User login
High readmits after peripheral arterial procedures
WASHINGTON – More than one in six patients who undergo a lower extremity arterial endovascular or surgical procedure are readmitted within 30 days, according to a large national study.
The annual total cost of these early readmissions is high, in excess of $360 million. But because there turned out to be surprisingly little difference in readmission rates between hospitals, 30-day readmissions may not be a rational quality measure on which to base institutional reimbursement or withholding of payment for peripheral arterial interventions, Eric A. Secemsky, MD, said at the annual meeting of the American College of Cardiology.

Forty-seven percent of patients had an endovascular procedure, 42% had surgery, and the remainder had hybrid procedures in which both endovascular and surgical interventions took place during the same admission. Patients with hybrid procedures contributed data to both treatment groups.
In-hospital mortality occurred in 2.5% of patients.
Of the patients who survived to discharge, 21,589, or 17.4%, were readmitted within 30 days. The early readmission rate was higher following endovascular procedures, at 18.7%, than the 16.1% rate in the surgical group. The average cost of a readmission was $15,876. Death during readmission occurred in 4.2% of patients.
The median rate ratio – a measure of the amount of variance in readmission rates between hospitals – was 1.12. That’s a low figure.
“If the median rate ratio is lower, like here, it says there’s not a lot of interhospital variability across the country. So overall this burden seems to be pretty uniform across the institutions included in our analysis,” Dr. Secemsky explained.
This observation drew the attention of session comoderator Naomi M. Hamburg, MD.
“It’s interesting that you didn’t see a lot of heterogeneity across hospitals, because we often think of readmissions as a potentially modifiable quality metric. Do you think it’s modifiable, or is this just the nature of the disease?” asked Dr. Hamburg of Boston Medical Center.
It’s the disease process, Dr. Secemsky replied.
“We were surprised by the lack of hospital variation,” he added. None of the institutional characteristics examined, including teaching hospital status, bed size, and procedural volume, had a significant impact on readmission rates.
But that doesn’t mean there aren’t opportunities to whittle down those readmissions, according to Dr. Secemsky.
He noted that the high readmission rates were driven by procedural complications such as graft or stent failure. Indeed, procedural complications accounted for 29% of all early readmissions. The procedural complication rate was about 20% following endovascular procedures and 39% after surgery. It’s likely that identification and implementation of best practices could trim those high rates. Unfortunately, however, the nationwide database relies upon ICD-9 codes, which don’t provide the granular level of detail required to home in on specific best practices. That will require further studies, according to Dr. Secemsky.
A distant second on the list of causes of early readmission was peripheral atherosclerosis, meaning persistent claudication or rest pain. This accounted for 8.8% of readmissions. Rounding out the top five causes of readmission were sepsis, which was the reason for 6.7% of readmissions; diabetes with complications, at 4.7%; and heart failure, at 4.6%.
The strongest predictors of readmission included having renal disease at baseline, Medicare rather than private insurance, and discharge to a subacute nursing facility or home with home care.
Dr. Hamburg commented that a focus on reducing readmissions for sepsis as well as for skin and soft tissue infections, which accounted for 2.1% of 30-day hospitalizations, could be fruitful.
Dr. Secemsky reported having no financial conflicts regarding his study.
WASHINGTON – More than one in six patients who undergo a lower extremity arterial endovascular or surgical procedure are readmitted within 30 days, according to a large national study.
The annual total cost of these early readmissions is high, in excess of $360 million. But because there turned out to be surprisingly little difference in readmission rates between hospitals, 30-day readmissions may not be a rational quality measure on which to base institutional reimbursement or withholding of payment for peripheral arterial interventions, Eric A. Secemsky, MD, said at the annual meeting of the American College of Cardiology.
Forty-seven percent of patients had an endovascular procedure, 42% had surgery, and the remainder had hybrid procedures in which both endovascular and surgical interventions took place during the same admission. Patients with hybrid procedures contributed data to both treatment groups.
In-hospital mortality occurred in 2.5% of patients.
Of the patients who survived to discharge, 21,589, or 17.4%, were readmitted within 30 days. The early readmission rate was higher following endovascular procedures, at 18.7%, than the 16.1% rate in the surgical group. The average cost of a readmission was $15,876. Death during readmission occurred in 4.2% of patients.
The median rate ratio – a measure of the amount of variance in readmission rates between hospitals – was 1.12. That’s a low figure.
“If the median rate ratio is lower, like here, it says there’s not a lot of interhospital variability across the country. So overall this burden seems to be pretty uniform across the institutions included in our analysis,” Dr. Secemsky explained.
This observation drew the attention of session comoderator Naomi M. Hamburg, MD.
“It’s interesting that you didn’t see a lot of heterogeneity across hospitals, because we often think of readmissions as a potentially modifiable quality metric. Do you think it’s modifiable, or is this just the nature of the disease?” asked Dr. Hamburg of Boston Medical Center.
It’s the disease process, Dr. Secemsky replied.
“We were surprised by the lack of hospital variation,” he added. None of the institutional characteristics examined, including teaching hospital status, bed size, and procedural volume, had a significant impact on readmission rates.
But that doesn’t mean there aren’t opportunities to whittle down those readmissions, according to Dr. Secemsky.
He noted that the high readmission rates were driven by procedural complications such as graft or stent failure. Indeed, procedural complications accounted for 29% of all early readmissions. The procedural complication rate was about 20% following endovascular procedures and 39% after surgery. It’s likely that identification and implementation of best practices could trim those high rates. Unfortunately, however, the nationwide database relies upon ICD-9 codes, which don’t provide the granular level of detail required to home in on specific best practices. That will require further studies, according to Dr. Secemsky.
A distant second on the list of causes of early readmission was peripheral atherosclerosis, meaning persistent claudication or rest pain. This accounted for 8.8% of readmissions. Rounding out the top five causes of readmission were sepsis, which was the reason for 6.7% of readmissions; diabetes with complications, at 4.7%; and heart failure, at 4.6%.
The strongest predictors of readmission included having renal disease at baseline, Medicare rather than private insurance, and discharge to a subacute nursing facility or home with home care.
Dr. Hamburg commented that a focus on reducing readmissions for sepsis as well as for skin and soft tissue infections, which accounted for 2.1% of 30-day hospitalizations, could be fruitful.
Dr. Secemsky reported having no financial conflicts regarding his study.
WASHINGTON – More than one in six patients who undergo a lower extremity arterial endovascular or surgical procedure are readmitted within 30 days, according to a large national study.
The annual total cost of these early readmissions is high, in excess of $360 million. But because there turned out to be surprisingly little difference in readmission rates between hospitals, 30-day readmissions may not be a rational quality measure on which to base institutional reimbursement or withholding of payment for peripheral arterial interventions, Eric A. Secemsky, MD, said at the annual meeting of the American College of Cardiology.
Forty-seven percent of patients had an endovascular procedure, 42% had surgery, and the remainder had hybrid procedures in which both endovascular and surgical interventions took place during the same admission. Patients with hybrid procedures contributed data to both treatment groups.
In-hospital mortality occurred in 2.5% of patients.
Of the patients who survived to discharge, 21,589, or 17.4%, were readmitted within 30 days. The early readmission rate was higher following endovascular procedures, at 18.7%, than the 16.1% rate in the surgical group. The average cost of a readmission was $15,876. Death during readmission occurred in 4.2% of patients.
The median rate ratio – a measure of the amount of variance in readmission rates between hospitals – was 1.12. That’s a low figure.
“If the median rate ratio is lower, like here, it says there’s not a lot of interhospital variability across the country. So overall this burden seems to be pretty uniform across the institutions included in our analysis,” Dr. Secemsky explained.
This observation drew the attention of session comoderator Naomi M. Hamburg, MD.
“It’s interesting that you didn’t see a lot of heterogeneity across hospitals, because we often think of readmissions as a potentially modifiable quality metric. Do you think it’s modifiable, or is this just the nature of the disease?” asked Dr. Hamburg of Boston Medical Center.
It’s the disease process, Dr. Secemsky replied.
“We were surprised by the lack of hospital variation,” he added. None of the institutional characteristics examined, including teaching hospital status, bed size, and procedural volume, had a significant impact on readmission rates.
But that doesn’t mean there aren’t opportunities to whittle down those readmissions, according to Dr. Secemsky.
He noted that the high readmission rates were driven by procedural complications such as graft or stent failure. Indeed, procedural complications accounted for 29% of all early readmissions. The procedural complication rate was about 20% following endovascular procedures and 39% after surgery. It’s likely that identification and implementation of best practices could trim those high rates. Unfortunately, however, the nationwide database relies upon ICD-9 codes, which don’t provide the granular level of detail required to home in on specific best practices. That will require further studies, according to Dr. Secemsky.
A distant second on the list of causes of early readmission was peripheral atherosclerosis, meaning persistent claudication or rest pain. This accounted for 8.8% of readmissions. Rounding out the top five causes of readmission were sepsis, which was the reason for 6.7% of readmissions; diabetes with complications, at 4.7%; and heart failure, at 4.6%.
The strongest predictors of readmission included having renal disease at baseline, Medicare rather than private insurance, and discharge to a subacute nursing facility or home with home care.
Dr. Hamburg commented that a focus on reducing readmissions for sepsis as well as for skin and soft tissue infections, which accounted for 2.1% of 30-day hospitalizations, could be fruitful.
Dr. Secemsky reported having no financial conflicts regarding his study.
AT ACC 2017
Key clinical point:
Major finding: Readmission within 30 days after a peripheral arterial procedure occurred nationally in 17.4% of patients, with little between-hospital variation in rates.
Data source: A retrospective analysis of nearly 124,000 hospital admissions for lower extremity arterial endovascular or surgical procedures.
Disclosures: The study presenter reported having no financial conflicts of interest.
Drugmakers Dramatically Boosted Lobbying Spending In Trump’s First Quarter
Eight pharmaceutical companies more than doubled their lobbying spending in the first three months of 2017, when the Affordable Care Act was on the chopping block and high drug prices were clearly in the crosshairs of Congress and President Donald Trump.
Congressional records show that those eight, including Celgene and Mylan, kicked in an extra $4.42 million versus that quarter last year. Industry giant Teva Pharmaceutical Industries spent $2.67 million, up 115% from a year ago as several companies embroiled in controversies raised their outlays significantly.
“It’s certainly a rare event” when lobbying dollars double, noted Timothy LaPira, PhD, an associate professor of political science at James Madison University. “These spikes are usually timed when Congress in particular is going to be really hammering home on a particular issue. Right now, that’s health care and taxes.”
Trump has come down hard on drugmakers, stating in a press conference before his inauguration that the industry is “getting away with murder.” He has promised to lower drug prices and increase competition with faster approvals and fewer regulations. Sen. Bernie Sanders (I-Vt.), Sen. John McCain (R-Ariz.), and Rep. Elijah E. Cummings (D-Md.) have introduced bills to allow lower-cost drug imports from Canada or other countries.
Lobbyists weren’t expecting much by way of big policy changes during the comparatively sleepy end of the Obama administration this time last year, but, with a surprise Trump administration and a Republican-controlled House and Senate, trade groups and companies are probably “going all in,” Dr. LaPira said.
