User login
New standard classification, pathophysiology of rosacea announced
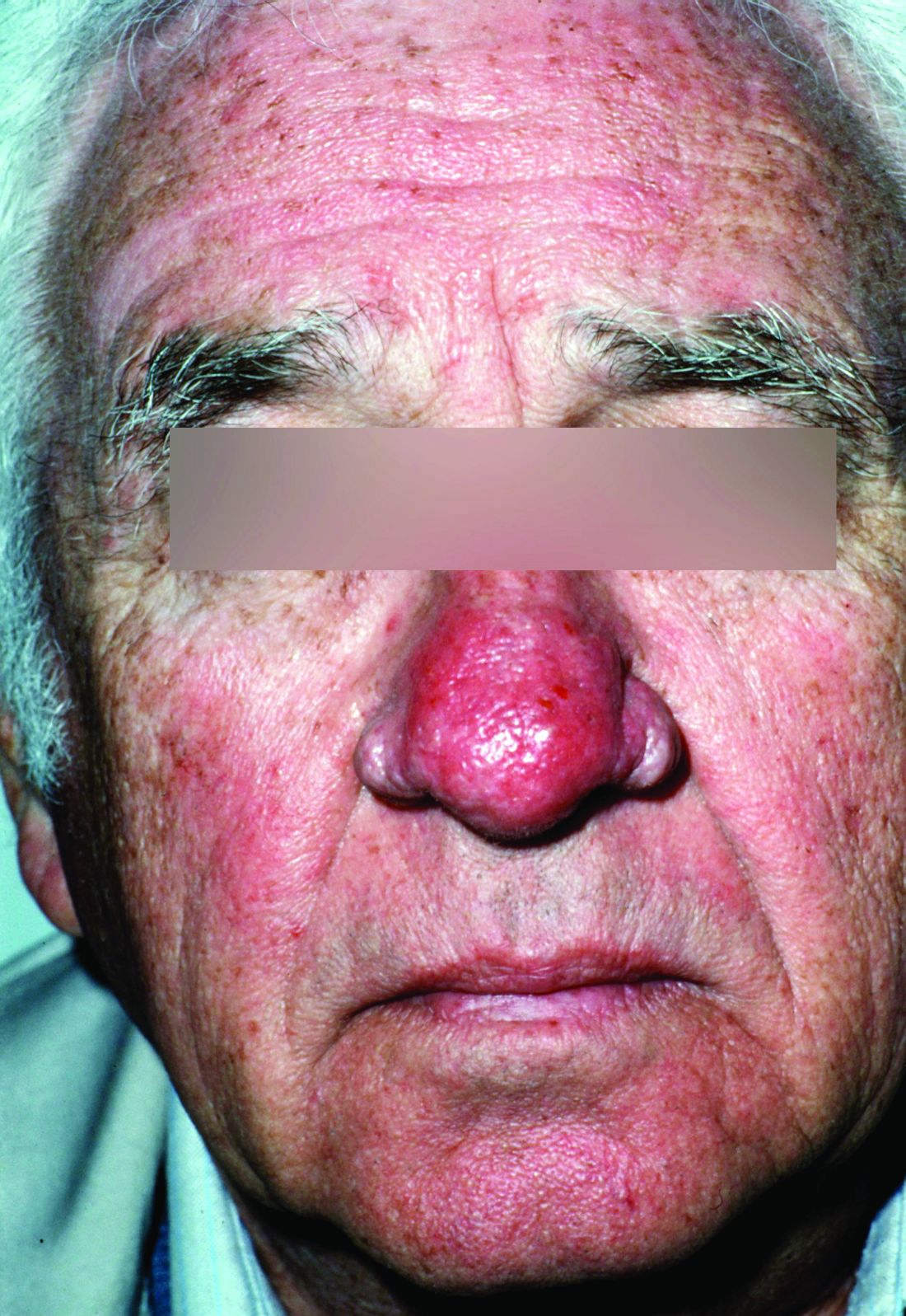
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).

Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY

Delay predicting outcome in comatose cardiac arrest
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.

The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.
The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
ANAHEIM, CALIF. – Withdrawal of life-sustaining systemic therapies in comatose patients after out-of-hospital cardiac arrest as advised in current guidelines often occurs too early, resulting in the death of many patients who could potentially survive with good outcome, according to the results of NORCAST, the Norwegian Cardiorespiratory Arrest Study.
“The take-home message is to be patient and wait. Three days may be too early to make decisions on the patient,” Kjetil Sunde, MD, said in presenting the study findings at the Resuscitation Science Symposium held during the American Heart Association scientific sessions.
The European Resuscitation Council and European Society of Intensive Care Medicine have jointly recommended a prognostic algorithm in which a multimodal assessment is made on patients who are still comatose on day 3 after cardiac arrest. But this advice is based on expert opinion and has never been validated. This was the impetus for the prospective NORCAST study.
Current practice in the management of out-of-hospital cardiac arrest patients who are comatose upon hospital admission is to induce therapeutic hypothermia, with targeted temperature management to 33° C for 24 hours under deep sedation. The study hypothesis was that this strategy delays the time to awakening and that, as a consequence, the recommended prognostic tests that are usually done on day 3 after withdrawal of sedation are rendered insufficiently reliable. Thus, decisions to withdraw life-supporting therapies at that point will reduce the survival potential of this population, Dr. Sunde explained.
NORCAST was a prospective observational study that included 259 patients admitted to Oslo University Hospital in a comatose state after out-of-hospital cardiac arrest. In this unselected group, 81% had a cardiac cause for their arrest; the remainder had hypoxic arrest. All patients underwent therapeutic hypothermia, then a period of nonhypothermia followed by sedation withdrawal.
