User login
Apremilast Effective in Early PsA With Limited Joint Involvement
Key clinical point: Patients with early oligoarticular psoriatic arthritis (PsA) treated with apremilast vs placebo showed greater disease control and minimal disease activity response with a maximum of one swollen joint and one tender joint count (MDA-Joints).
Major finding: At week 16, a higher proportion of patients receiving apremilast vs placebo achieved MDA-Joints response based on sentinel joints (33.9% vs 16.0%; P = .0008) and total joints (21.3% vs 7.9%; nominal P = .0028). No new safety signals were reported.
Study details: This phase 4 FOREMOST trial included 308 patients with early oligoarticular PsA previously treated with non-steroidal anti-inflammatory drugs or ≥2 conventional synthetic disease-modifying antirheumatic drugs and were randomly assigned to receive apremilast (n = 203) or placebo (n = 105).
Disclosures: This study was funded by Amgen. Five authors declared being employees and owning stocks of Amgen. Several authors have declared other ties with Amgen and other sources.
Source: Gossec L, Coates LC, Gladman DD, et al. Treatment of early oligoarticular psoriatic arthritis with apremilast: Primary outcomes at week 16 from the FOREMOST randomised controlled trial. Ann Rheum Dis. 2024 (Aug 20). doi: 10.1136/ard-2024-225833 Source
Key clinical point: Patients with early oligoarticular psoriatic arthritis (PsA) treated with apremilast vs placebo showed greater disease control and minimal disease activity response with a maximum of one swollen joint and one tender joint count (MDA-Joints).
Major finding: At week 16, a higher proportion of patients receiving apremilast vs placebo achieved MDA-Joints response based on sentinel joints (33.9% vs 16.0%; P = .0008) and total joints (21.3% vs 7.9%; nominal P = .0028). No new safety signals were reported.
Study details: This phase 4 FOREMOST trial included 308 patients with early oligoarticular PsA previously treated with non-steroidal anti-inflammatory drugs or ≥2 conventional synthetic disease-modifying antirheumatic drugs and were randomly assigned to receive apremilast (n = 203) or placebo (n = 105).
Disclosures: This study was funded by Amgen. Five authors declared being employees and owning stocks of Amgen. Several authors have declared other ties with Amgen and other sources.
Source: Gossec L, Coates LC, Gladman DD, et al. Treatment of early oligoarticular psoriatic arthritis with apremilast: Primary outcomes at week 16 from the FOREMOST randomised controlled trial. Ann Rheum Dis. 2024 (Aug 20). doi: 10.1136/ard-2024-225833 Source
Key clinical point: Patients with early oligoarticular psoriatic arthritis (PsA) treated with apremilast vs placebo showed greater disease control and minimal disease activity response with a maximum of one swollen joint and one tender joint count (MDA-Joints).
Major finding: At week 16, a higher proportion of patients receiving apremilast vs placebo achieved MDA-Joints response based on sentinel joints (33.9% vs 16.0%; P = .0008) and total joints (21.3% vs 7.9%; nominal P = .0028). No new safety signals were reported.
Study details: This phase 4 FOREMOST trial included 308 patients with early oligoarticular PsA previously treated with non-steroidal anti-inflammatory drugs or ≥2 conventional synthetic disease-modifying antirheumatic drugs and were randomly assigned to receive apremilast (n = 203) or placebo (n = 105).
Disclosures: This study was funded by Amgen. Five authors declared being employees and owning stocks of Amgen. Several authors have declared other ties with Amgen and other sources.
Source: Gossec L, Coates LC, Gladman DD, et al. Treatment of early oligoarticular psoriatic arthritis with apremilast: Primary outcomes at week 16 from the FOREMOST randomised controlled trial. Ann Rheum Dis. 2024 (Aug 20). doi: 10.1136/ard-2024-225833 Source
First Combined Face and Eye Transplant Performed
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
In a groundbreaking procedure, a team of surgeons from New York University Langone Health successfully performed the first combined face and eye transplant on a patient with extensive craniofacial tissue loss after an electrical accident.
The highly complex surgery lasted for 21 hours and involved more than 140 surgeons, nurses, and other healthcare professionals under the leadership of Eduardo D. Rodriguez. MD. It not only restored the patient’s facial features, but also integrated a functional eyeball, potentially setting a new standard for future treatments in similar cases.
The transplant took place in May 2023, and the case report was published on September 5 this year in JAMA.
The 46-year-old man lost a large part of his craniofacial tissue and his left eyeball. The approach was highly specialized. Advanced microsurgical techniques such as anastomoses of microscopic vessels and delicate suturing techniques were crucial for the transplant’s success.
Moreover, customized surgical devices, specific implants, and tissue manipulation tools were developed specifically for this case, thus ensuring the viability of the transplant and adequate perfusion of the transplanted ocular tissue.
The initial results are encouraging. Retinal arterial perfusion has been maintained, and retinal architecture has been preserved, as demonstrated by optical coherence tomography. Electroretinography confirmed retinal responses to light, suggesting that the transplanted eye may eventually contribute to the patient’s visual perception. These results are comparable to those of previous facial tissue transplants, but with the significant addition of ocular functionality, which is a notable advance.
