User login
Moving Beyond Readmission Penalties
Containing the rise of healthcare costs has taken on a new sense of urgency in the wake of the recent economic recession and continued growth in the cost of healthcare. Accordingly, many stakeholders seek solutions to improve value (reducing costs while improving care)[1]; hospital readmissions, which are common and costly,[2] have emerged as a key target. The Centers for Medicare and Medicaid Services (CMS) have instituted several programs intended to reduce readmissions, including funding for community‐based, care‐transition programs; penalties for hospitals with elevated risk‐adjusted readmission rates for selected diagnoses; pioneer Accountable Care Organizations (ACOs) with incentives to reduce global costs of care; and Hospital Engagement Networks (HENs) through the Partnership for Patients.[3] A primary aim of these initiatives is to enhance the quality of care transitions as patients are discharged from the hospital.
Though the recent focus on hospital readmissions has appropriately drawn attention to transitions in care, some have expressed concerns. Among these are questions about: 1) the extent to which readmissions truly reflect the quality of hospital care[4]; 2) the preventability of readmissions[5]; 3) limitations in risk‐adjustment techniques[6]; and 4) best practices for preventing readmissions.[7] We believe these concerns stem in part from deficiencies in the state of the science of transitional care, and that future efforts in this area will be hindered without a clear vision of an ideal transition in care. We propose the key components of an ideal transition in care and discuss the implications of this concept as it pertains to hospital readmissions.
THE IDEAL TRANSITION IN CARE
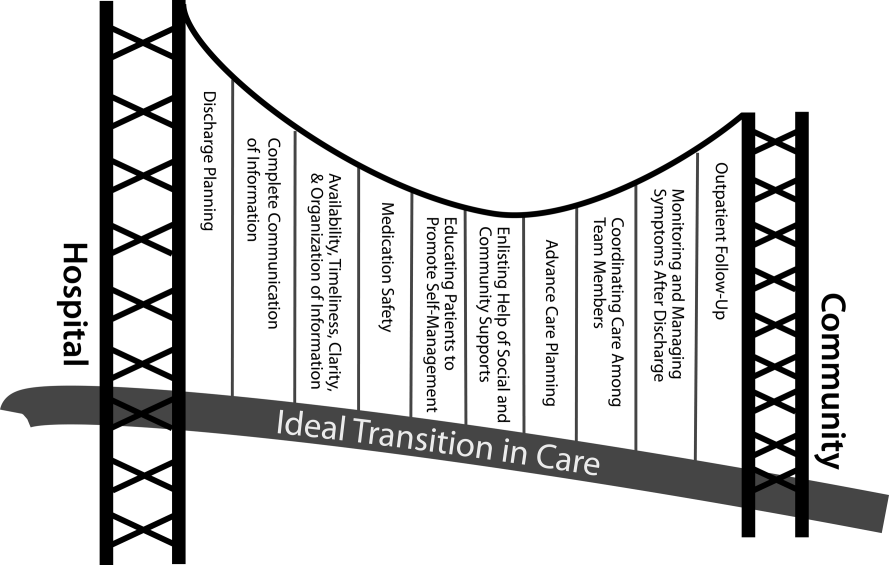
We propose the key components of an ideal transition in care in Figure 1 and Table 1. Figure 1 represents 10 domains described more fully below as structural supports of the bridge patients must cross from one care environment to another during a care transition. This figure highlights key domains and suggests that lack of a domain makes the bridge weaker and more prone to gaps in care and poor outcomes. It also implies that the more components are missing, the less safe is the bridge or transition. Those domains that mainly take place prior to discharge are placed closer to the hospital side of the bridge, those that mainly take place after discharge are placed closer to the community side of the bridge, while those that take place both prior to and after discharge are in the middle. Table 1 provides descriptions of the key content for each of these domains, as well as guidance about which personnel might be involved and where in the transition process that domain should be implemented. We support these domains with supporting evidence where available.
| Domain | Who | When | References |
|---|---|---|---|
| |||
| Discharge planning | |||
| Use a multidisciplinary team to create a discharge plan | Discharging clinician | Predischarge | 911 |
| Collaborate with PCP regarding discharge and follow‐up plan | Care managers/discharge planners | ||
| Arrange follow‐up appointments prior to discharge | Nurses | ||
| Make timely appointments for follow‐up care | |||
| Make appointments that take patient and caregiver's schedules and transportation needs into account | |||
| Complete communication of information | |||
| Includes: | Discharging clinician | Time of discharge | 1214 |
| Patient's full name | |||
| Age | |||
| Dates of admission and discharge | |||
| Names of responsible hospital physicians | |||
| Name of physician preparing discharge summary | |||
| Name of PCP | |||
| Main diagnosis | |||
| Other relevant diagnoses, procedures, and complications | |||
| Relevant findings at admission | |||
| Treatment and response for each active problem | |||
| Results of procedures and abnormal laboratory test results | |||
| Recommendations of any subspecialty consultants | |||
| Patient's functional status at discharge | |||
| Discharge medications | |||
| Follow‐up appointments made and those to be made | |||
| Tests to be ordered and pending tests to be followed‐up | |||
| Counseling provided to patient and caregiver, when applicable | |||
| Contingency planning | |||
| Code status | |||
| Availability, timeliness, clarity, and organization of information | |||
| Timely communication with postdischarge providers verbally (preferred) or by fax/e‐mail | Discharging clinician | Time of discharge | 1214 |
| Timely completion of discharge summary and reliable transmission to postdischarge providers | |||
| Availability of information in medical record | |||
| Use of a structured template with subheadings in discharge communication | |||
| Medication safety | |||
| Take an accurate preadmission medication history | Clinicians | Admission | 1521 |
| Reconcile preadmission medications with all ordered medications at all transfers in care, including discharge | Pharmacists | Throughout hospitalization | |
| Communicate discharge medications to all outpatient providers, including all changes and rationale for those changes | Nurses | Time of discharge | |
| Educating patients, promoting self‐management | |||
| Focus discharge counseling on major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, warning signs and symptoms, and who to contact for problems | Clinicians | Daily | 911, 2228, 30 |
| Include caregivers as appropriate | Nurses | Time of discharge | |
| Ensure staff members provide consistent messages | Care managers/discharge planners | Postdischarge | |
| Provide simply written patient‐centered materials with instructions | Transition coaches | ||
| Use teach‐back methods to confirm understanding | |||
| Encourage questions | |||
| Continue teaching during postdischarge follow‐up | |||
| Use transition coaches in high‐risk patients: focus on medication management, keeping a personal medical record, follow‐up appointments, and knowledge of red flags | |||
| Enlisting help of social and community supports | |||
| Assess needs and appropriately arrange for home services | Clinicians | Predischarge and postdischarge | 29, 30 |
| Enlist help of caregivers | Nurses | ||
| Enlist help of community supports | Care managers | ||
| Home health staff | |||
| Advanced care planning | |||
| Establish healthcare proxy | Clinicians | Predischarge and postdischarge | 31, 32 |
| Discuss goals of care | Palliative care staff | ||
| Palliative care consultation (if appropriate) | Social workers | ||
| Enlist hospice services (if appropriate) | Nurses | ||
| Hospice workers | |||
| Coordinating care among team members | |||
| Share medical records | Clinicians | Predischarge and postdischarge | 33 |
| Communicate involving all team members | Nurses | ||
| Optimize continuity of providers and formal handoffs of care | Office personnel | ||
| IT staff | |||
| Monitoring and managing symptoms after discharge | |||
| Monitor for: | Clinicians | Postdischarge | 1113, 28, 3436 |
| Worsening disease control | Nurses | ||
| Medication side effects, discrepancies, nonadherence | Pharmacists | ||
| Therapeutic drug monitoring | Care managers | ||
| Inability to manage conditions at home | Visiting nurses and other home health staff | ||
| Via: | |||
| Postdischarge phone calls | |||
| Home visits | |||
| Postdischarge clinic visits | |||
| Patient hotline | |||
| Availability of inpatient providers after discharge | |||
| Follow‐up with outpatient providers | |||
| Within an appropriate time frame (eg, 7 d or sooner for high‐risk patients) | Clinicians | Postdischarge | 3740 |
| With appropriate providers (eg, most related to reasons for hospitalization, who manage least stable conditions, and/or PCP) | Nurses Pharmacists | ||
| Utilize multidisciplinary teams as appropriate | Care managers | ||
| Ensure appropriate progress along plan of care and safe transition | Office personnel | ||
| Other clinical staff as appropriate | |||
Our concept of an ideal transition in care began with work by Naylor, who described several important components of a safe transition in care, including complete communication of information, patient education, enlisting the help of social and community supports, ensuring continuity of care, and coordinating care among team members.[8] It is supplemented by the Transitions of Care Consensus Policy Statement proposed by representatives from hospital medicine, primary care, and emergency medicine, which emphasized aspects of timeliness and content of communication between providers.[9] Our present articulation of these key components includes 10 organizing domains.
The Discharge Planning domain highlights the important principle of planning ahead for hospital discharge while the patient is still being treated in the hospital, a paradigm espoused by Project RED[10] and other successful care transitions interventions.[11, 12] Collaborating with the outpatient provider and taking the patient and caregiver's preferences for appointment scheduling into account can help ensure optimal outpatient follow‐up.
Complete Communication of Information refers to the content that should be included in discharge summaries and other means of information transfer from hospital to postdischarge care. The specific content areas are based on the Society of Hospital Medicine and Society of General Internal Medicine Continuity of Care Task Force systematic review and recommendations,[13] which takes into account information requested by primary care physicians after discharge.
Availability, Timeliness, Clarity, and Organization of that information is as important as the content because postdischarge providers must be able to access and quickly understand the information they have been provided before assuming care of the patient.[14, 15]
The Medication Safety domain is of central importance because medications are responsible for most postdischarge adverse events.[16] Taking an accurate medication history,[17] reconciling changes throughout the hospitalization,[18] and communicating the reconciled medication regimen to patients and providers across transitions of care can reduce medication errors and improve patient safety.[19, 20, 21, 22]
The Patient Education and Promotion of Self‐Management domain involves teaching patients and their caregivers about the main hospital diagnoses and instructions for self‐care, including medication changes, appointments, and whom to contact if issues arise. Confirming comprehension of instructions through assessments of acute (delirium) and chronic (dementia) cognitive impairments[23, 24, 25, 26] and teach‐back from the patient (or caregiver) is an important aspect of such counseling, as is providing patients and caregivers with educational materials that are appropriate for their level of health literacy and preferred language.[14] High‐risk patients may benefit from patient coaching to improve their self‐management skills.[12] These recommendations are based on years of health literacy research,[27, 28, 29] and such elements are generally included in effective interventions (including Project RED,[10] Naylor and colleagues' Transitional Care Model,[11] and Coleman and colleagues' Care Transitions Intervention[12]).
Enlisting the help of Social and Community Supports is an important adjunct to medical care and is the rationale for the recent increase in CMS funding for community‐based, care‐transition programs. These programs are crucial for assisting patients with household activities, meals, and other necessities during the period of recovery, though they should be distinguished from care management or care coordination interventions, which have not been found to be helpful in preventing readmissions unless high touch in nature.[30, 31]
The Advanced Care Planning domain may begin in the hospital or outpatient setting, and involves establishing goals of care and healthcare proxies, as well as engaging with palliative care or hospice services if appropriate. Emerging evidence supports the intuitive conclusion that this approach prevents readmissions, particularly in patients who do not benefit from hospital readmission.[32, 33]
Attention to the Coordinating Care Among Team Members domain is needed to synchronize efforts across settings and providers. Clearly, many healthcare professionals as well as other involved parties can be involved in helping a single patient during transitions in care. It is vital that they coordinate information, assessments, and plans as a team.[34]
We recognize the domain of Monitoring and Managing Symptoms After Discharge as increasingly crucial as reflected in our growing understanding of the reasons for readmission, especially among patients with fragile conditions such as heart failure, chronic lung disease, gastrointestinal disorders, dementia,[23, 24, 25, 26] and vascular disease.[35] Monitoring for new or worsening symptoms; medication side effects, discrepancies, or nonadherence; and other self‐management challenges will allow problems to be detected and addressed early, before they result in unplanned healthcare utilization. It is noteworthy that successful interventions in this regard rely on in‐home evaluation[13, 14, 29] by nurses rather than telemonitoring, which in isolation has not been effective to date.[36, 37]
Finally, optimal Outpatient Follow‐Up with appropriate postdischarge providers is crucial for providing ideal transitions. These appointments need to be prompt[38, 39] (eg, within 7 days if not sooner for high‐risk patients) and with providers who have a longitudinal relationship to the patient, as prior work has shown increased readmissions when the provider is unfamiliar with the patient.[40] The advantages and disadvantages of hospitalist‐run postdischarge clinics as one way to increase access and expedite follow‐up are currently being explored. Although the optimal content of a postdischarge visit has not been defined, logical tasks to be completed are myriad and imply the need for checklists, adequate time, and a multidisciplinary team of providers.[41]
IMPLICATIONS OF THE IDEAL TRANSITION IN CARE
Our conceptualization of an ideal transition in care provides insight for hospital and healthcare system leadership, policymakers, researchers, clinicians, and educators seeking to improve transitions of care and reduce hospital readmissions. In the sections below, we briefly review commonly cited concerns about the recent focus on readmissions as a quality measure, illustrate how the Ideal Transition in Care addresses these concerns, and propose fruitful areas for future work.
How Does the Framework Address the Extent to Which Readmissions Reflect Hospital Quality?
One of the chief problems with readmissionrates as a hospital quality measure is that many of the factors that influence readmission may not currently be under the hospital's control. The healthcare environment to which a patient is being discharged (and was admitted from in the first place) is an important determinant of readmission.[42] In this context, it is noteworthy that successful interventions to reduce readmission are generally those that focus on outpatient follow‐up, while inpatient‐only interventions have had less success.[7] This is reflected in our framework above, informed by the literature, highlighting the importance of coordination between inpatient and outpatient providers and the importance of postdischarge care, including monitoring and managing symptoms after discharge, prompt follow‐up appointments, the continuation of patient self‐management activities, monitoring for drug‐related problems after discharge, and the effective utilization of community supports. Accountable care organizations, once established, would be responsible for several components of this environment, including the provision of prompt and effective follow‐up care.
The implication of the framework is that if a hospital does not have control over most of the factors that influence its readmission rate, it should see financial incentives to reduce readmission rates as an opportunity to invest in relationships with the outpatient environment from which their patients are admitted and to which they are discharged. One can envision hospitals growing ever‐closer relationships with their network of primary care physician groups, community agencies, and home health services, rehabilitation facilities, and nursing homes through coordinated discharge planning, medication management, patient education, shared electronic medical records, structured handoffs in care, and systems of intensive outpatient monitoring. Our proposed framework, in other words, emphasizes that hospitals cannot reduce their readmission rates by focusing on aspects of care within their walls. They must forge new and stronger relationships with their communities if they are to be successful.
How Does the Framework Help Us Understand Which Readmissions Are Preventable?
Public reporting and financial penalties are currently tied to all‐cause readmission, but preventable readmissions are a more appealing outcome to target. In one study, the ranking of hospitals by all‐cause readmission rate had very little correlation with the ranking by preventable readmission rate.[5] However, researchers have struggled to establish standardized, valid, and reliable measures for determining what proportion of readmissions are in fact preventable, with estimates ranging from 5% to 79% in the published literature.[43]
The difficulty of accurately determining preventability stems from an inadequate understanding of the roles that patient comorbidities, transitional processes of care, individual patient behaviors, and social and environmental determinants of health play in the complex process of hospital recidivism. Our proposed elements of an ideal transition in care provide a structure to frame this discussion and suggest future research opportunities to allow a more accurate and reliable understanding of the spectrum of preventability. Care system leadership can use the framework to rigorously evaluate their readmissions and determine the extent to which the transitions process approached the ideal. For example, if a readmission occurs despite care processes that addressed most of the domains with high fidelity, it becomes much less likely that the readmission was preventable. It should be noted that the converse is not always true: When a transition falls well short of the ideal, it does not always imply that provision of a more ideal transition would necessarily have prevented the readmission, but it does make it more likely.
For educators, the framework may provide insights for trainees into the complexity of the transitions process and vulnerability of patients during this time, highlighting preventable aspects of readmissions that are within the grasp of the discharging clinician or team. It highlights the importance of medication reconciliation, synchronous communication, and predischarge teaching, which are measurable and teachable skills for non‐physician providers, housestaff, and medical students. It also may allow for more structured feedback, for example, on the quality of discharge summaries produced by trainees.
How Could the Framework Improve Risk Adjustment for Between‐Hospital Comparisons?
Under the Patient Protection and Affordable Care Act (PPACA), hospitals will be compared to one another using risk‐standardized readmission rates as a way to penalize poorly performing hospitals. However, risk‐adjustment models have only modest ability to predict hospital readmission.[6] Moreover, current approaches predominantly adjust for patients' medical comorbidities (which are easily measurable), but they do not adequately take into account the growing literature on other factors that influence readmission rates, including a patient's health literacy, visual or cognitive impairment, functional status, language barriers, and community‐level factors such as social supports.[44, 45]
The Ideal Transition of Care provides a comprehensive framework of hospital discharge quality that provides additional process measures on which hospitals could be compared rather than focusing solely on (inadequately) risk‐adjusted readmission rates. Indeed, most other quality and safety measures (such as the National Quality Forum's Safe Practices[46] and The Joint Commission's National Patient Safety Goals),[47] emphasize process over outcome, in part because of issues of fairness. Process measures are less subject to differences in patient populations and also change the focus from simply reducing readmissions to improving transitional care more broadly. These process measures should be based on our framework and should attempt to capture as many dimensions of an optimal care transition as possible.
Possible examples of process measures include: the accuracy of medication reconciliation at admission and discharge; provision of prompt outpatient follow‐up; provision of adequate systems to monitor and manage symptoms after discharge; advanced care planning in appropriate patients; and the quality of discharge education, incorporating measurements of the patient's understanding and ability to self‐manage their illness. At least some of these could be used now as part of a performance measurement set that highlights opportunities for immediate system change and can serve as performance milestones.
The framework could also be used to validate risk‐adjustment techniques. After accounting for patient factors, the remaining variability in outcomes should be accounted for by processes of care that are in the transitions framework. Once these processes are accurately measured, one can determine if indeed the remaining variability is due to transitions processes, or rather unaccounted factors that are not being measured and that hospitals may have little control over. Such work can lead to iterative refinement of patient risk‐adjustment models.
What Does the Framework Imply About Best Practices for Reducing Readmission Rates?
Despite the limitations of readmission rates as a quality measure noted above, hospitals presently face potentially large financial penalties for readmissions and are allocating resources to readmission reduction efforts. However, hospitals currently may not have enough guidance to know what actions to take to reduce readmissions, and thus could be spending money inefficiently and reducing the value proposition of focusing on readmissions.
A recent systematic review of interventions hospitals could employ to reduce readmissions identified several positive studies, but also many negative studies, and there were significant barriers to understanding what works to reduce readmissions.[7] For example, most of the interventions described in both positive and negative studies were multifaceted, and the authors were unable to identify which components of the intervention were most effective. Also, while several studies have identified risk factors for readmission,[6, 48, 49] very few studies have identified which subgroups of patients benefit most from specific interventions. Few of the studies described key contextual factors that may have led to successful or failed implementation, or the fidelity with which the intervention was implemented.[50, 51, 52]
Few if any of the studies were guided by a concept of the ideal transition in care.[10] Such a framework will better guide development of multifaceted interventions and provide an improved means for interpreting the results. Clearly, rigorously conducted, multicenter studies of readmission prevention interventions are needed to move the field forward. These studies should: 1) correlate implementation of specific intervention components with reductions in readmission rates to better understand the most effective components; 2) be adequately powered to show effect modification, ie, which patients benefit most from these interventions; and 3) rigorously measure environmental context and intervention fidelity, and employ mixed methods to better understand predictors of implementation success and failure.
Our framework can be used in the design and evaluation of such interventions. For example, interventions could be designed that incorporate as many of the domains of an ideal transition as possible, in particular those that span the inpatient and outpatient settings. Processes of care metrics can be developed that measure the extent to which each domain is delivered, analogous to the way the Joint Commission might aggregate individual scores on the 10 items in Acute Myocardial Infarction Core Measure Set[53] to provide a composite of the quality of care provided to patients with this diagnosis. These can be used to correlate certain intervention components with success in reducing readmissions and also in measuring intervention fidelity.
NEXT STEPS
For hospital and healthcare system leaders, who need to take action now to avoid financial penalties, we recommend starting with proven, high‐touch interventions such as Project RED and the Care Transitions Intervention, which are durable, cost‐effective, robustly address multiple domains of the Ideal Transition in Care, and have been implemented at numerous sites.[54, 55] Each hospital or group will need to decide on a bundle of interventions and customize them based on local workflow, resources, and culture.
Risk‐stratification, to match the intensity of the intervention to the risk of readmission of the patient, will undoubtedly be a key component for the efficient use of resources. We anticipate future research will allow risk stratification to be a robust part of any implementation plan. However, as noted above, current risk prediction models are imperfect,[6] and more work is needed to determine which patients benefit most from which interventions. Few if any studies have described interventions tailored to risk for this reason.
Based on our ideal transition in care, our collective experience, and published evidence,[7, 10, 11, 12] potential elements to start with include: early discharge planning; medication reconciliation[56]; patient/caregiver education using health literacy principles, cognitive assessments, and teach‐back to confirm understanding; synchronous communication (eg, by phone) between inpatient and postdischarge providers; follow‐up phone calls to patients within 72 hours of discharge; 24/7 availability of a responsible inpatient provider to address questions and problems (both from the patient/caregiver and from postdischarge providers); and prompt appointments for patients discharged home. High‐risk patients will likely require additional interventions, including in‐home assessments, disease‐monitoring programs, and/or patient coaching. Lastly, patients with certain conditions prone to readmission (such as heart failure and chronic obstructive pulmonary disease) may benefit from disease‐specific programs, including patient education, outpatient disease management, and monitoring protocols.
It is likely that the most effective interventions are those that come from combined, coordinated interventions shared between inpatient and outpatient settings, and are intensive in nature. We expect that the more domains in the framework that are addressed, the safer and more seamless transitions in care will be, with improvement in patient outcomes. To the extent that fragmentation of care has been a barrier to the implementation of these types of interventions in the past, ACOs, perhaps with imbedded Patient‐Centered Medical Homes, may be in the best position to take advantage of newly aligned financial incentives to design comprehensive transitional care. Indeed, we anticipate that Figure 1 may provide substrate for a discussion of postdischarge care and division of responsibilities between inpatient and outpatient care teams at the time of transition, so effort is not duplicated and multiple domains are addressed.
Other barriers to implementation of ideal transitions in care will continue to be an issue for most healthcare systems. Financial constraints that have been a barrier up until now will be partially overcome by penalties for high readmission rates and by ACOs, bundled payments, and alternative care contracts (ie, global payments), but the extent to which each institution feels rewarded for investing in transitional interventions will vary greatly. Healthcare leadership that sees the value of improving transitions in care will be critical to overcoming this barrier. Competing demands (such as lowering hospital length of stay and carrying out other patient care responsibilities),[57] lack of coordination and diffusion of responsibility among various clinical personnel, and lack of standards are other barriers[58] that will require clear prioritization from leadership, policy changes, team‐based care, provider education and feedback, and adequate allocation of personnel resources. In short, process redesign using continuous quality improvement efforts and effective tools will be required to maximize the possibility of success.
CONCLUSIONS
Readmissions are costly and undesirable. Intuition suggests they are a marker of poor care and that hospitals should be capable of reducing them, thereby improving care and decreasing costs. In a potential future world of ACOs based on global payments, financial incentives would be aligned for each system to reduce readmissions below their current baseline, therefore obviating the need for external financial rewards and penalties. In the meantime, financial penalties do exist, and controversy exists over their fairness and likelihood of driving appropriate behavior. To address these controversies and promote better transitional care, we call for the development and use of multifaceted, collaborative transitions interventions that span settings, risk‐adjustment models that allow for fairer comparisons among hospitals, better and more widespread measurement of processes of transitional care, a better understanding of what interventions are most effective and in whom, and better guidance in how to implement these interventions. Our conceptualization of an ideal transition of care serves as a guide and provides a common vocabulary for these efforts. Such research is likely to produce the knowledge needed for healthcare systems to improve transitions in care, reduce readmissions, and reduce costs.
Disclosure
Funding for Dr Vasilevskis has been provided by the National Institutes of Health (K23AG040157) and the VA Tennessee Valley Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging, the National Institutes of Health, or the US Department of Veterans Affairs.
- , . Redefining Health Care: Creating Value‐Based Competition on Results. Boston, MA:Harvard Business School Press;2006.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act (PPACA). Public Law 111–148; 2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/pdf/PLAW‐111publ148.pdf. Accessed on June 4, 2012.
- , . Hospital readmission as an accountability measure. JAMA. 2011;305(5):504–505.
- , , , et al. Incidence of potentially avoidable urgent readmissions and their relation to all‐cause urgent readmissions. Can Med Assoc J. 2011;183(14):E1067–E1072.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306(15):1688–1698.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- . A decade of transitional care research with vulnerable elders. J Cardiovasc Nurs. 2000;14(3):1–14.
- , , , et al;for the American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. Transitions of Care Consensus Policy Statement American College of Physicians–Society of General Internal Medicine–Society of Hospital Medicine–American Geriatrics Society–American College of Emergency Physicians–Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971–976.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial. JAMA. 1999;281(7):613–620.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , , , , , . Discharge documentation of patients discharged to subacute facilities: a three‐year quality improvement process across an integrated health care system. Jt Comm J Qual Patient Saf. 2010;36(6):243–251.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , , , . Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Can Med Assoc J. 2005;173(5):510–515.
- , , , et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–1422.
- , , et al;for the PILL‐CVD (Pharmacist Intervention for Low Literacy in Cardiovascular Disease) Study Group. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , . Hospital‐based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172(14):1057–1069.
- , , , et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster‐randomized trial. Arch Intern Med. 2009;169(8):771–780.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , , . Insufficient help for activity of daily living disabilities and risk of all–cause hospitalization. J Am Geriatr Soc. 2012;60(5):927–933.
- , , , et al. Transitions in care for older adults with and without dementia. J Am Geriatr Soc. 2012;60(5):813–820.
- , , , , . Association of incident dementia with hospitalizations. JAMA. 2012;307(2):165–172.
- , , , et al. Potentially avoidable hospitalizations of dually eligible Medicare and Medicaid beneficiaries from nursing facility and home– and community–based services waiver programs. J Am Geriatr Soc. 2012;60(5):821–829.
- , . Teaching about health literacy and clear communication. J Gen Intern Med. 2006;21(8):888–890.
- , , , et al. Health literacy and outcomes among patients with heart failure. JAMA. 2011;305(16):1695–1701.
- , , , , . Patient experiences of transitioning from hospital to home: an ethnographic quality improvement project. J Hosp Med. 2012;7(5):382–387.
- , , , . Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA. 2009;301(6):603–618.
- , , , , . How changes in Washington University's Medicare coordinated care demonstration pilot ultimately achieved savings. Health Aff (Millwood). 2012;31(6):1216–1226.
- , , , et al. Quality of care and rehospitalization rate in the last stage of disease in brain tumor patients assisted at home: a cost effectiveness study. J Palliat Med. 2012;15(2):225–227.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15(2):48–51.
- , , , et al. TeamSTEPPS™: team strategies and tools to enhance performance and patient safety. In: Henriksen K, Battles JB, Keyes MA, Grady ML, ed. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3: Performance and Tools. Rockville, MD:Agency for Healthcare Research and Quality; August2008.
- , , , et al. Factors contributing to all‐cause 30‐day readmissions: a structured case series across 18 hospitals. Med Care. 2012;50(7):599–605.
- , , , et al. Telemonitoring in patients with heart failure [erratum, N Engl J Med. 2011;364(5):490]. N Engl J Med. 2010;363(24):2301–2309.
- , , , et al. A randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visits. Arch Intern Med. 2012;172(10):773–779.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303(17):1716–1722.
- , , . Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , . Does increased access to primary care reduce hospital readmissions? Veterans Affairs Cooperative Study Group on Primary Care and Hospital Readmission. N Engl J Med. 1996;334(22):1441–1447.
- . The Post‐Hospital Follow‐Up Visit: A Physician Checklist to Reduce Readmissions. California Healthcare Foundation; October 2010. Available at: http://www.chcf.org/publications/2010/10/the‐post‐hospital‐follow‐up‐visit‐a‐physician‐checklist. Accessed on January 10, 2012.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , , . Proportion of hospital readmissions deemed avoidable: a systematic review. Can Med Assoc J. 2011;183(7):E391–E402.
- , , , et al. Postdischarge environmental and socioeconomic factors and the likelihood of early hospital readmission among community‐dwelling Medicare beneficiaries. Gerontologist. 2008;48(4):495–504.
- , , , , . Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107.
- National Quality Forum. Safe Practices for Better Healthcare—2010 Update: A Consensus Report. Washington, DC;2010.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation Program: Hospital 2010 National Patient Safety Goals (NPSGs). 2010. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed on March 20, 2012.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211–219.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. Can Med Assoc J. 2010;182(6):551–557.
- , . Evaluating service delivery interventions to enhance patient safety. BMJ. 2008;337:a2764.
- , , . Assessing the Evidence for Context‐Sensitive Effectiveness and Safety of Patient Safety Practices: Developing Criteria. Rockville, MD:Agency for Healthcare Research and Quality; December2010.
- , , , et al. Advancing the science of patient safety. Ann Intern Med. 2011;154(10):693–696.
- The Joint Commission. Acute Myocardial Infarction Core Measure Set. Available at: http://www.jointcommission.org/assets/1/6/Acute%20Myocardial%20Infarction.pdf. Accessed August 20,2012.
- , , , , , . The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171(14):1232–1237.
- Project RED toolkit, AHRQ Innovations Exchange. Available at:http://www.innovations.ahrq.gov/content.aspx?id=2180. Accessed on July 2, 2012.
- , , , et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894–900.
- , . Thirty‐day readmissions—truth and consequences. N Engl J Med. 2012;366(15):1366–1369.
- , , , , . “Out of sight, out of mind”: housestaff perceptions of quality‐limiting factors in discharge care at teaching hospitals. J Hosp Med. 2012;7(5):376–381.
Containing the rise of healthcare costs has taken on a new sense of urgency in the wake of the recent economic recession and continued growth in the cost of healthcare. Accordingly, many stakeholders seek solutions to improve value (reducing costs while improving care)[1]; hospital readmissions, which are common and costly,[2] have emerged as a key target. The Centers for Medicare and Medicaid Services (CMS) have instituted several programs intended to reduce readmissions, including funding for community‐based, care‐transition programs; penalties for hospitals with elevated risk‐adjusted readmission rates for selected diagnoses; pioneer Accountable Care Organizations (ACOs) with incentives to reduce global costs of care; and Hospital Engagement Networks (HENs) through the Partnership for Patients.[3] A primary aim of these initiatives is to enhance the quality of care transitions as patients are discharged from the hospital.
Though the recent focus on hospital readmissions has appropriately drawn attention to transitions in care, some have expressed concerns. Among these are questions about: 1) the extent to which readmissions truly reflect the quality of hospital care[4]; 2) the preventability of readmissions[5]; 3) limitations in risk‐adjustment techniques[6]; and 4) best practices for preventing readmissions.[7] We believe these concerns stem in part from deficiencies in the state of the science of transitional care, and that future efforts in this area will be hindered without a clear vision of an ideal transition in care. We propose the key components of an ideal transition in care and discuss the implications of this concept as it pertains to hospital readmissions.
THE IDEAL TRANSITION IN CARE
We propose the key components of an ideal transition in care in Figure 1 and Table 1. Figure 1 represents 10 domains described more fully below as structural supports of the bridge patients must cross from one care environment to another during a care transition. This figure highlights key domains and suggests that lack of a domain makes the bridge weaker and more prone to gaps in care and poor outcomes. It also implies that the more components are missing, the less safe is the bridge or transition. Those domains that mainly take place prior to discharge are placed closer to the hospital side of the bridge, those that mainly take place after discharge are placed closer to the community side of the bridge, while those that take place both prior to and after discharge are in the middle. Table 1 provides descriptions of the key content for each of these domains, as well as guidance about which personnel might be involved and where in the transition process that domain should be implemented. We support these domains with supporting evidence where available.
| Domain | Who | When | References |
|---|---|---|---|
| |||
| Discharge planning | |||
| Use a multidisciplinary team to create a discharge plan | Discharging clinician | Predischarge | 911 |
| Collaborate with PCP regarding discharge and follow‐up plan | Care managers/discharge planners | ||
| Arrange follow‐up appointments prior to discharge | Nurses | ||
| Make timely appointments for follow‐up care | |||
| Make appointments that take patient and caregiver's schedules and transportation needs into account | |||
| Complete communication of information | |||
| Includes: | Discharging clinician | Time of discharge | 1214 |
| Patient's full name | |||
| Age | |||
| Dates of admission and discharge | |||
| Names of responsible hospital physicians | |||
| Name of physician preparing discharge summary | |||
| Name of PCP | |||
| Main diagnosis | |||
| Other relevant diagnoses, procedures, and complications | |||
| Relevant findings at admission | |||
| Treatment and response for each active problem | |||
| Results of procedures and abnormal laboratory test results | |||
| Recommendations of any subspecialty consultants | |||
| Patient's functional status at discharge | |||
| Discharge medications | |||
| Follow‐up appointments made and those to be made | |||
| Tests to be ordered and pending tests to be followed‐up | |||
| Counseling provided to patient and caregiver, when applicable | |||
| Contingency planning | |||
| Code status | |||
| Availability, timeliness, clarity, and organization of information | |||
| Timely communication with postdischarge providers verbally (preferred) or by fax/e‐mail | Discharging clinician | Time of discharge | 1214 |
| Timely completion of discharge summary and reliable transmission to postdischarge providers | |||
| Availability of information in medical record | |||
| Use of a structured template with subheadings in discharge communication | |||
| Medication safety | |||
| Take an accurate preadmission medication history | Clinicians | Admission | 1521 |
| Reconcile preadmission medications with all ordered medications at all transfers in care, including discharge | Pharmacists | Throughout hospitalization | |
| Communicate discharge medications to all outpatient providers, including all changes and rationale for those changes | Nurses | Time of discharge | |
| Educating patients, promoting self‐management | |||
| Focus discharge counseling on major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, warning signs and symptoms, and who to contact for problems | Clinicians | Daily | 911, 2228, 30 |
| Include caregivers as appropriate | Nurses | Time of discharge | |
| Ensure staff members provide consistent messages | Care managers/discharge planners | Postdischarge | |
| Provide simply written patient‐centered materials with instructions | Transition coaches | ||
| Use teach‐back methods to confirm understanding | |||
| Encourage questions | |||
| Continue teaching during postdischarge follow‐up | |||
| Use transition coaches in high‐risk patients: focus on medication management, keeping a personal medical record, follow‐up appointments, and knowledge of red flags | |||
| Enlisting help of social and community supports | |||
| Assess needs and appropriately arrange for home services | Clinicians | Predischarge and postdischarge | 29, 30 |
| Enlist help of caregivers | Nurses | ||
| Enlist help of community supports | Care managers | ||
| Home health staff | |||
| Advanced care planning | |||
| Establish healthcare proxy | Clinicians | Predischarge and postdischarge | 31, 32 |
| Discuss goals of care | Palliative care staff | ||
| Palliative care consultation (if appropriate) | Social workers | ||
| Enlist hospice services (if appropriate) | Nurses | ||
| Hospice workers | |||
| Coordinating care among team members | |||
| Share medical records | Clinicians | Predischarge and postdischarge | 33 |
| Communicate involving all team members | Nurses | ||
| Optimize continuity of providers and formal handoffs of care | Office personnel | ||
| IT staff | |||
| Monitoring and managing symptoms after discharge | |||
| Monitor for: | Clinicians | Postdischarge | 1113, 28, 3436 |
| Worsening disease control | Nurses | ||
| Medication side effects, discrepancies, nonadherence | Pharmacists | ||
| Therapeutic drug monitoring | Care managers | ||
| Inability to manage conditions at home | Visiting nurses and other home health staff | ||
| Via: | |||
| Postdischarge phone calls | |||
| Home visits | |||
| Postdischarge clinic visits | |||
| Patient hotline | |||
| Availability of inpatient providers after discharge | |||
| Follow‐up with outpatient providers | |||
| Within an appropriate time frame (eg, 7 d or sooner for high‐risk patients) | Clinicians | Postdischarge | 3740 |
| With appropriate providers (eg, most related to reasons for hospitalization, who manage least stable conditions, and/or PCP) | Nurses Pharmacists | ||
| Utilize multidisciplinary teams as appropriate | Care managers | ||
| Ensure appropriate progress along plan of care and safe transition | Office personnel | ||
| Other clinical staff as appropriate | |||
Our concept of an ideal transition in care began with work by Naylor, who described several important components of a safe transition in care, including complete communication of information, patient education, enlisting the help of social and community supports, ensuring continuity of care, and coordinating care among team members.[8] It is supplemented by the Transitions of Care Consensus Policy Statement proposed by representatives from hospital medicine, primary care, and emergency medicine, which emphasized aspects of timeliness and content of communication between providers.[9] Our present articulation of these key components includes 10 organizing domains.
The Discharge Planning domain highlights the important principle of planning ahead for hospital discharge while the patient is still being treated in the hospital, a paradigm espoused by Project RED[10] and other successful care transitions interventions.[11, 12] Collaborating with the outpatient provider and taking the patient and caregiver's preferences for appointment scheduling into account can help ensure optimal outpatient follow‐up.
Complete Communication of Information refers to the content that should be included in discharge summaries and other means of information transfer from hospital to postdischarge care. The specific content areas are based on the Society of Hospital Medicine and Society of General Internal Medicine Continuity of Care Task Force systematic review and recommendations,[13] which takes into account information requested by primary care physicians after discharge.
Availability, Timeliness, Clarity, and Organization of that information is as important as the content because postdischarge providers must be able to access and quickly understand the information they have been provided before assuming care of the patient.[14, 15]
The Medication Safety domain is of central importance because medications are responsible for most postdischarge adverse events.[16] Taking an accurate medication history,[17] reconciling changes throughout the hospitalization,[18] and communicating the reconciled medication regimen to patients and providers across transitions of care can reduce medication errors and improve patient safety.[19, 20, 21, 22]
The Patient Education and Promotion of Self‐Management domain involves teaching patients and their caregivers about the main hospital diagnoses and instructions for self‐care, including medication changes, appointments, and whom to contact if issues arise. Confirming comprehension of instructions through assessments of acute (delirium) and chronic (dementia) cognitive impairments[23, 24, 25, 26] and teach‐back from the patient (or caregiver) is an important aspect of such counseling, as is providing patients and caregivers with educational materials that are appropriate for their level of health literacy and preferred language.[14] High‐risk patients may benefit from patient coaching to improve their self‐management skills.[12] These recommendations are based on years of health literacy research,[27, 28, 29] and such elements are generally included in effective interventions (including Project RED,[10] Naylor and colleagues' Transitional Care Model,[11] and Coleman and colleagues' Care Transitions Intervention[12]).
Enlisting the help of Social and Community Supports is an important adjunct to medical care and is the rationale for the recent increase in CMS funding for community‐based, care‐transition programs. These programs are crucial for assisting patients with household activities, meals, and other necessities during the period of recovery, though they should be distinguished from care management or care coordination interventions, which have not been found to be helpful in preventing readmissions unless high touch in nature.[30, 31]
The Advanced Care Planning domain may begin in the hospital or outpatient setting, and involves establishing goals of care and healthcare proxies, as well as engaging with palliative care or hospice services if appropriate. Emerging evidence supports the intuitive conclusion that this approach prevents readmissions, particularly in patients who do not benefit from hospital readmission.[32, 33]
Attention to the Coordinating Care Among Team Members domain is needed to synchronize efforts across settings and providers. Clearly, many healthcare professionals as well as other involved parties can be involved in helping a single patient during transitions in care. It is vital that they coordinate information, assessments, and plans as a team.[34]
We recognize the domain of Monitoring and Managing Symptoms After Discharge as increasingly crucial as reflected in our growing understanding of the reasons for readmission, especially among patients with fragile conditions such as heart failure, chronic lung disease, gastrointestinal disorders, dementia,[23, 24, 25, 26] and vascular disease.[35] Monitoring for new or worsening symptoms; medication side effects, discrepancies, or nonadherence; and other self‐management challenges will allow problems to be detected and addressed early, before they result in unplanned healthcare utilization. It is noteworthy that successful interventions in this regard rely on in‐home evaluation[13, 14, 29] by nurses rather than telemonitoring, which in isolation has not been effective to date.[36, 37]
Finally, optimal Outpatient Follow‐Up with appropriate postdischarge providers is crucial for providing ideal transitions. These appointments need to be prompt[38, 39] (eg, within 7 days if not sooner for high‐risk patients) and with providers who have a longitudinal relationship to the patient, as prior work has shown increased readmissions when the provider is unfamiliar with the patient.[40] The advantages and disadvantages of hospitalist‐run postdischarge clinics as one way to increase access and expedite follow‐up are currently being explored. Although the optimal content of a postdischarge visit has not been defined, logical tasks to be completed are myriad and imply the need for checklists, adequate time, and a multidisciplinary team of providers.[41]
IMPLICATIONS OF THE IDEAL TRANSITION IN CARE
Our conceptualization of an ideal transition in care provides insight for hospital and healthcare system leadership, policymakers, researchers, clinicians, and educators seeking to improve transitions of care and reduce hospital readmissions. In the sections below, we briefly review commonly cited concerns about the recent focus on readmissions as a quality measure, illustrate how the Ideal Transition in Care addresses these concerns, and propose fruitful areas for future work.
How Does the Framework Address the Extent to Which Readmissions Reflect Hospital Quality?
One of the chief problems with readmissionrates as a hospital quality measure is that many of the factors that influence readmission may not currently be under the hospital's control. The healthcare environment to which a patient is being discharged (and was admitted from in the first place) is an important determinant of readmission.[42] In this context, it is noteworthy that successful interventions to reduce readmission are generally those that focus on outpatient follow‐up, while inpatient‐only interventions have had less success.[7] This is reflected in our framework above, informed by the literature, highlighting the importance of coordination between inpatient and outpatient providers and the importance of postdischarge care, including monitoring and managing symptoms after discharge, prompt follow‐up appointments, the continuation of patient self‐management activities, monitoring for drug‐related problems after discharge, and the effective utilization of community supports. Accountable care organizations, once established, would be responsible for several components of this environment, including the provision of prompt and effective follow‐up care.
The implication of the framework is that if a hospital does not have control over most of the factors that influence its readmission rate, it should see financial incentives to reduce readmission rates as an opportunity to invest in relationships with the outpatient environment from which their patients are admitted and to which they are discharged. One can envision hospitals growing ever‐closer relationships with their network of primary care physician groups, community agencies, and home health services, rehabilitation facilities, and nursing homes through coordinated discharge planning, medication management, patient education, shared electronic medical records, structured handoffs in care, and systems of intensive outpatient monitoring. Our proposed framework, in other words, emphasizes that hospitals cannot reduce their readmission rates by focusing on aspects of care within their walls. They must forge new and stronger relationships with their communities if they are to be successful.
How Does the Framework Help Us Understand Which Readmissions Are Preventable?
Public reporting and financial penalties are currently tied to all‐cause readmission, but preventable readmissions are a more appealing outcome to target. In one study, the ranking of hospitals by all‐cause readmission rate had very little correlation with the ranking by preventable readmission rate.[5] However, researchers have struggled to establish standardized, valid, and reliable measures for determining what proportion of readmissions are in fact preventable, with estimates ranging from 5% to 79% in the published literature.[43]
The difficulty of accurately determining preventability stems from an inadequate understanding of the roles that patient comorbidities, transitional processes of care, individual patient behaviors, and social and environmental determinants of health play in the complex process of hospital recidivism. Our proposed elements of an ideal transition in care provide a structure to frame this discussion and suggest future research opportunities to allow a more accurate and reliable understanding of the spectrum of preventability. Care system leadership can use the framework to rigorously evaluate their readmissions and determine the extent to which the transitions process approached the ideal. For example, if a readmission occurs despite care processes that addressed most of the domains with high fidelity, it becomes much less likely that the readmission was preventable. It should be noted that the converse is not always true: When a transition falls well short of the ideal, it does not always imply that provision of a more ideal transition would necessarily have prevented the readmission, but it does make it more likely.
For educators, the framework may provide insights for trainees into the complexity of the transitions process and vulnerability of patients during this time, highlighting preventable aspects of readmissions that are within the grasp of the discharging clinician or team. It highlights the importance of medication reconciliation, synchronous communication, and predischarge teaching, which are measurable and teachable skills for non‐physician providers, housestaff, and medical students. It also may allow for more structured feedback, for example, on the quality of discharge summaries produced by trainees.
How Could the Framework Improve Risk Adjustment for Between‐Hospital Comparisons?
Under the Patient Protection and Affordable Care Act (PPACA), hospitals will be compared to one another using risk‐standardized readmission rates as a way to penalize poorly performing hospitals. However, risk‐adjustment models have only modest ability to predict hospital readmission.[6] Moreover, current approaches predominantly adjust for patients' medical comorbidities (which are easily measurable), but they do not adequately take into account the growing literature on other factors that influence readmission rates, including a patient's health literacy, visual or cognitive impairment, functional status, language barriers, and community‐level factors such as social supports.[44, 45]
The Ideal Transition of Care provides a comprehensive framework of hospital discharge quality that provides additional process measures on which hospitals could be compared rather than focusing solely on (inadequately) risk‐adjusted readmission rates. Indeed, most other quality and safety measures (such as the National Quality Forum's Safe Practices[46] and The Joint Commission's National Patient Safety Goals),[47] emphasize process over outcome, in part because of issues of fairness. Process measures are less subject to differences in patient populations and also change the focus from simply reducing readmissions to improving transitional care more broadly. These process measures should be based on our framework and should attempt to capture as many dimensions of an optimal care transition as possible.
Possible examples of process measures include: the accuracy of medication reconciliation at admission and discharge; provision of prompt outpatient follow‐up; provision of adequate systems to monitor and manage symptoms after discharge; advanced care planning in appropriate patients; and the quality of discharge education, incorporating measurements of the patient's understanding and ability to self‐manage their illness. At least some of these could be used now as part of a performance measurement set that highlights opportunities for immediate system change and can serve as performance milestones.
The framework could also be used to validate risk‐adjustment techniques. After accounting for patient factors, the remaining variability in outcomes should be accounted for by processes of care that are in the transitions framework. Once these processes are accurately measured, one can determine if indeed the remaining variability is due to transitions processes, or rather unaccounted factors that are not being measured and that hospitals may have little control over. Such work can lead to iterative refinement of patient risk‐adjustment models.
What Does the Framework Imply About Best Practices for Reducing Readmission Rates?
Despite the limitations of readmission rates as a quality measure noted above, hospitals presently face potentially large financial penalties for readmissions and are allocating resources to readmission reduction efforts. However, hospitals currently may not have enough guidance to know what actions to take to reduce readmissions, and thus could be spending money inefficiently and reducing the value proposition of focusing on readmissions.
A recent systematic review of interventions hospitals could employ to reduce readmissions identified several positive studies, but also many negative studies, and there were significant barriers to understanding what works to reduce readmissions.[7] For example, most of the interventions described in both positive and negative studies were multifaceted, and the authors were unable to identify which components of the intervention were most effective. Also, while several studies have identified risk factors for readmission,[6, 48, 49] very few studies have identified which subgroups of patients benefit most from specific interventions. Few of the studies described key contextual factors that may have led to successful or failed implementation, or the fidelity with which the intervention was implemented.[50, 51, 52]
Few if any of the studies were guided by a concept of the ideal transition in care.[10] Such a framework will better guide development of multifaceted interventions and provide an improved means for interpreting the results. Clearly, rigorously conducted, multicenter studies of readmission prevention interventions are needed to move the field forward. These studies should: 1) correlate implementation of specific intervention components with reductions in readmission rates to better understand the most effective components; 2) be adequately powered to show effect modification, ie, which patients benefit most from these interventions; and 3) rigorously measure environmental context and intervention fidelity, and employ mixed methods to better understand predictors of implementation success and failure.
Our framework can be used in the design and evaluation of such interventions. For example, interventions could be designed that incorporate as many of the domains of an ideal transition as possible, in particular those that span the inpatient and outpatient settings. Processes of care metrics can be developed that measure the extent to which each domain is delivered, analogous to the way the Joint Commission might aggregate individual scores on the 10 items in Acute Myocardial Infarction Core Measure Set[53] to provide a composite of the quality of care provided to patients with this diagnosis. These can be used to correlate certain intervention components with success in reducing readmissions and also in measuring intervention fidelity.
NEXT STEPS
For hospital and healthcare system leaders, who need to take action now to avoid financial penalties, we recommend starting with proven, high‐touch interventions such as Project RED and the Care Transitions Intervention, which are durable, cost‐effective, robustly address multiple domains of the Ideal Transition in Care, and have been implemented at numerous sites.[54, 55] Each hospital or group will need to decide on a bundle of interventions and customize them based on local workflow, resources, and culture.
Risk‐stratification, to match the intensity of the intervention to the risk of readmission of the patient, will undoubtedly be a key component for the efficient use of resources. We anticipate future research will allow risk stratification to be a robust part of any implementation plan. However, as noted above, current risk prediction models are imperfect,[6] and more work is needed to determine which patients benefit most from which interventions. Few if any studies have described interventions tailored to risk for this reason.
Based on our ideal transition in care, our collective experience, and published evidence,[7, 10, 11, 12] potential elements to start with include: early discharge planning; medication reconciliation[56]; patient/caregiver education using health literacy principles, cognitive assessments, and teach‐back to confirm understanding; synchronous communication (eg, by phone) between inpatient and postdischarge providers; follow‐up phone calls to patients within 72 hours of discharge; 24/7 availability of a responsible inpatient provider to address questions and problems (both from the patient/caregiver and from postdischarge providers); and prompt appointments for patients discharged home. High‐risk patients will likely require additional interventions, including in‐home assessments, disease‐monitoring programs, and/or patient coaching. Lastly, patients with certain conditions prone to readmission (such as heart failure and chronic obstructive pulmonary disease) may benefit from disease‐specific programs, including patient education, outpatient disease management, and monitoring protocols.
It is likely that the most effective interventions are those that come from combined, coordinated interventions shared between inpatient and outpatient settings, and are intensive in nature. We expect that the more domains in the framework that are addressed, the safer and more seamless transitions in care will be, with improvement in patient outcomes. To the extent that fragmentation of care has been a barrier to the implementation of these types of interventions in the past, ACOs, perhaps with imbedded Patient‐Centered Medical Homes, may be in the best position to take advantage of newly aligned financial incentives to design comprehensive transitional care. Indeed, we anticipate that Figure 1 may provide substrate for a discussion of postdischarge care and division of responsibilities between inpatient and outpatient care teams at the time of transition, so effort is not duplicated and multiple domains are addressed.
Other barriers to implementation of ideal transitions in care will continue to be an issue for most healthcare systems. Financial constraints that have been a barrier up until now will be partially overcome by penalties for high readmission rates and by ACOs, bundled payments, and alternative care contracts (ie, global payments), but the extent to which each institution feels rewarded for investing in transitional interventions will vary greatly. Healthcare leadership that sees the value of improving transitions in care will be critical to overcoming this barrier. Competing demands (such as lowering hospital length of stay and carrying out other patient care responsibilities),[57] lack of coordination and diffusion of responsibility among various clinical personnel, and lack of standards are other barriers[58] that will require clear prioritization from leadership, policy changes, team‐based care, provider education and feedback, and adequate allocation of personnel resources. In short, process redesign using continuous quality improvement efforts and effective tools will be required to maximize the possibility of success.
CONCLUSIONS
Readmissions are costly and undesirable. Intuition suggests they are a marker of poor care and that hospitals should be capable of reducing them, thereby improving care and decreasing costs. In a potential future world of ACOs based on global payments, financial incentives would be aligned for each system to reduce readmissions below their current baseline, therefore obviating the need for external financial rewards and penalties. In the meantime, financial penalties do exist, and controversy exists over their fairness and likelihood of driving appropriate behavior. To address these controversies and promote better transitional care, we call for the development and use of multifaceted, collaborative transitions interventions that span settings, risk‐adjustment models that allow for fairer comparisons among hospitals, better and more widespread measurement of processes of transitional care, a better understanding of what interventions are most effective and in whom, and better guidance in how to implement these interventions. Our conceptualization of an ideal transition of care serves as a guide and provides a common vocabulary for these efforts. Such research is likely to produce the knowledge needed for healthcare systems to improve transitions in care, reduce readmissions, and reduce costs.
Disclosure
Funding for Dr Vasilevskis has been provided by the National Institutes of Health (K23AG040157) and the VA Tennessee Valley Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging, the National Institutes of Health, or the US Department of Veterans Affairs.
Containing the rise of healthcare costs has taken on a new sense of urgency in the wake of the recent economic recession and continued growth in the cost of healthcare. Accordingly, many stakeholders seek solutions to improve value (reducing costs while improving care)[1]; hospital readmissions, which are common and costly,[2] have emerged as a key target. The Centers for Medicare and Medicaid Services (CMS) have instituted several programs intended to reduce readmissions, including funding for community‐based, care‐transition programs; penalties for hospitals with elevated risk‐adjusted readmission rates for selected diagnoses; pioneer Accountable Care Organizations (ACOs) with incentives to reduce global costs of care; and Hospital Engagement Networks (HENs) through the Partnership for Patients.[3] A primary aim of these initiatives is to enhance the quality of care transitions as patients are discharged from the hospital.
Though the recent focus on hospital readmissions has appropriately drawn attention to transitions in care, some have expressed concerns. Among these are questions about: 1) the extent to which readmissions truly reflect the quality of hospital care[4]; 2) the preventability of readmissions[5]; 3) limitations in risk‐adjustment techniques[6]; and 4) best practices for preventing readmissions.[7] We believe these concerns stem in part from deficiencies in the state of the science of transitional care, and that future efforts in this area will be hindered without a clear vision of an ideal transition in care. We propose the key components of an ideal transition in care and discuss the implications of this concept as it pertains to hospital readmissions.
THE IDEAL TRANSITION IN CARE
We propose the key components of an ideal transition in care in Figure 1 and Table 1. Figure 1 represents 10 domains described more fully below as structural supports of the bridge patients must cross from one care environment to another during a care transition. This figure highlights key domains and suggests that lack of a domain makes the bridge weaker and more prone to gaps in care and poor outcomes. It also implies that the more components are missing, the less safe is the bridge or transition. Those domains that mainly take place prior to discharge are placed closer to the hospital side of the bridge, those that mainly take place after discharge are placed closer to the community side of the bridge, while those that take place both prior to and after discharge are in the middle. Table 1 provides descriptions of the key content for each of these domains, as well as guidance about which personnel might be involved and where in the transition process that domain should be implemented. We support these domains with supporting evidence where available.
| Domain | Who | When | References |
|---|---|---|---|
| |||
| Discharge planning | |||
| Use a multidisciplinary team to create a discharge plan | Discharging clinician | Predischarge | 911 |
| Collaborate with PCP regarding discharge and follow‐up plan | Care managers/discharge planners | ||
| Arrange follow‐up appointments prior to discharge | Nurses | ||
| Make timely appointments for follow‐up care | |||
| Make appointments that take patient and caregiver's schedules and transportation needs into account | |||
| Complete communication of information | |||
| Includes: | Discharging clinician | Time of discharge | 1214 |
| Patient's full name | |||
| Age | |||
| Dates of admission and discharge | |||
| Names of responsible hospital physicians | |||
| Name of physician preparing discharge summary | |||
| Name of PCP | |||
| Main diagnosis | |||
| Other relevant diagnoses, procedures, and complications | |||
| Relevant findings at admission | |||
| Treatment and response for each active problem | |||
| Results of procedures and abnormal laboratory test results | |||
| Recommendations of any subspecialty consultants | |||
| Patient's functional status at discharge | |||
| Discharge medications | |||
| Follow‐up appointments made and those to be made | |||
| Tests to be ordered and pending tests to be followed‐up | |||
| Counseling provided to patient and caregiver, when applicable | |||
| Contingency planning | |||
| Code status | |||
| Availability, timeliness, clarity, and organization of information | |||
| Timely communication with postdischarge providers verbally (preferred) or by fax/e‐mail | Discharging clinician | Time of discharge | 1214 |
| Timely completion of discharge summary and reliable transmission to postdischarge providers | |||
| Availability of information in medical record | |||
| Use of a structured template with subheadings in discharge communication | |||
| Medication safety | |||
| Take an accurate preadmission medication history | Clinicians | Admission | 1521 |
| Reconcile preadmission medications with all ordered medications at all transfers in care, including discharge | Pharmacists | Throughout hospitalization | |
| Communicate discharge medications to all outpatient providers, including all changes and rationale for those changes | Nurses | Time of discharge | |
| Educating patients, promoting self‐management | |||
| Focus discharge counseling on major diagnoses, medication changes, dates of follow‐up appointments, self‐care instructions, warning signs and symptoms, and who to contact for problems | Clinicians | Daily | 911, 2228, 30 |
| Include caregivers as appropriate | Nurses | Time of discharge | |
| Ensure staff members provide consistent messages | Care managers/discharge planners | Postdischarge | |
| Provide simply written patient‐centered materials with instructions | Transition coaches | ||
| Use teach‐back methods to confirm understanding | |||
| Encourage questions | |||
| Continue teaching during postdischarge follow‐up | |||
| Use transition coaches in high‐risk patients: focus on medication management, keeping a personal medical record, follow‐up appointments, and knowledge of red flags | |||
| Enlisting help of social and community supports | |||
| Assess needs and appropriately arrange for home services | Clinicians | Predischarge and postdischarge | 29, 30 |
| Enlist help of caregivers | Nurses | ||
| Enlist help of community supports | Care managers | ||
| Home health staff | |||
| Advanced care planning | |||
| Establish healthcare proxy | Clinicians | Predischarge and postdischarge | 31, 32 |
| Discuss goals of care | Palliative care staff | ||
| Palliative care consultation (if appropriate) | Social workers | ||
| Enlist hospice services (if appropriate) | Nurses | ||
| Hospice workers | |||
| Coordinating care among team members | |||
| Share medical records | Clinicians | Predischarge and postdischarge | 33 |
| Communicate involving all team members | Nurses | ||
| Optimize continuity of providers and formal handoffs of care | Office personnel | ||
| IT staff | |||
| Monitoring and managing symptoms after discharge | |||
| Monitor for: | Clinicians | Postdischarge | 1113, 28, 3436 |
| Worsening disease control | Nurses | ||
| Medication side effects, discrepancies, nonadherence | Pharmacists | ||
| Therapeutic drug monitoring | Care managers | ||
| Inability to manage conditions at home | Visiting nurses and other home health staff | ||
| Via: | |||
| Postdischarge phone calls | |||
| Home visits | |||
| Postdischarge clinic visits | |||
| Patient hotline | |||
| Availability of inpatient providers after discharge | |||
| Follow‐up with outpatient providers | |||
| Within an appropriate time frame (eg, 7 d or sooner for high‐risk patients) | Clinicians | Postdischarge | 3740 |
| With appropriate providers (eg, most related to reasons for hospitalization, who manage least stable conditions, and/or PCP) | Nurses Pharmacists | ||
| Utilize multidisciplinary teams as appropriate | Care managers | ||
| Ensure appropriate progress along plan of care and safe transition | Office personnel | ||
| Other clinical staff as appropriate | |||
Our concept of an ideal transition in care began with work by Naylor, who described several important components of a safe transition in care, including complete communication of information, patient education, enlisting the help of social and community supports, ensuring continuity of care, and coordinating care among team members.[8] It is supplemented by the Transitions of Care Consensus Policy Statement proposed by representatives from hospital medicine, primary care, and emergency medicine, which emphasized aspects of timeliness and content of communication between providers.[9] Our present articulation of these key components includes 10 organizing domains.
The Discharge Planning domain highlights the important principle of planning ahead for hospital discharge while the patient is still being treated in the hospital, a paradigm espoused by Project RED[10] and other successful care transitions interventions.[11, 12] Collaborating with the outpatient provider and taking the patient and caregiver's preferences for appointment scheduling into account can help ensure optimal outpatient follow‐up.
Complete Communication of Information refers to the content that should be included in discharge summaries and other means of information transfer from hospital to postdischarge care. The specific content areas are based on the Society of Hospital Medicine and Society of General Internal Medicine Continuity of Care Task Force systematic review and recommendations,[13] which takes into account information requested by primary care physicians after discharge.
Availability, Timeliness, Clarity, and Organization of that information is as important as the content because postdischarge providers must be able to access and quickly understand the information they have been provided before assuming care of the patient.[14, 15]
The Medication Safety domain is of central importance because medications are responsible for most postdischarge adverse events.[16] Taking an accurate medication history,[17] reconciling changes throughout the hospitalization,[18] and communicating the reconciled medication regimen to patients and providers across transitions of care can reduce medication errors and improve patient safety.[19, 20, 21, 22]
The Patient Education and Promotion of Self‐Management domain involves teaching patients and their caregivers about the main hospital diagnoses and instructions for self‐care, including medication changes, appointments, and whom to contact if issues arise. Confirming comprehension of instructions through assessments of acute (delirium) and chronic (dementia) cognitive impairments[23, 24, 25, 26] and teach‐back from the patient (or caregiver) is an important aspect of such counseling, as is providing patients and caregivers with educational materials that are appropriate for their level of health literacy and preferred language.[14] High‐risk patients may benefit from patient coaching to improve their self‐management skills.[12] These recommendations are based on years of health literacy research,[27, 28, 29] and such elements are generally included in effective interventions (including Project RED,[10] Naylor and colleagues' Transitional Care Model,[11] and Coleman and colleagues' Care Transitions Intervention[12]).
Enlisting the help of Social and Community Supports is an important adjunct to medical care and is the rationale for the recent increase in CMS funding for community‐based, care‐transition programs. These programs are crucial for assisting patients with household activities, meals, and other necessities during the period of recovery, though they should be distinguished from care management or care coordination interventions, which have not been found to be helpful in preventing readmissions unless high touch in nature.[30, 31]
The Advanced Care Planning domain may begin in the hospital or outpatient setting, and involves establishing goals of care and healthcare proxies, as well as engaging with palliative care or hospice services if appropriate. Emerging evidence supports the intuitive conclusion that this approach prevents readmissions, particularly in patients who do not benefit from hospital readmission.[32, 33]
Attention to the Coordinating Care Among Team Members domain is needed to synchronize efforts across settings and providers. Clearly, many healthcare professionals as well as other involved parties can be involved in helping a single patient during transitions in care. It is vital that they coordinate information, assessments, and plans as a team.[34]
We recognize the domain of Monitoring and Managing Symptoms After Discharge as increasingly crucial as reflected in our growing understanding of the reasons for readmission, especially among patients with fragile conditions such as heart failure, chronic lung disease, gastrointestinal disorders, dementia,[23, 24, 25, 26] and vascular disease.[35] Monitoring for new or worsening symptoms; medication side effects, discrepancies, or nonadherence; and other self‐management challenges will allow problems to be detected and addressed early, before they result in unplanned healthcare utilization. It is noteworthy that successful interventions in this regard rely on in‐home evaluation[13, 14, 29] by nurses rather than telemonitoring, which in isolation has not been effective to date.[36, 37]
Finally, optimal Outpatient Follow‐Up with appropriate postdischarge providers is crucial for providing ideal transitions. These appointments need to be prompt[38, 39] (eg, within 7 days if not sooner for high‐risk patients) and with providers who have a longitudinal relationship to the patient, as prior work has shown increased readmissions when the provider is unfamiliar with the patient.[40] The advantages and disadvantages of hospitalist‐run postdischarge clinics as one way to increase access and expedite follow‐up are currently being explored. Although the optimal content of a postdischarge visit has not been defined, logical tasks to be completed are myriad and imply the need for checklists, adequate time, and a multidisciplinary team of providers.[41]
IMPLICATIONS OF THE IDEAL TRANSITION IN CARE
Our conceptualization of an ideal transition in care provides insight for hospital and healthcare system leadership, policymakers, researchers, clinicians, and educators seeking to improve transitions of care and reduce hospital readmissions. In the sections below, we briefly review commonly cited concerns about the recent focus on readmissions as a quality measure, illustrate how the Ideal Transition in Care addresses these concerns, and propose fruitful areas for future work.
How Does the Framework Address the Extent to Which Readmissions Reflect Hospital Quality?
One of the chief problems with readmissionrates as a hospital quality measure is that many of the factors that influence readmission may not currently be under the hospital's control. The healthcare environment to which a patient is being discharged (and was admitted from in the first place) is an important determinant of readmission.[42] In this context, it is noteworthy that successful interventions to reduce readmission are generally those that focus on outpatient follow‐up, while inpatient‐only interventions have had less success.[7] This is reflected in our framework above, informed by the literature, highlighting the importance of coordination between inpatient and outpatient providers and the importance of postdischarge care, including monitoring and managing symptoms after discharge, prompt follow‐up appointments, the continuation of patient self‐management activities, monitoring for drug‐related problems after discharge, and the effective utilization of community supports. Accountable care organizations, once established, would be responsible for several components of this environment, including the provision of prompt and effective follow‐up care.
The implication of the framework is that if a hospital does not have control over most of the factors that influence its readmission rate, it should see financial incentives to reduce readmission rates as an opportunity to invest in relationships with the outpatient environment from which their patients are admitted and to which they are discharged. One can envision hospitals growing ever‐closer relationships with their network of primary care physician groups, community agencies, and home health services, rehabilitation facilities, and nursing homes through coordinated discharge planning, medication management, patient education, shared electronic medical records, structured handoffs in care, and systems of intensive outpatient monitoring. Our proposed framework, in other words, emphasizes that hospitals cannot reduce their readmission rates by focusing on aspects of care within their walls. They must forge new and stronger relationships with their communities if they are to be successful.
How Does the Framework Help Us Understand Which Readmissions Are Preventable?
Public reporting and financial penalties are currently tied to all‐cause readmission, but preventable readmissions are a more appealing outcome to target. In one study, the ranking of hospitals by all‐cause readmission rate had very little correlation with the ranking by preventable readmission rate.[5] However, researchers have struggled to establish standardized, valid, and reliable measures for determining what proportion of readmissions are in fact preventable, with estimates ranging from 5% to 79% in the published literature.[43]
The difficulty of accurately determining preventability stems from an inadequate understanding of the roles that patient comorbidities, transitional processes of care, individual patient behaviors, and social and environmental determinants of health play in the complex process of hospital recidivism. Our proposed elements of an ideal transition in care provide a structure to frame this discussion and suggest future research opportunities to allow a more accurate and reliable understanding of the spectrum of preventability. Care system leadership can use the framework to rigorously evaluate their readmissions and determine the extent to which the transitions process approached the ideal. For example, if a readmission occurs despite care processes that addressed most of the domains with high fidelity, it becomes much less likely that the readmission was preventable. It should be noted that the converse is not always true: When a transition falls well short of the ideal, it does not always imply that provision of a more ideal transition would necessarily have prevented the readmission, but it does make it more likely.
