User login
Single-port laparoscopy has few complications but BMI matters
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.

“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
AT AAGL 2017
Key clinical point:
Major finding: Obese patients experienced a 1% increase in risk of surgical complications per unit value increase of BMI.
Data source: Retrospective cohort study of 587 consecutive patients undergoing single-port laparoscopy at a single academic institution.
Disclosures: Dr. Al-Niaimi reported having no financial disclosures.
Direct oral anticoagulants okay during AF device placement
ANAHEIM, CALIF. – Whether direct oral anticoagulants are continued or interrupted for device placement in atrial fibrillation patients, the risk of device pocket hematoma or stroke is very low, based on results of the BRUISE CONTROL–2 trial in more than 600 subjects.
Either strategy is reasonable depending on the clinical scenario, coprincipal investigator David Birnie, MD, said in presenting the results at the American Heart Association scientific sessions.
When atrial fibrillation (AF) patients on direct oral anticoagulants (DOACs) present for device surgery, there’s concern that keeping them on the drugs will increase the bleeding risk, but that taking them off will increase the stroke risk. “We sought to resolve this dilemma,” said Dr. Birnie, an electrophysiologist and director of the arrhythmia service at the University of Ottawa Heart Institute.
The subjects were on dabigatran, rivaroxaban, or apixaban, about a third in each group; 328 were randomized to continue their daily dosing, including on the day of surgery. The other 334 were randomized to interrupted treatment. For rivaroxaban and apixaban, that meant taking their last dose 2 days before surgery. Dabigatran patients discontinued the drug 1-2 days beforehand, depending on glomerular filtration rate. Patients resumed treatment about 24 hours after surgery. CHA2DS2-VASc scores were a mean of 3.9 in both arms, and at least 2 in all participants.
The rate of clinically significant hematoma – the primary outcome in the study, defined as a hematoma requiring prolonged hospitalization, interrupted postoperative anticoagulation, or reoperation to evacuate – was identical in both arms, 2.1% (seven patients each). There were two ischemic strokes, one in each arm. There was one delayed cardiac tamponade in the continuation arm and one pericardial effusion in the interrupted arm. The three deaths in the trial were not related to device placement.
So, what to do depends on the clinical scenario, Dr. Birnie said in an interview. If someone needs urgent placement and there’s no time to wait for DOAC washout, “it’s quite reasonable to go ahead.” Also, “if somebody is at extremely high risk for stroke, then it’s very reasonable to continue the drug.”
On the other hand, “if someone has a much lower stroke risk, then the risk-benefit ratio is probably in the opposite direction, so temporarily discontinuing the drug is the right thing to do,” he said.
Dr. Birnie cautioned that although continued DOAC may reduce the risk of thromboembolism, “this study was not designed with power to answer this.”
“We are already putting these findings into practice” in Ottawa, he said. “Our protocol” – as in many places – “ was always to stop anticoagulation for 2 or 3 days, but now, for very high-risk patients – high-risk AF, unstable temporary pacing, that type of thing – we are very comfortable continuing it,” he said. The study follows up a previous randomized trial by Dr. Birnie and his colleagues that pitted continued warfarin against heparin bridging for AF device placement. There were far fewer device pocket hematomas with uninterrupted warfarin (N Engl J Med. 2013 May 30;368[22]:2084-93).
The team wanted to repeat the study using DOACs, since their use has grown substantially, with the majority of AF patients now on them.
The arms in BRUISE CONTROL–2 (Strategy of Continued Versus Interrupted Novel Oral Anticoagulant at Time of Device Surgery in Patients With Moderate to High Risk of Arterial Thromboembolic Events) were well matched, with a mean age of about 74 years; men made up more than 70% of the subjects in both arms. About 17% of the participants were on chronic aspirin therapy and about 4% were on clopidogrel, in each arm. The uninterrupted DOAC group went about 14 hours between their last preop and first postop DOAC dose. The interrupted group went about 72 hours.
BRUISE CONTROL–2 was funded by the Heart and Stroke Foundation of Canada, Boehringer Ingelheim, Bayer, Pfizer, and Bristol-Myers Squibb, among others. Dr. Birnie had no relevant financial disclosures.
ANAHEIM, CALIF. – Whether direct oral anticoagulants are continued or interrupted for device placement in atrial fibrillation patients, the risk of device pocket hematoma or stroke is very low, based on results of the BRUISE CONTROL–2 trial in more than 600 subjects.
Either strategy is reasonable depending on the clinical scenario, coprincipal investigator David Birnie, MD, said in presenting the results at the American Heart Association scientific sessions.
When atrial fibrillation (AF) patients on direct oral anticoagulants (DOACs) present for device surgery, there’s concern that keeping them on the drugs will increase the bleeding risk, but that taking them off will increase the stroke risk. “We sought to resolve this dilemma,” said Dr. Birnie, an electrophysiologist and director of the arrhythmia service at the University of Ottawa Heart Institute.
The subjects were on dabigatran, rivaroxaban, or apixaban, about a third in each group; 328 were randomized to continue their daily dosing, including on the day of surgery. The other 334 were randomized to interrupted treatment. For rivaroxaban and apixaban, that meant taking their last dose 2 days before surgery. Dabigatran patients discontinued the drug 1-2 days beforehand, depending on glomerular filtration rate. Patients resumed treatment about 24 hours after surgery. CHA2DS2-VASc scores were a mean of 3.9 in both arms, and at least 2 in all participants.
The rate of clinically significant hematoma – the primary outcome in the study, defined as a hematoma requiring prolonged hospitalization, interrupted postoperative anticoagulation, or reoperation to evacuate – was identical in both arms, 2.1% (seven patients each). There were two ischemic strokes, one in each arm. There was one delayed cardiac tamponade in the continuation arm and one pericardial effusion in the interrupted arm. The three deaths in the trial were not related to device placement.
So, what to do depends on the clinical scenario, Dr. Birnie said in an interview. If someone needs urgent placement and there’s no time to wait for DOAC washout, “it’s quite reasonable to go ahead.” Also, “if somebody is at extremely high risk for stroke, then it’s very reasonable to continue the drug.”
On the other hand, “if someone has a much lower stroke risk, then the risk-benefit ratio is probably in the opposite direction, so temporarily discontinuing the drug is the right thing to do,” he said.
Dr. Birnie cautioned that although continued DOAC may reduce the risk of thromboembolism, “this study was not designed with power to answer this.”
“We are already putting these findings into practice” in Ottawa, he said. “Our protocol” – as in many places – “ was always to stop anticoagulation for 2 or 3 days, but now, for very high-risk patients – high-risk AF, unstable temporary pacing, that type of thing – we are very comfortable continuing it,” he said. The study follows up a previous randomized trial by Dr. Birnie and his colleagues that pitted continued warfarin against heparin bridging for AF device placement. There were far fewer device pocket hematomas with uninterrupted warfarin (N Engl J Med. 2013 May 30;368[22]:2084-93).
The team wanted to repeat the study using DOACs, since their use has grown substantially, with the majority of AF patients now on them.
The arms in BRUISE CONTROL–2 (Strategy of Continued Versus Interrupted Novel Oral Anticoagulant at Time of Device Surgery in Patients With Moderate to High Risk of Arterial Thromboembolic Events) were well matched, with a mean age of about 74 years; men made up more than 70% of the subjects in both arms. About 17% of the participants were on chronic aspirin therapy and about 4% were on clopidogrel, in each arm. The uninterrupted DOAC group went about 14 hours between their last preop and first postop DOAC dose. The interrupted group went about 72 hours.
BRUISE CONTROL–2 was funded by the Heart and Stroke Foundation of Canada, Boehringer Ingelheim, Bayer, Pfizer, and Bristol-Myers Squibb, among others. Dr. Birnie had no relevant financial disclosures.
ANAHEIM, CALIF. – Whether direct oral anticoagulants are continued or interrupted for device placement in atrial fibrillation patients, the risk of device pocket hematoma or stroke is very low, based on results of the BRUISE CONTROL–2 trial in more than 600 subjects.
Either strategy is reasonable depending on the clinical scenario, coprincipal investigator David Birnie, MD, said in presenting the results at the American Heart Association scientific sessions.
When atrial fibrillation (AF) patients on direct oral anticoagulants (DOACs) present for device surgery, there’s concern that keeping them on the drugs will increase the bleeding risk, but that taking them off will increase the stroke risk. “We sought to resolve this dilemma,” said Dr. Birnie, an electrophysiologist and director of the arrhythmia service at the University of Ottawa Heart Institute.
The subjects were on dabigatran, rivaroxaban, or apixaban, about a third in each group; 328 were randomized to continue their daily dosing, including on the day of surgery. The other 334 were randomized to interrupted treatment. For rivaroxaban and apixaban, that meant taking their last dose 2 days before surgery. Dabigatran patients discontinued the drug 1-2 days beforehand, depending on glomerular filtration rate. Patients resumed treatment about 24 hours after surgery. CHA2DS2-VASc scores were a mean of 3.9 in both arms, and at least 2 in all participants.
The rate of clinically significant hematoma – the primary outcome in the study, defined as a hematoma requiring prolonged hospitalization, interrupted postoperative anticoagulation, or reoperation to evacuate – was identical in both arms, 2.1% (seven patients each). There were two ischemic strokes, one in each arm. There was one delayed cardiac tamponade in the continuation arm and one pericardial effusion in the interrupted arm. The three deaths in the trial were not related to device placement.
So, what to do depends on the clinical scenario, Dr. Birnie said in an interview. If someone needs urgent placement and there’s no time to wait for DOAC washout, “it’s quite reasonable to go ahead.” Also, “if somebody is at extremely high risk for stroke, then it’s very reasonable to continue the drug.”
On the other hand, “if someone has a much lower stroke risk, then the risk-benefit ratio is probably in the opposite direction, so temporarily discontinuing the drug is the right thing to do,” he said.
Dr. Birnie cautioned that although continued DOAC may reduce the risk of thromboembolism, “this study was not designed with power to answer this.”
“We are already putting these findings into practice” in Ottawa, he said. “Our protocol” – as in many places – “ was always to stop anticoagulation for 2 or 3 days, but now, for very high-risk patients – high-risk AF, unstable temporary pacing, that type of thing – we are very comfortable continuing it,” he said. The study follows up a previous randomized trial by Dr. Birnie and his colleagues that pitted continued warfarin against heparin bridging for AF device placement. There were far fewer device pocket hematomas with uninterrupted warfarin (N Engl J Med. 2013 May 30;368[22]:2084-93).
The team wanted to repeat the study using DOACs, since their use has grown substantially, with the majority of AF patients now on them.
The arms in BRUISE CONTROL–2 (Strategy of Continued Versus Interrupted Novel Oral Anticoagulant at Time of Device Surgery in Patients With Moderate to High Risk of Arterial Thromboembolic Events) were well matched, with a mean age of about 74 years; men made up more than 70% of the subjects in both arms. About 17% of the participants were on chronic aspirin therapy and about 4% were on clopidogrel, in each arm. The uninterrupted DOAC group went about 14 hours between their last preop and first postop DOAC dose. The interrupted group went about 72 hours.
BRUISE CONTROL–2 was funded by the Heart and Stroke Foundation of Canada, Boehringer Ingelheim, Bayer, Pfizer, and Bristol-Myers Squibb, among others. Dr. Birnie had no relevant financial disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The rate of clinically significant hematoma was identical in both arms, at 2.1% (seven patients each).
Data source: BRUISE CONTROL-2, a randomized trial with more than 600 subjects.
Disclosures: The work was funded by the Heart and Stroke Foundation of Canada, Boehringer Ingelheim, Bayer, Pfizer, and Bristol-Myers Squibb, among others. The presenter had no relevant financial disclosures.
Pain is a risk factor for endometrial ablation failure
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
AT AAGL 2017
Key clinical point:
Major finding: Ablation had a hysterectomy rate of 19.2% when pain was an indication, compared with 13.5% for other indications.
Data source: Retrospective study of 5,818 endometrial ablations conducted between October 2003 and March 2016 at a single institution.
Disclosures: The researchers reported no relevant financial disclosures.
Herbal supplements offer value with cautions, caveats
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
EXPERT ANALYSIS FROM AAP 2017
Experts question insulin as top choice in GDM
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.

The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.
The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.
The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
EXPERT ANALYSIS FROM DPSG-NA 2017
Recommending efficacious cleansers for your patients
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates

Reference
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates
Reference
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates
Reference
Decreasing the Incidence of Surgical-Site Infections After Total Joint Arthroplasty
Take-Home Points
- SSIs after TJA pose a substantial burden on patients, surgeons, and the healthcare system.
- While different forms of preoperative skin preparation have shown varying outcomes after TJA, the importance of preoperative patient optimization (nutritional status, immune function, etc) cannot be overstated.
- Intraoperative infection prevention measures include cutaneous preparation, gloving, body exhaust suits, surgical drapes, OR staff traffic and ventilation flow, and antibiotic-loaded cement.
- Antibiotic prophylaxis for dental procedures in TJA patients continues to remain a controversial issue with conflicting recommendations.
- SSIs have considerable financial costs and require increased resource utilization. Given the significant economic burden associated with TJA infections, it is imperative for orthopedists to establish practical and cost-effective strategies to prevent these devastating complications.
Surgical-site infection (SSI), a potentially devastating complication of lower extremity total joint arthroplasty (TJA), is estimated to occur in 1% to 2.5% of cases annually.1 Infection after TJA places a significant burden on patients, surgeons, and the healthcare system. Revision procedures that address infection after total hip arthroplasty (THA) are associated with more hospitalizations, more operations, longer hospital stay, and higher outpatient costs in comparison with primary THAs and revision surgeries for aseptic loosening.2 If left untreated, a SSI can go deeper into the joint and develop into a periprosthetic infection, which can be disastrous and costly. A periprosthetic joint infection study that used 2001 to 2009 Nationwide Inpatient Sample (NIS) data found that the cost of revision procedures increased to $560 million from $320 million, and was projected to reach $1.62 billion by 2020.3 Furthermore, society incurs indirect costs as a result of patient disability and loss of wages and productivity.2 Therefore, the issue of infection after TJA is even more crucial in our cost-conscious healthcare environment.
Patient optimization, advances in surgical technique, sterile protocol, and operative procedures have been effective in reducing bacterial counts at incision sites and minimizing SSIs. As a result, infection rates have leveled off after rising for a decade.4 Although infection prevention modalities have their differences, routine use is fundamental and recommended by the Hospital Infection Control Practices Advisory Committee.5 Furthermore, both the US Centers for Disease Control and Prevention (CDC) and its Healthcare Infection Control Practices Advisory Committee6,7 recently updated their SSI prevention guidelines by incorporating evidence-based methodology, an element missing from earlier recommendations.
The etiologies of postoperative SSIs have been discussed ad nauseam, but there are few reports summarizing the literature on infection prevention modalities. In this review, we identify and examine SSI prevention strategies as they relate to lower extremity TJA. Specifically, we discuss the literature on the preoperative, intraoperative, and postoperative actions that can be taken to reduce the incidence of SSIs after TJA. We also highlight the economic implications of SSIs that occur after TJA.
Methods
For this review, we performed a literature search with PubMed, EBSCOhost, and Scopus. We looked for reports published between the inception of each database and July 2016. Combinations of various search terms were used: surgical site, infection, total joint arthroplasty, knee, hip, preoperative, intraoperative, perioperative, postoperative, preparation, nutrition, ventilation, antibiotic, body exhaust suit, gloves, drain, costs, economic, and payment.
Our search identified 195 abstracts. Drs. Mistry and Chughtai reviewed these to determine which articles were relevant. For any uncertainties, consensus was reached with the help of Dr. Delanois. Of the 195 articles, 103 were potentially relevant, and 54 of the 103 were excluded for being not relevant to preventing SSIs after TJA or for being written in a language other than English. The references in the remaining articles were assessed, and those with potentially relevant titles were selected for abstract review. This step provided another 35 articles. After all exclusions, 48 articles remained. We discuss these in the context of preoperative, intraoperative, and postoperative measures and economic impact.
Results
Preoperative Measures
Skin Preparation. Preoperative skin preparation methods include standard washing and rinsing, antiseptic soaps, and iodine-based or chlorhexidine gluconate-based antiseptic showers or skin cloths. Iodine-based antiseptics are effective against a wide range of Gram-positive and Gram-negative bacteria, fungi, and viruses. These agents penetrate the cell wall, oxidize the microbial contents, and replace those contents with free iodine molecules.8 Iodophors are free iodine molecules associated with a polymer (eg, polyvinylpyrrolidone); the iodophor povidone-iodine is bactericidal.9 Chlorhexidine gluconate-based solutions are effective against many types of yeast, Gram-positive and Gram-negative bacteria, and a wide variety of viruses.9 Both solutions are useful. Patients with an allergy to iodine can use chlorhexidine. Table 1 summarizes the studies on preoperative measures for preventing SSIs.
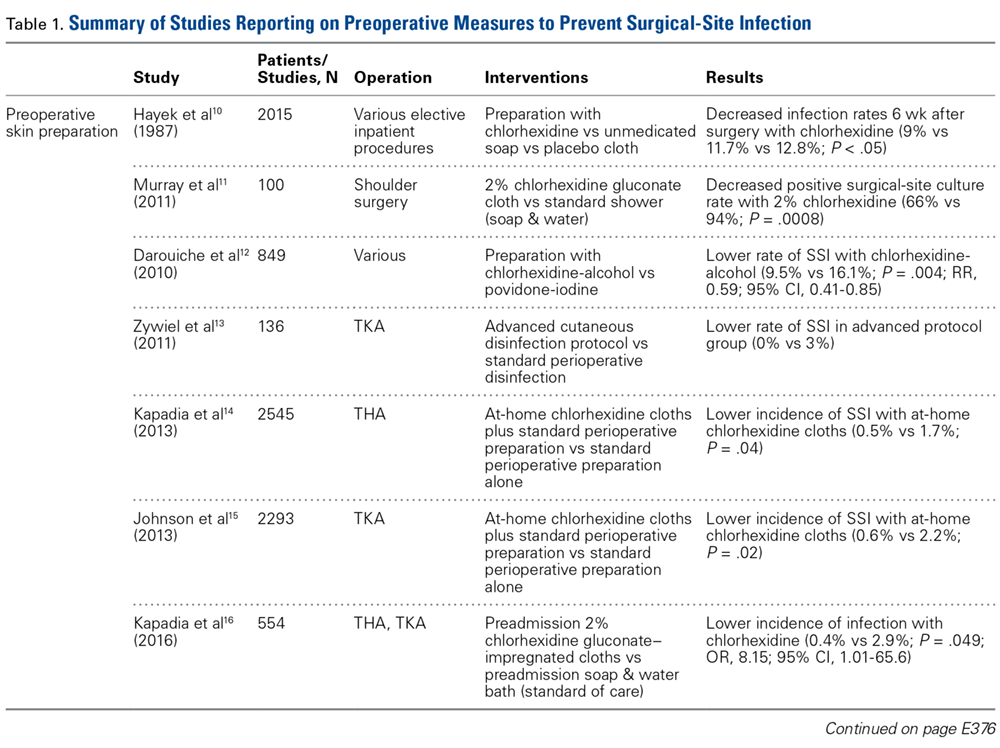
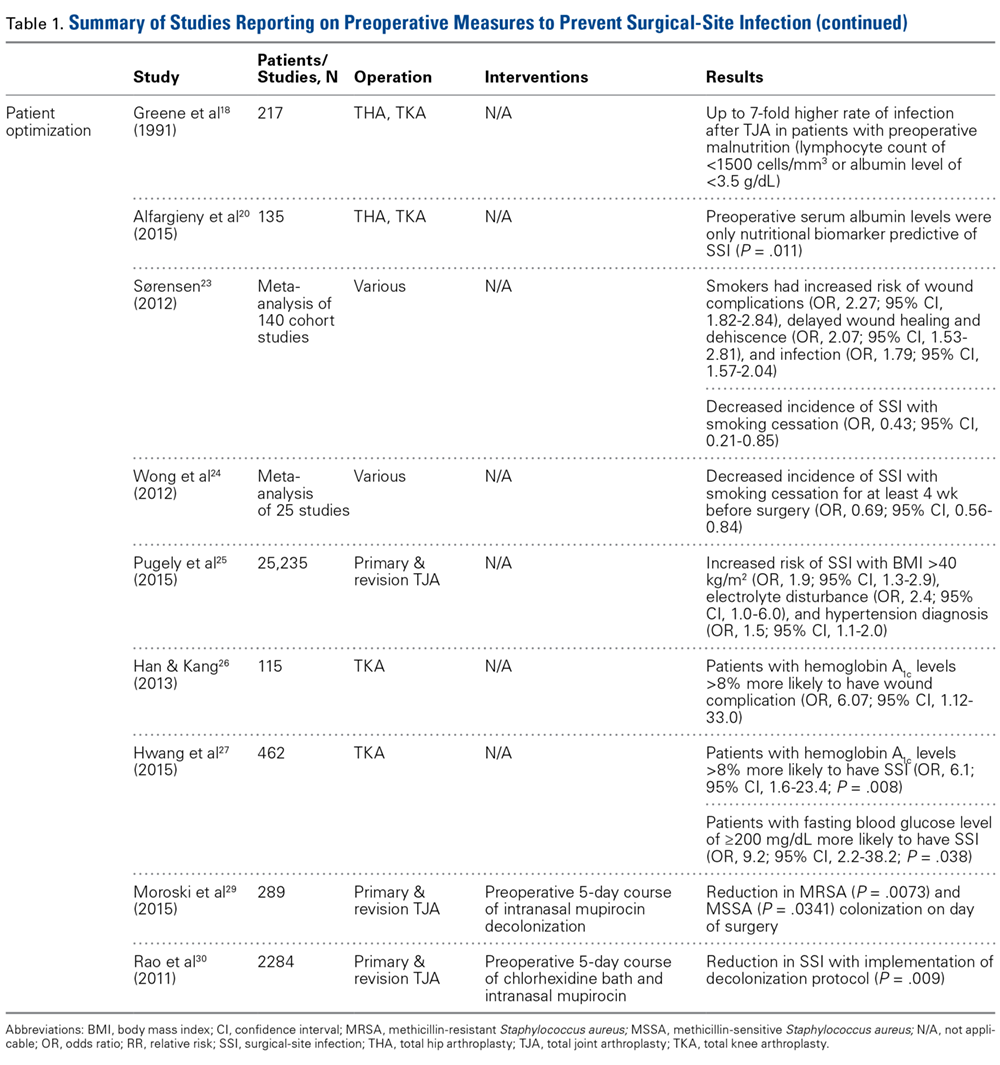
There is no shortage of evidence of the efficacy of these antiseptics in minimizing the incidence of SSIs. Hayek and colleagues10 prospectively analyzed use of different preoperative skin preparation methods in 2015 patients. Six weeks after surgery, the infection rate was significantly lower with use of chlorhexidine than with use of an unmedicated bar of soap or placebo cloth (9% vs 11.7% and 12.8%, respectively; P < .05). In a study of 100 patients, Murray and colleagues11 found the overall bacterial culture rate was significantly lower for those who used a 2% chlorhexidine gluconate cloth before shoulder surgery than for those who took a standard shower with soap (66% vs 94%; P = .0008). Darouiche and colleagues12 found the overall SSI rate was significantly lower for 409 surgical patients prepared with chlorhexidine-alcohol than for 440 prepared with povidone-iodine (9.5% vs 16.1%; P = .004; relative risk [RR], 0.59; 95% confidence interval [CI], 0.41-0.85).
