User login
Novel Agent First to Slow Disability in Nonrelapsing Secondary MS
COPENHAGEN — A new investigational drug has become the first agent to slow disability in patients with nonrelapsing secondary progressive multiple sclerosis (nrSPMS).
In addition, tolebrutinib almost doubled the number of patients who experienced confirmed disability improvement from 5% to 10%.
However, these benefits come with the potential safety issue of liver toxicity, with raised liver enzymes reported in 4% of patients and very severe liver enzyme rises occurring in 0.5% of patients, one of whom died after undergoing a liver transplant.
The results were presented by Robert Fox, MD, vice chair of research at the Cleveland Clinic’s Neurological Institute in Ohio, at the 2024 ECTRIMS annual meeting.
“We have finally found a therapy that can alter the compartmentalized inflammation that is driving progressive MS,” he said.
Dr. Fox pointed out that the population enrolled in the HERCULES trial had stopped having clinical relapses. “These are the patients for whom current immunomodulator therapies really don’t work at all — they don’t slow disability. This trial suggests that tolebrutinib can fill that void and now we have something to offer this patient group,” he said.
He estimated that up to 30% of patients with MS at his clinic may fall into this category.
A typical patient with nrSPMS who was included in this trial may have experienced a gradual decline in the distance they can walk or the ease with which they could climb stairs, he explained.
“I would project that this therapy will slow down that gradual decline, and, in some patients, it may actually stop the decline,” he added.
Dr. Fox said that BTK inhibitors are believed to have two main mechanisms of action relevant to MS — down-regulating B cells, probably mostly in the periphery, and, as these agents can cross the blood-brain barrier, they also appear to reduce the inflammatory activity of microglia and macrophages in the brain.
He noted that the disability progression in nrSPMS patients is thought to be caused by compartmentalized inflammation in the brain, which is what tolebrutinib may be targeting.
He noted that siponimod has also shown benefit in secondary progressive MS in the EXPAND trial, but the benefit was almost entirely restricted to patients who had experienced recent relapses.
Ocrelizumab has been shown to be beneficial in a trial in primary progressive MS, but again, a large proportion of patients in that study had active focal inflammation at baselineEngl J Med. 2017;376:209-220).
Trial Results
The HERCULES trial included 1131 patients with nrSPMS, defined as having an Expanded Disability Status Scale score (EDSS) between 3.0 and 6.5, no clinical relapses in the previous 24 months, and documented evidence of disability accumulation in the previous 12 months.
They were randomly assigned (2:1) to receive 60 mg tolebrutinib as an oral daily dose or placebo for up to approximately 48 months. This was an event-driven trial, with 288 6-month confirmed disability progression events required.
About 23% of patients in each group discontinued treatment and 12%-17% who had confirmed disability progression elected to crossover to open-label tolebrutinib.
The study population had an average age of 49 years, had a median EDSS score of 6, and a mean time since last clinical relapse of over 7 years.
“So, this was a really very quiescent patient population in terms of focal inflammation,” Dr. Fox noted.
Results showed that the primary endpoint showed a 31% reduction in the risk of 6-month confirmed disability progression (26.9% tolebrutinib vs. 37.2% placebo; hazard ratio [HR], 0.69; 95% CI, 0.55-0.88).
Rates of 3-month confirmed disability progression were 32.6% in the tolebrutinib group versus 41.5% with placebo — a 24% risk reduction.
In addition, 6-month confirmed disability improvement was achieved by 10% of tolebrutinib patients versus 5% in the placebo group (HR, 1.88; 95% CI, 1.10-3.21).
A ‘Head-scratcher’ Finding
Surprisingly, he noted, tolebrutinib did not appear to slow brain atrophy.
“Despite seeing a benefit on disability progression, we saw no significant slowing of brain atrophy or brain volume loss over the course of the study,” Dr. Fox reported.
He described this discordance between disability rates and brain volume loss rates as “a bit of a head-scratcher.”
In terms of safety, the main concern is liver enzyme elevations, which occurred at greater than three times the upper limit of normal (ULN) in 4.1% of the tolebrutinib group vs 1.6% in the placebo group.
A small (0.5%) proportion of patients treated with tolebrutinib experienced very severe elevations (> 20 x ULN) in liver enzymes, and one of these patients had to have a liver transplant and died because of postoperative complications, “a reminder that this can be a very serious complication of this drug,” said Dr. Fox.
However, he noted that all the very severe liver enzyme rises occurred in the first 3 months and it is now recommended that patients undergo weekly liver enzyme monitoring for the first 12 weeks of treatment.
Other adverse effects that were increased slightly in tolebrutinib group were upper respiratory infections and possibly hypertension.
Weekly Liver Enzyme Testing
Dr. Fox cautioned that patients starting tolebrutinib would need to undergo weekly liver enzyme testing in the first few months of treatment. “They would need to be very attentive to this monitoring, but if they are willing to do that, then I think many of these patients will be very eager to take this drug that may slow down their disability progression.”
The drug’s manufacturer, Sanofi, said the trial results will form the basis for applications to global regulatory authorities with submissions starting later in 2024.
Commenting on the trial, Ludwig Kappos, MD, professor of neurology at University Hospital and University of Basel, Switzerland, said the trial was important as it had shown “a robust effect on confirmed disability progression in a population of secondary progressive MS with no or very low signs of focal inflammation.”
“The effect is similar and probably more pronounced than that seen in the siponimod trial also in advanced secondary progressive MS,” he added.
Dr. Kappos believes more work will be needed to make sure the liver toxicity can be prevented, “but if that can be resolved then patients could have a significant delay in accumulating disability.”
GEMINI Trials Also Show Slowed Disability
Two other phase 3 trials of tolebrutinib were presented during the same ECTRIMS session — GEMINI 1 and 2 — which compared the new drug with teriflunomide, a standard of care treatment, in participants with relapsing MS. Neither study met the primary endpoint of an improvement in annualized relapse rates, compared with teriflunomide.
However, with respect to the key secondary endpoint, in a pooled analysis of data from GEMINI 1 and 2, tolebrutinib delayed the time to onset of 6-month confirmed disability worsening by 29%, a finding in line with the main results of the HERCULES trial.
“The significant impact of tolebrutinib on disability accumulation versus teriflunomide, in the absence of a statistically superior impact on relapses, also suggests that tolebrutinib may address smoldering neuroinflammation, which manifests as progression independent of relapses” Dr. Fox said.
The HERCULES trial was sponsored by Sanofi. Dr. Fox is a paid adviser to Sanofi. Dr. Kappos led the EXPAND trial of siponimod in SPMS.
A version of this article first appeared on Medscape.com.
COPENHAGEN — A new investigational drug has become the first agent to slow disability in patients with nonrelapsing secondary progressive multiple sclerosis (nrSPMS).
In addition, tolebrutinib almost doubled the number of patients who experienced confirmed disability improvement from 5% to 10%.
However, these benefits come with the potential safety issue of liver toxicity, with raised liver enzymes reported in 4% of patients and very severe liver enzyme rises occurring in 0.5% of patients, one of whom died after undergoing a liver transplant.
The results were presented by Robert Fox, MD, vice chair of research at the Cleveland Clinic’s Neurological Institute in Ohio, at the 2024 ECTRIMS annual meeting.
“We have finally found a therapy that can alter the compartmentalized inflammation that is driving progressive MS,” he said.
Dr. Fox pointed out that the population enrolled in the HERCULES trial had stopped having clinical relapses. “These are the patients for whom current immunomodulator therapies really don’t work at all — they don’t slow disability. This trial suggests that tolebrutinib can fill that void and now we have something to offer this patient group,” he said.
He estimated that up to 30% of patients with MS at his clinic may fall into this category.
A typical patient with nrSPMS who was included in this trial may have experienced a gradual decline in the distance they can walk or the ease with which they could climb stairs, he explained.
“I would project that this therapy will slow down that gradual decline, and, in some patients, it may actually stop the decline,” he added.
Dr. Fox said that BTK inhibitors are believed to have two main mechanisms of action relevant to MS — down-regulating B cells, probably mostly in the periphery, and, as these agents can cross the blood-brain barrier, they also appear to reduce the inflammatory activity of microglia and macrophages in the brain.
He noted that the disability progression in nrSPMS patients is thought to be caused by compartmentalized inflammation in the brain, which is what tolebrutinib may be targeting.
He noted that siponimod has also shown benefit in secondary progressive MS in the EXPAND trial, but the benefit was almost entirely restricted to patients who had experienced recent relapses.
Ocrelizumab has been shown to be beneficial in a trial in primary progressive MS, but again, a large proportion of patients in that study had active focal inflammation at baselineEngl J Med. 2017;376:209-220).
Trial Results
The HERCULES trial included 1131 patients with nrSPMS, defined as having an Expanded Disability Status Scale score (EDSS) between 3.0 and 6.5, no clinical relapses in the previous 24 months, and documented evidence of disability accumulation in the previous 12 months.
They were randomly assigned (2:1) to receive 60 mg tolebrutinib as an oral daily dose or placebo for up to approximately 48 months. This was an event-driven trial, with 288 6-month confirmed disability progression events required.
About 23% of patients in each group discontinued treatment and 12%-17% who had confirmed disability progression elected to crossover to open-label tolebrutinib.
The study population had an average age of 49 years, had a median EDSS score of 6, and a mean time since last clinical relapse of over 7 years.
“So, this was a really very quiescent patient population in terms of focal inflammation,” Dr. Fox noted.
Results showed that the primary endpoint showed a 31% reduction in the risk of 6-month confirmed disability progression (26.9% tolebrutinib vs. 37.2% placebo; hazard ratio [HR], 0.69; 95% CI, 0.55-0.88).
Rates of 3-month confirmed disability progression were 32.6% in the tolebrutinib group versus 41.5% with placebo — a 24% risk reduction.
In addition, 6-month confirmed disability improvement was achieved by 10% of tolebrutinib patients versus 5% in the placebo group (HR, 1.88; 95% CI, 1.10-3.21).
A ‘Head-scratcher’ Finding
Surprisingly, he noted, tolebrutinib did not appear to slow brain atrophy.
“Despite seeing a benefit on disability progression, we saw no significant slowing of brain atrophy or brain volume loss over the course of the study,” Dr. Fox reported.
He described this discordance between disability rates and brain volume loss rates as “a bit of a head-scratcher.”
In terms of safety, the main concern is liver enzyme elevations, which occurred at greater than three times the upper limit of normal (ULN) in 4.1% of the tolebrutinib group vs 1.6% in the placebo group.
A small (0.5%) proportion of patients treated with tolebrutinib experienced very severe elevations (> 20 x ULN) in liver enzymes, and one of these patients had to have a liver transplant and died because of postoperative complications, “a reminder that this can be a very serious complication of this drug,” said Dr. Fox.
However, he noted that all the very severe liver enzyme rises occurred in the first 3 months and it is now recommended that patients undergo weekly liver enzyme monitoring for the first 12 weeks of treatment.
Other adverse effects that were increased slightly in tolebrutinib group were upper respiratory infections and possibly hypertension.
Weekly Liver Enzyme Testing
Dr. Fox cautioned that patients starting tolebrutinib would need to undergo weekly liver enzyme testing in the first few months of treatment. “They would need to be very attentive to this monitoring, but if they are willing to do that, then I think many of these patients will be very eager to take this drug that may slow down their disability progression.”
The drug’s manufacturer, Sanofi, said the trial results will form the basis for applications to global regulatory authorities with submissions starting later in 2024.
Commenting on the trial, Ludwig Kappos, MD, professor of neurology at University Hospital and University of Basel, Switzerland, said the trial was important as it had shown “a robust effect on confirmed disability progression in a population of secondary progressive MS with no or very low signs of focal inflammation.”
“The effect is similar and probably more pronounced than that seen in the siponimod trial also in advanced secondary progressive MS,” he added.
Dr. Kappos believes more work will be needed to make sure the liver toxicity can be prevented, “but if that can be resolved then patients could have a significant delay in accumulating disability.”
GEMINI Trials Also Show Slowed Disability
Two other phase 3 trials of tolebrutinib were presented during the same ECTRIMS session — GEMINI 1 and 2 — which compared the new drug with teriflunomide, a standard of care treatment, in participants with relapsing MS. Neither study met the primary endpoint of an improvement in annualized relapse rates, compared with teriflunomide.
However, with respect to the key secondary endpoint, in a pooled analysis of data from GEMINI 1 and 2, tolebrutinib delayed the time to onset of 6-month confirmed disability worsening by 29%, a finding in line with the main results of the HERCULES trial.
“The significant impact of tolebrutinib on disability accumulation versus teriflunomide, in the absence of a statistically superior impact on relapses, also suggests that tolebrutinib may address smoldering neuroinflammation, which manifests as progression independent of relapses” Dr. Fox said.
The HERCULES trial was sponsored by Sanofi. Dr. Fox is a paid adviser to Sanofi. Dr. Kappos led the EXPAND trial of siponimod in SPMS.
A version of this article first appeared on Medscape.com.
COPENHAGEN — A new investigational drug has become the first agent to slow disability in patients with nonrelapsing secondary progressive multiple sclerosis (nrSPMS).
In addition, tolebrutinib almost doubled the number of patients who experienced confirmed disability improvement from 5% to 10%.
However, these benefits come with the potential safety issue of liver toxicity, with raised liver enzymes reported in 4% of patients and very severe liver enzyme rises occurring in 0.5% of patients, one of whom died after undergoing a liver transplant.
The results were presented by Robert Fox, MD, vice chair of research at the Cleveland Clinic’s Neurological Institute in Ohio, at the 2024 ECTRIMS annual meeting.
“We have finally found a therapy that can alter the compartmentalized inflammation that is driving progressive MS,” he said.
Dr. Fox pointed out that the population enrolled in the HERCULES trial had stopped having clinical relapses. “These are the patients for whom current immunomodulator therapies really don’t work at all — they don’t slow disability. This trial suggests that tolebrutinib can fill that void and now we have something to offer this patient group,” he said.
He estimated that up to 30% of patients with MS at his clinic may fall into this category.
A typical patient with nrSPMS who was included in this trial may have experienced a gradual decline in the distance they can walk or the ease with which they could climb stairs, he explained.
“I would project that this therapy will slow down that gradual decline, and, in some patients, it may actually stop the decline,” he added.
Dr. Fox said that BTK inhibitors are believed to have two main mechanisms of action relevant to MS — down-regulating B cells, probably mostly in the periphery, and, as these agents can cross the blood-brain barrier, they also appear to reduce the inflammatory activity of microglia and macrophages in the brain.
He noted that the disability progression in nrSPMS patients is thought to be caused by compartmentalized inflammation in the brain, which is what tolebrutinib may be targeting.
He noted that siponimod has also shown benefit in secondary progressive MS in the EXPAND trial, but the benefit was almost entirely restricted to patients who had experienced recent relapses.
Ocrelizumab has been shown to be beneficial in a trial in primary progressive MS, but again, a large proportion of patients in that study had active focal inflammation at baselineEngl J Med. 2017;376:209-220).
Trial Results
The HERCULES trial included 1131 patients with nrSPMS, defined as having an Expanded Disability Status Scale score (EDSS) between 3.0 and 6.5, no clinical relapses in the previous 24 months, and documented evidence of disability accumulation in the previous 12 months.
They were randomly assigned (2:1) to receive 60 mg tolebrutinib as an oral daily dose or placebo for up to approximately 48 months. This was an event-driven trial, with 288 6-month confirmed disability progression events required.
About 23% of patients in each group discontinued treatment and 12%-17% who had confirmed disability progression elected to crossover to open-label tolebrutinib.
The study population had an average age of 49 years, had a median EDSS score of 6, and a mean time since last clinical relapse of over 7 years.
“So, this was a really very quiescent patient population in terms of focal inflammation,” Dr. Fox noted.
Results showed that the primary endpoint showed a 31% reduction in the risk of 6-month confirmed disability progression (26.9% tolebrutinib vs. 37.2% placebo; hazard ratio [HR], 0.69; 95% CI, 0.55-0.88).
Rates of 3-month confirmed disability progression were 32.6% in the tolebrutinib group versus 41.5% with placebo — a 24% risk reduction.
In addition, 6-month confirmed disability improvement was achieved by 10% of tolebrutinib patients versus 5% in the placebo group (HR, 1.88; 95% CI, 1.10-3.21).
A ‘Head-scratcher’ Finding
Surprisingly, he noted, tolebrutinib did not appear to slow brain atrophy.
“Despite seeing a benefit on disability progression, we saw no significant slowing of brain atrophy or brain volume loss over the course of the study,” Dr. Fox reported.
He described this discordance between disability rates and brain volume loss rates as “a bit of a head-scratcher.”
In terms of safety, the main concern is liver enzyme elevations, which occurred at greater than three times the upper limit of normal (ULN) in 4.1% of the tolebrutinib group vs 1.6% in the placebo group.
A small (0.5%) proportion of patients treated with tolebrutinib experienced very severe elevations (> 20 x ULN) in liver enzymes, and one of these patients had to have a liver transplant and died because of postoperative complications, “a reminder that this can be a very serious complication of this drug,” said Dr. Fox.
However, he noted that all the very severe liver enzyme rises occurred in the first 3 months and it is now recommended that patients undergo weekly liver enzyme monitoring for the first 12 weeks of treatment.
Other adverse effects that were increased slightly in tolebrutinib group were upper respiratory infections and possibly hypertension.
Weekly Liver Enzyme Testing
Dr. Fox cautioned that patients starting tolebrutinib would need to undergo weekly liver enzyme testing in the first few months of treatment. “They would need to be very attentive to this monitoring, but if they are willing to do that, then I think many of these patients will be very eager to take this drug that may slow down their disability progression.”
The drug’s manufacturer, Sanofi, said the trial results will form the basis for applications to global regulatory authorities with submissions starting later in 2024.
Commenting on the trial, Ludwig Kappos, MD, professor of neurology at University Hospital and University of Basel, Switzerland, said the trial was important as it had shown “a robust effect on confirmed disability progression in a population of secondary progressive MS with no or very low signs of focal inflammation.”
“The effect is similar and probably more pronounced than that seen in the siponimod trial also in advanced secondary progressive MS,” he added.
Dr. Kappos believes more work will be needed to make sure the liver toxicity can be prevented, “but if that can be resolved then patients could have a significant delay in accumulating disability.”
GEMINI Trials Also Show Slowed Disability
Two other phase 3 trials of tolebrutinib were presented during the same ECTRIMS session — GEMINI 1 and 2 — which compared the new drug with teriflunomide, a standard of care treatment, in participants with relapsing MS. Neither study met the primary endpoint of an improvement in annualized relapse rates, compared with teriflunomide.
However, with respect to the key secondary endpoint, in a pooled analysis of data from GEMINI 1 and 2, tolebrutinib delayed the time to onset of 6-month confirmed disability worsening by 29%, a finding in line with the main results of the HERCULES trial.
“The significant impact of tolebrutinib on disability accumulation versus teriflunomide, in the absence of a statistically superior impact on relapses, also suggests that tolebrutinib may address smoldering neuroinflammation, which manifests as progression independent of relapses” Dr. Fox said.
The HERCULES trial was sponsored by Sanofi. Dr. Fox is a paid adviser to Sanofi. Dr. Kappos led the EXPAND trial of siponimod in SPMS.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2024
Muscle Relaxants for Chronic Pain: Where Is the Greatest Evidence?
TOPLINE:
The long-term use of muscle relaxants may benefit patients with painful spasms or cramps and neck pain, according to a systematic review of clinical studies, but they do not appear to be beneficial for low back pain, fibromyalgia, or headaches and can have adverse effects such as sedation and dry mouth.
METHODOLOGY:
- Researchers conducted a systematic review to evaluate the effectiveness of long-term use (≥ 4 weeks) of muscle relaxants for chronic pain lasting ≥ 3 months.
- They identified 30 randomized clinical trials involving 1314 patients and 14 cohort studies involving 1168 patients, grouped according to the categories of low back pain, fibromyalgia, painful cramps or spasticity, headaches, and other syndromes.
- Baclofen, tizanidine, cyclobenzaprine, eperisone, quinine, carisoprodol, orphenadrine, chlormezanone, and methocarbamol were the muscle relaxants assessed in comparison with placebo, other treatments, or untreated individuals.
TAKEAWAY:
- The long-term use of muscle relaxants reduced pain intensity in those with painful spasms or cramps and neck pain. Baclofen, orphenadrine, carisoprodol, and methocarbamol improved cramp frequency, while the use of eperisone and chlormezanone improved neck pain and enhanced the quality of sleep, respectively, in those with neck osteoarthritis.
- While some studies suggested that muscle relaxants reduced pain intensity in those with back pain and fibromyalgia, between-group differences were not observed. The benefits seen with some medications diminished after their discontinuation.
- Despite tizanidine improving pain severity in headaches, 25% participants dropped out owing to adverse effects. Although certain muscle relaxants demonstrated pain relief, others did not.
- The most common adverse effects of muscle relaxants were somnolence and dry mouth. Other adverse events included vomiting, diarrhea, nausea, weakness, and constipation.
