User login
Prenotification, unequivocal stroke promote ultra-fast door-to-needle time
BOSTON – Ultra-fast door-to-needle times of 10 minutes or less for intravenous acute ischemic stroke thrombolysis can be safely achieved in carefully selected cases, according to a review of cases at an Austrian teaching hospital.
Raffi Topakian, MD, and his colleagues at the Academic Teaching Hospital Wels-Grieskirchen in Wels, Austria, followed a multidisciplinary intervention to reinforce key components of the well-known Helsinki model of acute stroke care to improve the intravenous thrombolysis rate and the median door-to-needle time (DNT) at the teaching hospital and analyzed data from 361 patients who underwent intravenous thrombolysis (IVT) for stroke there between July 2014 and September 2016. The IVT rate increased from 19% to about 27% after intervention, and the DNT during the study period was 60 minutes or less in 316 patients (87.5%), 30 minutes or less in 181 patients (50.1%), and 10 minutes or less in 63 patients (17.5%).
“Over the study period, we reduced the DNT time from 49 minutes to 25 minutes. This was significant, and the door-to-needle times were astonishingly similar for the in-hours service and the out-of-hour service,” he said at the annual meeting of the American Academy of Neurology.
Further, the rate of prenotifications from emergency medical services rose from about 30% to 63% during the study period.
Patients with ultra-fast DNT vs. those with slower DNT were older, had more chronic heart failure, had more severe stroke (National Institutes of Health Stroke Scale score of 10 vs. 5), had more anterior circulation stroke and cardioembolic stroke, and had clear onset of stroke. Independent predictors of ultra-fast DNT included prenotification by EMS, anterior circulation syndrome, chronic heart failure, and having a stroke neurologist on duty, Dr. Topakian said.
“Ultra short DNTs can be achieved safely. The key is that we are prenotified by the EMS, that we can get all the relevant history details during transport, that there is a dedicated multidisciplinary stroke team and EMS staff, and that we have a seemingly unequivocal clinical scenario,” he said. “Out-of-hours DNT matched in-hours DNT, but the caveat is we’re talking about highly selected candidates; safety must not be sacrificed for the sake of speed, in all of our patients.”
Dr. Topakian has received personal compensation for activities with Novartis and Shire-Baxalta as an advisory board member; from Novartis, Pfizer, AbbVie, and Bayer for conference support; and from Pfizer as a speaker.
BOSTON – Ultra-fast door-to-needle times of 10 minutes or less for intravenous acute ischemic stroke thrombolysis can be safely achieved in carefully selected cases, according to a review of cases at an Austrian teaching hospital.
Raffi Topakian, MD, and his colleagues at the Academic Teaching Hospital Wels-Grieskirchen in Wels, Austria, followed a multidisciplinary intervention to reinforce key components of the well-known Helsinki model of acute stroke care to improve the intravenous thrombolysis rate and the median door-to-needle time (DNT) at the teaching hospital and analyzed data from 361 patients who underwent intravenous thrombolysis (IVT) for stroke there between July 2014 and September 2016. The IVT rate increased from 19% to about 27% after intervention, and the DNT during the study period was 60 minutes or less in 316 patients (87.5%), 30 minutes or less in 181 patients (50.1%), and 10 minutes or less in 63 patients (17.5%).
“Over the study period, we reduced the DNT time from 49 minutes to 25 minutes. This was significant, and the door-to-needle times were astonishingly similar for the in-hours service and the out-of-hour service,” he said at the annual meeting of the American Academy of Neurology.
Further, the rate of prenotifications from emergency medical services rose from about 30% to 63% during the study period.
Patients with ultra-fast DNT vs. those with slower DNT were older, had more chronic heart failure, had more severe stroke (National Institutes of Health Stroke Scale score of 10 vs. 5), had more anterior circulation stroke and cardioembolic stroke, and had clear onset of stroke. Independent predictors of ultra-fast DNT included prenotification by EMS, anterior circulation syndrome, chronic heart failure, and having a stroke neurologist on duty, Dr. Topakian said.
“Ultra short DNTs can be achieved safely. The key is that we are prenotified by the EMS, that we can get all the relevant history details during transport, that there is a dedicated multidisciplinary stroke team and EMS staff, and that we have a seemingly unequivocal clinical scenario,” he said. “Out-of-hours DNT matched in-hours DNT, but the caveat is we’re talking about highly selected candidates; safety must not be sacrificed for the sake of speed, in all of our patients.”
Dr. Topakian has received personal compensation for activities with Novartis and Shire-Baxalta as an advisory board member; from Novartis, Pfizer, AbbVie, and Bayer for conference support; and from Pfizer as a speaker.
BOSTON – Ultra-fast door-to-needle times of 10 minutes or less for intravenous acute ischemic stroke thrombolysis can be safely achieved in carefully selected cases, according to a review of cases at an Austrian teaching hospital.
Raffi Topakian, MD, and his colleagues at the Academic Teaching Hospital Wels-Grieskirchen in Wels, Austria, followed a multidisciplinary intervention to reinforce key components of the well-known Helsinki model of acute stroke care to improve the intravenous thrombolysis rate and the median door-to-needle time (DNT) at the teaching hospital and analyzed data from 361 patients who underwent intravenous thrombolysis (IVT) for stroke there between July 2014 and September 2016. The IVT rate increased from 19% to about 27% after intervention, and the DNT during the study period was 60 minutes or less in 316 patients (87.5%), 30 minutes or less in 181 patients (50.1%), and 10 minutes or less in 63 patients (17.5%).
“Over the study period, we reduced the DNT time from 49 minutes to 25 minutes. This was significant, and the door-to-needle times were astonishingly similar for the in-hours service and the out-of-hour service,” he said at the annual meeting of the American Academy of Neurology.
Further, the rate of prenotifications from emergency medical services rose from about 30% to 63% during the study period.
Patients with ultra-fast DNT vs. those with slower DNT were older, had more chronic heart failure, had more severe stroke (National Institutes of Health Stroke Scale score of 10 vs. 5), had more anterior circulation stroke and cardioembolic stroke, and had clear onset of stroke. Independent predictors of ultra-fast DNT included prenotification by EMS, anterior circulation syndrome, chronic heart failure, and having a stroke neurologist on duty, Dr. Topakian said.
“Ultra short DNTs can be achieved safely. The key is that we are prenotified by the EMS, that we can get all the relevant history details during transport, that there is a dedicated multidisciplinary stroke team and EMS staff, and that we have a seemingly unequivocal clinical scenario,” he said. “Out-of-hours DNT matched in-hours DNT, but the caveat is we’re talking about highly selected candidates; safety must not be sacrificed for the sake of speed, in all of our patients.”
Dr. Topakian has received personal compensation for activities with Novartis and Shire-Baxalta as an advisory board member; from Novartis, Pfizer, AbbVie, and Bayer for conference support; and from Pfizer as a speaker.
Key clinical point:
Major finding: Door-to-needle time of 10 minutes or less was achieved in 63 patients (17.5%).
Data source: A retrospective review of prospectively collected data from 361 patients.
Disclosures: Dr. Topakian has received personal compensation for activities with Novartis and Shire-Baxalta as an advisory board member; from Novartis, Pfizer, AbbVie, and Bayer for conference support; and from Pfizer as a speaker.
VHA warns of a ‘second epidemic’ of carbapenem-resistant E. cloacae complex
Veterans Health Administration monitoring of carbapenem-resistant Enterobacteriaceae (CRE) trends from 2006 to 2015 shows a rise in resistance rates of E. cloacae complex nationwide.
The first major CRE outbreak, Klebsiella pneumoniae, occurred in the eastern United States in the early 2000s and has since spread across the country. K. pneumoniae has recently shown a decrease in resistance rates in the region including New York, both in the current VHA-based study and in a 2016 study of three New York City hospitals.
“CRE trends during 2006-2015 in the VHA recapitulate the epidemic of carbapenem-resistant K. pneumoniae in the United States and indicate that a ‘second epidemic’ of carbapenem-resistant E. cloacae complex appears to be unfolding,” wrote Brigid M. Wilson, PhD, of Louis Stokes Cleveland Department of Veterans Affairs Medical Center, and her coauthors.
