User login
Second cancers take greater toll on younger patients

Second cancers take a greater toll on patients under the age of 40, according to research published in JAMA Oncology.
Researchers studied 14 types of cancer occurring in more than 1 million patients.
For nearly all of the cancers studied, 5-year survival rates were much higher if the cancer occurred as a first malignancy rather than a second cancer.
These survival differences were more pronounced in pediatric patients and adolescents and young adults (AYAs) than they were in patients age 40 and older.
Researchers hope these findings will help guide clinicians in providing age-specific recommendations on cancer prevention, screening, treatment, and survivorship, especially among the AYA population.
“Although the increased incidence of second cancers is well known among cancer survivors, less is known about outcomes of these cancers or the influence of age,” said Theresa Keegan, PhD, of the UC Davis Comprehensive Cancer Center in Sacramento, California.
With this in mind, Dr Keegan and her colleagues analyzed data on patients diagnosed with either a single cancer or a first and second malignancy during 1992 through 2008. The researchers used Surveillance, Epidemiology and End Results program data collected from 13 cancer registries.
The team collected data on the 14 most common cancer types that affect AYAs: acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), soft tissue sarcoma, and bone sarcoma, as well as female breast, thyroid, testicular, colorectal, central nervous system, cervical, and ovarian cancers.
There were a total of 15,954 pediatric patients (younger than 15 years at diagnosis), 125,750 AYAs (ages 15 to 39), and 878,370 older adult patients (age 40 and older).
Survival rates
For pediatric patients, the 5-year relative survival was 80% for a first cancer and 47% for a second primary malignancy.
For AYAs, the 5-year relative survival was 81% for a first cancer and 60% for a second primary malignancy.
For older adults, the 5-year relative survival was 70% for a first cancer and 61% for a second primary malignancy.
When the researchers looked at 5-year survival by age and individual cancer types, they found striking differences depending on whether it was a first or second malignancy in all but 2 of the 14 cancer types, testicular cancer and melanoma.
“For almost every type of cancer, the AYA population did worse with a secondary cancer,” said study author Melanie Goldfarb, MD, of John Wayne Cancer Institute at Providence Saint John’s Health Center in Santa Monica, California.
“What struck us was that the second cancer caused such an increased risk of death.”
Lymphomas
For pediatric patients with HL, the 5-year relative survival was 95% when patients had HL as a first cancer. There were no data on HL as a second primary malignancy.
For AYAs, the 5-year relative survival was 93% when patients had HL as a first cancer and 72% when they had HL as a second primary malignancy.
For older adults, the 5-year relative survival was 69% when patients had HL as a first cancer and 54% when they had HL as a second primary malignancy.
For pediatric patients with NHL, the 5-year relative survival was 84% when patients had NHL as a first cancer and 63% when they had NHL as a second primary malignancy.
For AYAs, the 5-year relative survival was 64% when patients had NHL as a first cancer and 22% when they had NHL as a second primary malignancy.
For older adults, the 5-year relative survival was 57% when patients had NHL as a first cancer and 54% when they had NHL as a second primary malignancy.
Leukemias
For pediatric patients with ALL, the 5-year relative survival was 87% when patients had ALL as a first cancer and 63% when they had ALL as a second primary malignancy.
For AYAs, the 5-year relative survival was 48% when patients had ALL as a first cancer and 26% when they had ALL as a second primary malignancy.
For older adults, the 5-year relative survival was 17% when patients had ALL as a first cancer and 11% when they had ALL as a second primary malignancy.
For pediatric patients with AML, the 5-year relative survival was 57% when patients had AML as a first cancer and 29% when they had AML as a second primary malignancy.
For AYAs, the 5-year relative survival was 46% when patients had AML as a first cancer and 23% when they had AML as a second primary malignancy.
For older adults, the 5-year relative survival was 12% when patients had AML as a first cancer and 10% when they had AML as a second primary malignancy.
Why younger patients tend to fare worse after a second cancer than older patients is not fully understood or specifically addressed in the current study, the researchers noted.
Now, the team plans to examine how the time between getting a first and second cancer affects survival and whether the type of treatment for the first cancer influences the outcome of a second cancer. ![]()
Second cancers take a greater toll on patients under the age of 40, according to research published in JAMA Oncology.
Researchers studied 14 types of cancer occurring in more than 1 million patients.
For nearly all of the cancers studied, 5-year survival rates were much higher if the cancer occurred as a first malignancy rather than a second cancer.
These survival differences were more pronounced in pediatric patients and adolescents and young adults (AYAs) than they were in patients age 40 and older.
Researchers hope these findings will help guide clinicians in providing age-specific recommendations on cancer prevention, screening, treatment, and survivorship, especially among the AYA population.
“Although the increased incidence of second cancers is well known among cancer survivors, less is known about outcomes of these cancers or the influence of age,” said Theresa Keegan, PhD, of the UC Davis Comprehensive Cancer Center in Sacramento, California.
With this in mind, Dr Keegan and her colleagues analyzed data on patients diagnosed with either a single cancer or a first and second malignancy during 1992 through 2008. The researchers used Surveillance, Epidemiology and End Results program data collected from 13 cancer registries.
The team collected data on the 14 most common cancer types that affect AYAs: acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), soft tissue sarcoma, and bone sarcoma, as well as female breast, thyroid, testicular, colorectal, central nervous system, cervical, and ovarian cancers.
There were a total of 15,954 pediatric patients (younger than 15 years at diagnosis), 125,750 AYAs (ages 15 to 39), and 878,370 older adult patients (age 40 and older).
Survival rates
For pediatric patients, the 5-year relative survival was 80% for a first cancer and 47% for a second primary malignancy.
For AYAs, the 5-year relative survival was 81% for a first cancer and 60% for a second primary malignancy.
For older adults, the 5-year relative survival was 70% for a first cancer and 61% for a second primary malignancy.
When the researchers looked at 5-year survival by age and individual cancer types, they found striking differences depending on whether it was a first or second malignancy in all but 2 of the 14 cancer types, testicular cancer and melanoma.
“For almost every type of cancer, the AYA population did worse with a secondary cancer,” said study author Melanie Goldfarb, MD, of John Wayne Cancer Institute at Providence Saint John’s Health Center in Santa Monica, California.
“What struck us was that the second cancer caused such an increased risk of death.”
Lymphomas
For pediatric patients with HL, the 5-year relative survival was 95% when patients had HL as a first cancer. There were no data on HL as a second primary malignancy.
For AYAs, the 5-year relative survival was 93% when patients had HL as a first cancer and 72% when they had HL as a second primary malignancy.
For older adults, the 5-year relative survival was 69% when patients had HL as a first cancer and 54% when they had HL as a second primary malignancy.
For pediatric patients with NHL, the 5-year relative survival was 84% when patients had NHL as a first cancer and 63% when they had NHL as a second primary malignancy.
For AYAs, the 5-year relative survival was 64% when patients had NHL as a first cancer and 22% when they had NHL as a second primary malignancy.
For older adults, the 5-year relative survival was 57% when patients had NHL as a first cancer and 54% when they had NHL as a second primary malignancy.
Leukemias
For pediatric patients with ALL, the 5-year relative survival was 87% when patients had ALL as a first cancer and 63% when they had ALL as a second primary malignancy.
For AYAs, the 5-year relative survival was 48% when patients had ALL as a first cancer and 26% when they had ALL as a second primary malignancy.
For older adults, the 5-year relative survival was 17% when patients had ALL as a first cancer and 11% when they had ALL as a second primary malignancy.
For pediatric patients with AML, the 5-year relative survival was 57% when patients had AML as a first cancer and 29% when they had AML as a second primary malignancy.
For AYAs, the 5-year relative survival was 46% when patients had AML as a first cancer and 23% when they had AML as a second primary malignancy.
For older adults, the 5-year relative survival was 12% when patients had AML as a first cancer and 10% when they had AML as a second primary malignancy.
Why younger patients tend to fare worse after a second cancer than older patients is not fully understood or specifically addressed in the current study, the researchers noted.
Now, the team plans to examine how the time between getting a first and second cancer affects survival and whether the type of treatment for the first cancer influences the outcome of a second cancer. ![]()
Second cancers take a greater toll on patients under the age of 40, according to research published in JAMA Oncology.
Researchers studied 14 types of cancer occurring in more than 1 million patients.
For nearly all of the cancers studied, 5-year survival rates were much higher if the cancer occurred as a first malignancy rather than a second cancer.
These survival differences were more pronounced in pediatric patients and adolescents and young adults (AYAs) than they were in patients age 40 and older.
Researchers hope these findings will help guide clinicians in providing age-specific recommendations on cancer prevention, screening, treatment, and survivorship, especially among the AYA population.
“Although the increased incidence of second cancers is well known among cancer survivors, less is known about outcomes of these cancers or the influence of age,” said Theresa Keegan, PhD, of the UC Davis Comprehensive Cancer Center in Sacramento, California.
With this in mind, Dr Keegan and her colleagues analyzed data on patients diagnosed with either a single cancer or a first and second malignancy during 1992 through 2008. The researchers used Surveillance, Epidemiology and End Results program data collected from 13 cancer registries.
The team collected data on the 14 most common cancer types that affect AYAs: acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), soft tissue sarcoma, and bone sarcoma, as well as female breast, thyroid, testicular, colorectal, central nervous system, cervical, and ovarian cancers.
There were a total of 15,954 pediatric patients (younger than 15 years at diagnosis), 125,750 AYAs (ages 15 to 39), and 878,370 older adult patients (age 40 and older).
Survival rates
For pediatric patients, the 5-year relative survival was 80% for a first cancer and 47% for a second primary malignancy.
For AYAs, the 5-year relative survival was 81% for a first cancer and 60% for a second primary malignancy.
For older adults, the 5-year relative survival was 70% for a first cancer and 61% for a second primary malignancy.
When the researchers looked at 5-year survival by age and individual cancer types, they found striking differences depending on whether it was a first or second malignancy in all but 2 of the 14 cancer types, testicular cancer and melanoma.
“For almost every type of cancer, the AYA population did worse with a secondary cancer,” said study author Melanie Goldfarb, MD, of John Wayne Cancer Institute at Providence Saint John’s Health Center in Santa Monica, California.
“What struck us was that the second cancer caused such an increased risk of death.”
Lymphomas
For pediatric patients with HL, the 5-year relative survival was 95% when patients had HL as a first cancer. There were no data on HL as a second primary malignancy.
For AYAs, the 5-year relative survival was 93% when patients had HL as a first cancer and 72% when they had HL as a second primary malignancy.
For older adults, the 5-year relative survival was 69% when patients had HL as a first cancer and 54% when they had HL as a second primary malignancy.
For pediatric patients with NHL, the 5-year relative survival was 84% when patients had NHL as a first cancer and 63% when they had NHL as a second primary malignancy.
For AYAs, the 5-year relative survival was 64% when patients had NHL as a first cancer and 22% when they had NHL as a second primary malignancy.
For older adults, the 5-year relative survival was 57% when patients had NHL as a first cancer and 54% when they had NHL as a second primary malignancy.
Leukemias
For pediatric patients with ALL, the 5-year relative survival was 87% when patients had ALL as a first cancer and 63% when they had ALL as a second primary malignancy.
For AYAs, the 5-year relative survival was 48% when patients had ALL as a first cancer and 26% when they had ALL as a second primary malignancy.