All of the widely used multimodal prognostic tests were ordered, including serial measurement of serum neuron-specific enolase; neurophysiologic testing using EEG and sensory-evoked potential readings obtained both during hypothermia and again at least 3 days after sedation withdrawal; a standardized clinical neurologic exam including assessment of brainstem reflexes and a Glasgow Coma Scale rating 3 days after sedation withdrawal; and a transcranial Doppler study and cerebral MRI on day 5-7. However, the treatment team was blinded to the results of these tests and was encouraged to delay withdrawal of life-supporting therapies as long as possible.
Key findings
Out of 259 patients who were comatose upon admission, 54% were alive at 6 months – and 91% of them had a CPC of 1 or 2.
The final tally at 6 months: 44% of patients were CPC 1, 5.5% were CPC 2, 4% were CPC 3, meaning severely disabled, and 46.5% were CPC 5, which is brain dead.
Withdrawal of life-supporting therapies occurred in 73 patients, or 28%, and 71% of those patients died, few of them in the early days.
Among patients with a CPC score of 1 or 2 at 6 months, only 20% were awake on day 1-3 following admission. Fifty-seven percent awoke on day 4-7, but importantly, 23% of patients with a good outcome at 6 months were not yet awake on day 8.
Three days after withdrawal of sedation, 49% of patients were rated as having a Glasgow Coma Scale score of 3-8, while 51% were Glasgow Coma Scale 9-15. Moreover, at that time 26% of patients with a good outcome as defined by a CPC of 1 or 2 at 6 months were still in a coma.
“So a lot of patients were still affected by their disease or by sedation at that point. That’s an important finding,” Dr. Sunde said.
Some prognostic tests were highly unreliable
A standout in poor performance was the widely utilized standard of a time to return of spontaneous circulation greater than 25 minutes as a predictor of poor cerebral outcome. In fact, it had a 34% false-positive rate.
“I think it’s really useless to use that. I would rather have return to spontaneous circulation after 40 minutes of good-quality CPR than not have it with 25 minutes of lesser-quality CPR,” he commented.
Similarly, a Glasgow Coma Scale score of 9 or less or a Glasgow Coma Scale-Motor score of 1-3 upon assessment 3 days after sedation withdrawal had false-positive rates of 30% and 34%, respectively.
During hypothermia, EEG abnormalities had a high false-positive rate, and sensory-evoked potential findings were difficult to interpret.
Predictors showing utility
Several clinical factors predicted poor cerebral outcome with low false-positive rates: Unwitnessed cardiac arrest had a false-positive rate of only 4%; initial presentation in asystole or with pulseless electrical activity had a false-positive rate of 6%; and no bystander CPR had a false-positive rate of 13%.
Abnormal sensory-evoked potential or EEG findings 3 days after sedation withdrawal had low false-positive rates as prognosticators of poor cerebral outcome. An EEG showing burst suppression or epileptiform activity had a “pretty good” false-positive rate of only 7%, Dr. Sunde noted. Bilaterally absent N20 sensory-evoked potential findings, while uncommon, had a false-positive rate of zero. A serum neuron-specific enolase level greater than 80 mcg/mL had a 3% false-positive rate, in sharp contrast to the previously recommended cutoff of more than 33 mcg/mL, which had an unacceptable 38% false-positive rate.
“We should avoid using single predictors in decision making and be patient, especially if we have a witnessed ventricular fibrillation with bystander CPR, independent of time to return of spontaneous circulation,” he concluded.
Dr. Sunde and his coinvestigators plan to present numerous further follow-up studies from NORCAST, including the results of comprehensive cognitive function testing 6-9 months after cardiac arrest in all survivors, coupled with interviews with their close relatives, as well as cognitive function and quality-of-life measurements 3-6 years after cardiac arrest along with interviews with relatives.
Several audience members rose to declare that they’ve been waiting for data such as this for a long time. Session chair Karl B. Kern, MD, professor of medicine at the University of Arizona, Tucson, and codirector of the University of Arizona Sarver Heart Center, commented, “We’ve been talking about whether 3 days is too early for a number of years, and clearly from your data it is. It was twice as long before most of them woke up.”
Dr. Sunde reported having no financial conflicts of interest regarding the NORCAST study, which was sponsored by Oslo University Hospital.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Patients with good cerebral function 6 months after admission in a comatose state stemming from out-of-hospital cardiac arrest awoke a mean of 6.2 days post cardiac arrest, far later than most prognostic assessments take place.
Data source: NORCAST, a prospective observational study, included 259 patients who were comatose upon hospital admission after out-of-hospital cardiac arrest.
Disclosures: NORCAST was sponsored by Oslo University Hospital. The presenter reported having no financial conflicts.
Frailty, not age, predicted complications after ambulatory surgery
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
Frailty was associated with a significant increase in 30-day complications after ambulatory hernia repair or ambulatory surgery of the breast, thyroid, or parathyroid, according to the results of a large retrospective cohort study.
The findings reinforce prior work indicating that frailty, not chronologic age, should be a primary factor when deciding about and preparing for surgery, Carolyn D. Seib, MD, and her associates at the University of California, San Francisco, wrote in JAMA Surgery. “Informed consent should be adjusted based on frailty to ensure that patients have an accurate assessment of their risk when making decisions about whether to undergo surgery,” the researchers said.
To test the hypothesis that frailty predicts morbidity and mortality after ambulatory general surgery, the researchers studied 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program (JAMA Surg. 2017 Oct 11. doi: 10.1001/jamasurg.2017.4007). Nearly 2,500 (1.7%) patients experienced perioperative complications, and 0.7% had serious complications, the researchers said. After controlling for age sex, race or ethnicity, smoking, type of anesthesia, and corticosteroid use, patients with an intermediate (0.18-0.35) frailty score had a 70% higher odds of any complication (odds ratio, 1.7; 95% confidence interval, 1.5-1.9) and a 100% higher odds of serious complications (OR, 2.0; 95% CI, 1.7-2.3), compared with patients with a low frailty score.
