User login
Ebola research update: March 2017
The struggle to defeat Ebola virus disease continues globally, although it may not always make the headlines. To catch up on what you may have missed, here are some notable news items and journal articles published over the past few weeks that are worth a second look.
Malaria parasite coinfections were common in patients presenting to Ebola treatment units in Sierra Leone and conferred an increased mortality risk in patients infected with Ebola virus, according to a study in the Lancet Infectious Diseases.
New oral vaccine technologies hold great promise as a tool for protecting endangered tropical wildlife from Ebola virus disease, according to a study on captive chimpanzees published in Scientific Reports.
A European study in JAMA found that immunity after heterologous primary and booster vaccination with Ebola virus vaccines Ad26.ZEBOV and MVA-BN-Filo persisted at 1 year. The researchers said a strategy of preemptive use of an Ad26.ZEBOV, followed by MVA-BN-Filo immunization schedule in at-risk populations may offer advantages over reactive use of single-dose vaccine regimens.
An analysis in Cell Host & Microbe concluded that the Ebola virus glycoprotein (GP) acquired an A82V change during the West Africa epidemic and that this change altered the capacity of GP to be activated by host factors, enhancing infection of human cells.
The overall decrease in bushmeat consumption in West Africa associated with the Ebola crisis may have had a short-term positive effect on vulnerable wildlife populations, according to a recent study.
A study in the Journal of Virology found that limiting the excessive TLR4-mediated proinflammatory response in Ebola virus infection should be considered as a potential supportive treatment option for Ebola virus disease.
The Clinical Data Interchange Standards Consortium and the Infectious Diseases Data Observatory have announced the availability of a new standard to assist in the collection, aggregation, and analysis of Ebola virus disease research data.
A small study published in PLOS One found that treatment with interferon beta-1a of people with Ebola virus disease may be associated with clearance of virus from blood, better clinical features, and potentially, improved survival.
Finally, medical evacuation of patients with suspected potentially fatal, infectious diseases such as Ebola virus is feasible using a light isolator containment pod for patients without critical dysfunctions, according to a study in BMC Emergency Medicine.
[email protected]
On Twitter @richpizzi
The struggle to defeat Ebola virus disease continues globally, although it may not always make the headlines. To catch up on what you may have missed, here are some notable news items and journal articles published over the past few weeks that are worth a second look.
Malaria parasite coinfections were common in patients presenting to Ebola treatment units in Sierra Leone and conferred an increased mortality risk in patients infected with Ebola virus, according to a study in the Lancet Infectious Diseases.
New oral vaccine technologies hold great promise as a tool for protecting endangered tropical wildlife from Ebola virus disease, according to a study on captive chimpanzees published in Scientific Reports.
A European study in JAMA found that immunity after heterologous primary and booster vaccination with Ebola virus vaccines Ad26.ZEBOV and MVA-BN-Filo persisted at 1 year. The researchers said a strategy of preemptive use of an Ad26.ZEBOV, followed by MVA-BN-Filo immunization schedule in at-risk populations may offer advantages over reactive use of single-dose vaccine regimens.
An analysis in Cell Host & Microbe concluded that the Ebola virus glycoprotein (GP) acquired an A82V change during the West Africa epidemic and that this change altered the capacity of GP to be activated by host factors, enhancing infection of human cells.
The overall decrease in bushmeat consumption in West Africa associated with the Ebola crisis may have had a short-term positive effect on vulnerable wildlife populations, according to a recent study.
A study in the Journal of Virology found that limiting the excessive TLR4-mediated proinflammatory response in Ebola virus infection should be considered as a potential supportive treatment option for Ebola virus disease.
The Clinical Data Interchange Standards Consortium and the Infectious Diseases Data Observatory have announced the availability of a new standard to assist in the collection, aggregation, and analysis of Ebola virus disease research data.
A small study published in PLOS One found that treatment with interferon beta-1a of people with Ebola virus disease may be associated with clearance of virus from blood, better clinical features, and potentially, improved survival.
Finally, medical evacuation of patients with suspected potentially fatal, infectious diseases such as Ebola virus is feasible using a light isolator containment pod for patients without critical dysfunctions, according to a study in BMC Emergency Medicine.
[email protected]
On Twitter @richpizzi
The struggle to defeat Ebola virus disease continues globally, although it may not always make the headlines. To catch up on what you may have missed, here are some notable news items and journal articles published over the past few weeks that are worth a second look.
Malaria parasite coinfections were common in patients presenting to Ebola treatment units in Sierra Leone and conferred an increased mortality risk in patients infected with Ebola virus, according to a study in the Lancet Infectious Diseases.
New oral vaccine technologies hold great promise as a tool for protecting endangered tropical wildlife from Ebola virus disease, according to a study on captive chimpanzees published in Scientific Reports.
A European study in JAMA found that immunity after heterologous primary and booster vaccination with Ebola virus vaccines Ad26.ZEBOV and MVA-BN-Filo persisted at 1 year. The researchers said a strategy of preemptive use of an Ad26.ZEBOV, followed by MVA-BN-Filo immunization schedule in at-risk populations may offer advantages over reactive use of single-dose vaccine regimens.
An analysis in Cell Host & Microbe concluded that the Ebola virus glycoprotein (GP) acquired an A82V change during the West Africa epidemic and that this change altered the capacity of GP to be activated by host factors, enhancing infection of human cells.
The overall decrease in bushmeat consumption in West Africa associated with the Ebola crisis may have had a short-term positive effect on vulnerable wildlife populations, according to a recent study.
A study in the Journal of Virology found that limiting the excessive TLR4-mediated proinflammatory response in Ebola virus infection should be considered as a potential supportive treatment option for Ebola virus disease.
The Clinical Data Interchange Standards Consortium and the Infectious Diseases Data Observatory have announced the availability of a new standard to assist in the collection, aggregation, and analysis of Ebola virus disease research data.
A small study published in PLOS One found that treatment with interferon beta-1a of people with Ebola virus disease may be associated with clearance of virus from blood, better clinical features, and potentially, improved survival.
Finally, medical evacuation of patients with suspected potentially fatal, infectious diseases such as Ebola virus is feasible using a light isolator containment pod for patients without critical dysfunctions, according to a study in BMC Emergency Medicine.
[email protected]
On Twitter @richpizzi
ACA brought down veterans’ uninsured rate
The percentage of uninsured veterans dropped by almost 40% in the first 2 years after the Affordable Care Act’s major coverage provisions were implemented, according to a report from the Robert Wood Johnson Foundation and the Urban Institute.
In 2015, 5.9% of the almost 9.4 million veterans aged 19-64 years were uninsured, down from 9.6% in 2013 – the statistically significant difference of 3.8 percentage points representing a relative decline of 38.5%. The difference was even greater for veterans living in the states that had expanded Medicaid by mid-2015, who saw their uninsured rate fall from 9% to 4.8%, compared with those in states that had not, whose uninsured rate declined from 10.3% to 7.1%, the report’s authors said.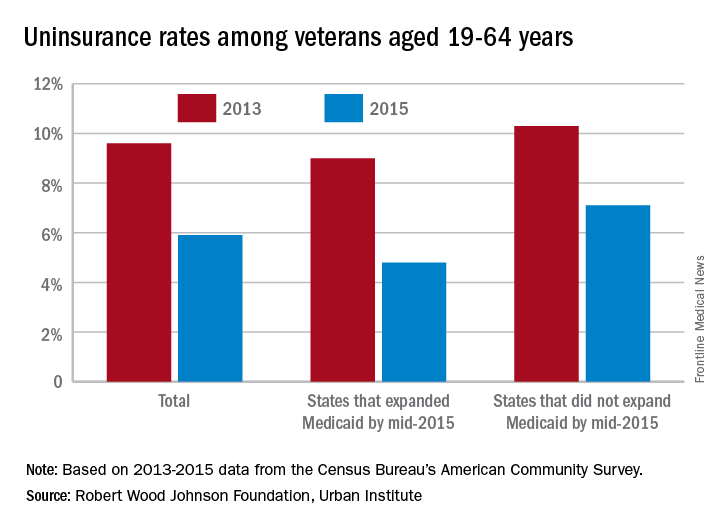
“These findings suggest that repeal of the ACA or particular components of the ACA (such as the Medicaid expansion) could reverse these coverage gains, increasing the number of veterans without health insurance coverage,” they wrote.
Of those currently uninsured, the report notes that “one-quarter are eligible for Medicaid but not enrolled, and … a number of uninsured veterans may qualify for VA care.” One option from the Department of Veterans Affairs, the Veterans Choice Program, was just extended beyond its expiration in August, ensuring that veterans will “continue to have access to care through local community providers [and] will not have to wait weeks or months, or drive long distances, to get the care they need,” Patrice A. Harris, MD, chair of the American Medical Association’s Board of Trustees, said in a statement.
The study was conducted by the Urban Institute with funding by the Robert Wood Johnson Foundation. Data for the analysis came from the Census Bureau’s American Community Survey and from the Centers for Disease Control and Prevention’s National Health Interview Survey.
The percentage of uninsured veterans dropped by almost 40% in the first 2 years after the Affordable Care Act’s major coverage provisions were implemented, according to a report from the Robert Wood Johnson Foundation and the Urban Institute.
In 2015, 5.9% of the almost 9.4 million veterans aged 19-64 years were uninsured, down from 9.6% in 2013 – the statistically significant difference of 3.8 percentage points representing a relative decline of 38.5%. The difference was even greater for veterans living in the states that had expanded Medicaid by mid-2015, who saw their uninsured rate fall from 9% to 4.8%, compared with those in states that had not, whose uninsured rate declined from 10.3% to 7.1%, the report’s authors said.
“These findings suggest that repeal of the ACA or particular components of the ACA (such as the Medicaid expansion) could reverse these coverage gains, increasing the number of veterans without health insurance coverage,” they wrote.
Of those currently uninsured, the report notes that “one-quarter are eligible for Medicaid but not enrolled, and … a number of uninsured veterans may qualify for VA care.” One option from the Department of Veterans Affairs, the Veterans Choice Program, was just extended beyond its expiration in August, ensuring that veterans will “continue to have access to care through local community providers [and] will not have to wait weeks or months, or drive long distances, to get the care they need,” Patrice A. Harris, MD, chair of the American Medical Association’s Board of Trustees, said in a statement.
