User login
Stopping TNF inhibitors for pregnancy may invite flares
Women with rheumatoid arthritis or axial spondyloarthritis who stop treatment with tumor necrosis factor inhibitors when they become pregnant may be inviting disease flares during the pregnancy, according to a report published in Arthritis Research & Therapy.
To examine the frequency of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) flares during pregnancy, researchers prospectively followed 136 women treated at the Center for Pregnancy in Rheumatic Diseases at Inselspital Bern (Switzerland) during a 5-year period. These patients – 75 with RA and 61 with axSpA – were assessed before conception, during each trimester, and 6-8 weeks postpartum for disease activity and medication use, said Stephanie van den Brandt, MD, of the department of rheumatology, immunology, and allergology at the University of Bern, and her associates.
The relative risk of a disease flare was 3.33 among RA patients and 3.08 among axSpA patients who discontinued TNF inhibitors at the time of a positive pregnancy test. In comparison, rheumatic disease remained stable throughout pregnancy in most women who were not taking TNF inhibitors before pregnancy, the investigators said (Arthritis Res Ther. 2017 Mar 20. doi: 10.1186/s13075-017-1269-1).
Most disease flares occurred in the first trimester among women with RA and in the second half of pregnancy among women with axSpA. Most women with RA who resumed taking TNF inhibitors when their disease flared responded well to the treatment, with CRP levels dropping by 70% and remission being achieved rapidly. In contrast, most women with axSpA who resumed taking TNF inhibitors did not respond as well, with CRP levels dropping by only 35%. Their disease was ameliorated but not controlled by restarting the therapy.
No sponsor was cited for this study. Dr. van den Brandt and her associates reported having no relevant financial disclosures.
Women with rheumatoid arthritis or axial spondyloarthritis who stop treatment with tumor necrosis factor inhibitors when they become pregnant may be inviting disease flares during the pregnancy, according to a report published in Arthritis Research & Therapy.
To examine the frequency of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) flares during pregnancy, researchers prospectively followed 136 women treated at the Center for Pregnancy in Rheumatic Diseases at Inselspital Bern (Switzerland) during a 5-year period. These patients – 75 with RA and 61 with axSpA – were assessed before conception, during each trimester, and 6-8 weeks postpartum for disease activity and medication use, said Stephanie van den Brandt, MD, of the department of rheumatology, immunology, and allergology at the University of Bern, and her associates.
The relative risk of a disease flare was 3.33 among RA patients and 3.08 among axSpA patients who discontinued TNF inhibitors at the time of a positive pregnancy test. In comparison, rheumatic disease remained stable throughout pregnancy in most women who were not taking TNF inhibitors before pregnancy, the investigators said (Arthritis Res Ther. 2017 Mar 20. doi: 10.1186/s13075-017-1269-1).
Most disease flares occurred in the first trimester among women with RA and in the second half of pregnancy among women with axSpA. Most women with RA who resumed taking TNF inhibitors when their disease flared responded well to the treatment, with CRP levels dropping by 70% and remission being achieved rapidly. In contrast, most women with axSpA who resumed taking TNF inhibitors did not respond as well, with CRP levels dropping by only 35%. Their disease was ameliorated but not controlled by restarting the therapy.
No sponsor was cited for this study. Dr. van den Brandt and her associates reported having no relevant financial disclosures.
Women with rheumatoid arthritis or axial spondyloarthritis who stop treatment with tumor necrosis factor inhibitors when they become pregnant may be inviting disease flares during the pregnancy, according to a report published in Arthritis Research & Therapy.
To examine the frequency of rheumatoid arthritis (RA) and axial spondyloarthritis (axSpA) flares during pregnancy, researchers prospectively followed 136 women treated at the Center for Pregnancy in Rheumatic Diseases at Inselspital Bern (Switzerland) during a 5-year period. These patients – 75 with RA and 61 with axSpA – were assessed before conception, during each trimester, and 6-8 weeks postpartum for disease activity and medication use, said Stephanie van den Brandt, MD, of the department of rheumatology, immunology, and allergology at the University of Bern, and her associates.
The relative risk of a disease flare was 3.33 among RA patients and 3.08 among axSpA patients who discontinued TNF inhibitors at the time of a positive pregnancy test. In comparison, rheumatic disease remained stable throughout pregnancy in most women who were not taking TNF inhibitors before pregnancy, the investigators said (Arthritis Res Ther. 2017 Mar 20. doi: 10.1186/s13075-017-1269-1).
Most disease flares occurred in the first trimester among women with RA and in the second half of pregnancy among women with axSpA. Most women with RA who resumed taking TNF inhibitors when their disease flared responded well to the treatment, with CRP levels dropping by 70% and remission being achieved rapidly. In contrast, most women with axSpA who resumed taking TNF inhibitors did not respond as well, with CRP levels dropping by only 35%. Their disease was ameliorated but not controlled by restarting the therapy.
No sponsor was cited for this study. Dr. van den Brandt and her associates reported having no relevant financial disclosures.
Key clinical point:
Major finding: The relative risk of a disease flare was 3.33 among RA patients and 3.08 among axSpA patients who discontinued TNF inhibitors at conception.
Data source: A prospective cohort study involving 75 pregnant women with RA and 61 with axial spondyloarthritis treated at one Swiss specialty center in 2000-2015.
Disclosures: No sponsor was cited for this study. Dr. van den Brandt and her associates reported having no relevant financial disclosures.
What’s old is new in topical psoriasis therapy
WAILEA, HAWAII – A fixed combination of halobetasol and tazarotene formulated as a once-daily lotion proved safe and effective for patients with moderate or severe plaque psoriasis in a phase II randomized clinical trial, Linda Stein Gold, MD, reported at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The rationale for developing this product is that it should provide the efficacy of a class 1 superpotent topical corticosteroid, albeit with the topical retinoid lessening concern about the possibility of steroid-induced skin atrophy and other long-term safety issues, explained Dr. Stein Gold, director of dermatology research at Henry Ford Health System in Detroit.
The double-blind, multicenter, 8-week, phase II study included 212 patients randomized 2:2:1 to once-daily application of fixed-combination halobetasol propionate 0.01% and tazarotene 0.045% lotion, either topical agent as monotherapy, or vehicle. Ninety percent of participants had moderate plaque psoriasis as defined by a baseline Investigator’s Global Assessment (IGA) score of 3 and a median 5% body surface area involvement. The remaining patients were classified as having severe psoriasis, with a baseline IGA of 4, but no one with psoriasis over more than 12% of their body surface area was eligible for the trial.
The fixed-combination lotion, known for now as IDP-118, established superior efficacy over placebo by 2 weeks. At week 8, treatment success, as defined by at least a two-grade improvement from baseline in IGA score plus a rating of clear or almost clear, was documented in 53% of the IDP-118 lotion group, compared with 33% on halobetasol propionate monotherapy, 19% with tazarotene alone, and 10% with vehicle, Dr. Stein Gold reported.
Each patient had a target lesion 25-32 cm2 in size, which was designated for careful assessment of changes in the domains of lesional erythema, plaque elevation, and scaling. At week 8, the IDP-118 had a target lesion treatment success rate of 54% for erythema, 68% for plaque elevation, and 64% for scaling, she said.
The treatment discontinuation rate was 3.4% in the IDP-118 group, 12.1% with tazarotene, zero for halobetasol propionate, and 3.2% for vehicle. The most frequently reported treatment-emergent adverse events were mild or moderate application-site reactions. Skin atrophy was rare. No treatment-related serious adverse events occurred.
A 555-patient, phase III, open-label, 12-month safety study of IDP-118 is due to be completed later in 2017.
The phase II study was funded by Valeant Pharmaceuticals. Dr. Stein Gold reported serving as an investigator, advisor, and speaker for the company. SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – A fixed combination of halobetasol and tazarotene formulated as a once-daily lotion proved safe and effective for patients with moderate or severe plaque psoriasis in a phase II randomized clinical trial, Linda Stein Gold, MD, reported at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The rationale for developing this product is that it should provide the efficacy of a class 1 superpotent topical corticosteroid, albeit with the topical retinoid lessening concern about the possibility of steroid-induced skin atrophy and other long-term safety issues, explained Dr. Stein Gold, director of dermatology research at Henry Ford Health System in Detroit.
The double-blind, multicenter, 8-week, phase II study included 212 patients randomized 2:2:1 to once-daily application of fixed-combination halobetasol propionate 0.01% and tazarotene 0.045% lotion, either topical agent as monotherapy, or vehicle. Ninety percent of participants had moderate plaque psoriasis as defined by a baseline Investigator’s Global Assessment (IGA) score of 3 and a median 5% body surface area involvement. The remaining patients were classified as having severe psoriasis, with a baseline IGA of 4, but no one with psoriasis over more than 12% of their body surface area was eligible for the trial.
