User login
Top 5 Medications That Can Increase Blood Glucose Levels
It’s that time of the year, when social media is rife with many top 5 and top 10 lists. Let’s revisit some of the most commonly used medications known to increase glucose levels and look at some practical tips on overcoming these.
1. Glucocorticoids
Without a doubt, corticosteroids are at the top of the list when it comes to the potential for increasing blood glucose levels. High-dose glucocorticoid therapy is known to lead to new-onset diabetes (steroid-induced diabetes). Similarly, people with preexisting diabetes may notice significant worsening of glycemic control when they start on glucocorticoid therapy. The extent of glucose elevation depends on their glycemic status prior to initiation on steroids, the dose and duration of glucocorticoid therapy, and comorbid conditions, among other factors.
Management tip: For those with previously well-controlled diabetes or borderline diabetes, glucocorticoid-induced hyperglycemia may be managed by metformin with or without sulfonylurea therapy, especially if corticosteroid treatment is low-dose and for a shorter duration. However, for many individuals with preexisting poorly controlled diabetes or those initiated on high-dose corticosteroids, insulin therapy would perhaps be the treatment of choice. Glucocorticoid therapy generally leads to more pronounced postprandial hyperglycemia compared with fasting hyperglycemia; hence, the use of short-acting insulin therapy or perhaps NPH insulin in the morning might be a better option for many individuals. Dietary modification plays an important role in limiting the extent of postprandial hyperglycemia. Use of continuous glucose monitoring (CGM) devices may also be very helpful for understanding glycemic excursions and how to adjust insulin. In individuals for whom glucocorticoid therapy is tapered down, it is important to adjust the dose of medications with potential to cause hypoglycemia, such as insulin/sulfonylurea therapy, as the degree of hyperglycemia may decrease with decreased dose of the glucocorticoid therapy.
2. Antipsychotic Therapy
Antipsychotic medications can be obesogenic; between 15% and 72% of people who take second-generation antipsychotics experience weight gain of 7% or more. Increases in weight are not the only factor contributing to an elevated risk of developing type 2 diabetes. Antipsychotics are thought to cause downregulation of intracellular insulin signaling, leading to insulin resistance. At the same time, there seems to be a direct effect on the pancreatic beta cells. Antagonism of the dopamine D2, serotonin 5-HT2C, and muscarinic M3 receptors impairs beta-cell response to changes in blood glucose. In addition to the pharmacologic effects, cell culture experiments have shown that antipsychotics increase apoptosis of beta cells. Increased weight and concomitant development of type 2 diabetes is seen particularly in agents that exhibit high muscarinic M3 and histamine H1 receptor blockade. The effect on glucose metabolism is seen the most with agents such as clozapine, olanzapine, and haloperidol and the least with agents such as ziprasidone.
Management tip: Given the ongoing change in the understanding of increases in weight and their association with the risk of developing type 2 diabetes, a metabolically safer approach involves starting with medications that have a lower propensity for weight gain, and the partial agonists/third-generation antipsychotics as a family presently have the best overall data.
3. Thiazide Diuretics
Thiazide diuretics are commonly used for the management of hypertension and are associated with metabolic complications including hypokalemia; higher cholesterol, triglycerides, and other circulating lipids; and elevated glucose. It’s thought that the reduced potassium level occurring as a result of these medications might contribute to new-onset diabetes. The hypokalemia occurring from these medications is thought to lead to a decrease in insulin secretion and sensitivity, which is dose dependent. Studies show that the number needed to harm for chlorthalidone-induced diabetes is 29 over 1 year. There is believed to be no additional risk beyond 1 year.
Management tip: It’s important to monitor potassium levels for those initiated on thiazide diuretics. If hypokalemia occurs, it would be pertinent to correct the hypokalemia with potassium supplements to mitigate the risk for new-onset diabetes.
4. Statin Therapy
Statin therapy is thought to be associated with decreased insulin sensitivity and impairment in insulin secretion. The overall incidence of diabetes is pegged to be between 9% and 12% on statin therapy on the basis of meta-analysis studies, and higher on the basis of population-based studies. Overall, the estimated number needed to harm is: 1 out of every 255 patients on statin therapy for 4 years may develop new-onset diabetes. Compare this with the extremely strong evidence for number needed to treat being 39 for 5 years with statin therapy in patients with preexisting heart disease to prevent one occurrence of a nonfatal myocardial infarction.
Management tip: Although statins are associated with a small incident increase in the risk of developing diabetes, the potential benefits of using statin therapy for both primary and secondary prevention of cardiovascular disease significantly outweigh any of the potential risks associated with hyperglycemia. This is an important discussion to have with patients who are reluctant to use statin therapy because of the potential risk for new-onset diabetes as a side effect.
5. Beta-Blockers
Beta-blockers are another commonly used group of medications for managing hypertension, heart failure, coronary artery disease, and arrhythmia. Nonvasodilating beta-blockers such as metoprolol and atenolol are more likely to be associated with increases in A1c, mean plasma glucose, body weight, and triglycerides compared with vasodilating beta-blockers such as carvedilol, nebivolol, and labetalol (Bakris GL et al; Giugliano D et al). Similarly, studies have also shown that atenolol and metoprolol are associated with increased odds of hypoglycemia compared with carvedilol. People on beta-blockers may have masking of some of the symptoms of hypoglycemia, such as tremor, irritability, and palpitations, while other symptoms such as diaphoresis may remain unaffected on beta-blockers.
Management tip: Education on recognizing and managing hypoglycemia would be important when starting patients on beta-blockers if they are on preexisting insulin/sulfonylurea therapy. Use of CGM devices may be helpful if there is a high risk for hypoglycemia, especially as symptoms of hypoglycemia are often masked.
Honorable Mention
Several other medications — including antiretroviral therapy, tyrosine kinase inhibitors, mechanistic target of rapamycin (mTOR) inhibitors, immunosuppressants, and interferon alpha — are associated with worsening glycemic control and new-onset diabetes. Consider these agents’ effects on blood glucose, especially in people with an elevated risk of developing diabetes or those with preexisting diabetes, when prescribing.
A special mention should also be made of androgen deprivation therapy. These include treatment options like goserelin and leuprolide, which are gonadotropin-releasing hormone (GnRH) agonist therapies and are commonly used for prostate cancer management. Depending on the patient, these agents may be used for prolonged duration. Androgen deprivation therapy, by definition, decreases testosterone levels in men, thereby leading to worsening insulin resistance. Increase in fat mass and concomitant muscle wasting have been associated with the use of these medications; these, in turn, lead to peripheral insulin resistance. Nearly 1 out of every 5 men treated with long-term androgen deprivation therapy may be prone to developing worsening of A1c by 1% or more.
Management tip: Men on androgen deprivation therapy should be encouraged to participate in regular physical activity to reduce the burden of insulin resistance and to promote cardiovascular health.
Drug-induced diabetes is potentially reversible in many cases. Similarly, worsening of glycemic control due to medications in people with preexisting diabetes may also attenuate once the effect of the drug wears off. Blood glucose should be monitored on an ongoing basis so that diabetes medications can be adjusted. For some individuals, however, the worsening of glycemic status may be more chronic and may require long-term use of antihyperglycemic agents, especially if the benefits of continuation of the medication leading to hyperglycemia far exceed any potential risks.
Dr. Jain is Clinical Instructor, Department of Endocrinology, University of British Columbia; Endocrinologist, Fraser River Endocrinology, Vancouver, British Columbia, Canada. He disclosed ties with Abbott, Amgen, Boehringer Ingelheim, Dexcom, Eli Lilly, Janssen, Medtronic, Merck, and Novo Nordisk.
A version of this article appeared on Medscape.com.
It’s that time of the year, when social media is rife with many top 5 and top 10 lists. Let’s revisit some of the most commonly used medications known to increase glucose levels and look at some practical tips on overcoming these.
1. Glucocorticoids
Without a doubt, corticosteroids are at the top of the list when it comes to the potential for increasing blood glucose levels. High-dose glucocorticoid therapy is known to lead to new-onset diabetes (steroid-induced diabetes). Similarly, people with preexisting diabetes may notice significant worsening of glycemic control when they start on glucocorticoid therapy. The extent of glucose elevation depends on their glycemic status prior to initiation on steroids, the dose and duration of glucocorticoid therapy, and comorbid conditions, among other factors.
Management tip: For those with previously well-controlled diabetes or borderline diabetes, glucocorticoid-induced hyperglycemia may be managed by metformin with or without sulfonylurea therapy, especially if corticosteroid treatment is low-dose and for a shorter duration. However, for many individuals with preexisting poorly controlled diabetes or those initiated on high-dose corticosteroids, insulin therapy would perhaps be the treatment of choice. Glucocorticoid therapy generally leads to more pronounced postprandial hyperglycemia compared with fasting hyperglycemia; hence, the use of short-acting insulin therapy or perhaps NPH insulin in the morning might be a better option for many individuals. Dietary modification plays an important role in limiting the extent of postprandial hyperglycemia. Use of continuous glucose monitoring (CGM) devices may also be very helpful for understanding glycemic excursions and how to adjust insulin. In individuals for whom glucocorticoid therapy is tapered down, it is important to adjust the dose of medications with potential to cause hypoglycemia, such as insulin/sulfonylurea therapy, as the degree of hyperglycemia may decrease with decreased dose of the glucocorticoid therapy.
2. Antipsychotic Therapy
Antipsychotic medications can be obesogenic; between 15% and 72% of people who take second-generation antipsychotics experience weight gain of 7% or more. Increases in weight are not the only factor contributing to an elevated risk of developing type 2 diabetes. Antipsychotics are thought to cause downregulation of intracellular insulin signaling, leading to insulin resistance. At the same time, there seems to be a direct effect on the pancreatic beta cells. Antagonism of the dopamine D2, serotonin 5-HT2C, and muscarinic M3 receptors impairs beta-cell response to changes in blood glucose. In addition to the pharmacologic effects, cell culture experiments have shown that antipsychotics increase apoptosis of beta cells. Increased weight and concomitant development of type 2 diabetes is seen particularly in agents that exhibit high muscarinic M3 and histamine H1 receptor blockade. The effect on glucose metabolism is seen the most with agents such as clozapine, olanzapine, and haloperidol and the least with agents such as ziprasidone.
Management tip: Given the ongoing change in the understanding of increases in weight and their association with the risk of developing type 2 diabetes, a metabolically safer approach involves starting with medications that have a lower propensity for weight gain, and the partial agonists/third-generation antipsychotics as a family presently have the best overall data.
3. Thiazide Diuretics
Thiazide diuretics are commonly used for the management of hypertension and are associated with metabolic complications including hypokalemia; higher cholesterol, triglycerides, and other circulating lipids; and elevated glucose. It’s thought that the reduced potassium level occurring as a result of these medications might contribute to new-onset diabetes. The hypokalemia occurring from these medications is thought to lead to a decrease in insulin secretion and sensitivity, which is dose dependent. Studies show that the number needed to harm for chlorthalidone-induced diabetes is 29 over 1 year. There is believed to be no additional risk beyond 1 year.
Management tip: It’s important to monitor potassium levels for those initiated on thiazide diuretics. If hypokalemia occurs, it would be pertinent to correct the hypokalemia with potassium supplements to mitigate the risk for new-onset diabetes.
4. Statin Therapy
Statin therapy is thought to be associated with decreased insulin sensitivity and impairment in insulin secretion. The overall incidence of diabetes is pegged to be between 9% and 12% on statin therapy on the basis of meta-analysis studies, and higher on the basis of population-based studies. Overall, the estimated number needed to harm is: 1 out of every 255 patients on statin therapy for 4 years may develop new-onset diabetes. Compare this with the extremely strong evidence for number needed to treat being 39 for 5 years with statin therapy in patients with preexisting heart disease to prevent one occurrence of a nonfatal myocardial infarction.
Management tip: Although statins are associated with a small incident increase in the risk of developing diabetes, the potential benefits of using statin therapy for both primary and secondary prevention of cardiovascular disease significantly outweigh any of the potential risks associated with hyperglycemia. This is an important discussion to have with patients who are reluctant to use statin therapy because of the potential risk for new-onset diabetes as a side effect.
