PARIS – Percutaneous left atrial appendage closure with an Amplatzer device in patients with nonvalvular atrial fibrillation was associated with significantly lower rates of all-cause and cardiovascular mortality, compared with oral anticoagulation, in a large propensity score–matched observational registry study.
Left atrial appendage closure (LAAC) also bested oral anticoagulation (OAC) with warfarin or a novel oral anticoagulant (NOAC) in terms of net clinical benefit on the basis of the device therapy’s greater protection against stroke and systemic embolism coupled with a trend, albeit not statistically significant, for fewer bleeding events, Steffen Gloekler, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The Watchman LAAC device, commercially available both in Europe and the United States, has previously been shown to be superior to OAC in terms of efficacy and noninferior regarding safety. But there have been no randomized trials of an Amplatzer device versus OAC. This lack of data was the impetus for Dr. Gloekler and his coinvestigators to create a meticulously propensity-matched observational registry.
Five hundred consecutive patients with AF who received an Amplatzer Cardiac Plug or its second-generation version, the Amplatzer Amulet, during 2009-2014 were tightly matched to an equal number of AF patients on OAC based on age, sex, body mass index, left ventricular ejection fraction, renal function, coronary artery disease status, hemoglobin level, CHA2DS2-VASc score, and HAS-BLED score. During a mean 2.7 years, or 2,645 patient-years, of follow-up, the composite primary efficacy endpoint, composed of stroke, systemic embolism, and cardiovascular or unexplained death occurred in 5.6% of the LAAC group, compared with 7.8% of controls in the OAC arm, for a statistically significant 30% relative risk reduction. Disabling stroke occurred in 0.7% of Amplatzer patients versus 1.5% of controls. The ischemic stroke rate was 1.5% in the device therapy group and 2% in the OAC arm.
All-cause mortality occurred in 8.3% of Amplatzer patients and 11.6% of the OAC group, for a 28% relative risk reduction. The cardiovascular death rate was 4% in the Amplatzer group, compared with 6.5% of controls, for a 36% risk reduction.
The composite safety endpoint, comprising all major procedural adverse events and major or life-threatening bleeding during follow-up, occurred in 3.6% of the Amplatzer group and 4.6% of the OAC group, for a 20% relative risk reduction that is not significant at this point because of the low number of events. Major, life-threatening, or fatal bleeding occurred in 2% of Amplatzer recipients versus 5.5% of controls, added Dr. Gloekler of University Hospital in Bern, Switzerland.
The net clinical benefit, a composite of death, bleeding, or stroke, occurred in 8.1% of the Amplatzer group, compared with 10.9% of controls, for a significant 24% reduction in relative risk in favor of device therapy.
Of note, at 2.7 years of follow-up only 55% of the OAC group were still taking an anticoagulant: 38% of the original 500 patients were on warfarin, and 17% were taking a NOAC. At that point, 8% of the Amplatzer group were on any anticoagulation therapy.
Discussion of the study focused on that low rate of medication adherence in the OAC arm. Dr. Gloekler’s response was that, after looking at the literature, he was no longer surprised by the finding that only 55% of the control group were on OAC at follow-up.
“If you look in the literature, that’s exactly the real-world adherence for OACs. Even in all four certification trials for the NOACs, the rate of discontinuation was 30% after 2 years – and these were controlled studies. Ours was observational, and it depicts a good deal of the problem with any OAC in my eyes,” Dr. Gloekler said.
Patients on warfarin in the real-world Amplatzer registry study spent on average a mere 30% of time in the therapeutic international normalized ratio range of 2-3.
“That means 70% of the time patients are higher and have an increased bleeding risk or they are lower and don’t have adequate stroke protection,” he noted.
This prompted one observer to comment, “We either have to do a better job in our clinics with OAC or we have to occlude more appendages.”
A large pivotal U.S. trial aimed at winning FDA approval for the Amplatzer Amulet for LAAC is underway. Patients with AF are being randomized to the approved Watchman or investigational Amulet at roughly 100 U.S. and 50 foreign sites.
Dr. Gloekler reported receiving research funds for the registry from the Swiss Heart Foundation and Abbott.
PARIS – Percutaneous left atrial appendage closure with an Amplatzer device in patients with nonvalvular atrial fibrillation was associated with significantly lower rates of all-cause and cardiovascular mortality, compared with oral anticoagulation, in a large propensity score–matched observational registry study.
Left atrial appendage closure (LAAC) also bested oral anticoagulation (OAC) with warfarin or a novel oral anticoagulant (NOAC) in terms of net clinical benefit on the basis of the device therapy’s greater protection against stroke and systemic embolism coupled with a trend, albeit not statistically significant, for fewer bleeding events, Steffen Gloekler, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The Watchman LAAC device, commercially available both in Europe and the United States, has previously been shown to be superior to OAC in terms of efficacy and noninferior regarding safety. But there have been no randomized trials of an Amplatzer device versus OAC. This lack of data was the impetus for Dr. Gloekler and his coinvestigators to create a meticulously propensity-matched observational registry.
Five hundred consecutive patients with AF who received an Amplatzer Cardiac Plug or its second-generation version, the Amplatzer Amulet, during 2009-2014 were tightly matched to an equal number of AF patients on OAC based on age, sex, body mass index, left ventricular ejection fraction, renal function, coronary artery disease status, hemoglobin level, CHA2DS2-VASc score, and HAS-BLED score. During a mean 2.7 years, or 2,645 patient-years, of follow-up, the composite primary efficacy endpoint, composed of stroke, systemic embolism, and cardiovascular or unexplained death occurred in 5.6% of the LAAC group, compared with 7.8% of controls in the OAC arm, for a statistically significant 30% relative risk reduction. Disabling stroke occurred in 0.7% of Amplatzer patients versus 1.5% of controls. The ischemic stroke rate was 1.5% in the device therapy group and 2% in the OAC arm.
All-cause mortality occurred in 8.3% of Amplatzer patients and 11.6% of the OAC group, for a 28% relative risk reduction. The cardiovascular death rate was 4% in the Amplatzer group, compared with 6.5% of controls, for a 36% risk reduction.
The composite safety endpoint, comprising all major procedural adverse events and major or life-threatening bleeding during follow-up, occurred in 3.6% of the Amplatzer group and 4.6% of the OAC group, for a 20% relative risk reduction that is not significant at this point because of the low number of events. Major, life-threatening, or fatal bleeding occurred in 2% of Amplatzer recipients versus 5.5% of controls, added Dr. Gloekler of University Hospital in Bern, Switzerland.
The net clinical benefit, a composite of death, bleeding, or stroke, occurred in 8.1% of the Amplatzer group, compared with 10.9% of controls, for a significant 24% reduction in relative risk in favor of device therapy.
Of note, at 2.7 years of follow-up only 55% of the OAC group were still taking an anticoagulant: 38% of the original 500 patients were on warfarin, and 17% were taking a NOAC. At that point, 8% of the Amplatzer group were on any anticoagulation therapy.
Discussion of the study focused on that low rate of medication adherence in the OAC arm. Dr. Gloekler’s response was that, after looking at the literature, he was no longer surprised by the finding that only 55% of the control group were on OAC at follow-up.
“If you look in the literature, that’s exactly the real-world adherence for OACs. Even in all four certification trials for the NOACs, the rate of discontinuation was 30% after 2 years – and these were controlled studies. Ours was observational, and it depicts a good deal of the problem with any OAC in my eyes,” Dr. Gloekler said.
Patients on warfarin in the real-world Amplatzer registry study spent on average a mere 30% of time in the therapeutic international normalized ratio range of 2-3.
“That means 70% of the time patients are higher and have an increased bleeding risk or they are lower and don’t have adequate stroke protection,” he noted.
This prompted one observer to comment, “We either have to do a better job in our clinics with OAC or we have to occlude more appendages.”
A large pivotal U.S. trial aimed at winning FDA approval for the Amplatzer Amulet for LAAC is underway. Patients with AF are being randomized to the approved Watchman or investigational Amulet at roughly 100 U.S. and 50 foreign sites.
Dr. Gloekler reported receiving research funds for the registry from the Swiss Heart Foundation and Abbott.
PARIS – Percutaneous left atrial appendage closure with an Amplatzer device in patients with nonvalvular atrial fibrillation was associated with significantly lower rates of all-cause and cardiovascular mortality, compared with oral anticoagulation, in a large propensity score–matched observational registry study.
Left atrial appendage closure (LAAC) also bested oral anticoagulation (OAC) with warfarin or a novel oral anticoagulant (NOAC) in terms of net clinical benefit on the basis of the device therapy’s greater protection against stroke and systemic embolism coupled with a trend, albeit not statistically significant, for fewer bleeding events, Steffen Gloekler, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The Watchman LAAC device, commercially available both in Europe and the United States, has previously been shown to be superior to OAC in terms of efficacy and noninferior regarding safety. But there have been no randomized trials of an Amplatzer device versus OAC. This lack of data was the impetus for Dr. Gloekler and his coinvestigators to create a meticulously propensity-matched observational registry.
Five hundred consecutive patients with AF who received an Amplatzer Cardiac Plug or its second-generation version, the Amplatzer Amulet, during 2009-2014 were tightly matched to an equal number of AF patients on OAC based on age, sex, body mass index, left ventricular ejection fraction, renal function, coronary artery disease status, hemoglobin level, CHA2DS2-VASc score, and HAS-BLED score. During a mean 2.7 years, or 2,645 patient-years, of follow-up, the composite primary efficacy endpoint, composed of stroke, systemic embolism, and cardiovascular or unexplained death occurred in 5.6% of the LAAC group, compared with 7.8% of controls in the OAC arm, for a statistically significant 30% relative risk reduction. Disabling stroke occurred in 0.7% of Amplatzer patients versus 1.5% of controls. The ischemic stroke rate was 1.5% in the device therapy group and 2% in the OAC arm.
All-cause mortality occurred in 8.3% of Amplatzer patients and 11.6% of the OAC group, for a 28% relative risk reduction. The cardiovascular death rate was 4% in the Amplatzer group, compared with 6.5% of controls, for a 36% risk reduction.
The composite safety endpoint, comprising all major procedural adverse events and major or life-threatening bleeding during follow-up, occurred in 3.6% of the Amplatzer group and 4.6% of the OAC group, for a 20% relative risk reduction that is not significant at this point because of the low number of events. Major, life-threatening, or fatal bleeding occurred in 2% of Amplatzer recipients versus 5.5% of controls, added Dr. Gloekler of University Hospital in Bern, Switzerland.
The net clinical benefit, a composite of death, bleeding, or stroke, occurred in 8.1% of the Amplatzer group, compared with 10.9% of controls, for a significant 24% reduction in relative risk in favor of device therapy.
Of note, at 2.7 years of follow-up only 55% of the OAC group were still taking an anticoagulant: 38% of the original 500 patients were on warfarin, and 17% were taking a NOAC. At that point, 8% of the Amplatzer group were on any anticoagulation therapy.
Discussion of the study focused on that low rate of medication adherence in the OAC arm. Dr. Gloekler’s response was that, after looking at the literature, he was no longer surprised by the finding that only 55% of the control group were on OAC at follow-up.
“If you look in the literature, that’s exactly the real-world adherence for OACs. Even in all four certification trials for the NOACs, the rate of discontinuation was 30% after 2 years – and these were controlled studies. Ours was observational, and it depicts a good deal of the problem with any OAC in my eyes,” Dr. Gloekler said.
Patients on warfarin in the real-world Amplatzer registry study spent on average a mere 30% of time in the therapeutic international normalized ratio range of 2-3.
“That means 70% of the time patients are higher and have an increased bleeding risk or they are lower and don’t have adequate stroke protection,” he noted.
This prompted one observer to comment, “We either have to do a better job in our clinics with OAC or we have to occlude more appendages.”
A large pivotal U.S. trial aimed at winning FDA approval for the Amplatzer Amulet for LAAC is underway. Patients with AF are being randomized to the approved Watchman or investigational Amulet at roughly 100 U.S. and 50 foreign sites.
Dr. Gloekler reported receiving research funds for the registry from the Swiss Heart Foundation and Abbott.
Key clinical point: Patients with atrial fibrillation who received an Amplatzer left atrial appendage closure device did significantly better over time than a matched group on oral anticoagulation.
Major finding: The primary composite efficacy endpoint of stroke, systemic embolism, or cardiovascular or unexplained death during a mean 2.7 years of follow-up occurred in 5.6% of Amplatzer device recipients, a 30% reduction, compared with the 7.8% rate in the oral anticoagulation group.
Data source: This observational registry included 500 patients with atrial fibrillation who received an Amplatzer left atrial appendage closure device and an equal number of carefully matched AF patients on oral anticoagulation.
Disclosures: The study presenter reported receiving research funds for the registry from the Swiss Heart Foundation and Abbott.
Outpatient care represents the largest share of mental health treatment expenditures, and it continues to get larger, while components such as retail drug prescriptions and inpatient care have declined, according to the National Center of Health Statistics.
In 2014, outpatient care took a $65.5-billion slice (about 35%) out of the $186-billion mental health care spending pie, compared with the $51.1 billion (27%) spent on retail drug prescriptions, which was the next-largest portion. Inpatient care was third with $30.3 billion in spending (16% of the total), followed by residential care at $23.2 billion (12%), and insurance administration at $15.9 billion (9%), the NCHS reported in “Health, United States, 2016.”
The distribution of spending has changed considerably since 1986, when mental health expenditures totaled $32.4 billion and inpatient care was the largest share at 41%, outpatient care was 24%, residential care was 22%, retail prescription drugs were 8%, and insurance administration was 5%, according to data from the Substance Abuse and Mental Health Services Administration’s Behavioral Health Spending and Use Accounts.
Outpatient care represents the largest share of mental health treatment expenditures, and it continues to get larger, while components such as retail drug prescriptions and inpatient care have declined, according to the National Center of Health Statistics.
In 2014, outpatient care took a $65.5-billion slice (about 35%) out of the $186-billion mental health care spending pie, compared with the $51.1 billion (27%) spent on retail drug prescriptions, which was the next-largest portion. Inpatient care was third with $30.3 billion in spending (16% of the total), followed by residential care at $23.2 billion (12%), and insurance administration at $15.9 billion (9%), the NCHS reported in “Health, United States, 2016.”
The distribution of spending has changed considerably since 1986, when mental health expenditures totaled $32.4 billion and inpatient care was the largest share at 41%, outpatient care was 24%, residential care was 22%, retail prescription drugs were 8%, and insurance administration was 5%, according to data from the Substance Abuse and Mental Health Services Administration’s Behavioral Health Spending and Use Accounts.
Outpatient care represents the largest share of mental health treatment expenditures, and it continues to get larger, while components such as retail drug prescriptions and inpatient care have declined, according to the National Center of Health Statistics.
In 2014, outpatient care took a $65.5-billion slice (about 35%) out of the $186-billion mental health care spending pie, compared with the $51.1 billion (27%) spent on retail drug prescriptions, which was the next-largest portion. Inpatient care was third with $30.3 billion in spending (16% of the total), followed by residential care at $23.2 billion (12%), and insurance administration at $15.9 billion (9%), the NCHS reported in “Health, United States, 2016.”
The distribution of spending has changed considerably since 1986, when mental health expenditures totaled $32.4 billion and inpatient care was the largest share at 41%, outpatient care was 24%, residential care was 22%, retail prescription drugs were 8%, and insurance administration was 5%, according to data from the Substance Abuse and Mental Health Services Administration’s Behavioral Health Spending and Use Accounts.
The Food and Drug Administration approved L-glutamine oral powder for reducing severe complications of sickle cell disease in patients aged 5 years and older.
The approval was based on placebo-controlled phase II and phase III trials suggesting that L-glutamate offered moderate benefit to patients with this rare, serious, and potentially fatal blood disorder.
This is only the second drug approved by FDA for sickle cell disease, and the first approval in nearly 20 years, Richard Pazdur, MD, acting director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research and director of the FDA’s Oncology Center of Excellence, said in the agency’s announcement.
L-glutamine oral powder will be marketed under the brand name Endari by Emmaus Medical. The FDA granted the approval through its orphan drug pathway, which is reserved for treatments of rare diseases or conditions. The National Institutes of Health estimates that sickle cell disorder affects approximately 100,000 individuals in the United States. Previously, the only drug approved for treating sickle cell disorder was hydroxyurea, which the FDA green-lighted in 1998.
The randomized, placebo-controlled, phase III trial on which the approval of L-glutamine was based (GLUSCC09-01) comprised patients aged 5-58 years with sickle cell disease or beta-0 thalassemia who had at least two episodes of painful crises during the 12 months before screening. A total of 152 patients were randomly assigned to receive oral L-glutamine (0.3 mg/kg per day) for 48 weeks followed by a 3-week tapering period, while 78 patients received placebo. Patients who received L-glutamine averaged three hospital visits for painful crises for which they received parenteral narcotics or ketorolac, while the placebo group averaged four such hospital visits. Additionally, the time to second crisis was delayed by 79 days in the treatment group, compared with the placebo group (hazard ratio, 0.68).
L-glutamine also was associated with fewer hospital days (median 6.5 vs. 11 days) and fewer occurrences of potentially life-threatening acute chest syndrome (8.6% vs. 23.1%), investigators reported to the FDA’s Oncologic Drugs Advisory Committee during a meeting on May 24.
Safety studies of L-glutamine included phase II and phase III data from 187 patients who received L-glutamine and 111 patients who received placebo, the investigators reported. Based on these analyses, rates of sickle cell anemia with crisis were 66% in the treatment population and 72% in placebo recipients. Rates of acute chest syndrome were 7% and 19%, respectively. Treatment-emergent adverse events led patients to drop out of the studies in 2.7% and 0.9% of cases. The most common adverse events of L-glutamine therapy were constipation, nausea, headache, cough, pain in the extremities, back pain, chest pain, and abdominal pain.
The FDA advisory committee voted 10-3 in favor of approving L-glutamate after hearing from industry and FDA representatives, physicians who treat patients with sickle cell disorder, and patients and their family members at the May 24 meeting. “No” voters expressed concerns about differing drop-out rates between the study groups, but other committee members emphasized the severe impact of sickle cell disorder on quality of life and the crucial need for more treatments.
The FDA Orphan Products Grants Program provided some of the funding to develop the drug. The FDA committee members had no relevant conflicts of interests.
The Food and Drug Administration approved L-glutamine oral powder for reducing severe complications of sickle cell disease in patients aged 5 years and older.
The approval was based on placebo-controlled phase II and phase III trials suggesting that L-glutamate offered moderate benefit to patients with this rare, serious, and potentially fatal blood disorder.
This is only the second drug approved by FDA for sickle cell disease, and the first approval in nearly 20 years, Richard Pazdur, MD, acting director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research and director of the FDA’s Oncology Center of Excellence, said in the agency’s announcement.
L-glutamine oral powder will be marketed under the brand name Endari by Emmaus Medical. The FDA granted the approval through its orphan drug pathway, which is reserved for treatments of rare diseases or conditions. The National Institutes of Health estimates that sickle cell disorder affects approximately 100,000 individuals in the United States. Previously, the only drug approved for treating sickle cell disorder was hydroxyurea, which the FDA green-lighted in 1998.
The randomized, placebo-controlled, phase III trial on which the approval of L-glutamine was based (GLUSCC09-01) comprised patients aged 5-58 years with sickle cell disease or beta-0 thalassemia who had at least two episodes of painful crises during the 12 months before screening. A total of 152 patients were randomly assigned to receive oral L-glutamine (0.3 mg/kg per day) for 48 weeks followed by a 3-week tapering period, while 78 patients received placebo. Patients who received L-glutamine averaged three hospital visits for painful crises for which they received parenteral narcotics or ketorolac, while the placebo group averaged four such hospital visits. Additionally, the time to second crisis was delayed by 79 days in the treatment group, compared with the placebo group (hazard ratio, 0.68).
L-glutamine also was associated with fewer hospital days (median 6.5 vs. 11 days) and fewer occurrences of potentially life-threatening acute chest syndrome (8.6% vs. 23.1%), investigators reported to the FDA’s Oncologic Drugs Advisory Committee during a meeting on May 24.
Safety studies of L-glutamine included phase II and phase III data from 187 patients who received L-glutamine and 111 patients who received placebo, the investigators reported. Based on these analyses, rates of sickle cell anemia with crisis were 66% in the treatment population and 72% in placebo recipients. Rates of acute chest syndrome were 7% and 19%, respectively. Treatment-emergent adverse events led patients to drop out of the studies in 2.7% and 0.9% of cases. The most common adverse events of L-glutamine therapy were constipation, nausea, headache, cough, pain in the extremities, back pain, chest pain, and abdominal pain.
The FDA advisory committee voted 10-3 in favor of approving L-glutamate after hearing from industry and FDA representatives, physicians who treat patients with sickle cell disorder, and patients and their family members at the May 24 meeting. “No” voters expressed concerns about differing drop-out rates between the study groups, but other committee members emphasized the severe impact of sickle cell disorder on quality of life and the crucial need for more treatments.
The FDA Orphan Products Grants Program provided some of the funding to develop the drug. The FDA committee members had no relevant conflicts of interests.
The Food and Drug Administration approved L-glutamine oral powder for reducing severe complications of sickle cell disease in patients aged 5 years and older.
The approval was based on placebo-controlled phase II and phase III trials suggesting that L-glutamate offered moderate benefit to patients with this rare, serious, and potentially fatal blood disorder.
This is only the second drug approved by FDA for sickle cell disease, and the first approval in nearly 20 years, Richard Pazdur, MD, acting director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research and director of the FDA’s Oncology Center of Excellence, said in the agency’s announcement.
L-glutamine oral powder will be marketed under the brand name Endari by Emmaus Medical. The FDA granted the approval through its orphan drug pathway, which is reserved for treatments of rare diseases or conditions. The National Institutes of Health estimates that sickle cell disorder affects approximately 100,000 individuals in the United States. Previously, the only drug approved for treating sickle cell disorder was hydroxyurea, which the FDA green-lighted in 1998.
The randomized, placebo-controlled, phase III trial on which the approval of L-glutamine was based (GLUSCC09-01) comprised patients aged 5-58 years with sickle cell disease or beta-0 thalassemia who had at least two episodes of painful crises during the 12 months before screening. A total of 152 patients were randomly assigned to receive oral L-glutamine (0.3 mg/kg per day) for 48 weeks followed by a 3-week tapering period, while 78 patients received placebo. Patients who received L-glutamine averaged three hospital visits for painful crises for which they received parenteral narcotics or ketorolac, while the placebo group averaged four such hospital visits. Additionally, the time to second crisis was delayed by 79 days in the treatment group, compared with the placebo group (hazard ratio, 0.68).
L-glutamine also was associated with fewer hospital days (median 6.5 vs. 11 days) and fewer occurrences of potentially life-threatening acute chest syndrome (8.6% vs. 23.1%), investigators reported to the FDA’s Oncologic Drugs Advisory Committee during a meeting on May 24.
Safety studies of L-glutamine included phase II and phase III data from 187 patients who received L-glutamine and 111 patients who received placebo, the investigators reported. Based on these analyses, rates of sickle cell anemia with crisis were 66% in the treatment population and 72% in placebo recipients. Rates of acute chest syndrome were 7% and 19%, respectively. Treatment-emergent adverse events led patients to drop out of the studies in 2.7% and 0.9% of cases. The most common adverse events of L-glutamine therapy were constipation, nausea, headache, cough, pain in the extremities, back pain, chest pain, and abdominal pain.
The FDA advisory committee voted 10-3 in favor of approving L-glutamate after hearing from industry and FDA representatives, physicians who treat patients with sickle cell disorder, and patients and their family members at the May 24 meeting. “No” voters expressed concerns about differing drop-out rates between the study groups, but other committee members emphasized the severe impact of sickle cell disorder on quality of life and the crucial need for more treatments.
The FDA Orphan Products Grants Program provided some of the funding to develop the drug. The FDA committee members had no relevant conflicts of interests.
LUGANO, SWITZERLAND – Tazemetostat, a first-in-class experimental agent that inhibits an oncogenic protein, shows efficacy in patients with heavily pretreated, relapsed/refractory follicular lymphoma (FL) and diffuse large B cell lymphoma (DLBCL), interim results from a phase II study suggest.
Among patients with relapsed/refractory FL who had mutations in EZH2 (enhancer of zeste homolog 2), a member of a family of proteins that are involved in epigenetic gene silencing, the overall response rate (ORR) was 92%, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.
Neil Osterweil/Frontline Medical News
Dr. Franck Morschhauser
Tazemetostat is an oral inhibitor of both the wild-type and mutated forms of the gene encoding for EZH2, a histone methyltransferase. The drug shows significantly more activity against the mutated form of the gene than the wild type, but some patients in the trial with the wild-type gene have had complete responses, Dr. Morschhauser said at the International Conference on Malignant Lymphoma.
“What we observed is a four-fold increase in [ORR in] follicular lymphoma-mutated patients compared to wild-type patients, a two-fold increase in DLBCL patients mutated compared to wild-type patients,” he said.
“But if we had focused [only] on the actionable mutation, we would have missed those other complete responders in the wild-type setting,” he added.
EZH2, an epigenetic regulator of gene expression, had been shown in preclinical studies to play an important role in multiple forms of cancers, and activating mutations of EZH2 have been shown to be oncogenic drivers in approximately 20% of FL and germinal center B-cell–like DLBCL, Dr. Morschhauser explained.
EZH2 has also been shown to be over-expressed in leukemia-initiating cells in patients with chronic myeloid leukemia, and EZH2 inhibitors are being explored as a possible therapy for patients with chronic myeloid leukemia that has become resistant to tyrosine kinase inhibitors.
Large multicenter study
Dr. Morschhauser reported interim results from a global, multi-center open-label study of tazemetostat in six cohorts of patients with relapsed/refractory FL (two monotherapy cohorts of 45 patients each) or DLBCL (three monotherapy cohorts of 60 patients each). A sixth cohort consisting of 70 patients with DLBCL treated with tazemetostat and prednisolone was added in 2017.
In the ongoing trial, patients receive oral tazemetostat 800 mg twice daily until disease progression or withdrawal from study, and are being followed for ORR, progression-free survival, overall survival, duration-of response, safety, and pharmacokinetics.
The longest follow-up at the time of data cutoff was approximately 18 months. Among 13 evaluable patients with FL with EZH2 mutations, the ORR was 92%, including one complete response (CR) and 11 partial responses (PR). In contrast, the ORR for 54 patients with FL and wild-type EZH2 was 28%, consisting of three CRs and 11 PRs. One patient with mutated EZH2 and 23 with wild-type EZH2 had stable disease.
Among 17 patients with DLBCL and EZH2 mutations, the ORR was 29%, consisting of 5 PR. For 119 patients with wild-type EZH2, the ORR was 15%, consisting of 10 CR and 8 PR. Six patients with mutations and 22 with wild-type EZH2 had stable disease.
Among the patients with FL, 75% had significant reduction in tumor burden.
The time to response ranged from 2 months to 1 year, with a median of approximately 4 months.
The variability in time to response “makes it a little bit tricky to calculate response duration,” Dr. Morschhauser said.
The drug had a “favorable” safety profile, with treatment-related adverse events of grade 3 or greater in more than 5% of patients including thrombocytopenias in 6% of patients, anemias in 4%, and neutropenias in 6%. Treatment-emergent adverse events leading to dose reductions occurred in 4% of patients, and those leading to drug discontinuation or study withdrawal occurred in 12% of patients.
In a retrospective analysis, the investigators performed molecular profiling studies using next-generation sequencing to look for predictors of response to tazemetostat. They found that patients most likely to respond to tazemetostat were those with activating mutations in EZH2 and MYD88. In contrast, patients with mutations HIST1H1E or MYC were not likely to respond.
Thomas E. Witzig, MD, of the Mayo Clinic in Rochester, Minn., the invited discussant, said that the study is important because “it provides proof of principle that attacking the methylation issue, attacking one of these enzymes, is very important and can produce single-agent responses.
“It also demonstrates the value of mutation status, and this trial knowledge of that mutation status has actually changed the trial design, so that now they are only putting patients on with mutations,” he said.
The trial also raises the possibility of targeting other parts of the methylation pathway to treat cancer, he added.
The study was sponsored by Epizyme, the maker of tazemetostat. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies. Dr. Witzig has disclosed grants for clinical trials from Novartis and Wyeth, and he has served on advisory boards for Cephalon, Novartis, and Wyeth.
LUGANO, SWITZERLAND – Tazemetostat, a first-in-class experimental agent that inhibits an oncogenic protein, shows efficacy in patients with heavily pretreated, relapsed/refractory follicular lymphoma (FL) and diffuse large B cell lymphoma (DLBCL), interim results from a phase II study suggest.
Among patients with relapsed/refractory FL who had mutations in EZH2 (enhancer of zeste homolog 2), a member of a family of proteins that are involved in epigenetic gene silencing, the overall response rate (ORR) was 92%, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.
Neil Osterweil/Frontline Medical News
Dr. Franck Morschhauser
Tazemetostat is an oral inhibitor of both the wild-type and mutated forms of the gene encoding for EZH2, a histone methyltransferase. The drug shows significantly more activity against the mutated form of the gene than the wild type, but some patients in the trial with the wild-type gene have had complete responses, Dr. Morschhauser said at the International Conference on Malignant Lymphoma.
“What we observed is a four-fold increase in [ORR in] follicular lymphoma-mutated patients compared to wild-type patients, a two-fold increase in DLBCL patients mutated compared to wild-type patients,” he said.
“But if we had focused [only] on the actionable mutation, we would have missed those other complete responders in the wild-type setting,” he added.
EZH2, an epigenetic regulator of gene expression, had been shown in preclinical studies to play an important role in multiple forms of cancers, and activating mutations of EZH2 have been shown to be oncogenic drivers in approximately 20% of FL and germinal center B-cell–like DLBCL, Dr. Morschhauser explained.
EZH2 has also been shown to be over-expressed in leukemia-initiating cells in patients with chronic myeloid leukemia, and EZH2 inhibitors are being explored as a possible therapy for patients with chronic myeloid leukemia that has become resistant to tyrosine kinase inhibitors.
Large multicenter study
Dr. Morschhauser reported interim results from a global, multi-center open-label study of tazemetostat in six cohorts of patients with relapsed/refractory FL (two monotherapy cohorts of 45 patients each) or DLBCL (three monotherapy cohorts of 60 patients each). A sixth cohort consisting of 70 patients with DLBCL treated with tazemetostat and prednisolone was added in 2017.
In the ongoing trial, patients receive oral tazemetostat 800 mg twice daily until disease progression or withdrawal from study, and are being followed for ORR, progression-free survival, overall survival, duration-of response, safety, and pharmacokinetics.
The longest follow-up at the time of data cutoff was approximately 18 months. Among 13 evaluable patients with FL with EZH2 mutations, the ORR was 92%, including one complete response (CR) and 11 partial responses (PR). In contrast, the ORR for 54 patients with FL and wild-type EZH2 was 28%, consisting of three CRs and 11 PRs. One patient with mutated EZH2 and 23 with wild-type EZH2 had stable disease.
Among 17 patients with DLBCL and EZH2 mutations, the ORR was 29%, consisting of 5 PR. For 119 patients with wild-type EZH2, the ORR was 15%, consisting of 10 CR and 8 PR. Six patients with mutations and 22 with wild-type EZH2 had stable disease.
Among the patients with FL, 75% had significant reduction in tumor burden.
The time to response ranged from 2 months to 1 year, with a median of approximately 4 months.
The variability in time to response “makes it a little bit tricky to calculate response duration,” Dr. Morschhauser said.
The drug had a “favorable” safety profile, with treatment-related adverse events of grade 3 or greater in more than 5% of patients including thrombocytopenias in 6% of patients, anemias in 4%, and neutropenias in 6%. Treatment-emergent adverse events leading to dose reductions occurred in 4% of patients, and those leading to drug discontinuation or study withdrawal occurred in 12% of patients.
In a retrospective analysis, the investigators performed molecular profiling studies using next-generation sequencing to look for predictors of response to tazemetostat. They found that patients most likely to respond to tazemetostat were those with activating mutations in EZH2 and MYD88. In contrast, patients with mutations HIST1H1E or MYC were not likely to respond.
