User login
Heart failure readmission metric not linked to care quality
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
[email protected]
On Twitter @legal_med
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.

Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.
Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
These authors add to a chorus of voices expressing concern regarding the appropriateness and validity of the 30-day readmission metric. Arguably, this metric has driven our entire provider workforce to construct machinery designed to reduce short-term posthospitalization utilization, while doing little to improve quality for the 5.7 million (and counting) Americans with heart failure.
Marvin A. Konstam, MD, of Tufts University, Boston, made these comments in an accompanying editorial (JACC: Heart Fail. 2016 Nov 15. doi: 10.1016/j.jchf.2016.10.004). He reported no relevant disclosures.
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
[email protected]
On Twitter @legal_med
Metrics used by the Centers for Medicare & Medicaid Services to determine penalties for heart failure hospital readmissions are not associated with quality of care or overall clinical outcomes, according to data presented at the annual scientific sessions of the American Heart Association.
Ambarish Pandey, MD, of the University of Texas Southwestern Medical Center in Dallas, and his colleagues analyzed data from centers participating in the American Heart Association’s Get With The Guidelines-Heart Failure (GWTG-HF) registry linked to Medicare claims from July 2008 to June 2011. Centers were stratified as having low risk-adjusted readmission rates and high risk-adjusted readmission rates based on publicly available data from 2013.
The study included 171 centers with 43,143 patients. Centers were almost evenly split between low- and high-risk–adjusted 30-day readmission rates, with just a few more (51%) falling in the low-risk–adjusted category.
Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures, as was the case for median percentage of defect-free care (90.0% vs. 91.1%, respectively) and composite 1-year outcome of death or all-cause readmission rates (median 62.9% vs. 65.3%, respectively). The higher readmission group had higher 1-year all-cause readmission rates (median, 59.1% vs. 54.7%), Dr. Pandey and his colleagues reported in the study that was published simultaneously in JACC: Heart Failure (2016 Nov 15. doi. org/10.1016/j.jchf.2016). One-year mortality rates were lower in the higher readmission group with a trend toward statistical significance (median, 28.2% vs. 31.7%; P = 0.07).
Taken together, the findings suggest the 30-day readmission metrics currently used by CMS to determine readmission penalties are not associated with quality of care or overall clinical outcomes, Dr. Pandey and his colleagues wrote. Results showing higher 30-day readmissions do not necessarily reflect poor quality of care and may be related to other factors.
“These findings question the usefulness of the [hospital readmission reduction program] metric in identifying and penalizing hospitals with low quality of care,” Dr. Pandey wrote, adding that the findings were consistent with previous studies that have demonstrated a lack of association between in-hospital quality of care and 30-day readmission rates.
CMS implemented the federal Hospital Readmissions Reduction Program (HRRP) in 2012 to provide financial incentives for hospitals to reduce readmissions. Under the program, CMS uses claims data to determine whether readmission rates for heart failure, acute myocardial infarction, and pneumonia at eligible hospitals are higher than would be predicted by CMS models. Centers with higher than expected readmission rates face up to a 3% reimbursement penalty.
[email protected]
On Twitter @legal_med
FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Performance was nearly equal (95.7% for centers with a low risk-adjusted readmission rate vs. 96.5% for those with high risk-adjusted rate) for median adherence to all performance measures.
Data source: Analysis of publicly available data reported to the CMS Hospital Readmission Reduction program.
Disclosures: No relevant conflicts of interest.
Application of Amniotic Tissue in Orthopedic Surgery
The amniotic membrane is a multilayer tissue forming the innermost layer of the amniotic sac that surrounds the developing fetus. It is comprised of 5 layers, from the inside out: a single layer of epithelial cells, a thick basement membrane, a compact layer, a fibroblast layer, and a spongy layer that abuts the surrounding chorion (Figure 1).1 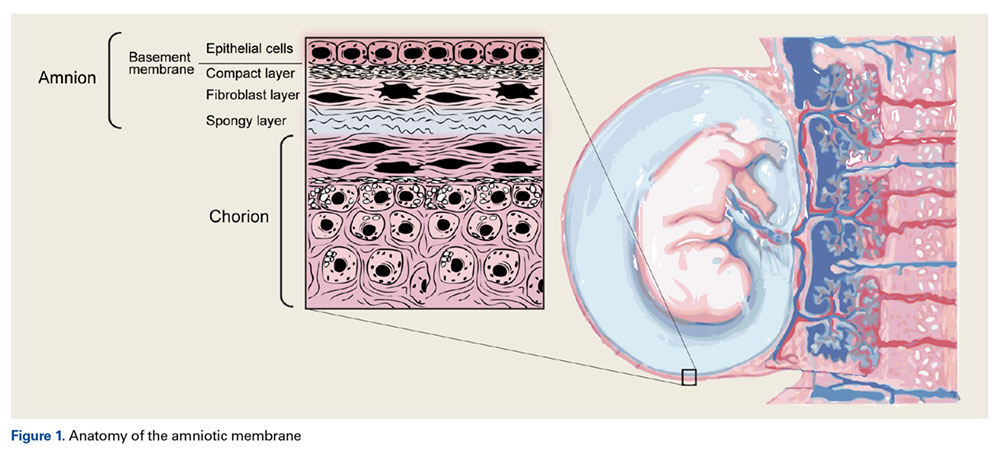
Amniotic epithelial cells are derived from the pluripotent epiblast at approximately day 8 of gestation. This is well before gastrulation occurs at days 15 to 17, considered the “tipping point” when pluripotent cells differentiate into ectoderm, mesoderm, and endoderm.3 These cells express Oct-4 and Nanog, 2 molecular markers that are indicative of pluripotency.3 Two cell types have been identified in amniotic tissues that possess stem cell-like characteristics: human amniotic epithelial cells and human amniotic mesenchymal stromal cells.4 Both of these cell types have demonstrated the ability to differentiate into various cell lineages, including endothelial cells, adipocytes, myogenic cells, neurogenic cells, chondrocytes, tenocytes, and osteogenic cells.5-7 These previously reported findings indicate that amniotic cells and tissue have the capability to generate mesenchymal tissues.
FDA Classification and Available Forms
The US Food and Drug Administration (FDA) classifies amnion as an allograft tissue under Human Cells, Tissues, and Cellular and Tissue-Based Products (HCT/Ps) 361. To meet criteria, the tissue needs to be minimally manipulated. It is to be for homologous use and cannot be combined with other cells or tissues. There can be no systemic effect or dependence on the metabolic activity of living cells to achieve its primary function. The tissue has to have a localized effect in vivo. Therefore, amnion allograft tissue can be commercialized, provided it is not marketed as a stem cell product or to contain viable cells.
Amniotic tissue is commercially available in several forms. 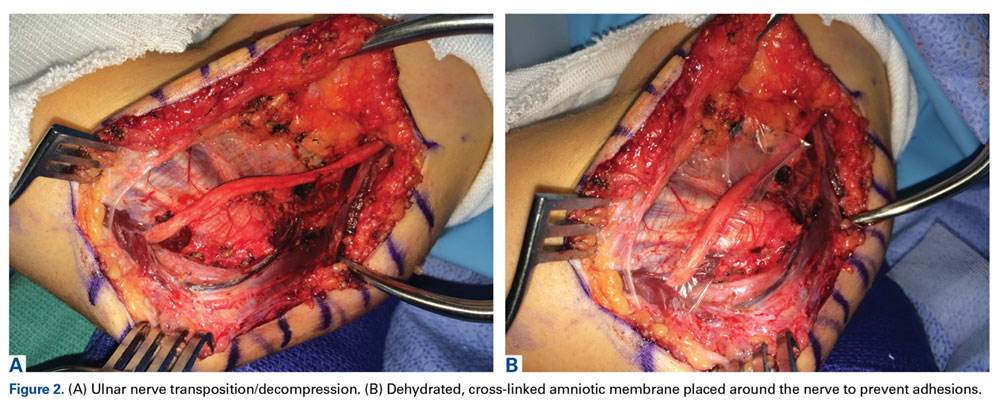
Safety
Amniotic tissue has been used for over 100 years in burn, ophthalmology, and chronic wound patients with favorable outcomes and no adverse effects reported in the literature. Unlike embryonic stem cells, which may be tumorigenic,8 amniotic cells do not possess any known tumorigenicity.9 In one study, 50 immunodeficient mice were injected with 1 to 2 million amniotic epithelial cells and observed for a maximum of 516 days with no tumorigenicity observed in any of the animals.10 In another study, amniotic epithelial cells were implanted into the forearms of healthy volunteers and no immunologic response was observed in any of the recipients.11 Furthermore, viable amniotic cells were recovered via biopsy 7 weeks following transplantation, demonstrating viability of the transplanted cells.11 The lack of tumorigenicity and immunologic response in hosts is due in part to the fact that amniotic cells do not express human leukocyte antigen class II antigens and only express class I antigens in small amounts.3
Advantages of Amnion Tissue
Amniotic tissue is readily available, as it is often discarded after childbirth. The use of this tissue poses no added risk to the fetus or mother, eliminating the ethical concerns associated with obtaining embryonic stem cells. Amniotic tissue is comprised of an extracellular matrix, which acts as a natural scaffold for cellular attachment and structural support for cells as well as collagen types I, III, IV, V, and VI, hyaluronic acid, and a host of growth factors.12 In addition, it possesses antimicrobial properties, including beta-defensins.13
Amniotic tissue has been shown to exert an anti-inflammatory effect by inhibiting the inflammatory cascade. Specifically, it has been shown to inhibit cytokines such as tumor necrosis factor-alpha in the presence of dendritic cells,14 as well as inhibiting transforming growth factor-beta, interleukin-8, and fibroblast proliferation.15 These findings indicate that amniotic tissue has the ability to dampen the “cytokine storm” that occurs after an injury in an adult, which would lead to beneficial impacts on healing and scar formation in patients.16
Basic Science and Animal Studies
Several studies have demonstrated promising outcomes for orthopedic applications in vitro. A comparison of osteogenic potential found that amniotic fluid-derived cells were able to produce approximately 5 times more mineralized matrix than bone marrow-derived mesenchymal stem cells.17 More recently, Si and colleagues18 compared the osteogenic potential of human amniotic epithelial cells, amniotic cells, and human bone marrow-derived mesenchymal stem cells. They found that all 3 cell lines were osteogenic, though the amniotic epithelial cells had better immunomodulatory properties and marginally less osteogenic potential than the other 2 cell types. Furthermore, several in vivo animal studies have demonstrated the ability of human amniotic cells to stimulate bone growth in rats,19,20 rabbits,21 and sheep.22
Amniotic tissue also possesses potential for chondrogenesis. Cryopreserved human amniotic membrane cells used for in vitro human osteoarthritis tissue scaffolds did not differentiate in culture, and they integrated and repaired damaged articular cartilage.23 Various in vitro24,25 and animal in vivo26,27 studies have reported similar supportive findings. Kunisaki and colleagues28 used sheep amniotic fluid mesenchymal stem cells to reconstruct lamb tracheal cartilage in utero, concluding that cells obtained from the amniotic fluid possess chondrogenic capabilities. Further in utero lamb studies of cartilage artificial defects, given 7 days to settle before adding a hypocellular matrix as a scaffold, showed chondrocyte density and cell architecture was restored at the defect site after 28 days without the formation of an inflammatory response or scar tissue.29
Amniotic tissue has had similar success in tendon repair studies in vivo.9,30,31 Barboni and colleagues32 implanted amniotic epithelial cells (AECs) into artificially created sheep Achilles tendon defects in situ, inducing superior structural and mechanical recovery in the defects at a faster rate compared to controls not receiving AECs. Healing via AECs started at the healthy tissue around the borders of the defect and progressed centrally, suggesting recruitment of native progenitor cells to the lesion.32 Kueckelhaus and colleagues33 investigated the role of amnion-derived cellular cytokine solution in the healing of transections of rat Achilles tendons, reporting improved mechanical properties of healing tendons at early time points compared to controls. Beredjiklian and colleagues34 compared the healing of transected extensor tendons of pregnant ewes and of their fetus in utero, reporting a reparative form of healing with scar formation in adult subjects and regenerative form of healing without scar formation or inflammation in fetal subjects.
Amniotic tissue has properties that prevent adhesion formation around tendons following injury and reconstruction.35 Ozgenel36 investigated the effects of hyaluronic acid and amniotic membrane alone and in combination on the presence of adhesions and the rate of healing following chicken flexor tendon repair. The study found amniotic membrane wrapped around the repaired tendon was superior in preventing adhesion formation. Kim and colleagues37 report a similar reduction in fibrosis and adhesion following application of a human amniotic membrane wrap to rabbit ulnar neurorrhaphy sites.
This barrier function of amniotic tissue has also been investigated in the prevention of surgical scarring and peridural fibrosis in animal models following spinal discectomy. A study in canine models showed a reduction of scarring following the application of cross-linked amniotic membrane compared to freeze dried amniotic membrane.38 Similar reductions in scarring in rat models with the application of freeze-dried amniotic membrane compared to negative controls have been reported.39
Human Studies
A randomized trial investigated the outcomes of prenatal vs postnatal repair of myelomeningocele in humans, finding a reduced need for implanted shunts and improved functional outcomes at 30 months of life in the prenatal intervention group compared to the postnatal group.40 This study was concluded early due to the efficacy of prenatal surgery and the benefit of nervous system repair in utero in the presence of amniotic growth factors.
Vines and colleagues41 performed a 6-patient feasibility study using amnion injections to treat symptomatic knee osteoarthritis. Each patient received a single intra-articular cryopreserved amniotic suspension allograft (ASA) injection and was followed for 1 year. No adverse outcomes were reported, with the only abnormal finding being a small increase in serum immunoglobulin G and immunoglobulin E levels. Intra-articular ASA injection was found to be safe, but a large-scale trial investigating symptomatic relief was recommended.41
Most of the human studies using amnion pertain to foot and ankle surgery. Its use as a treatment for diabetic foot ulcers and recalcitrant plantar fasciitis was one of the early-recognized successes.42-45 Zelen and colleagues46 investigated the applications of injectable micronized dehydrated human amniotic/chorionic membrane as an alternative to surgical intervention in the treatment of refractory plantar fasciitis. This prospective, randomized trial with 45 patients showed significant improvement in plantar fasciitis symptoms at 8 weeks compared to controls (saline injections). A similar study compared the use of cryopreserved human amniotic membrane (c-hAM) injections to corticosteroid injections in plantar fasciitis patients.47 The results indicated that c-hAM is safe and comparable to corticosteroids, with the authors noting that pain improvement was greatest in patients receiving 2 injections of c-hAM at 18 weeks.
Tendon wrapping, in which the amniotic membrane is laid over a tendon repair, has been reported with success. Amniotic membrane is superior to collagen for tendon wrapping as it actively contributes to healing while minimizing adhesions, which collagen alone cannot do.48 The membrane serves as a protective sheath around repaired tendons with anti-inflammatory, anti-adhesive, immunomodulatory, and antimicrobial benefits. A 124-patient study demonstrated the safety of using amnion in this manner, and the authors reported a decreased rate of complication compared to previously published data.49 Another study of 14 patients undergoing foot and ankle surgery with tendon wrapping reported clinical improvement with reduced pain and greater functional outcomes postoperatively compared to preoperative measurements.50
Conclusion
Amniotic membrane-derived tissues are safe and non-tumorigenic, producing an abundance of growth factors that have shown promise as tissue scaffolds and as aids in the regeneration of human bone and soft tissues. Amnion applications in orthopedic surgery may be numerous, but development is ongoing. Given the vast array of in vitro and in vivo animal data supporting the benefits of amnion in tissue regeneration, orthopedic surgeons and researchers should place emphasis on conducting clinical studies to validate the safety and efficacy of amniotic cells in the treatment of orthopedic conditions.
Am J Orthop. 2016;45(7):E421-E425. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Benirschke K, Kaufman P. Anatomy and pathology of the placental membranes. In: Pathology of the Human Placent., 4th ed. New York, NY: Springer-Verlag; 2000:281-334.
2. Mamede AC, Carvalho MJ, Abrantes AM, Laranjo M, Maia CJ, Botelho MF. Amniotic membrane: from structure and functions to clinical applications. Cell Tissue Res. 2012;349(2):447-458.
3. Miki T, Strom SC. Amnion-derived pluripotent/multipotent stem cells. Stem Cell Rev. 2006;2(2):133-142.
4. Parolini O, Alviano F, Bagnara GP, et al. Concise review: isolation and characterization of cells from human term placenta: outcome of the first international workshop on placenta derived stem cells. Stem Cells. 2008;26(2):300-311.
5. Ilancheran S, Michalska A, Peh G, Wallace EM, Pera M, Manuelpillai U. Stem cells derived from human fetal membranes display multilineage differentiation potential. Biol Reprod. 2007;77(3):577-588.
