User login
Monitoring Home BP Readings Just Got Easier
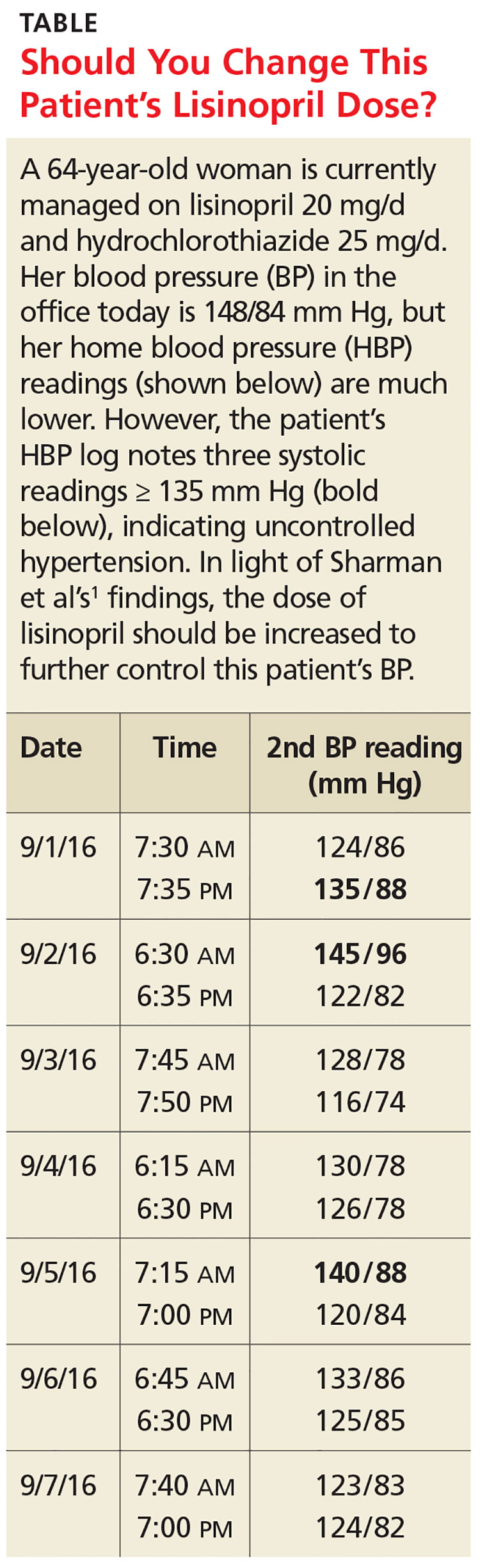
A 64-year-old woman presents to your office for a follow-up visit for her hypertension. She is currently managed on lisinopril 20 mg/d and hydrochlorothiazide 25 mg/d without any problems. The patient’s blood pressure (BP) in the office today is 148/84 mm Hg, but her home blood pressure (HBP) readings are much lower (see Table). Should you increase her lisinopril dose today?
Hypertension has been diagnosed on the basis of office readings of BP for almost a century, but the readings can be so inaccurate that they are not useful.2 The US Preventive Services Task Force recommends the use of ambulatory BP monitoring (ABPM) to accurately diagnose hypertension in all patients, while The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends ABPM for patients suspected of having white-coat hypertension and any patient with resistant hypertension, but ABPM is not always acceptable to patients.3-5
HBP monitoring for long-term follow-up
The European Society of Hypertension practice guideline on HBP monitoring suggests that HBP values < 130/80 mm Hg may be considered normal, while a mean HBP ≥ 135/85 mm Hg is considered elevated.9 The guideline recommends HBP monitoring for three to seven days prior to a patient’s follow-up appointment, with two readings taken one to two minutes apart in the morning and evening.9 In a busy clinic, averaging all of these home values can be time-consuming.
So how can primary care providers accurately and efficiently streamline the process? This study sought to answer that question.
STUDY SUMMARY
3 of 10 readings = predictive
This multicenter trial compared HBP monitoring to 24-hour ABPM in 286 patients with uncomplicated essential hypertension to determine the optimal percentage of HBP readings needed to diagnose uncontrolled BP (HBP ≥ 135/85 mm Hg). Patients were included if they were diagnosed with uncomplicated hypertension, not pregnant, age 18 or older, and taking three or fewer antihypertensive medications. Patients were excluded if they had a significant abnormal left ventricular mass index (women > 59 g/m2; men > 64 g/m2), coronary artery or renal disease, secondary hypertension, serum creatinine exceeding 1.6 mg/dL, aortic valve stenosis, upper limb obstructive atherosclerosis, or BP > 180/100 mm Hg.
Approximately half of the participants were women (53%). Average BMI was 29.4 kg/m2, and the average number of hypertension medications being taken was 2.4. Medication compliance was verified by a study nurse at a clinic visit.
The patients were instructed to take two BP readings (one minute apart) at home three times daily, in the morning (between 6
The primary outcome was to determine the optimal number of systolic HBP readings above goal (135 mm Hg), from the last 10 recordings, that would best predict elevated 24-hour ABP. Secondary outcomes were various cardiovascular markers of target end-organ damage.
The researchers found that if at least three of the last 10 HBP readings were elevated (≥ 135 mm Hg systolic), the patient was likely to have hypertension on 24-hour ABPM (≥ 130 mm Hg). When patients had less than three HBP elevations out of 10 readings, their mean (± standard deviation [SD]) 24-hour ambulatory daytime systolic BP was 132.7 (± 11.1) mm Hg and their mean systolic HBP value was 120.4 (± 9.8) mm Hg. When patients had three or more HBP elevations, their mean 24-hour ambulatory daytime systolic BP was 143.4 (± 11.2) mm Hg and their mean systolic HBP value was 147.4 (± 10.5) mm Hg.
The positive and negative predictive values of three or more HBP elevations were 0.85 and 0.56, respectively, for a 24-hour systolic ABP of ≥ 130 mm Hg. Three elevations or more in HBP, out of the last 10 readings, was also an indicator for target organ disease assessed by aortic stiffness and increased left ventricular mass and decreased function.
The sensitivity and specificity of three or more elevations for mean 24-hour ABP systolic readings ≥ 130 mm Hg were 62% and 80%, respectively, and for 24-hour ABP daytime systolic readings ≥ 135 mm Hg were 65% and 77%, respectively.
WHAT’S NEW
Monitoring home BP can be simplified
The researchers found that HBP monitoring correlates well with ABPM and that their method provides clinicians with a simple way (three of the past 10 measurements ≥ 135 mm Hg systolic) to use HBP readings to make clinical decisions regarding BP management.
CAVEATS
BP goals are hazy, patient education is required
Conflicting information and opinions remain regarding the ideal intensive and standard BP goals in different populations.10,11 Systolic BP goals in this study (≥ 130 mm Hg for overall 24-hour ABP and ≥ 135 mm Hg for 24-hour ABP daytime readings) are recommended by some experts but are not commonly recognized goals in the United States. This study found good correlation between HBP and ABPM at these goals, and it seems likely that this correlation could be extrapolated for similar BP goals.
Other limitations are that (1) The study focused only on systolic BP goals; (2) patients in the study adhered to precise instructions on BP monitoring; HBP monitoring requires significant patient education on the proper use of the equipment and the monitoring schedule; and (3) while end-organ complication outcomes showed numerical decreases in function, the clinical significance of these reductions for patients is unclear.
CHALLENGES TO IMPLEMENTATION
Cost, sizing of cuffs
The cost of HBP monitors ($40-$60) has decreased significantly over time, but the devices are not always covered by insurance and may be unobtainable for some people.
Additionally, patients should be counseled on how to determine the appropriate cuff size to ensure the accuracy of the measurements. The British Hypertension Society maintains a list of validated BP devices on its website: http://bhsoc.org/bp-monitors/bp-monitors.12
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(10):719-722.
1. Sharman JE, Blizzard L, Kosmala W, et al. Pragmatic method using blood pressure diaries to assess blood pressure control. Ann Fam Med. 2016;14:63-69.
2. Sebo P, Pechère-Bertschi A, Herrmann FR, et al. Blood pressure measurements are unreliable to diagnose hypertension in primary care. J Hypertens. 2014;32:509-517.
3. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163:778-786.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA. 2003;289:2560-2572.
5. Mallion JM, de Gaudemaris R, Baguet JP, et al. Acceptability and tolerance of ambulatory blood pressure measurement in the hypertensive patient. Blood Press Monit. 1996; 1:197-203.
6. Gaborieau V, Delarche N, Gosse P. Ambulatory blood pressure monitoring versus self-measurement of blood pressure at home: correlation with target organ damage. J Hypertens. 2008;26:1919-1927.
7. Ward AM, Takahashi O, Stevens R, et al. Home measurement of blood pressure and cardiovascular disease: systematic review and meta-analysis of prospective studies. J Hypertens. 2012;30:449-456.
8. Pickering TG, Miller NH, Ogedegbe G, et al. Call to action on use and reimbursement for home blood pressure monitoring: executive summary. A joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension. 2008;52:1-9.
9. Parati G, Stergiou GS, Asmar R, et al; ESH Working Group on Blood Pressure Monitoring. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens. 2010;24:779-785.
10. The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
11. Brunström M, Carlberg B. Effect of antihypertensive treatment at different blood pressure levels in patients with diabetes mellitus: systematic review and meta-analyses. BMJ. 2016;352:i717.
12. British Hypertension Society. BP Monitors. http://bhsoc.org/bp-monitors/bp-monitors. Accessed June 27, 2016.
A 64-year-old woman presents to your office for a follow-up visit for her hypertension. She is currently managed on lisinopril 20 mg/d and hydrochlorothiazide 25 mg/d without any problems. The patient’s blood pressure (BP) in the office today is 148/84 mm Hg, but her home blood pressure (HBP) readings are much lower (see Table). Should you increase her lisinopril dose today?
Hypertension has been diagnosed on the basis of office readings of BP for almost a century, but the readings can be so inaccurate that they are not useful.2 The US Preventive Services Task Force recommends the use of ambulatory BP monitoring (ABPM) to accurately diagnose hypertension in all patients, while The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends ABPM for patients suspected of having white-coat hypertension and any patient with resistant hypertension, but ABPM is not always acceptable to patients.3-5
HBP monitoring for long-term follow-up
The European Society of Hypertension practice guideline on HBP monitoring suggests that HBP values < 130/80 mm Hg may be considered normal, while a mean HBP ≥ 135/85 mm Hg is considered elevated.9 The guideline recommends HBP monitoring for three to seven days prior to a patient’s follow-up appointment, with two readings taken one to two minutes apart in the morning and evening.9 In a busy clinic, averaging all of these home values can be time-consuming.
So how can primary care providers accurately and efficiently streamline the process? This study sought to answer that question.
STUDY SUMMARY
3 of 10 readings = predictive
This multicenter trial compared HBP monitoring to 24-hour ABPM in 286 patients with uncomplicated essential hypertension to determine the optimal percentage of HBP readings needed to diagnose uncontrolled BP (HBP ≥ 135/85 mm Hg). Patients were included if they were diagnosed with uncomplicated hypertension, not pregnant, age 18 or older, and taking three or fewer antihypertensive medications. Patients were excluded if they had a significant abnormal left ventricular mass index (women > 59 g/m2; men > 64 g/m2), coronary artery or renal disease, secondary hypertension, serum creatinine exceeding 1.6 mg/dL, aortic valve stenosis, upper limb obstructive atherosclerosis, or BP > 180/100 mm Hg.
Approximately half of the participants were women (53%). Average BMI was 29.4 kg/m2, and the average number of hypertension medications being taken was 2.4. Medication compliance was verified by a study nurse at a clinic visit.
The patients were instructed to take two BP readings (one minute apart) at home three times daily, in the morning (between 6
The primary outcome was to determine the optimal number of systolic HBP readings above goal (135 mm Hg), from the last 10 recordings, that would best predict elevated 24-hour ABP. Secondary outcomes were various cardiovascular markers of target end-organ damage.
The researchers found that if at least three of the last 10 HBP readings were elevated (≥ 135 mm Hg systolic), the patient was likely to have hypertension on 24-hour ABPM (≥ 130 mm Hg). When patients had less than three HBP elevations out of 10 readings, their mean (± standard deviation [SD]) 24-hour ambulatory daytime systolic BP was 132.7 (± 11.1) mm Hg and their mean systolic HBP value was 120.4 (± 9.8) mm Hg. When patients had three or more HBP elevations, their mean 24-hour ambulatory daytime systolic BP was 143.4 (± 11.2) mm Hg and their mean systolic HBP value was 147.4 (± 10.5) mm Hg.
The positive and negative predictive values of three or more HBP elevations were 0.85 and 0.56, respectively, for a 24-hour systolic ABP of ≥ 130 mm Hg. Three elevations or more in HBP, out of the last 10 readings, was also an indicator for target organ disease assessed by aortic stiffness and increased left ventricular mass and decreased function.
The sensitivity and specificity of three or more elevations for mean 24-hour ABP systolic readings ≥ 130 mm Hg were 62% and 80%, respectively, and for 24-hour ABP daytime systolic readings ≥ 135 mm Hg were 65% and 77%, respectively.
WHAT’S NEW
Monitoring home BP can be simplified
The researchers found that HBP monitoring correlates well with ABPM and that their method provides clinicians with a simple way (three of the past 10 measurements ≥ 135 mm Hg systolic) to use HBP readings to make clinical decisions regarding BP management.
CAVEATS
BP goals are hazy, patient education is required
Conflicting information and opinions remain regarding the ideal intensive and standard BP goals in different populations.10,11 Systolic BP goals in this study (≥ 130 mm Hg for overall 24-hour ABP and ≥ 135 mm Hg for 24-hour ABP daytime readings) are recommended by some experts but are not commonly recognized goals in the United States. This study found good correlation between HBP and ABPM at these goals, and it seems likely that this correlation could be extrapolated for similar BP goals.
Other limitations are that (1) The study focused only on systolic BP goals; (2) patients in the study adhered to precise instructions on BP monitoring; HBP monitoring requires significant patient education on the proper use of the equipment and the monitoring schedule; and (3) while end-organ complication outcomes showed numerical decreases in function, the clinical significance of these reductions for patients is unclear.