Thomas E. Witzig, MD, of the Mayo Clinic in Rochester, Minn., the invited discussant, said that the study is important because “it provides proof of principle that attacking the methylation issue, attacking one of these enzymes, is very important and can produce single-agent responses.
“It also demonstrates the value of mutation status, and this trial knowledge of that mutation status has actually changed the trial design, so that now they are only putting patients on with mutations,” he said.
The trial also raises the possibility of targeting other parts of the methylation pathway to treat cancer, he added.
The study was sponsored by Epizyme, the maker of tazemetostat. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies. Dr. Witzig has disclosed grants for clinical trials from Novartis and Wyeth, and he has served on advisory boards for Cephalon, Novartis, and Wyeth.
LUGANO, SWITZERLAND – Tazemetostat, a first-in-class experimental agent that inhibits an oncogenic protein, shows efficacy in patients with heavily pretreated, relapsed/refractory follicular lymphoma (FL) and diffuse large B cell lymphoma (DLBCL), interim results from a phase II study suggest.
Among patients with relapsed/refractory FL who had mutations in EZH2 (enhancer of zeste homolog 2), a member of a family of proteins that are involved in epigenetic gene silencing, the overall response rate (ORR) was 92%, reported Franck Morschhauser, MD, PhD, of the University of Lille, France.
Neil Osterweil/Frontline Medical News
Dr. Franck Morschhauser
Tazemetostat is an oral inhibitor of both the wild-type and mutated forms of the gene encoding for EZH2, a histone methyltransferase. The drug shows significantly more activity against the mutated form of the gene than the wild type, but some patients in the trial with the wild-type gene have had complete responses, Dr. Morschhauser said at the International Conference on Malignant Lymphoma.
“What we observed is a four-fold increase in [ORR in] follicular lymphoma-mutated patients compared to wild-type patients, a two-fold increase in DLBCL patients mutated compared to wild-type patients,” he said.
“But if we had focused [only] on the actionable mutation, we would have missed those other complete responders in the wild-type setting,” he added.
EZH2, an epigenetic regulator of gene expression, had been shown in preclinical studies to play an important role in multiple forms of cancers, and activating mutations of EZH2 have been shown to be oncogenic drivers in approximately 20% of FL and germinal center B-cell–like DLBCL, Dr. Morschhauser explained.
EZH2 has also been shown to be over-expressed in leukemia-initiating cells in patients with chronic myeloid leukemia, and EZH2 inhibitors are being explored as a possible therapy for patients with chronic myeloid leukemia that has become resistant to tyrosine kinase inhibitors.
Large multicenter study
Dr. Morschhauser reported interim results from a global, multi-center open-label study of tazemetostat in six cohorts of patients with relapsed/refractory FL (two monotherapy cohorts of 45 patients each) or DLBCL (three monotherapy cohorts of 60 patients each). A sixth cohort consisting of 70 patients with DLBCL treated with tazemetostat and prednisolone was added in 2017.
In the ongoing trial, patients receive oral tazemetostat 800 mg twice daily until disease progression or withdrawal from study, and are being followed for ORR, progression-free survival, overall survival, duration-of response, safety, and pharmacokinetics.
The longest follow-up at the time of data cutoff was approximately 18 months. Among 13 evaluable patients with FL with EZH2 mutations, the ORR was 92%, including one complete response (CR) and 11 partial responses (PR). In contrast, the ORR for 54 patients with FL and wild-type EZH2 was 28%, consisting of three CRs and 11 PRs. One patient with mutated EZH2 and 23 with wild-type EZH2 had stable disease.
Among 17 patients with DLBCL and EZH2 mutations, the ORR was 29%, consisting of 5 PR. For 119 patients with wild-type EZH2, the ORR was 15%, consisting of 10 CR and 8 PR. Six patients with mutations and 22 with wild-type EZH2 had stable disease.
Among the patients with FL, 75% had significant reduction in tumor burden.
The time to response ranged from 2 months to 1 year, with a median of approximately 4 months.
The variability in time to response “makes it a little bit tricky to calculate response duration,” Dr. Morschhauser said.
The drug had a “favorable” safety profile, with treatment-related adverse events of grade 3 or greater in more than 5% of patients including thrombocytopenias in 6% of patients, anemias in 4%, and neutropenias in 6%. Treatment-emergent adverse events leading to dose reductions occurred in 4% of patients, and those leading to drug discontinuation or study withdrawal occurred in 12% of patients.
In a retrospective analysis, the investigators performed molecular profiling studies using next-generation sequencing to look for predictors of response to tazemetostat. They found that patients most likely to respond to tazemetostat were those with activating mutations in EZH2 and MYD88. In contrast, patients with mutations HIST1H1E or MYC were not likely to respond.
Thomas E. Witzig, MD, of the Mayo Clinic in Rochester, Minn., the invited discussant, said that the study is important because “it provides proof of principle that attacking the methylation issue, attacking one of these enzymes, is very important and can produce single-agent responses.
“It also demonstrates the value of mutation status, and this trial knowledge of that mutation status has actually changed the trial design, so that now they are only putting patients on with mutations,” he said.
The trial also raises the possibility of targeting other parts of the methylation pathway to treat cancer, he added.
The study was sponsored by Epizyme, the maker of tazemetostat. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies. Dr. Witzig has disclosed grants for clinical trials from Novartis and Wyeth, and he has served on advisory boards for Cephalon, Novartis, and Wyeth.
Key clinical point: The experimental drug tazemetostat induced responses in patients with heavily pretreated follicular lymphoma (FL) with mutations in EZH2.
Major finding: The overall response rate among patients with FL with mutated EZH2 was 92%.
Data source: Multicenter, open-label phase II study in patients with relapsed/refractory FL and diffuse large B cell lymphoma.
Disclosures: The study is sponsored by Epizyme. Dr. Morschhauser disclosed receiving honoraria from and serving on advisory boards for both companies. Dr. Witzig has disclosed grants for clinical trials from Novartis and Wyeth, and he has served on advisory boards for Cephalon, Novartis, and Wyeth.
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
Opioid prescribing in the United States declined overall between 2010 and 2015, but remained stable or increased in some counties, according to a report from the Centers for Disease Control and Prevention. The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
“The bottom line remains: We have too many people getting too many prescriptions at too high a dose,” Anne Schuchat, MD, acting director of the CDC, said in a July 6 teleconference.
Providers in the highest-prescribing counties prescribed six times more opioids per person than in the lowest-prescribing counties in 2015, she noted.
CDC researchers calculated prescribing rates from 2006 to 2015 by dividing the number of opioid prescriptions by the population estimates from the U.S. census for each year and created quartiles using morphine milligram equivalent per capita to analyze opioid distribution. Annual opioid prescribing rates increased from 72 to 81 prescriptions per 100 persons from 2006 to 2010 and remained relatively constant from 2010 to 2012 before showing a 13% decrease to 71 prescriptions per 100 persons from 2012 to 2015 (MMWR. 2017 Jul 7;66[26]:697-704. doi: 10.15585/mmwr.mm6626a4).
But despite these overall declines, “We are now experiencing the highest overdose death rates ever recorded in the United States,” Dr. Schuchat said. Quartiles were created using MME per capita to characterize the distribution of opioids prescribed.
In the report, areas associated with higher opioid prescribing rates on a county level included small cities or towns, areas that had a higher proportion of white residents, areas with more doctors and dentists, and areas with more cases of arthritis, diabetes, or other disabilities, she said.
The findings suggest a need for more consistency among health care providers about prescription opioids, Dr. Schuchat said. “Clinical practice is all over the place, which is a sign that you need better standards; we hope the 2016 guidelines are a turning point for better prescribing,” she said.
The CDC’s guidelines on opioid prescribing were released in 2016. The guidelines recommend alternatives when possible. Clinicians should instead consider nonopioid therapy, other types of pain medication, and nondrug pain relief options, such as physical therapy and cognitive-behavioral therapy. Other concerns include the length and strength of opioid prescriptions. Even taking opioids for a few months increases the risk for addiction, Dr. Schuchat said.
“Physicians must continue to lead efforts to reverse the epidemic by using prescription drug–monitoring programs, eliminating stigma, prescribing the overdose reversal drug naloxone, and enhancing their education about safe opioid prescribing and effective pain management,” Patrice A. Harris, MD, chair of the American Medical Association Opioid Task Force, said in a statement in response to the report. “Our country must do more to provide evidence-based, comprehensive treatment for pain and for substance use disorders,” she said.
“We really encourage clinicians to look to the guidelines and the tools that are available,” Dr. Schuchat said. “We do know that internists and other primary care physicians prescribe most of the opioids, so it is important for them to be aware.” The CDC has developed a checklist and a mobile app that have been downloaded by thousands of clinicians so far, she noted. Changes in annual prescribing hold promise that practices can improve, she said.
The researchers reported no conflicts of interest.
Opioid prescribing in the United States declined overall between 2010 and 2015, but remained stable or increased in some counties, according to a report from the Centers for Disease Control and Prevention. The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
“The bottom line remains: We have too many people getting too many prescriptions at too high a dose,” Anne Schuchat, MD, acting director of the CDC, said in a July 6 teleconference.
Providers in the highest-prescribing counties prescribed six times more opioids per person than in the lowest-prescribing counties in 2015, she noted.
CDC researchers calculated prescribing rates from 2006 to 2015 by dividing the number of opioid prescriptions by the population estimates from the U.S. census for each year and created quartiles using morphine milligram equivalent per capita to analyze opioid distribution. Annual opioid prescribing rates increased from 72 to 81 prescriptions per 100 persons from 2006 to 2010 and remained relatively constant from 2010 to 2012 before showing a 13% decrease to 71 prescriptions per 100 persons from 2012 to 2015 (MMWR. 2017 Jul 7;66[26]:697-704. doi: 10.15585/mmwr.mm6626a4).
But despite these overall declines, “We are now experiencing the highest overdose death rates ever recorded in the United States,” Dr. Schuchat said. Quartiles were created using MME per capita to characterize the distribution of opioids prescribed.
In the report, areas associated with higher opioid prescribing rates on a county level included small cities or towns, areas that had a higher proportion of white residents, areas with more doctors and dentists, and areas with more cases of arthritis, diabetes, or other disabilities, she said.
The findings suggest a need for more consistency among health care providers about prescription opioids, Dr. Schuchat said. “Clinical practice is all over the place, which is a sign that you need better standards; we hope the 2016 guidelines are a turning point for better prescribing,” she said.
The CDC’s guidelines on opioid prescribing were released in 2016. The guidelines recommend alternatives when possible. Clinicians should instead consider nonopioid therapy, other types of pain medication, and nondrug pain relief options, such as physical therapy and cognitive-behavioral therapy. Other concerns include the length and strength of opioid prescriptions. Even taking opioids for a few months increases the risk for addiction, Dr. Schuchat said.
“Physicians must continue to lead efforts to reverse the epidemic by using prescription drug–monitoring programs, eliminating stigma, prescribing the overdose reversal drug naloxone, and enhancing their education about safe opioid prescribing and effective pain management,” Patrice A. Harris, MD, chair of the American Medical Association Opioid Task Force, said in a statement in response to the report. “Our country must do more to provide evidence-based, comprehensive treatment for pain and for substance use disorders,” she said.
“We really encourage clinicians to look to the guidelines and the tools that are available,” Dr. Schuchat said. “We do know that internists and other primary care physicians prescribe most of the opioids, so it is important for them to be aware.” The CDC has developed a checklist and a mobile app that have been downloaded by thousands of clinicians so far, she noted. Changes in annual prescribing hold promise that practices can improve, she said.
The researchers reported no conflicts of interest.
Opioid prescribing in the United States declined overall between 2010 and 2015, but remained stable or increased in some counties, according to a report from the Centers for Disease Control and Prevention. The findings were published online in the CDC’s Morbidity and Mortality Weekly Report.
“The bottom line remains: We have too many people getting too many prescriptions at too high a dose,” Anne Schuchat, MD, acting director of the CDC, said in a July 6 teleconference.
Providers in the highest-prescribing counties prescribed six times more opioids per person than in the lowest-prescribing counties in 2015, she noted.
CDC researchers calculated prescribing rates from 2006 to 2015 by dividing the number of opioid prescriptions by the population estimates from the U.S. census for each year and created quartiles using morphine milligram equivalent per capita to analyze opioid distribution. Annual opioid prescribing rates increased from 72 to 81 prescriptions per 100 persons from 2006 to 2010 and remained relatively constant from 2010 to 2012 before showing a 13% decrease to 71 prescriptions per 100 persons from 2012 to 2015 (MMWR. 2017 Jul 7;66[26]:697-704. doi: 10.15585/mmwr.mm6626a4).
But despite these overall declines, “We are now experiencing the highest overdose death rates ever recorded in the United States,” Dr. Schuchat said. Quartiles were created using MME per capita to characterize the distribution of opioids prescribed.
In the report, areas associated with higher opioid prescribing rates on a county level included small cities or towns, areas that had a higher proportion of white residents, areas with more doctors and dentists, and areas with more cases of arthritis, diabetes, or other disabilities, she said.
The findings suggest a need for more consistency among health care providers about prescription opioids, Dr. Schuchat said. “Clinical practice is all over the place, which is a sign that you need better standards; we hope the 2016 guidelines are a turning point for better prescribing,” she said.
The CDC’s guidelines on opioid prescribing were released in 2016. The guidelines recommend alternatives when possible. Clinicians should instead consider nonopioid therapy, other types of pain medication, and nondrug pain relief options, such as physical therapy and cognitive-behavioral therapy. Other concerns include the length and strength of opioid prescriptions. Even taking opioids for a few months increases the risk for addiction, Dr. Schuchat said.
“Physicians must continue to lead efforts to reverse the epidemic by using prescription drug–monitoring programs, eliminating stigma, prescribing the overdose reversal drug naloxone, and enhancing their education about safe opioid prescribing and effective pain management,” Patrice A. Harris, MD, chair of the American Medical Association Opioid Task Force, said in a statement in response to the report. “Our country must do more to provide evidence-based, comprehensive treatment for pain and for substance use disorders,” she said.
“We really encourage clinicians to look to the guidelines and the tools that are available,” Dr. Schuchat said. “We do know that internists and other primary care physicians prescribe most of the opioids, so it is important for them to be aware.” The CDC has developed a checklist and a mobile app that have been downloaded by thousands of clinicians so far, she noted. Changes in annual prescribing hold promise that practices can improve, she said.
The researchers reported no conflicts of interest.
The Food and Drug Administration has approved abatacept, a selective T-cell costimulation modulator, for treating adults with active psoriatic arthritis (PsA), the manufacturer, Bristol-Myers Squibb, has announced.
Approval of abatacept (Orencia) was based on two randomized, double-blind, placebo-controlled studies (PsA-I and PsA-II) in 594 adults with PsA for more than 7 years, according to the July 6 announcement. Patients had active PsA (at least three swollen joints and at least three tender joints), despite previous disease-modifying antirheumatic drug (DMARD) therapy and had one qualifying psoriatic skin lesion measuring at least 2 cm in diameter. The studies included patients treated with TNF inhibitors (TNFi) previously.
In the PsA-I trial, 170 patients received abatacept administered intravenously (IV) at days 1, 15, 29, and then every 28 days for 24 weeks, followed by open-label abatacept every 28 days. Patients were then randomized to placebo or treatment with abatacept 3 mg/kg, 10 mg/kg, or two doses of 30 mg/kg followed by weight range–based dosing of 10 mg/kg without escape for 24 weeks.
In the PsA-II trial, 424 patients received weekly doses of placebo or abatacept 25 mg administered subcutaneously (SC) without a loading dose for 24 weeks, followed by open-label abatacept at a dose of 125 mg SC weekly.
Compared with those on placebo, more patients treated with abatacept 10 mg/kg IV or 125 mg SC achieved an ACR 20 (American College of Rheumatology 20) response at 24 weeks: 47.5% vs. 19.0% and 39.4% vs. 22.3%, respectively (P less than .05).
Other results included a greater proportion of abatacept SC patients with at least a 0.35 decrease from baseline on the Health Assessment Questionnaire-Disability Index: 31% vs. 24% on placebo at 24 weeks. Responses were seen regardless of prior anti-TNFi treatment and regardless of concomitant non-biologic DMARD treatment. In addition, patients on abatacept IV and SC had improvements in enthesitis and dactylitis at 24 weeks.
The safety profile of abatacept in the two studies was “consistent with the safety profile” in rheumatoid arthritis, according to the company release.
Abatacept, initially approved in 2005, was previously approved for RA in adults and for juvenile idiopathic arthritis
Find the updated prescribing information for abatacept here.
The Food and Drug Administration has approved abatacept, a selective T-cell costimulation modulator, for treating adults with active psoriatic arthritis (PsA), the manufacturer, Bristol-Myers Squibb, has announced.
Approval of abatacept (Orencia) was based on two randomized, double-blind, placebo-controlled studies (PsA-I and PsA-II) in 594 adults with PsA for more than 7 years, according to the July 6 announcement. Patients had active PsA (at least three swollen joints and at least three tender joints), despite previous disease-modifying antirheumatic drug (DMARD) therapy and had one qualifying psoriatic skin lesion measuring at least 2 cm in diameter. The studies included patients treated with TNF inhibitors (TNFi) previously.
In the PsA-I trial, 170 patients received abatacept administered intravenously (IV) at days 1, 15, 29, and then every 28 days for 24 weeks, followed by open-label abatacept every 28 days. Patients were then randomized to placebo or treatment with abatacept 3 mg/kg, 10 mg/kg, or two doses of 30 mg/kg followed by weight range–based dosing of 10 mg/kg without escape for 24 weeks.
In the PsA-II trial, 424 patients received weekly doses of placebo or abatacept 25 mg administered subcutaneously (SC) without a loading dose for 24 weeks, followed by open-label abatacept at a dose of 125 mg SC weekly.
Compared with those on placebo, more patients treated with abatacept 10 mg/kg IV or 125 mg SC achieved an ACR 20 (American College of Rheumatology 20) response at 24 weeks: 47.5% vs. 19.0% and 39.4% vs. 22.3%, respectively (P less than .05).
Other results included a greater proportion of abatacept SC patients with at least a 0.35 decrease from baseline on the Health Assessment Questionnaire-Disability Index: 31% vs. 24% on placebo at 24 weeks. Responses were seen regardless of prior anti-TNFi treatment and regardless of concomitant non-biologic DMARD treatment. In addition, patients on abatacept IV and SC had improvements in enthesitis and dactylitis at 24 weeks.
The safety profile of abatacept in the two studies was “consistent with the safety profile” in rheumatoid arthritis, according to the company release.
Abatacept, initially approved in 2005, was previously approved for RA in adults and for juvenile idiopathic arthritis
Find the updated prescribing information for abatacept here.
The Food and Drug Administration has approved abatacept, a selective T-cell costimulation modulator, for treating adults with active psoriatic arthritis (PsA), the manufacturer, Bristol-Myers Squibb, has announced.
Approval of abatacept (Orencia) was based on two randomized, double-blind, placebo-controlled studies (PsA-I and PsA-II) in 594 adults with PsA for more than 7 years, according to the July 6 announcement. Patients had active PsA (at least three swollen joints and at least three tender joints), despite previous disease-modifying antirheumatic drug (DMARD) therapy and had one qualifying psoriatic skin lesion measuring at least 2 cm in diameter. The studies included patients treated with TNF inhibitors (TNFi) previously.
In the PsA-I trial, 170 patients received abatacept administered intravenously (IV) at days 1, 15, 29, and then every 28 days for 24 weeks, followed by open-label abatacept every 28 days. Patients were then randomized to placebo or treatment with abatacept 3 mg/kg, 10 mg/kg, or two doses of 30 mg/kg followed by weight range–based dosing of 10 mg/kg without escape for 24 weeks.
In the PsA-II trial, 424 patients received weekly doses of placebo or abatacept 25 mg administered subcutaneously (SC) without a loading dose for 24 weeks, followed by open-label abatacept at a dose of 125 mg SC weekly.
Compared with those on placebo, more patients treated with abatacept 10 mg/kg IV or 125 mg SC achieved an ACR 20 (American College of Rheumatology 20) response at 24 weeks: 47.5% vs. 19.0% and 39.4% vs. 22.3%, respectively (P less than .05).
Other results included a greater proportion of abatacept SC patients with at least a 0.35 decrease from baseline on the Health Assessment Questionnaire-Disability Index: 31% vs. 24% on placebo at 24 weeks. Responses were seen regardless of prior anti-TNFi treatment and regardless of concomitant non-biologic DMARD treatment. In addition, patients on abatacept IV and SC had improvements in enthesitis and dactylitis at 24 weeks.
The safety profile of abatacept in the two studies was “consistent with the safety profile” in rheumatoid arthritis, according to the company release.
Abatacept, initially approved in 2005, was previously approved for RA in adults and for juvenile idiopathic arthritis
Find the updated prescribing information for abatacept here.
Interstitial lung disease (ILD) encompasses a diverse group of disorders that cause inflammation and fibrosis of the lung parenchyma. The clinical manifestations, disease course, management and prognosis of ILD vary depending on the underlying subtype, making accurate classification and diagnosis an important initial step. While a comprehensive list of ILD contains dozens of disorders, the majority of patients will fall into 1 of 3 categories: exposure-related ILD, connective tissue disease-related ILD (CT-ILD), and the idiopathic interstitial pneumonias (Table).
An essential first step in the evaluation of every hospitalized patient with ILD is establishing a diagnosis. A common mistake among clinicians who diagnose patients with ILD is not realizing that ILD is a collection of diseases with different etiologies, natural histories, and treatments. A careful evaluation should be performed in every hospitalized patient with ILD to ensure an accurate diagnosis, ideally in the context of a multidisciplinary conference with pulmonary, radiology, pathology, and other specialties, as appropriate. A multidisciplinary panel of the American Thoracic Society/European Respiratory Society recently published a revised classification of ILD based on a combination of clinical, radiologic, and histopathologic findings, which may aid in refining the diagnosis.1
There are 3 main scenarios in which the hospital physician will encounter patients with ILD.
Acute presentation of new-onset disease. While many ILDs present insidiously, some cases present acutely and require hospitalization. The most common of these are acute hypersensitivity pneumonitis (HP), CT-ILD (in particular, myositis-related and systemic lupus erythematosus-related), drug-induced ILD (eg, amiodarone, nitrofurantoin), cryptogenic organizing pneumonia (COP), acute eosinophilic pneumonia (AEP), and acute interstitial pneumonia (AIP).
Acute presentation of established (chronic) disease. Patients with chronic forms of ILD can present to the hospital with an acute exacerbation of disease. This can be caused by extra-parenchymal complications, including pulmonary embolism, pneumothorax, and pleural effusion; parenchymal complications such as infectious pneumonia, aspiration pneumonitis, and congestive heart failure; or without an identifiable cause. This latter presentation is most commonly seen in idiopathic pulmonary fibrosis (IPF).2,3
Elective hospitalization for diagnostic surgical lung biopsy. Patients with ILD may be hospitalized electively for a laparoscopic surgical lung biopsy as part of their diagnostic evaluations.
Physicians caring for a hospitalized ILD patient must be familiar with the clinical presentations, diagnostic approach, medical management, and outpatient follow-up recommended in these 3 settings. We will summarize these areas and provide answers to commonly encountered clinical questions in the hospitalized patient with ILD.
CLINICAL PRESENTATION
Acute onset (or worsening) of dyspnea is the primary presenting symptom in most patients hospitalized for ILD. This symptom should be further characterized by assessing the degree of dyspnea and the extent of exercise limitation, as both impact overall disease severity and prognosis.4 Cough is the second most common symptom, and can be nonproductive, as is common in IPF, or be associated with secretions if parenchymal infection or acute bronchitis is present.5 Pleuritic chest pain, pleural effusion, and/or the presence of extrapulmonary features, including dysphagia, joint pain and swelling, or cutaneous thickening may suggest the presence of a CT-ILD. Because most forms of ILD present with only nonspecific symptoms, a careful history and physical examination are essential.
DIAGNOSIS
History
A comprehensive patient history is the backbone of diagnosing any ILD. History-taking should focus on severity and temporal progression of symptoms, presence of pre-existing systemic conditions associated with ILD, symptoms of extrapulmonary disease, and exposures to substances that can cause pulmonary injury, including a detailed history of occupations and hobbies, medications, smoking, and familial lung disease.6-9 Physicians must try to exclude other diagnoses that could result in a similar acute presentation, including congestive heart failure and infection. Considering the complex and extensive recommended history-taking, physicians may find it helpful to use a standardized questionnaire, as provided by the American College of Chest Physicians.10
Laboratory Testing
All patients presenting to the hospital with a suspected ILD should undergo careful assessment for the presence of connective tissue disease, including patients without clear symptoms because ILD can be the presenting manifestation. We routinely test for antinuclear antibody titer and pattern, rheumatoid factor, anticyclic citrullinated peptide, creatinine kinase, and aldolase as the initial screening panel in most patients, with further testing directed by the findings on history and physical examination. Pulmonary function tests are used routinely to monitor disease progression in the outpatient setting; however, in the hospitalized ILD patient, they are often difficult to perform and have no real diagnostic value. Similarly, arterial blood gas is not routinely used as part of the initial inpatient evaluation.
Table
Imaging
All hospitalized patients with a known or suspected ILD should undergo chest imaging, assuming they are stable enough to do so. While the chest radiograph can provide a low-cost initial assessment of the degree of lung involvement and presence of accompanying abnormalities, computed tomography (CT) scanning is the diagnostic test of choice.11 The pattern and distribution of abnormalities on CT scan can greatly assist with the differential diagnosis in patients presenting with a new ILD, while the presence and pattern of new opacities superimposed on chronic changes can inform the differential and the prognosis of an ILD exacerbation.12 High-resolution CT provides the most sensitive imaging modality for diffuse ILD. The addition of prone and expiratory images are helpful in differentiating mild lung disease from atelectasis and detecting air trapping, respectively.13 However, since pulmonary embolism is a common extraparenchymal finding routinely considered in the differential of a patient presenting with a known or suspected ILD, physicians should consider ordering a CT pulmonary angiogram with additional high-resolution images. Most important, radiographic evaluation should include a review of all available prior chest imaging to assess both the tempo and the nature of radiographic findings.
Bronchoscopy
Bronchoscopy (with bronchoalveolar lavage [BAL], transbronchial lung biopsy [TBLB] and/or transbronchial needle aspiration [TBNA]) is not a routinely used diagnostic tool in the hospitalized ILD patient. However, it should be considered in certain circumstances.7 Cell count and differential can be helpful in diagnosing AEP (greater than 40% eosinophilia) or acute HP (greater than 50% lymphocytosis), while the addition of microbiologic and cytologic analysis can assist with the diagnosis of infectious etiologies (including pneumocystis pneumonia) or malignancy.14,15 Bronchoscopy with BAL has limited sensitivity for many infections and the procedure is associated with a small risk of worsened hypoxemia. Transbronchial lung biopsy, and to a lesser extent TBNA, carry the added risk of pneumothorax and bleeding. In the majority of cases of ILD, TBLB and TBNA have limited diagnostic utility given the small amount of lung tissue sampled. In cases of suspected IPF, where the identification of the histologic pattern is needed for definitive diagnosis, tissue from TBLB cannot be used to make a conclusive diagnosis.16,17 However, both TBNA and TBLB are useful in the diagnosis of granulomatous disorders, such as sarcoidosis, where the diagnostic yield ranges from 80% to 90% and 50% to 75%, respectively.18,19
A newer bronchoscopic approach to sampling the lung using a bronchoscopically-placed cryoprobe (termed transbronchial cryobiopsy) has uncertain diagnostic utility and safety in the acute setting. This procedure involves intubation, sedation, and bronchoscopy allowing for the passage of an endobronchial cryoprobe through the bronchoscope and into the periphery of the lung. Several cryobiopies are generally taken from the same pulmonary subsegment. Despite a large number of recent publications on this topic, none of them have provided a clear sense of the diagnostic yield and safety.20,21 Transbronchial cryobiopsy remains a highly controversial procedure in the clinical setting, and we would not recommend its use until further data are available.22
Surgical Lung Biopsy
In the outpatient setting, a surgical lung biopsy is often useful when the ILD diagnosis cannot be made from the clinical context and imaging. However, patients presenting with acute respiratory failure from ILD are at greatly increased risk of complications from nonelective biopsy including pneumothorax, hemothorax, acute exacerbation of ILD, ICU admission, mechanical ventilation, and in-hospital mortality.23,24 Acute histological findings can also make it difficult to appreciate the underlying pattern of fibrosis, reducing the diagnostic utility.25-27 In our experience, surgical lung biopsy rarely alters the treatment of ILD patients presenting in acute respiratory failure. We believe that surgical lung biopsy should be reserved for the rare hospitalized patients in whom the clinician believes the results would clearly change management and that the substantial risk is worth taking.5,28
INPATIENT MANAGEMENT
The inpatient management of ILD is a large topic and difficult to comprehensively cover in a single review. Therefore, in this section, we will review 6 key management questions that address both general and specific treatment decisions that frequently arise in the care of hospitalized ILD patients (Figure).
Figure
When should hospitalized ILD patients be treated with antibiotics?
Infection and acute presentations of ILD have many similar clinical and radiographic features, making it difficult to distinguish between the two, or exclude infection as the causative role in an acute exacerbation.2 In many ILD patients, the risk of infection is higher than in the general population, due to the acute and chronic use of immunosuppression. Until firm guidelines on the use of antibiotics in hospitalized patients with acute respiratory symptoms are available, we recommend considering the empiric use of antibiotics in ILD patients in respiratory failure, in addition to a thorough infectious workup.
When should hospitalized ILD patients be treated with corticosteroids?
Clinical experience supports the use of corticosteroids in the acute management of most rapidly progressive ILDs presenting with respiratory failure, including AEP, COP, acute HP, drug-induced ILD, and some cases of CT-ILD. Patients with AEP tend to respond rapidly to corticosteroids. In a series of 137 patients with AEP, 127 (92%) received corticosteroids, with defervescence and improved dyspnea within 48 to 72 hours and resolution of all symptoms after a median of 7 (4 to 10) days.29 Cryptogenic organizing pneumonia is similarly corticosteroid-responsive, with patients typically started on doses of 1mg/kg of prednisone followed by a slow taper due to the risk of relapse.30 For the majority of acute CT-ILD, oral prednisone is the initial treatment, often in combination with a second immunosuppressive agent such as mycophenolate.
No proven therapies are available for acute exacerbations of IPF (AE-IPF), including the use of corticosteroids. The most recent international guidelines on the management of AE-IPF conditionally recommends the use of corticosteroids, although this recommendation is largely based on anecdotal reports and clearly states that randomized studies are needed.3 When corticosteroids are used, we recommend high doses (eg, 1 to 2 mg/kg of prednisone) with close clinical monitoring. Consider stopping corticosteroids after 3 to 5 days if there is no evidence of clinical improvement. Prolonged courses of corticosteroids should be avoided.
What additional pharmacologic therapies should be considered in the treatment of hospitalized ILD patients?
Immunomodulators. Patients presenting acutely with a new-onset ILD or with an acute exacerbation of a chronic ILD often receive corticosteroids, sometimes in concert with an immunomodulator. This is most commonly seen in the acute management of CTD- ILD and in chronic HP, where mycophenolate mofetil, and to a lesser extent, cyclophosphamide and azathioprine for CT-ILD are used in combination with corticosteroids. The rationale for this is both therapeutic synergy and a desire to limit the long-term exposure to corticosteroids. Similarly, multiple observational cohort studies have investigated the role of combination or tandem immunosuppression in the treatment AE-IPF. Although cyclosporine, cyclophosphamide, azathioprine, rituximab and tacrolimus have all been studied, their efficacy remains uncertain.3 Until these therapies are better studied, they have no routine role in the management of AE-IPF.