The study was conducted by the Urban Institute with funding by the Robert Wood Johnson Foundation. Data for the analysis came from the Census Bureau’s American Community Survey and from the Centers for Disease Control and Prevention’s National Health Interview Survey.
The percentage of uninsured veterans dropped by almost 40% in the first 2 years after the Affordable Care Act’s major coverage provisions were implemented, according to a report from the Robert Wood Johnson Foundation and the Urban Institute.
In 2015, 5.9% of the almost 9.4 million veterans aged 19-64 years were uninsured, down from 9.6% in 2013 – the statistically significant difference of 3.8 percentage points representing a relative decline of 38.5%. The difference was even greater for veterans living in the states that had expanded Medicaid by mid-2015, who saw their uninsured rate fall from 9% to 4.8%, compared with those in states that had not, whose uninsured rate declined from 10.3% to 7.1%, the report’s authors said.
“These findings suggest that repeal of the ACA or particular components of the ACA (such as the Medicaid expansion) could reverse these coverage gains, increasing the number of veterans without health insurance coverage,” they wrote.
Of those currently uninsured, the report notes that “one-quarter are eligible for Medicaid but not enrolled, and … a number of uninsured veterans may qualify for VA care.” One option from the Department of Veterans Affairs, the Veterans Choice Program, was just extended beyond its expiration in August, ensuring that veterans will “continue to have access to care through local community providers [and] will not have to wait weeks or months, or drive long distances, to get the care they need,” Patrice A. Harris, MD, chair of the American Medical Association’s Board of Trustees, said in a statement.
The study was conducted by the Urban Institute with funding by the Robert Wood Johnson Foundation. Data for the analysis came from the Census Bureau’s American Community Survey and from the Centers for Disease Control and Prevention’s National Health Interview Survey.
VIDEO: Surgery succeeds with select hidradenitis suppurativa patients
WASHINGTON – Medication has its limits for some patients with more severe hidradenitis suppurativa, and these patients can often benefit from surgical treatment, Chris Sayed, MD, said at an educational session held by George Washington University.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Especially if patients have relatively limited areas of sinus, being able to do some local procedures [is] what will get the patient a lot better,” Dr. Sayed of the department of dermatology at the University of North Carolina, Chapel Hill, said in a video interview. “Whereas the medicines would never have made that sinus go away.”
The meeting was supported by AbbVie. Dr. Sayed disclosed financial relationships with the company.
WASHINGTON – Medication has its limits for some patients with more severe hidradenitis suppurativa, and these patients can often benefit from surgical treatment, Chris Sayed, MD, said at an educational session held by George Washington University.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Especially if patients have relatively limited areas of sinus, being able to do some local procedures [is] what will get the patient a lot better,” Dr. Sayed of the department of dermatology at the University of North Carolina, Chapel Hill, said in a video interview. “Whereas the medicines would never have made that sinus go away.”
The meeting was supported by AbbVie. Dr. Sayed disclosed financial relationships with the company.
WASHINGTON – Medication has its limits for some patients with more severe hidradenitis suppurativa, and these patients can often benefit from surgical treatment, Chris Sayed, MD, said at an educational session held by George Washington University.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Especially if patients have relatively limited areas of sinus, being able to do some local procedures [is] what will get the patient a lot better,” Dr. Sayed of the department of dermatology at the University of North Carolina, Chapel Hill, said in a video interview. “Whereas the medicines would never have made that sinus go away.”
The meeting was supported by AbbVie. Dr. Sayed disclosed financial relationships with the company.

Renflexis approved as second infliximab biosimilar
Infliximab-abda is the second infliximab biosimilar approved by the Food and Drug Administration, the agency announced April 21.
Infliximab-abda, to be marketed as Renflexis, is approved for all indications as the reference product, including Crohn’s diseases in adults and children, ulcerative colitis, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis, according to the product label.![]()
Like Remicade, Renflexis will come with a boxed warning and a Medication Guide that describes important information about its uses and risks, which include serious infections, lymphoma and other malignancies, liver injury, blood problems, lupuslike syndrome, psoriasis, and in rare cases, nervous system disorders.
Renflexis will be marketed by Merck Sharp & Dohme and is manufactured by Samsung Bioepis.
[email protected]
On Twitter @denisefulton
Infliximab-abda is the second infliximab biosimilar approved by the Food and Drug Administration, the agency announced April 21.
Infliximab-abda, to be marketed as Renflexis, is approved for all indications as the reference product, including Crohn’s diseases in adults and children, ulcerative colitis, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis, according to the product label.![]()
Like Remicade, Renflexis will come with a boxed warning and a Medication Guide that describes important information about its uses and risks, which include serious infections, lymphoma and other malignancies, liver injury, blood problems, lupuslike syndrome, psoriasis, and in rare cases, nervous system disorders.
Renflexis will be marketed by Merck Sharp & Dohme and is manufactured by Samsung Bioepis.
[email protected]
On Twitter @denisefulton
Infliximab-abda is the second infliximab biosimilar approved by the Food and Drug Administration, the agency announced April 21.
Infliximab-abda, to be marketed as Renflexis, is approved for all indications as the reference product, including Crohn’s diseases in adults and children, ulcerative colitis, rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and plaque psoriasis, according to the product label.![]()
Like Remicade, Renflexis will come with a boxed warning and a Medication Guide that describes important information about its uses and risks, which include serious infections, lymphoma and other malignancies, liver injury, blood problems, lupuslike syndrome, psoriasis, and in rare cases, nervous system disorders.
Renflexis will be marketed by Merck Sharp & Dohme and is manufactured by Samsung Bioepis.
[email protected]
On Twitter @denisefulton
New and Noteworthy Information—May 2017
The Biomarkers for Infant Brain Injury Score can identify infants with acute intracranial hemorrhage, according to a study published online ahead of print April 10 in JAMA Pediatrics. Binary logistic regression was used to develop a multivariable model incorporating three serum biomarkers and one clinical variable (total hemoglobin). The Biomarkers for Infant Brain Injury Score was applied to 599 infants (mean age, 4.7 months) at increased risk for abusive head trauma. Fifty-two percent were boys, 78% were white, and 8% were Hispanic. At a cutoff of 0.182, the model was 89.3% sensitive and 48.0% specific for acute intracranial hemorrhage. Positive and negative predictive values were 21.3% and 95.6%, respectively. The model was neither sensitive nor specific for atraumatic brain abnormalities, isolated skull fractures, or chronic intracranial hemorrhage.
The FDA has approved Ocrevus (ocrelizumab), an IV infusion, to treat adults with relapsing forms of multiple sclerosis (MS) and primary progressive MS. This drug is the first to be approved by the FDA for primary progressive MS. The efficacy of Ocrevus for the treatment of relapsing-remitting MS was shown in two clinical trials including 1,656 participants treated for 96 weeks. In both studies, patients receiving Ocrevus had reduced relapse rates and reduced worsening of disability, compared with patients receiving interferon beta-1a. In a study of 732 participants with primary progressive MS treated for at least 120 weeks, participants receiving Ocrevus had a longer time to the worsening of disability, compared with participants receiving placebo. Common side effects include infusion-related reactions and upper respiratory tract infection. Genentech markets Ocrevus.
Unemployed men and women and reemployed men have an increased risk of hemorrhagic and ischemic stroke and mortality, according to a study published online ahead of print April 6 in Stroke. This prospective study included 21,902 men and 19,826 women, ages 40 to 59, from nine public health centers across Japan. Participants were followed up from 1990–1993 to the end of 2009–2014. During the follow-up period, 973 incident strokes and 275 deaths from stroke occurred in men, as well as 460 strokes and 131 deaths from stroke in women. Compared with continuously employed subjects, the multivariable hazard ratio (HR) for total stroke incidence was 1.58 in unemployed men and 1.51 in unemployed women. HR for total stroke mortality was 2.22 in men and 2.48 in women.
In people with uncomplicated childhood-onset epilepsy and five-year terminal remission, young adult social outcomes are comparable to those of sibling controls, according to a study published online ahead of print April 4 in Epilepsia. Long-term social outcomes were assessed at the 15-year follow-up of the Connecticut Study of Epilepsy, which included 361 individuals with epilepsy and 173 controls. Social outcomes for cases with uncomplicated epilepsy with five or more years’ terminal remission were comparable to those of controls. Cases with uncomplicated epilepsy and less than five years of seizure freedom were more likely to be less productive and not to have a driver’s license. Complicated cases with epilepsy and less than five years of seizure freedom had worse outcomes across multiple domains, including not graduating high school.
Deep brain stimulation of the ventralis oralis internus and centromedian-parafascicular thalamus is an effective and relatively safe treatment for severe, refractory Tourette syndrome, according to a study published online ahead of print April 7 in the Journal of Neurosurgery. Researchers retrospectively reviewed outcomes in 13 patients with refractory Tourette syndrome who underwent medial thalamic deep brain stimulation for seven years. Patients were evaluated by a multidisciplinary team, and preoperative objective assessments were performed using the Yale Global Tic Severity Scale and Yale-Brown Obsessive Compulsive Scale. Patients showed an average decrease of 37% in total tic severity at their first postoperative visit. During their most recent visit, patient scores decreased from preoperative scores by an average of 50%, which was statistically significant. Device-related complications occurred in two patients, necessitating additional surgeries.
The FDA has approved Ingrezza (valbenazine) capsules for the treatment of adults with tardive dyskinesia. Ingrezza is a selective vesicular monoamine transporter 2 inhibitor. The approval of Ingrezza was based on data from the Kinect 3 study, a phase III, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study comparing once-daily Ingrezza (80 mg and 40 mg) to placebo over six weeks in patients with schizophrenia, schizoaffective disorder, or mood disorder. The mean change from baseline to week six in the AIMS dyskinesia total score was –3.2 for patients receiving 80 mg/day of Ingrezza, compared with –0.1 for controls. Ingrezza also was generally well tolerated, with somnolence as the only adverse event occurring at a rate of 5% or greater and twice the rate associated with placebo. Neurocrine Biosciences markets Ingrezza.