CHALLENGES TO IMPLEMENTATION
Cost, sizing of cuffs
The cost of HBP monitors ($40-$60) has decreased significantly over time, but the devices are not always covered by insurance and may be unobtainable for some people.
Additionally, patients should be counseled on how to determine the appropriate cuff size to ensure the accuracy of the measurements. The British Hypertension Society maintains a list of validated BP devices on its website: http://bhsoc.org/bp-monitors/bp-monitors.12
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(10):719-722.
A 64-year-old woman presents to your office for a follow-up visit for her hypertension. She is currently managed on lisinopril 20 mg/d and hydrochlorothiazide 25 mg/d without any problems. The patient’s blood pressure (BP) in the office today is 148/84 mm Hg, but her home blood pressure (HBP) readings are much lower (see Table). Should you increase her lisinopril dose today?
Hypertension has been diagnosed on the basis of office readings of BP for almost a century, but the readings can be so inaccurate that they are not useful.2 The US Preventive Services Task Force recommends the use of ambulatory BP monitoring (ABPM) to accurately diagnose hypertension in all patients, while The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends ABPM for patients suspected of having white-coat hypertension and any patient with resistant hypertension, but ABPM is not always acceptable to patients.3-5
HBP monitoring for long-term follow-up
The European Society of Hypertension practice guideline on HBP monitoring suggests that HBP values < 130/80 mm Hg may be considered normal, while a mean HBP ≥ 135/85 mm Hg is considered elevated.9 The guideline recommends HBP monitoring for three to seven days prior to a patient’s follow-up appointment, with two readings taken one to two minutes apart in the morning and evening.9 In a busy clinic, averaging all of these home values can be time-consuming.
So how can primary care providers accurately and efficiently streamline the process? This study sought to answer that question.
STUDY SUMMARY
3 of 10 readings = predictive
This multicenter trial compared HBP monitoring to 24-hour ABPM in 286 patients with uncomplicated essential hypertension to determine the optimal percentage of HBP readings needed to diagnose uncontrolled BP (HBP ≥ 135/85 mm Hg). Patients were included if they were diagnosed with uncomplicated hypertension, not pregnant, age 18 or older, and taking three or fewer antihypertensive medications. Patients were excluded if they had a significant abnormal left ventricular mass index (women > 59 g/m2; men > 64 g/m2), coronary artery or renal disease, secondary hypertension, serum creatinine exceeding 1.6 mg/dL, aortic valve stenosis, upper limb obstructive atherosclerosis, or BP > 180/100 mm Hg.
Approximately half of the participants were women (53%). Average BMI was 29.4 kg/m2, and the average number of hypertension medications being taken was 2.4. Medication compliance was verified by a study nurse at a clinic visit.
The patients were instructed to take two BP readings (one minute apart) at home three times daily, in the morning (between 6
The primary outcome was to determine the optimal number of systolic HBP readings above goal (135 mm Hg), from the last 10 recordings, that would best predict elevated 24-hour ABP. Secondary outcomes were various cardiovascular markers of target end-organ damage.
The researchers found that if at least three of the last 10 HBP readings were elevated (≥ 135 mm Hg systolic), the patient was likely to have hypertension on 24-hour ABPM (≥ 130 mm Hg). When patients had less than three HBP elevations out of 10 readings, their mean (± standard deviation [SD]) 24-hour ambulatory daytime systolic BP was 132.7 (± 11.1) mm Hg and their mean systolic HBP value was 120.4 (± 9.8) mm Hg. When patients had three or more HBP elevations, their mean 24-hour ambulatory daytime systolic BP was 143.4 (± 11.2) mm Hg and their mean systolic HBP value was 147.4 (± 10.5) mm Hg.
The positive and negative predictive values of three or more HBP elevations were 0.85 and 0.56, respectively, for a 24-hour systolic ABP of ≥ 130 mm Hg. Three elevations or more in HBP, out of the last 10 readings, was also an indicator for target organ disease assessed by aortic stiffness and increased left ventricular mass and decreased function.
The sensitivity and specificity of three or more elevations for mean 24-hour ABP systolic readings ≥ 130 mm Hg were 62% and 80%, respectively, and for 24-hour ABP daytime systolic readings ≥ 135 mm Hg were 65% and 77%, respectively.
WHAT’S NEW
Monitoring home BP can be simplified
The researchers found that HBP monitoring correlates well with ABPM and that their method provides clinicians with a simple way (three of the past 10 measurements ≥ 135 mm Hg systolic) to use HBP readings to make clinical decisions regarding BP management.
CAVEATS
BP goals are hazy, patient education is required
Conflicting information and opinions remain regarding the ideal intensive and standard BP goals in different populations.10,11 Systolic BP goals in this study (≥ 130 mm Hg for overall 24-hour ABP and ≥ 135 mm Hg for 24-hour ABP daytime readings) are recommended by some experts but are not commonly recognized goals in the United States. This study found good correlation between HBP and ABPM at these goals, and it seems likely that this correlation could be extrapolated for similar BP goals.
Other limitations are that (1) The study focused only on systolic BP goals; (2) patients in the study adhered to precise instructions on BP monitoring; HBP monitoring requires significant patient education on the proper use of the equipment and the monitoring schedule; and (3) while end-organ complication outcomes showed numerical decreases in function, the clinical significance of these reductions for patients is unclear.
CHALLENGES TO IMPLEMENTATION
Cost, sizing of cuffs
The cost of HBP monitors ($40-$60) has decreased significantly over time, but the devices are not always covered by insurance and may be unobtainable for some people.
Additionally, patients should be counseled on how to determine the appropriate cuff size to ensure the accuracy of the measurements. The British Hypertension Society maintains a list of validated BP devices on its website: http://bhsoc.org/bp-monitors/bp-monitors.12
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(10):719-722.
1. Sharman JE, Blizzard L, Kosmala W, et al. Pragmatic method using blood pressure diaries to assess blood pressure control. Ann Fam Med. 2016;14:63-69.
2. Sebo P, Pechère-Bertschi A, Herrmann FR, et al. Blood pressure measurements are unreliable to diagnose hypertension in primary care. J Hypertens. 2014;32:509-517.
3. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163:778-786.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA. 2003;289:2560-2572.
5. Mallion JM, de Gaudemaris R, Baguet JP, et al. Acceptability and tolerance of ambulatory blood pressure measurement in the hypertensive patient. Blood Press Monit. 1996; 1:197-203.
6. Gaborieau V, Delarche N, Gosse P. Ambulatory blood pressure monitoring versus self-measurement of blood pressure at home: correlation with target organ damage. J Hypertens. 2008;26:1919-1927.
7. Ward AM, Takahashi O, Stevens R, et al. Home measurement of blood pressure and cardiovascular disease: systematic review and meta-analysis of prospective studies. J Hypertens. 2012;30:449-456.
8. Pickering TG, Miller NH, Ogedegbe G, et al. Call to action on use and reimbursement for home blood pressure monitoring: executive summary. A joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension. 2008;52:1-9.
9. Parati G, Stergiou GS, Asmar R, et al; ESH Working Group on Blood Pressure Monitoring. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens. 2010;24:779-785.
10. The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
11. Brunström M, Carlberg B. Effect of antihypertensive treatment at different blood pressure levels in patients with diabetes mellitus: systematic review and meta-analyses. BMJ. 2016;352:i717.
12. British Hypertension Society. BP Monitors. http://bhsoc.org/bp-monitors/bp-monitors. Accessed June 27, 2016.
1. Sharman JE, Blizzard L, Kosmala W, et al. Pragmatic method using blood pressure diaries to assess blood pressure control. Ann Fam Med. 2016;14:63-69.
2. Sebo P, Pechère-Bertschi A, Herrmann FR, et al. Blood pressure measurements are unreliable to diagnose hypertension in primary care. J Hypertens. 2014;32:509-517.
3. Siu AL; US Preventive Services Task Force. Screening for high blood pressure in adults: US Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163:778-786.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA. 2003;289:2560-2572.
5. Mallion JM, de Gaudemaris R, Baguet JP, et al. Acceptability and tolerance of ambulatory blood pressure measurement in the hypertensive patient. Blood Press Monit. 1996; 1:197-203.
6. Gaborieau V, Delarche N, Gosse P. Ambulatory blood pressure monitoring versus self-measurement of blood pressure at home: correlation with target organ damage. J Hypertens. 2008;26:1919-1927.
7. Ward AM, Takahashi O, Stevens R, et al. Home measurement of blood pressure and cardiovascular disease: systematic review and meta-analysis of prospective studies. J Hypertens. 2012;30:449-456.
8. Pickering TG, Miller NH, Ogedegbe G, et al. Call to action on use and reimbursement for home blood pressure monitoring: executive summary. A joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension. 2008;52:1-9.
9. Parati G, Stergiou GS, Asmar R, et al; ESH Working Group on Blood Pressure Monitoring. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens. 2010;24:779-785.
10. The SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103-2116.
11. Brunström M, Carlberg B. Effect of antihypertensive treatment at different blood pressure levels in patients with diabetes mellitus: systematic review and meta-analyses. BMJ. 2016;352:i717.
12. British Hypertension Society. BP Monitors. http://bhsoc.org/bp-monitors/bp-monitors. Accessed June 27, 2016.
Release of the MACRA Final Rule
On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released the final rule pertaining to the Medicare Access and CHIP Reauthorization Act (MACRA). As I write, almost three weeks later, Division of Advocacy and Health Policy staff are generally pleased with the contents of the rule as there were no big “negative” surprises and stakeholder input in response to the proposed rule seems to have been broadly taken to heart by the administration at CMS.
As Fellows prepare for 2017, they should take note of several changes that were made to the original proposed rule. Some key changes are summarized below.

With regard to what was previously referred to as the Clinical Practice Improvement Activities (CPIA), the nomenclature as well as the associated requirement have been shortened and simplified. Now called simply Improvement Activities, to achieve full credit most physicians will need to report on between two to four of the nearly 100 possible activities as opposed to up to the six activities needed to meet the requirements as outlined in the proposed rule. Fortunately, the reporting requirement for the Improvement Activities component remains the simple attestation that one has participated in the selected activities for a period of 90 continuous days during the 2017 reporting period. Improvement Activities continues to comprise 15% of the Composite Score.
With release of the final rule, we now have a more concrete definition of what CMS Acting Administrator Andrew Slavitt meant by “Pick Your Pace” which was the topic of last month’s column (October 2016, p. 15). CMS is looking at the 2017 reporting period as a transition year with which it hopes to engage physicians in participation in its new Medicare physician payment plan. As such, surgeons and other physicians will NOT receive a negative assessment on their 2019 Medicare payment if they simply report on one Quality measure for 90 days, OR one Improvement Activity for 90 days (again by simple attestation) OR four required Advancing Care Information measures utilizing a certified electronic health record (EHR). Accordingly, it is entirely possible for ALL to avoid the 4% penalty prescribed for those who report nothing for 2017.
ACS has developed numerous resources to assist surgeons in preparing for the 2017 reporting period. In addition to articles published in ACS Surgery News and other ACS publications, a website has been launched at www.facs.org/qpp. The website contains a series of videos based on the requirements outlined in the proposed rule, downloadable Power Point presentations, a glossary of terms and acronyms and perhaps, most importantly, a list of activities that surgeons can undertake now in order to best prepare themselves for the changes outlined in the final rule for January 2017.
In the coming weeks, plans are in place to revise the slide presentations and videos to reflect the modifications of requirements found in the final rule, publish a series of fact sheets designed for surgeons in various practice circumstances (employed surgeons, private practice surgeons, surgeons in small and/or rural practice, surgeons in large group practice), revise and republish the booklet entitled Resources for the New Medicare Physician Payment System, first made available to attendees at Clinical Congress in Washington in October, as well as the recording of an instructional webinar.
Based on the requirements outlined in the MACRA final rule, I am very confident that with minimal effort surgeons will be able to avoid a negative payment adjustment in 2019 based on their performance in the 2017 reporting period. Further, for those surgeons who are already participating in quality reporting and/or are well familiar with the requirements of the electronic health record program, it is entirely possible they will receive a positive update. ACS staff continue to endeavor to provide resources to Fellows to ensure their success.
Until next month…
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released the final rule pertaining to the Medicare Access and CHIP Reauthorization Act (MACRA). As I write, almost three weeks later, Division of Advocacy and Health Policy staff are generally pleased with the contents of the rule as there were no big “negative” surprises and stakeholder input in response to the proposed rule seems to have been broadly taken to heart by the administration at CMS.
As Fellows prepare for 2017, they should take note of several changes that were made to the original proposed rule. Some key changes are summarized below.
With regard to what was previously referred to as the Clinical Practice Improvement Activities (CPIA), the nomenclature as well as the associated requirement have been shortened and simplified. Now called simply Improvement Activities, to achieve full credit most physicians will need to report on between two to four of the nearly 100 possible activities as opposed to up to the six activities needed to meet the requirements as outlined in the proposed rule. Fortunately, the reporting requirement for the Improvement Activities component remains the simple attestation that one has participated in the selected activities for a period of 90 continuous days during the 2017 reporting period. Improvement Activities continues to comprise 15% of the Composite Score.
With release of the final rule, we now have a more concrete definition of what CMS Acting Administrator Andrew Slavitt meant by “Pick Your Pace” which was the topic of last month’s column (October 2016, p. 15). CMS is looking at the 2017 reporting period as a transition year with which it hopes to engage physicians in participation in its new Medicare physician payment plan. As such, surgeons and other physicians will NOT receive a negative assessment on their 2019 Medicare payment if they simply report on one Quality measure for 90 days, OR one Improvement Activity for 90 days (again by simple attestation) OR four required Advancing Care Information measures utilizing a certified electronic health record (EHR). Accordingly, it is entirely possible for ALL to avoid the 4% penalty prescribed for those who report nothing for 2017.
ACS has developed numerous resources to assist surgeons in preparing for the 2017 reporting period. In addition to articles published in ACS Surgery News and other ACS publications, a website has been launched at www.facs.org/qpp. The website contains a series of videos based on the requirements outlined in the proposed rule, downloadable Power Point presentations, a glossary of terms and acronyms and perhaps, most importantly, a list of activities that surgeons can undertake now in order to best prepare themselves for the changes outlined in the final rule for January 2017.