The researchers used VHA network data to identify 128,431 K. pneumoniae and 38,219 E. cloacae complex (which refers to the species E. cloacae, E. asburiae, E. kobei, E. hormaechei, and E. xiafangensis) isolates from patients hospitalized in 140 facilities in 40 states, the District of Columbia, and Puerto Rico from 2006 to 2015. These isolates, paired with their carbapenem susceptibility test results, show the rise and geographic concentration of the CRE cases over the decade.
The increased E. cloacae complex resistance in 2014-2015 was centered around the Pacific Coast and Southwest regions. The researchers noted that E. cloacae complex has a less well defined genetic makeup, compared with K. pneumoniae.
“We hypothesize that E. cloacae complex contains genotypes with epidemic potential associated with increasing rates of carbapenem resistance observed in the VHA,” they wrote, concluding that “the VHA may serve as a vantage point for detecting nationwide trends in antimicrobial drug resistance” (Emerg Infect Dis. 2017 Mar. doi: 10.3201/eid2305.162034).
Veterans Health Administration monitoring of carbapenem-resistant Enterobacteriaceae (CRE) trends from 2006 to 2015 shows a rise in resistance rates of E. cloacae complex nationwide.
The first major CRE outbreak, Klebsiella pneumoniae, occurred in the eastern United States in the early 2000s and has since spread across the country. K. pneumoniae has recently shown a decrease in resistance rates in the region including New York, both in the current VHA-based study and in a 2016 study of three New York City hospitals.
“CRE trends during 2006-2015 in the VHA recapitulate the epidemic of carbapenem-resistant K. pneumoniae in the United States and indicate that a ‘second epidemic’ of carbapenem-resistant E. cloacae complex appears to be unfolding,” wrote Brigid M. Wilson, PhD, of Louis Stokes Cleveland Department of Veterans Affairs Medical Center, and her coauthors.
The researchers used VHA network data to identify 128,431 K. pneumoniae and 38,219 E. cloacae complex (which refers to the species E. cloacae, E. asburiae, E. kobei, E. hormaechei, and E. xiafangensis) isolates from patients hospitalized in 140 facilities in 40 states, the District of Columbia, and Puerto Rico from 2006 to 2015. These isolates, paired with their carbapenem susceptibility test results, show the rise and geographic concentration of the CRE cases over the decade.
The increased E. cloacae complex resistance in 2014-2015 was centered around the Pacific Coast and Southwest regions. The researchers noted that E. cloacae complex has a less well defined genetic makeup, compared with K. pneumoniae.
“We hypothesize that E. cloacae complex contains genotypes with epidemic potential associated with increasing rates of carbapenem resistance observed in the VHA,” they wrote, concluding that “the VHA may serve as a vantage point for detecting nationwide trends in antimicrobial drug resistance” (Emerg Infect Dis. 2017 Mar. doi: 10.3201/eid2305.162034).
Veterans Health Administration monitoring of carbapenem-resistant Enterobacteriaceae (CRE) trends from 2006 to 2015 shows a rise in resistance rates of E. cloacae complex nationwide.
The first major CRE outbreak, Klebsiella pneumoniae, occurred in the eastern United States in the early 2000s and has since spread across the country. K. pneumoniae has recently shown a decrease in resistance rates in the region including New York, both in the current VHA-based study and in a 2016 study of three New York City hospitals.
“CRE trends during 2006-2015 in the VHA recapitulate the epidemic of carbapenem-resistant K. pneumoniae in the United States and indicate that a ‘second epidemic’ of carbapenem-resistant E. cloacae complex appears to be unfolding,” wrote Brigid M. Wilson, PhD, of Louis Stokes Cleveland Department of Veterans Affairs Medical Center, and her coauthors.
The researchers used VHA network data to identify 128,431 K. pneumoniae and 38,219 E. cloacae complex (which refers to the species E. cloacae, E. asburiae, E. kobei, E. hormaechei, and E. xiafangensis) isolates from patients hospitalized in 140 facilities in 40 states, the District of Columbia, and Puerto Rico from 2006 to 2015. These isolates, paired with their carbapenem susceptibility test results, show the rise and geographic concentration of the CRE cases over the decade.
The increased E. cloacae complex resistance in 2014-2015 was centered around the Pacific Coast and Southwest regions. The researchers noted that E. cloacae complex has a less well defined genetic makeup, compared with K. pneumoniae.
“We hypothesize that E. cloacae complex contains genotypes with epidemic potential associated with increasing rates of carbapenem resistance observed in the VHA,” they wrote, concluding that “the VHA may serve as a vantage point for detecting nationwide trends in antimicrobial drug resistance” (Emerg Infect Dis. 2017 Mar. doi: 10.3201/eid2305.162034).
Science advocates take to D.C. streets in March for Science
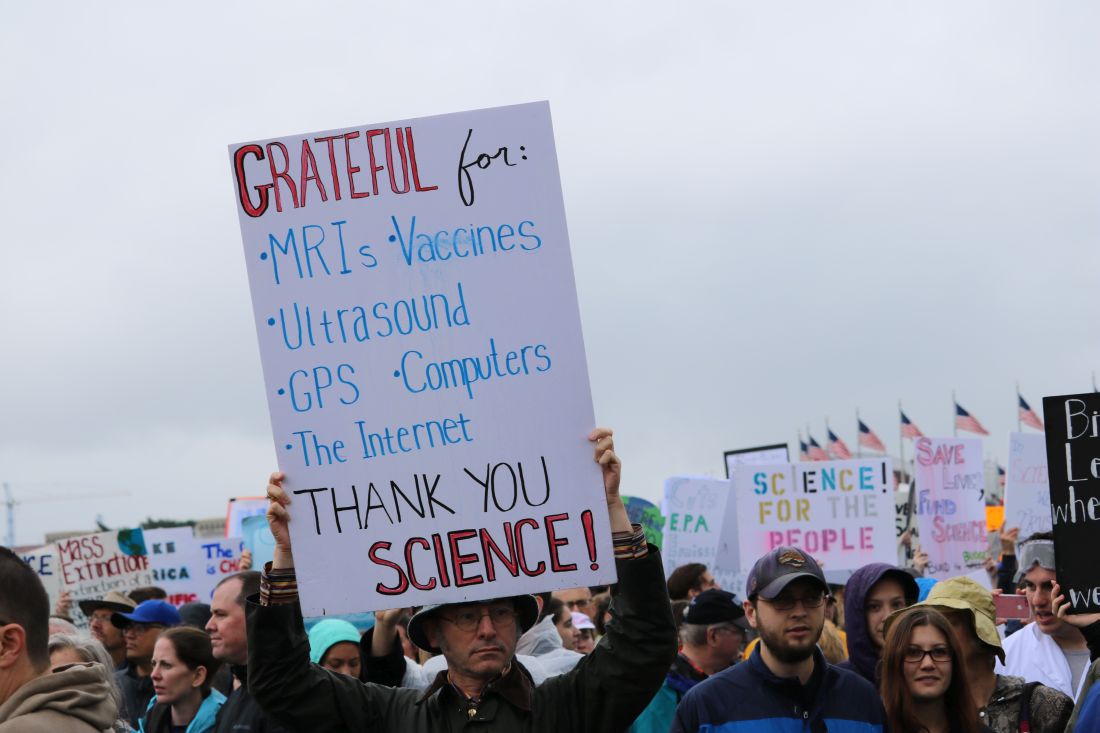
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.

“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.
“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
WASHINGTON – Crowds of protesters packed the Washington’s National Mall for the March for Science, joining participants in 600 cities across the world on Saturday, April 22.
Advocates came in droves, braving the rain armed with homemade signs, chants, and a passion for peer review, to champion the scientific method and the importance of its role in society and policy making.
The event, organized by March for Science, Earth Day Network, and a robust list of advocacy groups and think tanks, started with learning sessions hosted in tents located beyond the Washington Monument, where experts in topics from physics to environmental science informed attendees about the importance of their subjects.
To the left of the tents, directly across from the White House, scores gathered around a large stage, where 56 science professionals from different fields came together to promote the importance of scientific research and science-based policy.
The main stage event was emceed by musician Questlove and Tyler DeWitt, PhD, host of the YouTube science education show “Science with Tyler DeWitt.”
“You cannot criticize a public that doesn’t understand science if we can’t explain it,” said Dr. DeWitt.
