User login
Incompatible Type A plasma found safe for initial resuscitation of trauma patients
HOLLYWOOD, FLA. – Incompatible Type A plasma appears to be a safe and effective part of an initial resuscitation protocol for trauma patients who need a massive transfusion.
There were no increases in morbidity, mortality, or transfusion-related acute lung injury among 120 patients who received Type A plasma, compared with those who got compatible plasma, Bryan C. Morse, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Type AB blood products are preferred for initial transfusions for trauma patients with unknown blood type. While type AB blood products are universally acceptable to patients, they are also in short supply. In an attempt to mitigate this shortage, some trauma centers are relying on anecdotal data, much drawn from real-life combat experience dating from World War II to present times, suggesting that Type A plasma is safe for initial resuscitation protocols. But the body of data from well-constructed trials is small, said Dr. Morse of Emory University, Atlanta. Thus, EAST sponsored this retrospective registry study, which examined outcomes in 1,536 trauma patients who received plasma transfusions as part of a massive transfusion protocol from 2012 to 2016.
The primary endpoints were overall morbidity, and mortality at four time points: 6 and 24 hours, and 7 and 28 days. Eight trauma centers contributed data to the study.
The group was largely male (75%) with a mean age of 37 years. Patients were seriously injured, with a mean Injury Severity Score (ISS) of 25. About 60% suffered from blunt-force trauma. Among the entire group, 120 (8%) received incompatible type A plasma.
About 28% of patients (434) experienced an adverse event. These were numerically but not significantly more common among the incompatible A plasma group (35% vs. 28%; P = .14). Events included acute respiratory distress syndrome (6% vs. 7.6%), thromboembolism (9% vs. 7%), pneumonia (19% vs. 15%), and acute kidney injury (8% each).
There were two cases of transfusion-related acute lung injury, both of which occurred in the compatible type A group.
Mortality was similar at every time point: 6 hours (16% vs. 15%), 24 hours (25% vs. 22%), 7 days (35% vs. 32%), and 28 days (38% vs. 35%).
A multivariate regression model controlled for treatment center, ISS, units of packed red cells given by 4 hours, mechanism of injury, Type A plasma incompatibility, and age.
In the morbidity analysis, only ISS and units of red blood cells at 4 hours were associated with a significant increase in risk (odd ratio 1.02). Incompatible Type A plasma did not significantly increase the risk of morbidity.
In the mortality analysis, units of red cells, ISS, and age were significantly associated with increased risk. Again, incompatible Type A plasma did not significantly increase the risk of death.
Dr. Morse had no financial declaration.
[email protected]
On Twitter @Alz_Gal
HOLLYWOOD, FLA. – Incompatible Type A plasma appears to be a safe and effective part of an initial resuscitation protocol for trauma patients who need a massive transfusion.
There were no increases in morbidity, mortality, or transfusion-related acute lung injury among 120 patients who received Type A plasma, compared with those who got compatible plasma, Bryan C. Morse, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Type AB blood products are preferred for initial transfusions for trauma patients with unknown blood type. While type AB blood products are universally acceptable to patients, they are also in short supply. In an attempt to mitigate this shortage, some trauma centers are relying on anecdotal data, much drawn from real-life combat experience dating from World War II to present times, suggesting that Type A plasma is safe for initial resuscitation protocols. But the body of data from well-constructed trials is small, said Dr. Morse of Emory University, Atlanta. Thus, EAST sponsored this retrospective registry study, which examined outcomes in 1,536 trauma patients who received plasma transfusions as part of a massive transfusion protocol from 2012 to 2016.
The primary endpoints were overall morbidity, and mortality at four time points: 6 and 24 hours, and 7 and 28 days. Eight trauma centers contributed data to the study.
The group was largely male (75%) with a mean age of 37 years. Patients were seriously injured, with a mean Injury Severity Score (ISS) of 25. About 60% suffered from blunt-force trauma. Among the entire group, 120 (8%) received incompatible type A plasma.
About 28% of patients (434) experienced an adverse event. These were numerically but not significantly more common among the incompatible A plasma group (35% vs. 28%; P = .14). Events included acute respiratory distress syndrome (6% vs. 7.6%), thromboembolism (9% vs. 7%), pneumonia (19% vs. 15%), and acute kidney injury (8% each).
There were two cases of transfusion-related acute lung injury, both of which occurred in the compatible type A group.
Mortality was similar at every time point: 6 hours (16% vs. 15%), 24 hours (25% vs. 22%), 7 days (35% vs. 32%), and 28 days (38% vs. 35%).
A multivariate regression model controlled for treatment center, ISS, units of packed red cells given by 4 hours, mechanism of injury, Type A plasma incompatibility, and age.
In the morbidity analysis, only ISS and units of red blood cells at 4 hours were associated with a significant increase in risk (odd ratio 1.02). Incompatible Type A plasma did not significantly increase the risk of morbidity.
In the mortality analysis, units of red cells, ISS, and age were significantly associated with increased risk. Again, incompatible Type A plasma did not significantly increase the risk of death.
Dr. Morse had no financial declaration.
[email protected]
On Twitter @Alz_Gal
HOLLYWOOD, FLA. – Incompatible Type A plasma appears to be a safe and effective part of an initial resuscitation protocol for trauma patients who need a massive transfusion.
There were no increases in morbidity, mortality, or transfusion-related acute lung injury among 120 patients who received Type A plasma, compared with those who got compatible plasma, Bryan C. Morse, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Type AB blood products are preferred for initial transfusions for trauma patients with unknown blood type. While type AB blood products are universally acceptable to patients, they are also in short supply. In an attempt to mitigate this shortage, some trauma centers are relying on anecdotal data, much drawn from real-life combat experience dating from World War II to present times, suggesting that Type A plasma is safe for initial resuscitation protocols. But the body of data from well-constructed trials is small, said Dr. Morse of Emory University, Atlanta. Thus, EAST sponsored this retrospective registry study, which examined outcomes in 1,536 trauma patients who received plasma transfusions as part of a massive transfusion protocol from 2012 to 2016.
The primary endpoints were overall morbidity, and mortality at four time points: 6 and 24 hours, and 7 and 28 days. Eight trauma centers contributed data to the study.
The group was largely male (75%) with a mean age of 37 years. Patients were seriously injured, with a mean Injury Severity Score (ISS) of 25. About 60% suffered from blunt-force trauma. Among the entire group, 120 (8%) received incompatible type A plasma.
About 28% of patients (434) experienced an adverse event. These were numerically but not significantly more common among the incompatible A plasma group (35% vs. 28%; P = .14). Events included acute respiratory distress syndrome (6% vs. 7.6%), thromboembolism (9% vs. 7%), pneumonia (19% vs. 15%), and acute kidney injury (8% each).
There were two cases of transfusion-related acute lung injury, both of which occurred in the compatible type A group.
Mortality was similar at every time point: 6 hours (16% vs. 15%), 24 hours (25% vs. 22%), 7 days (35% vs. 32%), and 28 days (38% vs. 35%).
A multivariate regression model controlled for treatment center, ISS, units of packed red cells given by 4 hours, mechanism of injury, Type A plasma incompatibility, and age.
In the morbidity analysis, only ISS and units of red blood cells at 4 hours were associated with a significant increase in risk (odd ratio 1.02). Incompatible Type A plasma did not significantly increase the risk of morbidity.
In the mortality analysis, units of red cells, ISS, and age were significantly associated with increased risk. Again, incompatible Type A plasma did not significantly increase the risk of death.
Dr. Morse had no financial declaration.
[email protected]
On Twitter @Alz_Gal
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point:
Major finding: Adverse events were not significantly more common among the incompatible A plasma group (35% vs. 28%; P = .14).
Data source: The retrospective study comprised 1,536 patients.
Disclosures: Dr. Morse had no financial disclosures.
How to prepare to care for transgender adolescents
As pediatric and adolescent gynecologists, we are seeing an increasing number of adolescents with gender identity issues and have come to believe that all obstetrician-gynecologists need to have an understanding of varying gender identities, as well as their role in managing these patients’ care.
We had the honor to assist the American College of Obstetricians and Gynecologists’ (ACOG) Committee on Adolescent Health Care in the development of a new Committee Opinion to guide ob.gyns. in caring for transgender adolescents (Obstet Gynecol 2017;129:e11-6). As our culture grows more aware of the nuances and spectrum of gender identity, our health care practices must grow as well. Ob.gyns. are often uniquely positioned as being among the first people transgender adolescents present to – whether it’s signaling disassociation with their gender when answering routine medical questions or directly addressing gender with them as a trusted and private resource. Even when seeing a patient too young to consider hormone therapy, an ob.gyn. can offer vital early behavioral health support, educational and community resources, and specialist referrals.
Transgender adolescent patients have likely faced negative stereotypes and stigmas in social settings or through media that make them cautious and protective of their identity. They are also more likely to face social ostracism such as bullying and/or dissent and rejection from their parents, deepening the vulnerability of their situation. As a result, transgender adolescents can have increased instances of anxiety, depression, sexual harassment, homelessness, and risk-taking behavior. Medical practices can signal to transgender patients that they are safe and welcoming from the start by offering gender neutral forms, brochures, and information for LGBT patients in the waiting room, and having sensitive employees at every step – from the front desk onward.
As we’ve just outlined, transgender adolescent patients face unique challenges, including increased rates of social and mental health risks. In response, ob.gyns. must be prepared to have a comprehensive conversation about health and well-being beyond sexual and reproductive health. They must also be equipped to address the psychosocial issues associated with transgender adolescents. This includes knowledge of what to look for and offering patients resources, education, and referrals to guarantee their health and safety.
It is important that ob.gyns. are aware that transgender men have female reproductive organs and can present with common gynecological problems such as abnormal bleeding, ovarian cysts, and torsion, as well as pregnancy and pregnancy complications. Finally, ob.gyns. can serve a unique role in counseling about fertility and fertility preservation. Thus, not only do we provide essential health care, including ongoing primary care, but we can position ourselves as part of the support network for these adolescents and their families.
Most importantly, when addressing an adolescent transgender patient, we must understand there is no uniform transgender experience. Expressing gender, sexual identity, and behavior patterns will vary from patient to patient. There are a wide range of treatment options available for transgender patients, from hormone to surgical therapies. An ob.gyn.’s responsibility is to help each individual make an informed decision, and help that patient think ahead to the future.
While this all may seem like a lot, it’s important to remember the essential components of our role as health care providers do not change because an adolescent patient is transgender. Care should always include education about their bodies, safe sex, deliberate and thoughtful assessment of symptoms or concerns, and preventive care services such as STI screenings and contraception. We are simply adding more nuanced cultural and medical understanding to those practices.
Dr. Gomez-Lobo is director of pediatric and adolescent obstetrics and gynecology, Medstar Washington Hospital Center/Children’s National Health System, Washington, D.C. Dr. Sokkary is associate professor of ob.gyn. at Navicent Health Center/Mercer School of Medicine in Macon, Ga. They are members of the ACOG Committee on Adolescent Health Care. They reported having no relevant financial disclosures.
As pediatric and adolescent gynecologists, we are seeing an increasing number of adolescents with gender identity issues and have come to believe that all obstetrician-gynecologists need to have an understanding of varying gender identities, as well as their role in managing these patients’ care.
We had the honor to assist the American College of Obstetricians and Gynecologists’ (ACOG) Committee on Adolescent Health Care in the development of a new Committee Opinion to guide ob.gyns. in caring for transgender adolescents (Obstet Gynecol 2017;129:e11-6). As our culture grows more aware of the nuances and spectrum of gender identity, our health care practices must grow as well. Ob.gyns. are often uniquely positioned as being among the first people transgender adolescents present to – whether it’s signaling disassociation with their gender when answering routine medical questions or directly addressing gender with them as a trusted and private resource. Even when seeing a patient too young to consider hormone therapy, an ob.gyn. can offer vital early behavioral health support, educational and community resources, and specialist referrals.
Transgender adolescent patients have likely faced negative stereotypes and stigmas in social settings or through media that make them cautious and protective of their identity. They are also more likely to face social ostracism such as bullying and/or dissent and rejection from their parents, deepening the vulnerability of their situation. As a result, transgender adolescents can have increased instances of anxiety, depression, sexual harassment, homelessness, and risk-taking behavior. Medical practices can signal to transgender patients that they are safe and welcoming from the start by offering gender neutral forms, brochures, and information for LGBT patients in the waiting room, and having sensitive employees at every step – from the front desk onward.
As we’ve just outlined, transgender adolescent patients face unique challenges, including increased rates of social and mental health risks. In response, ob.gyns. must be prepared to have a comprehensive conversation about health and well-being beyond sexual and reproductive health. They must also be equipped to address the psychosocial issues associated with transgender adolescents. This includes knowledge of what to look for and offering patients resources, education, and referrals to guarantee their health and safety.
It is important that ob.gyns. are aware that transgender men have female reproductive organs and can present with common gynecological problems such as abnormal bleeding, ovarian cysts, and torsion, as well as pregnancy and pregnancy complications. Finally, ob.gyns. can serve a unique role in counseling about fertility and fertility preservation. Thus, not only do we provide essential health care, including ongoing primary care, but we can position ourselves as part of the support network for these adolescents and their families.
