth correctional facilities. Participants were young men and women, aged 12 to 21 years, who tested positive for chlamydia infection by a nucleic acid amplification test on entry to the correctional facility. Participants then were randomly assigned to receive either doxycycline or azithromycin in the doses described above. The primary outcome was the percent of individuals who still tested positive for chlamydia 28 days after treatment.
Of note, all patients took their medication under direct observation of corrections officers and, with rare exceptions, did not engage in sexual activity during the period of observation. Because this was a noninferiority trial, Geisler and colleagues analyzed the outcomes only of the individuals who actually took their medication in accordance with the assigned protocol. A priori, the authors established a 95% CI of <5% difference in effectiveness as indicative of noninferiority.
Overall, 155 patients in each treatment group completed the trial according to the assigned protocol. No treatment failures occurred in the doxycycline group (0%; 95% CI, 0.0-2.4). Five treatment failures occurred in the azithromycin group (3.2%; 95% CI, 0.4-7.4), in 1 female and 4 male participants. Because the 95% CI for the difference in treatment outcome exceeded 5%, the authors were unable to conclude that azithromycin was noninferior to doxycycline.
Consider real-world treatment adherence in these resultsFor several reasons, we do not conclude from this article that ObGyns should now stop using azithromycin to treat patients with chlamydia infection. First, the actual per protocol sample size was still relatively small. If there had been just 2 fewer failures in the azithromycin group, the 95% CI for the difference in outcomes would have been less than 5%, and the authors would have concluded that the 2 drug regimens were noninferior. Second, 4 of the 5 treatment failures in the azithromycin group were in male rather than female participants. Third, the unique study design resulted in almost perfect adherence with the 7-day doxycycline treatment regimen. Such adherence is very unlikely in other practice settings, and patients who do not complete their treatment regimen are significantly more likely to fail therapy. Finally, azithromycin is definitely preferred in pregnancy because we try to avoid maternal/fetal exposure to drugs such as tetracycline and doxycycline.
What this evidence means for practiceIn this study, both doxycycline and azithromycin were highly effective (100% and 97%, respectively) for treating chlamydia genital tract infection, and they are comparable in cost. In our opinion, the improved adherence that is possible with single-dose azithromycin, the greater safety in pregnancy, and the excellent tolerability of this drug outweigh its slightly deceased rate of microbiologic cure.
Vaccine effective against hepatitis E for 4+ yearsZhang J, Zhang XF, Huang SJ, et al. Long-term efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372(10):914-922.
This study conducted by Zhang and colleagues in Dongtai, China, is an extended follow-up study of the hepatitis E virus (HEV) vaccine (Hecolin; Xiamen Innovax Biotech). A recombinant vaccine directed against HEV genotype 1, Hecolin has been used in China since 2012.
In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine (vaccine group, 56,302 participants) or the hepatitis B vaccine (control group, 56,302 participants). Vaccine administration occurred at 0, 1, and 6 months, and participants were followed for a total of 19 months.
Details of the studyThe follow-up study was designed to assess the efficacy, immunogenicity, and safety of the HEV vaccine up to 4.5 years postvaccination. All health care centers (205 village and private clinics) in the study area were enrolled in the program. The treatment assignments of all patients remained double blinded. Unblinding occurred only after the data on safety, efficacy, and immunogenicity had been locked.
A diagnosis of HEV infection was made if at least 2 of the following markers were present: a positive test for immunoglobulin M antibodies against HEV, a positive test for HEV RNA, or a serum concentration of immunoglobulin G (IgG) antibodies against HEV that was at least 4 times higher than previously measured at any time during the same illness. Vaccine immunogenicity was assessed by testing serum samples for IgG antibodies against HEV at regular intervals after the vaccination was given.
Over the 4.5-year study period, 7 cases of hepatitis E occurred in the vaccine group, and 53 in the control group. Vaccine efficacy was 86.8% (P<.001) in the modified intention-to-treat analysis. Among patients who received 3 doses of HEV vaccine and who were seronegative at the start of the study, 87% maintained antibodies against HEV for 4.5 years. Within the control group, HEV titers developed in 9% of participants. The vaccine and control groups had similar rates of adverse events.
The authors concluded that the HEV vaccine induced antibodies against hepatitis E that lasted up to 4.5 years. Additionally, 2 doses of vaccine induced slightly lower levels of antibody than those produced by 3 doses of the vaccine. Finally, all participants in the vaccine group who developed HEV had antibodies with high or moderate avidity, indicating an anamnestic response from previous immunity. Most participants in the control group who developed HEV, however, had antibodies with low avidity, indicating no previous immunity.
The burden of HEVHepatitis E is a serious infection and is the most common waterborne illness in the world. It occurs mainly in developing countries with limited resources. HEV infection is caused by genotypes 1, 2, 3, or 4, although all 4 genotypes belong to the same serotype. Genotypes 1 and 2 are typically waterborne, and genotypes 3 and 4 are typically transmitted from animals and humans. In general, the case fatality rate associated with HEV infection is 1% to 3%.12 In pregnancy, this rate increases to 5% to 25%.13,14 In Bangladesh, for example, hepatitis E is responsible for more than 1,000 deaths per year among pregnant women.15
Clinical presentation of HEV infection is a spectrum, with most symptomatic patients presenting with acute, self-limited hepatitis. Severe cases may be associated with pancreatitis, arthritis, aplastic anemia, and neurologic complications, such as seizures. Populations at risk for more severe cases include pregnant women, elderly men, and patients with pre‑ existing, chronic liver disease.
What this evidence means for practiceStandard sanitary precautions, such as clean drinking water, traditionally have been considered the mainstay of hepatitis E prevention. However, as the study authors indicate, recent severe outbreaks of HEV infection in Sudan and Uganda have occurred despite these measures. Thus, an effective vaccine that produces long-standing immunity has great potential for reducing morbidity and mortality in these countries. The present vaccine appears to be highly effective and safe. The principal unanswered question is the duration of immunity.
My patients are asking, "What is the best insect repellent to try to avoid Zika virus?"
With summer upon us we have received questions from colleagues about the best over-the-counter insect repellents to advise their pregnant patients to use.
The preferred insect repellent for skin coverage is DEET (N,N-diethyl-meta-toluamide) (TABLE). Oil of lemon/eucalyptus/para-menthane-diol and IR3535 are also acceptable repellents to use on the skin that are safe for use in pregnancy. In addition, instruct patients to spray permethrin on their clothing or to buy clothing (boots, pants, socks) that has been pretreated with permethrin.1,2
Anushka Chelliah, MD, and Patrick Duff, MD.
