User login
Comorbidity Control Might Slow MS Activity
COPENHAGEN — The largest and perhaps most rigorous study to demonstrate an association between the presence of comorbidities and accelerated progression of multiple sclerosis (MS) is sufficiently compelling that both the study author and an independent expert maintained clinical practice should be adjusted.
Even while acknowledging that “it is hard to make causative statements” on the basis of these types of data, the findings are sufficiently compelling to suggest that comorbidities “should be a pressing concern” in MS management, according to Amber Salter, PhD, an associate professor of biostatistics at the University of Texas Southwestern Medical School, Dallas.

The strong association in this meta-analysis, presented at the 2024 ECTRIMS annual meeting, were drawn from 15 multicenter phase 3 treatment trials with 16,794 participants followed for at least 2 years, Dr. Salter reported. Her data were published simultaneously in JAMA Neurology.
“One of the strengths of this study is that the data on comorbidities were collected prospectively as part of these trials,” explained Mark S. Freedman, MD, director of the Multiple Sclerosis Research Center at Ottawa Hospital in Canada. He agreed with Dr. Salter that it is reasonable to apply these findings to clinical practice given their consistency with numerous other studies and the value of what he termed as “a holistic approach” to improving outcomes in MS.
Meta-Analysis Avoids Weaknesses of Previous Data
There are many potential weaknesses of past observational studies that the authors of this meta-analysis hoped to avoid. These include the possibility that MS patients with comorbidities might be less likely to take or adhere to disease-modifying therapies (DMT) or that comorbidity burden might masquerade or be misinterpreted as MS progression. By employing data from phase 3 DMT trials, Dr. Salter maintained that prospectively collected data monitored carefully over an extended follow-up allows the impact of comorbidities on outcome to be evaluated in a more controlled fashion.
Dr. Freedman liked the design of this study, but he admitted that he was surprised by the result.

“Phase 3 trials typically include exclusion criteria for significant comorbidities, so I did not think they would be able to show any meaningful differences,” Dr. Freedman said in an interview.
For the main outcome of evidence of disease activity (EDA), defined as confirmed disability worsening measured with the Expanded Disability Status Scale (EDSS), relapse activity, or any new or enlarging lesions on MRI, the differences reached significance even after adjustments for multiple potentially confounding factors.
MS Activity Increases Significantly with More Comorbidities
Compared with no comorbidity, the presence of three or more comorbidities were associated with a significant 14% increase in the adjusted hazard ratio (aHR) of EDA (aHR, 1.14; 95% CI, 1.02-1.28), Dr. Salter reported. If there were two or more cardiometabolic comorbidities, the risk of EDA was increased 21% (aHR, 1.21; 95% CI 1.08-1.37).
The list of comorbidities considered in this study was drawn from the International Advisory Committee on Clinical Trials in MS. It included numerous cardiometabolic comorbidities, such as hypertension, hyperlipidemia, diabetes, ischemic heart disease, cerebrovascular disease, and peripheral vascular disease. It also included chronic lung diseases, such as asthma and chronic obstructive pulmonary disease; psychiatric diseases, such as depression and anxiety; and miscellaneous autoimmune conditions.
The number of comorbidities was categorized for analysis as zero, one, two, or three or more. However, Dr. Salter acknowledged that these phase 3 trials did include comorbidity exclusion criteria. In fact, severe forms of most of these comorbidities were exclusion criteria in at least some studies. Yet, the prevalence of one or more comorbidities was still 45.4% in the total population from this meta-analysis.
By themselves alone, ischemic heart disease (aHR, 1.63), cerebrovascular disease (aHR, 1.70) and at least one psychiatric disorder (aHR, 1.14) were all significant for increased MS activity at the end of 2 years by a 95% confidence interval that did not cross the line of unity.
When the EDA endpoints were evaluated individually, not even three or more comorbidities was associated with an increased rate of active lesions on MRI at the end of follow-up, but two or more and three or more comorbidities were associated with a significantly increased risk of disability worsening (aHR, 1.16 and aHR, 1.31, respectively) and relapse (aHR, 1.16 for both).
An Underestimation of Associations?
Prospective trials are still needed to show that treating comorbidities improves outcome in MS, but randomization will be problematic if it means withholding treatment for conditions with risks independent of MS, Dr. Salter said. Although the data from this analysis did not permit an analysis of how relative severity of comorbidities affected MS outcome, she reiterated that most patients with severe comorbidities were likely excluded from inclusion in the studies anyway.
“We think that we are probably seeing an underestimation of an associations between comorbidity and increased MS activity,” Dr. Salter said. While she reported that confounding cannot be ruled out, the robust associations identified in a meta-analysis “limit the possibility of bias or chance findings.”
Asked if the message that clinicians should treat comorbidities to reduce MS activity is a reasonable conclusion in the absence of proof that treatment is beneficial, Dr. Freedman looked both to the body of evidence and to the common sense behind the recommendation.
Basically, Dr. Freedman believes that comorbidities should be addressed routinely and rigorously even if there was no evidence that they improve MS outcome. These data provide just one other source of support for a practice that should be conducted anyway.
Dr. Salter reported financial relationships with Abata Therapeutics, Gryphon Bio, and Owl Therapeutics. Dr. Freedman reported financial relationships with more than 10 pharmaceutical companies.
COPENHAGEN — The largest and perhaps most rigorous study to demonstrate an association between the presence of comorbidities and accelerated progression of multiple sclerosis (MS) is sufficiently compelling that both the study author and an independent expert maintained clinical practice should be adjusted.
Even while acknowledging that “it is hard to make causative statements” on the basis of these types of data, the findings are sufficiently compelling to suggest that comorbidities “should be a pressing concern” in MS management, according to Amber Salter, PhD, an associate professor of biostatistics at the University of Texas Southwestern Medical School, Dallas.
The strong association in this meta-analysis, presented at the 2024 ECTRIMS annual meeting, were drawn from 15 multicenter phase 3 treatment trials with 16,794 participants followed for at least 2 years, Dr. Salter reported. Her data were published simultaneously in JAMA Neurology.
“One of the strengths of this study is that the data on comorbidities were collected prospectively as part of these trials,” explained Mark S. Freedman, MD, director of the Multiple Sclerosis Research Center at Ottawa Hospital in Canada. He agreed with Dr. Salter that it is reasonable to apply these findings to clinical practice given their consistency with numerous other studies and the value of what he termed as “a holistic approach” to improving outcomes in MS.
Meta-Analysis Avoids Weaknesses of Previous Data
There are many potential weaknesses of past observational studies that the authors of this meta-analysis hoped to avoid. These include the possibility that MS patients with comorbidities might be less likely to take or adhere to disease-modifying therapies (DMT) or that comorbidity burden might masquerade or be misinterpreted as MS progression. By employing data from phase 3 DMT trials, Dr. Salter maintained that prospectively collected data monitored carefully over an extended follow-up allows the impact of comorbidities on outcome to be evaluated in a more controlled fashion.
Dr. Freedman liked the design of this study, but he admitted that he was surprised by the result.
“Phase 3 trials typically include exclusion criteria for significant comorbidities, so I did not think they would be able to show any meaningful differences,” Dr. Freedman said in an interview.
For the main outcome of evidence of disease activity (EDA), defined as confirmed disability worsening measured with the Expanded Disability Status Scale (EDSS), relapse activity, or any new or enlarging lesions on MRI, the differences reached significance even after adjustments for multiple potentially confounding factors.
MS Activity Increases Significantly with More Comorbidities
Compared with no comorbidity, the presence of three or more comorbidities were associated with a significant 14% increase in the adjusted hazard ratio (aHR) of EDA (aHR, 1.14; 95% CI, 1.02-1.28), Dr. Salter reported. If there were two or more cardiometabolic comorbidities, the risk of EDA was increased 21% (aHR, 1.21; 95% CI 1.08-1.37).
The list of comorbidities considered in this study was drawn from the International Advisory Committee on Clinical Trials in MS. It included numerous cardiometabolic comorbidities, such as hypertension, hyperlipidemia, diabetes, ischemic heart disease, cerebrovascular disease, and peripheral vascular disease. It also included chronic lung diseases, such as asthma and chronic obstructive pulmonary disease; psychiatric diseases, such as depression and anxiety; and miscellaneous autoimmune conditions.
The number of comorbidities was categorized for analysis as zero, one, two, or three or more. However, Dr. Salter acknowledged that these phase 3 trials did include comorbidity exclusion criteria. In fact, severe forms of most of these comorbidities were exclusion criteria in at least some studies. Yet, the prevalence of one or more comorbidities was still 45.4% in the total population from this meta-analysis.
By themselves alone, ischemic heart disease (aHR, 1.63), cerebrovascular disease (aHR, 1.70) and at least one psychiatric disorder (aHR, 1.14) were all significant for increased MS activity at the end of 2 years by a 95% confidence interval that did not cross the line of unity.
When the EDA endpoints were evaluated individually, not even three or more comorbidities was associated with an increased rate of active lesions on MRI at the end of follow-up, but two or more and three or more comorbidities were associated with a significantly increased risk of disability worsening (aHR, 1.16 and aHR, 1.31, respectively) and relapse (aHR, 1.16 for both).
An Underestimation of Associations?
Prospective trials are still needed to show that treating comorbidities improves outcome in MS, but randomization will be problematic if it means withholding treatment for conditions with risks independent of MS, Dr. Salter said. Although the data from this analysis did not permit an analysis of how relative severity of comorbidities affected MS outcome, she reiterated that most patients with severe comorbidities were likely excluded from inclusion in the studies anyway.
“We think that we are probably seeing an underestimation of an associations between comorbidity and increased MS activity,” Dr. Salter said. While she reported that confounding cannot be ruled out, the robust associations identified in a meta-analysis “limit the possibility of bias or chance findings.”
Asked if the message that clinicians should treat comorbidities to reduce MS activity is a reasonable conclusion in the absence of proof that treatment is beneficial, Dr. Freedman looked both to the body of evidence and to the common sense behind the recommendation.
Basically, Dr. Freedman believes that comorbidities should be addressed routinely and rigorously even if there was no evidence that they improve MS outcome. These data provide just one other source of support for a practice that should be conducted anyway.
Dr. Salter reported financial relationships with Abata Therapeutics, Gryphon Bio, and Owl Therapeutics. Dr. Freedman reported financial relationships with more than 10 pharmaceutical companies.
COPENHAGEN — The largest and perhaps most rigorous study to demonstrate an association between the presence of comorbidities and accelerated progression of multiple sclerosis (MS) is sufficiently compelling that both the study author and an independent expert maintained clinical practice should be adjusted.
Even while acknowledging that “it is hard to make causative statements” on the basis of these types of data, the findings are sufficiently compelling to suggest that comorbidities “should be a pressing concern” in MS management, according to Amber Salter, PhD, an associate professor of biostatistics at the University of Texas Southwestern Medical School, Dallas.
The strong association in this meta-analysis, presented at the 2024 ECTRIMS annual meeting, were drawn from 15 multicenter phase 3 treatment trials with 16,794 participants followed for at least 2 years, Dr. Salter reported. Her data were published simultaneously in JAMA Neurology.
“One of the strengths of this study is that the data on comorbidities were collected prospectively as part of these trials,” explained Mark S. Freedman, MD, director of the Multiple Sclerosis Research Center at Ottawa Hospital in Canada. He agreed with Dr. Salter that it is reasonable to apply these findings to clinical practice given their consistency with numerous other studies and the value of what he termed as “a holistic approach” to improving outcomes in MS.
Meta-Analysis Avoids Weaknesses of Previous Data
There are many potential weaknesses of past observational studies that the authors of this meta-analysis hoped to avoid. These include the possibility that MS patients with comorbidities might be less likely to take or adhere to disease-modifying therapies (DMT) or that comorbidity burden might masquerade or be misinterpreted as MS progression. By employing data from phase 3 DMT trials, Dr. Salter maintained that prospectively collected data monitored carefully over an extended follow-up allows the impact of comorbidities on outcome to be evaluated in a more controlled fashion.
Dr. Freedman liked the design of this study, but he admitted that he was surprised by the result.
“Phase 3 trials typically include exclusion criteria for significant comorbidities, so I did not think they would be able to show any meaningful differences,” Dr. Freedman said in an interview.
For the main outcome of evidence of disease activity (EDA), defined as confirmed disability worsening measured with the Expanded Disability Status Scale (EDSS), relapse activity, or any new or enlarging lesions on MRI, the differences reached significance even after adjustments for multiple potentially confounding factors.
MS Activity Increases Significantly with More Comorbidities
Compared with no comorbidity, the presence of three or more comorbidities were associated with a significant 14% increase in the adjusted hazard ratio (aHR) of EDA (aHR, 1.14; 95% CI, 1.02-1.28), Dr. Salter reported. If there were two or more cardiometabolic comorbidities, the risk of EDA was increased 21% (aHR, 1.21; 95% CI 1.08-1.37).
The list of comorbidities considered in this study was drawn from the International Advisory Committee on Clinical Trials in MS. It included numerous cardiometabolic comorbidities, such as hypertension, hyperlipidemia, diabetes, ischemic heart disease, cerebrovascular disease, and peripheral vascular disease. It also included chronic lung diseases, such as asthma and chronic obstructive pulmonary disease; psychiatric diseases, such as depression and anxiety; and miscellaneous autoimmune conditions.
The number of comorbidities was categorized for analysis as zero, one, two, or three or more. However, Dr. Salter acknowledged that these phase 3 trials did include comorbidity exclusion criteria. In fact, severe forms of most of these comorbidities were exclusion criteria in at least some studies. Yet, the prevalence of one or more comorbidities was still 45.4% in the total population from this meta-analysis.
By themselves alone, ischemic heart disease (aHR, 1.63), cerebrovascular disease (aHR, 1.70) and at least one psychiatric disorder (aHR, 1.14) were all significant for increased MS activity at the end of 2 years by a 95% confidence interval that did not cross the line of unity.
When the EDA endpoints were evaluated individually, not even three or more comorbidities was associated with an increased rate of active lesions on MRI at the end of follow-up, but two or more and three or more comorbidities were associated with a significantly increased risk of disability worsening (aHR, 1.16 and aHR, 1.31, respectively) and relapse (aHR, 1.16 for both).
An Underestimation of Associations?
Prospective trials are still needed to show that treating comorbidities improves outcome in MS, but randomization will be problematic if it means withholding treatment for conditions with risks independent of MS, Dr. Salter said. Although the data from this analysis did not permit an analysis of how relative severity of comorbidities affected MS outcome, she reiterated that most patients with severe comorbidities were likely excluded from inclusion in the studies anyway.
“We think that we are probably seeing an underestimation of an associations between comorbidity and increased MS activity,” Dr. Salter said. While she reported that confounding cannot be ruled out, the robust associations identified in a meta-analysis “limit the possibility of bias or chance findings.”
Asked if the message that clinicians should treat comorbidities to reduce MS activity is a reasonable conclusion in the absence of proof that treatment is beneficial, Dr. Freedman looked both to the body of evidence and to the common sense behind the recommendation.
Basically, Dr. Freedman believes that comorbidities should be addressed routinely and rigorously even if there was no evidence that they improve MS outcome. These data provide just one other source of support for a practice that should be conducted anyway.
Dr. Salter reported financial relationships with Abata Therapeutics, Gryphon Bio, and Owl Therapeutics. Dr. Freedman reported financial relationships with more than 10 pharmaceutical companies.
FROM ECTRIMS 2024
Rheumatology RCTs Have Lower Representation of Women as Authors
TOPLINE:
Women are underrepresented as authors in randomized controlled trials (RCTs) published in rheumatology from 2009 to 2023. RCTs from Africa had higher women representation as authors, while RCTs from Asia and Europe and industry-funded RCTs had lower representation of women.
METHODOLOGY:
- Researchers analyzed 1092 RCTs published in rheumatology from 2009 to 2023 involving 10,794 authors to evaluate the temporal trends and the factors influencing women’s authorship.
- The gender of authors was determined on the basis of their first names and countries of affiliation using a gender application programming interface service.
- The study assessed the association of women’s authorship with various factors using generalized estimating equations by considering women’s gender as the main binary outcome.
- Various covariates influencing women’s authorship such as geographic location, sponsorship type, intervention type, and journal impact factor were also evaluated.
TAKEAWAY:
- Overall, women accounted for 34.1% of authors in RCTs published in rheumatology from 2009 to 2023. They had less representation as first and last authors than men (36.8% vs 50.0% and 26.1% vs 61.2%, respectively).
- RCTs from Africa had higher odds of being authored by women than those from North America (odds ratio [OR], 2.34; 95% CI, 1.02-5.38). Women were also less represented as authors in RCTs from Asia and Europe.
- Their representation as authors was lower in industry-funded RCTs as well (OR, 0.64; 95% CI, 0.56-0.73).
- Women were less likely to be in senior author positions such as last (OR, 0.72) or penultimate (OR, 0.70; P < .001 for both) authors than in middle author positions.
IN PRACTICE:
“Implementing structured policies and supporting women through mentorship and leadership opportunities are crucial steps toward a more inclusive and dynamic research environment,” the authors wrote.