An intermediate score reflected the presence of two to three frailty traits, such as impaired functional status, history of diabetes, pneumonia, chronic cardiovascular or lung disease, or impaired sensorium, the investigators noted. Notably, having a high modified frailty index (four or more frailty traits) was associated with 3.3-fold higher odds of any complication and with nearly 4-fold higher odds of serious complications, even after controlling for potential confounders.
Among modifiable risk factors, only the use of local and monitored anesthesia was associated with a significant decrease in the likelihood of serious 30-day complications (adjusted OR, 0.66; 95% CI, 0.53-0.81). Single-center studies of elderly patients undergoing inguinal hernia repair have reported similar findings, the researchers said. “For frail patients who choose to undergo hernia repair, local and monitored anesthesia care should be used whenever possible,” they wrote. “The use of local with monitored anesthesia care may be challenging in complex surgical procedures for breast cancer, such as modified radical mastectomy or axillary dissection, but it should be considered for patients with increased anesthesia risk who are undergoing ambulatory breast surgery.”
The National Institute on Aging provided partial funding. The investigators reported having no conflicts of interest.
FROM JAMA SURGERY
Key clinical point: Frailty was an independent risk factor for 30-day complications of ambulatory surgery, independent of age and other correlates.
Major finding: Having an intermediate (0.18-0.35) frailty score increased the odds of any complication by 70% (OR, 1.7).
Data source: A single-center retrospective cohort study of 140,828 patients older than 40 years from the 2007-2010 American College of Surgeons National Surgical Quality Improvement Program.
Disclosures: The investigators had no disclosures.
Low-sodium DASH benefits increase with higher blood pressures
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).

It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).
It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
ANAHEIM, CALIF. – The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks, according to a new analysis of the DASH-Sodium trial.
The original 2001 study found that combining low sodium and the DASH [Dietary Approaches to Stop Hypertension] diet lowered blood pressure more than either alone, but results were not broken out by hypertension severity (N Engl J Med. 2001 Jan 4;344[1]:3-10).
It found that there were “progressively greater reductions at higher levels of baseline systolic BP (SBP). Among participants with baseline SBP at or above 150 mm Hg, “mean SBP reduction was striking,” said Dr. Juraschek, of Harvard Medical School/Beth Israel Deaconess Medical Center, Boston.
The original trial randomized 208 subjects to the DASH diet and 204 to a control diet similar to what most Americans eat. While on their diets, the subjects cycled through three sodium levels for 4 weeks each: 1.5 g/d, 2.4 g/d, and 3.3 g/d. Although deemed high sodium in the study, 3.3 g/d is typical of the American diet.
The new study analyzed outcomes according to four baseline SBP categories: 120-129, 130-139, 140-149, and 150-159 mm Hg.
Among subjects on the control diet, reducing sodium from high to low intake reduced SBP 3.20, 8.56, 8.99, and 7.04 mm Hg across the four baseline SBP categories (P = .004). Among patients consuming high sodium, the DASH diet, compared with the control diet, reduced SBP 4.5, 4.3, 4.7, and 10.6 mm Hg, but the trend was not statistically significant.
The low-sodium DASH diet, versus the high-sodium control diet, reduced SBP 5.3, 7.5, 9.7, and 20.8 mm Hg in subjects with baseline SBP at or above 150 mmHg (P < .001).
“The DASH diet with low sodium, compared with the control diet with high sodium, lowered SBP by nearly 10 mm Hg among those with a baseline SBP of 140-149 mm Hg and [greater than] 20 mm Hg among those with a baseline systolic BP [at or above] 150 mm Hg. SBP levels between 140 and 159 mm Hg represent the majority of patients with hypertension. Thus, our findings suggest that most adults with uncontrolled BP can experience substantial reductions in SBP from dietary changes alone,” the investigator said.
“To place our results in context, compared to placebo, angiotensin-converting enzyme inhibitors reduce SBP by 12 mm Hg, beta-blockers reduce SBP by 13 mm Hg, and calcium-channel blockers reduce SBP by 16 mm Hg,” he said.
“For many patients, it’s hard to take that step to be on a chronic medication. A lot of them want to talk about diet, but” find it hard to believe that something as simple as changing what you eat could beat drugs. “It’s important for both patients and physicians to realize that if you take this seriously, you can have significant reductions in your blood pressure. We should take it seriously as the first step. That’s the key take away,” Dr. Juraschek said in an interview.
None of the participants were on blood pressure medications; 57% were women, and 57% were black. The mean age was 48 years, and mean baseline BP was 135/86 mm Hg. The DASH diet includes whole grains, poultry, fish, and nuts, with reductions in red meat, sweets, and sugary drinks.
The results were published, online simultaneously with Dr. Juraschek’s presentation (J Am Coll Cardiol. 2017 Nov 12;doi: 10.1016/j.jacc.2017.10.011).
The original study was funded by the National Institutes of Health. Dr. Juraschek had no relevant disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The low-sodium DASH diet lowered systolic BP a mean of 20.8 mm Hg among patients with a baseline systolic pressure of 150-159 mm Hg, and did so in just 4 weeks.
Data source: New analysis of the landmark DASH-Sodium trial.
Disclosures: The original study was funded by the National Institutes of Health. The lead investigator in the new analysis didn’t have any relevant disclosures.
Virtual House Calls Are Feasible for Patients With Parkinson’s Disease
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of

Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
Providing remote neurologic care directly into the homes of patients with Parkinson’s disease is feasible and is neither more nor less efficacious than usual in-person care, according to research published in the September 12 issue of
Virtual house calls are becoming increasingly common for episodic conditions, but limited evidence supports their use for chronic conditions, according to the researchers. Approximately 40% of patients with Parkinson’s disease never receive care from a neurologist. These patients are more likely to have increased morbidity, to lose independence, and to die prematurely, they said.