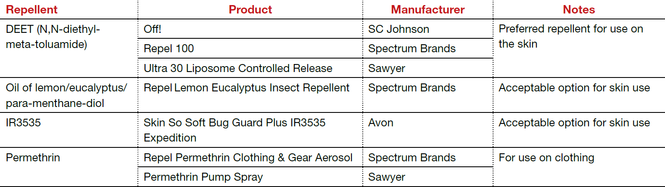
Abbreviation: OTC, over the counter.
Coming soon to OBG Management
Drs. Chelliah and Duff follow-up on their March 2016 examination of Zika virus infection with:
- Latest information on Zika virus-associated birth defects
- Ultrasonographic and radiologic evidence of abnormalities in the fetus and newborn exposed to Zika virus infection
- Link between Zika virus infection and serious neurologic complications in adults
- New recommendations for preventing sexual transmission of Zika virus infection
Dr. Chelliah is a Maternal Fetal Medicine-Fellow in the Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
References
- Peterson EE, Staples JE, Meaney-Delman D, et al. Interim guidelines for pregnant women during a Zika virus outbreak--United States, 2016. MMWR Morb Mortal Wkly Rep. 2016;65(2):30-33.
- Centers for Disease Control and Prevention. CDC Features: Avoid mosquito bites. http://www.cdc.gov/Features/stopmosquitoes/index.html. Updated March 18, 2016. Accessed May 10, 2016.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- DeFrances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13. 2007:165:1–209.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: final data for 2013. Natl Vital Stat Rep. 2015;64(1):1–65.
- Anderson DJ, Podgorny K, Berrios-Torres SI, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605–627.
- Conroy K, Koenig AF, Yu YH, Courtney A, Lee HJ, Norwitz ER. Infectious morbidity after cesarean delivery: 10 strategies to reduce risk. Rev Obstet Gynecol. 2012;5(2):69–77.
- Scifres CM, Leighton BL, Fogertey PJ, Macones GA, Stamilio DM. Supplemental oxygen for the prevention of postcesarean infectious morbidity: a randomized controlled trial. Am J Obstet Gynecol. 2011;205(3)267.e1–e9.
- Wloch C, Wilson J, Lamagni T, Harrington P, Charlett A, Sheridan E. Risk factors for surgical site infection following cesarean section in England: results from a multicenter cohort study. BJOG. 2012;119(11):1324–1333.
- Olsen MA, Butler AM, Willers DM, Gross GA, Hamilton BH, Fraser VJ. Attributable costs of surgical site infection and endometritis after low transverse cesarean delivery. Infect Control Hosp Epidemiol. 2010;31(3):276–282.
- Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18–26.
- Ngai IM, Van Arsdale A, Govindappagari S, et al. Skin preparation for prevention of surgical site infection after cesarean delivery: a randomized controlled trial. Obstet Gynecol. 2015;126(6):1251–1257.
- Duff P. Maternal and perinatal infection—bacterial. In: Gabbe SG, Niebyl JR, Simpson JL, et al, eds. Obstetrics: normal and problem pregnancies. 6th ed. Philadelphia, PA: Elsevier/Saunders; 2012.
- Workowski KA, Bolan GH; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1−137. Erratum in: MMWR Recomm Rep. 2015;64(33):924.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13(3):145–154.
- Khuroo MS, Teli MR, Skidmore S, Sofi MA, Khuroo MI. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70(2):252–255.
- Khuroo MS, Kamili S. Aetiology, clinical course and outcome of sporadic acute viral hepatitis in pregnancy. J Viral Hepat. 2003;10(1):61–69.
- Labrique AB, Sikder SS, Krain IJ, et al. Hepatitis E, a vaccine-preventable cause of maternal deaths. Emerg Infect Dis. 2012;18(9):1401–1404.

Dr. Jackson is a Maternal-Fetal Medicine Fellow in the Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.

Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Jackson is a Maternal-Fetal Medicine Fellow in the Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The authors report no financial relationships relevant to this article.
Dr. Jackson is a Maternal-Fetal Medicine Fellow in the Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The authors report no financial relationships relevant to this article.
Chlorhexidine-alcohol is superior to iodine-alcohol for reducing SSIs after cesarean deliveryTuuli Mg, Liu J, Stout Mj, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647-655.
In the United States, cesarean delivery is the most commonly performed major surgical procedure, with 32.7% of births--or 1.3 million--occurring in this fashion in 2013.1,2 In general, for all surgical procedures, the SSI rate is 2% to 5%, with the rate rising to 5% to 12% for cesarean delivery, especially in obese patients.3-6 Not only do SSIs increase morbidity for the patient but they also contribute to high medical costs, with an estimated additional expense of $3,529 per cesarean-associated infection.7
Skin pathogens are a major source of SSIs. Choosing the proper antiseptic has the potential to decrease infection risk. While current guidelines recommend use of an antiseptic containing alcohol, it is unclear which disinfectant is the most effective agent to combine with the alcohol.3
Most trials evaluating preoperative antiseptic skin preparation have studied patients undergoing general surgery procedures. A well-designed trial by Darouiche and coauthors demonstrated that chlorhexidine was superior to iodine when used as an antiseptic for skin preparation.8 Interestingly, however, this trial, like most others, compared chlorhexidine-alcohol to iodine without alcohol. It is therefore unclear whether the chlorhexidine or the alcohol is responsible for the enhanced antiseptic effect.
Details of the studyIn the single-center randomized trial conducted by Tuuli and colleagues, patients were assigned to preoperative skin antisepsis with either chlorhexidine-alcohol (2% chlorhexidine gluconate with 70% isopropyl alcohol) or iodine-alcohol (8.3% povidone-iodine with 72.5% isopropyl alcohol). Antiseptic was applied according to the manufacturer's instructions, with a standard wait time of 3 minutes between application and skin incision. However, wait time was eliminated for patients undergoing emergency cesarean delivery. Additionally, patients received standard, weight-based preoperative antibiotic prophylaxis (agent not specified).
The authors estimated the necessary sample size for the trial by assuming an 8% baseline SSI rate and an anticipated 50% reduction of infection in the chlorhexidine-alcohol group. Exclusion criteria included a known allergy to chlorhexidine, alcohol, iodine, or shellfish or a preexisting skin infection adjacent to the operative site.
In addition to assessing the primary outcome of SSI with the 2 preparations, the authors conducted 4 prespecified subgroup analyses. These subgroups were based on: type of cesarean delivery (scheduled vs unscheduled), body weight (obese vs nonobese), type of skin closure (subcuticular suture vs staples), and presence or absence of chronic medical conditions (diabetes, hypertension, renal disease). Additionally, a post hoc analysis was performed, comparing women with diabetes (gestational and pregestational) to those without diabetes.