Thirty-eight major drugmakers and trade groups spent a total of $50.9 million, up $10.1 million from the first quarter of last year, according to a Kaiser Health News analysis. They deployed 600 lobbyists in all.
PhRMA, the drug industry’s largest trade group, spent $7.98 million during the quarter – more than in any single quarter in almost a decade, congressional records show, topping even its quarterly lobbying ahead of the Affordable Care Act’s passage in 2010.
In their congressional disclosures, companies listed Medicare price negotiation, the American Health Care Act, drug importation, and the orphan drug program as issues they were lobbying for or against. They do not have to disclose on which side of an issue they lobbied.
When Medicare prices are on the table, it should come as no surprise that pharmaceutical companies are interested in influencing congress.
“It’s quite literally hitting their bottom line,” LaPira said.
Drugmakers, under fire, more than doubled their lobbying dollars. Mylan spent $1.45 million during the quarter, up from $610,000 last year. The company’s CEO faced a congressional hearing in the fall when it raised the price of EpiPen to over $600.
Marathon Pharmaceuticals spent $230,000, which was $120,000 more than last year. Marathon was criticized in February after setting the price of Emflaza, a steroid to treat Duchenne muscular dystrophy, at $89,000 a year. That angered advocates, Congress, and patients who had been importing the same drug for as little as $1,000 a year. Marathon has since sold the drug to another company, and the price may come down.
Teva and Shire also more than doubled their spending. Teva was accused, as part of an alleged generic price-fixing scheme in December, and the Federal Trade Commission sued Shire because one of its recently acquired companies allegedly filed “sham” petitions with the Food and Drug Administration to stave off generics.
Companies that make drugs for rare diseases also more than doubled lobbying dollars as congressional leaders and the Government Accountability Office work to determine whether the Orphan Drug Act is being abused. Those firms include BioMarin, Celgene, and Vertex Pharmaceuticals. Celgene, which makes a rare cancer drug, more than tripled its first quarter lobbying to more than $1 million.
Despite efforts to make good on campaign promises to repeal the Affordable Care Act, House Republicans canceled a floor vote on the American Health Care Act in March after multiple studies estimated that millions of people would lose coverage if it passed, and neither Democrats nor ultraconservatives lined up in opposition to the bill’s provisions. Drug prices weren’t a key part of the package.
KHN’s coverage of prescription drug development, costs, and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Eight pharmaceutical companies more than doubled their lobbying spending in the first three months of 2017, when the Affordable Care Act was on the chopping block and high drug prices were clearly in the crosshairs of Congress and President Donald Trump.
Congressional records show that those eight, including Celgene and Mylan, kicked in an extra $4.42 million versus that quarter last year. Industry giant Teva Pharmaceutical Industries spent $2.67 million, up 115% from a year ago as several companies embroiled in controversies raised their outlays significantly.
“It’s certainly a rare event” when lobbying dollars double, noted Timothy LaPira, PhD, an associate professor of political science at James Madison University. “These spikes are usually timed when Congress in particular is going to be really hammering home on a particular issue. Right now, that’s health care and taxes.”
Trump has come down hard on drugmakers, stating in a press conference before his inauguration that the industry is “getting away with murder.” He has promised to lower drug prices and increase competition with faster approvals and fewer regulations. Sen. Bernie Sanders (I-Vt.), Sen. John McCain (R-Ariz.), and Rep. Elijah E. Cummings (D-Md.) have introduced bills to allow lower-cost drug imports from Canada or other countries.
Lobbyists weren’t expecting much by way of big policy changes during the comparatively sleepy end of the Obama administration this time last year, but, with a surprise Trump administration and a Republican-controlled House and Senate, trade groups and companies are probably “going all in,” Dr. LaPira said.
Thirty-eight major drugmakers and trade groups spent a total of $50.9 million, up $10.1 million from the first quarter of last year, according to a Kaiser Health News analysis. They deployed 600 lobbyists in all.
PhRMA, the drug industry’s largest trade group, spent $7.98 million during the quarter – more than in any single quarter in almost a decade, congressional records show, topping even its quarterly lobbying ahead of the Affordable Care Act’s passage in 2010.
In their congressional disclosures, companies listed Medicare price negotiation, the American Health Care Act, drug importation, and the orphan drug program as issues they were lobbying for or against. They do not have to disclose on which side of an issue they lobbied.
When Medicare prices are on the table, it should come as no surprise that pharmaceutical companies are interested in influencing congress.
“It’s quite literally hitting their bottom line,” LaPira said.
Drugmakers, under fire, more than doubled their lobbying dollars. Mylan spent $1.45 million during the quarter, up from $610,000 last year. The company’s CEO faced a congressional hearing in the fall when it raised the price of EpiPen to over $600.
Marathon Pharmaceuticals spent $230,000, which was $120,000 more than last year. Marathon was criticized in February after setting the price of Emflaza, a steroid to treat Duchenne muscular dystrophy, at $89,000 a year. That angered advocates, Congress, and patients who had been importing the same drug for as little as $1,000 a year. Marathon has since sold the drug to another company, and the price may come down.
Teva and Shire also more than doubled their spending. Teva was accused, as part of an alleged generic price-fixing scheme in December, and the Federal Trade Commission sued Shire because one of its recently acquired companies allegedly filed “sham” petitions with the Food and Drug Administration to stave off generics.
Companies that make drugs for rare diseases also more than doubled lobbying dollars as congressional leaders and the Government Accountability Office work to determine whether the Orphan Drug Act is being abused. Those firms include BioMarin, Celgene, and Vertex Pharmaceuticals. Celgene, which makes a rare cancer drug, more than tripled its first quarter lobbying to more than $1 million.
Despite efforts to make good on campaign promises to repeal the Affordable Care Act, House Republicans canceled a floor vote on the American Health Care Act in March after multiple studies estimated that millions of people would lose coverage if it passed, and neither Democrats nor ultraconservatives lined up in opposition to the bill’s provisions. Drug prices weren’t a key part of the package.
KHN’s coverage of prescription drug development, costs, and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Eight pharmaceutical companies more than doubled their lobbying spending in the first three months of 2017, when the Affordable Care Act was on the chopping block and high drug prices were clearly in the crosshairs of Congress and President Donald Trump.
Congressional records show that those eight, including Celgene and Mylan, kicked in an extra $4.42 million versus that quarter last year. Industry giant Teva Pharmaceutical Industries spent $2.67 million, up 115% from a year ago as several companies embroiled in controversies raised their outlays significantly.
“It’s certainly a rare event” when lobbying dollars double, noted Timothy LaPira, PhD, an associate professor of political science at James Madison University. “These spikes are usually timed when Congress in particular is going to be really hammering home on a particular issue. Right now, that’s health care and taxes.”
Trump has come down hard on drugmakers, stating in a press conference before his inauguration that the industry is “getting away with murder.” He has promised to lower drug prices and increase competition with faster approvals and fewer regulations. Sen. Bernie Sanders (I-Vt.), Sen. John McCain (R-Ariz.), and Rep. Elijah E. Cummings (D-Md.) have introduced bills to allow lower-cost drug imports from Canada or other countries.
Lobbyists weren’t expecting much by way of big policy changes during the comparatively sleepy end of the Obama administration this time last year, but, with a surprise Trump administration and a Republican-controlled House and Senate, trade groups and companies are probably “going all in,” Dr. LaPira said.
Thirty-eight major drugmakers and trade groups spent a total of $50.9 million, up $10.1 million from the first quarter of last year, according to a Kaiser Health News analysis. They deployed 600 lobbyists in all.
PhRMA, the drug industry’s largest trade group, spent $7.98 million during the quarter – more than in any single quarter in almost a decade, congressional records show, topping even its quarterly lobbying ahead of the Affordable Care Act’s passage in 2010.
In their congressional disclosures, companies listed Medicare price negotiation, the American Health Care Act, drug importation, and the orphan drug program as issues they were lobbying for or against. They do not have to disclose on which side of an issue they lobbied.
When Medicare prices are on the table, it should come as no surprise that pharmaceutical companies are interested in influencing congress.
“It’s quite literally hitting their bottom line,” LaPira said.
Drugmakers, under fire, more than doubled their lobbying dollars. Mylan spent $1.45 million during the quarter, up from $610,000 last year. The company’s CEO faced a congressional hearing in the fall when it raised the price of EpiPen to over $600.
Marathon Pharmaceuticals spent $230,000, which was $120,000 more than last year. Marathon was criticized in February after setting the price of Emflaza, a steroid to treat Duchenne muscular dystrophy, at $89,000 a year. That angered advocates, Congress, and patients who had been importing the same drug for as little as $1,000 a year. Marathon has since sold the drug to another company, and the price may come down.
Teva and Shire also more than doubled their spending. Teva was accused, as part of an alleged generic price-fixing scheme in December, and the Federal Trade Commission sued Shire because one of its recently acquired companies allegedly filed “sham” petitions with the Food and Drug Administration to stave off generics.
Companies that make drugs for rare diseases also more than doubled lobbying dollars as congressional leaders and the Government Accountability Office work to determine whether the Orphan Drug Act is being abused. Those firms include BioMarin, Celgene, and Vertex Pharmaceuticals. Celgene, which makes a rare cancer drug, more than tripled its first quarter lobbying to more than $1 million.
Despite efforts to make good on campaign promises to repeal the Affordable Care Act, House Republicans canceled a floor vote on the American Health Care Act in March after multiple studies estimated that millions of people would lose coverage if it passed, and neither Democrats nor ultraconservatives lined up in opposition to the bill’s provisions. Drug prices weren’t a key part of the package.
KHN’s coverage of prescription drug development, costs, and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Targeted drugs transform CLL management
NEW YORK – New, targeted treatments, especially ibrutinib (Imbruvica), have sharply shifted prognosis for patients with chronic lymphocytic leukemia (CLL) and raised new issues for managing these patients now that they survive years longer.
“Ibrutinib has produced a profound change in survival” of patients with CLL, Timothy G. Call, MD, a hematologist/oncologist at the Mayo Clinic in Rochester, Minn., said at a conference held by Imedex. It “has changed the playing field.” No other new agent so far “has produced the same level of progression-free survival in CLL.”

An analysis published in early 2017 projected a greater than 50% jump in U.S. patients living with CLL from 2011, before the advent of targeted oral drugs, to 2025, when the study predicted that there will be nearly 200,000 U.S. patients living with CLL (J Clin Oncol. 2017 January;35[2]:166-74). With targeted drugs like ibrutinib and idelalisib (Zydelig) costing about $130,000 per patient each year, the projected cost for managing the U.S. CLL population is on track to rise to more than $5 billion by 2025, a nearly sixfold increase, compared with CLL patient expenditures in 2011, according to this analysis.
The impact of the higher cost of treatment is already being felt more acutely by many patients because of recent cuts in assistance from the Patient Access Network, which helps patients with copays but recently had to put a lid on CLL assistance availability when its funding availability hit a wall, Dr. Call said.
On the clinical side, there are new considerations triggered by greater patient longevity. “As we make patients live longer with CLL, we need to double down on the diagnosis and treatment of its complications,” such as watching for development of secondary cancers, Dr. Call said in an interview. This stems from the reduced immunosurveillance in patients with CLL and their resulting increased susceptibility to developing environmentally-triggered malignancies like lung and skin cancers. Other long-term implications of impaired immunosurveillance include increased infection susceptibility, an ongoing risk for Richter’s or Hodgkin lymphoma transformation, and a risk for autoimmune complications, such as red blood cell aplasia and transfusion-associated graft versus host disease.
