User login
Tips for Living With Suspected CTE
Click here to download the PDF. 
Click here to download the PDF.
Click here to download the PDF.
Migraine Increases the Risk of Perioperative Ischemic Stroke
Patients who undergo surgery have an increased risk of perioperative ischemic stroke if they have a history of migraine, according to a prospective study published January 10 in the BMJ. Surgical patients with a history of migraine also have an increased 30-day hospital readmission rate, compared with patients without migraine.
“Understanding this risk period offers unique opportunities to study ischemic stroke in migraine and might result in treatment considerations for patients at risk who are not undergoing surgical intervention,” said Matthias Eikermann, MD, PhD, Associate Professor of Anesthesia at Harvard Medical School in Boston, and colleagues. “An individual perioperative risk assessment for perioperative ischemic stroke in patients with migraine undergoing surgery may be crucial.”

Dr. Eikermann and colleagues conducted a prospective hospital registry study that encompassed 124,558 patients who underwent surgery at Massachusetts General Hospital and two community hospitals in Massachusetts between January 2007 and August 2014. The researchers determined participants’ history of migraine and migraine aura status using ICD-9 diagnosis codes. The primary outcome was perioperative ischemic stroke within 30 days after surgery. The secondary outcome was hospital readmission within 30 days of discharge.
The mean age of participants was 52.6. Approximately 55% of patients were women. The investigators identified 10,179 (8.2%) patients with migraine, of whom 1,278 (12.6%) had migraine with aura. Compared with participants without migraine, migraineurs were more often female, were younger, and had an overall lower frequency of vascular risk factors.
Among the 124,558 patients who underwent surgery, the investigators observed 771 (0.6%) perioperative ischemic strokes. Of all patients with perioperative ischemic stroke, 89 (11.5%) had migraine. Among migraineurs, 18 (2.3%) had migraine with aura, and 71 (9.2%) had migraine without aura. Patients with migraine had an increased risk for perioperative ischemic stroke, compared with patients without migraine (adjusted odds ratio, 1.75). The risk of ischemic stroke was higher for patients with migraine with aura (adjusted odds ratio, 2.61), but also was apparent for migraine without aura (adjusted odds ratio, 1.62), compared with surgical patients without migraine.
Dr. Eikermann and colleagues predicted that 2.4 ischemic strokes would occur for every 1,000 surgical patients. This risk increased to 4.3 strokes for every 1,000 patients with migraine. Stratified by migraine with aura status, these numbers are 3.9 strokes for migraine without aura and 6.3 strokes for migraine with aura.
A total of 10,088 participants were readmitted to the hospital within 30 days. The 30-day hospital readmission rate was higher for patients with migraine than for those with no migraine (adjusted odds ratio, 1.31). Migraine with aura (adjusted odds ratio, 1.59) and migraine without aura (adjusted odds ratio, 1.27) were associated with a higher risk of 30-day hospital readmission, compared with patients without migraine.
“The use of high-dose vasopressors during surgery, as well a history of a possible right-to-left shunt, may represent modifiable risk factors for perioperative ischemic stroke in patients with migraine with aura,” said Dr. Eikermann. “Early detection of symptoms of stroke through close postoperative monitoring of patients at high risk should be crucial to optimize the value of perioperative care in patients with migraine.”
—Erik Greb
Suggested Reading
Timm FP, Houle TT, Grabitz SD, et al. Migraine and risk of perioperative ischemic stroke and hospital readmission: hospital based registry study. BMJ. 2017 Jan 10;356:i6635.
Patients who undergo surgery have an increased risk of perioperative ischemic stroke if they have a history of migraine, according to a prospective study published January 10 in the BMJ. Surgical patients with a history of migraine also have an increased 30-day hospital readmission rate, compared with patients without migraine.
“Understanding this risk period offers unique opportunities to study ischemic stroke in migraine and might result in treatment considerations for patients at risk who are not undergoing surgical intervention,” said Matthias Eikermann, MD, PhD, Associate Professor of Anesthesia at Harvard Medical School in Boston, and colleagues. “An individual perioperative risk assessment for perioperative ischemic stroke in patients with migraine undergoing surgery may be crucial.”
