User login
A Call for Optimizing the Research Portfolio for Glioblastoma
The past 10 years have seen a rise in clinical trials for the treatment of primary and recurrent glioblastoma—but the “slightly positive trend” has been due to an increase in phase 2, not phase 3, studies, say researchers from University of Bern in Switzerland. Moreover, the majority of these trials focus on drugs designed for central nervous system (CNS) malignancies; trials addressing radiotherapy, surgery, imaging, and other therapeutic or diagnostic methods “appear to be rare.”
The researchers analyzed records of 208,777 studies registered at ClinicalTrials.gov. They classified trials according to disease setting (newly diagnosed glioblastoma, recurrent disease, and no differentiation) and by intervention (standard or experimental). All surgical approaches were considered experimental as were all radiotherapy approaches in the recurrent setting.
Related: Death Rates for Brain Cancer Trend Downward
Nearly all the trials (91%) evaluated forms of systemic therapy, with 44% in primary and 54% in recurrent disease. The majority of trials were phase 2 studies (88%); only 11% were phase 3.
Researchers identified 100 different molecular agents or biologics of which 40 had initially been approved for indications other than glioblastoma or CNS malignancies. Two agents (carmustine and lomustine) were approved for glioblastoma or other CNS or solid malignancies. Only 1 (temozolomide) was approved for glioblastoma. Of 57 compounds with investigational status, 19 were developed specifically for glioblastoma.
By contrast, the researchers say that surgery, radiotherapy, and imaging are “heavily underrepresented,” being the focus of > 10% of all phase 1 and 2 glioblastoma trials.
Industry “has displayed a strong interest in sponsoring trials for glioblastoma,” the researchers note. The fact that industry was a primary sponsor of one-fourth of the trials and a leading source of monetary support in 44% “indicates that glioblastoma is an attractive target even financially.” But the authors find “reason for concern” in the lack of industrial funding for research beyond forms of systemic therapy.
Related: Role of Radiosurgery in the Treatment of Brain Metastasis
They suggest, for instance, that learning more about alternative radiotherapy schedules along with dose or volume alterations could be of interest for glioblastoma treatment. They also note that imaging modalities rarely are evaluated in the prospective setting, and the size and role of the optimal radiotherapy margins are “a matter of debate”—of particular importance in recurrent glioblastoma.
The most probable cause for the upward trend of phase 2 trials in glioblastoma, the researchers say, is the failure of previous early investigative treatments to show a clinically significant advantage. Instead of starting more trials “unselectively,” they suggest, it might be better to enroll patients with glioblastoma in early phase trials with novel designs.
Source:
Cihoric N, Tsikkinis A, Minniti G, et al. Radiat Oncol. 2017;12(1):1.
doi: 10.1186/s13014-016-0740-5.
The past 10 years have seen a rise in clinical trials for the treatment of primary and recurrent glioblastoma—but the “slightly positive trend” has been due to an increase in phase 2, not phase 3, studies, say researchers from University of Bern in Switzerland. Moreover, the majority of these trials focus on drugs designed for central nervous system (CNS) malignancies; trials addressing radiotherapy, surgery, imaging, and other therapeutic or diagnostic methods “appear to be rare.”
The researchers analyzed records of 208,777 studies registered at ClinicalTrials.gov. They classified trials according to disease setting (newly diagnosed glioblastoma, recurrent disease, and no differentiation) and by intervention (standard or experimental). All surgical approaches were considered experimental as were all radiotherapy approaches in the recurrent setting.
Related: Death Rates for Brain Cancer Trend Downward
Nearly all the trials (91%) evaluated forms of systemic therapy, with 44% in primary and 54% in recurrent disease. The majority of trials were phase 2 studies (88%); only 11% were phase 3.
Researchers identified 100 different molecular agents or biologics of which 40 had initially been approved for indications other than glioblastoma or CNS malignancies. Two agents (carmustine and lomustine) were approved for glioblastoma or other CNS or solid malignancies. Only 1 (temozolomide) was approved for glioblastoma. Of 57 compounds with investigational status, 19 were developed specifically for glioblastoma.
By contrast, the researchers say that surgery, radiotherapy, and imaging are “heavily underrepresented,” being the focus of > 10% of all phase 1 and 2 glioblastoma trials.
Industry “has displayed a strong interest in sponsoring trials for glioblastoma,” the researchers note. The fact that industry was a primary sponsor of one-fourth of the trials and a leading source of monetary support in 44% “indicates that glioblastoma is an attractive target even financially.” But the authors find “reason for concern” in the lack of industrial funding for research beyond forms of systemic therapy.
Related: Role of Radiosurgery in the Treatment of Brain Metastasis
They suggest, for instance, that learning more about alternative radiotherapy schedules along with dose or volume alterations could be of interest for glioblastoma treatment. They also note that imaging modalities rarely are evaluated in the prospective setting, and the size and role of the optimal radiotherapy margins are “a matter of debate”—of particular importance in recurrent glioblastoma.
The most probable cause for the upward trend of phase 2 trials in glioblastoma, the researchers say, is the failure of previous early investigative treatments to show a clinically significant advantage. Instead of starting more trials “unselectively,” they suggest, it might be better to enroll patients with glioblastoma in early phase trials with novel designs.
Source:
Cihoric N, Tsikkinis A, Minniti G, et al. Radiat Oncol. 2017;12(1):1.
doi: 10.1186/s13014-016-0740-5.
The past 10 years have seen a rise in clinical trials for the treatment of primary and recurrent glioblastoma—but the “slightly positive trend” has been due to an increase in phase 2, not phase 3, studies, say researchers from University of Bern in Switzerland. Moreover, the majority of these trials focus on drugs designed for central nervous system (CNS) malignancies; trials addressing radiotherapy, surgery, imaging, and other therapeutic or diagnostic methods “appear to be rare.”
The researchers analyzed records of 208,777 studies registered at ClinicalTrials.gov. They classified trials according to disease setting (newly diagnosed glioblastoma, recurrent disease, and no differentiation) and by intervention (standard or experimental). All surgical approaches were considered experimental as were all radiotherapy approaches in the recurrent setting.
Related: Death Rates for Brain Cancer Trend Downward
Nearly all the trials (91%) evaluated forms of systemic therapy, with 44% in primary and 54% in recurrent disease. The majority of trials were phase 2 studies (88%); only 11% were phase 3.
Researchers identified 100 different molecular agents or biologics of which 40 had initially been approved for indications other than glioblastoma or CNS malignancies. Two agents (carmustine and lomustine) were approved for glioblastoma or other CNS or solid malignancies. Only 1 (temozolomide) was approved for glioblastoma. Of 57 compounds with investigational status, 19 were developed specifically for glioblastoma.
By contrast, the researchers say that surgery, radiotherapy, and imaging are “heavily underrepresented,” being the focus of > 10% of all phase 1 and 2 glioblastoma trials.
Industry “has displayed a strong interest in sponsoring trials for glioblastoma,” the researchers note. The fact that industry was a primary sponsor of one-fourth of the trials and a leading source of monetary support in 44% “indicates that glioblastoma is an attractive target even financially.” But the authors find “reason for concern” in the lack of industrial funding for research beyond forms of systemic therapy.
Related: Role of Radiosurgery in the Treatment of Brain Metastasis
They suggest, for instance, that learning more about alternative radiotherapy schedules along with dose or volume alterations could be of interest for glioblastoma treatment. They also note that imaging modalities rarely are evaluated in the prospective setting, and the size and role of the optimal radiotherapy margins are “a matter of debate”—of particular importance in recurrent glioblastoma.
The most probable cause for the upward trend of phase 2 trials in glioblastoma, the researchers say, is the failure of previous early investigative treatments to show a clinically significant advantage. Instead of starting more trials “unselectively,” they suggest, it might be better to enroll patients with glioblastoma in early phase trials with novel designs.
Source:
Cihoric N, Tsikkinis A, Minniti G, et al. Radiat Oncol. 2017;12(1):1.
doi: 10.1186/s13014-016-0740-5.
The Itch That Won't Quit
A 68-year-old woman with a very itchy rash is referred to dermatology for evaluation. She reports the itching to be constant—24 hours a day, seven days a week—but particularly severe at bedtime.
The rash has been totally unresponsive to numerous treatment attempts over the past year, including topical steroids (triamcinolone 0.1% cream bid), oral antibiotics (trimethoprim/sulfa), and oral steroids (prednisone).
The patient lives alone, apart from the occasional overnight visit from her grandchild.
EXAMINATION
The widespread rash spares only the patient’s legs below the knees. It is comprised of sparsely distributed excoriated foci, some surrounded by oval-to-round scales. The patient scratches the sites throughout the examination.
During a shave biopsy of one of the lesions on the patient’s arm, she mentions that occasionally lesions also manifest on her hands and fingers. Closer examination reveals a few unremarkable, scaly, 1- to 3-mm papules on her volar wrists. These are scraped with a #10 blade and placed on a slide, which is covered, filled with potassium hydroxide 10%, and examined under 10x magnification.

What is the diagnosis?
DISCUSSION
After a lengthy search, a single scabies adult (scabies sarcoptei var humanus) was found embedded in the scales. Scabies is one of the two most common ectoparasitic infestations in this country (the other being head lice).
Paradoxically, it is one of the most over- and under-diagnosed medical conditions worldwide. It is transmitted from person to person and can only be acquired from close, prolonged contact with another human who has the condition. This case illustrates some of the difficulties involved in making the diagnosis.
While it is vital to consider scabies in the differential for constant, severe itching, there are situations in which it can be ruled out. People who live alone and/or avoid physical contact with other people cannot get scabies. It can only be acquired from an infected person—not from a dog, cat, or inanimate object. In this case, the patient lived alone, but she hosted sleepovers with her grandchild—the likely source of this infestation.
Scabies can manifest as an eczematoid rash that will not respond to topical or systemic steroids. Conversely, when eczema patients are misdiagnosed with scabies, permethrin cream worsens the condition. Therefore, once scabies is considered in the differential, a KOH prep is indicated for a definitive diagnosis.
In terms of treatment, it does little good to simply treat the patient in question. The entire family (and/or close contacts) needs to be treated simultaneously—but before that, the source of the scabies needs to be identified. Failure to address all of these factors often leads to “treatment failure.”
