User login
‘Clear answer’: ALL study defies conventional wisdom
The same study also addressed two other issues related to standard care for these patients: 1) the dosage of dexamethasone used during the first treatment phase (results of which had already been reported some years ago) and 2) the impact of omitting monthly pulses of dexamethasone and vincristine after initial treatment.
“The trial did not give us the answers we were looking for, but that’s why we do randomized trials, and at least we have one clear answer, which is that high-dose methotrexate does not seem to have benefit in reducing the risk of CNS relapse,” reported study investigator Ajay Vora, MSc, from Great Ormond Street Hospital, London.
Among 1,570 patients randomly assigned in one group of the UKALL2011 trial, 5-year rates of CNS relapse were identical at 5.6% for patients treated with either high-dose methotrexate or standard interim maintenance with oral mercaptopurine and oral and intrathecal methotrexate.
There was a hint, however, that high-dose methotrexate could have a beneficial effect by reducing relapses in bone marrow for some subgroups of patients with B-lineage disease after dexamethasone induction, Dr. Vora commented.
He was speaking at a press briefing at the annual meeting of the American Society of Hematology, prior to the presentation of the data by Amy A. Kirkwood, MSc, from the University College London Cancer Institute.
Reacting to the results, Cynthia E. Dunbar, MD, chief of the Translational Stem Cell Biology Branch at the National Heart, Lung, and Blood Institute in Bethesda, Md., emphasized that “in patients treated with the UKALL regimen, high doses of methotrexate did not reduce the rate of CNS relapse, contrary to our long-standing beliefs.”
“Going forward, patients can be spared the risk of high-dose methotrexate without increasing their risk of recurrence in the central nervous system,” she said.
“As researchers in hematology, we look at it as our duty to question the standard approaches that we use to treat patients, even those that we thought of as tried-and-true,” said briefing moderator Mikkael Sekeres, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami. This is one of the abstracts that “challenge some of those standards and in fact reveal that in many cases, giving less therapy and being less restrictive is actually better for patients or at least no worse.”
Complex design
The UKALL2011 trial had a byzantine design, with the overarching goal of finding out which treatment and maintenance strategy best finds the sweet spot between efficacy and toxicity in children and young adults (up to age 25) with ALL and lymphoblastic lymphoma.
One question that was already answered, as investigators reported at the 2017 ASH annual meeting, came from the first randomization in the study, designed to see whether a shorter course of dexamethasone – 14 days versus the standard 28 days – could reduce induction toxicity. It did not.
Now, at ASH 2022, the investigators reported outcomes from the second phase of the trial, which included two randomizations: one comparing high-dose methotrexate with standard interim maintenance to reduce CNS relapse risk, and one to see whether forgoing pulses of vincristine/dexamethasone could reduce maintenance morbidity.
Patients were stratified by National Cancer Institute minimal residual disease (MRD) risk categories, cytogenetics, and end-of-induction MRD to receive one of three treatment regimens. Patients with MRD high risk, defined as MRD greater than 0.5% at the end of consolidation, were not eligible for second-phase randomization and instead received off-protocol therapies.The second randomization was factorial, stratified by NCI and MRD risk groups, resulting in four arms: high-dose methotrexate with or without pulses and standard interim maintenance with our without pulses.
Standard interim maintenance in this trial was 2 months of oral mercaptopurine/methotrexate monthly pulses and single intrathecal methotrexate in two of the regimens, as well as five doses of escalating intravenous methotrexate plus vincristine and two doses of pegylated asparaginase in the third.
High-dose methotrexate was given at a dose of 5 g/m2 for four doses 2 weeks apart, low dose 6-mercaptopurine, plus two doses of pegylated asparaginase in one regimen only.
Equivocal conclusions
As noted above, CNS relapse, the primary endpoint for the interim maintenance randomization, did not differ between the groups, with identical 5-year relapse rates. Similarly, 5-year event-free survival (EFS) rates were 90.3% in the high-dose group and 89.5% in the standard group, a difference that was not statistically significant (P = .68).
There was, however, an interaction between the first (short- vs. standard-course dexamethasone) and the interim maintenance randomizations, indicating significantly inferior EFS outcomes for patients who had received the short dose of dexamethasone followed by high-dose methotrexate, especially among patients who did not receive pulses (P = .006).
An analysis of patients treated with standard dexamethasone showed that those who received high-dose methotrexate had a lower risk for bone marrow relapse, with a hazard ratio of 0.62 (P = .029), and trends, albeit nonsignificant, toward better EFS and overall survival.
In addition, the overall results suggested that steroid pulses could be safely omitted without leading to an increase in bone marrow relapses: the 5-year rates of bone marrow relapse were 10.2% with pulses and 12.2% without, although omitting pulses was associated with a slight but significant decrease in EFS overall (P = .01). The effect was attenuated among patients who had received standard-course dexamethasone and high-dose methotrexate. Leaving out the pulses also reduced rates of grade 3 or 4 adverse events, including febrile neutropenia, Ms. Kirkwood noted in her presentation.
The investigators plan to analyze quality-of-life outcomes related to dexamethasone-vincristine pulses to see whether doing so could tip the balance in favor of leaving them out of therapy, and they will continue to follow patients to see whether their findings hold.
UKALL2011 was funded by Children with Cancer UK, Blood Cancer UK, and Cancer Research UK. Ms. Kirkwood disclosed consulting for and receiving honoraria from Kite. Dr. Vora reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The same study also addressed two other issues related to standard care for these patients: 1) the dosage of dexamethasone used during the first treatment phase (results of which had already been reported some years ago) and 2) the impact of omitting monthly pulses of dexamethasone and vincristine after initial treatment.
“The trial did not give us the answers we were looking for, but that’s why we do randomized trials, and at least we have one clear answer, which is that high-dose methotrexate does not seem to have benefit in reducing the risk of CNS relapse,” reported study investigator Ajay Vora, MSc, from Great Ormond Street Hospital, London.
Among 1,570 patients randomly assigned in one group of the UKALL2011 trial, 5-year rates of CNS relapse were identical at 5.6% for patients treated with either high-dose methotrexate or standard interim maintenance with oral mercaptopurine and oral and intrathecal methotrexate.
There was a hint, however, that high-dose methotrexate could have a beneficial effect by reducing relapses in bone marrow for some subgroups of patients with B-lineage disease after dexamethasone induction, Dr. Vora commented.
He was speaking at a press briefing at the annual meeting of the American Society of Hematology, prior to the presentation of the data by Amy A. Kirkwood, MSc, from the University College London Cancer Institute.
Reacting to the results, Cynthia E. Dunbar, MD, chief of the Translational Stem Cell Biology Branch at the National Heart, Lung, and Blood Institute in Bethesda, Md., emphasized that “in patients treated with the UKALL regimen, high doses of methotrexate did not reduce the rate of CNS relapse, contrary to our long-standing beliefs.”
“Going forward, patients can be spared the risk of high-dose methotrexate without increasing their risk of recurrence in the central nervous system,” she said.
“As researchers in hematology, we look at it as our duty to question the standard approaches that we use to treat patients, even those that we thought of as tried-and-true,” said briefing moderator Mikkael Sekeres, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami. This is one of the abstracts that “challenge some of those standards and in fact reveal that in many cases, giving less therapy and being less restrictive is actually better for patients or at least no worse.”
Complex design
The UKALL2011 trial had a byzantine design, with the overarching goal of finding out which treatment and maintenance strategy best finds the sweet spot between efficacy and toxicity in children and young adults (up to age 25) with ALL and lymphoblastic lymphoma.
One question that was already answered, as investigators reported at the 2017 ASH annual meeting, came from the first randomization in the study, designed to see whether a shorter course of dexamethasone – 14 days versus the standard 28 days – could reduce induction toxicity. It did not.
Now, at ASH 2022, the investigators reported outcomes from the second phase of the trial, which included two randomizations: one comparing high-dose methotrexate with standard interim maintenance to reduce CNS relapse risk, and one to see whether forgoing pulses of vincristine/dexamethasone could reduce maintenance morbidity.
Patients were stratified by National Cancer Institute minimal residual disease (MRD) risk categories, cytogenetics, and end-of-induction MRD to receive one of three treatment regimens. Patients with MRD high risk, defined as MRD greater than 0.5% at the end of consolidation, were not eligible for second-phase randomization and instead received off-protocol therapies.The second randomization was factorial, stratified by NCI and MRD risk groups, resulting in four arms: high-dose methotrexate with or without pulses and standard interim maintenance with our without pulses.
Standard interim maintenance in this trial was 2 months of oral mercaptopurine/methotrexate monthly pulses and single intrathecal methotrexate in two of the regimens, as well as five doses of escalating intravenous methotrexate plus vincristine and two doses of pegylated asparaginase in the third.
High-dose methotrexate was given at a dose of 5 g/m2 for four doses 2 weeks apart, low dose 6-mercaptopurine, plus two doses of pegylated asparaginase in one regimen only.
Equivocal conclusions
As noted above, CNS relapse, the primary endpoint for the interim maintenance randomization, did not differ between the groups, with identical 5-year relapse rates. Similarly, 5-year event-free survival (EFS) rates were 90.3% in the high-dose group and 89.5% in the standard group, a difference that was not statistically significant (P = .68).
There was, however, an interaction between the first (short- vs. standard-course dexamethasone) and the interim maintenance randomizations, indicating significantly inferior EFS outcomes for patients who had received the short dose of dexamethasone followed by high-dose methotrexate, especially among patients who did not receive pulses (P = .006).
An analysis of patients treated with standard dexamethasone showed that those who received high-dose methotrexate had a lower risk for bone marrow relapse, with a hazard ratio of 0.62 (P = .029), and trends, albeit nonsignificant, toward better EFS and overall survival.
In addition, the overall results suggested that steroid pulses could be safely omitted without leading to an increase in bone marrow relapses: the 5-year rates of bone marrow relapse were 10.2% with pulses and 12.2% without, although omitting pulses was associated with a slight but significant decrease in EFS overall (P = .01). The effect was attenuated among patients who had received standard-course dexamethasone and high-dose methotrexate. Leaving out the pulses also reduced rates of grade 3 or 4 adverse events, including febrile neutropenia, Ms. Kirkwood noted in her presentation.
The investigators plan to analyze quality-of-life outcomes related to dexamethasone-vincristine pulses to see whether doing so could tip the balance in favor of leaving them out of therapy, and they will continue to follow patients to see whether their findings hold.
UKALL2011 was funded by Children with Cancer UK, Blood Cancer UK, and Cancer Research UK. Ms. Kirkwood disclosed consulting for and receiving honoraria from Kite. Dr. Vora reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The same study also addressed two other issues related to standard care for these patients: 1) the dosage of dexamethasone used during the first treatment phase (results of which had already been reported some years ago) and 2) the impact of omitting monthly pulses of dexamethasone and vincristine after initial treatment.
“The trial did not give us the answers we were looking for, but that’s why we do randomized trials, and at least we have one clear answer, which is that high-dose methotrexate does not seem to have benefit in reducing the risk of CNS relapse,” reported study investigator Ajay Vora, MSc, from Great Ormond Street Hospital, London.
Among 1,570 patients randomly assigned in one group of the UKALL2011 trial, 5-year rates of CNS relapse were identical at 5.6% for patients treated with either high-dose methotrexate or standard interim maintenance with oral mercaptopurine and oral and intrathecal methotrexate.
There was a hint, however, that high-dose methotrexate could have a beneficial effect by reducing relapses in bone marrow for some subgroups of patients with B-lineage disease after dexamethasone induction, Dr. Vora commented.
He was speaking at a press briefing at the annual meeting of the American Society of Hematology, prior to the presentation of the data by Amy A. Kirkwood, MSc, from the University College London Cancer Institute.
Reacting to the results, Cynthia E. Dunbar, MD, chief of the Translational Stem Cell Biology Branch at the National Heart, Lung, and Blood Institute in Bethesda, Md., emphasized that “in patients treated with the UKALL regimen, high doses of methotrexate did not reduce the rate of CNS relapse, contrary to our long-standing beliefs.”
“Going forward, patients can be spared the risk of high-dose methotrexate without increasing their risk of recurrence in the central nervous system,” she said.
“As researchers in hematology, we look at it as our duty to question the standard approaches that we use to treat patients, even those that we thought of as tried-and-true,” said briefing moderator Mikkael Sekeres, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami. This is one of the abstracts that “challenge some of those standards and in fact reveal that in many cases, giving less therapy and being less restrictive is actually better for patients or at least no worse.”
Complex design
The UKALL2011 trial had a byzantine design, with the overarching goal of finding out which treatment and maintenance strategy best finds the sweet spot between efficacy and toxicity in children and young adults (up to age 25) with ALL and lymphoblastic lymphoma.
One question that was already answered, as investigators reported at the 2017 ASH annual meeting, came from the first randomization in the study, designed to see whether a shorter course of dexamethasone – 14 days versus the standard 28 days – could reduce induction toxicity. It did not.
Now, at ASH 2022, the investigators reported outcomes from the second phase of the trial, which included two randomizations: one comparing high-dose methotrexate with standard interim maintenance to reduce CNS relapse risk, and one to see whether forgoing pulses of vincristine/dexamethasone could reduce maintenance morbidity.
Patients were stratified by National Cancer Institute minimal residual disease (MRD) risk categories, cytogenetics, and end-of-induction MRD to receive one of three treatment regimens. Patients with MRD high risk, defined as MRD greater than 0.5% at the end of consolidation, were not eligible for second-phase randomization and instead received off-protocol therapies.The second randomization was factorial, stratified by NCI and MRD risk groups, resulting in four arms: high-dose methotrexate with or without pulses and standard interim maintenance with our without pulses.
Standard interim maintenance in this trial was 2 months of oral mercaptopurine/methotrexate monthly pulses and single intrathecal methotrexate in two of the regimens, as well as five doses of escalating intravenous methotrexate plus vincristine and two doses of pegylated asparaginase in the third.
High-dose methotrexate was given at a dose of 5 g/m2 for four doses 2 weeks apart, low dose 6-mercaptopurine, plus two doses of pegylated asparaginase in one regimen only.
Equivocal conclusions
As noted above, CNS relapse, the primary endpoint for the interim maintenance randomization, did not differ between the groups, with identical 5-year relapse rates. Similarly, 5-year event-free survival (EFS) rates were 90.3% in the high-dose group and 89.5% in the standard group, a difference that was not statistically significant (P = .68).
There was, however, an interaction between the first (short- vs. standard-course dexamethasone) and the interim maintenance randomizations, indicating significantly inferior EFS outcomes for patients who had received the short dose of dexamethasone followed by high-dose methotrexate, especially among patients who did not receive pulses (P = .006).
An analysis of patients treated with standard dexamethasone showed that those who received high-dose methotrexate had a lower risk for bone marrow relapse, with a hazard ratio of 0.62 (P = .029), and trends, albeit nonsignificant, toward better EFS and overall survival.
In addition, the overall results suggested that steroid pulses could be safely omitted without leading to an increase in bone marrow relapses: the 5-year rates of bone marrow relapse were 10.2% with pulses and 12.2% without, although omitting pulses was associated with a slight but significant decrease in EFS overall (P = .01). The effect was attenuated among patients who had received standard-course dexamethasone and high-dose methotrexate. Leaving out the pulses also reduced rates of grade 3 or 4 adverse events, including febrile neutropenia, Ms. Kirkwood noted in her presentation.
The investigators plan to analyze quality-of-life outcomes related to dexamethasone-vincristine pulses to see whether doing so could tip the balance in favor of leaving them out of therapy, and they will continue to follow patients to see whether their findings hold.
UKALL2011 was funded by Children with Cancer UK, Blood Cancer UK, and Cancer Research UK. Ms. Kirkwood disclosed consulting for and receiving honoraria from Kite. Dr. Vora reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ASH 2022
‘Astonishing’ results: Skip salvage chemo, proceed to HSCT
NEW ORLEANS –
The results come from the phase 3 ASAP Trial and were presented at the annual meeting of the American Society of Hematology.
“We selected this to be in the plenary because it completely changes how we’ve traditionally thought about acute myeloid leukemia,” commented press briefing moderator Mikkael A. Sekeres, MD, from the University of Miami, who also serves as chair of the ASH Committee on Communications.
“When we have a patient who has relapsed or refractory AML, that person is in a very, very difficult situation, and the mortality among those sort of patients is incredibly high,” Dr. Sekeres commented. “So traditionally we’ve given them very high doses of chemotherapy to try to reduce the tumor burden – at least that’s been the theory – to then get them successfully to a transplant.”
This new finding “completely upends that, if these results hold,” he said. The clinical implication is that “we no longer have to hospitalize these patients and give them very aggressive chemotherapy ... [and] we don’t introduce all the morbidity from giving them very high dose chemotherapy, which can actually prevent a transplant from happening if they get sick enough, and we can get them to a transplant quicker.”
The ASAP trial was conducted in patients with an unfavorable risk AML who either had a poor response to first induction therapy or a relapse after first induction therapy.
They were randomly assigned to either a remission-induction strategy aiming for a better response prior to an allogeneic hematopoietic stem cell transplant (alloHCT), or a disease-control strategy consisting primarily of watchful waiting with low-dose cytarabine and single doses of mitoxantrone as needed, followed by sequential conditioning and alloHCT.
The results after 4 years of follow-up showed no differences in either leukemia-free survival or overall survival between patients who underwent additional chemotherapy with the remission-induction strategy and those who went straight to transplant, reported Johannes Schetelig, MD, MSc, from the Clinical Trials Unit at DKMS, Dresden, Germany.
“We expected non-inferiority – this was what we tested, and of course this was based on an assumption that we could get close or even somewhat better with respect to the primary endpoint, disease-free survival, after transplantation,” he said.
“What we did not expect is that the early success, [complete response] on day 56 after transplantation, also translates into equal long-term benefit, so this is what I was really astonished about,” Dr. Schetelig said at a press briefing prior to his presentation.
