User login
Stroke hospitals owe all patients rapid thrombolysis
The best way to minimize death and disability in most patients having an acute ischemic stroke is rapid thrombolysis by infusion of tissue plasminogen activator. Mechanical clot removal – thrombectomy – has recently been shown even better, but it’s applicable to just a fraction of these stroke patients, and even for them thrombolysis remains, for the time being, the recommended first step, with thrombectomy following soon after.
The good news is that more eligible U.S. stroke patients than ever before get this effective treatment. As I reported recently from the International Stroke Conference, as of mid-2016, 68% of U.S. acute ischemic stroke patients treated at about 2,000 of the largest and most focused U.S. stroke hospitals received thrombolytic treatment within 60 minutes of their hospital arrival. That’s up from 30% in late 2009. Hooray! The sad news is that many eligible stroke patients seen at these hospitals don’t get treated this way. Simple math puts that figure at 32%. In other words, last year, nearly a third of U.S. stroke patients who should have received quick thrombolysis didn’t, even though they were taken to the country’s top stroke hospitals.
How do I know that more universal rapid thrombolysis is possible? The 2016 numbers reported from the Get With the Guidelines (GWTG)–Stroke hospitals showed that roughly 2% of the 788 hospitals included in this analysis treated 90% or more of their eligible stroke patients with thrombolysis within an hour. That’s about 16 hospitals. Another 8%, upward of 60 hospitals, treated 80%-89% of their eligible stroke patients within this window. So a high level of thrombolysis treatment is possible. It just isn’t being done everywhere. About 20% of the hospitals in the program treated 40% or fewer of eligible patients they saw within the 60-minute window.
I have no idea why some hospitals do so well while others don’t, despite being in the GWTG-Stroke program that promotes excellence in stroke care delivery. In the most recent iteration of the GWTG–Stroke Target Stroke program, phase II, the organization promoted 11 steps for hospitals to take to optimize rapid delivery of thrombolysis. The obvious inference is that some hospitals are doing all 11 steps very well and consistently, and many others aren’t. Underperforming hospitals owe it to their patients to do a much better job; the top-performing hospitals show it’s possible.
I have heard a lot recently at meetings about how research has established that a range of medical treatments, if used diligently by patients as directed, will substantially improve and prolong their life. Patient compliance then becomes a big issue, and so now I’m hearing more about new approaches to improve compliance. But what about hospital compliance?
Treating acute ischemic stroke as well as possible is different from most disorders – it’s not about patient compliance. It’s about the ambulance that picks up the patient and the hospital where the patient gets taken. The success or failure of the acute treatment that the roughly 700,000 annual U.S. acute ischemic stroke patients receive lies entirely in the hands of the hospital staff. Fewer than 10% of U.S. stroke hospitals offer the vast majority of these patients the best care currently available. Many others don’t do as well, and a huge fraction remain woefully slow, even though everyone knows the pathway to doing better. Underperforming hospitals owe it to patients to up their game, and they need to start doing it now.
[email protected]
On Twitter @mitchelzoler
The best way to minimize death and disability in most patients having an acute ischemic stroke is rapid thrombolysis by infusion of tissue plasminogen activator. Mechanical clot removal – thrombectomy – has recently been shown even better, but it’s applicable to just a fraction of these stroke patients, and even for them thrombolysis remains, for the time being, the recommended first step, with thrombectomy following soon after.
The good news is that more eligible U.S. stroke patients than ever before get this effective treatment. As I reported recently from the International Stroke Conference, as of mid-2016, 68% of U.S. acute ischemic stroke patients treated at about 2,000 of the largest and most focused U.S. stroke hospitals received thrombolytic treatment within 60 minutes of their hospital arrival. That’s up from 30% in late 2009. Hooray! The sad news is that many eligible stroke patients seen at these hospitals don’t get treated this way. Simple math puts that figure at 32%. In other words, last year, nearly a third of U.S. stroke patients who should have received quick thrombolysis didn’t, even though they were taken to the country’s top stroke hospitals.
How do I know that more universal rapid thrombolysis is possible? The 2016 numbers reported from the Get With the Guidelines (GWTG)–Stroke hospitals showed that roughly 2% of the 788 hospitals included in this analysis treated 90% or more of their eligible stroke patients with thrombolysis within an hour. That’s about 16 hospitals. Another 8%, upward of 60 hospitals, treated 80%-89% of their eligible stroke patients within this window. So a high level of thrombolysis treatment is possible. It just isn’t being done everywhere. About 20% of the hospitals in the program treated 40% or fewer of eligible patients they saw within the 60-minute window.
I have no idea why some hospitals do so well while others don’t, despite being in the GWTG-Stroke program that promotes excellence in stroke care delivery. In the most recent iteration of the GWTG–Stroke Target Stroke program, phase II, the organization promoted 11 steps for hospitals to take to optimize rapid delivery of thrombolysis. The obvious inference is that some hospitals are doing all 11 steps very well and consistently, and many others aren’t. Underperforming hospitals owe it to their patients to do a much better job; the top-performing hospitals show it’s possible.
I have heard a lot recently at meetings about how research has established that a range of medical treatments, if used diligently by patients as directed, will substantially improve and prolong their life. Patient compliance then becomes a big issue, and so now I’m hearing more about new approaches to improve compliance. But what about hospital compliance?
Treating acute ischemic stroke as well as possible is different from most disorders – it’s not about patient compliance. It’s about the ambulance that picks up the patient and the hospital where the patient gets taken. The success or failure of the acute treatment that the roughly 700,000 annual U.S. acute ischemic stroke patients receive lies entirely in the hands of the hospital staff. Fewer than 10% of U.S. stroke hospitals offer the vast majority of these patients the best care currently available. Many others don’t do as well, and a huge fraction remain woefully slow, even though everyone knows the pathway to doing better. Underperforming hospitals owe it to patients to up their game, and they need to start doing it now.
[email protected]
On Twitter @mitchelzoler
The best way to minimize death and disability in most patients having an acute ischemic stroke is rapid thrombolysis by infusion of tissue plasminogen activator. Mechanical clot removal – thrombectomy – has recently been shown even better, but it’s applicable to just a fraction of these stroke patients, and even for them thrombolysis remains, for the time being, the recommended first step, with thrombectomy following soon after.
The good news is that more eligible U.S. stroke patients than ever before get this effective treatment. As I reported recently from the International Stroke Conference, as of mid-2016, 68% of U.S. acute ischemic stroke patients treated at about 2,000 of the largest and most focused U.S. stroke hospitals received thrombolytic treatment within 60 minutes of their hospital arrival. That’s up from 30% in late 2009. Hooray! The sad news is that many eligible stroke patients seen at these hospitals don’t get treated this way. Simple math puts that figure at 32%. In other words, last year, nearly a third of U.S. stroke patients who should have received quick thrombolysis didn’t, even though they were taken to the country’s top stroke hospitals.
How do I know that more universal rapid thrombolysis is possible? The 2016 numbers reported from the Get With the Guidelines (GWTG)–Stroke hospitals showed that roughly 2% of the 788 hospitals included in this analysis treated 90% or more of their eligible stroke patients with thrombolysis within an hour. That’s about 16 hospitals. Another 8%, upward of 60 hospitals, treated 80%-89% of their eligible stroke patients within this window. So a high level of thrombolysis treatment is possible. It just isn’t being done everywhere. About 20% of the hospitals in the program treated 40% or fewer of eligible patients they saw within the 60-minute window.
I have no idea why some hospitals do so well while others don’t, despite being in the GWTG-Stroke program that promotes excellence in stroke care delivery. In the most recent iteration of the GWTG–Stroke Target Stroke program, phase II, the organization promoted 11 steps for hospitals to take to optimize rapid delivery of thrombolysis. The obvious inference is that some hospitals are doing all 11 steps very well and consistently, and many others aren’t. Underperforming hospitals owe it to their patients to do a much better job; the top-performing hospitals show it’s possible.
I have heard a lot recently at meetings about how research has established that a range of medical treatments, if used diligently by patients as directed, will substantially improve and prolong their life. Patient compliance then becomes a big issue, and so now I’m hearing more about new approaches to improve compliance. But what about hospital compliance?
Treating acute ischemic stroke as well as possible is different from most disorders – it’s not about patient compliance. It’s about the ambulance that picks up the patient and the hospital where the patient gets taken. The success or failure of the acute treatment that the roughly 700,000 annual U.S. acute ischemic stroke patients receive lies entirely in the hands of the hospital staff. Fewer than 10% of U.S. stroke hospitals offer the vast majority of these patients the best care currently available. Many others don’t do as well, and a huge fraction remain woefully slow, even though everyone knows the pathway to doing better. Underperforming hospitals owe it to patients to up their game, and they need to start doing it now.
[email protected]
On Twitter @mitchelzoler
Belimumab response at 2 years achieved by two-thirds of lupus patients
MELBOURNE – Two-thirds of patients with active systemic lupus erythematosus responded to treatment with belimumab at 2 years in a clinical practice setting, particularly those with higher disease activity or polyarthritis, according to data presented at an international conference on systemic lupus erythematosus.
In a multicenter prospective study of 188 patients with active systemic lupus erythematosus (SLE), Maddalena Larosa, MD, of the University of Padova (Italy) and her colleagues reported a 71.3% response rate with belimumab (Benlysta) at 12 months based on achieving SLE Responder Index (SRI-4) criteria. SRI-4 is a composite endpoint requiring at least a 4-point reduction in SLE Disease Activity Index 2000 (SLEDAI-2K) score, no worsening (less than 10-mm increase) from baseline in the Physician’s Global Assessment of Disease Activity score (PGA), and no new British Isles Lupus Assessment Group (BILAG) Domain A and no more than 1 new BILAG Domain B scores.

Patients were treated with belimumab as an add-on to standard care, with a treatment regimen of 10 mg/kg at day 0, 14, 28, and then every 28 days. The mean SLEDAI-2K score among patients was 8.3, all were positive for double-stranded DNA autoantibodies, and the mean Systemic Lupus International Collaborative Clinics (SLICC) Damage Index was 0.84. Nearly two-thirds of patients were also being treated with immunosuppressants.
Patients with a SLEDAI-2K score of 10 or above were 25 times more likely to respond by 12 months and 12 times more likely to respond by 24 months, both of which were statistically significant.
Similarly, patients with polyarthritis – who constituted nearly half of all patients in the study – were 8 times more likely to respond at 12 months, and 32 times more likely to respond at 24 months. Patients on a prednisone dose of 7.5 mg/day or greater were also significantly more likely to respond at 24 months.
“What was surprising in these patients who respond better are patients with higher disease activity,” Dr. Larosa said in an interview, noting that many patients had also had refractory disease.
Belimumab treatment was also associated with a plateauing of damage accrual, as measured by the SLICC Damage Index, she said.
“In the 5 years before belimumab initiation, we observed an increase of damage accrual related to SLE, but after the first belimumab infusion we did not observe any increase of damage accrual related to the disease,” Dr. Larosa told the audience.
The median duration of treatment was 12 months, but 58 patients (30.9%) discontinued belimumab, mainly because of adverse events. Eight patients also discontinued because of pregnancy, and two because of remission.
In response to a question on the effect of treatment on flare, Dr. Larosa said the treatment was also associated with a reduction in the number of patients who experienced flares, and a significant reduction in renal flares in patients with renal involvement.
No conflicts of interest were declared.
MELBOURNE – Two-thirds of patients with active systemic lupus erythematosus responded to treatment with belimumab at 2 years in a clinical practice setting, particularly those with higher disease activity or polyarthritis, according to data presented at an international conference on systemic lupus erythematosus.
