User login
Taking our own advice
Like many Americans, I’m overweight. Working 70-80 hours a week doesn’t leave much time for exercise. I try to do what I can, such as using stairs instead of the elevator, but in a two-story office building that doesn’t get you very far. And when I get home there are still tests to read, dictations to do, finances to catch up on ... which leaves little time for anything else other than eating and sleeping.

Eating better? Easier said than done. When I was single, back in residency, that was easy. I only had one person to shop for and feed, but in a family you need to find something that will keep everyone happy, and with three teenagers that ain’t easy. Everyone wants this, that, or the other, and none of it seems to be particularly good for you.
In the modern era convenience generally beats pretty much everything else. Our lives are hurried. At some point it’s just easier to pick something up or order out than to go to the effort of preparing your own meals. Of course, it’s possible to get something healthy for takeout, but the unhealthy menu items sound so much better, and by that time of day I’m tired, hungry, and stressed, and the will power I had in the morning is pretty much gone.
It’s kind of a medical paradox. Those of us taking care of others often don’t do the same for ourselves. Part of this, as noted in a recent Medscape article, is that we live on schedules that are unrelated to the typical 9-to-5 jobs that most other professionals have, not to mention a very different set of stressors.
At least I haven’t started smoking.
As the article points out, I’m not alone. In fact, it’s reassuring to know other physicians are dealing with the same situation. We often assume we’re alone in our struggles, when the actual truth is the opposite.
All of our medical training doesn’t mean we’re not human. It would be nice if the job made us better able to practice what we preach, but human nature is older than medicine, and we’re susceptible to the same faults and temptations as those of our patients.
And always will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Like many Americans, I’m overweight. Working 70-80 hours a week doesn’t leave much time for exercise. I try to do what I can, such as using stairs instead of the elevator, but in a two-story office building that doesn’t get you very far. And when I get home there are still tests to read, dictations to do, finances to catch up on ... which leaves little time for anything else other than eating and sleeping.
Eating better? Easier said than done. When I was single, back in residency, that was easy. I only had one person to shop for and feed, but in a family you need to find something that will keep everyone happy, and with three teenagers that ain’t easy. Everyone wants this, that, or the other, and none of it seems to be particularly good for you.
In the modern era convenience generally beats pretty much everything else. Our lives are hurried. At some point it’s just easier to pick something up or order out than to go to the effort of preparing your own meals. Of course, it’s possible to get something healthy for takeout, but the unhealthy menu items sound so much better, and by that time of day I’m tired, hungry, and stressed, and the will power I had in the morning is pretty much gone.
It’s kind of a medical paradox. Those of us taking care of others often don’t do the same for ourselves. Part of this, as noted in a recent Medscape article, is that we live on schedules that are unrelated to the typical 9-to-5 jobs that most other professionals have, not to mention a very different set of stressors.
At least I haven’t started smoking.
As the article points out, I’m not alone. In fact, it’s reassuring to know other physicians are dealing with the same situation. We often assume we’re alone in our struggles, when the actual truth is the opposite.
All of our medical training doesn’t mean we’re not human. It would be nice if the job made us better able to practice what we preach, but human nature is older than medicine, and we’re susceptible to the same faults and temptations as those of our patients.
And always will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Like many Americans, I’m overweight. Working 70-80 hours a week doesn’t leave much time for exercise. I try to do what I can, such as using stairs instead of the elevator, but in a two-story office building that doesn’t get you very far. And when I get home there are still tests to read, dictations to do, finances to catch up on ... which leaves little time for anything else other than eating and sleeping.
Eating better? Easier said than done. When I was single, back in residency, that was easy. I only had one person to shop for and feed, but in a family you need to find something that will keep everyone happy, and with three teenagers that ain’t easy. Everyone wants this, that, or the other, and none of it seems to be particularly good for you.
In the modern era convenience generally beats pretty much everything else. Our lives are hurried. At some point it’s just easier to pick something up or order out than to go to the effort of preparing your own meals. Of course, it’s possible to get something healthy for takeout, but the unhealthy menu items sound so much better, and by that time of day I’m tired, hungry, and stressed, and the will power I had in the morning is pretty much gone.
It’s kind of a medical paradox. Those of us taking care of others often don’t do the same for ourselves. Part of this, as noted in a recent Medscape article, is that we live on schedules that are unrelated to the typical 9-to-5 jobs that most other professionals have, not to mention a very different set of stressors.
At least I haven’t started smoking.
As the article points out, I’m not alone. In fact, it’s reassuring to know other physicians are dealing with the same situation. We often assume we’re alone in our struggles, when the actual truth is the opposite.
All of our medical training doesn’t mean we’re not human. It would be nice if the job made us better able to practice what we preach, but human nature is older than medicine, and we’re susceptible to the same faults and temptations as those of our patients.
And always will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Erythrasma
THE COMPARISON
A and B Axilla of a 65-year-old White man with erythrasma showing a well-demarcated erythematous plaque with fine scale (A). Wood-lamp examination of the area showed characteristic bright coral red fluorescence (B).
C and D A well-demarcated, red-brown plaque with fine scale in the antecubital fossa of an obese Hispanic woman (C). Wood-lamp examination revealed bright coral red fluorescence (D).
E Hypopigmented patches (with pruritus) in the groin of a Black man. He also had erythrasma between the toes.
Erythrasma is a skin condition caused by acute or chronic infection of the outermost layer of the epidermis (stratum corneum) with Corynebacterium minutissimum. It has a predilection for intertriginous regions such as the axillae, groin, and interdigital spaces of the toes. It can be associated with pruritus or can be asymptomatic.

Epidemiology
Erythrasma typically affects adults, with greater prevalence among those residing in shared living facilities, such as dormitories or nursing homes, or in humid climates.1 It is a common disorder with an estimated prevalence of 17.6% of bacterial skin infections in elderly patients and 44% of diabetic interdigital toe space infections.2,3
Key clinical features
Erythrasma can manifest as red-brown hyperpigmented plaques with fine scale and little central clearing (FIGURES A and C) or as a hypopigmented patch (FIGURE E) with a sharply marginated, hyperpigmented border in patients with skin of color. In the interdigital toe spaces, the skin often is white and macerated. These findings may appear in patients of all skin tones.
Worth noting
- C minutissimum produces coproporphyrin III, which glows fluorescent red under Wood-lamp examination (FIGURES B and D). A recent shower or bath may remove the fluorescent coproporphyrins and cause a false-negative result. The interdigital space between the fourth and fifth toes is a common location for C minutissimum; thus clinicians should consider examining these areas with a Wood lamp.
- Associated risk factors include obesity, immunosuppression, diabetes mellitus, and excessive sweating.1
- The differential diagnosis includes intertrigo, inverse psoriasis, confluent and reticulated papillomatosis (Gougerot-Carteaud syndrome), acanthosis nigricans, seborrheic dermatitis, and tinea pedis when present in the interdigital toe spaces. Plaques occurring in circular patterns may be mistaken for tinea corporis or pityriasis rotunda.
- There is a high prevalence of erythrasma in patients with inverse psoriasis, and it may exacerbate psoriatic plaques.4
- Treatment options include application of topical clindamycin or erythromycin to the affected area.1 Some patients have responded to topical mupiricin.2 For larger areas, a 1-g dose of clarithromycin5 or a 14-day course of erythromycin may be appropriate.1 Avoid prescribing clarithromycin to patients with preexisting heart disease due to its increased risk for cardiac events or death; consider other agents.
Health disparity highlight
Obesity, most prevalent in non-Hispanic Black adults (49.9%) and Hispanic adults (45.6%) followed by non-Hispanic White adults (41.4%),6 may cause velvety dark plaques on the neck called acanthosis nigricans. However, acute or chronic erythrasma also may cause hyperpigmentation of the body folds. Although the pathology of erythrasma is due to bacterial infection of the superficial layer of the stratum corneum, acanthosis nigricans is due to fibroblast proliferation and stimulation of epidermal keratinocytes, likely from increased growth factors and insulinlike growth factor.7 If erythrasma is mistaken for acanthosis nigricans, the patient may be counseled inappropriately that the hyperpigmentation is something not easily resolved and subsequently left with an active treatable condition that adversely affects their quality of life.
1. Groves JB, Nassereddin A, Freeman AM. Erythrasma. In: StatPearls. StatPearls Publishing; August 11, 2021. Accessed November 17, 2022. https://www.ncbi.nlm.nih.gov/books/NBK513352/
2. Forouzan P, Cohen PR. Erythrasma revisited: diagnosis, differential diagnoses, and comprehensive review of treatment. Cureus. 2020;12:E10733. doi:10.7759/cureus.10733
3. Polat M, I˙lhan MN. Dermatological complaints of the elderly attending a dermatology outpatient clinic in Turkey: a prospective study over a one-year period. Acta Dermatovenerol Croat. 2015;23:277-281.
4. Janeczek M, Kozel Z, Bhasin R, et al. High prevalence of erythrasma in patients with inverse psoriasis: a cross-sectional study. J Clin Aesthet Dermatol. 2020;13:12-14.
5. Khan MJ. Interdigital pedal erythrasma treated with one-time dose of oral clarithromycin 1 g: two case reports. Clin Case Rep. 2020;8:672-674. doi:10.1002/ccr3.2712
6. Stierman B, Afful J, Carroll M, et al. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes. National Health Statistics Reports. Published June 14, 2021. Accessed November 17, 2022. https://stacks.cdc.gov/view/cdc/106273
7. Brady MF, Rawla P. Acanthosis nigricans. In: StatPearls. Stat- Pearls Publishing; 2022. Updated October 9, 2022. Accessed November 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK431057
THE COMPARISON
A and B Axilla of a 65-year-old White man with erythrasma showing a well-demarcated erythematous plaque with fine scale (A). Wood-lamp examination of the area showed characteristic bright coral red fluorescence (B).
C and D A well-demarcated, red-brown plaque with fine scale in the antecubital fossa of an obese Hispanic woman (C). Wood-lamp examination revealed bright coral red fluorescence (D).
E Hypopigmented patches (with pruritus) in the groin of a Black man. He also had erythrasma between the toes.
Erythrasma is a skin condition caused by acute or chronic infection of the outermost layer of the epidermis (stratum corneum) with Corynebacterium minutissimum. It has a predilection for intertriginous regions such as the axillae, groin, and interdigital spaces of the toes. It can be associated with pruritus or can be asymptomatic.
Epidemiology
Erythrasma typically affects adults, with greater prevalence among those residing in shared living facilities, such as dormitories or nursing homes, or in humid climates.1 It is a common disorder with an estimated prevalence of 17.6% of bacterial skin infections in elderly patients and 44% of diabetic interdigital toe space infections.2,3
Key clinical features
Erythrasma can manifest as red-brown hyperpigmented plaques with fine scale and little central clearing (FIGURES A and C) or as a hypopigmented patch (FIGURE E) with a sharply marginated, hyperpigmented border in patients with skin of color. In the interdigital toe spaces, the skin often is white and macerated. These findings may appear in patients of all skin tones.
Worth noting
- C minutissimum produces coproporphyrin III, which glows fluorescent red under Wood-lamp examination (FIGURES B and D). A recent shower or bath may remove the fluorescent coproporphyrins and cause a false-negative result. The interdigital space between the fourth and fifth toes is a common location for C minutissimum; thus clinicians should consider examining these areas with a Wood lamp.
- Associated risk factors include obesity, immunosuppression, diabetes mellitus, and excessive sweating.1
- The differential diagnosis includes intertrigo, inverse psoriasis, confluent and reticulated papillomatosis (Gougerot-Carteaud syndrome), acanthosis nigricans, seborrheic dermatitis, and tinea pedis when present in the interdigital toe spaces. Plaques occurring in circular patterns may be mistaken for tinea corporis or pityriasis rotunda.
- There is a high prevalence of erythrasma in patients with inverse psoriasis, and it may exacerbate psoriatic plaques.4
- Treatment options include application of topical clindamycin or erythromycin to the affected area.1 Some patients have responded to topical mupiricin.2 For larger areas, a 1-g dose of clarithromycin5 or a 14-day course of erythromycin may be appropriate.1 Avoid prescribing clarithromycin to patients with preexisting heart disease due to its increased risk for cardiac events or death; consider other agents.
Health disparity highlight
Obesity, most prevalent in non-Hispanic Black adults (49.9%) and Hispanic adults (45.6%) followed by non-Hispanic White adults (41.4%),6 may cause velvety dark plaques on the neck called acanthosis nigricans. However, acute or chronic erythrasma also may cause hyperpigmentation of the body folds. Although the pathology of erythrasma is due to bacterial infection of the superficial layer of the stratum corneum, acanthosis nigricans is due to fibroblast proliferation and stimulation of epidermal keratinocytes, likely from increased growth factors and insulinlike growth factor.7 If erythrasma is mistaken for acanthosis nigricans, the patient may be counseled inappropriately that the hyperpigmentation is something not easily resolved and subsequently left with an active treatable condition that adversely affects their quality of life.
THE COMPARISON
A and B Axilla of a 65-year-old White man with erythrasma showing a well-demarcated erythematous plaque with fine scale (A). Wood-lamp examination of the area showed characteristic bright coral red fluorescence (B).
C and D A well-demarcated, red-brown plaque with fine scale in the antecubital fossa of an obese Hispanic woman (C). Wood-lamp examination revealed bright coral red fluorescence (D).
E Hypopigmented patches (with pruritus) in the groin of a Black man. He also had erythrasma between the toes.
Erythrasma is a skin condition caused by acute or chronic infection of the outermost layer of the epidermis (stratum corneum) with Corynebacterium minutissimum. It has a predilection for intertriginous regions such as the axillae, groin, and interdigital spaces of the toes. It can be associated with pruritus or can be asymptomatic.
Epidemiology
Erythrasma typically affects adults, with greater prevalence among those residing in shared living facilities, such as dormitories or nursing homes, or in humid climates.1 It is a common disorder with an estimated prevalence of 17.6% of bacterial skin infections in elderly patients and 44% of diabetic interdigital toe space infections.2,3
Key clinical features
Erythrasma can manifest as red-brown hyperpigmented plaques with fine scale and little central clearing (FIGURES A and C) or as a hypopigmented patch (FIGURE E) with a sharply marginated, hyperpigmented border in patients with skin of color. In the interdigital toe spaces, the skin often is white and macerated. These findings may appear in patients of all skin tones.
Worth noting
- C minutissimum produces coproporphyrin III, which glows fluorescent red under Wood-lamp examination (FIGURES B and D). A recent shower or bath may remove the fluorescent coproporphyrins and cause a false-negative result. The interdigital space between the fourth and fifth toes is a common location for C minutissimum; thus clinicians should consider examining these areas with a Wood lamp.
- Associated risk factors include obesity, immunosuppression, diabetes mellitus, and excessive sweating.1
- The differential diagnosis includes intertrigo, inverse psoriasis, confluent and reticulated papillomatosis (Gougerot-Carteaud syndrome), acanthosis nigricans, seborrheic dermatitis, and tinea pedis when present in the interdigital toe spaces. Plaques occurring in circular patterns may be mistaken for tinea corporis or pityriasis rotunda.
- There is a high prevalence of erythrasma in patients with inverse psoriasis, and it may exacerbate psoriatic plaques.4
- Treatment options include application of topical clindamycin or erythromycin to the affected area.1 Some patients have responded to topical mupiricin.2 For larger areas, a 1-g dose of clarithromycin5 or a 14-day course of erythromycin may be appropriate.1 Avoid prescribing clarithromycin to patients with preexisting heart disease due to its increased risk for cardiac events or death; consider other agents.
Health disparity highlight
Obesity, most prevalent in non-Hispanic Black adults (49.9%) and Hispanic adults (45.6%) followed by non-Hispanic White adults (41.4%),6 may cause velvety dark plaques on the neck called acanthosis nigricans. However, acute or chronic erythrasma also may cause hyperpigmentation of the body folds. Although the pathology of erythrasma is due to bacterial infection of the superficial layer of the stratum corneum, acanthosis nigricans is due to fibroblast proliferation and stimulation of epidermal keratinocytes, likely from increased growth factors and insulinlike growth factor.7 If erythrasma is mistaken for acanthosis nigricans, the patient may be counseled inappropriately that the hyperpigmentation is something not easily resolved and subsequently left with an active treatable condition that adversely affects their quality of life.
1. Groves JB, Nassereddin A, Freeman AM. Erythrasma. In: StatPearls. StatPearls Publishing; August 11, 2021. Accessed November 17, 2022. https://www.ncbi.nlm.nih.gov/books/NBK513352/
2. Forouzan P, Cohen PR. Erythrasma revisited: diagnosis, differential diagnoses, and comprehensive review of treatment. Cureus. 2020;12:E10733. doi:10.7759/cureus.10733
3. Polat M, I˙lhan MN. Dermatological complaints of the elderly attending a dermatology outpatient clinic in Turkey: a prospective study over a one-year period. Acta Dermatovenerol Croat. 2015;23:277-281.
