User login
‘Test all patients with cancer’: One in eight have inherited mutations
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
Don’t miss postpartum thyroiditis
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
FROM MEDS 2020
Nearly 10% of hospitalized patients with COVID-19 later readmitted
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
About 1 in 11 patients discharged after COVID-19 treatment is readmitted to the same hospital, according to researchers from the Centers for Disease Control and Prevention (CDC).
Older age and chronic diseases are associated with increased risk, said senior author Adi V. Gundlapalli, MD, PhD, chief public health informatics officer of the CDC’s Center for Surveillance, Epidemiology, and Laboratory Services.
Gundlapalli and colleagues published the finding November 9 in Morbidity and Mortality Weekly Report.
To get a picture of readmission after COVID-19 hospitalization, the researchers analyzed records of 126,137 patients hospitalized with COVID-19 between March and July and included in the Premier Healthcare Database, which covers discharge records from 865 nongovernmental, community, and teaching hospitals.
Overall, 15% of the patients died during hospitalization. Of those who survived to discharge, 9% were readmitted to the same hospital within 2 months of discharge; 1.6% of patients were readmitted more than once. The median interval from discharge to first readmission was 8 days (interquartile range, 3-20 days). This short interval suggests that patients are probably not suffering a relapse, Gundlapalli said in an interview. More likely they experienced some adverse event, such as difficulty breathing, that led their caretakers to send them back to the hospital.
Forty-five percent of the primary discharge diagnoses after readmission were infectious and parasitic diseases, primarily COVID-19. The next most common were circulatory system symptoms (11%) and digestive symptoms (7%).
After controlling for covariates, the researchers found that patients were more likely to be readmitted if they had chronic obstructive pulmonary disease (odds ratio [OR], 1.4), heart failure (OR, 1.6), diabetes (OR, 1.2), or chronic kidney disease (OR, 1.6).
They also found increased odds among patients discharged from the index hospitalization to a skilled nursing facility (OR, 1.4) or with home health organization support (OR, 1.3), compared with being discharged to home or self-care. Looked at another way, the rate of readmission was 15% among those discharged to a skilled nursing facility, 12% among those needing home health care and 7% of those discharged to home or self-care.
The researchers also found that people who had been hospitalized within 3 months prior to the index hospitalization were 2.6 times more likely to be readmitted than were those without prior inpatient care.
Further, the odds of readmission increased significantly among people over 65 years of age, compared with people aged 18 to 39 years.
“The results are not surprising,” Gundlapalli said. “We have known from before that elderly patients, especially with chronic conditions, certain clinical conditions, and those who have been hospitalized before, are at risk for readmission.”
But admitting COVID-19 patients requires special planning because they must be isolated and because more personal protective equipment (PPE) is required, he pointed out.
One unexpected finding from the report is that non-Hispanic White people were more likely to be readmitted than were people of other racial or ethnic groups. This contrasts with other research showing Hispanic and Black individuals are more severely affected by COVID-19 than White people. More research is needed to explain this result, Gundlapalli said.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Should our patients really go home for the holidays?
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States. 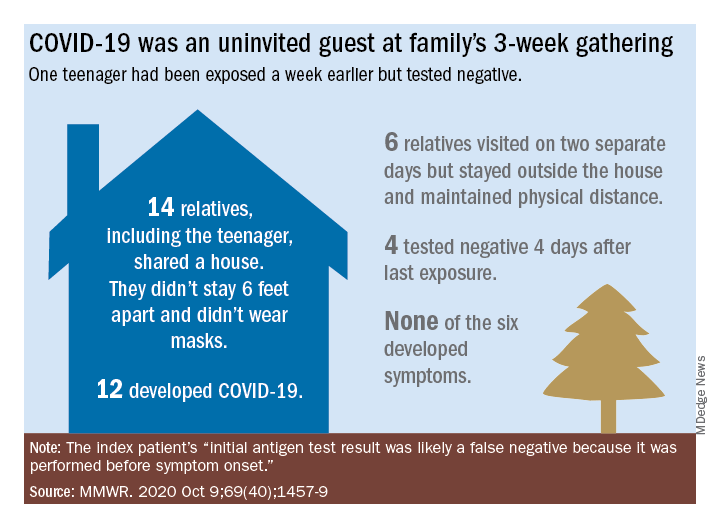
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.

In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States.
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.
In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
As an East Coast transplant residing in Texas, I look forward to the annual sojourn home to celebrate the holidays with family and friends – as do many of our patients and their families. But this is 2020. SARS-CoV-2, the causative agent of COVID-19, is still circulating. To make matters worse, cases are rising in 45 states and internationally. The day of this writing 102,831 new cases were reported in the United States.
Social distancing, wearing masks, and hand washing have been strategies recommended to help mitigate the spread of the virus. We know adherence is not always 100%. The reality is that several families will consider traveling and gathering with others over the holidays. Their actions may lead to increased infections, hospitalizations, and even deaths. It behooves us to at least remind them of the potential consequences of the activity, and if travel and/or holiday gatherings are inevitable, to provide some guidance to help them look at both the risks and benefits and offer strategies to minimize infection and spread.
