User login
To the limit
Do you believe that children whose parents can make and enforce rules are more likely to thrive than those children whose parents are hesitant to set limits? If you don’t see limit setting as a critical function of parenting, you and I are not only marching to different drummers, we aren’t even in the same parade.
You may be tempted to write me off as just another old school ranter because I believe that limit setting is one of the cornerstones of parenting. But, let’s look at some of the evidence. There are several studies demonstrating that children whose parents set bedtimes get more sleep. One recent survey also found that teenagers who got more sleep as a result of enforced bedtimes functioned better in school (Sleep. 2011 Jun 1;34[6]:797-800).
An important question is whether permissive parenting is a problem that warrants our concern as pediatricians. We always are on alert for the red flags of abusive parenting, and, obviously, failure to intervene in cases of abuse can be disastrous. However, if we can believe the results from the studies that have already been completed, it seems pretty clear that permissive parenting can spawn behavioral problems, sleep problems, and the myriad of downstream effects that can result from sleep deprivation. And I haven’t even touched on the possible relationship between permissive parenting and the obesity epidemic.
If we still consider ourselves the preventive medicine specialists, shouldn’t pediatricians and family medicine physicians be more invested in minimizing the unhealthy consequences of permissive parenting? If we can agree on a firm “Yes!” the next question is, When and how should we address the issue?
A more nuanced discussion can be the germ of a future Letters from Maine, but the short answer is that we need to sound as nonjudgmental as possible as we present our case for limit setting. We need to start early before the die is cast, and we should be better about publicizing our supporting evidence. Setting a bedtime can begin in the first 6 months of life. Helping parents learn to say, “No, we aren’t going to feed you only what you like to eat!” can start as an infant makes what can be an unsettling transition to solid food.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Do you believe that children whose parents can make and enforce rules are more likely to thrive than those children whose parents are hesitant to set limits? If you don’t see limit setting as a critical function of parenting, you and I are not only marching to different drummers, we aren’t even in the same parade.
You may be tempted to write me off as just another old school ranter because I believe that limit setting is one of the cornerstones of parenting. But, let’s look at some of the evidence. There are several studies demonstrating that children whose parents set bedtimes get more sleep. One recent survey also found that teenagers who got more sleep as a result of enforced bedtimes functioned better in school (Sleep. 2011 Jun 1;34[6]:797-800).
An important question is whether permissive parenting is a problem that warrants our concern as pediatricians. We always are on alert for the red flags of abusive parenting, and, obviously, failure to intervene in cases of abuse can be disastrous. However, if we can believe the results from the studies that have already been completed, it seems pretty clear that permissive parenting can spawn behavioral problems, sleep problems, and the myriad of downstream effects that can result from sleep deprivation. And I haven’t even touched on the possible relationship between permissive parenting and the obesity epidemic.
If we still consider ourselves the preventive medicine specialists, shouldn’t pediatricians and family medicine physicians be more invested in minimizing the unhealthy consequences of permissive parenting? If we can agree on a firm “Yes!” the next question is, When and how should we address the issue?
A more nuanced discussion can be the germ of a future Letters from Maine, but the short answer is that we need to sound as nonjudgmental as possible as we present our case for limit setting. We need to start early before the die is cast, and we should be better about publicizing our supporting evidence. Setting a bedtime can begin in the first 6 months of life. Helping parents learn to say, “No, we aren’t going to feed you only what you like to eat!” can start as an infant makes what can be an unsettling transition to solid food.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Do you believe that children whose parents can make and enforce rules are more likely to thrive than those children whose parents are hesitant to set limits? If you don’t see limit setting as a critical function of parenting, you and I are not only marching to different drummers, we aren’t even in the same parade.
You may be tempted to write me off as just another old school ranter because I believe that limit setting is one of the cornerstones of parenting. But, let’s look at some of the evidence. There are several studies demonstrating that children whose parents set bedtimes get more sleep. One recent survey also found that teenagers who got more sleep as a result of enforced bedtimes functioned better in school (Sleep. 2011 Jun 1;34[6]:797-800).
An important question is whether permissive parenting is a problem that warrants our concern as pediatricians. We always are on alert for the red flags of abusive parenting, and, obviously, failure to intervene in cases of abuse can be disastrous. However, if we can believe the results from the studies that have already been completed, it seems pretty clear that permissive parenting can spawn behavioral problems, sleep problems, and the myriad of downstream effects that can result from sleep deprivation. And I haven’t even touched on the possible relationship between permissive parenting and the obesity epidemic.
If we still consider ourselves the preventive medicine specialists, shouldn’t pediatricians and family medicine physicians be more invested in minimizing the unhealthy consequences of permissive parenting? If we can agree on a firm “Yes!” the next question is, When and how should we address the issue?
A more nuanced discussion can be the germ of a future Letters from Maine, but the short answer is that we need to sound as nonjudgmental as possible as we present our case for limit setting. We need to start early before the die is cast, and we should be better about publicizing our supporting evidence. Setting a bedtime can begin in the first 6 months of life. Helping parents learn to say, “No, we aren’t going to feed you only what you like to eat!” can start as an infant makes what can be an unsettling transition to solid food.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
NF-kB inhibitor IT-901 shows promise in Richter syndrome
NEW YORK – The novel NF-kB inhibitor IT-901 appears active against Richter syndrome, according to in vitro analyses of primary leukemic cells and in vivo analyses in patient-derived xenograft models.
The findings suggest that NF-kB inhibition should be considered as a therapeutic strategy for Richter syndrome patients, Tiziana Vaisitti, PhD, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
Several factors have been shown to be associated with the development of Richter syndrome (RS), including somatic and germline genetic characteristics, biologic and clinical features, and certain CLL therapies. Recent studies have identified a critical role of mutations in specific genes, such as CKN2A, TP53, and NOTCH1 in the transformation of CLL to RS, which ultimately results in the aberrant activation of selected pathways – including NF-kB, Dr. Vaisitti of the University of Turin and the Italian Institute for Genomic Medicine, Turin, Italy explained.
In an ongoing study on the effects of IT-901 in CLL, she and her colleagues showed that “this compound was able to interfere with NF-kB transcriptional activity.”
That effect is followed by rapid and marked reduction in “the oxidative phosphorylation capacity of CLL cells, determined also by the transcriptional regulation of genes that control this process.”
“Moreover, this compound induces a significant increase and release of mitochondrial reactive oxygen species,” she said, adding: “The final result of this cascade of events is that IT-901 is able to rapidly induce apoptosis selectively in primary CLL cells, independently of the clinical subgroup of patients we are considering, and with very little toxicity on normal lymphocytes.”
The experimental data indicated that IT-901 is effective not only on the leukemic side, but it also acts on the stromal bystander component of the disease, mainly on nurse-like cells, by modulating the expression of molecules critical for CLL survival, she said.
Those findings were reported at the 2016 American Society of Hematology annual meeting (Blood. 2016;128:304).
For the current analyses, she and her colleagues tested the effects of IT-901 in RS, which affects up to 10% of patients with CLL, and for which there is an unmet therapeutic need. They looked at the mechanisms of action of the compound in leukemic cells both in vitro and in vivo.
In line with previous data, NF-kB was “constitutively highly active in RS cells freshly isolated from patients,” she reported.
Exposure to IT-901 at a 5 microM dose for 6 hours significantly decreased binding of p50 and p65 to DNA, and western blotting analyses on nuclear extracts indicated impaired translocation of those subunits in the nucleus, and compromised expression of the whole NF-kB complex, she said.
IT-901 also induced apoptosis in primary RS cells in a dose- and time-dependent manner; significant efficacy was seen after 24 hours of treatment, with more than half of the cells dead.
These results were then confirmed in an RS cell line established in the lab from a patient-derived xenograft (PDX) model, and even in the presence of a protective stromal layer IT-901 was able to induce apoptosis, she said.
The effects of IT-901 treatment were then analyzed in vivo using 3 different PDX models established from primary cells of RS patients and characterized by different molecular and genetic features. RS cells obtained from the PDX-tumor mass, were subcutaneously injected in severely immune-compromised mice and left to engraft until a palpable mass was present. IT-901 was then administered at a dose of 15 mg/kg, every day for 2 weeks, with a 2 day break after 5 days of administration.
Tumor size was significantly reduced, and as was demonstrated in vitro, immune-histochemical analyses of the tumor mass showed diminished expression and localization of the p65 subunit into the nucleus of tumor cells and increased cleavage of Caspase-3 in the treated mice as compared with vehicle-treated mice.
The findings provide proof-of-principle that IT-901 is effective in RS cells, diminishing NF-kB transcriptional activity and expression, and finally inducing apoptosis, Dr. Vaisitti said.
Dr. Vaisitti has received research funding from Immune Target.
NEW YORK – The novel NF-kB inhibitor IT-901 appears active against Richter syndrome, according to in vitro analyses of primary leukemic cells and in vivo analyses in patient-derived xenograft models.
The findings suggest that NF-kB inhibition should be considered as a therapeutic strategy for Richter syndrome patients, Tiziana Vaisitti, PhD, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
Several factors have been shown to be associated with the development of Richter syndrome (RS), including somatic and germline genetic characteristics, biologic and clinical features, and certain CLL therapies. Recent studies have identified a critical role of mutations in specific genes, such as CKN2A, TP53, and NOTCH1 in the transformation of CLL to RS, which ultimately results in the aberrant activation of selected pathways – including NF-kB, Dr. Vaisitti of the University of Turin and the Italian Institute for Genomic Medicine, Turin, Italy explained.
In an ongoing study on the effects of IT-901 in CLL, she and her colleagues showed that “this compound was able to interfere with NF-kB transcriptional activity.”
That effect is followed by rapid and marked reduction in “the oxidative phosphorylation capacity of CLL cells, determined also by the transcriptional regulation of genes that control this process.”
“Moreover, this compound induces a significant increase and release of mitochondrial reactive oxygen species,” she said, adding: “The final result of this cascade of events is that IT-901 is able to rapidly induce apoptosis selectively in primary CLL cells, independently of the clinical subgroup of patients we are considering, and with very little toxicity on normal lymphocytes.”
The experimental data indicated that IT-901 is effective not only on the leukemic side, but it also acts on the stromal bystander component of the disease, mainly on nurse-like cells, by modulating the expression of molecules critical for CLL survival, she said.
Those findings were reported at the 2016 American Society of Hematology annual meeting (Blood. 2016;128:304).
For the current analyses, she and her colleagues tested the effects of IT-901 in RS, which affects up to 10% of patients with CLL, and for which there is an unmet therapeutic need. They looked at the mechanisms of action of the compound in leukemic cells both in vitro and in vivo.
In line with previous data, NF-kB was “constitutively highly active in RS cells freshly isolated from patients,” she reported.
Exposure to IT-901 at a 5 microM dose for 6 hours significantly decreased binding of p50 and p65 to DNA, and western blotting analyses on nuclear extracts indicated impaired translocation of those subunits in the nucleus, and compromised expression of the whole NF-kB complex, she said.
IT-901 also induced apoptosis in primary RS cells in a dose- and time-dependent manner; significant efficacy was seen after 24 hours of treatment, with more than half of the cells dead.
These results were then confirmed in an RS cell line established in the lab from a patient-derived xenograft (PDX) model, and even in the presence of a protective stromal layer IT-901 was able to induce apoptosis, she said.
The effects of IT-901 treatment were then analyzed in vivo using 3 different PDX models established from primary cells of RS patients and characterized by different molecular and genetic features. RS cells obtained from the PDX-tumor mass, were subcutaneously injected in severely immune-compromised mice and left to engraft until a palpable mass was present. IT-901 was then administered at a dose of 15 mg/kg, every day for 2 weeks, with a 2 day break after 5 days of administration.
Tumor size was significantly reduced, and as was demonstrated in vitro, immune-histochemical analyses of the tumor mass showed diminished expression and localization of the p65 subunit into the nucleus of tumor cells and increased cleavage of Caspase-3 in the treated mice as compared with vehicle-treated mice.
The findings provide proof-of-principle that IT-901 is effective in RS cells, diminishing NF-kB transcriptional activity and expression, and finally inducing apoptosis, Dr. Vaisitti said.
Dr. Vaisitti has received research funding from Immune Target.
NEW YORK – The novel NF-kB inhibitor IT-901 appears active against Richter syndrome, according to in vitro analyses of primary leukemic cells and in vivo analyses in patient-derived xenograft models.
The findings suggest that NF-kB inhibition should be considered as a therapeutic strategy for Richter syndrome patients, Tiziana Vaisitti, PhD, said at the annual International Workshop on Chronic Lymphocytic Leukemia.
Several factors have been shown to be associated with the development of Richter syndrome (RS), including somatic and germline genetic characteristics, biologic and clinical features, and certain CLL therapies. Recent studies have identified a critical role of mutations in specific genes, such as CKN2A, TP53, and NOTCH1 in the transformation of CLL to RS, which ultimately results in the aberrant activation of selected pathways – including NF-kB, Dr. Vaisitti of the University of Turin and the Italian Institute for Genomic Medicine, Turin, Italy explained.
In an ongoing study on the effects of IT-901 in CLL, she and her colleagues showed that “this compound was able to interfere with NF-kB transcriptional activity.”
That effect is followed by rapid and marked reduction in “the oxidative phosphorylation capacity of CLL cells, determined also by the transcriptional regulation of genes that control this process.”
“Moreover, this compound induces a significant increase and release of mitochondrial reactive oxygen species,” she said, adding: “The final result of this cascade of events is that IT-901 is able to rapidly induce apoptosis selectively in primary CLL cells, independently of the clinical subgroup of patients we are considering, and with very little toxicity on normal lymphocytes.”
The experimental data indicated that IT-901 is effective not only on the leukemic side, but it also acts on the stromal bystander component of the disease, mainly on nurse-like cells, by modulating the expression of molecules critical for CLL survival, she said.
Those findings were reported at the 2016 American Society of Hematology annual meeting (Blood. 2016;128:304).
For the current analyses, she and her colleagues tested the effects of IT-901 in RS, which affects up to 10% of patients with CLL, and for which there is an unmet therapeutic need. They looked at the mechanisms of action of the compound in leukemic cells both in vitro and in vivo.
In line with previous data, NF-kB was “constitutively highly active in RS cells freshly isolated from patients,” she reported.
Exposure to IT-901 at a 5 microM dose for 6 hours significantly decreased binding of p50 and p65 to DNA, and western blotting analyses on nuclear extracts indicated impaired translocation of those subunits in the nucleus, and compromised expression of the whole NF-kB complex, she said.