Most importantly, when addressing an adolescent transgender patient, we must understand there is no uniform transgender experience. Expressing gender, sexual identity, and behavior patterns will vary from patient to patient. There are a wide range of treatment options available for transgender patients, from hormone to surgical therapies. An ob.gyn.’s responsibility is to help each individual make an informed decision, and help that patient think ahead to the future.
While this all may seem like a lot, it’s important to remember the essential components of our role as health care providers do not change because an adolescent patient is transgender. Care should always include education about their bodies, safe sex, deliberate and thoughtful assessment of symptoms or concerns, and preventive care services such as STI screenings and contraception. We are simply adding more nuanced cultural and medical understanding to those practices.
Dr. Gomez-Lobo is director of pediatric and adolescent obstetrics and gynecology, Medstar Washington Hospital Center/Children’s National Health System, Washington, D.C. Dr. Sokkary is associate professor of ob.gyn. at Navicent Health Center/Mercer School of Medicine in Macon, Ga. They are members of the ACOG Committee on Adolescent Health Care. They reported having no relevant financial disclosures.
As pediatric and adolescent gynecologists, we are seeing an increasing number of adolescents with gender identity issues and have come to believe that all obstetrician-gynecologists need to have an understanding of varying gender identities, as well as their role in managing these patients’ care.
We had the honor to assist the American College of Obstetricians and Gynecologists’ (ACOG) Committee on Adolescent Health Care in the development of a new Committee Opinion to guide ob.gyns. in caring for transgender adolescents (Obstet Gynecol 2017;129:e11-6). As our culture grows more aware of the nuances and spectrum of gender identity, our health care practices must grow as well. Ob.gyns. are often uniquely positioned as being among the first people transgender adolescents present to – whether it’s signaling disassociation with their gender when answering routine medical questions or directly addressing gender with them as a trusted and private resource. Even when seeing a patient too young to consider hormone therapy, an ob.gyn. can offer vital early behavioral health support, educational and community resources, and specialist referrals.
Transgender adolescent patients have likely faced negative stereotypes and stigmas in social settings or through media that make them cautious and protective of their identity. They are also more likely to face social ostracism such as bullying and/or dissent and rejection from their parents, deepening the vulnerability of their situation. As a result, transgender adolescents can have increased instances of anxiety, depression, sexual harassment, homelessness, and risk-taking behavior. Medical practices can signal to transgender patients that they are safe and welcoming from the start by offering gender neutral forms, brochures, and information for LGBT patients in the waiting room, and having sensitive employees at every step – from the front desk onward.
As we’ve just outlined, transgender adolescent patients face unique challenges, including increased rates of social and mental health risks. In response, ob.gyns. must be prepared to have a comprehensive conversation about health and well-being beyond sexual and reproductive health. They must also be equipped to address the psychosocial issues associated with transgender adolescents. This includes knowledge of what to look for and offering patients resources, education, and referrals to guarantee their health and safety.
It is important that ob.gyns. are aware that transgender men have female reproductive organs and can present with common gynecological problems such as abnormal bleeding, ovarian cysts, and torsion, as well as pregnancy and pregnancy complications. Finally, ob.gyns. can serve a unique role in counseling about fertility and fertility preservation. Thus, not only do we provide essential health care, including ongoing primary care, but we can position ourselves as part of the support network for these adolescents and their families.
Most importantly, when addressing an adolescent transgender patient, we must understand there is no uniform transgender experience. Expressing gender, sexual identity, and behavior patterns will vary from patient to patient. There are a wide range of treatment options available for transgender patients, from hormone to surgical therapies. An ob.gyn.’s responsibility is to help each individual make an informed decision, and help that patient think ahead to the future.
While this all may seem like a lot, it’s important to remember the essential components of our role as health care providers do not change because an adolescent patient is transgender. Care should always include education about their bodies, safe sex, deliberate and thoughtful assessment of symptoms or concerns, and preventive care services such as STI screenings and contraception. We are simply adding more nuanced cultural and medical understanding to those practices.
Dr. Gomez-Lobo is director of pediatric and adolescent obstetrics and gynecology, Medstar Washington Hospital Center/Children’s National Health System, Washington, D.C. Dr. Sokkary is associate professor of ob.gyn. at Navicent Health Center/Mercer School of Medicine in Macon, Ga. They are members of the ACOG Committee on Adolescent Health Care. They reported having no relevant financial disclosures.
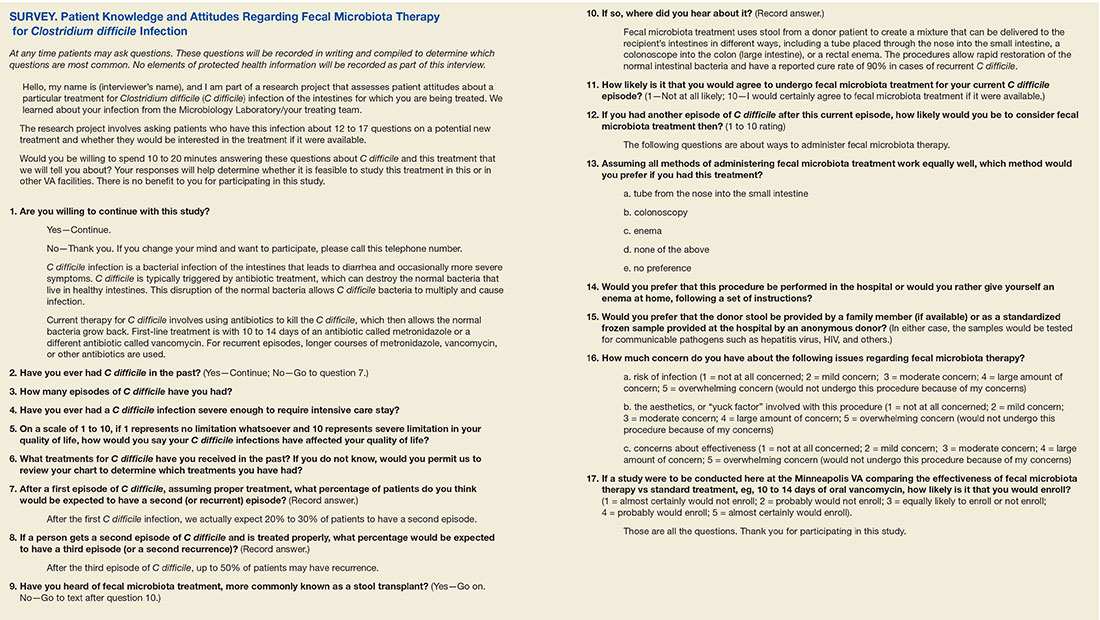
Patient Knowledge and Attitudes About Fecal Microbiota Therapy for Clostridium difficile Infection
Clostridium difficile (C difficile) infection (CDI) is a leading cause of infectious diarrhea among hospitalized patients and, increasingly, in ambulatory patients.1,2 The high prevalence of CDI and the high recurrence rates (15%-30%) led the CDC to categorize C difficile as an "urgent" threat (the highest category) in its 2013 Antimicrobial Resistance Threat Report.3-5 The Infectious Diseases Society of America guideline recommended treatment for CDI is vancomycin or metronidazole; more recent studies also support fidaxomicin use.4,6,7
Patients experiencing recurrent CDI are at risk for further recurrences, such that after the third CDI episode, the risk of subsequent recurrences exceeds 50%.8 This recurrence rate has stimulated research into other treatments, including fecal microbiota transplantation (FMT). A recent systematic review of FMT reports that 85% of patients have resolution of symptoms without recurrence after FMT, although this is based on data from case series and 2 small randomized clinical trials.9
A commonly cited barrier to FMT is patient acceptance. In response to this concern, a previous survey demonstrated that 81% of respondents would opt for FMT to treat a hypothetical case of recurrent CDI.10 However, the surveyed population did not have CDI, and the 48% response rate is concerning, since those with a favorable opinion of FMT might be more willing to complete a survey than would other patients. Accordingly, the authors systematically surveyed hospitalized veterans with active CDI to assess their knowledge, attitudes, and opinions about FMT as a treatment for CDI.
Methods
In-person patient interviews were conducted by one of the study authors at the Minneapolis VA Health Care System (MVAHCS), consisting of 13 to 18 questions. Questions addressed any prior CDI episodes and knowledge of the following: CDI, recurrence risk, and FMT; preferred route and location of FMT administration; concerns regarding FMT; likelihood of agreeing to undergo FMT (if available); and likelihood of enrollment in a hypothetical study comparing FMT to standard antibiotic treatment. The survey was developed internally and was not validated. Questions used the Likert-scale (Survey).
Patients with CDI were identified by monitoring for positive C difficile polymerase chain reaction (PCR) stool tests and then screened for inclusion by medical record review. Inclusion criteria were (1) MVAHCS hospitalization; and (2) written informed consent. Exclusion criteria were the inability to communicate or participate in an interview. Patient responses regarding their likelihood of agreeing to FMT for CDI treatment under different circumstances were compared using Wilcoxon rank sum test. These circumstances included FMT for their current episode of CDI, FMT for a subsequent episode, and FMT if recommended by their physician. Possible concerns regarding FMT also were solicited, including infection risk, effectiveness, and procedural aesthetics. The MVAHCS institutional review board approved the study.
Results
Stool PCR tests for CDI were monitored for 158 days from 2013 to 2014 (based on availability of study staff), yielding 106 positive results. Of those, 31 (29%) were from outpatients and not addressed further. Of the 75 positive CDI tests from 66 hospitalized patients (9 patients had duplicate tests), 18 of 66 (27%) were not able to provide consent and were excluded, leaving 48 eligible patients. Six (13%) were missed for logistic reasons (patient at a test or procedure, discharged before approached, etc), leaving 42 patients who were approached for participation. Among these, 34 (81%) consented to participate in the survey. Two subjects (6%) found the topic so unappealing that they terminated the interview.
The majority of enrolled subjects were men (32/34, 94%), with a mean age of 65.3 years (range, 31-89). Eleven subjects (32%) reported a prior CDI episode, with 10 reporting 1 such episode, and the other 2 episodes. Those with prior CDI reported the effect of CDI on their overall quality of life as 5.1 (1 = no limitation, 10 = severe limitation). Respondents were fairly accurate regarding the risk of recurrence after an initial episode of CDI, with the average expectedrecurrence rate estimated at 33%. In contrast, their estimation of the risk of recurrence after a second CDI episode was lower (28%), although the risk of recurrent episodes increases with each CDI recurrence.
Regarding FMT, 5 subjects indicated awareness of the procedure: 2 learning of it from a news source, 1 from family, 1 from a health care provider, and 1 was unsure of the source. After subjects received a description of FMT, their opinions regarding the procedure were elicited. When asked which route of delivery they would prefer if they were to undergo FMT, the 33 subjects who provided a response indicated a strong preference for either enema (15, 45%) or colonoscopy (10, 30%), compared with just 4 (12%) indicating no preference, 2 (6%) choosing nasogastric tube administration, and 2 (6%) indicating that they would not undergo FMT by any route (P < .001).
Regarding the location of FMT administration (hospital setting vs self-administered at home), 31 of 33 respondents (94%) indicated they would prefer FMT to occur in the hospital vs 2 (6%) preferring self-administration at home (P < .001). The preferred source of donor stool was more evenly distributed, with 14 of 32 respondents (44%) indicating a preference for an anonymous donor, 11 preferring a family member (34%), and 7 (21%) with no preference (P = .21).
Subjects were asked about concerns regarding FMT, and asked to rate each on a 5-point Likert scale (1 = not at all concerning; 5 = overwhelming concern). Concerns regarding risk of infection and effectiveness received an average score of 2.74 and 2.72, respectively, whereas concern regarding the aesthetics, or "yuck factor" was slightly lower (2.1: P = NS for all comparisons). Subjects also were asked to rate the likelihood of undergoing FMT, if it were available, for their current episode of CDI, a subsequent episode of CDI, or if their physician recommended undergoing FMT (10 point scale: 1 = not at all likely; 10 = certainly agree to FMT). The mean scores (SD) for agreeing to FMT for the current or a subsequent episode were 4.8 (SD 2.7) and 5.6 (SD 3.0); P = .12, but increased to 7.1 (SD 3.23) if FMT were recommended by their physician (P < .001 for FMT if physician recommended vs FMT for current episode; P = .001 for FMT if physician recommended vs FMT for a subsequent episode). Finally, subjects were asked about the likelihood of enrolling in a study comparing FMT to standard antimicrobial treatment, with answers ranging from 1 (almost certainly would not enroll) to 5 (almost certainly would enroll). Among the 32 respondents to this question, 17 (53%) answered either "probably would enroll" or "almost certainly would enroll," with a mean score of 3.2.
Discussion
Overall, VA patients with a current episode of CDI were not aware of FMT, with just 15% knowing about the procedure. However, after learning about FMT, patients expressed clear opinions regarding the route and setting of FMT administration, with enema or colonoscopy being the preferred routes, and a hospital the preferred setting. In contrast, subjects expressed ambivalence with regard to the source of donor stool, with no clear preference for stool from an anonymous donor vs from a family member.