SOURCE:
This study was led by Kim Lauper, MD, Geneva University Hospitals, Division of Rheumatology and Faculty of Medicine, University of Geneva, Switzerland, and was published online on August 26, 2024, in medRxiv.
LIMITATIONS:
This study relied on binary gender data, which did not encompass nonbinary or other gender identities. Moreover, the accuracy of gender determination from names, although robust, had inherent limitations that could have affected the interpretation of results.
DISCLOSURES:
This study did not receive any funding. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Women are underrepresented as authors in randomized controlled trials (RCTs) published in rheumatology from 2009 to 2023. RCTs from Africa had higher women representation as authors, while RCTs from Asia and Europe and industry-funded RCTs had lower representation of women.
METHODOLOGY:
- Researchers analyzed 1092 RCTs published in rheumatology from 2009 to 2023 involving 10,794 authors to evaluate the temporal trends and the factors influencing women’s authorship.
- The gender of authors was determined on the basis of their first names and countries of affiliation using a gender application programming interface service.
- The study assessed the association of women’s authorship with various factors using generalized estimating equations by considering women’s gender as the main binary outcome.
- Various covariates influencing women’s authorship such as geographic location, sponsorship type, intervention type, and journal impact factor were also evaluated.
TAKEAWAY:
- Overall, women accounted for 34.1% of authors in RCTs published in rheumatology from 2009 to 2023. They had less representation as first and last authors than men (36.8% vs 50.0% and 26.1% vs 61.2%, respectively).
- RCTs from Africa had higher odds of being authored by women than those from North America (odds ratio [OR], 2.34; 95% CI, 1.02-5.38). Women were also less represented as authors in RCTs from Asia and Europe.
- Their representation as authors was lower in industry-funded RCTs as well (OR, 0.64; 95% CI, 0.56-0.73).
- Women were less likely to be in senior author positions such as last (OR, 0.72) or penultimate (OR, 0.70; P < .001 for both) authors than in middle author positions.
IN PRACTICE:
“Implementing structured policies and supporting women through mentorship and leadership opportunities are crucial steps toward a more inclusive and dynamic research environment,” the authors wrote.
SOURCE:
This study was led by Kim Lauper, MD, Geneva University Hospitals, Division of Rheumatology and Faculty of Medicine, University of Geneva, Switzerland, and was published online on August 26, 2024, in medRxiv.
LIMITATIONS:
This study relied on binary gender data, which did not encompass nonbinary or other gender identities. Moreover, the accuracy of gender determination from names, although robust, had inherent limitations that could have affected the interpretation of results.
DISCLOSURES:
This study did not receive any funding. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Women are underrepresented as authors in randomized controlled trials (RCTs) published in rheumatology from 2009 to 2023. RCTs from Africa had higher women representation as authors, while RCTs from Asia and Europe and industry-funded RCTs had lower representation of women.
METHODOLOGY:
- Researchers analyzed 1092 RCTs published in rheumatology from 2009 to 2023 involving 10,794 authors to evaluate the temporal trends and the factors influencing women’s authorship.
- The gender of authors was determined on the basis of their first names and countries of affiliation using a gender application programming interface service.
- The study assessed the association of women’s authorship with various factors using generalized estimating equations by considering women’s gender as the main binary outcome.
- Various covariates influencing women’s authorship such as geographic location, sponsorship type, intervention type, and journal impact factor were also evaluated.
TAKEAWAY:
- Overall, women accounted for 34.1% of authors in RCTs published in rheumatology from 2009 to 2023. They had less representation as first and last authors than men (36.8% vs 50.0% and 26.1% vs 61.2%, respectively).
- RCTs from Africa had higher odds of being authored by women than those from North America (odds ratio [OR], 2.34; 95% CI, 1.02-5.38). Women were also less represented as authors in RCTs from Asia and Europe.
- Their representation as authors was lower in industry-funded RCTs as well (OR, 0.64; 95% CI, 0.56-0.73).
- Women were less likely to be in senior author positions such as last (OR, 0.72) or penultimate (OR, 0.70; P < .001 for both) authors than in middle author positions.
IN PRACTICE:
“Implementing structured policies and supporting women through mentorship and leadership opportunities are crucial steps toward a more inclusive and dynamic research environment,” the authors wrote.
SOURCE:
This study was led by Kim Lauper, MD, Geneva University Hospitals, Division of Rheumatology and Faculty of Medicine, University of Geneva, Switzerland, and was published online on August 26, 2024, in medRxiv.
LIMITATIONS:
This study relied on binary gender data, which did not encompass nonbinary or other gender identities. Moreover, the accuracy of gender determination from names, although robust, had inherent limitations that could have affected the interpretation of results.
DISCLOSURES:
This study did not receive any funding. The authors declared no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Rheumatology Clinic Interventions for Smoking, Blood Pressure ‘Make a Big Difference’
Two relatively simple interventions — addressing high blood pressure (BP) and smoking cessation — could make a huge difference for patients with rheumatic disease. Patients with autoimmune disease are up to three times more likely to develop cardiovascular disease (CVD) than the general population. In addition to compounding CVD, smoking is tied to the development of certain autoimmune conditions, as well as worse outcomes. Christie Bartels, MD, chief of the Division of Rheumatology at the University of Wisconsin School of Medicine and Public Health, Madison, has focused her research on improving cardiac health in inflammatory diseases. This news organization spoke with Bartels about two short interventions she developed that tackle hypertension and smoking cessation during regular visits, each taking less than 3 minutes.
How Do These Programs Address Cardiac Disease Prevention?
The BP and Quit Connect programs help clinics systematically address the two most modifiable risk factors for CVD: high BP and smoking. There’s also evidence that addressing these two risk factors improves outcomes in rheumatic diseases. Hypertension predicts an increase in lupus damage. Particularly in lupus nephritis, hypertension will increase the risk for CVD and kidney failure. People who use tobacco have worse outcomes in diseases like rheumatoid arthritis, psoriatic arthritis, and lupus, as well as more CVD, and antirheumatic drugs may not work as well.

In 90 seconds to 3 minutes, staff can do protocol-based care, which we’ve done across 20,000-plus visits. We showed we can improve population level rates of high BP and BP control, as well as increase smoking quitting rates across different patient settings.
What Is the Quit Connect Program?
The Quit Connect program is a 10- to 90-second point of care intervention. During rooming, staff (medical assistants and nurses) ask patients: “A) Do you smoke? and B) Have you thought about cutting back or quitting in the next 30 days?”
It turns out, when you ask the question that way, between a third and a half of people say that they’ve thought about cutting back or quitting. Then, we can get patients connected directly to Quitline, a free public service across all 50 states that smokers can use to get cessation support.
If patients are ready, we ask if we can arrange for them to receive a call from a Quitline coach about setting a quit date or receiving free nicotine replacement therapy. The beautiful thing is when that all happens, A) it’s free to the patient, and B) the results from the Quitline can be recorded right back to the electronic health record.
In our most recent publication in Arthritis Care & Research, we documented bringing Quit Connect to Grady Hospital in downtown Atlanta. It’s a safety net hospital, where 80% patients are Black and 70%-80% patients are on public insurance or uninsured. Using this protocol, we improved Quitline referrals 20-fold.
What Is the BP Connect Program?
At least half of the encounters in United States happen in specialty clinics. Unfortunately, when patients get their BP measured in a specialty clinic that’s not a cardiology or a vascular clinic, often, even if the pressure is high, the clinic doesn’t give patients feedback on that. The problem is because we haven’t said anything, that gives people the false reassurance that their BP is okay.
We’ve developed a 3-minute protocol to ask, advise, and connect. The idea is that if we measure a high BP, then we remeasure and confirm that it’s high. Then, we advise why it matters in rheumatic disease: Patients with rheumatic diseases are already at an increased risk for heart disease, and controlling BP can make a big difference. Then, we connect patients with high BP back to primary care.
Specifically, a SmartSet — an electronic medical record feature — prompts different actions based on confirmed high BP readings:
- If systolic BP ≥ 140-159, the SmartSet directs scheduling a visit to a nurse or primary care provider.
- If systolic BP ≥ 160-179, the next primary care visit anticipates the need to see a prescriber.
- If systolic BP ≥ 180, then the medical assistant or nurse at the visit is instructed to notify the provider who can arrange a provider-to-provider handoff for safety to exclude a hypertensive emergency.
That order goes to the scheduler to call primary care to coordinate follow-up. BP Connect doubled the likelihood of a guideline-recommended follow-up in primary care within 30 days. All patients benefited, and disparities decreased. BP Connect has had 1100 downloads, and both BP and Quit Connect programs are endorsed by the Centers for Disease Control and Prevention and Million Hearts.
How Do These Programs Affect Clinical Practice?
We developed these interventions with a health system engineer, and we time stamped everything. Part of the sustainability of this model is that it fits within a regular workflow. As a practicing rheumatologist, I understand that time is a precious commodity.
The interventions are in partnership with frontline staff. We’ve received feedback that they feel pride participating in these initiatives. They can say, because of me, 30 patients followed up last month for high BP, or 10 patients took a referral to the Quitline last year. We celebrate these accomplishments with the staff.
What Are the Next Steps for These Programs?
Public-facing toolkits for both BP and Quit Connect programs are available online. We have implemented [these programs] in a rural setting, in an urban setting, in Milwaukee and in Atlanta, and we are looking in the future to do a larger, multistate implementation study. If folks are interested, we’d love to partner with them to look at disseminating this further.
A version of this article appeared on Medscape.com.
Two relatively simple interventions — addressing high blood pressure (BP) and smoking cessation — could make a huge difference for patients with rheumatic disease. Patients with autoimmune disease are up to three times more likely to develop cardiovascular disease (CVD) than the general population. In addition to compounding CVD, smoking is tied to the development of certain autoimmune conditions, as well as worse outcomes. Christie Bartels, MD, chief of the Division of Rheumatology at the University of Wisconsin School of Medicine and Public Health, Madison, has focused her research on improving cardiac health in inflammatory diseases. This news organization spoke with Bartels about two short interventions she developed that tackle hypertension and smoking cessation during regular visits, each taking less than 3 minutes.
How Do These Programs Address Cardiac Disease Prevention?
The BP and Quit Connect programs help clinics systematically address the two most modifiable risk factors for CVD: high BP and smoking. There’s also evidence that addressing these two risk factors improves outcomes in rheumatic diseases. Hypertension predicts an increase in lupus damage. Particularly in lupus nephritis, hypertension will increase the risk for CVD and kidney failure. People who use tobacco have worse outcomes in diseases like rheumatoid arthritis, psoriatic arthritis, and lupus, as well as more CVD, and antirheumatic drugs may not work as well.
In 90 seconds to 3 minutes, staff can do protocol-based care, which we’ve done across 20,000-plus visits. We showed we can improve population level rates of high BP and BP control, as well as increase smoking quitting rates across different patient settings.
What Is the Quit Connect Program?
The Quit Connect program is a 10- to 90-second point of care intervention. During rooming, staff (medical assistants and nurses) ask patients: “A) Do you smoke? and B) Have you thought about cutting back or quitting in the next 30 days?”
It turns out, when you ask the question that way, between a third and a half of people say that they’ve thought about cutting back or quitting. Then, we can get patients connected directly to Quitline, a free public service across all 50 states that smokers can use to get cessation support.
If patients are ready, we ask if we can arrange for them to receive a call from a Quitline coach about setting a quit date or receiving free nicotine replacement therapy. The beautiful thing is when that all happens, A) it’s free to the patient, and B) the results from the Quitline can be recorded right back to the electronic health record.
In our most recent publication in Arthritis Care & Research, we documented bringing Quit Connect to Grady Hospital in downtown Atlanta. It’s a safety net hospital, where 80% patients are Black and 70%-80% patients are on public insurance or uninsured. Using this protocol, we improved Quitline referrals 20-fold.
What Is the BP Connect Program?
At least half of the encounters in United States happen in specialty clinics. Unfortunately, when patients get their BP measured in a specialty clinic that’s not a cardiology or a vascular clinic, often, even if the pressure is high, the clinic doesn’t give patients feedback on that. The problem is because we haven’t said anything, that gives people the false reassurance that their BP is okay.
We’ve developed a 3-minute protocol to ask, advise, and connect. The idea is that if we measure a high BP, then we remeasure and confirm that it’s high. Then, we advise why it matters in rheumatic disease: Patients with rheumatic diseases are already at an increased risk for heart disease, and controlling BP can make a big difference. Then, we connect patients with high BP back to primary care.
Specifically, a SmartSet — an electronic medical record feature — prompts different actions based on confirmed high BP readings:
- If systolic BP ≥ 140-159, the SmartSet directs scheduling a visit to a nurse or primary care provider.
- If systolic BP ≥ 160-179, the next primary care visit anticipates the need to see a prescriber.
- If systolic BP ≥ 180, then the medical assistant or nurse at the visit is instructed to notify the provider who can arrange a provider-to-provider handoff for safety to exclude a hypertensive emergency.
That order goes to the scheduler to call primary care to coordinate follow-up. BP Connect doubled the likelihood of a guideline-recommended follow-up in primary care within 30 days. All patients benefited, and disparities decreased. BP Connect has had 1100 downloads, and both BP and Quit Connect programs are endorsed by the Centers for Disease Control and Prevention and Million Hearts.
How Do These Programs Affect Clinical Practice?
We developed these interventions with a health system engineer, and we time stamped everything. Part of the sustainability of this model is that it fits within a regular workflow. As a practicing rheumatologist, I understand that time is a precious commodity.
The interventions are in partnership with frontline staff. We’ve received feedback that they feel pride participating in these initiatives. They can say, because of me, 30 patients followed up last month for high BP, or 10 patients took a referral to the Quitline last year. We celebrate these accomplishments with the staff.
What Are the Next Steps for These Programs?
Public-facing toolkits for both BP and Quit Connect programs are available online. We have implemented [these programs] in a rural setting, in an urban setting, in Milwaukee and in Atlanta, and we are looking in the future to do a larger, multistate implementation study. If folks are interested, we’d love to partner with them to look at disseminating this further.
A version of this article appeared on Medscape.com.
Two relatively simple interventions — addressing high blood pressure (BP) and smoking cessation — could make a huge difference for patients with rheumatic disease. Patients with autoimmune disease are up to three times more likely to develop cardiovascular disease (CVD) than the general population. In addition to compounding CVD, smoking is tied to the development of certain autoimmune conditions, as well as worse outcomes. Christie Bartels, MD, chief of the Division of Rheumatology at the University of Wisconsin School of Medicine and Public Health, Madison, has focused her research on improving cardiac health in inflammatory diseases. This news organization spoke with Bartels about two short interventions she developed that tackle hypertension and smoking cessation during regular visits, each taking less than 3 minutes.
How Do These Programs Address Cardiac Disease Prevention?
The BP and Quit Connect programs help clinics systematically address the two most modifiable risk factors for CVD: high BP and smoking. There’s also evidence that addressing these two risk factors improves outcomes in rheumatic diseases. Hypertension predicts an increase in lupus damage. Particularly in lupus nephritis, hypertension will increase the risk for CVD and kidney failure. People who use tobacco have worse outcomes in diseases like rheumatoid arthritis, psoriatic arthritis, and lupus, as well as more CVD, and antirheumatic drugs may not work as well.
In 90 seconds to 3 minutes, staff can do protocol-based care, which we’ve done across 20,000-plus visits. We showed we can improve population level rates of high BP and BP control, as well as increase smoking quitting rates across different patient settings.
What Is the Quit Connect Program?
The Quit Connect program is a 10- to 90-second point of care intervention. During rooming, staff (medical assistants and nurses) ask patients: “A) Do you smoke? and B) Have you thought about cutting back or quitting in the next 30 days?”
It turns out, when you ask the question that way, between a third and a half of people say that they’ve thought about cutting back or quitting. Then, we can get patients connected directly to Quitline, a free public service across all 50 states that smokers can use to get cessation support.
If patients are ready, we ask if we can arrange for them to receive a call from a Quitline coach about setting a quit date or receiving free nicotine replacement therapy. The beautiful thing is when that all happens, A) it’s free to the patient, and B) the results from the Quitline can be recorded right back to the electronic health record.
In our most recent publication in Arthritis Care & Research, we documented bringing Quit Connect to Grady Hospital in downtown Atlanta. It’s a safety net hospital, where 80% patients are Black and 70%-80% patients are on public insurance or uninsured. Using this protocol, we improved Quitline referrals 20-fold.
What Is the BP Connect Program?
At least half of the encounters in United States happen in specialty clinics. Unfortunately, when patients get their BP measured in a specialty clinic that’s not a cardiology or a vascular clinic, often, even if the pressure is high, the clinic doesn’t give patients feedback on that. The problem is because we haven’t said anything, that gives people the false reassurance that their BP is okay.
We’ve developed a 3-minute protocol to ask, advise, and connect. The idea is that if we measure a high BP, then we remeasure and confirm that it’s high. Then, we advise why it matters in rheumatic disease: Patients with rheumatic diseases are already at an increased risk for heart disease, and controlling BP can make a big difference. Then, we connect patients with high BP back to primary care.