4. Janeczek M, Kozel Z, Bhasin R, et al. High prevalence of erythrasma in patients with inverse psoriasis: a cross-sectional study. J Clin Aesthet Dermatol. 2020;13:12-14.
5. Khan MJ. Interdigital pedal erythrasma treated with one-time dose of oral clarithromycin 1 g: two case reports. Clin Case Rep. 2020;8:672-674. doi:10.1002/ccr3.2712
6. Stierman B, Afful J, Carroll M, et al. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes. National Health Statistics Reports. Published June 14, 2021. Accessed November 17, 2022. https://stacks.cdc.gov/view/cdc/106273
7. Brady MF, Rawla P. Acanthosis nigricans. In: StatPearls. Stat- Pearls Publishing; 2022. Updated October 9, 2022. Accessed November 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK431057
1. Groves JB, Nassereddin A, Freeman AM. Erythrasma. In: StatPearls. StatPearls Publishing; August 11, 2021. Accessed November 17, 2022. https://www.ncbi.nlm.nih.gov/books/NBK513352/
2. Forouzan P, Cohen PR. Erythrasma revisited: diagnosis, differential diagnoses, and comprehensive review of treatment. Cureus. 2020;12:E10733. doi:10.7759/cureus.10733
3. Polat M, I˙lhan MN. Dermatological complaints of the elderly attending a dermatology outpatient clinic in Turkey: a prospective study over a one-year period. Acta Dermatovenerol Croat. 2015;23:277-281.
4. Janeczek M, Kozel Z, Bhasin R, et al. High prevalence of erythrasma in patients with inverse psoriasis: a cross-sectional study. J Clin Aesthet Dermatol. 2020;13:12-14.
5. Khan MJ. Interdigital pedal erythrasma treated with one-time dose of oral clarithromycin 1 g: two case reports. Clin Case Rep. 2020;8:672-674. doi:10.1002/ccr3.2712
6. Stierman B, Afful J, Carroll M, et al. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes. National Health Statistics Reports. Published June 14, 2021. Accessed November 17, 2022. https://stacks.cdc.gov/view/cdc/106273
7. Brady MF, Rawla P. Acanthosis nigricans. In: StatPearls. Stat- Pearls Publishing; 2022. Updated October 9, 2022. Accessed November 30, 2022. https://www.ncbi.nlm.nih.gov/books/NBK431057

Let people take illegal drugs under medical supervision?
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m the director of the division of medical ethics at New York University.
One is up in Washington Heights in Manhattan; the other, I believe, is over in Harlem.
These two centers will supervise people taking drugs. They have available all of the anti-overdose medications, such as Narcan. If you overdose, they will help you and try to counsel you to get off drugs, but they don’t insist that you do so. You can go there, even if you’re an addict, and continue to take drugs under supervision. This is called a risk-reduction strategy.
Some people note that there are over 100 centers like this worldwide. They’re in Canada, Switzerland, and many other countries, and they seem to work. “Working” means more people seem to come off drugs slowly – not huge numbers, but some – than if you don’t do something like this, and death rates from overdose go way down.
By the way, having these centers in place has other benefits. They save money because when someone overdoses out in the community, you have to pay all the costs of the ambulances and emergency rooms, and there are risks to the first responders due to fentanyl or other things. There are fewer syringes littering parks and public places where people shoot up. You have everything controlled when they come into a center, so that’s less burden on the community.
It turns out that you have less crime because people just aren’t out there harming or robbing other people to get money to get their next fix. The drugs are provided for them. Crime rates in neighborhoods around the world where these centers operate seem to dip. There are many positives.
There are also some negatives. People say it shouldn’t be the job of the state to keep people addicted. It’s just not the right role. Everything should be aimed at getting people off drugs, maybe including criminal penalties if that’s what it takes to get them to stop using.
My own view is that hasn’t worked. Implementing tough prison sentences in trying to fight the war on drugs just doesn’t seem to work. We had 100,000 deaths last year from drug overdoses. That number has been climbing. We all know that we’ve got a terrible epidemic of deaths due to drug overdose.
It seems to me that these centers that are involved in risk reduction are a better option for now, until we figure out some interventions that can cut the desire or the drive to use drugs, or antidotes that are effective for months or years, to prevent people from getting high no matter what drugs they take.
I’m going to come out and say that I think the New York experiment has worked. I think it has saved upward of 600 lives, they estimate, in the past year that would have been overdoses. I think costwise, it’s effective. [Reductions in] related damages and injuries from syringes being scattered around, and robbery, and so forth, are all to the good. There are even a few people coming off drugs due to counseling, which is a better outcome than we get when they’re just out in the streets.
I think other cities want to try this. I know Philadelphia does. I know New York wants to expand its program. The federal government isn’t sure, but I think the time has come to try an expansion. I think we’ve got something that – although far from perfect and I wish we had other tools – may be the best we’ve got. In the war on drugs, little victories ought to be reinforced.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m the director of the division of medical ethics at New York University.
One is up in Washington Heights in Manhattan; the other, I believe, is over in Harlem.
These two centers will supervise people taking drugs. They have available all of the anti-overdose medications, such as Narcan. If you overdose, they will help you and try to counsel you to get off drugs, but they don’t insist that you do so. You can go there, even if you’re an addict, and continue to take drugs under supervision. This is called a risk-reduction strategy.
Some people note that there are over 100 centers like this worldwide. They’re in Canada, Switzerland, and many other countries, and they seem to work. “Working” means more people seem to come off drugs slowly – not huge numbers, but some – than if you don’t do something like this, and death rates from overdose go way down.
By the way, having these centers in place has other benefits. They save money because when someone overdoses out in the community, you have to pay all the costs of the ambulances and emergency rooms, and there are risks to the first responders due to fentanyl or other things. There are fewer syringes littering parks and public places where people shoot up. You have everything controlled when they come into a center, so that’s less burden on the community.
It turns out that you have less crime because people just aren’t out there harming or robbing other people to get money to get their next fix. The drugs are provided for them. Crime rates in neighborhoods around the world where these centers operate seem to dip. There are many positives.
There are also some negatives. People say it shouldn’t be the job of the state to keep people addicted. It’s just not the right role. Everything should be aimed at getting people off drugs, maybe including criminal penalties if that’s what it takes to get them to stop using.
My own view is that hasn’t worked. Implementing tough prison sentences in trying to fight the war on drugs just doesn’t seem to work. We had 100,000 deaths last year from drug overdoses. That number has been climbing. We all know that we’ve got a terrible epidemic of deaths due to drug overdose.
It seems to me that these centers that are involved in risk reduction are a better option for now, until we figure out some interventions that can cut the desire or the drive to use drugs, or antidotes that are effective for months or years, to prevent people from getting high no matter what drugs they take.
I’m going to come out and say that I think the New York experiment has worked. I think it has saved upward of 600 lives, they estimate, in the past year that would have been overdoses. I think costwise, it’s effective. [Reductions in] related damages and injuries from syringes being scattered around, and robbery, and so forth, are all to the good. There are even a few people coming off drugs due to counseling, which is a better outcome than we get when they’re just out in the streets.
I think other cities want to try this. I know Philadelphia does. I know New York wants to expand its program. The federal government isn’t sure, but I think the time has come to try an expansion. I think we’ve got something that – although far from perfect and I wish we had other tools – may be the best we’ve got. In the war on drugs, little victories ought to be reinforced.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m the director of the division of medical ethics at New York University.
One is up in Washington Heights in Manhattan; the other, I believe, is over in Harlem.
These two centers will supervise people taking drugs. They have available all of the anti-overdose medications, such as Narcan. If you overdose, they will help you and try to counsel you to get off drugs, but they don’t insist that you do so. You can go there, even if you’re an addict, and continue to take drugs under supervision. This is called a risk-reduction strategy.
Some people note that there are over 100 centers like this worldwide. They’re in Canada, Switzerland, and many other countries, and they seem to work. “Working” means more people seem to come off drugs slowly – not huge numbers, but some – than if you don’t do something like this, and death rates from overdose go way down.
By the way, having these centers in place has other benefits. They save money because when someone overdoses out in the community, you have to pay all the costs of the ambulances and emergency rooms, and there are risks to the first responders due to fentanyl or other things. There are fewer syringes littering parks and public places where people shoot up. You have everything controlled when they come into a center, so that’s less burden on the community.
It turns out that you have less crime because people just aren’t out there harming or robbing other people to get money to get their next fix. The drugs are provided for them. Crime rates in neighborhoods around the world where these centers operate seem to dip. There are many positives.
There are also some negatives. People say it shouldn’t be the job of the state to keep people addicted. It’s just not the right role. Everything should be aimed at getting people off drugs, maybe including criminal penalties if that’s what it takes to get them to stop using.
My own view is that hasn’t worked. Implementing tough prison sentences in trying to fight the war on drugs just doesn’t seem to work. We had 100,000 deaths last year from drug overdoses. That number has been climbing. We all know that we’ve got a terrible epidemic of deaths due to drug overdose.
It seems to me that these centers that are involved in risk reduction are a better option for now, until we figure out some interventions that can cut the desire or the drive to use drugs, or antidotes that are effective for months or years, to prevent people from getting high no matter what drugs they take.
I’m going to come out and say that I think the New York experiment has worked. I think it has saved upward of 600 lives, they estimate, in the past year that would have been overdoses. I think costwise, it’s effective. [Reductions in] related damages and injuries from syringes being scattered around, and robbery, and so forth, are all to the good. There are even a few people coming off drugs due to counseling, which is a better outcome than we get when they’re just out in the streets.
I think other cities want to try this. I know Philadelphia does. I know New York wants to expand its program. The federal government isn’t sure, but I think the time has come to try an expansion. I think we’ve got something that – although far from perfect and I wish we had other tools – may be the best we’ve got. In the war on drugs, little victories ought to be reinforced.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.

Why doctors are losing trust in patients; what should be done?
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University.
I want to talk about a paper that my colleagues in my division just published in Health Affairs.
As they pointed out, there’s a large amount of literature about what makes patients trust their doctor. There are many studies that show that, although patients sometimes have become more critical of the medical profession, in general they still try to trust their individual physician. Nurses remain in fairly high esteem among those who are getting hospital care.
What isn’t studied, as this paper properly points out, is, what can the doctor and the nurse do to trust the patient? How can that be assessed? Isn’t that just as important as saying that patients have to trust their doctors to do and comply with what they’re told?
What if doctors are afraid of violence? What if doctors are fearful that they can’t trust patients to listen, pay attention, or do what they’re being told? What if they think that patients are coming in with all kinds of disinformation, false information, or things they pick up on the Internet, so that even though you try your best to get across accurate and complete information about what to do about infectious diseases, taking care of a kid with strep throat, or whatever it might be, you’re thinking, Can I trust this patient to do what it is that I want them to do?
One particular problem that’s causing distrust is that more and more patients are showing stress and dependence on drugs and alcohol. That doesn’t make them less trustworthy per se, but it means they can’t regulate their own behavior as well.
That obviously has to be something that the physician or the nurse is thinking about. Is this person going to be able to contain anger? Is this person going to be able to handle bad news? Is this person going to deal with me when I tell them that some of the things they believe to be true about what’s good for their health care are false?
I think we have to really start to push administrators and people in positions of power to teach doctors and nurses how to defuse situations and how to make people more comfortable when they come in and the doctor suspects that they might be under the influence, impaired, or angry because of things they’ve seen on social media, whatever those might be – including concerns about racism, bigotry, and bias, which some patients are bringing into the clinic and the hospital setting.
We need more training. We’ve got to address this as a serious issue. What can we do to defuse situations where the doctor or the nurse rightly thinks that they can’t control or they can’t trust what the patient is thinking or how the patient might behave?
It’s also the case that I think we need more backup and quick access to security so that people feel safe and comfortable in providing care. We have to make sure that if you need someone to restrain a patient or to get somebody out of a situation, that they can get there quickly and respond rapidly, and that they know what to do to deescalate a situation.
It’s sad to say, but security in today’s health care world has to be something that we really test and check – not because we’re worried, as many places are, about a shooter entering the premises, which is its own bit of concern – but I’m just talking about when the doctor or the nurse says that this patient might be acting up, could get violent, or is someone I can’t trust.
My coauthors are basically saying that it’s not a one-way street. Yes, we have to figure out ways to make sure that our patients can trust what we say. Trust is absolutely the lubricant that makes health care flow. If patients don’t trust their doctors, they’re not going to do what they say. They’re not going to get their prescriptions filled. They’re not going to be compliant. They’re not going to try to lose weight or control their diabetes.
It also goes the other way. The doctor or the nurse has to trust the patient. They have to believe that they’re safe. They have to believe that the patient is capable of controlling themselves. They have to believe that the patient is capable of listening and hearing what they’re saying, and that they’re competent to follow up on instructions, including to come back if that’s what’s required.
Everybody has to feel secure in the environment in which they’re working. Security, sadly, has to be a priority if we’re going to have a health care workforce that really feels safe and comfortable dealing with a patient population that is increasingly aggressive and perhaps not as trustworthy.
That’s not news I like to read when my colleagues write it up, but it’s important and we have to take it seriously.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University.
I want to talk about a paper that my colleagues in my division just published in Health Affairs.
As they pointed out, there’s a large amount of literature about what makes patients trust their doctor. There are many studies that show that, although patients sometimes have become more critical of the medical profession, in general they still try to trust their individual physician. Nurses remain in fairly high esteem among those who are getting hospital care.
What isn’t studied, as this paper properly points out, is, what can the doctor and the nurse do to trust the patient? How can that be assessed? Isn’t that just as important as saying that patients have to trust their doctors to do and comply with what they’re told?
What if doctors are afraid of violence? What if doctors are fearful that they can’t trust patients to listen, pay attention, or do what they’re being told? What if they think that patients are coming in with all kinds of disinformation, false information, or things they pick up on the Internet, so that even though you try your best to get across accurate and complete information about what to do about infectious diseases, taking care of a kid with strep throat, or whatever it might be, you’re thinking, Can I trust this patient to do what it is that I want them to do?
One particular problem that’s causing distrust is that more and more patients are showing stress and dependence on drugs and alcohol. That doesn’t make them less trustworthy per se, but it means they can’t regulate their own behavior as well.
That obviously has to be something that the physician or the nurse is thinking about. Is this person going to be able to contain anger? Is this person going to be able to handle bad news? Is this person going to deal with me when I tell them that some of the things they believe to be true about what’s good for their health care are false?
I think we have to really start to push administrators and people in positions of power to teach doctors and nurses how to defuse situations and how to make people more comfortable when they come in and the doctor suspects that they might be under the influence, impaired, or angry because of things they’ve seen on social media, whatever those might be – including concerns about racism, bigotry, and bias, which some patients are bringing into the clinic and the hospital setting.
We need more training. We’ve got to address this as a serious issue. What can we do to defuse situations where the doctor or the nurse rightly thinks that they can’t control or they can’t trust what the patient is thinking or how the patient might behave?
It’s also the case that I think we need more backup and quick access to security so that people feel safe and comfortable in providing care. We have to make sure that if you need someone to restrain a patient or to get somebody out of a situation, that they can get there quickly and respond rapidly, and that they know what to do to deescalate a situation.
It’s sad to say, but security in today’s health care world has to be something that we really test and check – not because we’re worried, as many places are, about a shooter entering the premises, which is its own bit of concern – but I’m just talking about when the doctor or the nurse says that this patient might be acting up, could get violent, or is someone I can’t trust.
My coauthors are basically saying that it’s not a one-way street. Yes, we have to figure out ways to make sure that our patients can trust what we say. Trust is absolutely the lubricant that makes health care flow. If patients don’t trust their doctors, they’re not going to do what they say. They’re not going to get their prescriptions filled. They’re not going to be compliant. They’re not going to try to lose weight or control their diabetes.
It also goes the other way. The doctor or the nurse has to trust the patient. They have to believe that they’re safe. They have to believe that the patient is capable of controlling themselves. They have to believe that the patient is capable of listening and hearing what they’re saying, and that they’re competent to follow up on instructions, including to come back if that’s what’s required.
Everybody has to feel secure in the environment in which they’re working. Security, sadly, has to be a priority if we’re going to have a health care workforce that really feels safe and comfortable dealing with a patient population that is increasingly aggressive and perhaps not as trustworthy.
That’s not news I like to read when my colleagues write it up, but it’s important and we have to take it seriously.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University.
I want to talk about a paper that my colleagues in my division just published in Health Affairs.
As they pointed out, there’s a large amount of literature about what makes patients trust their doctor. There are many studies that show that, although patients sometimes have become more critical of the medical profession, in general they still try to trust their individual physician. Nurses remain in fairly high esteem among those who are getting hospital care.
What isn’t studied, as this paper properly points out, is, what can the doctor and the nurse do to trust the patient? How can that be assessed? Isn’t that just as important as saying that patients have to trust their doctors to do and comply with what they’re told?
