User login
Flashback to 2011
Barrett’s esophagus, named after Australian-born thoracic surgeon Norman Barrett in the 1950s, is now recognized as an important risk factor for esophageal adenocarcinoma. Estimating the magnitude of this risk has proved challenging; however, as early studies of Barrett’s esophagus tended to overestimate cancer risk because of small sample sizes and selection bias. Accurate risk estimation has profound implications for whether and how to identify and monitor patients with Barrett’s esophagus as part of a cancer-prevention strategy.
The December 2011 issue of GI & Hepatology News highlighted an influential study by Frederik Hvid-Jensen and his colleagues from Aarhus (Denmark) University that harnessed the power of Danish population-based registries to estimate the incidence of esophageal adenocarcinoma and high-grade dysplasia among patients with Barrett’s esophagus. Published in the New England Journal of Medicine (2011;365:1375-83), the study utilized data from Denmark’s national pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus, compared with the general population. The study was unique in that there was nearly no loss to follow-up and no referral bias because of the nature of the registry.

Megan A. Adams, MD, JD, MSc, is a general gastroenterologist at Veterans Affairs, an investigator in the VA Center for Clinical Management Research, and a lecturer in gastroenterology at the University of Michigan, all in Ann Arbor. She currently serves as chair-elect of the AGA Quality Measures Committee and is an associate editor of GI & Hepatology News.
Barrett’s esophagus, named after Australian-born thoracic surgeon Norman Barrett in the 1950s, is now recognized as an important risk factor for esophageal adenocarcinoma. Estimating the magnitude of this risk has proved challenging; however, as early studies of Barrett’s esophagus tended to overestimate cancer risk because of small sample sizes and selection bias. Accurate risk estimation has profound implications for whether and how to identify and monitor patients with Barrett’s esophagus as part of a cancer-prevention strategy.
The December 2011 issue of GI & Hepatology News highlighted an influential study by Frederik Hvid-Jensen and his colleagues from Aarhus (Denmark) University that harnessed the power of Danish population-based registries to estimate the incidence of esophageal adenocarcinoma and high-grade dysplasia among patients with Barrett’s esophagus. Published in the New England Journal of Medicine (2011;365:1375-83), the study utilized data from Denmark’s national pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus, compared with the general population. The study was unique in that there was nearly no loss to follow-up and no referral bias because of the nature of the registry.
Megan A. Adams, MD, JD, MSc, is a general gastroenterologist at Veterans Affairs, an investigator in the VA Center for Clinical Management Research, and a lecturer in gastroenterology at the University of Michigan, all in Ann Arbor. She currently serves as chair-elect of the AGA Quality Measures Committee and is an associate editor of GI & Hepatology News.
Barrett’s esophagus, named after Australian-born thoracic surgeon Norman Barrett in the 1950s, is now recognized as an important risk factor for esophageal adenocarcinoma. Estimating the magnitude of this risk has proved challenging; however, as early studies of Barrett’s esophagus tended to overestimate cancer risk because of small sample sizes and selection bias. Accurate risk estimation has profound implications for whether and how to identify and monitor patients with Barrett’s esophagus as part of a cancer-prevention strategy.
The December 2011 issue of GI & Hepatology News highlighted an influential study by Frederik Hvid-Jensen and his colleagues from Aarhus (Denmark) University that harnessed the power of Danish population-based registries to estimate the incidence of esophageal adenocarcinoma and high-grade dysplasia among patients with Barrett’s esophagus. Published in the New England Journal of Medicine (2011;365:1375-83), the study utilized data from Denmark’s national pathology and cancer registries to calculate the incidence of adenocarcinoma among patients with Barrett’s esophagus, compared with the general population. The study was unique in that there was nearly no loss to follow-up and no referral bias because of the nature of the registry.
Megan A. Adams, MD, JD, MSc, is a general gastroenterologist at Veterans Affairs, an investigator in the VA Center for Clinical Management Research, and a lecturer in gastroenterology at the University of Michigan, all in Ann Arbor. She currently serves as chair-elect of the AGA Quality Measures Committee and is an associate editor of GI & Hepatology News.
Letter from the Editor: Spring brings flowers and liver stories
Happy spring (finally, for many of us)! This month’s issue of GI & Hepatology News is “weighted” towards liver. The decrease in hepatitis C–related liver disease means that steatohepatitis will emerge as the most frequent cause of cirrhosis and transplantation. Finding medical therapies to slow obesity-related liver damage has proven challenging. Bariatric surgery may be the best option for patients, as pointed out by one of our lead stories. Another page one story lays out a roadmap to eliminate viral hepatitis in the United States, a situation unheard of until direct-acting antiviral agents were developed.
The AGA’s contribution to this month’s issue is excellent. First, there is the continuing controversy regarding maintenance of certification. AGA has worked hard to eliminate the 10-year high-impact closed book examination (now an anachronism). We will have the option of a 2-year exam (open book) and you will need to become familiar with testing proposals so we all can add voices of reason to the ABIM process.
Additionally, the AGA highlights the POWER guideline (weight management) and its obesity resources, DDSEP® 8 and a new clinical guideline concerning transient elastography.
We close this month’s issue with a discussion from Ray Cross and Sunanda Kane about telemedicine and its impact on gastroenterology. There are multiple examples of how telemedicine is changing our practices and the piece provides hope for increased efficiencies and leveraged resources.
I hope you enjoy this issue. I have avoided my usual hints about our chaotic politics and its impact on our practices. We all need some relief and should take time to note the spring flowers.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Happy spring (finally, for many of us)! This month’s issue of GI & Hepatology News is “weighted” towards liver. The decrease in hepatitis C–related liver disease means that steatohepatitis will emerge as the most frequent cause of cirrhosis and transplantation. Finding medical therapies to slow obesity-related liver damage has proven challenging. Bariatric surgery may be the best option for patients, as pointed out by one of our lead stories. Another page one story lays out a roadmap to eliminate viral hepatitis in the United States, a situation unheard of until direct-acting antiviral agents were developed.
The AGA’s contribution to this month’s issue is excellent. First, there is the continuing controversy regarding maintenance of certification. AGA has worked hard to eliminate the 10-year high-impact closed book examination (now an anachronism). We will have the option of a 2-year exam (open book) and you will need to become familiar with testing proposals so we all can add voices of reason to the ABIM process.
Additionally, the AGA highlights the POWER guideline (weight management) and its obesity resources, DDSEP® 8 and a new clinical guideline concerning transient elastography.
We close this month’s issue with a discussion from Ray Cross and Sunanda Kane about telemedicine and its impact on gastroenterology. There are multiple examples of how telemedicine is changing our practices and the piece provides hope for increased efficiencies and leveraged resources.
I hope you enjoy this issue. I have avoided my usual hints about our chaotic politics and its impact on our practices. We all need some relief and should take time to note the spring flowers.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Happy spring (finally, for many of us)! This month’s issue of GI & Hepatology News is “weighted” towards liver. The decrease in hepatitis C–related liver disease means that steatohepatitis will emerge as the most frequent cause of cirrhosis and transplantation. Finding medical therapies to slow obesity-related liver damage has proven challenging. Bariatric surgery may be the best option for patients, as pointed out by one of our lead stories. Another page one story lays out a roadmap to eliminate viral hepatitis in the United States, a situation unheard of until direct-acting antiviral agents were developed.
The AGA’s contribution to this month’s issue is excellent. First, there is the continuing controversy regarding maintenance of certification. AGA has worked hard to eliminate the 10-year high-impact closed book examination (now an anachronism). We will have the option of a 2-year exam (open book) and you will need to become familiar with testing proposals so we all can add voices of reason to the ABIM process.
Additionally, the AGA highlights the POWER guideline (weight management) and its obesity resources, DDSEP® 8 and a new clinical guideline concerning transient elastography.
We close this month’s issue with a discussion from Ray Cross and Sunanda Kane about telemedicine and its impact on gastroenterology. There are multiple examples of how telemedicine is changing our practices and the piece provides hope for increased efficiencies and leveraged resources.
I hope you enjoy this issue. I have avoided my usual hints about our chaotic politics and its impact on our practices. We all need some relief and should take time to note the spring flowers.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Preterm infants face increased pertussis risk
Pertussis is more likely in infants who are born prematurely, compared with infants carried to term, according to Dr. Øystein Rolandsen Riise of the Norwegian Institute of Public Health, Oslo, and associates.
Using data from the Medical Birth Registry of Norway, 713,166 children were monitored until the age of 2 years from 1998 to 2010, during which time 968 cases of pertussis were laboratory confirmed. The incidence rate in term infants was 67.9 cases per 100,000 person-years, and was 115.2 cases per 100,000 person-years for preterm infants. The overall incidence rate ratio (IRR) of pertussis for preterm infants was 1.65, compared with term infants.
Hospitalization due to pertussis also was significantly more likely in preterm infants, with an overall IRR of 1.99, and infants born at 23-27 weeks again faced a greatly increased risk, with an IRR of 5.28.
Three-dose vaccine effectiveness against reported pertussis was 88.8% in term infants and 93% in preterm infants.
“Early and timely pediatric vaccinations as well as other strategies to prevent transmission to preterm infants are of utmost importance,” the investigators wrote.
Find the full study in the Pediatric Infectious Disease Journal (2017 May. doi: 10.1097/INF.0000000000001545).
Pertussis is more likely in infants who are born prematurely, compared with infants carried to term, according to Dr. Øystein Rolandsen Riise of the Norwegian Institute of Public Health, Oslo, and associates.
Using data from the Medical Birth Registry of Norway, 713,166 children were monitored until the age of 2 years from 1998 to 2010, during which time 968 cases of pertussis were laboratory confirmed. The incidence rate in term infants was 67.9 cases per 100,000 person-years, and was 115.2 cases per 100,000 person-years for preterm infants. The overall incidence rate ratio (IRR) of pertussis for preterm infants was 1.65, compared with term infants.
Hospitalization due to pertussis also was significantly more likely in preterm infants, with an overall IRR of 1.99, and infants born at 23-27 weeks again faced a greatly increased risk, with an IRR of 5.28.
Three-dose vaccine effectiveness against reported pertussis was 88.8% in term infants and 93% in preterm infants.
“Early and timely pediatric vaccinations as well as other strategies to prevent transmission to preterm infants are of utmost importance,” the investigators wrote.
Find the full study in the Pediatric Infectious Disease Journal (2017 May. doi: 10.1097/INF.0000000000001545).
Pertussis is more likely in infants who are born prematurely, compared with infants carried to term, according to Dr. Øystein Rolandsen Riise of the Norwegian Institute of Public Health, Oslo, and associates.
Using data from the Medical Birth Registry of Norway, 713,166 children were monitored until the age of 2 years from 1998 to 2010, during which time 968 cases of pertussis were laboratory confirmed. The incidence rate in term infants was 67.9 cases per 100,000 person-years, and was 115.2 cases per 100,000 person-years for preterm infants. The overall incidence rate ratio (IRR) of pertussis for preterm infants was 1.65, compared with term infants.
Hospitalization due to pertussis also was significantly more likely in preterm infants, with an overall IRR of 1.99, and infants born at 23-27 weeks again faced a greatly increased risk, with an IRR of 5.28.
Three-dose vaccine effectiveness against reported pertussis was 88.8% in term infants and 93% in preterm infants.
“Early and timely pediatric vaccinations as well as other strategies to prevent transmission to preterm infants are of utmost importance,” the investigators wrote.
Find the full study in the Pediatric Infectious Disease Journal (2017 May. doi: 10.1097/INF.0000000000001545).
High early stroke risk for adult congenital heart disease
WASHINGTON – Adults with congenital heart disease are at fourfold greater risk of experiencing an ischemic stroke by age 60 than is the general population, Mette Glavind reported at the annual meeting of the American College of Cardiology.
She presented a population-based study that included all 14,710 Danish adults with congenital heart disease (ACHD) diagnosed in 1963-1994. Taking advantage of Denmark’s comprehensive system of linked national registries, she and her coinvestigators created a control group consisting of 144,735 age- and birth year–matched individuals from the general population.
During follow-up, a total of 2,868 Danes included in the study had an ischemic stroke. The cumulative incidence of ischemic stroke in the ACHD cohort was 0.8% by age 30 and 8.2% by age 60, compared with 0.09% and 2.9%, respectively, in controls, according to Ms. Glavind, a medical student at Aarhus (Denmark) University.
The median age at diagnosis of stroke was 52 years in the ACHD group and 69 years in controls. The risk of early ischemic stroke – defined as stroke at age 18-60 – was increased by 3.97-fold in the ACHD group, compared with controls. The risk of stroke after age 60 was increased by 1.68-fold.