The fixed-combination lotion, known for now as IDP-118, established superior efficacy over placebo by 2 weeks. At week 8, treatment success, as defined by at least a two-grade improvement from baseline in IGA score plus a rating of clear or almost clear, was documented in 53% of the IDP-118 lotion group, compared with 33% on halobetasol propionate monotherapy, 19% with tazarotene alone, and 10% with vehicle, Dr. Stein Gold reported.
Each patient had a target lesion 25-32 cm2 in size, which was designated for careful assessment of changes in the domains of lesional erythema, plaque elevation, and scaling. At week 8, the IDP-118 had a target lesion treatment success rate of 54% for erythema, 68% for plaque elevation, and 64% for scaling, she said.
The treatment discontinuation rate was 3.4% in the IDP-118 group, 12.1% with tazarotene, zero for halobetasol propionate, and 3.2% for vehicle. The most frequently reported treatment-emergent adverse events were mild or moderate application-site reactions. Skin atrophy was rare. No treatment-related serious adverse events occurred.
A 555-patient, phase III, open-label, 12-month safety study of IDP-118 is due to be completed later in 2017.
The phase II study was funded by Valeant Pharmaceuticals. Dr. Stein Gold reported serving as an investigator, advisor, and speaker for the company. SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – A fixed combination of halobetasol and tazarotene formulated as a once-daily lotion proved safe and effective for patients with moderate or severe plaque psoriasis in a phase II randomized clinical trial, Linda Stein Gold, MD, reported at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
The rationale for developing this product is that it should provide the efficacy of a class 1 superpotent topical corticosteroid, albeit with the topical retinoid lessening concern about the possibility of steroid-induced skin atrophy and other long-term safety issues, explained Dr. Stein Gold, director of dermatology research at Henry Ford Health System in Detroit.
The double-blind, multicenter, 8-week, phase II study included 212 patients randomized 2:2:1 to once-daily application of fixed-combination halobetasol propionate 0.01% and tazarotene 0.045% lotion, either topical agent as monotherapy, or vehicle. Ninety percent of participants had moderate plaque psoriasis as defined by a baseline Investigator’s Global Assessment (IGA) score of 3 and a median 5% body surface area involvement. The remaining patients were classified as having severe psoriasis, with a baseline IGA of 4, but no one with psoriasis over more than 12% of their body surface area was eligible for the trial.
The fixed-combination lotion, known for now as IDP-118, established superior efficacy over placebo by 2 weeks. At week 8, treatment success, as defined by at least a two-grade improvement from baseline in IGA score plus a rating of clear or almost clear, was documented in 53% of the IDP-118 lotion group, compared with 33% on halobetasol propionate monotherapy, 19% with tazarotene alone, and 10% with vehicle, Dr. Stein Gold reported.
Each patient had a target lesion 25-32 cm2 in size, which was designated for careful assessment of changes in the domains of lesional erythema, plaque elevation, and scaling. At week 8, the IDP-118 had a target lesion treatment success rate of 54% for erythema, 68% for plaque elevation, and 64% for scaling, she said.
The treatment discontinuation rate was 3.4% in the IDP-118 group, 12.1% with tazarotene, zero for halobetasol propionate, and 3.2% for vehicle. The most frequently reported treatment-emergent adverse events were mild or moderate application-site reactions. Skin atrophy was rare. No treatment-related serious adverse events occurred.
A 555-patient, phase III, open-label, 12-month safety study of IDP-118 is due to be completed later in 2017.
The phase II study was funded by Valeant Pharmaceuticals. Dr. Stein Gold reported serving as an investigator, advisor, and speaker for the company. SDEF and this news organization are owned by the same parent company.
Key clinical point:
Major finding: An investigational fixed-combination lotion consisting of halobetasol propionate 0.01% and tazarotene 0.045% achieved scores of clear or almost clear in 53% of patients, significantly better than either component as monotherapy.
Data source: This phase II, double-blind, multicenter, vehicle-controlled, 8-week randomized clinical trial included 212 patients with moderate or severe plaque psoriasis.
Disclosures: The study was funded by Valeant Pharmaceuticals. The presenter reported serving as an investigator, advisor, and speaker for the company.
Alpha-blockers deemed safe in heart failure
WASHINGTON – Prescribing alpha-adrenergic blocking agents for treatment of benign prostatic hypertrophy in men with heart failure proved to be not only safe, but also was associated with significantly reduced rates of both heart failure readmission and all-cause mortality in a large retrospective cohort study.
“These findings are associative, not necessarily causative. But the novel association between alpha-blocker treatment and improved outcomes may warrant further study,” Alberta L. Warner, MD, said at the annual meeting of the American College of Cardiology.

Many men with heart failure also have benign prostatic hypertrophy (BPH), for which they receive treatment with an alpha-blocker. Yet little is known about the impact of this drug class on safety and outcomes in the setting of heart failure. Of note, the use of alpha-blockers for treatment of hypertension was associated with increased risk of new-onset heart failure in the ALLHAT study.
To shed light on the safety of alpha-blockers in patients with prevalent heart failure, Dr. Warner and her coinvestigators analyzed data on nearly 170,000 men with a primary diagnosis of heart failure discharged from Veterans Affairs hospitals in 2002-2015. They determined that fully 28% of them left the hospital on an alpha-blocker. From this pool of nearly 48,000 heart failure patients, they were able to propensity-score match 38,991 on the basis of 54 baseline clinical characteristics to an equal number of VA heart failure patients who weren’t on an alpha-blocker. The study outcomes were time to first readmission for heart failure or all-cause mortality during 2 years of follow-up.
Patients on an alpha-blocker had a 38% heart failure readmission rate at 2 years, compared with 40% in nonusers, for a modest, albeit statistically significant, 6% reduction in relative risk. The all-cause mortality rate also was significantly lower in patients on an alpha-blocker: 40% versus 44%, for a 9% relative risk reduction.
In a subanalysis restricted to the heart failure patients on an alpha-blocker, higher-dose therapy was associated with a significantly lower incidence of all-cause mortality than was a lower-dose alpha-blocker during 2 years of follow-up, with a 9% relative risk reduction. A high-dose alpha-blocker, however, wasn’t significantly more effective than lower-dose therapy in terms of reducing heart failure readmissions, said Dr. Warner, a cardiologist at the Veterans Affairs Greater Los Angeles Healthcare System and the University of California, Los Angeles.
Similarly, patients treated with a nonspecific, peripherally vasoactive alpha-blocker had a significantly lower mortality rate than those on an alpha-1a-adrenergic–specific agent, with a highly significant 15% reduction in relative risk. The type of alpha-blocker, however, didn’t make a significant difference in terms of heart failure readmissions, where both types of agents were similarly better than not being on an alpha-blocker at all, she said.
Eighty-five percent of study participants were on a beta-blocker. Heart failure readmissions and all-cause mortality were significantly lower with alpha-blocker therapy, regardless of whether patients were on background beta-blocker therapy.
One audience member, however, noting that the beta-blocker carvedilol possesses some alpha-blocking effects, asked if outcomes differed depending on whether a patient was on carvedilol or metoprolol.
Dr. Warner replied that those numbers are still being crunched, and that the final answer isn’t in yet, but her preliminary impression is that the benefits of alpha-blocker therapy in terms of both heart failure readmissions and all-cause mortality were attenuated in the patients on carvedilol, possibly due to that beta-blocker’s alpha-blocking properties.
She reported having no financial conflicts regarding the study.
WASHINGTON – Prescribing alpha-adrenergic blocking agents for treatment of benign prostatic hypertrophy in men with heart failure proved to be not only safe, but also was associated with significantly reduced rates of both heart failure readmission and all-cause mortality in a large retrospective cohort study.
“These findings are associative, not necessarily causative. But the novel association between alpha-blocker treatment and improved outcomes may warrant further study,” Alberta L. Warner, MD, said at the annual meeting of the American College of Cardiology.
Many men with heart failure also have benign prostatic hypertrophy (BPH), for which they receive treatment with an alpha-blocker. Yet little is known about the impact of this drug class on safety and outcomes in the setting of heart failure. Of note, the use of alpha-blockers for treatment of hypertension was associated with increased risk of new-onset heart failure in the ALLHAT study.
To shed light on the safety of alpha-blockers in patients with prevalent heart failure, Dr. Warner and her coinvestigators analyzed data on nearly 170,000 men with a primary diagnosis of heart failure discharged from Veterans Affairs hospitals in 2002-2015. They determined that fully 28% of them left the hospital on an alpha-blocker. From this pool of nearly 48,000 heart failure patients, they were able to propensity-score match 38,991 on the basis of 54 baseline clinical characteristics to an equal number of VA heart failure patients who weren’t on an alpha-blocker. The study outcomes were time to first readmission for heart failure or all-cause mortality during 2 years of follow-up.
Patients on an alpha-blocker had a 38% heart failure readmission rate at 2 years, compared with 40% in nonusers, for a modest, albeit statistically significant, 6% reduction in relative risk. The all-cause mortality rate also was significantly lower in patients on an alpha-blocker: 40% versus 44%, for a 9% relative risk reduction.