Dr. Eikermann and colleagues conducted a prospective hospital registry study that encompassed 124,558 patients who underwent surgery at Massachusetts General Hospital and two community hospitals in Massachusetts between January 2007 and August 2014. The researchers determined participants’ history of migraine and migraine aura status using ICD-9 diagnosis codes. The primary outcome was perioperative ischemic stroke within 30 days after surgery. The secondary outcome was hospital readmission within 30 days of discharge.
The mean age of participants was 52.6. Approximately 55% of patients were women. The investigators identified 10,179 (8.2%) patients with migraine, of whom 1,278 (12.6%) had migraine with aura. Compared with participants without migraine, migraineurs were more often female, were younger, and had an overall lower frequency of vascular risk factors.
Among the 124,558 patients who underwent surgery, the investigators observed 771 (0.6%) perioperative ischemic strokes. Of all patients with perioperative ischemic stroke, 89 (11.5%) had migraine. Among migraineurs, 18 (2.3%) had migraine with aura, and 71 (9.2%) had migraine without aura. Patients with migraine had an increased risk for perioperative ischemic stroke, compared with patients without migraine (adjusted odds ratio, 1.75). The risk of ischemic stroke was higher for patients with migraine with aura (adjusted odds ratio, 2.61), but also was apparent for migraine without aura (adjusted odds ratio, 1.62), compared with surgical patients without migraine.
Dr. Eikermann and colleagues predicted that 2.4 ischemic strokes would occur for every 1,000 surgical patients. This risk increased to 4.3 strokes for every 1,000 patients with migraine. Stratified by migraine with aura status, these numbers are 3.9 strokes for migraine without aura and 6.3 strokes for migraine with aura.
A total of 10,088 participants were readmitted to the hospital within 30 days. The 30-day hospital readmission rate was higher for patients with migraine than for those with no migraine (adjusted odds ratio, 1.31). Migraine with aura (adjusted odds ratio, 1.59) and migraine without aura (adjusted odds ratio, 1.27) were associated with a higher risk of 30-day hospital readmission, compared with patients without migraine.
“The use of high-dose vasopressors during surgery, as well a history of a possible right-to-left shunt, may represent modifiable risk factors for perioperative ischemic stroke in patients with migraine with aura,” said Dr. Eikermann. “Early detection of symptoms of stroke through close postoperative monitoring of patients at high risk should be crucial to optimize the value of perioperative care in patients with migraine.”
—Erik Greb
Suggested Reading
Timm FP, Houle TT, Grabitz SD, et al. Migraine and risk of perioperative ischemic stroke and hospital readmission: hospital based registry study. BMJ. 2017 Jan 10;356:i6635.
Patients who undergo surgery have an increased risk of perioperative ischemic stroke if they have a history of migraine, according to a prospective study published January 10 in the BMJ. Surgical patients with a history of migraine also have an increased 30-day hospital readmission rate, compared with patients without migraine.
“Understanding this risk period offers unique opportunities to study ischemic stroke in migraine and might result in treatment considerations for patients at risk who are not undergoing surgical intervention,” said Matthias Eikermann, MD, PhD, Associate Professor of Anesthesia at Harvard Medical School in Boston, and colleagues. “An individual perioperative risk assessment for perioperative ischemic stroke in patients with migraine undergoing surgery may be crucial.”
Dr. Eikermann and colleagues conducted a prospective hospital registry study that encompassed 124,558 patients who underwent surgery at Massachusetts General Hospital and two community hospitals in Massachusetts between January 2007 and August 2014. The researchers determined participants’ history of migraine and migraine aura status using ICD-9 diagnosis codes. The primary outcome was perioperative ischemic stroke within 30 days after surgery. The secondary outcome was hospital readmission within 30 days of discharge.
The mean age of participants was 52.6. Approximately 55% of patients were women. The investigators identified 10,179 (8.2%) patients with migraine, of whom 1,278 (12.6%) had migraine with aura. Compared with participants without migraine, migraineurs were more often female, were younger, and had an overall lower frequency of vascular risk factors.
Among the 124,558 patients who underwent surgery, the investigators observed 771 (0.6%) perioperative ischemic strokes. Of all patients with perioperative ischemic stroke, 89 (11.5%) had migraine. Among migraineurs, 18 (2.3%) had migraine with aura, and 71 (9.2%) had migraine without aura. Patients with migraine had an increased risk for perioperative ischemic stroke, compared with patients without migraine (adjusted odds ratio, 1.75). The risk of ischemic stroke was higher for patients with migraine with aura (adjusted odds ratio, 2.61), but also was apparent for migraine without aura (adjusted odds ratio, 1.62), compared with surgical patients without migraine.