IN PRACTICE:
“For patients already prescribed long-term SMRs [skeletal muscle relaxants], interventions are needed to assist clinicians to engage in shared decision-making with patients about deprescribing SMRs. This may be particularly true for older patients for whom risks of adverse events may be greater,” the authors wrote. “Clinicians should be vigilant for adverse effects and consider deprescribing if pain-related goals are not met.”
SOURCE:
The study, led by Benjamin J. Oldfield, MD, MHS, Yale School of Medicine, New Haven, Connecticut, was published online on September 19, 2024, in JAMA Network Open
LIMITATIONS:
This systematic review was limited to publications written in English, Spanish, and Italian language, potentially excluding studies from other regions. Variations in clinical sites, definitions of pain syndromes, medications, and durations of therapy prevented the possibility of conducting meta-analyses. Only quantitative studies were included, excluding valuable insights into patient experiences offered by qualitative studies.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The long-term use of muscle relaxants may benefit patients with painful spasms or cramps and neck pain, according to a systematic review of clinical studies, but they do not appear to be beneficial for low back pain, fibromyalgia, or headaches and can have adverse effects such as sedation and dry mouth.
METHODOLOGY:
- Researchers conducted a systematic review to evaluate the effectiveness of long-term use (≥ 4 weeks) of muscle relaxants for chronic pain lasting ≥ 3 months.
- They identified 30 randomized clinical trials involving 1314 patients and 14 cohort studies involving 1168 patients, grouped according to the categories of low back pain, fibromyalgia, painful cramps or spasticity, headaches, and other syndromes.
- Baclofen, tizanidine, cyclobenzaprine, eperisone, quinine, carisoprodol, orphenadrine, chlormezanone, and methocarbamol were the muscle relaxants assessed in comparison with placebo, other treatments, or untreated individuals.
TAKEAWAY:
- The long-term use of muscle relaxants reduced pain intensity in those with painful spasms or cramps and neck pain. Baclofen, orphenadrine, carisoprodol, and methocarbamol improved cramp frequency, while the use of eperisone and chlormezanone improved neck pain and enhanced the quality of sleep, respectively, in those with neck osteoarthritis.
- While some studies suggested that muscle relaxants reduced pain intensity in those with back pain and fibromyalgia, between-group differences were not observed. The benefits seen with some medications diminished after their discontinuation.
- Despite tizanidine improving pain severity in headaches, 25% participants dropped out owing to adverse effects. Although certain muscle relaxants demonstrated pain relief, others did not.
- The most common adverse effects of muscle relaxants were somnolence and dry mouth. Other adverse events included vomiting, diarrhea, nausea, weakness, and constipation.
IN PRACTICE:
“For patients already prescribed long-term SMRs [skeletal muscle relaxants], interventions are needed to assist clinicians to engage in shared decision-making with patients about deprescribing SMRs. This may be particularly true for older patients for whom risks of adverse events may be greater,” the authors wrote. “Clinicians should be vigilant for adverse effects and consider deprescribing if pain-related goals are not met.”
SOURCE:
The study, led by Benjamin J. Oldfield, MD, MHS, Yale School of Medicine, New Haven, Connecticut, was published online on September 19, 2024, in JAMA Network Open
LIMITATIONS:
This systematic review was limited to publications written in English, Spanish, and Italian language, potentially excluding studies from other regions. Variations in clinical sites, definitions of pain syndromes, medications, and durations of therapy prevented the possibility of conducting meta-analyses. Only quantitative studies were included, excluding valuable insights into patient experiences offered by qualitative studies.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The long-term use of muscle relaxants may benefit patients with painful spasms or cramps and neck pain, according to a systematic review of clinical studies, but they do not appear to be beneficial for low back pain, fibromyalgia, or headaches and can have adverse effects such as sedation and dry mouth.
METHODOLOGY:
- Researchers conducted a systematic review to evaluate the effectiveness of long-term use (≥ 4 weeks) of muscle relaxants for chronic pain lasting ≥ 3 months.
- They identified 30 randomized clinical trials involving 1314 patients and 14 cohort studies involving 1168 patients, grouped according to the categories of low back pain, fibromyalgia, painful cramps or spasticity, headaches, and other syndromes.
- Baclofen, tizanidine, cyclobenzaprine, eperisone, quinine, carisoprodol, orphenadrine, chlormezanone, and methocarbamol were the muscle relaxants assessed in comparison with placebo, other treatments, or untreated individuals.
TAKEAWAY:
- The long-term use of muscle relaxants reduced pain intensity in those with painful spasms or cramps and neck pain. Baclofen, orphenadrine, carisoprodol, and methocarbamol improved cramp frequency, while the use of eperisone and chlormezanone improved neck pain and enhanced the quality of sleep, respectively, in those with neck osteoarthritis.
- While some studies suggested that muscle relaxants reduced pain intensity in those with back pain and fibromyalgia, between-group differences were not observed. The benefits seen with some medications diminished after their discontinuation.
- Despite tizanidine improving pain severity in headaches, 25% participants dropped out owing to adverse effects. Although certain muscle relaxants demonstrated pain relief, others did not.
- The most common adverse effects of muscle relaxants were somnolence and dry mouth. Other adverse events included vomiting, diarrhea, nausea, weakness, and constipation.
IN PRACTICE:
“For patients already prescribed long-term SMRs [skeletal muscle relaxants], interventions are needed to assist clinicians to engage in shared decision-making with patients about deprescribing SMRs. This may be particularly true for older patients for whom risks of adverse events may be greater,” the authors wrote. “Clinicians should be vigilant for adverse effects and consider deprescribing if pain-related goals are not met.”
SOURCE:
The study, led by Benjamin J. Oldfield, MD, MHS, Yale School of Medicine, New Haven, Connecticut, was published online on September 19, 2024, in JAMA Network Open
LIMITATIONS:
This systematic review was limited to publications written in English, Spanish, and Italian language, potentially excluding studies from other regions. Variations in clinical sites, definitions of pain syndromes, medications, and durations of therapy prevented the possibility of conducting meta-analyses. Only quantitative studies were included, excluding valuable insights into patient experiences offered by qualitative studies.
DISCLOSURES:
The study was supported by the National Institute on Drug Abuse. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Patient Navigators in Rheumatology Set to Expand in Importance, Scope With New Medicare Codes
When a large rheumatology clinic in Richmond, Virginia, heard that Medicare would be reimbursing patient navigators, they decided to launch their own virtual navigator program.
“We read about it and felt like it was the perfect representation of what we were already trying to do,” said Blake Wehman, founder and CEO of Remission Medical, which offers virtual diagnosis and longitudinal care in rheumatology.

Mr. Wehman has plans to start submitting for these principal illness navigation (PIN) codes in 2025.
The Centers for Medicare & Medicaid Services (CMS) in 2024 began paying navigators who assist Medicare patients with high-risk conditions, which could include rheumatologic diseases. “The codes are not limited to a specific set of diagnoses; rather, the definition of a serious, high-risk condition is dependent on clinical judgment,” the agency clarified.
CMS established this provision in the CY 2024 Physician Fee Schedule final rule.
Reimbursing patient navigators is long overdue, noted Edith Williams, PhD, MS, director of the Center for Community Health and Prevention and founding director of the Office of Health Equity Research at the University of Rochester in New York. “It’s something our patients need. It’s something that the science is telling us can impact outcomes as an adjunct to clinical care,” she said.

Dr. Williams said the new CMS codes “got our departments talking about what this policy is and how it would translate into patient care.”
The codes apply when navigators are assigned to support patients with high-risk conditions who need assistance connecting with clinical and other resources, including any unmet social determinants of health needs, or in diagnosis or treatment of their medical problems.
“Having a navigator by their side to help get through all the clinical and administrative challenges gives people an advocate and a partner who is with them and their families every step of the way to help make the journey easier,” said a CMS spokesperson.
Not all navigator programs may qualify for the new codes. Some are supported by grants and don’t bill patient insurance. However, they all share a common goal: to guide patients through the healthcare continuum and assist with appointments and medication adherence.
Identifying ‘Root Causes’ of Barriers
Navigators represent a wide variety of backgrounds, ranging from healthcare professionals to students or even patients themselves. They generally don’t provide medical advice. “However, we are responsible for making sure our patients and their families are educated and aware, then assist with guidance on their path,” said Katie Costillo, BSW, CPPN, patient navigator and program manager with the Lupus Foundation of America, Heartland Region.

“Training and experience in engaging and building rapport is essential to assisting patients overcome obstacles that limit their access to healthcare,” she said. Narrowing down with patients the root causes of their barriers and then identifying appropriate and available community resources is key.
Studies have demonstrated the effectiveness of adding a navigator to a rheumatology patient’s care plan. In one study, a group of Boston researchers determined that navigators played a useful role in reducing adherence barriers to oral disease-modifying antirheumatic drugs. The navigators uncovered several concerns among 107 rheumatology patients, including fear of adverse events and medication effectiveness.
They also helped to facilitate patient-physician communication, developed strategies to improve medication adherence, and provided medication and diagnosis education. Patients reported satisfaction with the navigator experience.
A study Dr. Williams coauthored that examined behavioral interventions to support African American women with systemic lupus erythematosus found that patient navigator participants had superior coping scores, compared with those engaged in peer-to-peer methodology and patient support groups.
“We had a lot of success with the mentorship program, too,” Dr. Williams said. Navigator services, however, offer more one-on-one attention, “and it’s more tailored to what the person needs rather than the set curriculum that the mentors delivered to their mentees.”
Supporting Patients With Lupus
Ideally, navigators should be able to relate to patients and know what they’re going through, Dr. Williams said. This is someone whom the patient can trust and depend on. “That’s where the benefit of having someone who is also a patient lies because they’re ultimately relatable to other patients. But different institutions have taken different approaches to this.”
Some programs focus on specific rheumatologic conditions. The Lupus Foundation of America, for example, established patient navigator programs to assist patients with lupus in four markets across the country.
The Heartland patient navigator program is available for all patients with lupus within its region, which includes Kansas, Missouri, and central and southern Illinois. As a navigator, Ms. Costillo has been assisting patients since 2022. In 2023, she began meeting with patients at the Washington University Lupus Clinic (WULC) in St. Louis, Missouri.
Navigators work directly with patients before and after their appointment to ensure follow-up and reduce missed appointments. “They help lupus patients connect with community services and overcoming barriers to access and care. The goal of this position is to improve overall disease management, which results in better health outcomes,” Ms. Costillo said.
Since its inception, the patient navigator program at WULC has shown a decrease in patient no-call no-shows and an increase in requests to reschedule as opposed to not showing up for their scheduled appointment, based on history.
Patients have reported fewer barriers to transportation and improvement in access to resources, support, and disease education. “Our patients have also stated [that] meeting with the navigator during their appointments has helped them to feel heard, understood, and supported,” Ms. Costillo said.
Navigator Work Is Not Without Challenges
A total of 90% of patients with lupus are women, and women of color are two to three times more likely to develop lupus in their lifetime.
“Based on socioeconomic statistics, lupus patients are in a demographic that is commonly underserved, underfunded, and often overlooked. Finding appropriate local community resources for a patient who must choose between feeding her family or paying for transportation to multiple physician appointments is a common problem,” Ms. Costillo said.
Much of the assistance that became available during the COVID pandemic is starting to disappear. “With the rising costs of daily living, we are having to find creative and alternative ways to break down barriers and find support to fill those gaps,” she continued.
Getting insurance coverage of patients is another challenge. Many patients with lupus will be prescribed a treatment that insurance refuses to cover even after the physician disputes it.
Additionally, many patients with lupus are unable to work to support their family. A majority who apply for Social Security Disability Insurance are denied on their first and second attempts, “requiring multiple hearings and pages of documentation from their physicians,” Ms. Costillo said.
Students Serve as Navigators
One inner-city program is seeking to increase access to healthcare services to patients with lupus and lupus nephritis in underserved communities. In 2021, SUNY Downstate Health Sciences University in New York City, in partnership with the Brooklyn Free Clinic and Brooklyn Health Disparities Center, launched a program to teach navigator skills to second-year medical students.
The students assist patients at the Arthritis Clinic at University Hospital at Downstate. “Many of our patients have either low medical literacy or difficulty with English. Many of them are immigrants,” said Ellen M. Ginzler, MD, MPH, SUNY Downstate’s professor emerita and former vice-chair for research and rheumatology division chief.
Dr. Ginzler sought out navigator candidates who showed a strong interest in working with underserved patients with complicated, severe disease who struggled with keeping appointments or adhering to medication regimens. The program also gave preference to students fluent in other languages such as Spanish.
All these efforts have generated improvements in care.
Assessing the program’s effectiveness in a cross-sectional study, Dr. Ginzler and colleagues reported that 94% of navigators were able to schedule appointments and 87% assisted with prescriptions. Navigators also had high success rates in answering medical questions, getting in touch with a patient’s doctor, and reminding patients of medical appointments.
Medical student Jeremy Wilson, a coauthor of the study, served as a navigator for a woman with lupus and scleroderma for many years, along with other comorbidities.
Mr. Wilson went above and beyond for this patient, helping to secure social services supports that included accompanying her to clinic visits and serving as her advocate. “She found an enormous difference in how she was treated when she went to these clinics because the doctors in those clinics took her much more seriously,” Dr. Ginzler said. Mr. Wilson ran interference to secure clinic appointments and worked with the patient’s rheumatology fellow in the clinic to get approval for medications.
Mr. Wilson and the patient formed a great bond. “It not only helped the patient, but it helped Jeremy tremendously in terms of how he felt about his medical career,” Dr. Ginzler said.
The program has since expanded to include patients with other rheumatic diseases, such as rheumatoid arthritis and psoriatic arthritis, and also offers navigator services in dermatology.
A total of 21 students to date have completed the second year of the program. “We’ve just selected eight more,” Dr. Ginzler said. Some of the students continue to do the program in their third or even fourth year as they’re applying for residencies.
A student-run, unpublished survey of nine students in the SUNY program found that all nine reported high confidence in identifying social factors that impact patient health and well-being, compared with four who reported high confidence prior to starting the program. “Additionally, students reported increased confidence in providing comprehensive care in rheumatology and dermatology, and interdisciplinary collaboration,” study author Alejandra K. Moncayo, MPH, and colleagues wrote.
When Navigators Go Virtual
Remission Medical offers its navigator service through its own standalone virtual clinic.
Pain associated with rheumatologic conditions increases the urgency to see a doctor. The goal of the virtual RemissionNavigator program is to meet rheumatology patients where they live, to bridge care gaps and reduce wait times, said Mr. Wehman.
RemissionNavigator accomplishes this through video visits and unlimited texting to its network of board-certified rheumatologists or rheumatology-focused advanced practice providers. Experts can answer questions about why labs are ordered, why a patient may have received a certain diagnosis, or provide detailed explanations of a rheumatic condition.
“There are instances where improvement for the patient means waiting a couple days for us versus 45 days for their brick-and-mortar choice,” Mr. Wehman said.
The program currently has 36 subscribers to Remission’s services, which include navigation. “We have 15 providers in a blend of employed and contracted relationships with Remission,” Mr. Wehman said.
Even in its infancy, the navigator program has produced some success stories. “We had a patient tell us that thanks to us, he was seen faster, found relief immediately through our diagnosis and prescription of methotrexate, felt better at work, lost weight, and was happier in general,” Mr. Wehman said.
Another patient was making monthly, 90-minute trips to Richmond for infusion services. Through the virtual program’s assistance, she is now receiving care from home and can get her monthly infusions at a local clinic.
Ultimately, the goal is to help rheumatology move into an era of value-based care where the transition from fee-for-service to per patient will enable optimized care models and better accessibility, Mr. Wehman said. “It will not happen overnight, but every day we work toward this future.”
VA Targets Rheumatology Care
The Department of Veterans Affairs (VA) has also explored the use of navigator services in rheumatology, including virtual services.
VA uses an integrated, interdisciplinary model that manages each veteran’s individual healthcare needs through a coordinated effort among providers, nurses, social workers, pharmacists, and other health professionals, according to VA press secretary Terrence Hayes.
Care coordination may include supporting scheduling appointments, managing chronic conditions, and coordinating care across different medical departments. “This coordination is particularly important in managing complex rheumatologic conditions, where multiple providers may be involved,” Mr. Hayes said.
Additionally, VA has launched a national telerheumatology initiative to improve access to rheumatology providers in rural areas. The initiative will assist veterans in understanding the telehealth system, navigating appointments, and ensuring they have the necessary technology for virtual consultations.
“It will also facilitate communication between rheumatologists, primary care providers, and other specialists, ensuring that all team members are aligned in their approach to the veteran’s care,” Mr. Hayes said.
Who Will Take Advantage of New Codes?
Currently, Remission Medical operates on a cash-pay model, but the company intends to transition to insurance-based coverage in 2025.
Remission Medical also partners directly with preexisting healthcare systems and clinics such as Sentara Health and OrthoVirginia, where a PIN program, powered by Remission Medical’s virtual rheumatology network, may be explored as well.
The company offers its partners synchronous virtual visits and e-consults. It’s likely that these larger organizations will explore coverage for navigator services for Medicare and private insurance. “We can be there to support them as they decide to implement this,” Mr. Wehman said.
Taking advantage of CMS’s navigator PIN codes is an eventual goal. Remission Medical has not submitted the codes yet, “but we do intend to as we continue to grow our membership count,” Mr. Wehman said. “We hope to provide coverage for most of the US and submit the codes to reimbursement by early to mid-2025.”
In terms of reimbursement, the VA operates under a different payment model than Medicare or private insurance, focusing on providing integrated care within the VA system rather than reimbursing for specific services such as patient navigation.
While the SUNY clinic takes care of Medicare patients, it’s unlikely that the new CMS codes for navigators would apply to medical students. Students get paid a monthly stipend for doing navigator work. “There’s a policy about what students can get paid, and how many hours they can work,” Dr. Ginzler clarified.
The SUNY Downstate and Lupus Foundation navigator programs rely on grants to sustain their services. Aurinia Pharmaceuticals has funded both programs, and the SUNY program received an additional grant from Janssen to expand its offerings.
Because it’s grant funded, the navigator position at the Lupus Foundation does not bill patient insurance, Ms. Costillo explained.
Navigator Work Requires Training
Before they start working with patients, navigators often go through a vetting or training process. At Remission Medical, a clinical leadership team does a synchronous interview, background check, and CV review of its potential navigators.
Even before she became a navigator, Ms. Costillo had a strong baseline education in this work. She has a bachelor’s degree in social work and 15 years of experience in social services working with disabled, vulnerable, and underserved populations. Some of her fellow navigators at the Lupus Foundation of America also have degrees in social work.
Ms. Costillo underwent training with the Patient-Centered Education & Research Institute to become a certified professional patient navigator. Her name is on the national registry. The curriculum covered various aspects of medical care such as patient and care team interactions and communications, health and clinical knowledge, patient care coordination and resources, and using evidence-based approaches.
“For our lupus patients, it is essential that navigators understand the disease and the impact on patients and families, treatments available and those in the pipelines, and also the ins and outs of various insurance options,” Ms. Costillo said.
Mr. Wehman, Dr. Williams, and Ms. Costillo reported no disclosures. Dr. Ginzler has been a consultant for Aurinia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
When a large rheumatology clinic in Richmond, Virginia, heard that Medicare would be reimbursing patient navigators, they decided to launch their own virtual navigator program.
“We read about it and felt like it was the perfect representation of what we were already trying to do,” said Blake Wehman, founder and CEO of Remission Medical, which offers virtual diagnosis and longitudinal care in rheumatology.
Mr. Wehman has plans to start submitting for these principal illness navigation (PIN) codes in 2025.
The Centers for Medicare & Medicaid Services (CMS) in 2024 began paying navigators who assist Medicare patients with high-risk conditions, which could include rheumatologic diseases. “The codes are not limited to a specific set of diagnoses; rather, the definition of a serious, high-risk condition is dependent on clinical judgment,” the agency clarified.
CMS established this provision in the CY 2024 Physician Fee Schedule final rule.
Reimbursing patient navigators is long overdue, noted Edith Williams, PhD, MS, director of the Center for Community Health and Prevention and founding director of the Office of Health Equity Research at the University of Rochester in New York. “It’s something our patients need. It’s something that the science is telling us can impact outcomes as an adjunct to clinical care,” she said.
Dr. Williams said the new CMS codes “got our departments talking about what this policy is and how it would translate into patient care.”
The codes apply when navigators are assigned to support patients with high-risk conditions who need assistance connecting with clinical and other resources, including any unmet social determinants of health needs, or in diagnosis or treatment of their medical problems.
“Having a navigator by their side to help get through all the clinical and administrative challenges gives people an advocate and a partner who is with them and their families every step of the way to help make the journey easier,” said a CMS spokesperson.
Not all navigator programs may qualify for the new codes. Some are supported by grants and don’t bill patient insurance. However, they all share a common goal: to guide patients through the healthcare continuum and assist with appointments and medication adherence.
Identifying ‘Root Causes’ of Barriers
Navigators represent a wide variety of backgrounds, ranging from healthcare professionals to students or even patients themselves. They generally don’t provide medical advice. “However, we are responsible for making sure our patients and their families are educated and aware, then assist with guidance on their path,” said Katie Costillo, BSW, CPPN, patient navigator and program manager with the Lupus Foundation of America, Heartland Region.
