User login
No Signal of Benefit for Simvastatin in Progressive MS
COPENHAGEN — There were high hopes that simvastatin, a well-tolerated lipid-lowering therapy, would reduce disability progression in patients with nonflaring secondary progressive multiple sclerosis (SPMS), but a definitive multicenter double-blind randomized trial found no benefit at all.
“There was no effect on the primary outcome of confirmed progression or on any of the secondary outcomes,” reported Jeremy Chataway, MD, PhD, consultant neurologist, National Hospital for Neurology and Neurosurgery, University College of London, England.
For the primary outcome of progression on the Expanded Disability Status Scale (EDSS), the nonsignificant hazard ratio (HR) was, in fact, in favor of placebo (HR, 1.13; P = .26) over 45 months of follow-up and 365 progression events.
No Meaningful Difference Between Study Arms
“There were wide confidence intervals [95% CI, 0.91-1.39], so, really, there were no differences between the two arms,” reported Dr. Chataway, who presented the simvastatin trial, called MS-STAT2, during the late-breaker session of the 2024 ECTRIMS annual meeting.
Over a period of more than 20 years, a series of experimental and clinical studies have indicated that simvastatin and other CoA reductase inhibitors have anti-inflammatory and neuroprotective effects. These studies were the basis for the first MED-STAT study, which was a placebo-controlled randomized trial published in 2014.
Although this study did not have a clinical endpoint, it associated simvastatin with a 43% reduction (P = .003) in the annualized rate of brain atrophy, which has been widely accepted as a surrogate measure of MS progression.
In MS-STAT2, 964 patients were available for the intention-to-treat analysis. An established diagnosis of SPMS, an age of 25-65, and an EDSS score of 4.0-6.5 were among the inclusion criteria. Patients were required to be relapse-free for at least 3 months prior to study entry.
Importantly, patients were excluded if they were taking statin-lowering therapies or were candidates for these therapies due to the presence of cardiovascular disease. They were also excluded from entering the trial if taking immunosuppressants, such as methotrexate or azathioprine, or had exposure to monoclonal antibodies employed in the treatment of MS, such as natalizumab and alemtuzumab, in the prior 12 months.
Randomized to 80 mg of simvastatin (40 mg in the first month followed by rapid upward titration) or placebo in a 1:1 fashion, patients remained on their assigned therapy for 3 years in the absence of progression. At the end of this time, patients who remained progression-free could continue for up to 45 months while still blinded to treatment assignment.
Even though a large proportion of patients who were eligible to remain in the study for the full 45 months did so, the retention did not reflect clinical improvement.
Indeed, the secondary endpoints also produced no signal of benefit. On a composite secondary endpoint of EDSS, ambulation in the form of the 25-foot walk, and upper extremity function in the form of the 9-hole peg test (9-HPT), the numerical odds ratio (OR) went in the wrong direction for simvastatin although the difference was not significant (OR, 1.17; P = .26).
Annualized Relapse Rate Numerically Higher on Simvastatin
The annualized relapse rate, another secondary endpoint, was low in both arms of the study at 0.05 relapses/year for placebo and 0.7 relapses/year for simvastatin. Again, this result, although numerically unfavorable for simvastatin did not reach statistical significance (OR, 1.43; P = .04).
Simvastatin had a placebo-like safety profile. The single case of rhabdomyolysis in the simvastatin arm, which occurred early after randomization, resolved. Otherwise, simvastatin was well tolerated.
Conducted before and through the period of the COVID-19 pandemic, the number of progression events tripled in the year after the COVID-19 pandemic started relative to the prior year. At the end of the pandemic, progression events returned to a level similar to that before its onset. However, although Dr. Chataway noted this was an interesting example of comorbidities exacerbating MS, he emphasized that this increase was similar in the simvastatin and placebo arms.
There are more analyses to come, including patient-reported outcomes, biomarker analyses, and further comparisons of change in MRIs, but Dr. Chataway acknowledged that the study provided no support for the underlying hypothesis.
Several experts commenting after the study was presented, including Ludwig Kappos, MD, PhD, Chair of Neurology at the University Hospital, Basel, Switzerland, agreed.
“Unfortunately, these results are quite disappointing,” he said. When asked if there is any rationale for further pursuing studies of simvastatin for the treatment of SPMS, he said no.
“These data are quite convincing that there is no benefit. I do not see where you could go from here,” Dr. Kappos said in an interview.
Dr. Chataway, asked the same question, reiterated that there are a number of preplanned analyses that will be completed, but he does not foresee further studies with simvastatin for the indication studied in MS-STAT-2 trial.
However, he also emphasized strongly that simvastatin or any other lipid-lowering therapy should not be withheld from MS patients that need these drugs for a cardiovascular indication.
“We saw no benefit seen from simvastatin for patients with stable SPMS, but these drugs were well tolerated and they can be life-saving therapies for patients with increased cardiovascular risk,” Dr. Chataway said.
Dr, Chataway reported financial relationships with Biogen, Genzyme, Ionis, Lucid, Merck NerveGen, Novartis, Roche, and Sanofi. Dr. Kappos reports financial relationships with more than 20 pharmaceutical companies. The MS-STAT2 trial received no funding from industry.
COPENHAGEN — There were high hopes that simvastatin, a well-tolerated lipid-lowering therapy, would reduce disability progression in patients with nonflaring secondary progressive multiple sclerosis (SPMS), but a definitive multicenter double-blind randomized trial found no benefit at all.
“There was no effect on the primary outcome of confirmed progression or on any of the secondary outcomes,” reported Jeremy Chataway, MD, PhD, consultant neurologist, National Hospital for Neurology and Neurosurgery, University College of London, England.
For the primary outcome of progression on the Expanded Disability Status Scale (EDSS), the nonsignificant hazard ratio (HR) was, in fact, in favor of placebo (HR, 1.13; P = .26) over 45 months of follow-up and 365 progression events.
No Meaningful Difference Between Study Arms
“There were wide confidence intervals [95% CI, 0.91-1.39], so, really, there were no differences between the two arms,” reported Dr. Chataway, who presented the simvastatin trial, called MS-STAT2, during the late-breaker session of the 2024 ECTRIMS annual meeting.
Over a period of more than 20 years, a series of experimental and clinical studies have indicated that simvastatin and other CoA reductase inhibitors have anti-inflammatory and neuroprotective effects. These studies were the basis for the first MED-STAT study, which was a placebo-controlled randomized trial published in 2014.
Although this study did not have a clinical endpoint, it associated simvastatin with a 43% reduction (P = .003) in the annualized rate of brain atrophy, which has been widely accepted as a surrogate measure of MS progression.
In MS-STAT2, 964 patients were available for the intention-to-treat analysis. An established diagnosis of SPMS, an age of 25-65, and an EDSS score of 4.0-6.5 were among the inclusion criteria. Patients were required to be relapse-free for at least 3 months prior to study entry.
Importantly, patients were excluded if they were taking statin-lowering therapies or were candidates for these therapies due to the presence of cardiovascular disease. They were also excluded from entering the trial if taking immunosuppressants, such as methotrexate or azathioprine, or had exposure to monoclonal antibodies employed in the treatment of MS, such as natalizumab and alemtuzumab, in the prior 12 months.
Randomized to 80 mg of simvastatin (40 mg in the first month followed by rapid upward titration) or placebo in a 1:1 fashion, patients remained on their assigned therapy for 3 years in the absence of progression. At the end of this time, patients who remained progression-free could continue for up to 45 months while still blinded to treatment assignment.
Even though a large proportion of patients who were eligible to remain in the study for the full 45 months did so, the retention did not reflect clinical improvement.
Indeed, the secondary endpoints also produced no signal of benefit. On a composite secondary endpoint of EDSS, ambulation in the form of the 25-foot walk, and upper extremity function in the form of the 9-hole peg test (9-HPT), the numerical odds ratio (OR) went in the wrong direction for simvastatin although the difference was not significant (OR, 1.17; P = .26).
Annualized Relapse Rate Numerically Higher on Simvastatin
The annualized relapse rate, another secondary endpoint, was low in both arms of the study at 0.05 relapses/year for placebo and 0.7 relapses/year for simvastatin. Again, this result, although numerically unfavorable for simvastatin did not reach statistical significance (OR, 1.43; P = .04).
Simvastatin had a placebo-like safety profile. The single case of rhabdomyolysis in the simvastatin arm, which occurred early after randomization, resolved. Otherwise, simvastatin was well tolerated.
Conducted before and through the period of the COVID-19 pandemic, the number of progression events tripled in the year after the COVID-19 pandemic started relative to the prior year. At the end of the pandemic, progression events returned to a level similar to that before its onset. However, although Dr. Chataway noted this was an interesting example of comorbidities exacerbating MS, he emphasized that this increase was similar in the simvastatin and placebo arms.
There are more analyses to come, including patient-reported outcomes, biomarker analyses, and further comparisons of change in MRIs, but Dr. Chataway acknowledged that the study provided no support for the underlying hypothesis.
Several experts commenting after the study was presented, including Ludwig Kappos, MD, PhD, Chair of Neurology at the University Hospital, Basel, Switzerland, agreed.
“Unfortunately, these results are quite disappointing,” he said. When asked if there is any rationale for further pursuing studies of simvastatin for the treatment of SPMS, he said no.
“These data are quite convincing that there is no benefit. I do not see where you could go from here,” Dr. Kappos said in an interview.
Dr. Chataway, asked the same question, reiterated that there are a number of preplanned analyses that will be completed, but he does not foresee further studies with simvastatin for the indication studied in MS-STAT-2 trial.
However, he also emphasized strongly that simvastatin or any other lipid-lowering therapy should not be withheld from MS patients that need these drugs for a cardiovascular indication.
“We saw no benefit seen from simvastatin for patients with stable SPMS, but these drugs were well tolerated and they can be life-saving therapies for patients with increased cardiovascular risk,” Dr. Chataway said.
Dr, Chataway reported financial relationships with Biogen, Genzyme, Ionis, Lucid, Merck NerveGen, Novartis, Roche, and Sanofi. Dr. Kappos reports financial relationships with more than 20 pharmaceutical companies. The MS-STAT2 trial received no funding from industry.
COPENHAGEN — There were high hopes that simvastatin, a well-tolerated lipid-lowering therapy, would reduce disability progression in patients with nonflaring secondary progressive multiple sclerosis (SPMS), but a definitive multicenter double-blind randomized trial found no benefit at all.
“There was no effect on the primary outcome of confirmed progression or on any of the secondary outcomes,” reported Jeremy Chataway, MD, PhD, consultant neurologist, National Hospital for Neurology and Neurosurgery, University College of London, England.
For the primary outcome of progression on the Expanded Disability Status Scale (EDSS), the nonsignificant hazard ratio (HR) was, in fact, in favor of placebo (HR, 1.13; P = .26) over 45 months of follow-up and 365 progression events.
No Meaningful Difference Between Study Arms
“There were wide confidence intervals [95% CI, 0.91-1.39], so, really, there were no differences between the two arms,” reported Dr. Chataway, who presented the simvastatin trial, called MS-STAT2, during the late-breaker session of the 2024 ECTRIMS annual meeting.
Over a period of more than 20 years, a series of experimental and clinical studies have indicated that simvastatin and other CoA reductase inhibitors have anti-inflammatory and neuroprotective effects. These studies were the basis for the first MED-STAT study, which was a placebo-controlled randomized trial published in 2014.
Although this study did not have a clinical endpoint, it associated simvastatin with a 43% reduction (P = .003) in the annualized rate of brain atrophy, which has been widely accepted as a surrogate measure of MS progression.
In MS-STAT2, 964 patients were available for the intention-to-treat analysis. An established diagnosis of SPMS, an age of 25-65, and an EDSS score of 4.0-6.5 were among the inclusion criteria. Patients were required to be relapse-free for at least 3 months prior to study entry.
Importantly, patients were excluded if they were taking statin-lowering therapies or were candidates for these therapies due to the presence of cardiovascular disease. They were also excluded from entering the trial if taking immunosuppressants, such as methotrexate or azathioprine, or had exposure to monoclonal antibodies employed in the treatment of MS, such as natalizumab and alemtuzumab, in the prior 12 months.
Randomized to 80 mg of simvastatin (40 mg in the first month followed by rapid upward titration) or placebo in a 1:1 fashion, patients remained on their assigned therapy for 3 years in the absence of progression. At the end of this time, patients who remained progression-free could continue for up to 45 months while still blinded to treatment assignment.
Even though a large proportion of patients who were eligible to remain in the study for the full 45 months did so, the retention did not reflect clinical improvement.
Indeed, the secondary endpoints also produced no signal of benefit. On a composite secondary endpoint of EDSS, ambulation in the form of the 25-foot walk, and upper extremity function in the form of the 9-hole peg test (9-HPT), the numerical odds ratio (OR) went in the wrong direction for simvastatin although the difference was not significant (OR, 1.17; P = .26).
Annualized Relapse Rate Numerically Higher on Simvastatin
The annualized relapse rate, another secondary endpoint, was low in both arms of the study at 0.05 relapses/year for placebo and 0.7 relapses/year for simvastatin. Again, this result, although numerically unfavorable for simvastatin did not reach statistical significance (OR, 1.43; P = .04).
Simvastatin had a placebo-like safety profile. The single case of rhabdomyolysis in the simvastatin arm, which occurred early after randomization, resolved. Otherwise, simvastatin was well tolerated.
Conducted before and through the period of the COVID-19 pandemic, the number of progression events tripled in the year after the COVID-19 pandemic started relative to the prior year. At the end of the pandemic, progression events returned to a level similar to that before its onset. However, although Dr. Chataway noted this was an interesting example of comorbidities exacerbating MS, he emphasized that this increase was similar in the simvastatin and placebo arms.
There are more analyses to come, including patient-reported outcomes, biomarker analyses, and further comparisons of change in MRIs, but Dr. Chataway acknowledged that the study provided no support for the underlying hypothesis.
Several experts commenting after the study was presented, including Ludwig Kappos, MD, PhD, Chair of Neurology at the University Hospital, Basel, Switzerland, agreed.
“Unfortunately, these results are quite disappointing,” he said. When asked if there is any rationale for further pursuing studies of simvastatin for the treatment of SPMS, he said no.
“These data are quite convincing that there is no benefit. I do not see where you could go from here,” Dr. Kappos said in an interview.
Dr. Chataway, asked the same question, reiterated that there are a number of preplanned analyses that will be completed, but he does not foresee further studies with simvastatin for the indication studied in MS-STAT-2 trial.
However, he also emphasized strongly that simvastatin or any other lipid-lowering therapy should not be withheld from MS patients that need these drugs for a cardiovascular indication.
“We saw no benefit seen from simvastatin for patients with stable SPMS, but these drugs were well tolerated and they can be life-saving therapies for patients with increased cardiovascular risk,” Dr. Chataway said.
Dr, Chataway reported financial relationships with Biogen, Genzyme, Ionis, Lucid, Merck NerveGen, Novartis, Roche, and Sanofi. Dr. Kappos reports financial relationships with more than 20 pharmaceutical companies. The MS-STAT2 trial received no funding from industry.
FROM ECTRIMS 2024
FDA OKs Adjuvant Ribociclib in Earlier Stage Breast Cancer
FDA also approved ribociclib and the aromatase inhibitor letrozole packaged together (Kisqali Femara Co-Pack, Novartis) for the same indication.
A rival cyclin-dependent kinase 4/6 (CDK4/6) inhibitor abemaciclib (Verzenio, Eli Lilly) carries a similar adjuvant indication, but use of this agent requires patients to be lymph node–positive.
There’s no such restriction for the new ribociclib indication, which “allows us to offer treatment with a CDK4/6 inhibitor to a significantly broader group of people,” lead investigator Dennis J. Slamon, MD, breast oncologist at the University of California Los Angeless, said in a Novartis press release.
The new indication joins ribociclib’s previous approval for advanced or metastatic HR-positive, HER2-negative breast cancer in combination with an aromatase inhibitor or fulvestrant.
The current approval was based on data from the NATALEE trial. NATALEE randomized 5101 patients with early-stage HR-positive, HER2-negative disease to either 400 mg ribociclib with an aromatase inhibitor or to an aromatase inhibitor alone following surgery.
Invasive disease-free survival at 36 months was 90.7% in the ribociclib arm vs 87.6% with aromatase inhibitor monotherapy (hazard ratio [HR], 0.749; P = .0006). The trial included patients with and without lymph node involvement.
At 4 years (well beyond NATALEE’s 3-year treatment window), the ribociclib group continued to do better, with an invasive disease-free survival rate of 88.5% vs 83.6% in the control arm.