6. Alviano F, Fossati V, Marchionni C, et al. Term amniotic membrane is a high throughput source for multipotent mesenchymal stem cells with the ability to differentiate into endothelial cells in vitro. BMC Dev Biol. 2007;7:11.
7. Barboni B, Curini V, Russo V, et al. Indirect co-culture with tendons or tenocytes can program amniotic epithelial cells towards stepwise tenogenic differentiation. PLoS One. 2012;7(2):e30974.
8. Ben-David U, Benvenisty N. The tumorigenicity of human embryonic and induced pluripotent stem cells. Nature Reviews Cancer. 2011;11(4):268-277.
9. Lange-Consiglio A, Rossi D, Tassan S, Perego R, Cremonesi F, Parolini O. Conditioned medium from horse amniotic membrane-derived multipotent progenitor cells: immunomodulatory activity in vitro and first clinical application in tendon and ligament injuries in vivo. Stem Cells Dev. 2013;22(22):3015-3024.
10. Miki T. Amnion-derived stem cells: in quest of clinical applications. Stem Cell Res Ther. 2011;2(3):25.
11. Akle CA, Adinolfi M, Welsh KI, Leibowitz S, McColl I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet. 1981;2(8254):1003-1035.
12. Gupta A, Kedige SD, Jain K. Amnion and chorion membranes: potential stem cell reservoir with wide applications in periodontics. Int J Biomater. 2015;2015:274082.
13. Buhimschi IA, Jabr M, Buhimschi CS, Petkova AP, Weiner CP, Saed GM. The novel antimicrobial peptide beta3-defensin is produced by the amnion: a possible role of the fetal membranes in innate immunity of the amniotic cavity. Am J Obstet Gynecol. 2004;191(5):1678-1687.
14. Magatti M, De Munari S, Vertua E, et al. Amniotic mesenchymal tissue cells inhibit dendritic cell differentiation of peripheral blood and amnion resident monocytes. Cell Transplant. 2009;18(8):899-914.
15. Solomon A, Wajngarten M, Alviano F, et al. Suppression of inflammatory and fibrotic responses in allergic inflammation by the amniotic membrane stromal matrix. Clin Exp Allergy. 2005;35(7):941-948.
16. Silini A, Parolini O, Huppertz B, Lang I. Soluble factors of amnion-derived cells in treatment of inflammatory and fibrotic pathologies. Curr Stem Cell Res Ther. 2013;8(1):6-14.
17. Peister A, Woodruff MA, Prince JJ, Gray DP, Hutmacher DW, Guldberg RE. Cell sourcing for bone tissue engineering: amniotic fluid stem cells have a delayed, robust differentiation compared to mesenchymal stem cells. Stem Cell Res. 2011;7(1):17-27.
18. Si J, Dai J, Zhang J, et al. Comparative investigation of human amniotic epithelial cells and mesenchymal stem cells for application in bone tissue engineering. Stem Cells Int. 2015;2015:565732.
19. Starecki M, Schwartz JA, Grande DA. Evaluation of amniotic-derived membrane biomaterial as an adjunct for repair of critical sized bone defects. Advances in Orthopedic Surgery. 2014;2014:572586.
20. Kerimoglu S, Livaoglu M, Sönmez B, et al. Effects of human amniotic fluid on fracture healing in rat tibia. J Surg Res. 2009;152(2):281-287.
21. Karaçal N, Kocucu P, Cobanglu U, Kutlu N. Effect of human amniotic fluid on bone healing. J Surg Res. 2005;129(2):283-287.
22. Barboni B, Mangano C, Valbonetti L, et al. Synthetic bone substitute engineered with amniotic epithelial cells enhances bone regeneration after maxillary sinus augmentation. PLoS One. 2013;8(5):e63256.
23. Díaz-Prado S, Rendal-Vázquez ME, Muiños-Lopez E, et al. Potential use of the human amniotic membrane as a scaffold in human articular cartilage repair. Cell Tissue Bank. 2010;11(2):183-195.
24. Krishnamurithy G, Shilpa PN, Ahmad RE, Sulaiman S, Ng CL, Kamarul T. Human amniotic membrane as a chondrocyte carrier vehicle/substrate: in vitro study. J Biomed Mater Res A. 2011;99(3):500-506.
25. Tan SL, Sulaiman S, Pingguan-Murphy B, Selvaratnam L, Tai CC, Kamarul T. Human amnion as a novel cell delivery vehicle for chondrogenic mesenchymal stem cells. Cell Tissue Bank. 2011;12(1):59-70.
26. Jin CZ, Park SR, Choi BH, Lee KY, Kang CK, Min BH. Human amniotic membrane as a delivery matrix for articular cartilage repair. Tissue Eng. 2007;13(4):693-702.
27. Garcia D, Longo UG, Vaquero J, et al. Amniotic membrane transplant for articular cartilage repair: an experimental study in sheep. Curr Stem Cell Res Ther. 2014;10(1):77-83.
28. Kunisaki SM, Freedman DA, Fauza DO. Fetal tracheal reconstruction with cartilaginous grafts engineered from mesenchymal amniocytes. J Pediatr Surg. 2006;41(4):675-682.
29. Namba RS, Meuli M, Sullivan KM, Le AX, Adzick NS. Spontaneous repair of superficial defects in articular cartilage in a fetal lamb model. J Bone Joint Surg Am. 1998;80(1):4-10.
30. Philip J, Hackl F, Canseco JA, et al. Amnion-derived multipotent progenitor cells improve achilles tendon repair in rats. Eplasty. 2013;13:e31.
31. Lange-Consiglio A, Tassan S, Corradetti B, et al. Investigating the efficacy of amnion-derived compared with bone marrow–derived mesenchymal stromal cells in equine tendon and ligament injuries. Cytotherapy. 2013;15(8):1011-1020.
32. Barboni B, Russo V, Curini V, et al. Achilles tendon regeneration can be improved by amniotic epithelial cell allotransplantation. Cell Transplant. 2012;21(11):2377-2395.
33. Kueckelhaus M, Philip J, Kamel RA, et al. Sustained release of amnion-derived cellular cytokine solution facilitates achilles tendon healing in rats. Eplasty. 2014;14:e29.
34. Beredjiklian PK, Favata M, Cartmell JS, Flanagan CL, Crombleholme TM, Soslowski LJ. Regenerative versus reparative healing in tendon: a study of biomechanical and histological properties in fetal sheep. Ann Biomed Eng. 2003;31(10):1143-1152.
35. Demirkan F, Colakoglu N, Herek O, Erkula G. The use of amniotic membrane in flexor tendon repair: an experimental model. Arch Orthop Trauma Surg. 2002;122(7):396-369.
36. Ozgenel GY. The effects of a combination of hyaluronic and amniotic membrane on the formation of peritendinous adhesions after flexor tendon surgery in chickens. J Bone Joint Surg Br. 2004;86(2):301-307.
37. Kim SS, Sohn SK, Lee KY, Lee MJ, Roh MS, Kim CH. Use of human amniotic membrane wrap in reducing perineural adhesions in a rabbit model of ulnar nerve neurorrhaphy. J Hand Surg Eur Vol. 2010;35(3):214-219.
38. Tao H, Fan H. Implantation of amniotic membrane to reduce postlaminectomy epidural adhesions. Eur Spine J. 2009;18(8):1202-1212.
39. Choi HJ, Kim KB, Kwon YM. Effect of amniotic membrane to reduce postlaminectomy epidural adhesion on a rat model. J Korean Neurosurg Soc. 2011;49(6):323-328.
40. Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011;364(11):993-1004.
41. Vines JB, Aliprantis AO, Gomoll AH, Farr J. Cryopreserved amniotic suspension for the treatment of knee osteoarthritis. J Knee Surg. 2016;29(6):443-450.
42. Zelen CM. An evaluation of dehydrated human amniotic membrane allografts in patients with DFUs. J Wound Care. 2013;22(7):347-348,350-351.
43. Zelen CM, Serena TE, Denoziere G, Fetterolf DE. A prospective randomised comparative parallel study of amniotic membrane wound graft in the management of diabetic foot ulcers. Int Wound J. 2013;10(5):502-507.
44. Zelen CM, Serena TE, Snyder RJ. A prospective, randomised comparative study of weekly versus biweekly application of dehydrated human amnion/chorion membrane allograft in the management of diabetic foot ulcers. Int Wound J. 2014;11(2):122-128.
45. Zelen CM, Snyder RJ, Serena TE, Li WW. The use of human amnion/chorion membrane in the clinical setting for lower extremity repair: a review. Clin Podiatr Med Surg. 2015;32(1):135-146.
46. Zelen CM, Poka A, Andrews J. Prospective, randomized, blinded, comparative study of injectable micronized dehydrated amniotic/chorionic membrane allograft for plantar fasciitis: a feasibility study. Foot Ankle Int. 2013;34(10):1332-1339.
47. Hanselman AE, Tidwell JE, Santrock RD. Cryopreserved human amniotic membrane injection for plantar fasciitis: a randomized, controlled, double-blind pilot study. Foot Ankle Int. 2015;36(2):151-158.
48. Jay RM. Initial clinical experience with the use of human amniotic membrane tissue during repair of posterior tibial and achilles tendons. 2009. http://encompassbiologics.com/wp-content/uploads/2015/07/DrJayClinicalExperience.pdf. Accessed September 29, 2016.
49. DeMill SL, Granata JD, McAlister JE, Berlet GC, Hyer CF. Safety analysis of cryopreserved amniotic membrane/umbilical cord tissue in foot and ankle surgery: a consecutive case series of 124 patients. Surg Technol Int. 2014;25:257-261.
50. Warner M, Lasyone L. An open-label, single-center, retrospective study of cryopreserved amniotic membrane and umbilical cord tissue as an adjunct for foot and ankle surgery. Surg Technol Int. 2014;25:251-255.
The amniotic membrane is a multilayer tissue forming the innermost layer of the amniotic sac that surrounds the developing fetus. It is comprised of 5 layers, from the inside out: a single layer of epithelial cells, a thick basement membrane, a compact layer, a fibroblast layer, and a spongy layer that abuts the surrounding chorion (Figure 1).1
Amniotic epithelial cells are derived from the pluripotent epiblast at approximately day 8 of gestation. This is well before gastrulation occurs at days 15 to 17, considered the “tipping point” when pluripotent cells differentiate into ectoderm, mesoderm, and endoderm.3 These cells express Oct-4 and Nanog, 2 molecular markers that are indicative of pluripotency.3 Two cell types have been identified in amniotic tissues that possess stem cell-like characteristics: human amniotic epithelial cells and human amniotic mesenchymal stromal cells.4 Both of these cell types have demonstrated the ability to differentiate into various cell lineages, including endothelial cells, adipocytes, myogenic cells, neurogenic cells, chondrocytes, tenocytes, and osteogenic cells.5-7 These previously reported findings indicate that amniotic cells and tissue have the capability to generate mesenchymal tissues.
FDA Classification and Available Forms
The US Food and Drug Administration (FDA) classifies amnion as an allograft tissue under Human Cells, Tissues, and Cellular and Tissue-Based Products (HCT/Ps) 361. To meet criteria, the tissue needs to be minimally manipulated. It is to be for homologous use and cannot be combined with other cells or tissues. There can be no systemic effect or dependence on the metabolic activity of living cells to achieve its primary function. The tissue has to have a localized effect in vivo. Therefore, amnion allograft tissue can be commercialized, provided it is not marketed as a stem cell product or to contain viable cells.
Amniotic tissue is commercially available in several forms.
Safety
Amniotic tissue has been used for over 100 years in burn, ophthalmology, and chronic wound patients with favorable outcomes and no adverse effects reported in the literature. Unlike embryonic stem cells, which may be tumorigenic,8 amniotic cells do not possess any known tumorigenicity.9 In one study, 50 immunodeficient mice were injected with 1 to 2 million amniotic epithelial cells and observed for a maximum of 516 days with no tumorigenicity observed in any of the animals.10 In another study, amniotic epithelial cells were implanted into the forearms of healthy volunteers and no immunologic response was observed in any of the recipients.11 Furthermore, viable amniotic cells were recovered via biopsy 7 weeks following transplantation, demonstrating viability of the transplanted cells.11 The lack of tumorigenicity and immunologic response in hosts is due in part to the fact that amniotic cells do not express human leukocyte antigen class II antigens and only express class I antigens in small amounts.3
Advantages of Amnion Tissue
Amniotic tissue is readily available, as it is often discarded after childbirth. The use of this tissue poses no added risk to the fetus or mother, eliminating the ethical concerns associated with obtaining embryonic stem cells. Amniotic tissue is comprised of an extracellular matrix, which acts as a natural scaffold for cellular attachment and structural support for cells as well as collagen types I, III, IV, V, and VI, hyaluronic acid, and a host of growth factors.12 In addition, it possesses antimicrobial properties, including beta-defensins.13
Amniotic tissue has been shown to exert an anti-inflammatory effect by inhibiting the inflammatory cascade. Specifically, it has been shown to inhibit cytokines such as tumor necrosis factor-alpha in the presence of dendritic cells,14 as well as inhibiting transforming growth factor-beta, interleukin-8, and fibroblast proliferation.15 These findings indicate that amniotic tissue has the ability to dampen the “cytokine storm” that occurs after an injury in an adult, which would lead to beneficial impacts on healing and scar formation in patients.16
Basic Science and Animal Studies
Several studies have demonstrated promising outcomes for orthopedic applications in vitro. A comparison of osteogenic potential found that amniotic fluid-derived cells were able to produce approximately 5 times more mineralized matrix than bone marrow-derived mesenchymal stem cells.17 More recently, Si and colleagues18 compared the osteogenic potential of human amniotic epithelial cells, amniotic cells, and human bone marrow-derived mesenchymal stem cells. They found that all 3 cell lines were osteogenic, though the amniotic epithelial cells had better immunomodulatory properties and marginally less osteogenic potential than the other 2 cell types. Furthermore, several in vivo animal studies have demonstrated the ability of human amniotic cells to stimulate bone growth in rats,19,20 rabbits,21 and sheep.22
Amniotic tissue also possesses potential for chondrogenesis. Cryopreserved human amniotic membrane cells used for in vitro human osteoarthritis tissue scaffolds did not differentiate in culture, and they integrated and repaired damaged articular cartilage.23 Various in vitro24,25 and animal in vivo26,27 studies have reported similar supportive findings. Kunisaki and colleagues28 used sheep amniotic fluid mesenchymal stem cells to reconstruct lamb tracheal cartilage in utero, concluding that cells obtained from the amniotic fluid possess chondrogenic capabilities. Further in utero lamb studies of cartilage artificial defects, given 7 days to settle before adding a hypocellular matrix as a scaffold, showed chondrocyte density and cell architecture was restored at the defect site after 28 days without the formation of an inflammatory response or scar tissue.29
Amniotic tissue has had similar success in tendon repair studies in vivo.9,30,31 Barboni and colleagues32 implanted amniotic epithelial cells (AECs) into artificially created sheep Achilles tendon defects in situ, inducing superior structural and mechanical recovery in the defects at a faster rate compared to controls not receiving AECs. Healing via AECs started at the healthy tissue around the borders of the defect and progressed centrally, suggesting recruitment of native progenitor cells to the lesion.32 Kueckelhaus and colleagues33 investigated the role of amnion-derived cellular cytokine solution in the healing of transections of rat Achilles tendons, reporting improved mechanical properties of healing tendons at early time points compared to controls. Beredjiklian and colleagues34 compared the healing of transected extensor tendons of pregnant ewes and of their fetus in utero, reporting a reparative form of healing with scar formation in adult subjects and regenerative form of healing without scar formation or inflammation in fetal subjects.
Amniotic tissue has properties that prevent adhesion formation around tendons following injury and reconstruction.35 Ozgenel36 investigated the effects of hyaluronic acid and amniotic membrane alone and in combination on the presence of adhesions and the rate of healing following chicken flexor tendon repair. The study found amniotic membrane wrapped around the repaired tendon was superior in preventing adhesion formation. Kim and colleagues37 report a similar reduction in fibrosis and adhesion following application of a human amniotic membrane wrap to rabbit ulnar neurorrhaphy sites.
This barrier function of amniotic tissue has also been investigated in the prevention of surgical scarring and peridural fibrosis in animal models following spinal discectomy. A study in canine models showed a reduction of scarring following the application of cross-linked amniotic membrane compared to freeze dried amniotic membrane.38 Similar reductions in scarring in rat models with the application of freeze-dried amniotic membrane compared to negative controls have been reported.39
Human Studies
A randomized trial investigated the outcomes of prenatal vs postnatal repair of myelomeningocele in humans, finding a reduced need for implanted shunts and improved functional outcomes at 30 months of life in the prenatal intervention group compared to the postnatal group.40 This study was concluded early due to the efficacy of prenatal surgery and the benefit of nervous system repair in utero in the presence of amniotic growth factors.