Specifically, a SmartSet — an electronic medical record feature — prompts different actions based on confirmed high BP readings:
- If systolic BP ≥ 140-159, the SmartSet directs scheduling a visit to a nurse or primary care provider.
- If systolic BP ≥ 160-179, the next primary care visit anticipates the need to see a prescriber.
- If systolic BP ≥ 180, then the medical assistant or nurse at the visit is instructed to notify the provider who can arrange a provider-to-provider handoff for safety to exclude a hypertensive emergency.
That order goes to the scheduler to call primary care to coordinate follow-up. BP Connect doubled the likelihood of a guideline-recommended follow-up in primary care within 30 days. All patients benefited, and disparities decreased. BP Connect has had 1100 downloads, and both BP and Quit Connect programs are endorsed by the Centers for Disease Control and Prevention and Million Hearts.
How Do These Programs Affect Clinical Practice?
We developed these interventions with a health system engineer, and we time stamped everything. Part of the sustainability of this model is that it fits within a regular workflow. As a practicing rheumatologist, I understand that time is a precious commodity.
The interventions are in partnership with frontline staff. We’ve received feedback that they feel pride participating in these initiatives. They can say, because of me, 30 patients followed up last month for high BP, or 10 patients took a referral to the Quitline last year. We celebrate these accomplishments with the staff.
What Are the Next Steps for These Programs?
Public-facing toolkits for both BP and Quit Connect programs are available online. We have implemented [these programs] in a rural setting, in an urban setting, in Milwaukee and in Atlanta, and we are looking in the future to do a larger, multistate implementation study. If folks are interested, we’d love to partner with them to look at disseminating this further.
A version of this article appeared on Medscape.com.
Short Interval Repeat Colonoscopy After Inadequate Bowel Preparation Is Low Among Veterans
Colorectal cancer (CRC) is the third-most diagnosed cancer after breast and lung cancer, and is the second leading cause of global cancer related deaths.1 In 2023 in the United States, > 150,000 individuals were diagnosed with CRC and 52,000 died.2
Colonoscopy is an effective CRC screening method and the lone method recommended for polyp surveillance. Inadequate bowel preparation (IBP) has been estimated to occur in about 6% to 26% of colonoscopies. 3,4 The prevalence varies based on a variety of comorbidities, including immobility, diabetes mellitus, neurologic disorders, and use of opioids, with more occurrences of IBP noted in older adult, non-English speaking, and male individuals.4-6
The quality of bowel preparation is integral to the effectiveness of screening and surveillance colonoscopies. IBP has been associated with missed adenomas and significantly lower adenoma detection rates.7-9 In particular, IBP is independently associated with an increased risk of CRC in the future.3 Accordingly, the US Multisociety Task Force recommends repeat colonoscopies for individuals with IBP within 1 year.10 Ensuring that these individuals receive repeat colonoscopies is an essential part of CRC prevention. The benefit of repeat colonoscopy after IBP is highlighted by a retrospective analysis from Fung and colleagues that showed 81% of repeat colonoscopies had adequate bowel preparation, with higher numbers of adenomas detected on repeat compared to initial colonoscopies.11
Given the impact of bowel preparation quality on the diagnostic capability of the colonoscopy, adherence to guidelines for repeat colonoscopies in cases of IBP is paramount for effective CRC prevention. This study aims to measure the frequency of repeat colonoscopy after IBP and the factors associated with adherence to recommendations.
METHODS
Individuals who underwent colonoscopy at the Minneapolis Veterans Affairs Medical Center (MVAMC) from January 1, 2016, to October 19, 2021, were identified to allow for 400 days of follow-up from the index colonoscopy to the data collection date. During the COVID-19 pandemic, the colonoscopy procedure capacity was reduced by 50% from June 1, 2020, to December 1, 2020, delaying nonurgent procedures, including screening and surveillance colonoscopies.
Individuals who underwent colonoscopy for CRC screening or polyp surveillance, or following a positive fecal immunohistochemistry test (FIT) or virtual computed tomography colonoscopy were included. Patients with colonoscopy indications for iron deficiency anemia, gastrointestinal bleeding, disease activity assessment of inflammatory bowel disease, abdominal pain, or changes in bowel movement pattern were excluded. IBP was defined as recording a Boston Bowel Preparation Scale (BBPS) score of < 6, or < 2 in any segment, or described as poor or inadequate using the Aronchick scale.
Age, sex, race, marital status, distance to MVAMC, smoking status, comorbidities, and concurrent medication use, including antiplatelet, anticoagulation, and prescription opiates at the time of index colonoscopy were obtained from the Veterans Health Administration (VHA) Corporate Data Warehouse (CDW) using structured query language processing of colonoscopy procedure notes to extract preparation scores and other procedure information. The CDW contains extracts from VHA clinical and administrative systems that contain complete clinical data from October 1999.12 Current smoking status was defined as any smoking activity at the time the questionnaire was administered during a routine clinic visit within 400 days from the index colonoscopy.
Only individuals who were recommended to have repeat colonoscopy within 1 year were included. The intervals of 365 days and 400 days (1 year + about 1 additional month) were used in the event that the individual had a delay in scheduling their 1-year repeat colonoscopy. For individuals who did not undergo a colonoscopy at MVAMC within 400 days, a manual chart review of all available records was performed to determine whether a colonoscopy was performed at a non-VA facility.
Patients received written instructions for bowel preparation 2 weeks prior to the procedure. The preparation included magnesium citrate and a split dose of 4 liters of polyethylene glycol. Patients were also advised to start a low-fiber diet 3 days prior to the procedure and a clear liquid diet the day before the procedure. Patients with a history of IBP or those undergoing procedures with anesthesia received an additional 2 liters for a total of 6 liters of polyethylene glycol.
Statistical analysis
Baseline characteristics were reported as mean (SD) or median and IQR for continuous variables and percentage for categorical variables. Individuals who returned for colonoscopy within 400 days were compared to those who did not identify factors associated with adherence to recommendations. The data on individuals who returned for colonoscopy within 400 days were also analyzed for additional minor delays in the timing of the repeat colonoscopy. Continuous data were compared using Mann-Whitney U tests. Categorical data were compared using X2 or Fisher exact tests. Missing data were imputed from the analyses. All analyses were performed using SAS JMP Pro version 16. P < .05 was considered statistically significant.
RESULTS
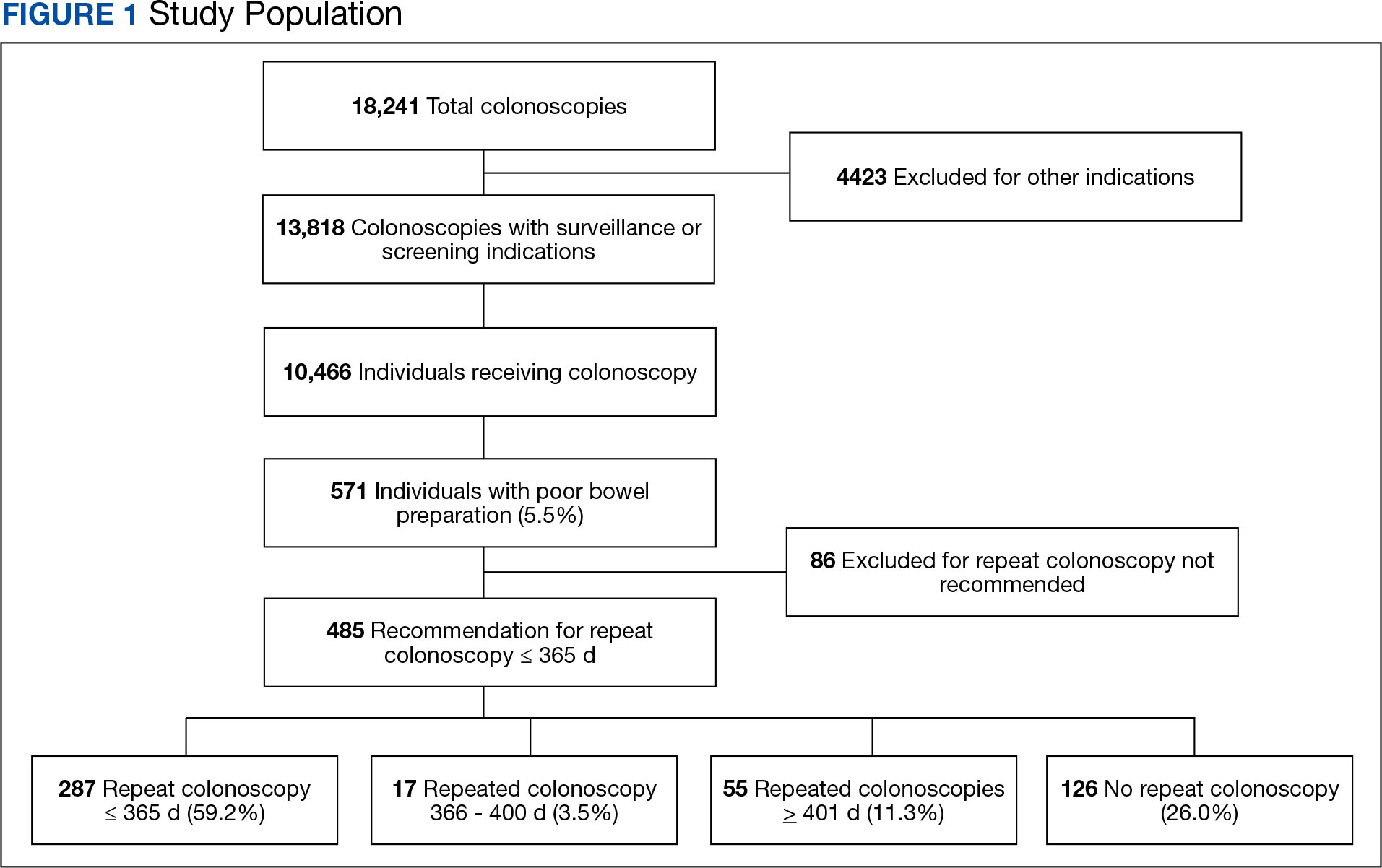
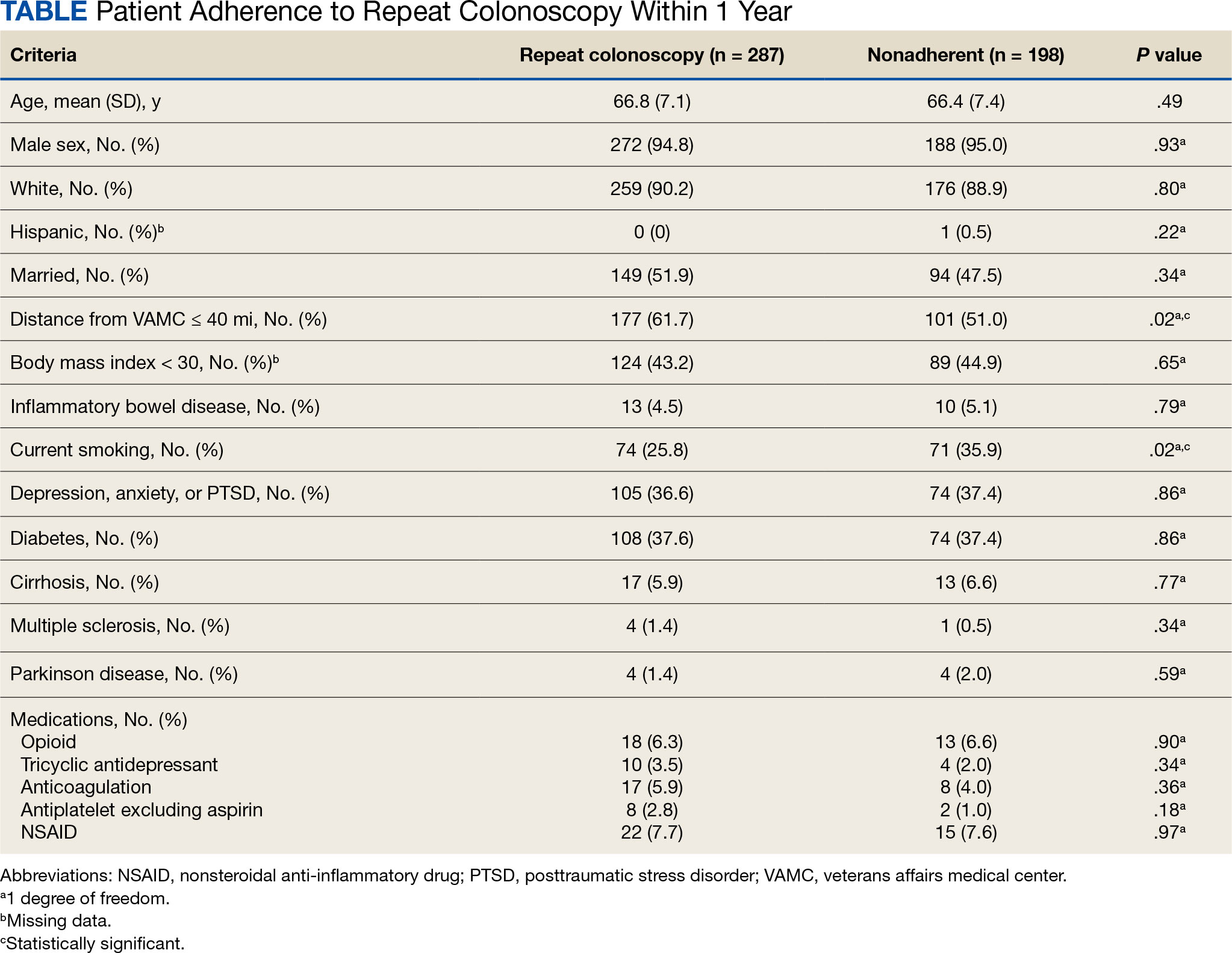
There were 18,241 total colonoscopies performed between January 1, 2016, to October 19, 2021, and 13,818 colonoscopies had indications for screening for colon cancer, positive FIT, virtual colonoscopy, or surveillance. Of the 10,466 unique patients there were 5369 patients for polyp surveillance, 4054 patients for CRC screening, and 1043 patients for positive FIT or virtual colonoscopy. Of these, 571 individuals (5.5%) had IBP. Repeat colonoscopy within 1 year was recommended for 485 individuals (84.9%) who were included in this study (153 CRC screenings and 46 positive FITs) but not for 86 individuals (15.1%) (Figure 1). Among included patients, the mean (SD) age was 66.6 (7.2) years, and the majority were male (460 [94.8%]) and White (435 [89.7%]) (Table). Two hundred and forty-three (50.1%) were married.
Adherence to Recommended Interval Colonoscopy
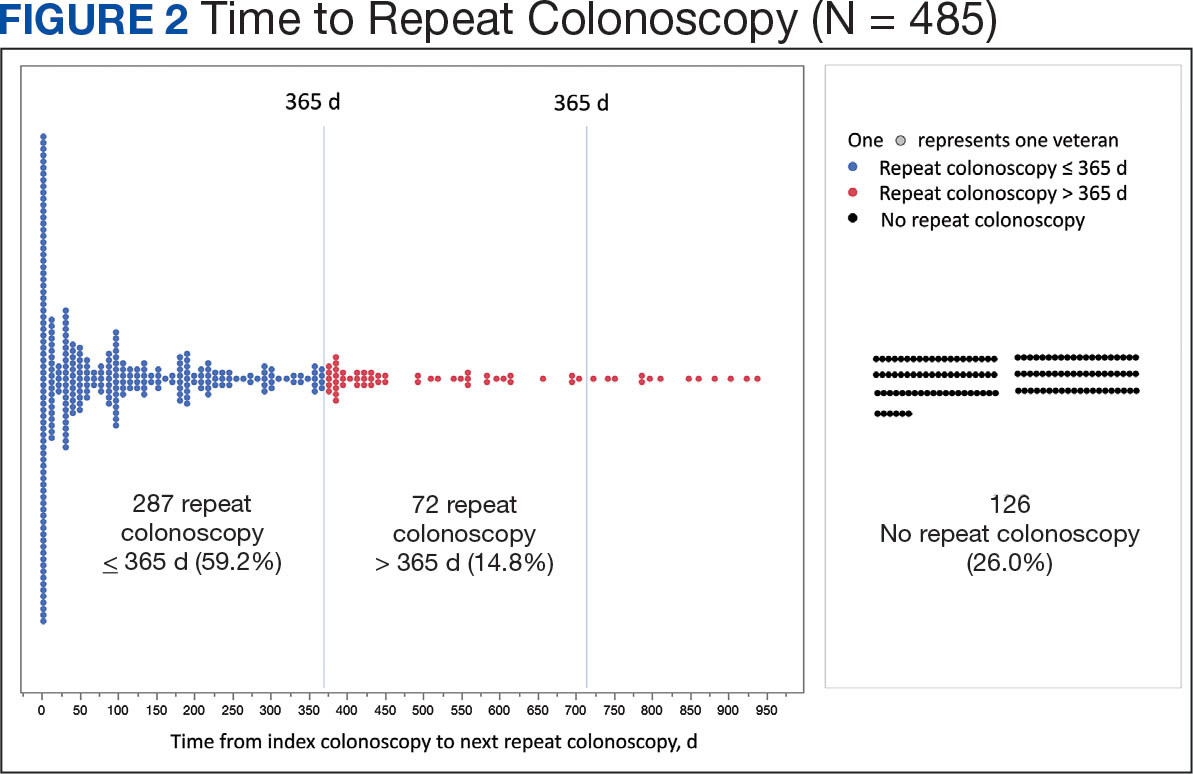
Of the 485 patients with IBP who were recommended for follow-up colonoscopy, 287 (59.2%) had a colonoscopy within 1 year, and 198 (40.8%) did not; 17 patients (13.5%) had repeat colonoscopy within 366 to 400 days. Five (1.0%) individuals had a repeat colonoscopy the next day, and 77 (15.9%) had a repeat colonoscopy within 7 days. One hundred and twentysix (26.0%) individuals underwent no repeat colonoscopy during the study period (Figure 2).