Standard Care Versus Virtual House Calls
To determine whether providing virtual house calls is feasible, valuable, and beneficial, Dr. Beck and colleagues conducted a one-year randomized controlled study. Eligible participants had a clinical diagnosis of Parkinson’s disease; had a private, Internet-enabled device; and lived in a state where a site investigator was licensed to practice. Patients currently hospitalized, who had a condition that would preclude study participation in the judgment of the site investigator, or who were currently enrolled in another telemedicine study were excluded.
Investigators compared usual care to usual care supplemented with four virtual visits via video conferencing from a remote specialist into patients’ homes. Primary outcome measures were feasibility, measured by the proportion of participants who completed at least one virtual visit and the proportion of virtual visits completed on time, and efficacy, measured by change in the Parkinson’s Disease Questionnaire-39, a quality of life scale. Secondary outcomes included quality of care, caregiver burden, and time and travel savings.
Most Participants Were Satisfied With Virtual Visits
A total of 927 patients indicated interest in the study. Of these, 732 were excluded because they did not meet eligibility requirements, did not consent, or withdrew prior to randomization. A total of 210 patients were enrolled, and 195 were randomized. In all, 73% of participants had recently visited a specialist, 73% were college-educated, and 96% were white. The mean age of participants was 66. Ninety-eight percent of participants randomized to the intervention arm completed at least one virtual visit; 91% of 388 virtual visits were completed.
Quality of life did not improve for patients who received virtual house calls, nor did quality of care or caregiver burden. However, each virtual house call saved patients a median of 88 minutes per visit and 38 miles per visit. Ninety-seven percent of patients and 86% of physicians were satisfied or very satisfied with virtual visits.
One limitation of this study was that the majority of participants were white, well educated, and more familiar with the Internet than the general population. “Dedicated outreach to underserved populations, including those with advanced disease and from underserved demographic groups, especially women, rural residents, minorities, the homebound, or those in assisted living facilities, will help determine if the results are more generalizable and whether the benefits are potentially greater for those with historically less access to care,” said Dr. Beck and colleagues.
“Virtual house calls generated great interest and provided substantial convenience,” the researchers said. “Future efforts must address the digital divide and policy barriers to ensure that this new care model can address inequities in access to care.”
—Erica Tricarico
Suggested Reading
Beck CA, Beran DB, Biglan KM, et al. National randomized controlled trial of virtual house calls for Parkinson disease. Neurology. 2017;89(11):1152-1161.
FDA approves Vimpat for POS treatment in children with epilepsy
The Food and Drug Administration has approved lacosamide for the treatment of partial-onset seizures in children with epilepsy, according to a statement by UCB, manufacturer of the drug.
The approval by the FDA is an extension of the drug’s previous indication, which was approved in 2009 for use in adults, and is based on four clinical trials and pharmacokinetic analyses from adult and pediatric data. The expanded indication is for children older than 4 years, and applies only to the oral tablet. Lacosamide (Vimpat) injections remain indicated only for adult patients older than 17 years.
“Until recently there were few effective treatment options approved for childhood epilepsy. This has contributed to poor seizure control for many, which can be detrimental to overall quality of life. The availability of lacosamide for children with epilepsy has the potential to change the lives of children and their families by providing an additional choice to support them in their epilepsy journey,” Raman Sankar, MD, PhD, professor of neurology and pediatrics and chief of pediatric neurology at the University of California, Los Angeles, said in the statement.
Find the full press release on the UCB website.
The Food and Drug Administration has approved lacosamide for the treatment of partial-onset seizures in children with epilepsy, according to a statement by UCB, manufacturer of the drug.
The approval by the FDA is an extension of the drug’s previous indication, which was approved in 2009 for use in adults, and is based on four clinical trials and pharmacokinetic analyses from adult and pediatric data. The expanded indication is for children older than 4 years, and applies only to the oral tablet. Lacosamide (Vimpat) injections remain indicated only for adult patients older than 17 years.
“Until recently there were few effective treatment options approved for childhood epilepsy. This has contributed to poor seizure control for many, which can be detrimental to overall quality of life. The availability of lacosamide for children with epilepsy has the potential to change the lives of children and their families by providing an additional choice to support them in their epilepsy journey,” Raman Sankar, MD, PhD, professor of neurology and pediatrics and chief of pediatric neurology at the University of California, Los Angeles, said in the statement.
Find the full press release on the UCB website.
The Food and Drug Administration has approved lacosamide for the treatment of partial-onset seizures in children with epilepsy, according to a statement by UCB, manufacturer of the drug.
The approval by the FDA is an extension of the drug’s previous indication, which was approved in 2009 for use in adults, and is based on four clinical trials and pharmacokinetic analyses from adult and pediatric data. The expanded indication is for children older than 4 years, and applies only to the oral tablet. Lacosamide (Vimpat) injections remain indicated only for adult patients older than 17 years.
“Until recently there were few effective treatment options approved for childhood epilepsy. This has contributed to poor seizure control for many, which can be detrimental to overall quality of life. The availability of lacosamide for children with epilepsy has the potential to change the lives of children and their families by providing an additional choice to support them in their epilepsy journey,” Raman Sankar, MD, PhD, professor of neurology and pediatrics and chief of pediatric neurology at the University of California, Los Angeles, said in the statement.
Find the full press release on the UCB website.
ARDS incidence is declining. Is it a preventable syndrome?
TORONTO – The incidence of acute respiratory distress syndrome (ARDS) is on the decline, according to a retrospective, population-based cohort study conducted at the Mayo Clinic in Rochester, Minn.
“This is very promising data in combating this syndrome,” reported Augustin Joseph of the Mayo Clinic, and “it suggests that ARDS may in part be a completely preventable disease.”

To see if ARDS incidence has continued to decline, Mr. Joseph’s group studied all patients admitted during 2009-2014 to the Mayo Clinic’s ICU, the only facility in the county that cares for ARDS patients. From 82,388 ICU admissions, they identified 505 patients with ARDS according to the Berlin definition of ARDS developed in 2012.