In a multicenter prospective study of 188 patients with active systemic lupus erythematosus (SLE), Maddalena Larosa, MD, of the University of Padova (Italy) and her colleagues reported a 71.3% response rate with belimumab (Benlysta) at 12 months based on achieving SLE Responder Index (SRI-4) criteria. SRI-4 is a composite endpoint requiring at least a 4-point reduction in SLE Disease Activity Index 2000 (SLEDAI-2K) score, no worsening (less than 10-mm increase) from baseline in the Physician’s Global Assessment of Disease Activity score (PGA), and no new British Isles Lupus Assessment Group (BILAG) Domain A and no more than 1 new BILAG Domain B scores.
Patients were treated with belimumab as an add-on to standard care, with a treatment regimen of 10 mg/kg at day 0, 14, 28, and then every 28 days. The mean SLEDAI-2K score among patients was 8.3, all were positive for double-stranded DNA autoantibodies, and the mean Systemic Lupus International Collaborative Clinics (SLICC) Damage Index was 0.84. Nearly two-thirds of patients were also being treated with immunosuppressants.
Patients with a SLEDAI-2K score of 10 or above were 25 times more likely to respond by 12 months and 12 times more likely to respond by 24 months, both of which were statistically significant.
Similarly, patients with polyarthritis – who constituted nearly half of all patients in the study – were 8 times more likely to respond at 12 months, and 32 times more likely to respond at 24 months. Patients on a prednisone dose of 7.5 mg/day or greater were also significantly more likely to respond at 24 months.
“What was surprising in these patients who respond better are patients with higher disease activity,” Dr. Larosa said in an interview, noting that many patients had also had refractory disease.
Belimumab treatment was also associated with a plateauing of damage accrual, as measured by the SLICC Damage Index, she said.
“In the 5 years before belimumab initiation, we observed an increase of damage accrual related to SLE, but after the first belimumab infusion we did not observe any increase of damage accrual related to the disease,” Dr. Larosa told the audience.
The median duration of treatment was 12 months, but 58 patients (30.9%) discontinued belimumab, mainly because of adverse events. Eight patients also discontinued because of pregnancy, and two because of remission.
In response to a question on the effect of treatment on flare, Dr. Larosa said the treatment was also associated with a reduction in the number of patients who experienced flares, and a significant reduction in renal flares in patients with renal involvement.
No conflicts of interest were declared.
MELBOURNE – Two-thirds of patients with active systemic lupus erythematosus responded to treatment with belimumab at 2 years in a clinical practice setting, particularly those with higher disease activity or polyarthritis, according to data presented at an international conference on systemic lupus erythematosus.
In a multicenter prospective study of 188 patients with active systemic lupus erythematosus (SLE), Maddalena Larosa, MD, of the University of Padova (Italy) and her colleagues reported a 71.3% response rate with belimumab (Benlysta) at 12 months based on achieving SLE Responder Index (SRI-4) criteria. SRI-4 is a composite endpoint requiring at least a 4-point reduction in SLE Disease Activity Index 2000 (SLEDAI-2K) score, no worsening (less than 10-mm increase) from baseline in the Physician’s Global Assessment of Disease Activity score (PGA), and no new British Isles Lupus Assessment Group (BILAG) Domain A and no more than 1 new BILAG Domain B scores.
Patients were treated with belimumab as an add-on to standard care, with a treatment regimen of 10 mg/kg at day 0, 14, 28, and then every 28 days. The mean SLEDAI-2K score among patients was 8.3, all were positive for double-stranded DNA autoantibodies, and the mean Systemic Lupus International Collaborative Clinics (SLICC) Damage Index was 0.84. Nearly two-thirds of patients were also being treated with immunosuppressants.
Patients with a SLEDAI-2K score of 10 or above were 25 times more likely to respond by 12 months and 12 times more likely to respond by 24 months, both of which were statistically significant.
Similarly, patients with polyarthritis – who constituted nearly half of all patients in the study – were 8 times more likely to respond at 12 months, and 32 times more likely to respond at 24 months. Patients on a prednisone dose of 7.5 mg/day or greater were also significantly more likely to respond at 24 months.
“What was surprising in these patients who respond better are patients with higher disease activity,” Dr. Larosa said in an interview, noting that many patients had also had refractory disease.
Belimumab treatment was also associated with a plateauing of damage accrual, as measured by the SLICC Damage Index, she said.
“In the 5 years before belimumab initiation, we observed an increase of damage accrual related to SLE, but after the first belimumab infusion we did not observe any increase of damage accrual related to the disease,” Dr. Larosa told the audience.
The median duration of treatment was 12 months, but 58 patients (30.9%) discontinued belimumab, mainly because of adverse events. Eight patients also discontinued because of pregnancy, and two because of remission.
In response to a question on the effect of treatment on flare, Dr. Larosa said the treatment was also associated with a reduction in the number of patients who experienced flares, and a significant reduction in renal flares in patients with renal involvement.
No conflicts of interest were declared.
AT LUPUS 2017
Key clinical point:
Major finding: Belimumab as an add-on therapy in systemic lupus erythematosus was associated with a 71.3% response rate at 12 months and 68.7% response rate at 24 months.
Data source: Prospective, multicenter cohort study of 188 patients with systemic lupus erythematosus.
Disclosures: No conflicts of interest were declared.
A new form of photodynamic therapy remains controversial
A new approach to photodynamic therapy (PDT) – where patients expose their skin to daylight after application of a photosensitizing agent – is gaining traction in Europe, and dermatologists in the United States could soon see more patients inquiring about daylight PDT.
While proponents of daylight PDT point to less pain and greater convenience for patients who have when acne or precancerous actinic keratosis (AK) lesions or are trying to improve the appearance of their skin, not everyone is convinced this approach is safe.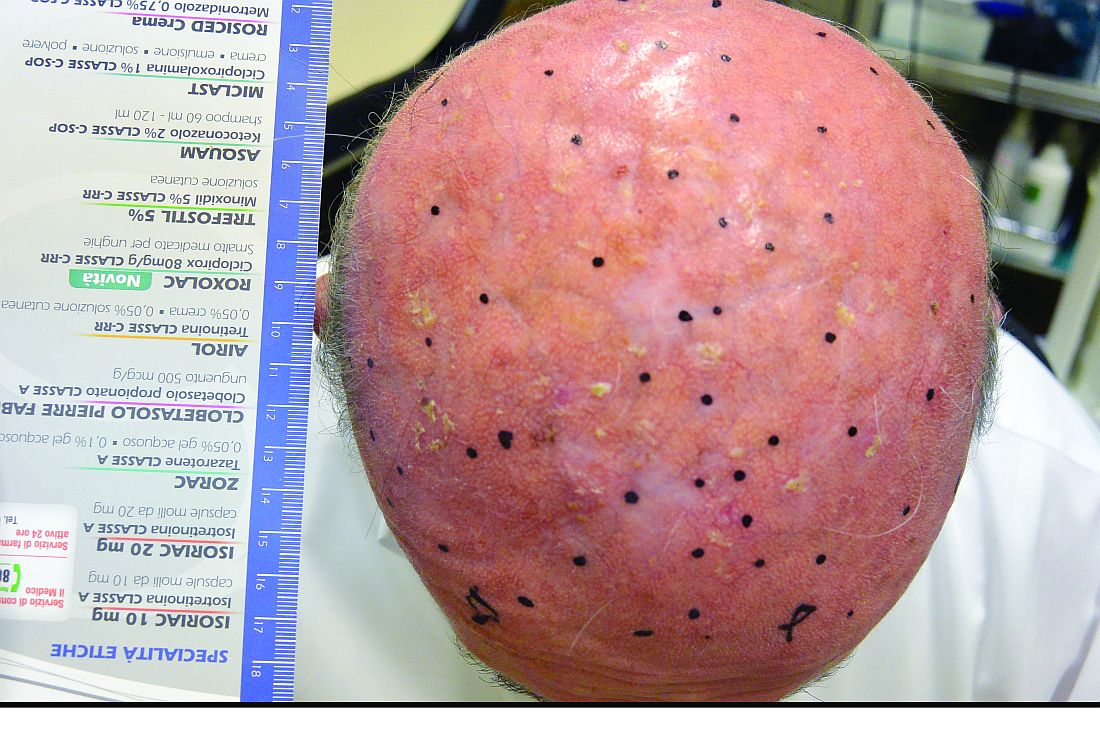
The European experience
Italy is among the European countries where daylight PDT has been evaluated in quality studies. In one Italian study, a split-face study of 35 patients with multiple grade 1 AKs of the face and scalp, no statistically significant difference in the complete response rate of grade 1 AKs at 3 months emerged between the side of the face treated with daylight PDT (87%) and the side treated with conventional PDT (91%). Most of the patients preferred the treatment with daylight PDT, reported the investigators, from the University of L’Aquila (Italy) and the University of Milan (J Eur Acad Dermatol Venereol. 2015 Oct;29[10]:1926-32).

Another advantage of daylight PDT is the ability to treat a larger surface area, he said, pointing out that it is possible to treat half of the face (200 cm2) in only one session. “The drawback is the cost, but, if you compare this with Picato [ingenol mebutate] and Aldara [imiquimod], you must calculate that they are approved for 25 cm2. Therefore, if you need to treat 200 cm2, you need eight packages,” added Dr. Calzavara-Pinton, who is also the president of the Italian Society of Dermatology.
“Daylight PDT with methyl aminolevulinate ... has proven to be efficacious in the treatment of mild to moderate actinic keratoses on the face and scalp,” agreed Rolf-Markus Szeimies, MD, PhD, head of the department of dermatology and allergology at Klinikum Vest, Recklinghausen, Germany.

He cited two randomized, controlled, split-face studies conducted in Australia and Europe, the COMET-1 and COMET-2 trials in patients with mild to moderate AKs of the face and scalp, which found that cure rates with daylight PDT “were not statistically inferior to conventional PDT with red light.” The biggest advantages “are the single-treatment setting, the possibility to treat large areas in one step, the excellent cosmesis, and the almost total lack of pain during the procedure,” he said in an interview.
While it is not approved by the Food and Drug Administration for use in the United States, daylight PDT is a registered treatment modality in Europe, Australia, and South America, said Dr. Szeimies, who presented an update on daylight PDT during a session on PDT at the 2017 annual meeting of the American Academy of Dermatology in Orlando.
U.S. dermatologists urge caution

The potential benefits of daylight PDT for patients mentioned in the published studies are less pain and fewer office visits, “so it’s more convenient,” said Dr. Spencer, a dermatologist and dermatologic surgeon in private practice in St. Petersburg, Fla. “I don’t think those benefits are strong [enough] to outweigh the potential risks.”
He added that most of the studies are from Norway and other Northern European countries where residents generally are exposed to less intense sun, so the generalizability of the findings could be an issue.
Nevertheless, Dr. Spencer predicted there will be more attention to daylight PDT in the United States soon. “This has certainly caught on in Europe. This is out there, and you’re definitely going to hear more about this.”
Some wavelengths of ultraviolet light are harmful to the skin, “and we don’t want to increase the sensitivity. If anything, you want to protect against it,” she noted. In her practice, when she treats patients with conventional PDT, using ALA (with the Levulan Kerastick) most often combined with blue light therapy, she said she cautions patients to avoid exposure to light for up to 24 hour post procedure.
“If you’re going to photosensitize someone, you need to control the amount of energy they are exposed to until that photosensitizer is deactivated, and sunlight is too broad and, in my view, causes more potential harm than good,” Dr. Day commented.
When administered in a controlled fashion, conventional PDT can improve patient outcomes and appearance, she said. “We use it for acne [and] for precancerous actinic keratoses, and, depending on what we do it with – different chromophores or different color light – you can have benefits for photorejuvenation as well.”