IT-901 also induced apoptosis in primary RS cells in a dose- and time-dependent manner; significant efficacy was seen after 24 hours of treatment, with more than half of the cells dead.
These results were then confirmed in an RS cell line established in the lab from a patient-derived xenograft (PDX) model, and even in the presence of a protective stromal layer IT-901 was able to induce apoptosis, she said.
The effects of IT-901 treatment were then analyzed in vivo using 3 different PDX models established from primary cells of RS patients and characterized by different molecular and genetic features. RS cells obtained from the PDX-tumor mass, were subcutaneously injected in severely immune-compromised mice and left to engraft until a palpable mass was present. IT-901 was then administered at a dose of 15 mg/kg, every day for 2 weeks, with a 2 day break after 5 days of administration.
Tumor size was significantly reduced, and as was demonstrated in vitro, immune-histochemical analyses of the tumor mass showed diminished expression and localization of the p65 subunit into the nucleus of tumor cells and increased cleavage of Caspase-3 in the treated mice as compared with vehicle-treated mice.
The findings provide proof-of-principle that IT-901 is effective in RS cells, diminishing NF-kB transcriptional activity and expression, and finally inducing apoptosis, Dr. Vaisitti said.
Dr. Vaisitti has received research funding from Immune Target.
AT THE iwCLL MEETING
Key clinical point:
Major finding: IT-901 induced apoptosis in primary RS cells in a dose- and time-dependent manner; significant efficacy was seen after 24 hours of treatment, with more than half of the cells dead.
Data source: In vitro and in vivo analyses.
Disclosures: Dr. Vaisitti has received research funding from Immune Target.
Consequence of change? Medicaid disenrollment delayed breast cancer diagnosis
A spike in later-stage breast cancers is a potential byproduct of the Republican-proposed Medicaid reductions, according to Wafa Tarazi, PhD, and her colleagues.
The team looked at breast cancer stage at diagnosis following the 2005 Medicaid disenrollment of nearly 170,000 nonelderly adults in Tennessee that occurred because of state financial issues.
“Overall, nonelderly women in Tennessee were diagnosed at later stages of disease and experienced more delays in treatment in the period after disenrollment,” wrote Dr. Tarazi of Virginia Commonwealth University, Richmond, and her colleagues. “Disenrollment was found to be associated with a 3.3 percentage point increase in late stage of disease at the time of diagnosis” (Cancer 2016 June 26. doi: 10.1002/cncr.30771).
The investigators offered a few explanations for why this could be the case.
While disenrollment was associated with later stage of breast cancer at diagnosis, it also was associated with a 1.9 percentage-point decrease in a 60-day–plus delay in surgical treatment and a 1.4 percentage-point decrease in a greater-than-90-day–plus delay in treatment for women living in low-income ZIP codes, compared with women living in high-income ZIP codes.
Contractions “in the availability of Medicaid coverage have important health consequences for low-income women, and may increase income-related disparities, morbidity, and mortality for those diagnosed with breast cancer,” the authors wrote. “These negative health consequences should be considered by policymakers who weigh the costs and benefits of implementing or discontinuing expanded Medicaid coverage under the Patient Protection and Affordable Care Act and future federal and state policies.”
The Susan G. Komen Breast Cancer Foundation funded the study. The authors reported no conflicts of interest.
A spike in later-stage breast cancers is a potential byproduct of the Republican-proposed Medicaid reductions, according to Wafa Tarazi, PhD, and her colleagues.
The team looked at breast cancer stage at diagnosis following the 2005 Medicaid disenrollment of nearly 170,000 nonelderly adults in Tennessee that occurred because of state financial issues.
“Overall, nonelderly women in Tennessee were diagnosed at later stages of disease and experienced more delays in treatment in the period after disenrollment,” wrote Dr. Tarazi of Virginia Commonwealth University, Richmond, and her colleagues. “Disenrollment was found to be associated with a 3.3 percentage point increase in late stage of disease at the time of diagnosis” (Cancer 2016 June 26. doi: 10.1002/cncr.30771).
The investigators offered a few explanations for why this could be the case.
While disenrollment was associated with later stage of breast cancer at diagnosis, it also was associated with a 1.9 percentage-point decrease in a 60-day–plus delay in surgical treatment and a 1.4 percentage-point decrease in a greater-than-90-day–plus delay in treatment for women living in low-income ZIP codes, compared with women living in high-income ZIP codes.
Contractions “in the availability of Medicaid coverage have important health consequences for low-income women, and may increase income-related disparities, morbidity, and mortality for those diagnosed with breast cancer,” the authors wrote. “These negative health consequences should be considered by policymakers who weigh the costs and benefits of implementing or discontinuing expanded Medicaid coverage under the Patient Protection and Affordable Care Act and future federal and state policies.”
The Susan G. Komen Breast Cancer Foundation funded the study. The authors reported no conflicts of interest.
A spike in later-stage breast cancers is a potential byproduct of the Republican-proposed Medicaid reductions, according to Wafa Tarazi, PhD, and her colleagues.
The team looked at breast cancer stage at diagnosis following the 2005 Medicaid disenrollment of nearly 170,000 nonelderly adults in Tennessee that occurred because of state financial issues.
“Overall, nonelderly women in Tennessee were diagnosed at later stages of disease and experienced more delays in treatment in the period after disenrollment,” wrote Dr. Tarazi of Virginia Commonwealth University, Richmond, and her colleagues. “Disenrollment was found to be associated with a 3.3 percentage point increase in late stage of disease at the time of diagnosis” (Cancer 2016 June 26. doi: 10.1002/cncr.30771).
The investigators offered a few explanations for why this could be the case.
While disenrollment was associated with later stage of breast cancer at diagnosis, it also was associated with a 1.9 percentage-point decrease in a 60-day–plus delay in surgical treatment and a 1.4 percentage-point decrease in a greater-than-90-day–plus delay in treatment for women living in low-income ZIP codes, compared with women living in high-income ZIP codes.
Contractions “in the availability of Medicaid coverage have important health consequences for low-income women, and may increase income-related disparities, morbidity, and mortality for those diagnosed with breast cancer,” the authors wrote. “These negative health consequences should be considered by policymakers who weigh the costs and benefits of implementing or discontinuing expanded Medicaid coverage under the Patient Protection and Affordable Care Act and future federal and state policies.”
The Susan G. Komen Breast Cancer Foundation funded the study. The authors reported no conflicts of interest.
FROM CANCER
Meta-analysis: Bisphosphonates mitigate glucocorticoid-induced bone loss
MADRID – Bisphosphonates mitigate the damaging effects of glucocorticoid on bone, boosting bone mineral density and reducing the risk of fracture by up to 33%, compared with placebo, according to a systematic review and meta-analysis.
The review of 11 randomized, controlled trials found that bisphosphonates consistently improved bone outcomes among patients taking prednisone, Anas Makhzoum, MD, said at the European Congress of Rheumatology.

The primary outcomes of these trials were mean percentage change in bone mineral density at lumbar spine and femoral neck, and fracture incidence.
The drugs examined were ibandronate, alendronate, risedronate, etidronate, and clodronate. The mean duration of these trials was 71 weeks. Patients took a mean steroid dose of 15 mg.
Dr. Makhzoum, a resident at Queen’s University, Kingston, Ont., pooled nine of these trials for the outcome of mean percentage change in lumbar spine bone mineral density. The pooled mean percentage change of lumbar spine consistently favored bisphosphonates, compared with placebo, with a mean, statistically significant difference of approximately 4%.
Six studies were pooled for the outcome of mean percentage change in femoral neck bone mineral density. The pooled mean percentage change consistently favored bisphosphonates, with a mean, statistically significant difference of 2.95% relative to placebo.
Seven studies were pooled for outcome of incident fracture and the results consistently favored bisphosphonates, with a mean, statistically significant 33% decrease in the risk of a new fracture, compared with the placebo group (relative risk, 0.66).
“Bisphosphonates remain the standard of care for prevention and treatment of bone loss in patients on chronic steroids treatment,” Dr. Makhzoum noted.
He had no financial disclosures.
[email protected]
On Twitter @alz_gal
MADRID – Bisphosphonates mitigate the damaging effects of glucocorticoid on bone, boosting bone mineral density and reducing the risk of fracture by up to 33%, compared with placebo, according to a systematic review and meta-analysis.
The review of 11 randomized, controlled trials found that bisphosphonates consistently improved bone outcomes among patients taking prednisone, Anas Makhzoum, MD, said at the European Congress of Rheumatology.
The primary outcomes of these trials were mean percentage change in bone mineral density at lumbar spine and femoral neck, and fracture incidence.
The drugs examined were ibandronate, alendronate, risedronate, etidronate, and clodronate. The mean duration of these trials was 71 weeks. Patients took a mean steroid dose of 15 mg.
Dr. Makhzoum, a resident at Queen’s University, Kingston, Ont., pooled nine of these trials for the outcome of mean percentage change in lumbar spine bone mineral density. The pooled mean percentage change of lumbar spine consistently favored bisphosphonates, compared with placebo, with a mean, statistically significant difference of approximately 4%.
Six studies were pooled for the outcome of mean percentage change in femoral neck bone mineral density. The pooled mean percentage change consistently favored bisphosphonates, with a mean, statistically significant difference of 2.95% relative to placebo.
Seven studies were pooled for outcome of incident fracture and the results consistently favored bisphosphonates, with a mean, statistically significant 33% decrease in the risk of a new fracture, compared with the placebo group (relative risk, 0.66).
“Bisphosphonates remain the standard of care for prevention and treatment of bone loss in patients on chronic steroids treatment,” Dr. Makhzoum noted.
He had no financial disclosures.
[email protected]
On Twitter @alz_gal
MADRID – Bisphosphonates mitigate the damaging effects of glucocorticoid on bone, boosting bone mineral density and reducing the risk of fracture by up to 33%, compared with placebo, according to a systematic review and meta-analysis.
The review of 11 randomized, controlled trials found that bisphosphonates consistently improved bone outcomes among patients taking prednisone, Anas Makhzoum, MD, said at the European Congress of Rheumatology.
The primary outcomes of these trials were mean percentage change in bone mineral density at lumbar spine and femoral neck, and fracture incidence.
The drugs examined were ibandronate, alendronate, risedronate, etidronate, and clodronate. The mean duration of these trials was 71 weeks. Patients took a mean steroid dose of 15 mg.
Dr. Makhzoum, a resident at Queen’s University, Kingston, Ont., pooled nine of these trials for the outcome of mean percentage change in lumbar spine bone mineral density. The pooled mean percentage change of lumbar spine consistently favored bisphosphonates, compared with placebo, with a mean, statistically significant difference of approximately 4%.
Six studies were pooled for the outcome of mean percentage change in femoral neck bone mineral density. The pooled mean percentage change consistently favored bisphosphonates, with a mean, statistically significant difference of 2.95% relative to placebo.
Seven studies were pooled for outcome of incident fracture and the results consistently favored bisphosphonates, with a mean, statistically significant 33% decrease in the risk of a new fracture, compared with the placebo group (relative risk, 0.66).
“Bisphosphonates remain the standard of care for prevention and treatment of bone loss in patients on chronic steroids treatment,” Dr. Makhzoum noted.
He had no financial disclosures.
[email protected]
On Twitter @alz_gal
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: Relative to placebo, bisphosphonates reduced the risk of fracture by up to 33%.
Data source: A meta-analysis comprising 11 randomized, placebo-controlled trials with more than 2,000 patients.
Disclosures: Dr. Makhzoum had no financial disclosures.