In a subanalysis restricted to the heart failure patients on an alpha-blocker, higher-dose therapy was associated with a significantly lower incidence of all-cause mortality than was a lower-dose alpha-blocker during 2 years of follow-up, with a 9% relative risk reduction. A high-dose alpha-blocker, however, wasn’t significantly more effective than lower-dose therapy in terms of reducing heart failure readmissions, said Dr. Warner, a cardiologist at the Veterans Affairs Greater Los Angeles Healthcare System and the University of California, Los Angeles.
Similarly, patients treated with a nonspecific, peripherally vasoactive alpha-blocker had a significantly lower mortality rate than those on an alpha-1a-adrenergic–specific agent, with a highly significant 15% reduction in relative risk. The type of alpha-blocker, however, didn’t make a significant difference in terms of heart failure readmissions, where both types of agents were similarly better than not being on an alpha-blocker at all, she said.
Eighty-five percent of study participants were on a beta-blocker. Heart failure readmissions and all-cause mortality were significantly lower with alpha-blocker therapy, regardless of whether patients were on background beta-blocker therapy.
One audience member, however, noting that the beta-blocker carvedilol possesses some alpha-blocking effects, asked if outcomes differed depending on whether a patient was on carvedilol or metoprolol.
Dr. Warner replied that those numbers are still being crunched, and that the final answer isn’t in yet, but her preliminary impression is that the benefits of alpha-blocker therapy in terms of both heart failure readmissions and all-cause mortality were attenuated in the patients on carvedilol, possibly due to that beta-blocker’s alpha-blocking properties.
She reported having no financial conflicts regarding the study.
WASHINGTON – Prescribing alpha-adrenergic blocking agents for treatment of benign prostatic hypertrophy in men with heart failure proved to be not only safe, but also was associated with significantly reduced rates of both heart failure readmission and all-cause mortality in a large retrospective cohort study.
“These findings are associative, not necessarily causative. But the novel association between alpha-blocker treatment and improved outcomes may warrant further study,” Alberta L. Warner, MD, said at the annual meeting of the American College of Cardiology.
Many men with heart failure also have benign prostatic hypertrophy (BPH), for which they receive treatment with an alpha-blocker. Yet little is known about the impact of this drug class on safety and outcomes in the setting of heart failure. Of note, the use of alpha-blockers for treatment of hypertension was associated with increased risk of new-onset heart failure in the ALLHAT study.
To shed light on the safety of alpha-blockers in patients with prevalent heart failure, Dr. Warner and her coinvestigators analyzed data on nearly 170,000 men with a primary diagnosis of heart failure discharged from Veterans Affairs hospitals in 2002-2015. They determined that fully 28% of them left the hospital on an alpha-blocker. From this pool of nearly 48,000 heart failure patients, they were able to propensity-score match 38,991 on the basis of 54 baseline clinical characteristics to an equal number of VA heart failure patients who weren’t on an alpha-blocker. The study outcomes were time to first readmission for heart failure or all-cause mortality during 2 years of follow-up.
Patients on an alpha-blocker had a 38% heart failure readmission rate at 2 years, compared with 40% in nonusers, for a modest, albeit statistically significant, 6% reduction in relative risk. The all-cause mortality rate also was significantly lower in patients on an alpha-blocker: 40% versus 44%, for a 9% relative risk reduction.
In a subanalysis restricted to the heart failure patients on an alpha-blocker, higher-dose therapy was associated with a significantly lower incidence of all-cause mortality than was a lower-dose alpha-blocker during 2 years of follow-up, with a 9% relative risk reduction. A high-dose alpha-blocker, however, wasn’t significantly more effective than lower-dose therapy in terms of reducing heart failure readmissions, said Dr. Warner, a cardiologist at the Veterans Affairs Greater Los Angeles Healthcare System and the University of California, Los Angeles.
Similarly, patients treated with a nonspecific, peripherally vasoactive alpha-blocker had a significantly lower mortality rate than those on an alpha-1a-adrenergic–specific agent, with a highly significant 15% reduction in relative risk. The type of alpha-blocker, however, didn’t make a significant difference in terms of heart failure readmissions, where both types of agents were similarly better than not being on an alpha-blocker at all, she said.
Eighty-five percent of study participants were on a beta-blocker. Heart failure readmissions and all-cause mortality were significantly lower with alpha-blocker therapy, regardless of whether patients were on background beta-blocker therapy.
One audience member, however, noting that the beta-blocker carvedilol possesses some alpha-blocking effects, asked if outcomes differed depending on whether a patient was on carvedilol or metoprolol.
Dr. Warner replied that those numbers are still being crunched, and that the final answer isn’t in yet, but her preliminary impression is that the benefits of alpha-blocker therapy in terms of both heart failure readmissions and all-cause mortality were attenuated in the patients on carvedilol, possibly due to that beta-blocker’s alpha-blocking properties.
She reported having no financial conflicts regarding the study.
Key clinical point:
Major finding: The risk of all-cause mortality in heart failure patients on an alpha-blocker was 9% lower than in extensively matched controls during 2 years of follow-up.
Data source: This retrospective cohort study included 38,991 heart failure patients taking an alpha-blocker for benign prostatic hypertrophy who were propensity matched on 54 clinical characteristics to an equal number of heart failure controls not on the medication.
Disclosures: The study presenter reported having no financial conflicts.
NCI to Study African-American Cancer Survivors
Studies have shown that African Americans have higher incidences of cancer than that of other racial/ethnic groups. They also are more likely to be diagnosed later and to die of the cancer. Compared with whites, African Americans have poorer survival rates for the 4 most common types of cancer (lung, breast, prostate, and colorectal). The ready-to-launch Detroit Research on Cancer Survivors study, funded by the National Cancer Institute (NCI), is “uniquely poised” to find out why, said Douglas Lowy, MD, acting director of NCI.
The largest such study to date will include 5,560 African American cancer survivors and 2,780 family members and will look at cancer progression, recurrence, mortality as well as quality of life for survivors and their families. The researchers will investigate the “myriad factors that may affect cancer survival,” including type of treatment, coexisting disease, genetics, social structure, support, neighborhood context, poverty, stress, racial discrimination, and literacy.
The participants are drawn from 3 counties around Detroit where about 21,000 people are diagnosed with cancer every year. The study also uses data from the Detroit area population-based cancer registry, part of NCI’s Surveillance, Epidemiology and End Results (SEER) Program. Joanne Elena, PhD, MPH, scientific program director for the grant funding the study, calls it a “great example of an efficient use of an existing structure to rapidly recruit cancer survivors into research studies.”
The grant is for $9 million over 5 years. “Investigating the complex factors that lead to disparities in cancer among underserved populations should lead to a greater understanding of the social and biologic causes of such differences,” said Robert Croyle, PhD, director of NCI’s Division of Cancer Control and Population Sciences. “And our hope is that this knowledge will lead to better outcomes.”
Studies have shown that African Americans have higher incidences of cancer than that of other racial/ethnic groups. They also are more likely to be diagnosed later and to die of the cancer. Compared with whites, African Americans have poorer survival rates for the 4 most common types of cancer (lung, breast, prostate, and colorectal). The ready-to-launch Detroit Research on Cancer Survivors study, funded by the National Cancer Institute (NCI), is “uniquely poised” to find out why, said Douglas Lowy, MD, acting director of NCI.
The largest such study to date will include 5,560 African American cancer survivors and 2,780 family members and will look at cancer progression, recurrence, mortality as well as quality of life for survivors and their families. The researchers will investigate the “myriad factors that may affect cancer survival,” including type of treatment, coexisting disease, genetics, social structure, support, neighborhood context, poverty, stress, racial discrimination, and literacy.
The participants are drawn from 3 counties around Detroit where about 21,000 people are diagnosed with cancer every year. The study also uses data from the Detroit area population-based cancer registry, part of NCI’s Surveillance, Epidemiology and End Results (SEER) Program. Joanne Elena, PhD, MPH, scientific program director for the grant funding the study, calls it a “great example of an efficient use of an existing structure to rapidly recruit cancer survivors into research studies.”
The grant is for $9 million over 5 years. “Investigating the complex factors that lead to disparities in cancer among underserved populations should lead to a greater understanding of the social and biologic causes of such differences,” said Robert Croyle, PhD, director of NCI’s Division of Cancer Control and Population Sciences. “And our hope is that this knowledge will lead to better outcomes.”
Studies have shown that African Americans have higher incidences of cancer than that of other racial/ethnic groups. They also are more likely to be diagnosed later and to die of the cancer. Compared with whites, African Americans have poorer survival rates for the 4 most common types of cancer (lung, breast, prostate, and colorectal). The ready-to-launch Detroit Research on Cancer Survivors study, funded by the National Cancer Institute (NCI), is “uniquely poised” to find out why, said Douglas Lowy, MD, acting director of NCI.
