User login
Highlights from the ASDS Annual Conference 2016
At this year’s American Society for Dermatologic Surgery (ASDS) annual meeting, many of the hot topics pertained to tightening and smoothness of the skin. More naturally derived skin care products were discussed, as well as skin-tightening devices, techniques for improving fat, microneedling, devices for improving cellulite, and some of the newer injectable fillers on the market.
Of all of these, the use of microneedling with and without radiofrequency energy to improve acne scars, rhytids, and pore size was the most prominent emerging trend. Microneedling devices with radiofrequency also are being used for skin tightening, in addition to improving skin texture.

There were also presentations on improvements in acne scars with a number of techniques, including fractional ablative and nonablative lasers, subcision, microneedling, and fillers.
Controversies addressed at the meeting included whether or not dermatologists should use the same lasers with different Food and Drug Administration–approved hand pieces for vaginal rejuvenation. In addition, controversies over whether Mohs surgeons should undergo board examination were discussed.

Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Write to them at [email protected].
At this year’s American Society for Dermatologic Surgery (ASDS) annual meeting, many of the hot topics pertained to tightening and smoothness of the skin. More naturally derived skin care products were discussed, as well as skin-tightening devices, techniques for improving fat, microneedling, devices for improving cellulite, and some of the newer injectable fillers on the market.
Of all of these, the use of microneedling with and without radiofrequency energy to improve acne scars, rhytids, and pore size was the most prominent emerging trend. Microneedling devices with radiofrequency also are being used for skin tightening, in addition to improving skin texture.
There were also presentations on improvements in acne scars with a number of techniques, including fractional ablative and nonablative lasers, subcision, microneedling, and fillers.
Controversies addressed at the meeting included whether or not dermatologists should use the same lasers with different Food and Drug Administration–approved hand pieces for vaginal rejuvenation. In addition, controversies over whether Mohs surgeons should undergo board examination were discussed.
Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Write to them at [email protected].
At this year’s American Society for Dermatologic Surgery (ASDS) annual meeting, many of the hot topics pertained to tightening and smoothness of the skin. More naturally derived skin care products were discussed, as well as skin-tightening devices, techniques for improving fat, microneedling, devices for improving cellulite, and some of the newer injectable fillers on the market.
Of all of these, the use of microneedling with and without radiofrequency energy to improve acne scars, rhytids, and pore size was the most prominent emerging trend. Microneedling devices with radiofrequency also are being used for skin tightening, in addition to improving skin texture.
There were also presentations on improvements in acne scars with a number of techniques, including fractional ablative and nonablative lasers, subcision, microneedling, and fillers.
Controversies addressed at the meeting included whether or not dermatologists should use the same lasers with different Food and Drug Administration–approved hand pieces for vaginal rejuvenation. In addition, controversies over whether Mohs surgeons should undergo board examination were discussed.
Dr. Talakoub and Dr. Wesley are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley. Write to them at [email protected].
Two Truths About Substance Use and One Hope Unite Us
Given the recently concluded election season, it may seem that there are few things Americans have in common or can agree on. And although I did not conduct a poll or hold a debate, I suspect that a majority of those who work in the VA, DoD, or PHS would agree that one of the most serious and prevalent public health problems facing those in federal service and in the country at large is the epidemic of substance use disorders (SUDs).
In 2013 the National Institute on Drug Abuse reported that “members of the armed forces are not immune to the substance use problems that affect the rest of society.”1 Although active-duty service members use illicit drugs less frequently, as would be expected given the potential disciplinary consequences, the prevalence of problematic use of the legal ones—tobacco, alcohol, and particularly prescription medications—is greater among individuals in the military.
Substance use disorders affect every sector of federal health care practice from military pediatrics and VA pathology to PHS primary care. Reflecting this ubiquity, in this special substance use disorders issue of Federal Practitioner we focus on several distinctive and significant efforts of health care practitioners who care for patients with SUDs. All of medicine is becoming more interdisciplinary, multidisciplinary, and team-based, but perhaps no other area has as long a legacy or as intrinsic a need for team approaches to care than does the diagnosis and treatment of SUDs. We see this need reflected in this issue’s articles authored by clinical pharmacists, nurse practitioners, physicians, and physicians in training, among others.
Prescription opioids are the subject of 3 articles from VA practitioners: a look at primary, secondary, and tertiary forms of prevention of morbidity and mortality from substance use. Pharmacists at the Salt Lake City VAMC studied the epidemiology of veterans seen in emergency departments who were given naloxone for unintentional opioid overdoses. A second article reviews the distribution of naloxone at a VA facility, providing an example of a successful implementation of the VA Overdose Education and Naloxone Distribution network (OEND)—the only national naloxone program in any health care system.
Even farther upstream in the effort to reduce the large doses of opioids that are directly related to overdose deaths is an article on an outpatient opioid-monitoring clinic that uses evidence-based medicine to diagnose patients with opioid use disorder. Research in the VHA showed that in a 4-year period of study, “the risk of overdose deaths was directly related to the maximum prescribed daily dose of opioid medication.”2
Our colleagues in active duty underscore the challenge that new and emerging substances present not only to federal regulatory agencies like the Drug Enforcement Agency, but also to state and local law enforcement agencies. When spice (synthetic cannabinoids) and bath salts (synthetic cathinones) first appeared, no drug tests were available to detect them. Technically not illegal in the early phase of their use, they became the perfect and popular drugs of young service men and women.3
Tragically, history has shown 2 truths about humans and the use of psychoactive products. The first is that as soon as one product is outlawed, creative chemists invent another mind-altering product. Practical education regarding the latest of these underground drugs, kratom, which threatens our service members, is introduced in this issue.
The second truth is that nearly every drug that is originally prescribed for legitimate medical reasons is eventually misused for a nonmedical purpose and can lead to SUDs. By the time the medical community realizes the dark side of the medication, many individuals have already developed a disorder, and sadly some have died.
One of the oldest classes of drugs that brings both relief and torment to human culture—opioid medication—is now the scourge of postmodern society. Our well-intentioned efforts to succor real pain for patients using prescription opioids have paved a road to hellish suffering for others. A recent study examined whether a resurgence of heroin use among veterans—the likes of which has not been seen since the Vietnam era—was associated with the nonmedical use of yes, prescribed narcotics. The same study found that solely having chronic pain was not correlated with the use of heroin.4 This finding offers the hope that practitioners and patients together can learn to treat chronic pain with opioids in selected patients, which can be life-restoring in appropriate cases for limited duration, safely and responsibly while avoiding and minimizing the death dealing blow of opioid use disorders.
In this issue, we also feature a discussion with Karen Drexler, MD, the newly appointed Mental Health Program Director, Addictive Disorders. Dr. Drexler expertly discusses a wide array of SUD subjects relevant to Federal Practitioner readers, including the approach to patients using medical marijuana in the VA, the 2016 VA/DoD Clinical Practice Guidelines, and an inside view of the challenges and successes of VA SUD programs, from the vantage point of the new leader of these critical initiatives.
Finally, astute readers may notice the editorial attempts to avoid use of the value-laden terms addiction and substance abuse. Instead, the less stigmatizing terminology of DSM-5 is employed, which jettisons the problematic abuse and dependence distinction for the unitary domain of SUDs. This approach is not just a change in semantics but as thought leaders have shown, a real and meaningful comprehension of the role of words in shaping culture.5 The VA as a health care entity is moving to adopt better scientific framing of SUDs as a salient step toward a recovery-oriented program.
In the coming months, we intend to expand our coverage of this public health crisis, and we invite readers who care every day for patients wrestling with SUDs for control of their health and very lives, to educate, advocate for resources for active-duty service personnel and veterans, and share innovative efforts to turn the tide toward recovery.
1. National Institute on Drug Abuse. DrugFacts—substance abuse in the military. https://www.drugabuse.gov/publications/drugfacts/substance-abuse-in-military. Revised March 2013. Accessed October 18, 2016.
2. Loeffler G, Hurst D, Penn A, Yung K. Spice, bath salts, and the U.S. military: the emergence of synthetic cannabinoid receptor agonists and cathinones in the U.S. Armed Forces. Mil Med. 2012;177(9):1041-1048.
3. Banerjee G, Edelman EJ, Barry DT, et al. Non-medical use of prescription opioids is associated with heroin initiation among U.S. veterans: a prospective cohort study. Addiction. 2016;111(11):2021-2031.
4. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid-related deaths. JAMA. 2011;305(13):1315-1321.
5. Botticelli MP, Koh HK. Changing the language of addiction. JAMA. 2016;316(13):1361-1362.
Given the recently concluded election season, it may seem that there are few things Americans have in common or can agree on. And although I did not conduct a poll or hold a debate, I suspect that a majority of those who work in the VA, DoD, or PHS would agree that one of the most serious and prevalent public health problems facing those in federal service and in the country at large is the epidemic of substance use disorders (SUDs).
In 2013 the National Institute on Drug Abuse reported that “members of the armed forces are not immune to the substance use problems that affect the rest of society.”1 Although active-duty service members use illicit drugs less frequently, as would be expected given the potential disciplinary consequences, the prevalence of problematic use of the legal ones—tobacco, alcohol, and particularly prescription medications—is greater among individuals in the military.
Substance use disorders affect every sector of federal health care practice from military pediatrics and VA pathology to PHS primary care. Reflecting this ubiquity, in this special substance use disorders issue of Federal Practitioner we focus on several distinctive and significant efforts of health care practitioners who care for patients with SUDs. All of medicine is becoming more interdisciplinary, multidisciplinary, and team-based, but perhaps no other area has as long a legacy or as intrinsic a need for team approaches to care than does the diagnosis and treatment of SUDs. We see this need reflected in this issue’s articles authored by clinical pharmacists, nurse practitioners, physicians, and physicians in training, among others.
Prescription opioids are the subject of 3 articles from VA practitioners: a look at primary, secondary, and tertiary forms of prevention of morbidity and mortality from substance use. Pharmacists at the Salt Lake City VAMC studied the epidemiology of veterans seen in emergency departments who were given naloxone for unintentional opioid overdoses. A second article reviews the distribution of naloxone at a VA facility, providing an example of a successful implementation of the VA Overdose Education and Naloxone Distribution network (OEND)—the only national naloxone program in any health care system.