The case patient was successfully treated with a combination of permethrin cream and oral ivermectin, according to the standard regimen (two treatments, seven to 10 days apart).
TAKE-HOME LEARNING POINTS
- Scabies can only be acquired from close, prolonged contact with another human who has the condition.
- Intractable itching and failure to respond to treatment (ie, topical and systemic steroids) are its dependable diagnostic features.
- Scraping suspected scabetic lesions (tiny vesicles, dried papules, or—if you’re lucky—a burrow) and examining them under 10x microscopy is preferable for confirmation of the diagnosis.
- The whole family must be treated in synchrony with the patient.
- It is essential to identify the source of the scabies (eg, spouse, boyfriend/girlfriend, child) to successfully eradicate the problem.
A 68-year-old woman with a very itchy rash is referred to dermatology for evaluation. She reports the itching to be constant—24 hours a day, seven days a week—but particularly severe at bedtime.
The rash has been totally unresponsive to numerous treatment attempts over the past year, including topical steroids (triamcinolone 0.1% cream bid), oral antibiotics (trimethoprim/sulfa), and oral steroids (prednisone).
The patient lives alone, apart from the occasional overnight visit from her grandchild.
EXAMINATION
The widespread rash spares only the patient’s legs below the knees. It is comprised of sparsely distributed excoriated foci, some surrounded by oval-to-round scales. The patient scratches the sites throughout the examination.
During a shave biopsy of one of the lesions on the patient’s arm, she mentions that occasionally lesions also manifest on her hands and fingers. Closer examination reveals a few unremarkable, scaly, 1- to 3-mm papules on her volar wrists. These are scraped with a #10 blade and placed on a slide, which is covered, filled with potassium hydroxide 10%, and examined under 10x magnification.
What is the diagnosis?
DISCUSSION
After a lengthy search, a single scabies adult (scabies sarcoptei var humanus) was found embedded in the scales. Scabies is one of the two most common ectoparasitic infestations in this country (the other being head lice).
Paradoxically, it is one of the most over- and under-diagnosed medical conditions worldwide. It is transmitted from person to person and can only be acquired from close, prolonged contact with another human who has the condition. This case illustrates some of the difficulties involved in making the diagnosis.
While it is vital to consider scabies in the differential for constant, severe itching, there are situations in which it can be ruled out. People who live alone and/or avoid physical contact with other people cannot get scabies. It can only be acquired from an infected person—not from a dog, cat, or inanimate object. In this case, the patient lived alone, but she hosted sleepovers with her grandchild—the likely source of this infestation.
Scabies can manifest as an eczematoid rash that will not respond to topical or systemic steroids. Conversely, when eczema patients are misdiagnosed with scabies, permethrin cream worsens the condition. Therefore, once scabies is considered in the differential, a KOH prep is indicated for a definitive diagnosis.
In terms of treatment, it does little good to simply treat the patient in question. The entire family (and/or close contacts) needs to be treated simultaneously—but before that, the source of the scabies needs to be identified. Failure to address all of these factors often leads to “treatment failure.”
The case patient was successfully treated with a combination of permethrin cream and oral ivermectin, according to the standard regimen (two treatments, seven to 10 days apart).
TAKE-HOME LEARNING POINTS
- Scabies can only be acquired from close, prolonged contact with another human who has the condition.
- Intractable itching and failure to respond to treatment (ie, topical and systemic steroids) are its dependable diagnostic features.
- Scraping suspected scabetic lesions (tiny vesicles, dried papules, or—if you’re lucky—a burrow) and examining them under 10x microscopy is preferable for confirmation of the diagnosis.
- The whole family must be treated in synchrony with the patient.
- It is essential to identify the source of the scabies (eg, spouse, boyfriend/girlfriend, child) to successfully eradicate the problem.
A 68-year-old woman with a very itchy rash is referred to dermatology for evaluation. She reports the itching to be constant—24 hours a day, seven days a week—but particularly severe at bedtime.
The rash has been totally unresponsive to numerous treatment attempts over the past year, including topical steroids (triamcinolone 0.1% cream bid), oral antibiotics (trimethoprim/sulfa), and oral steroids (prednisone).
The patient lives alone, apart from the occasional overnight visit from her grandchild.
EXAMINATION
The widespread rash spares only the patient’s legs below the knees. It is comprised of sparsely distributed excoriated foci, some surrounded by oval-to-round scales. The patient scratches the sites throughout the examination.
During a shave biopsy of one of the lesions on the patient’s arm, she mentions that occasionally lesions also manifest on her hands and fingers. Closer examination reveals a few unremarkable, scaly, 1- to 3-mm papules on her volar wrists. These are scraped with a #10 blade and placed on a slide, which is covered, filled with potassium hydroxide 10%, and examined under 10x magnification.
What is the diagnosis?
DISCUSSION
After a lengthy search, a single scabies adult (scabies sarcoptei var humanus) was found embedded in the scales. Scabies is one of the two most common ectoparasitic infestations in this country (the other being head lice).
Paradoxically, it is one of the most over- and under-diagnosed medical conditions worldwide. It is transmitted from person to person and can only be acquired from close, prolonged contact with another human who has the condition. This case illustrates some of the difficulties involved in making the diagnosis.
While it is vital to consider scabies in the differential for constant, severe itching, there are situations in which it can be ruled out. People who live alone and/or avoid physical contact with other people cannot get scabies. It can only be acquired from an infected person—not from a dog, cat, or inanimate object. In this case, the patient lived alone, but she hosted sleepovers with her grandchild—the likely source of this infestation.
Scabies can manifest as an eczematoid rash that will not respond to topical or systemic steroids. Conversely, when eczema patients are misdiagnosed with scabies, permethrin cream worsens the condition. Therefore, once scabies is considered in the differential, a KOH prep is indicated for a definitive diagnosis.
In terms of treatment, it does little good to simply treat the patient in question. The entire family (and/or close contacts) needs to be treated simultaneously—but before that, the source of the scabies needs to be identified. Failure to address all of these factors often leads to “treatment failure.”
The case patient was successfully treated with a combination of permethrin cream and oral ivermectin, according to the standard regimen (two treatments, seven to 10 days apart).
TAKE-HOME LEARNING POINTS
- Scabies can only be acquired from close, prolonged contact with another human who has the condition.
- Intractable itching and failure to respond to treatment (ie, topical and systemic steroids) are its dependable diagnostic features.
- Scraping suspected scabetic lesions (tiny vesicles, dried papules, or—if you’re lucky—a burrow) and examining them under 10x microscopy is preferable for confirmation of the diagnosis.
- The whole family must be treated in synchrony with the patient.
- It is essential to identify the source of the scabies (eg, spouse, boyfriend/girlfriend, child) to successfully eradicate the problem.
Pruritic nodules in axillae

The FP suspected scabies, realizing that in addition to the classic burrows seen between the fingers, scabies may present with pruritic nodules in the axilla or genital region. This child did not have any visible burrows between his fingers and there was no involvement of the genital area. Using dermoscopy, scabies mites were seen as triangular structures with trailing burrows over some of the nodules. The mother agreed to have her hands examined and scabies mites were seen between her fingers.
The child weighed less than 33 pounds, so he was not an appropriate candidate for oral ivermectin. The physician prescribed 5% permethrin cream for the child, mother, and other household members. The FP explained the importance of applying the cream from the neck down to the toes overnight and washing it off in the morning. Toddlers often have the scabies mites above the neck, so the mother was counseled to apply the 5% permethrin cream on her son’s head and face, being careful to avoid his mouth and eyes. The FP also gave the family directions to wash their clothes and bedclothes.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Chanoine P, Smith M. Scabies. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:575-580.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP suspected scabies, realizing that in addition to the classic burrows seen between the fingers, scabies may present with pruritic nodules in the axilla or genital region. This child did not have any visible burrows between his fingers and there was no involvement of the genital area. Using dermoscopy, scabies mites were seen as triangular structures with trailing burrows over some of the nodules. The mother agreed to have her hands examined and scabies mites were seen between her fingers.
The child weighed less than 33 pounds, so he was not an appropriate candidate for oral ivermectin. The physician prescribed 5% permethrin cream for the child, mother, and other household members. The FP explained the importance of applying the cream from the neck down to the toes overnight and washing it off in the morning. Toddlers often have the scabies mites above the neck, so the mother was counseled to apply the 5% permethrin cream on her son’s head and face, being careful to avoid his mouth and eyes. The FP also gave the family directions to wash their clothes and bedclothes.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Chanoine P, Smith M. Scabies. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:575-580.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP suspected scabies, realizing that in addition to the classic burrows seen between the fingers, scabies may present with pruritic nodules in the axilla or genital region. This child did not have any visible burrows between his fingers and there was no involvement of the genital area. Using dermoscopy, scabies mites were seen as triangular structures with trailing burrows over some of the nodules. The mother agreed to have her hands examined and scabies mites were seen between her fingers.
The child weighed less than 33 pounds, so he was not an appropriate candidate for oral ivermectin. The physician prescribed 5% permethrin cream for the child, mother, and other household members. The FP explained the importance of applying the cream from the neck down to the toes overnight and washing it off in the morning. Toddlers often have the scabies mites above the neck, so the mother was counseled to apply the 5% permethrin cream on her son’s head and face, being careful to avoid his mouth and eyes. The FP also gave the family directions to wash their clothes and bedclothes.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Chanoine P, Smith M. Scabies. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:575-580.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Hospital-acquired VTE with high risk of recurrence
Clinical question: Is the risk of recurrence for a venous thromboembolism (VTE) acquired as an inpatient higher than other reversible risk factors?
Background: In patients with acute VTE, transient provoking factors place patients at lower risks for recurrent VTE, while persistent factors (that is, cancer) increase risk for recurrence. Unprovoked VTE places patients at intermediate to high risk, but few data are present for VTE experienced while in the hospital.
Study design: Single-center, population-based, prospective cohort study.
Setting: Tromso, Norway.
Synopsis: Using repeat health surveys from 1994 to 2012, researchers followed 822 patients with a validated, first-lifetime VTE. Hospital-related VTE was defined as a VTE within 8 weeks of hospitalization related to medical illness, surgery, or in patients with active cancer.
This global definition of hospital-related VTE was not associated with an increased risk of recurrent VTE (hazard ratio, 0.99; 0.69-1.41). However, in separate groups, the cumulative risk of recurrence after 5 years in hospital-related VTE due to medical illness was similar to nonhospital-related VTE (20.1% vs. 18.4%), higher than VTE related to surgery (11%), and lower than VTE related to cancer (27.4%).