What if doctors are afraid of violence? What if doctors are fearful that they can’t trust patients to listen, pay attention, or do what they’re being told? What if they think that patients are coming in with all kinds of disinformation, false information, or things they pick up on the Internet, so that even though you try your best to get across accurate and complete information about what to do about infectious diseases, taking care of a kid with strep throat, or whatever it might be, you’re thinking, Can I trust this patient to do what it is that I want them to do?
One particular problem that’s causing distrust is that more and more patients are showing stress and dependence on drugs and alcohol. That doesn’t make them less trustworthy per se, but it means they can’t regulate their own behavior as well.
That obviously has to be something that the physician or the nurse is thinking about. Is this person going to be able to contain anger? Is this person going to be able to handle bad news? Is this person going to deal with me when I tell them that some of the things they believe to be true about what’s good for their health care are false?
I think we have to really start to push administrators and people in positions of power to teach doctors and nurses how to defuse situations and how to make people more comfortable when they come in and the doctor suspects that they might be under the influence, impaired, or angry because of things they’ve seen on social media, whatever those might be – including concerns about racism, bigotry, and bias, which some patients are bringing into the clinic and the hospital setting.
We need more training. We’ve got to address this as a serious issue. What can we do to defuse situations where the doctor or the nurse rightly thinks that they can’t control or they can’t trust what the patient is thinking or how the patient might behave?
It’s also the case that I think we need more backup and quick access to security so that people feel safe and comfortable in providing care. We have to make sure that if you need someone to restrain a patient or to get somebody out of a situation, that they can get there quickly and respond rapidly, and that they know what to do to deescalate a situation.
It’s sad to say, but security in today’s health care world has to be something that we really test and check – not because we’re worried, as many places are, about a shooter entering the premises, which is its own bit of concern – but I’m just talking about when the doctor or the nurse says that this patient might be acting up, could get violent, or is someone I can’t trust.
My coauthors are basically saying that it’s not a one-way street. Yes, we have to figure out ways to make sure that our patients can trust what we say. Trust is absolutely the lubricant that makes health care flow. If patients don’t trust their doctors, they’re not going to do what they say. They’re not going to get their prescriptions filled. They’re not going to be compliant. They’re not going to try to lose weight or control their diabetes.
It also goes the other way. The doctor or the nurse has to trust the patient. They have to believe that they’re safe. They have to believe that the patient is capable of controlling themselves. They have to believe that the patient is capable of listening and hearing what they’re saying, and that they’re competent to follow up on instructions, including to come back if that’s what’s required.
Everybody has to feel secure in the environment in which they’re working. Security, sadly, has to be a priority if we’re going to have a health care workforce that really feels safe and comfortable dealing with a patient population that is increasingly aggressive and perhaps not as trustworthy.
That’s not news I like to read when my colleagues write it up, but it’s important and we have to take it seriously.
Dr. Caplan disclosed that he has served as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape. A version of this article first appeared on Medscape.com.
Mood stabilizers, particularly lithium, potential lifesavers in bipolar disorder
Investigators led by Pao-Huan Chen, MD, of the department of psychiatry, Taipei Medical University Hospital, Taiwan, evaluated the association between the use of mood stabilizers and the risks for all-cause mortality, suicide, and natural mortality in more than 25,000 patients with BD and found that those with BD had higher mortality.
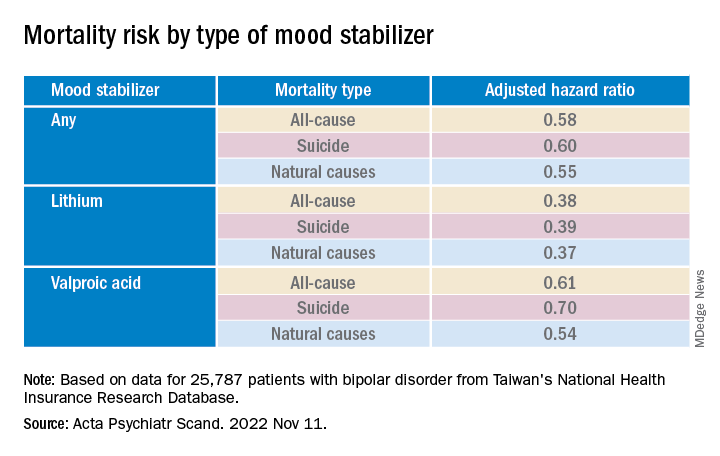
However, they also found that patients with BD had a significantly decreased adjusted 5-year risk of dying from any cause, suicide, and natural causes. Lithium was associated with the largest risk reduction compared with the other mood stabilizers.
“The present findings highlight the potential role of mood stabilizers, particularly lithium, in reducing mortality among patients with bipolar disorder,” the authors write.
“The findings of this study could inform future clinical and mechanistic research evaluating the multifaceted effects of mood stabilizers, particularly lithium, on the psychological and physiological statuses of patients with bipolar disorder,” they add.
The study was published online in Acta Psychiatrica Scandinavica.
Research gap
Patients with BD have an elevated risk for multiple comorbidities in addition to mood symptoms and neurocognitive dysfunction, with previous research suggesting a mortality rate due to suicide and natural causes that is at least twice as high as that of the general population, the authors write.
Lithium, in particular, has been associated with decreased risk for all-cause mortality and suicide in patients with BD, but findings regarding anticonvulsant mood stabilizers have been “inconsistent.”
To fill this research gap, the researchers evaluated 16 years of data from Taiwan’s National Health Insurance Research Database, which includes information about more than 23 million residents of Taiwan. The current study, which encompassed 25,787 patients with BD, looked at data from the 5-year period after index hospitalization.
The researchers hypothesized that mood stabilizers “would decrease the risk of mortality” among patients with BD and that “different mood stabilizers would exhibit different associations with mortality, owing to their varying effects on mood symptoms and physiological function.”
Covariates included sex, age, employment status, comorbidities, and concomitant drugs.
Of the patients with BD, 4,000 died within the 5-year period. Suicide and natural causes accounted for 19.0% and 73.7% of these deaths, respectively.
Cardioprotective effects?
The standardized mortality ratios (SMRs) – the ratios of observed mortality in the BD cohort to the number of expected deaths in the general population – were 5.26 for all causes (95% confidence interval, 5.10-5.43), 26.02 for suicide (95% CI, 24.20-27.93), and 4.68 for natural causes (95% CI, 4.51-4.85).
The cumulative mortality rate was higher among men vs. women, a difference that was even larger among patients who had died from any cause or natural causes (crude hazard ratios, .60 and .52, respectively; both Ps < .001).
The suicide risk peaked between ages 45 and 65 years, whereas the risks for all-cause and natural mortality increased with age and were highest in those older than 65 years.
Patients who had died from any cause or from natural causes had a higher risk for physical and psychiatric comorbidities, whereas those who had died by suicide had a higher risk for primarily psychiatric comorbidities.
Mood stabilizers were associated with decreased risks for all-cause mortality and natural mortality, with lithium and valproic acid tied to the lowest risk for all three mortality types (all Ps < .001).
Lamotrigine and carbamazepine were “not significantly associated with any type of mortality,” the authors report.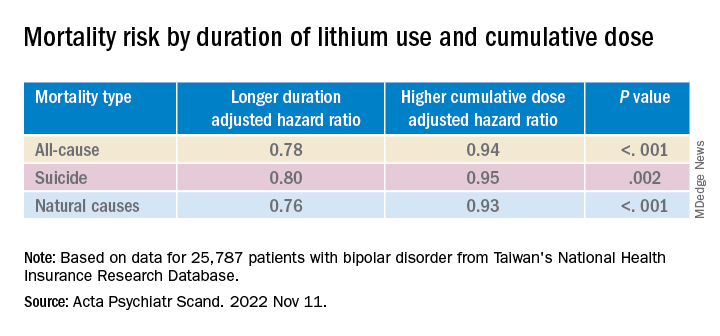
Longer duration of lithium use and a higher cumulative dose of lithium were both associated with lower risks for all three types of mortality (all Ps < .001).
Valproic acid was associated with dose-dependent decreases in all-cause and natural mortality risks.
The findings suggest that mood stabilizers “may improve not only psychosocial outcomes but also the physical health of patients with BD,” the investigators note.
The association between mood stabilizer use and reduced natural mortality risk “may be attributable to the potential benefits of psychiatric care” but may also “have resulted from the direct effects of mood stabilizers on physiological functions,” they add.
Some research suggests lithium treatment may reduce the risk for cardiovascular disease in patients with BD. Mechanistic studies have also pointed to potential cardioprotective effects from valproic acid.
The authors note several study limitations. Focusing on hospitalized patients “may have led to selection bias and overestimated mortality risk.” Moreover, the analyses were “based on the prescription, not the consumption, of mood stabilizers” and information regarding adherence was unavailable.
The absence of a protective mechanism of lamotrigine and carbamazepine may be attributable to “bias toward the relatively poor treatment responses” of these agents, neither of which is used as a first-line medication to treat BD in Taiwan. Patients taking these agents “may not receive medical care at a level equal to those taking lithium, who tend to receive closer surveillance, owing to the narrow therapeutic index.”
First-line treatment
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, said that the data “add to a growing confluence of data from observational studies indicating that lithium especially is capable of reducing all-cause mortality, suicide mortality, and natural mortality.”

Dr. McIntyre, chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study, agreed with the authors that lamotrigine is “not a very popular drug in Taiwan, therefore we may not have sufficient assay sensitivity to document the effect.”
But lamotrigine “does have recurrence prevention effects in BD, especially bipolar depression, and it would be expected that it would reduce suicide potentially especially in such a large sample.”
The study’s take-home message “is that the extant evidence now indicates that lithium should be a first-line treatment in persons who live with BD who are experiencing suicidal ideation and/or behavior and these data should inform algorithms of treatment selection and sequencing in clinical practice guidelines,” said Dr. McIntyre.
This research was supported by grants from the Ministry of Science and Technology in Taiwan and Taipei City Hospital. The authors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China, and the Milken Institute; and speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe Pharma, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
Investigators led by Pao-Huan Chen, MD, of the department of psychiatry, Taipei Medical University Hospital, Taiwan, evaluated the association between the use of mood stabilizers and the risks for all-cause mortality, suicide, and natural mortality in more than 25,000 patients with BD and found that those with BD had higher mortality.
However, they also found that patients with BD had a significantly decreased adjusted 5-year risk of dying from any cause, suicide, and natural causes. Lithium was associated with the largest risk reduction compared with the other mood stabilizers.
“The present findings highlight the potential role of mood stabilizers, particularly lithium, in reducing mortality among patients with bipolar disorder,” the authors write.
“The findings of this study could inform future clinical and mechanistic research evaluating the multifaceted effects of mood stabilizers, particularly lithium, on the psychological and physiological statuses of patients with bipolar disorder,” they add.
The study was published online in Acta Psychiatrica Scandinavica.
Research gap
Patients with BD have an elevated risk for multiple comorbidities in addition to mood symptoms and neurocognitive dysfunction, with previous research suggesting a mortality rate due to suicide and natural causes that is at least twice as high as that of the general population, the authors write.
Lithium, in particular, has been associated with decreased risk for all-cause mortality and suicide in patients with BD, but findings regarding anticonvulsant mood stabilizers have been “inconsistent.”
To fill this research gap, the researchers evaluated 16 years of data from Taiwan’s National Health Insurance Research Database, which includes information about more than 23 million residents of Taiwan. The current study, which encompassed 25,787 patients with BD, looked at data from the 5-year period after index hospitalization.
The researchers hypothesized that mood stabilizers “would decrease the risk of mortality” among patients with BD and that “different mood stabilizers would exhibit different associations with mortality, owing to their varying effects on mood symptoms and physiological function.”
Covariates included sex, age, employment status, comorbidities, and concomitant drugs.
Of the patients with BD, 4,000 died within the 5-year period. Suicide and natural causes accounted for 19.0% and 73.7% of these deaths, respectively.
Cardioprotective effects?
The standardized mortality ratios (SMRs) – the ratios of observed mortality in the BD cohort to the number of expected deaths in the general population – were 5.26 for all causes (95% confidence interval, 5.10-5.43), 26.02 for suicide (95% CI, 24.20-27.93), and 4.68 for natural causes (95% CI, 4.51-4.85).
The cumulative mortality rate was higher among men vs. women, a difference that was even larger among patients who had died from any cause or natural causes (crude hazard ratios, .60 and .52, respectively; both Ps < .001).
The suicide risk peaked between ages 45 and 65 years, whereas the risks for all-cause and natural mortality increased with age and were highest in those older than 65 years.
Patients who had died from any cause or from natural causes had a higher risk for physical and psychiatric comorbidities, whereas those who had died by suicide had a higher risk for primarily psychiatric comorbidities.
Mood stabilizers were associated with decreased risks for all-cause mortality and natural mortality, with lithium and valproic acid tied to the lowest risk for all three mortality types (all Ps < .001).
Lamotrigine and carbamazepine were “not significantly associated with any type of mortality,” the authors report.
Longer duration of lithium use and a higher cumulative dose of lithium were both associated with lower risks for all three types of mortality (all Ps < .001).
Valproic acid was associated with dose-dependent decreases in all-cause and natural mortality risks.
The findings suggest that mood stabilizers “may improve not only psychosocial outcomes but also the physical health of patients with BD,” the investigators note.
The association between mood stabilizer use and reduced natural mortality risk “may be attributable to the potential benefits of psychiatric care” but may also “have resulted from the direct effects of mood stabilizers on physiological functions,” they add.
Some research suggests lithium treatment may reduce the risk for cardiovascular disease in patients with BD. Mechanistic studies have also pointed to potential cardioprotective effects from valproic acid.
The authors note several study limitations. Focusing on hospitalized patients “may have led to selection bias and overestimated mortality risk.” Moreover, the analyses were “based on the prescription, not the consumption, of mood stabilizers” and information regarding adherence was unavailable.
The absence of a protective mechanism of lamotrigine and carbamazepine may be attributable to “bias toward the relatively poor treatment responses” of these agents, neither of which is used as a first-line medication to treat BD in Taiwan. Patients taking these agents “may not receive medical care at a level equal to those taking lithium, who tend to receive closer surveillance, owing to the narrow therapeutic index.”
First-line treatment
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, said that the data “add to a growing confluence of data from observational studies indicating that lithium especially is capable of reducing all-cause mortality, suicide mortality, and natural mortality.”
Dr. McIntyre, chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study, agreed with the authors that lamotrigine is “not a very popular drug in Taiwan, therefore we may not have sufficient assay sensitivity to document the effect.”
But lamotrigine “does have recurrence prevention effects in BD, especially bipolar depression, and it would be expected that it would reduce suicide potentially especially in such a large sample.”
The study’s take-home message “is that the extant evidence now indicates that lithium should be a first-line treatment in persons who live with BD who are experiencing suicidal ideation and/or behavior and these data should inform algorithms of treatment selection and sequencing in clinical practice guidelines,” said Dr. McIntyre.
This research was supported by grants from the Ministry of Science and Technology in Taiwan and Taipei City Hospital. The authors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China, and the Milken Institute; and speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe Pharma, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
Investigators led by Pao-Huan Chen, MD, of the department of psychiatry, Taipei Medical University Hospital, Taiwan, evaluated the association between the use of mood stabilizers and the risks for all-cause mortality, suicide, and natural mortality in more than 25,000 patients with BD and found that those with BD had higher mortality.
However, they also found that patients with BD had a significantly decreased adjusted 5-year risk of dying from any cause, suicide, and natural causes. Lithium was associated with the largest risk reduction compared with the other mood stabilizers.
“The present findings highlight the potential role of mood stabilizers, particularly lithium, in reducing mortality among patients with bipolar disorder,” the authors write.
“The findings of this study could inform future clinical and mechanistic research evaluating the multifaceted effects of mood stabilizers, particularly lithium, on the psychological and physiological statuses of patients with bipolar disorder,” they add.
The study was published online in Acta Psychiatrica Scandinavica.
Research gap
Patients with BD have an elevated risk for multiple comorbidities in addition to mood symptoms and neurocognitive dysfunction, with previous research suggesting a mortality rate due to suicide and natural causes that is at least twice as high as that of the general population, the authors write.
Lithium, in particular, has been associated with decreased risk for all-cause mortality and suicide in patients with BD, but findings regarding anticonvulsant mood stabilizers have been “inconsistent.”
To fill this research gap, the researchers evaluated 16 years of data from Taiwan’s National Health Insurance Research Database, which includes information about more than 23 million residents of Taiwan. The current study, which encompassed 25,787 patients with BD, looked at data from the 5-year period after index hospitalization.
The researchers hypothesized that mood stabilizers “would decrease the risk of mortality” among patients with BD and that “different mood stabilizers would exhibit different associations with mortality, owing to their varying effects on mood symptoms and physiological function.”
Covariates included sex, age, employment status, comorbidities, and concomitant drugs.
Of the patients with BD, 4,000 died within the 5-year period. Suicide and natural causes accounted for 19.0% and 73.7% of these deaths, respectively.