Even farther upstream in the effort to reduce the large doses of opioids that are directly related to overdose deaths is an article on an outpatient opioid-monitoring clinic that uses evidence-based medicine to diagnose patients with opioid use disorder. Research in the VHA showed that in a 4-year period of study, “the risk of overdose deaths was directly related to the maximum prescribed daily dose of opioid medication.”2
Our colleagues in active duty underscore the challenge that new and emerging substances present not only to federal regulatory agencies like the Drug Enforcement Agency, but also to state and local law enforcement agencies. When spice (synthetic cannabinoids) and bath salts (synthetic cathinones) first appeared, no drug tests were available to detect them. Technically not illegal in the early phase of their use, they became the perfect and popular drugs of young service men and women.3
Tragically, history has shown 2 truths about humans and the use of psychoactive products. The first is that as soon as one product is outlawed, creative chemists invent another mind-altering product. Practical education regarding the latest of these underground drugs, kratom, which threatens our service members, is introduced in this issue.
The second truth is that nearly every drug that is originally prescribed for legitimate medical reasons is eventually misused for a nonmedical purpose and can lead to SUDs. By the time the medical community realizes the dark side of the medication, many individuals have already developed a disorder, and sadly some have died.
One of the oldest classes of drugs that brings both relief and torment to human culture—opioid medication—is now the scourge of postmodern society. Our well-intentioned efforts to succor real pain for patients using prescription opioids have paved a road to hellish suffering for others. A recent study examined whether a resurgence of heroin use among veterans—the likes of which has not been seen since the Vietnam era—was associated with the nonmedical use of yes, prescribed narcotics. The same study found that solely having chronic pain was not correlated with the use of heroin.4 This finding offers the hope that practitioners and patients together can learn to treat chronic pain with opioids in selected patients, which can be life-restoring in appropriate cases for limited duration, safely and responsibly while avoiding and minimizing the death dealing blow of opioid use disorders.
In this issue, we also feature a discussion with Karen Drexler, MD, the newly appointed Mental Health Program Director, Addictive Disorders. Dr. Drexler expertly discusses a wide array of SUD subjects relevant to Federal Practitioner readers, including the approach to patients using medical marijuana in the VA, the 2016 VA/DoD Clinical Practice Guidelines, and an inside view of the challenges and successes of VA SUD programs, from the vantage point of the new leader of these critical initiatives.
Finally, astute readers may notice the editorial attempts to avoid use of the value-laden terms addiction and substance abuse. Instead, the less stigmatizing terminology of DSM-5 is employed, which jettisons the problematic abuse and dependence distinction for the unitary domain of SUDs. This approach is not just a change in semantics but as thought leaders have shown, a real and meaningful comprehension of the role of words in shaping culture.5 The VA as a health care entity is moving to adopt better scientific framing of SUDs as a salient step toward a recovery-oriented program.
In the coming months, we intend to expand our coverage of this public health crisis, and we invite readers who care every day for patients wrestling with SUDs for control of their health and very lives, to educate, advocate for resources for active-duty service personnel and veterans, and share innovative efforts to turn the tide toward recovery.
Given the recently concluded election season, it may seem that there are few things Americans have in common or can agree on. And although I did not conduct a poll or hold a debate, I suspect that a majority of those who work in the VA, DoD, or PHS would agree that one of the most serious and prevalent public health problems facing those in federal service and in the country at large is the epidemic of substance use disorders (SUDs).
In 2013 the National Institute on Drug Abuse reported that “members of the armed forces are not immune to the substance use problems that affect the rest of society.”1 Although active-duty service members use illicit drugs less frequently, as would be expected given the potential disciplinary consequences, the prevalence of problematic use of the legal ones—tobacco, alcohol, and particularly prescription medications—is greater among individuals in the military.
Substance use disorders affect every sector of federal health care practice from military pediatrics and VA pathology to PHS primary care. Reflecting this ubiquity, in this special substance use disorders issue of Federal Practitioner we focus on several distinctive and significant efforts of health care practitioners who care for patients with SUDs. All of medicine is becoming more interdisciplinary, multidisciplinary, and team-based, but perhaps no other area has as long a legacy or as intrinsic a need for team approaches to care than does the diagnosis and treatment of SUDs. We see this need reflected in this issue’s articles authored by clinical pharmacists, nurse practitioners, physicians, and physicians in training, among others.
Prescription opioids are the subject of 3 articles from VA practitioners: a look at primary, secondary, and tertiary forms of prevention of morbidity and mortality from substance use. Pharmacists at the Salt Lake City VAMC studied the epidemiology of veterans seen in emergency departments who were given naloxone for unintentional opioid overdoses. A second article reviews the distribution of naloxone at a VA facility, providing an example of a successful implementation of the VA Overdose Education and Naloxone Distribution network (OEND)—the only national naloxone program in any health care system.
Even farther upstream in the effort to reduce the large doses of opioids that are directly related to overdose deaths is an article on an outpatient opioid-monitoring clinic that uses evidence-based medicine to diagnose patients with opioid use disorder. Research in the VHA showed that in a 4-year period of study, “the risk of overdose deaths was directly related to the maximum prescribed daily dose of opioid medication.”2
Our colleagues in active duty underscore the challenge that new and emerging substances present not only to federal regulatory agencies like the Drug Enforcement Agency, but also to state and local law enforcement agencies. When spice (synthetic cannabinoids) and bath salts (synthetic cathinones) first appeared, no drug tests were available to detect them. Technically not illegal in the early phase of their use, they became the perfect and popular drugs of young service men and women.3
Tragically, history has shown 2 truths about humans and the use of psychoactive products. The first is that as soon as one product is outlawed, creative chemists invent another mind-altering product. Practical education regarding the latest of these underground drugs, kratom, which threatens our service members, is introduced in this issue.
The second truth is that nearly every drug that is originally prescribed for legitimate medical reasons is eventually misused for a nonmedical purpose and can lead to SUDs. By the time the medical community realizes the dark side of the medication, many individuals have already developed a disorder, and sadly some have died.
One of the oldest classes of drugs that brings both relief and torment to human culture—opioid medication—is now the scourge of postmodern society. Our well-intentioned efforts to succor real pain for patients using prescription opioids have paved a road to hellish suffering for others. A recent study examined whether a resurgence of heroin use among veterans—the likes of which has not been seen since the Vietnam era—was associated with the nonmedical use of yes, prescribed narcotics. The same study found that solely having chronic pain was not correlated with the use of heroin.4 This finding offers the hope that practitioners and patients together can learn to treat chronic pain with opioids in selected patients, which can be life-restoring in appropriate cases for limited duration, safely and responsibly while avoiding and minimizing the death dealing blow of opioid use disorders.
In this issue, we also feature a discussion with Karen Drexler, MD, the newly appointed Mental Health Program Director, Addictive Disorders. Dr. Drexler expertly discusses a wide array of SUD subjects relevant to Federal Practitioner readers, including the approach to patients using medical marijuana in the VA, the 2016 VA/DoD Clinical Practice Guidelines, and an inside view of the challenges and successes of VA SUD programs, from the vantage point of the new leader of these critical initiatives.
Finally, astute readers may notice the editorial attempts to avoid use of the value-laden terms addiction and substance abuse. Instead, the less stigmatizing terminology of DSM-5 is employed, which jettisons the problematic abuse and dependence distinction for the unitary domain of SUDs. This approach is not just a change in semantics but as thought leaders have shown, a real and meaningful comprehension of the role of words in shaping culture.5 The VA as a health care entity is moving to adopt better scientific framing of SUDs as a salient step toward a recovery-oriented program.
In the coming months, we intend to expand our coverage of this public health crisis, and we invite readers who care every day for patients wrestling with SUDs for control of their health and very lives, to educate, advocate for resources for active-duty service personnel and veterans, and share innovative efforts to turn the tide toward recovery.
1. National Institute on Drug Abuse. DrugFacts—substance abuse in the military. https://www.drugabuse.gov/publications/drugfacts/substance-abuse-in-military. Revised March 2013. Accessed October 18, 2016.
2. Loeffler G, Hurst D, Penn A, Yung K. Spice, bath salts, and the U.S. military: the emergence of synthetic cannabinoid receptor agonists and cathinones in the U.S. Armed Forces. Mil Med. 2012;177(9):1041-1048.
3. Banerjee G, Edelman EJ, Barry DT, et al. Non-medical use of prescription opioids is associated with heroin initiation among U.S. veterans: a prospective cohort study. Addiction. 2016;111(11):2021-2031.
4. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid-related deaths. JAMA. 2011;305(13):1315-1321.
5. Botticelli MP, Koh HK. Changing the language of addiction. JAMA. 2016;316(13):1361-1362.
1. National Institute on Drug Abuse. DrugFacts—substance abuse in the military. https://www.drugabuse.gov/publications/drugfacts/substance-abuse-in-military. Revised March 2013. Accessed October 18, 2016.
2. Loeffler G, Hurst D, Penn A, Yung K. Spice, bath salts, and the U.S. military: the emergence of synthetic cannabinoid receptor agonists and cathinones in the U.S. Armed Forces. Mil Med. 2012;177(9):1041-1048.
3. Banerjee G, Edelman EJ, Barry DT, et al. Non-medical use of prescription opioids is associated with heroin initiation among U.S. veterans: a prospective cohort study. Addiction. 2016;111(11):2021-2031.
4. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid-related deaths. JAMA. 2011;305(13):1315-1321.
5. Botticelli MP, Koh HK. Changing the language of addiction. JAMA. 2016;316(13):1361-1362.

Anecdotal Failures in the Diagnosis of Serotonin Syndrome
Clinical Question: What is the validity of commonly held beliefs regarding serotonin syndrome (SS)?

Background: SS is a potentially life-threatening condition caused by serotonin excess in the central nervous system. The authors tested the validity of four widely accepted tenets about SS: that the Hunter criteria are superior, that the onset of SS is rapid compared to neuroleptic malignant syndrome (NMS), that hyperthermia is common with SS, and that SS can be distinguished from NMS based on medication history.
Study Design: Systematic review and meta-analysis.
Setting: PubMed and Web of Science.