For older adults, the 5-year relative survival was 17% when patients had ALL as a first cancer and 11% when they had ALL as a second primary malignancy.
For pediatric patients with AML, the 5-year relative survival was 57% when patients had AML as a first cancer and 29% when they had AML as a second primary malignancy.
For AYAs, the 5-year relative survival was 46% when patients had AML as a first cancer and 23% when they had AML as a second primary malignancy.
For older adults, the 5-year relative survival was 12% when patients had AML as a first cancer and 10% when they had AML as a second primary malignancy.
Why younger patients tend to fare worse after a second cancer than older patients is not fully understood or specifically addressed in the current study, the researchers noted.
Now, the team plans to examine how the time between getting a first and second cancer affects survival and whether the type of treatment for the first cancer influences the outcome of a second cancer. ![]()
Cord blood product bests standard UCB transplant

The expanded umbilical cord blood (UCB) product NiCord can provide benefits over standard UCB transplant, according to research published in Biology of Blood and Marrow Transplantation.
NiCord is a stand-alone graft derived from a single UCB unit that has been expanded in culture and enriched with stem and progenitor cells.
The study showed that patients transplanted with NiCord had shorter time to engraftment, a lower risk of infection, and shorter hospital stays than patients who received standard UCB transplants.
On the other hand, there was no significant difference between the transplant groups when it came to grade 2-4 acute graft-versus-host disease (GVHD), relapse, or survival within 100 days of transplant.
“Our results indicate that rapid hematopoietic recovery from Gamida Cell’s NiCord transplantation approach is associated with clinical benefit,” said study author Mitchell Horwitz, MD, of Duke University School of Medicine in Durham, North Carolina.
Dr Horwitz receives research support from Gamida Cell Ltd., makers of NiCord.
Patient characteristics
The researchers compared 18 consecutive NiCord-transplanted patients and 86 consecutive patients who received standard UCB transplants. All of the patients received total body irradiation-based myeloablative conditioning.
In both arms, most patients received a double transplant. In the NiCord arm, 61.1% of patients (n=11) received NiCord along with a second unmanipulated UCB unit. In the standard UCB arm, 95.3% of patients (n=82) received a double UCB transplant.
Patients in the NiCord arm were older than patients in the standard UCB arm, with median ages of 45.5 (range, 42-57) and 37.5 (range, 28-51), respectively.
Most patients in both arms had acute leukemia or myelodysplastic syndromes (about 89%), although roughly 11% had lymphoid malignancies.
There were no significant differences between the arms when it came to patient sex, pre-transplant weight, cytomegalovirus serostatus, and Karnofsky Performance Status.
Results
The median time to neutrophil engraftment was 12.5 days (range, 10-18) in the NiCord arm and 27 days (range, 23-28) in the standard UCB arm (P<0.001).
All of the patients studied had at least 1 infection of any severity. However, patients in the NiCord arm had a significantly lower risk of infection than patients in the standard UCB arm.
In an analysis adjusted for age, disease stage, and grade 2-4 acute GVHD, the risk ratios (RRs) for NiCord versus standard UCB transplant were as follows:
- Total infection—RR=0.72, P=0.03
- Grade 2-3 infection—RR=0.38, P=0.001
- Bacterial infection—RR=0.42, P=0.008
- Grade 2-3 bacterial infection—RR=0.23, P=0.006.
Patients in the NiCord arm spent a mean of 72.4 days out of the hospital in the first 100 days after transplant, compared to 48.6 days for the standard UCB arm (P=0.001).
After the researchers adjusted for age and Karnofsky Performance Status, patients in the NiCord arm had a mean of 20.2 more days out of the hospital than their peers who received standard UCB (P=0.005).
The incidence of grade 2-4 acute GHVD was 55.6% in the NiCord arm and 41.9% in the standard UCB arm (P=0.31). The rate of second transplant was 5.6% and 11.6%, respectively (P=0.68).
The rate of relapse was 0% in the NiCord arm and 7% in the standard UCB arm (P=0.59). And the rate of death was 5.6% and 16.3%, respectively (P=0.46). ![]()
The expanded umbilical cord blood (UCB) product NiCord can provide benefits over standard UCB transplant, according to research published in Biology of Blood and Marrow Transplantation.
NiCord is a stand-alone graft derived from a single UCB unit that has been expanded in culture and enriched with stem and progenitor cells.
The study showed that patients transplanted with NiCord had shorter time to engraftment, a lower risk of infection, and shorter hospital stays than patients who received standard UCB transplants.
On the other hand, there was no significant difference between the transplant groups when it came to grade 2-4 acute graft-versus-host disease (GVHD), relapse, or survival within 100 days of transplant.
“Our results indicate that rapid hematopoietic recovery from Gamida Cell’s NiCord transplantation approach is associated with clinical benefit,” said study author Mitchell Horwitz, MD, of Duke University School of Medicine in Durham, North Carolina.
Dr Horwitz receives research support from Gamida Cell Ltd., makers of NiCord.
Patient characteristics
The researchers compared 18 consecutive NiCord-transplanted patients and 86 consecutive patients who received standard UCB transplants. All of the patients received total body irradiation-based myeloablative conditioning.
In both arms, most patients received a double transplant. In the NiCord arm, 61.1% of patients (n=11) received NiCord along with a second unmanipulated UCB unit. In the standard UCB arm, 95.3% of patients (n=82) received a double UCB transplant.
Patients in the NiCord arm were older than patients in the standard UCB arm, with median ages of 45.5 (range, 42-57) and 37.5 (range, 28-51), respectively.
Most patients in both arms had acute leukemia or myelodysplastic syndromes (about 89%), although roughly 11% had lymphoid malignancies.
There were no significant differences between the arms when it came to patient sex, pre-transplant weight, cytomegalovirus serostatus, and Karnofsky Performance Status.
Results
The median time to neutrophil engraftment was 12.5 days (range, 10-18) in the NiCord arm and 27 days (range, 23-28) in the standard UCB arm (P<0.001).
All of the patients studied had at least 1 infection of any severity. However, patients in the NiCord arm had a significantly lower risk of infection than patients in the standard UCB arm.
In an analysis adjusted for age, disease stage, and grade 2-4 acute GVHD, the risk ratios (RRs) for NiCord versus standard UCB transplant were as follows:
- Total infection—RR=0.72, P=0.03
- Grade 2-3 infection—RR=0.38, P=0.001
- Bacterial infection—RR=0.42, P=0.008
- Grade 2-3 bacterial infection—RR=0.23, P=0.006.
Patients in the NiCord arm spent a mean of 72.4 days out of the hospital in the first 100 days after transplant, compared to 48.6 days for the standard UCB arm (P=0.001).
After the researchers adjusted for age and Karnofsky Performance Status, patients in the NiCord arm had a mean of 20.2 more days out of the hospital than their peers who received standard UCB (P=0.005).
The incidence of grade 2-4 acute GHVD was 55.6% in the NiCord arm and 41.9% in the standard UCB arm (P=0.31). The rate of second transplant was 5.6% and 11.6%, respectively (P=0.68).
The rate of relapse was 0% in the NiCord arm and 7% in the standard UCB arm (P=0.59). And the rate of death was 5.6% and 16.3%, respectively (P=0.46). ![]()
The expanded umbilical cord blood (UCB) product NiCord can provide benefits over standard UCB transplant, according to research published in Biology of Blood and Marrow Transplantation.
NiCord is a stand-alone graft derived from a single UCB unit that has been expanded in culture and enriched with stem and progenitor cells.
The study showed that patients transplanted with NiCord had shorter time to engraftment, a lower risk of infection, and shorter hospital stays than patients who received standard UCB transplants.
On the other hand, there was no significant difference between the transplant groups when it came to grade 2-4 acute graft-versus-host disease (GVHD), relapse, or survival within 100 days of transplant.
“Our results indicate that rapid hematopoietic recovery from Gamida Cell’s NiCord transplantation approach is associated with clinical benefit,” said study author Mitchell Horwitz, MD, of Duke University School of Medicine in Durham, North Carolina.
Dr Horwitz receives research support from Gamida Cell Ltd., makers of NiCord.
Patient characteristics
The researchers compared 18 consecutive NiCord-transplanted patients and 86 consecutive patients who received standard UCB transplants. All of the patients received total body irradiation-based myeloablative conditioning.
In both arms, most patients received a double transplant. In the NiCord arm, 61.1% of patients (n=11) received NiCord along with a second unmanipulated UCB unit. In the standard UCB arm, 95.3% of patients (n=82) received a double UCB transplant.
Patients in the NiCord arm were older than patients in the standard UCB arm, with median ages of 45.5 (range, 42-57) and 37.5 (range, 28-51), respectively.
Most patients in both arms had acute leukemia or myelodysplastic syndromes (about 89%), although roughly 11% had lymphoid malignancies.
There were no significant differences between the arms when it came to patient sex, pre-transplant weight, cytomegalovirus serostatus, and Karnofsky Performance Status.
Results
The median time to neutrophil engraftment was 12.5 days (range, 10-18) in the NiCord arm and 27 days (range, 23-28) in the standard UCB arm (P<0.001).
All of the patients studied had at least 1 infection of any severity. However, patients in the NiCord arm had a significantly lower risk of infection than patients in the standard UCB arm.
In an analysis adjusted for age, disease stage, and grade 2-4 acute GVHD, the risk ratios (RRs) for NiCord versus standard UCB transplant were as follows:
- Total infection—RR=0.72, P=0.03
- Grade 2-3 infection—RR=0.38, P=0.001
- Bacterial infection—RR=0.42, P=0.008
- Grade 2-3 bacterial infection—RR=0.23, P=0.006.
Patients in the NiCord arm spent a mean of 72.4 days out of the hospital in the first 100 days after transplant, compared to 48.6 days for the standard UCB arm (P=0.001).
After the researchers adjusted for age and Karnofsky Performance Status, patients in the NiCord arm had a mean of 20.2 more days out of the hospital than their peers who received standard UCB (P=0.005).
The incidence of grade 2-4 acute GHVD was 55.6% in the NiCord arm and 41.9% in the standard UCB arm (P=0.31). The rate of second transplant was 5.6% and 11.6%, respectively (P=0.68).
The rate of relapse was 0% in the NiCord arm and 7% in the standard UCB arm (P=0.59). And the rate of death was 5.6% and 16.3%, respectively (P=0.46). ![]()
TGA approves therapy for hemophilia A

The Australian Therapeutic Goods Administration (TGA) has approved use of lonoctocog alfa (AFSTYLA®), a recombinant single-chain coagulation factor VIII (FVIII) therapy, in patients with hemophilia A.
The product is indicated for use as routine prophylaxis to prevent or reduce the frequency of bleeding episodes, for control and prevention of bleeding episodes, and for perioperative management.
Lonoctocog alfa is designed to provide long-lasting protection from bleeds with 2- to 3-times weekly dosing, according to CSL Behring, the company developing the product.
The company says lonoctocog alfa uses a covalent bond that forms one structural entity—a single polypeptide chain—to improve the stability of FVIII and provide FVIII activity with the option of twice-weekly dosing.
The TGA’s approval of lonoctocog alfa is based on results from the AFFINITY clinical development program, which includes a trial of children (n=84) and a trial of adolescents and adults (n=175).
Among patients who received lonoctocog alfa prophylactically in these trials, the median annualized bleeding rate was 1.14 in the adults/adolescents and 3.69 in children younger than 12.