“The successful revascularization of the transplanted eye achieved in this study may serve as a step toward the goal of globe transplant for restoration of vision,” wrote the authors.
The complexity of the combined transplant required a deep understanding of facial and ocular anatomy, as well as tissue preservation techniques. The surgical team reported significant challenges, including the need to align delicate anatomical structures and ensure immunological compatibility between the donor and recipient. Meticulous planning from donor selection to postoperative follow-up was considered essential to maximize the likelihood of success and minimize the risk for allograft rejection.
The patient will now be continuously monitored and receive treatment with immunosuppressants such as tacrolimus and prednisone, adjusted according to his response to the transplant. According to the researchers, further studies will be needed to assess the long-term functionality of the transplanted eye and its integration with the central nervous system.
Despite being the fifth facial transplant surgery performed under Dr. Rodriguez’s leadership, this is the first record of a whole-eye transplant. “The mere fact that we have successfully performed the first whole-eye transplant along with a face transplant is a tremendous achievement that many believed to be impossible,” the doctor said in a statement. “We have taken a giant step forward and paved the way for the next chapter in vision restoration.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Valsartan May Be as Effective as Propranolol for Preventing Migraines
Key clinical point: Although valsartan is not typically used for migraine treatment, it was found to reduce migraine frequency and severity as effectively as propranolol, and in some instances, more effectively.
Major findings: Valsartan vs propranolol significantly reduced the mean score of migraine frequency and severity (1.82 vs 2.39; P = .042), and a lower rate of grade 3 headaches (0% vs 7.14%; P = .029) and a lower Headache Index score (1.41 vs 3.22; P = .048) in patients with migraine. Conversely, propranolol was more effective than valsartan in lowering the Headache Unit Index score (0.06 vs 0.13; P = .025).
Study details: This double-blind trial included 56 adult patients with migraine who were randomly assigned to receive propranolol (20 mg twice daily) or valsartan (40 mg once daily) for 12 weeks.
Disclosure: This study was supported by a grant from Urmia University of Medical Sciences. The authors declared no conflicts of interest.
Source: Mosarrezaii A, Tahazadeh D, Soleimantabar H, Panahi P. Comparison of the efficacy of propranolol versus valsartan in the prevention of migraine: A randomized controlled trial. Pain Manag Nurs. 2024 (Aug 13). doi: 10.1016/j.pmn.2024.07.001 Source
Key clinical point: Although valsartan is not typically used for migraine treatment, it was found to reduce migraine frequency and severity as effectively as propranolol, and in some instances, more effectively.
Major findings: Valsartan vs propranolol significantly reduced the mean score of migraine frequency and severity (1.82 vs 2.39; P = .042), and a lower rate of grade 3 headaches (0% vs 7.14%; P = .029) and a lower Headache Index score (1.41 vs 3.22; P = .048) in patients with migraine. Conversely, propranolol was more effective than valsartan in lowering the Headache Unit Index score (0.06 vs 0.13; P = .025).
Study details: This double-blind trial included 56 adult patients with migraine who were randomly assigned to receive propranolol (20 mg twice daily) or valsartan (40 mg once daily) for 12 weeks.
Disclosure: This study was supported by a grant from Urmia University of Medical Sciences. The authors declared no conflicts of interest.
Source: Mosarrezaii A, Tahazadeh D, Soleimantabar H, Panahi P. Comparison of the efficacy of propranolol versus valsartan in the prevention of migraine: A randomized controlled trial. Pain Manag Nurs. 2024 (Aug 13). doi: 10.1016/j.pmn.2024.07.001 Source
Key clinical point: Although valsartan is not typically used for migraine treatment, it was found to reduce migraine frequency and severity as effectively as propranolol, and in some instances, more effectively.
Major findings: Valsartan vs propranolol significantly reduced the mean score of migraine frequency and severity (1.82 vs 2.39; P = .042), and a lower rate of grade 3 headaches (0% vs 7.14%; P = .029) and a lower Headache Index score (1.41 vs 3.22; P = .048) in patients with migraine. Conversely, propranolol was more effective than valsartan in lowering the Headache Unit Index score (0.06 vs 0.13; P = .025).
Study details: This double-blind trial included 56 adult patients with migraine who were randomly assigned to receive propranolol (20 mg twice daily) or valsartan (40 mg once daily) for 12 weeks.
Disclosure: This study was supported by a grant from Urmia University of Medical Sciences. The authors declared no conflicts of interest.
Source: Mosarrezaii A, Tahazadeh D, Soleimantabar H, Panahi P. Comparison of the efficacy of propranolol versus valsartan in the prevention of migraine: A randomized controlled trial. Pain Manag Nurs. 2024 (Aug 13). doi: 10.1016/j.pmn.2024.07.001 Source
Protective Relationship Between Migraine and Cardiovascular Disease
Key clinical point: Migraine may have a protective effect against some cardiovascular diseases, such as coronary artery disease (CAD) and ischemic stroke, in this Mendelian randomization (MR) analysis, with coronary atherosclerosis (CA) and myocardial infarction (MI), reducing the risk for migraine in reverse MR analysis.
