User login
Are You Using the Correct Medication or a Look-Alike?
Five years have passed since the member states of the World Health Organization (WHO) gathered at the 72nd World Health Assembly and decided that September 17 should be recognized as World Patient Safety Day, acknowledging it as a global health priority.
WHO data indicate the following findings related to medical safety:
- One in 10 patients is harmed while receiving healthcare, and 3 million die as a result.
- More than half of these incidents could be prevented.
- Indirect costs could amount to several billion US dollars annually.
Given the magnitude of preventable harm related to medication use, in 2017, the WHO launched the third Global Patient Safety Challenge: Medication Without Harm with the goal of reducing serious and preventable harm related to medication by 50%. In addition, considering the volume of medication packages prescribed in 2023 by physicians in Spain’s National Health System, it is necessary to understand the most common types of medication errors to provide an effective and efficient response.
According to Spain’s Institute for Safe Medication Practices (ISMP), the 10 types of medication errors detected in 2020 with the most serious consequences were the following:
- Errors due to omission or delay in medication.
- Administration of medication to the wrong patient.
- Errors related to allergies or known adverse effects of medications.
- Dosing errors in pediatric patients.
- Errors due to similarities in the labeling or packaging of marketed medications.
- Errors associated with the lack of use of smart infusion pumps.
- Errors due to accidental administration of neuromuscular blocking agents.
- Incorrect intravenous administration of oral liquid medications.
- Errors in medication reconciliation upon hospital admission and discharge.
- Errors due to patient misunderstandings regarding medication use.
I would like to focus on the fifth item, errors due to similarities in the labeling or packaging of marketed medications.
Medications with similar names or with similar labeling or packaging are known as “look alike–sound alike” medications. They are estimated to account for between 6.2% and 14.7% of all medication errors. Confusion can arise due to spelling and phonetic similarities.
As shown in bulletin no. 50 of the ISMP, difficulties in distinguishing different medications or different presentations of the same medication due to similar packaging and labeling have frequently been associated with reported incidents.
Most cases involve either medications marketed by the same laboratory with a design based on brand image or different medications marketed by different laboratories in screen-printed ampoules used in the same settings.
In 2020, the ISMP published 11 new cases of labeling or packaging that may promote errors on its website. It reported 49 incidents to the Spanish Agency for Medicines and Medical Devices.
Shortages caused by the COVID-19 pandemic have further contributed to these incidents, as healthcare facilities sometimes had to change the medications they usually acquired and purchase whatever was available, without being able to select products that would not be confused with existing medications in the facility.
The ISMP recommends the following general practices for healthcare institutions, professionals, and patients to prevent these errors:
- Develop short lists of easily confused medication names and distribute them among all healthcare professionals.
- Prioritize medication names by active ingredient instead of brand name.
- For similar names, highlight the differences in capital letters, eg, DOBUTamine, DOPamine.
- For similar active ingredients, use brand names.
- Avoid placing similar medications near each other.
- Prescribe all medications electronically to minimize the risk of selecting the wrong medication.
- Make manual prescriptions legible, with clearly written dosages and pharmaceutical forms.
- Encourage patients to actively participate in their treatment and consult a clinician if they have any questions about the medications they are receiving.
- Raise awareness among patients, family members, and caregivers about the issues caused by medication name confusion and inform them about how to avoid these errors.
- Instruct patients to focus on and always use the active ingredient name as an identifying element for the medications they are taking.
- Review treatments with patients to ensure they know the medications they are taking.
Julia María Ruiz Redondo is the regional nursing advisor inspector of Spanish Society of General and Family Physicians of Castilla-La Mancha (SEMG-CLM), coordinator of the National Working Group on Public Health in the SEMG, and director of the international public health master’s degree at TECH Technological University. This article is the result of an editorial collaboration between the SEMG and Univadis, which you can access here.
This story was translated from Univadis Spain, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Five years have passed since the member states of the World Health Organization (WHO) gathered at the 72nd World Health Assembly and decided that September 17 should be recognized as World Patient Safety Day, acknowledging it as a global health priority.
WHO data indicate the following findings related to medical safety:
- One in 10 patients is harmed while receiving healthcare, and 3 million die as a result.
- More than half of these incidents could be prevented.
- Indirect costs could amount to several billion US dollars annually.
Given the magnitude of preventable harm related to medication use, in 2017, the WHO launched the third Global Patient Safety Challenge: Medication Without Harm with the goal of reducing serious and preventable harm related to medication by 50%. In addition, considering the volume of medication packages prescribed in 2023 by physicians in Spain’s National Health System, it is necessary to understand the most common types of medication errors to provide an effective and efficient response.
According to Spain’s Institute for Safe Medication Practices (ISMP), the 10 types of medication errors detected in 2020 with the most serious consequences were the following:
- Errors due to omission or delay in medication.
- Administration of medication to the wrong patient.
- Errors related to allergies or known adverse effects of medications.
- Dosing errors in pediatric patients.
- Errors due to similarities in the labeling or packaging of marketed medications.
- Errors associated with the lack of use of smart infusion pumps.
- Errors due to accidental administration of neuromuscular blocking agents.
- Incorrect intravenous administration of oral liquid medications.
- Errors in medication reconciliation upon hospital admission and discharge.
- Errors due to patient misunderstandings regarding medication use.
I would like to focus on the fifth item, errors due to similarities in the labeling or packaging of marketed medications.
Medications with similar names or with similar labeling or packaging are known as “look alike–sound alike” medications. They are estimated to account for between 6.2% and 14.7% of all medication errors. Confusion can arise due to spelling and phonetic similarities.
As shown in bulletin no. 50 of the ISMP, difficulties in distinguishing different medications or different presentations of the same medication due to similar packaging and labeling have frequently been associated with reported incidents.
Most cases involve either medications marketed by the same laboratory with a design based on brand image or different medications marketed by different laboratories in screen-printed ampoules used in the same settings.
In 2020, the ISMP published 11 new cases of labeling or packaging that may promote errors on its website. It reported 49 incidents to the Spanish Agency for Medicines and Medical Devices.
Shortages caused by the COVID-19 pandemic have further contributed to these incidents, as healthcare facilities sometimes had to change the medications they usually acquired and purchase whatever was available, without being able to select products that would not be confused with existing medications in the facility.
The ISMP recommends the following general practices for healthcare institutions, professionals, and patients to prevent these errors:
- Develop short lists of easily confused medication names and distribute them among all healthcare professionals.
- Prioritize medication names by active ingredient instead of brand name.
- For similar names, highlight the differences in capital letters, eg, DOBUTamine, DOPamine.
- For similar active ingredients, use brand names.
- Avoid placing similar medications near each other.
- Prescribe all medications electronically to minimize the risk of selecting the wrong medication.
- Make manual prescriptions legible, with clearly written dosages and pharmaceutical forms.
- Encourage patients to actively participate in their treatment and consult a clinician if they have any questions about the medications they are receiving.
- Raise awareness among patients, family members, and caregivers about the issues caused by medication name confusion and inform them about how to avoid these errors.
- Instruct patients to focus on and always use the active ingredient name as an identifying element for the medications they are taking.
- Review treatments with patients to ensure they know the medications they are taking.
Julia María Ruiz Redondo is the regional nursing advisor inspector of Spanish Society of General and Family Physicians of Castilla-La Mancha (SEMG-CLM), coordinator of the National Working Group on Public Health in the SEMG, and director of the international public health master’s degree at TECH Technological University. This article is the result of an editorial collaboration between the SEMG and Univadis, which you can access here.
This story was translated from Univadis Spain, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Five years have passed since the member states of the World Health Organization (WHO) gathered at the 72nd World Health Assembly and decided that September 17 should be recognized as World Patient Safety Day, acknowledging it as a global health priority.
WHO data indicate the following findings related to medical safety:
- One in 10 patients is harmed while receiving healthcare, and 3 million die as a result.
- More than half of these incidents could be prevented.
- Indirect costs could amount to several billion US dollars annually.
Given the magnitude of preventable harm related to medication use, in 2017, the WHO launched the third Global Patient Safety Challenge: Medication Without Harm with the goal of reducing serious and preventable harm related to medication by 50%. In addition, considering the volume of medication packages prescribed in 2023 by physicians in Spain’s National Health System, it is necessary to understand the most common types of medication errors to provide an effective and efficient response.
According to Spain’s Institute for Safe Medication Practices (ISMP), the 10 types of medication errors detected in 2020 with the most serious consequences were the following:
- Errors due to omission or delay in medication.
- Administration of medication to the wrong patient.
- Errors related to allergies or known adverse effects of medications.
- Dosing errors in pediatric patients.
- Errors due to similarities in the labeling or packaging of marketed medications.
- Errors associated with the lack of use of smart infusion pumps.
- Errors due to accidental administration of neuromuscular blocking agents.
- Incorrect intravenous administration of oral liquid medications.
- Errors in medication reconciliation upon hospital admission and discharge.
- Errors due to patient misunderstandings regarding medication use.
I would like to focus on the fifth item, errors due to similarities in the labeling or packaging of marketed medications.
Medications with similar names or with similar labeling or packaging are known as “look alike–sound alike” medications. They are estimated to account for between 6.2% and 14.7% of all medication errors. Confusion can arise due to spelling and phonetic similarities.
As shown in bulletin no. 50 of the ISMP, difficulties in distinguishing different medications or different presentations of the same medication due to similar packaging and labeling have frequently been associated with reported incidents.
Most cases involve either medications marketed by the same laboratory with a design based on brand image or different medications marketed by different laboratories in screen-printed ampoules used in the same settings.
In 2020, the ISMP published 11 new cases of labeling or packaging that may promote errors on its website. It reported 49 incidents to the Spanish Agency for Medicines and Medical Devices.
Shortages caused by the COVID-19 pandemic have further contributed to these incidents, as healthcare facilities sometimes had to change the medications they usually acquired and purchase whatever was available, without being able to select products that would not be confused with existing medications in the facility.
The ISMP recommends the following general practices for healthcare institutions, professionals, and patients to prevent these errors:
- Develop short lists of easily confused medication names and distribute them among all healthcare professionals.
- Prioritize medication names by active ingredient instead of brand name.
- For similar names, highlight the differences in capital letters, eg, DOBUTamine, DOPamine.
- For similar active ingredients, use brand names.
- Avoid placing similar medications near each other.
- Prescribe all medications electronically to minimize the risk of selecting the wrong medication.
- Make manual prescriptions legible, with clearly written dosages and pharmaceutical forms.
- Encourage patients to actively participate in their treatment and consult a clinician if they have any questions about the medications they are receiving.
- Raise awareness among patients, family members, and caregivers about the issues caused by medication name confusion and inform them about how to avoid these errors.
- Instruct patients to focus on and always use the active ingredient name as an identifying element for the medications they are taking.
- Review treatments with patients to ensure they know the medications they are taking.
Julia María Ruiz Redondo is the regional nursing advisor inspector of Spanish Society of General and Family Physicians of Castilla-La Mancha (SEMG-CLM), coordinator of the National Working Group on Public Health in the SEMG, and director of the international public health master’s degree at TECH Technological University. This article is the result of an editorial collaboration between the SEMG and Univadis, which you can access here.
This story was translated from Univadis Spain, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Cancer Risk: Are Pesticides the New Smoking?
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Pesticides have transformed modern agriculture by boosting production yields and helping alleviate food insecurity amid rapid global population growth. However, from a public health perspective, exposure to pesticides has been linked to numerous harmful effects, including neurologic disorders like Parkinson’s disease, weakened immune function, and an increased risk for cancer.
thus offering a limited perspective.
A comprehensive assessment of how pesticide use affects cancer risk across a broader population has yet to be conducted.
A recent population-level study aimed to address this gap by evaluating cancer risks in the US population using a model that accounts for pesticide use and adjusts for various factors. The goal was to identify regional disparities in exposure and contribute to the development of public health policies that protect populations from potential harm.
Calculating Cancer Risk
Researchers developed a model using several data sources to estimate the additional cancer risk from agricultural pesticide use. Key data included:
- Pesticide use data from the US Geological Survey in 2019, which covered 69 agricultural pesticides across 3143 counties
- Cancer incidence rates per 100,000 people, which were collected between 2015 and 2019 by the National Institutes of Health and the Centers for Disease Control and Prevention; these data covered various cancers, including bladder, colorectal, leukemia, lung, non-Hodgkin lymphoma, and pancreatic cancers
- Covariates, including smoking prevalence, the Social Vulnerability Index, agricultural land use, and total US population in 2019
Pesticide use profile patterns were developed using latent class analysis, a statistical method used to identify homogeneous subgroups within a heterogeneous population. A generalized linear model then estimated how these pesticide use patterns and the covariates affected cancer incidence.
The model highlighted regions with the highest and lowest “additional” cancer risks linked to pesticide exposure, calculating the estimated increase in cancer cases per year that resulted from variations in agricultural pesticide use.
Midwest Most Affected
While this model doesn’t establish causality or assess individual risk, it reveals regional trends in the association between pesticide use patterns and cancer incidence from a population-based perspective.
The Midwest, known for its high corn production, emerged as the region most affected by pesticide use. Compared with regions with the lowest risk, the Midwest faced an additional 154,541 cancer cases annually across all types. For colorectal and pancreatic cancers, the yearly increases were 20,927 and 3835 cases, respectively. Similar trends were observed for leukemia and non-Hodgkin lymphoma.
Pesticides vs Smoking
The researchers also estimated the additional cancer risk related to smoking, using the same model. They found that pesticides contributed to a higher risk for cancer than smoking in several cases.
The most significant difference was observed with non-Hodgkin lymphoma, where pesticides were linked to 154.1% more cases than smoking. For all cancers combined, as well as bladder cancer and leukemia, the increases were moderate: 18.7%, 19.3%, and 21.0%, respectively.
This result highlights the importance of considering pesticide exposure alongside smoking when studying cancer risks.
Expanding Scope of Research
Some limitations of this study should be noted. Certain counties lacked complete data, and there was heterogeneity in the size and population of the counties studied. The research also did not account for seasonal and migrant workers, who are likely to be heavily exposed. In addition, the data used in the study were not independently validated, and they could not be used to assess individual risk.
The effect of pesticides on human health is a vast and critical field of research, often focusing on a limited range of pesticides or specific cancers. This study stands out by taking a broader, more holistic approach, aiming to highlight regional inequalities and identify less-studied pesticides that could be future research priorities.
Given the significant public health impact, the authors encouraged the authorities to share these findings with the most vulnerable communities to raise awareness.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Semaglutide Bests Liraglutide in Long-Term Weight Loss
Patients with obesity or type 2 diabetes (T2D) who stuck with their medication for a year lost more weight with semaglutide than with liraglutide, a new study reported.
Researchers at the Cleveland Clinic reviewed records for 3389 adult patients with obesity who were prescribed one of the glucagon-like peptide 1 (GLP-1) medications for either T2D or obesity between 2015 and 2022. They found that patients who took either semaglutide or liraglutide for obesity were more likely to lose weight than those prescribed the medications for T2D and that semaglutide was associated with greater weight loss.
The study, published in JAMA Network Open, identified “key characteristics that could inform the probability of achieving sustained weight loss of a magnitude large enough to provide clinically significant health benefits,” said lead author Hamlet Gasoyan, PhD, a staff investigator at the Center for Value-Based Care Research in the Department of Internal Medicine of Primary Care Institute, Cleveland Clinic, Cleveland.
Only about 40% of patients continued to take the medications at 1 year. Those who did not continue did not achieve the same level of weight loss, Dr. Gasoyan told this news organization. He and his colleagues will study the factors that lead patients to stop taking the medications in a future paper.
The results from the current paper give patients and clinicians reasonable expectations on the trajectory of weight loss when the drugs are prescribed for diabetes vs obesity, said Dr. Gasoyan, assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland.
Semaglutide Superior
Because of the study’s timeframe, the majority of GLP-1s were prescribed for T2D. Liraglutide was approved (as Saxenda) for obesity in December 2020 and semaglutide (as Wegovy) for obesity in June 2021.
The authors were able to capture fills under the brand names and doses approved by the US Food and Drug Administration (FDA) for obesity (Wegovy, 1.7 or 2.4 mg; Saxenda, 3.0 mg), as well as those approved for T2D (Ozempic, 0.5, 1.0, or 2.0 mg; Victoza, 1.2 or 1.8 mg).
The researchers reported that among the 3389 patients, 1341 (39.6%) were prescribed semaglutide and 1444 (42.6%) were prescribed liraglutide for T2D. For obesity, 227 (6.7%) were prescribed liraglutide, and 377 (11.1%) were prescribed semaglutide.
Overall, those with diabetes had a −3.2% mean weight change compared with those with obesity who had a −5.9% mean weight change.
Semaglutide consistently outperformed liraglutide, particularly in obesity.
Overall, at 1 year, the mean percentage weight change among those with obesity was −5.1% with semaglutide compared with −2.2% with liraglutide (P < .001).
At 1 year, among those with obesity who were persistent in semaglutide use (defined as 90-275 medication days) had a mean body weight of −12.9% vs −5.6% in those taking liraglutide.
Overall, about 40% of patients were persistent at 1 year. But the figure was higher for semaglutide (45.8%) and lower for liraglutide (35.6%).
Liraglutide requires daily injections compared with semaglutide that requires weekly injections. The authors did not study the reasons for medication adherence or discontinuation.
Key factors for achieving a greater than 10% weight loss — considered clinically meaningful — included taking semaglutide, receiving a GLP-1 for obesity, persistent medication use, high dosage, and being female.