Antifibrotics. Nintedanib and pirfenidone are 2 antifibrotic agents approved for the treatment of IPF. Clinical trials suggest that, in addition to slowing disease progression, these therapies may help prevent AE-IPF. The data are most robust in studies of nintedanib. A phase 2 trial with 432 subjects demonstrated a delay in time to the first investigator-reported acute exacerbation.31 Two follow-up phase 3 trials showed a reduction in centrally adjudicated AE-IPF in the pooled nintedanib groups compared to placebo.32 An initial phase 2 trial of pirfenidone showed a reduction in acute exacerbations in patients on pirfenidone, but this finding was not replicated in follow-up studies.33-35 Because of their potential role in preventing acute exacerbations and emerging evidence to suggest that continuation of antifibrotics may lead to better outcomes during an acute exacerbation, these drugs should not generally be stopped during a hospitalization for ILD. However, no evidence supports their initiation during acute exacerbations, and we do not recommend starting antifibrotics in the hospitalized setting for newly diagnosed patients. Starting and stopping antifibrotics should be reserved for outpatient management.
When should noninvasive and mechanical ventilation be considered?
We recommend carefully considering the use of noninvasive ventilation (NIV) and intubation in every ILD patient in respiratory distress, as an acutely reversible process may be present. In patients requiring mechanical ventilation, every effort should be made to minimize potential damage by reducing the fraction of inspired oxygen (to prevent potential hyperoxic injury) and reducing tidal volumes (to minimize barotrauma). Patients with a chronic ILD, particularly IPF, who require NIV or mechanical ventilation will generally have poor outcomes.
Studies suggest that NIV prevents mechanical ventilation in only the minority of patients presenting with an AE-IPF and is associated with high in-hospital mortality and a median survival following hospital discharge of only 60 days.36-38 The majority of patients with IPF requiring mechanical ventilation will not survive the intensive care unit. In a series of 23 patients presenting with acute respiratory failure and IPF, 22 of the 23 patients died while receiving mechanical ventilation, with a median survival of 3 days. In a more recent study of 34 patients with acute respiratory failure and IPF, 15 subjects underwent mechanical ventilation with an in-hospital mortality rate of 100%.39 Given the overall poor survival associated with AE-IPF, mechanical ventilation should be carefully considered with the patient and family as part of an overall goals-of-care conversation prior to initiation.
When should hospitalized ILD patients be referred for inpatient lung transplant evaluation?
A subset of hospitalized patients with ILD will not respond to supportive and pharmacologic care, particularly those with advanced lung fibrosis. In these cases, lung transplantation may be the only remaining treatment option. This is particularly true for patients presenting with IPF, and it is 1 of the most common indications for lung transplantation. Patients with respiratory failure and ILD should be evaluated early in the hospital course for transplantation or considered for transfer to a transplant center. General contraindications to transplant are age older than 70 years, underweight or elevated BMI (generally higher than 30), malignancy within the last 2 years (with the exception of cutaneous squamous and basal cell tumors), untreatable major organ dysfunction other than the lung, noncurable chronic extrapulmonary infection (chronic active viral hepatitis B, hepatitis C, human immunodeficiency virus), significant chest wall deformity, untreatable psychiatric or psychologic disease, substance addiction within the last 6 months, or lack of dependable social support.40 In select patients with ILD and gas exchange abnormalities, mechanical ventilation or extracorporeal membrane oxygenation may be used to bridge a patient to lung transplantation.41
What should you tell your ILD patient to expect at discharge?
Accurate diagnosis is important not only for acute inpatient management, but for informing long-term prognosis. Acute-onset ILD tends to be more reversible, to be responsive to medical therapy, and to have a more favorable overall outcome. On the other hand, acute exacerbations of established ILD, particularly IPF, can have a more unfavorable and treatment-refractory course. Once a diagnosis is established, it is important both to provide patients with information and ensure appropriate outpatient follow-up. The Pulmonary Fibrosis Foundation (the largest U.S. advocacy and support organization for patients with ILD) provides information on ILD to patients and families and can serve as an important educational source.42 Prior to discharge, it is important to evaluate the oxygen needs of patients at rest and with exertion. Referral to an ILD center at discharge is important whenever possible, to monitor clinical symptoms and lung function, initiate or assess response to treatment, and provide supportive care, including oxygen therapy, pulmonary rehabilitation, and outpatient lung transplant referral.
CONCLUSION
ILD is a group of heterogeneous disorders characterized by lung inflammation and fibrosis. Although the onset of disease is typically insidious, patients can present acutely requiring hospitalization. Inpatient management varies significantly depending on ILD subtype, and, therefore, accurate diagnosis is key in determining treatment and prognosis. As we develop an improved understanding of the mechanisms of acute presentations of ILD, and our approaches to detection and treatment improve as a result of clinical trials, we anticipate continued modifications to this shared framework.
Disclosure
Dr. Collard reports personal fees from Alkermes, aTyr Pharmaceuticals, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Global Blood Therapeutics, Genoa, ImmuneWorks, Moerae Matrix, Navitor, Parexel, Patara, Pharma Capital Partners, Prometic, Takeda, Toray, and Xfibra, outside the submitted work. Drs. Farrand and Shah report no financial conflicts of interest.
References
1. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733-748. PubMed 2. Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis. Clin Chest Med. 2012;33(1):59-68. PubMed 3. Collard HR, Ryerson CJ, Corte TJ, et al. Acute Exacerbation of Idiopathic Pulmonary Fibrosis. An International Working Group Report. Am J Respir Crit Care Med. 2016;194(3):265-275. PubMed 4. King TE Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med. 2001;164(7):1171-1181. PubMed 5. Behr J. Approach to the diagnosis of interstitial lung disease. Clin Chest Med. 2012;33(1):1-10. PubMed 6. Raghu G, Brown KK. Interstitial lung disease: clinical evaluation and keys to an accurate diagnosis. Clin Chest Med. 2004;25(3):409-419. PubMed 7. Bradley B, Branley HM, Egan JJ, et al. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63(suppl 5):v1-v58. PubMed 8. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 1: Cytotoxic drugs. Am Rev Respir Dis. 1986;133(2):321-340. PubMed 9. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 2: Noncytotoxic drugs. Am Rev Respir Dis. 1986;133(3):488-505. PubMed 10. Diffuse Lung Disease Questionnaire for Patients. Available at: https://www.chestnet.org/~/media/chesnetorg/Foundation/Documents/Lung Disease Questionaire.ashx. Accessed August 15, 2016. 11. Pipavath S, Godwin JD. Imaging of interstitial lung disease. Clin Chest Med. 2004;25(3):455-465, v-vi. PubMed 12. Fujimoto K, Taniguchi H, Johkoh T, et al. Acute exacerbation of idiopathic pulmonary fibrosis: high-resolution CT scores predict mortality. Eur Radiol. 2012;22(1):83-92. PubMed 13. Mayo JR. CT evaluation of diffuse infiltrative lung disease: dose considerations and optimal technique. J Thorac Imaging. 2009;24(4):252-259. PubMed 14. Allen JN, Pacht ER, Gadek JE, Davis WB. Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. New Engl J Med. 1989;321(9):569-574. PubMed 15. Selman M, Pardo A, King TE Jr. Hypersensitivity pneumonitis: insights in diagnosis and pathobiology. Am J Respir Crit Care Med. 2012;186(4):314-324. PubMed 16. Churg A, Schwarz M. Transbronchial biopsy and usual interstitial pneumonia: a new paradigm? Chest. 2006;129(5):1117-1118. PubMed 17. Shim HS, Park MS, Park IK. Histopathologic findings of transbronchial biopsy in usual interstitial pneumonia. Pathol Int. 2010;60(5):373-377. PubMed 18. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788-824. PubMed 19. Carmona EM, Kalra S, Ryu JH. Pulmonary sarcoidosis: diagnosis and treatment. Mayo Clin Proc. 2016;91(7):946-954. PubMed 20. Tomassetti S, Wells AU, Costabel U, et al. Bronchoscopic lung cryobiopsy increases diagnostic confidence in the multidisciplinary diagnosis of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2016;193(7):745-752. PubMed 21. Johannson KA, Marcoux VS, Ronksley PE, Ryerson CJ. Diagnostic yield and complications of transbronchial lung cryobiopsy for interstitial lung disease. A systematic review and metaanalysis. Ann Am Thorac Soc. 2016;13(10):1828-1838. PubMed 22. Patel NM, Borczuk AC, Lederer DJ. Cryobiopsy in the diagnosis of interstitial lung disease. A step forward or back? Am J Respir Crit Care Med. 2016;193(7):707-709. PubMed 23. Rishi Raj M, Kirtee Raparia, MD, David A. Lynch, MD, Kevin K. Brown, MD. Surgical lung biopsy for interstitial lung diseases. Chest. 2016. 24. Kreider ME, Hansen-Flaschen J, Ahmad NN, et al. Complications of video-assisted thoracoscopic lung biopsy in patients with interstitial lung disease. AnnAm Thor Surg. 2007;83(3):1140-1144. PubMed 25. Churg A, Wright JL, Tazelaar HD. Acute exacerbations of fibrotic interstitial lung disease. Histopathology. 2011;58(4):525-530. PubMed 26. Churg A, Muller NL, Silva CI, Wright JL. Acute exacerbation (acute lung injury of unknown cause) in UIP and other forms of fibrotic interstitial pneumonias. Am J Surg Pathol. 2007;31(2):277-284. PubMed 27. Jones KD, Urisman A. Histopathologic approach to the surgical lung biopsy in interstitial lung disease. Clin Chest Med. 2012;33(1):27-40. PubMed 28. Hutchinson JP, Fogarty AW, McKeever TM, Hubbard RB. In-hospital mortality after surgical lung biopsy for interstitial lung disease in the United States. 2000 to 2011. Am J Respir Crit Care Med. 2016;193(10):1161-1167. PubMed 29. Rhee CK, Min KH, Yim NY, et al. Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia. Eur Respir J. 2013;41(2):402-409. PubMed 30. Lazor R, Vandevenne A, Pelletier A, Leclerc P, Court-Fortune I, Cordier JF. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles “Orphelines” Pulmonaires (GERM”O”P). Am J Respir Crit Care Med. 2000;162(2 Pt 1):571-577. PubMed 31. Richeldi L, Costabel U, Selman M, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. New Engl J Med. 2011;365(12):1079-1087. PubMed 32. Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2071-2082. PubMed 33. Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040-1047. PubMed 34. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760-1769. PubMed 35. King TE Jr, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2083-2092. PubMed 36. Saydain G, Islam A, Afessa B, Ryu JH, Scott JP, Peters SG. Outcome of patients with idiopathic pulmonary fibrosis admitted to the intensive care unit. Am J Respir Crit Care Med. 2002;166(6):839-842. PubMed 37. Vianello A, Arcaro G, Battistella L, et al. Noninvasive ventilation in the event of acute respiratory failure in patients with idiopathic pulmonary fibrosis. J Crit Care. 2014;29(4):562-567. PubMed 38. Blivet S, Philit F, Sab JM, et al. Outcome of patients with idiopathic pulmonary fibrosis admitted to the ICU for respiratory failure. Chest. 2001;120(1):209-212. PubMed 39. Mollica C, Paone G, Conti V, et al. Mechanical ventilation in patients with endstage idiopathic pulmonary fibrosis. Respiration. 2010;79(3):209-215. PubMed 40. Orens JB, Estenne M, Arcasoy S, et al. International guidelines for the selection of lung transplant candidates: 2006 update--a consensus report from the Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2006;25(7):745-755. PubMed 41. Hoopes CW, Kukreja J, Golden J, Davenport DL, Diaz-Guzman E, Zwischenberger JB. Extracorporeal membrane oxygenation as a bridge to pulmonary transplantation. J Thorac Cardiovasc Surg. 2013;145(3):862-867; discussion 867-868. PubMed 42. Pulmonary Fibrosis Foundation. http://pulmonaryfibrosis.org/. Accessed August 31, 2016.
Interstitial lung disease (ILD) encompasses a diverse group of disorders that cause inflammation and fibrosis of the lung parenchyma. The clinical manifestations, disease course, management and prognosis of ILD vary depending on the underlying subtype, making accurate classification and diagnosis an important initial step. While a comprehensive list of ILD contains dozens of disorders, the majority of patients will fall into 1 of 3 categories: exposure-related ILD, connective tissue disease-related ILD (CT-ILD), and the idiopathic interstitial pneumonias (Table).
An essential first step in the evaluation of every hospitalized patient with ILD is establishing a diagnosis. A common mistake among clinicians who diagnose patients with ILD is not realizing that ILD is a collection of diseases with different etiologies, natural histories, and treatments. A careful evaluation should be performed in every hospitalized patient with ILD to ensure an accurate diagnosis, ideally in the context of a multidisciplinary conference with pulmonary, radiology, pathology, and other specialties, as appropriate. A multidisciplinary panel of the American Thoracic Society/European Respiratory Society recently published a revised classification of ILD based on a combination of clinical, radiologic, and histopathologic findings, which may aid in refining the diagnosis.1
There are 3 main scenarios in which the hospital physician will encounter patients with ILD.
Acute presentation of new-onset disease. While many ILDs present insidiously, some cases present acutely and require hospitalization. The most common of these are acute hypersensitivity pneumonitis (HP), CT-ILD (in particular, myositis-related and systemic lupus erythematosus-related), drug-induced ILD (eg, amiodarone, nitrofurantoin), cryptogenic organizing pneumonia (COP), acute eosinophilic pneumonia (AEP), and acute interstitial pneumonia (AIP).
Acute presentation of established (chronic) disease. Patients with chronic forms of ILD can present to the hospital with an acute exacerbation of disease. This can be caused by extra-parenchymal complications, including pulmonary embolism, pneumothorax, and pleural effusion; parenchymal complications such as infectious pneumonia, aspiration pneumonitis, and congestive heart failure; or without an identifiable cause. This latter presentation is most commonly seen in idiopathic pulmonary fibrosis (IPF).2,3
Elective hospitalization for diagnostic surgical lung biopsy. Patients with ILD may be hospitalized electively for a laparoscopic surgical lung biopsy as part of their diagnostic evaluations.
Physicians caring for a hospitalized ILD patient must be familiar with the clinical presentations, diagnostic approach, medical management, and outpatient follow-up recommended in these 3 settings. We will summarize these areas and provide answers to commonly encountered clinical questions in the hospitalized patient with ILD.
CLINICAL PRESENTATION
Acute onset (or worsening) of dyspnea is the primary presenting symptom in most patients hospitalized for ILD. This symptom should be further characterized by assessing the degree of dyspnea and the extent of exercise limitation, as both impact overall disease severity and prognosis.4 Cough is the second most common symptom, and can be nonproductive, as is common in IPF, or be associated with secretions if parenchymal infection or acute bronchitis is present.5 Pleuritic chest pain, pleural effusion, and/or the presence of extrapulmonary features, including dysphagia, joint pain and swelling, or cutaneous thickening may suggest the presence of a CT-ILD. Because most forms of ILD present with only nonspecific symptoms, a careful history and physical examination are essential.
DIAGNOSIS
History
A comprehensive patient history is the backbone of diagnosing any ILD. History-taking should focus on severity and temporal progression of symptoms, presence of pre-existing systemic conditions associated with ILD, symptoms of extrapulmonary disease, and exposures to substances that can cause pulmonary injury, including a detailed history of occupations and hobbies, medications, smoking, and familial lung disease.6-9 Physicians must try to exclude other diagnoses that could result in a similar acute presentation, including congestive heart failure and infection. Considering the complex and extensive recommended history-taking, physicians may find it helpful to use a standardized questionnaire, as provided by the American College of Chest Physicians.10
Laboratory Testing
All patients presenting to the hospital with a suspected ILD should undergo careful assessment for the presence of connective tissue disease, including patients without clear symptoms because ILD can be the presenting manifestation. We routinely test for antinuclear antibody titer and pattern, rheumatoid factor, anticyclic citrullinated peptide, creatinine kinase, and aldolase as the initial screening panel in most patients, with further testing directed by the findings on history and physical examination. Pulmonary function tests are used routinely to monitor disease progression in the outpatient setting; however, in the hospitalized ILD patient, they are often difficult to perform and have no real diagnostic value. Similarly, arterial blood gas is not routinely used as part of the initial inpatient evaluation.
Table
Imaging
All hospitalized patients with a known or suspected ILD should undergo chest imaging, assuming they are stable enough to do so. While the chest radiograph can provide a low-cost initial assessment of the degree of lung involvement and presence of accompanying abnormalities, computed tomography (CT) scanning is the diagnostic test of choice.11 The pattern and distribution of abnormalities on CT scan can greatly assist with the differential diagnosis in patients presenting with a new ILD, while the presence and pattern of new opacities superimposed on chronic changes can inform the differential and the prognosis of an ILD exacerbation.12 High-resolution CT provides the most sensitive imaging modality for diffuse ILD. The addition of prone and expiratory images are helpful in differentiating mild lung disease from atelectasis and detecting air trapping, respectively.13 However, since pulmonary embolism is a common extraparenchymal finding routinely considered in the differential of a patient presenting with a known or suspected ILD, physicians should consider ordering a CT pulmonary angiogram with additional high-resolution images. Most important, radiographic evaluation should include a review of all available prior chest imaging to assess both the tempo and the nature of radiographic findings.
Bronchoscopy
Bronchoscopy (with bronchoalveolar lavage [BAL], transbronchial lung biopsy [TBLB] and/or transbronchial needle aspiration [TBNA]) is not a routinely used diagnostic tool in the hospitalized ILD patient. However, it should be considered in certain circumstances.7 Cell count and differential can be helpful in diagnosing AEP (greater than 40% eosinophilia) or acute HP (greater than 50% lymphocytosis), while the addition of microbiologic and cytologic analysis can assist with the diagnosis of infectious etiologies (including pneumocystis pneumonia) or malignancy.14,15 Bronchoscopy with BAL has limited sensitivity for many infections and the procedure is associated with a small risk of worsened hypoxemia. Transbronchial lung biopsy, and to a lesser extent TBNA, carry the added risk of pneumothorax and bleeding. In the majority of cases of ILD, TBLB and TBNA have limited diagnostic utility given the small amount of lung tissue sampled. In cases of suspected IPF, where the identification of the histologic pattern is needed for definitive diagnosis, tissue from TBLB cannot be used to make a conclusive diagnosis.16,17 However, both TBNA and TBLB are useful in the diagnosis of granulomatous disorders, such as sarcoidosis, where the diagnostic yield ranges from 80% to 90% and 50% to 75%, respectively.18,19
A newer bronchoscopic approach to sampling the lung using a bronchoscopically-placed cryoprobe (termed transbronchial cryobiopsy) has uncertain diagnostic utility and safety in the acute setting. This procedure involves intubation, sedation, and bronchoscopy allowing for the passage of an endobronchial cryoprobe through the bronchoscope and into the periphery of the lung. Several cryobiopies are generally taken from the same pulmonary subsegment. Despite a large number of recent publications on this topic, none of them have provided a clear sense of the diagnostic yield and safety.20,21 Transbronchial cryobiopsy remains a highly controversial procedure in the clinical setting, and we would not recommend its use until further data are available.22
Surgical Lung Biopsy
In the outpatient setting, a surgical lung biopsy is often useful when the ILD diagnosis cannot be made from the clinical context and imaging. However, patients presenting with acute respiratory failure from ILD are at greatly increased risk of complications from nonelective biopsy including pneumothorax, hemothorax, acute exacerbation of ILD, ICU admission, mechanical ventilation, and in-hospital mortality.23,24 Acute histological findings can also make it difficult to appreciate the underlying pattern of fibrosis, reducing the diagnostic utility.25-27 In our experience, surgical lung biopsy rarely alters the treatment of ILD patients presenting in acute respiratory failure. We believe that surgical lung biopsy should be reserved for the rare hospitalized patients in whom the clinician believes the results would clearly change management and that the substantial risk is worth taking.5,28
INPATIENT MANAGEMENT
The inpatient management of ILD is a large topic and difficult to comprehensively cover in a single review. Therefore, in this section, we will review 6 key management questions that address both general and specific treatment decisions that frequently arise in the care of hospitalized ILD patients (Figure).
Figure
When should hospitalized ILD patients be treated with antibiotics?
Infection and acute presentations of ILD have many similar clinical and radiographic features, making it difficult to distinguish between the two, or exclude infection as the causative role in an acute exacerbation.2 In many ILD patients, the risk of infection is higher than in the general population, due to the acute and chronic use of immunosuppression. Until firm guidelines on the use of antibiotics in hospitalized patients with acute respiratory symptoms are available, we recommend considering the empiric use of antibiotics in ILD patients in respiratory failure, in addition to a thorough infectious workup.
When should hospitalized ILD patients be treated with corticosteroids?
Clinical experience supports the use of corticosteroids in the acute management of most rapidly progressive ILDs presenting with respiratory failure, including AEP, COP, acute HP, drug-induced ILD, and some cases of CT-ILD. Patients with AEP tend to respond rapidly to corticosteroids. In a series of 137 patients with AEP, 127 (92%) received corticosteroids, with defervescence and improved dyspnea within 48 to 72 hours and resolution of all symptoms after a median of 7 (4 to 10) days.29 Cryptogenic organizing pneumonia is similarly corticosteroid-responsive, with patients typically started on doses of 1mg/kg of prednisone followed by a slow taper due to the risk of relapse.30 For the majority of acute CT-ILD, oral prednisone is the initial treatment, often in combination with a second immunosuppressive agent such as mycophenolate.
No proven therapies are available for acute exacerbations of IPF (AE-IPF), including the use of corticosteroids. The most recent international guidelines on the management of AE-IPF conditionally recommends the use of corticosteroids, although this recommendation is largely based on anecdotal reports and clearly states that randomized studies are needed.3 When corticosteroids are used, we recommend high doses (eg, 1 to 2 mg/kg of prednisone) with close clinical monitoring. Consider stopping corticosteroids after 3 to 5 days if there is no evidence of clinical improvement. Prolonged courses of corticosteroids should be avoided.
What additional pharmacologic therapies should be considered in the treatment of hospitalized ILD patients?
Immunomodulators. Patients presenting acutely with a new-onset ILD or with an acute exacerbation of a chronic ILD often receive corticosteroids, sometimes in concert with an immunomodulator. This is most commonly seen in the acute management of CTD- ILD and in chronic HP, where mycophenolate mofetil, and to a lesser extent, cyclophosphamide and azathioprine for CT-ILD are used in combination with corticosteroids. The rationale for this is both therapeutic synergy and a desire to limit the long-term exposure to corticosteroids. Similarly, multiple observational cohort studies have investigated the role of combination or tandem immunosuppression in the treatment AE-IPF. Although cyclosporine, cyclophosphamide, azathioprine, rituximab and tacrolimus have all been studied, their efficacy remains uncertain.3 Until these therapies are better studied, they have no routine role in the management of AE-IPF.
Antifibrotics. Nintedanib and pirfenidone are 2 antifibrotic agents approved for the treatment of IPF. Clinical trials suggest that, in addition to slowing disease progression, these therapies may help prevent AE-IPF. The data are most robust in studies of nintedanib. A phase 2 trial with 432 subjects demonstrated a delay in time to the first investigator-reported acute exacerbation.31 Two follow-up phase 3 trials showed a reduction in centrally adjudicated AE-IPF in the pooled nintedanib groups compared to placebo.32 An initial phase 2 trial of pirfenidone showed a reduction in acute exacerbations in patients on pirfenidone, but this finding was not replicated in follow-up studies.33-35 Because of their potential role in preventing acute exacerbations and emerging evidence to suggest that continuation of antifibrotics may lead to better outcomes during an acute exacerbation, these drugs should not generally be stopped during a hospitalization for ILD. However, no evidence supports their initiation during acute exacerbations, and we do not recommend starting antifibrotics in the hospitalized setting for newly diagnosed patients. Starting and stopping antifibrotics should be reserved for outpatient management.
When should noninvasive and mechanical ventilation be considered?
We recommend carefully considering the use of noninvasive ventilation (NIV) and intubation in every ILD patient in respiratory distress, as an acutely reversible process may be present. In patients requiring mechanical ventilation, every effort should be made to minimize potential damage by reducing the fraction of inspired oxygen (to prevent potential hyperoxic injury) and reducing tidal volumes (to minimize barotrauma). Patients with a chronic ILD, particularly IPF, who require NIV or mechanical ventilation will generally have poor outcomes.
Studies suggest that NIV prevents mechanical ventilation in only the minority of patients presenting with an AE-IPF and is associated with high in-hospital mortality and a median survival following hospital discharge of only 60 days.36-38 The majority of patients with IPF requiring mechanical ventilation will not survive the intensive care unit. In a series of 23 patients presenting with acute respiratory failure and IPF, 22 of the 23 patients died while receiving mechanical ventilation, with a median survival of 3 days. In a more recent study of 34 patients with acute respiratory failure and IPF, 15 subjects underwent mechanical ventilation with an in-hospital mortality rate of 100%.39 Given the overall poor survival associated with AE-IPF, mechanical ventilation should be carefully considered with the patient and family as part of an overall goals-of-care conversation prior to initiation.
When should hospitalized ILD patients be referred for inpatient lung transplant evaluation?
A subset of hospitalized patients with ILD will not respond to supportive and pharmacologic care, particularly those with advanced lung fibrosis. In these cases, lung transplantation may be the only remaining treatment option. This is particularly true for patients presenting with IPF, and it is 1 of the most common indications for lung transplantation. Patients with respiratory failure and ILD should be evaluated early in the hospital course for transplantation or considered for transfer to a transplant center. General contraindications to transplant are age older than 70 years, underweight or elevated BMI (generally higher than 30), malignancy within the last 2 years (with the exception of cutaneous squamous and basal cell tumors), untreatable major organ dysfunction other than the lung, noncurable chronic extrapulmonary infection (chronic active viral hepatitis B, hepatitis C, human immunodeficiency virus), significant chest wall deformity, untreatable psychiatric or psychologic disease, substance addiction within the last 6 months, or lack of dependable social support.40 In select patients with ILD and gas exchange abnormalities, mechanical ventilation or extracorporeal membrane oxygenation may be used to bridge a patient to lung transplantation.41
What should you tell your ILD patient to expect at discharge?
Accurate diagnosis is important not only for acute inpatient management, but for informing long-term prognosis. Acute-onset ILD tends to be more reversible, to be responsive to medical therapy, and to have a more favorable overall outcome. On the other hand, acute exacerbations of established ILD, particularly IPF, can have a more unfavorable and treatment-refractory course. Once a diagnosis is established, it is important both to provide patients with information and ensure appropriate outpatient follow-up. The Pulmonary Fibrosis Foundation (the largest U.S. advocacy and support organization for patients with ILD) provides information on ILD to patients and families and can serve as an important educational source.42 Prior to discharge, it is important to evaluate the oxygen needs of patients at rest and with exertion. Referral to an ILD center at discharge is important whenever possible, to monitor clinical symptoms and lung function, initiate or assess response to treatment, and provide supportive care, including oxygen therapy, pulmonary rehabilitation, and outpatient lung transplant referral.
CONCLUSION
ILD is a group of heterogeneous disorders characterized by lung inflammation and fibrosis. Although the onset of disease is typically insidious, patients can present acutely requiring hospitalization. Inpatient management varies significantly depending on ILD subtype, and, therefore, accurate diagnosis is key in determining treatment and prognosis. As we develop an improved understanding of the mechanisms of acute presentations of ILD, and our approaches to detection and treatment improve as a result of clinical trials, we anticipate continued modifications to this shared framework.
Disclosure
Dr. Collard reports personal fees from Alkermes, aTyr Pharmaceuticals, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Global Blood Therapeutics, Genoa, ImmuneWorks, Moerae Matrix, Navitor, Parexel, Patara, Pharma Capital Partners, Prometic, Takeda, Toray, and Xfibra, outside the submitted work. Drs. Farrand and Shah report no financial conflicts of interest.
Interstitial lung disease (ILD) encompasses a diverse group of disorders that cause inflammation and fibrosis of the lung parenchyma. The clinical manifestations, disease course, management and prognosis of ILD vary depending on the underlying subtype, making accurate classification and diagnosis an important initial step. While a comprehensive list of ILD contains dozens of disorders, the majority of patients will fall into 1 of 3 categories: exposure-related ILD, connective tissue disease-related ILD (CT-ILD), and the idiopathic interstitial pneumonias (Table).
An essential first step in the evaluation of every hospitalized patient with ILD is establishing a diagnosis. A common mistake among clinicians who diagnose patients with ILD is not realizing that ILD is a collection of diseases with different etiologies, natural histories, and treatments. A careful evaluation should be performed in every hospitalized patient with ILD to ensure an accurate diagnosis, ideally in the context of a multidisciplinary conference with pulmonary, radiology, pathology, and other specialties, as appropriate. A multidisciplinary panel of the American Thoracic Society/European Respiratory Society recently published a revised classification of ILD based on a combination of clinical, radiologic, and histopathologic findings, which may aid in refining the diagnosis.1
There are 3 main scenarios in which the hospital physician will encounter patients with ILD.
Acute presentation of new-onset disease. While many ILDs present insidiously, some cases present acutely and require hospitalization. The most common of these are acute hypersensitivity pneumonitis (HP), CT-ILD (in particular, myositis-related and systemic lupus erythematosus-related), drug-induced ILD (eg, amiodarone, nitrofurantoin), cryptogenic organizing pneumonia (COP), acute eosinophilic pneumonia (AEP), and acute interstitial pneumonia (AIP).
Acute presentation of established (chronic) disease. Patients with chronic forms of ILD can present to the hospital with an acute exacerbation of disease. This can be caused by extra-parenchymal complications, including pulmonary embolism, pneumothorax, and pleural effusion; parenchymal complications such as infectious pneumonia, aspiration pneumonitis, and congestive heart failure; or without an identifiable cause. This latter presentation is most commonly seen in idiopathic pulmonary fibrosis (IPF).2,3
Elective hospitalization for diagnostic surgical lung biopsy. Patients with ILD may be hospitalized electively for a laparoscopic surgical lung biopsy as part of their diagnostic evaluations.
Physicians caring for a hospitalized ILD patient must be familiar with the clinical presentations, diagnostic approach, medical management, and outpatient follow-up recommended in these 3 settings. We will summarize these areas and provide answers to commonly encountered clinical questions in the hospitalized patient with ILD.
CLINICAL PRESENTATION
Acute onset (or worsening) of dyspnea is the primary presenting symptom in most patients hospitalized for ILD. This symptom should be further characterized by assessing the degree of dyspnea and the extent of exercise limitation, as both impact overall disease severity and prognosis.4 Cough is the second most common symptom, and can be nonproductive, as is common in IPF, or be associated with secretions if parenchymal infection or acute bronchitis is present.5 Pleuritic chest pain, pleural effusion, and/or the presence of extrapulmonary features, including dysphagia, joint pain and swelling, or cutaneous thickening may suggest the presence of a CT-ILD. Because most forms of ILD present with only nonspecific symptoms, a careful history and physical examination are essential.
DIAGNOSIS
History
A comprehensive patient history is the backbone of diagnosing any ILD. History-taking should focus on severity and temporal progression of symptoms, presence of pre-existing systemic conditions associated with ILD, symptoms of extrapulmonary disease, and exposures to substances that can cause pulmonary injury, including a detailed history of occupations and hobbies, medications, smoking, and familial lung disease.6-9 Physicians must try to exclude other diagnoses that could result in a similar acute presentation, including congestive heart failure and infection. Considering the complex and extensive recommended history-taking, physicians may find it helpful to use a standardized questionnaire, as provided by the American College of Chest Physicians.10
Laboratory Testing
All patients presenting to the hospital with a suspected ILD should undergo careful assessment for the presence of connective tissue disease, including patients without clear symptoms because ILD can be the presenting manifestation. We routinely test for antinuclear antibody titer and pattern, rheumatoid factor, anticyclic citrullinated peptide, creatinine kinase, and aldolase as the initial screening panel in most patients, with further testing directed by the findings on history and physical examination. Pulmonary function tests are used routinely to monitor disease progression in the outpatient setting; however, in the hospitalized ILD patient, they are often difficult to perform and have no real diagnostic value. Similarly, arterial blood gas is not routinely used as part of the initial inpatient evaluation.