Major findings: Genetically predicted risk of migraine was associated with a lower risk for CAD (odds ratio [OR] 0.881; P = .023) and ischemic stroke (OR 0.912; P = .006). Reciprocally, CA (OR 0.865; P = .001) and MI (OR 0.798; P = .012) were associated with a lower risk for migraine.
Study details: This bidirectional MR study analyzed the causal effect of migraine on CVD using data from 873,341 and 554,569 individuals, and the causal effect of CVD on migraine using data from 484,598 and 463,010 individuals, using large-scale Genome-Wide Association Study databases.
Disclosure: The study was supported by the National Natural Science Foundation of China, and others. The authors reported no conflicts of interest.
Source: Duan X, Du X, Zheng G, et al. Causality between migraine and cardiovascular disease: A bidirectional Mendelian randomization study. J Headache Pain. 2024;25:130 (Aug 13). doi: 10.1186/s10194-024-01836-w Source
Key clinical point: Migraine may have a protective effect against some cardiovascular diseases, such as coronary artery disease (CAD) and ischemic stroke, in this Mendelian randomization (MR) analysis, with coronary atherosclerosis (CA) and myocardial infarction (MI), reducing the risk for migraine in reverse MR analysis.
Major findings: Genetically predicted risk of migraine was associated with a lower risk for CAD (odds ratio [OR] 0.881; P = .023) and ischemic stroke (OR 0.912; P = .006). Reciprocally, CA (OR 0.865; P = .001) and MI (OR 0.798; P = .012) were associated with a lower risk for migraine.
Study details: This bidirectional MR study analyzed the causal effect of migraine on CVD using data from 873,341 and 554,569 individuals, and the causal effect of CVD on migraine using data from 484,598 and 463,010 individuals, using large-scale Genome-Wide Association Study databases.
Disclosure: The study was supported by the National Natural Science Foundation of China, and others. The authors reported no conflicts of interest.
Source: Duan X, Du X, Zheng G, et al. Causality between migraine and cardiovascular disease: A bidirectional Mendelian randomization study. J Headache Pain. 2024;25:130 (Aug 13). doi: 10.1186/s10194-024-01836-w Source
Key clinical point: Migraine may have a protective effect against some cardiovascular diseases, such as coronary artery disease (CAD) and ischemic stroke, in this Mendelian randomization (MR) analysis, with coronary atherosclerosis (CA) and myocardial infarction (MI), reducing the risk for migraine in reverse MR analysis.
Major findings: Genetically predicted risk of migraine was associated with a lower risk for CAD (odds ratio [OR] 0.881; P = .023) and ischemic stroke (OR 0.912; P = .006). Reciprocally, CA (OR 0.865; P = .001) and MI (OR 0.798; P = .012) were associated with a lower risk for migraine.
Study details: This bidirectional MR study analyzed the causal effect of migraine on CVD using data from 873,341 and 554,569 individuals, and the causal effect of CVD on migraine using data from 484,598 and 463,010 individuals, using large-scale Genome-Wide Association Study databases.
Disclosure: The study was supported by the National Natural Science Foundation of China, and others. The authors reported no conflicts of interest.
Source: Duan X, Du X, Zheng G, et al. Causality between migraine and cardiovascular disease: A bidirectional Mendelian randomization study. J Headache Pain. 2024;25:130 (Aug 13). doi: 10.1186/s10194-024-01836-w Source
Monthly or Quarterly Fremanezumab Effective Against Episodic Migraine
Key clinical point: Administration of monthly or quarterly fremanezumab reduced acute medication use and alleviated migraine-associated symptoms in patients with episodic migraine (EM).
Major findings: Fremanezumab, administered monthly vs placebo significantly reduced the acute medication use for headaches (–2.98 vs –0.01; P < .001) and number of days with nausea or vomiting (–1.59 vs –0.66; P = .023) in the first month after initial dosage, with continued benefits till months 2 and 3. Fremanezumab, administered quarterly, also yielded promising outcomes.
Study details: Findings are from an exploratory endpoint analysis of a phase 2b/3 randomized trial including patients with EM who were randomly assigned to receive either monthly fremanezumab (n = 121), quarterly fremanezumab (n = 119), or placebo (n = 117) in monthly intervals.
Disclosures: This study was funded by Otsuka Pharmaceutical Co., Ltd. Five authors declared being full-time employees of Otsuka Pharmaceutical Co., Ltd. Other authors declared having other ties with various sources, including Otsuka Pharmaceutical Co., Ltd.
Source: Tatsumoto M, Ishida M, Iba K, et al. Effects of fremanezumab on migraine-associated symptoms and medication use in Japanese and Korean patients with episodic migraine: Exploratory endpoint analysis of a multicenter, randomized, double-blind, placebo-controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14810 Source
Key clinical point: Administration of monthly or quarterly fremanezumab reduced acute medication use and alleviated migraine-associated symptoms in patients with episodic migraine (EM).
Major findings: Fremanezumab, administered monthly vs placebo significantly reduced the acute medication use for headaches (–2.98 vs –0.01; P < .001) and number of days with nausea or vomiting (–1.59 vs –0.66; P = .023) in the first month after initial dosage, with continued benefits till months 2 and 3. Fremanezumab, administered quarterly, also yielded promising outcomes.