Risk-adjusted analyses maintained these differences in recurrence risk dependent on reason for hospitalization (cancer, medical illness, surgery). When compared with non-hospital VTE, however, hospital-related VTE was associated with a threefold higher risk of death.
Study limitations included being from a single center, possibly underpowered due to low number of events.
Bottom line: Hospital-related VTE has a high risk of recurrence, but risk level is variable and dependent on the reason for hospitalization.
Citation: Bjøri E, Arshad N, Johnsen HS, Hansen J-B, Brækkan SK. Hospital-related first venous thromboembolism and risk of recurrence [published online ahead of print, Sept. 2, 2016]. J Thromb Haemost. doi: 10.1111/jth.13492
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Clinical question: Is the risk of recurrence for a venous thromboembolism (VTE) acquired as an inpatient higher than other reversible risk factors?
Background: In patients with acute VTE, transient provoking factors place patients at lower risks for recurrent VTE, while persistent factors (that is, cancer) increase risk for recurrence. Unprovoked VTE places patients at intermediate to high risk, but few data are present for VTE experienced while in the hospital.
Study design: Single-center, population-based, prospective cohort study.
Setting: Tromso, Norway.
Synopsis: Using repeat health surveys from 1994 to 2012, researchers followed 822 patients with a validated, first-lifetime VTE. Hospital-related VTE was defined as a VTE within 8 weeks of hospitalization related to medical illness, surgery, or in patients with active cancer.
This global definition of hospital-related VTE was not associated with an increased risk of recurrent VTE (hazard ratio, 0.99; 0.69-1.41). However, in separate groups, the cumulative risk of recurrence after 5 years in hospital-related VTE due to medical illness was similar to nonhospital-related VTE (20.1% vs. 18.4%), higher than VTE related to surgery (11%), and lower than VTE related to cancer (27.4%).
Risk-adjusted analyses maintained these differences in recurrence risk dependent on reason for hospitalization (cancer, medical illness, surgery). When compared with non-hospital VTE, however, hospital-related VTE was associated with a threefold higher risk of death.
Study limitations included being from a single center, possibly underpowered due to low number of events.
Bottom line: Hospital-related VTE has a high risk of recurrence, but risk level is variable and dependent on the reason for hospitalization.
Citation: Bjøri E, Arshad N, Johnsen HS, Hansen J-B, Brækkan SK. Hospital-related first venous thromboembolism and risk of recurrence [published online ahead of print, Sept. 2, 2016]. J Thromb Haemost. doi: 10.1111/jth.13492
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Clinical question: Is the risk of recurrence for a venous thromboembolism (VTE) acquired as an inpatient higher than other reversible risk factors?
Background: In patients with acute VTE, transient provoking factors place patients at lower risks for recurrent VTE, while persistent factors (that is, cancer) increase risk for recurrence. Unprovoked VTE places patients at intermediate to high risk, but few data are present for VTE experienced while in the hospital.
Study design: Single-center, population-based, prospective cohort study.
Setting: Tromso, Norway.
Synopsis: Using repeat health surveys from 1994 to 2012, researchers followed 822 patients with a validated, first-lifetime VTE. Hospital-related VTE was defined as a VTE within 8 weeks of hospitalization related to medical illness, surgery, or in patients with active cancer.
This global definition of hospital-related VTE was not associated with an increased risk of recurrent VTE (hazard ratio, 0.99; 0.69-1.41). However, in separate groups, the cumulative risk of recurrence after 5 years in hospital-related VTE due to medical illness was similar to nonhospital-related VTE (20.1% vs. 18.4%), higher than VTE related to surgery (11%), and lower than VTE related to cancer (27.4%).
Risk-adjusted analyses maintained these differences in recurrence risk dependent on reason for hospitalization (cancer, medical illness, surgery). When compared with non-hospital VTE, however, hospital-related VTE was associated with a threefold higher risk of death.
Study limitations included being from a single center, possibly underpowered due to low number of events.
Bottom line: Hospital-related VTE has a high risk of recurrence, but risk level is variable and dependent on the reason for hospitalization.
Citation: Bjøri E, Arshad N, Johnsen HS, Hansen J-B, Brækkan SK. Hospital-related first venous thromboembolism and risk of recurrence [published online ahead of print, Sept. 2, 2016]. J Thromb Haemost. doi: 10.1111/jth.13492
Dr. Ciarkowski is a clinical instructor at the University of Utah School of Medicine and an academic hospitalist at the University of Utah Hospital.
Bezlotoxumab prevents recurrent C. difficile infection
Adding bezlotoxumab to standard antibiotic treatment of primary or recurrent Clostridium difficile infection reduces recurrences by 38% (10 percentage points), according to a report published in the New England Journal of Medicine.
As many as 35% of patients who complete initial antibiotic treatment have at least one recurrence of C. difficile infection, and the rate of repeat recurrence rate jumps to 60% after the initial recurrence. Researchers performed two parallel international phase III trials to assess the efficacy and safety of bezlotoxumab, alone or in combination with actoxumab, for preventing such recurrences. Both monoclonal antibodies work by binding to and neutralizing C. difficile toxins; bezlotoxumab targets toxin B and actoxumab targets toxin A, said Mark H. Wilcox, MD, of the division of microbiology, Leeds (England) General Infirmary, and his associates.
The primary efficacy endpoint – the proportion of patients with recurrent C. difficile infection during 12 weeks of follow-up – was substantially lower with bezlotoxumab (17%) than with placebo (28%) in the first trial and in the second trial (16% vs. 26%). This treatment benefit was evident as early as 2 weeks after infusion and persisted throughout follow-up, the investigators said (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMoa1602615).
The agent’s persistent effect through 12 weeks is important to note because approximately 30% of the recurrences in this study “occurred beyond the conventional 4-week assessment period for treatment efficacy. The number needed to treat to prevent one episode of recurrent C. difficile infection was 10; it was 6 among participants 65 years of age or older and those with previous C. difficile infection,” Dr. Wilcox and his associates noted.
Bezlotoxumab was consistently effective in several sensitivity analyses. It also was effective in both trials individually as well as in pooled results. And the choice of oral antibiotic appeared to have no effect on bezlotoxumab’s efficacy.
In a post hoc analysis, bezlotoxumab was also effective in the subgroup of 1,964 patients at highest risk for C. difficile recurrence because they were elderly, had compromised immunity, had the most severe infections, had a history of C. difficile infection, or carried a strain of the organism associated with particularly poor outcomes. In this subgroup, 17% of patients given bezlotoxumab and 16% of those given bezlotoxumab plus actoxumab developed recurrences, compared with 30% of those given placebo.
Regarding adverse events, the agent had “a generally favorable safety profile,” and the rates of adverse events “were generally as expected, given the underlying disease severity, baseline coexisting conditions, and ages of the participants.” Two participants discontinued the infusion because of an adverse event. Drug-related adverse events occurred in 7% of the entire study population, serious drug-related adverse events occurred in 1%, and both occurred at similar rates across the study groups.
Both trials were funded by Merck, which also was involved in study design, data analysis and interpretation, and writing the reports. Dr. Wilcox and his associates reported ties to Merck and numerous other industry sources.
Bezlotoxumab must be placed in perspective, seen within the context of alternative options currently being evaluated in clinical trials.
These include recently developed drugs such as ridinilazole, surotomycin, cadazolid, RBX2660, and SER-109. Also under assessment is the oral administration of nontoxigenic C. difficile strains to compete with toxigenic strains, as well as three vaccines against the organism. Stool transplantation also is known to be highly successful in preventing recurrent C. difficile infection.
In addition, the cost-effectiveness of bezlotoxumab, especially in relation to these alternative treatments, hasn’t yet been determined.
John G. Bartlett, MD, is in the department of medicine at Johns Hopkins University, Baltimore. He reported having no relevant financial disclosures. Dr. Bartlett made these remarks in an editorial accompanying Dr. Wilcox’s report (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMe1614726).
Bezlotoxumab must be placed in perspective, seen within the context of alternative options currently being evaluated in clinical trials.
These include recently developed drugs such as ridinilazole, surotomycin, cadazolid, RBX2660, and SER-109. Also under assessment is the oral administration of nontoxigenic C. difficile strains to compete with toxigenic strains, as well as three vaccines against the organism. Stool transplantation also is known to be highly successful in preventing recurrent C. difficile infection.
In addition, the cost-effectiveness of bezlotoxumab, especially in relation to these alternative treatments, hasn’t yet been determined.
John G. Bartlett, MD, is in the department of medicine at Johns Hopkins University, Baltimore. He reported having no relevant financial disclosures. Dr. Bartlett made these remarks in an editorial accompanying Dr. Wilcox’s report (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMe1614726).
Bezlotoxumab must be placed in perspective, seen within the context of alternative options currently being evaluated in clinical trials.
These include recently developed drugs such as ridinilazole, surotomycin, cadazolid, RBX2660, and SER-109. Also under assessment is the oral administration of nontoxigenic C. difficile strains to compete with toxigenic strains, as well as three vaccines against the organism. Stool transplantation also is known to be highly successful in preventing recurrent C. difficile infection.
In addition, the cost-effectiveness of bezlotoxumab, especially in relation to these alternative treatments, hasn’t yet been determined.
John G. Bartlett, MD, is in the department of medicine at Johns Hopkins University, Baltimore. He reported having no relevant financial disclosures. Dr. Bartlett made these remarks in an editorial accompanying Dr. Wilcox’s report (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMe1614726).
Adding bezlotoxumab to standard antibiotic treatment of primary or recurrent Clostridium difficile infection reduces recurrences by 38% (10 percentage points), according to a report published in the New England Journal of Medicine.
As many as 35% of patients who complete initial antibiotic treatment have at least one recurrence of C. difficile infection, and the rate of repeat recurrence rate jumps to 60% after the initial recurrence. Researchers performed two parallel international phase III trials to assess the efficacy and safety of bezlotoxumab, alone or in combination with actoxumab, for preventing such recurrences. Both monoclonal antibodies work by binding to and neutralizing C. difficile toxins; bezlotoxumab targets toxin B and actoxumab targets toxin A, said Mark H. Wilcox, MD, of the division of microbiology, Leeds (England) General Infirmary, and his associates.