Synopsis: Researchers identified 299 case reports from 2004 to 2014 in which SS was the most likely diagnosis based on one of three available diagnostic systems. Rhabdomyolysis with creatine kinase >1,500 and ICU treatment were used as proxies for SS severity. The Hunter criteria (the current gold standard) identified fewer overdoses, episodes of rhabdomyolysis, and ICU cases than the Sternbach or Radomski criteria. Combinations of antidepressants with methylene blue, opiates, or linezolid were the most common reasons for ICU admission. Symptom onset was within six hours in only 27.5% of cases. Hyperthermia was present in only 9.2% of patients with SS.
Hospitalists cannot rely on any one set of criteria to diagnose SS. The typical combinations of opiates or linezolid with antidepressants should raise the level of suspicion for SS. Rigidity and rhabdomyolysis occur commonly in both NMS and SS. Hyperthermia and timing of onset are not good indicators to the diagnosis of SS.
Bottom line: A high index of suspicion rather than reliance on classification systems or anecdotal key symptoms is necessary when considering SS.
Citation: Werneke U, Jamshidi F, Taylor DM, Ott M. Conundrums in neurology: diagnosing serotonin syndrome – a meta-analysis of cases. BMC Neurol. 2016;16:97.
Clinical Question: What is the validity of commonly held beliefs regarding serotonin syndrome (SS)?
Background: SS is a potentially life-threatening condition caused by serotonin excess in the central nervous system. The authors tested the validity of four widely accepted tenets about SS: that the Hunter criteria are superior, that the onset of SS is rapid compared to neuroleptic malignant syndrome (NMS), that hyperthermia is common with SS, and that SS can be distinguished from NMS based on medication history.
Study Design: Systematic review and meta-analysis.
Setting: PubMed and Web of Science.
Synopsis: Researchers identified 299 case reports from 2004 to 2014 in which SS was the most likely diagnosis based on one of three available diagnostic systems. Rhabdomyolysis with creatine kinase >1,500 and ICU treatment were used as proxies for SS severity. The Hunter criteria (the current gold standard) identified fewer overdoses, episodes of rhabdomyolysis, and ICU cases than the Sternbach or Radomski criteria. Combinations of antidepressants with methylene blue, opiates, or linezolid were the most common reasons for ICU admission. Symptom onset was within six hours in only 27.5% of cases. Hyperthermia was present in only 9.2% of patients with SS.
Hospitalists cannot rely on any one set of criteria to diagnose SS. The typical combinations of opiates or linezolid with antidepressants should raise the level of suspicion for SS. Rigidity and rhabdomyolysis occur commonly in both NMS and SS. Hyperthermia and timing of onset are not good indicators to the diagnosis of SS.
Bottom line: A high index of suspicion rather than reliance on classification systems or anecdotal key symptoms is necessary when considering SS.
Citation: Werneke U, Jamshidi F, Taylor DM, Ott M. Conundrums in neurology: diagnosing serotonin syndrome – a meta-analysis of cases. BMC Neurol. 2016;16:97.
Clinical Question: What is the validity of commonly held beliefs regarding serotonin syndrome (SS)?
Background: SS is a potentially life-threatening condition caused by serotonin excess in the central nervous system. The authors tested the validity of four widely accepted tenets about SS: that the Hunter criteria are superior, that the onset of SS is rapid compared to neuroleptic malignant syndrome (NMS), that hyperthermia is common with SS, and that SS can be distinguished from NMS based on medication history.
Study Design: Systematic review and meta-analysis.
Setting: PubMed and Web of Science.
Synopsis: Researchers identified 299 case reports from 2004 to 2014 in which SS was the most likely diagnosis based on one of three available diagnostic systems. Rhabdomyolysis with creatine kinase >1,500 and ICU treatment were used as proxies for SS severity. The Hunter criteria (the current gold standard) identified fewer overdoses, episodes of rhabdomyolysis, and ICU cases than the Sternbach or Radomski criteria. Combinations of antidepressants with methylene blue, opiates, or linezolid were the most common reasons for ICU admission. Symptom onset was within six hours in only 27.5% of cases. Hyperthermia was present in only 9.2% of patients with SS.
Hospitalists cannot rely on any one set of criteria to diagnose SS. The typical combinations of opiates or linezolid with antidepressants should raise the level of suspicion for SS. Rigidity and rhabdomyolysis occur commonly in both NMS and SS. Hyperthermia and timing of onset are not good indicators to the diagnosis of SS.
Bottom line: A high index of suspicion rather than reliance on classification systems or anecdotal key symptoms is necessary when considering SS.
Citation: Werneke U, Jamshidi F, Taylor DM, Ott M. Conundrums in neurology: diagnosing serotonin syndrome – a meta-analysis of cases. BMC Neurol. 2016;16:97.

Restrictive Blood Transfusion Strategies May Increase the Risk of Mortality, Morbidity for Elderly Patients Undergoing Orthopedic Surgery
Clinical Question: Are there particular groups of patients in which lower transfusion thresholds (transfusion only at lower hemoglobin levels) may be harmful?
Background: Previously published meta-analyses have examined transfusion thresholds for critically ill, surgical, and medical patients. By combining these patients, previous meta-analyses are limited in the identification of intervention effects. A more refined understanding of how transfusion thresholds impact outcomes for a variety of patients in different clinical settings is needed.
Study Design: Context-specific systematic review and meta-analysis of randomized clinical trials.
Setting: Adult patients in perioperative, emergency, or intensive-care settings.
Synopsis: Patient information was extracted from 31 randomized clinical trials. The authors found that among 3,465 elderly patients undergoing orthopedic surgery, those given restrictive transfusion strategies had significantly more events reflecting inadequate oxygen supply (relative risk, 1.41; 95% CI, 1.03–1.92). No statistically significant effect from restrictive transfusions was seen in 3,322 patients with cardiovascular disease undergoing cardiac or vascular procedures; 3,590 mixed medical-surgical patients in emergency and intensive-care settings; and 823 patients in a combined group of postpartum women, hematologic malignancy patients, and younger patients with neurologic injury.
The authors argue that even statistically nonsignificant differences in morbidity and mortality should encourage more liberal transfusion; apart from orthopedic surgery patients, this argument is not well-supported by the available data.
Bottom Line: It remains unclear whether restrictive transfusion strategies have a negative impact on certain types of patients, although the authors argue that there may be a trend in that direction. Further study is needed for specific patient populations.
Citation: Hovaguimian F, Myles PS. Restrictive versus liberal transfusion strategy in the perioperative and acute care settings: a context-specific systematic review and meta-analysis of randomized clinical trials. Anesthesiology. 2016;125(1):46-61.
Clinical Question: Are there particular groups of patients in which lower transfusion thresholds (transfusion only at lower hemoglobin levels) may be harmful?
Background: Previously published meta-analyses have examined transfusion thresholds for critically ill, surgical, and medical patients. By combining these patients, previous meta-analyses are limited in the identification of intervention effects. A more refined understanding of how transfusion thresholds impact outcomes for a variety of patients in different clinical settings is needed.
Study Design: Context-specific systematic review and meta-analysis of randomized clinical trials.
Setting: Adult patients in perioperative, emergency, or intensive-care settings.
Synopsis: Patient information was extracted from 31 randomized clinical trials. The authors found that among 3,465 elderly patients undergoing orthopedic surgery, those given restrictive transfusion strategies had significantly more events reflecting inadequate oxygen supply (relative risk, 1.41; 95% CI, 1.03–1.92). No statistically significant effect from restrictive transfusions was seen in 3,322 patients with cardiovascular disease undergoing cardiac or vascular procedures; 3,590 mixed medical-surgical patients in emergency and intensive-care settings; and 823 patients in a combined group of postpartum women, hematologic malignancy patients, and younger patients with neurologic injury.
The authors argue that even statistically nonsignificant differences in morbidity and mortality should encourage more liberal transfusion; apart from orthopedic surgery patients, this argument is not well-supported by the available data.
Bottom Line: It remains unclear whether restrictive transfusion strategies have a negative impact on certain types of patients, although the authors argue that there may be a trend in that direction. Further study is needed for specific patient populations.
Citation: Hovaguimian F, Myles PS. Restrictive versus liberal transfusion strategy in the perioperative and acute care settings: a context-specific systematic review and meta-analysis of randomized clinical trials. Anesthesiology. 2016;125(1):46-61.
Clinical Question: Are there particular groups of patients in which lower transfusion thresholds (transfusion only at lower hemoglobin levels) may be harmful?
Background: Previously published meta-analyses have examined transfusion thresholds for critically ill, surgical, and medical patients. By combining these patients, previous meta-analyses are limited in the identification of intervention effects. A more refined understanding of how transfusion thresholds impact outcomes for a variety of patients in different clinical settings is needed.
Study Design: Context-specific systematic review and meta-analysis of randomized clinical trials.
Setting: Adult patients in perioperative, emergency, or intensive-care settings.
Synopsis: Patient information was extracted from 31 randomized clinical trials. The authors found that among 3,465 elderly patients undergoing orthopedic surgery, those given restrictive transfusion strategies had significantly more events reflecting inadequate oxygen supply (relative risk, 1.41; 95% CI, 1.03–1.92). No statistically significant effect from restrictive transfusions was seen in 3,322 patients with cardiovascular disease undergoing cardiac or vascular procedures; 3,590 mixed medical-surgical patients in emergency and intensive-care settings; and 823 patients in a combined group of postpartum women, hematologic malignancy patients, and younger patients with neurologic injury.
The authors argue that even statistically nonsignificant differences in morbidity and mortality should encourage more liberal transfusion; apart from orthopedic surgery patients, this argument is not well-supported by the available data.
Bottom Line: It remains unclear whether restrictive transfusion strategies have a negative impact on certain types of patients, although the authors argue that there may be a trend in that direction. Further study is needed for specific patient populations.
Citation: Hovaguimian F, Myles PS. Restrictive versus liberal transfusion strategy in the perioperative and acute care settings: a context-specific systematic review and meta-analysis of randomized clinical trials. Anesthesiology. 2016;125(1):46-61.
Team develops model of common infant ALL

Photo by Petr Kratochvil
After trying for nearly 2 decades, researchers have created a mouse model of t(4;11) pro-B acute lymphoblastic
leukemia (ALL).