For educators, the framework may provide insights for trainees into the complexity of the transitions process and vulnerability of patients during this time, highlighting preventable aspects of readmissions that are within the grasp of the discharging clinician or team. It highlights the importance of medication reconciliation, synchronous communication, and predischarge teaching, which are measurable and teachable skills for non‐physician providers, housestaff, and medical students. It also may allow for more structured feedback, for example, on the quality of discharge summaries produced by trainees.
How Could the Framework Improve Risk Adjustment for Between‐Hospital Comparisons?
Under the Patient Protection and Affordable Care Act (PPACA), hospitals will be compared to one another using risk‐standardized readmission rates as a way to penalize poorly performing hospitals. However, risk‐adjustment models have only modest ability to predict hospital readmission.[6] Moreover, current approaches predominantly adjust for patients' medical comorbidities (which are easily measurable), but they do not adequately take into account the growing literature on other factors that influence readmission rates, including a patient's health literacy, visual or cognitive impairment, functional status, language barriers, and community‐level factors such as social supports.[44, 45]
The Ideal Transition of Care provides a comprehensive framework of hospital discharge quality that provides additional process measures on which hospitals could be compared rather than focusing solely on (inadequately) risk‐adjusted readmission rates. Indeed, most other quality and safety measures (such as the National Quality Forum's Safe Practices[46] and The Joint Commission's National Patient Safety Goals),[47] emphasize process over outcome, in part because of issues of fairness. Process measures are less subject to differences in patient populations and also change the focus from simply reducing readmissions to improving transitional care more broadly. These process measures should be based on our framework and should attempt to capture as many dimensions of an optimal care transition as possible.
Possible examples of process measures include: the accuracy of medication reconciliation at admission and discharge; provision of prompt outpatient follow‐up; provision of adequate systems to monitor and manage symptoms after discharge; advanced care planning in appropriate patients; and the quality of discharge education, incorporating measurements of the patient's understanding and ability to self‐manage their illness. At least some of these could be used now as part of a performance measurement set that highlights opportunities for immediate system change and can serve as performance milestones.
The framework could also be used to validate risk‐adjustment techniques. After accounting for patient factors, the remaining variability in outcomes should be accounted for by processes of care that are in the transitions framework. Once these processes are accurately measured, one can determine if indeed the remaining variability is due to transitions processes, or rather unaccounted factors that are not being measured and that hospitals may have little control over. Such work can lead to iterative refinement of patient risk‐adjustment models.
What Does the Framework Imply About Best Practices for Reducing Readmission Rates?
Despite the limitations of readmission rates as a quality measure noted above, hospitals presently face potentially large financial penalties for readmissions and are allocating resources to readmission reduction efforts. However, hospitals currently may not have enough guidance to know what actions to take to reduce readmissions, and thus could be spending money inefficiently and reducing the value proposition of focusing on readmissions.
A recent systematic review of interventions hospitals could employ to reduce readmissions identified several positive studies, but also many negative studies, and there were significant barriers to understanding what works to reduce readmissions.[7] For example, most of the interventions described in both positive and negative studies were multifaceted, and the authors were unable to identify which components of the intervention were most effective. Also, while several studies have identified risk factors for readmission,[6, 48, 49] very few studies have identified which subgroups of patients benefit most from specific interventions. Few of the studies described key contextual factors that may have led to successful or failed implementation, or the fidelity with which the intervention was implemented.[50, 51, 52]
Few if any of the studies were guided by a concept of the ideal transition in care.[10] Such a framework will better guide development of multifaceted interventions and provide an improved means for interpreting the results. Clearly, rigorously conducted, multicenter studies of readmission prevention interventions are needed to move the field forward. These studies should: 1) correlate implementation of specific intervention components with reductions in readmission rates to better understand the most effective components; 2) be adequately powered to show effect modification, ie, which patients benefit most from these interventions; and 3) rigorously measure environmental context and intervention fidelity, and employ mixed methods to better understand predictors of implementation success and failure.
Our framework can be used in the design and evaluation of such interventions. For example, interventions could be designed that incorporate as many of the domains of an ideal transition as possible, in particular those that span the inpatient and outpatient settings. Processes of care metrics can be developed that measure the extent to which each domain is delivered, analogous to the way the Joint Commission might aggregate individual scores on the 10 items in Acute Myocardial Infarction Core Measure Set[53] to provide a composite of the quality of care provided to patients with this diagnosis. These can be used to correlate certain intervention components with success in reducing readmissions and also in measuring intervention fidelity.
NEXT STEPS
For hospital and healthcare system leaders, who need to take action now to avoid financial penalties, we recommend starting with proven, high‐touch interventions such as Project RED and the Care Transitions Intervention, which are durable, cost‐effective, robustly address multiple domains of the Ideal Transition in Care, and have been implemented at numerous sites.[54, 55] Each hospital or group will need to decide on a bundle of interventions and customize them based on local workflow, resources, and culture.
Risk‐stratification, to match the intensity of the intervention to the risk of readmission of the patient, will undoubtedly be a key component for the efficient use of resources. We anticipate future research will allow risk stratification to be a robust part of any implementation plan. However, as noted above, current risk prediction models are imperfect,[6] and more work is needed to determine which patients benefit most from which interventions. Few if any studies have described interventions tailored to risk for this reason.
Based on our ideal transition in care, our collective experience, and published evidence,[7, 10, 11, 12] potential elements to start with include: early discharge planning; medication reconciliation[56]; patient/caregiver education using health literacy principles, cognitive assessments, and teach‐back to confirm understanding; synchronous communication (eg, by phone) between inpatient and postdischarge providers; follow‐up phone calls to patients within 72 hours of discharge; 24/7 availability of a responsible inpatient provider to address questions and problems (both from the patient/caregiver and from postdischarge providers); and prompt appointments for patients discharged home. High‐risk patients will likely require additional interventions, including in‐home assessments, disease‐monitoring programs, and/or patient coaching. Lastly, patients with certain conditions prone to readmission (such as heart failure and chronic obstructive pulmonary disease) may benefit from disease‐specific programs, including patient education, outpatient disease management, and monitoring protocols.
It is likely that the most effective interventions are those that come from combined, coordinated interventions shared between inpatient and outpatient settings, and are intensive in nature. We expect that the more domains in the framework that are addressed, the safer and more seamless transitions in care will be, with improvement in patient outcomes. To the extent that fragmentation of care has been a barrier to the implementation of these types of interventions in the past, ACOs, perhaps with imbedded Patient‐Centered Medical Homes, may be in the best position to take advantage of newly aligned financial incentives to design comprehensive transitional care. Indeed, we anticipate that Figure 1 may provide substrate for a discussion of postdischarge care and division of responsibilities between inpatient and outpatient care teams at the time of transition, so effort is not duplicated and multiple domains are addressed.
Other barriers to implementation of ideal transitions in care will continue to be an issue for most healthcare systems. Financial constraints that have been a barrier up until now will be partially overcome by penalties for high readmission rates and by ACOs, bundled payments, and alternative care contracts (ie, global payments), but the extent to which each institution feels rewarded for investing in transitional interventions will vary greatly. Healthcare leadership that sees the value of improving transitions in care will be critical to overcoming this barrier. Competing demands (such as lowering hospital length of stay and carrying out other patient care responsibilities),[57] lack of coordination and diffusion of responsibility among various clinical personnel, and lack of standards are other barriers[58] that will require clear prioritization from leadership, policy changes, team‐based care, provider education and feedback, and adequate allocation of personnel resources. In short, process redesign using continuous quality improvement efforts and effective tools will be required to maximize the possibility of success.
CONCLUSIONS
Readmissions are costly and undesirable. Intuition suggests they are a marker of poor care and that hospitals should be capable of reducing them, thereby improving care and decreasing costs. In a potential future world of ACOs based on global payments, financial incentives would be aligned for each system to reduce readmissions below their current baseline, therefore obviating the need for external financial rewards and penalties. In the meantime, financial penalties do exist, and controversy exists over their fairness and likelihood of driving appropriate behavior. To address these controversies and promote better transitional care, we call for the development and use of multifaceted, collaborative transitions interventions that span settings, risk‐adjustment models that allow for fairer comparisons among hospitals, better and more widespread measurement of processes of transitional care, a better understanding of what interventions are most effective and in whom, and better guidance in how to implement these interventions. Our conceptualization of an ideal transition of care serves as a guide and provides a common vocabulary for these efforts. Such research is likely to produce the knowledge needed for healthcare systems to improve transitions in care, reduce readmissions, and reduce costs.
Disclosure
Funding for Dr Vasilevskis has been provided by the National Institutes of Health (K23AG040157) and the VA Tennessee Valley Geriatric Research, Education and Clinical Center (GRECC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging, the National Institutes of Health, or the US Department of Veterans Affairs.
- , . Redefining Health Care: Creating Value‐Based Competition on Results. Boston, MA:Harvard Business School Press;2006.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act (PPACA). Public Law 111–148; 2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/pdf/PLAW‐111publ148.pdf. Accessed on June 4, 2012.
- , . Hospital readmission as an accountability measure. JAMA. 2011;305(5):504–505.
- , , , et al. Incidence of potentially avoidable urgent readmissions and their relation to all‐cause urgent readmissions. Can Med Assoc J. 2011;183(14):E1067–E1072.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306(15):1688–1698.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- . A decade of transitional care research with vulnerable elders. J Cardiovasc Nurs. 2000;14(3):1–14.
- , , , et al;for the American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. Transitions of Care Consensus Policy Statement American College of Physicians–Society of General Internal Medicine–Society of Hospital Medicine–American Geriatrics Society–American College of Emergency Physicians–Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971–976.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial. JAMA. 1999;281(7):613–620.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , , , , , . Discharge documentation of patients discharged to subacute facilities: a three‐year quality improvement process across an integrated health care system. Jt Comm J Qual Patient Saf. 2010;36(6):243–251.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , , , . Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Can Med Assoc J. 2005;173(5):510–515.
- , , , et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–1422.
- , , et al;for the PILL‐CVD (Pharmacist Intervention for Low Literacy in Cardiovascular Disease) Study Group. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , . Hospital‐based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172(14):1057–1069.
- , , , et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster‐randomized trial. Arch Intern Med. 2009;169(8):771–780.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , , . Insufficient help for activity of daily living disabilities and risk of all–cause hospitalization. J Am Geriatr Soc. 2012;60(5):927–933.
- , , , et al. Transitions in care for older adults with and without dementia. J Am Geriatr Soc. 2012;60(5):813–820.
- , , , , . Association of incident dementia with hospitalizations. JAMA. 2012;307(2):165–172.
- , , , et al. Potentially avoidable hospitalizations of dually eligible Medicare and Medicaid beneficiaries from nursing facility and home– and community–based services waiver programs. J Am Geriatr Soc. 2012;60(5):821–829.
- , . Teaching about health literacy and clear communication. J Gen Intern Med. 2006;21(8):888–890.
- , , , et al. Health literacy and outcomes among patients with heart failure. JAMA. 2011;305(16):1695–1701.
- , , , , . Patient experiences of transitioning from hospital to home: an ethnographic quality improvement project. J Hosp Med. 2012;7(5):382–387.
- , , , . Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA. 2009;301(6):603–618.
- , , , , . How changes in Washington University's Medicare coordinated care demonstration pilot ultimately achieved savings. Health Aff (Millwood). 2012;31(6):1216–1226.
- , , , et al. Quality of care and rehospitalization rate in the last stage of disease in brain tumor patients assisted at home: a cost effectiveness study. J Palliat Med. 2012;15(2):225–227.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15(2):48–51.
- , , , et al. TeamSTEPPS™: team strategies and tools to enhance performance and patient safety. In: Henriksen K, Battles JB, Keyes MA, Grady ML, ed. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3: Performance and Tools. Rockville, MD:Agency for Healthcare Research and Quality; August2008.
- , , , et al. Factors contributing to all‐cause 30‐day readmissions: a structured case series across 18 hospitals. Med Care. 2012;50(7):599–605.
- , , , et al. Telemonitoring in patients with heart failure [erratum, N Engl J Med. 2011;364(5):490]. N Engl J Med. 2010;363(24):2301–2309.
- , , , et al. A randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visits. Arch Intern Med. 2012;172(10):773–779.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303(17):1716–1722.
- , , . Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , . Does increased access to primary care reduce hospital readmissions? Veterans Affairs Cooperative Study Group on Primary Care and Hospital Readmission. N Engl J Med. 1996;334(22):1441–1447.
- . The Post‐Hospital Follow‐Up Visit: A Physician Checklist to Reduce Readmissions. California Healthcare Foundation; October 2010. Available at: http://www.chcf.org/publications/2010/10/the‐post‐hospital‐follow‐up‐visit‐a‐physician‐checklist. Accessed on January 10, 2012.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , , . Proportion of hospital readmissions deemed avoidable: a systematic review. Can Med Assoc J. 2011;183(7):E391–E402.
- , , , et al. Postdischarge environmental and socioeconomic factors and the likelihood of early hospital readmission among community‐dwelling Medicare beneficiaries. Gerontologist. 2008;48(4):495–504.
- , , , , . Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107.
- National Quality Forum. Safe Practices for Better Healthcare—2010 Update: A Consensus Report. Washington, DC;2010.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation Program: Hospital 2010 National Patient Safety Goals (NPSGs). 2010. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed on March 20, 2012.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211–219.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. Can Med Assoc J. 2010;182(6):551–557.
- , . Evaluating service delivery interventions to enhance patient safety. BMJ. 2008;337:a2764.
- , , . Assessing the Evidence for Context‐Sensitive Effectiveness and Safety of Patient Safety Practices: Developing Criteria. Rockville, MD:Agency for Healthcare Research and Quality; December2010.
- , , , et al. Advancing the science of patient safety. Ann Intern Med. 2011;154(10):693–696.
- The Joint Commission. Acute Myocardial Infarction Core Measure Set. Available at: http://www.jointcommission.org/assets/1/6/Acute%20Myocardial%20Infarction.pdf. Accessed August 20,2012.
- , , , , , . The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171(14):1232–1237.
- Project RED toolkit, AHRQ Innovations Exchange. Available at:http://www.innovations.ahrq.gov/content.aspx?id=2180. Accessed on July 2, 2012.
- , , , et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894–900.
- , . Thirty‐day readmissions—truth and consequences. N Engl J Med. 2012;366(15):1366–1369.
- , , , , . “Out of sight, out of mind”: housestaff perceptions of quality‐limiting factors in discharge care at teaching hospitals. J Hosp Med. 2012;7(5):376–381.
- , . Redefining Health Care: Creating Value‐Based Competition on Results. Boston, MA:Harvard Business School Press;2006.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360(14):1418–1428.
- Patient Protection and Affordable Care Act (PPACA). Public Law 111–148; 2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/pdf/PLAW‐111publ148.pdf. Accessed on June 4, 2012.
- , . Hospital readmission as an accountability measure. JAMA. 2011;305(5):504–505.
- , , , et al. Incidence of potentially avoidable urgent readmissions and their relation to all‐cause urgent readmissions. Can Med Assoc J. 2011;183(14):E1067–E1072.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306(15):1688–1698.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- . A decade of transitional care research with vulnerable elders. J Cardiovasc Nurs. 2000;14(3):1–14.
- , , , et al;for the American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. Transitions of Care Consensus Policy Statement American College of Physicians–Society of General Internal Medicine–Society of Hospital Medicine–American Geriatrics Society–American College of Emergency Physicians–Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971–976.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. Comprehensive discharge planning and home follow‐up of hospitalized elders: a randomized clinical trial. JAMA. 1999;281(7):613–620.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , , , , , . Discharge documentation of patients discharged to subacute facilities: a three‐year quality improvement process across an integrated health care system. Jt Comm J Qual Patient Saf. 2010;36(6):243–251.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , , , . Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Can Med Assoc J. 2005;173(5):510–515.
- , , , et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–1422.
- , , et al;for the PILL‐CVD (Pharmacist Intervention for Low Literacy in Cardiovascular Disease) Study Group. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. 2012;157(1):1–10.
- , , , . Hospital‐based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172(14):1057–1069.
- , , , et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster‐randomized trial. Arch Intern Med. 2009;169(8):771–780.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , , . Insufficient help for activity of daily living disabilities and risk of all–cause hospitalization. J Am Geriatr Soc. 2012;60(5):927–933.
- , , , et al. Transitions in care for older adults with and without dementia. J Am Geriatr Soc. 2012;60(5):813–820.
- , , , , . Association of incident dementia with hospitalizations. JAMA. 2012;307(2):165–172.
- , , , et al. Potentially avoidable hospitalizations of dually eligible Medicare and Medicaid beneficiaries from nursing facility and home– and community–based services waiver programs. J Am Geriatr Soc. 2012;60(5):821–829.
- , . Teaching about health literacy and clear communication. J Gen Intern Med. 2006;21(8):888–890.
- , , , et al. Health literacy and outcomes among patients with heart failure. JAMA. 2011;305(16):1695–1701.
- , , , , . Patient experiences of transitioning from hospital to home: an ethnographic quality improvement project. J Hosp Med. 2012;7(5):382–387.
- , , , . Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. JAMA. 2009;301(6):603–618.
- , , , , . How changes in Washington University's Medicare coordinated care demonstration pilot ultimately achieved savings. Health Aff (Millwood). 2012;31(6):1216–1226.
- , , , et al. Quality of care and rehospitalization rate in the last stage of disease in brain tumor patients assisted at home: a cost effectiveness study. J Palliat Med. 2012;15(2):225–227.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15(2):48–51.
- , , , et al. TeamSTEPPS™: team strategies and tools to enhance performance and patient safety. In: Henriksen K, Battles JB, Keyes MA, Grady ML, ed. Advances in Patient Safety: New Directions and Alternative Approaches. Vol 3: Performance and Tools. Rockville, MD:Agency for Healthcare Research and Quality; August2008.
- , , , et al. Factors contributing to all‐cause 30‐day readmissions: a structured case series across 18 hospitals. Med Care. 2012;50(7):599–605.
- , , , et al. Telemonitoring in patients with heart failure [erratum, N Engl J Med. 2011;364(5):490]. N Engl J Med. 2010;363(24):2301–2309.
- , , , et al. A randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visits. Arch Intern Med. 2012;172(10):773–779.
- , , , et al. Relationship between early physician follow‐up and 30‐day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303(17):1716–1722.
- , , . Post‐hospitalization transitions: examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- , , . Does increased access to primary care reduce hospital readmissions? Veterans Affairs Cooperative Study Group on Primary Care and Hospital Readmission. N Engl J Med. 1996;334(22):1441–1447.
- . The Post‐Hospital Follow‐Up Visit: A Physician Checklist to Reduce Readmissions. California Healthcare Foundation; October 2010. Available at: http://www.chcf.org/publications/2010/10/the‐post‐hospital‐follow‐up‐visit‐a‐physician‐checklist. Accessed on January 10, 2012.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , , , , . Proportion of hospital readmissions deemed avoidable: a systematic review. Can Med Assoc J. 2011;183(7):E391–E402.
- , , , et al. Postdischarge environmental and socioeconomic factors and the likelihood of early hospital readmission among community‐dwelling Medicare beneficiaries. Gerontologist. 2008;48(4):495–504.
- , , , , . Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107.
- National Quality Forum. Safe Practices for Better Healthcare—2010 Update: A Consensus Report. Washington, DC;2010.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation Program: Hospital 2010 National Patient Safety Goals (NPSGs). 2010. Available at: http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. Accessed on March 20, 2012.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211–219.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. Can Med Assoc J. 2010;182(6):551–557.
- , . Evaluating service delivery interventions to enhance patient safety. BMJ. 2008;337:a2764.
- , , . Assessing the Evidence for Context‐Sensitive Effectiveness and Safety of Patient Safety Practices: Developing Criteria. Rockville, MD:Agency for Healthcare Research and Quality; December2010.
- , , , et al. Advancing the science of patient safety. Ann Intern Med. 2011;154(10):693–696.
- The Joint Commission. Acute Myocardial Infarction Core Measure Set. Available at: http://www.jointcommission.org/assets/1/6/Acute%20Myocardial%20Infarction.pdf. Accessed August 20,2012.
- , , , , , . The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171(14):1232–1237.
- Project RED toolkit, AHRQ Innovations Exchange. Available at:http://www.innovations.ahrq.gov/content.aspx?id=2180. Accessed on July 2, 2012.
- , , , et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894–900.
- , . Thirty‐day readmissions—truth and consequences. N Engl J Med. 2012;366(15):1366–1369.
- , , , , . “Out of sight, out of mind”: housestaff perceptions of quality‐limiting factors in discharge care at teaching hospitals. J Hosp Med. 2012;7(5):376–381.
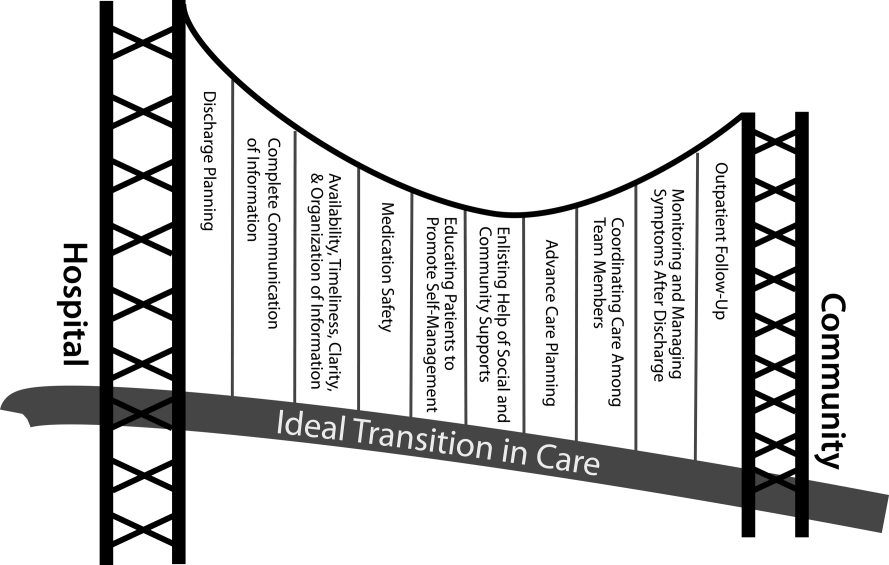
Patients with Aspiration Pneumonia
Pneumonia is a common clinical syndrome with well‐described epidemiology and microbiology. Aspiration pneumonia comprises 5% to 15% of patients with pneumonia,[1] but is less well‐characterized despite being a major syndrome of pneumonia in the elderly.[2, 3] Difficulties in studying aspiration pneumonia include the lack of a sensitive and specific marker for aspiration, the overlap between aspiration pneumonia and other forms of pneumonia, and the lack of differentiation between aspiration pneumonia and aspiration pneumonitis by many clinicians.[4, 5, 6] Aspiration pneumonia, which develops after the aspiration of oropharyngeal contents, differs from aspiration pneumonitis, wherein inhalation of gastric contents causes inflammation without the subsequent development of bacterial infection.[7, 8]
A number of validated mortality prediction models exist for community‐acquired pneumonia (CAP), using a variety of clinical predictors. One clinical prediction rule endorsed by the British Thoracic Society is the CURB‐65, which assigns a score for Confusion, Uremia >19 mg/dL, Respiratory rate >= 30 breaths/min, Blood Pressure < 90 mmHg systolic or < 60 mmHg diastolic, and age 65). We favor eCURB, a version of the CURB‐65 model that uses continuously weighted variables to more accurately predict mortality, validated in CAP populations.[9] Most studies validating pneumonia severity scoring systems excluded aspiration pneumonia from their study population.[10, 11, 12] Severity scoring systems for CAP may not accurately predict disease severity patients with aspiration pneumonia.
The aims of our study were to: (1) identify a population of patients with aspiration pneumonia; (2) compare characteristics and outcomes in patients with community‐acquired aspiration pneumonia to those with CAP; and (3) study the performance of eCURB and CURB‐65 in predicting mortality for patients with community‐acquired aspiration pneumonia.
PATIENTS AND METHODS
Study Design and Setting
The study was performed at LDS Hospital, a university‐affiliated community teaching hospital in Salt Lake City, Utah, with 520 beds. In retrospective analysis of data from the electronic medical records, we identified all patients older than 18 years who were evaluated in the emergency department at LDS Hospital or admitted patients from other sources (direct admission, transfer from another hospital) from 1996 to 2006 with International Statistical Classification of Disease and Health Related Problems, 9th Revision (ICD‐9) codes specific for aspiration pneumonia and pneumonitis (507.x). The treating physicians were mostly hospitalists and intensivists. Two physicians (M.L. and N.D.) manually reviewed the electronic medical records, including the emergency room physician's notes, the admission histories and physicals, the discharge summaries, and radiographic reports of the patients identified in the query. Consensus regarding the diagnosis of aspiration pneumonia was achieved in all patients reviewed using criteria listed in Table 1. This study was approved by the LDS Hospital institutional review board, and permission was granted to use the Utah Population Database for determining mortality (#1008505), with a waiver of informed consent. For the contemporaneous group of CAP patients, we used a previously described population identified using ICD‐9 codes 481.x to 487.x, captured from the same hospital during the same period.[13]
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| |
| 1. Age 18 years | 1. Absence of radiographic evidence of pneumonia within 48 hours after evaluation |
| 2. Either admitted to hospital or evaluated in emergency department | 2. Previous episode of aspiration pneumonia within 12 months |
| 3. 507.x code as primary diagnosis | 3. Initial admission date >48 hours before transfer to LDS Hospital |
| 4. 507.x code as secondary diagnosis with a primary diagnosis of pneumonia, respiratory failure, or septicemia | 4. AIDS 5. Receipt of antiretroviral therapy 6. History of solid organ transplant |
| 5. Treating physician indicated a diagnosis of aspiration pneumonia in the history and physical and/or discharge summary | 7. Hematologic malignancy 8. Witnessed isolated aspiration event within 24 hours prior to evaluation 9. Drug overdose, cardiopulmonary arrest, or seizure prior to hospital admission 10. Laryngoscopic or bronchoscopic evidence of food material in airway |
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria are listed in Table 1. To exclude patients with recurrent pneumonia, we included only the first episode of pneumonia in a given 12‐month period. LDS Hospital frequently receives patients transferred from surrounding emergency departments and intensive care units. We excluded patients who were transferred >48 hours from their initial emergency department admission and therefore were late in their disease course. Exclusion criteria 8 to 10 were used to exclude patients with clinical presentations more consistent with aspiration pneumonitis. We also excluded immunocompromised patients (criteria 4 to 7).
Healthcare‐associated aspiration pneumonia was defined as receipt of chronic hemodialysis, residence in a nursing facility, or hospitalization within any Intermountain Healthcare‐affiliated hospital within the past 90 days.[14] The remaining patients were defined as community‐acquired aspiration pneumonia.
Measurements
The first vital signs, orientation status, and first 12 hours of routine laboratory results were extracted from the electronic medical records and used to calculate predicted mortality by eCURB and CURB‐65. We determined 30‐day mortality from the merger of the electronic medical records with vital status information from the Utah Population Database.[15] The first measured SpO2 and FiO2 were used to estimate the PaO2/FiO2 ratio, using the Severinghaus calculation[16] if no arterial blood gas was available. Presence of American Thoracic Society/Infectious Diseases Society of America (IDSA/ATS) 2007 minor criteria for severe community‐acquired pneumonia (SCAP)[17] were obtained from baseline patient characteristics (Table 2). A Charlson comorbidity index was calculated from ICD‐9 codes using published methodology.[18, 19] Presence of an abnormal swallow was defined as dysphagia or aspiration on modified barium swallow study, fiberoptic endoscopic evaluation, or clinical determination by a speech language pathologist during the index hospitalization. We also looked for causative pathogens, defined by a positive pneumococcus or legionella urinary antigen, or a positive culture from blood, bronchoalveolar lavage, pleural fluid, or tracheal aspirate, collected within 24 hours of admission. Antibiotics administered within the first 24 hours of admission were classified into 4 broad groups based on local physician prescribing patterns. Clindamycin and metronidazole were considered anaerobic‐specific antibiotics. Vancomycin or linezolid were considered methicillin‐resistant Staphylococcus aureus (MRSA) antibiotics. Broad‐spectrum antibiotics included any of the following: carbapenems, aztreonam, piperacillin/tazobactam, ticarcillin/clavulanate, cefepime, and ceftazidime. Macrolides, respiratory fluoroquinolones, and third‐generation cephalosporins were considered standard‐care antibiotics.
| Respiratory rate 30 breaths/minute |
| PaO2/FiO2 250 |
| Multilobar infiltrates |
| Confusion/disorientation |
| Uremia (blood urea nitrogen 20 mg/dL) |
| Leukopenia (white blood cell count <4000 cells/mm3) |
| Thrombocytopenia (platelet count <100,000 cells/mm3) |
| Hypothermia (core temperature 36C) |
| Hypotension requiring aggressive fluid resuscitation |
Statistical Analysis
We compared baseline patient characteristics and clinical outcomes using the Fisher exact test to compare proportions of categorical variables, and Mann‐Whitney U test or Student t test to compare central tendencies of continuous variables, as dictated by the normality of the data. Receiver operating characteristic curves calculated the ability of eCURB and CURB‐65 to predict 30‐day mortality prediction in patients with community‐acquired aspiration pneumonia and CAP, as well as the ability of IDSA/ATS minor criteria for SCAP to predict admission to the intensive care unit (ICU). We performed multivariate logistic regression to predict 30‐day mortality in patients with community‐acquired aspiration pneumonia and CAP, using stepwise backward elimination. Confounders were included if they were significant at a 0.05 level or if they altered the coefficient of the main variable by more than 10%. For logistic models, we evaluated goodness of fit with the Hosmer‐Lemeshow technique; comparisons of area under the curve (AUC) among models were made using the technique of DeLong.[20] Two‐tailed P values of 0.05 were considered statistically significant. Stata version 12 (StataCorp, College Station, TX) was used for all analyses.
RESULTS
Our initial query identified 1165 patients. Physician review of the medical records resulted in 628 patients, 118 of whom were classified as healthcare‐associated aspiration pneumonia (Figure 1, Table 3). Of all aspiration pneumonia patients, 80% were seen in the emergency department, 12.5% were directly admitted from the community, and 7.5% were transferred from another healthcare facility. Almost all patients seen in the emergency department (99.0%) were admitted to the hospital, with median length of hospitalization 6.7 days among survivors.
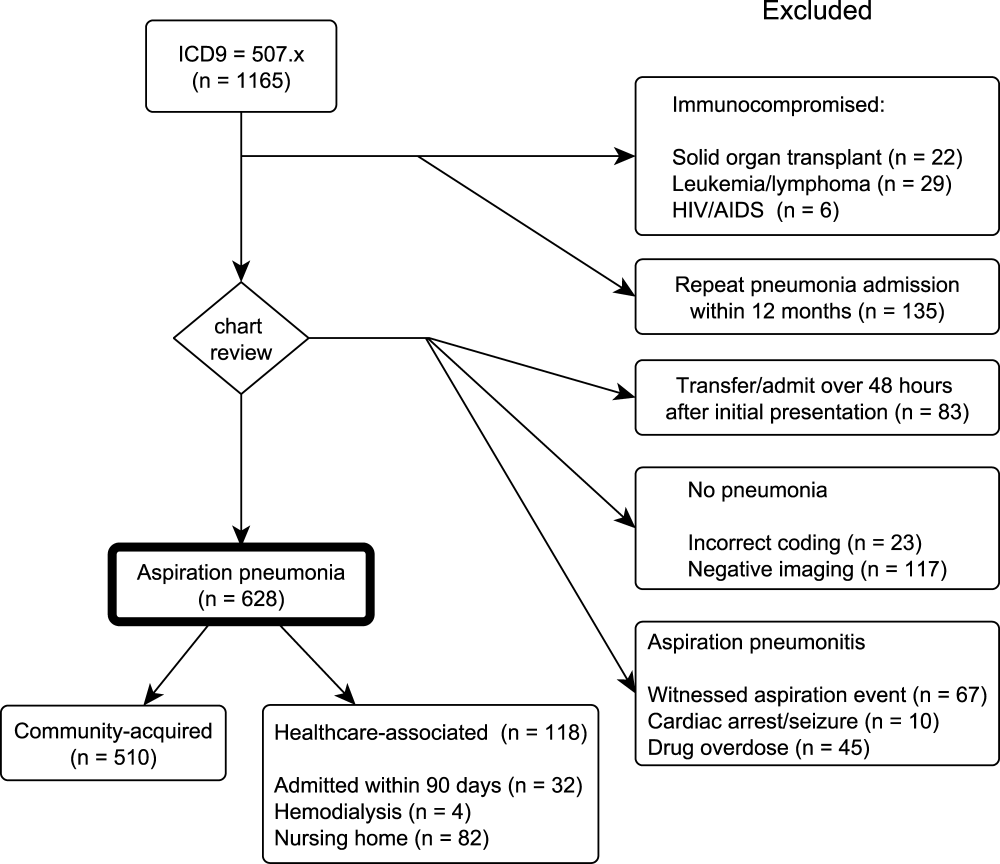
| Aspiration Pneumonia (N = 628) | Community‐Acquired Aspiration Pneumonia (N = 510) | Healthcare Associated Aspiration Pneumonia (N=118) | P Value | |
|---|---|---|---|---|
| ||||
| Age (range), y | 77 (6585) | 77 (6485) | 80 (6786) | 0.42 |
| Female, % | 49.8 | 50.2 | 48.3 | 0.76 |
| 30‐day mortality, % | 21.0% | 19.0% | 29.7% | 0.02 |
| CURB‐65 score | 2 (13) | 2 (13) | 2 (13) | 0.0012 |
| Confusion | 13.9% | 12.7% | 18.6% | 0.10 |
| Blood urea nitrogen (mg/dL) | 22 (1634) | 21 (1532) | 30 (2047) | <0.0001 |
| Respiratory rate (breaths/min) | 20 (1826) | 20 (1824) | 21 (1828) | 0.30 |
| Systolic blood pressure (mm Hg) | 128 (110149) | 129 (110150) | 127 (105146) | 0.28 |
| eCURB 30‐day mortality estimate (median, %) | 5.6 (2.414.2) | 5.2 (2.212.4) | 8.9 (4.222.5) | <0.0001 |
| eCURB 30‐day mortality estimate (mean, %) | 10.6 12.2 | 9.7 11.5 | 14.614.1 | <0.0001 |
| Hospital admission (of ED visits), % | 99.0 | 98.8 | 100 | 0.59 |
| Hospital LOS, d | 6.7 (4.111.1) | 6.5 (4.011.0) | 7.8 (5.412.3) | 0.05 |
| ICU admission, % | 37.9 | 37.1 | 41.5 | 0.21 |
| ICU LOS, d | 3.5 (1.98.8) | 3.1 (1.87.6) | 5.6 (3.810.8) | 0.02 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.28.3 | 25.97.7 | 22.710.0 | 0.01 |
| Receipt of mechanical ventilation, % | 18.6 | 17.2 | 24.6 | 0.09 |
| Duration of ventilation, d | 2.8 (0.96.5) | 3.1 (1.06.6) | 1.9 (0.86.3) | 0.05 |
| Receipt of vasopressor, % | 1.8 | 1.4 | 3.4 | 0.13 |
| Charlson comorbidity index | 4 (26) | 3 (26) | 4 (36) | 0.0024 |
| Cerebrovascular disease, % | 33.9 | 32.4 | 40.7 | 0.11 |
| Chronic pulmonary disease, % | 51.0 | 51.8 | 47.5 | 0.42 |
| Congestive heart failure, % | 52.4 | 50.0 | 62.7 | 0.01 |
| Connective tissue disease, % | 8.4 | 8.8 | 6.8 | 0.58 |
| Dementia, % | 14.2 | 12.0 | 23.7 | 0.0019 |
| Hemiplegia/paraplegia | 9.4 | 8.0 | 15.2 | 0.02 |
| Myocardial infarction, % | 21.0 | 17.8 | 29.7 | 0.02 |
| Peripheral vascular disease, % | 17.7 | 16.3 | 23.7 | 0.06 |
| Peptic ulcer disease, % | 18.8 | 19.2 | 16.9 | 0.70 |
| Diabetes without complications, % | 10.7 | 9.2 | 16.9 | 0.02 |
| Diabetes with complications, % | 31.5 | 30.4 | 36.4 | 0.23 |
| Mild liver disease, % | 8.6 | 8.0 | 11.0 | 0.28 |
| Moderate or severe liver disease, % | 1.8 | 1.6 | 2.5 | 0.44 |
| Malignant solid tumor, % | 16.6 | 17.3 | 13.6 | 0.41 |
| Metastatic cancer, % | 5.4 | 5.7 | 4.2 | 0.66 |
| Renal disease, % | 14.7 | 4.2 | 18.6 | 0.19 |
| 3 or more minor SCAP criteria, %* | 24.7 | 23.1 | 31.4 | 0.08 |
| PaO2/FiO2 ratio | 221 (161280) | 226 (169280) | 181 (133245) | 0.0004 |
| Multilobar disease, % | 46.3 | 43.2 | 53.9 | 0.11 |
| Presence of an effusion, % | 23.1 | 19.7 | 31.9 | 0.03 |
| Swallow impairment (of tested survivors), % | 34.1 | 34.1 | 34.1 | 0.22 |
| Presence of a DNR/DNI order, % | 26.4 | 23.7 | 38.1 | 0.0024 |
| Mortality of patients with DNR/DNI order, % | 39.1 | 38.8 | 40.0 | 1.00 |
| Receipt of broad‐spectrum antibiotic, % | 35.4 | 32.5 | 47.5 | 0.0028 |
| Receipt of MRSA antibiotic, % | 7.5 | 5.7 | 15.3 | 0.0014 |
| Receipt of anaerobe antibiotic, % | 28.7 | 27.6 | 33.1 | 0.26 |
Observed mortality was 21.0%. eCURB significantly underestimated mortality in this group, predicting a mortality rate of 10.6%. When classifying patients by the 2007 IDSA/ATS guidelines, 24.7% of the patients had 3 or more minor criteria for SCAP.[17] The PaO2/FiO2 ratio was obtained in 99.7% of patients. The median PaO2/FiO2 ratio observed in this population was 221 mm Hg (equivalent to 260 mm Hg at sea level barometric pressure, adjusted for our altitude of 1400 meters), near the threshold sea level definition (250 mm Hg) for SCAP.[13, 17] Admission to the ICU was common, as were admission orders for do not resuscitate (DNR) or do not intubate (DNI). Patients with healthcare‐associated aspiration pneumonia had a higher comorbidity index and had a higher mortality rate than patients with community‐acquired aspiration pneumonia, although we found no significant difference in the rate of hospital or ICU admission or the receipt of critical care therapies. Inpatient assessment of dysphagia and aspiration was conducted in 177 patients. Abnormal swallow was noted in 96% of those tested.
We found several differences between patients with community‐acquired aspiration pneumonia and 2584 patients with CAP identified during the same time period[13] (Table 4). Patients with community‐acquired aspiration pneumonia were older, more likely to have multilobar disease or effusion on imaging, and had greater disease severity. They also had a higher frequency of ICU and hospital admission, IDSA/ATS minor criteria for SCAP, and higher Charlson comorbidity indices. Patients with community‐acquired aspiration pneumonia were more likely to receive mechanical ventilation than CAP patients, although there was no difference in 30‐day mortality among intubated patients or a difference in ventilator‐free days.
| Community‐Acquired Aspiration Pneumonia (N = 510) | Community‐ Acquired Pneumonia (N = 2584) | P Value | |
|---|---|---|---|
| |||
| Age (range), y | 77 (6485) | 59 (4176) | <0.0001 |
| Female, % | 50.2 | 49.5 | 0.81 |
| 30‐day mortality, % | 19.0 | 4.2 | <0.0001 |
| CURB‐65 score | 2 (13) | 1 (02) | <0.0001 |
| Confusion, % | 12.7 | 5.1 | <0.0001 |
| Blood urea nitrogen | 21 (1532) | 16 (1124) | <0.0001 |
| Respiratory rate | 20 (1824) | 20 (1824) | <0.0001 |
| Systolic blood pressure | 129 (110150) | 130 (112146) | 0.67 |
| eCURB 30‐day mortality estimate, median, % | 5.2 (2.212.4) | 1.7 (0.94.3) | <0.0001 |
| eCURB 30‐day mortality estimate, mean, % | 9.7 11.5 | 4.4 7.5 | <0.0001 |
| AUC of eCURB versus mortality | 0.71 (0.660.75) | 0.86 (0.830.90) | <0.0001 |
| Excluding DNR/DNI patients | 0.69 (0.650.74) | 0.87 (0.830.90) | 0.0001 |
| AUC of CURB‐65 versus mortality | 0.66 (0.620.69) | 0.81 (0.780.85) | <0.0001 |
| Excluding DNR/DNI patients | 0.65 (0.600.70) | 0.81 (0.760.85) | 0.0003 |
| Hospital admission (of ED visits), % | 98.8 | 57.8 | <0.0001 |
| Hospital LOS, d | 6.5 (4.011.0) | 3.3 (2.25.2) | <0.0001 |
| ICU admission, % | 37.1 | 14.2 | <0.0001 |
| ICU LOS, d | 3.1 (1.87.6) | 2.5 (1.17.7) | 0.01 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.9 7.7 | 25 9 | 0.75 |
| Receipt of mechanical ventilation, % | 17.2 | 7.8 | <0.0001 |
| Duration of ventilation, d | 3.1 (1.06.6) | 3.5 (1.57.2) | 0.09 |
| Receipt of vasopressor, % | 1.4 | 3.3 | 0.02 |
| Charlson comorbidity index | 3 (26) | 1 (03) | <0.0001 |
| Cerebrovascular disease, % | 32.4 | 10.0 | <0.0001 |
| Chronic pulmonary disease, % | 51.8 | 42.5 | <0.0001 |
| Congestive heart failure, % | 50.0 | 22.1 | <0.0001 |
| Connective tissue disease, % | 8.8 | 5.6 | 0.0084 |
| Dementia, % | 12.0 | 2.8 | <0.0001 |
| Hemiplegia/paraplegia, % | 8.0 | 2.7 | <0.0001 |
| Myocardial infarction, % | 17.8 | 10.8 | <0.0001 |
| Peripheral vascular disease, % | 16.3 | 7.4 | <0.0001 |
| Peptic ulcer disease, % | 19.2 | 7.6 | <0.0001 |
| Diabetes without complications, % | 9.2 | 24.7 | <0.0001 |
| Diabetes with complications, % | 30.4 | 5.1 | <0.0001 |
| Mild liver disease, % | 8.0 | 6.2 | 0.14 |
| Moderate or severe liver disease, % | 1.6 | 0.8 | 0.13 |
| Malignant solid tumor, % | 17. | 8.9 | <0.0001 |
| Metastatic cancer, % | 5.7 | 1.3 | <0.0001 |
| Renal disease, % | 4.2 | 5.6 | <0.0001 |
| 3 or more minor SCAP criteria, %* | 24.7 | 19.1 | 0.01 |
| PaO2/FiO2 ratio | 226 (169280) | 260 (148338) | 0.0004 |
| Multilobar disease, % | 43.2 | 37.2 | 0.0012 |
| Presence of an effusion, % | 19.7 | 18.3 | <0.0001 |
| Presence of a DNR/DNI order, % | 23.7 | 9.7 | <0.0001 |
| Mortality of patients with DNR/DNI order, % | 38.8 | 12.4 | <0.0001 |
| Receipt of broad‐spectrum antibiotic, % | 32.5 | 8.4 | <0.0001 |
| Receipt of MRSA antibiotic, % | 5.7 | 2.2 | <0.0001 |
| Receipt of anaerobe antibiotic, % | 27.6 | 3.1 | <0.0001 |
Thirty‐day mortality for patients with community‐acquired aspiration pneumonia was significantly higher than in CAP patients. Patients with community‐acquired aspiration pneumonia also had higher eCURB and CURB‐65 scores. However, eCURB was a poor predictor of 30‐day mortality, with an AUC of 0.71, compared to 0.86 calculated for the CAP population (Figure 2). CURB‐65 performed similarly: AUC was 0.66 vs 0.81. The presence of a DNR/DNI order was twice as prevalent in the community‐acquired aspiration pneumonia population vs the CAP population; those patients with a DNR/DNI order were 3 times as likely to die. Excluding patients with a DNR/DNI order did not improve performance of eCURB or CURB‐65 (Table 4). The presence of IDSA/ATS minor criteria for SCAP was not predictive of triage to the ICU in the group of patients with community‐acquired aspiration pneumonia (AUC: 0.51), compared with CAP patients (AUC: 0.88, P < 0.01 for comparison, Figure 3). This finding persisted in the subset of patients without a DNR/DNI order (AUC: 0.52 in community‐acquired aspiration pneumonia vs 0.88 in CAP, P < 0.01).


Our regression model of mortality incorporated gender, presence of effusion or multilobar pneumonia, presence of a DNR/DNI order, and all the components of the CURB‐65, IDSA/ATS minor criteria for SCAP, and Charlson comorbidity index. The regression model demonstrated that even after adjustment for age, comorbidities, disease severity, and presence of a DNR/DNI order, the presence of aspiration pneumonia was associated with higher mortality than CAP (odds ratio [OR]: 3.46, P < 0.001, Table 5). In this model, systolic blood pressure did not predict mortality, and diabetes with complications was associated with decreased mortality.
| Odds Ratio | P Value | |
|---|---|---|
| ||
| Presence of aspiration pneumonia | 3.46 (2.115.67) | <0.001 |
| Age, y | 1.03 (1.011.04) | <0.001 |
| Confusion | 3.14 (1.955.05) | <0.001 |
| Blood urea nitrogen, mg/dL | 1.03 (1.021.04) | <0.001 |
| Respiratory rate, breaths/minute | 1.03 (1.001.06) | 0.04 |
| PaO2/FiO2 ratio, per 1 mm Hg | 0.99 (0.991.00) | <0.001 |
| Moderate or severe liver disease | 9.21 (3.1626.86) | <0.001 |
| Paraplegia/hemiplegia | 2.43 (1.135.27) | 0.02 |
| Diabetes with complications | 0.42 (0.200.87) | 0.02 |
| Leukocytosis | 4.47 (2.278.82) | <0.001 |
| DNR/DNI | 1.75 (1.112.75) | 0.02 |
Microbiological Findings
Blood cultures were performed at admission in 67.4% of aspiration‐pneumonia patients, and a tracheal aspirate in half (50.7%) of intubated patients with aspiration pneumonia. Organisms were recovered in 90 patients (14.3%), although 41 of those patients had tracheal aspirates of organisms commonly thought to be nonpathogenic (nonpneumococcal alpha‐hemolytic streptococcus, nonhemolytic streptococcus, diphtheroids, micrococci, coagulase negative staphylococccus). Tracheal aspirate was the most common method of recovering an organism (7.8% of patients), followed by blood culture (4.3%). Bronchoalveolar lavage, urinary antigen, and pleural fluid culture were less common (1.3%, 1.1%, 0.3%, respectively). The microbiologic results were grouped into: Staphylococcus aureus, Streptococcus pneumoniae, enteric bacilli, Haemophilus species, Neisseria species, Moraxella catarrhalis, and Pseudomonas aeruginosa (Figure 4). Comparing healthcare‐associated with community‐acquired aspiration pneumonia, healthcare‐associated patients were more likely to have a confirmed infection with MRSA (4.2% vs 1.4%, P = 0.06) and enteric bacteria (5.1% vs 1.6%, P = 0.03). There were no other statistically significant differences in microbiologic recovery between the 2 groups. Antibiotics targeting anaerobic pathogens were administered in 28.7% of patients with aspiration pneumonia, with no correlation to the presence of healthcare‐associated risks. Healthcare‐associated patients were more likely to receive broad‐spectrum antibiotics (47.5% vs 32.5%, P < 0.01) and MRSA coverage (15.3% vs 5.7%, P < 0.01) than patients with community‐acquired aspiration pneumonia.
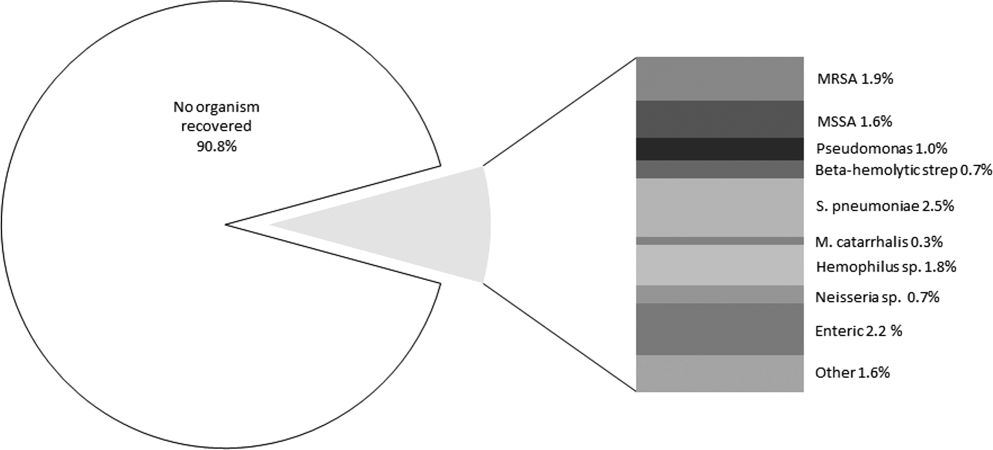
DISCUSSION
Our study identifies a larger cohort of patients with aspiration pneumonia than previous studies.[21, 22, 23, 24, 25] Patients with community‐acquired aspiration pneumonia are older and more likely to die than CAP patients. They are more likely to be admitted to the hospital or ICU. Thirty‐day mortality in this patient population was significantly underestimated by CURB‐65 and eCURB, models developed and validated in CAP populations.[9, 26] This finding supports a prior study.[27] It appears that a traditional prognostic model assessing mortality risk in the CAP patient does not apply to the aspiration‐pneumonia patient. One reason for eCURB and CURB‐65s poor utility in community‐acquired aspiration pneumonia may be their reliance on objective clinical features rather than comorbidities, which may influence mortality to a greater degree in aspiration pneumonia.
This study has several limitations. There is no gold standard for the definition of aspiration pneumonia, and it is difficult to distinguish aspiration pneumonia from typical pneumonia. It is plausible that older patients with greater comorbidities are being designated as aspiration pneumonia. If this is the case, then aspiration pneumonia merely represents the end of the pneumonia spectrum with highest mortality risk, and it is no surprise that these patients fare poorly.
It appears that the hospitalist or emergency department physician implicitly appreciates that aspiration pneumonia has a higher mortality risk than predicted by traditional severity assessment. With such high mortality and morbidity, a patient presenting to the emergency room with aspiration pneumonia is almost always admitted to the hospital. Further work in this area should investigate other factors to improve prognostic modeling in patients with aspiration pneumonia, although the utility of such a model may be limited to determining ICU admission. Our data indicate that IDSA/ATS minor criteria for SCAP are not useful in predicting admission to the ICU in patients with aspiration pneumonia.
In this study, a DNR/DNI order was twice as common in the community‐acquired aspiration pneumonia population than the CAP population. However, patients with community‐acquired aspiration pneumonia and a DNR/DNI order were more than 3 times more likely to die than patients with CAP and a DNR/DNI order. Our regression model suggested that the presence of a DNR/DNI order was an independent predictor of mortality (OR: 1.75, P < 0.001). Although a DNR/DNI order may correlate with the withholding or withdrawal of medical therapy, it is also a surrogate for increased age or comorbidities.[28] In our study, however, the increased prevalence of DNR/DNI orders did not explain the poor mortality prediction of the eCURB or CURB‐65, as exclusion of those patients did not significantly alter the AUCs in either the aspiration group or the CAP group.
Controversy exists regarding treatment of aspiration pneumonia. Historically, some have advocated for treatment of aspiration pneumonia with a regimen designed to cover anaerobic bacteria.[29] This recommendation was based on early microbiologic studies that obtained the samples late in the course of illness, or other studies where the sample was obtained transtracheally, where oropharyngeal flora may contaminate the sample.[30, 31, 32] Our clinically obtained microbiologic recovery of organisms was similar to the flora recovered in more recent CAP studies, in respect to both the incidence of pathogen recovery and the relative frequencies of recovered organisms.[33, 34] Our data do not support inferences regarding the prevalence of anaerobic infections, as the recovery of anaerobic organisms was limited to blood and pleural fluid cultures in this study, rather than techniques used in research settings that might have greater yield. As expected, patients with healthcare‐associated risk factors trended toward increased incidence of MRSA. Given the similarity of the organisms recovered to those recovered in CAP,[35] this study supports IDSA/ATS recommendations that antibiotic therapy in aspiration pneumonia be similar to that of higher‐risk CAP, with the addition of vancomycin or linezolid for MRSA coverage in patients with risk factors for healthcare‐associated pneumonia.[17]
Our study is limited by its single‐center retrospective design. However, beginning in 1995, the LDS Hospital emergency department initiated a standardized pneumonia therapy protocol and deployed electronic medical records, which prospectively recorded a wide array of clinical, therapeutic, and biometric data. Most data elements used in this analysis were routinely charted for clinical purposes in real time. Although the eCURB, CURB‐65, and some comorbidities could be extracted electronically for each patient, it was not possible to calculate the pneumonia severity index score due to our inability to rigorously identify the necessary comorbid illness elements. Other comorbidities, not present in our model, may have been identified by the physician who makes a diagnosis of aspiration pneumonia. Our identification of swallow impairment is also methodologically limited. The decision to obtain a swallow study was clinical, usually occurring upon convalescence. Therefore, it is not possible to distinguish between antecedent oropharyngeal dysfunction and post‐critical illness dysfunction.
Our definition of aspiration pneumonia required the treating physician to diagnose and code the patient as having aspiration pneumonia, followed by excluding patients more likely to have aspiration pneumonitis. Although we relied on ICD‐9 codes to initially identify aspiration pneumonia, all patients in our database were confirmed by physician chart review. Our incidence of community‐acquired aspiration pneumonia is congruent with other studies using different methodologies.[1, 36, 37] Unfortunately, there is no standard and widely accepted definition for separating aspiration pneumonia from usual CAP. A younger and healthier patient who has developed pneumonia subsequent to aspiration may be more likely to be diagnosed with CAP, resulting in selection bias for older patients with greater comorbidities.
CONCLUSION
Patients diagnosed with aspiration pneumonia are older, have more comorbid conditions, and demonstrate greater disease severity and higher 30‐day mortality than CAP patients. Mortality prediction using CURB‐65 and eCURB in this population was poor, possibly due to a greater effect of comorbidities on mortality. The pneumonia severity index, which incorporates patient comorbidities, might perform better than the eCURB or CURB‐65, and should be studied in aspiration pneumonia populations where comorbid illness information is prospectively collected. Further areas of study include creating an improved mortality prediction model for aspiration pneumonia that incorporates comorbid conditions, DNR/DNI status, and disease severity.
Acknowledgments
The authors acknowledge Al Jephson for database support, Yao Li for statistical analysis, and Anita Austin for help reviewing the medical records. Dr. Lanspa had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure
Preliminary versions of this work were presented as posters at the American Thoracic Society Meeting, Denver, Colorado, May 17, 2011. This study was supported by grants from the Intermountain Research and Medical Foundation. Dr. Brown is supported by a career development award from National Institute of General Medical Sciences (K23GM094465). Dr. Dean served on an advisory board for Merck, has been a paid consultant for Cerexa, and has received an investigator‐initiated competitive grant from Pfizer for development of an electronic pneumonia decision support tool. All other authors report no relevant financial disclosures.
- , , , et al. Severe community‐acquired pneumonia. Epidemiology and prognostic factors. Am Rev Respir Dis. 1991;144(2):312–318.
- , , . Risk factors for pneumonia in the elderly. Am J Med. 1994;96(4):313–320.
- , . Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124(1):328–336.
- , , . Pneumonia versus aspiration pneumonitis in nursing home residents: diagnosis and management. J Am Geriatr Soc. 2003;51(1):17–23.
- . Aspiration pneumonia: mixing apples with oranges and tangerines. Crit Care Med. 2004;32(5):1236; author reply 1236–1237.
- , , , , . Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999–2000. Crit Care Med. 2003;31(7):1930–1937.
- . Aspiration syndromes: aspiration pneumonia and pneumonitis. Hosp Pract (Minneap). 2010;38(1):35–42.
- . Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665–671.
- , , , et al. CURB‐65 pneumonia severity assessment adapted for electronic decision support. Chest. 2011;140(1):156–163.
- , , , et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382.
- , , , et al. Comparison of a disease‐specific and a generic severity of illness measure for patients with community‐acquired pneumonia. J Gen Intern Med. 1995;10(7):359–368.
- , , , et al. Development and validation of a clinical prediction rule for severe community‐acquired pneumonia. Am J Respir Crit Care Med. 2006;174(11):1249–1256.
- , , , . Validation of the Infectious Disease Society of America/American Thoracic Society 2007 guidelines for severe community‐acquired pneumonia. Crit Care Med. 2009;37(12):3010–3016.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416.
- .The Utah genealogical database: a resource for genetic epidemiology. In: Cairns JL, Skolnick M, eds. Banbury Report No 4; Cancer Incidence in Defined Populations. New York, NY:Cold Spring Harbor Laboratory;1980:285–297.
- . Simple, accurate equations for human blood O2 dissociation computations. J Appl Physiol. 1979;46(3):599–602.
- , , , et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27–S72.
- , , , . Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , . Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–845.
- , , . Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia. 1996;11(2):104–109.
- , , , . Predictors of aspiration pneumonia in nursing home residents. Dysphagia. 2002;17(4):298–307.
- , , , , , . Aspiration pneumonia: dental and oral risk factors in an older veteran population. J Am Geriatr Soc. 2001;49(5):557–563.
- , , , et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003;167(12):1650–1654.
- , , . Aspiration pneumonia in stroke. Arch Phys Med Rehabil. 1993;74(9):973–976.
- , , , et al. Validation of a predictive rule for the management of community‐acquired pneumonia. Eur Respir J. 2006;27(1):151–157.
- , , , , . Pneumonia Severity Index (PSI), CURB‐65, and mortality in hospitalized elderly patients with aspiration pneumonia [in German]. Zeitschrift fur Gerontologie und Geriatrie. 2011;44(4):229–234.
- , , , . Do‐not‐resuscitate orders for critically ill patients in the hospital. How are they used and what is their impact?JAMA. 1986;256(2):233–237.
- , , , , . The Sanford Guide to Antimicrobial Therapy: 2010.40th ed.Sperryville, VA:Antimicrobial Therapy, Inc.;2009.
- , , . The bacteriology of aspiration pneumonia. Am J Med. 1974;56(2):202–207.
- , , . Bacteriologic flora of aspiration‐induced pulmonary infections. Arch Intern Med. 1975;135(5):711–714.
- , . Bacteriology of aspiration pneumonia. A prospective study of community‐ and hospital‐acquired cases. Ann Intern Med. 1974;81(3):329–331.
- , . The role of anaerobes in patients with ventilator‐associated pneumonia and aspiration pneumonia: a prospective study. Chest. 1999;115(1):178–183.
- , , , et al. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279–284.
- , , , , . Community‐acquired pneumonia in the elderly. Semin Respir Infect. 1999;14(2):173–183.
- , , . Nursing home‐acquired pneumonia. A case‐control study. J Am Geriatr Soc. 1986;34(10):697–702.
- , , , , . Severe community‐acquired pneumonia. Etiology, epidemiology, and prognosis factors. French Study Group for Community‐Acquired Pneumonia in the Intensive Care Unit. Chest. 1994;105(5):1487–1495.
Pneumonia is a common clinical syndrome with well‐described epidemiology and microbiology. Aspiration pneumonia comprises 5% to 15% of patients with pneumonia,[1] but is less well‐characterized despite being a major syndrome of pneumonia in the elderly.[2, 3] Difficulties in studying aspiration pneumonia include the lack of a sensitive and specific marker for aspiration, the overlap between aspiration pneumonia and other forms of pneumonia, and the lack of differentiation between aspiration pneumonia and aspiration pneumonitis by many clinicians.[4, 5, 6] Aspiration pneumonia, which develops after the aspiration of oropharyngeal contents, differs from aspiration pneumonitis, wherein inhalation of gastric contents causes inflammation without the subsequent development of bacterial infection.[7, 8]
A number of validated mortality prediction models exist for community‐acquired pneumonia (CAP), using a variety of clinical predictors. One clinical prediction rule endorsed by the British Thoracic Society is the CURB‐65, which assigns a score for Confusion, Uremia >19 mg/dL, Respiratory rate >= 30 breaths/min, Blood Pressure < 90 mmHg systolic or < 60 mmHg diastolic, and age 65). We favor eCURB, a version of the CURB‐65 model that uses continuously weighted variables to more accurately predict mortality, validated in CAP populations.[9] Most studies validating pneumonia severity scoring systems excluded aspiration pneumonia from their study population.[10, 11, 12] Severity scoring systems for CAP may not accurately predict disease severity patients with aspiration pneumonia.
The aims of our study were to: (1) identify a population of patients with aspiration pneumonia; (2) compare characteristics and outcomes in patients with community‐acquired aspiration pneumonia to those with CAP; and (3) study the performance of eCURB and CURB‐65 in predicting mortality for patients with community‐acquired aspiration pneumonia.
PATIENTS AND METHODS
Study Design and Setting
The study was performed at LDS Hospital, a university‐affiliated community teaching hospital in Salt Lake City, Utah, with 520 beds. In retrospective analysis of data from the electronic medical records, we identified all patients older than 18 years who were evaluated in the emergency department at LDS Hospital or admitted patients from other sources (direct admission, transfer from another hospital) from 1996 to 2006 with International Statistical Classification of Disease and Health Related Problems, 9th Revision (ICD‐9) codes specific for aspiration pneumonia and pneumonitis (507.x). The treating physicians were mostly hospitalists and intensivists. Two physicians (M.L. and N.D.) manually reviewed the electronic medical records, including the emergency room physician's notes, the admission histories and physicals, the discharge summaries, and radiographic reports of the patients identified in the query. Consensus regarding the diagnosis of aspiration pneumonia was achieved in all patients reviewed using criteria listed in Table 1. This study was approved by the LDS Hospital institutional review board, and permission was granted to use the Utah Population Database for determining mortality (#1008505), with a waiver of informed consent. For the contemporaneous group of CAP patients, we used a previously described population identified using ICD‐9 codes 481.x to 487.x, captured from the same hospital during the same period.[13]
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| |
| 1. Age 18 years | 1. Absence of radiographic evidence of pneumonia within 48 hours after evaluation |
| 2. Either admitted to hospital or evaluated in emergency department | 2. Previous episode of aspiration pneumonia within 12 months |
| 3. 507.x code as primary diagnosis | 3. Initial admission date >48 hours before transfer to LDS Hospital |
| 4. 507.x code as secondary diagnosis with a primary diagnosis of pneumonia, respiratory failure, or septicemia | 4. AIDS 5. Receipt of antiretroviral therapy 6. History of solid organ transplant |
| 5. Treating physician indicated a diagnosis of aspiration pneumonia in the history and physical and/or discharge summary | 7. Hematologic malignancy 8. Witnessed isolated aspiration event within 24 hours prior to evaluation 9. Drug overdose, cardiopulmonary arrest, or seizure prior to hospital admission 10. Laryngoscopic or bronchoscopic evidence of food material in airway |
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria are listed in Table 1. To exclude patients with recurrent pneumonia, we included only the first episode of pneumonia in a given 12‐month period. LDS Hospital frequently receives patients transferred from surrounding emergency departments and intensive care units. We excluded patients who were transferred >48 hours from their initial emergency department admission and therefore were late in their disease course. Exclusion criteria 8 to 10 were used to exclude patients with clinical presentations more consistent with aspiration pneumonitis. We also excluded immunocompromised patients (criteria 4 to 7).
Healthcare‐associated aspiration pneumonia was defined as receipt of chronic hemodialysis, residence in a nursing facility, or hospitalization within any Intermountain Healthcare‐affiliated hospital within the past 90 days.[14] The remaining patients were defined as community‐acquired aspiration pneumonia.
Measurements
The first vital signs, orientation status, and first 12 hours of routine laboratory results were extracted from the electronic medical records and used to calculate predicted mortality by eCURB and CURB‐65. We determined 30‐day mortality from the merger of the electronic medical records with vital status information from the Utah Population Database.[15] The first measured SpO2 and FiO2 were used to estimate the PaO2/FiO2 ratio, using the Severinghaus calculation[16] if no arterial blood gas was available. Presence of American Thoracic Society/Infectious Diseases Society of America (IDSA/ATS) 2007 minor criteria for severe community‐acquired pneumonia (SCAP)[17] were obtained from baseline patient characteristics (Table 2). A Charlson comorbidity index was calculated from ICD‐9 codes using published methodology.[18, 19] Presence of an abnormal swallow was defined as dysphagia or aspiration on modified barium swallow study, fiberoptic endoscopic evaluation, or clinical determination by a speech language pathologist during the index hospitalization. We also looked for causative pathogens, defined by a positive pneumococcus or legionella urinary antigen, or a positive culture from blood, bronchoalveolar lavage, pleural fluid, or tracheal aspirate, collected within 24 hours of admission. Antibiotics administered within the first 24 hours of admission were classified into 4 broad groups based on local physician prescribing patterns. Clindamycin and metronidazole were considered anaerobic‐specific antibiotics. Vancomycin or linezolid were considered methicillin‐resistant Staphylococcus aureus (MRSA) antibiotics. Broad‐spectrum antibiotics included any of the following: carbapenems, aztreonam, piperacillin/tazobactam, ticarcillin/clavulanate, cefepime, and ceftazidime. Macrolides, respiratory fluoroquinolones, and third‐generation cephalosporins were considered standard‐care antibiotics.
| Respiratory rate 30 breaths/minute |
| PaO2/FiO2 250 |
| Multilobar infiltrates |
| Confusion/disorientation |
| Uremia (blood urea nitrogen 20 mg/dL) |
| Leukopenia (white blood cell count <4000 cells/mm3) |
| Thrombocytopenia (platelet count <100,000 cells/mm3) |
| Hypothermia (core temperature 36C) |
| Hypotension requiring aggressive fluid resuscitation |
Statistical Analysis
We compared baseline patient characteristics and clinical outcomes using the Fisher exact test to compare proportions of categorical variables, and Mann‐Whitney U test or Student t test to compare central tendencies of continuous variables, as dictated by the normality of the data. Receiver operating characteristic curves calculated the ability of eCURB and CURB‐65 to predict 30‐day mortality prediction in patients with community‐acquired aspiration pneumonia and CAP, as well as the ability of IDSA/ATS minor criteria for SCAP to predict admission to the intensive care unit (ICU). We performed multivariate logistic regression to predict 30‐day mortality in patients with community‐acquired aspiration pneumonia and CAP, using stepwise backward elimination. Confounders were included if they were significant at a 0.05 level or if they altered the coefficient of the main variable by more than 10%. For logistic models, we evaluated goodness of fit with the Hosmer‐Lemeshow technique; comparisons of area under the curve (AUC) among models were made using the technique of DeLong.[20] Two‐tailed P values of 0.05 were considered statistically significant. Stata version 12 (StataCorp, College Station, TX) was used for all analyses.