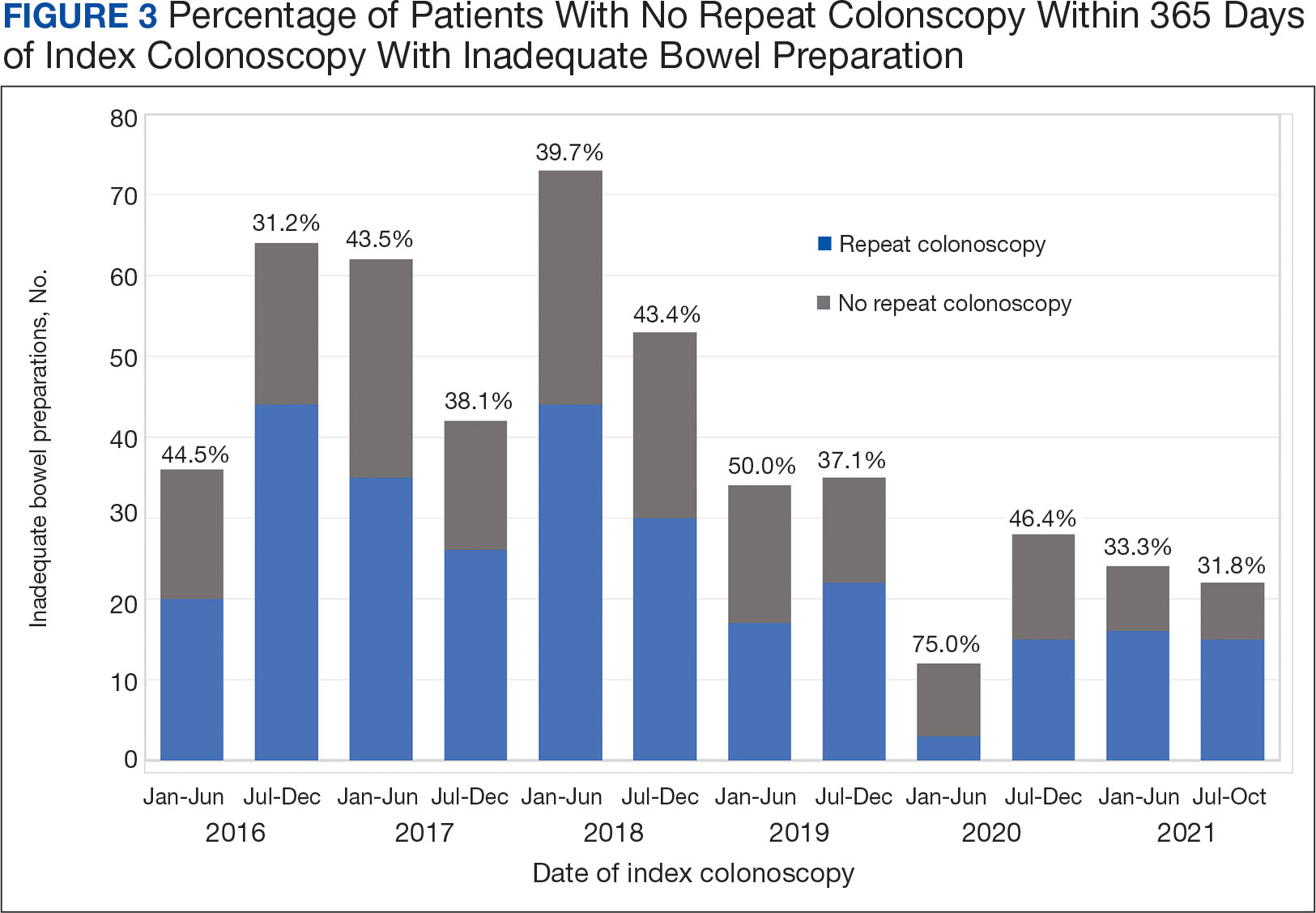
To account for the COVID-19 pandemic, the adherence rate of repeat colonoscopy within 1 year prepandemic (January 1, 2016, to December 1, 2018) was calculated along with the adherence rate postpandemic (January 1, 2019 to the end of the study). The rates were similar: 199 of 330 (60.3%) individuals prepandemic vs 88 of 155 (56.8%) individuals postpandemic (Figure 3).
Significant Associations
Age, sex, and race were not associated with adherence to repeat colonoscopy within 1 year. Individuals living ≤ 40 miles from the endoscopy center were more likely to undergo a repeat colonoscopy within 1 year compared with those who lived > 40 miles away (61.7% vs 51.0%, P = .02). Current smoking status was associated with a lower rate of repeat colonoscopy within 1 year (25.8% vs 35.9%; P = .02). There were no differences with respect to inflammatory bowel disease diagnosis, mental health diagnosis, diabetes mellitus, cirrhosis, or medications used, including opioids, anticoagulation, and antiplatelet therapy.
Outcomes
Among individuals who had a repeat colonoscopy the day after the index colonoscopy, 53 of 56 individuals (94.6%) had adequate bowel preparation. Among individuals who had a repeat colonoscopy within 7 days, 70 of 77 (90.9%) had adequate bowel preparation. Of 287 individuals with a repeat colonoscopy within 1 year, 251 (87.5%) had adequate bowel preparation on the repeat colonoscopy. By 400 days after the index colonoscopy, 268 of 304 individuals (88.2%) had adequate bowel preparation.
In this study conducted at a large VA medical center, we found that 5.6% of individuals undergoing colonoscopies had IBP, a rate comparable to prior studies (6% to 26%).3,4 Only 59.2% of individuals underwent repeat colonoscopies within 1 year, as recommended after an index colonoscopy with IBP. Smoking and living longer distances (> 40 miles) from the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation.
Current guidelines recommend repeat colonoscopy for individuals with IBP within 1 year.10 In cases of IBP, the advanced adenoma miss rate is 36% upon repeat colonoscopy within 1 year.13 Despite the importance of a follow-up colonoscopy, clinician adherence with this recommendation remains low.10,14,15 However, in this study cohort, 485 of 571 individuals with IBP (84.9%) received recommendations for a repeat colonoscopy within 1 year. In the US, only 31.9% of 260,314 colonoscopies with IBP included recommendations for a follow-up colonoscopy within 1 year.14 This could be related to variations in endoscopist practice as well as patient risk factors for developing polyps, including family history of cancer and personal history of prior polyps. The findings of multiple polyps, high-risk adenomas, and cancer on the index colonoscopy also influences the endoscopist for repeat colonoscopy within 1 year.14
The timing for repeat colonoscopies within 1 year will be determined by the patients, clinicians, and available scheduling. In this study, the earlier repeat colonoscopies, especially those occurring the day after the index colonoscopy, had the highest success rate of adequate bowel preparation. In a prior study, repeating colonoscopies within the same day or the next day was also found to have a higher rate of adequate bowel preparation than repeat colonoscopies within 1 year (88.9% vs 83.5%).16
Ensuring the return of individuals with IBP for repeat colonoscopy is a challenging task. We identified that individuals who live further away from MVAMC and current smokers had a decreased probability of returning for a repeat colonoscopy. Toro and colleagues found a 68.7% return rate for a repeat colonoscopy within 1 year with individuals age ≥ 60 years, and patients who were White were less likely to proceed with a repeat colonoscopy within 1 year.17 The study did not provide data regarding smoking status or distance to the endoscopy center.17 In a prior study of veterans, the dual diagnosis of psychiatric disorders and substance abuse was associated with missed and canceled colonoscopy appointments.18 The distance to the endoscopy center has also been previously identified as a barrier to a colonoscopy following an abnormal FIT.19 Although not identified in this study due to the homogenous demographic profile, social determinants of health such as socioeconomic status, education, and insurance coverage are known barriers to cancer screening but were not evaluated in this study.20
Based on the identified risk factors, we have created a model for utilizing those risk factors to identify individuals at higher risk for noncompliance (ie, those who live further away from the endoscopy center or currently smoke). These individuals are proactively offered to use an intraprocedural bowel cleansing device to achieve adequate bowel preparation or priority rescheduling for a next-day colonoscopy.
Limitations
This study was a single-center study of the veteran population, which is predominantly White and male, thus limiting generalizability. The study is also limited by minimal available data on adenoma detection and colon cancer incidence on subsequent colonoscopies.
CONCLUSIONS
The rate of IBP was 5.5% in individuals undergoing colonoscopy for colon cancer screening, surveillance, positive FIT, or computed tomography colonography. Only 59.2% of those with IBP underwent the recommended repeat colonoscopy within 1 year. Smoking and distance to the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation. Additional efforts are needed to ensure that individuals with IBP return for timely repeat colonoscopy.
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Atkin W, Wooldrage K, Brenner A, et al. Adenoma surveillance and colorectal cancer incidence: a retrospective, multicentre, cohort study. Lancet Oncol. 2017;18(6):823- 834. doi:10.1016/S1470-2045(17)30187-0
- Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;61(3):378- 384. doi:10.1016/s0016-5107(04)02776-2
- Mahmood S, Farooqui SM, Madhoun MF. Predictors of inadequate bowel preparation for colonoscopy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2018;30(8):819-826. doi:10.1097/MEG.0000000000001175
- ASGE Standards of Practice Committee, Saltzman JR, Cash BD, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81(4):781-794. doi:10.1016/j.gie.2014.09.048
- Clark BT, Protiva P, Nagar A, et al. Quantification of Adequate Bowel Preparation for Screening or Surveillance Colonoscopy in Men. Gastroenterology. 2016;150(2):396- e15. doi:10.1053/j.gastro.2015.09.041
- Sulz MC, Kröger A, Prakash M, Manser CN, Heinrich H, Misselwitz B. Meta-Analysis of the Effect of Bowel Preparation on Adenoma Detection: Early Adenomas Affected Stronger than Advanced Adenomas. PLoS One. 2016;11(6):e0154149. Published 2016 Jun 3. doi:10.1371/journal.pone.0154149
- Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75(6):1197-1203. doi:10.1016/j.gie.2012.01.005
- Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143(3):844-857. doi:10.1053/j.gastro.2012.06.001
- Fung P, Syed A, Cole R, Farah K. Poor bowel prep: are you really going to come back within a year? Abstract presented at American Gastroenterological Association DDW 2021, May 21-23, 2021. doi:10.1016/S0016-5085(21)01204-X
- US Department of Veterans Affairs, VA Health Systems Research. Corporate data warehouse (CDW). Updated January 11, 2023. Accessed August 6, 2024. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Lebwohl B, Kastrinos F, Glick M, Rosenbaum AJ, Wang T, Neugut AI. The impact of suboptimal bowel preparation on adenoma miss rates and the factors associated with early repeat colonoscopy. Gastrointest Endosc. 2011;73(6):1207-1214. doi:10.1016/j.gie.2011.01.051
- Calderwood AH, Holub JL, Greenwald DA. Recommendations for follow-up interval after colonoscopy with inadequate bowel preparation in a national colonoscopy quality registry. Gastrointest Endosc. 2022;95(2):360-367. e2. doi:10.1016/j.gie.2021.09.027
- Latorre M, Roy A, Spyrou E, Garcia-Carrasquillo R, Rosenberg R, Lebwohl B. Adherence to guidelines after poor colonoscopy preparation: experience from a patient navigator program. Gastroenterology. 2016;151(1):P196. doi:10.1053/j.gastro.2016.05.027
- Bouquet E, Tomal J, Choksi Y. Next-day screening colonoscopy following inadequate bowel preparation may improve quality of preparation and adenoma detection in a veteran population. Am J Gastroenterol. 2020;115:S259. doi:10.14309/ajg.0000000000000853
- Toro B, Dawkins G, Friedenberg FK, Ehrlich AC. Risk factors for failure to return after a poor preparation colonoscopy: experience in a safety-net hospital, 255. Abstract presented at ACG October 2016. https://journals.lww.com/ajg/fulltext/2016/10001/risk_factors_for_failure_to_return_after_a_poor.255.aspx
- Partin MR, Gravely A, Gellad ZF, et al. Factors Associated With Missed and Cancelled Colonoscopy Appointments at Veterans Health Administration Facilities. Clin Gastroenterol Hepatol. 2016;14(2):259-267. doi:10.1016/j.cgh.2015.07.051
- Idos GE, Bonner JD, Haghighat S, et al. Bridging the Gap: Patient Navigation Increases Colonoscopy Follow-up After Abnormal FIT. Clin Transl Gastroenterol. 2021;12(2):e00307. doi:10.14309/ctg.0000000000000307
- Islami F, Baeker Bispo J, Lee H, et al. American Cancer Society’s report on the status of cancer disparities in the United States, 2023. CA Cancer J Clin. 2024;74(2):136- 166. doi:10.3322/caac.21812
Colorectal cancer (CRC) is the third-most diagnosed cancer after breast and lung cancer, and is the second leading cause of global cancer related deaths.1 In 2023 in the United States, > 150,000 individuals were diagnosed with CRC and 52,000 died.2
Colonoscopy is an effective CRC screening method and the lone method recommended for polyp surveillance. Inadequate bowel preparation (IBP) has been estimated to occur in about 6% to 26% of colonoscopies. 3,4 The prevalence varies based on a variety of comorbidities, including immobility, diabetes mellitus, neurologic disorders, and use of opioids, with more occurrences of IBP noted in older adult, non-English speaking, and male individuals.4-6
The quality of bowel preparation is integral to the effectiveness of screening and surveillance colonoscopies. IBP has been associated with missed adenomas and significantly lower adenoma detection rates.7-9 In particular, IBP is independently associated with an increased risk of CRC in the future.3 Accordingly, the US Multisociety Task Force recommends repeat colonoscopies for individuals with IBP within 1 year.10 Ensuring that these individuals receive repeat colonoscopies is an essential part of CRC prevention. The benefit of repeat colonoscopy after IBP is highlighted by a retrospective analysis from Fung and colleagues that showed 81% of repeat colonoscopies had adequate bowel preparation, with higher numbers of adenomas detected on repeat compared to initial colonoscopies.11
Given the impact of bowel preparation quality on the diagnostic capability of the colonoscopy, adherence to guidelines for repeat colonoscopies in cases of IBP is paramount for effective CRC prevention. This study aims to measure the frequency of repeat colonoscopy after IBP and the factors associated with adherence to recommendations.
METHODS
Individuals who underwent colonoscopy at the Minneapolis Veterans Affairs Medical Center (MVAMC) from January 1, 2016, to October 19, 2021, were identified to allow for 400 days of follow-up from the index colonoscopy to the data collection date. During the COVID-19 pandemic, the colonoscopy procedure capacity was reduced by 50% from June 1, 2020, to December 1, 2020, delaying nonurgent procedures, including screening and surveillance colonoscopies.
Individuals who underwent colonoscopy for CRC screening or polyp surveillance, or following a positive fecal immunohistochemistry test (FIT) or virtual computed tomography colonoscopy were included. Patients with colonoscopy indications for iron deficiency anemia, gastrointestinal bleeding, disease activity assessment of inflammatory bowel disease, abdominal pain, or changes in bowel movement pattern were excluded. IBP was defined as recording a Boston Bowel Preparation Scale (BBPS) score of < 6, or < 2 in any segment, or described as poor or inadequate using the Aronchick scale.
Age, sex, race, marital status, distance to MVAMC, smoking status, comorbidities, and concurrent medication use, including antiplatelet, anticoagulation, and prescription opiates at the time of index colonoscopy were obtained from the Veterans Health Administration (VHA) Corporate Data Warehouse (CDW) using structured query language processing of colonoscopy procedure notes to extract preparation scores and other procedure information. The CDW contains extracts from VHA clinical and administrative systems that contain complete clinical data from October 1999.12 Current smoking status was defined as any smoking activity at the time the questionnaire was administered during a routine clinic visit within 400 days from the index colonoscopy.
Only individuals who were recommended to have repeat colonoscopy within 1 year were included. The intervals of 365 days and 400 days (1 year + about 1 additional month) were used in the event that the individual had a delay in scheduling their 1-year repeat colonoscopy. For individuals who did not undergo a colonoscopy at MVAMC within 400 days, a manual chart review of all available records was performed to determine whether a colonoscopy was performed at a non-VA facility.