The team said this model, described in Cancer Cell, mimics the human disease phenotypically and molecularly.
This type of ALL, which is common in infants, results from the translocation t(4;11)(q21;q23), which fuses the mixed-lineage leukemia (MLL) gene on chromosome 11 to the ALL-1 fused gene on chromosome 4 (AF4).
“For 20 years, scientists have repeatedly tried and consistently failed to make a model of MLL-AF4 pro-B acute lymphoblastic leukemia,” said study author Michael Thirman, MD, of the University of Chicago in Illinois.
“Even though we understood the basic genetic flaw, no one had been able create a mouse model that mimicked the human disease, which is crucial for evaluating potential therapies.”
That frustrated many researchers, who shifted their focus to test alternative hypotheses on the causes of t(4;11) pro-B ALL or refocused their laboratories to study different aspects of the disease.
However, Dr Thirman and his colleagues began working on this problem “years ago,” he said, and stayed with it.
The team identified 2 hurdles. The first was a problem with the retrovirus used to insert the MLL-AF4 fusion gene into mouse cells.
“We soon discovered that the virus wasn’t working,” Dr Thirman explained. “We knew that certain parts of human DNA can decrease viral titers. So we switched from the human version of AF4 to the mouse version, Af4, which is slightly different. This increased viral titers 30-fold.”
That worked, but it led to the second hurdle. The mice injected with virus transporting MLL-Af4 developed leukemia, but it was acute myeloid leukemia.
So the researchers inserted the fused MLL-Af4 gene into human CD34 cells, which were derived from cord blood or peripheral blood from volunteer donors.
The team then transferred those cells to mice, and, this time, the mice developed t(4;11) pro-B ALL.
The researchers said this model “fully recapitulates the immunophenotypic and molecular aspects” of human t(4;11) pro-B ALL and will therefore be “a valuable tool” for studying the disease. ![]()
Photo by Petr Kratochvil
After trying for nearly 2 decades, researchers have created a mouse model of t(4;11) pro-B acute lymphoblastic
leukemia (ALL).
The team said this model, described in Cancer Cell, mimics the human disease phenotypically and molecularly.
This type of ALL, which is common in infants, results from the translocation t(4;11)(q21;q23), which fuses the mixed-lineage leukemia (MLL) gene on chromosome 11 to the ALL-1 fused gene on chromosome 4 (AF4).
“For 20 years, scientists have repeatedly tried and consistently failed to make a model of MLL-AF4 pro-B acute lymphoblastic leukemia,” said study author Michael Thirman, MD, of the University of Chicago in Illinois.
“Even though we understood the basic genetic flaw, no one had been able create a mouse model that mimicked the human disease, which is crucial for evaluating potential therapies.”
That frustrated many researchers, who shifted their focus to test alternative hypotheses on the causes of t(4;11) pro-B ALL or refocused their laboratories to study different aspects of the disease.
However, Dr Thirman and his colleagues began working on this problem “years ago,” he said, and stayed with it.
The team identified 2 hurdles. The first was a problem with the retrovirus used to insert the MLL-AF4 fusion gene into mouse cells.
“We soon discovered that the virus wasn’t working,” Dr Thirman explained. “We knew that certain parts of human DNA can decrease viral titers. So we switched from the human version of AF4 to the mouse version, Af4, which is slightly different. This increased viral titers 30-fold.”
That worked, but it led to the second hurdle. The mice injected with virus transporting MLL-Af4 developed leukemia, but it was acute myeloid leukemia.
So the researchers inserted the fused MLL-Af4 gene into human CD34 cells, which were derived from cord blood or peripheral blood from volunteer donors.
The team then transferred those cells to mice, and, this time, the mice developed t(4;11) pro-B ALL.
The researchers said this model “fully recapitulates the immunophenotypic and molecular aspects” of human t(4;11) pro-B ALL and will therefore be “a valuable tool” for studying the disease. ![]()
Photo by Petr Kratochvil
After trying for nearly 2 decades, researchers have created a mouse model of t(4;11) pro-B acute lymphoblastic
leukemia (ALL).
The team said this model, described in Cancer Cell, mimics the human disease phenotypically and molecularly.
This type of ALL, which is common in infants, results from the translocation t(4;11)(q21;q23), which fuses the mixed-lineage leukemia (MLL) gene on chromosome 11 to the ALL-1 fused gene on chromosome 4 (AF4).
“For 20 years, scientists have repeatedly tried and consistently failed to make a model of MLL-AF4 pro-B acute lymphoblastic leukemia,” said study author Michael Thirman, MD, of the University of Chicago in Illinois.
“Even though we understood the basic genetic flaw, no one had been able create a mouse model that mimicked the human disease, which is crucial for evaluating potential therapies.”
That frustrated many researchers, who shifted their focus to test alternative hypotheses on the causes of t(4;11) pro-B ALL or refocused their laboratories to study different aspects of the disease.
However, Dr Thirman and his colleagues began working on this problem “years ago,” he said, and stayed with it.
The team identified 2 hurdles. The first was a problem with the retrovirus used to insert the MLL-AF4 fusion gene into mouse cells.
“We soon discovered that the virus wasn’t working,” Dr Thirman explained. “We knew that certain parts of human DNA can decrease viral titers. So we switched from the human version of AF4 to the mouse version, Af4, which is slightly different. This increased viral titers 30-fold.”
That worked, but it led to the second hurdle. The mice injected with virus transporting MLL-Af4 developed leukemia, but it was acute myeloid leukemia.
So the researchers inserted the fused MLL-Af4 gene into human CD34 cells, which were derived from cord blood or peripheral blood from volunteer donors.
The team then transferred those cells to mice, and, this time, the mice developed t(4;11) pro-B ALL.
The researchers said this model “fully recapitulates the immunophenotypic and molecular aspects” of human t(4;11) pro-B ALL and will therefore be “a valuable tool” for studying the disease. ![]()
Study shows lower bleeding risk with rivaroxaban

NEW ORLEANS—Results of the PIONEER AF-PCI trial suggest certain patients may have a lower risk of bleeding if they receive rivaroxaban rather than a vitamin K antagonist (VKA).
The study showed that patients with nonvalvular atrial fibrillation (NVAF) who underwent percutaneous coronary intervention (PCI) with stenting had a lower risk of clinically significant bleeding if they received rivaroxaban plus antiplatelet therapy rather than a VKA plus antiplatelet therapy.
However, the trial showed no significant difference between the treatment groups when it came to the risk of cardiovascular events.
These results were presented at the American Heart Association’s Scientific Sessions 2016 and simultaneously published in NEJM.
The trial was supported by Janssen Scientific Affairs LLC, and Bayer Health Care Pharmaceuticals.
“In managing the stented patient with atrial fibrillation, a pharmacologic strategy must carefully balance the risk of stent thrombosis, or blood clot, with the risk of bleeding complications,” said study investigator C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“This trial, which tested 2 entirely new strategies, now provides us with randomized clinical trial data demonstrating that a combination of rivaroxaban with antiplatelet therapy is successful in minimizing bleeding while preventing clotting.”
The trial included 2124 patients with NVAF who had undergone PCI with stenting. They were randomized to receive, in a 1:1:1 ratio:
- Low-dose rivaroxaban (15 mg once daily) plus a P2Y12 inhibitor for 12 months (group 1)
- Very-low-dose rivaroxaban (2.5 mg twice daily) plus dual antiplatelet therapy (DAPT) for 1, 6, or 12 months (group 2)
- Standard therapy with a dose-adjusted VKA (once daily) plus DAPT for 1, 6, or 12 months (group 3).
Key endpoints
The study’s primary safety endpoint was clinically significant bleeding, which was a composite of major bleeding according to Thrombolysis in Myocardial Infarction (TIMI) criteria, minor bleeding according to TIMI criteria, and bleeding requiring medical attention.
At 1 year, the rate of clinically significant bleeding was significantly lower in the 2 rivaroxaban groups than in the VKA group—16.8% in group 1, 18.0% in group 2, and 26.7% in group 3.
The hazard ratio for group 1 compared to group 3 was 0.59 (P<0.001). And the hazard ratio for group 2 compared to group 3 was 0.63 (P<0.001).
The researchers said this reduction in bleeding for the 2 rivaroxaban groups was consistent across multiple subgroups of patients.
The study’s key efficacy endpoint was major adverse cardiovascular events, which was a composite of death from cardiovascular causes, myocardial infarction, and stroke.
There was no significant difference between the groups with regard to this endpoint. It occurred in 6.5% of the patients in group 1, 5.6% in group 2, and 6.0% in group 3 (P>0.05 for both comparisons).
“For the first time in this population, a treatment regimen resulted in less bleeding than the current standard of care,” Dr Gibson said.
“Pairing rivaroxaban with single or dual antiplatelet therapy has the potential to transform current practice, as demonstrated in this study, with significantly less bleeding and numerically similar efficacy when compared to warfarin [VKA] with dual antiplatelet therapy.” ![]()
NEW ORLEANS—Results of the PIONEER AF-PCI trial suggest certain patients may have a lower risk of bleeding if they receive rivaroxaban rather than a vitamin K antagonist (VKA).
The study showed that patients with nonvalvular atrial fibrillation (NVAF) who underwent percutaneous coronary intervention (PCI) with stenting had a lower risk of clinically significant bleeding if they received rivaroxaban plus antiplatelet therapy rather than a VKA plus antiplatelet therapy.
However, the trial showed no significant difference between the treatment groups when it came to the risk of cardiovascular events.
These results were presented at the American Heart Association’s Scientific Sessions 2016 and simultaneously published in NEJM.
The trial was supported by Janssen Scientific Affairs LLC, and Bayer Health Care Pharmaceuticals.
“In managing the stented patient with atrial fibrillation, a pharmacologic strategy must carefully balance the risk of stent thrombosis, or blood clot, with the risk of bleeding complications,” said study investigator C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“This trial, which tested 2 entirely new strategies, now provides us with randomized clinical trial data demonstrating that a combination of rivaroxaban with antiplatelet therapy is successful in minimizing bleeding while preventing clotting.”