Real-World Data Welcomed
Michael Weintraub, MD, an obesity medicine specialist and clinical assistant professor at NYU Langone Health, New York City, said that having real-world data on GLP-1 effectiveness has been much needed.
The researchers “did a really good job at stratifying these patients,” he told this news organization, saying that the study “adds to the literature in terms of what we might expect and what things we should look out for when we want to obtain the maximum degree of weight loss and attain overall better metabolic health for our patients.”
One strength: The researchers were able to capture when someone actually filled a prescription, he said. Clinicians don’t always know whether a prescription for a GLP-1 has been filled because patients might go without the drug because of insurance hurdles or supply issues, he said.
Dr. Weintraub was not surprised that the study showed that both GLP-1s produced more weight loss in those with obesity than in those with T2D, as that has become a common finding. No one has been able to explain why there is such a difference, said Dr. Weintraub. “As a field, we actually don’t know the reason behind that yet,” he said.
Given the small number of patients prescribed semaglutide for obesity, that “limits the generalizability,” he said.
Even so, semaglutide is increasingly proving superior, Dr. Weintraub said. “I would reach towards semaglutide every time either for individuals with type 2 diabetes or individuals with obesity,” he said. “The major limitation, though, is insurance coverage rather than, unfortunately, my clinical decision-making.”
He also still sees a role for liraglutide. It will go off patent soon and that could “lead to a lower price point and hopefully greater access for patients,” he said.
Dr. Gasoyan and Dr. Weintraub reported no relevant financial relationships. One coauthor reported receiving advisory board fees from Novo Nordisk and research funding from Eli Lilly during the conduct of the study.
A version of this article first appeared on Medscape.com.
Patients with obesity or type 2 diabetes (T2D) who stuck with their medication for a year lost more weight with semaglutide than with liraglutide, a new study reported.
Researchers at the Cleveland Clinic reviewed records for 3389 adult patients with obesity who were prescribed one of the glucagon-like peptide 1 (GLP-1) medications for either T2D or obesity between 2015 and 2022. They found that patients who took either semaglutide or liraglutide for obesity were more likely to lose weight than those prescribed the medications for T2D and that semaglutide was associated with greater weight loss.
The study, published in JAMA Network Open, identified “key characteristics that could inform the probability of achieving sustained weight loss of a magnitude large enough to provide clinically significant health benefits,” said lead author Hamlet Gasoyan, PhD, a staff investigator at the Center for Value-Based Care Research in the Department of Internal Medicine of Primary Care Institute, Cleveland Clinic, Cleveland.
Only about 40% of patients continued to take the medications at 1 year. Those who did not continue did not achieve the same level of weight loss, Dr. Gasoyan told this news organization. He and his colleagues will study the factors that lead patients to stop taking the medications in a future paper.
The results from the current paper give patients and clinicians reasonable expectations on the trajectory of weight loss when the drugs are prescribed for diabetes vs obesity, said Dr. Gasoyan, assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland.
Semaglutide Superior
Because of the study’s timeframe, the majority of GLP-1s were prescribed for T2D. Liraglutide was approved (as Saxenda) for obesity in December 2020 and semaglutide (as Wegovy) for obesity in June 2021.
The authors were able to capture fills under the brand names and doses approved by the US Food and Drug Administration (FDA) for obesity (Wegovy, 1.7 or 2.4 mg; Saxenda, 3.0 mg), as well as those approved for T2D (Ozempic, 0.5, 1.0, or 2.0 mg; Victoza, 1.2 or 1.8 mg).
The researchers reported that among the 3389 patients, 1341 (39.6%) were prescribed semaglutide and 1444 (42.6%) were prescribed liraglutide for T2D. For obesity, 227 (6.7%) were prescribed liraglutide, and 377 (11.1%) were prescribed semaglutide.
Overall, those with diabetes had a −3.2% mean weight change compared with those with obesity who had a −5.9% mean weight change.
Semaglutide consistently outperformed liraglutide, particularly in obesity.
Overall, at 1 year, the mean percentage weight change among those with obesity was −5.1% with semaglutide compared with −2.2% with liraglutide (P < .001).
At 1 year, among those with obesity who were persistent in semaglutide use (defined as 90-275 medication days) had a mean body weight of −12.9% vs −5.6% in those taking liraglutide.
Overall, about 40% of patients were persistent at 1 year. But the figure was higher for semaglutide (45.8%) and lower for liraglutide (35.6%).
Liraglutide requires daily injections compared with semaglutide that requires weekly injections. The authors did not study the reasons for medication adherence or discontinuation.
Key factors for achieving a greater than 10% weight loss — considered clinically meaningful — included taking semaglutide, receiving a GLP-1 for obesity, persistent medication use, high dosage, and being female.
Real-World Data Welcomed
Michael Weintraub, MD, an obesity medicine specialist and clinical assistant professor at NYU Langone Health, New York City, said that having real-world data on GLP-1 effectiveness has been much needed.
The researchers “did a really good job at stratifying these patients,” he told this news organization, saying that the study “adds to the literature in terms of what we might expect and what things we should look out for when we want to obtain the maximum degree of weight loss and attain overall better metabolic health for our patients.”
One strength: The researchers were able to capture when someone actually filled a prescription, he said. Clinicians don’t always know whether a prescription for a GLP-1 has been filled because patients might go without the drug because of insurance hurdles or supply issues, he said.
Dr. Weintraub was not surprised that the study showed that both GLP-1s produced more weight loss in those with obesity than in those with T2D, as that has become a common finding. No one has been able to explain why there is such a difference, said Dr. Weintraub. “As a field, we actually don’t know the reason behind that yet,” he said.
Given the small number of patients prescribed semaglutide for obesity, that “limits the generalizability,” he said.
Even so, semaglutide is increasingly proving superior, Dr. Weintraub said. “I would reach towards semaglutide every time either for individuals with type 2 diabetes or individuals with obesity,” he said. “The major limitation, though, is insurance coverage rather than, unfortunately, my clinical decision-making.”
He also still sees a role for liraglutide. It will go off patent soon and that could “lead to a lower price point and hopefully greater access for patients,” he said.
Dr. Gasoyan and Dr. Weintraub reported no relevant financial relationships. One coauthor reported receiving advisory board fees from Novo Nordisk and research funding from Eli Lilly during the conduct of the study.
A version of this article first appeared on Medscape.com.
Patients with obesity or type 2 diabetes (T2D) who stuck with their medication for a year lost more weight with semaglutide than with liraglutide, a new study reported.
Researchers at the Cleveland Clinic reviewed records for 3389 adult patients with obesity who were prescribed one of the glucagon-like peptide 1 (GLP-1) medications for either T2D or obesity between 2015 and 2022. They found that patients who took either semaglutide or liraglutide for obesity were more likely to lose weight than those prescribed the medications for T2D and that semaglutide was associated with greater weight loss.
The study, published in JAMA Network Open, identified “key characteristics that could inform the probability of achieving sustained weight loss of a magnitude large enough to provide clinically significant health benefits,” said lead author Hamlet Gasoyan, PhD, a staff investigator at the Center for Value-Based Care Research in the Department of Internal Medicine of Primary Care Institute, Cleveland Clinic, Cleveland.
Only about 40% of patients continued to take the medications at 1 year. Those who did not continue did not achieve the same level of weight loss, Dr. Gasoyan told this news organization. He and his colleagues will study the factors that lead patients to stop taking the medications in a future paper.
The results from the current paper give patients and clinicians reasonable expectations on the trajectory of weight loss when the drugs are prescribed for diabetes vs obesity, said Dr. Gasoyan, assistant professor of medicine at Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland.
Semaglutide Superior
Because of the study’s timeframe, the majority of GLP-1s were prescribed for T2D. Liraglutide was approved (as Saxenda) for obesity in December 2020 and semaglutide (as Wegovy) for obesity in June 2021.
The authors were able to capture fills under the brand names and doses approved by the US Food and Drug Administration (FDA) for obesity (Wegovy, 1.7 or 2.4 mg; Saxenda, 3.0 mg), as well as those approved for T2D (Ozempic, 0.5, 1.0, or 2.0 mg; Victoza, 1.2 or 1.8 mg).
The researchers reported that among the 3389 patients, 1341 (39.6%) were prescribed semaglutide and 1444 (42.6%) were prescribed liraglutide for T2D. For obesity, 227 (6.7%) were prescribed liraglutide, and 377 (11.1%) were prescribed semaglutide.
Overall, those with diabetes had a −3.2% mean weight change compared with those with obesity who had a −5.9% mean weight change.
Semaglutide consistently outperformed liraglutide, particularly in obesity.
Overall, at 1 year, the mean percentage weight change among those with obesity was −5.1% with semaglutide compared with −2.2% with liraglutide (P < .001).
At 1 year, among those with obesity who were persistent in semaglutide use (defined as 90-275 medication days) had a mean body weight of −12.9% vs −5.6% in those taking liraglutide.
Overall, about 40% of patients were persistent at 1 year. But the figure was higher for semaglutide (45.8%) and lower for liraglutide (35.6%).
Liraglutide requires daily injections compared with semaglutide that requires weekly injections. The authors did not study the reasons for medication adherence or discontinuation.
Key factors for achieving a greater than 10% weight loss — considered clinically meaningful — included taking semaglutide, receiving a GLP-1 for obesity, persistent medication use, high dosage, and being female.
Real-World Data Welcomed
Michael Weintraub, MD, an obesity medicine specialist and clinical assistant professor at NYU Langone Health, New York City, said that having real-world data on GLP-1 effectiveness has been much needed.
The researchers “did a really good job at stratifying these patients,” he told this news organization, saying that the study “adds to the literature in terms of what we might expect and what things we should look out for when we want to obtain the maximum degree of weight loss and attain overall better metabolic health for our patients.”
One strength: The researchers were able to capture when someone actually filled a prescription, he said. Clinicians don’t always know whether a prescription for a GLP-1 has been filled because patients might go without the drug because of insurance hurdles or supply issues, he said.
Dr. Weintraub was not surprised that the study showed that both GLP-1s produced more weight loss in those with obesity than in those with T2D, as that has become a common finding. No one has been able to explain why there is such a difference, said Dr. Weintraub. “As a field, we actually don’t know the reason behind that yet,” he said.
Given the small number of patients prescribed semaglutide for obesity, that “limits the generalizability,” he said.
Even so, semaglutide is increasingly proving superior, Dr. Weintraub said. “I would reach towards semaglutide every time either for individuals with type 2 diabetes or individuals with obesity,” he said. “The major limitation, though, is insurance coverage rather than, unfortunately, my clinical decision-making.”
He also still sees a role for liraglutide. It will go off patent soon and that could “lead to a lower price point and hopefully greater access for patients,” he said.
Dr. Gasoyan and Dr. Weintraub reported no relevant financial relationships. One coauthor reported receiving advisory board fees from Novo Nordisk and research funding from Eli Lilly during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Nonscaly Red-Brown Macules on the Feet and Ankles
THE DIAGNOSIS: Secondary Syphilis
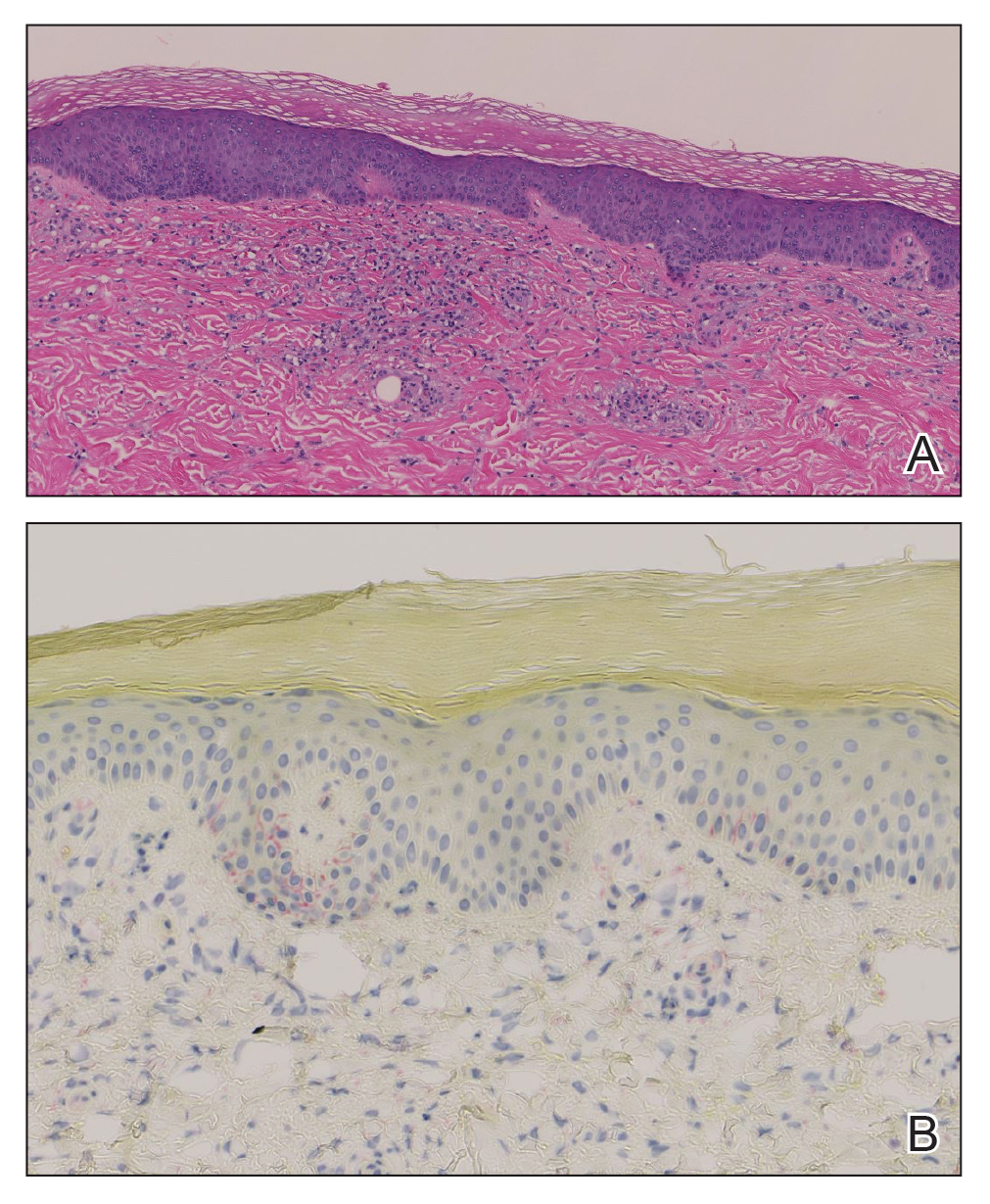
Histopathology demonstrated a mild superficial perivascular and interstitial infiltrate composed of lymphocytes, histiocytes, and rare plasma cells with a background of extravasated erythrocytes (Figure, A). Treponema pallidum staining highlighted multiple spirochetes along the dermoepidermal junction and in the superficial dermis (Figure, B). Direct immunofluorescence was negative. Laboratory workup revealed a reactive rapid plasma reagin screen with a titer of 1:16 and positive IgG and IgM treponemal antibodies. The patient was diagnosed with secondary syphilis and was treated with a single dose of 2.4 million U of intramuscular benzathine penicillin G, with notable improvement of the rash and arthritis symptoms at 2-week follow-up.
Syphilis is a sexually transmitted infection caused by the spirochete T pallidum that progresses through active and latent stages. The incidence of both the primary and secondary stages of syphilis was at a historic low in the year 2000 and has increased annually since then.1 Syphilis is more common in men, and men who have sex with men (MSM) are disproportionately affected. Although the incidence of syphilis in MSM has increased since 2000, rates have slowed, with slight decreases in this population between 2019 and 2020.1 Conversely, rates among women have increased substantially in recent years, suggesting a more recent epidemic affecting heterosexual men and women.2
Classically, the primary stage of syphilis manifests as an asymptomatic papule followed by a painless ulcer (chancre) that heals spontaneously. The secondary stage of syphilis results from dissemination of T pallidum and is characterized by a wide range of mucocutaneous manifestations and prodromal symptoms. The most common cutaneous manifestation is a diffuse, nonpruritic, papulosquamous rash with red-brown scaly macules or papules on the trunk and extremities.3 The palms and soles commonly are involved. Mucosal patches, “snail-track” ulcers in the mouth, and condylomata lata are the characteristic mucosal lesions of secondary syphilis. Mucocutaneous findings typically are preceded by systemic signs including fever, malaise, myalgia, and generalized lymphadenopathy. However, syphilis is considered “the great mimicker,” with new reports of unusual presentations of the disease. In addition to papulosquamous morphologies, pustular, targetoid, psoriasiform, and noduloulcerative (also known as lues maligna) forms of syphilis have been reported.3-5
The histopathologic features of secondary syphilis also are variable. Classically, secondary syphilis demonstrates vacuolar interface dermatitis and acanthosis with slender elongated rete ridges. Other well-known features include endothelial swelling and the presence of plasma cells in most cases.6 However, the histopathologic features of secondary syphilis may vary depending on the morphology of the skin eruption and when the biopsy is taken. Our patient lacked the classic histopathologic features of secondary syphilis. However, because syphilis was in the clinical differential diagnosis, a treponemal stain was ordered and confirmed the diagnosis. Immunohistochemical stains using antibodies to treponemal antigens have a reported sensitivity of 71% to 100% and are highly specific.7 Although the combination of endothelial swelling, interstitial inflammation, irregular acanthosis, and elongated rete ridges should raise the possibility of syphilis, a treponemal stain may be useful to identify spirochetes if clinical suspicion exists.8
Given our patient’s known history of GPA, leukocytoclastic vasculitis was high on the list of differential diagnoses. However, leukocytoclastic vasculitis most classically manifests as petechiae and palpable purpura, and unlike in secondary syphilis, the palms and soles are less commonly involved. Because our patient’s rash was mainly localized to the lower limbs, the differential also included 2 pigmented purpuric dermatoses (PPDs): progressive pigmentary purpura (Schamberg disease) and purpura annularis telangiectodes (Majocchi disease). Progressive pigmentary purpura is the most common manifestation of PPD and appears as cayenne pepper–colored macules that coalesce into golden brown–pigmented patches on the legs.9 Purpura annularis telangiectodes is another variant of PPD that manifests as pinpoint telangiectatic macules that progress to annular hyperpigmented patches with central clearing. Although PPDs frequently occur on the lower extremities, reports of plantar involvement are rare.10 Annular lichen planus manifests as violaceous papules with a clear center; however, it would be atypical for these lesions to be restricted to the feet and ankles. Palmoplantar lichen planus can mimic secondary syphilis clinically, but these cases manifest as hyperkeratotic pruritic papules on the palms and soles in contrast to the faint brown asymptomatic macules noted in our case.11
Our case highlights an unusual presentation of secondary syphilis and demonstrates the challenge of diagnosing this entity on clinical presentation alone. Because this patient lacked the classic clinical and histopathologic features of secondary syphilis, a skin biopsy with positive immunohistochemical staining for treponemal antigens was necessary to make the diagnosis. Given the variability in presentation of secondary syphilis, a biopsy or serologic testing may be necessary to make a proper diagnosis.