Less intensive approach
Dr. Schetelig explained that the rationale for the study was previous work by his group and others showing that alloHCT in patients with residual aplasia after first induction is feasible, with favorable outcomes, compared with standard of care. Additionally, the impetus for the research was evidence that sequential conditioning based on high-dose cytarabine or melphalan plus reduced-intensity conditioning and alloHCT resulted in long-term control for relapsed or refractory AML.
Dr. Schetelig also gave details of the two treatment arms of the ASAP trial. The remission-inducing arm consisted of cytarabine (3 g/m2 for younger patients or 1 g/m2 for patients over age 60) twice daily on days 1-3 plus 10 mitoxantrone mg/m2 on days 3-5 and subsequent alloHCT. In the other group – disease control prior to sequential conditioning and alloHCT – watchful waiting was recommended, but low-dose cytarabine (LDAC) and single doses of mitoxantrone were permitted for disease control.
Although, as Dr. Schetelig noted, the statistical goal of the study was to show non-inferiority of the disease control arm, this less intensive strategy exceeded expectations for meeting the primary endpoint of disease-free survival (DFS; a maintained complete response) by day 56 after alloHCT.
In an intention-to-treat and per-protocol analysis, the respective rates of DFS at 56 days in the disease control group were 83.5% and 84.1%. In comparison, the respective rates in the remission-induction group were 81% and 81.3%.
Further, after a median follow-up from randomization of 37 months, there were no differences in either leukemia-free survival or overall survival out to 4 years after DFS at day 56.
The disease-control strategy was also associated with significantly fewer adverse events grade 3 or greater (23% vs. 64%, P < .001), and fewer days in hospital prior to transplant (mean 19 vs. 42, P < .001). There were no significant differences between the trial arms in either deaths within 28 days of randomization or time to discharge from hospital (28 days in each arm).
“These data support sequential conditioning and alloHCT without prior remission-induction chemotherapy whenever a stem cell donor is readily available,” the researchers concluded.
“These results underline the importance of facilitating alloHCT as [the] most effective anti-leukemic therapy in patients with [relapsed or refractory] AML and stress the need for starting donor search at diagnosis,” they added.
The study was sponsored by DKMS gemeinnützige GmbH. Dr. Schetelig disclosed honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Sekkeres reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
The results come from the phase 3 ASAP Trial and were presented at the annual meeting of the American Society of Hematology.
“We selected this to be in the plenary because it completely changes how we’ve traditionally thought about acute myeloid leukemia,” commented press briefing moderator Mikkael A. Sekeres, MD, from the University of Miami, who also serves as chair of the ASH Committee on Communications.
“When we have a patient who has relapsed or refractory AML, that person is in a very, very difficult situation, and the mortality among those sort of patients is incredibly high,” Dr. Sekeres commented. “So traditionally we’ve given them very high doses of chemotherapy to try to reduce the tumor burden – at least that’s been the theory – to then get them successfully to a transplant.”
This new finding “completely upends that, if these results hold,” he said. The clinical implication is that “we no longer have to hospitalize these patients and give them very aggressive chemotherapy ... [and] we don’t introduce all the morbidity from giving them very high dose chemotherapy, which can actually prevent a transplant from happening if they get sick enough, and we can get them to a transplant quicker.”
The ASAP trial was conducted in patients with an unfavorable risk AML who either had a poor response to first induction therapy or a relapse after first induction therapy.
They were randomly assigned to either a remission-induction strategy aiming for a better response prior to an allogeneic hematopoietic stem cell transplant (alloHCT), or a disease-control strategy consisting primarily of watchful waiting with low-dose cytarabine and single doses of mitoxantrone as needed, followed by sequential conditioning and alloHCT.
The results after 4 years of follow-up showed no differences in either leukemia-free survival or overall survival between patients who underwent additional chemotherapy with the remission-induction strategy and those who went straight to transplant, reported Johannes Schetelig, MD, MSc, from the Clinical Trials Unit at DKMS, Dresden, Germany.
“We expected non-inferiority – this was what we tested, and of course this was based on an assumption that we could get close or even somewhat better with respect to the primary endpoint, disease-free survival, after transplantation,” he said.
“What we did not expect is that the early success, [complete response] on day 56 after transplantation, also translates into equal long-term benefit, so this is what I was really astonished about,” Dr. Schetelig said at a press briefing prior to his presentation.
Less intensive approach
Dr. Schetelig explained that the rationale for the study was previous work by his group and others showing that alloHCT in patients with residual aplasia after first induction is feasible, with favorable outcomes, compared with standard of care. Additionally, the impetus for the research was evidence that sequential conditioning based on high-dose cytarabine or melphalan plus reduced-intensity conditioning and alloHCT resulted in long-term control for relapsed or refractory AML.
Dr. Schetelig also gave details of the two treatment arms of the ASAP trial. The remission-inducing arm consisted of cytarabine (3 g/m2 for younger patients or 1 g/m2 for patients over age 60) twice daily on days 1-3 plus 10 mitoxantrone mg/m2 on days 3-5 and subsequent alloHCT. In the other group – disease control prior to sequential conditioning and alloHCT – watchful waiting was recommended, but low-dose cytarabine (LDAC) and single doses of mitoxantrone were permitted for disease control.
Although, as Dr. Schetelig noted, the statistical goal of the study was to show non-inferiority of the disease control arm, this less intensive strategy exceeded expectations for meeting the primary endpoint of disease-free survival (DFS; a maintained complete response) by day 56 after alloHCT.
In an intention-to-treat and per-protocol analysis, the respective rates of DFS at 56 days in the disease control group were 83.5% and 84.1%. In comparison, the respective rates in the remission-induction group were 81% and 81.3%.
Further, after a median follow-up from randomization of 37 months, there were no differences in either leukemia-free survival or overall survival out to 4 years after DFS at day 56.
The disease-control strategy was also associated with significantly fewer adverse events grade 3 or greater (23% vs. 64%, P < .001), and fewer days in hospital prior to transplant (mean 19 vs. 42, P < .001). There were no significant differences between the trial arms in either deaths within 28 days of randomization or time to discharge from hospital (28 days in each arm).
“These data support sequential conditioning and alloHCT without prior remission-induction chemotherapy whenever a stem cell donor is readily available,” the researchers concluded.
“These results underline the importance of facilitating alloHCT as [the] most effective anti-leukemic therapy in patients with [relapsed or refractory] AML and stress the need for starting donor search at diagnosis,” they added.
The study was sponsored by DKMS gemeinnützige GmbH. Dr. Schetelig disclosed honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Sekkeres reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
The results come from the phase 3 ASAP Trial and were presented at the annual meeting of the American Society of Hematology.
“We selected this to be in the plenary because it completely changes how we’ve traditionally thought about acute myeloid leukemia,” commented press briefing moderator Mikkael A. Sekeres, MD, from the University of Miami, who also serves as chair of the ASH Committee on Communications.
“When we have a patient who has relapsed or refractory AML, that person is in a very, very difficult situation, and the mortality among those sort of patients is incredibly high,” Dr. Sekeres commented. “So traditionally we’ve given them very high doses of chemotherapy to try to reduce the tumor burden – at least that’s been the theory – to then get them successfully to a transplant.”
This new finding “completely upends that, if these results hold,” he said. The clinical implication is that “we no longer have to hospitalize these patients and give them very aggressive chemotherapy ... [and] we don’t introduce all the morbidity from giving them very high dose chemotherapy, which can actually prevent a transplant from happening if they get sick enough, and we can get them to a transplant quicker.”
The ASAP trial was conducted in patients with an unfavorable risk AML who either had a poor response to first induction therapy or a relapse after first induction therapy.
They were randomly assigned to either a remission-induction strategy aiming for a better response prior to an allogeneic hematopoietic stem cell transplant (alloHCT), or a disease-control strategy consisting primarily of watchful waiting with low-dose cytarabine and single doses of mitoxantrone as needed, followed by sequential conditioning and alloHCT.
The results after 4 years of follow-up showed no differences in either leukemia-free survival or overall survival between patients who underwent additional chemotherapy with the remission-induction strategy and those who went straight to transplant, reported Johannes Schetelig, MD, MSc, from the Clinical Trials Unit at DKMS, Dresden, Germany.
“We expected non-inferiority – this was what we tested, and of course this was based on an assumption that we could get close or even somewhat better with respect to the primary endpoint, disease-free survival, after transplantation,” he said.
“What we did not expect is that the early success, [complete response] on day 56 after transplantation, also translates into equal long-term benefit, so this is what I was really astonished about,” Dr. Schetelig said at a press briefing prior to his presentation.
Less intensive approach
Dr. Schetelig explained that the rationale for the study was previous work by his group and others showing that alloHCT in patients with residual aplasia after first induction is feasible, with favorable outcomes, compared with standard of care. Additionally, the impetus for the research was evidence that sequential conditioning based on high-dose cytarabine or melphalan plus reduced-intensity conditioning and alloHCT resulted in long-term control for relapsed or refractory AML.
Dr. Schetelig also gave details of the two treatment arms of the ASAP trial. The remission-inducing arm consisted of cytarabine (3 g/m2 for younger patients or 1 g/m2 for patients over age 60) twice daily on days 1-3 plus 10 mitoxantrone mg/m2 on days 3-5 and subsequent alloHCT. In the other group – disease control prior to sequential conditioning and alloHCT – watchful waiting was recommended, but low-dose cytarabine (LDAC) and single doses of mitoxantrone were permitted for disease control.
Although, as Dr. Schetelig noted, the statistical goal of the study was to show non-inferiority of the disease control arm, this less intensive strategy exceeded expectations for meeting the primary endpoint of disease-free survival (DFS; a maintained complete response) by day 56 after alloHCT.
In an intention-to-treat and per-protocol analysis, the respective rates of DFS at 56 days in the disease control group were 83.5% and 84.1%. In comparison, the respective rates in the remission-induction group were 81% and 81.3%.
Further, after a median follow-up from randomization of 37 months, there were no differences in either leukemia-free survival or overall survival out to 4 years after DFS at day 56.
The disease-control strategy was also associated with significantly fewer adverse events grade 3 or greater (23% vs. 64%, P < .001), and fewer days in hospital prior to transplant (mean 19 vs. 42, P < .001). There were no significant differences between the trial arms in either deaths within 28 days of randomization or time to discharge from hospital (28 days in each arm).
“These data support sequential conditioning and alloHCT without prior remission-induction chemotherapy whenever a stem cell donor is readily available,” the researchers concluded.
“These results underline the importance of facilitating alloHCT as [the] most effective anti-leukemic therapy in patients with [relapsed or refractory] AML and stress the need for starting donor search at diagnosis,” they added.
The study was sponsored by DKMS gemeinnützige GmbH. Dr. Schetelig disclosed honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Sekkeres reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ASH 2022
Post-transplant diet: Gruel no longer rules
NEW ORLEANS – A new Italian study yields more evidence that stem-cell transplant patients need not lose their appetites along with their immune systems. Low-bacterial, gruel-like diets, once the mainstay of immunity-lowering surgeries, don’t actually provide any protection against infections, researchers reported.
University of Miami hematologist Mikkael A. Sekeres, MD, MS, expressed delight to hear these findings.
“Around the world, we should eliminate these silly neutropenic diets, let people eat what they want, and give them a much better quality of life while they’re in the hospital,” said Dr. Sekeres, moderator of the news briefing where these research results were discussed at the annual meeting of the American Society of Hematology.
In recent decades, physicians and nutritionists have questioned the value of low-bacterial/neutropenic menus, designed to protect people with compromised immune systems from germs in food. These diets can be quite strict, outlawing food such as deli, processed, and cured meats; yogurt; hummus; strawberries and raspberries; lettuce; raw nuts; certain kinds of seafood; and herbs and spices such as pepper, unless they were cooked. Patients may be urged to avoid salad bars, buffets, and potlucks.
MD Anderson Cancer Center pediatrician Karen Moody, MD, MS, who has studied the diet, said in an interview that the diet has been around since the 1970s, despite a lack of evidence supporting it. “Cancer patients often suffer from treatment-related side effects that affect taste, appetite, and tolerance of food,” she said. “Further restricting food options in this population can be burdensome and reduce diet-related satisfaction.”
For the new multi-center, phase 3 study, researchers led by hematology resident Federico Stella, MD, of the University of Milan, randomly assigned consecutive adult patients undergoing hematopoietic stem cells transplantation or high-dose induction chemotherapy to either a low-bacterial diet (n = 224) or a non-restrictive diet (n = 224).

The low-bacterial diet emphasized food cooked to at least 176 degrees Fahrenheit and thick-skinned fruit. Raw fruits/vegetables, yogurt, honey, cold cuts and sausages, and raw fish and meat were forbidden.
The two groups were similar in age (median = 56 years), gender (about 57% male), and reason for admission (97% stem-cell transplants and 3% high-dose chemotherapy). The plan was to follow the patients for 100 days (stem-cell transplant recipients) or 30 days (high-dose chemotherapy patients).
No statistically significant differences between the group were found in the rates of infections of higher than Grade 2 (per CTCAE 4.0): These infections occurred in 38 (34%) of those on the low-bacterial diet and 44 (39%) of those on the non-restrictive diet (P = 0.5).
There were also no statistically significant differences in rates of fever of unknown origin (P = 0.2), sepsis (P = 0.5), and gastrointestinal infection (P = 0.7).
The findings show that the “use of a restrictive diet is an unnecessary burden for our patients’ quality of life,” said study lead author Dr. Stella at the news briefing.
Dr. Sekeres, the news briefing moderator, noted that the findings reflect his own suspicions about the worthlessness of the low-bacterial diet. “I’ve never seen a patient die of an infection that was foodborne. So years ago, when I was still in Cleveland, I eliminated the neutropenic diet on the leukemia floor. That did face a lot of resistance, as you can imagine. There were decades of people saying we should do this.”
Now, Dr. Sekeres said, he feels validated. “I love this study because it formalizes what I thought was true,” he said.
Dr. Moody said it’s difficult to evaluate the study since it’s in abstract form, and details are limited. “However,” she said, “the sample size, study design, and outcomes appear very appropriate, and I think most likely the full-length study will provide additional evidence to support abandonment of the low-microbial diet in transplant patients.”
Also, Dr. Moody said, the study “replicates the same findings of other prospective randomized trials of this diet that say it confers no protection from infection and has no identified health benefit whatsoever. Bottom line? This diet has burden without benefit.”
Moving forward, she said, “we need a lot more research on diet in general for cancer patients. Recently, there is a lot more interest in this topic. I think we are going to learn a lot in the next few decades about the relationship between diet, epigenetics, the microbiome, and various cancer-related health issues.”
No study funding was reported. Dr. Stella reports no disclosures, and other authors report various relationships with industry. Dr. Moody reports no disclosures, and disclosures for Dr. Sekeres were not available.
NEW ORLEANS – A new Italian study yields more evidence that stem-cell transplant patients need not lose their appetites along with their immune systems. Low-bacterial, gruel-like diets, once the mainstay of immunity-lowering surgeries, don’t actually provide any protection against infections, researchers reported.
University of Miami hematologist Mikkael A. Sekeres, MD, MS, expressed delight to hear these findings.
“Around the world, we should eliminate these silly neutropenic diets, let people eat what they want, and give them a much better quality of life while they’re in the hospital,” said Dr. Sekeres, moderator of the news briefing where these research results were discussed at the annual meeting of the American Society of Hematology.
In recent decades, physicians and nutritionists have questioned the value of low-bacterial/neutropenic menus, designed to protect people with compromised immune systems from germs in food. These diets can be quite strict, outlawing food such as deli, processed, and cured meats; yogurt; hummus; strawberries and raspberries; lettuce; raw nuts; certain kinds of seafood; and herbs and spices such as pepper, unless they were cooked. Patients may be urged to avoid salad bars, buffets, and potlucks.
MD Anderson Cancer Center pediatrician Karen Moody, MD, MS, who has studied the diet, said in an interview that the diet has been around since the 1970s, despite a lack of evidence supporting it. “Cancer patients often suffer from treatment-related side effects that affect taste, appetite, and tolerance of food,” she said. “Further restricting food options in this population can be burdensome and reduce diet-related satisfaction.”
For the new multi-center, phase 3 study, researchers led by hematology resident Federico Stella, MD, of the University of Milan, randomly assigned consecutive adult patients undergoing hematopoietic stem cells transplantation or high-dose induction chemotherapy to either a low-bacterial diet (n = 224) or a non-restrictive diet (n = 224).
The low-bacterial diet emphasized food cooked to at least 176 degrees Fahrenheit and thick-skinned fruit. Raw fruits/vegetables, yogurt, honey, cold cuts and sausages, and raw fish and meat were forbidden.
The two groups were similar in age (median = 56 years), gender (about 57% male), and reason for admission (97% stem-cell transplants and 3% high-dose chemotherapy). The plan was to follow the patients for 100 days (stem-cell transplant recipients) or 30 days (high-dose chemotherapy patients).
No statistically significant differences between the group were found in the rates of infections of higher than Grade 2 (per CTCAE 4.0): These infections occurred in 38 (34%) of those on the low-bacterial diet and 44 (39%) of those on the non-restrictive diet (P = 0.5).
There were also no statistically significant differences in rates of fever of unknown origin (P = 0.2), sepsis (P = 0.5), and gastrointestinal infection (P = 0.7).
The findings show that the “use of a restrictive diet is an unnecessary burden for our patients’ quality of life,” said study lead author Dr. Stella at the news briefing.
Dr. Sekeres, the news briefing moderator, noted that the findings reflect his own suspicions about the worthlessness of the low-bacterial diet. “I’ve never seen a patient die of an infection that was foodborne. So years ago, when I was still in Cleveland, I eliminated the neutropenic diet on the leukemia floor. That did face a lot of resistance, as you can imagine. There were decades of people saying we should do this.”