What should be considered prior to travel?
Here is a list of points to ponder:
- Is your patient is in a high-risk group for developing severe disease or visiting someone who is in a high-risk group?
- What is their mode of transportation?
- What is their destination?
- How prevalent is the disease at their destination, compared with their community?
- What will be their accommodations?
- How will attendees prepare for the gathering, if at all?
- Will multiple families congregate after quarantining for 2 weeks or simply arrive?
- At the destination, will people wear masks and socially distance?
- Is an outdoor venue an option?
All of these questions should be considered by patients.
Review high-risk groups
In terms of high-risk groups, we usually focus on underlying medical conditions or extremes of age, but Black and LatinX children and their families have been diagnosed with COVID-19 and hospitalized more frequently than other racial/ ethnic groups in the United States. Of 277,285 school-aged children infected between March 1 and Sept. 19, 2020, 42% were LatinX, 32% White, and 17% Black, yet they comprise 18%, 60%, and 11% of the U.S. population, respectively. Of those hospitalized, 45% were LatinX, 22% White, and 24% Black. LatinX and Black children also have disproportionately higher mortality rates.
Think about transmission and how to mitigate it
Many patients erroneously think combining multiple households for small group gatherings is inconsequential. These types of gatherings serve as a continued source of SARS-CoV-2 spread. For example, a person in Illinois with mild upper respiratory infection symptoms attended a funeral; he reported embracing the family members after the funeral. He dined with two people the evening prior to the funeral, sharing the meal using common serving dishes. Four days later, he attended a birthday party with nine family members. Some of the family members with symptoms subsequently attended church, infecting another church attendee. A cluster of 16 cases of COVID-19 was subsequently identified, including three deaths likely resulting from this one introduction of COVID-19 at these two family gatherings.
In Tennessee and Wisconsin, household transmission of SARS-CoV-2 was studied prospectively. A total of 101 index cases and 191 asymptomatic household contacts were enrolled between April and Sept. 2020; 102 of 191 (53%) had SARS-CoV-2 detected during the 14-day follow-up. Most infections (75%) were identified within 5 days and occurred whether the index case was an adult or child.
Lastly, one adolescent was identified as the source for an outbreak at a family gathering where 15 persons from five households and four states shared a house between 8 and 25 days in July 2020. Six additional members visited the house. The index case had an exposure to COVID-19 and had a negative antigen test 4 days after exposure. She was asymptomatic when tested. She developed nasal congestion 2 days later, the same day she and her family departed for the gathering. A total of 11 household contacts developed confirmed, suspected, or probable COVID-19, and the teen developed symptoms. This report illustrates how easily SARS-CoV-2 is transmitted, and how when implemented, mitigation strategies work because none of the six who only visited the house was infected. It also serves as a reminder that antigen testing is indicated only for use within the first 5-12 days of onset of symptoms. In this case, the adolescent was asymptomatic when tested and had a false-negative test result.
Ponder modes of transportation
How will your patient arrive to their holiday destination? Nonstop travel by car with household members is probably the safest way. However, for many families, buses and trains are the only options, and social distancing may be challenging. Air travel is a must for others. Acquisition of COVID-19 during air travel appears to be low, but not absent based on how air enters and leaves the cabin. The challenge is socially distancing throughout the check in and boarding processes, as well as minimizing contact with common surfaces. There also is loss of social distancing once on board. Ideally, masks should be worn during the flight. Additionally, for those with international destinations, most countries now require a negative polymerase chain reaction COVID-19 test within a specified time frame for entry.
Essentially the safest place for your patients during the holidays is celebrating at home with their household contacts. The risk for disease acquisition increases with travel. You will not have the opportunity to discuss holiday plans with most parents. However, you can encourage them to consider the pros and cons of travel with reminders via telephone, e-mail, and /or social messaging directly from your practices similar to those sent for other medically necessary interventions. As for me, I will be celebrating virtually this year. There is a first time for everything.
For additional information that also is patient friendly, the Centers for Disease Control and Prevention offers information about travel within the United States and international travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at [email protected].
Patients with mental illness a priority for COVID vaccine, experts say
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
With this week’s announcement that Pfizer’s vaccine candidate against SARS-CoV-2 was 90% effective in preventing COVID-19, the world is one step closer to an effective vaccine.
Nevertheless, with a limited supply of initial doses, the question becomes, who should get it first? Individuals with severe mental illness should be a priority group to receive a COVID-19 vaccine, assert the authors of a perspective article published Nov. 1 in World Psychiatry.
Patients with underlying physical conditions, such as cardiovascular disease, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, obesity, immunodeficiency, and cancer, are particularly vulnerable to developing more severe illness and dying from COVID-19.
In these populations, the risk of a more severe course of infection or early death is significant enough for the U.S. National Academies of Sciences, Engineering, and Medicine to make these patients priority recipients of a vaccine against COVID-19.
Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors argued that those with severe mental illness also fit into this group.
