User login
Tick, Tick, Boom
1. A 16-year-old boy presents with a skin ulcer on the dorsum of his hand and swollen glands in the proximal axilla. He works as a camp counselor in South Dakota, leading nature walks and teaching the children to care for animals, including the camp’s rabbits. Several weeks ago, he developed a fever of 103°F, fatigue, and body aches, followed by the appearance of the skin lesion.

Diagnosis: Tularemia—also called rabbit fever or deer fly fever—is caused by the bacterium Francisella tularensis. It is an insect-borne pathogen of rabbits, squirrels, and other rodents, most commonly found in the western United States and Russia. Symptoms vary by mechanism of exposure but include skin ulcers; irritation and inflammation of the eye; sore throat, mouth ulcers, and tonsillitis; lung involvement with cough, chest pain, and difficulty breathing; and swelling of regional lymph nodes. Tularemia can be successfully treated with antibiotics.
For more information, see “Pneumonic Tularemia Presenting With a Vesicular Eruption.” Cutis. 2015;95(4):E17-E18.
2. About 10-12 days after hiking in the Appalachian Mountains, this young woman presents with a 7-in circular rash on her upper back that is slightly warm to the touch. She denies fever, pruritus, and joint pain.

Diagnosis: Lyme disease is the most common tick-borne illness in the United States, with more than 25,000 confirmed cases in 2014. It is concentrated mostly in the northeast and upper Midwest, although in 2014, only five states (Colorado, Hawaii, Louisiana, New Mexico, and Oklahoma) reported no incidence. Lyme disease is caused by Borrelia burgdorferi, which is transmitted to humans by the Ixodes tick.
For more information, see “Beyond the bull's eye: Recognizing Lyme disease.” J Fam Pract. 2016;65(6):373-379.
3. A 42-year-old Native American farmer in Arizona has a reddish purple petechial rash on his ankles and feet. Upon questioning, he reports that about three weeks ago he had a slight fever with headache and malaise. Then, last week, he noticed small, flat, pink, nonitchy macules on his wrists, forearms, and ankles; they are now spreading to the trunk.

Source: CDC
[https://www.cdc.gov/rmsf/symptoms/index.html]
Diagnosis: Rocky Mountain spotted fever, now reported to the CDC as spotted fever rickettsiosis, is a tick-borne illness caused by the gram-negative intracellular bacterium Rickettsia rickettsia. It is endemic in the Southeastern and South Central United States. Most cases occur between April and September, coinciding with the active season of the vector tick species. Early diagnosis is critical because untreated RMSF may progress to fulminant systemic illness.
For more information, see “Fever and Rash in a 3-Year-Old Girl: Rocky Mountain Spotted Fever.” Cutis. 2002;70(3):165-168.
1. A 16-year-old boy presents with a skin ulcer on the dorsum of his hand and swollen glands in the proximal axilla. He works as a camp counselor in South Dakota, leading nature walks and teaching the children to care for animals, including the camp’s rabbits. Several weeks ago, he developed a fever of 103°F, fatigue, and body aches, followed by the appearance of the skin lesion.
Diagnosis: Tularemia—also called rabbit fever or deer fly fever—is caused by the bacterium Francisella tularensis. It is an insect-borne pathogen of rabbits, squirrels, and other rodents, most commonly found in the western United States and Russia. Symptoms vary by mechanism of exposure but include skin ulcers; irritation and inflammation of the eye; sore throat, mouth ulcers, and tonsillitis; lung involvement with cough, chest pain, and difficulty breathing; and swelling of regional lymph nodes. Tularemia can be successfully treated with antibiotics.
For more information, see “Pneumonic Tularemia Presenting With a Vesicular Eruption.” Cutis. 2015;95(4):E17-E18.
2. About 10-12 days after hiking in the Appalachian Mountains, this young woman presents with a 7-in circular rash on her upper back that is slightly warm to the touch. She denies fever, pruritus, and joint pain.
Diagnosis: Lyme disease is the most common tick-borne illness in the United States, with more than 25,000 confirmed cases in 2014. It is concentrated mostly in the northeast and upper Midwest, although in 2014, only five states (Colorado, Hawaii, Louisiana, New Mexico, and Oklahoma) reported no incidence. Lyme disease is caused by Borrelia burgdorferi, which is transmitted to humans by the Ixodes tick.
For more information, see “Beyond the bull's eye: Recognizing Lyme disease.” J Fam Pract. 2016;65(6):373-379.
3. A 42-year-old Native American farmer in Arizona has a reddish purple petechial rash on his ankles and feet. Upon questioning, he reports that about three weeks ago he had a slight fever with headache and malaise. Then, last week, he noticed small, flat, pink, nonitchy macules on his wrists, forearms, and ankles; they are now spreading to the trunk.
Source: CDC
[https://www.cdc.gov/rmsf/symptoms/index.html]
Diagnosis: Rocky Mountain spotted fever, now reported to the CDC as spotted fever rickettsiosis, is a tick-borne illness caused by the gram-negative intracellular bacterium Rickettsia rickettsia. It is endemic in the Southeastern and South Central United States. Most cases occur between April and September, coinciding with the active season of the vector tick species. Early diagnosis is critical because untreated RMSF may progress to fulminant systemic illness.
For more information, see “Fever and Rash in a 3-Year-Old Girl: Rocky Mountain Spotted Fever.” Cutis. 2002;70(3):165-168.
1. A 16-year-old boy presents with a skin ulcer on the dorsum of his hand and swollen glands in the proximal axilla. He works as a camp counselor in South Dakota, leading nature walks and teaching the children to care for animals, including the camp’s rabbits. Several weeks ago, he developed a fever of 103°F, fatigue, and body aches, followed by the appearance of the skin lesion.
Diagnosis: Tularemia—also called rabbit fever or deer fly fever—is caused by the bacterium Francisella tularensis. It is an insect-borne pathogen of rabbits, squirrels, and other rodents, most commonly found in the western United States and Russia. Symptoms vary by mechanism of exposure but include skin ulcers; irritation and inflammation of the eye; sore throat, mouth ulcers, and tonsillitis; lung involvement with cough, chest pain, and difficulty breathing; and swelling of regional lymph nodes. Tularemia can be successfully treated with antibiotics.
For more information, see “Pneumonic Tularemia Presenting With a Vesicular Eruption.” Cutis. 2015;95(4):E17-E18.
2. About 10-12 days after hiking in the Appalachian Mountains, this young woman presents with a 7-in circular rash on her upper back that is slightly warm to the touch. She denies fever, pruritus, and joint pain.
Diagnosis: Lyme disease is the most common tick-borne illness in the United States, with more than 25,000 confirmed cases in 2014. It is concentrated mostly in the northeast and upper Midwest, although in 2014, only five states (Colorado, Hawaii, Louisiana, New Mexico, and Oklahoma) reported no incidence. Lyme disease is caused by Borrelia burgdorferi, which is transmitted to humans by the Ixodes tick.
For more information, see “Beyond the bull's eye: Recognizing Lyme disease.” J Fam Pract. 2016;65(6):373-379.
3. A 42-year-old Native American farmer in Arizona has a reddish purple petechial rash on his ankles and feet. Upon questioning, he reports that about three weeks ago he had a slight fever with headache and malaise. Then, last week, he noticed small, flat, pink, nonitchy macules on his wrists, forearms, and ankles; they are now spreading to the trunk.
Source: CDC
[https://www.cdc.gov/rmsf/symptoms/index.html]
Diagnosis: Rocky Mountain spotted fever, now reported to the CDC as spotted fever rickettsiosis, is a tick-borne illness caused by the gram-negative intracellular bacterium Rickettsia rickettsia. It is endemic in the Southeastern and South Central United States. Most cases occur between April and September, coinciding with the active season of the vector tick species. Early diagnosis is critical because untreated RMSF may progress to fulminant systemic illness.
For more information, see “Fever and Rash in a 3-Year-Old Girl: Rocky Mountain Spotted Fever.” Cutis. 2002;70(3):165-168.