5. Beta-Blockers
Beta-blockers are another commonly used group of medications for managing hypertension, heart failure, coronary artery disease, and arrhythmia. Nonvasodilating beta-blockers such as metoprolol and atenolol are more likely to be associated with increases in A1c, mean plasma glucose, body weight, and triglycerides compared with vasodilating beta-blockers such as carvedilol, nebivolol, and labetalol (Bakris GL et al; Giugliano D et al). Similarly, studies have also shown that atenolol and metoprolol are associated with increased odds of hypoglycemia compared with carvedilol. People on beta-blockers may have masking of some of the symptoms of hypoglycemia, such as tremor, irritability, and palpitations, while other symptoms such as diaphoresis may remain unaffected on beta-blockers.
Management tip: Education on recognizing and managing hypoglycemia would be important when starting patients on beta-blockers if they are on preexisting insulin/sulfonylurea therapy. Use of CGM devices may be helpful if there is a high risk for hypoglycemia, especially as symptoms of hypoglycemia are often masked.
Honorable Mention
Several other medications — including antiretroviral therapy, tyrosine kinase inhibitors, mechanistic target of rapamycin (mTOR) inhibitors, immunosuppressants, and interferon alpha — are associated with worsening glycemic control and new-onset diabetes. Consider these agents’ effects on blood glucose, especially in people with an elevated risk of developing diabetes or those with preexisting diabetes, when prescribing.
A special mention should also be made of androgen deprivation therapy. These include treatment options like goserelin and leuprolide, which are gonadotropin-releasing hormone (GnRH) agonist therapies and are commonly used for prostate cancer management. Depending on the patient, these agents may be used for prolonged duration. Androgen deprivation therapy, by definition, decreases testosterone levels in men, thereby leading to worsening insulin resistance. Increase in fat mass and concomitant muscle wasting have been associated with the use of these medications; these, in turn, lead to peripheral insulin resistance. Nearly 1 out of every 5 men treated with long-term androgen deprivation therapy may be prone to developing worsening of A1c by 1% or more.
Management tip: Men on androgen deprivation therapy should be encouraged to participate in regular physical activity to reduce the burden of insulin resistance and to promote cardiovascular health.
Drug-induced diabetes is potentially reversible in many cases. Similarly, worsening of glycemic control due to medications in people with preexisting diabetes may also attenuate once the effect of the drug wears off. Blood glucose should be monitored on an ongoing basis so that diabetes medications can be adjusted. For some individuals, however, the worsening of glycemic status may be more chronic and may require long-term use of antihyperglycemic agents, especially if the benefits of continuation of the medication leading to hyperglycemia far exceed any potential risks.
Dr. Jain is Clinical Instructor, Department of Endocrinology, University of British Columbia; Endocrinologist, Fraser River Endocrinology, Vancouver, British Columbia, Canada. He disclosed ties with Abbott, Amgen, Boehringer Ingelheim, Dexcom, Eli Lilly, Janssen, Medtronic, Merck, and Novo Nordisk.
A version of this article appeared on Medscape.com.
It’s that time of the year, when social media is rife with many top 5 and top 10 lists. Let’s revisit some of the most commonly used medications known to increase glucose levels and look at some practical tips on overcoming these.
1. Glucocorticoids
Without a doubt, corticosteroids are at the top of the list when it comes to the potential for increasing blood glucose levels. High-dose glucocorticoid therapy is known to lead to new-onset diabetes (steroid-induced diabetes). Similarly, people with preexisting diabetes may notice significant worsening of glycemic control when they start on glucocorticoid therapy. The extent of glucose elevation depends on their glycemic status prior to initiation on steroids, the dose and duration of glucocorticoid therapy, and comorbid conditions, among other factors.
Management tip: For those with previously well-controlled diabetes or borderline diabetes, glucocorticoid-induced hyperglycemia may be managed by metformin with or without sulfonylurea therapy, especially if corticosteroid treatment is low-dose and for a shorter duration. However, for many individuals with preexisting poorly controlled diabetes or those initiated on high-dose corticosteroids, insulin therapy would perhaps be the treatment of choice. Glucocorticoid therapy generally leads to more pronounced postprandial hyperglycemia compared with fasting hyperglycemia; hence, the use of short-acting insulin therapy or perhaps NPH insulin in the morning might be a better option for many individuals. Dietary modification plays an important role in limiting the extent of postprandial hyperglycemia. Use of continuous glucose monitoring (CGM) devices may also be very helpful for understanding glycemic excursions and how to adjust insulin. In individuals for whom glucocorticoid therapy is tapered down, it is important to adjust the dose of medications with potential to cause hypoglycemia, such as insulin/sulfonylurea therapy, as the degree of hyperglycemia may decrease with decreased dose of the glucocorticoid therapy.
2. Antipsychotic Therapy
Antipsychotic medications can be obesogenic; between 15% and 72% of people who take second-generation antipsychotics experience weight gain of 7% or more. Increases in weight are not the only factor contributing to an elevated risk of developing type 2 diabetes. Antipsychotics are thought to cause downregulation of intracellular insulin signaling, leading to insulin resistance. At the same time, there seems to be a direct effect on the pancreatic beta cells. Antagonism of the dopamine D2, serotonin 5-HT2C, and muscarinic M3 receptors impairs beta-cell response to changes in blood glucose. In addition to the pharmacologic effects, cell culture experiments have shown that antipsychotics increase apoptosis of beta cells. Increased weight and concomitant development of type 2 diabetes is seen particularly in agents that exhibit high muscarinic M3 and histamine H1 receptor blockade. The effect on glucose metabolism is seen the most with agents such as clozapine, olanzapine, and haloperidol and the least with agents such as ziprasidone.
Management tip: Given the ongoing change in the understanding of increases in weight and their association with the risk of developing type 2 diabetes, a metabolically safer approach involves starting with medications that have a lower propensity for weight gain, and the partial agonists/third-generation antipsychotics as a family presently have the best overall data.
3. Thiazide Diuretics
Thiazide diuretics are commonly used for the management of hypertension and are associated with metabolic complications including hypokalemia; higher cholesterol, triglycerides, and other circulating lipids; and elevated glucose. It’s thought that the reduced potassium level occurring as a result of these medications might contribute to new-onset diabetes. The hypokalemia occurring from these medications is thought to lead to a decrease in insulin secretion and sensitivity, which is dose dependent. Studies show that the number needed to harm for chlorthalidone-induced diabetes is 29 over 1 year. There is believed to be no additional risk beyond 1 year.
Management tip: It’s important to monitor potassium levels for those initiated on thiazide diuretics. If hypokalemia occurs, it would be pertinent to correct the hypokalemia with potassium supplements to mitigate the risk for new-onset diabetes.
4. Statin Therapy
Statin therapy is thought to be associated with decreased insulin sensitivity and impairment in insulin secretion. The overall incidence of diabetes is pegged to be between 9% and 12% on statin therapy on the basis of meta-analysis studies, and higher on the basis of population-based studies. Overall, the estimated number needed to harm is: 1 out of every 255 patients on statin therapy for 4 years may develop new-onset diabetes. Compare this with the extremely strong evidence for number needed to treat being 39 for 5 years with statin therapy in patients with preexisting heart disease to prevent one occurrence of a nonfatal myocardial infarction.
Management tip: Although statins are associated with a small incident increase in the risk of developing diabetes, the potential benefits of using statin therapy for both primary and secondary prevention of cardiovascular disease significantly outweigh any of the potential risks associated with hyperglycemia. This is an important discussion to have with patients who are reluctant to use statin therapy because of the potential risk for new-onset diabetes as a side effect.
5. Beta-Blockers
Beta-blockers are another commonly used group of medications for managing hypertension, heart failure, coronary artery disease, and arrhythmia. Nonvasodilating beta-blockers such as metoprolol and atenolol are more likely to be associated with increases in A1c, mean plasma glucose, body weight, and triglycerides compared with vasodilating beta-blockers such as carvedilol, nebivolol, and labetalol (Bakris GL et al; Giugliano D et al). Similarly, studies have also shown that atenolol and metoprolol are associated with increased odds of hypoglycemia compared with carvedilol. People on beta-blockers may have masking of some of the symptoms of hypoglycemia, such as tremor, irritability, and palpitations, while other symptoms such as diaphoresis may remain unaffected on beta-blockers.
Management tip: Education on recognizing and managing hypoglycemia would be important when starting patients on beta-blockers if they are on preexisting insulin/sulfonylurea therapy. Use of CGM devices may be helpful if there is a high risk for hypoglycemia, especially as symptoms of hypoglycemia are often masked.
Honorable Mention
Several other medications — including antiretroviral therapy, tyrosine kinase inhibitors, mechanistic target of rapamycin (mTOR) inhibitors, immunosuppressants, and interferon alpha — are associated with worsening glycemic control and new-onset diabetes. Consider these agents’ effects on blood glucose, especially in people with an elevated risk of developing diabetes or those with preexisting diabetes, when prescribing.
A special mention should also be made of androgen deprivation therapy. These include treatment options like goserelin and leuprolide, which are gonadotropin-releasing hormone (GnRH) agonist therapies and are commonly used for prostate cancer management. Depending on the patient, these agents may be used for prolonged duration. Androgen deprivation therapy, by definition, decreases testosterone levels in men, thereby leading to worsening insulin resistance. Increase in fat mass and concomitant muscle wasting have been associated with the use of these medications; these, in turn, lead to peripheral insulin resistance. Nearly 1 out of every 5 men treated with long-term androgen deprivation therapy may be prone to developing worsening of A1c by 1% or more.
Management tip: Men on androgen deprivation therapy should be encouraged to participate in regular physical activity to reduce the burden of insulin resistance and to promote cardiovascular health.
Drug-induced diabetes is potentially reversible in many cases. Similarly, worsening of glycemic control due to medications in people with preexisting diabetes may also attenuate once the effect of the drug wears off. Blood glucose should be monitored on an ongoing basis so that diabetes medications can be adjusted. For some individuals, however, the worsening of glycemic status may be more chronic and may require long-term use of antihyperglycemic agents, especially if the benefits of continuation of the medication leading to hyperglycemia far exceed any potential risks.
Dr. Jain is Clinical Instructor, Department of Endocrinology, University of British Columbia; Endocrinologist, Fraser River Endocrinology, Vancouver, British Columbia, Canada. He disclosed ties with Abbott, Amgen, Boehringer Ingelheim, Dexcom, Eli Lilly, Janssen, Medtronic, Merck, and Novo Nordisk.
A version of this article appeared on Medscape.com.
Migraine Associated With Increased Risk for IBD
TOPLINE:
Migraine is associated with a significantly increased risk of developing inflammatory bowel disease (IBD), including both Crohn’s disease (CD) and ulcerative colitis (UC), a new nationwide, population-based cohort study showed.
METHODOLOGY:
- Investigators analyzed data from South Korea’s National Health Insurance Service (NHIS) database, which houses data for the nationwide obligatory health system for South Korean citizens.
- Individuals aged ≥ 20 years who had at least one national health screening in 2009 were enrolled in the study and followed until December 2019.
- Investigators searched the data for International Classification of Diseases (10th Revision) codes corresponding to migraine and IBD. IBD diagnoses were also based on clinical manifestation, endoscopic findings, and pathologic findings.
TAKEAWAY:
- More than 10 million people were enrolled in the study (55% male; mean age, 47 years), and of these, 2.8% were diagnosed with migraine during the study period.
- During a median follow-up of 10 years, the incidence of IBD was significantly higher in patients with migraine (adjusted hazard ratio [aHR], 1.31; P < .001), CD (aHR, 1.58; P < .001) and UC (aHR, 1.26; P < .001) than in those without migraine.
- in men vs women (aHR, 1.43 vs 1.12; P = .042).
- Investigators could only speculate about the mechanisms underlying the association between migraine and IBD but suggest pathological processes underlying both migraine and IBD, including proinflammatory cytokines and tumor necrosis factor alpha, may be involved.
IN PRACTICE:
“Clinicians should be aware of the potential risk of IBD in patients diagnosed with migraine especially in men for the development of UC and in migraineurs with a long disease duration for a further risk of CD,” the authors wrote.
SOURCE:
Hyunjung Lee, MD, of Seoul National University College of Medicine, Seoul, South Korea, led the study, which was published online on January 12, 2024, in Scientific Reports.
LIMITATIONS:
Disease severity of migraine and IBD was not available. In addition, certain medications taken to relieve migraine, such as nonsteroidal anti-inflammatory drugs like ibuprofen, could cause intestinal inflammation, but there was no medication information available.
DISCLOSURES:
There was no information about study funding nor disclosures from study authors.
A version of this article appeared on Medscape.com.
