User login
Acute Pancreatitis
Acute pancreatitis accounts for more than 220,000 hospital admissions in the United States annually.1 In the following review, we outline the etiology of acute pancreatitis, discuss its complications, and provide an updated review on its management for the hospitalized patient.
Etiology
Gallstone disease and excess alcohol ingestion are the most common causes of acute pancreatitis in the United States. Gallstones account for roughly 45% of all cases, and the pathogenesis is due to transient obstruction of the pancreatic duct orifice to the flow of pancreatic exocrine secretions.2 Excess alcohol ingestion accounts for approximately 35% of all cases, yet the pathogenesis here is less understood.3 Most theories suggest a direct toxic effect of the ethanol upon the pancreatic parenchyma or its neurovascular supply.4
There are many other less common causes of acute pancreatitis including toxins, drugs, infections, trauma, vascular insults, anatomic abnormalities, and metabolic derangements. Hypertriglyceridemia and hypercalcemia are both implicated in acute pancreatitis. Serum triglyceride levels >1000 mg/dL can precipitate an attack of acute pancreatitis though the pathogenesis is not clearly understood.5 Hypercalcemia is also an uncommon cause of acute pancreatitis, and is thought to result from deposition of calcium in the pancreatic duct and calcium activation of trypsinogen.6
Idiopathic pancreatitis occurs in up to 20% of patients with acute pancreatitis, and by definition, the cause is not established by history, physical examination, routine laboratory tests, or imaging. The majority of idiopathic cases of pancreatitis are thought to have a biliary source. In patients with gallbladder in situ, it is estimated that up to 75% acquire pancreatitis from microlithiasis, or biliary sludge and stone debris, that causes obstruction of the distal common bile and main pancreatic ducts. Conversely, sphincter of Oddi dysfunction (SOD) resulting in transient pancreatic ductal obstruction is felt to be the most common cause in those patients who have undergone a previous cholecystectomy.7
An emerging entity, autoimmune pancreatitis (AIP), is more commonly associated with chronic pancreatitis but may cause episodes of acute pancreatitis or mimic pancreatic carcinoma. Typically, the diagnosis is based on elevated levels of serum gammaglobulin subgroup 4 (IgG4) populations, along with characteristic findings on computed tomography (CT) scan (eg, narrowed or wispy main pancreatic duct and an enlarged pancreatic parenchyma). Core‐needle biopsy may confirm the diagnosis of AIP with lymphoplasmacytic infiltration and dense fibrosis.8 Since AIP can mimic pancreatic cancer, the diagnosis may not be made until the time of surgical resection.
Diagnosis
Along with characteristic symptoms, the diagnosis of acute pancreatitis is often based on elevated serum levels of pancreatic enzymes that are at least twice the normal level. Amylase and lipase are the most frequently used serum markers for acute pancreatitis, though their elevation is not pathognomonic for the presence of disease. These enzymes may not always be significantly elevated during times of acute inflammation, and elevation of the enzymes can come from nonpancreatic origins as well (Table 1). Although there is no gold standard for the diagnosis of acute pancreatitis, using serum lipase (>250 IU/L) in conjunction with amylase (>160 IU/L) improves the overall diagnostic sensitivity from 81% to 94%.9 Isoamylase levels can be used to distinguish among pancreatic, salivary, and macroamylasemia though this is not often used if pancreatitis is suspected clinically. Similarly, serum isolipase can be measured, though this is not readily available.
| Nonpancreatic causes of hyperamylasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, intestinal obstruction, intestinal infarction, perforation, mesenteric thrombosis, pancreatic cancer, appendicitis, peritonitis, pyelonephritis, renal insufficiency, liver disease, pregnancy, ruptured ectopic pregnancy, aortic aneurysm dissection, prostatic disease, ovarian neoplasm |
| Thoracic | Esophagitis, myocardial infarction, pulmonary embolism, pneumonia, metastatic carcinoma of lung, breast cancer |
| Procedural | Abdominal operations, nonabdominal operations, post‐ERCP |
| Trauma | Brain trauma, burns, and traumatic shock |
| Metabolic | Diabetic ketoacidosis |
| Drugs | Opiate administration, oxyphenbutazone, phenylbutazone, aminosalicylic acid, aspirin, atovaquone, bethanecol, estrogens, lamivudine, meperidine, metoclopramide, ranitidine, thiazides, valproic acid, sulfonamides |
| Other | Parotitis, renal transplantation, alcoholism, human immunodeficiency virus, macroamylasemia |
| Nonpancreatic causes of hyperlipasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, spontaneous bacterial peritonitis, liver disease, pancreatic carcinoma, intestinal obstruction, ischemia, perforation, appendicitis, celiac disease |
| Thoracic | Esophagitis |
| Drugs | Furosemide, thiazides, metronidazole, valproic acid, bethanecol, oral contraceptives, indomethacin |
| Other | Renal insufficiency, macrolipasemia |
In order to improve the sensitivity and specificity of diagnosis, other tests have been studied to help predict disease presence and severity. Previously, serum tests for trypsin, elastase, phospholipase A2, and carboxylester lipase have all been evaluated but shown to have no significant improvement in diagnostic capability.1014 More recently, trypsinogen (a pancreatic proteinase) has proven to be a useful aid in the accurate diagnosis of acute disease. Trypsinogen undergoes activation into trypsin during acute pancreatic inflammation.3 It is comprised of 2 main isoenzymes (trypsinogen‐1 and trypsinogen‐2) that are secreted into the pancreatic fluid with a small proportion escaping into the circulation.15 Higher concentrations of trypsinogen‐1 are seen in healthy people, while higher concentrations of trypsinogen‐2 are seen in those with acute pancreatitis.16 Urinary trypsinogen‐2 dipstick tests detect acute pancreatitis more accurately than quantitative serum or urinary amylase, with a sensitivity as high as 94%, and a specificity of 95%.17 Studies have shown that in post‐endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis, serum trypsinogen‐2 levels begin to rise as early as 1 hour and peak at 6 hours.17 The Actim Pancreatitis (Medix Biomedica, Kauniainen, Finland) urine test strips measure concentrations of trypsinogen‐2 as low as 50 g/L, but is not a quantitative test and, thus, it does not predict severity. Some studies have advocated the use of urinary trypsinogen‐2 as a screening tool, with a positive result indicating a need for further evaluation of acute pancreatitis.1820 Urinary trypsinogen‐2 is less costly than serum tests, plus may result in additional cost savings with earlier patient discharge. Unfortunately, this test is not widely available for clinical use. Urinary trypsinogen activation peptide (TAP) is another test that has been studied in the diagnosis of acute pancreatitis, but may signify disease severity rather than the presence or absence of disease.21 Currently urinary assays for TAP are not widely available in the United States.
Choosing the Appropriate Imaging Modality
Along with the measurement of pancreatic release enzymes, abdominal imaging is often used, though not always necessary to confirm the diagnosis of acute pancreatitis. Imaging techniques such as CT, magnetic resonance imaging (MRI), and transabdominal ultrasonography may be used to rule out other causes of abdominal pain or elucidate the cause of the pancreatitis itself. Ultrasound may show pancreatic enlargement, diminished echogenicity, and possible adjacent fluid collections.22 In searching for evidence of gallstone pancreatitis, transabdominal ultrasound has a sensitivity of 67% and a specificity of 100%.23 However, it may be insensitive for detecting stones in the distal common bile duct near the ampulla due to acoustic interference from gas within the small bowel.24 Furthermore, ultrasound itself is operator‐dependent.
Contrast‐enhanced CT is the standard mode of imaging for diagnosing acute pancreatitis and provides superior imaging of the pancreas. Unfortunately it is more costly than ultrasound, involves radiation exposure, and requires intravenous contrast medium.25 Findings of acute pancreatitis frequently seen on CT include diffuse or segmental enlargement of the gland, irregular pancreatic contour, obliteration of peripancreatic fat planes, parenchymal heterogeneity, and ill‐defined fluid collections within the pancreas or in the lesser sac and pararenal spaces.26 CT scan may also be used to detect pancreatic necrosis, an important finding for the management and prognosis of this disease.27 Despite this, normal CT findings have been reported in patients with acute pancreatitis, and certain CT findings may be related to disease severity.25
Although MRI is less commonly used in the diagnosis of acute pancreatitis, it may provide a useful alternative to CT, especially in cases of renal failure or intravenous contrast hypersensitivity. When combined with magnetic resonance cholangiopancreatography (MRCP) imaging, MRI may even be able to detect a local area of pancreatic duct disruption.27 MRCP allows for a noninvasive cholangiogram and is frequently used to stratify patients who may benefit from ERCP. It can accurately identify common bile duct stones, with a higher sensitivity for choledocholithiasis than ultrasound or CT.2830 MRCP can also assist in the diagnosis of other disorders of the intrahepatic and extrahepatic biliary tree that may be related to the cause of pancreatitis. Overall, unless a patient has a contraindication, or the goal of the study is to diagnose choledocholithiasis, a contrast‐enhanced CT scan remains the imaging procedure of choice due to improved accessibility, lower cost, ease of performance, and increased sensitivity in the detection of gas bubbles (potentially indicating pancreatic infection).3133 Ordering a CT scan or other imaging at admission is not necessary in the diagnosis of acute pancreatitis if the patient's presentation is classic. At admission, however, a CT scan may be reasonable to exclude other serious causes of abdominal pain, such as a perforated ulcer. Imaging may also be ordered to define the cause of the episode of pancreatitis and to exclude occult malignancy. In addition, CT scan should be strongly considered in patients who do not improve within 2 to 3 days to assess for complications such as pancreatic necrosis, pseudocysts, or other complications.34
Most recently, endoscopic ultrasound (EUS) has risen to the forefront as a leader in accurate imaging of the pancreas and biliary tree. EUS is more sensitive than transabdominal ultrasound in detecting biliary stones,35 and it has been shown to have equivalent, and in some cases superior, sensitivity to ERCP and MRCP. Because EUS is able to detect smaller stones or sludge, it may have a role in those patients diagnosed with idiopathic pancreatitis.36 Like MRCP, EUS can also help stratify patients into those that are likely to benefit most from ERCP.37 Figure 1 reviews the evaluation of acute pancreatitis.
Prognosis
For the majority of patients with acute pancreatitis, the clinical course is mild and self‐limiting. In approximately 20% to 25% of patients, however, it is severe and associated with organ failure and significant morbidity and mortality.38, 39 Determining the severity of acute pancreatitis is critical, as patients at high‐risk for severe disease require closer monitoring and possible intervention. Several validated scoring systems are available that aim to predict the severity of acute pancreatitis including Ranson's criteria, the Imrie scoring system, the Acute Physiology and Chronic Health Evaluation (APACHE II) scale, and the CT Severity Index (CTSI) (Table 2).4043
| Ranson's Criteria | |
|---|---|
| |
| At admission or diagnosis | |
| Age | >55 years |
| WBC | >16,000/mm3 |
| Blood glucose | >200 mg/dL |
| Lactate dehydrogenase | >350 IU/L |
| AST | >250 IU/L |
| Within 48 hours after presentation | |
| Hematocrit decrease | >10% |
| Blood urea nitrogen increase | >5 mg/dL |
| Serum calcium | 8 mg/dL |
| Base deficit | >4 mEq/L |
| Fluid sequestration | >6 L |
| PaO2 | 60 mmHg |
| Scoring | 1 point for each criterion |
| APACHE II Scale | |
| Equation includes these factors: age, rectal temperature, mean arterial pressure, heart rate, PaO2, arterial pH, serum potassium, sodium, creatinine, hematocrit, WBC count, Glasgow coma scale score, chronic health status | |
| Scoring calculation available at |
|
| CT Severity Index (Balthazar Score) | |
| Grade of pancreatitis on CT | |
| A | Normal pancreas (0 points) |
| B | Pancreatic enlargement (1 point) |
| C | Pancreatic enlargement with peripancreatic inflammation (2 points) |
| D | Extrapancreatic changes plus 1 fluid collection (3 points) |
| E | More than 1 fluid collection (4 points) |
| Necrosis score | |
| None | 0 points |
| One‐third | 2 points |
| >One‐third but less than one‐half | 4 points |
| >One‐half | 6 points |
| Scoring | CT grade plus necrosis score |
| Imrie Scoring System | |
| Age | >55 years |
| WBC | >15,000/mm3 |
| Blood glucose | >180 mg/dL (absence of diabetes) |
| Lactate dehydrogenase | >600 IU/L |
| AST or ALT | >100 IU/L |
| Serum calcium | 8 mg/dl |
| PaO2 | 60 mm Hg |
| Serum albumin | 3.2 g/dL |
| Serum urea | >45 mg/dL |
| Scoring | 1 point for each criterion met after 48 hours of admission |
| Atlanta Criteria | |
| Ranson's score | 3 |
| APACHE II score | 8 |
| Presence of 1 or more organ failures: | |
| Shock | Blood pressure of 90 mmHg |
| Pulmonary insufficiency | PaO2 60 mmHg |
| Renal failure | Creatinine level >2 mg/dL after hydration |
| Gastrointestinal bleeding | Estimated >500‐mL blood loss/24 hours |
| Disseminated intravascular coagulation | Thrombocytopenia, hypofibrinogenemia, fibrin split products |
| Severe hypocalcemia | Calcium level 7.5 mg/dL |
| Presence of 1 or more local complications | |
| Pancreatic necrosis | |
| Pancreatic abscess | |
| Pancreatic pseudocyst | |
| Scoring | Severe pancreatitis indicated by any positive factor listed |
In 1992, the Atlanta Classification of acute pancreatitis was developed to provide a rational approach in predicting disease severity, thus allowing for comparison between clinical trials. It defines severe acute pancreatitis (SAP) on the basis of standard clinical manifestations, a Ranson's score 3, an APACHE II score 8, and evidence of organ failure and intrapancreatic pathological findings.44 Serum markers such as C‐reactive protein (CRP), interleukin‐6, and phospholipase A2 have all been studied to predict severity; however, only CRP is widely available. A cutoff level of 150 mg/L at 48 hours distinguishes mild disease from SAP.45 Clinical findings such as thirst, poor urine output, progressive tachycardia, tachypnea, hypoxemia, confusion, and a lack of improvement in symptoms within the first 48 hours are warning signs of impending severe disease, and thus warrant consideration of admission to an intensive care unit (ICU).34
Natural History and Complications
Despite initial aggressive intensive care treatment, 30% to 50% of patients with SAP do not respond promptly to ICU treatment and develop persistent multisystem organ failure.39 Severe organ failure in the first week of onset of acute pancreatitis is closely linked to the development of pancreatic infection occurring within 2 weeks of the initiation of symptoms.46 Early multiorgan dysfunction triggers additional mechanisms that render bacterial translocation into clinically manifested sepsis and septic shock.39 In most studied series, infection (including bacteremia, fungemia, and pancreatic abscess) remains the leading cause of death in patients with acute pancreatitis, accounting for up to 80% of fatal cases.4749 While sepsis is the more frequent cause of death in patients surviving beyond 7 days, death occurring early in the course of disease is more likely to be from respiratory complications such as pulmonary edema.50
In the spectrum of acute pancreatitis, ongoing pancreatic injury can lead to pancreatic necrosis, fluid collections, pseudocyst formation, and pancreatic duct disruption (Figures 24).51 In patients hospitalized with acute pancreatitis, up to 57% will have peripancreatic fluid collections that are initially ill‐defined.44, 52 Typically, these fluid collections may be managed conservatively; however, if they continue to enlarge, cause persistent abdominal pain, become infected, or compress adjacent organs, they may require further intervention.53 Ductal disruption may be diagnosed when fluid collections have high levels of pancreatic amylase, and their presence may lead to the formation of pseudocysts, persistent ascites, or pleural effusions.54 Pancreatic pseudocysts usually require 4 weeks for complete formation, and they classically contain fluid only without significant solid debris.55 Formation typically occurs as a result of limited pancreatic necrosis causing a pancreatic duct leak with subsequent organization, or from areas of necrosis that liquefy over time.56 Both pancreatic pseudocysts and necrotic pancreatic tissue may become infected leading to abscess formation.51

Pancreatic necrosis is defined as diffuse or focal areas of nonviable pancreatic parenchyma, and it is seen in approximately 20% of patients with acute pancreatitis.44, 57 While pseudocyst formation takes approximately 1 month to occur, pancreatic necrosis can occur within the first few days of initial symptoms and is associated with an increase in complications leading to an increased risk of morbidity and mortality.58 More than 80% of deaths in acute pancreatitis are associated with the presence of pancreatic necrosis.39 Patients at highest risk for complications are those with necrosis involving more than 50% of the gland based on MRI or contrast‐enhanced CT scan.59, 60
Patients with pancreatic infection may have infected necrosis, pancreatic abscess, and/or infected pseudocysts.39 The microbes most frequently involved are gram‐negative organisms including Escherichia coli, Enterococcus, and Klebsiella.61 Recently, gram‐positive bacteria have been implicated in pancreatic infection.62 Fungal infection with Candida species is seen in up to 15% of patients with infected necrosis and is associated with more serious systemic complications.63 The use of prophylactic antibiotics may increase the risk of fungal infection. It may be challenging to distinguish between infected and sterile pancreatic necrosis; hence, needle aspiration under EUS or radiologic guidance may be required.61, 64
Management
Supportive Care and Nutrition
The majority (80%) of cases of acute pancreatitis respond well to supportive care with fluid replacement, pain control, and controlled initiation of regular food intake.39 Aggressive intravenous fluid resuscitation is needed to overcome hypovolemia caused by intravascular fluid loss.65 Currently there is a paucity of data to support clinical recommendations regarding rate of fluid resuscitation, but previous studies have suggested a rate of at least 250 to 300 mL/hour for the first 48 hours if fluid status permits.65, 66 Typically, a diet is reintroduced when abdominal tenderness improves and appetite returns.34 Traditionally patients are started on a clear liquid diet and advanced either to a full‐liquid or lowfat diet as toleratedthough there is little data on this subject.67 A recent study randomized 121 subjects to initiate either a clear liquid diet or a lowfat solid diet once recovering from acute pancreatitis and found that the lowfat solid diet was as safe as the clear liquid diet and resulted in improved caloric intake.68
In patients with SAP or complicated disease, nutritional support is critical. In an effort to achieve pancreatic rest, total parenteral nutrition (TPN) has historically been used as the primary means of nutritional support in those patients who require it. TPN, however, carries significant risks of infection and metabolic disturbance,69 and recent studies have shown that enteral nutrition may improve outcomes by decreasing the rates of infection, need for surgical intervention, hospital length of stay, and overall total cost of care.7074 Research has shown that enteral nutrition prevents intestinal atrophy and improves the barrier function of the gut mucosa.75 Typically enteral feeds are given via the nasojejunal (NJ) route, though some data suggest that nasogastric (NG) feeding is also acceptable.76, 77 Despite good intentions by physicians to provide postpyloric feeding, often NJ tubes migrate back into the stomach, yet anecdotal reports showed patients continued to tolerate enteral feeding, prompting further studies. One randomized controlled trial of 49 patients showed NG feeds to be as good as NJ feeds in patients with SAP, plus they were less costly and easier to perform.78 Similarly, this was demonstrated in 16 patients receiving NJ feeds and 15 patients receiving NG feeds with no worsening of SAP in either group.77 In the 2 previous studies, patients with objective evidence of SAP were included and semielemental feeds were started within 24 to 72 hours after onset of pain. Presumably, NG feeds were given over oral feeds as semielemental feeds are not palatable. These are small studies and further research is needed comparing NG to NJ feeds. However, patients who have severe acute pancreatitis with prolonged pain and significant pancreatic necrosis on imaging may benefit from a trial of NJ feeds before advancing to oral feeds.79 TPN may be necessary in those patients who do not tolerate enteral feeding, or do not reach an adequate infusion rate within 2 to 4 days.80
When utilizing enteral feeding, the question of semielemental formula vs. polymeric formula frequently arises. Semielemental formulas seem to pose the advantage of less pancreatic stimulation while not requiring the presence of pancreatic enzymes for absorption.81, 82 Studies, however, have not uniformly supported this hypothesis.83
Antibiotics
Antibiotics do not have a role in mild acute pancreatitis. In SAP, the role of antibiotics is more controversial. Pancreatic or peripancreatic infection develops in a significant number of patients with acute pancreatitis and is associated with substantial morbidity and mortality, particularly in patients with pancreatic necrosis.84 Prophylactic antibiotics have been attempted to reduce infectious complications, but their role in SAP is not entirely clear. Two recent meta‐analyses showed that antibiotic prophylaxis had no significant effect on infection of pancreatic necrosis and mortality, though this did contradict earlier meta‐analyses.8587 Current American College of Gastroenterology guidelines recommend against the use of prophylactic antibiotics to prevent pancreatic infection.88 Though prophylactic antibiotics are not recommended, antibiotics may be given empirically for fever, leukocytosis, and/or sepsis while a possible infectious source is investigated, including fine needle aspiration of pancreatic necrosis.88 Imipenem, meropenem, and a combination of a quinolone and metronidazole have adequate penetration into pancreatic necrotic material and are the antibiotics of choice. Use of antibiotics may increase the risk of resistant organisms and possibly fungal infections.
Endoscopy
Urgent endoscopic therapy for acute pancreatitis is only indicated in gallstone, or biliary pancreatitis. Approximately 5% of patients with symptomatic gallstones will develop acute biliary pancreatitis.89 The risk of a recurrent attack is approximately 30% to 50% if definitive therapy is not sought.90, 91 Multiple studies have demonstrated that ERCP significantly reduces morbidity and mortality in acute biliary pancreatitis.92 Urgent ERCP (within 48 hours of symptom onset) should be considered in cases of cholangitis, or in the setting of severe symptoms of disease with ongoing biliary obstruction. Elective ERCP is indicated in patients with jaundice and imaging studies demonstrating choledocholithiasis, as well as those surgical patients with abnormal intraoperative cholangiography. ERCP should also be considered for suspected pancreatic duct disruption and for biliary sphincterotomy as primary therapy in poor operative candidates, or as temporary therapy during pregnancy.93 ERCP may also have a role in recurrent idiopathic acute pancreatitis if pancreas divisum or SOD is suspected. Sphincter of Oddi manometry may be performed, and if a diagnosis is confirmed, endoscopic sphincterotomy should be performed.94 For pancreas divisum, minor sphincterotomy and/or pancreatic duct stent may be performed.95 ERCP typically does not have a role in those patients with a single attack of acute pancreatitis, as significant complications may occur due to the ERCP itself. EUS, however, can be considered in a single attack of idiopathic pancreatitis in order to further investigate possible causes of the disease.7
Cholecystectomy
Cholecystectomy is indicated for appropriate operative candidates with resolving gallstone pancreatitis. Recurrent pancreatitis can be seen in up to 30% of patients if cholecystectomy is not performed.96, 97 Based on the American Gastroenterological Association (AGA) guidelines, definitive surgical management should be performed in the same hospitalization if possible, but no later than 2 to 4 weeks after discharge.98 In most patients with mild gallstone pancreatitis and no evidence of cholangitis, routine ERCP prior to cholecystectomy is not indicated, as long as pancreatitis is resolving and liver function abnormalities have normalized.88 As mentioned previously, for patients who are not candidates for surgery, endoscopic sphincterotomy should be considered. Cholecystectomy may also be indicated for those with 2 or more episodes of idiopathic pancreatitis, particularly if biliary pancreatitis is suspected.
Failure to Improve
In patients who fail to improve, contrast‐enhanced CT scan should be performed to evaluate for fluid collections, pancreatic necrosis, or other complications that may require intervention. Antibiotic therapy may need to be considered, and in any patient without rapid improvement, nutritional support should be addressed.34 The diagnosis of infected necrosis is typically made by fine‐needle aspiration of the necrotic area under EUS, CT, or transabdominal ultrasound guidance.64
Indications for Drainage of Pseudocysts
The indications for drainage of pancreatic pseudocysts are limited, but drainage is typically performed in those patients that are symptomatic, including abdominal pain, weight loss, gastric outlet obstruction, obstructive jaundice, pancreatic duct leakage, or infectious complications.55 Depending on the location of the pseudocyst and whether it communicates with the pancreatic duct, pseudocysts may be drained by transpapillary means (endoprosthesis placed in the pancreatic duct), or by transmural means (percutaneous, surgical, or endoscopic cyst‐gastrostomy, or endoscopic cyst‐duodenostomy).55 Prior to drainage the pseudocyst wall needs to be mature, which may require up to 4 to 6 weeks. Pancreatic duct leaks may occur as a result of acute or chronic pancreatitis, and they can arise from the head, tail, or body of the gland. Fluid may ultimately track into the mediastinum or peritoneum causing effusions or ascites.55 Treatment for such pancreatic duct leaks includes transpapillary therapy to cross, or bridge, the disrupted duct.
Management of Pancreatic Necrosis
Sterile pancreatic necrosis is typically managed conservatively without drainage. Generally, CT scans are repeated every 7 to 10 days to assess the necrosis and to evaluate for further complications.32 Patients who are clinically unstable with fever, tachycardia, leukocytosis, or organ failure may require percutaneous sampling to evaluate for infected necrosis.33 If the pancreatic tissue is sterile, the patient is determined to have sterile necrosis. If the patient with sterile necrosis is clinically unstable then prophylactic antibiotics may be indicated. If the pancreatic tissue is infected, the patient is deemed to have infected necrosis and treatment with antibiotics and necrosectomy is often indicated, especially in those with a poor clinical state. The antibiotic chosen should have adequate penetration into the necrotic material, such as imipenem, meropenem, or a combination of quinolone and metronidazole.99
It may be challenging to distinguish between sterile and infected pancreatic necrosis. A CT scan is unable to differentiate them with certainty; though, intrapancreatic, retroperitoneal, or lesser sac gas may indicate infection.31 In addition, inducing infection within a previously sterile collection is a potential risk of percutaneous sampling. As a result, sampling should not be performed unless completely indicated.31
In patients with sterile pancreatic necrosis who are symptomatic with refractory abdominal pain, gastric outlet obstruction, or failure to thrive at 4 or more weeks following the onset of acute pancreatitis, drainage and/or debridement is usually indicated. Pancreatic necrosectomy for sterile pancreatic necrosis may be accomplished endoscopically, or more traditionally by a surgical approach.55 Although endoscopic drainage is less invasive, it is technically difficult and has a higher rate of complication in the hands of inexperienced operators.100 Careful selection and evaluation of patients undergoing endoscopic drainage procedures is necessary. Bleeding, perforation, infection, pancreatitis, aspiration, stent migration, and pancreatic ductal damage are all possible complications during the drainage of necrotic pancreatic fluid collections.55 If pancreatic necrosis is infected, surgical necrosectomy should be performed as this is the gold standard for infected necrosis when debridement is necessary.55 Figure 5 reviews the management of acute pancreatitis.
Conclusion
Acute pancreatitis is a common disease frequently caused by choledocholithiasis or excess alcohol ingestion. In idiopathic acute pancreatitis, microlithiasis and SOD should be considered. Though CT scan remains the imaging modality of choice, newer methods such as MRCP and EUS may help to provide additional and improved diagnostic information.
The management of acute pancreatitis is frequently challenging, and severity scales help to predict the likelihood of complications, determine necessary interventions, and guide the appropriate level of care. Nutrition is critical in patients with SAP, and enteral feeding is clearly preferred over TPN. Currently, prophylactic antibiotics do not appear to have a role in SAP. Finally, though not always straightforward, recommendations do exist to guide the management of many of the complications of acute pancreatitis, such as pseudocyst formation and necrotizing disease. A multidisciplinary approach should be used in managing patients with severe disease, and the primary inpatient physician should not hesitate to involve specialists, including gastroenterologists, radiologists, and surgeons.
- ,.2005 National hospital discharge survey.Adv Data.2007;385:1–19.
- ,.Gallstones.BMJ.2007;335:295–299.
- ,.Acute pancreatitis.N Engl J Med.1994;330:1198–1210.
- ,.Pathobiology of alcoholic pancreatitis.Pancreatology.2007;7:105–114.
- .Hyperlipidemic pancreatitis.Gastroenterol Clin North Am.1990;19:783–791.
- ,,,,,.Acute hypercalcemia causes acute pancreatitis and ectopic trypsinogen activation in the rat.Gastroenterology.1995;109:239–246.
- ,,.Role of endoscopic evaluation in idiopathic pancreatitis: a systematic review.Gastrointest Endosc.2006;63:1037–1045.
- ,.Autoimmune pancreatitis: a review.World J Gastroenterol.2007;13:6327–6332.
- ,,, et al.Acute pancreatitis and normoamylasemia. not an uncommon combination.Ann Surg.1989;210:614–620.
- .Normal amylase levels in the presentation of acute pancreatitis.Am J Emerg Med.1994;12:21–24.
- .Diagnostic standards for acute pancreatitis.World J Surg.1997;21:136–142.
- .Support of the diagnosis of pancreatitis by enzyme tests — old problems, new techniques.Clinica Chimica Acta.1997;257:85–98.
- ,,,.What is the best biochemical test to diagnose acute pancreatitis? A prospective clinical study.Mayo Clin Proc.1996;71:1138–1144.
- .The value of clinical laboratory studies in acute pancreatitis.Arch Pathol Lab Med.1991;115:325–326.
- ,.Anionic and cationic trypsinogens (trypsins) in mammalian pancreas.Enzyme.1972/73;14:116–130.
- ,,,,,.Time‐resolved immunofluorometric assays for trypsinogen‐1 and 2 in serum reveal preferential elevation of trypsinogen‐2 in pancreatitis.J Lab Clin Med.1990;115:712–718.
- ,,, et al.Rapid measurement of urinary trypsinogen‐2 as a screening test for acute pancreatitis.N Engl J Med.1997;336:1788–1793.
- ,,,,.Rapid urinary trypsinogen‐2 test strip in the diagnosis of acute pancreatitis.Pancreas.2005;30:243–247.
- ,,, et al.Clinical value of rapid urine trypsinogen‐2 test strip, urinary trypsinogen activation peptide, and serum and urinary activation peptide of carboxypeptidase B in acute pancreatitis.World J Gastroenterol.2005;11:7261–7265.
- ,,,,.Use of the urinary trypsinogen‐2 dip stick test in early diagnosis of pancreatitis after endoscopic retrograde cholangiopancreatography.Surg Endosc.2007;21:1312–1315.
- ,,, et al.Early prediction of severity in acute pancreatitis by urinary trypsinogen activation peptide: a multicentre study.Lancet.2000;355:1955–1960.
- ,.The ultrasonic findings in inflammatory pancreatic disease.Semin Ultrasound.1980;1:178.
- ,,,,,.The urgent diagnosis of gallstones in acute pancreatitis: a prospective study of three methods.Br J Surg.1984;71:230–233.
- ,,.Gallstone pancreatitis: a community teaching hospital experience.J Clin Gastroenterol.2001;33:41–44.
- ,,,.Diagnostic imaging of acute pancreatitis: prospective study using CT and sonography.AJR Am J Roentgenol.1981;137:497–502.
- ,,,.Value of contrast‐enhanced computerized tomography in the early diagnosis and prognosis of acute pancreatitis: a prospective study of 202 patients.Am J Surg.1988;155:457–466.
- ,,, et al.Computed tomography and magnetic resonance imaging in the assessment of acute pancreatitis.Gastroenterology.2004;126:715–723.
- ,,, et al.The role of magnetic resonance cholangiography in the management of patients with gallstone pancreatitis.Ann Surg.2005;241:119–124.
- ,,.Magnetic resonance imaging of acute pancreatitis: the pancreatogram.JOP.2004;5:48–50.
- ,,.Magnetic resonance cholangiopancreatography.N Engl J Med.1999;341(4):258–264.
- ,,,,.Imaging and percutaneous management of acute complicated pancreatitis.Cardiovasc Intervent Radiol.2004;27:567–580.
- ,,.State‐of‐the‐art imaging of acute pancreatitis.JBR‐BTR.2003;86:193–208.
- ,,,.Acute necrotizing pancreatitis: Role of CT‐guided percutaneous catheter drainage.Abdom Imaging.2007;32:351–361.
- .Acute pancreatitis.N Engl J Med.2006;354:2142–2150.
- ,,, et al.Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients.Gastrointest Endosc.2001;54:325–330.
- ,.Endoscopic ultrasonography in the evaluation of idiopathic acute pancreatitis.Br J Surg.2000;87:1650–1655.
- ,; theCalgary Advanced Therapeutic Endoscopy Center (ATEC) Study Group.Noninvasive vs. selective invasive biliary imaging for acute biliary pancreatitis: an economic evaluation by using decision tree analysis.Gastrointest Endosc.2005;61:86–97.
- ,.Prognostic factors in acute pancreatitis.J Clin Gastroenterol.2002;34:167–176.
- ,.Severe acute pancreatitis: clinical course and management.World J Gastroenterol.2007;13:5043–5051.
- .Etiological and prognostic factors in human acute pancreatitis: a review.Am J Gastroenterol.1982;77:633–638.
- ,,,,.Prognostic factors in acute pancreatitis.Gut.1984;25:1340–1346.
- ,,,,.APACHE‐acute physiology and chronic health evaluation: a physiologically based classification system.Crit Care Med.1981;9:591–597.
- ,,,.Acute pancreatitis: value of CT in establishing prognosis.Radiology.1990;174:331–336.
- .A clinically based classification system for acute pancreatitis. summary of the international symposium on acute pancreatitis, Atlanta, GA, September 11 through 13, 1992.Arch Surg.1993;128:586–590.
- ,,, et al.Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini Consensus Conference.Int J Pancreatol.1999;25:195–210.
- ,,,.Role of early multisystem organ failure as major risk factor for pancreatic infections and death in severe acute pancreatitis.Clin Gastroenterol Hepatol.2006;4:1053–1061.
- ,.Lethal pancreatitis.Am J Gastroenterol.1983;78:810–814.
- ,,,.A randomized multicenter clinical trial of antibiotic prophylaxis of septic complications in acute necrotizing pancreatitis with imipenem.Surg Gynecol Obstet.1993;176:480–483.
- ,.Prevention, diagnosis, and treatment of pancreatic abscess.Surgery.1977;82:99–106.
- ,,,.Death due to acute pancreatitis. a retrospective analysis of 405 autopsy cases.Dig Dis Sci.1985;30:1005–1018.
- .Endoscopic drainage of pancreatic fluid collections and pancreatic necrosis.Gastrointest Endosc Clin North Am.2003;13:743–764.
- ,,, et al.Early prediction of acute pancreatitis: prospective study comparing computed tomography scans, Ranson, Glascow, Acute Physiology and Chronic Health Evaluation II scores, and various serum markers.World J Surg.2002;26:612–619.
- ,,, et al.ASGE guideline: the role of endoscopy in the diagnosis and the management of cystic lesions and inflammatory fluid collections of the pancreas.Gastrointest Endosc.2005;61:363–370.
- .Endoscopic therapy of complete and partial pancreatic duct disruptions.Gastrointest Endosc Clin N Am.1998;8:39–53.
- .Treatment of pancreatic pseudocysts, pancreatic necrosis, and pancreatic duct leaks.Gastrointest Endosc Clin North Am.2007;17:559–579.
- .Pathology of severe acute pancreatitis. In: Bradley EL III, ed.Acute Pancreatitis: Diagnosis and Therapy.New York, NY:Raven Press;1994:35–46.
- ,,,,,.Identification of pancreas necrosis in severe acute pancreatitis: imaging procedures versus clinical staging.Gut.1986;27:1035–1042.
- ,,,,.Results of surgical treatment of necrotizing pancreatitis.World J Surg.1985;9:972–979.
- ,,,,.Management of sterile necrosis in instances of severe acute pancreatitis.J Am Coll Surg.1995;181:279–288.
- ,,,.Prognostic factors in sterile pancreatic necrosis.Gastroenterology.1992;103:1636–1640.
- ,,,.Bacterial contamination of pancreatic necrosis. A prospective clinical study.Gastroenterology.1986;91:433–438.
- ,,.Surgical treatment of necrotizing pancreatitis by necrosectomy and closed lavage: changing patient characteristics and outcome in a 19‐year, single‐center series.Surgery.2005;138:28–39.
- ,,,,,.Characteristics of infection with Candida species in patients with necrotizing pancreatitis.World J Surg.2002;26:372–376.
- ,,,,,.CT‐guided aspiration of suspected pancreatic infection: bacteriology and clinical outcome.Int J Pancreatol.1995;18:265–270.
- .Initial management of acute pancreatitis: critical issues during the first 72 hours.Am J Gastroenterol.2004;99:2489–2494.
- ,,,.Fluid resuscitation in acute pancreatitis.Clin Gastroenterol Hepatol.2008;6:1070–1076.
- ,,, et al.ESPEN guidelines on nutrition in acute pancreatitis.Clin Nutr.2002;21:173–183.
- ,,,,,.A prospective, randomized trial of clear liquids versus low‐fat solid diet as the initial meal in mild acute pancreatitis.Clin Gastroenterol Hepatol.2007;5:946–951.
- ,,,,.Total parenteral nutrition in severe acute pancreatitis.J Am Coll Nutr.1991;10:156–162.
- ,,.Enteral versus parenteral nutrition for acute pancreatitis.Cochrane Database Syst Rev.2003; (1):CD002837.
- ,.Meta‐analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis.BMJ.2004;328:1407.
- ,,.Current management of acute pancreatitis.Nat Clin Pract Gastroenterol Hepatol.2005;2:473–483.
- ,,, et al.Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis.Gut.1998;42:431–435.
- ,,,,.Enteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial.Br J Surg.1997;84:1665–1669.
- ,,.Nutrition in patients with acute pancreatitis.Curr Opin Crit Care.2001;7:251–256.
- ,,,,.Early nasogastric enteral nutrition for severe acute pancreatitis: a systematic review.World J Gastroenterol.2007;13:5253–5260.
- ,,,,.Early enteral nutrition in severe acute pancreatitis: a prospective randomized controlled trial comparing nasojejunal and nasogastric routes.J Clin Gastroenterol.2006;40:431–434.
- ,,, et al.A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis.Am J Gastroenterol.2005;100:432–439.
- ,,,.Nutrition support in acute pancreatitis: a systematic review of the literature.JPEN J Parenter Enteral Nutr.2006;30:143–156.
- ,.Issues of nutritional support for the patient with acute pancreatitis.Semin Gastrointest Dis.2002;13:154–160.
- ,,,.Effect of continuous jejunal perfusion of elemental and complex nutritional solutions on pancreatic enzyme secretion in human subjects.Gut.1978;19:194–198.
- ,,, et al.Efficiency of enteral nitrogen support in surgical patients: small peptides v non‐degraded proteins.Gut.1990;31:1277–1283.
- ,,, et al.Semi‐elemental formula or polymeric formula: Is there a better choice for enteral nutrition in acute pancreatitis? randomized comparative study.JPEN J Parenter Enteral Nutr.2006;30:1–5.
- ,,, et al.IAP guidelines for the surgical management of acute pancreatitis.Pancreatology.2002;2:565–573.
- ,,, et al.Randomized controlled trials of antibiotic prophylaxis in severe acute pancreatitis: relationship between methodological quality and outcome.Pancreatology.2007;7:531–538.
- ,,,.Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta‐analysis of randomized controlled trials.Am J Gastroenterol.2008;103:104–110.
- ,.Prophylactic antibiotic administration reduces sepsis and mortality in acute necrotizing pancreatitis: a meta‐analysis.Pancreas.2001;22:28–31.
- ,,Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis.Am J Gastroenterol.2006;101:2379–2400.
- ,.Acute biliary pancreatitis.Ann Ital Chir.1995;66:197–202.
- .The timing of biliary surgery in acute pancreatitis.Ann Surg.1979;189:654–663.
- ,,,.Acute biliary pancreatitis. The roles of laparoscopic cholecystectomy and endoscopic retrograde cholangiopancreatography.Surg Endosc.1995;9:392–396.
- ,.Metaanalysis of randomized controlled trials of endoscopic retrograde cholangiography and endoscopic sphincterotomy for the treatment of acute biliary pancreatitis.Am J Gastroenterol.1999;94:3211–3214.
- ,.Endoscopic management of acute pancreatitis.Gastrointest Endosc Clin N Am.2007;17:307–322.
- ,.Review of idiopathic pancreatitis.World J Gastroenterol.2007;13:6296–6313.
- ,,,,.Does endoscopic therapy favorably affect the outcome of patients who have recurrent acute pancreatitis and pancreas divisum?Pancreas.2007;34:21–45.
- .The timing of cholecystectomy in patients with gallstone pancreatitis. A retrospective analysis of 89 patients.Acta Chir Scand.1978;144:487–490.
- ,,, et al.Recurrence of acute gallstone pancreatitis and relationship with cholecystectomy or endoscopic sphincterotomy.Am J Gastroenterol.2004;99:2417–2423.
- American Gastroenterological Association (AGA) Institute on “Management of Acute Pancreatitis” Clinical Practice and Economics Committee, AGA Institute Governing Board.AGA institute medical position statement on acute pancreatitis.Gastroenterology.2007;132:2019–2021.
- ,;AGA Institute Clinical Practice and Economics Committee, AGA Institute Governing Board. AGA institute technical review on acute pancreatitis.Gastroenterology.2007;132:2022–2044.
- .Endoscopic management of pancreatic necrosis: not for the uncommitted.Gastrointest Endosc.2005;62:101–104.
- ,,,.Serum amylase and lipase in the evaluation of acute abdominal pain.Am Surg.1996;62:1028–1033.
Acute pancreatitis accounts for more than 220,000 hospital admissions in the United States annually.1 In the following review, we outline the etiology of acute pancreatitis, discuss its complications, and provide an updated review on its management for the hospitalized patient.
Etiology
Gallstone disease and excess alcohol ingestion are the most common causes of acute pancreatitis in the United States. Gallstones account for roughly 45% of all cases, and the pathogenesis is due to transient obstruction of the pancreatic duct orifice to the flow of pancreatic exocrine secretions.2 Excess alcohol ingestion accounts for approximately 35% of all cases, yet the pathogenesis here is less understood.3 Most theories suggest a direct toxic effect of the ethanol upon the pancreatic parenchyma or its neurovascular supply.4
There are many other less common causes of acute pancreatitis including toxins, drugs, infections, trauma, vascular insults, anatomic abnormalities, and metabolic derangements. Hypertriglyceridemia and hypercalcemia are both implicated in acute pancreatitis. Serum triglyceride levels >1000 mg/dL can precipitate an attack of acute pancreatitis though the pathogenesis is not clearly understood.5 Hypercalcemia is also an uncommon cause of acute pancreatitis, and is thought to result from deposition of calcium in the pancreatic duct and calcium activation of trypsinogen.6
Idiopathic pancreatitis occurs in up to 20% of patients with acute pancreatitis, and by definition, the cause is not established by history, physical examination, routine laboratory tests, or imaging. The majority of idiopathic cases of pancreatitis are thought to have a biliary source. In patients with gallbladder in situ, it is estimated that up to 75% acquire pancreatitis from microlithiasis, or biliary sludge and stone debris, that causes obstruction of the distal common bile and main pancreatic ducts. Conversely, sphincter of Oddi dysfunction (SOD) resulting in transient pancreatic ductal obstruction is felt to be the most common cause in those patients who have undergone a previous cholecystectomy.7
An emerging entity, autoimmune pancreatitis (AIP), is more commonly associated with chronic pancreatitis but may cause episodes of acute pancreatitis or mimic pancreatic carcinoma. Typically, the diagnosis is based on elevated levels of serum gammaglobulin subgroup 4 (IgG4) populations, along with characteristic findings on computed tomography (CT) scan (eg, narrowed or wispy main pancreatic duct and an enlarged pancreatic parenchyma). Core‐needle biopsy may confirm the diagnosis of AIP with lymphoplasmacytic infiltration and dense fibrosis.8 Since AIP can mimic pancreatic cancer, the diagnosis may not be made until the time of surgical resection.
Diagnosis
Along with characteristic symptoms, the diagnosis of acute pancreatitis is often based on elevated serum levels of pancreatic enzymes that are at least twice the normal level. Amylase and lipase are the most frequently used serum markers for acute pancreatitis, though their elevation is not pathognomonic for the presence of disease. These enzymes may not always be significantly elevated during times of acute inflammation, and elevation of the enzymes can come from nonpancreatic origins as well (Table 1). Although there is no gold standard for the diagnosis of acute pancreatitis, using serum lipase (>250 IU/L) in conjunction with amylase (>160 IU/L) improves the overall diagnostic sensitivity from 81% to 94%.9 Isoamylase levels can be used to distinguish among pancreatic, salivary, and macroamylasemia though this is not often used if pancreatitis is suspected clinically. Similarly, serum isolipase can be measured, though this is not readily available.
| Nonpancreatic causes of hyperamylasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, intestinal obstruction, intestinal infarction, perforation, mesenteric thrombosis, pancreatic cancer, appendicitis, peritonitis, pyelonephritis, renal insufficiency, liver disease, pregnancy, ruptured ectopic pregnancy, aortic aneurysm dissection, prostatic disease, ovarian neoplasm |
| Thoracic | Esophagitis, myocardial infarction, pulmonary embolism, pneumonia, metastatic carcinoma of lung, breast cancer |
| Procedural | Abdominal operations, nonabdominal operations, post‐ERCP |
| Trauma | Brain trauma, burns, and traumatic shock |
| Metabolic | Diabetic ketoacidosis |
| Drugs | Opiate administration, oxyphenbutazone, phenylbutazone, aminosalicylic acid, aspirin, atovaquone, bethanecol, estrogens, lamivudine, meperidine, metoclopramide, ranitidine, thiazides, valproic acid, sulfonamides |
| Other | Parotitis, renal transplantation, alcoholism, human immunodeficiency virus, macroamylasemia |
| Nonpancreatic causes of hyperlipasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, spontaneous bacterial peritonitis, liver disease, pancreatic carcinoma, intestinal obstruction, ischemia, perforation, appendicitis, celiac disease |
| Thoracic | Esophagitis |
| Drugs | Furosemide, thiazides, metronidazole, valproic acid, bethanecol, oral contraceptives, indomethacin |
| Other | Renal insufficiency, macrolipasemia |
In order to improve the sensitivity and specificity of diagnosis, other tests have been studied to help predict disease presence and severity. Previously, serum tests for trypsin, elastase, phospholipase A2, and carboxylester lipase have all been evaluated but shown to have no significant improvement in diagnostic capability.1014 More recently, trypsinogen (a pancreatic proteinase) has proven to be a useful aid in the accurate diagnosis of acute disease. Trypsinogen undergoes activation into trypsin during acute pancreatic inflammation.3 It is comprised of 2 main isoenzymes (trypsinogen‐1 and trypsinogen‐2) that are secreted into the pancreatic fluid with a small proportion escaping into the circulation.15 Higher concentrations of trypsinogen‐1 are seen in healthy people, while higher concentrations of trypsinogen‐2 are seen in those with acute pancreatitis.16 Urinary trypsinogen‐2 dipstick tests detect acute pancreatitis more accurately than quantitative serum or urinary amylase, with a sensitivity as high as 94%, and a specificity of 95%.17 Studies have shown that in post‐endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis, serum trypsinogen‐2 levels begin to rise as early as 1 hour and peak at 6 hours.17 The Actim Pancreatitis (Medix Biomedica, Kauniainen, Finland) urine test strips measure concentrations of trypsinogen‐2 as low as 50 g/L, but is not a quantitative test and, thus, it does not predict severity. Some studies have advocated the use of urinary trypsinogen‐2 as a screening tool, with a positive result indicating a need for further evaluation of acute pancreatitis.1820 Urinary trypsinogen‐2 is less costly than serum tests, plus may result in additional cost savings with earlier patient discharge. Unfortunately, this test is not widely available for clinical use. Urinary trypsinogen activation peptide (TAP) is another test that has been studied in the diagnosis of acute pancreatitis, but may signify disease severity rather than the presence or absence of disease.21 Currently urinary assays for TAP are not widely available in the United States.
Choosing the Appropriate Imaging Modality
Along with the measurement of pancreatic release enzymes, abdominal imaging is often used, though not always necessary to confirm the diagnosis of acute pancreatitis. Imaging techniques such as CT, magnetic resonance imaging (MRI), and transabdominal ultrasonography may be used to rule out other causes of abdominal pain or elucidate the cause of the pancreatitis itself. Ultrasound may show pancreatic enlargement, diminished echogenicity, and possible adjacent fluid collections.22 In searching for evidence of gallstone pancreatitis, transabdominal ultrasound has a sensitivity of 67% and a specificity of 100%.23 However, it may be insensitive for detecting stones in the distal common bile duct near the ampulla due to acoustic interference from gas within the small bowel.24 Furthermore, ultrasound itself is operator‐dependent.
Contrast‐enhanced CT is the standard mode of imaging for diagnosing acute pancreatitis and provides superior imaging of the pancreas. Unfortunately it is more costly than ultrasound, involves radiation exposure, and requires intravenous contrast medium.25 Findings of acute pancreatitis frequently seen on CT include diffuse or segmental enlargement of the gland, irregular pancreatic contour, obliteration of peripancreatic fat planes, parenchymal heterogeneity, and ill‐defined fluid collections within the pancreas or in the lesser sac and pararenal spaces.26 CT scan may also be used to detect pancreatic necrosis, an important finding for the management and prognosis of this disease.27 Despite this, normal CT findings have been reported in patients with acute pancreatitis, and certain CT findings may be related to disease severity.25
Although MRI is less commonly used in the diagnosis of acute pancreatitis, it may provide a useful alternative to CT, especially in cases of renal failure or intravenous contrast hypersensitivity. When combined with magnetic resonance cholangiopancreatography (MRCP) imaging, MRI may even be able to detect a local area of pancreatic duct disruption.27 MRCP allows for a noninvasive cholangiogram and is frequently used to stratify patients who may benefit from ERCP. It can accurately identify common bile duct stones, with a higher sensitivity for choledocholithiasis than ultrasound or CT.2830 MRCP can also assist in the diagnosis of other disorders of the intrahepatic and extrahepatic biliary tree that may be related to the cause of pancreatitis. Overall, unless a patient has a contraindication, or the goal of the study is to diagnose choledocholithiasis, a contrast‐enhanced CT scan remains the imaging procedure of choice due to improved accessibility, lower cost, ease of performance, and increased sensitivity in the detection of gas bubbles (potentially indicating pancreatic infection).3133 Ordering a CT scan or other imaging at admission is not necessary in the diagnosis of acute pancreatitis if the patient's presentation is classic. At admission, however, a CT scan may be reasonable to exclude other serious causes of abdominal pain, such as a perforated ulcer. Imaging may also be ordered to define the cause of the episode of pancreatitis and to exclude occult malignancy. In addition, CT scan should be strongly considered in patients who do not improve within 2 to 3 days to assess for complications such as pancreatic necrosis, pseudocysts, or other complications.34
Most recently, endoscopic ultrasound (EUS) has risen to the forefront as a leader in accurate imaging of the pancreas and biliary tree. EUS is more sensitive than transabdominal ultrasound in detecting biliary stones,35 and it has been shown to have equivalent, and in some cases superior, sensitivity to ERCP and MRCP. Because EUS is able to detect smaller stones or sludge, it may have a role in those patients diagnosed with idiopathic pancreatitis.36 Like MRCP, EUS can also help stratify patients into those that are likely to benefit most from ERCP.37 Figure 1 reviews the evaluation of acute pancreatitis.