Dr. Eikermann and colleagues predicted that 2.4 ischemic strokes would occur for every 1,000 surgical patients. This risk increased to 4.3 strokes for every 1,000 patients with migraine. Stratified by migraine with aura status, these numbers are 3.9 strokes for migraine without aura and 6.3 strokes for migraine with aura.
A total of 10,088 participants were readmitted to the hospital within 30 days. The 30-day hospital readmission rate was higher for patients with migraine than for those with no migraine (adjusted odds ratio, 1.31). Migraine with aura (adjusted odds ratio, 1.59) and migraine without aura (adjusted odds ratio, 1.27) were associated with a higher risk of 30-day hospital readmission, compared with patients without migraine.
“The use of high-dose vasopressors during surgery, as well a history of a possible right-to-left shunt, may represent modifiable risk factors for perioperative ischemic stroke in patients with migraine with aura,” said Dr. Eikermann. “Early detection of symptoms of stroke through close postoperative monitoring of patients at high risk should be crucial to optimize the value of perioperative care in patients with migraine.”
—Erik Greb
Suggested Reading
Timm FP, Houle TT, Grabitz SD, et al. Migraine and risk of perioperative ischemic stroke and hospital readmission: hospital based registry study. BMJ. 2017 Jan 10;356:i6635.

Mobile Devices May Provide Accurate Seizure Detection and Help Prevent SUDEP
HOUSTON—Mobile or wearable devices that observe autonomic and motor changes may provide seizure detection, according to an overview presented at the 70th Annual Meeting of the American Epilepsy Society. Devices that monitor heart rate, electrodermal changes, and electromyogram (EMG) changes also may provide accurate detection of convulsive seizures. Many such devices are in development, and some already are available. They may be convenient for patients to use and could provide opportunities for interventions to prevent sudden unexpected death in epilepsy (SUDEP).
What Do Patients Want?
In 2015, Hoppe and colleagues published the results of their survey of patients’ preferences for automated seizure-detection devices. The authors found that patients want convenient devices such as wearable wristbands, but do not want devices that are conspicuous. Patients want devices that perform automatic seizure registration and make emergency calls to family members or caregivers. They do not, however, want devices that notify their doctors automatically about seizures, preferring to maintain control of their own medical data. On the other hand, patients do want to get help during medical appointments with controlling and using the devices. Finally, patients want devices that predict seizures, but this task “probably requires intracranial recording,” said Gregory Krauss, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore.

Another survey asked patients about the accuracy that they wanted from these devices. One survey suggested that patients would accept a false-positive or false-negative rate of less than 25%. Seizure-free patients would accept a false-positive rate of less than one per week. Patients with recurring seizures would accept a higher false-positive rate. “Most patients said [that] as long as the ratio of false detections to true detections was not more than 1:1, they would find that acceptable,” said Dr. Krauss.
Patients also want rapid detection of seizures so that they can protect themselves or quickly get help. “The majority of patients would like detection to occur with alerting within one minute” of seizure onset, said Dr. Krauss. Some patients want detection to occur within 30 seconds of seizure onset, and about 14% of patients said that detection within three minutes of onset would be sufficient.
Investigators have pursued various methods for seizure detection. The major methods are physiologic (eg, heart rate, pulse oximetry, and electrodermal activity), motion-related (eg, accelerometers, mattress sensors, EMG, and video motion detection), and responsive testing (eg, testing memory and responsiveness). The best technique may be to combine several of these methods to minimize the rate of false positives, said Dr. Krauss.
SmartWatch
One device that currently is available is SmartWatch, which is manufactured by SmartMonitor. The SmartWatch device is a wrist accelerometer that predominantly detects convulsive seizures. Data from epilepsy monitoring units (EMUs) on the device’s efficacy have been mixed. In a Stanford University study, SmartWatch recorded 62 seizures in 27 patients. Nine patients had 13 tonic–clonic seizures, and the device detected 12 of them. The device had a false positive rate of 87%. In a University of Tennessee study involving 41 patients who had 191 seizures, the SmartWatch device detected 31% of tonic–clonic seizures. These studies suggest that the device has “somewhat limited sensitivity without individualizing settings,” and its accuracy during real-world use is unclear, said Dr. Krauss.