TOPLINE:
Migraine is associated with a significantly increased risk of developing inflammatory bowel disease (IBD), including both Crohn’s disease (CD) and ulcerative colitis (UC), a new nationwide, population-based cohort study showed.
METHODOLOGY:
- Investigators analyzed data from South Korea’s National Health Insurance Service (NHIS) database, which houses data for the nationwide obligatory health system for South Korean citizens.
- Individuals aged ≥ 20 years who had at least one national health screening in 2009 were enrolled in the study and followed until December 2019.
- Investigators searched the data for International Classification of Diseases (10th Revision) codes corresponding to migraine and IBD. IBD diagnoses were also based on clinical manifestation, endoscopic findings, and pathologic findings.
TAKEAWAY:
- More than 10 million people were enrolled in the study (55% male; mean age, 47 years), and of these, 2.8% were diagnosed with migraine during the study period.
- During a median follow-up of 10 years, the incidence of IBD was significantly higher in patients with migraine (adjusted hazard ratio [aHR], 1.31; P < .001), CD (aHR, 1.58; P < .001) and UC (aHR, 1.26; P < .001) than in those without migraine.
- in men vs women (aHR, 1.43 vs 1.12; P = .042).
- Investigators could only speculate about the mechanisms underlying the association between migraine and IBD but suggest pathological processes underlying both migraine and IBD, including proinflammatory cytokines and tumor necrosis factor alpha, may be involved.
IN PRACTICE:
“Clinicians should be aware of the potential risk of IBD in patients diagnosed with migraine especially in men for the development of UC and in migraineurs with a long disease duration for a further risk of CD,” the authors wrote.
SOURCE:
Hyunjung Lee, MD, of Seoul National University College of Medicine, Seoul, South Korea, led the study, which was published online on January 12, 2024, in Scientific Reports.
LIMITATIONS:
Disease severity of migraine and IBD was not available. In addition, certain medications taken to relieve migraine, such as nonsteroidal anti-inflammatory drugs like ibuprofen, could cause intestinal inflammation, but there was no medication information available.
DISCLOSURES:
There was no information about study funding nor disclosures from study authors.
A version of this article appeared on Medscape.com.
TOPLINE:
Migraine is associated with a significantly increased risk of developing inflammatory bowel disease (IBD), including both Crohn’s disease (CD) and ulcerative colitis (UC), a new nationwide, population-based cohort study showed.
METHODOLOGY:
- Investigators analyzed data from South Korea’s National Health Insurance Service (NHIS) database, which houses data for the nationwide obligatory health system for South Korean citizens.
- Individuals aged ≥ 20 years who had at least one national health screening in 2009 were enrolled in the study and followed until December 2019.
- Investigators searched the data for International Classification of Diseases (10th Revision) codes corresponding to migraine and IBD. IBD diagnoses were also based on clinical manifestation, endoscopic findings, and pathologic findings.
TAKEAWAY:
- More than 10 million people were enrolled in the study (55% male; mean age, 47 years), and of these, 2.8% were diagnosed with migraine during the study period.
- During a median follow-up of 10 years, the incidence of IBD was significantly higher in patients with migraine (adjusted hazard ratio [aHR], 1.31; P < .001), CD (aHR, 1.58; P < .001) and UC (aHR, 1.26; P < .001) than in those without migraine.
- in men vs women (aHR, 1.43 vs 1.12; P = .042).
- Investigators could only speculate about the mechanisms underlying the association between migraine and IBD but suggest pathological processes underlying both migraine and IBD, including proinflammatory cytokines and tumor necrosis factor alpha, may be involved.
IN PRACTICE:
“Clinicians should be aware of the potential risk of IBD in patients diagnosed with migraine especially in men for the development of UC and in migraineurs with a long disease duration for a further risk of CD,” the authors wrote.
SOURCE:
Hyunjung Lee, MD, of Seoul National University College of Medicine, Seoul, South Korea, led the study, which was published online on January 12, 2024, in Scientific Reports.
LIMITATIONS:
Disease severity of migraine and IBD was not available. In addition, certain medications taken to relieve migraine, such as nonsteroidal anti-inflammatory drugs like ibuprofen, could cause intestinal inflammation, but there was no medication information available.
DISCLOSURES:
There was no information about study funding nor disclosures from study authors.
A version of this article appeared on Medscape.com.
Commentary: PsA in Women, February 2024

Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Another study investigated the persistence of targeted therapies for PsA in women compared with men. In a nationwide cohort study using administrative information from French health insurance, the study looked at 14,778 patients (57% women) with PsA who were new users of targeted therapies. The study showed that women had 20%-40% lower treatment persistence rates than men for tumour necrosis factor (TNF) inhibitors (adjusted hazard ratio [aHR] 1.4; 99% CI 1.3-1.5) and interleukin (IL)-17 inhibitors (aHR 1.2; 99% CI 1.1-1.3). However, the treatment persistence between both sexes was comparable for IL-12/23 inhibitor (aHR 1.1; 99% CI 0.9-1.3), IL-23 inhibitor (aHR 1.1; 99% CI 0.7-1.5), and Janus kinase (JAK) inhibitor (aHR 1.2; 99% CI 0.9-1.6) therapies. The paradigm that women have lower treatment persistence is based on studies done primarily in patients treated with TNF inhibitors. This study and a few other recent studies challenge this paradigm by indicating that other targeted therapies, especially JAK inhibitors, may not have lower persistence in women. Sex should be taken into consideration while choosing and counseling women about PsA therapies.
There are few studies on exercise and its impact on PsA. Functional training (FT) and resistance training (RT) may improve functional capacity and quality of life of patients with PsA. The safety of exercise is also not known, given that (micro)trauma is a risk factor for PsA. To evaluate this, Silva and colleagues conducted a 12-week, single-blind trial including 41 patients with PsA who were randomly assigned to undergo FT with elastic bands or RT with weight machines. They demonstrated that FT and RT led to similar improvements in functional capacity measured by the Bath Ankylosing Spondylitis Functional Index (P = .919), functional status measured by the Health Assessment Questionnaire for Spondyloarthritis (P = .932), disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (P = .700), and muscle strength. No adverse events occurred in either group. Thus, FT and RT improved functional capacity, functional status, disease activity, and muscle strength to a comparable extent in patients with PsA, with no adverse events. Both modalities may be recommended for PsA patients.
Finally, a cross-sectional study that included 503 patients with PsA, of whom 160 patients underwent treatment escalation, evaluated whether the patient-reported outcome (PsA Impact of Disease questionnaire [PsAID-12]) affected treatment decisions by the treating rheumatologist. Coyle and colleagues demonstrated that although PsAID-12 scores were higher in patients who did vs did not have a treatment escalation, physicians relied more on their assessment of disease activity rather than the PsAID-12 scores when making treatment-related decisions. Of note, physicians also reported that PsAID-12 scores influenced treatment reduction decisions.
Respiratory Virus Surge: Diagnosing COVID-19 vs RSV, Flu
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
OCD Tied to a Twofold Increased Risk for All-Cause Mortality
TOPLINE:
Obsessive-compulsive disorder (OCD) is linked to a twofold increased risk for all-cause mortality and a heightened risk for death from both natural and unnatural causes, a new study showed.
METHODOLOGY:
- Investigators studied a population-based cohort (58% female) of 61,378 people with OCD and 613,780 unaffected individuals from several Swedish population registers and a sibling cohort of 34,085 people with OCD (58% female) and 47,874 unaffected full siblings (48% female).
- The median 8.1-year follow-up and median age at first diagnosis of OCD were 27 years.
- The researchers used Cox proportional hazard models, adjusting for birth year, sex, county, country of birth (Sweden vs abroad), and sociodemographic variables.
TAKEAWAY:
- (adjusted hazard ratio [aHR], 1.82; 95% CI, 1.76-1.89), an almost threefold higher risk for mortality due to unnatural causes (aHR, 3.30; 95% CI, 3.05-3.57), and a higher risk for mortality due to natural causes (aHR, 1.31; 95% CI, 1.24-1.37).
- Of all the unnatural causes of death, suicide was most common (hazard ratio [HR], 4.90; 95% CI, 4.40-5.46), followed by accidents (HR, 1.92; 95% CI, 1.68-2.19).
- Similar results were found in the sibling comparison, where the HR of all-cause mortality was 1.85 (95% CI, 1.67-2.03), death from natural causes was 1.51 (95% CI, 1.35-1.68), and death from unnatural causes was 3.10 (95% CI, 2.52-3.80).
- Natural causes of death that were higher in the OCD vs non-OCD cohort included endocrine, nutritional, and metabolic diseases; mental and behavioral disorders; and diseases of the nervous, circulatory, respiratory, digestive, and genitourinary systems.
IN PRACTICE:
“Better surveillance, prevention, and early intervention strategies should be implemented to reduce the risk of fatal outcomes in people with OCD,” the authors wrote.
SOURCE:
Lorena Fernández de la Cruz, PhD, of Karolinska Institutet, Solna, Sweden, led the study, which was published online on January 17 in the British Medical Journal.
LIMITATIONS:
The study does not establish causality. Registry data used by the investigators only included diagnoses made in specialist care and may not have included diagnoses made in other settings. It is also unclear whether the findings, derived from a Swedish population, can be generalized to other populations, health systems, and medical practices.
DISCLOSURES:
The study was funded by the Swedish Council for Health, Working Life and Welfare, Region Stockholm, the Swedish Society of Medicine, and Karolinska Institutet. Dr. de la Cruz received royalties for contributing articles to UpToDate and Wolters Kluwer Health and for editorial work from Elsevier outside the submitted work. See the paper for disclosures of the other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
Obsessive-compulsive disorder (OCD) is linked to a twofold increased risk for all-cause mortality and a heightened risk for death from both natural and unnatural causes, a new study showed.
METHODOLOGY:
- Investigators studied a population-based cohort (58% female) of 61,378 people with OCD and 613,780 unaffected individuals from several Swedish population registers and a sibling cohort of 34,085 people with OCD (58% female) and 47,874 unaffected full siblings (48% female).
- The median 8.1-year follow-up and median age at first diagnosis of OCD were 27 years.
- The researchers used Cox proportional hazard models, adjusting for birth year, sex, county, country of birth (Sweden vs abroad), and sociodemographic variables.
TAKEAWAY:
- (adjusted hazard ratio [aHR], 1.82; 95% CI, 1.76-1.89), an almost threefold higher risk for mortality due to unnatural causes (aHR, 3.30; 95% CI, 3.05-3.57), and a higher risk for mortality due to natural causes (aHR, 1.31; 95% CI, 1.24-1.37).
- Of all the unnatural causes of death, suicide was most common (hazard ratio [HR], 4.90; 95% CI, 4.40-5.46), followed by accidents (HR, 1.92; 95% CI, 1.68-2.19).
- Similar results were found in the sibling comparison, where the HR of all-cause mortality was 1.85 (95% CI, 1.67-2.03), death from natural causes was 1.51 (95% CI, 1.35-1.68), and death from unnatural causes was 3.10 (95% CI, 2.52-3.80).
- Natural causes of death that were higher in the OCD vs non-OCD cohort included endocrine, nutritional, and metabolic diseases; mental and behavioral disorders; and diseases of the nervous, circulatory, respiratory, digestive, and genitourinary systems.
IN PRACTICE:
“Better surveillance, prevention, and early intervention strategies should be implemented to reduce the risk of fatal outcomes in people with OCD,” the authors wrote.
SOURCE:
Lorena Fernández de la Cruz, PhD, of Karolinska Institutet, Solna, Sweden, led the study, which was published online on January 17 in the British Medical Journal.
LIMITATIONS:
The study does not establish causality. Registry data used by the investigators only included diagnoses made in specialist care and may not have included diagnoses made in other settings. It is also unclear whether the findings, derived from a Swedish population, can be generalized to other populations, health systems, and medical practices.
DISCLOSURES:
The study was funded by the Swedish Council for Health, Working Life and Welfare, Region Stockholm, the Swedish Society of Medicine, and Karolinska Institutet. Dr. de la Cruz received royalties for contributing articles to UpToDate and Wolters Kluwer Health and for editorial work from Elsevier outside the submitted work. See the paper for disclosures of the other authors.
A version of this article appeared on Medscape.com.
TOPLINE:
Obsessive-compulsive disorder (OCD) is linked to a twofold increased risk for all-cause mortality and a heightened risk for death from both natural and unnatural causes, a new study showed.