Prognosis
For the majority of patients with acute pancreatitis, the clinical course is mild and self‐limiting. In approximately 20% to 25% of patients, however, it is severe and associated with organ failure and significant morbidity and mortality.38, 39 Determining the severity of acute pancreatitis is critical, as patients at high‐risk for severe disease require closer monitoring and possible intervention. Several validated scoring systems are available that aim to predict the severity of acute pancreatitis including Ranson's criteria, the Imrie scoring system, the Acute Physiology and Chronic Health Evaluation (APACHE II) scale, and the CT Severity Index (CTSI) (Table 2).4043
| Ranson's Criteria | |
|---|---|
| |
| At admission or diagnosis | |
| Age | >55 years |
| WBC | >16,000/mm3 |
| Blood glucose | >200 mg/dL |
| Lactate dehydrogenase | >350 IU/L |
| AST | >250 IU/L |
| Within 48 hours after presentation | |
| Hematocrit decrease | >10% |
| Blood urea nitrogen increase | >5 mg/dL |
| Serum calcium | 8 mg/dL |
| Base deficit | >4 mEq/L |
| Fluid sequestration | >6 L |
| PaO2 | 60 mmHg |
| Scoring | 1 point for each criterion |
| APACHE II Scale | |
| Equation includes these factors: age, rectal temperature, mean arterial pressure, heart rate, PaO2, arterial pH, serum potassium, sodium, creatinine, hematocrit, WBC count, Glasgow coma scale score, chronic health status | |
| Scoring calculation available at |
|
| CT Severity Index (Balthazar Score) | |
| Grade of pancreatitis on CT | |
| A | Normal pancreas (0 points) |
| B | Pancreatic enlargement (1 point) |
| C | Pancreatic enlargement with peripancreatic inflammation (2 points) |
| D | Extrapancreatic changes plus 1 fluid collection (3 points) |
| E | More than 1 fluid collection (4 points) |
| Necrosis score | |
| None | 0 points |
| One‐third | 2 points |
| >One‐third but less than one‐half | 4 points |
| >One‐half | 6 points |
| Scoring | CT grade plus necrosis score |
| Imrie Scoring System | |
| Age | >55 years |
| WBC | >15,000/mm3 |
| Blood glucose | >180 mg/dL (absence of diabetes) |
| Lactate dehydrogenase | >600 IU/L |
| AST or ALT | >100 IU/L |
| Serum calcium | 8 mg/dl |
| PaO2 | 60 mm Hg |
| Serum albumin | 3.2 g/dL |
| Serum urea | >45 mg/dL |
| Scoring | 1 point for each criterion met after 48 hours of admission |
| Atlanta Criteria | |
| Ranson's score | 3 |
| APACHE II score | 8 |
| Presence of 1 or more organ failures: | |
| Shock | Blood pressure of 90 mmHg |
| Pulmonary insufficiency | PaO2 60 mmHg |
| Renal failure | Creatinine level >2 mg/dL after hydration |
| Gastrointestinal bleeding | Estimated >500‐mL blood loss/24 hours |
| Disseminated intravascular coagulation | Thrombocytopenia, hypofibrinogenemia, fibrin split products |
| Severe hypocalcemia | Calcium level 7.5 mg/dL |
| Presence of 1 or more local complications | |
| Pancreatic necrosis | |
| Pancreatic abscess | |
| Pancreatic pseudocyst | |
| Scoring | Severe pancreatitis indicated by any positive factor listed |
In 1992, the Atlanta Classification of acute pancreatitis was developed to provide a rational approach in predicting disease severity, thus allowing for comparison between clinical trials. It defines severe acute pancreatitis (SAP) on the basis of standard clinical manifestations, a Ranson's score 3, an APACHE II score 8, and evidence of organ failure and intrapancreatic pathological findings.44 Serum markers such as C‐reactive protein (CRP), interleukin‐6, and phospholipase A2 have all been studied to predict severity; however, only CRP is widely available. A cutoff level of 150 mg/L at 48 hours distinguishes mild disease from SAP.45 Clinical findings such as thirst, poor urine output, progressive tachycardia, tachypnea, hypoxemia, confusion, and a lack of improvement in symptoms within the first 48 hours are warning signs of impending severe disease, and thus warrant consideration of admission to an intensive care unit (ICU).34
Natural History and Complications
Despite initial aggressive intensive care treatment, 30% to 50% of patients with SAP do not respond promptly to ICU treatment and develop persistent multisystem organ failure.39 Severe organ failure in the first week of onset of acute pancreatitis is closely linked to the development of pancreatic infection occurring within 2 weeks of the initiation of symptoms.46 Early multiorgan dysfunction triggers additional mechanisms that render bacterial translocation into clinically manifested sepsis and septic shock.39 In most studied series, infection (including bacteremia, fungemia, and pancreatic abscess) remains the leading cause of death in patients with acute pancreatitis, accounting for up to 80% of fatal cases.4749 While sepsis is the more frequent cause of death in patients surviving beyond 7 days, death occurring early in the course of disease is more likely to be from respiratory complications such as pulmonary edema.50
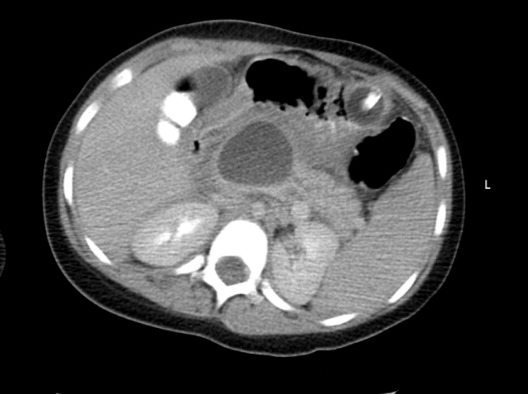
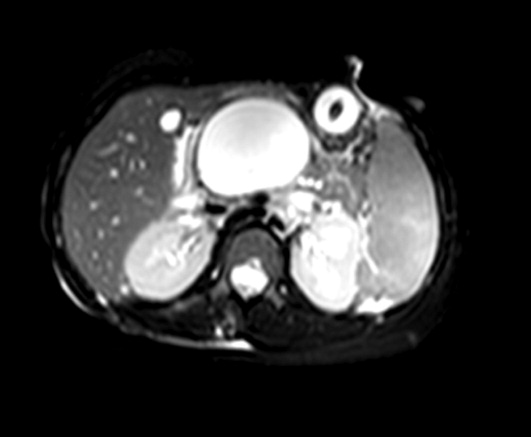
In the spectrum of acute pancreatitis, ongoing pancreatic injury can lead to pancreatic necrosis, fluid collections, pseudocyst formation, and pancreatic duct disruption (Figures 24).51 In patients hospitalized with acute pancreatitis, up to 57% will have peripancreatic fluid collections that are initially ill‐defined.44, 52 Typically, these fluid collections may be managed conservatively; however, if they continue to enlarge, cause persistent abdominal pain, become infected, or compress adjacent organs, they may require further intervention.53 Ductal disruption may be diagnosed when fluid collections have high levels of pancreatic amylase, and their presence may lead to the formation of pseudocysts, persistent ascites, or pleural effusions.54 Pancreatic pseudocysts usually require 4 weeks for complete formation, and they classically contain fluid only without significant solid debris.55 Formation typically occurs as a result of limited pancreatic necrosis causing a pancreatic duct leak with subsequent organization, or from areas of necrosis that liquefy over time.56 Both pancreatic pseudocysts and necrotic pancreatic tissue may become infected leading to abscess formation.51
Pancreatic necrosis is defined as diffuse or focal areas of nonviable pancreatic parenchyma, and it is seen in approximately 20% of patients with acute pancreatitis.44, 57 While pseudocyst formation takes approximately 1 month to occur, pancreatic necrosis can occur within the first few days of initial symptoms and is associated with an increase in complications leading to an increased risk of morbidity and mortality.58 More than 80% of deaths in acute pancreatitis are associated with the presence of pancreatic necrosis.39 Patients at highest risk for complications are those with necrosis involving more than 50% of the gland based on MRI or contrast‐enhanced CT scan.59, 60
Patients with pancreatic infection may have infected necrosis, pancreatic abscess, and/or infected pseudocysts.39 The microbes most frequently involved are gram‐negative organisms including Escherichia coli, Enterococcus, and Klebsiella.61 Recently, gram‐positive bacteria have been implicated in pancreatic infection.62 Fungal infection with Candida species is seen in up to 15% of patients with infected necrosis and is associated with more serious systemic complications.63 The use of prophylactic antibiotics may increase the risk of fungal infection. It may be challenging to distinguish between infected and sterile pancreatic necrosis; hence, needle aspiration under EUS or radiologic guidance may be required.61, 64
Management
Supportive Care and Nutrition
The majority (80%) of cases of acute pancreatitis respond well to supportive care with fluid replacement, pain control, and controlled initiation of regular food intake.39 Aggressive intravenous fluid resuscitation is needed to overcome hypovolemia caused by intravascular fluid loss.65 Currently there is a paucity of data to support clinical recommendations regarding rate of fluid resuscitation, but previous studies have suggested a rate of at least 250 to 300 mL/hour for the first 48 hours if fluid status permits.65, 66 Typically, a diet is reintroduced when abdominal tenderness improves and appetite returns.34 Traditionally patients are started on a clear liquid diet and advanced either to a full‐liquid or lowfat diet as toleratedthough there is little data on this subject.67 A recent study randomized 121 subjects to initiate either a clear liquid diet or a lowfat solid diet once recovering from acute pancreatitis and found that the lowfat solid diet was as safe as the clear liquid diet and resulted in improved caloric intake.68
In patients with SAP or complicated disease, nutritional support is critical. In an effort to achieve pancreatic rest, total parenteral nutrition (TPN) has historically been used as the primary means of nutritional support in those patients who require it. TPN, however, carries significant risks of infection and metabolic disturbance,69 and recent studies have shown that enteral nutrition may improve outcomes by decreasing the rates of infection, need for surgical intervention, hospital length of stay, and overall total cost of care.7074 Research has shown that enteral nutrition prevents intestinal atrophy and improves the barrier function of the gut mucosa.75 Typically enteral feeds are given via the nasojejunal (NJ) route, though some data suggest that nasogastric (NG) feeding is also acceptable.76, 77 Despite good intentions by physicians to provide postpyloric feeding, often NJ tubes migrate back into the stomach, yet anecdotal reports showed patients continued to tolerate enteral feeding, prompting further studies. One randomized controlled trial of 49 patients showed NG feeds to be as good as NJ feeds in patients with SAP, plus they were less costly and easier to perform.78 Similarly, this was demonstrated in 16 patients receiving NJ feeds and 15 patients receiving NG feeds with no worsening of SAP in either group.77 In the 2 previous studies, patients with objective evidence of SAP were included and semielemental feeds were started within 24 to 72 hours after onset of pain. Presumably, NG feeds were given over oral feeds as semielemental feeds are not palatable. These are small studies and further research is needed comparing NG to NJ feeds. However, patients who have severe acute pancreatitis with prolonged pain and significant pancreatic necrosis on imaging may benefit from a trial of NJ feeds before advancing to oral feeds.79 TPN may be necessary in those patients who do not tolerate enteral feeding, or do not reach an adequate infusion rate within 2 to 4 days.80
When utilizing enteral feeding, the question of semielemental formula vs. polymeric formula frequently arises. Semielemental formulas seem to pose the advantage of less pancreatic stimulation while not requiring the presence of pancreatic enzymes for absorption.81, 82 Studies, however, have not uniformly supported this hypothesis.83
Antibiotics
Antibiotics do not have a role in mild acute pancreatitis. In SAP, the role of antibiotics is more controversial. Pancreatic or peripancreatic infection develops in a significant number of patients with acute pancreatitis and is associated with substantial morbidity and mortality, particularly in patients with pancreatic necrosis.84 Prophylactic antibiotics have been attempted to reduce infectious complications, but their role in SAP is not entirely clear. Two recent meta‐analyses showed that antibiotic prophylaxis had no significant effect on infection of pancreatic necrosis and mortality, though this did contradict earlier meta‐analyses.8587 Current American College of Gastroenterology guidelines recommend against the use of prophylactic antibiotics to prevent pancreatic infection.88 Though prophylactic antibiotics are not recommended, antibiotics may be given empirically for fever, leukocytosis, and/or sepsis while a possible infectious source is investigated, including fine needle aspiration of pancreatic necrosis.88 Imipenem, meropenem, and a combination of a quinolone and metronidazole have adequate penetration into pancreatic necrotic material and are the antibiotics of choice. Use of antibiotics may increase the risk of resistant organisms and possibly fungal infections.
Endoscopy
Urgent endoscopic therapy for acute pancreatitis is only indicated in gallstone, or biliary pancreatitis. Approximately 5% of patients with symptomatic gallstones will develop acute biliary pancreatitis.89 The risk of a recurrent attack is approximately 30% to 50% if definitive therapy is not sought.90, 91 Multiple studies have demonstrated that ERCP significantly reduces morbidity and mortality in acute biliary pancreatitis.92 Urgent ERCP (within 48 hours of symptom onset) should be considered in cases of cholangitis, or in the setting of severe symptoms of disease with ongoing biliary obstruction. Elective ERCP is indicated in patients with jaundice and imaging studies demonstrating choledocholithiasis, as well as those surgical patients with abnormal intraoperative cholangiography. ERCP should also be considered for suspected pancreatic duct disruption and for biliary sphincterotomy as primary therapy in poor operative candidates, or as temporary therapy during pregnancy.93 ERCP may also have a role in recurrent idiopathic acute pancreatitis if pancreas divisum or SOD is suspected. Sphincter of Oddi manometry may be performed, and if a diagnosis is confirmed, endoscopic sphincterotomy should be performed.94 For pancreas divisum, minor sphincterotomy and/or pancreatic duct stent may be performed.95 ERCP typically does not have a role in those patients with a single attack of acute pancreatitis, as significant complications may occur due to the ERCP itself. EUS, however, can be considered in a single attack of idiopathic pancreatitis in order to further investigate possible causes of the disease.7
Cholecystectomy
Cholecystectomy is indicated for appropriate operative candidates with resolving gallstone pancreatitis. Recurrent pancreatitis can be seen in up to 30% of patients if cholecystectomy is not performed.96, 97 Based on the American Gastroenterological Association (AGA) guidelines, definitive surgical management should be performed in the same hospitalization if possible, but no later than 2 to 4 weeks after discharge.98 In most patients with mild gallstone pancreatitis and no evidence of cholangitis, routine ERCP prior to cholecystectomy is not indicated, as long as pancreatitis is resolving and liver function abnormalities have normalized.88 As mentioned previously, for patients who are not candidates for surgery, endoscopic sphincterotomy should be considered. Cholecystectomy may also be indicated for those with 2 or more episodes of idiopathic pancreatitis, particularly if biliary pancreatitis is suspected.
Failure to Improve
In patients who fail to improve, contrast‐enhanced CT scan should be performed to evaluate for fluid collections, pancreatic necrosis, or other complications that may require intervention. Antibiotic therapy may need to be considered, and in any patient without rapid improvement, nutritional support should be addressed.34 The diagnosis of infected necrosis is typically made by fine‐needle aspiration of the necrotic area under EUS, CT, or transabdominal ultrasound guidance.64
Indications for Drainage of Pseudocysts
The indications for drainage of pancreatic pseudocysts are limited, but drainage is typically performed in those patients that are symptomatic, including abdominal pain, weight loss, gastric outlet obstruction, obstructive jaundice, pancreatic duct leakage, or infectious complications.55 Depending on the location of the pseudocyst and whether it communicates with the pancreatic duct, pseudocysts may be drained by transpapillary means (endoprosthesis placed in the pancreatic duct), or by transmural means (percutaneous, surgical, or endoscopic cyst‐gastrostomy, or endoscopic cyst‐duodenostomy).55 Prior to drainage the pseudocyst wall needs to be mature, which may require up to 4 to 6 weeks. Pancreatic duct leaks may occur as a result of acute or chronic pancreatitis, and they can arise from the head, tail, or body of the gland. Fluid may ultimately track into the mediastinum or peritoneum causing effusions or ascites.55 Treatment for such pancreatic duct leaks includes transpapillary therapy to cross, or bridge, the disrupted duct.
Management of Pancreatic Necrosis
Sterile pancreatic necrosis is typically managed conservatively without drainage. Generally, CT scans are repeated every 7 to 10 days to assess the necrosis and to evaluate for further complications.32 Patients who are clinically unstable with fever, tachycardia, leukocytosis, or organ failure may require percutaneous sampling to evaluate for infected necrosis.33 If the pancreatic tissue is sterile, the patient is determined to have sterile necrosis. If the patient with sterile necrosis is clinically unstable then prophylactic antibiotics may be indicated. If the pancreatic tissue is infected, the patient is deemed to have infected necrosis and treatment with antibiotics and necrosectomy is often indicated, especially in those with a poor clinical state. The antibiotic chosen should have adequate penetration into the necrotic material, such as imipenem, meropenem, or a combination of quinolone and metronidazole.99
It may be challenging to distinguish between sterile and infected pancreatic necrosis. A CT scan is unable to differentiate them with certainty; though, intrapancreatic, retroperitoneal, or lesser sac gas may indicate infection.31 In addition, inducing infection within a previously sterile collection is a potential risk of percutaneous sampling. As a result, sampling should not be performed unless completely indicated.31
In patients with sterile pancreatic necrosis who are symptomatic with refractory abdominal pain, gastric outlet obstruction, or failure to thrive at 4 or more weeks following the onset of acute pancreatitis, drainage and/or debridement is usually indicated. Pancreatic necrosectomy for sterile pancreatic necrosis may be accomplished endoscopically, or more traditionally by a surgical approach.55 Although endoscopic drainage is less invasive, it is technically difficult and has a higher rate of complication in the hands of inexperienced operators.100 Careful selection and evaluation of patients undergoing endoscopic drainage procedures is necessary. Bleeding, perforation, infection, pancreatitis, aspiration, stent migration, and pancreatic ductal damage are all possible complications during the drainage of necrotic pancreatic fluid collections.55 If pancreatic necrosis is infected, surgical necrosectomy should be performed as this is the gold standard for infected necrosis when debridement is necessary.55 Figure 5 reviews the management of acute pancreatitis.
Conclusion
Acute pancreatitis is a common disease frequently caused by choledocholithiasis or excess alcohol ingestion. In idiopathic acute pancreatitis, microlithiasis and SOD should be considered. Though CT scan remains the imaging modality of choice, newer methods such as MRCP and EUS may help to provide additional and improved diagnostic information.
The management of acute pancreatitis is frequently challenging, and severity scales help to predict the likelihood of complications, determine necessary interventions, and guide the appropriate level of care. Nutrition is critical in patients with SAP, and enteral feeding is clearly preferred over TPN. Currently, prophylactic antibiotics do not appear to have a role in SAP. Finally, though not always straightforward, recommendations do exist to guide the management of many of the complications of acute pancreatitis, such as pseudocyst formation and necrotizing disease. A multidisciplinary approach should be used in managing patients with severe disease, and the primary inpatient physician should not hesitate to involve specialists, including gastroenterologists, radiologists, and surgeons.
Acute pancreatitis accounts for more than 220,000 hospital admissions in the United States annually.1 In the following review, we outline the etiology of acute pancreatitis, discuss its complications, and provide an updated review on its management for the hospitalized patient.
Etiology
Gallstone disease and excess alcohol ingestion are the most common causes of acute pancreatitis in the United States. Gallstones account for roughly 45% of all cases, and the pathogenesis is due to transient obstruction of the pancreatic duct orifice to the flow of pancreatic exocrine secretions.2 Excess alcohol ingestion accounts for approximately 35% of all cases, yet the pathogenesis here is less understood.3 Most theories suggest a direct toxic effect of the ethanol upon the pancreatic parenchyma or its neurovascular supply.4
There are many other less common causes of acute pancreatitis including toxins, drugs, infections, trauma, vascular insults, anatomic abnormalities, and metabolic derangements. Hypertriglyceridemia and hypercalcemia are both implicated in acute pancreatitis. Serum triglyceride levels >1000 mg/dL can precipitate an attack of acute pancreatitis though the pathogenesis is not clearly understood.5 Hypercalcemia is also an uncommon cause of acute pancreatitis, and is thought to result from deposition of calcium in the pancreatic duct and calcium activation of trypsinogen.6
Idiopathic pancreatitis occurs in up to 20% of patients with acute pancreatitis, and by definition, the cause is not established by history, physical examination, routine laboratory tests, or imaging. The majority of idiopathic cases of pancreatitis are thought to have a biliary source. In patients with gallbladder in situ, it is estimated that up to 75% acquire pancreatitis from microlithiasis, or biliary sludge and stone debris, that causes obstruction of the distal common bile and main pancreatic ducts. Conversely, sphincter of Oddi dysfunction (SOD) resulting in transient pancreatic ductal obstruction is felt to be the most common cause in those patients who have undergone a previous cholecystectomy.7
An emerging entity, autoimmune pancreatitis (AIP), is more commonly associated with chronic pancreatitis but may cause episodes of acute pancreatitis or mimic pancreatic carcinoma. Typically, the diagnosis is based on elevated levels of serum gammaglobulin subgroup 4 (IgG4) populations, along with characteristic findings on computed tomography (CT) scan (eg, narrowed or wispy main pancreatic duct and an enlarged pancreatic parenchyma). Core‐needle biopsy may confirm the diagnosis of AIP with lymphoplasmacytic infiltration and dense fibrosis.8 Since AIP can mimic pancreatic cancer, the diagnosis may not be made until the time of surgical resection.
Diagnosis
Along with characteristic symptoms, the diagnosis of acute pancreatitis is often based on elevated serum levels of pancreatic enzymes that are at least twice the normal level. Amylase and lipase are the most frequently used serum markers for acute pancreatitis, though their elevation is not pathognomonic for the presence of disease. These enzymes may not always be significantly elevated during times of acute inflammation, and elevation of the enzymes can come from nonpancreatic origins as well (Table 1). Although there is no gold standard for the diagnosis of acute pancreatitis, using serum lipase (>250 IU/L) in conjunction with amylase (>160 IU/L) improves the overall diagnostic sensitivity from 81% to 94%.9 Isoamylase levels can be used to distinguish among pancreatic, salivary, and macroamylasemia though this is not often used if pancreatitis is suspected clinically. Similarly, serum isolipase can be measured, though this is not readily available.
| Nonpancreatic causes of hyperamylasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, intestinal obstruction, intestinal infarction, perforation, mesenteric thrombosis, pancreatic cancer, appendicitis, peritonitis, pyelonephritis, renal insufficiency, liver disease, pregnancy, ruptured ectopic pregnancy, aortic aneurysm dissection, prostatic disease, ovarian neoplasm |
| Thoracic | Esophagitis, myocardial infarction, pulmonary embolism, pneumonia, metastatic carcinoma of lung, breast cancer |
| Procedural | Abdominal operations, nonabdominal operations, post‐ERCP |
| Trauma | Brain trauma, burns, and traumatic shock |
| Metabolic | Diabetic ketoacidosis |
| Drugs | Opiate administration, oxyphenbutazone, phenylbutazone, aminosalicylic acid, aspirin, atovaquone, bethanecol, estrogens, lamivudine, meperidine, metoclopramide, ranitidine, thiazides, valproic acid, sulfonamides |
| Other | Parotitis, renal transplantation, alcoholism, human immunodeficiency virus, macroamylasemia |
| Nonpancreatic causes of hyperlipasemia | |
| Abdominal/pelvic | Pancreatic pseudocyst, biliary tract disorders, gastritis, peptic ulcer disease, spontaneous bacterial peritonitis, liver disease, pancreatic carcinoma, intestinal obstruction, ischemia, perforation, appendicitis, celiac disease |
| Thoracic | Esophagitis |
| Drugs | Furosemide, thiazides, metronidazole, valproic acid, bethanecol, oral contraceptives, indomethacin |
| Other | Renal insufficiency, macrolipasemia |
In order to improve the sensitivity and specificity of diagnosis, other tests have been studied to help predict disease presence and severity. Previously, serum tests for trypsin, elastase, phospholipase A2, and carboxylester lipase have all been evaluated but shown to have no significant improvement in diagnostic capability.1014 More recently, trypsinogen (a pancreatic proteinase) has proven to be a useful aid in the accurate diagnosis of acute disease. Trypsinogen undergoes activation into trypsin during acute pancreatic inflammation.3 It is comprised of 2 main isoenzymes (trypsinogen‐1 and trypsinogen‐2) that are secreted into the pancreatic fluid with a small proportion escaping into the circulation.15 Higher concentrations of trypsinogen‐1 are seen in healthy people, while higher concentrations of trypsinogen‐2 are seen in those with acute pancreatitis.16 Urinary trypsinogen‐2 dipstick tests detect acute pancreatitis more accurately than quantitative serum or urinary amylase, with a sensitivity as high as 94%, and a specificity of 95%.17 Studies have shown that in post‐endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis, serum trypsinogen‐2 levels begin to rise as early as 1 hour and peak at 6 hours.17 The Actim Pancreatitis (Medix Biomedica, Kauniainen, Finland) urine test strips measure concentrations of trypsinogen‐2 as low as 50 g/L, but is not a quantitative test and, thus, it does not predict severity. Some studies have advocated the use of urinary trypsinogen‐2 as a screening tool, with a positive result indicating a need for further evaluation of acute pancreatitis.1820 Urinary trypsinogen‐2 is less costly than serum tests, plus may result in additional cost savings with earlier patient discharge. Unfortunately, this test is not widely available for clinical use. Urinary trypsinogen activation peptide (TAP) is another test that has been studied in the diagnosis of acute pancreatitis, but may signify disease severity rather than the presence or absence of disease.21 Currently urinary assays for TAP are not widely available in the United States.
Choosing the Appropriate Imaging Modality
Along with the measurement of pancreatic release enzymes, abdominal imaging is often used, though not always necessary to confirm the diagnosis of acute pancreatitis. Imaging techniques such as CT, magnetic resonance imaging (MRI), and transabdominal ultrasonography may be used to rule out other causes of abdominal pain or elucidate the cause of the pancreatitis itself. Ultrasound may show pancreatic enlargement, diminished echogenicity, and possible adjacent fluid collections.22 In searching for evidence of gallstone pancreatitis, transabdominal ultrasound has a sensitivity of 67% and a specificity of 100%.23 However, it may be insensitive for detecting stones in the distal common bile duct near the ampulla due to acoustic interference from gas within the small bowel.24 Furthermore, ultrasound itself is operator‐dependent.
Contrast‐enhanced CT is the standard mode of imaging for diagnosing acute pancreatitis and provides superior imaging of the pancreas. Unfortunately it is more costly than ultrasound, involves radiation exposure, and requires intravenous contrast medium.25 Findings of acute pancreatitis frequently seen on CT include diffuse or segmental enlargement of the gland, irregular pancreatic contour, obliteration of peripancreatic fat planes, parenchymal heterogeneity, and ill‐defined fluid collections within the pancreas or in the lesser sac and pararenal spaces.26 CT scan may also be used to detect pancreatic necrosis, an important finding for the management and prognosis of this disease.27 Despite this, normal CT findings have been reported in patients with acute pancreatitis, and certain CT findings may be related to disease severity.25
Although MRI is less commonly used in the diagnosis of acute pancreatitis, it may provide a useful alternative to CT, especially in cases of renal failure or intravenous contrast hypersensitivity. When combined with magnetic resonance cholangiopancreatography (MRCP) imaging, MRI may even be able to detect a local area of pancreatic duct disruption.27 MRCP allows for a noninvasive cholangiogram and is frequently used to stratify patients who may benefit from ERCP. It can accurately identify common bile duct stones, with a higher sensitivity for choledocholithiasis than ultrasound or CT.2830 MRCP can also assist in the diagnosis of other disorders of the intrahepatic and extrahepatic biliary tree that may be related to the cause of pancreatitis. Overall, unless a patient has a contraindication, or the goal of the study is to diagnose choledocholithiasis, a contrast‐enhanced CT scan remains the imaging procedure of choice due to improved accessibility, lower cost, ease of performance, and increased sensitivity in the detection of gas bubbles (potentially indicating pancreatic infection).3133 Ordering a CT scan or other imaging at admission is not necessary in the diagnosis of acute pancreatitis if the patient's presentation is classic. At admission, however, a CT scan may be reasonable to exclude other serious causes of abdominal pain, such as a perforated ulcer. Imaging may also be ordered to define the cause of the episode of pancreatitis and to exclude occult malignancy. In addition, CT scan should be strongly considered in patients who do not improve within 2 to 3 days to assess for complications such as pancreatic necrosis, pseudocysts, or other complications.34
Most recently, endoscopic ultrasound (EUS) has risen to the forefront as a leader in accurate imaging of the pancreas and biliary tree. EUS is more sensitive than transabdominal ultrasound in detecting biliary stones,35 and it has been shown to have equivalent, and in some cases superior, sensitivity to ERCP and MRCP. Because EUS is able to detect smaller stones or sludge, it may have a role in those patients diagnosed with idiopathic pancreatitis.36 Like MRCP, EUS can also help stratify patients into those that are likely to benefit most from ERCP.37 Figure 1 reviews the evaluation of acute pancreatitis.
Prognosis
For the majority of patients with acute pancreatitis, the clinical course is mild and self‐limiting. In approximately 20% to 25% of patients, however, it is severe and associated with organ failure and significant morbidity and mortality.38, 39 Determining the severity of acute pancreatitis is critical, as patients at high‐risk for severe disease require closer monitoring and possible intervention. Several validated scoring systems are available that aim to predict the severity of acute pancreatitis including Ranson's criteria, the Imrie scoring system, the Acute Physiology and Chronic Health Evaluation (APACHE II) scale, and the CT Severity Index (CTSI) (Table 2).4043
| Ranson's Criteria | |
|---|---|
| |
| At admission or diagnosis | |
| Age | >55 years |
| WBC | >16,000/mm3 |
| Blood glucose | >200 mg/dL |
| Lactate dehydrogenase | >350 IU/L |
| AST | >250 IU/L |
| Within 48 hours after presentation | |
| Hematocrit decrease | >10% |
| Blood urea nitrogen increase | >5 mg/dL |
| Serum calcium | 8 mg/dL |
| Base deficit | >4 mEq/L |
| Fluid sequestration | >6 L |
| PaO2 | 60 mmHg |
| Scoring | 1 point for each criterion |
| APACHE II Scale | |
| Equation includes these factors: age, rectal temperature, mean arterial pressure, heart rate, PaO2, arterial pH, serum potassium, sodium, creatinine, hematocrit, WBC count, Glasgow coma scale score, chronic health status | |
| Scoring calculation available at |
|
| CT Severity Index (Balthazar Score) | |
| Grade of pancreatitis on CT | |
| A | Normal pancreas (0 points) |
| B | Pancreatic enlargement (1 point) |
| C | Pancreatic enlargement with peripancreatic inflammation (2 points) |
| D | Extrapancreatic changes plus 1 fluid collection (3 points) |
| E | More than 1 fluid collection (4 points) |
| Necrosis score | |
| None | 0 points |
| One‐third | 2 points |
| >One‐third but less than one‐half | 4 points |
| >One‐half | 6 points |
| Scoring | CT grade plus necrosis score |
| Imrie Scoring System | |
| Age | >55 years |
| WBC | >15,000/mm3 |
| Blood glucose | >180 mg/dL (absence of diabetes) |
| Lactate dehydrogenase | >600 IU/L |
| AST or ALT | >100 IU/L |
| Serum calcium | 8 mg/dl |
| PaO2 | 60 mm Hg |
| Serum albumin | 3.2 g/dL |
| Serum urea | >45 mg/dL |
| Scoring | 1 point for each criterion met after 48 hours of admission |
| Atlanta Criteria | |
| Ranson's score | 3 |
| APACHE II score | 8 |
| Presence of 1 or more organ failures: | |
| Shock | Blood pressure of 90 mmHg |
| Pulmonary insufficiency | PaO2 60 mmHg |
| Renal failure | Creatinine level >2 mg/dL after hydration |
| Gastrointestinal bleeding | Estimated >500‐mL blood loss/24 hours |
| Disseminated intravascular coagulation | Thrombocytopenia, hypofibrinogenemia, fibrin split products |
| Severe hypocalcemia | Calcium level 7.5 mg/dL |
| Presence of 1 or more local complications | |
| Pancreatic necrosis | |
| Pancreatic abscess | |
| Pancreatic pseudocyst | |
| Scoring | Severe pancreatitis indicated by any positive factor listed |
In 1992, the Atlanta Classification of acute pancreatitis was developed to provide a rational approach in predicting disease severity, thus allowing for comparison between clinical trials. It defines severe acute pancreatitis (SAP) on the basis of standard clinical manifestations, a Ranson's score 3, an APACHE II score 8, and evidence of organ failure and intrapancreatic pathological findings.44 Serum markers such as C‐reactive protein (CRP), interleukin‐6, and phospholipase A2 have all been studied to predict severity; however, only CRP is widely available. A cutoff level of 150 mg/L at 48 hours distinguishes mild disease from SAP.45 Clinical findings such as thirst, poor urine output, progressive tachycardia, tachypnea, hypoxemia, confusion, and a lack of improvement in symptoms within the first 48 hours are warning signs of impending severe disease, and thus warrant consideration of admission to an intensive care unit (ICU).34
Natural History and Complications
Despite initial aggressive intensive care treatment, 30% to 50% of patients with SAP do not respond promptly to ICU treatment and develop persistent multisystem organ failure.39 Severe organ failure in the first week of onset of acute pancreatitis is closely linked to the development of pancreatic infection occurring within 2 weeks of the initiation of symptoms.46 Early multiorgan dysfunction triggers additional mechanisms that render bacterial translocation into clinically manifested sepsis and septic shock.39 In most studied series, infection (including bacteremia, fungemia, and pancreatic abscess) remains the leading cause of death in patients with acute pancreatitis, accounting for up to 80% of fatal cases.4749 While sepsis is the more frequent cause of death in patients surviving beyond 7 days, death occurring early in the course of disease is more likely to be from respiratory complications such as pulmonary edema.50
In the spectrum of acute pancreatitis, ongoing pancreatic injury can lead to pancreatic necrosis, fluid collections, pseudocyst formation, and pancreatic duct disruption (Figures 24).51 In patients hospitalized with acute pancreatitis, up to 57% will have peripancreatic fluid collections that are initially ill‐defined.44, 52 Typically, these fluid collections may be managed conservatively; however, if they continue to enlarge, cause persistent abdominal pain, become infected, or compress adjacent organs, they may require further intervention.53 Ductal disruption may be diagnosed when fluid collections have high levels of pancreatic amylase, and their presence may lead to the formation of pseudocysts, persistent ascites, or pleural effusions.54 Pancreatic pseudocysts usually require 4 weeks for complete formation, and they classically contain fluid only without significant solid debris.55 Formation typically occurs as a result of limited pancreatic necrosis causing a pancreatic duct leak with subsequent organization, or from areas of necrosis that liquefy over time.56 Both pancreatic pseudocysts and necrotic pancreatic tissue may become infected leading to abscess formation.51
Pancreatic necrosis is defined as diffuse or focal areas of nonviable pancreatic parenchyma, and it is seen in approximately 20% of patients with acute pancreatitis.44, 57 While pseudocyst formation takes approximately 1 month to occur, pancreatic necrosis can occur within the first few days of initial symptoms and is associated with an increase in complications leading to an increased risk of morbidity and mortality.58 More than 80% of deaths in acute pancreatitis are associated with the presence of pancreatic necrosis.39 Patients at highest risk for complications are those with necrosis involving more than 50% of the gland based on MRI or contrast‐enhanced CT scan.59, 60
Patients with pancreatic infection may have infected necrosis, pancreatic abscess, and/or infected pseudocysts.39 The microbes most frequently involved are gram‐negative organisms including Escherichia coli, Enterococcus, and Klebsiella.61 Recently, gram‐positive bacteria have been implicated in pancreatic infection.62 Fungal infection with Candida species is seen in up to 15% of patients with infected necrosis and is associated with more serious systemic complications.63 The use of prophylactic antibiotics may increase the risk of fungal infection. It may be challenging to distinguish between infected and sterile pancreatic necrosis; hence, needle aspiration under EUS or radiologic guidance may be required.61, 64
Management
Supportive Care and Nutrition
The majority (80%) of cases of acute pancreatitis respond well to supportive care with fluid replacement, pain control, and controlled initiation of regular food intake.39 Aggressive intravenous fluid resuscitation is needed to overcome hypovolemia caused by intravascular fluid loss.65 Currently there is a paucity of data to support clinical recommendations regarding rate of fluid resuscitation, but previous studies have suggested a rate of at least 250 to 300 mL/hour for the first 48 hours if fluid status permits.65, 66 Typically, a diet is reintroduced when abdominal tenderness improves and appetite returns.34 Traditionally patients are started on a clear liquid diet and advanced either to a full‐liquid or lowfat diet as toleratedthough there is little data on this subject.67 A recent study randomized 121 subjects to initiate either a clear liquid diet or a lowfat solid diet once recovering from acute pancreatitis and found that the lowfat solid diet was as safe as the clear liquid diet and resulted in improved caloric intake.68
In patients with SAP or complicated disease, nutritional support is critical. In an effort to achieve pancreatic rest, total parenteral nutrition (TPN) has historically been used as the primary means of nutritional support in those patients who require it. TPN, however, carries significant risks of infection and metabolic disturbance,69 and recent studies have shown that enteral nutrition may improve outcomes by decreasing the rates of infection, need for surgical intervention, hospital length of stay, and overall total cost of care.7074 Research has shown that enteral nutrition prevents intestinal atrophy and improves the barrier function of the gut mucosa.75 Typically enteral feeds are given via the nasojejunal (NJ) route, though some data suggest that nasogastric (NG) feeding is also acceptable.76, 77 Despite good intentions by physicians to provide postpyloric feeding, often NJ tubes migrate back into the stomach, yet anecdotal reports showed patients continued to tolerate enteral feeding, prompting further studies. One randomized controlled trial of 49 patients showed NG feeds to be as good as NJ feeds in patients with SAP, plus they were less costly and easier to perform.78 Similarly, this was demonstrated in 16 patients receiving NJ feeds and 15 patients receiving NG feeds with no worsening of SAP in either group.77 In the 2 previous studies, patients with objective evidence of SAP were included and semielemental feeds were started within 24 to 72 hours after onset of pain. Presumably, NG feeds were given over oral feeds as semielemental feeds are not palatable. These are small studies and further research is needed comparing NG to NJ feeds. However, patients who have severe acute pancreatitis with prolonged pain and significant pancreatic necrosis on imaging may benefit from a trial of NJ feeds before advancing to oral feeds.79 TPN may be necessary in those patients who do not tolerate enteral feeding, or do not reach an adequate infusion rate within 2 to 4 days.80
When utilizing enteral feeding, the question of semielemental formula vs. polymeric formula frequently arises. Semielemental formulas seem to pose the advantage of less pancreatic stimulation while not requiring the presence of pancreatic enzymes for absorption.81, 82 Studies, however, have not uniformly supported this hypothesis.83
Antibiotics
Antibiotics do not have a role in mild acute pancreatitis. In SAP, the role of antibiotics is more controversial. Pancreatic or peripancreatic infection develops in a significant number of patients with acute pancreatitis and is associated with substantial morbidity and mortality, particularly in patients with pancreatic necrosis.84 Prophylactic antibiotics have been attempted to reduce infectious complications, but their role in SAP is not entirely clear. Two recent meta‐analyses showed that antibiotic prophylaxis had no significant effect on infection of pancreatic necrosis and mortality, though this did contradict earlier meta‐analyses.8587 Current American College of Gastroenterology guidelines recommend against the use of prophylactic antibiotics to prevent pancreatic infection.88 Though prophylactic antibiotics are not recommended, antibiotics may be given empirically for fever, leukocytosis, and/or sepsis while a possible infectious source is investigated, including fine needle aspiration of pancreatic necrosis.88 Imipenem, meropenem, and a combination of a quinolone and metronidazole have adequate penetration into pancreatic necrotic material and are the antibiotics of choice. Use of antibiotics may increase the risk of resistant organisms and possibly fungal infections.
Endoscopy
Urgent endoscopic therapy for acute pancreatitis is only indicated in gallstone, or biliary pancreatitis. Approximately 5% of patients with symptomatic gallstones will develop acute biliary pancreatitis.89 The risk of a recurrent attack is approximately 30% to 50% if definitive therapy is not sought.90, 91 Multiple studies have demonstrated that ERCP significantly reduces morbidity and mortality in acute biliary pancreatitis.92 Urgent ERCP (within 48 hours of symptom onset) should be considered in cases of cholangitis, or in the setting of severe symptoms of disease with ongoing biliary obstruction. Elective ERCP is indicated in patients with jaundice and imaging studies demonstrating choledocholithiasis, as well as those surgical patients with abnormal intraoperative cholangiography. ERCP should also be considered for suspected pancreatic duct disruption and for biliary sphincterotomy as primary therapy in poor operative candidates, or as temporary therapy during pregnancy.93 ERCP may also have a role in recurrent idiopathic acute pancreatitis if pancreas divisum or SOD is suspected. Sphincter of Oddi manometry may be performed, and if a diagnosis is confirmed, endoscopic sphincterotomy should be performed.94 For pancreas divisum, minor sphincterotomy and/or pancreatic duct stent may be performed.95 ERCP typically does not have a role in those patients with a single attack of acute pancreatitis, as significant complications may occur due to the ERCP itself. EUS, however, can be considered in a single attack of idiopathic pancreatitis in order to further investigate possible causes of the disease.7
Cholecystectomy
Cholecystectomy is indicated for appropriate operative candidates with resolving gallstone pancreatitis. Recurrent pancreatitis can be seen in up to 30% of patients if cholecystectomy is not performed.96, 97 Based on the American Gastroenterological Association (AGA) guidelines, definitive surgical management should be performed in the same hospitalization if possible, but no later than 2 to 4 weeks after discharge.98 In most patients with mild gallstone pancreatitis and no evidence of cholangitis, routine ERCP prior to cholecystectomy is not indicated, as long as pancreatitis is resolving and liver function abnormalities have normalized.88 As mentioned previously, for patients who are not candidates for surgery, endoscopic sphincterotomy should be considered. Cholecystectomy may also be indicated for those with 2 or more episodes of idiopathic pancreatitis, particularly if biliary pancreatitis is suspected.
Failure to Improve
In patients who fail to improve, contrast‐enhanced CT scan should be performed to evaluate for fluid collections, pancreatic necrosis, or other complications that may require intervention. Antibiotic therapy may need to be considered, and in any patient without rapid improvement, nutritional support should be addressed.34 The diagnosis of infected necrosis is typically made by fine‐needle aspiration of the necrotic area under EUS, CT, or transabdominal ultrasound guidance.64
Indications for Drainage of Pseudocysts
The indications for drainage of pancreatic pseudocysts are limited, but drainage is typically performed in those patients that are symptomatic, including abdominal pain, weight loss, gastric outlet obstruction, obstructive jaundice, pancreatic duct leakage, or infectious complications.55 Depending on the location of the pseudocyst and whether it communicates with the pancreatic duct, pseudocysts may be drained by transpapillary means (endoprosthesis placed in the pancreatic duct), or by transmural means (percutaneous, surgical, or endoscopic cyst‐gastrostomy, or endoscopic cyst‐duodenostomy).55 Prior to drainage the pseudocyst wall needs to be mature, which may require up to 4 to 6 weeks. Pancreatic duct leaks may occur as a result of acute or chronic pancreatitis, and they can arise from the head, tail, or body of the gland. Fluid may ultimately track into the mediastinum or peritoneum causing effusions or ascites.55 Treatment for such pancreatic duct leaks includes transpapillary therapy to cross, or bridge, the disrupted duct.
Management of Pancreatic Necrosis
Sterile pancreatic necrosis is typically managed conservatively without drainage. Generally, CT scans are repeated every 7 to 10 days to assess the necrosis and to evaluate for further complications.32 Patients who are clinically unstable with fever, tachycardia, leukocytosis, or organ failure may require percutaneous sampling to evaluate for infected necrosis.33 If the pancreatic tissue is sterile, the patient is determined to have sterile necrosis. If the patient with sterile necrosis is clinically unstable then prophylactic antibiotics may be indicated. If the pancreatic tissue is infected, the patient is deemed to have infected necrosis and treatment with antibiotics and necrosectomy is often indicated, especially in those with a poor clinical state. The antibiotic chosen should have adequate penetration into the necrotic material, such as imipenem, meropenem, or a combination of quinolone and metronidazole.99
It may be challenging to distinguish between sterile and infected pancreatic necrosis. A CT scan is unable to differentiate them with certainty; though, intrapancreatic, retroperitoneal, or lesser sac gas may indicate infection.31 In addition, inducing infection within a previously sterile collection is a potential risk of percutaneous sampling. As a result, sampling should not be performed unless completely indicated.31
In patients with sterile pancreatic necrosis who are symptomatic with refractory abdominal pain, gastric outlet obstruction, or failure to thrive at 4 or more weeks following the onset of acute pancreatitis, drainage and/or debridement is usually indicated. Pancreatic necrosectomy for sterile pancreatic necrosis may be accomplished endoscopically, or more traditionally by a surgical approach.55 Although endoscopic drainage is less invasive, it is technically difficult and has a higher rate of complication in the hands of inexperienced operators.100 Careful selection and evaluation of patients undergoing endoscopic drainage procedures is necessary. Bleeding, perforation, infection, pancreatitis, aspiration, stent migration, and pancreatic ductal damage are all possible complications during the drainage of necrotic pancreatic fluid collections.55 If pancreatic necrosis is infected, surgical necrosectomy should be performed as this is the gold standard for infected necrosis when debridement is necessary.55 Figure 5 reviews the management of acute pancreatitis.
Conclusion
Acute pancreatitis is a common disease frequently caused by choledocholithiasis or excess alcohol ingestion. In idiopathic acute pancreatitis, microlithiasis and SOD should be considered. Though CT scan remains the imaging modality of choice, newer methods such as MRCP and EUS may help to provide additional and improved diagnostic information.
The management of acute pancreatitis is frequently challenging, and severity scales help to predict the likelihood of complications, determine necessary interventions, and guide the appropriate level of care. Nutrition is critical in patients with SAP, and enteral feeding is clearly preferred over TPN. Currently, prophylactic antibiotics do not appear to have a role in SAP. Finally, though not always straightforward, recommendations do exist to guide the management of many of the complications of acute pancreatitis, such as pseudocyst formation and necrotizing disease. A multidisciplinary approach should be used in managing patients with severe disease, and the primary inpatient physician should not hesitate to involve specialists, including gastroenterologists, radiologists, and surgeons.
- ,.2005 National hospital discharge survey.Adv Data.2007;385:1–19.
- ,.Gallstones.BMJ.2007;335:295–299.
- ,.Acute pancreatitis.N Engl J Med.1994;330:1198–1210.
- ,.Pathobiology of alcoholic pancreatitis.Pancreatology.2007;7:105–114.
- .Hyperlipidemic pancreatitis.Gastroenterol Clin North Am.1990;19:783–791.
- ,,,,,.Acute hypercalcemia causes acute pancreatitis and ectopic trypsinogen activation in the rat.Gastroenterology.1995;109:239–246.
- ,,.Role of endoscopic evaluation in idiopathic pancreatitis: a systematic review.Gastrointest Endosc.2006;63:1037–1045.
- ,.Autoimmune pancreatitis: a review.World J Gastroenterol.2007;13:6327–6332.
- ,,, et al.Acute pancreatitis and normoamylasemia. not an uncommon combination.Ann Surg.1989;210:614–620.
- .Normal amylase levels in the presentation of acute pancreatitis.Am J Emerg Med.1994;12:21–24.
- .Diagnostic standards for acute pancreatitis.World J Surg.1997;21:136–142.
- .Support of the diagnosis of pancreatitis by enzyme tests — old problems, new techniques.Clinica Chimica Acta.1997;257:85–98.
- ,,,.What is the best biochemical test to diagnose acute pancreatitis? A prospective clinical study.Mayo Clin Proc.1996;71:1138–1144.
- .The value of clinical laboratory studies in acute pancreatitis.Arch Pathol Lab Med.1991;115:325–326.
- ,.Anionic and cationic trypsinogens (trypsins) in mammalian pancreas.Enzyme.1972/73;14:116–130.
- ,,,,,.Time‐resolved immunofluorometric assays for trypsinogen‐1 and 2 in serum reveal preferential elevation of trypsinogen‐2 in pancreatitis.J Lab Clin Med.1990;115:712–718.
- ,,, et al.Rapid measurement of urinary trypsinogen‐2 as a screening test for acute pancreatitis.N Engl J Med.1997;336:1788–1793.
- ,,,,.Rapid urinary trypsinogen‐2 test strip in the diagnosis of acute pancreatitis.Pancreas.2005;30:243–247.
- ,,, et al.Clinical value of rapid urine trypsinogen‐2 test strip, urinary trypsinogen activation peptide, and serum and urinary activation peptide of carboxypeptidase B in acute pancreatitis.World J Gastroenterol.2005;11:7261–7265.
- ,,,,.Use of the urinary trypsinogen‐2 dip stick test in early diagnosis of pancreatitis after endoscopic retrograde cholangiopancreatography.Surg Endosc.2007;21:1312–1315.
- ,,, et al.Early prediction of severity in acute pancreatitis by urinary trypsinogen activation peptide: a multicentre study.Lancet.2000;355:1955–1960.
- ,.The ultrasonic findings in inflammatory pancreatic disease.Semin Ultrasound.1980;1:178.
- ,,,,,.The urgent diagnosis of gallstones in acute pancreatitis: a prospective study of three methods.Br J Surg.1984;71:230–233.
- ,,.Gallstone pancreatitis: a community teaching hospital experience.J Clin Gastroenterol.2001;33:41–44.
- ,,,.Diagnostic imaging of acute pancreatitis: prospective study using CT and sonography.AJR Am J Roentgenol.1981;137:497–502.
- ,,,.Value of contrast‐enhanced computerized tomography in the early diagnosis and prognosis of acute pancreatitis: a prospective study of 202 patients.Am J Surg.1988;155:457–466.
- ,,, et al.Computed tomography and magnetic resonance imaging in the assessment of acute pancreatitis.Gastroenterology.2004;126:715–723.
- ,,, et al.The role of magnetic resonance cholangiography in the management of patients with gallstone pancreatitis.Ann Surg.2005;241:119–124.
- ,,.Magnetic resonance imaging of acute pancreatitis: the pancreatogram.JOP.2004;5:48–50.
- ,,.Magnetic resonance cholangiopancreatography.N Engl J Med.1999;341(4):258–264.
- ,,,,.Imaging and percutaneous management of acute complicated pancreatitis.Cardiovasc Intervent Radiol.2004;27:567–580.
- ,,.State‐of‐the‐art imaging of acute pancreatitis.JBR‐BTR.2003;86:193–208.
- ,,,.Acute necrotizing pancreatitis: Role of CT‐guided percutaneous catheter drainage.Abdom Imaging.2007;32:351–361.
- .Acute pancreatitis.N Engl J Med.2006;354:2142–2150.
- ,,, et al.Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients.Gastrointest Endosc.2001;54:325–330.