Cardioprotective effects?
The standardized mortality ratios (SMRs) – the ratios of observed mortality in the BD cohort to the number of expected deaths in the general population – were 5.26 for all causes (95% confidence interval, 5.10-5.43), 26.02 for suicide (95% CI, 24.20-27.93), and 4.68 for natural causes (95% CI, 4.51-4.85).
The cumulative mortality rate was higher among men vs. women, a difference that was even larger among patients who had died from any cause or natural causes (crude hazard ratios, .60 and .52, respectively; both Ps < .001).
The suicide risk peaked between ages 45 and 65 years, whereas the risks for all-cause and natural mortality increased with age and were highest in those older than 65 years.
Patients who had died from any cause or from natural causes had a higher risk for physical and psychiatric comorbidities, whereas those who had died by suicide had a higher risk for primarily psychiatric comorbidities.
Mood stabilizers were associated with decreased risks for all-cause mortality and natural mortality, with lithium and valproic acid tied to the lowest risk for all three mortality types (all Ps < .001).
Lamotrigine and carbamazepine were “not significantly associated with any type of mortality,” the authors report.
Longer duration of lithium use and a higher cumulative dose of lithium were both associated with lower risks for all three types of mortality (all Ps < .001).
Valproic acid was associated with dose-dependent decreases in all-cause and natural mortality risks.
The findings suggest that mood stabilizers “may improve not only psychosocial outcomes but also the physical health of patients with BD,” the investigators note.
The association between mood stabilizer use and reduced natural mortality risk “may be attributable to the potential benefits of psychiatric care” but may also “have resulted from the direct effects of mood stabilizers on physiological functions,” they add.
Some research suggests lithium treatment may reduce the risk for cardiovascular disease in patients with BD. Mechanistic studies have also pointed to potential cardioprotective effects from valproic acid.
The authors note several study limitations. Focusing on hospitalized patients “may have led to selection bias and overestimated mortality risk.” Moreover, the analyses were “based on the prescription, not the consumption, of mood stabilizers” and information regarding adherence was unavailable.
The absence of a protective mechanism of lamotrigine and carbamazepine may be attributable to “bias toward the relatively poor treatment responses” of these agents, neither of which is used as a first-line medication to treat BD in Taiwan. Patients taking these agents “may not receive medical care at a level equal to those taking lithium, who tend to receive closer surveillance, owing to the narrow therapeutic index.”
First-line treatment
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, said that the data “add to a growing confluence of data from observational studies indicating that lithium especially is capable of reducing all-cause mortality, suicide mortality, and natural mortality.”
Dr. McIntyre, chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, who was not involved with the study, agreed with the authors that lamotrigine is “not a very popular drug in Taiwan, therefore we may not have sufficient assay sensitivity to document the effect.”
But lamotrigine “does have recurrence prevention effects in BD, especially bipolar depression, and it would be expected that it would reduce suicide potentially especially in such a large sample.”
The study’s take-home message “is that the extant evidence now indicates that lithium should be a first-line treatment in persons who live with BD who are experiencing suicidal ideation and/or behavior and these data should inform algorithms of treatment selection and sequencing in clinical practice guidelines,” said Dr. McIntyre.
This research was supported by grants from the Ministry of Science and Technology in Taiwan and Taipei City Hospital. The authors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China, and the Milken Institute; and speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe Pharma, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
FROM ACTA PSYCHIATRICA SCANDINAVICA
Race and spirometry
The European Respiratory Society (ERS) and American Thoracic Society (ATS) just published an update to their guidelines on lung function interpretation (Stanojevic S, et al. Eur Respir J. 2022; 60: 2101499). As with any update, the document builds on past work and integrates new advances the field has seen since 2005.
The current iteration comes at a time when academics, clinicians, and epidemiologists are re-analyzing what we think we know about the complex ways race and ethnicity intersect with the practice of medicine. Several experts on lung function testing, many if not most of whom are authors on the ERS/ATS guideline, have written letters or published reviews commenting on the way accounting for race or ethnicity affects lung function interpretation.
Race/ethnicity and lung function was also the topic of an excellent session at the recent CHEST 2022 Annual Meeting in Nashville, Tennessee. Here, we’ll provide a brief review and direct the reader to relevant sources for a more detailed analysis.
Spirometry is an integral part of the diagnosis and management of a wide range of pulmonary conditions. Dr. Aaron Baugh from the University of California San Francisco (UCSF) lectured on the spirometer’s history at CHEST 2022 and detailed its interactions with race over the past 2 centuries. Other authors have chronicled this history, as well (Braun L, et al. Can J Respir Ther. 2015;51[4]:99-101). The short version is that since the British surgeon John Hutchinson created the first spirometer in 1846, race has been a part of the discussion of lung function interpretation.
In 2022, we know far more about the factors that determine lung function than we did in the 19th century. Age, height, and sex assigned at birth all explain a high percentage of the variability seen in FEV1 and FVC. When modeled, race also explains a portion of the variability, and the NHANES III investigators found its inclusion in regression equations, along with age, height, and sex, improved their precision. Case closed, right? Modern medicine is defined by phenotyping, precision, and individualized care, so why shouldn’t race be a part of lung function interpretation?
Well, it’s complicated. As clinicians and academics, we must analyze the root cause of differences in health outcomes between racial groups.
Publications on pulse oximetry (Gottlieb ER, et al. JAMA Intern Med. 2022; 182:849-858) and glomerular filtration rate (Williams WW, et al. N Engl J Med. 2021;385:1804-1806) have revealed some of the ways our use of instruments and equations may exacerbate or perpetuate current disparities. Even small differences in a measure like pulse oximetry could have a profound impact on clinical decisions at the individual and population levels.
The 2022 ERS/ATS lung function interpretation guidelines have abandoned the use of NHANES III as a reference set. They now recommend the equations developed by the Global Lung Initiative (GLI) for referencing to normal for spirometry, diffusion capacity, and lung volumes. For spirometry the GLI was able to integrate data from countries around the world. This allowed ethnicity to be included in their regression equations and, similar to NHANES III, they found ethnicity improved the precision of their equations. They also published an equation that did not account for country of origin that could be applied to individuals of any race/ethnicity (Quanjer PH, et al. Eur Respir J. 2014;43:505-512). This allowed for applying the GLI equations to external data sets with or without ethnicity included as a co-variate.
Given well-established discrepancies in spirometry, it should come as no surprise that applying the race/ethnicity-neutral GLI equations to non-White populations increases the percentage of patients with pulmonary defects (Moffett AT, et al. Am J Respir Crit Care Med. 2021; A1030). Other data suggest that elimination of race/ethnicity as a co-variate improves the association between percent predicted lung function and important outcomes like mortality (McCormack MC, et al. Am J Respir Crit Care Med. 2022;205:723-724). The first analysis implies that by adjusting for race/ethnicity we may be missing abnormalities, and the second suggests accuracy for outcomes is lost. So case closed, right? Let’s abandon race/ethnicity as a co- variate for our spirometry reference equations.
Perhaps, but a few caveats are in order. It’s important to note that doing so would result in a dramatic increase in abnormal findings in otherwise healthy and asymptomatic non-White individuals. This could negatively affect eligibility for employment and military service (Townsend MC, et al. Am J Respir Crit Care Med. 2022;789-790). We’ve also yet to fully explain the factors driving differences in lung function between races. If socioeconomic factors explained the entirety of the difference, it would be easier to argue for elimination of using race/ethnicity in our equations. Currently, the etiology is thought to be multifactorial and is yet to be fully explained (Braun L, et al. Eur Respir J. 2013;41:1362-1370).
The more we look for institutional racism, the more we will find it. As we realize that attaining health and wellness is more difficult for the disenfranchised, we need to ensure our current practices are part of the solution.
The ERS/ATS guidelines suggest eliminating fixed correction factors for race but do not require elimination of race/ethnicity as a co-variate in the equations selected for use. This seems very reasonable given what we know now. As pulmonary medicine academics and researchers, we need to continue to study the impact integrating race/ethnicity has on precision, accuracy, and clinical outcomes. As pulmonary medicine clinicians, we need to be aware of the reference equations being used in our lab, understand how inclusion of race/ethnicity affects findings, and act accordingly, depending on the clinical situation.
Dr. Ghionni is a Pulmonary/Critical Care Fellow, and Dr. Woods is Program Director – PCCM Fellowship and Associate Program Director – IM Residency, Medstar Washington Hospital Center; Dr. Woods is Associate Professor of Medicine, Georgetown University School of Medicine, Washington, DC.
The European Respiratory Society (ERS) and American Thoracic Society (ATS) just published an update to their guidelines on lung function interpretation (Stanojevic S, et al. Eur Respir J. 2022; 60: 2101499). As with any update, the document builds on past work and integrates new advances the field has seen since 2005.
The current iteration comes at a time when academics, clinicians, and epidemiologists are re-analyzing what we think we know about the complex ways race and ethnicity intersect with the practice of medicine. Several experts on lung function testing, many if not most of whom are authors on the ERS/ATS guideline, have written letters or published reviews commenting on the way accounting for race or ethnicity affects lung function interpretation.
Race/ethnicity and lung function was also the topic of an excellent session at the recent CHEST 2022 Annual Meeting in Nashville, Tennessee. Here, we’ll provide a brief review and direct the reader to relevant sources for a more detailed analysis.
Spirometry is an integral part of the diagnosis and management of a wide range of pulmonary conditions. Dr. Aaron Baugh from the University of California San Francisco (UCSF) lectured on the spirometer’s history at CHEST 2022 and detailed its interactions with race over the past 2 centuries. Other authors have chronicled this history, as well (Braun L, et al. Can J Respir Ther. 2015;51[4]:99-101). The short version is that since the British surgeon John Hutchinson created the first spirometer in 1846, race has been a part of the discussion of lung function interpretation.
In 2022, we know far more about the factors that determine lung function than we did in the 19th century. Age, height, and sex assigned at birth all explain a high percentage of the variability seen in FEV1 and FVC. When modeled, race also explains a portion of the variability, and the NHANES III investigators found its inclusion in regression equations, along with age, height, and sex, improved their precision. Case closed, right? Modern medicine is defined by phenotyping, precision, and individualized care, so why shouldn’t race be a part of lung function interpretation?
Well, it’s complicated. As clinicians and academics, we must analyze the root cause of differences in health outcomes between racial groups.
Publications on pulse oximetry (Gottlieb ER, et al. JAMA Intern Med. 2022; 182:849-858) and glomerular filtration rate (Williams WW, et al. N Engl J Med. 2021;385:1804-1806) have revealed some of the ways our use of instruments and equations may exacerbate or perpetuate current disparities. Even small differences in a measure like pulse oximetry could have a profound impact on clinical decisions at the individual and population levels.
The 2022 ERS/ATS lung function interpretation guidelines have abandoned the use of NHANES III as a reference set. They now recommend the equations developed by the Global Lung Initiative (GLI) for referencing to normal for spirometry, diffusion capacity, and lung volumes. For spirometry the GLI was able to integrate data from countries around the world. This allowed ethnicity to be included in their regression equations and, similar to NHANES III, they found ethnicity improved the precision of their equations. They also published an equation that did not account for country of origin that could be applied to individuals of any race/ethnicity (Quanjer PH, et al. Eur Respir J. 2014;43:505-512). This allowed for applying the GLI equations to external data sets with or without ethnicity included as a co-variate.
Given well-established discrepancies in spirometry, it should come as no surprise that applying the race/ethnicity-neutral GLI equations to non-White populations increases the percentage of patients with pulmonary defects (Moffett AT, et al. Am J Respir Crit Care Med. 2021; A1030). Other data suggest that elimination of race/ethnicity as a co-variate improves the association between percent predicted lung function and important outcomes like mortality (McCormack MC, et al. Am J Respir Crit Care Med. 2022;205:723-724). The first analysis implies that by adjusting for race/ethnicity we may be missing abnormalities, and the second suggests accuracy for outcomes is lost. So case closed, right? Let’s abandon race/ethnicity as a co- variate for our spirometry reference equations.
Perhaps, but a few caveats are in order. It’s important to note that doing so would result in a dramatic increase in abnormal findings in otherwise healthy and asymptomatic non-White individuals. This could negatively affect eligibility for employment and military service (Townsend MC, et al. Am J Respir Crit Care Med. 2022;789-790). We’ve also yet to fully explain the factors driving differences in lung function between races. If socioeconomic factors explained the entirety of the difference, it would be easier to argue for elimination of using race/ethnicity in our equations. Currently, the etiology is thought to be multifactorial and is yet to be fully explained (Braun L, et al. Eur Respir J. 2013;41:1362-1370).
The more we look for institutional racism, the more we will find it. As we realize that attaining health and wellness is more difficult for the disenfranchised, we need to ensure our current practices are part of the solution.
The ERS/ATS guidelines suggest eliminating fixed correction factors for race but do not require elimination of race/ethnicity as a co-variate in the equations selected for use. This seems very reasonable given what we know now. As pulmonary medicine academics and researchers, we need to continue to study the impact integrating race/ethnicity has on precision, accuracy, and clinical outcomes. As pulmonary medicine clinicians, we need to be aware of the reference equations being used in our lab, understand how inclusion of race/ethnicity affects findings, and act accordingly, depending on the clinical situation.
Dr. Ghionni is a Pulmonary/Critical Care Fellow, and Dr. Woods is Program Director – PCCM Fellowship and Associate Program Director – IM Residency, Medstar Washington Hospital Center; Dr. Woods is Associate Professor of Medicine, Georgetown University School of Medicine, Washington, DC.
The European Respiratory Society (ERS) and American Thoracic Society (ATS) just published an update to their guidelines on lung function interpretation (Stanojevic S, et al. Eur Respir J. 2022; 60: 2101499). As with any update, the document builds on past work and integrates new advances the field has seen since 2005.
The current iteration comes at a time when academics, clinicians, and epidemiologists are re-analyzing what we think we know about the complex ways race and ethnicity intersect with the practice of medicine. Several experts on lung function testing, many if not most of whom are authors on the ERS/ATS guideline, have written letters or published reviews commenting on the way accounting for race or ethnicity affects lung function interpretation.
Race/ethnicity and lung function was also the topic of an excellent session at the recent CHEST 2022 Annual Meeting in Nashville, Tennessee. Here, we’ll provide a brief review and direct the reader to relevant sources for a more detailed analysis.
Spirometry is an integral part of the diagnosis and management of a wide range of pulmonary conditions. Dr. Aaron Baugh from the University of California San Francisco (UCSF) lectured on the spirometer’s history at CHEST 2022 and detailed its interactions with race over the past 2 centuries. Other authors have chronicled this history, as well (Braun L, et al. Can J Respir Ther. 2015;51[4]:99-101). The short version is that since the British surgeon John Hutchinson created the first spirometer in 1846, race has been a part of the discussion of lung function interpretation.
In 2022, we know far more about the factors that determine lung function than we did in the 19th century. Age, height, and sex assigned at birth all explain a high percentage of the variability seen in FEV1 and FVC. When modeled, race also explains a portion of the variability, and the NHANES III investigators found its inclusion in regression equations, along with age, height, and sex, improved their precision. Case closed, right? Modern medicine is defined by phenotyping, precision, and individualized care, so why shouldn’t race be a part of lung function interpretation?
Well, it’s complicated. As clinicians and academics, we must analyze the root cause of differences in health outcomes between racial groups.
Publications on pulse oximetry (Gottlieb ER, et al. JAMA Intern Med. 2022; 182:849-858) and glomerular filtration rate (Williams WW, et al. N Engl J Med. 2021;385:1804-1806) have revealed some of the ways our use of instruments and equations may exacerbate or perpetuate current disparities. Even small differences in a measure like pulse oximetry could have a profound impact on clinical decisions at the individual and population levels.
The 2022 ERS/ATS lung function interpretation guidelines have abandoned the use of NHANES III as a reference set. They now recommend the equations developed by the Global Lung Initiative (GLI) for referencing to normal for spirometry, diffusion capacity, and lung volumes. For spirometry the GLI was able to integrate data from countries around the world. This allowed ethnicity to be included in their regression equations and, similar to NHANES III, they found ethnicity improved the precision of their equations. They also published an equation that did not account for country of origin that could be applied to individuals of any race/ethnicity (Quanjer PH, et al. Eur Respir J. 2014;43:505-512). This allowed for applying the GLI equations to external data sets with or without ethnicity included as a co-variate.
Given well-established discrepancies in spirometry, it should come as no surprise that applying the race/ethnicity-neutral GLI equations to non-White populations increases the percentage of patients with pulmonary defects (Moffett AT, et al. Am J Respir Crit Care Med. 2021; A1030). Other data suggest that elimination of race/ethnicity as a co-variate improves the association between percent predicted lung function and important outcomes like mortality (McCormack MC, et al. Am J Respir Crit Care Med. 2022;205:723-724). The first analysis implies that by adjusting for race/ethnicity we may be missing abnormalities, and the second suggests accuracy for outcomes is lost. So case closed, right? Let’s abandon race/ethnicity as a co- variate for our spirometry reference equations.