RESULTS
Our initial query identified 1165 patients. Physician review of the medical records resulted in 628 patients, 118 of whom were classified as healthcare‐associated aspiration pneumonia (Figure 1, Table 3). Of all aspiration pneumonia patients, 80% were seen in the emergency department, 12.5% were directly admitted from the community, and 7.5% were transferred from another healthcare facility. Almost all patients seen in the emergency department (99.0%) were admitted to the hospital, with median length of hospitalization 6.7 days among survivors.
| Aspiration Pneumonia (N = 628) | Community‐Acquired Aspiration Pneumonia (N = 510) | Healthcare Associated Aspiration Pneumonia (N=118) | P Value | |
|---|---|---|---|---|
| ||||
| Age (range), y | 77 (6585) | 77 (6485) | 80 (6786) | 0.42 |
| Female, % | 49.8 | 50.2 | 48.3 | 0.76 |
| 30‐day mortality, % | 21.0% | 19.0% | 29.7% | 0.02 |
| CURB‐65 score | 2 (13) | 2 (13) | 2 (13) | 0.0012 |
| Confusion | 13.9% | 12.7% | 18.6% | 0.10 |
| Blood urea nitrogen (mg/dL) | 22 (1634) | 21 (1532) | 30 (2047) | <0.0001 |
| Respiratory rate (breaths/min) | 20 (1826) | 20 (1824) | 21 (1828) | 0.30 |
| Systolic blood pressure (mm Hg) | 128 (110149) | 129 (110150) | 127 (105146) | 0.28 |
| eCURB 30‐day mortality estimate (median, %) | 5.6 (2.414.2) | 5.2 (2.212.4) | 8.9 (4.222.5) | <0.0001 |
| eCURB 30‐day mortality estimate (mean, %) | 10.6 12.2 | 9.7 11.5 | 14.614.1 | <0.0001 |
| Hospital admission (of ED visits), % | 99.0 | 98.8 | 100 | 0.59 |
| Hospital LOS, d | 6.7 (4.111.1) | 6.5 (4.011.0) | 7.8 (5.412.3) | 0.05 |
| ICU admission, % | 37.9 | 37.1 | 41.5 | 0.21 |
| ICU LOS, d | 3.5 (1.98.8) | 3.1 (1.87.6) | 5.6 (3.810.8) | 0.02 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.28.3 | 25.97.7 | 22.710.0 | 0.01 |
| Receipt of mechanical ventilation, % | 18.6 | 17.2 | 24.6 | 0.09 |
| Duration of ventilation, d | 2.8 (0.96.5) | 3.1 (1.06.6) | 1.9 (0.86.3) | 0.05 |
| Receipt of vasopressor, % | 1.8 | 1.4 | 3.4 | 0.13 |
| Charlson comorbidity index | 4 (26) | 3 (26) | 4 (36) | 0.0024 |
| Cerebrovascular disease, % | 33.9 | 32.4 | 40.7 | 0.11 |
| Chronic pulmonary disease, % | 51.0 | 51.8 | 47.5 | 0.42 |
| Congestive heart failure, % | 52.4 | 50.0 | 62.7 | 0.01 |
| Connective tissue disease, % | 8.4 | 8.8 | 6.8 | 0.58 |
| Dementia, % | 14.2 | 12.0 | 23.7 | 0.0019 |
| Hemiplegia/paraplegia | 9.4 | 8.0 | 15.2 | 0.02 |
| Myocardial infarction, % | 21.0 | 17.8 | 29.7 | 0.02 |
| Peripheral vascular disease, % | 17.7 | 16.3 | 23.7 | 0.06 |
| Peptic ulcer disease, % | 18.8 | 19.2 | 16.9 | 0.70 |
| Diabetes without complications, % | 10.7 | 9.2 | 16.9 | 0.02 |
| Diabetes with complications, % | 31.5 | 30.4 | 36.4 | 0.23 |
| Mild liver disease, % | 8.6 | 8.0 | 11.0 | 0.28 |
| Moderate or severe liver disease, % | 1.8 | 1.6 | 2.5 | 0.44 |
| Malignant solid tumor, % | 16.6 | 17.3 | 13.6 | 0.41 |
| Metastatic cancer, % | 5.4 | 5.7 | 4.2 | 0.66 |
| Renal disease, % | 14.7 | 4.2 | 18.6 | 0.19 |
| 3 or more minor SCAP criteria, %* | 24.7 | 23.1 | 31.4 | 0.08 |
| PaO2/FiO2 ratio | 221 (161280) | 226 (169280) | 181 (133245) | 0.0004 |
| Multilobar disease, % | 46.3 | 43.2 | 53.9 | 0.11 |
| Presence of an effusion, % | 23.1 | 19.7 | 31.9 | 0.03 |
| Swallow impairment (of tested survivors), % | 34.1 | 34.1 | 34.1 | 0.22 |
| Presence of a DNR/DNI order, % | 26.4 | 23.7 | 38.1 | 0.0024 |
| Mortality of patients with DNR/DNI order, % | 39.1 | 38.8 | 40.0 | 1.00 |
| Receipt of broad‐spectrum antibiotic, % | 35.4 | 32.5 | 47.5 | 0.0028 |
| Receipt of MRSA antibiotic, % | 7.5 | 5.7 | 15.3 | 0.0014 |
| Receipt of anaerobe antibiotic, % | 28.7 | 27.6 | 33.1 | 0.26 |
Observed mortality was 21.0%. eCURB significantly underestimated mortality in this group, predicting a mortality rate of 10.6%. When classifying patients by the 2007 IDSA/ATS guidelines, 24.7% of the patients had 3 or more minor criteria for SCAP.[17] The PaO2/FiO2 ratio was obtained in 99.7% of patients. The median PaO2/FiO2 ratio observed in this population was 221 mm Hg (equivalent to 260 mm Hg at sea level barometric pressure, adjusted for our altitude of 1400 meters), near the threshold sea level definition (250 mm Hg) for SCAP.[13, 17] Admission to the ICU was common, as were admission orders for do not resuscitate (DNR) or do not intubate (DNI). Patients with healthcare‐associated aspiration pneumonia had a higher comorbidity index and had a higher mortality rate than patients with community‐acquired aspiration pneumonia, although we found no significant difference in the rate of hospital or ICU admission or the receipt of critical care therapies. Inpatient assessment of dysphagia and aspiration was conducted in 177 patients. Abnormal swallow was noted in 96% of those tested.
We found several differences between patients with community‐acquired aspiration pneumonia and 2584 patients with CAP identified during the same time period[13] (Table 4). Patients with community‐acquired aspiration pneumonia were older, more likely to have multilobar disease or effusion on imaging, and had greater disease severity. They also had a higher frequency of ICU and hospital admission, IDSA/ATS minor criteria for SCAP, and higher Charlson comorbidity indices. Patients with community‐acquired aspiration pneumonia were more likely to receive mechanical ventilation than CAP patients, although there was no difference in 30‐day mortality among intubated patients or a difference in ventilator‐free days.
| Community‐Acquired Aspiration Pneumonia (N = 510) | Community‐ Acquired Pneumonia (N = 2584) | P Value | |
|---|---|---|---|
| |||
| Age (range), y | 77 (6485) | 59 (4176) | <0.0001 |
| Female, % | 50.2 | 49.5 | 0.81 |
| 30‐day mortality, % | 19.0 | 4.2 | <0.0001 |
| CURB‐65 score | 2 (13) | 1 (02) | <0.0001 |
| Confusion, % | 12.7 | 5.1 | <0.0001 |
| Blood urea nitrogen | 21 (1532) | 16 (1124) | <0.0001 |
| Respiratory rate | 20 (1824) | 20 (1824) | <0.0001 |
| Systolic blood pressure | 129 (110150) | 130 (112146) | 0.67 |
| eCURB 30‐day mortality estimate, median, % | 5.2 (2.212.4) | 1.7 (0.94.3) | <0.0001 |
| eCURB 30‐day mortality estimate, mean, % | 9.7 11.5 | 4.4 7.5 | <0.0001 |
| AUC of eCURB versus mortality | 0.71 (0.660.75) | 0.86 (0.830.90) | <0.0001 |
| Excluding DNR/DNI patients | 0.69 (0.650.74) | 0.87 (0.830.90) | 0.0001 |
| AUC of CURB‐65 versus mortality | 0.66 (0.620.69) | 0.81 (0.780.85) | <0.0001 |
| Excluding DNR/DNI patients | 0.65 (0.600.70) | 0.81 (0.760.85) | 0.0003 |
| Hospital admission (of ED visits), % | 98.8 | 57.8 | <0.0001 |
| Hospital LOS, d | 6.5 (4.011.0) | 3.3 (2.25.2) | <0.0001 |
| ICU admission, % | 37.1 | 14.2 | <0.0001 |
| ICU LOS, d | 3.1 (1.87.6) | 2.5 (1.17.7) | 0.01 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.9 7.7 | 25 9 | 0.75 |
| Receipt of mechanical ventilation, % | 17.2 | 7.8 | <0.0001 |
| Duration of ventilation, d | 3.1 (1.06.6) | 3.5 (1.57.2) | 0.09 |
| Receipt of vasopressor, % | 1.4 | 3.3 | 0.02 |
| Charlson comorbidity index | 3 (26) | 1 (03) | <0.0001 |
| Cerebrovascular disease, % | 32.4 | 10.0 | <0.0001 |
| Chronic pulmonary disease, % | 51.8 | 42.5 | <0.0001 |
| Congestive heart failure, % | 50.0 | 22.1 | <0.0001 |
| Connective tissue disease, % | 8.8 | 5.6 | 0.0084 |
| Dementia, % | 12.0 | 2.8 | <0.0001 |
| Hemiplegia/paraplegia, % | 8.0 | 2.7 | <0.0001 |
| Myocardial infarction, % | 17.8 | 10.8 | <0.0001 |
| Peripheral vascular disease, % | 16.3 | 7.4 | <0.0001 |
| Peptic ulcer disease, % | 19.2 | 7.6 | <0.0001 |
| Diabetes without complications, % | 9.2 | 24.7 | <0.0001 |
| Diabetes with complications, % | 30.4 | 5.1 | <0.0001 |
| Mild liver disease, % | 8.0 | 6.2 | 0.14 |
| Moderate or severe liver disease, % | 1.6 | 0.8 | 0.13 |
| Malignant solid tumor, % | 17. | 8.9 | <0.0001 |
| Metastatic cancer, % | 5.7 | 1.3 | <0.0001 |
| Renal disease, % | 4.2 | 5.6 | <0.0001 |
| 3 or more minor SCAP criteria, %* | 24.7 | 19.1 | 0.01 |
| PaO2/FiO2 ratio | 226 (169280) | 260 (148338) | 0.0004 |
| Multilobar disease, % | 43.2 | 37.2 | 0.0012 |
| Presence of an effusion, % | 19.7 | 18.3 | <0.0001 |
| Presence of a DNR/DNI order, % | 23.7 | 9.7 | <0.0001 |
| Mortality of patients with DNR/DNI order, % | 38.8 | 12.4 | <0.0001 |
| Receipt of broad‐spectrum antibiotic, % | 32.5 | 8.4 | <0.0001 |
| Receipt of MRSA antibiotic, % | 5.7 | 2.2 | <0.0001 |
| Receipt of anaerobe antibiotic, % | 27.6 | 3.1 | <0.0001 |
Thirty‐day mortality for patients with community‐acquired aspiration pneumonia was significantly higher than in CAP patients. Patients with community‐acquired aspiration pneumonia also had higher eCURB and CURB‐65 scores. However, eCURB was a poor predictor of 30‐day mortality, with an AUC of 0.71, compared to 0.86 calculated for the CAP population (Figure 2). CURB‐65 performed similarly: AUC was 0.66 vs 0.81. The presence of a DNR/DNI order was twice as prevalent in the community‐acquired aspiration pneumonia population vs the CAP population; those patients with a DNR/DNI order were 3 times as likely to die. Excluding patients with a DNR/DNI order did not improve performance of eCURB or CURB‐65 (Table 4). The presence of IDSA/ATS minor criteria for SCAP was not predictive of triage to the ICU in the group of patients with community‐acquired aspiration pneumonia (AUC: 0.51), compared with CAP patients (AUC: 0.88, P < 0.01 for comparison, Figure 3). This finding persisted in the subset of patients without a DNR/DNI order (AUC: 0.52 in community‐acquired aspiration pneumonia vs 0.88 in CAP, P < 0.01).
Our regression model of mortality incorporated gender, presence of effusion or multilobar pneumonia, presence of a DNR/DNI order, and all the components of the CURB‐65, IDSA/ATS minor criteria for SCAP, and Charlson comorbidity index. The regression model demonstrated that even after adjustment for age, comorbidities, disease severity, and presence of a DNR/DNI order, the presence of aspiration pneumonia was associated with higher mortality than CAP (odds ratio [OR]: 3.46, P < 0.001, Table 5). In this model, systolic blood pressure did not predict mortality, and diabetes with complications was associated with decreased mortality.
| Odds Ratio | P Value | |
|---|---|---|
| ||
| Presence of aspiration pneumonia | 3.46 (2.115.67) | <0.001 |
| Age, y | 1.03 (1.011.04) | <0.001 |
| Confusion | 3.14 (1.955.05) | <0.001 |
| Blood urea nitrogen, mg/dL | 1.03 (1.021.04) | <0.001 |
| Respiratory rate, breaths/minute | 1.03 (1.001.06) | 0.04 |
| PaO2/FiO2 ratio, per 1 mm Hg | 0.99 (0.991.00) | <0.001 |
| Moderate or severe liver disease | 9.21 (3.1626.86) | <0.001 |
| Paraplegia/hemiplegia | 2.43 (1.135.27) | 0.02 |
| Diabetes with complications | 0.42 (0.200.87) | 0.02 |
| Leukocytosis | 4.47 (2.278.82) | <0.001 |
| DNR/DNI | 1.75 (1.112.75) | 0.02 |
Microbiological Findings
Blood cultures were performed at admission in 67.4% of aspiration‐pneumonia patients, and a tracheal aspirate in half (50.7%) of intubated patients with aspiration pneumonia. Organisms were recovered in 90 patients (14.3%), although 41 of those patients had tracheal aspirates of organisms commonly thought to be nonpathogenic (nonpneumococcal alpha‐hemolytic streptococcus, nonhemolytic streptococcus, diphtheroids, micrococci, coagulase negative staphylococccus). Tracheal aspirate was the most common method of recovering an organism (7.8% of patients), followed by blood culture (4.3%). Bronchoalveolar lavage, urinary antigen, and pleural fluid culture were less common (1.3%, 1.1%, 0.3%, respectively). The microbiologic results were grouped into: Staphylococcus aureus, Streptococcus pneumoniae, enteric bacilli, Haemophilus species, Neisseria species, Moraxella catarrhalis, and Pseudomonas aeruginosa (Figure 4). Comparing healthcare‐associated with community‐acquired aspiration pneumonia, healthcare‐associated patients were more likely to have a confirmed infection with MRSA (4.2% vs 1.4%, P = 0.06) and enteric bacteria (5.1% vs 1.6%, P = 0.03). There were no other statistically significant differences in microbiologic recovery between the 2 groups. Antibiotics targeting anaerobic pathogens were administered in 28.7% of patients with aspiration pneumonia, with no correlation to the presence of healthcare‐associated risks. Healthcare‐associated patients were more likely to receive broad‐spectrum antibiotics (47.5% vs 32.5%, P < 0.01) and MRSA coverage (15.3% vs 5.7%, P < 0.01) than patients with community‐acquired aspiration pneumonia.
DISCUSSION
Our study identifies a larger cohort of patients with aspiration pneumonia than previous studies.[21, 22, 23, 24, 25] Patients with community‐acquired aspiration pneumonia are older and more likely to die than CAP patients. They are more likely to be admitted to the hospital or ICU. Thirty‐day mortality in this patient population was significantly underestimated by CURB‐65 and eCURB, models developed and validated in CAP populations.[9, 26] This finding supports a prior study.[27] It appears that a traditional prognostic model assessing mortality risk in the CAP patient does not apply to the aspiration‐pneumonia patient. One reason for eCURB and CURB‐65s poor utility in community‐acquired aspiration pneumonia may be their reliance on objective clinical features rather than comorbidities, which may influence mortality to a greater degree in aspiration pneumonia.
This study has several limitations. There is no gold standard for the definition of aspiration pneumonia, and it is difficult to distinguish aspiration pneumonia from typical pneumonia. It is plausible that older patients with greater comorbidities are being designated as aspiration pneumonia. If this is the case, then aspiration pneumonia merely represents the end of the pneumonia spectrum with highest mortality risk, and it is no surprise that these patients fare poorly.
It appears that the hospitalist or emergency department physician implicitly appreciates that aspiration pneumonia has a higher mortality risk than predicted by traditional severity assessment. With such high mortality and morbidity, a patient presenting to the emergency room with aspiration pneumonia is almost always admitted to the hospital. Further work in this area should investigate other factors to improve prognostic modeling in patients with aspiration pneumonia, although the utility of such a model may be limited to determining ICU admission. Our data indicate that IDSA/ATS minor criteria for SCAP are not useful in predicting admission to the ICU in patients with aspiration pneumonia.
In this study, a DNR/DNI order was twice as common in the community‐acquired aspiration pneumonia population than the CAP population. However, patients with community‐acquired aspiration pneumonia and a DNR/DNI order were more than 3 times more likely to die than patients with CAP and a DNR/DNI order. Our regression model suggested that the presence of a DNR/DNI order was an independent predictor of mortality (OR: 1.75, P < 0.001). Although a DNR/DNI order may correlate with the withholding or withdrawal of medical therapy, it is also a surrogate for increased age or comorbidities.[28] In our study, however, the increased prevalence of DNR/DNI orders did not explain the poor mortality prediction of the eCURB or CURB‐65, as exclusion of those patients did not significantly alter the AUCs in either the aspiration group or the CAP group.
Controversy exists regarding treatment of aspiration pneumonia. Historically, some have advocated for treatment of aspiration pneumonia with a regimen designed to cover anaerobic bacteria.[29] This recommendation was based on early microbiologic studies that obtained the samples late in the course of illness, or other studies where the sample was obtained transtracheally, where oropharyngeal flora may contaminate the sample.[30, 31, 32] Our clinically obtained microbiologic recovery of organisms was similar to the flora recovered in more recent CAP studies, in respect to both the incidence of pathogen recovery and the relative frequencies of recovered organisms.[33, 34] Our data do not support inferences regarding the prevalence of anaerobic infections, as the recovery of anaerobic organisms was limited to blood and pleural fluid cultures in this study, rather than techniques used in research settings that might have greater yield. As expected, patients with healthcare‐associated risk factors trended toward increased incidence of MRSA. Given the similarity of the organisms recovered to those recovered in CAP,[35] this study supports IDSA/ATS recommendations that antibiotic therapy in aspiration pneumonia be similar to that of higher‐risk CAP, with the addition of vancomycin or linezolid for MRSA coverage in patients with risk factors for healthcare‐associated pneumonia.[17]
Our study is limited by its single‐center retrospective design. However, beginning in 1995, the LDS Hospital emergency department initiated a standardized pneumonia therapy protocol and deployed electronic medical records, which prospectively recorded a wide array of clinical, therapeutic, and biometric data. Most data elements used in this analysis were routinely charted for clinical purposes in real time. Although the eCURB, CURB‐65, and some comorbidities could be extracted electronically for each patient, it was not possible to calculate the pneumonia severity index score due to our inability to rigorously identify the necessary comorbid illness elements. Other comorbidities, not present in our model, may have been identified by the physician who makes a diagnosis of aspiration pneumonia. Our identification of swallow impairment is also methodologically limited. The decision to obtain a swallow study was clinical, usually occurring upon convalescence. Therefore, it is not possible to distinguish between antecedent oropharyngeal dysfunction and post‐critical illness dysfunction.
Our definition of aspiration pneumonia required the treating physician to diagnose and code the patient as having aspiration pneumonia, followed by excluding patients more likely to have aspiration pneumonitis. Although we relied on ICD‐9 codes to initially identify aspiration pneumonia, all patients in our database were confirmed by physician chart review. Our incidence of community‐acquired aspiration pneumonia is congruent with other studies using different methodologies.[1, 36, 37] Unfortunately, there is no standard and widely accepted definition for separating aspiration pneumonia from usual CAP. A younger and healthier patient who has developed pneumonia subsequent to aspiration may be more likely to be diagnosed with CAP, resulting in selection bias for older patients with greater comorbidities.
CONCLUSION
Patients diagnosed with aspiration pneumonia are older, have more comorbid conditions, and demonstrate greater disease severity and higher 30‐day mortality than CAP patients. Mortality prediction using CURB‐65 and eCURB in this population was poor, possibly due to a greater effect of comorbidities on mortality. The pneumonia severity index, which incorporates patient comorbidities, might perform better than the eCURB or CURB‐65, and should be studied in aspiration pneumonia populations where comorbid illness information is prospectively collected. Further areas of study include creating an improved mortality prediction model for aspiration pneumonia that incorporates comorbid conditions, DNR/DNI status, and disease severity.
Acknowledgments
The authors acknowledge Al Jephson for database support, Yao Li for statistical analysis, and Anita Austin for help reviewing the medical records. Dr. Lanspa had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure
Preliminary versions of this work were presented as posters at the American Thoracic Society Meeting, Denver, Colorado, May 17, 2011. This study was supported by grants from the Intermountain Research and Medical Foundation. Dr. Brown is supported by a career development award from National Institute of General Medical Sciences (K23GM094465). Dr. Dean served on an advisory board for Merck, has been a paid consultant for Cerexa, and has received an investigator‐initiated competitive grant from Pfizer for development of an electronic pneumonia decision support tool. All other authors report no relevant financial disclosures.
Pneumonia is a common clinical syndrome with well‐described epidemiology and microbiology. Aspiration pneumonia comprises 5% to 15% of patients with pneumonia,[1] but is less well‐characterized despite being a major syndrome of pneumonia in the elderly.[2, 3] Difficulties in studying aspiration pneumonia include the lack of a sensitive and specific marker for aspiration, the overlap between aspiration pneumonia and other forms of pneumonia, and the lack of differentiation between aspiration pneumonia and aspiration pneumonitis by many clinicians.[4, 5, 6] Aspiration pneumonia, which develops after the aspiration of oropharyngeal contents, differs from aspiration pneumonitis, wherein inhalation of gastric contents causes inflammation without the subsequent development of bacterial infection.[7, 8]
A number of validated mortality prediction models exist for community‐acquired pneumonia (CAP), using a variety of clinical predictors. One clinical prediction rule endorsed by the British Thoracic Society is the CURB‐65, which assigns a score for Confusion, Uremia >19 mg/dL, Respiratory rate >= 30 breaths/min, Blood Pressure < 90 mmHg systolic or < 60 mmHg diastolic, and age 65). We favor eCURB, a version of the CURB‐65 model that uses continuously weighted variables to more accurately predict mortality, validated in CAP populations.[9] Most studies validating pneumonia severity scoring systems excluded aspiration pneumonia from their study population.[10, 11, 12] Severity scoring systems for CAP may not accurately predict disease severity patients with aspiration pneumonia.
The aims of our study were to: (1) identify a population of patients with aspiration pneumonia; (2) compare characteristics and outcomes in patients with community‐acquired aspiration pneumonia to those with CAP; and (3) study the performance of eCURB and CURB‐65 in predicting mortality for patients with community‐acquired aspiration pneumonia.
PATIENTS AND METHODS
Study Design and Setting
The study was performed at LDS Hospital, a university‐affiliated community teaching hospital in Salt Lake City, Utah, with 520 beds. In retrospective analysis of data from the electronic medical records, we identified all patients older than 18 years who were evaluated in the emergency department at LDS Hospital or admitted patients from other sources (direct admission, transfer from another hospital) from 1996 to 2006 with International Statistical Classification of Disease and Health Related Problems, 9th Revision (ICD‐9) codes specific for aspiration pneumonia and pneumonitis (507.x). The treating physicians were mostly hospitalists and intensivists. Two physicians (M.L. and N.D.) manually reviewed the electronic medical records, including the emergency room physician's notes, the admission histories and physicals, the discharge summaries, and radiographic reports of the patients identified in the query. Consensus regarding the diagnosis of aspiration pneumonia was achieved in all patients reviewed using criteria listed in Table 1. This study was approved by the LDS Hospital institutional review board, and permission was granted to use the Utah Population Database for determining mortality (#1008505), with a waiver of informed consent. For the contemporaneous group of CAP patients, we used a previously described population identified using ICD‐9 codes 481.x to 487.x, captured from the same hospital during the same period.[13]
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| |
| 1. Age 18 years | 1. Absence of radiographic evidence of pneumonia within 48 hours after evaluation |
| 2. Either admitted to hospital or evaluated in emergency department | 2. Previous episode of aspiration pneumonia within 12 months |
| 3. 507.x code as primary diagnosis | 3. Initial admission date >48 hours before transfer to LDS Hospital |
| 4. 507.x code as secondary diagnosis with a primary diagnosis of pneumonia, respiratory failure, or septicemia | 4. AIDS 5. Receipt of antiretroviral therapy 6. History of solid organ transplant |
| 5. Treating physician indicated a diagnosis of aspiration pneumonia in the history and physical and/or discharge summary | 7. Hematologic malignancy 8. Witnessed isolated aspiration event within 24 hours prior to evaluation 9. Drug overdose, cardiopulmonary arrest, or seizure prior to hospital admission 10. Laryngoscopic or bronchoscopic evidence of food material in airway |
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria are listed in Table 1. To exclude patients with recurrent pneumonia, we included only the first episode of pneumonia in a given 12‐month period. LDS Hospital frequently receives patients transferred from surrounding emergency departments and intensive care units. We excluded patients who were transferred >48 hours from their initial emergency department admission and therefore were late in their disease course. Exclusion criteria 8 to 10 were used to exclude patients with clinical presentations more consistent with aspiration pneumonitis. We also excluded immunocompromised patients (criteria 4 to 7).
Healthcare‐associated aspiration pneumonia was defined as receipt of chronic hemodialysis, residence in a nursing facility, or hospitalization within any Intermountain Healthcare‐affiliated hospital within the past 90 days.[14] The remaining patients were defined as community‐acquired aspiration pneumonia.
Measurements
The first vital signs, orientation status, and first 12 hours of routine laboratory results were extracted from the electronic medical records and used to calculate predicted mortality by eCURB and CURB‐65. We determined 30‐day mortality from the merger of the electronic medical records with vital status information from the Utah Population Database.[15] The first measured SpO2 and FiO2 were used to estimate the PaO2/FiO2 ratio, using the Severinghaus calculation[16] if no arterial blood gas was available. Presence of American Thoracic Society/Infectious Diseases Society of America (IDSA/ATS) 2007 minor criteria for severe community‐acquired pneumonia (SCAP)[17] were obtained from baseline patient characteristics (Table 2). A Charlson comorbidity index was calculated from ICD‐9 codes using published methodology.[18, 19] Presence of an abnormal swallow was defined as dysphagia or aspiration on modified barium swallow study, fiberoptic endoscopic evaluation, or clinical determination by a speech language pathologist during the index hospitalization. We also looked for causative pathogens, defined by a positive pneumococcus or legionella urinary antigen, or a positive culture from blood, bronchoalveolar lavage, pleural fluid, or tracheal aspirate, collected within 24 hours of admission. Antibiotics administered within the first 24 hours of admission were classified into 4 broad groups based on local physician prescribing patterns. Clindamycin and metronidazole were considered anaerobic‐specific antibiotics. Vancomycin or linezolid were considered methicillin‐resistant Staphylococcus aureus (MRSA) antibiotics. Broad‐spectrum antibiotics included any of the following: carbapenems, aztreonam, piperacillin/tazobactam, ticarcillin/clavulanate, cefepime, and ceftazidime. Macrolides, respiratory fluoroquinolones, and third‐generation cephalosporins were considered standard‐care antibiotics.
| Respiratory rate 30 breaths/minute |
| PaO2/FiO2 250 |
| Multilobar infiltrates |
| Confusion/disorientation |
| Uremia (blood urea nitrogen 20 mg/dL) |
| Leukopenia (white blood cell count <4000 cells/mm3) |
| Thrombocytopenia (platelet count <100,000 cells/mm3) |
| Hypothermia (core temperature 36C) |
| Hypotension requiring aggressive fluid resuscitation |
Statistical Analysis
We compared baseline patient characteristics and clinical outcomes using the Fisher exact test to compare proportions of categorical variables, and Mann‐Whitney U test or Student t test to compare central tendencies of continuous variables, as dictated by the normality of the data. Receiver operating characteristic curves calculated the ability of eCURB and CURB‐65 to predict 30‐day mortality prediction in patients with community‐acquired aspiration pneumonia and CAP, as well as the ability of IDSA/ATS minor criteria for SCAP to predict admission to the intensive care unit (ICU). We performed multivariate logistic regression to predict 30‐day mortality in patients with community‐acquired aspiration pneumonia and CAP, using stepwise backward elimination. Confounders were included if they were significant at a 0.05 level or if they altered the coefficient of the main variable by more than 10%. For logistic models, we evaluated goodness of fit with the Hosmer‐Lemeshow technique; comparisons of area under the curve (AUC) among models were made using the technique of DeLong.[20] Two‐tailed P values of 0.05 were considered statistically significant. Stata version 12 (StataCorp, College Station, TX) was used for all analyses.
RESULTS
Our initial query identified 1165 patients. Physician review of the medical records resulted in 628 patients, 118 of whom were classified as healthcare‐associated aspiration pneumonia (Figure 1, Table 3). Of all aspiration pneumonia patients, 80% were seen in the emergency department, 12.5% were directly admitted from the community, and 7.5% were transferred from another healthcare facility. Almost all patients seen in the emergency department (99.0%) were admitted to the hospital, with median length of hospitalization 6.7 days among survivors.
| Aspiration Pneumonia (N = 628) | Community‐Acquired Aspiration Pneumonia (N = 510) | Healthcare Associated Aspiration Pneumonia (N=118) | P Value | |
|---|---|---|---|---|
| ||||
| Age (range), y | 77 (6585) | 77 (6485) | 80 (6786) | 0.42 |
| Female, % | 49.8 | 50.2 | 48.3 | 0.76 |
| 30‐day mortality, % | 21.0% | 19.0% | 29.7% | 0.02 |
| CURB‐65 score | 2 (13) | 2 (13) | 2 (13) | 0.0012 |
| Confusion | 13.9% | 12.7% | 18.6% | 0.10 |
| Blood urea nitrogen (mg/dL) | 22 (1634) | 21 (1532) | 30 (2047) | <0.0001 |
| Respiratory rate (breaths/min) | 20 (1826) | 20 (1824) | 21 (1828) | 0.30 |
| Systolic blood pressure (mm Hg) | 128 (110149) | 129 (110150) | 127 (105146) | 0.28 |
| eCURB 30‐day mortality estimate (median, %) | 5.6 (2.414.2) | 5.2 (2.212.4) | 8.9 (4.222.5) | <0.0001 |
| eCURB 30‐day mortality estimate (mean, %) | 10.6 12.2 | 9.7 11.5 | 14.614.1 | <0.0001 |
| Hospital admission (of ED visits), % | 99.0 | 98.8 | 100 | 0.59 |
| Hospital LOS, d | 6.7 (4.111.1) | 6.5 (4.011.0) | 7.8 (5.412.3) | 0.05 |
| ICU admission, % | 37.9 | 37.1 | 41.5 | 0.21 |
| ICU LOS, d | 3.5 (1.98.8) | 3.1 (1.87.6) | 5.6 (3.810.8) | 0.02 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.28.3 | 25.97.7 | 22.710.0 | 0.01 |
| Receipt of mechanical ventilation, % | 18.6 | 17.2 | 24.6 | 0.09 |
| Duration of ventilation, d | 2.8 (0.96.5) | 3.1 (1.06.6) | 1.9 (0.86.3) | 0.05 |
| Receipt of vasopressor, % | 1.8 | 1.4 | 3.4 | 0.13 |
| Charlson comorbidity index | 4 (26) | 3 (26) | 4 (36) | 0.0024 |
| Cerebrovascular disease, % | 33.9 | 32.4 | 40.7 | 0.11 |
| Chronic pulmonary disease, % | 51.0 | 51.8 | 47.5 | 0.42 |
| Congestive heart failure, % | 52.4 | 50.0 | 62.7 | 0.01 |
| Connective tissue disease, % | 8.4 | 8.8 | 6.8 | 0.58 |
| Dementia, % | 14.2 | 12.0 | 23.7 | 0.0019 |
| Hemiplegia/paraplegia | 9.4 | 8.0 | 15.2 | 0.02 |
| Myocardial infarction, % | 21.0 | 17.8 | 29.7 | 0.02 |
| Peripheral vascular disease, % | 17.7 | 16.3 | 23.7 | 0.06 |
| Peptic ulcer disease, % | 18.8 | 19.2 | 16.9 | 0.70 |
| Diabetes without complications, % | 10.7 | 9.2 | 16.9 | 0.02 |
| Diabetes with complications, % | 31.5 | 30.4 | 36.4 | 0.23 |
| Mild liver disease, % | 8.6 | 8.0 | 11.0 | 0.28 |
| Moderate or severe liver disease, % | 1.8 | 1.6 | 2.5 | 0.44 |
| Malignant solid tumor, % | 16.6 | 17.3 | 13.6 | 0.41 |
| Metastatic cancer, % | 5.4 | 5.7 | 4.2 | 0.66 |
| Renal disease, % | 14.7 | 4.2 | 18.6 | 0.19 |
| 3 or more minor SCAP criteria, %* | 24.7 | 23.1 | 31.4 | 0.08 |
| PaO2/FiO2 ratio | 221 (161280) | 226 (169280) | 181 (133245) | 0.0004 |
| Multilobar disease, % | 46.3 | 43.2 | 53.9 | 0.11 |
| Presence of an effusion, % | 23.1 | 19.7 | 31.9 | 0.03 |
| Swallow impairment (of tested survivors), % | 34.1 | 34.1 | 34.1 | 0.22 |
| Presence of a DNR/DNI order, % | 26.4 | 23.7 | 38.1 | 0.0024 |
| Mortality of patients with DNR/DNI order, % | 39.1 | 38.8 | 40.0 | 1.00 |
| Receipt of broad‐spectrum antibiotic, % | 35.4 | 32.5 | 47.5 | 0.0028 |
| Receipt of MRSA antibiotic, % | 7.5 | 5.7 | 15.3 | 0.0014 |
| Receipt of anaerobe antibiotic, % | 28.7 | 27.6 | 33.1 | 0.26 |
Observed mortality was 21.0%. eCURB significantly underestimated mortality in this group, predicting a mortality rate of 10.6%. When classifying patients by the 2007 IDSA/ATS guidelines, 24.7% of the patients had 3 or more minor criteria for SCAP.[17] The PaO2/FiO2 ratio was obtained in 99.7% of patients. The median PaO2/FiO2 ratio observed in this population was 221 mm Hg (equivalent to 260 mm Hg at sea level barometric pressure, adjusted for our altitude of 1400 meters), near the threshold sea level definition (250 mm Hg) for SCAP.[13, 17] Admission to the ICU was common, as were admission orders for do not resuscitate (DNR) or do not intubate (DNI). Patients with healthcare‐associated aspiration pneumonia had a higher comorbidity index and had a higher mortality rate than patients with community‐acquired aspiration pneumonia, although we found no significant difference in the rate of hospital or ICU admission or the receipt of critical care therapies. Inpatient assessment of dysphagia and aspiration was conducted in 177 patients. Abnormal swallow was noted in 96% of those tested.
We found several differences between patients with community‐acquired aspiration pneumonia and 2584 patients with CAP identified during the same time period[13] (Table 4). Patients with community‐acquired aspiration pneumonia were older, more likely to have multilobar disease or effusion on imaging, and had greater disease severity. They also had a higher frequency of ICU and hospital admission, IDSA/ATS minor criteria for SCAP, and higher Charlson comorbidity indices. Patients with community‐acquired aspiration pneumonia were more likely to receive mechanical ventilation than CAP patients, although there was no difference in 30‐day mortality among intubated patients or a difference in ventilator‐free days.
| Community‐Acquired Aspiration Pneumonia (N = 510) | Community‐ Acquired Pneumonia (N = 2584) | P Value | |
|---|---|---|---|
| |||
| Age (range), y | 77 (6485) | 59 (4176) | <0.0001 |
| Female, % | 50.2 | 49.5 | 0.81 |
| 30‐day mortality, % | 19.0 | 4.2 | <0.0001 |
| CURB‐65 score | 2 (13) | 1 (02) | <0.0001 |
| Confusion, % | 12.7 | 5.1 | <0.0001 |
| Blood urea nitrogen | 21 (1532) | 16 (1124) | <0.0001 |
| Respiratory rate | 20 (1824) | 20 (1824) | <0.0001 |
| Systolic blood pressure | 129 (110150) | 130 (112146) | 0.67 |
| eCURB 30‐day mortality estimate, median, % | 5.2 (2.212.4) | 1.7 (0.94.3) | <0.0001 |
| eCURB 30‐day mortality estimate, mean, % | 9.7 11.5 | 4.4 7.5 | <0.0001 |
| AUC of eCURB versus mortality | 0.71 (0.660.75) | 0.86 (0.830.90) | <0.0001 |
| Excluding DNR/DNI patients | 0.69 (0.650.74) | 0.87 (0.830.90) | 0.0001 |
| AUC of CURB‐65 versus mortality | 0.66 (0.620.69) | 0.81 (0.780.85) | <0.0001 |
| Excluding DNR/DNI patients | 0.65 (0.600.70) | 0.81 (0.760.85) | 0.0003 |
| Hospital admission (of ED visits), % | 98.8 | 57.8 | <0.0001 |
| Hospital LOS, d | 6.5 (4.011.0) | 3.3 (2.25.2) | <0.0001 |
| ICU admission, % | 37.1 | 14.2 | <0.0001 |
| ICU LOS, d | 3.1 (1.87.6) | 2.5 (1.17.7) | 0.01 |
| Mean ventilator‐free days (of ICU patients, out of 30 days) | 25.9 7.7 | 25 9 | 0.75 |
| Receipt of mechanical ventilation, % | 17.2 | 7.8 | <0.0001 |
| Duration of ventilation, d | 3.1 (1.06.6) | 3.5 (1.57.2) | 0.09 |
| Receipt of vasopressor, % | 1.4 | 3.3 | 0.02 |
| Charlson comorbidity index | 3 (26) | 1 (03) | <0.0001 |
| Cerebrovascular disease, % | 32.4 | 10.0 | <0.0001 |
| Chronic pulmonary disease, % | 51.8 | 42.5 | <0.0001 |
| Congestive heart failure, % | 50.0 | 22.1 | <0.0001 |
| Connective tissue disease, % | 8.8 | 5.6 | 0.0084 |
| Dementia, % | 12.0 | 2.8 | <0.0001 |
| Hemiplegia/paraplegia, % | 8.0 | 2.7 | <0.0001 |
| Myocardial infarction, % | 17.8 | 10.8 | <0.0001 |
| Peripheral vascular disease, % | 16.3 | 7.4 | <0.0001 |
| Peptic ulcer disease, % | 19.2 | 7.6 | <0.0001 |
| Diabetes without complications, % | 9.2 | 24.7 | <0.0001 |
| Diabetes with complications, % | 30.4 | 5.1 | <0.0001 |
| Mild liver disease, % | 8.0 | 6.2 | 0.14 |
| Moderate or severe liver disease, % | 1.6 | 0.8 | 0.13 |
| Malignant solid tumor, % | 17. | 8.9 | <0.0001 |
| Metastatic cancer, % | 5.7 | 1.3 | <0.0001 |
| Renal disease, % | 4.2 | 5.6 | <0.0001 |
| 3 or more minor SCAP criteria, %* | 24.7 | 19.1 | 0.01 |
| PaO2/FiO2 ratio | 226 (169280) | 260 (148338) | 0.0004 |
| Multilobar disease, % | 43.2 | 37.2 | 0.0012 |
| Presence of an effusion, % | 19.7 | 18.3 | <0.0001 |
| Presence of a DNR/DNI order, % | 23.7 | 9.7 | <0.0001 |
| Mortality of patients with DNR/DNI order, % | 38.8 | 12.4 | <0.0001 |
| Receipt of broad‐spectrum antibiotic, % | 32.5 | 8.4 | <0.0001 |
| Receipt of MRSA antibiotic, % | 5.7 | 2.2 | <0.0001 |
| Receipt of anaerobe antibiotic, % | 27.6 | 3.1 | <0.0001 |
Thirty‐day mortality for patients with community‐acquired aspiration pneumonia was significantly higher than in CAP patients. Patients with community‐acquired aspiration pneumonia also had higher eCURB and CURB‐65 scores. However, eCURB was a poor predictor of 30‐day mortality, with an AUC of 0.71, compared to 0.86 calculated for the CAP population (Figure 2). CURB‐65 performed similarly: AUC was 0.66 vs 0.81. The presence of a DNR/DNI order was twice as prevalent in the community‐acquired aspiration pneumonia population vs the CAP population; those patients with a DNR/DNI order were 3 times as likely to die. Excluding patients with a DNR/DNI order did not improve performance of eCURB or CURB‐65 (Table 4). The presence of IDSA/ATS minor criteria for SCAP was not predictive of triage to the ICU in the group of patients with community‐acquired aspiration pneumonia (AUC: 0.51), compared with CAP patients (AUC: 0.88, P < 0.01 for comparison, Figure 3). This finding persisted in the subset of patients without a DNR/DNI order (AUC: 0.52 in community‐acquired aspiration pneumonia vs 0.88 in CAP, P < 0.01).
Our regression model of mortality incorporated gender, presence of effusion or multilobar pneumonia, presence of a DNR/DNI order, and all the components of the CURB‐65, IDSA/ATS minor criteria for SCAP, and Charlson comorbidity index. The regression model demonstrated that even after adjustment for age, comorbidities, disease severity, and presence of a DNR/DNI order, the presence of aspiration pneumonia was associated with higher mortality than CAP (odds ratio [OR]: 3.46, P < 0.001, Table 5). In this model, systolic blood pressure did not predict mortality, and diabetes with complications was associated with decreased mortality.
| Odds Ratio | P Value | |
|---|---|---|
| ||
| Presence of aspiration pneumonia | 3.46 (2.115.67) | <0.001 |
| Age, y | 1.03 (1.011.04) | <0.001 |
| Confusion | 3.14 (1.955.05) | <0.001 |
| Blood urea nitrogen, mg/dL | 1.03 (1.021.04) | <0.001 |
| Respiratory rate, breaths/minute | 1.03 (1.001.06) | 0.04 |
| PaO2/FiO2 ratio, per 1 mm Hg | 0.99 (0.991.00) | <0.001 |
| Moderate or severe liver disease | 9.21 (3.1626.86) | <0.001 |
| Paraplegia/hemiplegia | 2.43 (1.135.27) | 0.02 |
| Diabetes with complications | 0.42 (0.200.87) | 0.02 |
| Leukocytosis | 4.47 (2.278.82) | <0.001 |
| DNR/DNI | 1.75 (1.112.75) | 0.02 |
Microbiological Findings
Blood cultures were performed at admission in 67.4% of aspiration‐pneumonia patients, and a tracheal aspirate in half (50.7%) of intubated patients with aspiration pneumonia. Organisms were recovered in 90 patients (14.3%), although 41 of those patients had tracheal aspirates of organisms commonly thought to be nonpathogenic (nonpneumococcal alpha‐hemolytic streptococcus, nonhemolytic streptococcus, diphtheroids, micrococci, coagulase negative staphylococccus). Tracheal aspirate was the most common method of recovering an organism (7.8% of patients), followed by blood culture (4.3%). Bronchoalveolar lavage, urinary antigen, and pleural fluid culture were less common (1.3%, 1.1%, 0.3%, respectively). The microbiologic results were grouped into: Staphylococcus aureus, Streptococcus pneumoniae, enteric bacilli, Haemophilus species, Neisseria species, Moraxella catarrhalis, and Pseudomonas aeruginosa (Figure 4). Comparing healthcare‐associated with community‐acquired aspiration pneumonia, healthcare‐associated patients were more likely to have a confirmed infection with MRSA (4.2% vs 1.4%, P = 0.06) and enteric bacteria (5.1% vs 1.6%, P = 0.03). There were no other statistically significant differences in microbiologic recovery between the 2 groups. Antibiotics targeting anaerobic pathogens were administered in 28.7% of patients with aspiration pneumonia, with no correlation to the presence of healthcare‐associated risks. Healthcare‐associated patients were more likely to receive broad‐spectrum antibiotics (47.5% vs 32.5%, P < 0.01) and MRSA coverage (15.3% vs 5.7%, P < 0.01) than patients with community‐acquired aspiration pneumonia.
DISCUSSION
Our study identifies a larger cohort of patients with aspiration pneumonia than previous studies.[21, 22, 23, 24, 25] Patients with community‐acquired aspiration pneumonia are older and more likely to die than CAP patients. They are more likely to be admitted to the hospital or ICU. Thirty‐day mortality in this patient population was significantly underestimated by CURB‐65 and eCURB, models developed and validated in CAP populations.[9, 26] This finding supports a prior study.[27] It appears that a traditional prognostic model assessing mortality risk in the CAP patient does not apply to the aspiration‐pneumonia patient. One reason for eCURB and CURB‐65s poor utility in community‐acquired aspiration pneumonia may be their reliance on objective clinical features rather than comorbidities, which may influence mortality to a greater degree in aspiration pneumonia.
This study has several limitations. There is no gold standard for the definition of aspiration pneumonia, and it is difficult to distinguish aspiration pneumonia from typical pneumonia. It is plausible that older patients with greater comorbidities are being designated as aspiration pneumonia. If this is the case, then aspiration pneumonia merely represents the end of the pneumonia spectrum with highest mortality risk, and it is no surprise that these patients fare poorly.
It appears that the hospitalist or emergency department physician implicitly appreciates that aspiration pneumonia has a higher mortality risk than predicted by traditional severity assessment. With such high mortality and morbidity, a patient presenting to the emergency room with aspiration pneumonia is almost always admitted to the hospital. Further work in this area should investigate other factors to improve prognostic modeling in patients with aspiration pneumonia, although the utility of such a model may be limited to determining ICU admission. Our data indicate that IDSA/ATS minor criteria for SCAP are not useful in predicting admission to the ICU in patients with aspiration pneumonia.
In this study, a DNR/DNI order was twice as common in the community‐acquired aspiration pneumonia population than the CAP population. However, patients with community‐acquired aspiration pneumonia and a DNR/DNI order were more than 3 times more likely to die than patients with CAP and a DNR/DNI order. Our regression model suggested that the presence of a DNR/DNI order was an independent predictor of mortality (OR: 1.75, P < 0.001). Although a DNR/DNI order may correlate with the withholding or withdrawal of medical therapy, it is also a surrogate for increased age or comorbidities.[28] In our study, however, the increased prevalence of DNR/DNI orders did not explain the poor mortality prediction of the eCURB or CURB‐65, as exclusion of those patients did not significantly alter the AUCs in either the aspiration group or the CAP group.
Controversy exists regarding treatment of aspiration pneumonia. Historically, some have advocated for treatment of aspiration pneumonia with a regimen designed to cover anaerobic bacteria.[29] This recommendation was based on early microbiologic studies that obtained the samples late in the course of illness, or other studies where the sample was obtained transtracheally, where oropharyngeal flora may contaminate the sample.[30, 31, 32] Our clinically obtained microbiologic recovery of organisms was similar to the flora recovered in more recent CAP studies, in respect to both the incidence of pathogen recovery and the relative frequencies of recovered organisms.[33, 34] Our data do not support inferences regarding the prevalence of anaerobic infections, as the recovery of anaerobic organisms was limited to blood and pleural fluid cultures in this study, rather than techniques used in research settings that might have greater yield. As expected, patients with healthcare‐associated risk factors trended toward increased incidence of MRSA. Given the similarity of the organisms recovered to those recovered in CAP,[35] this study supports IDSA/ATS recommendations that antibiotic therapy in aspiration pneumonia be similar to that of higher‐risk CAP, with the addition of vancomycin or linezolid for MRSA coverage in patients with risk factors for healthcare‐associated pneumonia.[17]
Our study is limited by its single‐center retrospective design. However, beginning in 1995, the LDS Hospital emergency department initiated a standardized pneumonia therapy protocol and deployed electronic medical records, which prospectively recorded a wide array of clinical, therapeutic, and biometric data. Most data elements used in this analysis were routinely charted for clinical purposes in real time. Although the eCURB, CURB‐65, and some comorbidities could be extracted electronically for each patient, it was not possible to calculate the pneumonia severity index score due to our inability to rigorously identify the necessary comorbid illness elements. Other comorbidities, not present in our model, may have been identified by the physician who makes a diagnosis of aspiration pneumonia. Our identification of swallow impairment is also methodologically limited. The decision to obtain a swallow study was clinical, usually occurring upon convalescence. Therefore, it is not possible to distinguish between antecedent oropharyngeal dysfunction and post‐critical illness dysfunction.
Our definition of aspiration pneumonia required the treating physician to diagnose and code the patient as having aspiration pneumonia, followed by excluding patients more likely to have aspiration pneumonitis. Although we relied on ICD‐9 codes to initially identify aspiration pneumonia, all patients in our database were confirmed by physician chart review. Our incidence of community‐acquired aspiration pneumonia is congruent with other studies using different methodologies.[1, 36, 37] Unfortunately, there is no standard and widely accepted definition for separating aspiration pneumonia from usual CAP. A younger and healthier patient who has developed pneumonia subsequent to aspiration may be more likely to be diagnosed with CAP, resulting in selection bias for older patients with greater comorbidities.
CONCLUSION
Patients diagnosed with aspiration pneumonia are older, have more comorbid conditions, and demonstrate greater disease severity and higher 30‐day mortality than CAP patients. Mortality prediction using CURB‐65 and eCURB in this population was poor, possibly due to a greater effect of comorbidities on mortality. The pneumonia severity index, which incorporates patient comorbidities, might perform better than the eCURB or CURB‐65, and should be studied in aspiration pneumonia populations where comorbid illness information is prospectively collected. Further areas of study include creating an improved mortality prediction model for aspiration pneumonia that incorporates comorbid conditions, DNR/DNI status, and disease severity.
Acknowledgments
The authors acknowledge Al Jephson for database support, Yao Li for statistical analysis, and Anita Austin for help reviewing the medical records. Dr. Lanspa had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Disclosure
Preliminary versions of this work were presented as posters at the American Thoracic Society Meeting, Denver, Colorado, May 17, 2011. This study was supported by grants from the Intermountain Research and Medical Foundation. Dr. Brown is supported by a career development award from National Institute of General Medical Sciences (K23GM094465). Dr. Dean served on an advisory board for Merck, has been a paid consultant for Cerexa, and has received an investigator‐initiated competitive grant from Pfizer for development of an electronic pneumonia decision support tool. All other authors report no relevant financial disclosures.
- , , , et al. Severe community‐acquired pneumonia. Epidemiology and prognostic factors. Am Rev Respir Dis. 1991;144(2):312–318.
- , , . Risk factors for pneumonia in the elderly. Am J Med. 1994;96(4):313–320.
- , . Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124(1):328–336.
- , , . Pneumonia versus aspiration pneumonitis in nursing home residents: diagnosis and management. J Am Geriatr Soc. 2003;51(1):17–23.
- . Aspiration pneumonia: mixing apples with oranges and tangerines. Crit Care Med. 2004;32(5):1236; author reply 1236–1237.
- , , , , . Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999–2000. Crit Care Med. 2003;31(7):1930–1937.
- . Aspiration syndromes: aspiration pneumonia and pneumonitis. Hosp Pract (Minneap). 2010;38(1):35–42.
- . Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665–671.
- , , , et al. CURB‐65 pneumonia severity assessment adapted for electronic decision support. Chest. 2011;140(1):156–163.
- , , , et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382.
- , , , et al. Comparison of a disease‐specific and a generic severity of illness measure for patients with community‐acquired pneumonia. J Gen Intern Med. 1995;10(7):359–368.
- , , , et al. Development and validation of a clinical prediction rule for severe community‐acquired pneumonia. Am J Respir Crit Care Med. 2006;174(11):1249–1256.
- , , , . Validation of the Infectious Disease Society of America/American Thoracic Society 2007 guidelines for severe community‐acquired pneumonia. Crit Care Med. 2009;37(12):3010–3016.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416.
- .The Utah genealogical database: a resource for genetic epidemiology. In: Cairns JL, Skolnick M, eds. Banbury Report No 4; Cancer Incidence in Defined Populations. New York, NY:Cold Spring Harbor Laboratory;1980:285–297.
- . Simple, accurate equations for human blood O2 dissociation computations. J Appl Physiol. 1979;46(3):599–602.
- , , , et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27–S72.
- , , , . Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , . Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–845.
- , , . Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia. 1996;11(2):104–109.
- , , , . Predictors of aspiration pneumonia in nursing home residents. Dysphagia. 2002;17(4):298–307.
- , , , , , . Aspiration pneumonia: dental and oral risk factors in an older veteran population. J Am Geriatr Soc. 2001;49(5):557–563.
- , , , et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003;167(12):1650–1654.
- , , . Aspiration pneumonia in stroke. Arch Phys Med Rehabil. 1993;74(9):973–976.
- , , , et al. Validation of a predictive rule for the management of community‐acquired pneumonia. Eur Respir J. 2006;27(1):151–157.
- , , , , . Pneumonia Severity Index (PSI), CURB‐65, and mortality in hospitalized elderly patients with aspiration pneumonia [in German]. Zeitschrift fur Gerontologie und Geriatrie. 2011;44(4):229–234.
- , , , . Do‐not‐resuscitate orders for critically ill patients in the hospital. How are they used and what is their impact?JAMA. 1986;256(2):233–237.
- , , , , . The Sanford Guide to Antimicrobial Therapy: 2010.40th ed.Sperryville, VA:Antimicrobial Therapy, Inc.;2009.
- , , . The bacteriology of aspiration pneumonia. Am J Med. 1974;56(2):202–207.
- , , . Bacteriologic flora of aspiration‐induced pulmonary infections. Arch Intern Med. 1975;135(5):711–714.
- , . Bacteriology of aspiration pneumonia. A prospective study of community‐ and hospital‐acquired cases. Ann Intern Med. 1974;81(3):329–331.
- , . The role of anaerobes in patients with ventilator‐associated pneumonia and aspiration pneumonia: a prospective study. Chest. 1999;115(1):178–183.
- , , , et al. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279–284.
- , , , , . Community‐acquired pneumonia in the elderly. Semin Respir Infect. 1999;14(2):173–183.
- , , . Nursing home‐acquired pneumonia. A case‐control study. J Am Geriatr Soc. 1986;34(10):697–702.
- , , , , . Severe community‐acquired pneumonia. Etiology, epidemiology, and prognosis factors. French Study Group for Community‐Acquired Pneumonia in the Intensive Care Unit. Chest. 1994;105(5):1487–1495.
- , , , et al. Severe community‐acquired pneumonia. Epidemiology and prognostic factors. Am Rev Respir Dis. 1991;144(2):312–318.
- , , . Risk factors for pneumonia in the elderly. Am J Med. 1994;96(4):313–320.
- , . Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124(1):328–336.
- , , . Pneumonia versus aspiration pneumonitis in nursing home residents: diagnosis and management. J Am Geriatr Soc. 2003;51(1):17–23.
- . Aspiration pneumonia: mixing apples with oranges and tangerines. Crit Care Med. 2004;32(5):1236; author reply 1236–1237.
- , , , , . Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999–2000. Crit Care Med. 2003;31(7):1930–1937.
- . Aspiration syndromes: aspiration pneumonia and pneumonitis. Hosp Pract (Minneap). 2010;38(1):35–42.
- . Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665–671.
- , , , et al. CURB‐65 pneumonia severity assessment adapted for electronic decision support. Chest. 2011;140(1):156–163.
- , , , et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382.
- , , , et al. Comparison of a disease‐specific and a generic severity of illness measure for patients with community‐acquired pneumonia. J Gen Intern Med. 1995;10(7):359–368.
- , , , et al. Development and validation of a clinical prediction rule for severe community‐acquired pneumonia. Am J Respir Crit Care Med. 2006;174(11):1249–1256.
- , , , . Validation of the Infectious Disease Society of America/American Thoracic Society 2007 guidelines for severe community‐acquired pneumonia. Crit Care Med. 2009;37(12):3010–3016.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416.
- .The Utah genealogical database: a resource for genetic epidemiology. In: Cairns JL, Skolnick M, eds. Banbury Report No 4; Cancer Incidence in Defined Populations. New York, NY:Cold Spring Harbor Laboratory;1980:285–297.
- . Simple, accurate equations for human blood O2 dissociation computations. J Appl Physiol. 1979;46(3):599–602.
- , , , et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27–S72.
- , , , . Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , . Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–845.
- , , . Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia. 1996;11(2):104–109.
- , , , . Predictors of aspiration pneumonia in nursing home residents. Dysphagia. 2002;17(4):298–307.
- , , , , , . Aspiration pneumonia: dental and oral risk factors in an older veteran population. J Am Geriatr Soc. 2001;49(5):557–563.
- , , , et al. Microbiology of severe aspiration pneumonia in institutionalized elderly. Am J Respir Crit Care Med. 2003;167(12):1650–1654.
- , , . Aspiration pneumonia in stroke. Arch Phys Med Rehabil. 1993;74(9):973–976.
- , , , et al. Validation of a predictive rule for the management of community‐acquired pneumonia. Eur Respir J. 2006;27(1):151–157.
- , , , , . Pneumonia Severity Index (PSI), CURB‐65, and mortality in hospitalized elderly patients with aspiration pneumonia [in German]. Zeitschrift fur Gerontologie und Geriatrie. 2011;44(4):229–234.
- , , , . Do‐not‐resuscitate orders for critically ill patients in the hospital. How are they used and what is their impact?JAMA. 1986;256(2):233–237.
- , , , , . The Sanford Guide to Antimicrobial Therapy: 2010.40th ed.Sperryville, VA:Antimicrobial Therapy, Inc.;2009.
- , , . The bacteriology of aspiration pneumonia. Am J Med. 1974;56(2):202–207.
- , , . Bacteriologic flora of aspiration‐induced pulmonary infections. Arch Intern Med. 1975;135(5):711–714.
- , . Bacteriology of aspiration pneumonia. A prospective study of community‐ and hospital‐acquired cases. Ann Intern Med. 1974;81(3):329–331.
- , . The role of anaerobes in patients with ventilator‐associated pneumonia and aspiration pneumonia: a prospective study. Chest. 1999;115(1):178–183.
- , , , et al. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993;19(5):279–284.
- , , , , . Community‐acquired pneumonia in the elderly. Semin Respir Infect. 1999;14(2):173–183.
- , , . Nursing home‐acquired pneumonia. A case‐control study. J Am Geriatr Soc. 1986;34(10):697–702.
- , , , , . Severe community‐acquired pneumonia. Etiology, epidemiology, and prognosis factors. French Study Group for Community‐Acquired Pneumonia in the Intensive Care Unit. Chest. 1994;105(5):1487–1495.
Copyright © 2012 Society of Hospital Medicine
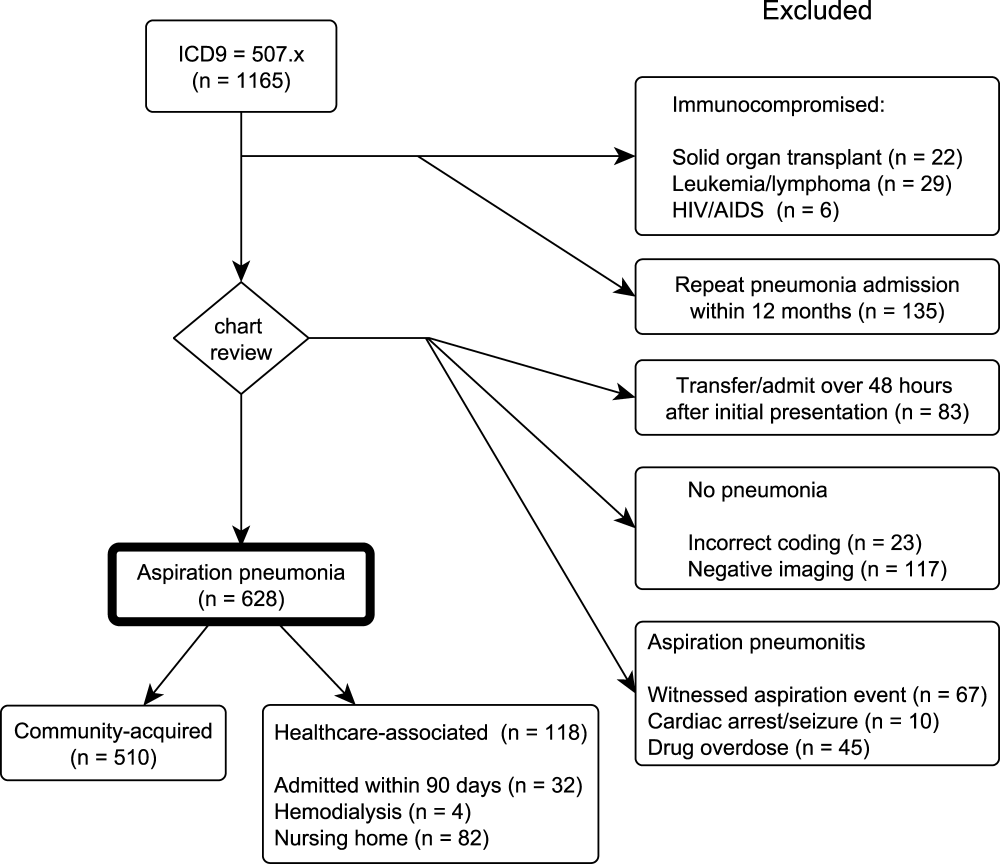
Chest Radiograph Interpretation
The inclusion of clinical information in diagnostic testing may influence the interpretation of the clinical findings. Historical and clinical findings may focus the reader's attention to the relevant details, thereby improving the accuracy of the interpretation. However, such information may cause the reader to have preconceived notions about the results, biasing the overall interpretation.
The impact of clinical information on the interpretation of radiographic studies remains an issue of debate. Previous studies have found that clinical information improves the accuracy of radiographic interpretation for a broad range of diagnoses,[1, 2, 3, 4] whereas others do not show improvement.[5, 6, 7] Additionally, clinical information may serve as a distraction that leads to more false‐positive interpretations.[8] For this reason, many radiologists prefer to review radiographs without knowledge of the clinical scenario prompting the study to avoid focusing on the expected findings and potentially missing other important abnormalities.[9]
The chest radiograph (CXR) is the most commonly used diagnostic imaging modality. Nevertheless, poor agreement exists among radiologists in the interpretation of chest radiographs for the diagnosis of pneumonia in both adults and children.[10, 11, 12, 13, 14, 15] Recent studies have found a high degree of agreement among pediatric radiologists with implementation of the World Health Organization (WHO) criteria for standardized CXR interpretation for diagnosis of bacterial pneumonia in children.[16, 17, 18] In these studies, participants were blinded to the clinical presentation. Data investigating the impact of clinical history on CXR interpretation in the pediatric population are limited.[19]
We conducted this prospective case‐based study to evaluate the impact of clinical information on the reliability of radiographic diagnosis of pneumonia among children presenting to a pediatric emergency department (ED) with clinical suspicion of pneumonia.
METHODS
Study Subjects
Six board‐certified radiologists at 2 academic children's hospitals (Children's Hospital of Philadelphia [n = 3] and Boston Children's Hospital [n = 3]) interpreted the same 110 chest radiographs (100 original and 10 duplicates) on 2 separate occasions. Clinical information was withheld during the first interpretation. The inter‐ and inter‐rater reliability for the interpretation of these 110 radiographs without clinical information have been previously reported.[18] After a period of 6 months, the radiologists reviewed the radiographs with access to clinical information provided by the physician ordering the CXR. This clinical information included age, sex, clinical indication for obtaining the radiograph, relevant history, and physical examination findings. The radiologists did not have access to the patients' medical records. The radiologists varied with respect to the number of years practicing pediatric radiology (median, 8 years; range, 336 years).
Radiographs were selected from children who presented to the ED at Boston Children's Hospital with concern of pneumonia. We selected radiographs with a spectrum of respiratory disease processes encountered in a pediatric population. The final radiographs included 50 radiographs with a final reading in the medical record without suspicion for pneumonia and 50 radiographs with suspicion of pneumonia. In the latter group, 25 radiographs had a final reading suggestive of an alveolar infiltrate, and 25 radiographs had a final reading suggestive of an interstitial infiltrate. Ten duplicate radiographs were included.
Radiograph Interpretation
The radiologists interpreted both anterior‐posterior and lateral views for each subject. Digital Imaging and Communications in Medicine images were downloaded from a registry at Boston Children's Hospital, and were copied to DVDs that were provided to each radiologist. Standardized radiographic imaging software (eFilm Lite; Merge Healthcare, Chicago, Illinois) was used by each radiologist.
Each radiologist completed a study questionnaire for each radiograph (see Supporting Information, Appendix 1, in the online version of this article). The questionnaire utilized radiographic descriptors of primary endpoint pneumonia described by the WHO to standardize the radiographic diagnosis of pneumonia.[20, 21] No additional training was provided to the radiologists. The main outcome of interest was the presence or absence of an infiltrate. Among radiographs in which an infiltrate was identified, radiologists selected whether there was an alveolar infiltrate, interstitial infiltrate, or both. Alveolar infiltrate and interstitial infiltrate are defined on the study questionnaire (Appendix 1). A radiograph classified as having either an alveolar infiltrate or interstitial infiltrate (not atelectasis) was considered to have any infiltrate. Additional findings including air bronchograms, hilar adenopathy, pleural effusion, and location of abnormalities were also recorded.
Statistical Analysis
Inter‐rater reliability was assessed using the kappa statistic to determine the overall agreement among the 6 radiologists for each outcome (eg, presence or absence of alveolar infiltrate). The kappa statistic for more than 2 raters utilizes an analysis of variance approach.[22] To calculate 95% confidence intervals (CI) for kappa statistics with more than 2 raters, we employed a bootstrapping method with 1000 replications of samples equal in size to the study sample. Intra‐rater reliability was evaluated by examining the agreement within each radiologist upon review of 10 duplicate radiographs. We used the following benchmarks to classify the strength of agreement: poor (<0.0), slight (00.20), fair (0.210.40), moderate (0.410.60), substantial (0.610.80), almost perfect (0.811.0).[23] Negative kappa values represent agreement less than would be predicted by chance alone.[24, 25] To calculate the kappa, a value must be recorded in 3 of 4 of the following categories: negative to positive, positive to negative, concordant negative, and concordant positive reporting of pneumonia. If raters did not fulfill 3 categories, the kappa could not be calculated.