Now, Dr. Sekeres said, he feels validated. “I love this study because it formalizes what I thought was true,” he said.
Dr. Moody said it’s difficult to evaluate the study since it’s in abstract form, and details are limited. “However,” she said, “the sample size, study design, and outcomes appear very appropriate, and I think most likely the full-length study will provide additional evidence to support abandonment of the low-microbial diet in transplant patients.”
Also, Dr. Moody said, the study “replicates the same findings of other prospective randomized trials of this diet that say it confers no protection from infection and has no identified health benefit whatsoever. Bottom line? This diet has burden without benefit.”
Moving forward, she said, “we need a lot more research on diet in general for cancer patients. Recently, there is a lot more interest in this topic. I think we are going to learn a lot in the next few decades about the relationship between diet, epigenetics, the microbiome, and various cancer-related health issues.”
No study funding was reported. Dr. Stella reports no disclosures, and other authors report various relationships with industry. Dr. Moody reports no disclosures, and disclosures for Dr. Sekeres were not available.
NEW ORLEANS – A new Italian study yields more evidence that stem-cell transplant patients need not lose their appetites along with their immune systems. Low-bacterial, gruel-like diets, once the mainstay of immunity-lowering surgeries, don’t actually provide any protection against infections, researchers reported.
University of Miami hematologist Mikkael A. Sekeres, MD, MS, expressed delight to hear these findings.
“Around the world, we should eliminate these silly neutropenic diets, let people eat what they want, and give them a much better quality of life while they’re in the hospital,” said Dr. Sekeres, moderator of the news briefing where these research results were discussed at the annual meeting of the American Society of Hematology.
In recent decades, physicians and nutritionists have questioned the value of low-bacterial/neutropenic menus, designed to protect people with compromised immune systems from germs in food. These diets can be quite strict, outlawing food such as deli, processed, and cured meats; yogurt; hummus; strawberries and raspberries; lettuce; raw nuts; certain kinds of seafood; and herbs and spices such as pepper, unless they were cooked. Patients may be urged to avoid salad bars, buffets, and potlucks.
MD Anderson Cancer Center pediatrician Karen Moody, MD, MS, who has studied the diet, said in an interview that the diet has been around since the 1970s, despite a lack of evidence supporting it. “Cancer patients often suffer from treatment-related side effects that affect taste, appetite, and tolerance of food,” she said. “Further restricting food options in this population can be burdensome and reduce diet-related satisfaction.”
For the new multi-center, phase 3 study, researchers led by hematology resident Federico Stella, MD, of the University of Milan, randomly assigned consecutive adult patients undergoing hematopoietic stem cells transplantation or high-dose induction chemotherapy to either a low-bacterial diet (n = 224) or a non-restrictive diet (n = 224).
The low-bacterial diet emphasized food cooked to at least 176 degrees Fahrenheit and thick-skinned fruit. Raw fruits/vegetables, yogurt, honey, cold cuts and sausages, and raw fish and meat were forbidden.
The two groups were similar in age (median = 56 years), gender (about 57% male), and reason for admission (97% stem-cell transplants and 3% high-dose chemotherapy). The plan was to follow the patients for 100 days (stem-cell transplant recipients) or 30 days (high-dose chemotherapy patients).
No statistically significant differences between the group were found in the rates of infections of higher than Grade 2 (per CTCAE 4.0): These infections occurred in 38 (34%) of those on the low-bacterial diet and 44 (39%) of those on the non-restrictive diet (P = 0.5).
There were also no statistically significant differences in rates of fever of unknown origin (P = 0.2), sepsis (P = 0.5), and gastrointestinal infection (P = 0.7).
The findings show that the “use of a restrictive diet is an unnecessary burden for our patients’ quality of life,” said study lead author Dr. Stella at the news briefing.
Dr. Sekeres, the news briefing moderator, noted that the findings reflect his own suspicions about the worthlessness of the low-bacterial diet. “I’ve never seen a patient die of an infection that was foodborne. So years ago, when I was still in Cleveland, I eliminated the neutropenic diet on the leukemia floor. That did face a lot of resistance, as you can imagine. There were decades of people saying we should do this.”
Now, Dr. Sekeres said, he feels validated. “I love this study because it formalizes what I thought was true,” he said.
Dr. Moody said it’s difficult to evaluate the study since it’s in abstract form, and details are limited. “However,” she said, “the sample size, study design, and outcomes appear very appropriate, and I think most likely the full-length study will provide additional evidence to support abandonment of the low-microbial diet in transplant patients.”
Also, Dr. Moody said, the study “replicates the same findings of other prospective randomized trials of this diet that say it confers no protection from infection and has no identified health benefit whatsoever. Bottom line? This diet has burden without benefit.”
Moving forward, she said, “we need a lot more research on diet in general for cancer patients. Recently, there is a lot more interest in this topic. I think we are going to learn a lot in the next few decades about the relationship between diet, epigenetics, the microbiome, and various cancer-related health issues.”
No study funding was reported. Dr. Stella reports no disclosures, and other authors report various relationships with industry. Dr. Moody reports no disclosures, and disclosures for Dr. Sekeres were not available.
AT ASH 2022
Incorporating medication abortion into your ObGyn practice: Why and how
The Supreme Court’s Dobbs decision on June 24, 2022, which nullified the federal protections of Roe v Wade, resulted in the swift and devastating dissolution of access to abortion care for hundreds of thousands of patients in the United States.1 Within days of the decision, 11 states in the South and Midwest implemented complete or 6-week abortion bans that, in part, led to the closure of over half the abortion clinics in these states.2 Abortion bans, severe restrictions, and clinic closures affect all patients and magnify existing health care inequities.
Medication abortion is becoming increasingly popular; as of 2020, approximately 50% of US abortions were performed using this method.3 Through a combination of mifepristone and misoprostol, medication abortion induces the physiologic process and symptoms similar to those of a miscarriage. Notably, this regimen is also the most effective medical management method for a missed abortion in the first trimester, and therefore, should already be incorporated into any general ObGyn practice.4
Although a recent study found that 97% of ObGyn physicians report encountering patients who seek an abortion, only 15% to 25% of them reported providing abortion services.5,6 Given our expertise, ObGyns are well-positioned to incorporate medication abortion into our practices. For those ObGyn providers who practice in states without extreme abortion bans, this article provides guidance on how to incorporate medication abortion into your practice (FIGURE). Several states now have early gestational limits on abortion, and the abortion-dedicated clinics that remain open are over capacity. Therefore, by incorporating medication abortion into your practice you can contribute to timely abortion access for your patients.
Medication abortion: The process
Determine your ability and patient’s eligibility
Abortion-specific laws for your state have now become the first determinant of your ability to provide medication abortion to your patients. The Guttmacher Institute is one reliable source of specific state laws that your practice can reference and is updated regularly.7
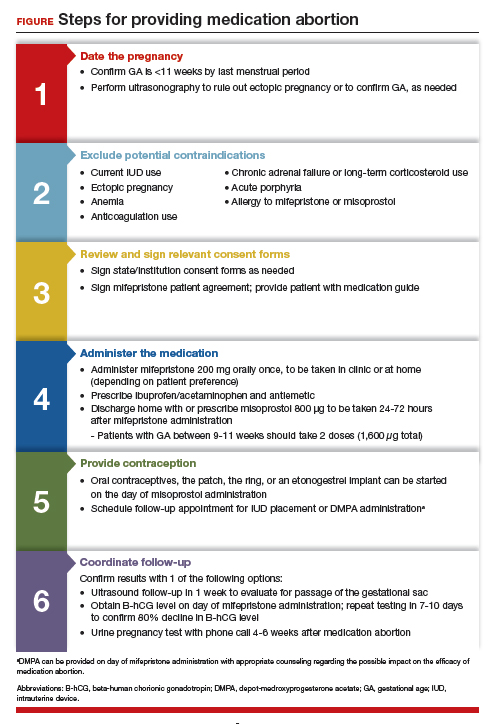
From a practice perspective, most ObGyn physicians already have the technical capabilities in place to provide medication abortion. First, you must be able to accurately determine the patient’s gestational age by their last menstrual period, which is often confirmed through ultrasonography.
Medication abortion is safe and routinely used in many practices up to 77 days, or 11 weeks, of gestation. Authors of a recent retrospective cohort study found that medication abortion also may be initiated for a pregnancy of unknown location in patients who are asymptomatic and determined to have low risk for an ectopic pregnancy. In this study, initiation of medication abortion on the day of presentation, with concurrent evaluation for ectopic pregnancy, was associated with a shorter time to a completed abortion, but a lower rate of successful medication abortion when compared with patients who delayed the initiation of medication abortion until a clear intrauterine pregnancy was diagnosed.8
Few medical contraindications exist for patients who seek a medication abortion. These contraindications include allergy to or medication interaction with mifepristone or misoprostol, chronic adrenal failure or long-term corticosteroid therapy, acute porphyria, anemia or the use of anticoagulation therapy, or current intrauterine device (IUD) use.
Continue to: Gather consents and administer treatment...
Gather consents and administer treatment
Historically, mifepristone has been dispensed directly at an ObGyn physician’s office. However, the US Food and Drug Administration (FDA) regulations requiring this were lifted during the COVID-19 pandemic, and as of December 2021, the inperson dispensing requirement was permanently removed.9 To provide mifepristone in a medical practice under current guidelines, a confidential prescriber agreement must be completed once by one person on behalf of the practice. Then each patient must read the manufacturer’s medication guide and sign the patient agreement form as part of the consent process (available on the FDA’s website).10 These agreement forms must be filled out by a physician and each patient if your practice uses mifepristone for any pregnancy indication, including induction of labor or medical management of miscarriage. Given the multiple evidence-based indications for mifepristone in pregnancy, it is hoped that these agreement forms will become a routine part of most ObGyn practices. Other consent requirements vary by state.
After signing consent forms, patients receive and often immediately take mifepristone 200 mg orally. Mifepristone is a progesterone receptor antagonist that sensitizes the uterine myometrium to the effects of prostaglandin.11 Rarely, patients may experience symptoms of bleeding or cramping after mifepristone administration alone.
Patients are discharged home with ibuprofen and an antiemetic for symptom relief to be taken around the time of administration of misoprostol. Misoprostol is a synthetic prostaglandin that causes uterine cramping and expulsion of the pregnancy typically within 4 hours of administration. Patients leave with the pills of misoprostol 800 μg (4 tablets, 200 µg each), which they self-administer buccally 24-48 hours after mifepristone administration. A prescription for misoprostol can be given instead of the actual pills, but geographic distance to the pharmacy and other potential barriers should be considered when evaluating the feasibility and convenience of providing pharmacy-dispensed misoprostol.
We instruct patients to place 2 tablets buccally between each gum and cheek, dosing all 4 tablets at the same time. Patients are instructed to let the tablets dissolve buccally and, after 30 minutes, to swallow the tablets with water. Administration of an automatic second dose of misoprostol 3-6 hours after the first dose for pregnancies between 9-11 weeks of gestation is recommended to increase success rate at these later gestational ages.12,13 Several different routes of administration, including buccal, vaginal, and sublingual, have been used for first trimester medication abortion with misoprostol.
Follow up and confirm the results
Patients can safely follow up after their medication abortion in several ways. In our practice, patients are offered 3 possible options.
- The first is ultrasound follow-up, whereby the patient returns to the clinic 1 week after their medication abortion for a pelvic ultrasound to confirm the gestational sac has passed.
- The second method is to test beta-human chorionic gonadotropin (B-hCG) levels. Patients interested in this option have a baseline B-hCG drawn on the day of presentation and follow up 7-10 days later for a repeat B-hCG test. An 80% drop in B-hCG level is consistent with a successful medication abortion.
- The third option, a phone checklist that is usually combined with a urine pregnancy test 4-6 weeks after a medication abortion, is an effective patient-centered approach. The COVID-19 pandemic and the subsequent compulsory shift to providing medical care via telemedicine highlighted the safety, acceptability, and patient preference for the provision of medication abortion using telehealth platforms.14
Outcomes and complications
Medication abortion using a combined regimen of mifepristone followed by misoprostol is approximately 95% effective at complete expulsion of the pregnancy.15,16 Complications after a first trimester medication abortion are rare. In a retrospective cohort study of 54,911 abortions, the most common complication was incomplete abortion.17 Symptoms concerning for incomplete abortion included persistent heavy vaginal bleeding and pelvic cramping. An incomplete or failed abortion should be managed with an additional dose of misoprostol or dilation and evacuation. Other possible complications such as infection are also rare, and prophylactic antibiotics are not encouraged.18
Future fertility and pregnancy implications
Patients should be counseled that a medication abortion is not associated with infertility or increased risk for adverse outcomes in future pregnancies.19 Contraceptive counseling should be provided to all interested patients at the time of a medication abortion and ideally provided to the patient on the day of their visit. Oral contraceptives, the patch, and the ring can be started on the day of misoprostol administration.20 The optimal timing of IUD insertion has been examined in 2 randomized control trials. Results indicated a higher uptake in the group of patients who received their IUD approximately 1 week after medication abortion versus delaying placement for several weeks, with no difference in IUD expulsion rates.21,22 Patients interested in depot-medroxyprogesterone acetate (DMPA) injection should be counseled on the theoretical decreased efficacy of medication abortion in the setting of concurrent DMPA administration. If possible, a follow-up plan should be made so that the patient can receive DMPA, if desired, at a later date.23 The etonogestrel implant (Nexplanon), however, can be placed on the day of mifepristone administration and does not affect the efficacy of a medication abortion.24,25
Summary
During this critical time for reproductive health care, it is essential that ObGyns consider how their professional position and expertise can assist with the provision of medication abortions. Most ObGyn practices already have the resources in place to effectively care for patients before, during, and after a medication abortion. Integrating abortion health care into your practice promotes patient-centered care, continuity, and patient satisfaction. Furthermore, by improving abortion referrals or offering information on safe, self-procured abortion, you can contribute to destigmatizing abortion care, while playing an integral role in connecting your patients with the care they need and desire. ●
- Jones RK, Philbin J, Kirstein M, et al. Long-term decline in US abortions reverses, showing rising need for abortion as Supreme Court is poised to overturn Roe v. Wade. Guttmacher Institute. August 30, 2022. https://www.gut. Accessed November 2, 2022. tmacher.org/article/2022/06 /long-term-decline-us-abortions-reverses-showing-rising -need-abortion-supreme-court.
- Kirstein M, Jones RK, Philbin J. One month post-roe: at least 43 abortion clinics across 11 states have stopped offering abortion care. Guttmacher Institute. September 5, 2022. https://www.guttmacher.org/article/2022/07/one-month -post-roe-least-43-abortion-clinics-across-11-states-have -stopped-offering. Accessed November 2, 2022.
- Jones RK, Nash E, Cross L, et al. Medication abortion now accounts for more than half of all US abortions. Guttmacher Institute. September 12, 2022. https://www.guttmacher.org /article/2022/02/medication-abortion-now-accounts-more-half-all-us-abortions. Accessed November 2, 2022.
- Schreiber CA, Creinin MD, Atrio J, et al. Mifepristone pretreatment for the medical management of early pregnancy loss. N Engl J Med. 2018;378:2161-2170. doi:10.1056/ nejmoa1715726.
- Stulberg DB, Dude AM, Dahlquist I, Curlin, FA. Abortion provision among practicing obstetrician-gynecologists. Obstet Gynecol. 2011;118:609-614. doi:10.1097/aog.0b013e31822ad973.
- Daniel S, Schulkin J, Grossman D. Obstetrician-gynecologist willingness to provide medication abortion with removal of the in-person dispensing requirement for mifepristone. Contraception. 2021;104:73-76. doi:10.1016/j. contraception.2021.03.026.
- Guttmacher Institute. State legislation tracker. Updated October 31, 2022. https://www.guttmacher.org/state-policy. Accessed November 2, 2022.
- Goldberg AB, Fulcher IR, Fortin J, et al. Mifepristone and misoprostol for undesired pregnancy of unknown location. Obstet Gynecol. 2022;139:771-780. doi:10.1097/ aog.0000000000004756.
- The American College of Obstetricians and Gynecologists. Understanding the practical implications of the FDA’s December 2021 mifepristone REMS decision: a Q&A with Dr. Nisha Verma and Vanessa Wellbery. March 28, 2022. https:// www.acog.org/news/news-articles/2022/03/understanding -the-practical-implications-of-the-fdas-december-2021 -mifepristone-rems-decision. Accessed November 2, 2022.
- US Food and Drug Administration. Mifeprex (mifepristone) information. December 16, 2021. https://www.fda.gov/ drugs/postmarket-drug-safety-information-patients-and-providers/ifeprex-mifepristone-information. Accessed November 2, 2022.
- Cadepond F, Ulmann A, Baulieu EE. Ru486 (mifepristone): mechanisms of action and clinical uses. Annu Rev Med. 1997;48:129-156. doi:10.1146/annurev.med.48.1.129.
- Ashok PW, Templeton A, Wagaarachchi PT, Flett GMM. Factors affecting the outcome of early medical abortion: a review of 4132 consecutive cases. BJOG. 2002;109:1281-1289. doi:10.1046/j.1471-0528.2002.02156.x.
- Coyaji K, Krishna U, Ambardekar S, et al. Are two doses of misoprostol after mifepristone for early abortion better than one? BJOG. 2007;114:271-278. doi:10.1111/j.14710528.2006.01208.x.
- Aiken A, Lohr PA, Lord J, et al. Effectiveness, safety and acceptability of no‐test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128:1464-1474. doi:10.1111/14710528.16668.
- Schaff EA, Eisinger SH, Stadalius LS, et al. Low-dose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception. 1999;59:1-6. doi:10.1016/s00107824(98)00150-4.
- Schaff EA, Fielding SL, Westhoff C. Randomized trial of oral versus vaginal misoprostol at one day after mifepristone for early medical abortion. Contraception. 2001;64:81-85. doi:10.1016/s0010-7824(01)00229-3.