A total of 1,636 pregnant women were screened for eligibility. Of these, 489 women were excluded because they did not meet inclusion criteria or declined to participate or because informed consent could not be obtained. Baseline characteristics were similar across both groups.
Patients were followed for 30 days after surgery. A total of 1,082 women (94.3% of sample size) completed the follow-up. Among these patients, the rate of SSI was significantly lower in the chlorhexidine-alcohol group (4.3%) compared with the iodine-alcohol group (7.7%, P = .02).
In the subgroup analyses, the frequency of SSI remained lower for the chlorhexidine-alcohol group than for the iodine-alcohol group. These reductions were not affected by whether the cesarean was scheduled or unscheduled, the presence or absence of obesity, the type of skin closure, the presence of chronic disease, or diabetes status.
Several secondary outcomes also were examined in this study. There were no significant differences between the 2 antiseptic groups with respect to rates of endometritis, hospital readmission for infection-related complications, length of hospital stay, use of other health care services (such as emergency department visits, additional wound surgery, and home health services), and rates of other wound complications (seroma, hematoma, and cellulitis). Patients in the chlorhexidine-alcohol group were significantly less likely than those in the iodine-alcohol group to have physician office visits for concerns about possible wound complications (P = .009).
The authors concluded that the use of chlorhexidine-alcohol was superior to iodine-alcohol in preventing SSI after cesarean delivery.
Study strengths and limitations The authors acknowledged that their study had some minor limitations. First, the trial was conducted at a single site, which may limit the generalizability of the findings. However, the study population was racially and economically diverse. Second, the lack of blinding among providers and participants may have introduced bias, although, as the authors explain, we would expect this bias to be largely nondirectional.
A major strength of this study is its randomized design. Another strength is that the authors included emergency cesarean deliveries in their analysis. Emergency procedures represent a substantial proportion of cesarean deliveries, and they place the patient at increased risk for SSIs because of limited time available to prepare the skin before surgery begins. Thus, it is of great interest that chlorhexidine-alcohol was so effective even in the highest-risk patients.
Several properties may make chlorhexidine superior to iodine as an antiseptic: high binding affinity for the skin, high antibacterial activity against both gram-positive and gram-negative bacteria, and longer residual effects than iodine. Additionally, iodine is inactivated by organic matter, such as body fluids, whereas chlorhexidine is not.
A recent study by Ngai and colleagues9 compared chlorhexidine-alcohol with iodine-alcohol for skin preparation before cesarean delivery. These authors found no difference in SSI when comparing the 2 solutions used separately or sequentially, except in morbidly obese women. In these women, sequential application of both solutions reduced the infection rate. However, this study specifically excluded emergency cesarean deliveries, making the generalizability of the results questionable.9
What this evidence means for practiceThis large, randomized study found chlorhexidine-alcohol to be superior to iodine-alchol in reducing the risk of SSIs after cesarean delivery. These results confirm those of previous studies from both the obstetric and general surgery literature. Although chlorhexidine-alcohol is more expensive than iodine-alcohol, we strongly recommend its use in patients having cesarean delivery.
Five effective oral and intramuscular antibiotic regimens for treating postpartum endometritisMeaney-Delman D, Bartlett LA, Gravett MG, Jamieson DJ. Oral and intramuscular treatment options for early postpartum endometritis in low-resource settings: a systematic review. Obstet Gynecol. 2015;125(4):789-800.
The authors of this excellent systematic review on antibiotic treatments for early postpartum endometritis conducted their study in 3 phases. Initially, Meaney-Delman and colleagues searched the literature for reports of prospective studies that evaluated the use of oral and intramuscular (IM) antibiotics for treatment of patients who developed endometritis following either cesarean or vaginal delivery. When they discovered that these initial trials were few in number and of relatively poor quality, they reviewed more rigorous trials of intravenous (IV) antibiotics. Finally, they evaluated clinical trials that specifically identified microorganisms isolated from the uterus in patients with endometritis and used this information to help inform their recommendations for treatment options.
Details of the studyIn evaluating the trials of oral and IM antibiotics, the authors set as a standard for effectiveness a cure rate of 85%, a figure comparable to that generally achieved with IV antibiotics. They identified 2 oral antibiotic regimens that met this standard of effectiveness: amoxicillin-clavulanate (100% cure in 36 patients; 95% confidence interval [CI], 90-100) and ampicillin plus metronidazole (97% cure in 37 patients; 95% CI, 86-100).
Two studies demonstrated acceptable levels of cure with single-agent IM antibiotics: aztreonam (100% cure in 16 patients; 95% CI, 81-100) and imipenem (91% cure in 23 patients; 95% CI, 73-98). One additional trial demonstrated an acceptable clinical response rate when IV clindamycin was combined with IM gentamicin (100% cure in 54 patients; 95% CI, 94-100). By contrast, the authors noted, many different IV regimens--either as a single agent or as a drug combination--provided cure rates that equaled or exceeded 85%.
In the study's final phase, the authors provided an excellent overview of the polymicrobial nature of puerperal endometritis. As documented in multiple prior reports, the most common pathogens are the gram-negative anaerobic bacilli, such as Bacteroides and Prevotella species; the anaerobic gram-positive organisms, including Peptococcus and Peptostreptococcus species; aerobic gram-negative bacilli, such as Escherichia coli, Klebsiella pneumoniae, and Proteus species; and aerobic gram-positive cocci, such as group B streptococci, enterococci, and staphylococci.
Recommended regimens. Based on their review of clinical and microbiological studies, the authors proposed 5 oral or combined oral-IM treatment regimens that could be used in low-resource settings:
- oral clindamycin (600 mg every 6 hours)
- plus IM gentamicin (4.5 g every 24 hours)
- oral amoxicillin-clavulanic acid (875 mg every 12 hours)
- IM cefotetan (2 g every 8 hours)
- IM meropenem or imipenem-cilastatin (500 mg every 8 hours)
- oral amoxicillin (500 mg every 8 hours) plus oral metronidazole (500 mg every 8 hours).
Typical endometritis treamentEndometritis is the single most common complication following cesarean delivery. The frequency of its occurrence depends on several factors, including: the socioeconomic characteristics of the patient population, length of labor, length of ruptured membranes, number of internal vaginal examinations, presence of preexisting lower genital tract infection, type of anesthesia, surgical technique, and use of prophylactic antibiotics. Endometritis is much less common after vaginal delivery but still may occur in 3% to 5% of patients.10
Endometritis is clearly a polymicrobial infection that includes multiple aerobic and anaerobic organisms. Accordingly, antibiotic therapy must target all the major groups of pathogens. The usual standard of care for treatment of early-onset endometritis is IV antibiotics, and patients typically are treated until they have been afebrile and asymptomatic for a minimum of 24 hours. Several different IV regimens provide acceptable treatment10:
- clindamycin plus gentamicin
- metronidazole plus ampicillin plus gentamicin
- extended-spectrum cephalosporins, such as cefepime, cefotetan, and cefoxitin
- extended-spectrum penicillins, such as ampicillin-sulbactam, piperacillin- tazobactam, and ticarcillin-clavulanic acid
- carbapenems, such as imipenem-cilastatin and meropenem.