In all, there were 1195 bleeding events—848 in the adults/adolescents and 347 in the children.
Ninety-four percent of bleeds in adults/adolescents and 96% of bleeds in pediatric patients were effectively controlled with no more than 2 infusions of lonoctocog alfa weekly.
Eighty-one percent of bleeds in adults/adolescents and 86% of bleeds in pediatric patients were controlled by a single infusion.
Researchers assessed safety in 258 patients from both studies. Adverse reactions occurred in 14 patients and included hypersensitivity (n=4), dizziness (n=2), paresthesia (n=1), rash (n=1), erythema (n=1), pruritus (n=1), pyrexia (n=1), injection-site pain (n=1), chills (n=1), and feeling hot (n=1).
One patient withdrew from treatment due to hypersensitivity.
None of the patients developed neutralizing antibodies to FVIII or antibodies to host cell proteins. There were no reports of anaphylaxis or thrombosis.
Results from the trial of adolescents/adults were published in Blood in August 2016. Results from the trial of children were published in the Journal of Thrombosis and Haemostasis in March 2017. ![]()
The Australian Therapeutic Goods Administration (TGA) has approved use of lonoctocog alfa (AFSTYLA®), a recombinant single-chain coagulation factor VIII (FVIII) therapy, in patients with hemophilia A.
The product is indicated for use as routine prophylaxis to prevent or reduce the frequency of bleeding episodes, for control and prevention of bleeding episodes, and for perioperative management.
Lonoctocog alfa is designed to provide long-lasting protection from bleeds with 2- to 3-times weekly dosing, according to CSL Behring, the company developing the product.
The company says lonoctocog alfa uses a covalent bond that forms one structural entity—a single polypeptide chain—to improve the stability of FVIII and provide FVIII activity with the option of twice-weekly dosing.
The TGA’s approval of lonoctocog alfa is based on results from the AFFINITY clinical development program, which includes a trial of children (n=84) and a trial of adolescents and adults (n=175).
Among patients who received lonoctocog alfa prophylactically in these trials, the median annualized bleeding rate was 1.14 in the adults/adolescents and 3.69 in children younger than 12.
In all, there were 1195 bleeding events—848 in the adults/adolescents and 347 in the children.
Ninety-four percent of bleeds in adults/adolescents and 96% of bleeds in pediatric patients were effectively controlled with no more than 2 infusions of lonoctocog alfa weekly.
Eighty-one percent of bleeds in adults/adolescents and 86% of bleeds in pediatric patients were controlled by a single infusion.
Researchers assessed safety in 258 patients from both studies. Adverse reactions occurred in 14 patients and included hypersensitivity (n=4), dizziness (n=2), paresthesia (n=1), rash (n=1), erythema (n=1), pruritus (n=1), pyrexia (n=1), injection-site pain (n=1), chills (n=1), and feeling hot (n=1).
One patient withdrew from treatment due to hypersensitivity.
None of the patients developed neutralizing antibodies to FVIII or antibodies to host cell proteins. There were no reports of anaphylaxis or thrombosis.
Results from the trial of adolescents/adults were published in Blood in August 2016. Results from the trial of children were published in the Journal of Thrombosis and Haemostasis in March 2017. ![]()
The Australian Therapeutic Goods Administration (TGA) has approved use of lonoctocog alfa (AFSTYLA®), a recombinant single-chain coagulation factor VIII (FVIII) therapy, in patients with hemophilia A.
The product is indicated for use as routine prophylaxis to prevent or reduce the frequency of bleeding episodes, for control and prevention of bleeding episodes, and for perioperative management.
Lonoctocog alfa is designed to provide long-lasting protection from bleeds with 2- to 3-times weekly dosing, according to CSL Behring, the company developing the product.
The company says lonoctocog alfa uses a covalent bond that forms one structural entity—a single polypeptide chain—to improve the stability of FVIII and provide FVIII activity with the option of twice-weekly dosing.
The TGA’s approval of lonoctocog alfa is based on results from the AFFINITY clinical development program, which includes a trial of children (n=84) and a trial of adolescents and adults (n=175).
Among patients who received lonoctocog alfa prophylactically in these trials, the median annualized bleeding rate was 1.14 in the adults/adolescents and 3.69 in children younger than 12.
In all, there were 1195 bleeding events—848 in the adults/adolescents and 347 in the children.
Ninety-four percent of bleeds in adults/adolescents and 96% of bleeds in pediatric patients were effectively controlled with no more than 2 infusions of lonoctocog alfa weekly.
Eighty-one percent of bleeds in adults/adolescents and 86% of bleeds in pediatric patients were controlled by a single infusion.
Researchers assessed safety in 258 patients from both studies. Adverse reactions occurred in 14 patients and included hypersensitivity (n=4), dizziness (n=2), paresthesia (n=1), rash (n=1), erythema (n=1), pruritus (n=1), pyrexia (n=1), injection-site pain (n=1), chills (n=1), and feeling hot (n=1).
One patient withdrew from treatment due to hypersensitivity.
None of the patients developed neutralizing antibodies to FVIII or antibodies to host cell proteins. There were no reports of anaphylaxis or thrombosis.
Results from the trial of adolescents/adults were published in Blood in August 2016. Results from the trial of children were published in the Journal of Thrombosis and Haemostasis in March 2017. ![]()
How malaria parasites weaken RBCs’ defenses

Malaria parasites change the properties of red blood cells (RBCs) in a way that helps the parasites achieve cell entry, according to research published in PNAS.
Researchers found that Plasmodium parasites, upon binding to the surface of RBCs, cause the cell membranes to become more pliable, making it easier for the parasites to push inside the cells.
This suggests that differences in RBC stiffness, due to age or increased cholesterol content, could influence the parasites’ ability to invade.
“We have discovered that red cell entry is not just down to the ability of the parasite itself but that parasite-initiated changes to the red blood cells appear to contribute to the process of invasion,” said study author Marion Koch, a PhD student at Imperial College London in the UK.
“This could also mean that naturally more flexible cells would be easier for parasites to invade, which raises some interesting questions. Are parasites choosy about which cells to invade, picking the most deformable? Is susceptibility to malaria modified by fat or cholesterol content, or the age of circulating red blood cells?”
In the PNAS paper, the researchers noted that erythrocyte-binding antigen 175 (EBA175), a protein that’s required for entry in most parasite strains, binds to glycophorin A (GPA) on the RBC surface. However, the function of this binding interaction was unknown.
The team took a closer look at the interaction using real-time deformability cytometry and flicker spectroscopy.
They filmed 1000 RBCs per second passing through a narrow channel. Using this approach, the researchers were able to determine cell deformability by measuring how elongated the cells became during transit through the channel.
The team then measured where this deformation came from. They measured how much the RBCs deviate from their normally circular shape as their membranes naturally fluctuate or flicker.
The researchers found that EBA175 binding to GPA leads to an increase in the cytoskeletal tension of the RBC and a reduction in the bending modulus of the cell’s membrane. (The bending modulus is a measure of how much energy it takes to bend the cell membrane.)
The team then showed that the reduction in the bending modulus was “directly correlated with parasite invasion efficiency.”
The researchers said these results suggest the parasite primes the RBC surface through its binding antigens, altering the cell and reducing a barrier to invasion.
“This suggests we should be investigating not just parasite biology, but also how the body’s own red blood cells respond,” said study author Jake Baum, PhD, of Imperial College London.
“There are therapies developed for diseases like HIV that strengthen the body’s responses in addition to tackling the ‘invader.’ It’s not impossible to imagine something similar for malaria; for example, looking at a host-directed drug target and not just the parasite.” ![]()
Malaria parasites change the properties of red blood cells (RBCs) in a way that helps the parasites achieve cell entry, according to research published in PNAS.
Researchers found that Plasmodium parasites, upon binding to the surface of RBCs, cause the cell membranes to become more pliable, making it easier for the parasites to push inside the cells.
This suggests that differences in RBC stiffness, due to age or increased cholesterol content, could influence the parasites’ ability to invade.
“We have discovered that red cell entry is not just down to the ability of the parasite itself but that parasite-initiated changes to the red blood cells appear to contribute to the process of invasion,” said study author Marion Koch, a PhD student at Imperial College London in the UK.
“This could also mean that naturally more flexible cells would be easier for parasites to invade, which raises some interesting questions. Are parasites choosy about which cells to invade, picking the most deformable? Is susceptibility to malaria modified by fat or cholesterol content, or the age of circulating red blood cells?”
In the PNAS paper, the researchers noted that erythrocyte-binding antigen 175 (EBA175), a protein that’s required for entry in most parasite strains, binds to glycophorin A (GPA) on the RBC surface. However, the function of this binding interaction was unknown.
The team took a closer look at the interaction using real-time deformability cytometry and flicker spectroscopy.
They filmed 1000 RBCs per second passing through a narrow channel. Using this approach, the researchers were able to determine cell deformability by measuring how elongated the cells became during transit through the channel.
The team then measured where this deformation came from. They measured how much the RBCs deviate from their normally circular shape as their membranes naturally fluctuate or flicker.
The researchers found that EBA175 binding to GPA leads to an increase in the cytoskeletal tension of the RBC and a reduction in the bending modulus of the cell’s membrane. (The bending modulus is a measure of how much energy it takes to bend the cell membrane.)
The team then showed that the reduction in the bending modulus was “directly correlated with parasite invasion efficiency.”
The researchers said these results suggest the parasite primes the RBC surface through its binding antigens, altering the cell and reducing a barrier to invasion.
“This suggests we should be investigating not just parasite biology, but also how the body’s own red blood cells respond,” said study author Jake Baum, PhD, of Imperial College London.
“There are therapies developed for diseases like HIV that strengthen the body’s responses in addition to tackling the ‘invader.’ It’s not impossible to imagine something similar for malaria; for example, looking at a host-directed drug target and not just the parasite.” ![]()
Malaria parasites change the properties of red blood cells (RBCs) in a way that helps the parasites achieve cell entry, according to research published in PNAS.
Researchers found that Plasmodium parasites, upon binding to the surface of RBCs, cause the cell membranes to become more pliable, making it easier for the parasites to push inside the cells.
This suggests that differences in RBC stiffness, due to age or increased cholesterol content, could influence the parasites’ ability to invade.
“We have discovered that red cell entry is not just down to the ability of the parasite itself but that parasite-initiated changes to the red blood cells appear to contribute to the process of invasion,” said study author Marion Koch, a PhD student at Imperial College London in the UK.
“This could also mean that naturally more flexible cells would be easier for parasites to invade, which raises some interesting questions. Are parasites choosy about which cells to invade, picking the most deformable? Is susceptibility to malaria modified by fat or cholesterol content, or the age of circulating red blood cells?”
In the PNAS paper, the researchers noted that erythrocyte-binding antigen 175 (EBA175), a protein that’s required for entry in most parasite strains, binds to glycophorin A (GPA) on the RBC surface. However, the function of this binding interaction was unknown.
The team took a closer look at the interaction using real-time deformability cytometry and flicker spectroscopy.
They filmed 1000 RBCs per second passing through a narrow channel. Using this approach, the researchers were able to determine cell deformability by measuring how elongated the cells became during transit through the channel.
The team then measured where this deformation came from. They measured how much the RBCs deviate from their normally circular shape as their membranes naturally fluctuate or flicker.