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2020. Accessed September 4, 2024. https://www.cdc.gov/std/statistics/2020/2020-SR-4-10-2023.pdf
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382:845-854. doi:10.1056/NEJMra1901593
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: historical aspects, microbiology, epidemiology, and clinical manifestations. J Am Acad Dermatol. 2020;82:1-14. doi:10.1016/j.jaad.2019.02.073
- Wu MC, Hsu CK, Lee JY, et al. Erythema multiforme-like secondary syphilis in a HIV-positive bisexual man. Acta Derm Venereol. 2010;90:647-648. doi:10.2340/00015555-0920
- Kopelman H, Lin A, Jorizzo JL. A pemphigus-like presentation of secondary syphilis. JAAD Case Rep. 2019;5:861-864. doi:10.1016/j.jdcr.2019.07.021
- Liu XK, Li J. Histologic features of secondary syphilis. Dermatology. 2020;236:145-150. doi:10.1159/000502641
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: laboratory diagnosis, management, and prevention. J Am Acad Dermatol. 2020;82:17-28. doi:10.1016/j.jaad.2019.02.074
- Flamm A, Parikh K, Xie Q, et al. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol. 2015;73:1025-1030. doi:10.1016/j.jaad.2015.08.062
- Kim DH, Seo SH, Ahn HH, et al. Characteristics and clinical manifestations of pigmented purpuric dermatosis. Ann Dermatol. 2015;27:404-410. doi:10.5021/ad.2015.27.4.404
- Sivendran M, Mowad C. Hyperpigmented patches on shins, palms, and soles. JAMA Dermatol. 2013;149:223. doi:10.1001/2013.jamadermatol.652a
- Kim YS, Kim MH, Kim CW, et al. A case of palmoplantar lichen planus mimicking secondary syphilis. Ann Dermatol. 2009;21:429-431.doi:10.5021/ad.2009.21.4.429
THE DIAGNOSIS: Secondary Syphilis
Histopathology demonstrated a mild superficial perivascular and interstitial infiltrate composed of lymphocytes, histiocytes, and rare plasma cells with a background of extravasated erythrocytes (Figure, A). Treponema pallidum staining highlighted multiple spirochetes along the dermoepidermal junction and in the superficial dermis (Figure, B). Direct immunofluorescence was negative. Laboratory workup revealed a reactive rapid plasma reagin screen with a titer of 1:16 and positive IgG and IgM treponemal antibodies. The patient was diagnosed with secondary syphilis and was treated with a single dose of 2.4 million U of intramuscular benzathine penicillin G, with notable improvement of the rash and arthritis symptoms at 2-week follow-up.
Syphilis is a sexually transmitted infection caused by the spirochete T pallidum that progresses through active and latent stages. The incidence of both the primary and secondary stages of syphilis was at a historic low in the year 2000 and has increased annually since then.1 Syphilis is more common in men, and men who have sex with men (MSM) are disproportionately affected. Although the incidence of syphilis in MSM has increased since 2000, rates have slowed, with slight decreases in this population between 2019 and 2020.1 Conversely, rates among women have increased substantially in recent years, suggesting a more recent epidemic affecting heterosexual men and women.2
Classically, the primary stage of syphilis manifests as an asymptomatic papule followed by a painless ulcer (chancre) that heals spontaneously. The secondary stage of syphilis results from dissemination of T pallidum and is characterized by a wide range of mucocutaneous manifestations and prodromal symptoms. The most common cutaneous manifestation is a diffuse, nonpruritic, papulosquamous rash with red-brown scaly macules or papules on the trunk and extremities.3 The palms and soles commonly are involved. Mucosal patches, “snail-track” ulcers in the mouth, and condylomata lata are the characteristic mucosal lesions of secondary syphilis. Mucocutaneous findings typically are preceded by systemic signs including fever, malaise, myalgia, and generalized lymphadenopathy. However, syphilis is considered “the great mimicker,” with new reports of unusual presentations of the disease. In addition to papulosquamous morphologies, pustular, targetoid, psoriasiform, and noduloulcerative (also known as lues maligna) forms of syphilis have been reported.3-5
The histopathologic features of secondary syphilis also are variable. Classically, secondary syphilis demonstrates vacuolar interface dermatitis and acanthosis with slender elongated rete ridges. Other well-known features include endothelial swelling and the presence of plasma cells in most cases.6 However, the histopathologic features of secondary syphilis may vary depending on the morphology of the skin eruption and when the biopsy is taken. Our patient lacked the classic histopathologic features of secondary syphilis. However, because syphilis was in the clinical differential diagnosis, a treponemal stain was ordered and confirmed the diagnosis. Immunohistochemical stains using antibodies to treponemal antigens have a reported sensitivity of 71% to 100% and are highly specific.7 Although the combination of endothelial swelling, interstitial inflammation, irregular acanthosis, and elongated rete ridges should raise the possibility of syphilis, a treponemal stain may be useful to identify spirochetes if clinical suspicion exists.8
Given our patient’s known history of GPA, leukocytoclastic vasculitis was high on the list of differential diagnoses. However, leukocytoclastic vasculitis most classically manifests as petechiae and palpable purpura, and unlike in secondary syphilis, the palms and soles are less commonly involved. Because our patient’s rash was mainly localized to the lower limbs, the differential also included 2 pigmented purpuric dermatoses (PPDs): progressive pigmentary purpura (Schamberg disease) and purpura annularis telangiectodes (Majocchi disease). Progressive pigmentary purpura is the most common manifestation of PPD and appears as cayenne pepper–colored macules that coalesce into golden brown–pigmented patches on the legs.9 Purpura annularis telangiectodes is another variant of PPD that manifests as pinpoint telangiectatic macules that progress to annular hyperpigmented patches with central clearing. Although PPDs frequently occur on the lower extremities, reports of plantar involvement are rare.10 Annular lichen planus manifests as violaceous papules with a clear center; however, it would be atypical for these lesions to be restricted to the feet and ankles. Palmoplantar lichen planus can mimic secondary syphilis clinically, but these cases manifest as hyperkeratotic pruritic papules on the palms and soles in contrast to the faint brown asymptomatic macules noted in our case.11
Our case highlights an unusual presentation of secondary syphilis and demonstrates the challenge of diagnosing this entity on clinical presentation alone. Because this patient lacked the classic clinical and histopathologic features of secondary syphilis, a skin biopsy with positive immunohistochemical staining for treponemal antigens was necessary to make the diagnosis. Given the variability in presentation of secondary syphilis, a biopsy or serologic testing may be necessary to make a proper diagnosis.
THE DIAGNOSIS: Secondary Syphilis
Histopathology demonstrated a mild superficial perivascular and interstitial infiltrate composed of lymphocytes, histiocytes, and rare plasma cells with a background of extravasated erythrocytes (Figure, A). Treponema pallidum staining highlighted multiple spirochetes along the dermoepidermal junction and in the superficial dermis (Figure, B). Direct immunofluorescence was negative. Laboratory workup revealed a reactive rapid plasma reagin screen with a titer of 1:16 and positive IgG and IgM treponemal antibodies. The patient was diagnosed with secondary syphilis and was treated with a single dose of 2.4 million U of intramuscular benzathine penicillin G, with notable improvement of the rash and arthritis symptoms at 2-week follow-up.
Syphilis is a sexually transmitted infection caused by the spirochete T pallidum that progresses through active and latent stages. The incidence of both the primary and secondary stages of syphilis was at a historic low in the year 2000 and has increased annually since then.1 Syphilis is more common in men, and men who have sex with men (MSM) are disproportionately affected. Although the incidence of syphilis in MSM has increased since 2000, rates have slowed, with slight decreases in this population between 2019 and 2020.1 Conversely, rates among women have increased substantially in recent years, suggesting a more recent epidemic affecting heterosexual men and women.2
Classically, the primary stage of syphilis manifests as an asymptomatic papule followed by a painless ulcer (chancre) that heals spontaneously. The secondary stage of syphilis results from dissemination of T pallidum and is characterized by a wide range of mucocutaneous manifestations and prodromal symptoms. The most common cutaneous manifestation is a diffuse, nonpruritic, papulosquamous rash with red-brown scaly macules or papules on the trunk and extremities.3 The palms and soles commonly are involved. Mucosal patches, “snail-track” ulcers in the mouth, and condylomata lata are the characteristic mucosal lesions of secondary syphilis. Mucocutaneous findings typically are preceded by systemic signs including fever, malaise, myalgia, and generalized lymphadenopathy. However, syphilis is considered “the great mimicker,” with new reports of unusual presentations of the disease. In addition to papulosquamous morphologies, pustular, targetoid, psoriasiform, and noduloulcerative (also known as lues maligna) forms of syphilis have been reported.3-5
The histopathologic features of secondary syphilis also are variable. Classically, secondary syphilis demonstrates vacuolar interface dermatitis and acanthosis with slender elongated rete ridges. Other well-known features include endothelial swelling and the presence of plasma cells in most cases.6 However, the histopathologic features of secondary syphilis may vary depending on the morphology of the skin eruption and when the biopsy is taken. Our patient lacked the classic histopathologic features of secondary syphilis. However, because syphilis was in the clinical differential diagnosis, a treponemal stain was ordered and confirmed the diagnosis. Immunohistochemical stains using antibodies to treponemal antigens have a reported sensitivity of 71% to 100% and are highly specific.7 Although the combination of endothelial swelling, interstitial inflammation, irregular acanthosis, and elongated rete ridges should raise the possibility of syphilis, a treponemal stain may be useful to identify spirochetes if clinical suspicion exists.8
Given our patient’s known history of GPA, leukocytoclastic vasculitis was high on the list of differential diagnoses. However, leukocytoclastic vasculitis most classically manifests as petechiae and palpable purpura, and unlike in secondary syphilis, the palms and soles are less commonly involved. Because our patient’s rash was mainly localized to the lower limbs, the differential also included 2 pigmented purpuric dermatoses (PPDs): progressive pigmentary purpura (Schamberg disease) and purpura annularis telangiectodes (Majocchi disease). Progressive pigmentary purpura is the most common manifestation of PPD and appears as cayenne pepper–colored macules that coalesce into golden brown–pigmented patches on the legs.9 Purpura annularis telangiectodes is another variant of PPD that manifests as pinpoint telangiectatic macules that progress to annular hyperpigmented patches with central clearing. Although PPDs frequently occur on the lower extremities, reports of plantar involvement are rare.10 Annular lichen planus manifests as violaceous papules with a clear center; however, it would be atypical for these lesions to be restricted to the feet and ankles. Palmoplantar lichen planus can mimic secondary syphilis clinically, but these cases manifest as hyperkeratotic pruritic papules on the palms and soles in contrast to the faint brown asymptomatic macules noted in our case.11
Our case highlights an unusual presentation of secondary syphilis and demonstrates the challenge of diagnosing this entity on clinical presentation alone. Because this patient lacked the classic clinical and histopathologic features of secondary syphilis, a skin biopsy with positive immunohistochemical staining for treponemal antigens was necessary to make the diagnosis. Given the variability in presentation of secondary syphilis, a biopsy or serologic testing may be necessary to make a proper diagnosis.
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2020. Accessed September 4, 2024. https://www.cdc.gov/std/statistics/2020/2020-SR-4-10-2023.pdf
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382:845-854. doi:10.1056/NEJMra1901593
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: historical aspects, microbiology, epidemiology, and clinical manifestations. J Am Acad Dermatol. 2020;82:1-14. doi:10.1016/j.jaad.2019.02.073
- Wu MC, Hsu CK, Lee JY, et al. Erythema multiforme-like secondary syphilis in a HIV-positive bisexual man. Acta Derm Venereol. 2010;90:647-648. doi:10.2340/00015555-0920
- Kopelman H, Lin A, Jorizzo JL. A pemphigus-like presentation of secondary syphilis. JAAD Case Rep. 2019;5:861-864. doi:10.1016/j.jdcr.2019.07.021
- Liu XK, Li J. Histologic features of secondary syphilis. Dermatology. 2020;236:145-150. doi:10.1159/000502641
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: laboratory diagnosis, management, and prevention. J Am Acad Dermatol. 2020;82:17-28. doi:10.1016/j.jaad.2019.02.074
- Flamm A, Parikh K, Xie Q, et al. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol. 2015;73:1025-1030. doi:10.1016/j.jaad.2015.08.062
- Kim DH, Seo SH, Ahn HH, et al. Characteristics and clinical manifestations of pigmented purpuric dermatosis. Ann Dermatol. 2015;27:404-410. doi:10.5021/ad.2015.27.4.404
- Sivendran M, Mowad C. Hyperpigmented patches on shins, palms, and soles. JAMA Dermatol. 2013;149:223. doi:10.1001/2013.jamadermatol.652a
- Kim YS, Kim MH, Kim CW, et al. A case of palmoplantar lichen planus mimicking secondary syphilis. Ann Dermatol. 2009;21:429-431.doi:10.5021/ad.2009.21.4.429
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2020. Accessed September 4, 2024. https://www.cdc.gov/std/statistics/2020/2020-SR-4-10-2023.pdf
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382:845-854. doi:10.1056/NEJMra1901593
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: historical aspects, microbiology, epidemiology, and clinical manifestations. J Am Acad Dermatol. 2020;82:1-14. doi:10.1016/j.jaad.2019.02.073
- Wu MC, Hsu CK, Lee JY, et al. Erythema multiforme-like secondary syphilis in a HIV-positive bisexual man. Acta Derm Venereol. 2010;90:647-648. doi:10.2340/00015555-0920
- Kopelman H, Lin A, Jorizzo JL. A pemphigus-like presentation of secondary syphilis. JAAD Case Rep. 2019;5:861-864. doi:10.1016/j.jdcr.2019.07.021
- Liu XK, Li J. Histologic features of secondary syphilis. Dermatology. 2020;236:145-150. doi:10.1159/000502641
- Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: laboratory diagnosis, management, and prevention. J Am Acad Dermatol. 2020;82:17-28. doi:10.1016/j.jaad.2019.02.074
- Flamm A, Parikh K, Xie Q, et al. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol. 2015;73:1025-1030. doi:10.1016/j.jaad.2015.08.062
- Kim DH, Seo SH, Ahn HH, et al. Characteristics and clinical manifestations of pigmented purpuric dermatosis. Ann Dermatol. 2015;27:404-410. doi:10.5021/ad.2015.27.4.404
- Sivendran M, Mowad C. Hyperpigmented patches on shins, palms, and soles. JAMA Dermatol. 2013;149:223. doi:10.1001/2013.jamadermatol.652a
- Kim YS, Kim MH, Kim CW, et al. A case of palmoplantar lichen planus mimicking secondary syphilis. Ann Dermatol. 2009;21:429-431.doi:10.5021/ad.2009.21.4.429
A 59-year-old man presented with a nontender nonpruritic rash on the feet of 2 days’ duration. The patient had a several-year history of granulomatosis with polyangiitis (GPA) and was taking methotrexate and prednisone. The rash appeared suddenly—first on the right foot and then on the left foot—and was preceded by 1 week of worsening polyarthralgia, most notably in the ankles. He denied any fever, chills, sore throat, or weight loss. His typical GPA symptoms included inflammatory arthritis, scleritis, leukocytoclastic vasculitis, and sinonasal and renal involvement. He recently experienced exacerbation of inflammatory arthritis that required an increase in the prednisone dosage (from 40 mg to 60 mg daily), but there were no other GPA symptoms. He had a history of multiple female sexual partners but no known history of HIV and no recent testing for sexually transmitted infections. Hepatitis C antibody testing performed 5 years earlier was nonreactive. He denied any illicit drug use, recent travel, sick contacts, or new medications.
Dermatologic examination revealed nonscaly, clustered, red-brown macules, some with central clearing, on the medial and lateral aspects of the feet and ankles with a few faint copper-colored macules on the palms and soles. The ankles had full range of motion with no edema or effusion. There were no oral or genital lesions. The remainder of the skin examination was normal. Punch biopsies of skin on the left foot were obtained for histopathology and direct immunofluorescence.