Vines and colleagues41 performed a 6-patient feasibility study using amnion injections to treat symptomatic knee osteoarthritis. Each patient received a single intra-articular cryopreserved amniotic suspension allograft (ASA) injection and was followed for 1 year. No adverse outcomes were reported, with the only abnormal finding being a small increase in serum immunoglobulin G and immunoglobulin E levels. Intra-articular ASA injection was found to be safe, but a large-scale trial investigating symptomatic relief was recommended.41
Most of the human studies using amnion pertain to foot and ankle surgery. Its use as a treatment for diabetic foot ulcers and recalcitrant plantar fasciitis was one of the early-recognized successes.42-45 Zelen and colleagues46 investigated the applications of injectable micronized dehydrated human amniotic/chorionic membrane as an alternative to surgical intervention in the treatment of refractory plantar fasciitis. This prospective, randomized trial with 45 patients showed significant improvement in plantar fasciitis symptoms at 8 weeks compared to controls (saline injections). A similar study compared the use of cryopreserved human amniotic membrane (c-hAM) injections to corticosteroid injections in plantar fasciitis patients.47 The results indicated that c-hAM is safe and comparable to corticosteroids, with the authors noting that pain improvement was greatest in patients receiving 2 injections of c-hAM at 18 weeks.
Tendon wrapping, in which the amniotic membrane is laid over a tendon repair, has been reported with success. Amniotic membrane is superior to collagen for tendon wrapping as it actively contributes to healing while minimizing adhesions, which collagen alone cannot do.48 The membrane serves as a protective sheath around repaired tendons with anti-inflammatory, anti-adhesive, immunomodulatory, and antimicrobial benefits. A 124-patient study demonstrated the safety of using amnion in this manner, and the authors reported a decreased rate of complication compared to previously published data.49 Another study of 14 patients undergoing foot and ankle surgery with tendon wrapping reported clinical improvement with reduced pain and greater functional outcomes postoperatively compared to preoperative measurements.50
Conclusion
Amniotic membrane-derived tissues are safe and non-tumorigenic, producing an abundance of growth factors that have shown promise as tissue scaffolds and as aids in the regeneration of human bone and soft tissues. Amnion applications in orthopedic surgery may be numerous, but development is ongoing. Given the vast array of in vitro and in vivo animal data supporting the benefits of amnion in tissue regeneration, orthopedic surgeons and researchers should place emphasis on conducting clinical studies to validate the safety and efficacy of amniotic cells in the treatment of orthopedic conditions.
Am J Orthop. 2016;45(7):E421-E425. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
The amniotic membrane is a multilayer tissue forming the innermost layer of the amniotic sac that surrounds the developing fetus. It is comprised of 5 layers, from the inside out: a single layer of epithelial cells, a thick basement membrane, a compact layer, a fibroblast layer, and a spongy layer that abuts the surrounding chorion (Figure 1).1
Amniotic epithelial cells are derived from the pluripotent epiblast at approximately day 8 of gestation. This is well before gastrulation occurs at days 15 to 17, considered the “tipping point” when pluripotent cells differentiate into ectoderm, mesoderm, and endoderm.3 These cells express Oct-4 and Nanog, 2 molecular markers that are indicative of pluripotency.3 Two cell types have been identified in amniotic tissues that possess stem cell-like characteristics: human amniotic epithelial cells and human amniotic mesenchymal stromal cells.4 Both of these cell types have demonstrated the ability to differentiate into various cell lineages, including endothelial cells, adipocytes, myogenic cells, neurogenic cells, chondrocytes, tenocytes, and osteogenic cells.5-7 These previously reported findings indicate that amniotic cells and tissue have the capability to generate mesenchymal tissues.
FDA Classification and Available Forms
The US Food and Drug Administration (FDA) classifies amnion as an allograft tissue under Human Cells, Tissues, and Cellular and Tissue-Based Products (HCT/Ps) 361. To meet criteria, the tissue needs to be minimally manipulated. It is to be for homologous use and cannot be combined with other cells or tissues. There can be no systemic effect or dependence on the metabolic activity of living cells to achieve its primary function. The tissue has to have a localized effect in vivo. Therefore, amnion allograft tissue can be commercialized, provided it is not marketed as a stem cell product or to contain viable cells.
Amniotic tissue is commercially available in several forms.
Safety
Amniotic tissue has been used for over 100 years in burn, ophthalmology, and chronic wound patients with favorable outcomes and no adverse effects reported in the literature. Unlike embryonic stem cells, which may be tumorigenic,8 amniotic cells do not possess any known tumorigenicity.9 In one study, 50 immunodeficient mice were injected with 1 to 2 million amniotic epithelial cells and observed for a maximum of 516 days with no tumorigenicity observed in any of the animals.10 In another study, amniotic epithelial cells were implanted into the forearms of healthy volunteers and no immunologic response was observed in any of the recipients.11 Furthermore, viable amniotic cells were recovered via biopsy 7 weeks following transplantation, demonstrating viability of the transplanted cells.11 The lack of tumorigenicity and immunologic response in hosts is due in part to the fact that amniotic cells do not express human leukocyte antigen class II antigens and only express class I antigens in small amounts.3
Advantages of Amnion Tissue
Amniotic tissue is readily available, as it is often discarded after childbirth. The use of this tissue poses no added risk to the fetus or mother, eliminating the ethical concerns associated with obtaining embryonic stem cells. Amniotic tissue is comprised of an extracellular matrix, which acts as a natural scaffold for cellular attachment and structural support for cells as well as collagen types I, III, IV, V, and VI, hyaluronic acid, and a host of growth factors.12 In addition, it possesses antimicrobial properties, including beta-defensins.13
Amniotic tissue has been shown to exert an anti-inflammatory effect by inhibiting the inflammatory cascade. Specifically, it has been shown to inhibit cytokines such as tumor necrosis factor-alpha in the presence of dendritic cells,14 as well as inhibiting transforming growth factor-beta, interleukin-8, and fibroblast proliferation.15 These findings indicate that amniotic tissue has the ability to dampen the “cytokine storm” that occurs after an injury in an adult, which would lead to beneficial impacts on healing and scar formation in patients.16
Basic Science and Animal Studies
Several studies have demonstrated promising outcomes for orthopedic applications in vitro. A comparison of osteogenic potential found that amniotic fluid-derived cells were able to produce approximately 5 times more mineralized matrix than bone marrow-derived mesenchymal stem cells.17 More recently, Si and colleagues18 compared the osteogenic potential of human amniotic epithelial cells, amniotic cells, and human bone marrow-derived mesenchymal stem cells. They found that all 3 cell lines were osteogenic, though the amniotic epithelial cells had better immunomodulatory properties and marginally less osteogenic potential than the other 2 cell types. Furthermore, several in vivo animal studies have demonstrated the ability of human amniotic cells to stimulate bone growth in rats,19,20 rabbits,21 and sheep.22
Amniotic tissue also possesses potential for chondrogenesis. Cryopreserved human amniotic membrane cells used for in vitro human osteoarthritis tissue scaffolds did not differentiate in culture, and they integrated and repaired damaged articular cartilage.23 Various in vitro24,25 and animal in vivo26,27 studies have reported similar supportive findings. Kunisaki and colleagues28 used sheep amniotic fluid mesenchymal stem cells to reconstruct lamb tracheal cartilage in utero, concluding that cells obtained from the amniotic fluid possess chondrogenic capabilities. Further in utero lamb studies of cartilage artificial defects, given 7 days to settle before adding a hypocellular matrix as a scaffold, showed chondrocyte density and cell architecture was restored at the defect site after 28 days without the formation of an inflammatory response or scar tissue.29
Amniotic tissue has had similar success in tendon repair studies in vivo.9,30,31 Barboni and colleagues32 implanted amniotic epithelial cells (AECs) into artificially created sheep Achilles tendon defects in situ, inducing superior structural and mechanical recovery in the defects at a faster rate compared to controls not receiving AECs. Healing via AECs started at the healthy tissue around the borders of the defect and progressed centrally, suggesting recruitment of native progenitor cells to the lesion.32 Kueckelhaus and colleagues33 investigated the role of amnion-derived cellular cytokine solution in the healing of transections of rat Achilles tendons, reporting improved mechanical properties of healing tendons at early time points compared to controls. Beredjiklian and colleagues34 compared the healing of transected extensor tendons of pregnant ewes and of their fetus in utero, reporting a reparative form of healing with scar formation in adult subjects and regenerative form of healing without scar formation or inflammation in fetal subjects.
Amniotic tissue has properties that prevent adhesion formation around tendons following injury and reconstruction.35 Ozgenel36 investigated the effects of hyaluronic acid and amniotic membrane alone and in combination on the presence of adhesions and the rate of healing following chicken flexor tendon repair. The study found amniotic membrane wrapped around the repaired tendon was superior in preventing adhesion formation. Kim and colleagues37 report a similar reduction in fibrosis and adhesion following application of a human amniotic membrane wrap to rabbit ulnar neurorrhaphy sites.
This barrier function of amniotic tissue has also been investigated in the prevention of surgical scarring and peridural fibrosis in animal models following spinal discectomy. A study in canine models showed a reduction of scarring following the application of cross-linked amniotic membrane compared to freeze dried amniotic membrane.38 Similar reductions in scarring in rat models with the application of freeze-dried amniotic membrane compared to negative controls have been reported.39
Human Studies
A randomized trial investigated the outcomes of prenatal vs postnatal repair of myelomeningocele in humans, finding a reduced need for implanted shunts and improved functional outcomes at 30 months of life in the prenatal intervention group compared to the postnatal group.40 This study was concluded early due to the efficacy of prenatal surgery and the benefit of nervous system repair in utero in the presence of amniotic growth factors.
Vines and colleagues41 performed a 6-patient feasibility study using amnion injections to treat symptomatic knee osteoarthritis. Each patient received a single intra-articular cryopreserved amniotic suspension allograft (ASA) injection and was followed for 1 year. No adverse outcomes were reported, with the only abnormal finding being a small increase in serum immunoglobulin G and immunoglobulin E levels. Intra-articular ASA injection was found to be safe, but a large-scale trial investigating symptomatic relief was recommended.41
Most of the human studies using amnion pertain to foot and ankle surgery. Its use as a treatment for diabetic foot ulcers and recalcitrant plantar fasciitis was one of the early-recognized successes.42-45 Zelen and colleagues46 investigated the applications of injectable micronized dehydrated human amniotic/chorionic membrane as an alternative to surgical intervention in the treatment of refractory plantar fasciitis. This prospective, randomized trial with 45 patients showed significant improvement in plantar fasciitis symptoms at 8 weeks compared to controls (saline injections). A similar study compared the use of cryopreserved human amniotic membrane (c-hAM) injections to corticosteroid injections in plantar fasciitis patients.47 The results indicated that c-hAM is safe and comparable to corticosteroids, with the authors noting that pain improvement was greatest in patients receiving 2 injections of c-hAM at 18 weeks.
Tendon wrapping, in which the amniotic membrane is laid over a tendon repair, has been reported with success. Amniotic membrane is superior to collagen for tendon wrapping as it actively contributes to healing while minimizing adhesions, which collagen alone cannot do.48 The membrane serves as a protective sheath around repaired tendons with anti-inflammatory, anti-adhesive, immunomodulatory, and antimicrobial benefits. A 124-patient study demonstrated the safety of using amnion in this manner, and the authors reported a decreased rate of complication compared to previously published data.49 Another study of 14 patients undergoing foot and ankle surgery with tendon wrapping reported clinical improvement with reduced pain and greater functional outcomes postoperatively compared to preoperative measurements.50
Conclusion
Amniotic membrane-derived tissues are safe and non-tumorigenic, producing an abundance of growth factors that have shown promise as tissue scaffolds and as aids in the regeneration of human bone and soft tissues. Amnion applications in orthopedic surgery may be numerous, but development is ongoing. Given the vast array of in vitro and in vivo animal data supporting the benefits of amnion in tissue regeneration, orthopedic surgeons and researchers should place emphasis on conducting clinical studies to validate the safety and efficacy of amniotic cells in the treatment of orthopedic conditions.
Am J Orthop. 2016;45(7):E421-E425. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Benirschke K, Kaufman P. Anatomy and pathology of the placental membranes. In: Pathology of the Human Placent., 4th ed. New York, NY: Springer-Verlag; 2000:281-334.
2. Mamede AC, Carvalho MJ, Abrantes AM, Laranjo M, Maia CJ, Botelho MF. Amniotic membrane: from structure and functions to clinical applications. Cell Tissue Res. 2012;349(2):447-458.
3. Miki T, Strom SC. Amnion-derived pluripotent/multipotent stem cells. Stem Cell Rev. 2006;2(2):133-142.
4. Parolini O, Alviano F, Bagnara GP, et al. Concise review: isolation and characterization of cells from human term placenta: outcome of the first international workshop on placenta derived stem cells. Stem Cells. 2008;26(2):300-311.
5. Ilancheran S, Michalska A, Peh G, Wallace EM, Pera M, Manuelpillai U. Stem cells derived from human fetal membranes display multilineage differentiation potential. Biol Reprod. 2007;77(3):577-588.
6. Alviano F, Fossati V, Marchionni C, et al. Term amniotic membrane is a high throughput source for multipotent mesenchymal stem cells with the ability to differentiate into endothelial cells in vitro. BMC Dev Biol. 2007;7:11.
7. Barboni B, Curini V, Russo V, et al. Indirect co-culture with tendons or tenocytes can program amniotic epithelial cells towards stepwise tenogenic differentiation. PLoS One. 2012;7(2):e30974.
8. Ben-David U, Benvenisty N. The tumorigenicity of human embryonic and induced pluripotent stem cells. Nature Reviews Cancer. 2011;11(4):268-277.
9. Lange-Consiglio A, Rossi D, Tassan S, Perego R, Cremonesi F, Parolini O. Conditioned medium from horse amniotic membrane-derived multipotent progenitor cells: immunomodulatory activity in vitro and first clinical application in tendon and ligament injuries in vivo. Stem Cells Dev. 2013;22(22):3015-3024.
10. Miki T. Amnion-derived stem cells: in quest of clinical applications. Stem Cell Res Ther. 2011;2(3):25.
11. Akle CA, Adinolfi M, Welsh KI, Leibowitz S, McColl I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet. 1981;2(8254):1003-1035.
12. Gupta A, Kedige SD, Jain K. Amnion and chorion membranes: potential stem cell reservoir with wide applications in periodontics. Int J Biomater. 2015;2015:274082.
13. Buhimschi IA, Jabr M, Buhimschi CS, Petkova AP, Weiner CP, Saed GM. The novel antimicrobial peptide beta3-defensin is produced by the amnion: a possible role of the fetal membranes in innate immunity of the amniotic cavity. Am J Obstet Gynecol. 2004;191(5):1678-1687.
14. Magatti M, De Munari S, Vertua E, et al. Amniotic mesenchymal tissue cells inhibit dendritic cell differentiation of peripheral blood and amnion resident monocytes. Cell Transplant. 2009;18(8):899-914.
15. Solomon A, Wajngarten M, Alviano F, et al. Suppression of inflammatory and fibrotic responses in allergic inflammation by the amniotic membrane stromal matrix. Clin Exp Allergy. 2005;35(7):941-948.
16. Silini A, Parolini O, Huppertz B, Lang I. Soluble factors of amnion-derived cells in treatment of inflammatory and fibrotic pathologies. Curr Stem Cell Res Ther. 2013;8(1):6-14.
17. Peister A, Woodruff MA, Prince JJ, Gray DP, Hutmacher DW, Guldberg RE. Cell sourcing for bone tissue engineering: amniotic fluid stem cells have a delayed, robust differentiation compared to mesenchymal stem cells. Stem Cell Res. 2011;7(1):17-27.
18. Si J, Dai J, Zhang J, et al. Comparative investigation of human amniotic epithelial cells and mesenchymal stem cells for application in bone tissue engineering. Stem Cells Int. 2015;2015:565732.
19. Starecki M, Schwartz JA, Grande DA. Evaluation of amniotic-derived membrane biomaterial as an adjunct for repair of critical sized bone defects. Advances in Orthopedic Surgery. 2014;2014:572586.
20. Kerimoglu S, Livaoglu M, Sönmez B, et al. Effects of human amniotic fluid on fracture healing in rat tibia. J Surg Res. 2009;152(2):281-287.
21. Karaçal N, Kocucu P, Cobanglu U, Kutlu N. Effect of human amniotic fluid on bone healing. J Surg Res. 2005;129(2):283-287.
22. Barboni B, Mangano C, Valbonetti L, et al. Synthetic bone substitute engineered with amniotic epithelial cells enhances bone regeneration after maxillary sinus augmentation. PLoS One. 2013;8(5):e63256.
23. Díaz-Prado S, Rendal-Vázquez ME, Muiños-Lopez E, et al. Potential use of the human amniotic membrane as a scaffold in human articular cartilage repair. Cell Tissue Bank. 2010;11(2):183-195.