Benzodiazepine use is associated with an increased risk of pneumonia among patients with Alzheimer’s disease, according to a study published April 10 in CMAJ. Researchers obtained data on all community-dwelling adults with a recent diagnosis of Alzheimer disease in Finland between 2005 and 2011 from the Medication use and Alzheimer’s disease cohort. Incident users of benzodiazepines and nonbenzodiazepines were identified using a one-year washout period and matched with nonusers through propensity scores. Among 49,484 eligible participants with Alzheimer’s disease, 5,232 taking benzodiazepines and 3,269 taking nonbenzodiazepines were matched 1:1 with people not taking these drugs. Benzodiazepine and nonbenzodiazepine use was associated with a 22% increased risk of pneumonia. When analyzed separately, benzodiazepine use was significantly associated with a 28% increased risk of pneumonia, but nonbenzodiazepine use was not.
Hospitalization rates for acute ischemic stroke in young adults are increasing, along with the prevalence of traditional stroke risk factors, according to a study published online ahead of print April 10 in JAMA Neurology. Hospitalization data from the National Inpatient Sample from 1995 through 2012 were used to analyze acute stroke hospitalization rates among people ages 18 to 64. The 2003–2004 set included 362,339 hospitalizations, and the 2011–2012 set included 421,815 hospitalizations. Acute ischemic stroke hospitalization rates increased significantly for men and women, and for certain racial and ethnic groups, among younger adults ages 18 to 54. The prevalence of stroke risk factors among people hospitalized for acute ischemic stroke continued to increase from 2003–2004 through 2011–2012 for men and women ages 18 to 64.
A polygenic hazard score may help quantify individual differences in age-specific genetic risk for Alzheimer’s disease, according to a study published March 21 in PLOS Medicine. The investigators reviewed single-nucleotide polymorphisms associated with Alzheimer’s disease risk. Using a Cox proportional hazard model, they calculated polygenic hazard scores for participants in the Alzheimer’s Disease Genetics Consortium and tested them in two independent cohorts. People in the top polygenic hazard score quartile developed Alzheimer’s disease at a considerably lower age and had the highest yearly Alzheimer’s disease incidence rate. Among people who did not have the APOE ε3 allele, polygenic hazard score modified the age of expected onset by more than 10 years between the lowest and highest deciles. In independent cohorts, the polygenic hazard score strongly predicted age of Alzheimer’s disease onset.
Generalized anxiety disorder (GAD) is associated with migraine, according to a study published in the March issue of Headache. Researchers performed a secondary data analysis of the 2012 Canadian Community Health Survey-Mental Health. The first subsample included people with and without migraine. The second subsample was restricted to people with migraine. Six percent of people with migraine had had GAD in the previous year, compared with 2.1% of people without migraine. The adjusted odds of previous year GAD were 2.5 times higher among people with migraine than among people without. In the sample containing only migraineurs, the factors associated with higher odds of 12-month GAD included having a university degree, having low income, being without a confidant, and being male.
The rates of childhood epilepsy increase with maternal overweight or obesity in a dose-response manner, according to a study published online ahead of print April 3 in JAMA Neurology. Researchers conducted a population-based cohort study of 1,441,623 live single births at 22 or more gestational weeks in Sweden from January 1, 1997, to December 31, 2011. The risk of childhood epilepsy increased by maternal BMI from 6.30 per 10,000 child-years among normal-weight women to 12.4 per 10,000 child-years among women with grade III obesity. Risk of epilepsy increased by 11% in children of overweight mothers, compared with children of normal-weight mothers. Grade I obesity was associated with a 20% increased risk, grade II obesity was associated with a 30% increased risk, and grade III obesity was associated with an 82% increased risk.
The FDA has approved a label expansion for Trokendi XR (topiramate) to include migraine prophylaxis in adults and adolescents age 12 and older. Trokendi XR is a once-daily extended release formulation. The drug previously was approved as initial monotherapy and adjunctive therapy in patients age 6 and older with partial onset or primary generalized tonic-clonic seizures and as adjunctive therapy in patients age 6 and older with seizures associated with Lennox-Gastaut syndrome. Trokendi XR is available in 25-mg, 50-mg, 100-mg, and 200-mg capsules. The drug may cause sudden decrease in vision, secondary angle closure glaucoma, or decreased sweating. Approximately one in 500 people who take Trokendi XR may have suicidal thoughts. Supernus Pharmaceuticals markets Trokendi XR.
The FDA has approved Austedo (deutetrabenazine) tablets for the treatment of chorea associated with Huntington’s disease. Austedo was previously referred to by the name SD-809 and was granted Orphan Drug Designation by the FDA. Austedo is the second product approved for Huntington’s disease. The approval was based on phase III results in a randomized, double-blind, placebo-controlled, multicenter trial conducted in 90 ambulatory patients with manifest chorea associated with Huntington’s disease. Total Maximal Chorea Scores for patients receiving Austedo improved by approximately 4.4 units from baseline to the maintenance period, compared with approximately 1.9 units in the placebo group. At the week 13 follow-up visit (one week after discontinuation of the study drug), the Total Maximal Chorea Scores of patients who had received Austedo returned to baseline levels. Teva Pharmaceutical Industries markets Austedo.
—Kimberly Williams
The Biomarkers for Infant Brain Injury Score can identify infants with acute intracranial hemorrhage, according to a study published online ahead of print April 10 in JAMA Pediatrics. Binary logistic regression was used to develop a multivariable model incorporating three serum biomarkers and one clinical variable (total hemoglobin). The Biomarkers for Infant Brain Injury Score was applied to 599 infants (mean age, 4.7 months) at increased risk for abusive head trauma. Fifty-two percent were boys, 78% were white, and 8% were Hispanic. At a cutoff of 0.182, the model was 89.3% sensitive and 48.0% specific for acute intracranial hemorrhage. Positive and negative predictive values were 21.3% and 95.6%, respectively. The model was neither sensitive nor specific for atraumatic brain abnormalities, isolated skull fractures, or chronic intracranial hemorrhage.
The FDA has approved Ocrevus (ocrelizumab), an IV infusion, to treat adults with relapsing forms of multiple sclerosis (MS) and primary progressive MS. This drug is the first to be approved by the FDA for primary progressive MS. The efficacy of Ocrevus for the treatment of relapsing-remitting MS was shown in two clinical trials including 1,656 participants treated for 96 weeks. In both studies, patients receiving Ocrevus had reduced relapse rates and reduced worsening of disability, compared with patients receiving interferon beta-1a. In a study of 732 participants with primary progressive MS treated for at least 120 weeks, participants receiving Ocrevus had a longer time to the worsening of disability, compared with participants receiving placebo. Common side effects include infusion-related reactions and upper respiratory tract infection. Genentech markets Ocrevus.
Unemployed men and women and reemployed men have an increased risk of hemorrhagic and ischemic stroke and mortality, according to a study published online ahead of print April 6 in Stroke. This prospective study included 21,902 men and 19,826 women, ages 40 to 59, from nine public health centers across Japan. Participants were followed up from 1990–1993 to the end of 2009–2014. During the follow-up period, 973 incident strokes and 275 deaths from stroke occurred in men, as well as 460 strokes and 131 deaths from stroke in women. Compared with continuously employed subjects, the multivariable hazard ratio (HR) for total stroke incidence was 1.58 in unemployed men and 1.51 in unemployed women. HR for total stroke mortality was 2.22 in men and 2.48 in women.
In people with uncomplicated childhood-onset epilepsy and five-year terminal remission, young adult social outcomes are comparable to those of sibling controls, according to a study published online ahead of print April 4 in Epilepsia. Long-term social outcomes were assessed at the 15-year follow-up of the Connecticut Study of Epilepsy, which included 361 individuals with epilepsy and 173 controls. Social outcomes for cases with uncomplicated epilepsy with five or more years’ terminal remission were comparable to those of controls. Cases with uncomplicated epilepsy and less than five years of seizure freedom were more likely to be less productive and not to have a driver’s license. Complicated cases with epilepsy and less than five years of seizure freedom had worse outcomes across multiple domains, including not graduating high school.
Deep brain stimulation of the ventralis oralis internus and centromedian-parafascicular thalamus is an effective and relatively safe treatment for severe, refractory Tourette syndrome, according to a study published online ahead of print April 7 in the Journal of Neurosurgery. Researchers retrospectively reviewed outcomes in 13 patients with refractory Tourette syndrome who underwent medial thalamic deep brain stimulation for seven years. Patients were evaluated by a multidisciplinary team, and preoperative objective assessments were performed using the Yale Global Tic Severity Scale and Yale-Brown Obsessive Compulsive Scale. Patients showed an average decrease of 37% in total tic severity at their first postoperative visit. During their most recent visit, patient scores decreased from preoperative scores by an average of 50%, which was statistically significant. Device-related complications occurred in two patients, necessitating additional surgeries.
The FDA has approved Ingrezza (valbenazine) capsules for the treatment of adults with tardive dyskinesia. Ingrezza is a selective vesicular monoamine transporter 2 inhibitor. The approval of Ingrezza was based on data from the Kinect 3 study, a phase III, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study comparing once-daily Ingrezza (80 mg and 40 mg) to placebo over six weeks in patients with schizophrenia, schizoaffective disorder, or mood disorder. The mean change from baseline to week six in the AIMS dyskinesia total score was –3.2 for patients receiving 80 mg/day of Ingrezza, compared with –0.1 for controls. Ingrezza also was generally well tolerated, with somnolence as the only adverse event occurring at a rate of 5% or greater and twice the rate associated with placebo. Neurocrine Biosciences markets Ingrezza.
Benzodiazepine use is associated with an increased risk of pneumonia among patients with Alzheimer’s disease, according to a study published April 10 in CMAJ. Researchers obtained data on all community-dwelling adults with a recent diagnosis of Alzheimer disease in Finland between 2005 and 2011 from the Medication use and Alzheimer’s disease cohort. Incident users of benzodiazepines and nonbenzodiazepines were identified using a one-year washout period and matched with nonusers through propensity scores. Among 49,484 eligible participants with Alzheimer’s disease, 5,232 taking benzodiazepines and 3,269 taking nonbenzodiazepines were matched 1:1 with people not taking these drugs. Benzodiazepine and nonbenzodiazepine use was associated with a 22% increased risk of pneumonia. When analyzed separately, benzodiazepine use was significantly associated with a 28% increased risk of pneumonia, but nonbenzodiazepine use was not.
Hospitalization rates for acute ischemic stroke in young adults are increasing, along with the prevalence of traditional stroke risk factors, according to a study published online ahead of print April 10 in JAMA Neurology. Hospitalization data from the National Inpatient Sample from 1995 through 2012 were used to analyze acute stroke hospitalization rates among people ages 18 to 64. The 2003–2004 set included 362,339 hospitalizations, and the 2011–2012 set included 421,815 hospitalizations. Acute ischemic stroke hospitalization rates increased significantly for men and women, and for certain racial and ethnic groups, among younger adults ages 18 to 54. The prevalence of stroke risk factors among people hospitalized for acute ischemic stroke continued to increase from 2003–2004 through 2011–2012 for men and women ages 18 to 64.