Patients received written instructions for bowel preparation 2 weeks prior to the procedure. The preparation included magnesium citrate and a split dose of 4 liters of polyethylene glycol. Patients were also advised to start a low-fiber diet 3 days prior to the procedure and a clear liquid diet the day before the procedure. Patients with a history of IBP or those undergoing procedures with anesthesia received an additional 2 liters for a total of 6 liters of polyethylene glycol.
Statistical analysis
Baseline characteristics were reported as mean (SD) or median and IQR for continuous variables and percentage for categorical variables. Individuals who returned for colonoscopy within 400 days were compared to those who did not identify factors associated with adherence to recommendations. The data on individuals who returned for colonoscopy within 400 days were also analyzed for additional minor delays in the timing of the repeat colonoscopy. Continuous data were compared using Mann-Whitney U tests. Categorical data were compared using X2 or Fisher exact tests. Missing data were imputed from the analyses. All analyses were performed using SAS JMP Pro version 16. P < .05 was considered statistically significant.
RESULTS
There were 18,241 total colonoscopies performed between January 1, 2016, to October 19, 2021, and 13,818 colonoscopies had indications for screening for colon cancer, positive FIT, virtual colonoscopy, or surveillance. Of the 10,466 unique patients there were 5369 patients for polyp surveillance, 4054 patients for CRC screening, and 1043 patients for positive FIT or virtual colonoscopy. Of these, 571 individuals (5.5%) had IBP. Repeat colonoscopy within 1 year was recommended for 485 individuals (84.9%) who were included in this study (153 CRC screenings and 46 positive FITs) but not for 86 individuals (15.1%) (Figure 1). Among included patients, the mean (SD) age was 66.6 (7.2) years, and the majority were male (460 [94.8%]) and White (435 [89.7%]) (Table). Two hundred and forty-three (50.1%) were married.
Adherence to Recommended Interval Colonoscopy
Of the 485 patients with IBP who were recommended for follow-up colonoscopy, 287 (59.2%) had a colonoscopy within 1 year, and 198 (40.8%) did not; 17 patients (13.5%) had repeat colonoscopy within 366 to 400 days. Five (1.0%) individuals had a repeat colonoscopy the next day, and 77 (15.9%) had a repeat colonoscopy within 7 days. One hundred and twentysix (26.0%) individuals underwent no repeat colonoscopy during the study period (Figure 2).
To account for the COVID-19 pandemic, the adherence rate of repeat colonoscopy within 1 year prepandemic (January 1, 2016, to December 1, 2018) was calculated along with the adherence rate postpandemic (January 1, 2019 to the end of the study). The rates were similar: 199 of 330 (60.3%) individuals prepandemic vs 88 of 155 (56.8%) individuals postpandemic (Figure 3).
Significant Associations
Age, sex, and race were not associated with adherence to repeat colonoscopy within 1 year. Individuals living ≤ 40 miles from the endoscopy center were more likely to undergo a repeat colonoscopy within 1 year compared with those who lived > 40 miles away (61.7% vs 51.0%, P = .02). Current smoking status was associated with a lower rate of repeat colonoscopy within 1 year (25.8% vs 35.9%; P = .02). There were no differences with respect to inflammatory bowel disease diagnosis, mental health diagnosis, diabetes mellitus, cirrhosis, or medications used, including opioids, anticoagulation, and antiplatelet therapy.
Outcomes
Among individuals who had a repeat colonoscopy the day after the index colonoscopy, 53 of 56 individuals (94.6%) had adequate bowel preparation. Among individuals who had a repeat colonoscopy within 7 days, 70 of 77 (90.9%) had adequate bowel preparation. Of 287 individuals with a repeat colonoscopy within 1 year, 251 (87.5%) had adequate bowel preparation on the repeat colonoscopy. By 400 days after the index colonoscopy, 268 of 304 individuals (88.2%) had adequate bowel preparation.
In this study conducted at a large VA medical center, we found that 5.6% of individuals undergoing colonoscopies had IBP, a rate comparable to prior studies (6% to 26%).3,4 Only 59.2% of individuals underwent repeat colonoscopies within 1 year, as recommended after an index colonoscopy with IBP. Smoking and living longer distances (> 40 miles) from the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation.
Current guidelines recommend repeat colonoscopy for individuals with IBP within 1 year.10 In cases of IBP, the advanced adenoma miss rate is 36% upon repeat colonoscopy within 1 year.13 Despite the importance of a follow-up colonoscopy, clinician adherence with this recommendation remains low.10,14,15 However, in this study cohort, 485 of 571 individuals with IBP (84.9%) received recommendations for a repeat colonoscopy within 1 year. In the US, only 31.9% of 260,314 colonoscopies with IBP included recommendations for a follow-up colonoscopy within 1 year.14 This could be related to variations in endoscopist practice as well as patient risk factors for developing polyps, including family history of cancer and personal history of prior polyps. The findings of multiple polyps, high-risk adenomas, and cancer on the index colonoscopy also influences the endoscopist for repeat colonoscopy within 1 year.14
The timing for repeat colonoscopies within 1 year will be determined by the patients, clinicians, and available scheduling. In this study, the earlier repeat colonoscopies, especially those occurring the day after the index colonoscopy, had the highest success rate of adequate bowel preparation. In a prior study, repeating colonoscopies within the same day or the next day was also found to have a higher rate of adequate bowel preparation than repeat colonoscopies within 1 year (88.9% vs 83.5%).16
Ensuring the return of individuals with IBP for repeat colonoscopy is a challenging task. We identified that individuals who live further away from MVAMC and current smokers had a decreased probability of returning for a repeat colonoscopy. Toro and colleagues found a 68.7% return rate for a repeat colonoscopy within 1 year with individuals age ≥ 60 years, and patients who were White were less likely to proceed with a repeat colonoscopy within 1 year.17 The study did not provide data regarding smoking status or distance to the endoscopy center.17 In a prior study of veterans, the dual diagnosis of psychiatric disorders and substance abuse was associated with missed and canceled colonoscopy appointments.18 The distance to the endoscopy center has also been previously identified as a barrier to a colonoscopy following an abnormal FIT.19 Although not identified in this study due to the homogenous demographic profile, social determinants of health such as socioeconomic status, education, and insurance coverage are known barriers to cancer screening but were not evaluated in this study.20
Based on the identified risk factors, we have created a model for utilizing those risk factors to identify individuals at higher risk for noncompliance (ie, those who live further away from the endoscopy center or currently smoke). These individuals are proactively offered to use an intraprocedural bowel cleansing device to achieve adequate bowel preparation or priority rescheduling for a next-day colonoscopy.
Limitations
This study was a single-center study of the veteran population, which is predominantly White and male, thus limiting generalizability. The study is also limited by minimal available data on adenoma detection and colon cancer incidence on subsequent colonoscopies.
CONCLUSIONS
The rate of IBP was 5.5% in individuals undergoing colonoscopy for colon cancer screening, surveillance, positive FIT, or computed tomography colonography. Only 59.2% of those with IBP underwent the recommended repeat colonoscopy within 1 year. Smoking and distance to the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation. Additional efforts are needed to ensure that individuals with IBP return for timely repeat colonoscopy.
Colorectal cancer (CRC) is the third-most diagnosed cancer after breast and lung cancer, and is the second leading cause of global cancer related deaths.1 In 2023 in the United States, > 150,000 individuals were diagnosed with CRC and 52,000 died.2
Colonoscopy is an effective CRC screening method and the lone method recommended for polyp surveillance. Inadequate bowel preparation (IBP) has been estimated to occur in about 6% to 26% of colonoscopies. 3,4 The prevalence varies based on a variety of comorbidities, including immobility, diabetes mellitus, neurologic disorders, and use of opioids, with more occurrences of IBP noted in older adult, non-English speaking, and male individuals.4-6
The quality of bowel preparation is integral to the effectiveness of screening and surveillance colonoscopies. IBP has been associated with missed adenomas and significantly lower adenoma detection rates.7-9 In particular, IBP is independently associated with an increased risk of CRC in the future.3 Accordingly, the US Multisociety Task Force recommends repeat colonoscopies for individuals with IBP within 1 year.10 Ensuring that these individuals receive repeat colonoscopies is an essential part of CRC prevention. The benefit of repeat colonoscopy after IBP is highlighted by a retrospective analysis from Fung and colleagues that showed 81% of repeat colonoscopies had adequate bowel preparation, with higher numbers of adenomas detected on repeat compared to initial colonoscopies.11
Given the impact of bowel preparation quality on the diagnostic capability of the colonoscopy, adherence to guidelines for repeat colonoscopies in cases of IBP is paramount for effective CRC prevention. This study aims to measure the frequency of repeat colonoscopy after IBP and the factors associated with adherence to recommendations.
METHODS
Individuals who underwent colonoscopy at the Minneapolis Veterans Affairs Medical Center (MVAMC) from January 1, 2016, to October 19, 2021, were identified to allow for 400 days of follow-up from the index colonoscopy to the data collection date. During the COVID-19 pandemic, the colonoscopy procedure capacity was reduced by 50% from June 1, 2020, to December 1, 2020, delaying nonurgent procedures, including screening and surveillance colonoscopies.
Individuals who underwent colonoscopy for CRC screening or polyp surveillance, or following a positive fecal immunohistochemistry test (FIT) or virtual computed tomography colonoscopy were included. Patients with colonoscopy indications for iron deficiency anemia, gastrointestinal bleeding, disease activity assessment of inflammatory bowel disease, abdominal pain, or changes in bowel movement pattern were excluded. IBP was defined as recording a Boston Bowel Preparation Scale (BBPS) score of < 6, or < 2 in any segment, or described as poor or inadequate using the Aronchick scale.
Age, sex, race, marital status, distance to MVAMC, smoking status, comorbidities, and concurrent medication use, including antiplatelet, anticoagulation, and prescription opiates at the time of index colonoscopy were obtained from the Veterans Health Administration (VHA) Corporate Data Warehouse (CDW) using structured query language processing of colonoscopy procedure notes to extract preparation scores and other procedure information. The CDW contains extracts from VHA clinical and administrative systems that contain complete clinical data from October 1999.12 Current smoking status was defined as any smoking activity at the time the questionnaire was administered during a routine clinic visit within 400 days from the index colonoscopy.
Only individuals who were recommended to have repeat colonoscopy within 1 year were included. The intervals of 365 days and 400 days (1 year + about 1 additional month) were used in the event that the individual had a delay in scheduling their 1-year repeat colonoscopy. For individuals who did not undergo a colonoscopy at MVAMC within 400 days, a manual chart review of all available records was performed to determine whether a colonoscopy was performed at a non-VA facility.
Patients received written instructions for bowel preparation 2 weeks prior to the procedure. The preparation included magnesium citrate and a split dose of 4 liters of polyethylene glycol. Patients were also advised to start a low-fiber diet 3 days prior to the procedure and a clear liquid diet the day before the procedure. Patients with a history of IBP or those undergoing procedures with anesthesia received an additional 2 liters for a total of 6 liters of polyethylene glycol.
Statistical analysis
Baseline characteristics were reported as mean (SD) or median and IQR for continuous variables and percentage for categorical variables. Individuals who returned for colonoscopy within 400 days were compared to those who did not identify factors associated with adherence to recommendations. The data on individuals who returned for colonoscopy within 400 days were also analyzed for additional minor delays in the timing of the repeat colonoscopy. Continuous data were compared using Mann-Whitney U tests. Categorical data were compared using X2 or Fisher exact tests. Missing data were imputed from the analyses. All analyses were performed using SAS JMP Pro version 16. P < .05 was considered statistically significant.
RESULTS
There were 18,241 total colonoscopies performed between January 1, 2016, to October 19, 2021, and 13,818 colonoscopies had indications for screening for colon cancer, positive FIT, virtual colonoscopy, or surveillance. Of the 10,466 unique patients there were 5369 patients for polyp surveillance, 4054 patients for CRC screening, and 1043 patients for positive FIT or virtual colonoscopy. Of these, 571 individuals (5.5%) had IBP. Repeat colonoscopy within 1 year was recommended for 485 individuals (84.9%) who were included in this study (153 CRC screenings and 46 positive FITs) but not for 86 individuals (15.1%) (Figure 1). Among included patients, the mean (SD) age was 66.6 (7.2) years, and the majority were male (460 [94.8%]) and White (435 [89.7%]) (Table). Two hundred and forty-three (50.1%) were married.
Adherence to Recommended Interval Colonoscopy
Of the 485 patients with IBP who were recommended for follow-up colonoscopy, 287 (59.2%) had a colonoscopy within 1 year, and 198 (40.8%) did not; 17 patients (13.5%) had repeat colonoscopy within 366 to 400 days. Five (1.0%) individuals had a repeat colonoscopy the next day, and 77 (15.9%) had a repeat colonoscopy within 7 days. One hundred and twentysix (26.0%) individuals underwent no repeat colonoscopy during the study period (Figure 2).
To account for the COVID-19 pandemic, the adherence rate of repeat colonoscopy within 1 year prepandemic (January 1, 2016, to December 1, 2018) was calculated along with the adherence rate postpandemic (January 1, 2019 to the end of the study). The rates were similar: 199 of 330 (60.3%) individuals prepandemic vs 88 of 155 (56.8%) individuals postpandemic (Figure 3).
Significant Associations
Age, sex, and race were not associated with adherence to repeat colonoscopy within 1 year. Individuals living ≤ 40 miles from the endoscopy center were more likely to undergo a repeat colonoscopy within 1 year compared with those who lived > 40 miles away (61.7% vs 51.0%, P = .02). Current smoking status was associated with a lower rate of repeat colonoscopy within 1 year (25.8% vs 35.9%; P = .02). There were no differences with respect to inflammatory bowel disease diagnosis, mental health diagnosis, diabetes mellitus, cirrhosis, or medications used, including opioids, anticoagulation, and antiplatelet therapy.
Outcomes
Among individuals who had a repeat colonoscopy the day after the index colonoscopy, 53 of 56 individuals (94.6%) had adequate bowel preparation. Among individuals who had a repeat colonoscopy within 7 days, 70 of 77 (90.9%) had adequate bowel preparation. Of 287 individuals with a repeat colonoscopy within 1 year, 251 (87.5%) had adequate bowel preparation on the repeat colonoscopy. By 400 days after the index colonoscopy, 268 of 304 individuals (88.2%) had adequate bowel preparation.
In this study conducted at a large VA medical center, we found that 5.6% of individuals undergoing colonoscopies had IBP, a rate comparable to prior studies (6% to 26%).3,4 Only 59.2% of individuals underwent repeat colonoscopies within 1 year, as recommended after an index colonoscopy with IBP. Smoking and living longer distances (> 40 miles) from the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation.
Current guidelines recommend repeat colonoscopy for individuals with IBP within 1 year.10 In cases of IBP, the advanced adenoma miss rate is 36% upon repeat colonoscopy within 1 year.13 Despite the importance of a follow-up colonoscopy, clinician adherence with this recommendation remains low.10,14,15 However, in this study cohort, 485 of 571 individuals with IBP (84.9%) received recommendations for a repeat colonoscopy within 1 year. In the US, only 31.9% of 260,314 colonoscopies with IBP included recommendations for a follow-up colonoscopy within 1 year.14 This could be related to variations in endoscopist practice as well as patient risk factors for developing polyps, including family history of cancer and personal history of prior polyps. The findings of multiple polyps, high-risk adenomas, and cancer on the index colonoscopy also influences the endoscopist for repeat colonoscopy within 1 year.14
The timing for repeat colonoscopies within 1 year will be determined by the patients, clinicians, and available scheduling. In this study, the earlier repeat colonoscopies, especially those occurring the day after the index colonoscopy, had the highest success rate of adequate bowel preparation. In a prior study, repeating colonoscopies within the same day or the next day was also found to have a higher rate of adequate bowel preparation than repeat colonoscopies within 1 year (88.9% vs 83.5%).16
Ensuring the return of individuals with IBP for repeat colonoscopy is a challenging task. We identified that individuals who live further away from MVAMC and current smokers had a decreased probability of returning for a repeat colonoscopy. Toro and colleagues found a 68.7% return rate for a repeat colonoscopy within 1 year with individuals age ≥ 60 years, and patients who were White were less likely to proceed with a repeat colonoscopy within 1 year.17 The study did not provide data regarding smoking status or distance to the endoscopy center.17 In a prior study of veterans, the dual diagnosis of psychiatric disorders and substance abuse was associated with missed and canceled colonoscopy appointments.18 The distance to the endoscopy center has also been previously identified as a barrier to a colonoscopy following an abnormal FIT.19 Although not identified in this study due to the homogenous demographic profile, social determinants of health such as socioeconomic status, education, and insurance coverage are known barriers to cancer screening but were not evaluated in this study.20
Based on the identified risk factors, we have created a model for utilizing those risk factors to identify individuals at higher risk for noncompliance (ie, those who live further away from the endoscopy center or currently smoke). These individuals are proactively offered to use an intraprocedural bowel cleansing device to achieve adequate bowel preparation or priority rescheduling for a next-day colonoscopy.