Stroke was more likely to prove fatal in the ACHD group. Their 30-day stroke mortality rate was 10%, compared with 9.6% in controls. This corresponded to an adjusted 44% increased risk of stroke mortality, which was statistically significant.
The severity of congenital heart disease modified the stroke risk. Patients with mild or moderate ACHD had a 3.25-fold increased risk of early stroke, compared with controls, while those with severe or univentricular ACHD were at 5.97-fold greater risk.
For purposes of this study, mild ACHD was defined as a biventricular defect that was not repaired surgically or percutaneously. Moderate ACHD was considered to have biventricular pathophysiology with surgical or percutaneous intervention. The severe ACHD category was reserved for cases involving complex biventricular abnormalities.
By these definitions, 41% of patients had mild ACHD, 21% moderate, 22% severe, and 1% univentricular ACHD; the rest of the patients were unclassified.
This study was supported by Aarhus University and Cincinnati Children’s Hospital. Ms. Glavind reported having no financial conflicts.
WASHINGTON – Adults with congenital heart disease are at fourfold greater risk of experiencing an ischemic stroke by age 60 than is the general population, Mette Glavind reported at the annual meeting of the American College of Cardiology.
She presented a population-based study that included all 14,710 Danish adults with congenital heart disease (ACHD) diagnosed in 1963-1994. Taking advantage of Denmark’s comprehensive system of linked national registries, she and her coinvestigators created a control group consisting of 144,735 age- and birth year–matched individuals from the general population.
During follow-up, a total of 2,868 Danes included in the study had an ischemic stroke. The cumulative incidence of ischemic stroke in the ACHD cohort was 0.8% by age 30 and 8.2% by age 60, compared with 0.09% and 2.9%, respectively, in controls, according to Ms. Glavind, a medical student at Aarhus (Denmark) University.
The median age at diagnosis of stroke was 52 years in the ACHD group and 69 years in controls. The risk of early ischemic stroke – defined as stroke at age 18-60 – was increased by 3.97-fold in the ACHD group, compared with controls. The risk of stroke after age 60 was increased by 1.68-fold.
Stroke was more likely to prove fatal in the ACHD group. Their 30-day stroke mortality rate was 10%, compared with 9.6% in controls. This corresponded to an adjusted 44% increased risk of stroke mortality, which was statistically significant.
The severity of congenital heart disease modified the stroke risk. Patients with mild or moderate ACHD had a 3.25-fold increased risk of early stroke, compared with controls, while those with severe or univentricular ACHD were at 5.97-fold greater risk.
For purposes of this study, mild ACHD was defined as a biventricular defect that was not repaired surgically or percutaneously. Moderate ACHD was considered to have biventricular pathophysiology with surgical or percutaneous intervention. The severe ACHD category was reserved for cases involving complex biventricular abnormalities.
By these definitions, 41% of patients had mild ACHD, 21% moderate, 22% severe, and 1% univentricular ACHD; the rest of the patients were unclassified.
This study was supported by Aarhus University and Cincinnati Children’s Hospital. Ms. Glavind reported having no financial conflicts.
WASHINGTON – Adults with congenital heart disease are at fourfold greater risk of experiencing an ischemic stroke by age 60 than is the general population, Mette Glavind reported at the annual meeting of the American College of Cardiology.
She presented a population-based study that included all 14,710 Danish adults with congenital heart disease (ACHD) diagnosed in 1963-1994. Taking advantage of Denmark’s comprehensive system of linked national registries, she and her coinvestigators created a control group consisting of 144,735 age- and birth year–matched individuals from the general population.
During follow-up, a total of 2,868 Danes included in the study had an ischemic stroke. The cumulative incidence of ischemic stroke in the ACHD cohort was 0.8% by age 30 and 8.2% by age 60, compared with 0.09% and 2.9%, respectively, in controls, according to Ms. Glavind, a medical student at Aarhus (Denmark) University.
The median age at diagnosis of stroke was 52 years in the ACHD group and 69 years in controls. The risk of early ischemic stroke – defined as stroke at age 18-60 – was increased by 3.97-fold in the ACHD group, compared with controls. The risk of stroke after age 60 was increased by 1.68-fold.
Stroke was more likely to prove fatal in the ACHD group. Their 30-day stroke mortality rate was 10%, compared with 9.6% in controls. This corresponded to an adjusted 44% increased risk of stroke mortality, which was statistically significant.
The severity of congenital heart disease modified the stroke risk. Patients with mild or moderate ACHD had a 3.25-fold increased risk of early stroke, compared with controls, while those with severe or univentricular ACHD were at 5.97-fold greater risk.
For purposes of this study, mild ACHD was defined as a biventricular defect that was not repaired surgically or percutaneously. Moderate ACHD was considered to have biventricular pathophysiology with surgical or percutaneous intervention. The severe ACHD category was reserved for cases involving complex biventricular abnormalities.
By these definitions, 41% of patients had mild ACHD, 21% moderate, 22% severe, and 1% univentricular ACHD; the rest of the patients were unclassified.
This study was supported by Aarhus University and Cincinnati Children’s Hospital. Ms. Glavind reported having no financial conflicts.
AT ACC 2017
Key clinical point:
Major finding: Danish adults with complex biventricular congenital heart disease were sixfold more likely to have an ischemic stroke by age 60 years, compared with the general population.
Data source: A population-based registry study that included all Danish adults with congenital heart disease diagnosed in 1963-1994 and nearly 145,000 age- and birth year–matched controls drawn from the general Danish population.
Disclosures: This study was supported by Aarhus University and Cincinnati Children’s Hospital. The presenter reported having no financial conflicts.
Pharmacist-run PrEP clinic proves effective, profitable
SEATTLE – A pharmacist-run HIV pre-exposure prophylaxis (PrEP) clinic had a retention rate of 75% and achieved a financial return within the first year of operation.
The Seattle-area project allowed individuals to leave their first appointment with medication in hand, and it drew in many men who had no primary care provider.
The approach is a departure from typical PrEP assignment, in which a patient must navigate a provider, lab testing, a pharmacist, and the need for prior authorization, explained Elyse Tung-Wisner, PharmD, director of clinical services at Kelley-Ross Pharmacy, Seattle. That process can take a few days to a few weeks.

“For years, pharmacists have done glucose testing. A finger stick for an HIV test is a similar model. We applied the same protocol to PrEP,” said Dr. Tung-Wisner, who presented an analysis of the program in a poster session at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
In the program, patients can come in, receive counseling, undergo all tests, and the pharmacist can work through all the prior authorizations and patient-assistance programs. “Oftentimes, a patient can leave with medication in hand within an hour,” said Dr. Tung-Wisner.
“As far as we know, we’re the first in the country to have a pharmacist-run HIV PrEP clinic in a community pharmacy setting,” she added.
She and her colleagues presented data on the effectiveness and financial viability of what they term One-Step PrEP. In the program, pharmacists take a medical and sexual history of each patient, perform a risk assessment and laboratory testing, provide education, and prescribe and dispense PrEP if appropriate. The pharmacist also performs all guideline-recommended follow-up care.
From March 2015 through March 2016, 373 patients inquired about PrEP services. A total of 251 patients were evaluated in person and 245 (98%) went on to begin PrEP. Among those who started PrEP, 88% identified as men who have sex with men (mean age, 34 years; range, 18-64).
The program had a 75% retention rate over the first year, with one HIV seroconversion.
The initial start-up costs were recouped at 9 months, suggesting that the program quickly became financially sustainable.
It also reached a highly vulnerable, underserved population. The average men who have sex with men index score was 20, which indicates that the patients were high risk, Dr. Tung-Wisner noted.
And just 23% of the patients who were evaluated in person had a primary care provider. “That suggests we were accessing a patient population that has not already established care anywhere else,” she explained.
The program was run by Kelley-Ross Pharmacye. Dr. Tung-Wisner is an employee of the pharmacy.
SEATTLE – A pharmacist-run HIV pre-exposure prophylaxis (PrEP) clinic had a retention rate of 75% and achieved a financial return within the first year of operation.
The Seattle-area project allowed individuals to leave their first appointment with medication in hand, and it drew in many men who had no primary care provider.
The approach is a departure from typical PrEP assignment, in which a patient must navigate a provider, lab testing, a pharmacist, and the need for prior authorization, explained Elyse Tung-Wisner, PharmD, director of clinical services at Kelley-Ross Pharmacy, Seattle. That process can take a few days to a few weeks.
“For years, pharmacists have done glucose testing. A finger stick for an HIV test is a similar model. We applied the same protocol to PrEP,” said Dr. Tung-Wisner, who presented an analysis of the program in a poster session at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
In the program, patients can come in, receive counseling, undergo all tests, and the pharmacist can work through all the prior authorizations and patient-assistance programs. “Oftentimes, a patient can leave with medication in hand within an hour,” said Dr. Tung-Wisner.
“As far as we know, we’re the first in the country to have a pharmacist-run HIV PrEP clinic in a community pharmacy setting,” she added.
She and her colleagues presented data on the effectiveness and financial viability of what they term One-Step PrEP. In the program, pharmacists take a medical and sexual history of each patient, perform a risk assessment and laboratory testing, provide education, and prescribe and dispense PrEP if appropriate. The pharmacist also performs all guideline-recommended follow-up care.
From March 2015 through March 2016, 373 patients inquired about PrEP services. A total of 251 patients were evaluated in person and 245 (98%) went on to begin PrEP. Among those who started PrEP, 88% identified as men who have sex with men (mean age, 34 years; range, 18-64).
The program had a 75% retention rate over the first year, with one HIV seroconversion.
The initial start-up costs were recouped at 9 months, suggesting that the program quickly became financially sustainable.
It also reached a highly vulnerable, underserved population. The average men who have sex with men index score was 20, which indicates that the patients were high risk, Dr. Tung-Wisner noted.
And just 23% of the patients who were evaluated in person had a primary care provider. “That suggests we were accessing a patient population that has not already established care anywhere else,” she explained.
The program was run by Kelley-Ross Pharmacye. Dr. Tung-Wisner is an employee of the pharmacy.
SEATTLE – A pharmacist-run HIV pre-exposure prophylaxis (PrEP) clinic had a retention rate of 75% and achieved a financial return within the first year of operation.
The Seattle-area project allowed individuals to leave their first appointment with medication in hand, and it drew in many men who had no primary care provider.
The approach is a departure from typical PrEP assignment, in which a patient must navigate a provider, lab testing, a pharmacist, and the need for prior authorization, explained Elyse Tung-Wisner, PharmD, director of clinical services at Kelley-Ross Pharmacy, Seattle. That process can take a few days to a few weeks.
“For years, pharmacists have done glucose testing. A finger stick for an HIV test is a similar model. We applied the same protocol to PrEP,” said Dr. Tung-Wisner, who presented an analysis of the program in a poster session at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
In the program, patients can come in, receive counseling, undergo all tests, and the pharmacist can work through all the prior authorizations and patient-assistance programs. “Oftentimes, a patient can leave with medication in hand within an hour,” said Dr. Tung-Wisner.
“As far as we know, we’re the first in the country to have a pharmacist-run HIV PrEP clinic in a community pharmacy setting,” she added.
She and her colleagues presented data on the effectiveness and financial viability of what they term One-Step PrEP. In the program, pharmacists take a medical and sexual history of each patient, perform a risk assessment and laboratory testing, provide education, and prescribe and dispense PrEP if appropriate. The pharmacist also performs all guideline-recommended follow-up care.
From March 2015 through March 2016, 373 patients inquired about PrEP services. A total of 251 patients were evaluated in person and 245 (98%) went on to begin PrEP. Among those who started PrEP, 88% identified as men who have sex with men (mean age, 34 years; range, 18-64).
The program had a 75% retention rate over the first year, with one HIV seroconversion.
The initial start-up costs were recouped at 9 months, suggesting that the program quickly became financially sustainable.
It also reached a highly vulnerable, underserved population. The average men who have sex with men index score was 20, which indicates that the patients were high risk, Dr. Tung-Wisner noted.
And just 23% of the patients who were evaluated in person had a primary care provider. “That suggests we were accessing a patient population that has not already established care anywhere else,” she explained.
The program was run by Kelley-Ross Pharmacye. Dr. Tung-Wisner is an employee of the pharmacy.
Key clinical point: A pharmacist-run HIV pre-exposure prophylaxis (PrEP) clinic had a retention rate of 75% and achieved a financial return within the first year of operation.
Major finding: The retention rate was 75%, and only 23% of patients had a primary care physician.
Data source: A retrospective analysis of a program that served 251 patients.
Disclosures: The program was run by Kelley-Ross Pharmacy in Seattle. Dr. Tung-Wisner is an employee of the pharmacy.