“Training and experience in engaging and building rapport is essential to assisting patients overcome obstacles that limit their access to healthcare,” she said. Narrowing down with patients the root causes of their barriers and then identifying appropriate and available community resources is key.
Studies have demonstrated the effectiveness of adding a navigator to a rheumatology patient’s care plan. In one study, a group of Boston researchers determined that navigators played a useful role in reducing adherence barriers to oral disease-modifying antirheumatic drugs. The navigators uncovered several concerns among 107 rheumatology patients, including fear of adverse events and medication effectiveness.
They also helped to facilitate patient-physician communication, developed strategies to improve medication adherence, and provided medication and diagnosis education. Patients reported satisfaction with the navigator experience.
A study Dr. Williams coauthored that examined behavioral interventions to support African American women with systemic lupus erythematosus found that patient navigator participants had superior coping scores, compared with those engaged in peer-to-peer methodology and patient support groups.
“We had a lot of success with the mentorship program, too,” Dr. Williams said. Navigator services, however, offer more one-on-one attention, “and it’s more tailored to what the person needs rather than the set curriculum that the mentors delivered to their mentees.”
Supporting Patients With Lupus
Ideally, navigators should be able to relate to patients and know what they’re going through, Dr. Williams said. This is someone whom the patient can trust and depend on. “That’s where the benefit of having someone who is also a patient lies because they’re ultimately relatable to other patients. But different institutions have taken different approaches to this.”
Some programs focus on specific rheumatologic conditions. The Lupus Foundation of America, for example, established patient navigator programs to assist patients with lupus in four markets across the country.
The Heartland patient navigator program is available for all patients with lupus within its region, which includes Kansas, Missouri, and central and southern Illinois. As a navigator, Ms. Costillo has been assisting patients since 2022. In 2023, she began meeting with patients at the Washington University Lupus Clinic (WULC) in St. Louis, Missouri.
Navigators work directly with patients before and after their appointment to ensure follow-up and reduce missed appointments. “They help lupus patients connect with community services and overcoming barriers to access and care. The goal of this position is to improve overall disease management, which results in better health outcomes,” Ms. Costillo said.
Since its inception, the patient navigator program at WULC has shown a decrease in patient no-call no-shows and an increase in requests to reschedule as opposed to not showing up for their scheduled appointment, based on history.
Patients have reported fewer barriers to transportation and improvement in access to resources, support, and disease education. “Our patients have also stated [that] meeting with the navigator during their appointments has helped them to feel heard, understood, and supported,” Ms. Costillo said.
Navigator Work Is Not Without Challenges
A total of 90% of patients with lupus are women, and women of color are two to three times more likely to develop lupus in their lifetime.
“Based on socioeconomic statistics, lupus patients are in a demographic that is commonly underserved, underfunded, and often overlooked. Finding appropriate local community resources for a patient who must choose between feeding her family or paying for transportation to multiple physician appointments is a common problem,” Ms. Costillo said.
Much of the assistance that became available during the COVID pandemic is starting to disappear. “With the rising costs of daily living, we are having to find creative and alternative ways to break down barriers and find support to fill those gaps,” she continued.
Getting insurance coverage of patients is another challenge. Many patients with lupus will be prescribed a treatment that insurance refuses to cover even after the physician disputes it.
Additionally, many patients with lupus are unable to work to support their family. A majority who apply for Social Security Disability Insurance are denied on their first and second attempts, “requiring multiple hearings and pages of documentation from their physicians,” Ms. Costillo said.
Students Serve as Navigators
One inner-city program is seeking to increase access to healthcare services to patients with lupus and lupus nephritis in underserved communities. In 2021, SUNY Downstate Health Sciences University in New York City, in partnership with the Brooklyn Free Clinic and Brooklyn Health Disparities Center, launched a program to teach navigator skills to second-year medical students.
The students assist patients at the Arthritis Clinic at University Hospital at Downstate. “Many of our patients have either low medical literacy or difficulty with English. Many of them are immigrants,” said Ellen M. Ginzler, MD, MPH, SUNY Downstate’s professor emerita and former vice-chair for research and rheumatology division chief.
Dr. Ginzler sought out navigator candidates who showed a strong interest in working with underserved patients with complicated, severe disease who struggled with keeping appointments or adhering to medication regimens. The program also gave preference to students fluent in other languages such as Spanish.
All these efforts have generated improvements in care.
Assessing the program’s effectiveness in a cross-sectional study, Dr. Ginzler and colleagues reported that 94% of navigators were able to schedule appointments and 87% assisted with prescriptions. Navigators also had high success rates in answering medical questions, getting in touch with a patient’s doctor, and reminding patients of medical appointments.
Medical student Jeremy Wilson, a coauthor of the study, served as a navigator for a woman with lupus and scleroderma for many years, along with other comorbidities.
Mr. Wilson went above and beyond for this patient, helping to secure social services supports that included accompanying her to clinic visits and serving as her advocate. “She found an enormous difference in how she was treated when she went to these clinics because the doctors in those clinics took her much more seriously,” Dr. Ginzler said. Mr. Wilson ran interference to secure clinic appointments and worked with the patient’s rheumatology fellow in the clinic to get approval for medications.
Mr. Wilson and the patient formed a great bond. “It not only helped the patient, but it helped Jeremy tremendously in terms of how he felt about his medical career,” Dr. Ginzler said.
The program has since expanded to include patients with other rheumatic diseases, such as rheumatoid arthritis and psoriatic arthritis, and also offers navigator services in dermatology.
A total of 21 students to date have completed the second year of the program. “We’ve just selected eight more,” Dr. Ginzler said. Some of the students continue to do the program in their third or even fourth year as they’re applying for residencies.
A student-run, unpublished survey of nine students in the SUNY program found that all nine reported high confidence in identifying social factors that impact patient health and well-being, compared with four who reported high confidence prior to starting the program. “Additionally, students reported increased confidence in providing comprehensive care in rheumatology and dermatology, and interdisciplinary collaboration,” study author Alejandra K. Moncayo, MPH, and colleagues wrote.
When Navigators Go Virtual
Remission Medical offers its navigator service through its own standalone virtual clinic.
Pain associated with rheumatologic conditions increases the urgency to see a doctor. The goal of the virtual RemissionNavigator program is to meet rheumatology patients where they live, to bridge care gaps and reduce wait times, said Mr. Wehman.
RemissionNavigator accomplishes this through video visits and unlimited texting to its network of board-certified rheumatologists or rheumatology-focused advanced practice providers. Experts can answer questions about why labs are ordered, why a patient may have received a certain diagnosis, or provide detailed explanations of a rheumatic condition.
“There are instances where improvement for the patient means waiting a couple days for us versus 45 days for their brick-and-mortar choice,” Mr. Wehman said.
The program currently has 36 subscribers to Remission’s services, which include navigation. “We have 15 providers in a blend of employed and contracted relationships with Remission,” Mr. Wehman said.
Even in its infancy, the navigator program has produced some success stories. “We had a patient tell us that thanks to us, he was seen faster, found relief immediately through our diagnosis and prescription of methotrexate, felt better at work, lost weight, and was happier in general,” Mr. Wehman said.
Another patient was making monthly, 90-minute trips to Richmond for infusion services. Through the virtual program’s assistance, she is now receiving care from home and can get her monthly infusions at a local clinic.
Ultimately, the goal is to help rheumatology move into an era of value-based care where the transition from fee-for-service to per patient will enable optimized care models and better accessibility, Mr. Wehman said. “It will not happen overnight, but every day we work toward this future.”
VA Targets Rheumatology Care
The Department of Veterans Affairs (VA) has also explored the use of navigator services in rheumatology, including virtual services.
VA uses an integrated, interdisciplinary model that manages each veteran’s individual healthcare needs through a coordinated effort among providers, nurses, social workers, pharmacists, and other health professionals, according to VA press secretary Terrence Hayes.
Care coordination may include supporting scheduling appointments, managing chronic conditions, and coordinating care across different medical departments. “This coordination is particularly important in managing complex rheumatologic conditions, where multiple providers may be involved,” Mr. Hayes said.
Additionally, VA has launched a national telerheumatology initiative to improve access to rheumatology providers in rural areas. The initiative will assist veterans in understanding the telehealth system, navigating appointments, and ensuring they have the necessary technology for virtual consultations.
“It will also facilitate communication between rheumatologists, primary care providers, and other specialists, ensuring that all team members are aligned in their approach to the veteran’s care,” Mr. Hayes said.
Who Will Take Advantage of New Codes?
Currently, Remission Medical operates on a cash-pay model, but the company intends to transition to insurance-based coverage in 2025.
Remission Medical also partners directly with preexisting healthcare systems and clinics such as Sentara Health and OrthoVirginia, where a PIN program, powered by Remission Medical’s virtual rheumatology network, may be explored as well.
The company offers its partners synchronous virtual visits and e-consults. It’s likely that these larger organizations will explore coverage for navigator services for Medicare and private insurance. “We can be there to support them as they decide to implement this,” Mr. Wehman said.
Taking advantage of CMS’s navigator PIN codes is an eventual goal. Remission Medical has not submitted the codes yet, “but we do intend to as we continue to grow our membership count,” Mr. Wehman said. “We hope to provide coverage for most of the US and submit the codes to reimbursement by early to mid-2025.”
In terms of reimbursement, the VA operates under a different payment model than Medicare or private insurance, focusing on providing integrated care within the VA system rather than reimbursing for specific services such as patient navigation.
While the SUNY clinic takes care of Medicare patients, it’s unlikely that the new CMS codes for navigators would apply to medical students. Students get paid a monthly stipend for doing navigator work. “There’s a policy about what students can get paid, and how many hours they can work,” Dr. Ginzler clarified.
The SUNY Downstate and Lupus Foundation navigator programs rely on grants to sustain their services. Aurinia Pharmaceuticals has funded both programs, and the SUNY program received an additional grant from Janssen to expand its offerings.
Because it’s grant funded, the navigator position at the Lupus Foundation does not bill patient insurance, Ms. Costillo explained.
Navigator Work Requires Training
Before they start working with patients, navigators often go through a vetting or training process. At Remission Medical, a clinical leadership team does a synchronous interview, background check, and CV review of its potential navigators.
Even before she became a navigator, Ms. Costillo had a strong baseline education in this work. She has a bachelor’s degree in social work and 15 years of experience in social services working with disabled, vulnerable, and underserved populations. Some of her fellow navigators at the Lupus Foundation of America also have degrees in social work.
Ms. Costillo underwent training with the Patient-Centered Education & Research Institute to become a certified professional patient navigator. Her name is on the national registry. The curriculum covered various aspects of medical care such as patient and care team interactions and communications, health and clinical knowledge, patient care coordination and resources, and using evidence-based approaches.
“For our lupus patients, it is essential that navigators understand the disease and the impact on patients and families, treatments available and those in the pipelines, and also the ins and outs of various insurance options,” Ms. Costillo said.
Mr. Wehman, Dr. Williams, and Ms. Costillo reported no disclosures. Dr. Ginzler has been a consultant for Aurinia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
When a large rheumatology clinic in Richmond, Virginia, heard that Medicare would be reimbursing patient navigators, they decided to launch their own virtual navigator program.
“We read about it and felt like it was the perfect representation of what we were already trying to do,” said Blake Wehman, founder and CEO of Remission Medical, which offers virtual diagnosis and longitudinal care in rheumatology.
Mr. Wehman has plans to start submitting for these principal illness navigation (PIN) codes in 2025.
The Centers for Medicare & Medicaid Services (CMS) in 2024 began paying navigators who assist Medicare patients with high-risk conditions, which could include rheumatologic diseases. “The codes are not limited to a specific set of diagnoses; rather, the definition of a serious, high-risk condition is dependent on clinical judgment,” the agency clarified.
CMS established this provision in the CY 2024 Physician Fee Schedule final rule.
Reimbursing patient navigators is long overdue, noted Edith Williams, PhD, MS, director of the Center for Community Health and Prevention and founding director of the Office of Health Equity Research at the University of Rochester in New York. “It’s something our patients need. It’s something that the science is telling us can impact outcomes as an adjunct to clinical care,” she said.
Dr. Williams said the new CMS codes “got our departments talking about what this policy is and how it would translate into patient care.”
The codes apply when navigators are assigned to support patients with high-risk conditions who need assistance connecting with clinical and other resources, including any unmet social determinants of health needs, or in diagnosis or treatment of their medical problems.
“Having a navigator by their side to help get through all the clinical and administrative challenges gives people an advocate and a partner who is with them and their families every step of the way to help make the journey easier,” said a CMS spokesperson.
Not all navigator programs may qualify for the new codes. Some are supported by grants and don’t bill patient insurance. However, they all share a common goal: to guide patients through the healthcare continuum and assist with appointments and medication adherence.
Identifying ‘Root Causes’ of Barriers
Navigators represent a wide variety of backgrounds, ranging from healthcare professionals to students or even patients themselves. They generally don’t provide medical advice. “However, we are responsible for making sure our patients and their families are educated and aware, then assist with guidance on their path,” said Katie Costillo, BSW, CPPN, patient navigator and program manager with the Lupus Foundation of America, Heartland Region.
“Training and experience in engaging and building rapport is essential to assisting patients overcome obstacles that limit their access to healthcare,” she said. Narrowing down with patients the root causes of their barriers and then identifying appropriate and available community resources is key.
Studies have demonstrated the effectiveness of adding a navigator to a rheumatology patient’s care plan. In one study, a group of Boston researchers determined that navigators played a useful role in reducing adherence barriers to oral disease-modifying antirheumatic drugs. The navigators uncovered several concerns among 107 rheumatology patients, including fear of adverse events and medication effectiveness.
They also helped to facilitate patient-physician communication, developed strategies to improve medication adherence, and provided medication and diagnosis education. Patients reported satisfaction with the navigator experience.
A study Dr. Williams coauthored that examined behavioral interventions to support African American women with systemic lupus erythematosus found that patient navigator participants had superior coping scores, compared with those engaged in peer-to-peer methodology and patient support groups.
“We had a lot of success with the mentorship program, too,” Dr. Williams said. Navigator services, however, offer more one-on-one attention, “and it’s more tailored to what the person needs rather than the set curriculum that the mentors delivered to their mentees.”
Supporting Patients With Lupus
Ideally, navigators should be able to relate to patients and know what they’re going through, Dr. Williams said. This is someone whom the patient can trust and depend on. “That’s where the benefit of having someone who is also a patient lies because they’re ultimately relatable to other patients. But different institutions have taken different approaches to this.”
Some programs focus on specific rheumatologic conditions. The Lupus Foundation of America, for example, established patient navigator programs to assist patients with lupus in four markets across the country.
The Heartland patient navigator program is available for all patients with lupus within its region, which includes Kansas, Missouri, and central and southern Illinois. As a navigator, Ms. Costillo has been assisting patients since 2022. In 2023, she began meeting with patients at the Washington University Lupus Clinic (WULC) in St. Louis, Missouri.
Navigators work directly with patients before and after their appointment to ensure follow-up and reduce missed appointments. “They help lupus patients connect with community services and overcoming barriers to access and care. The goal of this position is to improve overall disease management, which results in better health outcomes,” Ms. Costillo said.
Since its inception, the patient navigator program at WULC has shown a decrease in patient no-call no-shows and an increase in requests to reschedule as opposed to not showing up for their scheduled appointment, based on history.
Patients have reported fewer barriers to transportation and improvement in access to resources, support, and disease education. “Our patients have also stated [that] meeting with the navigator during their appointments has helped them to feel heard, understood, and supported,” Ms. Costillo said.
Navigator Work Is Not Without Challenges
A total of 90% of patients with lupus are women, and women of color are two to three times more likely to develop lupus in their lifetime.
“Based on socioeconomic statistics, lupus patients are in a demographic that is commonly underserved, underfunded, and often overlooked. Finding appropriate local community resources for a patient who must choose between feeding her family or paying for transportation to multiple physician appointments is a common problem,” Ms. Costillo said.
Much of the assistance that became available during the COVID pandemic is starting to disappear. “With the rising costs of daily living, we are having to find creative and alternative ways to break down barriers and find support to fill those gaps,” she continued.
Getting insurance coverage of patients is another challenge. Many patients with lupus will be prescribed a treatment that insurance refuses to cover even after the physician disputes it.
Additionally, many patients with lupus are unable to work to support their family. A majority who apply for Social Security Disability Insurance are denied on their first and second attempts, “requiring multiple hearings and pages of documentation from their physicians,” Ms. Costillo said.
Students Serve as Navigators
One inner-city program is seeking to increase access to healthcare services to patients with lupus and lupus nephritis in underserved communities. In 2021, SUNY Downstate Health Sciences University in New York City, in partnership with the Brooklyn Free Clinic and Brooklyn Health Disparities Center, launched a program to teach navigator skills to second-year medical students.
The students assist patients at the Arthritis Clinic at University Hospital at Downstate. “Many of our patients have either low medical literacy or difficulty with English. Many of them are immigrants,” said Ellen M. Ginzler, MD, MPH, SUNY Downstate’s professor emerita and former vice-chair for research and rheumatology division chief.
Dr. Ginzler sought out navigator candidates who showed a strong interest in working with underserved patients with complicated, severe disease who struggled with keeping appointments or adhering to medication regimens. The program also gave preference to students fluent in other languages such as Spanish.
All these efforts have generated improvements in care.
Assessing the program’s effectiveness in a cross-sectional study, Dr. Ginzler and colleagues reported that 94% of navigators were able to schedule appointments and 87% assisted with prescriptions. Navigators also had high success rates in answering medical questions, getting in touch with a patient’s doctor, and reminding patients of medical appointments.
Medical student Jeremy Wilson, a coauthor of the study, served as a navigator for a woman with lupus and scleroderma for many years, along with other comorbidities.
Mr. Wilson went above and beyond for this patient, helping to secure social services supports that included accompanying her to clinic visits and serving as her advocate. “She found an enormous difference in how she was treated when she went to these clinics because the doctors in those clinics took her much more seriously,” Dr. Ginzler said. Mr. Wilson ran interference to secure clinic appointments and worked with the patient’s rheumatology fellow in the clinic to get approval for medications.
Mr. Wilson and the patient formed a great bond. “It not only helped the patient, but it helped Jeremy tremendously in terms of how he felt about his medical career,” Dr. Ginzler said.
The program has since expanded to include patients with other rheumatic diseases, such as rheumatoid arthritis and psoriatic arthritis, and also offers navigator services in dermatology.
A total of 21 students to date have completed the second year of the program. “We’ve just selected eight more,” Dr. Ginzler said. Some of the students continue to do the program in their third or even fourth year as they’re applying for residencies.
A student-run, unpublished survey of nine students in the SUNY program found that all nine reported high confidence in identifying social factors that impact patient health and well-being, compared with four who reported high confidence prior to starting the program. “Additionally, students reported increased confidence in providing comprehensive care in rheumatology and dermatology, and interdisciplinary collaboration,” study author Alejandra K. Moncayo, MPH, and colleagues wrote.
When Navigators Go Virtual
Remission Medical offers its navigator service through its own standalone virtual clinic.
Pain associated with rheumatologic conditions increases the urgency to see a doctor. The goal of the virtual RemissionNavigator program is to meet rheumatology patients where they live, to bridge care gaps and reduce wait times, said Mr. Wehman.
RemissionNavigator accomplishes this through video visits and unlimited texting to its network of board-certified rheumatologists or rheumatology-focused advanced practice providers. Experts can answer questions about why labs are ordered, why a patient may have received a certain diagnosis, or provide detailed explanations of a rheumatic condition.
“There are instances where improvement for the patient means waiting a couple days for us versus 45 days for their brick-and-mortar choice,” Mr. Wehman said.
The program currently has 36 subscribers to Remission’s services, which include navigation. “We have 15 providers in a blend of employed and contracted relationships with Remission,” Mr. Wehman said.
Even in its infancy, the navigator program has produced some success stories. “We had a patient tell us that thanks to us, he was seen faster, found relief immediately through our diagnosis and prescription of methotrexate, felt better at work, lost weight, and was happier in general,” Mr. Wehman said.
Another patient was making monthly, 90-minute trips to Richmond for infusion services. Through the virtual program’s assistance, she is now receiving care from home and can get her monthly infusions at a local clinic.
Ultimately, the goal is to help rheumatology move into an era of value-based care where the transition from fee-for-service to per patient will enable optimized care models and better accessibility, Mr. Wehman said. “It will not happen overnight, but every day we work toward this future.”
VA Targets Rheumatology Care
The Department of Veterans Affairs (VA) has also explored the use of navigator services in rheumatology, including virtual services.
VA uses an integrated, interdisciplinary model that manages each veteran’s individual healthcare needs through a coordinated effort among providers, nurses, social workers, pharmacists, and other health professionals, according to VA press secretary Terrence Hayes.
Care coordination may include supporting scheduling appointments, managing chronic conditions, and coordinating care across different medical departments. “This coordination is particularly important in managing complex rheumatologic conditions, where multiple providers may be involved,” Mr. Hayes said.
Additionally, VA has launched a national telerheumatology initiative to improve access to rheumatology providers in rural areas. The initiative will assist veterans in understanding the telehealth system, navigating appointments, and ensuring they have the necessary technology for virtual consultations.
