User login
Hospitalists prepare for MACRA, seek more changes
“We heard you and will continue listening.”
Those were the words that Andrew Slavitt, then-acting administrator of the Centers for Medicare and Medicaid Services, used in a blog post on Oct. 14, 2016.1 (Slavitt no longer maintains that title since the new federal administration took office on Jan. 20, 2017.)

And, it seems they are still listening. Since issuing the final rule, CMS has continued to seek input from stakeholders. The SHM and other groups are working to clarify and pursue improvements to the bipartisan law. Reporting under MACRA begins this year and several changes that appeared in the final rule already may make living with the law less challenging for hospitalists.

For instance, 13 specialty measures were required under the final rule in order for hospitalists to begin reporting under the Quality category of the Merit-based Incentive Payment System (MIPS), one of two pathways to reimbursement available to all physicians under MACRA’s Quality Payment Program. However, of these, Dr. Greeno said that just seven are relevant to the hospitalist practice. The CMS now requires six reported measures in the Quality category, reduced from the initial nine.3
The measures include:
- Heart failure: ACE inhibitor/angiotensin receptor blocker for left ventricular systolic dysfunction
- Heart failure: Beta-blocker for LVSD
- Stroke: DC on antithrombotic therapy
- Advance Care Plan
- Prevention of catheter-related bloodstream infection: CVC (central venous catheter) Insertion Protocol
- Documentation of current medications
- Appropriate treatment of methicillin-susceptible Staphylococcus aureus bacteremia
“Of the seven available, not all will be reportable because hospitalist practices have a lot of variation, both in their practices and in their patient mix,” Dr. Greeno said. “Most hospitalists will only be able to successfully report on four measures, but we are seeking clarification on what they call a validation test and how that will function.”
In the final rule, CMS said that it will perform that “validation test” to evaluate physicians who cannot report the minimum number of measures to ensure they are not penalized for it.
In addition to Quality, the other reporting categories under the umbrella of MIPS include Advancing Care Information, Cost, and Improvement Activities. For 2017, CMS gave physicians the option to “pick your pace.”4 As long as doctors report just one quality measure, one improvement activity, or the required advancing care information measures (most hospitalists will be exempt from this category), they will avoid a penalty.1,5 Cost will not be included for 2017, the first performance year for MIPS. This year’s reporting will be used to determine payments in 2019, though all physicians will see a 0.5 percent fee increase between now and 2019.
Additionally, just for this year, physicians can choose to report for either a full or partial year (90 days). They will not be subject to the penalty and may be eligible for a positive payment adjustment. However, those who submit nothing are subject to a negative 4% adjustment penalty.

Additionally, CMS took steps to make MACRA easier on small and rural physician practices. The final rule exempts physicians who bill $30,000 or less in Medicare Part B or 100 or fewer Medicare patients, up from the previous $10,000 threshold.1
However, this is unlikely to apply to the majority of – if any – hospitalists, Dr. Dutta said. “By virtue of being a hospitalist, you are seeing all comers to your institution. We don’t really have the choice to see fewer Medicare patients, to be honest, and, [for] most hospitalists – whether employed by a hospital or contracting – one of the main reasons we are in place is to help the hospital and take the patients nobody else will take.”
The CMS has also allotted $20 million each year for five years to support training and education for practices of 15 providers or fewer, for rural providers, and for those working in geographic health professional shortage areas.1,6 According to CMS, as of December 2016, experienced organizations (regional health collaboratives, quality improvement organizations, and others) began receiving funds to help these practices choose appropriate quality measures, train in improvement techniques, select the right health information technology, and more.
Under MACRA, small practices (10 clinicians or fewer) may also join “virtual groups” in order to combine their MIPS reporting into a composite score. However, this is not yet well defined, and the option is not available in 2017. The CMS said that it will continue to seek feedback on the structure and implementation of virtual groups in future years.1
Hospitalists may find themselves presented with another option for performance measurement, Dr. Greeno said. The SHM has asked CMS to consider allowing hospitalists to align with their hospital facility instead of being measured separately.
“Hospitalists are in the unique position of working at only one acute care hospital, for the most part, and we actually floated this idea around years ago, to give hospitalists the option for all their quality metrics – not as a standalone physician group – to be judged on hospital performance metrics,” he said, adding, “It would be easier if we could do this for everybody, but not all hospitalist groups that work for hospitals may want to do that.”
Dr. Dutta said that this would be “a great and efficient option,” especially since hospitalists oversee the bulk of quality improvement activities in their hospitals.
“Hospital-level data would be a reflection of what we’re involved in, as the bulk of hospitalists not only provide clinical care but also participate in a multitude of hospital activities,” she said, like: “helping to develop and promote practices around high-value care, to serving on groups like safe transitions in care. It’s hospitalists who are usually the hospital leaders around quality improvement.”
This includes coming up with ways to work with pharmacists at patient admission and on medication reconciliation upon discharge, as well as providing input on clinical protocols, such as what should be done when someone falls or when potassium is high, Dr. Dutta said.
“Performance should be tied to the performance of the hospital. It moves in the right direction to force more collaboration and a joint fate,” Dr. Berenson added.
Alternative payment models
While MIPS is the pathway most physicians expect to find themselves on in 2017, the other option is the Alternative Payment Models (APMs) pathway, which moves away from the pay-for-performance, semi-fee-for-service structure of MIPS and, instead, follows the rules established by the models themselves, which include select qualified accountable care organizations and patient-centered medical homes.7 Participating physicians are eligible for a 5% incentive payment in 2019. Many health experts say that it’s clear CMS would like to ultimately steer most physicians from MIPS to APMs.
However, very few – if any – hospitalists will find themselves on an APM track. This is, in part, because models considered APMs require the use of Certified Electronic Health Record Technology (CEHRT) and must present “more than nominal risk” to providers.
“Right now, the only alternative payment model where hospitalists can directly take risk is BPCI [Bundled Payments for Care Improvement], but it does not qualify as an APM,” Dr. Greeno said.
It will also be difficult because CMS requires patient and payer thresholds under APMs that hospitalists simply are not poised to meet. In 2019, this means 25% of Medicare payments must come from an Advanced APM in 2017, or 20% of providers’ Medicare patients must be seen through an Advanced APM.8
Advanced APMs are those with which, at least in 2019 and 2020, providers face the risk of losing the lesser of 8% of their revenue or repaying CMS up to 3% of their total Medicare expenditures, if expenditures are higher than expected.8,9
“It is going to be very difficult for hospitalists to qualify for APMs because we’re not in the position to hit the thresholds,” said Dr. Dutta.
However, SHM has urged CMS to consider other BPCI models for qualification as APMs, and Dr. Greeno said that CMS is currently looking into developing bundles that may be appropriate for hospitalists. For instance, Dr. Dutta said, “What we do often in medicine is chronic disease management, and the time is coming to get into chronic disease bundles, such as [those for] management of heart failure or kidney disease.”
In December, SHM submitted a letter to PTAC (the Physician-Focused Payment Model Technical Advisory Committee) to show support for a model created by the American College of Surgeons, called ACS-Brandeis, which they hope will be considered as an Advanced Alternative Payment Model. In the proposal that ACS submitted, the authors noted, “The core model is focused on procedure episodes but can easily be expanded to include acute and chronic conditions.”
The SHM notes in its letter that, while the initial proposal is intended for surgical patients, the term-based nature of surgical care provides a platform for expanding the model more broadly to hospitalists and other specialties.
Some skepticism remains
Even if BPCI or other models are accepted as APMs, hospitalists may still be challenged to meet the required payment or patient thresholds, Dr. Greeno said. Additionally, Dr. Berenson is skeptical of bundled payments, particularly for hospitalists.
“Are hospitalists the right organization to be held accountable for the total cost of care for 90 days of spending, any more than oncologists under Oncology Care Models should be accountable for the total cost of cancer where some patients are getting palliative care and that’s not a driver of healthcare costs?” he asked. “I could see that as problematic for hospitalists.”
While he believes there are many positive aspects to MACRA, in general, Dr. Berenson considers it bad policy. While he does not want to see the Sustainable Growth Rate return, he believes many physicians would have seen reimbursement reductions sooner without MACRA (under the prior quality measurement programs) and that the law provides some perverse incentives.
For one thing, the Quality Payment Program is budget neutral, which means that, for every winner, there is also a loser. Before CMS expanded exemptions for smaller and rural practices, Dr. Berenson said that some larger groups – which are often better equipped to pursue APMs – were planning to stay in MIPS because they figured they were more likely to be the winners when compared with smaller physician practices. And MIPS comes with a 9% payment boost by 2022 (or 9% penalty), plus the possibility of an extra bonus for top performers, compared with the 5% incentive of APMs that same year.7
“There were literally groups saying they were going to go for the MIPS pathway because it’s a bigger upside,” Dr. Berenson said. “When CMS said it was exempting those [smaller, rural] groups, the [larger] groups turned around and said [that the smaller, rural groups] were the downside. ... That kind of game theory is bad public policy.”
Dr. Berenson also believes MACRA will be detrimental to some small and independent practices. Others may decide not to bill Medicare altogether, though that is not an option open to most hospitalists who care to stay in practice. It could, however, drive more hospitalists to consolidate or to become employees of their hospitals.10
“I don’t think there is any doubt this is going to drive consolidation,” Dr. Greeno said, citing numbers released by CMS that show an inverse relationship between practice size and the negative impact of MACRA.11 “I think it’s going to be pretty tough unless you’re big enough to commit the resources you need to do it right.”
At TeamHealth, where Dr. Greeno is senior advisor of medical affairs, he said that they have invested in information technology compliance, developed systems and trained providers to ensure the creation of favorable metrics for the organization’ and built the infrastructure to gather, report, and validate data. These are steps that may be out of reach for most smaller practices.
As Dr. Greeno said, no one expected this to be easy. “You’re trying to get doctors to change the way they practice. Anybody who has ever worked with doctors knows that’s not an easy things to do,” he said. “CMS is changing things to create enough incentive so the pain of not changing becomes greater than the pain of changing.”
While hospitalists may bear more of the pressure than other physician specialties, by virtue of their role in improving the quality of care in hospitals, they were born from reform efforts of the past, Dr. Greeno adds.
“If there had never been an attempt to change the way that physicians were paid, hospitalists wouldn’t exist,” he said. “We were created by physician groups who took capitated payments from HMOs, who had to find more efficient ways to treat patients in the hospital or go out of business.”
“Hospitalists are a delivery system reform and people look to us to lead. We can create a tremendous amount of value for whomever we work for,” Dr. Greeno said.
This is also why SHM continues to work with CMS to advocate for all its members. Dr. Greeno is in Washington at least once a month, participating in critical meetings and helping to guide decisions.
“The Public Policy Committee has to get into the weeds and get involved in advocating for measures that truly get at the work we do and push back on metrics and categories that do not relate to the care we are delivering for our patients,” said Dr. Dutta. “The group worked hard to push back on having to comply with Meaningful Use standards for hospitalists, and now we’re exempt from that category. CMS does listen. It sometimes just takes a while.”
References
1. Slavitt A. (2016 Oct 14). A letter from CMS to Medicare clinicians in the Quality Payment Program: We heard you and will continue listening. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123921/https://blog.cms.gov/2016/10/14/a-letter-from-cms-to-medicare-clinicians-in-the-quality-payment-program/.
2. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program executive summary. Retrieved from https://qpp.cms.gov/docs/QPP_Executive_Summary_of_Final_Rule.pdf.
3. American Medical Association. (2016 Oct 19). Medicare Access and CHIP Reauthorization Act (MACRA) Quality Payment Program final rule AMA summary. Retrieved from https://www.ama-assn.org/sites/default/files/media-browser/public/physicians/macra/macra-qpp-summary.pdf.
4. Slavitt A. (2016 Sept 8). Plans for the Quality Payment Program in 2017: Pick your pace. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123909/https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace/.
5. The Society of Hospital Medicine. Medicare physician payments are changing. Retrieved from http://www.macraforhm.org/.
6. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program fact sheet. Retrieved from https://qpp.cms.gov/docs/QPP_Small_Practice.pdf.