The trial included 2124 patients with NVAF who had undergone PCI with stenting. They were randomized to receive, in a 1:1:1 ratio:
- Low-dose rivaroxaban (15 mg once daily) plus a P2Y12 inhibitor for 12 months (group 1)
- Very-low-dose rivaroxaban (2.5 mg twice daily) plus dual antiplatelet therapy (DAPT) for 1, 6, or 12 months (group 2)
- Standard therapy with a dose-adjusted VKA (once daily) plus DAPT for 1, 6, or 12 months (group 3).
Key endpoints
The study’s primary safety endpoint was clinically significant bleeding, which was a composite of major bleeding according to Thrombolysis in Myocardial Infarction (TIMI) criteria, minor bleeding according to TIMI criteria, and bleeding requiring medical attention.
At 1 year, the rate of clinically significant bleeding was significantly lower in the 2 rivaroxaban groups than in the VKA group—16.8% in group 1, 18.0% in group 2, and 26.7% in group 3.
The hazard ratio for group 1 compared to group 3 was 0.59 (P<0.001). And the hazard ratio for group 2 compared to group 3 was 0.63 (P<0.001).
The researchers said this reduction in bleeding for the 2 rivaroxaban groups was consistent across multiple subgroups of patients.
The study’s key efficacy endpoint was major adverse cardiovascular events, which was a composite of death from cardiovascular causes, myocardial infarction, and stroke.
There was no significant difference between the groups with regard to this endpoint. It occurred in 6.5% of the patients in group 1, 5.6% in group 2, and 6.0% in group 3 (P>0.05 for both comparisons).
“For the first time in this population, a treatment regimen resulted in less bleeding than the current standard of care,” Dr Gibson said.
“Pairing rivaroxaban with single or dual antiplatelet therapy has the potential to transform current practice, as demonstrated in this study, with significantly less bleeding and numerically similar efficacy when compared to warfarin [VKA] with dual antiplatelet therapy.” ![]()
NEW ORLEANS—Results of the PIONEER AF-PCI trial suggest certain patients may have a lower risk of bleeding if they receive rivaroxaban rather than a vitamin K antagonist (VKA).
The study showed that patients with nonvalvular atrial fibrillation (NVAF) who underwent percutaneous coronary intervention (PCI) with stenting had a lower risk of clinically significant bleeding if they received rivaroxaban plus antiplatelet therapy rather than a VKA plus antiplatelet therapy.
However, the trial showed no significant difference between the treatment groups when it came to the risk of cardiovascular events.
These results were presented at the American Heart Association’s Scientific Sessions 2016 and simultaneously published in NEJM.
The trial was supported by Janssen Scientific Affairs LLC, and Bayer Health Care Pharmaceuticals.
“In managing the stented patient with atrial fibrillation, a pharmacologic strategy must carefully balance the risk of stent thrombosis, or blood clot, with the risk of bleeding complications,” said study investigator C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“This trial, which tested 2 entirely new strategies, now provides us with randomized clinical trial data demonstrating that a combination of rivaroxaban with antiplatelet therapy is successful in minimizing bleeding while preventing clotting.”
The trial included 2124 patients with NVAF who had undergone PCI with stenting. They were randomized to receive, in a 1:1:1 ratio:
- Low-dose rivaroxaban (15 mg once daily) plus a P2Y12 inhibitor for 12 months (group 1)
- Very-low-dose rivaroxaban (2.5 mg twice daily) plus dual antiplatelet therapy (DAPT) for 1, 6, or 12 months (group 2)
- Standard therapy with a dose-adjusted VKA (once daily) plus DAPT for 1, 6, or 12 months (group 3).
Key endpoints
The study’s primary safety endpoint was clinically significant bleeding, which was a composite of major bleeding according to Thrombolysis in Myocardial Infarction (TIMI) criteria, minor bleeding according to TIMI criteria, and bleeding requiring medical attention.
At 1 year, the rate of clinically significant bleeding was significantly lower in the 2 rivaroxaban groups than in the VKA group—16.8% in group 1, 18.0% in group 2, and 26.7% in group 3.
The hazard ratio for group 1 compared to group 3 was 0.59 (P<0.001). And the hazard ratio for group 2 compared to group 3 was 0.63 (P<0.001).
The researchers said this reduction in bleeding for the 2 rivaroxaban groups was consistent across multiple subgroups of patients.
The study’s key efficacy endpoint was major adverse cardiovascular events, which was a composite of death from cardiovascular causes, myocardial infarction, and stroke.
There was no significant difference between the groups with regard to this endpoint. It occurred in 6.5% of the patients in group 1, 5.6% in group 2, and 6.0% in group 3 (P>0.05 for both comparisons).
“For the first time in this population, a treatment regimen resulted in less bleeding than the current standard of care,” Dr Gibson said.
“Pairing rivaroxaban with single or dual antiplatelet therapy has the potential to transform current practice, as demonstrated in this study, with significantly less bleeding and numerically similar efficacy when compared to warfarin [VKA] with dual antiplatelet therapy.” ![]()
Hemophilia treatment falling short, study suggests

Results of a real-world, retrospective study suggest there may be a need to improve the standard of care for hemophilia A and B in some European countries.
Hemophilia treatment practices varied widely among the 7 countries studied, as did annual bleeding rates (ABRs).
Some countries had low median ABRs in hemophilia A and B patients receiving prophylaxis—in the range of 1.0 to 2.0.
However, the median ABR was as high as 8.0 for some patients, despite receiving prophylaxis. And these were patients with moderate disease.
The study, which was sponsored by Sobi, was published in Haemophilia.
“The overall results indicate that there is a significant need to advance standard of care within hemophilia,” said Stefan Lethagen, vice president medical & clinical sciences, haemophilia at Sobi.
“Even when prophylaxis is the norm, it appears that prophylactic treatment is driven to the minimal acceptable level or even lower, which increases the risk of joint injury and limits the ability to live a full and active life.”
The study was designed to provide insight into current hemophilia treatment practice and outcomes in 7 European countries—Belgium, France, Germany, Italy, Spain, Sweden, and the UK.
The researchers analyzed data on 1346 patients with hemophilia A and 312 with hemophilia B treated in these countries.
Treatment type, dosing
Prophylaxis was, overall, the most dominating treatment for patients with severe hemophilia A. It was the most common treatment regimen among children and decreased with increasing age.
On-demand treatment was reported to be most common in moderate hemophilia A, and there was no trend across age groups.
For patients with hemophilia B, prophylaxis was the most common treatment in 4 out of the 7 countries (France, Germany, Sweden, and UK).
Overall, a majority of patients received a recombinant antihemophilic factor product as opposed to a plasma-derived product. The one exception was patients with hemophilia B in Germany. A majority of these patients (66%) received a plasma-derived product.
The mean prescribed prophylactic treatment ranged from 67.9 IU kg-1 per week (Belgium) to 108.4 IU kg-1 per week (Germany) for hemophilia A and 32.3 IU kg-1 per week (Belgium) to 97.7 IU kg-1 per week (France) for hemophilia B.
Most patients on prophylaxis were treated 3 or more times a week if they had hemophilia A and 2 times a week if they had hemophilia B.
ABRs across countries
For hemophilia A patients on prophylaxis, the median ABR ranged from 1.0 (Belgium, Italy, Sweden) to 4.0 (France, UK) for patients with severe disease and from 2.0 (Sweden) to 8.0 (Belgium) for patients with moderate disease.
The researchers pointed out that ABRs were higher for patients with moderate hemophilia A, but low patient numbers should be taken into account when interpreting these data.
The median ABRs for hemophilia A patients who received on-demand treatment ranged from 4.5 (Sweden) to 18.0 (UK, Belgium) for patients with severe disease and from 1.0 (Spain, Sweden) to 12.0 (UK) for patients with moderate disease.
For hemophilia B patients on prophylaxis, the median ABRs ranged from 1.0 (Germany, Sweden) to 6.0 (Belgium) for patients with severe disease and from 1.5 (Sweden) to 8.0 (Belgium) for patients with moderate disease. Again, ABRs were higher for patients with moderate disease.
The median ABRs for hemophilia B patients who received on-demand treatment ranged from 1.5 (Germany) to 14.0 (UK) for patients with severe disease and from 1.0 (Belgium, France, Germany, Italy) to 6.5 (UK) for patients with moderate disease.
The researchers said the high number of bleeds observed in some patients likely reflects insufficient therapy, inappropriate dose-interval, presence of target joints, poor adherence, or patient difficulty in correctly assessing bleeds.
The team said the overall results of the study suggest there is room for improvement of hemophilia therapy, even for patients currently on prophylactic treatment. ![]()
Results of a real-world, retrospective study suggest there may be a need to improve the standard of care for hemophilia A and B in some European countries.
Hemophilia treatment practices varied widely among the 7 countries studied, as did annual bleeding rates (ABRs).
Some countries had low median ABRs in hemophilia A and B patients receiving prophylaxis—in the range of 1.0 to 2.0.
However, the median ABR was as high as 8.0 for some patients, despite receiving prophylaxis. And these were patients with moderate disease.
The study, which was sponsored by Sobi, was published in Haemophilia.
“The overall results indicate that there is a significant need to advance standard of care within hemophilia,” said Stefan Lethagen, vice president medical & clinical sciences, haemophilia at Sobi.
“Even when prophylaxis is the norm, it appears that prophylactic treatment is driven to the minimal acceptable level or even lower, which increases the risk of joint injury and limits the ability to live a full and active life.”
The study was designed to provide insight into current hemophilia treatment practice and outcomes in 7 European countries—Belgium, France, Germany, Italy, Spain, Sweden, and the UK.
The researchers analyzed data on 1346 patients with hemophilia A and 312 with hemophilia B treated in these countries.
Treatment type, dosing
Prophylaxis was, overall, the most dominating treatment for patients with severe hemophilia A. It was the most common treatment regimen among children and decreased with increasing age.
On-demand treatment was reported to be most common in moderate hemophilia A, and there was no trend across age groups.
For patients with hemophilia B, prophylaxis was the most common treatment in 4 out of the 7 countries (France, Germany, Sweden, and UK).
Overall, a majority of patients received a recombinant antihemophilic factor product as opposed to a plasma-derived product. The one exception was patients with hemophilia B in Germany. A majority of these patients (66%) received a plasma-derived product.