Large Hyperpigmented Nodule on the Leg
The Diagnosis: Dermatofibroma
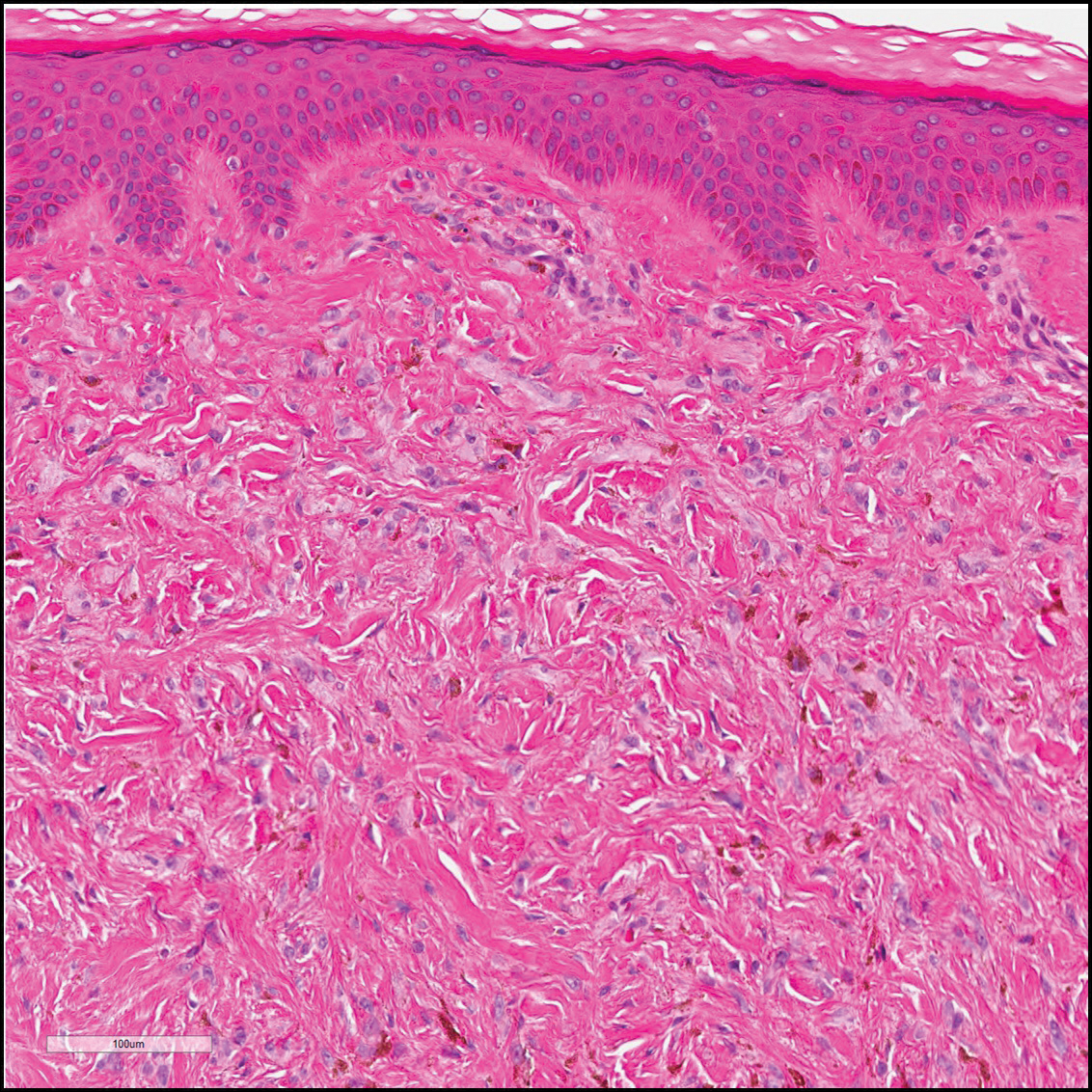
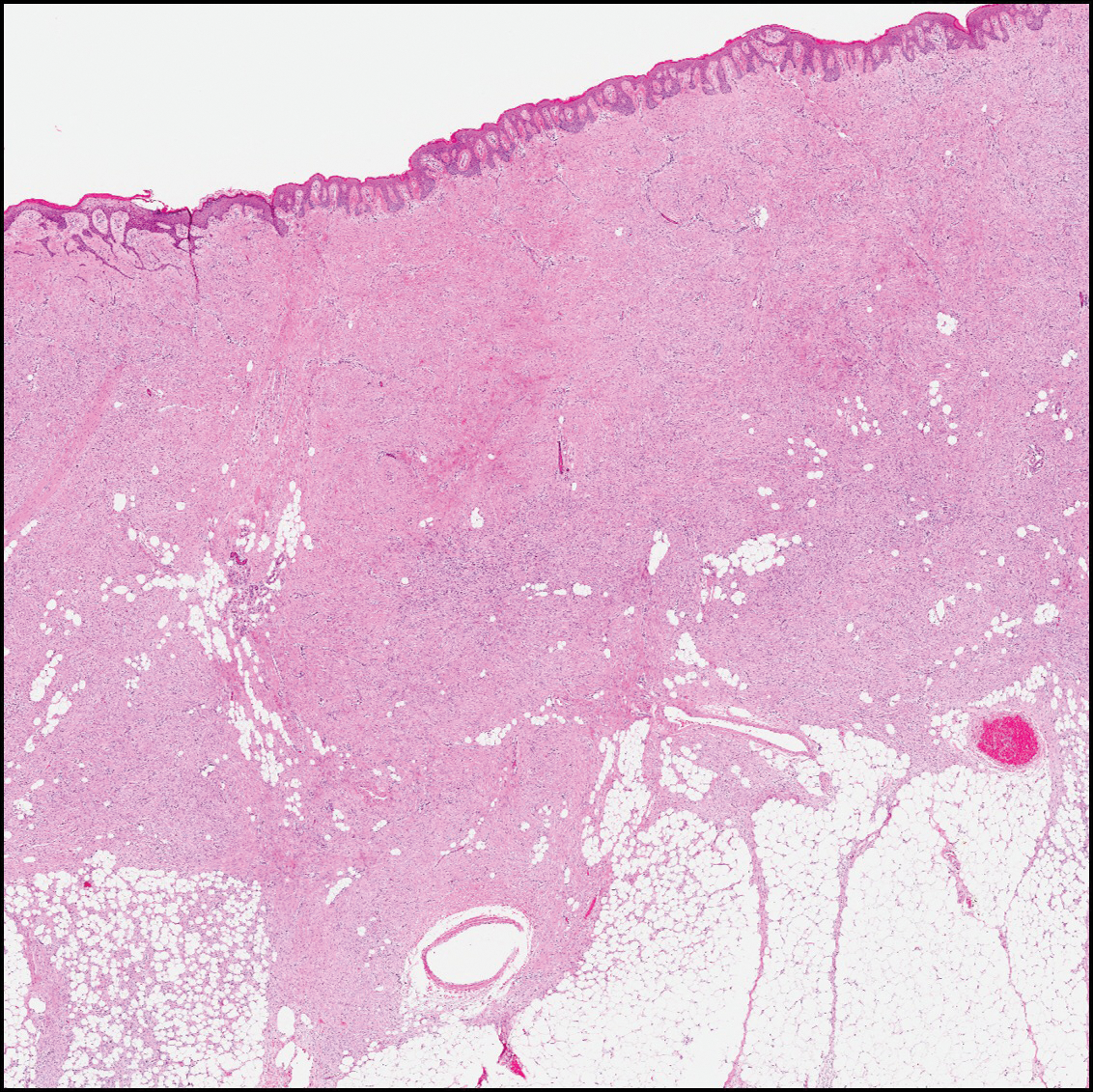
Dermatofibroma (DF) is a commonly encountered lesion. Although usually a straightforward clinical diagnosis, histopathological diagnosis is sometimes required. Conventional histologic findings of DF are hyperkeratosis, induction of the epidermis with acanthosis, and basal layer hyperpigmentation.1,2 Within the dermis there usually is proliferation of fibroblasts, histiocytes, and blood vessels that sometimes spares the overlying papillary dermis. Nomenclature of specific variants may be assigned based on the predominant component (eg, nodular subepidermal fibrosis, histiocytoma, sclerosing hemangioma) or histologic findings (eg, fibrocollagenous, sclerotic, cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, epithelioid).3-5 Of the histologic variants, fibrocollagenous is most common, but knowledge of other variants is important for accurate diagnosis, especially to exclude malignancy.
The sclerosing hemangioma variant of DF may pre-sent a diagnostic dilemma. In addition to typical features of DF, pseudovascular spaces, abundant hemosiderin, and reactive-appearing spindled cells are histologically demonstrated. The marked sclerosis and pigment deposition may mimic a blue nevus, and the dilated pseudovascular spaces may be reminiscent of a vascular neoplasm such as angiosarcoma or Kaposi sarcoma. However, the presence of characteristic features such as peripheral collagen trapping and overlying epidermal hyperplasia provide important clues for correct diagnosis.
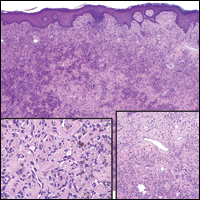
Angiosarcomas (Figure 1) are malignant neoplasms with vascular differentiation. Cutaneous angiosarcomas present as purple plaques or nodules on the head and/or neck in elderly individuals as well as in patients with chronic lymphedema or prior radiation exposure.6-9 They are aggressive neoplasms with high rates of recurrence and metastases. Microscopically, the tumor is composed of anastomosing vascular channels lined by atypical endothelial cells with a multilayered appearance. There is frequent red blood cell extravasation, and substantial hemosiderin deposition may be noted in long-standing lesions. Neoplastic cells are positive for vascular markers (CD34, CD31, ETS-related gene transcription factor). Notably, cases associated with radiation exposure and chronic lymphedema are positive for MYC.10

Blue nevi (Figure 2) are benign melanocytic tumors that occur most frequently in children but may pre-sent in any age group. Clinical presentation is a blue to black, slightly raised papule that may be found on any site of the body. Biopsy typically shows a wedge-shaped infiltrate of spindled melanocytes with elongated dendritic processes in a sclerotic collagenous stroma. There frequently is a striking population of heavily pigmented melanophages. The melanocytes are positive for melanoma antigen recognized by T cells (MART-1)/melan-A, S-100, and transcription factor SOX-10. In contrast to other benign nevi, human melanoma black-45 will be positive in the dermal component.
Dermatofibrosarcoma protuberans (Figure 3) is a dermal-based tumor of intermediate malignant potential with a high rate of local recurrence and potential for sarcomatous transformation. Dermatofibrosarcoma protuberans most commonly presents in young adults as firm, pink to brown plaques and can occur on any site of the body. Histologically, they show a dermal proliferation of spindled cells that infiltrate in a storiform fashion into the subcutaneous adipose tissue,11 which imparts a honeycomb or Swiss cheese pattern. The tumor characteristically demonstrates positive staining for CD34. Loss of CD34 staining, increased mitoses, nuclear atypia, and fascicular growth are features suggestive of sarcomatous transformation.11,12 Dermatofibrosarcoma protuberans is associated with chromosomal abnormalities of chromosomes 17 and 22, resulting in COL1A1 (collagen type 1 alpha 1 chain) and PDGF-β (platelet-derived growth factor subunit B) gene fusion.13
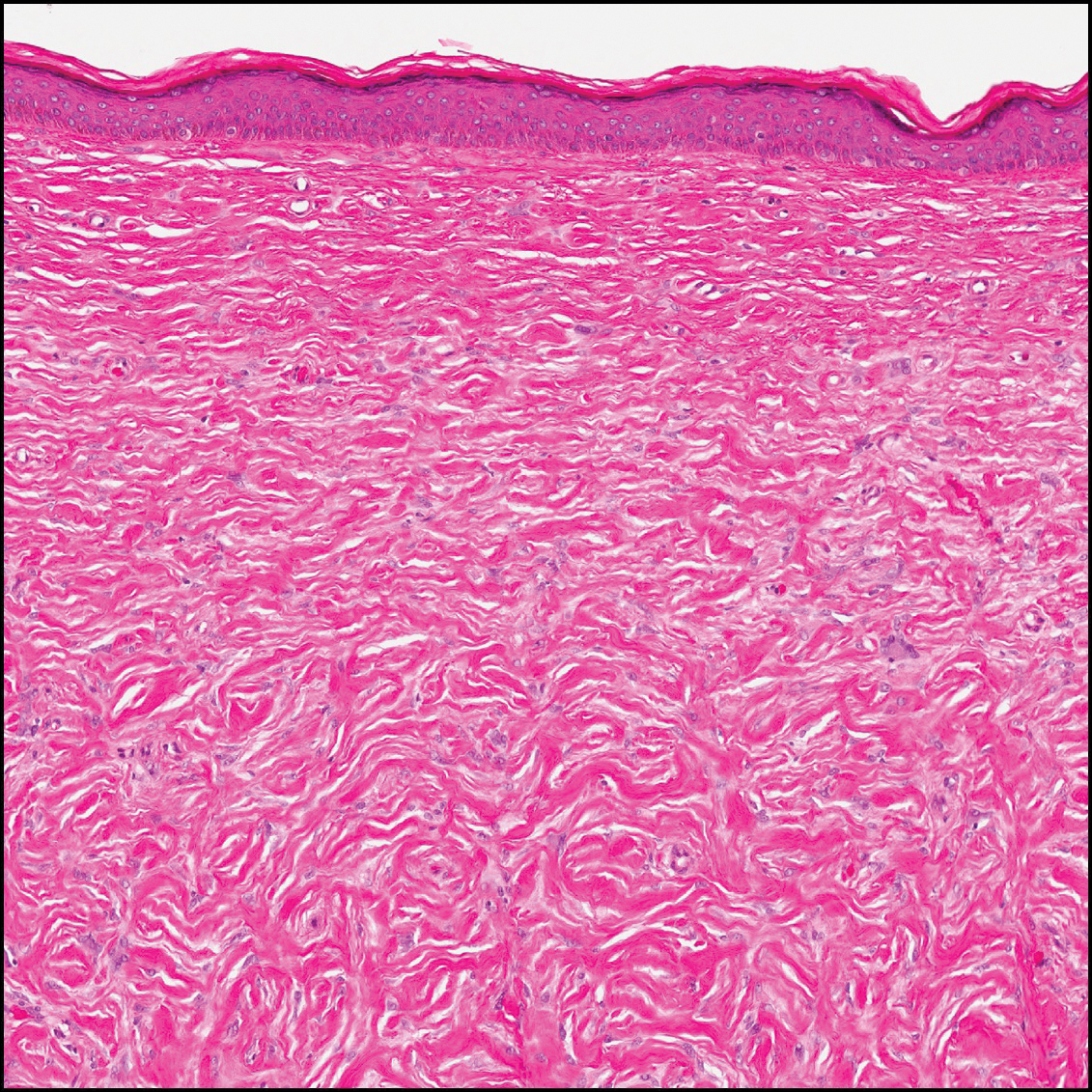
Sclerotic fibromas (also known as storiform collagenomas)(Figure 4) may represent regressed DFs and are frequently associated with prior trauma to the affected area.14,15 They usually appear as flesh-colored papules or nodules on the face and trunk. The presence of multiple sclerotic fibromas is associated with Cowden syndrome.16,17 Histologically, the lesions present as well-demarcated, nonencapsulated, dermal nodules composed of a storiform or whorled arrangement of collagen with spindled fibroblasts. The sclerotic collagen bundles often are separated by small clefts imparting a plywoodlike pattern.16
The differential diagnosis for DF expands once atypical clinical and histopathological findings are present. In this case, the nodule was much larger and darker than the usual appearance of DF (3-10 mm).2,4 Given the lesion's nodularity, the clinical dimple sign on lateral compression could not be seen. On biopsy, the predominance of blood vessels and sclerosis further complicated the diagnostic picture. In unusual cases such as this one, correlation of clinical history, histology, and immunophenotype is ever important.
- Zeidi M, North JP. Sebaceous induction in dermatofibroma: a common feature of dermatofibromas on the shoulder. J Cutan Pathol. 2015;42:400-405.
- Şenel E, Yuyucu Karabulut Y, Doğruer S¸enel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Dermatol Venereol. 2015;29:1958-1966.
- Vilanova JR, Flint A. The morphological variations of fibrous histiocytomas. J Cutan Pathol. 1974;1:155-164.
- Han TY, Chang HS, Lee JH, et al. A clinical and histopathological study of 122 cases of dermatofibroma (benign fibrous histiocytoma)[published online May 27, 2011]. Ann Dermatol. 2011;23:185-192.
- Alves JVP, Matos DM, Barreiros HF, et al. Variants of dermatofibroma--a histopathological study. An Bras Dermatol. 2014;89:472-477.
- Rosai J, Sumner HW, Major MC, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema: a report of six cases in elephantiasis chirurgica. Cancer. 1948;1:64-81.
- Goette DK, Detlefs RL. Postirradiation angiosarcoma. J Am Acad Dermatol. 1985;12(5 pt 2):922-926.
- Manner J, Radlwimmer B, Hohenberger P, et al. MYC high level gene amplification is a distinctive feature of angiosarcomas after irradiation or chronic lymphedema. Am J Pathol. 2010;176:34-39.
- Voth H, Landsberg J, Hinz T, et al. Management of dermatofibrosarcoma protuberans with fibrosarcomatous transformation: an evidence-based review of the literature. J Eur Acad Dermatol Venereol. 2011;25:1385-1391.