In the coming weeks, plans are in place to revise the slide presentations and videos to reflect the modifications of requirements found in the final rule, publish a series of fact sheets designed for surgeons in various practice circumstances (employed surgeons, private practice surgeons, surgeons in small and/or rural practice, surgeons in large group practice), revise and republish the booklet entitled Resources for the New Medicare Physician Payment System, first made available to attendees at Clinical Congress in Washington in October, as well as the recording of an instructional webinar.
Based on the requirements outlined in the MACRA final rule, I am very confident that with minimal effort surgeons will be able to avoid a negative payment adjustment in 2019 based on their performance in the 2017 reporting period. Further, for those surgeons who are already participating in quality reporting and/or are well familiar with the requirements of the electronic health record program, it is entirely possible they will receive a positive update. ACS staff continue to endeavor to provide resources to Fellows to ensure their success.
Until next month…
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
On October 14, 2016, the Centers for Medicare and Medicaid Services (CMS) released the final rule pertaining to the Medicare Access and CHIP Reauthorization Act (MACRA). As I write, almost three weeks later, Division of Advocacy and Health Policy staff are generally pleased with the contents of the rule as there were no big “negative” surprises and stakeholder input in response to the proposed rule seems to have been broadly taken to heart by the administration at CMS.
As Fellows prepare for 2017, they should take note of several changes that were made to the original proposed rule. Some key changes are summarized below.
With regard to what was previously referred to as the Clinical Practice Improvement Activities (CPIA), the nomenclature as well as the associated requirement have been shortened and simplified. Now called simply Improvement Activities, to achieve full credit most physicians will need to report on between two to four of the nearly 100 possible activities as opposed to up to the six activities needed to meet the requirements as outlined in the proposed rule. Fortunately, the reporting requirement for the Improvement Activities component remains the simple attestation that one has participated in the selected activities for a period of 90 continuous days during the 2017 reporting period. Improvement Activities continues to comprise 15% of the Composite Score.
With release of the final rule, we now have a more concrete definition of what CMS Acting Administrator Andrew Slavitt meant by “Pick Your Pace” which was the topic of last month’s column (October 2016, p. 15). CMS is looking at the 2017 reporting period as a transition year with which it hopes to engage physicians in participation in its new Medicare physician payment plan. As such, surgeons and other physicians will NOT receive a negative assessment on their 2019 Medicare payment if they simply report on one Quality measure for 90 days, OR one Improvement Activity for 90 days (again by simple attestation) OR four required Advancing Care Information measures utilizing a certified electronic health record (EHR). Accordingly, it is entirely possible for ALL to avoid the 4% penalty prescribed for those who report nothing for 2017.
ACS has developed numerous resources to assist surgeons in preparing for the 2017 reporting period. In addition to articles published in ACS Surgery News and other ACS publications, a website has been launched at www.facs.org/qpp. The website contains a series of videos based on the requirements outlined in the proposed rule, downloadable Power Point presentations, a glossary of terms and acronyms and perhaps, most importantly, a list of activities that surgeons can undertake now in order to best prepare themselves for the changes outlined in the final rule for January 2017.
In the coming weeks, plans are in place to revise the slide presentations and videos to reflect the modifications of requirements found in the final rule, publish a series of fact sheets designed for surgeons in various practice circumstances (employed surgeons, private practice surgeons, surgeons in small and/or rural practice, surgeons in large group practice), revise and republish the booklet entitled Resources for the New Medicare Physician Payment System, first made available to attendees at Clinical Congress in Washington in October, as well as the recording of an instructional webinar.
Based on the requirements outlined in the MACRA final rule, I am very confident that with minimal effort surgeons will be able to avoid a negative payment adjustment in 2019 based on their performance in the 2017 reporting period. Further, for those surgeons who are already participating in quality reporting and/or are well familiar with the requirements of the electronic health record program, it is entirely possible they will receive a positive update. ACS staff continue to endeavor to provide resources to Fellows to ensure their success.
Until next month…
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
From the Editors: Querencia
In the flood of emails, periodicals, Twitter, Facebook, Doximity, Medscape, and other information that washes over surgeons every day, why should they use their precious time to read ACS Surgery News? That question is foremost in the minds of the editors of this publication as we consider news stories and commentaries for inclusion. Is this an article our readers are going to find informative, pertinent, and stimulating? We want ACS Surgery News to be a querencia: a source of reliable, vetted information that gives surgeons a place of intellectual security along the information highway.


The editors of ACS Surgery News understand surgery from the scrub sink up. While our mission includes keeping our readers informed about these looming thunderstorms, we are also privileged to report progress and innovations that keep coming no matter how the forces of red tape and commerce play against our profession. Bringing news of both challenges and beacons of hope for our profession with commentary and perspective from our colleagues is our objective. For the editors, this is both a mission and a pleasure. Since most of the editors and our Editorial Advisory Board (EAB), like our readers, must focus primarily on our jobs as surgeons, teachers, and researchers, we cannot read every journal or attend every meeting. The role of ACS Surgery News is to find the relevant news of interest and importance to surgeons, wherever it may be found, and to report it succinctly and accurately in a readable form. Before an article appears in ACS Surgery News, it is reviewed by the author of the paper or presentation for accuracy and reviewed by the most appropriate member of the EAB as well as by both Co-Editors for importance and relevance to our surgeon readers. We do not want to shy away from controversial topics, but endeavor to present such topics with balance and sensitivity, just as the ACS itself always attempts to do: to shed light, rather than merely heat, on all subjects that we cover in our pages.
The editors of ACS Surgery News hope that in the months and years to come, this publication can be a querencia for the surgeon: a safe and secure place to engage all the forces that a surgeon must confront to be successful. In these pages we hope you will find knowledge, wisdom, camaraderie, and support for your practice, whatever that may be.
Surgery is a life of great joy and great sorrow, sometimes happening all within the same hour. We hope to be part of the joy and to soften the sorrow by being a publication you look forward to reading and wherein you find those things that contribute to your being a great surgeon and human being.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the Co-Editor of ACS Surgery News.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
In the flood of emails, periodicals, Twitter, Facebook, Doximity, Medscape, and other information that washes over surgeons every day, why should they use their precious time to read ACS Surgery News? That question is foremost in the minds of the editors of this publication as we consider news stories and commentaries for inclusion. Is this an article our readers are going to find informative, pertinent, and stimulating? We want ACS Surgery News to be a querencia: a source of reliable, vetted information that gives surgeons a place of intellectual security along the information highway.
The editors of ACS Surgery News understand surgery from the scrub sink up. While our mission includes keeping our readers informed about these looming thunderstorms, we are also privileged to report progress and innovations that keep coming no matter how the forces of red tape and commerce play against our profession. Bringing news of both challenges and beacons of hope for our profession with commentary and perspective from our colleagues is our objective. For the editors, this is both a mission and a pleasure. Since most of the editors and our Editorial Advisory Board (EAB), like our readers, must focus primarily on our jobs as surgeons, teachers, and researchers, we cannot read every journal or attend every meeting. The role of ACS Surgery News is to find the relevant news of interest and importance to surgeons, wherever it may be found, and to report it succinctly and accurately in a readable form. Before an article appears in ACS Surgery News, it is reviewed by the author of the paper or presentation for accuracy and reviewed by the most appropriate member of the EAB as well as by both Co-Editors for importance and relevance to our surgeon readers. We do not want to shy away from controversial topics, but endeavor to present such topics with balance and sensitivity, just as the ACS itself always attempts to do: to shed light, rather than merely heat, on all subjects that we cover in our pages.
The editors of ACS Surgery News hope that in the months and years to come, this publication can be a querencia for the surgeon: a safe and secure place to engage all the forces that a surgeon must confront to be successful. In these pages we hope you will find knowledge, wisdom, camaraderie, and support for your practice, whatever that may be.
Surgery is a life of great joy and great sorrow, sometimes happening all within the same hour. We hope to be part of the joy and to soften the sorrow by being a publication you look forward to reading and wherein you find those things that contribute to your being a great surgeon and human being.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the Co-Editor of ACS Surgery News.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
In the flood of emails, periodicals, Twitter, Facebook, Doximity, Medscape, and other information that washes over surgeons every day, why should they use their precious time to read ACS Surgery News? That question is foremost in the minds of the editors of this publication as we consider news stories and commentaries for inclusion. Is this an article our readers are going to find informative, pertinent, and stimulating? We want ACS Surgery News to be a querencia: a source of reliable, vetted information that gives surgeons a place of intellectual security along the information highway.
The editors of ACS Surgery News understand surgery from the scrub sink up. While our mission includes keeping our readers informed about these looming thunderstorms, we are also privileged to report progress and innovations that keep coming no matter how the forces of red tape and commerce play against our profession. Bringing news of both challenges and beacons of hope for our profession with commentary and perspective from our colleagues is our objective. For the editors, this is both a mission and a pleasure. Since most of the editors and our Editorial Advisory Board (EAB), like our readers, must focus primarily on our jobs as surgeons, teachers, and researchers, we cannot read every journal or attend every meeting. The role of ACS Surgery News is to find the relevant news of interest and importance to surgeons, wherever it may be found, and to report it succinctly and accurately in a readable form. Before an article appears in ACS Surgery News, it is reviewed by the author of the paper or presentation for accuracy and reviewed by the most appropriate member of the EAB as well as by both Co-Editors for importance and relevance to our surgeon readers. We do not want to shy away from controversial topics, but endeavor to present such topics with balance and sensitivity, just as the ACS itself always attempts to do: to shed light, rather than merely heat, on all subjects that we cover in our pages.
The editors of ACS Surgery News hope that in the months and years to come, this publication can be a querencia for the surgeon: a safe and secure place to engage all the forces that a surgeon must confront to be successful. In these pages we hope you will find knowledge, wisdom, camaraderie, and support for your practice, whatever that may be.
Surgery is a life of great joy and great sorrow, sometimes happening all within the same hour. We hope to be part of the joy and to soften the sorrow by being a publication you look forward to reading and wherein you find those things that contribute to your being a great surgeon and human being.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the Co-Editor of ACS Surgery News.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and Co-Editor of ACS Surgery News.
Courtney M. Townsend, Jr., MD, FACS, installed as 97th President of the ACS
Courtney M. Townsend, Jr., MD, FACS, a general surgeon from Galveston, TX, was installed as the 97th President of the American College of Surgeons (ACS) during the Convocation on October 16 at the Walter E. Washington Convention Center, Washington, DC.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery; professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB.
Dr. Townsend earned his bachelor’s degree in history and English from the University of Texas, Austin. He then earned his medical degree and completed his internship and general surgery training at UTMB. Dr. Townsend completed a surgical oncology fellowship at the University of California, Los Angeles (UCLA), and was a McLaughlin Fellow twice, a Jeane B. Kempner Fellow, an American Cancer Society clinical fellow, and an NIH postdoctoral fellow.
Dr. Townsend’s first teaching position was as an adjunct assistant professor of surgery, division of oncology, department of surgery, at UCLA (1974–1976). He then served in the U.S. Navy from 1976 to 1978 as a staff surgeon and surgical director in the intensive care unit at the National Naval Medical Center, Bethesda, MD.
In 1978, Dr. Townsend returned to UTMB as an associate professor in the department of surgery. In 1981, he was promoted to Robertson-Poth Associate Professor of Surgery, and the next year he became director of the surgical research laboratory at UTMB. From 1983 to 1995, Dr. Townsend was the Robertson-Poth Professor of Surgery, and from 1987 to 1995, he served as interim director of the UTMB Cancer Center. He assumed his current roles as professor of physician assistant studies in 1989, as graduate faculty in the cell biology program in 2001, and as Robertson-Poth Distinguished Chair in General Surgery in 2009. Dr. Townsend also served as John Woods Harris Distinguished Chairman from 1995 to 2013.
Dr. Townsend has served in many leadership roles at the College, including ACS Secretary (2006–2015). He held prominent positions on the Board of Governors (B/G), including Chair (2004–2005), B/G Executive Committee Member (1999–2003); and ACS Governor from the Society for Surgery of the Alimentary Tract (1986–1992). He has also served in various capacities on the Commission on Cancer (CoC) and on other ACS committees. Dr. Townsend served on the CoC Committee on Approvals (1989–1994), the CoC National Cancer Data Committee and the National Cancer Data Base Governing Board (1989–1995), the ACS Committee for the Forum on Fundamental Surgical Problems and the Committee on Special Issues (both 1991–1994), the Committee on Papers (2000–2003), the Member Services Liaison Committee (2003–2004), and the Nominating Committee of the Fellows (2000–2002).
Most recently, Dr. Townsend served on the ACS Surgical Research and Education Committee, which he chaired for two years (1998–2000). At the local level, he has served on the Southern Texas District #1 Committee on Applicants (1996–1999) and as President of the ACS South Texas Chapter (1988–1989).
Dr. Townsend has assumed leadership roles in several other medical organizations as well. He is past-director and chair of the American Board of Surgery (2000–2007); served on the Accreditation Council for Graduate Medical Education Residency Review Committee for Surgery (1994–1999); American Pancreatic Association president (1992−1993); American Surgical Association president (2007–2008); Southern Surgical Association president (2004); and Texas Surgical Society council member (1997–1999). He is an honorary member of the Society of Black Academic Surgeons and the Association of Women Surgeons (AWS) and is a recipient of UTMB’s John P. McGovern Lifetime Achievement Award in Oslerian Medicine.
Dr. Townsend has been editor-in-chief of the Sabiston Textbook for Surgery: The Biological Basis of Modern Surgical Practice since 2000 and was the editor of Surgical Oncology (1992−1999). He has served on the editorial board of the Journal of the American College of Surgeons (JACS), Surgery, and The American Journal of Surgery.
Vice-Presidents
In addition, during the Convocation, Hilary Sanfey, MB, BCh, MHPE, FACS, FRCSI, FRCS, was installed as ACS First Vice-President, and Mary C. McCarthy, MD, FACS, was installed as ACS Second Vice-President.