7. The Society of Hospital Medicine. (2017). MACRA and the Quality Payment Program. Retrieved from http://www.macraforhm.org/MACRA_FAQ_m1_final.pdf.
8. Department of Health & Human Services and Centers for Medicare & Medicaid Services. Quality Payment Program: Modernizing Medicare to provide better care and smarter spending for a healthier America. Retrieved from https://qpp.cms.gov/.
9. Wynne B. (2016 Oct 17). MACRA Final Rule: CMS strikes a balance; will docs hang on? Retrieved from http://healthaffairs.org/blog/2016/10/17/macra-final-rule-cms-strikes-a-balance-will-docs-hang-on/.
10. Quinn R. (2015 Aug). TeamHealth-IPC Deal Latest in consolidation trend. The Hospitalist. 2015(8). Retrieved from http://www.the-hospitalist.org/hospitalist/article/122210/teamhealth-ipc-deal-latest-consolidation-trend
11. Barkholz D. (2016 Jun 30). Potential MACRA byproduct: physician consolidation. Retrieved from http://www.modernhealthcare.com/article/20160630/NEWS/160639995.
“We heard you and will continue listening.”
Those were the words that Andrew Slavitt, then-acting administrator of the Centers for Medicare and Medicaid Services, used in a blog post on Oct. 14, 2016.1 (Slavitt no longer maintains that title since the new federal administration took office on Jan. 20, 2017.)
And, it seems they are still listening. Since issuing the final rule, CMS has continued to seek input from stakeholders. The SHM and other groups are working to clarify and pursue improvements to the bipartisan law. Reporting under MACRA begins this year and several changes that appeared in the final rule already may make living with the law less challenging for hospitalists.
For instance, 13 specialty measures were required under the final rule in order for hospitalists to begin reporting under the Quality category of the Merit-based Incentive Payment System (MIPS), one of two pathways to reimbursement available to all physicians under MACRA’s Quality Payment Program. However, of these, Dr. Greeno said that just seven are relevant to the hospitalist practice. The CMS now requires six reported measures in the Quality category, reduced from the initial nine.3
The measures include:
- Heart failure: ACE inhibitor/angiotensin receptor blocker for left ventricular systolic dysfunction
- Heart failure: Beta-blocker for LVSD
- Stroke: DC on antithrombotic therapy
- Advance Care Plan
- Prevention of catheter-related bloodstream infection: CVC (central venous catheter) Insertion Protocol
- Documentation of current medications
- Appropriate treatment of methicillin-susceptible Staphylococcus aureus bacteremia
“Of the seven available, not all will be reportable because hospitalist practices have a lot of variation, both in their practices and in their patient mix,” Dr. Greeno said. “Most hospitalists will only be able to successfully report on four measures, but we are seeking clarification on what they call a validation test and how that will function.”
In the final rule, CMS said that it will perform that “validation test” to evaluate physicians who cannot report the minimum number of measures to ensure they are not penalized for it.
In addition to Quality, the other reporting categories under the umbrella of MIPS include Advancing Care Information, Cost, and Improvement Activities. For 2017, CMS gave physicians the option to “pick your pace.”4 As long as doctors report just one quality measure, one improvement activity, or the required advancing care information measures (most hospitalists will be exempt from this category), they will avoid a penalty.1,5 Cost will not be included for 2017, the first performance year for MIPS. This year’s reporting will be used to determine payments in 2019, though all physicians will see a 0.5 percent fee increase between now and 2019.
Additionally, just for this year, physicians can choose to report for either a full or partial year (90 days). They will not be subject to the penalty and may be eligible for a positive payment adjustment. However, those who submit nothing are subject to a negative 4% adjustment penalty.
Additionally, CMS took steps to make MACRA easier on small and rural physician practices. The final rule exempts physicians who bill $30,000 or less in Medicare Part B or 100 or fewer Medicare patients, up from the previous $10,000 threshold.1
However, this is unlikely to apply to the majority of – if any – hospitalists, Dr. Dutta said. “By virtue of being a hospitalist, you are seeing all comers to your institution. We don’t really have the choice to see fewer Medicare patients, to be honest, and, [for] most hospitalists – whether employed by a hospital or contracting – one of the main reasons we are in place is to help the hospital and take the patients nobody else will take.”
The CMS has also allotted $20 million each year for five years to support training and education for practices of 15 providers or fewer, for rural providers, and for those working in geographic health professional shortage areas.1,6 According to CMS, as of December 2016, experienced organizations (regional health collaboratives, quality improvement organizations, and others) began receiving funds to help these practices choose appropriate quality measures, train in improvement techniques, select the right health information technology, and more.
Under MACRA, small practices (10 clinicians or fewer) may also join “virtual groups” in order to combine their MIPS reporting into a composite score. However, this is not yet well defined, and the option is not available in 2017. The CMS said that it will continue to seek feedback on the structure and implementation of virtual groups in future years.1
Hospitalists may find themselves presented with another option for performance measurement, Dr. Greeno said. The SHM has asked CMS to consider allowing hospitalists to align with their hospital facility instead of being measured separately.
“Hospitalists are in the unique position of working at only one acute care hospital, for the most part, and we actually floated this idea around years ago, to give hospitalists the option for all their quality metrics – not as a standalone physician group – to be judged on hospital performance metrics,” he said, adding, “It would be easier if we could do this for everybody, but not all hospitalist groups that work for hospitals may want to do that.”
Dr. Dutta said that this would be “a great and efficient option,” especially since hospitalists oversee the bulk of quality improvement activities in their hospitals.
“Hospital-level data would be a reflection of what we’re involved in, as the bulk of hospitalists not only provide clinical care but also participate in a multitude of hospital activities,” she said, like: “helping to develop and promote practices around high-value care, to serving on groups like safe transitions in care. It’s hospitalists who are usually the hospital leaders around quality improvement.”
This includes coming up with ways to work with pharmacists at patient admission and on medication reconciliation upon discharge, as well as providing input on clinical protocols, such as what should be done when someone falls or when potassium is high, Dr. Dutta said.
“Performance should be tied to the performance of the hospital. It moves in the right direction to force more collaboration and a joint fate,” Dr. Berenson added.
Alternative payment models
While MIPS is the pathway most physicians expect to find themselves on in 2017, the other option is the Alternative Payment Models (APMs) pathway, which moves away from the pay-for-performance, semi-fee-for-service structure of MIPS and, instead, follows the rules established by the models themselves, which include select qualified accountable care organizations and patient-centered medical homes.7 Participating physicians are eligible for a 5% incentive payment in 2019. Many health experts say that it’s clear CMS would like to ultimately steer most physicians from MIPS to APMs.
However, very few – if any – hospitalists will find themselves on an APM track. This is, in part, because models considered APMs require the use of Certified Electronic Health Record Technology (CEHRT) and must present “more than nominal risk” to providers.
“Right now, the only alternative payment model where hospitalists can directly take risk is BPCI [Bundled Payments for Care Improvement], but it does not qualify as an APM,” Dr. Greeno said.
It will also be difficult because CMS requires patient and payer thresholds under APMs that hospitalists simply are not poised to meet. In 2019, this means 25% of Medicare payments must come from an Advanced APM in 2017, or 20% of providers’ Medicare patients must be seen through an Advanced APM.8
Advanced APMs are those with which, at least in 2019 and 2020, providers face the risk of losing the lesser of 8% of their revenue or repaying CMS up to 3% of their total Medicare expenditures, if expenditures are higher than expected.8,9
“It is going to be very difficult for hospitalists to qualify for APMs because we’re not in the position to hit the thresholds,” said Dr. Dutta.
However, SHM has urged CMS to consider other BPCI models for qualification as APMs, and Dr. Greeno said that CMS is currently looking into developing bundles that may be appropriate for hospitalists. For instance, Dr. Dutta said, “What we do often in medicine is chronic disease management, and the time is coming to get into chronic disease bundles, such as [those for] management of heart failure or kidney disease.”
In December, SHM submitted a letter to PTAC (the Physician-Focused Payment Model Technical Advisory Committee) to show support for a model created by the American College of Surgeons, called ACS-Brandeis, which they hope will be considered as an Advanced Alternative Payment Model. In the proposal that ACS submitted, the authors noted, “The core model is focused on procedure episodes but can easily be expanded to include acute and chronic conditions.”
The SHM notes in its letter that, while the initial proposal is intended for surgical patients, the term-based nature of surgical care provides a platform for expanding the model more broadly to hospitalists and other specialties.
Some skepticism remains
Even if BPCI or other models are accepted as APMs, hospitalists may still be challenged to meet the required payment or patient thresholds, Dr. Greeno said. Additionally, Dr. Berenson is skeptical of bundled payments, particularly for hospitalists.
“Are hospitalists the right organization to be held accountable for the total cost of care for 90 days of spending, any more than oncologists under Oncology Care Models should be accountable for the total cost of cancer where some patients are getting palliative care and that’s not a driver of healthcare costs?” he asked. “I could see that as problematic for hospitalists.”
While he believes there are many positive aspects to MACRA, in general, Dr. Berenson considers it bad policy. While he does not want to see the Sustainable Growth Rate return, he believes many physicians would have seen reimbursement reductions sooner without MACRA (under the prior quality measurement programs) and that the law provides some perverse incentives.
For one thing, the Quality Payment Program is budget neutral, which means that, for every winner, there is also a loser. Before CMS expanded exemptions for smaller and rural practices, Dr. Berenson said that some larger groups – which are often better equipped to pursue APMs – were planning to stay in MIPS because they figured they were more likely to be the winners when compared with smaller physician practices. And MIPS comes with a 9% payment boost by 2022 (or 9% penalty), plus the possibility of an extra bonus for top performers, compared with the 5% incentive of APMs that same year.7
“There were literally groups saying they were going to go for the MIPS pathway because it’s a bigger upside,” Dr. Berenson said. “When CMS said it was exempting those [smaller, rural] groups, the [larger] groups turned around and said [that the smaller, rural groups] were the downside. ... That kind of game theory is bad public policy.”
Dr. Berenson also believes MACRA will be detrimental to some small and independent practices. Others may decide not to bill Medicare altogether, though that is not an option open to most hospitalists who care to stay in practice. It could, however, drive more hospitalists to consolidate or to become employees of their hospitals.10
“I don’t think there is any doubt this is going to drive consolidation,” Dr. Greeno said, citing numbers released by CMS that show an inverse relationship between practice size and the negative impact of MACRA.11 “I think it’s going to be pretty tough unless you’re big enough to commit the resources you need to do it right.”
At TeamHealth, where Dr. Greeno is senior advisor of medical affairs, he said that they have invested in information technology compliance, developed systems and trained providers to ensure the creation of favorable metrics for the organization’ and built the infrastructure to gather, report, and validate data. These are steps that may be out of reach for most smaller practices.
As Dr. Greeno said, no one expected this to be easy. “You’re trying to get doctors to change the way they practice. Anybody who has ever worked with doctors knows that’s not an easy things to do,” he said. “CMS is changing things to create enough incentive so the pain of not changing becomes greater than the pain of changing.”
While hospitalists may bear more of the pressure than other physician specialties, by virtue of their role in improving the quality of care in hospitals, they were born from reform efforts of the past, Dr. Greeno adds.
“If there had never been an attempt to change the way that physicians were paid, hospitalists wouldn’t exist,” he said. “We were created by physician groups who took capitated payments from HMOs, who had to find more efficient ways to treat patients in the hospital or go out of business.”
“Hospitalists are a delivery system reform and people look to us to lead. We can create a tremendous amount of value for whomever we work for,” Dr. Greeno said.
This is also why SHM continues to work with CMS to advocate for all its members. Dr. Greeno is in Washington at least once a month, participating in critical meetings and helping to guide decisions.
“The Public Policy Committee has to get into the weeds and get involved in advocating for measures that truly get at the work we do and push back on metrics and categories that do not relate to the care we are delivering for our patients,” said Dr. Dutta. “The group worked hard to push back on having to comply with Meaningful Use standards for hospitalists, and now we’re exempt from that category. CMS does listen. It sometimes just takes a while.”