“It will also facilitate communication between rheumatologists, primary care providers, and other specialists, ensuring that all team members are aligned in their approach to the veteran’s care,” Mr. Hayes said.
Who Will Take Advantage of New Codes?
Currently, Remission Medical operates on a cash-pay model, but the company intends to transition to insurance-based coverage in 2025.
Remission Medical also partners directly with preexisting healthcare systems and clinics such as Sentara Health and OrthoVirginia, where a PIN program, powered by Remission Medical’s virtual rheumatology network, may be explored as well.
The company offers its partners synchronous virtual visits and e-consults. It’s likely that these larger organizations will explore coverage for navigator services for Medicare and private insurance. “We can be there to support them as they decide to implement this,” Mr. Wehman said.
Taking advantage of CMS’s navigator PIN codes is an eventual goal. Remission Medical has not submitted the codes yet, “but we do intend to as we continue to grow our membership count,” Mr. Wehman said. “We hope to provide coverage for most of the US and submit the codes to reimbursement by early to mid-2025.”
In terms of reimbursement, the VA operates under a different payment model than Medicare or private insurance, focusing on providing integrated care within the VA system rather than reimbursing for specific services such as patient navigation.
While the SUNY clinic takes care of Medicare patients, it’s unlikely that the new CMS codes for navigators would apply to medical students. Students get paid a monthly stipend for doing navigator work. “There’s a policy about what students can get paid, and how many hours they can work,” Dr. Ginzler clarified.
The SUNY Downstate and Lupus Foundation navigator programs rely on grants to sustain their services. Aurinia Pharmaceuticals has funded both programs, and the SUNY program received an additional grant from Janssen to expand its offerings.
Because it’s grant funded, the navigator position at the Lupus Foundation does not bill patient insurance, Ms. Costillo explained.
Navigator Work Requires Training
Before they start working with patients, navigators often go through a vetting or training process. At Remission Medical, a clinical leadership team does a synchronous interview, background check, and CV review of its potential navigators.
Even before she became a navigator, Ms. Costillo had a strong baseline education in this work. She has a bachelor’s degree in social work and 15 years of experience in social services working with disabled, vulnerable, and underserved populations. Some of her fellow navigators at the Lupus Foundation of America also have degrees in social work.
Ms. Costillo underwent training with the Patient-Centered Education & Research Institute to become a certified professional patient navigator. Her name is on the national registry. The curriculum covered various aspects of medical care such as patient and care team interactions and communications, health and clinical knowledge, patient care coordination and resources, and using evidence-based approaches.
“For our lupus patients, it is essential that navigators understand the disease and the impact on patients and families, treatments available and those in the pipelines, and also the ins and outs of various insurance options,” Ms. Costillo said.
Mr. Wehman, Dr. Williams, and Ms. Costillo reported no disclosures. Dr. Ginzler has been a consultant for Aurinia Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FDA Expands Indication for Amivantamab in Lung Cancer
Amivantamab with carboplatin and pemetrexed is now indicated for adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after treatment with an EGFR tyrosine kinase inhibitor (TKI).
The FDA has already approved first-line use of amivantamab in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations, as reported by Medscape Medical News.
The second-line approval for amivantamab plus chemotherapy “may address the most common mechanisms of treatment resistance to third-generation EGFR TKIs, such as osimertinib, in the first line,” Martin Dietrich, MD, PhD, oncologist, Cancer Care Centers of Brevard in Florida, said in a company news release.
“This multitargeted combination extended progression-free survival (PFS) and improved overall response compared to chemotherapy alone, offering an important and effective new second-line option for patients,” Dr. Dietrich added.
The second-line indication is supported by the phase 3 MARIPOSA-2 study, which included 657 patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations and disease progression on or after receiving osimertinib.
The study demonstrated a 52% reduced risk of disease progression or death when amivantamab was added to carboplatin and pemetrexed (hazard ratio, 0.48).
Median PFS was 6.3 months with amivantamab vs 4.2 months with chemotherapy alone. The confirmed objective response rate was 53% in the amivantamab plus chemotherapy group vs 29% in the chemotherapy only group.
The most common adverse reactions, occurring in at least 20% of patients, were rash, infusion-related reactions, fatigue, nail toxicity, nausea, constipation, edema, stomatitis, decreased appetite, musculoskeletal pain, vomiting, and COVID-19 infection.
The company noted that amivantamab in combination with chemotherapy is the only category 1 treatment option in National Comprehensive Cancer Network clinical practice guidelines for patients with EGFR-mutated NSCLC who have progressed on osimertinib and who are symptomatic with multiple lesions.
A version of this article appeared on Medscape.com.
Amivantamab with carboplatin and pemetrexed is now indicated for adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after treatment with an EGFR tyrosine kinase inhibitor (TKI).
The FDA has already approved first-line use of amivantamab in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations, as reported by Medscape Medical News.
The second-line approval for amivantamab plus chemotherapy “may address the most common mechanisms of treatment resistance to third-generation EGFR TKIs, such as osimertinib, in the first line,” Martin Dietrich, MD, PhD, oncologist, Cancer Care Centers of Brevard in Florida, said in a company news release.
“This multitargeted combination extended progression-free survival (PFS) and improved overall response compared to chemotherapy alone, offering an important and effective new second-line option for patients,” Dr. Dietrich added.
The second-line indication is supported by the phase 3 MARIPOSA-2 study, which included 657 patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations and disease progression on or after receiving osimertinib.
The study demonstrated a 52% reduced risk of disease progression or death when amivantamab was added to carboplatin and pemetrexed (hazard ratio, 0.48).
Median PFS was 6.3 months with amivantamab vs 4.2 months with chemotherapy alone. The confirmed objective response rate was 53% in the amivantamab plus chemotherapy group vs 29% in the chemotherapy only group.
The most common adverse reactions, occurring in at least 20% of patients, were rash, infusion-related reactions, fatigue, nail toxicity, nausea, constipation, edema, stomatitis, decreased appetite, musculoskeletal pain, vomiting, and COVID-19 infection.
The company noted that amivantamab in combination with chemotherapy is the only category 1 treatment option in National Comprehensive Cancer Network clinical practice guidelines for patients with EGFR-mutated NSCLC who have progressed on osimertinib and who are symptomatic with multiple lesions.
A version of this article appeared on Medscape.com.
Amivantamab with carboplatin and pemetrexed is now indicated for adults with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after treatment with an EGFR tyrosine kinase inhibitor (TKI).
The FDA has already approved first-line use of amivantamab in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations, as reported by Medscape Medical News.
The second-line approval for amivantamab plus chemotherapy “may address the most common mechanisms of treatment resistance to third-generation EGFR TKIs, such as osimertinib, in the first line,” Martin Dietrich, MD, PhD, oncologist, Cancer Care Centers of Brevard in Florida, said in a company news release.
“This multitargeted combination extended progression-free survival (PFS) and improved overall response compared to chemotherapy alone, offering an important and effective new second-line option for patients,” Dr. Dietrich added.
The second-line indication is supported by the phase 3 MARIPOSA-2 study, which included 657 patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations and disease progression on or after receiving osimertinib.
The study demonstrated a 52% reduced risk of disease progression or death when amivantamab was added to carboplatin and pemetrexed (hazard ratio, 0.48).
Median PFS was 6.3 months with amivantamab vs 4.2 months with chemotherapy alone. The confirmed objective response rate was 53% in the amivantamab plus chemotherapy group vs 29% in the chemotherapy only group.
The most common adverse reactions, occurring in at least 20% of patients, were rash, infusion-related reactions, fatigue, nail toxicity, nausea, constipation, edema, stomatitis, decreased appetite, musculoskeletal pain, vomiting, and COVID-19 infection.
The company noted that amivantamab in combination with chemotherapy is the only category 1 treatment option in National Comprehensive Cancer Network clinical practice guidelines for patients with EGFR-mutated NSCLC who have progressed on osimertinib and who are symptomatic with multiple lesions.
A version of this article appeared on Medscape.com.
Biomarkers in Cord Blood May Predict AD Onset in Newborns, Study Suggests
TOPLINE:
and interleukin (IL) 31.
METHODOLOGY:
- Researchers conducted a prospective study to evaluate the predictive role of serologic biomarkers and cutaneous markers and the development of AD in 40 full-term newborns from a university hospital in Italy.
- Cord blood was collected at birth and analyzed for serum biomarkers such as CCL17/TARC and IL-31.
- TEWL and skin hydration rates were measured at 1, 6, and 12 months, and dermatological features such as dryness, cradle cap, and eczematous lesions were also monitored during visits.
TAKEAWAY:
- At 6 months, 16 infants had symptoms of AD, which included dry skin, pruritus, and keratosis pilaris, which persisted at 12 months. Their mean Eczema Area and Severity Index score was 6.6 at 6 months and 2.9 at 12 months.
- Infants with signs of AD had significantly higher TEWL levels at the anterior cubital fossa at 1, 6, and 12 months than those without AD.
- Cord blood levels of CCL17/TARC and IL-31 were significantly higher in infants with AD.
- A correlation was found between TEWL values and CCL17 levels at 1, 6, and 12 months.
IN PRACTICE:
“,” the authors wrote. “Stratified interventions based on these variables, family history, FLG [filaggrin] variations, and other biomarkers could offer more targeted approaches to AD prevention and management, especially during the first year of life,” they added.
SOURCE:
The study was led by Angelo Massimiliano D’Erme, MD, PhD, of the Dermatology Unit, in the Department of Medical and Oncology, University of Pisa, Pisa, Italy, and was published online in JAMA Dermatology.
LIMITATIONS:
The limitations included the observational design and small sample size, and it was a single-center study.
DISCLOSURES:
The authors did not disclose any funding information. One author disclosed receiving personal fees from various pharmaceutical companies and serving as a founder and chairman of a nonprofit organization.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
TOPLINE:
and interleukin (IL) 31.
METHODOLOGY:
- Researchers conducted a prospective study to evaluate the predictive role of serologic biomarkers and cutaneous markers and the development of AD in 40 full-term newborns from a university hospital in Italy.
- Cord blood was collected at birth and analyzed for serum biomarkers such as CCL17/TARC and IL-31.
- TEWL and skin hydration rates were measured at 1, 6, and 12 months, and dermatological features such as dryness, cradle cap, and eczematous lesions were also monitored during visits.
TAKEAWAY:
- At 6 months, 16 infants had symptoms of AD, which included dry skin, pruritus, and keratosis pilaris, which persisted at 12 months. Their mean Eczema Area and Severity Index score was 6.6 at 6 months and 2.9 at 12 months.
- Infants with signs of AD had significantly higher TEWL levels at the anterior cubital fossa at 1, 6, and 12 months than those without AD.
- Cord blood levels of CCL17/TARC and IL-31 were significantly higher in infants with AD.
- A correlation was found between TEWL values and CCL17 levels at 1, 6, and 12 months.
IN PRACTICE:
“,” the authors wrote. “Stratified interventions based on these variables, family history, FLG [filaggrin] variations, and other biomarkers could offer more targeted approaches to AD prevention and management, especially during the first year of life,” they added.
SOURCE:
The study was led by Angelo Massimiliano D’Erme, MD, PhD, of the Dermatology Unit, in the Department of Medical and Oncology, University of Pisa, Pisa, Italy, and was published online in JAMA Dermatology.
LIMITATIONS:
The limitations included the observational design and small sample size, and it was a single-center study.
DISCLOSURES:
The authors did not disclose any funding information. One author disclosed receiving personal fees from various pharmaceutical companies and serving as a founder and chairman of a nonprofit organization.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
TOPLINE:
and interleukin (IL) 31.
METHODOLOGY:
- Researchers conducted a prospective study to evaluate the predictive role of serologic biomarkers and cutaneous markers and the development of AD in 40 full-term newborns from a university hospital in Italy.
- Cord blood was collected at birth and analyzed for serum biomarkers such as CCL17/TARC and IL-31.
- TEWL and skin hydration rates were measured at 1, 6, and 12 months, and dermatological features such as dryness, cradle cap, and eczematous lesions were also monitored during visits.
TAKEAWAY:
- At 6 months, 16 infants had symptoms of AD, which included dry skin, pruritus, and keratosis pilaris, which persisted at 12 months. Their mean Eczema Area and Severity Index score was 6.6 at 6 months and 2.9 at 12 months.
- Infants with signs of AD had significantly higher TEWL levels at the anterior cubital fossa at 1, 6, and 12 months than those without AD.
- Cord blood levels of CCL17/TARC and IL-31 were significantly higher in infants with AD.
- A correlation was found between TEWL values and CCL17 levels at 1, 6, and 12 months.
IN PRACTICE:
“,” the authors wrote. “Stratified interventions based on these variables, family history, FLG [filaggrin] variations, and other biomarkers could offer more targeted approaches to AD prevention and management, especially during the first year of life,” they added.
SOURCE:
The study was led by Angelo Massimiliano D’Erme, MD, PhD, of the Dermatology Unit, in the Department of Medical and Oncology, University of Pisa, Pisa, Italy, and was published online in JAMA Dermatology.
LIMITATIONS:
The limitations included the observational design and small sample size, and it was a single-center study.
DISCLOSURES:
The authors did not disclose any funding information. One author disclosed receiving personal fees from various pharmaceutical companies and serving as a founder and chairman of a nonprofit organization.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
Elinzanetant Shows Significant Improvement in Menopausal Vasomotor and Sleep Symptoms
CHICAGO — The nonhormonal investigational drug elinzanetant led to significant improvement in hot flashes as well as sleep disturbance and quality of life, according to data from three randomized controlled trials presented at The Menopause Society 2024 Annual Meeting in Chicago. Two phase 3 trials, OASIS 1 and 2, were also published in JAMA, and the longer-term OASIS 3 trial was presented as a poster at the conference.
Elinzanetant is a selective neurokinin (NK) receptor antagonist, similar to fezolinetant, the first drug in this class approved by the US Food and Drug Administration (FDA) for vasomotor symptoms in May 2023. This class of medications targets the estrogen-sensitive kisspeptin/NK B/dynorphin (KNDy) neurons thought to play a role in thermoregulation and hot flashes during menopause. While fezolinetant targets only the NK-3 receptor, elinzanetant is a dual NK receptor antagonist that targets both NK-1 and NK-3. Bayer submitted a New Drug Application for elinzanetant to the FDA on August 1.
For those in whom hormone therapy is contraindicated, “it’s always been difficult for women with really severe symptoms to have a safe and effective therapy,” lead author JoAnn Pinkerton, MD, a professor of ob.gyn. at the University of Virginia in Charlottesville, Virginia, told this news organization. “The nonhormonal therapies we’ve used mostly off-label — the antidepressants, gabapentin, clonidine, oxybutynin — do help the hot flashes, but they don’t work nearly as effectively as these new NK receptor antagonists, and having one that looks like it might have a broader use for hot flashes, night sweats, mood, and sleep is just really exciting.”
Dr. Pinkerton said approximately 80% of the women in the OASIS 1 and 2 studies had at least a 50% reduction in hot flashes. “It was a very strong, dramatic positive finding, but the improvements in sleep and mood have really encouraged us to go further,” she said.
Declining estrogen levels during and after menopause can cause hypertrophy and hyperactivity of the KNDy neurons, which has been linked to thermoregulation disruptions that may trigger hot flashes, James Simon, MD, a clinical professor of ob.gyn. at The George Washington University School of Medicine & Health Sciences and medical director of IntimMedicine in Washington, DC, told attendees. He presented pooled data from OASIS 1 and 2. The NK-1 receptor, targeted by elinzanetant but not fezolinetant, is also thought to play a role in insomnia and possibly in mood.
“Oftentimes the focus on a lot of these drugs is hot flashes, hot flashes, hot flashes, but we know hot flashes do not occur in isolation,” Chrisandra Shufelt, MD, professor and chair of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Florida, told this news organization. Elinzanetant is “an interesting compound because it actually works on sleep, and that was critical because sleep disturbance precedes” many other menopausal symptoms, said Dr. Shufelt, who was not involved in the study.
“I think it is an outstanding option for women who don’t have the opportunity to get hormones,” Dr. Shufelt said, and she was particularly pleased to see there were no safety concerns for the liver in the trial data. The FDA issued a warning on September 12 about the risk for rare liver injury with fezolinetant, but the early signals that had been seen in fezolinetant data were not seen in these elinzanetant data.
The OASIS 1 and 2 trials enrolled postmenopausal women, aged 40-65 years, who had at least 50 moderate to severe vasomotor occurrences per week.
“A moderate hot flash is a hot flash that is also associated with sweating, and a severe hot flash is a moderate hot flash that stops a woman in her tracks,” Dr. Simon said. “Namely, it’s severe enough with sweating and central nervous system effects that she is interrupted in whatever it is that she’s doing at the time.”
Exclusion criteria for the trials included a history of arrhythmias, heart block, or QT prolongation; abnormal lab results; history of malignancy within the past 5 years; uncontrolled or treatment-resistant hypertension, hypothyroidism, or hyperthyroidism; unexplained postmenopausal bleeding; clinically relevant abnormal mammogram findings; or disordered proliferative endometrium, endometrial hyperplasia, polyp, or endometrial cancer.
The predominantly White (80%) women were an average 54 years old, with an average body mass index (BMI) of 27.8, and were an average 3.5 years from their last period. For the first 12 weeks of the trials, 399 women were assigned to receive 120 mg once daily of oral elinzanetant and 397 were assigned to once daily placebo. Then the women taking placebo switched to elinzanetant for the final 14 weeks of the study.
The endpoints included mean change in frequency and severity of vasomotor symptoms at weeks 1, 4, and 12 as well as change in sleep disturbance and quality of life at week 12. Sleep was assessed with the Patient-Reported Outcomes Measurement Information System Sleep Disturbance–Short Form score, which ranges from 28.9 to 76.5, with a higher number denoting greater sleep disturbance. The Menopause-Specific Quality-of-Life score ranges from 1 to 8, with a higher score indicating poorer quality of life.
Daily frequency of vasomotor symptoms was 14 per day at baseline in the elinzanetant group, decreasing by 4.8 per day at week 1, 8 per day at week 4, and 9.4 per day at week 12. In the placebo group, women had an average 15.2 occurrences per day at baseline, which decreased by 3.2 at week 1, 5.2 at week 4, and 6.4 at week 12. Comparing the groups at 12 weeks, those receiving elinzanetant had 3.2 fewer daily vasomotor symptoms than those receiving placebo (P < .0001).
The severity of vasomotor symptoms also improved more in the elinzanetant group than in the placebo group over 12 weeks, after which severity improved further in those who switched from placebo to elinzanetant (P < .0001).
Sleep disturbance scores, starting at a mean 61.5 in the elinzanetant group and 60.5 in the placebo group, fell 10.7 points in the elinzanetant group and 5.3 points in the placebo group at 12 weeks, for a difference of 4.9 points (P < .0001). Sleep then further improved in those who switched from placebo to elinzanetant. Quality-of-life scores improved 1.37 points (from 4.52 at baseline) in the elinzanetant group and 0.96 points (from 4.49 at baseline) in the placebo group, for a mean difference at 12 weeks of 0.36 (P < .0001).
Though no head-to-head data exist comparing elinzanetant and fezolinetant, Dr. Simon told this news organization the side effects with fezolinetant “tend to be gastrointestinal, whereas the side effects for elinzanetant tend to be central nervous system,” such as drowsiness and lethargy.
The women who are the best candidates for elinzanetant, Dr. Pinkerton told this news organization, include those who have had an estrogen-sensitive cancer, such as breast or endometrial cancer, or who have fear of it, a family history, or are otherwise high risk. Other ideal candidates include those with a history of venous thromboembolism, people who have migraine with aura (due to concerns about increased risk for stroke), and those who have endometriosis or large fibroids.
“Then the last group might be women who took hormone therapy in their 50s and want to continue, but they’re trying to go off, and they have a recurrence of their hot flashes or night sweats or sleep issues,” Dr. Pinkerton said. “This might be a great group to switch over.”
OASIS 3 assessed the drug for 1 year and “supported the results of OASIS 1 and 2, demonstrating efficacy over a longer study duration and in a population with a vasomotor symptom profile representative of that seen in clinical practice,” Nick Panay, BSc, MBBS, director of the Menopause & PMS Centre at Queen Charlotte’s Hospital & Imperial College London, London, England, and his colleague reported.
Among 628 postmenopausal women aged 40-65, the predominantly White (78.5%) women were an average 54 years old, with an average BMI of 27.6, and were an average 5 years past their last period. Half received 120 mg elinzanetant and half received a placebo for 52 weeks.
At 12 weeks, the women receiving elinzanetant reported an average 1.6 moderate to severe vasomotor symptoms per day, down from 6.7 at baseline. Daily average symptoms in the placebo group fell from 6.8 at baseline to 3.4 at 12 weeks, for a difference of 1.6 fewer occurrences per day in the elinzanetant group (P < .0001).
Sleep disturbances also improved, falling 9.4 points from a baseline 57.4 in the elinzanetant group and 5.7 points from a baseline 58 in the placebo group. Quality-of-life scores improved from 4.1 to 2.8 (−1.3 change) in the elinzanetant group and from 4.4 to 3.3 (−1.1 change) in the placebo group.