METHODOLOGY:
- Investigators studied a population-based cohort (58% female) of 61,378 people with OCD and 613,780 unaffected individuals from several Swedish population registers and a sibling cohort of 34,085 people with OCD (58% female) and 47,874 unaffected full siblings (48% female).
- The median 8.1-year follow-up and median age at first diagnosis of OCD were 27 years.
- The researchers used Cox proportional hazard models, adjusting for birth year, sex, county, country of birth (Sweden vs abroad), and sociodemographic variables.
TAKEAWAY:
- (adjusted hazard ratio [aHR], 1.82; 95% CI, 1.76-1.89), an almost threefold higher risk for mortality due to unnatural causes (aHR, 3.30; 95% CI, 3.05-3.57), and a higher risk for mortality due to natural causes (aHR, 1.31; 95% CI, 1.24-1.37).
- Of all the unnatural causes of death, suicide was most common (hazard ratio [HR], 4.90; 95% CI, 4.40-5.46), followed by accidents (HR, 1.92; 95% CI, 1.68-2.19).
- Similar results were found in the sibling comparison, where the HR of all-cause mortality was 1.85 (95% CI, 1.67-2.03), death from natural causes was 1.51 (95% CI, 1.35-1.68), and death from unnatural causes was 3.10 (95% CI, 2.52-3.80).
- Natural causes of death that were higher in the OCD vs non-OCD cohort included endocrine, nutritional, and metabolic diseases; mental and behavioral disorders; and diseases of the nervous, circulatory, respiratory, digestive, and genitourinary systems.
IN PRACTICE:
“Better surveillance, prevention, and early intervention strategies should be implemented to reduce the risk of fatal outcomes in people with OCD,” the authors wrote.
SOURCE:
Lorena Fernández de la Cruz, PhD, of Karolinska Institutet, Solna, Sweden, led the study, which was published online on January 17 in the British Medical Journal.
LIMITATIONS:
The study does not establish causality. Registry data used by the investigators only included diagnoses made in specialist care and may not have included diagnoses made in other settings. It is also unclear whether the findings, derived from a Swedish population, can be generalized to other populations, health systems, and medical practices.
DISCLOSURES:
The study was funded by the Swedish Council for Health, Working Life and Welfare, Region Stockholm, the Swedish Society of Medicine, and Karolinska Institutet. Dr. de la Cruz received royalties for contributing articles to UpToDate and Wolters Kluwer Health and for editorial work from Elsevier outside the submitted work. See the paper for disclosures of the other authors.
A version of this article appeared on Medscape.com.
Commentary: Benign Breast Disease, PD-L1+ TNBC, and Exercise in BC, February 2024

The benefit of immunotherapy in combination with chemotherapy for programmed death–ligand 1–positive (PD-L1+) metastatic triple-negative breast cancer (mTNBC) has been shown in both the IMpassion130 and KEYNOTE-355 trials.[2,3] However, the IMpassion131 trial, which evaluated atezolizumab plus paclitaxel, did not show a progression-free survival (PFS) or overall survival (OS) benefit vs paclitaxel alone in PD-L1+ mTNBC.[4] Various explanations for these divergent results have been proposed, including the inherent properties of the chemotherapy backbone, patient populations, and the heterogenous nature of TNBC, which can affect response to immunotherapy. Of present, the various KEYNOTE-355 regimens (pembrolizumab plus investigator's choice chemotherapy [nab-paclitaxel, paclitaxel, or gemcitabine-carboplatin]) are US Food and Drug Administration approved for PD-L1+ mTNBC in the first-line setting. The phase 2 randomized TBCRC 043 trial investigated the effect of atezolizumab with carboplatin in patients with mTNBC and further looked at clinical and molecular correlates of response (Lehmann et al). A total of 106 patients were randomly assigned to carboplatin or carboplatin plus atezolizumab; the combination improved PFS (median PFS, 4.1 vs 2.2 mo; hazard ratio [HR] 0.66; P = .05) and OS (12.6 vs 8.6 mo; HR 0.60; P = .03). Grade 3/4 serious adverse events were more common with carboplatin-atezolizumab vs carboplatin alone (41% vs 8%). In addition, an association of better responses with PD-L1 immunotherapy was seen in patients with obesity, uncontrolled blood glucose levels, high tumor mutation burden, and increased tumor infiltrating lymphocytes. These data support the role of immunotherapy in mTNBC, highlight tumor heterogeneity within this subtype and encourage correlative studies to better define which patients benefit from immunotherapy.
Various studies have demonstrated the favorable impact of physical activity on breast cancer risk in postmenopausal women.[5] However, data in premenopausal women is less clear. Various mechanisms connecting physical activity to premenopausal breast cancer risk have been proposed including the effect of exercise on sex steroid hormones, fasting insulin levels, and inflammation.[6] A pooled analysis from 19 cohort studies including 547,601 premenopausal women, with 10,231 incident cases of breast cancer, aimed to examine the relationship between leisure-time physical activity (sports, exercise, recreational walking) and breast cancer risk in young women (Timmins et al). Higher (90th percentile) vs lower (10th percentile) levels of leisure-time physical activity were associated with a 10% reduction in breast cancer risk after adjustment for body mass index (BMI; adjusted HR 0.90; 95% CI 0.85-0.95; P < .001). They also found a significant reduction in risk: 32% (HR 0.68; P = .01) and 9% (HR 0.91; P = .005) for women with underweight (BMI < 18.5) and with average weight (BMI 18.5-24.9), respectively. Further, the effect of physical activity was most pronounced in the human epidermal growth factor receptor 2 (HER2)–enriched breast cancer subtype, wherein higher vs lower levels of activity were associated with an estimated 45% reduction in breast cancer risk (adjusted HR 0.55; 95% CI 0.37-0.82). These findings support the beneficial role of aerobic exercise and healthy body weight on breast cancer risk among premenopausal women and highlight the value of incorporating this information into counseling for our patients.
Additional References
- Figueroa JD, Gierach GL, Duggan MA, et al. Risk factors for breast cancer development by tumor characteristics among women with benign breast disease. Breast Cancer Res. 2021;23:34. doi: 10.1186/s13058-021-01410-1 Source
- Schmid P, Adams S, Rugo HS, et al, for the IMpassion130 Trial Investigators. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379:2108-2121. doi: 10.1056/nejmoa1809615 Source
- Cortes J, Rugo HS, Cescon DW, et al, for the KEYNOTE-355 Investigators. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226. doi: 10.1056/NEJMoa2202809 Source
- Miles D, Gligorov J, André F, et al, on behalf of the IMpassion131 investigators. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32:994-1004. doi: 10.1016/j.annonc.2021.05.801 Source
- Eliassen AH, Hankinson SE, Rosner B, et al. Physical activity and risk of breast cancer among postmenopausal women. Arch Intern Med. 2010;170:1758-1764. doi: 10.1001/archinternmed.2010.363 Source
- Swain CTV, Drummond AE, Boing L, et al. Linking physical activity to breast cancer via sex hormones, part 1: The effect of physical activity on sex steroid hormones. Cancer Epidemiol Biomarkers Prev. 2022;31:16-27. doi: 10.1158/1055-9965.EPI-21-0437 Source
The benefit of immunotherapy in combination with chemotherapy for programmed death–ligand 1–positive (PD-L1+) metastatic triple-negative breast cancer (mTNBC) has been shown in both the IMpassion130 and KEYNOTE-355 trials.[2,3] However, the IMpassion131 trial, which evaluated atezolizumab plus paclitaxel, did not show a progression-free survival (PFS) or overall survival (OS) benefit vs paclitaxel alone in PD-L1+ mTNBC.[4] Various explanations for these divergent results have been proposed, including the inherent properties of the chemotherapy backbone, patient populations, and the heterogenous nature of TNBC, which can affect response to immunotherapy. Of present, the various KEYNOTE-355 regimens (pembrolizumab plus investigator's choice chemotherapy [nab-paclitaxel, paclitaxel, or gemcitabine-carboplatin]) are US Food and Drug Administration approved for PD-L1+ mTNBC in the first-line setting. The phase 2 randomized TBCRC 043 trial investigated the effect of atezolizumab with carboplatin in patients with mTNBC and further looked at clinical and molecular correlates of response (Lehmann et al). A total of 106 patients were randomly assigned to carboplatin or carboplatin plus atezolizumab; the combination improved PFS (median PFS, 4.1 vs 2.2 mo; hazard ratio [HR] 0.66; P = .05) and OS (12.6 vs 8.6 mo; HR 0.60; P = .03). Grade 3/4 serious adverse events were more common with carboplatin-atezolizumab vs carboplatin alone (41% vs 8%). In addition, an association of better responses with PD-L1 immunotherapy was seen in patients with obesity, uncontrolled blood glucose levels, high tumor mutation burden, and increased tumor infiltrating lymphocytes. These data support the role of immunotherapy in mTNBC, highlight tumor heterogeneity within this subtype and encourage correlative studies to better define which patients benefit from immunotherapy.
Various studies have demonstrated the favorable impact of physical activity on breast cancer risk in postmenopausal women.[5] However, data in premenopausal women is less clear. Various mechanisms connecting physical activity to premenopausal breast cancer risk have been proposed including the effect of exercise on sex steroid hormones, fasting insulin levels, and inflammation.[6] A pooled analysis from 19 cohort studies including 547,601 premenopausal women, with 10,231 incident cases of breast cancer, aimed to examine the relationship between leisure-time physical activity (sports, exercise, recreational walking) and breast cancer risk in young women (Timmins et al). Higher (90th percentile) vs lower (10th percentile) levels of leisure-time physical activity were associated with a 10% reduction in breast cancer risk after adjustment for body mass index (BMI; adjusted HR 0.90; 95% CI 0.85-0.95; P < .001). They also found a significant reduction in risk: 32% (HR 0.68; P = .01) and 9% (HR 0.91; P = .005) for women with underweight (BMI < 18.5) and with average weight (BMI 18.5-24.9), respectively. Further, the effect of physical activity was most pronounced in the human epidermal growth factor receptor 2 (HER2)–enriched breast cancer subtype, wherein higher vs lower levels of activity were associated with an estimated 45% reduction in breast cancer risk (adjusted HR 0.55; 95% CI 0.37-0.82). These findings support the beneficial role of aerobic exercise and healthy body weight on breast cancer risk among premenopausal women and highlight the value of incorporating this information into counseling for our patients.
Additional References
- Figueroa JD, Gierach GL, Duggan MA, et al. Risk factors for breast cancer development by tumor characteristics among women with benign breast disease. Breast Cancer Res. 2021;23:34. doi: 10.1186/s13058-021-01410-1 Source
- Schmid P, Adams S, Rugo HS, et al, for the IMpassion130 Trial Investigators. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379:2108-2121. doi: 10.1056/nejmoa1809615 Source
- Cortes J, Rugo HS, Cescon DW, et al, for the KEYNOTE-355 Investigators. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226. doi: 10.1056/NEJMoa2202809 Source
- Miles D, Gligorov J, André F, et al, on behalf of the IMpassion131 investigators. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32:994-1004. doi: 10.1016/j.annonc.2021.05.801 Source
- Eliassen AH, Hankinson SE, Rosner B, et al. Physical activity and risk of breast cancer among postmenopausal women. Arch Intern Med. 2010;170:1758-1764. doi: 10.1001/archinternmed.2010.363 Source
- Swain CTV, Drummond AE, Boing L, et al. Linking physical activity to breast cancer via sex hormones, part 1: The effect of physical activity on sex steroid hormones. Cancer Epidemiol Biomarkers Prev. 2022;31:16-27. doi: 10.1158/1055-9965.EPI-21-0437 Source
The benefit of immunotherapy in combination with chemotherapy for programmed death–ligand 1–positive (PD-L1+) metastatic triple-negative breast cancer (mTNBC) has been shown in both the IMpassion130 and KEYNOTE-355 trials.[2,3] However, the IMpassion131 trial, which evaluated atezolizumab plus paclitaxel, did not show a progression-free survival (PFS) or overall survival (OS) benefit vs paclitaxel alone in PD-L1+ mTNBC.[4] Various explanations for these divergent results have been proposed, including the inherent properties of the chemotherapy backbone, patient populations, and the heterogenous nature of TNBC, which can affect response to immunotherapy. Of present, the various KEYNOTE-355 regimens (pembrolizumab plus investigator's choice chemotherapy [nab-paclitaxel, paclitaxel, or gemcitabine-carboplatin]) are US Food and Drug Administration approved for PD-L1+ mTNBC in the first-line setting. The phase 2 randomized TBCRC 043 trial investigated the effect of atezolizumab with carboplatin in patients with mTNBC and further looked at clinical and molecular correlates of response (Lehmann et al). A total of 106 patients were randomly assigned to carboplatin or carboplatin plus atezolizumab; the combination improved PFS (median PFS, 4.1 vs 2.2 mo; hazard ratio [HR] 0.66; P = .05) and OS (12.6 vs 8.6 mo; HR 0.60; P = .03). Grade 3/4 serious adverse events were more common with carboplatin-atezolizumab vs carboplatin alone (41% vs 8%). In addition, an association of better responses with PD-L1 immunotherapy was seen in patients with obesity, uncontrolled blood glucose levels, high tumor mutation burden, and increased tumor infiltrating lymphocytes. These data support the role of immunotherapy in mTNBC, highlight tumor heterogeneity within this subtype and encourage correlative studies to better define which patients benefit from immunotherapy.