Dr. Sanfey is professor of surgery and vice-chair for educational affairs, department of surgery, and associate director, Academy for Scholarship and Education, Southern Illinois University (SIU) School of Medicine, Springfield. Dr. Sanfey, who hails from Ireland, graduated from Trinity College Dublin School of Medicine in 1976. She trained at the Royal College of Surgeons in Ireland (RCSI), spent three years as a research fellow at Johns Hopkins University, Baltimore, MD, and worked as a consultant transplant surgeon at the Royal Infirmary of Edinburgh for four years before moving to the University of Virginia, Charlottesville, in 1996. She remained on the clinical faculty at the University of Virginia, starting as an assistant professor of hepatobiliary surgery in 1991 and leaving in 2008 for SIU as a tenured professor of surgery. In 2009, she received a master’s degree in health professions education from the University of Illinois, Chicago.
Dr. Sanfey is the immediate past-president of the International Society of Surgery, U.S. chapter, and a member of the American Surgical Association. Dr. Sanfey serves as faculty for the ACS Residents as Teachers and Leaders Program and has served as a specialist advisor in postgraduate surgical training and education in the department of surgical affairs, RCSI.
An ACS Fellow since 2001, Dr. Sanfey served as the ACS Liaison to the American Medical Association (AMA) Women Physicians Congress (2006–2009) and an ACS Governor (2006–2012). As a Governor, she chaired the B/G Committee on Chapters Subcommittee on Diversity (2009–2011) and the Nominating Committee (2010–2012). In addition, she served on the Executive Committee of the Committee on Medical Student Education (2005–2011) and as a liaison to the Program Committee. She presently serves on the Executive Committee of the Scholarship Committee.
She has been active on the Women in Surgery Committee since 2005. She has held high-ranking positions in other prestigious surgical organizations as well, including the AWS (president, 2005–2006) and the U.S. chapter of the International Surgical Society (president, 2013–2015). In addition, she has served on key committees of the Association of Program Directors in Surgery, the Association for Surgical Education, and the American Society of Transplant Surgeons.
Dr. Sanfey is on the editorial boards of the Association for Surgical Education, Journal of the Royal Colleges of Edinburgh and Ireland, and JACS. She is an accomplished surgical investigator, has contributed to more than 100 peer-reviewed papers and 24 book chapters, and has been a frequent guest lecturer and visiting professor at international symposia and workshops.
She is the recipient of many awards in surgical education. The AWS in 2010 renamed its Outstanding Woman Resident Award as the Hilary Sanfey Outstanding Resident Award, and in 2013 and 2014, respectively, Dr. Sanfey was honored with the AWS Olga Jonasson Distinguished Member Award and Nina Starr Braunwald Award.
Dr. McCarthy is the Elizabeth Berry Gray Chair and Professor, department of surgery, Boonshoft School of Medicine, and adjunct graduate faculty, School of Engineering, Wright State University (WSU); and an acute care surgeon at Miami Valley Hospital, Dayton, OH. Before moving to WSU, she was assistant professor of surgery (1983–1988) at Indiana University (IU) School of Medicine, Indianapolis.
An ACS Fellow since 1986, Dr. McCarthy has served in a number of leadership positions within the organization, including as an ACS Governor (1995–2001). As a Specialty Society Governor for the AWS, she served on the Nominating Committee (member, 1996–1997, and Vice-Chair, 1997–1998); the Governors Committee on Chapter Activities (1995–2001), chairing the committee’s Subcommittee on Chapter Membership Recruitment, Retention, and Diversification (1998–2001); and Advisor to the Governors Committee on Chapter Activities Executive Committee (1995).
Dr. McCarthy also served on the ACS Advisory Council for General Surgery and is a current member of the Committee on Trauma. She has served on the Surgical Education and Self-Assessment Program (SESAP®) Committee, including as Co-Chair for SESAP XII, 1999; the Committee on Continuing Education (Member, 1994–1999, and Vice-Chair, 1995–1997); the Committee on Applicants for District 6 (present); and the Clinical Congress Abstract Selection Committee (2007–2009). While at IU, she was active in the Indiana Chapter, and she remains active in the Ohio chapter, having served on the Executive Committee (1995–2001) and the Ohio Committee on Trauma (1991–present).
She is a past-president of the AWS (1990–1992) and has served in prominent positions in the Association for Surgical Education, Eastern Association for the Surgery of Trauma, Halsted Surgical Society, Midwest Surgical Association, Parkland Surgical Society, and Society of Critical Care Medicine.
She is the recipient of numerous professional awards, including the American Hospital Association Nova Award, and AWS Distinguished Member, Olga Jonasson Award, and Nina Starr Braunwald Awards. She is a prolific author of peer-reviewed publications, book chapters, and abstracts on trauma and critical care.
Courtney M. Townsend, Jr., MD, FACS, a general surgeon from Galveston, TX, was installed as the 97th President of the American College of Surgeons (ACS) during the Convocation on October 16 at the Walter E. Washington Convention Center, Washington, DC.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery; professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB.
Dr. Townsend earned his bachelor’s degree in history and English from the University of Texas, Austin. He then earned his medical degree and completed his internship and general surgery training at UTMB. Dr. Townsend completed a surgical oncology fellowship at the University of California, Los Angeles (UCLA), and was a McLaughlin Fellow twice, a Jeane B. Kempner Fellow, an American Cancer Society clinical fellow, and an NIH postdoctoral fellow.
Dr. Townsend’s first teaching position was as an adjunct assistant professor of surgery, division of oncology, department of surgery, at UCLA (1974–1976). He then served in the U.S. Navy from 1976 to 1978 as a staff surgeon and surgical director in the intensive care unit at the National Naval Medical Center, Bethesda, MD.
In 1978, Dr. Townsend returned to UTMB as an associate professor in the department of surgery. In 1981, he was promoted to Robertson-Poth Associate Professor of Surgery, and the next year he became director of the surgical research laboratory at UTMB. From 1983 to 1995, Dr. Townsend was the Robertson-Poth Professor of Surgery, and from 1987 to 1995, he served as interim director of the UTMB Cancer Center. He assumed his current roles as professor of physician assistant studies in 1989, as graduate faculty in the cell biology program in 2001, and as Robertson-Poth Distinguished Chair in General Surgery in 2009. Dr. Townsend also served as John Woods Harris Distinguished Chairman from 1995 to 2013.
Dr. Townsend has served in many leadership roles at the College, including ACS Secretary (2006–2015). He held prominent positions on the Board of Governors (B/G), including Chair (2004–2005), B/G Executive Committee Member (1999–2003); and ACS Governor from the Society for Surgery of the Alimentary Tract (1986–1992). He has also served in various capacities on the Commission on Cancer (CoC) and on other ACS committees. Dr. Townsend served on the CoC Committee on Approvals (1989–1994), the CoC National Cancer Data Committee and the National Cancer Data Base Governing Board (1989–1995), the ACS Committee for the Forum on Fundamental Surgical Problems and the Committee on Special Issues (both 1991–1994), the Committee on Papers (2000–2003), the Member Services Liaison Committee (2003–2004), and the Nominating Committee of the Fellows (2000–2002).
Most recently, Dr. Townsend served on the ACS Surgical Research and Education Committee, which he chaired for two years (1998–2000). At the local level, he has served on the Southern Texas District #1 Committee on Applicants (1996–1999) and as President of the ACS South Texas Chapter (1988–1989).
Dr. Townsend has assumed leadership roles in several other medical organizations as well. He is past-director and chair of the American Board of Surgery (2000–2007); served on the Accreditation Council for Graduate Medical Education Residency Review Committee for Surgery (1994–1999); American Pancreatic Association president (1992−1993); American Surgical Association president (2007–2008); Southern Surgical Association president (2004); and Texas Surgical Society council member (1997–1999). He is an honorary member of the Society of Black Academic Surgeons and the Association of Women Surgeons (AWS) and is a recipient of UTMB’s John P. McGovern Lifetime Achievement Award in Oslerian Medicine.
Dr. Townsend has been editor-in-chief of the Sabiston Textbook for Surgery: The Biological Basis of Modern Surgical Practice since 2000 and was the editor of Surgical Oncology (1992−1999). He has served on the editorial board of the Journal of the American College of Surgeons (JACS), Surgery, and The American Journal of Surgery.
Vice-Presidents
In addition, during the Convocation, Hilary Sanfey, MB, BCh, MHPE, FACS, FRCSI, FRCS, was installed as ACS First Vice-President, and Mary C. McCarthy, MD, FACS, was installed as ACS Second Vice-President.
Dr. Sanfey is professor of surgery and vice-chair for educational affairs, department of surgery, and associate director, Academy for Scholarship and Education, Southern Illinois University (SIU) School of Medicine, Springfield. Dr. Sanfey, who hails from Ireland, graduated from Trinity College Dublin School of Medicine in 1976. She trained at the Royal College of Surgeons in Ireland (RCSI), spent three years as a research fellow at Johns Hopkins University, Baltimore, MD, and worked as a consultant transplant surgeon at the Royal Infirmary of Edinburgh for four years before moving to the University of Virginia, Charlottesville, in 1996. She remained on the clinical faculty at the University of Virginia, starting as an assistant professor of hepatobiliary surgery in 1991 and leaving in 2008 for SIU as a tenured professor of surgery. In 2009, she received a master’s degree in health professions education from the University of Illinois, Chicago.
Dr. Sanfey is the immediate past-president of the International Society of Surgery, U.S. chapter, and a member of the American Surgical Association. Dr. Sanfey serves as faculty for the ACS Residents as Teachers and Leaders Program and has served as a specialist advisor in postgraduate surgical training and education in the department of surgical affairs, RCSI.
An ACS Fellow since 2001, Dr. Sanfey served as the ACS Liaison to the American Medical Association (AMA) Women Physicians Congress (2006–2009) and an ACS Governor (2006–2012). As a Governor, she chaired the B/G Committee on Chapters Subcommittee on Diversity (2009–2011) and the Nominating Committee (2010–2012). In addition, she served on the Executive Committee of the Committee on Medical Student Education (2005–2011) and as a liaison to the Program Committee. She presently serves on the Executive Committee of the Scholarship Committee.
She has been active on the Women in Surgery Committee since 2005. She has held high-ranking positions in other prestigious surgical organizations as well, including the AWS (president, 2005–2006) and the U.S. chapter of the International Surgical Society (president, 2013–2015). In addition, she has served on key committees of the Association of Program Directors in Surgery, the Association for Surgical Education, and the American Society of Transplant Surgeons.
Dr. Sanfey is on the editorial boards of the Association for Surgical Education, Journal of the Royal Colleges of Edinburgh and Ireland, and JACS. She is an accomplished surgical investigator, has contributed to more than 100 peer-reviewed papers and 24 book chapters, and has been a frequent guest lecturer and visiting professor at international symposia and workshops.
She is the recipient of many awards in surgical education. The AWS in 2010 renamed its Outstanding Woman Resident Award as the Hilary Sanfey Outstanding Resident Award, and in 2013 and 2014, respectively, Dr. Sanfey was honored with the AWS Olga Jonasson Distinguished Member Award and Nina Starr Braunwald Award.
Dr. McCarthy is the Elizabeth Berry Gray Chair and Professor, department of surgery, Boonshoft School of Medicine, and adjunct graduate faculty, School of Engineering, Wright State University (WSU); and an acute care surgeon at Miami Valley Hospital, Dayton, OH. Before moving to WSU, she was assistant professor of surgery (1983–1988) at Indiana University (IU) School of Medicine, Indianapolis.
An ACS Fellow since 1986, Dr. McCarthy has served in a number of leadership positions within the organization, including as an ACS Governor (1995–2001). As a Specialty Society Governor for the AWS, she served on the Nominating Committee (member, 1996–1997, and Vice-Chair, 1997–1998); the Governors Committee on Chapter Activities (1995–2001), chairing the committee’s Subcommittee on Chapter Membership Recruitment, Retention, and Diversification (1998–2001); and Advisor to the Governors Committee on Chapter Activities Executive Committee (1995).
Dr. McCarthy also served on the ACS Advisory Council for General Surgery and is a current member of the Committee on Trauma. She has served on the Surgical Education and Self-Assessment Program (SESAP®) Committee, including as Co-Chair for SESAP XII, 1999; the Committee on Continuing Education (Member, 1994–1999, and Vice-Chair, 1995–1997); the Committee on Applicants for District 6 (present); and the Clinical Congress Abstract Selection Committee (2007–2009). While at IU, she was active in the Indiana Chapter, and she remains active in the Ohio chapter, having served on the Executive Committee (1995–2001) and the Ohio Committee on Trauma (1991–present).
She is a past-president of the AWS (1990–1992) and has served in prominent positions in the Association for Surgical Education, Eastern Association for the Surgery of Trauma, Halsted Surgical Society, Midwest Surgical Association, Parkland Surgical Society, and Society of Critical Care Medicine.
She is the recipient of numerous professional awards, including the American Hospital Association Nova Award, and AWS Distinguished Member, Olga Jonasson Award, and Nina Starr Braunwald Awards. She is a prolific author of peer-reviewed publications, book chapters, and abstracts on trauma and critical care.
Courtney M. Townsend, Jr., MD, FACS, a general surgeon from Galveston, TX, was installed as the 97th President of the American College of Surgeons (ACS) during the Convocation on October 16 at the Walter E. Washington Convention Center, Washington, DC.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery; professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB.
Dr. Townsend earned his bachelor’s degree in history and English from the University of Texas, Austin. He then earned his medical degree and completed his internship and general surgery training at UTMB. Dr. Townsend completed a surgical oncology fellowship at the University of California, Los Angeles (UCLA), and was a McLaughlin Fellow twice, a Jeane B. Kempner Fellow, an American Cancer Society clinical fellow, and an NIH postdoctoral fellow.
Dr. Townsend’s first teaching position was as an adjunct assistant professor of surgery, division of oncology, department of surgery, at UCLA (1974–1976). He then served in the U.S. Navy from 1976 to 1978 as a staff surgeon and surgical director in the intensive care unit at the National Naval Medical Center, Bethesda, MD.
In 1978, Dr. Townsend returned to UTMB as an associate professor in the department of surgery. In 1981, he was promoted to Robertson-Poth Associate Professor of Surgery, and the next year he became director of the surgical research laboratory at UTMB. From 1983 to 1995, Dr. Townsend was the Robertson-Poth Professor of Surgery, and from 1987 to 1995, he served as interim director of the UTMB Cancer Center. He assumed his current roles as professor of physician assistant studies in 1989, as graduate faculty in the cell biology program in 2001, and as Robertson-Poth Distinguished Chair in General Surgery in 2009. Dr. Townsend also served as John Woods Harris Distinguished Chairman from 1995 to 2013.