Embrace Watch
The device furthest along in development is Embrace Watch, which is being designed by Empatica. Embrace Watch is a smart watch that performs electrodermal and accelerometer measurements and is connected to a smart phone. It uses an app that graphically displays information about the user’s activity, stress level, and sleep. The watch is intended to detect convulsive seizures and send alerts to caregivers.
One reason that Embrace Watch measures electrodermal activity is that the latter correlates with postictal EEG suppression. Research indicates that postictal generalized EEG suppression corresponds with the risk of SUDEP. “That [finding] raises the possibility that the Empatica device may be useful for intervening in SUDEP,” said Dr. Krauss.
An ongoing study is evaluating Embrace Watch’s efficacy in an EMU. Investigators collected video EEG data for 69 patients and monitored electrodermal activity and movement with the Embrace Watch. The investigators reviewed the detection of 55 convulsive seizures in 22 patients. They tested two classifier models, which were different combinations of electrodermal activity and heart rate changes. One classifier model had 100% sensitivity, but a moderately high rate of false alarms (1.26/day). The other classifier model had a sensitivity of 95% and a rate of 0.2 false alarms per day, which may be acceptable for a patient with uncontrolled seizures, said Dr. Krauss. A separate case study suggests that Embrace Watch accurately detects major seizures in patients with Dravet syndrome.
Brain Sentinel
The FDA is reviewing the Brain Sentinel seizure-monitoring system, which uses EMG recordings to detect convulsive seizures. The device takes advantage of a characteristic firing pattern on EMG that is associated with convulsive seizures. Research has indicated that, when used properly, the system detects seizures with near-perfect accuracy. The system’s accuracy was slightly higher in adults than in a group of adults and children. The average time between seizure onset and alarm was 5.34 seconds in adults and 7.70 seconds in adults and children. The rate of false positives per eight-hour period was 0.51 in adults and 0.48 in adults and children. Most false alarms occurred in a minority of participants. “This device is probably going to be effective for detecting convulsive seizures in patients with uncontrolled epilepsy,” said Dr. Krauss.
EpiWatch App
Dr. Krauss and Nathan Crone, MD, Professor of Neurology at Johns Hopkins University School of Medicine, are developing a seizure-detection app called EpiWatch for use on the Apple Watch. Their objective is to use the Apple Watch’s ability to monitor heart rate, movement, and position to detect seizures. Through the Apple Watch’s user interface, the app asks patients to label seizures and attempts to reduce the number of false detections. During a seizure, the app tests the user’s responsiveness by asking him or her to tap the watch. The test occurs at 20 seconds after seizure onset and at one-minute intervals thereafter. If the user is responsive, the app administers a test of working memory that involves repeating a series of random numbers. At 10 minutes after the seizure ends, the app asks the user whether he or she had had a seizure, whether he or she had had an aura, and whether he or she had lost awareness. These data are logged into a journal that can be transmitted.
Drs. Krauss and Crone are using Apple ResearchKit to study the app’s efficacy. They have enrolled approximately 700 participants in the study, and about 40% of them were able to activate the app during a seizure. The seizure types recorded so far are representative of those of the general US population of patients with epilepsy. Approximately 30% of participants had a 50% increase in heart rate during their seizure. About two-thirds of patients had a 30% increase in heart rate. A significant number of patients with complex partial seizures had decreases in heart rate during their seizure. “Heart rate alone would probably not be a sensitive screening technique for seizures, but it could be one component of an algorithm,” said Dr. Krauss.
Can These Devices Prevent SUDEP?
Many of these devices were designed with the goal of enabling interventions, particularly during severe nocturnal convulsive seizures, to prevent SUDEP. The current understanding of SUDEP provides grounds for optimism that such interventions could be achieved, said Dr. Krauss. Many patients with tonic–clonic seizures have oxygen saturation, postictal generalized EEG suppression, and autonomic alterations. If patients become immobile during a seizure and are lying face down, they may become asphyxiated. “The question is whether we can intervene at that point to prevent the subsequent cardiac arrhythmias which lead to their death,” said Dr. Krauss. A caregiver, for example, could turn a patient on his or her side and stimulate him or her to promote breathing. If the caregiver finds the patient at a later time after seizure onset, he or she could attempt resuscitation. “This is our general concept of perhaps how SUDEP intervention could be performed using mobile device detectors,” Dr. Krauss concluded.