VIDEO: ERAS for minimally invasive surgery
Stacy A. Brethauer, MD, FACS, discusses the role of Enhanced Recovery After Surgery (ERAS) in minimally invasive surgical procedures. The goal of the ERAS approach is to minimize surgical stress on the patient, reduce length of stay, and reduce the use of opioids in the recovery phase. Dr. Brethauer discusses a pilot program, the Energy project, which will be conducted in more than 30 institutions for a year to look at an ERAS protocol designed to work with minimally invasive surgical procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Stacy A. Brethauer, MD, FACS, discusses the role of Enhanced Recovery After Surgery (ERAS) in minimally invasive surgical procedures. The goal of the ERAS approach is to minimize surgical stress on the patient, reduce length of stay, and reduce the use of opioids in the recovery phase. Dr. Brethauer discusses a pilot program, the Energy project, which will be conducted in more than 30 institutions for a year to look at an ERAS protocol designed to work with minimally invasive surgical procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Stacy A. Brethauer, MD, FACS, discusses the role of Enhanced Recovery After Surgery (ERAS) in minimally invasive surgical procedures. The goal of the ERAS approach is to minimize surgical stress on the patient, reduce length of stay, and reduce the use of opioids in the recovery phase. Dr. Brethauer discusses a pilot program, the Energy project, which will be conducted in more than 30 institutions for a year to look at an ERAS protocol designed to work with minimally invasive surgical procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Blindness linked to HCQ use rare in rheumatic patients
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
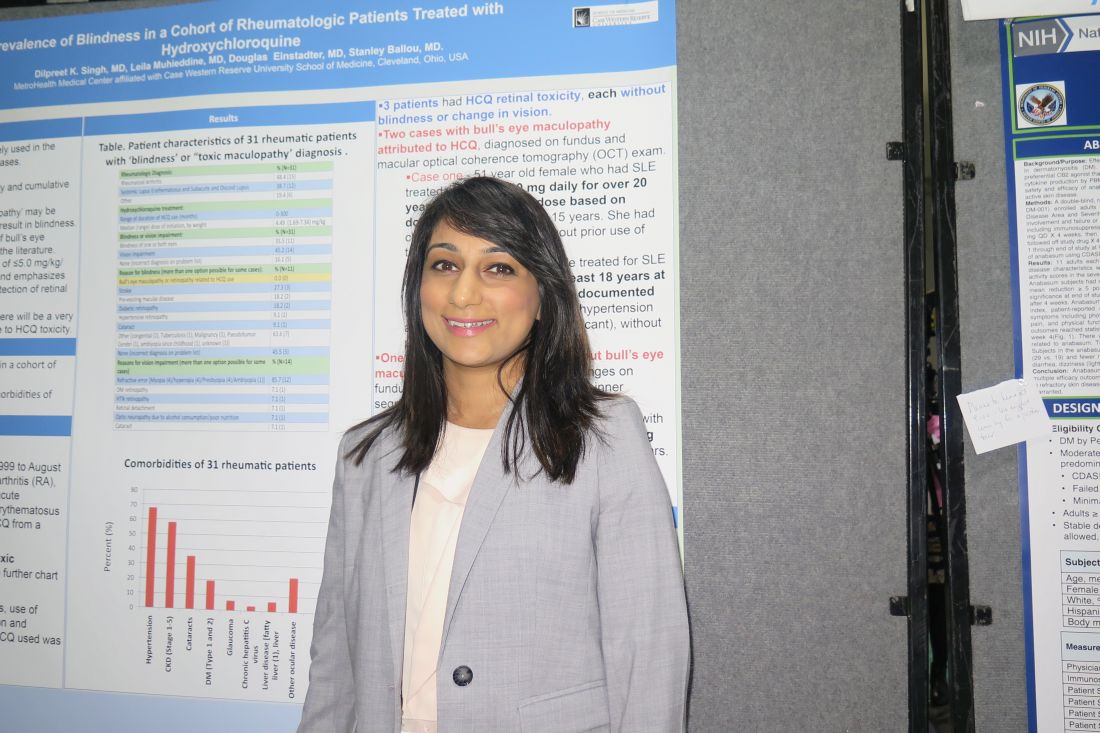
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
[email protected]
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
[email protected]
SAN DIEGO – Out of a cohort of nearly 2,900 rheumatic patients, none developed blindness attributable to toxic maculopathy from using hydroxychloroquine, in a single-center retrospective study.
“That’s very reassuring,” lead study author Dilpreet K. Singh, MD, said in an interview at the annual meeting of the American College of Rheumatology. “It’s still important to be vigilant with our screening and also to take note of the hydroxychloroquine dose that they’re on, because a lot of our patients have been on hydroxychloroquine for 10 or 15 years and there may not have been a dose adjustment. It’s also important to focus on the patients’ comorbidities and get them under better control.”
In an effort to assess the prevalence of blindness in a cohort of rheumatic patients and to identify the characteristics and comorbidities of those with HCQ retinal toxicity, Dr. Singh and her associates retrospectively evaluated 2,898 patients at MetroHealth Medical Center between January 1999 and August of 2017 with diagnoses of rheumatoid arthritis, inflammatory polyarthritis, systemic lupus erythematosus, subacute cutaneous lupus, and discoid lupus erythematosus who had a prescription written for HCQ.
In all, 31 had a diagnosis of “blindness” or “toxic maculopathy,” and these cases were further assessed for patient demographics, comorbidities, use of tamoxifen, weight and dose at initiation and discontinuation of HCQ, and duration of HCQ. Nearly 70% of these patients had hypertension, about 60% had chronic kidney disease, and 35% had cataracts. The researchers confirmed that in each of the cases the blindness was not caused by HCQ ocular toxicity, but instead by stroke, preexisting macular disease, diabetic retinopathy, hypertensive retinopathy, or cataracts.
Only 3 of the 31 patients were found to have HCQ retinal toxicity, each without blindness or change in vision. Two patients had bull’s-eye maculopathy and one had HCQ toxic maculopathy. Each of the three patients had received HCQ for more than 18 years at doses that ranged from 6.3 to 8.2 mg/kg based on documented weight, and none had functional vision loss at diagnosis.
“It’s reassuring to know that there’s a very small percentage of patients that will have HCQ-related toxicity,” Dr. Singh concluded. “We should also be focusing on the comorbidities [such as] diabetes, hypertension, and stroke-related vision loss that are common in our population of rheumatic patients, because these are contributing to visual impairment and blindness.”
She reported having no disclosures.
[email protected]
AT ACR 2017
Key clinical point: The incidence of blindness due to hydroxychloroquine toxicity is very low.
Major finding: No patients developed blindness attributable to toxic maculopathy from using hydroxychloroquine.
Study details: A single-center retrospective study of 2,898 rheumatic patients.
Disclosures: Dr. Singh reported having no disclosures.
TAP an alternative to epidural for colorectal surgery
SCOTTSDALE, ARIZ. – In colorectal surgery, transversus abdominis plane (TAP) block was associated with shorter hospital stays than epidural, according to a study that was conducted in patients undergoing both open and laparoscopic surgeries. TAP fared well in both groups.
There were higher rates of nausea/vomiting in the TAP group, suggesting the need for preoperative management in patients preparing to undergo TAP block. Urine retention was higher in the epidural group.
Physicians used liposomal bupivacaine, which is more costly than alternatives, and that fact met some resistance in the audience when the study was presented at the annual meeting of the Western Surgical Association. But patients receiving TAP had a 0.5-day shorter length of stay, which should reduce costs overall, and the drug component cost of TAP was less than $100 more than for the epidural.
“The biggest conclusion we drew from this study was that in patients where you would always consider an epidural historically, like an open procedure or a laparoscopic procedure where the conversion risk to open was higher, [favoring epidural] is now being called into question. We really believe that TAP block affords the length of stay benefit with no change in the pain control regimen after surgery,” Shawn Obi, DO, chief of surgery at Henry Ford Allegiance Health, Jackson, Mich., said in an interview.
The findings dovetail with an overall trend of improved protocols in colon surgery. “I think we’re working toward colorectal surgery as an outpatient operation, similar to what has happened in the joint arena,” said Dr. Obi.
His colleague, Matt Torgeson, DO, who is a surgical resident at Henry Ford Allegiance Health, noted that the hospital stay following colorectal surgery was once 6-8 days, and it has been shortened to 3-3.5 days. Enhanced recovery protocols made the biggest impact, shaving about 3 days. “Now we’re going to be seeing small, incremental changes,” said Dr. Torgeson.
The researchers randomized patients undergoing open or laparoscopic colorectal surgery to receive either an epidural (n = 37) or TAP block (n = 41). All patients entered an enhanced recovery pathway following surgery, with standardized discharge criteria. The two groups had similar times to return to normal bowel function (TAP, 1.7 days; epidural, 1.9 days) but the length of hospital stay was lower in the TAP group (2.8 days vs. 3.3 days; P = .023; 74.9 hours vs. 86.3 hours; P = .045). Subjects in the epidural group had a higher frequency of urinary retention (29.7% vs. 14.6%), though this did not reach statistical significance (P = .11). Postoperative nausea occurred at a higher rate in the TAP group (31.7% vs. 13.5%; odds ratio, 2.97), though this result just missed significance (P = .06).
In patients who had open surgery or laparoscopic surgery that converted to open, the length of stay was 2.9 days in the TAP group (n = 9) and 4.4 days in the epidural group (n = 5). Those numbers are small, but they suggest that TAP is effective even in open surgery. The cost of TAP was about $80 more than epidural medication ($406.16 vs. $322.73).
The study received no outside funding. Dr. Torgeson and Dr. Obi reported having no financial disclosures.