“A strong commitment to research is absolutely essential to crafting evidence-based policies to protect us from serious health threats,” said Georges C. Benjamin, MD, executive director of the America Public Health Association. “A nation that ignores science, that denies science, that underfunds science, does so at its own peril.”
Speakers like Kellan Baker, senior fellow with the LGBT Research and Communications Project at the Center for American Progress, promoted political action, echoing organizers’ intentions of being bipartisan but not shying away from promoting political action.
“Advocacy is not a dirty word” said Mr. Baker. “Science is objective, but it is not neutral.”
Other speakers included Mona Hanna-Attisha, MD, the pediatrician who helped expose the lead poisoning situation in Flint, Mich., and Bill Nye, CEO of the Planetary Society and host of the Netflix series “Bill Nye Saves the World.”
After speeches, protesters marched from the Washington Monument to the U.S. Capitol, chanting loudly and waving signs.
March for Science and its partners are continuing to promote advocacy through a “week of action” scheduled to run through April 29.
*This article was updated May 2, 2017.
[email protected]
On Twitter @eaztweets
Sepsis survivors may have high risk for seizures
BOSTON – Survivors of sepsis face a significantly increased risk of seizures following an index hospitalization, regardless of any previous history of seizures or seizures occurring during hospitalization, according to findings from a retrospective, population-based cohort study.
The risk for having subsequent seizures was highest for patients younger than 65 years but was still elevated above the general population for those aged 65 years or older, Michael Reznik, MD, reported at the annual meeting of the American Academy of Neurology.

Seizures are already a well-known complication of sepsis, and they also can occur alongside sepsis-associated encephalopathy, stroke, and neuromuscular disease. The frequency of sepsis-associated encephalopathy also has led to the recognition of postsepsis cognitive dysfunction, said Dr. Reznik, a neurocritical care fellow in the department of neurology at Weill Cornell Medicine and Columbia University Medical Center in New York.
It is unclear, however, how much of the risk for cognitive impairment after sepsis is due to pre-existing cognitive impairment, frailty, or lingering sedation effects, he said.
It’s possible, he noted, that “seizures may be more specific for structural brain injury, and I think our findings may support the hypothesis that sepsis could be associated with pathways leading to long-lasting brain injury that’s independent of other primary injuries that we have controlled for.”
Dr. Reznik and his coinvestigators used administrative claims data from all discharges from nonfederal emergency departments and acute care hospitals in California, New York, and Florida during 2005-2013 that had been collected as part of the federal Healthcare Cost and Utilization Project (HCUP). The HCUP assigns each patient a unique number that can be used to follow them anonymously through all subsequent hospitalizations. At each encounter, HCUP also tracks up to 25 discharge diagnoses that were present before hospital admission or developed during hospitalization, based on ICD-9-CM codes.
The investigators excluded patients with an ICD-9-CM diagnosis of seizures either before or during the index hospitalization for sepsis.
Overall, the 842,735 adult sepsis survivors in the study had a 6.67% cumulative rate of seizures over the 8-year period, compared with 1.27% in the general population. This translated to an incidence of about 1,288 per 100,000 patient-years in sepsis survivors, compared with 159 per 100,000 patient-years in the general population. The overall incidence rate ratio (IRR) for seizures among sepsis survivors was about 5, but was higher for those who also had neurologic dysfunction (such as encephalopathy, delirium, coma, or stupor) during their index hospitalization than in those without it (7.52 vs. 4.53). Sepsis survivors also had an elevated IRR of 5.42 for status epilepticus.
Sepsis survivors also had an elevated IRR of 4.35 for seizures when compared against control patients who were hospitalized for diagnoses other than sepsis and matched for age, sex, race, insurance, length of stay, discharge location, year of hospitalization, state, and the presence of codes for organ dysfunction.
The investigators confirmed the findings from the state-based HCUP analysis through inpatient and outpatient Medicare claims during 2008-1014 in a nationally representative sample of 5% of Medicare beneficiaries. These patients had an IRR for seizures of 2.72, and the IRR remained elevated (2.18) relative to patients who were hospitalized with diagnoses other than sepsis even when they excluded patients with ICD-9-CM codes for conditions that confer risk for seizures, including stroke, traumatic brain injury, CNS infection, or brain neoplasm. The seizure outcome in this analysis was defined as one or more inpatient claims for epilepsy or two or more outpatient claims within 3 months of each other.
Since the state-based HCUP data gave a much stronger association between sepsis and subsequent seizures than did the Medicare claims data, the investigators performed a post hoc stratified analysis according to age. Age proved to have a significant effect on the relationship between sepsis and subsequent seizures: Patients aged 65 years or older had an IRR of 2.83, compared with an IRR of 10.33 for those younger than 65.
In an interview, Dr. Reznik said that he sees the results as hypothesis generating and suggested they could serve as a “red flag” for neurologists that’s worth further investigation, given that studies suggest systemic infections and sepsis overall have long-term neurologic implications.
“I think there’s a possibility that, down the line, [sepsis] might be seen as a seizure risk factor, but unfortunately there are limitations from being based on an administrative data set,” he said.
The study was supported by a grant from the National Institute for Neurological Disorders and Stroke to one of the investigators and also by the Michael Goldberg Research Fund. Dr. Reznik had no disclosures to report.
BOSTON – Survivors of sepsis face a significantly increased risk of seizures following an index hospitalization, regardless of any previous history of seizures or seizures occurring during hospitalization, according to findings from a retrospective, population-based cohort study.
The risk for having subsequent seizures was highest for patients younger than 65 years but was still elevated above the general population for those aged 65 years or older, Michael Reznik, MD, reported at the annual meeting of the American Academy of Neurology.
Seizures are already a well-known complication of sepsis, and they also can occur alongside sepsis-associated encephalopathy, stroke, and neuromuscular disease. The frequency of sepsis-associated encephalopathy also has led to the recognition of postsepsis cognitive dysfunction, said Dr. Reznik, a neurocritical care fellow in the department of neurology at Weill Cornell Medicine and Columbia University Medical Center in New York.
It is unclear, however, how much of the risk for cognitive impairment after sepsis is due to pre-existing cognitive impairment, frailty, or lingering sedation effects, he said.
It’s possible, he noted, that “seizures may be more specific for structural brain injury, and I think our findings may support the hypothesis that sepsis could be associated with pathways leading to long-lasting brain injury that’s independent of other primary injuries that we have controlled for.”
Dr. Reznik and his coinvestigators used administrative claims data from all discharges from nonfederal emergency departments and acute care hospitals in California, New York, and Florida during 2005-2013 that had been collected as part of the federal Healthcare Cost and Utilization Project (HCUP). The HCUP assigns each patient a unique number that can be used to follow them anonymously through all subsequent hospitalizations. At each encounter, HCUP also tracks up to 25 discharge diagnoses that were present before hospital admission or developed during hospitalization, based on ICD-9-CM codes.
The investigators excluded patients with an ICD-9-CM diagnosis of seizures either before or during the index hospitalization for sepsis.
Overall, the 842,735 adult sepsis survivors in the study had a 6.67% cumulative rate of seizures over the 8-year period, compared with 1.27% in the general population. This translated to an incidence of about 1,288 per 100,000 patient-years in sepsis survivors, compared with 159 per 100,000 patient-years in the general population. The overall incidence rate ratio (IRR) for seizures among sepsis survivors was about 5, but was higher for those who also had neurologic dysfunction (such as encephalopathy, delirium, coma, or stupor) during their index hospitalization than in those without it (7.52 vs. 4.53). Sepsis survivors also had an elevated IRR of 5.42 for status epilepticus.
Sepsis survivors also had an elevated IRR of 4.35 for seizures when compared against control patients who were hospitalized for diagnoses other than sepsis and matched for age, sex, race, insurance, length of stay, discharge location, year of hospitalization, state, and the presence of codes for organ dysfunction.
The investigators confirmed the findings from the state-based HCUP analysis through inpatient and outpatient Medicare claims during 2008-1014 in a nationally representative sample of 5% of Medicare beneficiaries. These patients had an IRR for seizures of 2.72, and the IRR remained elevated (2.18) relative to patients who were hospitalized with diagnoses other than sepsis even when they excluded patients with ICD-9-CM codes for conditions that confer risk for seizures, including stroke, traumatic brain injury, CNS infection, or brain neoplasm. The seizure outcome in this analysis was defined as one or more inpatient claims for epilepsy or two or more outpatient claims within 3 months of each other.