Table
Imaging
All hospitalized patients with a known or suspected ILD should undergo chest imaging, assuming they are stable enough to do so. While the chest radiograph can provide a low-cost initial assessment of the degree of lung involvement and presence of accompanying abnormalities, computed tomography (CT) scanning is the diagnostic test of choice.11 The pattern and distribution of abnormalities on CT scan can greatly assist with the differential diagnosis in patients presenting with a new ILD, while the presence and pattern of new opacities superimposed on chronic changes can inform the differential and the prognosis of an ILD exacerbation.12 High-resolution CT provides the most sensitive imaging modality for diffuse ILD. The addition of prone and expiratory images are helpful in differentiating mild lung disease from atelectasis and detecting air trapping, respectively.13 However, since pulmonary embolism is a common extraparenchymal finding routinely considered in the differential of a patient presenting with a known or suspected ILD, physicians should consider ordering a CT pulmonary angiogram with additional high-resolution images. Most important, radiographic evaluation should include a review of all available prior chest imaging to assess both the tempo and the nature of radiographic findings.
Bronchoscopy
Bronchoscopy (with bronchoalveolar lavage [BAL], transbronchial lung biopsy [TBLB] and/or transbronchial needle aspiration [TBNA]) is not a routinely used diagnostic tool in the hospitalized ILD patient. However, it should be considered in certain circumstances.7 Cell count and differential can be helpful in diagnosing AEP (greater than 40% eosinophilia) or acute HP (greater than 50% lymphocytosis), while the addition of microbiologic and cytologic analysis can assist with the diagnosis of infectious etiologies (including pneumocystis pneumonia) or malignancy.14,15 Bronchoscopy with BAL has limited sensitivity for many infections and the procedure is associated with a small risk of worsened hypoxemia. Transbronchial lung biopsy, and to a lesser extent TBNA, carry the added risk of pneumothorax and bleeding. In the majority of cases of ILD, TBLB and TBNA have limited diagnostic utility given the small amount of lung tissue sampled. In cases of suspected IPF, where the identification of the histologic pattern is needed for definitive diagnosis, tissue from TBLB cannot be used to make a conclusive diagnosis.16,17 However, both TBNA and TBLB are useful in the diagnosis of granulomatous disorders, such as sarcoidosis, where the diagnostic yield ranges from 80% to 90% and 50% to 75%, respectively.18,19
A newer bronchoscopic approach to sampling the lung using a bronchoscopically-placed cryoprobe (termed transbronchial cryobiopsy) has uncertain diagnostic utility and safety in the acute setting. This procedure involves intubation, sedation, and bronchoscopy allowing for the passage of an endobronchial cryoprobe through the bronchoscope and into the periphery of the lung. Several cryobiopies are generally taken from the same pulmonary subsegment. Despite a large number of recent publications on this topic, none of them have provided a clear sense of the diagnostic yield and safety.20,21 Transbronchial cryobiopsy remains a highly controversial procedure in the clinical setting, and we would not recommend its use until further data are available.22
Surgical Lung Biopsy
In the outpatient setting, a surgical lung biopsy is often useful when the ILD diagnosis cannot be made from the clinical context and imaging. However, patients presenting with acute respiratory failure from ILD are at greatly increased risk of complications from nonelective biopsy including pneumothorax, hemothorax, acute exacerbation of ILD, ICU admission, mechanical ventilation, and in-hospital mortality.23,24 Acute histological findings can also make it difficult to appreciate the underlying pattern of fibrosis, reducing the diagnostic utility.25-27 In our experience, surgical lung biopsy rarely alters the treatment of ILD patients presenting in acute respiratory failure. We believe that surgical lung biopsy should be reserved for the rare hospitalized patients in whom the clinician believes the results would clearly change management and that the substantial risk is worth taking.5,28
INPATIENT MANAGEMENT
The inpatient management of ILD is a large topic and difficult to comprehensively cover in a single review. Therefore, in this section, we will review 6 key management questions that address both general and specific treatment decisions that frequently arise in the care of hospitalized ILD patients (Figure).
Figure
When should hospitalized ILD patients be treated with antibiotics?
Infection and acute presentations of ILD have many similar clinical and radiographic features, making it difficult to distinguish between the two, or exclude infection as the causative role in an acute exacerbation.2 In many ILD patients, the risk of infection is higher than in the general population, due to the acute and chronic use of immunosuppression. Until firm guidelines on the use of antibiotics in hospitalized patients with acute respiratory symptoms are available, we recommend considering the empiric use of antibiotics in ILD patients in respiratory failure, in addition to a thorough infectious workup.
When should hospitalized ILD patients be treated with corticosteroids?
Clinical experience supports the use of corticosteroids in the acute management of most rapidly progressive ILDs presenting with respiratory failure, including AEP, COP, acute HP, drug-induced ILD, and some cases of CT-ILD. Patients with AEP tend to respond rapidly to corticosteroids. In a series of 137 patients with AEP, 127 (92%) received corticosteroids, with defervescence and improved dyspnea within 48 to 72 hours and resolution of all symptoms after a median of 7 (4 to 10) days.29 Cryptogenic organizing pneumonia is similarly corticosteroid-responsive, with patients typically started on doses of 1mg/kg of prednisone followed by a slow taper due to the risk of relapse.30 For the majority of acute CT-ILD, oral prednisone is the initial treatment, often in combination with a second immunosuppressive agent such as mycophenolate.
No proven therapies are available for acute exacerbations of IPF (AE-IPF), including the use of corticosteroids. The most recent international guidelines on the management of AE-IPF conditionally recommends the use of corticosteroids, although this recommendation is largely based on anecdotal reports and clearly states that randomized studies are needed.3 When corticosteroids are used, we recommend high doses (eg, 1 to 2 mg/kg of prednisone) with close clinical monitoring. Consider stopping corticosteroids after 3 to 5 days if there is no evidence of clinical improvement. Prolonged courses of corticosteroids should be avoided.
What additional pharmacologic therapies should be considered in the treatment of hospitalized ILD patients?
Immunomodulators. Patients presenting acutely with a new-onset ILD or with an acute exacerbation of a chronic ILD often receive corticosteroids, sometimes in concert with an immunomodulator. This is most commonly seen in the acute management of CTD- ILD and in chronic HP, where mycophenolate mofetil, and to a lesser extent, cyclophosphamide and azathioprine for CT-ILD are used in combination with corticosteroids. The rationale for this is both therapeutic synergy and a desire to limit the long-term exposure to corticosteroids. Similarly, multiple observational cohort studies have investigated the role of combination or tandem immunosuppression in the treatment AE-IPF. Although cyclosporine, cyclophosphamide, azathioprine, rituximab and tacrolimus have all been studied, their efficacy remains uncertain.3 Until these therapies are better studied, they have no routine role in the management of AE-IPF.
Antifibrotics. Nintedanib and pirfenidone are 2 antifibrotic agents approved for the treatment of IPF. Clinical trials suggest that, in addition to slowing disease progression, these therapies may help prevent AE-IPF. The data are most robust in studies of nintedanib. A phase 2 trial with 432 subjects demonstrated a delay in time to the first investigator-reported acute exacerbation.31 Two follow-up phase 3 trials showed a reduction in centrally adjudicated AE-IPF in the pooled nintedanib groups compared to placebo.32 An initial phase 2 trial of pirfenidone showed a reduction in acute exacerbations in patients on pirfenidone, but this finding was not replicated in follow-up studies.33-35 Because of their potential role in preventing acute exacerbations and emerging evidence to suggest that continuation of antifibrotics may lead to better outcomes during an acute exacerbation, these drugs should not generally be stopped during a hospitalization for ILD. However, no evidence supports their initiation during acute exacerbations, and we do not recommend starting antifibrotics in the hospitalized setting for newly diagnosed patients. Starting and stopping antifibrotics should be reserved for outpatient management.
When should noninvasive and mechanical ventilation be considered?
We recommend carefully considering the use of noninvasive ventilation (NIV) and intubation in every ILD patient in respiratory distress, as an acutely reversible process may be present. In patients requiring mechanical ventilation, every effort should be made to minimize potential damage by reducing the fraction of inspired oxygen (to prevent potential hyperoxic injury) and reducing tidal volumes (to minimize barotrauma). Patients with a chronic ILD, particularly IPF, who require NIV or mechanical ventilation will generally have poor outcomes.
Studies suggest that NIV prevents mechanical ventilation in only the minority of patients presenting with an AE-IPF and is associated with high in-hospital mortality and a median survival following hospital discharge of only 60 days.36-38 The majority of patients with IPF requiring mechanical ventilation will not survive the intensive care unit. In a series of 23 patients presenting with acute respiratory failure and IPF, 22 of the 23 patients died while receiving mechanical ventilation, with a median survival of 3 days. In a more recent study of 34 patients with acute respiratory failure and IPF, 15 subjects underwent mechanical ventilation with an in-hospital mortality rate of 100%.39 Given the overall poor survival associated with AE-IPF, mechanical ventilation should be carefully considered with the patient and family as part of an overall goals-of-care conversation prior to initiation.
When should hospitalized ILD patients be referred for inpatient lung transplant evaluation?
A subset of hospitalized patients with ILD will not respond to supportive and pharmacologic care, particularly those with advanced lung fibrosis. In these cases, lung transplantation may be the only remaining treatment option. This is particularly true for patients presenting with IPF, and it is 1 of the most common indications for lung transplantation. Patients with respiratory failure and ILD should be evaluated early in the hospital course for transplantation or considered for transfer to a transplant center. General contraindications to transplant are age older than 70 years, underweight or elevated BMI (generally higher than 30), malignancy within the last 2 years (with the exception of cutaneous squamous and basal cell tumors), untreatable major organ dysfunction other than the lung, noncurable chronic extrapulmonary infection (chronic active viral hepatitis B, hepatitis C, human immunodeficiency virus), significant chest wall deformity, untreatable psychiatric or psychologic disease, substance addiction within the last 6 months, or lack of dependable social support.40 In select patients with ILD and gas exchange abnormalities, mechanical ventilation or extracorporeal membrane oxygenation may be used to bridge a patient to lung transplantation.41
What should you tell your ILD patient to expect at discharge?
Accurate diagnosis is important not only for acute inpatient management, but for informing long-term prognosis. Acute-onset ILD tends to be more reversible, to be responsive to medical therapy, and to have a more favorable overall outcome. On the other hand, acute exacerbations of established ILD, particularly IPF, can have a more unfavorable and treatment-refractory course. Once a diagnosis is established, it is important both to provide patients with information and ensure appropriate outpatient follow-up. The Pulmonary Fibrosis Foundation (the largest U.S. advocacy and support organization for patients with ILD) provides information on ILD to patients and families and can serve as an important educational source.42 Prior to discharge, it is important to evaluate the oxygen needs of patients at rest and with exertion. Referral to an ILD center at discharge is important whenever possible, to monitor clinical symptoms and lung function, initiate or assess response to treatment, and provide supportive care, including oxygen therapy, pulmonary rehabilitation, and outpatient lung transplant referral.
CONCLUSION
ILD is a group of heterogeneous disorders characterized by lung inflammation and fibrosis. Although the onset of disease is typically insidious, patients can present acutely requiring hospitalization. Inpatient management varies significantly depending on ILD subtype, and, therefore, accurate diagnosis is key in determining treatment and prognosis. As we develop an improved understanding of the mechanisms of acute presentations of ILD, and our approaches to detection and treatment improve as a result of clinical trials, we anticipate continued modifications to this shared framework.
Disclosure
Dr. Collard reports personal fees from Alkermes, aTyr Pharmaceuticals, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Global Blood Therapeutics, Genoa, ImmuneWorks, Moerae Matrix, Navitor, Parexel, Patara, Pharma Capital Partners, Prometic, Takeda, Toray, and Xfibra, outside the submitted work. Drs. Farrand and Shah report no financial conflicts of interest.
References
1. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733-748. PubMed 2. Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis. Clin Chest Med. 2012;33(1):59-68. PubMed 3. Collard HR, Ryerson CJ, Corte TJ, et al. Acute Exacerbation of Idiopathic Pulmonary Fibrosis. An International Working Group Report. Am J Respir Crit Care Med. 2016;194(3):265-275. PubMed 4. King TE Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med. 2001;164(7):1171-1181. PubMed 5. Behr J. Approach to the diagnosis of interstitial lung disease. Clin Chest Med. 2012;33(1):1-10. PubMed 6. Raghu G, Brown KK. Interstitial lung disease: clinical evaluation and keys to an accurate diagnosis. Clin Chest Med. 2004;25(3):409-419. PubMed 7. Bradley B, Branley HM, Egan JJ, et al. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63(suppl 5):v1-v58. PubMed 8. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 1: Cytotoxic drugs. Am Rev Respir Dis. 1986;133(2):321-340. PubMed 9. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 2: Noncytotoxic drugs. Am Rev Respir Dis. 1986;133(3):488-505. PubMed 10. Diffuse Lung Disease Questionnaire for Patients. Available at: https://www.chestnet.org/~/media/chesnetorg/Foundation/Documents/Lung Disease Questionaire.ashx. Accessed August 15, 2016. 11. Pipavath S, Godwin JD. Imaging of interstitial lung disease. Clin Chest Med. 2004;25(3):455-465, v-vi. PubMed 12. Fujimoto K, Taniguchi H, Johkoh T, et al. Acute exacerbation of idiopathic pulmonary fibrosis: high-resolution CT scores predict mortality. Eur Radiol. 2012;22(1):83-92. PubMed 13. Mayo JR. CT evaluation of diffuse infiltrative lung disease: dose considerations and optimal technique. J Thorac Imaging. 2009;24(4):252-259. PubMed 14. Allen JN, Pacht ER, Gadek JE, Davis WB. Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. New Engl J Med. 1989;321(9):569-574. PubMed 15. Selman M, Pardo A, King TE Jr. Hypersensitivity pneumonitis: insights in diagnosis and pathobiology. Am J Respir Crit Care Med. 2012;186(4):314-324. PubMed 16. Churg A, Schwarz M. Transbronchial biopsy and usual interstitial pneumonia: a new paradigm? Chest. 2006;129(5):1117-1118. PubMed 17. Shim HS, Park MS, Park IK. Histopathologic findings of transbronchial biopsy in usual interstitial pneumonia. Pathol Int. 2010;60(5):373-377. PubMed 18. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788-824. PubMed 19. Carmona EM, Kalra S, Ryu JH. Pulmonary sarcoidosis: diagnosis and treatment. Mayo Clin Proc. 2016;91(7):946-954. PubMed 20. Tomassetti S, Wells AU, Costabel U, et al. Bronchoscopic lung cryobiopsy increases diagnostic confidence in the multidisciplinary diagnosis of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2016;193(7):745-752. PubMed 21. Johannson KA, Marcoux VS, Ronksley PE, Ryerson CJ. Diagnostic yield and complications of transbronchial lung cryobiopsy for interstitial lung disease. A systematic review and metaanalysis. Ann Am Thorac Soc. 2016;13(10):1828-1838. PubMed 22. Patel NM, Borczuk AC, Lederer DJ. Cryobiopsy in the diagnosis of interstitial lung disease. A step forward or back? Am J Respir Crit Care Med. 2016;193(7):707-709. PubMed 23. Rishi Raj M, Kirtee Raparia, MD, David A. Lynch, MD, Kevin K. Brown, MD. Surgical lung biopsy for interstitial lung diseases. Chest. 2016. 24. Kreider ME, Hansen-Flaschen J, Ahmad NN, et al. Complications of video-assisted thoracoscopic lung biopsy in patients with interstitial lung disease. AnnAm Thor Surg. 2007;83(3):1140-1144. PubMed 25. Churg A, Wright JL, Tazelaar HD. Acute exacerbations of fibrotic interstitial lung disease. Histopathology. 2011;58(4):525-530. PubMed 26. Churg A, Muller NL, Silva CI, Wright JL. Acute exacerbation (acute lung injury of unknown cause) in UIP and other forms of fibrotic interstitial pneumonias. Am J Surg Pathol. 2007;31(2):277-284. PubMed 27. Jones KD, Urisman A. Histopathologic approach to the surgical lung biopsy in interstitial lung disease. Clin Chest Med. 2012;33(1):27-40. PubMed 28. Hutchinson JP, Fogarty AW, McKeever TM, Hubbard RB. In-hospital mortality after surgical lung biopsy for interstitial lung disease in the United States. 2000 to 2011. Am J Respir Crit Care Med. 2016;193(10):1161-1167. PubMed 29. Rhee CK, Min KH, Yim NY, et al. Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia. Eur Respir J. 2013;41(2):402-409. PubMed 30. Lazor R, Vandevenne A, Pelletier A, Leclerc P, Court-Fortune I, Cordier JF. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles “Orphelines” Pulmonaires (GERM”O”P). Am J Respir Crit Care Med. 2000;162(2 Pt 1):571-577. PubMed 31. Richeldi L, Costabel U, Selman M, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. New Engl J Med. 2011;365(12):1079-1087. PubMed 32. Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2071-2082. PubMed 33. Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040-1047. PubMed 34. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760-1769. PubMed 35. King TE Jr, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2083-2092. PubMed 36. Saydain G, Islam A, Afessa B, Ryu JH, Scott JP, Peters SG. Outcome of patients with idiopathic pulmonary fibrosis admitted to the intensive care unit. Am J Respir Crit Care Med. 2002;166(6):839-842. PubMed 37. Vianello A, Arcaro G, Battistella L, et al. Noninvasive ventilation in the event of acute respiratory failure in patients with idiopathic pulmonary fibrosis. J Crit Care. 2014;29(4):562-567. PubMed 38. Blivet S, Philit F, Sab JM, et al. Outcome of patients with idiopathic pulmonary fibrosis admitted to the ICU for respiratory failure. Chest. 2001;120(1):209-212. PubMed 39. Mollica C, Paone G, Conti V, et al. Mechanical ventilation in patients with endstage idiopathic pulmonary fibrosis. Respiration. 2010;79(3):209-215. PubMed 40. Orens JB, Estenne M, Arcasoy S, et al. International guidelines for the selection of lung transplant candidates: 2006 update--a consensus report from the Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2006;25(7):745-755. PubMed 41. Hoopes CW, Kukreja J, Golden J, Davenport DL, Diaz-Guzman E, Zwischenberger JB. Extracorporeal membrane oxygenation as a bridge to pulmonary transplantation. J Thorac Cardiovasc Surg. 2013;145(3):862-867; discussion 867-868. PubMed 42. Pulmonary Fibrosis Foundation. http://pulmonaryfibrosis.org/. Accessed August 31, 2016.
References
1. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733-748. PubMed 2. Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis. Clin Chest Med. 2012;33(1):59-68. PubMed 3. Collard HR, Ryerson CJ, Corte TJ, et al. Acute Exacerbation of Idiopathic Pulmonary Fibrosis. An International Working Group Report. Am J Respir Crit Care Med. 2016;194(3):265-275. PubMed 4. King TE Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med. 2001;164(7):1171-1181. PubMed 5. Behr J. Approach to the diagnosis of interstitial lung disease. Clin Chest Med. 2012;33(1):1-10. PubMed 6. Raghu G, Brown KK. Interstitial lung disease: clinical evaluation and keys to an accurate diagnosis. Clin Chest Med. 2004;25(3):409-419. PubMed 7. Bradley B, Branley HM, Egan JJ, et al. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63(suppl 5):v1-v58. PubMed 8. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 1: Cytotoxic drugs. Am Rev Respir Dis. 1986;133(2):321-340. PubMed 9. Cooper JA Jr, White DA, Matthay RA. Drug-induced pulmonary disease. Part 2: Noncytotoxic drugs. Am Rev Respir Dis. 1986;133(3):488-505. PubMed 10. Diffuse Lung Disease Questionnaire for Patients. Available at: https://www.chestnet.org/~/media/chesnetorg/Foundation/Documents/Lung Disease Questionaire.ashx. Accessed August 15, 2016. 11. Pipavath S, Godwin JD. Imaging of interstitial lung disease. Clin Chest Med. 2004;25(3):455-465, v-vi. PubMed 12. Fujimoto K, Taniguchi H, Johkoh T, et al. Acute exacerbation of idiopathic pulmonary fibrosis: high-resolution CT scores predict mortality. Eur Radiol. 2012;22(1):83-92. PubMed 13. Mayo JR. CT evaluation of diffuse infiltrative lung disease: dose considerations and optimal technique. J Thorac Imaging. 2009;24(4):252-259. PubMed 14. Allen JN, Pacht ER, Gadek JE, Davis WB. Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure. New Engl J Med. 1989;321(9):569-574. PubMed 15. Selman M, Pardo A, King TE Jr. Hypersensitivity pneumonitis: insights in diagnosis and pathobiology. Am J Respir Crit Care Med. 2012;186(4):314-324. PubMed 16. Churg A, Schwarz M. Transbronchial biopsy and usual interstitial pneumonia: a new paradigm? Chest. 2006;129(5):1117-1118. PubMed 17. Shim HS, Park MS, Park IK. Histopathologic findings of transbronchial biopsy in usual interstitial pneumonia. Pathol Int. 2010;60(5):373-377. PubMed 18. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788-824. PubMed 19. Carmona EM, Kalra S, Ryu JH. Pulmonary sarcoidosis: diagnosis and treatment. Mayo Clin Proc. 2016;91(7):946-954. PubMed 20. Tomassetti S, Wells AU, Costabel U, et al. Bronchoscopic lung cryobiopsy increases diagnostic confidence in the multidisciplinary diagnosis of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2016;193(7):745-752. PubMed 21. Johannson KA, Marcoux VS, Ronksley PE, Ryerson CJ. Diagnostic yield and complications of transbronchial lung cryobiopsy for interstitial lung disease. A systematic review and metaanalysis. Ann Am Thorac Soc. 2016;13(10):1828-1838. PubMed 22. Patel NM, Borczuk AC, Lederer DJ. Cryobiopsy in the diagnosis of interstitial lung disease. A step forward or back? Am J Respir Crit Care Med. 2016;193(7):707-709. PubMed 23. Rishi Raj M, Kirtee Raparia, MD, David A. Lynch, MD, Kevin K. Brown, MD. Surgical lung biopsy for interstitial lung diseases. Chest. 2016. 24. Kreider ME, Hansen-Flaschen J, Ahmad NN, et al. Complications of video-assisted thoracoscopic lung biopsy in patients with interstitial lung disease. AnnAm Thor Surg. 2007;83(3):1140-1144. PubMed 25. Churg A, Wright JL, Tazelaar HD. Acute exacerbations of fibrotic interstitial lung disease. Histopathology. 2011;58(4):525-530. PubMed 26. Churg A, Muller NL, Silva CI, Wright JL. Acute exacerbation (acute lung injury of unknown cause) in UIP and other forms of fibrotic interstitial pneumonias. Am J Surg Pathol. 2007;31(2):277-284. PubMed 27. Jones KD, Urisman A. Histopathologic approach to the surgical lung biopsy in interstitial lung disease. Clin Chest Med. 2012;33(1):27-40. PubMed 28. Hutchinson JP, Fogarty AW, McKeever TM, Hubbard RB. In-hospital mortality after surgical lung biopsy for interstitial lung disease in the United States. 2000 to 2011. Am J Respir Crit Care Med. 2016;193(10):1161-1167. PubMed 29. Rhee CK, Min KH, Yim NY, et al. Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia. Eur Respir J. 2013;41(2):402-409. PubMed 30. Lazor R, Vandevenne A, Pelletier A, Leclerc P, Court-Fortune I, Cordier JF. Cryptogenic organizing pneumonia. Characteristics of relapses in a series of 48 patients. The Groupe d’Etudes et de Recherche sur les Maladles “Orphelines” Pulmonaires (GERM”O”P). Am J Respir Crit Care Med. 2000;162(2 Pt 1):571-577. PubMed 31. Richeldi L, Costabel U, Selman M, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. New Engl J Med. 2011;365(12):1079-1087. PubMed 32. Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2071-2082. PubMed 33. Azuma A, Nukiwa T, Tsuboi E, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040-1047. PubMed 34. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760-1769. PubMed 35. King TE Jr, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. New Engl J Med. 2014;370(22):2083-2092. PubMed 36. Saydain G, Islam A, Afessa B, Ryu JH, Scott JP, Peters SG. Outcome of patients with idiopathic pulmonary fibrosis admitted to the intensive care unit. Am J Respir Crit Care Med. 2002;166(6):839-842. PubMed 37. Vianello A, Arcaro G, Battistella L, et al. Noninvasive ventilation in the event of acute respiratory failure in patients with idiopathic pulmonary fibrosis. J Crit Care. 2014;29(4):562-567. PubMed 38. Blivet S, Philit F, Sab JM, et al. Outcome of patients with idiopathic pulmonary fibrosis admitted to the ICU for respiratory failure. Chest. 2001;120(1):209-212. PubMed 39. Mollica C, Paone G, Conti V, et al. Mechanical ventilation in patients with endstage idiopathic pulmonary fibrosis. Respiration. 2010;79(3):209-215. PubMed 40. Orens JB, Estenne M, Arcasoy S, et al. International guidelines for the selection of lung transplant candidates: 2006 update--a consensus report from the Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2006;25(7):745-755. PubMed 41. Hoopes CW, Kukreja J, Golden J, Davenport DL, Diaz-Guzman E, Zwischenberger JB. Extracorporeal membrane oxygenation as a bridge to pulmonary transplantation. J Thorac Cardiovasc Surg. 2013;145(3):862-867; discussion 867-868. PubMed 42. Pulmonary Fibrosis Foundation. http://pulmonaryfibrosis.org/. Accessed August 31, 2016.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient’s case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
After losing consciousness at a supermarket, a 70-year-old man was brought to the emergency department by paramedics. He subsequently developed chest pain.
Syncope can be difficult to evaluate, but chest pain may help narrow an otherwise broad differential diagnosis. If this patient has aortic stenosis or hypertrophic cardiomyopathy, effort syncope is the culprit. Cardiac dysrhythmia (eg, ventricular tachycardia), complete heart block, and supraventricular tachycardia each can cause syncope along with chest pain. Myocardial infarction and associated ventricular arrhythmia might also explain both chest pain and syncope. The paramedics might have noted an arrhythmia on the cardiac monitor; if possible, the rhythm strip should be reviewed. A pulmonary embolus can cause chest pain and, if large enough to cause right ventricular compromise, syncope.
According to witnesses at the supermarket, the patient dropped to the ground, lost consciousness, and convulsed for 30 seconds. He had no head trauma, tongue biting, urinary incontinence, or confusion afterward. Electrocardiogram (ECG) performed at the scene showed ST elevations in leads V1 to V3 with ST depressions in the inferior leads. On arrival in the emergency department, the patient described nonradiating substernal chest pressure exacerbated by deep inhalation. The pain did not improve with nitroglycerin. He recalled feeling light-headed before the syncope.
He had not received medical care for 20 years and had no known illnesses other than hypertension. He was not taking any medications. He previously worked as a welder and never smoked tobacco, drank alcohol, or used illicit drugs.The patient’s temperature was 36.4°C. Heart rate was 88 beats per minute, blood pressure 128/72 mm Hg, oxygen saturation 100% on room air, and respiratory rate 22 breaths per minute. The patient had conjunctival pallor. There was a grade 3/6 crescendo-decrescendo systolic murmur loudest at the right upper sternal border without radiation to the carotids. There was no jugular venous distention. Lungs were clear to auscultation bilaterally. There was no peripheral edema, rash, or lymphadenopathy.
Convulsive movements commonly occur during episodes of unconsciousness lasting more than 15 seconds—a phenomenon termed convulsive syncope and often is confused with seizures. These movements are usually clonic jerks of the extremities and trunk and slight twitching of the face, and occasionally tonic extension of the trunk and clenching of the jaw. Absence of tongue biting, urinary incontinence, and confusion in this patient’s case makes seizures less likely.
The distribution of ST segment changes on his ECG are concerning for myocardial infarction in the septal and inferior regions. Right-sided ECG should be performed to assess for right ventricular infarction. Although myocardial ischemia is the primary concern, some features warrant consideration of other etiologies of syncope. First, syncope is an unusual presentation of cardiac ischemia or infarct. The complaint of chest pressure exacerbated by deep inhalation is another atypical feature for myocardial ischemia. Although the patient’s oxygen saturation and heart rate are normal, pulmonary embolism remains a possibility.
The prominent crescendo-decrescendo systolic murmur at the right upper sternal border could indicate aortic stenosis; the carotids should be palpated to assess for pulsus parvus et tardus. A high-flow state associated with anemia could also lead to a midsystolic murmur. Conjunctival pallor typically is seen with hemoglobin levels of 6 g/dL or less. This finding may indicate severe anemia, which has the potential to cause myocardial ischemia and syncope.
Laboratory testing revealed a troponin of 0.04 ng/dL, hemoglobin 4.1 g/dL with MCV of 84.7 fL, white blood cell count 6,500/μL and platelet count 179,000/μL. Serum sodium was 130 mEq/L, urea nitrogen 16 mg/dL, creatinine 1.6 mg/dL, calcium 7.8 mg/dL, total protein 11.4 g/dL (reference range, 6.0-8.2), and albumin 2.2 g/dL. Erythrocyte sedimentation rate (ESR) was 20 mm/h. Serum iron was 48 μg/mL, total iron binding capacity 275 μg/dL, percent iron saturation 17% (reference range, 20-55), and ferritin 10 ng/mL (reference range, 30-400). The international normalized ratio (INR) was 1.5, prothrombin time 15.5 sec (reference range, 9.4-11.6), and partial thromboplastin time 24.7 sec (reference range, 22.9-30.6). Hepatitis C and HIV antibodies were negative as was the urine toxicology screen. Urine protein to creatinine ratio was 0.07. His hemoglobinrose to 7.9 g/dL with transfusion of 4 units packed red blood cells (RBC). His chest pain improved and inferior ST depressions resolved on follow-up ECG. Further history revealed multiple episodes of melena and hematochezia in the preceding weeks without nausea, vomiting, or abdominal pain.
The patient has a strikingly large gamma gap: 9.2. A gap larger than 4 is concerning for the presence of paraproteins. Given the possibility of a paraproteinemia (eg, multiple myeloma, plasmacytoma, Waldenström macroglobulinemia), the first step is to check serum and urine protein electrophoresis. The patient’s anemia is significant and reticulocyte index low. The low ferritin level combined with the inappropriately low reticulocyte count could result from iron deficiency anemia, another bone marrow process, or both. The patient’s syncope likely resulted from severe anemia and hypovolemia associated with hematochezia. The prolonged prothrombin time could be caused by a coagulation factor production problem, from vitamin K deficiency or underlying liver disease, or by a consumptive problem, from low-grade disseminated intravascular coagulation. It is controversial whether inhaling welding fumes causes cancer, but the patient’s age alone makes malignancy a definite possibility.
Figure 1The patient was admitted to the progressive care unit with a plan for urgent endoscopy with cardiac anesthesia. Troponin level peaked at 0.84 ng/dL 10 hours after admission. Transthoracic echocardiogram revealed ejection fraction 40% with pseudo-normal filling pattern, right ventricular systolic blood pressure 60 to 65 mm Hg, and echodense material with overlying spontaneous echo contrast leading into the right atrium (a concern for thrombus or tumor); diffuse sclerosis and mild stenosis of the aortic valve were seen with mild to moderate tricuspid regurgitation. Intravenous-contrast computed tomography (CT) of chest, abdomen, and pelvis showed descending and sigmoid colon diverticulosis and an area of circumferential wall thickening of the rectum and anus with adjacent perirectal lymph nodes and inflammatory stranding. There was no evidence of pulmonary embolism.