A CRC Blood Test Is Here. What Does it Mean for Screening?
In July, the US Food and Drug Administration (FDA) approved the first blood-based test to screen for colorectal cancer (CRC).
The FDA’s approval of Shield (Guardant Health) marks a notable achievement, as individuals at average risk now have the option to receive a simple blood test for CRC screening, starting at age 45.
“No one has an excuse anymore not to be screened,” said John Marshall, MD, director of The Ruesch Center for the Cure of Gastrointestinal Cancers and chief medical officer of the Lombardi Comprehensive Cancer Center at the Georgetown University Medical Center in Washington, DC.
The approval was based on findings from the ECLIPSE study, which reported that Shield had 83% sensitivity for CRC and 90% specificity for advanced neoplasia, though only 13% sensitivity for advanced precancerous lesions.
While an exciting option, the test has its pros and cons.
The bad news, however, is that it does a poor job of detecting precancerous lesions. This could snowball if patients decide to replace a colonoscopy — which helps both detect and prevent CRC — with the blood test.
This news organization spoke to experts across three core specialties involved in the screening and treatment of CRC — primary care, gastroenterology, and oncology — to better understand both the potential value and potential pitfalls of this new option.
The interview responses have been condensed and edited for clarity.
What does this FDA approval mean for CRC screening?
David Lieberman, MD, gastroenterologist and professor emeritus at Oregon Health & Science University: Detecting circulating-free DNA associated with CRC in blood is a major scientific breakthrough. The ease of blood testing will appeal to patients and providers.
Folasade May, MD, director of the gastroenterology quality improvement program at the University of California, Los Angeles: The FDA approval means that we continue to broaden the scope of available tools to help reduce the impact of this largely preventable disease.
Dr. Marshall: Colonoscopy is still the gold standard, but we have to recognize that not everyone does it. And that not everyone wants to send their poop in the mail (with a stool-based test). Now there are no more excuses.
Alan Venook, MD, gastrointestinal medical oncologist at the University of California, San Francisco: Although it’s good to have a blood test that’s approved for CRC screening, I don’t think it moves the bar much in terms of screening. I worry about it overpromising and under-delivering. If it could find polyps or premalignant lesions, that would make a big difference; however, at 13%, that doesn’t really register, so this doesn’t really change anything.
Kenny Lin, MD, a family physician at Penn Medicine Lancaster General Health: I see this test as a good option for the 30% people of CRC screening age who are either not being screened or out of date for screening. I’m a little concerned about the people who are already getting recommended screening and may try to switch to this option.
William Golden, MD, internist and professor of medicine and public health at the University of Arkansas for Medical Sciences, Little Rock, Arkansas: On a scale of 1-10, I give it a 2. It’s expensive ($900 per test without insurance). It’s also not sensitive for early cancers, which would be its main value. Frankly, there are better strategies to get patients engaged.
What do you see as the pros and cons of this test?
Dr. Lin: The pros are that it’s very convenient for patients, and it’s especially easy for physicians if they have a lab in their office and can avoid a referral where patients may never get the test. However, the data I saw were disappointing, with sensitivity and specificity falling short of the stool-based Cologuard test, which is also not invasive and less likely to miss early cancers, precancerous lesions, and polyps.
Dr. Lieberman: A major con is the detection rate of only 13% for advanced precancerous lesions, which means that this test is not likely to result in much cancer prevention. There is good evidence that if advanced precancerous lesions are detected and removed, many — if not most — CRCs can be prevented.
Dr. Marshall: Another issue is the potential for a false-positive result (which occurs for 1 in every 10 tests). With this result, you would do a scope but can’t find what’s going on. This is a big deal. It’s the first of the blood tests that will be used for cancer screening, and it could be scary for a patient to receive a positive result but not be able to figure out where it’s coming from.
Will you be recommending this test or relying on its results?
Dr. Lieberman: Patients need to understand that the blood test is inferior to every other screening test and, if selected, would result in less protection against developing CRC or dying from CRC than other screening tests. But models suggest that this test will perform better than no screening. Therefore, it is reasonable to offer the test to individuals who decline any other form of screening.
Dr. May: I will do what I’ve always done — after the FDA approval, I wait for the US Preventive Services Task Force (USPSTF) to endorse it. If it does, then I feel it’s my responsibility to tell my patients about all the options they have and stay up to date on how the tests perform, what the pros and cons are, and what reliable information will help patients make the best decision.
Dr. Venook: No, but I could potentially see us moving it into surveillance mode, where CRC survivors or patients undergoing therapy could take it, which might give us a unique second bite of the apple. The test could potentially be of value in identifying early relapse or recurrence, which might give us a heads-up or jump start on follow-up.
Are you concerned that patients won’t return for a colonoscopy after a positive result?
Dr. Golden: This concern is relevant for all tests, including fecal immunochemical test (FIT), but I’ve found that if the patient is willing to do the initial test and it comes back positive, most are willing to do the follow-up. Of course, some folks have issues with this, but now we’ll have a marker in their medical records and can re-engage them through outreach.
Dr. Lieberman: I am concerned that a patient who previously declined to have a colonoscopy may not follow up an abnormal blood test with a colonoscopy. If this occurs, it will render a blood test program ineffective for those patients. Patients should be told upfront that if the test is abnormal, a colonoscopy would be recommended.
Dr. May: This is a big concern that I have. We already have two-step screening processes with FIT, Cologuard, and CT colonography, and strong data show there is attrition. All doctors and companies will need to make it clear that if patients have an abnormal test result, they must undergo a colonoscopy. We must have activated and involved systems of patient follow-up and navigation.
Dr. Lin: I already have some concerns, given that some patients with positive FIT tests don’t get timely follow-up. I see it in my own practice where we call patients to get a colonoscopy, but they don’t take it seriously or their initial counseling wasn’t clear about the possibility of needing a follow-up colonoscopy. If people aren’t being screened for whatever reason in the first place and they get a positive result on the Shield blood test, they might be even less likely to get the necessary follow-up testing afterward.
What might this mean for insurance coverage and costs for patients?
Dr. May: This is an important question because if we don’t have equal access, we create or widen disparities. For insurers to cover Shield, it’ll need to be endorsed by major medical societies, including USPSTF. But what will happen in the beginning is that wealthy patients who can pay out of pocket will use it, while lower-income individuals won’t have access until insurers cover it.
Dr. Golden: I could do 70 (or more) FIT tests for the cost of this one blood test. A FIT test should be offered first. We’re advising the Medicaid program that physicians should be required to explain why a patient doesn’t want a FIT test, prior to covering this blood test.
Dr. Venook: It’s too early to say. Although it’s approved, we now have to look at the monetization factor. At the end of the day, we still need a colonoscopy. The science is impressive, but it doesn’t mean we need to spend $900 doing a blood test.
Dr. Lin: I could see the coverage trajectory being similar to that for Cologuard, which had little coverage when it came out 10 years ago, but eventually, Medicare and commercial coverage happened. With Shield, initially, there will be some coverage gaps, especially with commercial insurance, and I can see insurance companies having concerns, especially because the test is expensive compared with other tests and the return isn’t well known. It could also be a waste of money if people with positive tests don’t receive follow-up colonoscopies.
What else would you like to share that people may not have considered?
Dr. Marshall: These tests could pick up other genes from other cancers. My worry is that people could have another cancer detected but not find it on a colonoscopy and think the blood test must be wrong. Or they’ll do a scan, which could lead to more scans and tests.
Dr. Golden: This test has received a lot of attention and coverage that didn’t discuss other screening options, limitations, or nuances. Let’s face it — we’ll see lots of TV ads about it, but once we start dealing with the total cost of care and alternate payment models, it’s going to be hard for this test to find a niche.
Dr. Venook: This test has only been validated in a population of ages 45 years or older, which is the conventional screening population. We desperately need something that can work in younger people, where CRC rates are increasing. I’d like to see the research move in that direction.
Dr. Lin: I thought it was unique that the FDA Advisory Panel clearly stated this was better than nothing but also should be used as second-line screening. The agency took pains to say this is not a colonoscopy or even equivalent to the fecal tests in use. But they appropriately did approve it because a lot of people aren’t getting anything at all, which is the biggest problem with CRC screening.
A version of this article first appeared on Medscape.com.
In July, the US Food and Drug Administration (FDA) approved the first blood-based test to screen for colorectal cancer (CRC).
The FDA’s approval of Shield (Guardant Health) marks a notable achievement, as individuals at average risk now have the option to receive a simple blood test for CRC screening, starting at age 45.
“No one has an excuse anymore not to be screened,” said John Marshall, MD, director of The Ruesch Center for the Cure of Gastrointestinal Cancers and chief medical officer of the Lombardi Comprehensive Cancer Center at the Georgetown University Medical Center in Washington, DC.
The approval was based on findings from the ECLIPSE study, which reported that Shield had 83% sensitivity for CRC and 90% specificity for advanced neoplasia, though only 13% sensitivity for advanced precancerous lesions.
While an exciting option, the test has its pros and cons.
The bad news, however, is that it does a poor job of detecting precancerous lesions. This could snowball if patients decide to replace a colonoscopy — which helps both detect and prevent CRC — with the blood test.
This news organization spoke to experts across three core specialties involved in the screening and treatment of CRC — primary care, gastroenterology, and oncology — to better understand both the potential value and potential pitfalls of this new option.
The interview responses have been condensed and edited for clarity.
What does this FDA approval mean for CRC screening?
David Lieberman, MD, gastroenterologist and professor emeritus at Oregon Health & Science University: Detecting circulating-free DNA associated with CRC in blood is a major scientific breakthrough. The ease of blood testing will appeal to patients and providers.
Folasade May, MD, director of the gastroenterology quality improvement program at the University of California, Los Angeles: The FDA approval means that we continue to broaden the scope of available tools to help reduce the impact of this largely preventable disease.
Dr. Marshall: Colonoscopy is still the gold standard, but we have to recognize that not everyone does it. And that not everyone wants to send their poop in the mail (with a stool-based test). Now there are no more excuses.
Alan Venook, MD, gastrointestinal medical oncologist at the University of California, San Francisco: Although it’s good to have a blood test that’s approved for CRC screening, I don’t think it moves the bar much in terms of screening. I worry about it overpromising and under-delivering. If it could find polyps or premalignant lesions, that would make a big difference; however, at 13%, that doesn’t really register, so this doesn’t really change anything.
Kenny Lin, MD, a family physician at Penn Medicine Lancaster General Health: I see this test as a good option for the 30% people of CRC screening age who are either not being screened or out of date for screening. I’m a little concerned about the people who are already getting recommended screening and may try to switch to this option.
William Golden, MD, internist and professor of medicine and public health at the University of Arkansas for Medical Sciences, Little Rock, Arkansas: On a scale of 1-10, I give it a 2. It’s expensive ($900 per test without insurance). It’s also not sensitive for early cancers, which would be its main value. Frankly, there are better strategies to get patients engaged.
What do you see as the pros and cons of this test?
Dr. Lin: The pros are that it’s very convenient for patients, and it’s especially easy for physicians if they have a lab in their office and can avoid a referral where patients may never get the test. However, the data I saw were disappointing, with sensitivity and specificity falling short of the stool-based Cologuard test, which is also not invasive and less likely to miss early cancers, precancerous lesions, and polyps.
Dr. Lieberman: A major con is the detection rate of only 13% for advanced precancerous lesions, which means that this test is not likely to result in much cancer prevention. There is good evidence that if advanced precancerous lesions are detected and removed, many — if not most — CRCs can be prevented.
Dr. Marshall: Another issue is the potential for a false-positive result (which occurs for 1 in every 10 tests). With this result, you would do a scope but can’t find what’s going on. This is a big deal. It’s the first of the blood tests that will be used for cancer screening, and it could be scary for a patient to receive a positive result but not be able to figure out where it’s coming from.
Will you be recommending this test or relying on its results?
Dr. Lieberman: Patients need to understand that the blood test is inferior to every other screening test and, if selected, would result in less protection against developing CRC or dying from CRC than other screening tests. But models suggest that this test will perform better than no screening. Therefore, it is reasonable to offer the test to individuals who decline any other form of screening.
Dr. May: I will do what I’ve always done — after the FDA approval, I wait for the US Preventive Services Task Force (USPSTF) to endorse it. If it does, then I feel it’s my responsibility to tell my patients about all the options they have and stay up to date on how the tests perform, what the pros and cons are, and what reliable information will help patients make the best decision.
Dr. Venook: No, but I could potentially see us moving it into surveillance mode, where CRC survivors or patients undergoing therapy could take it, which might give us a unique second bite of the apple. The test could potentially be of value in identifying early relapse or recurrence, which might give us a heads-up or jump start on follow-up.
Are you concerned that patients won’t return for a colonoscopy after a positive result?
Dr. Golden: This concern is relevant for all tests, including fecal immunochemical test (FIT), but I’ve found that if the patient is willing to do the initial test and it comes back positive, most are willing to do the follow-up. Of course, some folks have issues with this, but now we’ll have a marker in their medical records and can re-engage them through outreach.
Dr. Lieberman: I am concerned that a patient who previously declined to have a colonoscopy may not follow up an abnormal blood test with a colonoscopy. If this occurs, it will render a blood test program ineffective for those patients. Patients should be told upfront that if the test is abnormal, a colonoscopy would be recommended.
Dr. May: This is a big concern that I have. We already have two-step screening processes with FIT, Cologuard, and CT colonography, and strong data show there is attrition. All doctors and companies will need to make it clear that if patients have an abnormal test result, they must undergo a colonoscopy. We must have activated and involved systems of patient follow-up and navigation.
Dr. Lin: I already have some concerns, given that some patients with positive FIT tests don’t get timely follow-up. I see it in my own practice where we call patients to get a colonoscopy, but they don’t take it seriously or their initial counseling wasn’t clear about the possibility of needing a follow-up colonoscopy. If people aren’t being screened for whatever reason in the first place and they get a positive result on the Shield blood test, they might be even less likely to get the necessary follow-up testing afterward.
What might this mean for insurance coverage and costs for patients?
Dr. May: This is an important question because if we don’t have equal access, we create or widen disparities. For insurers to cover Shield, it’ll need to be endorsed by major medical societies, including USPSTF. But what will happen in the beginning is that wealthy patients who can pay out of pocket will use it, while lower-income individuals won’t have access until insurers cover it.
Dr. Golden: I could do 70 (or more) FIT tests for the cost of this one blood test. A FIT test should be offered first. We’re advising the Medicaid program that physicians should be required to explain why a patient doesn’t want a FIT test, prior to covering this blood test.
Dr. Venook: It’s too early to say. Although it’s approved, we now have to look at the monetization factor. At the end of the day, we still need a colonoscopy. The science is impressive, but it doesn’t mean we need to spend $900 doing a blood test.
Dr. Lin: I could see the coverage trajectory being similar to that for Cologuard, which had little coverage when it came out 10 years ago, but eventually, Medicare and commercial coverage happened. With Shield, initially, there will be some coverage gaps, especially with commercial insurance, and I can see insurance companies having concerns, especially because the test is expensive compared with other tests and the return isn’t well known. It could also be a waste of money if people with positive tests don’t receive follow-up colonoscopies.
What else would you like to share that people may not have considered?
Dr. Marshall: These tests could pick up other genes from other cancers. My worry is that people could have another cancer detected but not find it on a colonoscopy and think the blood test must be wrong. Or they’ll do a scan, which could lead to more scans and tests.
Dr. Golden: This test has received a lot of attention and coverage that didn’t discuss other screening options, limitations, or nuances. Let’s face it — we’ll see lots of TV ads about it, but once we start dealing with the total cost of care and alternate payment models, it’s going to be hard for this test to find a niche.
Dr. Venook: This test has only been validated in a population of ages 45 years or older, which is the conventional screening population. We desperately need something that can work in younger people, where CRC rates are increasing. I’d like to see the research move in that direction.
Dr. Lin: I thought it was unique that the FDA Advisory Panel clearly stated this was better than nothing but also should be used as second-line screening. The agency took pains to say this is not a colonoscopy or even equivalent to the fecal tests in use. But they appropriately did approve it because a lot of people aren’t getting anything at all, which is the biggest problem with CRC screening.
A version of this article first appeared on Medscape.com.
In July, the US Food and Drug Administration (FDA) approved the first blood-based test to screen for colorectal cancer (CRC).
The FDA’s approval of Shield (Guardant Health) marks a notable achievement, as individuals at average risk now have the option to receive a simple blood test for CRC screening, starting at age 45.
“No one has an excuse anymore not to be screened,” said John Marshall, MD, director of The Ruesch Center for the Cure of Gastrointestinal Cancers and chief medical officer of the Lombardi Comprehensive Cancer Center at the Georgetown University Medical Center in Washington, DC.
The approval was based on findings from the ECLIPSE study, which reported that Shield had 83% sensitivity for CRC and 90% specificity for advanced neoplasia, though only 13% sensitivity for advanced precancerous lesions.
While an exciting option, the test has its pros and cons.
The bad news, however, is that it does a poor job of detecting precancerous lesions. This could snowball if patients decide to replace a colonoscopy — which helps both detect and prevent CRC — with the blood test.
This news organization spoke to experts across three core specialties involved in the screening and treatment of CRC — primary care, gastroenterology, and oncology — to better understand both the potential value and potential pitfalls of this new option.
The interview responses have been condensed and edited for clarity.
What does this FDA approval mean for CRC screening?