A polygenic hazard score may help quantify individual differences in age-specific genetic risk for Alzheimer’s disease, according to a study published March 21 in PLOS Medicine. The investigators reviewed single-nucleotide polymorphisms associated with Alzheimer’s disease risk. Using a Cox proportional hazard model, they calculated polygenic hazard scores for participants in the Alzheimer’s Disease Genetics Consortium and tested them in two independent cohorts. People in the top polygenic hazard score quartile developed Alzheimer’s disease at a considerably lower age and had the highest yearly Alzheimer’s disease incidence rate. Among people who did not have the APOE ε3 allele, polygenic hazard score modified the age of expected onset by more than 10 years between the lowest and highest deciles. In independent cohorts, the polygenic hazard score strongly predicted age of Alzheimer’s disease onset.
Generalized anxiety disorder (GAD) is associated with migraine, according to a study published in the March issue of Headache. Researchers performed a secondary data analysis of the 2012 Canadian Community Health Survey-Mental Health. The first subsample included people with and without migraine. The second subsample was restricted to people with migraine. Six percent of people with migraine had had GAD in the previous year, compared with 2.1% of people without migraine. The adjusted odds of previous year GAD were 2.5 times higher among people with migraine than among people without. In the sample containing only migraineurs, the factors associated with higher odds of 12-month GAD included having a university degree, having low income, being without a confidant, and being male.
The rates of childhood epilepsy increase with maternal overweight or obesity in a dose-response manner, according to a study published online ahead of print April 3 in JAMA Neurology. Researchers conducted a population-based cohort study of 1,441,623 live single births at 22 or more gestational weeks in Sweden from January 1, 1997, to December 31, 2011. The risk of childhood epilepsy increased by maternal BMI from 6.30 per 10,000 child-years among normal-weight women to 12.4 per 10,000 child-years among women with grade III obesity. Risk of epilepsy increased by 11% in children of overweight mothers, compared with children of normal-weight mothers. Grade I obesity was associated with a 20% increased risk, grade II obesity was associated with a 30% increased risk, and grade III obesity was associated with an 82% increased risk.
The FDA has approved a label expansion for Trokendi XR (topiramate) to include migraine prophylaxis in adults and adolescents age 12 and older. Trokendi XR is a once-daily extended release formulation. The drug previously was approved as initial monotherapy and adjunctive therapy in patients age 6 and older with partial onset or primary generalized tonic-clonic seizures and as adjunctive therapy in patients age 6 and older with seizures associated with Lennox-Gastaut syndrome. Trokendi XR is available in 25-mg, 50-mg, 100-mg, and 200-mg capsules. The drug may cause sudden decrease in vision, secondary angle closure glaucoma, or decreased sweating. Approximately one in 500 people who take Trokendi XR may have suicidal thoughts. Supernus Pharmaceuticals markets Trokendi XR.
The FDA has approved Austedo (deutetrabenazine) tablets for the treatment of chorea associated with Huntington’s disease. Austedo was previously referred to by the name SD-809 and was granted Orphan Drug Designation by the FDA. Austedo is the second product approved for Huntington’s disease. The approval was based on phase III results in a randomized, double-blind, placebo-controlled, multicenter trial conducted in 90 ambulatory patients with manifest chorea associated with Huntington’s disease. Total Maximal Chorea Scores for patients receiving Austedo improved by approximately 4.4 units from baseline to the maintenance period, compared with approximately 1.9 units in the placebo group. At the week 13 follow-up visit (one week after discontinuation of the study drug), the Total Maximal Chorea Scores of patients who had received Austedo returned to baseline levels. Teva Pharmaceutical Industries markets Austedo.
—Kimberly Williams
The Biomarkers for Infant Brain Injury Score can identify infants with acute intracranial hemorrhage, according to a study published online ahead of print April 10 in JAMA Pediatrics. Binary logistic regression was used to develop a multivariable model incorporating three serum biomarkers and one clinical variable (total hemoglobin). The Biomarkers for Infant Brain Injury Score was applied to 599 infants (mean age, 4.7 months) at increased risk for abusive head trauma. Fifty-two percent were boys, 78% were white, and 8% were Hispanic. At a cutoff of 0.182, the model was 89.3% sensitive and 48.0% specific for acute intracranial hemorrhage. Positive and negative predictive values were 21.3% and 95.6%, respectively. The model was neither sensitive nor specific for atraumatic brain abnormalities, isolated skull fractures, or chronic intracranial hemorrhage.
The FDA has approved Ocrevus (ocrelizumab), an IV infusion, to treat adults with relapsing forms of multiple sclerosis (MS) and primary progressive MS. This drug is the first to be approved by the FDA for primary progressive MS. The efficacy of Ocrevus for the treatment of relapsing-remitting MS was shown in two clinical trials including 1,656 participants treated for 96 weeks. In both studies, patients receiving Ocrevus had reduced relapse rates and reduced worsening of disability, compared with patients receiving interferon beta-1a. In a study of 732 participants with primary progressive MS treated for at least 120 weeks, participants receiving Ocrevus had a longer time to the worsening of disability, compared with participants receiving placebo. Common side effects include infusion-related reactions and upper respiratory tract infection. Genentech markets Ocrevus.
Unemployed men and women and reemployed men have an increased risk of hemorrhagic and ischemic stroke and mortality, according to a study published online ahead of print April 6 in Stroke. This prospective study included 21,902 men and 19,826 women, ages 40 to 59, from nine public health centers across Japan. Participants were followed up from 1990–1993 to the end of 2009–2014. During the follow-up period, 973 incident strokes and 275 deaths from stroke occurred in men, as well as 460 strokes and 131 deaths from stroke in women. Compared with continuously employed subjects, the multivariable hazard ratio (HR) for total stroke incidence was 1.58 in unemployed men and 1.51 in unemployed women. HR for total stroke mortality was 2.22 in men and 2.48 in women.
In people with uncomplicated childhood-onset epilepsy and five-year terminal remission, young adult social outcomes are comparable to those of sibling controls, according to a study published online ahead of print April 4 in Epilepsia. Long-term social outcomes were assessed at the 15-year follow-up of the Connecticut Study of Epilepsy, which included 361 individuals with epilepsy and 173 controls. Social outcomes for cases with uncomplicated epilepsy with five or more years’ terminal remission were comparable to those of controls. Cases with uncomplicated epilepsy and less than five years of seizure freedom were more likely to be less productive and not to have a driver’s license. Complicated cases with epilepsy and less than five years of seizure freedom had worse outcomes across multiple domains, including not graduating high school.
Deep brain stimulation of the ventralis oralis internus and centromedian-parafascicular thalamus is an effective and relatively safe treatment for severe, refractory Tourette syndrome, according to a study published online ahead of print April 7 in the Journal of Neurosurgery. Researchers retrospectively reviewed outcomes in 13 patients with refractory Tourette syndrome who underwent medial thalamic deep brain stimulation for seven years. Patients were evaluated by a multidisciplinary team, and preoperative objective assessments were performed using the Yale Global Tic Severity Scale and Yale-Brown Obsessive Compulsive Scale. Patients showed an average decrease of 37% in total tic severity at their first postoperative visit. During their most recent visit, patient scores decreased from preoperative scores by an average of 50%, which was statistically significant. Device-related complications occurred in two patients, necessitating additional surgeries.
The FDA has approved Ingrezza (valbenazine) capsules for the treatment of adults with tardive dyskinesia. Ingrezza is a selective vesicular monoamine transporter 2 inhibitor. The approval of Ingrezza was based on data from the Kinect 3 study, a phase III, randomized, double-blind, placebo-controlled, parallel-group, fixed-dose study comparing once-daily Ingrezza (80 mg and 40 mg) to placebo over six weeks in patients with schizophrenia, schizoaffective disorder, or mood disorder. The mean change from baseline to week six in the AIMS dyskinesia total score was –3.2 for patients receiving 80 mg/day of Ingrezza, compared with –0.1 for controls. Ingrezza also was generally well tolerated, with somnolence as the only adverse event occurring at a rate of 5% or greater and twice the rate associated with placebo. Neurocrine Biosciences markets Ingrezza.
Benzodiazepine use is associated with an increased risk of pneumonia among patients with Alzheimer’s disease, according to a study published April 10 in CMAJ. Researchers obtained data on all community-dwelling adults with a recent diagnosis of Alzheimer disease in Finland between 2005 and 2011 from the Medication use and Alzheimer’s disease cohort. Incident users of benzodiazepines and nonbenzodiazepines were identified using a one-year washout period and matched with nonusers through propensity scores. Among 49,484 eligible participants with Alzheimer’s disease, 5,232 taking benzodiazepines and 3,269 taking nonbenzodiazepines were matched 1:1 with people not taking these drugs. Benzodiazepine and nonbenzodiazepine use was associated with a 22% increased risk of pneumonia. When analyzed separately, benzodiazepine use was significantly associated with a 28% increased risk of pneumonia, but nonbenzodiazepine use was not.
Hospitalization rates for acute ischemic stroke in young adults are increasing, along with the prevalence of traditional stroke risk factors, according to a study published online ahead of print April 10 in JAMA Neurology. Hospitalization data from the National Inpatient Sample from 1995 through 2012 were used to analyze acute stroke hospitalization rates among people ages 18 to 64. The 2003–2004 set included 362,339 hospitalizations, and the 2011–2012 set included 421,815 hospitalizations. Acute ischemic stroke hospitalization rates increased significantly for men and women, and for certain racial and ethnic groups, among younger adults ages 18 to 54. The prevalence of stroke risk factors among people hospitalized for acute ischemic stroke continued to increase from 2003–2004 through 2011–2012 for men and women ages 18 to 64.