Perhaps, but a few caveats are in order. It’s important to note that doing so would result in a dramatic increase in abnormal findings in otherwise healthy and asymptomatic non-White individuals. This could negatively affect eligibility for employment and military service (Townsend MC, et al. Am J Respir Crit Care Med. 2022;789-790). We’ve also yet to fully explain the factors driving differences in lung function between races. If socioeconomic factors explained the entirety of the difference, it would be easier to argue for elimination of using race/ethnicity in our equations. Currently, the etiology is thought to be multifactorial and is yet to be fully explained (Braun L, et al. Eur Respir J. 2013;41:1362-1370).
The more we look for institutional racism, the more we will find it. As we realize that attaining health and wellness is more difficult for the disenfranchised, we need to ensure our current practices are part of the solution.
The ERS/ATS guidelines suggest eliminating fixed correction factors for race but do not require elimination of race/ethnicity as a co-variate in the equations selected for use. This seems very reasonable given what we know now. As pulmonary medicine academics and researchers, we need to continue to study the impact integrating race/ethnicity has on precision, accuracy, and clinical outcomes. As pulmonary medicine clinicians, we need to be aware of the reference equations being used in our lab, understand how inclusion of race/ethnicity affects findings, and act accordingly, depending on the clinical situation.
Dr. Ghionni is a Pulmonary/Critical Care Fellow, and Dr. Woods is Program Director – PCCM Fellowship and Associate Program Director – IM Residency, Medstar Washington Hospital Center; Dr. Woods is Associate Professor of Medicine, Georgetown University School of Medicine, Washington, DC.
Have you heard of VEXAS syndrome?
Its name is an acronym: Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic. The prevalence of this syndrome is unknown, but it is not so rare. As it is an X-linked disease, men are predominantly affected.
First identification
The NIH team screened the exomes and genomes of 2,560 individuals. Of this group, 1,477 had been referred because of undiagnosed recurrent fevers, systemic inflammation, or both, and 1,083 were affected by atypical, unclassified disorders. The researchers identified 25 men with a somatic mutation in the ubiquitin-like modifier activating enzyme 1 (UBA1) gene, which is involved in the protein ubiquitylation system. This posttranslational modification has a pleiotropic function that likely explains the clinical heterogeneity seen in VEXAS patients: regulation of protein turnover, especially those involved in the cell cycle, cell death, and signal transduction. Ubiquitylation is also involved in nonproteolytic functions, such as assembly of multiprotein complexes, intracellular signaling, inflammatory signaling, and DNA repair.
Clinical presentation
The clinicobiological presentation of VEXAS syndrome is very heterogeneous. Typically, patients present with a systemic inflammatory disease with unexplained episodes of fever, involvement of the lungs, skin, blood vessels, and joints. Molecular diagnosis is made by the sequencing of UBA1.
Most patients present with the characteristic clinical signs of other inflammatory diseases, such as polyarteritis nodosa and recurrent polychondritis. But VEXAS patients are at high risk of developing hematologic conditions. Indeed, the following were seen among the 25 participants in the NIH study: macrocytic anemia (96%), venous thromboembolism (44%), myelodysplastic syndrome (24%), and multiple myeloma or monoclonal gammopathy of undetermined significance (20%).
In VEXAS patients, levels of serum inflammatory markers are increased. These markers include tumor necrosis factor, interleukin-8, interleukin-6, interferon-inducible protein-10, interferon-gamma, C-reactive protein. In addition, there is aberrant activation of innate immune-signaling pathways.
In a large-scale analysis of a multicenter case series of 116 French patients, researchers found that VEXAS syndrome primarily affected men. The disease was progressive, and onset occurred after age 50 years. These patients can be divided into three phenotypically distinct clusters on the basis of integration of clinical and biological data. In the 58 cases in which myelodysplastic syndrome was present, the mortality rates were higher. The researchers also reported that the UBA1 p.Met41L mutation was associated with a better prognosis.
Treatment data
VEXAS syndrome resists the classical therapeutic arsenal. Patients require high-dose glucocorticoids, and prognosis appears to be poor. The available treatment data are retrospective. Of the 25 participants in the NIH study, 40% died within 5 years from disease-related causes or complications related to treatment. Among the promising therapeutic avenues is the use of inhibitors of the Janus kinase pathway.
This article was translated from Univadis France. A version of this article appeared on Medscape.com.
Its name is an acronym: Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic. The prevalence of this syndrome is unknown, but it is not so rare. As it is an X-linked disease, men are predominantly affected.
First identification
The NIH team screened the exomes and genomes of 2,560 individuals. Of this group, 1,477 had been referred because of undiagnosed recurrent fevers, systemic inflammation, or both, and 1,083 were affected by atypical, unclassified disorders. The researchers identified 25 men with a somatic mutation in the ubiquitin-like modifier activating enzyme 1 (UBA1) gene, which is involved in the protein ubiquitylation system. This posttranslational modification has a pleiotropic function that likely explains the clinical heterogeneity seen in VEXAS patients: regulation of protein turnover, especially those involved in the cell cycle, cell death, and signal transduction. Ubiquitylation is also involved in nonproteolytic functions, such as assembly of multiprotein complexes, intracellular signaling, inflammatory signaling, and DNA repair.
Clinical presentation
The clinicobiological presentation of VEXAS syndrome is very heterogeneous. Typically, patients present with a systemic inflammatory disease with unexplained episodes of fever, involvement of the lungs, skin, blood vessels, and joints. Molecular diagnosis is made by the sequencing of UBA1.
Most patients present with the characteristic clinical signs of other inflammatory diseases, such as polyarteritis nodosa and recurrent polychondritis. But VEXAS patients are at high risk of developing hematologic conditions. Indeed, the following were seen among the 25 participants in the NIH study: macrocytic anemia (96%), venous thromboembolism (44%), myelodysplastic syndrome (24%), and multiple myeloma or monoclonal gammopathy of undetermined significance (20%).
In VEXAS patients, levels of serum inflammatory markers are increased. These markers include tumor necrosis factor, interleukin-8, interleukin-6, interferon-inducible protein-10, interferon-gamma, C-reactive protein. In addition, there is aberrant activation of innate immune-signaling pathways.
In a large-scale analysis of a multicenter case series of 116 French patients, researchers found that VEXAS syndrome primarily affected men. The disease was progressive, and onset occurred after age 50 years. These patients can be divided into three phenotypically distinct clusters on the basis of integration of clinical and biological data. In the 58 cases in which myelodysplastic syndrome was present, the mortality rates were higher. The researchers also reported that the UBA1 p.Met41L mutation was associated with a better prognosis.
Treatment data
VEXAS syndrome resists the classical therapeutic arsenal. Patients require high-dose glucocorticoids, and prognosis appears to be poor. The available treatment data are retrospective. Of the 25 participants in the NIH study, 40% died within 5 years from disease-related causes or complications related to treatment. Among the promising therapeutic avenues is the use of inhibitors of the Janus kinase pathway.
This article was translated from Univadis France. A version of this article appeared on Medscape.com.
Its name is an acronym: Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic. The prevalence of this syndrome is unknown, but it is not so rare. As it is an X-linked disease, men are predominantly affected.
First identification
The NIH team screened the exomes and genomes of 2,560 individuals. Of this group, 1,477 had been referred because of undiagnosed recurrent fevers, systemic inflammation, or both, and 1,083 were affected by atypical, unclassified disorders. The researchers identified 25 men with a somatic mutation in the ubiquitin-like modifier activating enzyme 1 (UBA1) gene, which is involved in the protein ubiquitylation system. This posttranslational modification has a pleiotropic function that likely explains the clinical heterogeneity seen in VEXAS patients: regulation of protein turnover, especially those involved in the cell cycle, cell death, and signal transduction. Ubiquitylation is also involved in nonproteolytic functions, such as assembly of multiprotein complexes, intracellular signaling, inflammatory signaling, and DNA repair.
Clinical presentation
The clinicobiological presentation of VEXAS syndrome is very heterogeneous. Typically, patients present with a systemic inflammatory disease with unexplained episodes of fever, involvement of the lungs, skin, blood vessels, and joints. Molecular diagnosis is made by the sequencing of UBA1.
Most patients present with the characteristic clinical signs of other inflammatory diseases, such as polyarteritis nodosa and recurrent polychondritis. But VEXAS patients are at high risk of developing hematologic conditions. Indeed, the following were seen among the 25 participants in the NIH study: macrocytic anemia (96%), venous thromboembolism (44%), myelodysplastic syndrome (24%), and multiple myeloma or monoclonal gammopathy of undetermined significance (20%).
In VEXAS patients, levels of serum inflammatory markers are increased. These markers include tumor necrosis factor, interleukin-8, interleukin-6, interferon-inducible protein-10, interferon-gamma, C-reactive protein. In addition, there is aberrant activation of innate immune-signaling pathways.
In a large-scale analysis of a multicenter case series of 116 French patients, researchers found that VEXAS syndrome primarily affected men. The disease was progressive, and onset occurred after age 50 years. These patients can be divided into three phenotypically distinct clusters on the basis of integration of clinical and biological data. In the 58 cases in which myelodysplastic syndrome was present, the mortality rates were higher. The researchers also reported that the UBA1 p.Met41L mutation was associated with a better prognosis.
Treatment data
VEXAS syndrome resists the classical therapeutic arsenal. Patients require high-dose glucocorticoids, and prognosis appears to be poor. The available treatment data are retrospective. Of the 25 participants in the NIH study, 40% died within 5 years from disease-related causes or complications related to treatment. Among the promising therapeutic avenues is the use of inhibitors of the Janus kinase pathway.
This article was translated from Univadis France. A version of this article appeared on Medscape.com.
Toward a healthy and sustainable critical care workforce in the COVID-19 era: A call for action
The COVID-19 pandemic has caused unprecedented and unpredictable strain on health care systems worldwide, forcing rapid organizational modifications and innovations to ensure availability of critical care resources during acute surge events. Yet, while much attention has been paid to the availability of ICU beds and ventilators, COVID-19 has insidiously and significantly harmed the most precious critical care resource of all – the human beings who are the lifeblood of critical care delivery. We are now at a crucial moment in history to better understand the pandemic’s impact on our human resources and enact changes to reverse the damage that it has inflicted on our workforce.
ICUs, where critical care delivery predominantly occurs, increasingly utilize interprofessional staffing models in which clinicians from multiple disciplines – physicians, nurses, clinical pharmacists, respiratory therapists, and dieticians, among others – bring their unique expertise to team-based clinical decisions and care delivery. Such a multidisciplinary approach helps enable the provision of more comprehensive, higher-quality critical care. In this way, the interprofessional ICU care team is an embodiment of the notion that the “whole” is more than just the sum of its parts. Therefore, we must consider the impact of the pandemic on interprofessional critical care clinicians as the team that they are.
Even before the COVID-19 pandemic, the well-being of critical care clinicians was compromised. Across multiple disciplines, they had among the highest rates of burnout syndrome of all health care professionals (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113). As the pandemic has dragged on, their well-being has only further declined. Burnout rates are at all-time highs, and symptoms of posttraumatic stress disorder, anxiety, and depression are common and have increased with each subsequent surge (Azoulay E, et al. Chest. 2021;160[3]:944-955). Offsets to burnout, such as fulfillment and recognition, have declined over time (Kerlin MP, et al. Ann Amer Thorac Soc. 2022;19[2]:329-331). These worrisome trends pose a significant threat to critical care delivery. Clinician burnout is associated with worse patient outcomes, increased medical errors, and lower patient satisfaction (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113; Poghosyan L, et al. Res Nurs Health. 2010;33[4]:288-298). It is also associated with mental illness and substance use disorders among clinicians (Dyrbye LN, et al. Ann Intern Med. 2008;149[5]:334-341). Finally, it has contributed to a workforce crisis: nearly 500,000 health care workers have left the US health care sector since the beginning of the pandemic, and approximately two-thirds of acute and critical care nurses have considered doing so (Wong E. “Why Healthcare Workers are Quitting in Droves”. The Atlantic. Accessed November 7, 2022). Such a “brain drain” of clinicians – whose expertise cannot be easily replicated or replaced – represents a staffing crisis that threatens our ability to provide high-quality, safe care for the foreseeable future.
To combat burnout, it is first necessary to identify the mechanisms by which the pandemic has induced harm. Early during the pandemic, critical care clinicians feared for their own safety with little information of how the virus was spread. At a time when the world was under lockdown, vaccines were not yet available, and hospitals were overwhelmed with surges of critically ill patients, clinicians struggled like the rest of the world to meet their own basic needs such as childcare, grocery shopping, and time with family. They experienced distress from high volumes of patients with extreme mortality rates, helplessness due to lack of treatment options, and moral injury over restrictive visitation policies (Vranas KC, et al. Chest. 2022;162[2]:331-345; Vranas KC, et al. Chest. 2021;160[5]:1714-1728). Over time, critical care clinicians have no doubt experienced further exhaustion related to the duration of the pandemic, often without adequate time to recover and process the trauma they have experienced. More recently, a new source of distress for clinicians has emerged from variability in vaccine uptake among the public. Clinicians have experienced compassion fatigue and even moral outrage toward those who chose not to receive a vaccine that is highly effective at preventing severe illness. They also suffered from ethical conflicts over how to treat unvaccinated patients and whether they should be given equal priority and access to limited therapies (Shaw D. Bioethics. 2022;36[8]:883-890).
Furthermore, the pandemic has damaged the relationship between clinicians and their institutions. Early in the pandemic, the widespread shortages of personal protective equipment harmed trust among clinicians due to their perception that their safety was not prioritized. Hospitals have also struggled with having to make rapid decisions on how to equitably allocate fixed resources in response to unanticipated and unpredictable demands, while also maintaining financial solvency. In some cases, these challenging policy decisions (eg, whether to continue elective procedures during acute surge events) lacked transparency and input from the team at the frontlines of patient care. As a result, clinicians have felt undervalued and without a voice in decisions that directly impact both the care they can provide their patients and their own well-being.
It is incumbent upon us now to take steps to repair the damage inflicted on our critical care workforce by the pandemic. To this end, there have been calls for the urgent implementation of strategies to mitigate the psychological burden experienced by critical care clinicians. However, many of these focus on interventions to increase coping strategies and resilience among individual clinicians. While programs such as mindfulness apps and resilience training are valuable, they are not sufficient. The very nature of these solutions implies that the solution (and therefore, the problem) of burnout lies in the individual clinician. Yet, as described above, many of the mechanisms of harm to clinicians’ well-being are systems-level issues that will necessarily require systems-level solutions.
Therefore, we propose a comprehensive, layered approach to begin to reverse the damage inflicted by the pandemic on critical care clinicians’ well-being, with solutions organized by ecological levels of individual clinicians, departments, institutions, and society. With this approach, we hope to address specific aspects of our critical care delivery system that, taken together, will fortify the well-being of our critical care workforce as a whole. We offer suggestions below that are both informed by existing evidence, as well as our own opinions as intensivists and researchers.
At the level of the individual clinician:
- Proactively provide access to mental health resources. Clinicians have limited time or energy to navigate mental health and support services and find it helpful when others proactively reach out to them.
- Provide opportunities for clinicians to experience community and support among peers. Clinicians find benefit in town halls, debrief sessions, and peer support groups, particularly during times of acute strain.
At the level of the department:
- Allow more flexibility in work schedules. Even prior to the pandemic, the lack of scheduling flexibility and the number of consecutive days worked had been identified as key contributors to burnout; these have been exacerbated during times of caseload surges, when clinicians have been asked or even required to increase their hours and work extra shifts.
- Promote a culture of psychological safety in which clinicians feel empowered to say “I cannot work” for whatever reason. This will require the establishment of formalized backup systems that easily accommodate call-outs without relying on individual clinicians to find their own coverage.
At the level of the health care system:
- Prioritize transparency, and bring administrators and clinicians together for policy decisions. Break down silos between the frontline workers involved in direct patient care and hospital executives, both to inform those decisions and demonstrate the value of clinicians’ perspectives.
- Compensate clinicians for extra work. Consider hazard pay or ensure extra time off for extra time worked.
- Make it “easier” for clinicians to do their jobs by helping them meet their basic needs. Create schedules with designated breaks during shifts. Provide adequate office space and call rooms. Facilitate access to childcare. Provide parking.
- Minimize moral injury. Develop protocols for scarce resource allocation that exclude the treatment team from making decisions about allocation of scarce resources. Avoid visitor restrictions given the harm these policies inflict on patients, families, and members of the care team.
At the level of society:
- Study mechanisms to improve communication about public health with the public. Both science and communication are essential to promoting and protecting public health; more research is needed to improve the way scientific knowledge and evidence-based recommendations are communicated to the public.
In conclusion, the COVID-19 pandemic has forever changed our critical care workforce and the way we deliver care. The time is now to act on the lessons learned from the COVID-19 pandemic through implementation of systems-level solutions to combat burnout and ensure both the health and sustainability of our critical care workforce for the season ahead.