Various studies have demonstrated the favorable impact of physical activity on breast cancer risk in postmenopausal women.[5] However, data in premenopausal women is less clear. Various mechanisms connecting physical activity to premenopausal breast cancer risk have been proposed including the effect of exercise on sex steroid hormones, fasting insulin levels, and inflammation.[6] A pooled analysis from 19 cohort studies including 547,601 premenopausal women, with 10,231 incident cases of breast cancer, aimed to examine the relationship between leisure-time physical activity (sports, exercise, recreational walking) and breast cancer risk in young women (Timmins et al). Higher (90th percentile) vs lower (10th percentile) levels of leisure-time physical activity were associated with a 10% reduction in breast cancer risk after adjustment for body mass index (BMI; adjusted HR 0.90; 95% CI 0.85-0.95; P < .001). They also found a significant reduction in risk: 32% (HR 0.68; P = .01) and 9% (HR 0.91; P = .005) for women with underweight (BMI < 18.5) and with average weight (BMI 18.5-24.9), respectively. Further, the effect of physical activity was most pronounced in the human epidermal growth factor receptor 2 (HER2)–enriched breast cancer subtype, wherein higher vs lower levels of activity were associated with an estimated 45% reduction in breast cancer risk (adjusted HR 0.55; 95% CI 0.37-0.82). These findings support the beneficial role of aerobic exercise and healthy body weight on breast cancer risk among premenopausal women and highlight the value of incorporating this information into counseling for our patients.
Additional References
- Figueroa JD, Gierach GL, Duggan MA, et al. Risk factors for breast cancer development by tumor characteristics among women with benign breast disease. Breast Cancer Res. 2021;23:34. doi: 10.1186/s13058-021-01410-1 Source
- Schmid P, Adams S, Rugo HS, et al, for the IMpassion130 Trial Investigators. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379:2108-2121. doi: 10.1056/nejmoa1809615 Source
- Cortes J, Rugo HS, Cescon DW, et al, for the KEYNOTE-355 Investigators. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387:217-226. doi: 10.1056/NEJMoa2202809 Source
- Miles D, Gligorov J, André F, et al, on behalf of the IMpassion131 investigators. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32:994-1004. doi: 10.1016/j.annonc.2021.05.801 Source
- Eliassen AH, Hankinson SE, Rosner B, et al. Physical activity and risk of breast cancer among postmenopausal women. Arch Intern Med. 2010;170:1758-1764. doi: 10.1001/archinternmed.2010.363 Source
- Swain CTV, Drummond AE, Boing L, et al. Linking physical activity to breast cancer via sex hormones, part 1: The effect of physical activity on sex steroid hormones. Cancer Epidemiol Biomarkers Prev. 2022;31:16-27. doi: 10.1158/1055-9965.EPI-21-0437 Source
Once-Weekly Insulin Better Than Daily in Type 2 Diabetes
TOPLINE:
Once-weekly insulin icodec shows a higher glycated A1c reduction than once-daily basal insulin analogs in patients with type 2 diabetes (T2D), without major safety concerns.
METHODOLOGY:
- A meta-analysis of five phase 3 ONWARDS randomized controlled trials included 3764 patients with T2D.
- The trials compared the effects of the weekly insulin icodec with those of the daily basal insulin analogs glargine and degludec over 26-78 months.
- The primary outcome was the change in A1c levels.
- Secondary outcomes included fasting plasma glucose levels, A1c levels < 7%, time in target glycemic range, body weight changes, insulin dose, hypoglycemia events, and adverse events.
TAKEAWAY:
- A1c levels < 7% were observed in a higher percentage of patients in the insulin icodec group than in the comparator group (odds ratio, 1.51; P = .004).
- In subgroup analyses, insulin icodec was superior to insulin degludec by several measures but comparatively similar to glargine.
- Insulin icodec was associated with no major safety concerns and had a slightly higher incidence of levels 1, 2, and combined 2/3 than degludec but no significant differences compared with glargine.
IN PRACTICE:
“Sustained glycemic control with once-weekly injections of insulin icodec would lead to better patient acceptance and treatment satisfaction,” the authors wrote.
SOURCE:
This study, authored by Sahana Shetty, MD, and Renuka Suvarna, MSc, Manipal Academy of Higher Education, Department of Endocrinology, Kasturba Medical College, Manipal, Karnataka, was published online on January 8, 2024, in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The comparator group included individuals who used different basal insulin analogs. This heterogeneity in the comparator group introduced a potential source of variability, making it challenging to isolate the specific effects of insulin icodec compared with a standardized comparator. Blinding or masking of participants was performed in only one of the five trials.
DISCLOSURES:
The authors declared no conflicts of interest. All five clinical trials in the meta-analysis were sponsored by Novo Nordisk.
A version of this article appeared on Medscape.com.
TOPLINE:
Once-weekly insulin icodec shows a higher glycated A1c reduction than once-daily basal insulin analogs in patients with type 2 diabetes (T2D), without major safety concerns.
METHODOLOGY:
- A meta-analysis of five phase 3 ONWARDS randomized controlled trials included 3764 patients with T2D.
- The trials compared the effects of the weekly insulin icodec with those of the daily basal insulin analogs glargine and degludec over 26-78 months.
- The primary outcome was the change in A1c levels.
- Secondary outcomes included fasting plasma glucose levels, A1c levels < 7%, time in target glycemic range, body weight changes, insulin dose, hypoglycemia events, and adverse events.
TAKEAWAY:
- A1c levels < 7% were observed in a higher percentage of patients in the insulin icodec group than in the comparator group (odds ratio, 1.51; P = .004).
- In subgroup analyses, insulin icodec was superior to insulin degludec by several measures but comparatively similar to glargine.
- Insulin icodec was associated with no major safety concerns and had a slightly higher incidence of levels 1, 2, and combined 2/3 than degludec but no significant differences compared with glargine.
IN PRACTICE:
“Sustained glycemic control with once-weekly injections of insulin icodec would lead to better patient acceptance and treatment satisfaction,” the authors wrote.
SOURCE:
This study, authored by Sahana Shetty, MD, and Renuka Suvarna, MSc, Manipal Academy of Higher Education, Department of Endocrinology, Kasturba Medical College, Manipal, Karnataka, was published online on January 8, 2024, in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The comparator group included individuals who used different basal insulin analogs. This heterogeneity in the comparator group introduced a potential source of variability, making it challenging to isolate the specific effects of insulin icodec compared with a standardized comparator. Blinding or masking of participants was performed in only one of the five trials.
DISCLOSURES:
The authors declared no conflicts of interest. All five clinical trials in the meta-analysis were sponsored by Novo Nordisk.
A version of this article appeared on Medscape.com.
TOPLINE:
Once-weekly insulin icodec shows a higher glycated A1c reduction than once-daily basal insulin analogs in patients with type 2 diabetes (T2D), without major safety concerns.
METHODOLOGY:
- A meta-analysis of five phase 3 ONWARDS randomized controlled trials included 3764 patients with T2D.
- The trials compared the effects of the weekly insulin icodec with those of the daily basal insulin analogs glargine and degludec over 26-78 months.
- The primary outcome was the change in A1c levels.
- Secondary outcomes included fasting plasma glucose levels, A1c levels < 7%, time in target glycemic range, body weight changes, insulin dose, hypoglycemia events, and adverse events.
TAKEAWAY:
- A1c levels < 7% were observed in a higher percentage of patients in the insulin icodec group than in the comparator group (odds ratio, 1.51; P = .004).
- In subgroup analyses, insulin icodec was superior to insulin degludec by several measures but comparatively similar to glargine.
- Insulin icodec was associated with no major safety concerns and had a slightly higher incidence of levels 1, 2, and combined 2/3 than degludec but no significant differences compared with glargine.
IN PRACTICE:
“Sustained glycemic control with once-weekly injections of insulin icodec would lead to better patient acceptance and treatment satisfaction,” the authors wrote.
SOURCE:
This study, authored by Sahana Shetty, MD, and Renuka Suvarna, MSc, Manipal Academy of Higher Education, Department of Endocrinology, Kasturba Medical College, Manipal, Karnataka, was published online on January 8, 2024, in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The comparator group included individuals who used different basal insulin analogs. This heterogeneity in the comparator group introduced a potential source of variability, making it challenging to isolate the specific effects of insulin icodec compared with a standardized comparator. Blinding or masking of participants was performed in only one of the five trials.
DISCLOSURES:
The authors declared no conflicts of interest. All five clinical trials in the meta-analysis were sponsored by Novo Nordisk.
A version of this article appeared on Medscape.com.
Combo Tx Best in Metastatic Prostate Cancer with HRR Mutations
That’s the conclusion of investigators in the phase 2 BRCAAway trial, which compared a combination of abiraterone (Zytiga) and prednisone plus olaparib (Lynparza) against sequential therapy with the same agents.
At the time of data cutoff, median progression-free survival (PFS), the primary endpoint, was 39 months for patients randomized to the combination, compared with 8.4 months for those assigned to abiraterone/prednisone, and 14 months for those assigned to olaparib monotherapy, reported Maha Hussain, MD, of the Robert H. Lurie Comprehensive Cancer Center in Chicago.
“In patients with metastatic castration-resistant prostate cancer [mCRPC] and BRCA1/2 or ATM alterations, abiraterone and prednisone plus olaparib was well tolerated and resulted in better progression-free survival and response rates vs. single-agent olaparib or abiraterone/prednisone,” she said in an oral abstract presentation at the ASCO Genitourinary Cancers Symposium.
Although the study allowed crossover between the single-agent arms at the time of progression, only a few patients made the switch. Nonetheless, in these patients the PFS with the frontline combination was superior to that of sequential therapy, she noted.
Study Rationale and Design
Germline or somatic mutations in genes encoding for homologous recombination-repair occur in about 20% of men with mCRPC. Olaparib, a PARP1 (poly-adp ribose polymerase-1) inhibitor, interacts with androgen signaling, and preclinical studies have shown that castration-resistant prostate tumor cells have increased PARP1 activity. In addition, PARP1 has been shown preclinically to synergize with androgen receptor pathway inhibitors (ARPIs) such as abiraterone, Dr. Hussain explained.
The BRCAAway trial was designed to test whether co-targeting the androgen receptor and PARP1 could result in higher and more durable responses than current frontline therapies in patients with mCRPC with DNA-damage response mutations.
Patients with mCRPC with no prior exposure to either a PARP1 inhibitor, androgen receptor inhibitor, or mCRPC-directed chemotherapy underwent next-generation sequencing and germline testing of tumor tissues, and those patients found to have inactivating BRCA1/2 and/or ATM alterations were randomized on a 1:1:1 basis to either abiraterone 1000 mg daily plus prednisone 5 mg twice daily (19 patients); olaparib 300 mg twice daily (21 patients); or to the combination (21 patients).
The primary endpoint was radiographic PFS according to RECIST 1.1 criteria, Prostate Cancer Working Group 3 criteria, clinical assessment, or death.
As noted, the median PFS was 8.4 months with abiraterone/prednisone, 14 months with olaparib, and 39 months with the combination.
Secondary endpoints also favored the combination therapy arm, with objective response rates of 22%, 14%, and 33%, respectively; PSA response rates of 61%, 67% and 95%; and undetectable PSA response rates of 17%, 14%, and 33%.
A total of 8 of 19 patients on abiraterone were crossed over to olaparib, and 8 of 21 initially assigned to olaparib were crossed over to abiraterone. In these patients the median PFS from crossover was 8.3 and 7.2 months, respectively. In each crossover group the median PFS from the time of randomization was 16 months.