A polygenic hazard score may help quantify individual differences in age-specific genetic risk for Alzheimer’s disease, according to a study published March 21 in PLOS Medicine. The investigators reviewed single-nucleotide polymorphisms associated with Alzheimer’s disease risk. Using a Cox proportional hazard model, they calculated polygenic hazard scores for participants in the Alzheimer’s Disease Genetics Consortium and tested them in two independent cohorts. People in the top polygenic hazard score quartile developed Alzheimer’s disease at a considerably lower age and had the highest yearly Alzheimer’s disease incidence rate. Among people who did not have the APOE ε3 allele, polygenic hazard score modified the age of expected onset by more than 10 years between the lowest and highest deciles. In independent cohorts, the polygenic hazard score strongly predicted age of Alzheimer’s disease onset.
Generalized anxiety disorder (GAD) is associated with migraine, according to a study published in the March issue of Headache. Researchers performed a secondary data analysis of the 2012 Canadian Community Health Survey-Mental Health. The first subsample included people with and without migraine. The second subsample was restricted to people with migraine. Six percent of people with migraine had had GAD in the previous year, compared with 2.1% of people without migraine. The adjusted odds of previous year GAD were 2.5 times higher among people with migraine than among people without. In the sample containing only migraineurs, the factors associated with higher odds of 12-month GAD included having a university degree, having low income, being without a confidant, and being male.
The rates of childhood epilepsy increase with maternal overweight or obesity in a dose-response manner, according to a study published online ahead of print April 3 in JAMA Neurology. Researchers conducted a population-based cohort study of 1,441,623 live single births at 22 or more gestational weeks in Sweden from January 1, 1997, to December 31, 2011. The risk of childhood epilepsy increased by maternal BMI from 6.30 per 10,000 child-years among normal-weight women to 12.4 per 10,000 child-years among women with grade III obesity. Risk of epilepsy increased by 11% in children of overweight mothers, compared with children of normal-weight mothers. Grade I obesity was associated with a 20% increased risk, grade II obesity was associated with a 30% increased risk, and grade III obesity was associated with an 82% increased risk.
The FDA has approved a label expansion for Trokendi XR (topiramate) to include migraine prophylaxis in adults and adolescents age 12 and older. Trokendi XR is a once-daily extended release formulation. The drug previously was approved as initial monotherapy and adjunctive therapy in patients age 6 and older with partial onset or primary generalized tonic-clonic seizures and as adjunctive therapy in patients age 6 and older with seizures associated with Lennox-Gastaut syndrome. Trokendi XR is available in 25-mg, 50-mg, 100-mg, and 200-mg capsules. The drug may cause sudden decrease in vision, secondary angle closure glaucoma, or decreased sweating. Approximately one in 500 people who take Trokendi XR may have suicidal thoughts. Supernus Pharmaceuticals markets Trokendi XR.
The FDA has approved Austedo (deutetrabenazine) tablets for the treatment of chorea associated with Huntington’s disease. Austedo was previously referred to by the name SD-809 and was granted Orphan Drug Designation by the FDA. Austedo is the second product approved for Huntington’s disease. The approval was based on phase III results in a randomized, double-blind, placebo-controlled, multicenter trial conducted in 90 ambulatory patients with manifest chorea associated with Huntington’s disease. Total Maximal Chorea Scores for patients receiving Austedo improved by approximately 4.4 units from baseline to the maintenance period, compared with approximately 1.9 units in the placebo group. At the week 13 follow-up visit (one week after discontinuation of the study drug), the Total Maximal Chorea Scores of patients who had received Austedo returned to baseline levels. Teva Pharmaceutical Industries markets Austedo.
—Kimberly Williams

For doctors, a clampdown on visas could have an uneven effect in the U.S.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Limiting the number of foreign doctors who can get visas to practice in the United States could have a significant impact on certain hospitals and states that rely on them, according to a new study.
The research, published online in JAMA this week, found that more than 2,100 U.S. employers were certified to fill nearly 10,500 physician jobs nationwide, in 2016. That represents 1.4% of the physician workforce overall. There were wide variations by state and employer, however (JAMA. 2017 Apr 17. doi: 10.1001/jama.2017.4877).
Employers in New York, Michigan and Illinois accounted for the most H-1B visa applications for foreign physicians, nearly a third of the total. North Dakota, however, had the most applicants as a percentage of its physician workforce: 4.7%.
The top three employers that submitted applications for the most doctors through the visa program were William Beaumont Hospital in Royal Oak, Mich., with 470 physician applications, Bronx-Lebanon (N.Y.) Hospital Center, with 213, and Cleveland Clinic Foundation, with 180.
“People underestimate the fragility of certain hospitals and their reliance on certain physicians for their functioning,” said study coauthor Peter Kahn, who graduates from Albert Einstein College of Medicine, New York, this spring.
The H-1B visa program allows employers to hire highly skilled professionals from abroad to fill employment gaps in the United States, typically in high-tech, science, engineering, and math jobs. But hospitals use the program as well, often to recruit doctors to serve in rural or underserved urban areas. The number of visas is capped at 85,000 annually.
That could change. On Tuesday, President Donald Trump signed an executive order reiterating his administration’s priority to buy American goods and hire American workers. Among other things, it requires federal agencies to suggest reforms to the H-1B visa program to ensure the visas are awarded appropriately.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Prognostic tool may allow tailored therapy for Hodgkin lymphoma
A newly developed “robust and inexpensive” prognostic tool, the Childhood Hodgkin International Prognostic Score (CHIPS), may allow better tailoring of therapy at the time of diagnosis for children and adolescents who have intermediate-risk Hodgkin lymphoma.
Researchers in the Children’s Oncology Group first assessed 562 patients receiving uniform standard treatment to identify which risk factors present at diagnosis best predicted response to therapy, and used them to develop the prognostic score. They considered such factors as patient age, the number of involved sites, hemoglobin level, albumin level, erythrocyte sedimentation rate, the presence or absence of a large mediastinal mass, nodal involvement, the total bulk of disease, and the presence or absence of B symptoms (fever, weight loss, and/or night sweats). The final CHIPS prognostic tool included four predictors of poor event-free survival that are easily ascertained at diagnosis: stage IV disease, a large mediastinal mass (one with a tumor to thoracic diameter ratio over 0.33), the presence of fever, and hypoalbuminemia (a level of less than 3.5 g/dL).
The investigators then confirmed the accuracy of that score in a validation cohort of 541 patients from the United States, Canada, Switzerland, Australia, New Zealand, the Netherlands, and Israel. All the study participants received four cycles of doxorubicin, bleomycin, vincristine, and etoposide (ABVE) with prednisone and cyclophosphamide (PC), followed by involved-field radiation therapy, said Cindy L. Schwartz, MD, of the division of pediatrics, University of Texas MD Anderson Cancer Center, Houston, and her associates.
Patients who had low a CHIPS of 0 or 1 had excellent 4-year event-free survival (93% and 89%, respectively), while patients with a high CHIPS of 2 or 3 had poorer 4-year event-free survival (78% and 69%, respectively). These findings remained consistent across all subgroups of patients, regardless of whether the tumors had nodular sclerosis histology or mixed cellular histology (Pediatr Blood Cancer. 2017 Apr;64[4]).
The study results suggest that patients with CHIPS 2 or 3 could be considered for high-risk Hodgkin lymphoma treatment such as higher-dose cyclophosphamide or the addition of brentuximab vedotin, while those with a CHIPS 0 or 1 could be considered for less aggressive treatment such as foregoing or reducing radiation therapy, Dr. Schwartz and her associates said.
This study was supported by a grant from the National Cancer Institute to the Children’s Oncology Group. Dr. Schwartz and her associates reported having no relevant financial disclosures.
A newly developed “robust and inexpensive” prognostic tool, the Childhood Hodgkin International Prognostic Score (CHIPS), may allow better tailoring of therapy at the time of diagnosis for children and adolescents who have intermediate-risk Hodgkin lymphoma.
Researchers in the Children’s Oncology Group first assessed 562 patients receiving uniform standard treatment to identify which risk factors present at diagnosis best predicted response to therapy, and used them to develop the prognostic score. They considered such factors as patient age, the number of involved sites, hemoglobin level, albumin level, erythrocyte sedimentation rate, the presence or absence of a large mediastinal mass, nodal involvement, the total bulk of disease, and the presence or absence of B symptoms (fever, weight loss, and/or night sweats). The final CHIPS prognostic tool included four predictors of poor event-free survival that are easily ascertained at diagnosis: stage IV disease, a large mediastinal mass (one with a tumor to thoracic diameter ratio over 0.33), the presence of fever, and hypoalbuminemia (a level of less than 3.5 g/dL).
The investigators then confirmed the accuracy of that score in a validation cohort of 541 patients from the United States, Canada, Switzerland, Australia, New Zealand, the Netherlands, and Israel. All the study participants received four cycles of doxorubicin, bleomycin, vincristine, and etoposide (ABVE) with prednisone and cyclophosphamide (PC), followed by involved-field radiation therapy, said Cindy L. Schwartz, MD, of the division of pediatrics, University of Texas MD Anderson Cancer Center, Houston, and her associates.
Patients who had low a CHIPS of 0 or 1 had excellent 4-year event-free survival (93% and 89%, respectively), while patients with a high CHIPS of 2 or 3 had poorer 4-year event-free survival (78% and 69%, respectively). These findings remained consistent across all subgroups of patients, regardless of whether the tumors had nodular sclerosis histology or mixed cellular histology (Pediatr Blood Cancer. 2017 Apr;64[4]).
The study results suggest that patients with CHIPS 2 or 3 could be considered for high-risk Hodgkin lymphoma treatment such as higher-dose cyclophosphamide or the addition of brentuximab vedotin, while those with a CHIPS 0 or 1 could be considered for less aggressive treatment such as foregoing or reducing radiation therapy, Dr. Schwartz and her associates said.
This study was supported by a grant from the National Cancer Institute to the Children’s Oncology Group. Dr. Schwartz and her associates reported having no relevant financial disclosures.
A newly developed “robust and inexpensive” prognostic tool, the Childhood Hodgkin International Prognostic Score (CHIPS), may allow better tailoring of therapy at the time of diagnosis for children and adolescents who have intermediate-risk Hodgkin lymphoma.
Researchers in the Children’s Oncology Group first assessed 562 patients receiving uniform standard treatment to identify which risk factors present at diagnosis best predicted response to therapy, and used them to develop the prognostic score. They considered such factors as patient age, the number of involved sites, hemoglobin level, albumin level, erythrocyte sedimentation rate, the presence or absence of a large mediastinal mass, nodal involvement, the total bulk of disease, and the presence or absence of B symptoms (fever, weight loss, and/or night sweats). The final CHIPS prognostic tool included four predictors of poor event-free survival that are easily ascertained at diagnosis: stage IV disease, a large mediastinal mass (one with a tumor to thoracic diameter ratio over 0.33), the presence of fever, and hypoalbuminemia (a level of less than 3.5 g/dL).