Patients with CLL can also be susceptible to complications from long-term use of the targeted drug they’re on. The new targeted agents can trigger bruising and bleeding, diarrhea, rash, fatigue, muscle and joint aches, and arrhythmia, he noted.
Potential adverse effects, specifically from ibrutinib, include a 3% risk for a major bleed, a 10% rate of new-onset atrial fibrillation, and a 20% risk for new hypertension, Dr. Call said. Before starting ibrutinib, patients should undergo screening for hepatitis B virus infection and receive prophylaxis against herpes zoster activation with acyclovir or valacyclovir. If the patient starts with a CD4 cell count below 200 cells/mm3, it might be prudent to prophylax the patient against Pneumocystis jirovecii pneumonia.
However, even if a toxicity develops on ibrutinib, Dr. Call recommended reducing the dosage rather than discontinuing the drug. “I rarely see a loss in response from a reduced dosage of ibrutinib,” he said.
Because ibrutinib is primarily metabolized via the liver enzyme cytochrome P450 3A (CYP3A), other drugs that enhance or reduce the activity of this enzyme produce significant changes in ibrutinib levels. The Food and Drug Administration considers ibrutinib a “sensitive substrate” for fluctuations in CYP3A activity. Strong CYP3A inhibitors include clarithromycin, ketoconazole, and various anti-HIV medications; moderate CYP3A4 inhibitors include ciprofloxacin, and verapamil; and inducers of CYP3A include phenytoin and rifampin. A more complete list of the drugs that inhibit or induce CYP3A activity can be found at the FDA website: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm#table2-2.
Dr. Call presented the combined experience from several U.S. Mayo Clinic centers for 118 patients treated with ibrutinib after the drug received FDA marketing approval in November 2013. The clinicians identified 75 patients (64%) who were on a concurrent medication that could potentially increase the risk for ibrutinib toxicity and 4 patients (3%) who were on a concurrent drug with the potential to reduce ibrutinib efficacy (Leukemia Lymphoma, 2017;58[6]:1376-83).
“We don’t change the dosage of ibrutinib when the patient is on a CYP3A inducer, but, if the patient is getting a CYP3A inhibitor, we change that to another drug or reduce the ibrutinib dosage,” Dr. Call said.
Dr. Call had no disclosures.
[email protected]
On Twitter @mitchelzoler
NEW YORK – New, targeted treatments, especially ibrutinib (Imbruvica), have sharply shifted prognosis for patients with chronic lymphocytic leukemia (CLL) and raised new issues for managing these patients now that they survive years longer.
“Ibrutinib has produced a profound change in survival” of patients with CLL, Timothy G. Call, MD, a hematologist/oncologist at the Mayo Clinic in Rochester, Minn., said at a conference held by Imedex. It “has changed the playing field.” No other new agent so far “has produced the same level of progression-free survival in CLL.”
An analysis published in early 2017 projected a greater than 50% jump in U.S. patients living with CLL from 2011, before the advent of targeted oral drugs, to 2025, when the study predicted that there will be nearly 200,000 U.S. patients living with CLL (J Clin Oncol. 2017 January;35[2]:166-74). With targeted drugs like ibrutinib and idelalisib (Zydelig) costing about $130,000 per patient each year, the projected cost for managing the U.S. CLL population is on track to rise to more than $5 billion by 2025, a nearly sixfold increase, compared with CLL patient expenditures in 2011, according to this analysis.
The impact of the higher cost of treatment is already being felt more acutely by many patients because of recent cuts in assistance from the Patient Access Network, which helps patients with copays but recently had to put a lid on CLL assistance availability when its funding availability hit a wall, Dr. Call said.
On the clinical side, there are new considerations triggered by greater patient longevity. “As we make patients live longer with CLL, we need to double down on the diagnosis and treatment of its complications,” such as watching for development of secondary cancers, Dr. Call said in an interview. This stems from the reduced immunosurveillance in patients with CLL and their resulting increased susceptibility to developing environmentally-triggered malignancies like lung and skin cancers. Other long-term implications of impaired immunosurveillance include increased infection susceptibility, an ongoing risk for Richter’s or Hodgkin lymphoma transformation, and a risk for autoimmune complications, such as red blood cell aplasia and transfusion-associated graft versus host disease.
Patients with CLL can also be susceptible to complications from long-term use of the targeted drug they’re on. The new targeted agents can trigger bruising and bleeding, diarrhea, rash, fatigue, muscle and joint aches, and arrhythmia, he noted.
Potential adverse effects, specifically from ibrutinib, include a 3% risk for a major bleed, a 10% rate of new-onset atrial fibrillation, and a 20% risk for new hypertension, Dr. Call said. Before starting ibrutinib, patients should undergo screening for hepatitis B virus infection and receive prophylaxis against herpes zoster activation with acyclovir or valacyclovir. If the patient starts with a CD4 cell count below 200 cells/mm3, it might be prudent to prophylax the patient against Pneumocystis jirovecii pneumonia.
However, even if a toxicity develops on ibrutinib, Dr. Call recommended reducing the dosage rather than discontinuing the drug. “I rarely see a loss in response from a reduced dosage of ibrutinib,” he said.
Because ibrutinib is primarily metabolized via the liver enzyme cytochrome P450 3A (CYP3A), other drugs that enhance or reduce the activity of this enzyme produce significant changes in ibrutinib levels. The Food and Drug Administration considers ibrutinib a “sensitive substrate” for fluctuations in CYP3A activity. Strong CYP3A inhibitors include clarithromycin, ketoconazole, and various anti-HIV medications; moderate CYP3A4 inhibitors include ciprofloxacin, and verapamil; and inducers of CYP3A include phenytoin and rifampin. A more complete list of the drugs that inhibit or induce CYP3A activity can be found at the FDA website: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm#table2-2.
Dr. Call presented the combined experience from several U.S. Mayo Clinic centers for 118 patients treated with ibrutinib after the drug received FDA marketing approval in November 2013. The clinicians identified 75 patients (64%) who were on a concurrent medication that could potentially increase the risk for ibrutinib toxicity and 4 patients (3%) who were on a concurrent drug with the potential to reduce ibrutinib efficacy (Leukemia Lymphoma, 2017;58[6]:1376-83).
“We don’t change the dosage of ibrutinib when the patient is on a CYP3A inducer, but, if the patient is getting a CYP3A inhibitor, we change that to another drug or reduce the ibrutinib dosage,” Dr. Call said.
Dr. Call had no disclosures.
[email protected]
On Twitter @mitchelzoler
NEW YORK – New, targeted treatments, especially ibrutinib (Imbruvica), have sharply shifted prognosis for patients with chronic lymphocytic leukemia (CLL) and raised new issues for managing these patients now that they survive years longer.
“Ibrutinib has produced a profound change in survival” of patients with CLL, Timothy G. Call, MD, a hematologist/oncologist at the Mayo Clinic in Rochester, Minn., said at a conference held by Imedex. It “has changed the playing field.” No other new agent so far “has produced the same level of progression-free survival in CLL.”
An analysis published in early 2017 projected a greater than 50% jump in U.S. patients living with CLL from 2011, before the advent of targeted oral drugs, to 2025, when the study predicted that there will be nearly 200,000 U.S. patients living with CLL (J Clin Oncol. 2017 January;35[2]:166-74). With targeted drugs like ibrutinib and idelalisib (Zydelig) costing about $130,000 per patient each year, the projected cost for managing the U.S. CLL population is on track to rise to more than $5 billion by 2025, a nearly sixfold increase, compared with CLL patient expenditures in 2011, according to this analysis.
The impact of the higher cost of treatment is already being felt more acutely by many patients because of recent cuts in assistance from the Patient Access Network, which helps patients with copays but recently had to put a lid on CLL assistance availability when its funding availability hit a wall, Dr. Call said.
On the clinical side, there are new considerations triggered by greater patient longevity. “As we make patients live longer with CLL, we need to double down on the diagnosis and treatment of its complications,” such as watching for development of secondary cancers, Dr. Call said in an interview. This stems from the reduced immunosurveillance in patients with CLL and their resulting increased susceptibility to developing environmentally-triggered malignancies like lung and skin cancers. Other long-term implications of impaired immunosurveillance include increased infection susceptibility, an ongoing risk for Richter’s or Hodgkin lymphoma transformation, and a risk for autoimmune complications, such as red blood cell aplasia and transfusion-associated graft versus host disease.
Patients with CLL can also be susceptible to complications from long-term use of the targeted drug they’re on. The new targeted agents can trigger bruising and bleeding, diarrhea, rash, fatigue, muscle and joint aches, and arrhythmia, he noted.
Potential adverse effects, specifically from ibrutinib, include a 3% risk for a major bleed, a 10% rate of new-onset atrial fibrillation, and a 20% risk for new hypertension, Dr. Call said. Before starting ibrutinib, patients should undergo screening for hepatitis B virus infection and receive prophylaxis against herpes zoster activation with acyclovir or valacyclovir. If the patient starts with a CD4 cell count below 200 cells/mm3, it might be prudent to prophylax the patient against Pneumocystis jirovecii pneumonia.
However, even if a toxicity develops on ibrutinib, Dr. Call recommended reducing the dosage rather than discontinuing the drug. “I rarely see a loss in response from a reduced dosage of ibrutinib,” he said.
Because ibrutinib is primarily metabolized via the liver enzyme cytochrome P450 3A (CYP3A), other drugs that enhance or reduce the activity of this enzyme produce significant changes in ibrutinib levels. The Food and Drug Administration considers ibrutinib a “sensitive substrate” for fluctuations in CYP3A activity. Strong CYP3A inhibitors include clarithromycin, ketoconazole, and various anti-HIV medications; moderate CYP3A4 inhibitors include ciprofloxacin, and verapamil; and inducers of CYP3A include phenytoin and rifampin. A more complete list of the drugs that inhibit or induce CYP3A activity can be found at the FDA website: https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm#table2-2.
Dr. Call presented the combined experience from several U.S. Mayo Clinic centers for 118 patients treated with ibrutinib after the drug received FDA marketing approval in November 2013. The clinicians identified 75 patients (64%) who were on a concurrent medication that could potentially increase the risk for ibrutinib toxicity and 4 patients (3%) who were on a concurrent drug with the potential to reduce ibrutinib efficacy (Leukemia Lymphoma, 2017;58[6]:1376-83).
“We don’t change the dosage of ibrutinib when the patient is on a CYP3A inducer, but, if the patient is getting a CYP3A inhibitor, we change that to another drug or reduce the ibrutinib dosage,” Dr. Call said.
Dr. Call had no disclosures.