Chlorhexidine gluconate-impregnated cloths have also had promising results, which may be attributed to general ease of use and potentially improved patient adherence. Zywiel and colleagues13 reported no SSIs in 136 patients who used these cloths at home before total knee arthroplasty (TKA) and 21 SSIs (3.0%) in 711 patients who did not use the cloths. In a study of 2545 THA patients, Kapadia and colleagues14 noted a significantly lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths than with only in-hospital perioperative skin preparation (0.5% vs 1.7%; P = .04). In 2293 TKAs, Johnson and colleagues15 similarly found a lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths (0.6% vs 2.2%; P = .02). In another prospective, randomized trial, Kapadia and colleagues16 compared 275 patients who used chlorhexidine cloths the night before and the morning of lower extremity TJA surgery with 279 patients who underwent standard-of-care preparation (preadmission bathing with antibacterial soap and water). The chlorhexidine cohort had a lower overall incidence of infection (0.4% vs 2.9%; P = .049), and the standard-of-care cohort had a stronger association with infection (odds ratio [OR], 8.15; 95% CI, 1.01-65.6).
Patient Optimization. Poor nutritional status may compromise immune function, potentially resulting in delayed healing, increased risk of infection, and, ultimately, negative postoperative outcomes. Malnutrition can be diagnosed on the basis of a prealbumin level of <15 mg/dL (normal, 15-30 mg/dL), a serum albumin level of <3.4 g/dL (normal, 3.4-5.4 g/dL), or a total lymphocyte count under 1200 cells/μL (normal, 3900-10,000 cells/μL).17-19 Greene and colleagues18 found that patients with preoperative malnutrition had up to a 7-fold higher rate of infection after TJA. In a study of 135 THAs and TKAs, Alfargieny and colleagues20 found preoperative serum albumin was the only nutritional biomarker predictive of SSI (P = .011). Furthermore, patients who take immunomodulating medications (eg, for inflammatory arthropathies) should temporarily discontinue them before surgery in order to lower their risk of infection.21
Smoking is well established as a major risk factor for poor outcomes after surgery. It is postulated that the vasoconstrictive effects of nicotine and the hypoxic effects of carbon monoxide contribute to poor wound healing.22 In a meta-analysis of 4 studies, Sørensen23 found smokers were at increased risk for wound complications (OR, 2.27; 95% CI, 1.82-2.84), delayed wound healing and dehiscence (OR, 2.07; 95% CI, 1.53-2.81), and infection (OR, 1.79; 95% CI, 1.57-2.04). Moreover, smoking cessation decreased the incidence of SSIs (OR, 0.43; 95% CI, 0.21-0.85). A meta- analysis by Wong and colleagues24 revealed an inflection point for improved outcomes in patients who abstained from smoking for at least 4 weeks before surgery. Risk of infection was lower for these patients than for current smokers (OR, 0.69; 95% CI, 0.56-0.84).
Other comorbidities contribute to SSIs as well. In their analysis of American College of Surgeons National Surgical Quality Improvement Program registry data on 25,235 patients who underwent primary and revision lower extremity TJA, Pugely and colleagues25 found that, in the primary TJA cohort, body mass index (BMI) of >40 kg/m2 (OR, 1.9; 95% CI, 1.3-2.9), electrolyte disturbance (OR, 2.4; 95% CI, 1.0-6.0), and hypertension diagnosis (OR, 1.5; 95% CI, 1.1-2.0) increased the risk of SSI within 30 days. Furthermore, diabetes mellitus delays collagen synthesis, impairs lymphocyte function, and impairs wound healing, which may lead to poor recovery and higher risk of infection.26 In a study of 167 TKAs performed in 115 patients with type 2 diabetes mellitus, Han and Kang26 found that wound complications were 6 times more likely in those with hemoglobin A1c (HbA1c) levels higher than 8% than in those with lower HbA1c levels (OR, 6.07; 95% CI, 1.12-33.0). In a similar study of 462 patients with diabetes, Hwang and colleagues27 found a higher likelihood of superficial SSIs in patients with HbA1c levels >8% (OR, 6.1; 95% CI, 1.6-23.4; P = .008). This association was also found in patients with a fasting blood glucose level of >200 mg/dL (OR, 9.2; 95% CI, 2.2-38.2; P = .038).
Methicillin-resistant Staphylococcus aureus (MRSA) is thought to account for 10% to 25% of all periprosthetic infections in the United States.28 Nasal colonization by this pathogen increases the risk for SSIs; however, decolonization protocols have proved useful in decreasing the rates of colonization. Moroski and colleagues29 assessed the efficacy of a preoperative 5-day course of intranasal mupirocin in 289 primary or revision TJA patients. Before surgery, 12 patients had positive MRSA cultures, and 44 had positive methicillin-sensitive S aureus (MSSA) cultures. On day of surgery, a significant reduction in MRSA (P = .0073) and MSSA (P = .0341) colonization was noted. Rao and colleagues30 found that the infection rate decreased from 2.7% to 1.2% in 2284 TJA patients treated with a decolonization protocol (P = .009).
Intraoperative Measures
Cutaneous Preparation. The solutions used in perioperative skin preparation are similar to those used preoperatively: povidone-iodine, alcohol, and chlorhexidine. The efficacy of these preparations varies. Table 2 summarizes the studies on intraoperative measures for preventing SSIs.
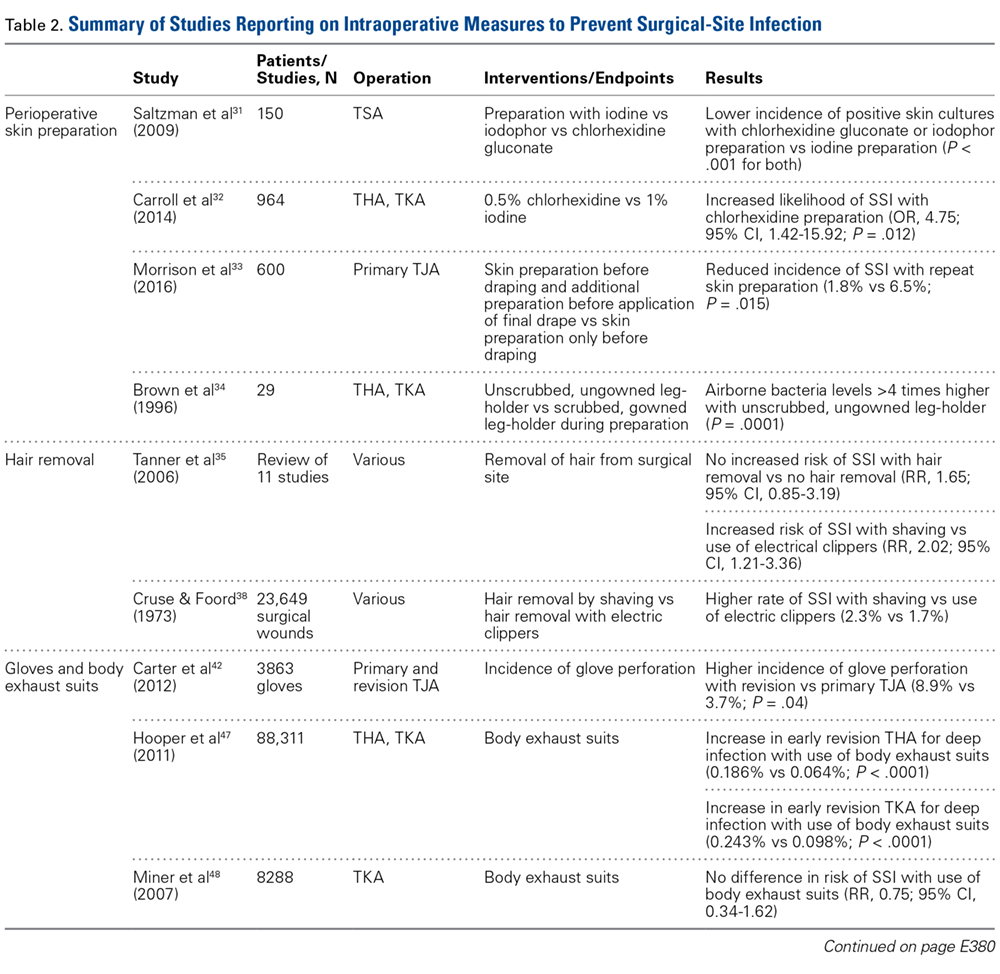
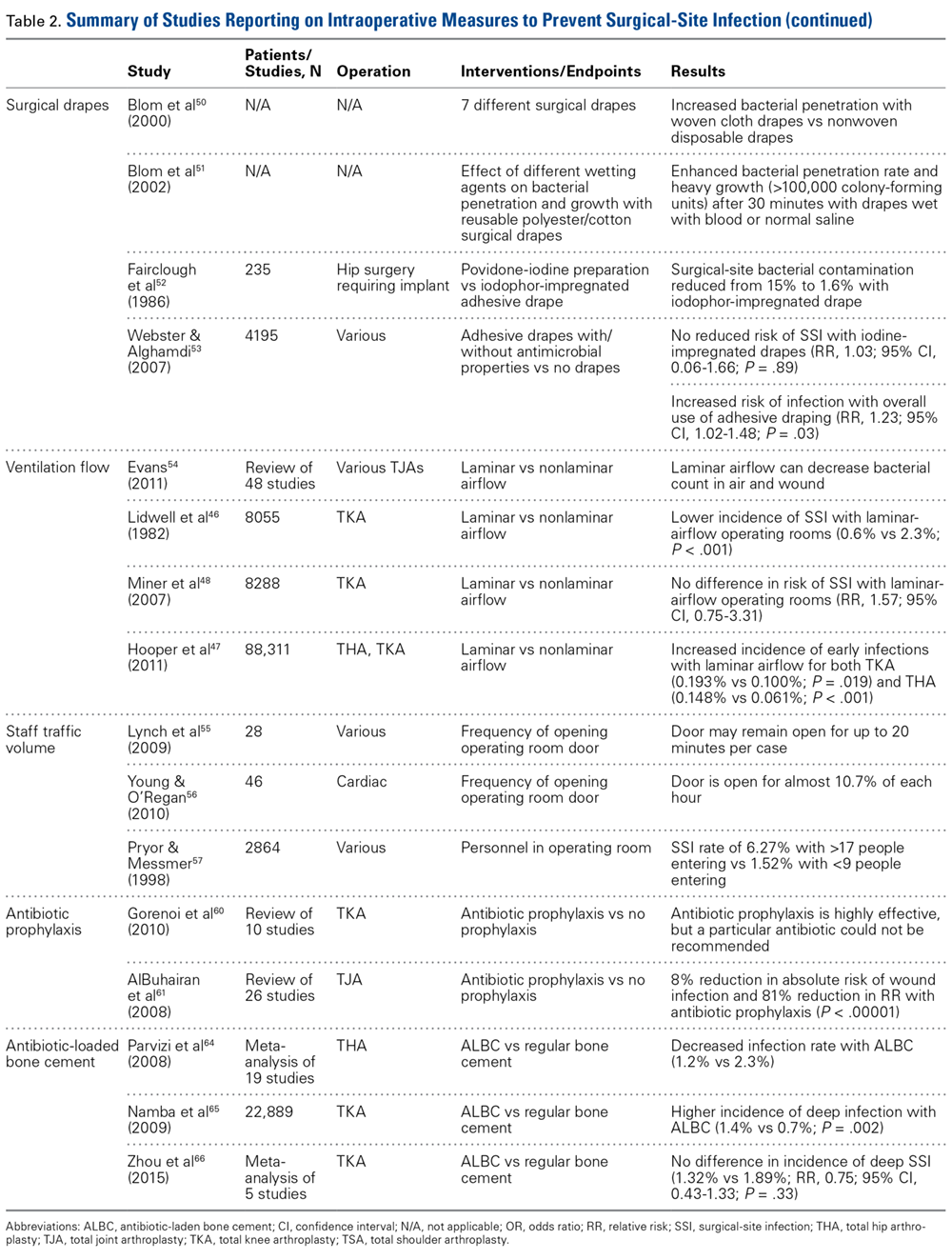
The literature also highlights the importance of technique in incision-site preparation. In a prospective study, Morrison and colleagues33 randomly assigned 600 primary TJA patients to either (1) use of alcohol and povidone-iodine before draping, with additional preparation with iodine povacrylex (DuraPrep) and isopropyl alcohol before application of the final drape (300-patient intervention group) or (2) only use of alcohol and povidone-iodine before draping (300-patient control group). At the final follow-up, the incidence of SSI was significantly lower in the intervention group than in the control group (1.8% vs 6.5%; P = .015). In another study that assessed perioperative skin preparation methods, Brown and colleagues34 found that airborne bacteria levels in operating rooms were >4 times higher with patients whose legs were prepared by a scrubbed, gowned leg-holder than with patients whose legs were prepared by an unscrubbed, ungowned leg-holder (P = .0001).
Hair Removal. Although removing hair from surgical sites is common practice, the literature advocating it varies. A large comprehensive review35 revealed no increased risk of SSI with removing vs not removing hair (RR, 1.65; 95% CI, 0.85-3.19). On the other hand, some hair removal methods may affect the incidence of infection. For example, use of electric hair clippers is presumed to reduce the risk of SSIs, whereas traditional razors may compromise the epidermal barriers and create a pathway for bacterial colonization.5,36,37 In the aforementioned review,35 SSIs were more than twice as likely to occur with hair removed by shaving than with hair removed by electric clippers (RR, 2.02; 95% CI, 1.21-3.36). Cruse and Foord38 found a higher rate of SSIs with hair removed by shaving than with hair removed by clipping (2.3% vs 1.7%). Most surgeons agree that, if given the choice, they would remove hair with electric clippers rather than razors.
Gloves. Almost all orthopedists double their gloves for TJA cases. Over several studies, the incidence of glove perforation during orthopedic procedures has ranged from 3.6% to 26%,39-41 depending on the operating room personnel and glove layering studied. Orthopedists must know this startling finding, as surgical glove perforation is associated with an increase in the rate of SSIs, from 1.7% to 5.7%.38 Carter and colleagues42 found the highest risk of glove perforation occurs when double-gloved attending surgeons, adult reconstruction fellows, and registered nurses initially assist during primary and revision TJA. In their study, outer and inner glove layers were perforated 2.5% of the time. All outer-layer perforations were noticed, but inner-layer perforations went unnoticed 81% of the time, which poses a potential hazard for both patients and healthcare personnel. In addition, there was a significant increase in the incidence of glove perforations for attending surgeons during revision TJA vs primary TJA (8.9% vs 3.7%; P = .04). This finding may be expected given the complexity of revision procedures, the presence of sharp bony and metal edges, and the longer operative times. Giving more attention to glove perforations during arthroplasties may mitigate the risk of SSI. As soon as a perforation is noticed, the glove should be removed and replaced.
Body Exhaust Suits. Early TJAs had infection rates approaching 10%.43 Bacterial-laden particles shed from surgical staff were postulated to be the cause,44,45 and this idea prompted the development of new technology, such as body exhaust suits, which have demonstrated up to a 20-fold reduction in airborne bacterial contamination and decreased incidence of deep infection, from 1% to 0.1%, as compared with conventional surgical attire.46 However, the efficacy of these suits was recently challenged. Hooper and colleagues47 assessed >88,000 TJA cases in the New Zealand Joint Registry and found a significant increase in early revision THA for deep infection with vs without use of body exhaust suits (0.186% vs 0.064%; P < .0001). The incidence of revision TKAs for deep infections with use of these suits was similar (0.243% vs 0.098%; P < .001). Many of the surgeons surveyed indicated their peripheral vision was limited by the suits, which may contribute to sterile field contamination. By contrast, Miner and colleagues48 were unable to determine an increased risk of SSI with use of body exhaust suits (RR, 0.75; 95% CI, 0.34-1.62), though there was a trend toward more infections without suits. Moreover, these suits are effective in reducing mean air bacterial counts (P = .014), but it is not known if this method correlates with mean wound bacterial counts (r = –.011) and therefore increases the risk of SSI.49
Surgical Drapes. Surgical draping, including cloths, iodine-impregnated materials, and woven or unwoven materials, is the standard of care worldwide. The particular draping technique usually varies by surgeon. Plastic drapes are better barriers than cloth drapes, as found in a study by Blom and colleagues50: Bacterial growth rates were almost 10 times higher with use of wet woven cloth drapes than with plastic surgical drapes. These findings were supported in another, similar study by Blom and colleagues51: Wetting drapes with blood or normal saline enhanced bacterial penetration. In addition, wetting drapes with chlorhexidine or iodine reduced but did not eliminate bacterial penetration. Fairclough and colleagues52 emphasized that iodine-impregnated drapes reduced surgical-site bacterial contamination from 15% to 1.6%. However, a Cochrane review53 found these drapes had no effect on the SSI rate (RR, 1.03; 95% CI, 0.06-1.66; P = .89), though the risk of infection was slightly higher with adhesive draping than with no drape (RR, 1.23; 95% CI, 1.02-1.48; P = .03).