Patient adherence to instructions is paramount
“The idea of taking this and applying it to a much broader population, because acne is so common, is interesting but a little bit scary in the sense that it’s such a poorly controlled experiment,” said Samantha B. Conrad, MD, a dermatologist at Northwestern Medicine in Chicago. “Every day, the sun is different, people’s habits are different, and, if people have irritated skin, they’re going to take up a lot more of the ALA. If people have thicker, more oily skin, they may not take as much up. It also depends on the climate – it would be different in Chicago than it would be in LA.”

“I always have patients stay indoors with the blinds closed for 24 hours after [therapy]. I try to schedule the treatments in the wintertime here in New York when the daytime is shorter,” Dr. Day said. “We do the treatment in the afternoon, they leave when it’s dark or almost dark, and then they stay indoors the next day.”
Exposure to sunlight after ALA is applied to the skin “will just increase the specific D-dimers and specific [matrix metalloproteinases] uptake that breaks down collagen, accelerates the aging of the skin, and increases your risk of skin cancer,” she pointed out.
“We’ve all had patients who received their Levulan but then didn’t follow instructions and, the day after, got significant burns from something that would not normally precipitate a severe sunburn,” Dr. Conrad added.
She cited a study recently published from South Korea in which 46 patients with facial acne applied a much lower concentration of ALA, a new variant of 5-aminolevulinate ester (1.5% 3-butenyl ALA-bu gel), compared with the 20% concentration in the Levulan Kerastick available in the United States. (J Dermatol. 2016 May;43[5]:515-21). “With this very low concentration, it’s something of a different ball game,” she said.
“Patients applied that gel every other day and then just basically went about their business, getting daily, normal amounts of sun,” she said. After 12 weeks, the researchers reported a 58% reduction in inflammatory acne lesions and a 34% decrease in noninflammatory acne lesions among those who applied the ALA-bu gel to acne lesions every other day and used daylight as the only light source. “There was very little pain involved, and it was relatively easy to do,” Dr. Conrad said.
“You know people are always looking for the next big thing for acne. The idea is interesting but very rough.”
Dr. Spencer, Dr. Day, and Dr. Conrad had no relevant financial disclosures. Dr. Calzavara-Pinton is a consultant for Leo Pharma, Galderma, Almirall, and Meda AB. Dr. Szeimies is an adviser for Almirall, Biofrontera, Galderma, and Pierre Fabre Dermo Cosmetique, France and is a member of the speakers bureau for Almirall, Desitin, Galderma, Janssen, Pierre Fabre Dermo Cosmetique, France.
A new approach to photodynamic therapy (PDT) – where patients expose their skin to daylight after application of a photosensitizing agent – is gaining traction in Europe, and dermatologists in the United States could soon see more patients inquiring about daylight PDT.
While proponents of daylight PDT point to less pain and greater convenience for patients who have when acne or precancerous actinic keratosis (AK) lesions or are trying to improve the appearance of their skin, not everyone is convinced this approach is safe.
The European experience
Italy is among the European countries where daylight PDT has been evaluated in quality studies. In one Italian study, a split-face study of 35 patients with multiple grade 1 AKs of the face and scalp, no statistically significant difference in the complete response rate of grade 1 AKs at 3 months emerged between the side of the face treated with daylight PDT (87%) and the side treated with conventional PDT (91%). Most of the patients preferred the treatment with daylight PDT, reported the investigators, from the University of L’Aquila (Italy) and the University of Milan (J Eur Acad Dermatol Venereol. 2015 Oct;29[10]:1926-32).
Another advantage of daylight PDT is the ability to treat a larger surface area, he said, pointing out that it is possible to treat half of the face (200 cm2) in only one session. “The drawback is the cost, but, if you compare this with Picato [ingenol mebutate] and Aldara [imiquimod], you must calculate that they are approved for 25 cm2. Therefore, if you need to treat 200 cm2, you need eight packages,” added Dr. Calzavara-Pinton, who is also the president of the Italian Society of Dermatology.
“Daylight PDT with methyl aminolevulinate ... has proven to be efficacious in the treatment of mild to moderate actinic keratoses on the face and scalp,” agreed Rolf-Markus Szeimies, MD, PhD, head of the department of dermatology and allergology at Klinikum Vest, Recklinghausen, Germany.
He cited two randomized, controlled, split-face studies conducted in Australia and Europe, the COMET-1 and COMET-2 trials in patients with mild to moderate AKs of the face and scalp, which found that cure rates with daylight PDT “were not statistically inferior to conventional PDT with red light.” The biggest advantages “are the single-treatment setting, the possibility to treat large areas in one step, the excellent cosmesis, and the almost total lack of pain during the procedure,” he said in an interview.
While it is not approved by the Food and Drug Administration for use in the United States, daylight PDT is a registered treatment modality in Europe, Australia, and South America, said Dr. Szeimies, who presented an update on daylight PDT during a session on PDT at the 2017 annual meeting of the American Academy of Dermatology in Orlando.
U.S. dermatologists urge caution
The potential benefits of daylight PDT for patients mentioned in the published studies are less pain and fewer office visits, “so it’s more convenient,” said Dr. Spencer, a dermatologist and dermatologic surgeon in private practice in St. Petersburg, Fla. “I don’t think those benefits are strong [enough] to outweigh the potential risks.”
He added that most of the studies are from Norway and other Northern European countries where residents generally are exposed to less intense sun, so the generalizability of the findings could be an issue.
Nevertheless, Dr. Spencer predicted there will be more attention to daylight PDT in the United States soon. “This has certainly caught on in Europe. This is out there, and you’re definitely going to hear more about this.”
Some wavelengths of ultraviolet light are harmful to the skin, “and we don’t want to increase the sensitivity. If anything, you want to protect against it,” she noted. In her practice, when she treats patients with conventional PDT, using ALA (with the Levulan Kerastick) most often combined with blue light therapy, she said she cautions patients to avoid exposure to light for up to 24 hour post procedure.
“If you’re going to photosensitize someone, you need to control the amount of energy they are exposed to until that photosensitizer is deactivated, and sunlight is too broad and, in my view, causes more potential harm than good,” Dr. Day commented.
When administered in a controlled fashion, conventional PDT can improve patient outcomes and appearance, she said. “We use it for acne [and] for precancerous actinic keratoses, and, depending on what we do it with – different chromophores or different color light – you can have benefits for photorejuvenation as well.”
Patient adherence to instructions is paramount
“The idea of taking this and applying it to a much broader population, because acne is so common, is interesting but a little bit scary in the sense that it’s such a poorly controlled experiment,” said Samantha B. Conrad, MD, a dermatologist at Northwestern Medicine in Chicago. “Every day, the sun is different, people’s habits are different, and, if people have irritated skin, they’re going to take up a lot more of the ALA. If people have thicker, more oily skin, they may not take as much up. It also depends on the climate – it would be different in Chicago than it would be in LA.”
“I always have patients stay indoors with the blinds closed for 24 hours after [therapy]. I try to schedule the treatments in the wintertime here in New York when the daytime is shorter,” Dr. Day said. “We do the treatment in the afternoon, they leave when it’s dark or almost dark, and then they stay indoors the next day.”
Exposure to sunlight after ALA is applied to the skin “will just increase the specific D-dimers and specific [matrix metalloproteinases] uptake that breaks down collagen, accelerates the aging of the skin, and increases your risk of skin cancer,” she pointed out.
“We’ve all had patients who received their Levulan but then didn’t follow instructions and, the day after, got significant burns from something that would not normally precipitate a severe sunburn,” Dr. Conrad added.
She cited a study recently published from South Korea in which 46 patients with facial acne applied a much lower concentration of ALA, a new variant of 5-aminolevulinate ester (1.5% 3-butenyl ALA-bu gel), compared with the 20% concentration in the Levulan Kerastick available in the United States. (J Dermatol. 2016 May;43[5]:515-21). “With this very low concentration, it’s something of a different ball game,” she said.
“Patients applied that gel every other day and then just basically went about their business, getting daily, normal amounts of sun,” she said. After 12 weeks, the researchers reported a 58% reduction in inflammatory acne lesions and a 34% decrease in noninflammatory acne lesions among those who applied the ALA-bu gel to acne lesions every other day and used daylight as the only light source. “There was very little pain involved, and it was relatively easy to do,” Dr. Conrad said.
“You know people are always looking for the next big thing for acne. The idea is interesting but very rough.”
Dr. Spencer, Dr. Day, and Dr. Conrad had no relevant financial disclosures. Dr. Calzavara-Pinton is a consultant for Leo Pharma, Galderma, Almirall, and Meda AB. Dr. Szeimies is an adviser for Almirall, Biofrontera, Galderma, and Pierre Fabre Dermo Cosmetique, France and is a member of the speakers bureau for Almirall, Desitin, Galderma, Janssen, Pierre Fabre Dermo Cosmetique, France.
A new approach to photodynamic therapy (PDT) – where patients expose their skin to daylight after application of a photosensitizing agent – is gaining traction in Europe, and dermatologists in the United States could soon see more patients inquiring about daylight PDT.
While proponents of daylight PDT point to less pain and greater convenience for patients who have when acne or precancerous actinic keratosis (AK) lesions or are trying to improve the appearance of their skin, not everyone is convinced this approach is safe.
The European experience
Italy is among the European countries where daylight PDT has been evaluated in quality studies. In one Italian study, a split-face study of 35 patients with multiple grade 1 AKs of the face and scalp, no statistically significant difference in the complete response rate of grade 1 AKs at 3 months emerged between the side of the face treated with daylight PDT (87%) and the side treated with conventional PDT (91%). Most of the patients preferred the treatment with daylight PDT, reported the investigators, from the University of L’Aquila (Italy) and the University of Milan (J Eur Acad Dermatol Venereol. 2015 Oct;29[10]:1926-32).
Another advantage of daylight PDT is the ability to treat a larger surface area, he said, pointing out that it is possible to treat half of the face (200 cm2) in only one session. “The drawback is the cost, but, if you compare this with Picato [ingenol mebutate] and Aldara [imiquimod], you must calculate that they are approved for 25 cm2. Therefore, if you need to treat 200 cm2, you need eight packages,” added Dr. Calzavara-Pinton, who is also the president of the Italian Society of Dermatology.
“Daylight PDT with methyl aminolevulinate ... has proven to be efficacious in the treatment of mild to moderate actinic keratoses on the face and scalp,” agreed Rolf-Markus Szeimies, MD, PhD, head of the department of dermatology and allergology at Klinikum Vest, Recklinghausen, Germany.
He cited two randomized, controlled, split-face studies conducted in Australia and Europe, the COMET-1 and COMET-2 trials in patients with mild to moderate AKs of the face and scalp, which found that cure rates with daylight PDT “were not statistically inferior to conventional PDT with red light.” The biggest advantages “are the single-treatment setting, the possibility to treat large areas in one step, the excellent cosmesis, and the almost total lack of pain during the procedure,” he said in an interview.
While it is not approved by the Food and Drug Administration for use in the United States, daylight PDT is a registered treatment modality in Europe, Australia, and South America, said Dr. Szeimies, who presented an update on daylight PDT during a session on PDT at the 2017 annual meeting of the American Academy of Dermatology in Orlando.
U.S. dermatologists urge caution
The potential benefits of daylight PDT for patients mentioned in the published studies are less pain and fewer office visits, “so it’s more convenient,” said Dr. Spencer, a dermatologist and dermatologic surgeon in private practice in St. Petersburg, Fla. “I don’t think those benefits are strong [enough] to outweigh the potential risks.”
He added that most of the studies are from Norway and other Northern European countries where residents generally are exposed to less intense sun, so the generalizability of the findings could be an issue.