References
1. Slavitt A. (2016 Oct 14). A letter from CMS to Medicare clinicians in the Quality Payment Program: We heard you and will continue listening. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123921/https://blog.cms.gov/2016/10/14/a-letter-from-cms-to-medicare-clinicians-in-the-quality-payment-program/.
2. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program executive summary. Retrieved from https://qpp.cms.gov/docs/QPP_Executive_Summary_of_Final_Rule.pdf.
3. American Medical Association. (2016 Oct 19). Medicare Access and CHIP Reauthorization Act (MACRA) Quality Payment Program final rule AMA summary. Retrieved from https://www.ama-assn.org/sites/default/files/media-browser/public/physicians/macra/macra-qpp-summary.pdf.
4. Slavitt A. (2016 Sept 8). Plans for the Quality Payment Program in 2017: Pick your pace. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123909/https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace/.
5. The Society of Hospital Medicine. Medicare physician payments are changing. Retrieved from http://www.macraforhm.org/.
6. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program fact sheet. Retrieved from https://qpp.cms.gov/docs/QPP_Small_Practice.pdf.
7. The Society of Hospital Medicine. (2017). MACRA and the Quality Payment Program. Retrieved from http://www.macraforhm.org/MACRA_FAQ_m1_final.pdf.
8. Department of Health & Human Services and Centers for Medicare & Medicaid Services. Quality Payment Program: Modernizing Medicare to provide better care and smarter spending for a healthier America. Retrieved from https://qpp.cms.gov/.
9. Wynne B. (2016 Oct 17). MACRA Final Rule: CMS strikes a balance; will docs hang on? Retrieved from http://healthaffairs.org/blog/2016/10/17/macra-final-rule-cms-strikes-a-balance-will-docs-hang-on/.
10. Quinn R. (2015 Aug). TeamHealth-IPC Deal Latest in consolidation trend. The Hospitalist. 2015(8). Retrieved from http://www.the-hospitalist.org/hospitalist/article/122210/teamhealth-ipc-deal-latest-consolidation-trend
11. Barkholz D. (2016 Jun 30). Potential MACRA byproduct: physician consolidation. Retrieved from http://www.modernhealthcare.com/article/20160630/NEWS/160639995.
“We heard you and will continue listening.”
Those were the words that Andrew Slavitt, then-acting administrator of the Centers for Medicare and Medicaid Services, used in a blog post on Oct. 14, 2016.1 (Slavitt no longer maintains that title since the new federal administration took office on Jan. 20, 2017.)
And, it seems they are still listening. Since issuing the final rule, CMS has continued to seek input from stakeholders. The SHM and other groups are working to clarify and pursue improvements to the bipartisan law. Reporting under MACRA begins this year and several changes that appeared in the final rule already may make living with the law less challenging for hospitalists.
For instance, 13 specialty measures were required under the final rule in order for hospitalists to begin reporting under the Quality category of the Merit-based Incentive Payment System (MIPS), one of two pathways to reimbursement available to all physicians under MACRA’s Quality Payment Program. However, of these, Dr. Greeno said that just seven are relevant to the hospitalist practice. The CMS now requires six reported measures in the Quality category, reduced from the initial nine.3
The measures include:
- Heart failure: ACE inhibitor/angiotensin receptor blocker for left ventricular systolic dysfunction
- Heart failure: Beta-blocker for LVSD
- Stroke: DC on antithrombotic therapy
- Advance Care Plan
- Prevention of catheter-related bloodstream infection: CVC (central venous catheter) Insertion Protocol
- Documentation of current medications
- Appropriate treatment of methicillin-susceptible Staphylococcus aureus bacteremia
“Of the seven available, not all will be reportable because hospitalist practices have a lot of variation, both in their practices and in their patient mix,” Dr. Greeno said. “Most hospitalists will only be able to successfully report on four measures, but we are seeking clarification on what they call a validation test and how that will function.”
In the final rule, CMS said that it will perform that “validation test” to evaluate physicians who cannot report the minimum number of measures to ensure they are not penalized for it.
In addition to Quality, the other reporting categories under the umbrella of MIPS include Advancing Care Information, Cost, and Improvement Activities. For 2017, CMS gave physicians the option to “pick your pace.”4 As long as doctors report just one quality measure, one improvement activity, or the required advancing care information measures (most hospitalists will be exempt from this category), they will avoid a penalty.1,5 Cost will not be included for 2017, the first performance year for MIPS. This year’s reporting will be used to determine payments in 2019, though all physicians will see a 0.5 percent fee increase between now and 2019.
Additionally, just for this year, physicians can choose to report for either a full or partial year (90 days). They will not be subject to the penalty and may be eligible for a positive payment adjustment. However, those who submit nothing are subject to a negative 4% adjustment penalty.
Additionally, CMS took steps to make MACRA easier on small and rural physician practices. The final rule exempts physicians who bill $30,000 or less in Medicare Part B or 100 or fewer Medicare patients, up from the previous $10,000 threshold.1
However, this is unlikely to apply to the majority of – if any – hospitalists, Dr. Dutta said. “By virtue of being a hospitalist, you are seeing all comers to your institution. We don’t really have the choice to see fewer Medicare patients, to be honest, and, [for] most hospitalists – whether employed by a hospital or contracting – one of the main reasons we are in place is to help the hospital and take the patients nobody else will take.”
The CMS has also allotted $20 million each year for five years to support training and education for practices of 15 providers or fewer, for rural providers, and for those working in geographic health professional shortage areas.1,6 According to CMS, as of December 2016, experienced organizations (regional health collaboratives, quality improvement organizations, and others) began receiving funds to help these practices choose appropriate quality measures, train in improvement techniques, select the right health information technology, and more.
Under MACRA, small practices (10 clinicians or fewer) may also join “virtual groups” in order to combine their MIPS reporting into a composite score. However, this is not yet well defined, and the option is not available in 2017. The CMS said that it will continue to seek feedback on the structure and implementation of virtual groups in future years.1
Hospitalists may find themselves presented with another option for performance measurement, Dr. Greeno said. The SHM has asked CMS to consider allowing hospitalists to align with their hospital facility instead of being measured separately.
“Hospitalists are in the unique position of working at only one acute care hospital, for the most part, and we actually floated this idea around years ago, to give hospitalists the option for all their quality metrics – not as a standalone physician group – to be judged on hospital performance metrics,” he said, adding, “It would be easier if we could do this for everybody, but not all hospitalist groups that work for hospitals may want to do that.”
Dr. Dutta said that this would be “a great and efficient option,” especially since hospitalists oversee the bulk of quality improvement activities in their hospitals.
“Hospital-level data would be a reflection of what we’re involved in, as the bulk of hospitalists not only provide clinical care but also participate in a multitude of hospital activities,” she said, like: “helping to develop and promote practices around high-value care, to serving on groups like safe transitions in care. It’s hospitalists who are usually the hospital leaders around quality improvement.”
This includes coming up with ways to work with pharmacists at patient admission and on medication reconciliation upon discharge, as well as providing input on clinical protocols, such as what should be done when someone falls or when potassium is high, Dr. Dutta said.
“Performance should be tied to the performance of the hospital. It moves in the right direction to force more collaboration and a joint fate,” Dr. Berenson added.
Alternative payment models
While MIPS is the pathway most physicians expect to find themselves on in 2017, the other option is the Alternative Payment Models (APMs) pathway, which moves away from the pay-for-performance, semi-fee-for-service structure of MIPS and, instead, follows the rules established by the models themselves, which include select qualified accountable care organizations and patient-centered medical homes.7 Participating physicians are eligible for a 5% incentive payment in 2019. Many health experts say that it’s clear CMS would like to ultimately steer most physicians from MIPS to APMs.
However, very few – if any – hospitalists will find themselves on an APM track. This is, in part, because models considered APMs require the use of Certified Electronic Health Record Technology (CEHRT) and must present “more than nominal risk” to providers.
“Right now, the only alternative payment model where hospitalists can directly take risk is BPCI [Bundled Payments for Care Improvement], but it does not qualify as an APM,” Dr. Greeno said.
It will also be difficult because CMS requires patient and payer thresholds under APMs that hospitalists simply are not poised to meet. In 2019, this means 25% of Medicare payments must come from an Advanced APM in 2017, or 20% of providers’ Medicare patients must be seen through an Advanced APM.8
Advanced APMs are those with which, at least in 2019 and 2020, providers face the risk of losing the lesser of 8% of their revenue or repaying CMS up to 3% of their total Medicare expenditures, if expenditures are higher than expected.8,9
“It is going to be very difficult for hospitalists to qualify for APMs because we’re not in the position to hit the thresholds,” said Dr. Dutta.
However, SHM has urged CMS to consider other BPCI models for qualification as APMs, and Dr. Greeno said that CMS is currently looking into developing bundles that may be appropriate for hospitalists. For instance, Dr. Dutta said, “What we do often in medicine is chronic disease management, and the time is coming to get into chronic disease bundles, such as [those for] management of heart failure or kidney disease.”
In December, SHM submitted a letter to PTAC (the Physician-Focused Payment Model Technical Advisory Committee) to show support for a model created by the American College of Surgeons, called ACS-Brandeis, which they hope will be considered as an Advanced Alternative Payment Model. In the proposal that ACS submitted, the authors noted, “The core model is focused on procedure episodes but can easily be expanded to include acute and chronic conditions.”
The SHM notes in its letter that, while the initial proposal is intended for surgical patients, the term-based nature of surgical care provides a platform for expanding the model more broadly to hospitalists and other specialties.
Some skepticism remains
Even if BPCI or other models are accepted as APMs, hospitalists may still be challenged to meet the required payment or patient thresholds, Dr. Greeno said. Additionally, Dr. Berenson is skeptical of bundled payments, particularly for hospitalists.
“Are hospitalists the right organization to be held accountable for the total cost of care for 90 days of spending, any more than oncologists under Oncology Care Models should be accountable for the total cost of cancer where some patients are getting palliative care and that’s not a driver of healthcare costs?” he asked. “I could see that as problematic for hospitalists.”
While he believes there are many positive aspects to MACRA, in general, Dr. Berenson considers it bad policy. While he does not want to see the Sustainable Growth Rate return, he believes many physicians would have seen reimbursement reductions sooner without MACRA (under the prior quality measurement programs) and that the law provides some perverse incentives.
For one thing, the Quality Payment Program is budget neutral, which means that, for every winner, there is also a loser. Before CMS expanded exemptions for smaller and rural practices, Dr. Berenson said that some larger groups – which are often better equipped to pursue APMs – were planning to stay in MIPS because they figured they were more likely to be the winners when compared with smaller physician practices. And MIPS comes with a 9% payment boost by 2022 (or 9% penalty), plus the possibility of an extra bonus for top performers, compared with the 5% incentive of APMs that same year.7
“There were literally groups saying they were going to go for the MIPS pathway because it’s a bigger upside,” Dr. Berenson said. “When CMS said it was exempting those [smaller, rural] groups, the [larger] groups turned around and said [that the smaller, rural groups] were the downside. ... That kind of game theory is bad public policy.”
Dr. Berenson also believes MACRA will be detrimental to some small and independent practices. Others may decide not to bill Medicare altogether, though that is not an option open to most hospitalists who care to stay in practice. It could, however, drive more hospitalists to consolidate or to become employees of their hospitals.10
“I don’t think there is any doubt this is going to drive consolidation,” Dr. Greeno said, citing numbers released by CMS that show an inverse relationship between practice size and the negative impact of MACRA.11 “I think it’s going to be pretty tough unless you’re big enough to commit the resources you need to do it right.”
At TeamHealth, where Dr. Greeno is senior advisor of medical affairs, he said that they have invested in information technology compliance, developed systems and trained providers to ensure the creation of favorable metrics for the organization’ and built the infrastructure to gather, report, and validate data. These are steps that may be out of reach for most smaller practices.
As Dr. Greeno said, no one expected this to be easy. “You’re trying to get doctors to change the way they practice. Anybody who has ever worked with doctors knows that’s not an easy things to do,” he said. “CMS is changing things to create enough incentive so the pain of not changing becomes greater than the pain of changing.”