Since the state-based HCUP data gave a much stronger association between sepsis and subsequent seizures than did the Medicare claims data, the investigators performed a post hoc stratified analysis according to age. Age proved to have a significant effect on the relationship between sepsis and subsequent seizures: Patients aged 65 years or older had an IRR of 2.83, compared with an IRR of 10.33 for those younger than 65.
In an interview, Dr. Reznik said that he sees the results as hypothesis generating and suggested they could serve as a “red flag” for neurologists that’s worth further investigation, given that studies suggest systemic infections and sepsis overall have long-term neurologic implications.
“I think there’s a possibility that, down the line, [sepsis] might be seen as a seizure risk factor, but unfortunately there are limitations from being based on an administrative data set,” he said.
The study was supported by a grant from the National Institute for Neurological Disorders and Stroke to one of the investigators and also by the Michael Goldberg Research Fund. Dr. Reznik had no disclosures to report.
BOSTON – Survivors of sepsis face a significantly increased risk of seizures following an index hospitalization, regardless of any previous history of seizures or seizures occurring during hospitalization, according to findings from a retrospective, population-based cohort study.
The risk for having subsequent seizures was highest for patients younger than 65 years but was still elevated above the general population for those aged 65 years or older, Michael Reznik, MD, reported at the annual meeting of the American Academy of Neurology.
Seizures are already a well-known complication of sepsis, and they also can occur alongside sepsis-associated encephalopathy, stroke, and neuromuscular disease. The frequency of sepsis-associated encephalopathy also has led to the recognition of postsepsis cognitive dysfunction, said Dr. Reznik, a neurocritical care fellow in the department of neurology at Weill Cornell Medicine and Columbia University Medical Center in New York.
It is unclear, however, how much of the risk for cognitive impairment after sepsis is due to pre-existing cognitive impairment, frailty, or lingering sedation effects, he said.
It’s possible, he noted, that “seizures may be more specific for structural brain injury, and I think our findings may support the hypothesis that sepsis could be associated with pathways leading to long-lasting brain injury that’s independent of other primary injuries that we have controlled for.”
Dr. Reznik and his coinvestigators used administrative claims data from all discharges from nonfederal emergency departments and acute care hospitals in California, New York, and Florida during 2005-2013 that had been collected as part of the federal Healthcare Cost and Utilization Project (HCUP). The HCUP assigns each patient a unique number that can be used to follow them anonymously through all subsequent hospitalizations. At each encounter, HCUP also tracks up to 25 discharge diagnoses that were present before hospital admission or developed during hospitalization, based on ICD-9-CM codes.
The investigators excluded patients with an ICD-9-CM diagnosis of seizures either before or during the index hospitalization for sepsis.
Overall, the 842,735 adult sepsis survivors in the study had a 6.67% cumulative rate of seizures over the 8-year period, compared with 1.27% in the general population. This translated to an incidence of about 1,288 per 100,000 patient-years in sepsis survivors, compared with 159 per 100,000 patient-years in the general population. The overall incidence rate ratio (IRR) for seizures among sepsis survivors was about 5, but was higher for those who also had neurologic dysfunction (such as encephalopathy, delirium, coma, or stupor) during their index hospitalization than in those without it (7.52 vs. 4.53). Sepsis survivors also had an elevated IRR of 5.42 for status epilepticus.
Sepsis survivors also had an elevated IRR of 4.35 for seizures when compared against control patients who were hospitalized for diagnoses other than sepsis and matched for age, sex, race, insurance, length of stay, discharge location, year of hospitalization, state, and the presence of codes for organ dysfunction.
The investigators confirmed the findings from the state-based HCUP analysis through inpatient and outpatient Medicare claims during 2008-1014 in a nationally representative sample of 5% of Medicare beneficiaries. These patients had an IRR for seizures of 2.72, and the IRR remained elevated (2.18) relative to patients who were hospitalized with diagnoses other than sepsis even when they excluded patients with ICD-9-CM codes for conditions that confer risk for seizures, including stroke, traumatic brain injury, CNS infection, or brain neoplasm. The seizure outcome in this analysis was defined as one or more inpatient claims for epilepsy or two or more outpatient claims within 3 months of each other.
Since the state-based HCUP data gave a much stronger association between sepsis and subsequent seizures than did the Medicare claims data, the investigators performed a post hoc stratified analysis according to age. Age proved to have a significant effect on the relationship between sepsis and subsequent seizures: Patients aged 65 years or older had an IRR of 2.83, compared with an IRR of 10.33 for those younger than 65.
In an interview, Dr. Reznik said that he sees the results as hypothesis generating and suggested they could serve as a “red flag” for neurologists that’s worth further investigation, given that studies suggest systemic infections and sepsis overall have long-term neurologic implications.
“I think there’s a possibility that, down the line, [sepsis] might be seen as a seizure risk factor, but unfortunately there are limitations from being based on an administrative data set,” he said.
The study was supported by a grant from the National Institute for Neurological Disorders and Stroke to one of the investigators and also by the Michael Goldberg Research Fund. Dr. Reznik had no disclosures to report.
Key clinical point:
Major finding: The overall incidence rate ratio for seizures among sepsis survivors was about 5, compared with the general population.
Data source: A retrospective, population-based cohort study of 842,735 sepsis survivors from three states during 2005-2013.
Disclosures: The study was supported by a grant from the National Institute for Neurological Disorders and Stroke to one of the investigators and also the Michael Goldberg Research Fund. Dr. Reznik had no disclosures to report.
VIDEO: Geeks brave rain to March for Science
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
WASHINGTON – Peaceful protesters in hundreds of cities around the globe gathered on Earth Day, April 22, to voice their support for evidence-based policies and funding for scientific research at the March for Science.
In Washington, thousands of participants gathered on the rainy National Mall for teach-ins and speeches, then marched from the Washington Monument to Capitol Hill. A key concern for marchers here was cuts in science agency funding in the Trump administration’s budget proposal for fiscal year 2018.
Organizers now are calling on supporters to participate in a week of action to continue to demonstrate widespread support for their positions.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @denisefulton
Everything We Say and Do: Hospitalists are leaders in designing inpatient experience
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively affect patients’ experience of care. This column highlights key takeaways from the SHM track of the upcoming 2017 Cleveland Clinic Patient Experience Empathy and Innovation Summit, May 22-24. Three hospitalist leaders describe their approach to leading the design of the inpatient experience.
What we say and do, and why
Like many forms of care improvement, we have found that health care providers and patients alike engage most proactively when they are directly involved in codesigning an approach or intervention for improving the experience of care. Here are some examples of how hospitalists can be effective leaders in cocreating the inpatient experience with patients and interdisciplinary colleagues.



Dr. Sliwka is medical director of patient and provider experience at University of California, San Francisco, Health; Dr. Kneeland is medical director for patient and provider experience at University of Colorado, Aurora, Hospital; Dr. Hoffman is medical director for patient relations at University of Wisconsin-Madison, Health.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively affect patients’ experience of care. This column highlights key takeaways from the SHM track of the upcoming 2017 Cleveland Clinic Patient Experience Empathy and Innovation Summit, May 22-24. Three hospitalist leaders describe their approach to leading the design of the inpatient experience.
What we say and do, and why
Like many forms of care improvement, we have found that health care providers and patients alike engage most proactively when they are directly involved in codesigning an approach or intervention for improving the experience of care. Here are some examples of how hospitalists can be effective leaders in cocreating the inpatient experience with patients and interdisciplinary colleagues.
Dr. Sliwka is medical director of patient and provider experience at University of California, San Francisco, Health; Dr. Kneeland is medical director for patient and provider experience at University of Colorado, Aurora, Hospital; Dr. Hoffman is medical director for patient relations at University of Wisconsin-Madison, Health.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively affect patients’ experience of care. This column highlights key takeaways from the SHM track of the upcoming 2017 Cleveland Clinic Patient Experience Empathy and Innovation Summit, May 22-24. Three hospitalist leaders describe their approach to leading the design of the inpatient experience.
What we say and do, and why
Like many forms of care improvement, we have found that health care providers and patients alike engage most proactively when they are directly involved in codesigning an approach or intervention for improving the experience of care. Here are some examples of how hospitalists can be effective leaders in cocreating the inpatient experience with patients and interdisciplinary colleagues.