24. Krishnamurithy G, Shilpa PN, Ahmad RE, Sulaiman S, Ng CL, Kamarul T. Human amniotic membrane as a chondrocyte carrier vehicle/substrate: in vitro study. J Biomed Mater Res A. 2011;99(3):500-506.
25. Tan SL, Sulaiman S, Pingguan-Murphy B, Selvaratnam L, Tai CC, Kamarul T. Human amnion as a novel cell delivery vehicle for chondrogenic mesenchymal stem cells. Cell Tissue Bank. 2011;12(1):59-70.
26. Jin CZ, Park SR, Choi BH, Lee KY, Kang CK, Min BH. Human amniotic membrane as a delivery matrix for articular cartilage repair. Tissue Eng. 2007;13(4):693-702.
27. Garcia D, Longo UG, Vaquero J, et al. Amniotic membrane transplant for articular cartilage repair: an experimental study in sheep. Curr Stem Cell Res Ther. 2014;10(1):77-83.
28. Kunisaki SM, Freedman DA, Fauza DO. Fetal tracheal reconstruction with cartilaginous grafts engineered from mesenchymal amniocytes. J Pediatr Surg. 2006;41(4):675-682.
29. Namba RS, Meuli M, Sullivan KM, Le AX, Adzick NS. Spontaneous repair of superficial defects in articular cartilage in a fetal lamb model. J Bone Joint Surg Am. 1998;80(1):4-10.
30. Philip J, Hackl F, Canseco JA, et al. Amnion-derived multipotent progenitor cells improve achilles tendon repair in rats. Eplasty. 2013;13:e31.
31. Lange-Consiglio A, Tassan S, Corradetti B, et al. Investigating the efficacy of amnion-derived compared with bone marrow–derived mesenchymal stromal cells in equine tendon and ligament injuries. Cytotherapy. 2013;15(8):1011-1020.
32. Barboni B, Russo V, Curini V, et al. Achilles tendon regeneration can be improved by amniotic epithelial cell allotransplantation. Cell Transplant. 2012;21(11):2377-2395.
33. Kueckelhaus M, Philip J, Kamel RA, et al. Sustained release of amnion-derived cellular cytokine solution facilitates achilles tendon healing in rats. Eplasty. 2014;14:e29.
34. Beredjiklian PK, Favata M, Cartmell JS, Flanagan CL, Crombleholme TM, Soslowski LJ. Regenerative versus reparative healing in tendon: a study of biomechanical and histological properties in fetal sheep. Ann Biomed Eng. 2003;31(10):1143-1152.
35. Demirkan F, Colakoglu N, Herek O, Erkula G. The use of amniotic membrane in flexor tendon repair: an experimental model. Arch Orthop Trauma Surg. 2002;122(7):396-369.
36. Ozgenel GY. The effects of a combination of hyaluronic and amniotic membrane on the formation of peritendinous adhesions after flexor tendon surgery in chickens. J Bone Joint Surg Br. 2004;86(2):301-307.
37. Kim SS, Sohn SK, Lee KY, Lee MJ, Roh MS, Kim CH. Use of human amniotic membrane wrap in reducing perineural adhesions in a rabbit model of ulnar nerve neurorrhaphy. J Hand Surg Eur Vol. 2010;35(3):214-219.
38. Tao H, Fan H. Implantation of amniotic membrane to reduce postlaminectomy epidural adhesions. Eur Spine J. 2009;18(8):1202-1212.
39. Choi HJ, Kim KB, Kwon YM. Effect of amniotic membrane to reduce postlaminectomy epidural adhesion on a rat model. J Korean Neurosurg Soc. 2011;49(6):323-328.
40. Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011;364(11):993-1004.
41. Vines JB, Aliprantis AO, Gomoll AH, Farr J. Cryopreserved amniotic suspension for the treatment of knee osteoarthritis. J Knee Surg. 2016;29(6):443-450.
42. Zelen CM. An evaluation of dehydrated human amniotic membrane allografts in patients with DFUs. J Wound Care. 2013;22(7):347-348,350-351.
43. Zelen CM, Serena TE, Denoziere G, Fetterolf DE. A prospective randomised comparative parallel study of amniotic membrane wound graft in the management of diabetic foot ulcers. Int Wound J. 2013;10(5):502-507.
44. Zelen CM, Serena TE, Snyder RJ. A prospective, randomised comparative study of weekly versus biweekly application of dehydrated human amnion/chorion membrane allograft in the management of diabetic foot ulcers. Int Wound J. 2014;11(2):122-128.
45. Zelen CM, Snyder RJ, Serena TE, Li WW. The use of human amnion/chorion membrane in the clinical setting for lower extremity repair: a review. Clin Podiatr Med Surg. 2015;32(1):135-146.
46. Zelen CM, Poka A, Andrews J. Prospective, randomized, blinded, comparative study of injectable micronized dehydrated amniotic/chorionic membrane allograft for plantar fasciitis: a feasibility study. Foot Ankle Int. 2013;34(10):1332-1339.
47. Hanselman AE, Tidwell JE, Santrock RD. Cryopreserved human amniotic membrane injection for plantar fasciitis: a randomized, controlled, double-blind pilot study. Foot Ankle Int. 2015;36(2):151-158.
48. Jay RM. Initial clinical experience with the use of human amniotic membrane tissue during repair of posterior tibial and achilles tendons. 2009. http://encompassbiologics.com/wp-content/uploads/2015/07/DrJayClinicalExperience.pdf. Accessed September 29, 2016.
49. DeMill SL, Granata JD, McAlister JE, Berlet GC, Hyer CF. Safety analysis of cryopreserved amniotic membrane/umbilical cord tissue in foot and ankle surgery: a consecutive case series of 124 patients. Surg Technol Int. 2014;25:257-261.
50. Warner M, Lasyone L. An open-label, single-center, retrospective study of cryopreserved amniotic membrane and umbilical cord tissue as an adjunct for foot and ankle surgery. Surg Technol Int. 2014;25:251-255.
1. Benirschke K, Kaufman P. Anatomy and pathology of the placental membranes. In: Pathology of the Human Placent., 4th ed. New York, NY: Springer-Verlag; 2000:281-334.
2. Mamede AC, Carvalho MJ, Abrantes AM, Laranjo M, Maia CJ, Botelho MF. Amniotic membrane: from structure and functions to clinical applications. Cell Tissue Res. 2012;349(2):447-458.
3. Miki T, Strom SC. Amnion-derived pluripotent/multipotent stem cells. Stem Cell Rev. 2006;2(2):133-142.
4. Parolini O, Alviano F, Bagnara GP, et al. Concise review: isolation and characterization of cells from human term placenta: outcome of the first international workshop on placenta derived stem cells. Stem Cells. 2008;26(2):300-311.
5. Ilancheran S, Michalska A, Peh G, Wallace EM, Pera M, Manuelpillai U. Stem cells derived from human fetal membranes display multilineage differentiation potential. Biol Reprod. 2007;77(3):577-588.
6. Alviano F, Fossati V, Marchionni C, et al. Term amniotic membrane is a high throughput source for multipotent mesenchymal stem cells with the ability to differentiate into endothelial cells in vitro. BMC Dev Biol. 2007;7:11.
7. Barboni B, Curini V, Russo V, et al. Indirect co-culture with tendons or tenocytes can program amniotic epithelial cells towards stepwise tenogenic differentiation. PLoS One. 2012;7(2):e30974.
8. Ben-David U, Benvenisty N. The tumorigenicity of human embryonic and induced pluripotent stem cells. Nature Reviews Cancer. 2011;11(4):268-277.
9. Lange-Consiglio A, Rossi D, Tassan S, Perego R, Cremonesi F, Parolini O. Conditioned medium from horse amniotic membrane-derived multipotent progenitor cells: immunomodulatory activity in vitro and first clinical application in tendon and ligament injuries in vivo. Stem Cells Dev. 2013;22(22):3015-3024.
10. Miki T. Amnion-derived stem cells: in quest of clinical applications. Stem Cell Res Ther. 2011;2(3):25.
11. Akle CA, Adinolfi M, Welsh KI, Leibowitz S, McColl I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet. 1981;2(8254):1003-1035.
12. Gupta A, Kedige SD, Jain K. Amnion and chorion membranes: potential stem cell reservoir with wide applications in periodontics. Int J Biomater. 2015;2015:274082.
13. Buhimschi IA, Jabr M, Buhimschi CS, Petkova AP, Weiner CP, Saed GM. The novel antimicrobial peptide beta3-defensin is produced by the amnion: a possible role of the fetal membranes in innate immunity of the amniotic cavity. Am J Obstet Gynecol. 2004;191(5):1678-1687.
14. Magatti M, De Munari S, Vertua E, et al. Amniotic mesenchymal tissue cells inhibit dendritic cell differentiation of peripheral blood and amnion resident monocytes. Cell Transplant. 2009;18(8):899-914.
15. Solomon A, Wajngarten M, Alviano F, et al. Suppression of inflammatory and fibrotic responses in allergic inflammation by the amniotic membrane stromal matrix. Clin Exp Allergy. 2005;35(7):941-948.
16. Silini A, Parolini O, Huppertz B, Lang I. Soluble factors of amnion-derived cells in treatment of inflammatory and fibrotic pathologies. Curr Stem Cell Res Ther. 2013;8(1):6-14.
17. Peister A, Woodruff MA, Prince JJ, Gray DP, Hutmacher DW, Guldberg RE. Cell sourcing for bone tissue engineering: amniotic fluid stem cells have a delayed, robust differentiation compared to mesenchymal stem cells. Stem Cell Res. 2011;7(1):17-27.
18. Si J, Dai J, Zhang J, et al. Comparative investigation of human amniotic epithelial cells and mesenchymal stem cells for application in bone tissue engineering. Stem Cells Int. 2015;2015:565732.
19. Starecki M, Schwartz JA, Grande DA. Evaluation of amniotic-derived membrane biomaterial as an adjunct for repair of critical sized bone defects. Advances in Orthopedic Surgery. 2014;2014:572586.
20. Kerimoglu S, Livaoglu M, Sönmez B, et al. Effects of human amniotic fluid on fracture healing in rat tibia. J Surg Res. 2009;152(2):281-287.
21. Karaçal N, Kocucu P, Cobanglu U, Kutlu N. Effect of human amniotic fluid on bone healing. J Surg Res. 2005;129(2):283-287.
22. Barboni B, Mangano C, Valbonetti L, et al. Synthetic bone substitute engineered with amniotic epithelial cells enhances bone regeneration after maxillary sinus augmentation. PLoS One. 2013;8(5):e63256.
23. Díaz-Prado S, Rendal-Vázquez ME, Muiños-Lopez E, et al. Potential use of the human amniotic membrane as a scaffold in human articular cartilage repair. Cell Tissue Bank. 2010;11(2):183-195.
24. Krishnamurithy G, Shilpa PN, Ahmad RE, Sulaiman S, Ng CL, Kamarul T. Human amniotic membrane as a chondrocyte carrier vehicle/substrate: in vitro study. J Biomed Mater Res A. 2011;99(3):500-506.
25. Tan SL, Sulaiman S, Pingguan-Murphy B, Selvaratnam L, Tai CC, Kamarul T. Human amnion as a novel cell delivery vehicle for chondrogenic mesenchymal stem cells. Cell Tissue Bank. 2011;12(1):59-70.
26. Jin CZ, Park SR, Choi BH, Lee KY, Kang CK, Min BH. Human amniotic membrane as a delivery matrix for articular cartilage repair. Tissue Eng. 2007;13(4):693-702.
27. Garcia D, Longo UG, Vaquero J, et al. Amniotic membrane transplant for articular cartilage repair: an experimental study in sheep. Curr Stem Cell Res Ther. 2014;10(1):77-83.
28. Kunisaki SM, Freedman DA, Fauza DO. Fetal tracheal reconstruction with cartilaginous grafts engineered from mesenchymal amniocytes. J Pediatr Surg. 2006;41(4):675-682.
29. Namba RS, Meuli M, Sullivan KM, Le AX, Adzick NS. Spontaneous repair of superficial defects in articular cartilage in a fetal lamb model. J Bone Joint Surg Am. 1998;80(1):4-10.
30. Philip J, Hackl F, Canseco JA, et al. Amnion-derived multipotent progenitor cells improve achilles tendon repair in rats. Eplasty. 2013;13:e31.
31. Lange-Consiglio A, Tassan S, Corradetti B, et al. Investigating the efficacy of amnion-derived compared with bone marrow–derived mesenchymal stromal cells in equine tendon and ligament injuries. Cytotherapy. 2013;15(8):1011-1020.
32. Barboni B, Russo V, Curini V, et al. Achilles tendon regeneration can be improved by amniotic epithelial cell allotransplantation. Cell Transplant. 2012;21(11):2377-2395.
33. Kueckelhaus M, Philip J, Kamel RA, et al. Sustained release of amnion-derived cellular cytokine solution facilitates achilles tendon healing in rats. Eplasty. 2014;14:e29.
34. Beredjiklian PK, Favata M, Cartmell JS, Flanagan CL, Crombleholme TM, Soslowski LJ. Regenerative versus reparative healing in tendon: a study of biomechanical and histological properties in fetal sheep. Ann Biomed Eng. 2003;31(10):1143-1152.
35. Demirkan F, Colakoglu N, Herek O, Erkula G. The use of amniotic membrane in flexor tendon repair: an experimental model. Arch Orthop Trauma Surg. 2002;122(7):396-369.
36. Ozgenel GY. The effects of a combination of hyaluronic and amniotic membrane on the formation of peritendinous adhesions after flexor tendon surgery in chickens. J Bone Joint Surg Br. 2004;86(2):301-307.
37. Kim SS, Sohn SK, Lee KY, Lee MJ, Roh MS, Kim CH. Use of human amniotic membrane wrap in reducing perineural adhesions in a rabbit model of ulnar nerve neurorrhaphy. J Hand Surg Eur Vol. 2010;35(3):214-219.
38. Tao H, Fan H. Implantation of amniotic membrane to reduce postlaminectomy epidural adhesions. Eur Spine J. 2009;18(8):1202-1212.
39. Choi HJ, Kim KB, Kwon YM. Effect of amniotic membrane to reduce postlaminectomy epidural adhesion on a rat model. J Korean Neurosurg Soc. 2011;49(6):323-328.
40. Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011;364(11):993-1004.
41. Vines JB, Aliprantis AO, Gomoll AH, Farr J. Cryopreserved amniotic suspension for the treatment of knee osteoarthritis. J Knee Surg. 2016;29(6):443-450.
42. Zelen CM. An evaluation of dehydrated human amniotic membrane allografts in patients with DFUs. J Wound Care. 2013;22(7):347-348,350-351.
43. Zelen CM, Serena TE, Denoziere G, Fetterolf DE. A prospective randomised comparative parallel study of amniotic membrane wound graft in the management of diabetic foot ulcers. Int Wound J. 2013;10(5):502-507.
44. Zelen CM, Serena TE, Snyder RJ. A prospective, randomised comparative study of weekly versus biweekly application of dehydrated human amnion/chorion membrane allograft in the management of diabetic foot ulcers. Int Wound J. 2014;11(2):122-128.
45. Zelen CM, Snyder RJ, Serena TE, Li WW. The use of human amnion/chorion membrane in the clinical setting for lower extremity repair: a review. Clin Podiatr Med Surg. 2015;32(1):135-146.
46. Zelen CM, Poka A, Andrews J. Prospective, randomized, blinded, comparative study of injectable micronized dehydrated amniotic/chorionic membrane allograft for plantar fasciitis: a feasibility study. Foot Ankle Int. 2013;34(10):1332-1339.
47. Hanselman AE, Tidwell JE, Santrock RD. Cryopreserved human amniotic membrane injection for plantar fasciitis: a randomized, controlled, double-blind pilot study. Foot Ankle Int. 2015;36(2):151-158.
48. Jay RM. Initial clinical experience with the use of human amniotic membrane tissue during repair of posterior tibial and achilles tendons. 2009. http://encompassbiologics.com/wp-content/uploads/2015/07/DrJayClinicalExperience.pdf. Accessed September 29, 2016.
49. DeMill SL, Granata JD, McAlister JE, Berlet GC, Hyer CF. Safety analysis of cryopreserved amniotic membrane/umbilical cord tissue in foot and ankle surgery: a consecutive case series of 124 patients. Surg Technol Int. 2014;25:257-261.
50. Warner M, Lasyone L. An open-label, single-center, retrospective study of cryopreserved amniotic membrane and umbilical cord tissue as an adjunct for foot and ankle surgery. Surg Technol Int. 2014;25:251-255.
VIDEO: Rivaroxaban gives safer protection to atrial fib patients post PCI
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.

Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”

The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
[email protected]
On Twitter @mitchelzoler
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
The results from PIONEER AF-PCI give us important and helpful information now that physicians increasingly prescribe a new oral anticoagulant to treat patients with nonvalvular atrial fibrillation. The trial provides strong evidence that one or two antiplatelet drugs can safely be combined with rivaroxaban when these patients undergo coronary stenting.
Until now, the only data we had on the safety and efficacy of combining an anticoagulant with one or more antiplatelet drugs in these patients involved warfarin-based regimens. Because of this limitation, some clinicians even switched atrial fibrillation patients who were on a new oral anticoagulant to warfarin if they received a coronary stent and therefore needed treatment with antiplatelet drugs.
The study results show that the rivaroxaban-based regimens were safe, even safer than the warfarin-based strategy, and there was no signal of harm in the form on increased strokes or stent thrombosis. Because of the study’s complex design, with many different regimens that included various thienopyridines and various durations of antiplatelet treatment, it is hard to decide from just these results the best approach among all the different combinations tested. But the PIONEER AF-PCI results start to build a data platform for the new oral anticoagulants that clinicians can use to help guide management of these patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Richard C. Becker, MD, is professor of medicine and director of the Heart, Lung and Vascular Institute at the University of Cincinnati. He has received research support from AstraZeneca and Janssen. He made these comments in an interview.
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.
Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”
The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
[email protected]
On Twitter @mitchelzoler
NEW ORLEANS – The puzzle of how to safely prevent thrombotic events in patients with atrial fibrillation who receive a coronary stent now has a little more clarity in the era of new oral anticoagulants.
The first randomized trial to compare the safety of a new oral anticoagulant (NOAC, in this case rivaroxaban) against warfarin when paired with one or more antiplatelet drugs showed that the NOAC edged out warfarin for safety by cutting the rate of clinically significant bleeding events while preventing thrombotic events roughly as well as warfarin.
Despite that, the incidence of all major adverse coronary events during the 1-year follow-up was virtually identical in the three groups, ranging from 5.6% to 6.5%, with very low rates of stroke in the three treatment arms, ranging from 1.2%-1.5%, said Dr. Gibson, a professor of medicine at Harvard Medical School and an interventional cardiologist at Beth Israel Deaconess Medical Center, both in Boston.
These results “are a huge step forward and will change practice,” commented Philippe Gabriel Steg, MD, discussant for the report and director of the coronary care unit of Bichat Hospital in Paris. “We’ve gone from having no evidence to having some evidence” for using a NOAC in this setting. “It was a difficult but very important study that truly advances the field.”
The trial randomized patients to any of three main treatment regimens: 2.5 mg rivaroxaban b.i.d., 15 mg rivaroxaban once daily, or warfarin taken to maintain an international normalized ratio of 2.0-3.0. During the study, patients in the warfarin arm were in this therapeutic range 65% of the time.
The trial’s design instructed physicians to treat patients who received the lower rivaroxaban dosage to also administer aspirin (75-100 mg daily) plus a thienopyridine of their choice. Patients on the higher rivaroxaban dosage received monotherapy with a thienopyridine of the physician’s choosing, while patients assigned to receive warfarin were also to get aspirin (75-100 mg daily) and a thienopyridine. It turned out that in each of the three treatment arms, 95% of patients received clopidogrel, 4% received ticagrelor (Brilinta), and 1% received prasugrel (Effient).
The trial also left it up to each physician to decide how long each patient should remain on dual antiplatelet therapy. In each of the two treatment arms that used dual therapy, 49% received 12 months of dual treatment, 35% received it for 6 months, and 16% received it for 1 month. Once the period of dual therapy ended, patients continued to receive aspirin (at 75-100 mg/day) for the balance of the 12-month study.
Leaving the choice of thienopyridine and duration of dual therapy up to each physician helped make this a “real world study,” Dr. Gibson said.
The trial was fully powered to prove a difference in safety based on rates of clinically significant bleeding events. The 1-year rates were 17% in patients who received 15 mg of rivaroxaban daily, 18% in those who received 2.5 mg rivaroxaban b.i.d., and 27% in the patients on warfarin: statistically significant differences between the warfarin arm and each of the two rivaroxaban arms. The study was not powered to prove noninferiority of the rivaroxaban regimens for efficacy at preventing stroke or major adverse events (cardiovascular death, MI, or stroke). To do that would require a trial with more than 30,000 patients, Dr. Gibson noted.
Also concurrently with Dr. Gibson’s report, a second article was published online with a post-hoc efficacy analysis that used as an efficacy endpoint the combined 1-year rate of death and all-cause hospitalization for an adverse event (Circulation. 2016 Nov 14. doi: 10.1161/CIRCULATIONAHA.116.025783). In this analysis, each of the two rivaroxaban arms cut the rate of this outcome by about 25% relative to the patients treated with warfarin, statistically significant differences. Both of the rivaroxaban regimens led to significant reductions in hospitalizations both for cardiovascular events and for bleeding events, Dr. Gibson reported.
He speculated that the vast majority of patients in the study wound up receiving clopidogrel because of cost consideration, because many physicians weren’t comfortable pairing a more potent thienopyridine with an anticoagulant, and because clopidogrel remains the most commonly used agent from this class in many parts of the world.
Dr. Gibson suggested that physicians who use these rivaroxaban-based regimens in routine practice tailor their thienopyridine selection and the duration of dual therapy to each patient based on these factors as well as whether the individual patient appears to face a greater danger from bleeding or from an ischemic event. The same approach should also guide choosing between the two rivaroxaban regimens tested. The 2.5-mg b.i.d. dosage used in a triple-therapy strategy that combines it with aspirin and a thienopyridine is better suited to patients at higher risk for ischemic events, while the 15-mg once daily dosage coupled with a thienopyridine but without aspirin is better suited to patients with a high bleeding risk, he said in an interview. Because the 2.5-mg formulation is not currently available for U.S. sales, most American physicians will be limited to only prescribing 15 mg of rivaroxaban daily. And for patients with very poor renal function, with a creatinine clearance rate of less than 15 mL/min, warfarin remains the best option, Dr. Gibson said.
PIONEER AF-PCI was sponsored by Johnson & Johnson (Janssen) and Bayer, the two companies that market rivaroxaban (Xarelto) worldwide. Dr. Gibson has received research support from and has been a consultant to Johnson & Johnson and Bayer and has also received research support and consulted for several other drug companies. Dr. Steg has been a consultant to Bayer and Janssen, and has received research support from or has been a consultant to several other drug companies.
[email protected]
On Twitter @mitchelzoler
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The two tested rivaroxaban regimens cut clinically significant bleeds by about 40%, compared with a warfarin-based regimen.
Data source: PIONEER AF-PCI, an international, multicenter randomized trial with 2,124 patients.
Disclosures: Dr. Gibson has received research support and consulted for Johnson & Johnson (Janssen) and Bayer, the study sponsors that also market rivaroxaban (Xarelto) worldwide, and several other drug companies.
VIDEO: Don’t be surprised by weight gain in men after HCV cure
BOSTON – In the new era of direct-acting antiviral (DAA) therapy, physicians will be seeing more and more patients who have achieved a cure of their hepatitis C virus (HCV). Once freed from the burden of a chronic illness, patients feel better and may eat better. Unexpected weight gain and potential associated health effects may be the next set of challenges patients and their physicians will face.
A single-center retrospective study of patients who had achieved sustained virologic response (SVR) after treatment for HCV found a small but significant weight gain in men, but not women. Additionally, according to noninvasive assessments, liver fat increased significantly in men, but not women, after SVR was achieved.
In a study of 63 patients (42 male, 67%) who received DAA treatment for HCV, mean weight gain for men after SVR was 2.8 pounds (range, –26 to +17; P = .0459), and body mass index (BMI) increased by a mean 0.50 kg/m2 (range, –3.6 to +3.33; P = .0176). No significant change was seen for women when pre- and posttreatment measures were compared.
Isaac Wasserman, a medical student at Mount Sinai Medical Center, New York, presented the results of the single-center retrospective study in a poster presentation at the annual meeting of the American Association for the Study of Liver Diseases.
To assess changes in liver fat, Mr. Wasserman and his coinvestigator used results of pre- and posttreatment transient elastography with controlled attenuation parameter (CAP). CAP measures the degree to which the ultrasound signal is attenuated by liver fat, he explained in a video interview.
For men, hepatic steatosis increased by this measure, with CAP measurements up by a mean 18 dB/m (range, –106 to +128, P = .0314). Mr. Wasserman and his colleagues wrote, “The change in liver fat was large enough to push 11% of the cohort (n = 7 of 63) into advanced steatosis (CAP greater than 300 dB/m).” Again, the women studied had no significant posttreatment change in liver fat.
Post-SVR weight gain appeared to be the culprit in the increased fat seen in the posttreatment livers. Mr. Wasserman and his colleagues in the abstract accompanying the presentation, “Changes in weight were positively correlated with changes in liver fat (P = .006).”
Mr. Wasserman said that he and his coinvestigators believe that social, and not biochemical or mechanistic, reasons underlie the weight gain and increased hepatic steatosis. They are planning further investigation of social and economic factors that may underlie the difference seen in this study, and hope to continue and expand data acquisition to validate their findings.
Mr. Wasserman reported no conflicts of interest or outside sources of funding for the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
BOSTON – In the new era of direct-acting antiviral (DAA) therapy, physicians will be seeing more and more patients who have achieved a cure of their hepatitis C virus (HCV). Once freed from the burden of a chronic illness, patients feel better and may eat better. Unexpected weight gain and potential associated health effects may be the next set of challenges patients and their physicians will face.
A single-center retrospective study of patients who had achieved sustained virologic response (SVR) after treatment for HCV found a small but significant weight gain in men, but not women. Additionally, according to noninvasive assessments, liver fat increased significantly in men, but not women, after SVR was achieved.
In a study of 63 patients (42 male, 67%) who received DAA treatment for HCV, mean weight gain for men after SVR was 2.8 pounds (range, –26 to +17; P = .0459), and body mass index (BMI) increased by a mean 0.50 kg/m2 (range, –3.6 to +3.33; P = .0176). No significant change was seen for women when pre- and posttreatment measures were compared.
Isaac Wasserman, a medical student at Mount Sinai Medical Center, New York, presented the results of the single-center retrospective study in a poster presentation at the annual meeting of the American Association for the Study of Liver Diseases.
To assess changes in liver fat, Mr. Wasserman and his coinvestigator used results of pre- and posttreatment transient elastography with controlled attenuation parameter (CAP). CAP measures the degree to which the ultrasound signal is attenuated by liver fat, he explained in a video interview.
For men, hepatic steatosis increased by this measure, with CAP measurements up by a mean 18 dB/m (range, –106 to +128, P = .0314). Mr. Wasserman and his colleagues wrote, “The change in liver fat was large enough to push 11% of the cohort (n = 7 of 63) into advanced steatosis (CAP greater than 300 dB/m).” Again, the women studied had no significant posttreatment change in liver fat.
Post-SVR weight gain appeared to be the culprit in the increased fat seen in the posttreatment livers. Mr. Wasserman and his colleagues in the abstract accompanying the presentation, “Changes in weight were positively correlated with changes in liver fat (P = .006).”
Mr. Wasserman said that he and his coinvestigators believe that social, and not biochemical or mechanistic, reasons underlie the weight gain and increased hepatic steatosis. They are planning further investigation of social and economic factors that may underlie the difference seen in this study, and hope to continue and expand data acquisition to validate their findings.
Mr. Wasserman reported no conflicts of interest or outside sources of funding for the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
BOSTON – In the new era of direct-acting antiviral (DAA) therapy, physicians will be seeing more and more patients who have achieved a cure of their hepatitis C virus (HCV). Once freed from the burden of a chronic illness, patients feel better and may eat better. Unexpected weight gain and potential associated health effects may be the next set of challenges patients and their physicians will face.
A single-center retrospective study of patients who had achieved sustained virologic response (SVR) after treatment for HCV found a small but significant weight gain in men, but not women. Additionally, according to noninvasive assessments, liver fat increased significantly in men, but not women, after SVR was achieved.
In a study of 63 patients (42 male, 67%) who received DAA treatment for HCV, mean weight gain for men after SVR was 2.8 pounds (range, –26 to +17; P = .0459), and body mass index (BMI) increased by a mean 0.50 kg/m2 (range, –3.6 to +3.33; P = .0176). No significant change was seen for women when pre- and posttreatment measures were compared.
Isaac Wasserman, a medical student at Mount Sinai Medical Center, New York, presented the results of the single-center retrospective study in a poster presentation at the annual meeting of the American Association for the Study of Liver Diseases.
To assess changes in liver fat, Mr. Wasserman and his coinvestigator used results of pre- and posttreatment transient elastography with controlled attenuation parameter (CAP). CAP measures the degree to which the ultrasound signal is attenuated by liver fat, he explained in a video interview.
For men, hepatic steatosis increased by this measure, with CAP measurements up by a mean 18 dB/m (range, –106 to +128, P = .0314). Mr. Wasserman and his colleagues wrote, “The change in liver fat was large enough to push 11% of the cohort (n = 7 of 63) into advanced steatosis (CAP greater than 300 dB/m).” Again, the women studied had no significant posttreatment change in liver fat.
Post-SVR weight gain appeared to be the culprit in the increased fat seen in the posttreatment livers. Mr. Wasserman and his colleagues in the abstract accompanying the presentation, “Changes in weight were positively correlated with changes in liver fat (P = .006).”
Mr. Wasserman said that he and his coinvestigators believe that social, and not biochemical or mechanistic, reasons underlie the weight gain and increased hepatic steatosis. They are planning further investigation of social and economic factors that may underlie the difference seen in this study, and hope to continue and expand data acquisition to validate their findings.
Mr. Wasserman reported no conflicts of interest or outside sources of funding for the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
AT THE LIVER MEETING

Time for transparency in skin cancer treatment
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.

In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.
In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
I heard Marty Makary, MD, speak at the annual meeting of the American College of Mohs Surgery (ACMS) a few months ago, and got to meet with him there. He is the author of the book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care,” published in 2013, and is a potent advocate for physicians, patients, and effective, safe, and efficient medical care.
His personal epiphany centered around the stubborn, continued use of open colonic resection of polyps by one of his professors, despite the availability of much safer and less expensive endoscopic removal. He is a powerful advocate for abandoning obsolete treatment techniques for safer and more effective ones. He insists on transparency in selecting the best treatments for patients.
In his writings, Dr. Makary points out that when looking for areas to improve, it is most productive to focus on treatments that have wide variations in treatment settings and modalities. Sometimes, this is due to a lack of data to support a consensus, a lack of information about a superior treatment modality – or more disturbing, stubbornness and ingrained patterns of behavior. This is the familiar, “This is the way we have always done it” syndrome that was behind his personal epiphany.
This is exactly the situation we face in the United States with the continued treatment of skin cancer in the hospital operating room. At least 40% of all skin cancers are excised in the hospital setting, in the face of overwhelming evidence that excision or destruction in the office setting is safer, yields higher cure rates, and is much less expensive.
It is time to speak up, and admit that 99% of all skin cancers should be treated in the office setting, under local anesthesia. Currently, this is most commonly done by a dermatologist, or a primary care physician, who is not operating room dependent. Those specialists who have been trained exclusively in hospital operating rooms need to become more knowledgeable about local anesthesia, and how to operate in their offices. This should be fertile ground for the government, insurers, patient advocates, and accountable care organizations looking to cut costs and improve quality of care. Moreover, the percentage of these conditions being treated in the office setting by a provider should be a quality indicator.
Maybe it is time for Dr. Makary, a surgical oncologist, to issue a shout out to physicians to stop treating thin melanomas (80% of those diagnosed), nonmelanoma skin cancer, and “lumps and bumps” in the operating room.
We need to publicly expound on the benefits of office-based surgery, and take this message to national patient advocacy groups and the public. New “bedless” hospitals are being built to perform outpatient surgery, and avoid the serious infections (think methicillin-resistant Staphylococcus aureus and Clostridium difficile) that are prevalent in hospitals. It is time to realize a properly equipped physician’s office is as good as a bedless hospital operating room for the treatment of skin cancer, with additional benefits of already being built and staffed.
Dr. Makary, this is a great opportunity to improve the health care of the United States, and at reduced cost.
Dr. Coldiron is past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Shea butter
Indigenous to Africa, Vitellaria paradoxa, better known as the shea or shi tree, is a member of the Sapotaceae family. It has long been used in traditional medicine in sub-Saharan West Africa (as far west as Mali) as well as parts of East Africa (as far east as Uganda and Ethiopia) for its anti-inflammatory and analgesic properties.1,2
Some indications in traditional Nigerian medicine include nasal congestion, scabies, and ulcers.2 In addition, anecdotal success in treating keloids has been reported in association with traditional African remedies, including shea butter and boa constrictor oil.3 Antioxidant activities have also been linked to V. paradoxa.4 Given such purported properties, it is not surprising that demand for shea kernels and butter has steadily increased in recent years for various purposes, including use as food (particularly as a cocoa butter additive in chocolate) and in medical and cosmetic products.2,4 The use of shea butter in skin care is attributed to its hydrating qualities and reputed effectiveness in softening scars.3
Constituents
Shea butter contains fatty acids that have been shown to improve the skin barrier. These include palmitic, stearic, and linoleic acid. It also contains the fatty acids oleic and arachidic. Shea butter also has phenolic components that function as antioxidants.