While hospitalists may bear more of the pressure than other physician specialties, by virtue of their role in improving the quality of care in hospitals, they were born from reform efforts of the past, Dr. Greeno adds.
“If there had never been an attempt to change the way that physicians were paid, hospitalists wouldn’t exist,” he said. “We were created by physician groups who took capitated payments from HMOs, who had to find more efficient ways to treat patients in the hospital or go out of business.”
“Hospitalists are a delivery system reform and people look to us to lead. We can create a tremendous amount of value for whomever we work for,” Dr. Greeno said.
This is also why SHM continues to work with CMS to advocate for all its members. Dr. Greeno is in Washington at least once a month, participating in critical meetings and helping to guide decisions.
“The Public Policy Committee has to get into the weeds and get involved in advocating for measures that truly get at the work we do and push back on metrics and categories that do not relate to the care we are delivering for our patients,” said Dr. Dutta. “The group worked hard to push back on having to comply with Meaningful Use standards for hospitalists, and now we’re exempt from that category. CMS does listen. It sometimes just takes a while.”
References
1. Slavitt A. (2016 Oct 14). A letter from CMS to Medicare clinicians in the Quality Payment Program: We heard you and will continue listening. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123921/https://blog.cms.gov/2016/10/14/a-letter-from-cms-to-medicare-clinicians-in-the-quality-payment-program/.
2. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program executive summary. Retrieved from https://qpp.cms.gov/docs/QPP_Executive_Summary_of_Final_Rule.pdf.
3. American Medical Association. (2016 Oct 19). Medicare Access and CHIP Reauthorization Act (MACRA) Quality Payment Program final rule AMA summary. Retrieved from https://www.ama-assn.org/sites/default/files/media-browser/public/physicians/macra/macra-qpp-summary.pdf.
4. Slavitt A. (2016 Sept 8). Plans for the Quality Payment Program in 2017: Pick your pace. The CMS Blog (archived). Retrieved from http://wayback.archive-it.org/2744/20161109123909/https://blog.cms.gov/2016/09/08/qualitypaymentprogram-pickyourpace/.
5. The Society of Hospital Medicine. Medicare physician payments are changing. Retrieved from http://www.macraforhm.org/.
6. Department of Health & Human Services and Centers for Medicare & Medicaid Services. (2016 Oct 14). Quality Payment Program fact sheet. Retrieved from https://qpp.cms.gov/docs/QPP_Small_Practice.pdf.
7. The Society of Hospital Medicine. (2017). MACRA and the Quality Payment Program. Retrieved from http://www.macraforhm.org/MACRA_FAQ_m1_final.pdf.
8. Department of Health & Human Services and Centers for Medicare & Medicaid Services. Quality Payment Program: Modernizing Medicare to provide better care and smarter spending for a healthier America. Retrieved from https://qpp.cms.gov/.
9. Wynne B. (2016 Oct 17). MACRA Final Rule: CMS strikes a balance; will docs hang on? Retrieved from http://healthaffairs.org/blog/2016/10/17/macra-final-rule-cms-strikes-a-balance-will-docs-hang-on/.
10. Quinn R. (2015 Aug). TeamHealth-IPC Deal Latest in consolidation trend. The Hospitalist. 2015(8). Retrieved from http://www.the-hospitalist.org/hospitalist/article/122210/teamhealth-ipc-deal-latest-consolidation-trend
11. Barkholz D. (2016 Jun 30). Potential MACRA byproduct: physician consolidation. Retrieved from http://www.modernhealthcare.com/article/20160630/NEWS/160639995.
Triple therapy found as ‘durable’ as biologic after methotrexate failure
People with active rheumatoid arthritis who have a suboptimal response to methotrexate and then switch to triple therapy with methotrexate, sulfasalazine, and hydroxychloroquine do just as well and stay on treatment just as long as do those who switch to methotrexate and etanercept, a follow-up study to the RACAT trial shows.
Although evidence shows that patients do well on combination disease-modifying antirheumatic drugs (DMARDs) following methotrexate failure, many rheumatologists still prefer to add a tumor necrosis factor inhibitor such as etanercept, wrote first author Shana M. Peper, MD, of the University of Nebraska, Omaha, and her colleagues (Arthritis Care Res. 2017 Apr 7. doi: 10.1002/acr.23255).
The observational, follow-up study involved 289 patients with active rheumatoid arthritis with a suboptimal response to methotrexate who had participated in the 48-week, multicenter, double-blind, Rheumatoid Arthritis Comparison of Active Therapies (RACAT) trial and then consented to an additional 72 weeks of open-label extended follow-up during which patients and their physicians were free to change or continue treatment. At the end of the double-blind portion, 145 were receiving triple therapy with the conventional DMARDs and 144 were receiving combination therapy with methotrexate and etanercept.
In the RACAT trial, the primary outcome was the 48-week change in 28-joint Disease Activity Score (DAS28). At 24 weeks, patients in both groups who had an inadequate response to their assigned therapy (defined by a change in DAS28 of less than 1.2) were switched to the other treatment arm in a blinded fashion.
After 1 year, 78% of patients on triple therapy remained on it, compared with 63% of patients who began the extended follow-up on the methotrexate-etanercept combination and remained on it.
More patients switched from methotrexate-etanercept to triple therapy than the other way around (P = .005), but when the researchers removed patients who switched at the start of the extended follow-up from the analysis, continuation rates were nearly identical. The results also did not change when the researchers performed analyses using only the patients who did not switch therapy at week 24 during the blinded trial and again with patients assigned to their original randomized groups.
Average DAS28 scores were similar for each group (3.8 ± 1.4 for triple therapy vs. 3.5 ± 1.3 for methotrexate-etanercept) and remained similar at follow-up. There were also no differences between swollen or tender joint counts, patient global health assessments, or erythrocyte sedimentation rates between the groups.
“Triple therapy remained at least as durable and effective as its biologic counterpart,” the authors concluded.
“Our findings suggest that the majority of patients with active disease despite methotrexate respond to triple therapy and will continue to do so with excellent tolerability,” they wrote.
The findings also supported the approach of reserving more costly biologics for patients who continue to have disease progression despite combination conventional DMARD therapy, they added.
The authors reported no relevant funding for the follow-up analysis. One author reported having consulted for Pfizer and received research support from Bristol-Myers Squibb and AstraZeneca. Another author reported having consulted for Medac, Antares, Lilly, Coherus, and GlaxoSmithKline.
People with active rheumatoid arthritis who have a suboptimal response to methotrexate and then switch to triple therapy with methotrexate, sulfasalazine, and hydroxychloroquine do just as well and stay on treatment just as long as do those who switch to methotrexate and etanercept, a follow-up study to the RACAT trial shows.
Although evidence shows that patients do well on combination disease-modifying antirheumatic drugs (DMARDs) following methotrexate failure, many rheumatologists still prefer to add a tumor necrosis factor inhibitor such as etanercept, wrote first author Shana M. Peper, MD, of the University of Nebraska, Omaha, and her colleagues (Arthritis Care Res. 2017 Apr 7. doi: 10.1002/acr.23255).
The observational, follow-up study involved 289 patients with active rheumatoid arthritis with a suboptimal response to methotrexate who had participated in the 48-week, multicenter, double-blind, Rheumatoid Arthritis Comparison of Active Therapies (RACAT) trial and then consented to an additional 72 weeks of open-label extended follow-up during which patients and their physicians were free to change or continue treatment. At the end of the double-blind portion, 145 were receiving triple therapy with the conventional DMARDs and 144 were receiving combination therapy with methotrexate and etanercept.
In the RACAT trial, the primary outcome was the 48-week change in 28-joint Disease Activity Score (DAS28). At 24 weeks, patients in both groups who had an inadequate response to their assigned therapy (defined by a change in DAS28 of less than 1.2) were switched to the other treatment arm in a blinded fashion.
After 1 year, 78% of patients on triple therapy remained on it, compared with 63% of patients who began the extended follow-up on the methotrexate-etanercept combination and remained on it.
More patients switched from methotrexate-etanercept to triple therapy than the other way around (P = .005), but when the researchers removed patients who switched at the start of the extended follow-up from the analysis, continuation rates were nearly identical. The results also did not change when the researchers performed analyses using only the patients who did not switch therapy at week 24 during the blinded trial and again with patients assigned to their original randomized groups.
Average DAS28 scores were similar for each group (3.8 ± 1.4 for triple therapy vs. 3.5 ± 1.3 for methotrexate-etanercept) and remained similar at follow-up. There were also no differences between swollen or tender joint counts, patient global health assessments, or erythrocyte sedimentation rates between the groups.
“Triple therapy remained at least as durable and effective as its biologic counterpart,” the authors concluded.
“Our findings suggest that the majority of patients with active disease despite methotrexate respond to triple therapy and will continue to do so with excellent tolerability,” they wrote.
The findings also supported the approach of reserving more costly biologics for patients who continue to have disease progression despite combination conventional DMARD therapy, they added.
The authors reported no relevant funding for the follow-up analysis. One author reported having consulted for Pfizer and received research support from Bristol-Myers Squibb and AstraZeneca. Another author reported having consulted for Medac, Antares, Lilly, Coherus, and GlaxoSmithKline.
People with active rheumatoid arthritis who have a suboptimal response to methotrexate and then switch to triple therapy with methotrexate, sulfasalazine, and hydroxychloroquine do just as well and stay on treatment just as long as do those who switch to methotrexate and etanercept, a follow-up study to the RACAT trial shows.
Although evidence shows that patients do well on combination disease-modifying antirheumatic drugs (DMARDs) following methotrexate failure, many rheumatologists still prefer to add a tumor necrosis factor inhibitor such as etanercept, wrote first author Shana M. Peper, MD, of the University of Nebraska, Omaha, and her colleagues (Arthritis Care Res. 2017 Apr 7. doi: 10.1002/acr.23255).
The observational, follow-up study involved 289 patients with active rheumatoid arthritis with a suboptimal response to methotrexate who had participated in the 48-week, multicenter, double-blind, Rheumatoid Arthritis Comparison of Active Therapies (RACAT) trial and then consented to an additional 72 weeks of open-label extended follow-up during which patients and their physicians were free to change or continue treatment. At the end of the double-blind portion, 145 were receiving triple therapy with the conventional DMARDs and 144 were receiving combination therapy with methotrexate and etanercept.
In the RACAT trial, the primary outcome was the 48-week change in 28-joint Disease Activity Score (DAS28). At 24 weeks, patients in both groups who had an inadequate response to their assigned therapy (defined by a change in DAS28 of less than 1.2) were switched to the other treatment arm in a blinded fashion.
After 1 year, 78% of patients on triple therapy remained on it, compared with 63% of patients who began the extended follow-up on the methotrexate-etanercept combination and remained on it.
More patients switched from methotrexate-etanercept to triple therapy than the other way around (P = .005), but when the researchers removed patients who switched at the start of the extended follow-up from the analysis, continuation rates were nearly identical. The results also did not change when the researchers performed analyses using only the patients who did not switch therapy at week 24 during the blinded trial and again with patients assigned to their original randomized groups.
Average DAS28 scores were similar for each group (3.8 ± 1.4 for triple therapy vs. 3.5 ± 1.3 for methotrexate-etanercept) and remained similar at follow-up. There were also no differences between swollen or tender joint counts, patient global health assessments, or erythrocyte sedimentation rates between the groups.
“Triple therapy remained at least as durable and effective as its biologic counterpart,” the authors concluded.
“Our findings suggest that the majority of patients with active disease despite methotrexate respond to triple therapy and will continue to do so with excellent tolerability,” they wrote.
The findings also supported the approach of reserving more costly biologics for patients who continue to have disease progression despite combination conventional DMARD therapy, they added.
The authors reported no relevant funding for the follow-up analysis. One author reported having consulted for Pfizer and received research support from Bristol-Myers Squibb and AstraZeneca. Another author reported having consulted for Medac, Antares, Lilly, Coherus, and GlaxoSmithKline.
Key clinical point:
Major finding: At 1 year, people with active RA with a suboptimal response to methotrexate were just as likely to remain on triple DMARD therapy as they were on etanercept plus methotrexate.