- ,.Endoscopic ultrasonography in the evaluation of idiopathic acute pancreatitis.Br J Surg.2000;87:1650–1655.
- ,; theCalgary Advanced Therapeutic Endoscopy Center (ATEC) Study Group.Noninvasive vs. selective invasive biliary imaging for acute biliary pancreatitis: an economic evaluation by using decision tree analysis.Gastrointest Endosc.2005;61:86–97.
- ,.Prognostic factors in acute pancreatitis.J Clin Gastroenterol.2002;34:167–176.
- ,.Severe acute pancreatitis: clinical course and management.World J Gastroenterol.2007;13:5043–5051.
- .Etiological and prognostic factors in human acute pancreatitis: a review.Am J Gastroenterol.1982;77:633–638.
- ,,,,.Prognostic factors in acute pancreatitis.Gut.1984;25:1340–1346.
- ,,,,.APACHE‐acute physiology and chronic health evaluation: a physiologically based classification system.Crit Care Med.1981;9:591–597.
- ,,,.Acute pancreatitis: value of CT in establishing prognosis.Radiology.1990;174:331–336.
- .A clinically based classification system for acute pancreatitis. summary of the international symposium on acute pancreatitis, Atlanta, GA, September 11 through 13, 1992.Arch Surg.1993;128:586–590.
- ,,, et al.Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini Consensus Conference.Int J Pancreatol.1999;25:195–210.
- ,,,.Role of early multisystem organ failure as major risk factor for pancreatic infections and death in severe acute pancreatitis.Clin Gastroenterol Hepatol.2006;4:1053–1061.
- ,.Lethal pancreatitis.Am J Gastroenterol.1983;78:810–814.
- ,,,.A randomized multicenter clinical trial of antibiotic prophylaxis of septic complications in acute necrotizing pancreatitis with imipenem.Surg Gynecol Obstet.1993;176:480–483.
- ,.Prevention, diagnosis, and treatment of pancreatic abscess.Surgery.1977;82:99–106.
- ,,,.Death due to acute pancreatitis. a retrospective analysis of 405 autopsy cases.Dig Dis Sci.1985;30:1005–1018.
- .Endoscopic drainage of pancreatic fluid collections and pancreatic necrosis.Gastrointest Endosc Clin North Am.2003;13:743–764.
- ,,, et al.Early prediction of acute pancreatitis: prospective study comparing computed tomography scans, Ranson, Glascow, Acute Physiology and Chronic Health Evaluation II scores, and various serum markers.World J Surg.2002;26:612–619.
- ,,, et al.ASGE guideline: the role of endoscopy in the diagnosis and the management of cystic lesions and inflammatory fluid collections of the pancreas.Gastrointest Endosc.2005;61:363–370.
- .Endoscopic therapy of complete and partial pancreatic duct disruptions.Gastrointest Endosc Clin N Am.1998;8:39–53.
- .Treatment of pancreatic pseudocysts, pancreatic necrosis, and pancreatic duct leaks.Gastrointest Endosc Clin North Am.2007;17:559–579.
- .Pathology of severe acute pancreatitis. In: Bradley EL III, ed.Acute Pancreatitis: Diagnosis and Therapy.New York, NY:Raven Press;1994:35–46.
- ,,,,,.Identification of pancreas necrosis in severe acute pancreatitis: imaging procedures versus clinical staging.Gut.1986;27:1035–1042.
- ,,,,.Results of surgical treatment of necrotizing pancreatitis.World J Surg.1985;9:972–979.
- ,,,,.Management of sterile necrosis in instances of severe acute pancreatitis.J Am Coll Surg.1995;181:279–288.
- ,,,.Prognostic factors in sterile pancreatic necrosis.Gastroenterology.1992;103:1636–1640.
- ,,,.Bacterial contamination of pancreatic necrosis. A prospective clinical study.Gastroenterology.1986;91:433–438.
- ,,.Surgical treatment of necrotizing pancreatitis by necrosectomy and closed lavage: changing patient characteristics and outcome in a 19‐year, single‐center series.Surgery.2005;138:28–39.
- ,,,,,.Characteristics of infection with Candida species in patients with necrotizing pancreatitis.World J Surg.2002;26:372–376.
- ,,,,,.CT‐guided aspiration of suspected pancreatic infection: bacteriology and clinical outcome.Int J Pancreatol.1995;18:265–270.
- .Initial management of acute pancreatitis: critical issues during the first 72 hours.Am J Gastroenterol.2004;99:2489–2494.
- ,,,.Fluid resuscitation in acute pancreatitis.Clin Gastroenterol Hepatol.2008;6:1070–1076.
- ,,, et al.ESPEN guidelines on nutrition in acute pancreatitis.Clin Nutr.2002;21:173–183.
- ,,,,,.A prospective, randomized trial of clear liquids versus low‐fat solid diet as the initial meal in mild acute pancreatitis.Clin Gastroenterol Hepatol.2007;5:946–951.
- ,,,,.Total parenteral nutrition in severe acute pancreatitis.J Am Coll Nutr.1991;10:156–162.
- ,,.Enteral versus parenteral nutrition for acute pancreatitis.Cochrane Database Syst Rev.2003; (1):CD002837.
- ,.Meta‐analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis.BMJ.2004;328:1407.
- ,,.Current management of acute pancreatitis.Nat Clin Pract Gastroenterol Hepatol.2005;2:473–483.
- ,,, et al.Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis.Gut.1998;42:431–435.
- ,,,,.Enteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial.Br J Surg.1997;84:1665–1669.
- ,,.Nutrition in patients with acute pancreatitis.Curr Opin Crit Care.2001;7:251–256.
- ,,,,.Early nasogastric enteral nutrition for severe acute pancreatitis: a systematic review.World J Gastroenterol.2007;13:5253–5260.
- ,,,,.Early enteral nutrition in severe acute pancreatitis: a prospective randomized controlled trial comparing nasojejunal and nasogastric routes.J Clin Gastroenterol.2006;40:431–434.
- ,,, et al.A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis.Am J Gastroenterol.2005;100:432–439.
- ,,,.Nutrition support in acute pancreatitis: a systematic review of the literature.JPEN J Parenter Enteral Nutr.2006;30:143–156.
- ,.Issues of nutritional support for the patient with acute pancreatitis.Semin Gastrointest Dis.2002;13:154–160.
- ,,,.Effect of continuous jejunal perfusion of elemental and complex nutritional solutions on pancreatic enzyme secretion in human subjects.Gut.1978;19:194–198.
- ,,, et al.Efficiency of enteral nitrogen support in surgical patients: small peptides v non‐degraded proteins.Gut.1990;31:1277–1283.
- ,,, et al.Semi‐elemental formula or polymeric formula: Is there a better choice for enteral nutrition in acute pancreatitis? randomized comparative study.JPEN J Parenter Enteral Nutr.2006;30:1–5.
- ,,, et al.IAP guidelines for the surgical management of acute pancreatitis.Pancreatology.2002;2:565–573.
- ,,, et al.Randomized controlled trials of antibiotic prophylaxis in severe acute pancreatitis: relationship between methodological quality and outcome.Pancreatology.2007;7:531–538.
- ,,,.Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta‐analysis of randomized controlled trials.Am J Gastroenterol.2008;103:104–110.
- ,.Prophylactic antibiotic administration reduces sepsis and mortality in acute necrotizing pancreatitis: a meta‐analysis.Pancreas.2001;22:28–31.
- ,,Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis.Am J Gastroenterol.2006;101:2379–2400.
- ,.Acute biliary pancreatitis.Ann Ital Chir.1995;66:197–202.
- .The timing of biliary surgery in acute pancreatitis.Ann Surg.1979;189:654–663.
- ,,,.Acute biliary pancreatitis. The roles of laparoscopic cholecystectomy and endoscopic retrograde cholangiopancreatography.Surg Endosc.1995;9:392–396.
- ,.Metaanalysis of randomized controlled trials of endoscopic retrograde cholangiography and endoscopic sphincterotomy for the treatment of acute biliary pancreatitis.Am J Gastroenterol.1999;94:3211–3214.
- ,.Endoscopic management of acute pancreatitis.Gastrointest Endosc Clin N Am.2007;17:307–322.
- ,.Review of idiopathic pancreatitis.World J Gastroenterol.2007;13:6296–6313.
- ,,,,.Does endoscopic therapy favorably affect the outcome of patients who have recurrent acute pancreatitis and pancreas divisum?Pancreas.2007;34:21–45.
- .The timing of cholecystectomy in patients with gallstone pancreatitis. A retrospective analysis of 89 patients.Acta Chir Scand.1978;144:487–490.
- ,,, et al.Recurrence of acute gallstone pancreatitis and relationship with cholecystectomy or endoscopic sphincterotomy.Am J Gastroenterol.2004;99:2417–2423.
- American Gastroenterological Association (AGA) Institute on “Management of Acute Pancreatitis” Clinical Practice and Economics Committee, AGA Institute Governing Board.AGA institute medical position statement on acute pancreatitis.Gastroenterology.2007;132:2019–2021.
- ,;AGA Institute Clinical Practice and Economics Committee, AGA Institute Governing Board. AGA institute technical review on acute pancreatitis.Gastroenterology.2007;132:2022–2044.
- .Endoscopic management of pancreatic necrosis: not for the uncommitted.Gastrointest Endosc.2005;62:101–104.
- ,,,.Serum amylase and lipase in the evaluation of acute abdominal pain.Am Surg.1996;62:1028–1033.
- ,.2005 National hospital discharge survey.Adv Data.2007;385:1–19.
- ,.Gallstones.BMJ.2007;335:295–299.
- ,.Acute pancreatitis.N Engl J Med.1994;330:1198–1210.
- ,.Pathobiology of alcoholic pancreatitis.Pancreatology.2007;7:105–114.
- .Hyperlipidemic pancreatitis.Gastroenterol Clin North Am.1990;19:783–791.
- ,,,,,.Acute hypercalcemia causes acute pancreatitis and ectopic trypsinogen activation in the rat.Gastroenterology.1995;109:239–246.
- ,,.Role of endoscopic evaluation in idiopathic pancreatitis: a systematic review.Gastrointest Endosc.2006;63:1037–1045.
- ,.Autoimmune pancreatitis: a review.World J Gastroenterol.2007;13:6327–6332.
- ,,, et al.Acute pancreatitis and normoamylasemia. not an uncommon combination.Ann Surg.1989;210:614–620.
- .Normal amylase levels in the presentation of acute pancreatitis.Am J Emerg Med.1994;12:21–24.
- .Diagnostic standards for acute pancreatitis.World J Surg.1997;21:136–142.
- .Support of the diagnosis of pancreatitis by enzyme tests — old problems, new techniques.Clinica Chimica Acta.1997;257:85–98.
- ,,,.What is the best biochemical test to diagnose acute pancreatitis? A prospective clinical study.Mayo Clin Proc.1996;71:1138–1144.
- .The value of clinical laboratory studies in acute pancreatitis.Arch Pathol Lab Med.1991;115:325–326.
- ,.Anionic and cationic trypsinogens (trypsins) in mammalian pancreas.Enzyme.1972/73;14:116–130.
- ,,,,,.Time‐resolved immunofluorometric assays for trypsinogen‐1 and 2 in serum reveal preferential elevation of trypsinogen‐2 in pancreatitis.J Lab Clin Med.1990;115:712–718.
- ,,, et al.Rapid measurement of urinary trypsinogen‐2 as a screening test for acute pancreatitis.N Engl J Med.1997;336:1788–1793.
- ,,,,.Rapid urinary trypsinogen‐2 test strip in the diagnosis of acute pancreatitis.Pancreas.2005;30:243–247.
- ,,, et al.Clinical value of rapid urine trypsinogen‐2 test strip, urinary trypsinogen activation peptide, and serum and urinary activation peptide of carboxypeptidase B in acute pancreatitis.World J Gastroenterol.2005;11:7261–7265.
- ,,,,.Use of the urinary trypsinogen‐2 dip stick test in early diagnosis of pancreatitis after endoscopic retrograde cholangiopancreatography.Surg Endosc.2007;21:1312–1315.
- ,,, et al.Early prediction of severity in acute pancreatitis by urinary trypsinogen activation peptide: a multicentre study.Lancet.2000;355:1955–1960.
- ,.The ultrasonic findings in inflammatory pancreatic disease.Semin Ultrasound.1980;1:178.
- ,,,,,.The urgent diagnosis of gallstones in acute pancreatitis: a prospective study of three methods.Br J Surg.1984;71:230–233.
- ,,.Gallstone pancreatitis: a community teaching hospital experience.J Clin Gastroenterol.2001;33:41–44.
- ,,,.Diagnostic imaging of acute pancreatitis: prospective study using CT and sonography.AJR Am J Roentgenol.1981;137:497–502.
- ,,,.Value of contrast‐enhanced computerized tomography in the early diagnosis and prognosis of acute pancreatitis: a prospective study of 202 patients.Am J Surg.1988;155:457–466.
- ,,, et al.Computed tomography and magnetic resonance imaging in the assessment of acute pancreatitis.Gastroenterology.2004;126:715–723.
- ,,, et al.The role of magnetic resonance cholangiography in the management of patients with gallstone pancreatitis.Ann Surg.2005;241:119–124.
- ,,.Magnetic resonance imaging of acute pancreatitis: the pancreatogram.JOP.2004;5:48–50.
- ,,.Magnetic resonance cholangiopancreatography.N Engl J Med.1999;341(4):258–264.
- ,,,,.Imaging and percutaneous management of acute complicated pancreatitis.Cardiovasc Intervent Radiol.2004;27:567–580.
- ,,.State‐of‐the‐art imaging of acute pancreatitis.JBR‐BTR.2003;86:193–208.
- ,,,.Acute necrotizing pancreatitis: Role of CT‐guided percutaneous catheter drainage.Abdom Imaging.2007;32:351–361.
- .Acute pancreatitis.N Engl J Med.2006;354:2142–2150.
- ,,, et al.Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients.Gastrointest Endosc.2001;54:325–330.
- ,.Endoscopic ultrasonography in the evaluation of idiopathic acute pancreatitis.Br J Surg.2000;87:1650–1655.
- ,; theCalgary Advanced Therapeutic Endoscopy Center (ATEC) Study Group.Noninvasive vs. selective invasive biliary imaging for acute biliary pancreatitis: an economic evaluation by using decision tree analysis.Gastrointest Endosc.2005;61:86–97.
- ,.Prognostic factors in acute pancreatitis.J Clin Gastroenterol.2002;34:167–176.
- ,.Severe acute pancreatitis: clinical course and management.World J Gastroenterol.2007;13:5043–5051.
- .Etiological and prognostic factors in human acute pancreatitis: a review.Am J Gastroenterol.1982;77:633–638.
- ,,,,.Prognostic factors in acute pancreatitis.Gut.1984;25:1340–1346.
- ,,,,.APACHE‐acute physiology and chronic health evaluation: a physiologically based classification system.Crit Care Med.1981;9:591–597.
- ,,,.Acute pancreatitis: value of CT in establishing prognosis.Radiology.1990;174:331–336.
- .A clinically based classification system for acute pancreatitis. summary of the international symposium on acute pancreatitis, Atlanta, GA, September 11 through 13, 1992.Arch Surg.1993;128:586–590.
- ,,, et al.Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini Consensus Conference.Int J Pancreatol.1999;25:195–210.
- ,,,.Role of early multisystem organ failure as major risk factor for pancreatic infections and death in severe acute pancreatitis.Clin Gastroenterol Hepatol.2006;4:1053–1061.
- ,.Lethal pancreatitis.Am J Gastroenterol.1983;78:810–814.
- ,,,.A randomized multicenter clinical trial of antibiotic prophylaxis of septic complications in acute necrotizing pancreatitis with imipenem.Surg Gynecol Obstet.1993;176:480–483.
- ,.Prevention, diagnosis, and treatment of pancreatic abscess.Surgery.1977;82:99–106.
- ,,,.Death due to acute pancreatitis. a retrospective analysis of 405 autopsy cases.Dig Dis Sci.1985;30:1005–1018.
- .Endoscopic drainage of pancreatic fluid collections and pancreatic necrosis.Gastrointest Endosc Clin North Am.2003;13:743–764.
- ,,, et al.Early prediction of acute pancreatitis: prospective study comparing computed tomography scans, Ranson, Glascow, Acute Physiology and Chronic Health Evaluation II scores, and various serum markers.World J Surg.2002;26:612–619.
- ,,, et al.ASGE guideline: the role of endoscopy in the diagnosis and the management of cystic lesions and inflammatory fluid collections of the pancreas.Gastrointest Endosc.2005;61:363–370.
- .Endoscopic therapy of complete and partial pancreatic duct disruptions.Gastrointest Endosc Clin N Am.1998;8:39–53.
- .Treatment of pancreatic pseudocysts, pancreatic necrosis, and pancreatic duct leaks.Gastrointest Endosc Clin North Am.2007;17:559–579.
- .Pathology of severe acute pancreatitis. In: Bradley EL III, ed.Acute Pancreatitis: Diagnosis and Therapy.New York, NY:Raven Press;1994:35–46.
- ,,,,,.Identification of pancreas necrosis in severe acute pancreatitis: imaging procedures versus clinical staging.Gut.1986;27:1035–1042.
- ,,,,.Results of surgical treatment of necrotizing pancreatitis.World J Surg.1985;9:972–979.
- ,,,,.Management of sterile necrosis in instances of severe acute pancreatitis.J Am Coll Surg.1995;181:279–288.
- ,,,.Prognostic factors in sterile pancreatic necrosis.Gastroenterology.1992;103:1636–1640.
- ,,,.Bacterial contamination of pancreatic necrosis. A prospective clinical study.Gastroenterology.1986;91:433–438.
- ,,.Surgical treatment of necrotizing pancreatitis by necrosectomy and closed lavage: changing patient characteristics and outcome in a 19‐year, single‐center series.Surgery.2005;138:28–39.
- ,,,,,.Characteristics of infection with Candida species in patients with necrotizing pancreatitis.World J Surg.2002;26:372–376.
- ,,,,,.CT‐guided aspiration of suspected pancreatic infection: bacteriology and clinical outcome.Int J Pancreatol.1995;18:265–270.
- .Initial management of acute pancreatitis: critical issues during the first 72 hours.Am J Gastroenterol.2004;99:2489–2494.
- ,,,.Fluid resuscitation in acute pancreatitis.Clin Gastroenterol Hepatol.2008;6:1070–1076.
- ,,, et al.ESPEN guidelines on nutrition in acute pancreatitis.Clin Nutr.2002;21:173–183.
- ,,,,,.A prospective, randomized trial of clear liquids versus low‐fat solid diet as the initial meal in mild acute pancreatitis.Clin Gastroenterol Hepatol.2007;5:946–951.
- ,,,,.Total parenteral nutrition in severe acute pancreatitis.J Am Coll Nutr.1991;10:156–162.
- ,,.Enteral versus parenteral nutrition for acute pancreatitis.Cochrane Database Syst Rev.2003; (1):CD002837.
- ,.Meta‐analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis.BMJ.2004;328:1407.
- ,,.Current management of acute pancreatitis.Nat Clin Pract Gastroenterol Hepatol.2005;2:473–483.
- ,,, et al.Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis.Gut.1998;42:431–435.
- ,,,,.Enteral nutrition is superior to parenteral nutrition in severe acute pancreatitis: Results of a randomized prospective trial.Br J Surg.1997;84:1665–1669.
- ,,.Nutrition in patients with acute pancreatitis.Curr Opin Crit Care.2001;7:251–256.
- ,,,,.Early nasogastric enteral nutrition for severe acute pancreatitis: a systematic review.World J Gastroenterol.2007;13:5253–5260.
- ,,,,.Early enteral nutrition in severe acute pancreatitis: a prospective randomized controlled trial comparing nasojejunal and nasogastric routes.J Clin Gastroenterol.2006;40:431–434.
- ,,, et al.A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis.Am J Gastroenterol.2005;100:432–439.
- ,,,.Nutrition support in acute pancreatitis: a systematic review of the literature.JPEN J Parenter Enteral Nutr.2006;30:143–156.
- ,.Issues of nutritional support for the patient with acute pancreatitis.Semin Gastrointest Dis.2002;13:154–160.
- ,,,.Effect of continuous jejunal perfusion of elemental and complex nutritional solutions on pancreatic enzyme secretion in human subjects.Gut.1978;19:194–198.
- ,,, et al.Efficiency of enteral nitrogen support in surgical patients: small peptides v non‐degraded proteins.Gut.1990;31:1277–1283.
- ,,, et al.Semi‐elemental formula or polymeric formula: Is there a better choice for enteral nutrition in acute pancreatitis? randomized comparative study.JPEN J Parenter Enteral Nutr.2006;30:1–5.
- ,,, et al.IAP guidelines for the surgical management of acute pancreatitis.Pancreatology.2002;2:565–573.
- ,,, et al.Randomized controlled trials of antibiotic prophylaxis in severe acute pancreatitis: relationship between methodological quality and outcome.Pancreatology.2007;7:531–538.
- ,,,.Prophylactic antibiotics cannot reduce infected pancreatic necrosis and mortality in acute necrotizing pancreatitis: evidence from a meta‐analysis of randomized controlled trials.Am J Gastroenterol.2008;103:104–110.
- ,.Prophylactic antibiotic administration reduces sepsis and mortality in acute necrotizing pancreatitis: a meta‐analysis.Pancreas.2001;22:28–31.
- ,,Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis.Am J Gastroenterol.2006;101:2379–2400.
- ,.Acute biliary pancreatitis.Ann Ital Chir.1995;66:197–202.
- .The timing of biliary surgery in acute pancreatitis.Ann Surg.1979;189:654–663.
- ,,,.Acute biliary pancreatitis. The roles of laparoscopic cholecystectomy and endoscopic retrograde cholangiopancreatography.Surg Endosc.1995;9:392–396.
- ,.Metaanalysis of randomized controlled trials of endoscopic retrograde cholangiography and endoscopic sphincterotomy for the treatment of acute biliary pancreatitis.Am J Gastroenterol.1999;94:3211–3214.
- ,.Endoscopic management of acute pancreatitis.Gastrointest Endosc Clin N Am.2007;17:307–322.
- ,.Review of idiopathic pancreatitis.World J Gastroenterol.2007;13:6296–6313.
- ,,,,.Does endoscopic therapy favorably affect the outcome of patients who have recurrent acute pancreatitis and pancreas divisum?Pancreas.2007;34:21–45.
- .The timing of cholecystectomy in patients with gallstone pancreatitis. A retrospective analysis of 89 patients.Acta Chir Scand.1978;144:487–490.
- ,,, et al.Recurrence of acute gallstone pancreatitis and relationship with cholecystectomy or endoscopic sphincterotomy.Am J Gastroenterol.2004;99:2417–2423.
- American Gastroenterological Association (AGA) Institute on “Management of Acute Pancreatitis” Clinical Practice and Economics Committee, AGA Institute Governing Board.AGA institute medical position statement on acute pancreatitis.Gastroenterology.2007;132:2019–2021.
- ,;AGA Institute Clinical Practice and Economics Committee, AGA Institute Governing Board. AGA institute technical review on acute pancreatitis.Gastroenterology.2007;132:2022–2044.
- .Endoscopic management of pancreatic necrosis: not for the uncommitted.Gastrointest Endosc.2005;62:101–104.
- ,,,.Serum amylase and lipase in the evaluation of acute abdominal pain.Am Surg.1996;62:1028–1033.
Electrical Alternans and Pulsus Paradoxus
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
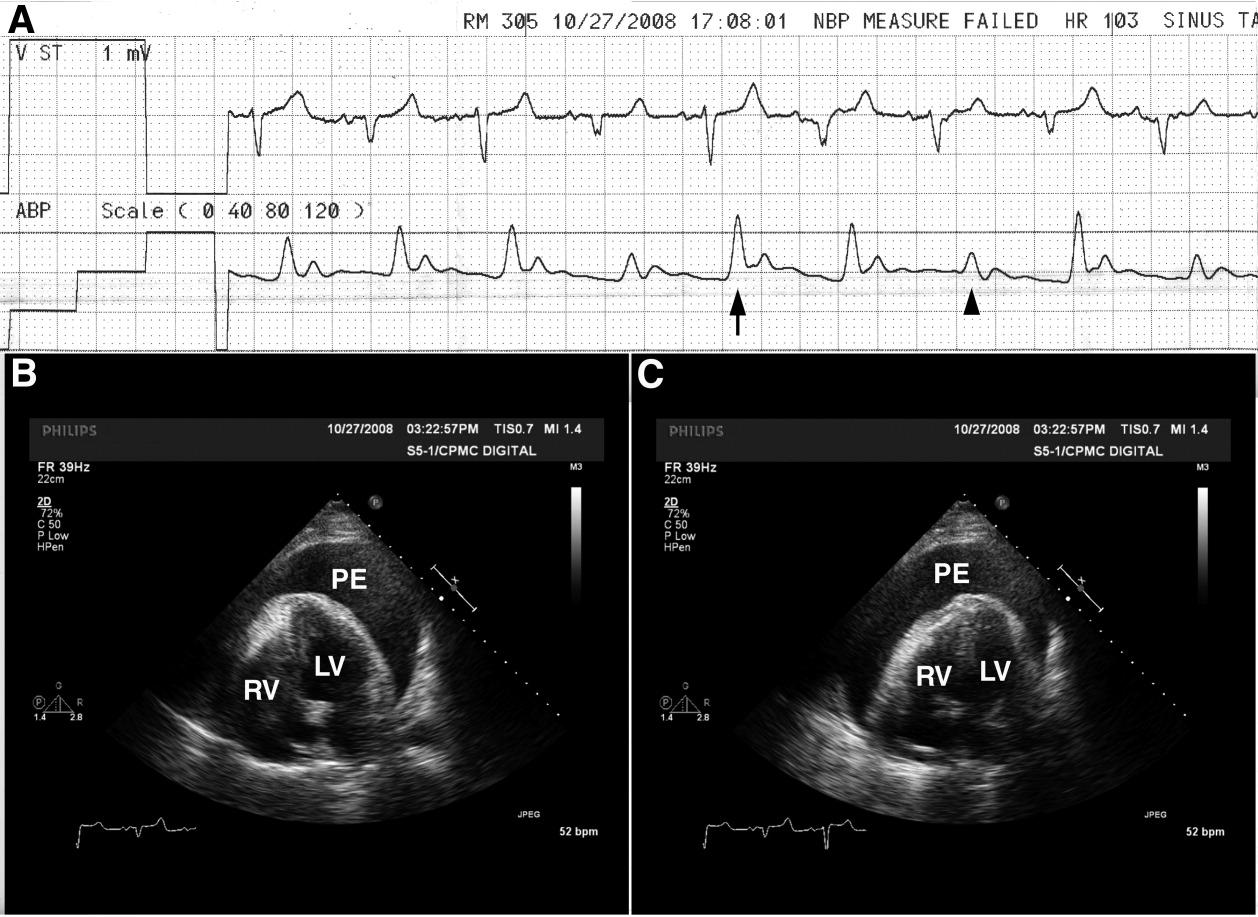
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.
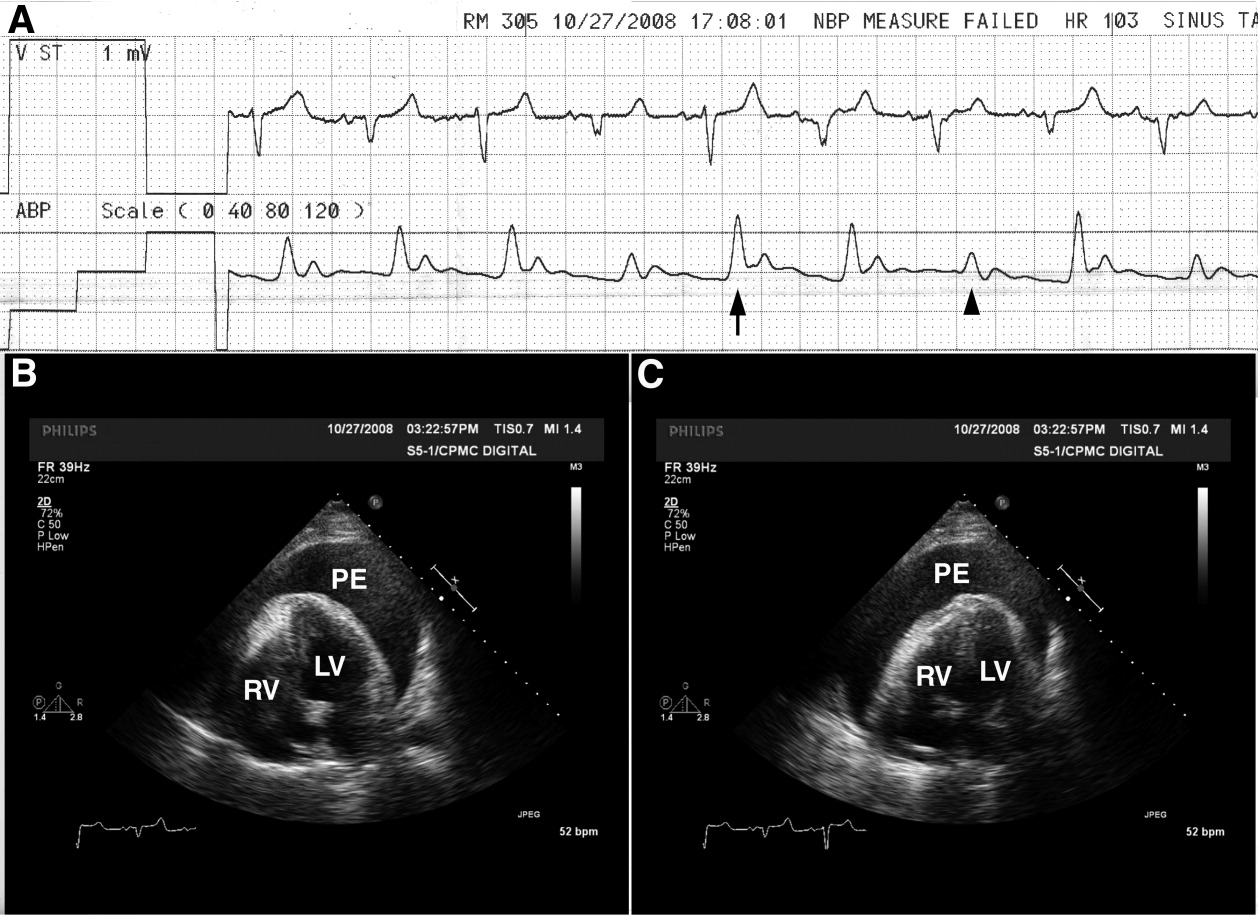
Significance of Bacteriuria
Staphylococcus aureus (SA) infection can cause a wide range of clinical syndromes, from folliculitis to life‐threatening endocarditis. Further, SA is second only to S. epidermidis as a cause of bacteremia in hospitalized patients.1, 2 Recent single‐institution studies suggests that SA could be the most frequent cause of nosocomial bacteremia,3, 4 but this needs to be validated in multicenter studies. SA bacteremia (SAB) is often complicated by hematogenous seeding into deep tissues or prosthetic material. The association of future hardware infection following SAB is well documented.5, 6 One study showed that SAB can precede and be associated with prosthetic joint infections in up to 34% of cases.6 Intravascular cardiac devices can also be infected by SAB, with rates from 28% to 75% depending on how early the bacteremia occurred in relation to the implantation of the device.5 Risk stratification for these complications is a clinical challenge. Fowler et al.7 postulated some clinical identifiers of complicated SAB; however, predicting which patients will develop a complication from SAB remains very difficult. Muder et al.8 demonstrated that the presence of SA bacteriuria (SABU) correlates with subsequent SAB, but a possible association of SABU with complicated bacteremia was not examined. A more recent study from Huggan et al.9 has suggested a possible association between SABU and poor clinical outcomes in adults with SAB.
We hypothesized that the presence of SABU would identify those patients at increased risk of complications from SAB. SABU may be a practical, economical, and readily available predictor of complicated SAB. Those patients at higher risk for complications may require a more aggressive diagnostic and therapeutic approach.
Methods
We conducted a retrospective cohort study of SAB patients with and without SA in the urine to investigate the association between SABU and the outcomes of the complications and mortality.
The study was conducted at Miami Valley Hospital (MVH, Dayton, OH), an 848‐bed, level 1 trauma center with 69 intensive care unit (ICU) beds. MVH is a community teaching hospital affiliated with Wright State University Boonshoft School of Medicine and averages 35,000 admissions per year. The same microbiology laboratory (Compunet Clinical Laboratories) processed all the blood and urine culture specimens of the patients in this study.
The inclusion criteria were as follows: 1) admission to MVH between January 1, 2004 and December 31, 2007 with a documented episode of SAB (at least 1 positive blood culture); and 2) a documented urine culture within 7 days of the episode of SAB. Patients without a documented urine culture or with inadequate/emncomplete treatment for SAB were excluded. A total of 118 patients were included based on the presence of a positive blood culture for SA and the presence of a documented urine culture. Patient electronic and paper records were reviewed by 3 of the investigators (E.V.P.‐J., S.D.B., and W.B.B.). Patients subsequently admitted to MVH and to MVH's companion medical center in Dayton, Good Samaritan Hospital, were followed through the electronic medical record common to both institutions.
Study patients were divided into 2 cohorts. One cohort included the patients with a urine culture that grew SA, either methicillin‐resistant SA (MRSA) or methicillin‐susceptible SA (MSSA). The other cohort included patients who had either a negative urine culture or a positive urine culture with organisms other than SA. The age, sex, date of admission, length of stay, and duration of follow‐up were recorded for each patient. Clinical variables included blood culture and urine culture results, presence of intravenous catheters, antibiotic therapy and duration, presence of comorbidities, and clinical outcomes (complications and death).
The primary outcome was complications during hospital admission. The 8 complications investigated were as follows: endocarditis, osteomyelitis, septic arthritis, thrombophlebitis, septic shock, septic embolism/abscess, persistent SAB (lasting more than 5 days after starting adequate SA treatment), and recurrent SAB. In addition, the 2 groups were compared on: 1) any complication, 2) average complications, 3) early complications (ie, within the current hospital admission), and 4) delayed complications (ie, complications diagnosed on subsequent admissions).
Statistical Methods
Means standard deviations (SDs) are reported for continuous variables while frequencies and percents are reported for categorical variables. The independent samples t test for continuous variables and the chi square test or Fisher's exact test for categorical variables were used to compare the two cohorts. Inferences were made at the 0.05 level of significance with no correction for multiple comparisons. SPSS 11.0 software (SPSS, Inc., Chicago, IL) was used for all analyses.
Results
Of the 118 patients, 58 were female (49.2%) and 60 male (50.8%). The age of the patients was 63.3 16.7 years (mean SD). The length of hospital stay was 19.3 17.0 days, and the duration of follow up was 8.3 5.7 months. MRSA was isolated in 75 patients (63.6%) and MSSA in 43 patients (36.4%). In the 28 patients with SA in urine cultures, MRSA was found more frequently than MSSA (20 vs. 8 patients). The acquisition of SAB was equally divided among outpatient (35.6%), healthcare‐associated (30.5%), and hospital‐acquired (33.9%) settings.
Table 1 shows that the group with SABU did not differ from the group without SABU in age (66 years vs. 62 years; P = 0.29), sex (43% male vs. 53% male; P = 0.33), length of hospital stay (18 days vs. 20 days; P = 0.59), and duration of follow‐up (6.6 months vs. 8.8 months; P = 0.064). The 2 cohorts also did not differ on the proportion with MRSA bacteremia (71% vs. 61%; P = 0.32), origin of SAB (P = 0.12), and the presence of comorbidities (diabetes mellitus, cardiomyopathy/congestive heart failure, malignancy, renal disease, and immunosuppression) (all P values > 0.30).
| Characteristic | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Age (years) (mean SD) | 66.3 16.3 | 62.4 16.8 | 0.29 |
| Male sex (n [%[) | 12 (42.9) | 48 (53.3) | 0.33 |
| Length of stay (days) (mean SD) | 17.8 16.1 | 19.7 17.3 | 0.59 |
| Follow‐up (months) (mean SD) | 6.6 5.3 | 8.8 5.7 | 0.064 |
| Blood culture (n [%]) | |||
| MRSA | 20 (71.4) | 55 (61.1) | 0.32 |
| MSSA | 8 (28.6) | 35 (38.9) | |
| Origin of the bacteremia [n (%)] | 0.12 | ||
| Community‐acquired | 13 (46.4) | 29 (32.2) | |
| Healthcare‐acquired | 10 (35.7) | 26 (28.9) | |
| Hospital‐acquired | 5 (17.9) | 35 (38.9) | |
| Comorbidities (n [%]) | |||
| DM | 11 (39.3) | 38 (42.2) | 0.78 |
| CHF | 5 (17.9) | 20 (22.2) | 0.62 |
| Cancer | 7 (25.0) | 15 (16.7) | 0.32 |
| ESRD | 4 (14.3) | 12 (13.3) | 1.00 |
| Immunosuppression | 6 (21.4) | 15 (16.7) | 0.58 |
| Patients lost to follow‐up (n [%]) | 5 (17.8) | 8 (8.8) | 0.19 |
Table 2 shows that patients in the SABU group were nearly twice as likely to have a complication as the group without SABU (64% vs. 33%; P = 0.004) and had a higher mean number of complications (0.89 vs. 0.48; P = 0.016). Patients in the SABU group also were more likely to have early complications (64% vs. 23%; P < 0.001) but no more likely to have a delayed complication (14% vs. 12%; P = 0.75). Of the 8 specific complications evaluated, the 2 groups differed only on the presence of septic shock, with the SABU group having 3 times more patients with this complication (21% vs. 7%; P = 0.035). Also, a higher proportion of patients died in the SABU group (32.1% vs. 14.4%; P = 0.036).
| Outcome | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Any complication (n [%]) | 18 (64.3) | 30 (33.3) | 0.004 |
| Average complications (mean SD) | 0.89 0.83 | 0.48 0.77 | 0.016 |
| Timing of complication (n [%]) | |||
| Early | 18 (64.3) | 21 (23.3) | <0.001 |
| Delayed | 4 (14.3) | 11 (12.2) | 0.75 |
| By specific complication, n (%) | |||
| Endocarditis | 1 (3.6) | 5 (5.6) | 1.00 |
| Osteomyelitis | 3 (10.7) | 5 (5.6) | 0.39 |
| Septic arthritis | 2 (7.1) | 3 (3.3) | 0.59 |
| Thrombophlebitis | 1 (3.6) | 3 (3.3) | 1.00 |
| Septic shock | 6 (21.4) | 6 (6.7) | 0.035 |
| Septic embolism/abscess | 6 (21.4) | 10 (11.1) | 0.21 |
| Persistent SAB | 3 (10.7) | 3 (3.3) | 0.14 |
| Recurrent SAB | 3 (10.7) | 8 (8.9) | 0.72 |
| Death (n [%]) | 9 (32.1) | 13 (14.4) | 0.036 |
Patients with MRSA (n = 75) and those with MSSA (n = 43) did not differ on any complication, average complications, early or late complications, or 7 of the specific complications (data not shown). Only with thrombophlebitis did the 2 groups differ; the MSSA group had 4 (9.3%) patients with this complication while none in the MRSA group were affected (P = 0.016).
Discussion
In our retrospective analysis, SAB with concomitant SABU was associated with more severe disease, complications, and death. Compared to SAB patients without SA in the urine, those with SAB and SA in the urine had more total complications and more early complications, especially septic shock. Further, the proportion of deaths in the SABU cohort was more than twice as high (32% vs. 14%). Therefore, the presence of SABU in patients with SAB could potentially be a useful predictor of complicated SAB and death.
The relationship between SABU and early complications and death remained after excluding the complication of septic shock/need for vasopressors from the analysis (data not shown). The lack of relationship between SABU and delayed complications might have been due to the adequacy of treatment for SAB. Appropriateness of therapy, a criterion for patient inclusion, may have lessened the likelihood of an insufficient treatment plan causing complications. Those patients with MRSA did not differ from those with MSSA on the mean number of complications or early and delayed complications. A greater proportion of MSSA patients had thrombophlebitis than MRSA patients.
Other investigations have identified predictors of mortality or complications from SAB,7, 912 but SABU was not included as a variable in most of these studies. Fowler et al.7 proposed a prognostic model of complicated SAB using the predictors from their study; community acquisition of organisms, persistent bacteremia, persistent fever over 72 hours, and skin examination suggestive of an acute systemic infection. Muder et al.8 reported a relationship between SABU and subsequent SAB, but they did not examine the association between SABU and the risk of complicated SAB. Huggan et al.9 found that concomitant SABU is associated with ICU admission and increased in‐hospital mortality in patients with SAB.
SAB patients with SABU may be at risk for early complications. Consequently, such patients may warrant more aggressive evaluation and treatment. Further, SABU in patients with SAB may be indicative of an endocarditis‐like condition. SA is rarely isolated from the urinary tract as a uropathogen, although it may colonize indwelling catheters and may cause catheter‐related urinary tract infections.13, 14 Thus, when present in urine, SA could be a marker of deep tissue dissemination with the potential to cause complications. Guidelines for the management of intravascular device‐associated bacteremia have been published by the Infectious Diseases Society of America (IDSA) and other organizations,15, 16 and recent studies have demonstrated the effectiveness of newer agents for the management of SAB.17 Nevertheless, there is still controversy regarding some aspects of the management of SAB (eg, duration of therapy, criteria for echocardiographic evaluation, role of combination therapy). The presence of SABU, the marker evaluated in our study, may be an additional factor to consider when deciding upon duration of therapy and whether to obtain echocardiography or other imaging.
Our study was limited by its retrospective nature. Patient records were not always complete. For example, not all patients had echocardiography to evaluate for endocarditis or venous ultrasound to evaluate for septic thrombophlebitis. Also, the presence (or proper removal) of intravascular or urinary catheters could not be documented reliably in all patients. In addition, the 7‐day cutoff for obtaining urine cultures may have been too lenient, leading to underdiagnosis of bacteriuria. Finally, while 13 patients were lost to follow‐up, the 2 groups (SABU and No SABU) did not differ in the proportion lost.
In conclusion, our study found that SABU may be a useful predictor of complicated SAB and death. SAB patients with SABU may be at risk for more and earlier complications. These patients may need closer monitoring due to the higher risk of septic shock and death. Additional therapeutic and management recommendations might include: 1) longer duration of therapy even if a removable source of the bacteremia is identified; 2) more frequent and better supervised follow‐up; and 3) imaging studies including either computed tomography (CT) scans or ultrasound for thorough evaluation of complications. Prospective studies including randomized controlled trials are required before implementing these suggested diagnostic and therapeutic recommendations.
Acknowledgements
The authors thank and acknowledge Logan McCool and Adam Woiwood for their administrative contributions to the study. E.V.P.‐J., as the principal investigator, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
- ,,, et al.Prevalence and drug susceptibility of pathogens causing bloodstream infections in northern Italy: a two‐year study in 16 hospitals.Eur J Clin Microbiol Infect Dis.2002;21(12):849–855.
- ,,, et al.Nosocomial bloodstream infections in ICU and non‐ICU patients.Am J Infec Control.2005;33(6):333–340.
- ,,, et al.Age‐ and sex‐associated trends in bloodstream infection: a population‐based study in Olmsted County, Minnesota.Arch Intern Med.2007;167(8):834–839.
- ,,.Bloodstream infections in a geriatric cohort: a population‐based study.Am J Med.2007;120(12):1078–1883.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104(9):1029–1033.
- ,,, et al.Infection of orthopedic prostheses after Staphylococcus aureus bacteremia.Clin Infect Dis.2001;32(4):647–649.
- ,,, et al.Clinical identifiers of complicated Staphylococcus aureus bacteremia.Arch Intern Med.2003;163(17):2066–2072.
- ,,, et al.Isolation of Staphylococcus aureus from the urinary tract: association of isolation with symptomatic UTI and subsequent staphylococcal bacteremia.Clin Infect Dis.2006;42(1):46–50.
- ,,, et al.Concomitant Staphylococcus aureus bacteriuria is associated with poor clinical outcome in adults with S. aureus bacteremia.J Hosp Infect.2008;69:345–349.
- ,,, et al.Persistent Staphylococcus aureus bacteremia. An analysis of risk factors and outcomes.Arch Int Med.2007;167(17):1861–1867.
- .Staphylococcus aureus bacteremia in older adults: predictors of 7‐day mortality and infection with a methicillin‐resistant strain.Infect Control Hosp Epidemiol.2006;27(11):1219–1225.
- ,,, et al.Infective endocarditis. Diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America.Circulation2005;111(23):e394–e434.
- ,,, et al.Antibiotic sensitivity of bacteria associated with community‐acquired urinary tract infection in Britain.J Antimicrob Chemother.1999;44(3):359–365.
- .Antibiotic susceptibility of bacterial strains isolated from patients with community‐acquired urinary tract infections in France.Eur J Clin Microbiol Infect Dis.2000;19(2):112–117.
- ,.Management of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46(suppl 5):S386–S393.
- ,,, et al.Guidelines for the management of intravascular catheter‐related infections.Clin Infect Dis.2001;32(9):1249–1272.
- ,,.Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus.N Engl J Med.2006;355(7):653–665.
Staphylococcus aureus (SA) infection can cause a wide range of clinical syndromes, from folliculitis to life‐threatening endocarditis. Further, SA is second only to S. epidermidis as a cause of bacteremia in hospitalized patients.1, 2 Recent single‐institution studies suggests that SA could be the most frequent cause of nosocomial bacteremia,3, 4 but this needs to be validated in multicenter studies. SA bacteremia (SAB) is often complicated by hematogenous seeding into deep tissues or prosthetic material. The association of future hardware infection following SAB is well documented.5, 6 One study showed that SAB can precede and be associated with prosthetic joint infections in up to 34% of cases.6 Intravascular cardiac devices can also be infected by SAB, with rates from 28% to 75% depending on how early the bacteremia occurred in relation to the implantation of the device.5 Risk stratification for these complications is a clinical challenge. Fowler et al.7 postulated some clinical identifiers of complicated SAB; however, predicting which patients will develop a complication from SAB remains very difficult. Muder et al.8 demonstrated that the presence of SA bacteriuria (SABU) correlates with subsequent SAB, but a possible association of SABU with complicated bacteremia was not examined. A more recent study from Huggan et al.9 has suggested a possible association between SABU and poor clinical outcomes in adults with SAB.
We hypothesized that the presence of SABU would identify those patients at increased risk of complications from SAB. SABU may be a practical, economical, and readily available predictor of complicated SAB. Those patients at higher risk for complications may require a more aggressive diagnostic and therapeutic approach.
Methods
We conducted a retrospective cohort study of SAB patients with and without SA in the urine to investigate the association between SABU and the outcomes of the complications and mortality.
The study was conducted at Miami Valley Hospital (MVH, Dayton, OH), an 848‐bed, level 1 trauma center with 69 intensive care unit (ICU) beds. MVH is a community teaching hospital affiliated with Wright State University Boonshoft School of Medicine and averages 35,000 admissions per year. The same microbiology laboratory (Compunet Clinical Laboratories) processed all the blood and urine culture specimens of the patients in this study.
The inclusion criteria were as follows: 1) admission to MVH between January 1, 2004 and December 31, 2007 with a documented episode of SAB (at least 1 positive blood culture); and 2) a documented urine culture within 7 days of the episode of SAB. Patients without a documented urine culture or with inadequate/emncomplete treatment for SAB were excluded. A total of 118 patients were included based on the presence of a positive blood culture for SA and the presence of a documented urine culture. Patient electronic and paper records were reviewed by 3 of the investigators (E.V.P.‐J., S.D.B., and W.B.B.). Patients subsequently admitted to MVH and to MVH's companion medical center in Dayton, Good Samaritan Hospital, were followed through the electronic medical record common to both institutions.
Study patients were divided into 2 cohorts. One cohort included the patients with a urine culture that grew SA, either methicillin‐resistant SA (MRSA) or methicillin‐susceptible SA (MSSA). The other cohort included patients who had either a negative urine culture or a positive urine culture with organisms other than SA. The age, sex, date of admission, length of stay, and duration of follow‐up were recorded for each patient. Clinical variables included blood culture and urine culture results, presence of intravenous catheters, antibiotic therapy and duration, presence of comorbidities, and clinical outcomes (complications and death).
The primary outcome was complications during hospital admission. The 8 complications investigated were as follows: endocarditis, osteomyelitis, septic arthritis, thrombophlebitis, septic shock, septic embolism/abscess, persistent SAB (lasting more than 5 days after starting adequate SA treatment), and recurrent SAB. In addition, the 2 groups were compared on: 1) any complication, 2) average complications, 3) early complications (ie, within the current hospital admission), and 4) delayed complications (ie, complications diagnosed on subsequent admissions).
Statistical Methods
Means standard deviations (SDs) are reported for continuous variables while frequencies and percents are reported for categorical variables. The independent samples t test for continuous variables and the chi square test or Fisher's exact test for categorical variables were used to compare the two cohorts. Inferences were made at the 0.05 level of significance with no correction for multiple comparisons. SPSS 11.0 software (SPSS, Inc., Chicago, IL) was used for all analyses.
Results
Of the 118 patients, 58 were female (49.2%) and 60 male (50.8%). The age of the patients was 63.3 16.7 years (mean SD). The length of hospital stay was 19.3 17.0 days, and the duration of follow up was 8.3 5.7 months. MRSA was isolated in 75 patients (63.6%) and MSSA in 43 patients (36.4%). In the 28 patients with SA in urine cultures, MRSA was found more frequently than MSSA (20 vs. 8 patients). The acquisition of SAB was equally divided among outpatient (35.6%), healthcare‐associated (30.5%), and hospital‐acquired (33.9%) settings.