[email protected]
On Twitter @mitchelzoler
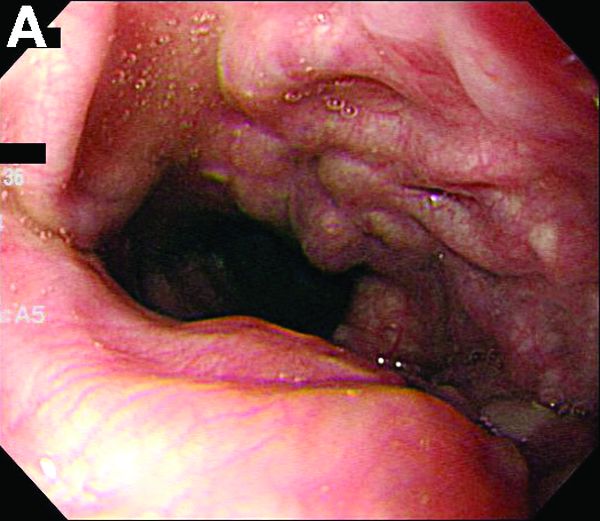
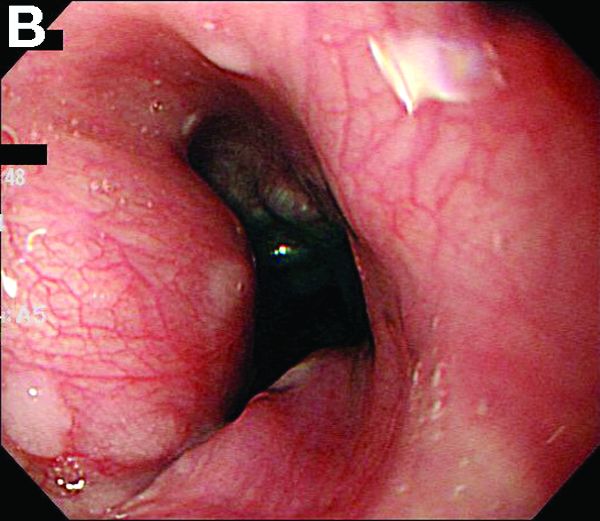
Clinical Challenges - May 2017 What's Your Diagnosis?
What's Your Diagnosis?
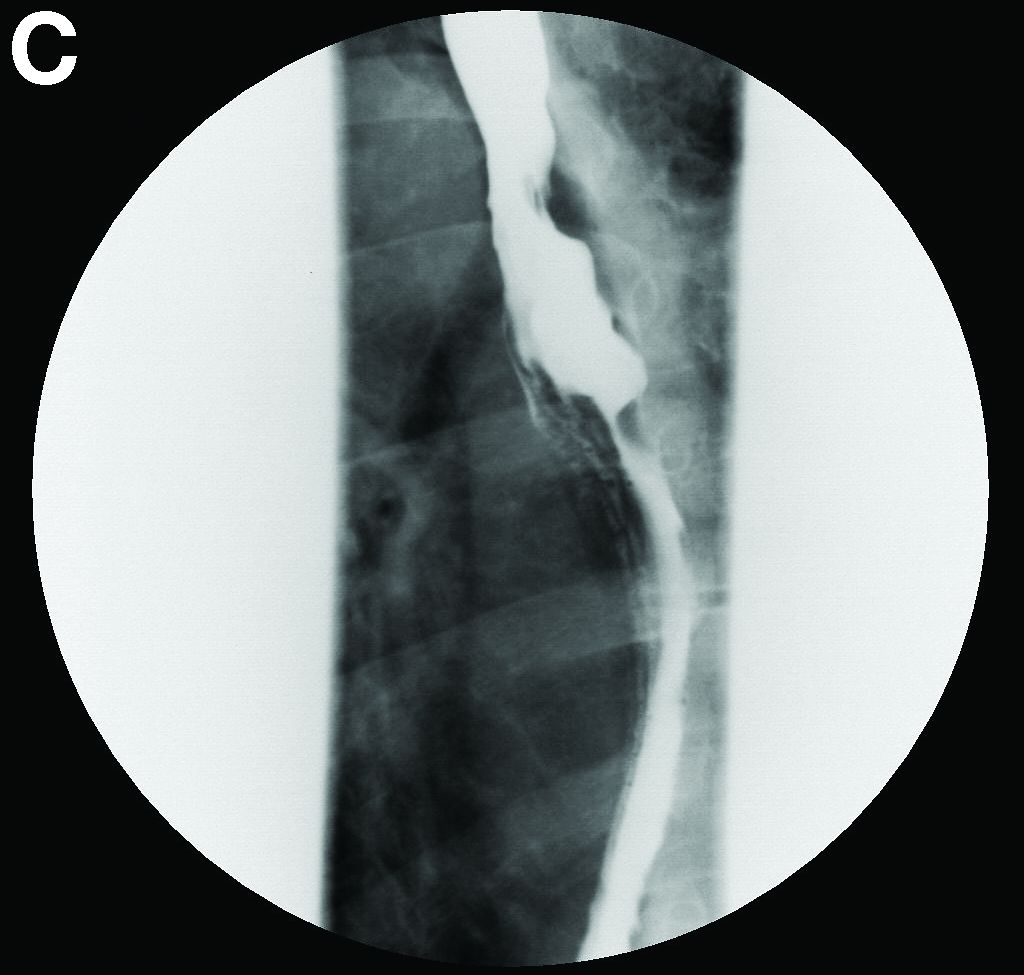
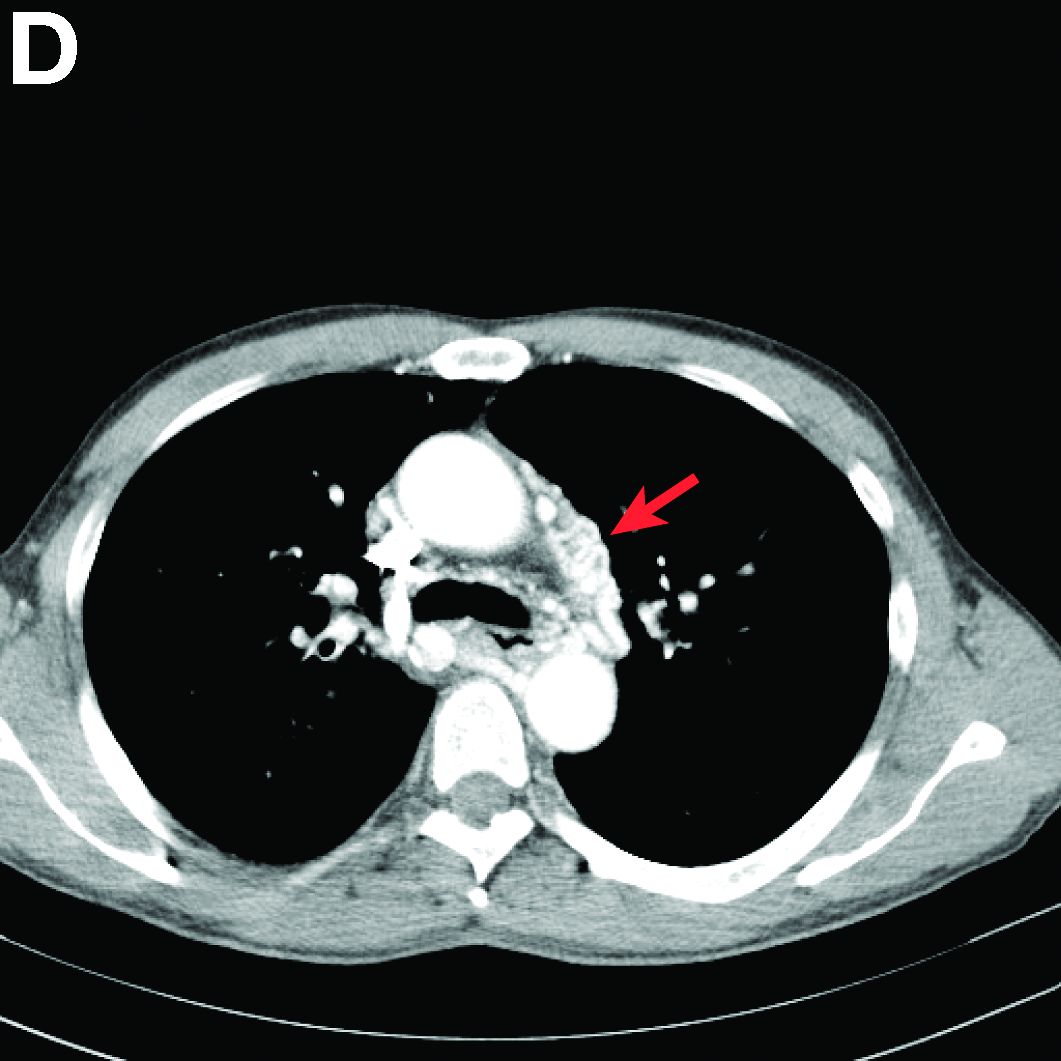
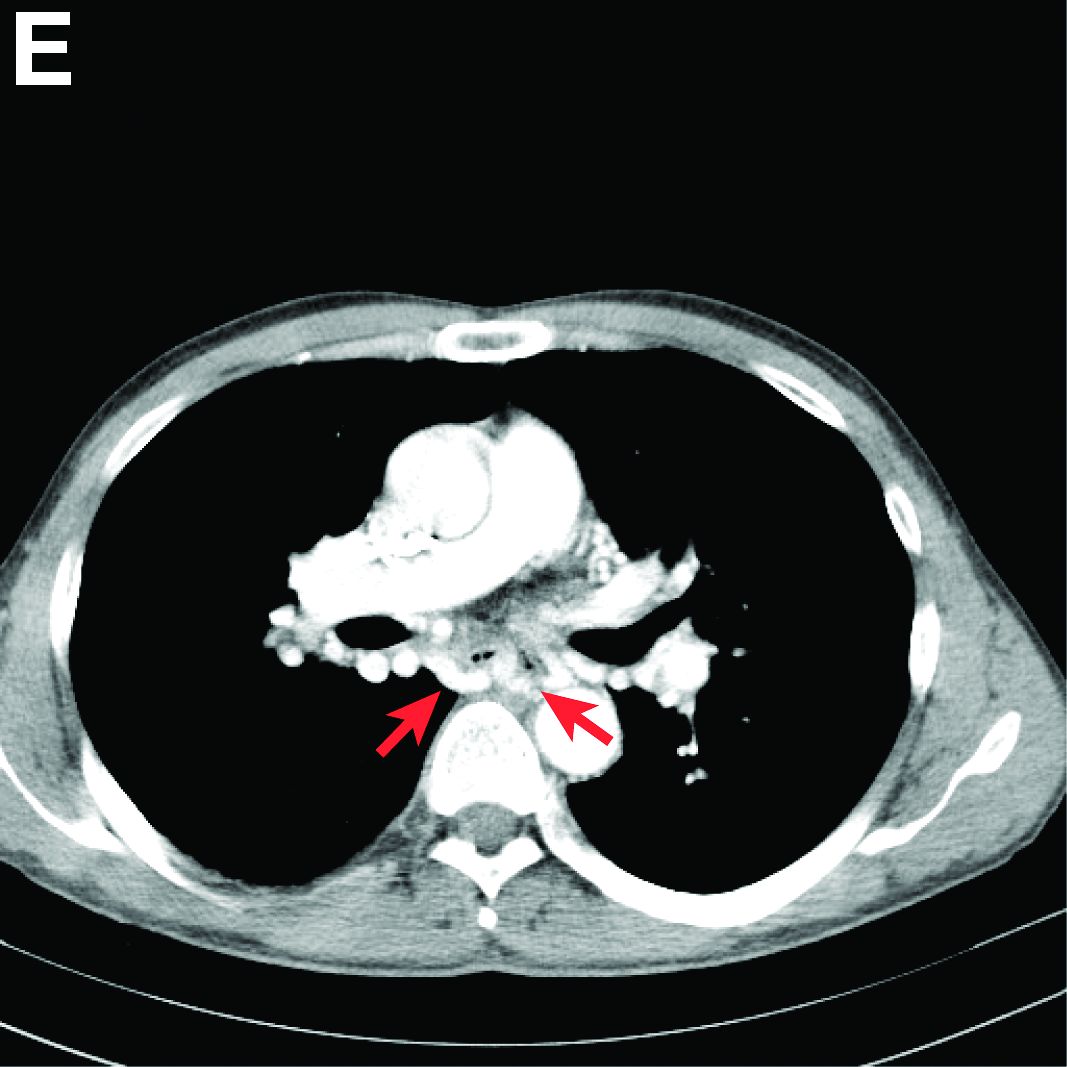
Answer to “What’s your diagnosis?” on page 2: Arteriovenous fistulas arising from the subclavian and coronary arteries
We performed aortography along with coronary angiography to find the feeding vessels for the vascular bundle (). There was an arteriovenous fistula that arose from the left subclavian artery, ran over the left mediastinum with the complex plexus, and emptied into the venous system of the left thorax. Multiple coronary artery fistulas originated in the left coronary artery, traversed the left and right mediastinum, and eventually emptied into the venous system of the mediastinum. The left anterior oblique view revealed a coronary artery fistula that arose from the distal right coronary artery and drained into the venous system of the thorax. In transthoracic echocardiography, the sizes of the left atrium and left ventricle were mildly dilated, but left ventricular systolic functions were preserved with an ejection fraction of 61%. We recommended surgery to the patient, but he refused invasive treatment. He will be followed with close observation.