When asked about concerns regarding FMT, none of the presented options (risk of infection, uncertain effectiveness, or procedural aesthetics) emerged as significantly more important than did others, although the oft-cited concern regarding FMT aesthetics engendered the lowest overall level of concern. In terms of FMT acceptance, 4 subjects (12%) were opposed to the procedure, indicating that they were not at all likely to agree to FMT for all scenarios (defined as a score of 1 or 2 on the 10-point Likert scale) or by terminating the survey because of the questions. However, 15 (44%) indicated that they would certainly agree to FMT (defined as a score of 9 or 10 on the 10-point Likert scale) if their physician recommended it. Physician recommendation for FMT resulted in the highest overall likelihood of agreeing to FMT, a finding in agreement with a previous survey of FMT for CDI.10 Most subjects indicated likely enrollment in a potential study comparing FMT with standard antimicrobial therapy.
Strengths/Limitations
Study strengths included surveying patients with current CDI, such that patients had personal experience with the disease in question. Use of in-person interviews also resulted in a robust response rate of 81% and allowed subjects to clarify any unclear questions with study personnel. Weaknesses included a relatively small sample size, underrepresentation of women, and lack of detail regarding respondent characteristics. Additionally, capsule delivery of FMT was not assessed since this method of delivery had not been published at the time of survey administration.
Conclusion
This survey of VA patients with CDI suggests that aesthetic concerns are not a critical deterrent for this population, and interest in FMT for the treatment of recurrent CDI exists. Physician recommendation to undergo FMT seems to be the most influential factor affecting the likelihood of agreeing to undergo FMT. These results support the feasibility of conducting clinical trials of FMT in the VA system.
1. Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile Infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32(4):387-390.
2. Centers for Disease Control and Prevention. Severe Clostridium difficile-associated disease in populations previously at low risk--four states, 2005. MMWR Morb Mortal Wkly Rep. 2005;54(47):1201-1205.
3. Johnson S, Louie TJ, Gerding DN, et al; Polymer Alternative for CDI Treatment (PACT) investigators. Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection: results from two multinational, randomized, controlled trials. Clin Infect Dis. 2014;59(3):345-354.
4. Louie TJ, Miller MA, Mullane KM, et al; OPT-80-003 Clinical Study Group. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med. 2011;364(5):422-431.
5. Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. http://www.cdc.gov/drugresistance/threat-report-2013. Updated July 17, 2014. Accessed November 16.2016.
6. Cohen SH, Gerding DN, Johnson S, et al; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31(5):431-455.
7. Cornely OA, Crook DW, Esposito R, et al; OPT-80-004 Clinical Study Group. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis. 2012;12(4):281-289.
8. Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect. 2009;58(6):403-410.
9. Drekonja DM, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection--a systematic review. Ann Intern Med. 2015;162(9):630-638.
10. Zipursky JS, Sidorsky TI, Freedman CA, Sidorsky MN, Kirkland KB. Patient attitudes toward the use of fecal microbiota transplantation in the treatment of recurrent Clostridium difficile infection. Clin Infect Dis. 2012;55(12):1652-1658.
Clostridium difficile (C difficile) infection (CDI) is a leading cause of infectious diarrhea among hospitalized patients and, increasingly, in ambulatory patients.1,2 The high prevalence of CDI and the high recurrence rates (15%-30%) led the CDC to categorize C difficile as an "urgent" threat (the highest category) in its 2013 Antimicrobial Resistance Threat Report.3-5 The Infectious Diseases Society of America guideline recommended treatment for CDI is vancomycin or metronidazole; more recent studies also support fidaxomicin use.4,6,7
Patients experiencing recurrent CDI are at risk for further recurrences, such that after the third CDI episode, the risk of subsequent recurrences exceeds 50%.8 This recurrence rate has stimulated research into other treatments, including fecal microbiota transplantation (FMT). A recent systematic review of FMT reports that 85% of patients have resolution of symptoms without recurrence after FMT, although this is based on data from case series and 2 small randomized clinical trials.9
A commonly cited barrier to FMT is patient acceptance. In response to this concern, a previous survey demonstrated that 81% of respondents would opt for FMT to treat a hypothetical case of recurrent CDI.10 However, the surveyed population did not have CDI, and the 48% response rate is concerning, since those with a favorable opinion of FMT might be more willing to complete a survey than would other patients. Accordingly, the authors systematically surveyed hospitalized veterans with active CDI to assess their knowledge, attitudes, and opinions about FMT as a treatment for CDI.
Methods
In-person patient interviews were conducted by one of the study authors at the Minneapolis VA Health Care System (MVAHCS), consisting of 13 to 18 questions. Questions addressed any prior CDI episodes and knowledge of the following: CDI, recurrence risk, and FMT; preferred route and location of FMT administration; concerns regarding FMT; likelihood of agreeing to undergo FMT (if available); and likelihood of enrollment in a hypothetical study comparing FMT to standard antibiotic treatment. The survey was developed internally and was not validated. Questions used the Likert-scale (Survey).
Patients with CDI were identified by monitoring for positive C difficile polymerase chain reaction (PCR) stool tests and then screened for inclusion by medical record review. Inclusion criteria were (1) MVAHCS hospitalization; and (2) written informed consent. Exclusion criteria were the inability to communicate or participate in an interview. Patient responses regarding their likelihood of agreeing to FMT for CDI treatment under different circumstances were compared using Wilcoxon rank sum test. These circumstances included FMT for their current episode of CDI, FMT for a subsequent episode, and FMT if recommended by their physician. Possible concerns regarding FMT also were solicited, including infection risk, effectiveness, and procedural aesthetics. The MVAHCS institutional review board approved the study.
Results
Stool PCR tests for CDI were monitored for 158 days from 2013 to 2014 (based on availability of study staff), yielding 106 positive results. Of those, 31 (29%) were from outpatients and not addressed further. Of the 75 positive CDI tests from 66 hospitalized patients (9 patients had duplicate tests), 18 of 66 (27%) were not able to provide consent and were excluded, leaving 48 eligible patients. Six (13%) were missed for logistic reasons (patient at a test or procedure, discharged before approached, etc), leaving 42 patients who were approached for participation. Among these, 34 (81%) consented to participate in the survey. Two subjects (6%) found the topic so unappealing that they terminated the interview.
The majority of enrolled subjects were men (32/34, 94%), with a mean age of 65.3 years (range, 31-89). Eleven subjects (32%) reported a prior CDI episode, with 10 reporting 1 such episode, and the other 2 episodes. Those with prior CDI reported the effect of CDI on their overall quality of life as 5.1 (1 = no limitation, 10 = severe limitation). Respondents were fairly accurate regarding the risk of recurrence after an initial episode of CDI, with the average expectedrecurrence rate estimated at 33%. In contrast, their estimation of the risk of recurrence after a second CDI episode was lower (28%), although the risk of recurrent episodes increases with each CDI recurrence.
Regarding FMT, 5 subjects indicated awareness of the procedure: 2 learning of it from a news source, 1 from family, 1 from a health care provider, and 1 was unsure of the source. After subjects received a description of FMT, their opinions regarding the procedure were elicited. When asked which route of delivery they would prefer if they were to undergo FMT, the 33 subjects who provided a response indicated a strong preference for either enema (15, 45%) or colonoscopy (10, 30%), compared with just 4 (12%) indicating no preference, 2 (6%) choosing nasogastric tube administration, and 2 (6%) indicating that they would not undergo FMT by any route (P < .001).
Regarding the location of FMT administration (hospital setting vs self-administered at home), 31 of 33 respondents (94%) indicated they would prefer FMT to occur in the hospital vs 2 (6%) preferring self-administration at home (P < .001). The preferred source of donor stool was more evenly distributed, with 14 of 32 respondents (44%) indicating a preference for an anonymous donor, 11 preferring a family member (34%), and 7 (21%) with no preference (P = .21).
Subjects were asked about concerns regarding FMT, and asked to rate each on a 5-point Likert scale (1 = not at all concerning; 5 = overwhelming concern). Concerns regarding risk of infection and effectiveness received an average score of 2.74 and 2.72, respectively, whereas concern regarding the aesthetics, or "yuck factor" was slightly lower (2.1: P = NS for all comparisons). Subjects also were asked to rate the likelihood of undergoing FMT, if it were available, for their current episode of CDI, a subsequent episode of CDI, or if their physician recommended undergoing FMT (10 point scale: 1 = not at all likely; 10 = certainly agree to FMT). The mean scores (SD) for agreeing to FMT for the current or a subsequent episode were 4.8 (SD 2.7) and 5.6 (SD 3.0); P = .12, but increased to 7.1 (SD 3.23) if FMT were recommended by their physician (P < .001 for FMT if physician recommended vs FMT for current episode; P = .001 for FMT if physician recommended vs FMT for a subsequent episode). Finally, subjects were asked about the likelihood of enrolling in a study comparing FMT to standard antimicrobial treatment, with answers ranging from 1 (almost certainly would not enroll) to 5 (almost certainly would enroll). Among the 32 respondents to this question, 17 (53%) answered either "probably would enroll" or "almost certainly would enroll," with a mean score of 3.2.
Discussion
Overall, VA patients with a current episode of CDI were not aware of FMT, with just 15% knowing about the procedure. However, after learning about FMT, patients expressed clear opinions regarding the route and setting of FMT administration, with enema or colonoscopy being the preferred routes, and a hospital the preferred setting. In contrast, subjects expressed ambivalence with regard to the source of donor stool, with no clear preference for stool from an anonymous donor vs from a family member.
When asked about concerns regarding FMT, none of the presented options (risk of infection, uncertain effectiveness, or procedural aesthetics) emerged as significantly more important than did others, although the oft-cited concern regarding FMT aesthetics engendered the lowest overall level of concern. In terms of FMT acceptance, 4 subjects (12%) were opposed to the procedure, indicating that they were not at all likely to agree to FMT for all scenarios (defined as a score of 1 or 2 on the 10-point Likert scale) or by terminating the survey because of the questions. However, 15 (44%) indicated that they would certainly agree to FMT (defined as a score of 9 or 10 on the 10-point Likert scale) if their physician recommended it. Physician recommendation for FMT resulted in the highest overall likelihood of agreeing to FMT, a finding in agreement with a previous survey of FMT for CDI.10 Most subjects indicated likely enrollment in a potential study comparing FMT with standard antimicrobial therapy.
Strengths/Limitations
Study strengths included surveying patients with current CDI, such that patients had personal experience with the disease in question. Use of in-person interviews also resulted in a robust response rate of 81% and allowed subjects to clarify any unclear questions with study personnel. Weaknesses included a relatively small sample size, underrepresentation of women, and lack of detail regarding respondent characteristics. Additionally, capsule delivery of FMT was not assessed since this method of delivery had not been published at the time of survey administration.
Conclusion
This survey of VA patients with CDI suggests that aesthetic concerns are not a critical deterrent for this population, and interest in FMT for the treatment of recurrent CDI exists. Physician recommendation to undergo FMT seems to be the most influential factor affecting the likelihood of agreeing to undergo FMT. These results support the feasibility of conducting clinical trials of FMT in the VA system.
Clostridium difficile (C difficile) infection (CDI) is a leading cause of infectious diarrhea among hospitalized patients and, increasingly, in ambulatory patients.1,2 The high prevalence of CDI and the high recurrence rates (15%-30%) led the CDC to categorize C difficile as an "urgent" threat (the highest category) in its 2013 Antimicrobial Resistance Threat Report.3-5 The Infectious Diseases Society of America guideline recommended treatment for CDI is vancomycin or metronidazole; more recent studies also support fidaxomicin use.4,6,7
Patients experiencing recurrent CDI are at risk for further recurrences, such that after the third CDI episode, the risk of subsequent recurrences exceeds 50%.8 This recurrence rate has stimulated research into other treatments, including fecal microbiota transplantation (FMT). A recent systematic review of FMT reports that 85% of patients have resolution of symptoms without recurrence after FMT, although this is based on data from case series and 2 small randomized clinical trials.9
A commonly cited barrier to FMT is patient acceptance. In response to this concern, a previous survey demonstrated that 81% of respondents would opt for FMT to treat a hypothetical case of recurrent CDI.10 However, the surveyed population did not have CDI, and the 48% response rate is concerning, since those with a favorable opinion of FMT might be more willing to complete a survey than would other patients. Accordingly, the authors systematically surveyed hospitalized veterans with active CDI to assess their knowledge, attitudes, and opinions about FMT as a treatment for CDI.
Methods
In-person patient interviews were conducted by one of the study authors at the Minneapolis VA Health Care System (MVAHCS), consisting of 13 to 18 questions. Questions addressed any prior CDI episodes and knowledge of the following: CDI, recurrence risk, and FMT; preferred route and location of FMT administration; concerns regarding FMT; likelihood of agreeing to undergo FMT (if available); and likelihood of enrollment in a hypothetical study comparing FMT to standard antibiotic treatment. The survey was developed internally and was not validated. Questions used the Likert-scale (Survey).