Dr. Sliwka is medical director of patient and provider experience at University of California, San Francisco, Health; Dr. Kneeland is medical director for patient and provider experience at University of Colorado, Aurora, Hospital; Dr. Hoffman is medical director for patient relations at University of Wisconsin-Madison, Health.
CHMP recommends inotuzumab ozogamicin for adult ALL

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of inotuzumab ozogamicin (Besponsa®).
The CHMP is recommending approval of inotuzumab ozogamicin for the treatment of adults with relapsed or refractory CD22-positive B-cell precursor acute lymphoblastic leukemia (ALL), including patients with Philadelphia chromosome-positive ALL who have failed treatment with at least one tyrosine kinase inhibitor.
The CHMP’s opinion will be reviewed by the European Commission, which is expected to issue a decision on approval within 67 days from adoption of the opinion.
Inotuzumab ozogamicin is an antibody-drug conjugate that consists of a monoclonal antibody targeting CD22 and a cytotoxic agent known as calicheamicin.
The product originates from a collaboration between Pfizer and Celltech (now UCB), but Pfizer has sole responsibility for all manufacturing and clinical development activities.
The application for inotuzumab ozogamicin is supported by results from a phase 3 trial, which were published in NEJM in June 2016.
The trial enrolled 326 adult patients with relapsed or refractory B-cell ALL and compared inotuzumab ozogamicin to standard of care chemotherapy.
The rate of complete remission, including incomplete hematologic recovery, was 80.7% in the inotuzumab ozogamicin arm and 29.4% in the chemotherapy arm (P<0.001). The median duration of remission was 4.6 months and 3.1 months, respectively (P=0.03).
Forty-one percent of patients treated with inotuzumab ozogamicin and 11% of those who received chemotherapy proceeded to stem cell transplant directly after treatment (P<0.001).
The median progression-free survival was 5.0 months in the inotuzumab ozogamicin arm and 1.8 months in the chemotherapy arm (P<0.001).
The median overall survival was 7.7 months and 6.7 months, respectively (P=0.04). This did not meet the prespecified boundary of significance (P=0.0208).
Liver-related adverse events were more common in the inotuzumab ozogamicin arm than the chemotherapy arm. The most frequent of these were increased aspartate aminotransferase level (20% vs 10%), hyperbilirubinemia (15% vs 10%), and increased alanine aminotransferase level (14% vs 11%).
Veno-occlusive liver disease occurred in 11% of patients in the inotuzumab ozogamicin arm and 1% in the chemotherapy arm.
There were 17 deaths during treatment in the inotuzumab ozogamicin arm and 11 in the chemotherapy arm. Four deaths were considered related to inotuzumab ozogamicin, and 2 were thought to be related to chemotherapy. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of inotuzumab ozogamicin (Besponsa®).
The CHMP is recommending approval of inotuzumab ozogamicin for the treatment of adults with relapsed or refractory CD22-positive B-cell precursor acute lymphoblastic leukemia (ALL), including patients with Philadelphia chromosome-positive ALL who have failed treatment with at least one tyrosine kinase inhibitor.
The CHMP’s opinion will be reviewed by the European Commission, which is expected to issue a decision on approval within 67 days from adoption of the opinion.
Inotuzumab ozogamicin is an antibody-drug conjugate that consists of a monoclonal antibody targeting CD22 and a cytotoxic agent known as calicheamicin.
The product originates from a collaboration between Pfizer and Celltech (now UCB), but Pfizer has sole responsibility for all manufacturing and clinical development activities.
The application for inotuzumab ozogamicin is supported by results from a phase 3 trial, which were published in NEJM in June 2016.
The trial enrolled 326 adult patients with relapsed or refractory B-cell ALL and compared inotuzumab ozogamicin to standard of care chemotherapy.
The rate of complete remission, including incomplete hematologic recovery, was 80.7% in the inotuzumab ozogamicin arm and 29.4% in the chemotherapy arm (P<0.001). The median duration of remission was 4.6 months and 3.1 months, respectively (P=0.03).
Forty-one percent of patients treated with inotuzumab ozogamicin and 11% of those who received chemotherapy proceeded to stem cell transplant directly after treatment (P<0.001).
The median progression-free survival was 5.0 months in the inotuzumab ozogamicin arm and 1.8 months in the chemotherapy arm (P<0.001).
The median overall survival was 7.7 months and 6.7 months, respectively (P=0.04). This did not meet the prespecified boundary of significance (P=0.0208).
Liver-related adverse events were more common in the inotuzumab ozogamicin arm than the chemotherapy arm. The most frequent of these were increased aspartate aminotransferase level (20% vs 10%), hyperbilirubinemia (15% vs 10%), and increased alanine aminotransferase level (14% vs 11%).
Veno-occlusive liver disease occurred in 11% of patients in the inotuzumab ozogamicin arm and 1% in the chemotherapy arm.
There were 17 deaths during treatment in the inotuzumab ozogamicin arm and 11 in the chemotherapy arm. Four deaths were considered related to inotuzumab ozogamicin, and 2 were thought to be related to chemotherapy. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of inotuzumab ozogamicin (Besponsa®).
The CHMP is recommending approval of inotuzumab ozogamicin for the treatment of adults with relapsed or refractory CD22-positive B-cell precursor acute lymphoblastic leukemia (ALL), including patients with Philadelphia chromosome-positive ALL who have failed treatment with at least one tyrosine kinase inhibitor.
The CHMP’s opinion will be reviewed by the European Commission, which is expected to issue a decision on approval within 67 days from adoption of the opinion.
Inotuzumab ozogamicin is an antibody-drug conjugate that consists of a monoclonal antibody targeting CD22 and a cytotoxic agent known as calicheamicin.
The product originates from a collaboration between Pfizer and Celltech (now UCB), but Pfizer has sole responsibility for all manufacturing and clinical development activities.
The application for inotuzumab ozogamicin is supported by results from a phase 3 trial, which were published in NEJM in June 2016.
The trial enrolled 326 adult patients with relapsed or refractory B-cell ALL and compared inotuzumab ozogamicin to standard of care chemotherapy.
The rate of complete remission, including incomplete hematologic recovery, was 80.7% in the inotuzumab ozogamicin arm and 29.4% in the chemotherapy arm (P<0.001). The median duration of remission was 4.6 months and 3.1 months, respectively (P=0.03).
Forty-one percent of patients treated with inotuzumab ozogamicin and 11% of those who received chemotherapy proceeded to stem cell transplant directly after treatment (P<0.001).
The median progression-free survival was 5.0 months in the inotuzumab ozogamicin arm and 1.8 months in the chemotherapy arm (P<0.001).
The median overall survival was 7.7 months and 6.7 months, respectively (P=0.04). This did not meet the prespecified boundary of significance (P=0.0208).
Liver-related adverse events were more common in the inotuzumab ozogamicin arm than the chemotherapy arm. The most frequent of these were increased aspartate aminotransferase level (20% vs 10%), hyperbilirubinemia (15% vs 10%), and increased alanine aminotransferase level (14% vs 11%).
Veno-occlusive liver disease occurred in 11% of patients in the inotuzumab ozogamicin arm and 1% in the chemotherapy arm.
There were 17 deaths during treatment in the inotuzumab ozogamicin arm and 11 in the chemotherapy arm. Four deaths were considered related to inotuzumab ozogamicin, and 2 were thought to be related to chemotherapy. ![]()
Elimination of urine culture screening prior to elective joint arthroplasty
Clinical question: What is the clinical impact of implementing a policy to no longer process urine specimens for perioperative screening in patients undergoing elective joint arthroplasty (EJA)?
Background: Despite prior studies indicating the lack of clinical benefit, preoperative urine cultures are still frequently obtained in patients undergoing EJA in attempts to reduce the risk of periprosthetic joint infections (PJI).
Study Design: Time series analysis.
Setting: Holland Orthopedic and Arthritic Center (HOAC) of Sunnybrook Health Sciences Centre.