There were no grade 4 adverse events or treatment-related deaths reported in any of the study arms, and “essentially when you look at the adverse events, they pretty much are consistent with what you would expect to see with these particular agents,” Dr. Hussain said.
“Overall the patients were tolerating the treatment well,” she added.
Practice Changing with Caveats
Kim N. Chi, MD, FRCPC, of the University of British Columbia in Vancouver, BC, Canada, the invited discussant, said that the strengths of the study included an olaparib monotherapy arm — something that was missing from phase 3 trials — that provides insights into how PARP inhibitors perform in this population. He also applauded the inclusion of clinical assessment as a primary endpoint, noting that “this is what we do in routine practice, and therefore, the generalizability of the trial becomes more evident.”
The crossover design provides important information about whether an upfront combination or a sequential therapy approach is more effective, as well, he added.
He pointed out, however, that the trial was limited by small sample size and by its “horse race” design rather than as a comparison trial.
“So how does the BRCAAway trial change our practice? Despite the limitations, I think it does support an upfront PARP inhibitor-ARPI combination as firstline therapy for HRR gene-mutated metastatic CRPC. These data suggest synergy, and most importantly, there is no loss of opportunity [for more effective therapies]. However, the limitations of the trial will not end this debate today,” he said.
The trial was funded by AstraZeneca. Both Dr. Hussain and Dr. Chi disclosed honoraria, consulting/advising, and institutional research funding from AstraZeneca and others.
That’s the conclusion of investigators in the phase 2 BRCAAway trial, which compared a combination of abiraterone (Zytiga) and prednisone plus olaparib (Lynparza) against sequential therapy with the same agents.
At the time of data cutoff, median progression-free survival (PFS), the primary endpoint, was 39 months for patients randomized to the combination, compared with 8.4 months for those assigned to abiraterone/prednisone, and 14 months for those assigned to olaparib monotherapy, reported Maha Hussain, MD, of the Robert H. Lurie Comprehensive Cancer Center in Chicago.
“In patients with metastatic castration-resistant prostate cancer [mCRPC] and BRCA1/2 or ATM alterations, abiraterone and prednisone plus olaparib was well tolerated and resulted in better progression-free survival and response rates vs. single-agent olaparib or abiraterone/prednisone,” she said in an oral abstract presentation at the ASCO Genitourinary Cancers Symposium.
Although the study allowed crossover between the single-agent arms at the time of progression, only a few patients made the switch. Nonetheless, in these patients the PFS with the frontline combination was superior to that of sequential therapy, she noted.
Study Rationale and Design
Germline or somatic mutations in genes encoding for homologous recombination-repair occur in about 20% of men with mCRPC. Olaparib, a PARP1 (poly-adp ribose polymerase-1) inhibitor, interacts with androgen signaling, and preclinical studies have shown that castration-resistant prostate tumor cells have increased PARP1 activity. In addition, PARP1 has been shown preclinically to synergize with androgen receptor pathway inhibitors (ARPIs) such as abiraterone, Dr. Hussain explained.
The BRCAAway trial was designed to test whether co-targeting the androgen receptor and PARP1 could result in higher and more durable responses than current frontline therapies in patients with mCRPC with DNA-damage response mutations.
Patients with mCRPC with no prior exposure to either a PARP1 inhibitor, androgen receptor inhibitor, or mCRPC-directed chemotherapy underwent next-generation sequencing and germline testing of tumor tissues, and those patients found to have inactivating BRCA1/2 and/or ATM alterations were randomized on a 1:1:1 basis to either abiraterone 1000 mg daily plus prednisone 5 mg twice daily (19 patients); olaparib 300 mg twice daily (21 patients); or to the combination (21 patients).
The primary endpoint was radiographic PFS according to RECIST 1.1 criteria, Prostate Cancer Working Group 3 criteria, clinical assessment, or death.
As noted, the median PFS was 8.4 months with abiraterone/prednisone, 14 months with olaparib, and 39 months with the combination.
Secondary endpoints also favored the combination therapy arm, with objective response rates of 22%, 14%, and 33%, respectively; PSA response rates of 61%, 67% and 95%; and undetectable PSA response rates of 17%, 14%, and 33%.
A total of 8 of 19 patients on abiraterone were crossed over to olaparib, and 8 of 21 initially assigned to olaparib were crossed over to abiraterone. In these patients the median PFS from crossover was 8.3 and 7.2 months, respectively. In each crossover group the median PFS from the time of randomization was 16 months.
There were no grade 4 adverse events or treatment-related deaths reported in any of the study arms, and “essentially when you look at the adverse events, they pretty much are consistent with what you would expect to see with these particular agents,” Dr. Hussain said.
“Overall the patients were tolerating the treatment well,” she added.
Practice Changing with Caveats
Kim N. Chi, MD, FRCPC, of the University of British Columbia in Vancouver, BC, Canada, the invited discussant, said that the strengths of the study included an olaparib monotherapy arm — something that was missing from phase 3 trials — that provides insights into how PARP inhibitors perform in this population. He also applauded the inclusion of clinical assessment as a primary endpoint, noting that “this is what we do in routine practice, and therefore, the generalizability of the trial becomes more evident.”
The crossover design provides important information about whether an upfront combination or a sequential therapy approach is more effective, as well, he added.
He pointed out, however, that the trial was limited by small sample size and by its “horse race” design rather than as a comparison trial.
“So how does the BRCAAway trial change our practice? Despite the limitations, I think it does support an upfront PARP inhibitor-ARPI combination as firstline therapy for HRR gene-mutated metastatic CRPC. These data suggest synergy, and most importantly, there is no loss of opportunity [for more effective therapies]. However, the limitations of the trial will not end this debate today,” he said.
The trial was funded by AstraZeneca. Both Dr. Hussain and Dr. Chi disclosed honoraria, consulting/advising, and institutional research funding from AstraZeneca and others.
That’s the conclusion of investigators in the phase 2 BRCAAway trial, which compared a combination of abiraterone (Zytiga) and prednisone plus olaparib (Lynparza) against sequential therapy with the same agents.
At the time of data cutoff, median progression-free survival (PFS), the primary endpoint, was 39 months for patients randomized to the combination, compared with 8.4 months for those assigned to abiraterone/prednisone, and 14 months for those assigned to olaparib monotherapy, reported Maha Hussain, MD, of the Robert H. Lurie Comprehensive Cancer Center in Chicago.
“In patients with metastatic castration-resistant prostate cancer [mCRPC] and BRCA1/2 or ATM alterations, abiraterone and prednisone plus olaparib was well tolerated and resulted in better progression-free survival and response rates vs. single-agent olaparib or abiraterone/prednisone,” she said in an oral abstract presentation at the ASCO Genitourinary Cancers Symposium.
Although the study allowed crossover between the single-agent arms at the time of progression, only a few patients made the switch. Nonetheless, in these patients the PFS with the frontline combination was superior to that of sequential therapy, she noted.
Study Rationale and Design
Germline or somatic mutations in genes encoding for homologous recombination-repair occur in about 20% of men with mCRPC. Olaparib, a PARP1 (poly-adp ribose polymerase-1) inhibitor, interacts with androgen signaling, and preclinical studies have shown that castration-resistant prostate tumor cells have increased PARP1 activity. In addition, PARP1 has been shown preclinically to synergize with androgen receptor pathway inhibitors (ARPIs) such as abiraterone, Dr. Hussain explained.
The BRCAAway trial was designed to test whether co-targeting the androgen receptor and PARP1 could result in higher and more durable responses than current frontline therapies in patients with mCRPC with DNA-damage response mutations.
Patients with mCRPC with no prior exposure to either a PARP1 inhibitor, androgen receptor inhibitor, or mCRPC-directed chemotherapy underwent next-generation sequencing and germline testing of tumor tissues, and those patients found to have inactivating BRCA1/2 and/or ATM alterations were randomized on a 1:1:1 basis to either abiraterone 1000 mg daily plus prednisone 5 mg twice daily (19 patients); olaparib 300 mg twice daily (21 patients); or to the combination (21 patients).
The primary endpoint was radiographic PFS according to RECIST 1.1 criteria, Prostate Cancer Working Group 3 criteria, clinical assessment, or death.
As noted, the median PFS was 8.4 months with abiraterone/prednisone, 14 months with olaparib, and 39 months with the combination.
Secondary endpoints also favored the combination therapy arm, with objective response rates of 22%, 14%, and 33%, respectively; PSA response rates of 61%, 67% and 95%; and undetectable PSA response rates of 17%, 14%, and 33%.
A total of 8 of 19 patients on abiraterone were crossed over to olaparib, and 8 of 21 initially assigned to olaparib were crossed over to abiraterone. In these patients the median PFS from crossover was 8.3 and 7.2 months, respectively. In each crossover group the median PFS from the time of randomization was 16 months.
There were no grade 4 adverse events or treatment-related deaths reported in any of the study arms, and “essentially when you look at the adverse events, they pretty much are consistent with what you would expect to see with these particular agents,” Dr. Hussain said.
“Overall the patients were tolerating the treatment well,” she added.
Practice Changing with Caveats
Kim N. Chi, MD, FRCPC, of the University of British Columbia in Vancouver, BC, Canada, the invited discussant, said that the strengths of the study included an olaparib monotherapy arm — something that was missing from phase 3 trials — that provides insights into how PARP inhibitors perform in this population. He also applauded the inclusion of clinical assessment as a primary endpoint, noting that “this is what we do in routine practice, and therefore, the generalizability of the trial becomes more evident.”
The crossover design provides important information about whether an upfront combination or a sequential therapy approach is more effective, as well, he added.
He pointed out, however, that the trial was limited by small sample size and by its “horse race” design rather than as a comparison trial.
“So how does the BRCAAway trial change our practice? Despite the limitations, I think it does support an upfront PARP inhibitor-ARPI combination as firstline therapy for HRR gene-mutated metastatic CRPC. These data suggest synergy, and most importantly, there is no loss of opportunity [for more effective therapies]. However, the limitations of the trial will not end this debate today,” he said.
The trial was funded by AstraZeneca. Both Dr. Hussain and Dr. Chi disclosed honoraria, consulting/advising, and institutional research funding from AstraZeneca and others.
FROM ASCO GU 2024
New Criteria Identify Sepsis in Children With Infection
New criteria for pediatric sepsis, based on a novel score that predicts mortality in children with suspected or confirmed infection, perform better than existing organ dysfunction scores and criteria and have the potential to improve clinical care globally, researchers say.
Current pediatric-specific criteria for sepsis were published in 2005, based on expert opinion. In 2016, sepsis was redefined for adults as life-threatening organ dysfunction caused by a dysregulated host response to infection, as opposed to an earlier focus on systemic inflammation. But the paradigm-shifting changes were not extended to children (< 18 years, but not newborns), setting the stage for the new initiative.
The new criteria, and their development and validation, were published in JAMA and presented the same day at the Society of Critical Care Medicine’s 2024 Critical Care Congress in Phoenix, Arizona.
International Consensus
“The new criteria we derived are based on data from electronic health records and analysis of more than 3 million pediatric healthcare encounters from 10 hospitals around the world, including in low-resource settings,” L. Nelson Sanchez-Pinto, MD, MBI, a critical care physician at the Ann and Robert H. Lurie Children’s Hospital of Chicago, told this news organization.
Dr. Sanchez-Pinto co-led the data group of the international expert task force convened by the Society of Critical Care Medicine (SCCM) to develop and validate the criteria, which are based on evidence from an international survey, systematic review and meta-analysis, a newly created organ dysfunction score (Phoenix Sepsis Score), and sites on four continents.
Based on the findings, the task force now suggests that pediatric sepsis be defined by a Phoenix Sepsis Score of at least 2 points in children with suspected infection, which indicates potentially life-threatening dysfunction of the respiratory, cardiovascular, coagulation, and/or neurological systems. Septic shock is defined as sepsis with at least 1 cardiovascular point in the score.
Disparities Across Settings
To derive and validate the new criteria across differently resourced settings, the researchers conducted a multicenter, international, retrospective cohort study involving 10 health systems in the United States, Colombia, Bangladesh, China, and Kenya, 3 of which were used as external validation sites.
Data were collected from pediatric emergency and inpatient encounters from 2010 to 2019. The development set comprised 3,049,699 children, and the external validation set included 581,317.
Stacked regression models to predict mortality in children with suspected infection were derived and validated using the best-performing organ dysfunction subscores from eight existing scores.