The investigators then confirmed the accuracy of that score in a validation cohort of 541 patients from the United States, Canada, Switzerland, Australia, New Zealand, the Netherlands, and Israel. All the study participants received four cycles of doxorubicin, bleomycin, vincristine, and etoposide (ABVE) with prednisone and cyclophosphamide (PC), followed by involved-field radiation therapy, said Cindy L. Schwartz, MD, of the division of pediatrics, University of Texas MD Anderson Cancer Center, Houston, and her associates.
Patients who had low a CHIPS of 0 or 1 had excellent 4-year event-free survival (93% and 89%, respectively), while patients with a high CHIPS of 2 or 3 had poorer 4-year event-free survival (78% and 69%, respectively). These findings remained consistent across all subgroups of patients, regardless of whether the tumors had nodular sclerosis histology or mixed cellular histology (Pediatr Blood Cancer. 2017 Apr;64[4]).
The study results suggest that patients with CHIPS 2 or 3 could be considered for high-risk Hodgkin lymphoma treatment such as higher-dose cyclophosphamide or the addition of brentuximab vedotin, while those with a CHIPS 0 or 1 could be considered for less aggressive treatment such as foregoing or reducing radiation therapy, Dr. Schwartz and her associates said.
This study was supported by a grant from the National Cancer Institute to the Children’s Oncology Group. Dr. Schwartz and her associates reported having no relevant financial disclosures.
Key clinical point: A newly developed “robust and inexpensive” prognostic tool, the Childhood Hodgkin International Prognostic Score, or CHIPS, may allow more tailored therapy for children and adolescents who have intermediate-risk Hodgkin lymphoma.
Major finding: Patients who had a low CHIPS of 0 or 1 had excellent 4-year event-free survival (93.1% and 88.5%, respectively), while patients with a high CHIPS of 2 or 3 had poorer 4-year event-free survival (77.6% and 69.2%).
Data source: A cohort study to develop (in 562 patients) and validate (in 541 patients) a score for predicting the response to standard treatment in pediatric Hodgkin lymphoma.
Disclosures: This study was supported by a grant from the National Cancer Institute to the Children’s Oncology Group. Dr. Schwartz and her associates reported having no relevant financial disclosures.
Pediatric Dermatology Consult - April 2017
BY JEREMY UDKOFF AND CATALINA MATIZ, MD
Juvenile xanthogranuloma (JXG), a non–Langerhans cell histiocytosis, is a common pediatric tumor that most commonly presents either at birth, in infants, or in young children – with the majority of cases occurring before 2 years. There is a male predominance with a 50% increased prevalence for solitary lesion disease and a 12 times higher prevalence in multilesion disease.1 Few lesions are concerning, and spontaneous regression of cutaneous lesions over the subsequent 1-5 years is a hallmark feature of JXG.2
Clinically, the JXGs are initially smooth, pinkish papules that may enlarge to 1-cm nodules and become yellowish in appearance before resolving to become atrophic macules or patches.2,3 JXGs are firm but rubbery and may become scaly and/or ulcerate as the lesion progresses.2 The JXGs most frequently occur superficially on the scalp and flexural areas of the upper extremities but infrequently present in the subcutaneous soft tissue, central nervous system, liver/spleen, eye/orbit, oropharynx, and muscle tissue.3,4 A well-described and concerning extracutaneous manifestations of JXG is ocular involvement and may be associated with bleeding into the anterior chamber of the eye. Despite this potentially disabling complication, screening for ocular involvement is recommended only in patients under age 2 years and in those with multiple skin lesions.5
The etiology of JXG is largely unknown. However, an association between neurofibromatosis type 1 (NF1) and the development of JXG and other diseases such as juvenile myelomonocytic leukemia, previously called juvenile chronic myelomonocytic leukemia, exists. It was thought that patients with NF1 and JXGs had a higher risk to develop juvenile myelomonocytic leukemia.6 However, a recent study showed that JXG alone does not appear to confer an increased risk for developing malignancy in children with NF1.6,7
Differential diagnosis and work-up
The clinical differential diagnosis for JXG includes dermatofibromas, Langerhans cell histiocytosis, mastocytosis, Spitz nevus, hemangioendothelioma, and other xanthomas. Because of the concerning nature of these look-alikes, equivocal cases should be referred to a pediatric dermatologist.
Although, altered laboratory values may be seen with systemic JXG with solid organ involvement, there are no systemic tests that can be used to determine if a cutaneous lesion is JXG. Thus, biopsy is the gold standard diagnostic for confirmatory testing. As a histiocytic disorder, JXG will display various macrophages on histologic examination. Additionally, one may observe a dense dermal infiltrate of vacuolated cells, along with wreathlike giant cells (Touton cells) and eosinophils.3 Although these Touton cells are thought to be pathognomonic of JXG, early lesions may lack these cells.8 Thus, their absence does not exclude the diagnosis of JXG. These are more serious cases, and the work-up conducted depends upon the organ system(s) involved. Systemic disease occurs in approximately 5% of patients.
Treatment and prognosis
Clinical monitoring is the only therapy required if there are only a few cutaneous JXGs present. However, systemic JXG is a concerning disease and various chemotherapy regimens have been recommended.3 Additionally, the use of a vinca alkaloid in conjunction with a steroid is associated with better outcomes than either of these agents alone.9 As a word of caution, in one study of 12 patients who received therapeutic systemic chemotherapy or radiation therapy to the brain, eye, skin, or heart, the patients had long-term disabilities and 2 patients died of their disease.4 In another study, children with systemic JXG, again, had a poor prognosis: Despite courses of multiagent chemotherapy, 2 of 17 patients died.9
Despite the poor results associated with systemic JXG, the vast majority of JXG patients have localized disease, which is associated with an excellent prognosis. The majority of these lesions spontaneously regress.
In conclusion, JXG is typically a benign, cutaneous disease. It presents in infants and children and involutes over a 1-5 year period. Lesions that are not classic for JXG should be referred to a pediatric dermatologist, and biopsy is the gold standard diagnosis. Most manifestations of JXG do not require therapy. However, systemic JXG may be difficult to treat and is associated with poor outcomes.
Dr. Catalina Matiz is assistant professor of dermatology at Rady Children’s Hospital-San Diego, associated with the University of California, San Diego. Jeremy Udkoff is a medical student at the university. Neither Dr. Matiz nor Mr. Udkoff have relevant financial disclosures.
References
1. Am J Surg Pathol. 2005 Jan;29(1):21-8.
2. Int J Dermatol. 2015 Oct;54(10):1109-23.
4. J Pediatr. 1996 Aug;129(2):227-37.
5. J Am Acad Dermatol. 1996 Mar;34(3):445-9.
6. J Am Acad Dermatol. 2017 Feb 8. pii: S0190-9622(16)31196-3.
7. Pediatr Dermatol. 2004 Mar-Apr;21(2):97-101.
BY JEREMY UDKOFF AND CATALINA MATIZ, MD
Juvenile xanthogranuloma (JXG), a non–Langerhans cell histiocytosis, is a common pediatric tumor that most commonly presents either at birth, in infants, or in young children – with the majority of cases occurring before 2 years. There is a male predominance with a 50% increased prevalence for solitary lesion disease and a 12 times higher prevalence in multilesion disease.1 Few lesions are concerning, and spontaneous regression of cutaneous lesions over the subsequent 1-5 years is a hallmark feature of JXG.2
Clinically, the JXGs are initially smooth, pinkish papules that may enlarge to 1-cm nodules and become yellowish in appearance before resolving to become atrophic macules or patches.2,3 JXGs are firm but rubbery and may become scaly and/or ulcerate as the lesion progresses.2 The JXGs most frequently occur superficially on the scalp and flexural areas of the upper extremities but infrequently present in the subcutaneous soft tissue, central nervous system, liver/spleen, eye/orbit, oropharynx, and muscle tissue.3,4 A well-described and concerning extracutaneous manifestations of JXG is ocular involvement and may be associated with bleeding into the anterior chamber of the eye. Despite this potentially disabling complication, screening for ocular involvement is recommended only in patients under age 2 years and in those with multiple skin lesions.5
The etiology of JXG is largely unknown. However, an association between neurofibromatosis type 1 (NF1) and the development of JXG and other diseases such as juvenile myelomonocytic leukemia, previously called juvenile chronic myelomonocytic leukemia, exists. It was thought that patients with NF1 and JXGs had a higher risk to develop juvenile myelomonocytic leukemia.6 However, a recent study showed that JXG alone does not appear to confer an increased risk for developing malignancy in children with NF1.6,7
Differential diagnosis and work-up
The clinical differential diagnosis for JXG includes dermatofibromas, Langerhans cell histiocytosis, mastocytosis, Spitz nevus, hemangioendothelioma, and other xanthomas. Because of the concerning nature of these look-alikes, equivocal cases should be referred to a pediatric dermatologist.
Although, altered laboratory values may be seen with systemic JXG with solid organ involvement, there are no systemic tests that can be used to determine if a cutaneous lesion is JXG. Thus, biopsy is the gold standard diagnostic for confirmatory testing. As a histiocytic disorder, JXG will display various macrophages on histologic examination. Additionally, one may observe a dense dermal infiltrate of vacuolated cells, along with wreathlike giant cells (Touton cells) and eosinophils.3 Although these Touton cells are thought to be pathognomonic of JXG, early lesions may lack these cells.8 Thus, their absence does not exclude the diagnosis of JXG. These are more serious cases, and the work-up conducted depends upon the organ system(s) involved. Systemic disease occurs in approximately 5% of patients.
Treatment and prognosis
Clinical monitoring is the only therapy required if there are only a few cutaneous JXGs present. However, systemic JXG is a concerning disease and various chemotherapy regimens have been recommended.3 Additionally, the use of a vinca alkaloid in conjunction with a steroid is associated with better outcomes than either of these agents alone.9 As a word of caution, in one study of 12 patients who received therapeutic systemic chemotherapy or radiation therapy to the brain, eye, skin, or heart, the patients had long-term disabilities and 2 patients died of their disease.4 In another study, children with systemic JXG, again, had a poor prognosis: Despite courses of multiagent chemotherapy, 2 of 17 patients died.9
Despite the poor results associated with systemic JXG, the vast majority of JXG patients have localized disease, which is associated with an excellent prognosis. The majority of these lesions spontaneously regress.