The inter‐rater concordance for identification of an alveolar infiltrate was calculated for each radiologist by comparing their reporting of alveolar infiltrate with and without clinical history for each of the 100 radiographs. Radiographs that were identified by an individual rater as no alveolar infiltrate when read without clinical history, but those subsequently identified as alveolar infiltrate with clinical history were categorized as negative to positive reporting of pneumonia with clinical history. Those that were identified as alveolar infiltrate but subsequently identified as no alveolar infiltrate were categorized as positive to negative reporting of pneumonia with clinical history. Those radiographs in which there was no change in identification of alveolar infiltrate with clinical information were categorized as concordant reporting of pneumonia.
The study was approved by the institutional review boards at both children's hospitals.
RESULTS
Patient Sample
The radiographs were from patients ranging in age from 1 week to 19 years (median, 3.5 years; interquartile range, 1.66.0 years). Fifty (50%) patients were male.
Inter‐rater Reliability
The kappa coefficients of inter‐rater reliability between the radiologists across the 6 clinical measures of interest with and without access to clinical history are plotted in Figure 1. Reliability improved from fair (k = 0.32, 95% CI: 0.24 to 0.42) to moderate (k = 0.53, 95% CI: 0.43 to 0.64) for identification of air bronchograms with the addition of clinical history. Although there was an increase in kappa values for identification of any infiltrate, alveolar infiltrate, interstitial infiltrate, and pleural effusion, and a decrease in the kappa value for identification of hilar adenopathy with the addition of clinical information, there was substantial overlap of the 95% CIs, suggesting that inclusion of clinical history did not result in a statistically significant change in the reliability of these findings.
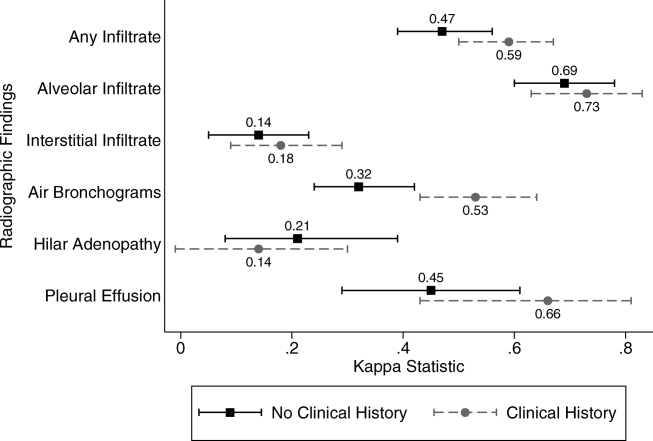
Intra‐rater Reliability
The estimates of inter‐rater reliability for the interpretation of the 10 duplicate images with and without clinical history are shown in Table 1. The inter‐rater reliability in the identification of alveolar infiltrate remained substantial to almost perfect for each rater with and without access to clinical history. Rater 1 had a decrease in inter‐rater reliability from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.21, 95% CI: 0.43 to 0.85) in the identification of interstitial infiltrate with the addition of clinical history. This rater also had a decrease in agreement from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.4, 95% CI: 0.16 to 0.96) in the identification of any infiltrate.
| Phase 1No Clinical History | Phase 2Access to Clinical History | |||
|---|---|---|---|---|
| Kappa | 95% Confidence Interval | Kappa | 95% Confidence Interval | |
| ||||
| Any infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.40 | 0.16 to 0.96 |
| Rater 2 | 0.60 | 0.10 to 1.00 | 0.58 | 0.07 to 1.00 |
| Rater 3 | 0.80 | 0.44 to 1.00 | 0.80 | 0.44 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | N/Aa | 0.11 | 0.36 to 0.14 | |
| Rater 6 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Alveolar infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 2 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 3 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | 0.78 | 0.39 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 6 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Interstitial infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.21 | 0.43 to 0.85 |
| Rater 2 | 0.21 | 0.43 to 0.85 | 0.11 | 0.36 to 0.14 |
| Rater 3 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 4 | N/A | N/A | ||
| Rater 5 | 0.58 | 0.07 to 1.00 | 0.52 | 0.05 to 1.00 |
| Rater 6 | 0.62 | 0.5 to 1.00 | N/Aa | |
Intra‐rater Concordance
The inter‐rater concordance of the radiologists for the identification of alveolar infiltrate during the interpretation of the 100 chest radiographs with and without access to clinical history is shown in Figure 2. The availability of clinical information impacted physicians differently in the evaluation of alveolar infiltrates. Raters 1, 4, and 6 appeared more likely to identify an alveolar infiltrate with access to the clinical information, whereas raters 3 and 5 appeared less likely to identify an alveolar infiltrate. Of the 100 films that were interpreted with and without clinical information, the mean number of discordant interpretations per rater was 10, with values ranging from 6 to 19 for the individual raters. Radiographs in which more than 3 raters changed their interpretation regarding the presence of an alveolar infiltrate are shown in Figure 3. For Figure 3D, 4 radiologists changed their interpretation from no alveolar infiltrate to alveolar infiltrate, and 1 radiologist changed from alveolar infiltrate to no alveolar infiltrate with the addition of clinical history.
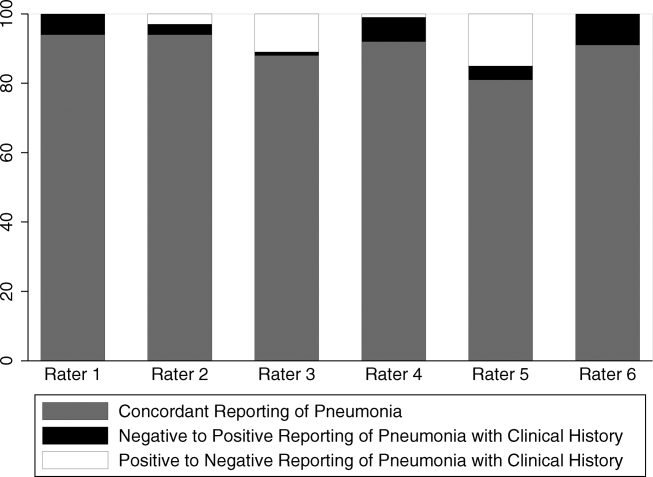
Comment
We investigated the impact of the availability of clinical information on the reliability of chest radiographic interpretation in the diagnosis of pneumonia. There was improved inter‐rater reliability in the identification of air bronchograms with the addition of clinical information; however, clinical history did not have a substantial impact on the inter‐rater reliability of other findings. The addition of clinical information did not alter the inter‐rater reliability in the identification of alveolar infiltrate. Clinical history affected individual raters differently in their interpretation of alveolar infiltrate, with 3 raters more likely to identify an alveolar infiltrate and 2 raters less likely to identify an alveolar infiltrate.
Most studies addressing the impact of clinical history on radiographic interpretation evaluated accuracy. In many of these studies, accuracy was defined as the raters' agreement with the final interpretation of each film as documented in the medical record or their agreement with the interpretation of the radiologists selecting the cases.[1, 2, 3, 5, 6, 7] Given the known inter‐rater variability in radiographic interpretation,[10, 11, 12, 13, 14, 15] accuracy of a radiologist's interpretation cannot be appropriately assessed through agreement with their peers. Because a true measure of accuracy in the radiographic diagnosis of pneumonia can only be determined through invasive testing, such as lung biopsy, reliability serves as a more appropriate measure of performance. Inclusion of clinical information in chest radiograph interpretation has been shown to improve reliability in the radiographic diagnosis of a broad range of conditions.[15]
The primary outcome in this study was the identification of an infiltrate. Previous studies have noted consistent identification of the radiographic features that are most suggestive of bacterial pneumonia, such as alveolar infiltrate, and less consistent identification of other radiographic findings, including interstitial infiltrate.[18, 26, 27] Among the radiologists in this study, the addition of clinical information did not have a meaningful impact on the reliability of either of these findings, as there was substantial inter‐rater agreement for the identification of alveolar infiltrate and only slight agreement for the identification of interstitial infiltrate, both with and without clinical history. Additionally, inter‐rater reliability for the identification of alveolar infiltrate remained substantial to almost perfect for all 6 raters with the addition of clinical information.
Clinical information impacted the raters differently in their pattern of alveolar infiltrate identification, suggesting that radiologists may differ in their approach to incorporating clinical history in the interpretation of chest radiographs. The inclusion of clinical information may impact a radiologist's perception, leading to improved identification of abnormalities; however, it may also guide their decision making about the relevance of previously identified abnormalities.[28] Some radiologists may use clinical information to support or suggest possible radiographic findings, whereas others may use the information to challenge potential findings. This study did not address the manner in which the individual raters utilized the clinical history. There were also several radiographs in which the clinical information resulted in a change in the identification of an alveolar infiltrate by 3 or more raters, with as many as 5 of 6 raters changing their interpretation for 1 particular radiograph. These changes in identification of an infiltrate suggest that unidentified aspects of a history may be likely to influence a rater's interpretation of a radiograph. Nevertheless, these changes did not result in improved reliability and it is not possible to determine if these changes resulted in improved accuracy in interpretation.
This study had several limitations. First, radiographs were purposefully selected to encompass a broad spectrum of radiographic findings. Thus, the prevalence of pneumonia and other abnormal findings was artificially higher than typically observed among a cohort of children for whom pneumonia is considered. Second, the radiologists recruited for this study all practice in an academic children's hospital setting. These factors may limit the generalizability of our findings. However, we would expect these results to be generalizable to pediatric radiologists from other academic institutions. Third, this study does not meet the criteria of a balanced study design as defined by Loy and Irwig.[19] A study was characterized as balanced if half of the radiographs were read with and half without clinical information in each of the 2 reading sessions. The proposed benefit of such a design is to control for possible changes in ability or reporting practices of the raters that may have occurred between study periods. The use of a standardized reporting tool likely minimized changes in reporting practices. Also, it is unlikely that the ability or reporting practices of an experienced radiologist would change over the study period. Fourth, the radiologists interpreted the films outside of their standard workflow and utilized a standardized reporting tool that focused on the presence or absence of pneumonia indicators. These factors may have increased the radiologists' suspicion for pneumonia even in the absence of clinical information. This may have biased the results toward finding no difference in the identification of pneumonia with the addition of detailed clinical history. Thus, the inclusion of clinical information in radiograph interpretation in clinical practice may have greater impact on the identification of these pneumonia indicators than was found in this study.[29] Finally, reliability does not imply accuracy, and it is unknown if changes in the identification of pneumonia indicators led to more accurate interpretation with respect to the clinical or pathologic diagnosis of pneumonia.
In conclusion, we observed high intra‐ and inter‐rater reliability among radiologists in the identification of an alveolar infiltrate, the radiographic finding most suggestive of bacterial pneumonia.[16, 17, 18, 30] The addition of clinical information did not have a substantial impact on the reliability of its identification.
- , , , et al. Tentative diagnoses facilitate the detection of diverse lesions in chest radiographs. Invest Radiol. 1986;21(7):532–539.
- , , , . Influence of clinical history upon detection of nodules and other lesions. Invest Radiol. 1988;23(1):48–55.
- , , , . Influence of clinical history on perception of abnormalities in pediatric radiographs. Acad Radiol. 1994;1(3):217–223.
- , , , et al. Impact of clinical history on film interpretation. Yonsei Med J. 1992;33(2):168–172.
- , , , et al. The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1990;25(6):670–674.
- , , , et al. Does knowledge of the clinical history affect the accuracy of chest radiograph interpretation?AJR Am J Roentgenol. 1990;154(4):709–712.
- , , , . Detection of lung cancer on the chest radiograph: impact of previous films, clinical information, double reading, and dual reading. J Clin Epidemiol. 2001;54(11):1146–1150.
- , , , . The effect of clinical bias on the interpretation of myelography and spinal computed tomography. Radiology. 1982;145(1):85–89.
- . A suggestion: look at the images first, before you read the history. Radiology. 2002;223(1):9–10.
- , , , et al. Interobserver reliability of the chest radiograph in community‐acquired pneumonia. PORT Investigators. Chest. 1996;110(2):343–350.
- , , , , . Inter‐ and intra‐observer variability in the assessment of atelectasis and consolidation in neonatal chest radiographs. Pediatr Radiol. 1999;29(6):459–462.
- , , , , . Chest radiographs in the emergency department: is the radiologist really necessary?Postgrad Med J. 2003;79(930):214–217.
- , , , . Inter‐observer variation in the interpretation of chest radiographs for pneumonia in community‐acquired lower respiratory tract infections. Clin Radiol. 2004;59(8):743–752.
- , , , , , . Disagreement in the interpretation of chest radiographs among specialists and clinical outcomes of patients hospitalized with suspected pneumonia. Eur J Intern Med. 2006;17(1):43–47.
- , , . An assessment of inter‐observer agreement and accuracy when reporting plain radiographs. Clin Radiol. 1997;52(3):235–238.
- , , , et al. Evaluation of the World Health Organization criteria for chest radiographs for pneumonia diagnosis in children. Eur J Pediatr. 2011;171(2):369–374.
- , , , et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ. 2005;83(5):353–359.
- , , , et al. Variability in the interpretation of chest radiographs for the diagnosis of pneumonia in children. J Hosp Med. 2012;7(4):294–298.
- , . Accuracy of diagnostic tests read with and without clinical information: a systematic review. JAMA. 2004;292(13):1602–1609.
- Standardization of interpretation of chest radiographs for the diagnosis of pneumonia in children. In:World Health Organization: Pneumonia Vaccine Trial Investigators' Group.Geneva: Department of Vaccine and Biologics;2001.
- , , , et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia: updated analysis using World Health Organization standardized interpretation of chest radiographs. Pediatr Infect Dis J. 2006;25(9):779–781.
- , . A one‐way components of variance model for categorical data. Biometrics. 1977;33:671–679.
- , . The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
- , . Kappa statistic. CMAJ. 2005;173(1):16.
- , . Clinical biostatistics. LIV. The biostatistics of concordance. Clin Pharmacol Ther. 1981;29(1):111–123.
- , , , , , . Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis. 2000;31(2):347–382.
- , , , et al. Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730–1754.
- , . Commentary does clinical history affect perception?Acad Radiol. 2006;13(3):402–403.
- , . The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1991;26(5):512–514.
- , , , . Comparison of radiological findings and microbial aetiology of childhood pneumonia. Acta Paediatr. 1993;82(4):360–363.
The inclusion of clinical information in diagnostic testing may influence the interpretation of the clinical findings. Historical and clinical findings may focus the reader's attention to the relevant details, thereby improving the accuracy of the interpretation. However, such information may cause the reader to have preconceived notions about the results, biasing the overall interpretation.
The impact of clinical information on the interpretation of radiographic studies remains an issue of debate. Previous studies have found that clinical information improves the accuracy of radiographic interpretation for a broad range of diagnoses,[1, 2, 3, 4] whereas others do not show improvement.[5, 6, 7] Additionally, clinical information may serve as a distraction that leads to more false‐positive interpretations.[8] For this reason, many radiologists prefer to review radiographs without knowledge of the clinical scenario prompting the study to avoid focusing on the expected findings and potentially missing other important abnormalities.[9]
The chest radiograph (CXR) is the most commonly used diagnostic imaging modality. Nevertheless, poor agreement exists among radiologists in the interpretation of chest radiographs for the diagnosis of pneumonia in both adults and children.[10, 11, 12, 13, 14, 15] Recent studies have found a high degree of agreement among pediatric radiologists with implementation of the World Health Organization (WHO) criteria for standardized CXR interpretation for diagnosis of bacterial pneumonia in children.[16, 17, 18] In these studies, participants were blinded to the clinical presentation. Data investigating the impact of clinical history on CXR interpretation in the pediatric population are limited.[19]
We conducted this prospective case‐based study to evaluate the impact of clinical information on the reliability of radiographic diagnosis of pneumonia among children presenting to a pediatric emergency department (ED) with clinical suspicion of pneumonia.
METHODS
Study Subjects
Six board‐certified radiologists at 2 academic children's hospitals (Children's Hospital of Philadelphia [n = 3] and Boston Children's Hospital [n = 3]) interpreted the same 110 chest radiographs (100 original and 10 duplicates) on 2 separate occasions. Clinical information was withheld during the first interpretation. The inter‐ and inter‐rater reliability for the interpretation of these 110 radiographs without clinical information have been previously reported.[18] After a period of 6 months, the radiologists reviewed the radiographs with access to clinical information provided by the physician ordering the CXR. This clinical information included age, sex, clinical indication for obtaining the radiograph, relevant history, and physical examination findings. The radiologists did not have access to the patients' medical records. The radiologists varied with respect to the number of years practicing pediatric radiology (median, 8 years; range, 336 years).
Radiographs were selected from children who presented to the ED at Boston Children's Hospital with concern of pneumonia. We selected radiographs with a spectrum of respiratory disease processes encountered in a pediatric population. The final radiographs included 50 radiographs with a final reading in the medical record without suspicion for pneumonia and 50 radiographs with suspicion of pneumonia. In the latter group, 25 radiographs had a final reading suggestive of an alveolar infiltrate, and 25 radiographs had a final reading suggestive of an interstitial infiltrate. Ten duplicate radiographs were included.
Radiograph Interpretation
The radiologists interpreted both anterior‐posterior and lateral views for each subject. Digital Imaging and Communications in Medicine images were downloaded from a registry at Boston Children's Hospital, and were copied to DVDs that were provided to each radiologist. Standardized radiographic imaging software (eFilm Lite; Merge Healthcare, Chicago, Illinois) was used by each radiologist.
Each radiologist completed a study questionnaire for each radiograph (see Supporting Information, Appendix 1, in the online version of this article). The questionnaire utilized radiographic descriptors of primary endpoint pneumonia described by the WHO to standardize the radiographic diagnosis of pneumonia.[20, 21] No additional training was provided to the radiologists. The main outcome of interest was the presence or absence of an infiltrate. Among radiographs in which an infiltrate was identified, radiologists selected whether there was an alveolar infiltrate, interstitial infiltrate, or both. Alveolar infiltrate and interstitial infiltrate are defined on the study questionnaire (Appendix 1). A radiograph classified as having either an alveolar infiltrate or interstitial infiltrate (not atelectasis) was considered to have any infiltrate. Additional findings including air bronchograms, hilar adenopathy, pleural effusion, and location of abnormalities were also recorded.
Statistical Analysis
Inter‐rater reliability was assessed using the kappa statistic to determine the overall agreement among the 6 radiologists for each outcome (eg, presence or absence of alveolar infiltrate). The kappa statistic for more than 2 raters utilizes an analysis of variance approach.[22] To calculate 95% confidence intervals (CI) for kappa statistics with more than 2 raters, we employed a bootstrapping method with 1000 replications of samples equal in size to the study sample. Intra‐rater reliability was evaluated by examining the agreement within each radiologist upon review of 10 duplicate radiographs. We used the following benchmarks to classify the strength of agreement: poor (<0.0), slight (00.20), fair (0.210.40), moderate (0.410.60), substantial (0.610.80), almost perfect (0.811.0).[23] Negative kappa values represent agreement less than would be predicted by chance alone.[24, 25] To calculate the kappa, a value must be recorded in 3 of 4 of the following categories: negative to positive, positive to negative, concordant negative, and concordant positive reporting of pneumonia. If raters did not fulfill 3 categories, the kappa could not be calculated.
The inter‐rater concordance for identification of an alveolar infiltrate was calculated for each radiologist by comparing their reporting of alveolar infiltrate with and without clinical history for each of the 100 radiographs. Radiographs that were identified by an individual rater as no alveolar infiltrate when read without clinical history, but those subsequently identified as alveolar infiltrate with clinical history were categorized as negative to positive reporting of pneumonia with clinical history. Those that were identified as alveolar infiltrate but subsequently identified as no alveolar infiltrate were categorized as positive to negative reporting of pneumonia with clinical history. Those radiographs in which there was no change in identification of alveolar infiltrate with clinical information were categorized as concordant reporting of pneumonia.
The study was approved by the institutional review boards at both children's hospitals.
RESULTS
Patient Sample
The radiographs were from patients ranging in age from 1 week to 19 years (median, 3.5 years; interquartile range, 1.66.0 years). Fifty (50%) patients were male.
Inter‐rater Reliability
The kappa coefficients of inter‐rater reliability between the radiologists across the 6 clinical measures of interest with and without access to clinical history are plotted in Figure 1. Reliability improved from fair (k = 0.32, 95% CI: 0.24 to 0.42) to moderate (k = 0.53, 95% CI: 0.43 to 0.64) for identification of air bronchograms with the addition of clinical history. Although there was an increase in kappa values for identification of any infiltrate, alveolar infiltrate, interstitial infiltrate, and pleural effusion, and a decrease in the kappa value for identification of hilar adenopathy with the addition of clinical information, there was substantial overlap of the 95% CIs, suggesting that inclusion of clinical history did not result in a statistically significant change in the reliability of these findings.
Intra‐rater Reliability
The estimates of inter‐rater reliability for the interpretation of the 10 duplicate images with and without clinical history are shown in Table 1. The inter‐rater reliability in the identification of alveolar infiltrate remained substantial to almost perfect for each rater with and without access to clinical history. Rater 1 had a decrease in inter‐rater reliability from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.21, 95% CI: 0.43 to 0.85) in the identification of interstitial infiltrate with the addition of clinical history. This rater also had a decrease in agreement from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.4, 95% CI: 0.16 to 0.96) in the identification of any infiltrate.
| Phase 1No Clinical History | Phase 2Access to Clinical History | |||
|---|---|---|---|---|
| Kappa | 95% Confidence Interval | Kappa | 95% Confidence Interval | |
| ||||
| Any infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.40 | 0.16 to 0.96 |
| Rater 2 | 0.60 | 0.10 to 1.00 | 0.58 | 0.07 to 1.00 |
| Rater 3 | 0.80 | 0.44 to 1.00 | 0.80 | 0.44 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | N/Aa | 0.11 | 0.36 to 0.14 | |
| Rater 6 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Alveolar infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 2 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 3 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | 0.78 | 0.39 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 6 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Interstitial infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.21 | 0.43 to 0.85 |
| Rater 2 | 0.21 | 0.43 to 0.85 | 0.11 | 0.36 to 0.14 |
| Rater 3 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 4 | N/A | N/A | ||
| Rater 5 | 0.58 | 0.07 to 1.00 | 0.52 | 0.05 to 1.00 |
| Rater 6 | 0.62 | 0.5 to 1.00 | N/Aa | |
Intra‐rater Concordance
The inter‐rater concordance of the radiologists for the identification of alveolar infiltrate during the interpretation of the 100 chest radiographs with and without access to clinical history is shown in Figure 2. The availability of clinical information impacted physicians differently in the evaluation of alveolar infiltrates. Raters 1, 4, and 6 appeared more likely to identify an alveolar infiltrate with access to the clinical information, whereas raters 3 and 5 appeared less likely to identify an alveolar infiltrate. Of the 100 films that were interpreted with and without clinical information, the mean number of discordant interpretations per rater was 10, with values ranging from 6 to 19 for the individual raters. Radiographs in which more than 3 raters changed their interpretation regarding the presence of an alveolar infiltrate are shown in Figure 3. For Figure 3D, 4 radiologists changed their interpretation from no alveolar infiltrate to alveolar infiltrate, and 1 radiologist changed from alveolar infiltrate to no alveolar infiltrate with the addition of clinical history.
Comment
We investigated the impact of the availability of clinical information on the reliability of chest radiographic interpretation in the diagnosis of pneumonia. There was improved inter‐rater reliability in the identification of air bronchograms with the addition of clinical information; however, clinical history did not have a substantial impact on the inter‐rater reliability of other findings. The addition of clinical information did not alter the inter‐rater reliability in the identification of alveolar infiltrate. Clinical history affected individual raters differently in their interpretation of alveolar infiltrate, with 3 raters more likely to identify an alveolar infiltrate and 2 raters less likely to identify an alveolar infiltrate.
Most studies addressing the impact of clinical history on radiographic interpretation evaluated accuracy. In many of these studies, accuracy was defined as the raters' agreement with the final interpretation of each film as documented in the medical record or their agreement with the interpretation of the radiologists selecting the cases.[1, 2, 3, 5, 6, 7] Given the known inter‐rater variability in radiographic interpretation,[10, 11, 12, 13, 14, 15] accuracy of a radiologist's interpretation cannot be appropriately assessed through agreement with their peers. Because a true measure of accuracy in the radiographic diagnosis of pneumonia can only be determined through invasive testing, such as lung biopsy, reliability serves as a more appropriate measure of performance. Inclusion of clinical information in chest radiograph interpretation has been shown to improve reliability in the radiographic diagnosis of a broad range of conditions.[15]
The primary outcome in this study was the identification of an infiltrate. Previous studies have noted consistent identification of the radiographic features that are most suggestive of bacterial pneumonia, such as alveolar infiltrate, and less consistent identification of other radiographic findings, including interstitial infiltrate.[18, 26, 27] Among the radiologists in this study, the addition of clinical information did not have a meaningful impact on the reliability of either of these findings, as there was substantial inter‐rater agreement for the identification of alveolar infiltrate and only slight agreement for the identification of interstitial infiltrate, both with and without clinical history. Additionally, inter‐rater reliability for the identification of alveolar infiltrate remained substantial to almost perfect for all 6 raters with the addition of clinical information.
Clinical information impacted the raters differently in their pattern of alveolar infiltrate identification, suggesting that radiologists may differ in their approach to incorporating clinical history in the interpretation of chest radiographs. The inclusion of clinical information may impact a radiologist's perception, leading to improved identification of abnormalities; however, it may also guide their decision making about the relevance of previously identified abnormalities.[28] Some radiologists may use clinical information to support or suggest possible radiographic findings, whereas others may use the information to challenge potential findings. This study did not address the manner in which the individual raters utilized the clinical history. There were also several radiographs in which the clinical information resulted in a change in the identification of an alveolar infiltrate by 3 or more raters, with as many as 5 of 6 raters changing their interpretation for 1 particular radiograph. These changes in identification of an infiltrate suggest that unidentified aspects of a history may be likely to influence a rater's interpretation of a radiograph. Nevertheless, these changes did not result in improved reliability and it is not possible to determine if these changes resulted in improved accuracy in interpretation.
This study had several limitations. First, radiographs were purposefully selected to encompass a broad spectrum of radiographic findings. Thus, the prevalence of pneumonia and other abnormal findings was artificially higher than typically observed among a cohort of children for whom pneumonia is considered. Second, the radiologists recruited for this study all practice in an academic children's hospital setting. These factors may limit the generalizability of our findings. However, we would expect these results to be generalizable to pediatric radiologists from other academic institutions. Third, this study does not meet the criteria of a balanced study design as defined by Loy and Irwig.[19] A study was characterized as balanced if half of the radiographs were read with and half without clinical information in each of the 2 reading sessions. The proposed benefit of such a design is to control for possible changes in ability or reporting practices of the raters that may have occurred between study periods. The use of a standardized reporting tool likely minimized changes in reporting practices. Also, it is unlikely that the ability or reporting practices of an experienced radiologist would change over the study period. Fourth, the radiologists interpreted the films outside of their standard workflow and utilized a standardized reporting tool that focused on the presence or absence of pneumonia indicators. These factors may have increased the radiologists' suspicion for pneumonia even in the absence of clinical information. This may have biased the results toward finding no difference in the identification of pneumonia with the addition of detailed clinical history. Thus, the inclusion of clinical information in radiograph interpretation in clinical practice may have greater impact on the identification of these pneumonia indicators than was found in this study.[29] Finally, reliability does not imply accuracy, and it is unknown if changes in the identification of pneumonia indicators led to more accurate interpretation with respect to the clinical or pathologic diagnosis of pneumonia.
In conclusion, we observed high intra‐ and inter‐rater reliability among radiologists in the identification of an alveolar infiltrate, the radiographic finding most suggestive of bacterial pneumonia.[16, 17, 18, 30] The addition of clinical information did not have a substantial impact on the reliability of its identification.
The inclusion of clinical information in diagnostic testing may influence the interpretation of the clinical findings. Historical and clinical findings may focus the reader's attention to the relevant details, thereby improving the accuracy of the interpretation. However, such information may cause the reader to have preconceived notions about the results, biasing the overall interpretation.
The impact of clinical information on the interpretation of radiographic studies remains an issue of debate. Previous studies have found that clinical information improves the accuracy of radiographic interpretation for a broad range of diagnoses,[1, 2, 3, 4] whereas others do not show improvement.[5, 6, 7] Additionally, clinical information may serve as a distraction that leads to more false‐positive interpretations.[8] For this reason, many radiologists prefer to review radiographs without knowledge of the clinical scenario prompting the study to avoid focusing on the expected findings and potentially missing other important abnormalities.[9]
The chest radiograph (CXR) is the most commonly used diagnostic imaging modality. Nevertheless, poor agreement exists among radiologists in the interpretation of chest radiographs for the diagnosis of pneumonia in both adults and children.[10, 11, 12, 13, 14, 15] Recent studies have found a high degree of agreement among pediatric radiologists with implementation of the World Health Organization (WHO) criteria for standardized CXR interpretation for diagnosis of bacterial pneumonia in children.[16, 17, 18] In these studies, participants were blinded to the clinical presentation. Data investigating the impact of clinical history on CXR interpretation in the pediatric population are limited.[19]
We conducted this prospective case‐based study to evaluate the impact of clinical information on the reliability of radiographic diagnosis of pneumonia among children presenting to a pediatric emergency department (ED) with clinical suspicion of pneumonia.
METHODS
Study Subjects
Six board‐certified radiologists at 2 academic children's hospitals (Children's Hospital of Philadelphia [n = 3] and Boston Children's Hospital [n = 3]) interpreted the same 110 chest radiographs (100 original and 10 duplicates) on 2 separate occasions. Clinical information was withheld during the first interpretation. The inter‐ and inter‐rater reliability for the interpretation of these 110 radiographs without clinical information have been previously reported.[18] After a period of 6 months, the radiologists reviewed the radiographs with access to clinical information provided by the physician ordering the CXR. This clinical information included age, sex, clinical indication for obtaining the radiograph, relevant history, and physical examination findings. The radiologists did not have access to the patients' medical records. The radiologists varied with respect to the number of years practicing pediatric radiology (median, 8 years; range, 336 years).
Radiographs were selected from children who presented to the ED at Boston Children's Hospital with concern of pneumonia. We selected radiographs with a spectrum of respiratory disease processes encountered in a pediatric population. The final radiographs included 50 radiographs with a final reading in the medical record without suspicion for pneumonia and 50 radiographs with suspicion of pneumonia. In the latter group, 25 radiographs had a final reading suggestive of an alveolar infiltrate, and 25 radiographs had a final reading suggestive of an interstitial infiltrate. Ten duplicate radiographs were included.
Radiograph Interpretation
The radiologists interpreted both anterior‐posterior and lateral views for each subject. Digital Imaging and Communications in Medicine images were downloaded from a registry at Boston Children's Hospital, and were copied to DVDs that were provided to each radiologist. Standardized radiographic imaging software (eFilm Lite; Merge Healthcare, Chicago, Illinois) was used by each radiologist.
Each radiologist completed a study questionnaire for each radiograph (see Supporting Information, Appendix 1, in the online version of this article). The questionnaire utilized radiographic descriptors of primary endpoint pneumonia described by the WHO to standardize the radiographic diagnosis of pneumonia.[20, 21] No additional training was provided to the radiologists. The main outcome of interest was the presence or absence of an infiltrate. Among radiographs in which an infiltrate was identified, radiologists selected whether there was an alveolar infiltrate, interstitial infiltrate, or both. Alveolar infiltrate and interstitial infiltrate are defined on the study questionnaire (Appendix 1). A radiograph classified as having either an alveolar infiltrate or interstitial infiltrate (not atelectasis) was considered to have any infiltrate. Additional findings including air bronchograms, hilar adenopathy, pleural effusion, and location of abnormalities were also recorded.
Statistical Analysis
Inter‐rater reliability was assessed using the kappa statistic to determine the overall agreement among the 6 radiologists for each outcome (eg, presence or absence of alveolar infiltrate). The kappa statistic for more than 2 raters utilizes an analysis of variance approach.[22] To calculate 95% confidence intervals (CI) for kappa statistics with more than 2 raters, we employed a bootstrapping method with 1000 replications of samples equal in size to the study sample. Intra‐rater reliability was evaluated by examining the agreement within each radiologist upon review of 10 duplicate radiographs. We used the following benchmarks to classify the strength of agreement: poor (<0.0), slight (00.20), fair (0.210.40), moderate (0.410.60), substantial (0.610.80), almost perfect (0.811.0).[23] Negative kappa values represent agreement less than would be predicted by chance alone.[24, 25] To calculate the kappa, a value must be recorded in 3 of 4 of the following categories: negative to positive, positive to negative, concordant negative, and concordant positive reporting of pneumonia. If raters did not fulfill 3 categories, the kappa could not be calculated.
The inter‐rater concordance for identification of an alveolar infiltrate was calculated for each radiologist by comparing their reporting of alveolar infiltrate with and without clinical history for each of the 100 radiographs. Radiographs that were identified by an individual rater as no alveolar infiltrate when read without clinical history, but those subsequently identified as alveolar infiltrate with clinical history were categorized as negative to positive reporting of pneumonia with clinical history. Those that were identified as alveolar infiltrate but subsequently identified as no alveolar infiltrate were categorized as positive to negative reporting of pneumonia with clinical history. Those radiographs in which there was no change in identification of alveolar infiltrate with clinical information were categorized as concordant reporting of pneumonia.
The study was approved by the institutional review boards at both children's hospitals.
RESULTS
Patient Sample
The radiographs were from patients ranging in age from 1 week to 19 years (median, 3.5 years; interquartile range, 1.66.0 years). Fifty (50%) patients were male.
Inter‐rater Reliability
The kappa coefficients of inter‐rater reliability between the radiologists across the 6 clinical measures of interest with and without access to clinical history are plotted in Figure 1. Reliability improved from fair (k = 0.32, 95% CI: 0.24 to 0.42) to moderate (k = 0.53, 95% CI: 0.43 to 0.64) for identification of air bronchograms with the addition of clinical history. Although there was an increase in kappa values for identification of any infiltrate, alveolar infiltrate, interstitial infiltrate, and pleural effusion, and a decrease in the kappa value for identification of hilar adenopathy with the addition of clinical information, there was substantial overlap of the 95% CIs, suggesting that inclusion of clinical history did not result in a statistically significant change in the reliability of these findings.
Intra‐rater Reliability
The estimates of inter‐rater reliability for the interpretation of the 10 duplicate images with and without clinical history are shown in Table 1. The inter‐rater reliability in the identification of alveolar infiltrate remained substantial to almost perfect for each rater with and without access to clinical history. Rater 1 had a decrease in inter‐rater reliability from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.21, 95% CI: 0.43 to 0.85) in the identification of interstitial infiltrate with the addition of clinical history. This rater also had a decrease in agreement from almost perfect (k = 1.0, 95% CI: 1.0 to 1.0) to fair (k = 0.4, 95% CI: 0.16 to 0.96) in the identification of any infiltrate.
| Phase 1No Clinical History | Phase 2Access to Clinical History | |||
|---|---|---|---|---|
| Kappa | 95% Confidence Interval | Kappa | 95% Confidence Interval | |
| ||||
| Any infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.40 | 0.16 to 0.96 |
| Rater 2 | 0.60 | 0.10 to 1.00 | 0.58 | 0.07 to 1.00 |
| Rater 3 | 0.80 | 0.44 to 1.00 | 0.80 | 0.44 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | N/Aa | 0.11 | 0.36 to 0.14 | |
| Rater 6 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Alveolar infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 2 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 3 | 1.00 | 1.00 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 4 | 1.00 | 1.00 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 5 | 0.78 | 0.39 to 1.00 | 1.00 | 1.00 to 1.00 |
| Rater 6 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Interstitial infiltrate | ||||
| Rater 1 | 1.00 | 1.00 to 1.00 | 0.21 | 0.43 to 0.85 |
| Rater 2 | 0.21 | 0.43 to 0.85 | 0.11 | 0.36 to 0.14 |
| Rater 3 | 0.74 | 0.27 to 1.00 | 0.78 | 0.39 to 1.00 |
| Rater 4 | N/A | N/A | ||
| Rater 5 | 0.58 | 0.07 to 1.00 | 0.52 | 0.05 to 1.00 |
| Rater 6 | 0.62 | 0.5 to 1.00 | N/Aa | |
Intra‐rater Concordance
The inter‐rater concordance of the radiologists for the identification of alveolar infiltrate during the interpretation of the 100 chest radiographs with and without access to clinical history is shown in Figure 2. The availability of clinical information impacted physicians differently in the evaluation of alveolar infiltrates. Raters 1, 4, and 6 appeared more likely to identify an alveolar infiltrate with access to the clinical information, whereas raters 3 and 5 appeared less likely to identify an alveolar infiltrate. Of the 100 films that were interpreted with and without clinical information, the mean number of discordant interpretations per rater was 10, with values ranging from 6 to 19 for the individual raters. Radiographs in which more than 3 raters changed their interpretation regarding the presence of an alveolar infiltrate are shown in Figure 3. For Figure 3D, 4 radiologists changed their interpretation from no alveolar infiltrate to alveolar infiltrate, and 1 radiologist changed from alveolar infiltrate to no alveolar infiltrate with the addition of clinical history.
Comment
We investigated the impact of the availability of clinical information on the reliability of chest radiographic interpretation in the diagnosis of pneumonia. There was improved inter‐rater reliability in the identification of air bronchograms with the addition of clinical information; however, clinical history did not have a substantial impact on the inter‐rater reliability of other findings. The addition of clinical information did not alter the inter‐rater reliability in the identification of alveolar infiltrate. Clinical history affected individual raters differently in their interpretation of alveolar infiltrate, with 3 raters more likely to identify an alveolar infiltrate and 2 raters less likely to identify an alveolar infiltrate.
Most studies addressing the impact of clinical history on radiographic interpretation evaluated accuracy. In many of these studies, accuracy was defined as the raters' agreement with the final interpretation of each film as documented in the medical record or their agreement with the interpretation of the radiologists selecting the cases.[1, 2, 3, 5, 6, 7] Given the known inter‐rater variability in radiographic interpretation,[10, 11, 12, 13, 14, 15] accuracy of a radiologist's interpretation cannot be appropriately assessed through agreement with their peers. Because a true measure of accuracy in the radiographic diagnosis of pneumonia can only be determined through invasive testing, such as lung biopsy, reliability serves as a more appropriate measure of performance. Inclusion of clinical information in chest radiograph interpretation has been shown to improve reliability in the radiographic diagnosis of a broad range of conditions.[15]
The primary outcome in this study was the identification of an infiltrate. Previous studies have noted consistent identification of the radiographic features that are most suggestive of bacterial pneumonia, such as alveolar infiltrate, and less consistent identification of other radiographic findings, including interstitial infiltrate.[18, 26, 27] Among the radiologists in this study, the addition of clinical information did not have a meaningful impact on the reliability of either of these findings, as there was substantial inter‐rater agreement for the identification of alveolar infiltrate and only slight agreement for the identification of interstitial infiltrate, both with and without clinical history. Additionally, inter‐rater reliability for the identification of alveolar infiltrate remained substantial to almost perfect for all 6 raters with the addition of clinical information.
Clinical information impacted the raters differently in their pattern of alveolar infiltrate identification, suggesting that radiologists may differ in their approach to incorporating clinical history in the interpretation of chest radiographs. The inclusion of clinical information may impact a radiologist's perception, leading to improved identification of abnormalities; however, it may also guide their decision making about the relevance of previously identified abnormalities.[28] Some radiologists may use clinical information to support or suggest possible radiographic findings, whereas others may use the information to challenge potential findings. This study did not address the manner in which the individual raters utilized the clinical history. There were also several radiographs in which the clinical information resulted in a change in the identification of an alveolar infiltrate by 3 or more raters, with as many as 5 of 6 raters changing their interpretation for 1 particular radiograph. These changes in identification of an infiltrate suggest that unidentified aspects of a history may be likely to influence a rater's interpretation of a radiograph. Nevertheless, these changes did not result in improved reliability and it is not possible to determine if these changes resulted in improved accuracy in interpretation.
This study had several limitations. First, radiographs were purposefully selected to encompass a broad spectrum of radiographic findings. Thus, the prevalence of pneumonia and other abnormal findings was artificially higher than typically observed among a cohort of children for whom pneumonia is considered. Second, the radiologists recruited for this study all practice in an academic children's hospital setting. These factors may limit the generalizability of our findings. However, we would expect these results to be generalizable to pediatric radiologists from other academic institutions. Third, this study does not meet the criteria of a balanced study design as defined by Loy and Irwig.[19] A study was characterized as balanced if half of the radiographs were read with and half without clinical information in each of the 2 reading sessions. The proposed benefit of such a design is to control for possible changes in ability or reporting practices of the raters that may have occurred between study periods. The use of a standardized reporting tool likely minimized changes in reporting practices. Also, it is unlikely that the ability or reporting practices of an experienced radiologist would change over the study period. Fourth, the radiologists interpreted the films outside of their standard workflow and utilized a standardized reporting tool that focused on the presence or absence of pneumonia indicators. These factors may have increased the radiologists' suspicion for pneumonia even in the absence of clinical information. This may have biased the results toward finding no difference in the identification of pneumonia with the addition of detailed clinical history. Thus, the inclusion of clinical information in radiograph interpretation in clinical practice may have greater impact on the identification of these pneumonia indicators than was found in this study.[29] Finally, reliability does not imply accuracy, and it is unknown if changes in the identification of pneumonia indicators led to more accurate interpretation with respect to the clinical or pathologic diagnosis of pneumonia.
In conclusion, we observed high intra‐ and inter‐rater reliability among radiologists in the identification of an alveolar infiltrate, the radiographic finding most suggestive of bacterial pneumonia.[16, 17, 18, 30] The addition of clinical information did not have a substantial impact on the reliability of its identification.
- , , , et al. Tentative diagnoses facilitate the detection of diverse lesions in chest radiographs. Invest Radiol. 1986;21(7):532–539.
- , , , . Influence of clinical history upon detection of nodules and other lesions. Invest Radiol. 1988;23(1):48–55.
- , , , . Influence of clinical history on perception of abnormalities in pediatric radiographs. Acad Radiol. 1994;1(3):217–223.
- , , , et al. Impact of clinical history on film interpretation. Yonsei Med J. 1992;33(2):168–172.
- , , , et al. The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1990;25(6):670–674.
- , , , et al. Does knowledge of the clinical history affect the accuracy of chest radiograph interpretation?AJR Am J Roentgenol. 1990;154(4):709–712.
- , , , . Detection of lung cancer on the chest radiograph: impact of previous films, clinical information, double reading, and dual reading. J Clin Epidemiol. 2001;54(11):1146–1150.
- , , , . The effect of clinical bias on the interpretation of myelography and spinal computed tomography. Radiology. 1982;145(1):85–89.
- . A suggestion: look at the images first, before you read the history. Radiology. 2002;223(1):9–10.
- , , , et al. Interobserver reliability of the chest radiograph in community‐acquired pneumonia. PORT Investigators. Chest. 1996;110(2):343–350.
- , , , , . Inter‐ and intra‐observer variability in the assessment of atelectasis and consolidation in neonatal chest radiographs. Pediatr Radiol. 1999;29(6):459–462.
- , , , , . Chest radiographs in the emergency department: is the radiologist really necessary?Postgrad Med J. 2003;79(930):214–217.
- , , , . Inter‐observer variation in the interpretation of chest radiographs for pneumonia in community‐acquired lower respiratory tract infections. Clin Radiol. 2004;59(8):743–752.
- , , , , , . Disagreement in the interpretation of chest radiographs among specialists and clinical outcomes of patients hospitalized with suspected pneumonia. Eur J Intern Med. 2006;17(1):43–47.
- , , . An assessment of inter‐observer agreement and accuracy when reporting plain radiographs. Clin Radiol. 1997;52(3):235–238.
- , , , et al. Evaluation of the World Health Organization criteria for chest radiographs for pneumonia diagnosis in children. Eur J Pediatr. 2011;171(2):369–374.
- , , , et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ. 2005;83(5):353–359.
- , , , et al. Variability in the interpretation of chest radiographs for the diagnosis of pneumonia in children. J Hosp Med. 2012;7(4):294–298.
- , . Accuracy of diagnostic tests read with and without clinical information: a systematic review. JAMA. 2004;292(13):1602–1609.
- Standardization of interpretation of chest radiographs for the diagnosis of pneumonia in children. In:World Health Organization: Pneumonia Vaccine Trial Investigators' Group.Geneva: Department of Vaccine and Biologics;2001.
- , , , et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia: updated analysis using World Health Organization standardized interpretation of chest radiographs. Pediatr Infect Dis J. 2006;25(9):779–781.
- , . A one‐way components of variance model for categorical data. Biometrics. 1977;33:671–679.
- , . The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
- , . Kappa statistic. CMAJ. 2005;173(1):16.
- , . Clinical biostatistics. LIV. The biostatistics of concordance. Clin Pharmacol Ther. 1981;29(1):111–123.
- , , , , , . Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis. 2000;31(2):347–382.
- , , , et al. Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730–1754.
- , . Commentary does clinical history affect perception?Acad Radiol. 2006;13(3):402–403.
- , . The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1991;26(5):512–514.
- , , , . Comparison of radiological findings and microbial aetiology of childhood pneumonia. Acta Paediatr. 1993;82(4):360–363.
- , , , et al. Tentative diagnoses facilitate the detection of diverse lesions in chest radiographs. Invest Radiol. 1986;21(7):532–539.
- , , , . Influence of clinical history upon detection of nodules and other lesions. Invest Radiol. 1988;23(1):48–55.
- , , , . Influence of clinical history on perception of abnormalities in pediatric radiographs. Acad Radiol. 1994;1(3):217–223.
- , , , et al. Impact of clinical history on film interpretation. Yonsei Med J. 1992;33(2):168–172.
- , , , et al. The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1990;25(6):670–674.
- , , , et al. Does knowledge of the clinical history affect the accuracy of chest radiograph interpretation?AJR Am J Roentgenol. 1990;154(4):709–712.
- , , , . Detection of lung cancer on the chest radiograph: impact of previous films, clinical information, double reading, and dual reading. J Clin Epidemiol. 2001;54(11):1146–1150.
- , , , . The effect of clinical bias on the interpretation of myelography and spinal computed tomography. Radiology. 1982;145(1):85–89.
- . A suggestion: look at the images first, before you read the history. Radiology. 2002;223(1):9–10.
- , , , et al. Interobserver reliability of the chest radiograph in community‐acquired pneumonia. PORT Investigators. Chest. 1996;110(2):343–350.
- , , , , . Inter‐ and intra‐observer variability in the assessment of atelectasis and consolidation in neonatal chest radiographs. Pediatr Radiol. 1999;29(6):459–462.
- , , , , . Chest radiographs in the emergency department: is the radiologist really necessary?Postgrad Med J. 2003;79(930):214–217.
- , , , . Inter‐observer variation in the interpretation of chest radiographs for pneumonia in community‐acquired lower respiratory tract infections. Clin Radiol. 2004;59(8):743–752.
- , , , , , . Disagreement in the interpretation of chest radiographs among specialists and clinical outcomes of patients hospitalized with suspected pneumonia. Eur J Intern Med. 2006;17(1):43–47.
- , , . An assessment of inter‐observer agreement and accuracy when reporting plain radiographs. Clin Radiol. 1997;52(3):235–238.
- , , , et al. Evaluation of the World Health Organization criteria for chest radiographs for pneumonia diagnosis in children. Eur J Pediatr. 2011;171(2):369–374.
- , , , et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull World Health Organ. 2005;83(5):353–359.
- , , , et al. Variability in the interpretation of chest radiographs for the diagnosis of pneumonia in children. J Hosp Med. 2012;7(4):294–298.
- , . Accuracy of diagnostic tests read with and without clinical information: a systematic review. JAMA. 2004;292(13):1602–1609.
- Standardization of interpretation of chest radiographs for the diagnosis of pneumonia in children. In:World Health Organization: Pneumonia Vaccine Trial Investigators' Group.Geneva: Department of Vaccine and Biologics;2001.
- , , , et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia: updated analysis using World Health Organization standardized interpretation of chest radiographs. Pediatr Infect Dis J. 2006;25(9):779–781.
- , . A one‐way components of variance model for categorical data. Biometrics. 1977;33:671–679.
- , . The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
- , . Kappa statistic. CMAJ. 2005;173(1):16.
- , . Clinical biostatistics. LIV. The biostatistics of concordance. Clin Pharmacol Ther. 1981;29(1):111–123.
- , , , , , . Practice guidelines for the management of community‐acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis. 2000;31(2):347–382.
- , , , et al. Guidelines for the management of adults with community‐acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163(7):1730–1754.
- , . Commentary does clinical history affect perception?Acad Radiol. 2006;13(3):402–403.
- , . The effect of clinical history on chest radiograph interpretations in a PACS environment. Invest Radiol. 1991;26(5):512–514.
- , , , . Comparison of radiological findings and microbial aetiology of childhood pneumonia. Acta Paediatr. 1993;82(4):360–363.
© 2012 Society of Hospital Medicine
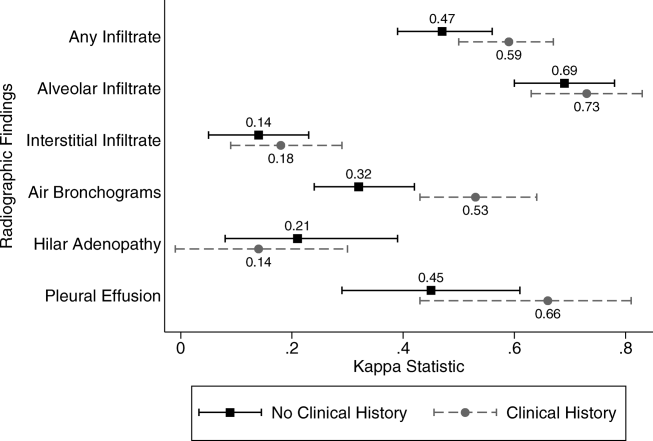
Pay-for-Performance Challenged as Best Model for Healthcare
Pushing healthcare toward pay-for-performance models that provide financial rewards for patient outcomes might not be the best direction for healthcare, according to an article published by a duo of doctors and a behavioral economist.
“Will Pay for Performance Backfire? Insights from Behavioral Economics” posted at Healthaffairs.org, questions the validity of paying for outcomes, particularly as there is no evidence yet that the model improves patient outcomes.
“You’re not actually paying for quality,” says David Himmelstein, MD, a professor at City University of New York School of Public Health at Hunter College, New York. “What you’re paying for is some very gameable measurement that doctors will find a way to cheat.”
The blog post notes that monetary rewards can actually undermine motivation for tasks that are intrinsically interesting or rewarding, a phenomenon known as “motivational crowd-out.” Dr. Himmelstein says it could focus attention on coding, rather than patients, or encourage providers to avoid noncompliant patients who will make their measured performances look bad.
“Injecting different monetary incentives into healthcare can certainly change it,” according to the article, “but not necessarily in the ways that policy makers would plan, much less hope for.”
Dr. Himmelstein says that without evidence for, or against, pay for performance, it’s difficult to say whether it will improve outcomes over the long term. Given the government push toward pay-for-performance programs—such as value-based purchasing (VBP)—he suggests physicians prepare themselves to comply. Accordingly, SHM supports policies that link "quality measurement to performance-based payment” and has created a toolkit to help hospitalists prepare for VBP, one of the most targeted pay-for-performance programs.
Even as HM moves toward adopting pay for performance as a mantra, Dr. Himmelstein believes hospitalists are in a good position to lead discussions on whether pay for performance is the only way to move forward.
“It can feel like a fait d’accompli, but things can change, and they can change rapidly,” Dr. Himmelstein adds. “The first step is to have real discussions about it. Up to now, much of the medical literature is saying, ‘It’s not working. We must have the wrong incentives.’ What if there are no right incentives?”
Visit our website for more information about pay-for-performance programs.
Pushing healthcare toward pay-for-performance models that provide financial rewards for patient outcomes might not be the best direction for healthcare, according to an article published by a duo of doctors and a behavioral economist.
“Will Pay for Performance Backfire? Insights from Behavioral Economics” posted at Healthaffairs.org, questions the validity of paying for outcomes, particularly as there is no evidence yet that the model improves patient outcomes.
“You’re not actually paying for quality,” says David Himmelstein, MD, a professor at City University of New York School of Public Health at Hunter College, New York. “What you’re paying for is some very gameable measurement that doctors will find a way to cheat.”
The blog post notes that monetary rewards can actually undermine motivation for tasks that are intrinsically interesting or rewarding, a phenomenon known as “motivational crowd-out.” Dr. Himmelstein says it could focus attention on coding, rather than patients, or encourage providers to avoid noncompliant patients who will make their measured performances look bad.
“Injecting different monetary incentives into healthcare can certainly change it,” according to the article, “but not necessarily in the ways that policy makers would plan, much less hope for.”
Dr. Himmelstein says that without evidence for, or against, pay for performance, it’s difficult to say whether it will improve outcomes over the long term. Given the government push toward pay-for-performance programs—such as value-based purchasing (VBP)—he suggests physicians prepare themselves to comply. Accordingly, SHM supports policies that link "quality measurement to performance-based payment” and has created a toolkit to help hospitalists prepare for VBP, one of the most targeted pay-for-performance programs.
Even as HM moves toward adopting pay for performance as a mantra, Dr. Himmelstein believes hospitalists are in a good position to lead discussions on whether pay for performance is the only way to move forward.
“It can feel like a fait d’accompli, but things can change, and they can change rapidly,” Dr. Himmelstein adds. “The first step is to have real discussions about it. Up to now, much of the medical literature is saying, ‘It’s not working. We must have the wrong incentives.’ What if there are no right incentives?”
Visit our website for more information about pay-for-performance programs.
Pushing healthcare toward pay-for-performance models that provide financial rewards for patient outcomes might not be the best direction for healthcare, according to an article published by a duo of doctors and a behavioral economist.
“Will Pay for Performance Backfire? Insights from Behavioral Economics” posted at Healthaffairs.org, questions the validity of paying for outcomes, particularly as there is no evidence yet that the model improves patient outcomes.
“You’re not actually paying for quality,” says David Himmelstein, MD, a professor at City University of New York School of Public Health at Hunter College, New York. “What you’re paying for is some very gameable measurement that doctors will find a way to cheat.”
The blog post notes that monetary rewards can actually undermine motivation for tasks that are intrinsically interesting or rewarding, a phenomenon known as “motivational crowd-out.” Dr. Himmelstein says it could focus attention on coding, rather than patients, or encourage providers to avoid noncompliant patients who will make their measured performances look bad.
“Injecting different monetary incentives into healthcare can certainly change it,” according to the article, “but not necessarily in the ways that policy makers would plan, much less hope for.”
Dr. Himmelstein says that without evidence for, or against, pay for performance, it’s difficult to say whether it will improve outcomes over the long term. Given the government push toward pay-for-performance programs—such as value-based purchasing (VBP)—he suggests physicians prepare themselves to comply. Accordingly, SHM supports policies that link "quality measurement to performance-based payment” and has created a toolkit to help hospitalists prepare for VBP, one of the most targeted pay-for-performance programs.
Even as HM moves toward adopting pay for performance as a mantra, Dr. Himmelstein believes hospitalists are in a good position to lead discussions on whether pay for performance is the only way to move forward.
“It can feel like a fait d’accompli, but things can change, and they can change rapidly,” Dr. Himmelstein adds. “The first step is to have real discussions about it. Up to now, much of the medical literature is saying, ‘It’s not working. We must have the wrong incentives.’ What if there are no right incentives?”
Visit our website for more information about pay-for-performance programs.
Not Sexy Enough
The annual meeting of the American College of Rheumatology has just ended. As usual, it was frenetic. So many lectures to choose from, so little time (and, as I age, energy) to get to them all.
The meeting is a great opportunity for the motivated rheumatologist if you know how to use it to your advantage – and that’s a skill that’s learned over a few years of attendance. Apart from catching up with old mentors and friends, you can catch up on the latest and greatest in basic science research. You can find out how experts manage difficult cases. There are sessions on how to manage your practice more efficiently. There are thousands of posters from all over the world to peruse.
Year after year there are several sessions on the autoimmune diseases, covering everything from basic science to bench and clinical research to clinical practice. An ever-growing pool of information about the genetic and molecular bases of disease has led to a rapid expansion of treatment targets – primarily for rheumatoid arthritis but extending to other autoimmune diseases as well.
But there are certain bread-and-butter illnesses that are not as sexy and, as such, do not get as much airtime.
This year, for example, there was only one clinical session on gout, and it was held in one of the smaller rooms. Slated for the same time slot were "Dermatology Topics for Rheumatologists" and "Preclinical Autoimmunity – Potential for Prevention," both much sexier-sounding and held in much larger venues. If my small cohort of friends and colleagues is a microcosm of the attendee population, it made complete sense to do this because I was the only one out of six who was interested in gout.
I understand that "Dermatology Topics for Rheumatologists" – by far the most popular in my small cohort – is indeed interesting, but I do not think it provides terribly useful information. No offense to the ACR or to my friends who picked this topic, but while you may see an interesting rash here and there and maybe remember seeing a similar picture from a lecture that you attended somewhere, I contend that it is more valuable for a clinician to be able to treat challenging gout cases, to learn more postmarketing information about pegloticase, and to understand what asymptomatic hyperuricemia might potentially indicate.
And what of osteoarthritis? There was a popular lecture on back pain, though I heard it was not very good. OA has become one of my biggest frustrations. It is never easy to tell patients that there is not much that can be done for their condition. Thankfully there was a basic science lecture on OA. Hopefully, this means more funding for more research, and ultimately perhaps a disease-modifier as well.
I appreciate that there was a session on paraneoplastic syndromes, one on polymyalgia rheumatica, and one on osteoporosis. I see more of these conditions in my practice than I do systemic lupus erythematosus, scleroderma, or vasculitis.
Without a doubt, ours is a wonderful field to be in. Our diseases have historically been very challenging to define, let alone treat. I feel lucky to be a rheumatologist at such a heady time, when it is now possible to go into drug-free remission if you have rheumatoid arthritis. We understand mechanisms of autoimmune disease better and are making great strides in therapeutics.
But there are other diseases that have been largely ignored, for reasons that are not entirely clear to me (perhaps the unfettered profit motivation that I talked about a few columns ago?), and I think it is about time we had a more equitable distribution of resources for research. Glamorous zebras aside, I will be grateful for the day that I can tell my patients: "yes, there is a nonsurgical option for your osteoarthritis, and no, it is not an antidepressant."
Dr. Chan practices rheumatology in Pawtucket, R.I. E-mail her at [email protected].
The annual meeting of the American College of Rheumatology has just ended. As usual, it was frenetic. So many lectures to choose from, so little time (and, as I age, energy) to get to them all.
The meeting is a great opportunity for the motivated rheumatologist if you know how to use it to your advantage – and that’s a skill that’s learned over a few years of attendance. Apart from catching up with old mentors and friends, you can catch up on the latest and greatest in basic science research. You can find out how experts manage difficult cases. There are sessions on how to manage your practice more efficiently. There are thousands of posters from all over the world to peruse.
Year after year there are several sessions on the autoimmune diseases, covering everything from basic science to bench and clinical research to clinical practice. An ever-growing pool of information about the genetic and molecular bases of disease has led to a rapid expansion of treatment targets – primarily for rheumatoid arthritis but extending to other autoimmune diseases as well.
But there are certain bread-and-butter illnesses that are not as sexy and, as such, do not get as much airtime.
This year, for example, there was only one clinical session on gout, and it was held in one of the smaller rooms. Slated for the same time slot were "Dermatology Topics for Rheumatologists" and "Preclinical Autoimmunity – Potential for Prevention," both much sexier-sounding and held in much larger venues. If my small cohort of friends and colleagues is a microcosm of the attendee population, it made complete sense to do this because I was the only one out of six who was interested in gout.
I understand that "Dermatology Topics for Rheumatologists" – by far the most popular in my small cohort – is indeed interesting, but I do not think it provides terribly useful information. No offense to the ACR or to my friends who picked this topic, but while you may see an interesting rash here and there and maybe remember seeing a similar picture from a lecture that you attended somewhere, I contend that it is more valuable for a clinician to be able to treat challenging gout cases, to learn more postmarketing information about pegloticase, and to understand what asymptomatic hyperuricemia might potentially indicate.
And what of osteoarthritis? There was a popular lecture on back pain, though I heard it was not very good. OA has become one of my biggest frustrations. It is never easy to tell patients that there is not much that can be done for their condition. Thankfully there was a basic science lecture on OA. Hopefully, this means more funding for more research, and ultimately perhaps a disease-modifier as well.
I appreciate that there was a session on paraneoplastic syndromes, one on polymyalgia rheumatica, and one on osteoporosis. I see more of these conditions in my practice than I do systemic lupus erythematosus, scleroderma, or vasculitis.
Without a doubt, ours is a wonderful field to be in. Our diseases have historically been very challenging to define, let alone treat. I feel lucky to be a rheumatologist at such a heady time, when it is now possible to go into drug-free remission if you have rheumatoid arthritis. We understand mechanisms of autoimmune disease better and are making great strides in therapeutics.
But there are other diseases that have been largely ignored, for reasons that are not entirely clear to me (perhaps the unfettered profit motivation that I talked about a few columns ago?), and I think it is about time we had a more equitable distribution of resources for research. Glamorous zebras aside, I will be grateful for the day that I can tell my patients: "yes, there is a nonsurgical option for your osteoarthritis, and no, it is not an antidepressant."
Dr. Chan practices rheumatology in Pawtucket, R.I. E-mail her at [email protected].
The annual meeting of the American College of Rheumatology has just ended. As usual, it was frenetic. So many lectures to choose from, so little time (and, as I age, energy) to get to them all.
The meeting is a great opportunity for the motivated rheumatologist if you know how to use it to your advantage – and that’s a skill that’s learned over a few years of attendance. Apart from catching up with old mentors and friends, you can catch up on the latest and greatest in basic science research. You can find out how experts manage difficult cases. There are sessions on how to manage your practice more efficiently. There are thousands of posters from all over the world to peruse.
Year after year there are several sessions on the autoimmune diseases, covering everything from basic science to bench and clinical research to clinical practice. An ever-growing pool of information about the genetic and molecular bases of disease has led to a rapid expansion of treatment targets – primarily for rheumatoid arthritis but extending to other autoimmune diseases as well.
But there are certain bread-and-butter illnesses that are not as sexy and, as such, do not get as much airtime.
This year, for example, there was only one clinical session on gout, and it was held in one of the smaller rooms. Slated for the same time slot were "Dermatology Topics for Rheumatologists" and "Preclinical Autoimmunity – Potential for Prevention," both much sexier-sounding and held in much larger venues. If my small cohort of friends and colleagues is a microcosm of the attendee population, it made complete sense to do this because I was the only one out of six who was interested in gout.
I understand that "Dermatology Topics for Rheumatologists" – by far the most popular in my small cohort – is indeed interesting, but I do not think it provides terribly useful information. No offense to the ACR or to my friends who picked this topic, but while you may see an interesting rash here and there and maybe remember seeing a similar picture from a lecture that you attended somewhere, I contend that it is more valuable for a clinician to be able to treat challenging gout cases, to learn more postmarketing information about pegloticase, and to understand what asymptomatic hyperuricemia might potentially indicate.
And what of osteoarthritis? There was a popular lecture on back pain, though I heard it was not very good. OA has become one of my biggest frustrations. It is never easy to tell patients that there is not much that can be done for their condition. Thankfully there was a basic science lecture on OA. Hopefully, this means more funding for more research, and ultimately perhaps a disease-modifier as well.
I appreciate that there was a session on paraneoplastic syndromes, one on polymyalgia rheumatica, and one on osteoporosis. I see more of these conditions in my practice than I do systemic lupus erythematosus, scleroderma, or vasculitis.
Without a doubt, ours is a wonderful field to be in. Our diseases have historically been very challenging to define, let alone treat. I feel lucky to be a rheumatologist at such a heady time, when it is now possible to go into drug-free remission if you have rheumatoid arthritis. We understand mechanisms of autoimmune disease better and are making great strides in therapeutics.
But there are other diseases that have been largely ignored, for reasons that are not entirely clear to me (perhaps the unfettered profit motivation that I talked about a few columns ago?), and I think it is about time we had a more equitable distribution of resources for research. Glamorous zebras aside, I will be grateful for the day that I can tell my patients: "yes, there is a nonsurgical option for your osteoarthritis, and no, it is not an antidepressant."
Dr. Chan practices rheumatology in Pawtucket, R.I. E-mail her at [email protected].

Triple Therapy Boosts HCV Response After Transplant
BOSTON – Liver transplant recipients with hepatitis C virus infection who underwent triple-drug therapy achieved a high extended rapid virologic response rate but often contended with treatment complications in a retrospective multicenter cohort study.
The extended rapid virologic response (eRVR) rate seen in 57% of patients was "encouraging, given a very difficult-to-cure population," Dr. James R. Burton, Jr., said at the annual meeting of the American Association for the Study of Liver Diseases. He noted, however, that it’s not clear if the encouraging eRVR rate will predict sustained virologic response (SVR) as it does in non-liver transplant patients.

The use of peginteferon plus ribavirin in liver transplant recipients with hepatitis C virus infection has an SVR of only 30%. While triple therapy with peginterferon, ribavirin, and a protease inhibitor (boceprevir or telaprevir) has significantly improved rates of SVR in patients infected with genotype 1 hepatitis C virus, its safety and efficacy in liver transplant recipients is unknown, said Dr. Burton, medical director of liver transplantation at the University of Colorado Hospital, Aurora.
With 101 patients, the five-center study is the largest involving triple therapy in liver transplant recipients with hepatitis C virus infection.
Telaprevir was the protease inhibitor used most often in patients (90% vs. 10% with boceprevir). Nearly all patients (96%) had a lead-in treatment phase with peginterferon plus ribavirin. A minority of patients (14%) had an extended lead-in phase of at least 90 days (median of 189 days) and were excluded from efficacy, but not safety, analyses. The other patients had a lead-in lasting a median of 29 days. The patients with a long lead-in phase had a median of 398 total treatment days, compared with a median of 154 days for those with a shorter lead-in time.
The efficacy study population involved genotype 1–infected patients (54% genotype 1a, 39% 1b, and 7% mixed) from five medical centers. Most patients were men (76%); they had a median age of 58 years and a median duration of 54 months from their liver transplant to starting a protease inhibitor. An unfavorable IL28B genotype was found in 69% of 45 patients tested. In the 60% of patients who had undergone previous antiviral therapy, 29% had a partial response. On liver biopsy, another 47% of patients had either bridging fibrosis or cirrhosis.
The immunosuppressive agents used by the patients included cyclosporine (66%) and tacrolimus (23%). A small percentage did not receive a calcineurin inhibitor or rapamycin. Another 27% were taking corticosteroids, and 72% were taking mycophenolate mofetil or mycophenolic acid.
On treatment, the percentage of patients who had an HCV RNA level less than the limit of detection increased from 55% at 4 weeks to 63% at 8 weeks. At 12 weeks the percentage was 71%. An eRVR, defined as negative HCV RNA tests at 4 and 12 weeks, occurred in 57%. An eRVR occurred significantly more often among patients who had at least a 1 log drop in HCV RNA levels during the lead-in phase than did those with less than a 1 log drop (76% vs. 35%).