The number of annual cases dropped from 108 in 2009 to 59 in 2014, and the incidence steadily declined from 74.5 cases per 100,000 in 2009 to 39.3 per 100,000 in 2014.
Median age was 67 years in 2009 and 62 years in 2014. Hospital mortality ranged from 15% to 26% during the study period, while hospital length of stay ranged from 8 to 15 days, with no clear decline in either.
“For hospital and ICU mortality and hospital and ICU length of stay, we did not see much difference [from 2009 to 2014], so the overall picture between the Guangxi Li study and mine was that we did not see much of a difference in the patients who had ARDS, but [in terms of] preventing ARDS, the incidence has continued to decline,” Mr. Joseph reported.
While the earlier study used the American-European Consensus Conference (AECC) definition of ARDS, Mr. Joseph and his colleagues diagnosed ARDS according to the Berlin definition. One of the major changes seen in the new Berlin rules is that acute lung injury no longer exists and patients with a P/F ratio (PaO2/FiO2 ratio, or the ratio of arterial oxygen partial pressure to fractional inspired oxygen) between 200 and 300 are now considered to have “mild ARDS,” Mr. Joseph explained. With the AECC definition, a P/F ratio in this range was classified as acute lung injury and only one less than 200 was considered ARDS.
The researchers are now trying to parse out how changing ARDS diagnosis and management at their institution might be contributing to declining incidence, said Mr. Joseph.
TORONTO – The incidence of acute respiratory distress syndrome (ARDS) is on the decline, according to a retrospective, population-based cohort study conducted at the Mayo Clinic in Rochester, Minn.
“This is very promising data in combating this syndrome,” reported Augustin Joseph of the Mayo Clinic, and “it suggests that ARDS may in part be a completely preventable disease.”
To see if ARDS incidence has continued to decline, Mr. Joseph’s group studied all patients admitted during 2009-2014 to the Mayo Clinic’s ICU, the only facility in the county that cares for ARDS patients. From 82,388 ICU admissions, they identified 505 patients with ARDS according to the Berlin definition of ARDS developed in 2012.
The number of annual cases dropped from 108 in 2009 to 59 in 2014, and the incidence steadily declined from 74.5 cases per 100,000 in 2009 to 39.3 per 100,000 in 2014.
Median age was 67 years in 2009 and 62 years in 2014. Hospital mortality ranged from 15% to 26% during the study period, while hospital length of stay ranged from 8 to 15 days, with no clear decline in either.
“For hospital and ICU mortality and hospital and ICU length of stay, we did not see much difference [from 2009 to 2014], so the overall picture between the Guangxi Li study and mine was that we did not see much of a difference in the patients who had ARDS, but [in terms of] preventing ARDS, the incidence has continued to decline,” Mr. Joseph reported.
While the earlier study used the American-European Consensus Conference (AECC) definition of ARDS, Mr. Joseph and his colleagues diagnosed ARDS according to the Berlin definition. One of the major changes seen in the new Berlin rules is that acute lung injury no longer exists and patients with a P/F ratio (PaO2/FiO2 ratio, or the ratio of arterial oxygen partial pressure to fractional inspired oxygen) between 200 and 300 are now considered to have “mild ARDS,” Mr. Joseph explained. With the AECC definition, a P/F ratio in this range was classified as acute lung injury and only one less than 200 was considered ARDS.
The researchers are now trying to parse out how changing ARDS diagnosis and management at their institution might be contributing to declining incidence, said Mr. Joseph.
TORONTO – The incidence of acute respiratory distress syndrome (ARDS) is on the decline, according to a retrospective, population-based cohort study conducted at the Mayo Clinic in Rochester, Minn.
“This is very promising data in combating this syndrome,” reported Augustin Joseph of the Mayo Clinic, and “it suggests that ARDS may in part be a completely preventable disease.”
To see if ARDS incidence has continued to decline, Mr. Joseph’s group studied all patients admitted during 2009-2014 to the Mayo Clinic’s ICU, the only facility in the county that cares for ARDS patients. From 82,388 ICU admissions, they identified 505 patients with ARDS according to the Berlin definition of ARDS developed in 2012.
The number of annual cases dropped from 108 in 2009 to 59 in 2014, and the incidence steadily declined from 74.5 cases per 100,000 in 2009 to 39.3 per 100,000 in 2014.
Median age was 67 years in 2009 and 62 years in 2014. Hospital mortality ranged from 15% to 26% during the study period, while hospital length of stay ranged from 8 to 15 days, with no clear decline in either.
“For hospital and ICU mortality and hospital and ICU length of stay, we did not see much difference [from 2009 to 2014], so the overall picture between the Guangxi Li study and mine was that we did not see much of a difference in the patients who had ARDS, but [in terms of] preventing ARDS, the incidence has continued to decline,” Mr. Joseph reported.
While the earlier study used the American-European Consensus Conference (AECC) definition of ARDS, Mr. Joseph and his colleagues diagnosed ARDS according to the Berlin definition. One of the major changes seen in the new Berlin rules is that acute lung injury no longer exists and patients with a P/F ratio (PaO2/FiO2 ratio, or the ratio of arterial oxygen partial pressure to fractional inspired oxygen) between 200 and 300 are now considered to have “mild ARDS,” Mr. Joseph explained. With the AECC definition, a P/F ratio in this range was classified as acute lung injury and only one less than 200 was considered ARDS.
The researchers are now trying to parse out how changing ARDS diagnosis and management at their institution might be contributing to declining incidence, said Mr. Joseph.
AT CHEST 2017
Key clinical point: The incidence of acute respiratory distress syndrome is declining, an indication that it may be preventable, according to researchers.
Major finding: The number of annual cases dropped from 108 in 2009 to 59 in 2014, and the incidence steadily declined from 74.5 cases per 100,000 in 2009 to 39.3 per 100,000 in 2014.