Ventilation Flow. Laminar-airflow systems are widely used to prevent SSIs after TJA. Horizontal-flow and vertical-flow ventilation provides and maintains ultra-clean air in the operating room. Evans54 found the bacterial counts in the air and the wound were lower with laminar airflow than without this airflow. The amount of airborne bacterial colony-forming units and dust large enough to carry bacteria was reduced to 1 or 2 particles more than 2 μm/m3 with use of a typical laminar- airflow system. In comparing 3922 TKA patients in laminar-airflow operating rooms with 4133 patients in conventional rooms, Lidwell and colleagues46 found a significantly lower incidence of SSIs in patients in laminar-airflow operating rooms (0.6% vs 2.3%; P < .001).
Conversely, Miner and colleagues48 did not find a lower risk of SSI with laminar-airflow systems (RR, 1.57; 95% CI, 0.75-3.31). In addition, in their analysis of >88,000 cases from the New Zealand Joint Registry, Hooper and colleagues47 found that the incidence of early infections was higher with laminar-airflow systems than with standard airflow systems for both TKA (0.193% vs 0.100%; P = .019) and THA (0.148% vs 0.061%; P < .001). They postulated that vertically oriented airflow may have transmitted contaminated particles into the surgical sites. Additional evidence may be needed to resolve these conflicting findings and determine whether clean-air practices provide significant clinical benefit in the operating room.
Staff Traffic Volume. When staff enters or exits the operating room or makes extra movements during a procedure, airflow near the wound is disturbed and no longer able to remove sufficient airborne pathogens from the sterile field. The laminar- airflow pattern may be disrupted each time the operating room doors open and close, potentially allowing airborne pathogens to be introduced near the patient. Lynch and colleagues55 found the operating room door opened almost 50 times per hour, and it took about 20 seconds to close each time. As a result, the door may remain open for up to 20 minutes per case, causing substantial airflow disruption and potentially ineffective removal of airborne bacterial particles. Similarly, Young and O’Regan56 found the operating room door opened about 19 times per hour and took 20 seconds to close each time. The theater door was open an estimated 10.7% of each hour of sterile procedure. Presence of more staff also increases airborne bacterial counts. Pryor and Messmer57 evaluated a cohort of 2864 patients to determine the effect of number of personnel in the operating theater on the incidence of SSIs. Infection rates were 6.27% with >17 different people entering the room and 1.52% with <9 different people entering the room. Restricting the number of people in the room may be one of the easiest and most efficient ways to prevent SSI.
Systemic Antibiotic Prophylaxis. Perioperative antibiotic use is vital in minimizing the risk of infection after TJA. The Surgical Care Improvement Project recommended beginning the first antimicrobial dose either within 60 minutes before surgical incision (for cephalosporin) or within 2 hours before incision (for vancomycin) and discontinuing the prophylactic antimicrobial agents within 24 hours after surgery ends.58,59 However, Gorenoi and colleagues60 were unable to recommend a way to select particular antibiotics, as they found no difference in the effectiveness of various antibiotic agents used in TKA. A systematic review by AlBuhairan and colleagues61 revealed that antibiotic prophylaxis (vs no prophylaxis) reduced the absolute risk of a SSI by 8% and the relative risk by 81% (P < 0.0001). These findings are supported by evidence of the efficacy of perioperative antibiotics in reducing the incidence of SSI.62,63 Antibiotic regimens should be based on susceptibility and availability, depending on hospital prevalence of infections. Even more, patients should receive prophylaxis in a timely manner. Finally, bacteriostatic antibiotics (vancomycin) should not be used on their own for preoperative prophylaxis.
Antibiotic Cement. Antibiotic-loaded bone cement (ALBC), which locally releases antimicrobials in high concentration, is often used in revision joint arthroplasty, but use in primary joint arthroplasty remains controversial. In a study of THA patients, Parvizi and colleagues64 found infection rates of 1.2% with 2.3% with and without use of ALBC, respectively. Other studies have had opposing results. Namba and colleagues65 evaluated 22,889 primary TKAs, 2030 (8.9%) of which used ALBC. The incidence of deep infection was significantly higher with ALBC than with regular bone cement (1.4% vs 0.7%; P = .002). In addition, a meta- analysis of >6500 primary TKA patients, by Zhou and colleagues,66 revealed no significant difference in the incidence of deep SSIs with use of ALBC vs regular cement (1.32% vs 1.89%; RR, 0.75; 95% CI, 0.43-1.33; P = .33). More evidence is needed to determine the efficacy of ALBC in primary TJA. International Consensus Meeting on Periprosthetic Joint Infection participants recommended use of ALBC in high-risk patients, including patients who are obese or immunosuppressed or have diabetes or a prior history of infection.67
Postoperative Measures
Antibiotic Prophylaxis. The American Academy of Orthopaedic Surgeons (AAOS) and the American Dental Association (ADA) have suggestions for antibiotic prophylaxis for patients at increased risk for infection. As of 2015, the ADA no longer recommends antibiotic prophylaxis for patients with prosthetic joint implants,68 whereas the AAOS considers all patients with TJA to be at risk.69
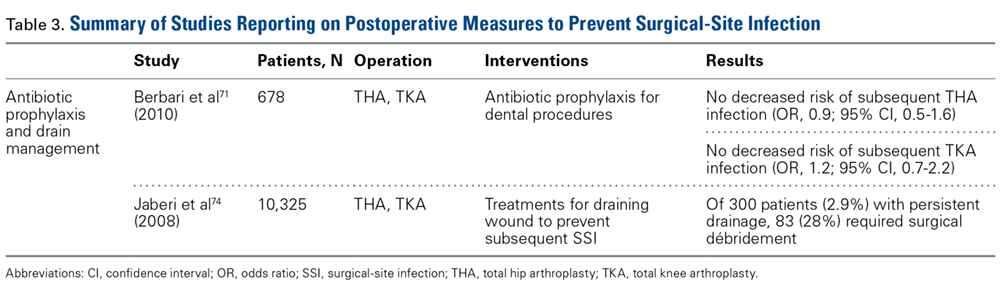
Although recommendations exist, the actual risk of infection resulting from dental procedures and the role of antibiotic prophylaxis are not well defined. Berbari and colleagues71 found that antibiotic prophylaxis in high- or low-risk dental procedures did not decrease the risk of subsequent THA infection (OR, 0.9; 95% CI, 0.5-1.6) or TKA infection (OR, 1.2; 95% CI, 0.7-2.2). Moreover, the risk of infection was no higher for patients who had a prosthetic hip or knee and underwent a high- or low-risk dental procedure without antibiotic prophylaxis (OR, 0.8; 95% CI, 0.4-1.6) than for similar patients who did not undergo a dental procedure (OR, 0.6; 95% CI, 0.4-1.1). Some studies highlight the low level of evidence supporting antibiotic prophylaxis during dental procedures.72,73 However, there is no evidence of adverse effects of antibiotic prophylaxis. Given the potential high risk of infection after such procedures, a more robust body of evidence is needed to reach consensus.
Evacuation Drain Management. Prolonged use of surgical evacuation drains may be a risk factor for SSI. Therefore, early drain removal is paramount. Higher infection rates with prolonged drain use have been found in patients with persistent wound drainage, including malnourished, obese, and over-anticoagulated patients. Patients with wounds persistently draining for >1 week should undergo superficial wound irrigation and débridement. Jaberi and colleagues74 assessed 10,325 TJA patients and found that the majority of persistent drainage ceased within 1 week with use of less invasive measures, including oral antibiotics and local wound care. Furthermore, only 28% of patients with persistent drainage underwent surgical débridement. It is unclear if this practice alone is appropriate. Infection should always be suspected and treated aggressively, and cultures should be obtained from synovial fluid before antibiotics are started, unless there is an obvious superficial infection that does not require further work-up.67
Economic Impact
SSIs remain a significant healthcare issue, and the social and financial costs are staggering. Without appropriate measures in place, these complications will place a larger burden on the healthcare system primarily as a result of longer hospital stays, multiple procedures, and increased resource utilization.75 Given the risk of progression to prosthetic joint infection, early preventive interventions must be explored.
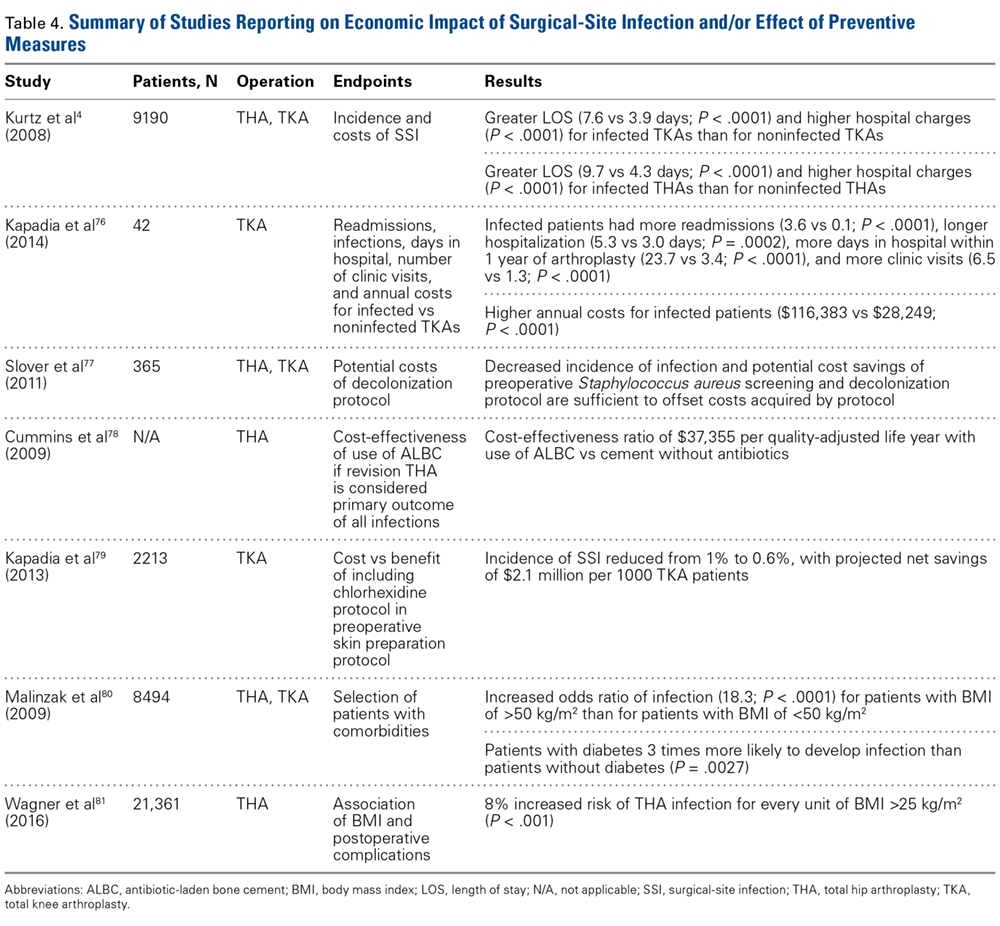
Improved patient selection may be an important factor in reducing SSIs. In an analysis of 8494 joint arthroplasties, Malinzak and colleagues80 noted that patients with a BMI of >50 kg/m2 had an increased OR of infection of 21.3 compared to those with BMI <50 kg/m2. Wagner and colleagues81 analyzed 21,361 THAs and found that, for every BMI unit over 25 kg/m2, there was an 8% increased risk of joint infection (P < .001). Although it is unknown if there is an association between reduction in preoperative BMI and reduction in postoperative complication risk, it may still be worthwhile and cost-effective to modify this and similar risk factors before elective procedures.
Market forces are becoming a larger consideration in healthcare and are being driven by provider competition.82 Treatment outcomes, quality of care, and healthcare prices have gained attention as a means of estimating potential costs.83 In 2011, the Centers for Medicare & Medicaid Services (CMS) advanced the Bundled Payments for Care Improvement (BPCI) initiative, which aimed to provide better coordinated care of higher quality and lower cost.84 This led to development of the Comprehensive Care for Joint Replacement (CJR) program, which gives beneficiaries flexibility in choosing services and ensures that providers adhere to required standards. During its 5-year test period beginning in 2016, the CJR program is projected to save CMS $153 million.84 Under this program, the institution where TJA is performed is responsible for all the costs of related care from time of surgery through 90 days after hospital discharge—which is known as an “episode of care.” If the cost incurred during an episode exceeds an established target cost (as determined by CMS), the hospital must repay Medicare the difference. Conversely, if the cost of an episode is less than the established target cost, the hospital is rewarded with the difference. Bundling payments for a single episode of care in this manner is thought to incentivize providers and hospitals to give patients more comprehensive and coordinated care. Given the substantial economic burden associated with joint arthroplasty infections, it is imperative for orthopedists to establish practical and cost-effective strategies that can prevent these disastrous complications.
Conclusion
SSIs are a devastating burden to patients, surgeons, and other healthcare providers. In recent years, new discoveries and innovations have helped mitigate the incidence of these complications of THA and TKA. However, the incidence of SSIs may rise with the increasing use of TJAs and with the development of new drug-resistant pathogens. In addition, the increasing number of TJAs performed on overweight and high-risk patients means the costs of postoperative infections will be substantial. With new reimbursement models in place, hospitals and providers are being held more accountable for the care they deliver during and after TJA. Consequently, more emphasis should be placed on techniques that are proved to minimize the incidence of SSIs.
1. National Nosocomial Infections Surveillance System. National Nosocomial Infections Surveillance (NNIS) System report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32(8):470-485.
2. Bozic KJ, Ries MD. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J Bone Joint Surg Am. 2005;87(8):1746-1751.
3. Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 suppl):61-65.e61.
4. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty. 2008;23(7):984-991.
5. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4):250-278.
6. Berrios-Torres SI. Evidence-based update to the U.S. Centers for Disease Control and Prevention and Healthcare Infection Control Practices Advisory Committee guideline for the prevention of surgical site infection: developmental process. Surg Infect (Larchmt). 2016;17(2):256-261.
7 Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27(2):97-132.
8. Marchetti MG, Kampf G, Finzi G, Salvatorelli G. Evaluation of the bactericidal effect of five products for surgical hand disinfection according to prEN 12054 and prEN 12791. J Hosp Infect. 2003;54(1):63-67.
9. Reichman DE, Greenberg JA. Reducing surgical site infections: a review. Rev Obstet Gynecol. 2009;2(4):212-221.
10. Hayek LJ, Emerson JM, Gardner AM. A placebo-controlled trial of the effect of two preoperative baths or showers with chlorhexidine detergent on postoperative wound infection rates. J Hosp Infect. 1987;10(2):165-172.
11. Murray MR, Saltzman MD, Gryzlo SM, Terry MA, Woodward CC, Nuber GW. Efficacy of preoperative home use of 2% chlorhexidine gluconate cloth before shoulder surgery. J Shoulder Elbow Surg. 2011;20(6):928-933.
12. Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18-26.
13. Zywiel MG, Daley JA, Delanois RE, Naziri Q, Johnson AJ, Mont MA. Advance pre-operative chlorhexidine reduces the incidence of surgical site infections in knee arthroplasty. Int Orthop. 2011;35(7):1001-1006.
14. Kapadia BH, Johnson AJ, Daley JA, Issa K, Mont MA. Pre-admission cutaneous chlorhexidine preparation reduces surgical site infections in total hip arthroplasty. J Arthroplasty. 2013;28(3):490-493.
15. Johnson AJ, Kapadia BH, Daley JA, Molina CB, Mont MA. Chlorhexidine reduces infections in knee arthroplasty. J Knee Surg. 2013;26(3):213-218.
16. Kapadia BH, Elmallah RK, Mont MA. A randomized, clinical trial of preadmission chlorhexidine skin preparation for lower extremity total joint arthroplasty. J Arthroplasty. 2016;31(12):2856-2861.
17. Mainous MR, Deitch EA. Nutrition and infection. Surg Clin North Am. 1994;74(3):659-676.
18. Greene KA, Wilde AH, Stulberg BN. Preoperative nutritional status of total joint patients. Relationship to postoperative wound complications. J Arthroplasty. 1991;6(4):321-325.
19. Del Savio GC, Zelicof SB, Wexler LM, et al. Preoperative nutritional status and outcome of elective total hip replacement. Clin Orthop Relat Res. 1996;(326):153-161.
20. Alfargieny R, Bodalal Z, Bendardaf R, El-Fadli M, Langhi S. Nutritional status as a predictive marker for surgical site infection in total joint arthroplasty. Avicenna J Med. 2015;5(4):117-122.
21. Bridges SL Jr, Lopez-Mendez A, Han KH, Tracy IC, Alarcon GS. Should methotrexate be discontinued before elective orthopedic surgery in patients with rheumatoid arthritis? J Rheumatol. 1991;18(7):984-988.
22. Silverstein P. Smoking and wound healing. Am J Med. 1992;93(1A):22S-24S.
23. Sørensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012;147(4):373-383.
24. Wong J, Lam DP, Abrishami A, Chan MT, Chung F. Short-term preoperative smoking cessation and postoperative complications: a systematic review and meta-analysis. Can J Anaesth. 2012;59(3):268-279.
25. Pugely AJ, Martin CT, Gao Y, Schweizer ML, Callaghan JJ. The incidence of and risk factors for 30-day surgical site infections following primary and revision total joint arthroplasty. J Arthroplasty. 2015;30(9 suppl):47-50.
26. Han HS, Kang SB. Relations between long-term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin Orthop Surg. 2013;5(2):118-123.
27. Hwang JS, Kim SJ, Bamne AB, Na YG, Kim TK. Do glycemic markers predict occurrence of complications after total knee arthroplasty in patients with diabetes? Clin Orthop Relat Res. 2015;473(5):1726-1731.
28. Whiteside LA, Peppers M, Nayfeh TA, Roy ME. Methicillin-resistant Staphylococcus aureus in TKA treated with revision and direct intra-articular antibiotic infusion. Clin Orthop Relat Res. 2011;469(1):26-33.
29. Moroski NM, Woolwine S, Schwarzkopf R. Is preoperative staphylococcal decolonization efficient in total joint arthroplasty. J Arthroplasty. 2015;30(3):444-446.
30. Rao N, Cannella BA, Crossett LS, Yates AJ Jr, McGough RL 3rd, Hamilton CW. Preoperative screening/decolonization for Staphylococcus aureus to prevent orthopedic surgical site infection: prospective cohort study with 2-year follow-up. J Arthroplasty. 2011;26(8):1501-1507.
31. Saltzman MD, Nuber GW, Gryzlo SM, Marecek GS, Koh JL. Efficacy of surgical preparation solutions in shoulder surgery. J Bone Joint Surg Am. 2009;91(8):1949-1953.
32. Carroll K, Dowsey M, Choong P, Peel T. Risk factors for superficial wound complications in hip and knee arthroplasty. Clin Microbiol Infect. 2014;20(2):130-135.
33. Morrison TN, Chen AF, Taneja M, Kucukdurmaz F, Rothman RH, Parvizi J. Single vs repeat surgical skin preparations for reducing surgical site infection after total joint arthroplasty: a prospective, randomized, double-blinded study. J Arthroplasty. 2016;31(6):1289-1294.
34. Brown AR, Taylor GJ, Gregg PJ. Air contamination during skin preparation and draping in joint replacement surgery. J Bone Joint Surg Br. 1996;78(1):92-94.
35. Tanner J, Woodings D, Moncaster K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2006;(3):CD004122.
36. Mishriki SF, Law DJ, Jeffery PJ. Factors affecting the incidence of postoperative wound infection. J Hosp Infect. 1990;16(3):223-230.
37. Harrop JS, Styliaras JC, Ooi YC, Radcliff KE, Vaccaro AR, Wu C. Contributing factors to surgical site infections. J Am Acad Orthop Surg. 2012;20(2):94-101.
38. Cruse PJ, Foord R. A five-year prospective study of 23,649 surgical wounds. Arch Surg. 1973;107(2):206-210.
39. Laine T, Aarnio P. Glove perforation in orthopaedic and trauma surgery. A comparison between single, double indicator gloving and double gloving with two regular gloves. J Bone Joint Surg Br. 2004;86(6):898-900.
40. Ersozlu S, Sahin O, Ozgur AF, Akkaya T, Tuncay C. Glove punctures in major and minor orthopaedic surgery with double gloving. Acta Orthop Belg. 2007;73(6):760-764.
41. Chan KY, Singh VA, Oun BH, To BH. The rate of glove perforations in orthopaedic procedures: single versus double gloving. A prospective study. Med J Malaysia. 2006;61(suppl B):3-7.