The researchers found that EBA175 binding to GPA leads to an increase in the cytoskeletal tension of the RBC and a reduction in the bending modulus of the cell’s membrane. (The bending modulus is a measure of how much energy it takes to bend the cell membrane.)
The team then showed that the reduction in the bending modulus was “directly correlated with parasite invasion efficiency.”
The researchers said these results suggest the parasite primes the RBC surface through its binding antigens, altering the cell and reducing a barrier to invasion.
“This suggests we should be investigating not just parasite biology, but also how the body’s own red blood cells respond,” said study author Jake Baum, PhD, of Imperial College London.
“There are therapies developed for diseases like HIV that strengthen the body’s responses in addition to tackling the ‘invader.’ It’s not impossible to imagine something similar for malaria; for example, looking at a host-directed drug target and not just the parasite.” ![]()
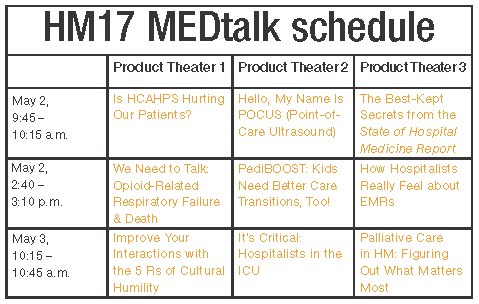
MEDtalk presentations
Is HCAHPS Hurting Our Patients?
Speakers: Suparna Dutta, MD, MS, MPH, and John Biebelhausen, MD, MBA
Explore the unintended consequences of assessing patient satisfaction and labeling pain as “the fifth vital sign” in the midst of a national opioid epidemic. The Hospital Consumer Assessment of Healthcare Providers and Systems, which was developed by the Centers for Medicare & Medicaid Services to assess the inpatient experience and impacts hospital reimbursement, includes directed questions about pain management.
Join us as we review the background of HCAHPS, its potential unintended impacts over the years, as well as current and future efforts of SHM toward improving health policy in this domain.
Hello, My Name Is POCUS (Point-of-Care Ultrasound)
Speaker: Nilam Soni, MD, MS, FHM
Point-of-care ultrasound is being used by more hospitalists to perform bedside diagnostics and to guide invasive procedures. However, most practicing hospitalists completed their training before point-of-care ultrasound education was common in medical school and residency curricula. This interactive session will:
- Explain what point-of-care ultrasonography is and how hospitalists are currently using it.
- Highlight some of the unique point-of-care ultrasound activities at HM17.
- Describe the launch of a new point-of-care ultrasound certification program offered by SHM & ACCP.
The Best-Kept Secrets from the State of Hospital Medicine Report
Speaker: Johnbuck Creamer, MD, SFHM
The State of Hospital Medicine Report is powered by SHM’s biannual survey that recently captured data from nearly 600 HM groups, augmented by additional hospitalist data licensed from MGMA. We’ll explore trends and difference among groups, including:
- Compensation per wRVU and use of nocturnists are increasing.
- Turnover rates are decreasing.
- Compensation for quality performance varies greatly among academic, nonacademic, and pediatric practice groups.
- NP/PA utilization rates are very different between East and West U.S. regions.
- Family Practice presence is increasing in adult-only practice groups.
- Academic groups are falling further behind in CPT coding levels.
We Need to Talk: Opioid-Related Respiratory Failure & Death
Speaker: Thomas Frederickson, MD, SFHM
Discussion topics:
- The opioid epidemic – not just an outpatient issue.
- How opioids can cause respiratory arrest and death, and why current screening and monitoring strategies can fail.
- What works – examples of successful strategies that have been implemented and have saved lives.
PediBOOST®: Kids Need Better Care Transitions, Too!
Speaker: James O’Callaghan, MD, SFHM
PediBOOST is a pediatric-specific adaption of the SHM Project BOOST® (Better Outcomes by Optimizing Safe Transitions) quality initiative. The goal is to improve poor discharge processes (demonstrated by low patient satisfaction and worse clinical outcomes, not just higher hospital readmission rates).
It considers unique problems for hospitalized children, including:
- Medication issues – palatability and adherence concerns, need for compounding.
- Equipment issues – portability use for home and school.
- Education issues – engagement of patient, as developmentally appropriate, along with training of all providers who might care for the patient (parents, teachers).
How Hospitalists Really Feel about EMRs
Speaker: Rupesh Prasad, MD, MPH, SFHM
Electronic medical record use has tremendously increased in the last few years.
- What are the potential benefits of use – have they been realized?
- What do the hospitalists think:
- How have EMRs impacted patient safety?
- How have EMRs impacted patient face to face time?
- What are hospitalists’ frustrations about EMRs?
Improve Your Interactions with the 5 Rs of Cultural Humility
Speaker: O’Neil Pyke, MD, SFHM
As the proverbial stranger at the bedside, HM providers are tasked with a very challenging proposition: meet a new patient in their most vulnerable state and quickly establish effective lines of communication and trust and provide patient-centric care, ultimately yielding a satisfied patient (and family) irrespective of the clinical outcome. With increased focus on patient experience and satisfaction, it is imperative that hospitals and health systems equip all hospitalists with the tools needed to deliver culturally competent care to all patients served.
The goal of the 5 Rs is to equip HM providers with tangible resources and easy to understand reminders that focus on encouraging awareness and, ultimately, deliver culturally “humble” care to all patients (and family members).
- Respect: Hospitalists will treat every person with the utmost respect and strive to preserve patient dignity.
- Regard: Hospitalists will hold every person in their highest regard and not allow unconscious biases to manifest, exercising utmost sensitivity to anticipated differences in beliefs, value systems, and preferences.
- Relevance: Hospitalists will expect cultural humility to be relevant and apply this practice to every encounter.
- Reflection: Hospitalists will approach every encounter with humility and understanding that there is always something to learn from everyone.
- Resiliency: In order to provide better care for hospitalized patients, hospitalists will embody the practice of cultural humility to enhance personal resiliency and compassion for all.
It’s Critical: Hospitalists in the ICU
Speaker: Joseph Sweigart, MD
We hope to:
- Describe formation of purpose of the critical care task force within the Education Committee.
- Discuss the creation and execution of the SHM critical care survey.
- Present selected results including:
- Introduce strategies to address the practice gaps identified including:
Palliative Care in Hospital Medicine: Figuring Out What Matters Most
Speaker: Rab Razzak, MBBS, MD
We aim to:
- Discuss the overall definition of palliative care. It is for all seriously ill patients and focuses on human-centered care and quality of life, best provided early in an illness.
- Idea of primary palliative care and role of hospitalists. Most palliative care is provided by frontline clinicians, and hospitalists are optimally positioned to support seriously ill patients and their families. It is crucial for HM to involve palliative care specialists when needed.
- Effective communication about serious illness – words that work and how to operationalize human-centered care while honestly discussing serious illness.
Is HCAHPS Hurting Our Patients?
Speakers: Suparna Dutta, MD, MS, MPH, and John Biebelhausen, MD, MBA
Explore the unintended consequences of assessing patient satisfaction and labeling pain as “the fifth vital sign” in the midst of a national opioid epidemic. The Hospital Consumer Assessment of Healthcare Providers and Systems, which was developed by the Centers for Medicare & Medicaid Services to assess the inpatient experience and impacts hospital reimbursement, includes directed questions about pain management.
Join us as we review the background of HCAHPS, its potential unintended impacts over the years, as well as current and future efforts of SHM toward improving health policy in this domain.
Hello, My Name Is POCUS (Point-of-Care Ultrasound)
Speaker: Nilam Soni, MD, MS, FHM
Point-of-care ultrasound is being used by more hospitalists to perform bedside diagnostics and to guide invasive procedures. However, most practicing hospitalists completed their training before point-of-care ultrasound education was common in medical school and residency curricula. This interactive session will:
- Explain what point-of-care ultrasonography is and how hospitalists are currently using it.
- Highlight some of the unique point-of-care ultrasound activities at HM17.
- Describe the launch of a new point-of-care ultrasound certification program offered by SHM & ACCP.
The Best-Kept Secrets from the State of Hospital Medicine Report
Speaker: Johnbuck Creamer, MD, SFHM
The State of Hospital Medicine Report is powered by SHM’s biannual survey that recently captured data from nearly 600 HM groups, augmented by additional hospitalist data licensed from MGMA. We’ll explore trends and difference among groups, including:
- Compensation per wRVU and use of nocturnists are increasing.
- Turnover rates are decreasing.
- Compensation for quality performance varies greatly among academic, nonacademic, and pediatric practice groups.
- NP/PA utilization rates are very different between East and West U.S. regions.
- Family Practice presence is increasing in adult-only practice groups.
- Academic groups are falling further behind in CPT coding levels.
We Need to Talk: Opioid-Related Respiratory Failure & Death
Speaker: Thomas Frederickson, MD, SFHM
Discussion topics:
- The opioid epidemic – not just an outpatient issue.
- How opioids can cause respiratory arrest and death, and why current screening and monitoring strategies can fail.
- What works – examples of successful strategies that have been implemented and have saved lives.
PediBOOST®: Kids Need Better Care Transitions, Too!
Speaker: James O’Callaghan, MD, SFHM
PediBOOST is a pediatric-specific adaption of the SHM Project BOOST® (Better Outcomes by Optimizing Safe Transitions) quality initiative. The goal is to improve poor discharge processes (demonstrated by low patient satisfaction and worse clinical outcomes, not just higher hospital readmission rates).
It considers unique problems for hospitalized children, including:
- Medication issues – palatability and adherence concerns, need for compounding.
- Equipment issues – portability use for home and school.
- Education issues – engagement of patient, as developmentally appropriate, along with training of all providers who might care for the patient (parents, teachers).
How Hospitalists Really Feel about EMRs
Speaker: Rupesh Prasad, MD, MPH, SFHM
Electronic medical record use has tremendously increased in the last few years.
- What are the potential benefits of use – have they been realized?
- What do the hospitalists think:
- How have EMRs impacted patient safety?
- How have EMRs impacted patient face to face time?
- What are hospitalists’ frustrations about EMRs?
Improve Your Interactions with the 5 Rs of Cultural Humility
Speaker: O’Neil Pyke, MD, SFHM
As the proverbial stranger at the bedside, HM providers are tasked with a very challenging proposition: meet a new patient in their most vulnerable state and quickly establish effective lines of communication and trust and provide patient-centric care, ultimately yielding a satisfied patient (and family) irrespective of the clinical outcome. With increased focus on patient experience and satisfaction, it is imperative that hospitals and health systems equip all hospitalists with the tools needed to deliver culturally competent care to all patients served.
The goal of the 5 Rs is to equip HM providers with tangible resources and easy to understand reminders that focus on encouraging awareness and, ultimately, deliver culturally “humble” care to all patients (and family members).
- Respect: Hospitalists will treat every person with the utmost respect and strive to preserve patient dignity.
- Regard: Hospitalists will hold every person in their highest regard and not allow unconscious biases to manifest, exercising utmost sensitivity to anticipated differences in beliefs, value systems, and preferences.
- Relevance: Hospitalists will expect cultural humility to be relevant and apply this practice to every encounter.
- Reflection: Hospitalists will approach every encounter with humility and understanding that there is always something to learn from everyone.
- Resiliency: In order to provide better care for hospitalized patients, hospitalists will embody the practice of cultural humility to enhance personal resiliency and compassion for all.
It’s Critical: Hospitalists in the ICU
Speaker: Joseph Sweigart, MD
We hope to:
- Describe formation of purpose of the critical care task force within the Education Committee.