Overall, 12% of patients experienced virologic breakthrough, and treatment was stopped. This occurred more often among those with a long lead-in vs. those with a short lead-in (21% vs. 10%, respectively). Another 14% discontinued treatment early because of an adverse event; discontinuations occurred more often among patients with a long lead-in (40% vs. 11%).
Protease inhibitors are known to inhibit the metabolism of calcineurin inhibitors, which was reflected in the study by the need to reduce the median daily doses of cyclosporine (from 200 mg to 50 mg) and tacrolimus (from 1.0 mg to 0.06 mg) after protease inhibitor therapy began.
Many patients (49%) required blood transfusions during triple therapy. During the first 16 weeks of therapy, these patients used a median of 2.5 units. The majority of patients (86%) used growth factors, including granulocyte-colony stimulating factor in 44% and erythropoietin in 79%. Medication dose reductions were most frequent for ribavirin (in 78%). A total of 7% were hospitalized for anemia, Dr. Burton said.
Renal insufficiency, defined as an increase in creatinine of greater than 0.5 mg/dL from baseline, developed in 32%. Of two rejection episodes in the study, one involved a patient coming off a protease inhibitor.
Dr. Burton suggested that future studies should focus on identifying predictors for nonresponse to avoid unnecessary treatment and associated toxicities such as complications of anemia and adverse events related to significant protease inhibitor–calcineurin inhibitor interactions, such as worsening renal function and graft rejection when transitioning off a protease inhibitor.
Dr. Burton disclosed that he is an investigator in a clinical trial sponsored by Vertex Pharmaceuticals, which makes telaprevir.☐
BOSTON – Liver transplant recipients with hepatitis C virus infection who underwent triple-drug therapy achieved a high extended rapid virologic response rate but often contended with treatment complications in a retrospective multicenter cohort study.
The extended rapid virologic response (eRVR) rate seen in 57% of patients was "encouraging, given a very difficult-to-cure population," Dr. James R. Burton, Jr., said at the annual meeting of the American Association for the Study of Liver Diseases. He noted, however, that it’s not clear if the encouraging eRVR rate will predict sustained virologic response (SVR) as it does in non-liver transplant patients.
The use of peginteferon plus ribavirin in liver transplant recipients with hepatitis C virus infection has an SVR of only 30%. While triple therapy with peginterferon, ribavirin, and a protease inhibitor (boceprevir or telaprevir) has significantly improved rates of SVR in patients infected with genotype 1 hepatitis C virus, its safety and efficacy in liver transplant recipients is unknown, said Dr. Burton, medical director of liver transplantation at the University of Colorado Hospital, Aurora.
With 101 patients, the five-center study is the largest involving triple therapy in liver transplant recipients with hepatitis C virus infection.
Telaprevir was the protease inhibitor used most often in patients (90% vs. 10% with boceprevir). Nearly all patients (96%) had a lead-in treatment phase with peginterferon plus ribavirin. A minority of patients (14%) had an extended lead-in phase of at least 90 days (median of 189 days) and were excluded from efficacy, but not safety, analyses. The other patients had a lead-in lasting a median of 29 days. The patients with a long lead-in phase had a median of 398 total treatment days, compared with a median of 154 days for those with a shorter lead-in time.
The efficacy study population involved genotype 1–infected patients (54% genotype 1a, 39% 1b, and 7% mixed) from five medical centers. Most patients were men (76%); they had a median age of 58 years and a median duration of 54 months from their liver transplant to starting a protease inhibitor. An unfavorable IL28B genotype was found in 69% of 45 patients tested. In the 60% of patients who had undergone previous antiviral therapy, 29% had a partial response. On liver biopsy, another 47% of patients had either bridging fibrosis or cirrhosis.
The immunosuppressive agents used by the patients included cyclosporine (66%) and tacrolimus (23%). A small percentage did not receive a calcineurin inhibitor or rapamycin. Another 27% were taking corticosteroids, and 72% were taking mycophenolate mofetil or mycophenolic acid.
On treatment, the percentage of patients who had an HCV RNA level less than the limit of detection increased from 55% at 4 weeks to 63% at 8 weeks. At 12 weeks the percentage was 71%. An eRVR, defined as negative HCV RNA tests at 4 and 12 weeks, occurred in 57%. An eRVR occurred significantly more often among patients who had at least a 1 log drop in HCV RNA levels during the lead-in phase than did those with less than a 1 log drop (76% vs. 35%).
Overall, 12% of patients experienced virologic breakthrough, and treatment was stopped. This occurred more often among those with a long lead-in vs. those with a short lead-in (21% vs. 10%, respectively). Another 14% discontinued treatment early because of an adverse event; discontinuations occurred more often among patients with a long lead-in (40% vs. 11%).
Protease inhibitors are known to inhibit the metabolism of calcineurin inhibitors, which was reflected in the study by the need to reduce the median daily doses of cyclosporine (from 200 mg to 50 mg) and tacrolimus (from 1.0 mg to 0.06 mg) after protease inhibitor therapy began.
Many patients (49%) required blood transfusions during triple therapy. During the first 16 weeks of therapy, these patients used a median of 2.5 units. The majority of patients (86%) used growth factors, including granulocyte-colony stimulating factor in 44% and erythropoietin in 79%. Medication dose reductions were most frequent for ribavirin (in 78%). A total of 7% were hospitalized for anemia, Dr. Burton said.
Renal insufficiency, defined as an increase in creatinine of greater than 0.5 mg/dL from baseline, developed in 32%. Of two rejection episodes in the study, one involved a patient coming off a protease inhibitor.
Dr. Burton suggested that future studies should focus on identifying predictors for nonresponse to avoid unnecessary treatment and associated toxicities such as complications of anemia and adverse events related to significant protease inhibitor–calcineurin inhibitor interactions, such as worsening renal function and graft rejection when transitioning off a protease inhibitor.
Dr. Burton disclosed that he is an investigator in a clinical trial sponsored by Vertex Pharmaceuticals, which makes telaprevir.☐
BOSTON – Liver transplant recipients with hepatitis C virus infection who underwent triple-drug therapy achieved a high extended rapid virologic response rate but often contended with treatment complications in a retrospective multicenter cohort study.
The extended rapid virologic response (eRVR) rate seen in 57% of patients was "encouraging, given a very difficult-to-cure population," Dr. James R. Burton, Jr., said at the annual meeting of the American Association for the Study of Liver Diseases. He noted, however, that it’s not clear if the encouraging eRVR rate will predict sustained virologic response (SVR) as it does in non-liver transplant patients.
The use of peginteferon plus ribavirin in liver transplant recipients with hepatitis C virus infection has an SVR of only 30%. While triple therapy with peginterferon, ribavirin, and a protease inhibitor (boceprevir or telaprevir) has significantly improved rates of SVR in patients infected with genotype 1 hepatitis C virus, its safety and efficacy in liver transplant recipients is unknown, said Dr. Burton, medical director of liver transplantation at the University of Colorado Hospital, Aurora.
With 101 patients, the five-center study is the largest involving triple therapy in liver transplant recipients with hepatitis C virus infection.
Telaprevir was the protease inhibitor used most often in patients (90% vs. 10% with boceprevir). Nearly all patients (96%) had a lead-in treatment phase with peginterferon plus ribavirin. A minority of patients (14%) had an extended lead-in phase of at least 90 days (median of 189 days) and were excluded from efficacy, but not safety, analyses. The other patients had a lead-in lasting a median of 29 days. The patients with a long lead-in phase had a median of 398 total treatment days, compared with a median of 154 days for those with a shorter lead-in time.
The efficacy study population involved genotype 1–infected patients (54% genotype 1a, 39% 1b, and 7% mixed) from five medical centers. Most patients were men (76%); they had a median age of 58 years and a median duration of 54 months from their liver transplant to starting a protease inhibitor. An unfavorable IL28B genotype was found in 69% of 45 patients tested. In the 60% of patients who had undergone previous antiviral therapy, 29% had a partial response. On liver biopsy, another 47% of patients had either bridging fibrosis or cirrhosis.
The immunosuppressive agents used by the patients included cyclosporine (66%) and tacrolimus (23%). A small percentage did not receive a calcineurin inhibitor or rapamycin. Another 27% were taking corticosteroids, and 72% were taking mycophenolate mofetil or mycophenolic acid.
On treatment, the percentage of patients who had an HCV RNA level less than the limit of detection increased from 55% at 4 weeks to 63% at 8 weeks. At 12 weeks the percentage was 71%. An eRVR, defined as negative HCV RNA tests at 4 and 12 weeks, occurred in 57%. An eRVR occurred significantly more often among patients who had at least a 1 log drop in HCV RNA levels during the lead-in phase than did those with less than a 1 log drop (76% vs. 35%).
Overall, 12% of patients experienced virologic breakthrough, and treatment was stopped. This occurred more often among those with a long lead-in vs. those with a short lead-in (21% vs. 10%, respectively). Another 14% discontinued treatment early because of an adverse event; discontinuations occurred more often among patients with a long lead-in (40% vs. 11%).
Protease inhibitors are known to inhibit the metabolism of calcineurin inhibitors, which was reflected in the study by the need to reduce the median daily doses of cyclosporine (from 200 mg to 50 mg) and tacrolimus (from 1.0 mg to 0.06 mg) after protease inhibitor therapy began.
Many patients (49%) required blood transfusions during triple therapy. During the first 16 weeks of therapy, these patients used a median of 2.5 units. The majority of patients (86%) used growth factors, including granulocyte-colony stimulating factor in 44% and erythropoietin in 79%. Medication dose reductions were most frequent for ribavirin (in 78%). A total of 7% were hospitalized for anemia, Dr. Burton said.
Renal insufficiency, defined as an increase in creatinine of greater than 0.5 mg/dL from baseline, developed in 32%. Of two rejection episodes in the study, one involved a patient coming off a protease inhibitor.
Dr. Burton suggested that future studies should focus on identifying predictors for nonresponse to avoid unnecessary treatment and associated toxicities such as complications of anemia and adverse events related to significant protease inhibitor–calcineurin inhibitor interactions, such as worsening renal function and graft rejection when transitioning off a protease inhibitor.
Dr. Burton disclosed that he is an investigator in a clinical trial sponsored by Vertex Pharmaceuticals, which makes telaprevir.☐
AT THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
Major Finding: An extended rapid virologic response occurred significantly more often among patients who had at least a 1 log drop in HCV RNA levels during the lead-in phase than did those with less than a 1 log drop (76% vs. 35%)
Data Source: This was a multicenter retrospective cohort study of triple therapy for hepatitis C virus infection in 101 patients with post liver transplant.
Disclosures: Dr. Burton disclosed that he is an investigator in a clinical trial sponsored by Vertex Pharmaceuticals, which makes telaprevir.

End‐of‐Life Discussions
Most patients prefer to die at home, pain free and without the use of life‐sustaining treatments[1, 2] yet the majority of patients with serious illness die in the hospital.[3, 4, 5] When hospitalized patient die, the care is frequently focused on life‐sustaining treatments[6]; pain, dyspnea, and agitation levels are higher when compared with patients who die in non‐hospital settings.[7, 8, 9] End‐of‐life discussions and their products (ie, advanced directives) can clarify treatment options with patients and family,[10] and help ensure that patients receive care consistent with their beliefs.[11, 12, 13] End‐of‐life discussions are associated with a decrease use of life‐sustaining treatments, improved quality of life, and reduced costs of care.[14, 15] For the majority of patients dying of cancer, the first end‐of‐life discussion takes place in the hospital setting.[16]
Conducting end‐of‐life conversations in the hospital setting can be challenging. Patients are acutely ill and nearly 40% are incapable of making their own medical decisions.[17] In order to participate in an end‐of‐life discussion, a physician must determine that a patient meets the 4 criteria of decisional capacity as outlined by Appelbaum and Grisso:[18] Does the patient (1) communicate a clear and consistent choice; (2) understand the relevant information surrounding that decision; (3) appreciate the consequences of that decision; and (4) communicate reasoning for that decision?[19] In practice, however, clinicians inaccurately assign capacity up to 25% of the time.[17] When a physician determines, accurately or inaccurately, that the patient does not meet this standard for decisional capacity, discussions must be held instead with a surrogate decision‐maker. Surrogate decision‐making can make communication with the physician more difficult,[20] delay important medical decisions,[21] and be stressful on the decision‐maker.[22] To our knowledge, no studies have examined patient and surrogate participation in end‐of‐life discussions at the time of terminal hospitalization and its association with end‐of‐life treatments received.
Our goals were to examine physician assessment of decisional capacity and the prevalence of end‐of‐life discussions during the terminal hospitalization of patients with advanced cancer. Our research questions were: (1) What proportion of patients were assessed to have decisional capacity by the clinical team at the time of their terminal hospital admission? (2) What proportion of these patients had a documented discussion about end‐of‐life care with the clinical team, and for what proportion was the conversation held instead by the patient's surrogate decision‐maker because the patient was considered to have lost decisional capacity? (3) Was patient participation in a discussion about end‐of‐life care associated with life‐sustaining and palliative treatments received?
METHODS
Design
This is a retrospective cohort study of consecutive adult patients with advanced cancer who died at the University of Michigan Hospital, Ann Arbor, MI, from January 1, 2004 through December 31, 2007. This study was exempted from review by the University of Michigan (UM) Institutional Review Board because decedent data were used.
Sample
The UM Cancer Registry is a database of all cancer patients treated at the UM Comprehensive Cancer Center. We used the Registry to identify patients who met the following criteria: (1) age 18 years at time of cancer diagnosis; (2) estimated probability of 5‐year survival 20% at time of diagnosis, as predicted by the SEER Cancer Statistics Review[23]; (3) the entirety of cancer treatment was received at University of Michigan Health System (UMHS); and (4) the patient died while admitted to the University Hospital between January 1, 2004 and December 31, 2007.
UMHS is a healthcare system and academic medical center consisting of hospitals, health centers, and clinics, including the University of Michigan Hospital and Comprehensive Cancer Center. Over 4000 cancer patients are admitted to University Hospital and 80,000 outpatient visits occur to the Cancer Center every year. It serves as a major cancer referral center for the patients of Michigan and the greater Midwest. The University of Michigan implemented a palliative care consult service that was started in 2005, during the time period of our study.
Data Collection
Data were abstracted by review of the medical record by an internist (M.Z.) using a comprehensive chart abstraction instrument based on a previously validated tool.[24] Demographic data abstracted from the medical record included age, religious affiliation, race, ethnicity, and marital status. The original abstraction tool, which included 83 items, was reduced to include 47 items focusing on information related to advanced care planning, hospital course, and end‐of‐life discussions. Specific items included: reasons for admission, primary hospital service, occurrence and timing of end‐of‐life decision‐making, whether patient or family preferences were elicited through an end‐of‐life discussion, clinician's assessment of patient's decisional capacity at time of admission and end‐of‐life conversations, whether a comfort care plan was made, and whether palliative morphine was used.
The chart abstraction tool was pilot tested on the medical records of 10 patients, who were not included in the study, and refined to improve completeness of data collection. A copy of the abstraction tool is available upon request.
Definition of Key Variables
Decisional Capacity Assessment
Decisional capacity assessment is a reflection of the clinical team's assessment of the patient's decisional capacity on admission, and was determined through examination of the medical record in the first 24 hours of admission. Positive decision‐making capacity assessment was assumed if the clinician assessment of decisional capacity was documented in the mental status exam, or if the clinician documented conversations between clinician and patient in the history that suggested intact decision‐making capacity (ie, clinician documented terms such as patient stated or patient described and then described a coherent or sensible statement which implied patient capacity and intact mental status), or if the clinician's documentation of the assessment and plan stated or suggested decisions were being made by the patient. Other supportive information from the record was used to corroborate the evidence used to determine the clinician's assessment of the patient's decisional capacity, including whether the patient signed consent forms.
End‐of‐Life Discussions
The presence of an end‐of‐life discussion was presumed when the clinician documented a discussion with the patient, discussion with family, or family meeting concerning treatment preferences, or when the clinician quoted the patient's preferences in a fashion that documents a face‐to‐face discussion or directly described the elicitation of preferences from the patient or family.
Living Will
A living will was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed a living will.
Health Care Proxy
Health Care Proxy or Durable Power of Attorney for Healthcare was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed such a document.
Do Not Resuscitate (DNR) on Admission
DNR status was identified as present if the patient had documents with established DNR orders, or if a physician explicitly documented code status as DNR in the admission note or other documents placed in the record within the first 24 hours of admission.
Intensive Care Unit (ICU)Treatment
Patients were defined as having received ICU treatment if they were admitted directly or subsequently transferred to the ICU during the hospital course.
Comfort Care
Comfort care was defined as present only if the phrases comfort care, palliative care, or supportive care, were documented.
Palliative Opioid Therapy
Treatments with morphine or other opioids were recorded as palliative only if it was explicitly stated that these medications were used in the context of palliative or end‐of‐life care.
Data Analysis
We report the proportion of patients who were documented to lack decisional capacity at the time of hospital admission. We compared patient characteristics for those with and without documentation of decisional capacity on admission, and patients with decisional capacity on admission who did and did not participate in discussions about end‐of‐life care using chi‐square tests for categorical data, t tests for normally distributed continuous variables, and MannWhitney U tests for non‐normally distributed continuous variables. We examined whether documentation of a discussion about end‐of‐life care was associated with life‐sustaining and palliative treatments received using chi‐square for categorical treatments, and MannWhitney U tests for days from admission to initiation of comfort care. We used P < 0.05 to signify statistical significance.
RESULTS
Characteristics of Population and Decisional Capacity on Admission
The characteristics of the 145 patients who met entry criteria are summarized in Table 1. The most common types of cancers were lung cancer and leukemia/lymphoma. Of the 145 patients, the medical team's assessment of the patient's decisional capacity on admission could be established for 142 patients. As documented within the first 24 hours of admission, 27 patients (19%) were considered not to have decisional capacity, and 115 patients (79%) were considered to have decisional capacity. Both of these groups had similar age and gender distributions. There were no significant differences in the distribution of cancer type between those with and without decisional capacity. In both groups, the majority of the cancer diagnoses were made prior to admission. There was no difference in DNR orders established prior to or on admission between the groups (Table 1).
| Decision‐Making Capacity on Admissiona | |||
|---|---|---|---|
| No (N = 27) | Yes (N = 115) | ||
| N (%) | N (%) | P Value | |
| |||
| Age >65 | 15 (55.6) | 60 (52.2) | 0.75 |
| Gender (male) | 14 (51.9) | 68 (59.1) | 0.46 |
| Cancer type | |||
| Lung | 12 (44.4) | 42 (36.5) | 0.67 |
| Bone marrow | 5 (18.5) | 35 (30.4) | |
| Liver | 3 (11.1) | 6 (5.2) | |
| Pancreas | 3 (11.1) | 7 (6.10) | |
| Esophagus | 1 (3.7) | 8 (7.0) | |
| Colon | 1 (3.7) | 6 (5.2) | |
| Otherb | 2 (7.4) | 11 (9.6) | |
| Prior to admission | |||
| Cancer diagnosis known | 23 (85.2) | 91 (79.1) | 0.48 |
| Living will completed | 6 (22.2) | 26 (22.6 | 0.97 |
| Health care proxy established | 3 (11.1) | 26 (22.6) | 0.18 |
| DNR established | 8 (29.6) | 27 (23.5) | 0.79 |
End‐of‐Life Discussion in Patients With Decisional Capacity on Admission
Of the 115 patients assessed to have intact decisional capacity on admission, 56 (48.7%) participated in an end‐of‐life discussion with the medical team during their terminal hospitalization. For the remaining 59 patients who did not participate in an end‐of‐life discussion during the terminal hospital course, 46 (40.0%) had documentation suggesting they lost decisional capacity prior to a conversation and that the end‐of‐life discussions were held instead with the patient's surrogate decision‐maker, and 13 (11.3%) had no evidence of any end‐of‐life discussion (with the patient or surrogate).
When comparing those patients who participated in an end‐of‐life discussion with those patients whose surrogate participated in the discussion, there were no significant differences in gender and age distributions (Table 2). There was a significant difference in the type of cancers between the 2 groups. Among patients who participated in their end‐of‐life discussions, bone marrow cancer was proportionately more prevalent (17.9% vs 2.2%; P <0.01) and lung cancer was less prevalent (16.1% vs 41.3%; P <0.01), when compared to those who required surrogate participation. Timing of cancer diagnosis and prevalence of advance directives were similar between the 2 groups. The proportion of patients who had an established DNR order prior to admission was higher among those who did participate in end‐of‐life discussions when compared to those who had surrogate participation in these discussions (30.4% vs 17.4%; P < 0.04).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | ||||
|---|---|---|---|---|
| N =13 | N = 102 | |||
| End‐of‐Life discussion not documented | End‐of‐Life discussion with surrogate (N = 46) | End‐of‐Life discussion with patient (N = 56) | ||
| N (%) | N (%) | N (%) | P Value | |
| ||||
| Age 65 | 9 (69.2) | 18 (39.1) | 27 (48.2) | 0.36 |
| Gender (male) | 10 (76.9) | 27 (60.0) | 31 (55.4) | 0.64 |
| Cancer type | ||||
| Lung | 3 (23.1) | 19 (41.3) | 9 (16.1) | |
| Bone marrow | 7 (53.9) | 1 (2.2) | 10 (17.9) | |
| Liver | 1 (7.7) | 3 (6.5) | 2 (3.6) | |
| Pancreas | 1 (7.7) | 2 (4.4) | 4 (7.1) | <0.01 |
| Esophagus | 0 | 6 (13.0) | 2 (3.6) | |
| Colon | 1 (7.7) | 1 (2.2) | 3 (5.4) | |
| Othera | 0 | 1 (2.2) | 10 (17.9) | |
| Prior to Admission | ||||
| Cancer diagnosis known | 10 (76.9) | 37 (80.4) | 43 (76.8) | 0.66 |
| Living will completed | 4 (30.8) | 10 (21.7) | 12 (21.4) | 0.97 |
| Health care proxy established | ||||
| 3 (23.1) | 13 (28.3) | 10 (17.9) | 0.21 | |
| DNR established | 2 (15.4) | 8 (17.4) | 17 (30.4) | 0.04 |
Life‐Prolonging and Palliative Care Treatments Received and Participation in End‐of‐Life Discussions
Life‐prolonging treatments were more likely to be used for patients whose end‐of‐life discussions were held by patient's surrogate decision‐maker, in comparison to those patients who participated in the discussions themselves. Patients who had conversations held by surrogates were more likely to receive ventilator support (56.5% vs 23.2%, P < 0.01), chemotherapy (39.1% vs 5.4%, P < 0.01), artificial nutrition or hydration (45.7% vs 25.0%, P = 0.03), and antibiotics (97.8% vs 78.6%, P < 0.01), when compared to patients who participated in their own end‐of‐life discussion. Intensive care treatment rates also differed significantly between the 2 groups; 56.5% of those who did not participate in end‐of‐life discussions, and only 23.2% of those patients who did participate, were admitted or transferred to the intensive care unit (P < 0.01). There was no significant difference in the proportion of patients who received cardiopulmonary resuscitation (CPR) (15.2% vs 7.1%, P = 0.56) (Table 3). Patients who lost decisional capacity and required a surrogate decision‐maker to participate in their end‐of‐life discussions had longer length of stay (15.8 vs 10.3 days, P = 0.03) and length of time to end‐of‐life discussions (14.0 vs 6.1 days, P < 0.01) (Table 3).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | |||
|---|---|---|---|
| End‐of‐Life Discussion With Surrogate (N =46) | End‐of‐Life Discussion With Patient (N = 56) | ||
| N (%) | N (%) | P Value | |
| |||
| Life‐Prolonging Treatment | |||
| Ventilatory support | 26 (56.5) | 13 (23.2) | <0.01 |
| Chemotherapy | 18 (39.1) | 3 (5.4) | <0.01 |
| Artificial nutrition or hydration | 21 (45.7) | 14 (25.0) | 0.03 |
| Antibiotics | 45 (97.8) | 44 (78.6) | <0.01 |
| Cardiopulmonary resuscitation | 7 (15.2) | 4 (7.1) | 0.19 |
| ICU treatment (admit or transfer) | 26 (56.5) | 13 (23.2) | <0.01 |
| Palliative Treatments | |||
| Comfort care | 39 (84.8) | 45 (80.4) | 0.56 |
| Palliative morphine drip | 24 (52.2) | 33 (57.1) | 0.62 |
| Mean (95% CI) [Range] | Mean (95% CI) [Range] | ||
| Timing of Advanced Care Planning | |||
| Length of hospitalization | 15.8 d (11.420.2) [157] | 10.3 d (146) [146] | 0.03 |
| Time to end‐of‐life discussion | 14.0 d (9.918.1) [055] | 6.1 d (3.88.4) [046] | <0.01 |
| Time to comfort care | 23.5 d (4.342.8) [1374] | 9.2 d (6.312.1) [046] | 0.12 |
A comparison of the proportion of patients receiving palliative treatments, such as palliative comfort care orders and morphine infusions, revealed no significant differences between those with and without a discussion about end‐of‐life care (Table 3). Furthermore, while the time interval from hospital admission to initiation of comfort care was shorter for those who did participate in end‐of‐life discussions compared with those had surrogate participation (9.3 vs 23.5 days, P = 0.13 for equality), this difference was not statistically significant (Table 3).
Since a higher proportion of those who participated in end‐of‐life discussions during the hospitalization were admitted with a DNR order established prior to or on admission, we also examined the use of life‐prolonging treatments in the subgroup of patients who did not have a DNR order prior to admission. The difference in life‐prolonging treatments between those who did and did not participate in end‐of‐life discussions was preserved among those patients who did not have DNR status on admission (data not shown).
DISCUSSION
In this retrospective study of 145 terminal cancer patients who died in the hospital, we found that half of the patients had documentation suggesting that they lost decisional capacity during hospitalization and did not participate in end‐of‐life discussion with their healthcare providers. Among cancer patients in our study, 19% were determined not to have decisional capacity on admission, and another 32% were determined to lose decisional capacity during the hospital course. When patients did participate in documented discussions about end‐of‐life care, they were less likely to receive intensive life‐sustaining treatments, less likely to be admitted or transferred to the ICU, and more likely to avoid prolonged hospitalization. The finding that the majority of cancer patients are assessed to have intact decisional capacity upon admission to their terminal hospitalization, but less than half of them participate in their own end‐of‐life conversation, suggests that there is an important lost opportunity to provide quality advanced care planning to hospitalized patients.
Advanced care planning is the act of defining a competent patient's wishes regarding their future healthcare in the event of loss of decisional capacity. For many of the patients who were determined to lose decisional capacity during their hospitalization in our study, a surrogate decision‐maker was involved in a subsequent end‐of‐life discussion. This represents a missed opportunity in 2 ways. First, because surrogates may incorrectly predict patients' end‐of‐life treatment preferences in approximately one‐third of the cases,[25] patients may receive care that is inconsistent with their beliefs. Second, reliance on surrogate decision‐making may result in a greater burden on family members. Surrogate decision‐making places a large burden on surrogates, and can lead to emotional and psychological stress that can last well beyond the death of the loved one.[16, 26]
Our results reinforce the growing body of evidence suggesting that communication with the dying patient, both before and during the terminal hospitalization, promotes end‐of‐life care that involves less invasive life‐prolonging treatments,[10, 11, 12, 13, 14, 15] which is a consistently stated goal of most patients at the end of life.[1, 2] Our findings are consistent with a recent randomized trial of hospitalized patients over the age of 80 which showed that advance care planning discussions were associated with decreased use of intensive life‐sustaining treatments, increased patient and family satisfaction with care, as well as decreased psychological symptoms among family members.[27] In addition, studies examining patients with advanced cancer have shown that discussions about end‐of‐life care in the outpatient setting resulted in less intensive life‐sustaining treatments.[14, 15] Nearly 20% of our cohort was determined by the clinical team to lack decisional capacity at the time of their terminal hospitalization, highlighting the importance of end‐of‐life discussion prior to hospitalization. Our results also extend these recent findings to the inpatient setting. Seventy‐nine percent of patients in our study were determined to have decisional capacity at the time of their terminal hospitalization, and end‐of‐life discussion conducted with these patients was associated with decreased use of life‐sustaining treatments.
Seriously ill patients, particularly in hospital settings, have high symptom burden and subsequent poor quality of life.[6] These patients and families often report inadequate pain and symptom relief.[8, 28, 29] It is therefore reassuring that we found no difference in the proportion of patients who received comfort care and palliative morphine infusions according to whether they or a surrogate participated in the end‐of‐life discussions. In fact, the majority of patients were made DNR and received some form of comfort measure prior to death, although these comfort measures were frequently initiated only hours prior to death.
While our findings are consistent with research that has demonstrated that end‐of‐life discussions with patients are associated with a decrease in life‐prolonging treatments, it is important to note that our observational study cannot establish a causal relationship between the end‐of‐life discussion and the subsequent use of life‐sustaining treatments. It is possible that patients who have discussions about end‐of‐life care inherently prefer to have less intensive life‐sustaining treatment at the end of life. Physicians may be more apt to engage in these types of discussions with patients who express interest in limited intervention. Interestingly, patients with a DNR order at the time of admission were more likely to participate in end‐of‐life care with their provider during their terminal hospitalization, which supports this alternate explanation. However, when we excluded all patients with a DNR on admission, our findings persisted. Regardless of the explanation for the association between end‐of‐life discussions and life‐sustaining treatments, our study identifies a cohort of hospitalized patients who could benefit from improved end‐of‐life communication, and a clinical setting where opportunities remain to improve the quality of advanced care planning.
Discussions about end‐of‐life care with patients result in earlier transition to care focused on palliation.[14] Although we examined the timing to initiation of comfort care between those who participated and those who did not participate in end‐of‐life discussions, we were not able to demonstrate a statistically significant difference. However, our cohort may not be suitable for an examination of this type of intervention, as early discussions about end‐of‐life care may have lead to early referral to hospice, and therefore death outside the hospital setting, making the patients ineligible for our study.
There are several additional limitations to our study. First, our study is subject to the potential biases inherent in retrospective chart review. For example, since we identified patients who died in the hospital, our study does not generalize to patients with advanced cancer who survive the hospitalization or who were discharged to die at home.[30] Furthermore, our use of the medical record to assess documentation of communication about end‐of‐life care and decisional capacity relies on the accuracy of clinician documentation. There may have been communication about end‐of‐life care that was not documented in the medical record, resulting in underestimation of the effects of end‐of‐life discussions. In clinical practice, the assessment of decisional capacity can be challenging.[19, 31, 32] Although clinicians are often accurate in identifying patients with capacity, in nearly one‐quarter of all assessments, they mistakenly assign capacity to patients who lack decision‐making capacity.[17] In our study, we examine clinician assessment of the patient's decisional capacity, but cannot assess either the accuracy of their clinical assessment or the accuracy of their documentation of this assessment. A second limitation is that the chart abstraction was conducted by a single reviewer without inter‐rater assessment, although the abstraction tool was modified from a well‐established tool.[24] A third limitation is that all of the patients were from a single academic center and the results may not generalize to other regions. Fourth, we did not assess for the potential effect of individual clinicians. Since most patients were cared for by multiple physicians, our study is not capable of assessing a clinician‐level effect. Finally, our study was not able to address whether the care received by patients was in accord with their informed preferences.
We have shown that opportunities exist for advanced care planning at the time of the terminal hospitalization of patients with advanced cancer. The majority of these patients have documentation of decisional capacity at the time of admission, suggesting that opportunities exist to conduct end‐of‐life discussion while the patient retains decisional capacity. Furthermore, we found that patients who participate in these discussions about end‐of‐life care with their clinicians have an associated decrease in the use of life‐sustaining treatments, which is consistent with prior studies.[11, 13, 14, 15, 27] Improving communication about end‐of‐life care for patients hospitalized with advanced cancer may represent an important opportunity to improve the concordance between patients' wishes for care at the end‐of‐life and the care that these patients actually receive. Such communication may also decrease the burden on family members who are frequently asked to play the role of surrogate decision‐maker without an opportunity to discuss these issues with the patient.
Acknowledgments
The authors acknowledge Melissa Braxton for her assistance with the preparation of this manuscript.
Disclosures: A portion of this data was presented at the annual meeting of the Society of Hospital Medicine, 2011, in Grapevine, TX. This work was supported by the National Cancer Institute at the National Institutes of Health (KO5 CA 104699 to J.G.E.) and the National Heart, Lung, and Blood Institute (K24HL68593 to J.R.C.). Dr Silveira's salary was supported by core funds from the Ann Arbor VA HSRD Center of Excellence. The authors have no relevant financial interest in the subject matter contained within this manuscript.
- , , , . Treatment decisions for breast carcinoma: patient preferences and physician perceptions. Cancer. 2002;94(7):2076–2080.
- , , , . Dying trajectory in the last year of life: does cancer trajectory fit other diseases?J Palliat Med. 2001;4(4):457–464.
- , , , . Trends and Variation in End‐of‐Life Care for Medicare Beneficiaries with Severe Chronic Illness.The Dartmouth Institute for Health Policy 32(3):638–643.
- , , , , . The symptom burden of seriously ill hospitalized patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcome and Risks of Treatment. J Pain Symptom Manage. 1999;17(4):248–255.
- , , , . Family reports of pain in dying hospitalized patients: a structured telephone survey. West J Med. 2000;172(6):374–377.
- , , , et al. Perceptions by family members of the dying experience of older and seriously ill patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. Ann Intern Med. 1997;126(2):97–106.
- , , , , . Death in the hospital. Arch Intern Med. 1998;158(14):1570–1572.
- , , , , . End‐of‐life discussions, goal attainment, and distress at the end of life: predictors and outcomes of receipt of care consistent with preferences. J Clin Oncol. 2010;28(7):1203–1208.
- , , . Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211–1218.
- , , , et al. Family perspectives on end‐of‐life care at the last place of care. JAMA. 2004;291(1):88–93.
- , , , , . Association between advance directives and quality of end‐of‐life care: a national study. J Am Geriatr Soc. 2007;55(2):189–194.
- , , , et al. Associations between end‐of‐life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300(14):1665–1673.
- , , , et al. Health care costs in the last week of life: associations with end‐of‐life conversations. Arch Intern Med. 2009;169(5):480–488.
- , , , et al. End‐of‐life care discussions among patients with advanced cancer: a cohort study. Ann Intern Med. 2012;156(3):204–210.
- , , , et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross‐sectional study. Lancet. 2004;364(9443):1421–1427.
- , . Assessing patients' capacities to consent to treatment. N Engl J Med 1998;319:1635–1638.
- . Clinical practice. Assessment of patients' competence to consent to treatment. N Engl J Med. 2007;357(18):1834–1840.
- , , , . The physician‐surrogate relationship. Arch Intern Med. 2007;167(11):1117–1121.
- , , , , . Physicians' experience with surrogate decision making for hospitalized adults. J Gen Intern Med. 2009;24(9):1023–1028.
- , , , . The surrogate's experience in authorizing a do not resuscitate order. Palliat Support Care. 2008;6(1):13–19.
- , , , et al. Surveillance Epidemiology and End Results (SEER) Cancer Statistics Review 1975–2004. Bethesda, MD:National Cancer Institute. Based on November 2006 SEER data submission, posted to the SEER Web site,2007. Available at: http://seer.cancer.gov/csr/1975_2004/. Accessed on November 1, 2007.
- , , , , , . End‐of‐life decision‐making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999;17(1):6–15.
- , , . The accuracy of surrogate decision makers: a systematic review. Arch Intern Med. 2006;166(5):493–497.
- , . Systematic review: the effect on surrogates of making treatment decisions for others. Ann Intern Med. 2011;154(5):336–346.
- , , , . The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
- , , , et al. Dying with lung cancer or chronic obstructive pulmonary disease: insights from SUPPORT. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc. 2000;48(5 suppl):S146–S153.
- , , , . The use of life‐sustaining treatments in hospitalized persons aged 80 and older. J Am Geriatr Soc. 2002;50(5):930–934.
- , , . Resurrecting treatment histories of dead patients: a study design that should be laid to rest. JAMA. 2004;292(22):2765–2770.
- , , , et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14(1):27–34.
- , , . The MacCAT‐T: a clinical tool to assess patients' capacities to make treatment decisions. Psychiatr Serv. 1997;48(11):1415–1419.
Most patients prefer to die at home, pain free and without the use of life‐sustaining treatments[1, 2] yet the majority of patients with serious illness die in the hospital.[3, 4, 5] When hospitalized patient die, the care is frequently focused on life‐sustaining treatments[6]; pain, dyspnea, and agitation levels are higher when compared with patients who die in non‐hospital settings.[7, 8, 9] End‐of‐life discussions and their products (ie, advanced directives) can clarify treatment options with patients and family,[10] and help ensure that patients receive care consistent with their beliefs.[11, 12, 13] End‐of‐life discussions are associated with a decrease use of life‐sustaining treatments, improved quality of life, and reduced costs of care.[14, 15] For the majority of patients dying of cancer, the first end‐of‐life discussion takes place in the hospital setting.[16]
Conducting end‐of‐life conversations in the hospital setting can be challenging. Patients are acutely ill and nearly 40% are incapable of making their own medical decisions.[17] In order to participate in an end‐of‐life discussion, a physician must determine that a patient meets the 4 criteria of decisional capacity as outlined by Appelbaum and Grisso:[18] Does the patient (1) communicate a clear and consistent choice; (2) understand the relevant information surrounding that decision; (3) appreciate the consequences of that decision; and (4) communicate reasoning for that decision?[19] In practice, however, clinicians inaccurately assign capacity up to 25% of the time.[17] When a physician determines, accurately or inaccurately, that the patient does not meet this standard for decisional capacity, discussions must be held instead with a surrogate decision‐maker. Surrogate decision‐making can make communication with the physician more difficult,[20] delay important medical decisions,[21] and be stressful on the decision‐maker.[22] To our knowledge, no studies have examined patient and surrogate participation in end‐of‐life discussions at the time of terminal hospitalization and its association with end‐of‐life treatments received.
Our goals were to examine physician assessment of decisional capacity and the prevalence of end‐of‐life discussions during the terminal hospitalization of patients with advanced cancer. Our research questions were: (1) What proportion of patients were assessed to have decisional capacity by the clinical team at the time of their terminal hospital admission? (2) What proportion of these patients had a documented discussion about end‐of‐life care with the clinical team, and for what proportion was the conversation held instead by the patient's surrogate decision‐maker because the patient was considered to have lost decisional capacity? (3) Was patient participation in a discussion about end‐of‐life care associated with life‐sustaining and palliative treatments received?
METHODS
Design
This is a retrospective cohort study of consecutive adult patients with advanced cancer who died at the University of Michigan Hospital, Ann Arbor, MI, from January 1, 2004 through December 31, 2007. This study was exempted from review by the University of Michigan (UM) Institutional Review Board because decedent data were used.
Sample
The UM Cancer Registry is a database of all cancer patients treated at the UM Comprehensive Cancer Center. We used the Registry to identify patients who met the following criteria: (1) age 18 years at time of cancer diagnosis; (2) estimated probability of 5‐year survival 20% at time of diagnosis, as predicted by the SEER Cancer Statistics Review[23]; (3) the entirety of cancer treatment was received at University of Michigan Health System (UMHS); and (4) the patient died while admitted to the University Hospital between January 1, 2004 and December 31, 2007.
UMHS is a healthcare system and academic medical center consisting of hospitals, health centers, and clinics, including the University of Michigan Hospital and Comprehensive Cancer Center. Over 4000 cancer patients are admitted to University Hospital and 80,000 outpatient visits occur to the Cancer Center every year. It serves as a major cancer referral center for the patients of Michigan and the greater Midwest. The University of Michigan implemented a palliative care consult service that was started in 2005, during the time period of our study.
Data Collection
Data were abstracted by review of the medical record by an internist (M.Z.) using a comprehensive chart abstraction instrument based on a previously validated tool.[24] Demographic data abstracted from the medical record included age, religious affiliation, race, ethnicity, and marital status. The original abstraction tool, which included 83 items, was reduced to include 47 items focusing on information related to advanced care planning, hospital course, and end‐of‐life discussions. Specific items included: reasons for admission, primary hospital service, occurrence and timing of end‐of‐life decision‐making, whether patient or family preferences were elicited through an end‐of‐life discussion, clinician's assessment of patient's decisional capacity at time of admission and end‐of‐life conversations, whether a comfort care plan was made, and whether palliative morphine was used.
The chart abstraction tool was pilot tested on the medical records of 10 patients, who were not included in the study, and refined to improve completeness of data collection. A copy of the abstraction tool is available upon request.
Definition of Key Variables
Decisional Capacity Assessment
Decisional capacity assessment is a reflection of the clinical team's assessment of the patient's decisional capacity on admission, and was determined through examination of the medical record in the first 24 hours of admission. Positive decision‐making capacity assessment was assumed if the clinician assessment of decisional capacity was documented in the mental status exam, or if the clinician documented conversations between clinician and patient in the history that suggested intact decision‐making capacity (ie, clinician documented terms such as patient stated or patient described and then described a coherent or sensible statement which implied patient capacity and intact mental status), or if the clinician's documentation of the assessment and plan stated or suggested decisions were being made by the patient. Other supportive information from the record was used to corroborate the evidence used to determine the clinician's assessment of the patient's decisional capacity, including whether the patient signed consent forms.
End‐of‐Life Discussions
The presence of an end‐of‐life discussion was presumed when the clinician documented a discussion with the patient, discussion with family, or family meeting concerning treatment preferences, or when the clinician quoted the patient's preferences in a fashion that documents a face‐to‐face discussion or directly described the elicitation of preferences from the patient or family.
Living Will
A living will was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed a living will.
Health Care Proxy
Health Care Proxy or Durable Power of Attorney for Healthcare was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed such a document.
Do Not Resuscitate (DNR) on Admission
DNR status was identified as present if the patient had documents with established DNR orders, or if a physician explicitly documented code status as DNR in the admission note or other documents placed in the record within the first 24 hours of admission.
Intensive Care Unit (ICU)Treatment
Patients were defined as having received ICU treatment if they were admitted directly or subsequently transferred to the ICU during the hospital course.
Comfort Care
Comfort care was defined as present only if the phrases comfort care, palliative care, or supportive care, were documented.
Palliative Opioid Therapy
Treatments with morphine or other opioids were recorded as palliative only if it was explicitly stated that these medications were used in the context of palliative or end‐of‐life care.
Data Analysis
We report the proportion of patients who were documented to lack decisional capacity at the time of hospital admission. We compared patient characteristics for those with and without documentation of decisional capacity on admission, and patients with decisional capacity on admission who did and did not participate in discussions about end‐of‐life care using chi‐square tests for categorical data, t tests for normally distributed continuous variables, and MannWhitney U tests for non‐normally distributed continuous variables. We examined whether documentation of a discussion about end‐of‐life care was associated with life‐sustaining and palliative treatments received using chi‐square for categorical treatments, and MannWhitney U tests for days from admission to initiation of comfort care. We used P < 0.05 to signify statistical significance.
RESULTS
Characteristics of Population and Decisional Capacity on Admission
The characteristics of the 145 patients who met entry criteria are summarized in Table 1. The most common types of cancers were lung cancer and leukemia/lymphoma. Of the 145 patients, the medical team's assessment of the patient's decisional capacity on admission could be established for 142 patients. As documented within the first 24 hours of admission, 27 patients (19%) were considered not to have decisional capacity, and 115 patients (79%) were considered to have decisional capacity. Both of these groups had similar age and gender distributions. There were no significant differences in the distribution of cancer type between those with and without decisional capacity. In both groups, the majority of the cancer diagnoses were made prior to admission. There was no difference in DNR orders established prior to or on admission between the groups (Table 1).
| Decision‐Making Capacity on Admissiona | |||
|---|---|---|---|
| No (N = 27) | Yes (N = 115) | ||
| N (%) | N (%) | P Value | |
| |||
| Age >65 | 15 (55.6) | 60 (52.2) | 0.75 |
| Gender (male) | 14 (51.9) | 68 (59.1) | 0.46 |
| Cancer type | |||
| Lung | 12 (44.4) | 42 (36.5) | 0.67 |
| Bone marrow | 5 (18.5) | 35 (30.4) | |
| Liver | 3 (11.1) | 6 (5.2) | |
| Pancreas | 3 (11.1) | 7 (6.10) | |
| Esophagus | 1 (3.7) | 8 (7.0) | |
| Colon | 1 (3.7) | 6 (5.2) | |
| Otherb | 2 (7.4) | 11 (9.6) | |
| Prior to admission | |||
| Cancer diagnosis known | 23 (85.2) | 91 (79.1) | 0.48 |
| Living will completed | 6 (22.2) | 26 (22.6 | 0.97 |
| Health care proxy established | 3 (11.1) | 26 (22.6) | 0.18 |
| DNR established | 8 (29.6) | 27 (23.5) | 0.79 |
End‐of‐Life Discussion in Patients With Decisional Capacity on Admission
Of the 115 patients assessed to have intact decisional capacity on admission, 56 (48.7%) participated in an end‐of‐life discussion with the medical team during their terminal hospitalization. For the remaining 59 patients who did not participate in an end‐of‐life discussion during the terminal hospital course, 46 (40.0%) had documentation suggesting they lost decisional capacity prior to a conversation and that the end‐of‐life discussions were held instead with the patient's surrogate decision‐maker, and 13 (11.3%) had no evidence of any end‐of‐life discussion (with the patient or surrogate).
When comparing those patients who participated in an end‐of‐life discussion with those patients whose surrogate participated in the discussion, there were no significant differences in gender and age distributions (Table 2). There was a significant difference in the type of cancers between the 2 groups. Among patients who participated in their end‐of‐life discussions, bone marrow cancer was proportionately more prevalent (17.9% vs 2.2%; P <0.01) and lung cancer was less prevalent (16.1% vs 41.3%; P <0.01), when compared to those who required surrogate participation. Timing of cancer diagnosis and prevalence of advance directives were similar between the 2 groups. The proportion of patients who had an established DNR order prior to admission was higher among those who did participate in end‐of‐life discussions when compared to those who had surrogate participation in these discussions (30.4% vs 17.4%; P < 0.04).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | ||||
|---|---|---|---|---|
| N =13 | N = 102 | |||
| End‐of‐Life discussion not documented | End‐of‐Life discussion with surrogate (N = 46) | End‐of‐Life discussion with patient (N = 56) | ||
| N (%) | N (%) | N (%) | P Value | |
| ||||
| Age 65 | 9 (69.2) | 18 (39.1) | 27 (48.2) | 0.36 |
| Gender (male) | 10 (76.9) | 27 (60.0) | 31 (55.4) | 0.64 |
| Cancer type | ||||
| Lung | 3 (23.1) | 19 (41.3) | 9 (16.1) | |
| Bone marrow | 7 (53.9) | 1 (2.2) | 10 (17.9) | |
| Liver | 1 (7.7) | 3 (6.5) | 2 (3.6) | |
| Pancreas | 1 (7.7) | 2 (4.4) | 4 (7.1) | <0.01 |
| Esophagus | 0 | 6 (13.0) | 2 (3.6) | |
| Colon | 1 (7.7) | 1 (2.2) | 3 (5.4) | |
| Othera | 0 | 1 (2.2) | 10 (17.9) | |
| Prior to Admission | ||||
| Cancer diagnosis known | 10 (76.9) | 37 (80.4) | 43 (76.8) | 0.66 |
| Living will completed | 4 (30.8) | 10 (21.7) | 12 (21.4) | 0.97 |
| Health care proxy established | ||||
| 3 (23.1) | 13 (28.3) | 10 (17.9) | 0.21 | |
| DNR established | 2 (15.4) | 8 (17.4) | 17 (30.4) | 0.04 |
Life‐Prolonging and Palliative Care Treatments Received and Participation in End‐of‐Life Discussions
Life‐prolonging treatments were more likely to be used for patients whose end‐of‐life discussions were held by patient's surrogate decision‐maker, in comparison to those patients who participated in the discussions themselves. Patients who had conversations held by surrogates were more likely to receive ventilator support (56.5% vs 23.2%, P < 0.01), chemotherapy (39.1% vs 5.4%, P < 0.01), artificial nutrition or hydration (45.7% vs 25.0%, P = 0.03), and antibiotics (97.8% vs 78.6%, P < 0.01), when compared to patients who participated in their own end‐of‐life discussion. Intensive care treatment rates also differed significantly between the 2 groups; 56.5% of those who did not participate in end‐of‐life discussions, and only 23.2% of those patients who did participate, were admitted or transferred to the intensive care unit (P < 0.01). There was no significant difference in the proportion of patients who received cardiopulmonary resuscitation (CPR) (15.2% vs 7.1%, P = 0.56) (Table 3). Patients who lost decisional capacity and required a surrogate decision‐maker to participate in their end‐of‐life discussions had longer length of stay (15.8 vs 10.3 days, P = 0.03) and length of time to end‐of‐life discussions (14.0 vs 6.1 days, P < 0.01) (Table 3).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | |||
|---|---|---|---|
| End‐of‐Life Discussion With Surrogate (N =46) | End‐of‐Life Discussion With Patient (N = 56) | ||
| N (%) | N (%) | P Value | |
| |||
| Life‐Prolonging Treatment | |||
| Ventilatory support | 26 (56.5) | 13 (23.2) | <0.01 |
| Chemotherapy | 18 (39.1) | 3 (5.4) | <0.01 |
| Artificial nutrition or hydration | 21 (45.7) | 14 (25.0) | 0.03 |
| Antibiotics | 45 (97.8) | 44 (78.6) | <0.01 |
| Cardiopulmonary resuscitation | 7 (15.2) | 4 (7.1) | 0.19 |
| ICU treatment (admit or transfer) | 26 (56.5) | 13 (23.2) | <0.01 |
| Palliative Treatments | |||
| Comfort care | 39 (84.8) | 45 (80.4) | 0.56 |
| Palliative morphine drip | 24 (52.2) | 33 (57.1) | 0.62 |
| Mean (95% CI) [Range] | Mean (95% CI) [Range] | ||
| Timing of Advanced Care Planning | |||
| Length of hospitalization | 15.8 d (11.420.2) [157] | 10.3 d (146) [146] | 0.03 |
| Time to end‐of‐life discussion | 14.0 d (9.918.1) [055] | 6.1 d (3.88.4) [046] | <0.01 |
| Time to comfort care | 23.5 d (4.342.8) [1374] | 9.2 d (6.312.1) [046] | 0.12 |
A comparison of the proportion of patients receiving palliative treatments, such as palliative comfort care orders and morphine infusions, revealed no significant differences between those with and without a discussion about end‐of‐life care (Table 3). Furthermore, while the time interval from hospital admission to initiation of comfort care was shorter for those who did participate in end‐of‐life discussions compared with those had surrogate participation (9.3 vs 23.5 days, P = 0.13 for equality), this difference was not statistically significant (Table 3).
Since a higher proportion of those who participated in end‐of‐life discussions during the hospitalization were admitted with a DNR order established prior to or on admission, we also examined the use of life‐prolonging treatments in the subgroup of patients who did not have a DNR order prior to admission. The difference in life‐prolonging treatments between those who did and did not participate in end‐of‐life discussions was preserved among those patients who did not have DNR status on admission (data not shown).
DISCUSSION
In this retrospective study of 145 terminal cancer patients who died in the hospital, we found that half of the patients had documentation suggesting that they lost decisional capacity during hospitalization and did not participate in end‐of‐life discussion with their healthcare providers. Among cancer patients in our study, 19% were determined not to have decisional capacity on admission, and another 32% were determined to lose decisional capacity during the hospital course. When patients did participate in documented discussions about end‐of‐life care, they were less likely to receive intensive life‐sustaining treatments, less likely to be admitted or transferred to the ICU, and more likely to avoid prolonged hospitalization. The finding that the majority of cancer patients are assessed to have intact decisional capacity upon admission to their terminal hospitalization, but less than half of them participate in their own end‐of‐life conversation, suggests that there is an important lost opportunity to provide quality advanced care planning to hospitalized patients.
Advanced care planning is the act of defining a competent patient's wishes regarding their future healthcare in the event of loss of decisional capacity. For many of the patients who were determined to lose decisional capacity during their hospitalization in our study, a surrogate decision‐maker was involved in a subsequent end‐of‐life discussion. This represents a missed opportunity in 2 ways. First, because surrogates may incorrectly predict patients' end‐of‐life treatment preferences in approximately one‐third of the cases,[25] patients may receive care that is inconsistent with their beliefs. Second, reliance on surrogate decision‐making may result in a greater burden on family members. Surrogate decision‐making places a large burden on surrogates, and can lead to emotional and psychological stress that can last well beyond the death of the loved one.[16, 26]
Our results reinforce the growing body of evidence suggesting that communication with the dying patient, both before and during the terminal hospitalization, promotes end‐of‐life care that involves less invasive life‐prolonging treatments,[10, 11, 12, 13, 14, 15] which is a consistently stated goal of most patients at the end of life.[1, 2] Our findings are consistent with a recent randomized trial of hospitalized patients over the age of 80 which showed that advance care planning discussions were associated with decreased use of intensive life‐sustaining treatments, increased patient and family satisfaction with care, as well as decreased psychological symptoms among family members.[27] In addition, studies examining patients with advanced cancer have shown that discussions about end‐of‐life care in the outpatient setting resulted in less intensive life‐sustaining treatments.[14, 15] Nearly 20% of our cohort was determined by the clinical team to lack decisional capacity at the time of their terminal hospitalization, highlighting the importance of end‐of‐life discussion prior to hospitalization. Our results also extend these recent findings to the inpatient setting. Seventy‐nine percent of patients in our study were determined to have decisional capacity at the time of their terminal hospitalization, and end‐of‐life discussion conducted with these patients was associated with decreased use of life‐sustaining treatments.
Seriously ill patients, particularly in hospital settings, have high symptom burden and subsequent poor quality of life.[6] These patients and families often report inadequate pain and symptom relief.[8, 28, 29] It is therefore reassuring that we found no difference in the proportion of patients who received comfort care and palliative morphine infusions according to whether they or a surrogate participated in the end‐of‐life discussions. In fact, the majority of patients were made DNR and received some form of comfort measure prior to death, although these comfort measures were frequently initiated only hours prior to death.
While our findings are consistent with research that has demonstrated that end‐of‐life discussions with patients are associated with a decrease in life‐prolonging treatments, it is important to note that our observational study cannot establish a causal relationship between the end‐of‐life discussion and the subsequent use of life‐sustaining treatments. It is possible that patients who have discussions about end‐of‐life care inherently prefer to have less intensive life‐sustaining treatment at the end of life. Physicians may be more apt to engage in these types of discussions with patients who express interest in limited intervention. Interestingly, patients with a DNR order at the time of admission were more likely to participate in end‐of‐life care with their provider during their terminal hospitalization, which supports this alternate explanation. However, when we excluded all patients with a DNR on admission, our findings persisted. Regardless of the explanation for the association between end‐of‐life discussions and life‐sustaining treatments, our study identifies a cohort of hospitalized patients who could benefit from improved end‐of‐life communication, and a clinical setting where opportunities remain to improve the quality of advanced care planning.
Discussions about end‐of‐life care with patients result in earlier transition to care focused on palliation.[14] Although we examined the timing to initiation of comfort care between those who participated and those who did not participate in end‐of‐life discussions, we were not able to demonstrate a statistically significant difference. However, our cohort may not be suitable for an examination of this type of intervention, as early discussions about end‐of‐life care may have lead to early referral to hospice, and therefore death outside the hospital setting, making the patients ineligible for our study.
There are several additional limitations to our study. First, our study is subject to the potential biases inherent in retrospective chart review. For example, since we identified patients who died in the hospital, our study does not generalize to patients with advanced cancer who survive the hospitalization or who were discharged to die at home.[30] Furthermore, our use of the medical record to assess documentation of communication about end‐of‐life care and decisional capacity relies on the accuracy of clinician documentation. There may have been communication about end‐of‐life care that was not documented in the medical record, resulting in underestimation of the effects of end‐of‐life discussions. In clinical practice, the assessment of decisional capacity can be challenging.[19, 31, 32] Although clinicians are often accurate in identifying patients with capacity, in nearly one‐quarter of all assessments, they mistakenly assign capacity to patients who lack decision‐making capacity.[17] In our study, we examine clinician assessment of the patient's decisional capacity, but cannot assess either the accuracy of their clinical assessment or the accuracy of their documentation of this assessment. A second limitation is that the chart abstraction was conducted by a single reviewer without inter‐rater assessment, although the abstraction tool was modified from a well‐established tool.[24] A third limitation is that all of the patients were from a single academic center and the results may not generalize to other regions. Fourth, we did not assess for the potential effect of individual clinicians. Since most patients were cared for by multiple physicians, our study is not capable of assessing a clinician‐level effect. Finally, our study was not able to address whether the care received by patients was in accord with their informed preferences.
We have shown that opportunities exist for advanced care planning at the time of the terminal hospitalization of patients with advanced cancer. The majority of these patients have documentation of decisional capacity at the time of admission, suggesting that opportunities exist to conduct end‐of‐life discussion while the patient retains decisional capacity. Furthermore, we found that patients who participate in these discussions about end‐of‐life care with their clinicians have an associated decrease in the use of life‐sustaining treatments, which is consistent with prior studies.[11, 13, 14, 15, 27] Improving communication about end‐of‐life care for patients hospitalized with advanced cancer may represent an important opportunity to improve the concordance between patients' wishes for care at the end‐of‐life and the care that these patients actually receive. Such communication may also decrease the burden on family members who are frequently asked to play the role of surrogate decision‐maker without an opportunity to discuss these issues with the patient.
Acknowledgments
The authors acknowledge Melissa Braxton for her assistance with the preparation of this manuscript.
Disclosures: A portion of this data was presented at the annual meeting of the Society of Hospital Medicine, 2011, in Grapevine, TX. This work was supported by the National Cancer Institute at the National Institutes of Health (KO5 CA 104699 to J.G.E.) and the National Heart, Lung, and Blood Institute (K24HL68593 to J.R.C.). Dr Silveira's salary was supported by core funds from the Ann Arbor VA HSRD Center of Excellence. The authors have no relevant financial interest in the subject matter contained within this manuscript.
Most patients prefer to die at home, pain free and without the use of life‐sustaining treatments[1, 2] yet the majority of patients with serious illness die in the hospital.[3, 4, 5] When hospitalized patient die, the care is frequently focused on life‐sustaining treatments[6]; pain, dyspnea, and agitation levels are higher when compared with patients who die in non‐hospital settings.[7, 8, 9] End‐of‐life discussions and their products (ie, advanced directives) can clarify treatment options with patients and family,[10] and help ensure that patients receive care consistent with their beliefs.[11, 12, 13] End‐of‐life discussions are associated with a decrease use of life‐sustaining treatments, improved quality of life, and reduced costs of care.[14, 15] For the majority of patients dying of cancer, the first end‐of‐life discussion takes place in the hospital setting.[16]
Conducting end‐of‐life conversations in the hospital setting can be challenging. Patients are acutely ill and nearly 40% are incapable of making their own medical decisions.[17] In order to participate in an end‐of‐life discussion, a physician must determine that a patient meets the 4 criteria of decisional capacity as outlined by Appelbaum and Grisso:[18] Does the patient (1) communicate a clear and consistent choice; (2) understand the relevant information surrounding that decision; (3) appreciate the consequences of that decision; and (4) communicate reasoning for that decision?[19] In practice, however, clinicians inaccurately assign capacity up to 25% of the time.[17] When a physician determines, accurately or inaccurately, that the patient does not meet this standard for decisional capacity, discussions must be held instead with a surrogate decision‐maker. Surrogate decision‐making can make communication with the physician more difficult,[20] delay important medical decisions,[21] and be stressful on the decision‐maker.[22] To our knowledge, no studies have examined patient and surrogate participation in end‐of‐life discussions at the time of terminal hospitalization and its association with end‐of‐life treatments received.
Our goals were to examine physician assessment of decisional capacity and the prevalence of end‐of‐life discussions during the terminal hospitalization of patients with advanced cancer. Our research questions were: (1) What proportion of patients were assessed to have decisional capacity by the clinical team at the time of their terminal hospital admission? (2) What proportion of these patients had a documented discussion about end‐of‐life care with the clinical team, and for what proportion was the conversation held instead by the patient's surrogate decision‐maker because the patient was considered to have lost decisional capacity? (3) Was patient participation in a discussion about end‐of‐life care associated with life‐sustaining and palliative treatments received?
METHODS
Design
This is a retrospective cohort study of consecutive adult patients with advanced cancer who died at the University of Michigan Hospital, Ann Arbor, MI, from January 1, 2004 through December 31, 2007. This study was exempted from review by the University of Michigan (UM) Institutional Review Board because decedent data were used.
Sample
The UM Cancer Registry is a database of all cancer patients treated at the UM Comprehensive Cancer Center. We used the Registry to identify patients who met the following criteria: (1) age 18 years at time of cancer diagnosis; (2) estimated probability of 5‐year survival 20% at time of diagnosis, as predicted by the SEER Cancer Statistics Review[23]; (3) the entirety of cancer treatment was received at University of Michigan Health System (UMHS); and (4) the patient died while admitted to the University Hospital between January 1, 2004 and December 31, 2007.
UMHS is a healthcare system and academic medical center consisting of hospitals, health centers, and clinics, including the University of Michigan Hospital and Comprehensive Cancer Center. Over 4000 cancer patients are admitted to University Hospital and 80,000 outpatient visits occur to the Cancer Center every year. It serves as a major cancer referral center for the patients of Michigan and the greater Midwest. The University of Michigan implemented a palliative care consult service that was started in 2005, during the time period of our study.
Data Collection
Data were abstracted by review of the medical record by an internist (M.Z.) using a comprehensive chart abstraction instrument based on a previously validated tool.[24] Demographic data abstracted from the medical record included age, religious affiliation, race, ethnicity, and marital status. The original abstraction tool, which included 83 items, was reduced to include 47 items focusing on information related to advanced care planning, hospital course, and end‐of‐life discussions. Specific items included: reasons for admission, primary hospital service, occurrence and timing of end‐of‐life decision‐making, whether patient or family preferences were elicited through an end‐of‐life discussion, clinician's assessment of patient's decisional capacity at time of admission and end‐of‐life conversations, whether a comfort care plan was made, and whether palliative morphine was used.
The chart abstraction tool was pilot tested on the medical records of 10 patients, who were not included in the study, and refined to improve completeness of data collection. A copy of the abstraction tool is available upon request.
Definition of Key Variables
Decisional Capacity Assessment
Decisional capacity assessment is a reflection of the clinical team's assessment of the patient's decisional capacity on admission, and was determined through examination of the medical record in the first 24 hours of admission. Positive decision‐making capacity assessment was assumed if the clinician assessment of decisional capacity was documented in the mental status exam, or if the clinician documented conversations between clinician and patient in the history that suggested intact decision‐making capacity (ie, clinician documented terms such as patient stated or patient described and then described a coherent or sensible statement which implied patient capacity and intact mental status), or if the clinician's documentation of the assessment and plan stated or suggested decisions were being made by the patient. Other supportive information from the record was used to corroborate the evidence used to determine the clinician's assessment of the patient's decisional capacity, including whether the patient signed consent forms.
End‐of‐Life Discussions
The presence of an end‐of‐life discussion was presumed when the clinician documented a discussion with the patient, discussion with family, or family meeting concerning treatment preferences, or when the clinician quoted the patient's preferences in a fashion that documents a face‐to‐face discussion or directly described the elicitation of preferences from the patient or family.
Living Will
A living will was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed a living will.
Health Care Proxy
Health Care Proxy or Durable Power of Attorney for Healthcare was identified as present if the document was scanned into the patient's medical record, or if the chart indicated that the patient or family stated that the patient had completed such a document.
Do Not Resuscitate (DNR) on Admission
DNR status was identified as present if the patient had documents with established DNR orders, or if a physician explicitly documented code status as DNR in the admission note or other documents placed in the record within the first 24 hours of admission.
Intensive Care Unit (ICU)Treatment
Patients were defined as having received ICU treatment if they were admitted directly or subsequently transferred to the ICU during the hospital course.
Comfort Care
Comfort care was defined as present only if the phrases comfort care, palliative care, or supportive care, were documented.
Palliative Opioid Therapy
Treatments with morphine or other opioids were recorded as palliative only if it was explicitly stated that these medications were used in the context of palliative or end‐of‐life care.
Data Analysis
We report the proportion of patients who were documented to lack decisional capacity at the time of hospital admission. We compared patient characteristics for those with and without documentation of decisional capacity on admission, and patients with decisional capacity on admission who did and did not participate in discussions about end‐of‐life care using chi‐square tests for categorical data, t tests for normally distributed continuous variables, and MannWhitney U tests for non‐normally distributed continuous variables. We examined whether documentation of a discussion about end‐of‐life care was associated with life‐sustaining and palliative treatments received using chi‐square for categorical treatments, and MannWhitney U tests for days from admission to initiation of comfort care. We used P < 0.05 to signify statistical significance.
RESULTS
Characteristics of Population and Decisional Capacity on Admission
The characteristics of the 145 patients who met entry criteria are summarized in Table 1. The most common types of cancers were lung cancer and leukemia/lymphoma. Of the 145 patients, the medical team's assessment of the patient's decisional capacity on admission could be established for 142 patients. As documented within the first 24 hours of admission, 27 patients (19%) were considered not to have decisional capacity, and 115 patients (79%) were considered to have decisional capacity. Both of these groups had similar age and gender distributions. There were no significant differences in the distribution of cancer type between those with and without decisional capacity. In both groups, the majority of the cancer diagnoses were made prior to admission. There was no difference in DNR orders established prior to or on admission between the groups (Table 1).
| Decision‐Making Capacity on Admissiona | |||
|---|---|---|---|
| No (N = 27) | Yes (N = 115) | ||
| N (%) | N (%) | P Value | |
| |||
| Age >65 | 15 (55.6) | 60 (52.2) | 0.75 |
| Gender (male) | 14 (51.9) | 68 (59.1) | 0.46 |
| Cancer type | |||
| Lung | 12 (44.4) | 42 (36.5) | 0.67 |
| Bone marrow | 5 (18.5) | 35 (30.4) | |
| Liver | 3 (11.1) | 6 (5.2) | |
| Pancreas | 3 (11.1) | 7 (6.10) | |
| Esophagus | 1 (3.7) | 8 (7.0) | |
| Colon | 1 (3.7) | 6 (5.2) | |
| Otherb | 2 (7.4) | 11 (9.6) | |
| Prior to admission | |||
| Cancer diagnosis known | 23 (85.2) | 91 (79.1) | 0.48 |
| Living will completed | 6 (22.2) | 26 (22.6 | 0.97 |
| Health care proxy established | 3 (11.1) | 26 (22.6) | 0.18 |
| DNR established | 8 (29.6) | 27 (23.5) | 0.79 |
End‐of‐Life Discussion in Patients With Decisional Capacity on Admission
Of the 115 patients assessed to have intact decisional capacity on admission, 56 (48.7%) participated in an end‐of‐life discussion with the medical team during their terminal hospitalization. For the remaining 59 patients who did not participate in an end‐of‐life discussion during the terminal hospital course, 46 (40.0%) had documentation suggesting they lost decisional capacity prior to a conversation and that the end‐of‐life discussions were held instead with the patient's surrogate decision‐maker, and 13 (11.3%) had no evidence of any end‐of‐life discussion (with the patient or surrogate).