Dr. Townsend has served in many leadership roles at the College, including ACS Secretary (2006–2015). He held prominent positions on the Board of Governors (B/G), including Chair (2004–2005), B/G Executive Committee Member (1999–2003); and ACS Governor from the Society for Surgery of the Alimentary Tract (1986–1992). He has also served in various capacities on the Commission on Cancer (CoC) and on other ACS committees. Dr. Townsend served on the CoC Committee on Approvals (1989–1994), the CoC National Cancer Data Committee and the National Cancer Data Base Governing Board (1989–1995), the ACS Committee for the Forum on Fundamental Surgical Problems and the Committee on Special Issues (both 1991–1994), the Committee on Papers (2000–2003), the Member Services Liaison Committee (2003–2004), and the Nominating Committee of the Fellows (2000–2002).
Most recently, Dr. Townsend served on the ACS Surgical Research and Education Committee, which he chaired for two years (1998–2000). At the local level, he has served on the Southern Texas District #1 Committee on Applicants (1996–1999) and as President of the ACS South Texas Chapter (1988–1989).
Dr. Townsend has assumed leadership roles in several other medical organizations as well. He is past-director and chair of the American Board of Surgery (2000–2007); served on the Accreditation Council for Graduate Medical Education Residency Review Committee for Surgery (1994–1999); American Pancreatic Association president (1992−1993); American Surgical Association president (2007–2008); Southern Surgical Association president (2004); and Texas Surgical Society council member (1997–1999). He is an honorary member of the Society of Black Academic Surgeons and the Association of Women Surgeons (AWS) and is a recipient of UTMB’s John P. McGovern Lifetime Achievement Award in Oslerian Medicine.
Dr. Townsend has been editor-in-chief of the Sabiston Textbook for Surgery: The Biological Basis of Modern Surgical Practice since 2000 and was the editor of Surgical Oncology (1992−1999). He has served on the editorial board of the Journal of the American College of Surgeons (JACS), Surgery, and The American Journal of Surgery.
Vice-Presidents
In addition, during the Convocation, Hilary Sanfey, MB, BCh, MHPE, FACS, FRCSI, FRCS, was installed as ACS First Vice-President, and Mary C. McCarthy, MD, FACS, was installed as ACS Second Vice-President.
Dr. Sanfey is professor of surgery and vice-chair for educational affairs, department of surgery, and associate director, Academy for Scholarship and Education, Southern Illinois University (SIU) School of Medicine, Springfield. Dr. Sanfey, who hails from Ireland, graduated from Trinity College Dublin School of Medicine in 1976. She trained at the Royal College of Surgeons in Ireland (RCSI), spent three years as a research fellow at Johns Hopkins University, Baltimore, MD, and worked as a consultant transplant surgeon at the Royal Infirmary of Edinburgh for four years before moving to the University of Virginia, Charlottesville, in 1996. She remained on the clinical faculty at the University of Virginia, starting as an assistant professor of hepatobiliary surgery in 1991 and leaving in 2008 for SIU as a tenured professor of surgery. In 2009, she received a master’s degree in health professions education from the University of Illinois, Chicago.
Dr. Sanfey is the immediate past-president of the International Society of Surgery, U.S. chapter, and a member of the American Surgical Association. Dr. Sanfey serves as faculty for the ACS Residents as Teachers and Leaders Program and has served as a specialist advisor in postgraduate surgical training and education in the department of surgical affairs, RCSI.
An ACS Fellow since 2001, Dr. Sanfey served as the ACS Liaison to the American Medical Association (AMA) Women Physicians Congress (2006–2009) and an ACS Governor (2006–2012). As a Governor, she chaired the B/G Committee on Chapters Subcommittee on Diversity (2009–2011) and the Nominating Committee (2010–2012). In addition, she served on the Executive Committee of the Committee on Medical Student Education (2005–2011) and as a liaison to the Program Committee. She presently serves on the Executive Committee of the Scholarship Committee.
She has been active on the Women in Surgery Committee since 2005. She has held high-ranking positions in other prestigious surgical organizations as well, including the AWS (president, 2005–2006) and the U.S. chapter of the International Surgical Society (president, 2013–2015). In addition, she has served on key committees of the Association of Program Directors in Surgery, the Association for Surgical Education, and the American Society of Transplant Surgeons.
Dr. Sanfey is on the editorial boards of the Association for Surgical Education, Journal of the Royal Colleges of Edinburgh and Ireland, and JACS. She is an accomplished surgical investigator, has contributed to more than 100 peer-reviewed papers and 24 book chapters, and has been a frequent guest lecturer and visiting professor at international symposia and workshops.
She is the recipient of many awards in surgical education. The AWS in 2010 renamed its Outstanding Woman Resident Award as the Hilary Sanfey Outstanding Resident Award, and in 2013 and 2014, respectively, Dr. Sanfey was honored with the AWS Olga Jonasson Distinguished Member Award and Nina Starr Braunwald Award.
Dr. McCarthy is the Elizabeth Berry Gray Chair and Professor, department of surgery, Boonshoft School of Medicine, and adjunct graduate faculty, School of Engineering, Wright State University (WSU); and an acute care surgeon at Miami Valley Hospital, Dayton, OH. Before moving to WSU, she was assistant professor of surgery (1983–1988) at Indiana University (IU) School of Medicine, Indianapolis.
An ACS Fellow since 1986, Dr. McCarthy has served in a number of leadership positions within the organization, including as an ACS Governor (1995–2001). As a Specialty Society Governor for the AWS, she served on the Nominating Committee (member, 1996–1997, and Vice-Chair, 1997–1998); the Governors Committee on Chapter Activities (1995–2001), chairing the committee’s Subcommittee on Chapter Membership Recruitment, Retention, and Diversification (1998–2001); and Advisor to the Governors Committee on Chapter Activities Executive Committee (1995).
Dr. McCarthy also served on the ACS Advisory Council for General Surgery and is a current member of the Committee on Trauma. She has served on the Surgical Education and Self-Assessment Program (SESAP®) Committee, including as Co-Chair for SESAP XII, 1999; the Committee on Continuing Education (Member, 1994–1999, and Vice-Chair, 1995–1997); the Committee on Applicants for District 6 (present); and the Clinical Congress Abstract Selection Committee (2007–2009). While at IU, she was active in the Indiana Chapter, and she remains active in the Ohio chapter, having served on the Executive Committee (1995–2001) and the Ohio Committee on Trauma (1991–present).
She is a past-president of the AWS (1990–1992) and has served in prominent positions in the Association for Surgical Education, Eastern Association for the Surgery of Trauma, Halsted Surgical Society, Midwest Surgical Association, Parkland Surgical Society, and Society of Critical Care Medicine.
She is the recipient of numerous professional awards, including the American Hospital Association Nova Award, and AWS Distinguished Member, Olga Jonasson Award, and Nina Starr Braunwald Awards. She is a prolific author of peer-reviewed publications, book chapters, and abstracts on trauma and critical care.
New history of ACS Bulletin reflects history of the College
To celebrate the centennial of the Bulletin of the American College of Surgeons (ACS), David L. Nahrwold, MD, FACS, has written a history of the ACS member magazine, titled, “A Mirror Reflecting Surgery, Surgeons, and their College: The Bulletin of the American College of Surgeons.”
“After studying the history of the College and the content of 100 years of Bulletins,” writes Dr. Nahrwold in the book’s foreword, “I soon realized that the Bulletin has conveyed the remarkable story of how the College and its members laid the foundation for our healthcare system.”
The Bulletin began in 1916 as a series of single-subject bulletins to the Fellowship from the College’s founders. The first issue described the mission of the College, listed the requirements for admission to Fellowship, and included a packet of blank case history forms for candidates to fill out and submit with their application. Subsequent issues established hospital standards, summarized external and internal meetings and conferences, and reported on credentialing, record keeping, education, specialization, ACS finances and structure, public health issues, scientific advances, international relations, and military surgery, among other subjects.
The book covers the history of the magazine through the end of World War II, and illuminates the background, concerns, and personalities of the College’s founders and leaders as they explained and defended their actions to the members and determined what role the ACS would play in the practice of surgery.
“Given the unpredictable fates of periodicals,” Dr. Nahrwold writes, “it is remarkable – indeed astonishing – that this mirror, the Bulletin, has not only existed, but has thrived, for one hundred years. Its fortunes, of course, have been tied to those of the College, but its editors and staff have continuously adjusted the mirror to make it informative, pertinent, and interesting, and its readers have found deep within the mirror a reservoir of truthfulness, accuracy, and good taste.”
Dr. Nahrwold is Emeritus Professor of Surgery at Northwestern University Feinberg School of Medicine, Chicago, IL, where he was the Loyal and Edith Davis Professor and Chairman, department of surgery, and surgeon-in-chief, Northwestern Memorial Hospital. He served as a Regent, Chairman of the Board of Governors, First Vice-President, and Interim Director of the ACS, and in 2001 he received its highest honor – the Distinguished Service Award. He represented the College at The Joint Commission, where he was chairman of the Board of Commissioners.
He was a director and chairman of the American Board of Surgery and president of the American Board of Medical Specialties.
Dr. Nahrwold is co-author, with Peter J. Kernahan, MD, PhD, FACS, of “A Century of Surgeons and Surgery: The American College of Surgeons 1913-2012.”
“A Mirror Reflecting Surgery, Surgeons, and their College” is available for purchase for $15.95 at amazon.com.
To celebrate the centennial of the Bulletin of the American College of Surgeons (ACS), David L. Nahrwold, MD, FACS, has written a history of the ACS member magazine, titled, “A Mirror Reflecting Surgery, Surgeons, and their College: The Bulletin of the American College of Surgeons.”
“After studying the history of the College and the content of 100 years of Bulletins,” writes Dr. Nahrwold in the book’s foreword, “I soon realized that the Bulletin has conveyed the remarkable story of how the College and its members laid the foundation for our healthcare system.”
The Bulletin began in 1916 as a series of single-subject bulletins to the Fellowship from the College’s founders. The first issue described the mission of the College, listed the requirements for admission to Fellowship, and included a packet of blank case history forms for candidates to fill out and submit with their application. Subsequent issues established hospital standards, summarized external and internal meetings and conferences, and reported on credentialing, record keeping, education, specialization, ACS finances and structure, public health issues, scientific advances, international relations, and military surgery, among other subjects.
The book covers the history of the magazine through the end of World War II, and illuminates the background, concerns, and personalities of the College’s founders and leaders as they explained and defended their actions to the members and determined what role the ACS would play in the practice of surgery.
“Given the unpredictable fates of periodicals,” Dr. Nahrwold writes, “it is remarkable – indeed astonishing – that this mirror, the Bulletin, has not only existed, but has thrived, for one hundred years. Its fortunes, of course, have been tied to those of the College, but its editors and staff have continuously adjusted the mirror to make it informative, pertinent, and interesting, and its readers have found deep within the mirror a reservoir of truthfulness, accuracy, and good taste.”
Dr. Nahrwold is Emeritus Professor of Surgery at Northwestern University Feinberg School of Medicine, Chicago, IL, where he was the Loyal and Edith Davis Professor and Chairman, department of surgery, and surgeon-in-chief, Northwestern Memorial Hospital. He served as a Regent, Chairman of the Board of Governors, First Vice-President, and Interim Director of the ACS, and in 2001 he received its highest honor – the Distinguished Service Award. He represented the College at The Joint Commission, where he was chairman of the Board of Commissioners.
He was a director and chairman of the American Board of Surgery and president of the American Board of Medical Specialties.
Dr. Nahrwold is co-author, with Peter J. Kernahan, MD, PhD, FACS, of “A Century of Surgeons and Surgery: The American College of Surgeons 1913-2012.”
“A Mirror Reflecting Surgery, Surgeons, and their College” is available for purchase for $15.95 at amazon.com.
To celebrate the centennial of the Bulletin of the American College of Surgeons (ACS), David L. Nahrwold, MD, FACS, has written a history of the ACS member magazine, titled, “A Mirror Reflecting Surgery, Surgeons, and their College: The Bulletin of the American College of Surgeons.”
“After studying the history of the College and the content of 100 years of Bulletins,” writes Dr. Nahrwold in the book’s foreword, “I soon realized that the Bulletin has conveyed the remarkable story of how the College and its members laid the foundation for our healthcare system.”
The Bulletin began in 1916 as a series of single-subject bulletins to the Fellowship from the College’s founders. The first issue described the mission of the College, listed the requirements for admission to Fellowship, and included a packet of blank case history forms for candidates to fill out and submit with their application. Subsequent issues established hospital standards, summarized external and internal meetings and conferences, and reported on credentialing, record keeping, education, specialization, ACS finances and structure, public health issues, scientific advances, international relations, and military surgery, among other subjects.
The book covers the history of the magazine through the end of World War II, and illuminates the background, concerns, and personalities of the College’s founders and leaders as they explained and defended their actions to the members and determined what role the ACS would play in the practice of surgery.
“Given the unpredictable fates of periodicals,” Dr. Nahrwold writes, “it is remarkable – indeed astonishing – that this mirror, the Bulletin, has not only existed, but has thrived, for one hundred years. Its fortunes, of course, have been tied to those of the College, but its editors and staff have continuously adjusted the mirror to make it informative, pertinent, and interesting, and its readers have found deep within the mirror a reservoir of truthfulness, accuracy, and good taste.”
Dr. Nahrwold is Emeritus Professor of Surgery at Northwestern University Feinberg School of Medicine, Chicago, IL, where he was the Loyal and Edith Davis Professor and Chairman, department of surgery, and surgeon-in-chief, Northwestern Memorial Hospital. He served as a Regent, Chairman of the Board of Governors, First Vice-President, and Interim Director of the ACS, and in 2001 he received its highest honor – the Distinguished Service Award. He represented the College at The Joint Commission, where he was chairman of the Board of Commissioners.
He was a director and chairman of the American Board of Surgery and president of the American Board of Medical Specialties.
Dr. Nahrwold is co-author, with Peter J. Kernahan, MD, PhD, FACS, of “A Century of Surgeons and Surgery: The American College of Surgeons 1913-2012.”