A coronary artery fistula is usually of congenital origin, and connects a major coronary artery directly with the cardiac chamber, coronary sinus, superior vena cava, or pulmonary artery. However, its connection with a systemic venous system is extremely rare. Congenital subclavian arteriovenous fistulas are rare because they usually occur as a complication of previous trauma, percutaneous catheterization, or surgery.1 Complications include “steal” from the adjacent myocardium causing myocardial ischemia, thrombosis/embolism, cardiac failure, atrial fibrillation, rupture, endocarditis/endarteritis, and arrhythmia.2 Treatment options include close medical observation, surgical ligation, and catheter embolization.3
References
1. Brountzos, E.N., Kelekis, N.L., Danassi-Afentaki, D. et al. Congenital subclavian artery-to-subclavian vein fistula in an adult: treatment with transcatheter embolization. Cardiovasc Intervent Radiol. 2004;27:675-7.
2. Wilde, P., Watt, I. Congenital coronary artery fistulae: six new cases with a collective review. Clin Radiol. 1980;31:301-11.
3. Mangukia, C.V. Coronary artery fistula. Ann Thorac Surg. 2012;93:2084-92.
Answer to “What’s your diagnosis?” on page 2: Arteriovenous fistulas arising from the subclavian and coronary arteries
We performed aortography along with coronary angiography to find the feeding vessels for the vascular bundle (). There was an arteriovenous fistula that arose from the left subclavian artery, ran over the left mediastinum with the complex plexus, and emptied into the venous system of the left thorax. Multiple coronary artery fistulas originated in the left coronary artery, traversed the left and right mediastinum, and eventually emptied into the venous system of the mediastinum. The left anterior oblique view revealed a coronary artery fistula that arose from the distal right coronary artery and drained into the venous system of the thorax. In transthoracic echocardiography, the sizes of the left atrium and left ventricle were mildly dilated, but left ventricular systolic functions were preserved with an ejection fraction of 61%. We recommended surgery to the patient, but he refused invasive treatment. He will be followed with close observation.
A coronary artery fistula is usually of congenital origin, and connects a major coronary artery directly with the cardiac chamber, coronary sinus, superior vena cava, or pulmonary artery. However, its connection with a systemic venous system is extremely rare. Congenital subclavian arteriovenous fistulas are rare because they usually occur as a complication of previous trauma, percutaneous catheterization, or surgery.1 Complications include “steal” from the adjacent myocardium causing myocardial ischemia, thrombosis/embolism, cardiac failure, atrial fibrillation, rupture, endocarditis/endarteritis, and arrhythmia.2 Treatment options include close medical observation, surgical ligation, and catheter embolization.3
References
1. Brountzos, E.N., Kelekis, N.L., Danassi-Afentaki, D. et al. Congenital subclavian artery-to-subclavian vein fistula in an adult: treatment with transcatheter embolization. Cardiovasc Intervent Radiol. 2004;27:675-7.
2. Wilde, P., Watt, I. Congenital coronary artery fistulae: six new cases with a collective review. Clin Radiol. 1980;31:301-11.
3. Mangukia, C.V. Coronary artery fistula. Ann Thorac Surg. 2012;93:2084-92.
Answer to “What’s your diagnosis?” on page 2: Arteriovenous fistulas arising from the subclavian and coronary arteries
We performed aortography along with coronary angiography to find the feeding vessels for the vascular bundle (). There was an arteriovenous fistula that arose from the left subclavian artery, ran over the left mediastinum with the complex plexus, and emptied into the venous system of the left thorax. Multiple coronary artery fistulas originated in the left coronary artery, traversed the left and right mediastinum, and eventually emptied into the venous system of the mediastinum. The left anterior oblique view revealed a coronary artery fistula that arose from the distal right coronary artery and drained into the venous system of the thorax. In transthoracic echocardiography, the sizes of the left atrium and left ventricle were mildly dilated, but left ventricular systolic functions were preserved with an ejection fraction of 61%. We recommended surgery to the patient, but he refused invasive treatment. He will be followed with close observation.
A coronary artery fistula is usually of congenital origin, and connects a major coronary artery directly with the cardiac chamber, coronary sinus, superior vena cava, or pulmonary artery. However, its connection with a systemic venous system is extremely rare. Congenital subclavian arteriovenous fistulas are rare because they usually occur as a complication of previous trauma, percutaneous catheterization, or surgery.1 Complications include “steal” from the adjacent myocardium causing myocardial ischemia, thrombosis/embolism, cardiac failure, atrial fibrillation, rupture, endocarditis/endarteritis, and arrhythmia.2 Treatment options include close medical observation, surgical ligation, and catheter embolization.3
References
1. Brountzos, E.N., Kelekis, N.L., Danassi-Afentaki, D. et al. Congenital subclavian artery-to-subclavian vein fistula in an adult: treatment with transcatheter embolization. Cardiovasc Intervent Radiol. 2004;27:675-7.
2. Wilde, P., Watt, I. Congenital coronary artery fistulae: six new cases with a collective review. Clin Radiol. 1980;31:301-11.
3. Mangukia, C.V. Coronary artery fistula. Ann Thorac Surg. 2012;93:2084-92.
What's Your Diagnosis?
What's Your Diagnosis?
What’s your diagnosis?
By Ki-Hyun Ryu, MD, Tae-Hee Lee, MD, and Taek-Geun Kwon, MD. Published previously in Gastroenterology (2013;144;35, 253).
Reflectance confocal microscopy offers one-stop solution for BCC
For selected patients with basal cell carcinoma, one-stop shopping – diagnosing, subtyping, and excising the lesion all in one visit – using reflectance confocal microscopy was found noninferior to the standard approach of obtaining a punch biopsy to diagnose and subtype the lesion in one visit and performing surgical excision in a separate visit.
Those were the findings of an open-label, randomized, noninferiority trial in the Netherlands comparing the two approaches in 95 adults with suspected basal cell carcinoma (BCC), investigators reported.
In addition to reducing the number of visits and the total time required for treatment, this new approach uses noninvasive reflectance confocal microscopy in the place of punch biopsy, which patients will likely prefer, said Daniel J. Kadouch, MD, of the department of dermatology, Academic Medical Center, Amsterdam, and his associates (British J Derm. 2017 Apr 9. doi: 10.1111/bjd.15559).
The study excluded patients who had lesions in a high-risk location of the face, lesions larger than 20 mm, recurrent lesions, and macroscopic ulcerating lesions, as well as patients who had basal cell nevus syndrome. Another 22 patients who were found to have non-BCC lesions (1 melanoma, 2 squamous cell carcinomas, 5 cases of Bowen’s disease, and 11 nonmalignant lesions) also were excluded, leaving 40 patients with BCC in the one-stop shopping group and 33 in the standard of care (control) group.
The primary outcome – the proportion of patients with tumor-free margins on the final pathology report after surgical excision – was 100% (40 of 40) in the one-stop shopping group and 94% (31 of 33) in the control group, which demonstrates the noninferiority of the new, less invasive approach, Dr. Kadouch and his associates said.
The mean total treatment time was 2 hours and 23 minutes for the one-stop shopping group. The total treatment time could not be determined for the control group because their surgical times weren’t recorded.
Adverse events included four postoperative wound infections in the one-stop shopping group, all of which were successfully treated with oral antibiotics, and one case of excessive postoperative bleeding in the control group, which required 3 days of hospitalization.
This study was limited in that it excluded patients with large lesions and those with BCC on high-risk areas of the face, which reduces the generalizability of the findings. In addition, a follow-up time of at least 1 year would be needed to detect signs of BCC recurrence in the study participants, the investigators said.
For selected patients with basal cell carcinoma, one-stop shopping – diagnosing, subtyping, and excising the lesion all in one visit – using reflectance confocal microscopy was found noninferior to the standard approach of obtaining a punch biopsy to diagnose and subtype the lesion in one visit and performing surgical excision in a separate visit.
Those were the findings of an open-label, randomized, noninferiority trial in the Netherlands comparing the two approaches in 95 adults with suspected basal cell carcinoma (BCC), investigators reported.
In addition to reducing the number of visits and the total time required for treatment, this new approach uses noninvasive reflectance confocal microscopy in the place of punch biopsy, which patients will likely prefer, said Daniel J. Kadouch, MD, of the department of dermatology, Academic Medical Center, Amsterdam, and his associates (British J Derm. 2017 Apr 9. doi: 10.1111/bjd.15559).
The study excluded patients who had lesions in a high-risk location of the face, lesions larger than 20 mm, recurrent lesions, and macroscopic ulcerating lesions, as well as patients who had basal cell nevus syndrome. Another 22 patients who were found to have non-BCC lesions (1 melanoma, 2 squamous cell carcinomas, 5 cases of Bowen’s disease, and 11 nonmalignant lesions) also were excluded, leaving 40 patients with BCC in the one-stop shopping group and 33 in the standard of care (control) group.
The primary outcome – the proportion of patients with tumor-free margins on the final pathology report after surgical excision – was 100% (40 of 40) in the one-stop shopping group and 94% (31 of 33) in the control group, which demonstrates the noninferiority of the new, less invasive approach, Dr. Kadouch and his associates said.
The mean total treatment time was 2 hours and 23 minutes for the one-stop shopping group. The total treatment time could not be determined for the control group because their surgical times weren’t recorded.