David Lieberman, MD, gastroenterologist and professor emeritus at Oregon Health & Science University: Detecting circulating-free DNA associated with CRC in blood is a major scientific breakthrough. The ease of blood testing will appeal to patients and providers.
Folasade May, MD, director of the gastroenterology quality improvement program at the University of California, Los Angeles: The FDA approval means that we continue to broaden the scope of available tools to help reduce the impact of this largely preventable disease.
Dr. Marshall: Colonoscopy is still the gold standard, but we have to recognize that not everyone does it. And that not everyone wants to send their poop in the mail (with a stool-based test). Now there are no more excuses.
Alan Venook, MD, gastrointestinal medical oncologist at the University of California, San Francisco: Although it’s good to have a blood test that’s approved for CRC screening, I don’t think it moves the bar much in terms of screening. I worry about it overpromising and under-delivering. If it could find polyps or premalignant lesions, that would make a big difference; however, at 13%, that doesn’t really register, so this doesn’t really change anything.
Kenny Lin, MD, a family physician at Penn Medicine Lancaster General Health: I see this test as a good option for the 30% people of CRC screening age who are either not being screened or out of date for screening. I’m a little concerned about the people who are already getting recommended screening and may try to switch to this option.
William Golden, MD, internist and professor of medicine and public health at the University of Arkansas for Medical Sciences, Little Rock, Arkansas: On a scale of 1-10, I give it a 2. It’s expensive ($900 per test without insurance). It’s also not sensitive for early cancers, which would be its main value. Frankly, there are better strategies to get patients engaged.
What do you see as the pros and cons of this test?
Dr. Lin: The pros are that it’s very convenient for patients, and it’s especially easy for physicians if they have a lab in their office and can avoid a referral where patients may never get the test. However, the data I saw were disappointing, with sensitivity and specificity falling short of the stool-based Cologuard test, which is also not invasive and less likely to miss early cancers, precancerous lesions, and polyps.
Dr. Lieberman: A major con is the detection rate of only 13% for advanced precancerous lesions, which means that this test is not likely to result in much cancer prevention. There is good evidence that if advanced precancerous lesions are detected and removed, many — if not most — CRCs can be prevented.
Dr. Marshall: Another issue is the potential for a false-positive result (which occurs for 1 in every 10 tests). With this result, you would do a scope but can’t find what’s going on. This is a big deal. It’s the first of the blood tests that will be used for cancer screening, and it could be scary for a patient to receive a positive result but not be able to figure out where it’s coming from.
Will you be recommending this test or relying on its results?
Dr. Lieberman: Patients need to understand that the blood test is inferior to every other screening test and, if selected, would result in less protection against developing CRC or dying from CRC than other screening tests. But models suggest that this test will perform better than no screening. Therefore, it is reasonable to offer the test to individuals who decline any other form of screening.
Dr. May: I will do what I’ve always done — after the FDA approval, I wait for the US Preventive Services Task Force (USPSTF) to endorse it. If it does, then I feel it’s my responsibility to tell my patients about all the options they have and stay up to date on how the tests perform, what the pros and cons are, and what reliable information will help patients make the best decision.
Dr. Venook: No, but I could potentially see us moving it into surveillance mode, where CRC survivors or patients undergoing therapy could take it, which might give us a unique second bite of the apple. The test could potentially be of value in identifying early relapse or recurrence, which might give us a heads-up or jump start on follow-up.
Are you concerned that patients won’t return for a colonoscopy after a positive result?
Dr. Golden: This concern is relevant for all tests, including fecal immunochemical test (FIT), but I’ve found that if the patient is willing to do the initial test and it comes back positive, most are willing to do the follow-up. Of course, some folks have issues with this, but now we’ll have a marker in their medical records and can re-engage them through outreach.
Dr. Lieberman: I am concerned that a patient who previously declined to have a colonoscopy may not follow up an abnormal blood test with a colonoscopy. If this occurs, it will render a blood test program ineffective for those patients. Patients should be told upfront that if the test is abnormal, a colonoscopy would be recommended.
Dr. May: This is a big concern that I have. We already have two-step screening processes with FIT, Cologuard, and CT colonography, and strong data show there is attrition. All doctors and companies will need to make it clear that if patients have an abnormal test result, they must undergo a colonoscopy. We must have activated and involved systems of patient follow-up and navigation.
Dr. Lin: I already have some concerns, given that some patients with positive FIT tests don’t get timely follow-up. I see it in my own practice where we call patients to get a colonoscopy, but they don’t take it seriously or their initial counseling wasn’t clear about the possibility of needing a follow-up colonoscopy. If people aren’t being screened for whatever reason in the first place and they get a positive result on the Shield blood test, they might be even less likely to get the necessary follow-up testing afterward.
What might this mean for insurance coverage and costs for patients?
Dr. May: This is an important question because if we don’t have equal access, we create or widen disparities. For insurers to cover Shield, it’ll need to be endorsed by major medical societies, including USPSTF. But what will happen in the beginning is that wealthy patients who can pay out of pocket will use it, while lower-income individuals won’t have access until insurers cover it.
Dr. Golden: I could do 70 (or more) FIT tests for the cost of this one blood test. A FIT test should be offered first. We’re advising the Medicaid program that physicians should be required to explain why a patient doesn’t want a FIT test, prior to covering this blood test.
Dr. Venook: It’s too early to say. Although it’s approved, we now have to look at the monetization factor. At the end of the day, we still need a colonoscopy. The science is impressive, but it doesn’t mean we need to spend $900 doing a blood test.
Dr. Lin: I could see the coverage trajectory being similar to that for Cologuard, which had little coverage when it came out 10 years ago, but eventually, Medicare and commercial coverage happened. With Shield, initially, there will be some coverage gaps, especially with commercial insurance, and I can see insurance companies having concerns, especially because the test is expensive compared with other tests and the return isn’t well known. It could also be a waste of money if people with positive tests don’t receive follow-up colonoscopies.
What else would you like to share that people may not have considered?
Dr. Marshall: These tests could pick up other genes from other cancers. My worry is that people could have another cancer detected but not find it on a colonoscopy and think the blood test must be wrong. Or they’ll do a scan, which could lead to more scans and tests.
Dr. Golden: This test has received a lot of attention and coverage that didn’t discuss other screening options, limitations, or nuances. Let’s face it — we’ll see lots of TV ads about it, but once we start dealing with the total cost of care and alternate payment models, it’s going to be hard for this test to find a niche.
Dr. Venook: This test has only been validated in a population of ages 45 years or older, which is the conventional screening population. We desperately need something that can work in younger people, where CRC rates are increasing. I’d like to see the research move in that direction.
Dr. Lin: I thought it was unique that the FDA Advisory Panel clearly stated this was better than nothing but also should be used as second-line screening. The agency took pains to say this is not a colonoscopy or even equivalent to the fecal tests in use. But they appropriately did approve it because a lot of people aren’t getting anything at all, which is the biggest problem with CRC screening.
A version of this article first appeared on Medscape.com.
Five Steps to Improved Colonoscopy Performance
According to several experts who spoke at the American Gastroenterological Association’s Postgraduate Course this spring, which was offered at Digestive Disease Week (DDW), gastroenterologists can take these five steps to improve their performance: Addressing poor bowel prep, improving polyp detection, following the best intervals for polyp surveillance, reducing the environmental impact of gastrointestinal (GI) practice, and implementing artificial intelligence (AI) tools for efficiency and quality.
Addressing Poor Prep
To improve bowel preparation rates, clinicians may consider identifying those at high risk for inadequate prep, which could include known risk factors such as age, body mass index, inpatient status, constipation, tobacco use, and hypertension. However, other variables tend to serve as bigger predictors of inadequate prep, such as the patient’s status regarding cirrhosis, Parkinson’s disease, dementia, diabetes, opioid use, gastroparesis, tricyclics, and colorectal surgery.
Although several prediction models are based on some of these factors — looking at comorbidities, antidepressant use, constipation, and prior abdominal or pelvic surgery — the data don’t indicate whether knowing about or addressing these risks actually leads to better bowel prep, said Brian Jacobson, MD, associate professor of medicine at Harvard Medical School, Boston, and director of program development for gastroenterology at Massachusetts General Hospital in Boston.
Instead, the biggest return-on-investment option is to maximize prep for all patients, he said, especially since every patient has at least some risk of poor prep, either due to the required diet changes, medication considerations, or purgative solution and timing.

To create a state-of-the-art bowel prep process, Dr. Jacobson recommended numerous tactics for all patients: Verbal and written instructions for all components of prep, patient navigation with phone or virtual messaging to guide patients through the process, a low-fiber or all-liquid diet on the day before colonoscopy, and a split-dose 2-L prep regimen. Patients should begin the second half of the split-dose regimen 4-6 hours before colonoscopy and complete it at least 2 hours before the procedure starts, and clinicians should use an irrigation pump during colonoscopy to improve visibility.
Beyond that, Dr. Jacobson noted, higher risk patients can take a split-dose 4-L prep regimen with bisacodyl, a low-fiber diet 2-3 days before colonoscopy, and a clear liquid diet the day before colonoscopy. Using simethicone as an adjunct solution can also reduce bubbles in the colon.
Future tech developments may help clinicians as well, he said, such as using AI to identify patients at high risk and modifying their prep process, creating a personalized prep on a digital platform with videos that guide patients through the process, and using a phone checklist tool to indicate when they’re ready for colonoscopy.
Improving Polyp Detection
Adenoma detection rates (ADR) can be highly variable due to different techniques, technical skills, pattern recognition, interpretation, and experience. New adjunct and AI-based tools can help improve ADR, especially if clinicians want to improve, receive training, and use best-practice techniques.
“In colonoscopy, it’s tricky because it’s not just a blood test or an x-ray. There’s really a lot of technique involved, both cognitive awareness and pattern recognition, as well as our technical skills,” said Tonya Kaltenbach, MD, professor of clinical medicine at the University of California San Francisco and director of advanced endoscopy at the San Francisco VA Health Care System in San Francisco.
For instance, multiple tools and techniques may be needed in real time to interpret a lesion, such as washing, retroflexing, and using better lighting, while paying attention to alerts and noting areas for further inspection and resection.

“This is not innate. It’s a learned skill,” she said. “It’s something we need to intentionally make efforts on and get feedback to improve.”
Improvement starts with using the right mindset for lesion detection, Dr. Kaltenbach said, by having a “reflexive recognition of deconstructed patterns of normal” — following the lines, vessels, and folds and looking for interruptions, abnormal thickness, and mucus caps. On top of that, adjunctive tools such as caps/cuffs and dye chromoendoscopy can help with proper ergonomics, irrigation, and mucosa exposure.
In the past 3 years, real-world studies using AI and computer-assisted detection have shown mixed results, with some demonstrating significant increases in ADR, while others haven’t, she said. However, being willing to try AI and other tools, such as the Endocuff cap, may help improve ADR, standardize interpretation, improve efficiency, and increase reproducibility.
“We’re always better with intentional feedback and deliberate practice,” she said. “Remember that if you improve, you’re protecting the patient from death and reducing interval cancer.”
Following Polyp Surveillance Intervals
The US Multi-Society Task Force on Colorectal Cancer’s recommendations for follow-up after colonoscopy and polypectomy provide valuable information and rationale for how to determine surveillance intervals for patients. However, clinicians still may be unsure what to recommend for some patients — or tell them to come back too soon, leading to unnecessary colonoscopy.
For instance, a 47-year-old woman who presents for her initial screening and has a single 6-mm polyp, which pathology returns as a single adenoma may be considered to be at average risk and suggested to return in 7-10 years. The guidelines seem more obvious for patients with one or two adenomas under 10 mm removed en bloc.
However, once the case details shift into gray areas and include three or four adenomas between 10 and 20 mm, or piecemeal removal, clinicians may differ on their recommendations, said Rajesh N. Keswani, MD, associate professor of medicine at the Northwestern University Feinberg School of Medicine and director of endoscopy for Northwestern Medicine in Chicago. At DDW 2024, Dr. Keswani presented several case examples, often finding various audience opinions.

In addition, he noted, recent studies have found that clinicians may estimate imprecise polyp measurements, struggle to identify sessile serrated polyposis syndrome, and often don’t follow evidence-based guidelines.
“Why do we ignore the guidelines? There’s this perception that a patient has risk factors that aren’t addressed by the guidelines, with regards to family history or a distant history of a large polyp that we don’t want to leave to the usual intervals,” he said. “We feel uncomfortable, even with our meticulous colonoscopy, telling people to come back in 10 years.”
To improve guideline adherence, Dr. Keswani suggested providing additional education, implementing an automated surveillance calculator, and using guidelines at the point of care. At Northwestern, for instance, clinicians use a hyperlink with an interpreted version of the guidelines with prior colonoscopy considerations. Overall though, practitioners should feel comfortable leaning toward longer surveillance intervals, he noted.
“More effort should be spent on getting unscreened patients in for colonoscopy than bringing back low-risk patients too early,” he said.
Reducing Environmental Effects
In recent waste audits of endoscopy rooms, providers generate 1-3 kg of waste per procedure, which would fill 117 soccer fields to a depth of 1 m, based on 18 million procedures in the United States per year. This waste comes from procedure-related equipment, administration, medications, travel of patients and staff, and infrastructure with systems such as air conditioning. Taking steps toward a green practice can reduce waste and the carbon footprint of healthcare.
“When we think about improving colonoscopy performance, the goal is to prevent colon cancer death, but when we expand that, we have to apply sustainable practices as a domain of quality,” said Heiko Pohl, MD, professor of medicine at the Geisel School of Medicine at Dartmouth in Hanover, New Hampshire, and a gastroenterologist at White River Junction VA Medical Center in White River Junction, Vermont.
The GI Multisociety Strategic Plan on Environmental Sustainability suggests a 5-year initiative to improve sustainability and reduce waste across seven domains — clinical setting, education, research, society efforts, intersociety efforts, industry, and advocacy.

For instance, clinicians can take the biggest step toward sustainability by avoiding unneeded colonoscopies, Dr. Pohl said, noting that between 20% and 30% aren’t appropriate or indicated. Instead, practitioners can implement longer surveillance intervals, adhere to guidelines, and consider alternative tests, such as the fecal immunochemical test, fecal DNA, blood-based tests, and CT colonography, where relevant.
Clinicians can also rethink their approach to resection, such as using a snare first instead of forceps to reduce single-instrument use, using clip closure only when it’s truly indicated, and implementing AI-assisted optical diagnosis to help with leaving rectosigmoid polyps in place.
In terms of physical waste, practices may also reconsider how they sort bins and biohazards, looking at new ways to dispose of regulated medical waste, sharps, recyclables, and typical trash. Waste audits can help find ways to reduce paper, combine procedures, and create more efficient use of endoscopy rooms.
“We are really in a very precarious situation,” Dr. Pohl said. “It’s our generation that has a responsibility to change the course for our children’s and grandchildren’s sake.”
AI for Quality And Efficiency
Moving forward, AI tools will likely become more popular in various parts of GI practice, by assisting with documentation, spotting polyps, tracking mucosal surfaces, providing optical histopathology, and supervising performance through high-quality feedback.
“Endoscopy has reached the limits of human visual capacity, where seeing more pixels won’t necessarily improve clinical diagnosis. What’s next for elevating the care of patients really is AI,” said Jason B. Samarasena, MD, professor of medicine and program director of the interventional endoscopy training program at the University of California Irvine in Irvine, California.
As practices adopt AI-based systems, however, clinicians should be cautious about a false sense of comfort or “alarm fatigue” if bounding boxes become distracting. Instead, new tools need to be adopted as a “physician-AI hybrid,” with the endoscopist in mind, particularly if helpful for performing a better exam by watching withdrawal time or endoscope slippage.

“In real-world practice, this is being implemented without attention to endoscopist inclination and behavior,” he said. “Having a better understanding of physician attitudes could yield more optimal results.”
Notably, AI-assisted tools should be viewed akin to spell-check, which signals to the endoscopist when to pay attention and double-check an area — but primarily relies on the expert to do a high-quality exam, said Aasma Shaukat, MD, professor of medicine and director of GI outcomes research at the NYU Grossman School of Medicine, New York City.
“This should be an adjunct or an additional tool, not a replacement tool,” she added. “This doesn’t mean to stop doing astute observation.”

Future tools show promise in terms of tracking additional data related to prep quality, cecal landmarks, polyp size, mucosa exposure, histology prediction, and complete resection. These automated reports could also link to real-time dashboards, hospital or national registries, and reimbursement systems, Dr. Shaukat noted.
“At the end of the day, our interests are aligned,” she said. “Everybody cares about quality, patient satisfaction, and reimbursement, and with that goal in mind, I think some of the tools can be applied to show how we can achieve those principles together.”
Dr. Jacobson, Dr. Kaltenbach, Dr. Keswani, Dr. Pohl, Dr. Samarasena, and Dr. Shaukat reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
According to several experts who spoke at the American Gastroenterological Association’s Postgraduate Course this spring, which was offered at Digestive Disease Week (DDW), gastroenterologists can take these five steps to improve their performance: Addressing poor bowel prep, improving polyp detection, following the best intervals for polyp surveillance, reducing the environmental impact of gastrointestinal (GI) practice, and implementing artificial intelligence (AI) tools for efficiency and quality.
Addressing Poor Prep
To improve bowel preparation rates, clinicians may consider identifying those at high risk for inadequate prep, which could include known risk factors such as age, body mass index, inpatient status, constipation, tobacco use, and hypertension. However, other variables tend to serve as bigger predictors of inadequate prep, such as the patient’s status regarding cirrhosis, Parkinson’s disease, dementia, diabetes, opioid use, gastroparesis, tricyclics, and colorectal surgery.