42. Carter AH, Casper DS, Parvizi J, Austin MS. A prospective analysis of glove perforation in primary and revision total hip and total knee arthroplasty. J Arthroplasty. 2012;27(7):1271-1275.
43. Charnley J. A clean-air operating enclosure. Br J Surg. 1964;51:202-205.
44. Whyte W, Hodgson R, Tinkler J. The importance of airborne bacterial contamination of wounds. J Hosp Infect. 1982;3(2):123-135.
45. Owers KL, James E, Bannister GC. Source of bacterial shedding in laminar flow theatres. J Hosp Infect. 2004;58(3):230-232.
46. Lidwell OM, Lowbury EJ, Whyte W, Blowers R, Stanley SJ, Lowe D. Effect of ultraclean air in operating rooms on deep sepsis in the joint after total hip or knee replacement: a randomised study. Br Med J (Clin Res Ed). 1982;285(6334):10-14.
47. Hooper GJ, Rothwell AG, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement? The ten-year results of the New Zealand Joint Registry. J Bone Joint Surg Br. 2011;93(1):85-90.
48. Miner AL, Losina E, Katz JN, Fossel AH, Platt R. Deep infection after total knee replacement: impact of laminar airflow systems and body exhaust suits in the modern operating room. Infect Control Hosp Epidemiol. 2007;28(2):222-226.
49. Der Tavitian J, Ong SM, Taub NA, Taylor GJ. Body-exhaust suit versus occlusive clothing. A randomised, prospective trial using air and wound bacterial counts. J Bone Joint Surg Br. 2003;85(4):490-494.
50. Blom A, Estela C, Bowker K, MacGowan A, Hardy JR. The passage of bacteria through surgical drapes. Ann R Coll Surg Engl. 2000;82(6):405-407.
51. Blom AW, Gozzard C, Heal J, Bowker K, Estela CM. Bacterial strike-through of re-usable surgical drapes: the effect of different wetting agents. J Hosp Infect. 2002;52(1):52-55.
52. Fairclough JA, Johnson D, Mackie I. The prevention of wound contamination by skin organisms by the pre-operative application of an iodophor impregnated plastic adhesive drape. J Int Med Res. 1986;14(2):105-109.
53. Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev. 2007;(4):CD006353.
54. Evans RP. Current concepts for clean air and total joint arthroplasty: laminar airflow and ultraviolet radiation: a systematic review. Clin Orthop Relat Res. 2011;469(4):945-953.
55. Lynch RJ, Englesbe MJ, Sturm L, et al. Measurement of foot traffic in the operating room: implications for infection control. Am J Med Qual. 2009;24(1):45-52.
56. Young RS, O’Regan DJ. Cardiac surgical theatre traffic: time for traffic calming measures? Interact Cardiovasc Thorac Surg. 2010;10(4):526-529.
57. Pryor F, Messmer PR. The effect of traffic patterns in the OR on surgical site infections. AORN J. 1998;68(4):649-660.
58. Bratzler DW, Houck PM; Surgical Infection Prevention Guidelines Writers Workgroup, American Academy of Orthopaedic Surgeons, American Association of Critical Care Nurses, et al. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis. 2004;38(12):1706-1715.
59. Rosenberger LH, Politano AD, Sawyer RG. The Surgical Care Improvement Project and prevention of post-operative infection, including surgical site infection. Surg Infect (Larchmt). 2011;12(3):163-168.
60. Gorenoi V, Schonermark MP, Hagen A. Prevention of infection after knee arthroplasty. GMS Health Technol Assess. 2010;6:Doc10.
61. AlBuhairan B, Hind D, Hutchinson A. Antibiotic prophylaxis for wound infections in total joint arthroplasty: a systematic review. J Bone Joint Surg Br. 2008;90(7):915-919.
62. Bratzler DW, Houck PM; Surgical Infection Prevention Guideline Writers Workgroup. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Am J Surg. 2005;189(4):395-404.
63. Quenon JL, Eveillard M, Vivien A, et al. Evaluation of current practices in surgical antimicrobial prophylaxis in primary total hip prosthesis—a multicentre survey in private and public French hospitals. J Hosp Infect. 2004;56(3):202-207.
64. Parvizi J, Saleh KJ, Ragland PS, Pour AE, Mont MA. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008;79(3):335-341.
65. Namba RS, Chen Y, Paxton EW, Slipchenko T, Fithian DC. Outcomes of routine use of antibiotic-loaded cement in primary total knee arthroplasty. J Arthroplasty. 2009;24(6 suppl):44-47.
66. Zhou Y, Li L, Zhou Q, et al. Lack of efficacy of prophylactic application of antibiotic-loaded bone cement for prevention of infection in primary total knee arthroplasty: results of a meta-analysis. Surg Infect (Larchmt). 2015;16(2):183-187.
67. Leopold SS. Consensus statement from the International Consensus Meeting on Periprosthetic Joint Infection. Clin Orthop Relat Res. 2013;471(12):3731-3732.
68. Sollecito TP, Abt E, Lockhart PB, et al. The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints: evidence-based clinical practice guideline for dental practitioners—a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146(1):11-16.e18.
69. Watters W 3rd, Rethman MP, Hanson NB, et al. Prevention of orthopaedic implant infection in patients undergoing dental procedures. J Am Acad Orthop Surg. 2013;21(3):180-189.
70. Merchant VA; American Academy of Orthopaedic Surgeons, American Dental Association. The new AAOS/ADA clinical practice guidelines for management of patients with prosthetic joint replacements. J Mich Dent Assoc. 2013;95(2):16, 74.
71. Berbari EF, Osmon DR, Carr A, et al. Dental procedures as risk factors for prosthetic hip or knee infection: a hospital-based prospective case–control study. Clin Infect Dis. 2010;50(1):8-16.
72. Little JW, Jacobson JJ, Lockhart PB; American Academy of Oral Medicine. The dental treatment of patients with joint replacements: a position paper from the American Academy of Oral Medicine. J Am Dent Assoc. 2010;141(6):667-671.
73. Curry S, Phillips H. Joint arthroplasty, dental treatment, and antibiotics: a review. J Arthroplasty. 2002;17(1):111-113.
74. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res. 2008;466(6):1368-1371.
75. Stone PW. Economic burden of healthcare-associated infections: an American perspective. Expert Rev Pharmacoecon Outcomes Res. 2009;9(5):417-422.
76. Kapadia BH, McElroy MJ, Issa K, Johnson AJ, Bozic KJ, Mont MA. The economic impact of periprosthetic infections following total knee arthroplasty at a specialized tertiary-care center. J Arthroplasty. 2014;29(5):929-932.
77. Slover J, Haas JP, Quirno M, Phillips MS, Bosco JA 3rd. Cost-effectiveness of a Staphylococcus aureus screening and decolonization program for high-risk orthopedic patients. J Arthroplasty. 2011;26(3):360-365.
78. Cummins JS, Tomek IM, Kantor SR, Furnes O, Engesaeter LB, Finlayson SR. Cost-effectiveness of antibiotic-impregnated bone cement used in primary total hip arthroplasty. J Bone Joint Surg Am. 2009;91(3):634-641.
79. Kapadia BH, Johnson AJ, Issa K, Mont MA. Economic evaluation of chlorhexidine cloths on healthcare costs due to surgical site infections following total knee arthroplasty. J Arthroplasty. 2013;28(7):1061-1065.
80. Malinzak RA, Ritter MA, Berend ME, Meding JB, Olberding EM, Davis KE. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24(6 suppl):84-88.
81. Wagner ER, Kamath AF, Fruth KM, Harmsen WS, Berry DJ. Effect of body mass index on complications and reoperations after total hip arthroplasty. J Bone Joint Surg Am. 2016;98(3):169-179.
82 Broex EC, van Asselt AD, Bruggeman CA, van Tiel FH. Surgical site infections: how high are the costs? J Hosp Infect. 2009;72(3):193-201.
83. Anderson DJ, Kirkland KB, Kaye KS, et al. Underresourced hospital infection control and prevention programs: penny wise, pound foolish? Infect Control Hosp Epidemiol. 2007;28(7):767-773.
84. Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program; comprehensive care for joint replacement payment model for acute care hospitals furnishing lower extremity joint replacement services. Final rule. Fed Regist. 2015;80(226):73273-73554.
Take-Home Points
- SSIs after TJA pose a substantial burden on patients, surgeons, and the healthcare system.
- While different forms of preoperative skin preparation have shown varying outcomes after TJA, the importance of preoperative patient optimization (nutritional status, immune function, etc) cannot be overstated.
- Intraoperative infection prevention measures include cutaneous preparation, gloving, body exhaust suits, surgical drapes, OR staff traffic and ventilation flow, and antibiotic-loaded cement.
- Antibiotic prophylaxis for dental procedures in TJA patients continues to remain a controversial issue with conflicting recommendations.
- SSIs have considerable financial costs and require increased resource utilization. Given the significant economic burden associated with TJA infections, it is imperative for orthopedists to establish practical and cost-effective strategies to prevent these devastating complications.
Surgical-site infection (SSI), a potentially devastating complication of lower extremity total joint arthroplasty (TJA), is estimated to occur in 1% to 2.5% of cases annually.1 Infection after TJA places a significant burden on patients, surgeons, and the healthcare system. Revision procedures that address infection after total hip arthroplasty (THA) are associated with more hospitalizations, more operations, longer hospital stay, and higher outpatient costs in comparison with primary THAs and revision surgeries for aseptic loosening.2 If left untreated, a SSI can go deeper into the joint and develop into a periprosthetic infection, which can be disastrous and costly. A periprosthetic joint infection study that used 2001 to 2009 Nationwide Inpatient Sample (NIS) data found that the cost of revision procedures increased to $560 million from $320 million, and was projected to reach $1.62 billion by 2020.3 Furthermore, society incurs indirect costs as a result of patient disability and loss of wages and productivity.2 Therefore, the issue of infection after TJA is even more crucial in our cost-conscious healthcare environment.
Patient optimization, advances in surgical technique, sterile protocol, and operative procedures have been effective in reducing bacterial counts at incision sites and minimizing SSIs. As a result, infection rates have leveled off after rising for a decade.4 Although infection prevention modalities have their differences, routine use is fundamental and recommended by the Hospital Infection Control Practices Advisory Committee.5 Furthermore, both the US Centers for Disease Control and Prevention (CDC) and its Healthcare Infection Control Practices Advisory Committee6,7 recently updated their SSI prevention guidelines by incorporating evidence-based methodology, an element missing from earlier recommendations.
The etiologies of postoperative SSIs have been discussed ad nauseam, but there are few reports summarizing the literature on infection prevention modalities. In this review, we identify and examine SSI prevention strategies as they relate to lower extremity TJA. Specifically, we discuss the literature on the preoperative, intraoperative, and postoperative actions that can be taken to reduce the incidence of SSIs after TJA. We also highlight the economic implications of SSIs that occur after TJA.
Methods
For this review, we performed a literature search with PubMed, EBSCOhost, and Scopus. We looked for reports published between the inception of each database and July 2016. Combinations of various search terms were used: surgical site, infection, total joint arthroplasty, knee, hip, preoperative, intraoperative, perioperative, postoperative, preparation, nutrition, ventilation, antibiotic, body exhaust suit, gloves, drain, costs, economic, and payment.
Our search identified 195 abstracts. Drs. Mistry and Chughtai reviewed these to determine which articles were relevant. For any uncertainties, consensus was reached with the help of Dr. Delanois. Of the 195 articles, 103 were potentially relevant, and 54 of the 103 were excluded for being not relevant to preventing SSIs after TJA or for being written in a language other than English. The references in the remaining articles were assessed, and those with potentially relevant titles were selected for abstract review. This step provided another 35 articles. After all exclusions, 48 articles remained. We discuss these in the context of preoperative, intraoperative, and postoperative measures and economic impact.
Results
Preoperative Measures
Skin Preparation. Preoperative skin preparation methods include standard washing and rinsing, antiseptic soaps, and iodine-based or chlorhexidine gluconate-based antiseptic showers or skin cloths. Iodine-based antiseptics are effective against a wide range of Gram-positive and Gram-negative bacteria, fungi, and viruses. These agents penetrate the cell wall, oxidize the microbial contents, and replace those contents with free iodine molecules.8 Iodophors are free iodine molecules associated with a polymer (eg, polyvinylpyrrolidone); the iodophor povidone-iodine is bactericidal.9 Chlorhexidine gluconate-based solutions are effective against many types of yeast, Gram-positive and Gram-negative bacteria, and a wide variety of viruses.9 Both solutions are useful. Patients with an allergy to iodine can use chlorhexidine. Table 1 summarizes the studies on preoperative measures for preventing SSIs.
There is no shortage of evidence of the efficacy of these antiseptics in minimizing the incidence of SSIs. Hayek and colleagues10 prospectively analyzed use of different preoperative skin preparation methods in 2015 patients. Six weeks after surgery, the infection rate was significantly lower with use of chlorhexidine than with use of an unmedicated bar of soap or placebo cloth (9% vs 11.7% and 12.8%, respectively; P < .05). In a study of 100 patients, Murray and colleagues11 found the overall bacterial culture rate was significantly lower for those who used a 2% chlorhexidine gluconate cloth before shoulder surgery than for those who took a standard shower with soap (66% vs 94%; P = .0008). Darouiche and colleagues12 found the overall SSI rate was significantly lower for 409 surgical patients prepared with chlorhexidine-alcohol than for 440 prepared with povidone-iodine (9.5% vs 16.1%; P = .004; relative risk [RR], 0.59; 95% confidence interval [CI], 0.41-0.85).
Chlorhexidine gluconate-impregnated cloths have also had promising results, which may be attributed to general ease of use and potentially improved patient adherence. Zywiel and colleagues13 reported no SSIs in 136 patients who used these cloths at home before total knee arthroplasty (TKA) and 21 SSIs (3.0%) in 711 patients who did not use the cloths. In a study of 2545 THA patients, Kapadia and colleagues14 noted a significantly lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths than with only in-hospital perioperative skin preparation (0.5% vs 1.7%; P = .04). In 2293 TKAs, Johnson and colleagues15 similarly found a lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths (0.6% vs 2.2%; P = .02). In another prospective, randomized trial, Kapadia and colleagues16 compared 275 patients who used chlorhexidine cloths the night before and the morning of lower extremity TJA surgery with 279 patients who underwent standard-of-care preparation (preadmission bathing with antibacterial soap and water). The chlorhexidine cohort had a lower overall incidence of infection (0.4% vs 2.9%; P = .049), and the standard-of-care cohort had a stronger association with infection (odds ratio [OR], 8.15; 95% CI, 1.01-65.6).
Patient Optimization. Poor nutritional status may compromise immune function, potentially resulting in delayed healing, increased risk of infection, and, ultimately, negative postoperative outcomes. Malnutrition can be diagnosed on the basis of a prealbumin level of <15 mg/dL (normal, 15-30 mg/dL), a serum albumin level of <3.4 g/dL (normal, 3.4-5.4 g/dL), or a total lymphocyte count under 1200 cells/μL (normal, 3900-10,000 cells/μL).17-19 Greene and colleagues18 found that patients with preoperative malnutrition had up to a 7-fold higher rate of infection after TJA. In a study of 135 THAs and TKAs, Alfargieny and colleagues20 found preoperative serum albumin was the only nutritional biomarker predictive of SSI (P = .011). Furthermore, patients who take immunomodulating medications (eg, for inflammatory arthropathies) should temporarily discontinue them before surgery in order to lower their risk of infection.21
Smoking is well established as a major risk factor for poor outcomes after surgery. It is postulated that the vasoconstrictive effects of nicotine and the hypoxic effects of carbon monoxide contribute to poor wound healing.22 In a meta-analysis of 4 studies, Sørensen23 found smokers were at increased risk for wound complications (OR, 2.27; 95% CI, 1.82-2.84), delayed wound healing and dehiscence (OR, 2.07; 95% CI, 1.53-2.81), and infection (OR, 1.79; 95% CI, 1.57-2.04). Moreover, smoking cessation decreased the incidence of SSIs (OR, 0.43; 95% CI, 0.21-0.85). A meta- analysis by Wong and colleagues24 revealed an inflection point for improved outcomes in patients who abstained from smoking for at least 4 weeks before surgery. Risk of infection was lower for these patients than for current smokers (OR, 0.69; 95% CI, 0.56-0.84).
Other comorbidities contribute to SSIs as well. In their analysis of American College of Surgeons National Surgical Quality Improvement Program registry data on 25,235 patients who underwent primary and revision lower extremity TJA, Pugely and colleagues25 found that, in the primary TJA cohort, body mass index (BMI) of >40 kg/m2 (OR, 1.9; 95% CI, 1.3-2.9), electrolyte disturbance (OR, 2.4; 95% CI, 1.0-6.0), and hypertension diagnosis (OR, 1.5; 95% CI, 1.1-2.0) increased the risk of SSI within 30 days. Furthermore, diabetes mellitus delays collagen synthesis, impairs lymphocyte function, and impairs wound healing, which may lead to poor recovery and higher risk of infection.26 In a study of 167 TKAs performed in 115 patients with type 2 diabetes mellitus, Han and Kang26 found that wound complications were 6 times more likely in those with hemoglobin A1c (HbA1c) levels higher than 8% than in those with lower HbA1c levels (OR, 6.07; 95% CI, 1.12-33.0). In a similar study of 462 patients with diabetes, Hwang and colleagues27 found a higher likelihood of superficial SSIs in patients with HbA1c levels >8% (OR, 6.1; 95% CI, 1.6-23.4; P = .008). This association was also found in patients with a fasting blood glucose level of >200 mg/dL (OR, 9.2; 95% CI, 2.2-38.2; P = .038).
Methicillin-resistant Staphylococcus aureus (MRSA) is thought to account for 10% to 25% of all periprosthetic infections in the United States.28 Nasal colonization by this pathogen increases the risk for SSIs; however, decolonization protocols have proved useful in decreasing the rates of colonization. Moroski and colleagues29 assessed the efficacy of a preoperative 5-day course of intranasal mupirocin in 289 primary or revision TJA patients. Before surgery, 12 patients had positive MRSA cultures, and 44 had positive methicillin-sensitive S aureus (MSSA) cultures. On day of surgery, a significant reduction in MRSA (P = .0073) and MSSA (P = .0341) colonization was noted. Rao and colleagues30 found that the infection rate decreased from 2.7% to 1.2% in 2284 TJA patients treated with a decolonization protocol (P = .009).
Intraoperative Measures
Cutaneous Preparation. The solutions used in perioperative skin preparation are similar to those used preoperatively: povidone-iodine, alcohol, and chlorhexidine. The efficacy of these preparations varies. Table 2 summarizes the studies on intraoperative measures for preventing SSIs.
The literature also highlights the importance of technique in incision-site preparation. In a prospective study, Morrison and colleagues33 randomly assigned 600 primary TJA patients to either (1) use of alcohol and povidone-iodine before draping, with additional preparation with iodine povacrylex (DuraPrep) and isopropyl alcohol before application of the final drape (300-patient intervention group) or (2) only use of alcohol and povidone-iodine before draping (300-patient control group). At the final follow-up, the incidence of SSI was significantly lower in the intervention group than in the control group (1.8% vs 6.5%; P = .015). In another study that assessed perioperative skin preparation methods, Brown and colleagues34 found that airborne bacteria levels in operating rooms were >4 times higher with patients whose legs were prepared by a scrubbed, gowned leg-holder than with patients whose legs were prepared by an unscrubbed, ungowned leg-holder (P = .0001).
Hair Removal. Although removing hair from surgical sites is common practice, the literature advocating it varies. A large comprehensive review35 revealed no increased risk of SSI with removing vs not removing hair (RR, 1.65; 95% CI, 0.85-3.19). On the other hand, some hair removal methods may affect the incidence of infection. For example, use of electric hair clippers is presumed to reduce the risk of SSIs, whereas traditional razors may compromise the epidermal barriers and create a pathway for bacterial colonization.5,36,37 In the aforementioned review,35 SSIs were more than twice as likely to occur with hair removed by shaving than with hair removed by electric clippers (RR, 2.02; 95% CI, 1.21-3.36). Cruse and Foord38 found a higher rate of SSIs with hair removed by shaving than with hair removed by clipping (2.3% vs 1.7%). Most surgeons agree that, if given the choice, they would remove hair with electric clippers rather than razors.