Patients with CDI were identified by monitoring for positive C difficile polymerase chain reaction (PCR) stool tests and then screened for inclusion by medical record review. Inclusion criteria were (1) MVAHCS hospitalization; and (2) written informed consent. Exclusion criteria were the inability to communicate or participate in an interview. Patient responses regarding their likelihood of agreeing to FMT for CDI treatment under different circumstances were compared using Wilcoxon rank sum test. These circumstances included FMT for their current episode of CDI, FMT for a subsequent episode, and FMT if recommended by their physician. Possible concerns regarding FMT also were solicited, including infection risk, effectiveness, and procedural aesthetics. The MVAHCS institutional review board approved the study.
Results
Stool PCR tests for CDI were monitored for 158 days from 2013 to 2014 (based on availability of study staff), yielding 106 positive results. Of those, 31 (29%) were from outpatients and not addressed further. Of the 75 positive CDI tests from 66 hospitalized patients (9 patients had duplicate tests), 18 of 66 (27%) were not able to provide consent and were excluded, leaving 48 eligible patients. Six (13%) were missed for logistic reasons (patient at a test or procedure, discharged before approached, etc), leaving 42 patients who were approached for participation. Among these, 34 (81%) consented to participate in the survey. Two subjects (6%) found the topic so unappealing that they terminated the interview.
The majority of enrolled subjects were men (32/34, 94%), with a mean age of 65.3 years (range, 31-89). Eleven subjects (32%) reported a prior CDI episode, with 10 reporting 1 such episode, and the other 2 episodes. Those with prior CDI reported the effect of CDI on their overall quality of life as 5.1 (1 = no limitation, 10 = severe limitation). Respondents were fairly accurate regarding the risk of recurrence after an initial episode of CDI, with the average expectedrecurrence rate estimated at 33%. In contrast, their estimation of the risk of recurrence after a second CDI episode was lower (28%), although the risk of recurrent episodes increases with each CDI recurrence.
Regarding FMT, 5 subjects indicated awareness of the procedure: 2 learning of it from a news source, 1 from family, 1 from a health care provider, and 1 was unsure of the source. After subjects received a description of FMT, their opinions regarding the procedure were elicited. When asked which route of delivery they would prefer if they were to undergo FMT, the 33 subjects who provided a response indicated a strong preference for either enema (15, 45%) or colonoscopy (10, 30%), compared with just 4 (12%) indicating no preference, 2 (6%) choosing nasogastric tube administration, and 2 (6%) indicating that they would not undergo FMT by any route (P < .001).
Regarding the location of FMT administration (hospital setting vs self-administered at home), 31 of 33 respondents (94%) indicated they would prefer FMT to occur in the hospital vs 2 (6%) preferring self-administration at home (P < .001). The preferred source of donor stool was more evenly distributed, with 14 of 32 respondents (44%) indicating a preference for an anonymous donor, 11 preferring a family member (34%), and 7 (21%) with no preference (P = .21).
Subjects were asked about concerns regarding FMT, and asked to rate each on a 5-point Likert scale (1 = not at all concerning; 5 = overwhelming concern). Concerns regarding risk of infection and effectiveness received an average score of 2.74 and 2.72, respectively, whereas concern regarding the aesthetics, or "yuck factor" was slightly lower (2.1: P = NS for all comparisons). Subjects also were asked to rate the likelihood of undergoing FMT, if it were available, for their current episode of CDI, a subsequent episode of CDI, or if their physician recommended undergoing FMT (10 point scale: 1 = not at all likely; 10 = certainly agree to FMT). The mean scores (SD) for agreeing to FMT for the current or a subsequent episode were 4.8 (SD 2.7) and 5.6 (SD 3.0); P = .12, but increased to 7.1 (SD 3.23) if FMT were recommended by their physician (P < .001 for FMT if physician recommended vs FMT for current episode; P = .001 for FMT if physician recommended vs FMT for a subsequent episode). Finally, subjects were asked about the likelihood of enrolling in a study comparing FMT to standard antimicrobial treatment, with answers ranging from 1 (almost certainly would not enroll) to 5 (almost certainly would enroll). Among the 32 respondents to this question, 17 (53%) answered either "probably would enroll" or "almost certainly would enroll," with a mean score of 3.2.
Discussion
Overall, VA patients with a current episode of CDI were not aware of FMT, with just 15% knowing about the procedure. However, after learning about FMT, patients expressed clear opinions regarding the route and setting of FMT administration, with enema or colonoscopy being the preferred routes, and a hospital the preferred setting. In contrast, subjects expressed ambivalence with regard to the source of donor stool, with no clear preference for stool from an anonymous donor vs from a family member.
When asked about concerns regarding FMT, none of the presented options (risk of infection, uncertain effectiveness, or procedural aesthetics) emerged as significantly more important than did others, although the oft-cited concern regarding FMT aesthetics engendered the lowest overall level of concern. In terms of FMT acceptance, 4 subjects (12%) were opposed to the procedure, indicating that they were not at all likely to agree to FMT for all scenarios (defined as a score of 1 or 2 on the 10-point Likert scale) or by terminating the survey because of the questions. However, 15 (44%) indicated that they would certainly agree to FMT (defined as a score of 9 or 10 on the 10-point Likert scale) if their physician recommended it. Physician recommendation for FMT resulted in the highest overall likelihood of agreeing to FMT, a finding in agreement with a previous survey of FMT for CDI.10 Most subjects indicated likely enrollment in a potential study comparing FMT with standard antimicrobial therapy.
Strengths/Limitations
Study strengths included surveying patients with current CDI, such that patients had personal experience with the disease in question. Use of in-person interviews also resulted in a robust response rate of 81% and allowed subjects to clarify any unclear questions with study personnel. Weaknesses included a relatively small sample size, underrepresentation of women, and lack of detail regarding respondent characteristics. Additionally, capsule delivery of FMT was not assessed since this method of delivery had not been published at the time of survey administration.
Conclusion
This survey of VA patients with CDI suggests that aesthetic concerns are not a critical deterrent for this population, and interest in FMT for the treatment of recurrent CDI exists. Physician recommendation to undergo FMT seems to be the most influential factor affecting the likelihood of agreeing to undergo FMT. These results support the feasibility of conducting clinical trials of FMT in the VA system.
1. Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile Infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32(4):387-390.
2. Centers for Disease Control and Prevention. Severe Clostridium difficile-associated disease in populations previously at low risk--four states, 2005. MMWR Morb Mortal Wkly Rep. 2005;54(47):1201-1205.
3. Johnson S, Louie TJ, Gerding DN, et al; Polymer Alternative for CDI Treatment (PACT) investigators. Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection: results from two multinational, randomized, controlled trials. Clin Infect Dis. 2014;59(3):345-354.
4. Louie TJ, Miller MA, Mullane KM, et al; OPT-80-003 Clinical Study Group. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med. 2011;364(5):422-431.
5. Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. http://www.cdc.gov/drugresistance/threat-report-2013. Updated July 17, 2014. Accessed November 16.2016.
6. Cohen SH, Gerding DN, Johnson S, et al; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31(5):431-455.
7. Cornely OA, Crook DW, Esposito R, et al; OPT-80-004 Clinical Study Group. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis. 2012;12(4):281-289.
8. Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect. 2009;58(6):403-410.
9. Drekonja DM, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection--a systematic review. Ann Intern Med. 2015;162(9):630-638.
10. Zipursky JS, Sidorsky TI, Freedman CA, Sidorsky MN, Kirkland KB. Patient attitudes toward the use of fecal microbiota transplantation in the treatment of recurrent Clostridium difficile infection. Clin Infect Dis. 2012;55(12):1652-1658.
1. Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile Infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32(4):387-390.
2. Centers for Disease Control and Prevention. Severe Clostridium difficile-associated disease in populations previously at low risk--four states, 2005. MMWR Morb Mortal Wkly Rep. 2005;54(47):1201-1205.
3. Johnson S, Louie TJ, Gerding DN, et al; Polymer Alternative for CDI Treatment (PACT) investigators. Vancomycin, metronidazole, or tolevamer for Clostridium difficile infection: results from two multinational, randomized, controlled trials. Clin Infect Dis. 2014;59(3):345-354.
4. Louie TJ, Miller MA, Mullane KM, et al; OPT-80-003 Clinical Study Group. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med. 2011;364(5):422-431.
5. Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. http://www.cdc.gov/drugresistance/threat-report-2013. Updated July 17, 2014. Accessed November 16.2016.
6. Cohen SH, Gerding DN, Johnson S, et al; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31(5):431-455.
7. Cornely OA, Crook DW, Esposito R, et al; OPT-80-004 Clinical Study Group. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis. 2012;12(4):281-289.
8. Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect. 2009;58(6):403-410.
9. Drekonja DM, Reich J, Gezahegn S, et al. Fecal microbiota transplantation for Clostridium difficile infection--a systematic review. Ann Intern Med. 2015;162(9):630-638.
10. Zipursky JS, Sidorsky TI, Freedman CA, Sidorsky MN, Kirkland KB. Patient attitudes toward the use of fecal microbiota transplantation in the treatment of recurrent Clostridium difficile infection. Clin Infect Dis. 2012;55(12):1652-1658.
Sexually Transmitted Disease Cases Hit a High
Cases of the most commonly reported STDs reached an “unprecedented” high in the US in 2015, with > 1.5 million chlamydia cases, nearly 400,000 gonorrhea cases, and nearly 24,000 cases of primary and secondary syphilis.
According to the CDC’s annual Sexually Transmitted Disease Surveillance Report, between 2014 and 2015, the number of syphilis cases rose by 19%, followed by gonorrhea (12.8%) and chlamydia (5.9%). Young people aged 15 to 24 accounted for nearly two thirds of chlamydia diagnoses and half of gonorrhea diagnoses. Men who have sex with men accounted for most new gonorrhea and syphilis cases. The report also notes that antibiotic-resistant gonorrhea may be higher in this group.
Syphilis diagnoses in women jumped by > 27% in 1 year, which presents a serious risk for infants. For example, reported congenital syphilis (transmitted from a pregnant woman to the baby) rose by 6%.
But all 3 of those STDs are not only treatable, they’re curable with antibiotics. Widespread access to screening and treatment would reduce the spread. Undiagnosed and untreated, these diseases pose severe and often irreversible health consequences, including infertility, chronic pain, and a greater risk of acquiring HIV. The CDC also estimates a ”substantial economic burden” of nearly $16 billion a year.
In recent years, > 50% of state and local STD programs have had their budgets cut, the report notes, and > 20 health department STD clinics closed their doors in 1 year alone. “STD prevention resources across the nation are stretched thin,” said Dr. Jonathan Mermin, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
The CDC says an effective national response to the epidemic requires engagement from many players. One suggestion: making screening a standard part of medical care, especially for pregnant women, and integrating STD prevention and treatment into prenatal care and other routine visits.
Cases of the most commonly reported STDs reached an “unprecedented” high in the US in 2015, with > 1.5 million chlamydia cases, nearly 400,000 gonorrhea cases, and nearly 24,000 cases of primary and secondary syphilis.
According to the CDC’s annual Sexually Transmitted Disease Surveillance Report, between 2014 and 2015, the number of syphilis cases rose by 19%, followed by gonorrhea (12.8%) and chlamydia (5.9%). Young people aged 15 to 24 accounted for nearly two thirds of chlamydia diagnoses and half of gonorrhea diagnoses. Men who have sex with men accounted for most new gonorrhea and syphilis cases. The report also notes that antibiotic-resistant gonorrhea may be higher in this group.
Syphilis diagnoses in women jumped by > 27% in 1 year, which presents a serious risk for infants. For example, reported congenital syphilis (transmitted from a pregnant woman to the baby) rose by 6%.
But all 3 of those STDs are not only treatable, they’re curable with antibiotics. Widespread access to screening and treatment would reduce the spread. Undiagnosed and untreated, these diseases pose severe and often irreversible health consequences, including infertility, chronic pain, and a greater risk of acquiring HIV. The CDC also estimates a ”substantial economic burden” of nearly $16 billion a year.
In recent years, > 50% of state and local STD programs have had their budgets cut, the report notes, and > 20 health department STD clinics closed their doors in 1 year alone. “STD prevention resources across the nation are stretched thin,” said Dr. Jonathan Mermin, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
The CDC says an effective national response to the epidemic requires engagement from many players. One suggestion: making screening a standard part of medical care, especially for pregnant women, and integrating STD prevention and treatment into prenatal care and other routine visits.
Cases of the most commonly reported STDs reached an “unprecedented” high in the US in 2015, with > 1.5 million chlamydia cases, nearly 400,000 gonorrhea cases, and nearly 24,000 cases of primary and secondary syphilis.
According to the CDC’s annual Sexually Transmitted Disease Surveillance Report, between 2014 and 2015, the number of syphilis cases rose by 19%, followed by gonorrhea (12.8%) and chlamydia (5.9%). Young people aged 15 to 24 accounted for nearly two thirds of chlamydia diagnoses and half of gonorrhea diagnoses. Men who have sex with men accounted for most new gonorrhea and syphilis cases. The report also notes that antibiotic-resistant gonorrhea may be higher in this group.