The largest such study to date will include 5,560 African American cancer survivors and 2,780 family members and will look at cancer progression, recurrence, mortality as well as quality of life for survivors and their families. The researchers will investigate the “myriad factors that may affect cancer survival,” including type of treatment, coexisting disease, genetics, social structure, support, neighborhood context, poverty, stress, racial discrimination, and literacy.
The participants are drawn from 3 counties around Detroit where about 21,000 people are diagnosed with cancer every year. The study also uses data from the Detroit area population-based cancer registry, part of NCI’s Surveillance, Epidemiology and End Results (SEER) Program. Joanne Elena, PhD, MPH, scientific program director for the grant funding the study, calls it a “great example of an efficient use of an existing structure to rapidly recruit cancer survivors into research studies.”
The grant is for $9 million over 5 years. “Investigating the complex factors that lead to disparities in cancer among underserved populations should lead to a greater understanding of the social and biologic causes of such differences,” said Robert Croyle, PhD, director of NCI’s Division of Cancer Control and Population Sciences. “And our hope is that this knowledge will lead to better outcomes.”
Inhibitor produces durable responses in rel/ref iNHL

WASHINGTON, DC—An investigational drug can produce durable responses and has a manageable safety profile in patients with relapsed or refractory indolent non-Hodgkin lymphoma (iNHL), according to researchers.
The drug is copanlisib, an intravenous pan-class I phosphatidylinositol-3-kinase (PI3K) inhibitor.
In the phase 2 CHRONOS-1 trial, copanlisib produced an objective response rate (ORR) of 59.2%, with a complete response (CR) rate of 12%, in patients with relapsed/refractory iNHL.
The median duration of response exceeded 98 weeks.
There were 3 deaths considered related to copanlisib, and the most common treatment-related adverse events (AEs) were transient hyperglycemia and hypertension.
These results were presented at the AACR Annual Meeting 2017 (abstract CT149). The study is supported by Bayer, the company developing copanlisib.
CHRONOS-1 included 141 patients with iNHL. Most (n=104) had follicular lymphoma (FL), 23 had marginal zone lymphoma (MZL), 8 had small lymphocytic lymphoma, and 6 had lymphoplasmacytoid/Waldenstrӧm’s macroglobulinemia.
All patients had relapsed after or were refractory to at least 2 prior lines of therapy, which included both rituximab and an alkylating agent.
For this study, the patients received 60 mg of intravenous copanlisib intermittently on days 1, 8, and 15 of a 28-day cycle.
At the time of analysis, the median duration of treatment was 22 weeks (range, 1-105), and 46 patients were still receiving copanlisib.
Efficacy
For the entire cohort, the ORR was 59.2%. Twelve percent of patients achieved a CR, 47.2% had a partial response (PR), 29.6% had stable disease, and 2.1% had progressive disease.
Among patients with FL, the ORR was 58.7%, the CR rate was 14.4%, and the PR rate was 44.2%.
Among patients with MZL, the ORR was 69.6%, with 8.7% of patients achieving a CR and 60.9% achieving a PR.
For the entire cohort, the estimated median duration of response was 687 days (range, 0-687). For patients with FL, it was 370 days (range, 0-687).
The estimated median progression-free survival was 340 days (range, 0-736), and the median overall survival had not been reached at the time of analysis.
Safety
The most common treatment-related AEs were transient hyperglycemia (all grades, 49%/grade 3+, 40%) and hypertension (all grades, 29%/grade 3+, 23%).
The researchers said other AEs of interest were neutropenia (all grades, 25%/grade 3+, 19%), diarrhea (all grades, 18%/grade 3+, 4%), lung infection (all grades, 14%/grade 3+, 11%), pneumonitis (all grades, 7%/grade 3+, 1.4%), and colitis (0.7%, all grade 3+).
Laboratory AEs of interest were alanine aminotransferase increase (all grades, 23%/grade 1, 19%) and aspartate aminotransferase increase (all grades, 28%/grade 1, 25%).
There were 2 non-fatal opportunistic infections.
There were 6 deaths, and 3 of them were considered related to copanlisib. These 3 deaths were due to lung infection, respiratory failure, and a thromboembolic event.
“[I]nhibition of the PI3K pathway has been shown to be an effective therapeutic strategy in treating indolent lymphomas . . .,” said study investigator Martin Dreyling, MD, of Klinikum der Universität München-Grosshadern in Munich, Germany.
“However, concerns exist about the safety of available oral PI3K inhibitors . . . . The results of CHRONOS-1 demonstrate that intermittent intravenous administration of copanlisib achieved durable efficacy with a manageable safety profile in this difficult-to-treat patient population.” ![]()
WASHINGTON, DC—An investigational drug can produce durable responses and has a manageable safety profile in patients with relapsed or refractory indolent non-Hodgkin lymphoma (iNHL), according to researchers.
The drug is copanlisib, an intravenous pan-class I phosphatidylinositol-3-kinase (PI3K) inhibitor.
In the phase 2 CHRONOS-1 trial, copanlisib produced an objective response rate (ORR) of 59.2%, with a complete response (CR) rate of 12%, in patients with relapsed/refractory iNHL.
The median duration of response exceeded 98 weeks.
There were 3 deaths considered related to copanlisib, and the most common treatment-related adverse events (AEs) were transient hyperglycemia and hypertension.
These results were presented at the AACR Annual Meeting 2017 (abstract CT149). The study is supported by Bayer, the company developing copanlisib.
CHRONOS-1 included 141 patients with iNHL. Most (n=104) had follicular lymphoma (FL), 23 had marginal zone lymphoma (MZL), 8 had small lymphocytic lymphoma, and 6 had lymphoplasmacytoid/Waldenstrӧm’s macroglobulinemia.
All patients had relapsed after or were refractory to at least 2 prior lines of therapy, which included both rituximab and an alkylating agent.
For this study, the patients received 60 mg of intravenous copanlisib intermittently on days 1, 8, and 15 of a 28-day cycle.
At the time of analysis, the median duration of treatment was 22 weeks (range, 1-105), and 46 patients were still receiving copanlisib.
Efficacy
For the entire cohort, the ORR was 59.2%. Twelve percent of patients achieved a CR, 47.2% had a partial response (PR), 29.6% had stable disease, and 2.1% had progressive disease.
Among patients with FL, the ORR was 58.7%, the CR rate was 14.4%, and the PR rate was 44.2%.
Among patients with MZL, the ORR was 69.6%, with 8.7% of patients achieving a CR and 60.9% achieving a PR.
For the entire cohort, the estimated median duration of response was 687 days (range, 0-687). For patients with FL, it was 370 days (range, 0-687).
The estimated median progression-free survival was 340 days (range, 0-736), and the median overall survival had not been reached at the time of analysis.
Safety
The most common treatment-related AEs were transient hyperglycemia (all grades, 49%/grade 3+, 40%) and hypertension (all grades, 29%/grade 3+, 23%).
The researchers said other AEs of interest were neutropenia (all grades, 25%/grade 3+, 19%), diarrhea (all grades, 18%/grade 3+, 4%), lung infection (all grades, 14%/grade 3+, 11%), pneumonitis (all grades, 7%/grade 3+, 1.4%), and colitis (0.7%, all grade 3+).
Laboratory AEs of interest were alanine aminotransferase increase (all grades, 23%/grade 1, 19%) and aspartate aminotransferase increase (all grades, 28%/grade 1, 25%).
There were 2 non-fatal opportunistic infections.
There were 6 deaths, and 3 of them were considered related to copanlisib. These 3 deaths were due to lung infection, respiratory failure, and a thromboembolic event.
“[I]nhibition of the PI3K pathway has been shown to be an effective therapeutic strategy in treating indolent lymphomas . . .,” said study investigator Martin Dreyling, MD, of Klinikum der Universität München-Grosshadern in Munich, Germany.
“However, concerns exist about the safety of available oral PI3K inhibitors . . . . The results of CHRONOS-1 demonstrate that intermittent intravenous administration of copanlisib achieved durable efficacy with a manageable safety profile in this difficult-to-treat patient population.” ![]()
WASHINGTON, DC—An investigational drug can produce durable responses and has a manageable safety profile in patients with relapsed or refractory indolent non-Hodgkin lymphoma (iNHL), according to researchers.
The drug is copanlisib, an intravenous pan-class I phosphatidylinositol-3-kinase (PI3K) inhibitor.
In the phase 2 CHRONOS-1 trial, copanlisib produced an objective response rate (ORR) of 59.2%, with a complete response (CR) rate of 12%, in patients with relapsed/refractory iNHL.
The median duration of response exceeded 98 weeks.
There were 3 deaths considered related to copanlisib, and the most common treatment-related adverse events (AEs) were transient hyperglycemia and hypertension.
These results were presented at the AACR Annual Meeting 2017 (abstract CT149). The study is supported by Bayer, the company developing copanlisib.
CHRONOS-1 included 141 patients with iNHL. Most (n=104) had follicular lymphoma (FL), 23 had marginal zone lymphoma (MZL), 8 had small lymphocytic lymphoma, and 6 had lymphoplasmacytoid/Waldenstrӧm’s macroglobulinemia.