Dr. Vranas is with the Center to Improve Veteran Involvement in Care, VA Portland Health Care System, the Division of Pulmonary and Critical Care, Oregon Health & Science University; Portland, OR; and the Palliative and Advanced Illness Research (PAIR) Center, University of Pennsylvania; Philadelphia, PA. Dr. Kerlin is with the Palliative and Advanced Illness Research (PAIR) Center, and Division of Pulmonary, Allergy and Critical Care, Perelman School of Medicine, University of Pennsylvania; Philadelphia, PA.
The COVID-19 pandemic has caused unprecedented and unpredictable strain on health care systems worldwide, forcing rapid organizational modifications and innovations to ensure availability of critical care resources during acute surge events. Yet, while much attention has been paid to the availability of ICU beds and ventilators, COVID-19 has insidiously and significantly harmed the most precious critical care resource of all – the human beings who are the lifeblood of critical care delivery. We are now at a crucial moment in history to better understand the pandemic’s impact on our human resources and enact changes to reverse the damage that it has inflicted on our workforce.
ICUs, where critical care delivery predominantly occurs, increasingly utilize interprofessional staffing models in which clinicians from multiple disciplines – physicians, nurses, clinical pharmacists, respiratory therapists, and dieticians, among others – bring their unique expertise to team-based clinical decisions and care delivery. Such a multidisciplinary approach helps enable the provision of more comprehensive, higher-quality critical care. In this way, the interprofessional ICU care team is an embodiment of the notion that the “whole” is more than just the sum of its parts. Therefore, we must consider the impact of the pandemic on interprofessional critical care clinicians as the team that they are.
Even before the COVID-19 pandemic, the well-being of critical care clinicians was compromised. Across multiple disciplines, they had among the highest rates of burnout syndrome of all health care professionals (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113). As the pandemic has dragged on, their well-being has only further declined. Burnout rates are at all-time highs, and symptoms of posttraumatic stress disorder, anxiety, and depression are common and have increased with each subsequent surge (Azoulay E, et al. Chest. 2021;160[3]:944-955). Offsets to burnout, such as fulfillment and recognition, have declined over time (Kerlin MP, et al. Ann Amer Thorac Soc. 2022;19[2]:329-331). These worrisome trends pose a significant threat to critical care delivery. Clinician burnout is associated with worse patient outcomes, increased medical errors, and lower patient satisfaction (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113; Poghosyan L, et al. Res Nurs Health. 2010;33[4]:288-298). It is also associated with mental illness and substance use disorders among clinicians (Dyrbye LN, et al. Ann Intern Med. 2008;149[5]:334-341). Finally, it has contributed to a workforce crisis: nearly 500,000 health care workers have left the US health care sector since the beginning of the pandemic, and approximately two-thirds of acute and critical care nurses have considered doing so (Wong E. “Why Healthcare Workers are Quitting in Droves”. The Atlantic. Accessed November 7, 2022). Such a “brain drain” of clinicians – whose expertise cannot be easily replicated or replaced – represents a staffing crisis that threatens our ability to provide high-quality, safe care for the foreseeable future.
To combat burnout, it is first necessary to identify the mechanisms by which the pandemic has induced harm. Early during the pandemic, critical care clinicians feared for their own safety with little information of how the virus was spread. At a time when the world was under lockdown, vaccines were not yet available, and hospitals were overwhelmed with surges of critically ill patients, clinicians struggled like the rest of the world to meet their own basic needs such as childcare, grocery shopping, and time with family. They experienced distress from high volumes of patients with extreme mortality rates, helplessness due to lack of treatment options, and moral injury over restrictive visitation policies (Vranas KC, et al. Chest. 2022;162[2]:331-345; Vranas KC, et al. Chest. 2021;160[5]:1714-1728). Over time, critical care clinicians have no doubt experienced further exhaustion related to the duration of the pandemic, often without adequate time to recover and process the trauma they have experienced. More recently, a new source of distress for clinicians has emerged from variability in vaccine uptake among the public. Clinicians have experienced compassion fatigue and even moral outrage toward those who chose not to receive a vaccine that is highly effective at preventing severe illness. They also suffered from ethical conflicts over how to treat unvaccinated patients and whether they should be given equal priority and access to limited therapies (Shaw D. Bioethics. 2022;36[8]:883-890).
Furthermore, the pandemic has damaged the relationship between clinicians and their institutions. Early in the pandemic, the widespread shortages of personal protective equipment harmed trust among clinicians due to their perception that their safety was not prioritized. Hospitals have also struggled with having to make rapid decisions on how to equitably allocate fixed resources in response to unanticipated and unpredictable demands, while also maintaining financial solvency. In some cases, these challenging policy decisions (eg, whether to continue elective procedures during acute surge events) lacked transparency and input from the team at the frontlines of patient care. As a result, clinicians have felt undervalued and without a voice in decisions that directly impact both the care they can provide their patients and their own well-being.
It is incumbent upon us now to take steps to repair the damage inflicted on our critical care workforce by the pandemic. To this end, there have been calls for the urgent implementation of strategies to mitigate the psychological burden experienced by critical care clinicians. However, many of these focus on interventions to increase coping strategies and resilience among individual clinicians. While programs such as mindfulness apps and resilience training are valuable, they are not sufficient. The very nature of these solutions implies that the solution (and therefore, the problem) of burnout lies in the individual clinician. Yet, as described above, many of the mechanisms of harm to clinicians’ well-being are systems-level issues that will necessarily require systems-level solutions.
Therefore, we propose a comprehensive, layered approach to begin to reverse the damage inflicted by the pandemic on critical care clinicians’ well-being, with solutions organized by ecological levels of individual clinicians, departments, institutions, and society. With this approach, we hope to address specific aspects of our critical care delivery system that, taken together, will fortify the well-being of our critical care workforce as a whole. We offer suggestions below that are both informed by existing evidence, as well as our own opinions as intensivists and researchers.
At the level of the individual clinician:
- Proactively provide access to mental health resources. Clinicians have limited time or energy to navigate mental health and support services and find it helpful when others proactively reach out to them.
- Provide opportunities for clinicians to experience community and support among peers. Clinicians find benefit in town halls, debrief sessions, and peer support groups, particularly during times of acute strain.
At the level of the department:
- Allow more flexibility in work schedules. Even prior to the pandemic, the lack of scheduling flexibility and the number of consecutive days worked had been identified as key contributors to burnout; these have been exacerbated during times of caseload surges, when clinicians have been asked or even required to increase their hours and work extra shifts.
- Promote a culture of psychological safety in which clinicians feel empowered to say “I cannot work” for whatever reason. This will require the establishment of formalized backup systems that easily accommodate call-outs without relying on individual clinicians to find their own coverage.
At the level of the health care system:
- Prioritize transparency, and bring administrators and clinicians together for policy decisions. Break down silos between the frontline workers involved in direct patient care and hospital executives, both to inform those decisions and demonstrate the value of clinicians’ perspectives.
- Compensate clinicians for extra work. Consider hazard pay or ensure extra time off for extra time worked.
- Make it “easier” for clinicians to do their jobs by helping them meet their basic needs. Create schedules with designated breaks during shifts. Provide adequate office space and call rooms. Facilitate access to childcare. Provide parking.
- Minimize moral injury. Develop protocols for scarce resource allocation that exclude the treatment team from making decisions about allocation of scarce resources. Avoid visitor restrictions given the harm these policies inflict on patients, families, and members of the care team.
At the level of society:
- Study mechanisms to improve communication about public health with the public. Both science and communication are essential to promoting and protecting public health; more research is needed to improve the way scientific knowledge and evidence-based recommendations are communicated to the public.
In conclusion, the COVID-19 pandemic has forever changed our critical care workforce and the way we deliver care. The time is now to act on the lessons learned from the COVID-19 pandemic through implementation of systems-level solutions to combat burnout and ensure both the health and sustainability of our critical care workforce for the season ahead.
Dr. Vranas is with the Center to Improve Veteran Involvement in Care, VA Portland Health Care System, the Division of Pulmonary and Critical Care, Oregon Health & Science University; Portland, OR; and the Palliative and Advanced Illness Research (PAIR) Center, University of Pennsylvania; Philadelphia, PA. Dr. Kerlin is with the Palliative and Advanced Illness Research (PAIR) Center, and Division of Pulmonary, Allergy and Critical Care, Perelman School of Medicine, University of Pennsylvania; Philadelphia, PA.
The COVID-19 pandemic has caused unprecedented and unpredictable strain on health care systems worldwide, forcing rapid organizational modifications and innovations to ensure availability of critical care resources during acute surge events. Yet, while much attention has been paid to the availability of ICU beds and ventilators, COVID-19 has insidiously and significantly harmed the most precious critical care resource of all – the human beings who are the lifeblood of critical care delivery. We are now at a crucial moment in history to better understand the pandemic’s impact on our human resources and enact changes to reverse the damage that it has inflicted on our workforce.
ICUs, where critical care delivery predominantly occurs, increasingly utilize interprofessional staffing models in which clinicians from multiple disciplines – physicians, nurses, clinical pharmacists, respiratory therapists, and dieticians, among others – bring their unique expertise to team-based clinical decisions and care delivery. Such a multidisciplinary approach helps enable the provision of more comprehensive, higher-quality critical care. In this way, the interprofessional ICU care team is an embodiment of the notion that the “whole” is more than just the sum of its parts. Therefore, we must consider the impact of the pandemic on interprofessional critical care clinicians as the team that they are.
Even before the COVID-19 pandemic, the well-being of critical care clinicians was compromised. Across multiple disciplines, they had among the highest rates of burnout syndrome of all health care professionals (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113). As the pandemic has dragged on, their well-being has only further declined. Burnout rates are at all-time highs, and symptoms of posttraumatic stress disorder, anxiety, and depression are common and have increased with each subsequent surge (Azoulay E, et al. Chest. 2021;160[3]:944-955). Offsets to burnout, such as fulfillment and recognition, have declined over time (Kerlin MP, et al. Ann Amer Thorac Soc. 2022;19[2]:329-331). These worrisome trends pose a significant threat to critical care delivery. Clinician burnout is associated with worse patient outcomes, increased medical errors, and lower patient satisfaction (Moss M, et al. Am J Respir Crit Care Med. 2016;194[1]:106-113; Poghosyan L, et al. Res Nurs Health. 2010;33[4]:288-298). It is also associated with mental illness and substance use disorders among clinicians (Dyrbye LN, et al. Ann Intern Med. 2008;149[5]:334-341). Finally, it has contributed to a workforce crisis: nearly 500,000 health care workers have left the US health care sector since the beginning of the pandemic, and approximately two-thirds of acute and critical care nurses have considered doing so (Wong E. “Why Healthcare Workers are Quitting in Droves”. The Atlantic. Accessed November 7, 2022). Such a “brain drain” of clinicians – whose expertise cannot be easily replicated or replaced – represents a staffing crisis that threatens our ability to provide high-quality, safe care for the foreseeable future.
To combat burnout, it is first necessary to identify the mechanisms by which the pandemic has induced harm. Early during the pandemic, critical care clinicians feared for their own safety with little information of how the virus was spread. At a time when the world was under lockdown, vaccines were not yet available, and hospitals were overwhelmed with surges of critically ill patients, clinicians struggled like the rest of the world to meet their own basic needs such as childcare, grocery shopping, and time with family. They experienced distress from high volumes of patients with extreme mortality rates, helplessness due to lack of treatment options, and moral injury over restrictive visitation policies (Vranas KC, et al. Chest. 2022;162[2]:331-345; Vranas KC, et al. Chest. 2021;160[5]:1714-1728). Over time, critical care clinicians have no doubt experienced further exhaustion related to the duration of the pandemic, often without adequate time to recover and process the trauma they have experienced. More recently, a new source of distress for clinicians has emerged from variability in vaccine uptake among the public. Clinicians have experienced compassion fatigue and even moral outrage toward those who chose not to receive a vaccine that is highly effective at preventing severe illness. They also suffered from ethical conflicts over how to treat unvaccinated patients and whether they should be given equal priority and access to limited therapies (Shaw D. Bioethics. 2022;36[8]:883-890).
Furthermore, the pandemic has damaged the relationship between clinicians and their institutions. Early in the pandemic, the widespread shortages of personal protective equipment harmed trust among clinicians due to their perception that their safety was not prioritized. Hospitals have also struggled with having to make rapid decisions on how to equitably allocate fixed resources in response to unanticipated and unpredictable demands, while also maintaining financial solvency. In some cases, these challenging policy decisions (eg, whether to continue elective procedures during acute surge events) lacked transparency and input from the team at the frontlines of patient care. As a result, clinicians have felt undervalued and without a voice in decisions that directly impact both the care they can provide their patients and their own well-being.
It is incumbent upon us now to take steps to repair the damage inflicted on our critical care workforce by the pandemic. To this end, there have been calls for the urgent implementation of strategies to mitigate the psychological burden experienced by critical care clinicians. However, many of these focus on interventions to increase coping strategies and resilience among individual clinicians. While programs such as mindfulness apps and resilience training are valuable, they are not sufficient. The very nature of these solutions implies that the solution (and therefore, the problem) of burnout lies in the individual clinician. Yet, as described above, many of the mechanisms of harm to clinicians’ well-being are systems-level issues that will necessarily require systems-level solutions.
Therefore, we propose a comprehensive, layered approach to begin to reverse the damage inflicted by the pandemic on critical care clinicians’ well-being, with solutions organized by ecological levels of individual clinicians, departments, institutions, and society. With this approach, we hope to address specific aspects of our critical care delivery system that, taken together, will fortify the well-being of our critical care workforce as a whole. We offer suggestions below that are both informed by existing evidence, as well as our own opinions as intensivists and researchers.
At the level of the individual clinician:
- Proactively provide access to mental health resources. Clinicians have limited time or energy to navigate mental health and support services and find it helpful when others proactively reach out to them.
- Provide opportunities for clinicians to experience community and support among peers. Clinicians find benefit in town halls, debrief sessions, and peer support groups, particularly during times of acute strain.
At the level of the department:
- Allow more flexibility in work schedules. Even prior to the pandemic, the lack of scheduling flexibility and the number of consecutive days worked had been identified as key contributors to burnout; these have been exacerbated during times of caseload surges, when clinicians have been asked or even required to increase their hours and work extra shifts.
- Promote a culture of psychological safety in which clinicians feel empowered to say “I cannot work” for whatever reason. This will require the establishment of formalized backup systems that easily accommodate call-outs without relying on individual clinicians to find their own coverage.
At the level of the health care system:
- Prioritize transparency, and bring administrators and clinicians together for policy decisions. Break down silos between the frontline workers involved in direct patient care and hospital executives, both to inform those decisions and demonstrate the value of clinicians’ perspectives.
- Compensate clinicians for extra work. Consider hazard pay or ensure extra time off for extra time worked.
- Make it “easier” for clinicians to do their jobs by helping them meet their basic needs. Create schedules with designated breaks during shifts. Provide adequate office space and call rooms. Facilitate access to childcare. Provide parking.
- Minimize moral injury. Develop protocols for scarce resource allocation that exclude the treatment team from making decisions about allocation of scarce resources. Avoid visitor restrictions given the harm these policies inflict on patients, families, and members of the care team.
At the level of society:
- Study mechanisms to improve communication about public health with the public. Both science and communication are essential to promoting and protecting public health; more research is needed to improve the way scientific knowledge and evidence-based recommendations are communicated to the public.
In conclusion, the COVID-19 pandemic has forever changed our critical care workforce and the way we deliver care. The time is now to act on the lessons learned from the COVID-19 pandemic through implementation of systems-level solutions to combat burnout and ensure both the health and sustainability of our critical care workforce for the season ahead.
Dr. Vranas is with the Center to Improve Veteran Involvement in Care, VA Portland Health Care System, the Division of Pulmonary and Critical Care, Oregon Health & Science University; Portland, OR; and the Palliative and Advanced Illness Research (PAIR) Center, University of Pennsylvania; Philadelphia, PA. Dr. Kerlin is with the Palliative and Advanced Illness Research (PAIR) Center, and Division of Pulmonary, Allergy and Critical Care, Perelman School of Medicine, University of Pennsylvania; Philadelphia, PA.
A single pediatric CT scan raises brain cancer risk
Children and young adults who are exposed to a single CT scan of the head or neck before age 22 years are at significantly increased risk of developing a brain tumor, particularly glioma, after at least 5 years, according to results of the large EPI-CT study.
“Translation of our risk estimates to the clinical setting indicates that per 10,000 children who received one head CT examination, about one radiation-induced brain cancer is expected during the 5-15 years following the CT examination,” noted lead author Michael Hauptmann, PhD, from the Institute of Biostatistics and Registry Research, Brandenburg Medical School, Neuruppin, Germany, and coauthors.
“Next to the clinical benefit of most CT scans, there is a small risk of cancer from the radiation exposure,” Dr. Hauptmann told this news organization.