Syphilis diagnoses in women jumped by > 27% in 1 year, which presents a serious risk for infants. For example, reported congenital syphilis (transmitted from a pregnant woman to the baby) rose by 6%.
But all 3 of those STDs are not only treatable, they’re curable with antibiotics. Widespread access to screening and treatment would reduce the spread. Undiagnosed and untreated, these diseases pose severe and often irreversible health consequences, including infertility, chronic pain, and a greater risk of acquiring HIV. The CDC also estimates a ”substantial economic burden” of nearly $16 billion a year.
In recent years, > 50% of state and local STD programs have had their budgets cut, the report notes, and > 20 health department STD clinics closed their doors in 1 year alone. “STD prevention resources across the nation are stretched thin,” said Dr. Jonathan Mermin, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention.
The CDC says an effective national response to the epidemic requires engagement from many players. One suggestion: making screening a standard part of medical care, especially for pregnant women, and integrating STD prevention and treatment into prenatal care and other routine visits.
Anticoagulants often unnecessary after surgery, analysis suggests

Many surgical patients may be receiving anticoagulants they don’t need, according to research published in Annals of Surgery.
The study challenges standard of care guidelines, which recommend that all general surgery patients receive treatment to prevent venous thromboembolism (VTE).
The new findings suggest that anticoagulants may be unnecessary for most surgical patients and could even be harmful to some.
“A ‘one-size-fits-all approach’ doesn’t always make sense,” said study author Christopher Pannucci, MD, of the University of Utah in Salt Lake City.
“A healthy 35-year-old is very different from someone who is 85 and has a history of clots. Our research indicates that there could be a substantial number of people who are being over-treated.”
Dr Pannucci and his colleagues reviewed data from 13 studies to determine which surgical patients were most likely, and least likely, to benefit from anticoagulants. There was data on VTE events in 11 studies (n=14,776) and data on clinically relevant bleeding in 8 studies (n=7590).
In most of the studies, patients received mechanical VTE prophylaxis, which meant elastic compression and/or sequential compression devices.
Some studies compared mechanical prophylaxis to anticoagulants, including heparin, low-molecular-weight heparin, direct factor Xa inhibitors, direct thrombin inhibitors, warfarin, dextran, and aspirin.
The studies included a broad range of surgical patients, from individuals with few VTE risk factors to those with multiple risk factors, such as obesity, advanced age, and personal or family history of VTE.
The patients were divided into 1 of 5 categories indicating overall VTE risk. Assessment was based on the Caprini score.
VTE risk without anticoagulant treatment
There were 11 studies in which some patients did not receive anticoagulants (n=6085).
Among these patients, those who were classified as having the highest risk of VTE were 14 times more likely to develop VTE than patients in the low-risk category—10.7% vs 0.7%.
These findings were independent of surgery type.
“It was eye-opening to see that there is this huge variability in risk among the overall group of patients that walk into your office,” Dr Pannucci said. “Unless you consider a patient’s risk based on their individual factors, you would never know.”
VTE outcomes by risk score
When given, anticoagulants did significantly reduce the risk of VTE for the overall study population and for high-risk patients.
The odds ratios (ORs) were 0.66 (P=0.001) for the overall population, 0.60 (P=0.04) for patients with Caprini scores of 7 to 8, and 0.41 (P=0.0002) for patients with scores higher than 8.
Unfortunately, anticoagulants did not make a significant difference in VTE rates for mid- or low-risk patients.
The ORs were 0.45 (P=0.31) for patients with Caprini scores of 0 to 2, 1.31 (P=0.57) for patients with scores of 3 to 4, and 0.96 (P=0.85) for patients with scores of 5 to 6.
Risk of bleeding
Anticoagulants significantly increased clinically relevant bleeding for the overall population. The OR was 1.69 (P=0.006).
Patients who received anticoagulants were not significantly more likely to have clinically relevant bleeding if they had risk scores of 0 to 2 (OR=2.47, P=0.61), 3 to 4 (OR=1.05, P=0.87), 5 to 6 (OR=2.10, P=0.06), 7 to 8 (OR=3.15, P=0.16), or >8 (OR=2.31, P=0.16).
“For the first time, we have data that prophylaxis for the highest-risk groups is beneficial, and data that suggests that lower-risk patients may need no prophylaxis,” said study author Peter Henke, MD, of the University of Michigan in Ann Arbor.
He and his colleagues noted, however, that prospective studies are needed to confirm these findings. ![]()
Many surgical patients may be receiving anticoagulants they don’t need, according to research published in Annals of Surgery.
The study challenges standard of care guidelines, which recommend that all general surgery patients receive treatment to prevent venous thromboembolism (VTE).
The new findings suggest that anticoagulants may be unnecessary for most surgical patients and could even be harmful to some.
“A ‘one-size-fits-all approach’ doesn’t always make sense,” said study author Christopher Pannucci, MD, of the University of Utah in Salt Lake City.
“A healthy 35-year-old is very different from someone who is 85 and has a history of clots. Our research indicates that there could be a substantial number of people who are being over-treated.”
Dr Pannucci and his colleagues reviewed data from 13 studies to determine which surgical patients were most likely, and least likely, to benefit from anticoagulants. There was data on VTE events in 11 studies (n=14,776) and data on clinically relevant bleeding in 8 studies (n=7590).
In most of the studies, patients received mechanical VTE prophylaxis, which meant elastic compression and/or sequential compression devices.
Some studies compared mechanical prophylaxis to anticoagulants, including heparin, low-molecular-weight heparin, direct factor Xa inhibitors, direct thrombin inhibitors, warfarin, dextran, and aspirin.
The studies included a broad range of surgical patients, from individuals with few VTE risk factors to those with multiple risk factors, such as obesity, advanced age, and personal or family history of VTE.
The patients were divided into 1 of 5 categories indicating overall VTE risk. Assessment was based on the Caprini score.
VTE risk without anticoagulant treatment
There were 11 studies in which some patients did not receive anticoagulants (n=6085).
Among these patients, those who were classified as having the highest risk of VTE were 14 times more likely to develop VTE than patients in the low-risk category—10.7% vs 0.7%.
These findings were independent of surgery type.
“It was eye-opening to see that there is this huge variability in risk among the overall group of patients that walk into your office,” Dr Pannucci said. “Unless you consider a patient’s risk based on their individual factors, you would never know.”
VTE outcomes by risk score
When given, anticoagulants did significantly reduce the risk of VTE for the overall study population and for high-risk patients.
The odds ratios (ORs) were 0.66 (P=0.001) for the overall population, 0.60 (P=0.04) for patients with Caprini scores of 7 to 8, and 0.41 (P=0.0002) for patients with scores higher than 8.
Unfortunately, anticoagulants did not make a significant difference in VTE rates for mid- or low-risk patients.
The ORs were 0.45 (P=0.31) for patients with Caprini scores of 0 to 2, 1.31 (P=0.57) for patients with scores of 3 to 4, and 0.96 (P=0.85) for patients with scores of 5 to 6.
Risk of bleeding
Anticoagulants significantly increased clinically relevant bleeding for the overall population. The OR was 1.69 (P=0.006).
Patients who received anticoagulants were not significantly more likely to have clinically relevant bleeding if they had risk scores of 0 to 2 (OR=2.47, P=0.61), 3 to 4 (OR=1.05, P=0.87), 5 to 6 (OR=2.10, P=0.06), 7 to 8 (OR=3.15, P=0.16), or >8 (OR=2.31, P=0.16).
“For the first time, we have data that prophylaxis for the highest-risk groups is beneficial, and data that suggests that lower-risk patients may need no prophylaxis,” said study author Peter Henke, MD, of the University of Michigan in Ann Arbor.
He and his colleagues noted, however, that prospective studies are needed to confirm these findings. ![]()
Many surgical patients may be receiving anticoagulants they don’t need, according to research published in Annals of Surgery.
The study challenges standard of care guidelines, which recommend that all general surgery patients receive treatment to prevent venous thromboembolism (VTE).
The new findings suggest that anticoagulants may be unnecessary for most surgical patients and could even be harmful to some.
“A ‘one-size-fits-all approach’ doesn’t always make sense,” said study author Christopher Pannucci, MD, of the University of Utah in Salt Lake City.
“A healthy 35-year-old is very different from someone who is 85 and has a history of clots. Our research indicates that there could be a substantial number of people who are being over-treated.”
Dr Pannucci and his colleagues reviewed data from 13 studies to determine which surgical patients were most likely, and least likely, to benefit from anticoagulants. There was data on VTE events in 11 studies (n=14,776) and data on clinically relevant bleeding in 8 studies (n=7590).
In most of the studies, patients received mechanical VTE prophylaxis, which meant elastic compression and/or sequential compression devices.
Some studies compared mechanical prophylaxis to anticoagulants, including heparin, low-molecular-weight heparin, direct factor Xa inhibitors, direct thrombin inhibitors, warfarin, dextran, and aspirin.
The studies included a broad range of surgical patients, from individuals with few VTE risk factors to those with multiple risk factors, such as obesity, advanced age, and personal or family history of VTE.
The patients were divided into 1 of 5 categories indicating overall VTE risk. Assessment was based on the Caprini score.
VTE risk without anticoagulant treatment
There were 11 studies in which some patients did not receive anticoagulants (n=6085).
Among these patients, those who were classified as having the highest risk of VTE were 14 times more likely to develop VTE than patients in the low-risk category—10.7% vs 0.7%.
These findings were independent of surgery type.
“It was eye-opening to see that there is this huge variability in risk among the overall group of patients that walk into your office,” Dr Pannucci said. “Unless you consider a patient’s risk based on their individual factors, you would never know.”
VTE outcomes by risk score
When given, anticoagulants did significantly reduce the risk of VTE for the overall study population and for high-risk patients.
The odds ratios (ORs) were 0.66 (P=0.001) for the overall population, 0.60 (P=0.04) for patients with Caprini scores of 7 to 8, and 0.41 (P=0.0002) for patients with scores higher than 8.
Unfortunately, anticoagulants did not make a significant difference in VTE rates for mid- or low-risk patients.
The ORs were 0.45 (P=0.31) for patients with Caprini scores of 0 to 2, 1.31 (P=0.57) for patients with scores of 3 to 4, and 0.96 (P=0.85) for patients with scores of 5 to 6.
Risk of bleeding
Anticoagulants significantly increased clinically relevant bleeding for the overall population. The OR was 1.69 (P=0.006).
Patients who received anticoagulants were not significantly more likely to have clinically relevant bleeding if they had risk scores of 0 to 2 (OR=2.47, P=0.61), 3 to 4 (OR=1.05, P=0.87), 5 to 6 (OR=2.10, P=0.06), 7 to 8 (OR=3.15, P=0.16), or >8 (OR=2.31, P=0.16).
“For the first time, we have data that prophylaxis for the highest-risk groups is beneficial, and data that suggests that lower-risk patients may need no prophylaxis,” said study author Peter Henke, MD, of the University of Michigan in Ann Arbor.
He and his colleagues noted, however, that prospective studies are needed to confirm these findings. ![]()
Study quantifies 5-year survival rates for blood cancers

chemotherapy
Photo by Rhoda Baer
A new study shows that 5-year survival rates for US patients with hematologic malignancies have increased greatly since the 1950s, but there is still room for improvement, particularly for patients with acute myeloid leukemia (AML).
Researchers found the absolute difference in improvement for 5-year survival from 1950-1954 to 2008-2013 ranged from 38.2% for non-Hodgkin lymphoma (NHL) to 56.6% for Hodgkin lymphoma.
And although the 5-year survival rate for Hodgkin lymphoma patients reached 86.6% for 2008-2013, the 5-year survival rate for patients with AML only reached 27.4%.
This study also revealed large disparities in overall cancer mortality rates between different counties across the country.
Ali H. Mokdad, PhD, of the Institute for Health Metrics and Evaluation in Seattle, Washington, and his colleagues reported these findings in JAMA.
Overall cancer deaths
The researchers found there were 19,511,910 cancer deaths recorded in the US between 1980 and 2014. Cancer mortality decreased by 20.1% between 1980 and 2014, from 240.2 deaths per 100,000 people to 192.0 deaths per 100,000 people.
In 1980, cancer mortality ranged from 130.6 per 100,000 in Summit County, Colorado, to 386.9 per 100,000 in North Slope Borough, Alaska.
In 2014, cancer mortality ranged from 70.7 per 100,000 in Summit County, Colorado, to 503.1 per 100,000 in Union County, Florida.
“Such significant disparities among US counties is unacceptable,” Dr Mokdad said. “Every person should have access to early screenings for cancer, as well as adequate treatment.”
Mortality rates for hematologic malignancies
In 2014, the mortality rates, per 100,000 people, for hematologic malignancies were:
- 0.4 for Hodgkin lymphoma (rank out of all cancers, 27)
- 8.3 for NHL (rank, 7)
- 3.9 for multiple myeloma (rank, 16)
- 9.0 for all leukemias (rank, 6)
- 0.7 for acute lymphoid leukemia (ALL)
- 2.6 for chronic lymphoid leukemia (CLL)
- 5.1 for AML
- 0.6 for chronic myeloid leukemia (CML).