Adverse events included four postoperative wound infections in the one-stop shopping group, all of which were successfully treated with oral antibiotics, and one case of excessive postoperative bleeding in the control group, which required 3 days of hospitalization.
This study was limited in that it excluded patients with large lesions and those with BCC on high-risk areas of the face, which reduces the generalizability of the findings. In addition, a follow-up time of at least 1 year would be needed to detect signs of BCC recurrence in the study participants, the investigators said.
For selected patients with basal cell carcinoma, one-stop shopping – diagnosing, subtyping, and excising the lesion all in one visit – using reflectance confocal microscopy was found noninferior to the standard approach of obtaining a punch biopsy to diagnose and subtype the lesion in one visit and performing surgical excision in a separate visit.
Those were the findings of an open-label, randomized, noninferiority trial in the Netherlands comparing the two approaches in 95 adults with suspected basal cell carcinoma (BCC), investigators reported.
In addition to reducing the number of visits and the total time required for treatment, this new approach uses noninvasive reflectance confocal microscopy in the place of punch biopsy, which patients will likely prefer, said Daniel J. Kadouch, MD, of the department of dermatology, Academic Medical Center, Amsterdam, and his associates (British J Derm. 2017 Apr 9. doi: 10.1111/bjd.15559).
The study excluded patients who had lesions in a high-risk location of the face, lesions larger than 20 mm, recurrent lesions, and macroscopic ulcerating lesions, as well as patients who had basal cell nevus syndrome. Another 22 patients who were found to have non-BCC lesions (1 melanoma, 2 squamous cell carcinomas, 5 cases of Bowen’s disease, and 11 nonmalignant lesions) also were excluded, leaving 40 patients with BCC in the one-stop shopping group and 33 in the standard of care (control) group.
The primary outcome – the proportion of patients with tumor-free margins on the final pathology report after surgical excision – was 100% (40 of 40) in the one-stop shopping group and 94% (31 of 33) in the control group, which demonstrates the noninferiority of the new, less invasive approach, Dr. Kadouch and his associates said.
The mean total treatment time was 2 hours and 23 minutes for the one-stop shopping group. The total treatment time could not be determined for the control group because their surgical times weren’t recorded.
Adverse events included four postoperative wound infections in the one-stop shopping group, all of which were successfully treated with oral antibiotics, and one case of excessive postoperative bleeding in the control group, which required 3 days of hospitalization.
This study was limited in that it excluded patients with large lesions and those with BCC on high-risk areas of the face, which reduces the generalizability of the findings. In addition, a follow-up time of at least 1 year would be needed to detect signs of BCC recurrence in the study participants, the investigators said.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Key clinical point: For selected patients with BCC, one-stop shopping – diagnosing, subtyping, and excising the lesion all in one visit – using reflectance confocal microscopy was found noninferior to the standard approach using punch biopsy.
Major finding: The percentage of patients with tumor-free margins after surgical excision was 100% (40 of 40) in the one-stop-shopping group and 94% (31 of 33) in the control group.
Data source: An open-label, randomized, controlled, noninferiority trial involving 95 adults.
Disclosures: The study received no outside funding. Dr. Kadouch and his associates reported having no relevant financial disclosures.
Blood donor age, sex do not affect recipient survival
The age and sex of blood donors do not affect the recipient’s survival and do not need to be considered in blood allocation, according to a report published online April 24 in JAMA Internal Medicine.
A recent observational Canadian study suggested that blood from young donors and female donors increased the recipients’ risk of death – a finding which, if confirmed, would have immediate implications for medical practice.
A separate group of Scandinavian researchers attempted to replicate these findings by performing a retrospective cohort study using similar but more nuanced statistical methods. Gustaf Edgren, MD, PhD, of the department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, and his associates analyzed information collected on 968,264 patients over a 10-year period from a Swedish and Danish transfusion database.
In initial, unadjusted analyses, both extremes of age (young and old) and female sex in the donor were associated with reduced survival in the recipient. However, that association disappeared when the data were adjusted to account for the total number of transfusions a patient received, a marker of their severity of illness. The hazard ratio per transfusion from a donor younger than age 20 was 0.98, and the hazard ratio per transfusion from a female donor was 0.99. This pattern also occurred in sensitivity analyses, the investigators noted (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0890).
“When studying associations between ... transfusions with a particular characteristic and the risk of death in the recipient, [the] underlying disease severity ... may still confound the association. However, with meticulous adjustment for total number of transfusions, it should be possible to block the confounding effect of patient disease severity entirely,” they noted.
“We believe that, rather than reflecting true biologic effects, the Canadian results can be explained by residual confounding (i.e., that the observations resulted from incomplete adjustment for the number of transfusions),” Dr. Edgren and his associates said.
“In addition, we believe these data reinforce the importance of extreme caution in assessing epidemiologic analyses in this field, given the tremendous clinical and logistical implications of false-positive findings,” they added.
The findings of Edgren et al. provide reassurance regarding the safety of current transfusion practice.
They present a convincing argument that differences in the statistical approach for controlling confounding likely explained the discrepant results of the Canadian study and their study.
This subtle confounding stems from the fact that increased transfusions expose the recipient to a greater total number of blood products, which in turn is associated with higher comorbidity, greater severity of illness, and higher mortality.
Nareg Roubinian, MD, is at the Blood Systems Research Institute, San Francisco, and in the division of research at Kaiser Permanente Northern California, Oakland. He and his associates reported having no relevant financial disclosures. They made these remarks in an invited commentary accompanying Dr. Edgren’s report (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0914).
The findings of Edgren et al. provide reassurance regarding the safety of current transfusion practice.
They present a convincing argument that differences in the statistical approach for controlling confounding likely explained the discrepant results of the Canadian study and their study.
This subtle confounding stems from the fact that increased transfusions expose the recipient to a greater total number of blood products, which in turn is associated with higher comorbidity, greater severity of illness, and higher mortality.
Nareg Roubinian, MD, is at the Blood Systems Research Institute, San Francisco, and in the division of research at Kaiser Permanente Northern California, Oakland. He and his associates reported having no relevant financial disclosures. They made these remarks in an invited commentary accompanying Dr. Edgren’s report (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0914).
The findings of Edgren et al. provide reassurance regarding the safety of current transfusion practice.
They present a convincing argument that differences in the statistical approach for controlling confounding likely explained the discrepant results of the Canadian study and their study.
This subtle confounding stems from the fact that increased transfusions expose the recipient to a greater total number of blood products, which in turn is associated with higher comorbidity, greater severity of illness, and higher mortality.
Nareg Roubinian, MD, is at the Blood Systems Research Institute, San Francisco, and in the division of research at Kaiser Permanente Northern California, Oakland. He and his associates reported having no relevant financial disclosures. They made these remarks in an invited commentary accompanying Dr. Edgren’s report (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0914).
The age and sex of blood donors do not affect the recipient’s survival and do not need to be considered in blood allocation, according to a report published online April 24 in JAMA Internal Medicine.
A recent observational Canadian study suggested that blood from young donors and female donors increased the recipients’ risk of death – a finding which, if confirmed, would have immediate implications for medical practice.
A separate group of Scandinavian researchers attempted to replicate these findings by performing a retrospective cohort study using similar but more nuanced statistical methods. Gustaf Edgren, MD, PhD, of the department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, and his associates analyzed information collected on 968,264 patients over a 10-year period from a Swedish and Danish transfusion database.
In initial, unadjusted analyses, both extremes of age (young and old) and female sex in the donor were associated with reduced survival in the recipient. However, that association disappeared when the data were adjusted to account for the total number of transfusions a patient received, a marker of their severity of illness. The hazard ratio per transfusion from a donor younger than age 20 was 0.98, and the hazard ratio per transfusion from a female donor was 0.99. This pattern also occurred in sensitivity analyses, the investigators noted (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0890).
“When studying associations between ... transfusions with a particular characteristic and the risk of death in the recipient, [the] underlying disease severity ... may still confound the association. However, with meticulous adjustment for total number of transfusions, it should be possible to block the confounding effect of patient disease severity entirely,” they noted.
“We believe that, rather than reflecting true biologic effects, the Canadian results can be explained by residual confounding (i.e., that the observations resulted from incomplete adjustment for the number of transfusions),” Dr. Edgren and his associates said.
“In addition, we believe these data reinforce the importance of extreme caution in assessing epidemiologic analyses in this field, given the tremendous clinical and logistical implications of false-positive findings,” they added.
The age and sex of blood donors do not affect the recipient’s survival and do not need to be considered in blood allocation, according to a report published online April 24 in JAMA Internal Medicine.
A recent observational Canadian study suggested that blood from young donors and female donors increased the recipients’ risk of death – a finding which, if confirmed, would have immediate implications for medical practice.
A separate group of Scandinavian researchers attempted to replicate these findings by performing a retrospective cohort study using similar but more nuanced statistical methods. Gustaf Edgren, MD, PhD, of the department of medical epidemiology and biostatistics, Karolinska Institutet, Stockholm, and his associates analyzed information collected on 968,264 patients over a 10-year period from a Swedish and Danish transfusion database.
In initial, unadjusted analyses, both extremes of age (young and old) and female sex in the donor were associated with reduced survival in the recipient. However, that association disappeared when the data were adjusted to account for the total number of transfusions a patient received, a marker of their severity of illness. The hazard ratio per transfusion from a donor younger than age 20 was 0.98, and the hazard ratio per transfusion from a female donor was 0.99. This pattern also occurred in sensitivity analyses, the investigators noted (JAMA Intern. Med. 2017 April 24. doi: 10.1001/jamainternmed.2017.0890).
“When studying associations between ... transfusions with a particular characteristic and the risk of death in the recipient, [the] underlying disease severity ... may still confound the association. However, with meticulous adjustment for total number of transfusions, it should be possible to block the confounding effect of patient disease severity entirely,” they noted.
“We believe that, rather than reflecting true biologic effects, the Canadian results can be explained by residual confounding (i.e., that the observations resulted from incomplete adjustment for the number of transfusions),” Dr. Edgren and his associates said.
“In addition, we believe these data reinforce the importance of extreme caution in assessing epidemiologic analyses in this field, given the tremendous clinical and logistical implications of false-positive findings,” they added.
Key clinical point: The age and sex of blood donors do not affect the recipient’s survival and do not need to be considered in blood allocation.
Major finding: The hazard ratio per transfusion from a donor younger than age 20 was 0.98, and the hazard ratio per transfusion from a female donor was 0.99.
Data source: A retrospective cohort study involving 968,264 transfusion recipients in Sweden and Denmark during a 10-year period.
Disclosures: The Swedish Research Council, the Swedish Heart-Lung Foundation, the Swedish Society for Medical Research, Karolinska Institutet’s Strategic Research Program, and the Danish Council for Independent Research supported the study. Dr. Edgren and his associates reported having no relevant financial disclosures.
Make the Diagnosis - May 2017
Dermatitis herpetiformis

The primary lesions of DH are vesicles and papules in a grouped or “herpetic” formation. However, as these lesions are extremely pruritic, the primary lesions may be absent in many cases and instead replaced by secondary excoriations and erosions. DH has a very classic distribution pattern, particularly involving the bilateral extensor surfaces, buttocks, and scalp. Although some cases of oral DH have been reported, mucosal involvement is generally considered to be very rare.