Dealing with stealing
A 7-year-old boy, Jacob, with a history of ADHD and frequent impulsive behavior, takes a calculator from another child’s desk. About 3 months before, he had come home after taking another child’s action figure. His parents have been working on parent training for ADHD, but don’t know how to respond to this behavior and are very upset at their son.
Discussion
Stealing is an issue of serious concern to parents. To understand how common this is in younger children, researchers need to rely on the reports of parents and teachers, which may be underestimates of the problem because stealing is usually a hidden or covert behavior. Research on older youth can include anonymous self-reports.

Stealing and dishonesty are such disappointing behaviors to adults that it is tempting to resort to harsh punishments, long lectures, or harshly disparaging words. But these kinds of punishments backfire. The goal is an overall positive relationship and a calm consistent response to undesired behaviors. Parents often need support in how to be positive with a child who is frustrating them. Taking 15 minutes a day to do some activity a child likes – playing catch, playing a board game, cooking together, or doing crafts – all while noticing the positive things a child is doing rather than teaching, criticizing, or grilling a child on what happened in school sets a happier tone to the relationship, which is a background for any discipline. Jacob’s parents had already been working on this through their parent training class, but it helped to encourage them to keep doing this.
Because of the covert nature of stealing, it is sometimes hard to know where an item has come from, and children are likely to lie about this, saying that a friend gave it to them or they found it. To avoid this, when working with a child who has been stealing, the expectation should be made clear in advance that it is the child’s responsibility to avoid suspicion by having nothing in his possession that is not known to the adult. It is important to avoid back and forth arguments. The adult’s decision is final. With frequent stealing, it is helpful to make an inventory of the child’s possessions as a baseline.
When it comes to consequences, the important thing is to be sure that they are consistent and predictable. Returning an item to the owner and apologizing are logical. Another excellent type of consequence for behaviors that happen rarely is an extra work chore of about half an hour.
So a parent might say something like, “Jacob, we know that a stealing monster has been getting you, and we want to fight against him. I have made up a list of everything you have right now, and it is going to be your responsibility to make sure you don’t bring home anything else. So that means even if you find something or someone gives you something, you shouldn’t take it. If I find anything that isn’t on the list, you are going to have to return it to the person it belongs to and apologize, and then do an extra work chore for half an hour. A habit can be hard to change, but I know we can do it together. Let’s go play catch.” Then when the child is found with something in his possession, the adult should remain calm, avoid a lecture, and just say something like, “Jacob, this is something that doesn’t belong to you. You need to return it to the person it belongs to, and you have an extra half hour of raking leaves. No TV until the leaves are done.” The parent also should be alert to opportunities to attend to or praise behaviors like the child saving money to spend on things he wants, or asking to borrow things from other family members rather than just taking them.
Stealing can be a tough problem and often goes along with other rule-breaking behavior. If a parent is struggling to stay calm and find the positive, referral to group or individual parent training through programs like the Incredible Years or Triple P can give a parent the chance to learn and practice skills step by step.
As children enter their teen years, stealing becomes much more common, and can be reinforced by peers as well as by the action itself. The same principles of finding positive activities, continuing positive interactions with parents, and predictable and consistent – rather than harsh – consequences continue to apply, but may require additional supports. Larger programs such as Multisystemic Therapy, which works with families, peers, and communities, have been demonstrated to be effective for young people with juvenile delinquency.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
Resource
Stealing, in “Children’s needs III: Development, prevention, and intervention,” (Washington: National Association of School Psychologists, 2006, pp. 171-83).
A 7-year-old boy, Jacob, with a history of ADHD and frequent impulsive behavior, takes a calculator from another child’s desk. About 3 months before, he had come home after taking another child’s action figure. His parents have been working on parent training for ADHD, but don’t know how to respond to this behavior and are very upset at their son.
Discussion
Stealing is an issue of serious concern to parents. To understand how common this is in younger children, researchers need to rely on the reports of parents and teachers, which may be underestimates of the problem because stealing is usually a hidden or covert behavior. Research on older youth can include anonymous self-reports.
Stealing and dishonesty are such disappointing behaviors to adults that it is tempting to resort to harsh punishments, long lectures, or harshly disparaging words. But these kinds of punishments backfire. The goal is an overall positive relationship and a calm consistent response to undesired behaviors. Parents often need support in how to be positive with a child who is frustrating them. Taking 15 minutes a day to do some activity a child likes – playing catch, playing a board game, cooking together, or doing crafts – all while noticing the positive things a child is doing rather than teaching, criticizing, or grilling a child on what happened in school sets a happier tone to the relationship, which is a background for any discipline. Jacob’s parents had already been working on this through their parent training class, but it helped to encourage them to keep doing this.
Because of the covert nature of stealing, it is sometimes hard to know where an item has come from, and children are likely to lie about this, saying that a friend gave it to them or they found it. To avoid this, when working with a child who has been stealing, the expectation should be made clear in advance that it is the child’s responsibility to avoid suspicion by having nothing in his possession that is not known to the adult. It is important to avoid back and forth arguments. The adult’s decision is final. With frequent stealing, it is helpful to make an inventory of the child’s possessions as a baseline.
When it comes to consequences, the important thing is to be sure that they are consistent and predictable. Returning an item to the owner and apologizing are logical. Another excellent type of consequence for behaviors that happen rarely is an extra work chore of about half an hour.
So a parent might say something like, “Jacob, we know that a stealing monster has been getting you, and we want to fight against him. I have made up a list of everything you have right now, and it is going to be your responsibility to make sure you don’t bring home anything else. So that means even if you find something or someone gives you something, you shouldn’t take it. If I find anything that isn’t on the list, you are going to have to return it to the person it belongs to and apologize, and then do an extra work chore for half an hour. A habit can be hard to change, but I know we can do it together. Let’s go play catch.” Then when the child is found with something in his possession, the adult should remain calm, avoid a lecture, and just say something like, “Jacob, this is something that doesn’t belong to you. You need to return it to the person it belongs to, and you have an extra half hour of raking leaves. No TV until the leaves are done.” The parent also should be alert to opportunities to attend to or praise behaviors like the child saving money to spend on things he wants, or asking to borrow things from other family members rather than just taking them.
Stealing can be a tough problem and often goes along with other rule-breaking behavior. If a parent is struggling to stay calm and find the positive, referral to group or individual parent training through programs like the Incredible Years or Triple P can give a parent the chance to learn and practice skills step by step.
As children enter their teen years, stealing becomes much more common, and can be reinforced by peers as well as by the action itself. The same principles of finding positive activities, continuing positive interactions with parents, and predictable and consistent – rather than harsh – consequences continue to apply, but may require additional supports. Larger programs such as Multisystemic Therapy, which works with families, peers, and communities, have been demonstrated to be effective for young people with juvenile delinquency.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
Resource
Stealing, in “Children’s needs III: Development, prevention, and intervention,” (Washington: National Association of School Psychologists, 2006, pp. 171-83).
A 7-year-old boy, Jacob, with a history of ADHD and frequent impulsive behavior, takes a calculator from another child’s desk. About 3 months before, he had come home after taking another child’s action figure. His parents have been working on parent training for ADHD, but don’t know how to respond to this behavior and are very upset at their son.
Discussion
Stealing is an issue of serious concern to parents. To understand how common this is in younger children, researchers need to rely on the reports of parents and teachers, which may be underestimates of the problem because stealing is usually a hidden or covert behavior. Research on older youth can include anonymous self-reports.
Stealing and dishonesty are such disappointing behaviors to adults that it is tempting to resort to harsh punishments, long lectures, or harshly disparaging words. But these kinds of punishments backfire. The goal is an overall positive relationship and a calm consistent response to undesired behaviors. Parents often need support in how to be positive with a child who is frustrating them. Taking 15 minutes a day to do some activity a child likes – playing catch, playing a board game, cooking together, or doing crafts – all while noticing the positive things a child is doing rather than teaching, criticizing, or grilling a child on what happened in school sets a happier tone to the relationship, which is a background for any discipline. Jacob’s parents had already been working on this through their parent training class, but it helped to encourage them to keep doing this.
Because of the covert nature of stealing, it is sometimes hard to know where an item has come from, and children are likely to lie about this, saying that a friend gave it to them or they found it. To avoid this, when working with a child who has been stealing, the expectation should be made clear in advance that it is the child’s responsibility to avoid suspicion by having nothing in his possession that is not known to the adult. It is important to avoid back and forth arguments. The adult’s decision is final. With frequent stealing, it is helpful to make an inventory of the child’s possessions as a baseline.
When it comes to consequences, the important thing is to be sure that they are consistent and predictable. Returning an item to the owner and apologizing are logical. Another excellent type of consequence for behaviors that happen rarely is an extra work chore of about half an hour.
So a parent might say something like, “Jacob, we know that a stealing monster has been getting you, and we want to fight against him. I have made up a list of everything you have right now, and it is going to be your responsibility to make sure you don’t bring home anything else. So that means even if you find something or someone gives you something, you shouldn’t take it. If I find anything that isn’t on the list, you are going to have to return it to the person it belongs to and apologize, and then do an extra work chore for half an hour. A habit can be hard to change, but I know we can do it together. Let’s go play catch.” Then when the child is found with something in his possession, the adult should remain calm, avoid a lecture, and just say something like, “Jacob, this is something that doesn’t belong to you. You need to return it to the person it belongs to, and you have an extra half hour of raking leaves. No TV until the leaves are done.” The parent also should be alert to opportunities to attend to or praise behaviors like the child saving money to spend on things he wants, or asking to borrow things from other family members rather than just taking them.
Stealing can be a tough problem and often goes along with other rule-breaking behavior. If a parent is struggling to stay calm and find the positive, referral to group or individual parent training through programs like the Incredible Years or Triple P can give a parent the chance to learn and practice skills step by step.
As children enter their teen years, stealing becomes much more common, and can be reinforced by peers as well as by the action itself. The same principles of finding positive activities, continuing positive interactions with parents, and predictable and consistent – rather than harsh – consequences continue to apply, but may require additional supports. Larger programs such as Multisystemic Therapy, which works with families, peers, and communities, have been demonstrated to be effective for young people with juvenile delinquency.
Dr. Hall is assistant professor of psychiatry and pediatrics at the University of Vermont, Burlington. She said she had no relevant financial disclosures.
Resource
Stealing, in “Children’s needs III: Development, prevention, and intervention,” (Washington: National Association of School Psychologists, 2006, pp. 171-83).
Recovery of Hair in the Psoriatic Plaques of a Patient With Coexistent Alopecia Universalis
To the Editor:
Both alopecia areata (AA) and psoriasis vulgaris are chronic relapsing autoimmune diseases, with AA causing nonscarring hair loss in approximately 0.1% to 0.2%1 of the population with a lifetime risk of 1.7%,2 and psoriasis more broadly impacting 1.5% to 2% of the population.3 The helper T cell (TH1) cytokine milieu is pathogenic in both conditions.4-6 IFN-γ knockout mice, unlike their wild-type counterparts, do not exhibit AA.7 Psoriasis is notably improved by IL-10 injections, which dampen the TH1 response.8 Distinct from AA, TH17 and TH22 cells have been implicated as key players in psoriasis pathogenesis, along with the associated IL-17 and IL-22 cytokines.9-12
Few cases of patients with concurrent AA and psoriasis have been described. Interestingly, these cases document normal hair regrowth in the areas of psoriasis.13-16 These cases may offer unique insight into the immune factors driving each disease. We describe a case of a man with both alopecia universalis (AU) and psoriasis who developed hair regrowth in some of the psoriatic plaques.
A 34-year-old man with concurrent AU and psoriasis who had not used any systemic or topical medication for either condition in the last year presented to our clinic seeking treatment. The patient had a history of alopecia totalis as a toddler that completely resolved by 4 years of age with the use of squaric acid dibutylester (SADBE). At 31 years of age, the alopecia recurred and was localized to the scalp. It was partially responsive to intralesional triamcinolone acetonide. The patient’s alopecia worsened over the 2 years following recurrence, ultimately progressing to AU. Two months after the alopecia recurrence, he developed the first psoriatic plaques. As the plaque psoriasis progressed, systemic therapy was initiated, first methotrexate and then etanercept. Shortly after developing AU, he lost his health insurance and discontinued all therapy. The patient’s psoriasis began to recur approximately 3 months after stopping etanercept. He was not using any other psoriasis medications. At that time, he noted terminal hair regrowth within some of the psoriatic plaques. No terminal hairs grew outside of the psoriatic plaques, and all regions with growth had previously been without hair for an extended period of time. The patient presented to our clinic approximately 1 year later. He had no other medical conditions and no relevant family history.