All patients had relapsed after or were refractory to at least 2 prior lines of therapy, which included both rituximab and an alkylating agent.
For this study, the patients received 60 mg of intravenous copanlisib intermittently on days 1, 8, and 15 of a 28-day cycle.
At the time of analysis, the median duration of treatment was 22 weeks (range, 1-105), and 46 patients were still receiving copanlisib.
Efficacy
For the entire cohort, the ORR was 59.2%. Twelve percent of patients achieved a CR, 47.2% had a partial response (PR), 29.6% had stable disease, and 2.1% had progressive disease.
Among patients with FL, the ORR was 58.7%, the CR rate was 14.4%, and the PR rate was 44.2%.
Among patients with MZL, the ORR was 69.6%, with 8.7% of patients achieving a CR and 60.9% achieving a PR.
For the entire cohort, the estimated median duration of response was 687 days (range, 0-687). For patients with FL, it was 370 days (range, 0-687).
The estimated median progression-free survival was 340 days (range, 0-736), and the median overall survival had not been reached at the time of analysis.
Safety
The most common treatment-related AEs were transient hyperglycemia (all grades, 49%/grade 3+, 40%) and hypertension (all grades, 29%/grade 3+, 23%).
The researchers said other AEs of interest were neutropenia (all grades, 25%/grade 3+, 19%), diarrhea (all grades, 18%/grade 3+, 4%), lung infection (all grades, 14%/grade 3+, 11%), pneumonitis (all grades, 7%/grade 3+, 1.4%), and colitis (0.7%, all grade 3+).
Laboratory AEs of interest were alanine aminotransferase increase (all grades, 23%/grade 1, 19%) and aspartate aminotransferase increase (all grades, 28%/grade 1, 25%).
There were 2 non-fatal opportunistic infections.
There were 6 deaths, and 3 of them were considered related to copanlisib. These 3 deaths were due to lung infection, respiratory failure, and a thromboembolic event.
“[I]nhibition of the PI3K pathway has been shown to be an effective therapeutic strategy in treating indolent lymphomas . . .,” said study investigator Martin Dreyling, MD, of Klinikum der Universität München-Grosshadern in Munich, Germany.
“However, concerns exist about the safety of available oral PI3K inhibitors . . . . The results of CHRONOS-1 demonstrate that intermittent intravenous administration of copanlisib achieved durable efficacy with a manageable safety profile in this difficult-to-treat patient population.” ![]()
First fossilized mammalian RBCs, Babesia-type pathogens found
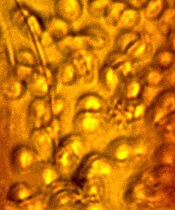
An amber specimen found in the Dominican Republic contained the first fossilized mammalian red blood cells (RBCs) and intraerythrocytic hemoparasites, according to an article published in the Journal of Medical Entomology.
The fossil contained an engorged tick and RBCs infected with parasites that resemble existing members of the Babesiidae and Theileriidae families of the order Piroplasmida.
It appears that 2 small holes in the back of the tick allowed blood to ooze out just as the tick became stuck in tree sap that later fossilized into amber.
“These 2 tiny holes indicate that something picked a tick off the mammal it was feeding on, puncturing it in the process and dropping it immediately into tree sap,” said study author George Poinar, Jr, PhD, of Oregon State University in Corvallis.
“This would be consistent with the grooming behavior of monkeys that we know lived at that time in this region. The fossilized blood cells, infected with these parasites, are simply amazing in their detail. This discovery provides the only known fossils of Babesia-type pathogens.”
Dr Poinar said the amber specimen came from mines located in the Cordillera Septentrional of the Dominican Republic. It may have originated anywhere from 15 to 45 million years ago.
The fossil contained an engorged nymphal tick of the genus Ambylomma. The parasites found in the RBCs were also found in the gut epithelial cells and body cavity of the tick.
“The life forms we find in amber can reveal so much about the history and evolution of diseases we still struggle with today,” Dr Poinar said. “This parasite, for instance, was clearly around millions of years before humans and appears to have evolved alongside primates, among other hosts.”
Part of what makes this fossil unique, Dr Poinar said, is the way in which the parasites and RBCs were preserved, almost as if they had been stained and otherwise treated in a lab.
The parasites were different enough in texture and density to stand out clearly within the RBCs during the natural embalming process for which amber is famous. ![]()
An amber specimen found in the Dominican Republic contained the first fossilized mammalian red blood cells (RBCs) and intraerythrocytic hemoparasites, according to an article published in the Journal of Medical Entomology.
The fossil contained an engorged tick and RBCs infected with parasites that resemble existing members of the Babesiidae and Theileriidae families of the order Piroplasmida.
It appears that 2 small holes in the back of the tick allowed blood to ooze out just as the tick became stuck in tree sap that later fossilized into amber.
“These 2 tiny holes indicate that something picked a tick off the mammal it was feeding on, puncturing it in the process and dropping it immediately into tree sap,” said study author George Poinar, Jr, PhD, of Oregon State University in Corvallis.
“This would be consistent with the grooming behavior of monkeys that we know lived at that time in this region. The fossilized blood cells, infected with these parasites, are simply amazing in their detail. This discovery provides the only known fossils of Babesia-type pathogens.”
Dr Poinar said the amber specimen came from mines located in the Cordillera Septentrional of the Dominican Republic. It may have originated anywhere from 15 to 45 million years ago.
The fossil contained an engorged nymphal tick of the genus Ambylomma. The parasites found in the RBCs were also found in the gut epithelial cells and body cavity of the tick.
“The life forms we find in amber can reveal so much about the history and evolution of diseases we still struggle with today,” Dr Poinar said. “This parasite, for instance, was clearly around millions of years before humans and appears to have evolved alongside primates, among other hosts.”
Part of what makes this fossil unique, Dr Poinar said, is the way in which the parasites and RBCs were preserved, almost as if they had been stained and otherwise treated in a lab.
The parasites were different enough in texture and density to stand out clearly within the RBCs during the natural embalming process for which amber is famous. ![]()
An amber specimen found in the Dominican Republic contained the first fossilized mammalian red blood cells (RBCs) and intraerythrocytic hemoparasites, according to an article published in the Journal of Medical Entomology.
The fossil contained an engorged tick and RBCs infected with parasites that resemble existing members of the Babesiidae and Theileriidae families of the order Piroplasmida.
It appears that 2 small holes in the back of the tick allowed blood to ooze out just as the tick became stuck in tree sap that later fossilized into amber.
“These 2 tiny holes indicate that something picked a tick off the mammal it was feeding on, puncturing it in the process and dropping it immediately into tree sap,” said study author George Poinar, Jr, PhD, of Oregon State University in Corvallis.
“This would be consistent with the grooming behavior of monkeys that we know lived at that time in this region. The fossilized blood cells, infected with these parasites, are simply amazing in their detail. This discovery provides the only known fossils of Babesia-type pathogens.”
Dr Poinar said the amber specimen came from mines located in the Cordillera Septentrional of the Dominican Republic. It may have originated anywhere from 15 to 45 million years ago.
The fossil contained an engorged nymphal tick of the genus Ambylomma. The parasites found in the RBCs were also found in the gut epithelial cells and body cavity of the tick.
“The life forms we find in amber can reveal so much about the history and evolution of diseases we still struggle with today,” Dr Poinar said. “This parasite, for instance, was clearly around millions of years before humans and appears to have evolved alongside primates, among other hosts.”
Part of what makes this fossil unique, Dr Poinar said, is the way in which the parasites and RBCs were preserved, almost as if they had been stained and otherwise treated in a lab.
The parasites were different enough in texture and density to stand out clearly within the RBCs during the natural embalming process for which amber is famous. ![]()
Rule identifies women at low risk of VTE recurrence

Results of the REVERSE-II study appear to validate the utility of the HERDOO2 rule to identify women who can safely stop taking anticoagulants after their first unprovoked venous thromboembolism (VTE).
Some women who were classified as low-risk according to HERDOO2 did experience VTE recurrence after they stopped taking anticoagulants.
However, their risk of recurrence was lower than that of women who were classified as high-risk and stopped taking anticoagulants.
These results were published in The BMJ.
“Patients can get very anxious trying to balance the risks of [anticoagulation] with the risks of another blood clot,” said study author Marc Rodger, MD, of Ottawa Hospital and University of Ottawa in Ontario, Canada.
“With this rule, we can confidently tell half of the women we see that they are at low risk of having another blood clot. This means they can stop taking blood thinners once their initial clot is treated, sparing them the cost, inconvenience, and risks of taking life-long medication.”
The HERDOO2 rule suggests a woman has a low risk of VTE if she has 1 or none of the following risk factors:
- HER=Hyperpigmentation, edema, or redness in either leg
- D=High levels of D-dimer in the blood
- O=Obesity (body mass index of 30 kg/m2 or more)
- O=Older age (65+).