Synopsis: After a multidisciplinary meeting, obtaining routine urine culture screening was removed from the preoperative order set. A time series analysis was performed to review the frequency of screening urine cultures obtained and processed, the number of patients treated for asymptomatic bacteriuria (ASB), and the incidence of PJI before and after the new policy was implemented. After the policy change, only 129 screening urine cultures were obtained prior to 1,891 EJAs (7 per 100 EJA; 95% CI 6-8; P less than .0001) which is a drastic decrease from the 3,069 screening urine cultures obtained prior to 3,523 EJAs (87 per 100 EJA; 95% CI, 86-88) before the policy change. Prior to the policy change, of the 352 positive urine cultures, 43 received perioperative treatment for ASB, and PJI incidence was 1/3523 (0.03%; 95% CI, 0.001-02). After the policy change, no perioperative antibiotics were prescribed for ASB, and PJI rate did not significantly change at 3/1891 (0.2%; 95% CI, 0.05-0.5; P = .1).
The study was limited by its low power to detect for small differences in rates because of its small PJI rate occurrence.
Bottom Line: A multidisciplinary approach in eliminating routine urine screening prior to EJA resulted in a decrease of urine cultures obtained and a decrease in treatment for asymptomatic bacteriuria, with no significant change in PJI rate. This change in clinical practice is supported by current evidence and has a significant impact on cost savings.
References: Lamb MJ, Baillie L, Pajak D, et al. “Elimination of Screening Urine Cultures Prior to Elective Joint Arthroplasty.”
Dr. Libot is assistant professor in the division of hospital medicine, Loyola University Chicago, Maywood, Ill.
Clinical question: What is the clinical impact of implementing a policy to no longer process urine specimens for perioperative screening in patients undergoing elective joint arthroplasty (EJA)?
Background: Despite prior studies indicating the lack of clinical benefit, preoperative urine cultures are still frequently obtained in patients undergoing EJA in attempts to reduce the risk of periprosthetic joint infections (PJI).
Study Design: Time series analysis.
Setting: Holland Orthopedic and Arthritic Center (HOAC) of Sunnybrook Health Sciences Centre.
Synopsis: After a multidisciplinary meeting, obtaining routine urine culture screening was removed from the preoperative order set. A time series analysis was performed to review the frequency of screening urine cultures obtained and processed, the number of patients treated for asymptomatic bacteriuria (ASB), and the incidence of PJI before and after the new policy was implemented. After the policy change, only 129 screening urine cultures were obtained prior to 1,891 EJAs (7 per 100 EJA; 95% CI 6-8; P less than .0001) which is a drastic decrease from the 3,069 screening urine cultures obtained prior to 3,523 EJAs (87 per 100 EJA; 95% CI, 86-88) before the policy change. Prior to the policy change, of the 352 positive urine cultures, 43 received perioperative treatment for ASB, and PJI incidence was 1/3523 (0.03%; 95% CI, 0.001-02). After the policy change, no perioperative antibiotics were prescribed for ASB, and PJI rate did not significantly change at 3/1891 (0.2%; 95% CI, 0.05-0.5; P = .1).
The study was limited by its low power to detect for small differences in rates because of its small PJI rate occurrence.
Bottom Line: A multidisciplinary approach in eliminating routine urine screening prior to EJA resulted in a decrease of urine cultures obtained and a decrease in treatment for asymptomatic bacteriuria, with no significant change in PJI rate. This change in clinical practice is supported by current evidence and has a significant impact on cost savings.
References: Lamb MJ, Baillie L, Pajak D, et al. “Elimination of Screening Urine Cultures Prior to Elective Joint Arthroplasty.”
Dr. Libot is assistant professor in the division of hospital medicine, Loyola University Chicago, Maywood, Ill.
Clinical question: What is the clinical impact of implementing a policy to no longer process urine specimens for perioperative screening in patients undergoing elective joint arthroplasty (EJA)?
Background: Despite prior studies indicating the lack of clinical benefit, preoperative urine cultures are still frequently obtained in patients undergoing EJA in attempts to reduce the risk of periprosthetic joint infections (PJI).
Study Design: Time series analysis.
Setting: Holland Orthopedic and Arthritic Center (HOAC) of Sunnybrook Health Sciences Centre.
Synopsis: After a multidisciplinary meeting, obtaining routine urine culture screening was removed from the preoperative order set. A time series analysis was performed to review the frequency of screening urine cultures obtained and processed, the number of patients treated for asymptomatic bacteriuria (ASB), and the incidence of PJI before and after the new policy was implemented. After the policy change, only 129 screening urine cultures were obtained prior to 1,891 EJAs (7 per 100 EJA; 95% CI 6-8; P less than .0001) which is a drastic decrease from the 3,069 screening urine cultures obtained prior to 3,523 EJAs (87 per 100 EJA; 95% CI, 86-88) before the policy change. Prior to the policy change, of the 352 positive urine cultures, 43 received perioperative treatment for ASB, and PJI incidence was 1/3523 (0.03%; 95% CI, 0.001-02). After the policy change, no perioperative antibiotics were prescribed for ASB, and PJI rate did not significantly change at 3/1891 (0.2%; 95% CI, 0.05-0.5; P = .1).
The study was limited by its low power to detect for small differences in rates because of its small PJI rate occurrence.
Bottom Line: A multidisciplinary approach in eliminating routine urine screening prior to EJA resulted in a decrease of urine cultures obtained and a decrease in treatment for asymptomatic bacteriuria, with no significant change in PJI rate. This change in clinical practice is supported by current evidence and has a significant impact on cost savings.
References: Lamb MJ, Baillie L, Pajak D, et al. “Elimination of Screening Urine Cultures Prior to Elective Joint Arthroplasty.”
Dr. Libot is assistant professor in the division of hospital medicine, Loyola University Chicago, Maywood, Ill.
In the lit: Short takes
Efficacy of ketorolac is similar at all the most commonly administered doses
A randomized, double-blind trial of IV ketorolac dosing found similar analgesic efficacy in patients aged 18-65 years with moderate to severe pain at the commonly ordered doses of 10 mg, 15 mg, and 30 mg with no increase in adverse effects.
Citation: Motov S, Yasavolian M, Likourezos A, et al. “Comparison of intravenous ketorolac at three single-dose regimens for treating acute pain in the emergency department: A randomized controlled trial.” Ann Emerg Med. 2016 Dec 16. doi: org/10.1016/j.annemergmed.2016.10.014.
-- Paula Marfia, MD, is assistant professor in the Division of Hospital Medicine, Loyola University Chicago, Maywood, Ill.
Viruses are common cause of nonventilated, hospital-acquired pneumonia

Retrospective analysis demonstrates that viruses are common etiology for nonventilated hospital-acquired pneumonia (NVHAP), as common as bacterial organisms. Clinicians should consider testing for viral etiologies in NVHAP in an effort to improve antibiotic stewardship.
Citation: Shorr AF, Zilberberg MD, Micek ST, Kollef MH. “Viruses are prevalent in non-ventilated hospital-acquired pneumonia.” Respir Med. 2017;122:76-80.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
FDA issues important safety precautions for use of implantable infusions pumps in MRI
Serious adverse events, including patient injury and death, have been reported with the use of implantable infusion pumps in the MRI environment. The Food and Drug Administration has issued a safety communication for patients, caregivers, health care providers, and MRI technologists, outlining safety precautions and recommendations.
Citation: “Implantable Infusion Pumps in the Magnetic Resonance (MR) Environment: FDA Safety Communication – Important Safety Precautions.” FDA.gov. 2017 Jan 11.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
Efficacy of ketorolac is similar at all the most commonly administered doses
A randomized, double-blind trial of IV ketorolac dosing found similar analgesic efficacy in patients aged 18-65 years with moderate to severe pain at the commonly ordered doses of 10 mg, 15 mg, and 30 mg with no increase in adverse effects.
Citation: Motov S, Yasavolian M, Likourezos A, et al. “Comparison of intravenous ketorolac at three single-dose regimens for treating acute pain in the emergency department: A randomized controlled trial.” Ann Emerg Med. 2016 Dec 16. doi: org/10.1016/j.annemergmed.2016.10.014.
-- Paula Marfia, MD, is assistant professor in the Division of Hospital Medicine, Loyola University Chicago, Maywood, Ill.
Viruses are common cause of nonventilated, hospital-acquired pneumonia
Retrospective analysis demonstrates that viruses are common etiology for nonventilated hospital-acquired pneumonia (NVHAP), as common as bacterial organisms. Clinicians should consider testing for viral etiologies in NVHAP in an effort to improve antibiotic stewardship.