What this evidence means for practiceClearly, IV antibiotics, even generic drugs, are more expensive than oral agents. They also are more difficult to administer than oral or IM drugs. The systematic review by Meaney-Delman and co-workers is therefore a very important contribution to the literature and should reassure clinicians practicing in low-resource settings that oral and oral-IM regimens can provide safe and effective treatment for endometritis. Until more rigorous comparative trials are conducted, however, we agree with the authors' caveat that, for now, such treatment should be limited to individuals whose infection occurred after vaginal delivery or who have evidence of only mild postcesarean endometritis.
Treatment options for chlamydia infection: How does azithromycin compare with doxycycline?Geisler WM, Uniyal A, Lee JY, et al. Azithromycin versus doxycycline for urogenital Chlamydia trachomatis infection. N Engl J Med. 2015;373(26):2512-2521.
The Centers for Disease Control and Prevention recommendations for treatment of chlamydia genital tract infection are either oral doxycycline, 100 mg twice daily for 7 days, or azithromycin, 1,000 mg in a single dose.11 Recent reports have raised questions about the relative effectiveness of single-dose azithromycin compared with the multiple-day doxycycline regimen. Accordingly, Geisler and colleagues conducted an interesting randomized controlled trial to determine if azithromycin is noninferior to doxycycline.
Details of the studyThe study took place in a unique institutional setting--the Los Angeles County youth correctional facilities. Participants were young men and women, aged 12 to 21 years, who tested positive for chlamydia infection by a nucleic acid amplification test on entry to the correctional facility. Participants then were randomly assigned to receive either doxycycline or azithromycin in the doses described above. The primary outcome was the percent of individuals who still tested positive for chlamydia 28 days after treatment.
Of note, all patients took their medication under direct observation of corrections officers and, with rare exceptions, did not engage in sexual activity during the period of observation. Because this was a noninferiority trial, Geisler and colleagues analyzed the outcomes only of the individuals who actually took their medication in accordance with the assigned protocol. A priori, the authors established a 95% CI of <5% difference in effectiveness as indicative of noninferiority.
Overall, 155 patients in each treatment group completed the trial according to the assigned protocol. No treatment failures occurred in the doxycycline group (0%; 95% CI, 0.0-2.4). Five treatment failures occurred in the azithromycin group (3.2%; 95% CI, 0.4-7.4), in 1 female and 4 male participants. Because the 95% CI for the difference in treatment outcome exceeded 5%, the authors were unable to conclude that azithromycin was noninferior to doxycycline.
Consider real-world treatment adherence in these resultsFor several reasons, we do not conclude from this article that ObGyns should now stop using azithromycin to treat patients with chlamydia infection. First, the actual per protocol sample size was still relatively small. If there had been just 2 fewer failures in the azithromycin group, the 95% CI for the difference in outcomes would have been less than 5%, and the authors would have concluded that the 2 drug regimens were noninferior. Second, 4 of the 5 treatment failures in the azithromycin group were in male rather than female participants. Third, the unique study design resulted in almost perfect adherence with the 7-day doxycycline treatment regimen. Such adherence is very unlikely in other practice settings, and patients who do not complete their treatment regimen are significantly more likely to fail therapy. Finally, azithromycin is definitely preferred in pregnancy because we try to avoid maternal/fetal exposure to drugs such as tetracycline and doxycycline.
What this evidence means for practiceIn this study, both doxycycline and azithromycin were highly effective (100% and 97%, respectively) for treating chlamydia genital tract infection, and they are comparable in cost. In our opinion, the improved adherence that is possible with single-dose azithromycin, the greater safety in pregnancy, and the excellent tolerability of this drug outweigh its slightly deceased rate of microbiologic cure.
Vaccine effective against hepatitis E for 4+ yearsZhang J, Zhang XF, Huang SJ, et al. Long-term efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372(10):914-922.
This study conducted by Zhang and colleagues in Dongtai, China, is an extended follow-up study of the hepatitis E virus (HEV) vaccine (Hecolin; Xiamen Innovax Biotech). A recombinant vaccine directed against HEV genotype 1, Hecolin has been used in China since 2012.
In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine (vaccine group, 56,302 participants) or the hepatitis B vaccine (control group, 56,302 participants). Vaccine administration occurred at 0, 1, and 6 months, and participants were followed for a total of 19 months.
Details of the studyThe follow-up study was designed to assess the efficacy, immunogenicity, and safety of the HEV vaccine up to 4.5 years postvaccination. All health care centers (205 village and private clinics) in the study area were enrolled in the program. The treatment assignments of all patients remained double blinded. Unblinding occurred only after the data on safety, efficacy, and immunogenicity had been locked.
A diagnosis of HEV infection was made if at least 2 of the following markers were present: a positive test for immunoglobulin M antibodies against HEV, a positive test for HEV RNA, or a serum concentration of immunoglobulin G (IgG) antibodies against HEV that was at least 4 times higher than previously measured at any time during the same illness. Vaccine immunogenicity was assessed by testing serum samples for IgG antibodies against HEV at regular intervals after the vaccination was given.
Over the 4.5-year study period, 7 cases of hepatitis E occurred in the vaccine group, and 53 in the control group. Vaccine efficacy was 86.8% (P<.001) in the modified intention-to-treat analysis. Among patients who received 3 doses of HEV vaccine and who were seronegative at the start of the study, 87% maintained antibodies against HEV for 4.5 years. Within the control group, HEV titers developed in 9% of participants. The vaccine and control groups had similar rates of adverse events.
The authors concluded that the HEV vaccine induced antibodies against hepatitis E that lasted up to 4.5 years. Additionally, 2 doses of vaccine induced slightly lower levels of antibody than those produced by 3 doses of the vaccine. Finally, all participants in the vaccine group who developed HEV had antibodies with high or moderate avidity, indicating an anamnestic response from previous immunity. Most participants in the control group who developed HEV, however, had antibodies with low avidity, indicating no previous immunity.