The mean prescribed prophylactic treatment ranged from 67.9 IU kg-1 per week (Belgium) to 108.4 IU kg-1 per week (Germany) for hemophilia A and 32.3 IU kg-1 per week (Belgium) to 97.7 IU kg-1 per week (France) for hemophilia B.
Most patients on prophylaxis were treated 3 or more times a week if they had hemophilia A and 2 times a week if they had hemophilia B.
ABRs across countries
For hemophilia A patients on prophylaxis, the median ABR ranged from 1.0 (Belgium, Italy, Sweden) to 4.0 (France, UK) for patients with severe disease and from 2.0 (Sweden) to 8.0 (Belgium) for patients with moderate disease.
The researchers pointed out that ABRs were higher for patients with moderate hemophilia A, but low patient numbers should be taken into account when interpreting these data.
The median ABRs for hemophilia A patients who received on-demand treatment ranged from 4.5 (Sweden) to 18.0 (UK, Belgium) for patients with severe disease and from 1.0 (Spain, Sweden) to 12.0 (UK) for patients with moderate disease.
For hemophilia B patients on prophylaxis, the median ABRs ranged from 1.0 (Germany, Sweden) to 6.0 (Belgium) for patients with severe disease and from 1.5 (Sweden) to 8.0 (Belgium) for patients with moderate disease. Again, ABRs were higher for patients with moderate disease.
The median ABRs for hemophilia B patients who received on-demand treatment ranged from 1.5 (Germany) to 14.0 (UK) for patients with severe disease and from 1.0 (Belgium, France, Germany, Italy) to 6.5 (UK) for patients with moderate disease.
The researchers said the high number of bleeds observed in some patients likely reflects insufficient therapy, inappropriate dose-interval, presence of target joints, poor adherence, or patient difficulty in correctly assessing bleeds.
The team said the overall results of the study suggest there is room for improvement of hemophilia therapy, even for patients currently on prophylactic treatment. ![]()
Results of a real-world, retrospective study suggest there may be a need to improve the standard of care for hemophilia A and B in some European countries.
Hemophilia treatment practices varied widely among the 7 countries studied, as did annual bleeding rates (ABRs).
Some countries had low median ABRs in hemophilia A and B patients receiving prophylaxis—in the range of 1.0 to 2.0.
However, the median ABR was as high as 8.0 for some patients, despite receiving prophylaxis. And these were patients with moderate disease.
The study, which was sponsored by Sobi, was published in Haemophilia.
“The overall results indicate that there is a significant need to advance standard of care within hemophilia,” said Stefan Lethagen, vice president medical & clinical sciences, haemophilia at Sobi.
“Even when prophylaxis is the norm, it appears that prophylactic treatment is driven to the minimal acceptable level or even lower, which increases the risk of joint injury and limits the ability to live a full and active life.”
The study was designed to provide insight into current hemophilia treatment practice and outcomes in 7 European countries—Belgium, France, Germany, Italy, Spain, Sweden, and the UK.
The researchers analyzed data on 1346 patients with hemophilia A and 312 with hemophilia B treated in these countries.
Treatment type, dosing
Prophylaxis was, overall, the most dominating treatment for patients with severe hemophilia A. It was the most common treatment regimen among children and decreased with increasing age.
On-demand treatment was reported to be most common in moderate hemophilia A, and there was no trend across age groups.
For patients with hemophilia B, prophylaxis was the most common treatment in 4 out of the 7 countries (France, Germany, Sweden, and UK).
Overall, a majority of patients received a recombinant antihemophilic factor product as opposed to a plasma-derived product. The one exception was patients with hemophilia B in Germany. A majority of these patients (66%) received a plasma-derived product.
The mean prescribed prophylactic treatment ranged from 67.9 IU kg-1 per week (Belgium) to 108.4 IU kg-1 per week (Germany) for hemophilia A and 32.3 IU kg-1 per week (Belgium) to 97.7 IU kg-1 per week (France) for hemophilia B.
Most patients on prophylaxis were treated 3 or more times a week if they had hemophilia A and 2 times a week if they had hemophilia B.
ABRs across countries
For hemophilia A patients on prophylaxis, the median ABR ranged from 1.0 (Belgium, Italy, Sweden) to 4.0 (France, UK) for patients with severe disease and from 2.0 (Sweden) to 8.0 (Belgium) for patients with moderate disease.
The researchers pointed out that ABRs were higher for patients with moderate hemophilia A, but low patient numbers should be taken into account when interpreting these data.
The median ABRs for hemophilia A patients who received on-demand treatment ranged from 4.5 (Sweden) to 18.0 (UK, Belgium) for patients with severe disease and from 1.0 (Spain, Sweden) to 12.0 (UK) for patients with moderate disease.
For hemophilia B patients on prophylaxis, the median ABRs ranged from 1.0 (Germany, Sweden) to 6.0 (Belgium) for patients with severe disease and from 1.5 (Sweden) to 8.0 (Belgium) for patients with moderate disease. Again, ABRs were higher for patients with moderate disease.
The median ABRs for hemophilia B patients who received on-demand treatment ranged from 1.5 (Germany) to 14.0 (UK) for patients with severe disease and from 1.0 (Belgium, France, Germany, Italy) to 6.5 (UK) for patients with moderate disease.
The researchers said the high number of bleeds observed in some patients likely reflects insufficient therapy, inappropriate dose-interval, presence of target joints, poor adherence, or patient difficulty in correctly assessing bleeds.
The team said the overall results of the study suggest there is room for improvement of hemophilia therapy, even for patients currently on prophylactic treatment. ![]()
Company withdraws application for eryaspase in ALL
ERYTECH Pharma has announced its decision to withdraw the European marketing authorization application (MAA) for eryaspase (GRASPA®) as a treatment for acute lymphoblastic leukemia (ALL).
The European Medicines Agency’s (EMA’s) Committee for Medicinal Products for Human Use (CHMP) asked for additional data on eryaspase, but ERYTECH said the time allowed by the EMA’s approval process is not sufficient to provide the data requested.
Therefore, the company decided to withdraw the MAA and resubmit it next year.
About eryaspase
Eryaspase consists of L-asparaginase encapsulated inside donor-derived red blood cells. These enzyme-loaded red blood cells function as bioreactors to eliminate circulating asparagine and “starve” cancer cells, thereby inducing their death.
Research has suggested this delivery system provides improved pharmacodynamics, protecting L-asparaginase from circulating proteolytic enzymes and preventing early liver or renal clearance.
The system also appears to reduce the risk of adverse events compared to native L-asparaginase.
The EMA and the US Food and Drug Administration have granted orphan drug designations for eryaspase for the treatment of ALL, acute myeloid
leukemia, and pancreatic cancer.
About the MAA
ERYTECH submitted an MAA for eryaspase in September 2015, based on positive results from a phase 2/3 study in which researchers compared eryaspase and native L-asparaginase in patients with relapsed and refractory ALL.
One year later (September 2016), the company received the CHMP’s Day 180 List of Outstanding Issues, which highlighted the need for additional data.
Specifically, the CHMP asked for data regarding the comparability between the old and new form of asparaginase encapsulated in eryaspase and the development of a new immunogenicity assay, as well as the pharmacodynamic effects of eryaspase.
Given the fact that the generation of these data will require more time than allowed in the EMA’s approval procedures, ERYTECH has notified the CHMP of the withdrawal of the MAA.
The company intends to resubmit the MAA in mid-2017, as soon as the newly generated data are available.
ERYTECH stressed that there have been no safety issues with eryaspase, and the withdrawal of this MAA will not affect any ongoing trials.
“We are committed to pursuing regulatory approval for GRASPA and intend to work closely with our investigators and advisors to generate the additional information requested and to resubmit an MAA next year,” said Iman El-Hariry, chief medical officer of ERYTECH.
“We believe we have generated strong clinical data in our different programs of eryaspase, and we continue to execute our plans towards making the product available to patients with aggressive forms of cancer, such as acute lymphoblastic leukemia, acute myeloid leukemia, and pancreatic cancer,” added Gil Beyen, ERYTECH’s chairman and chief executive officer. ![]()
ERYTECH Pharma has announced its decision to withdraw the European marketing authorization application (MAA) for eryaspase (GRASPA®) as a treatment for acute lymphoblastic leukemia (ALL).
The European Medicines Agency’s (EMA’s) Committee for Medicinal Products for Human Use (CHMP) asked for additional data on eryaspase, but ERYTECH said the time allowed by the EMA’s approval process is not sufficient to provide the data requested.
Therefore, the company decided to withdraw the MAA and resubmit it next year.
About eryaspase
Eryaspase consists of L-asparaginase encapsulated inside donor-derived red blood cells. These enzyme-loaded red blood cells function as bioreactors to eliminate circulating asparagine and “starve” cancer cells, thereby inducing their death.
Research has suggested this delivery system provides improved pharmacodynamics, protecting L-asparaginase from circulating proteolytic enzymes and preventing early liver or renal clearance.
The system also appears to reduce the risk of adverse events compared to native L-asparaginase.
The EMA and the US Food and Drug Administration have granted orphan drug designations for eryaspase for the treatment of ALL, acute myeloid
leukemia, and pancreatic cancer.
About the MAA
ERYTECH submitted an MAA for eryaspase in September 2015, based on positive results from a phase 2/3 study in which researchers compared eryaspase and native L-asparaginase in patients with relapsed and refractory ALL.
One year later (September 2016), the company received the CHMP’s Day 180 List of Outstanding Issues, which highlighted the need for additional data.
Specifically, the CHMP asked for data regarding the comparability between the old and new form of asparaginase encapsulated in eryaspase and the development of a new immunogenicity assay, as well as the pharmacodynamic effects of eryaspase.
Given the fact that the generation of these data will require more time than allowed in the EMA’s approval procedures, ERYTECH has notified the CHMP of the withdrawal of the MAA.
The company intends to resubmit the MAA in mid-2017, as soon as the newly generated data are available.
ERYTECH stressed that there have been no safety issues with eryaspase, and the withdrawal of this MAA will not affect any ongoing trials.