Citation: Shorr AF, Zilberberg MD, Micek ST, Kollef MH. “Viruses are prevalent in non-ventilated hospital-acquired pneumonia.” Respir Med. 2017;122:76-80.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
FDA issues important safety precautions for use of implantable infusions pumps in MRI
Serious adverse events, including patient injury and death, have been reported with the use of implantable infusion pumps in the MRI environment. The Food and Drug Administration has issued a safety communication for patients, caregivers, health care providers, and MRI technologists, outlining safety precautions and recommendations.
Citation: “Implantable Infusion Pumps in the Magnetic Resonance (MR) Environment: FDA Safety Communication – Important Safety Precautions.” FDA.gov. 2017 Jan 11.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
Efficacy of ketorolac is similar at all the most commonly administered doses
A randomized, double-blind trial of IV ketorolac dosing found similar analgesic efficacy in patients aged 18-65 years with moderate to severe pain at the commonly ordered doses of 10 mg, 15 mg, and 30 mg with no increase in adverse effects.
Citation: Motov S, Yasavolian M, Likourezos A, et al. “Comparison of intravenous ketorolac at three single-dose regimens for treating acute pain in the emergency department: A randomized controlled trial.” Ann Emerg Med. 2016 Dec 16. doi: org/10.1016/j.annemergmed.2016.10.014.
-- Paula Marfia, MD, is assistant professor in the Division of Hospital Medicine, Loyola University Chicago, Maywood, Ill.
Viruses are common cause of nonventilated, hospital-acquired pneumonia
Retrospective analysis demonstrates that viruses are common etiology for nonventilated hospital-acquired pneumonia (NVHAP), as common as bacterial organisms. Clinicians should consider testing for viral etiologies in NVHAP in an effort to improve antibiotic stewardship.
Citation: Shorr AF, Zilberberg MD, Micek ST, Kollef MH. “Viruses are prevalent in non-ventilated hospital-acquired pneumonia.” Respir Med. 2017;122:76-80.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
FDA issues important safety precautions for use of implantable infusions pumps in MRI
Serious adverse events, including patient injury and death, have been reported with the use of implantable infusion pumps in the MRI environment. The Food and Drug Administration has issued a safety communication for patients, caregivers, health care providers, and MRI technologists, outlining safety precautions and recommendations.
Citation: “Implantable Infusion Pumps in the Magnetic Resonance (MR) Environment: FDA Safety Communication – Important Safety Precautions.” FDA.gov. 2017 Jan 11.
-- Anar Mashruwala, MD, FACP, is assistant professor in the Department of Medicine, Division of Hospital Medicine at Loyola University Medical Center, Maywood, Ill.
WHO report sets baseline for viral hepatitis elimination
AMSTERDAM – An estimated 328 million people worldwide were living with chronic hepatitis B or C virus infection in 2015 according to a new report issued by the World Health Organization and launched at the International Liver Congress sponsored by the European Association for the Study of the Liver (EASL).
The WHO Global Hepatitis Report gives the worldwide prevalence of chronic hepatitis B (HBV) infection as 257 million and that of chronic hepatitis C (HCV) infection as 71 million at this time point, reported Yvan Hutin, MD, medical officer at the WHO Department of HIV and Global Hepatitis Programme (HIV/GHP) in Geneva.

Dr. Hutin explained that the report was needed as it sets the baseline or “year zero” for tracking the success of WHO’s new global health sector strategy on viral hepatitis, which aims to eliminate viral hepatitis as a public health threat, reduce the number of new HBV and HCV infections by 90%, and reduce viral hepatitis mortality by 65% by 2030.
The report was “a very important statement for all of us who work in this field,” said EASL Vice-Secretary Tom Hemming Karslen, MD, during a press briefing. “This is a wonderful initiative helping all the activities that are now already ongoing and need to be strengthened to move in a coordinated manner.”
The launch of the report at the International Liver Congress was “win-win situation”, Gottfried Hirnschall, MD, director of the WHO Department of HIV/GHP, said at the press briefing.
“We are in the era of elimination. It is not only the commitment of the WHO, it is the commitment of the 194 member states who have signed up for elimination,” he said.
“An important message is that people are still dying of hepatitis, the numbers are still going up,” Dr. Hirnschall said. There were an estimated 1.34 million viral hepatitis deaths worldwide in 2015, most (95%) were due to the development of cirrhosis or hepatocellular carcinoma, according to the new report. “We have a public health issue that obviously still needs to be addressed.”
Three decades ago, little could be done to prevent or treat infection with HBV or HCV, Dr. Hutin said during the opening general scientific session. A lot has changed since then, prevention of hepatitis B started to become a reality with the availability of a vaccine and understanding of the importance of improved blood safety and injection practices. Since 2010, there have also been improvements in the drugs available to treat, and potentially eliminate, HCV, notably direct-acting antiviral agents.
“To reach elimination, we modeled that we needed to reach sufficient service coverage for five core interventions,” Dr. Hutin said. Specifically:
- At least 90% of the world’s eligible population receives the three-dose hepatitis B vaccine
- 100% of blood donations are screened appropriately
- Proper injection technique is employed in 90% of cases
- Clean needles made available where they are needed
- 90% of people infected are diagnosed and 80% are treated.
Vaccination against HBV has been one success in the past 20 years, Ana Maria Henao Restrepo, MD, medical officer at the WHO Department of Immunization Vaccination and Biologicals, said at the press briefing.
Vaccination against HBV started in 1982, she said, “when the first safe and effective vaccine became available, and now four out of five children receive this life-saving vaccine. We are very pleased with this achievement but we know that there is still more work to do.”
The WHO report estimates that the global incidence of chronic HBV infection in children under 5 years of age was reduced from 4.7% in the pre-vaccination era to 1.3% in 2015 because of immunization.
But while uptake of the three-dose hepatitis B vaccine has increased, with 85% coverage of the worlds population in 2015, the number of children receiving this vaccine at birth is just 39% overall, with lower rates in the African region.
“Unsafe health care injections and injection drug use continue to transmit HCV, particularly in the eastern Mediterranean region and the European region,” Dr. Hutin said.
The WHO has already set up a campaign to improve blood and injection safety called “Get the Point,” but there is still a long way to go. The target is to provide 300 needle and syringe sets per person per year to people who inject drugs; the current rate is around 27 sets.
Of the 257 people infected with hepatitis B in 2015, only 9% were diagnosed and 1.7 million received treatment. As for hepatitis C, 20% of 71 million were diagnosed and 1.1 million received treatment.
“We need a public health approach that delivers all the basic services to all, including to specific groups that may differ from the general population in terms of incidence, prevalence, vulnerability, or needs,” said Dr. Hutin. This includes health care workers, intravenous drug users, prisoners, migrants, blood donors, men who have sex with men, sex workers, and indigenous populations.
“We have all the tools we need to eliminate hepatitis,” he said, adding that improved point of care tests, a functional cure for HBV, and a vaccine against HCV would accelerate the process.
“A year ago, elimination by 2030 looked very ambitious, but not that we’ve carefully looked at the baseline, it seems that we have a start. It’s going to be a lot of work but the train has left the station and we should get there,” Dr. Hutin concluded.
The U.S. Centers for Disease Control and Prevention provided funding for the production of the report. All speakers had no conflicts of interest.
AMSTERDAM – An estimated 328 million people worldwide were living with chronic hepatitis B or C virus infection in 2015 according to a new report issued by the World Health Organization and launched at the International Liver Congress sponsored by the European Association for the Study of the Liver (EASL).
The WHO Global Hepatitis Report gives the worldwide prevalence of chronic hepatitis B (HBV) infection as 257 million and that of chronic hepatitis C (HCV) infection as 71 million at this time point, reported Yvan Hutin, MD, medical officer at the WHO Department of HIV and Global Hepatitis Programme (HIV/GHP) in Geneva.
Dr. Hutin explained that the report was needed as it sets the baseline or “year zero” for tracking the success of WHO’s new global health sector strategy on viral hepatitis, which aims to eliminate viral hepatitis as a public health threat, reduce the number of new HBV and HCV infections by 90%, and reduce viral hepatitis mortality by 65% by 2030.