In addition to looking at treatment-emergent adverse events, the safety assessments also included endometrial biopsies; bone mineral density in the femoral neck, hip, and lumbar spine; weight; and labs. Adverse events related to the study drug occurred in 30.4% of those in the elinzanetant group and 14.6% of those in the placebo group. The most commonly reported adverse events were headache (9.6% elinzanetant vs 7% placebo), fatigue (7% vs 10.2%), and sleepiness (5.1% vs 1.3%). A higher proportion of women taking elinzanetant (12.5%) than those taking placebo (4.1%) discontinued the study.
No serious adverse events deemed to be treatment-related occurred in either group, and no endometrial hyperplasia or malignant neoplasm occurred in either group. Bone mineral density changes in both groups were within the expected range for the women’s age, and their weight remained stable over the 52 weeks.
Six women taking elinzanetant and four taking placebo met predefined criteria for close liver observation, but none showed hepatotoxicity or evidence of possible drug-induced liver injury.
The research was funded by Bayer. Dr. Pinkerton has run a trial funded by Bayer and is a consultant for Bayer and Pfizer. Dr. Shufelt had no disclosures. Dr. Simon had grant/research support, consulting/advisory board participation, and/or speaking disclosures with AbbVie, Bayer Healthcare, Besins Healthcare, California Institute of Integral Studies, Camargo Pharmaceutical Services, Covance, Daré Bioscience, DEKA M.E.L.A S.r.l., Femasys, Ipsen, KaNDy/NeRRe Therapeutics, Khyria, Madorra, Mayne Pharma, Mitsubishi Tanabe Pharma Development America, Mylan/Viatris Inc, Myovant Sciences, ObsEva SA, Pfizer, Pharmavite, QUE Oncology, Scynexis, Sebela Pharmaceuticals, Sprout Pharmaceuticals, TherapeuticsMD, Vella Bioscience, and Viveve Medical, and he is a stockholder in Sermonix Pharmaceuticals.
A version of this article first appeared on Medscape.com.
CHICAGO — The nonhormonal investigational drug elinzanetant led to significant improvement in hot flashes as well as sleep disturbance and quality of life, according to data from three randomized controlled trials presented at The Menopause Society 2024 Annual Meeting in Chicago. Two phase 3 trials, OASIS 1 and 2, were also published in JAMA, and the longer-term OASIS 3 trial was presented as a poster at the conference.
Elinzanetant is a selective neurokinin (NK) receptor antagonist, similar to fezolinetant, the first drug in this class approved by the US Food and Drug Administration (FDA) for vasomotor symptoms in May 2023. This class of medications targets the estrogen-sensitive kisspeptin/NK B/dynorphin (KNDy) neurons thought to play a role in thermoregulation and hot flashes during menopause. While fezolinetant targets only the NK-3 receptor, elinzanetant is a dual NK receptor antagonist that targets both NK-1 and NK-3. Bayer submitted a New Drug Application for elinzanetant to the FDA on August 1.
For those in whom hormone therapy is contraindicated, “it’s always been difficult for women with really severe symptoms to have a safe and effective therapy,” lead author JoAnn Pinkerton, MD, a professor of ob.gyn. at the University of Virginia in Charlottesville, Virginia, told this news organization. “The nonhormonal therapies we’ve used mostly off-label — the antidepressants, gabapentin, clonidine, oxybutynin — do help the hot flashes, but they don’t work nearly as effectively as these new NK receptor antagonists, and having one that looks like it might have a broader use for hot flashes, night sweats, mood, and sleep is just really exciting.”
Dr. Pinkerton said approximately 80% of the women in the OASIS 1 and 2 studies had at least a 50% reduction in hot flashes. “It was a very strong, dramatic positive finding, but the improvements in sleep and mood have really encouraged us to go further,” she said.
Declining estrogen levels during and after menopause can cause hypertrophy and hyperactivity of the KNDy neurons, which has been linked to thermoregulation disruptions that may trigger hot flashes, James Simon, MD, a clinical professor of ob.gyn. at The George Washington University School of Medicine & Health Sciences and medical director of IntimMedicine in Washington, DC, told attendees. He presented pooled data from OASIS 1 and 2. The NK-1 receptor, targeted by elinzanetant but not fezolinetant, is also thought to play a role in insomnia and possibly in mood.
“Oftentimes the focus on a lot of these drugs is hot flashes, hot flashes, hot flashes, but we know hot flashes do not occur in isolation,” Chrisandra Shufelt, MD, professor and chair of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Florida, told this news organization. Elinzanetant is “an interesting compound because it actually works on sleep, and that was critical because sleep disturbance precedes” many other menopausal symptoms, said Dr. Shufelt, who was not involved in the study.
“I think it is an outstanding option for women who don’t have the opportunity to get hormones,” Dr. Shufelt said, and she was particularly pleased to see there were no safety concerns for the liver in the trial data. The FDA issued a warning on September 12 about the risk for rare liver injury with fezolinetant, but the early signals that had been seen in fezolinetant data were not seen in these elinzanetant data.
The OASIS 1 and 2 trials enrolled postmenopausal women, aged 40-65 years, who had at least 50 moderate to severe vasomotor occurrences per week.
“A moderate hot flash is a hot flash that is also associated with sweating, and a severe hot flash is a moderate hot flash that stops a woman in her tracks,” Dr. Simon said. “Namely, it’s severe enough with sweating and central nervous system effects that she is interrupted in whatever it is that she’s doing at the time.”
Exclusion criteria for the trials included a history of arrhythmias, heart block, or QT prolongation; abnormal lab results; history of malignancy within the past 5 years; uncontrolled or treatment-resistant hypertension, hypothyroidism, or hyperthyroidism; unexplained postmenopausal bleeding; clinically relevant abnormal mammogram findings; or disordered proliferative endometrium, endometrial hyperplasia, polyp, or endometrial cancer.
The predominantly White (80%) women were an average 54 years old, with an average body mass index (BMI) of 27.8, and were an average 3.5 years from their last period. For the first 12 weeks of the trials, 399 women were assigned to receive 120 mg once daily of oral elinzanetant and 397 were assigned to once daily placebo. Then the women taking placebo switched to elinzanetant for the final 14 weeks of the study.
The endpoints included mean change in frequency and severity of vasomotor symptoms at weeks 1, 4, and 12 as well as change in sleep disturbance and quality of life at week 12. Sleep was assessed with the Patient-Reported Outcomes Measurement Information System Sleep Disturbance–Short Form score, which ranges from 28.9 to 76.5, with a higher number denoting greater sleep disturbance. The Menopause-Specific Quality-of-Life score ranges from 1 to 8, with a higher score indicating poorer quality of life.
Daily frequency of vasomotor symptoms was 14 per day at baseline in the elinzanetant group, decreasing by 4.8 per day at week 1, 8 per day at week 4, and 9.4 per day at week 12. In the placebo group, women had an average 15.2 occurrences per day at baseline, which decreased by 3.2 at week 1, 5.2 at week 4, and 6.4 at week 12. Comparing the groups at 12 weeks, those receiving elinzanetant had 3.2 fewer daily vasomotor symptoms than those receiving placebo (P < .0001).
The severity of vasomotor symptoms also improved more in the elinzanetant group than in the placebo group over 12 weeks, after which severity improved further in those who switched from placebo to elinzanetant (P < .0001).
Sleep disturbance scores, starting at a mean 61.5 in the elinzanetant group and 60.5 in the placebo group, fell 10.7 points in the elinzanetant group and 5.3 points in the placebo group at 12 weeks, for a difference of 4.9 points (P < .0001). Sleep then further improved in those who switched from placebo to elinzanetant. Quality-of-life scores improved 1.37 points (from 4.52 at baseline) in the elinzanetant group and 0.96 points (from 4.49 at baseline) in the placebo group, for a mean difference at 12 weeks of 0.36 (P < .0001).
Though no head-to-head data exist comparing elinzanetant and fezolinetant, Dr. Simon told this news organization the side effects with fezolinetant “tend to be gastrointestinal, whereas the side effects for elinzanetant tend to be central nervous system,” such as drowsiness and lethargy.
The women who are the best candidates for elinzanetant, Dr. Pinkerton told this news organization, include those who have had an estrogen-sensitive cancer, such as breast or endometrial cancer, or who have fear of it, a family history, or are otherwise high risk. Other ideal candidates include those with a history of venous thromboembolism, people who have migraine with aura (due to concerns about increased risk for stroke), and those who have endometriosis or large fibroids.
“Then the last group might be women who took hormone therapy in their 50s and want to continue, but they’re trying to go off, and they have a recurrence of their hot flashes or night sweats or sleep issues,” Dr. Pinkerton said. “This might be a great group to switch over.”
OASIS 3 assessed the drug for 1 year and “supported the results of OASIS 1 and 2, demonstrating efficacy over a longer study duration and in a population with a vasomotor symptom profile representative of that seen in clinical practice,” Nick Panay, BSc, MBBS, director of the Menopause & PMS Centre at Queen Charlotte’s Hospital & Imperial College London, London, England, and his colleague reported.
Among 628 postmenopausal women aged 40-65, the predominantly White (78.5%) women were an average 54 years old, with an average BMI of 27.6, and were an average 5 years past their last period. Half received 120 mg elinzanetant and half received a placebo for 52 weeks.
At 12 weeks, the women receiving elinzanetant reported an average 1.6 moderate to severe vasomotor symptoms per day, down from 6.7 at baseline. Daily average symptoms in the placebo group fell from 6.8 at baseline to 3.4 at 12 weeks, for a difference of 1.6 fewer occurrences per day in the elinzanetant group (P < .0001).
Sleep disturbances also improved, falling 9.4 points from a baseline 57.4 in the elinzanetant group and 5.7 points from a baseline 58 in the placebo group. Quality-of-life scores improved from 4.1 to 2.8 (−1.3 change) in the elinzanetant group and from 4.4 to 3.3 (−1.1 change) in the placebo group.
In addition to looking at treatment-emergent adverse events, the safety assessments also included endometrial biopsies; bone mineral density in the femoral neck, hip, and lumbar spine; weight; and labs. Adverse events related to the study drug occurred in 30.4% of those in the elinzanetant group and 14.6% of those in the placebo group. The most commonly reported adverse events were headache (9.6% elinzanetant vs 7% placebo), fatigue (7% vs 10.2%), and sleepiness (5.1% vs 1.3%). A higher proportion of women taking elinzanetant (12.5%) than those taking placebo (4.1%) discontinued the study.
No serious adverse events deemed to be treatment-related occurred in either group, and no endometrial hyperplasia or malignant neoplasm occurred in either group. Bone mineral density changes in both groups were within the expected range for the women’s age, and their weight remained stable over the 52 weeks.
Six women taking elinzanetant and four taking placebo met predefined criteria for close liver observation, but none showed hepatotoxicity or evidence of possible drug-induced liver injury.
The research was funded by Bayer. Dr. Pinkerton has run a trial funded by Bayer and is a consultant for Bayer and Pfizer. Dr. Shufelt had no disclosures. Dr. Simon had grant/research support, consulting/advisory board participation, and/or speaking disclosures with AbbVie, Bayer Healthcare, Besins Healthcare, California Institute of Integral Studies, Camargo Pharmaceutical Services, Covance, Daré Bioscience, DEKA M.E.L.A S.r.l., Femasys, Ipsen, KaNDy/NeRRe Therapeutics, Khyria, Madorra, Mayne Pharma, Mitsubishi Tanabe Pharma Development America, Mylan/Viatris Inc, Myovant Sciences, ObsEva SA, Pfizer, Pharmavite, QUE Oncology, Scynexis, Sebela Pharmaceuticals, Sprout Pharmaceuticals, TherapeuticsMD, Vella Bioscience, and Viveve Medical, and he is a stockholder in Sermonix Pharmaceuticals.
A version of this article first appeared on Medscape.com.
CHICAGO — The nonhormonal investigational drug elinzanetant led to significant improvement in hot flashes as well as sleep disturbance and quality of life, according to data from three randomized controlled trials presented at The Menopause Society 2024 Annual Meeting in Chicago. Two phase 3 trials, OASIS 1 and 2, were also published in JAMA, and the longer-term OASIS 3 trial was presented as a poster at the conference.
Elinzanetant is a selective neurokinin (NK) receptor antagonist, similar to fezolinetant, the first drug in this class approved by the US Food and Drug Administration (FDA) for vasomotor symptoms in May 2023. This class of medications targets the estrogen-sensitive kisspeptin/NK B/dynorphin (KNDy) neurons thought to play a role in thermoregulation and hot flashes during menopause. While fezolinetant targets only the NK-3 receptor, elinzanetant is a dual NK receptor antagonist that targets both NK-1 and NK-3. Bayer submitted a New Drug Application for elinzanetant to the FDA on August 1.
For those in whom hormone therapy is contraindicated, “it’s always been difficult for women with really severe symptoms to have a safe and effective therapy,” lead author JoAnn Pinkerton, MD, a professor of ob.gyn. at the University of Virginia in Charlottesville, Virginia, told this news organization. “The nonhormonal therapies we’ve used mostly off-label — the antidepressants, gabapentin, clonidine, oxybutynin — do help the hot flashes, but they don’t work nearly as effectively as these new NK receptor antagonists, and having one that looks like it might have a broader use for hot flashes, night sweats, mood, and sleep is just really exciting.”
Dr. Pinkerton said approximately 80% of the women in the OASIS 1 and 2 studies had at least a 50% reduction in hot flashes. “It was a very strong, dramatic positive finding, but the improvements in sleep and mood have really encouraged us to go further,” she said.
Declining estrogen levels during and after menopause can cause hypertrophy and hyperactivity of the KNDy neurons, which has been linked to thermoregulation disruptions that may trigger hot flashes, James Simon, MD, a clinical professor of ob.gyn. at The George Washington University School of Medicine & Health Sciences and medical director of IntimMedicine in Washington, DC, told attendees. He presented pooled data from OASIS 1 and 2. The NK-1 receptor, targeted by elinzanetant but not fezolinetant, is also thought to play a role in insomnia and possibly in mood.
“Oftentimes the focus on a lot of these drugs is hot flashes, hot flashes, hot flashes, but we know hot flashes do not occur in isolation,” Chrisandra Shufelt, MD, professor and chair of general internal medicine and associate director of the Women’s Health Research Center at Mayo Clinic in Jacksonville, Florida, told this news organization. Elinzanetant is “an interesting compound because it actually works on sleep, and that was critical because sleep disturbance precedes” many other menopausal symptoms, said Dr. Shufelt, who was not involved in the study.
“I think it is an outstanding option for women who don’t have the opportunity to get hormones,” Dr. Shufelt said, and she was particularly pleased to see there were no safety concerns for the liver in the trial data. The FDA issued a warning on September 12 about the risk for rare liver injury with fezolinetant, but the early signals that had been seen in fezolinetant data were not seen in these elinzanetant data.
The OASIS 1 and 2 trials enrolled postmenopausal women, aged 40-65 years, who had at least 50 moderate to severe vasomotor occurrences per week.
“A moderate hot flash is a hot flash that is also associated with sweating, and a severe hot flash is a moderate hot flash that stops a woman in her tracks,” Dr. Simon said. “Namely, it’s severe enough with sweating and central nervous system effects that she is interrupted in whatever it is that she’s doing at the time.”
Exclusion criteria for the trials included a history of arrhythmias, heart block, or QT prolongation; abnormal lab results; history of malignancy within the past 5 years; uncontrolled or treatment-resistant hypertension, hypothyroidism, or hyperthyroidism; unexplained postmenopausal bleeding; clinically relevant abnormal mammogram findings; or disordered proliferative endometrium, endometrial hyperplasia, polyp, or endometrial cancer.
The predominantly White (80%) women were an average 54 years old, with an average body mass index (BMI) of 27.8, and were an average 3.5 years from their last period. For the first 12 weeks of the trials, 399 women were assigned to receive 120 mg once daily of oral elinzanetant and 397 were assigned to once daily placebo. Then the women taking placebo switched to elinzanetant for the final 14 weeks of the study.
The endpoints included mean change in frequency and severity of vasomotor symptoms at weeks 1, 4, and 12 as well as change in sleep disturbance and quality of life at week 12. Sleep was assessed with the Patient-Reported Outcomes Measurement Information System Sleep Disturbance–Short Form score, which ranges from 28.9 to 76.5, with a higher number denoting greater sleep disturbance. The Menopause-Specific Quality-of-Life score ranges from 1 to 8, with a higher score indicating poorer quality of life.
Daily frequency of vasomotor symptoms was 14 per day at baseline in the elinzanetant group, decreasing by 4.8 per day at week 1, 8 per day at week 4, and 9.4 per day at week 12. In the placebo group, women had an average 15.2 occurrences per day at baseline, which decreased by 3.2 at week 1, 5.2 at week 4, and 6.4 at week 12. Comparing the groups at 12 weeks, those receiving elinzanetant had 3.2 fewer daily vasomotor symptoms than those receiving placebo (P < .0001).
The severity of vasomotor symptoms also improved more in the elinzanetant group than in the placebo group over 12 weeks, after which severity improved further in those who switched from placebo to elinzanetant (P < .0001).
Sleep disturbance scores, starting at a mean 61.5 in the elinzanetant group and 60.5 in the placebo group, fell 10.7 points in the elinzanetant group and 5.3 points in the placebo group at 12 weeks, for a difference of 4.9 points (P < .0001). Sleep then further improved in those who switched from placebo to elinzanetant. Quality-of-life scores improved 1.37 points (from 4.52 at baseline) in the elinzanetant group and 0.96 points (from 4.49 at baseline) in the placebo group, for a mean difference at 12 weeks of 0.36 (P < .0001).
Though no head-to-head data exist comparing elinzanetant and fezolinetant, Dr. Simon told this news organization the side effects with fezolinetant “tend to be gastrointestinal, whereas the side effects for elinzanetant tend to be central nervous system,” such as drowsiness and lethargy.
The women who are the best candidates for elinzanetant, Dr. Pinkerton told this news organization, include those who have had an estrogen-sensitive cancer, such as breast or endometrial cancer, or who have fear of it, a family history, or are otherwise high risk. Other ideal candidates include those with a history of venous thromboembolism, people who have migraine with aura (due to concerns about increased risk for stroke), and those who have endometriosis or large fibroids.
“Then the last group might be women who took hormone therapy in their 50s and want to continue, but they’re trying to go off, and they have a recurrence of their hot flashes or night sweats or sleep issues,” Dr. Pinkerton said. “This might be a great group to switch over.”
OASIS 3 assessed the drug for 1 year and “supported the results of OASIS 1 and 2, demonstrating efficacy over a longer study duration and in a population with a vasomotor symptom profile representative of that seen in clinical practice,” Nick Panay, BSc, MBBS, director of the Menopause & PMS Centre at Queen Charlotte’s Hospital & Imperial College London, London, England, and his colleague reported.
Among 628 postmenopausal women aged 40-65, the predominantly White (78.5%) women were an average 54 years old, with an average BMI of 27.6, and were an average 5 years past their last period. Half received 120 mg elinzanetant and half received a placebo for 52 weeks.
At 12 weeks, the women receiving elinzanetant reported an average 1.6 moderate to severe vasomotor symptoms per day, down from 6.7 at baseline. Daily average symptoms in the placebo group fell from 6.8 at baseline to 3.4 at 12 weeks, for a difference of 1.6 fewer occurrences per day in the elinzanetant group (P < .0001).
Sleep disturbances also improved, falling 9.4 points from a baseline 57.4 in the elinzanetant group and 5.7 points from a baseline 58 in the placebo group. Quality-of-life scores improved from 4.1 to 2.8 (−1.3 change) in the elinzanetant group and from 4.4 to 3.3 (−1.1 change) in the placebo group.
In addition to looking at treatment-emergent adverse events, the safety assessments also included endometrial biopsies; bone mineral density in the femoral neck, hip, and lumbar spine; weight; and labs. Adverse events related to the study drug occurred in 30.4% of those in the elinzanetant group and 14.6% of those in the placebo group. The most commonly reported adverse events were headache (9.6% elinzanetant vs 7% placebo), fatigue (7% vs 10.2%), and sleepiness (5.1% vs 1.3%). A higher proportion of women taking elinzanetant (12.5%) than those taking placebo (4.1%) discontinued the study.
No serious adverse events deemed to be treatment-related occurred in either group, and no endometrial hyperplasia or malignant neoplasm occurred in either group. Bone mineral density changes in both groups were within the expected range for the women’s age, and their weight remained stable over the 52 weeks.
Six women taking elinzanetant and four taking placebo met predefined criteria for close liver observation, but none showed hepatotoxicity or evidence of possible drug-induced liver injury.