Aortic stenosis is intriguing in light of the patient’s painless melena and hematochezia. Heyde syndrome is a phenomenon in which high shear stress causes a reduction in the size of von Willebrand factor predisposing to bleeding from submucosal angiodysplasia. However, Heyde syndrome has been reported to occur in the setting of severe or critical aortic stenosis and is unlikely to be the cause here. The patient needs to be examined with both upper and lower endoscopy to rule out gastrointestinal (GI) malignancy, gastric and esophageal varices, and painless peptic ulcers. High right ventricular systolic blood pressures along with echodense material in the inferior vena cava and right atrium suggest the possibility of malignancy with vascular invasion. Tricuspid regurgitation is consistent with high right-sided pressures. As left ventricular ejection fraction is reduced, some of the high right-sided pressures could also be attributable to left heart failure. CT findings of rectal wall thickening and perirectal lymph nodes could be attributable to cancer with locally metastatic disease. Blood loss caused by this cancer would explain the severe anemia on admission as well as the low ferritin level and the iron deficiency anemia. In this 70-year-old man who has not had routine health care maintenance, the leading diagnosis is colorectal cancer. However, the markedly elevated globulin gap and elevated INR strongly suggest another process (eg, multiple myeloma, other paraproteinemia) is also present.
INR remained elevated (1.5) despite vitamin K supplementation. Peripheral blood smear showed hypochromic and normocytic RBCs with moderate rouleaux formation (Figure 1). Intravenous pantoprazole and octreotide were started. Upper and lower endoscopy revealed multiple esophageal erosions and both a polypoid mass and an ulcer within the rectum with evidence of prior bleeding. The mass was resected and the ulcer biopsied.
Figure 2
On hospital day 3, the patient was transfused another unit of packed RBCs. Hemoglobin level increased from 7.4 g/dL to 8.2 g/dL, but he began to complain of headache, blurred vision, and worsened chest pain. He did not have weakness, numbness, diplopia, dysphagia, or dysarthria. External examination and extraocular movements of both eyes were normal. Visual acuity was 20/25 bilaterally. Funduscopic examination revealed mild dilation of retinal veins and retinal hemorrhages (Figure 2).
Rouleaux formation occurs as excess cathodal proteins, such as immunoglobulins or fibrinogen, adhere to RBCs and cause the cells to stack together in long chains. Classically this is associated with multiple myeloma, but can occur with Waldenström’s macroglobulinemia and other cancers or infections. It can also occur as an artifact in smear preparation but the large globulin gap in this patient supports pathologic rouleaux formation.
Venous retinopathy with hemorrhages may occur with occlusion of the arterial supply (eg, as with carotid artery obstruction) but also with hyperviscosity syndrome (HVS). Vascular disturbances throughout the body play a major role in HVS, but these changes are most easily visualized in the retina. It is interesting that the patient’s headache and blurred vision began after he received additional blood transfusions. Spuriously low hemoglobin and hematocrit levels may stem from increased plasma volume from high immunoglobulin M (IgM) concentrations in Waldenström macroglobulinemia; thus, RBC transfusions can exacerbate symptoms by elevating total RBC mass. Normocytic, normochromic anemia is characteristic of both multiple myeloma and Waldenström’s macroglobulinemia. That the patient’s chest pain recurred coincidentally with blurred vision and headache suggests the likely cause is cardiac ischemia from hyperviscosity. The serum viscosity level should be checked, and, if it is elevated, urgent serum plasmapheresis should be considered. Determining the source of excess globulin production and treating the underlying disease are crucial at this juncture.
In the general population, rectal adenocarcinoma is the most common cause of a rectal mass. In this patient, presence of a paraproteinemia may point to a different diagnosis. Extramedullary colorectal plasmacytoma can occur in the rectum but is exceedingly rare. Waldenström’s macroglobulinemia, a subtype of lymphoplasmacytic lymphoma, can be associated with a rectal lymphoma. At this point, it is not possible to confidently predict the etiology of the mass.
Figure 3Plasma viscosity was elevated at 4.0 (reference range, 1.6-1.9). Serum protein electrophoresis revealed an M-spike of 6.4 g/dL corresponding to IgG on immunofixation. The kappa/lambda light chain ratio was 2.2 with normal urine protein electrophoresis. Bone marrow core biopsy demonstrated 60 to 70% plasma cells (Figure 3) with aspirate flow cytometry showing 3% phenotypically abnormal monoclonal plasma cells that were kappa positive. Skeletal survey revealed possible small lytic lesions in right scapula and proximal humeri bilaterally. Hematoxylin and eosin stain of rectal ulcer was highly suggestive of amyloidosis. Pathology of the polypoid mass was consistent with at least high-grade dysplasia arising in a tubular adenoma. The initial colonoscopy was limited by poor colonic preparation. A sigmoidoscopy with biopsy 6 weeks later revealed a 4 cm rectal mass, which pathology showed moderately to poorly infiltrating adenocarcinoma with necrosis (clinical stage T3N1).
He was started on cyclophosphamide, bortezomib and dexamethasone for IgG κ myeloma with improvement in his headache, blurred vision, chest pain, and plasma viscosity (4 to 1.8). His hemoglobin remained stable at 10 g/dL. Neoadjuvant Capecitabine and radiation therapy were initiated for his rectal cancer.
DISCUSSION
Multiple myeloma is characterized by monoclonal proliferation of plasma cells, elevated circulating monoclonal immunoglobulin, and end-organ damage.1 It accounts for approximately 0.8% of all new cancer diagnoses; average age at onset is 70 years. The patient described here had an unusual presentation, with GI bleeding and progression to HVS, and known risk factors for multiple myeloma (male sex, low socioeconomic status, welding career).2,3
An early clue in the diagnosis was the patient’s large gamma gap and concurrent anemia. Gamma gap, calculated by subtracting serum albumin from serum total protein, is so named because it often reflects an elevated gamma globulin concentration. However, it actually reflects all nonalbumin serum protein. A gamma gap larger than 3.1 g/dL is an independent risk factor for death4 and may be associated with infection, autoimmunity, and malignancy. Although there are no screening guidelines for multiple myeloma, 73% of cases are brought to attention by anemia discovered on routine laboratory investigation.5 This patient’s lack of prior medical care likely contributed to his atypical presentation. Screening colonoscopy, recommended at age 50, might have identified his rectal cancer at an earlier stage.
The patient’s anemia was likely secondary to GI hemorrhage and bone marrow suppression. His hematochezia might have been partly related to the pathophysiologic interaction of paraproteins with platelets, coagulation factors, and blood vessels.6 Amyloidosis of the GI tract is seen in 8% of AL amyloidosis7 and most frequently manifests as gastrointestinal bleeding, which is thought to be due to ischemia, vascular friability, or mucosal lesions. It less commonly presents as malabsorption or dysmotility.8 Although gastrointestinal amyloid is not typically associated with radiologic abnormalities, occasionally it may cause luminal wall thickening, adenopathy, and inflammatory stranding.9 The gold standard for diagnosis is tissue biopsy. However, presence of amyloidosis does not change the overall treatment strategy for multiple myeloma.
An interesting feature of this case is the development of HVS, which typically manifests with mucosal bleeding, blurred vision, and headache.10 HVS can be diagnosed on retinal examination with findings of venous tortuosity, dilatation, and intraretinal hemorrhage, as occurred in this case,11 and is confirmed with serum viscosity measurement. The first evidence of HVS in this case might have been the spontaneous echo contrast, or “smoke,” detected on echocardiogram. Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates,12 and is associated with conditions that result in left atrial stasis, such as atrial arrhythmias and mitral stenosis. This patient did not have valvular pathology or arrhythmia, and thus the “smoke” likely reflected HVS.
Of the paraproteinemias, Waldenström’s macroglobulinemia is most often associated with HVS, likely because of the pentameric structure of IgM13 and the consequential large size that predisposes to vascular occlusion. Whereas HVS can occur with IgM levels as low as 3 g/dL, it typically does not occur with IgG concentrations under 15 g/dL. This patient presented with an IgG level of 8 g/dL and developed HVS symptoms only after multiple packed RBC transfusions. Elevated IgG level likely made him susceptible to HVS, which ultimately was precipitated by blood transfusion. Therefore, this patient’s initial chest pain most likely was caused by demand cardiac ischemia secondary to anemia, whereas his subsequent, posttransfusion chest pain likely resulted from hyperviscosity angina. Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—has been described in polycythemia and connective tissue disorders.14,15 To our knowledge, however, hyperviscosity angina has not been reported in patients with multiple myeloma. Treatment of hyperviscosity with end-organ damage typically consists of plasmapheresis, but this patient was started on urgent chemotherapy, and his symptoms improved. Untreated HVS can lead to end-organ ischemia and death.
This patient had a multitude of seemingly disparate symptoms and abnormalities that ultimately were united in a diagnosis of IgG κ multiple myeloma. Subsequently diagnosed rectal adenocarcinoma may have led to ongoing blood loss, which worsened the anemia, but had no evident relation to the primary diagnosis of multiple myeloma. This case exemplifies the fact that HVS is a rare but important iatrogenic complication of multiple myeloma treated with blood transfusion. As this patient’s hospital course progressed, the plot, and his blood, thickened.
KEY TEACHING POINTS
Multiple myeloma is occasionally associated with HVS, which manifests with mucosal bleeding, blurred vision, and headache.
Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—should be considered in patients with paraproteinemias and chest pain.
Plasmapheresis reverses the clinical manifestations of HVS but not the underlying disease process (eg, Waldenström’s macroglobulinemia, multiple myeloma, leukemia, polycythemia).
Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates, and is associated with left atrial stasis, commonly from atrial fibrillation or mitral stenosis, but might be present in HVS.
Acknowledgment
The authors thank Peter Campochiaro, MD, and Whitney Green, MD, for their contributions to the images used in this article.
Disclosure
Dr. Sedighi Manesh is supported by the Jeremiah A. Barondess Fellowship in the Clinical Transaction of the New York Academy of Medicine, in collaboration with the Accreditation Council for Graduate Medical Education (ACGME). The other authors have nothing to report.
References
1. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046-1060. PubMed 2. Koessel SL, Theis MK, Vaughan TL, et al. Socioeconomic status and the incidence of multiple myeloma. Epidemiology. 1996;7(1):4-8. PubMed 3. Fritschi L, Siemiatycki J. Lymphoma, myeloma and occupation: results of a case-control study. Int J Cancer. 1996;67(4):498-503. PubMed 4. Juraschek SP, Moliterno AR, Checkley W, Miller ER 3rd. The gamma gap and all-cause mortality. PLoS One. 2015;10(12):e0143494. PubMed 5. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. PubMed 6. Eby CS. Bleeding and thrombosis risks in plasma cell dyscrasias. Hematology Am Soc Hematol Educ Program. 2007:158-164. PubMed 7. Menke DM, Kyle RA, Fleming CR, Wolfe JT 3rd, Kurtin PJ, Oldenburg WA. Symptomatic gastric amyloidosis in patients with primary systemic amyloidosis. Mayo Clin Proc. 1993;68(8):763-767. PubMed 8. Levy DJ, Franklin GO, Rosenthal WS. Gastrointestinal bleeding and amyloidosis. Am J Gastroenterol. 1982;77(6):422-426. PubMed 9. Araoz PA, Batts KP, MacCarty RL. Amyloidosis of the alimentary canal: radiologic-pathologic correlation of CT findings. Abdom Imaging. 2000;25(1):38-44. PubMed 10. Stone MJ, Bogen SA. Evidence-based focused review of management of hyperviscosity syndrome. Blood. 2012;119(10):2205-2208. PubMed 11. Rajagopal R, Apte RS. Seeing through thick and through thin: retinal manifestations of thrombophilic and hyperviscosity syndromes. Surv Ophthalmol. 2016;61(2):236-247. PubMed 12. Black IW. Spontaneous echo contrast: where there’s smoke there’s fire. Echocardiography. 2000;17(4):373-382. PubMed 13. Kwaan HC. Hyperviscosity in plasma cell dyscrasias. Clin Hemorheol Microcirc. 2013;55(1):75-83. PubMed 14. Piccirillo G, Fimognari FL, Valdivia JL, Marigliano V. Effects of phlebotomy on a patient with secondary polycythemia and angina pectoris. Int J Cardiol. 1994;44(2):175-177. PubMed 15. Ovadia S, Lysyy L, Floru S. Emergency plasmapheresis for unstable angina in a patient with hyperviscosity syndrome. Am J Emerg Med. 2005;23(6):811-812. PubMed
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient’s case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
After losing consciousness at a supermarket, a 70-year-old man was brought to the emergency department by paramedics. He subsequently developed chest pain.
Syncope can be difficult to evaluate, but chest pain may help narrow an otherwise broad differential diagnosis. If this patient has aortic stenosis or hypertrophic cardiomyopathy, effort syncope is the culprit. Cardiac dysrhythmia (eg, ventricular tachycardia), complete heart block, and supraventricular tachycardia each can cause syncope along with chest pain. Myocardial infarction and associated ventricular arrhythmia might also explain both chest pain and syncope. The paramedics might have noted an arrhythmia on the cardiac monitor; if possible, the rhythm strip should be reviewed. A pulmonary embolus can cause chest pain and, if large enough to cause right ventricular compromise, syncope.
According to witnesses at the supermarket, the patient dropped to the ground, lost consciousness, and convulsed for 30 seconds. He had no head trauma, tongue biting, urinary incontinence, or confusion afterward. Electrocardiogram (ECG) performed at the scene showed ST elevations in leads V1 to V3 with ST depressions in the inferior leads. On arrival in the emergency department, the patient described nonradiating substernal chest pressure exacerbated by deep inhalation. The pain did not improve with nitroglycerin. He recalled feeling light-headed before the syncope.
He had not received medical care for 20 years and had no known illnesses other than hypertension. He was not taking any medications. He previously worked as a welder and never smoked tobacco, drank alcohol, or used illicit drugs.The patient’s temperature was 36.4°C. Heart rate was 88 beats per minute, blood pressure 128/72 mm Hg, oxygen saturation 100% on room air, and respiratory rate 22 breaths per minute. The patient had conjunctival pallor. There was a grade 3/6 crescendo-decrescendo systolic murmur loudest at the right upper sternal border without radiation to the carotids. There was no jugular venous distention. Lungs were clear to auscultation bilaterally. There was no peripheral edema, rash, or lymphadenopathy.
Convulsive movements commonly occur during episodes of unconsciousness lasting more than 15 seconds—a phenomenon termed convulsive syncope and often is confused with seizures. These movements are usually clonic jerks of the extremities and trunk and slight twitching of the face, and occasionally tonic extension of the trunk and clenching of the jaw. Absence of tongue biting, urinary incontinence, and confusion in this patient’s case makes seizures less likely.
The distribution of ST segment changes on his ECG are concerning for myocardial infarction in the septal and inferior regions. Right-sided ECG should be performed to assess for right ventricular infarction. Although myocardial ischemia is the primary concern, some features warrant consideration of other etiologies of syncope. First, syncope is an unusual presentation of cardiac ischemia or infarct. The complaint of chest pressure exacerbated by deep inhalation is another atypical feature for myocardial ischemia. Although the patient’s oxygen saturation and heart rate are normal, pulmonary embolism remains a possibility.
The prominent crescendo-decrescendo systolic murmur at the right upper sternal border could indicate aortic stenosis; the carotids should be palpated to assess for pulsus parvus et tardus. A high-flow state associated with anemia could also lead to a midsystolic murmur. Conjunctival pallor typically is seen with hemoglobin levels of 6 g/dL or less. This finding may indicate severe anemia, which has the potential to cause myocardial ischemia and syncope.
Laboratory testing revealed a troponin of 0.04 ng/dL, hemoglobin 4.1 g/dL with MCV of 84.7 fL, white blood cell count 6,500/μL and platelet count 179,000/μL. Serum sodium was 130 mEq/L, urea nitrogen 16 mg/dL, creatinine 1.6 mg/dL, calcium 7.8 mg/dL, total protein 11.4 g/dL (reference range, 6.0-8.2), and albumin 2.2 g/dL. Erythrocyte sedimentation rate (ESR) was 20 mm/h. Serum iron was 48 μg/mL, total iron binding capacity 275 μg/dL, percent iron saturation 17% (reference range, 20-55), and ferritin 10 ng/mL (reference range, 30-400). The international normalized ratio (INR) was 1.5, prothrombin time 15.5 sec (reference range, 9.4-11.6), and partial thromboplastin time 24.7 sec (reference range, 22.9-30.6). Hepatitis C and HIV antibodies were negative as was the urine toxicology screen. Urine protein to creatinine ratio was 0.07. His hemoglobinrose to 7.9 g/dL with transfusion of 4 units packed red blood cells (RBC). His chest pain improved and inferior ST depressions resolved on follow-up ECG. Further history revealed multiple episodes of melena and hematochezia in the preceding weeks without nausea, vomiting, or abdominal pain.
The patient has a strikingly large gamma gap: 9.2. A gap larger than 4 is concerning for the presence of paraproteins. Given the possibility of a paraproteinemia (eg, multiple myeloma, plasmacytoma, Waldenström macroglobulinemia), the first step is to check serum and urine protein electrophoresis. The patient’s anemia is significant and reticulocyte index low. The low ferritin level combined with the inappropriately low reticulocyte count could result from iron deficiency anemia, another bone marrow process, or both. The patient’s syncope likely resulted from severe anemia and hypovolemia associated with hematochezia. The prolonged prothrombin time could be caused by a coagulation factor production problem, from vitamin K deficiency or underlying liver disease, or by a consumptive problem, from low-grade disseminated intravascular coagulation. It is controversial whether inhaling welding fumes causes cancer, but the patient’s age alone makes malignancy a definite possibility.
Figure 1The patient was admitted to the progressive care unit with a plan for urgent endoscopy with cardiac anesthesia. Troponin level peaked at 0.84 ng/dL 10 hours after admission. Transthoracic echocardiogram revealed ejection fraction 40% with pseudo-normal filling pattern, right ventricular systolic blood pressure 60 to 65 mm Hg, and echodense material with overlying spontaneous echo contrast leading into the right atrium (a concern for thrombus or tumor); diffuse sclerosis and mild stenosis of the aortic valve were seen with mild to moderate tricuspid regurgitation. Intravenous-contrast computed tomography (CT) of chest, abdomen, and pelvis showed descending and sigmoid colon diverticulosis and an area of circumferential wall thickening of the rectum and anus with adjacent perirectal lymph nodes and inflammatory stranding. There was no evidence of pulmonary embolism.
Aortic stenosis is intriguing in light of the patient’s painless melena and hematochezia. Heyde syndrome is a phenomenon in which high shear stress causes a reduction in the size of von Willebrand factor predisposing to bleeding from submucosal angiodysplasia. However, Heyde syndrome has been reported to occur in the setting of severe or critical aortic stenosis and is unlikely to be the cause here. The patient needs to be examined with both upper and lower endoscopy to rule out gastrointestinal (GI) malignancy, gastric and esophageal varices, and painless peptic ulcers. High right ventricular systolic blood pressures along with echodense material in the inferior vena cava and right atrium suggest the possibility of malignancy with vascular invasion. Tricuspid regurgitation is consistent with high right-sided pressures. As left ventricular ejection fraction is reduced, some of the high right-sided pressures could also be attributable to left heart failure. CT findings of rectal wall thickening and perirectal lymph nodes could be attributable to cancer with locally metastatic disease. Blood loss caused by this cancer would explain the severe anemia on admission as well as the low ferritin level and the iron deficiency anemia. In this 70-year-old man who has not had routine health care maintenance, the leading diagnosis is colorectal cancer. However, the markedly elevated globulin gap and elevated INR strongly suggest another process (eg, multiple myeloma, other paraproteinemia) is also present.
INR remained elevated (1.5) despite vitamin K supplementation. Peripheral blood smear showed hypochromic and normocytic RBCs with moderate rouleaux formation (Figure 1). Intravenous pantoprazole and octreotide were started. Upper and lower endoscopy revealed multiple esophageal erosions and both a polypoid mass and an ulcer within the rectum with evidence of prior bleeding. The mass was resected and the ulcer biopsied.
Figure 2
On hospital day 3, the patient was transfused another unit of packed RBCs. Hemoglobin level increased from 7.4 g/dL to 8.2 g/dL, but he began to complain of headache, blurred vision, and worsened chest pain. He did not have weakness, numbness, diplopia, dysphagia, or dysarthria. External examination and extraocular movements of both eyes were normal. Visual acuity was 20/25 bilaterally. Funduscopic examination revealed mild dilation of retinal veins and retinal hemorrhages (Figure 2).
Rouleaux formation occurs as excess cathodal proteins, such as immunoglobulins or fibrinogen, adhere to RBCs and cause the cells to stack together in long chains. Classically this is associated with multiple myeloma, but can occur with Waldenström’s macroglobulinemia and other cancers or infections. It can also occur as an artifact in smear preparation but the large globulin gap in this patient supports pathologic rouleaux formation.
Venous retinopathy with hemorrhages may occur with occlusion of the arterial supply (eg, as with carotid artery obstruction) but also with hyperviscosity syndrome (HVS). Vascular disturbances throughout the body play a major role in HVS, but these changes are most easily visualized in the retina. It is interesting that the patient’s headache and blurred vision began after he received additional blood transfusions. Spuriously low hemoglobin and hematocrit levels may stem from increased plasma volume from high immunoglobulin M (IgM) concentrations in Waldenström macroglobulinemia; thus, RBC transfusions can exacerbate symptoms by elevating total RBC mass. Normocytic, normochromic anemia is characteristic of both multiple myeloma and Waldenström’s macroglobulinemia. That the patient’s chest pain recurred coincidentally with blurred vision and headache suggests the likely cause is cardiac ischemia from hyperviscosity. The serum viscosity level should be checked, and, if it is elevated, urgent serum plasmapheresis should be considered. Determining the source of excess globulin production and treating the underlying disease are crucial at this juncture.
In the general population, rectal adenocarcinoma is the most common cause of a rectal mass. In this patient, presence of a paraproteinemia may point to a different diagnosis. Extramedullary colorectal plasmacytoma can occur in the rectum but is exceedingly rare. Waldenström’s macroglobulinemia, a subtype of lymphoplasmacytic lymphoma, can be associated with a rectal lymphoma. At this point, it is not possible to confidently predict the etiology of the mass.
Figure 3Plasma viscosity was elevated at 4.0 (reference range, 1.6-1.9). Serum protein electrophoresis revealed an M-spike of 6.4 g/dL corresponding to IgG on immunofixation. The kappa/lambda light chain ratio was 2.2 with normal urine protein electrophoresis. Bone marrow core biopsy demonstrated 60 to 70% plasma cells (Figure 3) with aspirate flow cytometry showing 3% phenotypically abnormal monoclonal plasma cells that were kappa positive. Skeletal survey revealed possible small lytic lesions in right scapula and proximal humeri bilaterally. Hematoxylin and eosin stain of rectal ulcer was highly suggestive of amyloidosis. Pathology of the polypoid mass was consistent with at least high-grade dysplasia arising in a tubular adenoma. The initial colonoscopy was limited by poor colonic preparation. A sigmoidoscopy with biopsy 6 weeks later revealed a 4 cm rectal mass, which pathology showed moderately to poorly infiltrating adenocarcinoma with necrosis (clinical stage T3N1).
He was started on cyclophosphamide, bortezomib and dexamethasone for IgG κ myeloma with improvement in his headache, blurred vision, chest pain, and plasma viscosity (4 to 1.8). His hemoglobin remained stable at 10 g/dL. Neoadjuvant Capecitabine and radiation therapy were initiated for his rectal cancer.
DISCUSSION
Multiple myeloma is characterized by monoclonal proliferation of plasma cells, elevated circulating monoclonal immunoglobulin, and end-organ damage.1 It accounts for approximately 0.8% of all new cancer diagnoses; average age at onset is 70 years. The patient described here had an unusual presentation, with GI bleeding and progression to HVS, and known risk factors for multiple myeloma (male sex, low socioeconomic status, welding career).2,3
An early clue in the diagnosis was the patient’s large gamma gap and concurrent anemia. Gamma gap, calculated by subtracting serum albumin from serum total protein, is so named because it often reflects an elevated gamma globulin concentration. However, it actually reflects all nonalbumin serum protein. A gamma gap larger than 3.1 g/dL is an independent risk factor for death4 and may be associated with infection, autoimmunity, and malignancy. Although there are no screening guidelines for multiple myeloma, 73% of cases are brought to attention by anemia discovered on routine laboratory investigation.5 This patient’s lack of prior medical care likely contributed to his atypical presentation. Screening colonoscopy, recommended at age 50, might have identified his rectal cancer at an earlier stage.
The patient’s anemia was likely secondary to GI hemorrhage and bone marrow suppression. His hematochezia might have been partly related to the pathophysiologic interaction of paraproteins with platelets, coagulation factors, and blood vessels.6 Amyloidosis of the GI tract is seen in 8% of AL amyloidosis7 and most frequently manifests as gastrointestinal bleeding, which is thought to be due to ischemia, vascular friability, or mucosal lesions. It less commonly presents as malabsorption or dysmotility.8 Although gastrointestinal amyloid is not typically associated with radiologic abnormalities, occasionally it may cause luminal wall thickening, adenopathy, and inflammatory stranding.9 The gold standard for diagnosis is tissue biopsy. However, presence of amyloidosis does not change the overall treatment strategy for multiple myeloma.
An interesting feature of this case is the development of HVS, which typically manifests with mucosal bleeding, blurred vision, and headache.10 HVS can be diagnosed on retinal examination with findings of venous tortuosity, dilatation, and intraretinal hemorrhage, as occurred in this case,11 and is confirmed with serum viscosity measurement. The first evidence of HVS in this case might have been the spontaneous echo contrast, or “smoke,” detected on echocardiogram. Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates,12 and is associated with conditions that result in left atrial stasis, such as atrial arrhythmias and mitral stenosis. This patient did not have valvular pathology or arrhythmia, and thus the “smoke” likely reflected HVS.
Of the paraproteinemias, Waldenström’s macroglobulinemia is most often associated with HVS, likely because of the pentameric structure of IgM13 and the consequential large size that predisposes to vascular occlusion. Whereas HVS can occur with IgM levels as low as 3 g/dL, it typically does not occur with IgG concentrations under 15 g/dL. This patient presented with an IgG level of 8 g/dL and developed HVS symptoms only after multiple packed RBC transfusions. Elevated IgG level likely made him susceptible to HVS, which ultimately was precipitated by blood transfusion. Therefore, this patient’s initial chest pain most likely was caused by demand cardiac ischemia secondary to anemia, whereas his subsequent, posttransfusion chest pain likely resulted from hyperviscosity angina. Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—has been described in polycythemia and connective tissue disorders.14,15 To our knowledge, however, hyperviscosity angina has not been reported in patients with multiple myeloma. Treatment of hyperviscosity with end-organ damage typically consists of plasmapheresis, but this patient was started on urgent chemotherapy, and his symptoms improved. Untreated HVS can lead to end-organ ischemia and death.
This patient had a multitude of seemingly disparate symptoms and abnormalities that ultimately were united in a diagnosis of IgG κ multiple myeloma. Subsequently diagnosed rectal adenocarcinoma may have led to ongoing blood loss, which worsened the anemia, but had no evident relation to the primary diagnosis of multiple myeloma. This case exemplifies the fact that HVS is a rare but important iatrogenic complication of multiple myeloma treated with blood transfusion. As this patient’s hospital course progressed, the plot, and his blood, thickened.
KEY TEACHING POINTS
Multiple myeloma is occasionally associated with HVS, which manifests with mucosal bleeding, blurred vision, and headache.
Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—should be considered in patients with paraproteinemias and chest pain.
Plasmapheresis reverses the clinical manifestations of HVS but not the underlying disease process (eg, Waldenström’s macroglobulinemia, multiple myeloma, leukemia, polycythemia).
Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates, and is associated with left atrial stasis, commonly from atrial fibrillation or mitral stenosis, but might be present in HVS.
Acknowledgment
The authors thank Peter Campochiaro, MD, and Whitney Green, MD, for their contributions to the images used in this article.
Disclosure
Dr. Sedighi Manesh is supported by the Jeremiah A. Barondess Fellowship in the Clinical Transaction of the New York Academy of Medicine, in collaboration with the Accreditation Council for Graduate Medical Education (ACGME). The other authors have nothing to report.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient’s case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
After losing consciousness at a supermarket, a 70-year-old man was brought to the emergency department by paramedics. He subsequently developed chest pain.
Syncope can be difficult to evaluate, but chest pain may help narrow an otherwise broad differential diagnosis. If this patient has aortic stenosis or hypertrophic cardiomyopathy, effort syncope is the culprit. Cardiac dysrhythmia (eg, ventricular tachycardia), complete heart block, and supraventricular tachycardia each can cause syncope along with chest pain. Myocardial infarction and associated ventricular arrhythmia might also explain both chest pain and syncope. The paramedics might have noted an arrhythmia on the cardiac monitor; if possible, the rhythm strip should be reviewed. A pulmonary embolus can cause chest pain and, if large enough to cause right ventricular compromise, syncope.
According to witnesses at the supermarket, the patient dropped to the ground, lost consciousness, and convulsed for 30 seconds. He had no head trauma, tongue biting, urinary incontinence, or confusion afterward. Electrocardiogram (ECG) performed at the scene showed ST elevations in leads V1 to V3 with ST depressions in the inferior leads. On arrival in the emergency department, the patient described nonradiating substernal chest pressure exacerbated by deep inhalation. The pain did not improve with nitroglycerin. He recalled feeling light-headed before the syncope.
He had not received medical care for 20 years and had no known illnesses other than hypertension. He was not taking any medications. He previously worked as a welder and never smoked tobacco, drank alcohol, or used illicit drugs.The patient’s temperature was 36.4°C. Heart rate was 88 beats per minute, blood pressure 128/72 mm Hg, oxygen saturation 100% on room air, and respiratory rate 22 breaths per minute. The patient had conjunctival pallor. There was a grade 3/6 crescendo-decrescendo systolic murmur loudest at the right upper sternal border without radiation to the carotids. There was no jugular venous distention. Lungs were clear to auscultation bilaterally. There was no peripheral edema, rash, or lymphadenopathy.
Convulsive movements commonly occur during episodes of unconsciousness lasting more than 15 seconds—a phenomenon termed convulsive syncope and often is confused with seizures. These movements are usually clonic jerks of the extremities and trunk and slight twitching of the face, and occasionally tonic extension of the trunk and clenching of the jaw. Absence of tongue biting, urinary incontinence, and confusion in this patient’s case makes seizures less likely.
The distribution of ST segment changes on his ECG are concerning for myocardial infarction in the septal and inferior regions. Right-sided ECG should be performed to assess for right ventricular infarction. Although myocardial ischemia is the primary concern, some features warrant consideration of other etiologies of syncope. First, syncope is an unusual presentation of cardiac ischemia or infarct. The complaint of chest pressure exacerbated by deep inhalation is another atypical feature for myocardial ischemia. Although the patient’s oxygen saturation and heart rate are normal, pulmonary embolism remains a possibility.
The prominent crescendo-decrescendo systolic murmur at the right upper sternal border could indicate aortic stenosis; the carotids should be palpated to assess for pulsus parvus et tardus. A high-flow state associated with anemia could also lead to a midsystolic murmur. Conjunctival pallor typically is seen with hemoglobin levels of 6 g/dL or less. This finding may indicate severe anemia, which has the potential to cause myocardial ischemia and syncope.
Laboratory testing revealed a troponin of 0.04 ng/dL, hemoglobin 4.1 g/dL with MCV of 84.7 fL, white blood cell count 6,500/μL and platelet count 179,000/μL. Serum sodium was 130 mEq/L, urea nitrogen 16 mg/dL, creatinine 1.6 mg/dL, calcium 7.8 mg/dL, total protein 11.4 g/dL (reference range, 6.0-8.2), and albumin 2.2 g/dL. Erythrocyte sedimentation rate (ESR) was 20 mm/h. Serum iron was 48 μg/mL, total iron binding capacity 275 μg/dL, percent iron saturation 17% (reference range, 20-55), and ferritin 10 ng/mL (reference range, 30-400). The international normalized ratio (INR) was 1.5, prothrombin time 15.5 sec (reference range, 9.4-11.6), and partial thromboplastin time 24.7 sec (reference range, 22.9-30.6). Hepatitis C and HIV antibodies were negative as was the urine toxicology screen. Urine protein to creatinine ratio was 0.07. His hemoglobinrose to 7.9 g/dL with transfusion of 4 units packed red blood cells (RBC). His chest pain improved and inferior ST depressions resolved on follow-up ECG. Further history revealed multiple episodes of melena and hematochezia in the preceding weeks without nausea, vomiting, or abdominal pain.