Overall survival data remain immature but with a trend towards improved survival in the ribociclib arm (HR, 0.715; P < .0001), according to a recent report from the 2024 European Society for Medical Oncology Congress.
There were no new safety signals in the trial. Adverse events in the ribociclib group included neutropenia (62.5% overall; 44.3% grade 3/4), liver-related events (26.4% overall; 8.6% grade 3/4), QT prolongation (5.3% overall; 1.0% grade 3/4), and interstitial lung disease/pneumonitis (1.5% overall; 0.0% grade 3/4), according to Novartis.
Ribociclib dosing for the adjuvant indication is lower than for metastatic disease, but patients are on the same schedule — two 200 mg tablets once daily for 21 days followed by 7 days off in 28-day cycles. Treatment continues for 3 years.
Forty-two 200 mg tablets cost about $15,000, according to drugs.com. A patient assistance program is available through Novartis.
A version of this article appeared on Medscape.com.
FDA also approved ribociclib and the aromatase inhibitor letrozole packaged together (Kisqali Femara Co-Pack, Novartis) for the same indication.
A rival cyclin-dependent kinase 4/6 (CDK4/6) inhibitor abemaciclib (Verzenio, Eli Lilly) carries a similar adjuvant indication, but use of this agent requires patients to be lymph node–positive.
There’s no such restriction for the new ribociclib indication, which “allows us to offer treatment with a CDK4/6 inhibitor to a significantly broader group of people,” lead investigator Dennis J. Slamon, MD, breast oncologist at the University of California Los Angeless, said in a Novartis press release.
The new indication joins ribociclib’s previous approval for advanced or metastatic HR-positive, HER2-negative breast cancer in combination with an aromatase inhibitor or fulvestrant.
The current approval was based on data from the NATALEE trial. NATALEE randomized 5101 patients with early-stage HR-positive, HER2-negative disease to either 400 mg ribociclib with an aromatase inhibitor or to an aromatase inhibitor alone following surgery.
Invasive disease-free survival at 36 months was 90.7% in the ribociclib arm vs 87.6% with aromatase inhibitor monotherapy (hazard ratio [HR], 0.749; P = .0006). The trial included patients with and without lymph node involvement.
At 4 years (well beyond NATALEE’s 3-year treatment window), the ribociclib group continued to do better, with an invasive disease-free survival rate of 88.5% vs 83.6% in the control arm.
Overall survival data remain immature but with a trend towards improved survival in the ribociclib arm (HR, 0.715; P < .0001), according to a recent report from the 2024 European Society for Medical Oncology Congress.
There were no new safety signals in the trial. Adverse events in the ribociclib group included neutropenia (62.5% overall; 44.3% grade 3/4), liver-related events (26.4% overall; 8.6% grade 3/4), QT prolongation (5.3% overall; 1.0% grade 3/4), and interstitial lung disease/pneumonitis (1.5% overall; 0.0% grade 3/4), according to Novartis.
Ribociclib dosing for the adjuvant indication is lower than for metastatic disease, but patients are on the same schedule — two 200 mg tablets once daily for 21 days followed by 7 days off in 28-day cycles. Treatment continues for 3 years.
Forty-two 200 mg tablets cost about $15,000, according to drugs.com. A patient assistance program is available through Novartis.
A version of this article appeared on Medscape.com.
FDA also approved ribociclib and the aromatase inhibitor letrozole packaged together (Kisqali Femara Co-Pack, Novartis) for the same indication.
A rival cyclin-dependent kinase 4/6 (CDK4/6) inhibitor abemaciclib (Verzenio, Eli Lilly) carries a similar adjuvant indication, but use of this agent requires patients to be lymph node–positive.
There’s no such restriction for the new ribociclib indication, which “allows us to offer treatment with a CDK4/6 inhibitor to a significantly broader group of people,” lead investigator Dennis J. Slamon, MD, breast oncologist at the University of California Los Angeless, said in a Novartis press release.
The new indication joins ribociclib’s previous approval for advanced or metastatic HR-positive, HER2-negative breast cancer in combination with an aromatase inhibitor or fulvestrant.
The current approval was based on data from the NATALEE trial. NATALEE randomized 5101 patients with early-stage HR-positive, HER2-negative disease to either 400 mg ribociclib with an aromatase inhibitor or to an aromatase inhibitor alone following surgery.
Invasive disease-free survival at 36 months was 90.7% in the ribociclib arm vs 87.6% with aromatase inhibitor monotherapy (hazard ratio [HR], 0.749; P = .0006). The trial included patients with and without lymph node involvement.
At 4 years (well beyond NATALEE’s 3-year treatment window), the ribociclib group continued to do better, with an invasive disease-free survival rate of 88.5% vs 83.6% in the control arm.
Overall survival data remain immature but with a trend towards improved survival in the ribociclib arm (HR, 0.715; P < .0001), according to a recent report from the 2024 European Society for Medical Oncology Congress.
There were no new safety signals in the trial. Adverse events in the ribociclib group included neutropenia (62.5% overall; 44.3% grade 3/4), liver-related events (26.4% overall; 8.6% grade 3/4), QT prolongation (5.3% overall; 1.0% grade 3/4), and interstitial lung disease/pneumonitis (1.5% overall; 0.0% grade 3/4), according to Novartis.
Ribociclib dosing for the adjuvant indication is lower than for metastatic disease, but patients are on the same schedule — two 200 mg tablets once daily for 21 days followed by 7 days off in 28-day cycles. Treatment continues for 3 years.
Forty-two 200 mg tablets cost about $15,000, according to drugs.com. A patient assistance program is available through Novartis.
A version of this article appeared on Medscape.com.
Epilepsy Drug May Reduce Symptoms of OSA
An epilepsy drug sold in Europe as Ospolot and also known as sulthiame showed promise in reducing sleep disordered breathing and other symptoms of obstructive sleep apnea (OSA), based on data from nearly 300 individuals presented in a late-breaking study at the annual congress of the European Respiratory Society.
“Current therapies are mechanical and based on the notion of an airway splint,” presenting author Jan Hedner, MD, professor of respiratory medicine at Sahlgrenska University Hospital and the University of Gothenburg, both in Sweden, said in an interview. “In other words, applying an airflow at elevated pressure [continuous positive airway pressure] or advancing the jaw with a dental device. Adherence to this type of therapy is limited. In the case of continuous positive airway pressure [CPAP], it is < 50% after 3-4 years of therapy.” Therefore, there is a need for a better-tolerated therapy, such as a drug, and possibly a combination of mechanical and pharmaceutical therapies.
The use of medication has emerged as a viable option for OSA, with a high rate of compliance and acceptable safety profile, Dr. Hedner said in his presentation.
“Modified carbonic anhydrase activity may be a pathophysiological mechanism in OSA,” said Dr. Hedner. Sulthiame, a carbonic anhydrase inhibitor, showed safety and effectiveness for improving OSA in a previous phase 2b trial.
In the current study, the researchers sought to determine the most effective dose of sulthiame for patients with OSA. They randomized 298 adults with OSA who could not accept or tolerate oral splints or CPAP to 100 mg, 200 mg, or 300 mg of sulthiame daily (74, 74, and 75 patients, respectively) or placebo (75 patients).
The mean age of the patients was 56 years, 26.2% were women, and the average apnea-hypopnea index (AHI3a) at baseline was 29 n/h. Patients were treated at centers in Spain, France, Belgium, Germany, and the Czech Republic. Baseline demographics and clinical characteristics were similar among the treatment groups.
The primary endpoint was the change in AHI3a from baseline to 15 weeks, and significant changes occurred in patients who received the 100-mg, 200-mg, and 300-mg doses, with decreases of 17.8%, 34.8%, and 39.9%, respectively.
Dr. Hedner said in his presentation.
Notably, in a post hoc analysis, apnea improved by 47.1% at a 300-mg dose when the AHI4 measure (apnea/hypopnea with ≥ 4% O2 desaturation) was used in a placebo-adjusted dose-dependent reduction, the researchers wrote. The changes in AHI4 from baseline in this analysis also were significant for 200 mg and 100 mg doses (36.8% and 26.2%, respectively).
Patients underwent polysomnography at baseline and at weeks 4 and 12.
Mean overnight oxygen saturation also improved significantly from baseline with doses of 200 mg and 300 mg, compared with placebo (P < .0001 for both).
In addition, scores on the Epworth Sleepiness Scale (ESS) improved from baseline to week 15 in all dosage groups, and the subgroup of patients with ESS scores of ≥ 11 at baseline showed even greater improvement in ESS, Dr. Hedner said in his presentation.
Total arousal index and sleep quality also improved from baseline compared with placebo, and no clinically relevant reduction in REM sleep was noted, Dr. Hedner added.
Treatment-emergent adverse events were in line with the known safety profile of sulthiame and included paresthesia, headache, fatigue, and nausea; these were mainly moderate and dose-dependent, with no evidence of cardiovascular safety issues, he said.
Although the study results were not surprising given previous research, the investigators were pleased with the potency of the therapy. “We are also happy about potential added values such as a blood pressure lowering effect, which is beneficial in this group of patients; however, we need to further study these mechanisms in detail,” Dr. Hedner noted.
The study findings were limited by the relatively small scale, and larger studies on long-term efficacy and tolerability are also needed, he said.
“The current study was a dose-finding study, and we now have useful information on most suitable dose,” he said.
However, the results support sulthiame as an effective, well-tolerated, and promising novel candidate for drug therapy in patients with OSA, worthy of phase 3 studies, Dr. Hedner said.
Oral Option Could Be Game-Changer, But Not Yet
The gold standard of treatment for OSA is a CPAP machine, but the effectiveness is limited by patient tolerance, Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, said in an interview.
“Presently, there are no effective pharmacological treatments for OSA — having a pill that treats OSA would be a total game changer and huge advance for the treatment of OSA and the field of sleep medicine,” said Dr. Shamim-Uzzaman, who was not involved in the study. “More patients may be able to obtain treatment for OSA and thereby reduce the potential complications of untreated OSA.
“Carbonic anhydrase inhibitors such as acetazolamide and sulthiame have been studied with limited success for the treatment of other forms of sleep disordered breathing such as central sleep apnea [CSA] but have shown less efficacy for OSA and are presently not recommended in the treatment of OSA by the American Academy of Sleep Medicine,” Dr. Shamim-Uzzaman said.
Recently, emerging evidence about different phenotypes of OSA suggests that nonanatomic features (such as high loop gain) may play a role in patients with OSA, not only in those with CSA, she said. Whether carbonic anhydrase inhibitors could play a greater role in treating sleep apnea in patients with predominantly nonanatomic pathophysiologic traits remains to be seen.
The sulthiame data are promising, but more research is needed, Dr. Shamim-Uzzaman said. Although patients in the highest dose group showed a reduction in AHI of nearly 40%, they still would have moderate OSA, and the OSA did not appear to decrease to a normal range in any of the treatment groups.
“More research is needed to identify which types of patients would be responders to this form of therapy, to understand if these effects are maintained long term (beyond 15 weeks), to evaluate patient-centered outcomes, especially in different sleep apnea subgroups (such as phenotypes with high loop gain vs those without), and to assess interactions with other therapies,” she said.
The study was supported by manufacturer Desitin. Dr. Hedner disclosed serving as a consultant to AstraZeneca, Bayer, CereusScience, Jazz Pharmaceuticals, MSD, Weinmann, Desitin, SomnoMed, and Itamar Medical; serving on the speakers’ bureau for Almirall, AstraZeneca, Jazz Pharmaceuticals, ResMed, Philips Respironics, and Weinmann; and receiving grants or research support from Bayer, ResMed, Philips Respironics, and SomnoMed. He also disclosed shared ownership of intellectual property related to sleep apnea therapy. Dr. Shamim-Uzzaman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
An epilepsy drug sold in Europe as Ospolot and also known as sulthiame showed promise in reducing sleep disordered breathing and other symptoms of obstructive sleep apnea (OSA), based on data from nearly 300 individuals presented in a late-breaking study at the annual congress of the European Respiratory Society.
“Current therapies are mechanical and based on the notion of an airway splint,” presenting author Jan Hedner, MD, professor of respiratory medicine at Sahlgrenska University Hospital and the University of Gothenburg, both in Sweden, said in an interview. “In other words, applying an airflow at elevated pressure [continuous positive airway pressure] or advancing the jaw with a dental device. Adherence to this type of therapy is limited. In the case of continuous positive airway pressure [CPAP], it is < 50% after 3-4 years of therapy.” Therefore, there is a need for a better-tolerated therapy, such as a drug, and possibly a combination of mechanical and pharmaceutical therapies.
The use of medication has emerged as a viable option for OSA, with a high rate of compliance and acceptable safety profile, Dr. Hedner said in his presentation.
“Modified carbonic anhydrase activity may be a pathophysiological mechanism in OSA,” said Dr. Hedner. Sulthiame, a carbonic anhydrase inhibitor, showed safety and effectiveness for improving OSA in a previous phase 2b trial.
In the current study, the researchers sought to determine the most effective dose of sulthiame for patients with OSA. They randomized 298 adults with OSA who could not accept or tolerate oral splints or CPAP to 100 mg, 200 mg, or 300 mg of sulthiame daily (74, 74, and 75 patients, respectively) or placebo (75 patients).
The mean age of the patients was 56 years, 26.2% were women, and the average apnea-hypopnea index (AHI3a) at baseline was 29 n/h. Patients were treated at centers in Spain, France, Belgium, Germany, and the Czech Republic. Baseline demographics and clinical characteristics were similar among the treatment groups.
The primary endpoint was the change in AHI3a from baseline to 15 weeks, and significant changes occurred in patients who received the 100-mg, 200-mg, and 300-mg doses, with decreases of 17.8%, 34.8%, and 39.9%, respectively.
Dr. Hedner said in his presentation.
Notably, in a post hoc analysis, apnea improved by 47.1% at a 300-mg dose when the AHI4 measure (apnea/hypopnea with ≥ 4% O2 desaturation) was used in a placebo-adjusted dose-dependent reduction, the researchers wrote. The changes in AHI4 from baseline in this analysis also were significant for 200 mg and 100 mg doses (36.8% and 26.2%, respectively).
Patients underwent polysomnography at baseline and at weeks 4 and 12.
Mean overnight oxygen saturation also improved significantly from baseline with doses of 200 mg and 300 mg, compared with placebo (P < .0001 for both).
In addition, scores on the Epworth Sleepiness Scale (ESS) improved from baseline to week 15 in all dosage groups, and the subgroup of patients with ESS scores of ≥ 11 at baseline showed even greater improvement in ESS, Dr. Hedner said in his presentation.
Total arousal index and sleep quality also improved from baseline compared with placebo, and no clinically relevant reduction in REM sleep was noted, Dr. Hedner added.
Treatment-emergent adverse events were in line with the known safety profile of sulthiame and included paresthesia, headache, fatigue, and nausea; these were mainly moderate and dose-dependent, with no evidence of cardiovascular safety issues, he said.
Although the study results were not surprising given previous research, the investigators were pleased with the potency of the therapy. “We are also happy about potential added values such as a blood pressure lowering effect, which is beneficial in this group of patients; however, we need to further study these mechanisms in detail,” Dr. Hedner noted.
The study findings were limited by the relatively small scale, and larger studies on long-term efficacy and tolerability are also needed, he said.
“The current study was a dose-finding study, and we now have useful information on most suitable dose,” he said.
However, the results support sulthiame as an effective, well-tolerated, and promising novel candidate for drug therapy in patients with OSA, worthy of phase 3 studies, Dr. Hedner said.
Oral Option Could Be Game-Changer, But Not Yet
The gold standard of treatment for OSA is a CPAP machine, but the effectiveness is limited by patient tolerance, Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, said in an interview.
“Presently, there are no effective pharmacological treatments for OSA — having a pill that treats OSA would be a total game changer and huge advance for the treatment of OSA and the field of sleep medicine,” said Dr. Shamim-Uzzaman, who was not involved in the study. “More patients may be able to obtain treatment for OSA and thereby reduce the potential complications of untreated OSA.
“Carbonic anhydrase inhibitors such as acetazolamide and sulthiame have been studied with limited success for the treatment of other forms of sleep disordered breathing such as central sleep apnea [CSA] but have shown less efficacy for OSA and are presently not recommended in the treatment of OSA by the American Academy of Sleep Medicine,” Dr. Shamim-Uzzaman said.
Recently, emerging evidence about different phenotypes of OSA suggests that nonanatomic features (such as high loop gain) may play a role in patients with OSA, not only in those with CSA, she said. Whether carbonic anhydrase inhibitors could play a greater role in treating sleep apnea in patients with predominantly nonanatomic pathophysiologic traits remains to be seen.