When comparing those patients who participated in an end‐of‐life discussion with those patients whose surrogate participated in the discussion, there were no significant differences in gender and age distributions (Table 2). There was a significant difference in the type of cancers between the 2 groups. Among patients who participated in their end‐of‐life discussions, bone marrow cancer was proportionately more prevalent (17.9% vs 2.2%; P <0.01) and lung cancer was less prevalent (16.1% vs 41.3%; P <0.01), when compared to those who required surrogate participation. Timing of cancer diagnosis and prevalence of advance directives were similar between the 2 groups. The proportion of patients who had an established DNR order prior to admission was higher among those who did participate in end‐of‐life discussions when compared to those who had surrogate participation in these discussions (30.4% vs 17.4%; P < 0.04).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | ||||
|---|---|---|---|---|
| N =13 | N = 102 | |||
| End‐of‐Life discussion not documented | End‐of‐Life discussion with surrogate (N = 46) | End‐of‐Life discussion with patient (N = 56) | ||
| N (%) | N (%) | N (%) | P Value | |
| ||||
| Age 65 | 9 (69.2) | 18 (39.1) | 27 (48.2) | 0.36 |
| Gender (male) | 10 (76.9) | 27 (60.0) | 31 (55.4) | 0.64 |
| Cancer type | ||||
| Lung | 3 (23.1) | 19 (41.3) | 9 (16.1) | |
| Bone marrow | 7 (53.9) | 1 (2.2) | 10 (17.9) | |
| Liver | 1 (7.7) | 3 (6.5) | 2 (3.6) | |
| Pancreas | 1 (7.7) | 2 (4.4) | 4 (7.1) | <0.01 |
| Esophagus | 0 | 6 (13.0) | 2 (3.6) | |
| Colon | 1 (7.7) | 1 (2.2) | 3 (5.4) | |
| Othera | 0 | 1 (2.2) | 10 (17.9) | |
| Prior to Admission | ||||
| Cancer diagnosis known | 10 (76.9) | 37 (80.4) | 43 (76.8) | 0.66 |
| Living will completed | 4 (30.8) | 10 (21.7) | 12 (21.4) | 0.97 |
| Health care proxy established | ||||
| 3 (23.1) | 13 (28.3) | 10 (17.9) | 0.21 | |
| DNR established | 2 (15.4) | 8 (17.4) | 17 (30.4) | 0.04 |
Life‐Prolonging and Palliative Care Treatments Received and Participation in End‐of‐Life Discussions
Life‐prolonging treatments were more likely to be used for patients whose end‐of‐life discussions were held by patient's surrogate decision‐maker, in comparison to those patients who participated in the discussions themselves. Patients who had conversations held by surrogates were more likely to receive ventilator support (56.5% vs 23.2%, P < 0.01), chemotherapy (39.1% vs 5.4%, P < 0.01), artificial nutrition or hydration (45.7% vs 25.0%, P = 0.03), and antibiotics (97.8% vs 78.6%, P < 0.01), when compared to patients who participated in their own end‐of‐life discussion. Intensive care treatment rates also differed significantly between the 2 groups; 56.5% of those who did not participate in end‐of‐life discussions, and only 23.2% of those patients who did participate, were admitted or transferred to the intensive care unit (P < 0.01). There was no significant difference in the proportion of patients who received cardiopulmonary resuscitation (CPR) (15.2% vs 7.1%, P = 0.56) (Table 3). Patients who lost decisional capacity and required a surrogate decision‐maker to participate in their end‐of‐life discussions had longer length of stay (15.8 vs 10.3 days, P = 0.03) and length of time to end‐of‐life discussions (14.0 vs 6.1 days, P < 0.01) (Table 3).
| Patients With Documented Decision‐Making Capacity on Admission (N = 115) | |||
|---|---|---|---|
| End‐of‐Life Discussion With Surrogate (N =46) | End‐of‐Life Discussion With Patient (N = 56) | ||
| N (%) | N (%) | P Value | |
| |||
| Life‐Prolonging Treatment | |||
| Ventilatory support | 26 (56.5) | 13 (23.2) | <0.01 |
| Chemotherapy | 18 (39.1) | 3 (5.4) | <0.01 |
| Artificial nutrition or hydration | 21 (45.7) | 14 (25.0) | 0.03 |
| Antibiotics | 45 (97.8) | 44 (78.6) | <0.01 |
| Cardiopulmonary resuscitation | 7 (15.2) | 4 (7.1) | 0.19 |
| ICU treatment (admit or transfer) | 26 (56.5) | 13 (23.2) | <0.01 |
| Palliative Treatments | |||
| Comfort care | 39 (84.8) | 45 (80.4) | 0.56 |
| Palliative morphine drip | 24 (52.2) | 33 (57.1) | 0.62 |
| Mean (95% CI) [Range] | Mean (95% CI) [Range] | ||
| Timing of Advanced Care Planning | |||
| Length of hospitalization | 15.8 d (11.420.2) [157] | 10.3 d (146) [146] | 0.03 |
| Time to end‐of‐life discussion | 14.0 d (9.918.1) [055] | 6.1 d (3.88.4) [046] | <0.01 |
| Time to comfort care | 23.5 d (4.342.8) [1374] | 9.2 d (6.312.1) [046] | 0.12 |
A comparison of the proportion of patients receiving palliative treatments, such as palliative comfort care orders and morphine infusions, revealed no significant differences between those with and without a discussion about end‐of‐life care (Table 3). Furthermore, while the time interval from hospital admission to initiation of comfort care was shorter for those who did participate in end‐of‐life discussions compared with those had surrogate participation (9.3 vs 23.5 days, P = 0.13 for equality), this difference was not statistically significant (Table 3).
Since a higher proportion of those who participated in end‐of‐life discussions during the hospitalization were admitted with a DNR order established prior to or on admission, we also examined the use of life‐prolonging treatments in the subgroup of patients who did not have a DNR order prior to admission. The difference in life‐prolonging treatments between those who did and did not participate in end‐of‐life discussions was preserved among those patients who did not have DNR status on admission (data not shown).
DISCUSSION
In this retrospective study of 145 terminal cancer patients who died in the hospital, we found that half of the patients had documentation suggesting that they lost decisional capacity during hospitalization and did not participate in end‐of‐life discussion with their healthcare providers. Among cancer patients in our study, 19% were determined not to have decisional capacity on admission, and another 32% were determined to lose decisional capacity during the hospital course. When patients did participate in documented discussions about end‐of‐life care, they were less likely to receive intensive life‐sustaining treatments, less likely to be admitted or transferred to the ICU, and more likely to avoid prolonged hospitalization. The finding that the majority of cancer patients are assessed to have intact decisional capacity upon admission to their terminal hospitalization, but less than half of them participate in their own end‐of‐life conversation, suggests that there is an important lost opportunity to provide quality advanced care planning to hospitalized patients.
Advanced care planning is the act of defining a competent patient's wishes regarding their future healthcare in the event of loss of decisional capacity. For many of the patients who were determined to lose decisional capacity during their hospitalization in our study, a surrogate decision‐maker was involved in a subsequent end‐of‐life discussion. This represents a missed opportunity in 2 ways. First, because surrogates may incorrectly predict patients' end‐of‐life treatment preferences in approximately one‐third of the cases,[25] patients may receive care that is inconsistent with their beliefs. Second, reliance on surrogate decision‐making may result in a greater burden on family members. Surrogate decision‐making places a large burden on surrogates, and can lead to emotional and psychological stress that can last well beyond the death of the loved one.[16, 26]
Our results reinforce the growing body of evidence suggesting that communication with the dying patient, both before and during the terminal hospitalization, promotes end‐of‐life care that involves less invasive life‐prolonging treatments,[10, 11, 12, 13, 14, 15] which is a consistently stated goal of most patients at the end of life.[1, 2] Our findings are consistent with a recent randomized trial of hospitalized patients over the age of 80 which showed that advance care planning discussions were associated with decreased use of intensive life‐sustaining treatments, increased patient and family satisfaction with care, as well as decreased psychological symptoms among family members.[27] In addition, studies examining patients with advanced cancer have shown that discussions about end‐of‐life care in the outpatient setting resulted in less intensive life‐sustaining treatments.[14, 15] Nearly 20% of our cohort was determined by the clinical team to lack decisional capacity at the time of their terminal hospitalization, highlighting the importance of end‐of‐life discussion prior to hospitalization. Our results also extend these recent findings to the inpatient setting. Seventy‐nine percent of patients in our study were determined to have decisional capacity at the time of their terminal hospitalization, and end‐of‐life discussion conducted with these patients was associated with decreased use of life‐sustaining treatments.
Seriously ill patients, particularly in hospital settings, have high symptom burden and subsequent poor quality of life.[6] These patients and families often report inadequate pain and symptom relief.[8, 28, 29] It is therefore reassuring that we found no difference in the proportion of patients who received comfort care and palliative morphine infusions according to whether they or a surrogate participated in the end‐of‐life discussions. In fact, the majority of patients were made DNR and received some form of comfort measure prior to death, although these comfort measures were frequently initiated only hours prior to death.
While our findings are consistent with research that has demonstrated that end‐of‐life discussions with patients are associated with a decrease in life‐prolonging treatments, it is important to note that our observational study cannot establish a causal relationship between the end‐of‐life discussion and the subsequent use of life‐sustaining treatments. It is possible that patients who have discussions about end‐of‐life care inherently prefer to have less intensive life‐sustaining treatment at the end of life. Physicians may be more apt to engage in these types of discussions with patients who express interest in limited intervention. Interestingly, patients with a DNR order at the time of admission were more likely to participate in end‐of‐life care with their provider during their terminal hospitalization, which supports this alternate explanation. However, when we excluded all patients with a DNR on admission, our findings persisted. Regardless of the explanation for the association between end‐of‐life discussions and life‐sustaining treatments, our study identifies a cohort of hospitalized patients who could benefit from improved end‐of‐life communication, and a clinical setting where opportunities remain to improve the quality of advanced care planning.
Discussions about end‐of‐life care with patients result in earlier transition to care focused on palliation.[14] Although we examined the timing to initiation of comfort care between those who participated and those who did not participate in end‐of‐life discussions, we were not able to demonstrate a statistically significant difference. However, our cohort may not be suitable for an examination of this type of intervention, as early discussions about end‐of‐life care may have lead to early referral to hospice, and therefore death outside the hospital setting, making the patients ineligible for our study.
There are several additional limitations to our study. First, our study is subject to the potential biases inherent in retrospective chart review. For example, since we identified patients who died in the hospital, our study does not generalize to patients with advanced cancer who survive the hospitalization or who were discharged to die at home.[30] Furthermore, our use of the medical record to assess documentation of communication about end‐of‐life care and decisional capacity relies on the accuracy of clinician documentation. There may have been communication about end‐of‐life care that was not documented in the medical record, resulting in underestimation of the effects of end‐of‐life discussions. In clinical practice, the assessment of decisional capacity can be challenging.[19, 31, 32] Although clinicians are often accurate in identifying patients with capacity, in nearly one‐quarter of all assessments, they mistakenly assign capacity to patients who lack decision‐making capacity.[17] In our study, we examine clinician assessment of the patient's decisional capacity, but cannot assess either the accuracy of their clinical assessment or the accuracy of their documentation of this assessment. A second limitation is that the chart abstraction was conducted by a single reviewer without inter‐rater assessment, although the abstraction tool was modified from a well‐established tool.[24] A third limitation is that all of the patients were from a single academic center and the results may not generalize to other regions. Fourth, we did not assess for the potential effect of individual clinicians. Since most patients were cared for by multiple physicians, our study is not capable of assessing a clinician‐level effect. Finally, our study was not able to address whether the care received by patients was in accord with their informed preferences.
We have shown that opportunities exist for advanced care planning at the time of the terminal hospitalization of patients with advanced cancer. The majority of these patients have documentation of decisional capacity at the time of admission, suggesting that opportunities exist to conduct end‐of‐life discussion while the patient retains decisional capacity. Furthermore, we found that patients who participate in these discussions about end‐of‐life care with their clinicians have an associated decrease in the use of life‐sustaining treatments, which is consistent with prior studies.[11, 13, 14, 15, 27] Improving communication about end‐of‐life care for patients hospitalized with advanced cancer may represent an important opportunity to improve the concordance between patients' wishes for care at the end‐of‐life and the care that these patients actually receive. Such communication may also decrease the burden on family members who are frequently asked to play the role of surrogate decision‐maker without an opportunity to discuss these issues with the patient.
Acknowledgments
The authors acknowledge Melissa Braxton for her assistance with the preparation of this manuscript.
Disclosures: A portion of this data was presented at the annual meeting of the Society of Hospital Medicine, 2011, in Grapevine, TX. This work was supported by the National Cancer Institute at the National Institutes of Health (KO5 CA 104699 to J.G.E.) and the National Heart, Lung, and Blood Institute (K24HL68593 to J.R.C.). Dr Silveira's salary was supported by core funds from the Ann Arbor VA HSRD Center of Excellence. The authors have no relevant financial interest in the subject matter contained within this manuscript.
- , , , . Treatment decisions for breast carcinoma: patient preferences and physician perceptions. Cancer. 2002;94(7):2076–2080.
- , , , . Dying trajectory in the last year of life: does cancer trajectory fit other diseases?J Palliat Med. 2001;4(4):457–464.
- , , , . Trends and Variation in End‐of‐Life Care for Medicare Beneficiaries with Severe Chronic Illness.The Dartmouth Institute for Health Policy 32(3):638–643.
- , , , , . The symptom burden of seriously ill hospitalized patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcome and Risks of Treatment. J Pain Symptom Manage. 1999;17(4):248–255.
- , , , . Family reports of pain in dying hospitalized patients: a structured telephone survey. West J Med. 2000;172(6):374–377.
- , , , et al. Perceptions by family members of the dying experience of older and seriously ill patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. Ann Intern Med. 1997;126(2):97–106.
- , , , , . Death in the hospital. Arch Intern Med. 1998;158(14):1570–1572.
- , , , , . End‐of‐life discussions, goal attainment, and distress at the end of life: predictors and outcomes of receipt of care consistent with preferences. J Clin Oncol. 2010;28(7):1203–1208.
- , , . Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211–1218.
- , , , et al. Family perspectives on end‐of‐life care at the last place of care. JAMA. 2004;291(1):88–93.
- , , , , . Association between advance directives and quality of end‐of‐life care: a national study. J Am Geriatr Soc. 2007;55(2):189–194.
- , , , et al. Associations between end‐of‐life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300(14):1665–1673.
- , , , et al. Health care costs in the last week of life: associations with end‐of‐life conversations. Arch Intern Med. 2009;169(5):480–488.
- , , , et al. End‐of‐life care discussions among patients with advanced cancer: a cohort study. Ann Intern Med. 2012;156(3):204–210.
- , , , et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross‐sectional study. Lancet. 2004;364(9443):1421–1427.
- , . Assessing patients' capacities to consent to treatment. N Engl J Med 1998;319:1635–1638.
- . Clinical practice. Assessment of patients' competence to consent to treatment. N Engl J Med. 2007;357(18):1834–1840.
- , , , . The physician‐surrogate relationship. Arch Intern Med. 2007;167(11):1117–1121.
- , , , , . Physicians' experience with surrogate decision making for hospitalized adults. J Gen Intern Med. 2009;24(9):1023–1028.
- , , , . The surrogate's experience in authorizing a do not resuscitate order. Palliat Support Care. 2008;6(1):13–19.
- , , , et al. Surveillance Epidemiology and End Results (SEER) Cancer Statistics Review 1975–2004. Bethesda, MD:National Cancer Institute. Based on November 2006 SEER data submission, posted to the SEER Web site,2007. Available at: http://seer.cancer.gov/csr/1975_2004/. Accessed on November 1, 2007.
- , , , , , . End‐of‐life decision‐making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999;17(1):6–15.
- , , . The accuracy of surrogate decision makers: a systematic review. Arch Intern Med. 2006;166(5):493–497.
- , . Systematic review: the effect on surrogates of making treatment decisions for others. Ann Intern Med. 2011;154(5):336–346.
- , , , . The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
- , , , et al. Dying with lung cancer or chronic obstructive pulmonary disease: insights from SUPPORT. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc. 2000;48(5 suppl):S146–S153.
- , , , . The use of life‐sustaining treatments in hospitalized persons aged 80 and older. J Am Geriatr Soc. 2002;50(5):930–934.
- , , . Resurrecting treatment histories of dead patients: a study design that should be laid to rest. JAMA. 2004;292(22):2765–2770.
- , , , et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14(1):27–34.
- , , . The MacCAT‐T: a clinical tool to assess patients' capacities to make treatment decisions. Psychiatr Serv. 1997;48(11):1415–1419.
- , , , . Treatment decisions for breast carcinoma: patient preferences and physician perceptions. Cancer. 2002;94(7):2076–2080.
- , , , . Dying trajectory in the last year of life: does cancer trajectory fit other diseases?J Palliat Med. 2001;4(4):457–464.
- , , , . Trends and Variation in End‐of‐Life Care for Medicare Beneficiaries with Severe Chronic Illness.The Dartmouth Institute for Health Policy 32(3):638–643.
- , , , , . The symptom burden of seriously ill hospitalized patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcome and Risks of Treatment. J Pain Symptom Manage. 1999;17(4):248–255.
- , , , . Family reports of pain in dying hospitalized patients: a structured telephone survey. West J Med. 2000;172(6):374–377.
- , , , et al. Perceptions by family members of the dying experience of older and seriously ill patients. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. Ann Intern Med. 1997;126(2):97–106.
- , , , , . Death in the hospital. Arch Intern Med. 1998;158(14):1570–1572.
- , , , , . End‐of‐life discussions, goal attainment, and distress at the end of life: predictors and outcomes of receipt of care consistent with preferences. J Clin Oncol. 2010;28(7):1203–1208.
- , , . Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211–1218.
- , , , et al. Family perspectives on end‐of‐life care at the last place of care. JAMA. 2004;291(1):88–93.
- , , , , . Association between advance directives and quality of end‐of‐life care: a national study. J Am Geriatr Soc. 2007;55(2):189–194.
- , , , et al. Associations between end‐of‐life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300(14):1665–1673.
- , , , et al. Health care costs in the last week of life: associations with end‐of‐life conversations. Arch Intern Med. 2009;169(5):480–488.
- , , , et al. End‐of‐life care discussions among patients with advanced cancer: a cohort study. Ann Intern Med. 2012;156(3):204–210.
- , , , et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross‐sectional study. Lancet. 2004;364(9443):1421–1427.
- , . Assessing patients' capacities to consent to treatment. N Engl J Med 1998;319:1635–1638.
- . Clinical practice. Assessment of patients' competence to consent to treatment. N Engl J Med. 2007;357(18):1834–1840.
- , , , . The physician‐surrogate relationship. Arch Intern Med. 2007;167(11):1117–1121.
- , , , , . Physicians' experience with surrogate decision making for hospitalized adults. J Gen Intern Med. 2009;24(9):1023–1028.
- , , , . The surrogate's experience in authorizing a do not resuscitate order. Palliat Support Care. 2008;6(1):13–19.
- , , , et al. Surveillance Epidemiology and End Results (SEER) Cancer Statistics Review 1975–2004. Bethesda, MD:National Cancer Institute. Based on November 2006 SEER data submission, posted to the SEER Web site,2007. Available at: http://seer.cancer.gov/csr/1975_2004/. Accessed on November 1, 2007.
- , , , , , . End‐of‐life decision‐making in the hospital: current practice and future prospects. J Pain Symptom Manage. 1999;17(1):6–15.
- , , . The accuracy of surrogate decision makers: a systematic review. Arch Intern Med. 2006;166(5):493–497.
- , . Systematic review: the effect on surrogates of making treatment decisions for others. Ann Intern Med. 2011;154(5):336–346.
- , , , . The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
- , , , et al. Dying with lung cancer or chronic obstructive pulmonary disease: insights from SUPPORT. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc. 2000;48(5 suppl):S146–S153.
- , , , . The use of life‐sustaining treatments in hospitalized persons aged 80 and older. J Am Geriatr Soc. 2002;50(5):930–934.
- , , . Resurrecting treatment histories of dead patients: a study design that should be laid to rest. JAMA. 2004;292(22):2765–2770.
- , , , et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14(1):27–34.
- , , . The MacCAT‐T: a clinical tool to assess patients' capacities to make treatment decisions. Psychiatr Serv. 1997;48(11):1415–1419.
Copyright © 2012 Society of Hospital Medicine
Hospitalist‐Job Fit
Person‐organization fit concerns the conditions and consequences of compatibility between people and the organizations for which they work.[1] Studies of other industries have demonstrated that person‐organization fit informs the way individuals join, perform in, and are retained by organizations.[2] Person‐job fit is a closely related subordinate concept that concerns the alignment of workers and their job in as much as workers have needs that their job supplies, or conversely, jobs have requirements that certain workers' abilities can help meet.[3] Explorations of job fit in physicians and their work have recently emerged in a few investigations published in medical journals.[4, 5, 6, 7, 8] Further expanding the understanding of fit between physicians and their employment is important, because the decline of solo practices and recent emphasis on team‐based care have led to a growing number of US physicians working in organizations.[9]
The movement of physicians into employed situations may continue if certain types of Accountable Care Organizations take root.[10] And physicians may be primed to join employer organizations based on current career priorities of individuals in American society. Surveys of medical residents entering the workforce reveal more physicians preferring the security of being employees than starting their own practices.[11] Given these trends, job fit will inform our understanding of how personal and job characteristics facilitate recruitment, performance, satisfaction, and longevity of physician employees.
BACKGROUND
Virtually all hospitalists work in organizationshospitalsand are employees of hospitals, medical schools, physician group practices, or management companies, and therefore invariably function within organizational structures and systems.[7] In spite of their rapid growth in numbers, many employers have faced difficulties recruiting and retaining enough hospitalists to fill their staffing needs. Consequently, the US hospitalist workforce today is characterized by high salaries, work load, and attrition rates.[12]
In this evolving unsaturated market, the attraction‐selection‐attrition framework[13] provides a theoretical construct that predicts that hospitalists and their employers would seek congruence of goals and values early in their relationship through a process of trial and error. This framework assumes that early interactions between workers and organizations serve as opportunities for them to understand if job fit is poor and dissociate or remain affiliated as long as job fit is mutually acceptable. Therefore, job switching on average is expected to increase job fit because workers and organizations gain a better understanding of their own goals and values and choose more wisely the next time.
Other theoretical frameworks, such as the job characteristic model,[14] suggest that over time as workers stay at the same job, they continue to maintain and improve job fit through various workplace‐ or self‐modification strategies. For example, seniority status may have privileges (eg, less undesirable call), or workers may create privileged niches through the acquisition of new skills and abilities over time. Hospitalists' tendency to diversify their work‐related activities by incorporating administrative and teaching responsibilities[15] may thus contribute to improving job fit. Additionally, as a measure of complementarity among people who work together, job fit may be influenced by the quality of relationships among hospitalists and their coworkers through their reorientation to the prevailing organizational climate[16, 17] and increasing socialization.[18] Finally, given that experiential learning is known to contribute to better hospitalist work performance,[19] job fit may affect productivity and clinical outcomes vis‐‐vis quality of work life.
To test the validity of these assumptions in a sample of hospitalists, we critically appraised the following 4 hypotheses:
- Hypothesis 1 (H1): Job attrition and reselection improves job fit among hospitalists entering the job market.
- Hypothesis 2 (H2): Better job fit is achieved through hospitalists engaging a variety of personal skills and abilities.
- Hypothesis 3 (H3): Job fit increases with hospitalists' job duration together with socialization and internalization of organizational values.
- Hypothesis 4 (H4): Job fit is correlated with hospitalists' quality of work life.
METHODS
Analysis was performed on data from the 2009 to 2010 Hospital Medicine Physician Worklife Survey. The sample frame included nonmembers and members of Society of Hospital Medicine (SHM). Details about sampling strategy, data collection, and data quality are available in previous publications.[7, 20] The 118‐item survey instrument, including 9 demographic items and 24 practice and job characteristic items, was administered by mail. Examples of information solicited through these items included respondents' practice model, the number of hospitalist jobs they have held, and the specific kinds of clinical and nonclinical activities they performed as part of their current job.
We used a reliable but broad and generic measure of self‐perceived person‐job fit.[21] The survey items of the 5‐point Likert‐type scale anchored between strongly disagree and strongly agree were: I feel that my work utilizes my full abilities, I feel competent and fully able to handle my job, my job gives me the chance to do the things I feel I do best, I feel that my job and I are well‐matched, I feel I have adequate preparation for the job I now hold. The quality of hospitalists' relationships with physician colleagues, staff, and patients as well as job satisfaction was measured using scales adapted from the Physician Worklife Study.[22] Organizational climate was measured using an adapted scale from the Minimizing Error, Maximizing Outcome study incorporating 3 items from the cohesiveness subscale, 4 items from the organizational trust subscale, and 1 item from the quality emphasis subscale that were most pertinent to hospitalists' relationship with their organizations.[23] Intent to leave practice or reduce work hours was measured using 5 items from the Multi‐Center Hospitalist Survey Project.[24] Frequency of participation in suboptimal patient care was measured by adapting 3 items from the suboptimal reported practice subscale and 2 items from the suboptimal patient care subscale developed by Shanafelt et al.[25] Stress and job burnout were assessed using validated measures.[26, 27] Detailed descriptions of the response rate calculation and imputation of missing item data are available in previous publications.[7, 20]
Mean, variance, range, and skew were used to characterize the responses to the job fit survey scale. A table of respondent characteristics was constructed. A visual representation of job fit by individual hospitalist year in current practice was created, first, by plotting a locally weighted scatterplot smoothing curve to examine the shape of the general relationship, and second, by fitting a similarly contoured functional polynomial curve with 95% confidence intervals (CI) to a plot of the mean and interquartile range of job fit for each year in current practice. Spearman partial correlations were calculated for job fit and each of the 5 items addressing likelihood of leaving practice or reducing workload adjusted for gender to control for the higher proportion of women who plan to work part time. Median (interquartile range) job fit was calculated for categories defined by the number of job changes and compared with the reference category (no job change) using the nonparametric rank sum test for comparing non‐normally distributed data. Multivariate logistic regression models were used to calculate the odds ratio (OR) of participating in each of several clinical and nonclinical hospitalist activities between respondents whose job fit score was optimal (5 on a 5‐point scale) and less than optimal controlling for covariates that influence the likelihood of participating in these activities (years in current practice, practice model, and specialty training). A Spearman correlation matrix was created to assess interscale correlations among organizational parameters (years in current practice, job fit, organizational climate, and relationship with colleagues, staff, and patients). Finally, a separate Spearman correlation matrix was created to assess the interscale correlations among individual worker parameters (job fit, suboptimal patient care, job burnout, stress, and job satisfaction). Statistical significance was defined as P value <0.05, and all analyses were performed on Stata 11.0 (StataCorp, College Station, TX). The Northwestern University institutional review board approved this study.
RESULTS
Respondents included 816 hospitalists belonging to around 700 unique organizations. The adjusted response rate from the stratified sample was 26%. Respondents and nonrespondents were similar with regard to geographic region and model of practice, but respondents were more likely to be members of the SHM than nonrespondents. Panel A of Table 1 shows the demographic characteristics of the respondents. The mean age was 44.3 years, and about one‐third were women. The average hospitalist had about 7 years of experience in the specialty and about 5 years with their current hospitalist job. The majority were trained in internal medicine or one of its subspecialties, whereas pediatricians, family physicians, and physicians with other training made up the remainder.
| Panel A | Panel B | ||
|---|---|---|---|
| Total | Assimilation Period Hospitalists | Advancement Period Hospitalists | |
| |||
| Total, n | 816 | 103 | 713 |
| Female, n (%) | 284 (35) | 37 (36) | 247 (35) |
| Age, mean (SD) | 44.3 (9.0) | 41.9 (9.3) | 44.7 (8.9) |
| Years postresidency experience as hospitalist, mean (SD) | 6.9 (4.5) | 4.3 (3.1) | 7.2 (4.6) |
| Years in current practice, mean (SD) | 5.1 (3.9) | 0.9 (0.3) | 6.7 (3.8) |
| Specialty training, n (%) | |||
| Internal medicine | 555 (68) | 75 (73) | 480 (67) |
| Pediatrics | 117 (14) | 8 (8) | 109 (15.3) |
| Family medicine | 49 (6) | 7 (7) | 42 (6) |
| Other | 95 (11) | 13 (13) | 82 (12) |
Job fit was highly skewed toward optimum fit, with a mean of 4.3 on a scale of 1 to 5, with a narrow standard deviation of 0.7. The poorest job fit was reported by 0.3%, whereas optimal fit was reported by 21% of respondents. Job fit plotted against years in current practice had a logarithmic appearance typical of learning curves (Figure 1). An inflection point was visualized at around 2 years. For the purposes of this article, we refer to hospitalists' experience in the first 2 years of a job as an assimilation period, which is marked by a steep increase in job fit early when rapid learning or attrition took place. The years beyond the inflection point are characterized as an advancement period, when a more attenuated rise in job fit was experienced with time. The Spearman correlation between job fit and years in practice during the advancement period was 0.145 (n = 678, P < 0.001). Panel B of Table 1 displays the characteristics of respondents separately for the assimilation and advancement cohorts. Assimilation hospitalists in our sample had a mean age of 41.9 years and mean on‐the‐job experience of 4.3 years, reflecting that many hospitalists in the first 2 years of a job have made at least 1 job change in the past.
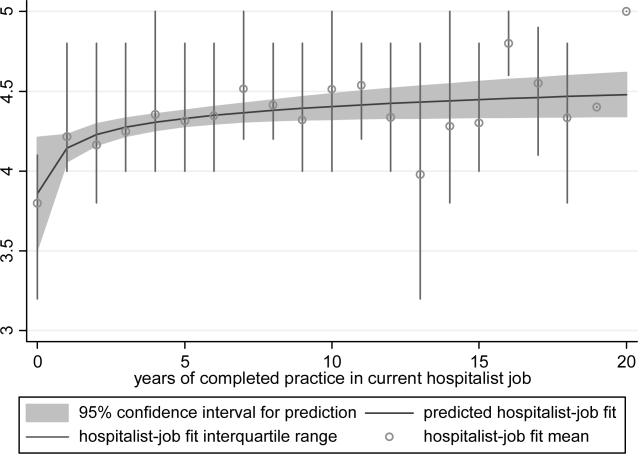
To show the effects of attrition and reselection, we first evaluated the proposition that hospitalists experience attrition (ie, intend to leave their jobs) in response to poor fit. Table 2 shows the correlations between job fit and the self‐reported intent to leave practice or reduce workload separately for the assimilation and advancement periods. For hospitalists in the assimilation period, job fit was negatively correlated with intent to leave current practice within 2 years and to leave hospital medicine within 5 years (P = 0.010 and 0.043, respectively). Hospitalists with <2 years in their current job, therefore, tended to consider attrition but not workload reduction to deal with poor job fit. On the other hand, hospitalists in the advancement period considered both attrition and workload reduction strategies in response to poor fit (all P < 0.001).
| Assimilation Period Hospitalists | Advancement Period Hospitalists | |||
|---|---|---|---|---|
| Rho | P Value | Rho | P Value | |
| Likelihood that a hospitalist will: | ||||
| Leave current practice within 2 years | 0.253 | 0.010 | 0.367 | <0.001 |
| Decrease total work hours within 5 years | 0.060 | 0.548 | 0.179 | <0.001 |
| Decrease clinical work hours within 5 years | 0.072 | 0.469 | 0.144 | <0.001 |
| Leave hospital medicine within 5 years | 0.200 | 0.043 | 0.231 | <0.001 |
| Leave direct patient care within 5 years | 0.040 | 0.691 | 0.212 | <0.001 |
In Table 3, we further compared the median job fit across categories for the number of job switches. The median job fit during the assimilation period of hospitalists who had made 1 job change was slightly but statistically higher than the job fit of their counterparts who never left their first job (4.4 vs 4.0, P = 0.046). This suggests that job switching by hospitalists early in their jobs is associated with improved job fit (H1). However, the fit during the assimilation period of hospitalists who switched jobs twice or more was statistically no different from the fit of those in their first jobs, suggesting that the effect of the attrition‐reselection strategy is weak or inconsistent. The job fit for advancement period hospitalists was also different across the job change and no‐change categories. However, in the case of hospitalists later in their jobs, the median job fit was slightly but statistically lower among those who made job changes, revealing the potential drop in job fit that occurs when a hospitalist already established in his or her job starts over again in a new setting.
| n | Age, Mean (95% CI), y | Hospitalist‐Job Fit, Median (IQR) | P Valuea | |
|---|---|---|---|---|
| ||||
| Assimilation period hospitalistsb | ||||
| No job change | 29 | 42.3 (37.347.3) | 4.0 (3.84.4) | Reference |
| 1 job change | 39 | 40.3 (38.142.5) | 4.4 (4.04.8) | 0.046 |
| 2 or more job changes | 27 | 43.8 (41.046.6) | 4.4 (3.84.8) | 0.153 |
| Advancement period hospitalistsc | ||||
| No job change | 390 | 44.5 (43.645.5) | 4.6 (4.05.0) | Reference |
| 1 job change | 183 | 45.0 (43.746.3) | 4.2 (4.04.8) | 0.002 |
| 2 or more job changes | 99 | 44.9 (43.146.6) | 4.2 (3.84.8) | 0.002 |
We hypothesized that hospitalists who achieved high job fit within a particular job were more likely to have engaged in activities that utilize a wider spectrum of their abilities. As shown in Table 4, hospitalists in the highest quartile of job fit were associated with a general trend toward higher odds of participating in a variety of common clinical and nonclinical hospitalist activities, but only the odds ratio associated with teaching achieved statistical significance (OR: 1.53, 95% CI: 1.01‐2.31) (H2).
| Participation, n/N (%) | Odds Ratio (95% CI) | P Value | |
|---|---|---|---|
| |||
| Administrative or committee work | 704/816 (86) | 0.73 (0.431.26) | 0.262 |
| Quality improvement or patient safety initiatives | 678/816 (83) | 1.13 (0.642.00) | 0.680 |
| Information technology design or implementation | 379/816 (46) | 1.18 (0.801.73) | 0.408 |
| Any of the above leadership activities | 758/816 (93) | 1.31 (0.563.05) | 0.535 |
| Teaching | 442/816 (54) | 1.53 (1.012.31) | 0.046 |
| Research | 120/816 (15) | 1.07 (0.601.92) | 0.816 |
| Any of the above academic activities | 457/816 (56) | 1.50 (0.992.27) | 0.057 |
| Code team or rapid response team | 437/816 (54) | 1.13 (0.771.68) | 0.533 |
| Intensive care unit | 254/816 (31) | 0.84 (0.531.35) | 0.469 |
| Skilled nursing facility or long‐term acute care facility | 126/816 (15) | 1.06 (0.621.81) | 0.835 |
| Outpatient general medical practice | 44/816 (5) | 1.75 (0.813.80) | 0.157 |
| Any of the above clinical activities | 681/816 (79) | 1.02 (0.601.76) | 0.930 |
Socialization with peers and the gradual sharing of values within organizations are hypothesized mechanisms for increasing job fit with time. We found that the number of years in current practice was positively correlated with job fit (Spearman coefficient R = 0.149, P < 0.001), organizational climate (R = 0.128, P < 0.001), and relationship with nonphysician staff (R = 0.102, P < 0.01). The association between years in practice and relationship with physician colleagues were weaker (R = 0.079, P < 0.05). Consistent with the episodic nature of patients' encounters with hospitalists, the measure of patient relationships was not significantly associated with length of time in job. In addition, we found substantial correlations among job fit, organizational climate, and all the relational measures (all R > 0.280, P < 0.001), indicating that hospitalists increasingly share the values of their organizations over time (H3).
Finally, we also hypothesized that poor job fit is associated with poor performance and quality of work life. Strong correlations with job fit were noted for stress (R = 0.307, P < 0.001), job burnout (R = 0.360, P < 0.001), and job satisfaction (R = 0.570, P < 0.001). Job fit (R = 0.147, P < 0.001), job burnout (R = 0.236, P < 0.001), stress (R = 0.305, P < 0.001), and job satisfaction (R = 0.224, P < 0.001) were all significantly correlated with the frequency of participating in suboptimal care (H4).
DISCUSSION
In this exploratory analysis, we validated in the hospitalist workforce several assumptions about person‐job fit that have been observed in workers of other industries. We observed attrition‐reselection (ie, job switching) as a strategy used by physicians to achieve better fit early in their job tenure, whereas job modification appeared to be more effective than attrition‐reselection among physicians already established in their jobs. We provided weak but plausible evidence that physicians with optimal job fit had a tendency to participate in activities (eg, teaching) that engage a wider set of interests and abilities. We also demonstrated the growth in hospitalists sharing the values of their organization through the time‐dependent associations among organizational climate, relational measures, and job fit. Finally, we found that physicians with suboptimal job fit were more likely to report poor performance in their work compared to those indicating optimal fit.
Our previous analysis of data from the Hospital Medicine Physician Worklife Survey exposed the widely variable work characteristics of hospitalist jobs in the US market and the equally variable preferences and priorities of individual hospitalists in selecting their work setting.[7] The implication of our present study is that hospitalists achieve the high levels of observed job fit using various strategies that aid their alignment with their employment. One of these strategies involves time, but physician longevity in practice may be both a determinant and product of good job fit. Although early job attrition may be necessary for fitting the right hospitalists to the right jobs, employers may appreciate the importance of retaining experienced hospitalists not only for cost and performance considerations but also for the growth of social capital in organizations consisting of enduring individuals. As our data suggest that hospitalists grow with their jobs, physicians may experience better fit with jobs that flexibly couple their work demands with benefits that address their individual work‐life needs over time. Another implication of this study is that job fit is a useful and predictive measure of job selection, performance, and retention. In light of studies that expose the limitations of job satisfaction as a measure influenced more by workers' dispositional affect (ie, their temperament and outlook) than their compatibility with their jobs,[28] job fit may add a functional dimension to traditional employee feedback measures.
There are limitations to this analysis. The most notable is the low survey response rate. Two reasons contributed to the fairly low rate of return. First, the original sampling frame included many outdated addresses and names of individuals who did not meet inclusion criteria. Although all sampled individuals who would have been excluded from the study could not be identified, we calculated our response rate without accounting for the proportion of potential ineligibles in the denominator population [Response Rate 2 (RR2) according to standards of the American Association of Public Opinion Research].[29] Second, the response rates of physician surveys have seen a steady decline over the years.[30] Respondents to our survey may be older and more experienced than US hospitalists in general. Although concerns about bias from under‐reporting cannot be fully addressed, we believe that the study sample is adequate for this preliminary study intended to translate the evidence of observed phenomena from the nonphysician to the physician workforces. The suboptimal response characteristics (high skew and low variability) of the generic person‐job fit survey scale used in this study indicate that a reliable survey instrument specifically designed to measure physician‐job fit need to be constructed de novo and validated for any future study. Although we performed simple analyses to support our assertions, few of our subanalyses may be underpowered, contributing to overinterpretation of the data. Additional empirical work is also necessary to assess the generalizability of this study's claims in other medical and surgical specialties. Such studies would also allow measurement of the sensitivity and specificity of physicians' self‐identification of poor job fit. Finally, additional investigations of this time‐dependent construct are more appropriately performed using a longitudinal study design to overcome the limitations inherent in this cross‐sectional analysis. Our conclusions about the time‐dependent features of job fit may be explained by other characteristics such as generational and cultural differences among hospitalists with varying experience.
As the US healthcare system reorganizes to bolster accountability,[31] we anticipate increasing interdependence between physicians and their employer organizations. Ultimately, the desired accountability in healthcare is likely to be obtained if physicians function not only as passive and interchangeable employees but as active stakeholders in the achievement of each organization's goals. A methodology for assessing the alignment of physicians and their jobs will continue to be important along the way.
Disclosure
Nothing to report.
- . Person‐organization fit: an integrative review of its conceptualizations, measurement, and implications. Personnel Psychol. 1996;49:1–49.
- , , . Consequences of individuals' fit at work: a meta‐analysis of person‐job, person‐organization, person‐group, and person‐supervisor fit. Personnel Psychol. 2005;58(2):281–342.
- .Person‐job fit: a conceptual integration, literature review and methodological critique. In: Cooper CL, Robertson IT, eds. International Review of Industrial and Organizational Psychology. Vol.6. New York, NY:John Wiley 1991.
- . Organizational culture, person‐culture fit, and turnover: a replication in the health care industry. J Organ Behav. 1999;20(2):175–184.
- , , , . Organizational culture and physician satisfaction with dimensions of group practice. Health Serv Res. 2007;42(3 pt 1):1150–1176.
- , , , et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169(10):990–995.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- . Provider‐hospital “fit” and patient outcomes: evidence from Massachusetts cardiac surgeons, 2002–2004. Health Serv Res. 2011;46(1 pt 1):1–26.
- . The evolving primary care physician. N Engl J Med. 2012;366(20):1849–1853.
- , . Hospitals' race to employ physicians—the logic behind a money‐losing proposition. N Engl J Med. 2011;364(19):1790–1793.
- 2011 Survey of Final‐Year Medical Residents. Irving, TX:Merritt Hawkins;2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO:Society of Hospital Medicine and the Medical Group Management Association;2010.
- , , . The ASA framework: an update. Personnel Psychol. 1995;48(4):747–773.
- , . Work Redesign. Reading. MA:Addison‐Wesley;1980.
- , . The expanding role of hospitalists in the United States. Swiss Med Wkly. 2006;136(37–38):591–596.
- , . Organizational socialization as a learning‐process—the role of information acquisition. Personnel Psychol. 1992;45(4):849–874.
- , . The moderating effect of tenure in person‐environment fit: a field study in educational organizations. J Occup Organ Psych. 1997;70:173–188.
- . Matching people and organizations—selection and socialization in public accounting firms. Admin Sci Quart. 1991;36(3):459–484.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- . Karasek's model in the People's Republic of China: effects of job demands, control, and individual differences. Acad Manage J. 1996;39(6):1594–1618.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO Study. Adv Patient Saf. 2005;1:65–77.
- , , , et al. Effects of inpatient experience on outcomes and costs in a multicenter trial of academic hospitalists. J Gen Intern Med. 2005;20(suppl 1):141–142.
- , , , . Burnout and self‐reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358–367.
- , . Effect of job demands and social support on worker stress—a study of VDT users. Behav Inform Technol. 1995;14(1):32–40.
- , , . Validation of a single‐item measure of burnout against the Maslach Burnout Inventory among physicians. Stress Health. 2004;20(2):75–79.
- , . Job satisfaction: a meta‐analysis of stabilities. J Organ Behav. 2001;22(5):483–504.
- The American Association for Public Opinion Research. Standard definitions: final dispositions of case codes and outcome rates for surveys.7th ed. Available at: http://www.aapor.org/Standard_Definitions2.htm. Accessed May 2,2012.
- , , , . Response rates and response bias for 50 surveys of pediatricians. Health Serv Res. 2005;40(1):213–226.
- , . Accountable care organizations: accountable for what, to whom, and how. JAMA. 2010;304(15):1715–6.
Person‐organization fit concerns the conditions and consequences of compatibility between people and the organizations for which they work.[1] Studies of other industries have demonstrated that person‐organization fit informs the way individuals join, perform in, and are retained by organizations.[2] Person‐job fit is a closely related subordinate concept that concerns the alignment of workers and their job in as much as workers have needs that their job supplies, or conversely, jobs have requirements that certain workers' abilities can help meet.[3] Explorations of job fit in physicians and their work have recently emerged in a few investigations published in medical journals.[4, 5, 6, 7, 8] Further expanding the understanding of fit between physicians and their employment is important, because the decline of solo practices and recent emphasis on team‐based care have led to a growing number of US physicians working in organizations.[9]
The movement of physicians into employed situations may continue if certain types of Accountable Care Organizations take root.[10] And physicians may be primed to join employer organizations based on current career priorities of individuals in American society. Surveys of medical residents entering the workforce reveal more physicians preferring the security of being employees than starting their own practices.[11] Given these trends, job fit will inform our understanding of how personal and job characteristics facilitate recruitment, performance, satisfaction, and longevity of physician employees.
BACKGROUND
Virtually all hospitalists work in organizationshospitalsand are employees of hospitals, medical schools, physician group practices, or management companies, and therefore invariably function within organizational structures and systems.[7] In spite of their rapid growth in numbers, many employers have faced difficulties recruiting and retaining enough hospitalists to fill their staffing needs. Consequently, the US hospitalist workforce today is characterized by high salaries, work load, and attrition rates.[12]
In this evolving unsaturated market, the attraction‐selection‐attrition framework[13] provides a theoretical construct that predicts that hospitalists and their employers would seek congruence of goals and values early in their relationship through a process of trial and error. This framework assumes that early interactions between workers and organizations serve as opportunities for them to understand if job fit is poor and dissociate or remain affiliated as long as job fit is mutually acceptable. Therefore, job switching on average is expected to increase job fit because workers and organizations gain a better understanding of their own goals and values and choose more wisely the next time.
Other theoretical frameworks, such as the job characteristic model,[14] suggest that over time as workers stay at the same job, they continue to maintain and improve job fit through various workplace‐ or self‐modification strategies. For example, seniority status may have privileges (eg, less undesirable call), or workers may create privileged niches through the acquisition of new skills and abilities over time. Hospitalists' tendency to diversify their work‐related activities by incorporating administrative and teaching responsibilities[15] may thus contribute to improving job fit. Additionally, as a measure of complementarity among people who work together, job fit may be influenced by the quality of relationships among hospitalists and their coworkers through their reorientation to the prevailing organizational climate[16, 17] and increasing socialization.[18] Finally, given that experiential learning is known to contribute to better hospitalist work performance,[19] job fit may affect productivity and clinical outcomes vis‐‐vis quality of work life.
To test the validity of these assumptions in a sample of hospitalists, we critically appraised the following 4 hypotheses:
- Hypothesis 1 (H1): Job attrition and reselection improves job fit among hospitalists entering the job market.
- Hypothesis 2 (H2): Better job fit is achieved through hospitalists engaging a variety of personal skills and abilities.
- Hypothesis 3 (H3): Job fit increases with hospitalists' job duration together with socialization and internalization of organizational values.
- Hypothesis 4 (H4): Job fit is correlated with hospitalists' quality of work life.
METHODS
Analysis was performed on data from the 2009 to 2010 Hospital Medicine Physician Worklife Survey. The sample frame included nonmembers and members of Society of Hospital Medicine (SHM). Details about sampling strategy, data collection, and data quality are available in previous publications.[7, 20] The 118‐item survey instrument, including 9 demographic items and 24 practice and job characteristic items, was administered by mail. Examples of information solicited through these items included respondents' practice model, the number of hospitalist jobs they have held, and the specific kinds of clinical and nonclinical activities they performed as part of their current job.
We used a reliable but broad and generic measure of self‐perceived person‐job fit.[21] The survey items of the 5‐point Likert‐type scale anchored between strongly disagree and strongly agree were: I feel that my work utilizes my full abilities, I feel competent and fully able to handle my job, my job gives me the chance to do the things I feel I do best, I feel that my job and I are well‐matched, I feel I have adequate preparation for the job I now hold. The quality of hospitalists' relationships with physician colleagues, staff, and patients as well as job satisfaction was measured using scales adapted from the Physician Worklife Study.[22] Organizational climate was measured using an adapted scale from the Minimizing Error, Maximizing Outcome study incorporating 3 items from the cohesiveness subscale, 4 items from the organizational trust subscale, and 1 item from the quality emphasis subscale that were most pertinent to hospitalists' relationship with their organizations.[23] Intent to leave practice or reduce work hours was measured using 5 items from the Multi‐Center Hospitalist Survey Project.[24] Frequency of participation in suboptimal patient care was measured by adapting 3 items from the suboptimal reported practice subscale and 2 items from the suboptimal patient care subscale developed by Shanafelt et al.[25] Stress and job burnout were assessed using validated measures.[26, 27] Detailed descriptions of the response rate calculation and imputation of missing item data are available in previous publications.[7, 20]
Mean, variance, range, and skew were used to characterize the responses to the job fit survey scale. A table of respondent characteristics was constructed. A visual representation of job fit by individual hospitalist year in current practice was created, first, by plotting a locally weighted scatterplot smoothing curve to examine the shape of the general relationship, and second, by fitting a similarly contoured functional polynomial curve with 95% confidence intervals (CI) to a plot of the mean and interquartile range of job fit for each year in current practice. Spearman partial correlations were calculated for job fit and each of the 5 items addressing likelihood of leaving practice or reducing workload adjusted for gender to control for the higher proportion of women who plan to work part time. Median (interquartile range) job fit was calculated for categories defined by the number of job changes and compared with the reference category (no job change) using the nonparametric rank sum test for comparing non‐normally distributed data. Multivariate logistic regression models were used to calculate the odds ratio (OR) of participating in each of several clinical and nonclinical hospitalist activities between respondents whose job fit score was optimal (5 on a 5‐point scale) and less than optimal controlling for covariates that influence the likelihood of participating in these activities (years in current practice, practice model, and specialty training). A Spearman correlation matrix was created to assess interscale correlations among organizational parameters (years in current practice, job fit, organizational climate, and relationship with colleagues, staff, and patients). Finally, a separate Spearman correlation matrix was created to assess the interscale correlations among individual worker parameters (job fit, suboptimal patient care, job burnout, stress, and job satisfaction). Statistical significance was defined as P value <0.05, and all analyses were performed on Stata 11.0 (StataCorp, College Station, TX). The Northwestern University institutional review board approved this study.
RESULTS
Respondents included 816 hospitalists belonging to around 700 unique organizations. The adjusted response rate from the stratified sample was 26%. Respondents and nonrespondents were similar with regard to geographic region and model of practice, but respondents were more likely to be members of the SHM than nonrespondents. Panel A of Table 1 shows the demographic characteristics of the respondents. The mean age was 44.3 years, and about one‐third were women. The average hospitalist had about 7 years of experience in the specialty and about 5 years with their current hospitalist job. The majority were trained in internal medicine or one of its subspecialties, whereas pediatricians, family physicians, and physicians with other training made up the remainder.
| Panel A | Panel B | ||
|---|---|---|---|
| Total | Assimilation Period Hospitalists | Advancement Period Hospitalists | |
| |||
| Total, n | 816 | 103 | 713 |
| Female, n (%) | 284 (35) | 37 (36) | 247 (35) |
| Age, mean (SD) | 44.3 (9.0) | 41.9 (9.3) | 44.7 (8.9) |
| Years postresidency experience as hospitalist, mean (SD) | 6.9 (4.5) | 4.3 (3.1) | 7.2 (4.6) |
| Years in current practice, mean (SD) | 5.1 (3.9) | 0.9 (0.3) | 6.7 (3.8) |
| Specialty training, n (%) | |||
| Internal medicine | 555 (68) | 75 (73) | 480 (67) |
| Pediatrics | 117 (14) | 8 (8) | 109 (15.3) |
| Family medicine | 49 (6) | 7 (7) | 42 (6) |
| Other | 95 (11) | 13 (13) | 82 (12) |
Job fit was highly skewed toward optimum fit, with a mean of 4.3 on a scale of 1 to 5, with a narrow standard deviation of 0.7. The poorest job fit was reported by 0.3%, whereas optimal fit was reported by 21% of respondents. Job fit plotted against years in current practice had a logarithmic appearance typical of learning curves (Figure 1). An inflection point was visualized at around 2 years. For the purposes of this article, we refer to hospitalists' experience in the first 2 years of a job as an assimilation period, which is marked by a steep increase in job fit early when rapid learning or attrition took place. The years beyond the inflection point are characterized as an advancement period, when a more attenuated rise in job fit was experienced with time. The Spearman correlation between job fit and years in practice during the advancement period was 0.145 (n = 678, P < 0.001). Panel B of Table 1 displays the characteristics of respondents separately for the assimilation and advancement cohorts. Assimilation hospitalists in our sample had a mean age of 41.9 years and mean on‐the‐job experience of 4.3 years, reflecting that many hospitalists in the first 2 years of a job have made at least 1 job change in the past.
To show the effects of attrition and reselection, we first evaluated the proposition that hospitalists experience attrition (ie, intend to leave their jobs) in response to poor fit. Table 2 shows the correlations between job fit and the self‐reported intent to leave practice or reduce workload separately for the assimilation and advancement periods. For hospitalists in the assimilation period, job fit was negatively correlated with intent to leave current practice within 2 years and to leave hospital medicine within 5 years (P = 0.010 and 0.043, respectively). Hospitalists with <2 years in their current job, therefore, tended to consider attrition but not workload reduction to deal with poor job fit. On the other hand, hospitalists in the advancement period considered both attrition and workload reduction strategies in response to poor fit (all P < 0.001).
| Assimilation Period Hospitalists | Advancement Period Hospitalists | |||
|---|---|---|---|---|
| Rho | P Value | Rho | P Value | |
| Likelihood that a hospitalist will: | ||||
| Leave current practice within 2 years | 0.253 | 0.010 | 0.367 | <0.001 |
| Decrease total work hours within 5 years | 0.060 | 0.548 | 0.179 | <0.001 |
| Decrease clinical work hours within 5 years | 0.072 | 0.469 | 0.144 | <0.001 |
| Leave hospital medicine within 5 years | 0.200 | 0.043 | 0.231 | <0.001 |
| Leave direct patient care within 5 years | 0.040 | 0.691 | 0.212 | <0.001 |
In Table 3, we further compared the median job fit across categories for the number of job switches. The median job fit during the assimilation period of hospitalists who had made 1 job change was slightly but statistically higher than the job fit of their counterparts who never left their first job (4.4 vs 4.0, P = 0.046). This suggests that job switching by hospitalists early in their jobs is associated with improved job fit (H1). However, the fit during the assimilation period of hospitalists who switched jobs twice or more was statistically no different from the fit of those in their first jobs, suggesting that the effect of the attrition‐reselection strategy is weak or inconsistent. The job fit for advancement period hospitalists was also different across the job change and no‐change categories. However, in the case of hospitalists later in their jobs, the median job fit was slightly but statistically lower among those who made job changes, revealing the potential drop in job fit that occurs when a hospitalist already established in his or her job starts over again in a new setting.
| n | Age, Mean (95% CI), y | Hospitalist‐Job Fit, Median (IQR) | P Valuea | |
|---|---|---|---|---|
| ||||
| Assimilation period hospitalistsb | ||||
| No job change | 29 | 42.3 (37.347.3) | 4.0 (3.84.4) | Reference |
| 1 job change | 39 | 40.3 (38.142.5) | 4.4 (4.04.8) | 0.046 |
| 2 or more job changes | 27 | 43.8 (41.046.6) | 4.4 (3.84.8) | 0.153 |
| Advancement period hospitalistsc | ||||
| No job change | 390 | 44.5 (43.645.5) | 4.6 (4.05.0) | Reference |
| 1 job change | 183 | 45.0 (43.746.3) | 4.2 (4.04.8) | 0.002 |
| 2 or more job changes | 99 | 44.9 (43.146.6) | 4.2 (3.84.8) | 0.002 |
We hypothesized that hospitalists who achieved high job fit within a particular job were more likely to have engaged in activities that utilize a wider spectrum of their abilities. As shown in Table 4, hospitalists in the highest quartile of job fit were associated with a general trend toward higher odds of participating in a variety of common clinical and nonclinical hospitalist activities, but only the odds ratio associated with teaching achieved statistical significance (OR: 1.53, 95% CI: 1.01‐2.31) (H2).
| Participation, n/N (%) | Odds Ratio (95% CI) | P Value | |
|---|---|---|---|
| |||
| Administrative or committee work | 704/816 (86) | 0.73 (0.431.26) | 0.262 |
| Quality improvement or patient safety initiatives | 678/816 (83) | 1.13 (0.642.00) | 0.680 |
| Information technology design or implementation | 379/816 (46) | 1.18 (0.801.73) | 0.408 |
| Any of the above leadership activities | 758/816 (93) | 1.31 (0.563.05) | 0.535 |
| Teaching | 442/816 (54) | 1.53 (1.012.31) | 0.046 |
| Research | 120/816 (15) | 1.07 (0.601.92) | 0.816 |
| Any of the above academic activities | 457/816 (56) | 1.50 (0.992.27) | 0.057 |
| Code team or rapid response team | 437/816 (54) | 1.13 (0.771.68) | 0.533 |
| Intensive care unit | 254/816 (31) | 0.84 (0.531.35) | 0.469 |
| Skilled nursing facility or long‐term acute care facility | 126/816 (15) | 1.06 (0.621.81) | 0.835 |
| Outpatient general medical practice | 44/816 (5) | 1.75 (0.813.80) | 0.157 |
| Any of the above clinical activities | 681/816 (79) | 1.02 (0.601.76) | 0.930 |
Socialization with peers and the gradual sharing of values within organizations are hypothesized mechanisms for increasing job fit with time. We found that the number of years in current practice was positively correlated with job fit (Spearman coefficient R = 0.149, P < 0.001), organizational climate (R = 0.128, P < 0.001), and relationship with nonphysician staff (R = 0.102, P < 0.01). The association between years in practice and relationship with physician colleagues were weaker (R = 0.079, P < 0.05). Consistent with the episodic nature of patients' encounters with hospitalists, the measure of patient relationships was not significantly associated with length of time in job. In addition, we found substantial correlations among job fit, organizational climate, and all the relational measures (all R > 0.280, P < 0.001), indicating that hospitalists increasingly share the values of their organizations over time (H3).
Finally, we also hypothesized that poor job fit is associated with poor performance and quality of work life. Strong correlations with job fit were noted for stress (R = 0.307, P < 0.001), job burnout (R = 0.360, P < 0.001), and job satisfaction (R = 0.570, P < 0.001). Job fit (R = 0.147, P < 0.001), job burnout (R = 0.236, P < 0.001), stress (R = 0.305, P < 0.001), and job satisfaction (R = 0.224, P < 0.001) were all significantly correlated with the frequency of participating in suboptimal care (H4).
DISCUSSION
In this exploratory analysis, we validated in the hospitalist workforce several assumptions about person‐job fit that have been observed in workers of other industries. We observed attrition‐reselection (ie, job switching) as a strategy used by physicians to achieve better fit early in their job tenure, whereas job modification appeared to be more effective than attrition‐reselection among physicians already established in their jobs. We provided weak but plausible evidence that physicians with optimal job fit had a tendency to participate in activities (eg, teaching) that engage a wider set of interests and abilities. We also demonstrated the growth in hospitalists sharing the values of their organization through the time‐dependent associations among organizational climate, relational measures, and job fit. Finally, we found that physicians with suboptimal job fit were more likely to report poor performance in their work compared to those indicating optimal fit.
Our previous analysis of data from the Hospital Medicine Physician Worklife Survey exposed the widely variable work characteristics of hospitalist jobs in the US market and the equally variable preferences and priorities of individual hospitalists in selecting their work setting.[7] The implication of our present study is that hospitalists achieve the high levels of observed job fit using various strategies that aid their alignment with their employment. One of these strategies involves time, but physician longevity in practice may be both a determinant and product of good job fit. Although early job attrition may be necessary for fitting the right hospitalists to the right jobs, employers may appreciate the importance of retaining experienced hospitalists not only for cost and performance considerations but also for the growth of social capital in organizations consisting of enduring individuals. As our data suggest that hospitalists grow with their jobs, physicians may experience better fit with jobs that flexibly couple their work demands with benefits that address their individual work‐life needs over time. Another implication of this study is that job fit is a useful and predictive measure of job selection, performance, and retention. In light of studies that expose the limitations of job satisfaction as a measure influenced more by workers' dispositional affect (ie, their temperament and outlook) than their compatibility with their jobs,[28] job fit may add a functional dimension to traditional employee feedback measures.
There are limitations to this analysis. The most notable is the low survey response rate. Two reasons contributed to the fairly low rate of return. First, the original sampling frame included many outdated addresses and names of individuals who did not meet inclusion criteria. Although all sampled individuals who would have been excluded from the study could not be identified, we calculated our response rate without accounting for the proportion of potential ineligibles in the denominator population [Response Rate 2 (RR2) according to standards of the American Association of Public Opinion Research].[29] Second, the response rates of physician surveys have seen a steady decline over the years.[30] Respondents to our survey may be older and more experienced than US hospitalists in general. Although concerns about bias from under‐reporting cannot be fully addressed, we believe that the study sample is adequate for this preliminary study intended to translate the evidence of observed phenomena from the nonphysician to the physician workforces. The suboptimal response characteristics (high skew and low variability) of the generic person‐job fit survey scale used in this study indicate that a reliable survey instrument specifically designed to measure physician‐job fit need to be constructed de novo and validated for any future study. Although we performed simple analyses to support our assertions, few of our subanalyses may be underpowered, contributing to overinterpretation of the data. Additional empirical work is also necessary to assess the generalizability of this study's claims in other medical and surgical specialties. Such studies would also allow measurement of the sensitivity and specificity of physicians' self‐identification of poor job fit. Finally, additional investigations of this time‐dependent construct are more appropriately performed using a longitudinal study design to overcome the limitations inherent in this cross‐sectional analysis. Our conclusions about the time‐dependent features of job fit may be explained by other characteristics such as generational and cultural differences among hospitalists with varying experience.
As the US healthcare system reorganizes to bolster accountability,[31] we anticipate increasing interdependence between physicians and their employer organizations. Ultimately, the desired accountability in healthcare is likely to be obtained if physicians function not only as passive and interchangeable employees but as active stakeholders in the achievement of each organization's goals. A methodology for assessing the alignment of physicians and their jobs will continue to be important along the way.
Disclosure
Nothing to report.
Person‐organization fit concerns the conditions and consequences of compatibility between people and the organizations for which they work.[1] Studies of other industries have demonstrated that person‐organization fit informs the way individuals join, perform in, and are retained by organizations.[2] Person‐job fit is a closely related subordinate concept that concerns the alignment of workers and their job in as much as workers have needs that their job supplies, or conversely, jobs have requirements that certain workers' abilities can help meet.[3] Explorations of job fit in physicians and their work have recently emerged in a few investigations published in medical journals.[4, 5, 6, 7, 8] Further expanding the understanding of fit between physicians and their employment is important, because the decline of solo practices and recent emphasis on team‐based care have led to a growing number of US physicians working in organizations.[9]
The movement of physicians into employed situations may continue if certain types of Accountable Care Organizations take root.[10] And physicians may be primed to join employer organizations based on current career priorities of individuals in American society. Surveys of medical residents entering the workforce reveal more physicians preferring the security of being employees than starting their own practices.[11] Given these trends, job fit will inform our understanding of how personal and job characteristics facilitate recruitment, performance, satisfaction, and longevity of physician employees.
BACKGROUND
Virtually all hospitalists work in organizationshospitalsand are employees of hospitals, medical schools, physician group practices, or management companies, and therefore invariably function within organizational structures and systems.[7] In spite of their rapid growth in numbers, many employers have faced difficulties recruiting and retaining enough hospitalists to fill their staffing needs. Consequently, the US hospitalist workforce today is characterized by high salaries, work load, and attrition rates.[12]
In this evolving unsaturated market, the attraction‐selection‐attrition framework[13] provides a theoretical construct that predicts that hospitalists and their employers would seek congruence of goals and values early in their relationship through a process of trial and error. This framework assumes that early interactions between workers and organizations serve as opportunities for them to understand if job fit is poor and dissociate or remain affiliated as long as job fit is mutually acceptable. Therefore, job switching on average is expected to increase job fit because workers and organizations gain a better understanding of their own goals and values and choose more wisely the next time.
Other theoretical frameworks, such as the job characteristic model,[14] suggest that over time as workers stay at the same job, they continue to maintain and improve job fit through various workplace‐ or self‐modification strategies. For example, seniority status may have privileges (eg, less undesirable call), or workers may create privileged niches through the acquisition of new skills and abilities over time. Hospitalists' tendency to diversify their work‐related activities by incorporating administrative and teaching responsibilities[15] may thus contribute to improving job fit. Additionally, as a measure of complementarity among people who work together, job fit may be influenced by the quality of relationships among hospitalists and their coworkers through their reorientation to the prevailing organizational climate[16, 17] and increasing socialization.[18] Finally, given that experiential learning is known to contribute to better hospitalist work performance,[19] job fit may affect productivity and clinical outcomes vis‐‐vis quality of work life.
To test the validity of these assumptions in a sample of hospitalists, we critically appraised the following 4 hypotheses:
- Hypothesis 1 (H1): Job attrition and reselection improves job fit among hospitalists entering the job market.
- Hypothesis 2 (H2): Better job fit is achieved through hospitalists engaging a variety of personal skills and abilities.
- Hypothesis 3 (H3): Job fit increases with hospitalists' job duration together with socialization and internalization of organizational values.
- Hypothesis 4 (H4): Job fit is correlated with hospitalists' quality of work life.
METHODS
Analysis was performed on data from the 2009 to 2010 Hospital Medicine Physician Worklife Survey. The sample frame included nonmembers and members of Society of Hospital Medicine (SHM). Details about sampling strategy, data collection, and data quality are available in previous publications.[7, 20] The 118‐item survey instrument, including 9 demographic items and 24 practice and job characteristic items, was administered by mail. Examples of information solicited through these items included respondents' practice model, the number of hospitalist jobs they have held, and the specific kinds of clinical and nonclinical activities they performed as part of their current job.
We used a reliable but broad and generic measure of self‐perceived person‐job fit.[21] The survey items of the 5‐point Likert‐type scale anchored between strongly disagree and strongly agree were: I feel that my work utilizes my full abilities, I feel competent and fully able to handle my job, my job gives me the chance to do the things I feel I do best, I feel that my job and I are well‐matched, I feel I have adequate preparation for the job I now hold. The quality of hospitalists' relationships with physician colleagues, staff, and patients as well as job satisfaction was measured using scales adapted from the Physician Worklife Study.[22] Organizational climate was measured using an adapted scale from the Minimizing Error, Maximizing Outcome study incorporating 3 items from the cohesiveness subscale, 4 items from the organizational trust subscale, and 1 item from the quality emphasis subscale that were most pertinent to hospitalists' relationship with their organizations.[23] Intent to leave practice or reduce work hours was measured using 5 items from the Multi‐Center Hospitalist Survey Project.[24] Frequency of participation in suboptimal patient care was measured by adapting 3 items from the suboptimal reported practice subscale and 2 items from the suboptimal patient care subscale developed by Shanafelt et al.[25] Stress and job burnout were assessed using validated measures.[26, 27] Detailed descriptions of the response rate calculation and imputation of missing item data are available in previous publications.[7, 20]
Mean, variance, range, and skew were used to characterize the responses to the job fit survey scale. A table of respondent characteristics was constructed. A visual representation of job fit by individual hospitalist year in current practice was created, first, by plotting a locally weighted scatterplot smoothing curve to examine the shape of the general relationship, and second, by fitting a similarly contoured functional polynomial curve with 95% confidence intervals (CI) to a plot of the mean and interquartile range of job fit for each year in current practice. Spearman partial correlations were calculated for job fit and each of the 5 items addressing likelihood of leaving practice or reducing workload adjusted for gender to control for the higher proportion of women who plan to work part time. Median (interquartile range) job fit was calculated for categories defined by the number of job changes and compared with the reference category (no job change) using the nonparametric rank sum test for comparing non‐normally distributed data. Multivariate logistic regression models were used to calculate the odds ratio (OR) of participating in each of several clinical and nonclinical hospitalist activities between respondents whose job fit score was optimal (5 on a 5‐point scale) and less than optimal controlling for covariates that influence the likelihood of participating in these activities (years in current practice, practice model, and specialty training). A Spearman correlation matrix was created to assess interscale correlations among organizational parameters (years in current practice, job fit, organizational climate, and relationship with colleagues, staff, and patients). Finally, a separate Spearman correlation matrix was created to assess the interscale correlations among individual worker parameters (job fit, suboptimal patient care, job burnout, stress, and job satisfaction). Statistical significance was defined as P value <0.05, and all analyses were performed on Stata 11.0 (StataCorp, College Station, TX). The Northwestern University institutional review board approved this study.