Although several prediction models are based on some of these factors — looking at comorbidities, antidepressant use, constipation, and prior abdominal or pelvic surgery — the data don’t indicate whether knowing about or addressing these risks actually leads to better bowel prep, said Brian Jacobson, MD, associate professor of medicine at Harvard Medical School, Boston, and director of program development for gastroenterology at Massachusetts General Hospital in Boston.
Instead, the biggest return-on-investment option is to maximize prep for all patients, he said, especially since every patient has at least some risk of poor prep, either due to the required diet changes, medication considerations, or purgative solution and timing.
To create a state-of-the-art bowel prep process, Dr. Jacobson recommended numerous tactics for all patients: Verbal and written instructions for all components of prep, patient navigation with phone or virtual messaging to guide patients through the process, a low-fiber or all-liquid diet on the day before colonoscopy, and a split-dose 2-L prep regimen. Patients should begin the second half of the split-dose regimen 4-6 hours before colonoscopy and complete it at least 2 hours before the procedure starts, and clinicians should use an irrigation pump during colonoscopy to improve visibility.
Beyond that, Dr. Jacobson noted, higher risk patients can take a split-dose 4-L prep regimen with bisacodyl, a low-fiber diet 2-3 days before colonoscopy, and a clear liquid diet the day before colonoscopy. Using simethicone as an adjunct solution can also reduce bubbles in the colon.
Future tech developments may help clinicians as well, he said, such as using AI to identify patients at high risk and modifying their prep process, creating a personalized prep on a digital platform with videos that guide patients through the process, and using a phone checklist tool to indicate when they’re ready for colonoscopy.
Improving Polyp Detection
Adenoma detection rates (ADR) can be highly variable due to different techniques, technical skills, pattern recognition, interpretation, and experience. New adjunct and AI-based tools can help improve ADR, especially if clinicians want to improve, receive training, and use best-practice techniques.
“In colonoscopy, it’s tricky because it’s not just a blood test or an x-ray. There’s really a lot of technique involved, both cognitive awareness and pattern recognition, as well as our technical skills,” said Tonya Kaltenbach, MD, professor of clinical medicine at the University of California San Francisco and director of advanced endoscopy at the San Francisco VA Health Care System in San Francisco.
For instance, multiple tools and techniques may be needed in real time to interpret a lesion, such as washing, retroflexing, and using better lighting, while paying attention to alerts and noting areas for further inspection and resection.
“This is not innate. It’s a learned skill,” she said. “It’s something we need to intentionally make efforts on and get feedback to improve.”
Improvement starts with using the right mindset for lesion detection, Dr. Kaltenbach said, by having a “reflexive recognition of deconstructed patterns of normal” — following the lines, vessels, and folds and looking for interruptions, abnormal thickness, and mucus caps. On top of that, adjunctive tools such as caps/cuffs and dye chromoendoscopy can help with proper ergonomics, irrigation, and mucosa exposure.
In the past 3 years, real-world studies using AI and computer-assisted detection have shown mixed results, with some demonstrating significant increases in ADR, while others haven’t, she said. However, being willing to try AI and other tools, such as the Endocuff cap, may help improve ADR, standardize interpretation, improve efficiency, and increase reproducibility.
“We’re always better with intentional feedback and deliberate practice,” she said. “Remember that if you improve, you’re protecting the patient from death and reducing interval cancer.”
Following Polyp Surveillance Intervals
The US Multi-Society Task Force on Colorectal Cancer’s recommendations for follow-up after colonoscopy and polypectomy provide valuable information and rationale for how to determine surveillance intervals for patients. However, clinicians still may be unsure what to recommend for some patients — or tell them to come back too soon, leading to unnecessary colonoscopy.
For instance, a 47-year-old woman who presents for her initial screening and has a single 6-mm polyp, which pathology returns as a single adenoma may be considered to be at average risk and suggested to return in 7-10 years. The guidelines seem more obvious for patients with one or two adenomas under 10 mm removed en bloc.
However, once the case details shift into gray areas and include three or four adenomas between 10 and 20 mm, or piecemeal removal, clinicians may differ on their recommendations, said Rajesh N. Keswani, MD, associate professor of medicine at the Northwestern University Feinberg School of Medicine and director of endoscopy for Northwestern Medicine in Chicago. At DDW 2024, Dr. Keswani presented several case examples, often finding various audience opinions.
In addition, he noted, recent studies have found that clinicians may estimate imprecise polyp measurements, struggle to identify sessile serrated polyposis syndrome, and often don’t follow evidence-based guidelines.
“Why do we ignore the guidelines? There’s this perception that a patient has risk factors that aren’t addressed by the guidelines, with regards to family history or a distant history of a large polyp that we don’t want to leave to the usual intervals,” he said. “We feel uncomfortable, even with our meticulous colonoscopy, telling people to come back in 10 years.”
To improve guideline adherence, Dr. Keswani suggested providing additional education, implementing an automated surveillance calculator, and using guidelines at the point of care. At Northwestern, for instance, clinicians use a hyperlink with an interpreted version of the guidelines with prior colonoscopy considerations. Overall though, practitioners should feel comfortable leaning toward longer surveillance intervals, he noted.
“More effort should be spent on getting unscreened patients in for colonoscopy than bringing back low-risk patients too early,” he said.
Reducing Environmental Effects
In recent waste audits of endoscopy rooms, providers generate 1-3 kg of waste per procedure, which would fill 117 soccer fields to a depth of 1 m, based on 18 million procedures in the United States per year. This waste comes from procedure-related equipment, administration, medications, travel of patients and staff, and infrastructure with systems such as air conditioning. Taking steps toward a green practice can reduce waste and the carbon footprint of healthcare.
“When we think about improving colonoscopy performance, the goal is to prevent colon cancer death, but when we expand that, we have to apply sustainable practices as a domain of quality,” said Heiko Pohl, MD, professor of medicine at the Geisel School of Medicine at Dartmouth in Hanover, New Hampshire, and a gastroenterologist at White River Junction VA Medical Center in White River Junction, Vermont.
The GI Multisociety Strategic Plan on Environmental Sustainability suggests a 5-year initiative to improve sustainability and reduce waste across seven domains — clinical setting, education, research, society efforts, intersociety efforts, industry, and advocacy.
For instance, clinicians can take the biggest step toward sustainability by avoiding unneeded colonoscopies, Dr. Pohl said, noting that between 20% and 30% aren’t appropriate or indicated. Instead, practitioners can implement longer surveillance intervals, adhere to guidelines, and consider alternative tests, such as the fecal immunochemical test, fecal DNA, blood-based tests, and CT colonography, where relevant.
Clinicians can also rethink their approach to resection, such as using a snare first instead of forceps to reduce single-instrument use, using clip closure only when it’s truly indicated, and implementing AI-assisted optical diagnosis to help with leaving rectosigmoid polyps in place.
In terms of physical waste, practices may also reconsider how they sort bins and biohazards, looking at new ways to dispose of regulated medical waste, sharps, recyclables, and typical trash. Waste audits can help find ways to reduce paper, combine procedures, and create more efficient use of endoscopy rooms.
“We are really in a very precarious situation,” Dr. Pohl said. “It’s our generation that has a responsibility to change the course for our children’s and grandchildren’s sake.”
AI for Quality And Efficiency
Moving forward, AI tools will likely become more popular in various parts of GI practice, by assisting with documentation, spotting polyps, tracking mucosal surfaces, providing optical histopathology, and supervising performance through high-quality feedback.
“Endoscopy has reached the limits of human visual capacity, where seeing more pixels won’t necessarily improve clinical diagnosis. What’s next for elevating the care of patients really is AI,” said Jason B. Samarasena, MD, professor of medicine and program director of the interventional endoscopy training program at the University of California Irvine in Irvine, California.
As practices adopt AI-based systems, however, clinicians should be cautious about a false sense of comfort or “alarm fatigue” if bounding boxes become distracting. Instead, new tools need to be adopted as a “physician-AI hybrid,” with the endoscopist in mind, particularly if helpful for performing a better exam by watching withdrawal time or endoscope slippage.
“In real-world practice, this is being implemented without attention to endoscopist inclination and behavior,” he said. “Having a better understanding of physician attitudes could yield more optimal results.”
Notably, AI-assisted tools should be viewed akin to spell-check, which signals to the endoscopist when to pay attention and double-check an area — but primarily relies on the expert to do a high-quality exam, said Aasma Shaukat, MD, professor of medicine and director of GI outcomes research at the NYU Grossman School of Medicine, New York City.
“This should be an adjunct or an additional tool, not a replacement tool,” she added. “This doesn’t mean to stop doing astute observation.”
Future tools show promise in terms of tracking additional data related to prep quality, cecal landmarks, polyp size, mucosa exposure, histology prediction, and complete resection. These automated reports could also link to real-time dashboards, hospital or national registries, and reimbursement systems, Dr. Shaukat noted.
“At the end of the day, our interests are aligned,” she said. “Everybody cares about quality, patient satisfaction, and reimbursement, and with that goal in mind, I think some of the tools can be applied to show how we can achieve those principles together.”
Dr. Jacobson, Dr. Kaltenbach, Dr. Keswani, Dr. Pohl, Dr. Samarasena, and Dr. Shaukat reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
According to several experts who spoke at the American Gastroenterological Association’s Postgraduate Course this spring, which was offered at Digestive Disease Week (DDW), gastroenterologists can take these five steps to improve their performance: Addressing poor bowel prep, improving polyp detection, following the best intervals for polyp surveillance, reducing the environmental impact of gastrointestinal (GI) practice, and implementing artificial intelligence (AI) tools for efficiency and quality.
Addressing Poor Prep
To improve bowel preparation rates, clinicians may consider identifying those at high risk for inadequate prep, which could include known risk factors such as age, body mass index, inpatient status, constipation, tobacco use, and hypertension. However, other variables tend to serve as bigger predictors of inadequate prep, such as the patient’s status regarding cirrhosis, Parkinson’s disease, dementia, diabetes, opioid use, gastroparesis, tricyclics, and colorectal surgery.
Although several prediction models are based on some of these factors — looking at comorbidities, antidepressant use, constipation, and prior abdominal or pelvic surgery — the data don’t indicate whether knowing about or addressing these risks actually leads to better bowel prep, said Brian Jacobson, MD, associate professor of medicine at Harvard Medical School, Boston, and director of program development for gastroenterology at Massachusetts General Hospital in Boston.
Instead, the biggest return-on-investment option is to maximize prep for all patients, he said, especially since every patient has at least some risk of poor prep, either due to the required diet changes, medication considerations, or purgative solution and timing.
To create a state-of-the-art bowel prep process, Dr. Jacobson recommended numerous tactics for all patients: Verbal and written instructions for all components of prep, patient navigation with phone or virtual messaging to guide patients through the process, a low-fiber or all-liquid diet on the day before colonoscopy, and a split-dose 2-L prep regimen. Patients should begin the second half of the split-dose regimen 4-6 hours before colonoscopy and complete it at least 2 hours before the procedure starts, and clinicians should use an irrigation pump during colonoscopy to improve visibility.
Beyond that, Dr. Jacobson noted, higher risk patients can take a split-dose 4-L prep regimen with bisacodyl, a low-fiber diet 2-3 days before colonoscopy, and a clear liquid diet the day before colonoscopy. Using simethicone as an adjunct solution can also reduce bubbles in the colon.
Future tech developments may help clinicians as well, he said, such as using AI to identify patients at high risk and modifying their prep process, creating a personalized prep on a digital platform with videos that guide patients through the process, and using a phone checklist tool to indicate when they’re ready for colonoscopy.
Improving Polyp Detection
Adenoma detection rates (ADR) can be highly variable due to different techniques, technical skills, pattern recognition, interpretation, and experience. New adjunct and AI-based tools can help improve ADR, especially if clinicians want to improve, receive training, and use best-practice techniques.
“In colonoscopy, it’s tricky because it’s not just a blood test or an x-ray. There’s really a lot of technique involved, both cognitive awareness and pattern recognition, as well as our technical skills,” said Tonya Kaltenbach, MD, professor of clinical medicine at the University of California San Francisco and director of advanced endoscopy at the San Francisco VA Health Care System in San Francisco.
For instance, multiple tools and techniques may be needed in real time to interpret a lesion, such as washing, retroflexing, and using better lighting, while paying attention to alerts and noting areas for further inspection and resection.
“This is not innate. It’s a learned skill,” she said. “It’s something we need to intentionally make efforts on and get feedback to improve.”
Improvement starts with using the right mindset for lesion detection, Dr. Kaltenbach said, by having a “reflexive recognition of deconstructed patterns of normal” — following the lines, vessels, and folds and looking for interruptions, abnormal thickness, and mucus caps. On top of that, adjunctive tools such as caps/cuffs and dye chromoendoscopy can help with proper ergonomics, irrigation, and mucosa exposure.
In the past 3 years, real-world studies using AI and computer-assisted detection have shown mixed results, with some demonstrating significant increases in ADR, while others haven’t, she said. However, being willing to try AI and other tools, such as the Endocuff cap, may help improve ADR, standardize interpretation, improve efficiency, and increase reproducibility.
“We’re always better with intentional feedback and deliberate practice,” she said. “Remember that if you improve, you’re protecting the patient from death and reducing interval cancer.”
Following Polyp Surveillance Intervals
The US Multi-Society Task Force on Colorectal Cancer’s recommendations for follow-up after colonoscopy and polypectomy provide valuable information and rationale for how to determine surveillance intervals for patients. However, clinicians still may be unsure what to recommend for some patients — or tell them to come back too soon, leading to unnecessary colonoscopy.
For instance, a 47-year-old woman who presents for her initial screening and has a single 6-mm polyp, which pathology returns as a single adenoma may be considered to be at average risk and suggested to return in 7-10 years. The guidelines seem more obvious for patients with one or two adenomas under 10 mm removed en bloc.
However, once the case details shift into gray areas and include three or four adenomas between 10 and 20 mm, or piecemeal removal, clinicians may differ on their recommendations, said Rajesh N. Keswani, MD, associate professor of medicine at the Northwestern University Feinberg School of Medicine and director of endoscopy for Northwestern Medicine in Chicago. At DDW 2024, Dr. Keswani presented several case examples, often finding various audience opinions.
In addition, he noted, recent studies have found that clinicians may estimate imprecise polyp measurements, struggle to identify sessile serrated polyposis syndrome, and often don’t follow evidence-based guidelines.
“Why do we ignore the guidelines? There’s this perception that a patient has risk factors that aren’t addressed by the guidelines, with regards to family history or a distant history of a large polyp that we don’t want to leave to the usual intervals,” he said. “We feel uncomfortable, even with our meticulous colonoscopy, telling people to come back in 10 years.”
To improve guideline adherence, Dr. Keswani suggested providing additional education, implementing an automated surveillance calculator, and using guidelines at the point of care. At Northwestern, for instance, clinicians use a hyperlink with an interpreted version of the guidelines with prior colonoscopy considerations. Overall though, practitioners should feel comfortable leaning toward longer surveillance intervals, he noted.
“More effort should be spent on getting unscreened patients in for colonoscopy than bringing back low-risk patients too early,” he said.
Reducing Environmental Effects
In recent waste audits of endoscopy rooms, providers generate 1-3 kg of waste per procedure, which would fill 117 soccer fields to a depth of 1 m, based on 18 million procedures in the United States per year. This waste comes from procedure-related equipment, administration, medications, travel of patients and staff, and infrastructure with systems such as air conditioning. Taking steps toward a green practice can reduce waste and the carbon footprint of healthcare.
“When we think about improving colonoscopy performance, the goal is to prevent colon cancer death, but when we expand that, we have to apply sustainable practices as a domain of quality,” said Heiko Pohl, MD, professor of medicine at the Geisel School of Medicine at Dartmouth in Hanover, New Hampshire, and a gastroenterologist at White River Junction VA Medical Center in White River Junction, Vermont.
The GI Multisociety Strategic Plan on Environmental Sustainability suggests a 5-year initiative to improve sustainability and reduce waste across seven domains — clinical setting, education, research, society efforts, intersociety efforts, industry, and advocacy.
For instance, clinicians can take the biggest step toward sustainability by avoiding unneeded colonoscopies, Dr. Pohl said, noting that between 20% and 30% aren’t appropriate or indicated. Instead, practitioners can implement longer surveillance intervals, adhere to guidelines, and consider alternative tests, such as the fecal immunochemical test, fecal DNA, blood-based tests, and CT colonography, where relevant.
Clinicians can also rethink their approach to resection, such as using a snare first instead of forceps to reduce single-instrument use, using clip closure only when it’s truly indicated, and implementing AI-assisted optical diagnosis to help with leaving rectosigmoid polyps in place.
In terms of physical waste, practices may also reconsider how they sort bins and biohazards, looking at new ways to dispose of regulated medical waste, sharps, recyclables, and typical trash. Waste audits can help find ways to reduce paper, combine procedures, and create more efficient use of endoscopy rooms.
“We are really in a very precarious situation,” Dr. Pohl said. “It’s our generation that has a responsibility to change the course for our children’s and grandchildren’s sake.”
AI for Quality And Efficiency
Moving forward, AI tools will likely become more popular in various parts of GI practice, by assisting with documentation, spotting polyps, tracking mucosal surfaces, providing optical histopathology, and supervising performance through high-quality feedback.