The sulthiame data are promising, but more research is needed, Dr. Shamim-Uzzaman said. Although patients in the highest dose group showed a reduction in AHI of nearly 40%, they still would have moderate OSA, and the OSA did not appear to decrease to a normal range in any of the treatment groups.
“More research is needed to identify which types of patients would be responders to this form of therapy, to understand if these effects are maintained long term (beyond 15 weeks), to evaluate patient-centered outcomes, especially in different sleep apnea subgroups (such as phenotypes with high loop gain vs those without), and to assess interactions with other therapies,” she said.
The study was supported by manufacturer Desitin. Dr. Hedner disclosed serving as a consultant to AstraZeneca, Bayer, CereusScience, Jazz Pharmaceuticals, MSD, Weinmann, Desitin, SomnoMed, and Itamar Medical; serving on the speakers’ bureau for Almirall, AstraZeneca, Jazz Pharmaceuticals, ResMed, Philips Respironics, and Weinmann; and receiving grants or research support from Bayer, ResMed, Philips Respironics, and SomnoMed. He also disclosed shared ownership of intellectual property related to sleep apnea therapy. Dr. Shamim-Uzzaman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
An epilepsy drug sold in Europe as Ospolot and also known as sulthiame showed promise in reducing sleep disordered breathing and other symptoms of obstructive sleep apnea (OSA), based on data from nearly 300 individuals presented in a late-breaking study at the annual congress of the European Respiratory Society.
“Current therapies are mechanical and based on the notion of an airway splint,” presenting author Jan Hedner, MD, professor of respiratory medicine at Sahlgrenska University Hospital and the University of Gothenburg, both in Sweden, said in an interview. “In other words, applying an airflow at elevated pressure [continuous positive airway pressure] or advancing the jaw with a dental device. Adherence to this type of therapy is limited. In the case of continuous positive airway pressure [CPAP], it is < 50% after 3-4 years of therapy.” Therefore, there is a need for a better-tolerated therapy, such as a drug, and possibly a combination of mechanical and pharmaceutical therapies.
The use of medication has emerged as a viable option for OSA, with a high rate of compliance and acceptable safety profile, Dr. Hedner said in his presentation.
“Modified carbonic anhydrase activity may be a pathophysiological mechanism in OSA,” said Dr. Hedner. Sulthiame, a carbonic anhydrase inhibitor, showed safety and effectiveness for improving OSA in a previous phase 2b trial.
In the current study, the researchers sought to determine the most effective dose of sulthiame for patients with OSA. They randomized 298 adults with OSA who could not accept or tolerate oral splints or CPAP to 100 mg, 200 mg, or 300 mg of sulthiame daily (74, 74, and 75 patients, respectively) or placebo (75 patients).
The mean age of the patients was 56 years, 26.2% were women, and the average apnea-hypopnea index (AHI3a) at baseline was 29 n/h. Patients were treated at centers in Spain, France, Belgium, Germany, and the Czech Republic. Baseline demographics and clinical characteristics were similar among the treatment groups.
The primary endpoint was the change in AHI3a from baseline to 15 weeks, and significant changes occurred in patients who received the 100-mg, 200-mg, and 300-mg doses, with decreases of 17.8%, 34.8%, and 39.9%, respectively.
Dr. Hedner said in his presentation.
Notably, in a post hoc analysis, apnea improved by 47.1% at a 300-mg dose when the AHI4 measure (apnea/hypopnea with ≥ 4% O2 desaturation) was used in a placebo-adjusted dose-dependent reduction, the researchers wrote. The changes in AHI4 from baseline in this analysis also were significant for 200 mg and 100 mg doses (36.8% and 26.2%, respectively).
Patients underwent polysomnography at baseline and at weeks 4 and 12.
Mean overnight oxygen saturation also improved significantly from baseline with doses of 200 mg and 300 mg, compared with placebo (P < .0001 for both).
In addition, scores on the Epworth Sleepiness Scale (ESS) improved from baseline to week 15 in all dosage groups, and the subgroup of patients with ESS scores of ≥ 11 at baseline showed even greater improvement in ESS, Dr. Hedner said in his presentation.
Total arousal index and sleep quality also improved from baseline compared with placebo, and no clinically relevant reduction in REM sleep was noted, Dr. Hedner added.
Treatment-emergent adverse events were in line with the known safety profile of sulthiame and included paresthesia, headache, fatigue, and nausea; these were mainly moderate and dose-dependent, with no evidence of cardiovascular safety issues, he said.
Although the study results were not surprising given previous research, the investigators were pleased with the potency of the therapy. “We are also happy about potential added values such as a blood pressure lowering effect, which is beneficial in this group of patients; however, we need to further study these mechanisms in detail,” Dr. Hedner noted.
The study findings were limited by the relatively small scale, and larger studies on long-term efficacy and tolerability are also needed, he said.
“The current study was a dose-finding study, and we now have useful information on most suitable dose,” he said.
However, the results support sulthiame as an effective, well-tolerated, and promising novel candidate for drug therapy in patients with OSA, worthy of phase 3 studies, Dr. Hedner said.
Oral Option Could Be Game-Changer, But Not Yet
The gold standard of treatment for OSA is a CPAP machine, but the effectiveness is limited by patient tolerance, Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, said in an interview.
“Presently, there are no effective pharmacological treatments for OSA — having a pill that treats OSA would be a total game changer and huge advance for the treatment of OSA and the field of sleep medicine,” said Dr. Shamim-Uzzaman, who was not involved in the study. “More patients may be able to obtain treatment for OSA and thereby reduce the potential complications of untreated OSA.
“Carbonic anhydrase inhibitors such as acetazolamide and sulthiame have been studied with limited success for the treatment of other forms of sleep disordered breathing such as central sleep apnea [CSA] but have shown less efficacy for OSA and are presently not recommended in the treatment of OSA by the American Academy of Sleep Medicine,” Dr. Shamim-Uzzaman said.
Recently, emerging evidence about different phenotypes of OSA suggests that nonanatomic features (such as high loop gain) may play a role in patients with OSA, not only in those with CSA, she said. Whether carbonic anhydrase inhibitors could play a greater role in treating sleep apnea in patients with predominantly nonanatomic pathophysiologic traits remains to be seen.
The sulthiame data are promising, but more research is needed, Dr. Shamim-Uzzaman said. Although patients in the highest dose group showed a reduction in AHI of nearly 40%, they still would have moderate OSA, and the OSA did not appear to decrease to a normal range in any of the treatment groups.
“More research is needed to identify which types of patients would be responders to this form of therapy, to understand if these effects are maintained long term (beyond 15 weeks), to evaluate patient-centered outcomes, especially in different sleep apnea subgroups (such as phenotypes with high loop gain vs those without), and to assess interactions with other therapies,” she said.
The study was supported by manufacturer Desitin. Dr. Hedner disclosed serving as a consultant to AstraZeneca, Bayer, CereusScience, Jazz Pharmaceuticals, MSD, Weinmann, Desitin, SomnoMed, and Itamar Medical; serving on the speakers’ bureau for Almirall, AstraZeneca, Jazz Pharmaceuticals, ResMed, Philips Respironics, and Weinmann; and receiving grants or research support from Bayer, ResMed, Philips Respironics, and SomnoMed. He also disclosed shared ownership of intellectual property related to sleep apnea therapy. Dr. Shamim-Uzzaman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
FROM ERS CONGRESS 2024
New Options for Treating Atopic Dermatitis Available, and in Development
HUNTINGTON BEACH, CALIFORNIA — If the number of recent drug approvals for atopic dermatitis (AD) is overwhelming, the future is unlikely to be any less challenging: According to the National Eczema Association, the current pipeline for AD includes 39 injectable medications, 21 oral agents, and 49 topicals, some with novel targets, like human umbilical cord blood derived stem cells.
“It’s amazing how many drugs are coming out for AD,” Robert Sidbury, MD, MPH, said at the annual meeting of the Pacific Dermatologic Association (PDA). and is approved in Europe for the treatment of moderate to severe AD in patients aged ≥ 12 years. (On September 13, after the PDA meeting, lebrikizumab was approved by the Food and Drug Administration [FDA] for treatment of moderate to severe AD in adults and adolescents aged ≥ 12 years.)

In two identical phase 3 trials known as ADvocate 1 and ADvocate 2, researchers randomly assigned 851 patients with moderate to severe AD in a 2:1 ratio to receive either lebrikizumab at a dose of 250 mg (loading dose of 500 mg at baseline and week 2) or placebo, administered subcutaneously every 2 weeks, through week 16. The primary outcome was an Investigator’s Global Assessment (IGA) score of 0 or 1, indicating clear or almost clear skin. The researchers reported that an IGA score of 0 or 1 was achieved by 43.1% of patients in the lebrikizumab arm compared with 12.7% of those in the placebo arm.
“Those are good numbers,” said Dr. Sidbury, who was not involved with the study. Conjunctivitis occurred more often in those who received lebrikizumab compared with those who received placebo (7.4% vs 2.8%, respectively), “which is not surprising because it is an IL-13 agent,” he said.
In a subsequent study presented during the Revolutionizing Atopic Dermatitis meeting in the fall of 2023, researchers presented data on Eczema Severity and Area Index (EASI)-90 responses in the ADvocate trial participants, showing EASI-90 responses were sustained up to 38 weeks after lebrikizumab withdrawal, while serum concentrations were negligible. They found that between week 14 and week 32, approximately five serum concentration half-lives of the medication had elapsed since patients randomized to the withdrawal arm received their last dose of lebrikizumab, extending to approximately 11 half-lives by week 52. “That durability of response with next to no blood levels of drug in many of the study participants is interesting,” said Dr. Sidbury, who cochairs the current iteration of the American Academy of Dermatology Atopic Dermatitis Guidelines.
Nemolizumab is a neuroimmune response modulator that inhibits the IL-31 receptor and is approved in Japan for the treatment of itch associated with AD in patients aged ≥ 13 years. Results from two identical phase 3, randomized, controlled trials known as ARCADIA 1 and ARCADIA 2 found that 36% of patients in ARCADIA 1 and 38% in ARCADIA 2 achieved clear skin, compared with 25% and 26% of patients in the placebo group, respectively. (Nemolizumab was recently approved by the FDA for treating prurigo nodularis and is under FDA review for AD.)
In terms of safety, Dr. Sidbury, who is a member of the steering committee for the ARCADIA trials, said that nemolizumab has been “generally well tolerated;” with 1%-3% of study participants experiencing at least one serious treatment-emergent adverse event that included asthma exacerbation, facial edema, and peripheral edema. “The latest data are reassuring but we are watching these safety concerns carefully,” he said.
Dr. Sidbury disclosed that he is an investigator for Regeneron, Pfizer, Galderma, UCB, and Castle; a consultant for Lilly, Leo, Arcutis, and Dermavant; and a member of the speaker’s bureau for Beiersdorf.
A version of this article appeared on Medscape.com.
HUNTINGTON BEACH, CALIFORNIA — If the number of recent drug approvals for atopic dermatitis (AD) is overwhelming, the future is unlikely to be any less challenging: According to the National Eczema Association, the current pipeline for AD includes 39 injectable medications, 21 oral agents, and 49 topicals, some with novel targets, like human umbilical cord blood derived stem cells.
“It’s amazing how many drugs are coming out for AD,” Robert Sidbury, MD, MPH, said at the annual meeting of the Pacific Dermatologic Association (PDA). and is approved in Europe for the treatment of moderate to severe AD in patients aged ≥ 12 years. (On September 13, after the PDA meeting, lebrikizumab was approved by the Food and Drug Administration [FDA] for treatment of moderate to severe AD in adults and adolescents aged ≥ 12 years.)
In two identical phase 3 trials known as ADvocate 1 and ADvocate 2, researchers randomly assigned 851 patients with moderate to severe AD in a 2:1 ratio to receive either lebrikizumab at a dose of 250 mg (loading dose of 500 mg at baseline and week 2) or placebo, administered subcutaneously every 2 weeks, through week 16. The primary outcome was an Investigator’s Global Assessment (IGA) score of 0 or 1, indicating clear or almost clear skin. The researchers reported that an IGA score of 0 or 1 was achieved by 43.1% of patients in the lebrikizumab arm compared with 12.7% of those in the placebo arm.
“Those are good numbers,” said Dr. Sidbury, who was not involved with the study. Conjunctivitis occurred more often in those who received lebrikizumab compared with those who received placebo (7.4% vs 2.8%, respectively), “which is not surprising because it is an IL-13 agent,” he said.
In a subsequent study presented during the Revolutionizing Atopic Dermatitis meeting in the fall of 2023, researchers presented data on Eczema Severity and Area Index (EASI)-90 responses in the ADvocate trial participants, showing EASI-90 responses were sustained up to 38 weeks after lebrikizumab withdrawal, while serum concentrations were negligible. They found that between week 14 and week 32, approximately five serum concentration half-lives of the medication had elapsed since patients randomized to the withdrawal arm received their last dose of lebrikizumab, extending to approximately 11 half-lives by week 52. “That durability of response with next to no blood levels of drug in many of the study participants is interesting,” said Dr. Sidbury, who cochairs the current iteration of the American Academy of Dermatology Atopic Dermatitis Guidelines.
Nemolizumab is a neuroimmune response modulator that inhibits the IL-31 receptor and is approved in Japan for the treatment of itch associated with AD in patients aged ≥ 13 years. Results from two identical phase 3, randomized, controlled trials known as ARCADIA 1 and ARCADIA 2 found that 36% of patients in ARCADIA 1 and 38% in ARCADIA 2 achieved clear skin, compared with 25% and 26% of patients in the placebo group, respectively. (Nemolizumab was recently approved by the FDA for treating prurigo nodularis and is under FDA review for AD.)
In terms of safety, Dr. Sidbury, who is a member of the steering committee for the ARCADIA trials, said that nemolizumab has been “generally well tolerated;” with 1%-3% of study participants experiencing at least one serious treatment-emergent adverse event that included asthma exacerbation, facial edema, and peripheral edema. “The latest data are reassuring but we are watching these safety concerns carefully,” he said.
Dr. Sidbury disclosed that he is an investigator for Regeneron, Pfizer, Galderma, UCB, and Castle; a consultant for Lilly, Leo, Arcutis, and Dermavant; and a member of the speaker’s bureau for Beiersdorf.
A version of this article appeared on Medscape.com.
HUNTINGTON BEACH, CALIFORNIA — If the number of recent drug approvals for atopic dermatitis (AD) is overwhelming, the future is unlikely to be any less challenging: According to the National Eczema Association, the current pipeline for AD includes 39 injectable medications, 21 oral agents, and 49 topicals, some with novel targets, like human umbilical cord blood derived stem cells.
“It’s amazing how many drugs are coming out for AD,” Robert Sidbury, MD, MPH, said at the annual meeting of the Pacific Dermatologic Association (PDA). and is approved in Europe for the treatment of moderate to severe AD in patients aged ≥ 12 years. (On September 13, after the PDA meeting, lebrikizumab was approved by the Food and Drug Administration [FDA] for treatment of moderate to severe AD in adults and adolescents aged ≥ 12 years.)
In two identical phase 3 trials known as ADvocate 1 and ADvocate 2, researchers randomly assigned 851 patients with moderate to severe AD in a 2:1 ratio to receive either lebrikizumab at a dose of 250 mg (loading dose of 500 mg at baseline and week 2) or placebo, administered subcutaneously every 2 weeks, through week 16. The primary outcome was an Investigator’s Global Assessment (IGA) score of 0 or 1, indicating clear or almost clear skin. The researchers reported that an IGA score of 0 or 1 was achieved by 43.1% of patients in the lebrikizumab arm compared with 12.7% of those in the placebo arm.
“Those are good numbers,” said Dr. Sidbury, who was not involved with the study. Conjunctivitis occurred more often in those who received lebrikizumab compared with those who received placebo (7.4% vs 2.8%, respectively), “which is not surprising because it is an IL-13 agent,” he said.
In a subsequent study presented during the Revolutionizing Atopic Dermatitis meeting in the fall of 2023, researchers presented data on Eczema Severity and Area Index (EASI)-90 responses in the ADvocate trial participants, showing EASI-90 responses were sustained up to 38 weeks after lebrikizumab withdrawal, while serum concentrations were negligible. They found that between week 14 and week 32, approximately five serum concentration half-lives of the medication had elapsed since patients randomized to the withdrawal arm received their last dose of lebrikizumab, extending to approximately 11 half-lives by week 52. “That durability of response with next to no blood levels of drug in many of the study participants is interesting,” said Dr. Sidbury, who cochairs the current iteration of the American Academy of Dermatology Atopic Dermatitis Guidelines.