Gloves. Almost all orthopedists double their gloves for TJA cases. Over several studies, the incidence of glove perforation during orthopedic procedures has ranged from 3.6% to 26%,39-41 depending on the operating room personnel and glove layering studied. Orthopedists must know this startling finding, as surgical glove perforation is associated with an increase in the rate of SSIs, from 1.7% to 5.7%.38 Carter and colleagues42 found the highest risk of glove perforation occurs when double-gloved attending surgeons, adult reconstruction fellows, and registered nurses initially assist during primary and revision TJA. In their study, outer and inner glove layers were perforated 2.5% of the time. All outer-layer perforations were noticed, but inner-layer perforations went unnoticed 81% of the time, which poses a potential hazard for both patients and healthcare personnel. In addition, there was a significant increase in the incidence of glove perforations for attending surgeons during revision TJA vs primary TJA (8.9% vs 3.7%; P = .04). This finding may be expected given the complexity of revision procedures, the presence of sharp bony and metal edges, and the longer operative times. Giving more attention to glove perforations during arthroplasties may mitigate the risk of SSI. As soon as a perforation is noticed, the glove should be removed and replaced.
Body Exhaust Suits. Early TJAs had infection rates approaching 10%.43 Bacterial-laden particles shed from surgical staff were postulated to be the cause,44,45 and this idea prompted the development of new technology, such as body exhaust suits, which have demonstrated up to a 20-fold reduction in airborne bacterial contamination and decreased incidence of deep infection, from 1% to 0.1%, as compared with conventional surgical attire.46 However, the efficacy of these suits was recently challenged. Hooper and colleagues47 assessed >88,000 TJA cases in the New Zealand Joint Registry and found a significant increase in early revision THA for deep infection with vs without use of body exhaust suits (0.186% vs 0.064%; P < .0001). The incidence of revision TKAs for deep infections with use of these suits was similar (0.243% vs 0.098%; P < .001). Many of the surgeons surveyed indicated their peripheral vision was limited by the suits, which may contribute to sterile field contamination. By contrast, Miner and colleagues48 were unable to determine an increased risk of SSI with use of body exhaust suits (RR, 0.75; 95% CI, 0.34-1.62), though there was a trend toward more infections without suits. Moreover, these suits are effective in reducing mean air bacterial counts (P = .014), but it is not known if this method correlates with mean wound bacterial counts (r = –.011) and therefore increases the risk of SSI.49
Surgical Drapes. Surgical draping, including cloths, iodine-impregnated materials, and woven or unwoven materials, is the standard of care worldwide. The particular draping technique usually varies by surgeon. Plastic drapes are better barriers than cloth drapes, as found in a study by Blom and colleagues50: Bacterial growth rates were almost 10 times higher with use of wet woven cloth drapes than with plastic surgical drapes. These findings were supported in another, similar study by Blom and colleagues51: Wetting drapes with blood or normal saline enhanced bacterial penetration. In addition, wetting drapes with chlorhexidine or iodine reduced but did not eliminate bacterial penetration. Fairclough and colleagues52 emphasized that iodine-impregnated drapes reduced surgical-site bacterial contamination from 15% to 1.6%. However, a Cochrane review53 found these drapes had no effect on the SSI rate (RR, 1.03; 95% CI, 0.06-1.66; P = .89), though the risk of infection was slightly higher with adhesive draping than with no drape (RR, 1.23; 95% CI, 1.02-1.48; P = .03).
Ventilation Flow. Laminar-airflow systems are widely used to prevent SSIs after TJA. Horizontal-flow and vertical-flow ventilation provides and maintains ultra-clean air in the operating room. Evans54 found the bacterial counts in the air and the wound were lower with laminar airflow than without this airflow. The amount of airborne bacterial colony-forming units and dust large enough to carry bacteria was reduced to 1 or 2 particles more than 2 μm/m3 with use of a typical laminar- airflow system. In comparing 3922 TKA patients in laminar-airflow operating rooms with 4133 patients in conventional rooms, Lidwell and colleagues46 found a significantly lower incidence of SSIs in patients in laminar-airflow operating rooms (0.6% vs 2.3%; P < .001).
Conversely, Miner and colleagues48 did not find a lower risk of SSI with laminar-airflow systems (RR, 1.57; 95% CI, 0.75-3.31). In addition, in their analysis of >88,000 cases from the New Zealand Joint Registry, Hooper and colleagues47 found that the incidence of early infections was higher with laminar-airflow systems than with standard airflow systems for both TKA (0.193% vs 0.100%; P = .019) and THA (0.148% vs 0.061%; P < .001). They postulated that vertically oriented airflow may have transmitted contaminated particles into the surgical sites. Additional evidence may be needed to resolve these conflicting findings and determine whether clean-air practices provide significant clinical benefit in the operating room.
Staff Traffic Volume. When staff enters or exits the operating room or makes extra movements during a procedure, airflow near the wound is disturbed and no longer able to remove sufficient airborne pathogens from the sterile field. The laminar- airflow pattern may be disrupted each time the operating room doors open and close, potentially allowing airborne pathogens to be introduced near the patient. Lynch and colleagues55 found the operating room door opened almost 50 times per hour, and it took about 20 seconds to close each time. As a result, the door may remain open for up to 20 minutes per case, causing substantial airflow disruption and potentially ineffective removal of airborne bacterial particles. Similarly, Young and O’Regan56 found the operating room door opened about 19 times per hour and took 20 seconds to close each time. The theater door was open an estimated 10.7% of each hour of sterile procedure. Presence of more staff also increases airborne bacterial counts. Pryor and Messmer57 evaluated a cohort of 2864 patients to determine the effect of number of personnel in the operating theater on the incidence of SSIs. Infection rates were 6.27% with >17 different people entering the room and 1.52% with <9 different people entering the room. Restricting the number of people in the room may be one of the easiest and most efficient ways to prevent SSI.
Systemic Antibiotic Prophylaxis. Perioperative antibiotic use is vital in minimizing the risk of infection after TJA. The Surgical Care Improvement Project recommended beginning the first antimicrobial dose either within 60 minutes before surgical incision (for cephalosporin) or within 2 hours before incision (for vancomycin) and discontinuing the prophylactic antimicrobial agents within 24 hours after surgery ends.58,59 However, Gorenoi and colleagues60 were unable to recommend a way to select particular antibiotics, as they found no difference in the effectiveness of various antibiotic agents used in TKA. A systematic review by AlBuhairan and colleagues61 revealed that antibiotic prophylaxis (vs no prophylaxis) reduced the absolute risk of a SSI by 8% and the relative risk by 81% (P < 0.0001). These findings are supported by evidence of the efficacy of perioperative antibiotics in reducing the incidence of SSI.62,63 Antibiotic regimens should be based on susceptibility and availability, depending on hospital prevalence of infections. Even more, patients should receive prophylaxis in a timely manner. Finally, bacteriostatic antibiotics (vancomycin) should not be used on their own for preoperative prophylaxis.
Antibiotic Cement. Antibiotic-loaded bone cement (ALBC), which locally releases antimicrobials in high concentration, is often used in revision joint arthroplasty, but use in primary joint arthroplasty remains controversial. In a study of THA patients, Parvizi and colleagues64 found infection rates of 1.2% with 2.3% with and without use of ALBC, respectively. Other studies have had opposing results. Namba and colleagues65 evaluated 22,889 primary TKAs, 2030 (8.9%) of which used ALBC. The incidence of deep infection was significantly higher with ALBC than with regular bone cement (1.4% vs 0.7%; P = .002). In addition, a meta- analysis of >6500 primary TKA patients, by Zhou and colleagues,66 revealed no significant difference in the incidence of deep SSIs with use of ALBC vs regular cement (1.32% vs 1.89%; RR, 0.75; 95% CI, 0.43-1.33; P = .33). More evidence is needed to determine the efficacy of ALBC in primary TJA. International Consensus Meeting on Periprosthetic Joint Infection participants recommended use of ALBC in high-risk patients, including patients who are obese or immunosuppressed or have diabetes or a prior history of infection.67
Postoperative Measures
Antibiotic Prophylaxis. The American Academy of Orthopaedic Surgeons (AAOS) and the American Dental Association (ADA) have suggestions for antibiotic prophylaxis for patients at increased risk for infection. As of 2015, the ADA no longer recommends antibiotic prophylaxis for patients with prosthetic joint implants,68 whereas the AAOS considers all patients with TJA to be at risk.69
Although recommendations exist, the actual risk of infection resulting from dental procedures and the role of antibiotic prophylaxis are not well defined. Berbari and colleagues71 found that antibiotic prophylaxis in high- or low-risk dental procedures did not decrease the risk of subsequent THA infection (OR, 0.9; 95% CI, 0.5-1.6) or TKA infection (OR, 1.2; 95% CI, 0.7-2.2). Moreover, the risk of infection was no higher for patients who had a prosthetic hip or knee and underwent a high- or low-risk dental procedure without antibiotic prophylaxis (OR, 0.8; 95% CI, 0.4-1.6) than for similar patients who did not undergo a dental procedure (OR, 0.6; 95% CI, 0.4-1.1). Some studies highlight the low level of evidence supporting antibiotic prophylaxis during dental procedures.72,73 However, there is no evidence of adverse effects of antibiotic prophylaxis. Given the potential high risk of infection after such procedures, a more robust body of evidence is needed to reach consensus.
Evacuation Drain Management. Prolonged use of surgical evacuation drains may be a risk factor for SSI. Therefore, early drain removal is paramount. Higher infection rates with prolonged drain use have been found in patients with persistent wound drainage, including malnourished, obese, and over-anticoagulated patients. Patients with wounds persistently draining for >1 week should undergo superficial wound irrigation and débridement. Jaberi and colleagues74 assessed 10,325 TJA patients and found that the majority of persistent drainage ceased within 1 week with use of less invasive measures, including oral antibiotics and local wound care. Furthermore, only 28% of patients with persistent drainage underwent surgical débridement. It is unclear if this practice alone is appropriate. Infection should always be suspected and treated aggressively, and cultures should be obtained from synovial fluid before antibiotics are started, unless there is an obvious superficial infection that does not require further work-up.67
Economic Impact
SSIs remain a significant healthcare issue, and the social and financial costs are staggering. Without appropriate measures in place, these complications will place a larger burden on the healthcare system primarily as a result of longer hospital stays, multiple procedures, and increased resource utilization.75 Given the risk of progression to prosthetic joint infection, early preventive interventions must be explored.
Improved patient selection may be an important factor in reducing SSIs. In an analysis of 8494 joint arthroplasties, Malinzak and colleagues80 noted that patients with a BMI of >50 kg/m2 had an increased OR of infection of 21.3 compared to those with BMI <50 kg/m2. Wagner and colleagues81 analyzed 21,361 THAs and found that, for every BMI unit over 25 kg/m2, there was an 8% increased risk of joint infection (P < .001). Although it is unknown if there is an association between reduction in preoperative BMI and reduction in postoperative complication risk, it may still be worthwhile and cost-effective to modify this and similar risk factors before elective procedures.
Market forces are becoming a larger consideration in healthcare and are being driven by provider competition.82 Treatment outcomes, quality of care, and healthcare prices have gained attention as a means of estimating potential costs.83 In 2011, the Centers for Medicare & Medicaid Services (CMS) advanced the Bundled Payments for Care Improvement (BPCI) initiative, which aimed to provide better coordinated care of higher quality and lower cost.84 This led to development of the Comprehensive Care for Joint Replacement (CJR) program, which gives beneficiaries flexibility in choosing services and ensures that providers adhere to required standards. During its 5-year test period beginning in 2016, the CJR program is projected to save CMS $153 million.84 Under this program, the institution where TJA is performed is responsible for all the costs of related care from time of surgery through 90 days after hospital discharge—which is known as an “episode of care.” If the cost incurred during an episode exceeds an established target cost (as determined by CMS), the hospital must repay Medicare the difference. Conversely, if the cost of an episode is less than the established target cost, the hospital is rewarded with the difference. Bundling payments for a single episode of care in this manner is thought to incentivize providers and hospitals to give patients more comprehensive and coordinated care. Given the substantial economic burden associated with joint arthroplasty infections, it is imperative for orthopedists to establish practical and cost-effective strategies that can prevent these disastrous complications.
Conclusion
SSIs are a devastating burden to patients, surgeons, and other healthcare providers. In recent years, new discoveries and innovations have helped mitigate the incidence of these complications of THA and TKA. However, the incidence of SSIs may rise with the increasing use of TJAs and with the development of new drug-resistant pathogens. In addition, the increasing number of TJAs performed on overweight and high-risk patients means the costs of postoperative infections will be substantial. With new reimbursement models in place, hospitals and providers are being held more accountable for the care they deliver during and after TJA. Consequently, more emphasis should be placed on techniques that are proved to minimize the incidence of SSIs.
Take-Home Points
- SSIs after TJA pose a substantial burden on patients, surgeons, and the healthcare system.
- While different forms of preoperative skin preparation have shown varying outcomes after TJA, the importance of preoperative patient optimization (nutritional status, immune function, etc) cannot be overstated.
- Intraoperative infection prevention measures include cutaneous preparation, gloving, body exhaust suits, surgical drapes, OR staff traffic and ventilation flow, and antibiotic-loaded cement.
- Antibiotic prophylaxis for dental procedures in TJA patients continues to remain a controversial issue with conflicting recommendations.
- SSIs have considerable financial costs and require increased resource utilization. Given the significant economic burden associated with TJA infections, it is imperative for orthopedists to establish practical and cost-effective strategies to prevent these devastating complications.
Surgical-site infection (SSI), a potentially devastating complication of lower extremity total joint arthroplasty (TJA), is estimated to occur in 1% to 2.5% of cases annually.1 Infection after TJA places a significant burden on patients, surgeons, and the healthcare system. Revision procedures that address infection after total hip arthroplasty (THA) are associated with more hospitalizations, more operations, longer hospital stay, and higher outpatient costs in comparison with primary THAs and revision surgeries for aseptic loosening.2 If left untreated, a SSI can go deeper into the joint and develop into a periprosthetic infection, which can be disastrous and costly. A periprosthetic joint infection study that used 2001 to 2009 Nationwide Inpatient Sample (NIS) data found that the cost of revision procedures increased to $560 million from $320 million, and was projected to reach $1.62 billion by 2020.3 Furthermore, society incurs indirect costs as a result of patient disability and loss of wages and productivity.2 Therefore, the issue of infection after TJA is even more crucial in our cost-conscious healthcare environment.
Patient optimization, advances in surgical technique, sterile protocol, and operative procedures have been effective in reducing bacterial counts at incision sites and minimizing SSIs. As a result, infection rates have leveled off after rising for a decade.4 Although infection prevention modalities have their differences, routine use is fundamental and recommended by the Hospital Infection Control Practices Advisory Committee.5 Furthermore, both the US Centers for Disease Control and Prevention (CDC) and its Healthcare Infection Control Practices Advisory Committee6,7 recently updated their SSI prevention guidelines by incorporating evidence-based methodology, an element missing from earlier recommendations.
The etiologies of postoperative SSIs have been discussed ad nauseam, but there are few reports summarizing the literature on infection prevention modalities. In this review, we identify and examine SSI prevention strategies as they relate to lower extremity TJA. Specifically, we discuss the literature on the preoperative, intraoperative, and postoperative actions that can be taken to reduce the incidence of SSIs after TJA. We also highlight the economic implications of SSIs that occur after TJA.
Methods
For this review, we performed a literature search with PubMed, EBSCOhost, and Scopus. We looked for reports published between the inception of each database and July 2016. Combinations of various search terms were used: surgical site, infection, total joint arthroplasty, knee, hip, preoperative, intraoperative, perioperative, postoperative, preparation, nutrition, ventilation, antibiotic, body exhaust suit, gloves, drain, costs, economic, and payment.
Our search identified 195 abstracts. Drs. Mistry and Chughtai reviewed these to determine which articles were relevant. For any uncertainties, consensus was reached with the help of Dr. Delanois. Of the 195 articles, 103 were potentially relevant, and 54 of the 103 were excluded for being not relevant to preventing SSIs after TJA or for being written in a language other than English. The references in the remaining articles were assessed, and those with potentially relevant titles were selected for abstract review. This step provided another 35 articles. After all exclusions, 48 articles remained. We discuss these in the context of preoperative, intraoperative, and postoperative measures and economic impact.
Results
Preoperative Measures
Skin Preparation. Preoperative skin preparation methods include standard washing and rinsing, antiseptic soaps, and iodine-based or chlorhexidine gluconate-based antiseptic showers or skin cloths. Iodine-based antiseptics are effective against a wide range of Gram-positive and Gram-negative bacteria, fungi, and viruses. These agents penetrate the cell wall, oxidize the microbial contents, and replace those contents with free iodine molecules.8 Iodophors are free iodine molecules associated with a polymer (eg, polyvinylpyrrolidone); the iodophor povidone-iodine is bactericidal.9 Chlorhexidine gluconate-based solutions are effective against many types of yeast, Gram-positive and Gram-negative bacteria, and a wide variety of viruses.9 Both solutions are useful. Patients with an allergy to iodine can use chlorhexidine. Table 1 summarizes the studies on preoperative measures for preventing SSIs.
There is no shortage of evidence of the efficacy of these antiseptics in minimizing the incidence of SSIs. Hayek and colleagues10 prospectively analyzed use of different preoperative skin preparation methods in 2015 patients. Six weeks after surgery, the infection rate was significantly lower with use of chlorhexidine than with use of an unmedicated bar of soap or placebo cloth (9% vs 11.7% and 12.8%, respectively; P < .05). In a study of 100 patients, Murray and colleagues11 found the overall bacterial culture rate was significantly lower for those who used a 2% chlorhexidine gluconate cloth before shoulder surgery than for those who took a standard shower with soap (66% vs 94%; P = .0008). Darouiche and colleagues12 found the overall SSI rate was significantly lower for 409 surgical patients prepared with chlorhexidine-alcohol than for 440 prepared with povidone-iodine (9.5% vs 16.1%; P = .004; relative risk [RR], 0.59; 95% confidence interval [CI], 0.41-0.85).
Chlorhexidine gluconate-impregnated cloths have also had promising results, which may be attributed to general ease of use and potentially improved patient adherence. Zywiel and colleagues13 reported no SSIs in 136 patients who used these cloths at home before total knee arthroplasty (TKA) and 21 SSIs (3.0%) in 711 patients who did not use the cloths. In a study of 2545 THA patients, Kapadia and colleagues14 noted a significantly lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths than with only in-hospital perioperative skin preparation (0.5% vs 1.7%; P = .04). In 2293 TKAs, Johnson and colleagues15 similarly found a lower incidence of SSIs with at-home preoperative use of chlorhexidine cloths (0.6% vs 2.2%; P = .02). In another prospective, randomized trial, Kapadia and colleagues16 compared 275 patients who used chlorhexidine cloths the night before and the morning of lower extremity TJA surgery with 279 patients who underwent standard-of-care preparation (preadmission bathing with antibacterial soap and water). The chlorhexidine cohort had a lower overall incidence of infection (0.4% vs 2.9%; P = .049), and the standard-of-care cohort had a stronger association with infection (odds ratio [OR], 8.15; 95% CI, 1.01-65.6).
Patient Optimization. Poor nutritional status may compromise immune function, potentially resulting in delayed healing, increased risk of infection, and, ultimately, negative postoperative outcomes. Malnutrition can be diagnosed on the basis of a prealbumin level of <15 mg/dL (normal, 15-30 mg/dL), a serum albumin level of <3.4 g/dL (normal, 3.4-5.4 g/dL), or a total lymphocyte count under 1200 cells/μL (normal, 3900-10,000 cells/μL).17-19 Greene and colleagues18 found that patients with preoperative malnutrition had up to a 7-fold higher rate of infection after TJA. In a study of 135 THAs and TKAs, Alfargieny and colleagues20 found preoperative serum albumin was the only nutritional biomarker predictive of SSI (P = .011). Furthermore, patients who take immunomodulating medications (eg, for inflammatory arthropathies) should temporarily discontinue them before surgery in order to lower their risk of infection.21
Smoking is well established as a major risk factor for poor outcomes after surgery. It is postulated that the vasoconstrictive effects of nicotine and the hypoxic effects of carbon monoxide contribute to poor wound healing.22 In a meta-analysis of 4 studies, Sørensen23 found smokers were at increased risk for wound complications (OR, 2.27; 95% CI, 1.82-2.84), delayed wound healing and dehiscence (OR, 2.07; 95% CI, 1.53-2.81), and infection (OR, 1.79; 95% CI, 1.57-2.04). Moreover, smoking cessation decreased the incidence of SSIs (OR, 0.43; 95% CI, 0.21-0.85). A meta- analysis by Wong and colleagues24 revealed an inflection point for improved outcomes in patients who abstained from smoking for at least 4 weeks before surgery. Risk of infection was lower for these patients than for current smokers (OR, 0.69; 95% CI, 0.56-0.84).