The final model was then translated into the integer-based Phoenix Sepsis Score and used to establish binary criteria for sepsis and septic shock.
Among 172,984 children with suspected infection in the first 24 hours (development set; 1.2% mortality), a four-organ-system model performed best. The Phoenix Sepsis Score — the integer version of the model — had areas under the precision recall curve of 0.23 to 0.38, and areas under the receiver operating characteristic curve of 0.71 to 0.92 to predict mortality in the validation sets.
A Phoenix Sepsis Score of 2 points or higher in children with suspected infection as criteria for sepsis, plus 1 or more cardiovascular points as criteria for septic shock, resulted in a higher positive predictive value and higher or similar sensitivity compared with the 2005 International Pediatric Sepsis Consensus Conference criteria across differently resourced settings.
Specifically, children with a Phoenix Sepsis Score of at least 2 points had in-hospital mortality of 7.1% in higher-resource settings and 28.5% in lower-resource settings — more than 8 times that of children with suspected infection not meeting these criteria.
Mortality also was higher in children who had organ dysfunction in at least one of four organ systems — respiratory, cardiovascular, coagulation, and/or neurological — that was not the primary site of infection.
Children with septic shock, indicated by at least 1 cardiovascular point in the Phoenix Sepsis Score, had severe hypotension for age, blood lactate exceeding 5 mmol/L, or need for vasoactive medication. These children had an in-hospital mortality rate of 10.8% in higher-resource settings and 33.5% in lower-resource settings.
A Better Score
Given the findings, the task force recommends that “the former criteria based on systemic inflammatory response syndrome should not be used to diagnose sepsis in children [and] the former term severe sepsis should no longer be used because sepsis is life-threatening organ dysfunction associated with infection and is thus indicative of a severe disease state.”
The task force cautions that although the four organs in the Phoenix Sepsis Score are most commonly involved in sepsis, “this does not diminish the crucial importance of the assessment and management of other organ dysfunction.”
Furthermore, they emphasize that the Phoenix score was designed to identify sepsis in children, not to screen children at risk for developing sepsis or early identification of children with suspected sepsis.
Additional Considerations
In related editorials, commentators noted some caveats and concerns with regard to the study design and the new criteria.
Roberto Jabornisky, MD, PhD, of National University of the Northeast, Corrientes, Argentina, and colleagues pointed out that “all the low-resource validation sites were institutions with electronic health records and most had PICUs [pediatric intensive care units], which does not adequately reflect conditions in most low-resource settings. These factors introduce a distinct bias favoring a ‘PICU-based consensus,’ potentially limiting the generalizability and adoption of the new criteria by health care practitioners in non-PICU and nonhospital settings responsible for recognizing and managing children with sepsis.” The editorialists called for additional prospective validation in differently resourced settings, especially those with the highest disease burdens.
“Until then,” they wrote, “it is essential to refrain from considering these criteria as an inflexible directive governing medical interventions for pediatric sepsis. No definition can fully substitute for the clinical judgment of an experienced, vigilant clinician caring for an unwell child.”
Erin F. Carlton, MD, MSc of the University of Michigan, Ann Arbor, and colleagues added in a separate editorial, “The Phoenix criteria identify a sicker subset of patients than prior SIRS [systemic inflammatory response syndrome]-based criteria. Some may worry this higher threshold could delay management of patients not meeting sepsis criteria. Just as patients with chest pain and a troponin leak warrant monitoring and treatment (but are not prioritized for immediate heart catheterization), patients with infection need monitoring and treatment. Improvements in care should thus be judged not only by improved outcomes among patients with sepsis but also by decreased progression to sepsis among patients with infection.”
The International Consensus Criteria paper was supported by the Society of Critical Care Medicine and a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development to Tellen C. Bennett, MD, MS, and Nelson Sanchez-Pinto, MD. Data for the Kenya site were collected with support of the Wellcome Trust to the Kenya Major Overseas Programme. Dr. Jabornisky reported no conflicts of interest. Dr. Carlton reported serving on the Pediatric Surviving Sepsis Campaign Guideline committee and receiving grant support from the NIH.
New criteria for pediatric sepsis, based on a novel score that predicts mortality in children with suspected or confirmed infection, perform better than existing organ dysfunction scores and criteria and have the potential to improve clinical care globally, researchers say.
Current pediatric-specific criteria for sepsis were published in 2005, based on expert opinion. In 2016, sepsis was redefined for adults as life-threatening organ dysfunction caused by a dysregulated host response to infection, as opposed to an earlier focus on systemic inflammation. But the paradigm-shifting changes were not extended to children (< 18 years, but not newborns), setting the stage for the new initiative.
The new criteria, and their development and validation, were published in JAMA and presented the same day at the Society of Critical Care Medicine’s 2024 Critical Care Congress in Phoenix, Arizona.
International Consensus
“The new criteria we derived are based on data from electronic health records and analysis of more than 3 million pediatric healthcare encounters from 10 hospitals around the world, including in low-resource settings,” L. Nelson Sanchez-Pinto, MD, MBI, a critical care physician at the Ann and Robert H. Lurie Children’s Hospital of Chicago, told this news organization.
Dr. Sanchez-Pinto co-led the data group of the international expert task force convened by the Society of Critical Care Medicine (SCCM) to develop and validate the criteria, which are based on evidence from an international survey, systematic review and meta-analysis, a newly created organ dysfunction score (Phoenix Sepsis Score), and sites on four continents.
Based on the findings, the task force now suggests that pediatric sepsis be defined by a Phoenix Sepsis Score of at least 2 points in children with suspected infection, which indicates potentially life-threatening dysfunction of the respiratory, cardiovascular, coagulation, and/or neurological systems. Septic shock is defined as sepsis with at least 1 cardiovascular point in the score.
Disparities Across Settings
To derive and validate the new criteria across differently resourced settings, the researchers conducted a multicenter, international, retrospective cohort study involving 10 health systems in the United States, Colombia, Bangladesh, China, and Kenya, 3 of which were used as external validation sites.
Data were collected from pediatric emergency and inpatient encounters from 2010 to 2019. The development set comprised 3,049,699 children, and the external validation set included 581,317.
Stacked regression models to predict mortality in children with suspected infection were derived and validated using the best-performing organ dysfunction subscores from eight existing scores.
The final model was then translated into the integer-based Phoenix Sepsis Score and used to establish binary criteria for sepsis and septic shock.
Among 172,984 children with suspected infection in the first 24 hours (development set; 1.2% mortality), a four-organ-system model performed best. The Phoenix Sepsis Score — the integer version of the model — had areas under the precision recall curve of 0.23 to 0.38, and areas under the receiver operating characteristic curve of 0.71 to 0.92 to predict mortality in the validation sets.
A Phoenix Sepsis Score of 2 points or higher in children with suspected infection as criteria for sepsis, plus 1 or more cardiovascular points as criteria for septic shock, resulted in a higher positive predictive value and higher or similar sensitivity compared with the 2005 International Pediatric Sepsis Consensus Conference criteria across differently resourced settings.
Specifically, children with a Phoenix Sepsis Score of at least 2 points had in-hospital mortality of 7.1% in higher-resource settings and 28.5% in lower-resource settings — more than 8 times that of children with suspected infection not meeting these criteria.
Mortality also was higher in children who had organ dysfunction in at least one of four organ systems — respiratory, cardiovascular, coagulation, and/or neurological — that was not the primary site of infection.
Children with septic shock, indicated by at least 1 cardiovascular point in the Phoenix Sepsis Score, had severe hypotension for age, blood lactate exceeding 5 mmol/L, or need for vasoactive medication. These children had an in-hospital mortality rate of 10.8% in higher-resource settings and 33.5% in lower-resource settings.
A Better Score
Given the findings, the task force recommends that “the former criteria based on systemic inflammatory response syndrome should not be used to diagnose sepsis in children [and] the former term severe sepsis should no longer be used because sepsis is life-threatening organ dysfunction associated with infection and is thus indicative of a severe disease state.”
The task force cautions that although the four organs in the Phoenix Sepsis Score are most commonly involved in sepsis, “this does not diminish the crucial importance of the assessment and management of other organ dysfunction.”
Furthermore, they emphasize that the Phoenix score was designed to identify sepsis in children, not to screen children at risk for developing sepsis or early identification of children with suspected sepsis.
Additional Considerations
In related editorials, commentators noted some caveats and concerns with regard to the study design and the new criteria.
Roberto Jabornisky, MD, PhD, of National University of the Northeast, Corrientes, Argentina, and colleagues pointed out that “all the low-resource validation sites were institutions with electronic health records and most had PICUs [pediatric intensive care units], which does not adequately reflect conditions in most low-resource settings. These factors introduce a distinct bias favoring a ‘PICU-based consensus,’ potentially limiting the generalizability and adoption of the new criteria by health care practitioners in non-PICU and nonhospital settings responsible for recognizing and managing children with sepsis.” The editorialists called for additional prospective validation in differently resourced settings, especially those with the highest disease burdens.
“Until then,” they wrote, “it is essential to refrain from considering these criteria as an inflexible directive governing medical interventions for pediatric sepsis. No definition can fully substitute for the clinical judgment of an experienced, vigilant clinician caring for an unwell child.”
Erin F. Carlton, MD, MSc of the University of Michigan, Ann Arbor, and colleagues added in a separate editorial, “The Phoenix criteria identify a sicker subset of patients than prior SIRS [systemic inflammatory response syndrome]-based criteria. Some may worry this higher threshold could delay management of patients not meeting sepsis criteria. Just as patients with chest pain and a troponin leak warrant monitoring and treatment (but are not prioritized for immediate heart catheterization), patients with infection need monitoring and treatment. Improvements in care should thus be judged not only by improved outcomes among patients with sepsis but also by decreased progression to sepsis among patients with infection.”
The International Consensus Criteria paper was supported by the Society of Critical Care Medicine and a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development to Tellen C. Bennett, MD, MS, and Nelson Sanchez-Pinto, MD. Data for the Kenya site were collected with support of the Wellcome Trust to the Kenya Major Overseas Programme. Dr. Jabornisky reported no conflicts of interest. Dr. Carlton reported serving on the Pediatric Surviving Sepsis Campaign Guideline committee and receiving grant support from the NIH.
New criteria for pediatric sepsis, based on a novel score that predicts mortality in children with suspected or confirmed infection, perform better than existing organ dysfunction scores and criteria and have the potential to improve clinical care globally, researchers say.
Current pediatric-specific criteria for sepsis were published in 2005, based on expert opinion. In 2016, sepsis was redefined for adults as life-threatening organ dysfunction caused by a dysregulated host response to infection, as opposed to an earlier focus on systemic inflammation. But the paradigm-shifting changes were not extended to children (< 18 years, but not newborns), setting the stage for the new initiative.
The new criteria, and their development and validation, were published in JAMA and presented the same day at the Society of Critical Care Medicine’s 2024 Critical Care Congress in Phoenix, Arizona.
International Consensus
“The new criteria we derived are based on data from electronic health records and analysis of more than 3 million pediatric healthcare encounters from 10 hospitals around the world, including in low-resource settings,” L. Nelson Sanchez-Pinto, MD, MBI, a critical care physician at the Ann and Robert H. Lurie Children’s Hospital of Chicago, told this news organization.
Dr. Sanchez-Pinto co-led the data group of the international expert task force convened by the Society of Critical Care Medicine (SCCM) to develop and validate the criteria, which are based on evidence from an international survey, systematic review and meta-analysis, a newly created organ dysfunction score (Phoenix Sepsis Score), and sites on four continents.
Based on the findings, the task force now suggests that pediatric sepsis be defined by a Phoenix Sepsis Score of at least 2 points in children with suspected infection, which indicates potentially life-threatening dysfunction of the respiratory, cardiovascular, coagulation, and/or neurological systems. Septic shock is defined as sepsis with at least 1 cardiovascular point in the score.
Disparities Across Settings
To derive and validate the new criteria across differently resourced settings, the researchers conducted a multicenter, international, retrospective cohort study involving 10 health systems in the United States, Colombia, Bangladesh, China, and Kenya, 3 of which were used as external validation sites.
Data were collected from pediatric emergency and inpatient encounters from 2010 to 2019. The development set comprised 3,049,699 children, and the external validation set included 581,317.
Stacked regression models to predict mortality in children with suspected infection were derived and validated using the best-performing organ dysfunction subscores from eight existing scores.
The final model was then translated into the integer-based Phoenix Sepsis Score and used to establish binary criteria for sepsis and septic shock.