Study details: Findings are from an exploratory endpoint analysis of a phase 2b/3 randomized trial including patients with EM who were randomly assigned to receive either monthly fremanezumab (n = 121), quarterly fremanezumab (n = 119), or placebo (n = 117) in monthly intervals.
Disclosures: This study was funded by Otsuka Pharmaceutical Co., Ltd. Five authors declared being full-time employees of Otsuka Pharmaceutical Co., Ltd. Other authors declared having other ties with various sources, including Otsuka Pharmaceutical Co., Ltd.
Source: Tatsumoto M, Ishida M, Iba K, et al. Effects of fremanezumab on migraine-associated symptoms and medication use in Japanese and Korean patients with episodic migraine: Exploratory endpoint analysis of a multicenter, randomized, double-blind, placebo-controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14810 Source
Key clinical point: Administration of monthly or quarterly fremanezumab reduced acute medication use and alleviated migraine-associated symptoms in patients with episodic migraine (EM).
Major findings: Fremanezumab, administered monthly vs placebo significantly reduced the acute medication use for headaches (–2.98 vs –0.01; P < .001) and number of days with nausea or vomiting (–1.59 vs –0.66; P = .023) in the first month after initial dosage, with continued benefits till months 2 and 3. Fremanezumab, administered quarterly, also yielded promising outcomes.
Study details: Findings are from an exploratory endpoint analysis of a phase 2b/3 randomized trial including patients with EM who were randomly assigned to receive either monthly fremanezumab (n = 121), quarterly fremanezumab (n = 119), or placebo (n = 117) in monthly intervals.
Disclosures: This study was funded by Otsuka Pharmaceutical Co., Ltd. Five authors declared being full-time employees of Otsuka Pharmaceutical Co., Ltd. Other authors declared having other ties with various sources, including Otsuka Pharmaceutical Co., Ltd.
Source: Tatsumoto M, Ishida M, Iba K, et al. Effects of fremanezumab on migraine-associated symptoms and medication use in Japanese and Korean patients with episodic migraine: Exploratory endpoint analysis of a multicenter, randomized, double-blind, placebo-controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14810 Source
Eicosapentaenoic Acid Is an Effective Adjunct Therapy for Chronic Migraine
Key clinical point: Eicosapentaenoic acid (EPA), used with standard prophylactic pharmacotherapy, significantly reduced migraine headache days (MHD) and migraine attacks in patients with chronic migraine (CM).
Major findings: The score relating to headache impact was significantly lower in the EPA vs placebo group at weeks 4 (P = .017) and 8 (P = .042). At 8 weeks, EPA treatment led to a greater reduction in mean MHD (−9.76 vs −4.60; P < .001) and mean number of attacks per month (3 vs 4; P = .012) than placebo. In the EPA group, only three patients experienced nausea and gastrointestinal upset.
Study details: This randomized controlled trial included 60 adult patients with CM who received 1000 mg EPA or placebo twice daily for 8 weeks and continued their first-line preventive pharmacotherapy throughout the trial.
Disclosure: The study was supported by the research committee of Shahid Beheshti University of Medical Sciences, Iran. The authors declared no conflicts of interest.
Source: Mohammadnezhad G, Assarzadegan F, Koosha M, Esmaily H. Eicosapentaenoic acid versus placebo as adjunctive therapy in chronic migraine: A randomized controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14808 Source
Key clinical point: Eicosapentaenoic acid (EPA), used with standard prophylactic pharmacotherapy, significantly reduced migraine headache days (MHD) and migraine attacks in patients with chronic migraine (CM).
Major findings: The score relating to headache impact was significantly lower in the EPA vs placebo group at weeks 4 (P = .017) and 8 (P = .042). At 8 weeks, EPA treatment led to a greater reduction in mean MHD (−9.76 vs −4.60; P < .001) and mean number of attacks per month (3 vs 4; P = .012) than placebo. In the EPA group, only three patients experienced nausea and gastrointestinal upset.
Study details: This randomized controlled trial included 60 adult patients with CM who received 1000 mg EPA or placebo twice daily for 8 weeks and continued their first-line preventive pharmacotherapy throughout the trial.
Disclosure: The study was supported by the research committee of Shahid Beheshti University of Medical Sciences, Iran. The authors declared no conflicts of interest.
Source: Mohammadnezhad G, Assarzadegan F, Koosha M, Esmaily H. Eicosapentaenoic acid versus placebo as adjunctive therapy in chronic migraine: A randomized controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14808 Source
Key clinical point: Eicosapentaenoic acid (EPA), used with standard prophylactic pharmacotherapy, significantly reduced migraine headache days (MHD) and migraine attacks in patients with chronic migraine (CM).
Major findings: The score relating to headache impact was significantly lower in the EPA vs placebo group at weeks 4 (P = .017) and 8 (P = .042). At 8 weeks, EPA treatment led to a greater reduction in mean MHD (−9.76 vs −4.60; P < .001) and mean number of attacks per month (3 vs 4; P = .012) than placebo. In the EPA group, only three patients experienced nausea and gastrointestinal upset.