Table 1 shows that the group with SABU did not differ from the group without SABU in age (66 years vs. 62 years; P = 0.29), sex (43% male vs. 53% male; P = 0.33), length of hospital stay (18 days vs. 20 days; P = 0.59), and duration of follow‐up (6.6 months vs. 8.8 months; P = 0.064). The 2 cohorts also did not differ on the proportion with MRSA bacteremia (71% vs. 61%; P = 0.32), origin of SAB (P = 0.12), and the presence of comorbidities (diabetes mellitus, cardiomyopathy/congestive heart failure, malignancy, renal disease, and immunosuppression) (all P values > 0.30).
| Characteristic | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Age (years) (mean SD) | 66.3 16.3 | 62.4 16.8 | 0.29 |
| Male sex (n [%[) | 12 (42.9) | 48 (53.3) | 0.33 |
| Length of stay (days) (mean SD) | 17.8 16.1 | 19.7 17.3 | 0.59 |
| Follow‐up (months) (mean SD) | 6.6 5.3 | 8.8 5.7 | 0.064 |
| Blood culture (n [%]) | |||
| MRSA | 20 (71.4) | 55 (61.1) | 0.32 |
| MSSA | 8 (28.6) | 35 (38.9) | |
| Origin of the bacteremia [n (%)] | 0.12 | ||
| Community‐acquired | 13 (46.4) | 29 (32.2) | |
| Healthcare‐acquired | 10 (35.7) | 26 (28.9) | |
| Hospital‐acquired | 5 (17.9) | 35 (38.9) | |
| Comorbidities (n [%]) | |||
| DM | 11 (39.3) | 38 (42.2) | 0.78 |
| CHF | 5 (17.9) | 20 (22.2) | 0.62 |
| Cancer | 7 (25.0) | 15 (16.7) | 0.32 |
| ESRD | 4 (14.3) | 12 (13.3) | 1.00 |
| Immunosuppression | 6 (21.4) | 15 (16.7) | 0.58 |
| Patients lost to follow‐up (n [%]) | 5 (17.8) | 8 (8.8) | 0.19 |
Table 2 shows that patients in the SABU group were nearly twice as likely to have a complication as the group without SABU (64% vs. 33%; P = 0.004) and had a higher mean number of complications (0.89 vs. 0.48; P = 0.016). Patients in the SABU group also were more likely to have early complications (64% vs. 23%; P < 0.001) but no more likely to have a delayed complication (14% vs. 12%; P = 0.75). Of the 8 specific complications evaluated, the 2 groups differed only on the presence of septic shock, with the SABU group having 3 times more patients with this complication (21% vs. 7%; P = 0.035). Also, a higher proportion of patients died in the SABU group (32.1% vs. 14.4%; P = 0.036).
| Outcome | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Any complication (n [%]) | 18 (64.3) | 30 (33.3) | 0.004 |
| Average complications (mean SD) | 0.89 0.83 | 0.48 0.77 | 0.016 |
| Timing of complication (n [%]) | |||
| Early | 18 (64.3) | 21 (23.3) | <0.001 |
| Delayed | 4 (14.3) | 11 (12.2) | 0.75 |
| By specific complication, n (%) | |||
| Endocarditis | 1 (3.6) | 5 (5.6) | 1.00 |
| Osteomyelitis | 3 (10.7) | 5 (5.6) | 0.39 |
| Septic arthritis | 2 (7.1) | 3 (3.3) | 0.59 |
| Thrombophlebitis | 1 (3.6) | 3 (3.3) | 1.00 |
| Septic shock | 6 (21.4) | 6 (6.7) | 0.035 |
| Septic embolism/abscess | 6 (21.4) | 10 (11.1) | 0.21 |
| Persistent SAB | 3 (10.7) | 3 (3.3) | 0.14 |
| Recurrent SAB | 3 (10.7) | 8 (8.9) | 0.72 |
| Death (n [%]) | 9 (32.1) | 13 (14.4) | 0.036 |
Patients with MRSA (n = 75) and those with MSSA (n = 43) did not differ on any complication, average complications, early or late complications, or 7 of the specific complications (data not shown). Only with thrombophlebitis did the 2 groups differ; the MSSA group had 4 (9.3%) patients with this complication while none in the MRSA group were affected (P = 0.016).
Discussion
In our retrospective analysis, SAB with concomitant SABU was associated with more severe disease, complications, and death. Compared to SAB patients without SA in the urine, those with SAB and SA in the urine had more total complications and more early complications, especially septic shock. Further, the proportion of deaths in the SABU cohort was more than twice as high (32% vs. 14%). Therefore, the presence of SABU in patients with SAB could potentially be a useful predictor of complicated SAB and death.
The relationship between SABU and early complications and death remained after excluding the complication of septic shock/need for vasopressors from the analysis (data not shown). The lack of relationship between SABU and delayed complications might have been due to the adequacy of treatment for SAB. Appropriateness of therapy, a criterion for patient inclusion, may have lessened the likelihood of an insufficient treatment plan causing complications. Those patients with MRSA did not differ from those with MSSA on the mean number of complications or early and delayed complications. A greater proportion of MSSA patients had thrombophlebitis than MRSA patients.
Other investigations have identified predictors of mortality or complications from SAB,7, 912 but SABU was not included as a variable in most of these studies. Fowler et al.7 proposed a prognostic model of complicated SAB using the predictors from their study; community acquisition of organisms, persistent bacteremia, persistent fever over 72 hours, and skin examination suggestive of an acute systemic infection. Muder et al.8 reported a relationship between SABU and subsequent SAB, but they did not examine the association between SABU and the risk of complicated SAB. Huggan et al.9 found that concomitant SABU is associated with ICU admission and increased in‐hospital mortality in patients with SAB.
SAB patients with SABU may be at risk for early complications. Consequently, such patients may warrant more aggressive evaluation and treatment. Further, SABU in patients with SAB may be indicative of an endocarditis‐like condition. SA is rarely isolated from the urinary tract as a uropathogen, although it may colonize indwelling catheters and may cause catheter‐related urinary tract infections.13, 14 Thus, when present in urine, SA could be a marker of deep tissue dissemination with the potential to cause complications. Guidelines for the management of intravascular device‐associated bacteremia have been published by the Infectious Diseases Society of America (IDSA) and other organizations,15, 16 and recent studies have demonstrated the effectiveness of newer agents for the management of SAB.17 Nevertheless, there is still controversy regarding some aspects of the management of SAB (eg, duration of therapy, criteria for echocardiographic evaluation, role of combination therapy). The presence of SABU, the marker evaluated in our study, may be an additional factor to consider when deciding upon duration of therapy and whether to obtain echocardiography or other imaging.
Our study was limited by its retrospective nature. Patient records were not always complete. For example, not all patients had echocardiography to evaluate for endocarditis or venous ultrasound to evaluate for septic thrombophlebitis. Also, the presence (or proper removal) of intravascular or urinary catheters could not be documented reliably in all patients. In addition, the 7‐day cutoff for obtaining urine cultures may have been too lenient, leading to underdiagnosis of bacteriuria. Finally, while 13 patients were lost to follow‐up, the 2 groups (SABU and No SABU) did not differ in the proportion lost.
In conclusion, our study found that SABU may be a useful predictor of complicated SAB and death. SAB patients with SABU may be at risk for more and earlier complications. These patients may need closer monitoring due to the higher risk of septic shock and death. Additional therapeutic and management recommendations might include: 1) longer duration of therapy even if a removable source of the bacteremia is identified; 2) more frequent and better supervised follow‐up; and 3) imaging studies including either computed tomography (CT) scans or ultrasound for thorough evaluation of complications. Prospective studies including randomized controlled trials are required before implementing these suggested diagnostic and therapeutic recommendations.
Acknowledgements
The authors thank and acknowledge Logan McCool and Adam Woiwood for their administrative contributions to the study. E.V.P.‐J., as the principal investigator, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Staphylococcus aureus (SA) infection can cause a wide range of clinical syndromes, from folliculitis to life‐threatening endocarditis. Further, SA is second only to S. epidermidis as a cause of bacteremia in hospitalized patients.1, 2 Recent single‐institution studies suggests that SA could be the most frequent cause of nosocomial bacteremia,3, 4 but this needs to be validated in multicenter studies. SA bacteremia (SAB) is often complicated by hematogenous seeding into deep tissues or prosthetic material. The association of future hardware infection following SAB is well documented.5, 6 One study showed that SAB can precede and be associated with prosthetic joint infections in up to 34% of cases.6 Intravascular cardiac devices can also be infected by SAB, with rates from 28% to 75% depending on how early the bacteremia occurred in relation to the implantation of the device.5 Risk stratification for these complications is a clinical challenge. Fowler et al.7 postulated some clinical identifiers of complicated SAB; however, predicting which patients will develop a complication from SAB remains very difficult. Muder et al.8 demonstrated that the presence of SA bacteriuria (SABU) correlates with subsequent SAB, but a possible association of SABU with complicated bacteremia was not examined. A more recent study from Huggan et al.9 has suggested a possible association between SABU and poor clinical outcomes in adults with SAB.
We hypothesized that the presence of SABU would identify those patients at increased risk of complications from SAB. SABU may be a practical, economical, and readily available predictor of complicated SAB. Those patients at higher risk for complications may require a more aggressive diagnostic and therapeutic approach.
Methods
We conducted a retrospective cohort study of SAB patients with and without SA in the urine to investigate the association between SABU and the outcomes of the complications and mortality.
The study was conducted at Miami Valley Hospital (MVH, Dayton, OH), an 848‐bed, level 1 trauma center with 69 intensive care unit (ICU) beds. MVH is a community teaching hospital affiliated with Wright State University Boonshoft School of Medicine and averages 35,000 admissions per year. The same microbiology laboratory (Compunet Clinical Laboratories) processed all the blood and urine culture specimens of the patients in this study.
The inclusion criteria were as follows: 1) admission to MVH between January 1, 2004 and December 31, 2007 with a documented episode of SAB (at least 1 positive blood culture); and 2) a documented urine culture within 7 days of the episode of SAB. Patients without a documented urine culture or with inadequate/emncomplete treatment for SAB were excluded. A total of 118 patients were included based on the presence of a positive blood culture for SA and the presence of a documented urine culture. Patient electronic and paper records were reviewed by 3 of the investigators (E.V.P.‐J., S.D.B., and W.B.B.). Patients subsequently admitted to MVH and to MVH's companion medical center in Dayton, Good Samaritan Hospital, were followed through the electronic medical record common to both institutions.
Study patients were divided into 2 cohorts. One cohort included the patients with a urine culture that grew SA, either methicillin‐resistant SA (MRSA) or methicillin‐susceptible SA (MSSA). The other cohort included patients who had either a negative urine culture or a positive urine culture with organisms other than SA. The age, sex, date of admission, length of stay, and duration of follow‐up were recorded for each patient. Clinical variables included blood culture and urine culture results, presence of intravenous catheters, antibiotic therapy and duration, presence of comorbidities, and clinical outcomes (complications and death).
The primary outcome was complications during hospital admission. The 8 complications investigated were as follows: endocarditis, osteomyelitis, septic arthritis, thrombophlebitis, septic shock, septic embolism/abscess, persistent SAB (lasting more than 5 days after starting adequate SA treatment), and recurrent SAB. In addition, the 2 groups were compared on: 1) any complication, 2) average complications, 3) early complications (ie, within the current hospital admission), and 4) delayed complications (ie, complications diagnosed on subsequent admissions).
Statistical Methods
Means standard deviations (SDs) are reported for continuous variables while frequencies and percents are reported for categorical variables. The independent samples t test for continuous variables and the chi square test or Fisher's exact test for categorical variables were used to compare the two cohorts. Inferences were made at the 0.05 level of significance with no correction for multiple comparisons. SPSS 11.0 software (SPSS, Inc., Chicago, IL) was used for all analyses.
Results
Of the 118 patients, 58 were female (49.2%) and 60 male (50.8%). The age of the patients was 63.3 16.7 years (mean SD). The length of hospital stay was 19.3 17.0 days, and the duration of follow up was 8.3 5.7 months. MRSA was isolated in 75 patients (63.6%) and MSSA in 43 patients (36.4%). In the 28 patients with SA in urine cultures, MRSA was found more frequently than MSSA (20 vs. 8 patients). The acquisition of SAB was equally divided among outpatient (35.6%), healthcare‐associated (30.5%), and hospital‐acquired (33.9%) settings.
Table 1 shows that the group with SABU did not differ from the group without SABU in age (66 years vs. 62 years; P = 0.29), sex (43% male vs. 53% male; P = 0.33), length of hospital stay (18 days vs. 20 days; P = 0.59), and duration of follow‐up (6.6 months vs. 8.8 months; P = 0.064). The 2 cohorts also did not differ on the proportion with MRSA bacteremia (71% vs. 61%; P = 0.32), origin of SAB (P = 0.12), and the presence of comorbidities (diabetes mellitus, cardiomyopathy/congestive heart failure, malignancy, renal disease, and immunosuppression) (all P values > 0.30).
| Characteristic | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Age (years) (mean SD) | 66.3 16.3 | 62.4 16.8 | 0.29 |
| Male sex (n [%[) | 12 (42.9) | 48 (53.3) | 0.33 |
| Length of stay (days) (mean SD) | 17.8 16.1 | 19.7 17.3 | 0.59 |
| Follow‐up (months) (mean SD) | 6.6 5.3 | 8.8 5.7 | 0.064 |
| Blood culture (n [%]) | |||
| MRSA | 20 (71.4) | 55 (61.1) | 0.32 |
| MSSA | 8 (28.6) | 35 (38.9) | |
| Origin of the bacteremia [n (%)] | 0.12 | ||
| Community‐acquired | 13 (46.4) | 29 (32.2) | |
| Healthcare‐acquired | 10 (35.7) | 26 (28.9) | |
| Hospital‐acquired | 5 (17.9) | 35 (38.9) | |
| Comorbidities (n [%]) | |||
| DM | 11 (39.3) | 38 (42.2) | 0.78 |
| CHF | 5 (17.9) | 20 (22.2) | 0.62 |
| Cancer | 7 (25.0) | 15 (16.7) | 0.32 |
| ESRD | 4 (14.3) | 12 (13.3) | 1.00 |
| Immunosuppression | 6 (21.4) | 15 (16.7) | 0.58 |
| Patients lost to follow‐up (n [%]) | 5 (17.8) | 8 (8.8) | 0.19 |
Table 2 shows that patients in the SABU group were nearly twice as likely to have a complication as the group without SABU (64% vs. 33%; P = 0.004) and had a higher mean number of complications (0.89 vs. 0.48; P = 0.016). Patients in the SABU group also were more likely to have early complications (64% vs. 23%; P < 0.001) but no more likely to have a delayed complication (14% vs. 12%; P = 0.75). Of the 8 specific complications evaluated, the 2 groups differed only on the presence of septic shock, with the SABU group having 3 times more patients with this complication (21% vs. 7%; P = 0.035). Also, a higher proportion of patients died in the SABU group (32.1% vs. 14.4%; P = 0.036).
| Outcome | S. aureus Bacteriuria (n = 28) | No S. aureus Bacteriuria (n = 90) | P Value* |
|---|---|---|---|
| |||
| Any complication (n [%]) | 18 (64.3) | 30 (33.3) | 0.004 |
| Average complications (mean SD) | 0.89 0.83 | 0.48 0.77 | 0.016 |
| Timing of complication (n [%]) | |||
| Early | 18 (64.3) | 21 (23.3) | <0.001 |
| Delayed | 4 (14.3) | 11 (12.2) | 0.75 |
| By specific complication, n (%) | |||
| Endocarditis | 1 (3.6) | 5 (5.6) | 1.00 |
| Osteomyelitis | 3 (10.7) | 5 (5.6) | 0.39 |
| Septic arthritis | 2 (7.1) | 3 (3.3) | 0.59 |
| Thrombophlebitis | 1 (3.6) | 3 (3.3) | 1.00 |
| Septic shock | 6 (21.4) | 6 (6.7) | 0.035 |
| Septic embolism/abscess | 6 (21.4) | 10 (11.1) | 0.21 |
| Persistent SAB | 3 (10.7) | 3 (3.3) | 0.14 |
| Recurrent SAB | 3 (10.7) | 8 (8.9) | 0.72 |
| Death (n [%]) | 9 (32.1) | 13 (14.4) | 0.036 |
Patients with MRSA (n = 75) and those with MSSA (n = 43) did not differ on any complication, average complications, early or late complications, or 7 of the specific complications (data not shown). Only with thrombophlebitis did the 2 groups differ; the MSSA group had 4 (9.3%) patients with this complication while none in the MRSA group were affected (P = 0.016).
Discussion
In our retrospective analysis, SAB with concomitant SABU was associated with more severe disease, complications, and death. Compared to SAB patients without SA in the urine, those with SAB and SA in the urine had more total complications and more early complications, especially septic shock. Further, the proportion of deaths in the SABU cohort was more than twice as high (32% vs. 14%). Therefore, the presence of SABU in patients with SAB could potentially be a useful predictor of complicated SAB and death.
The relationship between SABU and early complications and death remained after excluding the complication of septic shock/need for vasopressors from the analysis (data not shown). The lack of relationship between SABU and delayed complications might have been due to the adequacy of treatment for SAB. Appropriateness of therapy, a criterion for patient inclusion, may have lessened the likelihood of an insufficient treatment plan causing complications. Those patients with MRSA did not differ from those with MSSA on the mean number of complications or early and delayed complications. A greater proportion of MSSA patients had thrombophlebitis than MRSA patients.
Other investigations have identified predictors of mortality or complications from SAB,7, 912 but SABU was not included as a variable in most of these studies. Fowler et al.7 proposed a prognostic model of complicated SAB using the predictors from their study; community acquisition of organisms, persistent bacteremia, persistent fever over 72 hours, and skin examination suggestive of an acute systemic infection. Muder et al.8 reported a relationship between SABU and subsequent SAB, but they did not examine the association between SABU and the risk of complicated SAB. Huggan et al.9 found that concomitant SABU is associated with ICU admission and increased in‐hospital mortality in patients with SAB.
SAB patients with SABU may be at risk for early complications. Consequently, such patients may warrant more aggressive evaluation and treatment. Further, SABU in patients with SAB may be indicative of an endocarditis‐like condition. SA is rarely isolated from the urinary tract as a uropathogen, although it may colonize indwelling catheters and may cause catheter‐related urinary tract infections.13, 14 Thus, when present in urine, SA could be a marker of deep tissue dissemination with the potential to cause complications. Guidelines for the management of intravascular device‐associated bacteremia have been published by the Infectious Diseases Society of America (IDSA) and other organizations,15, 16 and recent studies have demonstrated the effectiveness of newer agents for the management of SAB.17 Nevertheless, there is still controversy regarding some aspects of the management of SAB (eg, duration of therapy, criteria for echocardiographic evaluation, role of combination therapy). The presence of SABU, the marker evaluated in our study, may be an additional factor to consider when deciding upon duration of therapy and whether to obtain echocardiography or other imaging.
Our study was limited by its retrospective nature. Patient records were not always complete. For example, not all patients had echocardiography to evaluate for endocarditis or venous ultrasound to evaluate for septic thrombophlebitis. Also, the presence (or proper removal) of intravascular or urinary catheters could not be documented reliably in all patients. In addition, the 7‐day cutoff for obtaining urine cultures may have been too lenient, leading to underdiagnosis of bacteriuria. Finally, while 13 patients were lost to follow‐up, the 2 groups (SABU and No SABU) did not differ in the proportion lost.
In conclusion, our study found that SABU may be a useful predictor of complicated SAB and death. SAB patients with SABU may be at risk for more and earlier complications. These patients may need closer monitoring due to the higher risk of septic shock and death. Additional therapeutic and management recommendations might include: 1) longer duration of therapy even if a removable source of the bacteremia is identified; 2) more frequent and better supervised follow‐up; and 3) imaging studies including either computed tomography (CT) scans or ultrasound for thorough evaluation of complications. Prospective studies including randomized controlled trials are required before implementing these suggested diagnostic and therapeutic recommendations.
Acknowledgements
The authors thank and acknowledge Logan McCool and Adam Woiwood for their administrative contributions to the study. E.V.P.‐J., as the principal investigator, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
- ,,, et al.Prevalence and drug susceptibility of pathogens causing bloodstream infections in northern Italy: a two‐year study in 16 hospitals.Eur J Clin Microbiol Infect Dis.2002;21(12):849–855.
- ,,, et al.Nosocomial bloodstream infections in ICU and non‐ICU patients.Am J Infec Control.2005;33(6):333–340.
- ,,, et al.Age‐ and sex‐associated trends in bloodstream infection: a population‐based study in Olmsted County, Minnesota.Arch Intern Med.2007;167(8):834–839.
- ,,.Bloodstream infections in a geriatric cohort: a population‐based study.Am J Med.2007;120(12):1078–1883.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104(9):1029–1033.
- ,,, et al.Infection of orthopedic prostheses after Staphylococcus aureus bacteremia.Clin Infect Dis.2001;32(4):647–649.
- ,,, et al.Clinical identifiers of complicated Staphylococcus aureus bacteremia.Arch Intern Med.2003;163(17):2066–2072.
- ,,, et al.Isolation of Staphylococcus aureus from the urinary tract: association of isolation with symptomatic UTI and subsequent staphylococcal bacteremia.Clin Infect Dis.2006;42(1):46–50.
- ,,, et al.Concomitant Staphylococcus aureus bacteriuria is associated with poor clinical outcome in adults with S. aureus bacteremia.J Hosp Infect.2008;69:345–349.
- ,,, et al.Persistent Staphylococcus aureus bacteremia. An analysis of risk factors and outcomes.Arch Int Med.2007;167(17):1861–1867.
- .Staphylococcus aureus bacteremia in older adults: predictors of 7‐day mortality and infection with a methicillin‐resistant strain.Infect Control Hosp Epidemiol.2006;27(11):1219–1225.
- ,,, et al.Infective endocarditis. Diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America.Circulation2005;111(23):e394–e434.
- ,,, et al.Antibiotic sensitivity of bacteria associated with community‐acquired urinary tract infection in Britain.J Antimicrob Chemother.1999;44(3):359–365.
- .Antibiotic susceptibility of bacterial strains isolated from patients with community‐acquired urinary tract infections in France.Eur J Clin Microbiol Infect Dis.2000;19(2):112–117.
- ,.Management of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46(suppl 5):S386–S393.
- ,,, et al.Guidelines for the management of intravascular catheter‐related infections.Clin Infect Dis.2001;32(9):1249–1272.
- ,,.Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus.N Engl J Med.2006;355(7):653–665.
- ,,, et al.Prevalence and drug susceptibility of pathogens causing bloodstream infections in northern Italy: a two‐year study in 16 hospitals.Eur J Clin Microbiol Infect Dis.2002;21(12):849–855.
- ,,, et al.Nosocomial bloodstream infections in ICU and non‐ICU patients.Am J Infec Control.2005;33(6):333–340.
- ,,, et al.Age‐ and sex‐associated trends in bloodstream infection: a population‐based study in Olmsted County, Minnesota.Arch Intern Med.2007;167(8):834–839.
- ,,.Bloodstream infections in a geriatric cohort: a population‐based study.Am J Med.2007;120(12):1078–1883.
- ,,, et al.Staphylococcus aureus bacteremia in patients with permanent pacemakers or implantable cardioverter‐defibrillators.Circulation.2001;104(9):1029–1033.
- ,,, et al.Infection of orthopedic prostheses after Staphylococcus aureus bacteremia.Clin Infect Dis.2001;32(4):647–649.
- ,,, et al.Clinical identifiers of complicated Staphylococcus aureus bacteremia.Arch Intern Med.2003;163(17):2066–2072.
- ,,, et al.Isolation of Staphylococcus aureus from the urinary tract: association of isolation with symptomatic UTI and subsequent staphylococcal bacteremia.Clin Infect Dis.2006;42(1):46–50.
- ,,, et al.Concomitant Staphylococcus aureus bacteriuria is associated with poor clinical outcome in adults with S. aureus bacteremia.J Hosp Infect.2008;69:345–349.
- ,,, et al.Persistent Staphylococcus aureus bacteremia. An analysis of risk factors and outcomes.Arch Int Med.2007;167(17):1861–1867.
- .Staphylococcus aureus bacteremia in older adults: predictors of 7‐day mortality and infection with a methicillin‐resistant strain.Infect Control Hosp Epidemiol.2006;27(11):1219–1225.
- ,,, et al.Infective endocarditis. Diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America.Circulation2005;111(23):e394–e434.
- ,,, et al.Antibiotic sensitivity of bacteria associated with community‐acquired urinary tract infection in Britain.J Antimicrob Chemother.1999;44(3):359–365.
- .Antibiotic susceptibility of bacterial strains isolated from patients with community‐acquired urinary tract infections in France.Eur J Clin Microbiol Infect Dis.2000;19(2):112–117.
- ,.Management of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46(suppl 5):S386–S393.
- ,,, et al.Guidelines for the management of intravascular catheter‐related infections.Clin Infect Dis.2001;32(9):1249–1272.
- ,,.Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus.N Engl J Med.2006;355(7):653–665.
Copyright © 2010 Society of Hospital Medicine
Hospital Approval of Human Research
Hospitals have important legal and ethical responsibilities for human participant research conducted within their facilities, such as ensuring that research complies with federal regulations and presents minimal risks to patients. Many hospitals accept as sufficient the federal requirement that human participant research studies have Institutional Review Board (IRB) review and approval. IRBs must review proposed research according to numerous criteria, such as scientific soundness, alignment with accepted ethics principles and weighing of benefit vs. risk to study participants.1, 2 The legally required aspects of IRB review do not, however, include considering practical matters in implementing and operating an interventional clinical trial in the complex environment of the modern acute care hospital.
Our hospital system established a broad policy requiring internal review and formal approval of any human participant research conducted within any of its hospitals, including studies that enroll hospital patients or hospital employees, utilize hospital medical records, or request hospital‐provided services for research tests or procedures. The purpose of this paper is to describe this formal hospital system review and approval process, the reasons for implementing it, and the types of issues considered prior to our hospital system granting a principal investigator permission to conduct a study.
Background
Surprisingly little healthcare or medical literature exists regarding hospital responsibilities toward human subject research conducted on its premises. Much of the literature focuses on ethics issues, the nature of informed consent, and study design. As critical as these discussions are, they seldom address the numerous complex operational issues and challenges that implementation of a clinical trial can create in a hospital setting.
Flanders et al.3 make the case for hospitalists and specialists to work together to support research that includes inpatients as study participants. Moore and Goldberg4 discuss the ingredients of successfully developing a research program in a community hospital and mention the need to involve all affected hospital departments in the initial hospital review of a study, evaluating study impact on hospital workflow, and establishing processes related to budgeting and billing. Jamerson5 also makes the case for hospital departmental review and involvement, assessment of the ability to integrate study activities into the hospital structure, assessment of the resources needed to support the research, determination of whether the hospital will contribute financially to the research, and explicit decision making regarding the assumption of institutional risk.
Despite the recognition that US patients increasingly live with multiple chronic conditions6 and that clinical trial protocols have become more procedure and resource intensive and costly,79 there has not been a corollary recognition of the increasing need for hospitals to understand and manage research activities occurring within their facilities.
Our organization is a hospital system with 9 acute care hospitals, including an academic teaching hospital (affiliated with a university medical school) with a Level 1 Trauma Center, 1 specialty rehabilitation hospital, numerous specialized clinics, and a LifeFlight Program with a 6‐helicopter fleet (Geisinger, Danville, PA). This system of hospitals serves the fourth largest metropolitan community in the US (Houston and Harris County in southeastern TX), with a population of nearly four million and a geographic spread of 1778 square miles.10, 11 The hospital system has approximately 140,700 inpatient admissions per year and 586,000 outpatient visits.
Eight years ago, our hospital system adopted a corporate policy requiring that any activity associated with human participant research receive prior hospital system review and approval. Our organization considers this review process vital to: (1) maintaining our commitment to our Federalwide Assurance with the Office for Human Research Protections, (2) abiding by the Joint Commission requirements related to research,12 (3) protecting the safety and confidentiality of patients and employees who are potential or actual research participants, (4) protecting the confidentiality of participants' medical information, (5) assuring that legal fundamentals and good clinical practice (GCH)13 are a part of study plans, (6) assuring that studies are operationally feasible, and (7) evaluating and minimizing risks to patients and risks to the organization.
Review and Approval Process
Overview
An investigator triggers a formal hospital system review by submitting study documents to 1 of the IRBs listed on the system's Federalwide Assurance through the electronic IRB system and completing the required hospital system's Research Application Form. The hospital system review occurs in parallel with the IRB review, not duplicating it but rather focusing separately on patient safety, operational and financial issues, and hospital risk issues.
Our Clinical Innovation and Research Institute manages the hospital system review. Upon electronic notification of a new study submission, an Institute Clinical Research Associate examines all study‐related documents, including the completed Research Application Form and other submitted documents, such as the study protocol, the investigational product's Investigator's Brochure, consent forms, Food and Drug Administration (FDA) letters, survey questions, and diary and other data collection forms. The Associate may spend considerable time communicating with the investigator's research team, collecting missing information and building a complete study file, including identifying the affected hospitals and hospital departments. The Institute then provides study documents to the individuals responsible for hospital‐level research review, and each affected hospital conducts its own internal review and approval process.
The hospital‐level review process varies depending on the hospitals involved. The academic teaching hospital has the most detailed review process, due to the complexities and risks associated with the full spectrum of human participant research which occurs there (Hospital A in Figure 1). If a study affects this hospital, the Institute provides study documents to each affected Department Manager, the affected Service Line Chief, the Chief Medical Officer or Medical Director of each Intensive Care Unit within which the study will recruit and enroll patients, and the Infection Control Officer and Radiation Safety Officer, as appropriate.
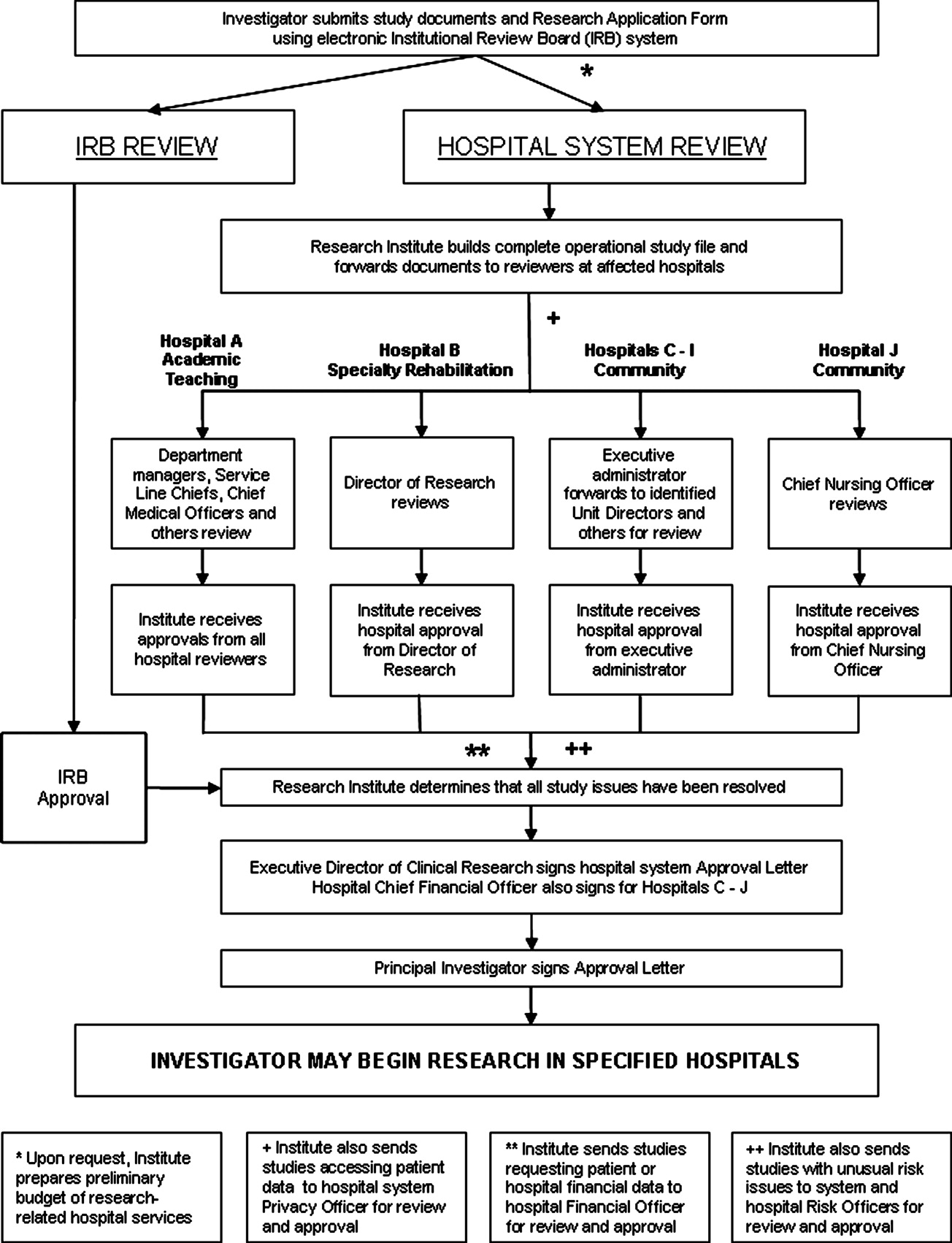
The specialty rehabilitation hospital has a long‐standing national reputation for its research programs; its Director of Research knows each investigator, reviews each study, and provides that hospital's administrative review (Hospital B). Seven of the system's community hospitals have either a Chief Executive Officer, Chief Nursing Officer, or Chief Financial Officer serve as the hospital's executive administrator responsible for research review, and this person distributes the study documents to the Chief Medical Officer, if deemed necessary, and to each affected department (Hospitals C‐I). One of the smaller community hospitals participates in relatively few studies; the Chief Nursing Officer reviews and provides hospital‐level approval (Hospital J). For retrospective studies requesting a clinical data set, the Institute provides the study documents to the Director of the Information Systems Department. All studies accessing patient data are provided to the system Privacy Officer for review and approval.
Studies may involve 1 or more hospitals; some have involved as many as 7 at once.
All reviewers also receive a standardized Research Study Evaluation Form for their written comments and recommendations (Approve, Disapprove, or Defer) regarding whether the hospital system should approve the study.
If a study requests hospital‐provided research services, the Institute's Research Financial Coordinator develops a research budget listing the hospital charges that the researcher will incur for these tests and procedures.
Once reviewers return completed Evaluation Forms, the Institute Clinical Research Associate makes an initial determination whether the review process has satisfactorily answered all questions and resolved all outstanding issues. The Manager of Clinical Research Operations then examines the study file to ensure a satisfactory review. Finally, the system Executive Director for Clinical Research provides a Letter of Approval to the Principal Investigator, which serves as the agreement of terms for conducting the study within the hospital system. The letter contains standard stipulations, such as requiring the Principal Investigator to abide by federal law and International Conference on Harmonization (ICH) GCPs and the budget for the hospital‐provided research tests and procedures. Additionally, it includes any stipulations unique to the studyfor example, that the Principal Investigator will provide training to hospital personnel who will be operating nonhospital equipment. The Institute provides affected hospital departments with copies of the approval letter. Upon signing and returning the letter, the Principal Investigator may begin the study in the designated hospitals.
Some details about the hospital system review are discussed in sections below.
Patient Safety and Human Participant Protections
Participant Recruitment Plans
Sometimes IRB submission documents do not adequately describe how researchers will identify potential study participants and approach them for consent. Key concerns which we address include how researchers will identify potential participants in a Health Insurance Portability and Accountability Act (HIPAA)‐compliant manner, the level and type of illnesses of the patients whom the investigator intends to recruit, whether the researcher must obtain the admitting or attending physician's permission, the qualifications of the person making the initial patient contact, and how and when that person will make contact, with special attention required if subjects may include very ill patients in an Intensive Care Unit (ICU).
In‐service for Unit Personnel and Pharmacists
For most interventional studies, we require that the principal investigator's research team provide a plan for study education in‐service for nurses, technicians, respiratory therapists, and pharmacists who may be involved in the care of a patient enrolled in the study. This is usually an in‐person presentation done at a regular unit meeting, with an additional investigational drug‐specific in‐service provided and available on the hospital system intranet for the pharmacists. We remind researchers that the plan must also include an in‐service for night shift personnel, who are often otherwise overlooked.
Personnel Administering the Investigational Product
Sometimes submitted protocols do not state who will administer the investigational productthe physician investigator, other members of the research team or unit nurses. If the investigator expects unit nurses to administer the product, the hospital needs to determine whether the nurses' experience and training qualifies them to administer it, assess for adverse events, and provide care for patients with these events. If the nurses are not qualified, then the hospital needs to decide whether the nurses should receive training or a member of the research team should administer the product. Some research studies involve investigational agents with novel administration techniques or risks of immediate severe adverse events, requiring the presence of a physician knowledgeable about the investigational product.
Care of Study Participants With Adverse Events
Studies with unusual investigational agents can also raise a Unit Director's or ICU Medical Director's concern as to whether bedside nurses can appropriately and adequately discern and respond to potential adverse events. If the investigational agent might result in an event not normally anticipated in patients in that particular unit, the hospital may need to consider additional preparation or staffing.
Consent Documentation
Federal law and ICH GCPs require that principal investigators have signed consent forms available in the research records, which may be off of the hospital premises in physician clinics or office areas. Our hospital system requires a copy of the consent form in the patient's medical chart if the research team conducted the consent process within the hospital or if the study participant will be an inpatient for a procedure included as part of the study protocol, whether the patient was recruited while an inpatient or prior to inpatient admission. This is important for meeting the Joint Commission's standards related to research. We established an internal monitoring program to verify that researchers were providing copies of consent, assent and parental permission forms to the Health Information Management Office for placement in medical charts.
IRB‐related Issues
Occasionally a hospital system review identifies an IRB‐related concern, such as a known possible adverse event missing from the consent form, unexplained medical terms in the consent form, exclusion criteria not mentioning pregnancy or a consent form not covering a pregnancy test even though the protocol text mentions these, or missing Investigational New Drug Application (IND) or Investigational Device Exemption (IDE) information. Institute staff route such concerns to the IRB for follow‐up with the researcher as necessary. If a hospital system review identifies an ethical concern, the Institute consults with the IRB Chair or ethicist member. Usually the Chair will assess the concern, raise options for addressing it, and recommend a course of action.
Operational Issues
Feasibility and Implementation
We urge researchers to meet with Institute staff to discuss implementation of a protocol as a real‐world, operationalized study and also encourage them to meet with managers of the primary units where the study will take place. Researchers, however, may develop and submit industry‐sponsored clinical trials or investigator‐initiated studies without such prior discussions and may not have adequately considered operational feasibility.
Given the increasing complexity of investigational agents, study designs, study procedures, and patient safety monitoring, hospital reviewers need to consider exactly who will perform study procedures and processes and how those people will do so. If a blood or tissue sample needs to be spun, packaged, and mailed on dry ice within a limited timeframe, for example, who will do this and will the supplies and equipment be available as needed? A study protocol can lead to a change in normal unit processes. Operating suite managers, for instance, may need to adjust schedules or work with research teams if research activities may prolong a procedure beyond average timeframes.
Other potential impacts abound. Research teams sometimes assume, without checking with hospital managers, that hospital staff, usually nurses or respiratory therapists, will perform research procedures of the kind they usually perform as standard clinical procedure. Most commonly, researchers assume that bedside nurses will perform frequent blood draws necessary for a pharmacokinetic substudy. Unit managers, however, may not agree to commit nurses' time to this task, depending on the number and timing of the draws. During surgery, a study may require recording of events or timelines which are not usually recorded. Researchers sometimes assume that operating room personnel will be able to focus on this data collection. Hospital managers and directors are often concerned that researchers assume that unit staff will transport patients within‐hospital for research procedures, which can involve repeatedly moving a patient from their home unit to Radiology or elsewhere and then back to the home unit. For a large hospital, this can involve considerable staff time spent away from the home unit, which may affect unit operations. Occasionally, an investigator requests that a hospital temporarily or permanently store blood or tissue samples. Since hospitals are not necessarily prepared to store large numbers of samples for extended periods, we address each such request on a case‐by‐case basis.
Investigational Product
Hospital reviewers need to consider an assortment of challenges relating to the receipt, storage, dispensing, and accountability recording of investigational products. If a hospital pharmacy will be dispensing an investigational drug, then pharmacists need to anticipate its arrival from the sponsor and know storage and other sponsor, study and FDA requirements. Pharmacists also need to know if they are expected to prepare placebo pills. If a drug is an agent that an external pharmacy needs to prepare and compound, the chain of custody documentation of the drug as it moves from manufacturer to external pharmacy to hospital pharmacy needs to be clear.
While academic hospitals usually have research‐knowledgeable pharmacists, community‐based hospital pharmacists may not be familiar with the special requirements of the FDA or sponsor, such as securing investigational products separately from marketed products, recording batch numbers, maintaining accountability logs, and following procedures for return or destruction of remaining product upon study closure. In our hospital system, 2 Research Pharmacists in the Investigational Drug Pharmacy at the academic teaching hospital serve as expert advisers to pharmacists of the community hospitals.
If a research study involves use of an investigational device, hospital reviewers need to consider what the device is, how it should be secured if stored on the unit, and how to document storage and accountability.
Biologics and radioactive materials can present unique challenges. For instance, our system requires researchers to provide hospitals with chain of custody documentation, similar to that used for organ transplants, when patient biologicals leave the hospital (for instance, for processing at a nearby accredited Cell Processing Facility) and returned to the hospital for infusion back into the patient, to confirm that the right product was returned to the hospital and infused into the right patient.
Unaffiliated Principal Investigators and Other Personnel
Increasingly, researchers who are not affiliated with our hospital system have inquired about conducting studies in 1 or more of our hospitals. We have been quite surprised by the number of inquiries from researchers or sponsors who presume we will grant immediate permission for them to access our patient lists for recruitment purposes, allow unidentified research team members to enter our hospitals, approve team members to conduct active recruitment of our hospital patients, and grant team members access to patient data.
Additionally, as clinical and translational research projects become increasingly multidisciplinary and involve cross‐organizational collaborations, many research teams include unaffiliated personnel from other organizations, such as faculty at local or distant universities, employees of a site management organization, and employees of the city or county health department.
We do not permit clinicians who are not clinically credentialed at our hospitals to engage in interventional research within our hospital system. For studies that include any intervention that qualifies as a clinical procedure, the Principal Investigator must become clinically credentialed by the hospital or an already credentialed clinician must become the local Principal Investigator for the study, and all team members who perform clinical procedures must also become clinically credentialed.
An unusual situation occurred when researchers from a university not formally affiliated with our hospital system sought to transfer a study to 1 of our hospitals following Hurricane Ike. For 15 years, the research team had performed needle muscle biopsies, for which they had received training and credentialing at their home institution. Our hospital's Chief Medical Officer, however, did not feel comfortable accepting the credentialing performed at another institution and required the external researchers to apply for privileges through our hospital's credentialing process. The original credentialing documentation at their home institution was unavailable, in any case, due to flooding and building closures, so the researchers worked through the night to complete our applications. The hospital credentialing committee came to order on short notice and completed the credentialing process in record time, allowing the research team to see the study participants at our hospital with only a few missed visits and few study deviations for the Principal Investigator.
For research team members who will be performing no clinical procedures, our hospital system has a research credentialing process, discussed below.
Financial Issues
Study Finances
Researchers are typically aware of charges for the procedures that their studies most frequently require, such as labs, radiology, and research pharmacy, although they often do not inquire about the hospital's current charges, so their information may be somewhat dated when they negotiate with sponsors or submit grant applications.
When researchers plan on utilizing hospital staff to perform research‐required tasks, such as blood draws or patient transport for tests or procedures, however, they rarely include financial support to the hospital in their study budgets, leaving these tasks unfunded, which can be a problem for hospital reviewers who must approve the research plan.
In our review and approval process, we seek clarification as to payment for research products. Sponsors are not permitted by law to seek payment for investigational drugs, but when a research protocol uses a standard‐of‐care drug for strictly research‐related purposes, determining whether the sponsor, hospital, or study participant incurs financial responsibility becomes an issue requiring careful consideration. We ensure that consent forms explicitly state any special charges to the study participant. An investigational device that falls into an FDA classification that permits charges can be especially problematic. Often the devices are expensive; the hospital must purchase them in batches and pay immediately. If the researcher does not use all the devices, the unused ones sometimes cannot be returned. If investigational devices are more costly than standard‐of‐care devices, then the hospital could incur substantial losses in billings, since hospital charges are diagnosis and procedure code dependent and usually not adjusted for device cost.
Our standardized financial assessment has led to more beneficial arrangements with sponsors for the return and reimbursement of unused products and more informed hospital decisions as to whether to conduct a specific medical device clinical trial.
We also carefully review consent form language to clarify who incurs costs for research‐related adverse events and research injuries. For investigational products with extensive potential side effects or studies enrolling very ill patients, the costs associated with adverse events can be extremely high.
Investigators are affiliated with our hospitals, not employed by them, so our hospital system does not have budget agreements with funding organizations, but relies on these external entities to fund the studies adequately. Some investigator‐initiated studies may be funded by the investigator's organization, such as a private practice or university, but in our experience such funds are sometimes depleted before study completion.
Hospital Financial Information as Study Data
As a part of the study protocol, researchers occasionally request patient‐related cost data pertinent to specific procedures or to the treatment of certain medical conditions, hospital charges and payments received, or other financial data. We forward these research requests to a hospital Finance Chief to determine the appropriateness of releasing the requested data and, if approved, how the hospital will extract and present the data sets to the investigator.
Hospital Risk Issues
Research Equipment
Our academic teaching hospital and the university medical school affiliated with it are distinct organizations, so a particular risk issue arises for the hospital when a researcher wishes to transport and use nonhospital equipment on the hospital premises. Our hospital system has responsibility to ensure appropriate and safe operation of equipment. Consequently, our hospital system review identifies any proposed use of externally‐owned equipment and involves the system and hospital Risk Officers in assessing such use for risk to patients. Specifics addressed include ownership of equipment, whether the research team or hospital staff will operate it; whether the operators have received or will receive training, and the potential risks to patients of equipment malfunctions. Upon determination that individuals will operate the equipment appropriately with minimal risks to study participants, the hospital's Biomedical Department performs their standard safety check prior to the equipment's use in the hospital.
Clinical Data Generated by NonHospital Equipment
Bringing external equipment into a hospital has a rarely anticipated consequence: the generation and storage of patient data. Our hospital system review determines whether these data constitute source data per FDA and ICH GCP definitions, whether the data are clinically pertinent, and whether the data need to go into the patient's hospital medical record. For example, if a university faculty researcher brings a vital signs monitor into the hospital to collect and electronically record data from hospital patients enrolled in a study, we may require that the research team print the data for insertion into the patient's hospital medical record.
Surveys of Hospital Employees
A research study that seeks to survey or interview hospital system employees raises a different type of institutional concern. In such a case, system and hospital Human Resources Department (HR) personnel review the planned study, paying close attention to how the research team will recruit employees and what type of information the team will request from them. HR does not want employees feeling that they must participate in a study simply because it takes place in their facility and wants to protect the identity of employees participating in anonymous surveys. On occasion, Institute staff distribute surveys (and sometimes collect them when completed), providing an identity firewall between the employee who elects to participate and the researcher.
HR may also limit researchers from asking especially personal questions or questions inquiring about the recruitment, hiring, and retention practices of their employer. HR must consider whether the study design and survey questions raise liability concerns. Studies that include employee focus groups or one‐on‐one interviews raise issues pertaining to the purpose and content of the focus groups or interviews, mechanisms to address special issues or complaints that may arise during them, and determination of whether the employees may participate during paid time as opposed to participating while off‐the‐clock.
Nonclinical Research Credentialing Process
It is vital that hospitals know who will be on hospital premises for a research study and what activities they will be engaging in. If a research team member is not already affiliated with our hospital system and will be engaging in noninterventional research activities, such as conducting the research consent process, administering a survey, or providing educational materials, our hospital system review initiates a nonclinical research credentialing process. The Institute's Manager of Clinical Research Operations assesses the team members' qualifications, reviews their resumes, interviews each of them, and discusses exactly what activities they will be engaging in and their training and experience. In addition to evaluating their qualifications, the hospital must determine how such individuals will be identified once inside the hospital, including what type of badge (employee, contractor, or visitor) the hospital will provide them. Upon successful completion of the research credentialing process, the Institute explicitly names the approved individuals in the Letter of Approval to the Principal Investigator, with copies to the affected hospitals' units.
Discussion
Our hospital research review and approval process is critical to ensuring that only safe and regulatory‐compliant research activities occur within our hospital system, but the review and approval process, with its many steps and numerous reviewers, can be cumbersome. There is no substitute for human beings reading and understanding the protocol, consent forms for patient involvement in a study, the proposed use of protected health information, Investigator's Brochure, Research Application Form, and other study documents and then identifying pertinent issues and resolving them, and this process does require significant staff time.
We have improved (continuously) the Research Application Form to help in the crucial initial gathering of information about studies' operational needs. We have also converted from a predominantly paper‐based review process to the widespread use of electronic documents, but we have not automated the distribution process for these electronic documents and a staff person must still do this through email.
Despite our efforts to improve the review process, investigators are sometimes frustrated with it, particularly if someone identifies a new issue late in the process, or if the hospital system's approval for the study lags behind the IRB approval by more than a few days.
Currently, the hospital system provides the majority of study approvals to the Principal Investigator within 2 weeks of IRB approval, with some approvals provided within 1 day of IRB approval and others as long as 3 months afterward. Delays in hospital approval can be due to a study lacking required approval from a Department of Defense IRB, the FDA not providing permission to proceed with a study, the absence of an executed contract with a vendor to pick up and dispose of radioactive waste from the investigational product and many other factors. Of course, when the research team can respond in timely fashion to inquiries or issues that we have raised, that assists all of us in completing the review and approval process as quickly as possible.
The review and approval process benefits hospital patients, hospital personnel who will be supporting studies, and hospitals as institutions. Thinking through, planning, and preparing for study operations, particularly for studies taking place in an ICU, benefits the research team, hospital personnel, and the patients. Overall, the hospital system's research review and approval process affords many protections to our patients and reduces risks to the hospital system while permitting research studies to be conducted within its varied healthcare facilities.
We encourage researchers not to view today's modern hospital as bricks and mortar, but as an institution with deep responsibility for safety on hospital premises. Hospitals must meet over a thousand Joint Commission standards, set goals for patient outcomes, measure and report on quality indicators, protect patient confidentiality, maintain the safety an ever‐expanding array of simple and complex equipment, maintain, check and document contents of adult and pediatric crash carts, have 24‐7 code teams at‐the‐ready, create, maintain and store patient medical records securely, transport patients, and much more.
Conclusion
Our hospital system, in accordance with a system‐wide policy, engages in a comprehensive review and approval process for any human participant research that has been proposed to be conducted within one or more of our facilities. The process focuses primarily on patient safety within the hospital premises, operational study issues, financial issues and hospital risk issues. This process decreases risks to the patients, researchers, and hospital facilities engaging in human participant research.
- Code of Federal Regulations Part 45, Title 46.
- Code of Federal Regulations Part 50, Title 21.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospital medicine research.J Hosp Med.2008;3:308–313.
- ,.Successfully developing a cardiovascular research program in a community hospital.J Cardiovasc Manag.2004;15:13–19.
- .Developing an infrastructure for research in a free‐standing hospital.J Nurs Adm.2007;37:295–301.
- ,,.Prevalence of multiple chronic conditions in the United States' Medicare population.Health Qual Life Outcomes.2009;7:82.
- ,,,,.Assessing the impact of protocol design changes on clinical trial performance.Am J Ther.2008;15:450–457.
- ,,, et al.Factors affecting workload of cancer clinical trials: results of a multicenter study of the National Cancer Institute of Canada Clinical Trials Group.J Clin Oncol.2002;20:545–556.
- ,,, et al.The changing face of Phase 1 Cancer Clinical Trials: new challenges in study requirements.Cancer.2009;115(8):1592–1597.
- U.S. Census Bureau. Annual Estimates of the Resident Population for Counties of Texas: April 1, 2000 to July 1, 2008. Available at: http://www.census.gov/popest/counties/tables/CO‐EST2008–01‐48.xls. Accessed February 2010.
- Harris County Texas. Available at: http://www.gis.hctx.net. Accessed February 2010.
- Accreditation Program: Hospital. Available by purchase from The Joint Commission on Accreditation of Healthcare Organizations.2008.
- International Conference on Harmonisation. Available at: www.ich.org/cache/compo/276–254‐1.html. Accessed February 2010.