Other comorbidities contribute to SSIs as well. In their analysis of American College of Surgeons National Surgical Quality Improvement Program registry data on 25,235 patients who underwent primary and revision lower extremity TJA, Pugely and colleagues25 found that, in the primary TJA cohort, body mass index (BMI) of >40 kg/m2 (OR, 1.9; 95% CI, 1.3-2.9), electrolyte disturbance (OR, 2.4; 95% CI, 1.0-6.0), and hypertension diagnosis (OR, 1.5; 95% CI, 1.1-2.0) increased the risk of SSI within 30 days. Furthermore, diabetes mellitus delays collagen synthesis, impairs lymphocyte function, and impairs wound healing, which may lead to poor recovery and higher risk of infection.26 In a study of 167 TKAs performed in 115 patients with type 2 diabetes mellitus, Han and Kang26 found that wound complications were 6 times more likely in those with hemoglobin A1c (HbA1c) levels higher than 8% than in those with lower HbA1c levels (OR, 6.07; 95% CI, 1.12-33.0). In a similar study of 462 patients with diabetes, Hwang and colleagues27 found a higher likelihood of superficial SSIs in patients with HbA1c levels >8% (OR, 6.1; 95% CI, 1.6-23.4; P = .008). This association was also found in patients with a fasting blood glucose level of >200 mg/dL (OR, 9.2; 95% CI, 2.2-38.2; P = .038).
Methicillin-resistant Staphylococcus aureus (MRSA) is thought to account for 10% to 25% of all periprosthetic infections in the United States.28 Nasal colonization by this pathogen increases the risk for SSIs; however, decolonization protocols have proved useful in decreasing the rates of colonization. Moroski and colleagues29 assessed the efficacy of a preoperative 5-day course of intranasal mupirocin in 289 primary or revision TJA patients. Before surgery, 12 patients had positive MRSA cultures, and 44 had positive methicillin-sensitive S aureus (MSSA) cultures. On day of surgery, a significant reduction in MRSA (P = .0073) and MSSA (P = .0341) colonization was noted. Rao and colleagues30 found that the infection rate decreased from 2.7% to 1.2% in 2284 TJA patients treated with a decolonization protocol (P = .009).
Intraoperative Measures
Cutaneous Preparation. The solutions used in perioperative skin preparation are similar to those used preoperatively: povidone-iodine, alcohol, and chlorhexidine. The efficacy of these preparations varies. Table 2 summarizes the studies on intraoperative measures for preventing SSIs.
The literature also highlights the importance of technique in incision-site preparation. In a prospective study, Morrison and colleagues33 randomly assigned 600 primary TJA patients to either (1) use of alcohol and povidone-iodine before draping, with additional preparation with iodine povacrylex (DuraPrep) and isopropyl alcohol before application of the final drape (300-patient intervention group) or (2) only use of alcohol and povidone-iodine before draping (300-patient control group). At the final follow-up, the incidence of SSI was significantly lower in the intervention group than in the control group (1.8% vs 6.5%; P = .015). In another study that assessed perioperative skin preparation methods, Brown and colleagues34 found that airborne bacteria levels in operating rooms were >4 times higher with patients whose legs were prepared by a scrubbed, gowned leg-holder than with patients whose legs were prepared by an unscrubbed, ungowned leg-holder (P = .0001).
Hair Removal. Although removing hair from surgical sites is common practice, the literature advocating it varies. A large comprehensive review35 revealed no increased risk of SSI with removing vs not removing hair (RR, 1.65; 95% CI, 0.85-3.19). On the other hand, some hair removal methods may affect the incidence of infection. For example, use of electric hair clippers is presumed to reduce the risk of SSIs, whereas traditional razors may compromise the epidermal barriers and create a pathway for bacterial colonization.5,36,37 In the aforementioned review,35 SSIs were more than twice as likely to occur with hair removed by shaving than with hair removed by electric clippers (RR, 2.02; 95% CI, 1.21-3.36). Cruse and Foord38 found a higher rate of SSIs with hair removed by shaving than with hair removed by clipping (2.3% vs 1.7%). Most surgeons agree that, if given the choice, they would remove hair with electric clippers rather than razors.
Gloves. Almost all orthopedists double their gloves for TJA cases. Over several studies, the incidence of glove perforation during orthopedic procedures has ranged from 3.6% to 26%,39-41 depending on the operating room personnel and glove layering studied. Orthopedists must know this startling finding, as surgical glove perforation is associated with an increase in the rate of SSIs, from 1.7% to 5.7%.38 Carter and colleagues42 found the highest risk of glove perforation occurs when double-gloved attending surgeons, adult reconstruction fellows, and registered nurses initially assist during primary and revision TJA. In their study, outer and inner glove layers were perforated 2.5% of the time. All outer-layer perforations were noticed, but inner-layer perforations went unnoticed 81% of the time, which poses a potential hazard for both patients and healthcare personnel. In addition, there was a significant increase in the incidence of glove perforations for attending surgeons during revision TJA vs primary TJA (8.9% vs 3.7%; P = .04). This finding may be expected given the complexity of revision procedures, the presence of sharp bony and metal edges, and the longer operative times. Giving more attention to glove perforations during arthroplasties may mitigate the risk of SSI. As soon as a perforation is noticed, the glove should be removed and replaced.
Body Exhaust Suits. Early TJAs had infection rates approaching 10%.43 Bacterial-laden particles shed from surgical staff were postulated to be the cause,44,45 and this idea prompted the development of new technology, such as body exhaust suits, which have demonstrated up to a 20-fold reduction in airborne bacterial contamination and decreased incidence of deep infection, from 1% to 0.1%, as compared with conventional surgical attire.46 However, the efficacy of these suits was recently challenged. Hooper and colleagues47 assessed >88,000 TJA cases in the New Zealand Joint Registry and found a significant increase in early revision THA for deep infection with vs without use of body exhaust suits (0.186% vs 0.064%; P < .0001). The incidence of revision TKAs for deep infections with use of these suits was similar (0.243% vs 0.098%; P < .001). Many of the surgeons surveyed indicated their peripheral vision was limited by the suits, which may contribute to sterile field contamination. By contrast, Miner and colleagues48 were unable to determine an increased risk of SSI with use of body exhaust suits (RR, 0.75; 95% CI, 0.34-1.62), though there was a trend toward more infections without suits. Moreover, these suits are effective in reducing mean air bacterial counts (P = .014), but it is not known if this method correlates with mean wound bacterial counts (r = –.011) and therefore increases the risk of SSI.49
Surgical Drapes. Surgical draping, including cloths, iodine-impregnated materials, and woven or unwoven materials, is the standard of care worldwide. The particular draping technique usually varies by surgeon. Plastic drapes are better barriers than cloth drapes, as found in a study by Blom and colleagues50: Bacterial growth rates were almost 10 times higher with use of wet woven cloth drapes than with plastic surgical drapes. These findings were supported in another, similar study by Blom and colleagues51: Wetting drapes with blood or normal saline enhanced bacterial penetration. In addition, wetting drapes with chlorhexidine or iodine reduced but did not eliminate bacterial penetration. Fairclough and colleagues52 emphasized that iodine-impregnated drapes reduced surgical-site bacterial contamination from 15% to 1.6%. However, a Cochrane review53 found these drapes had no effect on the SSI rate (RR, 1.03; 95% CI, 0.06-1.66; P = .89), though the risk of infection was slightly higher with adhesive draping than with no drape (RR, 1.23; 95% CI, 1.02-1.48; P = .03).
Ventilation Flow. Laminar-airflow systems are widely used to prevent SSIs after TJA. Horizontal-flow and vertical-flow ventilation provides and maintains ultra-clean air in the operating room. Evans54 found the bacterial counts in the air and the wound were lower with laminar airflow than without this airflow. The amount of airborne bacterial colony-forming units and dust large enough to carry bacteria was reduced to 1 or 2 particles more than 2 μm/m3 with use of a typical laminar- airflow system. In comparing 3922 TKA patients in laminar-airflow operating rooms with 4133 patients in conventional rooms, Lidwell and colleagues46 found a significantly lower incidence of SSIs in patients in laminar-airflow operating rooms (0.6% vs 2.3%; P < .001).
Conversely, Miner and colleagues48 did not find a lower risk of SSI with laminar-airflow systems (RR, 1.57; 95% CI, 0.75-3.31). In addition, in their analysis of >88,000 cases from the New Zealand Joint Registry, Hooper and colleagues47 found that the incidence of early infections was higher with laminar-airflow systems than with standard airflow systems for both TKA (0.193% vs 0.100%; P = .019) and THA (0.148% vs 0.061%; P < .001). They postulated that vertically oriented airflow may have transmitted contaminated particles into the surgical sites. Additional evidence may be needed to resolve these conflicting findings and determine whether clean-air practices provide significant clinical benefit in the operating room.
Staff Traffic Volume. When staff enters or exits the operating room or makes extra movements during a procedure, airflow near the wound is disturbed and no longer able to remove sufficient airborne pathogens from the sterile field. The laminar- airflow pattern may be disrupted each time the operating room doors open and close, potentially allowing airborne pathogens to be introduced near the patient. Lynch and colleagues55 found the operating room door opened almost 50 times per hour, and it took about 20 seconds to close each time. As a result, the door may remain open for up to 20 minutes per case, causing substantial airflow disruption and potentially ineffective removal of airborne bacterial particles. Similarly, Young and O’Regan56 found the operating room door opened about 19 times per hour and took 20 seconds to close each time. The theater door was open an estimated 10.7% of each hour of sterile procedure. Presence of more staff also increases airborne bacterial counts. Pryor and Messmer57 evaluated a cohort of 2864 patients to determine the effect of number of personnel in the operating theater on the incidence of SSIs. Infection rates were 6.27% with >17 different people entering the room and 1.52% with <9 different people entering the room. Restricting the number of people in the room may be one of the easiest and most efficient ways to prevent SSI.
Systemic Antibiotic Prophylaxis. Perioperative antibiotic use is vital in minimizing the risk of infection after TJA. The Surgical Care Improvement Project recommended beginning the first antimicrobial dose either within 60 minutes before surgical incision (for cephalosporin) or within 2 hours before incision (for vancomycin) and discontinuing the prophylactic antimicrobial agents within 24 hours after surgery ends.58,59 However, Gorenoi and colleagues60 were unable to recommend a way to select particular antibiotics, as they found no difference in the effectiveness of various antibiotic agents used in TKA. A systematic review by AlBuhairan and colleagues61 revealed that antibiotic prophylaxis (vs no prophylaxis) reduced the absolute risk of a SSI by 8% and the relative risk by 81% (P < 0.0001). These findings are supported by evidence of the efficacy of perioperative antibiotics in reducing the incidence of SSI.62,63 Antibiotic regimens should be based on susceptibility and availability, depending on hospital prevalence of infections. Even more, patients should receive prophylaxis in a timely manner. Finally, bacteriostatic antibiotics (vancomycin) should not be used on their own for preoperative prophylaxis.
Antibiotic Cement. Antibiotic-loaded bone cement (ALBC), which locally releases antimicrobials in high concentration, is often used in revision joint arthroplasty, but use in primary joint arthroplasty remains controversial. In a study of THA patients, Parvizi and colleagues64 found infection rates of 1.2% with 2.3% with and without use of ALBC, respectively. Other studies have had opposing results. Namba and colleagues65 evaluated 22,889 primary TKAs, 2030 (8.9%) of which used ALBC. The incidence of deep infection was significantly higher with ALBC than with regular bone cement (1.4% vs 0.7%; P = .002). In addition, a meta- analysis of >6500 primary TKA patients, by Zhou and colleagues,66 revealed no significant difference in the incidence of deep SSIs with use of ALBC vs regular cement (1.32% vs 1.89%; RR, 0.75; 95% CI, 0.43-1.33; P = .33). More evidence is needed to determine the efficacy of ALBC in primary TJA. International Consensus Meeting on Periprosthetic Joint Infection participants recommended use of ALBC in high-risk patients, including patients who are obese or immunosuppressed or have diabetes or a prior history of infection.67
Postoperative Measures
Antibiotic Prophylaxis. The American Academy of Orthopaedic Surgeons (AAOS) and the American Dental Association (ADA) have suggestions for antibiotic prophylaxis for patients at increased risk for infection. As of 2015, the ADA no longer recommends antibiotic prophylaxis for patients with prosthetic joint implants,68 whereas the AAOS considers all patients with TJA to be at risk.69
Although recommendations exist, the actual risk of infection resulting from dental procedures and the role of antibiotic prophylaxis are not well defined. Berbari and colleagues71 found that antibiotic prophylaxis in high- or low-risk dental procedures did not decrease the risk of subsequent THA infection (OR, 0.9; 95% CI, 0.5-1.6) or TKA infection (OR, 1.2; 95% CI, 0.7-2.2). Moreover, the risk of infection was no higher for patients who had a prosthetic hip or knee and underwent a high- or low-risk dental procedure without antibiotic prophylaxis (OR, 0.8; 95% CI, 0.4-1.6) than for similar patients who did not undergo a dental procedure (OR, 0.6; 95% CI, 0.4-1.1). Some studies highlight the low level of evidence supporting antibiotic prophylaxis during dental procedures.72,73 However, there is no evidence of adverse effects of antibiotic prophylaxis. Given the potential high risk of infection after such procedures, a more robust body of evidence is needed to reach consensus.
Evacuation Drain Management. Prolonged use of surgical evacuation drains may be a risk factor for SSI. Therefore, early drain removal is paramount. Higher infection rates with prolonged drain use have been found in patients with persistent wound drainage, including malnourished, obese, and over-anticoagulated patients. Patients with wounds persistently draining for >1 week should undergo superficial wound irrigation and débridement. Jaberi and colleagues74 assessed 10,325 TJA patients and found that the majority of persistent drainage ceased within 1 week with use of less invasive measures, including oral antibiotics and local wound care. Furthermore, only 28% of patients with persistent drainage underwent surgical débridement. It is unclear if this practice alone is appropriate. Infection should always be suspected and treated aggressively, and cultures should be obtained from synovial fluid before antibiotics are started, unless there is an obvious superficial infection that does not require further work-up.67
Economic Impact
SSIs remain a significant healthcare issue, and the social and financial costs are staggering. Without appropriate measures in place, these complications will place a larger burden on the healthcare system primarily as a result of longer hospital stays, multiple procedures, and increased resource utilization.75 Given the risk of progression to prosthetic joint infection, early preventive interventions must be explored.
Improved patient selection may be an important factor in reducing SSIs. In an analysis of 8494 joint arthroplasties, Malinzak and colleagues80 noted that patients with a BMI of >50 kg/m2 had an increased OR of infection of 21.3 compared to those with BMI <50 kg/m2. Wagner and colleagues81 analyzed 21,361 THAs and found that, for every BMI unit over 25 kg/m2, there was an 8% increased risk of joint infection (P < .001). Although it is unknown if there is an association between reduction in preoperative BMI and reduction in postoperative complication risk, it may still be worthwhile and cost-effective to modify this and similar risk factors before elective procedures.
Market forces are becoming a larger consideration in healthcare and are being driven by provider competition.82 Treatment outcomes, quality of care, and healthcare prices have gained attention as a means of estimating potential costs.83 In 2011, the Centers for Medicare & Medicaid Services (CMS) advanced the Bundled Payments for Care Improvement (BPCI) initiative, which aimed to provide better coordinated care of higher quality and lower cost.84 This led to development of the Comprehensive Care for Joint Replacement (CJR) program, which gives beneficiaries flexibility in choosing services and ensures that providers adhere to required standards. During its 5-year test period beginning in 2016, the CJR program is projected to save CMS $153 million.84 Under this program, the institution where TJA is performed is responsible for all the costs of related care from time of surgery through 90 days after hospital discharge—which is known as an “episode of care.” If the cost incurred during an episode exceeds an established target cost (as determined by CMS), the hospital must repay Medicare the difference. Conversely, if the cost of an episode is less than the established target cost, the hospital is rewarded with the difference. Bundling payments for a single episode of care in this manner is thought to incentivize providers and hospitals to give patients more comprehensive and coordinated care. Given the substantial economic burden associated with joint arthroplasty infections, it is imperative for orthopedists to establish practical and cost-effective strategies that can prevent these disastrous complications.
Conclusion
SSIs are a devastating burden to patients, surgeons, and other healthcare providers. In recent years, new discoveries and innovations have helped mitigate the incidence of these complications of THA and TKA. However, the incidence of SSIs may rise with the increasing use of TJAs and with the development of new drug-resistant pathogens. In addition, the increasing number of TJAs performed on overweight and high-risk patients means the costs of postoperative infections will be substantial. With new reimbursement models in place, hospitals and providers are being held more accountable for the care they deliver during and after TJA. Consequently, more emphasis should be placed on techniques that are proved to minimize the incidence of SSIs.
1. National Nosocomial Infections Surveillance System. National Nosocomial Infections Surveillance (NNIS) System report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32(8):470-485.
2. Bozic KJ, Ries MD. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J Bone Joint Surg Am. 2005;87(8):1746-1751.
3. Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 suppl):61-65.e61.
4. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty. 2008;23(7):984-991.
5. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4):250-278.
6. Berrios-Torres SI. Evidence-based update to the U.S. Centers for Disease Control and Prevention and Healthcare Infection Control Practices Advisory Committee guideline for the prevention of surgical site infection: developmental process. Surg Infect (Larchmt). 2016;17(2):256-261.
7 Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27(2):97-132.
8. Marchetti MG, Kampf G, Finzi G, Salvatorelli G. Evaluation of the bactericidal effect of five products for surgical hand disinfection according to prEN 12054 and prEN 12791. J Hosp Infect. 2003;54(1):63-67.
9. Reichman DE, Greenberg JA. Reducing surgical site infections: a review. Rev Obstet Gynecol. 2009;2(4):212-221.
10. Hayek LJ, Emerson JM, Gardner AM. A placebo-controlled trial of the effect of two preoperative baths or showers with chlorhexidine detergent on postoperative wound infection rates. J Hosp Infect. 1987;10(2):165-172.
11. Murray MR, Saltzman MD, Gryzlo SM, Terry MA, Woodward CC, Nuber GW. Efficacy of preoperative home use of 2% chlorhexidine gluconate cloth before shoulder surgery. J Shoulder Elbow Surg. 2011;20(6):928-933.
12. Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18-26.
13. Zywiel MG, Daley JA, Delanois RE, Naziri Q, Johnson AJ, Mont MA. Advance pre-operative chlorhexidine reduces the incidence of surgical site infections in knee arthroplasty. Int Orthop. 2011;35(7):1001-1006.
14. Kapadia BH, Johnson AJ, Daley JA, Issa K, Mont MA. Pre-admission cutaneous chlorhexidine preparation reduces surgical site infections in total hip arthroplasty. J Arthroplasty. 2013;28(3):490-493.
15. Johnson AJ, Kapadia BH, Daley JA, Molina CB, Mont MA. Chlorhexidine reduces infections in knee arthroplasty. J Knee Surg. 2013;26(3):213-218.
16. Kapadia BH, Elmallah RK, Mont MA. A randomized, clinical trial of preadmission chlorhexidine skin preparation for lower extremity total joint arthroplasty. J Arthroplasty. 2016;31(12):2856-2861.
17. Mainous MR, Deitch EA. Nutrition and infection. Surg Clin North Am. 1994;74(3):659-676.
18. Greene KA, Wilde AH, Stulberg BN. Preoperative nutritional status of total joint patients. Relationship to postoperative wound complications. J Arthroplasty. 1991;6(4):321-325.
19. Del Savio GC, Zelicof SB, Wexler LM, et al. Preoperative nutritional status and outcome of elective total hip replacement. Clin Orthop Relat Res. 1996;(326):153-161.