Even without factoring COVID-19 into the calculation, those with severe mental illness have a two- to threefold higher mortality rate than the general population, resulting in reduction in life expectancy of 10-20 years, they noted. This is largely because of physical diseases including cardiovascular disease, type 2 diabetes, and respiratory ailments.
Individuals with severe mental illness also have higher rates of obesity than the general population and obesity is a risk factor for dying from COVID-19.
High-risk population
Like their peers with physical illnesses, recent studies suggest that those with severe mental illness are also at increased risk of morbidity and mortality from COVID-19.
For example, a recent U.S. case-control study with over 61 million adults showed that those recently diagnosed with a mental health disorder had a significantly increased risk for COVID-19 infection, an effect strongest for depression and schizophrenia.
Other recent studies have confirmed these data, including one linking a psychiatric diagnosis in patients hospitalized with COVID-19 to a significantly increased risk for death, as reported by Medscape Medical News.
Dr. De Hert and colleagues put these findings into perspective with this example: In 2017, there were an estimated 11.2 million adults in the United States with severe mental illness. Taking into account the 8.5% death rate in COVID-19 patients recently diagnosed with a severe mental illness, this means that about 1 million patients with severe mental illness in the United States would die if all were infected with the virus.
In light of this knowledge, and taking into account published ethical principles that should guide vaccine allocation, Dr. De Hert and colleagues said it is “paramount” that persons with severe mental illness be prioritized to guarantee that they receive a COVID-19 vaccine during the first phase of its distribution.
“It is our responsibility as psychiatrists in this global health crisis to advocate for the needs of our patients with governments and public health policy bodies,” they wrote.
The authors also encourage public health agencies to develop and implement targeted programs to ensure that patients with severe mental illness and their health care providers “are made aware of these increased risks as well as the benefits of vaccination.”
An argument for fairness
Paul S. Appelbaum, MD, professor of psychiatry, medicine, and law at Columbia University, New York, also believes those with severe mental illness should be a priority group for a COVID vaccine.
“When we’re prioritizing groups for a COVID-19 vaccine, let’s not forget that people with serious mental illness have much lower life expectancies, more obesity, and more undiagnosed chronic conditions. They should be a priority group,” Dr. Appelbaum said in an interview.
“The argument for including people with severe mental illnesses among the vulnerable populations who should be prioritized for receipt of a COVID-19 vaccine is an argument for fairness in constructing that group,” he added.
“Like people with other chronic conditions associated with poor outcomes after SARS-CoV-2 infection, people with severe mental illnesses are more likely to be hospitalized and more likely to die. Although they are often systematically ignored when decisions are made about allocation of resources, there is some hope that, with enough public attention to this issue, they can be included this time,” Dr. Appelbaum said.
Dr. De Hert and Dr. Applebaum disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Tofacitinib effective for ankylosing spondylitis in phase 3
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ACR 2020
Fertility delay varied with contraceptive method in study
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
according to a new prospective cohort study.
Women who used hormonal intrauterine devices, copper intrauterine devices, and implants had the shortest delays, based on the same research project, which involved analyzing data from approximately 18,000 women in North America and Denmark.
“Most research on the use of contraceptives and fertility has focused on the effect of oral contraceptives on fecundability,” and data on the association between fertility and other contraceptive methods are limited, wrote Jennifer J. Yland, MS, of Boston University School of Public Health and colleagues.
“Given the increasing popularity of long acting reversible contraceptive methods and other alternatives to oral contraceptives, more research into their short- and long-term effects on fertility is needed,” the researchers noted.
In the study, which was published in the BMJ, the researchers reviewed data from a total of 17,954 women from three cohort studies of individuals planning pregnancies between 2007 and 2019. Participants reported their contraceptive use and typical menstrual cycle at baseline, then responded to questionnaires every 2 months for up to a year or until pregnancy.
On average, users of injectable contraceptives had the longest delay in return of normal fertility (five to eight menstrual cycles), compared with four cycles for patch contraceptives, three cycles for oral and ring contraceptives, and two cycles for hormonal and copper intrauterine devices and implants.
A total of 10,729 pregnancies were reported within 66,759 menstrual cycles; approximately 77% of the women conceived within 12 months, and 56% conceived within 6 months.
Oral contraceptives were the most common method of contraception (38%), followed by barrier methods (31%), natural methods (15%), and long-acting reversible contraceptives (13%). Intrauterine devices were the most frequently used of long-acting reversible contraceptives (8% hormonal, 4% copper).
The time until fertility returned after discontinuing contraceptives was not associated with duration of contraceptive use.
The study findings were limited by several factors including the potential misclassification of menstrual cycles and the use of self-reports for the time of contraceptive discontinuation, especially for users of injectable contraceptives, the researchers noted.
However, the results were strengthened by the large study size and show “little or no lasting effect” of long-term use of any of the reported contraceptive methods on fertility, the researchers noted. “Understanding the comparative effects of different contraceptives on fecundity is essential for family planning, counseling for contraception, and management of infertility,” they said.