Limitations
This study was a single-center study of the veteran population, which is predominantly White and male, thus limiting generalizability. The study is also limited by minimal available data on adenoma detection and colon cancer incidence on subsequent colonoscopies.
CONCLUSIONS
The rate of IBP was 5.5% in individuals undergoing colonoscopy for colon cancer screening, surveillance, positive FIT, or computed tomography colonography. Only 59.2% of those with IBP underwent the recommended repeat colonoscopy within 1 year. Smoking and distance to the endoscopy center were associated with a decreased adherence to the repeat colonoscopy recommendation. Additional efforts are needed to ensure that individuals with IBP return for timely repeat colonoscopy.
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Atkin W, Wooldrage K, Brenner A, et al. Adenoma surveillance and colorectal cancer incidence: a retrospective, multicentre, cohort study. Lancet Oncol. 2017;18(6):823- 834. doi:10.1016/S1470-2045(17)30187-0
- Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;61(3):378- 384. doi:10.1016/s0016-5107(04)02776-2
- Mahmood S, Farooqui SM, Madhoun MF. Predictors of inadequate bowel preparation for colonoscopy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2018;30(8):819-826. doi:10.1097/MEG.0000000000001175
- ASGE Standards of Practice Committee, Saltzman JR, Cash BD, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81(4):781-794. doi:10.1016/j.gie.2014.09.048
- Clark BT, Protiva P, Nagar A, et al. Quantification of Adequate Bowel Preparation for Screening or Surveillance Colonoscopy in Men. Gastroenterology. 2016;150(2):396- e15. doi:10.1053/j.gastro.2015.09.041
- Sulz MC, Kröger A, Prakash M, Manser CN, Heinrich H, Misselwitz B. Meta-Analysis of the Effect of Bowel Preparation on Adenoma Detection: Early Adenomas Affected Stronger than Advanced Adenomas. PLoS One. 2016;11(6):e0154149. Published 2016 Jun 3. doi:10.1371/journal.pone.0154149
- Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75(6):1197-1203. doi:10.1016/j.gie.2012.01.005
- Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143(3):844-857. doi:10.1053/j.gastro.2012.06.001
- Fung P, Syed A, Cole R, Farah K. Poor bowel prep: are you really going to come back within a year? Abstract presented at American Gastroenterological Association DDW 2021, May 21-23, 2021. doi:10.1016/S0016-5085(21)01204-X
- US Department of Veterans Affairs, VA Health Systems Research. Corporate data warehouse (CDW). Updated January 11, 2023. Accessed August 6, 2024. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Lebwohl B, Kastrinos F, Glick M, Rosenbaum AJ, Wang T, Neugut AI. The impact of suboptimal bowel preparation on adenoma miss rates and the factors associated with early repeat colonoscopy. Gastrointest Endosc. 2011;73(6):1207-1214. doi:10.1016/j.gie.2011.01.051
- Calderwood AH, Holub JL, Greenwald DA. Recommendations for follow-up interval after colonoscopy with inadequate bowel preparation in a national colonoscopy quality registry. Gastrointest Endosc. 2022;95(2):360-367. e2. doi:10.1016/j.gie.2021.09.027
- Latorre M, Roy A, Spyrou E, Garcia-Carrasquillo R, Rosenberg R, Lebwohl B. Adherence to guidelines after poor colonoscopy preparation: experience from a patient navigator program. Gastroenterology. 2016;151(1):P196. doi:10.1053/j.gastro.2016.05.027
- Bouquet E, Tomal J, Choksi Y. Next-day screening colonoscopy following inadequate bowel preparation may improve quality of preparation and adenoma detection in a veteran population. Am J Gastroenterol. 2020;115:S259. doi:10.14309/ajg.0000000000000853
- Toro B, Dawkins G, Friedenberg FK, Ehrlich AC. Risk factors for failure to return after a poor preparation colonoscopy: experience in a safety-net hospital, 255. Abstract presented at ACG October 2016. https://journals.lww.com/ajg/fulltext/2016/10001/risk_factors_for_failure_to_return_after_a_poor.255.aspx
- Partin MR, Gravely A, Gellad ZF, et al. Factors Associated With Missed and Cancelled Colonoscopy Appointments at Veterans Health Administration Facilities. Clin Gastroenterol Hepatol. 2016;14(2):259-267. doi:10.1016/j.cgh.2015.07.051
- Idos GE, Bonner JD, Haghighat S, et al. Bridging the Gap: Patient Navigation Increases Colonoscopy Follow-up After Abnormal FIT. Clin Transl Gastroenterol. 2021;12(2):e00307. doi:10.14309/ctg.0000000000000307
- Islami F, Baeker Bispo J, Lee H, et al. American Cancer Society’s report on the status of cancer disparities in the United States, 2023. CA Cancer J Clin. 2024;74(2):136- 166. doi:10.3322/caac.21812
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi:10.3322/caac.21660
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Atkin W, Wooldrage K, Brenner A, et al. Adenoma surveillance and colorectal cancer incidence: a retrospective, multicentre, cohort study. Lancet Oncol. 2017;18(6):823- 834. doi:10.1016/S1470-2045(17)30187-0
- Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;61(3):378- 384. doi:10.1016/s0016-5107(04)02776-2
- Mahmood S, Farooqui SM, Madhoun MF. Predictors of inadequate bowel preparation for colonoscopy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2018;30(8):819-826. doi:10.1097/MEG.0000000000001175
- ASGE Standards of Practice Committee, Saltzman JR, Cash BD, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81(4):781-794. doi:10.1016/j.gie.2014.09.048
- Clark BT, Protiva P, Nagar A, et al. Quantification of Adequate Bowel Preparation for Screening or Surveillance Colonoscopy in Men. Gastroenterology. 2016;150(2):396- e15. doi:10.1053/j.gastro.2015.09.041
- Sulz MC, Kröger A, Prakash M, Manser CN, Heinrich H, Misselwitz B. Meta-Analysis of the Effect of Bowel Preparation on Adenoma Detection: Early Adenomas Affected Stronger than Advanced Adenomas. PLoS One. 2016;11(6):e0154149. Published 2016 Jun 3. doi:10.1371/journal.pone.0154149
- Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc. 2012;75(6):1197-1203. doi:10.1016/j.gie.2012.01.005
- Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143(3):844-857. doi:10.1053/j.gastro.2012.06.001
- Fung P, Syed A, Cole R, Farah K. Poor bowel prep: are you really going to come back within a year? Abstract presented at American Gastroenterological Association DDW 2021, May 21-23, 2021. doi:10.1016/S0016-5085(21)01204-X
- US Department of Veterans Affairs, VA Health Systems Research. Corporate data warehouse (CDW). Updated January 11, 2023. Accessed August 6, 2024. https://www.hsrd.research.va.gov/for_researchers/cdw.cfm
- Lebwohl B, Kastrinos F, Glick M, Rosenbaum AJ, Wang T, Neugut AI. The impact of suboptimal bowel preparation on adenoma miss rates and the factors associated with early repeat colonoscopy. Gastrointest Endosc. 2011;73(6):1207-1214. doi:10.1016/j.gie.2011.01.051
- Calderwood AH, Holub JL, Greenwald DA. Recommendations for follow-up interval after colonoscopy with inadequate bowel preparation in a national colonoscopy quality registry. Gastrointest Endosc. 2022;95(2):360-367. e2. doi:10.1016/j.gie.2021.09.027
- Latorre M, Roy A, Spyrou E, Garcia-Carrasquillo R, Rosenberg R, Lebwohl B. Adherence to guidelines after poor colonoscopy preparation: experience from a patient navigator program. Gastroenterology. 2016;151(1):P196. doi:10.1053/j.gastro.2016.05.027
- Bouquet E, Tomal J, Choksi Y. Next-day screening colonoscopy following inadequate bowel preparation may improve quality of preparation and adenoma detection in a veteran population. Am J Gastroenterol. 2020;115:S259. doi:10.14309/ajg.0000000000000853
- Toro B, Dawkins G, Friedenberg FK, Ehrlich AC. Risk factors for failure to return after a poor preparation colonoscopy: experience in a safety-net hospital, 255. Abstract presented at ACG October 2016. https://journals.lww.com/ajg/fulltext/2016/10001/risk_factors_for_failure_to_return_after_a_poor.255.aspx
- Partin MR, Gravely A, Gellad ZF, et al. Factors Associated With Missed and Cancelled Colonoscopy Appointments at Veterans Health Administration Facilities. Clin Gastroenterol Hepatol. 2016;14(2):259-267. doi:10.1016/j.cgh.2015.07.051
- Idos GE, Bonner JD, Haghighat S, et al. Bridging the Gap: Patient Navigation Increases Colonoscopy Follow-up After Abnormal FIT. Clin Transl Gastroenterol. 2021;12(2):e00307. doi:10.14309/ctg.0000000000000307
- Islami F, Baeker Bispo J, Lee H, et al. American Cancer Society’s report on the status of cancer disparities in the United States, 2023. CA Cancer J Clin. 2024;74(2):136- 166. doi:10.3322/caac.21812
Expert Warns of Problems with Large Language Models in Dermatology
HUNTINGTON BEACH, CALIF. — and alarmed.
Of the 134 respondents who completed the survey, 87 (65%) reported using LLMs in a clinical setting. Of those 87 respondents, 17 (20%) used LMMs daily, 28 (32%) weekly, 5 (6%) monthly, and 37 (43%) rarely. That represents “pretty significant usage,” Dr. Daneshjou, assistant professor of biomedical data science and dermatology at Stanford University, Palo Alto, California, said at the annual meeting of the Pacific Dermatologic Association.

Most of the respondents reported using LLMs for patient care (79%), followed by administrative tasks (74%), medical records (43%), and education (18%), “which can be problematic,” she said. “These models are not appropriate to use for patient care.”
When asked about their thoughts on the accuracy of LLMs, 58% of respondents deemed them to be “somewhat accurate” and 7% viewed them as “extremely accurate.”
The overall survey responses raise concern because LLMs “are not trained for accuracy; they are trained initially as a next-word predictor on large bodies of tech data,” Dr. Daneshjou said. “LLMs are already being implemented but have the potential to cause harm and bias, and I believe they will if we implement them the way things are rolling out right now. I don’t understand why we’re implementing something without any clinical trial or showing that it improves care before we throw untested technology into our healthcare system.”
Meanwhile, Epic and Microsoft are collaborating to bring AI technology to electronic health records, she said, and Epic is building more than 100 new AI features for physicians and patients. “I think it’s important for every physician and trainee to understand what is going on in the realm of AI,” said Dr. Daneshjou, who is an associate editor for the monthly journal NEJM AI. “Be involved in the conversation because we are the clinical experts, and a lot of people making decisions and building tools do not have the clinical expertise.”
To further illustrate her concerns, Dr. Daneshjou referenced a red teaming event she and her colleagues held with computer scientists, biomedical data scientists, engineers, and physicians across multiple specialties to identify issues related to safety, bias, factual errors, and/or security issues in GPT-3.5, GPT-4, and GPT-4 with internet. The goal was to mimic clinical health scenarios, ask the LLM to respond, and have the team members review the accuracy of LLM responses.
The participants found that nearly 20% of LLM responses were inappropriate. For example, in one task, an LLM was asked to calculate a RegiSCAR score for Drug Reaction With Eosinophilia and Systemic Symptoms for a patient, but the response included an incorrect score for eosinophilia. “That’s why these tools can be so dangerous because you’re reading along and everything seems right, but there might be something so minor that can impact patient care and you might miss it,” Dr. Daneshjou said.
On a related note, she advised against dermatologists uploading images into GPT-4 Vision, an LLM that can analyze images and provide textual responses to questions about them, and she recommends not using GPT-4 Vision for any diagnostic support. At this time, “GPT-4 Vision overcalls malignancies, and the specificity and sensitivity are not very good,” she explained.
Dr. Daneshjou disclosed that she has served as an adviser to MDalgorithms and Revea and has received consulting fees from Pfizer, L’Oréal, Frazier Healthcare Partners, and DWA and research funding from UCB.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — and alarmed.
Of the 134 respondents who completed the survey, 87 (65%) reported using LLMs in a clinical setting. Of those 87 respondents, 17 (20%) used LMMs daily, 28 (32%) weekly, 5 (6%) monthly, and 37 (43%) rarely. That represents “pretty significant usage,” Dr. Daneshjou, assistant professor of biomedical data science and dermatology at Stanford University, Palo Alto, California, said at the annual meeting of the Pacific Dermatologic Association.
Most of the respondents reported using LLMs for patient care (79%), followed by administrative tasks (74%), medical records (43%), and education (18%), “which can be problematic,” she said. “These models are not appropriate to use for patient care.”
When asked about their thoughts on the accuracy of LLMs, 58% of respondents deemed them to be “somewhat accurate” and 7% viewed them as “extremely accurate.”
The overall survey responses raise concern because LLMs “are not trained for accuracy; they are trained initially as a next-word predictor on large bodies of tech data,” Dr. Daneshjou said. “LLMs are already being implemented but have the potential to cause harm and bias, and I believe they will if we implement them the way things are rolling out right now. I don’t understand why we’re implementing something without any clinical trial or showing that it improves care before we throw untested technology into our healthcare system.”
Meanwhile, Epic and Microsoft are collaborating to bring AI technology to electronic health records, she said, and Epic is building more than 100 new AI features for physicians and patients. “I think it’s important for every physician and trainee to understand what is going on in the realm of AI,” said Dr. Daneshjou, who is an associate editor for the monthly journal NEJM AI. “Be involved in the conversation because we are the clinical experts, and a lot of people making decisions and building tools do not have the clinical expertise.”
To further illustrate her concerns, Dr. Daneshjou referenced a red teaming event she and her colleagues held with computer scientists, biomedical data scientists, engineers, and physicians across multiple specialties to identify issues related to safety, bias, factual errors, and/or security issues in GPT-3.5, GPT-4, and GPT-4 with internet. The goal was to mimic clinical health scenarios, ask the LLM to respond, and have the team members review the accuracy of LLM responses.
The participants found that nearly 20% of LLM responses were inappropriate. For example, in one task, an LLM was asked to calculate a RegiSCAR score for Drug Reaction With Eosinophilia and Systemic Symptoms for a patient, but the response included an incorrect score for eosinophilia. “That’s why these tools can be so dangerous because you’re reading along and everything seems right, but there might be something so minor that can impact patient care and you might miss it,” Dr. Daneshjou said.
On a related note, she advised against dermatologists uploading images into GPT-4 Vision, an LLM that can analyze images and provide textual responses to questions about them, and she recommends not using GPT-4 Vision for any diagnostic support. At this time, “GPT-4 Vision overcalls malignancies, and the specificity and sensitivity are not very good,” she explained.
Dr. Daneshjou disclosed that she has served as an adviser to MDalgorithms and Revea and has received consulting fees from Pfizer, L’Oréal, Frazier Healthcare Partners, and DWA and research funding from UCB.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — and alarmed.
Of the 134 respondents who completed the survey, 87 (65%) reported using LLMs in a clinical setting. Of those 87 respondents, 17 (20%) used LMMs daily, 28 (32%) weekly, 5 (6%) monthly, and 37 (43%) rarely. That represents “pretty significant usage,” Dr. Daneshjou, assistant professor of biomedical data science and dermatology at Stanford University, Palo Alto, California, said at the annual meeting of the Pacific Dermatologic Association.
Most of the respondents reported using LLMs for patient care (79%), followed by administrative tasks (74%), medical records (43%), and education (18%), “which can be problematic,” she said. “These models are not appropriate to use for patient care.”
When asked about their thoughts on the accuracy of LLMs, 58% of respondents deemed them to be “somewhat accurate” and 7% viewed them as “extremely accurate.”
The overall survey responses raise concern because LLMs “are not trained for accuracy; they are trained initially as a next-word predictor on large bodies of tech data,” Dr. Daneshjou said. “LLMs are already being implemented but have the potential to cause harm and bias, and I believe they will if we implement them the way things are rolling out right now. I don’t understand why we’re implementing something without any clinical trial or showing that it improves care before we throw untested technology into our healthcare system.”
Meanwhile, Epic and Microsoft are collaborating to bring AI technology to electronic health records, she said, and Epic is building more than 100 new AI features for physicians and patients. “I think it’s important for every physician and trainee to understand what is going on in the realm of AI,” said Dr. Daneshjou, who is an associate editor for the monthly journal NEJM AI. “Be involved in the conversation because we are the clinical experts, and a lot of people making decisions and building tools do not have the clinical expertise.”
To further illustrate her concerns, Dr. Daneshjou referenced a red teaming event she and her colleagues held with computer scientists, biomedical data scientists, engineers, and physicians across multiple specialties to identify issues related to safety, bias, factual errors, and/or security issues in GPT-3.5, GPT-4, and GPT-4 with internet. The goal was to mimic clinical health scenarios, ask the LLM to respond, and have the team members review the accuracy of LLM responses.