The primary efficacy endpoint – the proportion of patients with recurrent C. difficile infection during 12 weeks of follow-up – was substantially lower with bezlotoxumab (17%) than with placebo (28%) in the first trial and in the second trial (16% vs. 26%). This treatment benefit was evident as early as 2 weeks after infusion and persisted throughout follow-up, the investigators said (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMoa1602615).
The agent’s persistent effect through 12 weeks is important to note because approximately 30% of the recurrences in this study “occurred beyond the conventional 4-week assessment period for treatment efficacy. The number needed to treat to prevent one episode of recurrent C. difficile infection was 10; it was 6 among participants 65 years of age or older and those with previous C. difficile infection,” Dr. Wilcox and his associates noted.
Bezlotoxumab was consistently effective in several sensitivity analyses. It also was effective in both trials individually as well as in pooled results. And the choice of oral antibiotic appeared to have no effect on bezlotoxumab’s efficacy.
In a post hoc analysis, bezlotoxumab was also effective in the subgroup of 1,964 patients at highest risk for C. difficile recurrence because they were elderly, had compromised immunity, had the most severe infections, had a history of C. difficile infection, or carried a strain of the organism associated with particularly poor outcomes. In this subgroup, 17% of patients given bezlotoxumab and 16% of those given bezlotoxumab plus actoxumab developed recurrences, compared with 30% of those given placebo.
Regarding adverse events, the agent had “a generally favorable safety profile,” and the rates of adverse events “were generally as expected, given the underlying disease severity, baseline coexisting conditions, and ages of the participants.” Two participants discontinued the infusion because of an adverse event. Drug-related adverse events occurred in 7% of the entire study population, serious drug-related adverse events occurred in 1%, and both occurred at similar rates across the study groups.
Both trials were funded by Merck, which also was involved in study design, data analysis and interpretation, and writing the reports. Dr. Wilcox and his associates reported ties to Merck and numerous other industry sources.
Adding bezlotoxumab to standard antibiotic treatment of primary or recurrent Clostridium difficile infection reduces recurrences by 38% (10 percentage points), according to a report published in the New England Journal of Medicine.
As many as 35% of patients who complete initial antibiotic treatment have at least one recurrence of C. difficile infection, and the rate of repeat recurrence rate jumps to 60% after the initial recurrence. Researchers performed two parallel international phase III trials to assess the efficacy and safety of bezlotoxumab, alone or in combination with actoxumab, for preventing such recurrences. Both monoclonal antibodies work by binding to and neutralizing C. difficile toxins; bezlotoxumab targets toxin B and actoxumab targets toxin A, said Mark H. Wilcox, MD, of the division of microbiology, Leeds (England) General Infirmary, and his associates.
The primary efficacy endpoint – the proportion of patients with recurrent C. difficile infection during 12 weeks of follow-up – was substantially lower with bezlotoxumab (17%) than with placebo (28%) in the first trial and in the second trial (16% vs. 26%). This treatment benefit was evident as early as 2 weeks after infusion and persisted throughout follow-up, the investigators said (N Engl J Med. 2017 Jan 25. doi: 10.1056/NEJMoa1602615).
The agent’s persistent effect through 12 weeks is important to note because approximately 30% of the recurrences in this study “occurred beyond the conventional 4-week assessment period for treatment efficacy. The number needed to treat to prevent one episode of recurrent C. difficile infection was 10; it was 6 among participants 65 years of age or older and those with previous C. difficile infection,” Dr. Wilcox and his associates noted.
Bezlotoxumab was consistently effective in several sensitivity analyses. It also was effective in both trials individually as well as in pooled results. And the choice of oral antibiotic appeared to have no effect on bezlotoxumab’s efficacy.
In a post hoc analysis, bezlotoxumab was also effective in the subgroup of 1,964 patients at highest risk for C. difficile recurrence because they were elderly, had compromised immunity, had the most severe infections, had a history of C. difficile infection, or carried a strain of the organism associated with particularly poor outcomes. In this subgroup, 17% of patients given bezlotoxumab and 16% of those given bezlotoxumab plus actoxumab developed recurrences, compared with 30% of those given placebo.
Regarding adverse events, the agent had “a generally favorable safety profile,” and the rates of adverse events “were generally as expected, given the underlying disease severity, baseline coexisting conditions, and ages of the participants.” Two participants discontinued the infusion because of an adverse event. Drug-related adverse events occurred in 7% of the entire study population, serious drug-related adverse events occurred in 1%, and both occurred at similar rates across the study groups.
Both trials were funded by Merck, which also was involved in study design, data analysis and interpretation, and writing the reports. Dr. Wilcox and his associates reported ties to Merck and numerous other industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Adding bezlotoxumab to standard antibiotic treatment of primary or recurrent Clostridium difficile infection reduced recurrences by 38% (10 percentage points).
Major finding: The number needed to treat to prevent one episode of recurrent C. difficile infection was 10; it was 6 among high-risk participants who were 65 years of age or older or who had previous C. difficile infection.
Data source: Two parallel randomized double-blind placebo-controlled international trials involving 2,655 adults followed for 12 weeks.
Disclosures: Both trials were funded by Merck, which also was involved in study design, data analysis and interpretation, and writing the reports. Dr. Wilcox and his associates reported ties to Merck and numerous other industry sources.
1 in 10 youths, 1 in 4 adults in U.S. use tobacco products
More than one in four U.S. adults are current users of at least one type of tobacco product, and nearly 1 in 10 youths report using tobacco in the previous month, according to a report published in the Jan. 26 edition of the New England Journal of Medicine.
Analysis of data from 45,971 adults and youths aged 12 years and older in Wave 1 of the national longitudinal Population Assessment of Tobacco and Health (PATH) study showed 28% of adults were current users of tobacco products, and 20% were daily users. Cigarettes were the most commonly used tobacco product: 18% of adults said they were current users of cigarettes and 16% were daily users. Cigars and e-cigarettes were the next most common tobacco products, with 8% of adults currently using cigars, and 6% currently using e-cigarettes. (N Eng J Med. 2016, Jan 26. doi: 10.1056/NEJMsa1607538).
“Among adults, tobacco use was generally higher among younger adults, men, members of racial minorities, members of sexual minorities, those with lower educational attainment and lower household income, and those living in the South or Midwest than among their counterparts,” wrote Karin A. Kasza of the department of health behavior at the Roswell Park Cancer Institute, Buffalo, N.Y., and coauthors. “Among youths, the prevalences of ever use and use in the previous 30 days were higher among older youths, male youths, and members of sexual minorities than among their counterparts.”
Many also reported using combinations of tobacco products in the previous 30 days, with 23% of adults and 15% of youths using cigarettes and e-cigarettes concurrently.
The authors noted that the estimates of tobacco use among youths obtained from this household-based survey were lower than those seen in previous school-based surveys, and suggested the survey method may have influenced young people’s responses.
“Surveys administered in a school-based environment may overestimate tobacco-use behaviors because of peer influences, whereas youths may underreport tobacco-use behaviors in a home-based survey out of fear that their parents will overhear answers or learn about them from the interviewer,” Ms. Kasza and her associates wrote.
The study was supported by the National Institute on Drug Abuse, National Institutes of Health, and the Food and Drug Administration and U.S. Department of Health and Human Services under a contract to Westat. One author declared grant support from a pharmaceutical company and having acted as an expert witness against the tobacco industry. Another declared advisory board positions and grant support from private industry, and a third declared stock in private industry. No other conflicts of interest were declared.
More than one in four U.S. adults are current users of at least one type of tobacco product, and nearly 1 in 10 youths report using tobacco in the previous month, according to a report published in the Jan. 26 edition of the New England Journal of Medicine.
Analysis of data from 45,971 adults and youths aged 12 years and older in Wave 1 of the national longitudinal Population Assessment of Tobacco and Health (PATH) study showed 28% of adults were current users of tobacco products, and 20% were daily users. Cigarettes were the most commonly used tobacco product: 18% of adults said they were current users of cigarettes and 16% were daily users. Cigars and e-cigarettes were the next most common tobacco products, with 8% of adults currently using cigars, and 6% currently using e-cigarettes. (N Eng J Med. 2016, Jan 26. doi: 10.1056/NEJMsa1607538).
“Among adults, tobacco use was generally higher among younger adults, men, members of racial minorities, members of sexual minorities, those with lower educational attainment and lower household income, and those living in the South or Midwest than among their counterparts,” wrote Karin A. Kasza of the department of health behavior at the Roswell Park Cancer Institute, Buffalo, N.Y., and coauthors. “Among youths, the prevalences of ever use and use in the previous 30 days were higher among older youths, male youths, and members of sexual minorities than among their counterparts.”
Many also reported using combinations of tobacco products in the previous 30 days, with 23% of adults and 15% of youths using cigarettes and e-cigarettes concurrently.
The authors noted that the estimates of tobacco use among youths obtained from this household-based survey were lower than those seen in previous school-based surveys, and suggested the survey method may have influenced young people’s responses.
“Surveys administered in a school-based environment may overestimate tobacco-use behaviors because of peer influences, whereas youths may underreport tobacco-use behaviors in a home-based survey out of fear that their parents will overhear answers or learn about them from the interviewer,” Ms. Kasza and her associates wrote.
The study was supported by the National Institute on Drug Abuse, National Institutes of Health, and the Food and Drug Administration and U.S. Department of Health and Human Services under a contract to Westat. One author declared grant support from a pharmaceutical company and having acted as an expert witness against the tobacco industry. Another declared advisory board positions and grant support from private industry, and a third declared stock in private industry. No other conflicts of interest were declared.
More than one in four U.S. adults are current users of at least one type of tobacco product, and nearly 1 in 10 youths report using tobacco in the previous month, according to a report published in the Jan. 26 edition of the New England Journal of Medicine.
Analysis of data from 45,971 adults and youths aged 12 years and older in Wave 1 of the national longitudinal Population Assessment of Tobacco and Health (PATH) study showed 28% of adults were current users of tobacco products, and 20% were daily users. Cigarettes were the most commonly used tobacco product: 18% of adults said they were current users of cigarettes and 16% were daily users. Cigars and e-cigarettes were the next most common tobacco products, with 8% of adults currently using cigars, and 6% currently using e-cigarettes. (N Eng J Med. 2016, Jan 26. doi: 10.1056/NEJMsa1607538).