Hospitals have important legal and ethical responsibilities for human participant research conducted within their facilities, such as ensuring that research complies with federal regulations and presents minimal risks to patients. Many hospitals accept as sufficient the federal requirement that human participant research studies have Institutional Review Board (IRB) review and approval. IRBs must review proposed research according to numerous criteria, such as scientific soundness, alignment with accepted ethics principles and weighing of benefit vs. risk to study participants.1, 2 The legally required aspects of IRB review do not, however, include considering practical matters in implementing and operating an interventional clinical trial in the complex environment of the modern acute care hospital.
Our hospital system established a broad policy requiring internal review and formal approval of any human participant research conducted within any of its hospitals, including studies that enroll hospital patients or hospital employees, utilize hospital medical records, or request hospital‐provided services for research tests or procedures. The purpose of this paper is to describe this formal hospital system review and approval process, the reasons for implementing it, and the types of issues considered prior to our hospital system granting a principal investigator permission to conduct a study.
Background
Surprisingly little healthcare or medical literature exists regarding hospital responsibilities toward human subject research conducted on its premises. Much of the literature focuses on ethics issues, the nature of informed consent, and study design. As critical as these discussions are, they seldom address the numerous complex operational issues and challenges that implementation of a clinical trial can create in a hospital setting.
Flanders et al.3 make the case for hospitalists and specialists to work together to support research that includes inpatients as study participants. Moore and Goldberg4 discuss the ingredients of successfully developing a research program in a community hospital and mention the need to involve all affected hospital departments in the initial hospital review of a study, evaluating study impact on hospital workflow, and establishing processes related to budgeting and billing. Jamerson5 also makes the case for hospital departmental review and involvement, assessment of the ability to integrate study activities into the hospital structure, assessment of the resources needed to support the research, determination of whether the hospital will contribute financially to the research, and explicit decision making regarding the assumption of institutional risk.
Despite the recognition that US patients increasingly live with multiple chronic conditions6 and that clinical trial protocols have become more procedure and resource intensive and costly,79 there has not been a corollary recognition of the increasing need for hospitals to understand and manage research activities occurring within their facilities.
Our organization is a hospital system with 9 acute care hospitals, including an academic teaching hospital (affiliated with a university medical school) with a Level 1 Trauma Center, 1 specialty rehabilitation hospital, numerous specialized clinics, and a LifeFlight Program with a 6‐helicopter fleet (Geisinger, Danville, PA). This system of hospitals serves the fourth largest metropolitan community in the US (Houston and Harris County in southeastern TX), with a population of nearly four million and a geographic spread of 1778 square miles.10, 11 The hospital system has approximately 140,700 inpatient admissions per year and 586,000 outpatient visits.
Eight years ago, our hospital system adopted a corporate policy requiring that any activity associated with human participant research receive prior hospital system review and approval. Our organization considers this review process vital to: (1) maintaining our commitment to our Federalwide Assurance with the Office for Human Research Protections, (2) abiding by the Joint Commission requirements related to research,12 (3) protecting the safety and confidentiality of patients and employees who are potential or actual research participants, (4) protecting the confidentiality of participants' medical information, (5) assuring that legal fundamentals and good clinical practice (GCH)13 are a part of study plans, (6) assuring that studies are operationally feasible, and (7) evaluating and minimizing risks to patients and risks to the organization.
Review and Approval Process
Overview
An investigator triggers a formal hospital system review by submitting study documents to 1 of the IRBs listed on the system's Federalwide Assurance through the electronic IRB system and completing the required hospital system's Research Application Form. The hospital system review occurs in parallel with the IRB review, not duplicating it but rather focusing separately on patient safety, operational and financial issues, and hospital risk issues.
Our Clinical Innovation and Research Institute manages the hospital system review. Upon electronic notification of a new study submission, an Institute Clinical Research Associate examines all study‐related documents, including the completed Research Application Form and other submitted documents, such as the study protocol, the investigational product's Investigator's Brochure, consent forms, Food and Drug Administration (FDA) letters, survey questions, and diary and other data collection forms. The Associate may spend considerable time communicating with the investigator's research team, collecting missing information and building a complete study file, including identifying the affected hospitals and hospital departments. The Institute then provides study documents to the individuals responsible for hospital‐level research review, and each affected hospital conducts its own internal review and approval process.
The hospital‐level review process varies depending on the hospitals involved. The academic teaching hospital has the most detailed review process, due to the complexities and risks associated with the full spectrum of human participant research which occurs there (Hospital A in Figure 1). If a study affects this hospital, the Institute provides study documents to each affected Department Manager, the affected Service Line Chief, the Chief Medical Officer or Medical Director of each Intensive Care Unit within which the study will recruit and enroll patients, and the Infection Control Officer and Radiation Safety Officer, as appropriate.
The specialty rehabilitation hospital has a long‐standing national reputation for its research programs; its Director of Research knows each investigator, reviews each study, and provides that hospital's administrative review (Hospital B). Seven of the system's community hospitals have either a Chief Executive Officer, Chief Nursing Officer, or Chief Financial Officer serve as the hospital's executive administrator responsible for research review, and this person distributes the study documents to the Chief Medical Officer, if deemed necessary, and to each affected department (Hospitals C‐I). One of the smaller community hospitals participates in relatively few studies; the Chief Nursing Officer reviews and provides hospital‐level approval (Hospital J). For retrospective studies requesting a clinical data set, the Institute provides the study documents to the Director of the Information Systems Department. All studies accessing patient data are provided to the system Privacy Officer for review and approval.
Studies may involve 1 or more hospitals; some have involved as many as 7 at once.
All reviewers also receive a standardized Research Study Evaluation Form for their written comments and recommendations (Approve, Disapprove, or Defer) regarding whether the hospital system should approve the study.
If a study requests hospital‐provided research services, the Institute's Research Financial Coordinator develops a research budget listing the hospital charges that the researcher will incur for these tests and procedures.
Once reviewers return completed Evaluation Forms, the Institute Clinical Research Associate makes an initial determination whether the review process has satisfactorily answered all questions and resolved all outstanding issues. The Manager of Clinical Research Operations then examines the study file to ensure a satisfactory review. Finally, the system Executive Director for Clinical Research provides a Letter of Approval to the Principal Investigator, which serves as the agreement of terms for conducting the study within the hospital system. The letter contains standard stipulations, such as requiring the Principal Investigator to abide by federal law and International Conference on Harmonization (ICH) GCPs and the budget for the hospital‐provided research tests and procedures. Additionally, it includes any stipulations unique to the studyfor example, that the Principal Investigator will provide training to hospital personnel who will be operating nonhospital equipment. The Institute provides affected hospital departments with copies of the approval letter. Upon signing and returning the letter, the Principal Investigator may begin the study in the designated hospitals.
Some details about the hospital system review are discussed in sections below.
Patient Safety and Human Participant Protections
Participant Recruitment Plans
Sometimes IRB submission documents do not adequately describe how researchers will identify potential study participants and approach them for consent. Key concerns which we address include how researchers will identify potential participants in a Health Insurance Portability and Accountability Act (HIPAA)‐compliant manner, the level and type of illnesses of the patients whom the investigator intends to recruit, whether the researcher must obtain the admitting or attending physician's permission, the qualifications of the person making the initial patient contact, and how and when that person will make contact, with special attention required if subjects may include very ill patients in an Intensive Care Unit (ICU).
In‐service for Unit Personnel and Pharmacists
For most interventional studies, we require that the principal investigator's research team provide a plan for study education in‐service for nurses, technicians, respiratory therapists, and pharmacists who may be involved in the care of a patient enrolled in the study. This is usually an in‐person presentation done at a regular unit meeting, with an additional investigational drug‐specific in‐service provided and available on the hospital system intranet for the pharmacists. We remind researchers that the plan must also include an in‐service for night shift personnel, who are often otherwise overlooked.
Personnel Administering the Investigational Product
Sometimes submitted protocols do not state who will administer the investigational productthe physician investigator, other members of the research team or unit nurses. If the investigator expects unit nurses to administer the product, the hospital needs to determine whether the nurses' experience and training qualifies them to administer it, assess for adverse events, and provide care for patients with these events. If the nurses are not qualified, then the hospital needs to decide whether the nurses should receive training or a member of the research team should administer the product. Some research studies involve investigational agents with novel administration techniques or risks of immediate severe adverse events, requiring the presence of a physician knowledgeable about the investigational product.
Care of Study Participants With Adverse Events
Studies with unusual investigational agents can also raise a Unit Director's or ICU Medical Director's concern as to whether bedside nurses can appropriately and adequately discern and respond to potential adverse events. If the investigational agent might result in an event not normally anticipated in patients in that particular unit, the hospital may need to consider additional preparation or staffing.
Consent Documentation
Federal law and ICH GCPs require that principal investigators have signed consent forms available in the research records, which may be off of the hospital premises in physician clinics or office areas. Our hospital system requires a copy of the consent form in the patient's medical chart if the research team conducted the consent process within the hospital or if the study participant will be an inpatient for a procedure included as part of the study protocol, whether the patient was recruited while an inpatient or prior to inpatient admission. This is important for meeting the Joint Commission's standards related to research. We established an internal monitoring program to verify that researchers were providing copies of consent, assent and parental permission forms to the Health Information Management Office for placement in medical charts.
IRB‐related Issues
Occasionally a hospital system review identifies an IRB‐related concern, such as a known possible adverse event missing from the consent form, unexplained medical terms in the consent form, exclusion criteria not mentioning pregnancy or a consent form not covering a pregnancy test even though the protocol text mentions these, or missing Investigational New Drug Application (IND) or Investigational Device Exemption (IDE) information. Institute staff route such concerns to the IRB for follow‐up with the researcher as necessary. If a hospital system review identifies an ethical concern, the Institute consults with the IRB Chair or ethicist member. Usually the Chair will assess the concern, raise options for addressing it, and recommend a course of action.
Operational Issues
Feasibility and Implementation
We urge researchers to meet with Institute staff to discuss implementation of a protocol as a real‐world, operationalized study and also encourage them to meet with managers of the primary units where the study will take place. Researchers, however, may develop and submit industry‐sponsored clinical trials or investigator‐initiated studies without such prior discussions and may not have adequately considered operational feasibility.
Given the increasing complexity of investigational agents, study designs, study procedures, and patient safety monitoring, hospital reviewers need to consider exactly who will perform study procedures and processes and how those people will do so. If a blood or tissue sample needs to be spun, packaged, and mailed on dry ice within a limited timeframe, for example, who will do this and will the supplies and equipment be available as needed? A study protocol can lead to a change in normal unit processes. Operating suite managers, for instance, may need to adjust schedules or work with research teams if research activities may prolong a procedure beyond average timeframes.
Other potential impacts abound. Research teams sometimes assume, without checking with hospital managers, that hospital staff, usually nurses or respiratory therapists, will perform research procedures of the kind they usually perform as standard clinical procedure. Most commonly, researchers assume that bedside nurses will perform frequent blood draws necessary for a pharmacokinetic substudy. Unit managers, however, may not agree to commit nurses' time to this task, depending on the number and timing of the draws. During surgery, a study may require recording of events or timelines which are not usually recorded. Researchers sometimes assume that operating room personnel will be able to focus on this data collection. Hospital managers and directors are often concerned that researchers assume that unit staff will transport patients within‐hospital for research procedures, which can involve repeatedly moving a patient from their home unit to Radiology or elsewhere and then back to the home unit. For a large hospital, this can involve considerable staff time spent away from the home unit, which may affect unit operations. Occasionally, an investigator requests that a hospital temporarily or permanently store blood or tissue samples. Since hospitals are not necessarily prepared to store large numbers of samples for extended periods, we address each such request on a case‐by‐case basis.
Investigational Product
Hospital reviewers need to consider an assortment of challenges relating to the receipt, storage, dispensing, and accountability recording of investigational products. If a hospital pharmacy will be dispensing an investigational drug, then pharmacists need to anticipate its arrival from the sponsor and know storage and other sponsor, study and FDA requirements. Pharmacists also need to know if they are expected to prepare placebo pills. If a drug is an agent that an external pharmacy needs to prepare and compound, the chain of custody documentation of the drug as it moves from manufacturer to external pharmacy to hospital pharmacy needs to be clear.
While academic hospitals usually have research‐knowledgeable pharmacists, community‐based hospital pharmacists may not be familiar with the special requirements of the FDA or sponsor, such as securing investigational products separately from marketed products, recording batch numbers, maintaining accountability logs, and following procedures for return or destruction of remaining product upon study closure. In our hospital system, 2 Research Pharmacists in the Investigational Drug Pharmacy at the academic teaching hospital serve as expert advisers to pharmacists of the community hospitals.
If a research study involves use of an investigational device, hospital reviewers need to consider what the device is, how it should be secured if stored on the unit, and how to document storage and accountability.
Biologics and radioactive materials can present unique challenges. For instance, our system requires researchers to provide hospitals with chain of custody documentation, similar to that used for organ transplants, when patient biologicals leave the hospital (for instance, for processing at a nearby accredited Cell Processing Facility) and returned to the hospital for infusion back into the patient, to confirm that the right product was returned to the hospital and infused into the right patient.
Unaffiliated Principal Investigators and Other Personnel
Increasingly, researchers who are not affiliated with our hospital system have inquired about conducting studies in 1 or more of our hospitals. We have been quite surprised by the number of inquiries from researchers or sponsors who presume we will grant immediate permission for them to access our patient lists for recruitment purposes, allow unidentified research team members to enter our hospitals, approve team members to conduct active recruitment of our hospital patients, and grant team members access to patient data.
Additionally, as clinical and translational research projects become increasingly multidisciplinary and involve cross‐organizational collaborations, many research teams include unaffiliated personnel from other organizations, such as faculty at local or distant universities, employees of a site management organization, and employees of the city or county health department.
We do not permit clinicians who are not clinically credentialed at our hospitals to engage in interventional research within our hospital system. For studies that include any intervention that qualifies as a clinical procedure, the Principal Investigator must become clinically credentialed by the hospital or an already credentialed clinician must become the local Principal Investigator for the study, and all team members who perform clinical procedures must also become clinically credentialed.
An unusual situation occurred when researchers from a university not formally affiliated with our hospital system sought to transfer a study to 1 of our hospitals following Hurricane Ike. For 15 years, the research team had performed needle muscle biopsies, for which they had received training and credentialing at their home institution. Our hospital's Chief Medical Officer, however, did not feel comfortable accepting the credentialing performed at another institution and required the external researchers to apply for privileges through our hospital's credentialing process. The original credentialing documentation at their home institution was unavailable, in any case, due to flooding and building closures, so the researchers worked through the night to complete our applications. The hospital credentialing committee came to order on short notice and completed the credentialing process in record time, allowing the research team to see the study participants at our hospital with only a few missed visits and few study deviations for the Principal Investigator.
For research team members who will be performing no clinical procedures, our hospital system has a research credentialing process, discussed below.
Financial Issues
Study Finances
Researchers are typically aware of charges for the procedures that their studies most frequently require, such as labs, radiology, and research pharmacy, although they often do not inquire about the hospital's current charges, so their information may be somewhat dated when they negotiate with sponsors or submit grant applications.
When researchers plan on utilizing hospital staff to perform research‐required tasks, such as blood draws or patient transport for tests or procedures, however, they rarely include financial support to the hospital in their study budgets, leaving these tasks unfunded, which can be a problem for hospital reviewers who must approve the research plan.
In our review and approval process, we seek clarification as to payment for research products. Sponsors are not permitted by law to seek payment for investigational drugs, but when a research protocol uses a standard‐of‐care drug for strictly research‐related purposes, determining whether the sponsor, hospital, or study participant incurs financial responsibility becomes an issue requiring careful consideration. We ensure that consent forms explicitly state any special charges to the study participant. An investigational device that falls into an FDA classification that permits charges can be especially problematic. Often the devices are expensive; the hospital must purchase them in batches and pay immediately. If the researcher does not use all the devices, the unused ones sometimes cannot be returned. If investigational devices are more costly than standard‐of‐care devices, then the hospital could incur substantial losses in billings, since hospital charges are diagnosis and procedure code dependent and usually not adjusted for device cost.
Our standardized financial assessment has led to more beneficial arrangements with sponsors for the return and reimbursement of unused products and more informed hospital decisions as to whether to conduct a specific medical device clinical trial.
We also carefully review consent form language to clarify who incurs costs for research‐related adverse events and research injuries. For investigational products with extensive potential side effects or studies enrolling very ill patients, the costs associated with adverse events can be extremely high.
Investigators are affiliated with our hospitals, not employed by them, so our hospital system does not have budget agreements with funding organizations, but relies on these external entities to fund the studies adequately. Some investigator‐initiated studies may be funded by the investigator's organization, such as a private practice or university, but in our experience such funds are sometimes depleted before study completion.
Hospital Financial Information as Study Data
As a part of the study protocol, researchers occasionally request patient‐related cost data pertinent to specific procedures or to the treatment of certain medical conditions, hospital charges and payments received, or other financial data. We forward these research requests to a hospital Finance Chief to determine the appropriateness of releasing the requested data and, if approved, how the hospital will extract and present the data sets to the investigator.
Hospital Risk Issues
Research Equipment
Our academic teaching hospital and the university medical school affiliated with it are distinct organizations, so a particular risk issue arises for the hospital when a researcher wishes to transport and use nonhospital equipment on the hospital premises. Our hospital system has responsibility to ensure appropriate and safe operation of equipment. Consequently, our hospital system review identifies any proposed use of externally‐owned equipment and involves the system and hospital Risk Officers in assessing such use for risk to patients. Specifics addressed include ownership of equipment, whether the research team or hospital staff will operate it; whether the operators have received or will receive training, and the potential risks to patients of equipment malfunctions. Upon determination that individuals will operate the equipment appropriately with minimal risks to study participants, the hospital's Biomedical Department performs their standard safety check prior to the equipment's use in the hospital.
Clinical Data Generated by NonHospital Equipment
Bringing external equipment into a hospital has a rarely anticipated consequence: the generation and storage of patient data. Our hospital system review determines whether these data constitute source data per FDA and ICH GCP definitions, whether the data are clinically pertinent, and whether the data need to go into the patient's hospital medical record. For example, if a university faculty researcher brings a vital signs monitor into the hospital to collect and electronically record data from hospital patients enrolled in a study, we may require that the research team print the data for insertion into the patient's hospital medical record.
Surveys of Hospital Employees
A research study that seeks to survey or interview hospital system employees raises a different type of institutional concern. In such a case, system and hospital Human Resources Department (HR) personnel review the planned study, paying close attention to how the research team will recruit employees and what type of information the team will request from them. HR does not want employees feeling that they must participate in a study simply because it takes place in their facility and wants to protect the identity of employees participating in anonymous surveys. On occasion, Institute staff distribute surveys (and sometimes collect them when completed), providing an identity firewall between the employee who elects to participate and the researcher.
HR may also limit researchers from asking especially personal questions or questions inquiring about the recruitment, hiring, and retention practices of their employer. HR must consider whether the study design and survey questions raise liability concerns. Studies that include employee focus groups or one‐on‐one interviews raise issues pertaining to the purpose and content of the focus groups or interviews, mechanisms to address special issues or complaints that may arise during them, and determination of whether the employees may participate during paid time as opposed to participating while off‐the‐clock.
Nonclinical Research Credentialing Process
It is vital that hospitals know who will be on hospital premises for a research study and what activities they will be engaging in. If a research team member is not already affiliated with our hospital system and will be engaging in noninterventional research activities, such as conducting the research consent process, administering a survey, or providing educational materials, our hospital system review initiates a nonclinical research credentialing process. The Institute's Manager of Clinical Research Operations assesses the team members' qualifications, reviews their resumes, interviews each of them, and discusses exactly what activities they will be engaging in and their training and experience. In addition to evaluating their qualifications, the hospital must determine how such individuals will be identified once inside the hospital, including what type of badge (employee, contractor, or visitor) the hospital will provide them. Upon successful completion of the research credentialing process, the Institute explicitly names the approved individuals in the Letter of Approval to the Principal Investigator, with copies to the affected hospitals' units.
Discussion
Our hospital research review and approval process is critical to ensuring that only safe and regulatory‐compliant research activities occur within our hospital system, but the review and approval process, with its many steps and numerous reviewers, can be cumbersome. There is no substitute for human beings reading and understanding the protocol, consent forms for patient involvement in a study, the proposed use of protected health information, Investigator's Brochure, Research Application Form, and other study documents and then identifying pertinent issues and resolving them, and this process does require significant staff time.
We have improved (continuously) the Research Application Form to help in the crucial initial gathering of information about studies' operational needs. We have also converted from a predominantly paper‐based review process to the widespread use of electronic documents, but we have not automated the distribution process for these electronic documents and a staff person must still do this through email.
Despite our efforts to improve the review process, investigators are sometimes frustrated with it, particularly if someone identifies a new issue late in the process, or if the hospital system's approval for the study lags behind the IRB approval by more than a few days.
Currently, the hospital system provides the majority of study approvals to the Principal Investigator within 2 weeks of IRB approval, with some approvals provided within 1 day of IRB approval and others as long as 3 months afterward. Delays in hospital approval can be due to a study lacking required approval from a Department of Defense IRB, the FDA not providing permission to proceed with a study, the absence of an executed contract with a vendor to pick up and dispose of radioactive waste from the investigational product and many other factors. Of course, when the research team can respond in timely fashion to inquiries or issues that we have raised, that assists all of us in completing the review and approval process as quickly as possible.
The review and approval process benefits hospital patients, hospital personnel who will be supporting studies, and hospitals as institutions. Thinking through, planning, and preparing for study operations, particularly for studies taking place in an ICU, benefits the research team, hospital personnel, and the patients. Overall, the hospital system's research review and approval process affords many protections to our patients and reduces risks to the hospital system while permitting research studies to be conducted within its varied healthcare facilities.
We encourage researchers not to view today's modern hospital as bricks and mortar, but as an institution with deep responsibility for safety on hospital premises. Hospitals must meet over a thousand Joint Commission standards, set goals for patient outcomes, measure and report on quality indicators, protect patient confidentiality, maintain the safety an ever‐expanding array of simple and complex equipment, maintain, check and document contents of adult and pediatric crash carts, have 24‐7 code teams at‐the‐ready, create, maintain and store patient medical records securely, transport patients, and much more.
Conclusion
Our hospital system, in accordance with a system‐wide policy, engages in a comprehensive review and approval process for any human participant research that has been proposed to be conducted within one or more of our facilities. The process focuses primarily on patient safety within the hospital premises, operational study issues, financial issues and hospital risk issues. This process decreases risks to the patients, researchers, and hospital facilities engaging in human participant research.
Hospitals have important legal and ethical responsibilities for human participant research conducted within their facilities, such as ensuring that research complies with federal regulations and presents minimal risks to patients. Many hospitals accept as sufficient the federal requirement that human participant research studies have Institutional Review Board (IRB) review and approval. IRBs must review proposed research according to numerous criteria, such as scientific soundness, alignment with accepted ethics principles and weighing of benefit vs. risk to study participants.1, 2 The legally required aspects of IRB review do not, however, include considering practical matters in implementing and operating an interventional clinical trial in the complex environment of the modern acute care hospital.
Our hospital system established a broad policy requiring internal review and formal approval of any human participant research conducted within any of its hospitals, including studies that enroll hospital patients or hospital employees, utilize hospital medical records, or request hospital‐provided services for research tests or procedures. The purpose of this paper is to describe this formal hospital system review and approval process, the reasons for implementing it, and the types of issues considered prior to our hospital system granting a principal investigator permission to conduct a study.
Background
Surprisingly little healthcare or medical literature exists regarding hospital responsibilities toward human subject research conducted on its premises. Much of the literature focuses on ethics issues, the nature of informed consent, and study design. As critical as these discussions are, they seldom address the numerous complex operational issues and challenges that implementation of a clinical trial can create in a hospital setting.
Flanders et al.3 make the case for hospitalists and specialists to work together to support research that includes inpatients as study participants. Moore and Goldberg4 discuss the ingredients of successfully developing a research program in a community hospital and mention the need to involve all affected hospital departments in the initial hospital review of a study, evaluating study impact on hospital workflow, and establishing processes related to budgeting and billing. Jamerson5 also makes the case for hospital departmental review and involvement, assessment of the ability to integrate study activities into the hospital structure, assessment of the resources needed to support the research, determination of whether the hospital will contribute financially to the research, and explicit decision making regarding the assumption of institutional risk.
Despite the recognition that US patients increasingly live with multiple chronic conditions6 and that clinical trial protocols have become more procedure and resource intensive and costly,79 there has not been a corollary recognition of the increasing need for hospitals to understand and manage research activities occurring within their facilities.
Our organization is a hospital system with 9 acute care hospitals, including an academic teaching hospital (affiliated with a university medical school) with a Level 1 Trauma Center, 1 specialty rehabilitation hospital, numerous specialized clinics, and a LifeFlight Program with a 6‐helicopter fleet (Geisinger, Danville, PA). This system of hospitals serves the fourth largest metropolitan community in the US (Houston and Harris County in southeastern TX), with a population of nearly four million and a geographic spread of 1778 square miles.10, 11 The hospital system has approximately 140,700 inpatient admissions per year and 586,000 outpatient visits.
Eight years ago, our hospital system adopted a corporate policy requiring that any activity associated with human participant research receive prior hospital system review and approval. Our organization considers this review process vital to: (1) maintaining our commitment to our Federalwide Assurance with the Office for Human Research Protections, (2) abiding by the Joint Commission requirements related to research,12 (3) protecting the safety and confidentiality of patients and employees who are potential or actual research participants, (4) protecting the confidentiality of participants' medical information, (5) assuring that legal fundamentals and good clinical practice (GCH)13 are a part of study plans, (6) assuring that studies are operationally feasible, and (7) evaluating and minimizing risks to patients and risks to the organization.
Review and Approval Process
Overview
An investigator triggers a formal hospital system review by submitting study documents to 1 of the IRBs listed on the system's Federalwide Assurance through the electronic IRB system and completing the required hospital system's Research Application Form. The hospital system review occurs in parallel with the IRB review, not duplicating it but rather focusing separately on patient safety, operational and financial issues, and hospital risk issues.
Our Clinical Innovation and Research Institute manages the hospital system review. Upon electronic notification of a new study submission, an Institute Clinical Research Associate examines all study‐related documents, including the completed Research Application Form and other submitted documents, such as the study protocol, the investigational product's Investigator's Brochure, consent forms, Food and Drug Administration (FDA) letters, survey questions, and diary and other data collection forms. The Associate may spend considerable time communicating with the investigator's research team, collecting missing information and building a complete study file, including identifying the affected hospitals and hospital departments. The Institute then provides study documents to the individuals responsible for hospital‐level research review, and each affected hospital conducts its own internal review and approval process.
The hospital‐level review process varies depending on the hospitals involved. The academic teaching hospital has the most detailed review process, due to the complexities and risks associated with the full spectrum of human participant research which occurs there (Hospital A in Figure 1). If a study affects this hospital, the Institute provides study documents to each affected Department Manager, the affected Service Line Chief, the Chief Medical Officer or Medical Director of each Intensive Care Unit within which the study will recruit and enroll patients, and the Infection Control Officer and Radiation Safety Officer, as appropriate.
The specialty rehabilitation hospital has a long‐standing national reputation for its research programs; its Director of Research knows each investigator, reviews each study, and provides that hospital's administrative review (Hospital B). Seven of the system's community hospitals have either a Chief Executive Officer, Chief Nursing Officer, or Chief Financial Officer serve as the hospital's executive administrator responsible for research review, and this person distributes the study documents to the Chief Medical Officer, if deemed necessary, and to each affected department (Hospitals C‐I). One of the smaller community hospitals participates in relatively few studies; the Chief Nursing Officer reviews and provides hospital‐level approval (Hospital J). For retrospective studies requesting a clinical data set, the Institute provides the study documents to the Director of the Information Systems Department. All studies accessing patient data are provided to the system Privacy Officer for review and approval.
Studies may involve 1 or more hospitals; some have involved as many as 7 at once.
All reviewers also receive a standardized Research Study Evaluation Form for their written comments and recommendations (Approve, Disapprove, or Defer) regarding whether the hospital system should approve the study.
If a study requests hospital‐provided research services, the Institute's Research Financial Coordinator develops a research budget listing the hospital charges that the researcher will incur for these tests and procedures.
Once reviewers return completed Evaluation Forms, the Institute Clinical Research Associate makes an initial determination whether the review process has satisfactorily answered all questions and resolved all outstanding issues. The Manager of Clinical Research Operations then examines the study file to ensure a satisfactory review. Finally, the system Executive Director for Clinical Research provides a Letter of Approval to the Principal Investigator, which serves as the agreement of terms for conducting the study within the hospital system. The letter contains standard stipulations, such as requiring the Principal Investigator to abide by federal law and International Conference on Harmonization (ICH) GCPs and the budget for the hospital‐provided research tests and procedures. Additionally, it includes any stipulations unique to the studyfor example, that the Principal Investigator will provide training to hospital personnel who will be operating nonhospital equipment. The Institute provides affected hospital departments with copies of the approval letter. Upon signing and returning the letter, the Principal Investigator may begin the study in the designated hospitals.
Some details about the hospital system review are discussed in sections below.
Patient Safety and Human Participant Protections
Participant Recruitment Plans
Sometimes IRB submission documents do not adequately describe how researchers will identify potential study participants and approach them for consent. Key concerns which we address include how researchers will identify potential participants in a Health Insurance Portability and Accountability Act (HIPAA)‐compliant manner, the level and type of illnesses of the patients whom the investigator intends to recruit, whether the researcher must obtain the admitting or attending physician's permission, the qualifications of the person making the initial patient contact, and how and when that person will make contact, with special attention required if subjects may include very ill patients in an Intensive Care Unit (ICU).
In‐service for Unit Personnel and Pharmacists
For most interventional studies, we require that the principal investigator's research team provide a plan for study education in‐service for nurses, technicians, respiratory therapists, and pharmacists who may be involved in the care of a patient enrolled in the study. This is usually an in‐person presentation done at a regular unit meeting, with an additional investigational drug‐specific in‐service provided and available on the hospital system intranet for the pharmacists. We remind researchers that the plan must also include an in‐service for night shift personnel, who are often otherwise overlooked.
Personnel Administering the Investigational Product
Sometimes submitted protocols do not state who will administer the investigational productthe physician investigator, other members of the research team or unit nurses. If the investigator expects unit nurses to administer the product, the hospital needs to determine whether the nurses' experience and training qualifies them to administer it, assess for adverse events, and provide care for patients with these events. If the nurses are not qualified, then the hospital needs to decide whether the nurses should receive training or a member of the research team should administer the product. Some research studies involve investigational agents with novel administration techniques or risks of immediate severe adverse events, requiring the presence of a physician knowledgeable about the investigational product.
Care of Study Participants With Adverse Events
Studies with unusual investigational agents can also raise a Unit Director's or ICU Medical Director's concern as to whether bedside nurses can appropriately and adequately discern and respond to potential adverse events. If the investigational agent might result in an event not normally anticipated in patients in that particular unit, the hospital may need to consider additional preparation or staffing.
Consent Documentation
Federal law and ICH GCPs require that principal investigators have signed consent forms available in the research records, which may be off of the hospital premises in physician clinics or office areas. Our hospital system requires a copy of the consent form in the patient's medical chart if the research team conducted the consent process within the hospital or if the study participant will be an inpatient for a procedure included as part of the study protocol, whether the patient was recruited while an inpatient or prior to inpatient admission. This is important for meeting the Joint Commission's standards related to research. We established an internal monitoring program to verify that researchers were providing copies of consent, assent and parental permission forms to the Health Information Management Office for placement in medical charts.
IRB‐related Issues
Occasionally a hospital system review identifies an IRB‐related concern, such as a known possible adverse event missing from the consent form, unexplained medical terms in the consent form, exclusion criteria not mentioning pregnancy or a consent form not covering a pregnancy test even though the protocol text mentions these, or missing Investigational New Drug Application (IND) or Investigational Device Exemption (IDE) information. Institute staff route such concerns to the IRB for follow‐up with the researcher as necessary. If a hospital system review identifies an ethical concern, the Institute consults with the IRB Chair or ethicist member. Usually the Chair will assess the concern, raise options for addressing it, and recommend a course of action.
Operational Issues
Feasibility and Implementation
We urge researchers to meet with Institute staff to discuss implementation of a protocol as a real‐world, operationalized study and also encourage them to meet with managers of the primary units where the study will take place. Researchers, however, may develop and submit industry‐sponsored clinical trials or investigator‐initiated studies without such prior discussions and may not have adequately considered operational feasibility.
Given the increasing complexity of investigational agents, study designs, study procedures, and patient safety monitoring, hospital reviewers need to consider exactly who will perform study procedures and processes and how those people will do so. If a blood or tissue sample needs to be spun, packaged, and mailed on dry ice within a limited timeframe, for example, who will do this and will the supplies and equipment be available as needed? A study protocol can lead to a change in normal unit processes. Operating suite managers, for instance, may need to adjust schedules or work with research teams if research activities may prolong a procedure beyond average timeframes.
Other potential impacts abound. Research teams sometimes assume, without checking with hospital managers, that hospital staff, usually nurses or respiratory therapists, will perform research procedures of the kind they usually perform as standard clinical procedure. Most commonly, researchers assume that bedside nurses will perform frequent blood draws necessary for a pharmacokinetic substudy. Unit managers, however, may not agree to commit nurses' time to this task, depending on the number and timing of the draws. During surgery, a study may require recording of events or timelines which are not usually recorded. Researchers sometimes assume that operating room personnel will be able to focus on this data collection. Hospital managers and directors are often concerned that researchers assume that unit staff will transport patients within‐hospital for research procedures, which can involve repeatedly moving a patient from their home unit to Radiology or elsewhere and then back to the home unit. For a large hospital, this can involve considerable staff time spent away from the home unit, which may affect unit operations. Occasionally, an investigator requests that a hospital temporarily or permanently store blood or tissue samples. Since hospitals are not necessarily prepared to store large numbers of samples for extended periods, we address each such request on a case‐by‐case basis.
Investigational Product
Hospital reviewers need to consider an assortment of challenges relating to the receipt, storage, dispensing, and accountability recording of investigational products. If a hospital pharmacy will be dispensing an investigational drug, then pharmacists need to anticipate its arrival from the sponsor and know storage and other sponsor, study and FDA requirements. Pharmacists also need to know if they are expected to prepare placebo pills. If a drug is an agent that an external pharmacy needs to prepare and compound, the chain of custody documentation of the drug as it moves from manufacturer to external pharmacy to hospital pharmacy needs to be clear.
While academic hospitals usually have research‐knowledgeable pharmacists, community‐based hospital pharmacists may not be familiar with the special requirements of the FDA or sponsor, such as securing investigational products separately from marketed products, recording batch numbers, maintaining accountability logs, and following procedures for return or destruction of remaining product upon study closure. In our hospital system, 2 Research Pharmacists in the Investigational Drug Pharmacy at the academic teaching hospital serve as expert advisers to pharmacists of the community hospitals.
If a research study involves use of an investigational device, hospital reviewers need to consider what the device is, how it should be secured if stored on the unit, and how to document storage and accountability.
Biologics and radioactive materials can present unique challenges. For instance, our system requires researchers to provide hospitals with chain of custody documentation, similar to that used for organ transplants, when patient biologicals leave the hospital (for instance, for processing at a nearby accredited Cell Processing Facility) and returned to the hospital for infusion back into the patient, to confirm that the right product was returned to the hospital and infused into the right patient.
Unaffiliated Principal Investigators and Other Personnel
Increasingly, researchers who are not affiliated with our hospital system have inquired about conducting studies in 1 or more of our hospitals. We have been quite surprised by the number of inquiries from researchers or sponsors who presume we will grant immediate permission for them to access our patient lists for recruitment purposes, allow unidentified research team members to enter our hospitals, approve team members to conduct active recruitment of our hospital patients, and grant team members access to patient data.
Additionally, as clinical and translational research projects become increasingly multidisciplinary and involve cross‐organizational collaborations, many research teams include unaffiliated personnel from other organizations, such as faculty at local or distant universities, employees of a site management organization, and employees of the city or county health department.
We do not permit clinicians who are not clinically credentialed at our hospitals to engage in interventional research within our hospital system. For studies that include any intervention that qualifies as a clinical procedure, the Principal Investigator must become clinically credentialed by the hospital or an already credentialed clinician must become the local Principal Investigator for the study, and all team members who perform clinical procedures must also become clinically credentialed.
An unusual situation occurred when researchers from a university not formally affiliated with our hospital system sought to transfer a study to 1 of our hospitals following Hurricane Ike. For 15 years, the research team had performed needle muscle biopsies, for which they had received training and credentialing at their home institution. Our hospital's Chief Medical Officer, however, did not feel comfortable accepting the credentialing performed at another institution and required the external researchers to apply for privileges through our hospital's credentialing process. The original credentialing documentation at their home institution was unavailable, in any case, due to flooding and building closures, so the researchers worked through the night to complete our applications. The hospital credentialing committee came to order on short notice and completed the credentialing process in record time, allowing the research team to see the study participants at our hospital with only a few missed visits and few study deviations for the Principal Investigator.
For research team members who will be performing no clinical procedures, our hospital system has a research credentialing process, discussed below.
Financial Issues
Study Finances
Researchers are typically aware of charges for the procedures that their studies most frequently require, such as labs, radiology, and research pharmacy, although they often do not inquire about the hospital's current charges, so their information may be somewhat dated when they negotiate with sponsors or submit grant applications.
When researchers plan on utilizing hospital staff to perform research‐required tasks, such as blood draws or patient transport for tests or procedures, however, they rarely include financial support to the hospital in their study budgets, leaving these tasks unfunded, which can be a problem for hospital reviewers who must approve the research plan.
In our review and approval process, we seek clarification as to payment for research products. Sponsors are not permitted by law to seek payment for investigational drugs, but when a research protocol uses a standard‐of‐care drug for strictly research‐related purposes, determining whether the sponsor, hospital, or study participant incurs financial responsibility becomes an issue requiring careful consideration. We ensure that consent forms explicitly state any special charges to the study participant. An investigational device that falls into an FDA classification that permits charges can be especially problematic. Often the devices are expensive; the hospital must purchase them in batches and pay immediately. If the researcher does not use all the devices, the unused ones sometimes cannot be returned. If investigational devices are more costly than standard‐of‐care devices, then the hospital could incur substantial losses in billings, since hospital charges are diagnosis and procedure code dependent and usually not adjusted for device cost.
Our standardized financial assessment has led to more beneficial arrangements with sponsors for the return and reimbursement of unused products and more informed hospital decisions as to whether to conduct a specific medical device clinical trial.
We also carefully review consent form language to clarify who incurs costs for research‐related adverse events and research injuries. For investigational products with extensive potential side effects or studies enrolling very ill patients, the costs associated with adverse events can be extremely high.
Investigators are affiliated with our hospitals, not employed by them, so our hospital system does not have budget agreements with funding organizations, but relies on these external entities to fund the studies adequately. Some investigator‐initiated studies may be funded by the investigator's organization, such as a private practice or university, but in our experience such funds are sometimes depleted before study completion.
Hospital Financial Information as Study Data
As a part of the study protocol, researchers occasionally request patient‐related cost data pertinent to specific procedures or to the treatment of certain medical conditions, hospital charges and payments received, or other financial data. We forward these research requests to a hospital Finance Chief to determine the appropriateness of releasing the requested data and, if approved, how the hospital will extract and present the data sets to the investigator.
Hospital Risk Issues
Research Equipment
Our academic teaching hospital and the university medical school affiliated with it are distinct organizations, so a particular risk issue arises for the hospital when a researcher wishes to transport and use nonhospital equipment on the hospital premises. Our hospital system has responsibility to ensure appropriate and safe operation of equipment. Consequently, our hospital system review identifies any proposed use of externally‐owned equipment and involves the system and hospital Risk Officers in assessing such use for risk to patients. Specifics addressed include ownership of equipment, whether the research team or hospital staff will operate it; whether the operators have received or will receive training, and the potential risks to patients of equipment malfunctions. Upon determination that individuals will operate the equipment appropriately with minimal risks to study participants, the hospital's Biomedical Department performs their standard safety check prior to the equipment's use in the hospital.
Clinical Data Generated by NonHospital Equipment
Bringing external equipment into a hospital has a rarely anticipated consequence: the generation and storage of patient data. Our hospital system review determines whether these data constitute source data per FDA and ICH GCP definitions, whether the data are clinically pertinent, and whether the data need to go into the patient's hospital medical record. For example, if a university faculty researcher brings a vital signs monitor into the hospital to collect and electronically record data from hospital patients enrolled in a study, we may require that the research team print the data for insertion into the patient's hospital medical record.
Surveys of Hospital Employees
A research study that seeks to survey or interview hospital system employees raises a different type of institutional concern. In such a case, system and hospital Human Resources Department (HR) personnel review the planned study, paying close attention to how the research team will recruit employees and what type of information the team will request from them. HR does not want employees feeling that they must participate in a study simply because it takes place in their facility and wants to protect the identity of employees participating in anonymous surveys. On occasion, Institute staff distribute surveys (and sometimes collect them when completed), providing an identity firewall between the employee who elects to participate and the researcher.
HR may also limit researchers from asking especially personal questions or questions inquiring about the recruitment, hiring, and retention practices of their employer. HR must consider whether the study design and survey questions raise liability concerns. Studies that include employee focus groups or one‐on‐one interviews raise issues pertaining to the purpose and content of the focus groups or interviews, mechanisms to address special issues or complaints that may arise during them, and determination of whether the employees may participate during paid time as opposed to participating while off‐the‐clock.
Nonclinical Research Credentialing Process
It is vital that hospitals know who will be on hospital premises for a research study and what activities they will be engaging in. If a research team member is not already affiliated with our hospital system and will be engaging in noninterventional research activities, such as conducting the research consent process, administering a survey, or providing educational materials, our hospital system review initiates a nonclinical research credentialing process. The Institute's Manager of Clinical Research Operations assesses the team members' qualifications, reviews their resumes, interviews each of them, and discusses exactly what activities they will be engaging in and their training and experience. In addition to evaluating their qualifications, the hospital must determine how such individuals will be identified once inside the hospital, including what type of badge (employee, contractor, or visitor) the hospital will provide them. Upon successful completion of the research credentialing process, the Institute explicitly names the approved individuals in the Letter of Approval to the Principal Investigator, with copies to the affected hospitals' units.
Discussion
Our hospital research review and approval process is critical to ensuring that only safe and regulatory‐compliant research activities occur within our hospital system, but the review and approval process, with its many steps and numerous reviewers, can be cumbersome. There is no substitute for human beings reading and understanding the protocol, consent forms for patient involvement in a study, the proposed use of protected health information, Investigator's Brochure, Research Application Form, and other study documents and then identifying pertinent issues and resolving them, and this process does require significant staff time.
We have improved (continuously) the Research Application Form to help in the crucial initial gathering of information about studies' operational needs. We have also converted from a predominantly paper‐based review process to the widespread use of electronic documents, but we have not automated the distribution process for these electronic documents and a staff person must still do this through email.
Despite our efforts to improve the review process, investigators are sometimes frustrated with it, particularly if someone identifies a new issue late in the process, or if the hospital system's approval for the study lags behind the IRB approval by more than a few days.
Currently, the hospital system provides the majority of study approvals to the Principal Investigator within 2 weeks of IRB approval, with some approvals provided within 1 day of IRB approval and others as long as 3 months afterward. Delays in hospital approval can be due to a study lacking required approval from a Department of Defense IRB, the FDA not providing permission to proceed with a study, the absence of an executed contract with a vendor to pick up and dispose of radioactive waste from the investigational product and many other factors. Of course, when the research team can respond in timely fashion to inquiries or issues that we have raised, that assists all of us in completing the review and approval process as quickly as possible.
The review and approval process benefits hospital patients, hospital personnel who will be supporting studies, and hospitals as institutions. Thinking through, planning, and preparing for study operations, particularly for studies taking place in an ICU, benefits the research team, hospital personnel, and the patients. Overall, the hospital system's research review and approval process affords many protections to our patients and reduces risks to the hospital system while permitting research studies to be conducted within its varied healthcare facilities.
We encourage researchers not to view today's modern hospital as bricks and mortar, but as an institution with deep responsibility for safety on hospital premises. Hospitals must meet over a thousand Joint Commission standards, set goals for patient outcomes, measure and report on quality indicators, protect patient confidentiality, maintain the safety an ever‐expanding array of simple and complex equipment, maintain, check and document contents of adult and pediatric crash carts, have 24‐7 code teams at‐the‐ready, create, maintain and store patient medical records securely, transport patients, and much more.
Conclusion
Our hospital system, in accordance with a system‐wide policy, engages in a comprehensive review and approval process for any human participant research that has been proposed to be conducted within one or more of our facilities. The process focuses primarily on patient safety within the hospital premises, operational study issues, financial issues and hospital risk issues. This process decreases risks to the patients, researchers, and hospital facilities engaging in human participant research.
- Code of Federal Regulations Part 45, Title 46.
- Code of Federal Regulations Part 50, Title 21.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospital medicine research.J Hosp Med.2008;3:308–313.
- ,.Successfully developing a cardiovascular research program in a community hospital.J Cardiovasc Manag.2004;15:13–19.
- .Developing an infrastructure for research in a free‐standing hospital.J Nurs Adm.2007;37:295–301.
- ,,.Prevalence of multiple chronic conditions in the United States' Medicare population.Health Qual Life Outcomes.2009;7:82.
- ,,,,.Assessing the impact of protocol design changes on clinical trial performance.Am J Ther.2008;15:450–457.
- ,,, et al.Factors affecting workload of cancer clinical trials: results of a multicenter study of the National Cancer Institute of Canada Clinical Trials Group.J Clin Oncol.2002;20:545–556.
- ,,, et al.The changing face of Phase 1 Cancer Clinical Trials: new challenges in study requirements.Cancer.2009;115(8):1592–1597.
- U.S. Census Bureau. Annual Estimates of the Resident Population for Counties of Texas: April 1, 2000 to July 1, 2008. Available at: http://www.census.gov/popest/counties/tables/CO‐EST2008–01‐48.xls. Accessed February 2010.
- Harris County Texas. Available at: http://www.gis.hctx.net. Accessed February 2010.
- Accreditation Program: Hospital. Available by purchase from The Joint Commission on Accreditation of Healthcare Organizations.2008.
- International Conference on Harmonisation. Available at: www.ich.org/cache/compo/276–254‐1.html. Accessed February 2010.
- Code of Federal Regulations Part 45, Title 46.
- Code of Federal Regulations Part 50, Title 21.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospital medicine research.J Hosp Med.2008;3:308–313.
- ,.Successfully developing a cardiovascular research program in a community hospital.J Cardiovasc Manag.2004;15:13–19.
- .Developing an infrastructure for research in a free‐standing hospital.J Nurs Adm.2007;37:295–301.
- ,,.Prevalence of multiple chronic conditions in the United States' Medicare population.Health Qual Life Outcomes.2009;7:82.
- ,,,,.Assessing the impact of protocol design changes on clinical trial performance.Am J Ther.2008;15:450–457.
- ,,, et al.Factors affecting workload of cancer clinical trials: results of a multicenter study of the National Cancer Institute of Canada Clinical Trials Group.J Clin Oncol.2002;20:545–556.
- ,,, et al.The changing face of Phase 1 Cancer Clinical Trials: new challenges in study requirements.Cancer.2009;115(8):1592–1597.
- U.S. Census Bureau. Annual Estimates of the Resident Population for Counties of Texas: April 1, 2000 to July 1, 2008. Available at: http://www.census.gov/popest/counties/tables/CO‐EST2008–01‐48.xls. Accessed February 2010.
- Harris County Texas. Available at: http://www.gis.hctx.net. Accessed February 2010.
- Accreditation Program: Hospital. Available by purchase from The Joint Commission on Accreditation of Healthcare Organizations.2008.
- International Conference on Harmonisation. Available at: www.ich.org/cache/compo/276–254‐1.html. Accessed February 2010.