“Endoscopy has reached the limits of human visual capacity, where seeing more pixels won’t necessarily improve clinical diagnosis. What’s next for elevating the care of patients really is AI,” said Jason B. Samarasena, MD, professor of medicine and program director of the interventional endoscopy training program at the University of California Irvine in Irvine, California.
As practices adopt AI-based systems, however, clinicians should be cautious about a false sense of comfort or “alarm fatigue” if bounding boxes become distracting. Instead, new tools need to be adopted as a “physician-AI hybrid,” with the endoscopist in mind, particularly if helpful for performing a better exam by watching withdrawal time or endoscope slippage.
“In real-world practice, this is being implemented without attention to endoscopist inclination and behavior,” he said. “Having a better understanding of physician attitudes could yield more optimal results.”
Notably, AI-assisted tools should be viewed akin to spell-check, which signals to the endoscopist when to pay attention and double-check an area — but primarily relies on the expert to do a high-quality exam, said Aasma Shaukat, MD, professor of medicine and director of GI outcomes research at the NYU Grossman School of Medicine, New York City.
“This should be an adjunct or an additional tool, not a replacement tool,” she added. “This doesn’t mean to stop doing astute observation.”
Future tools show promise in terms of tracking additional data related to prep quality, cecal landmarks, polyp size, mucosa exposure, histology prediction, and complete resection. These automated reports could also link to real-time dashboards, hospital or national registries, and reimbursement systems, Dr. Shaukat noted.
“At the end of the day, our interests are aligned,” she said. “Everybody cares about quality, patient satisfaction, and reimbursement, and with that goal in mind, I think some of the tools can be applied to show how we can achieve those principles together.”
Dr. Jacobson, Dr. Kaltenbach, Dr. Keswani, Dr. Pohl, Dr. Samarasena, and Dr. Shaukat reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
High-Dose Vitamin D Linked to Lower Disease Activity in CIS
COPENHAGEN — , results of a randomized, controlled trial suggest. In addition, cholecalciferol had a favorable safety profile and was well tolerated.
“These data support high-dose vitamin D supplementation in early MS and make vitamin D the best candidate for add-on therapy evaluation in the therapeutic strategy for multiple sclerosis [MS],” said study author Eric Thouvenot, MD, PhD, University Hospital of Nimes, Neurology Department, Nimes, France.
The study was presented at the 2024 ECTRIMS annual meeting.
Vitamin D Supplementation Versus Placebo
Research shows vitamin D deficiency is a risk factor for MS. However, results of previous research investigating vitamin D supplementation in MS, with different regimens and durations, have been contradictory.
The current double-blind study included 303 adults newly diagnosed with CIS (within 90 days) and a serum 25-hydroxy vitamin D concentration of less than 100 nmol/L at baseline. Participants had a median age of 34 years, and 70% were women.
About one third of participants had optic neuritis, two thirds had oligoclonal bands from cerebrospinal fluid analysis, and the median Expanded Disability Status Scale (EDSS) score was 1.0. Of the total, 89% fulfilled 2017 McDonald criteria for the diagnosis of relapsing-remitting MS (RRMS).
Participants were randomly assigned to receive high-dose (100,000 international units) oral cholecalciferol or placebo every 2 weeks for 24 months. Participants had a clinical visit at 3, 6, 12, 18, and 24 months, and brain and spinal cord MRI with and without gadolinium at 3, 12, and 24 months.
The primary outcome was occurrence of disease activity — relapse, new or enlarging T2 lesions, and presence of contrast-enhancing lesions.
Significant Difference
During follow-up, 60.3% in the vitamin group showed evidence of disease activity versus 74.1% in the placebo group (hazard ratio [HR], 0.66; 95% CI, 0.50-0.87; P = .004). In addition, the median time to evidence of disease activity was 432 days in the vitamin D group versus 224 days in the placebo group (P = .003).
“As you can see, the difference is really, really significant,” said Dr. Thouvenot, referring to a Kaplan-Meier curve. He said he was somewhat surprised by the “very rapid” effect of vitamin D.
He noted that the 34% reduction in relative risk for disease activity is “similar to that of some published platform therapies for CIS patients.”
An analysis of the 247 patients who met 2017 McDonald criteria for RRMS at baseline showed the same results.
Secondary analyses showed no significant reduction in relapses and no significant differences for annual change in EDSS, quality of life, fatigue, anxiety, or depression.
Additional analyses showed the HR was unchanged after adjusting for known prognostic factors including age, sex, number of lesions (< 9 vs ≥ 9), EDSS score at baseline, and delay between CIS and treatment onset.
Results showed vitamin D3 supplementation was safe and well tolerated. Dr. Thouvenot noted that 95% of participants completed the trial, and none of the 33 severe adverse events in 30 patients suggested hypercalcemia or were related to the study drug.
These encouraging new data support further studies of high-dose vitamin D supplementation as an add-on therapy in early MS, said Dr. Thouvenot. He noted that animal models suggest vitamin D added to interferon beta has a synergistic effect on the immune system.
‘Fabulous’ Research
During a question-and-answer session, delegates praised the study, with some describing it as “fantastic” or “fabulous.”
Addressing a query about why this study succeeded in showing the benefits of vitamin D while numerous previous studies did not, Dr. Thouvenot said it may be due to the longer duration or a design that was better powered to show differences.
Asked if researchers examined vitamin D blood levels during the study, Dr. Thouvenot said these measures are “ongoing.”
Responding to a question of whether high-dose vitamin D could be a lifelong treatment, he referred again to the “excellent” safety of the intervention. Not only is it well tolerated, but vitamin D benefits bones and the risk for hypercalcemia is low except perhaps for patients with tuberculosis or sarcoidosis, he said.
“When you exclude those patients, the safety is huge, so I don’t know why we should stop it once it’s started.”
This study was funded in part by the French Ministry of Health. Dr. Thouvenot reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
COPENHAGEN — , results of a randomized, controlled trial suggest. In addition, cholecalciferol had a favorable safety profile and was well tolerated.
“These data support high-dose vitamin D supplementation in early MS and make vitamin D the best candidate for add-on therapy evaluation in the therapeutic strategy for multiple sclerosis [MS],” said study author Eric Thouvenot, MD, PhD, University Hospital of Nimes, Neurology Department, Nimes, France.
The study was presented at the 2024 ECTRIMS annual meeting.
Vitamin D Supplementation Versus Placebo
Research shows vitamin D deficiency is a risk factor for MS. However, results of previous research investigating vitamin D supplementation in MS, with different regimens and durations, have been contradictory.
The current double-blind study included 303 adults newly diagnosed with CIS (within 90 days) and a serum 25-hydroxy vitamin D concentration of less than 100 nmol/L at baseline. Participants had a median age of 34 years, and 70% were women.
About one third of participants had optic neuritis, two thirds had oligoclonal bands from cerebrospinal fluid analysis, and the median Expanded Disability Status Scale (EDSS) score was 1.0. Of the total, 89% fulfilled 2017 McDonald criteria for the diagnosis of relapsing-remitting MS (RRMS).
Participants were randomly assigned to receive high-dose (100,000 international units) oral cholecalciferol or placebo every 2 weeks for 24 months. Participants had a clinical visit at 3, 6, 12, 18, and 24 months, and brain and spinal cord MRI with and without gadolinium at 3, 12, and 24 months.
The primary outcome was occurrence of disease activity — relapse, new or enlarging T2 lesions, and presence of contrast-enhancing lesions.
Significant Difference
During follow-up, 60.3% in the vitamin group showed evidence of disease activity versus 74.1% in the placebo group (hazard ratio [HR], 0.66; 95% CI, 0.50-0.87; P = .004). In addition, the median time to evidence of disease activity was 432 days in the vitamin D group versus 224 days in the placebo group (P = .003).
“As you can see, the difference is really, really significant,” said Dr. Thouvenot, referring to a Kaplan-Meier curve. He said he was somewhat surprised by the “very rapid” effect of vitamin D.
He noted that the 34% reduction in relative risk for disease activity is “similar to that of some published platform therapies for CIS patients.”
An analysis of the 247 patients who met 2017 McDonald criteria for RRMS at baseline showed the same results.
Secondary analyses showed no significant reduction in relapses and no significant differences for annual change in EDSS, quality of life, fatigue, anxiety, or depression.
Additional analyses showed the HR was unchanged after adjusting for known prognostic factors including age, sex, number of lesions (< 9 vs ≥ 9), EDSS score at baseline, and delay between CIS and treatment onset.
Results showed vitamin D3 supplementation was safe and well tolerated. Dr. Thouvenot noted that 95% of participants completed the trial, and none of the 33 severe adverse events in 30 patients suggested hypercalcemia or were related to the study drug.
These encouraging new data support further studies of high-dose vitamin D supplementation as an add-on therapy in early MS, said Dr. Thouvenot. He noted that animal models suggest vitamin D added to interferon beta has a synergistic effect on the immune system.
‘Fabulous’ Research
During a question-and-answer session, delegates praised the study, with some describing it as “fantastic” or “fabulous.”
Addressing a query about why this study succeeded in showing the benefits of vitamin D while numerous previous studies did not, Dr. Thouvenot said it may be due to the longer duration or a design that was better powered to show differences.
Asked if researchers examined vitamin D blood levels during the study, Dr. Thouvenot said these measures are “ongoing.”
Responding to a question of whether high-dose vitamin D could be a lifelong treatment, he referred again to the “excellent” safety of the intervention. Not only is it well tolerated, but vitamin D benefits bones and the risk for hypercalcemia is low except perhaps for patients with tuberculosis or sarcoidosis, he said.
“When you exclude those patients, the safety is huge, so I don’t know why we should stop it once it’s started.”
This study was funded in part by the French Ministry of Health. Dr. Thouvenot reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
COPENHAGEN — , results of a randomized, controlled trial suggest. In addition, cholecalciferol had a favorable safety profile and was well tolerated.
“These data support high-dose vitamin D supplementation in early MS and make vitamin D the best candidate for add-on therapy evaluation in the therapeutic strategy for multiple sclerosis [MS],” said study author Eric Thouvenot, MD, PhD, University Hospital of Nimes, Neurology Department, Nimes, France.
The study was presented at the 2024 ECTRIMS annual meeting.
Vitamin D Supplementation Versus Placebo
Research shows vitamin D deficiency is a risk factor for MS. However, results of previous research investigating vitamin D supplementation in MS, with different regimens and durations, have been contradictory.
The current double-blind study included 303 adults newly diagnosed with CIS (within 90 days) and a serum 25-hydroxy vitamin D concentration of less than 100 nmol/L at baseline. Participants had a median age of 34 years, and 70% were women.
About one third of participants had optic neuritis, two thirds had oligoclonal bands from cerebrospinal fluid analysis, and the median Expanded Disability Status Scale (EDSS) score was 1.0. Of the total, 89% fulfilled 2017 McDonald criteria for the diagnosis of relapsing-remitting MS (RRMS).
Participants were randomly assigned to receive high-dose (100,000 international units) oral cholecalciferol or placebo every 2 weeks for 24 months. Participants had a clinical visit at 3, 6, 12, 18, and 24 months, and brain and spinal cord MRI with and without gadolinium at 3, 12, and 24 months.
The primary outcome was occurrence of disease activity — relapse, new or enlarging T2 lesions, and presence of contrast-enhancing lesions.
Significant Difference
During follow-up, 60.3% in the vitamin group showed evidence of disease activity versus 74.1% in the placebo group (hazard ratio [HR], 0.66; 95% CI, 0.50-0.87; P = .004). In addition, the median time to evidence of disease activity was 432 days in the vitamin D group versus 224 days in the placebo group (P = .003).
“As you can see, the difference is really, really significant,” said Dr. Thouvenot, referring to a Kaplan-Meier curve. He said he was somewhat surprised by the “very rapid” effect of vitamin D.
He noted that the 34% reduction in relative risk for disease activity is “similar to that of some published platform therapies for CIS patients.”
An analysis of the 247 patients who met 2017 McDonald criteria for RRMS at baseline showed the same results.
Secondary analyses showed no significant reduction in relapses and no significant differences for annual change in EDSS, quality of life, fatigue, anxiety, or depression.
Additional analyses showed the HR was unchanged after adjusting for known prognostic factors including age, sex, number of lesions (< 9 vs ≥ 9), EDSS score at baseline, and delay between CIS and treatment onset.
Results showed vitamin D3 supplementation was safe and well tolerated. Dr. Thouvenot noted that 95% of participants completed the trial, and none of the 33 severe adverse events in 30 patients suggested hypercalcemia or were related to the study drug.
These encouraging new data support further studies of high-dose vitamin D supplementation as an add-on therapy in early MS, said Dr. Thouvenot. He noted that animal models suggest vitamin D added to interferon beta has a synergistic effect on the immune system.
‘Fabulous’ Research
During a question-and-answer session, delegates praised the study, with some describing it as “fantastic” or “fabulous.”
Addressing a query about why this study succeeded in showing the benefits of vitamin D while numerous previous studies did not, Dr. Thouvenot said it may be due to the longer duration or a design that was better powered to show differences.
Asked if researchers examined vitamin D blood levels during the study, Dr. Thouvenot said these measures are “ongoing.”
Responding to a question of whether high-dose vitamin D could be a lifelong treatment, he referred again to the “excellent” safety of the intervention. Not only is it well tolerated, but vitamin D benefits bones and the risk for hypercalcemia is low except perhaps for patients with tuberculosis or sarcoidosis, he said.
“When you exclude those patients, the safety is huge, so I don’t know why we should stop it once it’s started.”
This study was funded in part by the French Ministry of Health. Dr. Thouvenot reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2024
Harnessing Doxycycline for STI Prevention: A Vital Role for Primary Care Physicians
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.

Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.
Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Primary care physicians frequently offer postexposure prophylaxis for various infections, including influenza, pertussis, tetanus, hepatitis, and Lyme disease, among others. However, the scope of postexposure prophylaxis in primary care is expanding, presenting an opportunity to further integrate it into patient care. As primary care providers, we have the unique advantage of being involved in both preventive care and immediate response, particularly in urgent care or triage scenarios. This dual role is crucial, as timely administration of postexposure prophylaxis can prevent infections from taking hold, especially following high-risk exposures.
Recently, the use of doxycycline as a form of postexposure prophylaxis for sexually transmitted infections (STIs) has gained attention. Traditionally, doxycycline has been used as preexposure or postexposure prophylaxis for conditions like malaria and Lyme disease but has not been widely employed for STI prevention until now. Doxycycline is a relatively common medication, generally safe with side effects that typically resolve upon discontinuation. Several open-label studies have shown that taking 200 mg of doxycycline within 72 hours of condomless sex significantly reduces the incidence of chlamydia, gonorrhea, and syphilis among gay, bisexual, and other men who have sex with men, as well as transgender women who have previously had a bacterial STI. However, these benefits have not been consistently observed among cisgender women and heterosexual men.
Given these findings, the Centers for Disease Control and Prevention now recommends that clinicians discuss the risks and benefits of doxycycline PEP (Doxy PEP) with gay, bisexual, and other men who have sex with men, as well as transgender women who have had a bacterial STI in the past 12 months. This discussion should be part of a shared decision-making process, advising the use of 200 mg of doxycycline within 72 hours of oral, vaginal, or anal sex, with the recommendation not to exceed 200 mg every 24 hours and to reassess the need for continued use every 3-6 months. Doxy PEP can be safely prescribed with preexposure prophylaxis for HIV (PrEP). Patients who receive PrEP may often be eligible for Doxy PEP, though the groups are not always the same.
The shared decision-making process is essential when considering Doxy PEP. While cost-effective and proven to reduce the risk of gonorrhea, chlamydia, and syphilis, its benefits vary among different populations. Moreover, some patients may experience side effects such as photosensitivity and gastrointestinal discomfort. Since the effectiveness of prophylaxis is closely tied to the timing of exposure and the patient’s current risk factors, it is important to regularly evaluate whether Doxy PEP remains beneficial. As there is not yet clear benefit to heterosexual men and cisgender women, opportunities still need to be explored for them.
Integrating Doxy PEP into a primary care practice can be done efficiently. A standing order protocol could be established for telehealth visits or nurse triage, allowing timely administration when patients report an exposure within 72 hours. It could also be incorporated into electronic medical records as part of a smart set for easy access to orders and as standard educational material in after-visit instructions. As this option is new, it is also important to discuss it with patients before they may need it so that they are aware should the need arise. While concerns about antibiotic resistance are valid, studies have not yet shown significant resistance issues related to Doxy PEP use, though ongoing monitoring is necessary.
You might wonder why primary care should prioritize this intervention. As the first point of contact, primary care providers are well-positioned to identify the need for prophylaxis, particularly since its effectiveness diminishes over time. Furthermore, the established, trusting relationships that primary care physicians often have with their patients create a nonjudgmental environment that encourages disclosure of potential exposures. This trust, combined with easier access to care, can make a significant difference in the timely provision of postexposure prophylaxis. By offering comprehensive, holistic care, including prophylaxis, primary care physicians can prevent infections and address conditions before they lead to serious complications. Therefore, family medicine physicians should consider incorporating Doxy PEP into their practices as a standard of care.
Dr. Wheat is vice chair of Diversity, Equity, and Inclusion, Department of Family and Community Medicine, and associate professor, Family and Community Medicine, at Northwestern University’s Feinberg School of Medicine, Chicago. She has no relevant financial disclosures.
References
Bachmann LH et al. CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024. MMWR Recomm Rep 2024;73(No. RR-2):1-8.
Traeger MW et al. Potential Impact of Doxycycline Postexposure Prophylaxis Prescribing Strategies on Incidence of Bacterial Sexually Transmitted Infections. (Clin Infect Dis. 2023 Aug 18. doi: 10.1093/cid/ciad488).