The research was funded by Bayer. Dr. Pinkerton has run a trial funded by Bayer and is a consultant for Bayer and Pfizer. Dr. Shufelt had no disclosures. Dr. Simon had grant/research support, consulting/advisory board participation, and/or speaking disclosures with AbbVie, Bayer Healthcare, Besins Healthcare, California Institute of Integral Studies, Camargo Pharmaceutical Services, Covance, Daré Bioscience, DEKA M.E.L.A S.r.l., Femasys, Ipsen, KaNDy/NeRRe Therapeutics, Khyria, Madorra, Mayne Pharma, Mitsubishi Tanabe Pharma Development America, Mylan/Viatris Inc, Myovant Sciences, ObsEva SA, Pfizer, Pharmavite, QUE Oncology, Scynexis, Sebela Pharmaceuticals, Sprout Pharmaceuticals, TherapeuticsMD, Vella Bioscience, and Viveve Medical, and he is a stockholder in Sermonix Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM THE MENOPAUSE SOCIETY 2024
Environmental, Metabolic Factors Driving Global Rise in Stroke
Air pollution, high temperatures, and metabolic risk factors are driving global increases in stroke, contributing to 12 million cases and more than 7 million deaths from stroke each year, new data from the Global Burden of Disease (GBD) study showed.
Between 1990 and 2021, the number of people who experienced a stroke increased to 11.9 million (up by 70% since 1990), while the number of stroke survivors rose to 93.8 million (up by 86%), and stroke-related deaths rose to 7.3 million (up by 44%), making stroke the third leading cause of death worldwide after ischemic heart disease and COVID-19, investigators found.
Stroke is highly preventable, the investigators noted, with 84% of the stroke burden in 2021 attributable to 23 modifiable risk factors, including air pollution, excess body weight, high blood pressure, smoking, and physical inactivity.
This means there are “tremendous opportunities to alter the trajectory of stroke risk for the next generation,” Catherine O. Johnson, MPH, PhD, co-author and lead research scientist at the Institute for Health Metrics and Evaluation (IHME), University of Washington, Seattle, said in a news release.
The study was published online in The Lancet Neurology.
Top Risk Factor for Subarachnoid Hemorrhage
Since 1990, the contribution of high temperatures to poor health and early death due to stroke has risen 72%, a trend likely to increase in the future — underscoring the impact of environmental factors on the growing stroke burden, the authors said.
“Given that ambient air pollution is reciprocally linked with ambient temperature and climate change, the importance of urgent climate actions and measures to reduce air pollution cannot be overestimated,” Dr. Johnson said.
Mitchell S.V. Elkind, MD, MS, chief clinical science officer for the American Heart Association, who wasn’t involved in the study, told this news organization that environmental factors such as air pollution, particulate matter from wildfires and other sources, and excessive heat are now recognized as major contributors to the risk for stroke. “This should not be surprising as we have long recognized the risks of stroke associated with toxins in cigarette smoke, which likely share mechanisms for vascular damage with pollutants,” Dr. Elkind said.
The data also reveal for the first time that ambient particulate matter air pollution is a top risk factor for subarachnoid hemorrhage, contributing to 14% of the death and disability caused by this serious stroke subtype, on a par with smoking.
Dr. Elkind noted that smoking is “a major risk factor for subarachnoid hemorrhage. It makes sense that particulate air pollution would therefore similarly be a risk factor for subarachnoid hemorrhage, which similarly damages blood vessels. Prior studies were likely too small or did not assess the role of air pollution in subarachnoid hemorrhage.”
The analysis also showed substantial increases between 1990 and 2021 in the global stroke burden linked to high body mass index (up by 88%), high blood sugar (up 32%), a diet high in sugar-sweetened drinks (up 23%), low physical activity (up 11%), high systolic blood pressure (up 7%), and a diet low in omega-6 polyunsaturated fatty acids (up 5%).
“And with increasing exposure to risk factors such as high blood sugar and diet high in sugar-sweetened drinks, there is a critical need for interventions focused on obesity and metabolic syndromes,” Dr. Johnson said.
“Identifying sustainable ways to work with communities to take action to prevent and control modifiable risk factors for stroke is essential to address this growing crisis,” she added.
Prevention Strategies Fall Short
The data also showed that stroke-related disability-adjusted life-years rose from around 121.4 million years of healthy life lost in 1990 to 160.5 million years in 2021, making stroke the fourth leading cause of health loss worldwide after COVID-19, ischemic heart disease, and neonatal disorders.
“The global growth of the number of people who develop stroke and died from or remain disabled by stroke is growing fast, strongly suggesting that currently used stroke prevention strategies are not sufficiently effective,” lead author Valery L. Feigin, MD, PhD, from Auckland University of Technology, Auckland, New Zealand, and affiliate professor at IHME, said in the release.
“New, proven effective population-wide and motivational individual prevention strategies that could be applied to all people at risk of having a stroke, regardless of the level of risk, as recommended in the recent Lancet Neurology Commission on Stroke should be implemented across the globe urgently,” said Dr. Feigin.
Dr. Elkind said the AHA supports research on the effects of air quality on risk for vascular injury and stroke and has “long advocated for policies to mitigate the adverse health impacts of air pollutants, including reduction of vehicle emissions and renewable portfolio standards, taking into account racial, ethnic, and economic disparities.”
“AHA, and the healthcare sector more broadly, must take a leadership role in recommending policies to improve environmental air quality and in working with the private sector and industry to improve air quality,” Dr. Elkind said.
In an accompanying commentary, Ming Liu, MD, and Simiao Wu, MD, PhD, West China Hospital, Sichuan University, Chengdu, China, wrote that “pragmatic solutions to the enormous and increasing stroke burden include surveillance, prevention, acute care, and rehabilitation.”
“Surveillance strategies include establishing a national-level framework for regular monitoring of stroke burden, risk factors, and healthcare services via community-based surveys and health records,” they noted.
“Artificial intelligence and mobile technologies might not only facilitate the dissemination of evidence-based health services but also increase the number of data sources and encourage participation of multidisciplinary collaborators, potentially improving the validity and accuracy of future GBD estimates,” they added.
This study was funded by the Bill & Melinda Gates Foundation. Author disclosures are listed with the original article.
A version of this article first appeared on Medscape.com.
Air pollution, high temperatures, and metabolic risk factors are driving global increases in stroke, contributing to 12 million cases and more than 7 million deaths from stroke each year, new data from the Global Burden of Disease (GBD) study showed.
Between 1990 and 2021, the number of people who experienced a stroke increased to 11.9 million (up by 70% since 1990), while the number of stroke survivors rose to 93.8 million (up by 86%), and stroke-related deaths rose to 7.3 million (up by 44%), making stroke the third leading cause of death worldwide after ischemic heart disease and COVID-19, investigators found.
Stroke is highly preventable, the investigators noted, with 84% of the stroke burden in 2021 attributable to 23 modifiable risk factors, including air pollution, excess body weight, high blood pressure, smoking, and physical inactivity.
This means there are “tremendous opportunities to alter the trajectory of stroke risk for the next generation,” Catherine O. Johnson, MPH, PhD, co-author and lead research scientist at the Institute for Health Metrics and Evaluation (IHME), University of Washington, Seattle, said in a news release.
The study was published online in The Lancet Neurology.
Top Risk Factor for Subarachnoid Hemorrhage
Since 1990, the contribution of high temperatures to poor health and early death due to stroke has risen 72%, a trend likely to increase in the future — underscoring the impact of environmental factors on the growing stroke burden, the authors said.
“Given that ambient air pollution is reciprocally linked with ambient temperature and climate change, the importance of urgent climate actions and measures to reduce air pollution cannot be overestimated,” Dr. Johnson said.
Mitchell S.V. Elkind, MD, MS, chief clinical science officer for the American Heart Association, who wasn’t involved in the study, told this news organization that environmental factors such as air pollution, particulate matter from wildfires and other sources, and excessive heat are now recognized as major contributors to the risk for stroke. “This should not be surprising as we have long recognized the risks of stroke associated with toxins in cigarette smoke, which likely share mechanisms for vascular damage with pollutants,” Dr. Elkind said.
The data also reveal for the first time that ambient particulate matter air pollution is a top risk factor for subarachnoid hemorrhage, contributing to 14% of the death and disability caused by this serious stroke subtype, on a par with smoking.
Dr. Elkind noted that smoking is “a major risk factor for subarachnoid hemorrhage. It makes sense that particulate air pollution would therefore similarly be a risk factor for subarachnoid hemorrhage, which similarly damages blood vessels. Prior studies were likely too small or did not assess the role of air pollution in subarachnoid hemorrhage.”
The analysis also showed substantial increases between 1990 and 2021 in the global stroke burden linked to high body mass index (up by 88%), high blood sugar (up 32%), a diet high in sugar-sweetened drinks (up 23%), low physical activity (up 11%), high systolic blood pressure (up 7%), and a diet low in omega-6 polyunsaturated fatty acids (up 5%).
“And with increasing exposure to risk factors such as high blood sugar and diet high in sugar-sweetened drinks, there is a critical need for interventions focused on obesity and metabolic syndromes,” Dr. Johnson said.
“Identifying sustainable ways to work with communities to take action to prevent and control modifiable risk factors for stroke is essential to address this growing crisis,” she added.
Prevention Strategies Fall Short
The data also showed that stroke-related disability-adjusted life-years rose from around 121.4 million years of healthy life lost in 1990 to 160.5 million years in 2021, making stroke the fourth leading cause of health loss worldwide after COVID-19, ischemic heart disease, and neonatal disorders.
“The global growth of the number of people who develop stroke and died from or remain disabled by stroke is growing fast, strongly suggesting that currently used stroke prevention strategies are not sufficiently effective,” lead author Valery L. Feigin, MD, PhD, from Auckland University of Technology, Auckland, New Zealand, and affiliate professor at IHME, said in the release.
“New, proven effective population-wide and motivational individual prevention strategies that could be applied to all people at risk of having a stroke, regardless of the level of risk, as recommended in the recent Lancet Neurology Commission on Stroke should be implemented across the globe urgently,” said Dr. Feigin.
Dr. Elkind said the AHA supports research on the effects of air quality on risk for vascular injury and stroke and has “long advocated for policies to mitigate the adverse health impacts of air pollutants, including reduction of vehicle emissions and renewable portfolio standards, taking into account racial, ethnic, and economic disparities.”
“AHA, and the healthcare sector more broadly, must take a leadership role in recommending policies to improve environmental air quality and in working with the private sector and industry to improve air quality,” Dr. Elkind said.
In an accompanying commentary, Ming Liu, MD, and Simiao Wu, MD, PhD, West China Hospital, Sichuan University, Chengdu, China, wrote that “pragmatic solutions to the enormous and increasing stroke burden include surveillance, prevention, acute care, and rehabilitation.”
“Surveillance strategies include establishing a national-level framework for regular monitoring of stroke burden, risk factors, and healthcare services via community-based surveys and health records,” they noted.
“Artificial intelligence and mobile technologies might not only facilitate the dissemination of evidence-based health services but also increase the number of data sources and encourage participation of multidisciplinary collaborators, potentially improving the validity and accuracy of future GBD estimates,” they added.
This study was funded by the Bill & Melinda Gates Foundation. Author disclosures are listed with the original article.
A version of this article first appeared on Medscape.com.
Air pollution, high temperatures, and metabolic risk factors are driving global increases in stroke, contributing to 12 million cases and more than 7 million deaths from stroke each year, new data from the Global Burden of Disease (GBD) study showed.
Between 1990 and 2021, the number of people who experienced a stroke increased to 11.9 million (up by 70% since 1990), while the number of stroke survivors rose to 93.8 million (up by 86%), and stroke-related deaths rose to 7.3 million (up by 44%), making stroke the third leading cause of death worldwide after ischemic heart disease and COVID-19, investigators found.
Stroke is highly preventable, the investigators noted, with 84% of the stroke burden in 2021 attributable to 23 modifiable risk factors, including air pollution, excess body weight, high blood pressure, smoking, and physical inactivity.
This means there are “tremendous opportunities to alter the trajectory of stroke risk for the next generation,” Catherine O. Johnson, MPH, PhD, co-author and lead research scientist at the Institute for Health Metrics and Evaluation (IHME), University of Washington, Seattle, said in a news release.
The study was published online in The Lancet Neurology.
Top Risk Factor for Subarachnoid Hemorrhage
Since 1990, the contribution of high temperatures to poor health and early death due to stroke has risen 72%, a trend likely to increase in the future — underscoring the impact of environmental factors on the growing stroke burden, the authors said.
“Given that ambient air pollution is reciprocally linked with ambient temperature and climate change, the importance of urgent climate actions and measures to reduce air pollution cannot be overestimated,” Dr. Johnson said.
Mitchell S.V. Elkind, MD, MS, chief clinical science officer for the American Heart Association, who wasn’t involved in the study, told this news organization that environmental factors such as air pollution, particulate matter from wildfires and other sources, and excessive heat are now recognized as major contributors to the risk for stroke. “This should not be surprising as we have long recognized the risks of stroke associated with toxins in cigarette smoke, which likely share mechanisms for vascular damage with pollutants,” Dr. Elkind said.
The data also reveal for the first time that ambient particulate matter air pollution is a top risk factor for subarachnoid hemorrhage, contributing to 14% of the death and disability caused by this serious stroke subtype, on a par with smoking.
Dr. Elkind noted that smoking is “a major risk factor for subarachnoid hemorrhage. It makes sense that particulate air pollution would therefore similarly be a risk factor for subarachnoid hemorrhage, which similarly damages blood vessels. Prior studies were likely too small or did not assess the role of air pollution in subarachnoid hemorrhage.”
The analysis also showed substantial increases between 1990 and 2021 in the global stroke burden linked to high body mass index (up by 88%), high blood sugar (up 32%), a diet high in sugar-sweetened drinks (up 23%), low physical activity (up 11%), high systolic blood pressure (up 7%), and a diet low in omega-6 polyunsaturated fatty acids (up 5%).
“And with increasing exposure to risk factors such as high blood sugar and diet high in sugar-sweetened drinks, there is a critical need for interventions focused on obesity and metabolic syndromes,” Dr. Johnson said.
“Identifying sustainable ways to work with communities to take action to prevent and control modifiable risk factors for stroke is essential to address this growing crisis,” she added.
Prevention Strategies Fall Short
The data also showed that stroke-related disability-adjusted life-years rose from around 121.4 million years of healthy life lost in 1990 to 160.5 million years in 2021, making stroke the fourth leading cause of health loss worldwide after COVID-19, ischemic heart disease, and neonatal disorders.
“The global growth of the number of people who develop stroke and died from or remain disabled by stroke is growing fast, strongly suggesting that currently used stroke prevention strategies are not sufficiently effective,” lead author Valery L. Feigin, MD, PhD, from Auckland University of Technology, Auckland, New Zealand, and affiliate professor at IHME, said in the release.
“New, proven effective population-wide and motivational individual prevention strategies that could be applied to all people at risk of having a stroke, regardless of the level of risk, as recommended in the recent Lancet Neurology Commission on Stroke should be implemented across the globe urgently,” said Dr. Feigin.
Dr. Elkind said the AHA supports research on the effects of air quality on risk for vascular injury and stroke and has “long advocated for policies to mitigate the adverse health impacts of air pollutants, including reduction of vehicle emissions and renewable portfolio standards, taking into account racial, ethnic, and economic disparities.”
“AHA, and the healthcare sector more broadly, must take a leadership role in recommending policies to improve environmental air quality and in working with the private sector and industry to improve air quality,” Dr. Elkind said.
In an accompanying commentary, Ming Liu, MD, and Simiao Wu, MD, PhD, West China Hospital, Sichuan University, Chengdu, China, wrote that “pragmatic solutions to the enormous and increasing stroke burden include surveillance, prevention, acute care, and rehabilitation.”
“Surveillance strategies include establishing a national-level framework for regular monitoring of stroke burden, risk factors, and healthcare services via community-based surveys and health records,” they noted.
“Artificial intelligence and mobile technologies might not only facilitate the dissemination of evidence-based health services but also increase the number of data sources and encourage participation of multidisciplinary collaborators, potentially improving the validity and accuracy of future GBD estimates,” they added.
This study was funded by the Bill & Melinda Gates Foundation. Author disclosures are listed with the original article.
A version of this article first appeared on Medscape.com.
Black Women Have a Higher Risk for Death in BC Subtypes
TOPLINE:
The greatest disparity in BC-specific survival was observed in those with hormone receptor-positive (HR+), human epidermal growth factor 2–negative (HER2−) tumors, with Black women having a 50% higher risk for death.
METHODOLOGY:
- US Black women have a 40% higher risk for death from BC than White women, and many cancer specialists believe that disparities are worse among more treatable subtypes, such as HR+ tumors.
- Researchers conducted a systematic review and meta-analysis of 18 US studies published during 2009-2022 that included 228,885 women (34,262 Black women; 182,466 White women) and examined racial differences in BC survival by subtype.
- The analysis included hormone receptor and HER2/neu status to define subtypes: HR+ HER2+, HR+ HER2−, HR− HER2+, and HR− HER2−.
- Random-effects models were used to generate pooled relative risks and 95% CI for BC-specific survival and overall survival.
- The primary outcome was BC-specific survival, with overall survival as a secondary analysis.
TAKEAWAY:
- Black women had a higher risk for BC death across all tumor subtypes than White women, with the greatest disparity observed in HR+ HER2− tumors (hazard ratio [HR], 1.50; 95% CI, 1.30-1.72).
- The risk for BC death was also higher for Black women with HR+ HER2+ tumors (HR, 1.34; 95% CI, 1.10-1.64); HR− HER2+ tumors (HR, 1.20; 95% CI, 1.00-1.43); and HR− HER2− tumors (HR, 1.17; 95% CI, 1.10-1.25).
- Overall survival was poorer for Black women across all subtypes, although estimates for HR− HER2+ tumors did not reach statistical significance.
- In analysis of two subtypes with significant heterogeneity among studies, adjustments for socioeconomic status and number of Black participants explained about half and all the variance for HR+ HER2− and HR− HER2+ tumors, respectively.
IN PRACTICE:
“These results suggest there are both subtype-specific and subtype-independent mechanisms that contribute to disparities in breast cancer survival between Black and White women, which require multilevel interventions to address and achieve health equity,” wrote the authors.
SOURCE:
The study was led by Juliana M. Torres, Dana-Farber/Harvard Cancer Center, CURE Program, Boston. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
The study’s limitations included potential heterogeneity between studies as indicated by significant heterogeneity in some analyses. The use of different subtype definitions and potential overlap in data sets may have also affected the results. Many included studies did not capture the extent to which treatments were completed or detection and treatment of recurrences. Additionally, the study’s findings may not fully capture socioeconomic inequality and other unmeasured factors contributing to disparities. The racial and ethnic disparities analysis focused only on Black and White women.
DISCLOSURES:
Individual authors disclosed financial relationships with Pfizer, Healthix, Merck, AstraZeneca, LabCorp, and Takeda. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
TOPLINE:
The greatest disparity in BC-specific survival was observed in those with hormone receptor-positive (HR+), human epidermal growth factor 2–negative (HER2−) tumors, with Black women having a 50% higher risk for death.
METHODOLOGY:
- US Black women have a 40% higher risk for death from BC than White women, and many cancer specialists believe that disparities are worse among more treatable subtypes, such as HR+ tumors.
- Researchers conducted a systematic review and meta-analysis of 18 US studies published during 2009-2022 that included 228,885 women (34,262 Black women; 182,466 White women) and examined racial differences in BC survival by subtype.
- The analysis included hormone receptor and HER2/neu status to define subtypes: HR+ HER2+, HR+ HER2−, HR− HER2+, and HR− HER2−.
- Random-effects models were used to generate pooled relative risks and 95% CI for BC-specific survival and overall survival.
- The primary outcome was BC-specific survival, with overall survival as a secondary analysis.
TAKEAWAY:
- Black women had a higher risk for BC death across all tumor subtypes than White women, with the greatest disparity observed in HR+ HER2− tumors (hazard ratio [HR], 1.50; 95% CI, 1.30-1.72).
- The risk for BC death was also higher for Black women with HR+ HER2+ tumors (HR, 1.34; 95% CI, 1.10-1.64); HR− HER2+ tumors (HR, 1.20; 95% CI, 1.00-1.43); and HR− HER2− tumors (HR, 1.17; 95% CI, 1.10-1.25).
- Overall survival was poorer for Black women across all subtypes, although estimates for HR− HER2+ tumors did not reach statistical significance.
- In analysis of two subtypes with significant heterogeneity among studies, adjustments for socioeconomic status and number of Black participants explained about half and all the variance for HR+ HER2− and HR− HER2+ tumors, respectively.
IN PRACTICE:
“These results suggest there are both subtype-specific and subtype-independent mechanisms that contribute to disparities in breast cancer survival between Black and White women, which require multilevel interventions to address and achieve health equity,” wrote the authors.
SOURCE:
The study was led by Juliana M. Torres, Dana-Farber/Harvard Cancer Center, CURE Program, Boston. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
The study’s limitations included potential heterogeneity between studies as indicated by significant heterogeneity in some analyses. The use of different subtype definitions and potential overlap in data sets may have also affected the results. Many included studies did not capture the extent to which treatments were completed or detection and treatment of recurrences. Additionally, the study’s findings may not fully capture socioeconomic inequality and other unmeasured factors contributing to disparities. The racial and ethnic disparities analysis focused only on Black and White women.
DISCLOSURES:
Individual authors disclosed financial relationships with Pfizer, Healthix, Merck, AstraZeneca, LabCorp, and Takeda. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
TOPLINE:
The greatest disparity in BC-specific survival was observed in those with hormone receptor-positive (HR+), human epidermal growth factor 2–negative (HER2−) tumors, with Black women having a 50% higher risk for death.