Despite its strong association with underlying celiac disease, most patients with DH do not report any associated gastrointestinal symptoms. Those with DH may present with any variety of other autoimmune conditions, with hypothyroidism being the most common. Interestingly, patients with DH have been shown to be at an increased development of non-Hodgkin lymphoma. It is not certain whether adherence to a strict gluten-free diet reduces this risk in this population.
Diagnosis can be made with a proper clinical history and examination, tissue pathology, direct immunofluorescence microscopy (DIF), and/or serology, with DIF being the most definitive. Perilesional skin is preferred for DIF, as lesional biopsies have been found to have higher rates of false negative results. The characteristic DIF finding diagnostic of DH is granular IgA deposits within dermal papillae, which was seen in this patient’s DIF.
Adequate treatment of DH can usually be accomplished with a combination of dapsone and a gluten-free diet. Initially, dapsone may be used for more immediate relief of associated pruritus and other bothersome symptoms. A strict gluten-free diet should be implemented as soon as possible, and dapsone can be tapered approximately 2-3 months after initiation as to avoid potential adverse effects with longterm treatment at higher doses.
The case and photo were submitted by Natasha Cowan, BS, University of California, San Diego, School of Medicine, and Nick Celano, MD, of San Diego Family Dermatology.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Dermatitis herpetiformis
The primary lesions of DH are vesicles and papules in a grouped or “herpetic” formation. However, as these lesions are extremely pruritic, the primary lesions may be absent in many cases and instead replaced by secondary excoriations and erosions. DH has a very classic distribution pattern, particularly involving the bilateral extensor surfaces, buttocks, and scalp. Although some cases of oral DH have been reported, mucosal involvement is generally considered to be very rare.
Despite its strong association with underlying celiac disease, most patients with DH do not report any associated gastrointestinal symptoms. Those with DH may present with any variety of other autoimmune conditions, with hypothyroidism being the most common. Interestingly, patients with DH have been shown to be at an increased development of non-Hodgkin lymphoma. It is not certain whether adherence to a strict gluten-free diet reduces this risk in this population.
Diagnosis can be made with a proper clinical history and examination, tissue pathology, direct immunofluorescence microscopy (DIF), and/or serology, with DIF being the most definitive. Perilesional skin is preferred for DIF, as lesional biopsies have been found to have higher rates of false negative results. The characteristic DIF finding diagnostic of DH is granular IgA deposits within dermal papillae, which was seen in this patient’s DIF.
Adequate treatment of DH can usually be accomplished with a combination of dapsone and a gluten-free diet. Initially, dapsone may be used for more immediate relief of associated pruritus and other bothersome symptoms. A strict gluten-free diet should be implemented as soon as possible, and dapsone can be tapered approximately 2-3 months after initiation as to avoid potential adverse effects with longterm treatment at higher doses.
The case and photo were submitted by Natasha Cowan, BS, University of California, San Diego, School of Medicine, and Nick Celano, MD, of San Diego Family Dermatology.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Dermatitis herpetiformis
The primary lesions of DH are vesicles and papules in a grouped or “herpetic” formation. However, as these lesions are extremely pruritic, the primary lesions may be absent in many cases and instead replaced by secondary excoriations and erosions. DH has a very classic distribution pattern, particularly involving the bilateral extensor surfaces, buttocks, and scalp. Although some cases of oral DH have been reported, mucosal involvement is generally considered to be very rare.
Despite its strong association with underlying celiac disease, most patients with DH do not report any associated gastrointestinal symptoms. Those with DH may present with any variety of other autoimmune conditions, with hypothyroidism being the most common. Interestingly, patients with DH have been shown to be at an increased development of non-Hodgkin lymphoma. It is not certain whether adherence to a strict gluten-free diet reduces this risk in this population.
Diagnosis can be made with a proper clinical history and examination, tissue pathology, direct immunofluorescence microscopy (DIF), and/or serology, with DIF being the most definitive. Perilesional skin is preferred for DIF, as lesional biopsies have been found to have higher rates of false negative results. The characteristic DIF finding diagnostic of DH is granular IgA deposits within dermal papillae, which was seen in this patient’s DIF.
Adequate treatment of DH can usually be accomplished with a combination of dapsone and a gluten-free diet. Initially, dapsone may be used for more immediate relief of associated pruritus and other bothersome symptoms. A strict gluten-free diet should be implemented as soon as possible, and dapsone can be tapered approximately 2-3 months after initiation as to avoid potential adverse effects with longterm treatment at higher doses.
The case and photo were submitted by Natasha Cowan, BS, University of California, San Diego, School of Medicine, and Nick Celano, MD, of San Diego Family Dermatology.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Hepatitis B and C May Increase Risk of Parkinson’s Disease
Hepatitis B and C appear to increase the risk of later Parkinson’s disease, according to a report published online ahead of print March 29 in Neurology.

The etiology of Parkinson’s disease is complex, and several factors, including environmental toxins and head trauma, may increase the likelihood of the disorder. Two recent epidemiologic studies in Taiwan found an association between hepatitis C and Parkinson’s
To further explore that association, the investigators performed a retrospective cohort study using data from National Health Service hospitals across England for 1999 to 2011. They assessed the risk of Parkinson’s disease among 21,633 people with hepatitis B, 48,428 with hepatitis C, 6,225 with autoimmune hepatitis, 4,234 with chronic active hepatitis, 19,870 with HIV, and 6,132,124 control subjects with other disorders.
The risk of developing Parkinson’s disease was elevated following hospitalization for hepatitis B (relative risk [RR], 1.76) and hepatitis C (RR, 1.51). “These findings may be explained by a specific aspect of viral hepatitis (rather than a general hepatic inflammatory process or general use of antivirals), but whether this reflects shared disease mechanisms, shared genetic or environmental susceptibility, sequelae of viral hepatitis per se, or a consequence of treatment remains to be determined,” Dr. Pakpoor and her associates said.
The reason for this association is not yet known. “Neurotropic features of hepatitis C have been described previously and include the potential for cognitive impairment, independent of hepatic encephalopathy. Further, all essential hepatitis C virus receptors have been shown to be expressed on the brain microvascular endothelium … suggesting one mechanism by which the virus may affect the CNS,” they noted.
In addition, parkinsonism has been described as an adverse effect of treatment with interferon and ribavirin, which are commonly used in hepatitis C infection. Parkinsonism also is known to develop in association with liver cirrhosis. Cirrhosis status was not available for the members of this study cohort.
More studies are needed to confirm this association and verify that it is causal. Such research will also provide insight into pathophysiologic pathways of Parkinson’s disease, “which may be important to understanding the development of Parkinson’s disease more broadly,” Dr. Pakpoor and her associates said.
—Mary Ann Moon
Suggested Reading
Pakpoor J, Noyce A, Goldacre R, et al. Viral hepatitis and Parkinson disease: A national record-linkage study. Neurology. 2017 Mar 29 [Epub ahead of print].
Hepatitis B and C appear to increase the risk of later Parkinson’s disease, according to a report published online ahead of print March 29 in Neurology.
The etiology of Parkinson’s disease is complex, and several factors, including environmental toxins and head trauma, may increase the likelihood of the disorder. Two recent epidemiologic studies in Taiwan found an association between hepatitis C and Parkinson’s
To further explore that association, the investigators performed a retrospective cohort study using data from National Health Service hospitals across England for 1999 to 2011. They assessed the risk of Parkinson’s disease among 21,633 people with hepatitis B, 48,428 with hepatitis C, 6,225 with autoimmune hepatitis, 4,234 with chronic active hepatitis, 19,870 with HIV, and 6,132,124 control subjects with other disorders.
The risk of developing Parkinson’s disease was elevated following hospitalization for hepatitis B (relative risk [RR], 1.76) and hepatitis C (RR, 1.51). “These findings may be explained by a specific aspect of viral hepatitis (rather than a general hepatic inflammatory process or general use of antivirals), but whether this reflects shared disease mechanisms, shared genetic or environmental susceptibility, sequelae of viral hepatitis per se, or a consequence of treatment remains to be determined,” Dr. Pakpoor and her associates said.
The reason for this association is not yet known. “Neurotropic features of hepatitis C have been described previously and include the potential for cognitive impairment, independent of hepatic encephalopathy. Further, all essential hepatitis C virus receptors have been shown to be expressed on the brain microvascular endothelium … suggesting one mechanism by which the virus may affect the CNS,” they noted.
In addition, parkinsonism has been described as an adverse effect of treatment with interferon and ribavirin, which are commonly used in hepatitis C infection. Parkinsonism also is known to develop in association with liver cirrhosis. Cirrhosis status was not available for the members of this study cohort.
More studies are needed to confirm this association and verify that it is causal. Such research will also provide insight into pathophysiologic pathways of Parkinson’s disease, “which may be important to understanding the development of Parkinson’s disease more broadly,” Dr. Pakpoor and her associates said.
—Mary Ann Moon
Suggested Reading
Pakpoor J, Noyce A, Goldacre R, et al. Viral hepatitis and Parkinson disease: A national record-linkage study. Neurology. 2017 Mar 29 [Epub ahead of print].
Hepatitis B and C appear to increase the risk of later Parkinson’s disease, according to a report published online ahead of print March 29 in Neurology.
The etiology of Parkinson’s disease is complex, and several factors, including environmental toxins and head trauma, may increase the likelihood of the disorder. Two recent epidemiologic studies in Taiwan found an association between hepatitis C and Parkinson’s
To further explore that association, the investigators performed a retrospective cohort study using data from National Health Service hospitals across England for 1999 to 2011. They assessed the risk of Parkinson’s disease among 21,633 people with hepatitis B, 48,428 with hepatitis C, 6,225 with autoimmune hepatitis, 4,234 with chronic active hepatitis, 19,870 with HIV, and 6,132,124 control subjects with other disorders.
The risk of developing Parkinson’s disease was elevated following hospitalization for hepatitis B (relative risk [RR], 1.76) and hepatitis C (RR, 1.51). “These findings may be explained by a specific aspect of viral hepatitis (rather than a general hepatic inflammatory process or general use of antivirals), but whether this reflects shared disease mechanisms, shared genetic or environmental susceptibility, sequelae of viral hepatitis per se, or a consequence of treatment remains to be determined,” Dr. Pakpoor and her associates said.
The reason for this association is not yet known. “Neurotropic features of hepatitis C have been described previously and include the potential for cognitive impairment, independent of hepatic encephalopathy. Further, all essential hepatitis C virus receptors have been shown to be expressed on the brain microvascular endothelium … suggesting one mechanism by which the virus may affect the CNS,” they noted.
In addition, parkinsonism has been described as an adverse effect of treatment with interferon and ribavirin, which are commonly used in hepatitis C infection. Parkinsonism also is known to develop in association with liver cirrhosis. Cirrhosis status was not available for the members of this study cohort.
More studies are needed to confirm this association and verify that it is causal. Such research will also provide insight into pathophysiologic pathways of Parkinson’s disease, “which may be important to understanding the development of Parkinson’s disease more broadly,” Dr. Pakpoor and her associates said.
—Mary Ann Moon
Suggested Reading
Pakpoor J, Noyce A, Goldacre R, et al. Viral hepatitis and Parkinson disease: A national record-linkage study. Neurology. 2017 Mar 29 [Epub ahead of print].