“So, CT examinations should only be used when necessary, and if they are used, the lowest achievable dose should be applied,” he said.
The study was published online in The Lancet Oncology.
“This is a thoughtful and well-conducted study by an outstanding multinational team of scientists that adds further weight to the growing body of evidence that has found exposure to CT scanning increases a child’s risk of developing brain cancer,” commented Rebecca Bindman-Smith, MD, from the University of California, San Francisco, who was not involved in the research.
“The results are real, and important,” she told this news organization, adding that “the authors were conservative in their assumptions, and performed a very large number of sensitivity analyses ... to check that the results were robust to a large range of assumptions – and the results changed relatively little.”
“I do not think there is enough awareness [about this risk],” Dr. Hauptmann said. “There is evidence that a nonnegligible number of CTs is unjustified according to guidelines, and there is evidence that doses vary substantially for the same CT between institutions in the same or different countries.”
Indeed, particularly in the United States, “we perform many CT scans in children and even more so in adults that are simply unnecessary,” agreed Dr. Bindman-Smith, who is professor of epidemiology and biostatistics at the University of California, San Francisco. “It is important for patients and providers to understand that nothing we do in medicine is risk free, including CT scanning. If a CT is necessary, the benefit almost certainly outweighs the risk. But if [not], then it should not be obtained. Both patients and providers must make thoroughly considered decisions before asking for or agreeing to a CT.”
She also pointed out that while this study evaluated the risk only for brain cancer, children who undergo head CTs are also at increased risk for leukemia.
Dose/response relationship
The study included 658,752 individuals from nine European countries and 276 hospitals. Each patient had received at least one CT scan between 1977 and 2014 before they turned 22 years of age. Eligibility requirements included their being alive at least 5 years after the first scan and that they had not previously been diagnosed with cancer or benign brain tumor.
The radiation dose absorbed to the brain and 33 other organs and tissues was estimated for each participant using a dose reconstruction model that included historical information on CT machine settings, questionnaire data, and Digital Imaging and Communication in Medicine header metadata. “Mean brain dose per head or neck CT examination increased from 1984 until about 1991, following the introduction of multislice CT scanners at which point thereafter the mean dose decreased and then stabilized around 2010,” note the authors.
During a median follow-up of 5.6 years (starting 5 years after the first scan), 165 brain cancers occurred, including 121 (73%) gliomas, as well as a variety of other morphologic changes.
The mean cumulative brain dose, which lagged by 5 years, was 47.4 mGy overall and 76.0 mGy among people with brain cancer.
“We observed a significant positive association between the cumulative number of head or neck CT examinations and the risk of all brain cancers combined (P < .0001), and of gliomas separately (P = .0002),” the team reports, adding that, for a brain dose of 38 mGy, which was the average dose per head or neck CT in 2012-2014, the relative risk of developing brain cancer was 1.5, compared with not undergoing a CT scan, and the excess absolute risk per 100,000 person-years was 1.1.
These findings “can be used to give the patients and their parents important information on the risks of CT examination to balance against the known benefits,” noted Nobuyuki Hamada, PhD, from the Central Research Institute of Electric Power Industry, Tokyo, and Lydia B. Zablotska, MD, PhD, from the University of California, San Francisco, writing in a linked commentary.
“In recent years, rates of CT use have been steady or declined, and various efforts (for instance, in terms of diagnostic reference levels) have been made to justify and optimize CT examinations. Such continued efforts, along with extended epidemiological investigations, would be needed to minimize the risk of brain cancer after pediatric CT examination,” they add.
Keeping dose to a minimum
The study’s finding of a dose-response relationship underscores the importance of keeping doses to a minimum, Dr. Bindman-Smith commented. “I do not believe we are doing this nearly enough,” she added.
“In the UCSF International CT Dose Registry, where we have collected CT scans from 165 hospitals on many millions of patients, we found that the average brain dose for a head CT in a 1-year-old is 42 mGy but that this dose varies tremendously, where some children receive a dose of 100 mGy.
“So, a second message is that not only should CT scans be justified and used judiciously, but also they should be optimized, meaning using the lowest dose possible. I personally think there should be regulatory oversight to ensure that patients receive the absolutely lowest doses possible,” she added. “My team at UCSF has written quality measures endorsed by the National Quality Forum as a start for setting explicit standards for how CT should be performed in order to ensure the cancer risks are as low as possible.”
The study was funded through the Belgian Cancer Registry; La Ligue contre le Cancer, L’Institut National du Cancer, France; the Ministry of Health, Labour and Welfare of Japan; the German Federal Ministry of Education and Research; Worldwide Cancer Research; the Dutch Cancer Society; the Research Council of Norway; Consejo de Seguridad Nuclear, Generalitat deCatalunya, Spain; the U.S. National Cancer Institute; the U.K. National Institute for Health Research; and Public Health England. Dr. Hauptmann has disclosed no relevant financial relationships. Other investigators’ relevant financial relationships are listed in the original article. Dr. Hamada and Dr. Zablotska disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and young adults who are exposed to a single CT scan of the head or neck before age 22 years are at significantly increased risk of developing a brain tumor, particularly glioma, after at least 5 years, according to results of the large EPI-CT study.
“Translation of our risk estimates to the clinical setting indicates that per 10,000 children who received one head CT examination, about one radiation-induced brain cancer is expected during the 5-15 years following the CT examination,” noted lead author Michael Hauptmann, PhD, from the Institute of Biostatistics and Registry Research, Brandenburg Medical School, Neuruppin, Germany, and coauthors.
“Next to the clinical benefit of most CT scans, there is a small risk of cancer from the radiation exposure,” Dr. Hauptmann told this news organization.
“So, CT examinations should only be used when necessary, and if they are used, the lowest achievable dose should be applied,” he said.
The study was published online in The Lancet Oncology.
“This is a thoughtful and well-conducted study by an outstanding multinational team of scientists that adds further weight to the growing body of evidence that has found exposure to CT scanning increases a child’s risk of developing brain cancer,” commented Rebecca Bindman-Smith, MD, from the University of California, San Francisco, who was not involved in the research.
“The results are real, and important,” she told this news organization, adding that “the authors were conservative in their assumptions, and performed a very large number of sensitivity analyses ... to check that the results were robust to a large range of assumptions – and the results changed relatively little.”
“I do not think there is enough awareness [about this risk],” Dr. Hauptmann said. “There is evidence that a nonnegligible number of CTs is unjustified according to guidelines, and there is evidence that doses vary substantially for the same CT between institutions in the same or different countries.”
Indeed, particularly in the United States, “we perform many CT scans in children and even more so in adults that are simply unnecessary,” agreed Dr. Bindman-Smith, who is professor of epidemiology and biostatistics at the University of California, San Francisco. “It is important for patients and providers to understand that nothing we do in medicine is risk free, including CT scanning. If a CT is necessary, the benefit almost certainly outweighs the risk. But if [not], then it should not be obtained. Both patients and providers must make thoroughly considered decisions before asking for or agreeing to a CT.”
She also pointed out that while this study evaluated the risk only for brain cancer, children who undergo head CTs are also at increased risk for leukemia.
Dose/response relationship
The study included 658,752 individuals from nine European countries and 276 hospitals. Each patient had received at least one CT scan between 1977 and 2014 before they turned 22 years of age. Eligibility requirements included their being alive at least 5 years after the first scan and that they had not previously been diagnosed with cancer or benign brain tumor.
The radiation dose absorbed to the brain and 33 other organs and tissues was estimated for each participant using a dose reconstruction model that included historical information on CT machine settings, questionnaire data, and Digital Imaging and Communication in Medicine header metadata. “Mean brain dose per head or neck CT examination increased from 1984 until about 1991, following the introduction of multislice CT scanners at which point thereafter the mean dose decreased and then stabilized around 2010,” note the authors.
During a median follow-up of 5.6 years (starting 5 years after the first scan), 165 brain cancers occurred, including 121 (73%) gliomas, as well as a variety of other morphologic changes.
The mean cumulative brain dose, which lagged by 5 years, was 47.4 mGy overall and 76.0 mGy among people with brain cancer.
“We observed a significant positive association between the cumulative number of head or neck CT examinations and the risk of all brain cancers combined (P < .0001), and of gliomas separately (P = .0002),” the team reports, adding that, for a brain dose of 38 mGy, which was the average dose per head or neck CT in 2012-2014, the relative risk of developing brain cancer was 1.5, compared with not undergoing a CT scan, and the excess absolute risk per 100,000 person-years was 1.1.
These findings “can be used to give the patients and their parents important information on the risks of CT examination to balance against the known benefits,” noted Nobuyuki Hamada, PhD, from the Central Research Institute of Electric Power Industry, Tokyo, and Lydia B. Zablotska, MD, PhD, from the University of California, San Francisco, writing in a linked commentary.
“In recent years, rates of CT use have been steady or declined, and various efforts (for instance, in terms of diagnostic reference levels) have been made to justify and optimize CT examinations. Such continued efforts, along with extended epidemiological investigations, would be needed to minimize the risk of brain cancer after pediatric CT examination,” they add.
Keeping dose to a minimum
The study’s finding of a dose-response relationship underscores the importance of keeping doses to a minimum, Dr. Bindman-Smith commented. “I do not believe we are doing this nearly enough,” she added.
“In the UCSF International CT Dose Registry, where we have collected CT scans from 165 hospitals on many millions of patients, we found that the average brain dose for a head CT in a 1-year-old is 42 mGy but that this dose varies tremendously, where some children receive a dose of 100 mGy.
“So, a second message is that not only should CT scans be justified and used judiciously, but also they should be optimized, meaning using the lowest dose possible. I personally think there should be regulatory oversight to ensure that patients receive the absolutely lowest doses possible,” she added. “My team at UCSF has written quality measures endorsed by the National Quality Forum as a start for setting explicit standards for how CT should be performed in order to ensure the cancer risks are as low as possible.”
The study was funded through the Belgian Cancer Registry; La Ligue contre le Cancer, L’Institut National du Cancer, France; the Ministry of Health, Labour and Welfare of Japan; the German Federal Ministry of Education and Research; Worldwide Cancer Research; the Dutch Cancer Society; the Research Council of Norway; Consejo de Seguridad Nuclear, Generalitat deCatalunya, Spain; the U.S. National Cancer Institute; the U.K. National Institute for Health Research; and Public Health England. Dr. Hauptmann has disclosed no relevant financial relationships. Other investigators’ relevant financial relationships are listed in the original article. Dr. Hamada and Dr. Zablotska disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and young adults who are exposed to a single CT scan of the head or neck before age 22 years are at significantly increased risk of developing a brain tumor, particularly glioma, after at least 5 years, according to results of the large EPI-CT study.
“Translation of our risk estimates to the clinical setting indicates that per 10,000 children who received one head CT examination, about one radiation-induced brain cancer is expected during the 5-15 years following the CT examination,” noted lead author Michael Hauptmann, PhD, from the Institute of Biostatistics and Registry Research, Brandenburg Medical School, Neuruppin, Germany, and coauthors.
“Next to the clinical benefit of most CT scans, there is a small risk of cancer from the radiation exposure,” Dr. Hauptmann told this news organization.
“So, CT examinations should only be used when necessary, and if they are used, the lowest achievable dose should be applied,” he said.
The study was published online in The Lancet Oncology.
“This is a thoughtful and well-conducted study by an outstanding multinational team of scientists that adds further weight to the growing body of evidence that has found exposure to CT scanning increases a child’s risk of developing brain cancer,” commented Rebecca Bindman-Smith, MD, from the University of California, San Francisco, who was not involved in the research.
“The results are real, and important,” she told this news organization, adding that “the authors were conservative in their assumptions, and performed a very large number of sensitivity analyses ... to check that the results were robust to a large range of assumptions – and the results changed relatively little.”
“I do not think there is enough awareness [about this risk],” Dr. Hauptmann said. “There is evidence that a nonnegligible number of CTs is unjustified according to guidelines, and there is evidence that doses vary substantially for the same CT between institutions in the same or different countries.”
Indeed, particularly in the United States, “we perform many CT scans in children and even more so in adults that are simply unnecessary,” agreed Dr. Bindman-Smith, who is professor of epidemiology and biostatistics at the University of California, San Francisco. “It is important for patients and providers to understand that nothing we do in medicine is risk free, including CT scanning. If a CT is necessary, the benefit almost certainly outweighs the risk. But if [not], then it should not be obtained. Both patients and providers must make thoroughly considered decisions before asking for or agreeing to a CT.”
She also pointed out that while this study evaluated the risk only for brain cancer, children who undergo head CTs are also at increased risk for leukemia.
Dose/response relationship
The study included 658,752 individuals from nine European countries and 276 hospitals. Each patient had received at least one CT scan between 1977 and 2014 before they turned 22 years of age. Eligibility requirements included their being alive at least 5 years after the first scan and that they had not previously been diagnosed with cancer or benign brain tumor.
The radiation dose absorbed to the brain and 33 other organs and tissues was estimated for each participant using a dose reconstruction model that included historical information on CT machine settings, questionnaire data, and Digital Imaging and Communication in Medicine header metadata. “Mean brain dose per head or neck CT examination increased from 1984 until about 1991, following the introduction of multislice CT scanners at which point thereafter the mean dose decreased and then stabilized around 2010,” note the authors.
During a median follow-up of 5.6 years (starting 5 years after the first scan), 165 brain cancers occurred, including 121 (73%) gliomas, as well as a variety of other morphologic changes.
The mean cumulative brain dose, which lagged by 5 years, was 47.4 mGy overall and 76.0 mGy among people with brain cancer.
“We observed a significant positive association between the cumulative number of head or neck CT examinations and the risk of all brain cancers combined (P < .0001), and of gliomas separately (P = .0002),” the team reports, adding that, for a brain dose of 38 mGy, which was the average dose per head or neck CT in 2012-2014, the relative risk of developing brain cancer was 1.5, compared with not undergoing a CT scan, and the excess absolute risk per 100,000 person-years was 1.1.
These findings “can be used to give the patients and their parents important information on the risks of CT examination to balance against the known benefits,” noted Nobuyuki Hamada, PhD, from the Central Research Institute of Electric Power Industry, Tokyo, and Lydia B. Zablotska, MD, PhD, from the University of California, San Francisco, writing in a linked commentary.
“In recent years, rates of CT use have been steady or declined, and various efforts (for instance, in terms of diagnostic reference levels) have been made to justify and optimize CT examinations. Such continued efforts, along with extended epidemiological investigations, would be needed to minimize the risk of brain cancer after pediatric CT examination,” they add.
Keeping dose to a minimum
The study’s finding of a dose-response relationship underscores the importance of keeping doses to a minimum, Dr. Bindman-Smith commented. “I do not believe we are doing this nearly enough,” she added.
“In the UCSF International CT Dose Registry, where we have collected CT scans from 165 hospitals on many millions of patients, we found that the average brain dose for a head CT in a 1-year-old is 42 mGy but that this dose varies tremendously, where some children receive a dose of 100 mGy.
“So, a second message is that not only should CT scans be justified and used judiciously, but also they should be optimized, meaning using the lowest dose possible. I personally think there should be regulatory oversight to ensure that patients receive the absolutely lowest doses possible,” she added. “My team at UCSF has written quality measures endorsed by the National Quality Forum as a start for setting explicit standards for how CT should be performed in order to ensure the cancer risks are as low as possible.”
The study was funded through the Belgian Cancer Registry; La Ligue contre le Cancer, L’Institut National du Cancer, France; the Ministry of Health, Labour and Welfare of Japan; the German Federal Ministry of Education and Research; Worldwide Cancer Research; the Dutch Cancer Society; the Research Council of Norway; Consejo de Seguridad Nuclear, Generalitat deCatalunya, Spain; the U.S. National Cancer Institute; the U.K. National Institute for Health Research; and Public Health England. Dr. Hauptmann has disclosed no relevant financial relationships. Other investigators’ relevant financial relationships are listed in the original article. Dr. Hamada and Dr. Zablotska disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
Digital treatment may help relieve PTSD, panic disorder
The 28-day home-based treatment, known as the capnometry guided respiratory intervention (CGRI), uses an app-based feedback protocol to normalize respiration and increase patients’ ability to cope with symptoms of stress, anxiety, and panic by providing real time breath-to-breath feedback of respiratory rate and carbon dioxide (CO2) levels via a nasal cannula.
Results from the large real-world study showed that over 65% of patients with PD and over 72% of those with PTSD responded to the treatment. In addition, almost 75% of participants adhered to the study protocol, with low dropout rates.
“The brief duration of treatment, high adherence rates, and clinical benefit suggests that CGRI provides an important addition to treatment options for PD and PTSD,” the investigators write.
The study was published online in Frontiers in Digital Health.
‘New kid on the block’
The “respiratory dysregulation hypothesis” links CO2 sensitivity to panic attacks and PD, and similar reactivity has been identified in PTSD, but a “common limitation of psychotherapeutic and pharmacologic approaches to PD and PTSD is that neither address the role of respiratory physiology and breathing style,” the investigators note.