SCOTTSDALE, ARIZ. – In colorectal surgery, transversus abdominis plane (TAP) block was associated with shorter hospital stays than epidural, according to a study that was conducted in patients undergoing both open and laparoscopic surgeries. TAP fared well in both groups.
There were higher rates of nausea/vomiting in the TAP group, suggesting the need for preoperative management in patients preparing to undergo TAP block. Urine retention was higher in the epidural group.
Physicians used liposomal bupivacaine, which is more costly than alternatives, and that fact met some resistance in the audience when the study was presented at the annual meeting of the Western Surgical Association. But patients receiving TAP had a 0.5-day shorter length of stay, which should reduce costs overall, and the drug component cost of TAP was less than $100 more than for the epidural.
“The biggest conclusion we drew from this study was that in patients where you would always consider an epidural historically, like an open procedure or a laparoscopic procedure where the conversion risk to open was higher, [favoring epidural] is now being called into question. We really believe that TAP block affords the length of stay benefit with no change in the pain control regimen after surgery,” Shawn Obi, DO, chief of surgery at Henry Ford Allegiance Health, Jackson, Mich., said in an interview.
The findings dovetail with an overall trend of improved protocols in colon surgery. “I think we’re working toward colorectal surgery as an outpatient operation, similar to what has happened in the joint arena,” said Dr. Obi.
His colleague, Matt Torgeson, DO, who is a surgical resident at Henry Ford Allegiance Health, noted that the hospital stay following colorectal surgery was once 6-8 days, and it has been shortened to 3-3.5 days. Enhanced recovery protocols made the biggest impact, shaving about 3 days. “Now we’re going to be seeing small, incremental changes,” said Dr. Torgeson.
The researchers randomized patients undergoing open or laparoscopic colorectal surgery to receive either an epidural (n = 37) or TAP block (n = 41). All patients entered an enhanced recovery pathway following surgery, with standardized discharge criteria. The two groups had similar times to return to normal bowel function (TAP, 1.7 days; epidural, 1.9 days) but the length of hospital stay was lower in the TAP group (2.8 days vs. 3.3 days; P = .023; 74.9 hours vs. 86.3 hours; P = .045). Subjects in the epidural group had a higher frequency of urinary retention (29.7% vs. 14.6%), though this did not reach statistical significance (P = .11). Postoperative nausea occurred at a higher rate in the TAP group (31.7% vs. 13.5%; odds ratio, 2.97), though this result just missed significance (P = .06).
In patients who had open surgery or laparoscopic surgery that converted to open, the length of stay was 2.9 days in the TAP group (n = 9) and 4.4 days in the epidural group (n = 5). Those numbers are small, but they suggest that TAP is effective even in open surgery. The cost of TAP was about $80 more than epidural medication ($406.16 vs. $322.73).
The study received no outside funding. Dr. Torgeson and Dr. Obi reported having no financial disclosures.
SCOTTSDALE, ARIZ. – In colorectal surgery, transversus abdominis plane (TAP) block was associated with shorter hospital stays than epidural, according to a study that was conducted in patients undergoing both open and laparoscopic surgeries. TAP fared well in both groups.
There were higher rates of nausea/vomiting in the TAP group, suggesting the need for preoperative management in patients preparing to undergo TAP block. Urine retention was higher in the epidural group.
Physicians used liposomal bupivacaine, which is more costly than alternatives, and that fact met some resistance in the audience when the study was presented at the annual meeting of the Western Surgical Association. But patients receiving TAP had a 0.5-day shorter length of stay, which should reduce costs overall, and the drug component cost of TAP was less than $100 more than for the epidural.
“The biggest conclusion we drew from this study was that in patients where you would always consider an epidural historically, like an open procedure or a laparoscopic procedure where the conversion risk to open was higher, [favoring epidural] is now being called into question. We really believe that TAP block affords the length of stay benefit with no change in the pain control regimen after surgery,” Shawn Obi, DO, chief of surgery at Henry Ford Allegiance Health, Jackson, Mich., said in an interview.
The findings dovetail with an overall trend of improved protocols in colon surgery. “I think we’re working toward colorectal surgery as an outpatient operation, similar to what has happened in the joint arena,” said Dr. Obi.
His colleague, Matt Torgeson, DO, who is a surgical resident at Henry Ford Allegiance Health, noted that the hospital stay following colorectal surgery was once 6-8 days, and it has been shortened to 3-3.5 days. Enhanced recovery protocols made the biggest impact, shaving about 3 days. “Now we’re going to be seeing small, incremental changes,” said Dr. Torgeson.
The researchers randomized patients undergoing open or laparoscopic colorectal surgery to receive either an epidural (n = 37) or TAP block (n = 41). All patients entered an enhanced recovery pathway following surgery, with standardized discharge criteria. The two groups had similar times to return to normal bowel function (TAP, 1.7 days; epidural, 1.9 days) but the length of hospital stay was lower in the TAP group (2.8 days vs. 3.3 days; P = .023; 74.9 hours vs. 86.3 hours; P = .045). Subjects in the epidural group had a higher frequency of urinary retention (29.7% vs. 14.6%), though this did not reach statistical significance (P = .11). Postoperative nausea occurred at a higher rate in the TAP group (31.7% vs. 13.5%; odds ratio, 2.97), though this result just missed significance (P = .06).
In patients who had open surgery or laparoscopic surgery that converted to open, the length of stay was 2.9 days in the TAP group (n = 9) and 4.4 days in the epidural group (n = 5). Those numbers are small, but they suggest that TAP is effective even in open surgery. The cost of TAP was about $80 more than epidural medication ($406.16 vs. $322.73).
The study received no outside funding. Dr. Torgeson and Dr. Obi reported having no financial disclosures.
AT WSA 2017
Key clinical point: In appropriately selected patients, TAP may be a good alternative to epidural.
Major finding: TAP block was associated with a 0.5-day shorter hospital stay than epidurals.
Data source: Randomized, controlled trial (n = 78).
Disclosures: The study received no outside funding. Dr. Torgeson and Dr. Obi reported having no financial disclosures.
Acute cholecystitis guidelines need work
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.

The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.
The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
SCOTTSDALE, ARIZ. – In patients with right upper quadrant pain, the Tokyo Guidelines (TG13) failed to detect acute cholecystitis with adequate sensitivity, according to a single institution retrospective review.
Researchers at the University of Arizona, Tucson, also found that the Tokyo Guidelines’ advice to manage grade II and grade III cholecystitis patients conservatively may be unwarranted, because there were no differences in safety outcomes between grade I and grade II patients who underwent early cholecystectomy.
The Tokyo Guidelines were based on expert opinion rather than evidence, and may be limited by differences in practices in Japan and other countries. “There was no formal evaluation of the sensitivity and specificity in any other country,” Faisal Jehan, MD, a research fellow at the University of Arizona, said in an interview. Dr. Jehan presented the study at the annual meeting of the Western Surgical Association.
The study suggests there is additional work to be done before the guidelines are more generally applicable. They are being updated and the new version is slated to appear in 2018.
Cholecystectomy is one of the most common procedures in the United States, and hence represents a major source of health care expenditure. Useful guidelines will therefore be welcome to help standardize treatment, according to Dr. Riall. “I think while we’ve moved as a population toward earlier cholecystectomy, it isn’t uniformly practiced in the United States. So I think there is value in having guidelines that are relevant to our population and relevant to our practice,” she said.
But compared with the pathology report, the TG13 guidelines fared poorly in prediction of acute cholecystitis, with a sensitivity of just 53% (definitive 27%, suspected 26%, undiagnosed 53%). The underperformance of the guidelines may be due in part to recent changes in health-seeking behavior, as patients are likely to get to the hospital more quickly than in the past, and thus exhibit fewer clinical signs when first examined. “That could be decreasing the sensitivity,” said Dr. Jehan.
Suspicious that the guidelines were inadequate, the researchers analyzed their institution’s Emergency General Surgery registry, examining records from 952 patients who presented with right upper quadrant pain between 2013 and 2015. They compared diagnoses and severity assessed using the TG13 guidelines to the ensuing pathology reports, which were obtained from patient charts.
A total of 857 patients of the 952 had biliary disease. Of these, 779 patients went on to cholecystectomy, 15 had cholecystostomy-tube placement, and 63 were managed conservatively with no surgery. Among patients with biliary disease, the frequency of fever at presentation was just 4%, while 51.8% had leukocytosis. Right upper quadrant tenderness was the most sensitive predictor of acute cholecystitis (92%). Murphy’s sign occurred in 28.8% of patients and had a 72% sensitivity.
Following the TG13 guidelines resulted in classification of 414 patients as grade I, 400 as grade II, and 43 as grade III. A total of 92.5% of grade I patients underwent early cholecystectomy, as the TG-13 guidelines suggest. Nearly as many (89.3%) grade II patients also underwent early surgery, as did 50% of grade III patients. The complication rate was similar between grade I and grade II patients who underwent surgery (3.7% vs. 4.7%; P = .81). The rate of return to the operating room was also similar (0.6% vs. 0.7%; P = .95), as was mortality (0.3% vs. 0%; P = .96).