The report was “a very important statement for all of us who work in this field,” said EASL Vice-Secretary Tom Hemming Karslen, MD, during a press briefing. “This is a wonderful initiative helping all the activities that are now already ongoing and need to be strengthened to move in a coordinated manner.”
The launch of the report at the International Liver Congress was “win-win situation”, Gottfried Hirnschall, MD, director of the WHO Department of HIV/GHP, said at the press briefing.
“We are in the era of elimination. It is not only the commitment of the WHO, it is the commitment of the 194 member states who have signed up for elimination,” he said.
“An important message is that people are still dying of hepatitis, the numbers are still going up,” Dr. Hirnschall said. There were an estimated 1.34 million viral hepatitis deaths worldwide in 2015, most (95%) were due to the development of cirrhosis or hepatocellular carcinoma, according to the new report. “We have a public health issue that obviously still needs to be addressed.”
Three decades ago, little could be done to prevent or treat infection with HBV or HCV, Dr. Hutin said during the opening general scientific session. A lot has changed since then, prevention of hepatitis B started to become a reality with the availability of a vaccine and understanding of the importance of improved blood safety and injection practices. Since 2010, there have also been improvements in the drugs available to treat, and potentially eliminate, HCV, notably direct-acting antiviral agents.
“To reach elimination, we modeled that we needed to reach sufficient service coverage for five core interventions,” Dr. Hutin said. Specifically:
- At least 90% of the world’s eligible population receives the three-dose hepatitis B vaccine
- 100% of blood donations are screened appropriately
- Proper injection technique is employed in 90% of cases
- Clean needles made available where they are needed
- 90% of people infected are diagnosed and 80% are treated.
Vaccination against HBV has been one success in the past 20 years, Ana Maria Henao Restrepo, MD, medical officer at the WHO Department of Immunization Vaccination and Biologicals, said at the press briefing.
Vaccination against HBV started in 1982, she said, “when the first safe and effective vaccine became available, and now four out of five children receive this life-saving vaccine. We are very pleased with this achievement but we know that there is still more work to do.”
The WHO report estimates that the global incidence of chronic HBV infection in children under 5 years of age was reduced from 4.7% in the pre-vaccination era to 1.3% in 2015 because of immunization.
But while uptake of the three-dose hepatitis B vaccine has increased, with 85% coverage of the worlds population in 2015, the number of children receiving this vaccine at birth is just 39% overall, with lower rates in the African region.
“Unsafe health care injections and injection drug use continue to transmit HCV, particularly in the eastern Mediterranean region and the European region,” Dr. Hutin said.
The WHO has already set up a campaign to improve blood and injection safety called “Get the Point,” but there is still a long way to go. The target is to provide 300 needle and syringe sets per person per year to people who inject drugs; the current rate is around 27 sets.
Of the 257 people infected with hepatitis B in 2015, only 9% were diagnosed and 1.7 million received treatment. As for hepatitis C, 20% of 71 million were diagnosed and 1.1 million received treatment.
“We need a public health approach that delivers all the basic services to all, including to specific groups that may differ from the general population in terms of incidence, prevalence, vulnerability, or needs,” said Dr. Hutin. This includes health care workers, intravenous drug users, prisoners, migrants, blood donors, men who have sex with men, sex workers, and indigenous populations.
“We have all the tools we need to eliminate hepatitis,” he said, adding that improved point of care tests, a functional cure for HBV, and a vaccine against HCV would accelerate the process.
“A year ago, elimination by 2030 looked very ambitious, but not that we’ve carefully looked at the baseline, it seems that we have a start. It’s going to be a lot of work but the train has left the station and we should get there,” Dr. Hutin concluded.
The U.S. Centers for Disease Control and Prevention provided funding for the production of the report. All speakers had no conflicts of interest.
AMSTERDAM – An estimated 328 million people worldwide were living with chronic hepatitis B or C virus infection in 2015 according to a new report issued by the World Health Organization and launched at the International Liver Congress sponsored by the European Association for the Study of the Liver (EASL).
The WHO Global Hepatitis Report gives the worldwide prevalence of chronic hepatitis B (HBV) infection as 257 million and that of chronic hepatitis C (HCV) infection as 71 million at this time point, reported Yvan Hutin, MD, medical officer at the WHO Department of HIV and Global Hepatitis Programme (HIV/GHP) in Geneva.
Dr. Hutin explained that the report was needed as it sets the baseline or “year zero” for tracking the success of WHO’s new global health sector strategy on viral hepatitis, which aims to eliminate viral hepatitis as a public health threat, reduce the number of new HBV and HCV infections by 90%, and reduce viral hepatitis mortality by 65% by 2030.
The report was “a very important statement for all of us who work in this field,” said EASL Vice-Secretary Tom Hemming Karslen, MD, during a press briefing. “This is a wonderful initiative helping all the activities that are now already ongoing and need to be strengthened to move in a coordinated manner.”
The launch of the report at the International Liver Congress was “win-win situation”, Gottfried Hirnschall, MD, director of the WHO Department of HIV/GHP, said at the press briefing.
“We are in the era of elimination. It is not only the commitment of the WHO, it is the commitment of the 194 member states who have signed up for elimination,” he said.
“An important message is that people are still dying of hepatitis, the numbers are still going up,” Dr. Hirnschall said. There were an estimated 1.34 million viral hepatitis deaths worldwide in 2015, most (95%) were due to the development of cirrhosis or hepatocellular carcinoma, according to the new report. “We have a public health issue that obviously still needs to be addressed.”
Three decades ago, little could be done to prevent or treat infection with HBV or HCV, Dr. Hutin said during the opening general scientific session. A lot has changed since then, prevention of hepatitis B started to become a reality with the availability of a vaccine and understanding of the importance of improved blood safety and injection practices. Since 2010, there have also been improvements in the drugs available to treat, and potentially eliminate, HCV, notably direct-acting antiviral agents.
“To reach elimination, we modeled that we needed to reach sufficient service coverage for five core interventions,” Dr. Hutin said. Specifically:
- At least 90% of the world’s eligible population receives the three-dose hepatitis B vaccine
- 100% of blood donations are screened appropriately
- Proper injection technique is employed in 90% of cases
- Clean needles made available where they are needed
- 90% of people infected are diagnosed and 80% are treated.
Vaccination against HBV has been one success in the past 20 years, Ana Maria Henao Restrepo, MD, medical officer at the WHO Department of Immunization Vaccination and Biologicals, said at the press briefing.
Vaccination against HBV started in 1982, she said, “when the first safe and effective vaccine became available, and now four out of five children receive this life-saving vaccine. We are very pleased with this achievement but we know that there is still more work to do.”
The WHO report estimates that the global incidence of chronic HBV infection in children under 5 years of age was reduced from 4.7% in the pre-vaccination era to 1.3% in 2015 because of immunization.
But while uptake of the three-dose hepatitis B vaccine has increased, with 85% coverage of the worlds population in 2015, the number of children receiving this vaccine at birth is just 39% overall, with lower rates in the African region.
“Unsafe health care injections and injection drug use continue to transmit HCV, particularly in the eastern Mediterranean region and the European region,” Dr. Hutin said.
The WHO has already set up a campaign to improve blood and injection safety called “Get the Point,” but there is still a long way to go. The target is to provide 300 needle and syringe sets per person per year to people who inject drugs; the current rate is around 27 sets.
Of the 257 people infected with hepatitis B in 2015, only 9% were diagnosed and 1.7 million received treatment. As for hepatitis C, 20% of 71 million were diagnosed and 1.1 million received treatment.
“We need a public health approach that delivers all the basic services to all, including to specific groups that may differ from the general population in terms of incidence, prevalence, vulnerability, or needs,” said Dr. Hutin. This includes health care workers, intravenous drug users, prisoners, migrants, blood donors, men who have sex with men, sex workers, and indigenous populations.
“We have all the tools we need to eliminate hepatitis,” he said, adding that improved point of care tests, a functional cure for HBV, and a vaccine against HCV would accelerate the process.
“A year ago, elimination by 2030 looked very ambitious, but not that we’ve carefully looked at the baseline, it seems that we have a start. It’s going to be a lot of work but the train has left the station and we should get there,” Dr. Hutin concluded.
The U.S. Centers for Disease Control and Prevention provided funding for the production of the report. All speakers had no conflicts of interest.
AT ILC 2017