Nevertheless, Dr. Spencer predicted there will be more attention to daylight PDT in the United States soon. “This has certainly caught on in Europe. This is out there, and you’re definitely going to hear more about this.”
Some wavelengths of ultraviolet light are harmful to the skin, “and we don’t want to increase the sensitivity. If anything, you want to protect against it,” she noted. In her practice, when she treats patients with conventional PDT, using ALA (with the Levulan Kerastick) most often combined with blue light therapy, she said she cautions patients to avoid exposure to light for up to 24 hour post procedure.
“If you’re going to photosensitize someone, you need to control the amount of energy they are exposed to until that photosensitizer is deactivated, and sunlight is too broad and, in my view, causes more potential harm than good,” Dr. Day commented.
When administered in a controlled fashion, conventional PDT can improve patient outcomes and appearance, she said. “We use it for acne [and] for precancerous actinic keratoses, and, depending on what we do it with – different chromophores or different color light – you can have benefits for photorejuvenation as well.”
Patient adherence to instructions is paramount
“The idea of taking this and applying it to a much broader population, because acne is so common, is interesting but a little bit scary in the sense that it’s such a poorly controlled experiment,” said Samantha B. Conrad, MD, a dermatologist at Northwestern Medicine in Chicago. “Every day, the sun is different, people’s habits are different, and, if people have irritated skin, they’re going to take up a lot more of the ALA. If people have thicker, more oily skin, they may not take as much up. It also depends on the climate – it would be different in Chicago than it would be in LA.”
“I always have patients stay indoors with the blinds closed for 24 hours after [therapy]. I try to schedule the treatments in the wintertime here in New York when the daytime is shorter,” Dr. Day said. “We do the treatment in the afternoon, they leave when it’s dark or almost dark, and then they stay indoors the next day.”
Exposure to sunlight after ALA is applied to the skin “will just increase the specific D-dimers and specific [matrix metalloproteinases] uptake that breaks down collagen, accelerates the aging of the skin, and increases your risk of skin cancer,” she pointed out.
“We’ve all had patients who received their Levulan but then didn’t follow instructions and, the day after, got significant burns from something that would not normally precipitate a severe sunburn,” Dr. Conrad added.
She cited a study recently published from South Korea in which 46 patients with facial acne applied a much lower concentration of ALA, a new variant of 5-aminolevulinate ester (1.5% 3-butenyl ALA-bu gel), compared with the 20% concentration in the Levulan Kerastick available in the United States. (J Dermatol. 2016 May;43[5]:515-21). “With this very low concentration, it’s something of a different ball game,” she said.
“Patients applied that gel every other day and then just basically went about their business, getting daily, normal amounts of sun,” she said. After 12 weeks, the researchers reported a 58% reduction in inflammatory acne lesions and a 34% decrease in noninflammatory acne lesions among those who applied the ALA-bu gel to acne lesions every other day and used daylight as the only light source. “There was very little pain involved, and it was relatively easy to do,” Dr. Conrad said.
“You know people are always looking for the next big thing for acne. The idea is interesting but very rough.”
Dr. Spencer, Dr. Day, and Dr. Conrad had no relevant financial disclosures. Dr. Calzavara-Pinton is a consultant for Leo Pharma, Galderma, Almirall, and Meda AB. Dr. Szeimies is an adviser for Almirall, Biofrontera, Galderma, and Pierre Fabre Dermo Cosmetique, France and is a member of the speakers bureau for Almirall, Desitin, Galderma, Janssen, Pierre Fabre Dermo Cosmetique, France.
Perfluorodecalin-spiked patch improves tattoo removal results
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.

“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.
“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.
“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Key clinical point: Addition of a perfluorodecalin-infused patch to a laser treatment protocol allowed significantly more laser passes with no difference in adverse events.
Major finding: More laser treatment passes for tattoo removal were possible when the laser was combined with a perfluorodecalin patch vs. laser alone (an average of 3.7 vs. 1.4 passes in a 5-minute session, a significant difference).
Data source: A prospective, randomized study of 30 adults seeking removal of tattoos.
Disclosures: Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Update on the False Claims Act
Question: Which of the following is correct?
A. The False Claims Act dates back to the Civil War era.
B. The FCA covers only patently false statements.
C. Material misrepresentation is insufficient.
D. Negligence constitutes a violation.
E. A qui tam lawsuit under FCA refers to a third party who has suffered personal harm.
Answer: A. The False Claims Act (FCA) is an old law, enacted by Congress in 1863 to impose liability for submitting a payment demand to the federal government when there is actual or constructive knowledge that the claim is false.1 Many states now have their own versions of FCA.
Intent to defraud is not a required element, but knowing or reckless disregard of the truth or material misrepresentation are – whereas negligence is insufficient to constitute a violation.

In the health care field, FCA most commonly involves false claims made to Medicare or Medicaid. Pitfalls include billing for noncovered services such as experimental treatments, double billing, unnecessary services, billing the government as the primary payer when inappropriate, or regularly waiving deductibles and copayments.
Other activities that constitute wrongdoing in this context include knowingly using another patient’s name for purposes of federal drug coverage, billing for no-shows, and misrepresenting the diagnosis to justify services.
The electronic medical record enables easy check-offs as documentation of actual work done, and fraud is implicated if the information is deliberately misleading, as in the example of upcoding.
Importantly, physicians are liable for the actions of their office staff, so it is prudent to oversee and supervise all billing activities. Aggrieved or disgruntled employees or contractors, popularly known as whistle-blowers, can file a qui tam action. They stand to collect a substantial bounty, up to 30% of the proceeds. They do not have to show legal standing and need not sustain any personal injury.
FCA prosecutions are daily affairs, with egregious examples regularly making the news headlines. A few random pickings might give you an idea of the problem:
In 2015, in its largest case of health care fraud, the federal Department of Justice filed criminal charges against 243 individuals across the nation. Some of the violations included billings for intensive psychotherapy sessions for noncommunicative dementia patients, simply moving patients to different locations, and fraudulent prescriptions under Medicare Part D.
In 2016, a pain management clinic used “ill-equipped, desperate doctors in dire need of work” to write faked prescriptions for narcotics. The clinic owner, a doctor, was sentenced to 144 months in prison for running what was described as a “pill-mill zoo.”
Arguably, the most dramatic physician case occurred in 2017 and involved a Florida dermatologist who settled with the government for $18 million for treating patients for skin cancer they did not have. The action came from a qui tam lawsuit filed by another dermatologist.
A major development in the false claims law came with last year’s U.S. Supreme Court decision in Universal Health Services v. Escobar.2
This landmark case dealt with claims made by Arbour Counseling Services to the Massachusetts’ Medicaid program for mental health counseling and prescriptions, a satellite mental health facility of Universal Health Services. It turned out that relatively few Arbour employees were actually licensed to provide mental health counseling or authorized to prescribe medications. A death resulted from a reaction to an unlicensed prescription.
In a unanimous decision, the Supreme Court held that there can be FCA liability when a defendant submitting a claim makes specific representations about the goods or services provided but fails to disclose noncompliance with material statutory, regulatory, or contractual requirements. Technically referred to as “implied false certification,” such material omissions may amount to a misrepresentation and may be deemed fraudulent, even if the requirements were not expressly designated as conditions of payment.
In the words of the court, “Today’s decision holds that the claims at issue may be actionable because they do more than merely demand payment; they fall squarely within the rule that representations that state the truth only so far as it goes, while omitting critical qualifying information, can be actionable misrepresentations.”
The implied false certification, or implied fraud, ruling has widespread implications, as it does not require a patently false statement. A material misrepresentation or omission may suffice.
There is concern that this ruling will open the floodgates of FCA prosecution. However, the federal Ninth Circuit Court of Appeals has recently quashed an attempt to invoke the implied certification claim in an FCA suit against DJO Global and Biomet, brought by a medical device salesman and his private investigator. Their rejected whistle-blower suit alleged that the defendants were providing their spinal bone growth stimulation devices for use on the cervical spine, even though Food and Drug Administration approval was for use only on the lumbar spine.
Another concern is, can an alleged wrong prognosis regarding life expectancy amount to a false claim?
Under Medicare rules, a physician certifying that a patient is eligible for hospice care must attest that the condition is terminal, with death expected within 6 months.
AseraCare, a hospice company, was accused of knowingly submitting false claims to Medicare by certifying patients as eligible for hospice who did not have a life expectancy of 6 months or less. The government claimed that the medical records of the 123 patients at issue did not contain clinical information and other documentation that supported the medical prognosis. Thus, AseraCare’s claims for those patients were false.
The case brought out the conflicting views of physicians: Did the medical records supported AseraCare’s certifications that the patients were eligible? The defendants argued that, when hospice-certifying physicians and government medical experts look at the very same medical records and disagree about eligibility, the opinion of one medical expert alone cannot prove falsity without further evidence of an objective falsehood.
AseraCare won a summary judgment defending against the $200 million lawsuit in the U.S. District Court for the Northern District of Alabama.3 In a memorandum opinion, the court began with Blaise Pascal’s axiom that “Contradiction is not a sign of falsity, nor the lack of contradiction the sign of truth.” Federal prosecutors have appealed to the federal 11th Circuit Court of Appeals, which recently heard oral arguments. Its decision is pending.
In support of the hospice center physicians, the American Medical Association and other organizations have filed an amicus brief asserting that a physician’s opinion may be deemed false only if no reasonable physician could hold that opinion.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from earlier columns in Internal Medicine News. For additional information, readers may contact the author at [email protected].
References
1. 31 U.S. Code, Section 3729(a)(1)(A).
2. Universal Health Services v. United States ex rel. Escobar, 579 U.S. ____ (2016).
3. U.S. ex rel. Paradies et al. v. AseraCare Inc. et al., Case number 2:12-CV-245-KOB, in the U.S. District Court for the Northern District of Alabama.
Question: Which of the following is correct?
A. The False Claims Act dates back to the Civil War era.
B. The FCA covers only patently false statements.
C. Material misrepresentation is insufficient.
D. Negligence constitutes a violation.
E. A qui tam lawsuit under FCA refers to a third party who has suffered personal harm.
Answer: A. The False Claims Act (FCA) is an old law, enacted by Congress in 1863 to impose liability for submitting a payment demand to the federal government when there is actual or constructive knowledge that the claim is false.1 Many states now have their own versions of FCA.
Intent to defraud is not a required element, but knowing or reckless disregard of the truth or material misrepresentation are – whereas negligence is insufficient to constitute a violation.
In the health care field, FCA most commonly involves false claims made to Medicare or Medicaid. Pitfalls include billing for noncovered services such as experimental treatments, double billing, unnecessary services, billing the government as the primary payer when inappropriate, or regularly waiving deductibles and copayments.
Other activities that constitute wrongdoing in this context include knowingly using another patient’s name for purposes of federal drug coverage, billing for no-shows, and misrepresenting the diagnosis to justify services.
The electronic medical record enables easy check-offs as documentation of actual work done, and fraud is implicated if the information is deliberately misleading, as in the example of upcoding.
Importantly, physicians are liable for the actions of their office staff, so it is prudent to oversee and supervise all billing activities. Aggrieved or disgruntled employees or contractors, popularly known as whistle-blowers, can file a qui tam action. They stand to collect a substantial bounty, up to 30% of the proceeds. They do not have to show legal standing and need not sustain any personal injury.
FCA prosecutions are daily affairs, with egregious examples regularly making the news headlines. A few random pickings might give you an idea of the problem:
In 2015, in its largest case of health care fraud, the federal Department of Justice filed criminal charges against 243 individuals across the nation. Some of the violations included billings for intensive psychotherapy sessions for noncommunicative dementia patients, simply moving patients to different locations, and fraudulent prescriptions under Medicare Part D.