“We are committed to pursuing regulatory approval for GRASPA and intend to work closely with our investigators and advisors to generate the additional information requested and to resubmit an MAA next year,” said Iman El-Hariry, chief medical officer of ERYTECH.
“We believe we have generated strong clinical data in our different programs of eryaspase, and we continue to execute our plans towards making the product available to patients with aggressive forms of cancer, such as acute lymphoblastic leukemia, acute myeloid leukemia, and pancreatic cancer,” added Gil Beyen, ERYTECH’s chairman and chief executive officer. ![]()
ERYTECH Pharma has announced its decision to withdraw the European marketing authorization application (MAA) for eryaspase (GRASPA®) as a treatment for acute lymphoblastic leukemia (ALL).
The European Medicines Agency’s (EMA’s) Committee for Medicinal Products for Human Use (CHMP) asked for additional data on eryaspase, but ERYTECH said the time allowed by the EMA’s approval process is not sufficient to provide the data requested.
Therefore, the company decided to withdraw the MAA and resubmit it next year.
About eryaspase
Eryaspase consists of L-asparaginase encapsulated inside donor-derived red blood cells. These enzyme-loaded red blood cells function as bioreactors to eliminate circulating asparagine and “starve” cancer cells, thereby inducing their death.
Research has suggested this delivery system provides improved pharmacodynamics, protecting L-asparaginase from circulating proteolytic enzymes and preventing early liver or renal clearance.
The system also appears to reduce the risk of adverse events compared to native L-asparaginase.
The EMA and the US Food and Drug Administration have granted orphan drug designations for eryaspase for the treatment of ALL, acute myeloid
leukemia, and pancreatic cancer.
About the MAA
ERYTECH submitted an MAA for eryaspase in September 2015, based on positive results from a phase 2/3 study in which researchers compared eryaspase and native L-asparaginase in patients with relapsed and refractory ALL.
One year later (September 2016), the company received the CHMP’s Day 180 List of Outstanding Issues, which highlighted the need for additional data.
Specifically, the CHMP asked for data regarding the comparability between the old and new form of asparaginase encapsulated in eryaspase and the development of a new immunogenicity assay, as well as the pharmacodynamic effects of eryaspase.
Given the fact that the generation of these data will require more time than allowed in the EMA’s approval procedures, ERYTECH has notified the CHMP of the withdrawal of the MAA.
The company intends to resubmit the MAA in mid-2017, as soon as the newly generated data are available.
ERYTECH stressed that there have been no safety issues with eryaspase, and the withdrawal of this MAA will not affect any ongoing trials.
“We are committed to pursuing regulatory approval for GRASPA and intend to work closely with our investigators and advisors to generate the additional information requested and to resubmit an MAA next year,” said Iman El-Hariry, chief medical officer of ERYTECH.
“We believe we have generated strong clinical data in our different programs of eryaspase, and we continue to execute our plans towards making the product available to patients with aggressive forms of cancer, such as acute lymphoblastic leukemia, acute myeloid leukemia, and pancreatic cancer,” added Gil Beyen, ERYTECH’s chairman and chief executive officer. ![]()
Taking Steps to Reduce Arthritis Pain
Severe joint pain (SJP) is common in arthritis but it disproportionately affects certain groups, such as women, blacks, Hispanics, and people with comorbidities. In the US, it’s a leading cause of disability that affects nearly one quarter of adults in 2010-2012, according to data from the CDC, which also says an estimated 78 million people will have arthritis by 2040.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Severe joint pain can limit someone’s ability to perform basic functions, researchers note, and seriously compromise their quality of life. To find out how prevalent severe joint pain is among adults with arthritis, the CDC analyzed data from the National Health Interview Survey. In 2014, approximately one fourth of adults with arthritis had SJP.
Two major objectives of the 2016 National Pain Strategy are to reduce barriers to pain care and increase patient knowledge of treatment options and risks, the researchers say. They cite the CDC Guideline for Prescribing Opioids for Chronic Pain–United States, 2016, for guidance on managing arthritis pain. (The CDC also currently funds arthritis programs in 12 states.)
Related: Lessons Learned From the RACAT Trial: A Comparison of Rheumatoid Arthritis Therapies
But the researchers also point out that many non-drug options exist for managing arthritis pain. For example, low-impact physical activity, such as walking, biking, and swimming is a “nonpharmacological and underused way of reducing joint pain,” they comment. They also note that community-based programs such as EnhanceFitness and Walk with Ease, as well as self-management education interventions such as the Chronic Disease Self-Management Program, have been shown to improve health-related quality of life and confidence in managing health conditions.
Severe joint pain (SJP) is common in arthritis but it disproportionately affects certain groups, such as women, blacks, Hispanics, and people with comorbidities. In the US, it’s a leading cause of disability that affects nearly one quarter of adults in 2010-2012, according to data from the CDC, which also says an estimated 78 million people will have arthritis by 2040.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Severe joint pain can limit someone’s ability to perform basic functions, researchers note, and seriously compromise their quality of life. To find out how prevalent severe joint pain is among adults with arthritis, the CDC analyzed data from the National Health Interview Survey. In 2014, approximately one fourth of adults with arthritis had SJP.
Two major objectives of the 2016 National Pain Strategy are to reduce barriers to pain care and increase patient knowledge of treatment options and risks, the researchers say. They cite the CDC Guideline for Prescribing Opioids for Chronic Pain–United States, 2016, for guidance on managing arthritis pain. (The CDC also currently funds arthritis programs in 12 states.)
Related: Lessons Learned From the RACAT Trial: A Comparison of Rheumatoid Arthritis Therapies
But the researchers also point out that many non-drug options exist for managing arthritis pain. For example, low-impact physical activity, such as walking, biking, and swimming is a “nonpharmacological and underused way of reducing joint pain,” they comment. They also note that community-based programs such as EnhanceFitness and Walk with Ease, as well as self-management education interventions such as the Chronic Disease Self-Management Program, have been shown to improve health-related quality of life and confidence in managing health conditions.
Severe joint pain (SJP) is common in arthritis but it disproportionately affects certain groups, such as women, blacks, Hispanics, and people with comorbidities. In the US, it’s a leading cause of disability that affects nearly one quarter of adults in 2010-2012, according to data from the CDC, which also says an estimated 78 million people will have arthritis by 2040.
Related: Complementary and Alternative Medicine for Chronic Musculoskeletal Pain
Severe joint pain can limit someone’s ability to perform basic functions, researchers note, and seriously compromise their quality of life. To find out how prevalent severe joint pain is among adults with arthritis, the CDC analyzed data from the National Health Interview Survey. In 2014, approximately one fourth of adults with arthritis had SJP.
Two major objectives of the 2016 National Pain Strategy are to reduce barriers to pain care and increase patient knowledge of treatment options and risks, the researchers say. They cite the CDC Guideline for Prescribing Opioids for Chronic Pain–United States, 2016, for guidance on managing arthritis pain. (The CDC also currently funds arthritis programs in 12 states.)
Related: Lessons Learned From the RACAT Trial: A Comparison of Rheumatoid Arthritis Therapies
But the researchers also point out that many non-drug options exist for managing arthritis pain. For example, low-impact physical activity, such as walking, biking, and swimming is a “nonpharmacological and underused way of reducing joint pain,” they comment. They also note that community-based programs such as EnhanceFitness and Walk with Ease, as well as self-management education interventions such as the Chronic Disease Self-Management Program, have been shown to improve health-related quality of life and confidence in managing health conditions.
Kidney Disease & “Bad Teeth”
Q)Someone at a conference I attended said kidney disease and bad teeth go hand in hand. Is this true? What does that mean for my patients?
“Bad teeth” can refer to periodontitis, a chronic inflammation of the tissue and structures around the teeth. The sixth most common disease in the world, periodontitis often leads to shrinkage of the gums, infection, and subsequent loosening or loss of teeth.3
Patients with chronic kidney disease (CKD) are predisposed to oral lesions and tooth decay related to dryness of the mouth; alterations in taste; malnutrition; and low albumin. Certain medications—such as ß-blockers, diuretics, anticholinergics, anticonvulsants, and serotonin reuptake inhibitors—can increase the risk for dry mouth and negatively affect oral structures.4
Compared with community-dwelling adults, those with CKD have higher rates of periodontitis, which increase with disease progression.5 A systematic review found that periodontitis increases the risk for CKD; evidence was inconclusive for the impact of periodontal treatment on estimated glomerular filtration rates (eGFR) but suggested positive improvements in eGFR.6
There is growing evidence of a multifaceted relationship between CKD, diabetes, periodontitis, and cardiovascular disease (CVD), the leading cause of mortality in patients with CKD.7 Studies have shown that periodontitis can contribute to systemic inflammation, inhibiting glycemic control and elevating the risk for conditions such as CVD.8-10
Diabetes, the most common cause of CKD, is associated with adverse dental outcomes and poor glycemic control. Vice versa, severe periodontitis increases risk for diabetes and worsening glucose control. Mechanical periodontal treatment has been shown to improve glycemic control.8
A recent study showed an increased risk for both CVD events and all-cause mortality in those with stage III to stage V CKD (eGFR < 60 mL/min/1.73 m2). The study also found that periodontitis increased 10-year all-cause mortality in this population (see Figure).11
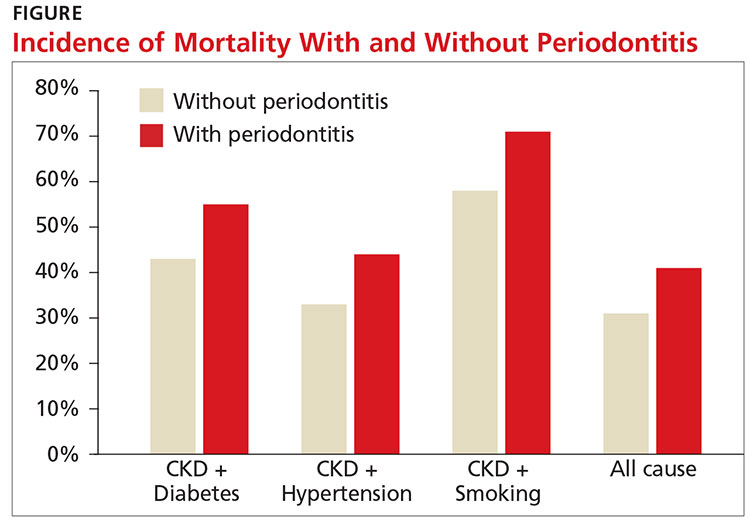
Research is ongoing regarding the complex relationship between CKD and oral health. For patients with CKD at any stage, evidence promotes the benefits of good oral health habits. Encourage smoking cessation, daily flossing and tooth brushing, regular dental cleanings, and prompt evaluation and treatment of any oral issues.12 —CS
Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN
Renal Consultants PLLC, South Charleston, West Virginia
3. Page RC, Eke PI. Case definitions for use in population-based surveillance of periodontitis. J Periodontol. 2007;78(7):1387-1399.