- Goldblum JR. CD34 positivity in fibrosarcomas which arise in dermatofibrosarcoma protuberans. Arch Pathol Lab Med. 1995;119:238-241.
- Patel KU, Szabo SS, Hernandez VS, et al. Dermatofibrosarcoma protuberans COL1A1-PDGFB fusion is identified in virtually all dermatofibrosarcoma protuberans cases when investigated by newly developed multiplex reverse transcription polymerase chain reaction and fluorescence in situ hybridization assays. Hum Pathol. 2008;39:184-193.
- Sohn IB, Hwang SM, Lee SH, et al. Dermatofibroma with sclerotic areas resembling a sclerotic fibroma of the skin. J Cutan Pathol. 2002;29:44-47.
- Pujol RM, de Castro F, Schroeter AL, et al. Solitary sclerotic fibroma of the skin: a sclerotic dermatofibroma? Am J Dermatopathol. 1996;18:620-624.
- Requena L, Gutiérrez J, Sánchez Yus E. Multiple sclerotic fibromas of the skin: a cutaneous marker of Cowden's disease. J Cutan Pathol. 1992;19:346-351.
- Weary PE, Gorlin RJ, Gentry WC Jr, et al. Multiple hamartoma syndrome (Cowden's disease). Arch Dermatol. 1972;106:682-690.
The Diagnosis: Dermatofibroma
Dermatofibroma (DF) is a commonly encountered lesion. Although usually a straightforward clinical diagnosis, histopathological diagnosis is sometimes required. Conventional histologic findings of DF are hyperkeratosis, induction of the epidermis with acanthosis, and basal layer hyperpigmentation.1,2 Within the dermis there usually is proliferation of fibroblasts, histiocytes, and blood vessels that sometimes spares the overlying papillary dermis. Nomenclature of specific variants may be assigned based on the predominant component (eg, nodular subepidermal fibrosis, histiocytoma, sclerosing hemangioma) or histologic findings (eg, fibrocollagenous, sclerotic, cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, epithelioid).3-5 Of the histologic variants, fibrocollagenous is most common, but knowledge of other variants is important for accurate diagnosis, especially to exclude malignancy.
The sclerosing hemangioma variant of DF may pre-sent a diagnostic dilemma. In addition to typical features of DF, pseudovascular spaces, abundant hemosiderin, and reactive-appearing spindled cells are histologically demonstrated. The marked sclerosis and pigment deposition may mimic a blue nevus, and the dilated pseudovascular spaces may be reminiscent of a vascular neoplasm such as angiosarcoma or Kaposi sarcoma. However, the presence of characteristic features such as peripheral collagen trapping and overlying epidermal hyperplasia provide important clues for correct diagnosis.
Angiosarcomas (Figure 1) are malignant neoplasms with vascular differentiation. Cutaneous angiosarcomas present as purple plaques or nodules on the head and/or neck in elderly individuals as well as in patients with chronic lymphedema or prior radiation exposure.6-9 They are aggressive neoplasms with high rates of recurrence and metastases. Microscopically, the tumor is composed of anastomosing vascular channels lined by atypical endothelial cells with a multilayered appearance. There is frequent red blood cell extravasation, and substantial hemosiderin deposition may be noted in long-standing lesions. Neoplastic cells are positive for vascular markers (CD34, CD31, ETS-related gene transcription factor). Notably, cases associated with radiation exposure and chronic lymphedema are positive for MYC.10
Blue nevi (Figure 2) are benign melanocytic tumors that occur most frequently in children but may pre-sent in any age group. Clinical presentation is a blue to black, slightly raised papule that may be found on any site of the body. Biopsy typically shows a wedge-shaped infiltrate of spindled melanocytes with elongated dendritic processes in a sclerotic collagenous stroma. There frequently is a striking population of heavily pigmented melanophages. The melanocytes are positive for melanoma antigen recognized by T cells (MART-1)/melan-A, S-100, and transcription factor SOX-10. In contrast to other benign nevi, human melanoma black-45 will be positive in the dermal component.
Dermatofibrosarcoma protuberans (Figure 3) is a dermal-based tumor of intermediate malignant potential with a high rate of local recurrence and potential for sarcomatous transformation. Dermatofibrosarcoma protuberans most commonly presents in young adults as firm, pink to brown plaques and can occur on any site of the body. Histologically, they show a dermal proliferation of spindled cells that infiltrate in a storiform fashion into the subcutaneous adipose tissue,11 which imparts a honeycomb or Swiss cheese pattern. The tumor characteristically demonstrates positive staining for CD34. Loss of CD34 staining, increased mitoses, nuclear atypia, and fascicular growth are features suggestive of sarcomatous transformation.11,12 Dermatofibrosarcoma protuberans is associated with chromosomal abnormalities of chromosomes 17 and 22, resulting in COL1A1 (collagen type 1 alpha 1 chain) and PDGF-β (platelet-derived growth factor subunit B) gene fusion.13
Sclerotic fibromas (also known as storiform collagenomas)(Figure 4) may represent regressed DFs and are frequently associated with prior trauma to the affected area.14,15 They usually appear as flesh-colored papules or nodules on the face and trunk. The presence of multiple sclerotic fibromas is associated with Cowden syndrome.16,17 Histologically, the lesions present as well-demarcated, nonencapsulated, dermal nodules composed of a storiform or whorled arrangement of collagen with spindled fibroblasts. The sclerotic collagen bundles often are separated by small clefts imparting a plywoodlike pattern.16
The differential diagnosis for DF expands once atypical clinical and histopathological findings are present. In this case, the nodule was much larger and darker than the usual appearance of DF (3-10 mm).2,4 Given the lesion's nodularity, the clinical dimple sign on lateral compression could not be seen. On biopsy, the predominance of blood vessels and sclerosis further complicated the diagnostic picture. In unusual cases such as this one, correlation of clinical history, histology, and immunophenotype is ever important.
The Diagnosis: Dermatofibroma
Dermatofibroma (DF) is a commonly encountered lesion. Although usually a straightforward clinical diagnosis, histopathological diagnosis is sometimes required. Conventional histologic findings of DF are hyperkeratosis, induction of the epidermis with acanthosis, and basal layer hyperpigmentation.1,2 Within the dermis there usually is proliferation of fibroblasts, histiocytes, and blood vessels that sometimes spares the overlying papillary dermis. Nomenclature of specific variants may be assigned based on the predominant component (eg, nodular subepidermal fibrosis, histiocytoma, sclerosing hemangioma) or histologic findings (eg, fibrocollagenous, sclerotic, cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, epithelioid).3-5 Of the histologic variants, fibrocollagenous is most common, but knowledge of other variants is important for accurate diagnosis, especially to exclude malignancy.
The sclerosing hemangioma variant of DF may pre-sent a diagnostic dilemma. In addition to typical features of DF, pseudovascular spaces, abundant hemosiderin, and reactive-appearing spindled cells are histologically demonstrated. The marked sclerosis and pigment deposition may mimic a blue nevus, and the dilated pseudovascular spaces may be reminiscent of a vascular neoplasm such as angiosarcoma or Kaposi sarcoma. However, the presence of characteristic features such as peripheral collagen trapping and overlying epidermal hyperplasia provide important clues for correct diagnosis.
Angiosarcomas (Figure 1) are malignant neoplasms with vascular differentiation. Cutaneous angiosarcomas present as purple plaques or nodules on the head and/or neck in elderly individuals as well as in patients with chronic lymphedema or prior radiation exposure.6-9 They are aggressive neoplasms with high rates of recurrence and metastases. Microscopically, the tumor is composed of anastomosing vascular channels lined by atypical endothelial cells with a multilayered appearance. There is frequent red blood cell extravasation, and substantial hemosiderin deposition may be noted in long-standing lesions. Neoplastic cells are positive for vascular markers (CD34, CD31, ETS-related gene transcription factor). Notably, cases associated with radiation exposure and chronic lymphedema are positive for MYC.10
Blue nevi (Figure 2) are benign melanocytic tumors that occur most frequently in children but may pre-sent in any age group. Clinical presentation is a blue to black, slightly raised papule that may be found on any site of the body. Biopsy typically shows a wedge-shaped infiltrate of spindled melanocytes with elongated dendritic processes in a sclerotic collagenous stroma. There frequently is a striking population of heavily pigmented melanophages. The melanocytes are positive for melanoma antigen recognized by T cells (MART-1)/melan-A, S-100, and transcription factor SOX-10. In contrast to other benign nevi, human melanoma black-45 will be positive in the dermal component.
Dermatofibrosarcoma protuberans (Figure 3) is a dermal-based tumor of intermediate malignant potential with a high rate of local recurrence and potential for sarcomatous transformation. Dermatofibrosarcoma protuberans most commonly presents in young adults as firm, pink to brown plaques and can occur on any site of the body. Histologically, they show a dermal proliferation of spindled cells that infiltrate in a storiform fashion into the subcutaneous adipose tissue,11 which imparts a honeycomb or Swiss cheese pattern. The tumor characteristically demonstrates positive staining for CD34. Loss of CD34 staining, increased mitoses, nuclear atypia, and fascicular growth are features suggestive of sarcomatous transformation.11,12 Dermatofibrosarcoma protuberans is associated with chromosomal abnormalities of chromosomes 17 and 22, resulting in COL1A1 (collagen type 1 alpha 1 chain) and PDGF-β (platelet-derived growth factor subunit B) gene fusion.13
Sclerotic fibromas (also known as storiform collagenomas)(Figure 4) may represent regressed DFs and are frequently associated with prior trauma to the affected area.14,15 They usually appear as flesh-colored papules or nodules on the face and trunk. The presence of multiple sclerotic fibromas is associated with Cowden syndrome.16,17 Histologically, the lesions present as well-demarcated, nonencapsulated, dermal nodules composed of a storiform or whorled arrangement of collagen with spindled fibroblasts. The sclerotic collagen bundles often are separated by small clefts imparting a plywoodlike pattern.16
The differential diagnosis for DF expands once atypical clinical and histopathological findings are present. In this case, the nodule was much larger and darker than the usual appearance of DF (3-10 mm).2,4 Given the lesion's nodularity, the clinical dimple sign on lateral compression could not be seen. On biopsy, the predominance of blood vessels and sclerosis further complicated the diagnostic picture. In unusual cases such as this one, correlation of clinical history, histology, and immunophenotype is ever important.
- Zeidi M, North JP. Sebaceous induction in dermatofibroma: a common feature of dermatofibromas on the shoulder. J Cutan Pathol. 2015;42:400-405.
- Şenel E, Yuyucu Karabulut Y, Doğruer S¸enel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Dermatol Venereol. 2015;29:1958-1966.
- Vilanova JR, Flint A. The morphological variations of fibrous histiocytomas. J Cutan Pathol. 1974;1:155-164.
- Han TY, Chang HS, Lee JH, et al. A clinical and histopathological study of 122 cases of dermatofibroma (benign fibrous histiocytoma)[published online May 27, 2011]. Ann Dermatol. 2011;23:185-192.
- Alves JVP, Matos DM, Barreiros HF, et al. Variants of dermatofibroma--a histopathological study. An Bras Dermatol. 2014;89:472-477.
- Rosai J, Sumner HW, Major MC, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema: a report of six cases in elephantiasis chirurgica. Cancer. 1948;1:64-81.
- Goette DK, Detlefs RL. Postirradiation angiosarcoma. J Am Acad Dermatol. 1985;12(5 pt 2):922-926.
- Manner J, Radlwimmer B, Hohenberger P, et al. MYC high level gene amplification is a distinctive feature of angiosarcomas after irradiation or chronic lymphedema. Am J Pathol. 2010;176:34-39.
- Voth H, Landsberg J, Hinz T, et al. Management of dermatofibrosarcoma protuberans with fibrosarcomatous transformation: an evidence-based review of the literature. J Eur Acad Dermatol Venereol. 2011;25:1385-1391.
- Goldblum JR. CD34 positivity in fibrosarcomas which arise in dermatofibrosarcoma protuberans. Arch Pathol Lab Med. 1995;119:238-241.
- Patel KU, Szabo SS, Hernandez VS, et al. Dermatofibrosarcoma protuberans COL1A1-PDGFB fusion is identified in virtually all dermatofibrosarcoma protuberans cases when investigated by newly developed multiplex reverse transcription polymerase chain reaction and fluorescence in situ hybridization assays. Hum Pathol. 2008;39:184-193.
- Sohn IB, Hwang SM, Lee SH, et al. Dermatofibroma with sclerotic areas resembling a sclerotic fibroma of the skin. J Cutan Pathol. 2002;29:44-47.
- Pujol RM, de Castro F, Schroeter AL, et al. Solitary sclerotic fibroma of the skin: a sclerotic dermatofibroma? Am J Dermatopathol. 1996;18:620-624.
- Requena L, Gutiérrez J, Sánchez Yus E. Multiple sclerotic fibromas of the skin: a cutaneous marker of Cowden's disease. J Cutan Pathol. 1992;19:346-351.
- Weary PE, Gorlin RJ, Gentry WC Jr, et al. Multiple hamartoma syndrome (Cowden's disease). Arch Dermatol. 1972;106:682-690.
- Zeidi M, North JP. Sebaceous induction in dermatofibroma: a common feature of dermatofibromas on the shoulder. J Cutan Pathol. 2015;42:400-405.
- Şenel E, Yuyucu Karabulut Y, Doğruer S¸enel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Dermatol Venereol. 2015;29:1958-1966.
- Vilanova JR, Flint A. The morphological variations of fibrous histiocytomas. J Cutan Pathol. 1974;1:155-164.
- Han TY, Chang HS, Lee JH, et al. A clinical and histopathological study of 122 cases of dermatofibroma (benign fibrous histiocytoma)[published online May 27, 2011]. Ann Dermatol. 2011;23:185-192.
- Alves JVP, Matos DM, Barreiros HF, et al. Variants of dermatofibroma--a histopathological study. An Bras Dermatol. 2014;89:472-477.
- Rosai J, Sumner HW, Major MC, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema: a report of six cases in elephantiasis chirurgica. Cancer. 1948;1:64-81.
- Goette DK, Detlefs RL. Postirradiation angiosarcoma. J Am Acad Dermatol. 1985;12(5 pt 2):922-926.
- Manner J, Radlwimmer B, Hohenberger P, et al. MYC high level gene amplification is a distinctive feature of angiosarcomas after irradiation or chronic lymphedema. Am J Pathol. 2010;176:34-39.
- Voth H, Landsberg J, Hinz T, et al. Management of dermatofibrosarcoma protuberans with fibrosarcomatous transformation: an evidence-based review of the literature. J Eur Acad Dermatol Venereol. 2011;25:1385-1391.