In 2016, a pain management clinic used “ill-equipped, desperate doctors in dire need of work” to write faked prescriptions for narcotics. The clinic owner, a doctor, was sentenced to 144 months in prison for running what was described as a “pill-mill zoo.”
Arguably, the most dramatic physician case occurred in 2017 and involved a Florida dermatologist who settled with the government for $18 million for treating patients for skin cancer they did not have. The action came from a qui tam lawsuit filed by another dermatologist.
A major development in the false claims law came with last year’s U.S. Supreme Court decision in Universal Health Services v. Escobar.2
This landmark case dealt with claims made by Arbour Counseling Services to the Massachusetts’ Medicaid program for mental health counseling and prescriptions, a satellite mental health facility of Universal Health Services. It turned out that relatively few Arbour employees were actually licensed to provide mental health counseling or authorized to prescribe medications. A death resulted from a reaction to an unlicensed prescription.
In a unanimous decision, the Supreme Court held that there can be FCA liability when a defendant submitting a claim makes specific representations about the goods or services provided but fails to disclose noncompliance with material statutory, regulatory, or contractual requirements. Technically referred to as “implied false certification,” such material omissions may amount to a misrepresentation and may be deemed fraudulent, even if the requirements were not expressly designated as conditions of payment.
In the words of the court, “Today’s decision holds that the claims at issue may be actionable because they do more than merely demand payment; they fall squarely within the rule that representations that state the truth only so far as it goes, while omitting critical qualifying information, can be actionable misrepresentations.”
The implied false certification, or implied fraud, ruling has widespread implications, as it does not require a patently false statement. A material misrepresentation or omission may suffice.
There is concern that this ruling will open the floodgates of FCA prosecution. However, the federal Ninth Circuit Court of Appeals has recently quashed an attempt to invoke the implied certification claim in an FCA suit against DJO Global and Biomet, brought by a medical device salesman and his private investigator. Their rejected whistle-blower suit alleged that the defendants were providing their spinal bone growth stimulation devices for use on the cervical spine, even though Food and Drug Administration approval was for use only on the lumbar spine.
Another concern is, can an alleged wrong prognosis regarding life expectancy amount to a false claim?
Under Medicare rules, a physician certifying that a patient is eligible for hospice care must attest that the condition is terminal, with death expected within 6 months.
AseraCare, a hospice company, was accused of knowingly submitting false claims to Medicare by certifying patients as eligible for hospice who did not have a life expectancy of 6 months or less. The government claimed that the medical records of the 123 patients at issue did not contain clinical information and other documentation that supported the medical prognosis. Thus, AseraCare’s claims for those patients were false.
The case brought out the conflicting views of physicians: Did the medical records supported AseraCare’s certifications that the patients were eligible? The defendants argued that, when hospice-certifying physicians and government medical experts look at the very same medical records and disagree about eligibility, the opinion of one medical expert alone cannot prove falsity without further evidence of an objective falsehood.
AseraCare won a summary judgment defending against the $200 million lawsuit in the U.S. District Court for the Northern District of Alabama.3 In a memorandum opinion, the court began with Blaise Pascal’s axiom that “Contradiction is not a sign of falsity, nor the lack of contradiction the sign of truth.” Federal prosecutors have appealed to the federal 11th Circuit Court of Appeals, which recently heard oral arguments. Its decision is pending.
In support of the hospice center physicians, the American Medical Association and other organizations have filed an amicus brief asserting that a physician’s opinion may be deemed false only if no reasonable physician could hold that opinion.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from earlier columns in Internal Medicine News. For additional information, readers may contact the author at [email protected].
References
1. 31 U.S. Code, Section 3729(a)(1)(A).
2. Universal Health Services v. United States ex rel. Escobar, 579 U.S. ____ (2016).
3. U.S. ex rel. Paradies et al. v. AseraCare Inc. et al., Case number 2:12-CV-245-KOB, in the U.S. District Court for the Northern District of Alabama.
Question: Which of the following is correct?
A. The False Claims Act dates back to the Civil War era.
B. The FCA covers only patently false statements.
C. Material misrepresentation is insufficient.
D. Negligence constitutes a violation.
E. A qui tam lawsuit under FCA refers to a third party who has suffered personal harm.
Answer: A. The False Claims Act (FCA) is an old law, enacted by Congress in 1863 to impose liability for submitting a payment demand to the federal government when there is actual or constructive knowledge that the claim is false.1 Many states now have their own versions of FCA.
Intent to defraud is not a required element, but knowing or reckless disregard of the truth or material misrepresentation are – whereas negligence is insufficient to constitute a violation.
In the health care field, FCA most commonly involves false claims made to Medicare or Medicaid. Pitfalls include billing for noncovered services such as experimental treatments, double billing, unnecessary services, billing the government as the primary payer when inappropriate, or regularly waiving deductibles and copayments.
Other activities that constitute wrongdoing in this context include knowingly using another patient’s name for purposes of federal drug coverage, billing for no-shows, and misrepresenting the diagnosis to justify services.
The electronic medical record enables easy check-offs as documentation of actual work done, and fraud is implicated if the information is deliberately misleading, as in the example of upcoding.
Importantly, physicians are liable for the actions of their office staff, so it is prudent to oversee and supervise all billing activities. Aggrieved or disgruntled employees or contractors, popularly known as whistle-blowers, can file a qui tam action. They stand to collect a substantial bounty, up to 30% of the proceeds. They do not have to show legal standing and need not sustain any personal injury.
FCA prosecutions are daily affairs, with egregious examples regularly making the news headlines. A few random pickings might give you an idea of the problem:
In 2015, in its largest case of health care fraud, the federal Department of Justice filed criminal charges against 243 individuals across the nation. Some of the violations included billings for intensive psychotherapy sessions for noncommunicative dementia patients, simply moving patients to different locations, and fraudulent prescriptions under Medicare Part D.
In 2016, a pain management clinic used “ill-equipped, desperate doctors in dire need of work” to write faked prescriptions for narcotics. The clinic owner, a doctor, was sentenced to 144 months in prison for running what was described as a “pill-mill zoo.”
Arguably, the most dramatic physician case occurred in 2017 and involved a Florida dermatologist who settled with the government for $18 million for treating patients for skin cancer they did not have. The action came from a qui tam lawsuit filed by another dermatologist.
A major development in the false claims law came with last year’s U.S. Supreme Court decision in Universal Health Services v. Escobar.2
This landmark case dealt with claims made by Arbour Counseling Services to the Massachusetts’ Medicaid program for mental health counseling and prescriptions, a satellite mental health facility of Universal Health Services. It turned out that relatively few Arbour employees were actually licensed to provide mental health counseling or authorized to prescribe medications. A death resulted from a reaction to an unlicensed prescription.
In a unanimous decision, the Supreme Court held that there can be FCA liability when a defendant submitting a claim makes specific representations about the goods or services provided but fails to disclose noncompliance with material statutory, regulatory, or contractual requirements. Technically referred to as “implied false certification,” such material omissions may amount to a misrepresentation and may be deemed fraudulent, even if the requirements were not expressly designated as conditions of payment.
In the words of the court, “Today’s decision holds that the claims at issue may be actionable because they do more than merely demand payment; they fall squarely within the rule that representations that state the truth only so far as it goes, while omitting critical qualifying information, can be actionable misrepresentations.”
The implied false certification, or implied fraud, ruling has widespread implications, as it does not require a patently false statement. A material misrepresentation or omission may suffice.
There is concern that this ruling will open the floodgates of FCA prosecution. However, the federal Ninth Circuit Court of Appeals has recently quashed an attempt to invoke the implied certification claim in an FCA suit against DJO Global and Biomet, brought by a medical device salesman and his private investigator. Their rejected whistle-blower suit alleged that the defendants were providing their spinal bone growth stimulation devices for use on the cervical spine, even though Food and Drug Administration approval was for use only on the lumbar spine.
Another concern is, can an alleged wrong prognosis regarding life expectancy amount to a false claim?
Under Medicare rules, a physician certifying that a patient is eligible for hospice care must attest that the condition is terminal, with death expected within 6 months.
AseraCare, a hospice company, was accused of knowingly submitting false claims to Medicare by certifying patients as eligible for hospice who did not have a life expectancy of 6 months or less. The government claimed that the medical records of the 123 patients at issue did not contain clinical information and other documentation that supported the medical prognosis. Thus, AseraCare’s claims for those patients were false.
The case brought out the conflicting views of physicians: Did the medical records supported AseraCare’s certifications that the patients were eligible? The defendants argued that, when hospice-certifying physicians and government medical experts look at the very same medical records and disagree about eligibility, the opinion of one medical expert alone cannot prove falsity without further evidence of an objective falsehood.
AseraCare won a summary judgment defending against the $200 million lawsuit in the U.S. District Court for the Northern District of Alabama.3 In a memorandum opinion, the court began with Blaise Pascal’s axiom that “Contradiction is not a sign of falsity, nor the lack of contradiction the sign of truth.” Federal prosecutors have appealed to the federal 11th Circuit Court of Appeals, which recently heard oral arguments. Its decision is pending.
In support of the hospice center physicians, the American Medical Association and other organizations have filed an amicus brief asserting that a physician’s opinion may be deemed false only if no reasonable physician could hold that opinion.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the materials have been taken from earlier columns in Internal Medicine News. For additional information, readers may contact the author at [email protected].
References
1. 31 U.S. Code, Section 3729(a)(1)(A).
2. Universal Health Services v. United States ex rel. Escobar, 579 U.S. ____ (2016).
3. U.S. ex rel. Paradies et al. v. AseraCare Inc. et al., Case number 2:12-CV-245-KOB, in the U.S. District Court for the Northern District of Alabama.
Oral Contraceptives for Acne Treatment: Prescribing Practices of US Dermatologists


Confirmatory blood typing unnecessary for closed prolapse repairs
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.

That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
A lot of people automatically order type and screen for vaginal prolapse repairs, but we really need to rethink that if there aren’t risk factors that warrant it. I defer to the anesthesiologists because they are the ones who usually want this, but most of the time we screen but don’t use the results. There’s room to improve clinical practice here.
Robert Gutman, MD, is a gynecologic surgeon in Washington, D.C., and the program chair for the 2017 Society of Gynecologic Surgeons annual scientific meeting. He wasn’t involved in the studies presented.
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.
That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
SAN ANTONIO – It was safe to skip preoperative blood type and antibody screening before vaginal and robotic apical prolapse surgeries at the University of North Carolina, Chapel Hill, so long as the women didn’t have hemorrhage risk factors.
The rate of blood transfusions was 0.5% for both the 204 women who had vaginal repairs and the 203 women who underwent robotic repairs; the rate of positive antibody tests was 1.6%. Given the 0.4% risk of transfusion reactions in unscreened women, the investigators calculated that the risk of serious transfusion reactions was 1 in 50,000 with closed vaginal prolapse repairs.
“The bottom line for us is that the risk in this situation is very low, even if preop type and screens are not performed, and women hemorrhage. This information provides insight to answer our key clinical question, which was if we should continue to order preop type and screens,” lead investigator Taylor Brueseke, MD, an ob.gyn. fellow at the University of North Carolina, Chapel Hill, said at the annual scientific meeting of the Society of Gynecologic Surgeons.
That question has been on the minds of gynecologic surgeons, and it’s probably never been parsed out before by route of surgery. The American College of Pathologists recommends two blood type and antibody screens from separate venipunctures before surgery. Often, the second, confirmatory test means that women have to come in even earlier on the morning of surgery and deal with another painful blood draw. It also adds a few hundred dollars to the bill.