Data source: Retrospective, population-based cohort study of all (505) patients admitted to the ICU for ARDS at a single center.
Disclosures: The authors reported having no relevant disclosures.
MACRA Monday: Documenting current medications
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
Measure #130: Documentation of Current Medications in the Medical Record
This measure is aimed at capturing the percentage of patients aged 18 years and older who had their current medications documented in the medical record, including nonprescription drugs, vitamins, and supplements.
What you need to do: Review and update the patient’s list of current medications, being sure to document all known prescriptions, over-the-counter medications, herbals, and vitamin/mineral/dietary supplements. This list must include the name, dosages, frequency, and route of administration for each drug.
Eligible cases include patients aged 18 years and older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 90791, 90792, 90832, 90834, 90837, 90839, 92002, 92004, 92012, 92014, 92507, 92508, 92526, 92537, 92538, 92540, 92541, 92542, 92544, 92545, 92547, 92548, 92550, 92557, 92567, 92568, 92570, 92585, 92588, 92626, 96116, 96150, 96151, 96152, 97161, 97162, 97163, 97164, 97165, 97166, 97167, 97168, 97532, 97802, 97803, 97804, 98960, 98961, 98962, 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99221, 99222, 99223, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99495, 99496, G0101, G0108, G0270, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, G8427 indicates that the patient’s medical record was updated with the current medications. Use exception code G8430 if you documented in the medical record that the patient is not eligible for a current list of medications being obtained and reviewed.
CMS has a full list of measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
- Those who enrolled in Medicare for the first time during a performance period.
- Those who have Medicare Part B allowed charges of $30,000 or less.
- Those who have 100 or fewer Medicare Part B patients.
- Those who are significantly participating in an Advanced Alternative Payment Model (APM).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
Measure #130: Documentation of Current Medications in the Medical Record
This measure is aimed at capturing the percentage of patients aged 18 years and older who had their current medications documented in the medical record, including nonprescription drugs, vitamins, and supplements.
What you need to do: Review and update the patient’s list of current medications, being sure to document all known prescriptions, over-the-counter medications, herbals, and vitamin/mineral/dietary supplements. This list must include the name, dosages, frequency, and route of administration for each drug.
Eligible cases include patients aged 18 years and older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 90791, 90792, 90832, 90834, 90837, 90839, 92002, 92004, 92012, 92014, 92507, 92508, 92526, 92537, 92538, 92540, 92541, 92542, 92544, 92545, 92547, 92548, 92550, 92557, 92567, 92568, 92570, 92585, 92588, 92626, 96116, 96150, 96151, 96152, 97161, 97162, 97163, 97164, 97165, 97166, 97167, 97168, 97532, 97802, 97803, 97804, 98960, 98961, 98962, 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99221, 99222, 99223, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99495, 99496, G0101, G0108, G0270, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, G8427 indicates that the patient’s medical record was updated with the current medications. Use exception code G8430 if you documented in the medical record that the patient is not eligible for a current list of medications being obtained and reviewed.
CMS has a full list of measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
- Those who enrolled in Medicare for the first time during a performance period.
- Those who have Medicare Part B allowed charges of $30,000 or less.
- Those who have 100 or fewer Medicare Part B patients.
- Those who are significantly participating in an Advanced Alternative Payment Model (APM).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
If you haven’t started reporting quality data for the Merit-Based Incentive Payment System (MIPS), there’s still time to avoid a 4% cut to your Medicare payments.
Under the Pick Your Pace approach being offered this year, Centers for Medicare & Medicaid Services allows clinicians to test the system by reporting on one quality measure for one patient through paper-based claims. Be sure to append a Quality Data Code (QDC) to the claim form for care provided up to Dec. 31, 2017, in order to avoid a penalty in payment year 2019.
Consider this measure:
Measure #130: Documentation of Current Medications in the Medical Record
This measure is aimed at capturing the percentage of patients aged 18 years and older who had their current medications documented in the medical record, including nonprescription drugs, vitamins, and supplements.
What you need to do: Review and update the patient’s list of current medications, being sure to document all known prescriptions, over-the-counter medications, herbals, and vitamin/mineral/dietary supplements. This list must include the name, dosages, frequency, and route of administration for each drug.
Eligible cases include patients aged 18 years and older on the date of the encounter and a patient encounter during the performance period. Applicable codes include (CPT or HCPCS): 90791, 90792, 90832, 90834, 90837, 90839, 92002, 92004, 92012, 92014, 92507, 92508, 92526, 92537, 92538, 92540, 92541, 92542, 92544, 92545, 92547, 92548, 92550, 92557, 92567, 92568, 92570, 92585, 92588, 92626, 96116, 96150, 96151, 96152, 97161, 97162, 97163, 97164, 97165, 97166, 97167, 97168, 97532, 97802, 97803, 97804, 98960, 98961, 98962, 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99221, 99222, 99223, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99495, 99496, G0101, G0108, G0270, G0402, G0438, G0439.
To get credit under MIPS, be sure to include a QDC that shows that you successfully performed the measure or had a good reason for not doing so. For instance, G8427 indicates that the patient’s medical record was updated with the current medications. Use exception code G8430 if you documented in the medical record that the patient is not eligible for a current list of medications being obtained and reviewed.
CMS has a full list of measures available for claims-based reporting at qpp.cms.gov. The American Medical Association has also created a step-by-step guide for reporting on one quality measure.
Certain clinicians are exempt from reporting and do not face a penalty under MIPS:
- Those who enrolled in Medicare for the first time during a performance period.
- Those who have Medicare Part B allowed charges of $30,000 or less.
- Those who have 100 or fewer Medicare Part B patients.
- Those who are significantly participating in an Advanced Alternative Payment Model (APM).
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Incidental lung nodules are frequently not mentioned in hospital discharge summary
Clinical question: How often are incidentally found pulmonary nodules and instructions for follow-up included in the discharge summary?