The leukemia subtypes were not assigned a rank.
5-year survival rates for hematologic malignancies
Hodgkin lymphoma
- 30% for 1950-54
- 68.6% for 1973-77
- 72.1% for 1978-82
- 86.6% for 2008-2013
- Absolute difference (between the first and latest year of data), 56.6%.
NHL
- 33% for 1950-54
- 45.3% for 1973-77
- 48.7% for 1978-82
- 71.2% for 2008-2013
- Absolute difference, 38.2%.
Multiple myeloma
- 6% for 1950-54
- 23.4% for 1973-77
- 26.6% for 1978-82
- 49.8% for 2008-2013
- Absolute difference, 43.8%.
Leukemia
- 10% for 1950-54
- 34% for 1973-77
- 36.3% for 1978-82
- 60.1% for 2008-2013
- Absolute difference, 50.1%.
ALL
- 39.2% for 1973-77
- 50.5% for 1978-82
- 68.1% for 2008-2013
- Absolute difference, 28.9%.
CLL
- 67% for 1973-77
- 66.3% for 1978-82
- 82.5% for 2008-2013
- Absolute difference, 15.5%.
AML
- 6.2% for 1973-77
- 7.9% for 1978-82
- 27.4% for 2008-2013
- Absolute difference, 21.2%.
CML
- 21.1% for 1973-77
- 25.8% for 1978-82
- 66.4% for 2008-2013
- Absolute difference, 45.3%.
For the leukemia subtypes, there was no data for 1950 to 1954. ![]()
chemotherapy
Photo by Rhoda Baer
A new study shows that 5-year survival rates for US patients with hematologic malignancies have increased greatly since the 1950s, but there is still room for improvement, particularly for patients with acute myeloid leukemia (AML).
Researchers found the absolute difference in improvement for 5-year survival from 1950-1954 to 2008-2013 ranged from 38.2% for non-Hodgkin lymphoma (NHL) to 56.6% for Hodgkin lymphoma.
And although the 5-year survival rate for Hodgkin lymphoma patients reached 86.6% for 2008-2013, the 5-year survival rate for patients with AML only reached 27.4%.
This study also revealed large disparities in overall cancer mortality rates between different counties across the country.
Ali H. Mokdad, PhD, of the Institute for Health Metrics and Evaluation in Seattle, Washington, and his colleagues reported these findings in JAMA.
Overall cancer deaths
The researchers found there were 19,511,910 cancer deaths recorded in the US between 1980 and 2014. Cancer mortality decreased by 20.1% between 1980 and 2014, from 240.2 deaths per 100,000 people to 192.0 deaths per 100,000 people.
In 1980, cancer mortality ranged from 130.6 per 100,000 in Summit County, Colorado, to 386.9 per 100,000 in North Slope Borough, Alaska.
In 2014, cancer mortality ranged from 70.7 per 100,000 in Summit County, Colorado, to 503.1 per 100,000 in Union County, Florida.
“Such significant disparities among US counties is unacceptable,” Dr Mokdad said. “Every person should have access to early screenings for cancer, as well as adequate treatment.”
Mortality rates for hematologic malignancies
In 2014, the mortality rates, per 100,000 people, for hematologic malignancies were:
- 0.4 for Hodgkin lymphoma (rank out of all cancers, 27)
- 8.3 for NHL (rank, 7)
- 3.9 for multiple myeloma (rank, 16)
- 9.0 for all leukemias (rank, 6)
- 0.7 for acute lymphoid leukemia (ALL)
- 2.6 for chronic lymphoid leukemia (CLL)
- 5.1 for AML
- 0.6 for chronic myeloid leukemia (CML).
The leukemia subtypes were not assigned a rank.
5-year survival rates for hematologic malignancies
Hodgkin lymphoma
- 30% for 1950-54
- 68.6% for 1973-77
- 72.1% for 1978-82
- 86.6% for 2008-2013
- Absolute difference (between the first and latest year of data), 56.6%.
NHL
- 33% for 1950-54
- 45.3% for 1973-77
- 48.7% for 1978-82
- 71.2% for 2008-2013
- Absolute difference, 38.2%.
Multiple myeloma
- 6% for 1950-54
- 23.4% for 1973-77
- 26.6% for 1978-82
- 49.8% for 2008-2013
- Absolute difference, 43.8%.
Leukemia
- 10% for 1950-54
- 34% for 1973-77
- 36.3% for 1978-82
- 60.1% for 2008-2013
- Absolute difference, 50.1%.
ALL
- 39.2% for 1973-77
- 50.5% for 1978-82
- 68.1% for 2008-2013
- Absolute difference, 28.9%.
CLL
- 67% for 1973-77
- 66.3% for 1978-82
- 82.5% for 2008-2013
- Absolute difference, 15.5%.
AML
- 6.2% for 1973-77
- 7.9% for 1978-82
- 27.4% for 2008-2013
- Absolute difference, 21.2%.
CML
- 21.1% for 1973-77
- 25.8% for 1978-82
- 66.4% for 2008-2013
- Absolute difference, 45.3%.
For the leukemia subtypes, there was no data for 1950 to 1954. ![]()
chemotherapy
Photo by Rhoda Baer
A new study shows that 5-year survival rates for US patients with hematologic malignancies have increased greatly since the 1950s, but there is still room for improvement, particularly for patients with acute myeloid leukemia (AML).
Researchers found the absolute difference in improvement for 5-year survival from 1950-1954 to 2008-2013 ranged from 38.2% for non-Hodgkin lymphoma (NHL) to 56.6% for Hodgkin lymphoma.
And although the 5-year survival rate for Hodgkin lymphoma patients reached 86.6% for 2008-2013, the 5-year survival rate for patients with AML only reached 27.4%.
This study also revealed large disparities in overall cancer mortality rates between different counties across the country.
Ali H. Mokdad, PhD, of the Institute for Health Metrics and Evaluation in Seattle, Washington, and his colleagues reported these findings in JAMA.
Overall cancer deaths
The researchers found there were 19,511,910 cancer deaths recorded in the US between 1980 and 2014. Cancer mortality decreased by 20.1% between 1980 and 2014, from 240.2 deaths per 100,000 people to 192.0 deaths per 100,000 people.
In 1980, cancer mortality ranged from 130.6 per 100,000 in Summit County, Colorado, to 386.9 per 100,000 in North Slope Borough, Alaska.
In 2014, cancer mortality ranged from 70.7 per 100,000 in Summit County, Colorado, to 503.1 per 100,000 in Union County, Florida.
“Such significant disparities among US counties is unacceptable,” Dr Mokdad said. “Every person should have access to early screenings for cancer, as well as adequate treatment.”
Mortality rates for hematologic malignancies
In 2014, the mortality rates, per 100,000 people, for hematologic malignancies were:
- 0.4 for Hodgkin lymphoma (rank out of all cancers, 27)
- 8.3 for NHL (rank, 7)
- 3.9 for multiple myeloma (rank, 16)
- 9.0 for all leukemias (rank, 6)
- 0.7 for acute lymphoid leukemia (ALL)
- 2.6 for chronic lymphoid leukemia (CLL)
- 5.1 for AML
- 0.6 for chronic myeloid leukemia (CML).
The leukemia subtypes were not assigned a rank.
5-year survival rates for hematologic malignancies
Hodgkin lymphoma
- 30% for 1950-54
- 68.6% for 1973-77
- 72.1% for 1978-82
- 86.6% for 2008-2013
- Absolute difference (between the first and latest year of data), 56.6%.
NHL
- 33% for 1950-54
- 45.3% for 1973-77
- 48.7% for 1978-82
- 71.2% for 2008-2013
- Absolute difference, 38.2%.
Multiple myeloma
- 6% for 1950-54
- 23.4% for 1973-77
- 26.6% for 1978-82
- 49.8% for 2008-2013
- Absolute difference, 43.8%.
Leukemia
- 10% for 1950-54
- 34% for 1973-77
- 36.3% for 1978-82
- 60.1% for 2008-2013
- Absolute difference, 50.1%.
ALL
- 39.2% for 1973-77
- 50.5% for 1978-82
- 68.1% for 2008-2013
- Absolute difference, 28.9%.
CLL
- 67% for 1973-77
- 66.3% for 1978-82
- 82.5% for 2008-2013
- Absolute difference, 15.5%.
AML
- 6.2% for 1973-77
- 7.9% for 1978-82
- 27.4% for 2008-2013
- Absolute difference, 21.2%.
CML
- 21.1% for 1973-77
- 25.8% for 1978-82
- 66.4% for 2008-2013
- Absolute difference, 45.3%.
For the leukemia subtypes, there was no data for 1950 to 1954. ![]()
Health Canada expands indication for lenalidomide

Photo courtesy of Celgene
Health Canada has expanded the approved indication for lenalidomide (Revlimid®) to include the treatment of patients with multiple myeloma (MM).
Lenalidomide is now approved for use in combination with dexamethasone to treat patients newly diagnosed with MM who are not eligible for stem cell transplant.
Lenalidomide was previously approved in Canada for the treatment of patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with a deletion 5q cytogenetic abnormality, with or without additional cytogenetic abnormalities.
Lenalidomide is a product of Celgene Corporation.
“The expanded indication of Revlimid® provides [MM] patients with a treatment much earlier in their disease and offers this patient population an all-oral, melphalan-free option for a disease that continues to be difficult to treat,” said Donna Reece, MD, of Princess Margaret Hospital in Toronto, Ontario, Canada.
The expanded approval of lenalidomide is based on safety and efficacy results from the phase 3 FIRST trial. Updated results from this study were published in the Journal of Clinical Oncology last November.
The trial included 1623 patients with newly diagnosed MM who were not eligible for stem cell transplant.
Patients were randomized to receive:
- Lenalidomide and low-dose dexamethasone (Rd) in 28-day cycles until disease progression (n=535)
- 18 cycles of Rd (Rd18) for 72 weeks (n=541)
- Melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
In the intent-to-treat population, the overall response rate was 81% for the continuous Rd group, 79% for the Rd18 group, and 67% in the MPT group. The complete response rates were 21%, 20%, and 12%, respectively.
The median progression-free survival (PFS) was 26.0 months in the continuous Rd group, 21.0 months in the Rd18 group, and 21.9 months in the MPT group. At 4 years, the PFS rates were 33%, 14%, and 13%, respectively.
The median overall survival (OS) was 58.9 months in the continuous Rd group, 56.7 months in the Rd18 group, and 48.5 months in the MPT group. At 4 years, the OS rates were 60%, 57%, and 51%, respectively.
The most frequent grade 3/4 hematologic treatment-emergent adverse events were neutropenia and anemia. The rate of grade 3/4 neutropenia was higher in the MPT group than the continuous Rd or Rd18 groups.
Infections were the most common grade 3/4 non-hematologic treatment-emergent adverse events. The rate of grade 3/4 infections was higher in the Rd groups than the MPT group.
“With this new clinical evidence, we know that keeping newly diagnosed multiple myeloma patients on Revlimid® may help delay disease progression and reduce the risk of death,” Dr Reece said. “As such, we are looking forward to having Revlimid® as a key option in the first-line setting for the appropriate patients.” ![]()
Photo courtesy of Celgene
Health Canada has expanded the approved indication for lenalidomide (Revlimid®) to include the treatment of patients with multiple myeloma (MM).
Lenalidomide is now approved for use in combination with dexamethasone to treat patients newly diagnosed with MM who are not eligible for stem cell transplant.
Lenalidomide was previously approved in Canada for the treatment of patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with a deletion 5q cytogenetic abnormality, with or without additional cytogenetic abnormalities.
Lenalidomide is a product of Celgene Corporation.
“The expanded indication of Revlimid® provides [MM] patients with a treatment much earlier in their disease and offers this patient population an all-oral, melphalan-free option for a disease that continues to be difficult to treat,” said Donna Reece, MD, of Princess Margaret Hospital in Toronto, Ontario, Canada.
The expanded approval of lenalidomide is based on safety and efficacy results from the phase 3 FIRST trial. Updated results from this study were published in the Journal of Clinical Oncology last November.
The trial included 1623 patients with newly diagnosed MM who were not eligible for stem cell transplant.
Patients were randomized to receive:
- Lenalidomide and low-dose dexamethasone (Rd) in 28-day cycles until disease progression (n=535)
- 18 cycles of Rd (Rd18) for 72 weeks (n=541)
- Melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
In the intent-to-treat population, the overall response rate was 81% for the continuous Rd group, 79% for the Rd18 group, and 67% in the MPT group. The complete response rates were 21%, 20%, and 12%, respectively.
The median progression-free survival (PFS) was 26.0 months in the continuous Rd group, 21.0 months in the Rd18 group, and 21.9 months in the MPT group. At 4 years, the PFS rates were 33%, 14%, and 13%, respectively.
The median overall survival (OS) was 58.9 months in the continuous Rd group, 56.7 months in the Rd18 group, and 48.5 months in the MPT group. At 4 years, the OS rates were 60%, 57%, and 51%, respectively.