The participants found that nearly 20% of LLM responses were inappropriate. For example, in one task, an LLM was asked to calculate a RegiSCAR score for Drug Reaction With Eosinophilia and Systemic Symptoms for a patient, but the response included an incorrect score for eosinophilia. “That’s why these tools can be so dangerous because you’re reading along and everything seems right, but there might be something so minor that can impact patient care and you might miss it,” Dr. Daneshjou said.
On a related note, she advised against dermatologists uploading images into GPT-4 Vision, an LLM that can analyze images and provide textual responses to questions about them, and she recommends not using GPT-4 Vision for any diagnostic support. At this time, “GPT-4 Vision overcalls malignancies, and the specificity and sensitivity are not very good,” she explained.
Dr. Daneshjou disclosed that she has served as an adviser to MDalgorithms and Revea and has received consulting fees from Pfizer, L’Oréal, Frazier Healthcare Partners, and DWA and research funding from UCB.
A version of this article first appeared on Medscape.com.
FROM PDA 2024
Diabetes Drug Improved Symptoms in Small Study of Women With Central Centrifugal Cicatricial Alopecia
TOPLINE:
in a retrospective case series.
METHODOLOGY:
- Researchers conducted a case series involving 12 Black women in their 30s, 40s, and 50s, with biopsy-confirmed, treatment-refractory CCCA, a chronic inflammatory hair disorder characterized by permanent hair loss, from the Johns Hopkins University alopecia clinic.
- Participants received CCCA treatment for at least 6 months and had stagnant or worsening symptoms before oral extended-release metformin (500 mg daily) was added to treatment. (Treatments included topical clobetasol, compounded minoxidil, and platelet-rich plasma injections.)
- Scalp biopsies were collected from four patients before and after metformin treatment to evaluate gene expression changes.
- Changes in clinical symptoms were assessed, including pruritus, inflammation, pain, scalp resistance, and hair regrowth, following initiation of metformin treatment.
TAKEAWAY:
- Metformin led to significant clinical improvement in eight patients, which included reductions in scalp pain, scalp resistance, pruritus, and inflammation. However, two patients experienced worsening symptoms.
- Six patients showed clinical evidence of hair regrowth after at least 6 months of metformin treatment with one experiencing hair loss again 3 months after discontinuing treatment.
- Transcriptomic analysis revealed 34 up-regulated genes, which included up-regulated of 23 hair keratin–associated proteins, and pathways related to keratinization, epidermis development, and the hair cycle. In addition, eight genes were down-regulated, with pathways that included those associated with extracellular matrix organization, collagen fibril organization, and collagen metabolism.
- Gene set variation analysis showed reduced expression of T helper 17 cell and epithelial-mesenchymal transition pathways and elevated adenosine monophosphate kinase signaling and keratin-associated proteins after treatment with metformin.
IN PRACTICE:
“Metformin’s ability to concomitantly target fibrosis and inflammation provides a plausible mechanism for its therapeutic effects in CCCA and other fibrosing alopecia disorders,” the authors concluded. But, they added, “larger prospective, placebo-controlled randomized clinical trials are needed to rigorously evaluate metformin’s efficacy and optimal dosing for treatment of cicatricial alopecias.”
SOURCE:
The study was led by Aaron Bao, Department of Dermatology, Johns Hopkins University School of Medicine, Baltimore, Maryland, and was published online on September 4 in JAMA Dermatology.
LIMITATIONS:
A small sample size, retrospective design, lack of a placebo control group, and the single-center setting limited the generalizability of the study findings. Additionally, the absence of a validated activity or severity scale for CCCA and the single posttreatment sampling limit the assessment and comparison of clinical symptoms and transcriptomic changes.
DISCLOSURES:
The study was supported by the American Academy of Dermatology. One author reported several ties with pharmaceutical companies, a pending patent, and authorship for the UpToDate section on CCCA.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
in a retrospective case series.
METHODOLOGY:
- Researchers conducted a case series involving 12 Black women in their 30s, 40s, and 50s, with biopsy-confirmed, treatment-refractory CCCA, a chronic inflammatory hair disorder characterized by permanent hair loss, from the Johns Hopkins University alopecia clinic.
- Participants received CCCA treatment for at least 6 months and had stagnant or worsening symptoms before oral extended-release metformin (500 mg daily) was added to treatment. (Treatments included topical clobetasol, compounded minoxidil, and platelet-rich plasma injections.)
- Scalp biopsies were collected from four patients before and after metformin treatment to evaluate gene expression changes.
- Changes in clinical symptoms were assessed, including pruritus, inflammation, pain, scalp resistance, and hair regrowth, following initiation of metformin treatment.
TAKEAWAY:
- Metformin led to significant clinical improvement in eight patients, which included reductions in scalp pain, scalp resistance, pruritus, and inflammation. However, two patients experienced worsening symptoms.
- Six patients showed clinical evidence of hair regrowth after at least 6 months of metformin treatment with one experiencing hair loss again 3 months after discontinuing treatment.
- Transcriptomic analysis revealed 34 up-regulated genes, which included up-regulated of 23 hair keratin–associated proteins, and pathways related to keratinization, epidermis development, and the hair cycle. In addition, eight genes were down-regulated, with pathways that included those associated with extracellular matrix organization, collagen fibril organization, and collagen metabolism.
- Gene set variation analysis showed reduced expression of T helper 17 cell and epithelial-mesenchymal transition pathways and elevated adenosine monophosphate kinase signaling and keratin-associated proteins after treatment with metformin.
IN PRACTICE:
“Metformin’s ability to concomitantly target fibrosis and inflammation provides a plausible mechanism for its therapeutic effects in CCCA and other fibrosing alopecia disorders,” the authors concluded. But, they added, “larger prospective, placebo-controlled randomized clinical trials are needed to rigorously evaluate metformin’s efficacy and optimal dosing for treatment of cicatricial alopecias.”
SOURCE:
The study was led by Aaron Bao, Department of Dermatology, Johns Hopkins University School of Medicine, Baltimore, Maryland, and was published online on September 4 in JAMA Dermatology.
LIMITATIONS:
A small sample size, retrospective design, lack of a placebo control group, and the single-center setting limited the generalizability of the study findings. Additionally, the absence of a validated activity or severity scale for CCCA and the single posttreatment sampling limit the assessment and comparison of clinical symptoms and transcriptomic changes.
DISCLOSURES:
The study was supported by the American Academy of Dermatology. One author reported several ties with pharmaceutical companies, a pending patent, and authorship for the UpToDate section on CCCA.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
in a retrospective case series.
METHODOLOGY:
- Researchers conducted a case series involving 12 Black women in their 30s, 40s, and 50s, with biopsy-confirmed, treatment-refractory CCCA, a chronic inflammatory hair disorder characterized by permanent hair loss, from the Johns Hopkins University alopecia clinic.
- Participants received CCCA treatment for at least 6 months and had stagnant or worsening symptoms before oral extended-release metformin (500 mg daily) was added to treatment. (Treatments included topical clobetasol, compounded minoxidil, and platelet-rich plasma injections.)
- Scalp biopsies were collected from four patients before and after metformin treatment to evaluate gene expression changes.
- Changes in clinical symptoms were assessed, including pruritus, inflammation, pain, scalp resistance, and hair regrowth, following initiation of metformin treatment.
TAKEAWAY:
- Metformin led to significant clinical improvement in eight patients, which included reductions in scalp pain, scalp resistance, pruritus, and inflammation. However, two patients experienced worsening symptoms.
- Six patients showed clinical evidence of hair regrowth after at least 6 months of metformin treatment with one experiencing hair loss again 3 months after discontinuing treatment.
- Transcriptomic analysis revealed 34 up-regulated genes, which included up-regulated of 23 hair keratin–associated proteins, and pathways related to keratinization, epidermis development, and the hair cycle. In addition, eight genes were down-regulated, with pathways that included those associated with extracellular matrix organization, collagen fibril organization, and collagen metabolism.
- Gene set variation analysis showed reduced expression of T helper 17 cell and epithelial-mesenchymal transition pathways and elevated adenosine monophosphate kinase signaling and keratin-associated proteins after treatment with metformin.
IN PRACTICE:
“Metformin’s ability to concomitantly target fibrosis and inflammation provides a plausible mechanism for its therapeutic effects in CCCA and other fibrosing alopecia disorders,” the authors concluded. But, they added, “larger prospective, placebo-controlled randomized clinical trials are needed to rigorously evaluate metformin’s efficacy and optimal dosing for treatment of cicatricial alopecias.”
SOURCE:
The study was led by Aaron Bao, Department of Dermatology, Johns Hopkins University School of Medicine, Baltimore, Maryland, and was published online on September 4 in JAMA Dermatology.
LIMITATIONS:
A small sample size, retrospective design, lack of a placebo control group, and the single-center setting limited the generalizability of the study findings. Additionally, the absence of a validated activity or severity scale for CCCA and the single posttreatment sampling limit the assessment and comparison of clinical symptoms and transcriptomic changes.
DISCLOSURES:
The study was supported by the American Academy of Dermatology. One author reported several ties with pharmaceutical companies, a pending patent, and authorship for the UpToDate section on CCCA.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Laser, Radiofrequency Therapies Offer Little Benefit for Genitourinary Syndrome of Menopause
CHICAGO — Use of CO2 lasers and similar “energy-based” treatments result in little to no benefit for genitourinary syndrome of menopause (GSM) symptoms, according to research presented at the The Menopause Society 2024 Annual Meeting in Chicago on September 12.
“There was a concern that menopausal women are being targeted for treatments that may not have a lot of benefit and might have significant harms,” Elisheva Danan, MD, MPH, a physician at the Minneapolis VA Health Care System and an assistant professor of medicine at the University of Minnesota Medical School in Minneapolis, told this news organization. While she was not surprised to find little evidence of benefit, “we were a little bit surprised that we also didn’t find significant evidence of harms.”
The study was unable to evaluate the potential for financial harms, but Dr. Danan noted that these therapies are often expensive and not typically covered by insurance. The treatments appear to be used primarily in private practice, she said, while “most academic clinicians were not familiar with these and do not use these lasers.”
The American Urological Association had requested the review, Dr. Danan said, “to inform clinical guidelines that they could put out for practitioners about treating genital urinary syndrome from menopause.” Yet the evidence available remains slim. “There’s a lot of outcomes that were not looked at by most of these [trials], or they were looked at in a way that we couldn’t separate out,” she said.
Kamalini Das, MD, a professor of ob.gyn. at the University of Minnesota who was not involved in the research, was surprised by the findings because studies to date have been variable, “but since this looks at multiple studies and they find no benefits, I would take these results as more significant than any of the small studies,” she told this news organization.
Dr. Das said she has patients who ask about using these therapies and have had them done. “So far, I’ve told them the jury is out on whether it will help or not, that there are some studies that say they’re beneficial and some studies that they’re not,” Dr. Das said.
But this new review changes what she will tell patients going forward, she said. “This is a good study because it consolidates lots of little studies, so I think I would use this to say, looking at all the studies together, this treatment is not beneficial.”
GSM occurs due to the body’s reduced production of estrogen and affects anywhere from 27% to 84% of postmenopausal women. It can involve a constellation of symptoms ranging from vaginal discomfort and irritation to painful urination or intercourse. Typical recommended treatments for GSM include systemic hormone therapy, localized hormonal treatments such as vaginal estrogen or dehydroepiandrosterone, nonhormonal creams and moisturizers, and the prescription drug ospemifene.
Most of these have been found effective, according to a recent systematic review Dr. Danan published in the Annals of Internal Medicine that this news organization covered. But recent years have also seen a rapid increase in interest and the availability of energy-based treatments for GSM, such as CO2 laser and radiofrequency interventions, particularly for those who cannot or do not want to use hormonal treatments. The idea behind these newer therapies is that they “heat tissue to cause a denaturation of collagen fibers and induce a wound-healing response,” with the aim of “enhancement of vaginal elasticity, restoration of premenopausal epithelial function, and symptom improvement,” the authors wrote.
Evidence has been scant and uneven for the safety and effectiveness of these treatments, and they have not been evaluated by the US Food and Drug Administration. The agency issued a warning in 2018 with remarks from then Commissioner Scott Gottlieb that the “products have serious risks and don’t have adequate evidence to support their use for these purposes.”
Much of the evidence has focused on CO2 lasers instead of other energy-based treatments, however, and a raft of new studies have been published on these interventions in the past 2 years. Dr. Danan and colleagues, therefore, assessed the most current state of the research with a systematic review of randomized controlled trials (RCTs) and prospective observational studies with control groups published through December 11, 2023.
Included studies needed to evaluate an energy-based treatment for at least 8 weeks in a minimum of 40 postmenopausal women (20 in each group) who had one or more GSM symptoms. The authors also included nonrandomized and uncontrolled studies with a follow-up of a year or more to assess possible adverse events. The studies also needed to assess at least one of eight core outcomes: Dyspareunia; vulvovaginal dryness; vulvovaginal discomfort/irritation; dysuria; change in most bothersome symptom; treatment satisfaction; adverse events; and distress, bother, or interference associated with genitourinary symptoms.
The authors identified 32 studies, including 16 RCTs, one quasi-RCT, and 15 nonrandomized studies. The researchers extracted and analyzed data from the 10 RCTs and one quasi-RCT that were rated as having low to moderate risk for bias.
Most of these studies assessed CO2 lasers alone, while three assessed erbium:yttrium-aluminum-garnet (Er:YAG) laser, and one looked at CO2 lasers vs radiofrequency treatments.
The average age of participants ranged from 56 to 64 years, and most trials were in the United States. Results showed that CO2 lasers led to little or no difference in dysuria, dyspareunia, or quality of life when compared with sham lasers. The CO2 laser therapy also showed little to no difference compared with vaginal estrogen creams for dyspareunia, dryness, discomfort/irritation, dysuria, or quality of life.
Most CO2 laser studies reported on most outcomes, but the Er:YAG studies tended to report only on quality of life and/or one or two other outcomes. The radiofrequency study only assessed dyspareunia and quality of life.
“Treatment effects on other outcomes and effects of Er:YAG laser or radiofrequency on any outcomes are very uncertain,” the authors reported. Few adverse events and no serious adverse events were reported based on 15 studies, including the additional non-RCTs that had follow-up for at least a year.
“There are case reports and other types of studies that have shown some bad outcomes using laser therapies, and we really wanted to be expansive and include anything, especially because this is such a new treatment and all these trials were in the last couple of years,” Dr. Danan said.
The review was limited by inconsistent or nonvalidated outcome reporting in the studies as well as small populations and short follow-up, typically less than 3 months.
The research was funded by the Agency for Healthcare Research and Quality and Patient-Centered Outcomes Research Institute. Dr. Danan and Dr. Das had no disclosures.
A version of this article first appeared on Medscape.com.
CHICAGO — Use of CO2 lasers and similar “energy-based” treatments result in little to no benefit for genitourinary syndrome of menopause (GSM) symptoms, according to research presented at the The Menopause Society 2024 Annual Meeting in Chicago on September 12.
“There was a concern that menopausal women are being targeted for treatments that may not have a lot of benefit and might have significant harms,” Elisheva Danan, MD, MPH, a physician at the Minneapolis VA Health Care System and an assistant professor of medicine at the University of Minnesota Medical School in Minneapolis, told this news organization. While she was not surprised to find little evidence of benefit, “we were a little bit surprised that we also didn’t find significant evidence of harms.”
The study was unable to evaluate the potential for financial harms, but Dr. Danan noted that these therapies are often expensive and not typically covered by insurance. The treatments appear to be used primarily in private practice, she said, while “most academic clinicians were not familiar with these and do not use these lasers.”
The American Urological Association had requested the review, Dr. Danan said, “to inform clinical guidelines that they could put out for practitioners about treating genital urinary syndrome from menopause.” Yet the evidence available remains slim. “There’s a lot of outcomes that were not looked at by most of these [trials], or they were looked at in a way that we couldn’t separate out,” she said.
Kamalini Das, MD, a professor of ob.gyn. at the University of Minnesota who was not involved in the research, was surprised by the findings because studies to date have been variable, “but since this looks at multiple studies and they find no benefits, I would take these results as more significant than any of the small studies,” she told this news organization.
Dr. Das said she has patients who ask about using these therapies and have had them done. “So far, I’ve told them the jury is out on whether it will help or not, that there are some studies that say they’re beneficial and some studies that they’re not,” Dr. Das said.
But this new review changes what she will tell patients going forward, she said. “This is a good study because it consolidates lots of little studies, so I think I would use this to say, looking at all the studies together, this treatment is not beneficial.”
GSM occurs due to the body’s reduced production of estrogen and affects anywhere from 27% to 84% of postmenopausal women. It can involve a constellation of symptoms ranging from vaginal discomfort and irritation to painful urination or intercourse. Typical recommended treatments for GSM include systemic hormone therapy, localized hormonal treatments such as vaginal estrogen or dehydroepiandrosterone, nonhormonal creams and moisturizers, and the prescription drug ospemifene.