AT WSA 2017
Key clinical point: Early surgery for acute cholecystitis appears safe in well selected patients.
Major finding: TG13 guidelines predicted acute cholecystitis with a sensitivity of 53%.
Data source: Analysis of a prospectively collected data on 952 patients at a single institution.
Disclosures: The study received no outside funding. Dr. Jehan and Dr. Riall reported having no financial disclosures.
Unblinded data show extent of verubecestat’s failure in mild-moderate Alzheimer’s
BOSTON – The Alzheimer’s research community absorbed yet another downer recently, when Merck scientists revealed the unblinded efficacy and safety data of EPOCH, the company’s failed verubecestat trial: The BACE inhibitor didn’t score in any endpoint, no matter how the data were sliced and diced.
Merck halted the study last February, when an interim analysis determined there was no chance of a positive outcome. No safety data played into the decision, officials said. At the time of discontinuation, Merck had not yet examined the unblinded data, which were released to a packed audience at the Clinical Trials on Alzheimer’s Disease conference in Boston.
Compared with placebo, the nonselective beta-secretase (BACE) inhibitor conferred no cognitive or functional benefit upon patients with mild-moderate Alzheimer’s disease, either in the overall analysis or in any age, disease stage, or genetic subgroup, Michael Egan, MD, said during a panel discussion. And although there was plenty of biomarker evidence that the drug did block beta amyloid production, there was also a plethora of concerning adverse events.

However, the failure of yet another antiamyloid drug doesn’t mean that researchers should abandon amyloid as a therapeutic target, said Dr. Egan, Merck’s associate vice president of clinical neuroscience. Verubecestat is still being investigated in the APECS study of patients with mild cognitive impairment, and a number of antiamyloid antibodies are still going forward in patients whose disease stages run from preclinical to moderate.
“It’s still possible that we may see a clinical benefit in some of these studies, so we have to keep an open mind,” Dr. Egan said.
EPOCH, a pivotal phase 2/3 trial, randomized about 1,200 patients with mild-moderate Alzheimer’s to either placebo or verubecestat 12 mg or 40 mg daily for 18 months. None of the patients had amyloid PET imaging, but in subsets of patients who had the imaging or lumbar puncture for Abeta levels, 90% were amyloid-positive. The primary efficacy outcomes were the change from baseline in the Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) score and the change from baseline in the Alzheimer’s Disease Cooperative Study–Activities of Daily Living (ADCS-ADL) score.
There were a number of secondary endpoints, including the Clinical Dementia Rating–Sum of Boxes (CDR-sb); total hippocampal volume; cerebrospinal fluid total and phosphorylated tau; changes on the Neuropsychiatric Index and Mini Mental State Exam; and brain amyloid burden.
In a nutshell, Dr. Egan said, there was virtually no efficacy signal on any of the primary or secondary endpoints. On the ADAS-Cog, all patients, regardless of treatment group, lost 7-8 points over the trial. The same was true for the ADCS-ADL, with everyone declining about 8 points over time. On the CDR-sb, all groups declined about 2 points.
“We also looked at a number of subgroups: younger subjects, those with earlier disease, and those who we knew were amyloid-positive, including all of our ApoE4 carriers. We found no evidence of efficacy in any subgroup.”
It is “worth noting,” Dr. Egan said, that in the amyloid PET substudy, there were treatment-related reductions in plaque burden. While those taking placebo showed no changes in brain amyloid, the 12-mg group experienced a mean 2% reduction in amyloid, and the 40-mg group, a 4% reduction. “While this is modest, it does show target engagement,” Dr. Egan said – an important and positive finding in light of the ongoing APECS study.
The study of cerebrospinal fluid showed no effect on either tau protein, but marked, dose-related reductions in Abeta1-40 and soluble amyloid precursor protein – both products of BACE cleavage of the amyloid precursor protein. “We saw a 70% reduction in the 12-mg group and more than an 80% reduction in the 40-mg group, but no change in the placebo group. This is an important finding, demonstrating that the drug got into the brain and turned off production of Abeta. EPOCH is the first phase 3 study of an antiamyloid agent where target engagement of this magnitude has been demonstrated.”
Verubecestat also had its share of adverse events, Dr. Egan said. The most common was rash, which developed in about 10%; 20% of those who developed rash discontinued treatment for that reason. More concerning were falls and injuries; diarrhea and weight loss; and a variety of neuropsychiatric events, including insomnia and sleep disorders, anxiety, depression, and suicidal ideation.*
The drug was also associated with more loss of hippocampal volume, compared with placebo (5.7% vs. 5%), Dr. Egan said in an interview. The etiology isn’t clear; he suggested that it could be related to amyloid plaque removal, resolution of neuroinflammation, or an actual worsening of neurodegeneration. “That is a concerning possibility, although if that were the case we would expect to see worsening cognition, which we did not.”
Falls and injuries occurred in 15% of the placebo group and 20%-23% of the active groups. A detailed analysis didn’t turn up any specific risk factors, though. The episodes of suicidal ideation were passive and more common in the first 6 months of treatment and among patients who had a history of depression or prior suicidal ideation. Four patients discontinued due to that side effect.
Verubecestat is a nonselective inhibitor of both BACE1 and BACE2, and it’s not clear if that wide-ranging inhibition increased the likelihood of adverse events over what might be seen with a more selective compound. “It’s difficult to attribute them to BACE2 over BACE1,” Dr. Egan said. “Any BACE inhibitor could potentially have similar side effects.”
Only time will provide those answers; BACE inhibition is an area of active investigation among several large companies. The newly announced Generation studies will test a selective BACE1 inhibitor called CNP520.
Eli Lilly is recruiting for a phase 2 study of its BACE1 inhibitor, dubbed LY3202626. AstraZeneca is also looking at BACE1 inhibition with its candidate, lanabecestat.
Dr. Egan remains hopeful, though, and said that Merck retains its commitment to bringing an effective Alzheimer’s treatment to market.
“It’s natural to get discouraged with negative trials, and there certainly have been a lot of them. But I think we have to continue to work very hard to try and find something to help patients, and we have more and more knowledge every year about how to do that. I believe BACE inhibition continues to offer the possibility that if we treat earlier that there could be benefit, but for those with dementia, BACE inhibition is just too late.”
Dr. Egan is employed by Merck Sharp & Dohme, which sponsored EPOCH.
This article was updated 11/16/17.
Correction, 11/20/17: An earlier version of this article misstated the percentage of patients who experienced rash.
[email protected]
On Twitter @Alz_Gal
BOSTON – The Alzheimer’s research community absorbed yet another downer recently, when Merck scientists revealed the unblinded efficacy and safety data of EPOCH, the company’s failed verubecestat trial: The BACE inhibitor didn’t score in any endpoint, no matter how the data were sliced and diced.
Merck halted the study last February, when an interim analysis determined there was no chance of a positive outcome. No safety data played into the decision, officials said. At the time of discontinuation, Merck had not yet examined the unblinded data, which were released to a packed audience at the Clinical Trials on Alzheimer’s Disease conference in Boston.
Compared with placebo, the nonselective beta-secretase (BACE) inhibitor conferred no cognitive or functional benefit upon patients with mild-moderate Alzheimer’s disease, either in the overall analysis or in any age, disease stage, or genetic subgroup, Michael Egan, MD, said during a panel discussion. And although there was plenty of biomarker evidence that the drug did block beta amyloid production, there was also a plethora of concerning adverse events.
However, the failure of yet another antiamyloid drug doesn’t mean that researchers should abandon amyloid as a therapeutic target, said Dr. Egan, Merck’s associate vice president of clinical neuroscience. Verubecestat is still being investigated in the APECS study of patients with mild cognitive impairment, and a number of antiamyloid antibodies are still going forward in patients whose disease stages run from preclinical to moderate.
“It’s still possible that we may see a clinical benefit in some of these studies, so we have to keep an open mind,” Dr. Egan said.
EPOCH, a pivotal phase 2/3 trial, randomized about 1,200 patients with mild-moderate Alzheimer’s to either placebo or verubecestat 12 mg or 40 mg daily for 18 months. None of the patients had amyloid PET imaging, but in subsets of patients who had the imaging or lumbar puncture for Abeta levels, 90% were amyloid-positive. The primary efficacy outcomes were the change from baseline in the Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) score and the change from baseline in the Alzheimer’s Disease Cooperative Study–Activities of Daily Living (ADCS-ADL) score.
There were a number of secondary endpoints, including the Clinical Dementia Rating–Sum of Boxes (CDR-sb); total hippocampal volume; cerebrospinal fluid total and phosphorylated tau; changes on the Neuropsychiatric Index and Mini Mental State Exam; and brain amyloid burden.