Every surgeon needs to draw their own line between risks and benefits, Dr. Brueseke said, but it seems reasonable in many cases to skip the second screening for closed repairs. Even if a woman has a transfusion reaction, “it doesn’t mean that the patient is going to die. It’s something that you can deal with,” he said.
However, the team reached a different conclusion for women who undergo open abdominal repairs. Among the 201 cases they reviewed, 10.5% had a transfusion, which translated to a transfusion reaction risk of 1 in 2,645 for unscreened women undergoing open apical prolapse surgery. The higher hemorrhage rate was probably due to concomitant Burch procedures and other open incontinence operations.
For abdominal cases, and for women who have had prior transfusions, surgeries, or anticoagulation, “consider type and screen,” Dr. Brueseke said at the meeting.
In a separate study presented at the conference, more than 50,000 pelvic floor disorder surgeries in the National Surgery Quality Improvement Program database further defined the hemorrhage risk.
Investigators at Ohio State University, Columbus, found that the overall incidence of blood transfusions was low at 1.26%, but open abdominal procedures again increased the risk. Other factors associated with an increased risk of blood transfusion included preoperative hematocrit less than 30%, an American Society of Anesthesiologists physical status score of 3 or higher, concomitant hysterectomy, body mass index below 18.5 kg/m2, age less than 30 and over 65 years, and a history of bleeding disorders.
In the UNC study, the median Pelvic Organ Prolapse Quantification was stage III. Patients with bleeding disorders, anticoagulant use, or combined surgery with other services were excluded.
There was no industry funding for the two studies, and the investigators reported having no relevant financial disclosures.
* The meeting sponsor information was updated 6/9/2017.
Key clinical point:
Major finding: Given the 0.4% risk of transfusion reactions in unscreened women, the risk of serious transfusion reactions was 1 in 50,000 women with closed apical prolapse repairs.
Data source: A review of more than 600 cases of apical prolapse surgery at a single center.
Disclosures: There was no industry funding, and the investigators reported having no relevant financial disclosures.
Neoadjuvant chemotherapy induces mutational, molecular shifts in ovarian cancers
NATIONAL HARBOR, MD. – Treatment of high-grade serous ovarian carcinomas with platinum-based neoadjuvant chemotherapy led to significant changes in the expression of genes encoding “canonical” cell cycle and DNA damage pathways, said Rebecca C. Arend, MD.
Analyses of cell-free (plasma) DNA also revealed mutations that matched those in tumor specimens obtained before and after platinum-based neoadjuvant chemotherapy, Dr. Arend reported at the annual meeting of the Society of Gynecologic Oncology. “Understanding the effect of chemotherapy on gene expression profiles may help guide therapy, and plasma cfDNA could provide a noninvasive approach for monitoring tumor mutations,” said Dr. Arend of the University of Alabama at Birmingham.
High-grade serous ovarian carcinoma is genetically heterogeneous, and chemotherapy further alters gene expression profiles and causes molecular derangement, Dr. Arend noted. “Neoadjuvant chemotherapy provides a unique opportunity to evaluate biospecimens before and afterward,” she added.
Both gene expression and mutational profiles have been used to characterize HGSC, but researchers lack solid methods to evaluate tumor heterogeneity and clonal evolution. To begin filling this gap, Dr. Arend and her associates analyzed plasma and tumor specimens from 19 patients with stage 3 or 4 high-grade serous ovarian carcinoma before and after they underwent three to six cycles of neoadjuvant chemotherapy. Biopsies yielded the baseline tumor specimens, and follow-up specimens were obtained during interval debulking.
The investigators used the NanoString PanCancer 770 gene pathway panel, the Ingenuity Pathway Analysis tool, and nSolver Analysis software to assess changes in gene expression. To quantify mutations, they performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens with a 50-gene Ion Torrent panel.
After neoadjuvant chemotherapy, the most up-regulated genes included NR4A1 and NR4A3, which regulate cellular proliferation, differentiation, and apoptosis, and SFRP2, which promotes resistance to chemotherapy by modulating Wnt signaling, Dr. Arend said. The most down-regulated genes included E2F1, which helps mediate the cell cycle and the activity of tumor suppressor genes, and BRCA2, the tumor suppressor gene that encodes a DNA repair protein.
Pathway analysis confirmed that the cell cycle pathway was most up-regulated after neoadjuvant chemotherapy, and that the DNA damage repair pathway was the most downregulated, Dr. Arend reported. Within the DNA damage repair pathway, no gene was significantly up-regulated, while RAD51C, BRCA1, BRCA2, and the FA core complex genes were down-regulated.
Next-generation sequencing of baseline plasma cfDNA identified 57 mutations, of which 6 persisted after neoadjuvant chemotherapy. In contrast, of 38 mutations in tumor at baseline, 33 persisted after chemotherapy.
Only 15 of the 38 mutations in tumor also appeared in cfDNA before treatment. At the time of interval debulking, tumor specimens yielded 36 mutations, of which 11 were detected in cfDNA.
At baseline and after treatment, all patients had TP53 mutations either tumor alone, or in both tumor and plasma. Among four patients whose cancer recurred, three had mutations in cfDNA that were previously detected in tumor. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Overall, the study suggests that gene expression profiling of ovarian HGSC tumor tissue taken at interval debulking could someday help guide treatment decisions after neoadjuvant chemotherapy, Dr. Arend said. “To be able to use cfDNA as liquid biopsy, more studies like this one, which match tumor and cfDNA from multiple time points, are needed,” she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Treatment of high-grade serous ovarian carcinomas with platinum-based neoadjuvant chemotherapy led to significant changes in the expression of genes encoding “canonical” cell cycle and DNA damage pathways, said Rebecca C. Arend, MD.
Analyses of cell-free (plasma) DNA also revealed mutations that matched those in tumor specimens obtained before and after platinum-based neoadjuvant chemotherapy, Dr. Arend reported at the annual meeting of the Society of Gynecologic Oncology. “Understanding the effect of chemotherapy on gene expression profiles may help guide therapy, and plasma cfDNA could provide a noninvasive approach for monitoring tumor mutations,” said Dr. Arend of the University of Alabama at Birmingham.
High-grade serous ovarian carcinoma is genetically heterogeneous, and chemotherapy further alters gene expression profiles and causes molecular derangement, Dr. Arend noted. “Neoadjuvant chemotherapy provides a unique opportunity to evaluate biospecimens before and afterward,” she added.
Both gene expression and mutational profiles have been used to characterize HGSC, but researchers lack solid methods to evaluate tumor heterogeneity and clonal evolution. To begin filling this gap, Dr. Arend and her associates analyzed plasma and tumor specimens from 19 patients with stage 3 or 4 high-grade serous ovarian carcinoma before and after they underwent three to six cycles of neoadjuvant chemotherapy. Biopsies yielded the baseline tumor specimens, and follow-up specimens were obtained during interval debulking.
The investigators used the NanoString PanCancer 770 gene pathway panel, the Ingenuity Pathway Analysis tool, and nSolver Analysis software to assess changes in gene expression. To quantify mutations, they performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens with a 50-gene Ion Torrent panel.
After neoadjuvant chemotherapy, the most up-regulated genes included NR4A1 and NR4A3, which regulate cellular proliferation, differentiation, and apoptosis, and SFRP2, which promotes resistance to chemotherapy by modulating Wnt signaling, Dr. Arend said. The most down-regulated genes included E2F1, which helps mediate the cell cycle and the activity of tumor suppressor genes, and BRCA2, the tumor suppressor gene that encodes a DNA repair protein.
Pathway analysis confirmed that the cell cycle pathway was most up-regulated after neoadjuvant chemotherapy, and that the DNA damage repair pathway was the most downregulated, Dr. Arend reported. Within the DNA damage repair pathway, no gene was significantly up-regulated, while RAD51C, BRCA1, BRCA2, and the FA core complex genes were down-regulated.
Next-generation sequencing of baseline plasma cfDNA identified 57 mutations, of which 6 persisted after neoadjuvant chemotherapy. In contrast, of 38 mutations in tumor at baseline, 33 persisted after chemotherapy.
Only 15 of the 38 mutations in tumor also appeared in cfDNA before treatment. At the time of interval debulking, tumor specimens yielded 36 mutations, of which 11 were detected in cfDNA.
At baseline and after treatment, all patients had TP53 mutations either tumor alone, or in both tumor and plasma. Among four patients whose cancer recurred, three had mutations in cfDNA that were previously detected in tumor. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Overall, the study suggests that gene expression profiling of ovarian HGSC tumor tissue taken at interval debulking could someday help guide treatment decisions after neoadjuvant chemotherapy, Dr. Arend said. “To be able to use cfDNA as liquid biopsy, more studies like this one, which match tumor and cfDNA from multiple time points, are needed,” she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Treatment of high-grade serous ovarian carcinomas with platinum-based neoadjuvant chemotherapy led to significant changes in the expression of genes encoding “canonical” cell cycle and DNA damage pathways, said Rebecca C. Arend, MD.
Analyses of cell-free (plasma) DNA also revealed mutations that matched those in tumor specimens obtained before and after platinum-based neoadjuvant chemotherapy, Dr. Arend reported at the annual meeting of the Society of Gynecologic Oncology. “Understanding the effect of chemotherapy on gene expression profiles may help guide therapy, and plasma cfDNA could provide a noninvasive approach for monitoring tumor mutations,” said Dr. Arend of the University of Alabama at Birmingham.
High-grade serous ovarian carcinoma is genetically heterogeneous, and chemotherapy further alters gene expression profiles and causes molecular derangement, Dr. Arend noted. “Neoadjuvant chemotherapy provides a unique opportunity to evaluate biospecimens before and afterward,” she added.
Both gene expression and mutational profiles have been used to characterize HGSC, but researchers lack solid methods to evaluate tumor heterogeneity and clonal evolution. To begin filling this gap, Dr. Arend and her associates analyzed plasma and tumor specimens from 19 patients with stage 3 or 4 high-grade serous ovarian carcinoma before and after they underwent three to six cycles of neoadjuvant chemotherapy. Biopsies yielded the baseline tumor specimens, and follow-up specimens were obtained during interval debulking.
The investigators used the NanoString PanCancer 770 gene pathway panel, the Ingenuity Pathway Analysis tool, and nSolver Analysis software to assess changes in gene expression. To quantify mutations, they performed longitudinal next-generation sequencing of 50 genes in tumor and plasma specimens with a 50-gene Ion Torrent panel.
After neoadjuvant chemotherapy, the most up-regulated genes included NR4A1 and NR4A3, which regulate cellular proliferation, differentiation, and apoptosis, and SFRP2, which promotes resistance to chemotherapy by modulating Wnt signaling, Dr. Arend said. The most down-regulated genes included E2F1, which helps mediate the cell cycle and the activity of tumor suppressor genes, and BRCA2, the tumor suppressor gene that encodes a DNA repair protein.
Pathway analysis confirmed that the cell cycle pathway was most up-regulated after neoadjuvant chemotherapy, and that the DNA damage repair pathway was the most downregulated, Dr. Arend reported. Within the DNA damage repair pathway, no gene was significantly up-regulated, while RAD51C, BRCA1, BRCA2, and the FA core complex genes were down-regulated.
Next-generation sequencing of baseline plasma cfDNA identified 57 mutations, of which 6 persisted after neoadjuvant chemotherapy. In contrast, of 38 mutations in tumor at baseline, 33 persisted after chemotherapy.
Only 15 of the 38 mutations in tumor also appeared in cfDNA before treatment. At the time of interval debulking, tumor specimens yielded 36 mutations, of which 11 were detected in cfDNA.
At baseline and after treatment, all patients had TP53 mutations either tumor alone, or in both tumor and plasma. Among four patients whose cancer recurred, three had mutations in cfDNA that were previously detected in tumor. Implicated genes included PIK3CA, TP53, KIT, and KDR.