Data source: An observational follow-up study of 289 patients with RA who had participated in the 48-week, multicenter, double-blind, RACAT trial.
Disclosures: The authors reported no relevant funding for the follow-up analysis. One author reported having consulted for Pfizer and received research support from Bristol-Myers Squibb and AstraZeneca. Another author reported having consulted for Medac, Antares, Lilly, Coherus, and GlaxoSmithKline.
Hospitalist specialty code goes live: What ‘C6’ means for you
The long wait for the introduction of the C6 hospitalist specialty code has ended. If you are a provider, hospital, or hospitalist administrator, this new specialty designation is important.
The Centers for Medicare & Medicaid Services tracks specialty utilization and compares providers across the country using codes attached to medical specialties, such as cardiology, emergency medicine, pediatrics, etc. Until the CMS designated hospital medicine as a unique specialty, hospitalists were grouped together with office-based internal medicine physicians and general practitioners. This lack of recognition of the hospitalist specialty created two issues.

The first is one of location. Hospitalists practice in hospitals and utilize codes that are hospital based, not office based. Yet hospitalists have been benchmarked against their primary care peers’ utilization for many years. At this point in time, most if not all primary care physicians practice exclusively in the office, so comparison of CPT utilization looks unusual when benchmarked nationally. What appeared as a ‘spike’ was actually normal utilization for a hospitalist; however, this coding anomaly can lead to pre- or postpayment audits.
The second issue is being able to benchmark utilization against one’s peers. For the first time, hospitalist utilization will be considered unique, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Hospitalists can use the C6 specialty code during initial enrollment or as an update, depending on the individual situation. Note that this is a designation for the individual, not the practice, organization, or billing company. The C6 specialty code was recognized as of April 1, 2017, on submitted claims. You may now change your designation and should avoid any disruption or denial of claims.
There are two places to designate the C6 specialty codes, depending on whether the provider is new to Medicare enrollment or is an existing provider:
• Paper: Initial enrollment in the Medicare program on form CMS-855I or CMS 855O (https://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/CMS-Forms-List.html).
• Electronically: Utilizing the PECOS system, provider credentialing offices can update existing specialty codes to C6 (https://pecos.cms.hhs.gov/PECOSWebMaintenance.htm).
This major milestone for hospital medicine demonstrates the continued growth and impact of the specialty. Ensure your self-election in the PECOS system reflects “C6,” your specialty as a hospitalist and your commitment to the hospital medicine movement.
For more information, visit www.hospitalmedicine.org/C6.
Dea Robinson is a member of SHM’s Practice Management Committee, Cultural Competency Workgroup and Physician Burnout Workgroup.
Reference: MLN Matters Number: MM9716 ( https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9716.pdf)
The long wait for the introduction of the C6 hospitalist specialty code has ended. If you are a provider, hospital, or hospitalist administrator, this new specialty designation is important.
The Centers for Medicare & Medicaid Services tracks specialty utilization and compares providers across the country using codes attached to medical specialties, such as cardiology, emergency medicine, pediatrics, etc. Until the CMS designated hospital medicine as a unique specialty, hospitalists were grouped together with office-based internal medicine physicians and general practitioners. This lack of recognition of the hospitalist specialty created two issues.
The first is one of location. Hospitalists practice in hospitals and utilize codes that are hospital based, not office based. Yet hospitalists have been benchmarked against their primary care peers’ utilization for many years. At this point in time, most if not all primary care physicians practice exclusively in the office, so comparison of CPT utilization looks unusual when benchmarked nationally. What appeared as a ‘spike’ was actually normal utilization for a hospitalist; however, this coding anomaly can lead to pre- or postpayment audits.
The second issue is being able to benchmark utilization against one’s peers. For the first time, hospitalist utilization will be considered unique, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Hospitalists can use the C6 specialty code during initial enrollment or as an update, depending on the individual situation. Note that this is a designation for the individual, not the practice, organization, or billing company. The C6 specialty code was recognized as of April 1, 2017, on submitted claims. You may now change your designation and should avoid any disruption or denial of claims.
There are two places to designate the C6 specialty codes, depending on whether the provider is new to Medicare enrollment or is an existing provider:
• Paper: Initial enrollment in the Medicare program on form CMS-855I or CMS 855O (https://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/CMS-Forms-List.html).
• Electronically: Utilizing the PECOS system, provider credentialing offices can update existing specialty codes to C6 (https://pecos.cms.hhs.gov/PECOSWebMaintenance.htm).
This major milestone for hospital medicine demonstrates the continued growth and impact of the specialty. Ensure your self-election in the PECOS system reflects “C6,” your specialty as a hospitalist and your commitment to the hospital medicine movement.
For more information, visit www.hospitalmedicine.org/C6.
Dea Robinson is a member of SHM’s Practice Management Committee, Cultural Competency Workgroup and Physician Burnout Workgroup.
Reference: MLN Matters Number: MM9716 ( https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9716.pdf)
The long wait for the introduction of the C6 hospitalist specialty code has ended. If you are a provider, hospital, or hospitalist administrator, this new specialty designation is important.
The Centers for Medicare & Medicaid Services tracks specialty utilization and compares providers across the country using codes attached to medical specialties, such as cardiology, emergency medicine, pediatrics, etc. Until the CMS designated hospital medicine as a unique specialty, hospitalists were grouped together with office-based internal medicine physicians and general practitioners. This lack of recognition of the hospitalist specialty created two issues.
The first is one of location. Hospitalists practice in hospitals and utilize codes that are hospital based, not office based. Yet hospitalists have been benchmarked against their primary care peers’ utilization for many years. At this point in time, most if not all primary care physicians practice exclusively in the office, so comparison of CPT utilization looks unusual when benchmarked nationally. What appeared as a ‘spike’ was actually normal utilization for a hospitalist; however, this coding anomaly can lead to pre- or postpayment audits.
The second issue is being able to benchmark utilization against one’s peers. For the first time, hospitalist utilization will be considered unique, facilitating more accurate comparisons and fairer assessments of hospitalist performance.
Hospitalists can use the C6 specialty code during initial enrollment or as an update, depending on the individual situation. Note that this is a designation for the individual, not the practice, organization, or billing company. The C6 specialty code was recognized as of April 1, 2017, on submitted claims. You may now change your designation and should avoid any disruption or denial of claims.
There are two places to designate the C6 specialty codes, depending on whether the provider is new to Medicare enrollment or is an existing provider:
• Paper: Initial enrollment in the Medicare program on form CMS-855I or CMS 855O (https://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/CMS-Forms-List.html).
• Electronically: Utilizing the PECOS system, provider credentialing offices can update existing specialty codes to C6 (https://pecos.cms.hhs.gov/PECOSWebMaintenance.htm).
This major milestone for hospital medicine demonstrates the continued growth and impact of the specialty. Ensure your self-election in the PECOS system reflects “C6,” your specialty as a hospitalist and your commitment to the hospital medicine movement.
For more information, visit www.hospitalmedicine.org/C6.
Dea Robinson is a member of SHM’s Practice Management Committee, Cultural Competency Workgroup and Physician Burnout Workgroup.
Reference: MLN Matters Number: MM9716 ( https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9716.pdf)
If you ask me ...
In a feature article in Pediatric News entitled “What do doctors want from health reform,” Alicia Gallegos reports on the results of a recent online Frontline Medical News poll of 390 physicians who were asked what one thing about the ACA they would change. The answers were scattered, but “Stabilize premiums and out of pocket expenses for patients” garnered 50% of the votes.
I suspect that this result was an anguished cry for some leadership in Washington. It could come from the left or the right or, even better, from a coalition. But please, we just need some clear leadership, some direction, and a plan that would allow all of us – physicians, patients, hospitals, and insurance companies – to get on with our various missions.

The cost of medication is another major driver of health care cost. Any new plan or adjustments to the ACA should more forcefully rein in or outright eliminate the pharmacy benefit managers who needlessly add cost to medication. Although most of us grumble when faced with cookbook recipes for care that constrain our prescribing choices, we must accept that, in most cases, these evidence-based guidelines are necessary evils. At the same time, we should vigorously support and cooperate with the efforts to discipline the flagrant overprescribers in our midst.
It is not surprising that the ACA has had difficulty attracting young healthy people to buy health insurance that is costly even at a discount. Offering a lower price, no frills, catastrophic care option might be more appealing to young people who still see themselves as invincible. While, as pediatricians, we can see the benefit of immunizations and preventive care in the first year of life, it may be time for a more critical look at the cost benefit ratio for other preventive initiatives in older age groups that may sound good but are making health insurance more expensive.
Finally, an improved ACA should make reduction of the administrative burden of prior authorizations a high priority. Michael L. Munger, MD, president-elect of the American Academy of Family Physicians, suggests that a standard process for both private and publicly funded patients would allow physicians to focus their time and talents on more efficient patient care. The failure of the ACA to mandate even basic standardization for electronic health records has left us with a nonsystem made up of mini-systems that are neither user friendly nor capable of effectively communicating with one another.
It appears that this country doesn’t yet have the stomach for a single payer model. While I usually believe that compromise will yield a good result, the ACA is an example of when a leadership vacuum can result in a collection of bad compromises.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
[polldaddy:9708248]
In a feature article in Pediatric News entitled “What do doctors want from health reform,” Alicia Gallegos reports on the results of a recent online Frontline Medical News poll of 390 physicians who were asked what one thing about the ACA they would change. The answers were scattered, but “Stabilize premiums and out of pocket expenses for patients” garnered 50% of the votes.
I suspect that this result was an anguished cry for some leadership in Washington. It could come from the left or the right or, even better, from a coalition. But please, we just need some clear leadership, some direction, and a plan that would allow all of us – physicians, patients, hospitals, and insurance companies – to get on with our various missions.
The cost of medication is another major driver of health care cost. Any new plan or adjustments to the ACA should more forcefully rein in or outright eliminate the pharmacy benefit managers who needlessly add cost to medication. Although most of us grumble when faced with cookbook recipes for care that constrain our prescribing choices, we must accept that, in most cases, these evidence-based guidelines are necessary evils. At the same time, we should vigorously support and cooperate with the efforts to discipline the flagrant overprescribers in our midst.
It is not surprising that the ACA has had difficulty attracting young healthy people to buy health insurance that is costly even at a discount. Offering a lower price, no frills, catastrophic care option might be more appealing to young people who still see themselves as invincible. While, as pediatricians, we can see the benefit of immunizations and preventive care in the first year of life, it may be time for a more critical look at the cost benefit ratio for other preventive initiatives in older age groups that may sound good but are making health insurance more expensive.
Finally, an improved ACA should make reduction of the administrative burden of prior authorizations a high priority. Michael L. Munger, MD, president-elect of the American Academy of Family Physicians, suggests that a standard process for both private and publicly funded patients would allow physicians to focus their time and talents on more efficient patient care. The failure of the ACA to mandate even basic standardization for electronic health records has left us with a nonsystem made up of mini-systems that are neither user friendly nor capable of effectively communicating with one another.
It appears that this country doesn’t yet have the stomach for a single payer model. While I usually believe that compromise will yield a good result, the ACA is an example of when a leadership vacuum can result in a collection of bad compromises.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
[polldaddy:9708248]
In a feature article in Pediatric News entitled “What do doctors want from health reform,” Alicia Gallegos reports on the results of a recent online Frontline Medical News poll of 390 physicians who were asked what one thing about the ACA they would change. The answers were scattered, but “Stabilize premiums and out of pocket expenses for patients” garnered 50% of the votes.
I suspect that this result was an anguished cry for some leadership in Washington. It could come from the left or the right or, even better, from a coalition. But please, we just need some clear leadership, some direction, and a plan that would allow all of us – physicians, patients, hospitals, and insurance companies – to get on with our various missions.
The cost of medication is another major driver of health care cost. Any new plan or adjustments to the ACA should more forcefully rein in or outright eliminate the pharmacy benefit managers who needlessly add cost to medication. Although most of us grumble when faced with cookbook recipes for care that constrain our prescribing choices, we must accept that, in most cases, these evidence-based guidelines are necessary evils. At the same time, we should vigorously support and cooperate with the efforts to discipline the flagrant overprescribers in our midst.