“Among adults, tobacco use was generally higher among younger adults, men, members of racial minorities, members of sexual minorities, those with lower educational attainment and lower household income, and those living in the South or Midwest than among their counterparts,” wrote Karin A. Kasza of the department of health behavior at the Roswell Park Cancer Institute, Buffalo, N.Y., and coauthors. “Among youths, the prevalences of ever use and use in the previous 30 days were higher among older youths, male youths, and members of sexual minorities than among their counterparts.”
Many also reported using combinations of tobacco products in the previous 30 days, with 23% of adults and 15% of youths using cigarettes and e-cigarettes concurrently.
The authors noted that the estimates of tobacco use among youths obtained from this household-based survey were lower than those seen in previous school-based surveys, and suggested the survey method may have influenced young people’s responses.
“Surveys administered in a school-based environment may overestimate tobacco-use behaviors because of peer influences, whereas youths may underreport tobacco-use behaviors in a home-based survey out of fear that their parents will overhear answers or learn about them from the interviewer,” Ms. Kasza and her associates wrote.
The study was supported by the National Institute on Drug Abuse, National Institutes of Health, and the Food and Drug Administration and U.S. Department of Health and Human Services under a contract to Westat. One author declared grant support from a pharmaceutical company and having acted as an expert witness against the tobacco industry. Another declared advisory board positions and grant support from private industry, and a third declared stock in private industry. No other conflicts of interest were declared.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: More than one in four U.S. adults are current users of at least one type of tobacco product, and nearly 1 in 10 youths report using tobacco in the previous month.
Major finding: The PATH study found 28% of adults are current users of tobacco products, and 20% are daily users.
Data source: Wave 1 of the national longitudinal Population Assessment of Tobacco and Health (PATH) study.
Disclosures: The study was supported by the National Institute on Drug Abuse, National Institutes of Health, and the Food and Drug Administration and U.S. Department of Health and Human Services. One author declared grant support from a pharmaceutical company and having acted as an expert witness against the tobacco industry. Another declared advisory board positions and grant support from private industry, and a third declared stock in private industry. No other conflicts of interest were declared.
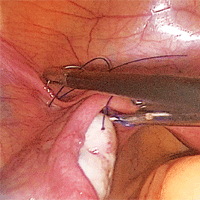
Strategies for prophylactic oophoropexy

Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
Visit the Society of Gynecologic Surgeons online: sgsonline.org
More videos from SGS:
- Tips and tricks for open laparoscopy
- Complete colpectomy & colpocleisis: Model for simulation
- Natural orifice sacral colpopexy
- Alternative options for visualizing ureteral patency during intraoperative cystoscopy
- Use of suprapubic Carter-Thomason needle to assist in cystoscopic excision of an intravesical foreign object
- Uterine artery ligation: Advanced techniques and considerations for the difficult laparoscopic hysterectomy
- Cervical injection of methylene blue for identification of sentinel lymph nodes in cervical cancer
- Misplaced hysteroscopic sterilization micro-insert in the peritoneal cavity: A corpus alienum
- Laparoscopic cystectomy for large, bilateral ovarian dermoids
- Small bowel surgery for the benign gynecologist
This video is brought to you by![]()
Vascular anomalies often misdiagnosed amidst confusion
CHICAGO – Thanks to convoluted terminology, not to mention confusion in the literature, physicians have been known to frequently misdiagnose vascular malformations as hemangiomas, but an evolving understanding of their differences may lead to more precise diagnoses, according to a report at a symposium on vascular surgery sponsored by Northwestern University.
“Historically there has been a great deal of confusion in the literature when it comes to the nomenclature used to describe vascular anomalies,” said Naiem Nassiri, MD, of Robert Wood Johnson Medical School, New Brunswick, N.J. He pointed out that the term hemangioma “or derivatives thereof” – cavernous hemangioma, cavernous angioma, lymphangioma and cystic hygroma – are “absolute misnomers and continue to be misused and applied almost haphazardly to any anomalous vascular lesion.”

He cited reports that 71% of vascular anomalies have been improperly called hemangiomas, 69% have initially been diagnosed incorrectly, and 21% received the wrong treatment (Pediatr Dermatol. 2008;25[1]:7-12; Plast Reconstr Surg. 2011:127[1]:347-51). “Erroneous terminology has prognostic as well as diagnostic and therapeutic implications, and these can actually be quite devastating for the patient, not only clinically and physically but psychologically as well,” Dr. Nassiri said.
Using the International Society for the Study of Vascular Anomalies classification for hemangiomas and vascular malformations can help physicians make the differential diagnosis, Dr. Nassiri said. Hemangiomas are neoplastic lesions of infancy, though not always congenital, with a finite growth phase, whereas vascular malformations (VMs) are nonneoplastic, congenital lesions that can appear at any age and do not regress spontaneously, he said.
Infantile hemangiomas typically appear as the classic strawberry birthmark in children, whereas VMs tend to appear later in life. “They require some environmental trigger, such as trauma, activity, or changes in the hormonal milieu to manifest onset,” he said of VMs.
Simply put, VMs fall into three broad categories: slow-flow malformations, which include lymphatic and venous malformations; high-flow arteriovenous malformations (AVMs) and fistulas; and congenital mixed syndromes, which can include combinations thereof.
Dr. Nassiri noted that contrast-enhanced MRI is the standard imaging modality for diagnosis of VMs, and can differentiate between slow-flow and high-flow lesions. However, vascular specialists must be vigilant in ordering imaging for slow-flow lesions. “Orders can be changed to MR venography, and I’ve had patients who’ve gone decades with multiple MR venograms and no one can figure out what’s going on as no identifiable lesion is readily detected,” he said. “MR venograms are fantastic for detecting truncular blood flow where there typically are no anomalies in the vast majority of patients with isolated venous malformations, but on contrast-enhanced MRI these convoluted cluster of anomalous veins light up like Christmas trees.”
Lymphatic malformations affect the head and neck more so than the extremities, trunk or viscera, and are prone to infection and bleeding. “You can think of these as fluid-filled balloons, and the goal of treatment is fairly simple: You want to puncture the balloon and drain the fluid inside so as to obtain maximum wall collapse,” Dr. Nassiri said. Infusion of a sclerosant causes an inflammatory reaction leading to fibrosis, which then prevents balloon re-expansion. Surgical excision is best used as a secondary adjunct.
Venous malformations, comprising about 80% of all VMs, typically present as soft, spongy blue or purple compressible masses with associated pain that worsens with exertion, Dr. Nassiri said. “The most dangerous thing that is often overlooked, even by some of the physicians that treat these on a regular basis, is localized intravascular coagulopathy, which if left untreated can progress to fulminant disseminated intravascular coagulopathy,” he said. This tends to occur more in the more widespread varieties of venous malformations.
A common misnomer associated with venous malformations in adults is “liver hemangioma,” owing to the confusing nomenclature, Dr. Nassiri said. “When interrogated angiographically,” he said, “what is often labeled as a hepatic hemangioma is in fact a venous malformation. Natural history of the two entities is completely different.”
Dr. Nassiri described congenital high-flow AVMs as “convoluted networks of blood vessels with poorly differentiated endothelial cells that have neither a venous nor an arterial designation; this entity, otherwise known as a nidus, sits between the feeding arteries and the draining veins.” Treatment aims to eliminate the flow within that nidus.
Super-selective microcatheterization is the best option for nidus access and embolization using liquid embolic agents, preferably those that polymerize when infused. “This is probably the most potent angiogenic entity I’ve ever seen,” Dr. Nassiri said of the nidus.
“It’s like a low-pressure sump and it will recruit collaterals vigorously, so you have to eliminate that nidus.” A variety of different embolic agents, some off label, may be used for high flow AVMs.
For congenital mixed syndromes, the same diagnostic and therapeutic concepts hold true depending on the type of VM involved. Dr. Nassiri advised a multidisciplinary approach, and noted that early trials have investigated the use of sirolimus in severe, life-threatening cases (Br J Clin Pharmacol. 2016;82[5]:1171-9. doi: 10.1111/bcp.13022).
Dr. Nassiri disclosed serving on the speakers bureaus for Boston Scientific, Penumbra, and Merritt Medical, and is a consultant to Merritt Medical.
CHICAGO – Thanks to convoluted terminology, not to mention confusion in the literature, physicians have been known to frequently misdiagnose vascular malformations as hemangiomas, but an evolving understanding of their differences may lead to more precise diagnoses, according to a report at a symposium on vascular surgery sponsored by Northwestern University.
“Historically there has been a great deal of confusion in the literature when it comes to the nomenclature used to describe vascular anomalies,” said Naiem Nassiri, MD, of Robert Wood Johnson Medical School, New Brunswick, N.J. He pointed out that the term hemangioma “or derivatives thereof” – cavernous hemangioma, cavernous angioma, lymphangioma and cystic hygroma – are “absolute misnomers and continue to be misused and applied almost haphazardly to any anomalous vascular lesion.”
He cited reports that 71% of vascular anomalies have been improperly called hemangiomas, 69% have initially been diagnosed incorrectly, and 21% received the wrong treatment (Pediatr Dermatol. 2008;25[1]:7-12; Plast Reconstr Surg. 2011:127[1]:347-51). “Erroneous terminology has prognostic as well as diagnostic and therapeutic implications, and these can actually be quite devastating for the patient, not only clinically and physically but psychologically as well,” Dr. Nassiri said.
Using the International Society for the Study of Vascular Anomalies classification for hemangiomas and vascular malformations can help physicians make the differential diagnosis, Dr. Nassiri said. Hemangiomas are neoplastic lesions of infancy, though not always congenital, with a finite growth phase, whereas vascular malformations (VMs) are nonneoplastic, congenital lesions that can appear at any age and do not regress spontaneously, he said.
Infantile hemangiomas typically appear as the classic strawberry birthmark in children, whereas VMs tend to appear later in life. “They require some environmental trigger, such as trauma, activity, or changes in the hormonal milieu to manifest onset,” he said of VMs.
Simply put, VMs fall into three broad categories: slow-flow malformations, which include lymphatic and venous malformations; high-flow arteriovenous malformations (AVMs) and fistulas; and congenital mixed syndromes, which can include combinations thereof.