—Erik Greb
Suggested Reading
Hoppe C, Feldmann M, Blachut B, et al. Novel techniques for automated seizure registration: Patients’ wants and needs. Epilepsy Behav. 2015;52(Pt A):1-7.
Lhatoo SD, Nei M, Raghavan M, et al. Nonseizure SUDEP: Sudden unexpected death in epilepsy without preceding epileptic seizures. Epilepsia. 2016;57(7):1161-1168.
Van de Vel A, Smets K, Wouters K, Ceulemans B. Automated non-EEG based seizure detection: Do users have a say? Epilepsy Behav. 2016;62:121-128.
Velez M, Fisher RS, Bartlett V, Le S. Tracking generalized tonic-clonic seizures with a wrist accelerometer linked to an online database. Seizure. 2016;39:13-18.
HOUSTON—Mobile or wearable devices that observe autonomic and motor changes may provide seizure detection, according to an overview presented at the 70th Annual Meeting of the American Epilepsy Society. Devices that monitor heart rate, electrodermal changes, and electromyogram (EMG) changes also may provide accurate detection of convulsive seizures. Many such devices are in development, and some already are available. They may be convenient for patients to use and could provide opportunities for interventions to prevent sudden unexpected death in epilepsy (SUDEP).
What Do Patients Want?
In 2015, Hoppe and colleagues published the results of their survey of patients’ preferences for automated seizure-detection devices. The authors found that patients want convenient devices such as wearable wristbands, but do not want devices that are conspicuous. Patients want devices that perform automatic seizure registration and make emergency calls to family members or caregivers. They do not, however, want devices that notify their doctors automatically about seizures, preferring to maintain control of their own medical data. On the other hand, patients do want to get help during medical appointments with controlling and using the devices. Finally, patients want devices that predict seizures, but this task “probably requires intracranial recording,” said Gregory Krauss, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore.
Another survey asked patients about the accuracy that they wanted from these devices. One survey suggested that patients would accept a false-positive or false-negative rate of less than 25%. Seizure-free patients would accept a false-positive rate of less than one per week. Patients with recurring seizures would accept a higher false-positive rate. “Most patients said [that] as long as the ratio of false detections to true detections was not more than 1:1, they would find that acceptable,” said Dr. Krauss.
Patients also want rapid detection of seizures so that they can protect themselves or quickly get help. “The majority of patients would like detection to occur with alerting within one minute” of seizure onset, said Dr. Krauss. Some patients want detection to occur within 30 seconds of seizure onset, and about 14% of patients said that detection within three minutes of onset would be sufficient.
Investigators have pursued various methods for seizure detection. The major methods are physiologic (eg, heart rate, pulse oximetry, and electrodermal activity), motion-related (eg, accelerometers, mattress sensors, EMG, and video motion detection), and responsive testing (eg, testing memory and responsiveness). The best technique may be to combine several of these methods to minimize the rate of false positives, said Dr. Krauss.
SmartWatch
One device that currently is available is SmartWatch, which is manufactured by SmartMonitor. The SmartWatch device is a wrist accelerometer that predominantly detects convulsive seizures. Data from epilepsy monitoring units (EMUs) on the device’s efficacy have been mixed. In a Stanford University study, SmartWatch recorded 62 seizures in 27 patients. Nine patients had 13 tonic–clonic seizures, and the device detected 12 of them. The device had a false positive rate of 87%. In a University of Tennessee study involving 41 patients who had 191 seizures, the SmartWatch device detected 31% of tonic–clonic seizures. These studies suggest that the device has “somewhat limited sensitivity without individualizing settings,” and its accuracy during real-world use is unclear, said Dr. Krauss.
Embrace Watch
The device furthest along in development is Embrace Watch, which is being designed by Empatica. Embrace Watch is a smart watch that performs electrodermal and accelerometer measurements and is connected to a smart phone. It uses an app that graphically displays information about the user’s activity, stress level, and sleep. The watch is intended to detect convulsive seizures and send alerts to caregivers.