On initial physical examination, he had nonscarring hair loss involving nearly 100% of the body with psoriatic plaques on approximately 30% of the body surface area. Regions of terminal hair growth were confined to some but not all of the psoriatic plaques (Figure). Interestingly, the terminal hairs were primarily localized to the thickest central regions of the plaques. The patient’s psoriasis was treated with a combination of topical clobetasol and calcipotriene. In addition, he was started on tacrolimus ointment to the face and eyebrows for the AA. Maintenance of terminal hair within a region of topically treated psoriasis on the forearm persisted at the 2-month follow-up despite complete clearance of the corresponding psoriatic plaque. A small psoriatic plaque on the scalp cleared early with topical therapy without noticeable hair regrowth. The patient subsequently was started on contact immunotherapy with SADBE and intralesional triamcinolone acetonide for the scalp alopecia without satisfactory response. He decided to discontinue further attempts at treating the alopecia and requested to be restarted on etanercept therapy for recalcitrant psoriatic plaques. His psoriasis responded well to this therapy and he continues to be followed in our psoriasis clinic. One year after clearance of the treated psoriatic plaques, the corresponding terminal hairs persist.

Contact immunotherapy, most commonly with diphenylcyclopropenone or SADBE, is reported to have a 50% to 60% success rate in extensive AA, with a broad range of 9% to 87%17; however, randomized controlled trials testing the efficacy of contact immunotherapy are lacking. Although the mechanism of action of these topical sensitizers is not clearly delineated, it has been postulated that by inducing a new type of inflammatory response in the region, the immunologic milieu is changed, allowing the hair to grow. Some proposed mechanisms include promoting perifollicular lymphocyte apoptosis, preventing new recruitment of autoreactive lymphocytes, and allowing for the correction of aberrant major histocompatibility complex expression on the hair matrix epithelium to regain follicle immune privilege.18-20
Iatrogenic immunotherapy may work analogously to the natural immune system deviation demonstrated in our patient. Psoriasis and AA are believed to form competing immune cells and cytokine milieus, thus explaining how an individual with AA could regain normal hair growth in areas of psoriasis.15,16 The Renbök phenomenon, or reverse Köbner phenomenon, coined by Happle et al13 can be used to describe both the iatrogenic and natural cases of dermatologic disease improvement in response to secondary insults.14
A complex cascade of immune cells and cytokines coordinate AA pathogenesis. In the acute stage of AA, an inflammatory infiltrate of CD4+ T cells, CD8+ T cells, and antigen-presenting cells target anagen phase follicles, with a higher CD4+:CD8+ ratio in clinically active disease.21-23 Subcutaneous injections of either CD4+ or CD8+ lymphocyte subsets from mice with AA into normal-haired mice induces disease. However, CD8+ T cell injections rapidly produce apparent hair loss, whereas CD4+ T cells cause hair loss after several weeks, suggesting that CD8+ T cells directly modulate AA hair loss and CD4+ T cells act as an aide.24 The growth, differentiation, and survival of CD8+ T cells are stimulated by IL-2 and IFN-γ. Alopecia areata biopsies demonstrate a prevalence of TH1 cytokines, and patients with localized AA, alopecia totalis, and AU have notably higher serum IFN-γ levels compared to controls.25 In murine models, IL-1α and IL-1β increase during the catagen phase of the hair cycle and peak during the telogen phase.26 Excessive IL-1β expression is detected in the early stages of human disease, and certain IL-1β polymorphisms are associated with severe forms of AA.26 The role of tumor necrosis factor (TNF) α in AA is not well understood. In vitro studies show it inhibits hair growth, suggesting the cytokine may play a role in AA.27 However, anti–TNF-α therapy is not effective in AA, and case reports propose these therapies rarely induce AA.28-31
The TH1 response is likewise critical to psoriatic plaque development. IFN-γ and TNF-α are overexpressed in psoriatic plaques.32 IFN-γ has an antiproliferative and differentiation-inducing effect on normal keratinocytes, but psoriatic epithelial cells in vitro respond differently to the cytokine with a notably diminished growth inhibition.33,34 One explanation for the role of IFN-γ is that it stimulates dendritic cells to produce IL-1 and IL-23.35 IL-23 activates TH17 cells36; TH1 and TH17 conditions produce IL-22 whose serum level correlates with disease severity.37-39 IL-22 induces keratinocyte proliferation and migration and inhibits keratinocyte differentiation, helping account for hallmarks of the disease.40 Patients with psoriasis have increased levels of TH1, TH17, and TH22 cells, as well as their associated cytokines, in the skin and blood compared to controls.4,11,32,39,41
Alopecia areata and psoriasis are regulated by complex and still not entirely understood immune interactions. The fact that many of the same therapies are used to treat both diseases emphasizes both their overlapping characteristics and the lack of targeted therapy. It is unclear if and how the topical or systemic therapies used in our patient to treat one disease affected the natural history of the other condition. It is important to highlight, however, that the patient had not been treated for months when he developed the psoriatic plaques with hair regrowth. Other case reports also document hair regrowth in untreated plaques,13,16 making it unlikely to be a side effect of the medication regimen. For both psoriasis and AA, the immune cell composition and cytokine levels in the skin or serum vary throughout a patient’s disease course depending on severity of disease or response to treatment.6,39,42,43 Therefore, we hypothesize that the 2 conditions interact in a similarly distinct manner based on each disease’s stage and intensity in the patient. Both our patient’s course thus far and the various presentations described by other groups support this hypothesis. Our patient had a small region of psoriasis on the scalp that cleared without any terminal hair growth. He also had larger plaques on the forearms that developed hair growth most predominantly within the thicker regions of the plaques. His unique presentation highlights the fluidity of the immune factors driving psoriasis vulgaris and AA.
- Safavi K. Prevalence of alopecia areata in the First National Health and Nutrition Examination Survey. Arch Dermatol. 1992;128:702.
- Safavi KH, Muller SA, Suman VJ, et al. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc. 1995;70:628-633.
- Wolff K, Johnson RA. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 6th ed. New York, NY: McGraw-Hill; 2009.
- Austin LM, Ozawa M, Kikuchi T, et al. The majority of epidermal T cells in psoriasis vulgaris lesions can produce type 1 cytokines, interferon-gamma, interleukin-2, and tumor necrosis factor-alpha, defining TC1 (cytotoxic T lymphocyte) and TH1 effector populations: a type 1 differentiation bias is also measured in circulating blood T cells in psoriatic patients. J Invest Dermatol. 1999;113:752-759.
- Ghoreishi M, Martinka M, Dutz JP. Type 1 interferon signature in the scalp lesions of alopecia areata. Br J Dermatol. 2010;163:57-62.
- Rossi A, Cantisani C, Carlesimo M, et al. Serum concentrations of IL-2, IL-6, IL-12 and TNF-α in patients with alopecia areata. Int J Immunopathol Pharmacol. 2012;25:781-788.
- Freyschmidt-Paul P, McElwee KJ, Hoffmann R, et al. Interferon-gamma-deficient mice are resistant to the development of alopecia areata. Br J Dermatol. 2006;155:515-521.
- Reich K, Garbe C, Blaschke V, et al. Response of psoriasis to interleukin-10 is associated with suppression of cutaneous type 1 inflammation, downregulation of the epidermal interleukin-8/CXCR2 pathway and normalization of keratinocyte maturation. J Invest Dermatol. 2001;116:319-329.
- Teunissen MB, Koomen CW, de Waal Malefyt R, et al. Interleukin-17 and interferon-gamma synergize in the enhancement of proinflammatory cytokine production by human keratinocytes. J Invest Dermatol. 1998;111:645-649.
- Zheng Y, Danilenko DM, Valdez P, et al. Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature. 2007;445:648-651.
- Boniface K, Guignouard E, Pedretti N, et al. A role for T cell-derived interleukin 22 in psoriatic skin inflammation. Clin Exp Immunol. 2007;150:407-415.
- Zaba LC, Suárez-Fariñas M, Fuentes-Duculan J, et al. Effective treatment of psoriasis with etanercept is linked to suppression of IL-17 signaling, not immediate response TNF genes. J Allergy Clin Immunol. 2009;124:1022-1030.e395.
- Happle R, van der Steen PHM, Perret CM. The Renbök phenomenon: an inverse Köebner reaction observed in alopecia areata. Eur J Dermatol. 1991;2:39-40.
- Ito T, Hashizume H, Takigawa M. Contact immunotherapy-induced Renbök phenomenon in a patient with alopecia areata and psoriasis vulgaris. Eur J Dermatol. 2010;20:126-127.
- Criado PR, Valente NY, Michalany NS, et al. An unusual association between scalp psoriasis and ophiasic alopecia areata: the Renbök phenomenon. Clin Exp Dermatol. 2007;32:320-321.
- Harris JE, Seykora JT, Lee RA. Renbök phenomenon and contact sensitization in a patient with alopecia universalis. Arch Dermatol. 2010;146:422-425.
- Alkhalifah A. Topical and intralesional therapies for alopecia areata. Dermatol Ther. 2011;24:355-363.
- Herbst V, Zöller M, Kissling S, et al. Diphenylcyclopropenone treatment of alopecia areata induces apoptosis of perifollicular lymphocytes. Eur J Dermatol. 2006;16:537-542.
- Zöller M, Freyschmidt-Paul P, Vitacolonna M, et al. Chronic delayed-type hypersensitivity reaction as a means to treat alopecia areata. Clin Exp Immunol. 2004;135:398-408.
- Bröcker EB, Echternacht-Happle K, Hamm H, et al. Abnormal expression of class I and class II major histocompatibility antigens in alopecia areata: modulation by topical immunotherapy. J Invest Dermatol. 1987;88:564-568.
- Todes-Taylor N, Turner R, Wood GS, et al. T cell subpopulations in alopecia areata. J Am Acad Dermatol. 1984;11:216-223.
- Perret C, Wiesner-Menzel L, Happle R. Immunohistochemical analysis of T-cell subsets in the peribulbar and intrabulbar infiltrates of alopecia areata. Acta Derm Venereol. 1984;64:26-30.
- Wiesner-Menzel L, Happle R. Intrabulbar and peribulbar accumulation of dendritic OKT 6-positive cells in alopecia areata. Arch Dermatol Res. 1984;276:333-334.
- McElwee KJ, Freyschmidt-Paul P, Hoffmann R, et al. Transfer of CD8+ cells induces localized hair loss whereas CD4+/CD25– cells promote systemic alopecia areata and CD4+/CD25+ cells blockade disease onset in the C3H/HeJ mouse model. J Invest Dermatol. 2005;124:947-957.
- Arca E, Muşabak U, Akar A, et al. Interferon-gamma in alopecia areata. Eur J Dermatol. 2004;14:33-36.
- Hoffmann R. The potential role of cytokines and T cells in alopecia areata. J Investig Dermatol Symp Proc. 1999;4:235-238.
- Philpott MP, Sanders DA, Bowen J, et al. Effects of interleukins, colony-stimulating factor and tumour necrosis factor on human hair follicle growth in vitro: a possible role for interleukin-1 and tumour necrosis factor-alpha in alopecia areata. Br J Dermatol. 1996;135:942-948.
- Le Bidre E, Chaby G, Martin L, et al. Alopecia areata during anti-TNF alpha therapy: nine cases. Ann Dermatol Venereol. 2011;138:285-293.
- Ferran M, Calvet J, Almirall M, et al. Alopecia areata as another immune-mediated disease developed in patients treated with tumour necrosis factor-α blocker agents: report of five cases and review of the literature. J Eur Acad Dermatol Venereol. 2011;25:479-484.
- Pan Y, Rao NA. Alopecia areata during etanercept therapy. Ocul Immunol Inflamm. 2009;17:127-129.
- Pelivani N, Hassan AS, Braathen LR, et al. Alopecia areata universalis elicited during treatment with adalimumab. Dermatology. 2008;216:320-323.
- Uyemura K, Yamamura M, Fivenson DF, et al. The cytokine network in lesional and lesion-free psoriatic skin is characterized by a T-helper type 1 cell-mediated response. J Invest Dermatol. 1993;101:701-705.
- Baker BS, Powles AV, Valdimarsson H, et al. An altered response by psoriatic keratinocytes to gamma interferon. Scan J Immunol. 1988;28:735-740.
- Jackson M, Howie SE, Weller R, et al. Psoriatic keratinocytes show reduced IRF-1 and STAT-1alpha activation in response to gamma-IFN. FASEB J. 1999;13:495-502.
- Perera GK, Di Meglio P, Nestle FO. Psoriasis. Annu Rev Pathol. 2012;7:385-422.
- McGeachy MJ, Chen Y, Tato CM, et al. The interleukin 23 receptor is essential for the terminal differentiation of interleukin 17-producing effector T helper cells in vivo. Nat Immunol. 2009;10:314-324.