In conclusion, JXG is typically a benign, cutaneous disease. It presents in infants and children and involutes over a 1-5 year period. Lesions that are not classic for JXG should be referred to a pediatric dermatologist, and biopsy is the gold standard diagnosis. Most manifestations of JXG do not require therapy. However, systemic JXG may be difficult to treat and is associated with poor outcomes.
Dr. Catalina Matiz is assistant professor of dermatology at Rady Children’s Hospital-San Diego, associated with the University of California, San Diego. Jeremy Udkoff is a medical student at the university. Neither Dr. Matiz nor Mr. Udkoff have relevant financial disclosures.
References
1. Am J Surg Pathol. 2005 Jan;29(1):21-8.
2. Int J Dermatol. 2015 Oct;54(10):1109-23.
4. J Pediatr. 1996 Aug;129(2):227-37.
5. J Am Acad Dermatol. 1996 Mar;34(3):445-9.
6. J Am Acad Dermatol. 2017 Feb 8. pii: S0190-9622(16)31196-3.
7. Pediatr Dermatol. 2004 Mar-Apr;21(2):97-101.
BY JEREMY UDKOFF AND CATALINA MATIZ, MD
Juvenile xanthogranuloma (JXG), a non–Langerhans cell histiocytosis, is a common pediatric tumor that most commonly presents either at birth, in infants, or in young children – with the majority of cases occurring before 2 years. There is a male predominance with a 50% increased prevalence for solitary lesion disease and a 12 times higher prevalence in multilesion disease.1 Few lesions are concerning, and spontaneous regression of cutaneous lesions over the subsequent 1-5 years is a hallmark feature of JXG.2
Clinically, the JXGs are initially smooth, pinkish papules that may enlarge to 1-cm nodules and become yellowish in appearance before resolving to become atrophic macules or patches.2,3 JXGs are firm but rubbery and may become scaly and/or ulcerate as the lesion progresses.2 The JXGs most frequently occur superficially on the scalp and flexural areas of the upper extremities but infrequently present in the subcutaneous soft tissue, central nervous system, liver/spleen, eye/orbit, oropharynx, and muscle tissue.3,4 A well-described and concerning extracutaneous manifestations of JXG is ocular involvement and may be associated with bleeding into the anterior chamber of the eye. Despite this potentially disabling complication, screening for ocular involvement is recommended only in patients under age 2 years and in those with multiple skin lesions.5
The etiology of JXG is largely unknown. However, an association between neurofibromatosis type 1 (NF1) and the development of JXG and other diseases such as juvenile myelomonocytic leukemia, previously called juvenile chronic myelomonocytic leukemia, exists. It was thought that patients with NF1 and JXGs had a higher risk to develop juvenile myelomonocytic leukemia.6 However, a recent study showed that JXG alone does not appear to confer an increased risk for developing malignancy in children with NF1.6,7
Differential diagnosis and work-up
The clinical differential diagnosis for JXG includes dermatofibromas, Langerhans cell histiocytosis, mastocytosis, Spitz nevus, hemangioendothelioma, and other xanthomas. Because of the concerning nature of these look-alikes, equivocal cases should be referred to a pediatric dermatologist.
Although, altered laboratory values may be seen with systemic JXG with solid organ involvement, there are no systemic tests that can be used to determine if a cutaneous lesion is JXG. Thus, biopsy is the gold standard diagnostic for confirmatory testing. As a histiocytic disorder, JXG will display various macrophages on histologic examination. Additionally, one may observe a dense dermal infiltrate of vacuolated cells, along with wreathlike giant cells (Touton cells) and eosinophils.3 Although these Touton cells are thought to be pathognomonic of JXG, early lesions may lack these cells.8 Thus, their absence does not exclude the diagnosis of JXG. These are more serious cases, and the work-up conducted depends upon the organ system(s) involved. Systemic disease occurs in approximately 5% of patients.
Treatment and prognosis
Clinical monitoring is the only therapy required if there are only a few cutaneous JXGs present. However, systemic JXG is a concerning disease and various chemotherapy regimens have been recommended.3 Additionally, the use of a vinca alkaloid in conjunction with a steroid is associated with better outcomes than either of these agents alone.9 As a word of caution, in one study of 12 patients who received therapeutic systemic chemotherapy or radiation therapy to the brain, eye, skin, or heart, the patients had long-term disabilities and 2 patients died of their disease.4 In another study, children with systemic JXG, again, had a poor prognosis: Despite courses of multiagent chemotherapy, 2 of 17 patients died.9
Despite the poor results associated with systemic JXG, the vast majority of JXG patients have localized disease, which is associated with an excellent prognosis. The majority of these lesions spontaneously regress.
In conclusion, JXG is typically a benign, cutaneous disease. It presents in infants and children and involutes over a 1-5 year period. Lesions that are not classic for JXG should be referred to a pediatric dermatologist, and biopsy is the gold standard diagnosis. Most manifestations of JXG do not require therapy. However, systemic JXG may be difficult to treat and is associated with poor outcomes.
Dr. Catalina Matiz is assistant professor of dermatology at Rady Children’s Hospital-San Diego, associated with the University of California, San Diego. Jeremy Udkoff is a medical student at the university. Neither Dr. Matiz nor Mr. Udkoff have relevant financial disclosures.
References
1. Am J Surg Pathol. 2005 Jan;29(1):21-8.
2. Int J Dermatol. 2015 Oct;54(10):1109-23.
4. J Pediatr. 1996 Aug;129(2):227-37.
5. J Am Acad Dermatol. 1996 Mar;34(3):445-9.
6. J Am Acad Dermatol. 2017 Feb 8. pii: S0190-9622(16)31196-3.
7. Pediatr Dermatol. 2004 Mar-Apr;21(2):97-101.

One month later, the patient returned to our clinic with an urgent concern. The patient accidentally scraped the lesion, and it bled heavily for 15 minutes before subsiding. The mother stated that the lesion grew rapidly since the prior visit and became painful. On repeat physical examination the lesion was a 1-cm fungiform, yellow to pink nodule, with central ulceration.
Approaches to isolating the uterine artery at its origin from the internal iliac artery

Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Advanced techniques in cystectomy for mature cystic teratomas
- Novel classification of labial anatomy and evaluation in the treatment of labial agglutination
- Strategies for prophylactic oophoropexy
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Advanced techniques in cystectomy for mature cystic teratomas
- Novel classification of labial anatomy and evaluation in the treatment of labial agglutination
- Strategies for prophylactic oophoropexy
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Advanced techniques in cystectomy for mature cystic teratomas
- Novel classification of labial anatomy and evaluation in the treatment of labial agglutination
- Strategies for prophylactic oophoropexy
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
This video is brought to you by![]()
Newly diagnosed mantle cell lymphoma is ‘one of the hardest consultations’
NEW YORK – Relatively young patients with newly diagnosed, average-risk mantle cell lymphoma who go into remission on induction therapy face a difficult choice on their next management step: undergo immediate autologous stem cell transplantation or defer the stem cell transplant and continue on maintenance therapy.
The choice is especially difficult because both are currently considered reasonable options and each choice has certain attractions and downsides, experts highlighted in discussing this fork-in-the-road decision patients face.

Immediate autologous stem cell transplantation (ASCT) has a good chance to allow the patient to remain treatment free and in remission for as long as about 10 years, but it involves intensive upfront treatment for 6-9 months, during which the patient will likely not be able to work or carry on many usual activities. Deferring the transplant with maintenance therapy puts off this life-disrupting initial period of intensive therapy for what may be several years, but relapse on maintenance therapy is inevitable and once it happens the patient may not have as successful an outcome from an ASCT. It also means several years of ongoing drug therapy with a maintenance regimen.
“I tell my fellows that patients with newly diagnosed mantle cell lymphoma [are] one of the hardest consultations because, unlike most other lymphomas, there is no established standard therapy but a range of options,” Timothy S. Fenske, MD, said at the conference held by Imedex. “I go through the pros and cons with patients, and it comes down to the patient’s perceived quality of life and their lifestyle.”
“It’s a very difficult decision [for patients] because we don’t have the data we’d like to have,” observed Peter Martin, MD, director of the clinical research program in lymphoma at Weill Cornell Medicine, New York.
“There is a lot of upfront toxicity with transplantation, with 6-9 months out of work in my experience. Patients often tell me that they can’t afford to do that; they’ll lose their employment insurance and won’t be able to pay for replacement insurance. But then they will hopefully go 6-10 years without more treatment, which is a real benefit. With less intensive upfront treatment they have a chance for similar overall survival, but they’ll need more ongoing treatment. It’s pretty complicated and challenging” for patients to make a decision, he said. “It depends a lot on where patients are in their lives and what they are willing to accept,” Dr. Martin said.
In general, Dr. Martin took a more skeptical view of ASCT than Dr. Fenske. “There is no evidence that ASCT cures patients or prolongs their survival. It improves progression-free survival, but not necessarily overall survival,” Dr. Martin noted.
In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “if you have good biology it doesn’t matter what the treatment is, you will do well,” he explained.

In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “less intense therapy works just as well” as more intense therapy, as long as the patient has a favorable genetic profile, he explained.
In contrast, Dr. Fenske put a much more positive spin on more intensive treatment upfront with ASCT.
“There is not much debate that you get longer progression-free survival with the more intensive approach. The question is, does progression-free survival matter in mantle cell lymphoma? I argue that it does because relapse in patients with mantle cell lymphoma is no picnic. What you can expect in patients with relapsed or refractory mantle cell lymphoma is a progression-free survival of about 1-2 years, and an overall survival of about 2-3 years,” said Dr. Fenske, head of the section of bone marrow transplant and hematologic malignancies at the Medical College of Wisconsin in Milwaukee.
As an example of the poor prognosis of relapsed or refractory mantle cell lymphoma patients Dr. Fenske cited a review he coauthored of 97 patients treated with ibrutinib (Imbruvica. Their median duration of response was 17 months and median progression-free survival was 15 months. Once ibrutinib treatment failure occurred their median overall survival was less than 3 months. (Hematol Oncol. 2017 Jan 8.doi:10.1002/hon.2380).