RESULTS
Respondents included 816 hospitalists belonging to around 700 unique organizations. The adjusted response rate from the stratified sample was 26%. Respondents and nonrespondents were similar with regard to geographic region and model of practice, but respondents were more likely to be members of the SHM than nonrespondents. Panel A of Table 1 shows the demographic characteristics of the respondents. The mean age was 44.3 years, and about one‐third were women. The average hospitalist had about 7 years of experience in the specialty and about 5 years with their current hospitalist job. The majority were trained in internal medicine or one of its subspecialties, whereas pediatricians, family physicians, and physicians with other training made up the remainder.
| Panel A | Panel B | ||
|---|---|---|---|
| Total | Assimilation Period Hospitalists | Advancement Period Hospitalists | |
| |||
| Total, n | 816 | 103 | 713 |
| Female, n (%) | 284 (35) | 37 (36) | 247 (35) |
| Age, mean (SD) | 44.3 (9.0) | 41.9 (9.3) | 44.7 (8.9) |
| Years postresidency experience as hospitalist, mean (SD) | 6.9 (4.5) | 4.3 (3.1) | 7.2 (4.6) |
| Years in current practice, mean (SD) | 5.1 (3.9) | 0.9 (0.3) | 6.7 (3.8) |
| Specialty training, n (%) | |||
| Internal medicine | 555 (68) | 75 (73) | 480 (67) |
| Pediatrics | 117 (14) | 8 (8) | 109 (15.3) |
| Family medicine | 49 (6) | 7 (7) | 42 (6) |
| Other | 95 (11) | 13 (13) | 82 (12) |
Job fit was highly skewed toward optimum fit, with a mean of 4.3 on a scale of 1 to 5, with a narrow standard deviation of 0.7. The poorest job fit was reported by 0.3%, whereas optimal fit was reported by 21% of respondents. Job fit plotted against years in current practice had a logarithmic appearance typical of learning curves (Figure 1). An inflection point was visualized at around 2 years. For the purposes of this article, we refer to hospitalists' experience in the first 2 years of a job as an assimilation period, which is marked by a steep increase in job fit early when rapid learning or attrition took place. The years beyond the inflection point are characterized as an advancement period, when a more attenuated rise in job fit was experienced with time. The Spearman correlation between job fit and years in practice during the advancement period was 0.145 (n = 678, P < 0.001). Panel B of Table 1 displays the characteristics of respondents separately for the assimilation and advancement cohorts. Assimilation hospitalists in our sample had a mean age of 41.9 years and mean on‐the‐job experience of 4.3 years, reflecting that many hospitalists in the first 2 years of a job have made at least 1 job change in the past.
To show the effects of attrition and reselection, we first evaluated the proposition that hospitalists experience attrition (ie, intend to leave their jobs) in response to poor fit. Table 2 shows the correlations between job fit and the self‐reported intent to leave practice or reduce workload separately for the assimilation and advancement periods. For hospitalists in the assimilation period, job fit was negatively correlated with intent to leave current practice within 2 years and to leave hospital medicine within 5 years (P = 0.010 and 0.043, respectively). Hospitalists with <2 years in their current job, therefore, tended to consider attrition but not workload reduction to deal with poor job fit. On the other hand, hospitalists in the advancement period considered both attrition and workload reduction strategies in response to poor fit (all P < 0.001).
| Assimilation Period Hospitalists | Advancement Period Hospitalists | |||
|---|---|---|---|---|
| Rho | P Value | Rho | P Value | |
| Likelihood that a hospitalist will: | ||||
| Leave current practice within 2 years | 0.253 | 0.010 | 0.367 | <0.001 |
| Decrease total work hours within 5 years | 0.060 | 0.548 | 0.179 | <0.001 |
| Decrease clinical work hours within 5 years | 0.072 | 0.469 | 0.144 | <0.001 |
| Leave hospital medicine within 5 years | 0.200 | 0.043 | 0.231 | <0.001 |
| Leave direct patient care within 5 years | 0.040 | 0.691 | 0.212 | <0.001 |
In Table 3, we further compared the median job fit across categories for the number of job switches. The median job fit during the assimilation period of hospitalists who had made 1 job change was slightly but statistically higher than the job fit of their counterparts who never left their first job (4.4 vs 4.0, P = 0.046). This suggests that job switching by hospitalists early in their jobs is associated with improved job fit (H1). However, the fit during the assimilation period of hospitalists who switched jobs twice or more was statistically no different from the fit of those in their first jobs, suggesting that the effect of the attrition‐reselection strategy is weak or inconsistent. The job fit for advancement period hospitalists was also different across the job change and no‐change categories. However, in the case of hospitalists later in their jobs, the median job fit was slightly but statistically lower among those who made job changes, revealing the potential drop in job fit that occurs when a hospitalist already established in his or her job starts over again in a new setting.
| n | Age, Mean (95% CI), y | Hospitalist‐Job Fit, Median (IQR) | P Valuea | |
|---|---|---|---|---|
| ||||
| Assimilation period hospitalistsb | ||||
| No job change | 29 | 42.3 (37.347.3) | 4.0 (3.84.4) | Reference |
| 1 job change | 39 | 40.3 (38.142.5) | 4.4 (4.04.8) | 0.046 |
| 2 or more job changes | 27 | 43.8 (41.046.6) | 4.4 (3.84.8) | 0.153 |
| Advancement period hospitalistsc | ||||
| No job change | 390 | 44.5 (43.645.5) | 4.6 (4.05.0) | Reference |
| 1 job change | 183 | 45.0 (43.746.3) | 4.2 (4.04.8) | 0.002 |
| 2 or more job changes | 99 | 44.9 (43.146.6) | 4.2 (3.84.8) | 0.002 |
We hypothesized that hospitalists who achieved high job fit within a particular job were more likely to have engaged in activities that utilize a wider spectrum of their abilities. As shown in Table 4, hospitalists in the highest quartile of job fit were associated with a general trend toward higher odds of participating in a variety of common clinical and nonclinical hospitalist activities, but only the odds ratio associated with teaching achieved statistical significance (OR: 1.53, 95% CI: 1.01‐2.31) (H2).
| Participation, n/N (%) | Odds Ratio (95% CI) | P Value | |
|---|---|---|---|
| |||
| Administrative or committee work | 704/816 (86) | 0.73 (0.431.26) | 0.262 |
| Quality improvement or patient safety initiatives | 678/816 (83) | 1.13 (0.642.00) | 0.680 |
| Information technology design or implementation | 379/816 (46) | 1.18 (0.801.73) | 0.408 |
| Any of the above leadership activities | 758/816 (93) | 1.31 (0.563.05) | 0.535 |
| Teaching | 442/816 (54) | 1.53 (1.012.31) | 0.046 |
| Research | 120/816 (15) | 1.07 (0.601.92) | 0.816 |
| Any of the above academic activities | 457/816 (56) | 1.50 (0.992.27) | 0.057 |
| Code team or rapid response team | 437/816 (54) | 1.13 (0.771.68) | 0.533 |
| Intensive care unit | 254/816 (31) | 0.84 (0.531.35) | 0.469 |
| Skilled nursing facility or long‐term acute care facility | 126/816 (15) | 1.06 (0.621.81) | 0.835 |
| Outpatient general medical practice | 44/816 (5) | 1.75 (0.813.80) | 0.157 |
| Any of the above clinical activities | 681/816 (79) | 1.02 (0.601.76) | 0.930 |
Socialization with peers and the gradual sharing of values within organizations are hypothesized mechanisms for increasing job fit with time. We found that the number of years in current practice was positively correlated with job fit (Spearman coefficient R = 0.149, P < 0.001), organizational climate (R = 0.128, P < 0.001), and relationship with nonphysician staff (R = 0.102, P < 0.01). The association between years in practice and relationship with physician colleagues were weaker (R = 0.079, P < 0.05). Consistent with the episodic nature of patients' encounters with hospitalists, the measure of patient relationships was not significantly associated with length of time in job. In addition, we found substantial correlations among job fit, organizational climate, and all the relational measures (all R > 0.280, P < 0.001), indicating that hospitalists increasingly share the values of their organizations over time (H3).
Finally, we also hypothesized that poor job fit is associated with poor performance and quality of work life. Strong correlations with job fit were noted for stress (R = 0.307, P < 0.001), job burnout (R = 0.360, P < 0.001), and job satisfaction (R = 0.570, P < 0.001). Job fit (R = 0.147, P < 0.001), job burnout (R = 0.236, P < 0.001), stress (R = 0.305, P < 0.001), and job satisfaction (R = 0.224, P < 0.001) were all significantly correlated with the frequency of participating in suboptimal care (H4).
DISCUSSION
In this exploratory analysis, we validated in the hospitalist workforce several assumptions about person‐job fit that have been observed in workers of other industries. We observed attrition‐reselection (ie, job switching) as a strategy used by physicians to achieve better fit early in their job tenure, whereas job modification appeared to be more effective than attrition‐reselection among physicians already established in their jobs. We provided weak but plausible evidence that physicians with optimal job fit had a tendency to participate in activities (eg, teaching) that engage a wider set of interests and abilities. We also demonstrated the growth in hospitalists sharing the values of their organization through the time‐dependent associations among organizational climate, relational measures, and job fit. Finally, we found that physicians with suboptimal job fit were more likely to report poor performance in their work compared to those indicating optimal fit.
Our previous analysis of data from the Hospital Medicine Physician Worklife Survey exposed the widely variable work characteristics of hospitalist jobs in the US market and the equally variable preferences and priorities of individual hospitalists in selecting their work setting.[7] The implication of our present study is that hospitalists achieve the high levels of observed job fit using various strategies that aid their alignment with their employment. One of these strategies involves time, but physician longevity in practice may be both a determinant and product of good job fit. Although early job attrition may be necessary for fitting the right hospitalists to the right jobs, employers may appreciate the importance of retaining experienced hospitalists not only for cost and performance considerations but also for the growth of social capital in organizations consisting of enduring individuals. As our data suggest that hospitalists grow with their jobs, physicians may experience better fit with jobs that flexibly couple their work demands with benefits that address their individual work‐life needs over time. Another implication of this study is that job fit is a useful and predictive measure of job selection, performance, and retention. In light of studies that expose the limitations of job satisfaction as a measure influenced more by workers' dispositional affect (ie, their temperament and outlook) than their compatibility with their jobs,[28] job fit may add a functional dimension to traditional employee feedback measures.
There are limitations to this analysis. The most notable is the low survey response rate. Two reasons contributed to the fairly low rate of return. First, the original sampling frame included many outdated addresses and names of individuals who did not meet inclusion criteria. Although all sampled individuals who would have been excluded from the study could not be identified, we calculated our response rate without accounting for the proportion of potential ineligibles in the denominator population [Response Rate 2 (RR2) according to standards of the American Association of Public Opinion Research].[29] Second, the response rates of physician surveys have seen a steady decline over the years.[30] Respondents to our survey may be older and more experienced than US hospitalists in general. Although concerns about bias from under‐reporting cannot be fully addressed, we believe that the study sample is adequate for this preliminary study intended to translate the evidence of observed phenomena from the nonphysician to the physician workforces. The suboptimal response characteristics (high skew and low variability) of the generic person‐job fit survey scale used in this study indicate that a reliable survey instrument specifically designed to measure physician‐job fit need to be constructed de novo and validated for any future study. Although we performed simple analyses to support our assertions, few of our subanalyses may be underpowered, contributing to overinterpretation of the data. Additional empirical work is also necessary to assess the generalizability of this study's claims in other medical and surgical specialties. Such studies would also allow measurement of the sensitivity and specificity of physicians' self‐identification of poor job fit. Finally, additional investigations of this time‐dependent construct are more appropriately performed using a longitudinal study design to overcome the limitations inherent in this cross‐sectional analysis. Our conclusions about the time‐dependent features of job fit may be explained by other characteristics such as generational and cultural differences among hospitalists with varying experience.
As the US healthcare system reorganizes to bolster accountability,[31] we anticipate increasing interdependence between physicians and their employer organizations. Ultimately, the desired accountability in healthcare is likely to be obtained if physicians function not only as passive and interchangeable employees but as active stakeholders in the achievement of each organization's goals. A methodology for assessing the alignment of physicians and their jobs will continue to be important along the way.
Disclosure
Nothing to report.
- . Person‐organization fit: an integrative review of its conceptualizations, measurement, and implications. Personnel Psychol. 1996;49:1–49.
- , , . Consequences of individuals' fit at work: a meta‐analysis of person‐job, person‐organization, person‐group, and person‐supervisor fit. Personnel Psychol. 2005;58(2):281–342.
- .Person‐job fit: a conceptual integration, literature review and methodological critique. In: Cooper CL, Robertson IT, eds. International Review of Industrial and Organizational Psychology. Vol.6. New York, NY:John Wiley 1991.
- . Organizational culture, person‐culture fit, and turnover: a replication in the health care industry. J Organ Behav. 1999;20(2):175–184.
- , , , . Organizational culture and physician satisfaction with dimensions of group practice. Health Serv Res. 2007;42(3 pt 1):1150–1176.
- , , , et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169(10):990–995.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- . Provider‐hospital “fit” and patient outcomes: evidence from Massachusetts cardiac surgeons, 2002–2004. Health Serv Res. 2011;46(1 pt 1):1–26.
- . The evolving primary care physician. N Engl J Med. 2012;366(20):1849–1853.
- , . Hospitals' race to employ physicians—the logic behind a money‐losing proposition. N Engl J Med. 2011;364(19):1790–1793.
- 2011 Survey of Final‐Year Medical Residents. Irving, TX:Merritt Hawkins;2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO:Society of Hospital Medicine and the Medical Group Management Association;2010.
- , , . The ASA framework: an update. Personnel Psychol. 1995;48(4):747–773.
- , . Work Redesign. Reading. MA:Addison‐Wesley;1980.
- , . The expanding role of hospitalists in the United States. Swiss Med Wkly. 2006;136(37–38):591–596.
- , . Organizational socialization as a learning‐process—the role of information acquisition. Personnel Psychol. 1992;45(4):849–874.
- , . The moderating effect of tenure in person‐environment fit: a field study in educational organizations. J Occup Organ Psych. 1997;70:173–188.
- . Matching people and organizations—selection and socialization in public accounting firms. Admin Sci Quart. 1991;36(3):459–484.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- . Karasek's model in the People's Republic of China: effects of job demands, control, and individual differences. Acad Manage J. 1996;39(6):1594–1618.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO Study. Adv Patient Saf. 2005;1:65–77.
- , , , et al. Effects of inpatient experience on outcomes and costs in a multicenter trial of academic hospitalists. J Gen Intern Med. 2005;20(suppl 1):141–142.
- , , , . Burnout and self‐reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358–367.
- , . Effect of job demands and social support on worker stress—a study of VDT users. Behav Inform Technol. 1995;14(1):32–40.
- , , . Validation of a single‐item measure of burnout against the Maslach Burnout Inventory among physicians. Stress Health. 2004;20(2):75–79.
- , . Job satisfaction: a meta‐analysis of stabilities. J Organ Behav. 2001;22(5):483–504.
- The American Association for Public Opinion Research. Standard definitions: final dispositions of case codes and outcome rates for surveys.7th ed. Available at: http://www.aapor.org/Standard_Definitions2.htm. Accessed May 2,2012.
- , , , . Response rates and response bias for 50 surveys of pediatricians. Health Serv Res. 2005;40(1):213–226.
- , . Accountable care organizations: accountable for what, to whom, and how. JAMA. 2010;304(15):1715–6.
- . Person‐organization fit: an integrative review of its conceptualizations, measurement, and implications. Personnel Psychol. 1996;49:1–49.
- , , . Consequences of individuals' fit at work: a meta‐analysis of person‐job, person‐organization, person‐group, and person‐supervisor fit. Personnel Psychol. 2005;58(2):281–342.
- .Person‐job fit: a conceptual integration, literature review and methodological critique. In: Cooper CL, Robertson IT, eds. International Review of Industrial and Organizational Psychology. Vol.6. New York, NY:John Wiley 1991.
- . Organizational culture, person‐culture fit, and turnover: a replication in the health care industry. J Organ Behav. 1999;20(2):175–184.
- , , , . Organizational culture and physician satisfaction with dimensions of group practice. Health Serv Res. 2007;42(3 pt 1):1150–1176.
- , , , et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169(10):990–995.
- , , , , . Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410.
- . Provider‐hospital “fit” and patient outcomes: evidence from Massachusetts cardiac surgeons, 2002–2004. Health Serv Res. 2011;46(1 pt 1):1–26.
- . The evolving primary care physician. N Engl J Med. 2012;366(20):1849–1853.
- , . Hospitals' race to employ physicians—the logic behind a money‐losing proposition. N Engl J Med. 2011;364(19):1790–1793.
- 2011 Survey of Final‐Year Medical Residents. Irving, TX:Merritt Hawkins;2011.
- State of Hospital Medicine: 2010 Report Based on 2009 Data. Englewood, CO:Society of Hospital Medicine and the Medical Group Management Association;2010.
- , , . The ASA framework: an update. Personnel Psychol. 1995;48(4):747–773.
- , . Work Redesign. Reading. MA:Addison‐Wesley;1980.
- , . The expanding role of hospitalists in the United States. Swiss Med Wkly. 2006;136(37–38):591–596.
- , . Organizational socialization as a learning‐process—the role of information acquisition. Personnel Psychol. 1992;45(4):849–874.
- , . The moderating effect of tenure in person‐environment fit: a field study in educational organizations. J Occup Organ Psych. 1997;70:173–188.
- . Matching people and organizations—selection and socialization in public accounting firms. Admin Sci Quart. 1991;36(3):459–484.
- , , , et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(11):866–874.
- , , , , . Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. 2012;27(1):28–36.
- . Karasek's model in the People's Republic of China: effects of job demands, control, and individual differences. Acad Manage J. 1996;39(6):1594–1618.
- , , , et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. 1999;37(11):1174–1182.
- , , , et al. Organizational climate, stress, and error in primary care: The MEMO Study. Adv Patient Saf. 2005;1:65–77.
- , , , et al. Effects of inpatient experience on outcomes and costs in a multicenter trial of academic hospitalists. J Gen Intern Med. 2005;20(suppl 1):141–142.
- , , , . Burnout and self‐reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358–367.
- , . Effect of job demands and social support on worker stress—a study of VDT users. Behav Inform Technol. 1995;14(1):32–40.
- , , . Validation of a single‐item measure of burnout against the Maslach Burnout Inventory among physicians. Stress Health. 2004;20(2):75–79.
- , . Job satisfaction: a meta‐analysis of stabilities. J Organ Behav. 2001;22(5):483–504.
- The American Association for Public Opinion Research. Standard definitions: final dispositions of case codes and outcome rates for surveys.7th ed. Available at: http://www.aapor.org/Standard_Definitions2.htm. Accessed May 2,2012.
- , , , . Response rates and response bias for 50 surveys of pediatricians. Health Serv Res. 2005;40(1):213–226.
- , . Accountable care organizations: accountable for what, to whom, and how. JAMA. 2010;304(15):1715–6.
Copyright © 2012 Society of Hospital Medicine
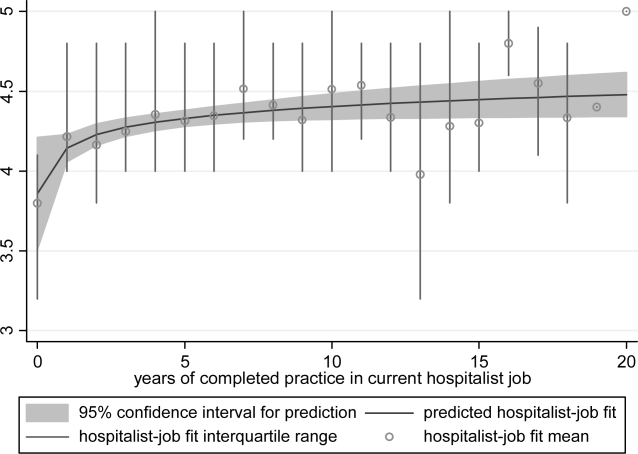
Analysis of Serum Folate Testing
Folate deficiency has been associated with a number of medical conditions. It is well established that folate deficiency leads to macrocytic anemia,[1, 2] and that supplementation of folic acid during pregnancy leads to decreased rates of neural tube defects.[3] Folate deficiency has also been hypothesized to affect other conditions including dementia, delirium, peripheral neuropathy, depression, cancer, and cardiovascular disease.[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18] Most of these latter assertions are based on case reports or observational studies, with randomized controlled trials failing to demonstrate benefit of folic acid supplementation.[19, 20, 21]
Prior to mandatory folic acid fortification in the United States, the prevalence of folate deficiency was estimated to be between 3% and 16%.[16, 22, 23] In a study conducted prior to fortification, serum folate levels were evaluated in patients presenting with macrocytosis and anemia.[24] The study found that 2.3% of patients were serum folate deficient, with a change in management occurring in 24% of the deficient patients. The study also found that patients were charged $9979 per result that changed physician management.
In 1998, mandatory folic acid fortification began in the United States, and the prevalence of folate deficiency in the general population decreased to an estimated 0.5%.[23, 25] In a postfortification study, serum folate levels were evaluated in patients with anemia, dementia, or altered mental status.[26] The overall rate of serum folate deficiency was 0.4%, with the authors concluding that there was a lack of utility in serum folate testing. Despite this, algorithms addressing the evaluation of anemia continue to include serum folate levels.[2, 27, 28]
To our knowledge, the use of serum folate testing in the inpatient and emergency department population has never been independently evaluated. In our study, we aimed to characterize the indications, rate of deficiency, charge and cost per deficient result, and change in management per deficient result in inpatient and emergency department serum folate testing. We hypothesized that serum folate testing in these populations would have poor utility and would not be cost‐effective for any indication.
METHODS
We conducted a retrospective review of all serum folate tests ordered in inpatient units and the emergency department at a large academic medical center in Boston, Massachusetts from January 1, 2011 through December 31, 2011. The test was considered to be an inpatient or emergency department test based on the location of the blood draw on which the test was performed. Serum folate values were determined using a chemiluminescent competitive binding protein assay on an E170 analyzer as prescribed by the manufacturer (Roche Diagnostics, Indianapolis, IN). We defined serum folate levels as deficient (3.0 ng/mL), low‐normal (3.0 ng/mL3.9 ng/mL),[26] normal (4.0 ng/mL20.0 ng/mL), and high (>20.0 ng/mL). Erythrocyte folate levels are not routinely ordered at our institution and were not measured in our study.[29] Macrocytosis was defined as mean corpuscular volume of >99 fL. Vitamin B12 deficiency was defined as vitamin B12 level of under 200 pg/mL or vitamin B12 level of 200 to 300 pg/mL, with a methylmalonic acid >270 nmol/L and a normal homocysteine level (514 mol/L).[30, 31]
We evaluated 250 randomly selected serum folate levels and all deficient or low‐normal serum folate levels and recorded indication, comorbidities, age, sex, race or ethnicity, hemoglobin, hematocrit, mean corpuscular volume, vitamin B12 level, folic acid supplement on presentation, and folic acid supplement on discharge. Indications were determined by chart review. If serum folate was checked at the same time as iron studies, it was assumed that the indication was anemia without macrocytosis or anemia with macrocytosis unless otherwise documented. Comorbidities were selected based on historical risk factors and included depression, peripheral neuropathy, intestinal surgery, gastric bypass, cirrhosis, inflammatory bowel disease, celiac disease, delirium, dementia, alcohol abuse, malnutrition, anemia, end‐stage renal disease, vitamin B12 deficiency, or current use of phenytoin, valproic acid, or methotrexate.[32]
A charge analysis was performed using the same methodology as Robinson and Mladenovic.[24] We defined the charge of serum folate testing as our institution's charge to the patient or payer, which was $151.00 per test. Because hospital charges are variable, we also made a second calculation based on the charge per patient or payer from the Robinson and Mladenovic study,[24] which was $71.00. The analytical cost to our hospital of performing each serum folate test was <$2.00. We determined the total charge and cost for all serum folate tests and the charge and cost per deficient result.
The study was reviewed by the institutional review board and determined to be exempt.
RESULTS
In 2011, a total of 2093 serum folate levels were obtained on 1944 inpatients and emergency department patients. Of the total patients, 79.9% were inpatients and 20.1% were emergency department patients. Of the patients with tests performed in the emergency department, 98.1% were admitted to an inpatient unit.
Of the 250 random chart reviews, all had normal or high serum folate levels. The demographics, indications, and comorbidities are listed in Table 1. The most common indications were anemia without macrocytosis (43.2%), anemia with macrocytosis (13.2%; mean corpuscular volume [MCV], 106.8 fL), delirium (12.0%), malnutrition (6.4%), and peripheral neuropathy (6.0%). The other indications included thrombocytopenia, macrocytosis (without anemia), methotrexate use, alcohol abuse, frequent falls, syncope, headache, lethargy, optic nerve neuropathy, paranoia, psychosis, leukopenia, anxiety, and suicidal ideation. All of these individual indications were 2% of total reviewed indications. There were 16 cases (6.4%) without a documented indication.
| |
| Age, median, y | 66.0 |
| Male sex, % | 50.8 |
| Race or ethnicity, % | |
| White | 76.0 |
| Black or African American | 12.0 |
| Asian | 4.4 |
| Hispanic | 4.0 |
| Unknown or declined | 2.0 |
| Other | 1.6 |
| Indications, %* | |
| Anemia without macrocytosis | 43.2 |
| Anemia with macrocytosis | 13.2 |
| Delirium | 12.0 |
| Malnutrition | 6.4 |
| Peripheral neuropathy | 6.0 |
| Depression | 3.6 |
| Dementia | 3.2 |
| Pancytopenia | 2.4 |
| Other | 10.4 |
| Unknown | 6.4 |
| Comorbidities, % | |
| Depression | 23.2 |
| Alcohol abuse | 18.4 |
| Chronic anemia | 11.2 |
| Malnutrition | 9.6 |
| Prior intestinal surgery | 8.8 |
| Peripheral neuropathy | 6.0 |
| Dementia | 5.6 |
| Gastric bypass surgery | 4.4 |
| End‐stage renal disease | 4.0 |
| End‐stage liver disease | 3.6 |
| Use of phenytoin | 3.2 |
| Inflammatory bowel disease | 2.4 |
| Use of valproic acid | 2.0 |
| Celiac disease | 1.2 |
Of the 2093 serum folate levels, there were 2 deficient (0.1%), 7 low‐normal (0.3%), 1487 normal (71.1%), and 597 high (28.5%) levels (Table 2). There were 128 patients (6.6%) who had more than 1 serum folate level checked within the prior 12 months, with 1 patient having 5 levels obtained during that time period. All of the deficient and low‐normal serum folate results are listed in Table 3. Of the 9 deficient or low‐normal serum folate levels, 8 had comorbid risk factors for folate deficiency. One of the deficient cases was on folic acid and multivitamin supplementation on presentation, although nonadherence with these supplements was documented in the medical record. The other deficient case was not on folic acid supplementation and did not receive folic acid supplementation for the deficient result. Vitamin B12 levels were checked simultaneously to serum folate levels in 85.2% of cases and within 6 months in 99.2% of cases. Of these patients, 2.0% were found to have vitamin B12 deficiency.
| |
| Total tests | 2093 |
| Total patients | 1944 |
| Low (%) | 2 (0.1) |
| Low‐normal (%) | 7 (0.3) |
| Normal (%) | 1487 (71.0) |
| High (%) | 597 (28.5) |
| MCV (StDev) | 92.1 (9.2) |
| Age, y | Sex | Folate (ng/mL) | Indication | Comorbidities | Hgb (g/dL) | MCV (fL) | |
|---|---|---|---|---|---|---|---|
| |||||||
| Deficient results | |||||||
| Case 1 | 35 | Male | 2.6 | Stroke workup | Phenytoin, depression | 16.0 | 91 |
| Case 2 | 63 | Male | 2.9 | Macrocytic anemia | Alcohol abuse, acute GI bleed | 7.7 | 119 |
| Low‐normal results | |||||||
| Case 3 | 64 | Male | 3.3 | Macrocytic anemia | Cirrhosis, alcohol abuse | 12.3 | 109 |
| Case 4 | 42 | Male | 3.4 | Pancytopenia | HIV, B12 deficiency | 7.5 | 93 |
| Case 5 | 58 | Male | 3.4 | Depression | Depression, alcohol abuse | 13.8 | 98 |
| Case 6 | 56 | Female | 3.5 | Depression | Alcohol abuse | ||
| Case 7 | 85 | Male | 3.6 | Delirium | Depression | 10.5 | 91 |
| Case 8 | 81 | Female | 3.6 | Anemia | Chronic anemia | 9.1 | 95 |
| Case 9 | 63 | Male | 3.9 | Anemia | Chronic anemia, malnutrition | 7.6 | 88 |
Based on our institution's charge for serum folate, a total of $316,043 was charged for the 2093 serum folate tests. The amount charged per deficient result was $158,022. Substituting the charge from the Robinson and Mladenovic study,[24] we calculated the corresponding total charge and charge per deficient result as $149,545 and $74,772, respectively. The actual total cost to our hospital was <$4186, with a cost per deficient test of <$2093.
DISCUSSION
Serum folate levels are often obtained when evaluating anemia without macrocytosis and anemia with macrocytosis.[2] They are also frequently obtained in the evaluation of delirium and dementia. A prior study evaluated both inpatient and outpatient serum folate levels in anemia, dementia, and altered mental status and found only 0.4% of serum folate results to be deficient.[26] In their study, the indications for serum folate tests were anemia or macrocytic anemia (60%) and dementia or altered mental status (30%).
We found the indications for serum folate testing in inpatients and emergency department patients to be different than prior studies. The majority of tests were done to evaluate anemia without macrocytosis (43.2%) or anemia with macrocytosis (13.2%). Lower percentages were done for the evaluation of delirium (12.0%) or dementia (3.2%). In addition, there were multiple indications that have not been noted in previous studies, including depression, peripheral neuropathy, malnutrition, pancytopenia, and others. These accounted for 28.0% of all indications. The reason for the difference in indications compared to prior studies is unknown but may be related to our cohort of exclusively inpatients and emergency department patients. Also, we observed a high concurrence of serum folate and vitamin B12 testing, with 85.2% of serum folate levels ordered at the same time as vitamin B12 levels. It appears that the tests are often ordered together even when the indication suggests that vitamin B12 alone may be more appropriate, such as peripheral neuropathy.
We found that serum folate deficiency was rare, occurring in only 2 of 2093 results. Furthermore, the deficient serum folate results may have been checked for inappropriate indications. The first deficient result was noted as part of a stroke workup in a patient not taking folic acid supplementation. Current guidelines do not recommend serum folate testing in patients with new stroke.[33] In the second deficient case, serum folate testing was performed for evaluation of macrocytic anemia with an MCV of 119 fL. Although reasonable, this was an alcoholic patient presenting with acute gastrointestinal bleeding already on folic acid and multivitamin supplementation and known nonadherence with these supplements. In neither case was there a change in management based on the deficient result.
Given the low rate of serum folate deficiency and the lack of change in management based on deficient results, we conclude that there is a low utility of serum folate testing for any indication in inpatients and emergency department patients in folic acid‐fortified countries. Based on prior studies, and supported by our results, there is no evidence for checking serum folate levels in delirium, dementia, peripheral neuropathy, malnutrition, or any of the other indications. In addition, our results demonstrate a low utility even in patients with anemia or macrocytic anemia.
The rate of serum folate deficiency in our study was significantly lower than prior studies.[24, 26] There may have been geographical factors that led to a lower prevalence of folate deficiency in our study population. Our cohort included inpatients and emergency department patients, whereas previous studies had a majority of outpatients. It is known that serum folate levels can rapidly fluctuate with proper nutrition.[34] It may be that our patients received nutrition in the hospital that corrected serum folate levels prior to laboratory testing.
In addition to the low utility of serum folate testing, the charge per deficient result in our study ($158,022) was more than 100‐fold higher than that in the Robinson and Mladenovic study ($1321).[24] Even when correcting for variability in hospital charges by using the charge from the latter study, the charge per deficient serum folate test remained 50‐fold higher ($74,772). This implies that the increase in charge per deficient result was driven in part by a decreased rate of deficient tests. Folic acid fortification is likely responsible for some of the decrease. However, we believe another source is the excessive ordering of serum folate tests in patients without previously accepted indications. Because no change in management was made for the deficient patients in our study, the charge per serum folate deficient result that changed management approached infinity. This compares to $9979 in the Robinson and Mladenovic analysis.[24]
The cost to the hospital of a serum folate test was much lower than the charge, and estimated to be <$2093 per deficient result. Because serum folate tests are performed on a highly automated, random access analyzer that performs thousands of other measurements daily, the capital and labor costs for each test was well below $0.50 combined. With the addition of reagent costs, our total cost for each serum folate measurement was <$2.00. It is somewhat difficult to extrapolate these values to other hospitals, as exact costs and charges are variable. Nonetheless, the exceptionally low utility of serum folate testing makes the costs associated with these tests excessive.
Our study has several limitations. We conducted our study at a single institution in a country with mandatory folic acid fortification. Our results may not be generalizable to other institutions or patient populations, such as those in countries without mandatory folic acid fortification. Only 259 (12.4%) charts were reviewed, and indications were determined in 93.6% of charts, which may have caused our frequency to vary from the true frequency. Additionally, the low rate of deficient serum folate results limited our ability to identify associations with deficiency. Further evaluation for geographic variations of serum folate deficiency may reveal variable rates.
We conclude that in folic acid fortified countries, the rate of serum folate deficiency is increasingly rare, and the charge to patients and payers per deficient result is exceptionally high. In addition, testing in our study did not change clinical management, which makes the costs associated with these test wasteful. Further evaluation of serum folate testing of inpatients and emergency department patients in folic acid fortified countries is warranted; however, based on our results the utility appears poor for all indications.
Disclosure
Nothing to report.
- , . The biochemical basis of cobalamin deficiency. Mayo Clin Proc. 1994;69(2):181–186.
- , , , et al. Harrison's Principles of Internal Medicine. New York, NY:McGraw‐Hill Professional;2004.
- , . Folic acid, pernicious anaemia, and prevention of neural tube defects. Lancet. 1994;343(8893):307.
- , , , et al. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high‐functioning adults: MacArthur Studies of Successful Aging. Am J Med. 2005;118(2):161–167.
- , . Folate and brain function in the elderly. Curr Opin Clin Nutr Metab Care. 2004;7(6):659–664.
- , , , , , . Plasma homocysteine levels and cognitive status in long‐term stay geriatric patients: a cross‐sectional study. Arch Gerontol Geriatr. 2005;40(2):129–138.
- . Folate responsive neuropathy. Presse Med. 1994;23(3):131–137.
- , . Treatment of depression: time to consider folic acid and vitamin B12. J Psychopharmacol (Oxford). 2005;19(1):59–65.
- , , , et al. Folate deficiency causes uracil misincorporation into human DNA and chromosome breakage: implications for cancer and neuronal damage. Proc Natl Acad Sci U S A. 1997;94(7):3290–3295.
- , , , et al. Folate deficiency in rats induces DNA strand breaks and hypomethylation within the p53 tumor suppressor gene. Am J Clin Nutr. 1997;65(1):46–52.
- , , , , , . Folate intake and carcinogenesis of the colon and rectum. Int J Epidemiol. 1991;20(2):368–374.
- , . Colorectal cancer protective effects and the dietary micronutrients folate, methionine, vitamins B6, B12, C, E, selenium, and lycopene. Nutr Cancer. 2006;56(1):11–21.
- , , , et al. Multivitamin use, folate, and colon cancer in women in the Nurses' Health Study. Ann Intern Med. 1998;129(7):517–524.
- , , , , . Serum homocysteine and folate but not vitamin B12 are predictors of CHD mortality in older adults [published online ahead of print September 29, 2011]. Eur J Cardiovasc Prev Rehabil. doi: 10.1177/1741826711424568.
- , , , , , . Plasma homocyst(e)ine levels in men with premature coronary artery disease. J Am Coll Cardiol. 1990;16(5):1114–1119.
- , , , et al. Low serum folate but normal homocysteine levels in patients with atherosclerotic vascular disease and matched healthy controls. Nutrition. 2000;16(6):434–438.
- , , , , , . Low serum folate concentrations are associated with an excess incidence of acute coronary events: the Kuopio Ischaemic Heart Disease Risk Factor Study. Eur J Clin Nutr. 2000;54(5):424–428.
- , , , , . Dietary folate and the risk of nonfatal myocardial infarction. Epidemiology. 2002;13(6):700–706.
- , , , et al.;Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators. Homocysteine lowering with folic acid and b vitamins in vascular disease. N Engl J Med. 2006;354(15):1567–1577.
- , , , , , . A controlled trial of homocysteine lowering and cognitive performance. N Engl J Med. 2006;354(26):2764–2772.
- , . Folic acid with or without vitamin B12 for the prevention and treatment of healthy elderly and demented people. Cochrane Database Syst Rev. 2008;(4):CD004514.
- , , , . Does the mean corpuscular volume help physicians evaluate hospitalized patients with anemia?J Gen Intern Med. 1990;5(3):187–191.
- , , , , . Biochemical indicators of B vitamin status in the US population after folic acid fortification: results from the National Health and Nutrition Examination Survey 1999–2000. Am J Clin Nutr. 2005;82(2):442–450.
- , . Lack of clinical utility of folate levels in the evaluation of macrocytosis or anemia. Am J Med. 2001;110(2):88–90.
- , , , et al. Blood folate levels: the latest NHANES results. NCHS Data Brief. 2008;(6):1–8.
- , , . Clinical utility of folic acid testing for patients with anemia or dementia. J Gen Intern Med. 2008;23(6):824–826.
- . Anemia in adults: a contemporary approach to diagnosis. Mayo Clin Proc 2003;78(10):1274–1280.
- . Anemia in the elderly. Am Fam Physician. 2000;62(7):1565–1572.
- , . Red cell or serum folate? Results from the National Pathology Alliance benchmarking review. J Clin Pathol. 2003;56(12):924–926.
- , , , , , . Hematology. Philadelphia, PA:Churchill Livingstone;2012.
- , , , . Sensitivity of serum methylmalonic acid and total homocysteine determinations for diagnosing cobalamin and folate deficiencies. Am J Med. 1994;96(3):239–246.
- . Laboratory diagnosis of vitamin B12 and folate deficiency: a guide for the primary care physician. Arch Intern Med. 1999;159(12):1289–1298.
- , , , et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38(5):1655–1711.
- , , , . Predicted serum folate concentrations based on in vitro studies and kinetic modeling are consistent with measured folate concentrations in humans. J Nutr. 2006;136(12):3074–3078.
Folate deficiency has been associated with a number of medical conditions. It is well established that folate deficiency leads to macrocytic anemia,[1, 2] and that supplementation of folic acid during pregnancy leads to decreased rates of neural tube defects.[3] Folate deficiency has also been hypothesized to affect other conditions including dementia, delirium, peripheral neuropathy, depression, cancer, and cardiovascular disease.[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18] Most of these latter assertions are based on case reports or observational studies, with randomized controlled trials failing to demonstrate benefit of folic acid supplementation.[19, 20, 21]
Prior to mandatory folic acid fortification in the United States, the prevalence of folate deficiency was estimated to be between 3% and 16%.[16, 22, 23] In a study conducted prior to fortification, serum folate levels were evaluated in patients presenting with macrocytosis and anemia.[24] The study found that 2.3% of patients were serum folate deficient, with a change in management occurring in 24% of the deficient patients. The study also found that patients were charged $9979 per result that changed physician management.
In 1998, mandatory folic acid fortification began in the United States, and the prevalence of folate deficiency in the general population decreased to an estimated 0.5%.[23, 25] In a postfortification study, serum folate levels were evaluated in patients with anemia, dementia, or altered mental status.[26] The overall rate of serum folate deficiency was 0.4%, with the authors concluding that there was a lack of utility in serum folate testing. Despite this, algorithms addressing the evaluation of anemia continue to include serum folate levels.[2, 27, 28]
To our knowledge, the use of serum folate testing in the inpatient and emergency department population has never been independently evaluated. In our study, we aimed to characterize the indications, rate of deficiency, charge and cost per deficient result, and change in management per deficient result in inpatient and emergency department serum folate testing. We hypothesized that serum folate testing in these populations would have poor utility and would not be cost‐effective for any indication.
METHODS
We conducted a retrospective review of all serum folate tests ordered in inpatient units and the emergency department at a large academic medical center in Boston, Massachusetts from January 1, 2011 through December 31, 2011. The test was considered to be an inpatient or emergency department test based on the location of the blood draw on which the test was performed. Serum folate values were determined using a chemiluminescent competitive binding protein assay on an E170 analyzer as prescribed by the manufacturer (Roche Diagnostics, Indianapolis, IN). We defined serum folate levels as deficient (3.0 ng/mL), low‐normal (3.0 ng/mL3.9 ng/mL),[26] normal (4.0 ng/mL20.0 ng/mL), and high (>20.0 ng/mL). Erythrocyte folate levels are not routinely ordered at our institution and were not measured in our study.[29] Macrocytosis was defined as mean corpuscular volume of >99 fL. Vitamin B12 deficiency was defined as vitamin B12 level of under 200 pg/mL or vitamin B12 level of 200 to 300 pg/mL, with a methylmalonic acid >270 nmol/L and a normal homocysteine level (514 mol/L).[30, 31]
We evaluated 250 randomly selected serum folate levels and all deficient or low‐normal serum folate levels and recorded indication, comorbidities, age, sex, race or ethnicity, hemoglobin, hematocrit, mean corpuscular volume, vitamin B12 level, folic acid supplement on presentation, and folic acid supplement on discharge. Indications were determined by chart review. If serum folate was checked at the same time as iron studies, it was assumed that the indication was anemia without macrocytosis or anemia with macrocytosis unless otherwise documented. Comorbidities were selected based on historical risk factors and included depression, peripheral neuropathy, intestinal surgery, gastric bypass, cirrhosis, inflammatory bowel disease, celiac disease, delirium, dementia, alcohol abuse, malnutrition, anemia, end‐stage renal disease, vitamin B12 deficiency, or current use of phenytoin, valproic acid, or methotrexate.[32]
A charge analysis was performed using the same methodology as Robinson and Mladenovic.[24] We defined the charge of serum folate testing as our institution's charge to the patient or payer, which was $151.00 per test. Because hospital charges are variable, we also made a second calculation based on the charge per patient or payer from the Robinson and Mladenovic study,[24] which was $71.00. The analytical cost to our hospital of performing each serum folate test was <$2.00. We determined the total charge and cost for all serum folate tests and the charge and cost per deficient result.
The study was reviewed by the institutional review board and determined to be exempt.
RESULTS
In 2011, a total of 2093 serum folate levels were obtained on 1944 inpatients and emergency department patients. Of the total patients, 79.9% were inpatients and 20.1% were emergency department patients. Of the patients with tests performed in the emergency department, 98.1% were admitted to an inpatient unit.
Of the 250 random chart reviews, all had normal or high serum folate levels. The demographics, indications, and comorbidities are listed in Table 1. The most common indications were anemia without macrocytosis (43.2%), anemia with macrocytosis (13.2%; mean corpuscular volume [MCV], 106.8 fL), delirium (12.0%), malnutrition (6.4%), and peripheral neuropathy (6.0%). The other indications included thrombocytopenia, macrocytosis (without anemia), methotrexate use, alcohol abuse, frequent falls, syncope, headache, lethargy, optic nerve neuropathy, paranoia, psychosis, leukopenia, anxiety, and suicidal ideation. All of these individual indications were 2% of total reviewed indications. There were 16 cases (6.4%) without a documented indication.
| |
| Age, median, y | 66.0 |
| Male sex, % | 50.8 |
| Race or ethnicity, % | |
| White | 76.0 |
| Black or African American | 12.0 |
| Asian | 4.4 |
| Hispanic | 4.0 |
| Unknown or declined | 2.0 |
| Other | 1.6 |
| Indications, %* | |
| Anemia without macrocytosis | 43.2 |
| Anemia with macrocytosis | 13.2 |
| Delirium | 12.0 |
| Malnutrition | 6.4 |
| Peripheral neuropathy | 6.0 |
| Depression | 3.6 |
| Dementia | 3.2 |
| Pancytopenia | 2.4 |
| Other | 10.4 |
| Unknown | 6.4 |
| Comorbidities, % | |
| Depression | 23.2 |
| Alcohol abuse | 18.4 |
| Chronic anemia | 11.2 |
| Malnutrition | 9.6 |
| Prior intestinal surgery | 8.8 |
| Peripheral neuropathy | 6.0 |
| Dementia | 5.6 |
| Gastric bypass surgery | 4.4 |
| End‐stage renal disease | 4.0 |
| End‐stage liver disease | 3.6 |
| Use of phenytoin | 3.2 |
| Inflammatory bowel disease | 2.4 |
| Use of valproic acid | 2.0 |
| Celiac disease | 1.2 |
Of the 2093 serum folate levels, there were 2 deficient (0.1%), 7 low‐normal (0.3%), 1487 normal (71.1%), and 597 high (28.5%) levels (Table 2). There were 128 patients (6.6%) who had more than 1 serum folate level checked within the prior 12 months, with 1 patient having 5 levels obtained during that time period. All of the deficient and low‐normal serum folate results are listed in Table 3. Of the 9 deficient or low‐normal serum folate levels, 8 had comorbid risk factors for folate deficiency. One of the deficient cases was on folic acid and multivitamin supplementation on presentation, although nonadherence with these supplements was documented in the medical record. The other deficient case was not on folic acid supplementation and did not receive folic acid supplementation for the deficient result. Vitamin B12 levels were checked simultaneously to serum folate levels in 85.2% of cases and within 6 months in 99.2% of cases. Of these patients, 2.0% were found to have vitamin B12 deficiency.
| |
| Total tests | 2093 |
| Total patients | 1944 |
| Low (%) | 2 (0.1) |
| Low‐normal (%) | 7 (0.3) |
| Normal (%) | 1487 (71.0) |
| High (%) | 597 (28.5) |
| MCV (StDev) | 92.1 (9.2) |
| Age, y | Sex | Folate (ng/mL) | Indication | Comorbidities | Hgb (g/dL) | MCV (fL) | |
|---|---|---|---|---|---|---|---|
| |||||||
| Deficient results | |||||||
| Case 1 | 35 | Male | 2.6 | Stroke workup | Phenytoin, depression | 16.0 | 91 |
| Case 2 | 63 | Male | 2.9 | Macrocytic anemia | Alcohol abuse, acute GI bleed | 7.7 | 119 |
| Low‐normal results | |||||||
| Case 3 | 64 | Male | 3.3 | Macrocytic anemia | Cirrhosis, alcohol abuse | 12.3 | 109 |
| Case 4 | 42 | Male | 3.4 | Pancytopenia | HIV, B12 deficiency | 7.5 | 93 |
| Case 5 | 58 | Male | 3.4 | Depression | Depression, alcohol abuse | 13.8 | 98 |
| Case 6 | 56 | Female | 3.5 | Depression | Alcohol abuse | ||
| Case 7 | 85 | Male | 3.6 | Delirium | Depression | 10.5 | 91 |
| Case 8 | 81 | Female | 3.6 | Anemia | Chronic anemia | 9.1 | 95 |
| Case 9 | 63 | Male | 3.9 | Anemia | Chronic anemia, malnutrition | 7.6 | 88 |
Based on our institution's charge for serum folate, a total of $316,043 was charged for the 2093 serum folate tests. The amount charged per deficient result was $158,022. Substituting the charge from the Robinson and Mladenovic study,[24] we calculated the corresponding total charge and charge per deficient result as $149,545 and $74,772, respectively. The actual total cost to our hospital was <$4186, with a cost per deficient test of <$2093.
DISCUSSION
Serum folate levels are often obtained when evaluating anemia without macrocytosis and anemia with macrocytosis.[2] They are also frequently obtained in the evaluation of delirium and dementia. A prior study evaluated both inpatient and outpatient serum folate levels in anemia, dementia, and altered mental status and found only 0.4% of serum folate results to be deficient.[26] In their study, the indications for serum folate tests were anemia or macrocytic anemia (60%) and dementia or altered mental status (30%).
We found the indications for serum folate testing in inpatients and emergency department patients to be different than prior studies. The majority of tests were done to evaluate anemia without macrocytosis (43.2%) or anemia with macrocytosis (13.2%). Lower percentages were done for the evaluation of delirium (12.0%) or dementia (3.2%). In addition, there were multiple indications that have not been noted in previous studies, including depression, peripheral neuropathy, malnutrition, pancytopenia, and others. These accounted for 28.0% of all indications. The reason for the difference in indications compared to prior studies is unknown but may be related to our cohort of exclusively inpatients and emergency department patients. Also, we observed a high concurrence of serum folate and vitamin B12 testing, with 85.2% of serum folate levels ordered at the same time as vitamin B12 levels. It appears that the tests are often ordered together even when the indication suggests that vitamin B12 alone may be more appropriate, such as peripheral neuropathy.
We found that serum folate deficiency was rare, occurring in only 2 of 2093 results. Furthermore, the deficient serum folate results may have been checked for inappropriate indications. The first deficient result was noted as part of a stroke workup in a patient not taking folic acid supplementation. Current guidelines do not recommend serum folate testing in patients with new stroke.[33] In the second deficient case, serum folate testing was performed for evaluation of macrocytic anemia with an MCV of 119 fL. Although reasonable, this was an alcoholic patient presenting with acute gastrointestinal bleeding already on folic acid and multivitamin supplementation and known nonadherence with these supplements. In neither case was there a change in management based on the deficient result.
Given the low rate of serum folate deficiency and the lack of change in management based on deficient results, we conclude that there is a low utility of serum folate testing for any indication in inpatients and emergency department patients in folic acid‐fortified countries. Based on prior studies, and supported by our results, there is no evidence for checking serum folate levels in delirium, dementia, peripheral neuropathy, malnutrition, or any of the other indications. In addition, our results demonstrate a low utility even in patients with anemia or macrocytic anemia.
The rate of serum folate deficiency in our study was significantly lower than prior studies.[24, 26] There may have been geographical factors that led to a lower prevalence of folate deficiency in our study population. Our cohort included inpatients and emergency department patients, whereas previous studies had a majority of outpatients. It is known that serum folate levels can rapidly fluctuate with proper nutrition.[34] It may be that our patients received nutrition in the hospital that corrected serum folate levels prior to laboratory testing.
In addition to the low utility of serum folate testing, the charge per deficient result in our study ($158,022) was more than 100‐fold higher than that in the Robinson and Mladenovic study ($1321).[24] Even when correcting for variability in hospital charges by using the charge from the latter study, the charge per deficient serum folate test remained 50‐fold higher ($74,772). This implies that the increase in charge per deficient result was driven in part by a decreased rate of deficient tests. Folic acid fortification is likely responsible for some of the decrease. However, we believe another source is the excessive ordering of serum folate tests in patients without previously accepted indications. Because no change in management was made for the deficient patients in our study, the charge per serum folate deficient result that changed management approached infinity. This compares to $9979 in the Robinson and Mladenovic analysis.[24]
The cost to the hospital of a serum folate test was much lower than the charge, and estimated to be <$2093 per deficient result. Because serum folate tests are performed on a highly automated, random access analyzer that performs thousands of other measurements daily, the capital and labor costs for each test was well below $0.50 combined. With the addition of reagent costs, our total cost for each serum folate measurement was <$2.00. It is somewhat difficult to extrapolate these values to other hospitals, as exact costs and charges are variable. Nonetheless, the exceptionally low utility of serum folate testing makes the costs associated with these tests excessive.
Our study has several limitations. We conducted our study at a single institution in a country with mandatory folic acid fortification. Our results may not be generalizable to other institutions or patient populations, such as those in countries without mandatory folic acid fortification. Only 259 (12.4%) charts were reviewed, and indications were determined in 93.6% of charts, which may have caused our frequency to vary from the true frequency. Additionally, the low rate of deficient serum folate results limited our ability to identify associations with deficiency. Further evaluation for geographic variations of serum folate deficiency may reveal variable rates.
We conclude that in folic acid fortified countries, the rate of serum folate deficiency is increasingly rare, and the charge to patients and payers per deficient result is exceptionally high. In addition, testing in our study did not change clinical management, which makes the costs associated with these test wasteful. Further evaluation of serum folate testing of inpatients and emergency department patients in folic acid fortified countries is warranted; however, based on our results the utility appears poor for all indications.
Disclosure
Nothing to report.
Folate deficiency has been associated with a number of medical conditions. It is well established that folate deficiency leads to macrocytic anemia,[1, 2] and that supplementation of folic acid during pregnancy leads to decreased rates of neural tube defects.[3] Folate deficiency has also been hypothesized to affect other conditions including dementia, delirium, peripheral neuropathy, depression, cancer, and cardiovascular disease.[4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18] Most of these latter assertions are based on case reports or observational studies, with randomized controlled trials failing to demonstrate benefit of folic acid supplementation.[19, 20, 21]
Prior to mandatory folic acid fortification in the United States, the prevalence of folate deficiency was estimated to be between 3% and 16%.[16, 22, 23] In a study conducted prior to fortification, serum folate levels were evaluated in patients presenting with macrocytosis and anemia.[24] The study found that 2.3% of patients were serum folate deficient, with a change in management occurring in 24% of the deficient patients. The study also found that patients were charged $9979 per result that changed physician management.
In 1998, mandatory folic acid fortification began in the United States, and the prevalence of folate deficiency in the general population decreased to an estimated 0.5%.[23, 25] In a postfortification study, serum folate levels were evaluated in patients with anemia, dementia, or altered mental status.[26] The overall rate of serum folate deficiency was 0.4%, with the authors concluding that there was a lack of utility in serum folate testing. Despite this, algorithms addressing the evaluation of anemia continue to include serum folate levels.[2, 27, 28]
To our knowledge, the use of serum folate testing in the inpatient and emergency department population has never been independently evaluated. In our study, we aimed to characterize the indications, rate of deficiency, charge and cost per deficient result, and change in management per deficient result in inpatient and emergency department serum folate testing. We hypothesized that serum folate testing in these populations would have poor utility and would not be cost‐effective for any indication.
METHODS
We conducted a retrospective review of all serum folate tests ordered in inpatient units and the emergency department at a large academic medical center in Boston, Massachusetts from January 1, 2011 through December 31, 2011. The test was considered to be an inpatient or emergency department test based on the location of the blood draw on which the test was performed. Serum folate values were determined using a chemiluminescent competitive binding protein assay on an E170 analyzer as prescribed by the manufacturer (Roche Diagnostics, Indianapolis, IN). We defined serum folate levels as deficient (3.0 ng/mL), low‐normal (3.0 ng/mL3.9 ng/mL),[26] normal (4.0 ng/mL20.0 ng/mL), and high (>20.0 ng/mL). Erythrocyte folate levels are not routinely ordered at our institution and were not measured in our study.[29] Macrocytosis was defined as mean corpuscular volume of >99 fL. Vitamin B12 deficiency was defined as vitamin B12 level of under 200 pg/mL or vitamin B12 level of 200 to 300 pg/mL, with a methylmalonic acid >270 nmol/L and a normal homocysteine level (514 mol/L).[30, 31]
We evaluated 250 randomly selected serum folate levels and all deficient or low‐normal serum folate levels and recorded indication, comorbidities, age, sex, race or ethnicity, hemoglobin, hematocrit, mean corpuscular volume, vitamin B12 level, folic acid supplement on presentation, and folic acid supplement on discharge. Indications were determined by chart review. If serum folate was checked at the same time as iron studies, it was assumed that the indication was anemia without macrocytosis or anemia with macrocytosis unless otherwise documented. Comorbidities were selected based on historical risk factors and included depression, peripheral neuropathy, intestinal surgery, gastric bypass, cirrhosis, inflammatory bowel disease, celiac disease, delirium, dementia, alcohol abuse, malnutrition, anemia, end‐stage renal disease, vitamin B12 deficiency, or current use of phenytoin, valproic acid, or methotrexate.[32]
A charge analysis was performed using the same methodology as Robinson and Mladenovic.[24] We defined the charge of serum folate testing as our institution's charge to the patient or payer, which was $151.00 per test. Because hospital charges are variable, we also made a second calculation based on the charge per patient or payer from the Robinson and Mladenovic study,[24] which was $71.00. The analytical cost to our hospital of performing each serum folate test was <$2.00. We determined the total charge and cost for all serum folate tests and the charge and cost per deficient result.
The study was reviewed by the institutional review board and determined to be exempt.
RESULTS
In 2011, a total of 2093 serum folate levels were obtained on 1944 inpatients and emergency department patients. Of the total patients, 79.9% were inpatients and 20.1% were emergency department patients. Of the patients with tests performed in the emergency department, 98.1% were admitted to an inpatient unit.
Of the 250 random chart reviews, all had normal or high serum folate levels. The demographics, indications, and comorbidities are listed in Table 1. The most common indications were anemia without macrocytosis (43.2%), anemia with macrocytosis (13.2%; mean corpuscular volume [MCV], 106.8 fL), delirium (12.0%), malnutrition (6.4%), and peripheral neuropathy (6.0%). The other indications included thrombocytopenia, macrocytosis (without anemia), methotrexate use, alcohol abuse, frequent falls, syncope, headache, lethargy, optic nerve neuropathy, paranoia, psychosis, leukopenia, anxiety, and suicidal ideation. All of these individual indications were 2% of total reviewed indications. There were 16 cases (6.4%) without a documented indication.
| |
| Age, median, y | 66.0 |
| Male sex, % | 50.8 |
| Race or ethnicity, % | |
| White | 76.0 |
| Black or African American | 12.0 |
| Asian | 4.4 |
| Hispanic | 4.0 |
| Unknown or declined | 2.0 |
| Other | 1.6 |
| Indications, %* | |
| Anemia without macrocytosis | 43.2 |
| Anemia with macrocytosis | 13.2 |
| Delirium | 12.0 |
| Malnutrition | 6.4 |
| Peripheral neuropathy | 6.0 |
| Depression | 3.6 |
| Dementia | 3.2 |
| Pancytopenia | 2.4 |
| Other | 10.4 |
| Unknown | 6.4 |
| Comorbidities, % | |
| Depression | 23.2 |
| Alcohol abuse | 18.4 |
| Chronic anemia | 11.2 |
| Malnutrition | 9.6 |
| Prior intestinal surgery | 8.8 |
| Peripheral neuropathy | 6.0 |
| Dementia | 5.6 |
| Gastric bypass surgery | 4.4 |
| End‐stage renal disease | 4.0 |
| End‐stage liver disease | 3.6 |
| Use of phenytoin | 3.2 |
| Inflammatory bowel disease | 2.4 |
| Use of valproic acid | 2.0 |
| Celiac disease | 1.2 |
Of the 2093 serum folate levels, there were 2 deficient (0.1%), 7 low‐normal (0.3%), 1487 normal (71.1%), and 597 high (28.5%) levels (Table 2). There were 128 patients (6.6%) who had more than 1 serum folate level checked within the prior 12 months, with 1 patient having 5 levels obtained during that time period. All of the deficient and low‐normal serum folate results are listed in Table 3. Of the 9 deficient or low‐normal serum folate levels, 8 had comorbid risk factors for folate deficiency. One of the deficient cases was on folic acid and multivitamin supplementation on presentation, although nonadherence with these supplements was documented in the medical record. The other deficient case was not on folic acid supplementation and did not receive folic acid supplementation for the deficient result. Vitamin B12 levels were checked simultaneously to serum folate levels in 85.2% of cases and within 6 months in 99.2% of cases. Of these patients, 2.0% were found to have vitamin B12 deficiency.
| |
| Total tests | 2093 |
| Total patients | 1944 |
| Low (%) | 2 (0.1) |
| Low‐normal (%) | 7 (0.3) |
| Normal (%) | 1487 (71.0) |
| High (%) | 597 (28.5) |
| MCV (StDev) | 92.1 (9.2) |
| Age, y | Sex | Folate (ng/mL) | Indication | Comorbidities | Hgb (g/dL) | MCV (fL) | |
|---|---|---|---|---|---|---|---|
| |||||||
| Deficient results | |||||||
| Case 1 | 35 | Male | 2.6 | Stroke workup | Phenytoin, depression | 16.0 | 91 |
| Case 2 | 63 | Male | 2.9 | Macrocytic anemia | Alcohol abuse, acute GI bleed | 7.7 | 119 |
| Low‐normal results | |||||||
| Case 3 | 64 | Male | 3.3 | Macrocytic anemia | Cirrhosis, alcohol abuse | 12.3 | 109 |
| Case 4 | 42 | Male | 3.4 | Pancytopenia | HIV, B12 deficiency | 7.5 | 93 |
| Case 5 | 58 | Male | 3.4 | Depression | Depression, alcohol abuse | 13.8 | 98 |
| Case 6 | 56 | Female | 3.5 | Depression | Alcohol abuse | ||
| Case 7 | 85 | Male | 3.6 | Delirium | Depression | 10.5 | 91 |
| Case 8 | 81 | Female | 3.6 | Anemia | Chronic anemia | 9.1 | 95 |
| Case 9 | 63 | Male | 3.9 | Anemia | Chronic anemia, malnutrition | 7.6 | 88 |
Based on our institution's charge for serum folate, a total of $316,043 was charged for the 2093 serum folate tests. The amount charged per deficient result was $158,022. Substituting the charge from the Robinson and Mladenovic study,[24] we calculated the corresponding total charge and charge per deficient result as $149,545 and $74,772, respectively. The actual total cost to our hospital was <$4186, with a cost per deficient test of <$2093.
DISCUSSION
Serum folate levels are often obtained when evaluating anemia without macrocytosis and anemia with macrocytosis.[2] They are also frequently obtained in the evaluation of delirium and dementia. A prior study evaluated both inpatient and outpatient serum folate levels in anemia, dementia, and altered mental status and found only 0.4% of serum folate results to be deficient.[26] In their study, the indications for serum folate tests were anemia or macrocytic anemia (60%) and dementia or altered mental status (30%).
We found the indications for serum folate testing in inpatients and emergency department patients to be different than prior studies. The majority of tests were done to evaluate anemia without macrocytosis (43.2%) or anemia with macrocytosis (13.2%). Lower percentages were done for the evaluation of delirium (12.0%) or dementia (3.2%). In addition, there were multiple indications that have not been noted in previous studies, including depression, peripheral neuropathy, malnutrition, pancytopenia, and others. These accounted for 28.0% of all indications. The reason for the difference in indications compared to prior studies is unknown but may be related to our cohort of exclusively inpatients and emergency department patients. Also, we observed a high concurrence of serum folate and vitamin B12 testing, with 85.2% of serum folate levels ordered at the same time as vitamin B12 levels. It appears that the tests are often ordered together even when the indication suggests that vitamin B12 alone may be more appropriate, such as peripheral neuropathy.
We found that serum folate deficiency was rare, occurring in only 2 of 2093 results. Furthermore, the deficient serum folate results may have been checked for inappropriate indications. The first deficient result was noted as part of a stroke workup in a patient not taking folic acid supplementation. Current guidelines do not recommend serum folate testing in patients with new stroke.[33] In the second deficient case, serum folate testing was performed for evaluation of macrocytic anemia with an MCV of 119 fL. Although reasonable, this was an alcoholic patient presenting with acute gastrointestinal bleeding already on folic acid and multivitamin supplementation and known nonadherence with these supplements. In neither case was there a change in management based on the deficient result.
Given the low rate of serum folate deficiency and the lack of change in management based on deficient results, we conclude that there is a low utility of serum folate testing for any indication in inpatients and emergency department patients in folic acid‐fortified countries. Based on prior studies, and supported by our results, there is no evidence for checking serum folate levels in delirium, dementia, peripheral neuropathy, malnutrition, or any of the other indications. In addition, our results demonstrate a low utility even in patients with anemia or macrocytic anemia.
The rate of serum folate deficiency in our study was significantly lower than prior studies.[24, 26] There may have been geographical factors that led to a lower prevalence of folate deficiency in our study population. Our cohort included inpatients and emergency department patients, whereas previous studies had a majority of outpatients. It is known that serum folate levels can rapidly fluctuate with proper nutrition.[34] It may be that our patients received nutrition in the hospital that corrected serum folate levels prior to laboratory testing.
In addition to the low utility of serum folate testing, the charge per deficient result in our study ($158,022) was more than 100‐fold higher than that in the Robinson and Mladenovic study ($1321).[24] Even when correcting for variability in hospital charges by using the charge from the latter study, the charge per deficient serum folate test remained 50‐fold higher ($74,772). This implies that the increase in charge per deficient result was driven in part by a decreased rate of deficient tests. Folic acid fortification is likely responsible for some of the decrease. However, we believe another source is the excessive ordering of serum folate tests in patients without previously accepted indications. Because no change in management was made for the deficient patients in our study, the charge per serum folate deficient result that changed management approached infinity. This compares to $9979 in the Robinson and Mladenovic analysis.[24]
The cost to the hospital of a serum folate test was much lower than the charge, and estimated to be <$2093 per deficient result. Because serum folate tests are performed on a highly automated, random access analyzer that performs thousands of other measurements daily, the capital and labor costs for each test was well below $0.50 combined. With the addition of reagent costs, our total cost for each serum folate measurement was <$2.00. It is somewhat difficult to extrapolate these values to other hospitals, as exact costs and charges are variable. Nonetheless, the exceptionally low utility of serum folate testing makes the costs associated with these tests excessive.
Our study has several limitations. We conducted our study at a single institution in a country with mandatory folic acid fortification. Our results may not be generalizable to other institutions or patient populations, such as those in countries without mandatory folic acid fortification. Only 259 (12.4%) charts were reviewed, and indications were determined in 93.6% of charts, which may have caused our frequency to vary from the true frequency. Additionally, the low rate of deficient serum folate results limited our ability to identify associations with deficiency. Further evaluation for geographic variations of serum folate deficiency may reveal variable rates.
We conclude that in folic acid fortified countries, the rate of serum folate deficiency is increasingly rare, and the charge to patients and payers per deficient result is exceptionally high. In addition, testing in our study did not change clinical management, which makes the costs associated with these test wasteful. Further evaluation of serum folate testing of inpatients and emergency department patients in folic acid fortified countries is warranted; however, based on our results the utility appears poor for all indications.