- Discuss the creation and execution of the SHM critical care survey.
- Present selected results including:
- Introduce strategies to address the practice gaps identified including:
Palliative Care in Hospital Medicine: Figuring Out What Matters Most
Speaker: Rab Razzak, MBBS, MD
We aim to:
- Discuss the overall definition of palliative care. It is for all seriously ill patients and focuses on human-centered care and quality of life, best provided early in an illness.
- Idea of primary palliative care and role of hospitalists. Most palliative care is provided by frontline clinicians, and hospitalists are optimally positioned to support seriously ill patients and their families. It is crucial for HM to involve palliative care specialists when needed.
- Effective communication about serious illness – words that work and how to operationalize human-centered care while honestly discussing serious illness.
Is HCAHPS Hurting Our Patients?
Speakers: Suparna Dutta, MD, MS, MPH, and John Biebelhausen, MD, MBA
Explore the unintended consequences of assessing patient satisfaction and labeling pain as “the fifth vital sign” in the midst of a national opioid epidemic. The Hospital Consumer Assessment of Healthcare Providers and Systems, which was developed by the Centers for Medicare & Medicaid Services to assess the inpatient experience and impacts hospital reimbursement, includes directed questions about pain management.
Join us as we review the background of HCAHPS, its potential unintended impacts over the years, as well as current and future efforts of SHM toward improving health policy in this domain.
Hello, My Name Is POCUS (Point-of-Care Ultrasound)
Speaker: Nilam Soni, MD, MS, FHM
Point-of-care ultrasound is being used by more hospitalists to perform bedside diagnostics and to guide invasive procedures. However, most practicing hospitalists completed their training before point-of-care ultrasound education was common in medical school and residency curricula. This interactive session will:
- Explain what point-of-care ultrasonography is and how hospitalists are currently using it.
- Highlight some of the unique point-of-care ultrasound activities at HM17.
- Describe the launch of a new point-of-care ultrasound certification program offered by SHM & ACCP.
The Best-Kept Secrets from the State of Hospital Medicine Report
Speaker: Johnbuck Creamer, MD, SFHM
The State of Hospital Medicine Report is powered by SHM’s biannual survey that recently captured data from nearly 600 HM groups, augmented by additional hospitalist data licensed from MGMA. We’ll explore trends and difference among groups, including:
- Compensation per wRVU and use of nocturnists are increasing.
- Turnover rates are decreasing.
- Compensation for quality performance varies greatly among academic, nonacademic, and pediatric practice groups.
- NP/PA utilization rates are very different between East and West U.S. regions.
- Family Practice presence is increasing in adult-only practice groups.
- Academic groups are falling further behind in CPT coding levels.
We Need to Talk: Opioid-Related Respiratory Failure & Death
Speaker: Thomas Frederickson, MD, SFHM
Discussion topics:
- The opioid epidemic – not just an outpatient issue.
- How opioids can cause respiratory arrest and death, and why current screening and monitoring strategies can fail.
- What works – examples of successful strategies that have been implemented and have saved lives.
PediBOOST®: Kids Need Better Care Transitions, Too!
Speaker: James O’Callaghan, MD, SFHM
PediBOOST is a pediatric-specific adaption of the SHM Project BOOST® (Better Outcomes by Optimizing Safe Transitions) quality initiative. The goal is to improve poor discharge processes (demonstrated by low patient satisfaction and worse clinical outcomes, not just higher hospital readmission rates).
It considers unique problems for hospitalized children, including:
- Medication issues – palatability and adherence concerns, need for compounding.
- Equipment issues – portability use for home and school.
- Education issues – engagement of patient, as developmentally appropriate, along with training of all providers who might care for the patient (parents, teachers).
How Hospitalists Really Feel about EMRs
Speaker: Rupesh Prasad, MD, MPH, SFHM
Electronic medical record use has tremendously increased in the last few years.
- What are the potential benefits of use – have they been realized?
- What do the hospitalists think:
- How have EMRs impacted patient safety?
- How have EMRs impacted patient face to face time?
- What are hospitalists’ frustrations about EMRs?
Improve Your Interactions with the 5 Rs of Cultural Humility
Speaker: O’Neil Pyke, MD, SFHM
As the proverbial stranger at the bedside, HM providers are tasked with a very challenging proposition: meet a new patient in their most vulnerable state and quickly establish effective lines of communication and trust and provide patient-centric care, ultimately yielding a satisfied patient (and family) irrespective of the clinical outcome. With increased focus on patient experience and satisfaction, it is imperative that hospitals and health systems equip all hospitalists with the tools needed to deliver culturally competent care to all patients served.
The goal of the 5 Rs is to equip HM providers with tangible resources and easy to understand reminders that focus on encouraging awareness and, ultimately, deliver culturally “humble” care to all patients (and family members).
- Respect: Hospitalists will treat every person with the utmost respect and strive to preserve patient dignity.
- Regard: Hospitalists will hold every person in their highest regard and not allow unconscious biases to manifest, exercising utmost sensitivity to anticipated differences in beliefs, value systems, and preferences.
- Relevance: Hospitalists will expect cultural humility to be relevant and apply this practice to every encounter.
- Reflection: Hospitalists will approach every encounter with humility and understanding that there is always something to learn from everyone.
- Resiliency: In order to provide better care for hospitalized patients, hospitalists will embody the practice of cultural humility to enhance personal resiliency and compassion for all.
It’s Critical: Hospitalists in the ICU
Speaker: Joseph Sweigart, MD
We hope to:
- Describe formation of purpose of the critical care task force within the Education Committee.
- Discuss the creation and execution of the SHM critical care survey.
- Present selected results including:
- Introduce strategies to address the practice gaps identified including:
Palliative Care in Hospital Medicine: Figuring Out What Matters Most
Speaker: Rab Razzak, MBBS, MD
We aim to:
- Discuss the overall definition of palliative care. It is for all seriously ill patients and focuses on human-centered care and quality of life, best provided early in an illness.
- Idea of primary palliative care and role of hospitalists. Most palliative care is provided by frontline clinicians, and hospitalists are optimally positioned to support seriously ill patients and their families. It is crucial for HM to involve palliative care specialists when needed.
- Effective communication about serious illness – words that work and how to operationalize human-centered care while honestly discussing serious illness.
AATS publishes guidelines for infective endocarditis
Infective endocarditis (IE) is a devastating complication of heart valve disease that, left untreated, can be fatal. Management requires a multidisciplinary approach, and many of the respective medical societies that represent the participating specialties have developed guidelines. Now, the American Association for Thoracic Surgery has published “Consensus Guidelines for the Surgical Treatment of Infective Endocarditis” to guide thoracic and cardiovascular surgeons in making decisions of when to operate in cases of IE (J Thorac Cardiovasc Surg. 2017 Jan 24. doi: 10.1016/j.jtcvs.2016.09.093).

The rationale for developing the guidelines is a growing prevalence of IE, including in patients with normal valves and no previous diagnosis of heart disease. “These new AATS consensus guidelines primarily address questions related to active and suspected active IE affective valves and intracardiac structures,” Dr. Pettersson and his coauthors said. The AATS guidelines for infective endocarditis address complications including risk of embolism and the timing of surgery in patients with neurological complications, while acknowledging the the need for additional research into these topics.* “It is understood that surgery is beneficial only if the patient’s complications and other comorbidities do not preclude survival and meaningful recovery,” the guideline authors said.
The guidelines confirm the team approach for managing patients with IE. The team should include cardiology, infectious disease, cardiac surgery, and other specialties needed to handle IE-related complications (class of recommendation [COR] I, level of evidence [LOE] B). Before surgery, the surgeon should know the patient is on effective antimicrobial therapy (COR I, LOE B). Transesophageal echocardiography (TEE) is indicated to yield the clearest understanding of the pathology (COR I, LOE B).
Dr. Pettersson and the guideline writing team also clarified indications for surgery in patients with IE. They include when valve dysfunction causes heart failure (COR I, LOE B); when, after a full course of antibiotics, the patient has signs of heart block, annular or aortic abscess or destructive penetrating lesions (COR I, LOE B); and in the setting of recurrent emboli and persistent vegetations despite appropriate antibiotic therapy (COR IIA, LOE B).
The guideline writers acknowledged potential disagreement between the AATS guidelines and those of the American College of Cardiology/American Heart Association with regard to early surgery in IE. Debate surrounds whether to operate early or wait for symptoms of heart failure to manifest in patients with native valve endocarditis (NVE). The AATS guideline authors cite work by Duk-Hyun Kang, MD, PhD, and coauthors in South Korea (N Engl J Med. 2012;366;2466-73) and others advocating for early surgery. “For this reason, once a surgical indication is evident, surgery should not be delayed,” Dr. Pettersson and his coauthors said.
Several conditions can influence the timing of surgery. Patients with cerebral mycotic aneurysm should be managed closely with neurology or neurosurgery (COR I, LOE C). Patients with a recent intracranial hemorrhage should wait at least 3 weeks for surgery (COR IIA, LOE B), but those with nonhemorrhagic strokes could go in for urgent surgery (COR IIA, LOE B). Brain imaging is indicated for IE patients with neurological symptoms (COR I, LOE B), but anticoagulation management requires a nuanced approach that takes all risks and benefits into consideration (COR I, LOE C).
Key steps during surgery involve mandatory intraoperative TEE (COR I, LOE B), median sternotomy with few exceptions (COR I, LOE B), and radical debridement and removal of all infected and necrotic tissue (COR I, LOE B). The writers also provided four guidelines for reconstruction and valve replacement:
- Repair when possible for patients with NVE (COR I, LOE B).
- When replacement is indicated, the surgeon should base valve choice on normal criteria – age, life expectancy, comorbidities, and expected compliance with anticoagulation (COR I, LOE B).
- Avoid use of mechanical valves in patients with intracranial bleeding or who have had a major stroke (COR IIA, LOE C).
- In patients with invasive disease and deconstruction, reconstruction should depend on the involved valve, severity of destruction, and available options for cardiac reconstruction (COR I, LOE B).
The AATS guidelines also challenge conventional thinking on the practice of soaking a gel-impregnated graft with antimicrobials targeting a specific organism. “We found no evidence to support this practice,” Dr. Pettersson and his coauthors said (COR IIB, LOE B). They came to the same conclusion with regard to the use of local antimicrobials or antiseptics during irrigation after debridement and local injection of antimicrobials around the infected area (COR I, LOE C).
The guidelines provide direction on a host of other surgical issues in IE: use of aortic valve grafts; when to remove or replace noninfected grafts; when to remove pacemakers; the role of drainage; postoperative management; follow-up; and additional screening. They also shed insight into what the guideline authors call “residual controversies,” including surgery for injection drug users (use “all available resources and options for drug rehabilitation”) and dialysis patients (“it is reasonable to offer surgery when the additional burden of comorbidities is not overwhelming”). They also acknowledge seven different scenarios that lack clear evidence for intervention but require the surgeon to determine the need for surgery, ranging from timing of surgery for IE in patients with neurologic complications to how to treat patients with functional valve issues after being cured of IE.
The guideline writers acknowledged that institutional funds supported the work. Dr. Pettersson had no financial relationships to disclose.