In a nutshell, Dr. Egan said, there was virtually no efficacy signal on any of the primary or secondary endpoints. On the ADAS-Cog, all patients, regardless of treatment group, lost 7-8 points over the trial. The same was true for the ADCS-ADL, with everyone declining about 8 points over time. On the CDR-sb, all groups declined about 2 points.
“We also looked at a number of subgroups: younger subjects, those with earlier disease, and those who we knew were amyloid-positive, including all of our ApoE4 carriers. We found no evidence of efficacy in any subgroup.”
It is “worth noting,” Dr. Egan said, that in the amyloid PET substudy, there were treatment-related reductions in plaque burden. While those taking placebo showed no changes in brain amyloid, the 12-mg group experienced a mean 2% reduction in amyloid, and the 40-mg group, a 4% reduction. “While this is modest, it does show target engagement,” Dr. Egan said – an important and positive finding in light of the ongoing APECS study.
The study of cerebrospinal fluid showed no effect on either tau protein, but marked, dose-related reductions in Abeta1-40 and soluble amyloid precursor protein – both products of BACE cleavage of the amyloid precursor protein. “We saw a 70% reduction in the 12-mg group and more than an 80% reduction in the 40-mg group, but no change in the placebo group. This is an important finding, demonstrating that the drug got into the brain and turned off production of Abeta. EPOCH is the first phase 3 study of an antiamyloid agent where target engagement of this magnitude has been demonstrated.”
Verubecestat also had its share of adverse events, Dr. Egan said. The most common was rash, which developed in about 10%; 20% of those who developed rash discontinued treatment for that reason. More concerning were falls and injuries; diarrhea and weight loss; and a variety of neuropsychiatric events, including insomnia and sleep disorders, anxiety, depression, and suicidal ideation.*
The drug was also associated with more loss of hippocampal volume, compared with placebo (5.7% vs. 5%), Dr. Egan said in an interview. The etiology isn’t clear; he suggested that it could be related to amyloid plaque removal, resolution of neuroinflammation, or an actual worsening of neurodegeneration. “That is a concerning possibility, although if that were the case we would expect to see worsening cognition, which we did not.”
Falls and injuries occurred in 15% of the placebo group and 20%-23% of the active groups. A detailed analysis didn’t turn up any specific risk factors, though. The episodes of suicidal ideation were passive and more common in the first 6 months of treatment and among patients who had a history of depression or prior suicidal ideation. Four patients discontinued due to that side effect.
Verubecestat is a nonselective inhibitor of both BACE1 and BACE2, and it’s not clear if that wide-ranging inhibition increased the likelihood of adverse events over what might be seen with a more selective compound. “It’s difficult to attribute them to BACE2 over BACE1,” Dr. Egan said. “Any BACE inhibitor could potentially have similar side effects.”
Only time will provide those answers; BACE inhibition is an area of active investigation among several large companies. The newly announced Generation studies will test a selective BACE1 inhibitor called CNP520.
Eli Lilly is recruiting for a phase 2 study of its BACE1 inhibitor, dubbed LY3202626. AstraZeneca is also looking at BACE1 inhibition with its candidate, lanabecestat.
Dr. Egan remains hopeful, though, and said that Merck retains its commitment to bringing an effective Alzheimer’s treatment to market.
“It’s natural to get discouraged with negative trials, and there certainly have been a lot of them. But I think we have to continue to work very hard to try and find something to help patients, and we have more and more knowledge every year about how to do that. I believe BACE inhibition continues to offer the possibility that if we treat earlier that there could be benefit, but for those with dementia, BACE inhibition is just too late.”
Dr. Egan is employed by Merck Sharp & Dohme, which sponsored EPOCH.
This article was updated 11/16/17.
Correction, 11/20/17: An earlier version of this article misstated the percentage of patients who experienced rash.
[email protected]
On Twitter @Alz_Gal
BOSTON – The Alzheimer’s research community absorbed yet another downer recently, when Merck scientists revealed the unblinded efficacy and safety data of EPOCH, the company’s failed verubecestat trial: The BACE inhibitor didn’t score in any endpoint, no matter how the data were sliced and diced.
Merck halted the study last February, when an interim analysis determined there was no chance of a positive outcome. No safety data played into the decision, officials said. At the time of discontinuation, Merck had not yet examined the unblinded data, which were released to a packed audience at the Clinical Trials on Alzheimer’s Disease conference in Boston.
Compared with placebo, the nonselective beta-secretase (BACE) inhibitor conferred no cognitive or functional benefit upon patients with mild-moderate Alzheimer’s disease, either in the overall analysis or in any age, disease stage, or genetic subgroup, Michael Egan, MD, said during a panel discussion. And although there was plenty of biomarker evidence that the drug did block beta amyloid production, there was also a plethora of concerning adverse events.
However, the failure of yet another antiamyloid drug doesn’t mean that researchers should abandon amyloid as a therapeutic target, said Dr. Egan, Merck’s associate vice president of clinical neuroscience. Verubecestat is still being investigated in the APECS study of patients with mild cognitive impairment, and a number of antiamyloid antibodies are still going forward in patients whose disease stages run from preclinical to moderate.
“It’s still possible that we may see a clinical benefit in some of these studies, so we have to keep an open mind,” Dr. Egan said.
EPOCH, a pivotal phase 2/3 trial, randomized about 1,200 patients with mild-moderate Alzheimer’s to either placebo or verubecestat 12 mg or 40 mg daily for 18 months. None of the patients had amyloid PET imaging, but in subsets of patients who had the imaging or lumbar puncture for Abeta levels, 90% were amyloid-positive. The primary efficacy outcomes were the change from baseline in the Alzheimer’s Disease Assessment Scale Cognitive Subscale (ADAS-Cog) score and the change from baseline in the Alzheimer’s Disease Cooperative Study–Activities of Daily Living (ADCS-ADL) score.
There were a number of secondary endpoints, including the Clinical Dementia Rating–Sum of Boxes (CDR-sb); total hippocampal volume; cerebrospinal fluid total and phosphorylated tau; changes on the Neuropsychiatric Index and Mini Mental State Exam; and brain amyloid burden.
In a nutshell, Dr. Egan said, there was virtually no efficacy signal on any of the primary or secondary endpoints. On the ADAS-Cog, all patients, regardless of treatment group, lost 7-8 points over the trial. The same was true for the ADCS-ADL, with everyone declining about 8 points over time. On the CDR-sb, all groups declined about 2 points.
“We also looked at a number of subgroups: younger subjects, those with earlier disease, and those who we knew were amyloid-positive, including all of our ApoE4 carriers. We found no evidence of efficacy in any subgroup.”
It is “worth noting,” Dr. Egan said, that in the amyloid PET substudy, there were treatment-related reductions in plaque burden. While those taking placebo showed no changes in brain amyloid, the 12-mg group experienced a mean 2% reduction in amyloid, and the 40-mg group, a 4% reduction. “While this is modest, it does show target engagement,” Dr. Egan said – an important and positive finding in light of the ongoing APECS study.
The study of cerebrospinal fluid showed no effect on either tau protein, but marked, dose-related reductions in Abeta1-40 and soluble amyloid precursor protein – both products of BACE cleavage of the amyloid precursor protein. “We saw a 70% reduction in the 12-mg group and more than an 80% reduction in the 40-mg group, but no change in the placebo group. This is an important finding, demonstrating that the drug got into the brain and turned off production of Abeta. EPOCH is the first phase 3 study of an antiamyloid agent where target engagement of this magnitude has been demonstrated.”
Verubecestat also had its share of adverse events, Dr. Egan said. The most common was rash, which developed in about 10%; 20% of those who developed rash discontinued treatment for that reason. More concerning were falls and injuries; diarrhea and weight loss; and a variety of neuropsychiatric events, including insomnia and sleep disorders, anxiety, depression, and suicidal ideation.*
The drug was also associated with more loss of hippocampal volume, compared with placebo (5.7% vs. 5%), Dr. Egan said in an interview. The etiology isn’t clear; he suggested that it could be related to amyloid plaque removal, resolution of neuroinflammation, or an actual worsening of neurodegeneration. “That is a concerning possibility, although if that were the case we would expect to see worsening cognition, which we did not.”
Falls and injuries occurred in 15% of the placebo group and 20%-23% of the active groups. A detailed analysis didn’t turn up any specific risk factors, though. The episodes of suicidal ideation were passive and more common in the first 6 months of treatment and among patients who had a history of depression or prior suicidal ideation. Four patients discontinued due to that side effect.
Verubecestat is a nonselective inhibitor of both BACE1 and BACE2, and it’s not clear if that wide-ranging inhibition increased the likelihood of adverse events over what might be seen with a more selective compound. “It’s difficult to attribute them to BACE2 over BACE1,” Dr. Egan said. “Any BACE inhibitor could potentially have similar side effects.”
Only time will provide those answers; BACE inhibition is an area of active investigation among several large companies. The newly announced Generation studies will test a selective BACE1 inhibitor called CNP520.