- Volpe E, Servant N, Zollinger R, et al. A critical function for transforming growth factor-beta, interleukin 23 and proinflammatory cytokines in driving and modulating human T(H)-17 responses. Nat Immunol. 2008;9:650-657.
- Boniface K, Blumenschein WM, Brovont-Porth K, et al. Human Th17 cells comprise heterogeneous subsets including IFN-gamma-producing cells with distinct properties from the Th1 lineage. J Immunol. 2010;185:679-687.
- Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
- Boniface K, Bernard FX, Garcia M, et al. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J Immunol. 2005;174:3695-3702.
- Harper EG, Guo C, Rizzo H, et al. Th17 cytokines stimulate CCL20 expression in keratinocytes in vitro and in vivo: implications for psoriasis pathogenesis. J Invest Dermatol. 2009;129:2175-2183.
- Bowcock AM, Krueger JG. Getting under the skin: the immunogenetics of psoriasis. Nat Rev Immunol. 2005;5:699-711.
- Hoffmann R, Wenzel E, Huth A, et al. Cytokine mRNA levels in alopecia areata before and after treatment with the contact allergen diphenylcyclopropenone. J Invest Dermatol. 1994;103:530-533.
To the Editor:
Both alopecia areata (AA) and psoriasis vulgaris are chronic relapsing autoimmune diseases, with AA causing nonscarring hair loss in approximately 0.1% to 0.2%1 of the population with a lifetime risk of 1.7%,2 and psoriasis more broadly impacting 1.5% to 2% of the population.3 The helper T cell (TH1) cytokine milieu is pathogenic in both conditions.4-6 IFN-γ knockout mice, unlike their wild-type counterparts, do not exhibit AA.7 Psoriasis is notably improved by IL-10 injections, which dampen the TH1 response.8 Distinct from AA, TH17 and TH22 cells have been implicated as key players in psoriasis pathogenesis, along with the associated IL-17 and IL-22 cytokines.9-12
Few cases of patients with concurrent AA and psoriasis have been described. Interestingly, these cases document normal hair regrowth in the areas of psoriasis.13-16 These cases may offer unique insight into the immune factors driving each disease. We describe a case of a man with both alopecia universalis (AU) and psoriasis who developed hair regrowth in some of the psoriatic plaques.
A 34-year-old man with concurrent AU and psoriasis who had not used any systemic or topical medication for either condition in the last year presented to our clinic seeking treatment. The patient had a history of alopecia totalis as a toddler that completely resolved by 4 years of age with the use of squaric acid dibutylester (SADBE). At 31 years of age, the alopecia recurred and was localized to the scalp. It was partially responsive to intralesional triamcinolone acetonide. The patient’s alopecia worsened over the 2 years following recurrence, ultimately progressing to AU. Two months after the alopecia recurrence, he developed the first psoriatic plaques. As the plaque psoriasis progressed, systemic therapy was initiated, first methotrexate and then etanercept. Shortly after developing AU, he lost his health insurance and discontinued all therapy. The patient’s psoriasis began to recur approximately 3 months after stopping etanercept. He was not using any other psoriasis medications. At that time, he noted terminal hair regrowth within some of the psoriatic plaques. No terminal hairs grew outside of the psoriatic plaques, and all regions with growth had previously been without hair for an extended period of time. The patient presented to our clinic approximately 1 year later. He had no other medical conditions and no relevant family history.
On initial physical examination, he had nonscarring hair loss involving nearly 100% of the body with psoriatic plaques on approximately 30% of the body surface area. Regions of terminal hair growth were confined to some but not all of the psoriatic plaques (Figure). Interestingly, the terminal hairs were primarily localized to the thickest central regions of the plaques. The patient’s psoriasis was treated with a combination of topical clobetasol and calcipotriene. In addition, he was started on tacrolimus ointment to the face and eyebrows for the AA. Maintenance of terminal hair within a region of topically treated psoriasis on the forearm persisted at the 2-month follow-up despite complete clearance of the corresponding psoriatic plaque. A small psoriatic plaque on the scalp cleared early with topical therapy without noticeable hair regrowth. The patient subsequently was started on contact immunotherapy with SADBE and intralesional triamcinolone acetonide for the scalp alopecia without satisfactory response. He decided to discontinue further attempts at treating the alopecia and requested to be restarted on etanercept therapy for recalcitrant psoriatic plaques. His psoriasis responded well to this therapy and he continues to be followed in our psoriasis clinic. One year after clearance of the treated psoriatic plaques, the corresponding terminal hairs persist.
Contact immunotherapy, most commonly with diphenylcyclopropenone or SADBE, is reported to have a 50% to 60% success rate in extensive AA, with a broad range of 9% to 87%17; however, randomized controlled trials testing the efficacy of contact immunotherapy are lacking. Although the mechanism of action of these topical sensitizers is not clearly delineated, it has been postulated that by inducing a new type of inflammatory response in the region, the immunologic milieu is changed, allowing the hair to grow. Some proposed mechanisms include promoting perifollicular lymphocyte apoptosis, preventing new recruitment of autoreactive lymphocytes, and allowing for the correction of aberrant major histocompatibility complex expression on the hair matrix epithelium to regain follicle immune privilege.18-20
Iatrogenic immunotherapy may work analogously to the natural immune system deviation demonstrated in our patient. Psoriasis and AA are believed to form competing immune cells and cytokine milieus, thus explaining how an individual with AA could regain normal hair growth in areas of psoriasis.15,16 The Renbök phenomenon, or reverse Köbner phenomenon, coined by Happle et al13 can be used to describe both the iatrogenic and natural cases of dermatologic disease improvement in response to secondary insults.14
A complex cascade of immune cells and cytokines coordinate AA pathogenesis. In the acute stage of AA, an inflammatory infiltrate of CD4+ T cells, CD8+ T cells, and antigen-presenting cells target anagen phase follicles, with a higher CD4+:CD8+ ratio in clinically active disease.21-23 Subcutaneous injections of either CD4+ or CD8+ lymphocyte subsets from mice with AA into normal-haired mice induces disease. However, CD8+ T cell injections rapidly produce apparent hair loss, whereas CD4+ T cells cause hair loss after several weeks, suggesting that CD8+ T cells directly modulate AA hair loss and CD4+ T cells act as an aide.24 The growth, differentiation, and survival of CD8+ T cells are stimulated by IL-2 and IFN-γ. Alopecia areata biopsies demonstrate a prevalence of TH1 cytokines, and patients with localized AA, alopecia totalis, and AU have notably higher serum IFN-γ levels compared to controls.25 In murine models, IL-1α and IL-1β increase during the catagen phase of the hair cycle and peak during the telogen phase.26 Excessive IL-1β expression is detected in the early stages of human disease, and certain IL-1β polymorphisms are associated with severe forms of AA.26 The role of tumor necrosis factor (TNF) α in AA is not well understood. In vitro studies show it inhibits hair growth, suggesting the cytokine may play a role in AA.27 However, anti–TNF-α therapy is not effective in AA, and case reports propose these therapies rarely induce AA.28-31
The TH1 response is likewise critical to psoriatic plaque development. IFN-γ and TNF-α are overexpressed in psoriatic plaques.32 IFN-γ has an antiproliferative and differentiation-inducing effect on normal keratinocytes, but psoriatic epithelial cells in vitro respond differently to the cytokine with a notably diminished growth inhibition.33,34 One explanation for the role of IFN-γ is that it stimulates dendritic cells to produce IL-1 and IL-23.35 IL-23 activates TH17 cells36; TH1 and TH17 conditions produce IL-22 whose serum level correlates with disease severity.37-39 IL-22 induces keratinocyte proliferation and migration and inhibits keratinocyte differentiation, helping account for hallmarks of the disease.40 Patients with psoriasis have increased levels of TH1, TH17, and TH22 cells, as well as their associated cytokines, in the skin and blood compared to controls.4,11,32,39,41
Alopecia areata and psoriasis are regulated by complex and still not entirely understood immune interactions. The fact that many of the same therapies are used to treat both diseases emphasizes both their overlapping characteristics and the lack of targeted therapy. It is unclear if and how the topical or systemic therapies used in our patient to treat one disease affected the natural history of the other condition. It is important to highlight, however, that the patient had not been treated for months when he developed the psoriatic plaques with hair regrowth. Other case reports also document hair regrowth in untreated plaques,13,16 making it unlikely to be a side effect of the medication regimen. For both psoriasis and AA, the immune cell composition and cytokine levels in the skin or serum vary throughout a patient’s disease course depending on severity of disease or response to treatment.6,39,42,43 Therefore, we hypothesize that the 2 conditions interact in a similarly distinct manner based on each disease’s stage and intensity in the patient. Both our patient’s course thus far and the various presentations described by other groups support this hypothesis. Our patient had a small region of psoriasis on the scalp that cleared without any terminal hair growth. He also had larger plaques on the forearms that developed hair growth most predominantly within the thicker regions of the plaques. His unique presentation highlights the fluidity of the immune factors driving psoriasis vulgaris and AA.
To the Editor:
Both alopecia areata (AA) and psoriasis vulgaris are chronic relapsing autoimmune diseases, with AA causing nonscarring hair loss in approximately 0.1% to 0.2%1 of the population with a lifetime risk of 1.7%,2 and psoriasis more broadly impacting 1.5% to 2% of the population.3 The helper T cell (TH1) cytokine milieu is pathogenic in both conditions.4-6 IFN-γ knockout mice, unlike their wild-type counterparts, do not exhibit AA.7 Psoriasis is notably improved by IL-10 injections, which dampen the TH1 response.8 Distinct from AA, TH17 and TH22 cells have been implicated as key players in psoriasis pathogenesis, along with the associated IL-17 and IL-22 cytokines.9-12
Few cases of patients with concurrent AA and psoriasis have been described. Interestingly, these cases document normal hair regrowth in the areas of psoriasis.13-16 These cases may offer unique insight into the immune factors driving each disease. We describe a case of a man with both alopecia universalis (AU) and psoriasis who developed hair regrowth in some of the psoriatic plaques.
A 34-year-old man with concurrent AU and psoriasis who had not used any systemic or topical medication for either condition in the last year presented to our clinic seeking treatment. The patient had a history of alopecia totalis as a toddler that completely resolved by 4 years of age with the use of squaric acid dibutylester (SADBE). At 31 years of age, the alopecia recurred and was localized to the scalp. It was partially responsive to intralesional triamcinolone acetonide. The patient’s alopecia worsened over the 2 years following recurrence, ultimately progressing to AU. Two months after the alopecia recurrence, he developed the first psoriatic plaques. As the plaque psoriasis progressed, systemic therapy was initiated, first methotrexate and then etanercept. Shortly after developing AU, he lost his health insurance and discontinued all therapy. The patient’s psoriasis began to recur approximately 3 months after stopping etanercept. He was not using any other psoriasis medications. At that time, he noted terminal hair regrowth within some of the psoriatic plaques. No terminal hairs grew outside of the psoriatic plaques, and all regions with growth had previously been without hair for an extended period of time. The patient presented to our clinic approximately 1 year later. He had no other medical conditions and no relevant family history.
On initial physical examination, he had nonscarring hair loss involving nearly 100% of the body with psoriatic plaques on approximately 30% of the body surface area. Regions of terminal hair growth were confined to some but not all of the psoriatic plaques (Figure). Interestingly, the terminal hairs were primarily localized to the thickest central regions of the plaques. The patient’s psoriasis was treated with a combination of topical clobetasol and calcipotriene. In addition, he was started on tacrolimus ointment to the face and eyebrows for the AA. Maintenance of terminal hair within a region of topically treated psoriasis on the forearm persisted at the 2-month follow-up despite complete clearance of the corresponding psoriatic plaque. A small psoriatic plaque on the scalp cleared early with topical therapy without noticeable hair regrowth. The patient subsequently was started on contact immunotherapy with SADBE and intralesional triamcinolone acetonide for the scalp alopecia without satisfactory response. He decided to discontinue further attempts at treating the alopecia and requested to be restarted on etanercept therapy for recalcitrant psoriatic plaques. His psoriasis responded well to this therapy and he continues to be followed in our psoriasis clinic. One year after clearance of the treated psoriatic plaques, the corresponding terminal hairs persist.