Dr. Nassiri noted that contrast-enhanced MRI is the standard imaging modality for diagnosis of VMs, and can differentiate between slow-flow and high-flow lesions. However, vascular specialists must be vigilant in ordering imaging for slow-flow lesions. “Orders can be changed to MR venography, and I’ve had patients who’ve gone decades with multiple MR venograms and no one can figure out what’s going on as no identifiable lesion is readily detected,” he said. “MR venograms are fantastic for detecting truncular blood flow where there typically are no anomalies in the vast majority of patients with isolated venous malformations, but on contrast-enhanced MRI these convoluted cluster of anomalous veins light up like Christmas trees.”
Lymphatic malformations affect the head and neck more so than the extremities, trunk or viscera, and are prone to infection and bleeding. “You can think of these as fluid-filled balloons, and the goal of treatment is fairly simple: You want to puncture the balloon and drain the fluid inside so as to obtain maximum wall collapse,” Dr. Nassiri said. Infusion of a sclerosant causes an inflammatory reaction leading to fibrosis, which then prevents balloon re-expansion. Surgical excision is best used as a secondary adjunct.
Venous malformations, comprising about 80% of all VMs, typically present as soft, spongy blue or purple compressible masses with associated pain that worsens with exertion, Dr. Nassiri said. “The most dangerous thing that is often overlooked, even by some of the physicians that treat these on a regular basis, is localized intravascular coagulopathy, which if left untreated can progress to fulminant disseminated intravascular coagulopathy,” he said. This tends to occur more in the more widespread varieties of venous malformations.
A common misnomer associated with venous malformations in adults is “liver hemangioma,” owing to the confusing nomenclature, Dr. Nassiri said. “When interrogated angiographically,” he said, “what is often labeled as a hepatic hemangioma is in fact a venous malformation. Natural history of the two entities is completely different.”
Dr. Nassiri described congenital high-flow AVMs as “convoluted networks of blood vessels with poorly differentiated endothelial cells that have neither a venous nor an arterial designation; this entity, otherwise known as a nidus, sits between the feeding arteries and the draining veins.” Treatment aims to eliminate the flow within that nidus.
Super-selective microcatheterization is the best option for nidus access and embolization using liquid embolic agents, preferably those that polymerize when infused. “This is probably the most potent angiogenic entity I’ve ever seen,” Dr. Nassiri said of the nidus.
“It’s like a low-pressure sump and it will recruit collaterals vigorously, so you have to eliminate that nidus.” A variety of different embolic agents, some off label, may be used for high flow AVMs.
For congenital mixed syndromes, the same diagnostic and therapeutic concepts hold true depending on the type of VM involved. Dr. Nassiri advised a multidisciplinary approach, and noted that early trials have investigated the use of sirolimus in severe, life-threatening cases (Br J Clin Pharmacol. 2016;82[5]:1171-9. doi: 10.1111/bcp.13022).
Dr. Nassiri disclosed serving on the speakers bureaus for Boston Scientific, Penumbra, and Merritt Medical, and is a consultant to Merritt Medical.
CHICAGO – Thanks to convoluted terminology, not to mention confusion in the literature, physicians have been known to frequently misdiagnose vascular malformations as hemangiomas, but an evolving understanding of their differences may lead to more precise diagnoses, according to a report at a symposium on vascular surgery sponsored by Northwestern University.
“Historically there has been a great deal of confusion in the literature when it comes to the nomenclature used to describe vascular anomalies,” said Naiem Nassiri, MD, of Robert Wood Johnson Medical School, New Brunswick, N.J. He pointed out that the term hemangioma “or derivatives thereof” – cavernous hemangioma, cavernous angioma, lymphangioma and cystic hygroma – are “absolute misnomers and continue to be misused and applied almost haphazardly to any anomalous vascular lesion.”
He cited reports that 71% of vascular anomalies have been improperly called hemangiomas, 69% have initially been diagnosed incorrectly, and 21% received the wrong treatment (Pediatr Dermatol. 2008;25[1]:7-12; Plast Reconstr Surg. 2011:127[1]:347-51). “Erroneous terminology has prognostic as well as diagnostic and therapeutic implications, and these can actually be quite devastating for the patient, not only clinically and physically but psychologically as well,” Dr. Nassiri said.
Using the International Society for the Study of Vascular Anomalies classification for hemangiomas and vascular malformations can help physicians make the differential diagnosis, Dr. Nassiri said. Hemangiomas are neoplastic lesions of infancy, though not always congenital, with a finite growth phase, whereas vascular malformations (VMs) are nonneoplastic, congenital lesions that can appear at any age and do not regress spontaneously, he said.
Infantile hemangiomas typically appear as the classic strawberry birthmark in children, whereas VMs tend to appear later in life. “They require some environmental trigger, such as trauma, activity, or changes in the hormonal milieu to manifest onset,” he said of VMs.
Simply put, VMs fall into three broad categories: slow-flow malformations, which include lymphatic and venous malformations; high-flow arteriovenous malformations (AVMs) and fistulas; and congenital mixed syndromes, which can include combinations thereof.
Dr. Nassiri noted that contrast-enhanced MRI is the standard imaging modality for diagnosis of VMs, and can differentiate between slow-flow and high-flow lesions. However, vascular specialists must be vigilant in ordering imaging for slow-flow lesions. “Orders can be changed to MR venography, and I’ve had patients who’ve gone decades with multiple MR venograms and no one can figure out what’s going on as no identifiable lesion is readily detected,” he said. “MR venograms are fantastic for detecting truncular blood flow where there typically are no anomalies in the vast majority of patients with isolated venous malformations, but on contrast-enhanced MRI these convoluted cluster of anomalous veins light up like Christmas trees.”
Lymphatic malformations affect the head and neck more so than the extremities, trunk or viscera, and are prone to infection and bleeding. “You can think of these as fluid-filled balloons, and the goal of treatment is fairly simple: You want to puncture the balloon and drain the fluid inside so as to obtain maximum wall collapse,” Dr. Nassiri said. Infusion of a sclerosant causes an inflammatory reaction leading to fibrosis, which then prevents balloon re-expansion. Surgical excision is best used as a secondary adjunct.
Venous malformations, comprising about 80% of all VMs, typically present as soft, spongy blue or purple compressible masses with associated pain that worsens with exertion, Dr. Nassiri said. “The most dangerous thing that is often overlooked, even by some of the physicians that treat these on a regular basis, is localized intravascular coagulopathy, which if left untreated can progress to fulminant disseminated intravascular coagulopathy,” he said. This tends to occur more in the more widespread varieties of venous malformations.
A common misnomer associated with venous malformations in adults is “liver hemangioma,” owing to the confusing nomenclature, Dr. Nassiri said. “When interrogated angiographically,” he said, “what is often labeled as a hepatic hemangioma is in fact a venous malformation. Natural history of the two entities is completely different.”
Dr. Nassiri described congenital high-flow AVMs as “convoluted networks of blood vessels with poorly differentiated endothelial cells that have neither a venous nor an arterial designation; this entity, otherwise known as a nidus, sits between the feeding arteries and the draining veins.” Treatment aims to eliminate the flow within that nidus.
Super-selective microcatheterization is the best option for nidus access and embolization using liquid embolic agents, preferably those that polymerize when infused. “This is probably the most potent angiogenic entity I’ve ever seen,” Dr. Nassiri said of the nidus.
“It’s like a low-pressure sump and it will recruit collaterals vigorously, so you have to eliminate that nidus.” A variety of different embolic agents, some off label, may be used for high flow AVMs.
For congenital mixed syndromes, the same diagnostic and therapeutic concepts hold true depending on the type of VM involved. Dr. Nassiri advised a multidisciplinary approach, and noted that early trials have investigated the use of sirolimus in severe, life-threatening cases (Br J Clin Pharmacol. 2016;82[5]:1171-9. doi: 10.1111/bcp.13022).
Dr. Nassiri disclosed serving on the speakers bureaus for Boston Scientific, Penumbra, and Merritt Medical, and is a consultant to Merritt Medical.
AT THE NORTHWESTERN VASCULAR SYMPOSIUM
Key clinical point:
Major finding: Use of imaging and a clearer understanding of the lack of neoplastic activity are key to more precisely diagnosing vascular malformations.
Data source: Review of literature and center experience.
Disclosure: Dr. Nassiri disclosed serving on the speakers bureaus for Boston Scientific, Penumbra, and Merritt Medical, and is a consultant to Merritt Medical.
But you told me...
“The other doctor I went to told me that the spot he biopsied on my nose was a skin cancer,” Larry said. “But he told me just to keep an eye on it.”
I always try not to roll my eyes when a patient quotes another doctor, especially if the quote doesn’t make much sense. In the first place, it’s bad form to act like you’re smarter than somebody else. In the second place, you probably aren’t.
In the third place, what the patient says the doctor said may not be what the doctor actually said. I have many chances to learn this firsthand, such as when patients quote me incorrectly to myself.

No, I didn’t.
I point out to students that, to patients, calling a mole benign is always provisional. They’re happy that it’s benign today. Tomorrow, who knows?
That’s why when I reassure people about moles I’m not worried about, I say, “It’s benign... and it will always be benign.” When they look startled – as they often do – I elaborate: “Because if I thought it could turn into skin cancer, I would have to remove it right now.” Then they nod, somewhat tentatively. What I just said clearly made sense, only it contradicts what they always assumed was true, which is that you should always keep an eye on things.
Since I thought Steve’s mole was benign, I did not tell him that we need to keep an eye on it, any more than Larry’s previous doctor had told him just to keep an eye on a biopsy-proved skin cancer. Steve just thought that’s what I must have said, because that’s what makes sense to him.
Then there was Amanda, who had stopped her acne gel weeks before. “It was making me worse,” she explained, “and you told me to stop the medicine if anything happened.”
Nope, not even close.
What I did say – what I always say – was this: “These are the reactions you might experience. If you think you’re getting them or any others, call me right away, so I can consider changing to something different.” I never tell patients to just stop treatment and not tell anyone. Who would?
The opposite happens too. Just as some people stop medication without telling their doctors, others find it just as hard to stop treatment even when they’re instructed to.
“When your seborrhea quiets down,” I say, “you can stop the cream. Resume it when you need to, but stop again as soon as you clear up.”
Easy for me to say. But in walks Phillip. He’s been using applying desonide daily for 6 years. “You said I should keep using it,” he explains.