The burden of HEVHepatitis E is a serious infection and is the most common waterborne illness in the world. It occurs mainly in developing countries with limited resources. HEV infection is caused by genotypes 1, 2, 3, or 4, although all 4 genotypes belong to the same serotype. Genotypes 1 and 2 are typically waterborne, and genotypes 3 and 4 are typically transmitted from animals and humans. In general, the case fatality rate associated with HEV infection is 1% to 3%.12 In pregnancy, this rate increases to 5% to 25%.13,14 In Bangladesh, for example, hepatitis E is responsible for more than 1,000 deaths per year among pregnant women.15
Clinical presentation of HEV infection is a spectrum, with most symptomatic patients presenting with acute, self-limited hepatitis. Severe cases may be associated with pancreatitis, arthritis, aplastic anemia, and neurologic complications, such as seizures. Populations at risk for more severe cases include pregnant women, elderly men, and patients with pre‑ existing, chronic liver disease.
What this evidence means for practiceStandard sanitary precautions, such as clean drinking water, traditionally have been considered the mainstay of hepatitis E prevention. However, as the study authors indicate, recent severe outbreaks of HEV infection in Sudan and Uganda have occurred despite these measures. Thus, an effective vaccine that produces long-standing immunity has great potential for reducing morbidity and mortality in these countries. The present vaccine appears to be highly effective and safe. The principal unanswered question is the duration of immunity.
My patients are asking, "What is the best insect repellent to try to avoid Zika virus?"
With summer upon us we have received questions from colleagues about the best over-the-counter insect repellents to advise their pregnant patients to use.
The preferred insect repellent for skin coverage is DEET (N,N-diethyl-meta-toluamide) (TABLE). Oil of lemon/eucalyptus/para-menthane-diol and IR3535 are also acceptable repellents to use on the skin that are safe for use in pregnancy. In addition, instruct patients to spray permethrin on their clothing or to buy clothing (boots, pants, socks) that has been pretreated with permethrin.1,2
Anushka Chelliah, MD, and Patrick Duff, MD.
Abbreviation: OTC, over the counter.
Coming soon to OBG Management
Drs. Chelliah and Duff follow-up on their March 2016 examination of Zika virus infection with:
- Latest information on Zika virus-associated birth defects
- Ultrasonographic and radiologic evidence of abnormalities in the fetus and newborn exposed to Zika virus infection
- Link between Zika virus infection and serious neurologic complications in adults
- New recommendations for preventing sexual transmission of Zika virus infection
Dr. Chelliah is a Maternal Fetal Medicine-Fellow in the Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
References
- Peterson EE, Staples JE, Meaney-Delman D, et al. Interim guidelines for pregnant women during a Zika virus outbreak--United States, 2016. MMWR Morb Mortal Wkly Rep. 2016;65(2):30-33.
- Centers for Disease Control and Prevention. CDC Features: Avoid mosquito bites. http://www.cdc.gov/Features/stopmosquitoes/index.html. Updated March 18, 2016. Accessed May 10, 2016.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Chlorhexidine-alcohol is superior to iodine-alcohol for reducing SSIs after cesarean deliveryTuuli Mg, Liu J, Stout Mj, et al. A randomized trial comparing skin antiseptic agents at cesarean delivery. N Engl J Med. 2016;374(7):647-655.
In the United States, cesarean delivery is the most commonly performed major surgical procedure, with 32.7% of births--or 1.3 million--occurring in this fashion in 2013.1,2 In general, for all surgical procedures, the SSI rate is 2% to 5%, with the rate rising to 5% to 12% for cesarean delivery, especially in obese patients.3-6 Not only do SSIs increase morbidity for the patient but they also contribute to high medical costs, with an estimated additional expense of $3,529 per cesarean-associated infection.7
Skin pathogens are a major source of SSIs. Choosing the proper antiseptic has the potential to decrease infection risk. While current guidelines recommend use of an antiseptic containing alcohol, it is unclear which disinfectant is the most effective agent to combine with the alcohol.3
Most trials evaluating preoperative antiseptic skin preparation have studied patients undergoing general surgery procedures. A well-designed trial by Darouiche and coauthors demonstrated that chlorhexidine was superior to iodine when used as an antiseptic for skin preparation.8 Interestingly, however, this trial, like most others, compared chlorhexidine-alcohol to iodine without alcohol. It is therefore unclear whether the chlorhexidine or the alcohol is responsible for the enhanced antiseptic effect.
Details of the studyIn the single-center randomized trial conducted by Tuuli and colleagues, patients were assigned to preoperative skin antisepsis with either chlorhexidine-alcohol (2% chlorhexidine gluconate with 70% isopropyl alcohol) or iodine-alcohol (8.3% povidone-iodine with 72.5% isopropyl alcohol). Antiseptic was applied according to the manufacturer's instructions, with a standard wait time of 3 minutes between application and skin incision. However, wait time was eliminated for patients undergoing emergency cesarean delivery. Additionally, patients received standard, weight-based preoperative antibiotic prophylaxis (agent not specified).
The authors estimated the necessary sample size for the trial by assuming an 8% baseline SSI rate and an anticipated 50% reduction of infection in the chlorhexidine-alcohol group. Exclusion criteria included a known allergy to chlorhexidine, alcohol, iodine, or shellfish or a preexisting skin infection adjacent to the operative site.
In addition to assessing the primary outcome of SSI with the 2 preparations, the authors conducted 4 prespecified subgroup analyses. These subgroups were based on: type of cesarean delivery (scheduled vs unscheduled), body weight (obese vs nonobese), type of skin closure (subcuticular suture vs staples), and presence or absence of chronic medical conditions (diabetes, hypertension, renal disease). Additionally, a post hoc analysis was performed, comparing women with diabetes (gestational and pregestational) to those without diabetes.
A total of 1,636 pregnant women were screened for eligibility. Of these, 489 women were excluded because they did not meet inclusion criteria or declined to participate or because informed consent could not be obtained. Baseline characteristics were similar across both groups.
Patients were followed for 30 days after surgery. A total of 1,082 women (94.3% of sample size) completed the follow-up. Among these patients, the rate of SSI was significantly lower in the chlorhexidine-alcohol group (4.3%) compared with the iodine-alcohol group (7.7%, P = .02).
In the subgroup analyses, the frequency of SSI remained lower for the chlorhexidine-alcohol group than for the iodine-alcohol group. These reductions were not affected by whether the cesarean was scheduled or unscheduled, the presence or absence of obesity, the type of skin closure, the presence of chronic disease, or diabetes status.
Several secondary outcomes also were examined in this study. There were no significant differences between the 2 antiseptic groups with respect to rates of endometritis, hospital readmission for infection-related complications, length of hospital stay, use of other health care services (such as emergency department visits, additional wound surgery, and home health services), and rates of other wound complications (seroma, hematoma, and cellulitis). Patients in the chlorhexidine-alcohol group were significantly less likely than those in the iodine-alcohol group to have physician office visits for concerns about possible wound complications (P = .009).