Eli Lilly is recruiting for a phase 2 study of its BACE1 inhibitor, dubbed LY3202626. AstraZeneca is also looking at BACE1 inhibition with its candidate, lanabecestat.
Dr. Egan remains hopeful, though, and said that Merck retains its commitment to bringing an effective Alzheimer’s treatment to market.
“It’s natural to get discouraged with negative trials, and there certainly have been a lot of them. But I think we have to continue to work very hard to try and find something to help patients, and we have more and more knowledge every year about how to do that. I believe BACE inhibition continues to offer the possibility that if we treat earlier that there could be benefit, but for those with dementia, BACE inhibition is just too late.”
Dr. Egan is employed by Merck Sharp & Dohme, which sponsored EPOCH.
This article was updated 11/16/17.
Correction, 11/20/17: An earlier version of this article misstated the percentage of patients who experienced rash.
[email protected]
On Twitter @Alz_Gal
AT CTAD
Key clinical point:
Major finding: On the ADAS-Cog score, all patients, regardless of treatment group, lost 7-8 points over the trial. The same was true for the ADCS-ADL score, with everyone declining about 8 points over time. On the CDR-sb, all groups declined about 2 points.
Data source: EPOCH, a pivotal phase 2/3 trial, randomized about 1,200 patients with mild-moderate Alzheimer’s to either placebo or verubecestat 12 mg or 40 mg daily for 18 months.
Disclosures: Dr. Egan is employed by Merck Sharp & Dohme, which sponsored EPOCH.
VIDEO: Evidence mounts for pulmonary embolism benefit from catheter thrombolysis
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
BY MITCHEL L. ZOLER
Frontline Medical News
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
TORONTO – Catheter-directed thrombolysis of pulmonary embolism using an ultrasound-assisted device led to significantly better outcomes in patients hospitalized for pulmonary embolism, compared with conventional systemic thrombolytic treatment, in a propensity score–adjusted analysis of nearly 3,400 patients.
Catheter-directed thrombolysis (CDT) “represents an opportunity to locally treat pulmonary embolism with significant thrombus burden with lower bleeding complications,” Abhishek Mishra, MD, said at the CHEST annual meeting. “I think we are underusing CDT,” said Dr. Mishra, a cardiovascular disease physician at Guthrie Robert Packer Hospital in Sayre, Pa.
Although one CDT device, the EKOS endovascular system that uses ultrasound to facilitate pulmonary embolism (PE) thrombolysis, received Food & Drug Administration approval for U.S. marketing in 2014, the trials that have compared it with systemic thrombolysis have been small, noted Dr. Mishra, and none have looked at whether CDT improves patient survival, compared with standard treatments. The largest report on CDT treatment of PE came from a single-arm, uncontrolled study with 150 patients who received ultrasound-facilitated CDT (JACC Cardiovasc Interv. 2015 Aug;8[10]:1382-92).
To better document the incremental benefit from CDT, Dr. Mishra and his associates used data collected by the Nationwide Readmissions Database during 2013 and 2014, both before and after a CDT device became available for U.S. use. From among 4,426 patients hospitalized with a primary diagnosis of PE and treated with thrombolytic therapy, they used propensity score matching to compare 2,256 patients treated with systemic thrombolysis with 1,128 matched patients treated with CDT using tissue plasminogen activator.
The analysis showed that in-hospital death was 15% in the systemic patients and 6% in the CDT group, a relative risk reduction of 63%, and 30-day readmissions occurred in 11% of the systemic patients and in 8% of those treated with CDT, a 30% relative risk reduction. Both were statistically significant differences for the study’s two primary endpoints, Dr. Mishra reported at the meeting. Rates of intracerebral hemorrhage and gastrointestinal bleeds were both numerically lower with CDT, and significantly lower for gastrointestinal bleeds.
The researchers also ran a multivariate analysis on their data that showed CDT was linked with significant relative reductions of about 60% for both in-hospital death and 30-day readmissions, compared with patients on systemic therapy. The results Dr. Mishra reported also appeared in a published report (Am J Cardiol. 2017 Nov 1;120[9]:1653-61).
These findings help buttress the case for using CDT for at least some PE patients. “The key is which patients need it. What is the best way to stratify patients?” commented Victor F. Tapson, MD, a pulmonologist at Cedars-Sinai Medical Center in Los Angeles.
“Patients with PE and a normal right ventricle generally don’t need anything more aggressive than anticoagulation, and really sick patients with massive PE need systemic thrombolytics. Intermediate-risk patients” are best suited to CDT, but “the problem is that intermediate-risk patients are heterogeneous,” Dr. Tapson said in a video interview. Future studies should establish a more specific subgroup of intermediate-risk patients who benefit from routinely employed CDT, he suggested.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
AT CHEST 2017
Key clinical point:
Major finding: Catheter-directed thrombolysis cut in-hospital mortality by 63%, compared with conventional systemic thrombolysis.
Data source: The National Readmission Database, which included 4,426 patients hospitalized during 2013 and 2014 with primary pulmonary embolism and treated with thrombolysis.
Disclosures: Dr. Mishra had no disclosures. Dr. Tapson has been a consultant to and had received research funding from Ekos/BTG, a company that markets a catheter-directed thrombolysis device. He has also ties to Daiichi Sankyo, Inari, Janssen, and Portola.

HPV vaccination cuts incidence of juvenile respiratory papillomatosis
Introduction of a national human papillomavirus vaccination program in Australia has been associated with declines in the incidence of juvenile-onset recurrent respiratory papillomatosis, according to a nationwide study.
Juvenile-onset recurrent respiratory papillomatosis (JORRP) is a rare condition characterized by recurring growths in the larynx that often require multiple operations to remove. The disease typically emerges around age 3-4 years and most cases are thought to be caused by human papillomavirus (HPV) subtypes 6 and 11, which are acquired from the mother during birth.
Overall, just 15 cases were reported during the course of the study; 7 in the 1st year, 3 in the 2nd year, 2 each in the 3rd and 4th years, and 1 case in the last year. The annual rates declined from 0.16 per 100,000 children aged 0-14 years in 2012 to 0.02 per 100,000 in 2016.
Of the cases identified, none of the mothers had been vaccinated against HPV before pregnancy and 20% had a history of genital warts. Seven cases were genotyped; 4 were HPV-6 and 3 were HPV-11, and 13 of the 15 cases were born vaginally.
“Our data strongly suggest that the previously documented impact of quadrivalent HPV vaccination in dramatically reducing the prevalence of HPV-6 and HPV-11 genital infection in the Australian population is translating to a reduction in the risk of transmission to infants intrapartum and subsequent development in some of these children of JORRP,” wrote Daniel Novakovic, MD, of the University of Sydney Medical School, and his coinvestigators.
The authors noted that their initial estimate of infection rates was lower than that seen in other studies, such as the 0.5 per 100,000 rate seen in private health insurance data, and the 1.0 per 100,000 seen with Medicaid data in the United States.
Given that the study period started nearly 5 years after the vaccination program began, they suggested that this lower prevalence may reflect the early impact of the vaccine, particularly given that the prevalence of genital warts had already dramatically declined by that point.
However they also stressed that their study relied on clinicians actively reporting cases, and that given surveillance only began after the introduction of the vaccination program, no data were available on the incidence before that point.
The study was supported by a research grant from Merck and by the Australian Paediatric Surveillance Unit, which is supported by the Australian Government Department of Health. Three authors declared research funding from Merck/Seqirus for HPV studies. Two authors declared funding, speaking fees, and other support from a range of pharmaceutical companies. No other conflicts of interest were declared.
Introduction of a national human papillomavirus vaccination program in Australia has been associated with declines in the incidence of juvenile-onset recurrent respiratory papillomatosis, according to a nationwide study.
Juvenile-onset recurrent respiratory papillomatosis (JORRP) is a rare condition characterized by recurring growths in the larynx that often require multiple operations to remove. The disease typically emerges around age 3-4 years and most cases are thought to be caused by human papillomavirus (HPV) subtypes 6 and 11, which are acquired from the mother during birth.
Overall, just 15 cases were reported during the course of the study; 7 in the 1st year, 3 in the 2nd year, 2 each in the 3rd and 4th years, and 1 case in the last year. The annual rates declined from 0.16 per 100,000 children aged 0-14 years in 2012 to 0.02 per 100,000 in 2016.
Of the cases identified, none of the mothers had been vaccinated against HPV before pregnancy and 20% had a history of genital warts. Seven cases were genotyped; 4 were HPV-6 and 3 were HPV-11, and 13 of the 15 cases were born vaginally.
“Our data strongly suggest that the previously documented impact of quadrivalent HPV vaccination in dramatically reducing the prevalence of HPV-6 and HPV-11 genital infection in the Australian population is translating to a reduction in the risk of transmission to infants intrapartum and subsequent development in some of these children of JORRP,” wrote Daniel Novakovic, MD, of the University of Sydney Medical School, and his coinvestigators.