Study details: This randomized controlled trial included 60 adult patients with CM who received 1000 mg EPA or placebo twice daily for 8 weeks and continued their first-line preventive pharmacotherapy throughout the trial.
Disclosure: The study was supported by the research committee of Shahid Beheshti University of Medical Sciences, Iran. The authors declared no conflicts of interest.
Source: Mohammadnezhad G, Assarzadegan F, Koosha M, Esmaily H. Eicosapentaenoic acid versus placebo as adjunctive therapy in chronic migraine: A randomized controlled trial. Headache. 2024 (Sept 2). doi: 10.1111/head.14808 Source
Long-term Safety of Intranasal Zavegepant for Acute Treatment of Migraine
Key clinical point: Zavegepant nasal spray, administered as needed for up to eight doses per month, demonstrated long-term safety in the acute treatment of migraine over 1 year.
Major finding: The most common adverse events (AE), reported in ≥5% patients receiving zavegepant, were dysgeusia, nasal discomfort, COVID-19, nausea, nasal congestion, throat irritation, and back pain. In the 1-year period, only 6.8% patients discontinued treatment due to AE; dysgeusia was the most common cause, accounting for 1.5% of discontinuations. No deaths were reported.
Study details: This phase 2/3, open-label safety study included 603 adults with moderate to severe migraine who had a history of 2 to 8 moderate to severe attacks per month and were treated with intranasal 10 mg zavegepant daily for 1 year.
Disclosures: This study was funded by Biohaven Pharmaceuticals. Some authors declared being employees of or holding stocks of or stock options in Biohaven Pharmaceuticals. Some others declared having ties with various sources, including Biohaven Pharmaceuticals.
Source: Mullin K, Croop R, Mosher L, et al. Long-term safety of zavegepant nasal spray for acute treatment of migraine: A phase 2/3 open-label study. Cephalalgia. 2024 (Aug 30). doi: 10.1177/033310242412594 Source
Key clinical point: Zavegepant nasal spray, administered as needed for up to eight doses per month, demonstrated long-term safety in the acute treatment of migraine over 1 year.
Major finding: The most common adverse events (AE), reported in ≥5% patients receiving zavegepant, were dysgeusia, nasal discomfort, COVID-19, nausea, nasal congestion, throat irritation, and back pain. In the 1-year period, only 6.8% patients discontinued treatment due to AE; dysgeusia was the most common cause, accounting for 1.5% of discontinuations. No deaths were reported.
Study details: This phase 2/3, open-label safety study included 603 adults with moderate to severe migraine who had a history of 2 to 8 moderate to severe attacks per month and were treated with intranasal 10 mg zavegepant daily for 1 year.
Disclosures: This study was funded by Biohaven Pharmaceuticals. Some authors declared being employees of or holding stocks of or stock options in Biohaven Pharmaceuticals. Some others declared having ties with various sources, including Biohaven Pharmaceuticals.
Source: Mullin K, Croop R, Mosher L, et al. Long-term safety of zavegepant nasal spray for acute treatment of migraine: A phase 2/3 open-label study. Cephalalgia. 2024 (Aug 30). doi: 10.1177/033310242412594 Source
Key clinical point: Zavegepant nasal spray, administered as needed for up to eight doses per month, demonstrated long-term safety in the acute treatment of migraine over 1 year.
Major finding: The most common adverse events (AE), reported in ≥5% patients receiving zavegepant, were dysgeusia, nasal discomfort, COVID-19, nausea, nasal congestion, throat irritation, and back pain. In the 1-year period, only 6.8% patients discontinued treatment due to AE; dysgeusia was the most common cause, accounting for 1.5% of discontinuations. No deaths were reported.
Study details: This phase 2/3, open-label safety study included 603 adults with moderate to severe migraine who had a history of 2 to 8 moderate to severe attacks per month and were treated with intranasal 10 mg zavegepant daily for 1 year.
Disclosures: This study was funded by Biohaven Pharmaceuticals. Some authors declared being employees of or holding stocks of or stock options in Biohaven Pharmaceuticals. Some others declared having ties with various sources, including Biohaven Pharmaceuticals.
Source: Mullin K, Croop R, Mosher L, et al. Long-term safety of zavegepant nasal spray for acute treatment of migraine: A phase 2/3 open-label study. Cephalalgia. 2024 (Aug 30). doi: 10.1177/033310242412594 Source
Migraine and GDM Raise Risk for Major Cerebro- and Cardiovascular Events in Women
Key clinical point: Women with either migraine or gestational diabetes mellitus (GDM) faced an increased long-term risk for developing major adverse cardiovascular and cerebrovascular events (MACCE) at a premature age (≤60 years), with the risk being significantly higher among those with both conditions.
Major findings: Women with migraine or GDM had a significantly higher 20-year risk for premature MACCE than women without these conditions (adjusted hazard ratio [aHR] 1.65; 95% CI 1.49-1.82 for migraine and aHR 1.64; 95% CI 1.37-1.96 for GDM). The risk was highest among women with both migraine and GDM (aHR 2.35; 95% CI 1.03-5.36).