The patient has a strikingly large gamma gap: 9.2. A gap larger than 4 is concerning for the presence of paraproteins. Given the possibility of a paraproteinemia (eg, multiple myeloma, plasmacytoma, Waldenström macroglobulinemia), the first step is to check serum and urine protein electrophoresis. The patient’s anemia is significant and reticulocyte index low. The low ferritin level combined with the inappropriately low reticulocyte count could result from iron deficiency anemia, another bone marrow process, or both. The patient’s syncope likely resulted from severe anemia and hypovolemia associated with hematochezia. The prolonged prothrombin time could be caused by a coagulation factor production problem, from vitamin K deficiency or underlying liver disease, or by a consumptive problem, from low-grade disseminated intravascular coagulation. It is controversial whether inhaling welding fumes causes cancer, but the patient’s age alone makes malignancy a definite possibility.
Figure 1The patient was admitted to the progressive care unit with a plan for urgent endoscopy with cardiac anesthesia. Troponin level peaked at 0.84 ng/dL 10 hours after admission. Transthoracic echocardiogram revealed ejection fraction 40% with pseudo-normal filling pattern, right ventricular systolic blood pressure 60 to 65 mm Hg, and echodense material with overlying spontaneous echo contrast leading into the right atrium (a concern for thrombus or tumor); diffuse sclerosis and mild stenosis of the aortic valve were seen with mild to moderate tricuspid regurgitation. Intravenous-contrast computed tomography (CT) of chest, abdomen, and pelvis showed descending and sigmoid colon diverticulosis and an area of circumferential wall thickening of the rectum and anus with adjacent perirectal lymph nodes and inflammatory stranding. There was no evidence of pulmonary embolism.
Aortic stenosis is intriguing in light of the patient’s painless melena and hematochezia. Heyde syndrome is a phenomenon in which high shear stress causes a reduction in the size of von Willebrand factor predisposing to bleeding from submucosal angiodysplasia. However, Heyde syndrome has been reported to occur in the setting of severe or critical aortic stenosis and is unlikely to be the cause here. The patient needs to be examined with both upper and lower endoscopy to rule out gastrointestinal (GI) malignancy, gastric and esophageal varices, and painless peptic ulcers. High right ventricular systolic blood pressures along with echodense material in the inferior vena cava and right atrium suggest the possibility of malignancy with vascular invasion. Tricuspid regurgitation is consistent with high right-sided pressures. As left ventricular ejection fraction is reduced, some of the high right-sided pressures could also be attributable to left heart failure. CT findings of rectal wall thickening and perirectal lymph nodes could be attributable to cancer with locally metastatic disease. Blood loss caused by this cancer would explain the severe anemia on admission as well as the low ferritin level and the iron deficiency anemia. In this 70-year-old man who has not had routine health care maintenance, the leading diagnosis is colorectal cancer. However, the markedly elevated globulin gap and elevated INR strongly suggest another process (eg, multiple myeloma, other paraproteinemia) is also present.
INR remained elevated (1.5) despite vitamin K supplementation. Peripheral blood smear showed hypochromic and normocytic RBCs with moderate rouleaux formation (Figure 1). Intravenous pantoprazole and octreotide were started. Upper and lower endoscopy revealed multiple esophageal erosions and both a polypoid mass and an ulcer within the rectum with evidence of prior bleeding. The mass was resected and the ulcer biopsied.
Figure 2
On hospital day 3, the patient was transfused another unit of packed RBCs. Hemoglobin level increased from 7.4 g/dL to 8.2 g/dL, but he began to complain of headache, blurred vision, and worsened chest pain. He did not have weakness, numbness, diplopia, dysphagia, or dysarthria. External examination and extraocular movements of both eyes were normal. Visual acuity was 20/25 bilaterally. Funduscopic examination revealed mild dilation of retinal veins and retinal hemorrhages (Figure 2).
Rouleaux formation occurs as excess cathodal proteins, such as immunoglobulins or fibrinogen, adhere to RBCs and cause the cells to stack together in long chains. Classically this is associated with multiple myeloma, but can occur with Waldenström’s macroglobulinemia and other cancers or infections. It can also occur as an artifact in smear preparation but the large globulin gap in this patient supports pathologic rouleaux formation.
Venous retinopathy with hemorrhages may occur with occlusion of the arterial supply (eg, as with carotid artery obstruction) but also with hyperviscosity syndrome (HVS). Vascular disturbances throughout the body play a major role in HVS, but these changes are most easily visualized in the retina. It is interesting that the patient’s headache and blurred vision began after he received additional blood transfusions. Spuriously low hemoglobin and hematocrit levels may stem from increased plasma volume from high immunoglobulin M (IgM) concentrations in Waldenström macroglobulinemia; thus, RBC transfusions can exacerbate symptoms by elevating total RBC mass. Normocytic, normochromic anemia is characteristic of both multiple myeloma and Waldenström’s macroglobulinemia. That the patient’s chest pain recurred coincidentally with blurred vision and headache suggests the likely cause is cardiac ischemia from hyperviscosity. The serum viscosity level should be checked, and, if it is elevated, urgent serum plasmapheresis should be considered. Determining the source of excess globulin production and treating the underlying disease are crucial at this juncture.
In the general population, rectal adenocarcinoma is the most common cause of a rectal mass. In this patient, presence of a paraproteinemia may point to a different diagnosis. Extramedullary colorectal plasmacytoma can occur in the rectum but is exceedingly rare. Waldenström’s macroglobulinemia, a subtype of lymphoplasmacytic lymphoma, can be associated with a rectal lymphoma. At this point, it is not possible to confidently predict the etiology of the mass.
Figure 3Plasma viscosity was elevated at 4.0 (reference range, 1.6-1.9). Serum protein electrophoresis revealed an M-spike of 6.4 g/dL corresponding to IgG on immunofixation. The kappa/lambda light chain ratio was 2.2 with normal urine protein electrophoresis. Bone marrow core biopsy demonstrated 60 to 70% plasma cells (Figure 3) with aspirate flow cytometry showing 3% phenotypically abnormal monoclonal plasma cells that were kappa positive. Skeletal survey revealed possible small lytic lesions in right scapula and proximal humeri bilaterally. Hematoxylin and eosin stain of rectal ulcer was highly suggestive of amyloidosis. Pathology of the polypoid mass was consistent with at least high-grade dysplasia arising in a tubular adenoma. The initial colonoscopy was limited by poor colonic preparation. A sigmoidoscopy with biopsy 6 weeks later revealed a 4 cm rectal mass, which pathology showed moderately to poorly infiltrating adenocarcinoma with necrosis (clinical stage T3N1).
He was started on cyclophosphamide, bortezomib and dexamethasone for IgG κ myeloma with improvement in his headache, blurred vision, chest pain, and plasma viscosity (4 to 1.8). His hemoglobin remained stable at 10 g/dL. Neoadjuvant Capecitabine and radiation therapy were initiated for his rectal cancer.
DISCUSSION
Multiple myeloma is characterized by monoclonal proliferation of plasma cells, elevated circulating monoclonal immunoglobulin, and end-organ damage.1 It accounts for approximately 0.8% of all new cancer diagnoses; average age at onset is 70 years. The patient described here had an unusual presentation, with GI bleeding and progression to HVS, and known risk factors for multiple myeloma (male sex, low socioeconomic status, welding career).2,3
An early clue in the diagnosis was the patient’s large gamma gap and concurrent anemia. Gamma gap, calculated by subtracting serum albumin from serum total protein, is so named because it often reflects an elevated gamma globulin concentration. However, it actually reflects all nonalbumin serum protein. A gamma gap larger than 3.1 g/dL is an independent risk factor for death4 and may be associated with infection, autoimmunity, and malignancy. Although there are no screening guidelines for multiple myeloma, 73% of cases are brought to attention by anemia discovered on routine laboratory investigation.5 This patient’s lack of prior medical care likely contributed to his atypical presentation. Screening colonoscopy, recommended at age 50, might have identified his rectal cancer at an earlier stage.
The patient’s anemia was likely secondary to GI hemorrhage and bone marrow suppression. His hematochezia might have been partly related to the pathophysiologic interaction of paraproteins with platelets, coagulation factors, and blood vessels.6 Amyloidosis of the GI tract is seen in 8% of AL amyloidosis7 and most frequently manifests as gastrointestinal bleeding, which is thought to be due to ischemia, vascular friability, or mucosal lesions. It less commonly presents as malabsorption or dysmotility.8 Although gastrointestinal amyloid is not typically associated with radiologic abnormalities, occasionally it may cause luminal wall thickening, adenopathy, and inflammatory stranding.9 The gold standard for diagnosis is tissue biopsy. However, presence of amyloidosis does not change the overall treatment strategy for multiple myeloma.
An interesting feature of this case is the development of HVS, which typically manifests with mucosal bleeding, blurred vision, and headache.10 HVS can be diagnosed on retinal examination with findings of venous tortuosity, dilatation, and intraretinal hemorrhage, as occurred in this case,11 and is confirmed with serum viscosity measurement. The first evidence of HVS in this case might have been the spontaneous echo contrast, or “smoke,” detected on echocardiogram. Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates,12 and is associated with conditions that result in left atrial stasis, such as atrial arrhythmias and mitral stenosis. This patient did not have valvular pathology or arrhythmia, and thus the “smoke” likely reflected HVS.
Of the paraproteinemias, Waldenström’s macroglobulinemia is most often associated with HVS, likely because of the pentameric structure of IgM13 and the consequential large size that predisposes to vascular occlusion. Whereas HVS can occur with IgM levels as low as 3 g/dL, it typically does not occur with IgG concentrations under 15 g/dL. This patient presented with an IgG level of 8 g/dL and developed HVS symptoms only after multiple packed RBC transfusions. Elevated IgG level likely made him susceptible to HVS, which ultimately was precipitated by blood transfusion. Therefore, this patient’s initial chest pain most likely was caused by demand cardiac ischemia secondary to anemia, whereas his subsequent, posttransfusion chest pain likely resulted from hyperviscosity angina. Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—has been described in polycythemia and connective tissue disorders.14,15 To our knowledge, however, hyperviscosity angina has not been reported in patients with multiple myeloma. Treatment of hyperviscosity with end-organ damage typically consists of plasmapheresis, but this patient was started on urgent chemotherapy, and his symptoms improved. Untreated HVS can lead to end-organ ischemia and death.
This patient had a multitude of seemingly disparate symptoms and abnormalities that ultimately were united in a diagnosis of IgG κ multiple myeloma. Subsequently diagnosed rectal adenocarcinoma may have led to ongoing blood loss, which worsened the anemia, but had no evident relation to the primary diagnosis of multiple myeloma. This case exemplifies the fact that HVS is a rare but important iatrogenic complication of multiple myeloma treated with blood transfusion. As this patient’s hospital course progressed, the plot, and his blood, thickened.
KEY TEACHING POINTS
Multiple myeloma is occasionally associated with HVS, which manifests with mucosal bleeding, blurred vision, and headache.
Hyperviscosity angina—cardiac ischemia resulting from poor coronary perfusion caused by hyperviscous blood—should be considered in patients with paraproteinemias and chest pain.
Plasmapheresis reverses the clinical manifestations of HVS but not the underlying disease process (eg, Waldenström’s macroglobulinemia, multiple myeloma, leukemia, polycythemia).
Spontaneous echo contrast represents increased RBC aggregation, from interaction of RBCs and plasma proteins, at low shear rates, and is associated with left atrial stasis, commonly from atrial fibrillation or mitral stenosis, but might be present in HVS.
Acknowledgment
The authors thank Peter Campochiaro, MD, and Whitney Green, MD, for their contributions to the images used in this article.
Disclosure
Dr. Sedighi Manesh is supported by the Jeremiah A. Barondess Fellowship in the Clinical Transaction of the New York Academy of Medicine, in collaboration with the Accreditation Council for Graduate Medical Education (ACGME). The other authors have nothing to report.
References
1. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046-1060. PubMed 2. Koessel SL, Theis MK, Vaughan TL, et al. Socioeconomic status and the incidence of multiple myeloma. Epidemiology. 1996;7(1):4-8. PubMed 3. Fritschi L, Siemiatycki J. Lymphoma, myeloma and occupation: results of a case-control study. Int J Cancer. 1996;67(4):498-503. PubMed 4. Juraschek SP, Moliterno AR, Checkley W, Miller ER 3rd. The gamma gap and all-cause mortality. PLoS One. 2015;10(12):e0143494. PubMed 5. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. PubMed 6. Eby CS. Bleeding and thrombosis risks in plasma cell dyscrasias. Hematology Am Soc Hematol Educ Program. 2007:158-164. PubMed 7. Menke DM, Kyle RA, Fleming CR, Wolfe JT 3rd, Kurtin PJ, Oldenburg WA. Symptomatic gastric amyloidosis in patients with primary systemic amyloidosis. Mayo Clin Proc. 1993;68(8):763-767. PubMed 8. Levy DJ, Franklin GO, Rosenthal WS. Gastrointestinal bleeding and amyloidosis. Am J Gastroenterol. 1982;77(6):422-426. PubMed 9. Araoz PA, Batts KP, MacCarty RL. Amyloidosis of the alimentary canal: radiologic-pathologic correlation of CT findings. Abdom Imaging. 2000;25(1):38-44. PubMed 10. Stone MJ, Bogen SA. Evidence-based focused review of management of hyperviscosity syndrome. Blood. 2012;119(10):2205-2208. PubMed 11. Rajagopal R, Apte RS. Seeing through thick and through thin: retinal manifestations of thrombophilic and hyperviscosity syndromes. Surv Ophthalmol. 2016;61(2):236-247. PubMed 12. Black IW. Spontaneous echo contrast: where there’s smoke there’s fire. Echocardiography. 2000;17(4):373-382. PubMed 13. Kwaan HC. Hyperviscosity in plasma cell dyscrasias. Clin Hemorheol Microcirc. 2013;55(1):75-83. PubMed 14. Piccirillo G, Fimognari FL, Valdivia JL, Marigliano V. Effects of phlebotomy on a patient with secondary polycythemia and angina pectoris. Int J Cardiol. 1994;44(2):175-177. PubMed 15. Ovadia S, Lysyy L, Floru S. Emergency plasmapheresis for unstable angina in a patient with hyperviscosity syndrome. Am J Emerg Med. 2005;23(6):811-812. PubMed
References
1. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046-1060. PubMed 2. Koessel SL, Theis MK, Vaughan TL, et al. Socioeconomic status and the incidence of multiple myeloma. Epidemiology. 1996;7(1):4-8. PubMed 3. Fritschi L, Siemiatycki J. Lymphoma, myeloma and occupation: results of a case-control study. Int J Cancer. 1996;67(4):498-503. PubMed 4. Juraschek SP, Moliterno AR, Checkley W, Miller ER 3rd. The gamma gap and all-cause mortality. PLoS One. 2015;10(12):e0143494. PubMed 5. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33. PubMed 6. Eby CS. Bleeding and thrombosis risks in plasma cell dyscrasias. Hematology Am Soc Hematol Educ Program. 2007:158-164. PubMed 7. Menke DM, Kyle RA, Fleming CR, Wolfe JT 3rd, Kurtin PJ, Oldenburg WA. Symptomatic gastric amyloidosis in patients with primary systemic amyloidosis. Mayo Clin Proc. 1993;68(8):763-767. PubMed 8. Levy DJ, Franklin GO, Rosenthal WS. Gastrointestinal bleeding and amyloidosis. Am J Gastroenterol. 1982;77(6):422-426. PubMed 9. Araoz PA, Batts KP, MacCarty RL. Amyloidosis of the alimentary canal: radiologic-pathologic correlation of CT findings. Abdom Imaging. 2000;25(1):38-44. PubMed 10. Stone MJ, Bogen SA. Evidence-based focused review of management of hyperviscosity syndrome. Blood. 2012;119(10):2205-2208. PubMed 11. Rajagopal R, Apte RS. Seeing through thick and through thin: retinal manifestations of thrombophilic and hyperviscosity syndromes. Surv Ophthalmol. 2016;61(2):236-247. PubMed 12. Black IW. Spontaneous echo contrast: where there’s smoke there’s fire. Echocardiography. 2000;17(4):373-382. PubMed 13. Kwaan HC. Hyperviscosity in plasma cell dyscrasias. Clin Hemorheol Microcirc. 2013;55(1):75-83. PubMed 14. Piccirillo G, Fimognari FL, Valdivia JL, Marigliano V. Effects of phlebotomy on a patient with secondary polycythemia and angina pectoris. Int J Cardiol. 1994;44(2):175-177. PubMed 15. Ovadia S, Lysyy L, Floru S. Emergency plasmapheresis for unstable angina in a patient with hyperviscosity syndrome. Am J Emerg Med. 2005;23(6):811-812. PubMed
Reza Sedighi Manesh, MD, Division of General Internal Medicine, Johns Hopkins University School of Medicine, 600 N Wolfe St, Nelson 215, Baltimore, MD 21287; Telephone: 412-708-6944; Fax: 410-502-0923; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
Alternative CME
Disqus Comments
Default
Consolidated Pubs: Do Not Show Source Publication Logo
For over 3 decades, AcademyHealth and its predecessor organizations and members have been studying how the healthcare system works and ways to improve health outcomes. The value of health services research (HSR) training programs that emphasize learning opportunities in delivery system settings was initially articulated at the 2009 AcademyHealth Summit on the Future of HSR Data and Methods.1 Two years later, the need for such programs was reiterated as a priority for AcademyHealth’s HSR Learning Consortium in their strategic plan.2 While HSR methods have become increasingly sophisticated, historical approaches largely relied on extant (usually academic-based) researchers.
To realize the goal of building learning health systems (considered here to be entities where applied, operationally relevant research is systematically designed, generated, and translated into high-quality care delivery), many healthcare organizations have begun to use researchers as an internal resource to inform and support higher quality and more efficient care delivery operations. However, there is a current dearth of scientists trained in research disciplines (eg, comparative effectiveness research, patient-centered outcomes research, implementation science) more directly applicable to operational settings.3,4 Conducting research within these “real-world” environments is challenging for a variety of well-documented reasons,5,6 and many important questions cannot be answered using traditional study designs and/or methodologies. Until more researchers are trained in research approaches that align better with care delivery needs, the field will continue to fall short of addressing topics identified by the National Academy of Medicine (NAM; formerly the Institute of Medicine) as priorities for real system improvement.
While researchers in academic and consulting settings play critical roles in knowledge generation, a substantial area for expansion is support for “embedded researchers” who work more directly with operational leaders and understand local context, data, and organizational-level goals of delivery systems. AcademyHealth’s Delivery System Science Fellowship (DSSF) was developed to forge a stronger link between rigorous research practice and pragmatic aspects of care delivery.
Since inception of the DSSF, national attention has further emphasized the need for specialized, experiential learning with specific competencies that extend formal HSR training. The Agency for Healthcare Research and Quality (AHRQ) is currently convening a Technical Expert Panel to guide Training the Next Generation of Learning Health System Researchers as part of its larger effort to provide support for evidence generation and uptake in these applied settings (see http://www.ahrq.gov/news/blog/ahrqviews/supporting-learning-health-systems.html for more information).This work is reinforced by an ongoing project at AcademyHealth focused on Understanding the Current Health Services Research Workforce and Maximizing Its Future,7 partially sponsored by AHRQ. These efforts aim to inform AHRQ-funded career and training program requirements in order to build a workforce in partnership with academia and delivery organizations in support of developing high-functioning researchers directly positioned to drive progress toward learning healthcare systems.
Table
ACADEMYHEALTH’S DSSF
The AcademyHealth DSSF Program is a pioneering effort designed to meet the needs of learning healthcare systems for a human capital resource capable of generating insights from operational data and deploying this knowledge effectively. Established in 2012 in partnership with 3 initial host sites, the DSSF provides a paid, postdoctoral training opportunity to help highly qualified, early-career researchers gain applied experience in delivery system settings.8 The goal is to provide hands-on experience and professional leadership opportunities to enhance the array of skills needed to generate and apply evidence in delivery systems. The long-term program objective is for graduates to employ the methods and training garnered during the DSSF to produce new, practical insights required to transform healthcare delivery and achieve the “Triple Aim.”9
Sixteen delivery systems have participated in the DSSF program over the course of 5 years. These organizations represent a diverse group of innovative, high-performing systems that serve populations across the rural-urban continuum. Host site preceptors are nationally recognized experts in areas such as health economics, comparative effectiveness, pragmatic trials, clinical decision support, and implementation science. The fellowship is guided by an advisory committee that provides strategic direction and plays a key role in selecting fellows. AcademyHealth partners with 8 to 10 health systems annually, accepting new partnerships as interest and availability allows. The Figure summarizes program inputs, elements, antecedents, outputs, and intended outcomes. As a relatively new and evolving program, the DSSF is using a disciplined approach to assess both mid- and long-term outcomes. The Table is a comparative matrix that depicts the range in areas of investment offered by a sample of host sites during the fellowship program. Complementing development of the common core competencies and exposures presented in the Table, specific project choice at a host site is mutually determined according to system needs and the fellow’s interests.
To apply for DSSF, researchers must hold a doctoral degree in any relevant aspect of clinical medicine, HSR, or a related field. The review committee evaluates applicants based on their qualifications, a clear statement of professional goals, appropriateness for placement, the quality of a writing sample, and letters of recommendation. Host sites select a fellow based on their individual preferences and recommendations from the review committee. The minimum duration of the fellowship is 1 year, during which the fellow works full time at the host site. Host sites provide the fellows’ salary and benefits, financial support to attend AcademyHealth’s Annual Research Meeting, and mentorship and/or training. To ensure general continuity across sites, each fellow’s work focuses on “delivery system science (DSS),” with a significant part of the work intended for public dissemination (eg, a conference presentation) or publication in a peer-reviewed journal.
Host sites additionally provide AcademyHealth financial support to manage the process of recruiting promising candidates. AcademyHealth manages and convenes the advisory committee proceedings, facilitates the application cycle (including peer review of applicants), markets the fellowship, guides the interview and match process, and promotes placement of fellows upon program completion. AcademyHealth also convenes active and graduate fellows to foster engagement and professional development.
Figure To date, 118 individuals have applied to the program and 25 fellows have been accepted. Nineteen have completed the fellowship, 2 are continuing as second-year fellows, and 4 started their fellowship in the fall of 2016. Fellows have a wide range of expertise in areas such as epidemiology, exercise physiology, health psychology, anthropology, clinical medicine, qualitative methods, organizational behavior, and systems engineering. Once individuals complete their fellowship, they become DSSF “alumni” and remain involved in program activities and as peer mentors.
EARLY EXPERIENCE WITH OUTCOMES
Program Level
AcademyHealth administers an annual evaluation to assess the program, understand impact on the fellow’s professional development and growth, track publications, and inform programmatic goals. To date, we have identified over 50 peer-reviewed publications resulting from work conducted through the fellowship (visit http://www.academyhealth.org/dssfpublications for a full listing of publications stemming from the DSSF program). As an example of continuous program improvement, this year staff implemented a fellow-led monthly call in response to requests to connect fellows. This has proven to be a useful response for fellows to understand how to enhance their own experience by learning from fellows in other systems to incorporate focused areas of development via cross-system sharing. As an indicator of continued value, of the 16 sites that have participated to date, 10 have participated in the DSSF for more than 1 cycle; 3 are new host sites currently participating in their first year of the program; and 3 host sites participated for 1 year. The 3 inaugural host sites that helped launch the DSSF continue to serve as host sites to date.
As a marker of longitudinal success, staff will continue to follow up with preceptors and fellows to understand fellows’ contributions to the host site and the field, as well as impact on the fellow career trajectory. Of the 19 fellow alumni to date, 8 have moved on to academic or research positions, and 11 have remained in care delivery systems to provide local expertise in study design, execution, and evidence uptake.
The program has also made some general contributions to advance the discipline of delivery system science, including:
1. Defining DSS and clarifying training needs for “embedded researchers” and health system analysts.To characterize the fellowship, AcademyHealth and the program advisory committee jointly developed the following definition for delivery system science (DSS):
“DSS includes research that seeks to understand how delivery systems operate, influence, change, and respond to external stimulus, among other topics. DSS may include efforts to examine how and under what circumstances interventions work and how delivery systems effectively implement evidence-based innovations. For the DSSF, DSS is conducted by researchers who are ‘embedded’ in delivery systems and respond to the decision-making needs of those systems.”
Additionally, closer connections with DSS leaders have led to a better understanding of challenges, opportunities, and needs of delivery systems.10,11
2. Cultivating a network of delivery systems and system leadersinterested in expanding the cadre of embedded researchers, and trainees who intend to build careers in DSS. The DSSF also aims to enhance fellows’ skills and knowledge base, career opportunities, and professional network. To extend these relationships and support delivery system analytics, AcademyHealth worked with preceptors and fellows to inform creation of a new Community of Practice supported by AcademyHealth’s EDM Forum and guide planning for AcademyHealth’s Concordium conference to provide a national meeting to showcase DSS.
3. Strategic planning to ensure sustainable support for embedded research within delivery systems.Substantial interest in the program developed quickly, with rapid learning over the first few cycles to refine the program to meet host sites’ and fellows’ needs. Both efforts were critical to demonstrate that the DSSF fulfills an important need for our health system partners and members. As indicated previously, strong, sustained interest from prospective host sites and applicants demonstrates the program has created a win-win to jointly assess fit while building skills and supporting continuous learning.
Likewise, Lisa Simpson, President and CEO of AcademyHealth, and Lucy Savitz, DSSF host site preceptor at Intermountain Healthcare, participated in the Canadian Institutes of Health Research (CIHR) Invitational Workshop, “Modernizing Health Services and Policy Research Training in Canada” in March 2016. Shared learning largely informed by the DSSF led to CIHR creating a similar fellowship program with initial awards to be made in 2017 (see https://www.researchnet-recherchenet.ca/rnr16/vwOpprtntyDtls.do?prog=2540&view=browseActive&sponsor=CIHR-8&type=EXACT&resultCount=25 for more information). We are working to thread these efforts together in a way to leverage our learning community of government agencies, academia, and employers as a long-term funding stream for training in delivery science.
Participant Host Site Level
Two selected examples of how DSSF researchers have engaged high-priority topics that contributed to health system operations are provided here.
Kaiser Permanente Southern California: Assessing adherence with “Choosing Wisely” recommendations in oncology. In partnership with preceptor Dr. Michael Gould, 2013-2014 DSSF fellow Dr. Erin Hahn worked with the Kaiser Permanente Southern California (KPSC) Care Improvement Research Team to lead a project addressing several KPSC priority areas. Focusing on “Choosing Wisely” recommendations from the American Society of Clinical Oncology,12 the project evaluated appropriateness of imaging and laboratory services for early-stage cancer patients and survivors between and within 2 integrated health systems, Kaiser Permanente (KP) and Intermountain Healthcare.13,14 Results were presented to KP national leaders, including an external health policy advisory board. In close collaboration with clinical and operational leaders in medical oncology, this multiregional, multisystem project is contributing to targeted quality improvement efforts and improved healthcare value, including audit and feedback of nonrecommended labs.
Dr. Hahn subsequently received a KPSC Incubator Award, a competitive internal grant, to further study factors associated with use of nonrecommended surveillance lab tests for early-stage breast cancer patients. The study focused on medical oncologists within KPSC, categorizing them as high or low utilizers of the tests.15 Results indicate that high utilizers perceive that the tests help manage patient anxiety about recurrence, while acknowledging that the tests do not provide clinical utility. These findings are contributing to the development of targeted survivorship services across the organization.
Intermountain Healthcare: Formative evaluation of large-scale implementation of shared decision-making.Preceptor Dr. Lucy Savitz assembled a team to conduct a formative evaluation of Intermountain Healthcare’s efforts to implement shared decision-making (SDM) as part of its Center for Medicare and Medicaid Innovation Challenge Award. The 2015-2017 DSSF fellow at Intermountain Healthcare, Dr. Kim Brunisholz, served as a core member of the project team, focusing primarily on a mixed-methods evaluation of the SDM program.
Dr. Brunisholz engaged operational leads, clinical teams, patient and family advisory councils, and senior executives to conduct the program assessment. Results demonstrated significant variation in invited participation in SDM among eligible patient populations: preference sensitive conditions (1 in 30 patients), oncology-related diagnosis (1 in 3 patients), and chronic conditions (1 in 74 patients). Provisional analysis of patient-level clinical outcomes demonstrated that among those invited to the SDM program compared to those that were not, total joint replacement was decreased (10.1% vs 17.3%; P < 0.001) and a trend towards breast conservation emerged (61.8% vs 56.4%; P = 0.10). No difference in treatment choice for lower back pain was observed. Qualitative program analysis suggested need for improvements in the areas of (1) routine and continuous staff training, (2) workflow standardization, and (3) active data monitoring with meaningful, actionable feedback to caregivers. In response to these results, a chartered SDM Steering Committee was created (Dr. Brunisholz is a member of that group) to develop a strategic plan for SDM, with an accompanying organizational response to reimplement SDM in a targeted manner. Learning from this program is being leveraged to support a subproject analysis on a large scale using data from the High Value Healthcare Collaborative as part of an AHRQ-funded Center of Excellence award. (See https://www.ahrq.gov/news/newsroom/press-releases/2015/pcorawards.html. For more information on the High Value Healthcare Collaborative, please visit: https://www.highvaluehealthcare.org.)
CONCLUSION
Moving forward, the DSSF will continue working with progressive delivery systems. Partnerships between organizations that are interested in integrating rigorous research practice to drive continuous system improvement and maximize the value of care will have substantial need for technical skills and analytic capacity. They will also need to ensure that researchers working in their systems have sufficient understanding of cultural and political context within the organization to be effective leaders who can manage change.
AcademyHealth created the DSSF in response to the field’s request to build a research workforce that reflects the vision for a 21st Century Health System, as laid out by the NAM.16 We anticipate that as the US Department of Health & Human Services’ goals for payment reform and new measures to promote quality and high-value care are implemented, the DSSF trainees’ skill set will be increasingly valuable and will provide needed thought leadership on strategies to generate and apply evidence in practice.
Disclosure
Ms. Kanani received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship. Drs. Hahn, Gould, and Brunisholz have no conflicts to disclose. Dr. Savitz has received funding from HRQ COE, PCORI LHSNet; received funding for lectures from the Institute from Healthcare Improvement, Department of Epidemiology, University of Utah; received funding for travel, accommodations, and meeting expenses from AHRQ NAC, EDM Forum, AH CAPP, AARP NPC, and PROM TEP; and received additional funding from Dartmouth University. Dr. Holve received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship, provided by our delivery system partners, several of whom are coauthors on this manuscript.