- Upadhyay UD, Desai S, Zlidar V, et al. Incidence of emergency department visits and complications after abortion. Obstet Gynecol. 2015;125:175-183. doi:10.1097/ aog.0000000000000603.
- Shannon C, Brothers LP, Philip NM, Winikoff B. Infection after medical abortion: a review of the literature. Contraception. 2004;70:183-190. doi:10.1016/j.contraception.2004.04.009.
- Virk J, Zhang J, Olsen J. Medical abortion and the risk of subsequent adverse pregnancy outcomes. N Engl J Med. 2007;357:648-653. doi:10.1056/nejmoa070445.
- Mittal S. Contraception after medical abortion. Contraception. 2006;74:56-60. doi:10.1016/j.contraception.2006.03.006.
- Shimoni N, Davis A, Ramos ME, et al. Timing of copper intrauterine device insertion after medical abortion. Obstet Gynecol. 2011;118:623-628. doi:10.1097/aog.0b013e31822ade67.
- Sääv I, Stephansson O, Gemzell-Danielsson K. Early versus delayed insertion of intrauterine contraception after medical abortion—a randomized controlled trial. PloS ONE. 2012;7:e48948. doi:10.1371/journal.pone.0048948.
- Raymond EG, Weaver MA, Louie KS, et al. Effects of depot medroxyprogesterone acetate injection timing on medical abortion efficacy and repeat pregnancy: a randomized controlled trial. Obstet Gynecol. 2016;128:739-745. doi:10.1097/aog.0000000000001627.
- Hognert H, Kopp Kallner H, Cameron S, et al. Immediate versus delayed insertion of an etonogestrel releasing implant at medical abortion—a randomized controlled equivalence trial. Hum Reprod. 2016;31:2484-2490. doi:10.1093/humrep/ dew238.
- Raymond EG, Weaver MA, Tan Y-L, et al. Effect of immediate compared with delayed insertion of etonogestrel implants on medical abortion efficacy and repeat pregnancy. Obstet Gynecol. 2016;127:306-312. doi:10.1097/ aog.0000000000001274.

Dr. Wright is Complex Family Planning Fellow, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts.

Dr. Bartz is Associate Professor, Harvard Medical School, Brigham and Women’s Hospital.
The authors report no financial relationships relevant to this article.
Dr. Wright is Complex Family Planning Fellow, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts.
Dr. Bartz is Associate Professor, Harvard Medical School, Brigham and Women’s Hospital.
The authors report no financial relationships relevant to this article.
Dr. Wright is Complex Family Planning Fellow, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts.
Dr. Bartz is Associate Professor, Harvard Medical School, Brigham and Women’s Hospital.
The authors report no financial relationships relevant to this article.
The Supreme Court’s Dobbs decision on June 24, 2022, which nullified the federal protections of Roe v Wade, resulted in the swift and devastating dissolution of access to abortion care for hundreds of thousands of patients in the United States.1 Within days of the decision, 11 states in the South and Midwest implemented complete or 6-week abortion bans that, in part, led to the closure of over half the abortion clinics in these states.2 Abortion bans, severe restrictions, and clinic closures affect all patients and magnify existing health care inequities.
Medication abortion is becoming increasingly popular; as of 2020, approximately 50% of US abortions were performed using this method.3 Through a combination of mifepristone and misoprostol, medication abortion induces the physiologic process and symptoms similar to those of a miscarriage. Notably, this regimen is also the most effective medical management method for a missed abortion in the first trimester, and therefore, should already be incorporated into any general ObGyn practice.4
Although a recent study found that 97% of ObGyn physicians report encountering patients who seek an abortion, only 15% to 25% of them reported providing abortion services.5,6 Given our expertise, ObGyns are well-positioned to incorporate medication abortion into our practices. For those ObGyn providers who practice in states without extreme abortion bans, this article provides guidance on how to incorporate medication abortion into your practice (FIGURE). Several states now have early gestational limits on abortion, and the abortion-dedicated clinics that remain open are over capacity. Therefore, by incorporating medication abortion into your practice you can contribute to timely abortion access for your patients.
Medication abortion: The process
Determine your ability and patient’s eligibility
Abortion-specific laws for your state have now become the first determinant of your ability to provide medication abortion to your patients. The Guttmacher Institute is one reliable source of specific state laws that your practice can reference and is updated regularly.7
From a practice perspective, most ObGyn physicians already have the technical capabilities in place to provide medication abortion. First, you must be able to accurately determine the patient’s gestational age by their last menstrual period, which is often confirmed through ultrasonography.
Medication abortion is safe and routinely used in many practices up to 77 days, or 11 weeks, of gestation. Authors of a recent retrospective cohort study found that medication abortion also may be initiated for a pregnancy of unknown location in patients who are asymptomatic and determined to have low risk for an ectopic pregnancy. In this study, initiation of medication abortion on the day of presentation, with concurrent evaluation for ectopic pregnancy, was associated with a shorter time to a completed abortion, but a lower rate of successful medication abortion when compared with patients who delayed the initiation of medication abortion until a clear intrauterine pregnancy was diagnosed.8
Few medical contraindications exist for patients who seek a medication abortion. These contraindications include allergy to or medication interaction with mifepristone or misoprostol, chronic adrenal failure or long-term corticosteroid therapy, acute porphyria, anemia or the use of anticoagulation therapy, or current intrauterine device (IUD) use.
Continue to: Gather consents and administer treatment...
Gather consents and administer treatment
Historically, mifepristone has been dispensed directly at an ObGyn physician’s office. However, the US Food and Drug Administration (FDA) regulations requiring this were lifted during the COVID-19 pandemic, and as of December 2021, the inperson dispensing requirement was permanently removed.9 To provide mifepristone in a medical practice under current guidelines, a confidential prescriber agreement must be completed once by one person on behalf of the practice. Then each patient must read the manufacturer’s medication guide and sign the patient agreement form as part of the consent process (available on the FDA’s website).10 These agreement forms must be filled out by a physician and each patient if your practice uses mifepristone for any pregnancy indication, including induction of labor or medical management of miscarriage. Given the multiple evidence-based indications for mifepristone in pregnancy, it is hoped that these agreement forms will become a routine part of most ObGyn practices. Other consent requirements vary by state.
After signing consent forms, patients receive and often immediately take mifepristone 200 mg orally. Mifepristone is a progesterone receptor antagonist that sensitizes the uterine myometrium to the effects of prostaglandin.11 Rarely, patients may experience symptoms of bleeding or cramping after mifepristone administration alone.
Patients are discharged home with ibuprofen and an antiemetic for symptom relief to be taken around the time of administration of misoprostol. Misoprostol is a synthetic prostaglandin that causes uterine cramping and expulsion of the pregnancy typically within 4 hours of administration. Patients leave with the pills of misoprostol 800 μg (4 tablets, 200 µg each), which they self-administer buccally 24-48 hours after mifepristone administration. A prescription for misoprostol can be given instead of the actual pills, but geographic distance to the pharmacy and other potential barriers should be considered when evaluating the feasibility and convenience of providing pharmacy-dispensed misoprostol.
We instruct patients to place 2 tablets buccally between each gum and cheek, dosing all 4 tablets at the same time. Patients are instructed to let the tablets dissolve buccally and, after 30 minutes, to swallow the tablets with water. Administration of an automatic second dose of misoprostol 3-6 hours after the first dose for pregnancies between 9-11 weeks of gestation is recommended to increase success rate at these later gestational ages.12,13 Several different routes of administration, including buccal, vaginal, and sublingual, have been used for first trimester medication abortion with misoprostol.
Follow up and confirm the results
Patients can safely follow up after their medication abortion in several ways. In our practice, patients are offered 3 possible options.
- The first is ultrasound follow-up, whereby the patient returns to the clinic 1 week after their medication abortion for a pelvic ultrasound to confirm the gestational sac has passed.
- The second method is to test beta-human chorionic gonadotropin (B-hCG) levels. Patients interested in this option have a baseline B-hCG drawn on the day of presentation and follow up 7-10 days later for a repeat B-hCG test. An 80% drop in B-hCG level is consistent with a successful medication abortion.
- The third option, a phone checklist that is usually combined with a urine pregnancy test 4-6 weeks after a medication abortion, is an effective patient-centered approach. The COVID-19 pandemic and the subsequent compulsory shift to providing medical care via telemedicine highlighted the safety, acceptability, and patient preference for the provision of medication abortion using telehealth platforms.14
Outcomes and complications
Medication abortion using a combined regimen of mifepristone followed by misoprostol is approximately 95% effective at complete expulsion of the pregnancy.15,16 Complications after a first trimester medication abortion are rare. In a retrospective cohort study of 54,911 abortions, the most common complication was incomplete abortion.17 Symptoms concerning for incomplete abortion included persistent heavy vaginal bleeding and pelvic cramping. An incomplete or failed abortion should be managed with an additional dose of misoprostol or dilation and evacuation. Other possible complications such as infection are also rare, and prophylactic antibiotics are not encouraged.18
Future fertility and pregnancy implications
Patients should be counseled that a medication abortion is not associated with infertility or increased risk for adverse outcomes in future pregnancies.19 Contraceptive counseling should be provided to all interested patients at the time of a medication abortion and ideally provided to the patient on the day of their visit. Oral contraceptives, the patch, and the ring can be started on the day of misoprostol administration.20 The optimal timing of IUD insertion has been examined in 2 randomized control trials. Results indicated a higher uptake in the group of patients who received their IUD approximately 1 week after medication abortion versus delaying placement for several weeks, with no difference in IUD expulsion rates.21,22 Patients interested in depot-medroxyprogesterone acetate (DMPA) injection should be counseled on the theoretical decreased efficacy of medication abortion in the setting of concurrent DMPA administration. If possible, a follow-up plan should be made so that the patient can receive DMPA, if desired, at a later date.23 The etonogestrel implant (Nexplanon), however, can be placed on the day of mifepristone administration and does not affect the efficacy of a medication abortion.24,25
Summary
During this critical time for reproductive health care, it is essential that ObGyns consider how their professional position and expertise can assist with the provision of medication abortions. Most ObGyn practices already have the resources in place to effectively care for patients before, during, and after a medication abortion. Integrating abortion health care into your practice promotes patient-centered care, continuity, and patient satisfaction. Furthermore, by improving abortion referrals or offering information on safe, self-procured abortion, you can contribute to destigmatizing abortion care, while playing an integral role in connecting your patients with the care they need and desire. ●
The Supreme Court’s Dobbs decision on June 24, 2022, which nullified the federal protections of Roe v Wade, resulted in the swift and devastating dissolution of access to abortion care for hundreds of thousands of patients in the United States.1 Within days of the decision, 11 states in the South and Midwest implemented complete or 6-week abortion bans that, in part, led to the closure of over half the abortion clinics in these states.2 Abortion bans, severe restrictions, and clinic closures affect all patients and magnify existing health care inequities.
Medication abortion is becoming increasingly popular; as of 2020, approximately 50% of US abortions were performed using this method.3 Through a combination of mifepristone and misoprostol, medication abortion induces the physiologic process and symptoms similar to those of a miscarriage. Notably, this regimen is also the most effective medical management method for a missed abortion in the first trimester, and therefore, should already be incorporated into any general ObGyn practice.4
Although a recent study found that 97% of ObGyn physicians report encountering patients who seek an abortion, only 15% to 25% of them reported providing abortion services.5,6 Given our expertise, ObGyns are well-positioned to incorporate medication abortion into our practices. For those ObGyn providers who practice in states without extreme abortion bans, this article provides guidance on how to incorporate medication abortion into your practice (FIGURE). Several states now have early gestational limits on abortion, and the abortion-dedicated clinics that remain open are over capacity. Therefore, by incorporating medication abortion into your practice you can contribute to timely abortion access for your patients.
Medication abortion: The process
Determine your ability and patient’s eligibility
Abortion-specific laws for your state have now become the first determinant of your ability to provide medication abortion to your patients. The Guttmacher Institute is one reliable source of specific state laws that your practice can reference and is updated regularly.7
From a practice perspective, most ObGyn physicians already have the technical capabilities in place to provide medication abortion. First, you must be able to accurately determine the patient’s gestational age by their last menstrual period, which is often confirmed through ultrasonography.
Medication abortion is safe and routinely used in many practices up to 77 days, or 11 weeks, of gestation. Authors of a recent retrospective cohort study found that medication abortion also may be initiated for a pregnancy of unknown location in patients who are asymptomatic and determined to have low risk for an ectopic pregnancy. In this study, initiation of medication abortion on the day of presentation, with concurrent evaluation for ectopic pregnancy, was associated with a shorter time to a completed abortion, but a lower rate of successful medication abortion when compared with patients who delayed the initiation of medication abortion until a clear intrauterine pregnancy was diagnosed.8
Few medical contraindications exist for patients who seek a medication abortion. These contraindications include allergy to or medication interaction with mifepristone or misoprostol, chronic adrenal failure or long-term corticosteroid therapy, acute porphyria, anemia or the use of anticoagulation therapy, or current intrauterine device (IUD) use.
Continue to: Gather consents and administer treatment...
Gather consents and administer treatment
Historically, mifepristone has been dispensed directly at an ObGyn physician’s office. However, the US Food and Drug Administration (FDA) regulations requiring this were lifted during the COVID-19 pandemic, and as of December 2021, the inperson dispensing requirement was permanently removed.9 To provide mifepristone in a medical practice under current guidelines, a confidential prescriber agreement must be completed once by one person on behalf of the practice. Then each patient must read the manufacturer’s medication guide and sign the patient agreement form as part of the consent process (available on the FDA’s website).10 These agreement forms must be filled out by a physician and each patient if your practice uses mifepristone for any pregnancy indication, including induction of labor or medical management of miscarriage. Given the multiple evidence-based indications for mifepristone in pregnancy, it is hoped that these agreement forms will become a routine part of most ObGyn practices. Other consent requirements vary by state.
After signing consent forms, patients receive and often immediately take mifepristone 200 mg orally. Mifepristone is a progesterone receptor antagonist that sensitizes the uterine myometrium to the effects of prostaglandin.11 Rarely, patients may experience symptoms of bleeding or cramping after mifepristone administration alone.
Patients are discharged home with ibuprofen and an antiemetic for symptom relief to be taken around the time of administration of misoprostol. Misoprostol is a synthetic prostaglandin that causes uterine cramping and expulsion of the pregnancy typically within 4 hours of administration. Patients leave with the pills of misoprostol 800 μg (4 tablets, 200 µg each), which they self-administer buccally 24-48 hours after mifepristone administration. A prescription for misoprostol can be given instead of the actual pills, but geographic distance to the pharmacy and other potential barriers should be considered when evaluating the feasibility and convenience of providing pharmacy-dispensed misoprostol.
We instruct patients to place 2 tablets buccally between each gum and cheek, dosing all 4 tablets at the same time. Patients are instructed to let the tablets dissolve buccally and, after 30 minutes, to swallow the tablets with water. Administration of an automatic second dose of misoprostol 3-6 hours after the first dose for pregnancies between 9-11 weeks of gestation is recommended to increase success rate at these later gestational ages.12,13 Several different routes of administration, including buccal, vaginal, and sublingual, have been used for first trimester medication abortion with misoprostol.
Follow up and confirm the results
Patients can safely follow up after their medication abortion in several ways. In our practice, patients are offered 3 possible options.
- The first is ultrasound follow-up, whereby the patient returns to the clinic 1 week after their medication abortion for a pelvic ultrasound to confirm the gestational sac has passed.
- The second method is to test beta-human chorionic gonadotropin (B-hCG) levels. Patients interested in this option have a baseline B-hCG drawn on the day of presentation and follow up 7-10 days later for a repeat B-hCG test. An 80% drop in B-hCG level is consistent with a successful medication abortion.
- The third option, a phone checklist that is usually combined with a urine pregnancy test 4-6 weeks after a medication abortion, is an effective patient-centered approach. The COVID-19 pandemic and the subsequent compulsory shift to providing medical care via telemedicine highlighted the safety, acceptability, and patient preference for the provision of medication abortion using telehealth platforms.14
Outcomes and complications
Medication abortion using a combined regimen of mifepristone followed by misoprostol is approximately 95% effective at complete expulsion of the pregnancy.15,16 Complications after a first trimester medication abortion are rare. In a retrospective cohort study of 54,911 abortions, the most common complication was incomplete abortion.17 Symptoms concerning for incomplete abortion included persistent heavy vaginal bleeding and pelvic cramping. An incomplete or failed abortion should be managed with an additional dose of misoprostol or dilation and evacuation. Other possible complications such as infection are also rare, and prophylactic antibiotics are not encouraged.18
Future fertility and pregnancy implications
Patients should be counseled that a medication abortion is not associated with infertility or increased risk for adverse outcomes in future pregnancies.19 Contraceptive counseling should be provided to all interested patients at the time of a medication abortion and ideally provided to the patient on the day of their visit. Oral contraceptives, the patch, and the ring can be started on the day of misoprostol administration.20 The optimal timing of IUD insertion has been examined in 2 randomized control trials. Results indicated a higher uptake in the group of patients who received their IUD approximately 1 week after medication abortion versus delaying placement for several weeks, with no difference in IUD expulsion rates.21,22 Patients interested in depot-medroxyprogesterone acetate (DMPA) injection should be counseled on the theoretical decreased efficacy of medication abortion in the setting of concurrent DMPA administration. If possible, a follow-up plan should be made so that the patient can receive DMPA, if desired, at a later date.23 The etonogestrel implant (Nexplanon), however, can be placed on the day of mifepristone administration and does not affect the efficacy of a medication abortion.24,25
Summary
During this critical time for reproductive health care, it is essential that ObGyns consider how their professional position and expertise can assist with the provision of medication abortions. Most ObGyn practices already have the resources in place to effectively care for patients before, during, and after a medication abortion. Integrating abortion health care into your practice promotes patient-centered care, continuity, and patient satisfaction. Furthermore, by improving abortion referrals or offering information on safe, self-procured abortion, you can contribute to destigmatizing abortion care, while playing an integral role in connecting your patients with the care they need and desire. ●
- Jones RK, Philbin J, Kirstein M, et al. Long-term decline in US abortions reverses, showing rising need for abortion as Supreme Court is poised to overturn Roe v. Wade. Guttmacher Institute. August 30, 2022. https://www.gut. Accessed November 2, 2022. tmacher.org/article/2022/06 /long-term-decline-us-abortions-reverses-showing-rising -need-abortion-supreme-court.