- Goldblum JR. CD34 positivity in fibrosarcomas which arise in dermatofibrosarcoma protuberans. Arch Pathol Lab Med. 1995;119:238-241.
- Patel KU, Szabo SS, Hernandez VS, et al. Dermatofibrosarcoma protuberans COL1A1-PDGFB fusion is identified in virtually all dermatofibrosarcoma protuberans cases when investigated by newly developed multiplex reverse transcription polymerase chain reaction and fluorescence in situ hybridization assays. Hum Pathol. 2008;39:184-193.
- Sohn IB, Hwang SM, Lee SH, et al. Dermatofibroma with sclerotic areas resembling a sclerotic fibroma of the skin. J Cutan Pathol. 2002;29:44-47.
- Pujol RM, de Castro F, Schroeter AL, et al. Solitary sclerotic fibroma of the skin: a sclerotic dermatofibroma? Am J Dermatopathol. 1996;18:620-624.
- Requena L, Gutiérrez J, Sánchez Yus E. Multiple sclerotic fibromas of the skin: a cutaneous marker of Cowden's disease. J Cutan Pathol. 1992;19:346-351.
- Weary PE, Gorlin RJ, Gentry WC Jr, et al. Multiple hamartoma syndrome (Cowden's disease). Arch Dermatol. 1972;106:682-690.

A 61-year-old woman presented with a 2.5-cm hyperpigmented exophytic nodule on the anterior aspect of the left shin of approximately 2 years' duration. The patient initially noticed a small lesion following a bee sting, but it subsequently grew over the ensuing 2 years. A shave biopsy was obtained.
VIDEO: Autoimmune hepatitis with cirrhosis tied to hepatocellular carcinoma
The presence of cirrhosis in patients with autoimmune hepatitis markedly increased their risk of hepatocellular carcinoma, according to a systematic review and meta-analysis of 25 cohort studies and 6,528 patients.
Estimated rates of hepatocellular carcinoma (HCC) were 10.1 (6.9-14.7) cases per 1,000 person-years in these patients versus 1.1 (0.6-2.2) cases per 1,000 person-years in patients without cirrhosis at diagnosis, Aylin Tansel, MD, of Baylor College of Medicine in Houston, and associates reported in Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.02.006). Thus, surveillance for HCC “might be cost effective in this population,” they wrote. “However, patients with AIH [autoimmune hepatitis] without cirrhosis at index diagnosis, particularly those identified from general populations, are at an extremely low risk of HCC.”
Source: American Gastroenterological Association
Autoimmune hepatitis may be asymptomatic at presentation or may cause severe acute hepatitis or even fulminant liver failure. Even with immunosuppressive therapy, patients progress to cirrhosis at reported annual rates of 0.1%-8%. HCC is the fastest-growing cause of cancer mortality, and the American Association for the Study of Liver Diseases (AASLD) recommends enhanced surveillance for this disease in patients whose annual estimated risk is at least 1.5%. Although the European Association for the Study of Liver Diseases recommends screening for HCC in patients with autoimmune hepatitis and cirrhosis, AASLD makes no such recommendation, the reviewers noted. To study the risk of HCC in patients with autoimmune hepatitis, they searched PubMed, Embase, and reference lists for relevant cohort studies published through June 2016. This work yielded 20 papers and five abstracts with a pooled median follow-up period of 8 years.
The overall pooled incidence of HCC was 3.1 (95% confidence interval, 2.2-4.2) cases per 1,000 person-years, or 1.007% per year, the reviewers wrote. However, the 95% confidence interval for the annual incidence rate nearly encompassed the 1.5% cutoff recommended by AASLD, they said. Furthermore, 5 of 16 studies that investigated the risk of HCC in patients with concurrent cirrhosis reported incidence rates above 1.5%. Among 93 patients who developed HCC in the meta-analysis, only 1 did not have cirrhosis by the time autoimmune hepatitis was diagnosed.
The meta-analysis also linked HCC to older age and Asian ethnicity among patients with autoimmune hepatitis, as has been reported before. Male sex only slightly increased the risk of HCC, but the studies included only about 1,130 men, the reviewers noted. Although the severity of autoimmune hepatitis varied among studies, higher rates of relapse predicted HCC in two cohorts. Additionally, one study linked alcohol abuse to a sixfold higher risk of HCC among patients with autoimmune hepatitis. “These data support careful monitoring of patients with autoimmune hepatitis, particularly older men, patients with multiple autoimmune hepatitis relapses, and those with ongoing alcohol abuse,” the investigators wrote.
They found no evidence of publication bias, but each individual study included at most 15 cases of HCC, so pooled incidence rates were probably imprecise, especially for subgroups, they said. Studies also inconsistently reported HCC risk factors, often lacked comparison groups, and usually did not report the effects of surveillance for HCC.
Dr. Tansel reported receiving support from the National Institutes of Health. The reviewers had no conflicts of interest.
Serial imaging surveillance facilitates detection of hepatocellular carcinoma (HCC) at a stage amenable to potentially curative resection or liver transplantation. The AASLD, EASL, and APASL recommend surveillance for cirrhotic patients; however, the AASLD stipulates that the incidence of HCC exceed the threshold of cost-effectiveness of 1.5% per year. Whether HCC surveillance in cirrhotic patients with autoimmune hepatitis (AIH) is cost effective remains controversial. The systematic review and meta-analysis by Tansel et al. of 25 rigorously selected cohort studies of AIH addresses this question by calculating incidence rates of HCC per 1,000 person-years using 95% confidence intervals derived from event rates in relation to the duration of follow-up. 
John M. Vierling, MD, FACP, FAASLD, is professor of medicine and surgery, chief of hepatology, Baylor College of Medicine, Houston. He has received grant support from Taiwan J and Novartis and is on the scientific advisory board for Novartis.
Serial imaging surveillance facilitates detection of hepatocellular carcinoma (HCC) at a stage amenable to potentially curative resection or liver transplantation. The AASLD, EASL, and APASL recommend surveillance for cirrhotic patients; however, the AASLD stipulates that the incidence of HCC exceed the threshold of cost-effectiveness of 1.5% per year. Whether HCC surveillance in cirrhotic patients with autoimmune hepatitis (AIH) is cost effective remains controversial. The systematic review and meta-analysis by Tansel et al. of 25 rigorously selected cohort studies of AIH addresses this question by calculating incidence rates of HCC per 1,000 person-years using 95% confidence intervals derived from event rates in relation to the duration of follow-up.
John M. Vierling, MD, FACP, FAASLD, is professor of medicine and surgery, chief of hepatology, Baylor College of Medicine, Houston. He has received grant support from Taiwan J and Novartis and is on the scientific advisory board for Novartis.
Serial imaging surveillance facilitates detection of hepatocellular carcinoma (HCC) at a stage amenable to potentially curative resection or liver transplantation. The AASLD, EASL, and APASL recommend surveillance for cirrhotic patients; however, the AASLD stipulates that the incidence of HCC exceed the threshold of cost-effectiveness of 1.5% per year. Whether HCC surveillance in cirrhotic patients with autoimmune hepatitis (AIH) is cost effective remains controversial. The systematic review and meta-analysis by Tansel et al. of 25 rigorously selected cohort studies of AIH addresses this question by calculating incidence rates of HCC per 1,000 person-years using 95% confidence intervals derived from event rates in relation to the duration of follow-up.
John M. Vierling, MD, FACP, FAASLD, is professor of medicine and surgery, chief of hepatology, Baylor College of Medicine, Houston. He has received grant support from Taiwan J and Novartis and is on the scientific advisory board for Novartis.
The presence of cirrhosis in patients with autoimmune hepatitis markedly increased their risk of hepatocellular carcinoma, according to a systematic review and meta-analysis of 25 cohort studies and 6,528 patients.
Estimated rates of hepatocellular carcinoma (HCC) were 10.1 (6.9-14.7) cases per 1,000 person-years in these patients versus 1.1 (0.6-2.2) cases per 1,000 person-years in patients without cirrhosis at diagnosis, Aylin Tansel, MD, of Baylor College of Medicine in Houston, and associates reported in Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.02.006). Thus, surveillance for HCC “might be cost effective in this population,” they wrote. “However, patients with AIH [autoimmune hepatitis] without cirrhosis at index diagnosis, particularly those identified from general populations, are at an extremely low risk of HCC.”
Source: American Gastroenterological Association
Autoimmune hepatitis may be asymptomatic at presentation or may cause severe acute hepatitis or even fulminant liver failure. Even with immunosuppressive therapy, patients progress to cirrhosis at reported annual rates of 0.1%-8%. HCC is the fastest-growing cause of cancer mortality, and the American Association for the Study of Liver Diseases (AASLD) recommends enhanced surveillance for this disease in patients whose annual estimated risk is at least 1.5%. Although the European Association for the Study of Liver Diseases recommends screening for HCC in patients with autoimmune hepatitis and cirrhosis, AASLD makes no such recommendation, the reviewers noted. To study the risk of HCC in patients with autoimmune hepatitis, they searched PubMed, Embase, and reference lists for relevant cohort studies published through June 2016. This work yielded 20 papers and five abstracts with a pooled median follow-up period of 8 years.
The overall pooled incidence of HCC was 3.1 (95% confidence interval, 2.2-4.2) cases per 1,000 person-years, or 1.007% per year, the reviewers wrote. However, the 95% confidence interval for the annual incidence rate nearly encompassed the 1.5% cutoff recommended by AASLD, they said. Furthermore, 5 of 16 studies that investigated the risk of HCC in patients with concurrent cirrhosis reported incidence rates above 1.5%. Among 93 patients who developed HCC in the meta-analysis, only 1 did not have cirrhosis by the time autoimmune hepatitis was diagnosed.
The meta-analysis also linked HCC to older age and Asian ethnicity among patients with autoimmune hepatitis, as has been reported before. Male sex only slightly increased the risk of HCC, but the studies included only about 1,130 men, the reviewers noted. Although the severity of autoimmune hepatitis varied among studies, higher rates of relapse predicted HCC in two cohorts. Additionally, one study linked alcohol abuse to a sixfold higher risk of HCC among patients with autoimmune hepatitis. “These data support careful monitoring of patients with autoimmune hepatitis, particularly older men, patients with multiple autoimmune hepatitis relapses, and those with ongoing alcohol abuse,” the investigators wrote.
They found no evidence of publication bias, but each individual study included at most 15 cases of HCC, so pooled incidence rates were probably imprecise, especially for subgroups, they said. Studies also inconsistently reported HCC risk factors, often lacked comparison groups, and usually did not report the effects of surveillance for HCC.
Dr. Tansel reported receiving support from the National Institutes of Health. The reviewers had no conflicts of interest.
The presence of cirrhosis in patients with autoimmune hepatitis markedly increased their risk of hepatocellular carcinoma, according to a systematic review and meta-analysis of 25 cohort studies and 6,528 patients.
Estimated rates of hepatocellular carcinoma (HCC) were 10.1 (6.9-14.7) cases per 1,000 person-years in these patients versus 1.1 (0.6-2.2) cases per 1,000 person-years in patients without cirrhosis at diagnosis, Aylin Tansel, MD, of Baylor College of Medicine in Houston, and associates reported in Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2017.02.006). Thus, surveillance for HCC “might be cost effective in this population,” they wrote. “However, patients with AIH [autoimmune hepatitis] without cirrhosis at index diagnosis, particularly those identified from general populations, are at an extremely low risk of HCC.”
Source: American Gastroenterological Association
Autoimmune hepatitis may be asymptomatic at presentation or may cause severe acute hepatitis or even fulminant liver failure. Even with immunosuppressive therapy, patients progress to cirrhosis at reported annual rates of 0.1%-8%. HCC is the fastest-growing cause of cancer mortality, and the American Association for the Study of Liver Diseases (AASLD) recommends enhanced surveillance for this disease in patients whose annual estimated risk is at least 1.5%. Although the European Association for the Study of Liver Diseases recommends screening for HCC in patients with autoimmune hepatitis and cirrhosis, AASLD makes no such recommendation, the reviewers noted. To study the risk of HCC in patients with autoimmune hepatitis, they searched PubMed, Embase, and reference lists for relevant cohort studies published through June 2016. This work yielded 20 papers and five abstracts with a pooled median follow-up period of 8 years.
The overall pooled incidence of HCC was 3.1 (95% confidence interval, 2.2-4.2) cases per 1,000 person-years, or 1.007% per year, the reviewers wrote. However, the 95% confidence interval for the annual incidence rate nearly encompassed the 1.5% cutoff recommended by AASLD, they said. Furthermore, 5 of 16 studies that investigated the risk of HCC in patients with concurrent cirrhosis reported incidence rates above 1.5%. Among 93 patients who developed HCC in the meta-analysis, only 1 did not have cirrhosis by the time autoimmune hepatitis was diagnosed.
The meta-analysis also linked HCC to older age and Asian ethnicity among patients with autoimmune hepatitis, as has been reported before. Male sex only slightly increased the risk of HCC, but the studies included only about 1,130 men, the reviewers noted. Although the severity of autoimmune hepatitis varied among studies, higher rates of relapse predicted HCC in two cohorts. Additionally, one study linked alcohol abuse to a sixfold higher risk of HCC among patients with autoimmune hepatitis. “These data support careful monitoring of patients with autoimmune hepatitis, particularly older men, patients with multiple autoimmune hepatitis relapses, and those with ongoing alcohol abuse,” the investigators wrote.
They found no evidence of publication bias, but each individual study included at most 15 cases of HCC, so pooled incidence rates were probably imprecise, especially for subgroups, they said. Studies also inconsistently reported HCC risk factors, often lacked comparison groups, and usually did not report the effects of surveillance for HCC.
Dr. Tansel reported receiving support from the National Institutes of Health. The reviewers had no conflicts of interest.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Patients with autoimmune hepatitis and cirrhosis are at increased risk of hepatocellular carcinoma.
Major finding: For every 1,000 person-years, there were 3.1 (95% CI, 2.2-4.2) cases of hepatocellular carcinoma overall, 10.1 (6.9-14.7) cases in patients who also had cirrhosis at diagnosis, and 1.1 (0.6-2.2) cases in patients who did not have cirrhosis at diagnosis.
Data source: A systematic review and meta-analysis of 25 studies of 6,528 patients with autoimmune hepatitis.
Disclosures: Dr. Tansel reported receiving support from the National Institutes of Health. The investigators disclosed no conflicts.