References
1. AcademyHealth. Health Services Research in 2020: Summit on the Future of HSR Data and Methods. http://www.academyhealth.org/About/content.cfm?ItemNumber=2529. Accessed March 21, 2016. 2. AcademyHealth. Health Services Research (HSR) Learning Consortium Strategic Plan. http://www.academyhealth.org/files/ProfDev/Files/HSRstrategicplan2011FINAL.pdf. Accessed March 21, 2016. 3. Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. http://www.nationalacademies.org/hmd/~/media/Files/Report%20Files/2009/ComparativeEffectivenessResearchPriorities/CER%20report%20brief%2008-13-09.pdf. Accessed March 21, 2016. 4. Bonham A, Rich E, Davis D, Longnecker D, Heinig S. Putting evidence to work: an expanded research agenda for academic medicine in the era of health care reform. Acad Med. 2010;85(10):1551-1553. PubMed 5. Zerhouni E. Translational and clinical science—time for a new vision. N Engl J Med. 2005;353(15):1621-1623. PubMed 6. AcademyHealth. “Getting Answers We Can Believe In: Methodological Considerations When Using Electronic Clinical Data for Research,” EDM Forum, December 2012. 7. Rich G, Collins A. Current and Future Demand for Health Services Researchers. Funded by the Agency for Healthcare Research and Quality (AHRQ). Presented at the AcademyHealth HSR Workforce Conference, Understanding the Current Health Services Research Workforce and Maximizing Its Future, funded by AHRQ, Patient-Centered Outcomes Research Institute, and the Robert Wood Johnson Foundation. October 2016. 8. AcademyHealth. Delivery System Science Fellowship. http://www.academyhealth.org/dssf. Accessed March 21, 2016. 9. Institute for Healthcare Improvement. IHI Triple Aim Initiative. http://www.ihi.org/engage/initiatives/tripleaim/Pages/default.aspx. Accessed March 21, 2016. 10. Psek W, Stametz R, Bailey-Davis L, et al. Operationalizing the learning health care system in an integrated delivery system. eGEMs. 2015;3(1):1122. PubMed 11. Thompson C, Kurian A, Luft H. Linking electronic health records to better understand breast cancer patient pathways within and between two health systems. eGEMs. 2015;3(1):1127. PubMed 12. Schnipper L, Smith TJ, Raghavan D, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: The top five list for oncology. J Clin Oncol. 2012;30(14):1715-1724. PubMed 13. Hahn E, Tang T, Lee JS, et al. Use of posttreatment imaging and biomarkers in survivors of early‐stage breast cancer: Inappropriate surveillance or necessary care? Cancer. 2015;122(6):908-916. PubMed 14. Hahn E, Tang T, Lee JS, et al. Use of imaging for staging of early-stage breast cancer in two integrated health care systems: Adherence with a choosing wisely recommendation. J Oncol Pract. 2015;11(3):e320-e328. PubMed 15. Hahn EE, Munoz-Plaza C, Wang J, et al. Anxiety, culture, expectations: Oncologist-perceived factors associated with use of non-recommended serum tumor marker tests for surveillance of early stage breast cancer. J Oncol Pract. 2016;13(1):e77-e290. PubMed 16. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences; 2000.
For over 3 decades, AcademyHealth and its predecessor organizations and members have been studying how the healthcare system works and ways to improve health outcomes. The value of health services research (HSR) training programs that emphasize learning opportunities in delivery system settings was initially articulated at the 2009 AcademyHealth Summit on the Future of HSR Data and Methods.1 Two years later, the need for such programs was reiterated as a priority for AcademyHealth’s HSR Learning Consortium in their strategic plan.2 While HSR methods have become increasingly sophisticated, historical approaches largely relied on extant (usually academic-based) researchers.
To realize the goal of building learning health systems (considered here to be entities where applied, operationally relevant research is systematically designed, generated, and translated into high-quality care delivery), many healthcare organizations have begun to use researchers as an internal resource to inform and support higher quality and more efficient care delivery operations. However, there is a current dearth of scientists trained in research disciplines (eg, comparative effectiveness research, patient-centered outcomes research, implementation science) more directly applicable to operational settings.3,4 Conducting research within these “real-world” environments is challenging for a variety of well-documented reasons,5,6 and many important questions cannot be answered using traditional study designs and/or methodologies. Until more researchers are trained in research approaches that align better with care delivery needs, the field will continue to fall short of addressing topics identified by the National Academy of Medicine (NAM; formerly the Institute of Medicine) as priorities for real system improvement.
While researchers in academic and consulting settings play critical roles in knowledge generation, a substantial area for expansion is support for “embedded researchers” who work more directly with operational leaders and understand local context, data, and organizational-level goals of delivery systems. AcademyHealth’s Delivery System Science Fellowship (DSSF) was developed to forge a stronger link between rigorous research practice and pragmatic aspects of care delivery.
Since inception of the DSSF, national attention has further emphasized the need for specialized, experiential learning with specific competencies that extend formal HSR training. The Agency for Healthcare Research and Quality (AHRQ) is currently convening a Technical Expert Panel to guide Training the Next Generation of Learning Health System Researchers as part of its larger effort to provide support for evidence generation and uptake in these applied settings (see http://www.ahrq.gov/news/blog/ahrqviews/supporting-learning-health-systems.html for more information).This work is reinforced by an ongoing project at AcademyHealth focused on Understanding the Current Health Services Research Workforce and Maximizing Its Future,7 partially sponsored by AHRQ. These efforts aim to inform AHRQ-funded career and training program requirements in order to build a workforce in partnership with academia and delivery organizations in support of developing high-functioning researchers directly positioned to drive progress toward learning healthcare systems.
Table
ACADEMYHEALTH’S DSSF
The AcademyHealth DSSF Program is a pioneering effort designed to meet the needs of learning healthcare systems for a human capital resource capable of generating insights from operational data and deploying this knowledge effectively. Established in 2012 in partnership with 3 initial host sites, the DSSF provides a paid, postdoctoral training opportunity to help highly qualified, early-career researchers gain applied experience in delivery system settings.8 The goal is to provide hands-on experience and professional leadership opportunities to enhance the array of skills needed to generate and apply evidence in delivery systems. The long-term program objective is for graduates to employ the methods and training garnered during the DSSF to produce new, practical insights required to transform healthcare delivery and achieve the “Triple Aim.”9
Sixteen delivery systems have participated in the DSSF program over the course of 5 years. These organizations represent a diverse group of innovative, high-performing systems that serve populations across the rural-urban continuum. Host site preceptors are nationally recognized experts in areas such as health economics, comparative effectiveness, pragmatic trials, clinical decision support, and implementation science. The fellowship is guided by an advisory committee that provides strategic direction and plays a key role in selecting fellows. AcademyHealth partners with 8 to 10 health systems annually, accepting new partnerships as interest and availability allows. The Figure summarizes program inputs, elements, antecedents, outputs, and intended outcomes. As a relatively new and evolving program, the DSSF is using a disciplined approach to assess both mid- and long-term outcomes. The Table is a comparative matrix that depicts the range in areas of investment offered by a sample of host sites during the fellowship program. Complementing development of the common core competencies and exposures presented in the Table, specific project choice at a host site is mutually determined according to system needs and the fellow’s interests.
To apply for DSSF, researchers must hold a doctoral degree in any relevant aspect of clinical medicine, HSR, or a related field. The review committee evaluates applicants based on their qualifications, a clear statement of professional goals, appropriateness for placement, the quality of a writing sample, and letters of recommendation. Host sites select a fellow based on their individual preferences and recommendations from the review committee. The minimum duration of the fellowship is 1 year, during which the fellow works full time at the host site. Host sites provide the fellows’ salary and benefits, financial support to attend AcademyHealth’s Annual Research Meeting, and mentorship and/or training. To ensure general continuity across sites, each fellow’s work focuses on “delivery system science (DSS),” with a significant part of the work intended for public dissemination (eg, a conference presentation) or publication in a peer-reviewed journal.
Host sites additionally provide AcademyHealth financial support to manage the process of recruiting promising candidates. AcademyHealth manages and convenes the advisory committee proceedings, facilitates the application cycle (including peer review of applicants), markets the fellowship, guides the interview and match process, and promotes placement of fellows upon program completion. AcademyHealth also convenes active and graduate fellows to foster engagement and professional development.
Figure To date, 118 individuals have applied to the program and 25 fellows have been accepted. Nineteen have completed the fellowship, 2 are continuing as second-year fellows, and 4 started their fellowship in the fall of 2016. Fellows have a wide range of expertise in areas such as epidemiology, exercise physiology, health psychology, anthropology, clinical medicine, qualitative methods, organizational behavior, and systems engineering. Once individuals complete their fellowship, they become DSSF “alumni” and remain involved in program activities and as peer mentors.
EARLY EXPERIENCE WITH OUTCOMES
Program Level
AcademyHealth administers an annual evaluation to assess the program, understand impact on the fellow’s professional development and growth, track publications, and inform programmatic goals. To date, we have identified over 50 peer-reviewed publications resulting from work conducted through the fellowship (visit http://www.academyhealth.org/dssfpublications for a full listing of publications stemming from the DSSF program). As an example of continuous program improvement, this year staff implemented a fellow-led monthly call in response to requests to connect fellows. This has proven to be a useful response for fellows to understand how to enhance their own experience by learning from fellows in other systems to incorporate focused areas of development via cross-system sharing. As an indicator of continued value, of the 16 sites that have participated to date, 10 have participated in the DSSF for more than 1 cycle; 3 are new host sites currently participating in their first year of the program; and 3 host sites participated for 1 year. The 3 inaugural host sites that helped launch the DSSF continue to serve as host sites to date.
As a marker of longitudinal success, staff will continue to follow up with preceptors and fellows to understand fellows’ contributions to the host site and the field, as well as impact on the fellow career trajectory. Of the 19 fellow alumni to date, 8 have moved on to academic or research positions, and 11 have remained in care delivery systems to provide local expertise in study design, execution, and evidence uptake.
The program has also made some general contributions to advance the discipline of delivery system science, including:
1. Defining DSS and clarifying training needs for “embedded researchers” and health system analysts.To characterize the fellowship, AcademyHealth and the program advisory committee jointly developed the following definition for delivery system science (DSS):
“DSS includes research that seeks to understand how delivery systems operate, influence, change, and respond to external stimulus, among other topics. DSS may include efforts to examine how and under what circumstances interventions work and how delivery systems effectively implement evidence-based innovations. For the DSSF, DSS is conducted by researchers who are ‘embedded’ in delivery systems and respond to the decision-making needs of those systems.”
Additionally, closer connections with DSS leaders have led to a better understanding of challenges, opportunities, and needs of delivery systems.10,11
2. Cultivating a network of delivery systems and system leadersinterested in expanding the cadre of embedded researchers, and trainees who intend to build careers in DSS. The DSSF also aims to enhance fellows’ skills and knowledge base, career opportunities, and professional network. To extend these relationships and support delivery system analytics, AcademyHealth worked with preceptors and fellows to inform creation of a new Community of Practice supported by AcademyHealth’s EDM Forum and guide planning for AcademyHealth’s Concordium conference to provide a national meeting to showcase DSS.
3. Strategic planning to ensure sustainable support for embedded research within delivery systems.Substantial interest in the program developed quickly, with rapid learning over the first few cycles to refine the program to meet host sites’ and fellows’ needs. Both efforts were critical to demonstrate that the DSSF fulfills an important need for our health system partners and members. As indicated previously, strong, sustained interest from prospective host sites and applicants demonstrates the program has created a win-win to jointly assess fit while building skills and supporting continuous learning.
Likewise, Lisa Simpson, President and CEO of AcademyHealth, and Lucy Savitz, DSSF host site preceptor at Intermountain Healthcare, participated in the Canadian Institutes of Health Research (CIHR) Invitational Workshop, “Modernizing Health Services and Policy Research Training in Canada” in March 2016. Shared learning largely informed by the DSSF led to CIHR creating a similar fellowship program with initial awards to be made in 2017 (see https://www.researchnet-recherchenet.ca/rnr16/vwOpprtntyDtls.do?prog=2540&view=browseActive&sponsor=CIHR-8&type=EXACT&resultCount=25 for more information). We are working to thread these efforts together in a way to leverage our learning community of government agencies, academia, and employers as a long-term funding stream for training in delivery science.
Participant Host Site Level
Two selected examples of how DSSF researchers have engaged high-priority topics that contributed to health system operations are provided here.
Kaiser Permanente Southern California: Assessing adherence with “Choosing Wisely” recommendations in oncology. In partnership with preceptor Dr. Michael Gould, 2013-2014 DSSF fellow Dr. Erin Hahn worked with the Kaiser Permanente Southern California (KPSC) Care Improvement Research Team to lead a project addressing several KPSC priority areas. Focusing on “Choosing Wisely” recommendations from the American Society of Clinical Oncology,12 the project evaluated appropriateness of imaging and laboratory services for early-stage cancer patients and survivors between and within 2 integrated health systems, Kaiser Permanente (KP) and Intermountain Healthcare.13,14 Results were presented to KP national leaders, including an external health policy advisory board. In close collaboration with clinical and operational leaders in medical oncology, this multiregional, multisystem project is contributing to targeted quality improvement efforts and improved healthcare value, including audit and feedback of nonrecommended labs.
Dr. Hahn subsequently received a KPSC Incubator Award, a competitive internal grant, to further study factors associated with use of nonrecommended surveillance lab tests for early-stage breast cancer patients. The study focused on medical oncologists within KPSC, categorizing them as high or low utilizers of the tests.15 Results indicate that high utilizers perceive that the tests help manage patient anxiety about recurrence, while acknowledging that the tests do not provide clinical utility. These findings are contributing to the development of targeted survivorship services across the organization.
Intermountain Healthcare: Formative evaluation of large-scale implementation of shared decision-making.Preceptor Dr. Lucy Savitz assembled a team to conduct a formative evaluation of Intermountain Healthcare’s efforts to implement shared decision-making (SDM) as part of its Center for Medicare and Medicaid Innovation Challenge Award. The 2015-2017 DSSF fellow at Intermountain Healthcare, Dr. Kim Brunisholz, served as a core member of the project team, focusing primarily on a mixed-methods evaluation of the SDM program.
Dr. Brunisholz engaged operational leads, clinical teams, patient and family advisory councils, and senior executives to conduct the program assessment. Results demonstrated significant variation in invited participation in SDM among eligible patient populations: preference sensitive conditions (1 in 30 patients), oncology-related diagnosis (1 in 3 patients), and chronic conditions (1 in 74 patients). Provisional analysis of patient-level clinical outcomes demonstrated that among those invited to the SDM program compared to those that were not, total joint replacement was decreased (10.1% vs 17.3%; P < 0.001) and a trend towards breast conservation emerged (61.8% vs 56.4%; P = 0.10). No difference in treatment choice for lower back pain was observed. Qualitative program analysis suggested need for improvements in the areas of (1) routine and continuous staff training, (2) workflow standardization, and (3) active data monitoring with meaningful, actionable feedback to caregivers. In response to these results, a chartered SDM Steering Committee was created (Dr. Brunisholz is a member of that group) to develop a strategic plan for SDM, with an accompanying organizational response to reimplement SDM in a targeted manner. Learning from this program is being leveraged to support a subproject analysis on a large scale using data from the High Value Healthcare Collaborative as part of an AHRQ-funded Center of Excellence award. (See https://www.ahrq.gov/news/newsroom/press-releases/2015/pcorawards.html. For more information on the High Value Healthcare Collaborative, please visit: https://www.highvaluehealthcare.org.)
CONCLUSION
Moving forward, the DSSF will continue working with progressive delivery systems. Partnerships between organizations that are interested in integrating rigorous research practice to drive continuous system improvement and maximize the value of care will have substantial need for technical skills and analytic capacity. They will also need to ensure that researchers working in their systems have sufficient understanding of cultural and political context within the organization to be effective leaders who can manage change.
AcademyHealth created the DSSF in response to the field’s request to build a research workforce that reflects the vision for a 21st Century Health System, as laid out by the NAM.16 We anticipate that as the US Department of Health & Human Services’ goals for payment reform and new measures to promote quality and high-value care are implemented, the DSSF trainees’ skill set will be increasingly valuable and will provide needed thought leadership on strategies to generate and apply evidence in practice.
Disclosure
Ms. Kanani received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship. Drs. Hahn, Gould, and Brunisholz have no conflicts to disclose. Dr. Savitz has received funding from HRQ COE, PCORI LHSNet; received funding for lectures from the Institute from Healthcare Improvement, Department of Epidemiology, University of Utah; received funding for travel, accommodations, and meeting expenses from AHRQ NAC, EDM Forum, AH CAPP, AARP NPC, and PROM TEP; and received additional funding from Dartmouth University. Dr. Holve received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship, provided by our delivery system partners, several of whom are coauthors on this manuscript.
For over 3 decades, AcademyHealth and its predecessor organizations and members have been studying how the healthcare system works and ways to improve health outcomes. The value of health services research (HSR) training programs that emphasize learning opportunities in delivery system settings was initially articulated at the 2009 AcademyHealth Summit on the Future of HSR Data and Methods.1 Two years later, the need for such programs was reiterated as a priority for AcademyHealth’s HSR Learning Consortium in their strategic plan.2 While HSR methods have become increasingly sophisticated, historical approaches largely relied on extant (usually academic-based) researchers.
To realize the goal of building learning health systems (considered here to be entities where applied, operationally relevant research is systematically designed, generated, and translated into high-quality care delivery), many healthcare organizations have begun to use researchers as an internal resource to inform and support higher quality and more efficient care delivery operations. However, there is a current dearth of scientists trained in research disciplines (eg, comparative effectiveness research, patient-centered outcomes research, implementation science) more directly applicable to operational settings.3,4 Conducting research within these “real-world” environments is challenging for a variety of well-documented reasons,5,6 and many important questions cannot be answered using traditional study designs and/or methodologies. Until more researchers are trained in research approaches that align better with care delivery needs, the field will continue to fall short of addressing topics identified by the National Academy of Medicine (NAM; formerly the Institute of Medicine) as priorities for real system improvement.
While researchers in academic and consulting settings play critical roles in knowledge generation, a substantial area for expansion is support for “embedded researchers” who work more directly with operational leaders and understand local context, data, and organizational-level goals of delivery systems. AcademyHealth’s Delivery System Science Fellowship (DSSF) was developed to forge a stronger link between rigorous research practice and pragmatic aspects of care delivery.
Since inception of the DSSF, national attention has further emphasized the need for specialized, experiential learning with specific competencies that extend formal HSR training. The Agency for Healthcare Research and Quality (AHRQ) is currently convening a Technical Expert Panel to guide Training the Next Generation of Learning Health System Researchers as part of its larger effort to provide support for evidence generation and uptake in these applied settings (see http://www.ahrq.gov/news/blog/ahrqviews/supporting-learning-health-systems.html for more information).This work is reinforced by an ongoing project at AcademyHealth focused on Understanding the Current Health Services Research Workforce and Maximizing Its Future,7 partially sponsored by AHRQ. These efforts aim to inform AHRQ-funded career and training program requirements in order to build a workforce in partnership with academia and delivery organizations in support of developing high-functioning researchers directly positioned to drive progress toward learning healthcare systems.
Table
ACADEMYHEALTH’S DSSF
The AcademyHealth DSSF Program is a pioneering effort designed to meet the needs of learning healthcare systems for a human capital resource capable of generating insights from operational data and deploying this knowledge effectively. Established in 2012 in partnership with 3 initial host sites, the DSSF provides a paid, postdoctoral training opportunity to help highly qualified, early-career researchers gain applied experience in delivery system settings.8 The goal is to provide hands-on experience and professional leadership opportunities to enhance the array of skills needed to generate and apply evidence in delivery systems. The long-term program objective is for graduates to employ the methods and training garnered during the DSSF to produce new, practical insights required to transform healthcare delivery and achieve the “Triple Aim.”9
Sixteen delivery systems have participated in the DSSF program over the course of 5 years. These organizations represent a diverse group of innovative, high-performing systems that serve populations across the rural-urban continuum. Host site preceptors are nationally recognized experts in areas such as health economics, comparative effectiveness, pragmatic trials, clinical decision support, and implementation science. The fellowship is guided by an advisory committee that provides strategic direction and plays a key role in selecting fellows. AcademyHealth partners with 8 to 10 health systems annually, accepting new partnerships as interest and availability allows. The Figure summarizes program inputs, elements, antecedents, outputs, and intended outcomes. As a relatively new and evolving program, the DSSF is using a disciplined approach to assess both mid- and long-term outcomes. The Table is a comparative matrix that depicts the range in areas of investment offered by a sample of host sites during the fellowship program. Complementing development of the common core competencies and exposures presented in the Table, specific project choice at a host site is mutually determined according to system needs and the fellow’s interests.
To apply for DSSF, researchers must hold a doctoral degree in any relevant aspect of clinical medicine, HSR, or a related field. The review committee evaluates applicants based on their qualifications, a clear statement of professional goals, appropriateness for placement, the quality of a writing sample, and letters of recommendation. Host sites select a fellow based on their individual preferences and recommendations from the review committee. The minimum duration of the fellowship is 1 year, during which the fellow works full time at the host site. Host sites provide the fellows’ salary and benefits, financial support to attend AcademyHealth’s Annual Research Meeting, and mentorship and/or training. To ensure general continuity across sites, each fellow’s work focuses on “delivery system science (DSS),” with a significant part of the work intended for public dissemination (eg, a conference presentation) or publication in a peer-reviewed journal.
Host sites additionally provide AcademyHealth financial support to manage the process of recruiting promising candidates. AcademyHealth manages and convenes the advisory committee proceedings, facilitates the application cycle (including peer review of applicants), markets the fellowship, guides the interview and match process, and promotes placement of fellows upon program completion. AcademyHealth also convenes active and graduate fellows to foster engagement and professional development.
Figure To date, 118 individuals have applied to the program and 25 fellows have been accepted. Nineteen have completed the fellowship, 2 are continuing as second-year fellows, and 4 started their fellowship in the fall of 2016. Fellows have a wide range of expertise in areas such as epidemiology, exercise physiology, health psychology, anthropology, clinical medicine, qualitative methods, organizational behavior, and systems engineering. Once individuals complete their fellowship, they become DSSF “alumni” and remain involved in program activities and as peer mentors.
EARLY EXPERIENCE WITH OUTCOMES
Program Level
AcademyHealth administers an annual evaluation to assess the program, understand impact on the fellow’s professional development and growth, track publications, and inform programmatic goals. To date, we have identified over 50 peer-reviewed publications resulting from work conducted through the fellowship (visit http://www.academyhealth.org/dssfpublications for a full listing of publications stemming from the DSSF program). As an example of continuous program improvement, this year staff implemented a fellow-led monthly call in response to requests to connect fellows. This has proven to be a useful response for fellows to understand how to enhance their own experience by learning from fellows in other systems to incorporate focused areas of development via cross-system sharing. As an indicator of continued value, of the 16 sites that have participated to date, 10 have participated in the DSSF for more than 1 cycle; 3 are new host sites currently participating in their first year of the program; and 3 host sites participated for 1 year. The 3 inaugural host sites that helped launch the DSSF continue to serve as host sites to date.
As a marker of longitudinal success, staff will continue to follow up with preceptors and fellows to understand fellows’ contributions to the host site and the field, as well as impact on the fellow career trajectory. Of the 19 fellow alumni to date, 8 have moved on to academic or research positions, and 11 have remained in care delivery systems to provide local expertise in study design, execution, and evidence uptake.
The program has also made some general contributions to advance the discipline of delivery system science, including:
1. Defining DSS and clarifying training needs for “embedded researchers” and health system analysts.To characterize the fellowship, AcademyHealth and the program advisory committee jointly developed the following definition for delivery system science (DSS):
“DSS includes research that seeks to understand how delivery systems operate, influence, change, and respond to external stimulus, among other topics. DSS may include efforts to examine how and under what circumstances interventions work and how delivery systems effectively implement evidence-based innovations. For the DSSF, DSS is conducted by researchers who are ‘embedded’ in delivery systems and respond to the decision-making needs of those systems.”
Additionally, closer connections with DSS leaders have led to a better understanding of challenges, opportunities, and needs of delivery systems.10,11
2. Cultivating a network of delivery systems and system leadersinterested in expanding the cadre of embedded researchers, and trainees who intend to build careers in DSS. The DSSF also aims to enhance fellows’ skills and knowledge base, career opportunities, and professional network. To extend these relationships and support delivery system analytics, AcademyHealth worked with preceptors and fellows to inform creation of a new Community of Practice supported by AcademyHealth’s EDM Forum and guide planning for AcademyHealth’s Concordium conference to provide a national meeting to showcase DSS.
3. Strategic planning to ensure sustainable support for embedded research within delivery systems.Substantial interest in the program developed quickly, with rapid learning over the first few cycles to refine the program to meet host sites’ and fellows’ needs. Both efforts were critical to demonstrate that the DSSF fulfills an important need for our health system partners and members. As indicated previously, strong, sustained interest from prospective host sites and applicants demonstrates the program has created a win-win to jointly assess fit while building skills and supporting continuous learning.
Likewise, Lisa Simpson, President and CEO of AcademyHealth, and Lucy Savitz, DSSF host site preceptor at Intermountain Healthcare, participated in the Canadian Institutes of Health Research (CIHR) Invitational Workshop, “Modernizing Health Services and Policy Research Training in Canada” in March 2016. Shared learning largely informed by the DSSF led to CIHR creating a similar fellowship program with initial awards to be made in 2017 (see https://www.researchnet-recherchenet.ca/rnr16/vwOpprtntyDtls.do?prog=2540&view=browseActive&sponsor=CIHR-8&type=EXACT&resultCount=25 for more information). We are working to thread these efforts together in a way to leverage our learning community of government agencies, academia, and employers as a long-term funding stream for training in delivery science.
Participant Host Site Level
Two selected examples of how DSSF researchers have engaged high-priority topics that contributed to health system operations are provided here.
Kaiser Permanente Southern California: Assessing adherence with “Choosing Wisely” recommendations in oncology. In partnership with preceptor Dr. Michael Gould, 2013-2014 DSSF fellow Dr. Erin Hahn worked with the Kaiser Permanente Southern California (KPSC) Care Improvement Research Team to lead a project addressing several KPSC priority areas. Focusing on “Choosing Wisely” recommendations from the American Society of Clinical Oncology,12 the project evaluated appropriateness of imaging and laboratory services for early-stage cancer patients and survivors between and within 2 integrated health systems, Kaiser Permanente (KP) and Intermountain Healthcare.13,14 Results were presented to KP national leaders, including an external health policy advisory board. In close collaboration with clinical and operational leaders in medical oncology, this multiregional, multisystem project is contributing to targeted quality improvement efforts and improved healthcare value, including audit and feedback of nonrecommended labs.
Dr. Hahn subsequently received a KPSC Incubator Award, a competitive internal grant, to further study factors associated with use of nonrecommended surveillance lab tests for early-stage breast cancer patients. The study focused on medical oncologists within KPSC, categorizing them as high or low utilizers of the tests.15 Results indicate that high utilizers perceive that the tests help manage patient anxiety about recurrence, while acknowledging that the tests do not provide clinical utility. These findings are contributing to the development of targeted survivorship services across the organization.
Intermountain Healthcare: Formative evaluation of large-scale implementation of shared decision-making.Preceptor Dr. Lucy Savitz assembled a team to conduct a formative evaluation of Intermountain Healthcare’s efforts to implement shared decision-making (SDM) as part of its Center for Medicare and Medicaid Innovation Challenge Award. The 2015-2017 DSSF fellow at Intermountain Healthcare, Dr. Kim Brunisholz, served as a core member of the project team, focusing primarily on a mixed-methods evaluation of the SDM program.
Dr. Brunisholz engaged operational leads, clinical teams, patient and family advisory councils, and senior executives to conduct the program assessment. Results demonstrated significant variation in invited participation in SDM among eligible patient populations: preference sensitive conditions (1 in 30 patients), oncology-related diagnosis (1 in 3 patients), and chronic conditions (1 in 74 patients). Provisional analysis of patient-level clinical outcomes demonstrated that among those invited to the SDM program compared to those that were not, total joint replacement was decreased (10.1% vs 17.3%; P < 0.001) and a trend towards breast conservation emerged (61.8% vs 56.4%; P = 0.10). No difference in treatment choice for lower back pain was observed. Qualitative program analysis suggested need for improvements in the areas of (1) routine and continuous staff training, (2) workflow standardization, and (3) active data monitoring with meaningful, actionable feedback to caregivers. In response to these results, a chartered SDM Steering Committee was created (Dr. Brunisholz is a member of that group) to develop a strategic plan for SDM, with an accompanying organizational response to reimplement SDM in a targeted manner. Learning from this program is being leveraged to support a subproject analysis on a large scale using data from the High Value Healthcare Collaborative as part of an AHRQ-funded Center of Excellence award. (See https://www.ahrq.gov/news/newsroom/press-releases/2015/pcorawards.html. For more information on the High Value Healthcare Collaborative, please visit: https://www.highvaluehealthcare.org.)
CONCLUSION
Moving forward, the DSSF will continue working with progressive delivery systems. Partnerships between organizations that are interested in integrating rigorous research practice to drive continuous system improvement and maximize the value of care will have substantial need for technical skills and analytic capacity. They will also need to ensure that researchers working in their systems have sufficient understanding of cultural and political context within the organization to be effective leaders who can manage change.
AcademyHealth created the DSSF in response to the field’s request to build a research workforce that reflects the vision for a 21st Century Health System, as laid out by the NAM.16 We anticipate that as the US Department of Health & Human Services’ goals for payment reform and new measures to promote quality and high-value care are implemented, the DSSF trainees’ skill set will be increasingly valuable and will provide needed thought leadership on strategies to generate and apply evidence in practice.
Disclosure
Ms. Kanani received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship. Drs. Hahn, Gould, and Brunisholz have no conflicts to disclose. Dr. Savitz has received funding from HRQ COE, PCORI LHSNet; received funding for lectures from the Institute from Healthcare Improvement, Department of Epidemiology, University of Utah; received funding for travel, accommodations, and meeting expenses from AHRQ NAC, EDM Forum, AH CAPP, AARP NPC, and PROM TEP; and received additional funding from Dartmouth University. Dr. Holve received funding from Intermountain Healthcare, Kaiser Permanente Southern California for support for the Delivery System Science Fellowship, provided by our delivery system partners, several of whom are coauthors on this manuscript.
References
1. AcademyHealth. Health Services Research in 2020: Summit on the Future of HSR Data and Methods. http://www.academyhealth.org/About/content.cfm?ItemNumber=2529. Accessed March 21, 2016. 2. AcademyHealth. Health Services Research (HSR) Learning Consortium Strategic Plan. http://www.academyhealth.org/files/ProfDev/Files/HSRstrategicplan2011FINAL.pdf. Accessed March 21, 2016. 3. Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. http://www.nationalacademies.org/hmd/~/media/Files/Report%20Files/2009/ComparativeEffectivenessResearchPriorities/CER%20report%20brief%2008-13-09.pdf. Accessed March 21, 2016. 4. Bonham A, Rich E, Davis D, Longnecker D, Heinig S. Putting evidence to work: an expanded research agenda for academic medicine in the era of health care reform. Acad Med. 2010;85(10):1551-1553. PubMed 5. Zerhouni E. Translational and clinical science—time for a new vision. N Engl J Med. 2005;353(15):1621-1623. PubMed 6. AcademyHealth. “Getting Answers We Can Believe In: Methodological Considerations When Using Electronic Clinical Data for Research,” EDM Forum, December 2012. 7. Rich G, Collins A. Current and Future Demand for Health Services Researchers. Funded by the Agency for Healthcare Research and Quality (AHRQ). Presented at the AcademyHealth HSR Workforce Conference, Understanding the Current Health Services Research Workforce and Maximizing Its Future, funded by AHRQ, Patient-Centered Outcomes Research Institute, and the Robert Wood Johnson Foundation. October 2016. 8. AcademyHealth. Delivery System Science Fellowship. http://www.academyhealth.org/dssf. Accessed March 21, 2016. 9. Institute for Healthcare Improvement. IHI Triple Aim Initiative. http://www.ihi.org/engage/initiatives/tripleaim/Pages/default.aspx. Accessed March 21, 2016. 10. Psek W, Stametz R, Bailey-Davis L, et al. Operationalizing the learning health care system in an integrated delivery system. eGEMs. 2015;3(1):1122. PubMed 11. Thompson C, Kurian A, Luft H. Linking electronic health records to better understand breast cancer patient pathways within and between two health systems. eGEMs. 2015;3(1):1127. PubMed 12. Schnipper L, Smith TJ, Raghavan D, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: The top five list for oncology. J Clin Oncol. 2012;30(14):1715-1724. PubMed 13. Hahn E, Tang T, Lee JS, et al. Use of posttreatment imaging and biomarkers in survivors of early‐stage breast cancer: Inappropriate surveillance or necessary care? Cancer. 2015;122(6):908-916. PubMed 14. Hahn E, Tang T, Lee JS, et al. Use of imaging for staging of early-stage breast cancer in two integrated health care systems: Adherence with a choosing wisely recommendation. J Oncol Pract. 2015;11(3):e320-e328. PubMed 15. Hahn EE, Munoz-Plaza C, Wang J, et al. Anxiety, culture, expectations: Oncologist-perceived factors associated with use of non-recommended serum tumor marker tests for surveillance of early stage breast cancer. J Oncol Pract. 2016;13(1):e77-e290. PubMed 16. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences; 2000.