Study details: This population-based longitudinal cohort study included 1,390,451 women, of which 56,811 had migraine, 24,700 had GDM, 1484 had both migraine and GDM, and 1,307,456 women had neither migraine nor GDM.
Disclosure: The study was funded by Aarhus University. The authors declared no conflicts of interest.
Source: Fuglsang CH, Pedersen L, Schmidt M, et al. The combined impact of migraine and gestational diabetes on long-term risk of premature myocardial infarction and stroke: A population-based cohort study. Headache. 2024 (Aug 28). doi: 10.1111/head.14821 Source
Key clinical point: Women with either migraine or gestational diabetes mellitus (GDM) faced an increased long-term risk for developing major adverse cardiovascular and cerebrovascular events (MACCE) at a premature age (≤60 years), with the risk being significantly higher among those with both conditions.
Major findings: Women with migraine or GDM had a significantly higher 20-year risk for premature MACCE than women without these conditions (adjusted hazard ratio [aHR] 1.65; 95% CI 1.49-1.82 for migraine and aHR 1.64; 95% CI 1.37-1.96 for GDM). The risk was highest among women with both migraine and GDM (aHR 2.35; 95% CI 1.03-5.36).
Study details: This population-based longitudinal cohort study included 1,390,451 women, of which 56,811 had migraine, 24,700 had GDM, 1484 had both migraine and GDM, and 1,307,456 women had neither migraine nor GDM.
Disclosure: The study was funded by Aarhus University. The authors declared no conflicts of interest.
Source: Fuglsang CH, Pedersen L, Schmidt M, et al. The combined impact of migraine and gestational diabetes on long-term risk of premature myocardial infarction and stroke: A population-based cohort study. Headache. 2024 (Aug 28). doi: 10.1111/head.14821 Source
Key clinical point: Women with either migraine or gestational diabetes mellitus (GDM) faced an increased long-term risk for developing major adverse cardiovascular and cerebrovascular events (MACCE) at a premature age (≤60 years), with the risk being significantly higher among those with both conditions.
Major findings: Women with migraine or GDM had a significantly higher 20-year risk for premature MACCE than women without these conditions (adjusted hazard ratio [aHR] 1.65; 95% CI 1.49-1.82 for migraine and aHR 1.64; 95% CI 1.37-1.96 for GDM). The risk was highest among women with both migraine and GDM (aHR 2.35; 95% CI 1.03-5.36).
Study details: This population-based longitudinal cohort study included 1,390,451 women, of which 56,811 had migraine, 24,700 had GDM, 1484 had both migraine and GDM, and 1,307,456 women had neither migraine nor GDM.
Disclosure: The study was funded by Aarhus University. The authors declared no conflicts of interest.
Source: Fuglsang CH, Pedersen L, Schmidt M, et al. The combined impact of migraine and gestational diabetes on long-term risk of premature myocardial infarction and stroke: A population-based cohort study. Headache. 2024 (Aug 28). doi: 10.1111/head.14821 Source
Meta-Analysis Shows Increased Neck Pain and Disability in Migraine
Key clinical point: Patients with migraine experienced considerable neck pain–related disability, with the effect being more prominent among patients with chronic vs episodic migraine.
Major findings: Patients with migraine reported a mean Neck Disability Index (NDI) score of 16.2, indicative of moderate disability. The NDI scores were 12.1 points higher among patients with migraine vs control individuals without headache (P < .001) and 5.5 points higher among patients with chronic vs episodic migraine (P < .001).
Study details: Findings are from a meta-analysis of 33 observational studies including patients with migraine, patients with tension-type headache, and healthy individuals without headache.
Disclosure: The study did not receive any funding. Four authors declared receiving personal fees or honoraria for consultation from or having other ties with various sources; others declared no conflicts of interest.
Source: Al-Khazali HM, Al-Sayegh Z, Younis S, et al. Systematic review and meta-analysis of Neck Disability Index and Numeric Pain Rating Scale in patients with migraine and tension-type headache. Cephalalgia. 2024 (Aug 28). doi: 10.1177/033310242412742 Source
Key clinical point: Patients with migraine experienced considerable neck pain–related disability, with the effect being more prominent among patients with chronic vs episodic migraine.
Major findings: Patients with migraine reported a mean Neck Disability Index (NDI) score of 16.2, indicative of moderate disability. The NDI scores were 12.1 points higher among patients with migraine vs control individuals without headache (P < .001) and 5.5 points higher among patients with chronic vs episodic migraine (P < .001).
Study details: Findings are from a meta-analysis of 33 observational studies including patients with migraine, patients with tension-type headache, and healthy individuals without headache.
Disclosure: The study did not receive any funding. Four authors declared receiving personal fees or honoraria for consultation from or having other ties with various sources; others declared no conflicts of interest.
Source: Al-Khazali HM, Al-Sayegh Z, Younis S, et al. Systematic review and meta-analysis of Neck Disability Index and Numeric Pain Rating Scale in patients with migraine and tension-type headache. Cephalalgia. 2024 (Aug 28). doi: 10.1177/033310242412742 Source
Key clinical point: Patients with migraine experienced considerable neck pain–related disability, with the effect being more prominent among patients with chronic vs episodic migraine.