Black Adherence Nodules on the Scalp Hair Shaft
The Diagnosis: Piedra
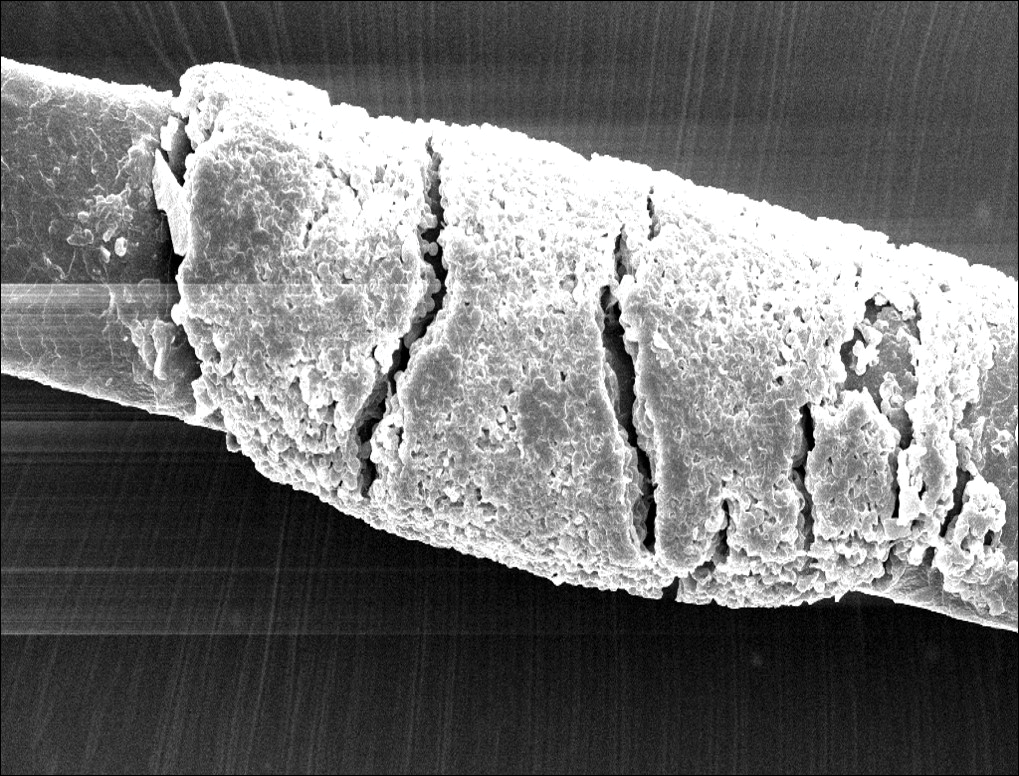
Microscopic examination of the hair shafts revealed brown to black, firmly adherent concretions (Figure 1). Scanning electron microscopy of the nodules was performed, which allowed for greater definition of the constituent hyphae and arthrospores (Figure 2).
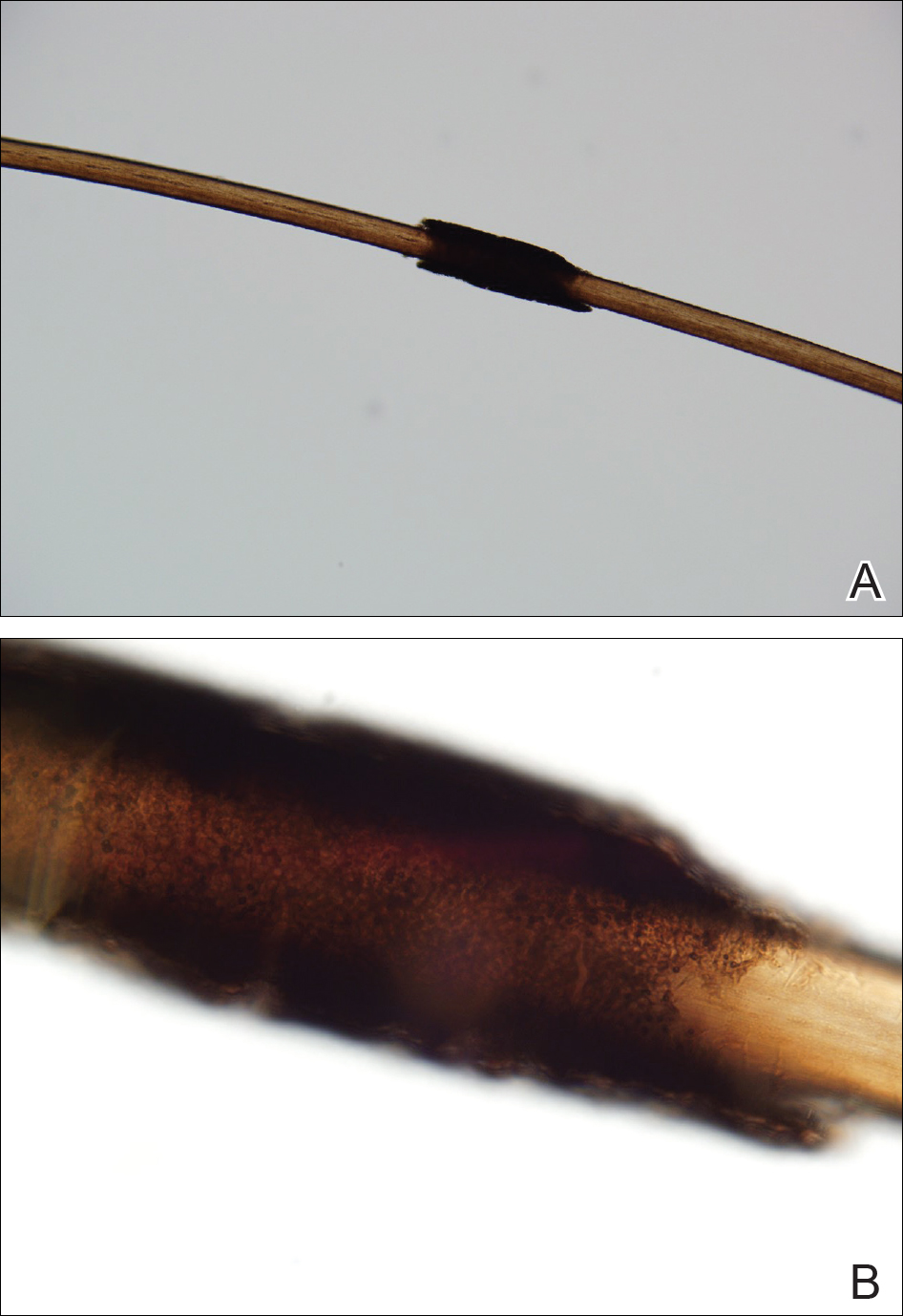
Fungal cultures grew Trichosporon inkin along with other dematiaceous molds. The patient initially was treated with a combination of ketoconazole shampoo and weekly application of topical terbinafine. She trimmed 15.2 cm of the hair of her own volition. At 2-month follow-up the nodules were still present, though smaller and less numerous. Repeat cultures were obtained, which again grew T inkin. She then began taking oral terbinafine 250 mg daily for 6 weeks.
This case of piedra is unique in that our patient presented with black nodules clinically, but cultures grew only the causative agent of white piedra, T inkin. A search of PubMed articles indexed for MEDLINE using the terms black piedra, white piedra, or piedra, and mixed infection or coinfection yielded one other similar case.1 Kanitakis et al1 speculated that perhaps there was coinfection of black and white piedra and that Piedraia hortae, the causative agent of black piedra, was unable to flourish in culture facing competition from other fungi. This scenario also could apply to our patient. However, the original culture taken from our patient also grew other dematiaceous molds including Cladosporium and Exophiala species. It also is possible that these other fungi could have contributed pigment to the nodules, giving it the appearance of black piedra when only T inkin was present as the true pathogen.
White piedra is a rare fungal infection of the hair shaft caused by organisms of the genus Trichosporon, with Trichosporon ovoides most likely to infect the scalp.2 Black piedra is a similar fungal infection caused by P hortae. Piedra means stone in Spanish, reflecting the appearance of these organisms on the hair shaft. It is common in tropical regions of the world such as Southeast Asia and South America, flourishing in the high temperatures and humidity.2 Both infectious agents are found in the soil or in standing water.3 White piedra most commonly is found in facial, axilla, or pubic hair, while black piedra most often is found in the hair of the scalp.2,4 Local cultural practices may contribute to transfer of Trichosporon or P hortae to the scalp, including the use of Brazilian plant oils in the hair or tying a veil or hijab to wet hair. Interestingly, some groups intentionally introduce the fungus to their hair for cosmetic reasons in endemic areas.2,3,5
Patients with white or black piedra generally are asymptomatic.4 Some may notice a rough texture to the hair or hear a characteristic metallic rattling sound as the nodules make contact with brush bristles.2,3 On inspection of the scalp, white piedra will appear to be white to light brown nodules, while black piedra presents as brown to black in color. The nodules are often firm on palpation.2,3 The nodules of white piedra generally are easy to remove in contrast to black piedra, which involves nodules that securely attach to the hair shaft but can be removed with pressure.3,5 Piedra has natural keratolytic activities and with prolonged infection can penetrate the hair cuticle, causing weakness and eventual breakage of the hair. This invasion into the hair cortex also can complicate treatment regimens, contributing to the chronic course of these infections.6
Diagnosis is based on clinical and microscopic findings. Nodules on hair shafts can be prepared with potassium hydroxide and placed on glass slides for examination.4 Dyes such as toluidine blue or chlorazol black E stain can be used to assist in identifying fungal structures.2 Sabouraud agar with cycloheximide may be the best choice for culture medium.2 Black piedra slowly grows into small dome-shaped colonies. White piedra will grow more quickly into cream-colored colonies with wrinkles and sometimes mucinous characteristics.3
The best treatment of black or white piedra is to cut the hair, thereby eliminating the fungi,7 which is not an easy option for many patients, such as ours, because of the aesthetic implications. Alternative treatments include azole shampoos such as ketoconazole.2,4 Treatment with oral terbinafine 250 mg daily for 6 weeks has been successfully used for black piedra.7 Patients must be careful to thoroughly clean or discard hairbrushes, as they can serve as reservoirs of fungi to reinfect patients or spread to others.5,7
- Kanitakis J, Persat F, Piens MA, et al. Black piedra: report of a French case associated with Trichosporon asahii. Int J Dermatol. 2006;45:1258-1260.
- Schwartz RA. Superficial fungal infections. Lancet. 2004;364:1173-1182.
- Khatu SS, Poojary SA, Nagpur NG. Nodules on the hair: a rare case of mixed piedra. Int J Trichology. 2013;5:220-223.
- Elewski BE, Hughey LC, Sobera JO, et al. Fungal diseases. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Health Sciences; 2012:1251-1284.
- Desai DH, Nadkarni NJ. Piedra: an ethnicity-related trichosis? Int J Dermatol. 2013;53:1008-1011.
- Figueras M, Guarro J, Zaror L. New findings in black piedra infection. Br J Dermatol. 1996;135:157-158.
- Gip L. Black piedra: the first case treated with terbinafine (Lamisil). Br J Dermatol. 1994;130(suppl 43):26-28.
The Diagnosis: Piedra
Microscopic examination of the hair shafts revealed brown to black, firmly adherent concretions (Figure 1). Scanning electron microscopy of the nodules was performed, which allowed for greater definition of the constituent hyphae and arthrospores (Figure 2).
Fungal cultures grew Trichosporon inkin along with other dematiaceous molds. The patient initially was treated with a combination of ketoconazole shampoo and weekly application of topical terbinafine. She trimmed 15.2 cm of the hair of her own volition. At 2-month follow-up the nodules were still present, though smaller and less numerous. Repeat cultures were obtained, which again grew T inkin. She then began taking oral terbinafine 250 mg daily for 6 weeks.
This case of piedra is unique in that our patient presented with black nodules clinically, but cultures grew only the causative agent of white piedra, T inkin. A search of PubMed articles indexed for MEDLINE using the terms black piedra, white piedra, or piedra, and mixed infection or coinfection yielded one other similar case.1 Kanitakis et al1 speculated that perhaps there was coinfection of black and white piedra and that Piedraia hortae, the causative agent of black piedra, was unable to flourish in culture facing competition from other fungi. This scenario also could apply to our patient. However, the original culture taken from our patient also grew other dematiaceous molds including Cladosporium and Exophiala species. It also is possible that these other fungi could have contributed pigment to the nodules, giving it the appearance of black piedra when only T inkin was present as the true pathogen.
White piedra is a rare fungal infection of the hair shaft caused by organisms of the genus Trichosporon, with Trichosporon ovoides most likely to infect the scalp.2 Black piedra is a similar fungal infection caused by P hortae. Piedra means stone in Spanish, reflecting the appearance of these organisms on the hair shaft. It is common in tropical regions of the world such as Southeast Asia and South America, flourishing in the high temperatures and humidity.2 Both infectious agents are found in the soil or in standing water.3 White piedra most commonly is found in facial, axilla, or pubic hair, while black piedra most often is found in the hair of the scalp.2,4 Local cultural practices may contribute to transfer of Trichosporon or P hortae to the scalp, including the use of Brazilian plant oils in the hair or tying a veil or hijab to wet hair. Interestingly, some groups intentionally introduce the fungus to their hair for cosmetic reasons in endemic areas.2,3,5
Patients with white or black piedra generally are asymptomatic.4 Some may notice a rough texture to the hair or hear a characteristic metallic rattling sound as the nodules make contact with brush bristles.2,3 On inspection of the scalp, white piedra will appear to be white to light brown nodules, while black piedra presents as brown to black in color. The nodules are often firm on palpation.2,3 The nodules of white piedra generally are easy to remove in contrast to black piedra, which involves nodules that securely attach to the hair shaft but can be removed with pressure.3,5 Piedra has natural keratolytic activities and with prolonged infection can penetrate the hair cuticle, causing weakness and eventual breakage of the hair. This invasion into the hair cortex also can complicate treatment regimens, contributing to the chronic course of these infections.6
Diagnosis is based on clinical and microscopic findings. Nodules on hair shafts can be prepared with potassium hydroxide and placed on glass slides for examination.4 Dyes such as toluidine blue or chlorazol black E stain can be used to assist in identifying fungal structures.2 Sabouraud agar with cycloheximide may be the best choice for culture medium.2 Black piedra slowly grows into small dome-shaped colonies. White piedra will grow more quickly into cream-colored colonies with wrinkles and sometimes mucinous characteristics.3
The best treatment of black or white piedra is to cut the hair, thereby eliminating the fungi,7 which is not an easy option for many patients, such as ours, because of the aesthetic implications. Alternative treatments include azole shampoos such as ketoconazole.2,4 Treatment with oral terbinafine 250 mg daily for 6 weeks has been successfully used for black piedra.7 Patients must be careful to thoroughly clean or discard hairbrushes, as they can serve as reservoirs of fungi to reinfect patients or spread to others.5,7
The Diagnosis: Piedra
Microscopic examination of the hair shafts revealed brown to black, firmly adherent concretions (Figure 1). Scanning electron microscopy of the nodules was performed, which allowed for greater definition of the constituent hyphae and arthrospores (Figure 2).