Comparison of contraceptives can inform counseling
The study is important because the use of long-acting reversible contraceptive (LARC) methods (IUDs, implants, patches, and injectable contraceptives) has become increasingly common worldwide, corresponding author Jennifer J. Yland, MS, said in an interview. “Many women are concerned about the potential effects of contraception on future fertility. However, previous research on this topic has focused mostly on oral contraceptives,” she said.
Ms. Yland said that the findings on oral and injectable contraceptives were consistent with previous publications. However, “we were surprised to find that women who had recently used the hormonal IUD had a shorter time to pregnancy, compared with women who used barrier methods,” she said.
The take-home message for clinicians is that delays in the return to normal fertility were temporary for all hormonal contraceptive methods, Ms. Yland emphasized. “However, delays in the return of fertility after discontinuing certain hormonal methods, such as injectables, were considerably longer than that shown for oral contraceptives. These findings should be taken into account when women are considering contraceptive choice in the context of family planning and infertility management,” she noted.
“Future research should evaluate the potential associations between recent use of hormonal contraceptives and perinatal outcomes,” she added.
Managing expectations helps patients plan
“The question of return to fertility is one that many patients who use contraception have unless they have completed their child bearing,” said Sarah W. Prager, MD, of the University of Washington, Seattle, in an interview. “For patients who want to plan a pregnancy, knowing what to expect in terms of return to fertility is important so they can make sure they are in the space and place they want to be with their health, life, job, and partner,” she said.
Dr. Prager said she was not surprised by the study findings because they agree with previously published data. “Overall, except for the injection, people using any form of contraception are back to their baseline fertility within a few months,” she noted. “It also makes perfect sense for return to fertility to be longer with the injection, as it is designed to prevent pregnancy for 16 weeks after the injection is given. Unlike all the other methods, it cannot be removed from the body once given,” she said.
“Clinicians should continue to advise patients that their return to baseline fertility is relatively rapid with any contraception other than the Depo-Provera injection,” said Dr. Prager. “There are no data to support a benefit in switching from an IUD or implant to a combination hormonal method (pills, patch, ring) before starting to try to conceive,” she said.
“This study tries to account for differences in baseline fertility for people using the different methods, but since the choice of method was not randomized, there could still be baseline differences that were not measured or accounted for,” Dr. Prager noted. “A randomized study would certainly eliminate some of these biases; however, I don’t think the differences found in this study are so profound as to require such study,” she said. “Generally speaking, almost 80% of people using any form of contraception were able to conceive within 1 year of trying, which has been the stated fertility data for decades,” she said.
The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health. Lead author Ms. Yland had no financial conflicts to disclose. Dr. Prager had no financial conflicts to disclose.
SOURCE: Yland JJ et al. BMJ. 2020 Nov 12. doi: 10.1136/bmj.m3966.
FROM THE BMJ
Postpartum Depression Recommendations: Screen More Women and Lengthen the Screening Period
Clinical practice guidelines advise screening women for perinatal depression twice prenatally and once postpartum, but providers at the US Department of Veterans Affairs (VA) may not be adhering closely to those recommendations. In a multisite cohort study, the researchers enrolled women veterans who were pregnant and delivered newborns between January 1, 2016 and December 31, 2019. The researchers combined electronic health record and claims data with information collected from prenatal and postpartum telephone surveys.
Of the 663 women involved, 93% received primary care at a VA facility during pregnancy; 41% saw a VA mental health provider. Less than half of the sample had been screened for depression during the perinatal period, despite contact with VA providers. Only 13% of the women had both prenatal and postnatal screens.
Screened veterans were less likely to be diagnosed with depression by a VA provider in either the preconception or pregnancy periods, compared with those not screened (11% vs 24% and 14% vs 23%, respectively).
Among unscreened women, 18% scored positive for depression prenatally and 9% postnatally on the Edinburgh Postnatal Depression scale. The researchers note that lack of screening can hinder connection to VA mental health treatment and referral resources.
The American Academy of Pediatrics recommends that pediatricians screen mothers for postpartum depression at 1, 2, 4, and 6 months after childbirth. But extending that into toddlerhood could pick up more women at risk, say National Institutes of Health researchers. “[S]ix months may not be long enough to gauge depressive symptoms,” said Diane Putnick, PhD, primary author.
In their study of 4,866 women, the researchers analyzed data from the Upstate KIDS study, which included babies born between 2008 and 2010 in New York State. The researchers found that approximately 1 in 4 women experienced high levels of depressive symptoms at some point during the 3 postnatal years.
In addition to extending the screening period to 36 months, the researchers advise keeping watch on women with underlying conditions, such as mood disorders and/or gestational diabetes, who were more likely to have higher levels of depressive symptoms that persisted.
Clinical practice guidelines advise screening women for perinatal depression twice prenatally and once postpartum, but providers at the US Department of Veterans Affairs (VA) may not be adhering closely to those recommendations. In a multisite cohort study, the researchers enrolled women veterans who were pregnant and delivered newborns between January 1, 2016 and December 31, 2019. The researchers combined electronic health record and claims data with information collected from prenatal and postpartum telephone surveys.