Anti-inflammatory effects
In 2010, Akihisa et al. evaluated the inhibitory effects of four triterpene acetates and four triterpene cinnamates isolated from the kernel fat of V. paradoxa against 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced inflammation in mice. All of the tested compounds showed considerable anti-inflammatory activity (ID50 values ranged from 0.15 to 0.75 micromol/ear). Lupeol cinnamate displayed the greatest anti-inflammatory activity, on carrageenan-induced edema on rat hind paws. All eight substances also exhibited moderate inhibitory effects on Epstein-Barr virus early antigen (EBV-EA) in Raji cells as a primary screening test for tumor promoter inhibitors. Using 7,12-dimethylbenz[a]anthracene (DMBA) as an initiator and TPA as a promoter in a two-stage carcinogenesis model in mice, the investigators also found that lupeol cinnamate inhibited skin tumor promotion. They concluded that the triterpenes and triterpene esters found in shea nuts and shea butter are significant anti-inflammatory and antitumor-promoting agents.2
The next year, Akihisa et al. determined the triacylglycerol and triterpene ester fraction composition of the kernel fats of the shea tree from 36 samples from Cote d’Ivoire, Ghana, Nigeria, Cameroon, Chad, Sudan, and Uganda. There were no significant differences in the composition of the triterpene ester fractions between West African and East African plants. Generally, though, West African shea kernel fats contained higher levels of high-melting triacylglycerols (e.g., stearic-oleic-stearic) and triterpene esters.6
Also that year, Olaitan et al. found that shea butter (as well as boa constrictor oil) was effective in suppressing the in vitro growth of normal and keloid fibroblasts.3
In 2012, Verma et al. used the lipopolysaccharide (LPS)-induced murine macrophage cell line J774 to investigate the anti-inflammatory properties of the methanolic extract of shea butter. They found that shea butter extract dose-dependently reduced, to a significant degree, the levels of nitric oxide, tumor necrosis factor (TNF)–alpha, as well as interleukin (IL)-1beta and IL-12 in the culture supernatants. In addition, the botanical extract suppressed IkappaB phosphorylation and NF-kappaB nuclear translocation as well as the expression of pro-inflammatory enzymes, inducible nitric oxide synthase (iNOS), and cyclooxygenase (COX)-2. The investigators attributed the anti-inflammatory activity of the extract to its inhibitory impact on LPS-induced iNOS, COX-2, TNF-alpha, IL-1beta, and IL-12 mRNA expression.1
In 2014, Honfo et al. conducted a literature review indicating that shea pulp is laden with vitamin C and the kernels contain copious fat (butter), which is used in food, drugs, and cosmetics.4
Notably, shea butter is also an ingredient in the topical nonsteroidal anti-inflammatory drug (NSAID) atopiclair, which has shown efficacy in alleviating pruritus in adults with mild to-moderate atopic dermatitis.7
Conclusion
Shea butter has long been incorporated into traditional medical practice in West and East Africa based on observed anti-inflammatory and analgesic characteristics. Such uses are compelling and often the basis for systematic scientific investigation. That said, there remains a dearth of experimental and clinical research on the potential cutaneous benefits of topically applied shea butter. Current data and traditional applications provide ample reason for continued research into this popular botanical agent.
References
1. J Complement Integr Med. 2012;9:Article 4.
2. J Oleo Sci. 2010;59[6]:273-80)
3. Wounds. 2011;23[4]:97-106.
4. Crit Rev Food Sci Nutr. 2014;54[5]:673-86.
5. J Agric Food Chem. 2003;51[21]:6268-73.
6. J Oleo Sci. 2011;60[8]:385-91.
7. J Drugs Dermatol. 2009 Jun;8[6]:537-9.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Indigenous to Africa, Vitellaria paradoxa, better known as the shea or shi tree, is a member of the Sapotaceae family. It has long been used in traditional medicine in sub-Saharan West Africa (as far west as Mali) as well as parts of East Africa (as far east as Uganda and Ethiopia) for its anti-inflammatory and analgesic properties.1,2
Some indications in traditional Nigerian medicine include nasal congestion, scabies, and ulcers.2 In addition, anecdotal success in treating keloids has been reported in association with traditional African remedies, including shea butter and boa constrictor oil.3 Antioxidant activities have also been linked to V. paradoxa.4 Given such purported properties, it is not surprising that demand for shea kernels and butter has steadily increased in recent years for various purposes, including use as food (particularly as a cocoa butter additive in chocolate) and in medical and cosmetic products.2,4 The use of shea butter in skin care is attributed to its hydrating qualities and reputed effectiveness in softening scars.3
Constituents
Shea butter contains fatty acids that have been shown to improve the skin barrier. These include palmitic, stearic, and linoleic acid. It also contains the fatty acids oleic and arachidic. Shea butter also has phenolic components that function as antioxidants.
Anti-inflammatory effects
In 2010, Akihisa et al. evaluated the inhibitory effects of four triterpene acetates and four triterpene cinnamates isolated from the kernel fat of V. paradoxa against 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced inflammation in mice. All of the tested compounds showed considerable anti-inflammatory activity (ID50 values ranged from 0.15 to 0.75 micromol/ear). Lupeol cinnamate displayed the greatest anti-inflammatory activity, on carrageenan-induced edema on rat hind paws. All eight substances also exhibited moderate inhibitory effects on Epstein-Barr virus early antigen (EBV-EA) in Raji cells as a primary screening test for tumor promoter inhibitors. Using 7,12-dimethylbenz[a]anthracene (DMBA) as an initiator and TPA as a promoter in a two-stage carcinogenesis model in mice, the investigators also found that lupeol cinnamate inhibited skin tumor promotion. They concluded that the triterpenes and triterpene esters found in shea nuts and shea butter are significant anti-inflammatory and antitumor-promoting agents.2
The next year, Akihisa et al. determined the triacylglycerol and triterpene ester fraction composition of the kernel fats of the shea tree from 36 samples from Cote d’Ivoire, Ghana, Nigeria, Cameroon, Chad, Sudan, and Uganda. There were no significant differences in the composition of the triterpene ester fractions between West African and East African plants. Generally, though, West African shea kernel fats contained higher levels of high-melting triacylglycerols (e.g., stearic-oleic-stearic) and triterpene esters.6
Also that year, Olaitan et al. found that shea butter (as well as boa constrictor oil) was effective in suppressing the in vitro growth of normal and keloid fibroblasts.3
In 2012, Verma et al. used the lipopolysaccharide (LPS)-induced murine macrophage cell line J774 to investigate the anti-inflammatory properties of the methanolic extract of shea butter. They found that shea butter extract dose-dependently reduced, to a significant degree, the levels of nitric oxide, tumor necrosis factor (TNF)–alpha, as well as interleukin (IL)-1beta and IL-12 in the culture supernatants. In addition, the botanical extract suppressed IkappaB phosphorylation and NF-kappaB nuclear translocation as well as the expression of pro-inflammatory enzymes, inducible nitric oxide synthase (iNOS), and cyclooxygenase (COX)-2. The investigators attributed the anti-inflammatory activity of the extract to its inhibitory impact on LPS-induced iNOS, COX-2, TNF-alpha, IL-1beta, and IL-12 mRNA expression.1
In 2014, Honfo et al. conducted a literature review indicating that shea pulp is laden with vitamin C and the kernels contain copious fat (butter), which is used in food, drugs, and cosmetics.4
Notably, shea butter is also an ingredient in the topical nonsteroidal anti-inflammatory drug (NSAID) atopiclair, which has shown efficacy in alleviating pruritus in adults with mild to-moderate atopic dermatitis.7
Conclusion
Shea butter has long been incorporated into traditional medical practice in West and East Africa based on observed anti-inflammatory and analgesic characteristics. Such uses are compelling and often the basis for systematic scientific investigation. That said, there remains a dearth of experimental and clinical research on the potential cutaneous benefits of topically applied shea butter. Current data and traditional applications provide ample reason for continued research into this popular botanical agent.
References
1. J Complement Integr Med. 2012;9:Article 4.
2. J Oleo Sci. 2010;59[6]:273-80)
3. Wounds. 2011;23[4]:97-106.
4. Crit Rev Food Sci Nutr. 2014;54[5]:673-86.
5. J Agric Food Chem. 2003;51[21]:6268-73.
6. J Oleo Sci. 2011;60[8]:385-91.
7. J Drugs Dermatol. 2009 Jun;8[6]:537-9.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.
Indigenous to Africa, Vitellaria paradoxa, better known as the shea or shi tree, is a member of the Sapotaceae family. It has long been used in traditional medicine in sub-Saharan West Africa (as far west as Mali) as well as parts of East Africa (as far east as Uganda and Ethiopia) for its anti-inflammatory and analgesic properties.1,2
Some indications in traditional Nigerian medicine include nasal congestion, scabies, and ulcers.2 In addition, anecdotal success in treating keloids has been reported in association with traditional African remedies, including shea butter and boa constrictor oil.3 Antioxidant activities have also been linked to V. paradoxa.4 Given such purported properties, it is not surprising that demand for shea kernels and butter has steadily increased in recent years for various purposes, including use as food (particularly as a cocoa butter additive in chocolate) and in medical and cosmetic products.2,4 The use of shea butter in skin care is attributed to its hydrating qualities and reputed effectiveness in softening scars.3
Constituents
Shea butter contains fatty acids that have been shown to improve the skin barrier. These include palmitic, stearic, and linoleic acid. It also contains the fatty acids oleic and arachidic. Shea butter also has phenolic components that function as antioxidants.
Anti-inflammatory effects
In 2010, Akihisa et al. evaluated the inhibitory effects of four triterpene acetates and four triterpene cinnamates isolated from the kernel fat of V. paradoxa against 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced inflammation in mice. All of the tested compounds showed considerable anti-inflammatory activity (ID50 values ranged from 0.15 to 0.75 micromol/ear). Lupeol cinnamate displayed the greatest anti-inflammatory activity, on carrageenan-induced edema on rat hind paws. All eight substances also exhibited moderate inhibitory effects on Epstein-Barr virus early antigen (EBV-EA) in Raji cells as a primary screening test for tumor promoter inhibitors. Using 7,12-dimethylbenz[a]anthracene (DMBA) as an initiator and TPA as a promoter in a two-stage carcinogenesis model in mice, the investigators also found that lupeol cinnamate inhibited skin tumor promotion. They concluded that the triterpenes and triterpene esters found in shea nuts and shea butter are significant anti-inflammatory and antitumor-promoting agents.2
The next year, Akihisa et al. determined the triacylglycerol and triterpene ester fraction composition of the kernel fats of the shea tree from 36 samples from Cote d’Ivoire, Ghana, Nigeria, Cameroon, Chad, Sudan, and Uganda. There were no significant differences in the composition of the triterpene ester fractions between West African and East African plants. Generally, though, West African shea kernel fats contained higher levels of high-melting triacylglycerols (e.g., stearic-oleic-stearic) and triterpene esters.6
Also that year, Olaitan et al. found that shea butter (as well as boa constrictor oil) was effective in suppressing the in vitro growth of normal and keloid fibroblasts.3
In 2012, Verma et al. used the lipopolysaccharide (LPS)-induced murine macrophage cell line J774 to investigate the anti-inflammatory properties of the methanolic extract of shea butter. They found that shea butter extract dose-dependently reduced, to a significant degree, the levels of nitric oxide, tumor necrosis factor (TNF)–alpha, as well as interleukin (IL)-1beta and IL-12 in the culture supernatants. In addition, the botanical extract suppressed IkappaB phosphorylation and NF-kappaB nuclear translocation as well as the expression of pro-inflammatory enzymes, inducible nitric oxide synthase (iNOS), and cyclooxygenase (COX)-2. The investigators attributed the anti-inflammatory activity of the extract to its inhibitory impact on LPS-induced iNOS, COX-2, TNF-alpha, IL-1beta, and IL-12 mRNA expression.1
In 2014, Honfo et al. conducted a literature review indicating that shea pulp is laden with vitamin C and the kernels contain copious fat (butter), which is used in food, drugs, and cosmetics.4
Notably, shea butter is also an ingredient in the topical nonsteroidal anti-inflammatory drug (NSAID) atopiclair, which has shown efficacy in alleviating pruritus in adults with mild to-moderate atopic dermatitis.7
Conclusion
Shea butter has long been incorporated into traditional medical practice in West and East Africa based on observed anti-inflammatory and analgesic characteristics. Such uses are compelling and often the basis for systematic scientific investigation. That said, there remains a dearth of experimental and clinical research on the potential cutaneous benefits of topically applied shea butter. Current data and traditional applications provide ample reason for continued research into this popular botanical agent.
References
1. J Complement Integr Med. 2012;9:Article 4.
2. J Oleo Sci. 2010;59[6]:273-80)
3. Wounds. 2011;23[4]:97-106.
4. Crit Rev Food Sci Nutr. 2014;54[5]:673-86.
5. J Agric Food Chem. 2003;51[21]:6268-73.
6. J Oleo Sci. 2011;60[8]:385-91.
7. J Drugs Dermatol. 2009 Jun;8[6]:537-9.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever. Dr. Baumann also developed and owns the Baumann Skin Type Solution skin typing systems and related products.

Simulation model favors hernia surgery over watchful waiting
WASHINGTON – Surgical repair of ventral hernias at time of diagnosis is a more cost-effective approach than watchful waiting, according to the results of a state-transition microsimulation model presented by Lindsey Wolf, MD, at the annual clinical congress of the American College of Surgeons.
The benefit of surgical intervention, compared with observation or watchful waiting for reducible ventral hernias is not well described, reported Dr. Wolf, a general surgery resident at Brigham and Women’s Hospital, Boston.

In the model, cost was represented in U.S. dollars and benefit was indicated by quality-adjusted life years (QALY). Both measures accumulated for individual patients over time and then were averaged and reported for an entire cohort of simulated patients, Dr. Wolf explained. Incremental cost effectiveness, a measure represented as a ratio of cost per QALY gained for each strategy, “provides context by allowing us to compare each strategy to the next best strategy,” explained Dr. Wolf.
Willingness to pay, a threshold set by the government that represents the maximum amount a payer is willing to spend for additional quality, was set at a threshold of $50,000 dollars per QALY, which is a “commonly accepted willingness-to pay-threshold,” she said.
The model’s primary outcomes were lifetime costs, QALYs from time of diagnosis, and incremental cost-effectiveness ratios.
“We built a state-transition microsimulation model which represents the different health states a patient can occupy at any point in time,” Dr. Wolf reported. “Using a yearly cycle, a cohort of patients were simulated through the model one at a time.”
All patients entered the model in an asymptomatic state. For each year there was a probability for a patient to transition from the current state to another state in the model.
Patients who underwent surgical repair at diagnosis were transitioned to the no-hernia state in the first year after undergoing surgery. Those in the watchful-waiting group stayed in the asymptotic state and each year there was a probability of becoming symptomatic. Of those who became symptomatic, there was a small probability that they would present with an incarcerated hernia and would require emergent surgery rather than elective surgery. Patients were subjected to perioperative mortality rates, as well as background yearly risk of death.
Cohort characteristics, hospital and other costs, perioperative mortality, and quality of life were derived from best available published studies and the Nationwide Inpatient Sample, the largest all-payer inpatient care database in the United States.
Overall, laparoscopic surgery at diagnosis was the optimal hernia repair strategy, reported Dr. Wolf.
Although laparoscopic surgery was the most expensive, it was also the most effective and, compared with watchful waiting – the least expensive and least effective strategy – the incremental cost-effectiveness ratio was about $14,800 per QALY.
Open repair at diagnosis fell between the watchful-waiting and laparoscopic-repair strategies in terms of cost and effectiveness.
To understand the conditions in which the optimal strategy changed, the researchers performed sensitivity analysis using the net monetary benefit metric, which represented both costs and benefits in a single unit at a given willingness to pay threshold.
“For a cohort of high-risk patients, once the perioperative risk of death exceeds 3.4%, watchful waiting becomes the preferred strategy,” Dr. Wolf said. Watchful waiting also was the preferred strategy when the yearly risk of recurrence exceeded 24%.
A sensitivity analysis comparing quality of life for elective open and laparoscopic repair revealed that, when quality-of-life measures were similar between the two surgical repair groups, the open repair became the preferred strategy.