To test the rule, Dr Rodgers and his colleagues evaluated 2785 men and women with a first, unprovoked VTE. The patients were recruited between 2008 and 2015 from 44 healthcare centers in 7 countries.
Patients who were found to be at low risk of VTE recurrence were told to stop taking anticoagulants after they completed the initial treatment for their first VTE.
For patients considered at high risk for VTE recurrence, the researchers left the decision of continuing anticoagulation to the patients and their doctors.
Low-risk patients
None of the men in this trial could be identified as low-risk using the HERDOO2 rule.
However, 631 women had a low risk of VTE recurrence according to HERDOO2. Most of these women (n=591) stopped anticoagulant therapy.
Twenty-seven low-risk women decided to continue anticoagulation, 1 patient’s physician decided she required continued anticoagulation, and 3 patients continued for “other” reasons.
Nine patients in this group were lost to follow-up.
High-risk patients
There were 2148 men and women considered at high risk for VTE recurrence. Most of these patients (n=1802) continued anticoagulation.
Of the 323 high-risk patients who stopped anticoagulation, 279 did so because of their own preference, 9 due to physician decision, 15 had a high risk of bleeding, and 20 stopped for “other” reasons.
Twenty-three patients in this group were lost to follow-up.
Results
The researchers followed the patients for a year after they had finished treatment for their first VTE.
The risk of recurrent major VTE per 100 patient-years was:
- 3.0% among low-risk women who discontinued anticoagulants
- 8.1% among men and high-risk women who discontinued anticoagulants
- 7.4% among high-risk women (only) who discontinued anticoagulants
- 1.6% among men and high-risk women who continued anticoagulants.
Among the low-risk women who continued to receive anticoagulants, there were no cases of recurrent, symptomatic VTE.
“We see 2 to 3 patients with unexplained blood clots every day at The Ottawa Hospital,” Dr Rodger said. “If this rule was applied across Canada, we estimate that over 10,000 women a year would be identified as low risk and be able to come off blood thinners.” ![]()
Results of the REVERSE-II study appear to validate the utility of the HERDOO2 rule to identify women who can safely stop taking anticoagulants after their first unprovoked venous thromboembolism (VTE).
Some women who were classified as low-risk according to HERDOO2 did experience VTE recurrence after they stopped taking anticoagulants.
However, their risk of recurrence was lower than that of women who were classified as high-risk and stopped taking anticoagulants.
These results were published in The BMJ.
“Patients can get very anxious trying to balance the risks of [anticoagulation] with the risks of another blood clot,” said study author Marc Rodger, MD, of Ottawa Hospital and University of Ottawa in Ontario, Canada.
“With this rule, we can confidently tell half of the women we see that they are at low risk of having another blood clot. This means they can stop taking blood thinners once their initial clot is treated, sparing them the cost, inconvenience, and risks of taking life-long medication.”
The HERDOO2 rule suggests a woman has a low risk of VTE if she has 1 or none of the following risk factors:
- HER=Hyperpigmentation, edema, or redness in either leg
- D=High levels of D-dimer in the blood
- O=Obesity (body mass index of 30 kg/m2 or more)
- O=Older age (65+).
To test the rule, Dr Rodgers and his colleagues evaluated 2785 men and women with a first, unprovoked VTE. The patients were recruited between 2008 and 2015 from 44 healthcare centers in 7 countries.
Patients who were found to be at low risk of VTE recurrence were told to stop taking anticoagulants after they completed the initial treatment for their first VTE.
For patients considered at high risk for VTE recurrence, the researchers left the decision of continuing anticoagulation to the patients and their doctors.
Low-risk patients
None of the men in this trial could be identified as low-risk using the HERDOO2 rule.
However, 631 women had a low risk of VTE recurrence according to HERDOO2. Most of these women (n=591) stopped anticoagulant therapy.
Twenty-seven low-risk women decided to continue anticoagulation, 1 patient’s physician decided she required continued anticoagulation, and 3 patients continued for “other” reasons.
Nine patients in this group were lost to follow-up.
High-risk patients
There were 2148 men and women considered at high risk for VTE recurrence. Most of these patients (n=1802) continued anticoagulation.
Of the 323 high-risk patients who stopped anticoagulation, 279 did so because of their own preference, 9 due to physician decision, 15 had a high risk of bleeding, and 20 stopped for “other” reasons.
Twenty-three patients in this group were lost to follow-up.
Results
The researchers followed the patients for a year after they had finished treatment for their first VTE.
The risk of recurrent major VTE per 100 patient-years was:
- 3.0% among low-risk women who discontinued anticoagulants
- 8.1% among men and high-risk women who discontinued anticoagulants
- 7.4% among high-risk women (only) who discontinued anticoagulants
- 1.6% among men and high-risk women who continued anticoagulants.
Among the low-risk women who continued to receive anticoagulants, there were no cases of recurrent, symptomatic VTE.
“We see 2 to 3 patients with unexplained blood clots every day at The Ottawa Hospital,” Dr Rodger said. “If this rule was applied across Canada, we estimate that over 10,000 women a year would be identified as low risk and be able to come off blood thinners.” ![]()
Results of the REVERSE-II study appear to validate the utility of the HERDOO2 rule to identify women who can safely stop taking anticoagulants after their first unprovoked venous thromboembolism (VTE).
Some women who were classified as low-risk according to HERDOO2 did experience VTE recurrence after they stopped taking anticoagulants.
However, their risk of recurrence was lower than that of women who were classified as high-risk and stopped taking anticoagulants.
These results were published in The BMJ.
“Patients can get very anxious trying to balance the risks of [anticoagulation] with the risks of another blood clot,” said study author Marc Rodger, MD, of Ottawa Hospital and University of Ottawa in Ontario, Canada.
“With this rule, we can confidently tell half of the women we see that they are at low risk of having another blood clot. This means they can stop taking blood thinners once their initial clot is treated, sparing them the cost, inconvenience, and risks of taking life-long medication.”
The HERDOO2 rule suggests a woman has a low risk of VTE if she has 1 or none of the following risk factors:
- HER=Hyperpigmentation, edema, or redness in either leg
- D=High levels of D-dimer in the blood
- O=Obesity (body mass index of 30 kg/m2 or more)
- O=Older age (65+).
To test the rule, Dr Rodgers and his colleagues evaluated 2785 men and women with a first, unprovoked VTE. The patients were recruited between 2008 and 2015 from 44 healthcare centers in 7 countries.
Patients who were found to be at low risk of VTE recurrence were told to stop taking anticoagulants after they completed the initial treatment for their first VTE.
For patients considered at high risk for VTE recurrence, the researchers left the decision of continuing anticoagulation to the patients and their doctors.
Low-risk patients
None of the men in this trial could be identified as low-risk using the HERDOO2 rule.
However, 631 women had a low risk of VTE recurrence according to HERDOO2. Most of these women (n=591) stopped anticoagulant therapy.
Twenty-seven low-risk women decided to continue anticoagulation, 1 patient’s physician decided she required continued anticoagulation, and 3 patients continued for “other” reasons.
Nine patients in this group were lost to follow-up.
High-risk patients
There were 2148 men and women considered at high risk for VTE recurrence. Most of these patients (n=1802) continued anticoagulation.
Of the 323 high-risk patients who stopped anticoagulation, 279 did so because of their own preference, 9 due to physician decision, 15 had a high risk of bleeding, and 20 stopped for “other” reasons.
Twenty-three patients in this group were lost to follow-up.
Results
The researchers followed the patients for a year after they had finished treatment for their first VTE.
The risk of recurrent major VTE per 100 patient-years was:
- 3.0% among low-risk women who discontinued anticoagulants
- 8.1% among men and high-risk women who discontinued anticoagulants
- 7.4% among high-risk women (only) who discontinued anticoagulants
- 1.6% among men and high-risk women who continued anticoagulants.
Among the low-risk women who continued to receive anticoagulants, there were no cases of recurrent, symptomatic VTE.