Of the 663 women involved, 93% received primary care at a VA facility during pregnancy; 41% saw a VA mental health provider. Less than half of the sample had been screened for depression during the perinatal period, despite contact with VA providers. Only 13% of the women had both prenatal and postnatal screens.
Screened veterans were less likely to be diagnosed with depression by a VA provider in either the preconception or pregnancy periods, compared with those not screened (11% vs 24% and 14% vs 23%, respectively).
Among unscreened women, 18% scored positive for depression prenatally and 9% postnatally on the Edinburgh Postnatal Depression scale. The researchers note that lack of screening can hinder connection to VA mental health treatment and referral resources.
The American Academy of Pediatrics recommends that pediatricians screen mothers for postpartum depression at 1, 2, 4, and 6 months after childbirth. But extending that into toddlerhood could pick up more women at risk, say National Institutes of Health researchers. “[S]ix months may not be long enough to gauge depressive symptoms,” said Diane Putnick, PhD, primary author.
In their study of 4,866 women, the researchers analyzed data from the Upstate KIDS study, which included babies born between 2008 and 2010 in New York State. The researchers found that approximately 1 in 4 women experienced high levels of depressive symptoms at some point during the 3 postnatal years.
In addition to extending the screening period to 36 months, the researchers advise keeping watch on women with underlying conditions, such as mood disorders and/or gestational diabetes, who were more likely to have higher levels of depressive symptoms that persisted.
Clinical practice guidelines advise screening women for perinatal depression twice prenatally and once postpartum, but providers at the US Department of Veterans Affairs (VA) may not be adhering closely to those recommendations. In a multisite cohort study, the researchers enrolled women veterans who were pregnant and delivered newborns between January 1, 2016 and December 31, 2019. The researchers combined electronic health record and claims data with information collected from prenatal and postpartum telephone surveys.
Of the 663 women involved, 93% received primary care at a VA facility during pregnancy; 41% saw a VA mental health provider. Less than half of the sample had been screened for depression during the perinatal period, despite contact with VA providers. Only 13% of the women had both prenatal and postnatal screens.
Screened veterans were less likely to be diagnosed with depression by a VA provider in either the preconception or pregnancy periods, compared with those not screened (11% vs 24% and 14% vs 23%, respectively).
Among unscreened women, 18% scored positive for depression prenatally and 9% postnatally on the Edinburgh Postnatal Depression scale. The researchers note that lack of screening can hinder connection to VA mental health treatment and referral resources.
The American Academy of Pediatrics recommends that pediatricians screen mothers for postpartum depression at 1, 2, 4, and 6 months after childbirth. But extending that into toddlerhood could pick up more women at risk, say National Institutes of Health researchers. “[S]ix months may not be long enough to gauge depressive symptoms,” said Diane Putnick, PhD, primary author.
In their study of 4,866 women, the researchers analyzed data from the Upstate KIDS study, which included babies born between 2008 and 2010 in New York State. The researchers found that approximately 1 in 4 women experienced high levels of depressive symptoms at some point during the 3 postnatal years.
In addition to extending the screening period to 36 months, the researchers advise keeping watch on women with underlying conditions, such as mood disorders and/or gestational diabetes, who were more likely to have higher levels of depressive symptoms that persisted.
Electronic Reminders Extend the Reach of Health Care
Many health care providers (HCPs) view the US Department of Veterans Affairs (VA) system of electronic reminders as a model. User experience and improvements that make clinical life easier (like automated text messaging, which requires no hands-on staff involvement) have brought more HCPs into the fold. And during a viral pandemic, preventive care is ever more important, as are the ways to provide it. But a recent Centers for Disease Control and Prevention (CDC) study shows some non-VA providers have some catching up to do.
Although the CDC researchers noted that electronic reminders can improve preventive and follow-up care, they also pointed out that HCPs must first have the computing capabilities to accomplish this. They analyzed 2017 data (the most recent available) from the National Electronic Health Records Survey of > 10,000 physicians and found only 65% of office-based physicians did.
Not surprisingly, practices that used electronic health record (EHR) systems were more than 3 times as likely to also have computerized capability to identify patients who needed preventive care or follow-up (71% vs 23% of practices without EHR). Primary care physicians were more likely than surgeons and other nonprimary care physicians to have the capability (73% vs 55% and 59%, respectively). Age also entered into it, with 70% of physicians aged between 45 and 54 years having the capability, compared with 57% of those aged 65 to 84 years. Offices with multiple physicians were more likely to have computerized capability.
The VA began using computerized clinical reminders 20 years ago to encourage patients to take better care of themselves to, for example, moderate alcohol use, manage cholesterol, or stop smoking. In 2006, the Veterans Health Information Systems and Technology Architecture (VistA) won an Innovations in American Government Award from Harvard University. The committee called VistA innovative because of its “unique linkage with standardized, consistent performance measurement.” VistA, the committee said, “substantially improves efficiency, reduces costs and demonstrably improves clinical decision-making.”