Nemolizumab is a neuroimmune response modulator that inhibits the IL-31 receptor and is approved in Japan for the treatment of itch associated with AD in patients aged ≥ 13 years. Results from two identical phase 3, randomized, controlled trials known as ARCADIA 1 and ARCADIA 2 found that 36% of patients in ARCADIA 1 and 38% in ARCADIA 2 achieved clear skin, compared with 25% and 26% of patients in the placebo group, respectively. (Nemolizumab was recently approved by the FDA for treating prurigo nodularis and is under FDA review for AD.)
In terms of safety, Dr. Sidbury, who is a member of the steering committee for the ARCADIA trials, said that nemolizumab has been “generally well tolerated;” with 1%-3% of study participants experiencing at least one serious treatment-emergent adverse event that included asthma exacerbation, facial edema, and peripheral edema. “The latest data are reassuring but we are watching these safety concerns carefully,” he said.
Dr. Sidbury disclosed that he is an investigator for Regeneron, Pfizer, Galderma, UCB, and Castle; a consultant for Lilly, Leo, Arcutis, and Dermavant; and a member of the speaker’s bureau for Beiersdorf.
A version of this article appeared on Medscape.com.
FROM PDA 2024
Whooping Cough Rising Fast, Especially Among Teens
Whooping cough is surging in the United States, with four times as many cases reported so far this year, compared to all of 2023.
The CDC said 14,569 cases had been reported as of Sept. 14, compared to 3475 in all of 2023.
Whooping cough, also called pertussis, is a respiratory illness spread through coughing, sneezing, or breathing very close to another person. Babies are given the DTaP vaccine to protect against whooping cough, diphtheria, and tetanus. Because the vaccine effectiveness wanes faster for whooping cough than the two other illnesses, boosters are recommended every decade or so.
Why the Whooping Cough Vaccine Is Important
Whooping cough is a very contagious bacteria, so vaccination is an important step to avoid it.
But many children in their tweens aren’t getting boosters, and that age group is driving the whooping cough outbreak.
“With the increase in vaccine hesitancy that has been going on since the COVID-19 pandemic, we’re seeing outbreaks occurring in kids who are not vaccinated,” Tina Tan, MD, president-elect of the Infectious Diseases Society of America, told NBC News.
Also, people are not social distancing the way they did during the height of the COVID pandemic, when whooping cough numbers went down.
“Levels of pertussis dropped dramatically when we were all masking, and now this huge increase is getting us back to pre-pandemic levels, and probably a little above that,” Thomas Murray, MD, a Yale Medicine pediatric infectious diseases specialist, said in a news release from the school. “It’s a contagious respiratory virus that can spread fairly quickly through the population.”
FDA advisers were scheduled to meet Sept. 20 to discuss developing more effective boosters for whooping cough.
A version of this article appeared on WebMD.com.
Whooping cough is surging in the United States, with four times as many cases reported so far this year, compared to all of 2023.
The CDC said 14,569 cases had been reported as of Sept. 14, compared to 3475 in all of 2023.
Whooping cough, also called pertussis, is a respiratory illness spread through coughing, sneezing, or breathing very close to another person. Babies are given the DTaP vaccine to protect against whooping cough, diphtheria, and tetanus. Because the vaccine effectiveness wanes faster for whooping cough than the two other illnesses, boosters are recommended every decade or so.
Why the Whooping Cough Vaccine Is Important
Whooping cough is a very contagious bacteria, so vaccination is an important step to avoid it.
But many children in their tweens aren’t getting boosters, and that age group is driving the whooping cough outbreak.
“With the increase in vaccine hesitancy that has been going on since the COVID-19 pandemic, we’re seeing outbreaks occurring in kids who are not vaccinated,” Tina Tan, MD, president-elect of the Infectious Diseases Society of America, told NBC News.
Also, people are not social distancing the way they did during the height of the COVID pandemic, when whooping cough numbers went down.
“Levels of pertussis dropped dramatically when we were all masking, and now this huge increase is getting us back to pre-pandemic levels, and probably a little above that,” Thomas Murray, MD, a Yale Medicine pediatric infectious diseases specialist, said in a news release from the school. “It’s a contagious respiratory virus that can spread fairly quickly through the population.”
FDA advisers were scheduled to meet Sept. 20 to discuss developing more effective boosters for whooping cough.
A version of this article appeared on WebMD.com.
Whooping cough is surging in the United States, with four times as many cases reported so far this year, compared to all of 2023.
The CDC said 14,569 cases had been reported as of Sept. 14, compared to 3475 in all of 2023.
Whooping cough, also called pertussis, is a respiratory illness spread through coughing, sneezing, or breathing very close to another person. Babies are given the DTaP vaccine to protect against whooping cough, diphtheria, and tetanus. Because the vaccine effectiveness wanes faster for whooping cough than the two other illnesses, boosters are recommended every decade or so.
Why the Whooping Cough Vaccine Is Important
Whooping cough is a very contagious bacteria, so vaccination is an important step to avoid it.
But many children in their tweens aren’t getting boosters, and that age group is driving the whooping cough outbreak.
“With the increase in vaccine hesitancy that has been going on since the COVID-19 pandemic, we’re seeing outbreaks occurring in kids who are not vaccinated,” Tina Tan, MD, president-elect of the Infectious Diseases Society of America, told NBC News.
Also, people are not social distancing the way they did during the height of the COVID pandemic, when whooping cough numbers went down.
“Levels of pertussis dropped dramatically when we were all masking, and now this huge increase is getting us back to pre-pandemic levels, and probably a little above that,” Thomas Murray, MD, a Yale Medicine pediatric infectious diseases specialist, said in a news release from the school. “It’s a contagious respiratory virus that can spread fairly quickly through the population.”
FDA advisers were scheduled to meet Sept. 20 to discuss developing more effective boosters for whooping cough.
A version of this article appeared on WebMD.com.
Feds Sue Three Biggest Pharmacy Benefit Managers Over Insulin Costs
The US Federal Trade Commission (FTC) has sued the nation’s three largest pharmacy benefit managers (PBMs), alleging that they have steered patients to buying higher-priced insulins so that they can reap more profits.
The three PBMs administer 80% of prescriptions in the United States, the FTC said in a statement announcing the action.
The agency filed an administrative complaint, which means its allegations will be tried in a formal hearing before an administrative law judge. It will not be heard in a criminal court.
The three PBMs “have extracted millions of dollars off the backs of patients who need life-saving medications,” Rahul Rao, deputy director of the FTC’s Bureau of Competition, said in the statement.
The FTC action is not the first taken by a government agency against PBMs. Ohio Attorney General Dave Yost sued Express Scripts and Prime Therapeutics in March 2023, alleging antitrust violations.
The FTC’s complaint, which is not yet public, alleges that PBMs excluded lower-priced insulins from their formularies “in favor of high list price, highly rebated insulin products.”
The FTC describes a market in which PBMs, as they consolidated market power, began to extract higher rebates from drug makers. In turn, insulin manufacturers started raising their prices. That allowed PBMs to collect larger rebates, even as drug makers profited, according to the FTC.
The PBMs “engaged in unfair methods of competition and unfair acts or practices under Section 5 of the FTC Act by incentivizing manufacturers to inflate insulin list prices, restricting patients’ access to more affordable insulins on drug formularies and shifting the cost of high list price insulins to vulnerable patient populations,” said the FTC, in its statement.
Andrea Nelson, chief legal officer for The Cigna Group, said in a statement that the lawsuit “continues a troubling pattern from the FTC of unsubstantiated and ideologically-driven attacks on pharmacy benefit managers, following the FTC’s biased and misleading July 2024 report, which Express Scripts demanded the Commission retract earlier this week.”
Conduct ‘Raises Serious Concerns’
Drug makers are not off the hook, said the FTC. Mr. Rao said in a separate statement that “all drug manufacturers should be on notice that their participation in the type of conduct challenged here raises serious concerns and that the Bureau of Competition may recommend suing drug manufacturers in any future enforcement actions.”
The lawsuit comes on the heels of a report issued by the FTC in July, in which it accused the industry of driving small pharmacies out of business and of having extraordinary control over where Americans access prescription drugs and how much they pay.
The agency also noted in that report that some PBMs had still not responded to its requests for information, some 2 years after first asking.
Cigna’s Express Scripts sued the FTC on September 17, 2024, claiming that the report hurt the company’s reputation.
The report is “74 pages of unsupported innuendo leveled against Express Scripts and other PBMs under a false and defamatory headline and accompanied by a false and defamatory press release,” said the Cigna suit.
Cigna is seeking to have the report scrubbed from the FTC website and an injunction that would bar FTC Chairwoman Lina Khan from participating in any FTC business relating to Express Scripts.
Cigna’s Ms. Nelson accused the FTC of trying to “score political points” and said that forcing PBMs to include some drugs on its formularies “will drive drug prices higher in this country.”
CVS Health’s Caremark and UnitedHealth’s Optum also pushed back, as did the industry trade group, the Pharmaceutical Care Management Association.
“This action not only fails to accurately consider the role of the entire prescription drug supply chain, but disregards positive progress, supported by PBMs, in making insulin more affordable for patients,” the association said in a statement. “In contrast to the rhetoric, the current insulin market is actually working, with PBMs effectively leveraging greater competition to drive down insulin prices and doing their part to make insulin affordable for patients through innovative programs,” said the group.
“The FTC has missed the mark entirely,” David Whitrap, vice president for external affairs at CVS Health, said in a statement emailed to this news organization.
CVS Health members “on average pay less than $25, far below list prices and far below the Biden Administration’s $35 cap,” said Mr. Whitrap, who added that the PBM had protected customers from “pharma price-gouging.”
UnitedHealth’s Optum also said that it had reduced insulin prices for members to an average of less than $18 per month. “This baseless action demonstrates a profound misunderstanding of how drug pricing works,” wrote Elizabeth Hoff, a spokesperson for UnitedHealth’s Optum Rx, in an email to this news organization.
A version of this article appeared on Medscape.com.
The US Federal Trade Commission (FTC) has sued the nation’s three largest pharmacy benefit managers (PBMs), alleging that they have steered patients to buying higher-priced insulins so that they can reap more profits.
The three PBMs administer 80% of prescriptions in the United States, the FTC said in a statement announcing the action.
The agency filed an administrative complaint, which means its allegations will be tried in a formal hearing before an administrative law judge. It will not be heard in a criminal court.
The three PBMs “have extracted millions of dollars off the backs of patients who need life-saving medications,” Rahul Rao, deputy director of the FTC’s Bureau of Competition, said in the statement.
The FTC action is not the first taken by a government agency against PBMs. Ohio Attorney General Dave Yost sued Express Scripts and Prime Therapeutics in March 2023, alleging antitrust violations.
The FTC’s complaint, which is not yet public, alleges that PBMs excluded lower-priced insulins from their formularies “in favor of high list price, highly rebated insulin products.”
The FTC describes a market in which PBMs, as they consolidated market power, began to extract higher rebates from drug makers. In turn, insulin manufacturers started raising their prices. That allowed PBMs to collect larger rebates, even as drug makers profited, according to the FTC.
The PBMs “engaged in unfair methods of competition and unfair acts or practices under Section 5 of the FTC Act by incentivizing manufacturers to inflate insulin list prices, restricting patients’ access to more affordable insulins on drug formularies and shifting the cost of high list price insulins to vulnerable patient populations,” said the FTC, in its statement.
Andrea Nelson, chief legal officer for The Cigna Group, said in a statement that the lawsuit “continues a troubling pattern from the FTC of unsubstantiated and ideologically-driven attacks on pharmacy benefit managers, following the FTC’s biased and misleading July 2024 report, which Express Scripts demanded the Commission retract earlier this week.”
Conduct ‘Raises Serious Concerns’
Drug makers are not off the hook, said the FTC. Mr. Rao said in a separate statement that “all drug manufacturers should be on notice that their participation in the type of conduct challenged here raises serious concerns and that the Bureau of Competition may recommend suing drug manufacturers in any future enforcement actions.”
The lawsuit comes on the heels of a report issued by the FTC in July, in which it accused the industry of driving small pharmacies out of business and of having extraordinary control over where Americans access prescription drugs and how much they pay.
The agency also noted in that report that some PBMs had still not responded to its requests for information, some 2 years after first asking.
Cigna’s Express Scripts sued the FTC on September 17, 2024, claiming that the report hurt the company’s reputation.
The report is “74 pages of unsupported innuendo leveled against Express Scripts and other PBMs under a false and defamatory headline and accompanied by a false and defamatory press release,” said the Cigna suit.
Cigna is seeking to have the report scrubbed from the FTC website and an injunction that would bar FTC Chairwoman Lina Khan from participating in any FTC business relating to Express Scripts.
Cigna’s Ms. Nelson accused the FTC of trying to “score political points” and said that forcing PBMs to include some drugs on its formularies “will drive drug prices higher in this country.”
CVS Health’s Caremark and UnitedHealth’s Optum also pushed back, as did the industry trade group, the Pharmaceutical Care Management Association.
“This action not only fails to accurately consider the role of the entire prescription drug supply chain, but disregards positive progress, supported by PBMs, in making insulin more affordable for patients,” the association said in a statement. “In contrast to the rhetoric, the current insulin market is actually working, with PBMs effectively leveraging greater competition to drive down insulin prices and doing their part to make insulin affordable for patients through innovative programs,” said the group.
“The FTC has missed the mark entirely,” David Whitrap, vice president for external affairs at CVS Health, said in a statement emailed to this news organization.
CVS Health members “on average pay less than $25, far below list prices and far below the Biden Administration’s $35 cap,” said Mr. Whitrap, who added that the PBM had protected customers from “pharma price-gouging.”
UnitedHealth’s Optum also said that it had reduced insulin prices for members to an average of less than $18 per month. “This baseless action demonstrates a profound misunderstanding of how drug pricing works,” wrote Elizabeth Hoff, a spokesperson for UnitedHealth’s Optum Rx, in an email to this news organization.
A version of this article appeared on Medscape.com.
The US Federal Trade Commission (FTC) has sued the nation’s three largest pharmacy benefit managers (PBMs), alleging that they have steered patients to buying higher-priced insulins so that they can reap more profits.
The three PBMs administer 80% of prescriptions in the United States, the FTC said in a statement announcing the action.
The agency filed an administrative complaint, which means its allegations will be tried in a formal hearing before an administrative law judge. It will not be heard in a criminal court.
The three PBMs “have extracted millions of dollars off the backs of patients who need life-saving medications,” Rahul Rao, deputy director of the FTC’s Bureau of Competition, said in the statement.
The FTC action is not the first taken by a government agency against PBMs. Ohio Attorney General Dave Yost sued Express Scripts and Prime Therapeutics in March 2023, alleging antitrust violations.
The FTC’s complaint, which is not yet public, alleges that PBMs excluded lower-priced insulins from their formularies “in favor of high list price, highly rebated insulin products.”
The FTC describes a market in which PBMs, as they consolidated market power, began to extract higher rebates from drug makers. In turn, insulin manufacturers started raising their prices. That allowed PBMs to collect larger rebates, even as drug makers profited, according to the FTC.
The PBMs “engaged in unfair methods of competition and unfair acts or practices under Section 5 of the FTC Act by incentivizing manufacturers to inflate insulin list prices, restricting patients’ access to more affordable insulins on drug formularies and shifting the cost of high list price insulins to vulnerable patient populations,” said the FTC, in its statement.
Andrea Nelson, chief legal officer for The Cigna Group, said in a statement that the lawsuit “continues a troubling pattern from the FTC of unsubstantiated and ideologically-driven attacks on pharmacy benefit managers, following the FTC’s biased and misleading July 2024 report, which Express Scripts demanded the Commission retract earlier this week.”
Conduct ‘Raises Serious Concerns’
Drug makers are not off the hook, said the FTC. Mr. Rao said in a separate statement that “all drug manufacturers should be on notice that their participation in the type of conduct challenged here raises serious concerns and that the Bureau of Competition may recommend suing drug manufacturers in any future enforcement actions.”
The lawsuit comes on the heels of a report issued by the FTC in July, in which it accused the industry of driving small pharmacies out of business and of having extraordinary control over where Americans access prescription drugs and how much they pay.
The agency also noted in that report that some PBMs had still not responded to its requests for information, some 2 years after first asking.
Cigna’s Express Scripts sued the FTC on September 17, 2024, claiming that the report hurt the company’s reputation.