METHODOLOGY:
- US Black women have a 40% higher risk for death from BC than White women, and many cancer specialists believe that disparities are worse among more treatable subtypes, such as HR+ tumors.
- Researchers conducted a systematic review and meta-analysis of 18 US studies published during 2009-2022 that included 228,885 women (34,262 Black women; 182,466 White women) and examined racial differences in BC survival by subtype.
- The analysis included hormone receptor and HER2/neu status to define subtypes: HR+ HER2+, HR+ HER2−, HR− HER2+, and HR− HER2−.
- Random-effects models were used to generate pooled relative risks and 95% CI for BC-specific survival and overall survival.
- The primary outcome was BC-specific survival, with overall survival as a secondary analysis.
TAKEAWAY:
- Black women had a higher risk for BC death across all tumor subtypes than White women, with the greatest disparity observed in HR+ HER2− tumors (hazard ratio [HR], 1.50; 95% CI, 1.30-1.72).
- The risk for BC death was also higher for Black women with HR+ HER2+ tumors (HR, 1.34; 95% CI, 1.10-1.64); HR− HER2+ tumors (HR, 1.20; 95% CI, 1.00-1.43); and HR− HER2− tumors (HR, 1.17; 95% CI, 1.10-1.25).
- Overall survival was poorer for Black women across all subtypes, although estimates for HR− HER2+ tumors did not reach statistical significance.
- In analysis of two subtypes with significant heterogeneity among studies, adjustments for socioeconomic status and number of Black participants explained about half and all the variance for HR+ HER2− and HR− HER2+ tumors, respectively.
IN PRACTICE:
“These results suggest there are both subtype-specific and subtype-independent mechanisms that contribute to disparities in breast cancer survival between Black and White women, which require multilevel interventions to address and achieve health equity,” wrote the authors.
SOURCE:
The study was led by Juliana M. Torres, Dana-Farber/Harvard Cancer Center, CURE Program, Boston. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
The study’s limitations included potential heterogeneity between studies as indicated by significant heterogeneity in some analyses. The use of different subtype definitions and potential overlap in data sets may have also affected the results. Many included studies did not capture the extent to which treatments were completed or detection and treatment of recurrences. Additionally, the study’s findings may not fully capture socioeconomic inequality and other unmeasured factors contributing to disparities. The racial and ethnic disparities analysis focused only on Black and White women.
DISCLOSURES:
Individual authors disclosed financial relationships with Pfizer, Healthix, Merck, AstraZeneca, LabCorp, and Takeda. Additional disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article appeared on Medscape.com.
Trial Looks at Early Use of Mycophenolate to Reduce Flares, Nephritis
Early use of mycophenolate mofetil (MMF), a drug used to dampen the immune system in organ transplant recipients, may reduce the risk for severe flares in patients with newly diagnosed systemic lupus erythematosus (SLE), according to results from a randomized, open-label, observer-blinded clinical trial.
In interviews, two SLE specialists who were not involved with the study said the research is preliminary but promising. However, another specialist criticized the paper’s reliance on unusual doses of prednisone and MMF, saying it “puts people on a treatment regimen that nobody ever uses.”

The Lupus Foundation of America estimates that about 16,000 people in the United States are diagnosed with lupus each year. “Our current treatment paradigm is to go pretty slowly and start treatment for new-onset, mild SLE with glucocorticoids, if necessary, and hydroxychloroquine,” said Karen H. Costenbader, MD, MPH, of Harvard Medical School and Harvard School of Public Health, Boston, Massachusetts.
Stronger immunosuppressive agents may be added as patients progress, she said.
Off-label use of MMF, which is approved by the Food and Drug Administration only for patients with certain organ transplants, may be appropriate in some cases, she said. “There is a big push to start immunosuppressives earlier, but we currently would reserve mycophenolate for those with severe manifestations — lupus nephritis; vasculitis; or lung, brain, or heart inflammation.”
In the trial, adult patients who received oral prednisone (starting at 0.5 mg/kg per day) and hydroxychloroquine sulfate (5 mg/kg per day) plus MMF (500 mg twice daily) for 96 weeks were less likely to develop severe flares than those who took the regimen without MMF (relative risk [RR], 0.39; 95% CI, 0.17-0.87; P = .01). Severe flares occurred in 10.8% of the MMF group (7 of 65 patients) and in 27.7% of the control group (18 of 65), Yijun You, MD, of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, and colleagues reported in JAMA Network Open.
Patients in the MMF group also had 89% lower risk for lupus nephritis than those in the control group (RR, 0.11; 95% CI, 0.01-0.85; P = .008), with kidney involvement occurring in 1.5% (1 of 65) vs 13.8% (9 of 65).
During 2018-2021, researchers recruited 130 patients in China aged 18-65 years with newly diagnosed SLE, a high titer of anti–double-stranded DNA (dsDNA) antibodies, and no major organ involvement (mean age, 34.5 years; 86.2% women). Patients’ initial 0.5–mg/kg per day prednisone dose was maintained for 4 weeks, then tapered by 5.0 mg every 2 weeks, and when the dose had been reduced to 20.0 mg/day, it was tapered by 5 mg every month and then gradually to 0.1-0.2 mg/kg per day. If patients had severe flares, they stopped taking MMF. (The study authors did not respond to requests for comment on the study.)
‘A Treatment Regimen That Nobody Ever Uses’
While Dr. Costenbader called the study “very interesting” and said “every person diagnosing or taking care of patients with lupus should be familiar” with it, she noted that the prednisone doses were high. “I am wondering why they used quite so much glucocorticoid for everyone. This may have masked some of the MMF effect and biased toward the null. They also used a low dose of MMF and did not ramp it up as we would normally to a full dose. That being said, it is remarkable that it was well-tolerated and resulted in better outcomes over the period of the trial.”
Daniel J. Wallace, MD, of Cedars-Sinai Medical Center, Los Angeles, California, and the University of California, Los Angeles, also highlighted the high doses of prednisone and low doses of MMF. “It’s a useless paper that puts people on a treatment regimen that nobody ever uses,” he said.
The rates of mild to moderate flares were similar between the control and intervention groups (38.5% vs 36.9%, respectively; RR, 0.96; P = .90). This finding is surprising, said Judith A. James, MD, PhD, executive vice president, chief medical officer, and head of the rheumatology clinic and Arthritis and Clinical Immunology Research Program at the Oklahoma Medical Research Foundation in Oklahoma City and also the Associate Vice Provost of Clinical & Translational Science, professor of medicine, and George Lynn Cross Research Professor at the University of Oklahoma Health Sciences Center in Oklahoma City. “It may be that mild flares have a different mechanism or are caused by noninflammatory endotypes that don’t respond to MMF.”
Dr. Costenbader noted that a risk-benefit analysis will need to be done to take the risks of MMF into account. “However, every time that a person flares or is not in lupus low-disease activity state, potentially permanent organ damage is done and the patient suffers,” she said. “Preventing lupus nephritis de novo was also seen — nine cases potentially prevented — and that is also really interesting. It would be amazing if we could completely avoid that life-threatening complication.”
MMF can cause miscarriage and boost the risk for birth defects, and the manufacturer says it can lower the effectiveness of birth control pills. It can also boost the risk for some cancers such as lymphoma and increase the risk for infections.
Surprisingly, the number of adverse events in the control and intervention groups were similar (35.4% vs 46.2%, respectively; RR, 1.30; 95% CI, 0.86-1.99; P = .20). They included infection (30.8% vs 33.8%, respectively; P = .70) and gastrointestinal tract events (16.9% for both; P > .99).
“There were overall pretty similar rates of side effects, but maybe this was because MMF dose was pretty low in the treated group, or the glucocorticoid dose was not so low in both groups,” Dr. Costenbader said. She also noted that “the risk of malignancy with MMF is longer term than this study. It may not show up for 5-10 or even more years, but we know it exists. Infections are also increased with MMF — some of which can be avoided with vaccines for COVID, pneumonia, influenza, shingles, etc. MMF also causes gastrointestinal intolerance, and people often are not able to take it because of nausea, vomiting, diarrhea, and elevated liver function tests.”
Dr. James said the infection rates “may be due to the higher doses of steroids patients in both groups are on for several months at the beginning of the study.”
A total of 12 patients in the MMF group discontinued the intervention for various reasons, and 6 were lost to follow-up. In the control group, 20 discontinued the intervention and two were lost to follow-up. However, all 130 patients in the trial were included in the primary and secondary outcome analyses.
Should clinicians consider prescribing MMF to patients with new-onset SLE? “We usually wait until later when there are indications of more severe disease, but here they started it from the time of diagnosis if the patient was anti-dsDNA positive. Given insurance restrictions in this country, we would be unlikely to be able to do that for many patients,” Dr. Costenbader said. “They likely also overtreated a lot of patients who didn’t need it. Due to our lack of more specific biomarkers and precision medicine for lupus, we do currently undertreat a lot of patients, as this study highlights, as well as overtreat others.”
How Much Might Cost Factor Into Treatment Decisions?
The study did not examine cost. Prednisone and hydroxychloroquine sulfate are inexpensive, but Dr. James said MMF can cost about $450 a month at the study dosage. However, “the average hospitalization without an ICU [intensive care unit] visit for an SLE patient is about $15,000-$20,000. If you can avoid one hospitalization, you can pay for nearly 4 years of MMF. More importantly, from a financial perspective, if you can convert a severe lupus patient to a mild/moderate lupus patient, then the annual costs of lupus decrease nearly by half, from about $52,000 per year to $25,000 per year.”
The study authors noted various limitations such as the small number of subjects, the need for a longer trial “to determine the advantages and disadvantages of early application of MMF,” and the fact that all subjects were Asian. The authors also called for confirmation via a double-blind, placebo-controlled study.
The study was funded by grants to the authors by the National Natural Science Foundation of China, Shanghai Rising-Star Program, Natural Science Foundation of Shanghai, Five-Year National Key R&D Program, and Ruijin–Zhongmei Huadong Lupus Funding. The authors had no disclosures. Dr. Costenbader disclosed consulting/research collaboration relationships with AstraZeneca, Amgen, Biogen, Bristol-Myers Squibb, GSK, Merck, Gilead, and Cabaletta. Dr. James and Dr. Wallace had no disclosures.
A version of this article first appeared on Medscape.com.
Early use of mycophenolate mofetil (MMF), a drug used to dampen the immune system in organ transplant recipients, may reduce the risk for severe flares in patients with newly diagnosed systemic lupus erythematosus (SLE), according to results from a randomized, open-label, observer-blinded clinical trial.
In interviews, two SLE specialists who were not involved with the study said the research is preliminary but promising. However, another specialist criticized the paper’s reliance on unusual doses of prednisone and MMF, saying it “puts people on a treatment regimen that nobody ever uses.”
The Lupus Foundation of America estimates that about 16,000 people in the United States are diagnosed with lupus each year. “Our current treatment paradigm is to go pretty slowly and start treatment for new-onset, mild SLE with glucocorticoids, if necessary, and hydroxychloroquine,” said Karen H. Costenbader, MD, MPH, of Harvard Medical School and Harvard School of Public Health, Boston, Massachusetts.
Stronger immunosuppressive agents may be added as patients progress, she said.
Off-label use of MMF, which is approved by the Food and Drug Administration only for patients with certain organ transplants, may be appropriate in some cases, she said. “There is a big push to start immunosuppressives earlier, but we currently would reserve mycophenolate for those with severe manifestations — lupus nephritis; vasculitis; or lung, brain, or heart inflammation.”
In the trial, adult patients who received oral prednisone (starting at 0.5 mg/kg per day) and hydroxychloroquine sulfate (5 mg/kg per day) plus MMF (500 mg twice daily) for 96 weeks were less likely to develop severe flares than those who took the regimen without MMF (relative risk [RR], 0.39; 95% CI, 0.17-0.87; P = .01). Severe flares occurred in 10.8% of the MMF group (7 of 65 patients) and in 27.7% of the control group (18 of 65), Yijun You, MD, of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, and colleagues reported in JAMA Network Open.
Patients in the MMF group also had 89% lower risk for lupus nephritis than those in the control group (RR, 0.11; 95% CI, 0.01-0.85; P = .008), with kidney involvement occurring in 1.5% (1 of 65) vs 13.8% (9 of 65).
During 2018-2021, researchers recruited 130 patients in China aged 18-65 years with newly diagnosed SLE, a high titer of anti–double-stranded DNA (dsDNA) antibodies, and no major organ involvement (mean age, 34.5 years; 86.2% women). Patients’ initial 0.5–mg/kg per day prednisone dose was maintained for 4 weeks, then tapered by 5.0 mg every 2 weeks, and when the dose had been reduced to 20.0 mg/day, it was tapered by 5 mg every month and then gradually to 0.1-0.2 mg/kg per day. If patients had severe flares, they stopped taking MMF. (The study authors did not respond to requests for comment on the study.)
‘A Treatment Regimen That Nobody Ever Uses’
While Dr. Costenbader called the study “very interesting” and said “every person diagnosing or taking care of patients with lupus should be familiar” with it, she noted that the prednisone doses were high. “I am wondering why they used quite so much glucocorticoid for everyone. This may have masked some of the MMF effect and biased toward the null. They also used a low dose of MMF and did not ramp it up as we would normally to a full dose. That being said, it is remarkable that it was well-tolerated and resulted in better outcomes over the period of the trial.”
Daniel J. Wallace, MD, of Cedars-Sinai Medical Center, Los Angeles, California, and the University of California, Los Angeles, also highlighted the high doses of prednisone and low doses of MMF. “It’s a useless paper that puts people on a treatment regimen that nobody ever uses,” he said.
The rates of mild to moderate flares were similar between the control and intervention groups (38.5% vs 36.9%, respectively; RR, 0.96; P = .90). This finding is surprising, said Judith A. James, MD, PhD, executive vice president, chief medical officer, and head of the rheumatology clinic and Arthritis and Clinical Immunology Research Program at the Oklahoma Medical Research Foundation in Oklahoma City and also the Associate Vice Provost of Clinical & Translational Science, professor of medicine, and George Lynn Cross Research Professor at the University of Oklahoma Health Sciences Center in Oklahoma City. “It may be that mild flares have a different mechanism or are caused by noninflammatory endotypes that don’t respond to MMF.”
Dr. Costenbader noted that a risk-benefit analysis will need to be done to take the risks of MMF into account. “However, every time that a person flares or is not in lupus low-disease activity state, potentially permanent organ damage is done and the patient suffers,” she said. “Preventing lupus nephritis de novo was also seen — nine cases potentially prevented — and that is also really interesting. It would be amazing if we could completely avoid that life-threatening complication.”
MMF can cause miscarriage and boost the risk for birth defects, and the manufacturer says it can lower the effectiveness of birth control pills. It can also boost the risk for some cancers such as lymphoma and increase the risk for infections.
Surprisingly, the number of adverse events in the control and intervention groups were similar (35.4% vs 46.2%, respectively; RR, 1.30; 95% CI, 0.86-1.99; P = .20). They included infection (30.8% vs 33.8%, respectively; P = .70) and gastrointestinal tract events (16.9% for both; P > .99).
“There were overall pretty similar rates of side effects, but maybe this was because MMF dose was pretty low in the treated group, or the glucocorticoid dose was not so low in both groups,” Dr. Costenbader said. She also noted that “the risk of malignancy with MMF is longer term than this study. It may not show up for 5-10 or even more years, but we know it exists. Infections are also increased with MMF — some of which can be avoided with vaccines for COVID, pneumonia, influenza, shingles, etc. MMF also causes gastrointestinal intolerance, and people often are not able to take it because of nausea, vomiting, diarrhea, and elevated liver function tests.”
Dr. James said the infection rates “may be due to the higher doses of steroids patients in both groups are on for several months at the beginning of the study.”
A total of 12 patients in the MMF group discontinued the intervention for various reasons, and 6 were lost to follow-up. In the control group, 20 discontinued the intervention and two were lost to follow-up. However, all 130 patients in the trial were included in the primary and secondary outcome analyses.
Should clinicians consider prescribing MMF to patients with new-onset SLE? “We usually wait until later when there are indications of more severe disease, but here they started it from the time of diagnosis if the patient was anti-dsDNA positive. Given insurance restrictions in this country, we would be unlikely to be able to do that for many patients,” Dr. Costenbader said. “They likely also overtreated a lot of patients who didn’t need it. Due to our lack of more specific biomarkers and precision medicine for lupus, we do currently undertreat a lot of patients, as this study highlights, as well as overtreat others.”
How Much Might Cost Factor Into Treatment Decisions?
The study did not examine cost. Prednisone and hydroxychloroquine sulfate are inexpensive, but Dr. James said MMF can cost about $450 a month at the study dosage. However, “the average hospitalization without an ICU [intensive care unit] visit for an SLE patient is about $15,000-$20,000. If you can avoid one hospitalization, you can pay for nearly 4 years of MMF. More importantly, from a financial perspective, if you can convert a severe lupus patient to a mild/moderate lupus patient, then the annual costs of lupus decrease nearly by half, from about $52,000 per year to $25,000 per year.”
The study authors noted various limitations such as the small number of subjects, the need for a longer trial “to determine the advantages and disadvantages of early application of MMF,” and the fact that all subjects were Asian. The authors also called for confirmation via a double-blind, placebo-controlled study.
The study was funded by grants to the authors by the National Natural Science Foundation of China, Shanghai Rising-Star Program, Natural Science Foundation of Shanghai, Five-Year National Key R&D Program, and Ruijin–Zhongmei Huadong Lupus Funding. The authors had no disclosures. Dr. Costenbader disclosed consulting/research collaboration relationships with AstraZeneca, Amgen, Biogen, Bristol-Myers Squibb, GSK, Merck, Gilead, and Cabaletta. Dr. James and Dr. Wallace had no disclosures.
A version of this article first appeared on Medscape.com.
Early use of mycophenolate mofetil (MMF), a drug used to dampen the immune system in organ transplant recipients, may reduce the risk for severe flares in patients with newly diagnosed systemic lupus erythematosus (SLE), according to results from a randomized, open-label, observer-blinded clinical trial.
In interviews, two SLE specialists who were not involved with the study said the research is preliminary but promising. However, another specialist criticized the paper’s reliance on unusual doses of prednisone and MMF, saying it “puts people on a treatment regimen that nobody ever uses.”
The Lupus Foundation of America estimates that about 16,000 people in the United States are diagnosed with lupus each year. “Our current treatment paradigm is to go pretty slowly and start treatment for new-onset, mild SLE with glucocorticoids, if necessary, and hydroxychloroquine,” said Karen H. Costenbader, MD, MPH, of Harvard Medical School and Harvard School of Public Health, Boston, Massachusetts.
Stronger immunosuppressive agents may be added as patients progress, she said.
Off-label use of MMF, which is approved by the Food and Drug Administration only for patients with certain organ transplants, may be appropriate in some cases, she said. “There is a big push to start immunosuppressives earlier, but we currently would reserve mycophenolate for those with severe manifestations — lupus nephritis; vasculitis; or lung, brain, or heart inflammation.”
In the trial, adult patients who received oral prednisone (starting at 0.5 mg/kg per day) and hydroxychloroquine sulfate (5 mg/kg per day) plus MMF (500 mg twice daily) for 96 weeks were less likely to develop severe flares than those who took the regimen without MMF (relative risk [RR], 0.39; 95% CI, 0.17-0.87; P = .01). Severe flares occurred in 10.8% of the MMF group (7 of 65 patients) and in 27.7% of the control group (18 of 65), Yijun You, MD, of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, and colleagues reported in JAMA Network Open.
Patients in the MMF group also had 89% lower risk for lupus nephritis than those in the control group (RR, 0.11; 95% CI, 0.01-0.85; P = .008), with kidney involvement occurring in 1.5% (1 of 65) vs 13.8% (9 of 65).
During 2018-2021, researchers recruited 130 patients in China aged 18-65 years with newly diagnosed SLE, a high titer of anti–double-stranded DNA (dsDNA) antibodies, and no major organ involvement (mean age, 34.5 years; 86.2% women). Patients’ initial 0.5–mg/kg per day prednisone dose was maintained for 4 weeks, then tapered by 5.0 mg every 2 weeks, and when the dose had been reduced to 20.0 mg/day, it was tapered by 5 mg every month and then gradually to 0.1-0.2 mg/kg per day. If patients had severe flares, they stopped taking MMF. (The study authors did not respond to requests for comment on the study.)
‘A Treatment Regimen That Nobody Ever Uses’
While Dr. Costenbader called the study “very interesting” and said “every person diagnosing or taking care of patients with lupus should be familiar” with it, she noted that the prednisone doses were high. “I am wondering why they used quite so much glucocorticoid for everyone. This may have masked some of the MMF effect and biased toward the null. They also used a low dose of MMF and did not ramp it up as we would normally to a full dose. That being said, it is remarkable that it was well-tolerated and resulted in better outcomes over the period of the trial.”
Daniel J. Wallace, MD, of Cedars-Sinai Medical Center, Los Angeles, California, and the University of California, Los Angeles, also highlighted the high doses of prednisone and low doses of MMF. “It’s a useless paper that puts people on a treatment regimen that nobody ever uses,” he said.