Contact immunotherapy, most commonly with diphenylcyclopropenone or SADBE, is reported to have a 50% to 60% success rate in extensive AA, with a broad range of 9% to 87%17; however, randomized controlled trials testing the efficacy of contact immunotherapy are lacking. Although the mechanism of action of these topical sensitizers is not clearly delineated, it has been postulated that by inducing a new type of inflammatory response in the region, the immunologic milieu is changed, allowing the hair to grow. Some proposed mechanisms include promoting perifollicular lymphocyte apoptosis, preventing new recruitment of autoreactive lymphocytes, and allowing for the correction of aberrant major histocompatibility complex expression on the hair matrix epithelium to regain follicle immune privilege.18-20
Iatrogenic immunotherapy may work analogously to the natural immune system deviation demonstrated in our patient. Psoriasis and AA are believed to form competing immune cells and cytokine milieus, thus explaining how an individual with AA could regain normal hair growth in areas of psoriasis.15,16 The Renbök phenomenon, or reverse Köbner phenomenon, coined by Happle et al13 can be used to describe both the iatrogenic and natural cases of dermatologic disease improvement in response to secondary insults.14
A complex cascade of immune cells and cytokines coordinate AA pathogenesis. In the acute stage of AA, an inflammatory infiltrate of CD4+ T cells, CD8+ T cells, and antigen-presenting cells target anagen phase follicles, with a higher CD4+:CD8+ ratio in clinically active disease.21-23 Subcutaneous injections of either CD4+ or CD8+ lymphocyte subsets from mice with AA into normal-haired mice induces disease. However, CD8+ T cell injections rapidly produce apparent hair loss, whereas CD4+ T cells cause hair loss after several weeks, suggesting that CD8+ T cells directly modulate AA hair loss and CD4+ T cells act as an aide.24 The growth, differentiation, and survival of CD8+ T cells are stimulated by IL-2 and IFN-γ. Alopecia areata biopsies demonstrate a prevalence of TH1 cytokines, and patients with localized AA, alopecia totalis, and AU have notably higher serum IFN-γ levels compared to controls.25 In murine models, IL-1α and IL-1β increase during the catagen phase of the hair cycle and peak during the telogen phase.26 Excessive IL-1β expression is detected in the early stages of human disease, and certain IL-1β polymorphisms are associated with severe forms of AA.26 The role of tumor necrosis factor (TNF) α in AA is not well understood. In vitro studies show it inhibits hair growth, suggesting the cytokine may play a role in AA.27 However, anti–TNF-α therapy is not effective in AA, and case reports propose these therapies rarely induce AA.28-31
The TH1 response is likewise critical to psoriatic plaque development. IFN-γ and TNF-α are overexpressed in psoriatic plaques.32 IFN-γ has an antiproliferative and differentiation-inducing effect on normal keratinocytes, but psoriatic epithelial cells in vitro respond differently to the cytokine with a notably diminished growth inhibition.33,34 One explanation for the role of IFN-γ is that it stimulates dendritic cells to produce IL-1 and IL-23.35 IL-23 activates TH17 cells36; TH1 and TH17 conditions produce IL-22 whose serum level correlates with disease severity.37-39 IL-22 induces keratinocyte proliferation and migration and inhibits keratinocyte differentiation, helping account for hallmarks of the disease.40 Patients with psoriasis have increased levels of TH1, TH17, and TH22 cells, as well as their associated cytokines, in the skin and blood compared to controls.4,11,32,39,41
Alopecia areata and psoriasis are regulated by complex and still not entirely understood immune interactions. The fact that many of the same therapies are used to treat both diseases emphasizes both their overlapping characteristics and the lack of targeted therapy. It is unclear if and how the topical or systemic therapies used in our patient to treat one disease affected the natural history of the other condition. It is important to highlight, however, that the patient had not been treated for months when he developed the psoriatic plaques with hair regrowth. Other case reports also document hair regrowth in untreated plaques,13,16 making it unlikely to be a side effect of the medication regimen. For both psoriasis and AA, the immune cell composition and cytokine levels in the skin or serum vary throughout a patient’s disease course depending on severity of disease or response to treatment.6,39,42,43 Therefore, we hypothesize that the 2 conditions interact in a similarly distinct manner based on each disease’s stage and intensity in the patient. Both our patient’s course thus far and the various presentations described by other groups support this hypothesis. Our patient had a small region of psoriasis on the scalp that cleared without any terminal hair growth. He also had larger plaques on the forearms that developed hair growth most predominantly within the thicker regions of the plaques. His unique presentation highlights the fluidity of the immune factors driving psoriasis vulgaris and AA.
- Safavi K. Prevalence of alopecia areata in the First National Health and Nutrition Examination Survey. Arch Dermatol. 1992;128:702.
- Safavi KH, Muller SA, Suman VJ, et al. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc. 1995;70:628-633.
- Wolff K, Johnson RA. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 6th ed. New York, NY: McGraw-Hill; 2009.
- Austin LM, Ozawa M, Kikuchi T, et al. The majority of epidermal T cells in psoriasis vulgaris lesions can produce type 1 cytokines, interferon-gamma, interleukin-2, and tumor necrosis factor-alpha, defining TC1 (cytotoxic T lymphocyte) and TH1 effector populations: a type 1 differentiation bias is also measured in circulating blood T cells in psoriatic patients. J Invest Dermatol. 1999;113:752-759.
- Ghoreishi M, Martinka M, Dutz JP. Type 1 interferon signature in the scalp lesions of alopecia areata. Br J Dermatol. 2010;163:57-62.
- Rossi A, Cantisani C, Carlesimo M, et al. Serum concentrations of IL-2, IL-6, IL-12 and TNF-α in patients with alopecia areata. Int J Immunopathol Pharmacol. 2012;25:781-788.
- Freyschmidt-Paul P, McElwee KJ, Hoffmann R, et al. Interferon-gamma-deficient mice are resistant to the development of alopecia areata. Br J Dermatol. 2006;155:515-521.
- Reich K, Garbe C, Blaschke V, et al. Response of psoriasis to interleukin-10 is associated with suppression of cutaneous type 1 inflammation, downregulation of the epidermal interleukin-8/CXCR2 pathway and normalization of keratinocyte maturation. J Invest Dermatol. 2001;116:319-329.
- Teunissen MB, Koomen CW, de Waal Malefyt R, et al. Interleukin-17 and interferon-gamma synergize in the enhancement of proinflammatory cytokine production by human keratinocytes. J Invest Dermatol. 1998;111:645-649.
- Zheng Y, Danilenko DM, Valdez P, et al. Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature. 2007;445:648-651.
- Boniface K, Guignouard E, Pedretti N, et al. A role for T cell-derived interleukin 22 in psoriatic skin inflammation. Clin Exp Immunol. 2007;150:407-415.
- Zaba LC, Suárez-Fariñas M, Fuentes-Duculan J, et al. Effective treatment of psoriasis with etanercept is linked to suppression of IL-17 signaling, not immediate response TNF genes. J Allergy Clin Immunol. 2009;124:1022-1030.e395.
- Happle R, van der Steen PHM, Perret CM. The Renbök phenomenon: an inverse Köebner reaction observed in alopecia areata. Eur J Dermatol. 1991;2:39-40.
- Ito T, Hashizume H, Takigawa M. Contact immunotherapy-induced Renbök phenomenon in a patient with alopecia areata and psoriasis vulgaris. Eur J Dermatol. 2010;20:126-127.
- Criado PR, Valente NY, Michalany NS, et al. An unusual association between scalp psoriasis and ophiasic alopecia areata: the Renbök phenomenon. Clin Exp Dermatol. 2007;32:320-321.
- Harris JE, Seykora JT, Lee RA. Renbök phenomenon and contact sensitization in a patient with alopecia universalis. Arch Dermatol. 2010;146:422-425.
- Alkhalifah A. Topical and intralesional therapies for alopecia areata. Dermatol Ther. 2011;24:355-363.
- Herbst V, Zöller M, Kissling S, et al. Diphenylcyclopropenone treatment of alopecia areata induces apoptosis of perifollicular lymphocytes. Eur J Dermatol. 2006;16:537-542.
- Zöller M, Freyschmidt-Paul P, Vitacolonna M, et al. Chronic delayed-type hypersensitivity reaction as a means to treat alopecia areata. Clin Exp Immunol. 2004;135:398-408.
- Bröcker EB, Echternacht-Happle K, Hamm H, et al. Abnormal expression of class I and class II major histocompatibility antigens in alopecia areata: modulation by topical immunotherapy. J Invest Dermatol. 1987;88:564-568.
- Todes-Taylor N, Turner R, Wood GS, et al. T cell subpopulations in alopecia areata. J Am Acad Dermatol. 1984;11:216-223.
- Perret C, Wiesner-Menzel L, Happle R. Immunohistochemical analysis of T-cell subsets in the peribulbar and intrabulbar infiltrates of alopecia areata. Acta Derm Venereol. 1984;64:26-30.
- Wiesner-Menzel L, Happle R. Intrabulbar and peribulbar accumulation of dendritic OKT 6-positive cells in alopecia areata. Arch Dermatol Res. 1984;276:333-334.
- McElwee KJ, Freyschmidt-Paul P, Hoffmann R, et al. Transfer of CD8+ cells induces localized hair loss whereas CD4+/CD25– cells promote systemic alopecia areata and CD4+/CD25+ cells blockade disease onset in the C3H/HeJ mouse model. J Invest Dermatol. 2005;124:947-957.
- Arca E, Muşabak U, Akar A, et al. Interferon-gamma in alopecia areata. Eur J Dermatol. 2004;14:33-36.
- Hoffmann R. The potential role of cytokines and T cells in alopecia areata. J Investig Dermatol Symp Proc. 1999;4:235-238.
- Philpott MP, Sanders DA, Bowen J, et al. Effects of interleukins, colony-stimulating factor and tumour necrosis factor on human hair follicle growth in vitro: a possible role for interleukin-1 and tumour necrosis factor-alpha in alopecia areata. Br J Dermatol. 1996;135:942-948.
- Le Bidre E, Chaby G, Martin L, et al. Alopecia areata during anti-TNF alpha therapy: nine cases. Ann Dermatol Venereol. 2011;138:285-293.
- Ferran M, Calvet J, Almirall M, et al. Alopecia areata as another immune-mediated disease developed in patients treated with tumour necrosis factor-α blocker agents: report of five cases and review of the literature. J Eur Acad Dermatol Venereol. 2011;25:479-484.
- Pan Y, Rao NA. Alopecia areata during etanercept therapy. Ocul Immunol Inflamm. 2009;17:127-129.
- Pelivani N, Hassan AS, Braathen LR, et al. Alopecia areata universalis elicited during treatment with adalimumab. Dermatology. 2008;216:320-323.
- Uyemura K, Yamamura M, Fivenson DF, et al. The cytokine network in lesional and lesion-free psoriatic skin is characterized by a T-helper type 1 cell-mediated response. J Invest Dermatol. 1993;101:701-705.
- Baker BS, Powles AV, Valdimarsson H, et al. An altered response by psoriatic keratinocytes to gamma interferon. Scan J Immunol. 1988;28:735-740.
- Jackson M, Howie SE, Weller R, et al. Psoriatic keratinocytes show reduced IRF-1 and STAT-1alpha activation in response to gamma-IFN. FASEB J. 1999;13:495-502.
- Perera GK, Di Meglio P, Nestle FO. Psoriasis. Annu Rev Pathol. 2012;7:385-422.
- McGeachy MJ, Chen Y, Tato CM, et al. The interleukin 23 receptor is essential for the terminal differentiation of interleukin 17-producing effector T helper cells in vivo. Nat Immunol. 2009;10:314-324.
- Volpe E, Servant N, Zollinger R, et al. A critical function for transforming growth factor-beta, interleukin 23 and proinflammatory cytokines in driving and modulating human T(H)-17 responses. Nat Immunol. 2008;9:650-657.
- Boniface K, Blumenschein WM, Brovont-Porth K, et al. Human Th17 cells comprise heterogeneous subsets including IFN-gamma-producing cells with distinct properties from the Th1 lineage. J Immunol. 2010;185:679-687.
- Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
- Boniface K, Bernard FX, Garcia M, et al. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J Immunol. 2005;174:3695-3702.
- Harper EG, Guo C, Rizzo H, et al. Th17 cytokines stimulate CCL20 expression in keratinocytes in vitro and in vivo: implications for psoriasis pathogenesis. J Invest Dermatol. 2009;129:2175-2183.
- Bowcock AM, Krueger JG. Getting under the skin: the immunogenetics of psoriasis. Nat Rev Immunol. 2005;5:699-711.
- Hoffmann R, Wenzel E, Huth A, et al. Cytokine mRNA levels in alopecia areata before and after treatment with the contact allergen diphenylcyclopropenone. J Invest Dermatol. 1994;103:530-533.
- Safavi K. Prevalence of alopecia areata in the First National Health and Nutrition Examination Survey. Arch Dermatol. 1992;128:702.
- Safavi KH, Muller SA, Suman VJ, et al. Incidence of alopecia areata in Olmsted County, Minnesota, 1975 through 1989. Mayo Clin Proc. 1995;70:628-633.
- Wolff K, Johnson RA. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 6th ed. New York, NY: McGraw-Hill; 2009.