However, when the VA was getting its electronic reminder system up to speed, not all users were comfortable with it. Researchers who studied uptake of a system that sent reminders about lipid management to patients with ischemic heart disease found “substantial barriers” to implementation, including a possibly significant effect of “prior culture and attitudes” toward reminders.
Four years after the VA began using computerized reminders, attendees at “Camp CPRS,” a week-long meeting to train employees in the Computerized Patient Record System, were asked about facilitation and barriers. More than half of respondents could report at least 1 situation in which reminders helped them deliver care more effectively. But “[w]hile the potential benefits of such a system are significant,” the researchers said, “and in fact some VA hospitals are showing an increase in compliance with some best practices…it is generally understood that some providers within the VA do not use the clinical reminders.” Some HCPs said they were hard to use and cited insufficient training.
Experience and consistent use pay off, though. For instance, researchers from the VA Puget Sound Health Care System in Washington evaluated the effectiveness of an electronic clinical reminder for brief alcohol counseling at 8 VA sites. They wanted to determine how often the HCPs used the reminder, and whether it helped patients resolve unhealthy alcohol use. The study, involving 4,198 participants who screened positive for alcohol use, found 71% of the patients had the clinical reminder documented in the EHR—a high rate, the researchers noted, relative to other studies. The results were similar across the 2-year period, even in the first 8 months.
Sustainability also is a factor. At the time of their study, the researchers said, no health care system had achieved sustained implementation of brief alcohol counseling for patients who screened positive. Moreover, the patients who had reminders were significantly more likely to report having resolved unhealthy alcohol use at follow-up.
Do electronic daily reminders really improve adherence? Valentin Rivish, DNP, RN, NE-BC, telehealth specialist and facility e-consult coordinator with the Phoenix VA Health Care System in Arizona, wanted to see what evidence exists on telehealth adherence and utilization. He enlisted 40 veterans whose home-telehealth response rates were < 70%. Over 4 weeks, the veterans received an electronic daily reminder sent to their home-telehealth device, with the goal of having them respond daily.
As Rivish expected, daily reminders did improve adherence. After 4 weeks, 24 participants (60%) showed an increased response rate, and 14 (35%) achieved at least a 70% response rate pos-intervention. As a result, the Phoenix telehealth department has included the cost-effective intervention in its standard operating procedure.
The VA has continued to add to its repertoire of ways to stay in touch with patients. In 2018, for instance, it launched VEText, a text messaging appointment-reminder system. According to the Veterans Health Administration Office of Veterans Access to Care, in just the first few months more than 3.24 million patients had received VEText messages (and had canceled 319,504 appointments, freeing up time slots for other veterans).
This year, the VA, US Department of Defense, and US Coast Guard launched a joint health information exchange (HIE) that allows partners to quickly and securely share EHR data bidirectionally with participating community healthcare providers. To that end, the 46,000-member HIE is collaborating with the CommonWell Health Alliance, adding a nationwide network of more than 15,000 hospitals and clinics.
“As a clinician who is using the joint HIE, the more patient information I have access to, the more I can understand the full picture of my patients’ care and better meet their needs,” says Dr. Neil Evans, a VA primary care physician and clinical leader with the Federal Electronic Health Record Modernization office. “During the COVID-19 pandemic, efficient electronic health information is more important than ever.”
Many health care providers (HCPs) view the US Department of Veterans Affairs (VA) system of electronic reminders as a model. User experience and improvements that make clinical life easier (like automated text messaging, which requires no hands-on staff involvement) have brought more HCPs into the fold. And during a viral pandemic, preventive care is ever more important, as are the ways to provide it. But a recent Centers for Disease Control and Prevention (CDC) study shows some non-VA providers have some catching up to do.
Although the CDC researchers noted that electronic reminders can improve preventive and follow-up care, they also pointed out that HCPs must first have the computing capabilities to accomplish this. They analyzed 2017 data (the most recent available) from the National Electronic Health Records Survey of > 10,000 physicians and found only 65% of office-based physicians did.
Not surprisingly, practices that used electronic health record (EHR) systems were more than 3 times as likely to also have computerized capability to identify patients who needed preventive care or follow-up (71% vs 23% of practices without EHR). Primary care physicians were more likely than surgeons and other nonprimary care physicians to have the capability (73% vs 55% and 59%, respectively). Age also entered into it, with 70% of physicians aged between 45 and 54 years having the capability, compared with 57% of those aged 65 to 84 years. Offices with multiple physicians were more likely to have computerized capability.
The VA began using computerized clinical reminders 20 years ago to encourage patients to take better care of themselves to, for example, moderate alcohol use, manage cholesterol, or stop smoking. In 2006, the Veterans Health Information Systems and Technology Architecture (VistA) won an Innovations in American Government Award from Harvard University. The committee called VistA innovative because of its “unique linkage with standardized, consistent performance measurement.” VistA, the committee said, “substantially improves efficiency, reduces costs and demonstrably improves clinical decision-making.”