It is not surprising that the ACA has had difficulty attracting young healthy people to buy health insurance that is costly even at a discount. Offering a lower price, no frills, catastrophic care option might be more appealing to young people who still see themselves as invincible. While, as pediatricians, we can see the benefit of immunizations and preventive care in the first year of life, it may be time for a more critical look at the cost benefit ratio for other preventive initiatives in older age groups that may sound good but are making health insurance more expensive.
Finally, an improved ACA should make reduction of the administrative burden of prior authorizations a high priority. Michael L. Munger, MD, president-elect of the American Academy of Family Physicians, suggests that a standard process for both private and publicly funded patients would allow physicians to focus their time and talents on more efficient patient care. The failure of the ACA to mandate even basic standardization for electronic health records has left us with a nonsystem made up of mini-systems that are neither user friendly nor capable of effectively communicating with one another.
It appears that this country doesn’t yet have the stomach for a single payer model. While I usually believe that compromise will yield a good result, the ACA is an example of when a leadership vacuum can result in a collection of bad compromises.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
[polldaddy:9708248]
Genital HPV prevalence tops 42% in adults
The overall prevalence of genital human papillomavirus (HPV) among adults aged 18-59 years was 42.5% in 2013-2014, with more than half of that representing infection with high-risk types, according to the National Center for Health Statistics.
Prevalence of the 14 HPV types (out of 37 total) considered to be high risk was almost 23% in 2013-2014. Men were significantly more likely than women to have any genital HPV (45% vs. 40%) and high-risk genital HPV (25% vs. 20%), the NCHS reported.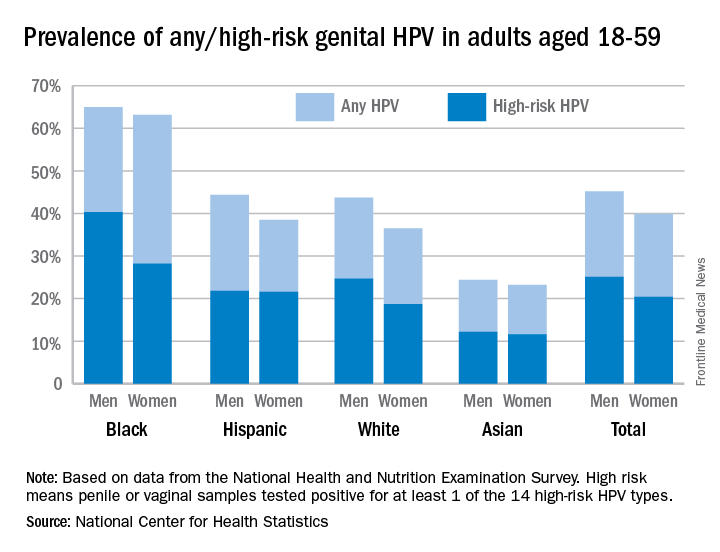
Oral rinse samples were collected as well for adults aged 18-69 years, and the overall prevalence was 7.3% for any oral HPV and 4% for high-risk HPV in 2011-2014. Prevalence among men was significantly higher than among women for all oral HPV (11.5% vs. 3.3%) and for high-risk HPV (6.8% vs. 1.2%), the NCHS said.
The overall prevalence of genital human papillomavirus (HPV) among adults aged 18-59 years was 42.5% in 2013-2014, with more than half of that representing infection with high-risk types, according to the National Center for Health Statistics.
Prevalence of the 14 HPV types (out of 37 total) considered to be high risk was almost 23% in 2013-2014. Men were significantly more likely than women to have any genital HPV (45% vs. 40%) and high-risk genital HPV (25% vs. 20%), the NCHS reported.
Oral rinse samples were collected as well for adults aged 18-69 years, and the overall prevalence was 7.3% for any oral HPV and 4% for high-risk HPV in 2011-2014. Prevalence among men was significantly higher than among women for all oral HPV (11.5% vs. 3.3%) and for high-risk HPV (6.8% vs. 1.2%), the NCHS said.
The overall prevalence of genital human papillomavirus (HPV) among adults aged 18-59 years was 42.5% in 2013-2014, with more than half of that representing infection with high-risk types, according to the National Center for Health Statistics.
Prevalence of the 14 HPV types (out of 37 total) considered to be high risk was almost 23% in 2013-2014. Men were significantly more likely than women to have any genital HPV (45% vs. 40%) and high-risk genital HPV (25% vs. 20%), the NCHS reported.
Oral rinse samples were collected as well for adults aged 18-69 years, and the overall prevalence was 7.3% for any oral HPV and 4% for high-risk HPV in 2011-2014. Prevalence among men was significantly higher than among women for all oral HPV (11.5% vs. 3.3%) and for high-risk HPV (6.8% vs. 1.2%), the NCHS said.
Hepatitis Outlook: March 2017
If you work on the front lines of medical care, treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month, covering the major hepatitis viruses.
Preliver transplant treatment with a highly effective, all-oral direct-acting antiviral agent regimen provides the best health outcomes and is the most cost-effective strategy for the treatment of patients with hepatitis C virus with hepatocellular carcinoma or decompensated cirrhosis who are waitlisted for liver transplant, a study in Hepatology revealed.
A recent study in the Journal of Viral Hepatitis found that patients with chronic HCV and compensated or decompensated cirrhosis who achieve sustained viral response can have clinically meaningful reductions in hepatic venous pressure gradient at long-term follow-up.
The hepatic expressions of cannabinoid receptor 1 and cannabinoid receptor 2 play important roles during the progression of fibrosis induced by chronic hepatitis B virus, according to a study in the International Journal of Infectious Diseases.
A study in the Journal of Viral Hepatitis found that the Pooled Cohort atherosclerotic cardiovascular disease risk equation overestimated the risk of cardiovascular disease among lower-risk patients and underestimated risk among higher-risk patients in both HCV-infected and uninfected groups.
A multinational study in Hepatology found that hemoglobin levels and international normalized ratio values were similar in patients with inherited bleeding disorders and HCV infection who received elbasvir/grazoprevir and placebo.
The number of HBV patients in the United States requiring liver transplantation remained stable, according to a recent study in the Journal of Viral Hepatitis, but the proportion of HBV patients with hepatocellular carcinoma continues to rise.
A research letter in the Morbidity and Mortality Weekly Report reported the transmission of HCV from the inappropriate reuse of saline flush syringes for multiple patients in an acute care hospital in Texas.
A large German study in the Journal of Viral Hepatitis found that ombitasvir/paritaprevir/ritonavir plus/minus dasabuvir plus/minus ribavirin for treatment of HCV genotype 1 and genotype 4 infection was effective and generally well tolerated in clinical practice.
A study, conducted in South Korea, in Hepatology found that monotherapy with tenofovir disoproxil fumarate was efficacious and safe for up to 144 weeks in heavily pretreated patients with multidrug-resistant HBV infection.
Overt and occult HBV infection of children was more serious in underdeveloped northwest regions of China, a study in the Journal of Viral Hepatitis found, suggesting that HBV neonatal immunization and catch-up programs should be strengthened and supplemented.
A study in Hepatology found that long-term entecavir monotherapy is highly effective in preventing HBV reactivation after liver transplantation for chronic HBV, with a durable HBV surface antigen seroclearance rate of 92%, undetectable HBV DNA rate of 100% at 8 years, and excellent long-term survival of 85% at 9 years.
An Italian study in the Journal of Viral Hepatitis found that treatment with direct-acting antivirals was effective and well tolerated in people who inject drugs, although cirrhotic subjects with Model For End-Stage Liver Disease scores greater than 10 and albumin levels below 3 g/dL showed a higher risk of developing serious adverse events and treatment failure.
Direct-acting antiviral–based treatments for severe posttransplant HCV recurrence, comprising fibrosing cholestatic hepatitis, significantly improves liver function even without viral clearance and permits excellent long-term survival, according to a study in the Journal of Viral Hepatitis.
[email protected]
On Twitter @richpizzi
If you work on the front lines of medical care, treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month, covering the major hepatitis viruses.
Preliver transplant treatment with a highly effective, all-oral direct-acting antiviral agent regimen provides the best health outcomes and is the most cost-effective strategy for the treatment of patients with hepatitis C virus with hepatocellular carcinoma or decompensated cirrhosis who are waitlisted for liver transplant, a study in Hepatology revealed.
A recent study in the Journal of Viral Hepatitis found that patients with chronic HCV and compensated or decompensated cirrhosis who achieve sustained viral response can have clinically meaningful reductions in hepatic venous pressure gradient at long-term follow-up.
The hepatic expressions of cannabinoid receptor 1 and cannabinoid receptor 2 play important roles during the progression of fibrosis induced by chronic hepatitis B virus, according to a study in the International Journal of Infectious Diseases.
A study in the Journal of Viral Hepatitis found that the Pooled Cohort atherosclerotic cardiovascular disease risk equation overestimated the risk of cardiovascular disease among lower-risk patients and underestimated risk among higher-risk patients in both HCV-infected and uninfected groups.
A multinational study in Hepatology found that hemoglobin levels and international normalized ratio values were similar in patients with inherited bleeding disorders and HCV infection who received elbasvir/grazoprevir and placebo.
The number of HBV patients in the United States requiring liver transplantation remained stable, according to a recent study in the Journal of Viral Hepatitis, but the proportion of HBV patients with hepatocellular carcinoma continues to rise.
A research letter in the Morbidity and Mortality Weekly Report reported the transmission of HCV from the inappropriate reuse of saline flush syringes for multiple patients in an acute care hospital in Texas.
A large German study in the Journal of Viral Hepatitis found that ombitasvir/paritaprevir/ritonavir plus/minus dasabuvir plus/minus ribavirin for treatment of HCV genotype 1 and genotype 4 infection was effective and generally well tolerated in clinical practice.
A study, conducted in South Korea, in Hepatology found that monotherapy with tenofovir disoproxil fumarate was efficacious and safe for up to 144 weeks in heavily pretreated patients with multidrug-resistant HBV infection.
Overt and occult HBV infection of children was more serious in underdeveloped northwest regions of China, a study in the Journal of Viral Hepatitis found, suggesting that HBV neonatal immunization and catch-up programs should be strengthened and supplemented.
A study in Hepatology found that long-term entecavir monotherapy is highly effective in preventing HBV reactivation after liver transplantation for chronic HBV, with a durable HBV surface antigen seroclearance rate of 92%, undetectable HBV DNA rate of 100% at 8 years, and excellent long-term survival of 85% at 9 years.
An Italian study in the Journal of Viral Hepatitis found that treatment with direct-acting antivirals was effective and well tolerated in people who inject drugs, although cirrhotic subjects with Model For End-Stage Liver Disease scores greater than 10 and albumin levels below 3 g/dL showed a higher risk of developing serious adverse events and treatment failure.
Direct-acting antiviral–based treatments for severe posttransplant HCV recurrence, comprising fibrosing cholestatic hepatitis, significantly improves liver function even without viral clearance and permits excellent long-term survival, according to a study in the Journal of Viral Hepatitis.
[email protected]
On Twitter @richpizzi
If you work on the front lines of medical care, treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month, covering the major hepatitis viruses.
Preliver transplant treatment with a highly effective, all-oral direct-acting antiviral agent regimen provides the best health outcomes and is the most cost-effective strategy for the treatment of patients with hepatitis C virus with hepatocellular carcinoma or decompensated cirrhosis who are waitlisted for liver transplant, a study in Hepatology revealed.
A recent study in the Journal of Viral Hepatitis found that patients with chronic HCV and compensated or decompensated cirrhosis who achieve sustained viral response can have clinically meaningful reductions in hepatic venous pressure gradient at long-term follow-up.
The hepatic expressions of cannabinoid receptor 1 and cannabinoid receptor 2 play important roles during the progression of fibrosis induced by chronic hepatitis B virus, according to a study in the International Journal of Infectious Diseases.
A study in the Journal of Viral Hepatitis found that the Pooled Cohort atherosclerotic cardiovascular disease risk equation overestimated the risk of cardiovascular disease among lower-risk patients and underestimated risk among higher-risk patients in both HCV-infected and uninfected groups.