- Kirstein M, Jones RK, Philbin J. One month post-roe: at least 43 abortion clinics across 11 states have stopped offering abortion care. Guttmacher Institute. September 5, 2022. https://www.guttmacher.org/article/2022/07/one-month -post-roe-least-43-abortion-clinics-across-11-states-have -stopped-offering. Accessed November 2, 2022.
- Jones RK, Nash E, Cross L, et al. Medication abortion now accounts for more than half of all US abortions. Guttmacher Institute. September 12, 2022. https://www.guttmacher.org /article/2022/02/medication-abortion-now-accounts-more-half-all-us-abortions. Accessed November 2, 2022.
- Schreiber CA, Creinin MD, Atrio J, et al. Mifepristone pretreatment for the medical management of early pregnancy loss. N Engl J Med. 2018;378:2161-2170. doi:10.1056/ nejmoa1715726.
- Stulberg DB, Dude AM, Dahlquist I, Curlin, FA. Abortion provision among practicing obstetrician-gynecologists. Obstet Gynecol. 2011;118:609-614. doi:10.1097/aog.0b013e31822ad973.
- Daniel S, Schulkin J, Grossman D. Obstetrician-gynecologist willingness to provide medication abortion with removal of the in-person dispensing requirement for mifepristone. Contraception. 2021;104:73-76. doi:10.1016/j. contraception.2021.03.026.
- Guttmacher Institute. State legislation tracker. Updated October 31, 2022. https://www.guttmacher.org/state-policy. Accessed November 2, 2022.
- Goldberg AB, Fulcher IR, Fortin J, et al. Mifepristone and misoprostol for undesired pregnancy of unknown location. Obstet Gynecol. 2022;139:771-780. doi:10.1097/ aog.0000000000004756.
- The American College of Obstetricians and Gynecologists. Understanding the practical implications of the FDA’s December 2021 mifepristone REMS decision: a Q&A with Dr. Nisha Verma and Vanessa Wellbery. March 28, 2022. https:// www.acog.org/news/news-articles/2022/03/understanding -the-practical-implications-of-the-fdas-december-2021 -mifepristone-rems-decision. Accessed November 2, 2022.
- US Food and Drug Administration. Mifeprex (mifepristone) information. December 16, 2021. https://www.fda.gov/ drugs/postmarket-drug-safety-information-patients-and-providers/ifeprex-mifepristone-information. Accessed November 2, 2022.
- Cadepond F, Ulmann A, Baulieu EE. Ru486 (mifepristone): mechanisms of action and clinical uses. Annu Rev Med. 1997;48:129-156. doi:10.1146/annurev.med.48.1.129.
- Ashok PW, Templeton A, Wagaarachchi PT, Flett GMM. Factors affecting the outcome of early medical abortion: a review of 4132 consecutive cases. BJOG. 2002;109:1281-1289. doi:10.1046/j.1471-0528.2002.02156.x.
- Coyaji K, Krishna U, Ambardekar S, et al. Are two doses of misoprostol after mifepristone for early abortion better than one? BJOG. 2007;114:271-278. doi:10.1111/j.14710528.2006.01208.x.
- Aiken A, Lohr PA, Lord J, et al. Effectiveness, safety and acceptability of no‐test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128:1464-1474. doi:10.1111/14710528.16668.
- Schaff EA, Eisinger SH, Stadalius LS, et al. Low-dose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception. 1999;59:1-6. doi:10.1016/s00107824(98)00150-4.
- Schaff EA, Fielding SL, Westhoff C. Randomized trial of oral versus vaginal misoprostol at one day after mifepristone for early medical abortion. Contraception. 2001;64:81-85. doi:10.1016/s0010-7824(01)00229-3.
- Upadhyay UD, Desai S, Zlidar V, et al. Incidence of emergency department visits and complications after abortion. Obstet Gynecol. 2015;125:175-183. doi:10.1097/ aog.0000000000000603.
- Shannon C, Brothers LP, Philip NM, Winikoff B. Infection after medical abortion: a review of the literature. Contraception. 2004;70:183-190. doi:10.1016/j.contraception.2004.04.009.
- Virk J, Zhang J, Olsen J. Medical abortion and the risk of subsequent adverse pregnancy outcomes. N Engl J Med. 2007;357:648-653. doi:10.1056/nejmoa070445.
- Mittal S. Contraception after medical abortion. Contraception. 2006;74:56-60. doi:10.1016/j.contraception.2006.03.006.
- Shimoni N, Davis A, Ramos ME, et al. Timing of copper intrauterine device insertion after medical abortion. Obstet Gynecol. 2011;118:623-628. doi:10.1097/aog.0b013e31822ade67.
- Sääv I, Stephansson O, Gemzell-Danielsson K. Early versus delayed insertion of intrauterine contraception after medical abortion—a randomized controlled trial. PloS ONE. 2012;7:e48948. doi:10.1371/journal.pone.0048948.
- Raymond EG, Weaver MA, Louie KS, et al. Effects of depot medroxyprogesterone acetate injection timing on medical abortion efficacy and repeat pregnancy: a randomized controlled trial. Obstet Gynecol. 2016;128:739-745. doi:10.1097/aog.0000000000001627.
- Hognert H, Kopp Kallner H, Cameron S, et al. Immediate versus delayed insertion of an etonogestrel releasing implant at medical abortion—a randomized controlled equivalence trial. Hum Reprod. 2016;31:2484-2490. doi:10.1093/humrep/ dew238.
- Raymond EG, Weaver MA, Tan Y-L, et al. Effect of immediate compared with delayed insertion of etonogestrel implants on medical abortion efficacy and repeat pregnancy. Obstet Gynecol. 2016;127:306-312. doi:10.1097/ aog.0000000000001274.
- Jones RK, Philbin J, Kirstein M, et al. Long-term decline in US abortions reverses, showing rising need for abortion as Supreme Court is poised to overturn Roe v. Wade. Guttmacher Institute. August 30, 2022. https://www.gut. Accessed November 2, 2022. tmacher.org/article/2022/06 /long-term-decline-us-abortions-reverses-showing-rising -need-abortion-supreme-court.
- Kirstein M, Jones RK, Philbin J. One month post-roe: at least 43 abortion clinics across 11 states have stopped offering abortion care. Guttmacher Institute. September 5, 2022. https://www.guttmacher.org/article/2022/07/one-month -post-roe-least-43-abortion-clinics-across-11-states-have -stopped-offering. Accessed November 2, 2022.
- Jones RK, Nash E, Cross L, et al. Medication abortion now accounts for more than half of all US abortions. Guttmacher Institute. September 12, 2022. https://www.guttmacher.org /article/2022/02/medication-abortion-now-accounts-more-half-all-us-abortions. Accessed November 2, 2022.
- Schreiber CA, Creinin MD, Atrio J, et al. Mifepristone pretreatment for the medical management of early pregnancy loss. N Engl J Med. 2018;378:2161-2170. doi:10.1056/ nejmoa1715726.
- Stulberg DB, Dude AM, Dahlquist I, Curlin, FA. Abortion provision among practicing obstetrician-gynecologists. Obstet Gynecol. 2011;118:609-614. doi:10.1097/aog.0b013e31822ad973.
- Daniel S, Schulkin J, Grossman D. Obstetrician-gynecologist willingness to provide medication abortion with removal of the in-person dispensing requirement for mifepristone. Contraception. 2021;104:73-76. doi:10.1016/j. contraception.2021.03.026.
- Guttmacher Institute. State legislation tracker. Updated October 31, 2022. https://www.guttmacher.org/state-policy. Accessed November 2, 2022.
- Goldberg AB, Fulcher IR, Fortin J, et al. Mifepristone and misoprostol for undesired pregnancy of unknown location. Obstet Gynecol. 2022;139:771-780. doi:10.1097/ aog.0000000000004756.
- The American College of Obstetricians and Gynecologists. Understanding the practical implications of the FDA’s December 2021 mifepristone REMS decision: a Q&A with Dr. Nisha Verma and Vanessa Wellbery. March 28, 2022. https:// www.acog.org/news/news-articles/2022/03/understanding -the-practical-implications-of-the-fdas-december-2021 -mifepristone-rems-decision. Accessed November 2, 2022.
- US Food and Drug Administration. Mifeprex (mifepristone) information. December 16, 2021. https://www.fda.gov/ drugs/postmarket-drug-safety-information-patients-and-providers/ifeprex-mifepristone-information. Accessed November 2, 2022.
- Cadepond F, Ulmann A, Baulieu EE. Ru486 (mifepristone): mechanisms of action and clinical uses. Annu Rev Med. 1997;48:129-156. doi:10.1146/annurev.med.48.1.129.
- Ashok PW, Templeton A, Wagaarachchi PT, Flett GMM. Factors affecting the outcome of early medical abortion: a review of 4132 consecutive cases. BJOG. 2002;109:1281-1289. doi:10.1046/j.1471-0528.2002.02156.x.
- Coyaji K, Krishna U, Ambardekar S, et al. Are two doses of misoprostol after mifepristone for early abortion better than one? BJOG. 2007;114:271-278. doi:10.1111/j.14710528.2006.01208.x.
- Aiken A, Lohr PA, Lord J, et al. Effectiveness, safety and acceptability of no‐test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128:1464-1474. doi:10.1111/14710528.16668.
- Schaff EA, Eisinger SH, Stadalius LS, et al. Low-dose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception. 1999;59:1-6. doi:10.1016/s00107824(98)00150-4.
- Schaff EA, Fielding SL, Westhoff C. Randomized trial of oral versus vaginal misoprostol at one day after mifepristone for early medical abortion. Contraception. 2001;64:81-85. doi:10.1016/s0010-7824(01)00229-3.
- Upadhyay UD, Desai S, Zlidar V, et al. Incidence of emergency department visits and complications after abortion. Obstet Gynecol. 2015;125:175-183. doi:10.1097/ aog.0000000000000603.
- Shannon C, Brothers LP, Philip NM, Winikoff B. Infection after medical abortion: a review of the literature. Contraception. 2004;70:183-190. doi:10.1016/j.contraception.2004.04.009.
- Virk J, Zhang J, Olsen J. Medical abortion and the risk of subsequent adverse pregnancy outcomes. N Engl J Med. 2007;357:648-653. doi:10.1056/nejmoa070445.
- Mittal S. Contraception after medical abortion. Contraception. 2006;74:56-60. doi:10.1016/j.contraception.2006.03.006.
- Shimoni N, Davis A, Ramos ME, et al. Timing of copper intrauterine device insertion after medical abortion. Obstet Gynecol. 2011;118:623-628. doi:10.1097/aog.0b013e31822ade67.
- Sääv I, Stephansson O, Gemzell-Danielsson K. Early versus delayed insertion of intrauterine contraception after medical abortion—a randomized controlled trial. PloS ONE. 2012;7:e48948. doi:10.1371/journal.pone.0048948.
- Raymond EG, Weaver MA, Louie KS, et al. Effects of depot medroxyprogesterone acetate injection timing on medical abortion efficacy and repeat pregnancy: a randomized controlled trial. Obstet Gynecol. 2016;128:739-745. doi:10.1097/aog.0000000000001627.
- Hognert H, Kopp Kallner H, Cameron S, et al. Immediate versus delayed insertion of an etonogestrel releasing implant at medical abortion—a randomized controlled equivalence trial. Hum Reprod. 2016;31:2484-2490. doi:10.1093/humrep/ dew238.
- Raymond EG, Weaver MA, Tan Y-L, et al. Effect of immediate compared with delayed insertion of etonogestrel implants on medical abortion efficacy and repeat pregnancy. Obstet Gynecol. 2016;127:306-312. doi:10.1097/ aog.0000000000001274.
Global effort needed to widen access to HSCT
The use of HSCT, the main curative option for AML, “remains unacceptably low,” commented Molly Tokaz, MD, a hematology/oncology fellow at the Fred Hutchinson Cancer Center, Seattle.
She was presenting the findings from a study of worldwide HSCT utilization at the annual meeting of the American Society of Hematology.
Globally, the incidence of AML has increased 16.2% – from 101,867 cases in 2009 to 118,404 in 2016, she noted. This in turn has led to a 54.9% increase in the worldwide use of HSCT for AML, from 9,659 to 14,965 transplants per year over the same period.
North America and Europe have the highest utilization rates of allogeneic HSCT for AML, but even so, fewer than 40% of patients have the procedure, raising a “question of how [well] we are prioritizing the use of HSCT, even in these resource-abundant health systems,” Dr. Tokaz said.
Meanwhile, in Africa, South America, and the Eastern Mediterranean, fewer than 5% of AML patients undergo transplant. Although “resource-constrained regions have the largest growth in HSCT use” in recent years, utilization rates remain abysmally low, “which has profound effects on the expected outcomes for patients in these regions,” she said.
Overall, “patients from lower- and middle-income countries face substantial barriers to accessing stem cell transplantation for AML,” commented Chancellor Donald, MD, a hematologist/oncologist at Tulane University, New Orleans, who moderated the session.
The “stark regional differences” illustrate “inequities in the delivery of stem cell transplants” but also opportunities “to improve access to this potentially curative treatment,” he said.
The goal of the study was to establish a global baseline of HSCT utilization to help focus future expansion efforts aimed at closing regional access gaps. It shows there is much work to be done, Dr. Tokaz said.
An international effort is needed to address the issue, including better data collection, implementation of regional HSCT programs, increased representation of ethnic and racial minorities in international donor registries, and other measures. In many cases, telemedicine can help with sharing cross-border expertise.
In short, what’s needed is a “comprehensive global effort to improve outcomes for patients with AML” worldwide, Dr. Tokaz said.
Timing of transplant is similar across regions, generally coming during the first complete remission, and there’s also been a global shift toward collecting stem cells from peripheral blood.
There has also been a marked shift away from autologous procedures and toward allogeneic transplants, she said.
A key difference between regions, however, is that while more than half of transplants are from unrelated donors in Europe and North America, almost all are from related donors in Africa and the Eastern Mediterranean, with an increasing proportion of haploidentical donors. In addition, the majority of transplants in Asia, the western Pacific, and South America are from related donors.
The use of related donors has implications for HSCT treatment algorithms and outcomes, Dr. Tokaz said.
The estimates of AML incidence were obtained from the 2019 Global Burden of Disease study. Data on HSCT utilization came from the Worldwide Network for Blood and Marrow Transplantation. No funding source was reported. Dr. Tokaz reports no relevant financial relationships, but some co-authors had numerous industry ties. Dr. Donald reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The use of HSCT, the main curative option for AML, “remains unacceptably low,” commented Molly Tokaz, MD, a hematology/oncology fellow at the Fred Hutchinson Cancer Center, Seattle.
She was presenting the findings from a study of worldwide HSCT utilization at the annual meeting of the American Society of Hematology.
Globally, the incidence of AML has increased 16.2% – from 101,867 cases in 2009 to 118,404 in 2016, she noted. This in turn has led to a 54.9% increase in the worldwide use of HSCT for AML, from 9,659 to 14,965 transplants per year over the same period.
North America and Europe have the highest utilization rates of allogeneic HSCT for AML, but even so, fewer than 40% of patients have the procedure, raising a “question of how [well] we are prioritizing the use of HSCT, even in these resource-abundant health systems,” Dr. Tokaz said.
Meanwhile, in Africa, South America, and the Eastern Mediterranean, fewer than 5% of AML patients undergo transplant. Although “resource-constrained regions have the largest growth in HSCT use” in recent years, utilization rates remain abysmally low, “which has profound effects on the expected outcomes for patients in these regions,” she said.
Overall, “patients from lower- and middle-income countries face substantial barriers to accessing stem cell transplantation for AML,” commented Chancellor Donald, MD, a hematologist/oncologist at Tulane University, New Orleans, who moderated the session.
The “stark regional differences” illustrate “inequities in the delivery of stem cell transplants” but also opportunities “to improve access to this potentially curative treatment,” he said.
The goal of the study was to establish a global baseline of HSCT utilization to help focus future expansion efforts aimed at closing regional access gaps. It shows there is much work to be done, Dr. Tokaz said.
An international effort is needed to address the issue, including better data collection, implementation of regional HSCT programs, increased representation of ethnic and racial minorities in international donor registries, and other measures. In many cases, telemedicine can help with sharing cross-border expertise.
In short, what’s needed is a “comprehensive global effort to improve outcomes for patients with AML” worldwide, Dr. Tokaz said.
Timing of transplant is similar across regions, generally coming during the first complete remission, and there’s also been a global shift toward collecting stem cells from peripheral blood.
There has also been a marked shift away from autologous procedures and toward allogeneic transplants, she said.
A key difference between regions, however, is that while more than half of transplants are from unrelated donors in Europe and North America, almost all are from related donors in Africa and the Eastern Mediterranean, with an increasing proportion of haploidentical donors. In addition, the majority of transplants in Asia, the western Pacific, and South America are from related donors.
The use of related donors has implications for HSCT treatment algorithms and outcomes, Dr. Tokaz said.
The estimates of AML incidence were obtained from the 2019 Global Burden of Disease study. Data on HSCT utilization came from the Worldwide Network for Blood and Marrow Transplantation. No funding source was reported. Dr. Tokaz reports no relevant financial relationships, but some co-authors had numerous industry ties. Dr. Donald reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The use of HSCT, the main curative option for AML, “remains unacceptably low,” commented Molly Tokaz, MD, a hematology/oncology fellow at the Fred Hutchinson Cancer Center, Seattle.