References
1. AcademyHealth. Health Services Research in 2020: Summit on the Future of HSR Data and Methods. http://www.academyhealth.org/About/content.cfm?ItemNumber=2529. Accessed March 21, 2016. 2. AcademyHealth. Health Services Research (HSR) Learning Consortium Strategic Plan. http://www.academyhealth.org/files/ProfDev/Files/HSRstrategicplan2011FINAL.pdf. Accessed March 21, 2016. 3. Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. http://www.nationalacademies.org/hmd/~/media/Files/Report%20Files/2009/ComparativeEffectivenessResearchPriorities/CER%20report%20brief%2008-13-09.pdf. Accessed March 21, 2016. 4. Bonham A, Rich E, Davis D, Longnecker D, Heinig S. Putting evidence to work: an expanded research agenda for academic medicine in the era of health care reform. Acad Med. 2010;85(10):1551-1553. PubMed 5. Zerhouni E. Translational and clinical science—time for a new vision. N Engl J Med. 2005;353(15):1621-1623. PubMed 6. AcademyHealth. “Getting Answers We Can Believe In: Methodological Considerations When Using Electronic Clinical Data for Research,” EDM Forum, December 2012. 7. Rich G, Collins A. Current and Future Demand for Health Services Researchers. Funded by the Agency for Healthcare Research and Quality (AHRQ). Presented at the AcademyHealth HSR Workforce Conference, Understanding the Current Health Services Research Workforce and Maximizing Its Future, funded by AHRQ, Patient-Centered Outcomes Research Institute, and the Robert Wood Johnson Foundation. October 2016. 8. AcademyHealth. Delivery System Science Fellowship. http://www.academyhealth.org/dssf. Accessed March 21, 2016. 9. Institute for Healthcare Improvement. IHI Triple Aim Initiative. http://www.ihi.org/engage/initiatives/tripleaim/Pages/default.aspx. Accessed March 21, 2016. 10. Psek W, Stametz R, Bailey-Davis L, et al. Operationalizing the learning health care system in an integrated delivery system. eGEMs. 2015;3(1):1122. PubMed 11. Thompson C, Kurian A, Luft H. Linking electronic health records to better understand breast cancer patient pathways within and between two health systems. eGEMs. 2015;3(1):1127. PubMed 12. Schnipper L, Smith TJ, Raghavan D, et al. American Society of Clinical Oncology identifies five key opportunities to improve care and reduce costs: The top five list for oncology. J Clin Oncol. 2012;30(14):1715-1724. PubMed 13. Hahn E, Tang T, Lee JS, et al. Use of posttreatment imaging and biomarkers in survivors of early‐stage breast cancer: Inappropriate surveillance or necessary care? Cancer. 2015;122(6):908-916. PubMed 14. Hahn E, Tang T, Lee JS, et al. Use of imaging for staging of early-stage breast cancer in two integrated health care systems: Adherence with a choosing wisely recommendation. J Oncol Pract. 2015;11(3):e320-e328. PubMed 15. Hahn EE, Munoz-Plaza C, Wang J, et al. Anxiety, culture, expectations: Oncologist-perceived factors associated with use of non-recommended serum tumor marker tests for surveillance of early stage breast cancer. J Oncol Pract. 2016;13(1):e77-e290. PubMed 16. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences; 2000.
Nisha Kanani, MPH, AcademyHealth, 1666 K Street NW Suite 1100, Washington, DC 20006; Telephone: 202-292-6762; Fax: 202-292-6862; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
Hospitalists must create rapport and communicate large amounts of information in a short amount of time without having a prior relationship with the patient.1 High-quality communication can improve satisfaction and compliance, while poor communication leaves patients ill prepared to transition back to the community.2–10
Many medical schools use standardized patients (SPs) to both train and evaluate their students’ communication skills. To our knowledge, no published studies describe using SPs to assess or teach communication skills for hospitalists.
Our objective in this study was to use SPs to assess for deficits in our hospitalists’ communication skills and to determine whether feedback provided by SPs could improve hospitalist confidence in and performance of optimal communication behaviors.
METHODS
Setting and Participants
Table 1
The study took place at the Morchand Center at Icahn School of Medicine at Mount Sinai, an SP center that trains medical students and residents. All 23 hospitalists had prior experience with SPs during their training and their main clinical duties were as attendings on teaching and non-teaching services at The Mount Sinai Hospital in New York City, a large academic center. Participation in the standardized encounters was required.
Scenario and Checklist Development
We developed 3 SP encounters around common hospitalist-patient interactions: daily rounding, discharge, and interacting with a difficult patient. In order to assess communication skills, we developed a checklist with 3 core domains: Courtesy and Respect, Listen, and Explain. Each domain corresponded to 1 of 3 questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that pertained to doctor’s communications skills: (1) How often did doctors treat you with courtesy and respect? (2) How often did doctors listen carefully to you? (3) How often did doctors explain things in a way you could understand? We then developed checklist items that corresponded to essential communication skills within each of the 3 domains. These communication skills were based on best practices and published literature.
Table 2
Discharge Encounter (Table 2): Patient admitted the night before with abdominal pain by another hospitalist. The checklist was based on AIDET®, an effective communication skills training protocol that our hospitalist group had been trained on.11
Daily Rounding Encounter (Table 3): Patient being discharged after an admission for congestive heart failure. The checklist was developed from the Society of Hospital Medicine discharge toolkit.12
Table 3 Difficult Patient Encounter (Table 4): A patient and his daughter who were unhappy because of a previously missed lung mass that was now found to be cancer. Our checklist was based on characteristics of therapeutic bedside manner.13
The checklist items were each scored using a 3-point scale of adequate, partial, or inadequate performance. A description of checklist items within each of the 3 domains is listed in Table 1. A postintervention survey was filled out by all hospitalists after the 3 encounters.
Table 4
Simulated Encounters
All 3 encounters occurred on the same day and each one lasted 1 hour (20 minutes for the encounter, 10 minutes for a posttest survey, and 30 minutes of feedback from the SP). For each case, a task list was given to the hospitalist before walking into the room (Appendix 1). During the feedback session, the SP gave the hospitalist feedback using the case checklist items. They then watched a video of the encounter and the SP further emphasized areas for improvement.
SP Training
SP training consisted of three 3-hour training sessions, which included review of the case, script, guidance on scoring the checklist items, role plays with attending hospitalists, and feedback training. Each SP was assigned to only 1 case.
Seven of the 24 encounters for each SP were reviewed independently by 2 investigators who created a final score for each checklist item which was compared to the SP’s checklist item score. The kappa (k) statistic was used to evaluate inter-observer reliability using the SAS system software (SAS Institute Inc.).
Analysis
The percent of hospitalists who performed each checklist item adequately within in each of the 3 domains (Courtesy and Respect, Listen, and Explain) was calculated. To compare the 3 domains, t tests were used.
We calculated the percent that our hospitalist group received on the 3 HCAHPS doctor’s questions 1 year prior to our SP exercise and 1 year after the SP exercise.
RESULTS
Twenty-three hospitalists completed all 3 encounters. For the 3 domains (Courtesy and Respect, Listen, and Explain), hospitalists performed significantly better in the Listen domain compared to the other 2 domains, with a mean percent adequate score of 90.2 % (95% confidence interval [CI], 72.2%-100%; P < 0.05), and significantly worse in the Explain domain compared to the other 2 domains, with a mean percent adequate score of 65.0% (95% CI, 49.2%-83.6%; P < 0.05). The mean percent adequate score for the Courtesy and Respect domain was 81.6% (95% CI, 56%-100%). This was significantly higher than the Explain domain and significantly lower than the Listen domain.
Posttest survey results showed that hospitalists had an increased level of confidence in their bedside manner, patient satisfaction skills, and high-quality discharge discussion skills.
Inter-Rater Reliability
Inter-rater reliability for the discharge encounter, the daily rounding encounter, and the difficult patient encounter were 0.74 (95% CI, 0.64-0.84), 0.73 (95% CI, 0.63-0.82), and 0.73 (95% CI, 0.63-0.83), respectively.
HCAHPS
Four hundred sixteen HCAHPS surveys were returned in the year prior to our SP exercise, and the percent of patients who answered always to the questions on Courtesy and Respect, Listen, and Explain were 80.4%, 74.2 %, and 69.4 %, respectively. In the year after our SP exercise, 492 surveys were returned, and there was no significant change in HCAHP scores for the group (80.9% for Courtesy and Respect, 70.2% for the Listen question, and 70.5% for Explain).
DISCUSSION
We have shown that SPs can be used to assess deficits in hospitalist communication skills and provide feedback that can improve hospitalist confidence in performing optimal communication behaviors. We have also shown that hospitalists perceive the exercise as beneficial in improving their communication skills and perceive them as similar to their real patient encounters.
The Explain domain was significantly worse than the Courtesy and Respect and Listen domains for our hospitalists. Analysis of the checklist items within the Explain domain found that the items within this domain that were most problematic for hospitalists were summarizing information at the end of the encounter, using teach-back (a communication confirmation method where a healthcare provider asks a patient to repeat what was said to confirm understanding), encouraging additional questions by using open-ended statements (What questions do you have?) instead of close ended statements (Do you have any questions?), managing team and self-up, setting expectations on length of stay, and timing of tests. This correlated with our patient satisfaction HCAHPS data, which showed that patients consistently rated our hospitalists’ ability to explain things in a way they could understand lowest among the 3 questions. HCAHPS scores did not change after our SP exercise, and this lack of improvement may indicate that meaningful improvement in communication skills requires longitudinal interventions and real-time feedback rather than a single exercise, as was shown in a recent study looking at daily patient satisfaction score feedback given to internal medicine residents.14
Our study had several limitations. First, hospitalists knew they were being videotaped and observed, which may have altered their behaviors and may not reflect our hospitalists’ actual behaviors with patients. Furthermore, we did not examine whether the feedback given was incorporated into our hospitalists’ daily patient communications and whether this impacted our patients care other than examining HCAHPS scores.
CONCLUSION
SPs can be used to identify deficiencies in communication skills and provide specific guidance that improves hospitalist confidence in their communication skills.
Acknowledgment
This trial was funded by a grant from The Doctor’s Company Foundation.
Disclosure
None of the authors report any conflicts of interest.
1. Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111(9B):31S-35S. PubMed 2. Kurtz S, Silverman J, Draper J. Teaching and learning communication skills in medicine. 2nd ed. London, UK: Radcliffe Publishing Ltd.; 2009. 3. Stewart MA. What is a successful doctor–patient interview? A study of interactions and outcomes. Soc Sci Med. 1984;9:167-175. PubMed 4. Kaplan SH, Greenfield S, Ware JE. Assessing the effects of physician–patient interactions on the outcomes of chronic disease. Med Care. 1989;27:S110-S127. PubMed 5. Levinson W, Lesser CS, Epstein RM. Developing physician communication skills for patient-centered care. Health Aff (Millwood). 2010;29:1310-1318. PubMed 6. Griffin SJ, Kinmonth AL, Veltman MWM, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2: 595-608. PubMed 7. Levinson W, Roter DL, Mullooly JP, Dull V, Frankel R. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559. PubMed 8. Levinson W. Physician-patient communication: a key to malpractice prevention. [Editorial]. JAMA. 1994;272:1619-1620. PubMed 9. Beckman HB, Markakis KM, Suchman AL, Frankel RM. The doctor–patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370. PubMed 10. Wofford MM, Wofford JL, Bothra J, Kendrick SB, Patient complaints about physician behaviors: a qualitative study. Acad Med. 2004;79(2):134-138. PubMed 11. Studer Group. Acknowledge, Introduce, Duration, Explanation and Thank You. http://www.studergroup.com/aidet. Accessed November 5, 2012. 12. SHM Discharge/Heart Failure Implementation Toolkit. https://www.hospitalmedicine. org/Web/Quality_Innovation/Implementation_Toolkits/Congestive_Heart_ Failure/Web/Quality___Innovation/Implementation_Toolkit/CHF/CHF_overview. aspx?hkey=f91120e3-6c8f-4a55-90e7-9b6a4b5472ef. 13. Carkhuff, RR. Helping and Human Relations: A Primer for Lay and Professional Helpers. Volume I. New York, NY: Holt, Rinehart & Winston; 1969. 14. Banka G, Edgington S, Kyulo N, et al. Improving patient satisfaction through physician education, feedback, and incentives. J Hosp Med. 2015;10:497-502. PubMed
Hospitalists must create rapport and communicate large amounts of information in a short amount of time without having a prior relationship with the patient.1 High-quality communication can improve satisfaction and compliance, while poor communication leaves patients ill prepared to transition back to the community.2–10
Many medical schools use standardized patients (SPs) to both train and evaluate their students’ communication skills. To our knowledge, no published studies describe using SPs to assess or teach communication skills for hospitalists.
Our objective in this study was to use SPs to assess for deficits in our hospitalists’ communication skills and to determine whether feedback provided by SPs could improve hospitalist confidence in and performance of optimal communication behaviors.
METHODS
Setting and Participants
Table 1
The study took place at the Morchand Center at Icahn School of Medicine at Mount Sinai, an SP center that trains medical students and residents. All 23 hospitalists had prior experience with SPs during their training and their main clinical duties were as attendings on teaching and non-teaching services at The Mount Sinai Hospital in New York City, a large academic center. Participation in the standardized encounters was required.
Scenario and Checklist Development
We developed 3 SP encounters around common hospitalist-patient interactions: daily rounding, discharge, and interacting with a difficult patient. In order to assess communication skills, we developed a checklist with 3 core domains: Courtesy and Respect, Listen, and Explain. Each domain corresponded to 1 of 3 questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that pertained to doctor’s communications skills: (1) How often did doctors treat you with courtesy and respect? (2) How often did doctors listen carefully to you? (3) How often did doctors explain things in a way you could understand? We then developed checklist items that corresponded to essential communication skills within each of the 3 domains. These communication skills were based on best practices and published literature.
Table 2
Discharge Encounter (Table 2): Patient admitted the night before with abdominal pain by another hospitalist. The checklist was based on AIDET®, an effective communication skills training protocol that our hospitalist group had been trained on.11
Daily Rounding Encounter (Table 3): Patient being discharged after an admission for congestive heart failure. The checklist was developed from the Society of Hospital Medicine discharge toolkit.12
Table 3 Difficult Patient Encounter (Table 4): A patient and his daughter who were unhappy because of a previously missed lung mass that was now found to be cancer. Our checklist was based on characteristics of therapeutic bedside manner.13
The checklist items were each scored using a 3-point scale of adequate, partial, or inadequate performance. A description of checklist items within each of the 3 domains is listed in Table 1. A postintervention survey was filled out by all hospitalists after the 3 encounters.
Table 4
Simulated Encounters
All 3 encounters occurred on the same day and each one lasted 1 hour (20 minutes for the encounter, 10 minutes for a posttest survey, and 30 minutes of feedback from the SP). For each case, a task list was given to the hospitalist before walking into the room (Appendix 1). During the feedback session, the SP gave the hospitalist feedback using the case checklist items. They then watched a video of the encounter and the SP further emphasized areas for improvement.
SP Training
SP training consisted of three 3-hour training sessions, which included review of the case, script, guidance on scoring the checklist items, role plays with attending hospitalists, and feedback training. Each SP was assigned to only 1 case.
Seven of the 24 encounters for each SP were reviewed independently by 2 investigators who created a final score for each checklist item which was compared to the SP’s checklist item score. The kappa (k) statistic was used to evaluate inter-observer reliability using the SAS system software (SAS Institute Inc.).
Analysis
The percent of hospitalists who performed each checklist item adequately within in each of the 3 domains (Courtesy and Respect, Listen, and Explain) was calculated. To compare the 3 domains, t tests were used.
We calculated the percent that our hospitalist group received on the 3 HCAHPS doctor’s questions 1 year prior to our SP exercise and 1 year after the SP exercise.
RESULTS
Twenty-three hospitalists completed all 3 encounters. For the 3 domains (Courtesy and Respect, Listen, and Explain), hospitalists performed significantly better in the Listen domain compared to the other 2 domains, with a mean percent adequate score of 90.2 % (95% confidence interval [CI], 72.2%-100%; P < 0.05), and significantly worse in the Explain domain compared to the other 2 domains, with a mean percent adequate score of 65.0% (95% CI, 49.2%-83.6%; P < 0.05). The mean percent adequate score for the Courtesy and Respect domain was 81.6% (95% CI, 56%-100%). This was significantly higher than the Explain domain and significantly lower than the Listen domain.
Posttest survey results showed that hospitalists had an increased level of confidence in their bedside manner, patient satisfaction skills, and high-quality discharge discussion skills.
Inter-Rater Reliability
Inter-rater reliability for the discharge encounter, the daily rounding encounter, and the difficult patient encounter were 0.74 (95% CI, 0.64-0.84), 0.73 (95% CI, 0.63-0.82), and 0.73 (95% CI, 0.63-0.83), respectively.
HCAHPS
Four hundred sixteen HCAHPS surveys were returned in the year prior to our SP exercise, and the percent of patients who answered always to the questions on Courtesy and Respect, Listen, and Explain were 80.4%, 74.2 %, and 69.4 %, respectively. In the year after our SP exercise, 492 surveys were returned, and there was no significant change in HCAHP scores for the group (80.9% for Courtesy and Respect, 70.2% for the Listen question, and 70.5% for Explain).
DISCUSSION
We have shown that SPs can be used to assess deficits in hospitalist communication skills and provide feedback that can improve hospitalist confidence in performing optimal communication behaviors. We have also shown that hospitalists perceive the exercise as beneficial in improving their communication skills and perceive them as similar to their real patient encounters.
The Explain domain was significantly worse than the Courtesy and Respect and Listen domains for our hospitalists. Analysis of the checklist items within the Explain domain found that the items within this domain that were most problematic for hospitalists were summarizing information at the end of the encounter, using teach-back (a communication confirmation method where a healthcare provider asks a patient to repeat what was said to confirm understanding), encouraging additional questions by using open-ended statements (What questions do you have?) instead of close ended statements (Do you have any questions?), managing team and self-up, setting expectations on length of stay, and timing of tests. This correlated with our patient satisfaction HCAHPS data, which showed that patients consistently rated our hospitalists’ ability to explain things in a way they could understand lowest among the 3 questions. HCAHPS scores did not change after our SP exercise, and this lack of improvement may indicate that meaningful improvement in communication skills requires longitudinal interventions and real-time feedback rather than a single exercise, as was shown in a recent study looking at daily patient satisfaction score feedback given to internal medicine residents.14
Our study had several limitations. First, hospitalists knew they were being videotaped and observed, which may have altered their behaviors and may not reflect our hospitalists’ actual behaviors with patients. Furthermore, we did not examine whether the feedback given was incorporated into our hospitalists’ daily patient communications and whether this impacted our patients care other than examining HCAHPS scores.
CONCLUSION
SPs can be used to identify deficiencies in communication skills and provide specific guidance that improves hospitalist confidence in their communication skills.
Acknowledgment
This trial was funded by a grant from The Doctor’s Company Foundation.
Disclosure
None of the authors report any conflicts of interest.
Hospitalists must create rapport and communicate large amounts of information in a short amount of time without having a prior relationship with the patient.1 High-quality communication can improve satisfaction and compliance, while poor communication leaves patients ill prepared to transition back to the community.2–10
Many medical schools use standardized patients (SPs) to both train and evaluate their students’ communication skills. To our knowledge, no published studies describe using SPs to assess or teach communication skills for hospitalists.
Our objective in this study was to use SPs to assess for deficits in our hospitalists’ communication skills and to determine whether feedback provided by SPs could improve hospitalist confidence in and performance of optimal communication behaviors.
METHODS
Setting and Participants
Table 1
The study took place at the Morchand Center at Icahn School of Medicine at Mount Sinai, an SP center that trains medical students and residents. All 23 hospitalists had prior experience with SPs during their training and their main clinical duties were as attendings on teaching and non-teaching services at The Mount Sinai Hospital in New York City, a large academic center. Participation in the standardized encounters was required.
Scenario and Checklist Development
We developed 3 SP encounters around common hospitalist-patient interactions: daily rounding, discharge, and interacting with a difficult patient. In order to assess communication skills, we developed a checklist with 3 core domains: Courtesy and Respect, Listen, and Explain. Each domain corresponded to 1 of 3 questions on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that pertained to doctor’s communications skills: (1) How often did doctors treat you with courtesy and respect? (2) How often did doctors listen carefully to you? (3) How often did doctors explain things in a way you could understand? We then developed checklist items that corresponded to essential communication skills within each of the 3 domains. These communication skills were based on best practices and published literature.
Table 2
Discharge Encounter (Table 2): Patient admitted the night before with abdominal pain by another hospitalist. The checklist was based on AIDET®, an effective communication skills training protocol that our hospitalist group had been trained on.11
Daily Rounding Encounter (Table 3): Patient being discharged after an admission for congestive heart failure. The checklist was developed from the Society of Hospital Medicine discharge toolkit.12
Table 3 Difficult Patient Encounter (Table 4): A patient and his daughter who were unhappy because of a previously missed lung mass that was now found to be cancer. Our checklist was based on characteristics of therapeutic bedside manner.13
The checklist items were each scored using a 3-point scale of adequate, partial, or inadequate performance. A description of checklist items within each of the 3 domains is listed in Table 1. A postintervention survey was filled out by all hospitalists after the 3 encounters.
Table 4
Simulated Encounters
All 3 encounters occurred on the same day and each one lasted 1 hour (20 minutes for the encounter, 10 minutes for a posttest survey, and 30 minutes of feedback from the SP). For each case, a task list was given to the hospitalist before walking into the room (Appendix 1). During the feedback session, the SP gave the hospitalist feedback using the case checklist items. They then watched a video of the encounter and the SP further emphasized areas for improvement.
SP Training
SP training consisted of three 3-hour training sessions, which included review of the case, script, guidance on scoring the checklist items, role plays with attending hospitalists, and feedback training. Each SP was assigned to only 1 case.
Seven of the 24 encounters for each SP were reviewed independently by 2 investigators who created a final score for each checklist item which was compared to the SP’s checklist item score. The kappa (k) statistic was used to evaluate inter-observer reliability using the SAS system software (SAS Institute Inc.).
Analysis
The percent of hospitalists who performed each checklist item adequately within in each of the 3 domains (Courtesy and Respect, Listen, and Explain) was calculated. To compare the 3 domains, t tests were used.
We calculated the percent that our hospitalist group received on the 3 HCAHPS doctor’s questions 1 year prior to our SP exercise and 1 year after the SP exercise.
RESULTS
Twenty-three hospitalists completed all 3 encounters. For the 3 domains (Courtesy and Respect, Listen, and Explain), hospitalists performed significantly better in the Listen domain compared to the other 2 domains, with a mean percent adequate score of 90.2 % (95% confidence interval [CI], 72.2%-100%; P < 0.05), and significantly worse in the Explain domain compared to the other 2 domains, with a mean percent adequate score of 65.0% (95% CI, 49.2%-83.6%; P < 0.05). The mean percent adequate score for the Courtesy and Respect domain was 81.6% (95% CI, 56%-100%). This was significantly higher than the Explain domain and significantly lower than the Listen domain.
Posttest survey results showed that hospitalists had an increased level of confidence in their bedside manner, patient satisfaction skills, and high-quality discharge discussion skills.
Inter-Rater Reliability
Inter-rater reliability for the discharge encounter, the daily rounding encounter, and the difficult patient encounter were 0.74 (95% CI, 0.64-0.84), 0.73 (95% CI, 0.63-0.82), and 0.73 (95% CI, 0.63-0.83), respectively.
HCAHPS
Four hundred sixteen HCAHPS surveys were returned in the year prior to our SP exercise, and the percent of patients who answered always to the questions on Courtesy and Respect, Listen, and Explain were 80.4%, 74.2 %, and 69.4 %, respectively. In the year after our SP exercise, 492 surveys were returned, and there was no significant change in HCAHP scores for the group (80.9% for Courtesy and Respect, 70.2% for the Listen question, and 70.5% for Explain).
DISCUSSION
We have shown that SPs can be used to assess deficits in hospitalist communication skills and provide feedback that can improve hospitalist confidence in performing optimal communication behaviors. We have also shown that hospitalists perceive the exercise as beneficial in improving their communication skills and perceive them as similar to their real patient encounters.
The Explain domain was significantly worse than the Courtesy and Respect and Listen domains for our hospitalists. Analysis of the checklist items within the Explain domain found that the items within this domain that were most problematic for hospitalists were summarizing information at the end of the encounter, using teach-back (a communication confirmation method where a healthcare provider asks a patient to repeat what was said to confirm understanding), encouraging additional questions by using open-ended statements (What questions do you have?) instead of close ended statements (Do you have any questions?), managing team and self-up, setting expectations on length of stay, and timing of tests. This correlated with our patient satisfaction HCAHPS data, which showed that patients consistently rated our hospitalists’ ability to explain things in a way they could understand lowest among the 3 questions. HCAHPS scores did not change after our SP exercise, and this lack of improvement may indicate that meaningful improvement in communication skills requires longitudinal interventions and real-time feedback rather than a single exercise, as was shown in a recent study looking at daily patient satisfaction score feedback given to internal medicine residents.14
Our study had several limitations. First, hospitalists knew they were being videotaped and observed, which may have altered their behaviors and may not reflect our hospitalists’ actual behaviors with patients. Furthermore, we did not examine whether the feedback given was incorporated into our hospitalists’ daily patient communications and whether this impacted our patients care other than examining HCAHPS scores.
CONCLUSION
SPs can be used to identify deficiencies in communication skills and provide specific guidance that improves hospitalist confidence in their communication skills.
Acknowledgment
This trial was funded by a grant from The Doctor’s Company Foundation.
Disclosure
None of the authors report any conflicts of interest.
References
1. Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111(9B):31S-35S. PubMed 2. Kurtz S, Silverman J, Draper J. Teaching and learning communication skills in medicine. 2nd ed. London, UK: Radcliffe Publishing Ltd.; 2009. 3. Stewart MA. What is a successful doctor–patient interview? A study of interactions and outcomes. Soc Sci Med. 1984;9:167-175. PubMed 4. Kaplan SH, Greenfield S, Ware JE. Assessing the effects of physician–patient interactions on the outcomes of chronic disease. Med Care. 1989;27:S110-S127. PubMed 5. Levinson W, Lesser CS, Epstein RM. Developing physician communication skills for patient-centered care. Health Aff (Millwood). 2010;29:1310-1318. PubMed 6. Griffin SJ, Kinmonth AL, Veltman MWM, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2: 595-608. PubMed 7. Levinson W, Roter DL, Mullooly JP, Dull V, Frankel R. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559. PubMed 8. Levinson W. Physician-patient communication: a key to malpractice prevention. [Editorial]. JAMA. 1994;272:1619-1620. PubMed 9. Beckman HB, Markakis KM, Suchman AL, Frankel RM. The doctor–patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370. PubMed 10. Wofford MM, Wofford JL, Bothra J, Kendrick SB, Patient complaints about physician behaviors: a qualitative study. Acad Med. 2004;79(2):134-138. PubMed 11. Studer Group. Acknowledge, Introduce, Duration, Explanation and Thank You. http://www.studergroup.com/aidet. Accessed November 5, 2012. 12. SHM Discharge/Heart Failure Implementation Toolkit. https://www.hospitalmedicine. org/Web/Quality_Innovation/Implementation_Toolkits/Congestive_Heart_ Failure/Web/Quality___Innovation/Implementation_Toolkit/CHF/CHF_overview. aspx?hkey=f91120e3-6c8f-4a55-90e7-9b6a4b5472ef. 13. Carkhuff, RR. Helping and Human Relations: A Primer for Lay and Professional Helpers. Volume I. New York, NY: Holt, Rinehart & Winston; 1969. 14. Banka G, Edgington S, Kyulo N, et al. Improving patient satisfaction through physician education, feedback, and incentives. J Hosp Med. 2015;10:497-502. PubMed
References
1. Barnett PB. Rapport and the hospitalist. Am J Med. 2001;111(9B):31S-35S. PubMed 2. Kurtz S, Silverman J, Draper J. Teaching and learning communication skills in medicine. 2nd ed. London, UK: Radcliffe Publishing Ltd.; 2009. 3. Stewart MA. What is a successful doctor–patient interview? A study of interactions and outcomes. Soc Sci Med. 1984;9:167-175. PubMed 4. Kaplan SH, Greenfield S, Ware JE. Assessing the effects of physician–patient interactions on the outcomes of chronic disease. Med Care. 1989;27:S110-S127. PubMed 5. Levinson W, Lesser CS, Epstein RM. Developing physician communication skills for patient-centered care. Health Aff (Millwood). 2010;29:1310-1318. PubMed 6. Griffin SJ, Kinmonth AL, Veltman MWM, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2: 595-608. PubMed 7. Levinson W, Roter DL, Mullooly JP, Dull V, Frankel R. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277:553-559. PubMed 8. Levinson W. Physician-patient communication: a key to malpractice prevention. [Editorial]. JAMA. 1994;272:1619-1620. PubMed 9. Beckman HB, Markakis KM, Suchman AL, Frankel RM. The doctor–patient relationship and malpractice. Lessons from plaintiff depositions. Arch Intern Med. 1994;154:1365-1370. PubMed 10. Wofford MM, Wofford JL, Bothra J, Kendrick SB, Patient complaints about physician behaviors: a qualitative study. Acad Med. 2004;79(2):134-138. PubMed 11. Studer Group. Acknowledge, Introduce, Duration, Explanation and Thank You. http://www.studergroup.com/aidet. Accessed November 5, 2012. 12. SHM Discharge/Heart Failure Implementation Toolkit. https://www.hospitalmedicine. org/Web/Quality_Innovation/Implementation_Toolkits/Congestive_Heart_ Failure/Web/Quality___Innovation/Implementation_Toolkit/CHF/CHF_overview. aspx?hkey=f91120e3-6c8f-4a55-90e7-9b6a4b5472ef. 13. Carkhuff, RR. Helping and Human Relations: A Primer for Lay and Professional Helpers. Volume I. New York, NY: Holt, Rinehart & Winston; 1969. 14. Banka G, Edgington S, Kyulo N, et al. Improving patient satisfaction through physician education, feedback, and incentives. J Hosp Med. 2015;10:497-502. PubMed
Dennis T. Chang, MD, Division of Hospital Medicine, Mount Sinai Health System, One Gustave L Levy Place, Box 1087, New York NY 10019; Telephone: 212-241-1653; Fax: 212-289-6393; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
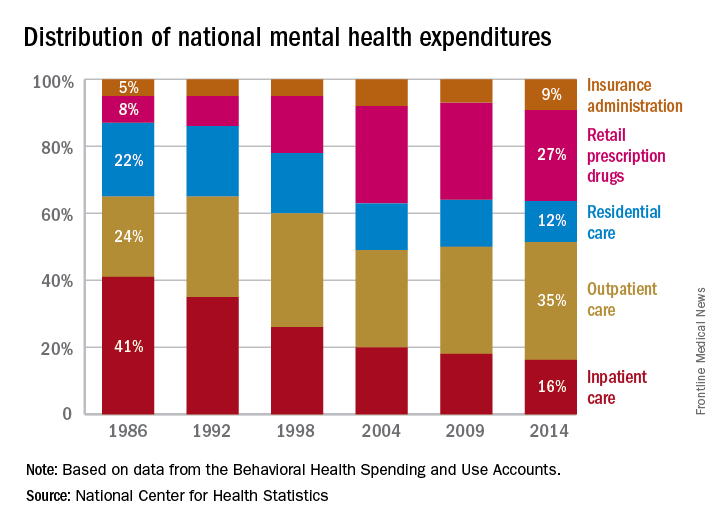






 and increased background staining secondary to hypergammaglobulinemia.")
 Color fundus photographs show mild dilatation of patient’s retinal veins and retinal hemorrhages. (C,D) Red-free fundus photographs show round blot hemorrhages occurring from vessels within retina (arrow) and linear, fl ame-shaped hemorrhages occurr")
.")



")
")
")