Overall, the study suggests that gene expression profiling of ovarian HGSC tumor tissue taken at interval debulking could someday help guide treatment decisions after neoadjuvant chemotherapy, Dr. Arend said. “To be able to use cfDNA as liquid biopsy, more studies like this one, which match tumor and cfDNA from multiple time points, are needed,” she added.
Dr. Arend cited no funding sources and reported having no conflicts of interest.
Key clinical point. Neoadjuvant chemotherapy was associated with changes in gene expression and associated pathways in high-grade serous ovarian carcinomas. Some mutations in tumors were also present in plasma cell-free DNA.
Major finding: Pathway analysis confirmed that the cell cycle and apoptosis pathway was the most up-regulated after neoadjuvant chemotherapy, while the DNA damage repair pathway was the most down-regulated. Among 38 baseline mutations in tumor specimens, 15 of 38 appeared in plasma cell-free DNA. At interval debulking, tumor specimens yielded 36 mutations, of which 11 were detected in cfDNA.
Data source: Gene expression profiling, pathway analysis, and next-generation sequencing of 19 patients with high-grade serous ovarian carcinomas.
Disclosures: Dr. Arend cited no funding sources and reported having no conflicts of interest.
Uptake of new heart failure drugs slow despite guidelines
SNOWMASS, COLO. – As William T. Abraham, MD, speaks to colleagues around the country about heart failure therapy, he has noticed that the first-in-class drug ivabradine remains below the radar of most physicians.
“I’ve found that this is an agent that very few people know about, even though it’s been FDA [Food and Drug Administration] approved for about 3 years. It’s used fairly extensively in Europe because that’s where the pivotal SHIFT trial was done, but not very much in the United States,” according to Dr. Abraham, professor of medicine, physiology, and cell biology and director of the division of cardiovascular medicine at Ohio State University in Columbus.
That’s likely to change as word spreads about the May 2016 update of the American College of Cardiology/American Heart Association Guideline for the Management of Heart Failure. The update incorporated evidence-based recommendations on the use of two important new heart failure medications: ivabradine (Corlanor), which received a moderate class IIa recommendation, meaning the drug “should be considered,” and sacubitril/valsartan (Entresto), which received the strongest class I recommendation.
In the right patients, these two oral medications improve heart failure morbidity and mortality significantly beyond what’s achievable with what has been the gold standard, guideline-directed medical therapy. Dr. Abraham described how to get started using the two medications at the Annual Cardiovascular Conference at Snowmass.
Ivabradine
Ivabradine is a selective inhibitor of the sinoatrial pacemaker modulating I(f) current. It acts by slowing the sinus rate without reducing myocardial contractility.
“This agent does one thing and one thing alone: It lowers heart rate,” the cardiologist explained.
And that, he added, was sufficient to significantly reduce the risks of death due to heart failure and recurrent hospitalization for worsening heart failure in the pivotal SHIFT trial.
SHIFT included 6,505 patients with moderate to severe heart failure with reduced left ventricular ejection fraction (LVEF) and a resting heart rate above 70 bpm despite background guideline-directed medical therapy. Participants were randomized double blind to ivabradine titrated to a maximum of 7.5 mg twice daily or placebo and followed for a median of about 23 months. The rate of death due to heart failure was 3% with ivabradine and 5% with placebo, for a statistically significant 26% relative risk reduction favoring ivabradine.
But the drug’s main benefit was in reducing recurrent hospitalizations for heart failure, an endpoint of particular interest to health policy officials given that heart failure hospitalizations chew up a substantial proportion of the Medicare budget. Ivabradine reduced first hospitalizations for heart failure during the study period by 25%, second hospitalizations by 34%, and third hospitalizations by 29% (Eur Heart J. 2012 Nov;33[22]:2813-20).
The ACC/AHA guideline update stresses the importance of reserving ivabradine for heart failure patients whose resting heart rate exceeds 70 bpm, despite being on their maximum tolerated dose of a beta-blocker, Dr. Abraham noted.
Ivabradine is contraindicated in the setting of acute decompensated heart failure, severe liver disease, or hypotension, in patients on any of the numerous agents that strongly inhibit the enzyme cytochrome P450 3A4, and in those who have sick sinus syndrome, have sinoatrial block, or are pacemaker dependent.
Sacubitril/valsartan
Sacubitril inhibits neprilysin, an enzyme that blocks the action of endogenous vasoactive peptides including bradykinin, substance P, and natriuretic peptides, all of which counter important maladaptive mechanisms in heart failure. Sacubitril has been combined with the angiotensin receptor blocker valsartan to form the first-in-class angiotensin receptor neprilysin inhibitor, or ARNI, formerly known as LCZ696 and now marketed as Entresto.
In the pivotal double-blind PARADIGM-HF trial, 8,442 patients with heart failure with reduced ejection fraction were randomized to the ARNI at 200 mg b.i.d. or to enalapril at 10 mg b.i.d. on top of background guideline-directed medical therapy. The trial was stopped early because of evidence of overwhelming benefit: a 20% relative risk reduction in cardiovascular death and a 21% decrease in the risk of heart failure hospitalizations in the sacubitril/valsartan group, as well as significant reductions in heart failure symptoms and physical limitations (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
The updated heart failure guidelines strongly recommend that patients with heart failure should be treated with either an ACE inhibitor, an angiotensin receptor blocker, or an ARNI. Further, patients who remain symptomatic on an ACE inhibitor or angiotensin receptor blocker should be switched to an ARNI; that’s a class Ib recommendation based upon the results of PARADIGM-HF.
In getting started using the ARNI, Dr. Abraham said it’s important to understand as background the selective nature of the PARADIGM-HF study design. During the single-blind run-in period of 5-8 weeks, roughly 10% of patients dropped out because they couldn’t tolerate enalapril at 10 mg b.i.d., and a similar percentage dropped out during the ARNI run-in. Thus, patients who couldn’t tolerate a low dose of an ACE inhibitor weren’t in the study. And patients capable of tolerating guideline-recommended full-dose ACE inhibitor therapy were not specifically sought for participation.
“So there are some unanswered questions about the ARNI. If you’re just getting started with this compound in treating your heart failure patients, my own feeling is you should maybe aim for the type of patient that was included in this trial: patients who could tolerate a moderate dose of an ACE inhibitor and had generally good blood pressure. That’s a great way to begin to get experience with this agent in heart failure,” the cardiologist advised.
He reported serving as a consultant to Abbott Vascular, Medtronic, Novartis, and St. Jude Medical.
SNOWMASS, COLO. – As William T. Abraham, MD, speaks to colleagues around the country about heart failure therapy, he has noticed that the first-in-class drug ivabradine remains below the radar of most physicians.
“I’ve found that this is an agent that very few people know about, even though it’s been FDA [Food and Drug Administration] approved for about 3 years. It’s used fairly extensively in Europe because that’s where the pivotal SHIFT trial was done, but not very much in the United States,” according to Dr. Abraham, professor of medicine, physiology, and cell biology and director of the division of cardiovascular medicine at Ohio State University in Columbus.
That’s likely to change as word spreads about the May 2016 update of the American College of Cardiology/American Heart Association Guideline for the Management of Heart Failure. The update incorporated evidence-based recommendations on the use of two important new heart failure medications: ivabradine (Corlanor), which received a moderate class IIa recommendation, meaning the drug “should be considered,” and sacubitril/valsartan (Entresto), which received the strongest class I recommendation.
In the right patients, these two oral medications improve heart failure morbidity and mortality significantly beyond what’s achievable with what has been the gold standard, guideline-directed medical therapy. Dr. Abraham described how to get started using the two medications at the Annual Cardiovascular Conference at Snowmass.
Ivabradine
Ivabradine is a selective inhibitor of the sinoatrial pacemaker modulating I(f) current. It acts by slowing the sinus rate without reducing myocardial contractility.
“This agent does one thing and one thing alone: It lowers heart rate,” the cardiologist explained.
And that, he added, was sufficient to significantly reduce the risks of death due to heart failure and recurrent hospitalization for worsening heart failure in the pivotal SHIFT trial.
SHIFT included 6,505 patients with moderate to severe heart failure with reduced left ventricular ejection fraction (LVEF) and a resting heart rate above 70 bpm despite background guideline-directed medical therapy. Participants were randomized double blind to ivabradine titrated to a maximum of 7.5 mg twice daily or placebo and followed for a median of about 23 months. The rate of death due to heart failure was 3% with ivabradine and 5% with placebo, for a statistically significant 26% relative risk reduction favoring ivabradine.
But the drug’s main benefit was in reducing recurrent hospitalizations for heart failure, an endpoint of particular interest to health policy officials given that heart failure hospitalizations chew up a substantial proportion of the Medicare budget. Ivabradine reduced first hospitalizations for heart failure during the study period by 25%, second hospitalizations by 34%, and third hospitalizations by 29% (Eur Heart J. 2012 Nov;33[22]:2813-20).
The ACC/AHA guideline update stresses the importance of reserving ivabradine for heart failure patients whose resting heart rate exceeds 70 bpm, despite being on their maximum tolerated dose of a beta-blocker, Dr. Abraham noted.
Ivabradine is contraindicated in the setting of acute decompensated heart failure, severe liver disease, or hypotension, in patients on any of the numerous agents that strongly inhibit the enzyme cytochrome P450 3A4, and in those who have sick sinus syndrome, have sinoatrial block, or are pacemaker dependent.
Sacubitril/valsartan
Sacubitril inhibits neprilysin, an enzyme that blocks the action of endogenous vasoactive peptides including bradykinin, substance P, and natriuretic peptides, all of which counter important maladaptive mechanisms in heart failure. Sacubitril has been combined with the angiotensin receptor blocker valsartan to form the first-in-class angiotensin receptor neprilysin inhibitor, or ARNI, formerly known as LCZ696 and now marketed as Entresto.
In the pivotal double-blind PARADIGM-HF trial, 8,442 patients with heart failure with reduced ejection fraction were randomized to the ARNI at 200 mg b.i.d. or to enalapril at 10 mg b.i.d. on top of background guideline-directed medical therapy. The trial was stopped early because of evidence of overwhelming benefit: a 20% relative risk reduction in cardiovascular death and a 21% decrease in the risk of heart failure hospitalizations in the sacubitril/valsartan group, as well as significant reductions in heart failure symptoms and physical limitations (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
The updated heart failure guidelines strongly recommend that patients with heart failure should be treated with either an ACE inhibitor, an angiotensin receptor blocker, or an ARNI. Further, patients who remain symptomatic on an ACE inhibitor or angiotensin receptor blocker should be switched to an ARNI; that’s a class Ib recommendation based upon the results of PARADIGM-HF.
In getting started using the ARNI, Dr. Abraham said it’s important to understand as background the selective nature of the PARADIGM-HF study design. During the single-blind run-in period of 5-8 weeks, roughly 10% of patients dropped out because they couldn’t tolerate enalapril at 10 mg b.i.d., and a similar percentage dropped out during the ARNI run-in. Thus, patients who couldn’t tolerate a low dose of an ACE inhibitor weren’t in the study. And patients capable of tolerating guideline-recommended full-dose ACE inhibitor therapy were not specifically sought for participation.
“So there are some unanswered questions about the ARNI. If you’re just getting started with this compound in treating your heart failure patients, my own feeling is you should maybe aim for the type of patient that was included in this trial: patients who could tolerate a moderate dose of an ACE inhibitor and had generally good blood pressure. That’s a great way to begin to get experience with this agent in heart failure,” the cardiologist advised.
He reported serving as a consultant to Abbott Vascular, Medtronic, Novartis, and St. Jude Medical.