Fungal cultures grew Trichosporon inkin along with other dematiaceous molds. The patient initially was treated with a combination of ketoconazole shampoo and weekly application of topical terbinafine. She trimmed 15.2 cm of the hair of her own volition. At 2-month follow-up the nodules were still present, though smaller and less numerous. Repeat cultures were obtained, which again grew T inkin. She then began taking oral terbinafine 250 mg daily for 6 weeks.
This case of piedra is unique in that our patient presented with black nodules clinically, but cultures grew only the causative agent of white piedra, T inkin. A search of PubMed articles indexed for MEDLINE using the terms black piedra, white piedra, or piedra, and mixed infection or coinfection yielded one other similar case.1 Kanitakis et al1 speculated that perhaps there was coinfection of black and white piedra and that Piedraia hortae, the causative agent of black piedra, was unable to flourish in culture facing competition from other fungi. This scenario also could apply to our patient. However, the original culture taken from our patient also grew other dematiaceous molds including Cladosporium and Exophiala species. It also is possible that these other fungi could have contributed pigment to the nodules, giving it the appearance of black piedra when only T inkin was present as the true pathogen.
White piedra is a rare fungal infection of the hair shaft caused by organisms of the genus Trichosporon, with Trichosporon ovoides most likely to infect the scalp.2 Black piedra is a similar fungal infection caused by P hortae. Piedra means stone in Spanish, reflecting the appearance of these organisms on the hair shaft. It is common in tropical regions of the world such as Southeast Asia and South America, flourishing in the high temperatures and humidity.2 Both infectious agents are found in the soil or in standing water.3 White piedra most commonly is found in facial, axilla, or pubic hair, while black piedra most often is found in the hair of the scalp.2,4 Local cultural practices may contribute to transfer of Trichosporon or P hortae to the scalp, including the use of Brazilian plant oils in the hair or tying a veil or hijab to wet hair. Interestingly, some groups intentionally introduce the fungus to their hair for cosmetic reasons in endemic areas.2,3,5
Patients with white or black piedra generally are asymptomatic.4 Some may notice a rough texture to the hair or hear a characteristic metallic rattling sound as the nodules make contact with brush bristles.2,3 On inspection of the scalp, white piedra will appear to be white to light brown nodules, while black piedra presents as brown to black in color. The nodules are often firm on palpation.2,3 The nodules of white piedra generally are easy to remove in contrast to black piedra, which involves nodules that securely attach to the hair shaft but can be removed with pressure.3,5 Piedra has natural keratolytic activities and with prolonged infection can penetrate the hair cuticle, causing weakness and eventual breakage of the hair. This invasion into the hair cortex also can complicate treatment regimens, contributing to the chronic course of these infections.6
Diagnosis is based on clinical and microscopic findings. Nodules on hair shafts can be prepared with potassium hydroxide and placed on glass slides for examination.4 Dyes such as toluidine blue or chlorazol black E stain can be used to assist in identifying fungal structures.2 Sabouraud agar with cycloheximide may be the best choice for culture medium.2 Black piedra slowly grows into small dome-shaped colonies. White piedra will grow more quickly into cream-colored colonies with wrinkles and sometimes mucinous characteristics.3
The best treatment of black or white piedra is to cut the hair, thereby eliminating the fungi,7 which is not an easy option for many patients, such as ours, because of the aesthetic implications. Alternative treatments include azole shampoos such as ketoconazole.2,4 Treatment with oral terbinafine 250 mg daily for 6 weeks has been successfully used for black piedra.7 Patients must be careful to thoroughly clean or discard hairbrushes, as they can serve as reservoirs of fungi to reinfect patients or spread to others.5,7
- Kanitakis J, Persat F, Piens MA, et al. Black piedra: report of a French case associated with Trichosporon asahii. Int J Dermatol. 2006;45:1258-1260.
- Schwartz RA. Superficial fungal infections. Lancet. 2004;364:1173-1182.
- Khatu SS, Poojary SA, Nagpur NG. Nodules on the hair: a rare case of mixed piedra. Int J Trichology. 2013;5:220-223.
- Elewski BE, Hughey LC, Sobera JO, et al. Fungal diseases. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Health Sciences; 2012:1251-1284.
- Desai DH, Nadkarni NJ. Piedra: an ethnicity-related trichosis? Int J Dermatol. 2013;53:1008-1011.
- Figueras M, Guarro J, Zaror L. New findings in black piedra infection. Br J Dermatol. 1996;135:157-158.
- Gip L. Black piedra: the first case treated with terbinafine (Lamisil). Br J Dermatol. 1994;130(suppl 43):26-28.
- Kanitakis J, Persat F, Piens MA, et al. Black piedra: report of a French case associated with Trichosporon asahii. Int J Dermatol. 2006;45:1258-1260.
- Schwartz RA. Superficial fungal infections. Lancet. 2004;364:1173-1182.
- Khatu SS, Poojary SA, Nagpur NG. Nodules on the hair: a rare case of mixed piedra. Int J Trichology. 2013;5:220-223.
- Elewski BE, Hughey LC, Sobera JO, et al. Fungal diseases. Dermatology. 3rd ed. Philadelphia, PA: Elsevier Health Sciences; 2012:1251-1284.
- Desai DH, Nadkarni NJ. Piedra: an ethnicity-related trichosis? Int J Dermatol. 2013;53:1008-1011.
- Figueras M, Guarro J, Zaror L. New findings in black piedra infection. Br J Dermatol. 1996;135:157-158.
- Gip L. Black piedra: the first case treated with terbinafine (Lamisil). Br J Dermatol. 1994;130(suppl 43):26-28.
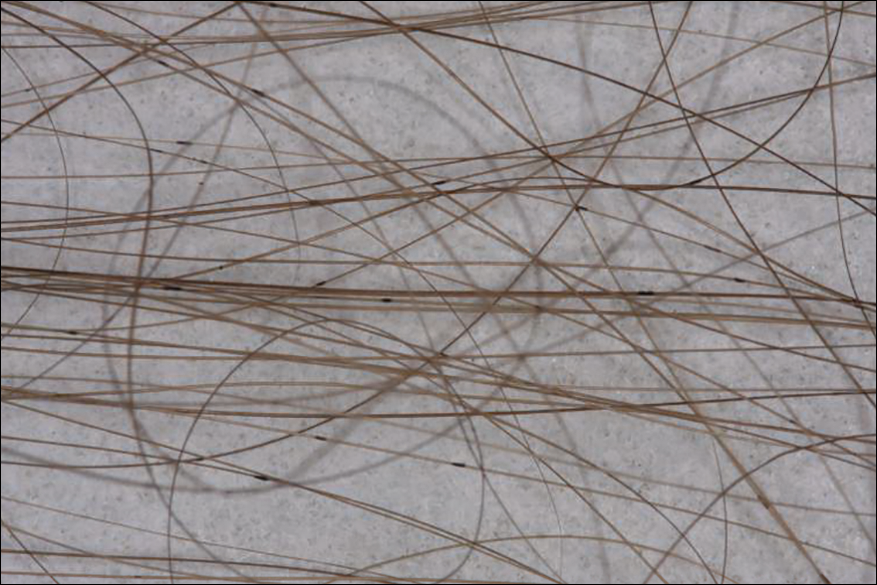
A 21-year-old woman presented to the dermatology clinic with what she described as small black dots in her hair that she first noted 3 months prior to presentation. The black nodules were asymptomatic, but the patient noted that they seemed to be moving up the hair shaft. They were firmly attached and great effort was required to remove them. The patient's sister recently developed similar nodules. The patient and her sister work as missionaries and had spent time in India, Southeast Asia, and Central America within the last few years. Physical examination revealed firmly adherent black nodules involving the mid to distal portions of the hair shafts on the scalp. There were no nail or skin findings. Cultures were obtained, and microscopic examination was performed.
Statins might protect against rectal anastomotic leaks
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.

Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.
Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.
Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
AT ASCRS 2017
Key clinical point:
Major finding: The statin group had a reduced risk of sepsis (OR, 0.712; 95% CI, 0.535-0.948; P = .020), and, while statins were not associated with a reduction in anastomotic leaks overall, they were protective in subgroup analysis of patients who had rectal resections, which are especially prone to leakage (OR, 0.260; 95% CI, 0.112-0.605, P = .002).
Data source: A review of 7,285 elective colorectal surgery patients.
Disclosures: The lead investigator had no disclosures.
VIDEO: Meta-analysis favors anticoagulation for patients with cirrhosis and portal vein thrombosis
Patients with cirrhosis and portal vein thrombosis (PVT) who received anticoagulation therapy had nearly fivefold greater odds of recanalization compared with untreated patients, and were no more likely to experience major or minor bleeding, in a pooled analysis of eight studies published in the August issue of Gastroenterology (doi: 10.1053/j.gastro.2017.04.042).
Rates of any recanalization were 71% in treated patients and 42% in untreated patients (P less than .0001), wrote Lorenzo Loffredo, MD, of Sapienza University, Rome, and his coinvestigators. Rates of complete recanalization were 53% and 33%, respectively (P = .002), rates of spontaneous variceal bleeding were 2% and 12% (P = .04), and bleeding affected 11% of patients in each group. Together, the findings “show that anticoagulants are efficacious and safe for treatment of portal vein thrombosis in cirrhotic patients,” although larger, interventional clinical trials are needed to pinpoint the clinical role of anticoagulation in cirrhotic patients with PVT, the reviewers reported.
Source: American Gastroenterological Association
Bleeding from portal hypertension is a major complication in cirrhosis, but PVT affects about 20% of patients and predicts poor outcomes, they noted. Anticoagulation in this setting can be difficult because patients often have concurrent coagulopathies that are hard to assess with standard techniques, such as PT-INR (international normalized ratio). Although some studies support anticoagulating these patients, data are limited. Therefore, the reviewers searched PubMed, the ISI Web of Science, SCOPUS, and the Cochrane database through Feb. 14, 2017, for trials comparing anticoagulation with no treatment in patients with cirrhosis and PVT.
This search yielded eight trials of 353 patients who received low-molecular-weight heparin, warfarin, or no treatment for about 6 months, with a typical follow-up period of 2 years. The reviewers found no evidence of publication bias or significant heterogeneity among the trials. Six studies evaluated complete recanalization, another set of six studies tracked progression of PVT, a third set of six studies evaluated major or minor bleeding events, and four studies evaluated spontaneous variceal bleeding. Compared with no treatment, anticoagulation was tied to a significantly greater likelihood of complete recanalization (pooled odds ratio, 3.4; 95% confidence interval, 1.5-7.4; P = .002), a significantly lower chance of PVT progressing (9% vs. 33%; pooled odds ratio, 0.14; 95% CI, 0.06-0.31; P less than .0001), no difference in bleeding rates (11% in each pooled group), and a significantly lower risk of spontaneous variceal bleeding (OR, 0.23; 95% CI, 0.06-0.94; P = .04).
“Metaregression analysis showed that duration of anticoagulation did not influence outcomes,” the reviewers wrote. “Low-molecular-weight heparin, but not warfarin, was significantly associated with a complete PVT resolution as compared to untreated patients, while both low-molecular-weight heparin and warfarin were effective in reducing PVT progression.” That finding merits careful interpretation, however, because most studies on warfarin were retrospective and lacked data on the quality of anticoagulation, they added.
“It is a challenge to treat patients with cirrhosis using anticoagulants because of the perception that the coexistent coagulopathy could promote bleeding,” the researchers wrote. Nonetheless, their analysis suggests that anticoagulation has significant benefits and does not increase bleeding risk, regardless of the severity of liver failure, they concluded.
The reviewers reported having no funding sources or conflicts of interest.
Patients with cirrhosis and portal vein thrombosis (PVT) who received anticoagulation therapy had nearly fivefold greater odds of recanalization compared with untreated patients, and were no more likely to experience major or minor bleeding, in a pooled analysis of eight studies published in the August issue of Gastroenterology (doi: 10.1053/j.gastro.2017.04.042).
Rates of any recanalization were 71% in treated patients and 42% in untreated patients (P less than .0001), wrote Lorenzo Loffredo, MD, of Sapienza University, Rome, and his coinvestigators. Rates of complete recanalization were 53% and 33%, respectively (P = .002), rates of spontaneous variceal bleeding were 2% and 12% (P = .04), and bleeding affected 11% of patients in each group. Together, the findings “show that anticoagulants are efficacious and safe for treatment of portal vein thrombosis in cirrhotic patients,” although larger, interventional clinical trials are needed to pinpoint the clinical role of anticoagulation in cirrhotic patients with PVT, the reviewers reported.
Source: American Gastroenterological Association
Bleeding from portal hypertension is a major complication in cirrhosis, but PVT affects about 20% of patients and predicts poor outcomes, they noted. Anticoagulation in this setting can be difficult because patients often have concurrent coagulopathies that are hard to assess with standard techniques, such as PT-INR (international normalized ratio). Although some studies support anticoagulating these patients, data are limited. Therefore, the reviewers searched PubMed, the ISI Web of Science, SCOPUS, and the Cochrane database through Feb. 14, 2017, for trials comparing anticoagulation with no treatment in patients with cirrhosis and PVT.
This search yielded eight trials of 353 patients who received low-molecular-weight heparin, warfarin, or no treatment for about 6 months, with a typical follow-up period of 2 years. The reviewers found no evidence of publication bias or significant heterogeneity among the trials. Six studies evaluated complete recanalization, another set of six studies tracked progression of PVT, a third set of six studies evaluated major or minor bleeding events, and four studies evaluated spontaneous variceal bleeding. Compared with no treatment, anticoagulation was tied to a significantly greater likelihood of complete recanalization (pooled odds ratio, 3.4; 95% confidence interval, 1.5-7.4; P = .002), a significantly lower chance of PVT progressing (9% vs. 33%; pooled odds ratio, 0.14; 95% CI, 0.06-0.31; P less than .0001), no difference in bleeding rates (11% in each pooled group), and a significantly lower risk of spontaneous variceal bleeding (OR, 0.23; 95% CI, 0.06-0.94; P = .04).