4. Akar H, Akar GC, Carrero JJ, et al. Systemic consequences of poor oral health in chronic kidney disease patients. Clin J Am Soc Nephrol. 2011;6(1):218-226.
5. Borawski J, Wilczyn´ska-Borawska M, Stokowska W, Mys´liwiec M. The periodontal status of pre-dialysis chronic kidney disease and maintenance dialysis patients. Nephrol Dial Transplant. 2007;22(2):457-464.
6. Chambrone L, Foz AM, Guglielmetti MR, et al. Periodontitis and chronic kidney disease: a systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J Clin Periodontol. 2013;40(5):443-456.
7. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305.
8. Kassebaum NJ, Bernabé E, Dahiya M, et al. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045-1053.
9. Chapple IL, Genco R; Working Group 2 of Joint EFP/AAP Workshop. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol. 2013; 40(14):S106-S112.
10. Menon V, Greene T, Wang X, et al. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005;68(2):766-772.
11. Sharma P, Dietrich T, Ferro CJ, et al. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J Clin Periodontol. 2016;43(2):104-113.
12. Ariyamuthu VK, Nolph KD, Ringdahl BE. Periodontal disease in chronic kidney disease and end-stage renal disease patients: a review. Cardiorenal Med. 2013;3(1):71-78.
Clinician Reviews in partnership with

Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a semi-retired PA who works with the American Academy of Nephrology PAs and is a past chair of the NKF-CAP. This month’s responses were authored by Sherry Mathes, NP-C, who practices at Georgia Nephrology LLC in Lawrenceville, Georgia, and Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN, who practices with Renal Consultants PLLC in South Charleston, West Virginia.
Clinician Reviews in partnership with
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a semi-retired PA who works with the American Academy of Nephrology PAs and is a past chair of the NKF-CAP. This month’s responses were authored by Sherry Mathes, NP-C, who practices at Georgia Nephrology LLC in Lawrenceville, Georgia, and Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN, who practices with Renal Consultants PLLC in South Charleston, West Virginia.
Clinician Reviews in partnership with
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a semi-retired PA who works with the American Academy of Nephrology PAs and is a past chair of the NKF-CAP. This month’s responses were authored by Sherry Mathes, NP-C, who practices at Georgia Nephrology LLC in Lawrenceville, Georgia, and Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN, who practices with Renal Consultants PLLC in South Charleston, West Virginia.
Q)Someone at a conference I attended said kidney disease and bad teeth go hand in hand. Is this true? What does that mean for my patients?
“Bad teeth” can refer to periodontitis, a chronic inflammation of the tissue and structures around the teeth. The sixth most common disease in the world, periodontitis often leads to shrinkage of the gums, infection, and subsequent loosening or loss of teeth.3
Patients with chronic kidney disease (CKD) are predisposed to oral lesions and tooth decay related to dryness of the mouth; alterations in taste; malnutrition; and low albumin. Certain medications—such as ß-blockers, diuretics, anticholinergics, anticonvulsants, and serotonin reuptake inhibitors—can increase the risk for dry mouth and negatively affect oral structures.4
Compared with community-dwelling adults, those with CKD have higher rates of periodontitis, which increase with disease progression.5 A systematic review found that periodontitis increases the risk for CKD; evidence was inconclusive for the impact of periodontal treatment on estimated glomerular filtration rates (eGFR) but suggested positive improvements in eGFR.6
There is growing evidence of a multifaceted relationship between CKD, diabetes, periodontitis, and cardiovascular disease (CVD), the leading cause of mortality in patients with CKD.7 Studies have shown that periodontitis can contribute to systemic inflammation, inhibiting glycemic control and elevating the risk for conditions such as CVD.8-10
Diabetes, the most common cause of CKD, is associated with adverse dental outcomes and poor glycemic control. Vice versa, severe periodontitis increases risk for diabetes and worsening glucose control. Mechanical periodontal treatment has been shown to improve glycemic control.8
A recent study showed an increased risk for both CVD events and all-cause mortality in those with stage III to stage V CKD (eGFR < 60 mL/min/1.73 m2). The study also found that periodontitis increased 10-year all-cause mortality in this population (see Figure).11
Research is ongoing regarding the complex relationship between CKD and oral health. For patients with CKD at any stage, evidence promotes the benefits of good oral health habits. Encourage smoking cessation, daily flossing and tooth brushing, regular dental cleanings, and prompt evaluation and treatment of any oral issues.12 —CS
Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN
Renal Consultants PLLC, South Charleston, West Virginia
Q)Someone at a conference I attended said kidney disease and bad teeth go hand in hand. Is this true? What does that mean for my patients?
“Bad teeth” can refer to periodontitis, a chronic inflammation of the tissue and structures around the teeth. The sixth most common disease in the world, periodontitis often leads to shrinkage of the gums, infection, and subsequent loosening or loss of teeth.3
Patients with chronic kidney disease (CKD) are predisposed to oral lesions and tooth decay related to dryness of the mouth; alterations in taste; malnutrition; and low albumin. Certain medications—such as ß-blockers, diuretics, anticholinergics, anticonvulsants, and serotonin reuptake inhibitors—can increase the risk for dry mouth and negatively affect oral structures.4
Compared with community-dwelling adults, those with CKD have higher rates of periodontitis, which increase with disease progression.5 A systematic review found that periodontitis increases the risk for CKD; evidence was inconclusive for the impact of periodontal treatment on estimated glomerular filtration rates (eGFR) but suggested positive improvements in eGFR.6
There is growing evidence of a multifaceted relationship between CKD, diabetes, periodontitis, and cardiovascular disease (CVD), the leading cause of mortality in patients with CKD.7 Studies have shown that periodontitis can contribute to systemic inflammation, inhibiting glycemic control and elevating the risk for conditions such as CVD.8-10
Diabetes, the most common cause of CKD, is associated with adverse dental outcomes and poor glycemic control. Vice versa, severe periodontitis increases risk for diabetes and worsening glucose control. Mechanical periodontal treatment has been shown to improve glycemic control.8
A recent study showed an increased risk for both CVD events and all-cause mortality in those with stage III to stage V CKD (eGFR < 60 mL/min/1.73 m2). The study also found that periodontitis increased 10-year all-cause mortality in this population (see Figure).11
Research is ongoing regarding the complex relationship between CKD and oral health. For patients with CKD at any stage, evidence promotes the benefits of good oral health habits. Encourage smoking cessation, daily flossing and tooth brushing, regular dental cleanings, and prompt evaluation and treatment of any oral issues.12 —CS
Cynthia Smith, DNP, CNN-NP, FNP-BC, APRN
Renal Consultants PLLC, South Charleston, West Virginia
3. Page RC, Eke PI. Case definitions for use in population-based surveillance of periodontitis. J Periodontol. 2007;78(7):1387-1399.
4. Akar H, Akar GC, Carrero JJ, et al. Systemic consequences of poor oral health in chronic kidney disease patients. Clin J Am Soc Nephrol. 2011;6(1):218-226.
5. Borawski J, Wilczyn´ska-Borawska M, Stokowska W, Mys´liwiec M. The periodontal status of pre-dialysis chronic kidney disease and maintenance dialysis patients. Nephrol Dial Transplant. 2007;22(2):457-464.
6. Chambrone L, Foz AM, Guglielmetti MR, et al. Periodontitis and chronic kidney disease: a systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J Clin Periodontol. 2013;40(5):443-456.
7. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305.
8. Kassebaum NJ, Bernabé E, Dahiya M, et al. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045-1053.
9. Chapple IL, Genco R; Working Group 2 of Joint EFP/AAP Workshop. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol. 2013; 40(14):S106-S112.
10. Menon V, Greene T, Wang X, et al. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005;68(2):766-772.
11. Sharma P, Dietrich T, Ferro CJ, et al. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J Clin Periodontol. 2016;43(2):104-113.
12. Ariyamuthu VK, Nolph KD, Ringdahl BE. Periodontal disease in chronic kidney disease and end-stage renal disease patients: a review. Cardiorenal Med. 2013;3(1):71-78.
3. Page RC, Eke PI. Case definitions for use in population-based surveillance of periodontitis. J Periodontol. 2007;78(7):1387-1399.
4. Akar H, Akar GC, Carrero JJ, et al. Systemic consequences of poor oral health in chronic kidney disease patients. Clin J Am Soc Nephrol. 2011;6(1):218-226.
5. Borawski J, Wilczyn´ska-Borawska M, Stokowska W, Mys´liwiec M. The periodontal status of pre-dialysis chronic kidney disease and maintenance dialysis patients. Nephrol Dial Transplant. 2007;22(2):457-464.
6. Chambrone L, Foz AM, Guglielmetti MR, et al. Periodontitis and chronic kidney disease: a systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J Clin Periodontol. 2013;40(5):443-456.
7. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305.
8. Kassebaum NJ, Bernabé E, Dahiya M, et al. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045-1053.
9. Chapple IL, Genco R; Working Group 2 of Joint EFP/AAP Workshop. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J Clin Periodontol. 2013; 40(14):S106-S112.
10. Menon V, Greene T, Wang X, et al. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005;68(2):766-772.
11. Sharma P, Dietrich T, Ferro CJ, et al. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J Clin Periodontol. 2016;43(2):104-113.
12. Ariyamuthu VK, Nolph KD, Ringdahl BE. Periodontal disease in chronic kidney disease and end-stage renal disease patients: a review. Cardiorenal Med. 2013;3(1):71-78.