- Austin LM, Ozawa M, Kikuchi T, et al. The majority of epidermal T cells in psoriasis vulgaris lesions can produce type 1 cytokines, interferon-gamma, interleukin-2, and tumor necrosis factor-alpha, defining TC1 (cytotoxic T lymphocyte) and TH1 effector populations: a type 1 differentiation bias is also measured in circulating blood T cells in psoriatic patients. J Invest Dermatol. 1999;113:752-759.
- Ghoreishi M, Martinka M, Dutz JP. Type 1 interferon signature in the scalp lesions of alopecia areata. Br J Dermatol. 2010;163:57-62.
- Rossi A, Cantisani C, Carlesimo M, et al. Serum concentrations of IL-2, IL-6, IL-12 and TNF-α in patients with alopecia areata. Int J Immunopathol Pharmacol. 2012;25:781-788.
- Freyschmidt-Paul P, McElwee KJ, Hoffmann R, et al. Interferon-gamma-deficient mice are resistant to the development of alopecia areata. Br J Dermatol. 2006;155:515-521.
- Reich K, Garbe C, Blaschke V, et al. Response of psoriasis to interleukin-10 is associated with suppression of cutaneous type 1 inflammation, downregulation of the epidermal interleukin-8/CXCR2 pathway and normalization of keratinocyte maturation. J Invest Dermatol. 2001;116:319-329.
- Teunissen MB, Koomen CW, de Waal Malefyt R, et al. Interleukin-17 and interferon-gamma synergize in the enhancement of proinflammatory cytokine production by human keratinocytes. J Invest Dermatol. 1998;111:645-649.
- Zheng Y, Danilenko DM, Valdez P, et al. Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature. 2007;445:648-651.
- Boniface K, Guignouard E, Pedretti N, et al. A role for T cell-derived interleukin 22 in psoriatic skin inflammation. Clin Exp Immunol. 2007;150:407-415.
- Zaba LC, Suárez-Fariñas M, Fuentes-Duculan J, et al. Effective treatment of psoriasis with etanercept is linked to suppression of IL-17 signaling, not immediate response TNF genes. J Allergy Clin Immunol. 2009;124:1022-1030.e395.
- Happle R, van der Steen PHM, Perret CM. The Renbök phenomenon: an inverse Köebner reaction observed in alopecia areata. Eur J Dermatol. 1991;2:39-40.
- Ito T, Hashizume H, Takigawa M. Contact immunotherapy-induced Renbök phenomenon in a patient with alopecia areata and psoriasis vulgaris. Eur J Dermatol. 2010;20:126-127.
- Criado PR, Valente NY, Michalany NS, et al. An unusual association between scalp psoriasis and ophiasic alopecia areata: the Renbök phenomenon. Clin Exp Dermatol. 2007;32:320-321.
- Harris JE, Seykora JT, Lee RA. Renbök phenomenon and contact sensitization in a patient with alopecia universalis. Arch Dermatol. 2010;146:422-425.
- Alkhalifah A. Topical and intralesional therapies for alopecia areata. Dermatol Ther. 2011;24:355-363.
- Herbst V, Zöller M, Kissling S, et al. Diphenylcyclopropenone treatment of alopecia areata induces apoptosis of perifollicular lymphocytes. Eur J Dermatol. 2006;16:537-542.
- Zöller M, Freyschmidt-Paul P, Vitacolonna M, et al. Chronic delayed-type hypersensitivity reaction as a means to treat alopecia areata. Clin Exp Immunol. 2004;135:398-408.
- Bröcker EB, Echternacht-Happle K, Hamm H, et al. Abnormal expression of class I and class II major histocompatibility antigens in alopecia areata: modulation by topical immunotherapy. J Invest Dermatol. 1987;88:564-568.
- Todes-Taylor N, Turner R, Wood GS, et al. T cell subpopulations in alopecia areata. J Am Acad Dermatol. 1984;11:216-223.
- Perret C, Wiesner-Menzel L, Happle R. Immunohistochemical analysis of T-cell subsets in the peribulbar and intrabulbar infiltrates of alopecia areata. Acta Derm Venereol. 1984;64:26-30.
- Wiesner-Menzel L, Happle R. Intrabulbar and peribulbar accumulation of dendritic OKT 6-positive cells in alopecia areata. Arch Dermatol Res. 1984;276:333-334.
- McElwee KJ, Freyschmidt-Paul P, Hoffmann R, et al. Transfer of CD8+ cells induces localized hair loss whereas CD4+/CD25– cells promote systemic alopecia areata and CD4+/CD25+ cells blockade disease onset in the C3H/HeJ mouse model. J Invest Dermatol. 2005;124:947-957.
- Arca E, Muşabak U, Akar A, et al. Interferon-gamma in alopecia areata. Eur J Dermatol. 2004;14:33-36.
- Hoffmann R. The potential role of cytokines and T cells in alopecia areata. J Investig Dermatol Symp Proc. 1999;4:235-238.
- Philpott MP, Sanders DA, Bowen J, et al. Effects of interleukins, colony-stimulating factor and tumour necrosis factor on human hair follicle growth in vitro: a possible role for interleukin-1 and tumour necrosis factor-alpha in alopecia areata. Br J Dermatol. 1996;135:942-948.
- Le Bidre E, Chaby G, Martin L, et al. Alopecia areata during anti-TNF alpha therapy: nine cases. Ann Dermatol Venereol. 2011;138:285-293.
- Ferran M, Calvet J, Almirall M, et al. Alopecia areata as another immune-mediated disease developed in patients treated with tumour necrosis factor-α blocker agents: report of five cases and review of the literature. J Eur Acad Dermatol Venereol. 2011;25:479-484.
- Pan Y, Rao NA. Alopecia areata during etanercept therapy. Ocul Immunol Inflamm. 2009;17:127-129.
- Pelivani N, Hassan AS, Braathen LR, et al. Alopecia areata universalis elicited during treatment with adalimumab. Dermatology. 2008;216:320-323.
- Uyemura K, Yamamura M, Fivenson DF, et al. The cytokine network in lesional and lesion-free psoriatic skin is characterized by a T-helper type 1 cell-mediated response. J Invest Dermatol. 1993;101:701-705.
- Baker BS, Powles AV, Valdimarsson H, et al. An altered response by psoriatic keratinocytes to gamma interferon. Scan J Immunol. 1988;28:735-740.
- Jackson M, Howie SE, Weller R, et al. Psoriatic keratinocytes show reduced IRF-1 and STAT-1alpha activation in response to gamma-IFN. FASEB J. 1999;13:495-502.
- Perera GK, Di Meglio P, Nestle FO. Psoriasis. Annu Rev Pathol. 2012;7:385-422.
- McGeachy MJ, Chen Y, Tato CM, et al. The interleukin 23 receptor is essential for the terminal differentiation of interleukin 17-producing effector T helper cells in vivo. Nat Immunol. 2009;10:314-324.
- Volpe E, Servant N, Zollinger R, et al. A critical function for transforming growth factor-beta, interleukin 23 and proinflammatory cytokines in driving and modulating human T(H)-17 responses. Nat Immunol. 2008;9:650-657.
- Boniface K, Blumenschein WM, Brovont-Porth K, et al. Human Th17 cells comprise heterogeneous subsets including IFN-gamma-producing cells with distinct properties from the Th1 lineage. J Immunol. 2010;185:679-687.
- Kagami S, Rizzo HL, Lee JJ, et al. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J Invest Dermatol. 2010;130:1373-1383.
- Boniface K, Bernard FX, Garcia M, et al. IL-22 inhibits epidermal differentiation and induces proinflammatory gene expression and migration of human keratinocytes. J Immunol. 2005;174:3695-3702.
- Harper EG, Guo C, Rizzo H, et al. Th17 cytokines stimulate CCL20 expression in keratinocytes in vitro and in vivo: implications for psoriasis pathogenesis. J Invest Dermatol. 2009;129:2175-2183.
- Bowcock AM, Krueger JG. Getting under the skin: the immunogenetics of psoriasis. Nat Rev Immunol. 2005;5:699-711.
- Hoffmann R, Wenzel E, Huth A, et al. Cytokine mRNA levels in alopecia areata before and after treatment with the contact allergen diphenylcyclopropenone. J Invest Dermatol. 1994;103:530-533.
Practice Points
- The Renbök phenomenon, or reverse Köbner phenomenon, describes cases where secondary insults improve dermatologic disease.
- Current evidence suggests that alopecia areata (AA) is driven by a helper T cell (TH1) response whereas psoriasis vulgaris is driven by TH1, TH17, and TH22.
- Patients with concurrent AA and psoriasis can develop normal hair regrowth confined to the psoriatic plaques. Developing methods to artificially alter the cytokine milieu in affected skin may lead to new therapeutic options for each condition.
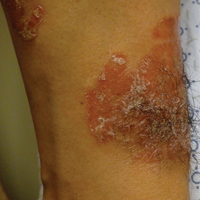
Beyond Residency: No more black and white
The obstetrics and gynecology written board exam made everything seem cut and dry. A patient with fibroids causing heavy bleeding? Management options include hormone treatment, minor surgical procedures, or major surgical procedures like myomectomy or hysterectomy. A pregnant patient in labor with a fetal heart rate deceleration? The next step is to shut off the oxytocin infusion, turn the patient on her left side, administer intravenous fluids, and give her oxygen via a nasal cannula. A patient who has ruptured her membranes at 28 weeks? That’s an easy one: magnesium for neuroprotection, latency antibiotics, prenatal steroids, neonatalogy consult. Straightforward.
At the end of June, I was grateful for my residency experience – even though some of it seemed hectic and haphazard – because it ensured that I understood the reasoning behind these multiple-choice questions. But then I started my maternal-fetal medicine fellowship this past July. I was learning the names of new residents, attendings, and nurses, and having to orient myself to an entirely different hospital system. Even labor and delivery board sign-out was completely different. I reassured myself by thinking: Obstetrics is obstetrics. The rules and guidelines of obstetrics are universal, practiced at every level, and always make sense, right?
One day I had a patient come in with chronic, refractory immune thrombocytopenia. Her plan for delivery was induction at 37 weeks after our hematology colleagues used medications we had never heard of to finally get her platelets into the 100s. But upon admission, her platelets were down to the 70s. I wondered, should we induce anyway because her platelets are likely to drop even further if we wait? Or do we give her the slew of medications that didn’t completely work initially as a last-ditch effort to boost her platelets again before delivery? I looked at practice bulletins, hematology guidelines, and numerous other publications and still I could not find a protocol for this specific kind of patient. After discussion with anesthesiologists, hematologists, maternal-fetal medicine specialists, labor and delivery nurses, and the patient herself, we came up with a plan. We gave her additional doses of thrombopoietic agents and steroids and continued to monitor her platelet count. Within a week, she had an uncomplicated vaginal delivery with an epidural.*
Taking a lead role in the decision-making process and organizing a management plan made me feel like I was the quarterback of a football team, with a healthy mother and baby substituting for a game-winning touchdown. The decisions we make in maternal-fetal medicine are not supposed to be easy. However, I’ve heard over and over that when our colleagues ask for our input, the guidance they want to hear is “deliver” or “don’t deliver.” Over the last several months, I’ve learned that there is so much more to it than that. I now examine the entire patient and fetus in two ways: as one physiologically inseparable unit, and as two patients, weighing the neonatal risks of delivery against the maternal risks of the pregnancy itself. Determining an appropriate time for delivery is just part of it.
There are also the questions about antepartum fetal testing. Should we do additional monitoring for patients with isolated polyhydramnios? What about patients who are at advanced maternal age? What about patients whose fetuses have “decreased growth velocity” but not growth restriction? Should these patients get umbilical artery Dopplers, too? ACOG and the SMFM often do not give us specific monitoring guidelines, which forces us to make a plan based on each individual clinical scenario.
In other words, we must practice in that ever-changing, ever-frustrating, and confusing gray area. I hope in fellowship I learn to not only navigate through this area effectively, but to one day confidently hold out my hand to others to help guide them through it, too.
Dr. Grossman recently completed her residency in obstetrics and gynecology at Albert Einstein College of Medicine–Montefiore Hospital in the Bronx, N.Y., and is currently a first-year maternal-fetal medicine fellow at Weill Cornell Medical College in New York. She reported having no financial disclosures.
*This article was update April 21, 2107.
The obstetrics and gynecology written board exam made everything seem cut and dry. A patient with fibroids causing heavy bleeding? Management options include hormone treatment, minor surgical procedures, or major surgical procedures like myomectomy or hysterectomy. A pregnant patient in labor with a fetal heart rate deceleration? The next step is to shut off the oxytocin infusion, turn the patient on her left side, administer intravenous fluids, and give her oxygen via a nasal cannula. A patient who has ruptured her membranes at 28 weeks? That’s an easy one: magnesium for neuroprotection, latency antibiotics, prenatal steroids, neonatalogy consult. Straightforward.