“We see 2 to 3 patients with unexplained blood clots every day at The Ottawa Hospital,” Dr Rodger said. “If this rule was applied across Canada, we estimate that over 10,000 women a year would be identified as low risk and be able to come off blood thinners.” ![]()
Pilot Has a Flighty Heart
ANSWER
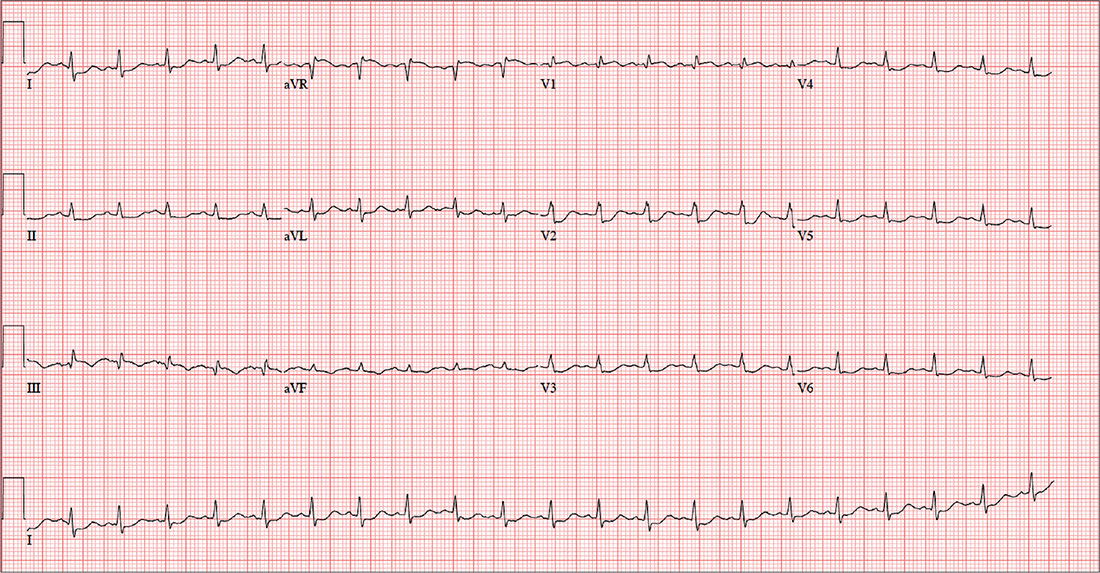
This ECG is consistent with sinus tachycardia, low-voltage QRS complexes, a posterior infarction, and ST- and T-wave abnormalities suggestive of inferior ischemia.
Sinus tachycardia is evidenced by the equal number of P and QRS complexes with a consistent PR interval. QRS complexes of lower amplitude than one would expect for the patient’s body habitus are deemed low voltage.
A posterior infarct is demonstrated by an R wave with no S wave in V1. Additionally, leads V2 and V3 show a pattern of a dominant R wave wit
Finally, inferior ischemia is identified by ST depressions in anterolateral leads I, aVL, V5, and V6, and T-wave inversions in inferior leads III and aVF.
ANSWER
This ECG is consistent with sinus tachycardia, low-voltage QRS complexes, a posterior infarction, and ST- and T-wave abnormalities suggestive of inferior ischemia.
Sinus tachycardia is evidenced by the equal number of P and QRS complexes with a consistent PR interval. QRS complexes of lower amplitude than one would expect for the patient’s body habitus are deemed low voltage.
A posterior infarct is demonstrated by an R wave with no S wave in V1. Additionally, leads V2 and V3 show a pattern of a dominant R wave wit
Finally, inferior ischemia is identified by ST depressions in anterolateral leads I, aVL, V5, and V6, and T-wave inversions in inferior leads III and aVF.
ANSWER
This ECG is consistent with sinus tachycardia, low-voltage QRS complexes, a posterior infarction, and ST- and T-wave abnormalities suggestive of inferior ischemia.
Sinus tachycardia is evidenced by the equal number of P and QRS complexes with a consistent PR interval. QRS complexes of lower amplitude than one would expect for the patient’s body habitus are deemed low voltage.
A posterior infarct is demonstrated by an R wave with no S wave in V1. Additionally, leads V2 and V3 show a pattern of a dominant R wave wit
Finally, inferior ischemia is identified by ST depressions in anterolateral leads I, aVL, V5, and V6, and T-wave inversions in inferior leads III and aVF.
For the past six hours, a 58-year-old man has been experiencing substernal chest discomfort. He is a commercial airline pilot for a regional carrier. Earlier today, he served as co-pilot on a roundtrip flight; about one hour before take-off, he started to feel a dull aching sensation in his chest that he attributed to his recently diagnosed gastroesophageal reflux disease (GERD). After landing, he purchased antacids in the airport terminal and took several, which provided only mild relief for the return trip. The pilot in command suggested he “get checked out” to make certain he didn’t have a bleeding ulcer.
Upon arrival at your facility, the patient appears uncomfortable but denies pain in his chest; there is no radiation to the neck, back, or arm. He denies palpitations, nausea, vomiting, diarrhea, and constipation. He says he feels more short of breath now than he did earlier, adding that “something just doesn’t feel right.”
The patient is a widower; his wife died of breast cancer at age 40. His daughter and son-in-law live in the same neighborhood so he can be close to his grandson. An avid triathlon participant, he has his own gym at home.
His medical history is remarkable for GERD, which was confirmed two months ago by upper endoscopy following several episodes of epigastric pain. He was prescribed a proton pump inhibitor, which he has forgotten to take for the past two days. His last flight physical, performed one year ago, was normal. Surgical history is remarkable for a tonsillectomy and a left inguinal hernia repair, both during childhood.
His current medication list includes lansoprazole and ibuprofen (as needed for musculoskeletal pain). He does not smoke, and he occasionally has a beer on the weekends when he isn’t working. The review of systems is noncontributory apart from his previously detailed symptoms.
Vital signs include a blood pressure of 130/86 mm Hg; pulse, 128 beats/min; respiratory rate, 12 breaths/min-1; and temperature, 97.9°F. His weight is 189 lb and his height, 73 in.
Physical exam reveals an uncomfortable, anxious-appearing male who is otherwise in excellent physical shape. Pertinent findings include a normal thyroid, no evidence of jugular venous distention, and clear lung fields bilaterally. The cardiac exam reveals a regular rate of 130 beats/min with no evidence of murmurs or rubs. The abdomen is flat and nontender, with no organomegaly. Peripheral pulses are equal bilaterally, and there is no peripheral edema. The neurologic exam is grossly intact.
A chest x-ray, ECG, and bloodwork are obtained. The ECG reveals a ventricular rate of 128 beats/min; PR interval, 136 ms; QRS duration, 72 ms; QT/QTc interval, 326/475 ms; P axis, 44°; R axis, 40°; and T axis, –47°. The ECG obtained during his flight physical one year ago showed normal sinus rhythm with nonspecific ST- and T-wave changes but was otherwise normal. With this history in mind, what is your interpretation of today’s ECG?

Defining high reliability
When the Joint Commission on Accreditation of Healthcare Organizations came to our hospital for a survey last fall, our administration was confident that the review would be favorable. The Joint Commission was stressing the reliability of hospitals and so were we. We had chartered a “High-Reliability Organization Enterprise Steering Committee” that was “empowered to make recommendations to the (executive board) on what is needed to achieve the goals of high reliability across the enterprise.” High reliability was a priority for our administration and for the Joint Commission. Unfortunately, nearly no one else knew what high reliability meant.

In 2001, Karl E. Weick and Kathleen M. Sutcliffe published their book, “Managing the Unexpected: Resilient Performance in an Age of Uncertainty,” (Hoboken, N.J.: Jossey-Bass, 2001), which defined high-reliability organizations as those that reliably prevent error. They included examples from the military and from aviation. They proffered five principles to guide those organizations wishing to become highly reliable:
1. Preoccupation with failure.
2. Reluctance to simplify interpretations.
3. Sensitivity to operations.
4. Commitment to resilience.
5. Deference to expertise.
In September 2005, the Agency for Healthcare Research and Quality created a document to adapt the concepts developed by Mr. Weick and Ms. Sutcliffe to the health care industry, where opportunities to avoid error and prevent catastrophe abound. The eventual result has been steady progress in measuring avoidable health care errors, such as avoiding central line–associated blood stream infections and holding health care organizations accountable for their reduction. However, organizational cultures are difficult to change, and there is still a long way to go.
In contrast to large systems, individual providers can change quickly, especially if there is incentive to do so. What principles would increase our own ability to become a high-reliability individuals (HRIs):
• Recognize failure as systemic, not personal. Health care providers are humans, and humans make mistakes. Unfortunately, we come from a tradition that rewards success and penalizes failure. Research shows that is better to recognize failure as something to be prevented next time rather than to be punished now. Admonitions to pay attention, focus more, and remember better rely on fallible humans and reliably fail. Systems solutions, such as checklists, timeouts, and hard stops reliably succeed. HRIs should blame error less often on people, and more often on system failures.
• Simple solutions are preferred to complex requirements. Chemotherapy was once calculated and written by hand. Every cancer center can recall tragic disasters that occurred as a result of errors either by the ordering physician or by interpretations made by pharmacists and nurses. The introduction of electronic chemotherapy ordering has nearly eliminated these mistakes. HRIs can initiate technology solutions to their work to help reduce the risk of errors.
• Sensitivity to patients. Patients often desire to be included as partners in their care. In addition to being present and attentive to patients, why not enlist them as colleagues in care? For example, the patient who has their own calendar of chemotherapy treatments – complete with agents, doses, and schedules – will be more likely to question perceived errors. HRIs are transparent.
• Resilience in character. Learning to accept the potential for error requires acceptance that others also are trying to prevent error and are not judging your competence. The physician who attacks those who are trying to help reduces the psychological safety required for colleagues to speak up when potential errors are identified. Physicians will become HRIs only when they lower their defenses and become more teammates rather than a soloists.