One reason that Embrace Watch measures electrodermal activity is that the latter correlates with postictal EEG suppression. Research indicates that postictal generalized EEG suppression corresponds with the risk of SUDEP. “That [finding] raises the possibility that the Empatica device may be useful for intervening in SUDEP,” said Dr. Krauss.
An ongoing study is evaluating Embrace Watch’s efficacy in an EMU. Investigators collected video EEG data for 69 patients and monitored electrodermal activity and movement with the Embrace Watch. The investigators reviewed the detection of 55 convulsive seizures in 22 patients. They tested two classifier models, which were different combinations of electrodermal activity and heart rate changes. One classifier model had 100% sensitivity, but a moderately high rate of false alarms (1.26/day). The other classifier model had a sensitivity of 95% and a rate of 0.2 false alarms per day, which may be acceptable for a patient with uncontrolled seizures, said Dr. Krauss. A separate case study suggests that Embrace Watch accurately detects major seizures in patients with Dravet syndrome.
Brain Sentinel
The FDA is reviewing the Brain Sentinel seizure-monitoring system, which uses EMG recordings to detect convulsive seizures. The device takes advantage of a characteristic firing pattern on EMG that is associated with convulsive seizures. Research has indicated that, when used properly, the system detects seizures with near-perfect accuracy. The system’s accuracy was slightly higher in adults than in a group of adults and children. The average time between seizure onset and alarm was 5.34 seconds in adults and 7.70 seconds in adults and children. The rate of false positives per eight-hour period was 0.51 in adults and 0.48 in adults and children. Most false alarms occurred in a minority of participants. “This device is probably going to be effective for detecting convulsive seizures in patients with uncontrolled epilepsy,” said Dr. Krauss.
EpiWatch App
Dr. Krauss and Nathan Crone, MD, Professor of Neurology at Johns Hopkins University School of Medicine, are developing a seizure-detection app called EpiWatch for use on the Apple Watch. Their objective is to use the Apple Watch’s ability to monitor heart rate, movement, and position to detect seizures. Through the Apple Watch’s user interface, the app asks patients to label seizures and attempts to reduce the number of false detections. During a seizure, the app tests the user’s responsiveness by asking him or her to tap the watch. The test occurs at 20 seconds after seizure onset and at one-minute intervals thereafter. If the user is responsive, the app administers a test of working memory that involves repeating a series of random numbers. At 10 minutes after the seizure ends, the app asks the user whether he or she had had a seizure, whether he or she had had an aura, and whether he or she had lost awareness. These data are logged into a journal that can be transmitted.
Drs. Krauss and Crone are using Apple ResearchKit to study the app’s efficacy. They have enrolled approximately 700 participants in the study, and about 40% of them were able to activate the app during a seizure. The seizure types recorded so far are representative of those of the general US population of patients with epilepsy. Approximately 30% of participants had a 50% increase in heart rate during their seizure. About two-thirds of patients had a 30% increase in heart rate. A significant number of patients with complex partial seizures had decreases in heart rate during their seizure. “Heart rate alone would probably not be a sensitive screening technique for seizures, but it could be one component of an algorithm,” said Dr. Krauss.
Can These Devices Prevent SUDEP?
Many of these devices were designed with the goal of enabling interventions, particularly during severe nocturnal convulsive seizures, to prevent SUDEP. The current understanding of SUDEP provides grounds for optimism that such interventions could be achieved, said Dr. Krauss. Many patients with tonic–clonic seizures have oxygen saturation, postictal generalized EEG suppression, and autonomic alterations. If patients become immobile during a seizure and are lying face down, they may become asphyxiated. “The question is whether we can intervene at that point to prevent the subsequent cardiac arrhythmias which lead to their death,” said Dr. Krauss. A caregiver, for example, could turn a patient on his or her side and stimulate him or her to promote breathing. If the caregiver finds the patient at a later time after seizure onset, he or she could attempt resuscitation. “This is our general concept of perhaps how SUDEP intervention could be performed using mobile device detectors,” Dr. Krauss concluded.
—Erik Greb
Suggested Reading
Hoppe C, Feldmann M, Blachut B, et al. Novel techniques for automated seizure registration: Patients’ wants and needs. Epilepsy Behav. 2015;52(Pt A):1-7.