The authors noted that their initial estimate of infection rates was lower than that seen in other studies, such as the 0.5 per 100,000 rate seen in private health insurance data, and the 1.0 per 100,000 seen with Medicaid data in the United States.
Given that the study period started nearly 5 years after the vaccination program began, they suggested that this lower prevalence may reflect the early impact of the vaccine, particularly given that the prevalence of genital warts had already dramatically declined by that point.
However they also stressed that their study relied on clinicians actively reporting cases, and that given surveillance only began after the introduction of the vaccination program, no data were available on the incidence before that point.
The study was supported by a research grant from Merck and by the Australian Paediatric Surveillance Unit, which is supported by the Australian Government Department of Health. Three authors declared research funding from Merck/Seqirus for HPV studies. Two authors declared funding, speaking fees, and other support from a range of pharmaceutical companies. No other conflicts of interest were declared.
Introduction of a national human papillomavirus vaccination program in Australia has been associated with declines in the incidence of juvenile-onset recurrent respiratory papillomatosis, according to a nationwide study.
Juvenile-onset recurrent respiratory papillomatosis (JORRP) is a rare condition characterized by recurring growths in the larynx that often require multiple operations to remove. The disease typically emerges around age 3-4 years and most cases are thought to be caused by human papillomavirus (HPV) subtypes 6 and 11, which are acquired from the mother during birth.
Overall, just 15 cases were reported during the course of the study; 7 in the 1st year, 3 in the 2nd year, 2 each in the 3rd and 4th years, and 1 case in the last year. The annual rates declined from 0.16 per 100,000 children aged 0-14 years in 2012 to 0.02 per 100,000 in 2016.
Of the cases identified, none of the mothers had been vaccinated against HPV before pregnancy and 20% had a history of genital warts. Seven cases were genotyped; 4 were HPV-6 and 3 were HPV-11, and 13 of the 15 cases were born vaginally.
“Our data strongly suggest that the previously documented impact of quadrivalent HPV vaccination in dramatically reducing the prevalence of HPV-6 and HPV-11 genital infection in the Australian population is translating to a reduction in the risk of transmission to infants intrapartum and subsequent development in some of these children of JORRP,” wrote Daniel Novakovic, MD, of the University of Sydney Medical School, and his coinvestigators.
The authors noted that their initial estimate of infection rates was lower than that seen in other studies, such as the 0.5 per 100,000 rate seen in private health insurance data, and the 1.0 per 100,000 seen with Medicaid data in the United States.
Given that the study period started nearly 5 years after the vaccination program began, they suggested that this lower prevalence may reflect the early impact of the vaccine, particularly given that the prevalence of genital warts had already dramatically declined by that point.
However they also stressed that their study relied on clinicians actively reporting cases, and that given surveillance only began after the introduction of the vaccination program, no data were available on the incidence before that point.
The study was supported by a research grant from Merck and by the Australian Paediatric Surveillance Unit, which is supported by the Australian Government Department of Health. Three authors declared research funding from Merck/Seqirus for HPV studies. Two authors declared funding, speaking fees, and other support from a range of pharmaceutical companies. No other conflicts of interest were declared.
FROM THE JOURNAL OF INFECTIOUS DISEASES
Key clinical point: The introduction of a human papillomavirus vaccination program in Australia has seen a decline in the incidence of juvenile-onset recurrent respiratory papillomatosis.
Major finding: The incidence of juvenile recurrent respiratory papillomatosis decreased from 0.16 per 100,000 children aged 0-14 years to 0.02 per 100,000 over 5 years shortly after the national HPV vaccination program was introduced.
Data source: Prospective study using data from the Australian Paediatric Surveillance Unit.
Disclosures: The study was supported by a research grant from Merck and by the Australian Paediatric Surveillance Unit, which is supported by the Australian Government Department of Health. Three authors declared research funding from Merck/Seqirus for HPV studies. Two authors declared funding, speaking fees, and other support from a range of pharmaceutical companies. No other conflicts of interest were declared.
CHMP recommends approval of romiplostim in kids

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the approved indication for romiplostim (Nplate®) to include children.
The CHMP is recommending authorization of romiplostim to treat patients age 1 and older who have chronic immune thrombocytopenia (ITP) that is refractory to other treatments.
The committee’s opinion will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, a centralized marketing authorization will be granted that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The recommendation for romiplostim was based on 5 studies of the drug in children with ITP. This includes 4 completed studies—a phase 1/2, a phase 3, and 2 long-term safety and efficacy studies—and 1 ongoing long-term study.
Results from the phase 1/2 trial were published in Blood in 2011. Phase 3 results were published in The Lancet in April of last year.
And results from 2 of the long-term trials were presented at 22nd Congress of the European Hematology Association in June (abstract P367 and abstract P727). ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the approved indication for romiplostim (Nplate®) to include children.
The CHMP is recommending authorization of romiplostim to treat patients age 1 and older who have chronic immune thrombocytopenia (ITP) that is refractory to other treatments.
The committee’s opinion will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, a centralized marketing authorization will be granted that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The recommendation for romiplostim was based on 5 studies of the drug in children with ITP. This includes 4 completed studies—a phase 1/2, a phase 3, and 2 long-term safety and efficacy studies—and 1 ongoing long-term study.
Results from the phase 1/2 trial were published in Blood in 2011. Phase 3 results were published in The Lancet in April of last year.
And results from 2 of the long-term trials were presented at 22nd Congress of the European Hematology Association in June (abstract P367 and abstract P727). ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended expanding the approved indication for romiplostim (Nplate®) to include children.
The CHMP is recommending authorization of romiplostim to treat patients age 1 and older who have chronic immune thrombocytopenia (ITP) that is refractory to other treatments.
The committee’s opinion will be reviewed by the European Commission (EC).
If the EC agrees with the CHMP, a centralized marketing authorization will be granted that will be valid in the European Union. Norway, Iceland, and Liechtenstein will make corresponding decisions on the basis of the EC’s decision.
The EC typically makes a decision within 67 days of the CHMP’s recommendation.
The recommendation for romiplostim was based on 5 studies of the drug in children with ITP. This includes 4 completed studies—a phase 1/2, a phase 3, and 2 long-term safety and efficacy studies—and 1 ongoing long-term study.
Results from the phase 1/2 trial were published in Blood in 2011. Phase 3 results were published in The Lancet in April of last year.
And results from 2 of the long-term trials were presented at 22nd Congress of the European Hematology Association in June (abstract P367 and abstract P727). ![]()
PCI outcomes not better at top-ranked hospitals
Outcomes after percutaneous coronary intervention (PCI) are not superior when performed in U.S. hospitals ranked as “best” in a prominent national rating system as compared with nonranked hospitals, according to results of a recent retrospective analysis.
Rates of in-hospital mortality, acute kidney injury, and bleeding were similar for hospitals in the 2015 U.S. News & World Report’s “Best Hospitals” rankings and nonranked hospitals, Devraj Sukul, MD, reported at the American Heart Association Scientific Sessions.
“These findings should reassure patients that safe and appropriate PCI is being performed across the country,” said Dr. Sukul of the Division of Cardiovascular Medicine, University of Michigan, Ann Arbor.
The findings, published simultaneously (JACC Cardiovasc Interv. 2017 Nov 12. doi: 10.1016/j.jcin.2017.10.042) were based on a retrospective analysis of PCIs documented in the National Cardiovascular Data Registry CathPCI Registry.
Dr. Sukul and his colleagues limited their analysis to hospitals that both participated in that registry and performed at least 400 PCIs during July 2014–June 2015. That narrowed it down to 654 hospitals, including 44 out of the 50 hospitals ranked by U.S. News & World Report in 2015.
A total of 509,153 PCIs were performed over the 1-year study period, including 55,550 (10.9%) performed at the top-ranked hospitals.
After adjusting for patient risk, there was no difference in post-PCI in-hospital mortality between top-ranked and nonranked hospitals investigators reported (adjusted odds ratio, 0.96; P = .64).
There were also no differences in acute kidney injury (adjusted OR, 1.10; P = .1) or bleeding (adjusted OR, 1.15; P = .052) for top-ranked vs. nonranked hospitals, according to investigators.
In addition, top-ranked hospitals had a “slightly lower proportion” of appropriate PCI, Dr. Sukul reported.
Though rates of appropriate PCI were relatively high in both groups, odds of appropriate PCI were nevertheless significantly higher at nonranked hospitals (89.2% for ranked and 92.8% for nonranked hospitals; P less than .001).
Appropriate PCIs – those based on evidence-based indications – have been increasingly emphasized over the past decade.
Although some recent reports suggest hospital-level appropriateness may not necessarily correlate with clinical outcomes, Dr. Sukul remarked, “we believe that PCI appropriateness is an important indicator of quality, serving as a measure of physician decision-making when faced with treating the vast array of coronary artery disease presentations.”