No, I didn’t. “What I was trying to say,” I politely explain, “is that when your skin feels fine, it’s OK to stop. They you can use it again when the rash comes back. Keeping up applying the cream doesn’t stop the rash from coming back if it’s going to.”
Philip nods. I think he understands. But I thought so last time too, didn’t I?
I should also give a shout-out to the patients who say, “I’ve been using the clotrimazole-betamethasone cream you prescribed...”
No, I did not prescribe clotrimazole-betamethasone! I would lose my membership in the dermatologists’ union.
Researchers who study cross-cultural practice look into issues of miscommunication between providers and consumers who come from distant cultures, where basic notions get in the way of each party’s understanding the other. No one seems that interested in studying all the miscommunication that goes on between educated native-English speakers, in medical offices no less than in the halls of the legislature.
I got hold of Larry’s biopsy report, by the way. It was read out as “actinic keratosis,” which is why Larry’s former doctor had told him that they would just watch it.
I called Larry. “It was not an actual cancer,” I told him. “Just precancerous. Come back in 6 months. We’ll keep an eye on it.”
That was clear. I think.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
“The other doctor I went to told me that the spot he biopsied on my nose was a skin cancer,” Larry said. “But he told me just to keep an eye on it.”
I always try not to roll my eyes when a patient quotes another doctor, especially if the quote doesn’t make much sense. In the first place, it’s bad form to act like you’re smarter than somebody else. In the second place, you probably aren’t.
In the third place, what the patient says the doctor said may not be what the doctor actually said. I have many chances to learn this firsthand, such as when patients quote me incorrectly to myself.
No, I didn’t.
I point out to students that, to patients, calling a mole benign is always provisional. They’re happy that it’s benign today. Tomorrow, who knows?
That’s why when I reassure people about moles I’m not worried about, I say, “It’s benign... and it will always be benign.” When they look startled – as they often do – I elaborate: “Because if I thought it could turn into skin cancer, I would have to remove it right now.” Then they nod, somewhat tentatively. What I just said clearly made sense, only it contradicts what they always assumed was true, which is that you should always keep an eye on things.
Since I thought Steve’s mole was benign, I did not tell him that we need to keep an eye on it, any more than Larry’s previous doctor had told him just to keep an eye on a biopsy-proved skin cancer. Steve just thought that’s what I must have said, because that’s what makes sense to him.
Then there was Amanda, who had stopped her acne gel weeks before. “It was making me worse,” she explained, “and you told me to stop the medicine if anything happened.”
Nope, not even close.
What I did say – what I always say – was this: “These are the reactions you might experience. If you think you’re getting them or any others, call me right away, so I can consider changing to something different.” I never tell patients to just stop treatment and not tell anyone. Who would?
The opposite happens too. Just as some people stop medication without telling their doctors, others find it just as hard to stop treatment even when they’re instructed to.
“When your seborrhea quiets down,” I say, “you can stop the cream. Resume it when you need to, but stop again as soon as you clear up.”
Easy for me to say. But in walks Phillip. He’s been using applying desonide daily for 6 years. “You said I should keep using it,” he explains.
No, I didn’t. “What I was trying to say,” I politely explain, “is that when your skin feels fine, it’s OK to stop. They you can use it again when the rash comes back. Keeping up applying the cream doesn’t stop the rash from coming back if it’s going to.”
Philip nods. I think he understands. But I thought so last time too, didn’t I?
I should also give a shout-out to the patients who say, “I’ve been using the clotrimazole-betamethasone cream you prescribed...”
No, I did not prescribe clotrimazole-betamethasone! I would lose my membership in the dermatologists’ union.
Researchers who study cross-cultural practice look into issues of miscommunication between providers and consumers who come from distant cultures, where basic notions get in the way of each party’s understanding the other. No one seems that interested in studying all the miscommunication that goes on between educated native-English speakers, in medical offices no less than in the halls of the legislature.
I got hold of Larry’s biopsy report, by the way. It was read out as “actinic keratosis,” which is why Larry’s former doctor had told him that they would just watch it.
I called Larry. “It was not an actual cancer,” I told him. “Just precancerous. Come back in 6 months. We’ll keep an eye on it.”
That was clear. I think.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
“The other doctor I went to told me that the spot he biopsied on my nose was a skin cancer,” Larry said. “But he told me just to keep an eye on it.”
I always try not to roll my eyes when a patient quotes another doctor, especially if the quote doesn’t make much sense. In the first place, it’s bad form to act like you’re smarter than somebody else. In the second place, you probably aren’t.
In the third place, what the patient says the doctor said may not be what the doctor actually said. I have many chances to learn this firsthand, such as when patients quote me incorrectly to myself.
No, I didn’t.
I point out to students that, to patients, calling a mole benign is always provisional. They’re happy that it’s benign today. Tomorrow, who knows?
That’s why when I reassure people about moles I’m not worried about, I say, “It’s benign... and it will always be benign.” When they look startled – as they often do – I elaborate: “Because if I thought it could turn into skin cancer, I would have to remove it right now.” Then they nod, somewhat tentatively. What I just said clearly made sense, only it contradicts what they always assumed was true, which is that you should always keep an eye on things.
Since I thought Steve’s mole was benign, I did not tell him that we need to keep an eye on it, any more than Larry’s previous doctor had told him just to keep an eye on a biopsy-proved skin cancer. Steve just thought that’s what I must have said, because that’s what makes sense to him.
Then there was Amanda, who had stopped her acne gel weeks before. “It was making me worse,” she explained, “and you told me to stop the medicine if anything happened.”
Nope, not even close.
What I did say – what I always say – was this: “These are the reactions you might experience. If you think you’re getting them or any others, call me right away, so I can consider changing to something different.” I never tell patients to just stop treatment and not tell anyone. Who would?
The opposite happens too. Just as some people stop medication without telling their doctors, others find it just as hard to stop treatment even when they’re instructed to.
“When your seborrhea quiets down,” I say, “you can stop the cream. Resume it when you need to, but stop again as soon as you clear up.”
Easy for me to say. But in walks Phillip. He’s been using applying desonide daily for 6 years. “You said I should keep using it,” he explains.
No, I didn’t. “What I was trying to say,” I politely explain, “is that when your skin feels fine, it’s OK to stop. They you can use it again when the rash comes back. Keeping up applying the cream doesn’t stop the rash from coming back if it’s going to.”
Philip nods. I think he understands. But I thought so last time too, didn’t I?
I should also give a shout-out to the patients who say, “I’ve been using the clotrimazole-betamethasone cream you prescribed...”
No, I did not prescribe clotrimazole-betamethasone! I would lose my membership in the dermatologists’ union.
Researchers who study cross-cultural practice look into issues of miscommunication between providers and consumers who come from distant cultures, where basic notions get in the way of each party’s understanding the other. No one seems that interested in studying all the miscommunication that goes on between educated native-English speakers, in medical offices no less than in the halls of the legislature.
I got hold of Larry’s biopsy report, by the way. It was read out as “actinic keratosis,” which is why Larry’s former doctor had told him that they would just watch it.
I called Larry. “It was not an actual cancer,” I told him. “Just precancerous. Come back in 6 months. We’ll keep an eye on it.”
That was clear. I think.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Ramucirumab benefits gastric cancer patients across age groups
SAN FRANCISCO – Patients with metastatic gastric or gastroesophageal junction adenocarcinoma benefit from treatment with ramucirumab regardless of their age, according to findings from an exploratory subgroup analysis of the phase III RAINBOW and REGARD studies.
The findings, which show at least a trend toward improvements in most age categories, are important given that nearly two-thirds of patients with these cancers are diagnosed at over age 65 years, and more than half of those are over age 75 years, Kei Muro, MD, reported at the symposium sponsored by ASCO, ASTRO, the American Gastroenterological Association, and the Society of Surgical Oncology.
“At the other end of the age spectrum, there is evidence that young age can also be an unfavorable prognostic characteristic for gastric cancer,” said Dr. Muro of Aichi Cancer Center Hospital in Nagoya, Japan.
Both RAINBOW and REGARD demonstrated statistically significant and clinically meaningful overall and progression-free survival benefits and acceptable and manageable toxicity with ramucirumab among patients with advanced gastric cancer who were randomized, in the second-line treatment setting, to receive active treatment with the fully humanized monoclonal antibody directed against vascular endothelial growth factor receptor–2 or placebo.
RAINBOW subjects were randomized 1:1 to receive 8 mg/kg of ramucirumab plus paclitaxel, or placebo plus paclitaxel. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 months for treatment vs. 4.2 months for placebo (hazard ratio, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
The corresponding median overall survival rates for those aged 45-70 (225 and 230 patients in the groups, respectively), 70 or older (68 patients in each group), and 75 or older (20 and 16 patients in the groups, respectively) were 9.6 vs. 7.6 months (HR, 0.860), 10.8 vs. 8.6 months (HR, 0.881), and 11.0 vs. 11.0 months (HR, 0.971). The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 4.6 vs. 2.8 months (HR, 0.649), 4.7 vs. 2.9 months (HR, 0.676), and 4.2 vs. 2.8 months (HR, 0.330).
REGARD subjects were randomized 2:1 to receive 8 mg/kg of ramucirumab plus best supportive care, or placebo plus best supportive care. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 vs. 4.2 months for treatment vs. placebo (HR, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
Among REGARD subjects aged 45 years or less (28 and 12 patients in the groups, respectively), the median overall survival was 5.8 vs. 2.9 months for treatment vs. placebo (HR, 0.586), and the median progression-free survival was 1.9 vs. 1.4 months (HR, 0.270).
The corresponding median overall survival rates for those aged 45-70 (166 and 70 patients in the groups, respectively), 70 or older (44 and 35 patients in the groups, respectively), and 75 or older (21 and 13 patients in the groups, respectively) were 4.9 vs. 4.1 months (HR, 0.780), 5.9 vs. 3.8 months (HR, 0.730), and 9.3 vs. 5.1 months (HR, 0.588).
The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 2.2 vs. 1.3 months (HR, 0.451), 2.1 vs. 1.4 months (HR, 0.559), 2.8 vs. 1.4 (HR, 0.420).