*Correction 5/172017: It was incorrectly stated that these complications were not addressed in the guidelines due to lack of evidence
Whether they’re intended to or not, guidelines like the AATS Consensus Guidelines for the Surgical Treatment of Infected Endocarditis “can evolve into hard and fast principles, sometimes leading to incorrect decision making and even creating medicolegal problems for treating physicians,” Gus J. Vlahakes, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in his invited commentary (J Thorac Cardiovasc Surg. 2016 Nov 3. doi: 10.1016/j.jtcvs.2016.10.041).
Guidelines cannot “integrate all the necessary considerations,” Dr. Vlahakes said, so surgeons should view them as “a set of general principles to guide decision making.” In IE, that means having an experienced cardiac surgeon who can apply the guidelines on a case-by-case basis and a multidisciplinary team that includes an infectious disease specialist, he said. The surgeon must participate in preoperative management.
Dr. Vlahakes had no relevant financial disclosures.
Whether they’re intended to or not, guidelines like the AATS Consensus Guidelines for the Surgical Treatment of Infected Endocarditis “can evolve into hard and fast principles, sometimes leading to incorrect decision making and even creating medicolegal problems for treating physicians,” Gus J. Vlahakes, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in his invited commentary (J Thorac Cardiovasc Surg. 2016 Nov 3. doi: 10.1016/j.jtcvs.2016.10.041).
Guidelines cannot “integrate all the necessary considerations,” Dr. Vlahakes said, so surgeons should view them as “a set of general principles to guide decision making.” In IE, that means having an experienced cardiac surgeon who can apply the guidelines on a case-by-case basis and a multidisciplinary team that includes an infectious disease specialist, he said. The surgeon must participate in preoperative management.
Dr. Vlahakes had no relevant financial disclosures.
Whether they’re intended to or not, guidelines like the AATS Consensus Guidelines for the Surgical Treatment of Infected Endocarditis “can evolve into hard and fast principles, sometimes leading to incorrect decision making and even creating medicolegal problems for treating physicians,” Gus J. Vlahakes, MD, of Harvard Medical School and Massachusetts General Hospital, Boston, said in his invited commentary (J Thorac Cardiovasc Surg. 2016 Nov 3. doi: 10.1016/j.jtcvs.2016.10.041).
Guidelines cannot “integrate all the necessary considerations,” Dr. Vlahakes said, so surgeons should view them as “a set of general principles to guide decision making.” In IE, that means having an experienced cardiac surgeon who can apply the guidelines on a case-by-case basis and a multidisciplinary team that includes an infectious disease specialist, he said. The surgeon must participate in preoperative management.
Dr. Vlahakes had no relevant financial disclosures.
Infective endocarditis (IE) is a devastating complication of heart valve disease that, left untreated, can be fatal. Management requires a multidisciplinary approach, and many of the respective medical societies that represent the participating specialties have developed guidelines. Now, the American Association for Thoracic Surgery has published “Consensus Guidelines for the Surgical Treatment of Infective Endocarditis” to guide thoracic and cardiovascular surgeons in making decisions of when to operate in cases of IE (J Thorac Cardiovasc Surg. 2017 Jan 24. doi: 10.1016/j.jtcvs.2016.09.093).
The rationale for developing the guidelines is a growing prevalence of IE, including in patients with normal valves and no previous diagnosis of heart disease. “These new AATS consensus guidelines primarily address questions related to active and suspected active IE affective valves and intracardiac structures,” Dr. Pettersson and his coauthors said. The AATS guidelines for infective endocarditis address complications including risk of embolism and the timing of surgery in patients with neurological complications, while acknowledging the the need for additional research into these topics.* “It is understood that surgery is beneficial only if the patient’s complications and other comorbidities do not preclude survival and meaningful recovery,” the guideline authors said.
The guidelines confirm the team approach for managing patients with IE. The team should include cardiology, infectious disease, cardiac surgery, and other specialties needed to handle IE-related complications (class of recommendation [COR] I, level of evidence [LOE] B). Before surgery, the surgeon should know the patient is on effective antimicrobial therapy (COR I, LOE B). Transesophageal echocardiography (TEE) is indicated to yield the clearest understanding of the pathology (COR I, LOE B).
Dr. Pettersson and the guideline writing team also clarified indications for surgery in patients with IE. They include when valve dysfunction causes heart failure (COR I, LOE B); when, after a full course of antibiotics, the patient has signs of heart block, annular or aortic abscess or destructive penetrating lesions (COR I, LOE B); and in the setting of recurrent emboli and persistent vegetations despite appropriate antibiotic therapy (COR IIA, LOE B).
The guideline writers acknowledged potential disagreement between the AATS guidelines and those of the American College of Cardiology/American Heart Association with regard to early surgery in IE. Debate surrounds whether to operate early or wait for symptoms of heart failure to manifest in patients with native valve endocarditis (NVE). The AATS guideline authors cite work by Duk-Hyun Kang, MD, PhD, and coauthors in South Korea (N Engl J Med. 2012;366;2466-73) and others advocating for early surgery. “For this reason, once a surgical indication is evident, surgery should not be delayed,” Dr. Pettersson and his coauthors said.
Several conditions can influence the timing of surgery. Patients with cerebral mycotic aneurysm should be managed closely with neurology or neurosurgery (COR I, LOE C). Patients with a recent intracranial hemorrhage should wait at least 3 weeks for surgery (COR IIA, LOE B), but those with nonhemorrhagic strokes could go in for urgent surgery (COR IIA, LOE B). Brain imaging is indicated for IE patients with neurological symptoms (COR I, LOE B), but anticoagulation management requires a nuanced approach that takes all risks and benefits into consideration (COR I, LOE C).
Key steps during surgery involve mandatory intraoperative TEE (COR I, LOE B), median sternotomy with few exceptions (COR I, LOE B), and radical debridement and removal of all infected and necrotic tissue (COR I, LOE B). The writers also provided four guidelines for reconstruction and valve replacement:
- Repair when possible for patients with NVE (COR I, LOE B).
- When replacement is indicated, the surgeon should base valve choice on normal criteria – age, life expectancy, comorbidities, and expected compliance with anticoagulation (COR I, LOE B).
- Avoid use of mechanical valves in patients with intracranial bleeding or who have had a major stroke (COR IIA, LOE C).
- In patients with invasive disease and deconstruction, reconstruction should depend on the involved valve, severity of destruction, and available options for cardiac reconstruction (COR I, LOE B).
The AATS guidelines also challenge conventional thinking on the practice of soaking a gel-impregnated graft with antimicrobials targeting a specific organism. “We found no evidence to support this practice,” Dr. Pettersson and his coauthors said (COR IIB, LOE B). They came to the same conclusion with regard to the use of local antimicrobials or antiseptics during irrigation after debridement and local injection of antimicrobials around the infected area (COR I, LOE C).
The guidelines provide direction on a host of other surgical issues in IE: use of aortic valve grafts; when to remove or replace noninfected grafts; when to remove pacemakers; the role of drainage; postoperative management; follow-up; and additional screening. They also shed insight into what the guideline authors call “residual controversies,” including surgery for injection drug users (use “all available resources and options for drug rehabilitation”) and dialysis patients (“it is reasonable to offer surgery when the additional burden of comorbidities is not overwhelming”). They also acknowledge seven different scenarios that lack clear evidence for intervention but require the surgeon to determine the need for surgery, ranging from timing of surgery for IE in patients with neurologic complications to how to treat patients with functional valve issues after being cured of IE.
The guideline writers acknowledged that institutional funds supported the work. Dr. Pettersson had no financial relationships to disclose.
*Correction 5/172017: It was incorrectly stated that these complications were not addressed in the guidelines due to lack of evidence
Infective endocarditis (IE) is a devastating complication of heart valve disease that, left untreated, can be fatal. Management requires a multidisciplinary approach, and many of the respective medical societies that represent the participating specialties have developed guidelines. Now, the American Association for Thoracic Surgery has published “Consensus Guidelines for the Surgical Treatment of Infective Endocarditis” to guide thoracic and cardiovascular surgeons in making decisions of when to operate in cases of IE (J Thorac Cardiovasc Surg. 2017 Jan 24. doi: 10.1016/j.jtcvs.2016.09.093).
The rationale for developing the guidelines is a growing prevalence of IE, including in patients with normal valves and no previous diagnosis of heart disease. “These new AATS consensus guidelines primarily address questions related to active and suspected active IE affective valves and intracardiac structures,” Dr. Pettersson and his coauthors said. The AATS guidelines for infective endocarditis address complications including risk of embolism and the timing of surgery in patients with neurological complications, while acknowledging the the need for additional research into these topics.* “It is understood that surgery is beneficial only if the patient’s complications and other comorbidities do not preclude survival and meaningful recovery,” the guideline authors said.
The guidelines confirm the team approach for managing patients with IE. The team should include cardiology, infectious disease, cardiac surgery, and other specialties needed to handle IE-related complications (class of recommendation [COR] I, level of evidence [LOE] B). Before surgery, the surgeon should know the patient is on effective antimicrobial therapy (COR I, LOE B). Transesophageal echocardiography (TEE) is indicated to yield the clearest understanding of the pathology (COR I, LOE B).
Dr. Pettersson and the guideline writing team also clarified indications for surgery in patients with IE. They include when valve dysfunction causes heart failure (COR I, LOE B); when, after a full course of antibiotics, the patient has signs of heart block, annular or aortic abscess or destructive penetrating lesions (COR I, LOE B); and in the setting of recurrent emboli and persistent vegetations despite appropriate antibiotic therapy (COR IIA, LOE B).
The guideline writers acknowledged potential disagreement between the AATS guidelines and those of the American College of Cardiology/American Heart Association with regard to early surgery in IE. Debate surrounds whether to operate early or wait for symptoms of heart failure to manifest in patients with native valve endocarditis (NVE). The AATS guideline authors cite work by Duk-Hyun Kang, MD, PhD, and coauthors in South Korea (N Engl J Med. 2012;366;2466-73) and others advocating for early surgery. “For this reason, once a surgical indication is evident, surgery should not be delayed,” Dr. Pettersson and his coauthors said.
Several conditions can influence the timing of surgery. Patients with cerebral mycotic aneurysm should be managed closely with neurology or neurosurgery (COR I, LOE C). Patients with a recent intracranial hemorrhage should wait at least 3 weeks for surgery (COR IIA, LOE B), but those with nonhemorrhagic strokes could go in for urgent surgery (COR IIA, LOE B). Brain imaging is indicated for IE patients with neurological symptoms (COR I, LOE B), but anticoagulation management requires a nuanced approach that takes all risks and benefits into consideration (COR I, LOE C).
Key steps during surgery involve mandatory intraoperative TEE (COR I, LOE B), median sternotomy with few exceptions (COR I, LOE B), and radical debridement and removal of all infected and necrotic tissue (COR I, LOE B). The writers also provided four guidelines for reconstruction and valve replacement:
- Repair when possible for patients with NVE (COR I, LOE B).
- When replacement is indicated, the surgeon should base valve choice on normal criteria – age, life expectancy, comorbidities, and expected compliance with anticoagulation (COR I, LOE B).
- Avoid use of mechanical valves in patients with intracranial bleeding or who have had a major stroke (COR IIA, LOE C).
- In patients with invasive disease and deconstruction, reconstruction should depend on the involved valve, severity of destruction, and available options for cardiac reconstruction (COR I, LOE B).