20. Alfargieny R, Bodalal Z, Bendardaf R, El-Fadli M, Langhi S. Nutritional status as a predictive marker for surgical site infection in total joint arthroplasty. Avicenna J Med. 2015;5(4):117-122.
21. Bridges SL Jr, Lopez-Mendez A, Han KH, Tracy IC, Alarcon GS. Should methotrexate be discontinued before elective orthopedic surgery in patients with rheumatoid arthritis? J Rheumatol. 1991;18(7):984-988.
22. Silverstein P. Smoking and wound healing. Am J Med. 1992;93(1A):22S-24S.
23. Sørensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012;147(4):373-383.
24. Wong J, Lam DP, Abrishami A, Chan MT, Chung F. Short-term preoperative smoking cessation and postoperative complications: a systematic review and meta-analysis. Can J Anaesth. 2012;59(3):268-279.
25. Pugely AJ, Martin CT, Gao Y, Schweizer ML, Callaghan JJ. The incidence of and risk factors for 30-day surgical site infections following primary and revision total joint arthroplasty. J Arthroplasty. 2015;30(9 suppl):47-50.
26. Han HS, Kang SB. Relations between long-term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin Orthop Surg. 2013;5(2):118-123.
27. Hwang JS, Kim SJ, Bamne AB, Na YG, Kim TK. Do glycemic markers predict occurrence of complications after total knee arthroplasty in patients with diabetes? Clin Orthop Relat Res. 2015;473(5):1726-1731.
28. Whiteside LA, Peppers M, Nayfeh TA, Roy ME. Methicillin-resistant Staphylococcus aureus in TKA treated with revision and direct intra-articular antibiotic infusion. Clin Orthop Relat Res. 2011;469(1):26-33.
29. Moroski NM, Woolwine S, Schwarzkopf R. Is preoperative staphylococcal decolonization efficient in total joint arthroplasty. J Arthroplasty. 2015;30(3):444-446.
30. Rao N, Cannella BA, Crossett LS, Yates AJ Jr, McGough RL 3rd, Hamilton CW. Preoperative screening/decolonization for Staphylococcus aureus to prevent orthopedic surgical site infection: prospective cohort study with 2-year follow-up. J Arthroplasty. 2011;26(8):1501-1507.
31. Saltzman MD, Nuber GW, Gryzlo SM, Marecek GS, Koh JL. Efficacy of surgical preparation solutions in shoulder surgery. J Bone Joint Surg Am. 2009;91(8):1949-1953.
32. Carroll K, Dowsey M, Choong P, Peel T. Risk factors for superficial wound complications in hip and knee arthroplasty. Clin Microbiol Infect. 2014;20(2):130-135.
33. Morrison TN, Chen AF, Taneja M, Kucukdurmaz F, Rothman RH, Parvizi J. Single vs repeat surgical skin preparations for reducing surgical site infection after total joint arthroplasty: a prospective, randomized, double-blinded study. J Arthroplasty. 2016;31(6):1289-1294.
34. Brown AR, Taylor GJ, Gregg PJ. Air contamination during skin preparation and draping in joint replacement surgery. J Bone Joint Surg Br. 1996;78(1):92-94.
35. Tanner J, Woodings D, Moncaster K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2006;(3):CD004122.
36. Mishriki SF, Law DJ, Jeffery PJ. Factors affecting the incidence of postoperative wound infection. J Hosp Infect. 1990;16(3):223-230.
37. Harrop JS, Styliaras JC, Ooi YC, Radcliff KE, Vaccaro AR, Wu C. Contributing factors to surgical site infections. J Am Acad Orthop Surg. 2012;20(2):94-101.
38. Cruse PJ, Foord R. A five-year prospective study of 23,649 surgical wounds. Arch Surg. 1973;107(2):206-210.
39. Laine T, Aarnio P. Glove perforation in orthopaedic and trauma surgery. A comparison between single, double indicator gloving and double gloving with two regular gloves. J Bone Joint Surg Br. 2004;86(6):898-900.
40. Ersozlu S, Sahin O, Ozgur AF, Akkaya T, Tuncay C. Glove punctures in major and minor orthopaedic surgery with double gloving. Acta Orthop Belg. 2007;73(6):760-764.
41. Chan KY, Singh VA, Oun BH, To BH. The rate of glove perforations in orthopaedic procedures: single versus double gloving. A prospective study. Med J Malaysia. 2006;61(suppl B):3-7.
42. Carter AH, Casper DS, Parvizi J, Austin MS. A prospective analysis of glove perforation in primary and revision total hip and total knee arthroplasty. J Arthroplasty. 2012;27(7):1271-1275.
43. Charnley J. A clean-air operating enclosure. Br J Surg. 1964;51:202-205.
44. Whyte W, Hodgson R, Tinkler J. The importance of airborne bacterial contamination of wounds. J Hosp Infect. 1982;3(2):123-135.
45. Owers KL, James E, Bannister GC. Source of bacterial shedding in laminar flow theatres. J Hosp Infect. 2004;58(3):230-232.
46. Lidwell OM, Lowbury EJ, Whyte W, Blowers R, Stanley SJ, Lowe D. Effect of ultraclean air in operating rooms on deep sepsis in the joint after total hip or knee replacement: a randomised study. Br Med J (Clin Res Ed). 1982;285(6334):10-14.
47. Hooper GJ, Rothwell AG, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement? The ten-year results of the New Zealand Joint Registry. J Bone Joint Surg Br. 2011;93(1):85-90.
48. Miner AL, Losina E, Katz JN, Fossel AH, Platt R. Deep infection after total knee replacement: impact of laminar airflow systems and body exhaust suits in the modern operating room. Infect Control Hosp Epidemiol. 2007;28(2):222-226.
49. Der Tavitian J, Ong SM, Taub NA, Taylor GJ. Body-exhaust suit versus occlusive clothing. A randomised, prospective trial using air and wound bacterial counts. J Bone Joint Surg Br. 2003;85(4):490-494.
50. Blom A, Estela C, Bowker K, MacGowan A, Hardy JR. The passage of bacteria through surgical drapes. Ann R Coll Surg Engl. 2000;82(6):405-407.
51. Blom AW, Gozzard C, Heal J, Bowker K, Estela CM. Bacterial strike-through of re-usable surgical drapes: the effect of different wetting agents. J Hosp Infect. 2002;52(1):52-55.
52. Fairclough JA, Johnson D, Mackie I. The prevention of wound contamination by skin organisms by the pre-operative application of an iodophor impregnated plastic adhesive drape. J Int Med Res. 1986;14(2):105-109.
53. Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev. 2007;(4):CD006353.
54. Evans RP. Current concepts for clean air and total joint arthroplasty: laminar airflow and ultraviolet radiation: a systematic review. Clin Orthop Relat Res. 2011;469(4):945-953.
55. Lynch RJ, Englesbe MJ, Sturm L, et al. Measurement of foot traffic in the operating room: implications for infection control. Am J Med Qual. 2009;24(1):45-52.
56. Young RS, O’Regan DJ. Cardiac surgical theatre traffic: time for traffic calming measures? Interact Cardiovasc Thorac Surg. 2010;10(4):526-529.
57. Pryor F, Messmer PR. The effect of traffic patterns in the OR on surgical site infections. AORN J. 1998;68(4):649-660.
58. Bratzler DW, Houck PM; Surgical Infection Prevention Guidelines Writers Workgroup, American Academy of Orthopaedic Surgeons, American Association of Critical Care Nurses, et al. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis. 2004;38(12):1706-1715.
59. Rosenberger LH, Politano AD, Sawyer RG. The Surgical Care Improvement Project and prevention of post-operative infection, including surgical site infection. Surg Infect (Larchmt). 2011;12(3):163-168.
60. Gorenoi V, Schonermark MP, Hagen A. Prevention of infection after knee arthroplasty. GMS Health Technol Assess. 2010;6:Doc10.
61. AlBuhairan B, Hind D, Hutchinson A. Antibiotic prophylaxis for wound infections in total joint arthroplasty: a systematic review. J Bone Joint Surg Br. 2008;90(7):915-919.
62. Bratzler DW, Houck PM; Surgical Infection Prevention Guideline Writers Workgroup. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Am J Surg. 2005;189(4):395-404.
63. Quenon JL, Eveillard M, Vivien A, et al. Evaluation of current practices in surgical antimicrobial prophylaxis in primary total hip prosthesis—a multicentre survey in private and public French hospitals. J Hosp Infect. 2004;56(3):202-207.
64. Parvizi J, Saleh KJ, Ragland PS, Pour AE, Mont MA. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008;79(3):335-341.
65. Namba RS, Chen Y, Paxton EW, Slipchenko T, Fithian DC. Outcomes of routine use of antibiotic-loaded cement in primary total knee arthroplasty. J Arthroplasty. 2009;24(6 suppl):44-47.
66. Zhou Y, Li L, Zhou Q, et al. Lack of efficacy of prophylactic application of antibiotic-loaded bone cement for prevention of infection in primary total knee arthroplasty: results of a meta-analysis. Surg Infect (Larchmt). 2015;16(2):183-187.
67. Leopold SS. Consensus statement from the International Consensus Meeting on Periprosthetic Joint Infection. Clin Orthop Relat Res. 2013;471(12):3731-3732.
68. Sollecito TP, Abt E, Lockhart PB, et al. The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints: evidence-based clinical practice guideline for dental practitioners—a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146(1):11-16.e18.
69. Watters W 3rd, Rethman MP, Hanson NB, et al. Prevention of orthopaedic implant infection in patients undergoing dental procedures. J Am Acad Orthop Surg. 2013;21(3):180-189.
70. Merchant VA; American Academy of Orthopaedic Surgeons, American Dental Association. The new AAOS/ADA clinical practice guidelines for management of patients with prosthetic joint replacements. J Mich Dent Assoc. 2013;95(2):16, 74.
71. Berbari EF, Osmon DR, Carr A, et al. Dental procedures as risk factors for prosthetic hip or knee infection: a hospital-based prospective case–control study. Clin Infect Dis. 2010;50(1):8-16.
72. Little JW, Jacobson JJ, Lockhart PB; American Academy of Oral Medicine. The dental treatment of patients with joint replacements: a position paper from the American Academy of Oral Medicine. J Am Dent Assoc. 2010;141(6):667-671.
73. Curry S, Phillips H. Joint arthroplasty, dental treatment, and antibiotics: a review. J Arthroplasty. 2002;17(1):111-113.
74. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res. 2008;466(6):1368-1371.
75. Stone PW. Economic burden of healthcare-associated infections: an American perspective. Expert Rev Pharmacoecon Outcomes Res. 2009;9(5):417-422.
76. Kapadia BH, McElroy MJ, Issa K, Johnson AJ, Bozic KJ, Mont MA. The economic impact of periprosthetic infections following total knee arthroplasty at a specialized tertiary-care center. J Arthroplasty. 2014;29(5):929-932.
77. Slover J, Haas JP, Quirno M, Phillips MS, Bosco JA 3rd. Cost-effectiveness of a Staphylococcus aureus screening and decolonization program for high-risk orthopedic patients. J Arthroplasty. 2011;26(3):360-365.
78. Cummins JS, Tomek IM, Kantor SR, Furnes O, Engesaeter LB, Finlayson SR. Cost-effectiveness of antibiotic-impregnated bone cement used in primary total hip arthroplasty. J Bone Joint Surg Am. 2009;91(3):634-641.
79. Kapadia BH, Johnson AJ, Issa K, Mont MA. Economic evaluation of chlorhexidine cloths on healthcare costs due to surgical site infections following total knee arthroplasty. J Arthroplasty. 2013;28(7):1061-1065.
80. Malinzak RA, Ritter MA, Berend ME, Meding JB, Olberding EM, Davis KE. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24(6 suppl):84-88.
81. Wagner ER, Kamath AF, Fruth KM, Harmsen WS, Berry DJ. Effect of body mass index on complications and reoperations after total hip arthroplasty. J Bone Joint Surg Am. 2016;98(3):169-179.
82 Broex EC, van Asselt AD, Bruggeman CA, van Tiel FH. Surgical site infections: how high are the costs? J Hosp Infect. 2009;72(3):193-201.
83. Anderson DJ, Kirkland KB, Kaye KS, et al. Underresourced hospital infection control and prevention programs: penny wise, pound foolish? Infect Control Hosp Epidemiol. 2007;28(7):767-773.
84. Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program; comprehensive care for joint replacement payment model for acute care hospitals furnishing lower extremity joint replacement services. Final rule. Fed Regist. 2015;80(226):73273-73554.
1. National Nosocomial Infections Surveillance System. National Nosocomial Infections Surveillance (NNIS) System report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32(8):470-485.
2. Bozic KJ, Ries MD. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J Bone Joint Surg Am. 2005;87(8):1746-1751.
3. Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 suppl):61-65.e61.
4. Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty. 2008;23(7):984-991.
5. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4):250-278.
6. Berrios-Torres SI. Evidence-based update to the U.S. Centers for Disease Control and Prevention and Healthcare Infection Control Practices Advisory Committee guideline for the prevention of surgical site infection: developmental process. Surg Infect (Larchmt). 2016;17(2):256-261.
7 Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27(2):97-132.
8. Marchetti MG, Kampf G, Finzi G, Salvatorelli G. Evaluation of the bactericidal effect of five products for surgical hand disinfection according to prEN 12054 and prEN 12791. J Hosp Infect. 2003;54(1):63-67.
9. Reichman DE, Greenberg JA. Reducing surgical site infections: a review. Rev Obstet Gynecol. 2009;2(4):212-221.
10. Hayek LJ, Emerson JM, Gardner AM. A placebo-controlled trial of the effect of two preoperative baths or showers with chlorhexidine detergent on postoperative wound infection rates. J Hosp Infect. 1987;10(2):165-172.
11. Murray MR, Saltzman MD, Gryzlo SM, Terry MA, Woodward CC, Nuber GW. Efficacy of preoperative home use of 2% chlorhexidine gluconate cloth before shoulder surgery. J Shoulder Elbow Surg. 2011;20(6):928-933.
12. Darouiche RO, Wall MJ Jr, Itani KM, et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med. 2010;362(1):18-26.
13. Zywiel MG, Daley JA, Delanois RE, Naziri Q, Johnson AJ, Mont MA. Advance pre-operative chlorhexidine reduces the incidence of surgical site infections in knee arthroplasty. Int Orthop. 2011;35(7):1001-1006.
14. Kapadia BH, Johnson AJ, Daley JA, Issa K, Mont MA. Pre-admission cutaneous chlorhexidine preparation reduces surgical site infections in total hip arthroplasty. J Arthroplasty. 2013;28(3):490-493.
15. Johnson AJ, Kapadia BH, Daley JA, Molina CB, Mont MA. Chlorhexidine reduces infections in knee arthroplasty. J Knee Surg. 2013;26(3):213-218.
16. Kapadia BH, Elmallah RK, Mont MA. A randomized, clinical trial of preadmission chlorhexidine skin preparation for lower extremity total joint arthroplasty. J Arthroplasty. 2016;31(12):2856-2861.
17. Mainous MR, Deitch EA. Nutrition and infection. Surg Clin North Am. 1994;74(3):659-676.
18. Greene KA, Wilde AH, Stulberg BN. Preoperative nutritional status of total joint patients. Relationship to postoperative wound complications. J Arthroplasty. 1991;6(4):321-325.
19. Del Savio GC, Zelicof SB, Wexler LM, et al. Preoperative nutritional status and outcome of elective total hip replacement. Clin Orthop Relat Res. 1996;(326):153-161.
20. Alfargieny R, Bodalal Z, Bendardaf R, El-Fadli M, Langhi S. Nutritional status as a predictive marker for surgical site infection in total joint arthroplasty. Avicenna J Med. 2015;5(4):117-122.
21. Bridges SL Jr, Lopez-Mendez A, Han KH, Tracy IC, Alarcon GS. Should methotrexate be discontinued before elective orthopedic surgery in patients with rheumatoid arthritis? J Rheumatol. 1991;18(7):984-988.
22. Silverstein P. Smoking and wound healing. Am J Med. 1992;93(1A):22S-24S.
23. Sørensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012;147(4):373-383.
24. Wong J, Lam DP, Abrishami A, Chan MT, Chung F. Short-term preoperative smoking cessation and postoperative complications: a systematic review and meta-analysis. Can J Anaesth. 2012;59(3):268-279.
25. Pugely AJ, Martin CT, Gao Y, Schweizer ML, Callaghan JJ. The incidence of and risk factors for 30-day surgical site infections following primary and revision total joint arthroplasty. J Arthroplasty. 2015;30(9 suppl):47-50.
26. Han HS, Kang SB. Relations between long-term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin Orthop Surg. 2013;5(2):118-123.
27. Hwang JS, Kim SJ, Bamne AB, Na YG, Kim TK. Do glycemic markers predict occurrence of complications after total knee arthroplasty in patients with diabetes? Clin Orthop Relat Res. 2015;473(5):1726-1731.
28. Whiteside LA, Peppers M, Nayfeh TA, Roy ME. Methicillin-resistant Staphylococcus aureus in TKA treated with revision and direct intra-articular antibiotic infusion. Clin Orthop Relat Res. 2011;469(1):26-33.
29. Moroski NM, Woolwine S, Schwarzkopf R. Is preoperative staphylococcal decolonization efficient in total joint arthroplasty. J Arthroplasty. 2015;30(3):444-446.
30. Rao N, Cannella BA, Crossett LS, Yates AJ Jr, McGough RL 3rd, Hamilton CW. Preoperative screening/decolonization for Staphylococcus aureus to prevent orthopedic surgical site infection: prospective cohort study with 2-year follow-up. J Arthroplasty. 2011;26(8):1501-1507.
31. Saltzman MD, Nuber GW, Gryzlo SM, Marecek GS, Koh JL. Efficacy of surgical preparation solutions in shoulder surgery. J Bone Joint Surg Am. 2009;91(8):1949-1953.
32. Carroll K, Dowsey M, Choong P, Peel T. Risk factors for superficial wound complications in hip and knee arthroplasty. Clin Microbiol Infect. 2014;20(2):130-135.
33. Morrison TN, Chen AF, Taneja M, Kucukdurmaz F, Rothman RH, Parvizi J. Single vs repeat surgical skin preparations for reducing surgical site infection after total joint arthroplasty: a prospective, randomized, double-blinded study. J Arthroplasty. 2016;31(6):1289-1294.
34. Brown AR, Taylor GJ, Gregg PJ. Air contamination during skin preparation and draping in joint replacement surgery. J Bone Joint Surg Br. 1996;78(1):92-94.
35. Tanner J, Woodings D, Moncaster K. Preoperative hair removal to reduce surgical site infection. Cochrane Database Syst Rev. 2006;(3):CD004122.
36. Mishriki SF, Law DJ, Jeffery PJ. Factors affecting the incidence of postoperative wound infection. J Hosp Infect. 1990;16(3):223-230.
37. Harrop JS, Styliaras JC, Ooi YC, Radcliff KE, Vaccaro AR, Wu C. Contributing factors to surgical site infections. J Am Acad Orthop Surg. 2012;20(2):94-101.
38. Cruse PJ, Foord R. A five-year prospective study of 23,649 surgical wounds. Arch Surg. 1973;107(2):206-210.
39. Laine T, Aarnio P. Glove perforation in orthopaedic and trauma surgery. A comparison between single, double indicator gloving and double gloving with two regular gloves. J Bone Joint Surg Br. 2004;86(6):898-900.
40. Ersozlu S, Sahin O, Ozgur AF, Akkaya T, Tuncay C. Glove punctures in major and minor orthopaedic surgery with double gloving. Acta Orthop Belg. 2007;73(6):760-764.
41. Chan KY, Singh VA, Oun BH, To BH. The rate of glove perforations in orthopaedic procedures: single versus double gloving. A prospective study. Med J Malaysia. 2006;61(suppl B):3-7.
42. Carter AH, Casper DS, Parvizi J, Austin MS. A prospective analysis of glove perforation in primary and revision total hip and total knee arthroplasty. J Arthroplasty. 2012;27(7):1271-1275.
43. Charnley J. A clean-air operating enclosure. Br J Surg. 1964;51:202-205.
44. Whyte W, Hodgson R, Tinkler J. The importance of airborne bacterial contamination of wounds. J Hosp Infect. 1982;3(2):123-135.
45. Owers KL, James E, Bannister GC. Source of bacterial shedding in laminar flow theatres. J Hosp Infect. 2004;58(3):230-232.