The authors concluded that the use of chlorhexidine-alcohol was superior to iodine-alcohol in preventing SSI after cesarean delivery.
Study strengths and limitations The authors acknowledged that their study had some minor limitations. First, the trial was conducted at a single site, which may limit the generalizability of the findings. However, the study population was racially and economically diverse. Second, the lack of blinding among providers and participants may have introduced bias, although, as the authors explain, we would expect this bias to be largely nondirectional.
A major strength of this study is its randomized design. Another strength is that the authors included emergency cesarean deliveries in their analysis. Emergency procedures represent a substantial proportion of cesarean deliveries, and they place the patient at increased risk for SSIs because of limited time available to prepare the skin before surgery begins. Thus, it is of great interest that chlorhexidine-alcohol was so effective even in the highest-risk patients.
Several properties may make chlorhexidine superior to iodine as an antiseptic: high binding affinity for the skin, high antibacterial activity against both gram-positive and gram-negative bacteria, and longer residual effects than iodine. Additionally, iodine is inactivated by organic matter, such as body fluids, whereas chlorhexidine is not.
A recent study by Ngai and colleagues9 compared chlorhexidine-alcohol with iodine-alcohol for skin preparation before cesarean delivery. These authors found no difference in SSI when comparing the 2 solutions used separately or sequentially, except in morbidly obese women. In these women, sequential application of both solutions reduced the infection rate. However, this study specifically excluded emergency cesarean deliveries, making the generalizability of the results questionable.9
What this evidence means for practiceThis large, randomized study found chlorhexidine-alcohol to be superior to iodine-alchol in reducing the risk of SSIs after cesarean delivery. These results confirm those of previous studies from both the obstetric and general surgery literature. Although chlorhexidine-alcohol is more expensive than iodine-alcohol, we strongly recommend its use in patients having cesarean delivery.
Five effective oral and intramuscular antibiotic regimens for treating postpartum endometritisMeaney-Delman D, Bartlett LA, Gravett MG, Jamieson DJ. Oral and intramuscular treatment options for early postpartum endometritis in low-resource settings: a systematic review. Obstet Gynecol. 2015;125(4):789-800.
The authors of this excellent systematic review on antibiotic treatments for early postpartum endometritis conducted their study in 3 phases. Initially, Meaney-Delman and colleagues searched the literature for reports of prospective studies that evaluated the use of oral and intramuscular (IM) antibiotics for treatment of patients who developed endometritis following either cesarean or vaginal delivery. When they discovered that these initial trials were few in number and of relatively poor quality, they reviewed more rigorous trials of intravenous (IV) antibiotics. Finally, they evaluated clinical trials that specifically identified microorganisms isolated from the uterus in patients with endometritis and used this information to help inform their recommendations for treatment options.
Details of the studyIn evaluating the trials of oral and IM antibiotics, the authors set as a standard for effectiveness a cure rate of 85%, a figure comparable to that generally achieved with IV antibiotics. They identified 2 oral antibiotic regimens that met this standard of effectiveness: amoxicillin-clavulanate (100% cure in 36 patients; 95% confidence interval [CI], 90-100) and ampicillin plus metronidazole (97% cure in 37 patients; 95% CI, 86-100).
Two studies demonstrated acceptable levels of cure with single-agent IM antibiotics: aztreonam (100% cure in 16 patients; 95% CI, 81-100) and imipenem (91% cure in 23 patients; 95% CI, 73-98). One additional trial demonstrated an acceptable clinical response rate when IV clindamycin was combined with IM gentamicin (100% cure in 54 patients; 95% CI, 94-100). By contrast, the authors noted, many different IV regimens--either as a single agent or as a drug combination--provided cure rates that equaled or exceeded 85%.
In the study's final phase, the authors provided an excellent overview of the polymicrobial nature of puerperal endometritis. As documented in multiple prior reports, the most common pathogens are the gram-negative anaerobic bacilli, such as Bacteroides and Prevotella species; the anaerobic gram-positive organisms, including Peptococcus and Peptostreptococcus species; aerobic gram-negative bacilli, such as Escherichia coli, Klebsiella pneumoniae, and Proteus species; and aerobic gram-positive cocci, such as group B streptococci, enterococci, and staphylococci.
Recommended regimens. Based on their review of clinical and microbiological studies, the authors proposed 5 oral or combined oral-IM treatment regimens that could be used in low-resource settings:
- oral clindamycin (600 mg every 6 hours)
- plus IM gentamicin (4.5 g every 24 hours)
- oral amoxicillin-clavulanic acid (875 mg every 12 hours)
- IM cefotetan (2 g every 8 hours)
- IM meropenem or imipenem-cilastatin (500 mg every 8 hours)
- oral amoxicillin (500 mg every 8 hours) plus oral metronidazole (500 mg every 8 hours).
Typical endometritis treamentEndometritis is the single most common complication following cesarean delivery. The frequency of its occurrence depends on several factors, including: the socioeconomic characteristics of the patient population, length of labor, length of ruptured membranes, number of internal vaginal examinations, presence of preexisting lower genital tract infection, type of anesthesia, surgical technique, and use of prophylactic antibiotics. Endometritis is much less common after vaginal delivery but still may occur in 3% to 5% of patients.10
Endometritis is clearly a polymicrobial infection that includes multiple aerobic and anaerobic organisms. Accordingly, antibiotic therapy must target all the major groups of pathogens. The usual standard of care for treatment of early-onset endometritis is IV antibiotics, and patients typically are treated until they have been afebrile and asymptomatic for a minimum of 24 hours. Several different IV regimens provide acceptable treatment10:
- clindamycin plus gentamicin
- metronidazole plus ampicillin plus gentamicin
- extended-spectrum cephalosporins, such as cefepime, cefotetan, and cefoxitin
- extended-spectrum penicillins, such as ampicillin-sulbactam, piperacillin- tazobactam, and ticarcillin-clavulanic acid
- carbapenems, such as imipenem-cilastatin and meropenem.
What this evidence means for practiceClearly, IV antibiotics, even generic drugs, are more expensive than oral agents. They also are more difficult to administer than oral or IM drugs. The systematic review by Meaney-Delman and co-workers is therefore a very important contribution to the literature and should reassure clinicians practicing in low-resource settings that oral and oral-IM regimens can provide safe and effective treatment for endometritis. Until more rigorous comparative trials are conducted, however, we agree with the authors' caveat that, for now, such treatment should be limited to individuals whose infection occurred after vaginal delivery or who have evidence of only mild postcesarean endometritis.
Treatment options for chlamydia infection: How does azithromycin compare with doxycycline?Geisler WM, Uniyal A, Lee JY, et al. Azithromycin versus doxycycline for urogenital Chlamydia trachomatis infection. N Engl J Med. 2015;373(26):2512-2521.