Dr. Sukul is supported by a National Institutes of Health postdoctoral research training grant.
It should be welcome news to the public that outcomes of PCI conducted at top-ranked hospitals were not superior to those of procedures performed at nonranked hospitals.
This study addresses what is often the foremost question of a patient and their family in their hometown: Is my local hospital doing a good job? To the extent measured by the variables in this study, it is reassuring that the answer appears to be “Yes.”
It is hard to argue that health care should be immune from rankings in an era where consumers have access to ratings for just about every product and service available.
However, the public may be confused regarding the multiple national hospital ranking systems that are available today, particularly since these rating systems do not consistently identify hospitals as top performers.
Each rating system uses different data sources, has its own rating methodology, defines different measures of performance, and has a different focus. Many have argued that transparency will improve health care but, for the public, this is getting to the point of “too much information.”
Gregory J. Dehmer, MD, of the Department of Medicine (Cardiology Division) Texas A&M University, and Baylor Scott & White Health, Temple, made the comments above in an accompanying editorial (JACC Cardiovasc Interv. 2017 Nov 1. doi: 10.1016/j.jcin.2017.11.001). He reported no financial relationships relevant to the topic.
It should be welcome news to the public that outcomes of PCI conducted at top-ranked hospitals were not superior to those of procedures performed at nonranked hospitals.
This study addresses what is often the foremost question of a patient and their family in their hometown: Is my local hospital doing a good job? To the extent measured by the variables in this study, it is reassuring that the answer appears to be “Yes.”
It is hard to argue that health care should be immune from rankings in an era where consumers have access to ratings for just about every product and service available.
However, the public may be confused regarding the multiple national hospital ranking systems that are available today, particularly since these rating systems do not consistently identify hospitals as top performers.
Each rating system uses different data sources, has its own rating methodology, defines different measures of performance, and has a different focus. Many have argued that transparency will improve health care but, for the public, this is getting to the point of “too much information.”
Gregory J. Dehmer, MD, of the Department of Medicine (Cardiology Division) Texas A&M University, and Baylor Scott & White Health, Temple, made the comments above in an accompanying editorial (JACC Cardiovasc Interv. 2017 Nov 1. doi: 10.1016/j.jcin.2017.11.001). He reported no financial relationships relevant to the topic.
It should be welcome news to the public that outcomes of PCI conducted at top-ranked hospitals were not superior to those of procedures performed at nonranked hospitals.
This study addresses what is often the foremost question of a patient and their family in their hometown: Is my local hospital doing a good job? To the extent measured by the variables in this study, it is reassuring that the answer appears to be “Yes.”
It is hard to argue that health care should be immune from rankings in an era where consumers have access to ratings for just about every product and service available.
However, the public may be confused regarding the multiple national hospital ranking systems that are available today, particularly since these rating systems do not consistently identify hospitals as top performers.
Each rating system uses different data sources, has its own rating methodology, defines different measures of performance, and has a different focus. Many have argued that transparency will improve health care but, for the public, this is getting to the point of “too much information.”
Gregory J. Dehmer, MD, of the Department of Medicine (Cardiology Division) Texas A&M University, and Baylor Scott & White Health, Temple, made the comments above in an accompanying editorial (JACC Cardiovasc Interv. 2017 Nov 1. doi: 10.1016/j.jcin.2017.11.001). He reported no financial relationships relevant to the topic.
Outcomes after percutaneous coronary intervention (PCI) are not superior when performed in U.S. hospitals ranked as “best” in a prominent national rating system as compared with nonranked hospitals, according to results of a recent retrospective analysis.
Rates of in-hospital mortality, acute kidney injury, and bleeding were similar for hospitals in the 2015 U.S. News & World Report’s “Best Hospitals” rankings and nonranked hospitals, Devraj Sukul, MD, reported at the American Heart Association Scientific Sessions.
“These findings should reassure patients that safe and appropriate PCI is being performed across the country,” said Dr. Sukul of the Division of Cardiovascular Medicine, University of Michigan, Ann Arbor.
The findings, published simultaneously (JACC Cardiovasc Interv. 2017 Nov 12. doi: 10.1016/j.jcin.2017.10.042) were based on a retrospective analysis of PCIs documented in the National Cardiovascular Data Registry CathPCI Registry.
Dr. Sukul and his colleagues limited their analysis to hospitals that both participated in that registry and performed at least 400 PCIs during July 2014–June 2015. That narrowed it down to 654 hospitals, including 44 out of the 50 hospitals ranked by U.S. News & World Report in 2015.
A total of 509,153 PCIs were performed over the 1-year study period, including 55,550 (10.9%) performed at the top-ranked hospitals.
After adjusting for patient risk, there was no difference in post-PCI in-hospital mortality between top-ranked and nonranked hospitals investigators reported (adjusted odds ratio, 0.96; P = .64).
There were also no differences in acute kidney injury (adjusted OR, 1.10; P = .1) or bleeding (adjusted OR, 1.15; P = .052) for top-ranked vs. nonranked hospitals, according to investigators.
In addition, top-ranked hospitals had a “slightly lower proportion” of appropriate PCI, Dr. Sukul reported.
Though rates of appropriate PCI were relatively high in both groups, odds of appropriate PCI were nevertheless significantly higher at nonranked hospitals (89.2% for ranked and 92.8% for nonranked hospitals; P less than .001).
Appropriate PCIs – those based on evidence-based indications – have been increasingly emphasized over the past decade.
Although some recent reports suggest hospital-level appropriateness may not necessarily correlate with clinical outcomes, Dr. Sukul remarked, “we believe that PCI appropriateness is an important indicator of quality, serving as a measure of physician decision-making when faced with treating the vast array of coronary artery disease presentations.”
Dr. Sukul is supported by a National Institutes of Health postdoctoral research training grant.
Outcomes after percutaneous coronary intervention (PCI) are not superior when performed in U.S. hospitals ranked as “best” in a prominent national rating system as compared with nonranked hospitals, according to results of a recent retrospective analysis.
Rates of in-hospital mortality, acute kidney injury, and bleeding were similar for hospitals in the 2015 U.S. News & World Report’s “Best Hospitals” rankings and nonranked hospitals, Devraj Sukul, MD, reported at the American Heart Association Scientific Sessions.
“These findings should reassure patients that safe and appropriate PCI is being performed across the country,” said Dr. Sukul of the Division of Cardiovascular Medicine, University of Michigan, Ann Arbor.
The findings, published simultaneously (JACC Cardiovasc Interv. 2017 Nov 12. doi: 10.1016/j.jcin.2017.10.042) were based on a retrospective analysis of PCIs documented in the National Cardiovascular Data Registry CathPCI Registry.
Dr. Sukul and his colleagues limited their analysis to hospitals that both participated in that registry and performed at least 400 PCIs during July 2014–June 2015. That narrowed it down to 654 hospitals, including 44 out of the 50 hospitals ranked by U.S. News & World Report in 2015.
A total of 509,153 PCIs were performed over the 1-year study period, including 55,550 (10.9%) performed at the top-ranked hospitals.
After adjusting for patient risk, there was no difference in post-PCI in-hospital mortality between top-ranked and nonranked hospitals investigators reported (adjusted odds ratio, 0.96; P = .64).
There were also no differences in acute kidney injury (adjusted OR, 1.10; P = .1) or bleeding (adjusted OR, 1.15; P = .052) for top-ranked vs. nonranked hospitals, according to investigators.
In addition, top-ranked hospitals had a “slightly lower proportion” of appropriate PCI, Dr. Sukul reported.
Though rates of appropriate PCI were relatively high in both groups, odds of appropriate PCI were nevertheless significantly higher at nonranked hospitals (89.2% for ranked and 92.8% for nonranked hospitals; P less than .001).
Appropriate PCIs – those based on evidence-based indications – have been increasingly emphasized over the past decade.
Although some recent reports suggest hospital-level appropriateness may not necessarily correlate with clinical outcomes, Dr. Sukul remarked, “we believe that PCI appropriateness is an important indicator of quality, serving as a measure of physician decision-making when faced with treating the vast array of coronary artery disease presentations.”
Dr. Sukul is supported by a National Institutes of Health postdoctoral research training grant.
FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point: Percutaneous coronary intervention (PCI) performed at the 50 “Best Hospitals” in U.S. News & World Report rankings was not associated with better outcomes, compared with PCI at other hospitals.
Major finding: There was no significant difference between ranked and nonranked hospitals for PCI-associated in-hospital mortality (adjusted OR, 0.96; 95% CI, 0.83-1.12; P = 0.64), acute kidney injury, or bleeding.
Data source: A retrospective analysis of 509,153 PCIs included in the National Cardiovascular Data Registry CathPCI Registry.
Disclosures: First author Dr. Devraj Sukul is supported by a National Institutes of Health postdoctoral research training grant. Coauthors reported disclosures including AstraZeneca, Regado Biosciences, and Pfizer, among others.