She was presenting the findings from a study of worldwide HSCT utilization at the annual meeting of the American Society of Hematology.
Globally, the incidence of AML has increased 16.2% – from 101,867 cases in 2009 to 118,404 in 2016, she noted. This in turn has led to a 54.9% increase in the worldwide use of HSCT for AML, from 9,659 to 14,965 transplants per year over the same period.
North America and Europe have the highest utilization rates of allogeneic HSCT for AML, but even so, fewer than 40% of patients have the procedure, raising a “question of how [well] we are prioritizing the use of HSCT, even in these resource-abundant health systems,” Dr. Tokaz said.
Meanwhile, in Africa, South America, and the Eastern Mediterranean, fewer than 5% of AML patients undergo transplant. Although “resource-constrained regions have the largest growth in HSCT use” in recent years, utilization rates remain abysmally low, “which has profound effects on the expected outcomes for patients in these regions,” she said.
Overall, “patients from lower- and middle-income countries face substantial barriers to accessing stem cell transplantation for AML,” commented Chancellor Donald, MD, a hematologist/oncologist at Tulane University, New Orleans, who moderated the session.
The “stark regional differences” illustrate “inequities in the delivery of stem cell transplants” but also opportunities “to improve access to this potentially curative treatment,” he said.
The goal of the study was to establish a global baseline of HSCT utilization to help focus future expansion efforts aimed at closing regional access gaps. It shows there is much work to be done, Dr. Tokaz said.
An international effort is needed to address the issue, including better data collection, implementation of regional HSCT programs, increased representation of ethnic and racial minorities in international donor registries, and other measures. In many cases, telemedicine can help with sharing cross-border expertise.
In short, what’s needed is a “comprehensive global effort to improve outcomes for patients with AML” worldwide, Dr. Tokaz said.
Timing of transplant is similar across regions, generally coming during the first complete remission, and there’s also been a global shift toward collecting stem cells from peripheral blood.
There has also been a marked shift away from autologous procedures and toward allogeneic transplants, she said.
A key difference between regions, however, is that while more than half of transplants are from unrelated donors in Europe and North America, almost all are from related donors in Africa and the Eastern Mediterranean, with an increasing proportion of haploidentical donors. In addition, the majority of transplants in Asia, the western Pacific, and South America are from related donors.
The use of related donors has implications for HSCT treatment algorithms and outcomes, Dr. Tokaz said.
The estimates of AML incidence were obtained from the 2019 Global Burden of Disease study. Data on HSCT utilization came from the Worldwide Network for Blood and Marrow Transplantation. No funding source was reported. Dr. Tokaz reports no relevant financial relationships, but some co-authors had numerous industry ties. Dr. Donald reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASH 2022
Poorly matched stem cell transplants linked to ancestry
There is “an intersectionality between ancestry and socioeconomic status and an association with donor type, with the most vulnerable patients” – those of non-European ancestry with low socioeconomic status (SES), especially people of African ancestry – “receiving the most complex [i.e., human leukocyte antigen (HLA)–disparate] transplants,” said lead investigator Warren Fingrut, MD, a research fellow in the Adult Bone Marrow Transplantation Service at Memorial Sloan Kettering Cancer Center, New York.
“Successful extension of transplant access to minority patients will be contingent on addressing [their] financial hardship,” said Dr. Fingrut, who presented the findings at the meeting.
To better channel support services and ensure that resources are available, he also noted that centers will have to do a better job of identifying patients with financial struggles.
“Household income data is not collected at our center, and neither is it collected at most centers,” hence assessments of SES are based on imperfect surrogates, such as neighborhood poverty by zip code. “Interventions to advance equity will require better SES classifications or detailed recording of household income,” Dr. Fingrut said.
Overall, the study highlights “inequities in the delivery of stem cell transplants,” pointing to opportunities “to improve access to this potentially curative treatment,” said hematologist/oncologist Chancellor Donald, MD, of Tulane University, New Orleans, who moderated the study presentation.
Dr. Donald said that the new research shows “how interactions between racial backgrounds and socioeconomic status relate to the type of allogenic stem cell transplant patients receive.” The team “identified that [people] of non-European ancestry and especially those of low SES, are more likely to receive the most specialized type of allogeneic stem cell transplantation, which notably require the highest level of care,” Dr. Donald said.
The investigators reviewed 372 consecutive adults transplanted at MSKCC from March 2020 to February 2022, mostly for myeloid malignancies.
Thirty-one percent of patients had non-European ancestry, including 11% of African, 9% of Asian, and 8% of White Hispanic descent.
With no information about household income, the team used neighborhood poverty (which affected 5% of patients); Medicaid as the primary insurance (6% of patients), and financial support for living and medical expenses (19%) as surrogates of lower SES. Classification depended largely on what criteria were used, with only 20 patients meeting two criteria and only one patient meeting all three.
Overall, more than half (58%) of non-European ancestry patients received HLA-disparate grafts, compared with 24% of people with European ancestry, including 48% of White Hispanic patients, 58% of Asian patients, and 78% of patients of African decent.
Markers of lower SES were more common among non-European patients. For instance, among people of European ancestry, 4% were on Medicaid and 15% were on financial aid, versus 10% on Medicaid and 29% on financial support among people of other ancestries. Medicaid use (12.5%) and financial aid (42.5%) were highest among patients of African descent.
Among patients who received HLA-disparate grafts, patients of non-European descent were three times more likely to be on Medicaid (12% versus 4%) and more than twice as likely to be on financial support (33% versus 15%).
People of African ancestry who received HLA-disparate grafts had the highest proportions of Medicaid reliance (16%) and financial support (45%).
There is “an intersectionality between ancestry and socioeconomic status and an association with donor type, with the most vulnerable patients” – those of non-European ancestry with low socioeconomic status (SES), especially people of African ancestry – “receiving the most complex [i.e., human leukocyte antigen (HLA)–disparate] transplants,” said lead investigator Warren Fingrut, MD, a research fellow in the Adult Bone Marrow Transplantation Service at Memorial Sloan Kettering Cancer Center, New York.
“Successful extension of transplant access to minority patients will be contingent on addressing [their] financial hardship,” said Dr. Fingrut, who presented the findings at the meeting.
To better channel support services and ensure that resources are available, he also noted that centers will have to do a better job of identifying patients with financial struggles.
“Household income data is not collected at our center, and neither is it collected at most centers,” hence assessments of SES are based on imperfect surrogates, such as neighborhood poverty by zip code. “Interventions to advance equity will require better SES classifications or detailed recording of household income,” Dr. Fingrut said.
Overall, the study highlights “inequities in the delivery of stem cell transplants,” pointing to opportunities “to improve access to this potentially curative treatment,” said hematologist/oncologist Chancellor Donald, MD, of Tulane University, New Orleans, who moderated the study presentation.
Dr. Donald said that the new research shows “how interactions between racial backgrounds and socioeconomic status relate to the type of allogenic stem cell transplant patients receive.” The team “identified that [people] of non-European ancestry and especially those of low SES, are more likely to receive the most specialized type of allogeneic stem cell transplantation, which notably require the highest level of care,” Dr. Donald said.
The investigators reviewed 372 consecutive adults transplanted at MSKCC from March 2020 to February 2022, mostly for myeloid malignancies.
Thirty-one percent of patients had non-European ancestry, including 11% of African, 9% of Asian, and 8% of White Hispanic descent.
With no information about household income, the team used neighborhood poverty (which affected 5% of patients); Medicaid as the primary insurance (6% of patients), and financial support for living and medical expenses (19%) as surrogates of lower SES. Classification depended largely on what criteria were used, with only 20 patients meeting two criteria and only one patient meeting all three.
Overall, more than half (58%) of non-European ancestry patients received HLA-disparate grafts, compared with 24% of people with European ancestry, including 48% of White Hispanic patients, 58% of Asian patients, and 78% of patients of African decent.
Markers of lower SES were more common among non-European patients. For instance, among people of European ancestry, 4% were on Medicaid and 15% were on financial aid, versus 10% on Medicaid and 29% on financial support among people of other ancestries. Medicaid use (12.5%) and financial aid (42.5%) were highest among patients of African descent.
Among patients who received HLA-disparate grafts, patients of non-European descent were three times more likely to be on Medicaid (12% versus 4%) and more than twice as likely to be on financial support (33% versus 15%).
People of African ancestry who received HLA-disparate grafts had the highest proportions of Medicaid reliance (16%) and financial support (45%).
There is “an intersectionality between ancestry and socioeconomic status and an association with donor type, with the most vulnerable patients” – those of non-European ancestry with low socioeconomic status (SES), especially people of African ancestry – “receiving the most complex [i.e., human leukocyte antigen (HLA)–disparate] transplants,” said lead investigator Warren Fingrut, MD, a research fellow in the Adult Bone Marrow Transplantation Service at Memorial Sloan Kettering Cancer Center, New York.
“Successful extension of transplant access to minority patients will be contingent on addressing [their] financial hardship,” said Dr. Fingrut, who presented the findings at the meeting.
To better channel support services and ensure that resources are available, he also noted that centers will have to do a better job of identifying patients with financial struggles.
“Household income data is not collected at our center, and neither is it collected at most centers,” hence assessments of SES are based on imperfect surrogates, such as neighborhood poverty by zip code. “Interventions to advance equity will require better SES classifications or detailed recording of household income,” Dr. Fingrut said.
Overall, the study highlights “inequities in the delivery of stem cell transplants,” pointing to opportunities “to improve access to this potentially curative treatment,” said hematologist/oncologist Chancellor Donald, MD, of Tulane University, New Orleans, who moderated the study presentation.
Dr. Donald said that the new research shows “how interactions between racial backgrounds and socioeconomic status relate to the type of allogenic stem cell transplant patients receive.” The team “identified that [people] of non-European ancestry and especially those of low SES, are more likely to receive the most specialized type of allogeneic stem cell transplantation, which notably require the highest level of care,” Dr. Donald said.
The investigators reviewed 372 consecutive adults transplanted at MSKCC from March 2020 to February 2022, mostly for myeloid malignancies.
Thirty-one percent of patients had non-European ancestry, including 11% of African, 9% of Asian, and 8% of White Hispanic descent.
With no information about household income, the team used neighborhood poverty (which affected 5% of patients); Medicaid as the primary insurance (6% of patients), and financial support for living and medical expenses (19%) as surrogates of lower SES. Classification depended largely on what criteria were used, with only 20 patients meeting two criteria and only one patient meeting all three.
Overall, more than half (58%) of non-European ancestry patients received HLA-disparate grafts, compared with 24% of people with European ancestry, including 48% of White Hispanic patients, 58% of Asian patients, and 78% of patients of African decent.
Markers of lower SES were more common among non-European patients. For instance, among people of European ancestry, 4% were on Medicaid and 15% were on financial aid, versus 10% on Medicaid and 29% on financial support among people of other ancestries. Medicaid use (12.5%) and financial aid (42.5%) were highest among patients of African descent.
Among patients who received HLA-disparate grafts, patients of non-European descent were three times more likely to be on Medicaid (12% versus 4%) and more than twice as likely to be on financial support (33% versus 15%).
People of African ancestry who received HLA-disparate grafts had the highest proportions of Medicaid reliance (16%) and financial support (45%).
FROM ASH 2022
For minorities with PE: Less advanced treatment, more mortality
NEW ORLEANS –
According to the research, released at the annual meeting of the American Society of Hematology, the biggest disparities affected Asian/Pacific Islander patients with PE. While they were the least likely among ethnic groups to be hospitalized for PE, the odds were 53% higher that they’d die in the hospital (adjusted odds ratio, 1.53; 95% confidence interval, 1.32-1.78), and 24% lower that they would get advanced therapies (aOR, 0.76; 95% CI, 0.59-0.98, P values not provided in this study).
“The findings really raise the importance of this research area and call for vigorous future research to try to better identify why we see these patterns and then come up with solutions to solve them,” said hematologist and study coauthor Mary Cushman, MD, of the University of Vermont, Burlington, at an ASH news briefing.

As Dr. Cushman noted, details about disparities in PE care are limited. It’s known that “Black people have a twofold greater mortality from pulmonary embolism compared to other groups, and this is a persistently observed disparity over many years,” she said. However, “little is known about the relationships of social determinants with treatment and course of pulmonary embolism,” she added.
The researchers used data from the Nationwide Inpatient Sample to track 1.1 million U.S. hospitalized patients with PE from 2016 to 2018. PE was the primary diagnosis in 615,570 patients (54.8%), and 66,570 (5.9%) had high-risk PE.
Among ethnic groups, hospitalization rates “differed pretty dramatically,” Dr. Cushman said. The researchers found that Blacks had the highest rate of PE hospitalization (20.1 per 10,000 person-years; 95% CI, 20.0-20.2), followed by Whites (13.1 per 10,000 person-years; 95% CI, 13.1-13.2), Hispanics (6.0 per 10,000 person-years; 95% CI, 5.9-6.1), Native Americans (5.6 per 10,000 person-years, 95% CI, 5.4-5.7) and Asians/Pacific Islanders (3.0 per 10,000 person-years; 95% CI, 2.9-3.1). Overall, the rate was 14.9/10,000 person-years.
With regard to treatment, therapies defined by the researchers as advanced – systemic thrombolysis, catheter-directed therapy, surgical embolectomy, and venoarterial extracorporeal membrane oxygenation – were also less commonly used in treating ethnic minorities.
These treatments were used in 5.5% of all patients, and 19% of those with high-risk PE. After adjusting for nearly 20 factors such as age, sex, and place of residence, researchers found that the odds that a patient would receive advanced treatment were lower in Blacks (aOR, 0.87; 95% CI, 0.81-0.92) and Asians/Pacific Islanders (aOR, 0.76; 95% CI, 0.59-0.98) compared with Whites. The differences in Hispanics and Native Americans were not statistically significant.
As for insurance, those with Medicare and Medicaid were less likely to get advanced treatment vs. those with private insurance (aOR, 0.73; 95% CI, 0.69-0.77 and aOR, 0.68; 95% CI, 0.63-0.74, respectively). Differences among income levels were not statistically significant.
In the hospital, 6.4% of patients with PE died, as did 50% of those with high-risk PE. There was no statistically significant difference in death rates overall between Whites and Blacks or Native Americans. However, Asians/Pacific Islanders had a much higher death rate (aOR, 1.53; 95% CI, 1.32-1.78), as did Hispanics (aOR, 1.10; 95% CI, 1.00-1.22).
Why are Asians/Pacific Islanders at such high risk of death? Dr. Cushman noted that, while their hospitalization rate is low, they are especially likely to present with high-risk PE.
The difference in death rates between patients with Medicare/Medicaid insurance and those with private insurance was not statistically significant. Neither was the difference in death rates among income groups vs. the highest quartile with one exception: The lowest quartile (aOR, 1.09; 95% CI, 1.02-1.17).
As for the reasons for the higher risks among various groups, Dr. Cushman said there are several possible theories. “It could be due to differences in awareness of PE symptoms: They don’t know how ill they are, so they present later in the course. Or they might have less trust in the system, which might lead to delayed care. Or it could be that they have misdiagnosis of PE symptoms when they present initially.”
Alternatively, she noted, the differences “could be rooted in structural racism and other social determinants of health that weren’t measured, such as education level and quality of education.”
In an interview, Dr. Cushman expressed the hope that “clinicians will think about these findings in terms of how they take care of patients and try their best to recognize any unconscious biases that might creep into their approach. In addition, as a society we need more education of the general public about PE. Some of our findings might be caused by delayed care due to lack of recognition of a need to seek care.”
In an interview, University of Pittsburgh vascular surgeon Rabih Chaer, MD, MSc, who didn’t take part in the study, said it relies on a "large dataset which offers valuable information but with limited granularity and follow-up. This limits the accurate categorization of PE severity, as well as comorbidities, all of which impact outcomes and survival.”
For example, Dr. Chaer said, PE treatments can be limited in some patients due to their comorbidities that cause bleeding risk. Still, Dr. Chaer said the findings mesh with his own research that has shown racial disparities in PE treatment and outcomes, including a 2021 study. "While we did not see a difference by race in in-hospital mortality, Black patients hospitalized with PE are younger with a higher severity of disease compared with White patients,” he said. "Although Black patients are less likely to receive an intervention overall, this differed depending on PE severity with higher risk of intervention only for life-threatening PE." And a 2022 study found that “patients with PE from deprived neighborhoods have worse survival beyond the index [first] admission and were more likely to suffer from cardiovascular or PE-related causes of death in the first year after the index pulmonary embolism,” he said.
Dr. Chaer noted that his research team “is actively working on the next steps beyond identifying the fact that there are racial disparities in PE treatment and outcomes. We are fortunate to have access to a large granular database with long-term follow up and are currently reviewing the medical record details to identify causes for disparities and potential solutions.”
Dr. Cushman received funding from the National Institutes of Health. Other study authors report various disclosures. Dr. Chaer has no disclosures.
NEW ORLEANS –
According to the research, released at the annual meeting of the American Society of Hematology, the biggest disparities affected Asian/Pacific Islander patients with PE. While they were the least likely among ethnic groups to be hospitalized for PE, the odds were 53% higher that they’d die in the hospital (adjusted odds ratio, 1.53; 95% confidence interval, 1.32-1.78), and 24% lower that they would get advanced therapies (aOR, 0.76; 95% CI, 0.59-0.98, P values not provided in this study).
“The findings really raise the importance of this research area and call for vigorous future research to try to better identify why we see these patterns and then come up with solutions to solve them,” said hematologist and study coauthor Mary Cushman, MD, of the University of Vermont, Burlington, at an ASH news briefing.