The Centers for Disease Control and Prevention recommendations for treatment of chlamydia genital tract infection are either oral doxycycline, 100 mg twice daily for 7 days, or azithromycin, 1,000 mg in a single dose.11 Recent reports have raised questions about the relative effectiveness of single-dose azithromycin compared with the multiple-day doxycycline regimen. Accordingly, Geisler and colleagues conducted an interesting randomized controlled trial to determine if azithromycin is noninferior to doxycycline.
Details of the studyThe study took place in a unique institutional setting--the Los Angeles County youth correctional facilities. Participants were young men and women, aged 12 to 21 years, who tested positive for chlamydia infection by a nucleic acid amplification test on entry to the correctional facility. Participants then were randomly assigned to receive either doxycycline or azithromycin in the doses described above. The primary outcome was the percent of individuals who still tested positive for chlamydia 28 days after treatment.
Of note, all patients took their medication under direct observation of corrections officers and, with rare exceptions, did not engage in sexual activity during the period of observation. Because this was a noninferiority trial, Geisler and colleagues analyzed the outcomes only of the individuals who actually took their medication in accordance with the assigned protocol. A priori, the authors established a 95% CI of <5% difference in effectiveness as indicative of noninferiority.
Overall, 155 patients in each treatment group completed the trial according to the assigned protocol. No treatment failures occurred in the doxycycline group (0%; 95% CI, 0.0-2.4). Five treatment failures occurred in the azithromycin group (3.2%; 95% CI, 0.4-7.4), in 1 female and 4 male participants. Because the 95% CI for the difference in treatment outcome exceeded 5%, the authors were unable to conclude that azithromycin was noninferior to doxycycline.
Consider real-world treatment adherence in these resultsFor several reasons, we do not conclude from this article that ObGyns should now stop using azithromycin to treat patients with chlamydia infection. First, the actual per protocol sample size was still relatively small. If there had been just 2 fewer failures in the azithromycin group, the 95% CI for the difference in outcomes would have been less than 5%, and the authors would have concluded that the 2 drug regimens were noninferior. Second, 4 of the 5 treatment failures in the azithromycin group were in male rather than female participants. Third, the unique study design resulted in almost perfect adherence with the 7-day doxycycline treatment regimen. Such adherence is very unlikely in other practice settings, and patients who do not complete their treatment regimen are significantly more likely to fail therapy. Finally, azithromycin is definitely preferred in pregnancy because we try to avoid maternal/fetal exposure to drugs such as tetracycline and doxycycline.
What this evidence means for practiceIn this study, both doxycycline and azithromycin were highly effective (100% and 97%, respectively) for treating chlamydia genital tract infection, and they are comparable in cost. In our opinion, the improved adherence that is possible with single-dose azithromycin, the greater safety in pregnancy, and the excellent tolerability of this drug outweigh its slightly deceased rate of microbiologic cure.
Vaccine effective against hepatitis E for 4+ yearsZhang J, Zhang XF, Huang SJ, et al. Long-term efficacy of a hepatitis E vaccine. N Engl J Med. 2015;372(10):914-922.
This study conducted by Zhang and colleagues in Dongtai, China, is an extended follow-up study of the hepatitis E virus (HEV) vaccine (Hecolin; Xiamen Innovax Biotech). A recombinant vaccine directed against HEV genotype 1, Hecolin has been used in China since 2012.
In the initial efficacy study, healthy adults aged 16 to 65 years were randomly assigned to receive either the hepatitis E vaccine (vaccine group, 56,302 participants) or the hepatitis B vaccine (control group, 56,302 participants). Vaccine administration occurred at 0, 1, and 6 months, and participants were followed for a total of 19 months.
Details of the studyThe follow-up study was designed to assess the efficacy, immunogenicity, and safety of the HEV vaccine up to 4.5 years postvaccination. All health care centers (205 village and private clinics) in the study area were enrolled in the program. The treatment assignments of all patients remained double blinded. Unblinding occurred only after the data on safety, efficacy, and immunogenicity had been locked.
A diagnosis of HEV infection was made if at least 2 of the following markers were present: a positive test for immunoglobulin M antibodies against HEV, a positive test for HEV RNA, or a serum concentration of immunoglobulin G (IgG) antibodies against HEV that was at least 4 times higher than previously measured at any time during the same illness. Vaccine immunogenicity was assessed by testing serum samples for IgG antibodies against HEV at regular intervals after the vaccination was given.
Over the 4.5-year study period, 7 cases of hepatitis E occurred in the vaccine group, and 53 in the control group. Vaccine efficacy was 86.8% (P<.001) in the modified intention-to-treat analysis. Among patients who received 3 doses of HEV vaccine and who were seronegative at the start of the study, 87% maintained antibodies against HEV for 4.5 years. Within the control group, HEV titers developed in 9% of participants. The vaccine and control groups had similar rates of adverse events.
The authors concluded that the HEV vaccine induced antibodies against hepatitis E that lasted up to 4.5 years. Additionally, 2 doses of vaccine induced slightly lower levels of antibody than those produced by 3 doses of the vaccine. Finally, all participants in the vaccine group who developed HEV had antibodies with high or moderate avidity, indicating an anamnestic response from previous immunity. Most participants in the control group who developed HEV, however, had antibodies with low avidity, indicating no previous immunity.
The burden of HEVHepatitis E is a serious infection and is the most common waterborne illness in the world. It occurs mainly in developing countries with limited resources. HEV infection is caused by genotypes 1, 2, 3, or 4, although all 4 genotypes belong to the same serotype. Genotypes 1 and 2 are typically waterborne, and genotypes 3 and 4 are typically transmitted from animals and humans. In general, the case fatality rate associated with HEV infection is 1% to 3%.12 In pregnancy, this rate increases to 5% to 25%.13,14 In Bangladesh, for example, hepatitis E is responsible for more than 1,000 deaths per year among pregnant women.15
Clinical presentation of HEV infection is a spectrum, with most symptomatic patients presenting with acute, self-limited hepatitis. Severe cases may be associated with pancreatitis, arthritis, aplastic anemia, and neurologic complications, such as seizures. Populations at risk for more severe cases include pregnant women, elderly men, and patients with pre‑ existing, chronic liver disease.
What this evidence means for practiceStandard sanitary precautions, such as clean drinking water, traditionally have been considered the mainstay of hepatitis E prevention. However, as the study authors indicate, recent severe outbreaks of HEV infection in Sudan and Uganda have occurred despite these measures. Thus, an effective vaccine that produces long-standing immunity has great potential for reducing morbidity and mortality in these countries. The present vaccine appears to be highly effective and safe. The principal unanswered question is the duration of immunity.