Background: Lung nodules are frequent incidental findings on imaging, but it is unclear whether patients are subsequently receiving the recommended follow-up.
Study design: Retrospective cohort study.
Synopsis: The authors identified 7,173 patients who had undergone abdominal CT scans during their admission and reviewed charts of 402 patients who had incidentally found pulmonary nodules identified on the scans. For each of the patients, discharge summaries were evaluated to determine whether they made reference to the nodules and whether follow-up instructions were included. Of the 208 patients noted to have nodules requiring follow-up, only 48 (23%) had discharge summaries that mentioned the nodules. Factors associated with including the nodules in the discharge summary were the radiologist recommending further surveillance, radiologist including the nodule in the summary heading of the report, and being on a medical as opposed to a surgical service. The authors concluded that systems-based approaches to incidentally found lung nodules are needed to ensure adequate follow-up.
Bottom line: Incidentally found lung nodules are often not included in discharge documentation and therefore may not receive the recommended follow-up.
Citation: Bates R, Plooster C, Croghan I, et al. Incidental pulmonary nodules reported on CT abdominal imaging: Frequency and factors affecting inclusion in the hospital discharge summary. J Hosp Med. 2017;6:454-7.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: How often are incidentally found pulmonary nodules and instructions for follow-up included in the discharge summary?
Background: Lung nodules are frequent incidental findings on imaging, but it is unclear whether patients are subsequently receiving the recommended follow-up.
Study design: Retrospective cohort study.
Synopsis: The authors identified 7,173 patients who had undergone abdominal CT scans during their admission and reviewed charts of 402 patients who had incidentally found pulmonary nodules identified on the scans. For each of the patients, discharge summaries were evaluated to determine whether they made reference to the nodules and whether follow-up instructions were included. Of the 208 patients noted to have nodules requiring follow-up, only 48 (23%) had discharge summaries that mentioned the nodules. Factors associated with including the nodules in the discharge summary were the radiologist recommending further surveillance, radiologist including the nodule in the summary heading of the report, and being on a medical as opposed to a surgical service. The authors concluded that systems-based approaches to incidentally found lung nodules are needed to ensure adequate follow-up.
Bottom line: Incidentally found lung nodules are often not included in discharge documentation and therefore may not receive the recommended follow-up.
Citation: Bates R, Plooster C, Croghan I, et al. Incidental pulmonary nodules reported on CT abdominal imaging: Frequency and factors affecting inclusion in the hospital discharge summary. J Hosp Med. 2017;6:454-7.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: How often are incidentally found pulmonary nodules and instructions for follow-up included in the discharge summary?
Background: Lung nodules are frequent incidental findings on imaging, but it is unclear whether patients are subsequently receiving the recommended follow-up.
Study design: Retrospective cohort study.
Synopsis: The authors identified 7,173 patients who had undergone abdominal CT scans during their admission and reviewed charts of 402 patients who had incidentally found pulmonary nodules identified on the scans. For each of the patients, discharge summaries were evaluated to determine whether they made reference to the nodules and whether follow-up instructions were included. Of the 208 patients noted to have nodules requiring follow-up, only 48 (23%) had discharge summaries that mentioned the nodules. Factors associated with including the nodules in the discharge summary were the radiologist recommending further surveillance, radiologist including the nodule in the summary heading of the report, and being on a medical as opposed to a surgical service. The authors concluded that systems-based approaches to incidentally found lung nodules are needed to ensure adequate follow-up.
Bottom line: Incidentally found lung nodules are often not included in discharge documentation and therefore may not receive the recommended follow-up.
Citation: Bates R, Plooster C, Croghan I, et al. Incidental pulmonary nodules reported on CT abdominal imaging: Frequency and factors affecting inclusion in the hospital discharge summary. J Hosp Med. 2017;6:454-7.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
Results support using MTD of HU in kids with SCA

Dosing of hydroxyurea (HU) in young patients with sickle cell anemia (SCA) should target a fetal hemoglobin (HbF) level above 20%, according to researchers.
Their study, HUSTLE, showed that children and adolescents who received a maximum tolerated dose (MTD) of HU were able to achieve HbF levels above 20%.
And patients who achieved such HbF levels had a significantly lower risk of hospitalization for any reason, including vaso-occlusive crisis, acute chest syndrome, and fever.
Jeremie Estepp, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these results in the American Journal of Hematology.
“Our analysis showed that, using this approach, hospitalizations for the average patient fell to less than 1 every couple of years rather than 4 to 6 annually,” Dr Estepp said. “This frees children from the fevers, pain, and other symptoms of this disease and gives them and their families more chances to enjoy childhood and adolescence.”
The study enrolled 230 SCA patients. Most had the HbSS genotype (n=214; 93%), although 7% (n=16) had HbSb0 thalassemia. The patients’ median age at HU initiation was 7.4 years (range, 6 months to 17.9 years). The mean HbF level at enrollment was 9.7%, and the median was 7.9% (range, 1.0-32.9%).
The researchers used a dose-escalation approach to determine the MTD of HU for each of the patients in this study. The MTD was defined by an absolute neutrophil count of 2000-4000 x 106/L or the presence of hematologic toxicity. The maximum absolute dose was 35 mg/kg/day or 2000 mg/day (whichever came first).
The mean daily dose of HU at the MTD was 26.7 mg/kg/day, and the median was 28.0 mg/kg/day (range, 13.0 to 35.0 mg/kg/day).
Three-quarters of patients (75.2%, 173/230) attained the MTD at the time of data censoring. Patients were followed for up to 4 years after study entry.
As far as treatment compliance, there were complete medication dispensation records available for 96% (220/230) of patients. And the patients were in possession of HU a mean of 93.6% of the time.
The researchers found that administering HU at the MTD resulted in a mean HbF of 26.7% and a median of 21.7% (interquartile range, 16.2% to 27.8%).