46. Lidwell OM, Lowbury EJ, Whyte W, Blowers R, Stanley SJ, Lowe D. Effect of ultraclean air in operating rooms on deep sepsis in the joint after total hip or knee replacement: a randomised study. Br Med J (Clin Res Ed). 1982;285(6334):10-14.
47. Hooper GJ, Rothwell AG, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement? The ten-year results of the New Zealand Joint Registry. J Bone Joint Surg Br. 2011;93(1):85-90.
48. Miner AL, Losina E, Katz JN, Fossel AH, Platt R. Deep infection after total knee replacement: impact of laminar airflow systems and body exhaust suits in the modern operating room. Infect Control Hosp Epidemiol. 2007;28(2):222-226.
49. Der Tavitian J, Ong SM, Taub NA, Taylor GJ. Body-exhaust suit versus occlusive clothing. A randomised, prospective trial using air and wound bacterial counts. J Bone Joint Surg Br. 2003;85(4):490-494.
50. Blom A, Estela C, Bowker K, MacGowan A, Hardy JR. The passage of bacteria through surgical drapes. Ann R Coll Surg Engl. 2000;82(6):405-407.
51. Blom AW, Gozzard C, Heal J, Bowker K, Estela CM. Bacterial strike-through of re-usable surgical drapes: the effect of different wetting agents. J Hosp Infect. 2002;52(1):52-55.
52. Fairclough JA, Johnson D, Mackie I. The prevention of wound contamination by skin organisms by the pre-operative application of an iodophor impregnated plastic adhesive drape. J Int Med Res. 1986;14(2):105-109.
53. Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev. 2007;(4):CD006353.
54. Evans RP. Current concepts for clean air and total joint arthroplasty: laminar airflow and ultraviolet radiation: a systematic review. Clin Orthop Relat Res. 2011;469(4):945-953.
55. Lynch RJ, Englesbe MJ, Sturm L, et al. Measurement of foot traffic in the operating room: implications for infection control. Am J Med Qual. 2009;24(1):45-52.
56. Young RS, O’Regan DJ. Cardiac surgical theatre traffic: time for traffic calming measures? Interact Cardiovasc Thorac Surg. 2010;10(4):526-529.
57. Pryor F, Messmer PR. The effect of traffic patterns in the OR on surgical site infections. AORN J. 1998;68(4):649-660.
58. Bratzler DW, Houck PM; Surgical Infection Prevention Guidelines Writers Workgroup, American Academy of Orthopaedic Surgeons, American Association of Critical Care Nurses, et al. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Clin Infect Dis. 2004;38(12):1706-1715.
59. Rosenberger LH, Politano AD, Sawyer RG. The Surgical Care Improvement Project and prevention of post-operative infection, including surgical site infection. Surg Infect (Larchmt). 2011;12(3):163-168.
60. Gorenoi V, Schonermark MP, Hagen A. Prevention of infection after knee arthroplasty. GMS Health Technol Assess. 2010;6:Doc10.
61. AlBuhairan B, Hind D, Hutchinson A. Antibiotic prophylaxis for wound infections in total joint arthroplasty: a systematic review. J Bone Joint Surg Br. 2008;90(7):915-919.
62. Bratzler DW, Houck PM; Surgical Infection Prevention Guideline Writers Workgroup. Antimicrobial prophylaxis for surgery: an advisory statement from the National Surgical Infection Prevention Project. Am J Surg. 2005;189(4):395-404.
63. Quenon JL, Eveillard M, Vivien A, et al. Evaluation of current practices in surgical antimicrobial prophylaxis in primary total hip prosthesis—a multicentre survey in private and public French hospitals. J Hosp Infect. 2004;56(3):202-207.
64. Parvizi J, Saleh KJ, Ragland PS, Pour AE, Mont MA. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008;79(3):335-341.
65. Namba RS, Chen Y, Paxton EW, Slipchenko T, Fithian DC. Outcomes of routine use of antibiotic-loaded cement in primary total knee arthroplasty. J Arthroplasty. 2009;24(6 suppl):44-47.
66. Zhou Y, Li L, Zhou Q, et al. Lack of efficacy of prophylactic application of antibiotic-loaded bone cement for prevention of infection in primary total knee arthroplasty: results of a meta-analysis. Surg Infect (Larchmt). 2015;16(2):183-187.
67. Leopold SS. Consensus statement from the International Consensus Meeting on Periprosthetic Joint Infection. Clin Orthop Relat Res. 2013;471(12):3731-3732.
68. Sollecito TP, Abt E, Lockhart PB, et al. The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints: evidence-based clinical practice guideline for dental practitioners—a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146(1):11-16.e18.
69. Watters W 3rd, Rethman MP, Hanson NB, et al. Prevention of orthopaedic implant infection in patients undergoing dental procedures. J Am Acad Orthop Surg. 2013;21(3):180-189.
70. Merchant VA; American Academy of Orthopaedic Surgeons, American Dental Association. The new AAOS/ADA clinical practice guidelines for management of patients with prosthetic joint replacements. J Mich Dent Assoc. 2013;95(2):16, 74.
71. Berbari EF, Osmon DR, Carr A, et al. Dental procedures as risk factors for prosthetic hip or knee infection: a hospital-based prospective case–control study. Clin Infect Dis. 2010;50(1):8-16.
72. Little JW, Jacobson JJ, Lockhart PB; American Academy of Oral Medicine. The dental treatment of patients with joint replacements: a position paper from the American Academy of Oral Medicine. J Am Dent Assoc. 2010;141(6):667-671.
73. Curry S, Phillips H. Joint arthroplasty, dental treatment, and antibiotics: a review. J Arthroplasty. 2002;17(1):111-113.
74. Jaberi FM, Parvizi J, Haytmanek CT, Joshi A, Purtill J. Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res. 2008;466(6):1368-1371.
75. Stone PW. Economic burden of healthcare-associated infections: an American perspective. Expert Rev Pharmacoecon Outcomes Res. 2009;9(5):417-422.
76. Kapadia BH, McElroy MJ, Issa K, Johnson AJ, Bozic KJ, Mont MA. The economic impact of periprosthetic infections following total knee arthroplasty at a specialized tertiary-care center. J Arthroplasty. 2014;29(5):929-932.
77. Slover J, Haas JP, Quirno M, Phillips MS, Bosco JA 3rd. Cost-effectiveness of a Staphylococcus aureus screening and decolonization program for high-risk orthopedic patients. J Arthroplasty. 2011;26(3):360-365.
78. Cummins JS, Tomek IM, Kantor SR, Furnes O, Engesaeter LB, Finlayson SR. Cost-effectiveness of antibiotic-impregnated bone cement used in primary total hip arthroplasty. J Bone Joint Surg Am. 2009;91(3):634-641.
79. Kapadia BH, Johnson AJ, Issa K, Mont MA. Economic evaluation of chlorhexidine cloths on healthcare costs due to surgical site infections following total knee arthroplasty. J Arthroplasty. 2013;28(7):1061-1065.
80. Malinzak RA, Ritter MA, Berend ME, Meding JB, Olberding EM, Davis KE. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. J Arthroplasty. 2009;24(6 suppl):84-88.
81. Wagner ER, Kamath AF, Fruth KM, Harmsen WS, Berry DJ. Effect of body mass index on complications and reoperations after total hip arthroplasty. J Bone Joint Surg Am. 2016;98(3):169-179.
82 Broex EC, van Asselt AD, Bruggeman CA, van Tiel FH. Surgical site infections: how high are the costs? J Hosp Infect. 2009;72(3):193-201.
83. Anderson DJ, Kirkland KB, Kaye KS, et al. Underresourced hospital infection control and prevention programs: penny wise, pound foolish? Infect Control Hosp Epidemiol. 2007;28(7):767-773.
84. Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program; comprehensive care for joint replacement payment model for acute care hospitals furnishing lower extremity joint replacement services. Final rule. Fed Regist. 2015;80(226):73273-73554.
Doctors’ and nurses’ predictions of ICU outcomes have variable accuracy
Clinical question: How accurate are doctors and nurses at predicting survival and functional outcomes in critically ill patients?
Background: Doctors have been shown to have moderate accuracy at predicting in-hospital mortality in critically ill patients; however, little is known about their ability to predict longer-term outcomes.
Study design: Prospective cohort study.
Synopsis: Physicians and nurses predicted survival and functional outcomes for critically ill patients requiring mechanical ventilation or vasopressors. Outcomes predicted were in-hospital and 6-month mortality and ability to return to original residence, toilet independently, ambulate stairs, remember most things, think clearly, and solve problems.
Six-month follow-up was completed for 299 patients. Accuracy was highest when either physicians or nurses expressed confidence in their predictions; doctors confident in their predications of 6-month survival had a positive likelihood ratio of 33.00 (95% CI, 8.34-130.63). Both doctors and nurses least accurately predicted cognitive function (positive LR, 2.36; 95% CI, 1.36-4.12; negative LR, 0.75; 95% CI, 0.61-0.92 for doctors, positive LR, 1.50; 95% CI, 0.86-2.60; negative LR, 0.88; 95% CI, 0.73-1.06 for nurses), while doctors most accurately predicated 6-month mortality (positive LR, 5.91; 95% CI, 3.74-9.32; negative LR, 0.41; 95% CI, 0.33-0.52) and nurses most accurately predicted in-hospital mortality (positive LR, 4.71; 95% CI, 2.94-7.56; negative LR, 0.6; 95% CI,0.49-0.75).
Bottom line: Doctors and nurses were better at predicting mortality than they were at predicting cognition, and their predicted outcomes were most accurate when they expressed a high degree of confidence in the predictions.
Citation: Detsky ME, Harhay MO, Bayard DF, et al. Discriminative accuracy of physician and nurse predictions for survival and functional outcomes 6 months after an ICU admission. JAMA. 2017;317(21):2187-95.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: How accurate are doctors and nurses at predicting survival and functional outcomes in critically ill patients?
Background: Doctors have been shown to have moderate accuracy at predicting in-hospital mortality in critically ill patients; however, little is known about their ability to predict longer-term outcomes.
Study design: Prospective cohort study.
Synopsis: Physicians and nurses predicted survival and functional outcomes for critically ill patients requiring mechanical ventilation or vasopressors. Outcomes predicted were in-hospital and 6-month mortality and ability to return to original residence, toilet independently, ambulate stairs, remember most things, think clearly, and solve problems.
Six-month follow-up was completed for 299 patients. Accuracy was highest when either physicians or nurses expressed confidence in their predictions; doctors confident in their predications of 6-month survival had a positive likelihood ratio of 33.00 (95% CI, 8.34-130.63). Both doctors and nurses least accurately predicted cognitive function (positive LR, 2.36; 95% CI, 1.36-4.12; negative LR, 0.75; 95% CI, 0.61-0.92 for doctors, positive LR, 1.50; 95% CI, 0.86-2.60; negative LR, 0.88; 95% CI, 0.73-1.06 for nurses), while doctors most accurately predicated 6-month mortality (positive LR, 5.91; 95% CI, 3.74-9.32; negative LR, 0.41; 95% CI, 0.33-0.52) and nurses most accurately predicted in-hospital mortality (positive LR, 4.71; 95% CI, 2.94-7.56; negative LR, 0.6; 95% CI,0.49-0.75).
Bottom line: Doctors and nurses were better at predicting mortality than they were at predicting cognition, and their predicted outcomes were most accurate when they expressed a high degree of confidence in the predictions.
Citation: Detsky ME, Harhay MO, Bayard DF, et al. Discriminative accuracy of physician and nurse predictions for survival and functional outcomes 6 months after an ICU admission. JAMA. 2017;317(21):2187-95.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
Clinical question: How accurate are doctors and nurses at predicting survival and functional outcomes in critically ill patients?
Background: Doctors have been shown to have moderate accuracy at predicting in-hospital mortality in critically ill patients; however, little is known about their ability to predict longer-term outcomes.
Study design: Prospective cohort study.
Synopsis: Physicians and nurses predicted survival and functional outcomes for critically ill patients requiring mechanical ventilation or vasopressors. Outcomes predicted were in-hospital and 6-month mortality and ability to return to original residence, toilet independently, ambulate stairs, remember most things, think clearly, and solve problems.
Six-month follow-up was completed for 299 patients. Accuracy was highest when either physicians or nurses expressed confidence in their predictions; doctors confident in their predications of 6-month survival had a positive likelihood ratio of 33.00 (95% CI, 8.34-130.63). Both doctors and nurses least accurately predicted cognitive function (positive LR, 2.36; 95% CI, 1.36-4.12; negative LR, 0.75; 95% CI, 0.61-0.92 for doctors, positive LR, 1.50; 95% CI, 0.86-2.60; negative LR, 0.88; 95% CI, 0.73-1.06 for nurses), while doctors most accurately predicated 6-month mortality (positive LR, 5.91; 95% CI, 3.74-9.32; negative LR, 0.41; 95% CI, 0.33-0.52) and nurses most accurately predicted in-hospital mortality (positive LR, 4.71; 95% CI, 2.94-7.56; negative LR, 0.6; 95% CI,0.49-0.75).
Bottom line: Doctors and nurses were better at predicting mortality than they were at predicting cognition, and their predicted outcomes were most accurate when they expressed a high degree of confidence in the predictions.
Citation: Detsky ME, Harhay MO, Bayard DF, et al. Discriminative accuracy of physician and nurse predictions for survival and functional outcomes 6 months after an ICU admission. JAMA. 2017;317(21):2187-95.
Dr. Herscher is assistant professor, division of hospital medicine, Icahn School of Medicine of the Mount Sinai Health System.
The Return of Scarlet Fever?
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”
Is scarlet fever—long thought to be eradicated—reemerging as a health threat? China, the United Kingdom, and Hong Kong have seen upsurges in scarlet fever cases in the past few years.
Hong Kong has seen a more than 10-fold increase over the previous incidence rate. In a study of 7,266 patients aged ≤ 14 years (3,304 with laboratory-confirmed diagnosis), researchers from University of Hong Kong found a “sharp peak” in 2011: 1,438 cases were reported, exceeding the total number of 1,117 in the previous 6 years. Since then, the annual number of reported cases has remained at a “relatively high level,” the researchers say, with an average of 14.5 cases per 10,000 children during 2012-2015.
The elevated pattern was more apparent in children aged ≤ 5 years. In that age group, annual incidence averaged 3.3 per 10,000 during 2005-2010, then jumped dramatically to 23.9 per 10,000 in 2011. It dropped slightly to 18.1 per 10,000 in 2012-2015.
The cause is unclear, the researchers say. They cite 1 report that suggests toxin acquisition and multidrug resistance may have contributed. School is probably a major transmission site. Incidence was higher among younger children entering school and during school days. The researchers say boys were more at risk than girls, possibly because they have more physical interactions or poorer personal hygiene. Thus, school-based control measures—especially for boys aged 3 to 5 years—could be “particularly important.”
TV time linked to VTE risk, even among active viewers

ANAHEIM, CA—New research suggests a person’s risk of developing venous thromboembolism (VTE) increases with the amount of time he or she spends watching television, even if that person is physically active.
Study participants who reported watching TV “very often” were more likely to develop VTE than those who reported watching TV “never or seldom,” and this was true even among subjects who met a recommended level of physical activity.
Mary Cushman, MD, of the Larner College of Medicine at the University of Vermont in Burlington, and her colleagues presented these findings in a poster at the American Heart Association’s Scientific Sessions 2017 (presentation S5169).
The researchers analyzed 15,158 middle-aged (45-64 years) subjects participating in the Atherosclerosis Risk in Communities Study.
TV viewing habits and other information on these individuals was collected in 1987-1989, 1993-1995, and 2009-2011.
The researchers used a Cox proportional hazards models to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of incident VTE according to subjects’ frequency of TV viewing.
Options for TV viewing included “never or seldom,” “sometimes,” “often,” or “very often.”
The researchers identified 691 VTEs during the 299,767 person-years of follow-up.
A multivariable analysis revealed an increased risk of VTE with increased TV viewing. The HR was 1.71 (95% CI: 1.26-2.32; P for trend=0.036) for subjects who reported watching TV “very often,” compared to subjects who watched TV “never or seldom.”
Among subjects who met a recommended level of physical activity, the HR was 1.80 (95% CI: 1.04-3.09) for those who watched TV “very often,” compared to those who watched TV “never or seldom.”
The researchers noted that obesity was more common in subjects who watched more TV. However, only about 25% (95% CI: 10.7-27.5) of the increased VTE risk could be explained by the presence of obesity.
“Watching TV itself isn’t likely bad, but we tend to snack and sit still for prolonged periods while watching,” Dr Cushman noted.
“Health professionals should take the time to ask patients about their fitness and sedentary time, such as prolonged sitting watching TV or at a computer.” ![]()
ANAHEIM, CA—New research suggests a person’s risk of developing venous thromboembolism (VTE) increases with the amount of time he or she spends watching television, even if that person is physically active.
Study participants who reported watching TV “very often” were more likely to develop VTE than those who reported watching TV “never or seldom,” and this was true even among subjects who met a recommended level of physical activity.
Mary Cushman, MD, of the Larner College of Medicine at the University of Vermont in Burlington, and her colleagues presented these findings in a poster at the American Heart Association’s Scientific Sessions 2017 (presentation S5169).
The researchers analyzed 15,158 middle-aged (45-64 years) subjects participating in the Atherosclerosis Risk in Communities Study.
TV viewing habits and other information on these individuals was collected in 1987-1989, 1993-1995, and 2009-2011.
The researchers used a Cox proportional hazards models to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of incident VTE according to subjects’ frequency of TV viewing.
Options for TV viewing included “never or seldom,” “sometimes,” “often,” or “very often.”
The researchers identified 691 VTEs during the 299,767 person-years of follow-up.
A multivariable analysis revealed an increased risk of VTE with increased TV viewing. The HR was 1.71 (95% CI: 1.26-2.32; P for trend=0.036) for subjects who reported watching TV “very often,” compared to subjects who watched TV “never or seldom.”
Among subjects who met a recommended level of physical activity, the HR was 1.80 (95% CI: 1.04-3.09) for those who watched TV “very often,” compared to those who watched TV “never or seldom.”
The researchers noted that obesity was more common in subjects who watched more TV. However, only about 25% (95% CI: 10.7-27.5) of the increased VTE risk could be explained by the presence of obesity.
“Watching TV itself isn’t likely bad, but we tend to snack and sit still for prolonged periods while watching,” Dr Cushman noted.
“Health professionals should take the time to ask patients about their fitness and sedentary time, such as prolonged sitting watching TV or at a computer.” ![]()
ANAHEIM, CA—New research suggests a person’s risk of developing venous thromboembolism (VTE) increases with the amount of time he or she spends watching television, even if that person is physically active.
Study participants who reported watching TV “very often” were more likely to develop VTE than those who reported watching TV “never or seldom,” and this was true even among subjects who met a recommended level of physical activity.
Mary Cushman, MD, of the Larner College of Medicine at the University of Vermont in Burlington, and her colleagues presented these findings in a poster at the American Heart Association’s Scientific Sessions 2017 (presentation S5169).
The researchers analyzed 15,158 middle-aged (45-64 years) subjects participating in the Atherosclerosis Risk in Communities Study.
TV viewing habits and other information on these individuals was collected in 1987-1989, 1993-1995, and 2009-2011.
The researchers used a Cox proportional hazards models to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of incident VTE according to subjects’ frequency of TV viewing.
Options for TV viewing included “never or seldom,” “sometimes,” “often,” or “very often.”
The researchers identified 691 VTEs during the 299,767 person-years of follow-up.
A multivariable analysis revealed an increased risk of VTE with increased TV viewing. The HR was 1.71 (95% CI: 1.26-2.32; P for trend=0.036) for subjects who reported watching TV “very often,” compared to subjects who watched TV “never or seldom.”
Among subjects who met a recommended level of physical activity, the HR was 1.80 (95% CI: 1.04-3.09) for those who watched TV “very often,” compared to those who watched TV “never or seldom.”
The researchers noted that obesity was more common in subjects who watched more TV. However, only about 25% (95% CI: 10.7-27.5) of the increased VTE risk could be explained by the presence of obesity.
“Watching TV itself isn’t likely bad, but we tend to snack and sit still for prolonged periods while watching,” Dr Cushman noted.
“Health professionals should take the time to ask patients about their fitness and sedentary time, such as prolonged sitting watching TV or at a computer.” ![]()