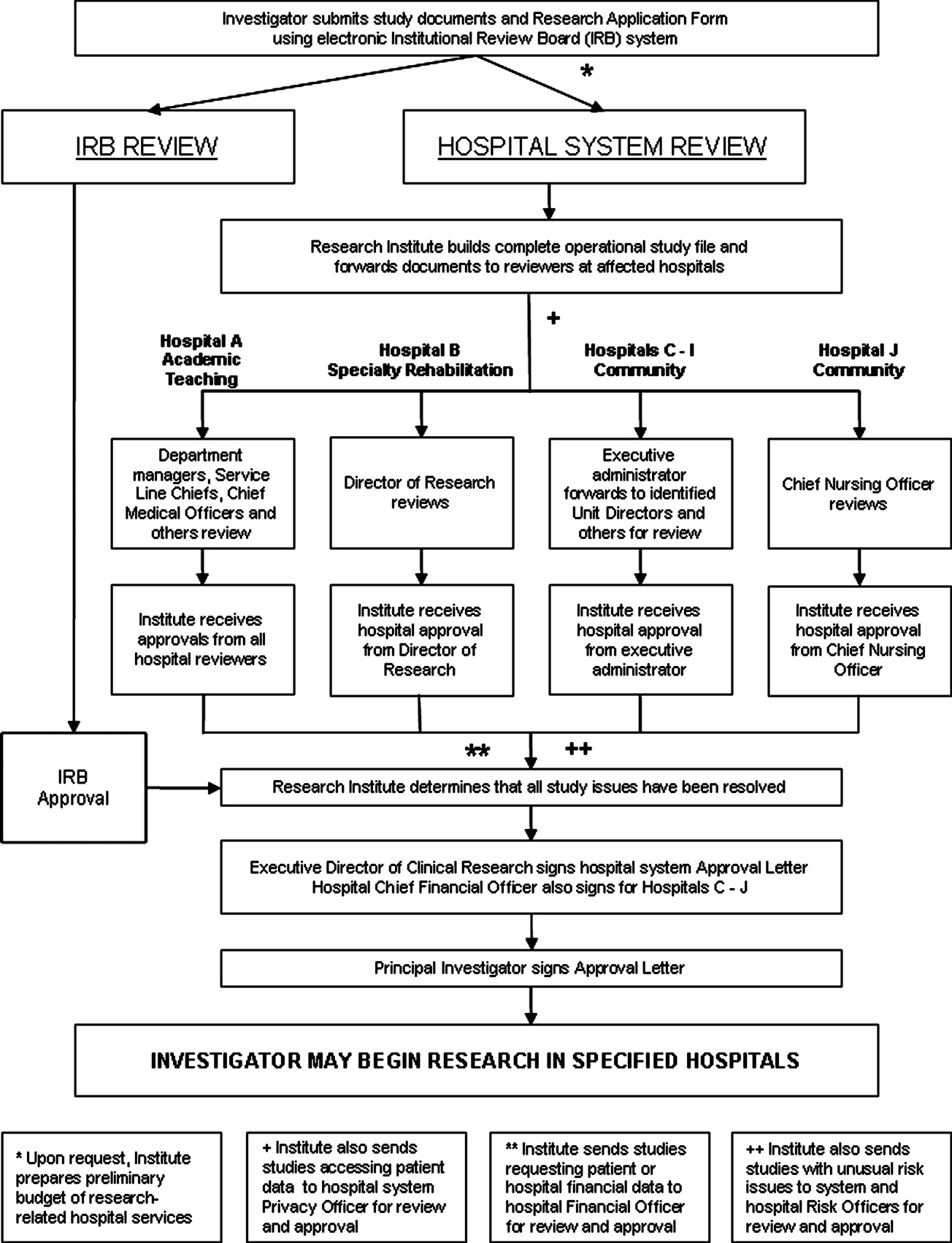
FDA‐warning for IV Haloperidol: A Review
Haloperidol is Food and Drug Administration (FDA)‐approved in the United States for the management of acute and chronic psychotic disorders and widely used in the management of delirium‐associated agitation in hospitalized patients.1 Delirium in the hospital is an acute confusional state that frequently arises from multiple complex factors and may affect up to 30% of hospitalized patients.2 Although the first step in the management of delirium involves identification and treatment of underlying causes and offering supportive behavioral care; medications may be needed to control severe agitation.2 Low dose intravenous (IV) haloperidol (ie, 0.250.5 mg every 4 hours) is a commonly used medication in this setting as recommended by expert‐groups including the Cochrane Collaboration and the American Psychiatric Association.2, 3
Although injectable haloperidol, a butyrophenone‐derived antipsychotic agent pharmacologically related to the piperazine phenothiazines,4 is approved for IV use in many countries (Table 1), parenteral use is approved only for intramuscular (IM) administration in the US. Thus, IV administration of the drug in the US is considered an off‐label use.5
| Indication | Country | |||||
|---|---|---|---|---|---|---|
| Canada24 | France29 | Germany25 | Great Britain37 | Italy30 | Switzerland31 | |
| ||||||
| Mainly delirium (schizophrenia, other psychosis, short‐term management of psychomotor agitation, excitement, violent or dangerously impulsive behavior, vomiting, hiccup) | Short term treatment of agitation and aggressiveness during an acute or chronic psychotic episode, vomiting along with antimitotic post‐radiotherapy treatment | Acute and chronic schizophrenia, psycho‐motorical agitation of psychotic genesis | Schizophrenia, other psychosis, short‐term adjunctive management if psychomotor agitation, violent or dangerous impulsive behavior | Resistant forms of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis' chronic psychosis High doses restrictions: syndrome of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis, chronic psychosis | Acute schizophrenic episode, mania, vomiting | |
| IV dosing in adults | 12 mg every 24 hours | The use is limited to adult patients and the drug can be administered IM or IV. The IV route is restricted to the treatment of vomiting. | 510 mg/day, daily max.: 30(100) mg | 210 mg initially, PRN every 48 hours, daily max. 18 mg | 510 mg initially, PRN every hour, daily max. 60 mg | 5 mg PRN every 30 minutes |
| IV dosing in geriatric care | 0.250.5 mg | Single dose of 0.51.5 mg, daily max. 5 mg | Half adult dose | Adjust to appropriate dose | 0.5 mg, than PRN | |
| Risk factors for the development of cardiac adverse events | QT prolonging drugs, diabetes, obesity, hypokalemia, congenital long QT syndrome | Bradycardia 55 beats per minute, hypokalemia, congenital QT prolongation, other medications provoking bradycardia, deceleration of the intra‐cardiac transition or prolonged QT interval | QT syndrome, hypokalemia, other electrolyte imbalance, cardiovascular diseases, QT prolongation in the family history | Cardiovalscular disease, drugs that can prolong the QTc, diabetes, obesity, hypokalemia, congenital long QT syndrome | Contraindications: recent cardiac infarction, uncompensated cardiac insufficiency, cardiac arrhythmias, antiarrhythmic drugs, pre‐existing QT prolongation, cases of arrhythmia or torsades de pointes in the family history, untreated potassium imbalance, QTc prolonging drugs | QT syndrome, hypokalemia, hypomagnesemia, other electrolyte imbalances, cardiovascular diseases, hypothyreosis, QT prolongation in the family history |
| Monitoring recommendations | Electrolytes | ECG monitoring at admission time, electrolytes | ECG monitoring, electrolytes | Metabolic parameters | ECG at baseline and regular ECG monitoring, electrolytes | Close ECG monitoring, electrolytes |
| General recommendations | Regular reevaluation in long‐term use | Apply the lowest effective dose | Apply the lowest effective dose | Application per mouth is the route of choice | Decrease dose if QTc >500 msec | Switch to PO as soon as possible |
Haloperidol is often preferred over other antipsychotics as a result of its effectiveness, low rate of anticholinergic side effects, familiarity with dosing and usage, and minimal respiratory or sedative properties.6 Use of the IV route in patients with acute delirium has several advantages over the IM or oral route,7 including rapid onset, immediate bioavailability, and ease and safety of administration.
Prior to September 2007, the package insert for haloperidol alerted healthcare professionals to the risk of cardiovascular side effects. Based on case reports of potentially fatal cardiac events, the FDA revised the label, warning that the QT prolongation (QTP) and risk of torsades de pointes (TdP) were increased with IV administration of haloperidol or administration of the drug at greater than recommended doses. Unfortunately, neither the typical dosing range nor the minimum dose associated with these cardiac side effects were specified in this recommendation.5
It is well‐established that haloperidol may prolong the QT interval by blocking the repolarizing potassium IKr current.8 Although drugs that block the IKr channel can produce arrhythmia in healthy individuals, additional risk factors, such as underlying heart conditions, electrolyte imbalances (ie, hypokalemia and hypomagnesemia), concomitant proarrhythmic drug use, and mechanical ventilation may increase this risk.9 Prolongation of the QT interval has been associated with subsequent malignant cardiac arrhythmias including ventricular fibrillation and TdP.10 Prolongation of the QT interval is considered the strongest risk factor for TdP, particularly with a baseline QTc > 450 msec.9
Based on the increased risk for QTP and TdP and the case reports of cardiac events, the FDA advisory recommended continuous electrocardiogram (ECG) monitoring in patients receiving IV haloperidol.5 However, such monitoring may be impractical and costly in hospitalized patients who require low doses of IV haloperidol to manage acute delirium and who are not in telemetry or intensive care units.
The aim of this review was to evaluate the case reports leading to the recent FDA warning for IV haloperidol, specifically focusing on the presence of risk factors for arrhythmias. Based upon the evidence, an additional aim was to provide an institutional response to this warning toward the optimal use of this agent.
Method
Two search pathways were used to evaluate reports of haloperidol‐associated TdP and/or QT prolongation:
Literature Review
We searched for published literature in humans indexed in Pubmed (1966April 2009), EMBASE (1972April 2009), and Scopus (1823April 2009) using the search terms haloperidol or Haldol combined with intravenous or infusion and at least one of the following terms: QT prolongation, TdP, torsades de pointes, torsades with a specific focus on case reports.
References from the retrieved articles were also reviewed to search for additional case reports.
In addition to cases reported in English journals, several of our reports originated from Japan11 (translation provided by the FDA), Spain12 and Germany13 (translated by the primary author).
Search of the FDA Database
We reviewed all adverse drug events reported through MedWatch or those submitted by the manufacturer from November 1997 to April 2008 through the Freedom of Information Act (FOIA) request. The FDA provided a full‐text summary of 5944 reports involving oral, intramuscular and IV use of haloperidol. The FDA data were transferred to a Microsoft Access database and screened for the key terms torsade, QT, prolongation, wave. Incident report number, date of report, age, gender, origin of report, medication name, role of drug as categorized by the FDA (suspect, concomitant, primary suspect, secondary suspect), route, dose, units, duration, symptoms and FDA outcome category (death, life‐threatening, hospitalization initial or prolonged, disability, congenital anomaly, required intervention to prevent permanent damage, other) were recorded. Only those reports in which IV haloperidol was considered by the reporter to be the primary causative agent for the adverse event were reviewed. Available information included diagnosis, laboratory parameters, QTc measurement, cardiac symptoms, outcomes and a description of recovery. No peer review was applied to the MedWatch reports and the data reported in this publication reflect the original information from the FDA MedWatch database. Baseline QTc was either the value defined as such in the original report or the lowest QTc reported. Haloperidol doses administered were defined as cumulative dose at event, encompassing all doses administered during the hospital stay until the occurrence of the adverse cardiac event.
The drugs listed in the case reports were assessed for proarrhythmic potential using 2 references: the individual package insert and the website of the Arizona Center for Education and Research on Therapeutics.14
The drugs were only considered proarrhythmic when the 2 resources were in agreement.
Duplicates and/or previously published cases, as well as reports involving adverse cardiac effects not associated with QTP or TdP, were identified and excluded.
In their advisory, the FDA does not state the exact origin of the reports, their specific search strategy to identify haloperidol‐associated adverse events, or the role IV haloperidol played in the individual events included in the extended warning. Consequently, the number of events identified in this review may differ from that published in the FDA extended warning.
Results
A total of 70 reported cases of IV haloperidol associated TdP and/or QTP were identified. Of these 70, 41 were identified through the PubMed/EMBASE/Scopus review, while an additional 29 cases were identified through the FDA database search.
Of the 29 cases in the FDA database, 21 were reported by health care professionals and 8 by manufacturers.
A total of 35 publications described cases originating from the US. Three cases took place in Japan and 1 case each in Canada, Germany and Spain. Several cases in the MedWatch database were reported outside the US: 1 case each originated from Austria, Canada, France, Japan, Spain, Switzerland and the United Kingdom. A summary of the published case reports is displayed in Table 2 and the FDA cases are summarized in Table 3.
| Case | Source (reference#) | Date | Age, Years | Gender | Drugs Pro‐arrhyth. | Venti‐ lated | Max. Daily Dose (mg) | Total Dose at Event (mg) | Time to Event | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | ECG Normalization, Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
| 1 | 35 | 1991 | 56 | m | No | Yes | 1200 | 1540 | NR | Yes | 584 (400) | 184 | NR | NR, uneventful |
| 2 | 13 | 1992 | 36 | m | Yes | No | 11.5 | 11.5 | 20 hours after start | Yes | 714 (428) | 286 | Yes | QTc normalization (440 msec), NR |
| 3 | 38 | 1993 | 39 | f | Yes | Yes | NR | 580 | Max. QTc 72 hours after start | Yes | 650 (420) | 230 | Yes | QTc normalization after 6 days, uneventful |
| 4 | 38 | 1993 | 19 | f | Yes | No | 170 | 170 | Max. QT 12 hours after start | Yes | 600 (480) | 120 | Yes | QTc normalization after 8 days, uneventful |
| 5 | 38 | 1993 | 63 | f | Yes | No | NR | 489 | Max. QT 48 hours after start | Yes | 670 (520) | 150 | Yes | QTc normalization after 8 days, uneventful |
| 6 | 38 | 1993 | 74 | f | Yes | Yes | NR | 10 | NR | No | 430 (410) | 20 | Yes | QTc unchanged after 8 days, uneventful |
| 7 | 17 | 1993 | 39 | m | Yes | Yes | NR | >490 | NR | Yes | 457 (348) | 109 | Yes | QTc normalization within 2 to 3 days, no further TdP, NR |
| 8 | 17 | 1993 | 61 | m | Yes | Yes | 115 | 211 | NR | Yes | 500 (390) | 110 | NR | QTc normalization within 2 days, death |
| 9 | 17 | 1993 | 48 | m | Yes | Yes | 825 | 825 | NR | Yes | 538 (441) | 97 | NR | QTc normalization in 3 days, rehabilitation |
| 10 | 39 | 1994 | 23 | f | Yes | Yes | 120 | 300 | 12 hours after dose increase | Yes | NR (550) | NR | Yes | NR, uneventful, extubation after 5 days, discharge after 10 days |
| 11 | 39 | 1994 | 28 | m | Yes | Yes | 300 | >300 | 24 hours after dose increase | Yes | NR (>520) | NR | Yes | No recurrence of arrhythmia, patient death (multi‐organ failure) |
| 12 | 40 | 1994 | 65 | m | Yes | NR | 230 | 410 | Worsening from day 2 to day 5 | Yes | 594 (490) | 104 | Yes | QTc normalization (406 msec), no cardiac problems at discharge |
| 13 | 40 | 1994 | 65 | f | Yes | NR | 500 | 980 | After the last 60mg | Yes | 628 (403) | 225 | Yes | QTc normalization (400 msec), recurrence with oral haloperidol, rehabilitation |
| 14 | 40 | 1994 | 76 | f | Yes | NR | 21 | 26 | Day 2 after several boluses | Yes | 670 (450) | 220 | Yes | QTc normalization within several days (412 msec), rehabilitation |
| 15 | 41 | 1994 | 59 | m | NR | Yes | 865 | 1013 | NR | Yes | 640 (480) | 160 | NR | QTc normalization in 24 hours, survived |
| 16 | 16 | 1995 | 76 | f | Yes | No | NR | 44.5 plus 1 PO | 15 minutes | Yes | 670 (409) | 261 | Yes | ECG normalized the next morning, no further events |
| 17 | 16 | 1995 | 49 | m | Yes | No | NR | 1150 plus 20 IM | 45 minutes | Yes | 648 (380) | 268 | Yes | QTc normalization in 24 hours, anoxic brain insult/rehabilitation |
| 18 | 16 | 1995 | 65 | f | Yes | No | 600 | 965 | 30 minutes | Yes | 628 (403) | 225 | Yes | 3 more episodes of TdP in 3 hours, QTc normalization in 2 days, no recurrence with further haloperidol, NR |
| 19 | 42 | 1995 | 42 | m | Yes | No | 28 | 28 | 20 minutes | Yes | 610 (533) | 77 | Yes | QTc normalization in 5 days, uneventful, ECG normal |
| 20 | 42 | 1995 | 39 | m | Yes | No | 45 | 45 | 5 minutes | Yes | 654 (NR) | NR | Yes | QTc normalization after 24 hours, uneventful |
| 21 | 11 | 1997 | 56 | f | No | No | 10 | 10 | Shortly after | NR | NR (NR) | NR | Yes | TdP resolved after 8 hours, NR |
| 22 | 11 | 1997 | 82 | f | NR | No | 10 | 10 | Shortly after | Yes | 680 (NR) | NR | Yes | QTc normalization on day 6 after admission (470 msec), NR |
| 23 | 11 | 1997 | 35 | m | NR | No | NR | 90 | After 20 mg | Yes | 520 (NR) | NR | Yes | TdP disappeared 12 hours later, NR |
| 24 | 43,44 | 1998 | 45 | m | NR | Yes* | NR | 9 | 203 minutes | Yes | 638 (560) | 78 | Yes | NR, overall survival 100%, significantly prolonged hospital stay |
| 25 | 43,44 | 1998 | 64 | f | NR | NR | 115 | 220 minutes | Yes | 605 (424) | 181 | Yes | ||
| 26 | 43,44 | 1998 | 75 | f | NR | NR | 85 | 60 minutes | Yes | 567 (508) | 59 | Yes | ||
| 27 | 43,44 | 1998 | 71 | f | NR | NR | 55 | 120 minutes | Paced | Paced | Paced | Yes | ||
| 28 | 43,44 | 1998 | 58 | f | NR | NR | 75 | 38 minutes | Yes | 657 (542) | 115 | Yes | ||
| 29 | 43,44 | 1998 | 40 | m | NR | NR | 35 | 15 minutes | Yes | 679 (475) | 204 | Yes | ||
| 30 | 43,44 | 1998 | 71 | m | NR | NR | 70 | 58 minutes | Yes | 521 (478) | 43 | Yes | ||
| 31 | 43,44 | 1998 | 47 | m | NR | 400 | 400 | 79 minutes | Yes | 574 (444) | 130 | Yes | ||
| 32 | 21 | 1999 | 41 | f | Yes | Yes | 320 | 915 | 55 minutes | Yes | 610 (426) | 184 | Yes | QTc normalization after 5 day, uneventful |
| 33 | 21 | 1999 | 31 | m | Yes | Yes | 480 | 1700 | 40 minutes | Yes | 599 (491) | 108 | Yes | QTc normalized in 4 days, NR |
| 34 | 18 | 2000 | 64 | f | Yes | Yes | 175 | 175 | NR | No | 413 (418) | (‐5) | Yes | QTc remained unchanged, uneventful |
| 35 | 8 | 2000 | 75 | m | No | NR | >2 | >2 | NR | Yes | 615 (435) | 180 | No | QTc normalization in 48 hours, uneventful |
| 36 | 8 | 2000 | 68 | m | Yes | Yes | >2 | >2 | NR | Yes | 650 (407) | 243 | No | QTc normalization after 4 day, uneventful after extubation |
| 37 | 8 | 2000 | 77 | m | NR | NR | (4) | 2 | NR | Yes | 550 (393) | 157 | No | QTc normalization in 24 to 36 hours, NR |
| 38 | 12 | 2004 | 34 | m | Yes | NR | 24.5 | 24.5 | 20 minutes | Yes | 560 (420) | 140 | Yes | QTc normalization (440 msec), ECG normal |
| 39 | 23 | 2004 | 58 | f | Yes | NR | 340 | 1010 | NR | Yes | 533 (460) | 73 | Yes | QTc normalization 7 days later discharge after 27days |
| 40 | 45 | 2008 | 86 | f | Yes | No | 2 mg | 2 mg | 8 hours after last dose | Yes | 524 (NR) | Probably 79 | No | QTc normalization (445 msec), NR |
| 41 | 46 | 2009 | 74 | m | Yes | No | 2 | 2 | Shortly after | Yes | NR (579) | NR | Yes | Pre‐existing heart block and fibrillation resolved, nursing home/rehabilitation |
| Report | MedWatch Identifier | Report Date | Age, Years | Gender | Drugs Pro‐arrh. | Maximum Daily Dose (mg) | Total Dose at Event (mg) | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | Outcome; Recovery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
| 1 | 3122988‐1 | 1998 | 61 | m | No | 48 | 48 | Yes | NR | NR | Yes | Intervention; NR |
| 2 | 3157827‐6 | 1998 | 44 | f | No | 160 | 160 | Yes | 550 (440) | 110 | Yes | Intervention; uneventful |
| 3 | 3178715‐5 | 1999 | 60 | m | NR | 415 | 645 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization in 1 day, no recurrence |
| 4 | 3271261‐X | 1999 | 56 | m | NR | NR | 20 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization |
| 5 | 3271080‐4 | 1999 | 35 | m | Yes | 7 | 7 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced, hospitalization prolonged |
| 6 | 3325391‐4 | 1999 | 55 | f | Yes | 75 | 75 | NR | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 7 | 3381921‐8 | 1999 | 52 | m | No | 320 | 634 | Yes | 458 (430) | 28 | Yes | Death; NA |
| 8 | 3483869‐7 | 2000 | 18 | m | No | >200 | >310 | Yes | NR | NR | Yes | Intervention; no recurrence after haloperidol reinstitution |
| 9 | 3516342‐8 | 2000 | NR | NR | NR | NR | NR | NR | NR | NR | Yes | NR; NR |
| 10 | 3516320‐9 | 2000 | 34 | m | Yes | 5 | 5 | Yes | NR | NR | No | Life‐threatening; event abated after dose stopped |
| 11 | 3552263‐2 | 2000 | 46 | f | Yes | NR | 97.5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 12 | 3574705‐9 | 2000 | 78 | m | Yes | NR | 160 | Yes | 603 (453) | 50 | Yes | Intervention; event abated after dose stopped/reduced |
| 13 | 3703871‐7 | 2001 | 27 | m | NR | 530 | 530 | Yes | NR | NR | Yes | Death, NA |
| 14 | 3724567‐1 | 2001 | 31 | m | Yes | 6 | 6 | Yes | 496 (449) | 47 | No | Life‐threatening; ECG returned to baseline |
| 15 | 3851984‐1 | 2002 | 72 | f | NR | 18 | 18 | NR | NR | NR | Yes | Hospitalization; NR |
| 16 | 3942407‐2 | 2002 | 51 | m | Yes | 14 | 14 | Yes | 461 (444) | 17 | Yes | Life‐threatening; no recurrence |
| 17 | 4066580‐3 | 2003 | >60 | f | NR | 50 | 50 | Yes | >600 (480) | >120 | No | Hospitalization; QTc normalization, patient recovered |
| 18 | 4126280‐8 | 2003 | 47 | f | NR | 60 | 180 | Yes | 550 (450) | 100 | No (bradycardia) | Hospitalization; patient recovered |
| 19 | 4150700‐6 | 2003 | NR | m | NR | 5 | 5 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced |
| 20 | 4340092‐1 | 2004 | 52 | m | Yes | 5 | 5 | Yes | >500 (490) | >10 | NR (polymorphous VT) | Life‐threatening; NR |
| 21 | 4714692‐0 | 2005 | NR | m | NR | NR | NR | Yes | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 22 | 4881813‐9 | 2006 | NR | m | NR | NR | 40 | NR | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 23 | 4892225‐6 | 2006 | NR | f | Yes | 10 | >10 | Yes | 493 (300) | 193 | No | Hospitalization; QTc normalization (403 msec) |
| 24 | 4911873‐8 | 2006 | 69 | m | Yes | 6 | 6 | NR | NR | NR | Yes | Cardiac arrest, death; NA |
| 25 | 5366448‐6 | 2007 | 53 | m | Yes | NR | 35 | Yes | NR | NR | NR | Cardiac arrest, life‐threatening; patient recovered |
| 26 | 5563440‐3 | 2007 | 58 | m | Possible | 5 | 5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 27 | 5642929‐2 | 2008 | 42 | m | Yes | 165 | 165 | Yes | 640 (350) | 290 | Yes | Death; NA |
| 28 | 5697758‐0 | 2008 | 38 | m | Yes | NR | 620 | NR | NR | NR | Yes | Hospitalization; patient recovered |
| 29 | 5254840‐X | 2008 | 19 | f | Possible | 15 | 25 | Yes | 461 | NR | NR | Cardiac arrest, hospitalization; patient recovered |
Of the 70 cases, 54 cases of TdP were reported. The remaining 16 of 70 cases involved cases of QTP, 9 of which did not progress to TdP and 7 of which the progression to TdP was unclear. Of note, 42 of 54 of the cases of TdP were reported as preceded by documented QTP. Presence of QTP was unknown in the other 12 original reports. Three out of 70 patients experienced sudden cardiac arrest, 1 of which was fatal. One arrest was preceded by TdP and 2 by QTP (Figure 1).
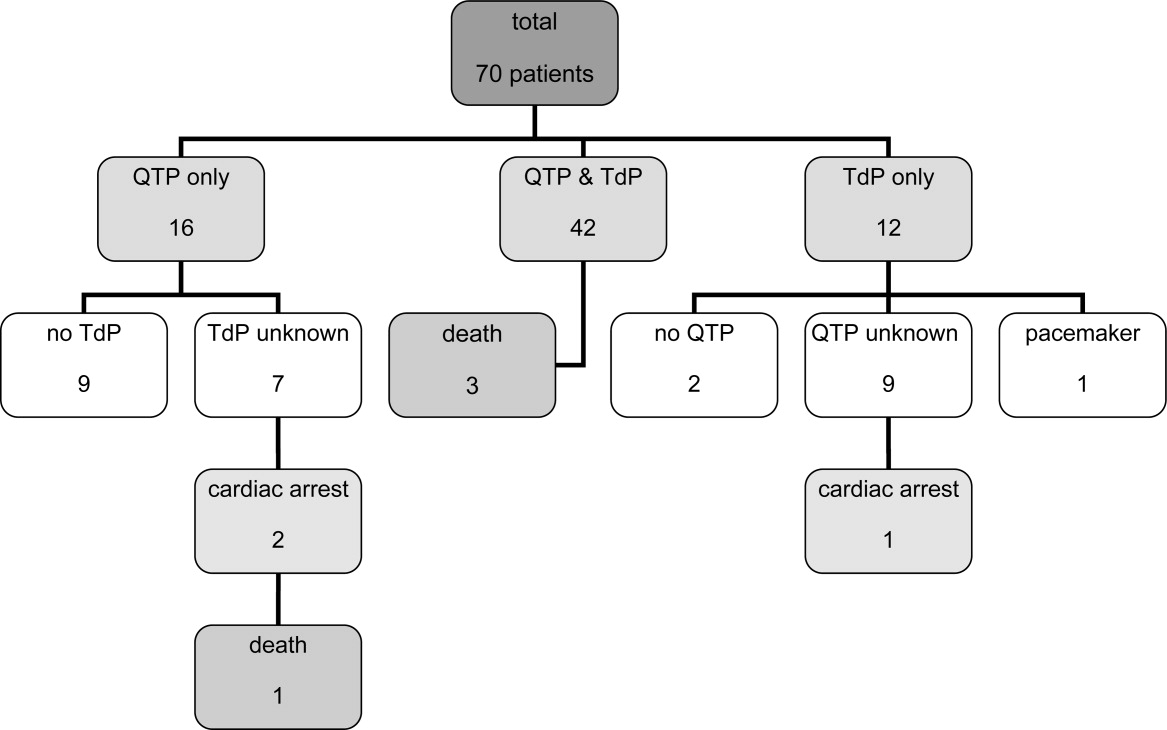
The patient ages ranged from 18 years to 86 years. Of note, 17 patients experiencing TdP and/or QTP were 40 years old, and 2 of those patients were 30 years old.
Haloperidol‐associated QTP and/or TdP were observed in 27 female and 42 male patients; the gender was not stated in one report. Of the 54 patients experiencing TdP (with or without report of previous QTP), 22 were female and 31 were male (1 gender unknown).
A total of 68 of 70 patients were determined to have associated risk factors15 for QTP/TdP (see Table 4). The circumstances of the remaining 2 patients were not described in sufficient detail to identify associated risk factors.
| Risk Factor | Patients, n (%) |
|---|---|
| |
| Any risk factor | 68/70 (97) |
| Unknown | 2/70 (3) |
| Specific risk factors | |
| Electrolyte imbalance | 27/68 (40) |
| Underlying cardiac disease | 32/68 (47) |
| Concomitant proarrhythmic agents | 39/68 (57) |
| Other drugs influencing cardiac function | 23/68 (34) |
| Baseline QTc >450 msec | 18/68 (26) |
| QTc known: 44 patients | 18/44 (41) |
Overall, 32 patients had underlying heart conditions. Electrolyte imbalances, including hypokalemia, hypomagnesemia, and hypocalcemia, were present in 17 patients. At least 39 patients were receiving potentially proarrhythmic agents (1‐8 proarrhythmic drugs per patient) in addition to IV haloperidol. At least 23 patients were receiving additional drugs with a potential for other cardiac adverse events than QTP and TdP.
A wide range of other disease states previously reported to be associated with QTP15 were identified in these patients: asthma (5 patients), diabetes (5 patients), obesity (3 patients), impaired renal and/or liver function (3 patients each), human immunodeficiency virus (HIV) (2 patients); chronic obstructive pulmonary disease (COPD), pancreatitis and hypothyroidism (1 patient each). A total of 22 patients had a history of substance abuse (alcohol and/or drugs), and 4 patients were smokers.
The administered doses of IV haloperidol varied widely. Considering that information regarding the maximal daily dose was missing in 22 reports and ambiguous in another 20 cases, the results have been presented using cumulative IV haloperidol doses. Patients experiencing TdP without preceding QTP received a cumulative dose (= total dose at event) ranging from 5 mg to 645 mg. Patients with both confirmed QTP and TdP were administered a cumulative dose of 2 mg to 1700 mg. Patients who experienced QTP without TdP received a cumulative dose of 2 mg to 1540 mg of IV haloperidol.
Sudden cardiac arrest following administration of IV haloperidol was observed in cumulative doses ranging from 6 mg to 35 mg. The cardiac arrest leading to a fatal outcome was preceded by an administration of at least 6 mg of IV haloperidol. Overall, 14 out of 70 patients received cumulative doses of 10 mg IV haloperidol.
The time from administration to documentation of QTP and/or TdP ranged from immediately post administration to 8 hours after administration of the last dose of IV haloperidol.
Baseline QTc was known in 44 patients. Baseline QTc was >450 msec in 18 of these 44 patients.
The change from baseline QTc varied widely from 20 msec to 286 msec; 36 patients demonstrated a prolongation of >50 msec.
In those patients with reported haloperidol‐associated QTP, 25 patients demonstrated a QTc >600 msec and 38 patients >520 msec.9 Of the cases with known specific QTc values, the QTc was prolonged >450 msec in 48 out of 50 cases. The lowest reported QTc leading to TdP was 413 msec.
A total of 20 patients were reported as having a normalization of QTc (as defined by the original reports) within several hours to 8 days; minimal QTP was reported as persisting in 2 patients. The specifics of the other patients were unknown, although 25 patients were categorized as recovered, 13 were stated as having an uneventful remainder of hospitalization, and 5 patients were discharged to a rehabilitation facility or a nursing home.
Discussion
The current review was performed in response to the FDA warning recommending the use of continuous ECG monitoring associated with the administration of intravenous haloperiodol.5 This warning has resulted in substantial dilemmas for health care organizations, additional resource allocation, and increased scrutiny from regulatory agencies. The results of our review reveal that intravenous haloperidol‐associated QTP and TdP almost uniformly take place in patients with concomitant risk factors and with cumulative doses 2 mg. In light of these findings, it is possible that hospitals may be able to administer intravenous haloperidol in patients without risk factors without continuous ECG monitoring. In reviewing these published reports, it is important to note that the FDA identified 28 published cases of haloperidol‐associated QTP and TdP, while our review yielded a total of 41 published case reports.
The FDA database included 73 cases of haloperidol‐associated TdP in their database. However, these cases included both oral as well as IV administration; using our methodology, we identified 29 additional case reports associated with intravenous haloperidol from this database. Consequently, our review included 41 published case reports and 29 FDA database cases, resulting in the total of 70 patients.
Our review revealed a number of practical findings. First, our summary demonstrated that neither QTP nor TdP has been documented with a cumulative dose of IV haloperidol of 2 mg. The majority of patients (80%) received cumulative IV doses 10 mg. The lowest dose associated with sudden cardiac arrest was 6 mg and this took place in a 69‐year‐old male patient. Second, the majority (97%) of our patients had additional risk factors for QTP and/or TdP. Pre‐existing heart disease,1619 electrolyte imbalance,17, 1921 concomitant proarrhythmic drugs16, 17, 1922 and mechanical ventilation17, 23 were identified as the most commonly observed risk factors (Table 4). Lastly, in those cases in which the data were reported, baseline QTc was >450 msec in 41% of the patients, and 96% had a QTc at the time of the event >450 msec. Therefore, we conclude that patients: (1) receiving low cumulative doses (2 mg) with (2) no risk factors for prolonged QTc or TdP, and (3) with a normal QTc on baseline EKG can safely be given IV haloperidol in the hospital setting.
This dosage range is consistent with the labelling for IV haloperidol dosing in Canada24 and Germany25 (Table 1), where single doses of 0.25 mg to 1.5 mg are recommended for the treatment of delirium or acute agitation in the geriatric population.24, 25
In a recent Cochrane review, low‐dose IV haloperidol (3 mg per day) was concluded to be as safe and effective as atypical antipsychotics in the treatment of acute delirium with respect to extrapyramidal adverse effects.2
The American Psychiatric Association recommends an initial IV dose of 12 mg every 24 hours as needed (0.250.50 mg every 4 hours as needed for elderly patients), with titration to higher doses for patients who continue to be agitated for the treatment of patients with delirium (issued 1999, updated 2004).3
While several expert‐groups and investigators currently consider IV haloperidol as an important therapeutic option for treating acute delirium and agitation in the dose range presented above, less consensus exists regarding monitoring requirements.2, 3, 26, 27
The American Psychiatric Association recommends IV haloperidol only after a baseline ECG is obtained. These guidelines have not been updated since the release of the FDA extended warning.3 In their recent review, Morandi et al.28 support the dosage recommendation of the 1999 American Psychiatric Association's practice guidelines for treatment of delirium,3 ie, administration of IV haloperidol in single doses of 0.5 mg to 2 mg in elderly patients, however, only after a baseline ECG is obtained.28 While the package insert of IV haloperidol in France29 recommends a baseline ECG, Germany,25 Italy30 and Switzerland's31 package information states the need for regular ECG monitoring. Guidelines for the treatment of delirium in the intensive care unit published by the American College of Critical Care Medicine and the Society of Critical Care Medicine in collaboration with the American Society of Health‐System Pharmacists consider IV haloperidol as the preferred agent for the treatment of delirium in critically ill patients (grade of recommendation = C). These expert groups recommend that patients should be monitored for electrocardiographic changes (QT interval prolongation and arrhythmias) when receiving haloperidol (Grade of recommendation = B).32
Nevertheless, continuous ECG monitoring (ie, telemetry) is expensive, labor‐intensive and, potentially overutilized.33, 34 Requiring clinicians to place all patients receiving intravenous haloperidol on telemetry is impractical and potentially costly. Mandating telemetry could also lead to unintended harm, ie, use of a less effective or less safe drug to avoid compliance with the telemetry mandate.
Based on our findings and the current recommendations in the literature, inpatient providers should be thoughtful and deliberate in the use of haloperidol to treat acute delirium with agitation. Patients requiring pharmacologic management of their delirium should be screened for risk factors for QTP and TdP (Table 4) and a baseline ECG should be obtained prior to haloperidol administration. If significant risk factors exist or the baseline ECG reveals a prolonged QTc, then the patient should receive continuous ECG monitoring. Similarly, if cumulative doses of 2 mg are needed, the patient should be placed on telemetry.
There are some limitations to our study design. Our findings are based upon previously published case reports or data submitted to the FDA MedWatch. While the content of the FDA's MedWatch database is accessible to the public via the Freedom of Information Act (FOIA), the events are neither categorized nor peer‐reviewed upon entry into the database. Consequently, information may be incomplete or inaccurate. In addition, the denominator representing the overall use of IV haloperidol is unknown, thus a rate of event cannot be assigned and the true scope of the problem cannot be determined. Despite these limitations, this summary represents the most comprehensive review of the literature to date, expanding on the analysis performed by the FDA. Of note, in our review of the FDA database, we noted several cases of haloperidol‐associated QTP or TdP associated with other routes of administration. Thus, it is unknown whether this complication is any greater with IV vs. the IM or per os (PO) routes of administration.
Conclusion
Although the proarrhythmic potential of haloperidol and other antipsychotics has been well established in the literature, IV haloperidol has been considered relatively safe with respect to this complication from the time of its approval in 1967.5, 1722, 35, 36 In reviewing all reported cases of cardiac complications associated with IV haloperidol, as well as the current literature, an association with QTP and TdP is likely. However, the case reports reveal that QTP and TdP generally occur in the setting of concomitant risk factors, and no cases have been reported utilizing a cumulative IV dose of 2 mg. It may therefore be safe to administer a cumulative dose of IV haloperidol of 2 mg without ECG monitoring in patients without risk factors for QTP. However, ECG monitoring should take place with IV haloperidol doses 2 mg and/or in those patients with additional risk factors of developing QTP and/or TdP.
Based on the findings of this review complemented by the guidelines of various expert‐groups and the official labelling information of different countries, the Pharmacy & Therapeutics Committee of the UCSF Medical Center revised the IV haloperidol policy: administration of a total dose of 2 mg IV haloperidol without concurrent telemetry is allowed in a noncritical care setting in patients without risk factors for QTP and TdP.
Acknowledgements
The authors acknowledge Gloria Won of the Fishbon Library at UCSF Medical Center at Mount Zion for her support.
- Haldol® injection (for immediate release) Package Insert.Raritan, NJ:Ortho‐McNeil Pharmaceutical Inc.;2005;rev. 05.2007.
- ,,,. Antipsychotics for delirium (review), the Cochrane collaboration2008;2. Available at: www. cochrane.org. Accessed February 2010.
- American Psychiatric Association: practice guideline for the treatment of patients with delirium.Am J Psychiatry.1999;156(5 suppl):1–20, updated 2004.
- Thomson Micromedex.2008. Micromedex healthcare series: “haloperidol” Thomson Micromedex, Greenwood Village.
- FDA alert: haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate).2007. This alert highlights revisions to the labeling for haloperidol. Available at: www.fda.gov. Accessed February 2010.
- ,,.Use of high‐dose intravenous haloperidol in the treatment of agitated cardiac patients,J Clin Psychopharmacol.1985;5(6):344–347.
- ,,, et al.Postoperative delirium,Am J Psychiatry.2008;165:7.
- ,.Corrected QT interval prolongation associated with intravenous haloperidol in acute coronary syndromes,Catheter Cardiovasc Interv.2000;50(3):352–355.
- ,.Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death.Am J Psych.2001;158(11):1774–1782.
- ,,, et al.Accuracy of uncorrected versus corrected QT Interval for Prediction of torsade de pointes associated with intravenous haloperidol.Pharmacotherapy.2007;27(2):175–182.
- ,,.Three cases of ventricular tachycardia and torsades de pointes induced by antipsychotic drugs.Shinzo.1997;29(1):68–74.
- ,,,.Haloperidol por via intravenosa y torsade de pointes.Medicina intensive.2004;28(2):89.
- ,,, et al.QT‐Verlängerung und Kammerflimmern unter Haloperidol‐ und Clonidin‐Therapie des Alkoholentzugssyndroms.Intensivmedizin und Notfallmedizin.1992;29(4):178–183.
- ARIZONA CERT, Arizona Center for Education and Research on Therapeutics. Available at: www.azcert.org. Accessed February 2010.
- ,.Cardiac arrhythmias—a clinical approach.Edinburgh:Mosby;2003.
- ,.The association between intravenous haloperidol and torsades de pointes—three cases and a literature review.Psychosomatics.1995;36:541–549.
- ,.Prolongation of the corrected QT and torsades de pointes cardiac arrhythmia associated with intravenous haloperidol in the medically ill.J Clin Psychopharmacol.1993;13(2):128–132.
- ,,,,.Torsades de pointes secondary to intravenous haloperidol after coronary bypass grafting surgery.Can J Anesth.2000;47(3):251–254.
- ,.Torsade de pointes associated with the administration of intravenous haloperidol: a review of the literature and practical guidelines for use,Expert Opin Drug Saf.2003;2(6):543–547.
- ,.Conduction disturbances associated with administration of butyrophenone antipsychotics in the critically ill: a review of the literature,Pharmacotherapy.1997;17(3):531–537.
- ,,.Haloperidol‐induced torsades de pointes.Ann Pharacother.1999;33(10):1046–1050.
- ,,, et al.Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary,Crit Care Med.1995;23(9):1596–1600.
- ,,,,,.Prolonged cardiac repolarization after tacrolimus and haloperidol administration in the critically ill patient.Pharmacotherapy.2004;24(3):404–408.
- CPS Compendium of Pharmaceuticals and Specialties, the Canadian drug reference for health professionals, 2007, Canadian pharmacists association.
- Rote Liste Deutschland2008, Rote Liste Service GmbH Frankfurt am Main. Available at: www.rote‐liste.de. Accessed February 2010.
- ,.Delirium in the hospitalized patient: a primer for the pharmacist clinician.J Pharm Pract.2007;20(5):368–372.
- ,,, et al.Delirium: guidelines for general hospitals.J Psychosom Res.2007;62(3):371–383.
- ,,,.The pharmacological management of delirium in critical illness.Current Drug Therapy.2008,3:148–157.
- VIDAL‐l'information sur les produits de santé2008, Issy les Moulineaux Cedex. Available at: www.vidal.fr. Accessed February 2010.
- Haldol iniettabile—ufficiale monografia italiana. Available at: www. informatorefarmaceutico.it. Accessed February 2010.
- Arzneimittelkompendium der Schweiz2008, documed Verlag Basel. Availabla at: www.kompendium.ch. Accessed February 2010.
- ,,, et al.Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill, American College of Critical Care Medicine ACCM, Society of Critical Care Medicine SCCM, American Society of Health‐System Pharmacists ASHP.Crit Care Med.2002;30(1):119–141.
- ,,,,.Is telemetry overused? Is it as helpful as thought?Cleve Clin J Med.2009;76(6):368–372.
- ,,.Telemetry outside critical care units: patterns of utilization and influence on management decisions.Clin Cardiol.1998;21(7):503–505.
- ,,.High‐dose intravenous haloperidol for agitated delirium in a cardiac patient on intra‐aortic balloon pump.J Clin Psychopharmacol.1991;11(2):146–147.
- .Haloperidol, midazolam and intravenous sedation.Aust NZ J Psychiatry.1999;33(6):942–943.
- BNF British National Formulary, compendium of pharmaceuticals and specialties of the UK.2007. Available at: www.bnf.org. Accessed February 2010.
- ,,,.Torsade de pointes associated with the use of intravenous haloperidol.Ann Intern Med.1993;119(5):391–394.
- ,.Torsades de pointes: potential consequence of intravenous haloperidol in the intensive care unit.Intensive Care World.1994;11(3):109–112.
- ,.Torsade de pointes caused by high‐dose intravenous haloperidol in cardiac patients.Clin Cardiol.1995;18:285–290.
- ,,.Continuous infusion of haloperidol controls agitation in critically ill patients.Crit Care Med.1994:22(3):433–440.
- ,,.Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalances.Am J Gastroenterol.1995;90(5):822–824.
- ,,,.Torsades de pointes associated with intravenous haloperidol in critically ill patients.Am J Cardiol.1998;81(2):238–240.
- ,,,,.The effect of intravenous haloperidol on QT interval dispersion in critically ill patients: comparison with QT interval prolongation for assessment of risk of torsades de pointes.J Clin Pharmacol.2001;41:1310–1318.
- ,,.Low‐dose haloperidol associated QTc prolongation.J Am Geriatr Soc.2008;56(10):1963–1964.
- ,,.Torsade de pointes following intravenous haloperidol administration in a patient with complete heart block.WMJ.2009;108(1):48–50.
Haloperidol is Food and Drug Administration (FDA)‐approved in the United States for the management of acute and chronic psychotic disorders and widely used in the management of delirium‐associated agitation in hospitalized patients.1 Delirium in the hospital is an acute confusional state that frequently arises from multiple complex factors and may affect up to 30% of hospitalized patients.2 Although the first step in the management of delirium involves identification and treatment of underlying causes and offering supportive behavioral care; medications may be needed to control severe agitation.2 Low dose intravenous (IV) haloperidol (ie, 0.250.5 mg every 4 hours) is a commonly used medication in this setting as recommended by expert‐groups including the Cochrane Collaboration and the American Psychiatric Association.2, 3
Although injectable haloperidol, a butyrophenone‐derived antipsychotic agent pharmacologically related to the piperazine phenothiazines,4 is approved for IV use in many countries (Table 1), parenteral use is approved only for intramuscular (IM) administration in the US. Thus, IV administration of the drug in the US is considered an off‐label use.5
| Indication | Country | |||||
|---|---|---|---|---|---|---|
| Canada24 | France29 | Germany25 | Great Britain37 | Italy30 | Switzerland31 | |
| ||||||
| Mainly delirium (schizophrenia, other psychosis, short‐term management of psychomotor agitation, excitement, violent or dangerously impulsive behavior, vomiting, hiccup) | Short term treatment of agitation and aggressiveness during an acute or chronic psychotic episode, vomiting along with antimitotic post‐radiotherapy treatment | Acute and chronic schizophrenia, psycho‐motorical agitation of psychotic genesis | Schizophrenia, other psychosis, short‐term adjunctive management if psychomotor agitation, violent or dangerous impulsive behavior | Resistant forms of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis' chronic psychosis High doses restrictions: syndrome of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis, chronic psychosis | Acute schizophrenic episode, mania, vomiting | |
| IV dosing in adults | 12 mg every 24 hours | The use is limited to adult patients and the drug can be administered IM or IV. The IV route is restricted to the treatment of vomiting. | 510 mg/day, daily max.: 30(100) mg | 210 mg initially, PRN every 48 hours, daily max. 18 mg | 510 mg initially, PRN every hour, daily max. 60 mg | 5 mg PRN every 30 minutes |
| IV dosing in geriatric care | 0.250.5 mg | Single dose of 0.51.5 mg, daily max. 5 mg | Half adult dose | Adjust to appropriate dose | 0.5 mg, than PRN | |
| Risk factors for the development of cardiac adverse events | QT prolonging drugs, diabetes, obesity, hypokalemia, congenital long QT syndrome | Bradycardia 55 beats per minute, hypokalemia, congenital QT prolongation, other medications provoking bradycardia, deceleration of the intra‐cardiac transition or prolonged QT interval | QT syndrome, hypokalemia, other electrolyte imbalance, cardiovascular diseases, QT prolongation in the family history | Cardiovalscular disease, drugs that can prolong the QTc, diabetes, obesity, hypokalemia, congenital long QT syndrome | Contraindications: recent cardiac infarction, uncompensated cardiac insufficiency, cardiac arrhythmias, antiarrhythmic drugs, pre‐existing QT prolongation, cases of arrhythmia or torsades de pointes in the family history, untreated potassium imbalance, QTc prolonging drugs | QT syndrome, hypokalemia, hypomagnesemia, other electrolyte imbalances, cardiovascular diseases, hypothyreosis, QT prolongation in the family history |
| Monitoring recommendations | Electrolytes | ECG monitoring at admission time, electrolytes | ECG monitoring, electrolytes | Metabolic parameters | ECG at baseline and regular ECG monitoring, electrolytes | Close ECG monitoring, electrolytes |
| General recommendations | Regular reevaluation in long‐term use | Apply the lowest effective dose | Apply the lowest effective dose | Application per mouth is the route of choice | Decrease dose if QTc >500 msec | Switch to PO as soon as possible |
Haloperidol is often preferred over other antipsychotics as a result of its effectiveness, low rate of anticholinergic side effects, familiarity with dosing and usage, and minimal respiratory or sedative properties.6 Use of the IV route in patients with acute delirium has several advantages over the IM or oral route,7 including rapid onset, immediate bioavailability, and ease and safety of administration.
Prior to September 2007, the package insert for haloperidol alerted healthcare professionals to the risk of cardiovascular side effects. Based on case reports of potentially fatal cardiac events, the FDA revised the label, warning that the QT prolongation (QTP) and risk of torsades de pointes (TdP) were increased with IV administration of haloperidol or administration of the drug at greater than recommended doses. Unfortunately, neither the typical dosing range nor the minimum dose associated with these cardiac side effects were specified in this recommendation.5
It is well‐established that haloperidol may prolong the QT interval by blocking the repolarizing potassium IKr current.8 Although drugs that block the IKr channel can produce arrhythmia in healthy individuals, additional risk factors, such as underlying heart conditions, electrolyte imbalances (ie, hypokalemia and hypomagnesemia), concomitant proarrhythmic drug use, and mechanical ventilation may increase this risk.9 Prolongation of the QT interval has been associated with subsequent malignant cardiac arrhythmias including ventricular fibrillation and TdP.10 Prolongation of the QT interval is considered the strongest risk factor for TdP, particularly with a baseline QTc > 450 msec.9
Based on the increased risk for QTP and TdP and the case reports of cardiac events, the FDA advisory recommended continuous electrocardiogram (ECG) monitoring in patients receiving IV haloperidol.5 However, such monitoring may be impractical and costly in hospitalized patients who require low doses of IV haloperidol to manage acute delirium and who are not in telemetry or intensive care units.
The aim of this review was to evaluate the case reports leading to the recent FDA warning for IV haloperidol, specifically focusing on the presence of risk factors for arrhythmias. Based upon the evidence, an additional aim was to provide an institutional response to this warning toward the optimal use of this agent.
Method
Two search pathways were used to evaluate reports of haloperidol‐associated TdP and/or QT prolongation:
Literature Review
We searched for published literature in humans indexed in Pubmed (1966April 2009), EMBASE (1972April 2009), and Scopus (1823April 2009) using the search terms haloperidol or Haldol combined with intravenous or infusion and at least one of the following terms: QT prolongation, TdP, torsades de pointes, torsades with a specific focus on case reports.
References from the retrieved articles were also reviewed to search for additional case reports.
In addition to cases reported in English journals, several of our reports originated from Japan11 (translation provided by the FDA), Spain12 and Germany13 (translated by the primary author).
Search of the FDA Database
We reviewed all adverse drug events reported through MedWatch or those submitted by the manufacturer from November 1997 to April 2008 through the Freedom of Information Act (FOIA) request. The FDA provided a full‐text summary of 5944 reports involving oral, intramuscular and IV use of haloperidol. The FDA data were transferred to a Microsoft Access database and screened for the key terms torsade, QT, prolongation, wave. Incident report number, date of report, age, gender, origin of report, medication name, role of drug as categorized by the FDA (suspect, concomitant, primary suspect, secondary suspect), route, dose, units, duration, symptoms and FDA outcome category (death, life‐threatening, hospitalization initial or prolonged, disability, congenital anomaly, required intervention to prevent permanent damage, other) were recorded. Only those reports in which IV haloperidol was considered by the reporter to be the primary causative agent for the adverse event were reviewed. Available information included diagnosis, laboratory parameters, QTc measurement, cardiac symptoms, outcomes and a description of recovery. No peer review was applied to the MedWatch reports and the data reported in this publication reflect the original information from the FDA MedWatch database. Baseline QTc was either the value defined as such in the original report or the lowest QTc reported. Haloperidol doses administered were defined as cumulative dose at event, encompassing all doses administered during the hospital stay until the occurrence of the adverse cardiac event.
The drugs listed in the case reports were assessed for proarrhythmic potential using 2 references: the individual package insert and the website of the Arizona Center for Education and Research on Therapeutics.14
The drugs were only considered proarrhythmic when the 2 resources were in agreement.
Duplicates and/or previously published cases, as well as reports involving adverse cardiac effects not associated with QTP or TdP, were identified and excluded.
In their advisory, the FDA does not state the exact origin of the reports, their specific search strategy to identify haloperidol‐associated adverse events, or the role IV haloperidol played in the individual events included in the extended warning. Consequently, the number of events identified in this review may differ from that published in the FDA extended warning.
Results
A total of 70 reported cases of IV haloperidol associated TdP and/or QTP were identified. Of these 70, 41 were identified through the PubMed/EMBASE/Scopus review, while an additional 29 cases were identified through the FDA database search.
Of the 29 cases in the FDA database, 21 were reported by health care professionals and 8 by manufacturers.