Finally, researchers performed probabilistic sensitivity analysis by simulating the cohort of 100,000 patients 100 times and each time deriving results that were similar – an indication of robust results.
“In conclusion, we found that, for a typical cohort of patients with ventral hernia, laparoscopic repair at diagnosis is very cost effective. As long-term outcomes for open and laparoscopic repair were very similar in the model, the decision between laparoscopic and open surgery depends on surgeon experience and preference for one method over another,” said Dr. Wolf.
This study was funded by the Resident Research Scholarship awarded by the American College of Surgeons. Dr. Wolf reported having no disclosures.
[email protected]
On Twitter @jessnicolecraig
WASHINGTON – Surgical repair of ventral hernias at time of diagnosis is a more cost-effective approach than watchful waiting, according to the results of a state-transition microsimulation model presented by Lindsey Wolf, MD, at the annual clinical congress of the American College of Surgeons.
The benefit of surgical intervention, compared with observation or watchful waiting for reducible ventral hernias is not well described, reported Dr. Wolf, a general surgery resident at Brigham and Women’s Hospital, Boston.
In the model, cost was represented in U.S. dollars and benefit was indicated by quality-adjusted life years (QALY). Both measures accumulated for individual patients over time and then were averaged and reported for an entire cohort of simulated patients, Dr. Wolf explained. Incremental cost effectiveness, a measure represented as a ratio of cost per QALY gained for each strategy, “provides context by allowing us to compare each strategy to the next best strategy,” explained Dr. Wolf.
Willingness to pay, a threshold set by the government that represents the maximum amount a payer is willing to spend for additional quality, was set at a threshold of $50,000 dollars per QALY, which is a “commonly accepted willingness-to pay-threshold,” she said.
The model’s primary outcomes were lifetime costs, QALYs from time of diagnosis, and incremental cost-effectiveness ratios.
“We built a state-transition microsimulation model which represents the different health states a patient can occupy at any point in time,” Dr. Wolf reported. “Using a yearly cycle, a cohort of patients were simulated through the model one at a time.”
All patients entered the model in an asymptomatic state. For each year there was a probability for a patient to transition from the current state to another state in the model.
Patients who underwent surgical repair at diagnosis were transitioned to the no-hernia state in the first year after undergoing surgery. Those in the watchful-waiting group stayed in the asymptotic state and each year there was a probability of becoming symptomatic. Of those who became symptomatic, there was a small probability that they would present with an incarcerated hernia and would require emergent surgery rather than elective surgery. Patients were subjected to perioperative mortality rates, as well as background yearly risk of death.
Cohort characteristics, hospital and other costs, perioperative mortality, and quality of life were derived from best available published studies and the Nationwide Inpatient Sample, the largest all-payer inpatient care database in the United States.
Overall, laparoscopic surgery at diagnosis was the optimal hernia repair strategy, reported Dr. Wolf.
Although laparoscopic surgery was the most expensive, it was also the most effective and, compared with watchful waiting – the least expensive and least effective strategy – the incremental cost-effectiveness ratio was about $14,800 per QALY.
Open repair at diagnosis fell between the watchful-waiting and laparoscopic-repair strategies in terms of cost and effectiveness.
To understand the conditions in which the optimal strategy changed, the researchers performed sensitivity analysis using the net monetary benefit metric, which represented both costs and benefits in a single unit at a given willingness to pay threshold.
“For a cohort of high-risk patients, once the perioperative risk of death exceeds 3.4%, watchful waiting becomes the preferred strategy,” Dr. Wolf said. Watchful waiting also was the preferred strategy when the yearly risk of recurrence exceeded 24%.
A sensitivity analysis comparing quality of life for elective open and laparoscopic repair revealed that, when quality-of-life measures were similar between the two surgical repair groups, the open repair became the preferred strategy.
Finally, researchers performed probabilistic sensitivity analysis by simulating the cohort of 100,000 patients 100 times and each time deriving results that were similar – an indication of robust results.
“In conclusion, we found that, for a typical cohort of patients with ventral hernia, laparoscopic repair at diagnosis is very cost effective. As long-term outcomes for open and laparoscopic repair were very similar in the model, the decision between laparoscopic and open surgery depends on surgeon experience and preference for one method over another,” said Dr. Wolf.
This study was funded by the Resident Research Scholarship awarded by the American College of Surgeons. Dr. Wolf reported having no disclosures.
[email protected]
On Twitter @jessnicolecraig
WASHINGTON – Surgical repair of ventral hernias at time of diagnosis is a more cost-effective approach than watchful waiting, according to the results of a state-transition microsimulation model presented by Lindsey Wolf, MD, at the annual clinical congress of the American College of Surgeons.
The benefit of surgical intervention, compared with observation or watchful waiting for reducible ventral hernias is not well described, reported Dr. Wolf, a general surgery resident at Brigham and Women’s Hospital, Boston.
In the model, cost was represented in U.S. dollars and benefit was indicated by quality-adjusted life years (QALY). Both measures accumulated for individual patients over time and then were averaged and reported for an entire cohort of simulated patients, Dr. Wolf explained. Incremental cost effectiveness, a measure represented as a ratio of cost per QALY gained for each strategy, “provides context by allowing us to compare each strategy to the next best strategy,” explained Dr. Wolf.
Willingness to pay, a threshold set by the government that represents the maximum amount a payer is willing to spend for additional quality, was set at a threshold of $50,000 dollars per QALY, which is a “commonly accepted willingness-to pay-threshold,” she said.
The model’s primary outcomes were lifetime costs, QALYs from time of diagnosis, and incremental cost-effectiveness ratios.
“We built a state-transition microsimulation model which represents the different health states a patient can occupy at any point in time,” Dr. Wolf reported. “Using a yearly cycle, a cohort of patients were simulated through the model one at a time.”
All patients entered the model in an asymptomatic state. For each year there was a probability for a patient to transition from the current state to another state in the model.
Patients who underwent surgical repair at diagnosis were transitioned to the no-hernia state in the first year after undergoing surgery. Those in the watchful-waiting group stayed in the asymptotic state and each year there was a probability of becoming symptomatic. Of those who became symptomatic, there was a small probability that they would present with an incarcerated hernia and would require emergent surgery rather than elective surgery. Patients were subjected to perioperative mortality rates, as well as background yearly risk of death.
Cohort characteristics, hospital and other costs, perioperative mortality, and quality of life were derived from best available published studies and the Nationwide Inpatient Sample, the largest all-payer inpatient care database in the United States.
Overall, laparoscopic surgery at diagnosis was the optimal hernia repair strategy, reported Dr. Wolf.
Although laparoscopic surgery was the most expensive, it was also the most effective and, compared with watchful waiting – the least expensive and least effective strategy – the incremental cost-effectiveness ratio was about $14,800 per QALY.
Open repair at diagnosis fell between the watchful-waiting and laparoscopic-repair strategies in terms of cost and effectiveness.
To understand the conditions in which the optimal strategy changed, the researchers performed sensitivity analysis using the net monetary benefit metric, which represented both costs and benefits in a single unit at a given willingness to pay threshold.
“For a cohort of high-risk patients, once the perioperative risk of death exceeds 3.4%, watchful waiting becomes the preferred strategy,” Dr. Wolf said. Watchful waiting also was the preferred strategy when the yearly risk of recurrence exceeded 24%.
A sensitivity analysis comparing quality of life for elective open and laparoscopic repair revealed that, when quality-of-life measures were similar between the two surgical repair groups, the open repair became the preferred strategy.
Finally, researchers performed probabilistic sensitivity analysis by simulating the cohort of 100,000 patients 100 times and each time deriving results that were similar – an indication of robust results.
“In conclusion, we found that, for a typical cohort of patients with ventral hernia, laparoscopic repair at diagnosis is very cost effective. As long-term outcomes for open and laparoscopic repair were very similar in the model, the decision between laparoscopic and open surgery depends on surgeon experience and preference for one method over another,” said Dr. Wolf.
This study was funded by the Resident Research Scholarship awarded by the American College of Surgeons. Dr. Wolf reported having no disclosures.
[email protected]
On Twitter @jessnicolecraig
AT THE ACS CLINICAL CONGRESS
Key clinical point:
Major finding: The incremental cost-effectiveness ratio for laparoscopic surgery, compared with watchful waiting, was about $14,800 per QALY.
Data source: A state-transition microsimulation model of 100,000 people.
Disclosures: This study was funded by the Resident Research Scholarship awarded by the American College of Surgeons. Dr. Wolf reported having no disclosures.
Lack of health literacy and normal routine implicated in hepatitis B virus treatment nonadherence
BOSTON – Lack of health literacy, lack of routine, and being a nonnative speaker of English were predictors of treatment nonadherence in one-quarter of adults with hepatitis B virus in Australia, according to a study.
“Clinicians don’t know this is happening. We overlook it. Because it’s just one tablet a day, we think it’s quite easy, but when I took up this project, I completely underestimated the complexity of adherence and how many different factors can play into why a patient does or doesn’t adhere,” Suzanne Sheppard-Law, RN, MPH, PhD, a senior research fellow at the University of Technology Sydney, said in an interview about her prize-winning poster presentation at this year’s annual meeting of the American Association for the Study of Liver Diseases.
The findings grew from Dr. Sheppard-Law’s clinical practice where she noticed a trend in some patients whose treatment regimen would lose efficacy over time. When switched to other therapies, the pattern would be repeated. Dr. Sheppard-Law interviewed 29 of these patients in person to see if there were commonalities she could address.
“The deeper I dug, the more it all unfolded before me,” she said. It turned out that patients who’d been endorsing adherence were not. In some cases, patients were skipping their medications for days at a time.
This informal study lead to a more formal one focused on a patient’s level of health literacy. Dr. Sheppard-Law and her colleagues examined factors the World Health Organization says are implicated in adherence, including ones that are social and economic, and others that are related to clinical worker interactions, health systems, individual therapy and condition, and patient considerations. They conducted in-person interviews and worked with the patients as they completed the Newest Vital Sign health literacy survey online.
Just over a fifth of respondents said they followed a regular routine when taking their medication, such as taking it at a certain time every day; however, three-quarters of those surveyed said they didn’t think having a routine made any difference (P less than .001). Half of respondents were prescribed at least one additional daily medication to their antiretroviral pill. A third had no idea what type of medication was prescribed for their hepatitis B.
Whether the person was proficient in English, and the impact this had on perceived communication between the patient and clinician was another factor, as most of the patients in the study were immigrants to Australia who’d been living there, on average, about 19 years. Only 27% of the study group reported that they spoke English at home as their primary language.
“It has to be individually focused, person-centered care, is the conclusion I came to,” Dr. Sheppard-Law said. Although her findings do not indicate a need for more resources in the clinic, she did say that clinicians could help patients by asking them to repeat back to them what they have heard.
“I don’t believe it has to be more resource intense; you just need to be sure the patient understands at the beginning what they need to do. Then you have a better chance [they will adhere],” she said. Because patients with poor health literacy are unlikely to tell their clinician that they do not fully grasp what they are being told about their condition and their treatment, Dr. Sheppard-Law suggested asking patients at the end of their consultation to detail what their routine will be, what they will do if they lose their prescription, what they will do if they run out of medication, and asking if they understand that their medication must be taken daily. “They need to understand it’s not okay to skip a day,” she said. “It’s our responsibility to ensure they know that.”
[email protected]
On Twitter @whitneymcknight
BOSTON – Lack of health literacy, lack of routine, and being a nonnative speaker of English were predictors of treatment nonadherence in one-quarter of adults with hepatitis B virus in Australia, according to a study.
“Clinicians don’t know this is happening. We overlook it. Because it’s just one tablet a day, we think it’s quite easy, but when I took up this project, I completely underestimated the complexity of adherence and how many different factors can play into why a patient does or doesn’t adhere,” Suzanne Sheppard-Law, RN, MPH, PhD, a senior research fellow at the University of Technology Sydney, said in an interview about her prize-winning poster presentation at this year’s annual meeting of the American Association for the Study of Liver Diseases.
The findings grew from Dr. Sheppard-Law’s clinical practice where she noticed a trend in some patients whose treatment regimen would lose efficacy over time. When switched to other therapies, the pattern would be repeated. Dr. Sheppard-Law interviewed 29 of these patients in person to see if there were commonalities she could address.
“The deeper I dug, the more it all unfolded before me,” she said. It turned out that patients who’d been endorsing adherence were not. In some cases, patients were skipping their medications for days at a time.
This informal study lead to a more formal one focused on a patient’s level of health literacy. Dr. Sheppard-Law and her colleagues examined factors the World Health Organization says are implicated in adherence, including ones that are social and economic, and others that are related to clinical worker interactions, health systems, individual therapy and condition, and patient considerations. They conducted in-person interviews and worked with the patients as they completed the Newest Vital Sign health literacy survey online.
Just over a fifth of respondents said they followed a regular routine when taking their medication, such as taking it at a certain time every day; however, three-quarters of those surveyed said they didn’t think having a routine made any difference (P less than .001). Half of respondents were prescribed at least one additional daily medication to their antiretroviral pill. A third had no idea what type of medication was prescribed for their hepatitis B.
Whether the person was proficient in English, and the impact this had on perceived communication between the patient and clinician was another factor, as most of the patients in the study were immigrants to Australia who’d been living there, on average, about 19 years. Only 27% of the study group reported that they spoke English at home as their primary language.
“It has to be individually focused, person-centered care, is the conclusion I came to,” Dr. Sheppard-Law said. Although her findings do not indicate a need for more resources in the clinic, she did say that clinicians could help patients by asking them to repeat back to them what they have heard.
“I don’t believe it has to be more resource intense; you just need to be sure the patient understands at the beginning what they need to do. Then you have a better chance [they will adhere],” she said. Because patients with poor health literacy are unlikely to tell their clinician that they do not fully grasp what they are being told about their condition and their treatment, Dr. Sheppard-Law suggested asking patients at the end of their consultation to detail what their routine will be, what they will do if they lose their prescription, what they will do if they run out of medication, and asking if they understand that their medication must be taken daily. “They need to understand it’s not okay to skip a day,” she said. “It’s our responsibility to ensure they know that.”
[email protected]
On Twitter @whitneymcknight
BOSTON – Lack of health literacy, lack of routine, and being a nonnative speaker of English were predictors of treatment nonadherence in one-quarter of adults with hepatitis B virus in Australia, according to a study.
“Clinicians don’t know this is happening. We overlook it. Because it’s just one tablet a day, we think it’s quite easy, but when I took up this project, I completely underestimated the complexity of adherence and how many different factors can play into why a patient does or doesn’t adhere,” Suzanne Sheppard-Law, RN, MPH, PhD, a senior research fellow at the University of Technology Sydney, said in an interview about her prize-winning poster presentation at this year’s annual meeting of the American Association for the Study of Liver Diseases.
The findings grew from Dr. Sheppard-Law’s clinical practice where she noticed a trend in some patients whose treatment regimen would lose efficacy over time. When switched to other therapies, the pattern would be repeated. Dr. Sheppard-Law interviewed 29 of these patients in person to see if there were commonalities she could address.
“The deeper I dug, the more it all unfolded before me,” she said. It turned out that patients who’d been endorsing adherence were not. In some cases, patients were skipping their medications for days at a time.
This informal study lead to a more formal one focused on a patient’s level of health literacy. Dr. Sheppard-Law and her colleagues examined factors the World Health Organization says are implicated in adherence, including ones that are social and economic, and others that are related to clinical worker interactions, health systems, individual therapy and condition, and patient considerations. They conducted in-person interviews and worked with the patients as they completed the Newest Vital Sign health literacy survey online.
Just over a fifth of respondents said they followed a regular routine when taking their medication, such as taking it at a certain time every day; however, three-quarters of those surveyed said they didn’t think having a routine made any difference (P less than .001). Half of respondents were prescribed at least one additional daily medication to their antiretroviral pill. A third had no idea what type of medication was prescribed for their hepatitis B.
Whether the person was proficient in English, and the impact this had on perceived communication between the patient and clinician was another factor, as most of the patients in the study were immigrants to Australia who’d been living there, on average, about 19 years. Only 27% of the study group reported that they spoke English at home as their primary language.
“It has to be individually focused, person-centered care, is the conclusion I came to,” Dr. Sheppard-Law said. Although her findings do not indicate a need for more resources in the clinic, she did say that clinicians could help patients by asking them to repeat back to them what they have heard.
“I don’t believe it has to be more resource intense; you just need to be sure the patient understands at the beginning what they need to do. Then you have a better chance [they will adhere],” she said. Because patients with poor health literacy are unlikely to tell their clinician that they do not fully grasp what they are being told about their condition and their treatment, Dr. Sheppard-Law suggested asking patients at the end of their consultation to detail what their routine will be, what they will do if they lose their prescription, what they will do if they run out of medication, and asking if they understand that their medication must be taken daily. “They need to understand it’s not okay to skip a day,” she said. “It’s our responsibility to ensure they know that.”