Baseline characteristics were generally well balanced between arms in each of the age subgroups, Dr. Muro said, noting that no obvious patterns for differential risks in terms of efficacy and adverse events of any grade or of grade 3 or greater were seen according to age. Discontinuation rates for adverse events were similar across different age groups, and quality of life, as determined by global health status, was satisfactory in all age groups.
“Despite some limitations regarding patient numbers in some age subgroups, this exploratory subgroup analysis supports the use of ramucirumab for the treatment of our patients with gastric cancer irrespective of age,” he concluded.
RAINBOW was funded by Eli Lilly. REGARD was funded by ImClone Systems. Dr. Muro reported receiving honoraria from Chugai Pharma, Merck Serono, Taiho Pharmaceutical, Takeda, Eli Lilly, and Yakult Honsha, as well as serving in a consulting or an advisory role for Ono, Merck Serono, and Eli Lilly, and receiving research funding from MSD, Daiichi Sankyo, Ono, Eisai, Pfizer, Chugai, Dainippon Sumitomo, Merck Serono, Janssen Pharmaceutical K.K., AstraZeneca, GlaxoSmithKline, and Kyowa Hakko Kirin.
SAN FRANCISCO – Patients with metastatic gastric or gastroesophageal junction adenocarcinoma benefit from treatment with ramucirumab regardless of their age, according to findings from an exploratory subgroup analysis of the phase III RAINBOW and REGARD studies.
The findings, which show at least a trend toward improvements in most age categories, are important given that nearly two-thirds of patients with these cancers are diagnosed at over age 65 years, and more than half of those are over age 75 years, Kei Muro, MD, reported at the symposium sponsored by ASCO, ASTRO, the American Gastroenterological Association, and the Society of Surgical Oncology.
“At the other end of the age spectrum, there is evidence that young age can also be an unfavorable prognostic characteristic for gastric cancer,” said Dr. Muro of Aichi Cancer Center Hospital in Nagoya, Japan.
Both RAINBOW and REGARD demonstrated statistically significant and clinically meaningful overall and progression-free survival benefits and acceptable and manageable toxicity with ramucirumab among patients with advanced gastric cancer who were randomized, in the second-line treatment setting, to receive active treatment with the fully humanized monoclonal antibody directed against vascular endothelial growth factor receptor–2 or placebo.
RAINBOW subjects were randomized 1:1 to receive 8 mg/kg of ramucirumab plus paclitaxel, or placebo plus paclitaxel. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 months for treatment vs. 4.2 months for placebo (hazard ratio, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
The corresponding median overall survival rates for those aged 45-70 (225 and 230 patients in the groups, respectively), 70 or older (68 patients in each group), and 75 or older (20 and 16 patients in the groups, respectively) were 9.6 vs. 7.6 months (HR, 0.860), 10.8 vs. 8.6 months (HR, 0.881), and 11.0 vs. 11.0 months (HR, 0.971). The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 4.6 vs. 2.8 months (HR, 0.649), 4.7 vs. 2.9 months (HR, 0.676), and 4.2 vs. 2.8 months (HR, 0.330).
REGARD subjects were randomized 2:1 to receive 8 mg/kg of ramucirumab plus best supportive care, or placebo plus best supportive care. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 vs. 4.2 months for treatment vs. placebo (HR, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
Among REGARD subjects aged 45 years or less (28 and 12 patients in the groups, respectively), the median overall survival was 5.8 vs. 2.9 months for treatment vs. placebo (HR, 0.586), and the median progression-free survival was 1.9 vs. 1.4 months (HR, 0.270).
The corresponding median overall survival rates for those aged 45-70 (166 and 70 patients in the groups, respectively), 70 or older (44 and 35 patients in the groups, respectively), and 75 or older (21 and 13 patients in the groups, respectively) were 4.9 vs. 4.1 months (HR, 0.780), 5.9 vs. 3.8 months (HR, 0.730), and 9.3 vs. 5.1 months (HR, 0.588).
The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 2.2 vs. 1.3 months (HR, 0.451), 2.1 vs. 1.4 months (HR, 0.559), 2.8 vs. 1.4 (HR, 0.420).
Baseline characteristics were generally well balanced between arms in each of the age subgroups, Dr. Muro said, noting that no obvious patterns for differential risks in terms of efficacy and adverse events of any grade or of grade 3 or greater were seen according to age. Discontinuation rates for adverse events were similar across different age groups, and quality of life, as determined by global health status, was satisfactory in all age groups.
“Despite some limitations regarding patient numbers in some age subgroups, this exploratory subgroup analysis supports the use of ramucirumab for the treatment of our patients with gastric cancer irrespective of age,” he concluded.
RAINBOW was funded by Eli Lilly. REGARD was funded by ImClone Systems. Dr. Muro reported receiving honoraria from Chugai Pharma, Merck Serono, Taiho Pharmaceutical, Takeda, Eli Lilly, and Yakult Honsha, as well as serving in a consulting or an advisory role for Ono, Merck Serono, and Eli Lilly, and receiving research funding from MSD, Daiichi Sankyo, Ono, Eisai, Pfizer, Chugai, Dainippon Sumitomo, Merck Serono, Janssen Pharmaceutical K.K., AstraZeneca, GlaxoSmithKline, and Kyowa Hakko Kirin.
SAN FRANCISCO – Patients with metastatic gastric or gastroesophageal junction adenocarcinoma benefit from treatment with ramucirumab regardless of their age, according to findings from an exploratory subgroup analysis of the phase III RAINBOW and REGARD studies.
The findings, which show at least a trend toward improvements in most age categories, are important given that nearly two-thirds of patients with these cancers are diagnosed at over age 65 years, and more than half of those are over age 75 years, Kei Muro, MD, reported at the symposium sponsored by ASCO, ASTRO, the American Gastroenterological Association, and the Society of Surgical Oncology.
“At the other end of the age spectrum, there is evidence that young age can also be an unfavorable prognostic characteristic for gastric cancer,” said Dr. Muro of Aichi Cancer Center Hospital in Nagoya, Japan.
Both RAINBOW and REGARD demonstrated statistically significant and clinically meaningful overall and progression-free survival benefits and acceptable and manageable toxicity with ramucirumab among patients with advanced gastric cancer who were randomized, in the second-line treatment setting, to receive active treatment with the fully humanized monoclonal antibody directed against vascular endothelial growth factor receptor–2 or placebo.
RAINBOW subjects were randomized 1:1 to receive 8 mg/kg of ramucirumab plus paclitaxel, or placebo plus paclitaxel. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 months for treatment vs. 4.2 months for placebo (hazard ratio, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
The corresponding median overall survival rates for those aged 45-70 (225 and 230 patients in the groups, respectively), 70 or older (68 patients in each group), and 75 or older (20 and 16 patients in the groups, respectively) were 9.6 vs. 7.6 months (HR, 0.860), 10.8 vs. 8.6 months (HR, 0.881), and 11.0 vs. 11.0 months (HR, 0.971). The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 4.6 vs. 2.8 months (HR, 0.649), 4.7 vs. 2.9 months (HR, 0.676), and 4.2 vs. 2.8 months (HR, 0.330).
REGARD subjects were randomized 2:1 to receive 8 mg/kg of ramucirumab plus best supportive care, or placebo plus best supportive care. Among those aged 45 years or less (37 patients in each group), the median overall survival was 9.0 vs. 4.2 months for treatment vs. placebo (HR, 0.555), and the median progression-free survival was 3.9 vs. 2.8 months (HR, 0.299).
Among REGARD subjects aged 45 years or less (28 and 12 patients in the groups, respectively), the median overall survival was 5.8 vs. 2.9 months for treatment vs. placebo (HR, 0.586), and the median progression-free survival was 1.9 vs. 1.4 months (HR, 0.270).
The corresponding median overall survival rates for those aged 45-70 (166 and 70 patients in the groups, respectively), 70 or older (44 and 35 patients in the groups, respectively), and 75 or older (21 and 13 patients in the groups, respectively) were 4.9 vs. 4.1 months (HR, 0.780), 5.9 vs. 3.8 months (HR, 0.730), and 9.3 vs. 5.1 months (HR, 0.588).
The corresponding progression-free survival rates for those aged 45-70, 70 or older, and 75 or older were 2.2 vs. 1.3 months (HR, 0.451), 2.1 vs. 1.4 months (HR, 0.559), 2.8 vs. 1.4 (HR, 0.420).
Baseline characteristics were generally well balanced between arms in each of the age subgroups, Dr. Muro said, noting that no obvious patterns for differential risks in terms of efficacy and adverse events of any grade or of grade 3 or greater were seen according to age. Discontinuation rates for adverse events were similar across different age groups, and quality of life, as determined by global health status, was satisfactory in all age groups.
“Despite some limitations regarding patient numbers in some age subgroups, this exploratory subgroup analysis supports the use of ramucirumab for the treatment of our patients with gastric cancer irrespective of age,” he concluded.
RAINBOW was funded by Eli Lilly. REGARD was funded by ImClone Systems. Dr. Muro reported receiving honoraria from Chugai Pharma, Merck Serono, Taiho Pharmaceutical, Takeda, Eli Lilly, and Yakult Honsha, as well as serving in a consulting or an advisory role for Ono, Merck Serono, and Eli Lilly, and receiving research funding from MSD, Daiichi Sankyo, Ono, Eisai, Pfizer, Chugai, Dainippon Sumitomo, Merck Serono, Janssen Pharmaceutical K.K., AstraZeneca, GlaxoSmithKline, and Kyowa Hakko Kirin.
AT THE 2017 GASTROINTESTINAL CANCERS SYMPOSIUM
Key clinical point:
Major finding: Among patients 45-70 years and 70 and older, the hazard ratios for overall survival were 0.860 and 0.881 with ramucirumab vs. placebo in RAINBOW, and 0.780 and 0.730 in REGARD
Data source: The phase III RAINBOW and REGARD trials, including a total of more than 1,000 patients.
Disclosures: Dr. Muro reported receiving honoraria from Chugai Pharma, Merck Serono, Taiho Pharmaceutical, Takeda, Eli Lilly, and Yakult Honsha, as well as serving in a consulting or an advisory role for Ono, Merck Serono, and Eli Lilly, and receiving research funding from MSD, Daiichi Sankyo, Ono, Eisai, Pfizer, Chugai, Dainippon Sumitomo, Merck Serono, Janssen Pharmaceutical K.K., AstraZeneca, GlaxoSmithKline, and Kyowa Hakko Kirin.