Major findings: Patients with migraine reported a mean Neck Disability Index (NDI) score of 16.2, indicative of moderate disability. The NDI scores were 12.1 points higher among patients with migraine vs control individuals without headache (P < .001) and 5.5 points higher among patients with chronic vs episodic migraine (P < .001).
Study details: Findings are from a meta-analysis of 33 observational studies including patients with migraine, patients with tension-type headache, and healthy individuals without headache.
Disclosure: The study did not receive any funding. Four authors declared receiving personal fees or honoraria for consultation from or having other ties with various sources; others declared no conflicts of interest.
Source: Al-Khazali HM, Al-Sayegh Z, Younis S, et al. Systematic review and meta-analysis of Neck Disability Index and Numeric Pain Rating Scale in patients with migraine and tension-type headache. Cephalalgia. 2024 (Aug 28). doi: 10.1177/033310242412742 Source
Coffee’s ‘Sweet Spot’: Daily Consumption and Cardiometabolic Risk
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.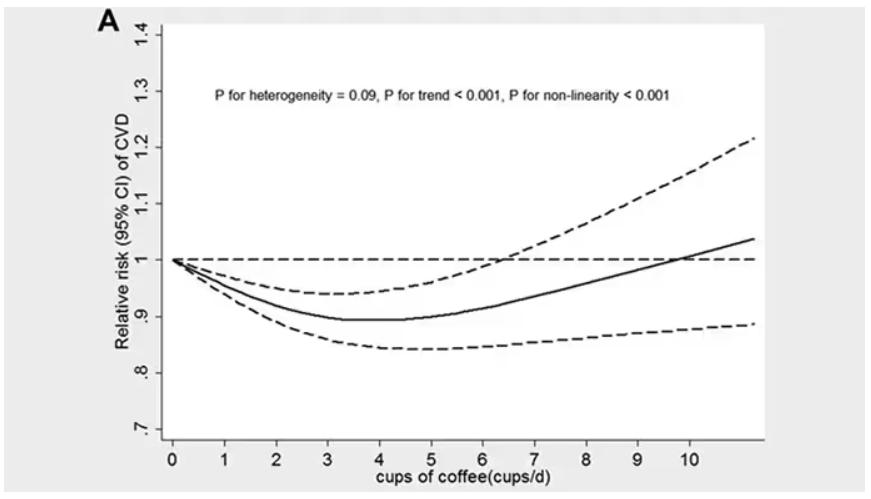
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.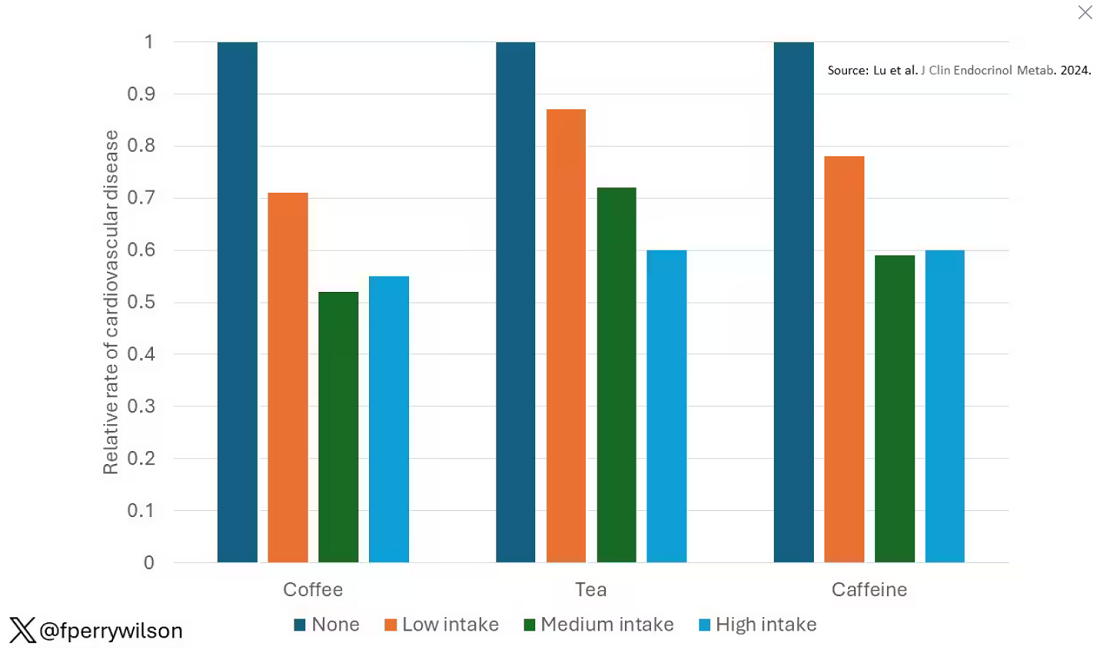
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine. 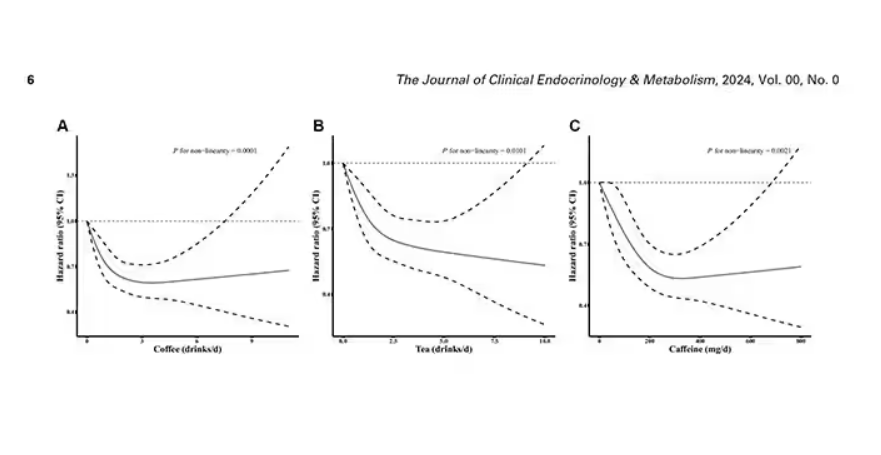
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated. 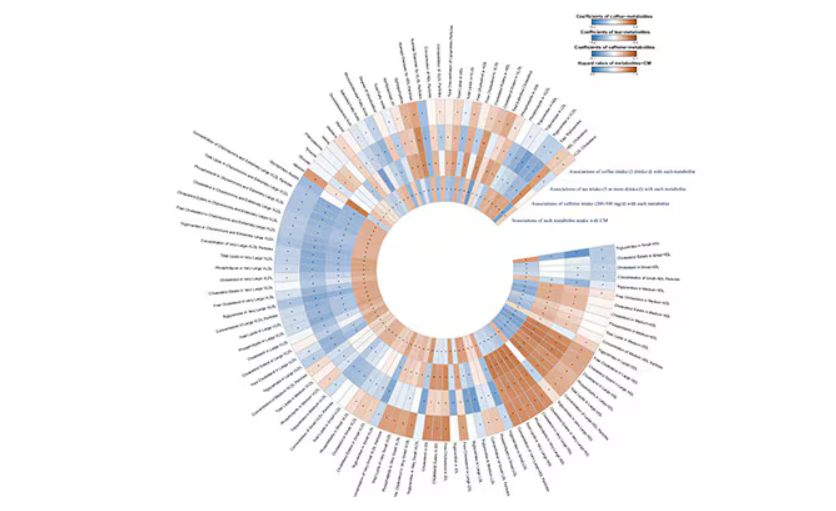
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.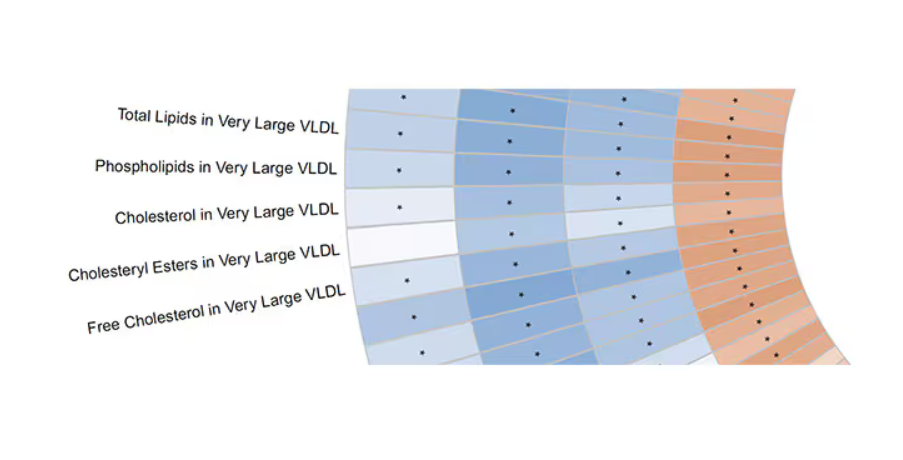
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.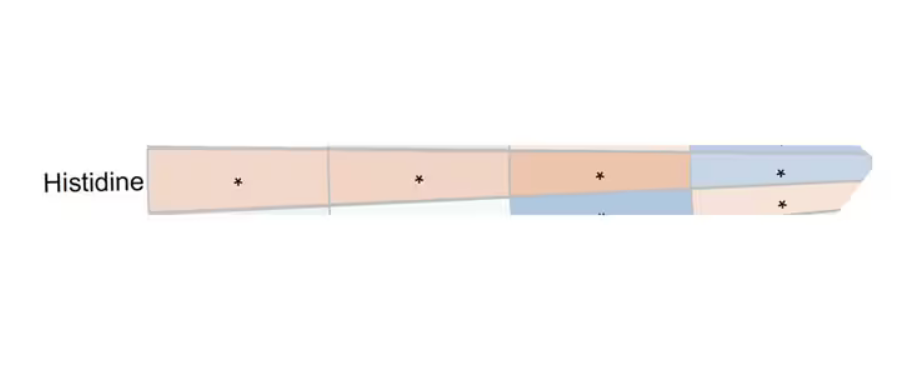
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.