At the end of June, I was grateful for my residency experience – even though some of it seemed hectic and haphazard – because it ensured that I understood the reasoning behind these multiple-choice questions. But then I started my maternal-fetal medicine fellowship this past July. I was learning the names of new residents, attendings, and nurses, and having to orient myself to an entirely different hospital system. Even labor and delivery board sign-out was completely different. I reassured myself by thinking: Obstetrics is obstetrics. The rules and guidelines of obstetrics are universal, practiced at every level, and always make sense, right?
One day I had a patient come in with chronic, refractory immune thrombocytopenia. Her plan for delivery was induction at 37 weeks after our hematology colleagues used medications we had never heard of to finally get her platelets into the 100s. But upon admission, her platelets were down to the 70s. I wondered, should we induce anyway because her platelets are likely to drop even further if we wait? Or do we give her the slew of medications that didn’t completely work initially as a last-ditch effort to boost her platelets again before delivery? I looked at practice bulletins, hematology guidelines, and numerous other publications and still I could not find a protocol for this specific kind of patient. After discussion with anesthesiologists, hematologists, maternal-fetal medicine specialists, labor and delivery nurses, and the patient herself, we came up with a plan. We gave her additional doses of thrombopoietic agents and steroids and continued to monitor her platelet count. Within a week, she had an uncomplicated vaginal delivery with an epidural.*
Taking a lead role in the decision-making process and organizing a management plan made me feel like I was the quarterback of a football team, with a healthy mother and baby substituting for a game-winning touchdown. The decisions we make in maternal-fetal medicine are not supposed to be easy. However, I’ve heard over and over that when our colleagues ask for our input, the guidance they want to hear is “deliver” or “don’t deliver.” Over the last several months, I’ve learned that there is so much more to it than that. I now examine the entire patient and fetus in two ways: as one physiologically inseparable unit, and as two patients, weighing the neonatal risks of delivery against the maternal risks of the pregnancy itself. Determining an appropriate time for delivery is just part of it.
There are also the questions about antepartum fetal testing. Should we do additional monitoring for patients with isolated polyhydramnios? What about patients who are at advanced maternal age? What about patients whose fetuses have “decreased growth velocity” but not growth restriction? Should these patients get umbilical artery Dopplers, too? ACOG and the SMFM often do not give us specific monitoring guidelines, which forces us to make a plan based on each individual clinical scenario.
In other words, we must practice in that ever-changing, ever-frustrating, and confusing gray area. I hope in fellowship I learn to not only navigate through this area effectively, but to one day confidently hold out my hand to others to help guide them through it, too.
Dr. Grossman recently completed her residency in obstetrics and gynecology at Albert Einstein College of Medicine–Montefiore Hospital in the Bronx, N.Y., and is currently a first-year maternal-fetal medicine fellow at Weill Cornell Medical College in New York. She reported having no financial disclosures.
*This article was update April 21, 2107.
The obstetrics and gynecology written board exam made everything seem cut and dry. A patient with fibroids causing heavy bleeding? Management options include hormone treatment, minor surgical procedures, or major surgical procedures like myomectomy or hysterectomy. A pregnant patient in labor with a fetal heart rate deceleration? The next step is to shut off the oxytocin infusion, turn the patient on her left side, administer intravenous fluids, and give her oxygen via a nasal cannula. A patient who has ruptured her membranes at 28 weeks? That’s an easy one: magnesium for neuroprotection, latency antibiotics, prenatal steroids, neonatalogy consult. Straightforward.
At the end of June, I was grateful for my residency experience – even though some of it seemed hectic and haphazard – because it ensured that I understood the reasoning behind these multiple-choice questions. But then I started my maternal-fetal medicine fellowship this past July. I was learning the names of new residents, attendings, and nurses, and having to orient myself to an entirely different hospital system. Even labor and delivery board sign-out was completely different. I reassured myself by thinking: Obstetrics is obstetrics. The rules and guidelines of obstetrics are universal, practiced at every level, and always make sense, right?
One day I had a patient come in with chronic, refractory immune thrombocytopenia. Her plan for delivery was induction at 37 weeks after our hematology colleagues used medications we had never heard of to finally get her platelets into the 100s. But upon admission, her platelets were down to the 70s. I wondered, should we induce anyway because her platelets are likely to drop even further if we wait? Or do we give her the slew of medications that didn’t completely work initially as a last-ditch effort to boost her platelets again before delivery? I looked at practice bulletins, hematology guidelines, and numerous other publications and still I could not find a protocol for this specific kind of patient. After discussion with anesthesiologists, hematologists, maternal-fetal medicine specialists, labor and delivery nurses, and the patient herself, we came up with a plan. We gave her additional doses of thrombopoietic agents and steroids and continued to monitor her platelet count. Within a week, she had an uncomplicated vaginal delivery with an epidural.*
Taking a lead role in the decision-making process and organizing a management plan made me feel like I was the quarterback of a football team, with a healthy mother and baby substituting for a game-winning touchdown. The decisions we make in maternal-fetal medicine are not supposed to be easy. However, I’ve heard over and over that when our colleagues ask for our input, the guidance they want to hear is “deliver” or “don’t deliver.” Over the last several months, I’ve learned that there is so much more to it than that. I now examine the entire patient and fetus in two ways: as one physiologically inseparable unit, and as two patients, weighing the neonatal risks of delivery against the maternal risks of the pregnancy itself. Determining an appropriate time for delivery is just part of it.
There are also the questions about antepartum fetal testing. Should we do additional monitoring for patients with isolated polyhydramnios? What about patients who are at advanced maternal age? What about patients whose fetuses have “decreased growth velocity” but not growth restriction? Should these patients get umbilical artery Dopplers, too? ACOG and the SMFM often do not give us specific monitoring guidelines, which forces us to make a plan based on each individual clinical scenario.
In other words, we must practice in that ever-changing, ever-frustrating, and confusing gray area. I hope in fellowship I learn to not only navigate through this area effectively, but to one day confidently hold out my hand to others to help guide them through it, too.
Dr. Grossman recently completed her residency in obstetrics and gynecology at Albert Einstein College of Medicine–Montefiore Hospital in the Bronx, N.Y., and is currently a first-year maternal-fetal medicine fellow at Weill Cornell Medical College in New York. She reported having no financial disclosures.
*This article was update April 21, 2107.
AGA tools help GIs manage patients with obesity
Patients with obesity need a multidisciplinary approach to achieve a healthy weight. AGA understands the importance of embracing obesity as a chronic, relapsing disease and supports a multidisciplinary approach to the management of obesity led by gastroenterologists.
To watch
AGA Solutions to Successful Obesity Program Integration: Andres Acosta, MD, PhD, assistant professor in medicine, clinical enteric neuroscience translational and epidemiological research, division of gastroenterology and hepatology, Mayo Clinic, Rochester, MN, and Sarah Streett, MD, AGAF, clinical associate professor and director of IBD, Stanford (Calif.) University, discuss the AGA Obesity Guide and how GIs can begin to implement the program in their practices. Watch the on-demand webinar in the AGA Community resource library.
To read
POWER: Practice Guide on Obesity and Weight Management, Education and Resources: This practice guide on obesity and weight management will help you develop a multidisciplinary team and obesity care model for your practice.
Episode-of-Care Framework for the Management of Obesity: Moving toward high-value, high-quality care – AGA established an obesity episode-of-care model to develop a framework to support value-based management of patients with obesity, focusing on the provision of nonsurgical and endoscopic services.
These resources are available at www.gastro.org/obesity.
To discuss
Visit the AGA Community to join the discussion on managing your patient with obesity.
Patients with obesity need a multidisciplinary approach to achieve a healthy weight. AGA understands the importance of embracing obesity as a chronic, relapsing disease and supports a multidisciplinary approach to the management of obesity led by gastroenterologists.
To watch
AGA Solutions to Successful Obesity Program Integration: Andres Acosta, MD, PhD, assistant professor in medicine, clinical enteric neuroscience translational and epidemiological research, division of gastroenterology and hepatology, Mayo Clinic, Rochester, MN, and Sarah Streett, MD, AGAF, clinical associate professor and director of IBD, Stanford (Calif.) University, discuss the AGA Obesity Guide and how GIs can begin to implement the program in their practices. Watch the on-demand webinar in the AGA Community resource library.
To read
POWER: Practice Guide on Obesity and Weight Management, Education and Resources: This practice guide on obesity and weight management will help you develop a multidisciplinary team and obesity care model for your practice.
Episode-of-Care Framework for the Management of Obesity: Moving toward high-value, high-quality care – AGA established an obesity episode-of-care model to develop a framework to support value-based management of patients with obesity, focusing on the provision of nonsurgical and endoscopic services.
These resources are available at www.gastro.org/obesity.
To discuss
Visit the AGA Community to join the discussion on managing your patient with obesity.
Patients with obesity need a multidisciplinary approach to achieve a healthy weight. AGA understands the importance of embracing obesity as a chronic, relapsing disease and supports a multidisciplinary approach to the management of obesity led by gastroenterologists.
To watch
AGA Solutions to Successful Obesity Program Integration: Andres Acosta, MD, PhD, assistant professor in medicine, clinical enteric neuroscience translational and epidemiological research, division of gastroenterology and hepatology, Mayo Clinic, Rochester, MN, and Sarah Streett, MD, AGAF, clinical associate professor and director of IBD, Stanford (Calif.) University, discuss the AGA Obesity Guide and how GIs can begin to implement the program in their practices. Watch the on-demand webinar in the AGA Community resource library.
To read
POWER: Practice Guide on Obesity and Weight Management, Education and Resources: This practice guide on obesity and weight management will help you develop a multidisciplinary team and obesity care model for your practice.
Episode-of-Care Framework for the Management of Obesity: Moving toward high-value, high-quality care – AGA established an obesity episode-of-care model to develop a framework to support value-based management of patients with obesity, focusing on the provision of nonsurgical and endoscopic services.
These resources are available at www.gastro.org/obesity.
To discuss
Visit the AGA Community to join the discussion on managing your patient with obesity.
DTC genetic health risk tests: Beware
The Food and Drug Administration recently authorized 23andMe to provide consumers with results of germline DNA sequence variants associated with risk for 10 health conditions, among them hereditary hemochromatosis, alpha-1 antitrypsin deficiency, celiac disease, Alzheimer’s disease, and Parkinson’s disease. After they submit a saliva sample and pay a test fee, customers ordering the online test will receive a report delineating their ancestry markers and informing them whether they carry any of the genetic variants associated with selected health risks included on the targeted DNA sequencing panel.

As more consumers partake in “recreational genomic testing,” clinicians should understand the limitations of DTC genetic tests and should be prepared to discuss with patients why these should not supersede clinical diagnostic evaluations.
Dr. Stoffel is a gastroenterologist, assistant professor of internal medicine, and director of the cancer genetics clinic at the University of Michigan, Ann Arbor. She has no disclosures.
The Food and Drug Administration recently authorized 23andMe to provide consumers with results of germline DNA sequence variants associated with risk for 10 health conditions, among them hereditary hemochromatosis, alpha-1 antitrypsin deficiency, celiac disease, Alzheimer’s disease, and Parkinson’s disease. After they submit a saliva sample and pay a test fee, customers ordering the online test will receive a report delineating their ancestry markers and informing them whether they carry any of the genetic variants associated with selected health risks included on the targeted DNA sequencing panel.
As more consumers partake in “recreational genomic testing,” clinicians should understand the limitations of DTC genetic tests and should be prepared to discuss with patients why these should not supersede clinical diagnostic evaluations.
Dr. Stoffel is a gastroenterologist, assistant professor of internal medicine, and director of the cancer genetics clinic at the University of Michigan, Ann Arbor. She has no disclosures.
The Food and Drug Administration recently authorized 23andMe to provide consumers with results of germline DNA sequence variants associated with risk for 10 health conditions, among them hereditary hemochromatosis, alpha-1 antitrypsin deficiency, celiac disease, Alzheimer’s disease, and Parkinson’s disease. After they submit a saliva sample and pay a test fee, customers ordering the online test will receive a report delineating their ancestry markers and informing them whether they carry any of the genetic variants associated with selected health risks included on the targeted DNA sequencing panel.
As more consumers partake in “recreational genomic testing,” clinicians should understand the limitations of DTC genetic tests and should be prepared to discuss with patients why these should not supersede clinical diagnostic evaluations.
Dr. Stoffel is a gastroenterologist, assistant professor of internal medicine, and director of the cancer genetics clinic at the University of Michigan, Ann Arbor. She has no disclosures.