Among 172,984 children with suspected infection in the first 24 hours (development set; 1.2% mortality), a four-organ-system model performed best. The Phoenix Sepsis Score — the integer version of the model — had areas under the precision recall curve of 0.23 to 0.38, and areas under the receiver operating characteristic curve of 0.71 to 0.92 to predict mortality in the validation sets.
A Phoenix Sepsis Score of 2 points or higher in children with suspected infection as criteria for sepsis, plus 1 or more cardiovascular points as criteria for septic shock, resulted in a higher positive predictive value and higher or similar sensitivity compared with the 2005 International Pediatric Sepsis Consensus Conference criteria across differently resourced settings.
Specifically, children with a Phoenix Sepsis Score of at least 2 points had in-hospital mortality of 7.1% in higher-resource settings and 28.5% in lower-resource settings — more than 8 times that of children with suspected infection not meeting these criteria.
Mortality also was higher in children who had organ dysfunction in at least one of four organ systems — respiratory, cardiovascular, coagulation, and/or neurological — that was not the primary site of infection.
Children with septic shock, indicated by at least 1 cardiovascular point in the Phoenix Sepsis Score, had severe hypotension for age, blood lactate exceeding 5 mmol/L, or need for vasoactive medication. These children had an in-hospital mortality rate of 10.8% in higher-resource settings and 33.5% in lower-resource settings.
A Better Score
Given the findings, the task force recommends that “the former criteria based on systemic inflammatory response syndrome should not be used to diagnose sepsis in children [and] the former term severe sepsis should no longer be used because sepsis is life-threatening organ dysfunction associated with infection and is thus indicative of a severe disease state.”
The task force cautions that although the four organs in the Phoenix Sepsis Score are most commonly involved in sepsis, “this does not diminish the crucial importance of the assessment and management of other organ dysfunction.”
Furthermore, they emphasize that the Phoenix score was designed to identify sepsis in children, not to screen children at risk for developing sepsis or early identification of children with suspected sepsis.
Additional Considerations
In related editorials, commentators noted some caveats and concerns with regard to the study design and the new criteria.
Roberto Jabornisky, MD, PhD, of National University of the Northeast, Corrientes, Argentina, and colleagues pointed out that “all the low-resource validation sites were institutions with electronic health records and most had PICUs [pediatric intensive care units], which does not adequately reflect conditions in most low-resource settings. These factors introduce a distinct bias favoring a ‘PICU-based consensus,’ potentially limiting the generalizability and adoption of the new criteria by health care practitioners in non-PICU and nonhospital settings responsible for recognizing and managing children with sepsis.” The editorialists called for additional prospective validation in differently resourced settings, especially those with the highest disease burdens.
“Until then,” they wrote, “it is essential to refrain from considering these criteria as an inflexible directive governing medical interventions for pediatric sepsis. No definition can fully substitute for the clinical judgment of an experienced, vigilant clinician caring for an unwell child.”
Erin F. Carlton, MD, MSc of the University of Michigan, Ann Arbor, and colleagues added in a separate editorial, “The Phoenix criteria identify a sicker subset of patients than prior SIRS [systemic inflammatory response syndrome]-based criteria. Some may worry this higher threshold could delay management of patients not meeting sepsis criteria. Just as patients with chest pain and a troponin leak warrant monitoring and treatment (but are not prioritized for immediate heart catheterization), patients with infection need monitoring and treatment. Improvements in care should thus be judged not only by improved outcomes among patients with sepsis but also by decreased progression to sepsis among patients with infection.”
The International Consensus Criteria paper was supported by the Society of Critical Care Medicine and a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development to Tellen C. Bennett, MD, MS, and Nelson Sanchez-Pinto, MD. Data for the Kenya site were collected with support of the Wellcome Trust to the Kenya Major Overseas Programme. Dr. Jabornisky reported no conflicts of interest. Dr. Carlton reported serving on the Pediatric Surviving Sepsis Campaign Guideline committee and receiving grant support from the NIH.
FROM JAMA
Breaking the Diagnostic Bottleneck in RA
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).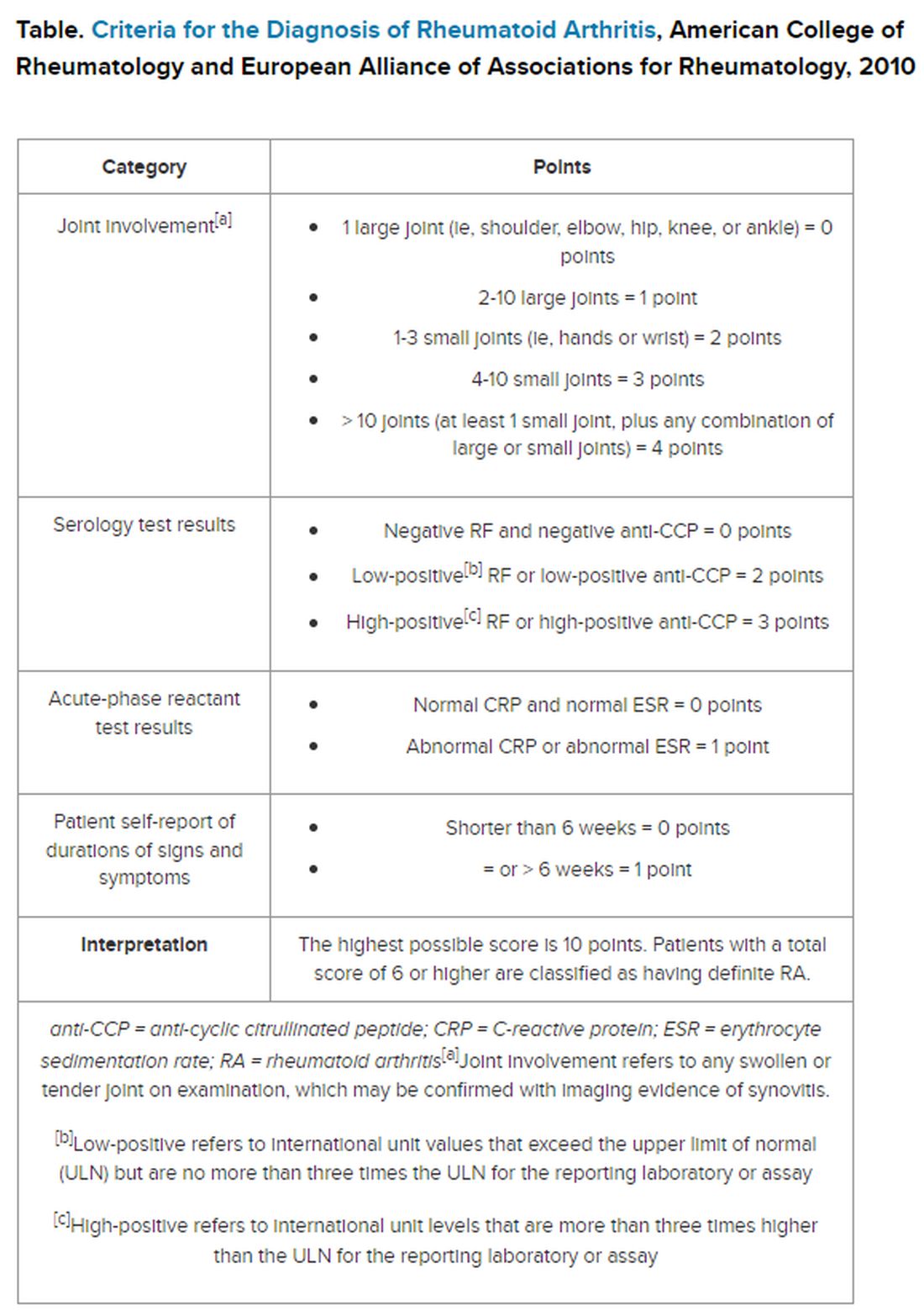
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
As head of the clinical laboratory at the San Juan University Hospital in Alicante, Spain, Maria Salinas, PhD, is passionate about the role she and her colleagues can play in clinical decision-making.
Her mission is the identification of “hidden diseases,” as she calls them, chronic conditions for which early identification and intervention can change the course of the illness. Her lab has been a leader over the past decade in using technology to partner with clinicians to promote the appropriate use of testing and clinical decision-making.
An example of a disease ripe for this type of intervention is rheumatoid arthritis (RA), the most common form of autoimmune arthritis, affecting around 1.3 million people in the United States. The prognosis for patients is better the earlier treatment begins.
But the
Amy S. Kehl, MD, an attending rheumatologist at Cedars-Sinai Medical Center in Los Angeles, who also sees patients at Saint John’s Physician Partners in Santa Monica, California, recommends a workup for inflammatory arthritis for patients presenting with the new onset of joint pain and swelling, primarily of small joints, although larger joints can be involved. The workup includes markers of inflammation such as an erythrocyte sedimentation rate and C-reactive protein, which are typically elevated and can be used to monitor the progression of the disease. Similarly, the presence of anemia is consistent with RA and helpful in tracking response to treatment.
But pinning down the diagnosis requires the presence of autoimmune antibodies. Guidelines from the American College of Rheumatology require a positive result for either rheumatoid factor (RF) or anti-cyclic citrullinated peptide (anti-CCP) antibody to definitively determine whether a patient has RA (Table).
“Classically, I find that the primary care physicians include a rheumatoid factor, not always a CCP, and may include other antibodies, including an ANA [antinuclear antibody] test, as part of that workup,” Dr. Kehl said. The problem with that strategy is that although the RF test does detect 60%-80% of patients with RA, it is positive in many other autoimmune conditions. Although the ANA might be positive in patients with RA, it is nonspecific and does not confirm the diagnosis of RA.
Up to 50% of autoimmune antibody tests are inappropriately ordered. And for rheumatologists, that leads to unnecessary referrals of patients with musculoskeletal complaints who do not meet objective clinical criteria for joint disease.
“These tests get ordered almost reflexively, and sometimes they’re ordered as part of a panel that includes a rheumatoid factor and an ANA, and it’s not necessarily going to be a high-yield test,” Dr. Kehl said. Superfluous tests and referrals often cause unnecessary anxiety in patients, as well as drive up costs, she added.
Dr. Salinas made the same observation in her hospital lab, which also serves nine primary care centers. She documented an upward trend in orders for RF testing in her hospital lab between 2011 and 2019. Dr. Salinas also noted that the anti-CCP antibody test was not commonly requested, although it has more utility in the diagnosis. Like the RF, it detects 50%-70% of patients with RA but has 95% specificity, resulting in far fewer false-positive results.
The appearance of both RF and anti-CCP antibodies often predicts a rapid progression to clinical disease. Dr. Kehl wants symptomatic patients with positive results for both markers to be seen right away by a rheumatologist. “We do know from studies that bony erosions can develop as early as a month or months after the onset of an inflammatory arthritis,” she said.
To address this need, Dr. Salinas worked with rheumatologists and primary care clinicians to develop an algorithm that called for reflex testing of samples from patients with positive RF results (> 30 IU/mL) for anti-CCP antibodies. If the anti-CCP antibody result was > 40 IU/mL, a comment in the lab report suggested rheumatology referral. The lab turned down requests to test sample for RF if the patient had a negative result in the previous 12 months — but it would perform the test if the clinician repeated the request.
The results were encouraging, Dr. Salinas said. “The main result in this study was that we really identified more hidden cases of patients with rheumatoid arthritis,” she told this news organization.
Compared with baseline trends, during the study period from April 2019 to January 2021 her lab demonstrated:
- Reduced RF tests conducted by canceling 16% of tests ordered for patients with negative RF result in the previous 12 months
- Fewer unnecessary referrals, from 22% in the baseline period to 8% during the intervention period
- A smaller percentage of missed patients, from 21% to 16%
To be sure, pre- and post-implementation comparisons are difficult when the implementation period happens to coincide with the emergence of SARS-CoV-2.
Although fewer patients were seen and fewer lab tests were ordered overall in Alicante during the COVID-19 pandemic, the proportion of tests ordered for RF testing dropped, and all the patients identified with double positives for RF and anti-CCP antibodies were referred to rheumatology, suggesting evidence of benefit.
Dr. Kehl said the practice of using clinical decision support systems could be used in the United States. “I thought this was an important study,” she said. Electronic health records systems “have all these capabilities where we can include best practice alerts when you order a test to make sure that it’s clinically warranted and cost-effective.”
Dr. Salinas and Dr. Kehl reported no relevant financial relationships.
A version of this article appeared on Medscape.com.