• Deference to evidence. The “way it has always been” must give way to the way things are. Anecdotes and personal conviction do not meet scientific standards and should be abandoned in the face of evidence. Yet, this seemingly obvious principle often is disregarded when clinicians are presented with standardized treatment pathways and limited formularies in the name of autonomy; autonomy is fine until patients are endangered by it. The HRI practices evidence-based medicine.
Marty Makary, MD, explores most of these principles in his book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care”(London: Bloomsbury Publishing, 2012). While written from a surgeon’s perspective, Dr. Makary exposes the dangerous state of modern medical care across all specialties. I recommend it as a sobering assessment of the way things are and as a prescription for health care systems and physicians to help them become more reliable.
How are you driving safety in your area? What are some best practices we can share with others? I invite you to reply to [email protected] to initiate a broader discussion of patient safety and reliability. Responses will be posted to hematologynews.com.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].
When the Joint Commission on Accreditation of Healthcare Organizations came to our hospital for a survey last fall, our administration was confident that the review would be favorable. The Joint Commission was stressing the reliability of hospitals and so were we. We had chartered a “High-Reliability Organization Enterprise Steering Committee” that was “empowered to make recommendations to the (executive board) on what is needed to achieve the goals of high reliability across the enterprise.” High reliability was a priority for our administration and for the Joint Commission. Unfortunately, nearly no one else knew what high reliability meant.
In 2001, Karl E. Weick and Kathleen M. Sutcliffe published their book, “Managing the Unexpected: Resilient Performance in an Age of Uncertainty,” (Hoboken, N.J.: Jossey-Bass, 2001), which defined high-reliability organizations as those that reliably prevent error. They included examples from the military and from aviation. They proffered five principles to guide those organizations wishing to become highly reliable:
1. Preoccupation with failure.
2. Reluctance to simplify interpretations.
3. Sensitivity to operations.
4. Commitment to resilience.
5. Deference to expertise.
In September 2005, the Agency for Healthcare Research and Quality created a document to adapt the concepts developed by Mr. Weick and Ms. Sutcliffe to the health care industry, where opportunities to avoid error and prevent catastrophe abound. The eventual result has been steady progress in measuring avoidable health care errors, such as avoiding central line–associated blood stream infections and holding health care organizations accountable for their reduction. However, organizational cultures are difficult to change, and there is still a long way to go.
In contrast to large systems, individual providers can change quickly, especially if there is incentive to do so. What principles would increase our own ability to become a high-reliability individuals (HRIs):
• Recognize failure as systemic, not personal. Health care providers are humans, and humans make mistakes. Unfortunately, we come from a tradition that rewards success and penalizes failure. Research shows that is better to recognize failure as something to be prevented next time rather than to be punished now. Admonitions to pay attention, focus more, and remember better rely on fallible humans and reliably fail. Systems solutions, such as checklists, timeouts, and hard stops reliably succeed. HRIs should blame error less often on people, and more often on system failures.
• Simple solutions are preferred to complex requirements. Chemotherapy was once calculated and written by hand. Every cancer center can recall tragic disasters that occurred as a result of errors either by the ordering physician or by interpretations made by pharmacists and nurses. The introduction of electronic chemotherapy ordering has nearly eliminated these mistakes. HRIs can initiate technology solutions to their work to help reduce the risk of errors.
• Sensitivity to patients. Patients often desire to be included as partners in their care. In addition to being present and attentive to patients, why not enlist them as colleagues in care? For example, the patient who has their own calendar of chemotherapy treatments – complete with agents, doses, and schedules – will be more likely to question perceived errors. HRIs are transparent.
• Resilience in character. Learning to accept the potential for error requires acceptance that others also are trying to prevent error and are not judging your competence. The physician who attacks those who are trying to help reduces the psychological safety required for colleagues to speak up when potential errors are identified. Physicians will become HRIs only when they lower their defenses and become more teammates rather than a soloists.
• Deference to evidence. The “way it has always been” must give way to the way things are. Anecdotes and personal conviction do not meet scientific standards and should be abandoned in the face of evidence. Yet, this seemingly obvious principle often is disregarded when clinicians are presented with standardized treatment pathways and limited formularies in the name of autonomy; autonomy is fine until patients are endangered by it. The HRI practices evidence-based medicine.
Marty Makary, MD, explores most of these principles in his book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care”(London: Bloomsbury Publishing, 2012). While written from a surgeon’s perspective, Dr. Makary exposes the dangerous state of modern medical care across all specialties. I recommend it as a sobering assessment of the way things are and as a prescription for health care systems and physicians to help them become more reliable.
How are you driving safety in your area? What are some best practices we can share with others? I invite you to reply to [email protected] to initiate a broader discussion of patient safety and reliability. Responses will be posted to hematologynews.com.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].
When the Joint Commission on Accreditation of Healthcare Organizations came to our hospital for a survey last fall, our administration was confident that the review would be favorable. The Joint Commission was stressing the reliability of hospitals and so were we. We had chartered a “High-Reliability Organization Enterprise Steering Committee” that was “empowered to make recommendations to the (executive board) on what is needed to achieve the goals of high reliability across the enterprise.” High reliability was a priority for our administration and for the Joint Commission. Unfortunately, nearly no one else knew what high reliability meant.
In 2001, Karl E. Weick and Kathleen M. Sutcliffe published their book, “Managing the Unexpected: Resilient Performance in an Age of Uncertainty,” (Hoboken, N.J.: Jossey-Bass, 2001), which defined high-reliability organizations as those that reliably prevent error. They included examples from the military and from aviation. They proffered five principles to guide those organizations wishing to become highly reliable:
1. Preoccupation with failure.
2. Reluctance to simplify interpretations.
3. Sensitivity to operations.
4. Commitment to resilience.
5. Deference to expertise.
In September 2005, the Agency for Healthcare Research and Quality created a document to adapt the concepts developed by Mr. Weick and Ms. Sutcliffe to the health care industry, where opportunities to avoid error and prevent catastrophe abound. The eventual result has been steady progress in measuring avoidable health care errors, such as avoiding central line–associated blood stream infections and holding health care organizations accountable for their reduction. However, organizational cultures are difficult to change, and there is still a long way to go.
In contrast to large systems, individual providers can change quickly, especially if there is incentive to do so. What principles would increase our own ability to become a high-reliability individuals (HRIs):
• Recognize failure as systemic, not personal. Health care providers are humans, and humans make mistakes. Unfortunately, we come from a tradition that rewards success and penalizes failure. Research shows that is better to recognize failure as something to be prevented next time rather than to be punished now. Admonitions to pay attention, focus more, and remember better rely on fallible humans and reliably fail. Systems solutions, such as checklists, timeouts, and hard stops reliably succeed. HRIs should blame error less often on people, and more often on system failures.
• Simple solutions are preferred to complex requirements. Chemotherapy was once calculated and written by hand. Every cancer center can recall tragic disasters that occurred as a result of errors either by the ordering physician or by interpretations made by pharmacists and nurses. The introduction of electronic chemotherapy ordering has nearly eliminated these mistakes. HRIs can initiate technology solutions to their work to help reduce the risk of errors.
• Sensitivity to patients. Patients often desire to be included as partners in their care. In addition to being present and attentive to patients, why not enlist them as colleagues in care? For example, the patient who has their own calendar of chemotherapy treatments – complete with agents, doses, and schedules – will be more likely to question perceived errors. HRIs are transparent.
• Resilience in character. Learning to accept the potential for error requires acceptance that others also are trying to prevent error and are not judging your competence. The physician who attacks those who are trying to help reduces the psychological safety required for colleagues to speak up when potential errors are identified. Physicians will become HRIs only when they lower their defenses and become more teammates rather than a soloists.
• Deference to evidence. The “way it has always been” must give way to the way things are. Anecdotes and personal conviction do not meet scientific standards and should be abandoned in the face of evidence. Yet, this seemingly obvious principle often is disregarded when clinicians are presented with standardized treatment pathways and limited formularies in the name of autonomy; autonomy is fine until patients are endangered by it. The HRI practices evidence-based medicine.
Marty Makary, MD, explores most of these principles in his book “Unaccountable: What Hospitals Won’t Tell You and How Transparency Can Revolutionize Health Care”(London: Bloomsbury Publishing, 2012). While written from a surgeon’s perspective, Dr. Makary exposes the dangerous state of modern medical care across all specialties. I recommend it as a sobering assessment of the way things are and as a prescription for health care systems and physicians to help them become more reliable.
How are you driving safety in your area? What are some best practices we can share with others? I invite you to reply to [email protected] to initiate a broader discussion of patient safety and reliability. Responses will be posted to hematologynews.com.
Dr. Kalaycio is Editor in Chief of Hematology News. Dr. Kalaycio chairs the department of hematologic oncology and blood disorders at Cleveland Clinic Taussig Cancer Institute. Contact him at [email protected].

Cosmetic Corner: Dermatologists Weigh in on Products for Hyperhidrosis
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