Most of these have been found effective, according to a recent systematic review Dr. Danan published in the Annals of Internal Medicine that this news organization covered. But recent years have also seen a rapid increase in interest and the availability of energy-based treatments for GSM, such as CO2 laser and radiofrequency interventions, particularly for those who cannot or do not want to use hormonal treatments. The idea behind these newer therapies is that they “heat tissue to cause a denaturation of collagen fibers and induce a wound-healing response,” with the aim of “enhancement of vaginal elasticity, restoration of premenopausal epithelial function, and symptom improvement,” the authors wrote.
Evidence has been scant and uneven for the safety and effectiveness of these treatments, and they have not been evaluated by the US Food and Drug Administration. The agency issued a warning in 2018 with remarks from then Commissioner Scott Gottlieb that the “products have serious risks and don’t have adequate evidence to support their use for these purposes.”
Much of the evidence has focused on CO2 lasers instead of other energy-based treatments, however, and a raft of new studies have been published on these interventions in the past 2 years. Dr. Danan and colleagues, therefore, assessed the most current state of the research with a systematic review of randomized controlled trials (RCTs) and prospective observational studies with control groups published through December 11, 2023.
Included studies needed to evaluate an energy-based treatment for at least 8 weeks in a minimum of 40 postmenopausal women (20 in each group) who had one or more GSM symptoms. The authors also included nonrandomized and uncontrolled studies with a follow-up of a year or more to assess possible adverse events. The studies also needed to assess at least one of eight core outcomes: Dyspareunia; vulvovaginal dryness; vulvovaginal discomfort/irritation; dysuria; change in most bothersome symptom; treatment satisfaction; adverse events; and distress, bother, or interference associated with genitourinary symptoms.
The authors identified 32 studies, including 16 RCTs, one quasi-RCT, and 15 nonrandomized studies. The researchers extracted and analyzed data from the 10 RCTs and one quasi-RCT that were rated as having low to moderate risk for bias.
Most of these studies assessed CO2 lasers alone, while three assessed erbium:yttrium-aluminum-garnet (Er:YAG) laser, and one looked at CO2 lasers vs radiofrequency treatments.
The average age of participants ranged from 56 to 64 years, and most trials were in the United States. Results showed that CO2 lasers led to little or no difference in dysuria, dyspareunia, or quality of life when compared with sham lasers. The CO2 laser therapy also showed little to no difference compared with vaginal estrogen creams for dyspareunia, dryness, discomfort/irritation, dysuria, or quality of life.
Most CO2 laser studies reported on most outcomes, but the Er:YAG studies tended to report only on quality of life and/or one or two other outcomes. The radiofrequency study only assessed dyspareunia and quality of life.
“Treatment effects on other outcomes and effects of Er:YAG laser or radiofrequency on any outcomes are very uncertain,” the authors reported. Few adverse events and no serious adverse events were reported based on 15 studies, including the additional non-RCTs that had follow-up for at least a year.
“There are case reports and other types of studies that have shown some bad outcomes using laser therapies, and we really wanted to be expansive and include anything, especially because this is such a new treatment and all these trials were in the last couple of years,” Dr. Danan said.
The review was limited by inconsistent or nonvalidated outcome reporting in the studies as well as small populations and short follow-up, typically less than 3 months.
The research was funded by the Agency for Healthcare Research and Quality and Patient-Centered Outcomes Research Institute. Dr. Danan and Dr. Das had no disclosures.
A version of this article first appeared on Medscape.com.
CHICAGO — Use of CO2 lasers and similar “energy-based” treatments result in little to no benefit for genitourinary syndrome of menopause (GSM) symptoms, according to research presented at the The Menopause Society 2024 Annual Meeting in Chicago on September 12.
“There was a concern that menopausal women are being targeted for treatments that may not have a lot of benefit and might have significant harms,” Elisheva Danan, MD, MPH, a physician at the Minneapolis VA Health Care System and an assistant professor of medicine at the University of Minnesota Medical School in Minneapolis, told this news organization. While she was not surprised to find little evidence of benefit, “we were a little bit surprised that we also didn’t find significant evidence of harms.”
The study was unable to evaluate the potential for financial harms, but Dr. Danan noted that these therapies are often expensive and not typically covered by insurance. The treatments appear to be used primarily in private practice, she said, while “most academic clinicians were not familiar with these and do not use these lasers.”
The American Urological Association had requested the review, Dr. Danan said, “to inform clinical guidelines that they could put out for practitioners about treating genital urinary syndrome from menopause.” Yet the evidence available remains slim. “There’s a lot of outcomes that were not looked at by most of these [trials], or they were looked at in a way that we couldn’t separate out,” she said.
Kamalini Das, MD, a professor of ob.gyn. at the University of Minnesota who was not involved in the research, was surprised by the findings because studies to date have been variable, “but since this looks at multiple studies and they find no benefits, I would take these results as more significant than any of the small studies,” she told this news organization.
Dr. Das said she has patients who ask about using these therapies and have had them done. “So far, I’ve told them the jury is out on whether it will help or not, that there are some studies that say they’re beneficial and some studies that they’re not,” Dr. Das said.
But this new review changes what she will tell patients going forward, she said. “This is a good study because it consolidates lots of little studies, so I think I would use this to say, looking at all the studies together, this treatment is not beneficial.”
GSM occurs due to the body’s reduced production of estrogen and affects anywhere from 27% to 84% of postmenopausal women. It can involve a constellation of symptoms ranging from vaginal discomfort and irritation to painful urination or intercourse. Typical recommended treatments for GSM include systemic hormone therapy, localized hormonal treatments such as vaginal estrogen or dehydroepiandrosterone, nonhormonal creams and moisturizers, and the prescription drug ospemifene.
Most of these have been found effective, according to a recent systematic review Dr. Danan published in the Annals of Internal Medicine that this news organization covered. But recent years have also seen a rapid increase in interest and the availability of energy-based treatments for GSM, such as CO2 laser and radiofrequency interventions, particularly for those who cannot or do not want to use hormonal treatments. The idea behind these newer therapies is that they “heat tissue to cause a denaturation of collagen fibers and induce a wound-healing response,” with the aim of “enhancement of vaginal elasticity, restoration of premenopausal epithelial function, and symptom improvement,” the authors wrote.
Evidence has been scant and uneven for the safety and effectiveness of these treatments, and they have not been evaluated by the US Food and Drug Administration. The agency issued a warning in 2018 with remarks from then Commissioner Scott Gottlieb that the “products have serious risks and don’t have adequate evidence to support their use for these purposes.”
Much of the evidence has focused on CO2 lasers instead of other energy-based treatments, however, and a raft of new studies have been published on these interventions in the past 2 years. Dr. Danan and colleagues, therefore, assessed the most current state of the research with a systematic review of randomized controlled trials (RCTs) and prospective observational studies with control groups published through December 11, 2023.
Included studies needed to evaluate an energy-based treatment for at least 8 weeks in a minimum of 40 postmenopausal women (20 in each group) who had one or more GSM symptoms. The authors also included nonrandomized and uncontrolled studies with a follow-up of a year or more to assess possible adverse events. The studies also needed to assess at least one of eight core outcomes: Dyspareunia; vulvovaginal dryness; vulvovaginal discomfort/irritation; dysuria; change in most bothersome symptom; treatment satisfaction; adverse events; and distress, bother, or interference associated with genitourinary symptoms.
The authors identified 32 studies, including 16 RCTs, one quasi-RCT, and 15 nonrandomized studies. The researchers extracted and analyzed data from the 10 RCTs and one quasi-RCT that were rated as having low to moderate risk for bias.
Most of these studies assessed CO2 lasers alone, while three assessed erbium:yttrium-aluminum-garnet (Er:YAG) laser, and one looked at CO2 lasers vs radiofrequency treatments.
The average age of participants ranged from 56 to 64 years, and most trials were in the United States. Results showed that CO2 lasers led to little or no difference in dysuria, dyspareunia, or quality of life when compared with sham lasers. The CO2 laser therapy also showed little to no difference compared with vaginal estrogen creams for dyspareunia, dryness, discomfort/irritation, dysuria, or quality of life.
Most CO2 laser studies reported on most outcomes, but the Er:YAG studies tended to report only on quality of life and/or one or two other outcomes. The radiofrequency study only assessed dyspareunia and quality of life.
“Treatment effects on other outcomes and effects of Er:YAG laser or radiofrequency on any outcomes are very uncertain,” the authors reported. Few adverse events and no serious adverse events were reported based on 15 studies, including the additional non-RCTs that had follow-up for at least a year.
“There are case reports and other types of studies that have shown some bad outcomes using laser therapies, and we really wanted to be expansive and include anything, especially because this is such a new treatment and all these trials were in the last couple of years,” Dr. Danan said.
The review was limited by inconsistent or nonvalidated outcome reporting in the studies as well as small populations and short follow-up, typically less than 3 months.
The research was funded by the Agency for Healthcare Research and Quality and Patient-Centered Outcomes Research Institute. Dr. Danan and Dr. Das had no disclosures.
A version of this article first appeared on Medscape.com.
FROM THE MENOPAUSE SOCIETY 2024
Study Helps Define Patient-Centered Definition of Atopic Dermatitis Flares
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
, which most agreed would help when communicating with their healthcare providers (HCPs).
METHODOLOGY:
- To develop a patient-centered definition of AD flare, researchers used a modified eDelphi method, which involved a focus group and survey to reach consensus on key aspects of an AD flare.
- The focus group included 26 US adults aged ≥ 18 years with AD who had experienced a flare within the past 12 months. The survey was conducted among 631 adults with AD to validate the identified concepts and assess their agreement with the consensus statements.
- Participants rated 98 statements on a scale from 1 to 9, with consensus defined as at least 70% rating a statement as 7-9 and less than 15% rating it as 1-3.
- In focus groups, participants identified six key concepts for a patient-centered definition of flare, including changes from baseline, mental and emotional consequences, and physical changes in skin.
TAKEAWAY:
- The focus group reached consensus on 15 statements, and survey participants reached consensus on 12 of those statements defining an AD flare, with the highest agreement on symptoms taking more attention than normal, worsening of physical symptoms associated with AD, and worsening of itching associated with AD.
- The statement “acute worsening of symptoms of AD” was ranked as the most important, while “a worsening of physical symptoms” was ranked the least important.
- Most participants (79.7%) reported that prior definitions of AD flare did not resonate with them.
- More than half (52.9%) agreed with their HCP on what constitutes an AD flare, and the majority (77.6%) indicated that a patient-centered definition would be useful for communication with their HCP and for self-management.
IN PRACTICE:
“In this consensus survey study, we identified statements that are critical to the definition of an AD flare from the patient perspective,” the authors wrote. These findings, they added, “may be useful in clinical practice to improve communication between patients and HCPs who may be using the term flare without a mutual understanding of its meaning” and “may also be applied to the development of outcome measures focused on AD flares, which is an important treatment outcome for people with AD.”
SOURCE:
The study was led by Aaron M. Drucker, MD, ScM, of the Division of Dermatology, Department of Medicine, University of Toronto, Ontario, Canada, and was published online September 11 in JAMA Dermatology.
LIMITATIONS:
Participants had higher-than-average knowledge about AD, and the study’s findings may not be generalizable to all people with AD. The study included a higher proportion of moderate to severe AD cases than the general population, which may introduce responder bias. The findings may not be applicable to children, caregivers, or individuals in other countries.
DISCLOSURES:
This work was supported by a grant to the National Eczema Association from Pfizer. Dr. Drucker disclosed received compensation from the British Journal of Dermatology, American Academy of Dermatology, and Canadian Dermatology Today, and consultant fees from the National Eczema Association and Canadian Agency for Drugs and Technologies in Health. Another author reported receiving personal fees from pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Imaging Tool Helps Identify Features of Nail Disorders
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The single-center, observational cross-sectional pilot study evaluated patients aged ≥ 7 years with newly diagnosed nail disorders between January 2022 and May 2023.
- A total of 128 patients (average age, 46.1 years; range, 8-84 years) with nail psoriasis, onychomycosis, idiopathic/traumatic onycholysis, brittle nail syndrome, nail lichen planus, retronychia, and other nail conditions and those with no nail findings (controls) were enrolled.
- Researchers performed nailfold capillaroscopy imaging and compared capillary features between patients with nail conditions and the controls.
TAKEAWAY:
- Patients with nail psoriasis had decreased capillary density and length (P < .001), more crossed and tortuous capillaries (P < .02), and increased abnormal capillary morphology (P = .03) compared with controls. Specific abnormalities, such as branching and meandering capillaries, were more common among those with nail psoriasis (both 26.5%).
- Patients with fingernail and toenail onychomycosis had a higher frequency of abnormal capillary morphology (P < .02), particularly meandering capillaries (75.0% for fingernails and 76.9% for toenails). However, other abnormalities were less frequently observed.
- Patients with nail lichen planus (P < .01), onychopapilloma (P = .01), and retronychia (P = .03) showed significantly shorter capillaries than controls. Retronychia was also associated with increased disorganized polymorphic capillaries (P = .02).
- Patients with brittle nail syndrome and eczema showed no significant differences compared with controls.
IN PRACTICE:
“Our findings highlight nailfold capillaroscopy as a potentially quick, cost-effective, and noninvasive imaging modality as an adjunct for diagnosis and treatment initiation for patients with onychodystrophies,” the authors wrote.
SOURCE:
This study was led by Jonathan K. Hwang, MD, Weill Cornell Medicine, New York City, and was published online in The Journal of the American Academy of Dermatology.
LIMITATIONS:
The study’s limitations included a small sample size for certain nail conditions and the single-center design, which limited generalizability. Additionally, the uneven surface, scaling, onycholysis, and thickening of toenails made some capillaroscopy images difficult to capture and interpret.
DISCLOSURES:
The study did not receive any funding. One author reported serving as a consultant for Eli Lilly, Ortho-Dermatologics, BelleTorus, and Moberg Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Presence of Central Sensitization Should Be Considered During PsA Treatment
Key clinical point: Nearly two out of three patients with psoriatic arthritis (PsA) had clinically significant central sensitization (CS), with the severity of psoriasis, anxiety level, and sleep quality being independent predictors of worse CS Inventory (CSI) scores.
Major finding: Overall, 65.1% patients had clinically significant CS, with a CSI score ≥ 40, with the severity of psoriasis and disease activity scores for PsA being positively associated with CSI scores (correlation coefficient 0.393-0.652; P < .001). The Psoriasis Area Severity Index (odds ratio [OR] 9.70; P = .017), General Anxiety Disorder-7 (OR 2.89; P = .014), and Insomnia Severity Index (OR 5.56; P = .041) scores were independent predictors of CS.
Study details: This cross-sectional observational study included 103 patients with PsA (age 18-75 years) with a mean CSI score of 45.4.
Disclosures: This study did not receive any financial support. The authors declared no conflicts of interest.
Source: Kaya MN, Tecer D, Kılıç Ö, et al. Impact of central sensitization on clinical and functional aspects of psoriatic arthritis. Medicina. 2024;60(9):1449 (Sept 4). Source
Key clinical point: Nearly two out of three patients with psoriatic arthritis (PsA) had clinically significant central sensitization (CS), with the severity of psoriasis, anxiety level, and sleep quality being independent predictors of worse CS Inventory (CSI) scores.
Major finding: Overall, 65.1% patients had clinically significant CS, with a CSI score ≥ 40, with the severity of psoriasis and disease activity scores for PsA being positively associated with CSI scores (correlation coefficient 0.393-0.652; P < .001). The Psoriasis Area Severity Index (odds ratio [OR] 9.70; P = .017), General Anxiety Disorder-7 (OR 2.89; P = .014), and Insomnia Severity Index (OR 5.56; P = .041) scores were independent predictors of CS.
Study details: This cross-sectional observational study included 103 patients with PsA (age 18-75 years) with a mean CSI score of 45.4.
Disclosures: This study did not receive any financial support. The authors declared no conflicts of interest.
Source: Kaya MN, Tecer D, Kılıç Ö, et al. Impact of central sensitization on clinical and functional aspects of psoriatic arthritis. Medicina. 2024;60(9):1449 (Sept 4). Source
Key clinical point: Nearly two out of three patients with psoriatic arthritis (PsA) had clinically significant central sensitization (CS), with the severity of psoriasis, anxiety level, and sleep quality being independent predictors of worse CS Inventory (CSI) scores.
Major finding: Overall, 65.1% patients had clinically significant CS, with a CSI score ≥ 40, with the severity of psoriasis and disease activity scores for PsA being positively associated with CSI scores (correlation coefficient 0.393-0.652; P < .001). The Psoriasis Area Severity Index (odds ratio [OR] 9.70; P = .017), General Anxiety Disorder-7 (OR 2.89; P = .014), and Insomnia Severity Index (OR 5.56; P = .041) scores were independent predictors of CS.
Study details: This cross-sectional observational study included 103 patients with PsA (age 18-75 years) with a mean CSI score of 45.4.
Disclosures: This study did not receive any financial support. The authors declared no conflicts of interest.
Source: Kaya MN, Tecer D, Kılıç Ö, et al. Impact of central sensitization on clinical and functional aspects of psoriatic arthritis. Medicina. 2024;60(9):1449 (Sept 4). Source