[email protected]
On Twitter @whitneymcknight
AT THE LIVER MEETING 2016
Key clinical point:
Major finding: A quarter of adults with hepatitis B virus were treatment noncompliant in the past 30 days.
Data source: In-person and online survey of 277 adults with hepatitis B virus.
Disclosures: Dr. Sheppard-Law did not have any relevant disclosures.
Urate-lowering therapy poses no harm to kidney function
WASHINGTON – Evidence supporting the renal benefits of urate-lowering therapy in patients with hyperuricemia and gout comes from two separate studies presented at the annual meeting of the American College of Rheumatology.
In the first study, allopurinol did not increase the risk of developing chronic kidney disease (CKD) in newly diagnosed patients with gout and normal or near-normal kidney function. The second study found that urate-lowering therapy (ULT) improved kidney function in patients who already had CKD.
Allopurinol in gout
The study was prompted by the recognition that gout patients are underdiagnosed and undertreated, and even when they have a diagnosis, both patients and primary care physicians who treat the majority of gout patients shy away from ULT.

“Further exacerbating the poor management of gout is the common practice of lowering the dose or stopping allopurinol when a patient with gout begins to have a decline in kidney function, which inevitably adds to the poor control of gout,” Dr. Vargas-Santos explained.
The study was based on electronic health records from the Health Improvement Network (THIN) database that includes patients treated by general practitioners in the United Kingdom. The study enrolled 13,608 patients with newly diagnosed gout and normal kidney function who initiated ULT with allopurinol; these patients were compared with 13,608 gout patients (matched by propensity score) in the THIN database who did not start ULT.
Patients were aged 18-89 years (mean age, 58 years) with incident gout diagnosed between 2000 and 2014 who had at least one contact with a general practitioner within a year of study enrollment. The investigators analyzed the relationship between allopurinol use by gout patients and the development of CKD stage 3 or higher.
At a mean follow-up of 4 years, there was no increased risk of developing CKD stage 3 or higher in the allopurinol users: 1,401 of the allopurinol initiators versus 1,319 of nonusers developed CKD stage 3 or higher. The relative risk of developing CKD stage 3 or higher on allopurinol was 1.05, which was not statistically significant. “Our study shows that there was no risk of harm to the kidney with allopurinol. This suggests that if a patient on gout presents with declining kidney function, it is better to look for other causes and keep the patient on allopurinol to lower serum urate. Accumulating evidence supports this. Doctors have to be less fearful of prescribing allopurinol. Gout patients deserve better,” Dr. Vargas-Santos said.
ULT in CKD
ULT improved kidney function in patients with CKD in a large retrospective study, with the greatest improvement observed in patients with CKD stage 3 and some improvement observed in patients with CKD stage 2. ULT had no benefit in patients with CKD stage 4, suggesting that these patients are too advanced to improve.

The study was conducted from 2008 to 2014 and included 12,751 patients with serum urate levels of greater than 7 mg/dL and CKD stages 2, 3, and 4 at the index date (the first time this test result was reported). Patients were drawn from the Kaiser Permanente database and treated by primary care physicians. Patients were followed for 1 year from the index date. The primary outcome measure was a 30% increase or a 30% decrease in glomerular filtration rate (GFR) from baseline to the last available result.
Of the 12,751 patients, 2,690 were on ULT and 10,061 were not. Goal serum urate (sUA) was achieved in 1,118 (42%) of patients on ULT. Among patients who achieved goal sUA, a 30% improvement in GFR was observed in 17.1% versus 10.4% of patients who did not achieve goal sUA, for an absolute difference of 6.7% (P less than .001).
For patients at goal versus those not at goal, the ratio of improvement was 3.4 and 3.8, respectively.
“This study suggests that patients with CKD should be tested for uric acid independent of whether they have gout or not. Getting to goal is important. Stage 3 CKD is the sweet spot where patients got the most pronounced benefit from urate-lowering therapy,” he said. “Stage 4 CDK is too late.”
The authors of both studies had no relevant financial disclosures to report.
WASHINGTON – Evidence supporting the renal benefits of urate-lowering therapy in patients with hyperuricemia and gout comes from two separate studies presented at the annual meeting of the American College of Rheumatology.
In the first study, allopurinol did not increase the risk of developing chronic kidney disease (CKD) in newly diagnosed patients with gout and normal or near-normal kidney function. The second study found that urate-lowering therapy (ULT) improved kidney function in patients who already had CKD.
Allopurinol in gout
The study was prompted by the recognition that gout patients are underdiagnosed and undertreated, and even when they have a diagnosis, both patients and primary care physicians who treat the majority of gout patients shy away from ULT.
“Further exacerbating the poor management of gout is the common practice of lowering the dose or stopping allopurinol when a patient with gout begins to have a decline in kidney function, which inevitably adds to the poor control of gout,” Dr. Vargas-Santos explained.
The study was based on electronic health records from the Health Improvement Network (THIN) database that includes patients treated by general practitioners in the United Kingdom. The study enrolled 13,608 patients with newly diagnosed gout and normal kidney function who initiated ULT with allopurinol; these patients were compared with 13,608 gout patients (matched by propensity score) in the THIN database who did not start ULT.
Patients were aged 18-89 years (mean age, 58 years) with incident gout diagnosed between 2000 and 2014 who had at least one contact with a general practitioner within a year of study enrollment. The investigators analyzed the relationship between allopurinol use by gout patients and the development of CKD stage 3 or higher.
At a mean follow-up of 4 years, there was no increased risk of developing CKD stage 3 or higher in the allopurinol users: 1,401 of the allopurinol initiators versus 1,319 of nonusers developed CKD stage 3 or higher. The relative risk of developing CKD stage 3 or higher on allopurinol was 1.05, which was not statistically significant. “Our study shows that there was no risk of harm to the kidney with allopurinol. This suggests that if a patient on gout presents with declining kidney function, it is better to look for other causes and keep the patient on allopurinol to lower serum urate. Accumulating evidence supports this. Doctors have to be less fearful of prescribing allopurinol. Gout patients deserve better,” Dr. Vargas-Santos said.
ULT in CKD
ULT improved kidney function in patients with CKD in a large retrospective study, with the greatest improvement observed in patients with CKD stage 3 and some improvement observed in patients with CKD stage 2. ULT had no benefit in patients with CKD stage 4, suggesting that these patients are too advanced to improve.
The study was conducted from 2008 to 2014 and included 12,751 patients with serum urate levels of greater than 7 mg/dL and CKD stages 2, 3, and 4 at the index date (the first time this test result was reported). Patients were drawn from the Kaiser Permanente database and treated by primary care physicians. Patients were followed for 1 year from the index date. The primary outcome measure was a 30% increase or a 30% decrease in glomerular filtration rate (GFR) from baseline to the last available result.
Of the 12,751 patients, 2,690 were on ULT and 10,061 were not. Goal serum urate (sUA) was achieved in 1,118 (42%) of patients on ULT. Among patients who achieved goal sUA, a 30% improvement in GFR was observed in 17.1% versus 10.4% of patients who did not achieve goal sUA, for an absolute difference of 6.7% (P less than .001).
For patients at goal versus those not at goal, the ratio of improvement was 3.4 and 3.8, respectively.
“This study suggests that patients with CKD should be tested for uric acid independent of whether they have gout or not. Getting to goal is important. Stage 3 CKD is the sweet spot where patients got the most pronounced benefit from urate-lowering therapy,” he said. “Stage 4 CDK is too late.”
The authors of both studies had no relevant financial disclosures to report.
WASHINGTON – Evidence supporting the renal benefits of urate-lowering therapy in patients with hyperuricemia and gout comes from two separate studies presented at the annual meeting of the American College of Rheumatology.
In the first study, allopurinol did not increase the risk of developing chronic kidney disease (CKD) in newly diagnosed patients with gout and normal or near-normal kidney function. The second study found that urate-lowering therapy (ULT) improved kidney function in patients who already had CKD.
Allopurinol in gout
The study was prompted by the recognition that gout patients are underdiagnosed and undertreated, and even when they have a diagnosis, both patients and primary care physicians who treat the majority of gout patients shy away from ULT.
“Further exacerbating the poor management of gout is the common practice of lowering the dose or stopping allopurinol when a patient with gout begins to have a decline in kidney function, which inevitably adds to the poor control of gout,” Dr. Vargas-Santos explained.
The study was based on electronic health records from the Health Improvement Network (THIN) database that includes patients treated by general practitioners in the United Kingdom. The study enrolled 13,608 patients with newly diagnosed gout and normal kidney function who initiated ULT with allopurinol; these patients were compared with 13,608 gout patients (matched by propensity score) in the THIN database who did not start ULT.
Patients were aged 18-89 years (mean age, 58 years) with incident gout diagnosed between 2000 and 2014 who had at least one contact with a general practitioner within a year of study enrollment. The investigators analyzed the relationship between allopurinol use by gout patients and the development of CKD stage 3 or higher.
At a mean follow-up of 4 years, there was no increased risk of developing CKD stage 3 or higher in the allopurinol users: 1,401 of the allopurinol initiators versus 1,319 of nonusers developed CKD stage 3 or higher. The relative risk of developing CKD stage 3 or higher on allopurinol was 1.05, which was not statistically significant. “Our study shows that there was no risk of harm to the kidney with allopurinol. This suggests that if a patient on gout presents with declining kidney function, it is better to look for other causes and keep the patient on allopurinol to lower serum urate. Accumulating evidence supports this. Doctors have to be less fearful of prescribing allopurinol. Gout patients deserve better,” Dr. Vargas-Santos said.
ULT in CKD
ULT improved kidney function in patients with CKD in a large retrospective study, with the greatest improvement observed in patients with CKD stage 3 and some improvement observed in patients with CKD stage 2. ULT had no benefit in patients with CKD stage 4, suggesting that these patients are too advanced to improve.
The study was conducted from 2008 to 2014 and included 12,751 patients with serum urate levels of greater than 7 mg/dL and CKD stages 2, 3, and 4 at the index date (the first time this test result was reported). Patients were drawn from the Kaiser Permanente database and treated by primary care physicians. Patients were followed for 1 year from the index date. The primary outcome measure was a 30% increase or a 30% decrease in glomerular filtration rate (GFR) from baseline to the last available result.
Of the 12,751 patients, 2,690 were on ULT and 10,061 were not. Goal serum urate (sUA) was achieved in 1,118 (42%) of patients on ULT. Among patients who achieved goal sUA, a 30% improvement in GFR was observed in 17.1% versus 10.4% of patients who did not achieve goal sUA, for an absolute difference of 6.7% (P less than .001).
For patients at goal versus those not at goal, the ratio of improvement was 3.4 and 3.8, respectively.
“This study suggests that patients with CKD should be tested for uric acid independent of whether they have gout or not. Getting to goal is important. Stage 3 CKD is the sweet spot where patients got the most pronounced benefit from urate-lowering therapy,” he said. “Stage 4 CDK is too late.”
The authors of both studies had no relevant financial disclosures to report.
AT THE ACR ANNUAL MEETING
Key clinical point:
Major finding: The first study found that allopurinol did not increase the risk of developing CKD stage 3 or higher in gout patients with normal or near-normal kidney function. The second study found that reaching goal with urate-lowering therapy led to improved kidney function, especially in patients with stage 3 CKD.
Data source: Two population-based studies based on the U.K.’s THIN database. The first included 13,608 patients and 13,608 matched controls. The second study included 12,751 patients with serum urate levels of greater than 7 mg/dL.
Disclosures: The authors of both studies had no relevant financial disclosures to report.
VIDEO: For CABG, double arterial grafts found no better than single
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions

The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions
The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
NEW ORLEANS – Patients undergoing coronary artery bypass graft (CABG) surgery do not see any 5-year survival advantage when their surgeon uses both internal mammary (thoracic) arteries for grafting rather than just one of them along with a vein, finds an interim analysis from the randomized Arterial Revascularization Trial (ART).
Overall, about 8.5% of the 3,102 patients randomized had died 5 years after surgery, with no significant difference between the bilateral graft and single graft groups, according to data reported at the American Heart Association scientific sessions and simultaneously published (N Engl J Med. 2016 Nov 14. doi: 10.1056/NEJMoa1610021). The former had roughly triple the rate of sternal reconstruction, mainly driven by complications in insulin-dependent diabetes patients having high body mass index.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
There is strong angiographic evidence that vein grafts have a high rate of failure over time because of atherosclerosis, but internal mammary artery grafts retain excellent patency, he elaborated. “People have speculated that this superior patency of internal mammary arteries will translate into a clinical survival benefit,” and observational data indeed suggest that the bilateral artery strategy reduces mortality by about one-fifth relative to the single artery strategy.
Yet uptake of the bilateral procedure has been low. It is used in fewer than 5% of patients undergoing CABG in the United States and fewer than 10% of those in Europe, reflecting concerns about its greater technical complexity, potentially increased mortality and morbidity, and – until now – lack of evidence from randomized trials.
“What I think we can conclude today is that there are excellent 5-year outcomes of CABG in both groups. This study confirms that it’s at least safe to use bilateral grafts over the medium term,” Dr. Taggart commented. He discussed the results in a video interview conducted at the meeting.
These interim ART data probably won’t sway practice one way or the other, he said. “People who believe in arterial grafts will continue to do them, and those who are not enthusiastic about the prospect of a slightly technically more difficult operation [can now] remain comfortable as to why they are not using both internal mammary arteries.”
Pointed questions
The lack of difference was possibly due to a very high level of guideline-based medical therapy in the trial (which may have especially protected the vein grafts) or to the fact that the annual failure rate of vein grafts is modest and steady up to 5 years but accelerates thereafter, Dr. Taggart proposed. The trial’s primary outcome of 10-year survival, expected in 2018, will likely differ, speculated Dr. Sellke, who is also program chair for the AHA scientific sessions.
“Do you think multiple arterial grafting is superior to single internal mammary artery grafting considering the lack of improvement in survival and other outcomes in the study, with the increase in sternal wound infections?” he asked.
“I personally, if I needed the operation, would insist on having bilateral internal mammary artery grafts done by an experienced operator because it is totally counterintuitive to believe that having more patent grafts in your heart at 10 to 20 years of follow-up is of no benefit,” Dr. Taggart maintained.
When data meet clinical practice
It may require time for the benefit of the bilateral artery graft to emerge, he agreed. “I’m undeterred from my belief that ... in patients who are getting CABG done in their 40s or 50s or early 60s, betting on a graft that’s going to outperform vein grafts is the better strategy.”
Until the trial’s 10-year results become available, physicians may wish to put these interim results in the context when counseling patients, according to Dr. Gardner.
“We have indisputable evidence that arterial grafts have better long-term patency than vein grafts,” he elaborated. “If we had a very sophisticated patient, we might tell them that we were a little surprised that this head-to-head trial of single versus double didn’t show any survival benefit at 5 years, but we still are persuaded by the data that shows the better patency, and we think in the situation that the patient’s in, that we would still recommend a double mammary, assuming that the patient doesn’t have comorbidities that would make that more dangerous.”
Trial details
ART enrolled patients from 28 cardiac surgical centers in seven countries. The patients, all of whom had multivessel coronary disease and were scheduled to undergo CABG, were randomized evenly to single or bilateral internal thoracic artery grafts.
The interim results showed differences in nonadherence to the randomized operation: 2.4% of patients in the single graft group ultimately underwent got bilateral grafts, whereas 14% of patients in the bilateral graft group ultimately got a single graft.
“This raises questions about how experienced some surgeons were with the use of bilateral internal mammary artery grafts,” Dr. Taggart commented.
At 5 years of follow-up, 8.7% of patients in the bilateral graft group and 8.4% of patients in the single graft group had died, a nonsignificant difference. “Those mortalities are similar to what has been observed in other contemporary trials of CABG,” he noted. There was no difference between diabetic and nondiabetic patients with respect to this outcome.
The rate of the composite outcome of death, myocardial infarction, or stroke was 12.2% in the bilateral graft group and 12.7% in the single graft group, also a nonsignificant difference.
On the other hand, patients in the bilateral graft group had higher rates of sternal wound complications (3.5% vs. 1.9%; P = .005) and sternal reconstruction (1.9% vs. 0.6%; P = .002).
The groups were statistically indistinguishable with respect to rates of mortality, major bleeding, or need for repeat revascularization, as well as angina status and quality of life measures, according to Dr. Taggart, who disclosed that he had no relevant conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: At 5 years, the rate of all-cause mortality was 8.7% in the bilateral graft group and 8.4% in the single graft group, a nonsignificant difference.
Data source: ART, a randomized trial among 3,102 patients with multivessel coronary disease undergoing CABG.
Disclosures: Dr. Taggart had no relevant conflicts of interest. The trial was funded by the U.K. Medical Research Council, the British Heart Foundation, and the U.K. National Institute of Health Research Efficacy and Mechanistic Evaluation.