The report is “74 pages of unsupported innuendo leveled against Express Scripts and other PBMs under a false and defamatory headline and accompanied by a false and defamatory press release,” said the Cigna suit.
Cigna is seeking to have the report scrubbed from the FTC website and an injunction that would bar FTC Chairwoman Lina Khan from participating in any FTC business relating to Express Scripts.
Cigna’s Ms. Nelson accused the FTC of trying to “score political points” and said that forcing PBMs to include some drugs on its formularies “will drive drug prices higher in this country.”
CVS Health’s Caremark and UnitedHealth’s Optum also pushed back, as did the industry trade group, the Pharmaceutical Care Management Association.
“This action not only fails to accurately consider the role of the entire prescription drug supply chain, but disregards positive progress, supported by PBMs, in making insulin more affordable for patients,” the association said in a statement. “In contrast to the rhetoric, the current insulin market is actually working, with PBMs effectively leveraging greater competition to drive down insulin prices and doing their part to make insulin affordable for patients through innovative programs,” said the group.
“The FTC has missed the mark entirely,” David Whitrap, vice president for external affairs at CVS Health, said in a statement emailed to this news organization.
CVS Health members “on average pay less than $25, far below list prices and far below the Biden Administration’s $35 cap,” said Mr. Whitrap, who added that the PBM had protected customers from “pharma price-gouging.”
UnitedHealth’s Optum also said that it had reduced insulin prices for members to an average of less than $18 per month. “This baseless action demonstrates a profound misunderstanding of how drug pricing works,” wrote Elizabeth Hoff, a spokesperson for UnitedHealth’s Optum Rx, in an email to this news organization.
A version of this article appeared on Medscape.com.
Isatuximab Approved First-Line for Transplant-Ineligible MM
The new first-line indication joins two previous approvals of the CD38 antibody for later-line indications, one for relapsed disease with carfilzomib and dexamethasone, the other with pomalidomide and dexamethasone after at least two prior regimens that include lenalidomide and a proteasome inhibitor.
In addition to other MM indications, isatuximab’s anti-CD38 competitor on the US market, daratumumab (Darzalex — Johnson & Johnson), also carries a first-line indication for transplant-ineligible MM in combination with either lenalidomide and dexamethasone or bortezomib, melphalan, and prednisone.
Isatuximab’s new approval is based on the open-label IMROZ trial in 446 patients randomized 3:2 to either isatuximab or placebo on a background of bortezomib, lenalidomide, and dexamethasone.
At a median follow-up of 59.7 months, estimated progression-free survival (PFS) was 63.2% with isatuximab add-on vs 45.2% in the placebo arm. Median PFS was not reached in the isatuximab group but 54.3 months with placebo (hazard ratio, 0.60; 98.5% CI, 0.41-0.88; P < .001).
In a press release announcing the results, Sanofi said “IMROZ is the first global phase 3 study of an anti-CD38 monoclonal antibody” to show benefit in combination with bortezomib, lenalidomide, and dexamethasone, the current standard of care for transplant-ineligible MM.
Upper respiratory tract infections, diarrhea, fatigue, peripheral sensory neuropathy, pneumonia, musculoskeletal pain, cataract, constipation, peripheral edema, rash, infusion-related reaction, insomnia, and COVID-19 were the most common adverse events in the isatuximab arm of IMROZ, occurring in 20% or more of subjects.
Eleven percent of isatuximab patients died during treatment vs 5.5% in the placebo group, driven primarily by infections.
The recommended dose of isatuximab is 10 mg/kg every week for 4 weeks followed by every 2 weeks until disease progression or unacceptable toxicity.
The cost is approximately $843 for 5 mL of the 20 mg/mL intravenous solution, according to Drugs.com.
A version of this article appeared on Medscape.com.
The new first-line indication joins two previous approvals of the CD38 antibody for later-line indications, one for relapsed disease with carfilzomib and dexamethasone, the other with pomalidomide and dexamethasone after at least two prior regimens that include lenalidomide and a proteasome inhibitor.
In addition to other MM indications, isatuximab’s anti-CD38 competitor on the US market, daratumumab (Darzalex — Johnson & Johnson), also carries a first-line indication for transplant-ineligible MM in combination with either lenalidomide and dexamethasone or bortezomib, melphalan, and prednisone.
Isatuximab’s new approval is based on the open-label IMROZ trial in 446 patients randomized 3:2 to either isatuximab or placebo on a background of bortezomib, lenalidomide, and dexamethasone.
At a median follow-up of 59.7 months, estimated progression-free survival (PFS) was 63.2% with isatuximab add-on vs 45.2% in the placebo arm. Median PFS was not reached in the isatuximab group but 54.3 months with placebo (hazard ratio, 0.60; 98.5% CI, 0.41-0.88; P < .001).
In a press release announcing the results, Sanofi said “IMROZ is the first global phase 3 study of an anti-CD38 monoclonal antibody” to show benefit in combination with bortezomib, lenalidomide, and dexamethasone, the current standard of care for transplant-ineligible MM.
Upper respiratory tract infections, diarrhea, fatigue, peripheral sensory neuropathy, pneumonia, musculoskeletal pain, cataract, constipation, peripheral edema, rash, infusion-related reaction, insomnia, and COVID-19 were the most common adverse events in the isatuximab arm of IMROZ, occurring in 20% or more of subjects.
Eleven percent of isatuximab patients died during treatment vs 5.5% in the placebo group, driven primarily by infections.
The recommended dose of isatuximab is 10 mg/kg every week for 4 weeks followed by every 2 weeks until disease progression or unacceptable toxicity.
The cost is approximately $843 for 5 mL of the 20 mg/mL intravenous solution, according to Drugs.com.
A version of this article appeared on Medscape.com.
The new first-line indication joins two previous approvals of the CD38 antibody for later-line indications, one for relapsed disease with carfilzomib and dexamethasone, the other with pomalidomide and dexamethasone after at least two prior regimens that include lenalidomide and a proteasome inhibitor.
In addition to other MM indications, isatuximab’s anti-CD38 competitor on the US market, daratumumab (Darzalex — Johnson & Johnson), also carries a first-line indication for transplant-ineligible MM in combination with either lenalidomide and dexamethasone or bortezomib, melphalan, and prednisone.
Isatuximab’s new approval is based on the open-label IMROZ trial in 446 patients randomized 3:2 to either isatuximab or placebo on a background of bortezomib, lenalidomide, and dexamethasone.
At a median follow-up of 59.7 months, estimated progression-free survival (PFS) was 63.2% with isatuximab add-on vs 45.2% in the placebo arm. Median PFS was not reached in the isatuximab group but 54.3 months with placebo (hazard ratio, 0.60; 98.5% CI, 0.41-0.88; P < .001).
In a press release announcing the results, Sanofi said “IMROZ is the first global phase 3 study of an anti-CD38 monoclonal antibody” to show benefit in combination with bortezomib, lenalidomide, and dexamethasone, the current standard of care for transplant-ineligible MM.
Upper respiratory tract infections, diarrhea, fatigue, peripheral sensory neuropathy, pneumonia, musculoskeletal pain, cataract, constipation, peripheral edema, rash, infusion-related reaction, insomnia, and COVID-19 were the most common adverse events in the isatuximab arm of IMROZ, occurring in 20% or more of subjects.
Eleven percent of isatuximab patients died during treatment vs 5.5% in the placebo group, driven primarily by infections.
The recommended dose of isatuximab is 10 mg/kg every week for 4 weeks followed by every 2 weeks until disease progression or unacceptable toxicity.
The cost is approximately $843 for 5 mL of the 20 mg/mL intravenous solution, according to Drugs.com.
A version of this article appeared on Medscape.com.
Hypnosis May Offer Relief During Sharp Debridement of Skin Ulcers
TOPLINE:
Hypnosis reduces pain during sharp debridement of skin ulcers in patients with immune-mediated inflammatory diseases, with most patients reporting decreased pain awareness and lasting pain relief for 2-3 days after the procedure.
METHODOLOGY:
- Researchers reported their experience with the anecdotal use of hypnosis for pain management in debridement of skin ulcers in immune-mediated inflammatory diseases.
- They studied 16 participants (14 women; mean age, 56 years; 14 with systemic sclerosis or morphea) with recurrent skin ulcerations requiring sharp debridement, who presented to a wound care clinic at the Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom. The participants had negative experiences with pharmacologic pain management.
- Participants consented to hypnosis during debridement as the only mode of analgesia, conducted by the same hypnosis-trained, experienced healthcare professional in charge of their ulcer care.
- Ulcer pain scores were recorded using a numerical rating pain scale before and immediately after debridement, with a score of 0 indicating no pain and 10 indicating worst pain.
TAKEAWAY:
- Hypnosis reduced the median pre-debridement ulcer pain score from 8 (interquartile range [IQR], 7-10) to 0.5 (IQR, 0-2) immediately after the procedure.
- Of 16 participants, 14 reported being aware of the procedure but not feeling the pain, with only two participants experiencing a brief spike in pain.
- The other two participants reported experiencing reduced awareness and being pain-free during the procedure.
- Five participants reported a lasting decrease in pain perception for 2-3 days after the procedure.
IN PRACTICE:
“These preliminary data underscore the potential for the integration of hypnosis into the management of intervention-related pain in clinical care,” the authors wrote.
SOURCE:
The study was led by Begonya Alcacer-Pitarch, PhD, Leeds Institute of Rheumatic and Musculoskeletal Medicine, the University of Leeds, and Chapel Allerton Hospital in Leeds, United Kingdom. It was published as a correspondence on September 10, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The small sample size may limit the generalizability of the findings. The methods used for data collection were not standardized, and the individuals included in the study may have introduced selection bias.
DISCLOSURES:
The study did not have a funding source. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Hypnosis reduces pain during sharp debridement of skin ulcers in patients with immune-mediated inflammatory diseases, with most patients reporting decreased pain awareness and lasting pain relief for 2-3 days after the procedure.
METHODOLOGY:
- Researchers reported their experience with the anecdotal use of hypnosis for pain management in debridement of skin ulcers in immune-mediated inflammatory diseases.
- They studied 16 participants (14 women; mean age, 56 years; 14 with systemic sclerosis or morphea) with recurrent skin ulcerations requiring sharp debridement, who presented to a wound care clinic at the Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom. The participants had negative experiences with pharmacologic pain management.
- Participants consented to hypnosis during debridement as the only mode of analgesia, conducted by the same hypnosis-trained, experienced healthcare professional in charge of their ulcer care.
- Ulcer pain scores were recorded using a numerical rating pain scale before and immediately after debridement, with a score of 0 indicating no pain and 10 indicating worst pain.
TAKEAWAY:
- Hypnosis reduced the median pre-debridement ulcer pain score from 8 (interquartile range [IQR], 7-10) to 0.5 (IQR, 0-2) immediately after the procedure.
- Of 16 participants, 14 reported being aware of the procedure but not feeling the pain, with only two participants experiencing a brief spike in pain.
- The other two participants reported experiencing reduced awareness and being pain-free during the procedure.
- Five participants reported a lasting decrease in pain perception for 2-3 days after the procedure.
IN PRACTICE:
“These preliminary data underscore the potential for the integration of hypnosis into the management of intervention-related pain in clinical care,” the authors wrote.
SOURCE:
The study was led by Begonya Alcacer-Pitarch, PhD, Leeds Institute of Rheumatic and Musculoskeletal Medicine, the University of Leeds, and Chapel Allerton Hospital in Leeds, United Kingdom. It was published as a correspondence on September 10, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The small sample size may limit the generalizability of the findings. The methods used for data collection were not standardized, and the individuals included in the study may have introduced selection bias.
DISCLOSURES:
The study did not have a funding source. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Hypnosis reduces pain during sharp debridement of skin ulcers in patients with immune-mediated inflammatory diseases, with most patients reporting decreased pain awareness and lasting pain relief for 2-3 days after the procedure.
METHODOLOGY:
- Researchers reported their experience with the anecdotal use of hypnosis for pain management in debridement of skin ulcers in immune-mediated inflammatory diseases.
- They studied 16 participants (14 women; mean age, 56 years; 14 with systemic sclerosis or morphea) with recurrent skin ulcerations requiring sharp debridement, who presented to a wound care clinic at the Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom. The participants had negative experiences with pharmacologic pain management.
- Participants consented to hypnosis during debridement as the only mode of analgesia, conducted by the same hypnosis-trained, experienced healthcare professional in charge of their ulcer care.
- Ulcer pain scores were recorded using a numerical rating pain scale before and immediately after debridement, with a score of 0 indicating no pain and 10 indicating worst pain.
TAKEAWAY:
- Hypnosis reduced the median pre-debridement ulcer pain score from 8 (interquartile range [IQR], 7-10) to 0.5 (IQR, 0-2) immediately after the procedure.
- Of 16 participants, 14 reported being aware of the procedure but not feeling the pain, with only two participants experiencing a brief spike in pain.
- The other two participants reported experiencing reduced awareness and being pain-free during the procedure.
- Five participants reported a lasting decrease in pain perception for 2-3 days after the procedure.
IN PRACTICE:
“These preliminary data underscore the potential for the integration of hypnosis into the management of intervention-related pain in clinical care,” the authors wrote.
SOURCE:
The study was led by Begonya Alcacer-Pitarch, PhD, Leeds Institute of Rheumatic and Musculoskeletal Medicine, the University of Leeds, and Chapel Allerton Hospital in Leeds, United Kingdom. It was published as a correspondence on September 10, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The small sample size may limit the generalizability of the findings. The methods used for data collection were not standardized, and the individuals included in the study may have introduced selection bias.
DISCLOSURES:
The study did not have a funding source. The authors declared no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Treating Family: Ethicist Discusses Whether It’s Appropriate
This transcript has been edited for clarity.
There’s a very interesting story in the medical press. A few years ago, a plastic surgeon named Edmond Cabbabe was preparing to do a follow-up cosmetic procedure on his wife at Mercy Hospital South, which is a big hospital in the St. Louis, Missouri, area.
He put her on the operating schedule, and he had done that when he had performed the original operation on her. On the day of the surgery, he got a call from the hospital saying the procedure was canceled. They said that the hospital’s policy, maybe a new one, would not allow doctors to operate on family members.
This physician was a past president of the Missouri State Medical Association. I think he was also on the board or president of the American Medical Association (AMA) Foundation. This was a physician not only in a skilled area where he felt confident he could take care of his wife, but also someone who was prominent in medical politics and medical policy.
The AMA forever has had a policy that says don’t treat relatives. This physician basically said, I think that policy is too restrictive, too cautious, and it doesn’t make much sense to continue to say that you can’t treat family and friends.
By implication, he was saying, I know exactly what I’m doing in my field and I know exactly what I’m doing with her procedure. I should have a right to perform it. I think I do a great job and I’d be best for her.
If you look at medical boards, every once in a while in some state, someone is brought up on a charge of doing different things with family members and saying that they’re going to get censured. They don’t usually lose their license, but they get a reprimand or get told that is just not ethical to do.
I think, in the long run, the policy about not treating your family and friends makes sense. The problem is, as is well known from the social sciences and psychology, people get biased when they deal with those they care about, love, and hold close to them.
It’s hard for the doctor to be objective when dealing with people that they really like or love. It’s also difficult for patients because they may not want to bring up something or they are uncomfortable talking with a doctor who’s a family member or close friend. They may not want to complain. They may be a little bit embarrassed about things. It just adds an emotional edge, I think, that’s difficult.
All that said, do I know doctors who regularly prescribe, say, an ointment for something that’s itchy or some kind of a pill when allergy season breaks out? I do. Do I think they’re acting in a horribly unethical manner? I don’t.
You need some judgment here. There are absolutely minor things where objectivity, fear, and anxiety are not in play. You’re going to be able to prescribe the routine thing for the routine itch without worrying too much about whether it’s a stranger, a friend, or your daughter.
What sorts of things am I really talking about when I say that minor variability ought to be allowed? It’s one thing when someone has poison ivy and they’re going to need some kind of standard medicine to treat it. A very different area that’s much more dangerous, and one I would avoid, is in the mental health field, and for that matter, the pain field.
It’s tempting to say: “Oh, my relative is just having a bad time. I’ll give her a little bit of antidepressant medicine,” or “They seem to be having pain after an operation or something, and I’m going to give them a little bit of pain meds just to get them through.”
Those areas are flying red flags. It’s easy to abuse and easy for someone to become a user and manipulate a friend or a doctor who’s a relative into getting things that another doctor wouldn’t be giving. I think that’s the space where you’ve got to exercise extreme caution.