A total of 35 publications described cases originating from the US. Three cases took place in Japan and 1 case each in Canada, Germany and Spain. Several cases in the MedWatch database were reported outside the US: 1 case each originated from Austria, Canada, France, Japan, Spain, Switzerland and the United Kingdom. A summary of the published case reports is displayed in Table 2 and the FDA cases are summarized in Table 3.
| Case | Source (reference#) | Date | Age, Years | Gender | Drugs Pro‐arrhyth. | Venti‐ lated | Max. Daily Dose (mg) | Total Dose at Event (mg) | Time to Event | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | ECG Normalization, Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
| 1 | 35 | 1991 | 56 | m | No | Yes | 1200 | 1540 | NR | Yes | 584 (400) | 184 | NR | NR, uneventful |
| 2 | 13 | 1992 | 36 | m | Yes | No | 11.5 | 11.5 | 20 hours after start | Yes | 714 (428) | 286 | Yes | QTc normalization (440 msec), NR |
| 3 | 38 | 1993 | 39 | f | Yes | Yes | NR | 580 | Max. QTc 72 hours after start | Yes | 650 (420) | 230 | Yes | QTc normalization after 6 days, uneventful |
| 4 | 38 | 1993 | 19 | f | Yes | No | 170 | 170 | Max. QT 12 hours after start | Yes | 600 (480) | 120 | Yes | QTc normalization after 8 days, uneventful |
| 5 | 38 | 1993 | 63 | f | Yes | No | NR | 489 | Max. QT 48 hours after start | Yes | 670 (520) | 150 | Yes | QTc normalization after 8 days, uneventful |
| 6 | 38 | 1993 | 74 | f | Yes | Yes | NR | 10 | NR | No | 430 (410) | 20 | Yes | QTc unchanged after 8 days, uneventful |
| 7 | 17 | 1993 | 39 | m | Yes | Yes | NR | >490 | NR | Yes | 457 (348) | 109 | Yes | QTc normalization within 2 to 3 days, no further TdP, NR |
| 8 | 17 | 1993 | 61 | m | Yes | Yes | 115 | 211 | NR | Yes | 500 (390) | 110 | NR | QTc normalization within 2 days, death |
| 9 | 17 | 1993 | 48 | m | Yes | Yes | 825 | 825 | NR | Yes | 538 (441) | 97 | NR | QTc normalization in 3 days, rehabilitation |
| 10 | 39 | 1994 | 23 | f | Yes | Yes | 120 | 300 | 12 hours after dose increase | Yes | NR (550) | NR | Yes | NR, uneventful, extubation after 5 days, discharge after 10 days |
| 11 | 39 | 1994 | 28 | m | Yes | Yes | 300 | >300 | 24 hours after dose increase | Yes | NR (>520) | NR | Yes | No recurrence of arrhythmia, patient death (multi‐organ failure) |
| 12 | 40 | 1994 | 65 | m | Yes | NR | 230 | 410 | Worsening from day 2 to day 5 | Yes | 594 (490) | 104 | Yes | QTc normalization (406 msec), no cardiac problems at discharge |
| 13 | 40 | 1994 | 65 | f | Yes | NR | 500 | 980 | After the last 60mg | Yes | 628 (403) | 225 | Yes | QTc normalization (400 msec), recurrence with oral haloperidol, rehabilitation |
| 14 | 40 | 1994 | 76 | f | Yes | NR | 21 | 26 | Day 2 after several boluses | Yes | 670 (450) | 220 | Yes | QTc normalization within several days (412 msec), rehabilitation |
| 15 | 41 | 1994 | 59 | m | NR | Yes | 865 | 1013 | NR | Yes | 640 (480) | 160 | NR | QTc normalization in 24 hours, survived |
| 16 | 16 | 1995 | 76 | f | Yes | No | NR | 44.5 plus 1 PO | 15 minutes | Yes | 670 (409) | 261 | Yes | ECG normalized the next morning, no further events |
| 17 | 16 | 1995 | 49 | m | Yes | No | NR | 1150 plus 20 IM | 45 minutes | Yes | 648 (380) | 268 | Yes | QTc normalization in 24 hours, anoxic brain insult/rehabilitation |
| 18 | 16 | 1995 | 65 | f | Yes | No | 600 | 965 | 30 minutes | Yes | 628 (403) | 225 | Yes | 3 more episodes of TdP in 3 hours, QTc normalization in 2 days, no recurrence with further haloperidol, NR |
| 19 | 42 | 1995 | 42 | m | Yes | No | 28 | 28 | 20 minutes | Yes | 610 (533) | 77 | Yes | QTc normalization in 5 days, uneventful, ECG normal |
| 20 | 42 | 1995 | 39 | m | Yes | No | 45 | 45 | 5 minutes | Yes | 654 (NR) | NR | Yes | QTc normalization after 24 hours, uneventful |
| 21 | 11 | 1997 | 56 | f | No | No | 10 | 10 | Shortly after | NR | NR (NR) | NR | Yes | TdP resolved after 8 hours, NR |
| 22 | 11 | 1997 | 82 | f | NR | No | 10 | 10 | Shortly after | Yes | 680 (NR) | NR | Yes | QTc normalization on day 6 after admission (470 msec), NR |
| 23 | 11 | 1997 | 35 | m | NR | No | NR | 90 | After 20 mg | Yes | 520 (NR) | NR | Yes | TdP disappeared 12 hours later, NR |
| 24 | 43,44 | 1998 | 45 | m | NR | Yes* | NR | 9 | 203 minutes | Yes | 638 (560) | 78 | Yes | NR, overall survival 100%, significantly prolonged hospital stay |
| 25 | 43,44 | 1998 | 64 | f | NR | NR | 115 | 220 minutes | Yes | 605 (424) | 181 | Yes | ||
| 26 | 43,44 | 1998 | 75 | f | NR | NR | 85 | 60 minutes | Yes | 567 (508) | 59 | Yes | ||
| 27 | 43,44 | 1998 | 71 | f | NR | NR | 55 | 120 minutes | Paced | Paced | Paced | Yes | ||
| 28 | 43,44 | 1998 | 58 | f | NR | NR | 75 | 38 minutes | Yes | 657 (542) | 115 | Yes | ||
| 29 | 43,44 | 1998 | 40 | m | NR | NR | 35 | 15 minutes | Yes | 679 (475) | 204 | Yes | ||
| 30 | 43,44 | 1998 | 71 | m | NR | NR | 70 | 58 minutes | Yes | 521 (478) | 43 | Yes | ||
| 31 | 43,44 | 1998 | 47 | m | NR | 400 | 400 | 79 minutes | Yes | 574 (444) | 130 | Yes | ||
| 32 | 21 | 1999 | 41 | f | Yes | Yes | 320 | 915 | 55 minutes | Yes | 610 (426) | 184 | Yes | QTc normalization after 5 day, uneventful |
| 33 | 21 | 1999 | 31 | m | Yes | Yes | 480 | 1700 | 40 minutes | Yes | 599 (491) | 108 | Yes | QTc normalized in 4 days, NR |
| 34 | 18 | 2000 | 64 | f | Yes | Yes | 175 | 175 | NR | No | 413 (418) | (‐5) | Yes | QTc remained unchanged, uneventful |
| 35 | 8 | 2000 | 75 | m | No | NR | >2 | >2 | NR | Yes | 615 (435) | 180 | No | QTc normalization in 48 hours, uneventful |
| 36 | 8 | 2000 | 68 | m | Yes | Yes | >2 | >2 | NR | Yes | 650 (407) | 243 | No | QTc normalization after 4 day, uneventful after extubation |
| 37 | 8 | 2000 | 77 | m | NR | NR | (4) | 2 | NR | Yes | 550 (393) | 157 | No | QTc normalization in 24 to 36 hours, NR |
| 38 | 12 | 2004 | 34 | m | Yes | NR | 24.5 | 24.5 | 20 minutes | Yes | 560 (420) | 140 | Yes | QTc normalization (440 msec), ECG normal |
| 39 | 23 | 2004 | 58 | f | Yes | NR | 340 | 1010 | NR | Yes | 533 (460) | 73 | Yes | QTc normalization 7 days later discharge after 27days |
| 40 | 45 | 2008 | 86 | f | Yes | No | 2 mg | 2 mg | 8 hours after last dose | Yes | 524 (NR) | Probably 79 | No | QTc normalization (445 msec), NR |
| 41 | 46 | 2009 | 74 | m | Yes | No | 2 | 2 | Shortly after | Yes | NR (579) | NR | Yes | Pre‐existing heart block and fibrillation resolved, nursing home/rehabilitation |
| Report | MedWatch Identifier | Report Date | Age, Years | Gender | Drugs Pro‐arrh. | Maximum Daily Dose (mg) | Total Dose at Event (mg) | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | Outcome; Recovery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
| 1 | 3122988‐1 | 1998 | 61 | m | No | 48 | 48 | Yes | NR | NR | Yes | Intervention; NR |
| 2 | 3157827‐6 | 1998 | 44 | f | No | 160 | 160 | Yes | 550 (440) | 110 | Yes | Intervention; uneventful |
| 3 | 3178715‐5 | 1999 | 60 | m | NR | 415 | 645 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization in 1 day, no recurrence |
| 4 | 3271261‐X | 1999 | 56 | m | NR | NR | 20 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization |
| 5 | 3271080‐4 | 1999 | 35 | m | Yes | 7 | 7 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced, hospitalization prolonged |
| 6 | 3325391‐4 | 1999 | 55 | f | Yes | 75 | 75 | NR | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 7 | 3381921‐8 | 1999 | 52 | m | No | 320 | 634 | Yes | 458 (430) | 28 | Yes | Death; NA |
| 8 | 3483869‐7 | 2000 | 18 | m | No | >200 | >310 | Yes | NR | NR | Yes | Intervention; no recurrence after haloperidol reinstitution |
| 9 | 3516342‐8 | 2000 | NR | NR | NR | NR | NR | NR | NR | NR | Yes | NR; NR |
| 10 | 3516320‐9 | 2000 | 34 | m | Yes | 5 | 5 | Yes | NR | NR | No | Life‐threatening; event abated after dose stopped |
| 11 | 3552263‐2 | 2000 | 46 | f | Yes | NR | 97.5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 12 | 3574705‐9 | 2000 | 78 | m | Yes | NR | 160 | Yes | 603 (453) | 50 | Yes | Intervention; event abated after dose stopped/reduced |
| 13 | 3703871‐7 | 2001 | 27 | m | NR | 530 | 530 | Yes | NR | NR | Yes | Death, NA |
| 14 | 3724567‐1 | 2001 | 31 | m | Yes | 6 | 6 | Yes | 496 (449) | 47 | No | Life‐threatening; ECG returned to baseline |
| 15 | 3851984‐1 | 2002 | 72 | f | NR | 18 | 18 | NR | NR | NR | Yes | Hospitalization; NR |
| 16 | 3942407‐2 | 2002 | 51 | m | Yes | 14 | 14 | Yes | 461 (444) | 17 | Yes | Life‐threatening; no recurrence |
| 17 | 4066580‐3 | 2003 | >60 | f | NR | 50 | 50 | Yes | >600 (480) | >120 | No | Hospitalization; QTc normalization, patient recovered |
| 18 | 4126280‐8 | 2003 | 47 | f | NR | 60 | 180 | Yes | 550 (450) | 100 | No (bradycardia) | Hospitalization; patient recovered |
| 19 | 4150700‐6 | 2003 | NR | m | NR | 5 | 5 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced |
| 20 | 4340092‐1 | 2004 | 52 | m | Yes | 5 | 5 | Yes | >500 (490) | >10 | NR (polymorphous VT) | Life‐threatening; NR |
| 21 | 4714692‐0 | 2005 | NR | m | NR | NR | NR | Yes | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 22 | 4881813‐9 | 2006 | NR | m | NR | NR | 40 | NR | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 23 | 4892225‐6 | 2006 | NR | f | Yes | 10 | >10 | Yes | 493 (300) | 193 | No | Hospitalization; QTc normalization (403 msec) |
| 24 | 4911873‐8 | 2006 | 69 | m | Yes | 6 | 6 | NR | NR | NR | Yes | Cardiac arrest, death; NA |
| 25 | 5366448‐6 | 2007 | 53 | m | Yes | NR | 35 | Yes | NR | NR | NR | Cardiac arrest, life‐threatening; patient recovered |
| 26 | 5563440‐3 | 2007 | 58 | m | Possible | 5 | 5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 27 | 5642929‐2 | 2008 | 42 | m | Yes | 165 | 165 | Yes | 640 (350) | 290 | Yes | Death; NA |
| 28 | 5697758‐0 | 2008 | 38 | m | Yes | NR | 620 | NR | NR | NR | Yes | Hospitalization; patient recovered |
| 29 | 5254840‐X | 2008 | 19 | f | Possible | 15 | 25 | Yes | 461 | NR | NR | Cardiac arrest, hospitalization; patient recovered |
Of the 70 cases, 54 cases of TdP were reported. The remaining 16 of 70 cases involved cases of QTP, 9 of which did not progress to TdP and 7 of which the progression to TdP was unclear. Of note, 42 of 54 of the cases of TdP were reported as preceded by documented QTP. Presence of QTP was unknown in the other 12 original reports. Three out of 70 patients experienced sudden cardiac arrest, 1 of which was fatal. One arrest was preceded by TdP and 2 by QTP (Figure 1).
The patient ages ranged from 18 years to 86 years. Of note, 17 patients experiencing TdP and/or QTP were 40 years old, and 2 of those patients were 30 years old.
Haloperidol‐associated QTP and/or TdP were observed in 27 female and 42 male patients; the gender was not stated in one report. Of the 54 patients experiencing TdP (with or without report of previous QTP), 22 were female and 31 were male (1 gender unknown).
A total of 68 of 70 patients were determined to have associated risk factors15 for QTP/TdP (see Table 4). The circumstances of the remaining 2 patients were not described in sufficient detail to identify associated risk factors.
| Risk Factor | Patients, n (%) |
|---|---|
| |
| Any risk factor | 68/70 (97) |
| Unknown | 2/70 (3) |
| Specific risk factors | |
| Electrolyte imbalance | 27/68 (40) |
| Underlying cardiac disease | 32/68 (47) |
| Concomitant proarrhythmic agents | 39/68 (57) |
| Other drugs influencing cardiac function | 23/68 (34) |
| Baseline QTc >450 msec | 18/68 (26) |
| QTc known: 44 patients | 18/44 (41) |
Overall, 32 patients had underlying heart conditions. Electrolyte imbalances, including hypokalemia, hypomagnesemia, and hypocalcemia, were present in 17 patients. At least 39 patients were receiving potentially proarrhythmic agents (1‐8 proarrhythmic drugs per patient) in addition to IV haloperidol. At least 23 patients were receiving additional drugs with a potential for other cardiac adverse events than QTP and TdP.
A wide range of other disease states previously reported to be associated with QTP15 were identified in these patients: asthma (5 patients), diabetes (5 patients), obesity (3 patients), impaired renal and/or liver function (3 patients each), human immunodeficiency virus (HIV) (2 patients); chronic obstructive pulmonary disease (COPD), pancreatitis and hypothyroidism (1 patient each). A total of 22 patients had a history of substance abuse (alcohol and/or drugs), and 4 patients were smokers.
The administered doses of IV haloperidol varied widely. Considering that information regarding the maximal daily dose was missing in 22 reports and ambiguous in another 20 cases, the results have been presented using cumulative IV haloperidol doses. Patients experiencing TdP without preceding QTP received a cumulative dose (= total dose at event) ranging from 5 mg to 645 mg. Patients with both confirmed QTP and TdP were administered a cumulative dose of 2 mg to 1700 mg. Patients who experienced QTP without TdP received a cumulative dose of 2 mg to 1540 mg of IV haloperidol.
Sudden cardiac arrest following administration of IV haloperidol was observed in cumulative doses ranging from 6 mg to 35 mg. The cardiac arrest leading to a fatal outcome was preceded by an administration of at least 6 mg of IV haloperidol. Overall, 14 out of 70 patients received cumulative doses of 10 mg IV haloperidol.
The time from administration to documentation of QTP and/or TdP ranged from immediately post administration to 8 hours after administration of the last dose of IV haloperidol.
Baseline QTc was known in 44 patients. Baseline QTc was >450 msec in 18 of these 44 patients.
The change from baseline QTc varied widely from 20 msec to 286 msec; 36 patients demonstrated a prolongation of >50 msec.
In those patients with reported haloperidol‐associated QTP, 25 patients demonstrated a QTc >600 msec and 38 patients >520 msec.9 Of the cases with known specific QTc values, the QTc was prolonged >450 msec in 48 out of 50 cases. The lowest reported QTc leading to TdP was 413 msec.
A total of 20 patients were reported as having a normalization of QTc (as defined by the original reports) within several hours to 8 days; minimal QTP was reported as persisting in 2 patients. The specifics of the other patients were unknown, although 25 patients were categorized as recovered, 13 were stated as having an uneventful remainder of hospitalization, and 5 patients were discharged to a rehabilitation facility or a nursing home.
Discussion
The current review was performed in response to the FDA warning recommending the use of continuous ECG monitoring associated with the administration of intravenous haloperiodol.5 This warning has resulted in substantial dilemmas for health care organizations, additional resource allocation, and increased scrutiny from regulatory agencies. The results of our review reveal that intravenous haloperidol‐associated QTP and TdP almost uniformly take place in patients with concomitant risk factors and with cumulative doses 2 mg. In light of these findings, it is possible that hospitals may be able to administer intravenous haloperidol in patients without risk factors without continuous ECG monitoring. In reviewing these published reports, it is important to note that the FDA identified 28 published cases of haloperidol‐associated QTP and TdP, while our review yielded a total of 41 published case reports.
The FDA database included 73 cases of haloperidol‐associated TdP in their database. However, these cases included both oral as well as IV administration; using our methodology, we identified 29 additional case reports associated with intravenous haloperidol from this database. Consequently, our review included 41 published case reports and 29 FDA database cases, resulting in the total of 70 patients.
Our review revealed a number of practical findings. First, our summary demonstrated that neither QTP nor TdP has been documented with a cumulative dose of IV haloperidol of 2 mg. The majority of patients (80%) received cumulative IV doses 10 mg. The lowest dose associated with sudden cardiac arrest was 6 mg and this took place in a 69‐year‐old male patient. Second, the majority (97%) of our patients had additional risk factors for QTP and/or TdP. Pre‐existing heart disease,1619 electrolyte imbalance,17, 1921 concomitant proarrhythmic drugs16, 17, 1922 and mechanical ventilation17, 23 were identified as the most commonly observed risk factors (Table 4). Lastly, in those cases in which the data were reported, baseline QTc was >450 msec in 41% of the patients, and 96% had a QTc at the time of the event >450 msec. Therefore, we conclude that patients: (1) receiving low cumulative doses (2 mg) with (2) no risk factors for prolonged QTc or TdP, and (3) with a normal QTc on baseline EKG can safely be given IV haloperidol in the hospital setting.
This dosage range is consistent with the labelling for IV haloperidol dosing in Canada24 and Germany25 (Table 1), where single doses of 0.25 mg to 1.5 mg are recommended for the treatment of delirium or acute agitation in the geriatric population.24, 25
In a recent Cochrane review, low‐dose IV haloperidol (3 mg per day) was concluded to be as safe and effective as atypical antipsychotics in the treatment of acute delirium with respect to extrapyramidal adverse effects.2
The American Psychiatric Association recommends an initial IV dose of 12 mg every 24 hours as needed (0.250.50 mg every 4 hours as needed for elderly patients), with titration to higher doses for patients who continue to be agitated for the treatment of patients with delirium (issued 1999, updated 2004).3
While several expert‐groups and investigators currently consider IV haloperidol as an important therapeutic option for treating acute delirium and agitation in the dose range presented above, less consensus exists regarding monitoring requirements.2, 3, 26, 27
The American Psychiatric Association recommends IV haloperidol only after a baseline ECG is obtained. These guidelines have not been updated since the release of the FDA extended warning.3 In their recent review, Morandi et al.28 support the dosage recommendation of the 1999 American Psychiatric Association's practice guidelines for treatment of delirium,3 ie, administration of IV haloperidol in single doses of 0.5 mg to 2 mg in elderly patients, however, only after a baseline ECG is obtained.28 While the package insert of IV haloperidol in France29 recommends a baseline ECG, Germany,25 Italy30 and Switzerland's31 package information states the need for regular ECG monitoring. Guidelines for the treatment of delirium in the intensive care unit published by the American College of Critical Care Medicine and the Society of Critical Care Medicine in collaboration with the American Society of Health‐System Pharmacists consider IV haloperidol as the preferred agent for the treatment of delirium in critically ill patients (grade of recommendation = C). These expert groups recommend that patients should be monitored for electrocardiographic changes (QT interval prolongation and arrhythmias) when receiving haloperidol (Grade of recommendation = B).32
Nevertheless, continuous ECG monitoring (ie, telemetry) is expensive, labor‐intensive and, potentially overutilized.33, 34 Requiring clinicians to place all patients receiving intravenous haloperidol on telemetry is impractical and potentially costly. Mandating telemetry could also lead to unintended harm, ie, use of a less effective or less safe drug to avoid compliance with the telemetry mandate.
Based on our findings and the current recommendations in the literature, inpatient providers should be thoughtful and deliberate in the use of haloperidol to treat acute delirium with agitation. Patients requiring pharmacologic management of their delirium should be screened for risk factors for QTP and TdP (Table 4) and a baseline ECG should be obtained prior to haloperidol administration. If significant risk factors exist or the baseline ECG reveals a prolonged QTc, then the patient should receive continuous ECG monitoring. Similarly, if cumulative doses of 2 mg are needed, the patient should be placed on telemetry.
There are some limitations to our study design. Our findings are based upon previously published case reports or data submitted to the FDA MedWatch. While the content of the FDA's MedWatch database is accessible to the public via the Freedom of Information Act (FOIA), the events are neither categorized nor peer‐reviewed upon entry into the database. Consequently, information may be incomplete or inaccurate. In addition, the denominator representing the overall use of IV haloperidol is unknown, thus a rate of event cannot be assigned and the true scope of the problem cannot be determined. Despite these limitations, this summary represents the most comprehensive review of the literature to date, expanding on the analysis performed by the FDA. Of note, in our review of the FDA database, we noted several cases of haloperidol‐associated QTP or TdP associated with other routes of administration. Thus, it is unknown whether this complication is any greater with IV vs. the IM or per os (PO) routes of administration.
Conclusion
Although the proarrhythmic potential of haloperidol and other antipsychotics has been well established in the literature, IV haloperidol has been considered relatively safe with respect to this complication from the time of its approval in 1967.5, 1722, 35, 36 In reviewing all reported cases of cardiac complications associated with IV haloperidol, as well as the current literature, an association with QTP and TdP is likely. However, the case reports reveal that QTP and TdP generally occur in the setting of concomitant risk factors, and no cases have been reported utilizing a cumulative IV dose of 2 mg. It may therefore be safe to administer a cumulative dose of IV haloperidol of 2 mg without ECG monitoring in patients without risk factors for QTP. However, ECG monitoring should take place with IV haloperidol doses 2 mg and/or in those patients with additional risk factors of developing QTP and/or TdP.
Based on the findings of this review complemented by the guidelines of various expert‐groups and the official labelling information of different countries, the Pharmacy & Therapeutics Committee of the UCSF Medical Center revised the IV haloperidol policy: administration of a total dose of 2 mg IV haloperidol without concurrent telemetry is allowed in a noncritical care setting in patients without risk factors for QTP and TdP.
Acknowledgements
The authors acknowledge Gloria Won of the Fishbon Library at UCSF Medical Center at Mount Zion for her support.
Haloperidol is Food and Drug Administration (FDA)‐approved in the United States for the management of acute and chronic psychotic disorders and widely used in the management of delirium‐associated agitation in hospitalized patients.1 Delirium in the hospital is an acute confusional state that frequently arises from multiple complex factors and may affect up to 30% of hospitalized patients.2 Although the first step in the management of delirium involves identification and treatment of underlying causes and offering supportive behavioral care; medications may be needed to control severe agitation.2 Low dose intravenous (IV) haloperidol (ie, 0.250.5 mg every 4 hours) is a commonly used medication in this setting as recommended by expert‐groups including the Cochrane Collaboration and the American Psychiatric Association.2, 3
Although injectable haloperidol, a butyrophenone‐derived antipsychotic agent pharmacologically related to the piperazine phenothiazines,4 is approved for IV use in many countries (Table 1), parenteral use is approved only for intramuscular (IM) administration in the US. Thus, IV administration of the drug in the US is considered an off‐label use.5
| Indication | Country | |||||
|---|---|---|---|---|---|---|
| Canada24 | France29 | Germany25 | Great Britain37 | Italy30 | Switzerland31 | |
| ||||||
| Mainly delirium (schizophrenia, other psychosis, short‐term management of psychomotor agitation, excitement, violent or dangerously impulsive behavior, vomiting, hiccup) | Short term treatment of agitation and aggressiveness during an acute or chronic psychotic episode, vomiting along with antimitotic post‐radiotherapy treatment | Acute and chronic schizophrenia, psycho‐motorical agitation of psychotic genesis | Schizophrenia, other psychosis, short‐term adjunctive management if psychomotor agitation, violent or dangerous impulsive behavior | Resistant forms of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis' chronic psychosis High doses restrictions: syndrome of psycho‐motorical excitement, acute delirious and/or hallucinatory psychosis, chronic psychosis | Acute schizophrenic episode, mania, vomiting | |
| IV dosing in adults | 12 mg every 24 hours | The use is limited to adult patients and the drug can be administered IM or IV. The IV route is restricted to the treatment of vomiting. | 510 mg/day, daily max.: 30(100) mg | 210 mg initially, PRN every 48 hours, daily max. 18 mg | 510 mg initially, PRN every hour, daily max. 60 mg | 5 mg PRN every 30 minutes |
| IV dosing in geriatric care | 0.250.5 mg | Single dose of 0.51.5 mg, daily max. 5 mg | Half adult dose | Adjust to appropriate dose | 0.5 mg, than PRN | |
| Risk factors for the development of cardiac adverse events | QT prolonging drugs, diabetes, obesity, hypokalemia, congenital long QT syndrome | Bradycardia 55 beats per minute, hypokalemia, congenital QT prolongation, other medications provoking bradycardia, deceleration of the intra‐cardiac transition or prolonged QT interval | QT syndrome, hypokalemia, other electrolyte imbalance, cardiovascular diseases, QT prolongation in the family history | Cardiovalscular disease, drugs that can prolong the QTc, diabetes, obesity, hypokalemia, congenital long QT syndrome | Contraindications: recent cardiac infarction, uncompensated cardiac insufficiency, cardiac arrhythmias, antiarrhythmic drugs, pre‐existing QT prolongation, cases of arrhythmia or torsades de pointes in the family history, untreated potassium imbalance, QTc prolonging drugs | QT syndrome, hypokalemia, hypomagnesemia, other electrolyte imbalances, cardiovascular diseases, hypothyreosis, QT prolongation in the family history |
| Monitoring recommendations | Electrolytes | ECG monitoring at admission time, electrolytes | ECG monitoring, electrolytes | Metabolic parameters | ECG at baseline and regular ECG monitoring, electrolytes | Close ECG monitoring, electrolytes |
| General recommendations | Regular reevaluation in long‐term use | Apply the lowest effective dose | Apply the lowest effective dose | Application per mouth is the route of choice | Decrease dose if QTc >500 msec | Switch to PO as soon as possible |
Haloperidol is often preferred over other antipsychotics as a result of its effectiveness, low rate of anticholinergic side effects, familiarity with dosing and usage, and minimal respiratory or sedative properties.6 Use of the IV route in patients with acute delirium has several advantages over the IM or oral route,7 including rapid onset, immediate bioavailability, and ease and safety of administration.
Prior to September 2007, the package insert for haloperidol alerted healthcare professionals to the risk of cardiovascular side effects. Based on case reports of potentially fatal cardiac events, the FDA revised the label, warning that the QT prolongation (QTP) and risk of torsades de pointes (TdP) were increased with IV administration of haloperidol or administration of the drug at greater than recommended doses. Unfortunately, neither the typical dosing range nor the minimum dose associated with these cardiac side effects were specified in this recommendation.5
It is well‐established that haloperidol may prolong the QT interval by blocking the repolarizing potassium IKr current.8 Although drugs that block the IKr channel can produce arrhythmia in healthy individuals, additional risk factors, such as underlying heart conditions, electrolyte imbalances (ie, hypokalemia and hypomagnesemia), concomitant proarrhythmic drug use, and mechanical ventilation may increase this risk.9 Prolongation of the QT interval has been associated with subsequent malignant cardiac arrhythmias including ventricular fibrillation and TdP.10 Prolongation of the QT interval is considered the strongest risk factor for TdP, particularly with a baseline QTc > 450 msec.9
Based on the increased risk for QTP and TdP and the case reports of cardiac events, the FDA advisory recommended continuous electrocardiogram (ECG) monitoring in patients receiving IV haloperidol.5 However, such monitoring may be impractical and costly in hospitalized patients who require low doses of IV haloperidol to manage acute delirium and who are not in telemetry or intensive care units.
The aim of this review was to evaluate the case reports leading to the recent FDA warning for IV haloperidol, specifically focusing on the presence of risk factors for arrhythmias. Based upon the evidence, an additional aim was to provide an institutional response to this warning toward the optimal use of this agent.
Method
Two search pathways were used to evaluate reports of haloperidol‐associated TdP and/or QT prolongation:
Literature Review
We searched for published literature in humans indexed in Pubmed (1966April 2009), EMBASE (1972April 2009), and Scopus (1823April 2009) using the search terms haloperidol or Haldol combined with intravenous or infusion and at least one of the following terms: QT prolongation, TdP, torsades de pointes, torsades with a specific focus on case reports.
References from the retrieved articles were also reviewed to search for additional case reports.
In addition to cases reported in English journals, several of our reports originated from Japan11 (translation provided by the FDA), Spain12 and Germany13 (translated by the primary author).
Search of the FDA Database
We reviewed all adverse drug events reported through MedWatch or those submitted by the manufacturer from November 1997 to April 2008 through the Freedom of Information Act (FOIA) request. The FDA provided a full‐text summary of 5944 reports involving oral, intramuscular and IV use of haloperidol. The FDA data were transferred to a Microsoft Access database and screened for the key terms torsade, QT, prolongation, wave. Incident report number, date of report, age, gender, origin of report, medication name, role of drug as categorized by the FDA (suspect, concomitant, primary suspect, secondary suspect), route, dose, units, duration, symptoms and FDA outcome category (death, life‐threatening, hospitalization initial or prolonged, disability, congenital anomaly, required intervention to prevent permanent damage, other) were recorded. Only those reports in which IV haloperidol was considered by the reporter to be the primary causative agent for the adverse event were reviewed. Available information included diagnosis, laboratory parameters, QTc measurement, cardiac symptoms, outcomes and a description of recovery. No peer review was applied to the MedWatch reports and the data reported in this publication reflect the original information from the FDA MedWatch database. Baseline QTc was either the value defined as such in the original report or the lowest QTc reported. Haloperidol doses administered were defined as cumulative dose at event, encompassing all doses administered during the hospital stay until the occurrence of the adverse cardiac event.
The drugs listed in the case reports were assessed for proarrhythmic potential using 2 references: the individual package insert and the website of the Arizona Center for Education and Research on Therapeutics.14
The drugs were only considered proarrhythmic when the 2 resources were in agreement.
Duplicates and/or previously published cases, as well as reports involving adverse cardiac effects not associated with QTP or TdP, were identified and excluded.
In their advisory, the FDA does not state the exact origin of the reports, their specific search strategy to identify haloperidol‐associated adverse events, or the role IV haloperidol played in the individual events included in the extended warning. Consequently, the number of events identified in this review may differ from that published in the FDA extended warning.
Results
A total of 70 reported cases of IV haloperidol associated TdP and/or QTP were identified. Of these 70, 41 were identified through the PubMed/EMBASE/Scopus review, while an additional 29 cases were identified through the FDA database search.
Of the 29 cases in the FDA database, 21 were reported by health care professionals and 8 by manufacturers.
A total of 35 publications described cases originating from the US. Three cases took place in Japan and 1 case each in Canada, Germany and Spain. Several cases in the MedWatch database were reported outside the US: 1 case each originated from Austria, Canada, France, Japan, Spain, Switzerland and the United Kingdom. A summary of the published case reports is displayed in Table 2 and the FDA cases are summarized in Table 3.
| Case | Source (reference#) | Date | Age, Years | Gender | Drugs Pro‐arrhyth. | Venti‐ lated | Max. Daily Dose (mg) | Total Dose at Event (mg) | Time to Event | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | ECG Normalization, Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
| 1 | 35 | 1991 | 56 | m | No | Yes | 1200 | 1540 | NR | Yes | 584 (400) | 184 | NR | NR, uneventful |
| 2 | 13 | 1992 | 36 | m | Yes | No | 11.5 | 11.5 | 20 hours after start | Yes | 714 (428) | 286 | Yes | QTc normalization (440 msec), NR |
| 3 | 38 | 1993 | 39 | f | Yes | Yes | NR | 580 | Max. QTc 72 hours after start | Yes | 650 (420) | 230 | Yes | QTc normalization after 6 days, uneventful |
| 4 | 38 | 1993 | 19 | f | Yes | No | 170 | 170 | Max. QT 12 hours after start | Yes | 600 (480) | 120 | Yes | QTc normalization after 8 days, uneventful |
| 5 | 38 | 1993 | 63 | f | Yes | No | NR | 489 | Max. QT 48 hours after start | Yes | 670 (520) | 150 | Yes | QTc normalization after 8 days, uneventful |
| 6 | 38 | 1993 | 74 | f | Yes | Yes | NR | 10 | NR | No | 430 (410) | 20 | Yes | QTc unchanged after 8 days, uneventful |
| 7 | 17 | 1993 | 39 | m | Yes | Yes | NR | >490 | NR | Yes | 457 (348) | 109 | Yes | QTc normalization within 2 to 3 days, no further TdP, NR |
| 8 | 17 | 1993 | 61 | m | Yes | Yes | 115 | 211 | NR | Yes | 500 (390) | 110 | NR | QTc normalization within 2 days, death |
| 9 | 17 | 1993 | 48 | m | Yes | Yes | 825 | 825 | NR | Yes | 538 (441) | 97 | NR | QTc normalization in 3 days, rehabilitation |
| 10 | 39 | 1994 | 23 | f | Yes | Yes | 120 | 300 | 12 hours after dose increase | Yes | NR (550) | NR | Yes | NR, uneventful, extubation after 5 days, discharge after 10 days |
| 11 | 39 | 1994 | 28 | m | Yes | Yes | 300 | >300 | 24 hours after dose increase | Yes | NR (>520) | NR | Yes | No recurrence of arrhythmia, patient death (multi‐organ failure) |
| 12 | 40 | 1994 | 65 | m | Yes | NR | 230 | 410 | Worsening from day 2 to day 5 | Yes | 594 (490) | 104 | Yes | QTc normalization (406 msec), no cardiac problems at discharge |
| 13 | 40 | 1994 | 65 | f | Yes | NR | 500 | 980 | After the last 60mg | Yes | 628 (403) | 225 | Yes | QTc normalization (400 msec), recurrence with oral haloperidol, rehabilitation |
| 14 | 40 | 1994 | 76 | f | Yes | NR | 21 | 26 | Day 2 after several boluses | Yes | 670 (450) | 220 | Yes | QTc normalization within several days (412 msec), rehabilitation |
| 15 | 41 | 1994 | 59 | m | NR | Yes | 865 | 1013 | NR | Yes | 640 (480) | 160 | NR | QTc normalization in 24 hours, survived |
| 16 | 16 | 1995 | 76 | f | Yes | No | NR | 44.5 plus 1 PO | 15 minutes | Yes | 670 (409) | 261 | Yes | ECG normalized the next morning, no further events |
| 17 | 16 | 1995 | 49 | m | Yes | No | NR | 1150 plus 20 IM | 45 minutes | Yes | 648 (380) | 268 | Yes | QTc normalization in 24 hours, anoxic brain insult/rehabilitation |
| 18 | 16 | 1995 | 65 | f | Yes | No | 600 | 965 | 30 minutes | Yes | 628 (403) | 225 | Yes | 3 more episodes of TdP in 3 hours, QTc normalization in 2 days, no recurrence with further haloperidol, NR |
| 19 | 42 | 1995 | 42 | m | Yes | No | 28 | 28 | 20 minutes | Yes | 610 (533) | 77 | Yes | QTc normalization in 5 days, uneventful, ECG normal |
| 20 | 42 | 1995 | 39 | m | Yes | No | 45 | 45 | 5 minutes | Yes | 654 (NR) | NR | Yes | QTc normalization after 24 hours, uneventful |
| 21 | 11 | 1997 | 56 | f | No | No | 10 | 10 | Shortly after | NR | NR (NR) | NR | Yes | TdP resolved after 8 hours, NR |
| 22 | 11 | 1997 | 82 | f | NR | No | 10 | 10 | Shortly after | Yes | 680 (NR) | NR | Yes | QTc normalization on day 6 after admission (470 msec), NR |
| 23 | 11 | 1997 | 35 | m | NR | No | NR | 90 | After 20 mg | Yes | 520 (NR) | NR | Yes | TdP disappeared 12 hours later, NR |
| 24 | 43,44 | 1998 | 45 | m | NR | Yes* | NR | 9 | 203 minutes | Yes | 638 (560) | 78 | Yes | NR, overall survival 100%, significantly prolonged hospital stay |
| 25 | 43,44 | 1998 | 64 | f | NR | NR | 115 | 220 minutes | Yes | 605 (424) | 181 | Yes | ||
| 26 | 43,44 | 1998 | 75 | f | NR | NR | 85 | 60 minutes | Yes | 567 (508) | 59 | Yes | ||
| 27 | 43,44 | 1998 | 71 | f | NR | NR | 55 | 120 minutes | Paced | Paced | Paced | Yes | ||
| 28 | 43,44 | 1998 | 58 | f | NR | NR | 75 | 38 minutes | Yes | 657 (542) | 115 | Yes | ||
| 29 | 43,44 | 1998 | 40 | m | NR | NR | 35 | 15 minutes | Yes | 679 (475) | 204 | Yes | ||
| 30 | 43,44 | 1998 | 71 | m | NR | NR | 70 | 58 minutes | Yes | 521 (478) | 43 | Yes | ||
| 31 | 43,44 | 1998 | 47 | m | NR | 400 | 400 | 79 minutes | Yes | 574 (444) | 130 | Yes | ||
| 32 | 21 | 1999 | 41 | f | Yes | Yes | 320 | 915 | 55 minutes | Yes | 610 (426) | 184 | Yes | QTc normalization after 5 day, uneventful |
| 33 | 21 | 1999 | 31 | m | Yes | Yes | 480 | 1700 | 40 minutes | Yes | 599 (491) | 108 | Yes | QTc normalized in 4 days, NR |
| 34 | 18 | 2000 | 64 | f | Yes | Yes | 175 | 175 | NR | No | 413 (418) | (‐5) | Yes | QTc remained unchanged, uneventful |
| 35 | 8 | 2000 | 75 | m | No | NR | >2 | >2 | NR | Yes | 615 (435) | 180 | No | QTc normalization in 48 hours, uneventful |
| 36 | 8 | 2000 | 68 | m | Yes | Yes | >2 | >2 | NR | Yes | 650 (407) | 243 | No | QTc normalization after 4 day, uneventful after extubation |
| 37 | 8 | 2000 | 77 | m | NR | NR | (4) | 2 | NR | Yes | 550 (393) | 157 | No | QTc normalization in 24 to 36 hours, NR |
| 38 | 12 | 2004 | 34 | m | Yes | NR | 24.5 | 24.5 | 20 minutes | Yes | 560 (420) | 140 | Yes | QTc normalization (440 msec), ECG normal |
| 39 | 23 | 2004 | 58 | f | Yes | NR | 340 | 1010 | NR | Yes | 533 (460) | 73 | Yes | QTc normalization 7 days later discharge after 27days |
| 40 | 45 | 2008 | 86 | f | Yes | No | 2 mg | 2 mg | 8 hours after last dose | Yes | 524 (NR) | Probably 79 | No | QTc normalization (445 msec), NR |
| 41 | 46 | 2009 | 74 | m | Yes | No | 2 | 2 | Shortly after | Yes | NR (579) | NR | Yes | Pre‐existing heart block and fibrillation resolved, nursing home/rehabilitation |
| Report | MedWatch Identifier | Report Date | Age, Years | Gender | Drugs Pro‐arrh. | Maximum Daily Dose (mg) | Total Dose at Event (mg) | Prolonged QT | QTc Maximal (baseline), msec | Change in QTc (msec) | TdP | Outcome; Recovery |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
| 1 | 3122988‐1 | 1998 | 61 | m | No | 48 | 48 | Yes | NR | NR | Yes | Intervention; NR |
| 2 | 3157827‐6 | 1998 | 44 | f | No | 160 | 160 | Yes | 550 (440) | 110 | Yes | Intervention; uneventful |
| 3 | 3178715‐5 | 1999 | 60 | m | NR | 415 | 645 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization in 1 day, no recurrence |
| 4 | 3271261‐X | 1999 | 56 | m | NR | NR | 20 | Yes | NR | NR | Yes | Life‐threatening; QTc normalization |
| 5 | 3271080‐4 | 1999 | 35 | m | Yes | 7 | 7 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced, hospitalization prolonged |
| 6 | 3325391‐4 | 1999 | 55 | f | Yes | 75 | 75 | NR | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 7 | 3381921‐8 | 1999 | 52 | m | No | 320 | 634 | Yes | 458 (430) | 28 | Yes | Death; NA |
| 8 | 3483869‐7 | 2000 | 18 | m | No | >200 | >310 | Yes | NR | NR | Yes | Intervention; no recurrence after haloperidol reinstitution |
| 9 | 3516342‐8 | 2000 | NR | NR | NR | NR | NR | NR | NR | NR | Yes | NR; NR |
| 10 | 3516320‐9 | 2000 | 34 | m | Yes | 5 | 5 | Yes | NR | NR | No | Life‐threatening; event abated after dose stopped |
| 11 | 3552263‐2 | 2000 | 46 | f | Yes | NR | 97.5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 12 | 3574705‐9 | 2000 | 78 | m | Yes | NR | 160 | Yes | 603 (453) | 50 | Yes | Intervention; event abated after dose stopped/reduced |
| 13 | 3703871‐7 | 2001 | 27 | m | NR | 530 | 530 | Yes | NR | NR | Yes | Death, NA |
| 14 | 3724567‐1 | 2001 | 31 | m | Yes | 6 | 6 | Yes | 496 (449) | 47 | No | Life‐threatening; ECG returned to baseline |
| 15 | 3851984‐1 | 2002 | 72 | f | NR | 18 | 18 | NR | NR | NR | Yes | Hospitalization; NR |
| 16 | 3942407‐2 | 2002 | 51 | m | Yes | 14 | 14 | Yes | 461 (444) | 17 | Yes | Life‐threatening; no recurrence |
| 17 | 4066580‐3 | 2003 | >60 | f | NR | 50 | 50 | Yes | >600 (480) | >120 | No | Hospitalization; QTc normalization, patient recovered |
| 18 | 4126280‐8 | 2003 | 47 | f | NR | 60 | 180 | Yes | 550 (450) | 100 | No (bradycardia) | Hospitalization; patient recovered |
| 19 | 4150700‐6 | 2003 | NR | m | NR | 5 | 5 | NR | NR | NR | Yes | NR; event abated after dose stopped/reduced |
| 20 | 4340092‐1 | 2004 | 52 | m | Yes | 5 | 5 | Yes | >500 (490) | >10 | NR (polymorphous VT) | Life‐threatening; NR |
| 21 | 4714692‐0 | 2005 | NR | m | NR | NR | NR | Yes | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 22 | 4881813‐9 | 2006 | NR | m | NR | NR | 40 | NR | NR | NR | Yes | Hospitalization; event abated after dose stopped/reduced |
| 23 | 4892225‐6 | 2006 | NR | f | Yes | 10 | >10 | Yes | 493 (300) | 193 | No | Hospitalization; QTc normalization (403 msec) |
| 24 | 4911873‐8 | 2006 | 69 | m | Yes | 6 | 6 | NR | NR | NR | Yes | Cardiac arrest, death; NA |
| 25 | 5366448‐6 | 2007 | 53 | m | Yes | NR | 35 | Yes | NR | NR | NR | Cardiac arrest, life‐threatening; patient recovered |
| 26 | 5563440‐3 | 2007 | 58 | m | Possible | 5 | 5 | Yes | NR | NR | Yes | Life‐threatening; event abated after dose stopped/reduced |
| 27 | 5642929‐2 | 2008 | 42 | m | Yes | 165 | 165 | Yes | 640 (350) | 290 | Yes | Death; NA |
| 28 | 5697758‐0 | 2008 | 38 | m | Yes | NR | 620 | NR | NR | NR | Yes | Hospitalization; patient recovered |
| 29 | 5254840‐X | 2008 | 19 | f | Possible | 15 | 25 | Yes | 461 | NR | NR | Cardiac arrest, hospitalization; patient recovered |
Of the 70 cases, 54 cases of TdP were reported. The remaining 16 of 70 cases involved cases of QTP, 9 of which did not progress to TdP and 7 of which the progression to TdP was unclear. Of note, 42 of 54 of the cases of TdP were reported as preceded by documented QTP. Presence of QTP was unknown in the other 12 original reports. Three out of 70 patients experienced sudden cardiac arrest, 1 of which was fatal. One arrest was preceded by TdP and 2 by QTP (Figure 1).
The patient ages ranged from 18 years to 86 years. Of note, 17 patients experiencing TdP and/or QTP were 40 years old, and 2 of those patients were 30 years old.
Haloperidol‐associated QTP and/or TdP were observed in 27 female and 42 male patients; the gender was not stated in one report. Of the 54 patients experiencing TdP (with or without report of previous QTP), 22 were female and 31 were male (1 gender unknown).
A total of 68 of 70 patients were determined to have associated risk factors15 for QTP/TdP (see Table 4). The circumstances of the remaining 2 patients were not described in sufficient detail to identify associated risk factors.
| Risk Factor | Patients, n (%) |
|---|---|
| |
| Any risk factor | 68/70 (97) |
| Unknown | 2/70 (3) |
| Specific risk factors | |
| Electrolyte imbalance | 27/68 (40) |
| Underlying cardiac disease | 32/68 (47) |
| Concomitant proarrhythmic agents | 39/68 (57) |
| Other drugs influencing cardiac function | 23/68 (34) |
| Baseline QTc >450 msec | 18/68 (26) |
| QTc known: 44 patients | 18/44 (41) |
Overall, 32 patients had underlying heart conditions. Electrolyte imbalances, including hypokalemia, hypomagnesemia, and hypocalcemia, were present in 17 patients. At least 39 patients were receiving potentially proarrhythmic agents (1‐8 proarrhythmic drugs per patient) in addition to IV haloperidol. At least 23 patients were receiving additional drugs with a potential for other cardiac adverse events than QTP and TdP.
A wide range of other disease states previously reported to be associated with QTP15 were identified in these patients: asthma (5 patients), diabetes (5 patients), obesity (3 patients), impaired renal and/or liver function (3 patients each), human immunodeficiency virus (HIV) (2 patients); chronic obstructive pulmonary disease (COPD), pancreatitis and hypothyroidism (1 patient each). A total of 22 patients had a history of substance abuse (alcohol and/or drugs), and 4 patients were smokers.
The administered doses of IV haloperidol varied widely. Considering that information regarding the maximal daily dose was missing in 22 reports and ambiguous in another 20 cases, the results have been presented using cumulative IV haloperidol doses. Patients experiencing TdP without preceding QTP received a cumulative dose (= total dose at event) ranging from 5 mg to 645 mg. Patients with both confirmed QTP and TdP were administered a cumulative dose of 2 mg to 1700 mg. Patients who experienced QTP without TdP received a cumulative dose of 2 mg to 1540 mg of IV haloperidol.
Sudden cardiac arrest following administration of IV haloperidol was observed in cumulative doses ranging from 6 mg to 35 mg. The cardiac arrest leading to a fatal outcome was preceded by an administration of at least 6 mg of IV haloperidol. Overall, 14 out of 70 patients received cumulative doses of 10 mg IV haloperidol.
The time from administration to documentation of QTP and/or TdP ranged from immediately post administration to 8 hours after administration of the last dose of IV haloperidol.
Baseline QTc was known in 44 patients. Baseline QTc was >450 msec in 18 of these 44 patients.
The change from baseline QTc varied widely from 20 msec to 286 msec; 36 patients demonstrated a prolongation of >50 msec.
In those patients with reported haloperidol‐associated QTP, 25 patients demonstrated a QTc >600 msec and 38 patients >520 msec.9 Of the cases with known specific QTc values, the QTc was prolonged >450 msec in 48 out of 50 cases. The lowest reported QTc leading to TdP was 413 msec.
A total of 20 patients were reported as having a normalization of QTc (as defined by the original reports) within several hours to 8 days; minimal QTP was reported as persisting in 2 patients. The specifics of the other patients were unknown, although 25 patients were categorized as recovered, 13 were stated as having an uneventful remainder of hospitalization, and 5 patients were discharged to a rehabilitation facility or a nursing home.
Discussion
The current review was performed in response to the FDA warning recommending the use of continuous ECG monitoring associated with the administration of intravenous haloperiodol.5 This warning has resulted in substantial dilemmas for health care organizations, additional resource allocation, and increased scrutiny from regulatory agencies. The results of our review reveal that intravenous haloperidol‐associated QTP and TdP almost uniformly take place in patients with concomitant risk factors and with cumulative doses 2 mg. In light of these findings, it is possible that hospitals may be able to administer intravenous haloperidol in patients without risk factors without continuous ECG monitoring. In reviewing these published reports, it is important to note that the FDA identified 28 published cases of haloperidol‐associated QTP and TdP, while our review yielded a total of 41 published case reports.
The FDA database included 73 cases of haloperidol‐associated TdP in their database. However, these cases included both oral as well as IV administration; using our methodology, we identified 29 additional case reports associated with intravenous haloperidol from this database. Consequently, our review included 41 published case reports and 29 FDA database cases, resulting in the total of 70 patients.
Our review revealed a number of practical findings. First, our summary demonstrated that neither QTP nor TdP has been documented with a cumulative dose of IV haloperidol of 2 mg. The majority of patients (80%) received cumulative IV doses 10 mg. The lowest dose associated with sudden cardiac arrest was 6 mg and this took place in a 69‐year‐old male patient. Second, the majority (97%) of our patients had additional risk factors for QTP and/or TdP. Pre‐existing heart disease,1619 electrolyte imbalance,17, 1921 concomitant proarrhythmic drugs16, 17, 1922 and mechanical ventilation17, 23 were identified as the most commonly observed risk factors (Table 4). Lastly, in those cases in which the data were reported, baseline QTc was >450 msec in 41% of the patients, and 96% had a QTc at the time of the event >450 msec. Therefore, we conclude that patients: (1) receiving low cumulative doses (2 mg) with (2) no risk factors for prolonged QTc or TdP, and (3) with a normal QTc on baseline EKG can safely be given IV haloperidol in the hospital setting.
This dosage range is consistent with the labelling for IV haloperidol dosing in Canada24 and Germany25 (Table 1), where single doses of 0.25 mg to 1.5 mg are recommended for the treatment of delirium or acute agitation in the geriatric population.24, 25
In a recent Cochrane review, low‐dose IV haloperidol (3 mg per day) was concluded to be as safe and effective as atypical antipsychotics in the treatment of acute delirium with respect to extrapyramidal adverse effects.2
The American Psychiatric Association recommends an initial IV dose of 12 mg every 24 hours as needed (0.250.50 mg every 4 hours as needed for elderly patients), with titration to higher doses for patients who continue to be agitated for the treatment of patients with delirium (issued 1999, updated 2004).3
While several expert‐groups and investigators currently consider IV haloperidol as an important therapeutic option for treating acute delirium and agitation in the dose range presented above, less consensus exists regarding monitoring requirements.2, 3, 26, 27
The American Psychiatric Association recommends IV haloperidol only after a baseline ECG is obtained. These guidelines have not been updated since the release of the FDA extended warning.3 In their recent review, Morandi et al.28 support the dosage recommendation of the 1999 American Psychiatric Association's practice guidelines for treatment of delirium,3 ie, administration of IV haloperidol in single doses of 0.5 mg to 2 mg in elderly patients, however, only after a baseline ECG is obtained.28 While the package insert of IV haloperidol in France29 recommends a baseline ECG, Germany,25 Italy30 and Switzerland's31 package information states the need for regular ECG monitoring. Guidelines for the treatment of delirium in the intensive care unit published by the American College of Critical Care Medicine and the Society of Critical Care Medicine in collaboration with the American Society of Health‐System Pharmacists consider IV haloperidol as the preferred agent for the treatment of delirium in critically ill patients (grade of recommendation = C). These expert groups recommend that patients should be monitored for electrocardiographic changes (QT interval prolongation and arrhythmias) when receiving haloperidol (Grade of recommendation = B).32
Nevertheless, continuous ECG monitoring (ie, telemetry) is expensive, labor‐intensive and, potentially overutilized.33, 34 Requiring clinicians to place all patients receiving intravenous haloperidol on telemetry is impractical and potentially costly. Mandating telemetry could also lead to unintended harm, ie, use of a less effective or less safe drug to avoid compliance with the telemetry mandate.