A multinational study in Hepatology found that hemoglobin levels and international normalized ratio values were similar in patients with inherited bleeding disorders and HCV infection who received elbasvir/grazoprevir and placebo.
The number of HBV patients in the United States requiring liver transplantation remained stable, according to a recent study in the Journal of Viral Hepatitis, but the proportion of HBV patients with hepatocellular carcinoma continues to rise.
A research letter in the Morbidity and Mortality Weekly Report reported the transmission of HCV from the inappropriate reuse of saline flush syringes for multiple patients in an acute care hospital in Texas.
A large German study in the Journal of Viral Hepatitis found that ombitasvir/paritaprevir/ritonavir plus/minus dasabuvir plus/minus ribavirin for treatment of HCV genotype 1 and genotype 4 infection was effective and generally well tolerated in clinical practice.
A study, conducted in South Korea, in Hepatology found that monotherapy with tenofovir disoproxil fumarate was efficacious and safe for up to 144 weeks in heavily pretreated patients with multidrug-resistant HBV infection.
Overt and occult HBV infection of children was more serious in underdeveloped northwest regions of China, a study in the Journal of Viral Hepatitis found, suggesting that HBV neonatal immunization and catch-up programs should be strengthened and supplemented.
A study in Hepatology found that long-term entecavir monotherapy is highly effective in preventing HBV reactivation after liver transplantation for chronic HBV, with a durable HBV surface antigen seroclearance rate of 92%, undetectable HBV DNA rate of 100% at 8 years, and excellent long-term survival of 85% at 9 years.
An Italian study in the Journal of Viral Hepatitis found that treatment with direct-acting antivirals was effective and well tolerated in people who inject drugs, although cirrhotic subjects with Model For End-Stage Liver Disease scores greater than 10 and albumin levels below 3 g/dL showed a higher risk of developing serious adverse events and treatment failure.
Direct-acting antiviral–based treatments for severe posttransplant HCV recurrence, comprising fibrosing cholestatic hepatitis, significantly improves liver function even without viral clearance and permits excellent long-term survival, according to a study in the Journal of Viral Hepatitis.
[email protected]
On Twitter @richpizzi
FDA approves new treatment for episodic cluster headaches in adults
The Food and Drug Administration announced April 18 the approval of the gammaCore device to treat pain associated with episodic cluster headache in adult patients.
The agency based its approval of the noninvasive vagus nerve stimulator device on subgroup analyses of episodic cluster headache patients in the ACT1 and ACT2 trials, which were double-blind, placebo-controlled, randomized studies.
In the ACT1 trial of 85 patients, 34.2% experienced a reduction in pain (defined as the percentage of patients who reported mild or no pain 15 minutes after treatment initiation with gammaCore), compared with 10.6% of patients treated with placebo (P = .008). Of 27 patients in the ACT2 trial, 47.5% of patients using the device were pain free at 15 minutes after the onset of pain from cluster headache, with no use of rescue medication through the 30-minute treatment period, which was significantly greater than for placebo (6.2%; P = .003).
“Cluster headache is a rare, debilitating, and difficult to treat disorder with few effective acute therapies,” Stephen Silberstein, MD, director of the Headache Center at Jefferson University, Philadelphia, said in a statement from the manufacturer, electroCore. “The FDA release of gammaCore is an important advance in the treatment of the pain associated with cluster headache. It is a way for patients to treat their symptoms as often as they need to use the device. It does not have the side effects or dose limitations of commonly prescribed treatments or the need for invasive implantation procedures, which can be inconvenient, costly, and high-risk.”
The gammaCore device works by transmitting a mild electrical stimulation to the vagus nerve through the skin, resulting in a reduction of pain. Currently, gammaCore is in use only outside of the United States, including in the European Union. Commercial availability of gammaCore in the United States is expected to begin early in the third quarter of 2017, the company said.
The Food and Drug Administration announced April 18 the approval of the gammaCore device to treat pain associated with episodic cluster headache in adult patients.
The agency based its approval of the noninvasive vagus nerve stimulator device on subgroup analyses of episodic cluster headache patients in the ACT1 and ACT2 trials, which were double-blind, placebo-controlled, randomized studies.
In the ACT1 trial of 85 patients, 34.2% experienced a reduction in pain (defined as the percentage of patients who reported mild or no pain 15 minutes after treatment initiation with gammaCore), compared with 10.6% of patients treated with placebo (P = .008). Of 27 patients in the ACT2 trial, 47.5% of patients using the device were pain free at 15 minutes after the onset of pain from cluster headache, with no use of rescue medication through the 30-minute treatment period, which was significantly greater than for placebo (6.2%; P = .003).
“Cluster headache is a rare, debilitating, and difficult to treat disorder with few effective acute therapies,” Stephen Silberstein, MD, director of the Headache Center at Jefferson University, Philadelphia, said in a statement from the manufacturer, electroCore. “The FDA release of gammaCore is an important advance in the treatment of the pain associated with cluster headache. It is a way for patients to treat their symptoms as often as they need to use the device. It does not have the side effects or dose limitations of commonly prescribed treatments or the need for invasive implantation procedures, which can be inconvenient, costly, and high-risk.”
The gammaCore device works by transmitting a mild electrical stimulation to the vagus nerve through the skin, resulting in a reduction of pain. Currently, gammaCore is in use only outside of the United States, including in the European Union. Commercial availability of gammaCore in the United States is expected to begin early in the third quarter of 2017, the company said.
The Food and Drug Administration announced April 18 the approval of the gammaCore device to treat pain associated with episodic cluster headache in adult patients.
The agency based its approval of the noninvasive vagus nerve stimulator device on subgroup analyses of episodic cluster headache patients in the ACT1 and ACT2 trials, which were double-blind, placebo-controlled, randomized studies.
In the ACT1 trial of 85 patients, 34.2% experienced a reduction in pain (defined as the percentage of patients who reported mild or no pain 15 minutes after treatment initiation with gammaCore), compared with 10.6% of patients treated with placebo (P = .008). Of 27 patients in the ACT2 trial, 47.5% of patients using the device were pain free at 15 minutes after the onset of pain from cluster headache, with no use of rescue medication through the 30-minute treatment period, which was significantly greater than for placebo (6.2%; P = .003).
“Cluster headache is a rare, debilitating, and difficult to treat disorder with few effective acute therapies,” Stephen Silberstein, MD, director of the Headache Center at Jefferson University, Philadelphia, said in a statement from the manufacturer, electroCore. “The FDA release of gammaCore is an important advance in the treatment of the pain associated with cluster headache. It is a way for patients to treat their symptoms as often as they need to use the device. It does not have the side effects or dose limitations of commonly prescribed treatments or the need for invasive implantation procedures, which can be inconvenient, costly, and high-risk.”
The gammaCore device works by transmitting a mild electrical stimulation to the vagus nerve through the skin, resulting in a reduction of pain. Currently, gammaCore is in use only outside of the United States, including in the European Union. Commercial availability of gammaCore in the United States is expected to begin early in the third quarter of 2017, the company said.
Infantile hemangiomas: Calculating dose for propranolol is tricky
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.

“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.
“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
Use of Hemangeol was associated with fewer dosing errors than use of generic propranolol hydrochloride oral solutions in treating infantile hemangiomas, according to an online questionnaire survey.
Anastasia O. Kurta, DO, of Saint Louis University and her associates emailed a questionnaire to 531 physicians who were members of the Society for Pediatric Dermatology and physicians known to treat infantile hemangiomas. Most of the 220 physicians who responded were pediatric dermatologists. Of those, 90% had prescribed generic propranolol available in concentrations of 4 mg/mL and 8 mg/mL, and 58.6% had prescribed Hemangeol, the Food and Drug Administration-approved formulation of propranolol hydrochloride available in a concentration of 4.28 mg/mL.
“A dosing chart accompanies propranolol 4.28 mg/mL [Hemangeol] using mL/kg doses, which eliminates conversion from milligrams to milliliters and could potentially explain the lower reported dose calculation error reported with propranolol 4.28 mg/mL,” Dr. Kurta and her associates said. “The risk of dispensing errors is increased for medications that are commercially available in different concentrations. Liquid medications prescribed for pediatric patients require additional computation for weight-based dosing and conversion, increasing the possibility of miscalculation.”
Daisy Dai, PhD, is employed by Pierre Fabre Pharmaceuticals and Elaine C. Siegfried, PhD, is a consultant for the company. Dr. Kurta and Eric S. Ambrecht, PhD, have no relevant financial disclosures.
Read more at J Am Acad Dermatol. 2017 May;76(5):999-1000.
Dr. Kurta reported no relevant financial disclosures.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Three-strategy combo reduces pancreatoduodenectomy fistula risk
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
MIAMI BEACH – Pancreaticojejunostomy reconstruction, use of stents, and avoidance of prophylactic octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Failure of the anastomosis is “of greatest concern” to surgeons performing a pancreatoduodenectomy, said Brett L. Ecker, MD, a surgical resident at the University of Pennsylvania, Philadelphia.
“There is no shortage of high-quality data to help guide the use of [fistula reduction] strategies,” he added. However, “the utility of these strategies in patients most vulnerable to fistula … has rarely been particularly explored.”
Dr. Ecker and his colleagues conducted a study with 62 surgeons at 17 institutions to compare various fistula mitigation strategies in this higher-risk population. They assessed surgical reconstruction, dunking, tissue patches, intraperitoneal drains, stents, prophylactic octreotide, and use of tissue sealants.
“Ultimately, we want to know the best way to deal with this high-stakes situation, and whether outcomes might be optimized by bundling these proactive strategies,” Dr. Ecker explained.
“We found the combination of externalized stents and PJ [pancreaticojejunostomy] reconstruction with the omission of prophylactic octreotide was associated with significant improvements in fistula that exceeded the benefit of any individual mitigation approach or any other combination of strategies,” he said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
“The mitigation of risk in real-life practice is often the result of multiple moving parts,” Dr. Ecker said. “The best outcomes [may result from] the synergistic effects of multiple strategies.”
Of the approximately 10% of patients with a Fistula Risk Score of 7-10, 152 ended up with clinically relevant postoperative pancreatic fistula (CR-POPF). “An FRS score of 7 or higher is associated with worse outcomes, including a fistula rate approaching 30%,” Dr. Ecker said. Grade B or C fistula based on International Study Group on Pancreatic Surgery criteria were considered clinically relevant. All patients had surgery from 2003 to 2016 in the retrospective, multinational study.
“This represents the only series of high-risk cases where current international standards were used to define both the risk and the outcome,” he noted.
“Almost all [of the 522] patients had a soft gland and a small duct, a median of 2 mm,” Dr. Ecker added. “High-risk pathology was common, in 86%.”
Surgeons contributing to the series were at high-volume centers and had performed more than 200 Whipple procedures in their careers. “Both institutional and surgeon volume were associated with improved fistula outcomes,” Dr. Ecker said. “We found that intraperitoneal drains were not associated with improved fistula outcomes, but that is limited by the fact that drains were rarely omitted in these cases.”
Four strategies compared
The investigators compared the outcomes of four fistula strategies among the patients considered high risk prior to surgery. When they combined pancreaticogastrostomy, prophylactic octreotide, and no stent, the CR-POPF rate was 47%. “This was associated with an alarming fistula rate approaching 50%,” Dr. Ecker said.
When surgeons combined pancreaticojejunostomy, octreotide, and no stent, the CR-POPF rate declined to 34%. Furthermore, pancreaticojejunostomy without octreotide or a stent yielded a 26% CR-POPF rate.
Ultimately, the most effective strategy to avoid clinically relevant fistula was pancreaticojejunostomy with an external stent and no octreotide.
“The use of PJ reconstruction with an external stent and omission of octreotide was associated with a fistula rate of about 13%, which was a greater than 50% risk reduction from the overall cohort,” Dr. Ecker said.
The researchers also performed propensity score matching to reduce bias associated with surgeon or patient factors. They matched 167 participants in the study with 155 controls. Dr. Ecker said, “Still, we observed that patients managed this way had significantly lower fistula rates.”