The most frequent grade 3/4 hematologic treatment-emergent adverse events were neutropenia and anemia. The rate of grade 3/4 neutropenia was higher in the MPT group than the continuous Rd or Rd18 groups.
Infections were the most common grade 3/4 non-hematologic treatment-emergent adverse events. The rate of grade 3/4 infections was higher in the Rd groups than the MPT group.
“With this new clinical evidence, we know that keeping newly diagnosed multiple myeloma patients on Revlimid® may help delay disease progression and reduce the risk of death,” Dr Reece said. “As such, we are looking forward to having Revlimid® as a key option in the first-line setting for the appropriate patients.” ![]()
Photo courtesy of Celgene
Health Canada has expanded the approved indication for lenalidomide (Revlimid®) to include the treatment of patients with multiple myeloma (MM).
Lenalidomide is now approved for use in combination with dexamethasone to treat patients newly diagnosed with MM who are not eligible for stem cell transplant.
Lenalidomide was previously approved in Canada for the treatment of patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with a deletion 5q cytogenetic abnormality, with or without additional cytogenetic abnormalities.
Lenalidomide is a product of Celgene Corporation.
“The expanded indication of Revlimid® provides [MM] patients with a treatment much earlier in their disease and offers this patient population an all-oral, melphalan-free option for a disease that continues to be difficult to treat,” said Donna Reece, MD, of Princess Margaret Hospital in Toronto, Ontario, Canada.
The expanded approval of lenalidomide is based on safety and efficacy results from the phase 3 FIRST trial. Updated results from this study were published in the Journal of Clinical Oncology last November.
The trial included 1623 patients with newly diagnosed MM who were not eligible for stem cell transplant.
Patients were randomized to receive:
- Lenalidomide and low-dose dexamethasone (Rd) in 28-day cycles until disease progression (n=535)
- 18 cycles of Rd (Rd18) for 72 weeks (n=541)
- Melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
In the intent-to-treat population, the overall response rate was 81% for the continuous Rd group, 79% for the Rd18 group, and 67% in the MPT group. The complete response rates were 21%, 20%, and 12%, respectively.
The median progression-free survival (PFS) was 26.0 months in the continuous Rd group, 21.0 months in the Rd18 group, and 21.9 months in the MPT group. At 4 years, the PFS rates were 33%, 14%, and 13%, respectively.
The median overall survival (OS) was 58.9 months in the continuous Rd group, 56.7 months in the Rd18 group, and 48.5 months in the MPT group. At 4 years, the OS rates were 60%, 57%, and 51%, respectively.
The most frequent grade 3/4 hematologic treatment-emergent adverse events were neutropenia and anemia. The rate of grade 3/4 neutropenia was higher in the MPT group than the continuous Rd or Rd18 groups.
Infections were the most common grade 3/4 non-hematologic treatment-emergent adverse events. The rate of grade 3/4 infections was higher in the Rd groups than the MPT group.
“With this new clinical evidence, we know that keeping newly diagnosed multiple myeloma patients on Revlimid® may help delay disease progression and reduce the risk of death,” Dr Reece said. “As such, we are looking forward to having Revlimid® as a key option in the first-line setting for the appropriate patients.” ![]()
Do not use steroids in patients with severe sepsis without shock
Clinical question: Does hydrocortisone therapy prevent progression to septic shock in patients with severe sepsis without shock?
Background: Current sepsis management guidelines recommend use of hydrocortisone in patients with septic shock who are unable to restore hemodynamic stability with IV fluids and pressors; current guidelines also recommend against use of corticosteroids without shock. However, these recommendations are based on two RCTs and remain controversial.
Study design: Multicenter, placebo-controlled, double-blind RCT.
Setting: Thirty-four intermediate or intensive care units in German university and community hospitals.
Synopsis: Investigators randomly assigned 380 patients to hydrocortisone or placebo. Patients were included if they had clinical evidence of infection, evidence of SIRS (systemic inflammatory response syndrome), and evidence of organ dysfunction. Patients were excluded if they had any of the following: sepsis-induced hypotension, separate indication for systemic steroid use, or hypersensitivity to steroids. Primary outcome was the occurrence of septic shock within 14 days. Secondary outcomes included time to septic shock or death, death in the ICU or hospital, organ dysfunction, ventilator therapy, renal replacement therapy, and secondary infection.
Study results showed no significant difference in the primary outcome between groups, or in any of the secondary outcomes. In a post-hoc analysis, there was more hyperglycemia and less delirium in the study group.
Study limitations are inclusion of patients only after consent, potentially missing early septic shock, and the fact that many analyses were done post-hoc.
Bottom line: Steroids should be avoided in severe sepsis without shock.
Citation: Keh D, Trips E, Marx G, et al. Effect of hydrocortisone on development of shock among patients with severe sepsis. JAMA. 2016;316(17):1775-85.
Dr. Graves is an assistant professor at the University of Utah School of Medicine and associate program director of quality and patient safety for the University of Utah Internal Medicine residency training program.
Clinical question: Does hydrocortisone therapy prevent progression to septic shock in patients with severe sepsis without shock?
Background: Current sepsis management guidelines recommend use of hydrocortisone in patients with septic shock who are unable to restore hemodynamic stability with IV fluids and pressors; current guidelines also recommend against use of corticosteroids without shock. However, these recommendations are based on two RCTs and remain controversial.
Study design: Multicenter, placebo-controlled, double-blind RCT.
Setting: Thirty-four intermediate or intensive care units in German university and community hospitals.
Synopsis: Investigators randomly assigned 380 patients to hydrocortisone or placebo. Patients were included if they had clinical evidence of infection, evidence of SIRS (systemic inflammatory response syndrome), and evidence of organ dysfunction. Patients were excluded if they had any of the following: sepsis-induced hypotension, separate indication for systemic steroid use, or hypersensitivity to steroids. Primary outcome was the occurrence of septic shock within 14 days. Secondary outcomes included time to septic shock or death, death in the ICU or hospital, organ dysfunction, ventilator therapy, renal replacement therapy, and secondary infection.
Study results showed no significant difference in the primary outcome between groups, or in any of the secondary outcomes. In a post-hoc analysis, there was more hyperglycemia and less delirium in the study group.
Study limitations are inclusion of patients only after consent, potentially missing early septic shock, and the fact that many analyses were done post-hoc.
Bottom line: Steroids should be avoided in severe sepsis without shock.
Citation: Keh D, Trips E, Marx G, et al. Effect of hydrocortisone on development of shock among patients with severe sepsis. JAMA. 2016;316(17):1775-85.
Dr. Graves is an assistant professor at the University of Utah School of Medicine and associate program director of quality and patient safety for the University of Utah Internal Medicine residency training program.
Clinical question: Does hydrocortisone therapy prevent progression to septic shock in patients with severe sepsis without shock?
Background: Current sepsis management guidelines recommend use of hydrocortisone in patients with septic shock who are unable to restore hemodynamic stability with IV fluids and pressors; current guidelines also recommend against use of corticosteroids without shock. However, these recommendations are based on two RCTs and remain controversial.
Study design: Multicenter, placebo-controlled, double-blind RCT.
Setting: Thirty-four intermediate or intensive care units in German university and community hospitals.
Synopsis: Investigators randomly assigned 380 patients to hydrocortisone or placebo. Patients were included if they had clinical evidence of infection, evidence of SIRS (systemic inflammatory response syndrome), and evidence of organ dysfunction. Patients were excluded if they had any of the following: sepsis-induced hypotension, separate indication for systemic steroid use, or hypersensitivity to steroids. Primary outcome was the occurrence of septic shock within 14 days. Secondary outcomes included time to septic shock or death, death in the ICU or hospital, organ dysfunction, ventilator therapy, renal replacement therapy, and secondary infection.
Study results showed no significant difference in the primary outcome between groups, or in any of the secondary outcomes. In a post-hoc analysis, there was more hyperglycemia and less delirium in the study group.
Study limitations are inclusion of patients only after consent, potentially missing early septic shock, and the fact that many analyses were done post-hoc.
Bottom line: Steroids should be avoided in severe sepsis without shock.
Citation: Keh D, Trips E, Marx G, et al. Effect of hydrocortisone on development of shock among patients with severe sepsis. JAMA. 2016;316(17):1775-85.
Dr. Graves is an assistant professor at the University of Utah School of Medicine and associate program director of quality and patient safety for the University of Utah Internal Medicine residency training program.
HHS Secretary-nominee avoids specifics on Medicaid funding during second hearing
WASHINGTON – Rep. Tom Price, MD (R-Ga.), dodged specifics on Medicaid reform and the issue of block grants for funding Medicaid during a hearing Jan. 24 before the Senate Financing Committee.
The committee will be voting to move forward to the full Senate his nomination as secretary of the Department of Health & Human Services.

Sen. Robert Casey (D-Penn.) queried Rep. Price about guarantees as to whether people with disabilities covered by Medicaid would continue to be covered under a block grant program. Rep. Price responded that the “metrics that we will use ... [are] the quality of care and whether or not they are receiving that care.”
Rep. Price added that he is committed “to make it so they have that [current level of existing] coverage or greater.” Sen. Casey questioned whether that goal could be achieved, considering the amount of funding that could potentially be lost to a block grant program.
When further pressed on the 2017 budget he prepared as House Budget Committee chairman that included block grants for Medicaid, Rep. Price would not state clearly his promotion of the concept. Instead, he said he was committed to creating a system that is affordable, accessible, of high quality, and responsive to patient needs, as well as one that incentivizes innovation and provides choice.
Rep. Price was also pressed on his advocacy of high-risk pools, particularly for those who have high-cost, preexisting conditions and might not be able to get coverage in other areas of the reformed market. He voiced his support for such pools as well as for pools that would allow people without a common economic link, such as an employer, to band together for insurance coverage.
Sen. Debbie Stabenow (D-Mich.) noted that the history of high-risk pools has been less than stellar, with insurance rates typically 150%-200% higher than the rates of other plans and, typically, lifetime caps on coverage.
Rep. Price additionally called for a “better” system that puts patients at the center of health care decisions. In response to discussion with Sen. Chuck Grassley (R-Iowa), Rep. Price said transparency, specifically in relation to the Physician Payments Sunshine Act, was “vital,” and expanded the notion of transparency to include outcomes and pricing so that patients could have the best information to make decisions about their own health care.
It is “virtually impossible” for patients to know their true health care costs, Rep. Price said. To be informed, patients need better outcome measures, which would be “a priority” if he is confirmed as secretary.
Rep. Price also agreed that the Children’s Health Insurance Plan should be extended, and when asked about extending the program for 5 years, he responded that “8 years would be better.”
In the area of mental health, he suggested treatment models similar to those used to address physical health.
Rep. Price was not grilled on his investments at the Finance Committee hearing as he was at the Health, Education, Labor and Pensions Committee hearing, where he maintained he did nothing unethical or against the rules of the Senate.
Separate from the hearing, eight Democratic senators, led by Ranking Member Patty Murray of Washington, sent a Jan. 23 letter to the U.S. Securities and Exchange Commission to investigate whether Rep. Price potentially engaged in insider trading or other violations in relation to his specific purchase of stock in Innate Immunotherapeutics.
WASHINGTON – Rep. Tom Price, MD (R-Ga.), dodged specifics on Medicaid reform and the issue of block grants for funding Medicaid during a hearing Jan. 24 before the Senate Financing Committee.
The committee will be voting to move forward to the full Senate his nomination as secretary of the Department of Health & Human Services.
Sen. Robert Casey (D-Penn.) queried Rep. Price about guarantees as to whether people with disabilities covered by Medicaid would continue to be covered under a block grant program. Rep. Price responded that the “metrics that we will use ... [are] the quality of care and whether or not they are receiving that care.”
Rep. Price added that he is committed “to make it so they have that [current level of existing] coverage or greater.” Sen. Casey questioned whether that goal could be achieved, considering the amount of funding that could potentially be lost to a block grant program.
When further pressed on the 2017 budget he prepared as House Budget Committee chairman that included block grants for Medicaid, Rep. Price would not state clearly his promotion of the concept. Instead, he said he was committed to creating a system that is affordable, accessible, of high quality, and responsive to patient needs, as well as one that incentivizes innovation and provides choice.
Rep. Price was also pressed on his advocacy of high-risk pools, particularly for those who have high-cost, preexisting conditions and might not be able to get coverage in other areas of the reformed market. He voiced his support for such pools as well as for pools that would allow people without a common economic link, such as an employer, to band together for insurance coverage.
Sen. Debbie Stabenow (D-Mich.) noted that the history of high-risk pools has been less than stellar, with insurance rates typically 150%-200% higher than the rates of other plans and, typically, lifetime caps on coverage.
Rep. Price additionally called for a “better” system that puts patients at the center of health care decisions. In response to discussion with Sen. Chuck Grassley (R-Iowa), Rep. Price said transparency, specifically in relation to the Physician Payments Sunshine Act, was “vital,” and expanded the notion of transparency to include outcomes and pricing so that patients could have the best information to make decisions about their own health care.
It is “virtually impossible” for patients to know their true health care costs, Rep. Price said. To be informed, patients need better outcome measures, which would be “a priority” if he is confirmed as secretary.