Time and again, when those people get called up in front of the boards for treating relatives, it’s in those spaces of mental health, anxiety, and pain control. Again, when you know that there’s a likelihood of abuse, I think that’s the place where the line has to hold. Don’t treat the relative. Don’t treat the friend.
At the end of the day, I wouldn’t change the AMA policy. I think we should keep it in place and morally try to discourage doctors from caring for those they’re close to or they have emotional ties to.
At the same time, as with all ethical situations, there has to be a little bit of wiggle room for those super-minor cases where it just makes sense to say: “You don’t have to go find somebody else to do this. I can prescribe this ointment or this minor thing for you. No one’s objectivity is going to be soured, and you’re not going to feel in any way at risk because I’m going to prescribe this for you.”
Common sense ought to prevail. The default position is don’t do it; however, maybe with a tiny bit of space for what’s minor, what’s routine, and what really does just save people some inconvenience, there I might just give a little.
Dr. Caplan, Director, Division of Medical Ethics, New York University Langone Medical Center, New York City, has disclosed relationships with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There’s a very interesting story in the medical press. A few years ago, a plastic surgeon named Edmond Cabbabe was preparing to do a follow-up cosmetic procedure on his wife at Mercy Hospital South, which is a big hospital in the St. Louis, Missouri, area.
He put her on the operating schedule, and he had done that when he had performed the original operation on her. On the day of the surgery, he got a call from the hospital saying the procedure was canceled. They said that the hospital’s policy, maybe a new one, would not allow doctors to operate on family members.
This physician was a past president of the Missouri State Medical Association. I think he was also on the board or president of the American Medical Association (AMA) Foundation. This was a physician not only in a skilled area where he felt confident he could take care of his wife, but also someone who was prominent in medical politics and medical policy.
The AMA forever has had a policy that says don’t treat relatives. This physician basically said, I think that policy is too restrictive, too cautious, and it doesn’t make much sense to continue to say that you can’t treat family and friends.
By implication, he was saying, I know exactly what I’m doing in my field and I know exactly what I’m doing with her procedure. I should have a right to perform it. I think I do a great job and I’d be best for her.
If you look at medical boards, every once in a while in some state, someone is brought up on a charge of doing different things with family members and saying that they’re going to get censured. They don’t usually lose their license, but they get a reprimand or get told that is just not ethical to do.
I think, in the long run, the policy about not treating your family and friends makes sense. The problem is, as is well known from the social sciences and psychology, people get biased when they deal with those they care about, love, and hold close to them.
It’s hard for the doctor to be objective when dealing with people that they really like or love. It’s also difficult for patients because they may not want to bring up something or they are uncomfortable talking with a doctor who’s a family member or close friend. They may not want to complain. They may be a little bit embarrassed about things. It just adds an emotional edge, I think, that’s difficult.
All that said, do I know doctors who regularly prescribe, say, an ointment for something that’s itchy or some kind of a pill when allergy season breaks out? I do. Do I think they’re acting in a horribly unethical manner? I don’t.
You need some judgment here. There are absolutely minor things where objectivity, fear, and anxiety are not in play. You’re going to be able to prescribe the routine thing for the routine itch without worrying too much about whether it’s a stranger, a friend, or your daughter.
What sorts of things am I really talking about when I say that minor variability ought to be allowed? It’s one thing when someone has poison ivy and they’re going to need some kind of standard medicine to treat it. A very different area that’s much more dangerous, and one I would avoid, is in the mental health field, and for that matter, the pain field.
It’s tempting to say: “Oh, my relative is just having a bad time. I’ll give her a little bit of antidepressant medicine,” or “They seem to be having pain after an operation or something, and I’m going to give them a little bit of pain meds just to get them through.”
Those areas are flying red flags. It’s easy to abuse and easy for someone to become a user and manipulate a friend or a doctor who’s a relative into getting things that another doctor wouldn’t be giving. I think that’s the space where you’ve got to exercise extreme caution.
Time and again, when those people get called up in front of the boards for treating relatives, it’s in those spaces of mental health, anxiety, and pain control. Again, when you know that there’s a likelihood of abuse, I think that’s the place where the line has to hold. Don’t treat the relative. Don’t treat the friend.
At the end of the day, I wouldn’t change the AMA policy. I think we should keep it in place and morally try to discourage doctors from caring for those they’re close to or they have emotional ties to.
At the same time, as with all ethical situations, there has to be a little bit of wiggle room for those super-minor cases where it just makes sense to say: “You don’t have to go find somebody else to do this. I can prescribe this ointment or this minor thing for you. No one’s objectivity is going to be soured, and you’re not going to feel in any way at risk because I’m going to prescribe this for you.”
Common sense ought to prevail. The default position is don’t do it; however, maybe with a tiny bit of space for what’s minor, what’s routine, and what really does just save people some inconvenience, there I might just give a little.
Dr. Caplan, Director, Division of Medical Ethics, New York University Langone Medical Center, New York City, has disclosed relationships with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There’s a very interesting story in the medical press. A few years ago, a plastic surgeon named Edmond Cabbabe was preparing to do a follow-up cosmetic procedure on his wife at Mercy Hospital South, which is a big hospital in the St. Louis, Missouri, area.
He put her on the operating schedule, and he had done that when he had performed the original operation on her. On the day of the surgery, he got a call from the hospital saying the procedure was canceled. They said that the hospital’s policy, maybe a new one, would not allow doctors to operate on family members.
This physician was a past president of the Missouri State Medical Association. I think he was also on the board or president of the American Medical Association (AMA) Foundation. This was a physician not only in a skilled area where he felt confident he could take care of his wife, but also someone who was prominent in medical politics and medical policy.
The AMA forever has had a policy that says don’t treat relatives. This physician basically said, I think that policy is too restrictive, too cautious, and it doesn’t make much sense to continue to say that you can’t treat family and friends.
By implication, he was saying, I know exactly what I’m doing in my field and I know exactly what I’m doing with her procedure. I should have a right to perform it. I think I do a great job and I’d be best for her.
If you look at medical boards, every once in a while in some state, someone is brought up on a charge of doing different things with family members and saying that they’re going to get censured. They don’t usually lose their license, but they get a reprimand or get told that is just not ethical to do.
I think, in the long run, the policy about not treating your family and friends makes sense. The problem is, as is well known from the social sciences and psychology, people get biased when they deal with those they care about, love, and hold close to them.
It’s hard for the doctor to be objective when dealing with people that they really like or love. It’s also difficult for patients because they may not want to bring up something or they are uncomfortable talking with a doctor who’s a family member or close friend. They may not want to complain. They may be a little bit embarrassed about things. It just adds an emotional edge, I think, that’s difficult.
All that said, do I know doctors who regularly prescribe, say, an ointment for something that’s itchy or some kind of a pill when allergy season breaks out? I do. Do I think they’re acting in a horribly unethical manner? I don’t.
You need some judgment here. There are absolutely minor things where objectivity, fear, and anxiety are not in play. You’re going to be able to prescribe the routine thing for the routine itch without worrying too much about whether it’s a stranger, a friend, or your daughter.
What sorts of things am I really talking about when I say that minor variability ought to be allowed? It’s one thing when someone has poison ivy and they’re going to need some kind of standard medicine to treat it. A very different area that’s much more dangerous, and one I would avoid, is in the mental health field, and for that matter, the pain field.
It’s tempting to say: “Oh, my relative is just having a bad time. I’ll give her a little bit of antidepressant medicine,” or “They seem to be having pain after an operation or something, and I’m going to give them a little bit of pain meds just to get them through.”
Those areas are flying red flags. It’s easy to abuse and easy for someone to become a user and manipulate a friend or a doctor who’s a relative into getting things that another doctor wouldn’t be giving. I think that’s the space where you’ve got to exercise extreme caution.
Time and again, when those people get called up in front of the boards for treating relatives, it’s in those spaces of mental health, anxiety, and pain control. Again, when you know that there’s a likelihood of abuse, I think that’s the place where the line has to hold. Don’t treat the relative. Don’t treat the friend.
At the end of the day, I wouldn’t change the AMA policy. I think we should keep it in place and morally try to discourage doctors from caring for those they’re close to or they have emotional ties to.
At the same time, as with all ethical situations, there has to be a little bit of wiggle room for those super-minor cases where it just makes sense to say: “You don’t have to go find somebody else to do this. I can prescribe this ointment or this minor thing for you. No one’s objectivity is going to be soured, and you’re not going to feel in any way at risk because I’m going to prescribe this for you.”
Common sense ought to prevail. The default position is don’t do it; however, maybe with a tiny bit of space for what’s minor, what’s routine, and what really does just save people some inconvenience, there I might just give a little.
Dr. Caplan, Director, Division of Medical Ethics, New York University Langone Medical Center, New York City, has disclosed relationships with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
Reflectance Confocal Microscopy as a Diagnostic Aid in Allergic Contact Dermatitis to Mango Sap
The mango tree (Mangifera indica) produces nutrient-dense fruit—known colloquially as the “king of fruits”—that is widely consumed across the world. Native to southern Asia, the mango tree is a member of the Anacardiaceae family, a large family of flowering, fruit-bearing plants.1 Many members of the Anacardiaceae family, which includes poison ivy and poison oak, are known to produce urushiol, a skin irritant associated with allergic contact dermatitis (ACD).2 Interestingly, despite its widespread consumption and categorization in the Anacardiaceae family, allergic reactions to mango are comparatively rare; they occur as either immediate type I hypersensitivity reactions manifesting with rapid-onset symptoms such as urticaria, wheezing, and angioedema, or delayed type IV hypersensitivity reactions manifesting as ACD.3 Although exposure to components of the mango tree has been most characteristically linked to type IV hypersensitivity reactions, there remain fewer than 40 reported cases of mango-induced ACD since it was first described in 1939.4
Evaluation of ACD most commonly includes a thorough clinical assessment with diagnostic support from patch testing and histopathologic review following skin biopsy. In recent years, reflectance confocal microscopy (RCM) has shown promising potential to join the repertoire of diagnostic tools for ACD by enabling dynamic and high-resolution imaging of contact dermatitis in vivo.5-10 Reflectance confocal microscopy is a noninvasive optical imaging technique that uses a low-energy diode laser to penetrate the layers of the skin. The resulting reflected light generates images that facilitate visualization of cutaneous structures to the depth of the papillary dermis.11 While it is most commonly used in skin cancer diagnostics, preliminary studies also have shown an emerging role for RCM in the evaluation of eczematous and inflammatory skin disease, including contact dermatitis.5-10 Herein, we present a unique case of mango sap–induced ACD imaged and diagnosed in real time via RCM.
Case Report
A 39-year-old woman presented to our clinic with a pruritic vesicular eruption on the right leg of 2 weeks’ duration that initially had developed within 7 days of exposure to mango tree sap (Figure 1). The patient reported having experienced similar pruritic eruptions in the past following contact with mango sap while eating mangos but denied any history of reactions from ingestion of the fruit. She also reported a history of robust reactions to poison ivy; however, a timeline specifying the order of first exposure to these irritants was unknown. She denied any personal or family history of atopic conditions.

The affected skin was imaged in real time during clinic using RCM, which showed an inflammatory infiltrate represented by dark spongiotic vesicles containing bright cells (Figure 2). Additional RCM imaging at the level of the stratum spinosum showed dark spongiotic areas with bright inflammatory cells infiltrating the vesicles, which were surrounded by normal skin showing a typical epidermal honeycomb pattern (Figure 3). These findings were diagnostic of ACD secondary to exposure to mango sap. The patient was advised to apply clobetasol cream 0.05% to the affected area. Notable improvement of the rash was noted within 10 days of treatment.
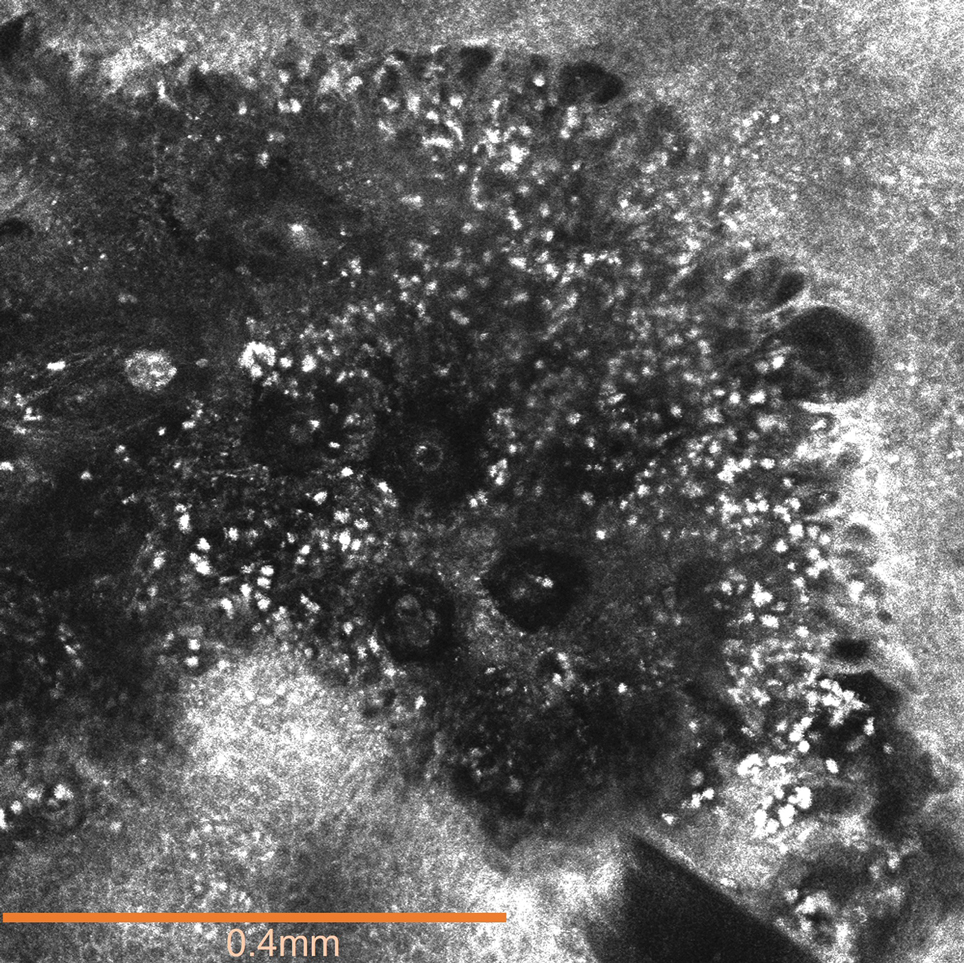
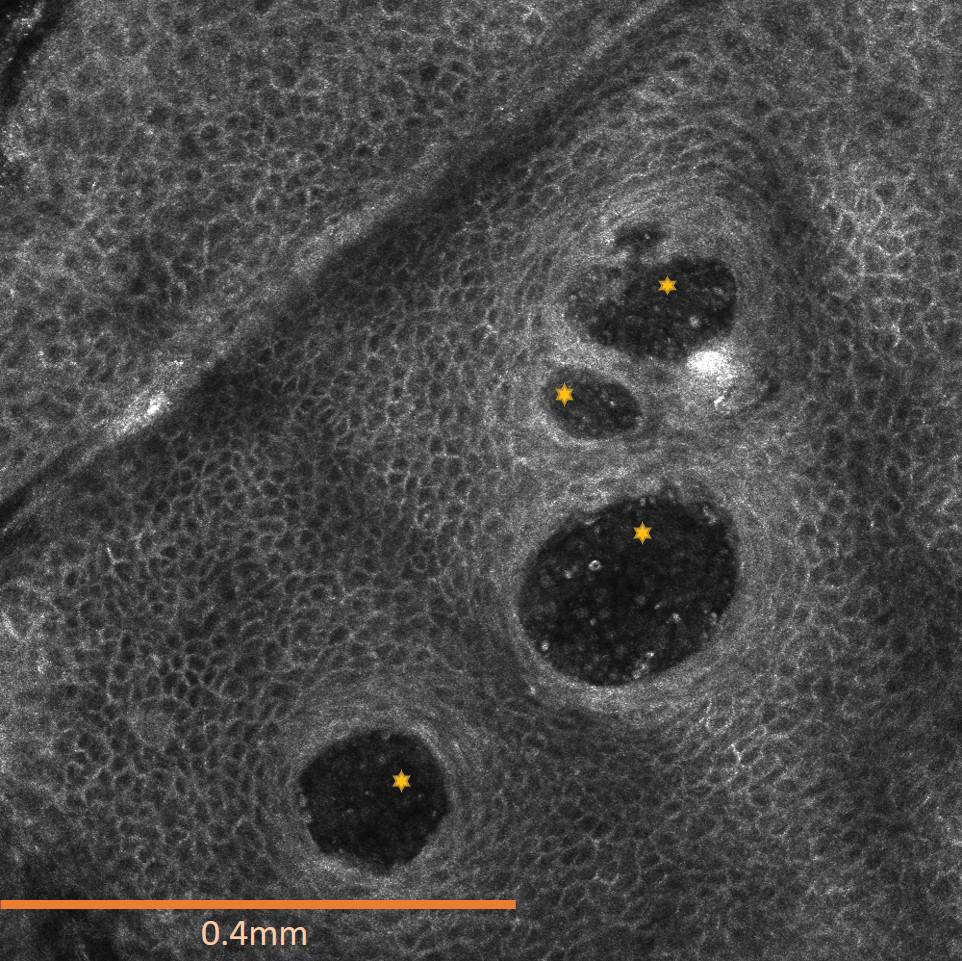
Comment
Exposure to the mango tree and its fruit is a rare cause of ACD, with few reported cases in the literature. The majority of known instances have occurred in non–mango-cultivating countries, largely the United States, although cases also have been reported in Canada, Australia, France, Japan, and Thailand.3,12 Mango-induced contact allergy follows a roughly equal distribution between males and females and most often occurs in young adults during the third and fourth decades of life.4,12-21 Importantly, delayed-type hypersensitivity reactions to mango can manifest as either localized or systemic ACD. Localized ACD can be induced via direct contact with the mango tree and its components or ingestion of the fruit.3,12,22 Conversely, systemic ACD is primarily stimulated by ingestion of the fruit. In our case, the patient had no history of allergy following mango ingestion, and her ACD was prompted by isolated contact with mango sap. The time from exposure to symptom onset of known instances of mango ACD varies widely, ranging from less than 24 hours to as long as 9 days.3,12 Diagnosis of mango-induced ACD largely is guided by clinical findings. Presenting symptoms often include an eczematous, vesicular, pruritic rash on affected areas of the skin, frequently the head, neck, and extremities. Patients also commonly present with linear papulovesicular lesions and periorbital or perioral edema.