Based on our findings and the current recommendations in the literature, inpatient providers should be thoughtful and deliberate in the use of haloperidol to treat acute delirium with agitation. Patients requiring pharmacologic management of their delirium should be screened for risk factors for QTP and TdP (Table 4) and a baseline ECG should be obtained prior to haloperidol administration. If significant risk factors exist or the baseline ECG reveals a prolonged QTc, then the patient should receive continuous ECG monitoring. Similarly, if cumulative doses of 2 mg are needed, the patient should be placed on telemetry.
There are some limitations to our study design. Our findings are based upon previously published case reports or data submitted to the FDA MedWatch. While the content of the FDA's MedWatch database is accessible to the public via the Freedom of Information Act (FOIA), the events are neither categorized nor peer‐reviewed upon entry into the database. Consequently, information may be incomplete or inaccurate. In addition, the denominator representing the overall use of IV haloperidol is unknown, thus a rate of event cannot be assigned and the true scope of the problem cannot be determined. Despite these limitations, this summary represents the most comprehensive review of the literature to date, expanding on the analysis performed by the FDA. Of note, in our review of the FDA database, we noted several cases of haloperidol‐associated QTP or TdP associated with other routes of administration. Thus, it is unknown whether this complication is any greater with IV vs. the IM or per os (PO) routes of administration.
Conclusion
Although the proarrhythmic potential of haloperidol and other antipsychotics has been well established in the literature, IV haloperidol has been considered relatively safe with respect to this complication from the time of its approval in 1967.5, 1722, 35, 36 In reviewing all reported cases of cardiac complications associated with IV haloperidol, as well as the current literature, an association with QTP and TdP is likely. However, the case reports reveal that QTP and TdP generally occur in the setting of concomitant risk factors, and no cases have been reported utilizing a cumulative IV dose of 2 mg. It may therefore be safe to administer a cumulative dose of IV haloperidol of 2 mg without ECG monitoring in patients without risk factors for QTP. However, ECG monitoring should take place with IV haloperidol doses 2 mg and/or in those patients with additional risk factors of developing QTP and/or TdP.
Based on the findings of this review complemented by the guidelines of various expert‐groups and the official labelling information of different countries, the Pharmacy & Therapeutics Committee of the UCSF Medical Center revised the IV haloperidol policy: administration of a total dose of 2 mg IV haloperidol without concurrent telemetry is allowed in a noncritical care setting in patients without risk factors for QTP and TdP.
Acknowledgements
The authors acknowledge Gloria Won of the Fishbon Library at UCSF Medical Center at Mount Zion for her support.
- Haldol® injection (for immediate release) Package Insert.Raritan, NJ:Ortho‐McNeil Pharmaceutical Inc.;2005;rev. 05.2007.
- ,,,. Antipsychotics for delirium (review), the Cochrane collaboration2008;2. Available at: www. cochrane.org. Accessed February 2010.
- American Psychiatric Association: practice guideline for the treatment of patients with delirium.Am J Psychiatry.1999;156(5 suppl):1–20, updated 2004.
- Thomson Micromedex.2008. Micromedex healthcare series: “haloperidol” Thomson Micromedex, Greenwood Village.
- FDA alert: haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate).2007. This alert highlights revisions to the labeling for haloperidol. Available at: www.fda.gov. Accessed February 2010.
- ,,.Use of high‐dose intravenous haloperidol in the treatment of agitated cardiac patients,J Clin Psychopharmacol.1985;5(6):344–347.
- ,,, et al.Postoperative delirium,Am J Psychiatry.2008;165:7.
- ,.Corrected QT interval prolongation associated with intravenous haloperidol in acute coronary syndromes,Catheter Cardiovasc Interv.2000;50(3):352–355.
- ,.Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death.Am J Psych.2001;158(11):1774–1782.
- ,,, et al.Accuracy of uncorrected versus corrected QT Interval for Prediction of torsade de pointes associated with intravenous haloperidol.Pharmacotherapy.2007;27(2):175–182.
- ,,.Three cases of ventricular tachycardia and torsades de pointes induced by antipsychotic drugs.Shinzo.1997;29(1):68–74.
- ,,,.Haloperidol por via intravenosa y torsade de pointes.Medicina intensive.2004;28(2):89.
- ,,, et al.QT‐Verlängerung und Kammerflimmern unter Haloperidol‐ und Clonidin‐Therapie des Alkoholentzugssyndroms.Intensivmedizin und Notfallmedizin.1992;29(4):178–183.
- ARIZONA CERT, Arizona Center for Education and Research on Therapeutics. Available at: www.azcert.org. Accessed February 2010.
- ,.Cardiac arrhythmias—a clinical approach.Edinburgh:Mosby;2003.
- ,.The association between intravenous haloperidol and torsades de pointes—three cases and a literature review.Psychosomatics.1995;36:541–549.
- ,.Prolongation of the corrected QT and torsades de pointes cardiac arrhythmia associated with intravenous haloperidol in the medically ill.J Clin Psychopharmacol.1993;13(2):128–132.
- ,,,,.Torsades de pointes secondary to intravenous haloperidol after coronary bypass grafting surgery.Can J Anesth.2000;47(3):251–254.
- ,.Torsade de pointes associated with the administration of intravenous haloperidol: a review of the literature and practical guidelines for use,Expert Opin Drug Saf.2003;2(6):543–547.
- ,.Conduction disturbances associated with administration of butyrophenone antipsychotics in the critically ill: a review of the literature,Pharmacotherapy.1997;17(3):531–537.
- ,,.Haloperidol‐induced torsades de pointes.Ann Pharacother.1999;33(10):1046–1050.
- ,,, et al.Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary,Crit Care Med.1995;23(9):1596–1600.
- ,,,,,.Prolonged cardiac repolarization after tacrolimus and haloperidol administration in the critically ill patient.Pharmacotherapy.2004;24(3):404–408.
- CPS Compendium of Pharmaceuticals and Specialties, the Canadian drug reference for health professionals, 2007, Canadian pharmacists association.
- Rote Liste Deutschland2008, Rote Liste Service GmbH Frankfurt am Main. Available at: www.rote‐liste.de. Accessed February 2010.
- ,.Delirium in the hospitalized patient: a primer for the pharmacist clinician.J Pharm Pract.2007;20(5):368–372.
- ,,, et al.Delirium: guidelines for general hospitals.J Psychosom Res.2007;62(3):371–383.
- ,,,.The pharmacological management of delirium in critical illness.Current Drug Therapy.2008,3:148–157.
- VIDAL‐l'information sur les produits de santé2008, Issy les Moulineaux Cedex. Available at: www.vidal.fr. Accessed February 2010.
- Haldol iniettabile—ufficiale monografia italiana. Available at: www. informatorefarmaceutico.it. Accessed February 2010.
- Arzneimittelkompendium der Schweiz2008, documed Verlag Basel. Availabla at: www.kompendium.ch. Accessed February 2010.
- ,,, et al.Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill, American College of Critical Care Medicine ACCM, Society of Critical Care Medicine SCCM, American Society of Health‐System Pharmacists ASHP.Crit Care Med.2002;30(1):119–141.
- ,,,,.Is telemetry overused? Is it as helpful as thought?Cleve Clin J Med.2009;76(6):368–372.
- ,,.Telemetry outside critical care units: patterns of utilization and influence on management decisions.Clin Cardiol.1998;21(7):503–505.
- ,,.High‐dose intravenous haloperidol for agitated delirium in a cardiac patient on intra‐aortic balloon pump.J Clin Psychopharmacol.1991;11(2):146–147.
- .Haloperidol, midazolam and intravenous sedation.Aust NZ J Psychiatry.1999;33(6):942–943.
- BNF British National Formulary, compendium of pharmaceuticals and specialties of the UK.2007. Available at: www.bnf.org. Accessed February 2010.
- ,,,.Torsade de pointes associated with the use of intravenous haloperidol.Ann Intern Med.1993;119(5):391–394.
- ,.Torsades de pointes: potential consequence of intravenous haloperidol in the intensive care unit.Intensive Care World.1994;11(3):109–112.
- ,.Torsade de pointes caused by high‐dose intravenous haloperidol in cardiac patients.Clin Cardiol.1995;18:285–290.
- ,,.Continuous infusion of haloperidol controls agitation in critically ill patients.Crit Care Med.1994:22(3):433–440.
- ,,.Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalances.Am J Gastroenterol.1995;90(5):822–824.
- ,,,.Torsades de pointes associated with intravenous haloperidol in critically ill patients.Am J Cardiol.1998;81(2):238–240.
- ,,,,.The effect of intravenous haloperidol on QT interval dispersion in critically ill patients: comparison with QT interval prolongation for assessment of risk of torsades de pointes.J Clin Pharmacol.2001;41:1310–1318.
- ,,.Low‐dose haloperidol associated QTc prolongation.J Am Geriatr Soc.2008;56(10):1963–1964.
- ,,.Torsade de pointes following intravenous haloperidol administration in a patient with complete heart block.WMJ.2009;108(1):48–50.
- Haldol® injection (for immediate release) Package Insert.Raritan, NJ:Ortho‐McNeil Pharmaceutical Inc.;2005;rev. 05.2007.
- ,,,. Antipsychotics for delirium (review), the Cochrane collaboration2008;2. Available at: www. cochrane.org. Accessed February 2010.
- American Psychiatric Association: practice guideline for the treatment of patients with delirium.Am J Psychiatry.1999;156(5 suppl):1–20, updated 2004.
- Thomson Micromedex.2008. Micromedex healthcare series: “haloperidol” Thomson Micromedex, Greenwood Village.
- FDA alert: haloperidol (marketed as Haldol, Haldol Decanoate and Haldol Lactate).2007. This alert highlights revisions to the labeling for haloperidol. Available at: www.fda.gov. Accessed February 2010.
- ,,.Use of high‐dose intravenous haloperidol in the treatment of agitated cardiac patients,J Clin Psychopharmacol.1985;5(6):344–347.
- ,,, et al.Postoperative delirium,Am J Psychiatry.2008;165:7.
- ,.Corrected QT interval prolongation associated with intravenous haloperidol in acute coronary syndromes,Catheter Cardiovasc Interv.2000;50(3):352–355.
- ,.Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death.Am J Psych.2001;158(11):1774–1782.
- ,,, et al.Accuracy of uncorrected versus corrected QT Interval for Prediction of torsade de pointes associated with intravenous haloperidol.Pharmacotherapy.2007;27(2):175–182.
- ,,.Three cases of ventricular tachycardia and torsades de pointes induced by antipsychotic drugs.Shinzo.1997;29(1):68–74.
- ,,,.Haloperidol por via intravenosa y torsade de pointes.Medicina intensive.2004;28(2):89.
- ,,, et al.QT‐Verlängerung und Kammerflimmern unter Haloperidol‐ und Clonidin‐Therapie des Alkoholentzugssyndroms.Intensivmedizin und Notfallmedizin.1992;29(4):178–183.
- ARIZONA CERT, Arizona Center for Education and Research on Therapeutics. Available at: www.azcert.org. Accessed February 2010.
- ,.Cardiac arrhythmias—a clinical approach.Edinburgh:Mosby;2003.
- ,.The association between intravenous haloperidol and torsades de pointes—three cases and a literature review.Psychosomatics.1995;36:541–549.
- ,.Prolongation of the corrected QT and torsades de pointes cardiac arrhythmia associated with intravenous haloperidol in the medically ill.J Clin Psychopharmacol.1993;13(2):128–132.
- ,,,,.Torsades de pointes secondary to intravenous haloperidol after coronary bypass grafting surgery.Can J Anesth.2000;47(3):251–254.
- ,.Torsade de pointes associated with the administration of intravenous haloperidol: a review of the literature and practical guidelines for use,Expert Opin Drug Saf.2003;2(6):543–547.
- ,.Conduction disturbances associated with administration of butyrophenone antipsychotics in the critically ill: a review of the literature,Pharmacotherapy.1997;17(3):531–537.
- ,,.Haloperidol‐induced torsades de pointes.Ann Pharacother.1999;33(10):1046–1050.
- ,,, et al.Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: an executive summary,Crit Care Med.1995;23(9):1596–1600.
- ,,,,,.Prolonged cardiac repolarization after tacrolimus and haloperidol administration in the critically ill patient.Pharmacotherapy.2004;24(3):404–408.
- CPS Compendium of Pharmaceuticals and Specialties, the Canadian drug reference for health professionals, 2007, Canadian pharmacists association.
- Rote Liste Deutschland2008, Rote Liste Service GmbH Frankfurt am Main. Available at: www.rote‐liste.de. Accessed February 2010.
- ,.Delirium in the hospitalized patient: a primer for the pharmacist clinician.J Pharm Pract.2007;20(5):368–372.
- ,,, et al.Delirium: guidelines for general hospitals.J Psychosom Res.2007;62(3):371–383.
- ,,,.The pharmacological management of delirium in critical illness.Current Drug Therapy.2008,3:148–157.
- VIDAL‐l'information sur les produits de santé2008, Issy les Moulineaux Cedex. Available at: www.vidal.fr. Accessed February 2010.
- Haldol iniettabile—ufficiale monografia italiana. Available at: www. informatorefarmaceutico.it. Accessed February 2010.
- Arzneimittelkompendium der Schweiz2008, documed Verlag Basel. Availabla at: www.kompendium.ch. Accessed February 2010.
- ,,, et al.Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill, American College of Critical Care Medicine ACCM, Society of Critical Care Medicine SCCM, American Society of Health‐System Pharmacists ASHP.Crit Care Med.2002;30(1):119–141.
- ,,,,.Is telemetry overused? Is it as helpful as thought?Cleve Clin J Med.2009;76(6):368–372.
- ,,.Telemetry outside critical care units: patterns of utilization and influence on management decisions.Clin Cardiol.1998;21(7):503–505.
- ,,.High‐dose intravenous haloperidol for agitated delirium in a cardiac patient on intra‐aortic balloon pump.J Clin Psychopharmacol.1991;11(2):146–147.
- .Haloperidol, midazolam and intravenous sedation.Aust NZ J Psychiatry.1999;33(6):942–943.
- BNF British National Formulary, compendium of pharmaceuticals and specialties of the UK.2007. Available at: www.bnf.org. Accessed February 2010.
- ,,,.Torsade de pointes associated with the use of intravenous haloperidol.Ann Intern Med.1993;119(5):391–394.
- ,.Torsades de pointes: potential consequence of intravenous haloperidol in the intensive care unit.Intensive Care World.1994;11(3):109–112.
- ,.Torsade de pointes caused by high‐dose intravenous haloperidol in cardiac patients.Clin Cardiol.1995;18:285–290.
- ,,.Continuous infusion of haloperidol controls agitation in critically ill patients.Crit Care Med.1994:22(3):433–440.
- ,,.Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalances.Am J Gastroenterol.1995;90(5):822–824.
- ,,,.Torsades de pointes associated with intravenous haloperidol in critically ill patients.Am J Cardiol.1998;81(2):238–240.
- ,,,,.The effect of intravenous haloperidol on QT interval dispersion in critically ill patients: comparison with QT interval prolongation for assessment of risk of torsades de pointes.J Clin Pharmacol.2001;41:1310–1318.
- ,,.Low‐dose haloperidol associated QTc prolongation.J Am Geriatr Soc.2008;56(10):1963–1964.
- ,,.Torsade de pointes following intravenous haloperidol administration in a patient with complete heart block.WMJ.2009;108(1):48–50.
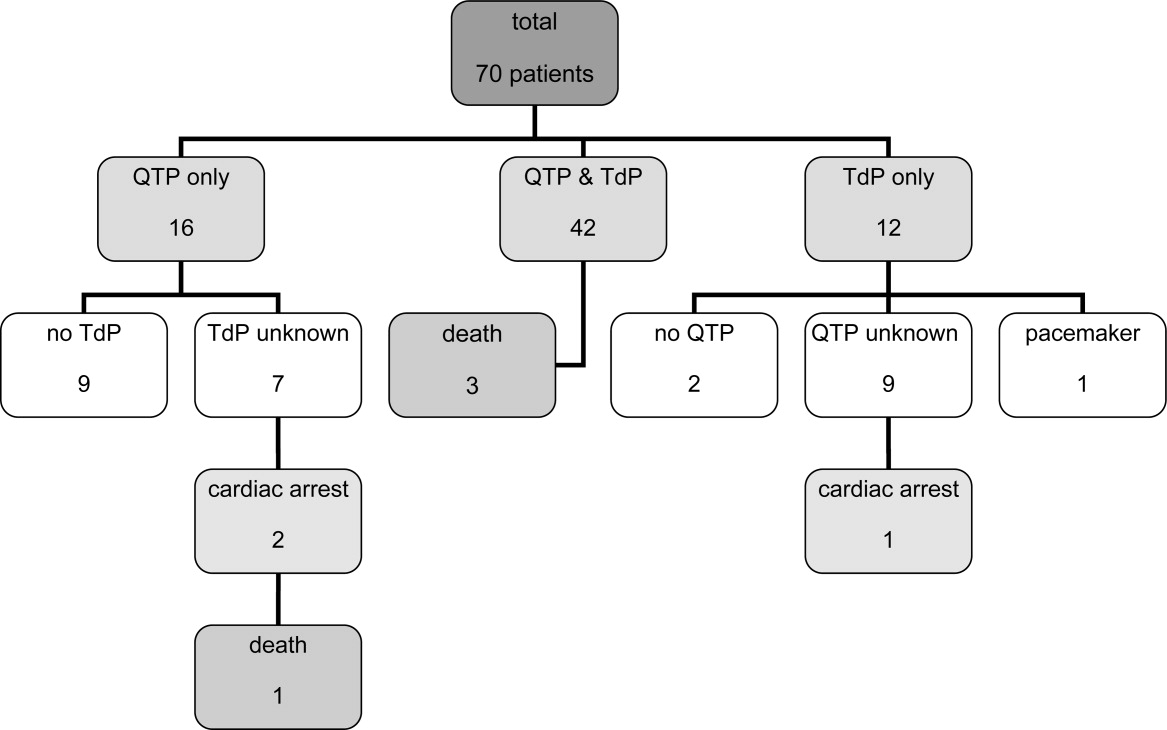
CVS in an Adult Patient
We present a 26‐year‐old white male with a chief complaint of nausea and vomiting. The patient described prodromal nausea followed by intractable vomiting for 2 days. Over the past 2 years he has experienced similar episodes occurring every 3 to 6 months. He has been hospitalized 5 times for this problem with no diagnosis given. There are no obvious precipitants. The symptoms consistently last 2 to 3 days and resolve with supportive care including intravenous fluids and antiemetics. The patient enjoys good health between the periods of sickness. He has never experienced coffee‐ground emesis or hematemesis. His past medical history is significant for attention deficit disorder and cholecystectomy. He takes no prescription medications. Social history is remarkable for tobacco abuse, binge drinking on weekends, and daily marijuana use. He is unemployed. His family history is unremarkable.
Physical examination at the time of admission was notable for tachycardia, orthostatic hypotension, and hypoactive bowel sounds. Otherwise physical examination was normal.
Diagnostic testing done on admission was notable for white blood cell count of 25,000, hemoglobin of 17.3, blood urea nitrogen 18, creatinine 1.4, aspartate aminotransferase (AST) 64, and alanine aminotransferase (ALT) 55. Pancreatic enzymes and acute abdominal series were normal.
The patient was admitted to the hospital with the presumptive diagnosis of viral gastroenteritis. Initial therapy included intravenous fluids and promethazine. Throughout hospital day 1, he remained nauseated and had multiple bouts of emesis. Records from the patient's hospitalization 5 months ago were obtained and reviewed. During this previous hospitalization, computed tomography (CT) scans of the abdomen and esophagogastroduodenoscopy (EGD) were performed, both of which were negative. Upon review of this recent workup, the diagnosis of cyclic vomiting syndrome (CVS) was entertained and the patient received a therapeutic trial of subcutaneous sumatriptan. His symptoms abated dramatically. Subsequently, he was able to keep oral liquids down and his orthostatic hypotension resolved. On hospital day 2, his white blood cell count normalized without intervention. Blood, urine, and stool cultures remained negative, and workup for acute intermittent porphyria was negative. Upon discharge from the hospital he was counseled to discontinue all marijuana use and was scheduled for follow‐up in the residents' clinic. He failed to keep this appointment. After being lost to follow‐up for 17 months, he presented to the emergency department with nausea and vomiting. As before, his symptoms promptly improved with sumatriptan.
Discussion
CVS, initially described in 1861 as a pediatric illness, is being increasingly recognized in adults.1 It has been estimated that up to 1.6% of children experience symptoms consistent with this disorder, but the prevalence in adults is unknown.2 The essential features of CVS, as noted in our patient, are multiple discrete episodes of nausea and vomiting lasting less than 1 week with absence of nausea and vomiting between episodes. The presentation of adults with CVS often differs from the pediatric form in that adults have longer, less frequent episodes, and the triggers are less evident.3
The etiology and pathogenesis of CVS remain unknown. A variety of physical and psychological stresses, including infection, overexertion, and emotional distress, have been noted to precipitate episodes.4 CVS has variably been associated with autonomic, mitochondrial, and endocrine disorders. The most prevalent theory in the literature, however, is that CVS and migraine headaches are different presentations of the same diathesis.5 Patients with both are noted to have similar patterns of symptoms and positive family history of migraines. The progression from CVS to migraines is noted frequently in individual patients. As many as 82% of the 214 children in a case series of CVS were noted to have a family history of migraines or to have or subsequently develop migraines.6 In addition, electroencephalogram findings and adrenergic autonomic abnormalities are similar in both sets of patients.3 In 1 case series of 17 patients with CVS, patients noted the possible association of episodes with menses (in 57% of women of reproductive age), and the improvement of symptoms with sleep (in 24%), clinical factors common in patients with migraines.3
CVS is one of the functional gastrointestinal disorders for which the diagnosis is clinical, with criteria based upon the consensus of expert opinion in the Rome III Criteria for Functional Gastrointestinal (GI) Disorders.7 At least 3 months, with onset at least 6 months previously of:
-
Stereotypical episodes of vomiting regarding onset (acute) and duration (less than 1 week);
-
3 or more discrete episodes in the prior year; and
-
Absence of nausea and vomiting between episodes.
Supportive criteria: History of migraine headaches or family history of migraine headaches.7
Making the diagnosis of CVS requires the exclusion of other disorders associated with recurrent vomiting. Examples include gastric outlet or small bowel obstruction, gastroparesis, vestibular neuritis, elevated intracranial pressure, inborn errors of metabolism, dysautonomia, porphyria, and alterations in the hypothalamic pituitary adrenal axis. The other functional nausea and vomiting disorders described in Rome III, specifically chronic idiopathic nausea and functional vomiting, also need to be considered.7 Many drugs can cause nausea and vomiting, and chronic marijuana use has been associated with cyclical hyperemesis.8 Our patient meets the diagnostic criteria for CVS, but his frequent marijuana use would preclude a diagnosis of functional vomiting, which by definition requires an absence of chronic cannabinoid use.
Determining which tests and procedures should be performed in the initial evaluation is based on clinical judgment, but commonly includes complete metabolic profile, urinalysis, upper GI series, EGD, neurological imaging, acute abdominal series, and CT of the abdomen and pelvis. In addition, pertinent metabolic screening including serum lactate, cortisol, pyruvate, ammonia, creatinine phosphokinase, carnitine, urinary organic acids, and porphobilinogen may be considered.5
Evidence‐based treatment of CVS is limited by the lack of controlled trials. Acutely, patients often require hospitalization and symptom management with aggressive hydration, antiemetics, and sometimes even sedative agents. Empiric abortive treatment with antimigraine mediations (sumitriptan, prochlorperazine, tricyclic antidepressants, and ketorolac) has been effective in case reports.911 Patients in whom a history of chronic cannabinoid use is elicited should be counseled that cessation may lead to an improvement in symptoms.
Just as with migraines, patients who experience frequent episodes of cyclic vomiting can benefit from prophylactic medications. Tricyclic antidepressants (TCAs) have been reported to be effective as prophylactic agents in children with CVS.12 An open‐label treatment group of 17 adult patients with CVS noted that 17% of patients had a complete remission with TCA therapy and almost 60% had a partial response.3 More recently, a retrospective case series of patients who had failed TCAs as maintenance therapy reported that 15 out of the 20 patients studied had improvement in the frequency of their vomiting episodes with the newer antiepileptic drugs zonisamide and levetiracem. However, moderate or severe side effects were reported in 45%.13
Conclusions
In summary, although CVS is still an uncommon diagnosis, it is being made more frequently in adults. Although recognition is increasing, there remains a significant delay between onset of symptoms and diagnosis in adults.4 CVS is a diagnosis of exclusion and should be considered when initial evaluation for recurrent nausea and vomiting are unrevealing. A wide range of medications show benefit for both abortive and prophylactic therapy. Increasing awareness of this disorder can lead to a reduction in invasive and costly diagnostic workups.
- .Evrose de la digestion, caracteriseo par des crises periodiques de vomissements et une profonde modification de l'assimilation.Gazette Medicale de Paris1861:312. [French]
- ,.Cyclical vomiting syndrome in children: a population‐based study.J Pediatr Gastroenterol Nutr.1995;21(4):454–458.
- ,.Cyclic vomiting syndrome in adults: clinical features and response to tricyclic antidepressants.Am J Gastroenterol.1999;94(10):2855–2860.
- ,,,.Cyclic vomiting syndrome in 41 adults: the illness, the patients, and problems of management.BMC Med.2005;3:20.
- ,,.Consensus statement—2nd International Scientific Symposium on CVS. The Faculty of The 2nd International Scientific Symposium on Cyclic Vomiting Syndrome.Dig Dis Sci.1999;44(8 suppl):9S–11S.
- ,,,,.Is cyclic vomiting syndrome related to migraine?J Pediatr.1999;134(5):567–572.
- ,,, et al.Functional gastroduodenal disorders.Gastroenterology.2006;130:1466–1479.
- ,,,.Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis use.Gut.2004;53:1566–1570.
- ,,.Sumatriptan in the treatment of cyclic vomiting.Ann Pharmacother.1995;29(10):997–999.
- .Recurrent vomiting in adults. A syndrome?Med J Aust.1983;1(7):329–331.
- ,,,,.Cyclic vomiting: association with multiple homeostatic abnormalities and response to ketorolac.Am J Gastroenterol.1996;91(10):2228–2232.
- .Effective prophylactic therapy for cyclic vomiting syndrome in children using amitriptyline or cyproheptadine.Pediatrics.1997;100(6):977–981.
- ,,,.Zonisamide or levetiracetam for adults with cyclic vomiting syndrome: a case series.Clin Gastroenterol Hepatol.2007;5(1):44–48.
We present a 26‐year‐old white male with a chief complaint of nausea and vomiting. The patient described prodromal nausea followed by intractable vomiting for 2 days. Over the past 2 years he has experienced similar episodes occurring every 3 to 6 months. He has been hospitalized 5 times for this problem with no diagnosis given. There are no obvious precipitants. The symptoms consistently last 2 to 3 days and resolve with supportive care including intravenous fluids and antiemetics. The patient enjoys good health between the periods of sickness. He has never experienced coffee‐ground emesis or hematemesis. His past medical history is significant for attention deficit disorder and cholecystectomy. He takes no prescription medications. Social history is remarkable for tobacco abuse, binge drinking on weekends, and daily marijuana use. He is unemployed. His family history is unremarkable.
Physical examination at the time of admission was notable for tachycardia, orthostatic hypotension, and hypoactive bowel sounds. Otherwise physical examination was normal.
Diagnostic testing done on admission was notable for white blood cell count of 25,000, hemoglobin of 17.3, blood urea nitrogen 18, creatinine 1.4, aspartate aminotransferase (AST) 64, and alanine aminotransferase (ALT) 55. Pancreatic enzymes and acute abdominal series were normal.
The patient was admitted to the hospital with the presumptive diagnosis of viral gastroenteritis. Initial therapy included intravenous fluids and promethazine. Throughout hospital day 1, he remained nauseated and had multiple bouts of emesis. Records from the patient's hospitalization 5 months ago were obtained and reviewed. During this previous hospitalization, computed tomography (CT) scans of the abdomen and esophagogastroduodenoscopy (EGD) were performed, both of which were negative. Upon review of this recent workup, the diagnosis of cyclic vomiting syndrome (CVS) was entertained and the patient received a therapeutic trial of subcutaneous sumatriptan. His symptoms abated dramatically. Subsequently, he was able to keep oral liquids down and his orthostatic hypotension resolved. On hospital day 2, his white blood cell count normalized without intervention. Blood, urine, and stool cultures remained negative, and workup for acute intermittent porphyria was negative. Upon discharge from the hospital he was counseled to discontinue all marijuana use and was scheduled for follow‐up in the residents' clinic. He failed to keep this appointment. After being lost to follow‐up for 17 months, he presented to the emergency department with nausea and vomiting. As before, his symptoms promptly improved with sumatriptan.
Discussion
CVS, initially described in 1861 as a pediatric illness, is being increasingly recognized in adults.1 It has been estimated that up to 1.6% of children experience symptoms consistent with this disorder, but the prevalence in adults is unknown.2 The essential features of CVS, as noted in our patient, are multiple discrete episodes of nausea and vomiting lasting less than 1 week with absence of nausea and vomiting between episodes. The presentation of adults with CVS often differs from the pediatric form in that adults have longer, less frequent episodes, and the triggers are less evident.3
The etiology and pathogenesis of CVS remain unknown. A variety of physical and psychological stresses, including infection, overexertion, and emotional distress, have been noted to precipitate episodes.4 CVS has variably been associated with autonomic, mitochondrial, and endocrine disorders. The most prevalent theory in the literature, however, is that CVS and migraine headaches are different presentations of the same diathesis.5 Patients with both are noted to have similar patterns of symptoms and positive family history of migraines. The progression from CVS to migraines is noted frequently in individual patients. As many as 82% of the 214 children in a case series of CVS were noted to have a family history of migraines or to have or subsequently develop migraines.6 In addition, electroencephalogram findings and adrenergic autonomic abnormalities are similar in both sets of patients.3 In 1 case series of 17 patients with CVS, patients noted the possible association of episodes with menses (in 57% of women of reproductive age), and the improvement of symptoms with sleep (in 24%), clinical factors common in patients with migraines.3
CVS is one of the functional gastrointestinal disorders for which the diagnosis is clinical, with criteria based upon the consensus of expert opinion in the Rome III Criteria for Functional Gastrointestinal (GI) Disorders.7 At least 3 months, with onset at least 6 months previously of:
-
Stereotypical episodes of vomiting regarding onset (acute) and duration (less than 1 week);
-
3 or more discrete episodes in the prior year; and
-
Absence of nausea and vomiting between episodes.
Supportive criteria: History of migraine headaches or family history of migraine headaches.7
Making the diagnosis of CVS requires the exclusion of other disorders associated with recurrent vomiting. Examples include gastric outlet or small bowel obstruction, gastroparesis, vestibular neuritis, elevated intracranial pressure, inborn errors of metabolism, dysautonomia, porphyria, and alterations in the hypothalamic pituitary adrenal axis. The other functional nausea and vomiting disorders described in Rome III, specifically chronic idiopathic nausea and functional vomiting, also need to be considered.7 Many drugs can cause nausea and vomiting, and chronic marijuana use has been associated with cyclical hyperemesis.8 Our patient meets the diagnostic criteria for CVS, but his frequent marijuana use would preclude a diagnosis of functional vomiting, which by definition requires an absence of chronic cannabinoid use.
Determining which tests and procedures should be performed in the initial evaluation is based on clinical judgment, but commonly includes complete metabolic profile, urinalysis, upper GI series, EGD, neurological imaging, acute abdominal series, and CT of the abdomen and pelvis. In addition, pertinent metabolic screening including serum lactate, cortisol, pyruvate, ammonia, creatinine phosphokinase, carnitine, urinary organic acids, and porphobilinogen may be considered.5
Evidence‐based treatment of CVS is limited by the lack of controlled trials. Acutely, patients often require hospitalization and symptom management with aggressive hydration, antiemetics, and sometimes even sedative agents. Empiric abortive treatment with antimigraine mediations (sumitriptan, prochlorperazine, tricyclic antidepressants, and ketorolac) has been effective in case reports.911 Patients in whom a history of chronic cannabinoid use is elicited should be counseled that cessation may lead to an improvement in symptoms.
Just as with migraines, patients who experience frequent episodes of cyclic vomiting can benefit from prophylactic medications. Tricyclic antidepressants (TCAs) have been reported to be effective as prophylactic agents in children with CVS.12 An open‐label treatment group of 17 adult patients with CVS noted that 17% of patients had a complete remission with TCA therapy and almost 60% had a partial response.3 More recently, a retrospective case series of patients who had failed TCAs as maintenance therapy reported that 15 out of the 20 patients studied had improvement in the frequency of their vomiting episodes with the newer antiepileptic drugs zonisamide and levetiracem. However, moderate or severe side effects were reported in 45%.13
Conclusions
In summary, although CVS is still an uncommon diagnosis, it is being made more frequently in adults. Although recognition is increasing, there remains a significant delay between onset of symptoms and diagnosis in adults.4 CVS is a diagnosis of exclusion and should be considered when initial evaluation for recurrent nausea and vomiting are unrevealing. A wide range of medications show benefit for both abortive and prophylactic therapy. Increasing awareness of this disorder can lead to a reduction in invasive and costly diagnostic workups.
We present a 26‐year‐old white male with a chief complaint of nausea and vomiting. The patient described prodromal nausea followed by intractable vomiting for 2 days. Over the past 2 years he has experienced similar episodes occurring every 3 to 6 months. He has been hospitalized 5 times for this problem with no diagnosis given. There are no obvious precipitants. The symptoms consistently last 2 to 3 days and resolve with supportive care including intravenous fluids and antiemetics. The patient enjoys good health between the periods of sickness. He has never experienced coffee‐ground emesis or hematemesis. His past medical history is significant for attention deficit disorder and cholecystectomy. He takes no prescription medications. Social history is remarkable for tobacco abuse, binge drinking on weekends, and daily marijuana use. He is unemployed. His family history is unremarkable.
Physical examination at the time of admission was notable for tachycardia, orthostatic hypotension, and hypoactive bowel sounds. Otherwise physical examination was normal.
Diagnostic testing done on admission was notable for white blood cell count of 25,000, hemoglobin of 17.3, blood urea nitrogen 18, creatinine 1.4, aspartate aminotransferase (AST) 64, and alanine aminotransferase (ALT) 55. Pancreatic enzymes and acute abdominal series were normal.
The patient was admitted to the hospital with the presumptive diagnosis of viral gastroenteritis. Initial therapy included intravenous fluids and promethazine. Throughout hospital day 1, he remained nauseated and had multiple bouts of emesis. Records from the patient's hospitalization 5 months ago were obtained and reviewed. During this previous hospitalization, computed tomography (CT) scans of the abdomen and esophagogastroduodenoscopy (EGD) were performed, both of which were negative. Upon review of this recent workup, the diagnosis of cyclic vomiting syndrome (CVS) was entertained and the patient received a therapeutic trial of subcutaneous sumatriptan. His symptoms abated dramatically. Subsequently, he was able to keep oral liquids down and his orthostatic hypotension resolved. On hospital day 2, his white blood cell count normalized without intervention. Blood, urine, and stool cultures remained negative, and workup for acute intermittent porphyria was negative. Upon discharge from the hospital he was counseled to discontinue all marijuana use and was scheduled for follow‐up in the residents' clinic. He failed to keep this appointment. After being lost to follow‐up for 17 months, he presented to the emergency department with nausea and vomiting. As before, his symptoms promptly improved with sumatriptan.
Discussion
CVS, initially described in 1861 as a pediatric illness, is being increasingly recognized in adults.1 It has been estimated that up to 1.6% of children experience symptoms consistent with this disorder, but the prevalence in adults is unknown.2 The essential features of CVS, as noted in our patient, are multiple discrete episodes of nausea and vomiting lasting less than 1 week with absence of nausea and vomiting between episodes. The presentation of adults with CVS often differs from the pediatric form in that adults have longer, less frequent episodes, and the triggers are less evident.3
The etiology and pathogenesis of CVS remain unknown. A variety of physical and psychological stresses, including infection, overexertion, and emotional distress, have been noted to precipitate episodes.4 CVS has variably been associated with autonomic, mitochondrial, and endocrine disorders. The most prevalent theory in the literature, however, is that CVS and migraine headaches are different presentations of the same diathesis.5 Patients with both are noted to have similar patterns of symptoms and positive family history of migraines. The progression from CVS to migraines is noted frequently in individual patients. As many as 82% of the 214 children in a case series of CVS were noted to have a family history of migraines or to have or subsequently develop migraines.6 In addition, electroencephalogram findings and adrenergic autonomic abnormalities are similar in both sets of patients.3 In 1 case series of 17 patients with CVS, patients noted the possible association of episodes with menses (in 57% of women of reproductive age), and the improvement of symptoms with sleep (in 24%), clinical factors common in patients with migraines.3
CVS is one of the functional gastrointestinal disorders for which the diagnosis is clinical, with criteria based upon the consensus of expert opinion in the Rome III Criteria for Functional Gastrointestinal (GI) Disorders.7 At least 3 months, with onset at least 6 months previously of:
-
Stereotypical episodes of vomiting regarding onset (acute) and duration (less than 1 week);
-
3 or more discrete episodes in the prior year; and
-
Absence of nausea and vomiting between episodes.
Supportive criteria: History of migraine headaches or family history of migraine headaches.7
Making the diagnosis of CVS requires the exclusion of other disorders associated with recurrent vomiting. Examples include gastric outlet or small bowel obstruction, gastroparesis, vestibular neuritis, elevated intracranial pressure, inborn errors of metabolism, dysautonomia, porphyria, and alterations in the hypothalamic pituitary adrenal axis. The other functional nausea and vomiting disorders described in Rome III, specifically chronic idiopathic nausea and functional vomiting, also need to be considered.7 Many drugs can cause nausea and vomiting, and chronic marijuana use has been associated with cyclical hyperemesis.8 Our patient meets the diagnostic criteria for CVS, but his frequent marijuana use would preclude a diagnosis of functional vomiting, which by definition requires an absence of chronic cannabinoid use.
Determining which tests and procedures should be performed in the initial evaluation is based on clinical judgment, but commonly includes complete metabolic profile, urinalysis, upper GI series, EGD, neurological imaging, acute abdominal series, and CT of the abdomen and pelvis. In addition, pertinent metabolic screening including serum lactate, cortisol, pyruvate, ammonia, creatinine phosphokinase, carnitine, urinary organic acids, and porphobilinogen may be considered.5
Evidence‐based treatment of CVS is limited by the lack of controlled trials. Acutely, patients often require hospitalization and symptom management with aggressive hydration, antiemetics, and sometimes even sedative agents. Empiric abortive treatment with antimigraine mediations (sumitriptan, prochlorperazine, tricyclic antidepressants, and ketorolac) has been effective in case reports.911 Patients in whom a history of chronic cannabinoid use is elicited should be counseled that cessation may lead to an improvement in symptoms.
Just as with migraines, patients who experience frequent episodes of cyclic vomiting can benefit from prophylactic medications. Tricyclic antidepressants (TCAs) have been reported to be effective as prophylactic agents in children with CVS.12 An open‐label treatment group of 17 adult patients with CVS noted that 17% of patients had a complete remission with TCA therapy and almost 60% had a partial response.3 More recently, a retrospective case series of patients who had failed TCAs as maintenance therapy reported that 15 out of the 20 patients studied had improvement in the frequency of their vomiting episodes with the newer antiepileptic drugs zonisamide and levetiracem. However, moderate or severe side effects were reported in 45%.13
Conclusions
In summary, although CVS is still an uncommon diagnosis, it is being made more frequently in adults. Although recognition is increasing, there remains a significant delay between onset of symptoms and diagnosis in adults.4 CVS is a diagnosis of exclusion and should be considered when initial evaluation for recurrent nausea and vomiting are unrevealing. A wide range of medications show benefit for both abortive and prophylactic therapy. Increasing awareness of this disorder can lead to a reduction in invasive and costly diagnostic workups.
- .Evrose de la digestion, caracteriseo par des crises periodiques de vomissements et une profonde modification de l'assimilation.Gazette Medicale de Paris1861:312. [French]
- ,.Cyclical vomiting syndrome in children: a population‐based study.J Pediatr Gastroenterol Nutr.1995;21(4):454–458.
- ,.Cyclic vomiting syndrome in adults: clinical features and response to tricyclic antidepressants.Am J Gastroenterol.1999;94(10):2855–2860.
- ,,,.Cyclic vomiting syndrome in 41 adults: the illness, the patients, and problems of management.BMC Med.2005;3:20.
- ,,.Consensus statement—2nd International Scientific Symposium on CVS. The Faculty of The 2nd International Scientific Symposium on Cyclic Vomiting Syndrome.Dig Dis Sci.1999;44(8 suppl):9S–11S.
- ,,,,.Is cyclic vomiting syndrome related to migraine?J Pediatr.1999;134(5):567–572.
- ,,, et al.Functional gastroduodenal disorders.Gastroenterology.2006;130:1466–1479.
- ,,,.Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis use.Gut.2004;53:1566–1570.
- ,,.Sumatriptan in the treatment of cyclic vomiting.Ann Pharmacother.1995;29(10):997–999.
- .Recurrent vomiting in adults. A syndrome?Med J Aust.1983;1(7):329–331.
- ,,,,.Cyclic vomiting: association with multiple homeostatic abnormalities and response to ketorolac.Am J Gastroenterol.1996;91(10):2228–2232.
- .Effective prophylactic therapy for cyclic vomiting syndrome in children using amitriptyline or cyproheptadine.Pediatrics.1997;100(6):977–981.
- ,,,.Zonisamide or levetiracetam for adults with cyclic vomiting syndrome: a case series.Clin Gastroenterol Hepatol.2007;5(1):44–48.
- .Evrose de la digestion, caracteriseo par des crises periodiques de vomissements et une profonde modification de l'assimilation.Gazette Medicale de Paris1861:312. [French]
- ,.Cyclical vomiting syndrome in children: a population‐based study.J Pediatr Gastroenterol Nutr.1995;21(4):454–458.
- ,.Cyclic vomiting syndrome in adults: clinical features and response to tricyclic antidepressants.Am J Gastroenterol.1999;94(10):2855–2860.
- ,,,.Cyclic vomiting syndrome in 41 adults: the illness, the patients, and problems of management.BMC Med.2005;3:20.
- ,,.Consensus statement—2nd International Scientific Symposium on CVS. The Faculty of The 2nd International Scientific Symposium on Cyclic Vomiting Syndrome.Dig Dis Sci.1999;44(8 suppl):9S–11S.
- ,,,,.Is cyclic vomiting syndrome related to migraine?J Pediatr.1999;134(5):567–572.
- ,,, et al.Functional gastroduodenal disorders.Gastroenterology.2006;130:1466–1479.
- ,,,.Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis use.Gut.2004;53:1566–1570.
- ,,.Sumatriptan in the treatment of cyclic vomiting.Ann Pharmacother.1995;29(10):997–999.
- .Recurrent vomiting in adults. A syndrome?Med J Aust.1983;1(7):329–331.
- ,,,,.Cyclic vomiting: association with multiple homeostatic abnormalities and response to ketorolac.Am J Gastroenterol.1996;91(10):2228–2232.
- .Effective prophylactic therapy for cyclic vomiting syndrome in children using amitriptyline or cyproheptadine.Pediatrics.1997;100(6):977–981.
- ,,,.Zonisamide or levetiracetam for adults with cyclic vomiting syndrome: a case series.Clin Gastroenterol Hepatol.2007;5(1):44–48.
Short Title
A long‐term tunneled subclavian venous catheter of a 32‐year‐old leukaemia patient blocked. Chest x‐ray (CXR) showed a fracture, with the proximal end underneath the first rib and clavicle (Figure 1, arrow, right panel), and distal fragment at the left hila (broken arrow). A CXR 3 months ago showed catheter kinking and narrowing at the same site, constituting the pinch‐off sign (arrow, left panel).1 The broken fragment was retrieved from the left pulmonary artery by cardiac catheterization. Fractured ends were smooth (central insert).
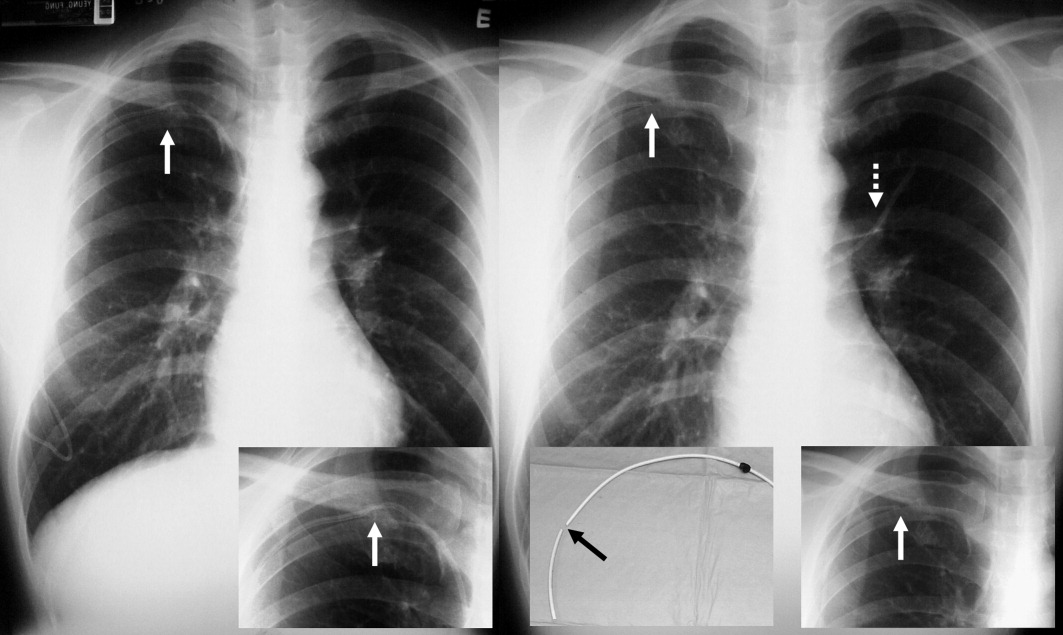
Spontaneous central venous catheter fracture occurs in 0.1% to 1% of cases.2 The catheter fracture is postulated to be related to compression between the clavicle and first rib due to vigorous movement or heavy object lifting,3 activities that should be avoided. Fractures at other sites are exceptional. The pinch‐off sign may precede fracture; if detected, catheter removal is warranted,4 a fact both clinicians and radiologists should be aware of.
- ,.The “pinch‐off sign”: a warning of impending problems with permanent subclavian catheters.Am J Surg.1984;148:633–636.
- ,,,.Spontaneous leak and transection of permanent subclavian catheters.J Surg Oncol.1998;68:166–168.
- ,,.Pinch‐off syndrome: case report and collective review of the literature.Am Surg.2004;70:635–644.
- ,.Prevention of complications in permanent central venous catheters.Surg Gynecol Obstet.1988;167:6–11.
A long‐term tunneled subclavian venous catheter of a 32‐year‐old leukaemia patient blocked. Chest x‐ray (CXR) showed a fracture, with the proximal end underneath the first rib and clavicle (Figure 1, arrow, right panel), and distal fragment at the left hila (broken arrow). A CXR 3 months ago showed catheter kinking and narrowing at the same site, constituting the pinch‐off sign (arrow, left panel).1 The broken fragment was retrieved from the left pulmonary artery by cardiac catheterization. Fractured ends were smooth (central insert).
Spontaneous central venous catheter fracture occurs in 0.1% to 1% of cases.2 The catheter fracture is postulated to be related to compression between the clavicle and first rib due to vigorous movement or heavy object lifting,3 activities that should be avoided. Fractures at other sites are exceptional. The pinch‐off sign may precede fracture; if detected, catheter removal is warranted,4 a fact both clinicians and radiologists should be aware of.
A long‐term tunneled subclavian venous catheter of a 32‐year‐old leukaemia patient blocked. Chest x‐ray (CXR) showed a fracture, with the proximal end underneath the first rib and clavicle (Figure 1, arrow, right panel), and distal fragment at the left hila (broken arrow). A CXR 3 months ago showed catheter kinking and narrowing at the same site, constituting the pinch‐off sign (arrow, left panel).1 The broken fragment was retrieved from the left pulmonary artery by cardiac catheterization. Fractured ends were smooth (central insert).
Spontaneous central venous catheter fracture occurs in 0.1% to 1% of cases.2 The catheter fracture is postulated to be related to compression between the clavicle and first rib due to vigorous movement or heavy object lifting,3 activities that should be avoided. Fractures at other sites are exceptional. The pinch‐off sign may precede fracture; if detected, catheter removal is warranted,4 a fact both clinicians and radiologists should be aware of.
- ,.The “pinch‐off sign”: a warning of impending problems with permanent subclavian catheters.Am J Surg.1984;148:633–636.
- ,,,.Spontaneous leak and transection of permanent subclavian catheters.J Surg Oncol.1998;68:166–168.
- ,,.Pinch‐off syndrome: case report and collective review of the literature.Am Surg.2004;70:635–644.
- ,.Prevention of complications in permanent central venous catheters.Surg Gynecol Obstet.1988;167:6–11.
- ,.The “pinch‐off sign”: a warning of impending problems with permanent subclavian catheters.Am J Surg.1984;148:633–636.
- ,,,.Spontaneous leak and transection of permanent subclavian catheters.J Surg Oncol.1998;68:166–168.
- ,,.Pinch‐off syndrome: case report and collective review of the literature.Am Surg.2004;70:635–644.
- ,.Prevention of complications in permanent central venous catheters.Surg Gynecol Obstet.1988;167:6–11.
Continuing Medical Education Program in
If you wish to receive credit for this activity, which begins on the next page, please refer to the website: www. blackwellpublishing.com/cme.
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which begins on the next page, please refer to the website: www. blackwellpublishing.com/cme.
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which begins on the next page, please refer to the website: www. blackwellpublishing.com/cme.
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to www.blackwellpublishing.com/cme.
-
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
Myth: LBBB Masks Hyperkalemia
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.

Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.
Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.
Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
Hospitalists in the AHSC
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
Copyright © 2010 Society of Hospital Medicine