As Dr. Cushman noted, details about disparities in PE care are limited. It’s known that “Black people have a twofold greater mortality from pulmonary embolism compared to other groups, and this is a persistently observed disparity over many years,” she said. However, “little is known about the relationships of social determinants with treatment and course of pulmonary embolism,” she added.
The researchers used data from the Nationwide Inpatient Sample to track 1.1 million U.S. hospitalized patients with PE from 2016 to 2018. PE was the primary diagnosis in 615,570 patients (54.8%), and 66,570 (5.9%) had high-risk PE.
Among ethnic groups, hospitalization rates “differed pretty dramatically,” Dr. Cushman said. The researchers found that Blacks had the highest rate of PE hospitalization (20.1 per 10,000 person-years; 95% CI, 20.0-20.2), followed by Whites (13.1 per 10,000 person-years; 95% CI, 13.1-13.2), Hispanics (6.0 per 10,000 person-years; 95% CI, 5.9-6.1), Native Americans (5.6 per 10,000 person-years, 95% CI, 5.4-5.7) and Asians/Pacific Islanders (3.0 per 10,000 person-years; 95% CI, 2.9-3.1). Overall, the rate was 14.9/10,000 person-years.
With regard to treatment, therapies defined by the researchers as advanced – systemic thrombolysis, catheter-directed therapy, surgical embolectomy, and venoarterial extracorporeal membrane oxygenation – were also less commonly used in treating ethnic minorities.
These treatments were used in 5.5% of all patients, and 19% of those with high-risk PE. After adjusting for nearly 20 factors such as age, sex, and place of residence, researchers found that the odds that a patient would receive advanced treatment were lower in Blacks (aOR, 0.87; 95% CI, 0.81-0.92) and Asians/Pacific Islanders (aOR, 0.76; 95% CI, 0.59-0.98) compared with Whites. The differences in Hispanics and Native Americans were not statistically significant.
As for insurance, those with Medicare and Medicaid were less likely to get advanced treatment vs. those with private insurance (aOR, 0.73; 95% CI, 0.69-0.77 and aOR, 0.68; 95% CI, 0.63-0.74, respectively). Differences among income levels were not statistically significant.
In the hospital, 6.4% of patients with PE died, as did 50% of those with high-risk PE. There was no statistically significant difference in death rates overall between Whites and Blacks or Native Americans. However, Asians/Pacific Islanders had a much higher death rate (aOR, 1.53; 95% CI, 1.32-1.78), as did Hispanics (aOR, 1.10; 95% CI, 1.00-1.22).
Why are Asians/Pacific Islanders at such high risk of death? Dr. Cushman noted that, while their hospitalization rate is low, they are especially likely to present with high-risk PE.
The difference in death rates between patients with Medicare/Medicaid insurance and those with private insurance was not statistically significant. Neither was the difference in death rates among income groups vs. the highest quartile with one exception: The lowest quartile (aOR, 1.09; 95% CI, 1.02-1.17).
As for the reasons for the higher risks among various groups, Dr. Cushman said there are several possible theories. “It could be due to differences in awareness of PE symptoms: They don’t know how ill they are, so they present later in the course. Or they might have less trust in the system, which might lead to delayed care. Or it could be that they have misdiagnosis of PE symptoms when they present initially.”
Alternatively, she noted, the differences “could be rooted in structural racism and other social determinants of health that weren’t measured, such as education level and quality of education.”
In an interview, Dr. Cushman expressed the hope that “clinicians will think about these findings in terms of how they take care of patients and try their best to recognize any unconscious biases that might creep into their approach. In addition, as a society we need more education of the general public about PE. Some of our findings might be caused by delayed care due to lack of recognition of a need to seek care.”
In an interview, University of Pittsburgh vascular surgeon Rabih Chaer, MD, MSc, who didn’t take part in the study, said it relies on a "large dataset which offers valuable information but with limited granularity and follow-up. This limits the accurate categorization of PE severity, as well as comorbidities, all of which impact outcomes and survival.”
For example, Dr. Chaer said, PE treatments can be limited in some patients due to their comorbidities that cause bleeding risk. Still, Dr. Chaer said the findings mesh with his own research that has shown racial disparities in PE treatment and outcomes, including a 2021 study. "While we did not see a difference by race in in-hospital mortality, Black patients hospitalized with PE are younger with a higher severity of disease compared with White patients,” he said. "Although Black patients are less likely to receive an intervention overall, this differed depending on PE severity with higher risk of intervention only for life-threatening PE." And a 2022 study found that “patients with PE from deprived neighborhoods have worse survival beyond the index [first] admission and were more likely to suffer from cardiovascular or PE-related causes of death in the first year after the index pulmonary embolism,” he said.
Dr. Chaer noted that his research team “is actively working on the next steps beyond identifying the fact that there are racial disparities in PE treatment and outcomes. We are fortunate to have access to a large granular database with long-term follow up and are currently reviewing the medical record details to identify causes for disparities and potential solutions.”
Dr. Cushman received funding from the National Institutes of Health. Other study authors report various disclosures. Dr. Chaer has no disclosures.
NEW ORLEANS –
According to the research, released at the annual meeting of the American Society of Hematology, the biggest disparities affected Asian/Pacific Islander patients with PE. While they were the least likely among ethnic groups to be hospitalized for PE, the odds were 53% higher that they’d die in the hospital (adjusted odds ratio, 1.53; 95% confidence interval, 1.32-1.78), and 24% lower that they would get advanced therapies (aOR, 0.76; 95% CI, 0.59-0.98, P values not provided in this study).
“The findings really raise the importance of this research area and call for vigorous future research to try to better identify why we see these patterns and then come up with solutions to solve them,” said hematologist and study coauthor Mary Cushman, MD, of the University of Vermont, Burlington, at an ASH news briefing.
As Dr. Cushman noted, details about disparities in PE care are limited. It’s known that “Black people have a twofold greater mortality from pulmonary embolism compared to other groups, and this is a persistently observed disparity over many years,” she said. However, “little is known about the relationships of social determinants with treatment and course of pulmonary embolism,” she added.
The researchers used data from the Nationwide Inpatient Sample to track 1.1 million U.S. hospitalized patients with PE from 2016 to 2018. PE was the primary diagnosis in 615,570 patients (54.8%), and 66,570 (5.9%) had high-risk PE.
Among ethnic groups, hospitalization rates “differed pretty dramatically,” Dr. Cushman said. The researchers found that Blacks had the highest rate of PE hospitalization (20.1 per 10,000 person-years; 95% CI, 20.0-20.2), followed by Whites (13.1 per 10,000 person-years; 95% CI, 13.1-13.2), Hispanics (6.0 per 10,000 person-years; 95% CI, 5.9-6.1), Native Americans (5.6 per 10,000 person-years, 95% CI, 5.4-5.7) and Asians/Pacific Islanders (3.0 per 10,000 person-years; 95% CI, 2.9-3.1). Overall, the rate was 14.9/10,000 person-years.
With regard to treatment, therapies defined by the researchers as advanced – systemic thrombolysis, catheter-directed therapy, surgical embolectomy, and venoarterial extracorporeal membrane oxygenation – were also less commonly used in treating ethnic minorities.
These treatments were used in 5.5% of all patients, and 19% of those with high-risk PE. After adjusting for nearly 20 factors such as age, sex, and place of residence, researchers found that the odds that a patient would receive advanced treatment were lower in Blacks (aOR, 0.87; 95% CI, 0.81-0.92) and Asians/Pacific Islanders (aOR, 0.76; 95% CI, 0.59-0.98) compared with Whites. The differences in Hispanics and Native Americans were not statistically significant.
As for insurance, those with Medicare and Medicaid were less likely to get advanced treatment vs. those with private insurance (aOR, 0.73; 95% CI, 0.69-0.77 and aOR, 0.68; 95% CI, 0.63-0.74, respectively). Differences among income levels were not statistically significant.
In the hospital, 6.4% of patients with PE died, as did 50% of those with high-risk PE. There was no statistically significant difference in death rates overall between Whites and Blacks or Native Americans. However, Asians/Pacific Islanders had a much higher death rate (aOR, 1.53; 95% CI, 1.32-1.78), as did Hispanics (aOR, 1.10; 95% CI, 1.00-1.22).
Why are Asians/Pacific Islanders at such high risk of death? Dr. Cushman noted that, while their hospitalization rate is low, they are especially likely to present with high-risk PE.
The difference in death rates between patients with Medicare/Medicaid insurance and those with private insurance was not statistically significant. Neither was the difference in death rates among income groups vs. the highest quartile with one exception: The lowest quartile (aOR, 1.09; 95% CI, 1.02-1.17).
As for the reasons for the higher risks among various groups, Dr. Cushman said there are several possible theories. “It could be due to differences in awareness of PE symptoms: They don’t know how ill they are, so they present later in the course. Or they might have less trust in the system, which might lead to delayed care. Or it could be that they have misdiagnosis of PE symptoms when they present initially.”
Alternatively, she noted, the differences “could be rooted in structural racism and other social determinants of health that weren’t measured, such as education level and quality of education.”
In an interview, Dr. Cushman expressed the hope that “clinicians will think about these findings in terms of how they take care of patients and try their best to recognize any unconscious biases that might creep into their approach. In addition, as a society we need more education of the general public about PE. Some of our findings might be caused by delayed care due to lack of recognition of a need to seek care.”
In an interview, University of Pittsburgh vascular surgeon Rabih Chaer, MD, MSc, who didn’t take part in the study, said it relies on a "large dataset which offers valuable information but with limited granularity and follow-up. This limits the accurate categorization of PE severity, as well as comorbidities, all of which impact outcomes and survival.”
For example, Dr. Chaer said, PE treatments can be limited in some patients due to their comorbidities that cause bleeding risk. Still, Dr. Chaer said the findings mesh with his own research that has shown racial disparities in PE treatment and outcomes, including a 2021 study. "While we did not see a difference by race in in-hospital mortality, Black patients hospitalized with PE are younger with a higher severity of disease compared with White patients,” he said. "Although Black patients are less likely to receive an intervention overall, this differed depending on PE severity with higher risk of intervention only for life-threatening PE." And a 2022 study found that “patients with PE from deprived neighborhoods have worse survival beyond the index [first] admission and were more likely to suffer from cardiovascular or PE-related causes of death in the first year after the index pulmonary embolism,” he said.
Dr. Chaer noted that his research team “is actively working on the next steps beyond identifying the fact that there are racial disparities in PE treatment and outcomes. We are fortunate to have access to a large granular database with long-term follow up and are currently reviewing the medical record details to identify causes for disparities and potential solutions.”
Dr. Cushman received funding from the National Institutes of Health. Other study authors report various disclosures. Dr. Chaer has no disclosures.
AT ASH 2022
Randomized trial finds DMARD therapy for RA has a beneficial effect on vascular inflammation, CV risk
Use of a tumor necrosis factor inhibitor (TNFi) or triple therapy with conventional, synthetic disease-modifying antirheumatic drugs (DMARDs) for rheumatoid arthritis have similar beneficial effects in reducing patients’ vascular inflammation and cardiovascular (CV) risk, according to results from a randomized, active comparator trial.
“The good news is, providers can rest assured that aggressive treatment for RA does reduce vascular inflammation and therefore cardiovascular risk,” lead author Daniel H. Solomon, MD, MPH, of Brigham and Women’s Hospital in Boston, told this news organization. “Part of the reason that treating people with potent disease-modifying agents is important is not only because of reductions in pain and improvements in function on the level of arthritis, but also because of the vascular impact.”

The small study, published in Annals of the Rheumatic Diseases, randomly assigned 115 patients with active RA despite methotrexate use to one of two treatment protocols for 24 weeks: addition of a TNFi or triple therapy with the addition of sulfasalazine and hydroxychloroquine. Participants had 18F-fluorodeoxyglucose (FDG)–PET/CT scans at baseline and 24 weeks to assess change in arterial inflammation, measured as an arterial target-to-background ratio (TBR) in the carotid arteries and aorta. The study achieved its outcomes despite a low 56.5% rate of adherence to 80% or more of randomized treatments.
Dr. Solomon said this is the first randomized trial comparing the effects of DMARDs on vascular inflammation in RA. The researchers hypothesized that TNFi would be superior to triple therapy for reducing vascular inflammation. “We found that they both reduced vascular inflammation on PET scanning to the same degree,” Dr. Solomon said.
Study results
In the TNFi group, the mean of the maximum of the TBR in the most diseased segment (MDS) of the index vessel declined from 2.72 to 2.47 for a delta of –0.24. In the triple-therapy patients, MDS declined from 2.62 to 2.43 for a delta of –0.19 (difference in deltas –0.02; 95% confidence interval, –0.19 to 0.15; P = .79).
Dr. Solomon explained the choice of FDG-PET/CT scanning to evaluate vascular inflammation in the study participants. “We know that FDG-PET/CT scanning correlates with CV risk, and we know that treatments like statins that impact CV risk reduce the inflammation as observed on FDG-PET/CT,” he said.
Although the study found no difference between the TNFi and triple therapy in terms of vascular outcomes, the conclusion is “a bit more nuanced,” Dr. Solomon said. “It tells us first that reducing inflammation with different strategies in rheumatoid arthritis can similarly impact vascular inflammation. That’s great news. These are aggressive treatment strategies, so if you can reduce vascular inflammation in a significant manner, that should result in reduced cardiovascular risk over time.”
Although the choice of TNFi or triple therapy may not matter for reducing CV risk, Dr. Solomon said, “It matters that you choose something that’s aggressive and that you use it in people who have active disease. That’s another part of the story: People who have active disease have worse vascular inflammation, which translates into a reduction in cardiovascular risk – but it’s not differentially reduced.”
Underlying mechanisms of CVD in RA
Commenting on the research for this news organization, Lihi Eder, MD, PhD, codirector of the cardio-rheumatology program at Women’s College Hospital in Toronto, said the study findings build on what’s known about some of the underlying mechanisms of cardiovascular diseases in RA and how to optimize treatments to reduce the risk.

“Importantly,” she said, “none of these treatment strategies was superior, suggesting that both treatment options are acceptable when considering cardiovascular risk reduction, in addition to controlling RA activity.”
The strengths of the study are its randomized, controlled design “conducted by a strong team of investigators,” and that it addressed questions relevant to routine practice, said Dr. Eder, who was not involved with the study.
The study’s use of FDG-PET/CT as a surrogate outcome is a limitation, she noted. “Although it would have been very challenging to perform a similar study that will include clinical events as a study outcome.” Another limitation, she said, was the low adherence rate to randomized treatments.
“Additional studies that will compare other modes of action [for example, interleukin-6 inhibitors, Janus kinase inhibitors, anti-CD20 monoclonal antibodies] could broaden our understanding regarding the inflammatory pathways driving CV risk in RA,” Dr. Eder added.
The study received funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. AbbVie and Amgen supplied drugs used in the study. Dr. Solomon disclosed receiving research support from AbbVie, Amgen, CorEvitas, and Moderna, and royalties from UpToDate. Dr. Eder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of a tumor necrosis factor inhibitor (TNFi) or triple therapy with conventional, synthetic disease-modifying antirheumatic drugs (DMARDs) for rheumatoid arthritis have similar beneficial effects in reducing patients’ vascular inflammation and cardiovascular (CV) risk, according to results from a randomized, active comparator trial.
“The good news is, providers can rest assured that aggressive treatment for RA does reduce vascular inflammation and therefore cardiovascular risk,” lead author Daniel H. Solomon, MD, MPH, of Brigham and Women’s Hospital in Boston, told this news organization. “Part of the reason that treating people with potent disease-modifying agents is important is not only because of reductions in pain and improvements in function on the level of arthritis, but also because of the vascular impact.”
The small study, published in Annals of the Rheumatic Diseases, randomly assigned 115 patients with active RA despite methotrexate use to one of two treatment protocols for 24 weeks: addition of a TNFi or triple therapy with the addition of sulfasalazine and hydroxychloroquine. Participants had 18F-fluorodeoxyglucose (FDG)–PET/CT scans at baseline and 24 weeks to assess change in arterial inflammation, measured as an arterial target-to-background ratio (TBR) in the carotid arteries and aorta. The study achieved its outcomes despite a low 56.5% rate of adherence to 80% or more of randomized treatments.
Dr. Solomon said this is the first randomized trial comparing the effects of DMARDs on vascular inflammation in RA. The researchers hypothesized that TNFi would be superior to triple therapy for reducing vascular inflammation. “We found that they both reduced vascular inflammation on PET scanning to the same degree,” Dr. Solomon said.
Study results
In the TNFi group, the mean of the maximum of the TBR in the most diseased segment (MDS) of the index vessel declined from 2.72 to 2.47 for a delta of –0.24. In the triple-therapy patients, MDS declined from 2.62 to 2.43 for a delta of –0.19 (difference in deltas –0.02; 95% confidence interval, –0.19 to 0.15; P = .79).
Dr. Solomon explained the choice of FDG-PET/CT scanning to evaluate vascular inflammation in the study participants. “We know that FDG-PET/CT scanning correlates with CV risk, and we know that treatments like statins that impact CV risk reduce the inflammation as observed on FDG-PET/CT,” he said.
Although the study found no difference between the TNFi and triple therapy in terms of vascular outcomes, the conclusion is “a bit more nuanced,” Dr. Solomon said. “It tells us first that reducing inflammation with different strategies in rheumatoid arthritis can similarly impact vascular inflammation. That’s great news. These are aggressive treatment strategies, so if you can reduce vascular inflammation in a significant manner, that should result in reduced cardiovascular risk over time.”
Although the choice of TNFi or triple therapy may not matter for reducing CV risk, Dr. Solomon said, “It matters that you choose something that’s aggressive and that you use it in people who have active disease. That’s another part of the story: People who have active disease have worse vascular inflammation, which translates into a reduction in cardiovascular risk – but it’s not differentially reduced.”