The suspected allergens responsible for mango-induced ACD are derived from resorcinol—specifically heptadecadienyl resorcinol, heptadecenyl resorcinol, and pentadecyl resorcinol, which are collectively known as mango allergens.23 These allergens can be found within the pulp and skin of the mango fruit as well as in the bark and leaves of the mango tree, which may explain observed allergic reactions to components of both the mango fruit and tree.12 Similar to these resorcinol derivatives, the urushiol resin found in poison ivy and poison oak is a catechol derivative.2 Importantly, both resorcinols and catechols are isomers of the same aromatic phenol—dihydroxybenzene. Because of these similarities, it is thought that the allergens in mangos may cross-react with urushiol in poison ivy or poison oak.23 Alongside their shared categorization in the Anacardiaceae family, it is hypothesized that this cross-reactivity underlies the sensitization that has been noted between mango and poison ivy or poison oak exposure.12,23,24 Thus, ACD often can occur on initial contact with the mango tree or its components, as a prior exposure to poison ivy or poison oak may serve as the inciting factor for hypersensitization. The majority of reported cases in the literature also occurred in countries where exposure to poison ivy and poison oak are common, further supporting the notion that these compounds may provide a sensitizing trigger for a future mango contact allergy.12
A detailed clinical history combined with adjunctive diagnostic support from patch testing and histopathology of biopsied skin lesions classically are used in the diagnosis of mango-induced ACD. Due to its ability to provide quick and noninvasive in vivo imaging of cutaneous lesions, RCM's applications have expanded to include evaluation of inflammatory skin diseases such as contact dermatitis. Many features of contact dermatitis identified via RCM are common between ACD and irritant contact dermatitis (ICD) and include disruption of the stratum corneum, parakeratosis, vesiculation, spongiosis, and exocytosis.6,10,25 Studies also have described features shown via RCM that are unique to ACD, including vasodilation and intercellular edema, compared to more distinct targetoid keratinocytes and detached corneocytes seen in ICD.6,10,25 Studies by Astner et al5,6 demonstrated a wide range of sensitivity from 52% to 96% and a high specificity of RCM greater than 95% for many of the aforementioned features of contact dermatitis, including disruption of the stratum corneum, parakeratosis, spongiosis, and exocytosis. Additional studies have further strengthened these findings, demonstrating sensitivity and specificity values of 83% and 92% for contact dermatitis under RCM, respectively.26 Importantly, given the similarities and potentially large overlap of features between ACD and ICD identified via RCM as well as findings seen on physical examination and histopathology, an emphasis on clinical correlation is essential when differentiating between these 2 variants of contact dermatitis. Thus, taken in consideration with clinical contexts, RCM has shown potent diagnostic accuracy and great potential to support the evaluation of ACD alongside patch testing and histopathology.
Final Thoughts
Contact allergy to the mango tree and its components is uncommon. We report a unique case of mango sap–induced ACD evaluated and diagnosed via dynamic visualization under RCM. As a noninvasive and reproducible imaging technique with resolutions comparable to histopathologic analysis, RCM is a promising tool that can be used to support the diagnostic evaluation of ACD.
- Shah KA, Patel MB, Patel RJ, et al. Mangifera indica (mango). Pharmacogn Rev. 2010;4:42-48.
- Lofgran T, Mahabal GD. Toxicodendron toxicity. StatPearls [Internet]. Updated May 16, 2023. Accessed September 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK557866
- Sareen R, Shah A. Hypersensitivity manifestations to the fruit mango. Asia Pac Allergy. 2011;1:43-49.
- Zakon SJ. Contact dermatitis due to mango. JAMA. 1939;113:1808.
- Astner S, Gonzalez E, Cheung A, et al. Pilot study on the sensitivity and specificity of in vivo reflectance confocal microscopy in the diagnosis of allergic contact dermatitis. J Am Acad Dermatol. 2005;53:986-992.
- Astner S, Gonzalez S, Gonzalez E. Noninvasive evaluation of allergic and irritant contact dermatitis by in vivo reflectance confocal microscopy. Dermatitis. 2006;17:182-191.
- Csuka EA, Ward SC, Ekelem C, et al. Reflectance confocal microscopy, optical coherence tomography, and multiphoton microscopy in inflammatory skin disease diagnosis. Lasers Surg Med. 2021;53:776-797.
- Guichard A, Fanian F, Girardin P, et al. Allergic patch test and contact dermatitis by in vivo reflectance confocal microscopy [in French]. Ann Dermatol Venereol. 2014;141:805-807.
- Sakanashi EN, Matsumura M, Kikuchi K, et al. A comparative study of allergic contact dermatitis by patch test versus reflectance confocal laser microscopy, with nickel and cobalt. Eur J Dermatol. 2010;20:705-711.
- Swindells K, Burnett N, Rius-Diaz F, et al. Reflectance confocal microscopy may differentiate acute allergic and irritant contact dermatitis in vivo. J Am Acad Dermatol. 2004;50:220-228.
- Shahriari N, Grant-Kels JM, Rabinovitz H, et al. Reflectance confocal microscopy: principles, basic terminology, clinical indications, limitations, and practical considerations. J Am Acad Dermatol. 2021;84:1-14.
- Berghea EC, Craiu M, Ali S, et al. Contact allergy induced by mango (Mangifera indica): a relevant topic? Medicina (Kaunas). 2021;57:1240.
- O’Hern K, Zhang F, Zug KA, et al. “Mango slice” dermatitis: pediatric allergic contact dermatitis to mango pulp and skin. Dermatitis. 2022;33:E46-E47.
- Raison-Peyron N, Aljaber F, Al Ali OA, et al. Mango dermatitis: an unusual cause of eyelid dermatitis in France. Contact Dermatitis. 2021;85:599-600.
- Alipour Tehrany Y, Coulombe J. Mango allergic contact dermatitis. Contact Dermatitis. 2021;85:241-242.
- Yoo MJ, Carius BM. Mango dermatitis after urushiol sensitization. Clin Pract Cases Emerg Med. 2019;3:361-363.
- Miyazawa H, Nishie W, Hata H, et al. A severe case of mango dermatitis. J Eur Acad Dermatol Venereol. 2018;32:E160-E161.
- Trehan I, Meuli GJ. Mango contact allergy. J Travel Med. 2010;17:284.
- Wiwanitkit V. Mango dermatitis. Indian J Dermatol. 2008;53:158.
- Weinstein S, Bassiri-Tehrani S, Cohen DE. Allergic contact dermatitis to mango flesh. Int J Dermatol. 2004;43:195-196.
- Calvert ML, Robertson I, Samaratunga H. Mango dermatitis: allergic contact dermatitis to Mangifera indica. Australas J Dermatol. 1996;37:59-60.
- Thoo CH, Freeman S. Hypersensitivity reaction to the ingestion of mango flesh. Australas J Dermatol. 2008;49:116-119.
- Oka K, Saito F, Yasuhara T, et al. A study of cross-reactions between mango contact allergens and urushiol. Contact Dermatitis. 2004;51:292-296.
- Keil H, Wasserman D, Dawson CR. Mango dermatitis and its relationship to poison ivy hypersensitivity. Ann Allergy. 1946;4: 268-281.
- Maarouf M, Costello CM, Gonzalez S, et al. In vivo reflectance confocal microscopy: emerging role in noninvasive diagnosis and monitoring of eczematous dermatoses. Actas Dermosifiliogr (Engl Ed). 2019;110:626-636.
- Koller S, Gerger A, Ahlgrimm-Siess V, et al. In vivo reflectance confocal microscopy of erythematosquamous skin diseases. Exp Dermatol. 2009;18:536-540.
The mango tree (Mangifera indica) produces nutrient-dense fruit—known colloquially as the “king of fruits”—that is widely consumed across the world. Native to southern Asia, the mango tree is a member of the Anacardiaceae family, a large family of flowering, fruit-bearing plants.1 Many members of the Anacardiaceae family, which includes poison ivy and poison oak, are known to produce urushiol, a skin irritant associated with allergic contact dermatitis (ACD).2 Interestingly, despite its widespread consumption and categorization in the Anacardiaceae family, allergic reactions to mango are comparatively rare; they occur as either immediate type I hypersensitivity reactions manifesting with rapid-onset symptoms such as urticaria, wheezing, and angioedema, or delayed type IV hypersensitivity reactions manifesting as ACD.3 Although exposure to components of the mango tree has been most characteristically linked to type IV hypersensitivity reactions, there remain fewer than 40 reported cases of mango-induced ACD since it was first described in 1939.4
Evaluation of ACD most commonly includes a thorough clinical assessment with diagnostic support from patch testing and histopathologic review following skin biopsy. In recent years, reflectance confocal microscopy (RCM) has shown promising potential to join the repertoire of diagnostic tools for ACD by enabling dynamic and high-resolution imaging of contact dermatitis in vivo.5-10 Reflectance confocal microscopy is a noninvasive optical imaging technique that uses a low-energy diode laser to penetrate the layers of the skin. The resulting reflected light generates images that facilitate visualization of cutaneous structures to the depth of the papillary dermis.11 While it is most commonly used in skin cancer diagnostics, preliminary studies also have shown an emerging role for RCM in the evaluation of eczematous and inflammatory skin disease, including contact dermatitis.5-10 Herein, we present a unique case of mango sap–induced ACD imaged and diagnosed in real time via RCM.
Case Report
A 39-year-old woman presented to our clinic with a pruritic vesicular eruption on the right leg of 2 weeks’ duration that initially had developed within 7 days of exposure to mango tree sap (Figure 1). The patient reported having experienced similar pruritic eruptions in the past following contact with mango sap while eating mangos but denied any history of reactions from ingestion of the fruit. She also reported a history of robust reactions to poison ivy; however, a timeline specifying the order of first exposure to these irritants was unknown. She denied any personal or family history of atopic conditions.
The affected skin was imaged in real time during clinic using RCM, which showed an inflammatory infiltrate represented by dark spongiotic vesicles containing bright cells (Figure 2). Additional RCM imaging at the level of the stratum spinosum showed dark spongiotic areas with bright inflammatory cells infiltrating the vesicles, which were surrounded by normal skin showing a typical epidermal honeycomb pattern (Figure 3). These findings were diagnostic of ACD secondary to exposure to mango sap. The patient was advised to apply clobetasol cream 0.05% to the affected area. Notable improvement of the rash was noted within 10 days of treatment.
Comment
Exposure to the mango tree and its fruit is a rare cause of ACD, with few reported cases in the literature. The majority of known instances have occurred in non–mango-cultivating countries, largely the United States, although cases also have been reported in Canada, Australia, France, Japan, and Thailand.3,12 Mango-induced contact allergy follows a roughly equal distribution between males and females and most often occurs in young adults during the third and fourth decades of life.4,12-21 Importantly, delayed-type hypersensitivity reactions to mango can manifest as either localized or systemic ACD. Localized ACD can be induced via direct contact with the mango tree and its components or ingestion of the fruit.3,12,22 Conversely, systemic ACD is primarily stimulated by ingestion of the fruit. In our case, the patient had no history of allergy following mango ingestion, and her ACD was prompted by isolated contact with mango sap. The time from exposure to symptom onset of known instances of mango ACD varies widely, ranging from less than 24 hours to as long as 9 days.3,12 Diagnosis of mango-induced ACD largely is guided by clinical findings. Presenting symptoms often include an eczematous, vesicular, pruritic rash on affected areas of the skin, frequently the head, neck, and extremities. Patients also commonly present with linear papulovesicular lesions and periorbital or perioral edema.
The suspected allergens responsible for mango-induced ACD are derived from resorcinol—specifically heptadecadienyl resorcinol, heptadecenyl resorcinol, and pentadecyl resorcinol, which are collectively known as mango allergens.23 These allergens can be found within the pulp and skin of the mango fruit as well as in the bark and leaves of the mango tree, which may explain observed allergic reactions to components of both the mango fruit and tree.12 Similar to these resorcinol derivatives, the urushiol resin found in poison ivy and poison oak is a catechol derivative.2 Importantly, both resorcinols and catechols are isomers of the same aromatic phenol—dihydroxybenzene. Because of these similarities, it is thought that the allergens in mangos may cross-react with urushiol in poison ivy or poison oak.23 Alongside their shared categorization in the Anacardiaceae family, it is hypothesized that this cross-reactivity underlies the sensitization that has been noted between mango and poison ivy or poison oak exposure.12,23,24 Thus, ACD often can occur on initial contact with the mango tree or its components, as a prior exposure to poison ivy or poison oak may serve as the inciting factor for hypersensitization. The majority of reported cases in the literature also occurred in countries where exposure to poison ivy and poison oak are common, further supporting the notion that these compounds may provide a sensitizing trigger for a future mango contact allergy.12
A detailed clinical history combined with adjunctive diagnostic support from patch testing and histopathology of biopsied skin lesions classically are used in the diagnosis of mango-induced ACD. Due to its ability to provide quick and noninvasive in vivo imaging of cutaneous lesions, RCM's applications have expanded to include evaluation of inflammatory skin diseases such as contact dermatitis. Many features of contact dermatitis identified via RCM are common between ACD and irritant contact dermatitis (ICD) and include disruption of the stratum corneum, parakeratosis, vesiculation, spongiosis, and exocytosis.6,10,25 Studies also have described features shown via RCM that are unique to ACD, including vasodilation and intercellular edema, compared to more distinct targetoid keratinocytes and detached corneocytes seen in ICD.6,10,25 Studies by Astner et al5,6 demonstrated a wide range of sensitivity from 52% to 96% and a high specificity of RCM greater than 95% for many of the aforementioned features of contact dermatitis, including disruption of the stratum corneum, parakeratosis, spongiosis, and exocytosis. Additional studies have further strengthened these findings, demonstrating sensitivity and specificity values of 83% and 92% for contact dermatitis under RCM, respectively.26 Importantly, given the similarities and potentially large overlap of features between ACD and ICD identified via RCM as well as findings seen on physical examination and histopathology, an emphasis on clinical correlation is essential when differentiating between these 2 variants of contact dermatitis. Thus, taken in consideration with clinical contexts, RCM has shown potent diagnostic accuracy and great potential to support the evaluation of ACD alongside patch testing and histopathology.
Final Thoughts
Contact allergy to the mango tree and its components is uncommon. We report a unique case of mango sap–induced ACD evaluated and diagnosed via dynamic visualization under RCM. As a noninvasive and reproducible imaging technique with resolutions comparable to histopathologic analysis, RCM is a promising tool that can be used to support the diagnostic evaluation of ACD.