“Metaregression analysis showed that duration of anticoagulation did not influence outcomes,” the reviewers wrote. “Low-molecular-weight heparin, but not warfarin, was significantly associated with a complete PVT resolution as compared to untreated patients, while both low-molecular-weight heparin and warfarin were effective in reducing PVT progression.” That finding merits careful interpretation, however, because most studies on warfarin were retrospective and lacked data on the quality of anticoagulation, they added.
“It is a challenge to treat patients with cirrhosis using anticoagulants because of the perception that the coexistent coagulopathy could promote bleeding,” the researchers wrote. Nonetheless, their analysis suggests that anticoagulation has significant benefits and does not increase bleeding risk, regardless of the severity of liver failure, they concluded.
The reviewers reported having no funding sources or conflicts of interest.
Patients with cirrhosis and portal vein thrombosis (PVT) who received anticoagulation therapy had nearly fivefold greater odds of recanalization compared with untreated patients, and were no more likely to experience major or minor bleeding, in a pooled analysis of eight studies published in the August issue of Gastroenterology (doi: 10.1053/j.gastro.2017.04.042).
Rates of any recanalization were 71% in treated patients and 42% in untreated patients (P less than .0001), wrote Lorenzo Loffredo, MD, of Sapienza University, Rome, and his coinvestigators. Rates of complete recanalization were 53% and 33%, respectively (P = .002), rates of spontaneous variceal bleeding were 2% and 12% (P = .04), and bleeding affected 11% of patients in each group. Together, the findings “show that anticoagulants are efficacious and safe for treatment of portal vein thrombosis in cirrhotic patients,” although larger, interventional clinical trials are needed to pinpoint the clinical role of anticoagulation in cirrhotic patients with PVT, the reviewers reported.
Source: American Gastroenterological Association
Bleeding from portal hypertension is a major complication in cirrhosis, but PVT affects about 20% of patients and predicts poor outcomes, they noted. Anticoagulation in this setting can be difficult because patients often have concurrent coagulopathies that are hard to assess with standard techniques, such as PT-INR (international normalized ratio). Although some studies support anticoagulating these patients, data are limited. Therefore, the reviewers searched PubMed, the ISI Web of Science, SCOPUS, and the Cochrane database through Feb. 14, 2017, for trials comparing anticoagulation with no treatment in patients with cirrhosis and PVT.
This search yielded eight trials of 353 patients who received low-molecular-weight heparin, warfarin, or no treatment for about 6 months, with a typical follow-up period of 2 years. The reviewers found no evidence of publication bias or significant heterogeneity among the trials. Six studies evaluated complete recanalization, another set of six studies tracked progression of PVT, a third set of six studies evaluated major or minor bleeding events, and four studies evaluated spontaneous variceal bleeding. Compared with no treatment, anticoagulation was tied to a significantly greater likelihood of complete recanalization (pooled odds ratio, 3.4; 95% confidence interval, 1.5-7.4; P = .002), a significantly lower chance of PVT progressing (9% vs. 33%; pooled odds ratio, 0.14; 95% CI, 0.06-0.31; P less than .0001), no difference in bleeding rates (11% in each pooled group), and a significantly lower risk of spontaneous variceal bleeding (OR, 0.23; 95% CI, 0.06-0.94; P = .04).
“Metaregression analysis showed that duration of anticoagulation did not influence outcomes,” the reviewers wrote. “Low-molecular-weight heparin, but not warfarin, was significantly associated with a complete PVT resolution as compared to untreated patients, while both low-molecular-weight heparin and warfarin were effective in reducing PVT progression.” That finding merits careful interpretation, however, because most studies on warfarin were retrospective and lacked data on the quality of anticoagulation, they added.
“It is a challenge to treat patients with cirrhosis using anticoagulants because of the perception that the coexistent coagulopathy could promote bleeding,” the researchers wrote. Nonetheless, their analysis suggests that anticoagulation has significant benefits and does not increase bleeding risk, regardless of the severity of liver failure, they concluded.
The reviewers reported having no funding sources or conflicts of interest.
FROM GASTROENTEROLOGY
Key clinical point: Anticoagulation produced favorable outcomes with no increase in bleeding risk in patients with cirrhosis and portal vein thrombosis.
Major finding: Rates of any recanalization were 71% in treated patients and 42% in untreated patients (P less than .0001); rates of complete recanalization were 53% and 33%, respectively (P = .002), rates of spontaneous variceal bleeding were 2% and 12% (P = .04), and bleeding affected 11% of patients in each group.
Data source: A systematic review and meta-analysis of eight studies of 353 patients with cirrhosis and portal vein thrombosis.
Disclosures: The reviewers reported having no funding sources or conflicts of interest.

Cosmeceuticals and Alternative Therapies for Rosacea
What do your patients need to know?
Vascular instability associated with rosacea is exacerbated by triggers such as sunlight, hot drinks, spicy foods, stress, and rapid changing weather, which make patients flush and blush, increase the appearance of telangiectasia, and disrupt the normal skin barrier. Because the patients feel on fire, an anti-inflammatory approach is indicated. The regimen I recommend includes mild cleansers, barrier repair creams and supplements, antioxidants (topical and oral), and sun protection, all without parabens and harsh chemicals. I always recommend a product that I dispense at the office and another one of similar effectiveness that can be found over-the-counter.
What are your go-to treatments?
Cleansing is indispensable to maintain the normal flow in and out of the skin. I recommend mild cleansers without potentially sensitizing agents such as propylene glycol or parabens. It also should have calming agents (eg, fruit extracts) that remove the contaminants from the skin surface without stripping the important layers of lipids that constitute the barrier of the skin as well as ingredients (eg, prebiotics) that promote the healthy skin biome. Selenium in thermal spring water has free radical scavenging and anti-inflammatory properties as well as protection against heavy metals.
After cleansing, I recommend a product to repair, maintain, and improve the barrier of the skin. A healthy skin barrier has an equal ratio of cholesterol, ceramides, and free fatty acids, the building blocks of the skin. In a barrier repair cream I look for ingredients that stop and prevent damaging inflammation, improve the skin's natural ability to repair and heal (eg, niacinamide), and protect against environmental insults. It should contain petrolatum and/or dimethicone to form a protective barrier on the skin to seal in moisture.
Oral niacinamide should be taken as a photoprotective agent. Oral supplementation (500 mg twice daily) is effective in reducing skin cancer. Because UV light is a trigger factor, oral photoprotection is recommended.
Topical antioxidants also are important. Free radical formation has been documented even in photoprotected skin. These free radicals have been implicated in skin cancer development and metalloproteinase production and are triggers of rosacea. As a result, I advise my patients to apply topical encapsulated vitamin C every night. The encapsulated form prevents oxidation of the product before application. In addition, I recommend oral vitamin C (1 g daily) and vitamin E (400 U daily).
For sun protection I recommend sunblocks with titanium dioxide and zinc oxide for total UVA and UVB protection. If the patient has a darker skin type, sun protection should contain iron oxide. Chemical agents can cause irritation, photocontact dermatitis, and exacerbation of rosacea symptoms. Daily application of sun protection with reapplication every 2 hours is reinforced.
What holistic therapies do you recommend?
Stress reduction activities, including yoga, relaxation, massages, and meditation, can help. Oral consumption of trigger factors is discouraged. Antioxidant green tea is recommended instead of caffeinated beverages.
Suggested Readings
Baldwin HE, Bathia ND, Friedman A, et al. The role of cutaneous microbiota harmony in maintaining functional skin barrier. J Drugs Dermatol. 2017;16:12-18.
Celerier P, Richard A, Litoux P, et al. Modulatory effects of selenium and strontium salts on keratinocyte-derived inflammatory cytokines. Arch Dermatol Res. 1995;287:680-682.
Chen AC, Martin AJ, Choy B, et al. A phase 3 randomized trial of nicotinamide for skin cancer chemoprevention. N Engl J Med. 2015;373:1618-1626.
Jones D. Reactive oxygen species and rosacea. Cutis. 2004;74(suppl 3):17-20.
What do your patients need to know?
Vascular instability associated with rosacea is exacerbated by triggers such as sunlight, hot drinks, spicy foods, stress, and rapid changing weather, which make patients flush and blush, increase the appearance of telangiectasia, and disrupt the normal skin barrier. Because the patients feel on fire, an anti-inflammatory approach is indicated. The regimen I recommend includes mild cleansers, barrier repair creams and supplements, antioxidants (topical and oral), and sun protection, all without parabens and harsh chemicals. I always recommend a product that I dispense at the office and another one of similar effectiveness that can be found over-the-counter.
What are your go-to treatments?
Cleansing is indispensable to maintain the normal flow in and out of the skin. I recommend mild cleansers without potentially sensitizing agents such as propylene glycol or parabens. It also should have calming agents (eg, fruit extracts) that remove the contaminants from the skin surface without stripping the important layers of lipids that constitute the barrier of the skin as well as ingredients (eg, prebiotics) that promote the healthy skin biome. Selenium in thermal spring water has free radical scavenging and anti-inflammatory properties as well as protection against heavy metals.
After cleansing, I recommend a product to repair, maintain, and improve the barrier of the skin. A healthy skin barrier has an equal ratio of cholesterol, ceramides, and free fatty acids, the building blocks of the skin. In a barrier repair cream I look for ingredients that stop and prevent damaging inflammation, improve the skin's natural ability to repair and heal (eg, niacinamide), and protect against environmental insults. It should contain petrolatum and/or dimethicone to form a protective barrier on the skin to seal in moisture.
Oral niacinamide should be taken as a photoprotective agent. Oral supplementation (500 mg twice daily) is effective in reducing skin cancer. Because UV light is a trigger factor, oral photoprotection is recommended.
Topical antioxidants also are important. Free radical formation has been documented even in photoprotected skin. These free radicals have been implicated in skin cancer development and metalloproteinase production and are triggers of rosacea. As a result, I advise my patients to apply topical encapsulated vitamin C every night. The encapsulated form prevents oxidation of the product before application. In addition, I recommend oral vitamin C (1 g daily) and vitamin E (400 U daily).
For sun protection I recommend sunblocks with titanium dioxide and zinc oxide for total UVA and UVB protection. If the patient has a darker skin type, sun protection should contain iron oxide. Chemical agents can cause irritation, photocontact dermatitis, and exacerbation of rosacea symptoms. Daily application of sun protection with reapplication every 2 hours is reinforced.
What holistic therapies do you recommend?
Stress reduction activities, including yoga, relaxation, massages, and meditation, can help. Oral consumption of trigger factors is discouraged. Antioxidant green tea is recommended instead of caffeinated beverages.
Suggested Readings
Baldwin HE, Bathia ND, Friedman A, et al. The role of cutaneous microbiota harmony in maintaining functional skin barrier. J Drugs Dermatol. 2017;16:12-18.
Celerier P, Richard A, Litoux P, et al. Modulatory effects of selenium and strontium salts on keratinocyte-derived inflammatory cytokines. Arch Dermatol Res. 1995;287:680-682.
Chen AC, Martin AJ, Choy B, et al. A phase 3 randomized trial of nicotinamide for skin cancer chemoprevention. N Engl J Med. 2015;373:1618-1626.
Jones D. Reactive oxygen species and rosacea. Cutis. 2004;74(suppl 3):17-20.
What do your patients need to know?
Vascular instability associated with rosacea is exacerbated by triggers such as sunlight, hot drinks, spicy foods, stress, and rapid changing weather, which make patients flush and blush, increase the appearance of telangiectasia, and disrupt the normal skin barrier. Because the patients feel on fire, an anti-inflammatory approach is indicated. The regimen I recommend includes mild cleansers, barrier repair creams and supplements, antioxidants (topical and oral), and sun protection, all without parabens and harsh chemicals. I always recommend a product that I dispense at the office and another one of similar effectiveness that can be found over-the-counter.
What are your go-to treatments?
Cleansing is indispensable to maintain the normal flow in and out of the skin. I recommend mild cleansers without potentially sensitizing agents such as propylene glycol or parabens. It also should have calming agents (eg, fruit extracts) that remove the contaminants from the skin surface without stripping the important layers of lipids that constitute the barrier of the skin as well as ingredients (eg, prebiotics) that promote the healthy skin biome. Selenium in thermal spring water has free radical scavenging and anti-inflammatory properties as well as protection against heavy metals.
After cleansing, I recommend a product to repair, maintain, and improve the barrier of the skin. A healthy skin barrier has an equal ratio of cholesterol, ceramides, and free fatty acids, the building blocks of the skin. In a barrier repair cream I look for ingredients that stop and prevent damaging inflammation, improve the skin's natural ability to repair and heal (eg, niacinamide), and protect against environmental insults. It should contain petrolatum and/or dimethicone to form a protective barrier on the skin to seal in moisture.
Oral niacinamide should be taken as a photoprotective agent. Oral supplementation (500 mg twice daily) is effective in reducing skin cancer. Because UV light is a trigger factor, oral photoprotection is recommended.
Topical antioxidants also are important. Free radical formation has been documented even in photoprotected skin. These free radicals have been implicated in skin cancer development and metalloproteinase production and are triggers of rosacea. As a result, I advise my patients to apply topical encapsulated vitamin C every night. The encapsulated form prevents oxidation of the product before application. In addition, I recommend oral vitamin C (1 g daily) and vitamin E (400 U daily).
For sun protection I recommend sunblocks with titanium dioxide and zinc oxide for total UVA and UVB protection. If the patient has a darker skin type, sun protection should contain iron oxide. Chemical agents can cause irritation, photocontact dermatitis, and exacerbation of rosacea symptoms. Daily application of sun protection with reapplication every 2 hours is reinforced.
What holistic therapies do you recommend?
Stress reduction activities, including yoga, relaxation, massages, and meditation, can help. Oral consumption of trigger factors is discouraged. Antioxidant green tea is recommended instead of caffeinated beverages.
Suggested Readings
Baldwin HE, Bathia ND, Friedman A, et al. The role of cutaneous microbiota harmony in maintaining functional skin barrier. J Drugs Dermatol. 2017;16:12-18.
Celerier P, Richard A, Litoux P, et al. Modulatory effects of selenium and strontium salts on keratinocyte-derived inflammatory cytokines. Arch Dermatol Res. 1995;287:680-682.
Chen AC, Martin AJ, Choy B, et al. A phase 3 randomized trial of nicotinamide for skin cancer chemoprevention. N Engl J Med. 2015;373:1618-1626.
Jones D. Reactive oxygen species and rosacea. Cutis. 2004;74(suppl 3):17-20.