The AATS guidelines also challenge conventional thinking on the practice of soaking a gel-impregnated graft with antimicrobials targeting a specific organism. “We found no evidence to support this practice,” Dr. Pettersson and his coauthors said (COR IIB, LOE B). They came to the same conclusion with regard to the use of local antimicrobials or antiseptics during irrigation after debridement and local injection of antimicrobials around the infected area (COR I, LOE C).
The guidelines provide direction on a host of other surgical issues in IE: use of aortic valve grafts; when to remove or replace noninfected grafts; when to remove pacemakers; the role of drainage; postoperative management; follow-up; and additional screening. They also shed insight into what the guideline authors call “residual controversies,” including surgery for injection drug users (use “all available resources and options for drug rehabilitation”) and dialysis patients (“it is reasonable to offer surgery when the additional burden of comorbidities is not overwhelming”). They also acknowledge seven different scenarios that lack clear evidence for intervention but require the surgeon to determine the need for surgery, ranging from timing of surgery for IE in patients with neurologic complications to how to treat patients with functional valve issues after being cured of IE.
The guideline writers acknowledged that institutional funds supported the work. Dr. Pettersson had no financial relationships to disclose.
*Correction 5/172017: It was incorrectly stated that these complications were not addressed in the guidelines due to lack of evidence
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: The American Association for Thoracic Surgery charged a committee of eight members to author “Consensus Guidelines: Surgical Treatment of Infective Endocarditis.”
Major finding: Patients with infective endocarditis need early input from the responsible cardiac surgeon, who must also lead the care team in evaluation, decision- making, and ultimately carrying out surgery as needed.
Data source: The writing committee followed Institute of Medicine standards for clinical practice guidelines, invited comment from a group of 12 multidisciplinary specialists and reviewed 288 articles in drafting the guidelines.
Disclosures: Institutional funds supported the work. Dr. Pettersson and his coauthors had no financial relationships to disclose.
FDA warns against use of codeine, tramadol in children
The Food and Drug Administration is restricting the use of two opiates – codeine and tramadol – in children, and also warns they are potentially dangerous to infants of breastfeeding women.
Codeine is approved to treat pain and cough; tramadol is approved to treat pain.
“We understand that there are limited options when it comes to treating pain or cough in children, and that these changes may raise some questions for health care providers and parents. However, please know that our decision today was made based on the latest evidence and with this goal in mind: keeping our kids safe,” Douglas Throckmorton, MD, the deputy center director for regulatory programs at the FDA Center for Drug Evaluation and Research, said in a statement.
In 2013, the FDA updated prescription codeine labeling to contain a boxed warning and contraindication for children up to age 18 years regarding the risk of slowed breathing from codeine prescribed after tonsillectomy and/or adenoidectomy. And in 2015, the agency issued warnings about the risk of serious breathing problems in children who had ultrarapid metabolism of codeine and tramadol.
In the current safety statement, the FDA said it will require additional labeling changes, including contraindications for use of codeine or tramadol in all children younger than 12 years of age and a new contraindication for tramadol in children younger than 18 years being treated for pain after tonsillectomy and/or adenoidectomy, warnings about their use in children 12-18 years of age with certain medical conditions, and a stronger warning recommending against their use in nursing mothers.
Single-ingredient codeine and all tramadol-containing products are FDA-approved only for use in adults, the agency noted.
The agency cited particular concerns over those who are “ultra-rapid metabolizers” of substrates of the cytochrome P450 isoenzyme 2D6 (CYP2D6) genotype. These people more quickly convert codeine into potentially dangerously high levels of morphine, which can lead to fatal respiratory depression.
Supporting the restrictions and warning were data on 64 cases of respiratory depression that occurred worldwide between 1969 and 2015, when a codeine-based medicine was used in children younger than 18 years. Twenty-four of these children died.
The most frequently cited medicines in the cases were acetaminophen with codeine and promethazine with codeine with or without phenylephrine, either given to soothe postoperative pain, general pain, sore or strep throat pain, or cough and cold.
Ten of the 64 cases implicated the CYP2D6 genotype. Seven of the patients were “ultrarapid metabolizers,” five of whom died.
Data cited on tramadol included nine worldwide cases of tramadol-related respiratory depression occurring between 1969 and 2016, resulting in the deaths of three children, all under the age of 6 years, and all of whom were taking the drug for postoperative pain or fever.
All but one case of respiratory depression occurred within the first 24 hours of taking the drug. One of the patients was genotyped for CYP2D6, and found to have three functional alleles consistent with ultrarapid metabolism.
Mothers who are ultrarapid metabolizers of codeine can have high levels of morphine in their breast milk that are dangerous to their breastfed infants, whereas there is less of a threat posed by women with normal codeine metabolism because the amount of codeine secreted into the breast milk is low and dose dependent.
The FDA stated that data reveal numerous reports of respiratory depression and at least one death in infants of breastfeeding mothers taking these medicines, particularly mothers with the CYP2D6 genotype. Although there are FDA-cleared tests for ultrarapid metabolism, they are not commonly used.
The agency stated that breastfeeding women taking any opioid pain medicine, including codeine or tramadol should contact their health care provider if they notice the infant is sleeping more than 4 hours at a time, or if the infant is having difficulty breastfeeding or seems limp.
Clinicians are urged to report side effects that occur while using codeine or tramadol to the FDA’s MedWatch Adverse Event Reporting program.
[email protected]
On Twitter @whitneymcknight
The Food and Drug Administration is restricting the use of two opiates – codeine and tramadol – in children, and also warns they are potentially dangerous to infants of breastfeeding women.
Codeine is approved to treat pain and cough; tramadol is approved to treat pain.
“We understand that there are limited options when it comes to treating pain or cough in children, and that these changes may raise some questions for health care providers and parents. However, please know that our decision today was made based on the latest evidence and with this goal in mind: keeping our kids safe,” Douglas Throckmorton, MD, the deputy center director for regulatory programs at the FDA Center for Drug Evaluation and Research, said in a statement.
In 2013, the FDA updated prescription codeine labeling to contain a boxed warning and contraindication for children up to age 18 years regarding the risk of slowed breathing from codeine prescribed after tonsillectomy and/or adenoidectomy. And in 2015, the agency issued warnings about the risk of serious breathing problems in children who had ultrarapid metabolism of codeine and tramadol.
In the current safety statement, the FDA said it will require additional labeling changes, including contraindications for use of codeine or tramadol in all children younger than 12 years of age and a new contraindication for tramadol in children younger than 18 years being treated for pain after tonsillectomy and/or adenoidectomy, warnings about their use in children 12-18 years of age with certain medical conditions, and a stronger warning recommending against their use in nursing mothers.
Single-ingredient codeine and all tramadol-containing products are FDA-approved only for use in adults, the agency noted.
The agency cited particular concerns over those who are “ultra-rapid metabolizers” of substrates of the cytochrome P450 isoenzyme 2D6 (CYP2D6) genotype. These people more quickly convert codeine into potentially dangerously high levels of morphine, which can lead to fatal respiratory depression.
Supporting the restrictions and warning were data on 64 cases of respiratory depression that occurred worldwide between 1969 and 2015, when a codeine-based medicine was used in children younger than 18 years. Twenty-four of these children died.
The most frequently cited medicines in the cases were acetaminophen with codeine and promethazine with codeine with or without phenylephrine, either given to soothe postoperative pain, general pain, sore or strep throat pain, or cough and cold.
Ten of the 64 cases implicated the CYP2D6 genotype. Seven of the patients were “ultrarapid metabolizers,” five of whom died.
Data cited on tramadol included nine worldwide cases of tramadol-related respiratory depression occurring between 1969 and 2016, resulting in the deaths of three children, all under the age of 6 years, and all of whom were taking the drug for postoperative pain or fever.
All but one case of respiratory depression occurred within the first 24 hours of taking the drug. One of the patients was genotyped for CYP2D6, and found to have three functional alleles consistent with ultrarapid metabolism.
Mothers who are ultrarapid metabolizers of codeine can have high levels of morphine in their breast milk that are dangerous to their breastfed infants, whereas there is less of a threat posed by women with normal codeine metabolism because the amount of codeine secreted into the breast milk is low and dose dependent.
The FDA stated that data reveal numerous reports of respiratory depression and at least one death in infants of breastfeeding mothers taking these medicines, particularly mothers with the CYP2D6 genotype. Although there are FDA-cleared tests for ultrarapid metabolism, they are not commonly used.
The agency stated that breastfeeding women taking any opioid pain medicine, including codeine or tramadol should contact their health care provider if they notice the infant is sleeping more than 4 hours at a time, or if the infant is having difficulty breastfeeding or seems limp.
Clinicians are urged to report side effects that occur while using codeine or tramadol to the FDA’s MedWatch Adverse Event Reporting program.
[email protected]
On Twitter @whitneymcknight
The Food and Drug Administration is restricting the use of two opiates – codeine and tramadol – in children, and also warns they are potentially dangerous to infants of breastfeeding women.
Codeine is approved to treat pain and cough; tramadol is approved to treat pain.
“We understand that there are limited options when it comes to treating pain or cough in children, and that these changes may raise some questions for health care providers and parents. However, please know that our decision today was made based on the latest evidence and with this goal in mind: keeping our kids safe,” Douglas Throckmorton, MD, the deputy center director for regulatory programs at the FDA Center for Drug Evaluation and Research, said in a statement.
In 2013, the FDA updated prescription codeine labeling to contain a boxed warning and contraindication for children up to age 18 years regarding the risk of slowed breathing from codeine prescribed after tonsillectomy and/or adenoidectomy. And in 2015, the agency issued warnings about the risk of serious breathing problems in children who had ultrarapid metabolism of codeine and tramadol.
In the current safety statement, the FDA said it will require additional labeling changes, including contraindications for use of codeine or tramadol in all children younger than 12 years of age and a new contraindication for tramadol in children younger than 18 years being treated for pain after tonsillectomy and/or adenoidectomy, warnings about their use in children 12-18 years of age with certain medical conditions, and a stronger warning recommending against their use in nursing mothers.
Single-ingredient codeine and all tramadol-containing products are FDA-approved only for use in adults, the agency noted.
The agency cited particular concerns over those who are “ultra-rapid metabolizers” of substrates of the cytochrome P450 isoenzyme 2D6 (CYP2D6) genotype. These people more quickly convert codeine into potentially dangerously high levels of morphine, which can lead to fatal respiratory depression.
Supporting the restrictions and warning were data on 64 cases of respiratory depression that occurred worldwide between 1969 and 2015, when a codeine-based medicine was used in children younger than 18 years. Twenty-four of these children died.
The most frequently cited medicines in the cases were acetaminophen with codeine and promethazine with codeine with or without phenylephrine, either given to soothe postoperative pain, general pain, sore or strep throat pain, or cough and cold.
Ten of the 64 cases implicated the CYP2D6 genotype. Seven of the patients were “ultrarapid metabolizers,” five of whom died.
Data cited on tramadol included nine worldwide cases of tramadol-related respiratory depression occurring between 1969 and 2016, resulting in the deaths of three children, all under the age of 6 years, and all of whom were taking the drug for postoperative pain or fever.
All but one case of respiratory depression occurred within the first 24 hours of taking the drug. One of the patients was genotyped for CYP2D6, and found to have three functional alleles consistent with ultrarapid metabolism.
Mothers who are ultrarapid metabolizers of codeine can have high levels of morphine in their breast milk that are dangerous to their breastfed infants, whereas there is less of a threat posed by women with normal codeine metabolism because the amount of codeine secreted into the breast milk is low and dose dependent.