“This is an excellent paper and an important topic,” said study discussant Michael L. Kendrick, MD, a general surgeon at the Mayo Clinic in Rochester, Minn.
“At our institution, we’ve used the same Fistula Risk Score and found it very helpful for a mitigation strategy in a separate protocol, and we found that reduced our leak rates as well,” Dr. Kendrick noted.
Dr. Ecker and Dr. Kendrick had no relevant disclosures.
AT AHPBA 2017
Key clinical point: Reconstruction, use of stents, and avoidance of octreotide, especially in combination, could reduce the fistula rate associated with pancreatoduodenectomy.
Major finding: The incidence of fistula decreased from 33% to 13% by combining the three strategies.
Data source: Multicenter retrospective study from 2003 to 2016 with 522 patients undergoing pancreatoduodenectomy.
Disclosures: Dr. Ecker and Dr. Kendrick had no relevant disclosures.
The psychiatric care system of the future
Yogi Berra once said, “It’s tough to make predictions, especially about the future.” It is particularly difficult to talk about the future of psychiatric care and the profession of psychiatry given the current state of affairs and the dysfunction of the mental health services system in America today.
The current system is broken. Needs are not being met. Care is underfunded and uncoordinated. Patients fall through the cracks and are criminalized or homeless. And although there are some early signs of reform, such as the push for integration of psychiatry in medical care systems, it is unclear with the potential repeal of the Affordable Care Act and the undoing of parity whether the situation for our patients and the profession might get even worse.

In the year 2067, most physicians will be employees of one out of four major health care nonprofit corporations that are vertically or horizontally integrated systems of care. All Americans will be enrolled through a government-financed universal single payer plan of care, as employer-based health insurance will have disappeared for the last 25 years. Americans will choose which of the four health systems they wish to join during an annual open season and be able to select their primary and specialty care physicians. Many of the services provided will be in the home or workplace through broad and interactive computing and telemedicine capacity and high-tech centers. Hospitals will provide sophisticated gene therapy, organ transplantation, and biomedical engineering. Approximately 30% of the gross national product will be spent on health care.
Americans will live to an average age of 125 years, but it would not be unusual to find some individuals living to age 150. These Americans will have had many of their organs replaced by either genetically programmed animal organs or harvested organs from special banks. However, the brain is the only irreplaceable organ, and psychiatrists will be prominently involved in the interface of brain and behavior as they have been for the past 200 years.
In the year 2067, an expanded specialty of psychiatric physicians will be certified in one of four major categories of practice. Those certifications will be in neuroscience, medical psychiatry, psychotherapy, and social psychiatry.
The neuroscience psychiatrists will combine an MD with a PhD, and will be the most highly technical and specialized and the most highly compensated psychiatrists. They will be the clinician scientists. The neuroscience psychiatrist will be an expert on the human genome, sophisticated brain imaging and mapping, and the differential use of a variety of neurochemicals, as well as the application of technology such as magnetic fields for the treatment of mental illness and direct intervention into the brain with psychosurgery.
The medical psychiatrists will most resemble the early 21st century psychiatrists with subspecialties in geriatrics, adult, child and adolescent, and substance use. The medical psychiatrists will be integrated with other medical colleagues in many ambulatory as well as residential settings. Geriatrics will be the specialty for the treatment of the very old working with the neuroscience psychiatrist in the treatment of dementias and similarly, the child psychiatrist will work with the neuroscience psychiatrists in early preventive interventions at the intrauterine level with genetic abnormalities being corrected before birth. The medical psychiatrist will be a very popular area for all physicians, with more than 20% of all medical graduates specializing in medical psychiatry.
The psychotherapy psychiatrists will combine the MD degree with psychology education, religion, and the humanities. This psychotherapist will work one to one and in group settings on the age-old problems of individuation, separation, grief, loss, insight, and self-actualization.
The social psychiatrists will combine the MD degree with a degree in sociology or criminology and/or a law degree. They will focus on the social control issues of the day. Forensic prisons will be an area of government-sponsored treatment and will dominate the criminal justice system with interventions in an effort to reduce criminal behavior.
Managed care will not exist 50 years from now. It will be perceived as a regrettable experiment of the late 20th century ending in the first part of the 21st century. With the enactment of a universal single payer system of care, the high-cost intrusive middle management of carve-out behavioral health care companies will become moot.
Human progress comes in many forms. By the year 2067, psychiatry will have made significant advances that will make the prior 200 years of psychiatric care seem crude, quaint, and absurd.
Dr. Sharfstein, a past president of the American Psychiatric Association, is president emeritus of the Sheppard Pratt Health System, Baltimore. This essay is based on a presentation he made in February 2017 at the annual meeting of the American College of Psychiatrists in Scottsdale, Ariz.
Yogi Berra once said, “It’s tough to make predictions, especially about the future.” It is particularly difficult to talk about the future of psychiatric care and the profession of psychiatry given the current state of affairs and the dysfunction of the mental health services system in America today.
The current system is broken. Needs are not being met. Care is underfunded and uncoordinated. Patients fall through the cracks and are criminalized or homeless. And although there are some early signs of reform, such as the push for integration of psychiatry in medical care systems, it is unclear with the potential repeal of the Affordable Care Act and the undoing of parity whether the situation for our patients and the profession might get even worse.
In the year 2067, most physicians will be employees of one out of four major health care nonprofit corporations that are vertically or horizontally integrated systems of care. All Americans will be enrolled through a government-financed universal single payer plan of care, as employer-based health insurance will have disappeared for the last 25 years. Americans will choose which of the four health systems they wish to join during an annual open season and be able to select their primary and specialty care physicians. Many of the services provided will be in the home or workplace through broad and interactive computing and telemedicine capacity and high-tech centers. Hospitals will provide sophisticated gene therapy, organ transplantation, and biomedical engineering. Approximately 30% of the gross national product will be spent on health care.
Americans will live to an average age of 125 years, but it would not be unusual to find some individuals living to age 150. These Americans will have had many of their organs replaced by either genetically programmed animal organs or harvested organs from special banks. However, the brain is the only irreplaceable organ, and psychiatrists will be prominently involved in the interface of brain and behavior as they have been for the past 200 years.
In the year 2067, an expanded specialty of psychiatric physicians will be certified in one of four major categories of practice. Those certifications will be in neuroscience, medical psychiatry, psychotherapy, and social psychiatry.
The neuroscience psychiatrists will combine an MD with a PhD, and will be the most highly technical and specialized and the most highly compensated psychiatrists. They will be the clinician scientists. The neuroscience psychiatrist will be an expert on the human genome, sophisticated brain imaging and mapping, and the differential use of a variety of neurochemicals, as well as the application of technology such as magnetic fields for the treatment of mental illness and direct intervention into the brain with psychosurgery.
The medical psychiatrists will most resemble the early 21st century psychiatrists with subspecialties in geriatrics, adult, child and adolescent, and substance use. The medical psychiatrists will be integrated with other medical colleagues in many ambulatory as well as residential settings. Geriatrics will be the specialty for the treatment of the very old working with the neuroscience psychiatrist in the treatment of dementias and similarly, the child psychiatrist will work with the neuroscience psychiatrists in early preventive interventions at the intrauterine level with genetic abnormalities being corrected before birth. The medical psychiatrist will be a very popular area for all physicians, with more than 20% of all medical graduates specializing in medical psychiatry.
The psychotherapy psychiatrists will combine the MD degree with psychology education, religion, and the humanities. This psychotherapist will work one to one and in group settings on the age-old problems of individuation, separation, grief, loss, insight, and self-actualization.
The social psychiatrists will combine the MD degree with a degree in sociology or criminology and/or a law degree. They will focus on the social control issues of the day. Forensic prisons will be an area of government-sponsored treatment and will dominate the criminal justice system with interventions in an effort to reduce criminal behavior.
Managed care will not exist 50 years from now. It will be perceived as a regrettable experiment of the late 20th century ending in the first part of the 21st century. With the enactment of a universal single payer system of care, the high-cost intrusive middle management of carve-out behavioral health care companies will become moot.
Human progress comes in many forms. By the year 2067, psychiatry will have made significant advances that will make the prior 200 years of psychiatric care seem crude, quaint, and absurd.
Dr. Sharfstein, a past president of the American Psychiatric Association, is president emeritus of the Sheppard Pratt Health System, Baltimore. This essay is based on a presentation he made in February 2017 at the annual meeting of the American College of Psychiatrists in Scottsdale, Ariz.
Yogi Berra once said, “It’s tough to make predictions, especially about the future.” It is particularly difficult to talk about the future of psychiatric care and the profession of psychiatry given the current state of affairs and the dysfunction of the mental health services system in America today.
The current system is broken. Needs are not being met. Care is underfunded and uncoordinated. Patients fall through the cracks and are criminalized or homeless. And although there are some early signs of reform, such as the push for integration of psychiatry in medical care systems, it is unclear with the potential repeal of the Affordable Care Act and the undoing of parity whether the situation for our patients and the profession might get even worse.
In the year 2067, most physicians will be employees of one out of four major health care nonprofit corporations that are vertically or horizontally integrated systems of care. All Americans will be enrolled through a government-financed universal single payer plan of care, as employer-based health insurance will have disappeared for the last 25 years. Americans will choose which of the four health systems they wish to join during an annual open season and be able to select their primary and specialty care physicians. Many of the services provided will be in the home or workplace through broad and interactive computing and telemedicine capacity and high-tech centers. Hospitals will provide sophisticated gene therapy, organ transplantation, and biomedical engineering. Approximately 30% of the gross national product will be spent on health care.
Americans will live to an average age of 125 years, but it would not be unusual to find some individuals living to age 150. These Americans will have had many of their organs replaced by either genetically programmed animal organs or harvested organs from special banks. However, the brain is the only irreplaceable organ, and psychiatrists will be prominently involved in the interface of brain and behavior as they have been for the past 200 years.
In the year 2067, an expanded specialty of psychiatric physicians will be certified in one of four major categories of practice. Those certifications will be in neuroscience, medical psychiatry, psychotherapy, and social psychiatry.
The neuroscience psychiatrists will combine an MD with a PhD, and will be the most highly technical and specialized and the most highly compensated psychiatrists. They will be the clinician scientists. The neuroscience psychiatrist will be an expert on the human genome, sophisticated brain imaging and mapping, and the differential use of a variety of neurochemicals, as well as the application of technology such as magnetic fields for the treatment of mental illness and direct intervention into the brain with psychosurgery.
The medical psychiatrists will most resemble the early 21st century psychiatrists with subspecialties in geriatrics, adult, child and adolescent, and substance use. The medical psychiatrists will be integrated with other medical colleagues in many ambulatory as well as residential settings. Geriatrics will be the specialty for the treatment of the very old working with the neuroscience psychiatrist in the treatment of dementias and similarly, the child psychiatrist will work with the neuroscience psychiatrists in early preventive interventions at the intrauterine level with genetic abnormalities being corrected before birth. The medical psychiatrist will be a very popular area for all physicians, with more than 20% of all medical graduates specializing in medical psychiatry.
The psychotherapy psychiatrists will combine the MD degree with psychology education, religion, and the humanities. This psychotherapist will work one to one and in group settings on the age-old problems of individuation, separation, grief, loss, insight, and self-actualization.
The social psychiatrists will combine the MD degree with a degree in sociology or criminology and/or a law degree. They will focus on the social control issues of the day. Forensic prisons will be an area of government-sponsored treatment and will dominate the criminal justice system with interventions in an effort to reduce criminal behavior.
Managed care will not exist 50 years from now. It will be perceived as a regrettable experiment of the late 20th century ending in the first part of the 21st century. With the enactment of a universal single payer system of care, the high-cost intrusive middle management of carve-out behavioral health care companies will become moot.
Human progress comes in many forms. By the year 2067, psychiatry will have made significant advances that will make the prior 200 years of psychiatric care seem crude, quaint, and absurd.
Dr. Sharfstein, a past president of the American Psychiatric Association, is president emeritus of the Sheppard Pratt Health System, Baltimore. This essay is based on a presentation he made in February 2017 at the annual meeting of the American College of Psychiatrists in Scottsdale, Ariz.