Underlying mechanisms of CVD in RA
Commenting on the research for this news organization, Lihi Eder, MD, PhD, codirector of the cardio-rheumatology program at Women’s College Hospital in Toronto, said the study findings build on what’s known about some of the underlying mechanisms of cardiovascular diseases in RA and how to optimize treatments to reduce the risk.
“Importantly,” she said, “none of these treatment strategies was superior, suggesting that both treatment options are acceptable when considering cardiovascular risk reduction, in addition to controlling RA activity.”
The strengths of the study are its randomized, controlled design “conducted by a strong team of investigators,” and that it addressed questions relevant to routine practice, said Dr. Eder, who was not involved with the study.
The study’s use of FDG-PET/CT as a surrogate outcome is a limitation, she noted. “Although it would have been very challenging to perform a similar study that will include clinical events as a study outcome.” Another limitation, she said, was the low adherence rate to randomized treatments.
“Additional studies that will compare other modes of action [for example, interleukin-6 inhibitors, Janus kinase inhibitors, anti-CD20 monoclonal antibodies] could broaden our understanding regarding the inflammatory pathways driving CV risk in RA,” Dr. Eder added.
The study received funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. AbbVie and Amgen supplied drugs used in the study. Dr. Solomon disclosed receiving research support from AbbVie, Amgen, CorEvitas, and Moderna, and royalties from UpToDate. Dr. Eder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of a tumor necrosis factor inhibitor (TNFi) or triple therapy with conventional, synthetic disease-modifying antirheumatic drugs (DMARDs) for rheumatoid arthritis have similar beneficial effects in reducing patients’ vascular inflammation and cardiovascular (CV) risk, according to results from a randomized, active comparator trial.
“The good news is, providers can rest assured that aggressive treatment for RA does reduce vascular inflammation and therefore cardiovascular risk,” lead author Daniel H. Solomon, MD, MPH, of Brigham and Women’s Hospital in Boston, told this news organization. “Part of the reason that treating people with potent disease-modifying agents is important is not only because of reductions in pain and improvements in function on the level of arthritis, but also because of the vascular impact.”
The small study, published in Annals of the Rheumatic Diseases, randomly assigned 115 patients with active RA despite methotrexate use to one of two treatment protocols for 24 weeks: addition of a TNFi or triple therapy with the addition of sulfasalazine and hydroxychloroquine. Participants had 18F-fluorodeoxyglucose (FDG)–PET/CT scans at baseline and 24 weeks to assess change in arterial inflammation, measured as an arterial target-to-background ratio (TBR) in the carotid arteries and aorta. The study achieved its outcomes despite a low 56.5% rate of adherence to 80% or more of randomized treatments.
Dr. Solomon said this is the first randomized trial comparing the effects of DMARDs on vascular inflammation in RA. The researchers hypothesized that TNFi would be superior to triple therapy for reducing vascular inflammation. “We found that they both reduced vascular inflammation on PET scanning to the same degree,” Dr. Solomon said.
Study results
In the TNFi group, the mean of the maximum of the TBR in the most diseased segment (MDS) of the index vessel declined from 2.72 to 2.47 for a delta of –0.24. In the triple-therapy patients, MDS declined from 2.62 to 2.43 for a delta of –0.19 (difference in deltas –0.02; 95% confidence interval, –0.19 to 0.15; P = .79).
Dr. Solomon explained the choice of FDG-PET/CT scanning to evaluate vascular inflammation in the study participants. “We know that FDG-PET/CT scanning correlates with CV risk, and we know that treatments like statins that impact CV risk reduce the inflammation as observed on FDG-PET/CT,” he said.
Although the study found no difference between the TNFi and triple therapy in terms of vascular outcomes, the conclusion is “a bit more nuanced,” Dr. Solomon said. “It tells us first that reducing inflammation with different strategies in rheumatoid arthritis can similarly impact vascular inflammation. That’s great news. These are aggressive treatment strategies, so if you can reduce vascular inflammation in a significant manner, that should result in reduced cardiovascular risk over time.”
Although the choice of TNFi or triple therapy may not matter for reducing CV risk, Dr. Solomon said, “It matters that you choose something that’s aggressive and that you use it in people who have active disease. That’s another part of the story: People who have active disease have worse vascular inflammation, which translates into a reduction in cardiovascular risk – but it’s not differentially reduced.”
Underlying mechanisms of CVD in RA
Commenting on the research for this news organization, Lihi Eder, MD, PhD, codirector of the cardio-rheumatology program at Women’s College Hospital in Toronto, said the study findings build on what’s known about some of the underlying mechanisms of cardiovascular diseases in RA and how to optimize treatments to reduce the risk.
“Importantly,” she said, “none of these treatment strategies was superior, suggesting that both treatment options are acceptable when considering cardiovascular risk reduction, in addition to controlling RA activity.”
The strengths of the study are its randomized, controlled design “conducted by a strong team of investigators,” and that it addressed questions relevant to routine practice, said Dr. Eder, who was not involved with the study.
The study’s use of FDG-PET/CT as a surrogate outcome is a limitation, she noted. “Although it would have been very challenging to perform a similar study that will include clinical events as a study outcome.” Another limitation, she said, was the low adherence rate to randomized treatments.
“Additional studies that will compare other modes of action [for example, interleukin-6 inhibitors, Janus kinase inhibitors, anti-CD20 monoclonal antibodies] could broaden our understanding regarding the inflammatory pathways driving CV risk in RA,” Dr. Eder added.
The study received funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. AbbVie and Amgen supplied drugs used in the study. Dr. Solomon disclosed receiving research support from AbbVie, Amgen, CorEvitas, and Moderna, and royalties from UpToDate. Dr. Eder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF THE RHEUMATIC DISEASES
Rheumatology Match Day follows same pattern as previous years
Rheumatology joined six other Medicine specialties that filled more than 95% of fellowship positions in 2022.
The National Resident Matching Program in its 2022 Medicine and Pediatric Specialties Match reported that rheumatology filled 123 of 127 certified programs (96.9%) along with 265 certified positions (97.8%).
Matched applicants for adult rheumatology programs included 40 U.S. foreign applicants (15.1%), 123 MD graduates (46.4%), 66 foreign (24.9%), and 36 DO graduates (13.6%).
A total of 352 applicants showed a preference for this specialty, and 75% matched to the specialty. Another 23% did not match to any program.
2022 was the first year that NRMP combined medical specialties, pediatric specialties, and adolescent medicine fellowship matches into the “Medicine and Pediatric Specialties Match.”
“We engaged the leadership of both pediatrics and internal medicine organizations to work with the NRMP to brainstorm solutions and were successful in combining pediatrics and internal medicine into one fellowship match,” said Jill Fussell, MD, immediate past chair of the Council of Pediatric Subspecialties in a statement. “It was an incredibly rewarding experience to work across pediatrics and internal medicine on behalf of resident well-being to make this collaborative change happen.”
Similar to 2021, pediatric rheumatology didn’t do as well as adult programs, filling just 18 of 32 certified programs (56.3%) and 27 out of 43 certified positions (62.8%). More than 66% of the applicants represented MD graduates. Eight were foreign, and one was a DO graduate.
The 2022 match was the largest on record, comprising 39 subspecialties in internal medicine, pediatrics, addiction, and multidisciplinary specialties. A total of 3,361 programs filled 7,648 (87.7%) of 8,724 positions in 2022. Three specialties – cardiovascular disease, interventional pulmonology, and oncology – filled all their positions offered in the match.
In addition to rheumatology, six other specialties filled 95% or more of their positions. This included clinical cardiac electrophysiology, critical care medicine, endocrinology, gastroenterology, hematology/oncology, and pulmonary/critical care medicine. Allergy and immunology, which accepts applicants from either internal medicine or pediatrics, also filled more than 95% of positions offered.
Matched applicants will start fellowship training in July 2023.
Rheumatology joined six other Medicine specialties that filled more than 95% of fellowship positions in 2022.
The National Resident Matching Program in its 2022 Medicine and Pediatric Specialties Match reported that rheumatology filled 123 of 127 certified programs (96.9%) along with 265 certified positions (97.8%).
Matched applicants for adult rheumatology programs included 40 U.S. foreign applicants (15.1%), 123 MD graduates (46.4%), 66 foreign (24.9%), and 36 DO graduates (13.6%).
A total of 352 applicants showed a preference for this specialty, and 75% matched to the specialty. Another 23% did not match to any program.
2022 was the first year that NRMP combined medical specialties, pediatric specialties, and adolescent medicine fellowship matches into the “Medicine and Pediatric Specialties Match.”
“We engaged the leadership of both pediatrics and internal medicine organizations to work with the NRMP to brainstorm solutions and were successful in combining pediatrics and internal medicine into one fellowship match,” said Jill Fussell, MD, immediate past chair of the Council of Pediatric Subspecialties in a statement. “It was an incredibly rewarding experience to work across pediatrics and internal medicine on behalf of resident well-being to make this collaborative change happen.”
Similar to 2021, pediatric rheumatology didn’t do as well as adult programs, filling just 18 of 32 certified programs (56.3%) and 27 out of 43 certified positions (62.8%). More than 66% of the applicants represented MD graduates. Eight were foreign, and one was a DO graduate.
The 2022 match was the largest on record, comprising 39 subspecialties in internal medicine, pediatrics, addiction, and multidisciplinary specialties. A total of 3,361 programs filled 7,648 (87.7%) of 8,724 positions in 2022. Three specialties – cardiovascular disease, interventional pulmonology, and oncology – filled all their positions offered in the match.
In addition to rheumatology, six other specialties filled 95% or more of their positions. This included clinical cardiac electrophysiology, critical care medicine, endocrinology, gastroenterology, hematology/oncology, and pulmonary/critical care medicine. Allergy and immunology, which accepts applicants from either internal medicine or pediatrics, also filled more than 95% of positions offered.
Matched applicants will start fellowship training in July 2023.
Rheumatology joined six other Medicine specialties that filled more than 95% of fellowship positions in 2022.
The National Resident Matching Program in its 2022 Medicine and Pediatric Specialties Match reported that rheumatology filled 123 of 127 certified programs (96.9%) along with 265 certified positions (97.8%).
Matched applicants for adult rheumatology programs included 40 U.S. foreign applicants (15.1%), 123 MD graduates (46.4%), 66 foreign (24.9%), and 36 DO graduates (13.6%).
A total of 352 applicants showed a preference for this specialty, and 75% matched to the specialty. Another 23% did not match to any program.
2022 was the first year that NRMP combined medical specialties, pediatric specialties, and adolescent medicine fellowship matches into the “Medicine and Pediatric Specialties Match.”
“We engaged the leadership of both pediatrics and internal medicine organizations to work with the NRMP to brainstorm solutions and were successful in combining pediatrics and internal medicine into one fellowship match,” said Jill Fussell, MD, immediate past chair of the Council of Pediatric Subspecialties in a statement. “It was an incredibly rewarding experience to work across pediatrics and internal medicine on behalf of resident well-being to make this collaborative change happen.”
Similar to 2021, pediatric rheumatology didn’t do as well as adult programs, filling just 18 of 32 certified programs (56.3%) and 27 out of 43 certified positions (62.8%). More than 66% of the applicants represented MD graduates. Eight were foreign, and one was a DO graduate.
The 2022 match was the largest on record, comprising 39 subspecialties in internal medicine, pediatrics, addiction, and multidisciplinary specialties. A total of 3,361 programs filled 7,648 (87.7%) of 8,724 positions in 2022. Three specialties – cardiovascular disease, interventional pulmonology, and oncology – filled all their positions offered in the match.
In addition to rheumatology, six other specialties filled 95% or more of their positions. This included clinical cardiac electrophysiology, critical care medicine, endocrinology, gastroenterology, hematology/oncology, and pulmonary/critical care medicine. Allergy and immunology, which accepts applicants from either internal medicine or pediatrics, also filled more than 95% of positions offered.
Matched applicants will start fellowship training in July 2023.
Researchers use AI to diagnose infantile hemangioma
a proof-of-concept study reported.
Early diagnosis of infantile hemangiomas “is essential, as there is a narrow window of opportunity to treat high-risk lesions,” April J. Zhang, MD, and coauthors noted in the study. “AI algorithms optimized for image classification through use of convolutional neural networks have been widely utilized to classify lesions in which images are readily standardized, such as skin cancers and onychomycosis.”
The results were published in Pediatric Dermatology.
Dr. Zhang, of the department of dermatology at the Medical College of Wisconsin, Milwaukee, and colleagues trained a convoluted neural network to diagnose infantile hemangiomas based on clinical images from pediatric dermatology patients treated at Children’s Wisconsin between 2002 and 2019.
They used Microsoft’s ResNet-50, a publicly available network architecture, to train a binary infantile hemangioma classifier to group images as infantile hemangiomas or non–infantile hemangiomas. The team randomly split data from the model into training, validation, and test groups.
The preliminary data set contained 14,811 images, about half of which were facial lesions. The training group of images achieved an accuracy of 61.5%. Next, Dr. Zhang and colleagues limited the data set to facial-only lesions and removed poor-quality images, which left 5,834 images in the final data set: 4,110 infantile hemangiomas and 1,724 non–infantile hemangiomas. This model achieved an overall accuracy of 91.7%, with a sensitivity of 93% and a specificity of 90.5%.
“Our study is the first to demonstrate the applicability of AI in the pediatric dermatology population,” the authors wrote. “With current nationwide shortages in pediatric dermatologists, AI has the potential to improve patient access and outcomes through enhanced rapid diagnostic capabilities.”
They acknowledged certain limitations of the study, including a data set with greater numbers of infantile hemangiomas, compared with non–infantile hemangiomas.
“Random oversampling of the non–infantile hemangioma data set was used to combat this but may lead to model overfitting, where a model performs well on its training data but is unable to generalize to new data,” they wrote. “As infantile hemangiomas are rarely biopsied, expert clinical diagnoses were used as the gold standard without pathologic confirmation.”
The authors reported having no financial disclosures.
a proof-of-concept study reported.
Early diagnosis of infantile hemangiomas “is essential, as there is a narrow window of opportunity to treat high-risk lesions,” April J. Zhang, MD, and coauthors noted in the study. “AI algorithms optimized for image classification through use of convolutional neural networks have been widely utilized to classify lesions in which images are readily standardized, such as skin cancers and onychomycosis.”
The results were published in Pediatric Dermatology.
Dr. Zhang, of the department of dermatology at the Medical College of Wisconsin, Milwaukee, and colleagues trained a convoluted neural network to diagnose infantile hemangiomas based on clinical images from pediatric dermatology patients treated at Children’s Wisconsin between 2002 and 2019.
They used Microsoft’s ResNet-50, a publicly available network architecture, to train a binary infantile hemangioma classifier to group images as infantile hemangiomas or non–infantile hemangiomas. The team randomly split data from the model into training, validation, and test groups.
The preliminary data set contained 14,811 images, about half of which were facial lesions. The training group of images achieved an accuracy of 61.5%. Next, Dr. Zhang and colleagues limited the data set to facial-only lesions and removed poor-quality images, which left 5,834 images in the final data set: 4,110 infantile hemangiomas and 1,724 non–infantile hemangiomas. This model achieved an overall accuracy of 91.7%, with a sensitivity of 93% and a specificity of 90.5%.
“Our study is the first to demonstrate the applicability of AI in the pediatric dermatology population,” the authors wrote. “With current nationwide shortages in pediatric dermatologists, AI has the potential to improve patient access and outcomes through enhanced rapid diagnostic capabilities.”
They acknowledged certain limitations of the study, including a data set with greater numbers of infantile hemangiomas, compared with non–infantile hemangiomas.
“Random oversampling of the non–infantile hemangioma data set was used to combat this but may lead to model overfitting, where a model performs well on its training data but is unable to generalize to new data,” they wrote. “As infantile hemangiomas are rarely biopsied, expert clinical diagnoses were used as the gold standard without pathologic confirmation.”
The authors reported having no financial disclosures.
a proof-of-concept study reported.
Early diagnosis of infantile hemangiomas “is essential, as there is a narrow window of opportunity to treat high-risk lesions,” April J. Zhang, MD, and coauthors noted in the study. “AI algorithms optimized for image classification through use of convolutional neural networks have been widely utilized to classify lesions in which images are readily standardized, such as skin cancers and onychomycosis.”
The results were published in Pediatric Dermatology.
Dr. Zhang, of the department of dermatology at the Medical College of Wisconsin, Milwaukee, and colleagues trained a convoluted neural network to diagnose infantile hemangiomas based on clinical images from pediatric dermatology patients treated at Children’s Wisconsin between 2002 and 2019.
They used Microsoft’s ResNet-50, a publicly available network architecture, to train a binary infantile hemangioma classifier to group images as infantile hemangiomas or non–infantile hemangiomas. The team randomly split data from the model into training, validation, and test groups.
The preliminary data set contained 14,811 images, about half of which were facial lesions. The training group of images achieved an accuracy of 61.5%. Next, Dr. Zhang and colleagues limited the data set to facial-only lesions and removed poor-quality images, which left 5,834 images in the final data set: 4,110 infantile hemangiomas and 1,724 non–infantile hemangiomas. This model achieved an overall accuracy of 91.7%, with a sensitivity of 93% and a specificity of 90.5%.
“Our study is the first to demonstrate the applicability of AI in the pediatric dermatology population,” the authors wrote. “With current nationwide shortages in pediatric dermatologists, AI has the potential to improve patient access and outcomes through enhanced rapid diagnostic capabilities.”
They acknowledged certain limitations of the study, including a data set with greater numbers of infantile hemangiomas, compared with non–infantile hemangiomas.
“Random oversampling of the non–infantile hemangioma data set was used to combat this but may lead to model overfitting, where a model performs well on its training data but is unable to generalize to new data,” they wrote. “As infantile hemangiomas are rarely biopsied, expert clinical diagnoses were used as the gold standard without pathologic confirmation.”
The authors reported having no financial disclosures.
FROM PEDIATRIC DERMATOLOGY