My patients are asking, "What is the best insect repellent to try to avoid Zika virus?"
With summer upon us we have received questions from colleagues about the best over-the-counter insect repellents to advise their pregnant patients to use.
The preferred insect repellent for skin coverage is DEET (N,N-diethyl-meta-toluamide) (TABLE). Oil of lemon/eucalyptus/para-menthane-diol and IR3535 are also acceptable repellents to use on the skin that are safe for use in pregnancy. In addition, instruct patients to spray permethrin on their clothing or to buy clothing (boots, pants, socks) that has been pretreated with permethrin.1,2
Anushka Chelliah, MD, and Patrick Duff, MD.
Abbreviation: OTC, over the counter.
Coming soon to OBG Management
Drs. Chelliah and Duff follow-up on their March 2016 examination of Zika virus infection with:
- Latest information on Zika virus-associated birth defects
- Ultrasonographic and radiologic evidence of abnormalities in the fetus and newborn exposed to Zika virus infection
- Link between Zika virus infection and serious neurologic complications in adults
- New recommendations for preventing sexual transmission of Zika virus infection
Dr. Chelliah is a Maternal Fetal Medicine-Fellow in the Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
Dr. Duff is Associate Dean for Student Affairs and Professor of Obstetrics and Gynecology in the Division of Maternal-Fetal Medicine, University of Florida College of Medicine.
The author reports no financial relationships relevant to this article.
References
- Peterson EE, Staples JE, Meaney-Delman D, et al. Interim guidelines for pregnant women during a Zika virus outbreak--United States, 2016. MMWR Morb Mortal Wkly Rep. 2016;65(2):30-33.
- Centers for Disease Control and Prevention. CDC Features: Avoid mosquito bites. http://www.cdc.gov/Features/stopmosquitoes/index.html. Updated March 18, 2016. Accessed May 10, 2016.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- DeFrances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13. 2007:165:1–209.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: final data for 2013. Natl Vital Stat Rep. 2015;64(1):1–65.
- Anderson DJ, Podgorny K, Berrios-Torres SI, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605–627.
- Conroy K, Koenig AF, Yu YH, Courtney A, Lee HJ, Norwitz ER. Infectious morbidity after cesarean delivery: 10 strategies to reduce risk. Rev Obstet Gynecol. 2012;5(2):69–77.
- Scifres CM, Leighton BL, Fogertey PJ, Macones GA, Stamilio DM. Supplemental oxygen for the prevention of postcesarean infectious morbidity: a randomized controlled trial. Am J Obstet Gynecol. 2011;205(3)267.e1–e9.
- Wloch C, Wilson J, Lamagni T, Harrington P, Charlett A, Sheridan E. Risk factors for surgical site infection following cesarean section in England: results from a multicenter cohort study. BJOG. 2012;119(11):1324–1333.
- Olsen MA, Butler AM, Willers DM, Gross GA, Hamilton BH, Fraser VJ. Attributable costs of surgical site infection and endometritis after low transverse cesarean delivery. Infect Control Hosp Epidemiol. 2010;31(3):276–282.
- Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18–26.
- Ngai IM, Van Arsdale A, Govindappagari S, et al. Skin preparation for prevention of surgical site infection after cesarean delivery: a randomized controlled trial. Obstet Gynecol. 2015;126(6):1251–1257.
- Duff P. Maternal and perinatal infection—bacterial. In: Gabbe SG, Niebyl JR, Simpson JL, et al, eds. Obstetrics: normal and problem pregnancies. 6th ed. Philadelphia, PA: Elsevier/Saunders; 2012.
- Workowski KA, Bolan GH; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1−137. Erratum in: MMWR Recomm Rep. 2015;64(33):924.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13(3):145–154.
- Khuroo MS, Teli MR, Skidmore S, Sofi MA, Khuroo MI. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70(2):252–255.
- Khuroo MS, Kamili S. Aetiology, clinical course and outcome of sporadic acute viral hepatitis in pregnancy. J Viral Hepat. 2003;10(1):61–69.
- Labrique AB, Sikder SS, Krain IJ, et al. Hepatitis E, a vaccine-preventable cause of maternal deaths. Emerg Infect Dis. 2012;18(9):1401–1404.
- DeFrances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13. 2007:165:1–209.
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: final data for 2013. Natl Vital Stat Rep. 2015;64(1):1–65.
- Anderson DJ, Podgorny K, Berrios-Torres SI, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605–627.
- Conroy K, Koenig AF, Yu YH, Courtney A, Lee HJ, Norwitz ER. Infectious morbidity after cesarean delivery: 10 strategies to reduce risk. Rev Obstet Gynecol. 2012;5(2):69–77.
- Scifres CM, Leighton BL, Fogertey PJ, Macones GA, Stamilio DM. Supplemental oxygen for the prevention of postcesarean infectious morbidity: a randomized controlled trial. Am J Obstet Gynecol. 2011;205(3)267.e1–e9.
- Wloch C, Wilson J, Lamagni T, Harrington P, Charlett A, Sheridan E. Risk factors for surgical site infection following cesarean section in England: results from a multicenter cohort study. BJOG. 2012;119(11):1324–1333.
- Olsen MA, Butler AM, Willers DM, Gross GA, Hamilton BH, Fraser VJ. Attributable costs of surgical site infection and endometritis after low transverse cesarean delivery. Infect Control Hosp Epidemiol. 2010;31(3):276–282.
- Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18–26.
- Ngai IM, Van Arsdale A, Govindappagari S, et al. Skin preparation for prevention of surgical site infection after cesarean delivery: a randomized controlled trial. Obstet Gynecol. 2015;126(6):1251–1257.
- Duff P. Maternal and perinatal infection—bacterial. In: Gabbe SG, Niebyl JR, Simpson JL, et al, eds. Obstetrics: normal and problem pregnancies. 6th ed. Philadelphia, PA: Elsevier/Saunders; 2012.
- Workowski KA, Bolan GH; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1−137. Erratum in: MMWR Recomm Rep. 2015;64(33):924.
- Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13(3):145–154.
- Khuroo MS, Teli MR, Skidmore S, Sofi MA, Khuroo MI. Incidence and severity of viral hepatitis in pregnancy. Am J Med. 1981;70(2):252–255.
- Khuroo MS, Kamili S. Aetiology, clinical course and outcome of sporadic acute viral hepatitis in pregnancy. J Viral Hepat. 2003;10(1):61–69.
- Labrique AB, Sikder SS, Krain IJ, et al. Hepatitis E, a vaccine-preventable cause of maternal deaths. Emerg Infect Dis. 2012;18(9):1401–1404.
In this article
• Azithromycin vs doxycycline for chlamydia
• Insect repellents to prevent Zika virus