“A Mirror Reflecting Surgery, Surgeons, and their College” is available for purchase for $15.95 at amazon.com.
Five outstanding surgeons conferred Honorary Fellowship in the ACS
Honorary Fellowship in the American College of Surgeons (ACS) was awarded to five prominent surgeons from Colombia, France, Pakistan, Japan, and Australia at the October 16 Convocation that preceded the official opening of Clinical Congress 2016 in Washington, DC. The granting of Honorary Fellowships is one of the highlights of the Clinical Congress. This year’s recipients were as follows.
Hernando Abaúnza Orjuela, MD, FACS, MACC(Hon), Bogotá, Colombia, is the founder, past-president, and current executive director of the Colombian Association of Surgery. He also is past-president of the Latin American Federation of Surgery (FELAC), which promotes research, teaching, and the practice of surgery among surgeons in Latin America. He became a Fellow of the ACS in 1970 and served on the ACS Board of Governors (1993–1999) and as President of the ACS Colombia Chapter (1990–1991). Dr. Abaúnza has written several articles on breast cancer and complex abdominal surgery problems, as well as more than 120 scientific papers and book chapters on gastric cancer, pancreaticoduodenectomy, laparoscopy, and other clinical topics. Dr. Abaúnza became professor of general surgery and chief, department of surgery, San Pedro Claver Hospital, and professor, National University of Colombia, Bogota. Dr. Abaúnza is a member of the International Society of Surgery and past-president of the Colombian Association of Gastroenterology.
Jacques Belghiti, MD, PhD, Paris, France, has made significant contributions to the fields of hepatocellular carcinoma and liver transplantation and has conducted vital studies in liver resection and hepatobiliary surgical oncology. His technical innovations include preservation of portal and caval flows during liver transplantation, the hanging maneuver to facilitate liver resection, and the use of peritoneal patch to provide an immediate and safe vascular graft. Dr. Belghiti was chief, department of hepato-bilio-pancreatic surgery and liver transplantation, Beaujon Hospital, University of Paris, for 20 years. In 2014, the department was classified as the first French surgical digestive center. French President François Hollande invited Dr. Belghiti to serve on the board of the National Health Authority in 2014; he now chairs the board’s medical devices and health technology committee for reimbursement. Dr. Belghiti is associate editor, liver surgery and biliary section, World Journal of Surgery.
S. Adibul Hasan Rizvi, MB, BS, FRCSEng, FRCSEd, Karachi, Pakistan, is the founder of the Sindh Institute of Urology and Transplantation (SIUT) and a leader of transplantation in Pakistan. He started SIUT, which has become one of the fastest-growing urological and transplant centers in the region, in 1972. SIUT offers procedures such as dialysis, lithotripsy, surgery, and transplantation. Pakistan’s first successful liver transplant was performed there in 2003, eight years after Dr. Rizvi and his team performed the first deceased renal transplant in the country. SIUT’s Dewan Farooque Medical Complex trains nurses, technical staff, and postgraduate physicians. All patient care is provided free of charge. The SIUT’s Hanifa Sulaiman Dawood Oncology Center now treats patients with post-transplant cancers and other malignancies. SIUT opened its first satellite unit in 2000, and three other dialysis centers that are part of the institute offer free dialysis to medically indigent patients in Karachi. Dr. Rizvi is a member of the World Health Organization advisory panel on organ transplantation and the Global Alliance for Transplantation.
Sachiyo Suita, MD, PhD, Fukuoka, Japan, was the first woman professor to head a surgery department at a Japanese national university. Dr. Suita realized she wanted to become a surgeon during the Vietnam War, when she interned at the American Air Force Hospital, Tachikawa, Japan. A mentor at Kyushu University, Fukuoka, encouraged her interest in pediatric surgery. Dr. Suita became surgeon-in-chief at Fukuoka Children’s Hospital in 1983 and professor of pediatric surgery at Kyushu University in 1989. Her promotion to professor marked the first time a woman had been on the faculty of medicine at the university. Dr. Suita’s areas of interest include fetal surgery, neonatal surgery, pediatric oncology, clinical nutrition, liver and small bowel transplantation, and grief care. In 2004, Dr. Suita became the first woman director of Kyushu University Hospital.
John Francis Thompson, AO, MD, FACS, FRACS, FAHMS, Sydney, Australia, has provided distinguished service in the field of oncology research, particularly melanoma, in international and national professional organizations, and in medical education. Dr. Thompson has written more than 700 peer-reviewed scientific articles, which led to his appointment as an Officer of the Order of Australia in 2014. His research interests are in lymphatic mapping and regional node management of patients with melanoma and other malignancies, and local and regional therapies for recurrent and advanced limb tumors. He is executive director and research director, Melanoma Institute Australia, and professor, melanoma and surgical oncology, University of Sydney. Dr. Thompson is a member of the Melanoma Staging Committee of the American Joint Committee on Cancer and chairs the workgroup to update Australia’s clinical practice guidelines for management of cutaneous melanoma in Australia.
Presenting on behalf of the College, respectively, were Marco Patti, MD, FACS, Chicago, IL; Leslie H. Blumgart, MD, FACS, FRCS, New York, NY; Prof. Mehmet A. Haberal, MD, FACS(Hon), FICS (Hon), FASA(Hon), Ankara, Turkey; Arnold G. Coran, MD, FACS, Ann Arbor, MI; and Jeffrey E. Gershenwald, MD, FACS, Houston, TX.
Sir Rickman Godlee, president of the Royal College of Surgeons of England, was awarded the first Honorary Fellowship in the ACS during the College’s first Convocation in 1913. Since then, 458 internationally prominent surgeons, including the five chosen this year, have been named Honorary Fellows of the ACS. The citations presented at the Convocation follow.
Honorary Fellowship in the American College of Surgeons (ACS) was awarded to five prominent surgeons from Colombia, France, Pakistan, Japan, and Australia at the October 16 Convocation that preceded the official opening of Clinical Congress 2016 in Washington, DC. The granting of Honorary Fellowships is one of the highlights of the Clinical Congress. This year’s recipients were as follows.
Hernando Abaúnza Orjuela, MD, FACS, MACC(Hon), Bogotá, Colombia, is the founder, past-president, and current executive director of the Colombian Association of Surgery. He also is past-president of the Latin American Federation of Surgery (FELAC), which promotes research, teaching, and the practice of surgery among surgeons in Latin America. He became a Fellow of the ACS in 1970 and served on the ACS Board of Governors (1993–1999) and as President of the ACS Colombia Chapter (1990–1991). Dr. Abaúnza has written several articles on breast cancer and complex abdominal surgery problems, as well as more than 120 scientific papers and book chapters on gastric cancer, pancreaticoduodenectomy, laparoscopy, and other clinical topics. Dr. Abaúnza became professor of general surgery and chief, department of surgery, San Pedro Claver Hospital, and professor, National University of Colombia, Bogota. Dr. Abaúnza is a member of the International Society of Surgery and past-president of the Colombian Association of Gastroenterology.
Jacques Belghiti, MD, PhD, Paris, France, has made significant contributions to the fields of hepatocellular carcinoma and liver transplantation and has conducted vital studies in liver resection and hepatobiliary surgical oncology. His technical innovations include preservation of portal and caval flows during liver transplantation, the hanging maneuver to facilitate liver resection, and the use of peritoneal patch to provide an immediate and safe vascular graft. Dr. Belghiti was chief, department of hepato-bilio-pancreatic surgery and liver transplantation, Beaujon Hospital, University of Paris, for 20 years. In 2014, the department was classified as the first French surgical digestive center. French President François Hollande invited Dr. Belghiti to serve on the board of the National Health Authority in 2014; he now chairs the board’s medical devices and health technology committee for reimbursement. Dr. Belghiti is associate editor, liver surgery and biliary section, World Journal of Surgery.
S. Adibul Hasan Rizvi, MB, BS, FRCSEng, FRCSEd, Karachi, Pakistan, is the founder of the Sindh Institute of Urology and Transplantation (SIUT) and a leader of transplantation in Pakistan. He started SIUT, which has become one of the fastest-growing urological and transplant centers in the region, in 1972. SIUT offers procedures such as dialysis, lithotripsy, surgery, and transplantation. Pakistan’s first successful liver transplant was performed there in 2003, eight years after Dr. Rizvi and his team performed the first deceased renal transplant in the country. SIUT’s Dewan Farooque Medical Complex trains nurses, technical staff, and postgraduate physicians. All patient care is provided free of charge. The SIUT’s Hanifa Sulaiman Dawood Oncology Center now treats patients with post-transplant cancers and other malignancies. SIUT opened its first satellite unit in 2000, and three other dialysis centers that are part of the institute offer free dialysis to medically indigent patients in Karachi. Dr. Rizvi is a member of the World Health Organization advisory panel on organ transplantation and the Global Alliance for Transplantation.
Sachiyo Suita, MD, PhD, Fukuoka, Japan, was the first woman professor to head a surgery department at a Japanese national university. Dr. Suita realized she wanted to become a surgeon during the Vietnam War, when she interned at the American Air Force Hospital, Tachikawa, Japan. A mentor at Kyushu University, Fukuoka, encouraged her interest in pediatric surgery. Dr. Suita became surgeon-in-chief at Fukuoka Children’s Hospital in 1983 and professor of pediatric surgery at Kyushu University in 1989. Her promotion to professor marked the first time a woman had been on the faculty of medicine at the university. Dr. Suita’s areas of interest include fetal surgery, neonatal surgery, pediatric oncology, clinical nutrition, liver and small bowel transplantation, and grief care. In 2004, Dr. Suita became the first woman director of Kyushu University Hospital.
John Francis Thompson, AO, MD, FACS, FRACS, FAHMS, Sydney, Australia, has provided distinguished service in the field of oncology research, particularly melanoma, in international and national professional organizations, and in medical education. Dr. Thompson has written more than 700 peer-reviewed scientific articles, which led to his appointment as an Officer of the Order of Australia in 2014. His research interests are in lymphatic mapping and regional node management of patients with melanoma and other malignancies, and local and regional therapies for recurrent and advanced limb tumors. He is executive director and research director, Melanoma Institute Australia, and professor, melanoma and surgical oncology, University of Sydney. Dr. Thompson is a member of the Melanoma Staging Committee of the American Joint Committee on Cancer and chairs the workgroup to update Australia’s clinical practice guidelines for management of cutaneous melanoma in Australia.
Presenting on behalf of the College, respectively, were Marco Patti, MD, FACS, Chicago, IL; Leslie H. Blumgart, MD, FACS, FRCS, New York, NY; Prof. Mehmet A. Haberal, MD, FACS(Hon), FICS (Hon), FASA(Hon), Ankara, Turkey; Arnold G. Coran, MD, FACS, Ann Arbor, MI; and Jeffrey E. Gershenwald, MD, FACS, Houston, TX.
Sir Rickman Godlee, president of the Royal College of Surgeons of England, was awarded the first Honorary Fellowship in the ACS during the College’s first Convocation in 1913. Since then, 458 internationally prominent surgeons, including the five chosen this year, have been named Honorary Fellows of the ACS. The citations presented at the Convocation follow.
Honorary Fellowship in the American College of Surgeons (ACS) was awarded to five prominent surgeons from Colombia, France, Pakistan, Japan, and Australia at the October 16 Convocation that preceded the official opening of Clinical Congress 2016 in Washington, DC. The granting of Honorary Fellowships is one of the highlights of the Clinical Congress. This year’s recipients were as follows.
Hernando Abaúnza Orjuela, MD, FACS, MACC(Hon), Bogotá, Colombia, is the founder, past-president, and current executive director of the Colombian Association of Surgery. He also is past-president of the Latin American Federation of Surgery (FELAC), which promotes research, teaching, and the practice of surgery among surgeons in Latin America. He became a Fellow of the ACS in 1970 and served on the ACS Board of Governors (1993–1999) and as President of the ACS Colombia Chapter (1990–1991). Dr. Abaúnza has written several articles on breast cancer and complex abdominal surgery problems, as well as more than 120 scientific papers and book chapters on gastric cancer, pancreaticoduodenectomy, laparoscopy, and other clinical topics. Dr. Abaúnza became professor of general surgery and chief, department of surgery, San Pedro Claver Hospital, and professor, National University of Colombia, Bogota. Dr. Abaúnza is a member of the International Society of Surgery and past-president of the Colombian Association of Gastroenterology.
Jacques Belghiti, MD, PhD, Paris, France, has made significant contributions to the fields of hepatocellular carcinoma and liver transplantation and has conducted vital studies in liver resection and hepatobiliary surgical oncology. His technical innovations include preservation of portal and caval flows during liver transplantation, the hanging maneuver to facilitate liver resection, and the use of peritoneal patch to provide an immediate and safe vascular graft. Dr. Belghiti was chief, department of hepato-bilio-pancreatic surgery and liver transplantation, Beaujon Hospital, University of Paris, for 20 years. In 2014, the department was classified as the first French surgical digestive center. French President François Hollande invited Dr. Belghiti to serve on the board of the National Health Authority in 2014; he now chairs the board’s medical devices and health technology committee for reimbursement. Dr. Belghiti is associate editor, liver surgery and biliary section, World Journal of Surgery.
S. Adibul Hasan Rizvi, MB, BS, FRCSEng, FRCSEd, Karachi, Pakistan, is the founder of the Sindh Institute of Urology and Transplantation (SIUT) and a leader of transplantation in Pakistan. He started SIUT, which has become one of the fastest-growing urological and transplant centers in the region, in 1972. SIUT offers procedures such as dialysis, lithotripsy, surgery, and transplantation. Pakistan’s first successful liver transplant was performed there in 2003, eight years after Dr. Rizvi and his team performed the first deceased renal transplant in the country. SIUT’s Dewan Farooque Medical Complex trains nurses, technical staff, and postgraduate physicians. All patient care is provided free of charge. The SIUT’s Hanifa Sulaiman Dawood Oncology Center now treats patients with post-transplant cancers and other malignancies. SIUT opened its first satellite unit in 2000, and three other dialysis centers that are part of the institute offer free dialysis to medically indigent patients in Karachi. Dr. Rizvi is a member of the World Health Organization advisory panel on organ transplantation and the Global Alliance for Transplantation.