“It’s easy to get carried away” when patients temporarily respond to a drug like ibrutinib or other new agents with a degree of efficacy for lymphomas, Dr. Fenske said, but these transient responses “don’t solve the problem. The patient is headed for trouble,” usually within a couple of years.
“I would argue that, especially for younger patients, the goal is to try to achieve the longest first remission, and that means an ASCT.” Dr. Fenske admitted that this strategy won’t work for very-high-risk patients, but for these patients no good treatment options currently exist.
He also stressed that research is just beginning to explore using measurement of negative minimal residual disease to identify patients with the best outcomes following initial induction treatment. It is possible that patients with undetectable minimal residual disease can avoid immediate ASCT and instead receive maintenance therapy, a hypothesis slated for testing in a randomized trial, he said.
Dr. Martin has been a consultant to Celgene, Gilead, Janssen, Novartis, Pharmacyclics, and Verastem. Dr. Fenske has been a consultant to Abbvie, Celgene, Pharmacyclics, Sanofi, and Seattle Genetics.
[email protected]
On Twitter @mitchelzoler
This article was updated May 30, 2017 .
NEW YORK – Relatively young patients with newly diagnosed, average-risk mantle cell lymphoma who go into remission on induction therapy face a difficult choice on their next management step: undergo immediate autologous stem cell transplantation or defer the stem cell transplant and continue on maintenance therapy.
The choice is especially difficult because both are currently considered reasonable options and each choice has certain attractions and downsides, experts highlighted in discussing this fork-in-the-road decision patients face.
Immediate autologous stem cell transplantation (ASCT) has a good chance to allow the patient to remain treatment free and in remission for as long as about 10 years, but it involves intensive upfront treatment for 6-9 months, during which the patient will likely not be able to work or carry on many usual activities. Deferring the transplant with maintenance therapy puts off this life-disrupting initial period of intensive therapy for what may be several years, but relapse on maintenance therapy is inevitable and once it happens the patient may not have as successful an outcome from an ASCT. It also means several years of ongoing drug therapy with a maintenance regimen.
“I tell my fellows that patients with newly diagnosed mantle cell lymphoma [are] one of the hardest consultations because, unlike most other lymphomas, there is no established standard therapy but a range of options,” Timothy S. Fenske, MD, said at the conference held by Imedex. “I go through the pros and cons with patients, and it comes down to the patient’s perceived quality of life and their lifestyle.”
“It’s a very difficult decision [for patients] because we don’t have the data we’d like to have,” observed Peter Martin, MD, director of the clinical research program in lymphoma at Weill Cornell Medicine, New York.
“There is a lot of upfront toxicity with transplantation, with 6-9 months out of work in my experience. Patients often tell me that they can’t afford to do that; they’ll lose their employment insurance and won’t be able to pay for replacement insurance. But then they will hopefully go 6-10 years without more treatment, which is a real benefit. With less intensive upfront treatment they have a chance for similar overall survival, but they’ll need more ongoing treatment. It’s pretty complicated and challenging” for patients to make a decision, he said. “It depends a lot on where patients are in their lives and what they are willing to accept,” Dr. Martin said.
In general, Dr. Martin took a more skeptical view of ASCT than Dr. Fenske. “There is no evidence that ASCT cures patients or prolongs their survival. It improves progression-free survival, but not necessarily overall survival,” Dr. Martin noted.
In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “if you have good biology it doesn’t matter what the treatment is, you will do well,” he explained.
In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “less intense therapy works just as well” as more intense therapy, as long as the patient has a favorable genetic profile, he explained.
In contrast, Dr. Fenske put a much more positive spin on more intensive treatment upfront with ASCT.
“There is not much debate that you get longer progression-free survival with the more intensive approach. The question is, does progression-free survival matter in mantle cell lymphoma? I argue that it does because relapse in patients with mantle cell lymphoma is no picnic. What you can expect in patients with relapsed or refractory mantle cell lymphoma is a progression-free survival of about 1-2 years, and an overall survival of about 2-3 years,” said Dr. Fenske, head of the section of bone marrow transplant and hematologic malignancies at the Medical College of Wisconsin in Milwaukee.
As an example of the poor prognosis of relapsed or refractory mantle cell lymphoma patients Dr. Fenske cited a review he coauthored of 97 patients treated with ibrutinib (Imbruvica. Their median duration of response was 17 months and median progression-free survival was 15 months. Once ibrutinib treatment failure occurred their median overall survival was less than 3 months. (Hematol Oncol. 2017 Jan 8.doi:10.1002/hon.2380).
“It’s easy to get carried away” when patients temporarily respond to a drug like ibrutinib or other new agents with a degree of efficacy for lymphomas, Dr. Fenske said, but these transient responses “don’t solve the problem. The patient is headed for trouble,” usually within a couple of years.
“I would argue that, especially for younger patients, the goal is to try to achieve the longest first remission, and that means an ASCT.” Dr. Fenske admitted that this strategy won’t work for very-high-risk patients, but for these patients no good treatment options currently exist.
He also stressed that research is just beginning to explore using measurement of negative minimal residual disease to identify patients with the best outcomes following initial induction treatment. It is possible that patients with undetectable minimal residual disease can avoid immediate ASCT and instead receive maintenance therapy, a hypothesis slated for testing in a randomized trial, he said.
Dr. Martin has been a consultant to Celgene, Gilead, Janssen, Novartis, Pharmacyclics, and Verastem. Dr. Fenske has been a consultant to Abbvie, Celgene, Pharmacyclics, Sanofi, and Seattle Genetics.
[email protected]
On Twitter @mitchelzoler
This article was updated May 30, 2017 .
NEW YORK – Relatively young patients with newly diagnosed, average-risk mantle cell lymphoma who go into remission on induction therapy face a difficult choice on their next management step: undergo immediate autologous stem cell transplantation or defer the stem cell transplant and continue on maintenance therapy.
The choice is especially difficult because both are currently considered reasonable options and each choice has certain attractions and downsides, experts highlighted in discussing this fork-in-the-road decision patients face.
Immediate autologous stem cell transplantation (ASCT) has a good chance to allow the patient to remain treatment free and in remission for as long as about 10 years, but it involves intensive upfront treatment for 6-9 months, during which the patient will likely not be able to work or carry on many usual activities. Deferring the transplant with maintenance therapy puts off this life-disrupting initial period of intensive therapy for what may be several years, but relapse on maintenance therapy is inevitable and once it happens the patient may not have as successful an outcome from an ASCT. It also means several years of ongoing drug therapy with a maintenance regimen.
“I tell my fellows that patients with newly diagnosed mantle cell lymphoma [are] one of the hardest consultations because, unlike most other lymphomas, there is no established standard therapy but a range of options,” Timothy S. Fenske, MD, said at the conference held by Imedex. “I go through the pros and cons with patients, and it comes down to the patient’s perceived quality of life and their lifestyle.”
“It’s a very difficult decision [for patients] because we don’t have the data we’d like to have,” observed Peter Martin, MD, director of the clinical research program in lymphoma at Weill Cornell Medicine, New York.
“There is a lot of upfront toxicity with transplantation, with 6-9 months out of work in my experience. Patients often tell me that they can’t afford to do that; they’ll lose their employment insurance and won’t be able to pay for replacement insurance. But then they will hopefully go 6-10 years without more treatment, which is a real benefit. With less intensive upfront treatment they have a chance for similar overall survival, but they’ll need more ongoing treatment. It’s pretty complicated and challenging” for patients to make a decision, he said. “It depends a lot on where patients are in their lives and what they are willing to accept,” Dr. Martin said.
In general, Dr. Martin took a more skeptical view of ASCT than Dr. Fenske. “There is no evidence that ASCT cures patients or prolongs their survival. It improves progression-free survival, but not necessarily overall survival,” Dr. Martin noted.
In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “if you have good biology it doesn’t matter what the treatment is, you will do well,” he explained.
In fact, a report in December 2016 at the American Society of Hematology annual meeting (Blood. 2016 Dec 5;abstract 1095) suggested that “biology is the primary driver of outcomes in mantle cell lymphoma, not treatment,” said Dr. Martin. The results from a limited number of patients enrolled in the Nordic mantle cell lymphoma trials provided good but preliminary evidence that “less intense therapy works just as well” as more intense therapy, as long as the patient has a favorable genetic profile, he explained.
In contrast, Dr. Fenske put a much more positive spin on more intensive treatment upfront with ASCT.
“There is not much debate that you get longer progression-free survival with the more intensive approach. The question is, does progression-free survival matter in mantle cell lymphoma? I argue that it does because relapse in patients with mantle cell lymphoma is no picnic. What you can expect in patients with relapsed or refractory mantle cell lymphoma is a progression-free survival of about 1-2 years, and an overall survival of about 2-3 years,” said Dr. Fenske, head of the section of bone marrow transplant and hematologic malignancies at the Medical College of Wisconsin in Milwaukee.
As an example of the poor prognosis of relapsed or refractory mantle cell lymphoma patients Dr. Fenske cited a review he coauthored of 97 patients treated with ibrutinib (Imbruvica. Their median duration of response was 17 months and median progression-free survival was 15 months. Once ibrutinib treatment failure occurred their median overall survival was less than 3 months. (Hematol Oncol. 2017 Jan 8.doi:10.1002/hon.2380).
“It’s easy to get carried away” when patients temporarily respond to a drug like ibrutinib or other new agents with a degree of efficacy for lymphomas, Dr. Fenske said, but these transient responses “don’t solve the problem. The patient is headed for trouble,” usually within a couple of years.
“I would argue that, especially for younger patients, the goal is to try to achieve the longest first remission, and that means an ASCT.” Dr. Fenske admitted that this strategy won’t work for very-high-risk patients, but for these patients no good treatment options currently exist.
He also stressed that research is just beginning to explore using measurement of negative minimal residual disease to identify patients with the best outcomes following initial induction treatment. It is possible that patients with undetectable minimal residual disease can avoid immediate ASCT and instead receive maintenance therapy, a hypothesis slated for testing in a randomized trial, he said.
Dr. Martin has been a consultant to Celgene, Gilead, Janssen, Novartis, Pharmacyclics, and Verastem. Dr. Fenske has been a consultant to Abbvie, Celgene, Pharmacyclics, Sanofi, and Seattle Genetics.
[email protected]
On Twitter @mitchelzoler
This article was updated May 30, 2017 .
EXPERT ANALYSIS FROM A MEETING ON HEMATOLOGIC MALIGNANCIES