The FDA stated that data reveal numerous reports of respiratory depression and at least one death in infants of breastfeeding mothers taking these medicines, particularly mothers with the CYP2D6 genotype. Although there are FDA-cleared tests for ultrarapid metabolism, they are not commonly used.
The agency stated that breastfeeding women taking any opioid pain medicine, including codeine or tramadol should contact their health care provider if they notice the infant is sleeping more than 4 hours at a time, or if the infant is having difficulty breastfeeding or seems limp.
Clinicians are urged to report side effects that occur while using codeine or tramadol to the FDA’s MedWatch Adverse Event Reporting program.
[email protected]
On Twitter @whitneymcknight
Dactylitis, enthesitis, anterior uveitis less frequent in IBD-SpA
In patients with inflammatory bowel disease and spondyloarthritis (IBD-SpA), dactylitis, enthesitis, and anterior uveitis (AU) are significantly less frequent than in patients with other types of SpA, according to Fabrizio Cantini, MD, and his associates.
In a 12-month, case-control study, 88 patients with IBD-SpA, 29 with ulcerative colitis (UC), and 59 with Crohn’s disease (CD) were examined along with the 176 patients with SpA in the control group. Results showed a significantly lower occurrence of dactylitis in case patients, with 4 episodes (4.5%) in IBD-SpA patients and 30 (17.4%) in controls (P = .008). The comparison of the frequency of dactylitis in patients with UC-SpA and in patients with CD-SpA found no significant differences between the two (3.4% and 5.08%, respectively; P = .843). Enthesitis was significantly lower in IBD-SpA, occurring in 16 out of 88 patients (18.1%), compared with in 78 out of 176 controls (44.3%; P less than .001). AU was also recorded in 3 (3.4%) of the patients with IBD-SpA and in 26 controls (14.7%; P = .010), and B27 positivity was recorded in 10 (11.3%) of patients with IBD-SpA and in 70 (39.8%) of patients with SpA (P less than .001).
There was a significantly lower occurrence of dactylitis reported in IBD-SpA patients without psoriasis (1 case in 74 patients; P = .001) compared with the control group, while dactylitis occurrence was not significantly different in 3 out of 14 patients (21.4%) with coexistent psoriasis (P = .960). Enthesitis was significantly higher in 14 IBD-SpA patients with associated psoriasis (50%), compared with the remaining 74 cases (12.1%; P = .003). It was noted that enthesitis occurrence was not different in patients with UC and in those with CD (P = .103).
“The results of our case-control study show that dactylitis, enthesitis, and AU are significantly less frequent in IBD-SpA, compared with other types of SpA,” researchers concluded. “Owing to the frequent association of psoriasis with IBD, and especially with CD, the coexistence of skin disease should be taken into account when evaluating the prevalence of dactylitis and enthesitis in patients with IBD-SpA.”
Find the full study in the Journal of Rheumatology (doi: 10.3899/jrheum.161518).
In patients with inflammatory bowel disease and spondyloarthritis (IBD-SpA), dactylitis, enthesitis, and anterior uveitis (AU) are significantly less frequent than in patients with other types of SpA, according to Fabrizio Cantini, MD, and his associates.
In a 12-month, case-control study, 88 patients with IBD-SpA, 29 with ulcerative colitis (UC), and 59 with Crohn’s disease (CD) were examined along with the 176 patients with SpA in the control group. Results showed a significantly lower occurrence of dactylitis in case patients, with 4 episodes (4.5%) in IBD-SpA patients and 30 (17.4%) in controls (P = .008). The comparison of the frequency of dactylitis in patients with UC-SpA and in patients with CD-SpA found no significant differences between the two (3.4% and 5.08%, respectively; P = .843). Enthesitis was significantly lower in IBD-SpA, occurring in 16 out of 88 patients (18.1%), compared with in 78 out of 176 controls (44.3%; P less than .001). AU was also recorded in 3 (3.4%) of the patients with IBD-SpA and in 26 controls (14.7%; P = .010), and B27 positivity was recorded in 10 (11.3%) of patients with IBD-SpA and in 70 (39.8%) of patients with SpA (P less than .001).
There was a significantly lower occurrence of dactylitis reported in IBD-SpA patients without psoriasis (1 case in 74 patients; P = .001) compared with the control group, while dactylitis occurrence was not significantly different in 3 out of 14 patients (21.4%) with coexistent psoriasis (P = .960). Enthesitis was significantly higher in 14 IBD-SpA patients with associated psoriasis (50%), compared with the remaining 74 cases (12.1%; P = .003). It was noted that enthesitis occurrence was not different in patients with UC and in those with CD (P = .103).
“The results of our case-control study show that dactylitis, enthesitis, and AU are significantly less frequent in IBD-SpA, compared with other types of SpA,” researchers concluded. “Owing to the frequent association of psoriasis with IBD, and especially with CD, the coexistence of skin disease should be taken into account when evaluating the prevalence of dactylitis and enthesitis in patients with IBD-SpA.”
Find the full study in the Journal of Rheumatology (doi: 10.3899/jrheum.161518).
In patients with inflammatory bowel disease and spondyloarthritis (IBD-SpA), dactylitis, enthesitis, and anterior uveitis (AU) are significantly less frequent than in patients with other types of SpA, according to Fabrizio Cantini, MD, and his associates.
In a 12-month, case-control study, 88 patients with IBD-SpA, 29 with ulcerative colitis (UC), and 59 with Crohn’s disease (CD) were examined along with the 176 patients with SpA in the control group. Results showed a significantly lower occurrence of dactylitis in case patients, with 4 episodes (4.5%) in IBD-SpA patients and 30 (17.4%) in controls (P = .008). The comparison of the frequency of dactylitis in patients with UC-SpA and in patients with CD-SpA found no significant differences between the two (3.4% and 5.08%, respectively; P = .843). Enthesitis was significantly lower in IBD-SpA, occurring in 16 out of 88 patients (18.1%), compared with in 78 out of 176 controls (44.3%; P less than .001). AU was also recorded in 3 (3.4%) of the patients with IBD-SpA and in 26 controls (14.7%; P = .010), and B27 positivity was recorded in 10 (11.3%) of patients with IBD-SpA and in 70 (39.8%) of patients with SpA (P less than .001).
There was a significantly lower occurrence of dactylitis reported in IBD-SpA patients without psoriasis (1 case in 74 patients; P = .001) compared with the control group, while dactylitis occurrence was not significantly different in 3 out of 14 patients (21.4%) with coexistent psoriasis (P = .960). Enthesitis was significantly higher in 14 IBD-SpA patients with associated psoriasis (50%), compared with the remaining 74 cases (12.1%; P = .003). It was noted that enthesitis occurrence was not different in patients with UC and in those with CD (P = .103).
“The results of our case-control study show that dactylitis, enthesitis, and AU are significantly less frequent in IBD-SpA, compared with other types of SpA,” researchers concluded. “Owing to the frequent association of psoriasis with IBD, and especially with CD, the coexistence of skin disease should be taken into account when evaluating the prevalence of dactylitis and enthesitis in patients with IBD-SpA.”
Find the full study in the Journal of Rheumatology (doi: 10.3899/jrheum.161518).
Management of chronic insomnia in adults
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.

As some holdout states revisit Medicaid expansion, new data show it pays off
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Although the GOP-controlled Congress is pledging its continued interest – despite stalls and snags – in dismantling Obamacare, some “red state” legislatures are changing course and showing a newfound interest in embracing the health law’s Medicaid expansion.
And a study published April 12 in Health Affairs adds to these discussions, percolating in places such as Kansas, Georgia, Virginia, North Carolina, and Maine. Thirty-one states plus the District of Columbia already opted to pursue the expansion, which provided federal funding to broaden eligibility to include most low-income adults with incomes up to 138 percent of the federal poverty level (about $16,000 for an individual).
Researchers analyzed data from the National Association of State Budget Officers for fiscal years 2010-2015 to assess the fiscal effects of expansion’s first 2 years.
Their findings address arguments put forth by some GOP lawmakers, who say the expansion will add to the nation’s budget deficit and saddle states with additional coverage costs, forcing them to skimp on other budget priorities like education or transportation.
The researchers concluded that when states expanded eligibility for the low-income health insurance program they did see larger health care expenditures – but those costs were covered with federal funding. In addition, expansion states didn’t have to skimp on other policy priorities – such as environment, housing, and other public health initiatives – to make ends meet.
“This is a potential big benefit, not only to people who get coverage, but to state economies,” said Benjamin Sommers, MD, PhD, an associate professor of health policy and economics at Harvard University’s public health school, and the study’s first author.
This finding – that states expanding Medicaid didn’t encounter unforeseen budget problems – shouldn’t be surprising.
“Expansion is basically free” to the states, agreed Massachusetts Institute of Technology economist Jonathan Gruber, PhD, one of Obamacare’s architects who worked with Dr. Sommers to systematically compare the budgets of all 50 states to examine Medicaid expansion’s impact. “That’s the big insight,” he said. “There’s no sort of hidden downside.”
And that may be part of what’s fueling this renewed interest, said Edwin Park, vice president for health policy at the left-leaning Center for Budget and Policy Priorities. These states are seeing the federal windfall their neighbors received while trying to navigate public health concerns like opioid addiction, he said. They “are looking at how their neighbors or expansion states have done and see the benefits,” Mr. Park said. “The primary argument against the expansion on the state level has been it’s going to break the bank. The research demonstrates that’s not the case.”
But a caveat: The data used in this analysis reflected only years during which the federal government picked up 100% of the tab for expanding Medicaid eligibility and therefore could overestimate the benefit to state budgets. That’s because in 2017 that federal support begins to taper off, and by 2020 states have to pay 10 percent of the expansion costs themselves.
That means policymakers should exert caution in reading too much into this study, said Tom Miller, a resident fellow at the conservative American Enterprise Institute. Because states will eventually shoulder more of the cost, he said, studies that assess its budgetary impact are preliminary at best. Plus, Miller said, other factors such as relative economic growth could have padded state budgets in the years studied – masking any unintended costs with a bigger Medicaid program. It’s unclear whether in times of downturn Medicaid would take a bigger bite out of state budgets.
“It’s just the beginning of this – it’s an early snapshot,” he said.
Dr. Sommers argued the limited data set means researchers should continue to track how state budgets compare between expansion and nonexpansion states. But even when states do take on more of Medicaid’s cost, that may not pose such a burden, suggested Sara Rosenbaum, a professor of health law and policy at George Washington University. Expanding Medicaid brings in other potential economic benefits that this paper doesn’t account for – less uncompensated care in hospitals, for instance – that could offset the expenditures states ultimately take up.
A bigger concern, some experts say, is that – even without the Obamacare repeal – some GOP health proposals would change the federal government’s Medicaid funding mechanism from being an open-ended match to a block grant or per-capita cap in an effort to curb national spending. Those proposals would take away at least some of the federal dollars that have insulated state budgets.
“Ironically, all the arguments that have been made against expansion for years – like creating a hole in the state budget or breaking the bank – that’s exactly what a per-capita grant or block grant does,” Park said.
As more states take on the Medicaid debate, those consequences matter, both Dr. Sommers and Dr. Gruber said. And not just for state budgets – for consumers, too.
“The main lesson is there’s no sort of big hidden cost of expanding Medicaid. What you see is what you get,” Dr. Gruber said. “You get free health insurance for your citizens.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.