Sachiyo Suita, MD, PhD, Fukuoka, Japan, was the first woman professor to head a surgery department at a Japanese national university. Dr. Suita realized she wanted to become a surgeon during the Vietnam War, when she interned at the American Air Force Hospital, Tachikawa, Japan. A mentor at Kyushu University, Fukuoka, encouraged her interest in pediatric surgery. Dr. Suita became surgeon-in-chief at Fukuoka Children’s Hospital in 1983 and professor of pediatric surgery at Kyushu University in 1989. Her promotion to professor marked the first time a woman had been on the faculty of medicine at the university. Dr. Suita’s areas of interest include fetal surgery, neonatal surgery, pediatric oncology, clinical nutrition, liver and small bowel transplantation, and grief care. In 2004, Dr. Suita became the first woman director of Kyushu University Hospital.
John Francis Thompson, AO, MD, FACS, FRACS, FAHMS, Sydney, Australia, has provided distinguished service in the field of oncology research, particularly melanoma, in international and national professional organizations, and in medical education. Dr. Thompson has written more than 700 peer-reviewed scientific articles, which led to his appointment as an Officer of the Order of Australia in 2014. His research interests are in lymphatic mapping and regional node management of patients with melanoma and other malignancies, and local and regional therapies for recurrent and advanced limb tumors. He is executive director and research director, Melanoma Institute Australia, and professor, melanoma and surgical oncology, University of Sydney. Dr. Thompson is a member of the Melanoma Staging Committee of the American Joint Committee on Cancer and chairs the workgroup to update Australia’s clinical practice guidelines for management of cutaneous melanoma in Australia.
Presenting on behalf of the College, respectively, were Marco Patti, MD, FACS, Chicago, IL; Leslie H. Blumgart, MD, FACS, FRCS, New York, NY; Prof. Mehmet A. Haberal, MD, FACS(Hon), FICS (Hon), FASA(Hon), Ankara, Turkey; Arnold G. Coran, MD, FACS, Ann Arbor, MI; and Jeffrey E. Gershenwald, MD, FACS, Houston, TX.
Sir Rickman Godlee, president of the Royal College of Surgeons of England, was awarded the first Honorary Fellowship in the ACS during the College’s first Convocation in 1913. Since then, 458 internationally prominent surgeons, including the five chosen this year, have been named Honorary Fellows of the ACS. The citations presented at the Convocation follow.
ACS leads efforts to improve quality of care for older surgical patients
The December issue of the Bulletin will feature an in-depth exploration of past, present, and future American College of Surgeons (ACS) efforts to improve the quality of surgical care for older adults. The following is a brief summary of these initiatives.
Decades of progress
Over the years, the College has been a leader in responding to the growing need for the aging American population to have access to high-quality surgical care. People older than 65 years of age represent a rapidly growing segment of the U.S. population and a disproportionate share of individuals who undergo surgical procedures. Older adults have unique physiology, which often puts them at risk for complications after surgery. At a time when the quality and value of health care are under increasing scrutiny, the need for high-quality standards to improve surgical care delivery for this vulnerable population is on the rise.
The ACS has invested in improving surgical care for older adults over several decades. The ACS has partnered with the American Geriatrics Society (AGS) and The John A. Hartford Foundation since 1995 and has had a standing Geriatric Surgery Task Force since 2004. In an interdisciplinary effort, the ACS, the AGS, and The John A. Hartford Foundation issued a set of guidelines for preoperative care of geriatric patients in 2012, with a follow-up set of guidelines for perioperative and postoperative care in 2016. Through the College’s National Surgical Quality Improvement Program (ACS NSQIP®), members of the Geriatric Surgery Task Force began collecting 14 patient-centered, geriatric-specific variables to better appreciate the unique risk factors and outcomes of older adults.
Coalition for Quality in Geriatric Surgery
Most recently, the ACS, with support from The John A. Hartford Foundation, convened a group of more than 50 stakeholders as the Coalition for Quality in Geriatric Surgery. This interdisciplinary, patient- and family-centered coalition aims to systematically improve surgical care for older adults. These improvements are intended for all geriatric surgical care programs, regardless of hospital size, location, or academic status. After an extensive standards evaluation process, the interdisciplinary panel is preparing to release the first iteration of high-quality geriatric surgery standards.
The project has garnered 74 mentions in the media as of press time, in addition to interviews on SiriusXM Doctor Radio, featuring Julia Berian, MD, ACS Clinical Scholar in Residence; Clifford Y. Ko, MD, MS, MSHS, FACS, FASCRS, Principal Investigator, and Director, ACS Division of Research and Optimal Patient Care; and Ronnie Rosenthal, MD, MS, FACS, Chair, ACS Geriatric Surgery Task Force and Co-Principal Investigator, Standards Subcommittee Co-Chair. Media outlets that have reported on the project include FOX News, Reuters, Medscape, and Surgical Products.
The December issue of the Bulletin will feature an in-depth exploration of past, present, and future American College of Surgeons (ACS) efforts to improve the quality of surgical care for older adults. The following is a brief summary of these initiatives.
Decades of progress
Over the years, the College has been a leader in responding to the growing need for the aging American population to have access to high-quality surgical care. People older than 65 years of age represent a rapidly growing segment of the U.S. population and a disproportionate share of individuals who undergo surgical procedures. Older adults have unique physiology, which often puts them at risk for complications after surgery. At a time when the quality and value of health care are under increasing scrutiny, the need for high-quality standards to improve surgical care delivery for this vulnerable population is on the rise.
The ACS has invested in improving surgical care for older adults over several decades. The ACS has partnered with the American Geriatrics Society (AGS) and The John A. Hartford Foundation since 1995 and has had a standing Geriatric Surgery Task Force since 2004. In an interdisciplinary effort, the ACS, the AGS, and The John A. Hartford Foundation issued a set of guidelines for preoperative care of geriatric patients in 2012, with a follow-up set of guidelines for perioperative and postoperative care in 2016. Through the College’s National Surgical Quality Improvement Program (ACS NSQIP®), members of the Geriatric Surgery Task Force began collecting 14 patient-centered, geriatric-specific variables to better appreciate the unique risk factors and outcomes of older adults.
Coalition for Quality in Geriatric Surgery
Most recently, the ACS, with support from The John A. Hartford Foundation, convened a group of more than 50 stakeholders as the Coalition for Quality in Geriatric Surgery. This interdisciplinary, patient- and family-centered coalition aims to systematically improve surgical care for older adults. These improvements are intended for all geriatric surgical care programs, regardless of hospital size, location, or academic status. After an extensive standards evaluation process, the interdisciplinary panel is preparing to release the first iteration of high-quality geriatric surgery standards.
The project has garnered 74 mentions in the media as of press time, in addition to interviews on SiriusXM Doctor Radio, featuring Julia Berian, MD, ACS Clinical Scholar in Residence; Clifford Y. Ko, MD, MS, MSHS, FACS, FASCRS, Principal Investigator, and Director, ACS Division of Research and Optimal Patient Care; and Ronnie Rosenthal, MD, MS, FACS, Chair, ACS Geriatric Surgery Task Force and Co-Principal Investigator, Standards Subcommittee Co-Chair. Media outlets that have reported on the project include FOX News, Reuters, Medscape, and Surgical Products.
The December issue of the Bulletin will feature an in-depth exploration of past, present, and future American College of Surgeons (ACS) efforts to improve the quality of surgical care for older adults. The following is a brief summary of these initiatives.
Decades of progress
Over the years, the College has been a leader in responding to the growing need for the aging American population to have access to high-quality surgical care. People older than 65 years of age represent a rapidly growing segment of the U.S. population and a disproportionate share of individuals who undergo surgical procedures. Older adults have unique physiology, which often puts them at risk for complications after surgery. At a time when the quality and value of health care are under increasing scrutiny, the need for high-quality standards to improve surgical care delivery for this vulnerable population is on the rise.
The ACS has invested in improving surgical care for older adults over several decades. The ACS has partnered with the American Geriatrics Society (AGS) and The John A. Hartford Foundation since 1995 and has had a standing Geriatric Surgery Task Force since 2004. In an interdisciplinary effort, the ACS, the AGS, and The John A. Hartford Foundation issued a set of guidelines for preoperative care of geriatric patients in 2012, with a follow-up set of guidelines for perioperative and postoperative care in 2016. Through the College’s National Surgical Quality Improvement Program (ACS NSQIP®), members of the Geriatric Surgery Task Force began collecting 14 patient-centered, geriatric-specific variables to better appreciate the unique risk factors and outcomes of older adults.
Coalition for Quality in Geriatric Surgery
Most recently, the ACS, with support from The John A. Hartford Foundation, convened a group of more than 50 stakeholders as the Coalition for Quality in Geriatric Surgery. This interdisciplinary, patient- and family-centered coalition aims to systematically improve surgical care for older adults. These improvements are intended for all geriatric surgical care programs, regardless of hospital size, location, or academic status. After an extensive standards evaluation process, the interdisciplinary panel is preparing to release the first iteration of high-quality geriatric surgery standards.
The project has garnered 74 mentions in the media as of press time, in addition to interviews on SiriusXM Doctor Radio, featuring Julia Berian, MD, ACS Clinical Scholar in Residence; Clifford Y. Ko, MD, MS, MSHS, FACS, FASCRS, Principal Investigator, and Director, ACS Division of Research and Optimal Patient Care; and Ronnie Rosenthal, MD, MS, FACS, Chair, ACS Geriatric Surgery Task Force and Co-Principal Investigator, Standards Subcommittee Co-Chair. Media outlets that have reported on the project include FOX News, Reuters, Medscape, and Surgical Products.
From the Washington Office: CMS says, “Pick Your Pace”
This month, we continue our discussion of the Quality Payment Program (QPP). Specifically, I write about a blog post from CMS Acting Administrator, Andy Slavitt, on Sept. 8, 2016. In that post Mr. Slavitt announced “plans for timing of reporting for the first year of the [quality payment] program” and stated that CMS “intend[s] for the Quality Payment Program to allow physicians to pick their pace of participation for the first performance period that begins Jan. 1, 2017.”
Though specific details are unknown at this time pending the release of the QPP final rule on or about Nov. 1, 2016, Mr. Slavitt’s post would seem to indicate that it will be possible for providers to avoid payment penalties and further that it should also be possible to receive a positive update in Medicare payment depending upon the level of one’s participation in the new program in 2017.
Options for Participation
Acting Administrator Slavitt’s post states, “During 2017, eligible physicians and other clinicians will have multiple options for participation. Choosing one of these options would ensure you do not receive a negative payment adjustment in 2019.”
Outlined below are those four options:
Option 1: Test the Quality Payment Program
With this option, one will be able to avoid a negative payment adjustment, “as long as you submit some data to the Quality Payment Program, including data from after January 1, 2017.”
This option is designed to ensure preparation for broader participation in 2018. As with all types of regulation, the “devil is in the details” and specifically, what constitutes “some data” is not defined at this time. As mentioned above, we expect such details to be described fully in the final rule, but I believe surgeons have reason to be optimistic that all should be able to avoid penalties under the first year of the QPP.
Option 2: Participate for part of the calendar year
For providers who choose to submit data for the QPP for less than a full year, i.e., “a reduced number of days,” their performance period could begin sometime after Jan. 1, 2017, and their “practice could still qualify for a small positive payment adjustment.”
For surgeons who are already participating in the current PQRS (Physician Quality Reporting System) program via the American College of Surgeons’ Surgeon Specific Registry (SSR) or other certified registry, this option presents an opportunity to be rewarded for those efforts. To reiterate, details relative to the threshold of participation required for the positive adjustment will not be known until the final rule is released. However, it is entirely possible that many surgeons will be eligible for a positive update based upon what they are already doing or could easily begin doing in 2017.
Option 3: Participate for the full calendar year
Option three is for practices that are ready to fully participate in all four components of the QPP for the entire calendar year of 2017. Those practices that submit information for the entire year on quality, the use of electronic health record technology, and their practice’s improvement activities “could qualify for a modest positive payment adjustment.”
For those practices that have invested in electronic health record technology and are already reporting PQRS data, “gearing up” to participate for the full calendar year may not be an arduous endeavor. Once the final rule is released and specific details are known, they may find that their previous efforts toward preparation for the QPP puts it well within their capability to fully participate in 2017 and receive a positive payment adjustment.
Option 4: Participate in an Advanced Alternative Payment Model (APM)
“Instead of reporting quality data and other information, the law allows you to participate in the Quality Payment Program by joining an Advanced Alternative Payment Model …” Mr. Slavitt stated.
As has been stated in previous editions of this column, for the first few years of the QPP we expect that most surgeons will participate in the QPP via the Merit-based Incentive Payment System (MIPS) pathway and not in APMs. However, the development of Advanced Alternative Payment Models widely applicable for surgeons is the object of significant and ongoing policy development efforts by the Division of Advocacy and Health Policy of the American College of Surgeons.
For those wishing to read Acting Administrator Slavitt’s post in its entirety, it may be found here: https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace.
Until next month.
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
This month, we continue our discussion of the Quality Payment Program (QPP). Specifically, I write about a blog post from CMS Acting Administrator, Andy Slavitt, on Sept. 8, 2016. In that post Mr. Slavitt announced “plans for timing of reporting for the first year of the [quality payment] program” and stated that CMS “intend[s] for the Quality Payment Program to allow physicians to pick their pace of participation for the first performance period that begins Jan. 1, 2017.”
Though specific details are unknown at this time pending the release of the QPP final rule on or about Nov. 1, 2016, Mr. Slavitt’s post would seem to indicate that it will be possible for providers to avoid payment penalties and further that it should also be possible to receive a positive update in Medicare payment depending upon the level of one’s participation in the new program in 2017.
Options for Participation
Acting Administrator Slavitt’s post states, “During 2017, eligible physicians and other clinicians will have multiple options for participation. Choosing one of these options would ensure you do not receive a negative payment adjustment in 2019.”
Outlined below are those four options:
Option 1: Test the Quality Payment Program
With this option, one will be able to avoid a negative payment adjustment, “as long as you submit some data to the Quality Payment Program, including data from after January 1, 2017.”