Disclosure
Nothing to report.
- , . The biochemical basis of cobalamin deficiency. Mayo Clin Proc. 1994;69(2):181–186.
- , , , et al. Harrison's Principles of Internal Medicine. New York, NY:McGraw‐Hill Professional;2004.
- , . Folic acid, pernicious anaemia, and prevention of neural tube defects. Lancet. 1994;343(8893):307.
- , , , et al. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high‐functioning adults: MacArthur Studies of Successful Aging. Am J Med. 2005;118(2):161–167.
- , . Folate and brain function in the elderly. Curr Opin Clin Nutr Metab Care. 2004;7(6):659–664.
- , , , , , . Plasma homocysteine levels and cognitive status in long‐term stay geriatric patients: a cross‐sectional study. Arch Gerontol Geriatr. 2005;40(2):129–138.
- . Folate responsive neuropathy. Presse Med. 1994;23(3):131–137.
- , . Treatment of depression: time to consider folic acid and vitamin B12. J Psychopharmacol (Oxford). 2005;19(1):59–65.
- , , , et al. Folate deficiency causes uracil misincorporation into human DNA and chromosome breakage: implications for cancer and neuronal damage. Proc Natl Acad Sci U S A. 1997;94(7):3290–3295.
- , , , et al. Folate deficiency in rats induces DNA strand breaks and hypomethylation within the p53 tumor suppressor gene. Am J Clin Nutr. 1997;65(1):46–52.
- , , , , , . Folate intake and carcinogenesis of the colon and rectum. Int J Epidemiol. 1991;20(2):368–374.
- , . Colorectal cancer protective effects and the dietary micronutrients folate, methionine, vitamins B6, B12, C, E, selenium, and lycopene. Nutr Cancer. 2006;56(1):11–21.
- , , , et al. Multivitamin use, folate, and colon cancer in women in the Nurses' Health Study. Ann Intern Med. 1998;129(7):517–524.
- , , , , . Serum homocysteine and folate but not vitamin B12 are predictors of CHD mortality in older adults [published online ahead of print September 29, 2011]. Eur J Cardiovasc Prev Rehabil. doi: 10.1177/1741826711424568.
- , , , , , . Plasma homocyst(e)ine levels in men with premature coronary artery disease. J Am Coll Cardiol. 1990;16(5):1114–1119.
- , , , et al. Low serum folate but normal homocysteine levels in patients with atherosclerotic vascular disease and matched healthy controls. Nutrition. 2000;16(6):434–438.
- , , , , , . Low serum folate concentrations are associated with an excess incidence of acute coronary events: the Kuopio Ischaemic Heart Disease Risk Factor Study. Eur J Clin Nutr. 2000;54(5):424–428.
- , , , , . Dietary folate and the risk of nonfatal myocardial infarction. Epidemiology. 2002;13(6):700–706.
- , , , et al.;Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators. Homocysteine lowering with folic acid and b vitamins in vascular disease. N Engl J Med. 2006;354(15):1567–1577.
- , , , , , . A controlled trial of homocysteine lowering and cognitive performance. N Engl J Med. 2006;354(26):2764–2772.
- , . Folic acid with or without vitamin B12 for the prevention and treatment of healthy elderly and demented people. Cochrane Database Syst Rev. 2008;(4):CD004514.
- , , , . Does the mean corpuscular volume help physicians evaluate hospitalized patients with anemia?J Gen Intern Med. 1990;5(3):187–191.
- , , , , . Biochemical indicators of B vitamin status in the US population after folic acid fortification: results from the National Health and Nutrition Examination Survey 1999–2000. Am J Clin Nutr. 2005;82(2):442–450.
- , . Lack of clinical utility of folate levels in the evaluation of macrocytosis or anemia. Am J Med. 2001;110(2):88–90.
- , , , et al. Blood folate levels: the latest NHANES results. NCHS Data Brief. 2008;(6):1–8.
- , , . Clinical utility of folic acid testing for patients with anemia or dementia. J Gen Intern Med. 2008;23(6):824–826.
- . Anemia in adults: a contemporary approach to diagnosis. Mayo Clin Proc 2003;78(10):1274–1280.
- . Anemia in the elderly. Am Fam Physician. 2000;62(7):1565–1572.
- , . Red cell or serum folate? Results from the National Pathology Alliance benchmarking review. J Clin Pathol. 2003;56(12):924–926.
- , , , , , . Hematology. Philadelphia, PA:Churchill Livingstone;2012.
- , , , . Sensitivity of serum methylmalonic acid and total homocysteine determinations for diagnosing cobalamin and folate deficiencies. Am J Med. 1994;96(3):239–246.
- . Laboratory diagnosis of vitamin B12 and folate deficiency: a guide for the primary care physician. Arch Intern Med. 1999;159(12):1289–1298.
- , , , et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38(5):1655–1711.
- , , , . Predicted serum folate concentrations based on in vitro studies and kinetic modeling are consistent with measured folate concentrations in humans. J Nutr. 2006;136(12):3074–3078.
- , . The biochemical basis of cobalamin deficiency. Mayo Clin Proc. 1994;69(2):181–186.
- , , , et al. Harrison's Principles of Internal Medicine. New York, NY:McGraw‐Hill Professional;2004.
- , . Folic acid, pernicious anaemia, and prevention of neural tube defects. Lancet. 1994;343(8893):307.
- , , , et al. Homocysteine versus the vitamins folate, B6, and B12 as predictors of cognitive function and decline in older high‐functioning adults: MacArthur Studies of Successful Aging. Am J Med. 2005;118(2):161–167.
- , . Folate and brain function in the elderly. Curr Opin Clin Nutr Metab Care. 2004;7(6):659–664.
- , , , , , . Plasma homocysteine levels and cognitive status in long‐term stay geriatric patients: a cross‐sectional study. Arch Gerontol Geriatr. 2005;40(2):129–138.
- . Folate responsive neuropathy. Presse Med. 1994;23(3):131–137.
- , . Treatment of depression: time to consider folic acid and vitamin B12. J Psychopharmacol (Oxford). 2005;19(1):59–65.
- , , , et al. Folate deficiency causes uracil misincorporation into human DNA and chromosome breakage: implications for cancer and neuronal damage. Proc Natl Acad Sci U S A. 1997;94(7):3290–3295.
- , , , et al. Folate deficiency in rats induces DNA strand breaks and hypomethylation within the p53 tumor suppressor gene. Am J Clin Nutr. 1997;65(1):46–52.
- , , , , , . Folate intake and carcinogenesis of the colon and rectum. Int J Epidemiol. 1991;20(2):368–374.
- , . Colorectal cancer protective effects and the dietary micronutrients folate, methionine, vitamins B6, B12, C, E, selenium, and lycopene. Nutr Cancer. 2006;56(1):11–21.
- , , , et al. Multivitamin use, folate, and colon cancer in women in the Nurses' Health Study. Ann Intern Med. 1998;129(7):517–524.
- , , , , . Serum homocysteine and folate but not vitamin B12 are predictors of CHD mortality in older adults [published online ahead of print September 29, 2011]. Eur J Cardiovasc Prev Rehabil. doi: 10.1177/1741826711424568.
- , , , , , . Plasma homocyst(e)ine levels in men with premature coronary artery disease. J Am Coll Cardiol. 1990;16(5):1114–1119.
- , , , et al. Low serum folate but normal homocysteine levels in patients with atherosclerotic vascular disease and matched healthy controls. Nutrition. 2000;16(6):434–438.
- , , , , , . Low serum folate concentrations are associated with an excess incidence of acute coronary events: the Kuopio Ischaemic Heart Disease Risk Factor Study. Eur J Clin Nutr. 2000;54(5):424–428.
- , , , , . Dietary folate and the risk of nonfatal myocardial infarction. Epidemiology. 2002;13(6):700–706.
- , , , et al.;Heart Outcomes Prevention Evaluation (HOPE) 2 Investigators. Homocysteine lowering with folic acid and b vitamins in vascular disease. N Engl J Med. 2006;354(15):1567–1577.
- , , , , , . A controlled trial of homocysteine lowering and cognitive performance. N Engl J Med. 2006;354(26):2764–2772.
- , . Folic acid with or without vitamin B12 for the prevention and treatment of healthy elderly and demented people. Cochrane Database Syst Rev. 2008;(4):CD004514.
- , , , . Does the mean corpuscular volume help physicians evaluate hospitalized patients with anemia?J Gen Intern Med. 1990;5(3):187–191.
- , , , , . Biochemical indicators of B vitamin status in the US population after folic acid fortification: results from the National Health and Nutrition Examination Survey 1999–2000. Am J Clin Nutr. 2005;82(2):442–450.
- , . Lack of clinical utility of folate levels in the evaluation of macrocytosis or anemia. Am J Med. 2001;110(2):88–90.
- , , , et al. Blood folate levels: the latest NHANES results. NCHS Data Brief. 2008;(6):1–8.
- , , . Clinical utility of folic acid testing for patients with anemia or dementia. J Gen Intern Med. 2008;23(6):824–826.
- . Anemia in adults: a contemporary approach to diagnosis. Mayo Clin Proc 2003;78(10):1274–1280.
- . Anemia in the elderly. Am Fam Physician. 2000;62(7):1565–1572.
- , . Red cell or serum folate? Results from the National Pathology Alliance benchmarking review. J Clin Pathol. 2003;56(12):924–926.
- , , , , , . Hematology. Philadelphia, PA:Churchill Livingstone;2012.
- , , , . Sensitivity of serum methylmalonic acid and total homocysteine determinations for diagnosing cobalamin and folate deficiencies. Am J Med. 1994;96(3):239–246.
- . Laboratory diagnosis of vitamin B12 and folate deficiency: a guide for the primary care physician. Arch Intern Med. 1999;159(12):1289–1298.
- , , , et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38(5):1655–1711.
- , , , . Predicted serum folate concentrations based on in vitro studies and kinetic modeling are consistent with measured folate concentrations in humans. J Nutr. 2006;136(12):3074–3078.
Copyright © 2012 Society of Hospital Medicine
“I'm Talking About Pain”
Sickle cell disease (SCD) accounts for approximately 113,000 hospital admissions annually in the United States, at a cost of approximately $500 million.1 The majority of these hospital admissions are due to painful episodes, vaso‐occlusive crises, often triggered by a psychological or physical stressor.2 Most individuals manage these crises at home,3 with sporadic admissions occurring, on average, 1.5 times per year.4 However, a minority of patients are admitted as often as several times per month, persistent over successive years,5, 6 a phenomenon we call extremely high hospital use (EHHU). These patients account for a disproportionate share of total costs, and may suffer worse health outcomes. Three or more hospital admissions per year has been correlated with a lower 5‐year survival rate,7 and high emergency room utilization was found to be associated with more reported pain, and more opioid use at home.8
To improve patient quality of life and to decrease healthcare costs in the management of SCD, there has been increased focus on predicting high utilization9 and identifying strategies to decrease hospitalization rates, especially among patients with EHHU.10 Although SCD patients with EHHU have been identified as a small group of outliers,5 the psychosocial factors associated with EHHU in adults with SCD have not been investigated. The objective of this qualitative study is to characterize the subjective experience of patients with sickle cell disease and EHHU, and generate hypotheses about its antecedents and consequences.
METHODS
The institutional review board (IRB) of Yale University School of Medicine, New Haven, CT, approved the research protocol.
Participants
We accessed the Yale‐New Haven Hospital administrative database to identify the number of patients with SCD who demonstrated EHHU that did not remit over successive years.5 We identified the 10 highest inpatient utilizing individuals with sickle cell disease over the period January 1, 2008December 31, 2010; 8 individuals consented to participate. We collected the following data on each participant through chart review: hemoglobinopathy, length of stay, primary diagnosis for each admission, and SCD‐related comorbidities (eg, avascular necrosis, leg ulcer, etc). No research team member was involved in the care of any of the participants.
Interviews
Based on literature review of other qualitative research in SCD, we created an interview guide to include the following themes: 1) disease, pain, and medication; 2) hospitalization; 3) support structures; 4) daily life; and 5) personal relationships (see Supporting Information, Appendix I, in the online version of this article). Applying Grounded Theory in qualitative research, the interview guide underwent several minor modifications based on field‐testing interviews with 4 interviews of patients not enrolled in the study and early interviews with study participants.11 Tape‐recorded interviews, each lasting at least an hour,12 were conducted by 1 researcher (D.W.) during inpatient hospitalizations, at least several days after admission to ensure that participants were comfortable enough to participate. When the interview exceeded an hour, it was continued at a later time. Recordings were transcribed by a professional transcription service and verified for accuracy by the interviewer. Participants were compensated $25 for completed interviews.
Narrative Analysis
The analysis team consisted of 2 psychiatrists (1 with additional training in internal medicine), 1 medical student, and 1 internist with additional training in addiction medicine. Analysts read each transcript, became thoroughly familiar with its content, and met to discuss preliminary findings. Then, we created patient experts among the group, assigning each analyst 2 interviews with which s/he prepared a detailed summary in the first person, using the participant's own words, according to an established process in phenomenological research13 (Figure 1). These narrative summaries allowed for the development of a holistic view of the participant, the creation of a narrative structure, and the fostering of an empathic bridge,13 a connection between the experiences of the participant and those of the reviewer. The summaries were read aloud at research meetings allowing for discussion, and the content of the summaries were modified based on the consensus of the group.
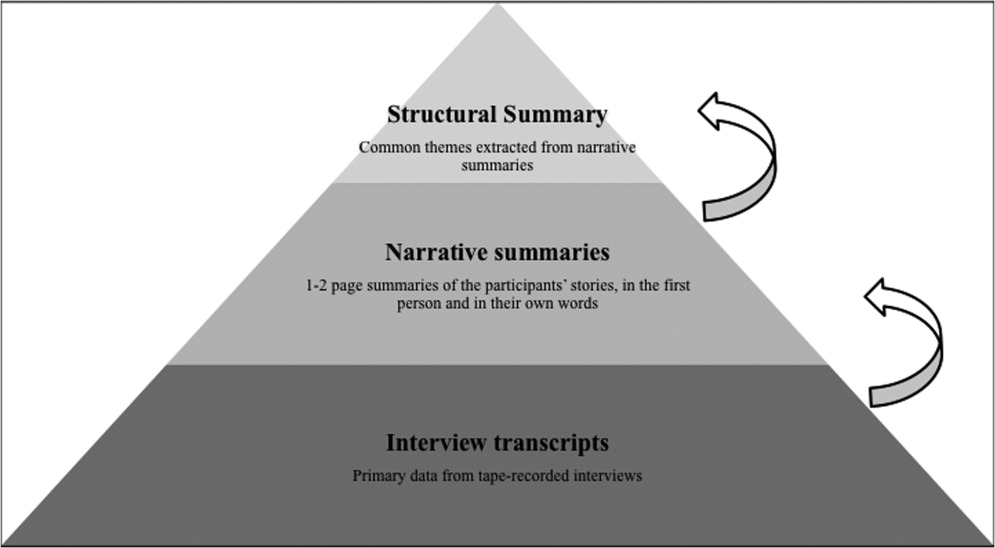
Next, we randomly rotated the narrative summaries so that each of the 4 analysts became an expert for 2 additional participants in order to critically evaluate the compiled narratives, and develop a structural summary14a summary of the prevalent themes. We extracted content from the narrative summaries based on these common themes, and returned to the transcripts as needed for relevant quotations. This inductive process allowed unique participant narratives to come through unconstrained by a predetermined coding structure.
The team reached consensus on organizing themes following the chronology of childhood to adulthood. This model was utilized to preserve the narrative basis of the methodology, and to ultimately elucidate the antecedents, subjective experience, and consequences of EHHU. An audit trail was maintained throughout the data analysis process.
RESULTS
Table 1 displays demographic, clinical, and hospitalization data for the 8 participants. These patients represented approximately 8% of the population with sickle cell disease at the study institution, but accounted for 57% of hospital days among sickle cell disease patients over a 3‐year period, with cumulative hospital days near or above 100 days per patient each year. Greater than 90% of admissions were for vaso‐occlusive crises without other SCD‐related complications. However, many participants had complicated medical histories, including avascular necrosis, acute chest syndrome, and leg ulcers.
| Participant | Age at Interview Date | Gender | Hemoglobin Diagnosis* | Average Hospital Days per Year 20082010 |
|---|---|---|---|---|
| ||||
| 1 | 34 | F | HbSS | 171 |
| 2 | 27 | F | HbSS | 263 |
| 3 | 26 | M | HbS‐B thalassemia | 151 |
| 4 | 34 | M | HbSC | 111 |
| 5 | 37 | F | HbSS | 202 |
| 6 | 25 | F | HbS‐B thalassemia | 104 |
| 7 | 24 | F | HbSS | 123 |
| 10 | 32 | M | HbSS | 94 |
Participant interviews presented a common narrative of the evolution of EHHU from a young age, culminating in a universally negative description of hospitalization: It's like jail. (participant 2); It's like a massacre, coming in the hospital; I get tortured. (participant 1). Saturation was reached on major themes, which fit into 3 general categories: pain and opioid medication use, interpersonal relationships, and personal development.
Pain and Opioid Medication Use
Participants reported hospital use dating back to childhood, which was the first exposure to intravenous opioid medications and the beginning of a trajectory of accelerating use, tolerance, and dependence: You know, I came in the hospital when I was two years old I stayed 'til I was like five and a half. I started school here. (participant 1); I started taking that medicine when I was on the pedi side. So my body's already used to it it doesn't really touch me. They're gonna have to up my doses. (participant 7).
As adults, participants expressed awareness of the potential problems of opioids. During interviews, many participants exhibited side effects of these medications, such as itching and somnolence. Moreover, participants expressed awareness of the skepticism and mistrust from providers, and acknowledged that such sentiments may be justified toward certain patients: That's all our body knows, is meds, meds, meds. And because your body is addicted to this level, you gotta go up another level, but some doctors think we're taking too much. How can we be taking too much when we need it? (participant 5); The oxy which I'm on [oxycontin 240 mg per day] when you take that, you going to sleep. And then some of them will say when you go home you're not taking the medicine like you should. (participant 5).
Opioids were taken in and out of the hospital by all participants, and were identified as necessary in combating debilitating pain. Many participants expressed a reluctance to try other forms of therapy, such as hydroxyurea: These new chemicals, you come across doctors who say there's this new medicine out, and it's been out for such and such amount of timeI think it would be good, can we try it with you? No. I'm not a guinea. (participant 2).
While all participants described unpredictable pain crises, some also described an underlying, constant pain syndrome: You know, like, I could be fine right now; the next minute I could be Oh, my God crying, so much pain. You never know when you're gonna have a crisis. (participant 1); There's never no pain. There's always pain. It's just a fact of life. I wake up and I can deal with the pain, it's not that bad today. But then when the crisis hits, that's when it gets unbearable. (participant 10); I'm not in pain every day, every second. To me, I don't think that any sickle cell patient is in pain every day. They make theirselves to [be] it saddens me sometimes. (participant 6).
Interpersonal Relationships
In childhood, participants developed close relationships with the staff of the children's hospital and an attachment to this institution: I loved pediatrics. It's the adult side I can't stand. They treat you better. (participant 7); Some people in the ER, they know us; and I call them my family they already know what I need. (participant 5).
In contrast, the hospital experience during adulthood was often punctuated by bitter relationships with staff, and distrust over possible excessive use of opioids. Moreover, participants raised the possibility of racism in their interactions with hospital staff. Overall, participants highlighted a lack of empathy among caregivers: Some doctors, they're rude, like, they're rough. They'll just pull out the scope bang it onto my back, or just push on my body or areas where it hurts. (participant 6); I'm your doctor. And I say I think you're doing a lot better, how would you feel about going home today? And you can say I don't think I'm ready. And I can say Well, you can't live here in the hospital. Why do you think you're not ready for home yet? You're never, ever going to be pain free, and that's when you turn around to me and say I know that. I've been dealing with this for all my life. I know I'm never gonna be pain free! (participant 2).
Such negative interactions extended to friends and family members, leading to a sense of social isolation and a reluctance to discuss their disease with others: I just don't think people will understand where I'm coming from. So I just don't talk to anybody, I keep it inside. Or I write it in my diary. (participant 5); I don't have any friends. I have associates. I'm always by myself. (participant 1).
Even though participants expressed dismay at dysfunctional relationships within the hospital, they also voiced affection for staff members. Participant 1 described hospital stays that were loving, and participant 3 described his hematologist as his brother from another mother, and a nurse practitioner as his aunt.
Personal Development
Hospitalization in childhood was linked to EHHU as an adult by the derailment that participants described in their personal development. Prolonged hospitalization and illness were barriers to education, interfering with the development of social as well as academic skills: I couldn't spell me being in a hospital for so much I was like, no, I don't want that bookwork like everybody else. (participant 3); I stopped going to school. I told [my mom] that I was not going back to school because the kids made fun of me Oh, she has a disease. Be careful, you might get the cooties. (participant 2).
Participants also described a sense of foreshortened future. Many were told that they would not survive their teens: They told my mother I would die before I was 12 years old. And I would be scared to go to sleep, because I would think I was gonna die in my sleep. (participant 2)
As an adult, numerous and/or prolonged hospitalizations interfered with participants' ability to remain employed, and they experienced strains on fulfilling family roles: I would love to work again, but who gonna hire somebody that's always out, more than you're working. Nobody. (participant 5); Sometimes I feel like I'm neglecting my son, being here. You have to take care of yourself in order for you to be there for him. But it just stresses me out. (participant 6).
The struggles of hospitalization and pain management took their toll on participants' mental health. Participants described difficulty sleeping, depression, and suicidal thoughts: Sorrow. That's what [sickle cell] means to me. Unhappy. Everything's depressing. It takes over your body and your mind and your soul. (participant 5); I really was gonna kill myself cause it's like, sometime, the pain, you be in so much pain, you be like, fuck this, man. My pain was bothering me so much, I laid down on the highway, wishin a car would run me over. (participant 4).
Despite fragile mental and physical health, many participants described feelings of strength and resilience, and some described hope in the future for employment, education, travel, and family: I don't know why God picked me, but for some strange, mysterious reason he picked me. I still don't know what that reason may be, but I ain't gonna give up. Maybe he got some kind of plan in store. (participant 2).
DISCUSSION
Our study population represents a unique and understudied group among patients with SCD. While several themes from prior research on individuals with SCD were presentreciprocal mistrust between patients and providers surrounding opioid analgesics and pain reporting,15, 16 racial and disease‐related bias,17 patient dissatisfaction with clinical services,18the common narrative of thwarted personal development in the setting of a long history of hospitalization and opioid use was striking.
The developmental perspective posits that age‐appropriate tasks govern basic capacities and skills (academic, interpersonal, affective, and cognitive) honed through institutional interactions (family, school, and community), which allow individuals to develop autonomy that guides them into effective participation in social groups and civil society, and eventually to becoming guarantors for the next generation. Our participants described problems such as social isolation, depression, and dependence on medications, all linked to their description of recurrent stays in the hospital during childhood and adolescence, where missed vocational and social opportunities left their indelible mark. Participants expressed an awareness of their inability to lead productive lives, and the perception that they were burdensome to their caregivers and the hospital.
While previous research has correlated high hospital utilization in SCD with factors like poor coping strategies,1921 high levels of stress,22 and inadequate support,17 our interviews suggest that such psychosocial difficulties may be consequences as well as causes of hospitalization, creating an accelerating downward spiral of dysfunction. At the center of this spiral is participants' ongoing experience of pain, which may be related to SCD, medications, or neither.23 Additionally, chronic anemia, opioid exposure, airway disease, and cerebrovascular disease are all implicated in impaired neuropsychological functioning in children and adolescents with sickle cell disease.24, 25
Clinical features of SCD remain relevant to hospitalization in adulthood. Chart review revealed that the vast majority of inpatient admissions were due to vaso‐occlusive crises uncomplicated by SCD‐related pathology, such as aseptic necrosis of bone or acute chest syndrome. This finding is consistent with previous work,9 which correlated new onset of high hospital use with SCD‐related complications, but not reliably with persistent EHHU, our study population.
The double‐edged sword of opioid use26 was starkly evident in participants' narratives. Crippling vaso‐occlusive crises were competently treated with opioids starting in childhood, but then a cycle of increasing outpatient doses of opioids and more frequent and longer courses of inpatient intravenous opioids followed. Participants felt judged and stigmatized for seeking one of the few treatment options they had been offered, resulting in confusion and bitterness at times. Other potential complications of long‐term opioid therapy less well known to patients and providers such as hypogonadism and hyperalgesia27may have played a role in the patient experience and should be examined in future research. In addition, undertreatment of pain may lead to pseudoaddiction,28 underscoring the complexity of delineating the pathologies of dependence, addiction, withdrawal, acute pain, and chronic pain.
Our study is limited primarily by the fact that it was conducted with a small number of participants. It is also possible that institutional variation, especially with regard to pain management, makes it difficult to generalize our hypotheses. Similarly, our participants grew up in similar environments outside the hospital, which may differ significantly from environments of other individuals with EHHU. Lastly, participants were all interviewed as inpatients, and the acuteness of their illness may have influenced responses. Despite these limitations, we achieved saturation on the major themes, and there was substantial agreement in their experiences of their illness.
Breaking the cycle of alienation from the external world and dependence on the hospital necessitates an acknowledgement of the role of the hospital, pain, and opioid use in the long‐term development of individuals with EHHU. Further research should test this developmental hypothesis, and focus on early interventions and the critical transition from pediatric to adult care.25 Longitudinal quantitative analysis could include psychosocial variables in SCD in the attempt to predict EHHU as has been accomplished in the chronic pain literature.29 Additionally, a comprehensive qualitative approach including the perspectives of caregivers, family members, and comparison to low hospital utilizers will better inform interventions aimed at ameliorating EHHU. It is particularly important to understand the similarities and differences in the long‐term development of patients with SCD who demonstrate EHHU versus low hospital use. The optimal strategy for opioid use in the long‐term management of pain in patients with SCD remains to be determined. Alternatives to opioids should be investigated in a controlled trial, and institutional differences should be examined as they relate to EHHU and pain‐management strategies. Lastly, our results suggest that psychosocial and skill rehabilitation may mitigate EHHU, and that multidisciplinary resources proactively directed towards this population will reduce hospitalization.30
- ,,,.The number of people with sickle‐cell disease in the United States: national and state estimates.Am J Hematol.2009;85:77–78.
- .Current issues in sickle cell pain and its management.Hematology Am Soc Hematol Educ Program.2007:97–105.
- ,,, et al.Daily assessment of pain in adults with sickle cell disease.Ann Intern Med.2008;148:94–101.
- ,,,,.Acute care utilization and rehospitalizations for sickle cell disease.JAMA.2010;303:1288–1294.
- ,,,.The course and correlates of high hospital utilization in sickle cell disease: evidence from a large, urban Medicaid managed care organization.Am J Hematol.2009;84:666–670.
- ,,,,,.Medical care utilization and mortality in sickle cell disease: a population‐based study.Am J Hematol.2005;80:262–270.
- ,,, et al.Pain in sickle cell disease. Rates and risk factors.N Engl J Med.1991;325:11–16.
- ,,, et al.Comparisons of high versus low emergency department utilizers in sickle cell disease.Ann Emerg Med.2009;53:587–593.
- ,,.Prediction of onset and course of high hospital utilization in sickle cell disease.J Hosp Med.2011;6:248–255.
- ,,.A review of empirically supported psychosocial interventions for pain and adherence outcomes in sickle cell disease.J Pediatr Psychol.2004;29:197–209.
- .More Grounded Theory Methodology: A Reader.Mill Valley, CA:Sociology Press;1994.
- .The Long Interview.Newbury Park, CA:Sage;1988.
- ,,.Generating coherence out of chaos: examples of the utility of empathic bridges in phenomenological research.J Phenomenolog Psychol.2004;35:253–271.
- ,,,.Using qualitative methods in clinical research. In: McKay D, ed.Handbook of Research Methods in Abnormal and Clinical Psychology.Los Angeles, CA:Sage;2008:263–269.
- ,,,.Sickle cell‐related pain: perceptions of medical practitioners.J Pain Symptom Manage.1997;14:168–174.
- ,,,.Pain management in sickle cell disease.Chronic Illn.2006;2:39–50.
- ,,.Experiences of hospital care and treatment‐seeking behavior for pain from sickle cell disease: qualitative study.West J Med.1999;171:306–313.
- ,,,,.Dissatisfaction with hospital care for children with sickle cell disease not due only to race and chronic disease.Pediatr Blood Cancer.2009;53:174–178.
- ,,,.Sickle cell disease pain: relation of coping strategies to adjustment.J Consult Clin Psychol.1989;57:725–731.
- ,,,.Sickle cell disease pain: 2. Predicting health care use and activity level at 9‐month follow‐up.J Consult Clin Psychol.1992;60:267–273.
- ,,,,.Coping and health service utilisation in a UK study of paediatric sickle cell pain.Arch Dis Child.2002;86:325–329.
- ,,,,,.Daily mood and stress predict pain, health care use, and work activity in African American adults with sickle‐cell disease.Health Psychol.2004;23:267–274.
- .Pain management in sickle cell disease: palliative care begins at birth?Hematology Am Soc Hematol Educ Program.2008:466–474.
- ,,,.Cognitive functioning in children with sickle cell disease: a meta‐analysis.J Pediatr Psychol.2002;27:739–748.
- ,,, et al.Transition planning for youth with sickle cell disease: embedding neuropsychological assessment into comprehensive care.Pediatrics.2010;126(suppl 3):S151–S159.
- .Increases in opioid medication use: balancing the good with the bad.Pain.2008;138:245–246.
- ,,,.Hyperalgesia: an emerging iatrogenic syndrome.J Pain Symptom Manage.2003;26:769–775.
- ,,,,.Understanding the causes of problematic pain management in sickle cell disease: evidence that pseudoaddiction plays a more important role than genuine analgesic dependence.J Pain Symptom Manage.2004;27:156–169.
- ,,,,.Functional abdominal pain patient subtypes in childhood predict functional gastrointestinal disorders with chronic pain and psychiatric comorbidities in adolescence and adulthood.Pain.2012;153:1798–1806.
- ,,.Caring for the adult with sickle cell disease: results of a multidisciplinary pilot program.J Natl Med Assoc.2010;102:1009–1016.
Sickle cell disease (SCD) accounts for approximately 113,000 hospital admissions annually in the United States, at a cost of approximately $500 million.1 The majority of these hospital admissions are due to painful episodes, vaso‐occlusive crises, often triggered by a psychological or physical stressor.2 Most individuals manage these crises at home,3 with sporadic admissions occurring, on average, 1.5 times per year.4 However, a minority of patients are admitted as often as several times per month, persistent over successive years,5, 6 a phenomenon we call extremely high hospital use (EHHU). These patients account for a disproportionate share of total costs, and may suffer worse health outcomes. Three or more hospital admissions per year has been correlated with a lower 5‐year survival rate,7 and high emergency room utilization was found to be associated with more reported pain, and more opioid use at home.8
To improve patient quality of life and to decrease healthcare costs in the management of SCD, there has been increased focus on predicting high utilization9 and identifying strategies to decrease hospitalization rates, especially among patients with EHHU.10 Although SCD patients with EHHU have been identified as a small group of outliers,5 the psychosocial factors associated with EHHU in adults with SCD have not been investigated. The objective of this qualitative study is to characterize the subjective experience of patients with sickle cell disease and EHHU, and generate hypotheses about its antecedents and consequences.
METHODS
The institutional review board (IRB) of Yale University School of Medicine, New Haven, CT, approved the research protocol.
Participants
We accessed the Yale‐New Haven Hospital administrative database to identify the number of patients with SCD who demonstrated EHHU that did not remit over successive years.5 We identified the 10 highest inpatient utilizing individuals with sickle cell disease over the period January 1, 2008December 31, 2010; 8 individuals consented to participate. We collected the following data on each participant through chart review: hemoglobinopathy, length of stay, primary diagnosis for each admission, and SCD‐related comorbidities (eg, avascular necrosis, leg ulcer, etc). No research team member was involved in the care of any of the participants.
Interviews
Based on literature review of other qualitative research in SCD, we created an interview guide to include the following themes: 1) disease, pain, and medication; 2) hospitalization; 3) support structures; 4) daily life; and 5) personal relationships (see Supporting Information, Appendix I, in the online version of this article). Applying Grounded Theory in qualitative research, the interview guide underwent several minor modifications based on field‐testing interviews with 4 interviews of patients not enrolled in the study and early interviews with study participants.11 Tape‐recorded interviews, each lasting at least an hour,12 were conducted by 1 researcher (D.W.) during inpatient hospitalizations, at least several days after admission to ensure that participants were comfortable enough to participate. When the interview exceeded an hour, it was continued at a later time. Recordings were transcribed by a professional transcription service and verified for accuracy by the interviewer. Participants were compensated $25 for completed interviews.
Narrative Analysis
The analysis team consisted of 2 psychiatrists (1 with additional training in internal medicine), 1 medical student, and 1 internist with additional training in addiction medicine. Analysts read each transcript, became thoroughly familiar with its content, and met to discuss preliminary findings. Then, we created patient experts among the group, assigning each analyst 2 interviews with which s/he prepared a detailed summary in the first person, using the participant's own words, according to an established process in phenomenological research13 (Figure 1). These narrative summaries allowed for the development of a holistic view of the participant, the creation of a narrative structure, and the fostering of an empathic bridge,13 a connection between the experiences of the participant and those of the reviewer. The summaries were read aloud at research meetings allowing for discussion, and the content of the summaries were modified based on the consensus of the group.
Next, we randomly rotated the narrative summaries so that each of the 4 analysts became an expert for 2 additional participants in order to critically evaluate the compiled narratives, and develop a structural summary14a summary of the prevalent themes. We extracted content from the narrative summaries based on these common themes, and returned to the transcripts as needed for relevant quotations. This inductive process allowed unique participant narratives to come through unconstrained by a predetermined coding structure.
The team reached consensus on organizing themes following the chronology of childhood to adulthood. This model was utilized to preserve the narrative basis of the methodology, and to ultimately elucidate the antecedents, subjective experience, and consequences of EHHU. An audit trail was maintained throughout the data analysis process.
RESULTS
Table 1 displays demographic, clinical, and hospitalization data for the 8 participants. These patients represented approximately 8% of the population with sickle cell disease at the study institution, but accounted for 57% of hospital days among sickle cell disease patients over a 3‐year period, with cumulative hospital days near or above 100 days per patient each year. Greater than 90% of admissions were for vaso‐occlusive crises without other SCD‐related complications. However, many participants had complicated medical histories, including avascular necrosis, acute chest syndrome, and leg ulcers.
| Participant | Age at Interview Date | Gender | Hemoglobin Diagnosis* | Average Hospital Days per Year 20082010 |
|---|---|---|---|---|
| ||||
| 1 | 34 | F | HbSS | 171 |
| 2 | 27 | F | HbSS | 263 |
| 3 | 26 | M | HbS‐B thalassemia | 151 |
| 4 | 34 | M | HbSC | 111 |
| 5 | 37 | F | HbSS | 202 |
| 6 | 25 | F | HbS‐B thalassemia | 104 |
| 7 | 24 | F | HbSS | 123 |
| 10 | 32 | M | HbSS | 94 |
Participant interviews presented a common narrative of the evolution of EHHU from a young age, culminating in a universally negative description of hospitalization: It's like jail. (participant 2); It's like a massacre, coming in the hospital; I get tortured. (participant 1). Saturation was reached on major themes, which fit into 3 general categories: pain and opioid medication use, interpersonal relationships, and personal development.
Pain and Opioid Medication Use
Participants reported hospital use dating back to childhood, which was the first exposure to intravenous opioid medications and the beginning of a trajectory of accelerating use, tolerance, and dependence: You know, I came in the hospital when I was two years old I stayed 'til I was like five and a half. I started school here. (participant 1); I started taking that medicine when I was on the pedi side. So my body's already used to it it doesn't really touch me. They're gonna have to up my doses. (participant 7).
As adults, participants expressed awareness of the potential problems of opioids. During interviews, many participants exhibited side effects of these medications, such as itching and somnolence. Moreover, participants expressed awareness of the skepticism and mistrust from providers, and acknowledged that such sentiments may be justified toward certain patients: That's all our body knows, is meds, meds, meds. And because your body is addicted to this level, you gotta go up another level, but some doctors think we're taking too much. How can we be taking too much when we need it? (participant 5); The oxy which I'm on [oxycontin 240 mg per day] when you take that, you going to sleep. And then some of them will say when you go home you're not taking the medicine like you should. (participant 5).
Opioids were taken in and out of the hospital by all participants, and were identified as necessary in combating debilitating pain. Many participants expressed a reluctance to try other forms of therapy, such as hydroxyurea: These new chemicals, you come across doctors who say there's this new medicine out, and it's been out for such and such amount of timeI think it would be good, can we try it with you? No. I'm not a guinea. (participant 2).
While all participants described unpredictable pain crises, some also described an underlying, constant pain syndrome: You know, like, I could be fine right now; the next minute I could be Oh, my God crying, so much pain. You never know when you're gonna have a crisis. (participant 1); There's never no pain. There's always pain. It's just a fact of life. I wake up and I can deal with the pain, it's not that bad today. But then when the crisis hits, that's when it gets unbearable. (participant 10); I'm not in pain every day, every second. To me, I don't think that any sickle cell patient is in pain every day. They make theirselves to [be] it saddens me sometimes. (participant 6).
Interpersonal Relationships
In childhood, participants developed close relationships with the staff of the children's hospital and an attachment to this institution: I loved pediatrics. It's the adult side I can't stand. They treat you better. (participant 7); Some people in the ER, they know us; and I call them my family they already know what I need. (participant 5).
In contrast, the hospital experience during adulthood was often punctuated by bitter relationships with staff, and distrust over possible excessive use of opioids. Moreover, participants raised the possibility of racism in their interactions with hospital staff. Overall, participants highlighted a lack of empathy among caregivers: Some doctors, they're rude, like, they're rough. They'll just pull out the scope bang it onto my back, or just push on my body or areas where it hurts. (participant 6); I'm your doctor. And I say I think you're doing a lot better, how would you feel about going home today? And you can say I don't think I'm ready. And I can say Well, you can't live here in the hospital. Why do you think you're not ready for home yet? You're never, ever going to be pain free, and that's when you turn around to me and say I know that. I've been dealing with this for all my life. I know I'm never gonna be pain free! (participant 2).
Such negative interactions extended to friends and family members, leading to a sense of social isolation and a reluctance to discuss their disease with others: I just don't think people will understand where I'm coming from. So I just don't talk to anybody, I keep it inside. Or I write it in my diary. (participant 5); I don't have any friends. I have associates. I'm always by myself. (participant 1).
Even though participants expressed dismay at dysfunctional relationships within the hospital, they also voiced affection for staff members. Participant 1 described hospital stays that were loving, and participant 3 described his hematologist as his brother from another mother, and a nurse practitioner as his aunt.
Personal Development
Hospitalization in childhood was linked to EHHU as an adult by the derailment that participants described in their personal development. Prolonged hospitalization and illness were barriers to education, interfering with the development of social as well as academic skills: I couldn't spell me being in a hospital for so much I was like, no, I don't want that bookwork like everybody else. (participant 3); I stopped going to school. I told [my mom] that I was not going back to school because the kids made fun of me Oh, she has a disease. Be careful, you might get the cooties. (participant 2).
Participants also described a sense of foreshortened future. Many were told that they would not survive their teens: They told my mother I would die before I was 12 years old. And I would be scared to go to sleep, because I would think I was gonna die in my sleep. (participant 2)
As an adult, numerous and/or prolonged hospitalizations interfered with participants' ability to remain employed, and they experienced strains on fulfilling family roles: I would love to work again, but who gonna hire somebody that's always out, more than you're working. Nobody. (participant 5); Sometimes I feel like I'm neglecting my son, being here. You have to take care of yourself in order for you to be there for him. But it just stresses me out. (participant 6).
The struggles of hospitalization and pain management took their toll on participants' mental health. Participants described difficulty sleeping, depression, and suicidal thoughts: Sorrow. That's what [sickle cell] means to me. Unhappy. Everything's depressing. It takes over your body and your mind and your soul. (participant 5); I really was gonna kill myself cause it's like, sometime, the pain, you be in so much pain, you be like, fuck this, man. My pain was bothering me so much, I laid down on the highway, wishin a car would run me over. (participant 4).
Despite fragile mental and physical health, many participants described feelings of strength and resilience, and some described hope in the future for employment, education, travel, and family: I don't know why God picked me, but for some strange, mysterious reason he picked me. I still don't know what that reason may be, but I ain't gonna give up. Maybe he got some kind of plan in store. (participant 2).
DISCUSSION
Our study population represents a unique and understudied group among patients with SCD. While several themes from prior research on individuals with SCD were presentreciprocal mistrust between patients and providers surrounding opioid analgesics and pain reporting,15, 16 racial and disease‐related bias,17 patient dissatisfaction with clinical services,18the common narrative of thwarted personal development in the setting of a long history of hospitalization and opioid use was striking.
The developmental perspective posits that age‐appropriate tasks govern basic capacities and skills (academic, interpersonal, affective, and cognitive) honed through institutional interactions (family, school, and community), which allow individuals to develop autonomy that guides them into effective participation in social groups and civil society, and eventually to becoming guarantors for the next generation. Our participants described problems such as social isolation, depression, and dependence on medications, all linked to their description of recurrent stays in the hospital during childhood and adolescence, where missed vocational and social opportunities left their indelible mark. Participants expressed an awareness of their inability to lead productive lives, and the perception that they were burdensome to their caregivers and the hospital.
While previous research has correlated high hospital utilization in SCD with factors like poor coping strategies,1921 high levels of stress,22 and inadequate support,17 our interviews suggest that such psychosocial difficulties may be consequences as well as causes of hospitalization, creating an accelerating downward spiral of dysfunction. At the center of this spiral is participants' ongoing experience of pain, which may be related to SCD, medications, or neither.23 Additionally, chronic anemia, opioid exposure, airway disease, and cerebrovascular disease are all implicated in impaired neuropsychological functioning in children and adolescents with sickle cell disease.24, 25
Clinical features of SCD remain relevant to hospitalization in adulthood. Chart review revealed that the vast majority of inpatient admissions were due to vaso‐occlusive crises uncomplicated by SCD‐related pathology, such as aseptic necrosis of bone or acute chest syndrome. This finding is consistent with previous work,9 which correlated new onset of high hospital use with SCD‐related complications, but not reliably with persistent EHHU, our study population.
The double‐edged sword of opioid use26 was starkly evident in participants' narratives. Crippling vaso‐occlusive crises were competently treated with opioids starting in childhood, but then a cycle of increasing outpatient doses of opioids and more frequent and longer courses of inpatient intravenous opioids followed. Participants felt judged and stigmatized for seeking one of the few treatment options they had been offered, resulting in confusion and bitterness at times. Other potential complications of long‐term opioid therapy less well known to patients and providers such as hypogonadism and hyperalgesia27may have played a role in the patient experience and should be examined in future research. In addition, undertreatment of pain may lead to pseudoaddiction,28 underscoring the complexity of delineating the pathologies of dependence, addiction, withdrawal, acute pain, and chronic pain.
Our study is limited primarily by the fact that it was conducted with a small number of participants. It is also possible that institutional variation, especially with regard to pain management, makes it difficult to generalize our hypotheses. Similarly, our participants grew up in similar environments outside the hospital, which may differ significantly from environments of other individuals with EHHU. Lastly, participants were all interviewed as inpatients, and the acuteness of their illness may have influenced responses. Despite these limitations, we achieved saturation on the major themes, and there was substantial agreement in their experiences of their illness.
Breaking the cycle of alienation from the external world and dependence on the hospital necessitates an acknowledgement of the role of the hospital, pain, and opioid use in the long‐term development of individuals with EHHU. Further research should test this developmental hypothesis, and focus on early interventions and the critical transition from pediatric to adult care.25 Longitudinal quantitative analysis could include psychosocial variables in SCD in the attempt to predict EHHU as has been accomplished in the chronic pain literature.29 Additionally, a comprehensive qualitative approach including the perspectives of caregivers, family members, and comparison to low hospital utilizers will better inform interventions aimed at ameliorating EHHU. It is particularly important to understand the similarities and differences in the long‐term development of patients with SCD who demonstrate EHHU versus low hospital use. The optimal strategy for opioid use in the long‐term management of pain in patients with SCD remains to be determined. Alternatives to opioids should be investigated in a controlled trial, and institutional differences should be examined as they relate to EHHU and pain‐management strategies. Lastly, our results suggest that psychosocial and skill rehabilitation may mitigate EHHU, and that multidisciplinary resources proactively directed towards this population will reduce hospitalization.30
Sickle cell disease (SCD) accounts for approximately 113,000 hospital admissions annually in the United States, at a cost of approximately $500 million.1 The majority of these hospital admissions are due to painful episodes, vaso‐occlusive crises, often triggered by a psychological or physical stressor.2 Most individuals manage these crises at home,3 with sporadic admissions occurring, on average, 1.5 times per year.4 However, a minority of patients are admitted as often as several times per month, persistent over successive years,5, 6 a phenomenon we call extremely high hospital use (EHHU). These patients account for a disproportionate share of total costs, and may suffer worse health outcomes. Three or more hospital admissions per year has been correlated with a lower 5‐year survival rate,7 and high emergency room utilization was found to be associated with more reported pain, and more opioid use at home.8
To improve patient quality of life and to decrease healthcare costs in the management of SCD, there has been increased focus on predicting high utilization9 and identifying strategies to decrease hospitalization rates, especially among patients with EHHU.10 Although SCD patients with EHHU have been identified as a small group of outliers,5 the psychosocial factors associated with EHHU in adults with SCD have not been investigated. The objective of this qualitative study is to characterize the subjective experience of patients with sickle cell disease and EHHU, and generate hypotheses about its antecedents and consequences.
METHODS
The institutional review board (IRB) of Yale University School of Medicine, New Haven, CT, approved the research protocol.
Participants
We accessed the Yale‐New Haven Hospital administrative database to identify the number of patients with SCD who demonstrated EHHU that did not remit over successive years.5 We identified the 10 highest inpatient utilizing individuals with sickle cell disease over the period January 1, 2008December 31, 2010; 8 individuals consented to participate. We collected the following data on each participant through chart review: hemoglobinopathy, length of stay, primary diagnosis for each admission, and SCD‐related comorbidities (eg, avascular necrosis, leg ulcer, etc). No research team member was involved in the care of any of the participants.
Interviews
Based on literature review of other qualitative research in SCD, we created an interview guide to include the following themes: 1) disease, pain, and medication; 2) hospitalization; 3) support structures; 4) daily life; and 5) personal relationships (see Supporting Information, Appendix I, in the online version of this article). Applying Grounded Theory in qualitative research, the interview guide underwent several minor modifications based on field‐testing interviews with 4 interviews of patients not enrolled in the study and early interviews with study participants.11 Tape‐recorded interviews, each lasting at least an hour,12 were conducted by 1 researcher (D.W.) during inpatient hospitalizations, at least several days after admission to ensure that participants were comfortable enough to participate. When the interview exceeded an hour, it was continued at a later time. Recordings were transcribed by a professional transcription service and verified for accuracy by the interviewer. Participants were compensated $25 for completed interviews.
Narrative Analysis
The analysis team consisted of 2 psychiatrists (1 with additional training in internal medicine), 1 medical student, and 1 internist with additional training in addiction medicine. Analysts read each transcript, became thoroughly familiar with its content, and met to discuss preliminary findings. Then, we created patient experts among the group, assigning each analyst 2 interviews with which s/he prepared a detailed summary in the first person, using the participant's own words, according to an established process in phenomenological research13 (Figure 1). These narrative summaries allowed for the development of a holistic view of the participant, the creation of a narrative structure, and the fostering of an empathic bridge,13 a connection between the experiences of the participant and those of the reviewer. The summaries were read aloud at research meetings allowing for discussion, and the content of the summaries were modified based on the consensus of the group.
Next, we randomly rotated the narrative summaries so that each of the 4 analysts became an expert for 2 additional participants in order to critically evaluate the compiled narratives, and develop a structural summary14a summary of the prevalent themes. We extracted content from the narrative summaries based on these common themes, and returned to the transcripts as needed for relevant quotations. This inductive process allowed unique participant narratives to come through unconstrained by a predetermined coding structure.
The team reached consensus on organizing themes following the chronology of childhood to adulthood. This model was utilized to preserve the narrative basis of the methodology, and to ultimately elucidate the antecedents, subjective experience, and consequences of EHHU. An audit trail was maintained throughout the data analysis process.
RESULTS
Table 1 displays demographic, clinical, and hospitalization data for the 8 participants. These patients represented approximately 8% of the population with sickle cell disease at the study institution, but accounted for 57% of hospital days among sickle cell disease patients over a 3‐year period, with cumulative hospital days near or above 100 days per patient each year. Greater than 90% of admissions were for vaso‐occlusive crises without other SCD‐related complications. However, many participants had complicated medical histories, including avascular necrosis, acute chest syndrome, and leg ulcers.
| Participant | Age at Interview Date | Gender | Hemoglobin Diagnosis* | Average Hospital Days per Year 20082010 |
|---|---|---|---|---|
| ||||
| 1 | 34 | F | HbSS | 171 |
| 2 | 27 | F | HbSS | 263 |
| 3 | 26 | M | HbS‐B thalassemia | 151 |
| 4 | 34 | M | HbSC | 111 |
| 5 | 37 | F | HbSS | 202 |
| 6 | 25 | F | HbS‐B thalassemia | 104 |
| 7 | 24 | F | HbSS | 123 |
| 10 | 32 | M | HbSS | 94 |
Participant interviews presented a common narrative of the evolution of EHHU from a young age, culminating in a universally negative description of hospitalization: It's like jail. (participant 2); It's like a massacre, coming in the hospital; I get tortured. (participant 1). Saturation was reached on major themes, which fit into 3 general categories: pain and opioid medication use, interpersonal relationships, and personal development.
Pain and Opioid Medication Use
Participants reported hospital use dating back to childhood, which was the first exposure to intravenous opioid medications and the beginning of a trajectory of accelerating use, tolerance, and dependence: You know, I came in the hospital when I was two years old I stayed 'til I was like five and a half. I started school here. (participant 1); I started taking that medicine when I was on the pedi side. So my body's already used to it it doesn't really touch me. They're gonna have to up my doses. (participant 7).
As adults, participants expressed awareness of the potential problems of opioids. During interviews, many participants exhibited side effects of these medications, such as itching and somnolence. Moreover, participants expressed awareness of the skepticism and mistrust from providers, and acknowledged that such sentiments may be justified toward certain patients: That's all our body knows, is meds, meds, meds. And because your body is addicted to this level, you gotta go up another level, but some doctors think we're taking too much. How can we be taking too much when we need it? (participant 5); The oxy which I'm on [oxycontin 240 mg per day] when you take that, you going to sleep. And then some of them will say when you go home you're not taking the medicine like you should. (participant 5).
Opioids were taken in and out of the hospital by all participants, and were identified as necessary in combating debilitating pain. Many participants expressed a reluctance to try other forms of therapy, such as hydroxyurea: These new chemicals, you come across doctors who say there's this new medicine out, and it's been out for such and such amount of timeI think it would be good, can we try it with you? No. I'm not a guinea. (participant 2).
While all participants described unpredictable pain crises, some also described an underlying, constant pain syndrome: You know, like, I could be fine right now; the next minute I could be Oh, my God crying, so much pain. You never know when you're gonna have a crisis. (participant 1); There's never no pain. There's always pain. It's just a fact of life. I wake up and I can deal with the pain, it's not that bad today. But then when the crisis hits, that's when it gets unbearable. (participant 10); I'm not in pain every day, every second. To me, I don't think that any sickle cell patient is in pain every day. They make theirselves to [be] it saddens me sometimes. (participant 6).
Interpersonal Relationships
In childhood, participants developed close relationships with the staff of the children's hospital and an attachment to this institution: I loved pediatrics. It's the adult side I can't stand. They treat you better. (participant 7); Some people in the ER, they know us; and I call them my family they already know what I need. (participant 5).
In contrast, the hospital experience during adulthood was often punctuated by bitter relationships with staff, and distrust over possible excessive use of opioids. Moreover, participants raised the possibility of racism in their interactions with hospital staff. Overall, participants highlighted a lack of empathy among caregivers: Some doctors, they're rude, like, they're rough. They'll just pull out the scope bang it onto my back, or just push on my body or areas where it hurts. (participant 6); I'm your doctor. And I say I think you're doing a lot better, how would you feel about going home today? And you can say I don't think I'm ready. And I can say Well, you can't live here in the hospital. Why do you think you're not ready for home yet? You're never, ever going to be pain free, and that's when you turn around to me and say I know that. I've been dealing with this for all my life. I know I'm never gonna be pain free! (participant 2).
Such negative interactions extended to friends and family members, leading to a sense of social isolation and a reluctance to discuss their disease with others: I just don't think people will understand where I'm coming from. So I just don't talk to anybody, I keep it inside. Or I write it in my diary. (participant 5); I don't have any friends. I have associates. I'm always by myself. (participant 1).
Even though participants expressed dismay at dysfunctional relationships within the hospital, they also voiced affection for staff members. Participant 1 described hospital stays that were loving, and participant 3 described his hematologist as his brother from another mother, and a nurse practitioner as his aunt.
Personal Development
Hospitalization in childhood was linked to EHHU as an adult by the derailment that participants described in their personal development. Prolonged hospitalization and illness were barriers to education, interfering with the development of social as well as academic skills: I couldn't spell me being in a hospital for so much I was like, no, I don't want that bookwork like everybody else. (participant 3); I stopped going to school. I told [my mom] that I was not going back to school because the kids made fun of me Oh, she has a disease. Be careful, you might get the cooties. (participant 2).
Participants also described a sense of foreshortened future. Many were told that they would not survive their teens: They told my mother I would die before I was 12 years old. And I would be scared to go to sleep, because I would think I was gonna die in my sleep. (participant 2)
As an adult, numerous and/or prolonged hospitalizations interfered with participants' ability to remain employed, and they experienced strains on fulfilling family roles: I would love to work again, but who gonna hire somebody that's always out, more than you're working. Nobody. (participant 5); Sometimes I feel like I'm neglecting my son, being here. You have to take care of yourself in order for you to be there for him. But it just stresses me out. (participant 6).
The struggles of hospitalization and pain management took their toll on participants' mental health. Participants described difficulty sleeping, depression, and suicidal thoughts: Sorrow. That's what [sickle cell] means to me. Unhappy. Everything's depressing. It takes over your body and your mind and your soul. (participant 5); I really was gonna kill myself cause it's like, sometime, the pain, you be in so much pain, you be like, fuck this, man. My pain was bothering me so much, I laid down on the highway, wishin a car would run me over. (participant 4).
Despite fragile mental and physical health, many participants described feelings of strength and resilience, and some described hope in the future for employment, education, travel, and family: I don't know why God picked me, but for some strange, mysterious reason he picked me. I still don't know what that reason may be, but I ain't gonna give up. Maybe he got some kind of plan in store. (participant 2).
DISCUSSION
Our study population represents a unique and understudied group among patients with SCD. While several themes from prior research on individuals with SCD were presentreciprocal mistrust between patients and providers surrounding opioid analgesics and pain reporting,15, 16 racial and disease‐related bias,17 patient dissatisfaction with clinical services,18the common narrative of thwarted personal development in the setting of a long history of hospitalization and opioid use was striking.
The developmental perspective posits that age‐appropriate tasks govern basic capacities and skills (academic, interpersonal, affective, and cognitive) honed through institutional interactions (family, school, and community), which allow individuals to develop autonomy that guides them into effective participation in social groups and civil society, and eventually to becoming guarantors for the next generation. Our participants described problems such as social isolation, depression, and dependence on medications, all linked to their description of recurrent stays in the hospital during childhood and adolescence, where missed vocational and social opportunities left their indelible mark. Participants expressed an awareness of their inability to lead productive lives, and the perception that they were burdensome to their caregivers and the hospital.
While previous research has correlated high hospital utilization in SCD with factors like poor coping strategies,1921 high levels of stress,22 and inadequate support,17 our interviews suggest that such psychosocial difficulties may be consequences as well as causes of hospitalization, creating an accelerating downward spiral of dysfunction. At the center of this spiral is participants' ongoing experience of pain, which may be related to SCD, medications, or neither.23 Additionally, chronic anemia, opioid exposure, airway disease, and cerebrovascular disease are all implicated in impaired neuropsychological functioning in children and adolescents with sickle cell disease.24, 25
Clinical features of SCD remain relevant to hospitalization in adulthood. Chart review revealed that the vast majority of inpatient admissions were due to vaso‐occlusive crises uncomplicated by SCD‐related pathology, such as aseptic necrosis of bone or acute chest syndrome. This finding is consistent with previous work,9 which correlated new onset of high hospital use with SCD‐related complications, but not reliably with persistent EHHU, our study population.
The double‐edged sword of opioid use26 was starkly evident in participants' narratives. Crippling vaso‐occlusive crises were competently treated with opioids starting in childhood, but then a cycle of increasing outpatient doses of opioids and more frequent and longer courses of inpatient intravenous opioids followed. Participants felt judged and stigmatized for seeking one of the few treatment options they had been offered, resulting in confusion and bitterness at times. Other potential complications of long‐term opioid therapy less well known to patients and providers such as hypogonadism and hyperalgesia27may have played a role in the patient experience and should be examined in future research. In addition, undertreatment of pain may lead to pseudoaddiction,28 underscoring the complexity of delineating the pathologies of dependence, addiction, withdrawal, acute pain, and chronic pain.
Our study is limited primarily by the fact that it was conducted with a small number of participants. It is also possible that institutional variation, especially with regard to pain management, makes it difficult to generalize our hypotheses. Similarly, our participants grew up in similar environments outside the hospital, which may differ significantly from environments of other individuals with EHHU. Lastly, participants were all interviewed as inpatients, and the acuteness of their illness may have influenced responses. Despite these limitations, we achieved saturation on the major themes, and there was substantial agreement in their experiences of their illness.
Breaking the cycle of alienation from the external world and dependence on the hospital necessitates an acknowledgement of the role of the hospital, pain, and opioid use in the long‐term development of individuals with EHHU. Further research should test this developmental hypothesis, and focus on early interventions and the critical transition from pediatric to adult care.25 Longitudinal quantitative analysis could include psychosocial variables in SCD in the attempt to predict EHHU as has been accomplished in the chronic pain literature.29 Additionally, a comprehensive qualitative approach including the perspectives of caregivers, family members, and comparison to low hospital utilizers will better inform interventions aimed at ameliorating EHHU. It is particularly important to understand the similarities and differences in the long‐term development of patients with SCD who demonstrate EHHU versus low hospital use. The optimal strategy for opioid use in the long‐term management of pain in patients with SCD remains to be determined. Alternatives to opioids should be investigated in a controlled trial, and institutional differences should be examined as they relate to EHHU and pain‐management strategies. Lastly, our results suggest that psychosocial and skill rehabilitation may mitigate EHHU, and that multidisciplinary resources proactively directed towards this population will reduce hospitalization.30
- ,,,.The number of people with sickle‐cell disease in the United States: national and state estimates.Am J Hematol.2009;85:77–78.
- .Current issues in sickle cell pain and its management.Hematology Am Soc Hematol Educ Program.2007:97–105.
- ,,, et al.Daily assessment of pain in adults with sickle cell disease.Ann Intern Med.2008;148:94–101.
- ,,,,.Acute care utilization and rehospitalizations for sickle cell disease.JAMA.2010;303:1288–1294.
- ,,,.The course and correlates of high hospital utilization in sickle cell disease: evidence from a large, urban Medicaid managed care organization.Am J Hematol.2009;84:666–670.
- ,,,,,.Medical care utilization and mortality in sickle cell disease: a population‐based study.Am J Hematol.2005;80:262–270.
- ,,, et al.Pain in sickle cell disease. Rates and risk factors.N Engl J Med.1991;325:11–16.
- ,,, et al.Comparisons of high versus low emergency department utilizers in sickle cell disease.Ann Emerg Med.2009;53:587–593.
- ,,.Prediction of onset and course of high hospital utilization in sickle cell disease.J Hosp Med.2011;6:248–255.
- ,,.A review of empirically supported psychosocial interventions for pain and adherence outcomes in sickle cell disease.J Pediatr Psychol.2004;29:197–209.
- .More Grounded Theory Methodology: A Reader.Mill Valley, CA:Sociology Press;1994.
- .The Long Interview.Newbury Park, CA:Sage;1988.
- ,,.Generating coherence out of chaos: examples of the utility of empathic bridges in phenomenological research.J Phenomenolog Psychol.2004;35:253–271.
- ,,,.Using qualitative methods in clinical research. In: McKay D, ed.Handbook of Research Methods in Abnormal and Clinical Psychology.Los Angeles, CA:Sage;2008:263–269.
- ,,,.Sickle cell‐related pain: perceptions of medical practitioners.J Pain Symptom Manage.1997;14:168–174.
- ,,,.Pain management in sickle cell disease.Chronic Illn.2006;2:39–50.
- ,,.Experiences of hospital care and treatment‐seeking behavior for pain from sickle cell disease: qualitative study.West J Med.1999;171:306–313.
- ,,,,.Dissatisfaction with hospital care for children with sickle cell disease not due only to race and chronic disease.Pediatr Blood Cancer.2009;53:174–178.
- ,,,.Sickle cell disease pain: relation of coping strategies to adjustment.J Consult Clin Psychol.1989;57:725–731.
- ,,,.Sickle cell disease pain: 2. Predicting health care use and activity level at 9‐month follow‐up.J Consult Clin Psychol.1992;60:267–273.
- ,,,,.Coping and health service utilisation in a UK study of paediatric sickle cell pain.Arch Dis Child.2002;86:325–329.
- ,,,,,.Daily mood and stress predict pain, health care use, and work activity in African American adults with sickle‐cell disease.Health Psychol.2004;23:267–274.
- .Pain management in sickle cell disease: palliative care begins at birth?Hematology Am Soc Hematol Educ Program.2008:466–474.
- ,,,.Cognitive functioning in children with sickle cell disease: a meta‐analysis.J Pediatr Psychol.2002;27:739–748.
- ,,, et al.Transition planning for youth with sickle cell disease: embedding neuropsychological assessment into comprehensive care.Pediatrics.2010;126(suppl 3):S151–S159.
- .Increases in opioid medication use: balancing the good with the bad.Pain.2008;138:245–246.
- ,,,.Hyperalgesia: an emerging iatrogenic syndrome.J Pain Symptom Manage.2003;26:769–775.
- ,,,,.Understanding the causes of problematic pain management in sickle cell disease: evidence that pseudoaddiction plays a more important role than genuine analgesic dependence.J Pain Symptom Manage.2004;27:156–169.
- ,,,,.Functional abdominal pain patient subtypes in childhood predict functional gastrointestinal disorders with chronic pain and psychiatric comorbidities in adolescence and adulthood.Pain.2012;153:1798–1806.
- ,,.Caring for the adult with sickle cell disease: results of a multidisciplinary pilot program.J Natl Med Assoc.2010;102:1009–1016.
- ,,,.The number of people with sickle‐cell disease in the United States: national and state estimates.Am J Hematol.2009;85:77–78.
- .Current issues in sickle cell pain and its management.Hematology Am Soc Hematol Educ Program.2007:97–105.
- ,,, et al.Daily assessment of pain in adults with sickle cell disease.Ann Intern Med.2008;148:94–101.
- ,,,,.Acute care utilization and rehospitalizations for sickle cell disease.JAMA.2010;303:1288–1294.
- ,,,.The course and correlates of high hospital utilization in sickle cell disease: evidence from a large, urban Medicaid managed care organization.Am J Hematol.2009;84:666–670.
- ,,,,,.Medical care utilization and mortality in sickle cell disease: a population‐based study.Am J Hematol.2005;80:262–270.
- ,,, et al.Pain in sickle cell disease. Rates and risk factors.N Engl J Med.1991;325:11–16.
- ,,, et al.Comparisons of high versus low emergency department utilizers in sickle cell disease.Ann Emerg Med.2009;53:587–593.
- ,,.Prediction of onset and course of high hospital utilization in sickle cell disease.J Hosp Med.2011;6:248–255.
- ,,.A review of empirically supported psychosocial interventions for pain and adherence outcomes in sickle cell disease.J Pediatr Psychol.2004;29:197–209.
- .More Grounded Theory Methodology: A Reader.Mill Valley, CA:Sociology Press;1994.
- .The Long Interview.Newbury Park, CA:Sage;1988.
- ,,.Generating coherence out of chaos: examples of the utility of empathic bridges in phenomenological research.J Phenomenolog Psychol.2004;35:253–271.
- ,,,.Using qualitative methods in clinical research. In: McKay D, ed.Handbook of Research Methods in Abnormal and Clinical Psychology.Los Angeles, CA:Sage;2008:263–269.
- ,,,.Sickle cell‐related pain: perceptions of medical practitioners.J Pain Symptom Manage.1997;14:168–174.
- ,,,.Pain management in sickle cell disease.Chronic Illn.2006;2:39–50.
- ,,.Experiences of hospital care and treatment‐seeking behavior for pain from sickle cell disease: qualitative study.West J Med.1999;171:306–313.
- ,,,,.Dissatisfaction with hospital care for children with sickle cell disease not due only to race and chronic disease.Pediatr Blood Cancer.2009;53:174–178.
- ,,,.Sickle cell disease pain: relation of coping strategies to adjustment.J Consult Clin Psychol.1989;57:725–731.
- ,,,.Sickle cell disease pain: 2. Predicting health care use and activity level at 9‐month follow‐up.J Consult Clin Psychol.1992;60:267–273.
- ,,,,.Coping and health service utilisation in a UK study of paediatric sickle cell pain.Arch Dis Child.2002;86:325–329.
- ,,,,,.Daily mood and stress predict pain, health care use, and work activity in African American adults with sickle‐cell disease.Health Psychol.2004;23:267–274.
- .Pain management in sickle cell disease: palliative care begins at birth?Hematology Am Soc Hematol Educ Program.2008:466–474.
- ,,,.Cognitive functioning in children with sickle cell disease: a meta‐analysis.J Pediatr Psychol.2002;27:739–748.
- ,,, et al.Transition planning for youth with sickle cell disease: embedding neuropsychological assessment into comprehensive care.Pediatrics.2010;126(suppl 3):S151–S159.
- .Increases in opioid medication use: balancing the good with the bad.Pain.2008;138:245–246.
- ,,,.Hyperalgesia: an emerging iatrogenic syndrome.J Pain Symptom Manage.2003;26:769–775.
- ,,,,.Understanding the causes of problematic pain management in sickle cell disease: evidence that pseudoaddiction plays a more important role than genuine analgesic dependence.J Pain Symptom Manage.2004;27:156–169.
- ,,,,.Functional abdominal pain patient subtypes in childhood predict functional gastrointestinal disorders with chronic pain and psychiatric comorbidities in adolescence and adulthood.Pain.2012;153:1798–1806.
- ,,.Caring for the adult with sickle cell disease: results of a multidisciplinary pilot program.J Natl Med Assoc.2010;102:1009–1016.
Copyright © 2012 Society of Hospital Medicine