The most widely studied treatment for PTSD is trauma-focused psychotherapy, in which the patient reviews and revisits the trauma, but it has a high dropout rate, study investigator Michael Telch, PhD, director of the Laboratory for the Study of Anxiety Disorders, University of Texas, Austin, told this news organization.
He described CGRI for PTSD as a “relatively new kid on the block, so to speak.” The intervention was cleared by the U.S. Food and Drug Administration for treatment of PD and PTSD in 2013 and 2018, respectively, and is currently available through the Veterans Administration for veterans with PTSD. It is also covered by some commercial insurance plans.
“The underlying assumption [of CGRI] is that a person can learn to develop skills for controlling some of their physiological reactions that are triggered as a result of trauma,” said Dr. Telch.
The device uses a biofeedback approach to give patients “greater control over their physiological reactions, such as hyperventilation and increased respiration rate, and the focus is on providing a sense of mastery,” he said.
Participants with PTSD were assigned to a health coach. The device was delivered to the patient’s home, and patients met with the trained coach weekly and could check in between visits via text or e-mail. Twice-daily sessions were recommended.
“The coach gets feedback about what’s happening with the patient’s respiration and end-tidal CO2 levels [etCO2] and instructs participants how to keep their respiration rate and etCO2 at a more normal level,” said Dr. Telch.
The CGRI “teaches a specific breathing style via a system providing real-time feedback of respiratory rate (RR) and exhaled carbon dioxide levels facilitated by data capture,” the authors note.
Sense of mastery
Of the 1,569 participants, 1,395 had PD and 174 had PTSD (mean age, 39.2 [standard deviation, 13.9] years and 40.9 [SD, 14.9] years, respectively; 76% and 73% female, respectively). Those with PD completed the Panic Disorder Severity Scale (PDSS) and those with PTSD completed the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5), before and after the intervention.
The treatment response rate for PD was defined as a 40% or greater reduction in PDSS total scores, whereas treatment response rate for PTSD was defined as a 10-point or greater reduction in PCL-5 scores.
At baseline, patients were classified either as normocapnic or hypocapnic (etCO2 ≥ 37 or < 37, respectively), with 65% classified as normocapnic and 35% classified as hypocapnic.
Among patients with PD, there was a 50.2% mean pre- to posttreatment reduction in total PDSS scores (P < .001; d = 1.31), with a treatment response rate of 65.3% of patients.
Among patients with PTSD, there was a 41.1% pre- to posttreatment reduction in total PCL-5 scores (P < .001; d = 1.16), with a treatment response rate of 72.4%.
When investigators analyzed the response at the individual level, they found that 55.7% of patients with PD and 53.5% of those with PTSD were classified as treatment responders. This determination was based on a two-pronged approach that first calculated the Reliable Change Index (RCI) for each participant, and, in participants showing statistically reliable improvement, whether the posttreatment score was closer to the distribution of scores for patients without or with the given disorder.
“Patients with both normal and below-normal baseline exhaled CO2 levels experienced comparable benefit,” the authors report.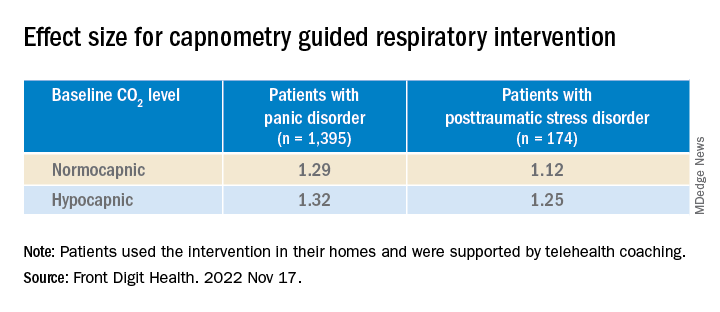
There were high levels of adherence across the full treatment period in both the PD and the PTSD groups (74.8% and 74.9%, respectively), with low dropout rates (10% and 11%, respectively).
“Not every single patient who undergoes any treatment has a perfect response, but the response rates to this treatment have, surprisingly, been quite positive and there have been no negative side effects,” Dr. Telch remarked.
He noted that one of the effects of PTSD is that the “patient has negative beliefs about their ability to control the world. ‘I can’t control my reactions. At any time, I could have a flashback.’ Helping the patient to develop any sense of mastery over some of their reactions can spill over and give them a greater sense of mastery and control, which can have a positive effect in reducing PTSD symptoms.”
‘A viable alternative’
Commenting on the research, Charles Marmar, MD, chair and Peter H. Schub Professor of Psychiatry, department of psychiatry, New York University, said that the study has some limitations, probably the most significant of which is that most participants had normal baseline CO2 levels.

“The treatment is fundamentally designed for people who hyperventilate and blow off too much CO2 so they can breathe in a more calm, relaxed way, but most people in the trial had normal CO2 to begin with,” said Dr. Marmar, who was not involved with the study.
“It’s likely that the major benefits were the relaxation from doing the breathing exercises rather than the change in CO2 levels,” he speculated.
The treatment is “probably a good thing for those patients who actually have abnormal CO2 levels. This treatment could be used in precision medicine, where you tailor treatments to those who actually need them rather than giving the same treatment to everyone,” he said.
“For patients who don’t respond to trauma-focused therapy or it’s too aversive for them to undergo, this new intervention provides a viable alternative,” Dr. Telch added.
The study was internally funded by Freespira. Dr. Telch is a scientific advisor at Freespira and receives compensation by way of stock options. The other authors’ disclosures are listed on the original paper. Dr. Marmar has declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The 28-day home-based treatment, known as the capnometry guided respiratory intervention (CGRI), uses an app-based feedback protocol to normalize respiration and increase patients’ ability to cope with symptoms of stress, anxiety, and panic by providing real time breath-to-breath feedback of respiratory rate and carbon dioxide (CO2) levels via a nasal cannula.
Results from the large real-world study showed that over 65% of patients with PD and over 72% of those with PTSD responded to the treatment. In addition, almost 75% of participants adhered to the study protocol, with low dropout rates.
“The brief duration of treatment, high adherence rates, and clinical benefit suggests that CGRI provides an important addition to treatment options for PD and PTSD,” the investigators write.
The study was published online in Frontiers in Digital Health.
‘New kid on the block’
The “respiratory dysregulation hypothesis” links CO2 sensitivity to panic attacks and PD, and similar reactivity has been identified in PTSD, but a “common limitation of psychotherapeutic and pharmacologic approaches to PD and PTSD is that neither address the role of respiratory physiology and breathing style,” the investigators note.
The most widely studied treatment for PTSD is trauma-focused psychotherapy, in which the patient reviews and revisits the trauma, but it has a high dropout rate, study investigator Michael Telch, PhD, director of the Laboratory for the Study of Anxiety Disorders, University of Texas, Austin, told this news organization.
He described CGRI for PTSD as a “relatively new kid on the block, so to speak.” The intervention was cleared by the U.S. Food and Drug Administration for treatment of PD and PTSD in 2013 and 2018, respectively, and is currently available through the Veterans Administration for veterans with PTSD. It is also covered by some commercial insurance plans.
“The underlying assumption [of CGRI] is that a person can learn to develop skills for controlling some of their physiological reactions that are triggered as a result of trauma,” said Dr. Telch.
The device uses a biofeedback approach to give patients “greater control over their physiological reactions, such as hyperventilation and increased respiration rate, and the focus is on providing a sense of mastery,” he said.
Participants with PTSD were assigned to a health coach. The device was delivered to the patient’s home, and patients met with the trained coach weekly and could check in between visits via text or e-mail. Twice-daily sessions were recommended.
“The coach gets feedback about what’s happening with the patient’s respiration and end-tidal CO2 levels [etCO2] and instructs participants how to keep their respiration rate and etCO2 at a more normal level,” said Dr. Telch.
The CGRI “teaches a specific breathing style via a system providing real-time feedback of respiratory rate (RR) and exhaled carbon dioxide levels facilitated by data capture,” the authors note.
Sense of mastery
Of the 1,569 participants, 1,395 had PD and 174 had PTSD (mean age, 39.2 [standard deviation, 13.9] years and 40.9 [SD, 14.9] years, respectively; 76% and 73% female, respectively). Those with PD completed the Panic Disorder Severity Scale (PDSS) and those with PTSD completed the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5), before and after the intervention.
The treatment response rate for PD was defined as a 40% or greater reduction in PDSS total scores, whereas treatment response rate for PTSD was defined as a 10-point or greater reduction in PCL-5 scores.
At baseline, patients were classified either as normocapnic or hypocapnic (etCO2 ≥ 37 or < 37, respectively), with 65% classified as normocapnic and 35% classified as hypocapnic.
Among patients with PD, there was a 50.2% mean pre- to posttreatment reduction in total PDSS scores (P < .001; d = 1.31), with a treatment response rate of 65.3% of patients.
Among patients with PTSD, there was a 41.1% pre- to posttreatment reduction in total PCL-5 scores (P < .001; d = 1.16), with a treatment response rate of 72.4%.
When investigators analyzed the response at the individual level, they found that 55.7% of patients with PD and 53.5% of those with PTSD were classified as treatment responders. This determination was based on a two-pronged approach that first calculated the Reliable Change Index (RCI) for each participant, and, in participants showing statistically reliable improvement, whether the posttreatment score was closer to the distribution of scores for patients without or with the given disorder.
“Patients with both normal and below-normal baseline exhaled CO2 levels experienced comparable benefit,” the authors report.
There were high levels of adherence across the full treatment period in both the PD and the PTSD groups (74.8% and 74.9%, respectively), with low dropout rates (10% and 11%, respectively).
“Not every single patient who undergoes any treatment has a perfect response, but the response rates to this treatment have, surprisingly, been quite positive and there have been no negative side effects,” Dr. Telch remarked.
He noted that one of the effects of PTSD is that the “patient has negative beliefs about their ability to control the world. ‘I can’t control my reactions. At any time, I could have a flashback.’ Helping the patient to develop any sense of mastery over some of their reactions can spill over and give them a greater sense of mastery and control, which can have a positive effect in reducing PTSD symptoms.”
‘A viable alternative’
Commenting on the research, Charles Marmar, MD, chair and Peter H. Schub Professor of Psychiatry, department of psychiatry, New York University, said that the study has some limitations, probably the most significant of which is that most participants had normal baseline CO2 levels.
“The treatment is fundamentally designed for people who hyperventilate and blow off too much CO2 so they can breathe in a more calm, relaxed way, but most people in the trial had normal CO2 to begin with,” said Dr. Marmar, who was not involved with the study.
“It’s likely that the major benefits were the relaxation from doing the breathing exercises rather than the change in CO2 levels,” he speculated.
The treatment is “probably a good thing for those patients who actually have abnormal CO2 levels. This treatment could be used in precision medicine, where you tailor treatments to those who actually need them rather than giving the same treatment to everyone,” he said.
“For patients who don’t respond to trauma-focused therapy or it’s too aversive for them to undergo, this new intervention provides a viable alternative,” Dr. Telch added.
The study was internally funded by Freespira. Dr. Telch is a scientific advisor at Freespira and receives compensation by way of stock options. The other authors’ disclosures are listed on the original paper. Dr. Marmar has declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The 28-day home-based treatment, known as the capnometry guided respiratory intervention (CGRI), uses an app-based feedback protocol to normalize respiration and increase patients’ ability to cope with symptoms of stress, anxiety, and panic by providing real time breath-to-breath feedback of respiratory rate and carbon dioxide (CO2) levels via a nasal cannula.
Results from the large real-world study showed that over 65% of patients with PD and over 72% of those with PTSD responded to the treatment. In addition, almost 75% of participants adhered to the study protocol, with low dropout rates.
“The brief duration of treatment, high adherence rates, and clinical benefit suggests that CGRI provides an important addition to treatment options for PD and PTSD,” the investigators write.
The study was published online in Frontiers in Digital Health.
‘New kid on the block’
The “respiratory dysregulation hypothesis” links CO2 sensitivity to panic attacks and PD, and similar reactivity has been identified in PTSD, but a “common limitation of psychotherapeutic and pharmacologic approaches to PD and PTSD is that neither address the role of respiratory physiology and breathing style,” the investigators note.
The most widely studied treatment for PTSD is trauma-focused psychotherapy, in which the patient reviews and revisits the trauma, but it has a high dropout rate, study investigator Michael Telch, PhD, director of the Laboratory for the Study of Anxiety Disorders, University of Texas, Austin, told this news organization.
He described CGRI for PTSD as a “relatively new kid on the block, so to speak.” The intervention was cleared by the U.S. Food and Drug Administration for treatment of PD and PTSD in 2013 and 2018, respectively, and is currently available through the Veterans Administration for veterans with PTSD. It is also covered by some commercial insurance plans.
“The underlying assumption [of CGRI] is that a person can learn to develop skills for controlling some of their physiological reactions that are triggered as a result of trauma,” said Dr. Telch.
The device uses a biofeedback approach to give patients “greater control over their physiological reactions, such as hyperventilation and increased respiration rate, and the focus is on providing a sense of mastery,” he said.
Participants with PTSD were assigned to a health coach. The device was delivered to the patient’s home, and patients met with the trained coach weekly and could check in between visits via text or e-mail. Twice-daily sessions were recommended.
“The coach gets feedback about what’s happening with the patient’s respiration and end-tidal CO2 levels [etCO2] and instructs participants how to keep their respiration rate and etCO2 at a more normal level,” said Dr. Telch.
The CGRI “teaches a specific breathing style via a system providing real-time feedback of respiratory rate (RR) and exhaled carbon dioxide levels facilitated by data capture,” the authors note.
Sense of mastery
Of the 1,569 participants, 1,395 had PD and 174 had PTSD (mean age, 39.2 [standard deviation, 13.9] years and 40.9 [SD, 14.9] years, respectively; 76% and 73% female, respectively). Those with PD completed the Panic Disorder Severity Scale (PDSS) and those with PTSD completed the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5), before and after the intervention.
The treatment response rate for PD was defined as a 40% or greater reduction in PDSS total scores, whereas treatment response rate for PTSD was defined as a 10-point or greater reduction in PCL-5 scores.
At baseline, patients were classified either as normocapnic or hypocapnic (etCO2 ≥ 37 or < 37, respectively), with 65% classified as normocapnic and 35% classified as hypocapnic.
Among patients with PD, there was a 50.2% mean pre- to posttreatment reduction in total PDSS scores (P < .001; d = 1.31), with a treatment response rate of 65.3% of patients.
Among patients with PTSD, there was a 41.1% pre- to posttreatment reduction in total PCL-5 scores (P < .001; d = 1.16), with a treatment response rate of 72.4%.
When investigators analyzed the response at the individual level, they found that 55.7% of patients with PD and 53.5% of those with PTSD were classified as treatment responders. This determination was based on a two-pronged approach that first calculated the Reliable Change Index (RCI) for each participant, and, in participants showing statistically reliable improvement, whether the posttreatment score was closer to the distribution of scores for patients without or with the given disorder.
“Patients with both normal and below-normal baseline exhaled CO2 levels experienced comparable benefit,” the authors report.
There were high levels of adherence across the full treatment period in both the PD and the PTSD groups (74.8% and 74.9%, respectively), with low dropout rates (10% and 11%, respectively).
“Not every single patient who undergoes any treatment has a perfect response, but the response rates to this treatment have, surprisingly, been quite positive and there have been no negative side effects,” Dr. Telch remarked.
He noted that one of the effects of PTSD is that the “patient has negative beliefs about their ability to control the world. ‘I can’t control my reactions. At any time, I could have a flashback.’ Helping the patient to develop any sense of mastery over some of their reactions can spill over and give them a greater sense of mastery and control, which can have a positive effect in reducing PTSD symptoms.”
‘A viable alternative’
Commenting on the research, Charles Marmar, MD, chair and Peter H. Schub Professor of Psychiatry, department of psychiatry, New York University, said that the study has some limitations, probably the most significant of which is that most participants had normal baseline CO2 levels.
“The treatment is fundamentally designed for people who hyperventilate and blow off too much CO2 so they can breathe in a more calm, relaxed way, but most people in the trial had normal CO2 to begin with,” said Dr. Marmar, who was not involved with the study.
“It’s likely that the major benefits were the relaxation from doing the breathing exercises rather than the change in CO2 levels,” he speculated.
The treatment is “probably a good thing for those patients who actually have abnormal CO2 levels. This treatment could be used in precision medicine, where you tailor treatments to those who actually need them rather than giving the same treatment to everyone,” he said.
“For patients who don’t respond to trauma-focused therapy or it’s too aversive for them to undergo, this new intervention provides a viable alternative,” Dr. Telch added.
The study was internally funded by Freespira. Dr. Telch is a scientific advisor at Freespira and receives compensation by way of stock options. The other authors’ disclosures are listed on the original paper. Dr. Marmar has declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM FRONTIERS IN DIGITAL HEALTH