However, when the VA was getting its electronic reminder system up to speed, not all users were comfortable with it. Researchers who studied uptake of a system that sent reminders about lipid management to patients with ischemic heart disease found “substantial barriers” to implementation, including a possibly significant effect of “prior culture and attitudes” toward reminders.
Four years after the VA began using computerized reminders, attendees at “Camp CPRS,” a week-long meeting to train employees in the Computerized Patient Record System, were asked about facilitation and barriers. More than half of respondents could report at least 1 situation in which reminders helped them deliver care more effectively. But “[w]hile the potential benefits of such a system are significant,” the researchers said, “and in fact some VA hospitals are showing an increase in compliance with some best practices…it is generally understood that some providers within the VA do not use the clinical reminders.” Some HCPs said they were hard to use and cited insufficient training.
Experience and consistent use pay off, though. For instance, researchers from the VA Puget Sound Health Care System in Washington evaluated the effectiveness of an electronic clinical reminder for brief alcohol counseling at 8 VA sites. They wanted to determine how often the HCPs used the reminder, and whether it helped patients resolve unhealthy alcohol use. The study, involving 4,198 participants who screened positive for alcohol use, found 71% of the patients had the clinical reminder documented in the EHR—a high rate, the researchers noted, relative to other studies. The results were similar across the 2-year period, even in the first 8 months.
Sustainability also is a factor. At the time of their study, the researchers said, no health care system had achieved sustained implementation of brief alcohol counseling for patients who screened positive. Moreover, the patients who had reminders were significantly more likely to report having resolved unhealthy alcohol use at follow-up.
Do electronic daily reminders really improve adherence? Valentin Rivish, DNP, RN, NE-BC, telehealth specialist and facility e-consult coordinator with the Phoenix VA Health Care System in Arizona, wanted to see what evidence exists on telehealth adherence and utilization. He enlisted 40 veterans whose home-telehealth response rates were < 70%. Over 4 weeks, the veterans received an electronic daily reminder sent to their home-telehealth device, with the goal of having them respond daily.
As Rivish expected, daily reminders did improve adherence. After 4 weeks, 24 participants (60%) showed an increased response rate, and 14 (35%) achieved at least a 70% response rate pos-intervention. As a result, the Phoenix telehealth department has included the cost-effective intervention in its standard operating procedure.
The VA has continued to add to its repertoire of ways to stay in touch with patients. In 2018, for instance, it launched VEText, a text messaging appointment-reminder system. According to the Veterans Health Administration Office of Veterans Access to Care, in just the first few months more than 3.24 million patients had received VEText messages (and had canceled 319,504 appointments, freeing up time slots for other veterans).
This year, the VA, US Department of Defense, and US Coast Guard launched a joint health information exchange (HIE) that allows partners to quickly and securely share EHR data bidirectionally with participating community healthcare providers. To that end, the 46,000-member HIE is collaborating with the CommonWell Health Alliance, adding a nationwide network of more than 15,000 hospitals and clinics.
“As a clinician who is using the joint HIE, the more patient information I have access to, the more I can understand the full picture of my patients’ care and better meet their needs,” says Dr. Neil Evans, a VA primary care physician and clinical leader with the Federal Electronic Health Record Modernization office. “During the COVID-19 pandemic, efficient electronic health information is more important than ever.”
Many health care providers (HCPs) view the US Department of Veterans Affairs (VA) system of electronic reminders as a model. User experience and improvements that make clinical life easier (like automated text messaging, which requires no hands-on staff involvement) have brought more HCPs into the fold. And during a viral pandemic, preventive care is ever more important, as are the ways to provide it. But a recent Centers for Disease Control and Prevention (CDC) study shows some non-VA providers have some catching up to do.
Although the CDC researchers noted that electronic reminders can improve preventive and follow-up care, they also pointed out that HCPs must first have the computing capabilities to accomplish this. They analyzed 2017 data (the most recent available) from the National Electronic Health Records Survey of > 10,000 physicians and found only 65% of office-based physicians did.
Not surprisingly, practices that used electronic health record (EHR) systems were more than 3 times as likely to also have computerized capability to identify patients who needed preventive care or follow-up (71% vs 23% of practices without EHR). Primary care physicians were more likely than surgeons and other nonprimary care physicians to have the capability (73% vs 55% and 59%, respectively). Age also entered into it, with 70% of physicians aged between 45 and 54 years having the capability, compared with 57% of those aged 65 to 84 years. Offices with multiple physicians were more likely to have computerized capability.
The VA began using computerized clinical reminders 20 years ago to encourage patients to take better care of themselves to, for example, moderate alcohol use, manage cholesterol, or stop smoking. In 2006, the Veterans Health Information Systems and Technology Architecture (VistA) won an Innovations in American Government Award from Harvard University. The committee called VistA innovative because of its “unique linkage with standardized, consistent performance measurement.” VistA, the committee said, “substantially improves efficiency, reduces costs and demonstrably improves clinical decision-making.”
However, when the VA was getting its electronic reminder system up to speed, not all users were comfortable with it. Researchers who studied uptake of a system that sent reminders about lipid management to patients with ischemic heart disease found “substantial barriers” to implementation, including a possibly significant effect of “prior culture and attitudes” toward reminders.