The mango tree (Mangifera indica) produces nutrient-dense fruit—known colloquially as the “king of fruits”—that is widely consumed across the world. Native to southern Asia, the mango tree is a member of the Anacardiaceae family, a large family of flowering, fruit-bearing plants.1 Many members of the Anacardiaceae family, which includes poison ivy and poison oak, are known to produce urushiol, a skin irritant associated with allergic contact dermatitis (ACD).2 Interestingly, despite its widespread consumption and categorization in the Anacardiaceae family, allergic reactions to mango are comparatively rare; they occur as either immediate type I hypersensitivity reactions manifesting with rapid-onset symptoms such as urticaria, wheezing, and angioedema, or delayed type IV hypersensitivity reactions manifesting as ACD.3 Although exposure to components of the mango tree has been most characteristically linked to type IV hypersensitivity reactions, there remain fewer than 40 reported cases of mango-induced ACD since it was first described in 1939.4
Evaluation of ACD most commonly includes a thorough clinical assessment with diagnostic support from patch testing and histopathologic review following skin biopsy. In recent years, reflectance confocal microscopy (RCM) has shown promising potential to join the repertoire of diagnostic tools for ACD by enabling dynamic and high-resolution imaging of contact dermatitis in vivo.5-10 Reflectance confocal microscopy is a noninvasive optical imaging technique that uses a low-energy diode laser to penetrate the layers of the skin. The resulting reflected light generates images that facilitate visualization of cutaneous structures to the depth of the papillary dermis.11 While it is most commonly used in skin cancer diagnostics, preliminary studies also have shown an emerging role for RCM in the evaluation of eczematous and inflammatory skin disease, including contact dermatitis.5-10 Herein, we present a unique case of mango sap–induced ACD imaged and diagnosed in real time via RCM.
Case Report
A 39-year-old woman presented to our clinic with a pruritic vesicular eruption on the right leg of 2 weeks’ duration that initially had developed within 7 days of exposure to mango tree sap (Figure 1). The patient reported having experienced similar pruritic eruptions in the past following contact with mango sap while eating mangos but denied any history of reactions from ingestion of the fruit. She also reported a history of robust reactions to poison ivy; however, a timeline specifying the order of first exposure to these irritants was unknown. She denied any personal or family history of atopic conditions.
The affected skin was imaged in real time during clinic using RCM, which showed an inflammatory infiltrate represented by dark spongiotic vesicles containing bright cells (Figure 2). Additional RCM imaging at the level of the stratum spinosum showed dark spongiotic areas with bright inflammatory cells infiltrating the vesicles, which were surrounded by normal skin showing a typical epidermal honeycomb pattern (Figure 3). These findings were diagnostic of ACD secondary to exposure to mango sap. The patient was advised to apply clobetasol cream 0.05% to the affected area. Notable improvement of the rash was noted within 10 days of treatment.
Comment
Exposure to the mango tree and its fruit is a rare cause of ACD, with few reported cases in the literature. The majority of known instances have occurred in non–mango-cultivating countries, largely the United States, although cases also have been reported in Canada, Australia, France, Japan, and Thailand.3,12 Mango-induced contact allergy follows a roughly equal distribution between males and females and most often occurs in young adults during the third and fourth decades of life.4,12-21 Importantly, delayed-type hypersensitivity reactions to mango can manifest as either localized or systemic ACD. Localized ACD can be induced via direct contact with the mango tree and its components or ingestion of the fruit.3,12,22 Conversely, systemic ACD is primarily stimulated by ingestion of the fruit. In our case, the patient had no history of allergy following mango ingestion, and her ACD was prompted by isolated contact with mango sap. The time from exposure to symptom onset of known instances of mango ACD varies widely, ranging from less than 24 hours to as long as 9 days.3,12 Diagnosis of mango-induced ACD largely is guided by clinical findings. Presenting symptoms often include an eczematous, vesicular, pruritic rash on affected areas of the skin, frequently the head, neck, and extremities. Patients also commonly present with linear papulovesicular lesions and periorbital or perioral edema.
The suspected allergens responsible for mango-induced ACD are derived from resorcinol—specifically heptadecadienyl resorcinol, heptadecenyl resorcinol, and pentadecyl resorcinol, which are collectively known as mango allergens.23 These allergens can be found within the pulp and skin of the mango fruit as well as in the bark and leaves of the mango tree, which may explain observed allergic reactions to components of both the mango fruit and tree.12 Similar to these resorcinol derivatives, the urushiol resin found in poison ivy and poison oak is a catechol derivative.2 Importantly, both resorcinols and catechols are isomers of the same aromatic phenol—dihydroxybenzene. Because of these similarities, it is thought that the allergens in mangos may cross-react with urushiol in poison ivy or poison oak.23 Alongside their shared categorization in the Anacardiaceae family, it is hypothesized that this cross-reactivity underlies the sensitization that has been noted between mango and poison ivy or poison oak exposure.12,23,24 Thus, ACD often can occur on initial contact with the mango tree or its components, as a prior exposure to poison ivy or poison oak may serve as the inciting factor for hypersensitization. The majority of reported cases in the literature also occurred in countries where exposure to poison ivy and poison oak are common, further supporting the notion that these compounds may provide a sensitizing trigger for a future mango contact allergy.12
A detailed clinical history combined with adjunctive diagnostic support from patch testing and histopathology of biopsied skin lesions classically are used in the diagnosis of mango-induced ACD. Due to its ability to provide quick and noninvasive in vivo imaging of cutaneous lesions, RCM's applications have expanded to include evaluation of inflammatory skin diseases such as contact dermatitis. Many features of contact dermatitis identified via RCM are common between ACD and irritant contact dermatitis (ICD) and include disruption of the stratum corneum, parakeratosis, vesiculation, spongiosis, and exocytosis.6,10,25 Studies also have described features shown via RCM that are unique to ACD, including vasodilation and intercellular edema, compared to more distinct targetoid keratinocytes and detached corneocytes seen in ICD.6,10,25 Studies by Astner et al5,6 demonstrated a wide range of sensitivity from 52% to 96% and a high specificity of RCM greater than 95% for many of the aforementioned features of contact dermatitis, including disruption of the stratum corneum, parakeratosis, spongiosis, and exocytosis. Additional studies have further strengthened these findings, demonstrating sensitivity and specificity values of 83% and 92% for contact dermatitis under RCM, respectively.26 Importantly, given the similarities and potentially large overlap of features between ACD and ICD identified via RCM as well as findings seen on physical examination and histopathology, an emphasis on clinical correlation is essential when differentiating between these 2 variants of contact dermatitis. Thus, taken in consideration with clinical contexts, RCM has shown potent diagnostic accuracy and great potential to support the evaluation of ACD alongside patch testing and histopathology.
Final Thoughts
Contact allergy to the mango tree and its components is uncommon. We report a unique case of mango sap–induced ACD evaluated and diagnosed via dynamic visualization under RCM. As a noninvasive and reproducible imaging technique with resolutions comparable to histopathologic analysis, RCM is a promising tool that can be used to support the diagnostic evaluation of ACD.
- Shah KA, Patel MB, Patel RJ, et al. Mangifera indica (mango). Pharmacogn Rev. 2010;4:42-48.
- Lofgran T, Mahabal GD. Toxicodendron toxicity. StatPearls [Internet]. Updated May 16, 2023. Accessed September 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK557866
- Sareen R, Shah A. Hypersensitivity manifestations to the fruit mango. Asia Pac Allergy. 2011;1:43-49.
- Zakon SJ. Contact dermatitis due to mango. JAMA. 1939;113:1808.
- Astner S, Gonzalez E, Cheung A, et al. Pilot study on the sensitivity and specificity of in vivo reflectance confocal microscopy in the diagnosis of allergic contact dermatitis. J Am Acad Dermatol. 2005;53:986-992.
- Astner S, Gonzalez S, Gonzalez E. Noninvasive evaluation of allergic and irritant contact dermatitis by in vivo reflectance confocal microscopy. Dermatitis. 2006;17:182-191.
- Csuka EA, Ward SC, Ekelem C, et al. Reflectance confocal microscopy, optical coherence tomography, and multiphoton microscopy in inflammatory skin disease diagnosis. Lasers Surg Med. 2021;53:776-797.
- Guichard A, Fanian F, Girardin P, et al. Allergic patch test and contact dermatitis by in vivo reflectance confocal microscopy [in French]. Ann Dermatol Venereol. 2014;141:805-807.
- Sakanashi EN, Matsumura M, Kikuchi K, et al. A comparative study of allergic contact dermatitis by patch test versus reflectance confocal laser microscopy, with nickel and cobalt. Eur J Dermatol. 2010;20:705-711.
- Swindells K, Burnett N, Rius-Diaz F, et al. Reflectance confocal microscopy may differentiate acute allergic and irritant contact dermatitis in vivo. J Am Acad Dermatol. 2004;50:220-228.
- Shahriari N, Grant-Kels JM, Rabinovitz H, et al. Reflectance confocal microscopy: principles, basic terminology, clinical indications, limitations, and practical considerations. J Am Acad Dermatol. 2021;84:1-14.
- Berghea EC, Craiu M, Ali S, et al. Contact allergy induced by mango (Mangifera indica): a relevant topic? Medicina (Kaunas). 2021;57:1240.
- O’Hern K, Zhang F, Zug KA, et al. “Mango slice” dermatitis: pediatric allergic contact dermatitis to mango pulp and skin. Dermatitis. 2022;33:E46-E47.
- Raison-Peyron N, Aljaber F, Al Ali OA, et al. Mango dermatitis: an unusual cause of eyelid dermatitis in France. Contact Dermatitis. 2021;85:599-600.
- Alipour Tehrany Y, Coulombe J. Mango allergic contact dermatitis. Contact Dermatitis. 2021;85:241-242.
- Yoo MJ, Carius BM. Mango dermatitis after urushiol sensitization. Clin Pract Cases Emerg Med. 2019;3:361-363.
- Miyazawa H, Nishie W, Hata H, et al. A severe case of mango dermatitis. J Eur Acad Dermatol Venereol. 2018;32:E160-E161.
- Trehan I, Meuli GJ. Mango contact allergy. J Travel Med. 2010;17:284.
- Wiwanitkit V. Mango dermatitis. Indian J Dermatol. 2008;53:158.
- Weinstein S, Bassiri-Tehrani S, Cohen DE. Allergic contact dermatitis to mango flesh. Int J Dermatol. 2004;43:195-196.
- Calvert ML, Robertson I, Samaratunga H. Mango dermatitis: allergic contact dermatitis to Mangifera indica. Australas J Dermatol. 1996;37:59-60.
- Thoo CH, Freeman S. Hypersensitivity reaction to the ingestion of mango flesh. Australas J Dermatol. 2008;49:116-119.
- Oka K, Saito F, Yasuhara T, et al. A study of cross-reactions between mango contact allergens and urushiol. Contact Dermatitis. 2004;51:292-296.
- Keil H, Wasserman D, Dawson CR. Mango dermatitis and its relationship to poison ivy hypersensitivity. Ann Allergy. 1946;4: 268-281.
- Maarouf M, Costello CM, Gonzalez S, et al. In vivo reflectance confocal microscopy: emerging role in noninvasive diagnosis and monitoring of eczematous dermatoses. Actas Dermosifiliogr (Engl Ed). 2019;110:626-636.
- Koller S, Gerger A, Ahlgrimm-Siess V, et al. In vivo reflectance confocal microscopy of erythematosquamous skin diseases. Exp Dermatol. 2009;18:536-540.
- Shah KA, Patel MB, Patel RJ, et al. Mangifera indica (mango). Pharmacogn Rev. 2010;4:42-48.
- Lofgran T, Mahabal GD. Toxicodendron toxicity. StatPearls [Internet]. Updated May 16, 2023. Accessed September 19, 2024. https://www.ncbi.nlm.nih.gov/books/NBK557866
- Sareen R, Shah A. Hypersensitivity manifestations to the fruit mango. Asia Pac Allergy. 2011;1:43-49.
- Zakon SJ. Contact dermatitis due to mango. JAMA. 1939;113:1808.
- Astner S, Gonzalez E, Cheung A, et al. Pilot study on the sensitivity and specificity of in vivo reflectance confocal microscopy in the diagnosis of allergic contact dermatitis. J Am Acad Dermatol. 2005;53:986-992.
- Astner S, Gonzalez S, Gonzalez E. Noninvasive evaluation of allergic and irritant contact dermatitis by in vivo reflectance confocal microscopy. Dermatitis. 2006;17:182-191.
- Csuka EA, Ward SC, Ekelem C, et al. Reflectance confocal microscopy, optical coherence tomography, and multiphoton microscopy in inflammatory skin disease diagnosis. Lasers Surg Med. 2021;53:776-797.
- Guichard A, Fanian F, Girardin P, et al. Allergic patch test and contact dermatitis by in vivo reflectance confocal microscopy [in French]. Ann Dermatol Venereol. 2014;141:805-807.
- Sakanashi EN, Matsumura M, Kikuchi K, et al. A comparative study of allergic contact dermatitis by patch test versus reflectance confocal laser microscopy, with nickel and cobalt. Eur J Dermatol. 2010;20:705-711.
- Swindells K, Burnett N, Rius-Diaz F, et al. Reflectance confocal microscopy may differentiate acute allergic and irritant contact dermatitis in vivo. J Am Acad Dermatol. 2004;50:220-228.
- Shahriari N, Grant-Kels JM, Rabinovitz H, et al. Reflectance confocal microscopy: principles, basic terminology, clinical indications, limitations, and practical considerations. J Am Acad Dermatol. 2021;84:1-14.
- Berghea EC, Craiu M, Ali S, et al. Contact allergy induced by mango (Mangifera indica): a relevant topic? Medicina (Kaunas). 2021;57:1240.
- O’Hern K, Zhang F, Zug KA, et al. “Mango slice” dermatitis: pediatric allergic contact dermatitis to mango pulp and skin. Dermatitis. 2022;33:E46-E47.
- Raison-Peyron N, Aljaber F, Al Ali OA, et al. Mango dermatitis: an unusual cause of eyelid dermatitis in France. Contact Dermatitis. 2021;85:599-600.
- Alipour Tehrany Y, Coulombe J. Mango allergic contact dermatitis. Contact Dermatitis. 2021;85:241-242.
- Yoo MJ, Carius BM. Mango dermatitis after urushiol sensitization. Clin Pract Cases Emerg Med. 2019;3:361-363.
- Miyazawa H, Nishie W, Hata H, et al. A severe case of mango dermatitis. J Eur Acad Dermatol Venereol. 2018;32:E160-E161.
- Trehan I, Meuli GJ. Mango contact allergy. J Travel Med. 2010;17:284.
- Wiwanitkit V. Mango dermatitis. Indian J Dermatol. 2008;53:158.
- Weinstein S, Bassiri-Tehrani S, Cohen DE. Allergic contact dermatitis to mango flesh. Int J Dermatol. 2004;43:195-196.
- Calvert ML, Robertson I, Samaratunga H. Mango dermatitis: allergic contact dermatitis to Mangifera indica. Australas J Dermatol. 1996;37:59-60.
- Thoo CH, Freeman S. Hypersensitivity reaction to the ingestion of mango flesh. Australas J Dermatol. 2008;49:116-119.
- Oka K, Saito F, Yasuhara T, et al. A study of cross-reactions between mango contact allergens and urushiol. Contact Dermatitis. 2004;51:292-296.
- Keil H, Wasserman D, Dawson CR. Mango dermatitis and its relationship to poison ivy hypersensitivity. Ann Allergy. 1946;4: 268-281.
- Maarouf M, Costello CM, Gonzalez S, et al. In vivo reflectance confocal microscopy: emerging role in noninvasive diagnosis and monitoring of eczematous dermatoses. Actas Dermosifiliogr (Engl Ed). 2019;110:626-636.
- Koller S, Gerger A, Ahlgrimm-Siess V, et al. In vivo reflectance confocal microscopy of erythematosquamous skin diseases. Exp Dermatol. 2009;18:536-540.
Practice Points
- Contact with mango tree sap can induce allergic contact dermatitis.
- Reflectance confocal microscopy (RCM) is a noninvasive imaging technique that can provide real-time in vivo visualization of affected skin in contact dermatitis.
- Predominant findings of contact dermatitis under RCM include disruption of the stratum corneum; parakeratosis; vesiculation; spongiosis; and exocytosis, vasodilation, and intercellular edema more specific to the allergic subtype.