SNOWMASS, COLO. – As William T. Abraham, MD, speaks to colleagues around the country about heart failure therapy, he has noticed that the first-in-class drug ivabradine remains below the radar of most physicians.
“I’ve found that this is an agent that very few people know about, even though it’s been FDA [Food and Drug Administration] approved for about 3 years. It’s used fairly extensively in Europe because that’s where the pivotal SHIFT trial was done, but not very much in the United States,” according to Dr. Abraham, professor of medicine, physiology, and cell biology and director of the division of cardiovascular medicine at Ohio State University in Columbus.
That’s likely to change as word spreads about the May 2016 update of the American College of Cardiology/American Heart Association Guideline for the Management of Heart Failure. The update incorporated evidence-based recommendations on the use of two important new heart failure medications: ivabradine (Corlanor), which received a moderate class IIa recommendation, meaning the drug “should be considered,” and sacubitril/valsartan (Entresto), which received the strongest class I recommendation.
In the right patients, these two oral medications improve heart failure morbidity and mortality significantly beyond what’s achievable with what has been the gold standard, guideline-directed medical therapy. Dr. Abraham described how to get started using the two medications at the Annual Cardiovascular Conference at Snowmass.
Ivabradine
Ivabradine is a selective inhibitor of the sinoatrial pacemaker modulating I(f) current. It acts by slowing the sinus rate without reducing myocardial contractility.
“This agent does one thing and one thing alone: It lowers heart rate,” the cardiologist explained.
And that, he added, was sufficient to significantly reduce the risks of death due to heart failure and recurrent hospitalization for worsening heart failure in the pivotal SHIFT trial.
SHIFT included 6,505 patients with moderate to severe heart failure with reduced left ventricular ejection fraction (LVEF) and a resting heart rate above 70 bpm despite background guideline-directed medical therapy. Participants were randomized double blind to ivabradine titrated to a maximum of 7.5 mg twice daily or placebo and followed for a median of about 23 months. The rate of death due to heart failure was 3% with ivabradine and 5% with placebo, for a statistically significant 26% relative risk reduction favoring ivabradine.
But the drug’s main benefit was in reducing recurrent hospitalizations for heart failure, an endpoint of particular interest to health policy officials given that heart failure hospitalizations chew up a substantial proportion of the Medicare budget. Ivabradine reduced first hospitalizations for heart failure during the study period by 25%, second hospitalizations by 34%, and third hospitalizations by 29% (Eur Heart J. 2012 Nov;33[22]:2813-20).
The ACC/AHA guideline update stresses the importance of reserving ivabradine for heart failure patients whose resting heart rate exceeds 70 bpm, despite being on their maximum tolerated dose of a beta-blocker, Dr. Abraham noted.
Ivabradine is contraindicated in the setting of acute decompensated heart failure, severe liver disease, or hypotension, in patients on any of the numerous agents that strongly inhibit the enzyme cytochrome P450 3A4, and in those who have sick sinus syndrome, have sinoatrial block, or are pacemaker dependent.
Sacubitril/valsartan
Sacubitril inhibits neprilysin, an enzyme that blocks the action of endogenous vasoactive peptides including bradykinin, substance P, and natriuretic peptides, all of which counter important maladaptive mechanisms in heart failure. Sacubitril has been combined with the angiotensin receptor blocker valsartan to form the first-in-class angiotensin receptor neprilysin inhibitor, or ARNI, formerly known as LCZ696 and now marketed as Entresto.
In the pivotal double-blind PARADIGM-HF trial, 8,442 patients with heart failure with reduced ejection fraction were randomized to the ARNI at 200 mg b.i.d. or to enalapril at 10 mg b.i.d. on top of background guideline-directed medical therapy. The trial was stopped early because of evidence of overwhelming benefit: a 20% relative risk reduction in cardiovascular death and a 21% decrease in the risk of heart failure hospitalizations in the sacubitril/valsartan group, as well as significant reductions in heart failure symptoms and physical limitations (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
The updated heart failure guidelines strongly recommend that patients with heart failure should be treated with either an ACE inhibitor, an angiotensin receptor blocker, or an ARNI. Further, patients who remain symptomatic on an ACE inhibitor or angiotensin receptor blocker should be switched to an ARNI; that’s a class Ib recommendation based upon the results of PARADIGM-HF.
In getting started using the ARNI, Dr. Abraham said it’s important to understand as background the selective nature of the PARADIGM-HF study design. During the single-blind run-in period of 5-8 weeks, roughly 10% of patients dropped out because they couldn’t tolerate enalapril at 10 mg b.i.d., and a similar percentage dropped out during the ARNI run-in. Thus, patients who couldn’t tolerate a low dose of an ACE inhibitor weren’t in the study. And patients capable of tolerating guideline-recommended full-dose ACE inhibitor therapy were not specifically sought for participation.
“So there are some unanswered questions about the ARNI. If you’re just getting started with this compound in treating your heart failure patients, my own feeling is you should maybe aim for the type of patient that was included in this trial: patients who could tolerate a moderate dose of an ACE inhibitor and had generally good blood pressure. That’s a great way to begin to get experience with this agent in heart failure,” the cardiologist advised.
He reported serving as a consultant to Abbott Vascular, Medtronic, Novartis, and St. Jude Medical.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Boston - Rich History, Lively Cultural Scene
There is history around every corner in Boston. This vibrant city is rich with art, music, and dance institutions, theatre and cultural attractions, distinguished dining and nightlife venues, world-class shopping and championship sports teams that attract millions of visitors each year.
The city’s downtown neighborhoods, each with its own personality, offer endless unique experiences, and Boston’s proximity to other must-see sites all around New England make it one of the country’s most diverse and exciting locales.Each of the city’s neighborhoods has a remarkably different style and tone. From the Back Bay’s cosmopolitan streets and ornate Victorian townhouses to the aromas spilling into the narrow and jumbled 17th-century streets of Boston’s North End to the spirited and funky neighborhood squares of Cambridge – all within easy distance from one another.Boston is “America’s Walking City.” Even though it is one of the largest cities in the country, its accessibility is unparalleled. And while sightseeing on foot is easy, Boston also has an excellent public transportation system to help you get around.
Boston is also known as the mecca of medicine. Boston is home to some of the most prestigious hospitals and medical schools, physicians, and medical scientists in the world. Thoralf M. Sundt, III, MD, and the AATS Centennial Committee have organized an engaging social program for the AATS Centennial.
Tour 1: ITALIAN GASTRONOMY NORTH END MARKET TOUR
Sunday, April 30, 2017
10:30 a.m.– 1:15 p.m.
Cost: $95 per person

Tour 2: A VISIT TO THE ISABELLA STEWART GARDNER MUSEUM
Monday, May 1, 2017
12:15 p.m. – 2:45 p.m.
Cost: $85 per person

Enjoy the Gardners’ compilation of tapestries, exquisite antique furniture, and famous collections while hearing wonderful anecdotes about Mrs. Gardner’s sophisticated and eclectic life and the famous heist. A docent will be available to guidevisitors.
Tour 3: BEACON HILL CIRCLE “BEHIND THE BRAHMIN DOORS”
Tuesday, May 2, 2017
9:15 a.m. – 11:45 a.m.
Cost: $110 per person
![]()
*Preregistration for social events and tours are required. Tours require a minimum number of participants. All tours will depart from the Hynes Convention Center.
For additional visit information and things to do in Boston, go to https://www.bostonusa.com/things-to-do.
There is history around every corner in Boston. This vibrant city is rich with art, music, and dance institutions, theatre and cultural attractions, distinguished dining and nightlife venues, world-class shopping and championship sports teams that attract millions of visitors each year.
The city’s downtown neighborhoods, each with its own personality, offer endless unique experiences, and Boston’s proximity to other must-see sites all around New England make it one of the country’s most diverse and exciting locales.Each of the city’s neighborhoods has a remarkably different style and tone. From the Back Bay’s cosmopolitan streets and ornate Victorian townhouses to the aromas spilling into the narrow and jumbled 17th-century streets of Boston’s North End to the spirited and funky neighborhood squares of Cambridge – all within easy distance from one another.Boston is “America’s Walking City.” Even though it is one of the largest cities in the country, its accessibility is unparalleled. And while sightseeing on foot is easy, Boston also has an excellent public transportation system to help you get around.
Boston is also known as the mecca of medicine. Boston is home to some of the most prestigious hospitals and medical schools, physicians, and medical scientists in the world. Thoralf M. Sundt, III, MD, and the AATS Centennial Committee have organized an engaging social program for the AATS Centennial.
Tour 1: ITALIAN GASTRONOMY NORTH END MARKET TOUR
Sunday, April 30, 2017
10:30 a.m.– 1:15 p.m.
Cost: $95 per person
Tour 2: A VISIT TO THE ISABELLA STEWART GARDNER MUSEUM
Monday, May 1, 2017
12:15 p.m. – 2:45 p.m.
Cost: $85 per person
Enjoy the Gardners’ compilation of tapestries, exquisite antique furniture, and famous collections while hearing wonderful anecdotes about Mrs. Gardner’s sophisticated and eclectic life and the famous heist. A docent will be available to guidevisitors.
Tour 3: BEACON HILL CIRCLE “BEHIND THE BRAHMIN DOORS”
Tuesday, May 2, 2017
9:15 a.m. – 11:45 a.m.
Cost: $110 per person
![]()
*Preregistration for social events and tours are required. Tours require a minimum number of participants. All tours will depart from the Hynes Convention Center.
For additional visit information and things to do in Boston, go to https://www.bostonusa.com/things-to-do.
There is history around every corner in Boston. This vibrant city is rich with art, music, and dance institutions, theatre and cultural attractions, distinguished dining and nightlife venues, world-class shopping and championship sports teams that attract millions of visitors each year.
The city’s downtown neighborhoods, each with its own personality, offer endless unique experiences, and Boston’s proximity to other must-see sites all around New England make it one of the country’s most diverse and exciting locales.Each of the city’s neighborhoods has a remarkably different style and tone. From the Back Bay’s cosmopolitan streets and ornate Victorian townhouses to the aromas spilling into the narrow and jumbled 17th-century streets of Boston’s North End to the spirited and funky neighborhood squares of Cambridge – all within easy distance from one another.Boston is “America’s Walking City.” Even though it is one of the largest cities in the country, its accessibility is unparalleled. And while sightseeing on foot is easy, Boston also has an excellent public transportation system to help you get around.
Boston is also known as the mecca of medicine. Boston is home to some of the most prestigious hospitals and medical schools, physicians, and medical scientists in the world. Thoralf M. Sundt, III, MD, and the AATS Centennial Committee have organized an engaging social program for the AATS Centennial.
Tour 1: ITALIAN GASTRONOMY NORTH END MARKET TOUR
Sunday, April 30, 2017
10:30 a.m.– 1:15 p.m.
Cost: $95 per person
Tour 2: A VISIT TO THE ISABELLA STEWART GARDNER MUSEUM
Monday, May 1, 2017
12:15 p.m. – 2:45 p.m.
Cost: $85 per person
Enjoy the Gardners’ compilation of tapestries, exquisite antique furniture, and famous collections while hearing wonderful anecdotes about Mrs. Gardner’s sophisticated and eclectic life and the famous heist. A docent will be available to guidevisitors.
Tour 3: BEACON HILL CIRCLE “BEHIND THE BRAHMIN DOORS”
Tuesday, May 2, 2017
9:15 a.m. – 11:45 a.m.
Cost: $110 per person
![]()
*Preregistration for social events and tours are required. Tours require a minimum number of participants. All tours will depart from the Hynes Convention Center.
For additional visit information and things to do in Boston, go to https://www.bostonusa.com/things-to-do.