Rep. Price also agreed that the Children’s Health Insurance Plan should be extended, and when asked about extending the program for 5 years, he responded that “8 years would be better.”
In the area of mental health, he suggested treatment models similar to those used to address physical health.
Rep. Price was not grilled on his investments at the Finance Committee hearing as he was at the Health, Education, Labor and Pensions Committee hearing, where he maintained he did nothing unethical or against the rules of the Senate.
Separate from the hearing, eight Democratic senators, led by Ranking Member Patty Murray of Washington, sent a Jan. 23 letter to the U.S. Securities and Exchange Commission to investigate whether Rep. Price potentially engaged in insider trading or other violations in relation to his specific purchase of stock in Innate Immunotherapeutics.
WASHINGTON – Rep. Tom Price, MD (R-Ga.), dodged specifics on Medicaid reform and the issue of block grants for funding Medicaid during a hearing Jan. 24 before the Senate Financing Committee.
The committee will be voting to move forward to the full Senate his nomination as secretary of the Department of Health & Human Services.
Sen. Robert Casey (D-Penn.) queried Rep. Price about guarantees as to whether people with disabilities covered by Medicaid would continue to be covered under a block grant program. Rep. Price responded that the “metrics that we will use ... [are] the quality of care and whether or not they are receiving that care.”
Rep. Price added that he is committed “to make it so they have that [current level of existing] coverage or greater.” Sen. Casey questioned whether that goal could be achieved, considering the amount of funding that could potentially be lost to a block grant program.
When further pressed on the 2017 budget he prepared as House Budget Committee chairman that included block grants for Medicaid, Rep. Price would not state clearly his promotion of the concept. Instead, he said he was committed to creating a system that is affordable, accessible, of high quality, and responsive to patient needs, as well as one that incentivizes innovation and provides choice.
Rep. Price was also pressed on his advocacy of high-risk pools, particularly for those who have high-cost, preexisting conditions and might not be able to get coverage in other areas of the reformed market. He voiced his support for such pools as well as for pools that would allow people without a common economic link, such as an employer, to band together for insurance coverage.
Sen. Debbie Stabenow (D-Mich.) noted that the history of high-risk pools has been less than stellar, with insurance rates typically 150%-200% higher than the rates of other plans and, typically, lifetime caps on coverage.
Rep. Price additionally called for a “better” system that puts patients at the center of health care decisions. In response to discussion with Sen. Chuck Grassley (R-Iowa), Rep. Price said transparency, specifically in relation to the Physician Payments Sunshine Act, was “vital,” and expanded the notion of transparency to include outcomes and pricing so that patients could have the best information to make decisions about their own health care.
It is “virtually impossible” for patients to know their true health care costs, Rep. Price said. To be informed, patients need better outcome measures, which would be “a priority” if he is confirmed as secretary.
Rep. Price also agreed that the Children’s Health Insurance Plan should be extended, and when asked about extending the program for 5 years, he responded that “8 years would be better.”
In the area of mental health, he suggested treatment models similar to those used to address physical health.
Rep. Price was not grilled on his investments at the Finance Committee hearing as he was at the Health, Education, Labor and Pensions Committee hearing, where he maintained he did nothing unethical or against the rules of the Senate.
Separate from the hearing, eight Democratic senators, led by Ranking Member Patty Murray of Washington, sent a Jan. 23 letter to the U.S. Securities and Exchange Commission to investigate whether Rep. Price potentially engaged in insider trading or other violations in relation to his specific purchase of stock in Innate Immunotherapeutics.
Intracardiac echo safely guides LAA occluder placement
ORLANDO – Intracardiac echocardiography (ICE) can be safely substituted for transesophageal echocardiography (TEE) as a less invasive option in the placement of an investigational percutaneous device for left atrial appendage (LAA) occlusion, according to data presented at the annual International AF Symposium.
The relative safety and efficacy of ICE and TEE for placement of the device, called the Amplatzer Amulet, was evaluated as a subanalysis of a large, nonrandomized, observational study, according to Boris Schmidt, MD, of Cardiovascular Center Bethanien, Frankfurt, Germany.
The Amplatzer Amulet device, which is designed to prevent LAA-associated thromboembolism in patients with nonvalvular atrial fibrillation (AF), has been available in Europe for several years. It functions much like Boston Scientific’s Watchman implant. A registration trial in the United States was initiated in 2016.
In the study that provided the basis for this analysis, 1,088 AF patients were implanted. The average age was 75 years, and the population was relatively high risk for both stroke and bleeding. The CHA2DS2-VASc score was at least 4 in 65% of patients, with an average score of 4.2. Prior stroke (28%) and transient ischemic attack (11%) had occurred in more than one-third. Reflecting the fact that 72% had a history of a major bleed, the average HAS-BLED score was 3.3. More than 80% were hypertensive.
The decision to place the device with TEE, which Dr. Schmidt characterized as the standard, or ICE was left up to the discretion of the implanter. Ultimately, 958 (88.4%) of the devices were placed with TEE and 126 (11.6%) with ICE.
There were no significant differences in implant success or safety when the two methods for guiding implantation were compared. Specifically, success was achieved in 99.2% of the ICE group with 90.5% of cases requiring only one device. In the TEE group, the device was successfully implanted in 98.4%, and 94.4% needed only one device. The first device to be selected was ultimately implanted in 96.5% of the ICE group and 94.4% of the TEE group. The LAA closure rate, defined as gap of less than 3 mm, was 100% at implant and 3 months after transplant in the ICE group, when evaluated by an independent core laboratory. The closure rates in the TEE group at the time of implant and 3 months later were 99.8% and 98.6%, respectively. No difference between imaging methods approached statistical significance.
Adverse events, which were also adjudicated by independent investigators, occurred at low rates and also did not differ by imaging strategy. In the ICE and TEE groups, respectively, these included vascular complications in 0.9% and 1.6%, pericardial effusion in 1.0% and 0.8%, stroke in 0.3% and 0%, and embolization in 0.1% and 0%. With a median follow-up of 6.6 months, there have been four deaths. Two were considered to be device related by the adjudicators. One involved a perforation and another a cardiac arrest. Both were observed in the TEE group.
The Amplatzer Amulet device consists of a lobe that is designed to fit inside the LAA neck and a disk that provides a complete seal at the orifice. It was first introduced in Europe in 2008 but has undergone several modifications. In the United States, the Watchman, which opens like an umbrella in order to block passage of thromboemboli when deployed in the LAA, received FDA approval in 2015. Other LAA closure strategies are in development. There are no large randomized trials in which LAA closure devices have been compared.
Dr. Schmidt has financial relationships with Boston Scientific and St. Jude Medical.
ORLANDO – Intracardiac echocardiography (ICE) can be safely substituted for transesophageal echocardiography (TEE) as a less invasive option in the placement of an investigational percutaneous device for left atrial appendage (LAA) occlusion, according to data presented at the annual International AF Symposium.
The relative safety and efficacy of ICE and TEE for placement of the device, called the Amplatzer Amulet, was evaluated as a subanalysis of a large, nonrandomized, observational study, according to Boris Schmidt, MD, of Cardiovascular Center Bethanien, Frankfurt, Germany.
The Amplatzer Amulet device, which is designed to prevent LAA-associated thromboembolism in patients with nonvalvular atrial fibrillation (AF), has been available in Europe for several years. It functions much like Boston Scientific’s Watchman implant. A registration trial in the United States was initiated in 2016.
In the study that provided the basis for this analysis, 1,088 AF patients were implanted. The average age was 75 years, and the population was relatively high risk for both stroke and bleeding. The CHA2DS2-VASc score was at least 4 in 65% of patients, with an average score of 4.2. Prior stroke (28%) and transient ischemic attack (11%) had occurred in more than one-third. Reflecting the fact that 72% had a history of a major bleed, the average HAS-BLED score was 3.3. More than 80% were hypertensive.
The decision to place the device with TEE, which Dr. Schmidt characterized as the standard, or ICE was left up to the discretion of the implanter. Ultimately, 958 (88.4%) of the devices were placed with TEE and 126 (11.6%) with ICE.
There were no significant differences in implant success or safety when the two methods for guiding implantation were compared. Specifically, success was achieved in 99.2% of the ICE group with 90.5% of cases requiring only one device. In the TEE group, the device was successfully implanted in 98.4%, and 94.4% needed only one device. The first device to be selected was ultimately implanted in 96.5% of the ICE group and 94.4% of the TEE group. The LAA closure rate, defined as gap of less than 3 mm, was 100% at implant and 3 months after transplant in the ICE group, when evaluated by an independent core laboratory. The closure rates in the TEE group at the time of implant and 3 months later were 99.8% and 98.6%, respectively. No difference between imaging methods approached statistical significance.
Adverse events, which were also adjudicated by independent investigators, occurred at low rates and also did not differ by imaging strategy. In the ICE and TEE groups, respectively, these included vascular complications in 0.9% and 1.6%, pericardial effusion in 1.0% and 0.8%, stroke in 0.3% and 0%, and embolization in 0.1% and 0%. With a median follow-up of 6.6 months, there have been four deaths. Two were considered to be device related by the adjudicators. One involved a perforation and another a cardiac arrest. Both were observed in the TEE group.
The Amplatzer Amulet device consists of a lobe that is designed to fit inside the LAA neck and a disk that provides a complete seal at the orifice. It was first introduced in Europe in 2008 but has undergone several modifications. In the United States, the Watchman, which opens like an umbrella in order to block passage of thromboemboli when deployed in the LAA, received FDA approval in 2015. Other LAA closure strategies are in development. There are no large randomized trials in which LAA closure devices have been compared.
Dr. Schmidt has financial relationships with Boston Scientific and St. Jude Medical.
ORLANDO – Intracardiac echocardiography (ICE) can be safely substituted for transesophageal echocardiography (TEE) as a less invasive option in the placement of an investigational percutaneous device for left atrial appendage (LAA) occlusion, according to data presented at the annual International AF Symposium.
The relative safety and efficacy of ICE and TEE for placement of the device, called the Amplatzer Amulet, was evaluated as a subanalysis of a large, nonrandomized, observational study, according to Boris Schmidt, MD, of Cardiovascular Center Bethanien, Frankfurt, Germany.
The Amplatzer Amulet device, which is designed to prevent LAA-associated thromboembolism in patients with nonvalvular atrial fibrillation (AF), has been available in Europe for several years. It functions much like Boston Scientific’s Watchman implant. A registration trial in the United States was initiated in 2016.
In the study that provided the basis for this analysis, 1,088 AF patients were implanted. The average age was 75 years, and the population was relatively high risk for both stroke and bleeding. The CHA2DS2-VASc score was at least 4 in 65% of patients, with an average score of 4.2. Prior stroke (28%) and transient ischemic attack (11%) had occurred in more than one-third. Reflecting the fact that 72% had a history of a major bleed, the average HAS-BLED score was 3.3. More than 80% were hypertensive.
The decision to place the device with TEE, which Dr. Schmidt characterized as the standard, or ICE was left up to the discretion of the implanter. Ultimately, 958 (88.4%) of the devices were placed with TEE and 126 (11.6%) with ICE.
There were no significant differences in implant success or safety when the two methods for guiding implantation were compared. Specifically, success was achieved in 99.2% of the ICE group with 90.5% of cases requiring only one device. In the TEE group, the device was successfully implanted in 98.4%, and 94.4% needed only one device. The first device to be selected was ultimately implanted in 96.5% of the ICE group and 94.4% of the TEE group. The LAA closure rate, defined as gap of less than 3 mm, was 100% at implant and 3 months after transplant in the ICE group, when evaluated by an independent core laboratory. The closure rates in the TEE group at the time of implant and 3 months later were 99.8% and 98.6%, respectively. No difference between imaging methods approached statistical significance.
Adverse events, which were also adjudicated by independent investigators, occurred at low rates and also did not differ by imaging strategy. In the ICE and TEE groups, respectively, these included vascular complications in 0.9% and 1.6%, pericardial effusion in 1.0% and 0.8%, stroke in 0.3% and 0%, and embolization in 0.1% and 0%. With a median follow-up of 6.6 months, there have been four deaths. Two were considered to be device related by the adjudicators. One involved a perforation and another a cardiac arrest. Both were observed in the TEE group.
The Amplatzer Amulet device consists of a lobe that is designed to fit inside the LAA neck and a disk that provides a complete seal at the orifice. It was first introduced in Europe in 2008 but has undergone several modifications. In the United States, the Watchman, which opens like an umbrella in order to block passage of thromboemboli when deployed in the LAA, received FDA approval in 2015. Other LAA closure strategies are in development. There are no large randomized trials in which LAA closure devices have been compared.
Dr. Schmidt has financial relationships with Boston Scientific and St. Jude Medical.
Key clinical point: Intracardiac echocardiography is a viable option for guiding placement of an experimental left atrial appendage thromboembolism blocker.
Major finding: LAA closure rates at 3 months were 100% with ICE and 98.6% with transesophageal echocardiograph.
Data source: Prospective, multicenter, observational study.
Disclosures: Dr. Schmidt has financial relationships with Boston Scientific and St. Jude Medical.