Decrease in Blood Pressure During Thrombectomy Under General Anesthesia Influences Outcome
HOUSTON—Among patients who undergo thrombectomy under general anesthesia, a decrease in blood pressure during treatment is associated with worse functional outcome, according to research presented at the International Stroke Conference 2017. The data suggest the importance of stringent blood pressure targets for improving outcome in patients treated under general anesthesia, said Kilian M. Treurniet, MD, a physician-researcher at the Academic Medical Center in Amsterdam.
The MR CLEAN trial indicated that intra-arterial treatment, including mechanical thrombectomy, is an effective and safe treatment for acute ischemic stroke. The investigators noticed, however, a loss of treatment effect when the procedure was performed on patients under general anesthesia. The researchers hypothesized that decreases in blood pressure might explain this loss of effect, said Dr. Treurniet.
To test this hypothesis, he and his colleagues performed a post hoc analysis of the MR CLEAN data to examine whether decreases from baseline in blood pressure during intervention under general anesthesia were associated with functional outcome. Patients were included in the analysis if their baseline blood pressure had been recorded and if they had regular blood pressure measurements during induction and maintenance anesthesia. The investigators focused on mean arterial pressure on the presumption that it most closely approximates cerebral perfusion pressure. The primary outcome was modified Rankin Scale (mRS) score at 90 days. The investigators performed a primary analysis before adjusting the data for known prognostic factors such as NIH Stroke Scale score and occlusion location.
In all, 60 patients treated under general anesthesia were included in the analysis. Age, sex, and occlusion location were similarly distributed in this population, compared with the larger MR CLEAN population. The majority of patients received propofol as an induction anesthetic and sevoflurane as a maintenance anesthetic.
At baseline, patients’ median systolic blood pressure was 140 mm Hg, and median mean arterial pressure was 100 mm Hg. The average decline in mean arterial pressure during the intervention, compared with baseline blood pressure, was 17 mm Hg. Patients with greater decreases in blood pressure had higher mRS scores at 90 days. Few patients in the analysis had low mRS scores, however, which makes the estimation of the association less precise, said Dr. Treurniet.
In the primary analysis, average mean arterial pressure during the intervention and lowest mean arterial pressure during the intervention were significantly associated with functional outcome. After adjustment, the association between average mean arterial pressure and functional outcome remained significant.
One of the limitations of the analysis is that the data came from nine centers and thus were heterogeneous. Blood pressure was not measured with the same frequency at every center. In addition, the sample size was small, and patients were not randomized to general anesthesia or to local anesthesia. Baseline blood pressure was based on a single manual measurement that could incorporate variability. Finally, the centers used invasive and noninvasive measurements during the procedure, and this heterogeneity could have influenced the results, said Dr. Treurniet.
“A decrease in mean arterial pressure during intervention under general anesthesia is associated with worse outcome in our study,” he added. “It might be that blood pressure management in those patients is of the utmost importance. We are looking forward to possible post hoc analyses of the SIESTA trial on this topic, and the upcoming results of the GOLIATH trial for [more] information.”
—Erik Greb
Suggested Reading
Simonsen CZ, Sørensen LH, Juul N, et al. Anesthetic strategy during endovascular therapy: General anesthesia or conscious sedation? (GOLIATH - General or Local Anesthesia in Intra Arterial Therapy) A single-center randomized trial. Int J Stroke. 2016;11(9):1045-1052.
Sivasankar C, Stiefel M, Miano TA, et al. Anesthetic variation and potential impact of anesthetics used during endovascular management of acute ischemic stroke. J Neurointerv Surg. 2016;8(11):1101-1106.
Treurniet KM, Berkhemer OA, Immink RV, et al.
Whalin MK, Lopian S, Wyatt K, et al. Dexmedetomidine: a safe alternative to general anesthesia for endovascular stroke treatment. J Neurointerv Surg. 2014;6(4):270-275.
HOUSTON—Among patients who undergo thrombectomy under general anesthesia, a decrease in blood pressure during treatment is associated with worse functional outcome, according to research presented at the International Stroke Conference 2017. The data suggest the importance of stringent blood pressure targets for improving outcome in patients treated under general anesthesia, said Kilian M. Treurniet, MD, a physician-researcher at the Academic Medical Center in Amsterdam.
The MR CLEAN trial indicated that intra-arterial treatment, including mechanical thrombectomy, is an effective and safe treatment for acute ischemic stroke. The investigators noticed, however, a loss of treatment effect when the procedure was performed on patients under general anesthesia. The researchers hypothesized that decreases in blood pressure might explain this loss of effect, said Dr. Treurniet.
To test this hypothesis, he and his colleagues performed a post hoc analysis of the MR CLEAN data to examine whether decreases from baseline in blood pressure during intervention under general anesthesia were associated with functional outcome. Patients were included in the analysis if their baseline blood pressure had been recorded and if they had regular blood pressure measurements during induction and maintenance anesthesia. The investigators focused on mean arterial pressure on the presumption that it most closely approximates cerebral perfusion pressure. The primary outcome was modified Rankin Scale (mRS) score at 90 days. The investigators performed a primary analysis before adjusting the data for known prognostic factors such as NIH Stroke Scale score and occlusion location.
In all, 60 patients treated under general anesthesia were included in the analysis. Age, sex, and occlusion location were similarly distributed in this population, compared with the larger MR CLEAN population. The majority of patients received propofol as an induction anesthetic and sevoflurane as a maintenance anesthetic.
At baseline, patients’ median systolic blood pressure was 140 mm Hg, and median mean arterial pressure was 100 mm Hg. The average decline in mean arterial pressure during the intervention, compared with baseline blood pressure, was 17 mm Hg. Patients with greater decreases in blood pressure had higher mRS scores at 90 days. Few patients in the analysis had low mRS scores, however, which makes the estimation of the association less precise, said Dr. Treurniet.
In the primary analysis, average mean arterial pressure during the intervention and lowest mean arterial pressure during the intervention were significantly associated with functional outcome. After adjustment, the association between average mean arterial pressure and functional outcome remained significant.
One of the limitations of the analysis is that the data came from nine centers and thus were heterogeneous. Blood pressure was not measured with the same frequency at every center. In addition, the sample size was small, and patients were not randomized to general anesthesia or to local anesthesia. Baseline blood pressure was based on a single manual measurement that could incorporate variability. Finally, the centers used invasive and noninvasive measurements during the procedure, and this heterogeneity could have influenced the results, said Dr. Treurniet.
“A decrease in mean arterial pressure during intervention under general anesthesia is associated with worse outcome in our study,” he added. “It might be that blood pressure management in those patients is of the utmost importance. We are looking forward to possible post hoc analyses of the SIESTA trial on this topic, and the upcoming results of the GOLIATH trial for [more] information.”
—Erik Greb
Suggested Reading
Simonsen CZ, Sørensen LH, Juul N, et al. Anesthetic strategy during endovascular therapy: General anesthesia or conscious sedation? (GOLIATH - General or Local Anesthesia in Intra Arterial Therapy) A single-center randomized trial. Int J Stroke. 2016;11(9):1045-1052.
Sivasankar C, Stiefel M, Miano TA, et al. Anesthetic variation and potential impact of anesthetics used during endovascular management of acute ischemic stroke. J Neurointerv Surg. 2016;8(11):1101-1106.
Treurniet KM, Berkhemer OA, Immink RV, et al.
Whalin MK, Lopian S, Wyatt K, et al. Dexmedetomidine: a safe alternative to general anesthesia for endovascular stroke treatment. J Neurointerv Surg. 2014;6(4):270-275.
HOUSTON—Among patients who undergo thrombectomy under general anesthesia, a decrease in blood pressure during treatment is associated with worse functional outcome, according to research presented at the International Stroke Conference 2017. The data suggest the importance of stringent blood pressure targets for improving outcome in patients treated under general anesthesia, said Kilian M. Treurniet, MD, a physician-researcher at the Academic Medical Center in Amsterdam.
The MR CLEAN trial indicated that intra-arterial treatment, including mechanical thrombectomy, is an effective and safe treatment for acute ischemic stroke. The investigators noticed, however, a loss of treatment effect when the procedure was performed on patients under general anesthesia. The researchers hypothesized that decreases in blood pressure might explain this loss of effect, said Dr. Treurniet.
To test this hypothesis, he and his colleagues performed a post hoc analysis of the MR CLEAN data to examine whether decreases from baseline in blood pressure during intervention under general anesthesia were associated with functional outcome. Patients were included in the analysis if their baseline blood pressure had been recorded and if they had regular blood pressure measurements during induction and maintenance anesthesia. The investigators focused on mean arterial pressure on the presumption that it most closely approximates cerebral perfusion pressure. The primary outcome was modified Rankin Scale (mRS) score at 90 days. The investigators performed a primary analysis before adjusting the data for known prognostic factors such as NIH Stroke Scale score and occlusion location.
In all, 60 patients treated under general anesthesia were included in the analysis. Age, sex, and occlusion location were similarly distributed in this population, compared with the larger MR CLEAN population. The majority of patients received propofol as an induction anesthetic and sevoflurane as a maintenance anesthetic.
At baseline, patients’ median systolic blood pressure was 140 mm Hg, and median mean arterial pressure was 100 mm Hg. The average decline in mean arterial pressure during the intervention, compared with baseline blood pressure, was 17 mm Hg. Patients with greater decreases in blood pressure had higher mRS scores at 90 days. Few patients in the analysis had low mRS scores, however, which makes the estimation of the association less precise, said Dr. Treurniet.
In the primary analysis, average mean arterial pressure during the intervention and lowest mean arterial pressure during the intervention were significantly associated with functional outcome. After adjustment, the association between average mean arterial pressure and functional outcome remained significant.
One of the limitations of the analysis is that the data came from nine centers and thus were heterogeneous. Blood pressure was not measured with the same frequency at every center. In addition, the sample size was small, and patients were not randomized to general anesthesia or to local anesthesia. Baseline blood pressure was based on a single manual measurement that could incorporate variability. Finally, the centers used invasive and noninvasive measurements during the procedure, and this heterogeneity could have influenced the results, said Dr. Treurniet.
“A decrease in mean arterial pressure during intervention under general anesthesia is associated with worse outcome in our study,” he added. “It might be that blood pressure management in those patients is of the utmost importance. We are looking forward to possible post hoc analyses of the SIESTA trial on this topic, and the upcoming results of the GOLIATH trial for [more] information.”
—Erik Greb
Suggested Reading
Simonsen CZ, Sørensen LH, Juul N, et al. Anesthetic strategy during endovascular therapy: General anesthesia or conscious sedation? (GOLIATH - General or Local Anesthesia in Intra Arterial Therapy) A single-center randomized trial. Int J Stroke. 2016;11(9):1045-1052.
Sivasankar C, Stiefel M, Miano TA, et al. Anesthetic variation and potential impact of anesthetics used during endovascular management of acute ischemic stroke. J Neurointerv Surg. 2016;8(11):1101-1106.
Treurniet KM, Berkhemer OA, Immink RV, et al.
Whalin MK, Lopian S, Wyatt K, et al. Dexmedetomidine: a safe alternative to general anesthesia for endovascular stroke treatment. J Neurointerv Surg. 2014;6(4):270-275.