This option is designed to ensure preparation for broader participation in 2018. As with all types of regulation, the “devil is in the details” and specifically, what constitutes “some data” is not defined at this time. As mentioned above, we expect such details to be described fully in the final rule, but I believe surgeons have reason to be optimistic that all should be able to avoid penalties under the first year of the QPP.
Option 2: Participate for part of the calendar year
For providers who choose to submit data for the QPP for less than a full year, i.e., “a reduced number of days,” their performance period could begin sometime after Jan. 1, 2017, and their “practice could still qualify for a small positive payment adjustment.”
For surgeons who are already participating in the current PQRS (Physician Quality Reporting System) program via the American College of Surgeons’ Surgeon Specific Registry (SSR) or other certified registry, this option presents an opportunity to be rewarded for those efforts. To reiterate, details relative to the threshold of participation required for the positive adjustment will not be known until the final rule is released. However, it is entirely possible that many surgeons will be eligible for a positive update based upon what they are already doing or could easily begin doing in 2017.
Option 3: Participate for the full calendar year
Option three is for practices that are ready to fully participate in all four components of the QPP for the entire calendar year of 2017. Those practices that submit information for the entire year on quality, the use of electronic health record technology, and their practice’s improvement activities “could qualify for a modest positive payment adjustment.”
For those practices that have invested in electronic health record technology and are already reporting PQRS data, “gearing up” to participate for the full calendar year may not be an arduous endeavor. Once the final rule is released and specific details are known, they may find that their previous efforts toward preparation for the QPP puts it well within their capability to fully participate in 2017 and receive a positive payment adjustment.
Option 4: Participate in an Advanced Alternative Payment Model (APM)
“Instead of reporting quality data and other information, the law allows you to participate in the Quality Payment Program by joining an Advanced Alternative Payment Model …” Mr. Slavitt stated.
As has been stated in previous editions of this column, for the first few years of the QPP we expect that most surgeons will participate in the QPP via the Merit-based Incentive Payment System (MIPS) pathway and not in APMs. However, the development of Advanced Alternative Payment Models widely applicable for surgeons is the object of significant and ongoing policy development efforts by the Division of Advocacy and Health Policy of the American College of Surgeons.
For those wishing to read Acting Administrator Slavitt’s post in its entirety, it may be found here: https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace.
Until next month.
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
This month, we continue our discussion of the Quality Payment Program (QPP). Specifically, I write about a blog post from CMS Acting Administrator, Andy Slavitt, on Sept. 8, 2016. In that post Mr. Slavitt announced “plans for timing of reporting for the first year of the [quality payment] program” and stated that CMS “intend[s] for the Quality Payment Program to allow physicians to pick their pace of participation for the first performance period that begins Jan. 1, 2017.”
Though specific details are unknown at this time pending the release of the QPP final rule on or about Nov. 1, 2016, Mr. Slavitt’s post would seem to indicate that it will be possible for providers to avoid payment penalties and further that it should also be possible to receive a positive update in Medicare payment depending upon the level of one’s participation in the new program in 2017.
Options for Participation
Acting Administrator Slavitt’s post states, “During 2017, eligible physicians and other clinicians will have multiple options for participation. Choosing one of these options would ensure you do not receive a negative payment adjustment in 2019.”
Outlined below are those four options:
Option 1: Test the Quality Payment Program
With this option, one will be able to avoid a negative payment adjustment, “as long as you submit some data to the Quality Payment Program, including data from after January 1, 2017.”
This option is designed to ensure preparation for broader participation in 2018. As with all types of regulation, the “devil is in the details” and specifically, what constitutes “some data” is not defined at this time. As mentioned above, we expect such details to be described fully in the final rule, but I believe surgeons have reason to be optimistic that all should be able to avoid penalties under the first year of the QPP.
Option 2: Participate for part of the calendar year
For providers who choose to submit data for the QPP for less than a full year, i.e., “a reduced number of days,” their performance period could begin sometime after Jan. 1, 2017, and their “practice could still qualify for a small positive payment adjustment.”
For surgeons who are already participating in the current PQRS (Physician Quality Reporting System) program via the American College of Surgeons’ Surgeon Specific Registry (SSR) or other certified registry, this option presents an opportunity to be rewarded for those efforts. To reiterate, details relative to the threshold of participation required for the positive adjustment will not be known until the final rule is released. However, it is entirely possible that many surgeons will be eligible for a positive update based upon what they are already doing or could easily begin doing in 2017.
Option 3: Participate for the full calendar year
Option three is for practices that are ready to fully participate in all four components of the QPP for the entire calendar year of 2017. Those practices that submit information for the entire year on quality, the use of electronic health record technology, and their practice’s improvement activities “could qualify for a modest positive payment adjustment.”
For those practices that have invested in electronic health record technology and are already reporting PQRS data, “gearing up” to participate for the full calendar year may not be an arduous endeavor. Once the final rule is released and specific details are known, they may find that their previous efforts toward preparation for the QPP puts it well within their capability to fully participate in 2017 and receive a positive payment adjustment.
Option 4: Participate in an Advanced Alternative Payment Model (APM)
“Instead of reporting quality data and other information, the law allows you to participate in the Quality Payment Program by joining an Advanced Alternative Payment Model …” Mr. Slavitt stated.
As has been stated in previous editions of this column, for the first few years of the QPP we expect that most surgeons will participate in the QPP via the Merit-based Incentive Payment System (MIPS) pathway and not in APMs. However, the development of Advanced Alternative Payment Models widely applicable for surgeons is the object of significant and ongoing policy development efforts by the Division of Advocacy and Health Policy of the American College of Surgeons.
For those wishing to read Acting Administrator Slavitt’s post in its entirety, it may be found here: https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace.
Until next month.
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, D.C.
Bulletin moves online for most readers beginning with January 2017 issue
In light of production costs, American College of Surgeons (ACS) Regents and the leadership of the Board of Governors, Young Fellows Association, and Resident and Associate Society have determined that the College would be best served by transitioning readers of the Bulletin to an online publication, effective with the January 2017 issue. The Bulletin will continue to offer the same array of features, news stories, and columns online, with the added benefit of providing more timely access to the Bulletin.
Members for whom we have an e-mail address will be notified each month when the new issue of the Bulletin becomes available. The e-mail notification will include a link that takes you directly to the Bulletin home page. (If your e-mail address is not on file or you need to update it, do so now via “My Profile” on the ACS website.)
From the Bulletin home page, bulletin.facs.org, you have three options: (1) start reading the current issue right there; (2) click the link on the right-hand side of the page, which will take you to a digital version that looks exactly like the print edition; or (3) download the Bulletin app, which will notify you each month when a new issue is available.
Note that, for a limited time, dues-paying members who do not have access to the Internet or who have a strong preference for print media may opt to continue receiving print copies of the Bulletin. Members who transition to non–dues-paying status will no longer receive the print edition. Dues-paying members (active Fellows, Associate Fellows, and Residents) should have received a notification from the College offering them the print option. If you do not recall receiving this notification e-mail or letter, you may request continuation of your print subscription via e-mail at [email protected] or by calling 800-621-4111. All requests should be made by December 9, 2016.
In light of production costs, American College of Surgeons (ACS) Regents and the leadership of the Board of Governors, Young Fellows Association, and Resident and Associate Society have determined that the College would be best served by transitioning readers of the Bulletin to an online publication, effective with the January 2017 issue. The Bulletin will continue to offer the same array of features, news stories, and columns online, with the added benefit of providing more timely access to the Bulletin.
Members for whom we have an e-mail address will be notified each month when the new issue of the Bulletin becomes available. The e-mail notification will include a link that takes you directly to the Bulletin home page. (If your e-mail address is not on file or you need to update it, do so now via “My Profile” on the ACS website.)
From the Bulletin home page, bulletin.facs.org, you have three options: (1) start reading the current issue right there; (2) click the link on the right-hand side of the page, which will take you to a digital version that looks exactly like the print edition; or (3) download the Bulletin app, which will notify you each month when a new issue is available.
Note that, for a limited time, dues-paying members who do not have access to the Internet or who have a strong preference for print media may opt to continue receiving print copies of the Bulletin. Members who transition to non–dues-paying status will no longer receive the print edition. Dues-paying members (active Fellows, Associate Fellows, and Residents) should have received a notification from the College offering them the print option. If you do not recall receiving this notification e-mail or letter, you may request continuation of your print subscription via e-mail at [email protected] or by calling 800-621-4111. All requests should be made by December 9, 2016.
In light of production costs, American College of Surgeons (ACS) Regents and the leadership of the Board of Governors, Young Fellows Association, and Resident and Associate Society have determined that the College would be best served by transitioning readers of the Bulletin to an online publication, effective with the January 2017 issue. The Bulletin will continue to offer the same array of features, news stories, and columns online, with the added benefit of providing more timely access to the Bulletin.
Members for whom we have an e-mail address will be notified each month when the new issue of the Bulletin becomes available. The e-mail notification will include a link that takes you directly to the Bulletin home page. (If your e-mail address is not on file or you need to update it, do so now via “My Profile” on the ACS website.)
From the Bulletin home page, bulletin.facs.org, you have three options: (1) start reading the current issue right there; (2) click the link on the right-hand side of the page, which will take you to a digital version that looks exactly like the print edition; or (3) download the Bulletin app, which will notify you each month when a new issue is available.
Note that, for a limited time, dues-paying members who do not have access to the Internet or who have a strong preference for print media may opt to continue receiving print copies of the Bulletin. Members who transition to non–dues-paying status will no longer receive the print edition. Dues-paying members (active Fellows, Associate Fellows, and Residents) should have received a notification from the College offering them the print option. If you do not recall receiving this notification e-mail or letter, you may request continuation of your print subscription via e-mail at [email protected] or by calling 800-621-4111. All requests should be made by December 9, 2016.
AJCC Releases Cancer Staging Manual, Eighth Edition
The American Joint Committee on Cancer (AJCC) has released the eighth edition of TNM Cancer Staging Manual, which reflects current understanding of cancer biology concepts and emphasizes a more individualized approach to cancer classification and treatment. This edition presents evidence-based revisions for staging cancer for a number of organ sites and includes the rationales and rules for staging; the definitions of tumor, lymph node involvement, and metastasis; stage groupings; and histologic grade.
Cancer staging provides patients and physicians with the standards for determining the best treatment approach for their disease and their prognosis. Mahul B. Amin, MD, FCAP, Editor-in-Chief of the Eighth Edition, noted that 430 experts from 184 institutions in 22 countries on six continents collaborated to produce this resource. Dr. Amin is professor and chairman emeritus, department of pathology and laboratory medicine, Cedars-Sinai Medical Center, Los Angeles, CA, and incoming chairman and endowed professor of the department of pathology and laboratory medicine at the University of Tennessee Health Sciences Center, Memphis.
Since the Seventh Edition of the manual was published in 2009, researchers and medical practitioners have learned that genomic alterations drive cancer and may vary considerably among tumors that, in the past, were thought to be in the same category, Dr. Amin said.
The American College of Surgeons Commission on Cancer will require accredited hospitals to use the Eighth Edition for all cancer cases diagnosed on or after January 1, 2017. The manual, developed in cooperation with the TNM Committee of the Union for International Cancer Control (UICC), is available for purchase online at http://www.springer.com/us/book/9783319406176.
Find additional information on licensing the content for electronic products at www.cancerstaging.org
The American Joint Committee on Cancer (AJCC) has released the eighth edition of TNM Cancer Staging Manual, which reflects current understanding of cancer biology concepts and emphasizes a more individualized approach to cancer classification and treatment. This edition presents evidence-based revisions for staging cancer for a number of organ sites and includes the rationales and rules for staging; the definitions of tumor, lymph node involvement, and metastasis; stage groupings; and histologic grade.
Cancer staging provides patients and physicians with the standards for determining the best treatment approach for their disease and their prognosis. Mahul B. Amin, MD, FCAP, Editor-in-Chief of the Eighth Edition, noted that 430 experts from 184 institutions in 22 countries on six continents collaborated to produce this resource. Dr. Amin is professor and chairman emeritus, department of pathology and laboratory medicine, Cedars-Sinai Medical Center, Los Angeles, CA, and incoming chairman and endowed professor of the department of pathology and laboratory medicine at the University of Tennessee Health Sciences Center, Memphis.
Since the Seventh Edition of the manual was published in 2009, researchers and medical practitioners have learned that genomic alterations drive cancer and may vary considerably among tumors that, in the past, were thought to be in the same category, Dr. Amin said.
The American College of Surgeons Commission on Cancer will require accredited hospitals to use the Eighth Edition for all cancer cases diagnosed on or after January 1, 2017. The manual, developed in cooperation with the TNM Committee of the Union for International Cancer Control (UICC), is available for purchase online at http://www.springer.com/us/book/9783319406176.
Find additional information on licensing the content for electronic products at www.cancerstaging.org
The American Joint Committee on Cancer (AJCC) has released the eighth edition of TNM Cancer Staging Manual, which reflects current understanding of cancer biology concepts and emphasizes a more individualized approach to cancer classification and treatment. This edition presents evidence-based revisions for staging cancer for a number of organ sites and includes the rationales and rules for staging; the definitions of tumor, lymph node involvement, and metastasis; stage groupings; and histologic grade.
Cancer staging provides patients and physicians with the standards for determining the best treatment approach for their disease and their prognosis. Mahul B. Amin, MD, FCAP, Editor-in-Chief of the Eighth Edition, noted that 430 experts from 184 institutions in 22 countries on six continents collaborated to produce this resource. Dr. Amin is professor and chairman emeritus, department of pathology and laboratory medicine, Cedars-Sinai Medical Center, Los Angeles, CA, and incoming chairman and endowed professor of the department of pathology and laboratory medicine at the University of Tennessee Health Sciences Center, Memphis.
Since the Seventh Edition of the manual was published in 2009, researchers and medical practitioners have learned that genomic alterations drive cancer and may vary considerably among tumors that, in the past, were thought to be in the same category, Dr. Amin said.
The American College of Surgeons Commission on Cancer will require accredited hospitals to use the Eighth Edition for all cancer cases diagnosed on or after January 1, 2017. The manual, developed in cooperation with the TNM Committee of the Union for International Cancer Control (UICC), is available for purchase online at http://www.springer.com/us/book/9783319406176.
Find additional information on licensing the content for electronic products at www.cancerstaging.org