Controlling Six Risk Factors Can Combat CKD in Obesity
TOPLINE:
Optimal management of blood pressure, A1c levels, low-density lipoprotein cholesterol (LDL-C), albuminuria, smoking, and physical activity may reduce the excess risk for chronic kidney disease (CKD) typically linked to obesity. The protective effect is more pronounced in men, in those with lower healthy food scores, and in users of diabetes medication.
METHODOLOGY:
- Obesity is a significant risk factor for CKD, but it is unknown if managing multiple other obesity-related CKD risk factors can mitigate the excess CKD risk.
- Researchers assessed CKD risk factor control in 97,538 participants with obesity from the UK Biobank and compared them with an equal number of age- and sex-matched control participants with normal body weight and no CKD at baseline.
- Participants with obesity were assessed for six modifiable risk factors: Blood pressure, A1c levels, LDL-C, albuminuria, smoking, and physical activity.
- Overall, 2487, 12,720, 32,388, 36,988, and 15,381 participants with obesity had at most two, three, four, five, and six risk factors under combined control, respectively, with the two or fewer group serving as the reference.
- The primary outcome was incident CKD and the degree of combined risk factor control in persons. The CKD risk and risk factor control in participants with obesity were also compared with CKD incidence in matched normal weight participants.
TAKEAWAY:
- During a median follow-up period of 10.8 years, 3954 cases of incident CKD were reported in participants with obesity and 1498 cases in matched persons of normal body mass index (BMI).
- In a stepwise pattern, optimal control of each additional risk factor was associated with 11% (adjusted hazard ratio [aHR], 0.89; 95% CI, 0.86-0.91) reduction in the incidence of CKD events, down to a 49% reduction in CKD incidence (aHR, 0.51; 95% CI, 0.43-0.61) for combined control of all six risk factors in participants with obesity.
- The protective effect of combined control of risk factors was more pronounced in men vs women, in those with lower vs higher healthy diet scores, and in users vs nonusers of diabetes medication.
- A similar stepwise pattern emerged between the number of risk factors controlled and CKD risk in participants with obesity compared with matched individuals of normal BMI, with the excess CKD risk eliminated in participants with obesity with six risk factors under control.
IN PRACTICE:
“Comprehensive control of risk factors might effectively neutralize the excessive CKD risk associated with obesity, emphasizing the potential of a joint management approach in the prevention of CKD in this population,” the authors wrote.
SOURCE:
The study was led by Rui Tang, MS, Department of Epidemiology, School of Public Health and Tropical Medicine, Tulane University, New Orleans, Louisiana. It was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The evaluated risk factors for CKD were arbitrarily selected, which may not represent the ideal group. The study did not consider the time-varying effect of joint risk factor control owing to the lack of some variables such as A1c. The generalizability of the findings was limited because over 90% of the UK Biobank cohort is composed of White people and individuals with healthier behaviors compared with the overall UK population.
DISCLOSURES:
The study was supported by grants from the US National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Optimal management of blood pressure, A1c levels, low-density lipoprotein cholesterol (LDL-C), albuminuria, smoking, and physical activity may reduce the excess risk for chronic kidney disease (CKD) typically linked to obesity. The protective effect is more pronounced in men, in those with lower healthy food scores, and in users of diabetes medication.
METHODOLOGY:
- Obesity is a significant risk factor for CKD, but it is unknown if managing multiple other obesity-related CKD risk factors can mitigate the excess CKD risk.
- Researchers assessed CKD risk factor control in 97,538 participants with obesity from the UK Biobank and compared them with an equal number of age- and sex-matched control participants with normal body weight and no CKD at baseline.
- Participants with obesity were assessed for six modifiable risk factors: Blood pressure, A1c levels, LDL-C, albuminuria, smoking, and physical activity.
- Overall, 2487, 12,720, 32,388, 36,988, and 15,381 participants with obesity had at most two, three, four, five, and six risk factors under combined control, respectively, with the two or fewer group serving as the reference.
- The primary outcome was incident CKD and the degree of combined risk factor control in persons. The CKD risk and risk factor control in participants with obesity were also compared with CKD incidence in matched normal weight participants.
TAKEAWAY:
- During a median follow-up period of 10.8 years, 3954 cases of incident CKD were reported in participants with obesity and 1498 cases in matched persons of normal body mass index (BMI).
- In a stepwise pattern, optimal control of each additional risk factor was associated with 11% (adjusted hazard ratio [aHR], 0.89; 95% CI, 0.86-0.91) reduction in the incidence of CKD events, down to a 49% reduction in CKD incidence (aHR, 0.51; 95% CI, 0.43-0.61) for combined control of all six risk factors in participants with obesity.
- The protective effect of combined control of risk factors was more pronounced in men vs women, in those with lower vs higher healthy diet scores, and in users vs nonusers of diabetes medication.
- A similar stepwise pattern emerged between the number of risk factors controlled and CKD risk in participants with obesity compared with matched individuals of normal BMI, with the excess CKD risk eliminated in participants with obesity with six risk factors under control.
IN PRACTICE:
“Comprehensive control of risk factors might effectively neutralize the excessive CKD risk associated with obesity, emphasizing the potential of a joint management approach in the prevention of CKD in this population,” the authors wrote.
SOURCE:
The study was led by Rui Tang, MS, Department of Epidemiology, School of Public Health and Tropical Medicine, Tulane University, New Orleans, Louisiana. It was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The evaluated risk factors for CKD were arbitrarily selected, which may not represent the ideal group. The study did not consider the time-varying effect of joint risk factor control owing to the lack of some variables such as A1c. The generalizability of the findings was limited because over 90% of the UK Biobank cohort is composed of White people and individuals with healthier behaviors compared with the overall UK population.
DISCLOSURES:
The study was supported by grants from the US National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Optimal management of blood pressure, A1c levels, low-density lipoprotein cholesterol (LDL-C), albuminuria, smoking, and physical activity may reduce the excess risk for chronic kidney disease (CKD) typically linked to obesity. The protective effect is more pronounced in men, in those with lower healthy food scores, and in users of diabetes medication.
METHODOLOGY:
- Obesity is a significant risk factor for CKD, but it is unknown if managing multiple other obesity-related CKD risk factors can mitigate the excess CKD risk.
- Researchers assessed CKD risk factor control in 97,538 participants with obesity from the UK Biobank and compared them with an equal number of age- and sex-matched control participants with normal body weight and no CKD at baseline.
- Participants with obesity were assessed for six modifiable risk factors: Blood pressure, A1c levels, LDL-C, albuminuria, smoking, and physical activity.
- Overall, 2487, 12,720, 32,388, 36,988, and 15,381 participants with obesity had at most two, three, four, five, and six risk factors under combined control, respectively, with the two or fewer group serving as the reference.
- The primary outcome was incident CKD and the degree of combined risk factor control in persons. The CKD risk and risk factor control in participants with obesity were also compared with CKD incidence in matched normal weight participants.
TAKEAWAY:
- During a median follow-up period of 10.8 years, 3954 cases of incident CKD were reported in participants with obesity and 1498 cases in matched persons of normal body mass index (BMI).
- In a stepwise pattern, optimal control of each additional risk factor was associated with 11% (adjusted hazard ratio [aHR], 0.89; 95% CI, 0.86-0.91) reduction in the incidence of CKD events, down to a 49% reduction in CKD incidence (aHR, 0.51; 95% CI, 0.43-0.61) for combined control of all six risk factors in participants with obesity.
- The protective effect of combined control of risk factors was more pronounced in men vs women, in those with lower vs higher healthy diet scores, and in users vs nonusers of diabetes medication.
- A similar stepwise pattern emerged between the number of risk factors controlled and CKD risk in participants with obesity compared with matched individuals of normal BMI, with the excess CKD risk eliminated in participants with obesity with six risk factors under control.
IN PRACTICE:
“Comprehensive control of risk factors might effectively neutralize the excessive CKD risk associated with obesity, emphasizing the potential of a joint management approach in the prevention of CKD in this population,” the authors wrote.
SOURCE:
The study was led by Rui Tang, MS, Department of Epidemiology, School of Public Health and Tropical Medicine, Tulane University, New Orleans, Louisiana. It was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The evaluated risk factors for CKD were arbitrarily selected, which may not represent the ideal group. The study did not consider the time-varying effect of joint risk factor control owing to the lack of some variables such as A1c. The generalizability of the findings was limited because over 90% of the UK Biobank cohort is composed of White people and individuals with healthier behaviors compared with the overall UK population.
DISCLOSURES:
The study was supported by grants from the US National Heart, Lung, and Blood Institute and the National Institute of Diabetes and Digestive and Kidney Diseases. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Starting Mammography at Age 40 May Backfire Due to False Positives
Earlier this year, I wrote a Medscape commentary to explain my disagreement with the US Preventive Services Task Force (USPSTF)’s updated recommendation that all women at average risk for breast cancer start screening mammography at age 40. The bottom line is that when the evidence doesn’t change, the guidelines shouldn’t change. Since then, other screening experts have criticized the USPSTF guideline on similar grounds, and a national survey reported that nearly 4 out of 10 women in their 40s preferred to delay breast cancer screening after viewing a decision aid and a personalized breast cancer risk estimate.
The decision analysis performed for the USPSTF guideline estimated that compared with having mammography beginning at age 50, 1000 women who begin at age 40 experience 519 more false-positive results and 62 more benign breast biopsies. Another study suggested that anxiety and other psychosocial harms resulting from a false-positive test are similar between patients who require a biopsy vs additional imaging only. Of greater concern, women who have false-positive results are less likely to return for their next scheduled screening exam.
A recent analysis of 2005-2017 data from the US Breast Cancer Surveillance Consortium found that about 1 in 10 mammograms had a false-positive result. Sixty percent of these patients underwent immediate additional imaging, 27% were recalled for diagnostic imaging within the next few days to weeks, and 13% were advised to have a biopsy. While patients who had additional imaging at the same visit were only 1.9% less likely to return for screening mammography within 30 months compared with those with normal mammograms, women who were recalled for short-interval follow-up or recommended for biopsy were 15.9% and 10% less likely to return, respectively. For unclear reasons, women who identified as Asian or Hispanic had even lower rates of return screening after false-positive results.
These differences matter because women in their 40s, with the lowest incidence of breast cancer among those undergoing screening, have a lot of false positives. A patient who follows the USPSTF recommendation and starts screening at age 40 has a 42% chance of having at least one false positive with every-other-year screening, or a 61% chance with annual screening, by the time she turns 50. If some of these patients are so turned off by false positives that they don’t return for regular mammography in their 50s and 60s, when screening is the most likely to catch clinically significant cancers at treatable stages, then moving up the starting age may backfire and cause net harm.
The recently implemented FDA rule requiring mammography reports to include breast density could compound this problem. Because younger women are more likely to have dense breasts, more of them will probably decide to have supplemental imaging for cancer. I previously pointed out that we don’t know whether supplemental imaging with breast ultrasonography or MRI reduces cancer deaths, but we do know that it increases false-positive results.
I have personally cared for several patients who abandoned screening mammography for long stretches, or permanently, after having endured one or more benign biopsies prompted by a false-positive result. I vividly recall one woman in her 60s who was very reluctant to have screening tests in general, and mammography in particular, for that reason. After she had been my patient for a few years, I finally persuaded her to resume screening. We were both surprised when her first mammogram in more than a decade revealed an early-stage breast cancer. Fortunately, the tumor was successfully treated, but for her, an earlier false-positive result nearly ended up having critical health consequences.
Dr. Lin is associate director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has no relevant financial relationships.
A version of this article appeared on Medscape.com.
Earlier this year, I wrote a Medscape commentary to explain my disagreement with the US Preventive Services Task Force (USPSTF)’s updated recommendation that all women at average risk for breast cancer start screening mammography at age 40. The bottom line is that when the evidence doesn’t change, the guidelines shouldn’t change. Since then, other screening experts have criticized the USPSTF guideline on similar grounds, and a national survey reported that nearly 4 out of 10 women in their 40s preferred to delay breast cancer screening after viewing a decision aid and a personalized breast cancer risk estimate.
The decision analysis performed for the USPSTF guideline estimated that compared with having mammography beginning at age 50, 1000 women who begin at age 40 experience 519 more false-positive results and 62 more benign breast biopsies. Another study suggested that anxiety and other psychosocial harms resulting from a false-positive test are similar between patients who require a biopsy vs additional imaging only. Of greater concern, women who have false-positive results are less likely to return for their next scheduled screening exam.
A recent analysis of 2005-2017 data from the US Breast Cancer Surveillance Consortium found that about 1 in 10 mammograms had a false-positive result. Sixty percent of these patients underwent immediate additional imaging, 27% were recalled for diagnostic imaging within the next few days to weeks, and 13% were advised to have a biopsy. While patients who had additional imaging at the same visit were only 1.9% less likely to return for screening mammography within 30 months compared with those with normal mammograms, women who were recalled for short-interval follow-up or recommended for biopsy were 15.9% and 10% less likely to return, respectively. For unclear reasons, women who identified as Asian or Hispanic had even lower rates of return screening after false-positive results.
These differences matter because women in their 40s, with the lowest incidence of breast cancer among those undergoing screening, have a lot of false positives. A patient who follows the USPSTF recommendation and starts screening at age 40 has a 42% chance of having at least one false positive with every-other-year screening, or a 61% chance with annual screening, by the time she turns 50. If some of these patients are so turned off by false positives that they don’t return for regular mammography in their 50s and 60s, when screening is the most likely to catch clinically significant cancers at treatable stages, then moving up the starting age may backfire and cause net harm.
The recently implemented FDA rule requiring mammography reports to include breast density could compound this problem. Because younger women are more likely to have dense breasts, more of them will probably decide to have supplemental imaging for cancer. I previously pointed out that we don’t know whether supplemental imaging with breast ultrasonography or MRI reduces cancer deaths, but we do know that it increases false-positive results.
I have personally cared for several patients who abandoned screening mammography for long stretches, or permanently, after having endured one or more benign biopsies prompted by a false-positive result. I vividly recall one woman in her 60s who was very reluctant to have screening tests in general, and mammography in particular, for that reason. After she had been my patient for a few years, I finally persuaded her to resume screening. We were both surprised when her first mammogram in more than a decade revealed an early-stage breast cancer. Fortunately, the tumor was successfully treated, but for her, an earlier false-positive result nearly ended up having critical health consequences.
Dr. Lin is associate director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has no relevant financial relationships.
A version of this article appeared on Medscape.com.
Earlier this year, I wrote a Medscape commentary to explain my disagreement with the US Preventive Services Task Force (USPSTF)’s updated recommendation that all women at average risk for breast cancer start screening mammography at age 40. The bottom line is that when the evidence doesn’t change, the guidelines shouldn’t change. Since then, other screening experts have criticized the USPSTF guideline on similar grounds, and a national survey reported that nearly 4 out of 10 women in their 40s preferred to delay breast cancer screening after viewing a decision aid and a personalized breast cancer risk estimate.
The decision analysis performed for the USPSTF guideline estimated that compared with having mammography beginning at age 50, 1000 women who begin at age 40 experience 519 more false-positive results and 62 more benign breast biopsies. Another study suggested that anxiety and other psychosocial harms resulting from a false-positive test are similar between patients who require a biopsy vs additional imaging only. Of greater concern, women who have false-positive results are less likely to return for their next scheduled screening exam.
A recent analysis of 2005-2017 data from the US Breast Cancer Surveillance Consortium found that about 1 in 10 mammograms had a false-positive result. Sixty percent of these patients underwent immediate additional imaging, 27% were recalled for diagnostic imaging within the next few days to weeks, and 13% were advised to have a biopsy. While patients who had additional imaging at the same visit were only 1.9% less likely to return for screening mammography within 30 months compared with those with normal mammograms, women who were recalled for short-interval follow-up or recommended for biopsy were 15.9% and 10% less likely to return, respectively. For unclear reasons, women who identified as Asian or Hispanic had even lower rates of return screening after false-positive results.
These differences matter because women in their 40s, with the lowest incidence of breast cancer among those undergoing screening, have a lot of false positives. A patient who follows the USPSTF recommendation and starts screening at age 40 has a 42% chance of having at least one false positive with every-other-year screening, or a 61% chance with annual screening, by the time she turns 50. If some of these patients are so turned off by false positives that they don’t return for regular mammography in their 50s and 60s, when screening is the most likely to catch clinically significant cancers at treatable stages, then moving up the starting age may backfire and cause net harm.
The recently implemented FDA rule requiring mammography reports to include breast density could compound this problem. Because younger women are more likely to have dense breasts, more of them will probably decide to have supplemental imaging for cancer. I previously pointed out that we don’t know whether supplemental imaging with breast ultrasonography or MRI reduces cancer deaths, but we do know that it increases false-positive results.
I have personally cared for several patients who abandoned screening mammography for long stretches, or permanently, after having endured one or more benign biopsies prompted by a false-positive result. I vividly recall one woman in her 60s who was very reluctant to have screening tests in general, and mammography in particular, for that reason. After she had been my patient for a few years, I finally persuaded her to resume screening. We were both surprised when her first mammogram in more than a decade revealed an early-stage breast cancer. Fortunately, the tumor was successfully treated, but for her, an earlier false-positive result nearly ended up having critical health consequences.
Dr. Lin is associate director, Family Medicine Residency Program, Lancaster General Hospital, Lancaster, Pennsylvania. He blogs at Common Sense Family Doctor. He has no relevant financial relationships.
A version of this article appeared on Medscape.com.