And the odds of being hospitalized were higher when a patient’s HbF level was less than 21%. The odds ratios for hospitalization were as follows:
- 4.1 for fever
- 2.6 for acute chest syndrome
- 2.2 for vaso-occlusive crisis
- 2.1 for any reason.
“These results support a hydroxyurea dosing strategy designed to produce fetal hemoglobin levels that exceed 20% in an effort to decrease hospitalization of children with sickle cell disease,” Dr Estepp said.
He and his colleagues are now conducting a multicenter trial to determine if toddlers with SCA would benefit from a similar dosing strategy or would respond better to a standard dose. ![]()
Dosing of hydroxyurea (HU) in young patients with sickle cell anemia (SCA) should target a fetal hemoglobin (HbF) level above 20%, according to researchers.
Their study, HUSTLE, showed that children and adolescents who received a maximum tolerated dose (MTD) of HU were able to achieve HbF levels above 20%.
And patients who achieved such HbF levels had a significantly lower risk of hospitalization for any reason, including vaso-occlusive crisis, acute chest syndrome, and fever.
Jeremie Estepp, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these results in the American Journal of Hematology.
“Our analysis showed that, using this approach, hospitalizations for the average patient fell to less than 1 every couple of years rather than 4 to 6 annually,” Dr Estepp said. “This frees children from the fevers, pain, and other symptoms of this disease and gives them and their families more chances to enjoy childhood and adolescence.”
The study enrolled 230 SCA patients. Most had the HbSS genotype (n=214; 93%), although 7% (n=16) had HbSb0 thalassemia. The patients’ median age at HU initiation was 7.4 years (range, 6 months to 17.9 years). The mean HbF level at enrollment was 9.7%, and the median was 7.9% (range, 1.0-32.9%).
The researchers used a dose-escalation approach to determine the MTD of HU for each of the patients in this study. The MTD was defined by an absolute neutrophil count of 2000-4000 x 106/L or the presence of hematologic toxicity. The maximum absolute dose was 35 mg/kg/day or 2000 mg/day (whichever came first).
The mean daily dose of HU at the MTD was 26.7 mg/kg/day, and the median was 28.0 mg/kg/day (range, 13.0 to 35.0 mg/kg/day).
Three-quarters of patients (75.2%, 173/230) attained the MTD at the time of data censoring. Patients were followed for up to 4 years after study entry.
As far as treatment compliance, there were complete medication dispensation records available for 96% (220/230) of patients. And the patients were in possession of HU a mean of 93.6% of the time.
The researchers found that administering HU at the MTD resulted in a mean HbF of 26.7% and a median of 21.7% (interquartile range, 16.2% to 27.8%).
And the odds of being hospitalized were higher when a patient’s HbF level was less than 21%. The odds ratios for hospitalization were as follows:
- 4.1 for fever
- 2.6 for acute chest syndrome
- 2.2 for vaso-occlusive crisis
- 2.1 for any reason.
“These results support a hydroxyurea dosing strategy designed to produce fetal hemoglobin levels that exceed 20% in an effort to decrease hospitalization of children with sickle cell disease,” Dr Estepp said.
He and his colleagues are now conducting a multicenter trial to determine if toddlers with SCA would benefit from a similar dosing strategy or would respond better to a standard dose. ![]()
Dosing of hydroxyurea (HU) in young patients with sickle cell anemia (SCA) should target a fetal hemoglobin (HbF) level above 20%, according to researchers.
Their study, HUSTLE, showed that children and adolescents who received a maximum tolerated dose (MTD) of HU were able to achieve HbF levels above 20%.
And patients who achieved such HbF levels had a significantly lower risk of hospitalization for any reason, including vaso-occlusive crisis, acute chest syndrome, and fever.
Jeremie Estepp, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these results in the American Journal of Hematology.
“Our analysis showed that, using this approach, hospitalizations for the average patient fell to less than 1 every couple of years rather than 4 to 6 annually,” Dr Estepp said. “This frees children from the fevers, pain, and other symptoms of this disease and gives them and their families more chances to enjoy childhood and adolescence.”
The study enrolled 230 SCA patients. Most had the HbSS genotype (n=214; 93%), although 7% (n=16) had HbSb0 thalassemia. The patients’ median age at HU initiation was 7.4 years (range, 6 months to 17.9 years). The mean HbF level at enrollment was 9.7%, and the median was 7.9% (range, 1.0-32.9%).
The researchers used a dose-escalation approach to determine the MTD of HU for each of the patients in this study. The MTD was defined by an absolute neutrophil count of 2000-4000 x 106/L or the presence of hematologic toxicity. The maximum absolute dose was 35 mg/kg/day or 2000 mg/day (whichever came first).
The mean daily dose of HU at the MTD was 26.7 mg/kg/day, and the median was 28.0 mg/kg/day (range, 13.0 to 35.0 mg/kg/day).
Three-quarters of patients (75.2%, 173/230) attained the MTD at the time of data censoring. Patients were followed for up to 4 years after study entry.
As far as treatment compliance, there were complete medication dispensation records available for 96% (220/230) of patients. And the patients were in possession of HU a mean of 93.6% of the time.
The researchers found that administering HU at the MTD resulted in a mean HbF of 26.7% and a median of 21.7% (interquartile range, 16.2% to 27.8%).
And the odds of being hospitalized were higher when a patient’s HbF level was less than 21%. The odds ratios for hospitalization were as follows:
- 4.1 for fever
- 2.6 for acute chest syndrome
- 2.2 for vaso-occlusive crisis
- 2.1 for any reason.
“These results support a hydroxyurea dosing strategy designed to produce fetal hemoglobin levels that exceed 20% in an effort to decrease hospitalization of children with sickle cell disease,” Dr Estepp said.
He and his colleagues are now conducting a multicenter trial to determine if toddlers with SCA would benefit from a similar dosing strategy or would respond better to a standard dose. ![]()