The rates of mild to moderate flares were similar between the control and intervention groups (38.5% vs 36.9%, respectively; RR, 0.96; P = .90). This finding is surprising, said Judith A. James, MD, PhD, executive vice president, chief medical officer, and head of the rheumatology clinic and Arthritis and Clinical Immunology Research Program at the Oklahoma Medical Research Foundation in Oklahoma City and also the Associate Vice Provost of Clinical & Translational Science, professor of medicine, and George Lynn Cross Research Professor at the University of Oklahoma Health Sciences Center in Oklahoma City. “It may be that mild flares have a different mechanism or are caused by noninflammatory endotypes that don’t respond to MMF.”
Dr. Costenbader noted that a risk-benefit analysis will need to be done to take the risks of MMF into account. “However, every time that a person flares or is not in lupus low-disease activity state, potentially permanent organ damage is done and the patient suffers,” she said. “Preventing lupus nephritis de novo was also seen — nine cases potentially prevented — and that is also really interesting. It would be amazing if we could completely avoid that life-threatening complication.”
MMF can cause miscarriage and boost the risk for birth defects, and the manufacturer says it can lower the effectiveness of birth control pills. It can also boost the risk for some cancers such as lymphoma and increase the risk for infections.
Surprisingly, the number of adverse events in the control and intervention groups were similar (35.4% vs 46.2%, respectively; RR, 1.30; 95% CI, 0.86-1.99; P = .20). They included infection (30.8% vs 33.8%, respectively; P = .70) and gastrointestinal tract events (16.9% for both; P > .99).
“There were overall pretty similar rates of side effects, but maybe this was because MMF dose was pretty low in the treated group, or the glucocorticoid dose was not so low in both groups,” Dr. Costenbader said. She also noted that “the risk of malignancy with MMF is longer term than this study. It may not show up for 5-10 or even more years, but we know it exists. Infections are also increased with MMF — some of which can be avoided with vaccines for COVID, pneumonia, influenza, shingles, etc. MMF also causes gastrointestinal intolerance, and people often are not able to take it because of nausea, vomiting, diarrhea, and elevated liver function tests.”
Dr. James said the infection rates “may be due to the higher doses of steroids patients in both groups are on for several months at the beginning of the study.”
A total of 12 patients in the MMF group discontinued the intervention for various reasons, and 6 were lost to follow-up. In the control group, 20 discontinued the intervention and two were lost to follow-up. However, all 130 patients in the trial were included in the primary and secondary outcome analyses.
Should clinicians consider prescribing MMF to patients with new-onset SLE? “We usually wait until later when there are indications of more severe disease, but here they started it from the time of diagnosis if the patient was anti-dsDNA positive. Given insurance restrictions in this country, we would be unlikely to be able to do that for many patients,” Dr. Costenbader said. “They likely also overtreated a lot of patients who didn’t need it. Due to our lack of more specific biomarkers and precision medicine for lupus, we do currently undertreat a lot of patients, as this study highlights, as well as overtreat others.”
How Much Might Cost Factor Into Treatment Decisions?
The study did not examine cost. Prednisone and hydroxychloroquine sulfate are inexpensive, but Dr. James said MMF can cost about $450 a month at the study dosage. However, “the average hospitalization without an ICU [intensive care unit] visit for an SLE patient is about $15,000-$20,000. If you can avoid one hospitalization, you can pay for nearly 4 years of MMF. More importantly, from a financial perspective, if you can convert a severe lupus patient to a mild/moderate lupus patient, then the annual costs of lupus decrease nearly by half, from about $52,000 per year to $25,000 per year.”
The study authors noted various limitations such as the small number of subjects, the need for a longer trial “to determine the advantages and disadvantages of early application of MMF,” and the fact that all subjects were Asian. The authors also called for confirmation via a double-blind, placebo-controlled study.
The study was funded by grants to the authors by the National Natural Science Foundation of China, Shanghai Rising-Star Program, Natural Science Foundation of Shanghai, Five-Year National Key R&D Program, and Ruijin–Zhongmei Huadong Lupus Funding. The authors had no disclosures. Dr. Costenbader disclosed consulting/research collaboration relationships with AstraZeneca, Amgen, Biogen, Bristol-Myers Squibb, GSK, Merck, Gilead, and Cabaletta. Dr. James and Dr. Wallace had no disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Inspection of Deep Tumor Margins for Accurate Cutaneous Squamous Cell Carcinoma Staging
To the Editor:
Histopathologic analysis of debulk specimens in Mohs micrographic surgery (MMS) may augment identification of high-risk factors in cutaneous squamous cell carcinoma (cSCC), which may warrant tumor upstaging.1 Intratumor location has not been studied when looking at these high-risk factors. Herein, we report 4 cSCCs initially categorized as well differentiated that were reclassified as moderate to poorly differentiated on analysis of debulk specimens obtained via shave removal.
An 80-year-old man (patient 1) presented with a tender 2-cm erythematous plaque with dried hemorrhagic crusting on the frontal scalp. He had a history of nonmelanoma skin cancers. A biopsy revealed a well-differentiated cSCC, which was upgraded from a T2a tumor to T2b during MMS due to galea involvement. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells at the deep margin (Figure 1A). Given T2b staging, baseline imaging and radiation therapy were recommended.
A 75-year-old man (patient 2) presented with a 2-cm erythematous plaque on the left vertex scalp with hemorrhagic crusting, yellow scale, and purulent drainage. He had a history of cSCCs. A biopsy revealed well-differentiated invasive cSCC, which was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Examination of the second Mohs stage revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, infiltration beyond the subcutaneous fat, and perineural invasion (Figure 1B). Given T2b staging, baseline imaging and radiation therapy were recommended.
An 86-year-old woman (patient 3) presented with a tender 2.4-cm plum-colored nodule on the right lower leg. She had a history of basal cell carcinoma. A biopsy revealed a well-differentiated invasive cSCC staged at T2a. Debulk analysis revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, though the staging remained the same (Figure 1C).
An 82-year-old man (patient 4) presented with a 2.7-cm ulcerated nodule with adjacent scaling on the vertex scalp. He had no history of skin cancer. A biopsy revealed a well-differentiated cSCC (Figure 2) that was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells with single-cell extension at the deep margin in the galea (Figure 1D). Given T2b staging, baseline imaging and radiation therapy were recommended.
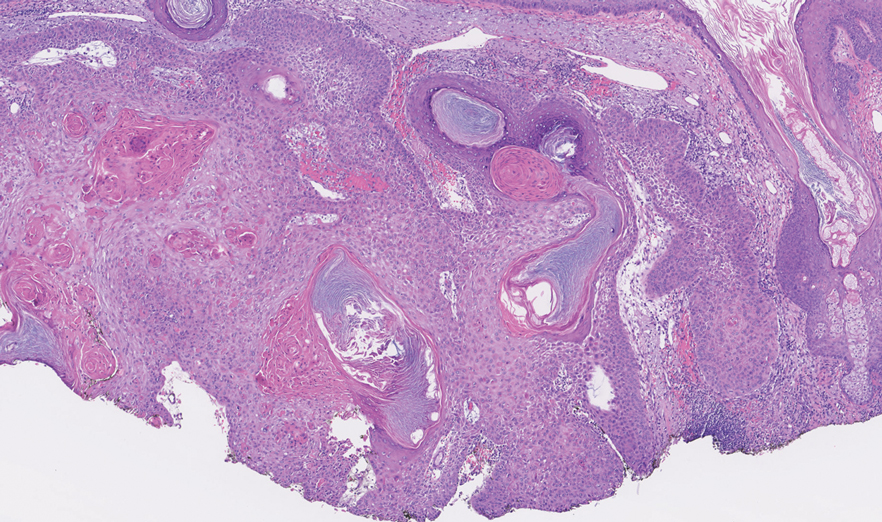
Tumor differentiation is a factor included in the Brigham and Women’s Hospital staging system, and intratumor variability can be clinically relevant for tumor staging.1 Specifically, cSCCs may exhibit intratumor heterogeneity in which predominantly well-differentiated tumors contain focal areas of poorer differentiation.2 This intratumor heterogeneity complicates estimation of tumor risk, as a well-differentiated tumor on biopsy may exhibit poor differentiation at a deeper margin. Our cases highlight that the cells at the deeper margin indeed can show poorer differentiation or other higher-risk tumor features. Thus, the most clinically relevant cells for tumor staging and prognostication may not be visible on initial biopsy, underscoring the utility of close examination of the deep layer of the debulk specimen and Mohs layer for comprehensive staging.
Genetic studies have attempted to identify gene expression patterns in cSCCs that predispose to invasion.3 Three of the top 6 genes in this “invasion signature gene set” were matrix metalloproteases; additionally, IL-24 messenger RNA was upregulated in both the cSCC invasion front and in situ cSCCs. IL-24 has been shown to upregulate the expression of matrix metalloprotease 7 in vitro, suggesting that it may influence tumor progression.3 Although gene expression was not included in this series, the identification of genetic variability in the most poorly differentiated cells residing in the deep margins is of great interest and may reveal mutations contributing to irregular cell morphology and cSCC invasiveness.
Prior studies have indicated that a proportion of cSCCs are histopathologically upgraded from the initial biopsy during MMS due to evidence of perineural invasion, bony invasion, or lesser differentiation noted during MMS stages or debulk analysis.1,4 However, the majority of Mohs surgeons report immediately discarding debulk specimens without further evaluation.5 Herein, we highlight 4 cSCC cases in which the deep margins of the debulk specimen contained the most dedifferentiated cells. Our findings emphasize the importance of thoroughly examining deep tumor margins for complete staging yet also highlight that identifying cells at these margins may not change patient management when high-risk criteria are already met.
- McIlwee BE, Abidi NY, Ravi M, et al. Utility of debulk specimens during Mohs micrographic surgery for cutaneous squamous cell carcinoma. Dermatol Surg. 2021;47:599-604.
- Ramón y Cajal S, Sesé M, Capdevila C, et al. Clinical implications of intratumor heterogeneity: challenges and opportunities. J Mol Med. 2020;98:161-177.
- Mitsui H, Suárez-Fariñas M, Gulati N, et al. Gene expression profiling of the leading edge of cutaneous squamous cell carcinoma: IL-24-driven MMP-7. J Invest Dermatol. 2014;134:1418-1427.
- Chung E, Hoang S, McEvoy AM, et al. Histopathologic upgrading of cutaneous squamous cell carcinomas during Mohs micrographic surgery: a retrospective cohort study. J Am Acad Dermatol. 2021;85:923-930.
- Alniemi DT, Swanson AM, Lasarev M, et al. Tumor debulking trends for keratinocyte carcinomas among Mohs surgeons. Dermatol Surg. 2021;47:1660-1661.
To the Editor:
Histopathologic analysis of debulk specimens in Mohs micrographic surgery (MMS) may augment identification of high-risk factors in cutaneous squamous cell carcinoma (cSCC), which may warrant tumor upstaging.1 Intratumor location has not been studied when looking at these high-risk factors. Herein, we report 4 cSCCs initially categorized as well differentiated that were reclassified as moderate to poorly differentiated on analysis of debulk specimens obtained via shave removal.
An 80-year-old man (patient 1) presented with a tender 2-cm erythematous plaque with dried hemorrhagic crusting on the frontal scalp. He had a history of nonmelanoma skin cancers. A biopsy revealed a well-differentiated cSCC, which was upgraded from a T2a tumor to T2b during MMS due to galea involvement. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells at the deep margin (Figure 1A). Given T2b staging, baseline imaging and radiation therapy were recommended.
A 75-year-old man (patient 2) presented with a 2-cm erythematous plaque on the left vertex scalp with hemorrhagic crusting, yellow scale, and purulent drainage. He had a history of cSCCs. A biopsy revealed well-differentiated invasive cSCC, which was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Examination of the second Mohs stage revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, infiltration beyond the subcutaneous fat, and perineural invasion (Figure 1B). Given T2b staging, baseline imaging and radiation therapy were recommended.
An 86-year-old woman (patient 3) presented with a tender 2.4-cm plum-colored nodule on the right lower leg. She had a history of basal cell carcinoma. A biopsy revealed a well-differentiated invasive cSCC staged at T2a. Debulk analysis revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, though the staging remained the same (Figure 1C).
An 82-year-old man (patient 4) presented with a 2.7-cm ulcerated nodule with adjacent scaling on the vertex scalp. He had no history of skin cancer. A biopsy revealed a well-differentiated cSCC (Figure 2) that was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells with single-cell extension at the deep margin in the galea (Figure 1D). Given T2b staging, baseline imaging and radiation therapy were recommended.
Tumor differentiation is a factor included in the Brigham and Women’s Hospital staging system, and intratumor variability can be clinically relevant for tumor staging.1 Specifically, cSCCs may exhibit intratumor heterogeneity in which predominantly well-differentiated tumors contain focal areas of poorer differentiation.2 This intratumor heterogeneity complicates estimation of tumor risk, as a well-differentiated tumor on biopsy may exhibit poor differentiation at a deeper margin. Our cases highlight that the cells at the deeper margin indeed can show poorer differentiation or other higher-risk tumor features. Thus, the most clinically relevant cells for tumor staging and prognostication may not be visible on initial biopsy, underscoring the utility of close examination of the deep layer of the debulk specimen and Mohs layer for comprehensive staging.
Genetic studies have attempted to identify gene expression patterns in cSCCs that predispose to invasion.3 Three of the top 6 genes in this “invasion signature gene set” were matrix metalloproteases; additionally, IL-24 messenger RNA was upregulated in both the cSCC invasion front and in situ cSCCs. IL-24 has been shown to upregulate the expression of matrix metalloprotease 7 in vitro, suggesting that it may influence tumor progression.3 Although gene expression was not included in this series, the identification of genetic variability in the most poorly differentiated cells residing in the deep margins is of great interest and may reveal mutations contributing to irregular cell morphology and cSCC invasiveness.
Prior studies have indicated that a proportion of cSCCs are histopathologically upgraded from the initial biopsy during MMS due to evidence of perineural invasion, bony invasion, or lesser differentiation noted during MMS stages or debulk analysis.1,4 However, the majority of Mohs surgeons report immediately discarding debulk specimens without further evaluation.5 Herein, we highlight 4 cSCC cases in which the deep margins of the debulk specimen contained the most dedifferentiated cells. Our findings emphasize the importance of thoroughly examining deep tumor margins for complete staging yet also highlight that identifying cells at these margins may not change patient management when high-risk criteria are already met.
To the Editor:
Histopathologic analysis of debulk specimens in Mohs micrographic surgery (MMS) may augment identification of high-risk factors in cutaneous squamous cell carcinoma (cSCC), which may warrant tumor upstaging.1 Intratumor location has not been studied when looking at these high-risk factors. Herein, we report 4 cSCCs initially categorized as well differentiated that were reclassified as moderate to poorly differentiated on analysis of debulk specimens obtained via shave removal.
An 80-year-old man (patient 1) presented with a tender 2-cm erythematous plaque with dried hemorrhagic crusting on the frontal scalp. He had a history of nonmelanoma skin cancers. A biopsy revealed a well-differentiated cSCC, which was upgraded from a T2a tumor to T2b during MMS due to galea involvement. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells at the deep margin (Figure 1A). Given T2b staging, baseline imaging and radiation therapy were recommended.
A 75-year-old man (patient 2) presented with a 2-cm erythematous plaque on the left vertex scalp with hemorrhagic crusting, yellow scale, and purulent drainage. He had a history of cSCCs. A biopsy revealed well-differentiated invasive cSCC, which was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Examination of the second Mohs stage revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, infiltration beyond the subcutaneous fat, and perineural invasion (Figure 1B). Given T2b staging, baseline imaging and radiation therapy were recommended.
An 86-year-old woman (patient 3) presented with a tender 2.4-cm plum-colored nodule on the right lower leg. She had a history of basal cell carcinoma. A biopsy revealed a well-differentiated invasive cSCC staged at T2a. Debulk analysis revealed moderately differentiated cSCC, with the least-differentiated cells at the deep margin, though the staging remained the same (Figure 1C).
An 82-year-old man (patient 4) presented with a 2.7-cm ulcerated nodule with adjacent scaling on the vertex scalp. He had no history of skin cancer. A biopsy revealed a well-differentiated cSCC (Figure 2) that was upgraded from a T2a tumor to T2b during MMS due to tumor extension beyond the subcutaneous fat. Debulk analysis revealed moderate to poorly differentiated cSCC, with the least-differentiated cells with single-cell extension at the deep margin in the galea (Figure 1D). Given T2b staging, baseline imaging and radiation therapy were recommended.
Tumor differentiation is a factor included in the Brigham and Women’s Hospital staging system, and intratumor variability can be clinically relevant for tumor staging.1 Specifically, cSCCs may exhibit intratumor heterogeneity in which predominantly well-differentiated tumors contain focal areas of poorer differentiation.2 This intratumor heterogeneity complicates estimation of tumor risk, as a well-differentiated tumor on biopsy may exhibit poor differentiation at a deeper margin. Our cases highlight that the cells at the deeper margin indeed can show poorer differentiation or other higher-risk tumor features. Thus, the most clinically relevant cells for tumor staging and prognostication may not be visible on initial biopsy, underscoring the utility of close examination of the deep layer of the debulk specimen and Mohs layer for comprehensive staging.
Genetic studies have attempted to identify gene expression patterns in cSCCs that predispose to invasion.3 Three of the top 6 genes in this “invasion signature gene set” were matrix metalloproteases; additionally, IL-24 messenger RNA was upregulated in both the cSCC invasion front and in situ cSCCs. IL-24 has been shown to upregulate the expression of matrix metalloprotease 7 in vitro, suggesting that it may influence tumor progression.3 Although gene expression was not included in this series, the identification of genetic variability in the most poorly differentiated cells residing in the deep margins is of great interest and may reveal mutations contributing to irregular cell morphology and cSCC invasiveness.
Prior studies have indicated that a proportion of cSCCs are histopathologically upgraded from the initial biopsy during MMS due to evidence of perineural invasion, bony invasion, or lesser differentiation noted during MMS stages or debulk analysis.1,4 However, the majority of Mohs surgeons report immediately discarding debulk specimens without further evaluation.5 Herein, we highlight 4 cSCC cases in which the deep margins of the debulk specimen contained the most dedifferentiated cells. Our findings emphasize the importance of thoroughly examining deep tumor margins for complete staging yet also highlight that identifying cells at these margins may not change patient management when high-risk criteria are already met.
- McIlwee BE, Abidi NY, Ravi M, et al. Utility of debulk specimens during Mohs micrographic surgery for cutaneous squamous cell carcinoma. Dermatol Surg. 2021;47:599-604.
- Ramón y Cajal S, Sesé M, Capdevila C, et al. Clinical implications of intratumor heterogeneity: challenges and opportunities. J Mol Med. 2020;98:161-177.
- Mitsui H, Suárez-Fariñas M, Gulati N, et al. Gene expression profiling of the leading edge of cutaneous squamous cell carcinoma: IL-24-driven MMP-7. J Invest Dermatol. 2014;134:1418-1427.
- Chung E, Hoang S, McEvoy AM, et al. Histopathologic upgrading of cutaneous squamous cell carcinomas during Mohs micrographic surgery: a retrospective cohort study. J Am Acad Dermatol. 2021;85:923-930.
- Alniemi DT, Swanson AM, Lasarev M, et al. Tumor debulking trends for keratinocyte carcinomas among Mohs surgeons. Dermatol Surg. 2021;47:1660-1661.
- McIlwee BE, Abidi NY, Ravi M, et al. Utility of debulk specimens during Mohs micrographic surgery for cutaneous squamous cell carcinoma. Dermatol Surg. 2021;47:599-604.
- Ramón y Cajal S, Sesé M, Capdevila C, et al. Clinical implications of intratumor heterogeneity: challenges and opportunities. J Mol Med. 2020;98:161-177.
- Mitsui H, Suárez-Fariñas M, Gulati N, et al. Gene expression profiling of the leading edge of cutaneous squamous cell carcinoma: IL-24-driven MMP-7. J Invest Dermatol. 2014;134:1418-1427.
- Chung E, Hoang S, McEvoy AM, et al. Histopathologic upgrading of cutaneous squamous cell carcinomas during Mohs micrographic surgery: a retrospective cohort study. J Am Acad Dermatol. 2021;85:923-930.
- Alniemi DT, Swanson AM, Lasarev M, et al. Tumor debulking trends for keratinocyte carcinomas among Mohs surgeons. Dermatol Surg. 2021;47:1660-1661.
Practice Points
- A proportion of cutaneous squamous cell carcinomas are upgraded from the initial biopsy during Mohs micrographic surgery due to evidence of perineural invasion, bony invasion, or lesser differentiation noted on Mohs stages or debulk analysis.
- Thorough inspection of the deep tumor margins may be required for accurate tumor staging and evaluation of metastatic risk. Cells at the deep margin of the tumor may demonstrate poorer differentiation and/or other higher-risk tumor features than those closer to the surface.
- Tumor staging may be incomplete until the deep margins are assessed to find the most dysplastic and likely clinically relevant cells, which may be missed without evaluation of the debulked tumor.