Four years after the VA began using computerized reminders, attendees at “Camp CPRS,” a week-long meeting to train employees in the Computerized Patient Record System, were asked about facilitation and barriers. More than half of respondents could report at least 1 situation in which reminders helped them deliver care more effectively. But “[w]hile the potential benefits of such a system are significant,” the researchers said, “and in fact some VA hospitals are showing an increase in compliance with some best practices…it is generally understood that some providers within the VA do not use the clinical reminders.” Some HCPs said they were hard to use and cited insufficient training.
Experience and consistent use pay off, though. For instance, researchers from the VA Puget Sound Health Care System in Washington evaluated the effectiveness of an electronic clinical reminder for brief alcohol counseling at 8 VA sites. They wanted to determine how often the HCPs used the reminder, and whether it helped patients resolve unhealthy alcohol use. The study, involving 4,198 participants who screened positive for alcohol use, found 71% of the patients had the clinical reminder documented in the EHR—a high rate, the researchers noted, relative to other studies. The results were similar across the 2-year period, even in the first 8 months.
Sustainability also is a factor. At the time of their study, the researchers said, no health care system had achieved sustained implementation of brief alcohol counseling for patients who screened positive. Moreover, the patients who had reminders were significantly more likely to report having resolved unhealthy alcohol use at follow-up.
Do electronic daily reminders really improve adherence? Valentin Rivish, DNP, RN, NE-BC, telehealth specialist and facility e-consult coordinator with the Phoenix VA Health Care System in Arizona, wanted to see what evidence exists on telehealth adherence and utilization. He enlisted 40 veterans whose home-telehealth response rates were < 70%. Over 4 weeks, the veterans received an electronic daily reminder sent to their home-telehealth device, with the goal of having them respond daily.
As Rivish expected, daily reminders did improve adherence. After 4 weeks, 24 participants (60%) showed an increased response rate, and 14 (35%) achieved at least a 70% response rate pos-intervention. As a result, the Phoenix telehealth department has included the cost-effective intervention in its standard operating procedure.
The VA has continued to add to its repertoire of ways to stay in touch with patients. In 2018, for instance, it launched VEText, a text messaging appointment-reminder system. According to the Veterans Health Administration Office of Veterans Access to Care, in just the first few months more than 3.24 million patients had received VEText messages (and had canceled 319,504 appointments, freeing up time slots for other veterans).
This year, the VA, US Department of Defense, and US Coast Guard launched a joint health information exchange (HIE) that allows partners to quickly and securely share EHR data bidirectionally with participating community healthcare providers. To that end, the 46,000-member HIE is collaborating with the CommonWell Health Alliance, adding a nationwide network of more than 15,000 hospitals and clinics.
“As a clinician who is using the joint HIE, the more patient information I have access to, the more I can understand the full picture of my patients’ care and better meet their needs,” says Dr. Neil Evans, a VA primary care physician and clinical leader with the Federal Electronic Health Record Modernization office. “During the COVID-19 pandemic, efficient electronic health information is more important than ever.”
The Cell’s Waste Disposal System May be Key to Killing Coronavirus
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”
Normally, the lysosome, known as the cells’ “trash compactor,” destroys viruses before they can leave the cell. However, researchers at the National Institutes of Health (NIH) have discovered that SARS-CoV-2 is not like other viruses. The virus can deactivate that waste disposal system, exit without hindrance, and spread freely throughout the body.
“To our shock, these coronaviruses got out of the cells just fine,” said Nihal Altan-Bonnet, PhD, chief of the Laboratory of Host-Pathogen Dynamics at the National Heart, Lung, and Blood Institute, who coauthored the study report.
Most viruses exit via the biosynthetic secretory pathway, used to transport hormones, growth factors and other materials. The researchers wanted to learn whether coronaviruses took an alternate route. To find out, they conducted further studies, using microscopy and virus-specific markers. They discovered that coronaviruses somehow target the lysosome and congregate there. Although lysosomes are highly acidic, the coronaviruses were not destroyed.
That question led to more experiments. The researchers next found that lysosomes get “de-acidified” in coronavirus-infected cells, which weakens their destructive enzymes. The result: The coronavirus remains intact, ready to infect other cells upon exiting.
The coronaviruses are “very sneaky,” Altan-Bonnet says. “They’re using these lysosomes to get out, but they’re also disrupting the lysosome so it can’t do its job or function.” It’s possible that the way the coronavirus interferes with the lysosome’s “immunological machinery” underlies some of the immune system abnormalities seen in COVID-19 patients, such as cytokine storms.
Studying this coronavirus's heterodox ways may mean that researchers can figure out how to keep it from getting out unscathed, or restore the lysosome’s killing ability by re-acidifying it. Altan-Bonnet and coauthor Sourish Ghosh, PhD, say they have already identified one experimental enzyme inhibitor that potently blocks coronaviruses from exiting the cell.
The lysosome pathway, Altan-Bonnet says, “offers a whole different way of thinking about targeted therapeutics.”