Lhatoo SD, Nei M, Raghavan M, et al. Nonseizure SUDEP: Sudden unexpected death in epilepsy without preceding epileptic seizures. Epilepsia. 2016;57(7):1161-1168.
Van de Vel A, Smets K, Wouters K, Ceulemans B. Automated non-EEG based seizure detection: Do users have a say? Epilepsy Behav. 2016;62:121-128.
Velez M, Fisher RS, Bartlett V, Le S. Tracking generalized tonic-clonic seizures with a wrist accelerometer linked to an online database. Seizure. 2016;39:13-18.
HOUSTON—Mobile or wearable devices that observe autonomic and motor changes may provide seizure detection, according to an overview presented at the 70th Annual Meeting of the American Epilepsy Society. Devices that monitor heart rate, electrodermal changes, and electromyogram (EMG) changes also may provide accurate detection of convulsive seizures. Many such devices are in development, and some already are available. They may be convenient for patients to use and could provide opportunities for interventions to prevent sudden unexpected death in epilepsy (SUDEP).
What Do Patients Want?
In 2015, Hoppe and colleagues published the results of their survey of patients’ preferences for automated seizure-detection devices. The authors found that patients want convenient devices such as wearable wristbands, but do not want devices that are conspicuous. Patients want devices that perform automatic seizure registration and make emergency calls to family members or caregivers. They do not, however, want devices that notify their doctors automatically about seizures, preferring to maintain control of their own medical data. On the other hand, patients do want to get help during medical appointments with controlling and using the devices. Finally, patients want devices that predict seizures, but this task “probably requires intracranial recording,” said Gregory Krauss, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore.
Another survey asked patients about the accuracy that they wanted from these devices. One survey suggested that patients would accept a false-positive or false-negative rate of less than 25%. Seizure-free patients would accept a false-positive rate of less than one per week. Patients with recurring seizures would accept a higher false-positive rate. “Most patients said [that] as long as the ratio of false detections to true detections was not more than 1:1, they would find that acceptable,” said Dr. Krauss.
Patients also want rapid detection of seizures so that they can protect themselves or quickly get help. “The majority of patients would like detection to occur with alerting within one minute” of seizure onset, said Dr. Krauss. Some patients want detection to occur within 30 seconds of seizure onset, and about 14% of patients said that detection within three minutes of onset would be sufficient.
Investigators have pursued various methods for seizure detection. The major methods are physiologic (eg, heart rate, pulse oximetry, and electrodermal activity), motion-related (eg, accelerometers, mattress sensors, EMG, and video motion detection), and responsive testing (eg, testing memory and responsiveness). The best technique may be to combine several of these methods to minimize the rate of false positives, said Dr. Krauss.
SmartWatch
One device that currently is available is SmartWatch, which is manufactured by SmartMonitor. The SmartWatch device is a wrist accelerometer that predominantly detects convulsive seizures. Data from epilepsy monitoring units (EMUs) on the device’s efficacy have been mixed. In a Stanford University study, SmartWatch recorded 62 seizures in 27 patients. Nine patients had 13 tonic–clonic seizures, and the device detected 12 of them. The device had a false positive rate of 87%. In a University of Tennessee study involving 41 patients who had 191 seizures, the SmartWatch device detected 31% of tonic–clonic seizures. These studies suggest that the device has “somewhat limited sensitivity without individualizing settings,” and its accuracy during real-world use is unclear, said Dr. Krauss.
Embrace Watch
The device furthest along in development is Embrace Watch, which is being designed by Empatica. Embrace Watch is a smart watch that performs electrodermal and accelerometer measurements and is connected to a smart phone. It uses an app that graphically displays information about the user’s activity, stress level, and sleep. The watch is intended to detect convulsive seizures and send alerts to caregivers.
One reason that Embrace Watch measures electrodermal activity is that the latter correlates with postictal EEG suppression. Research indicates that postictal generalized EEG suppression corresponds with the risk of SUDEP. “That [finding] raises the possibility that the Empatica device may be useful for intervening in SUDEP,” said Dr. Krauss.
An ongoing study is evaluating Embrace Watch’s efficacy in an EMU. Investigators collected video EEG data for 69 patients and monitored electrodermal activity and movement with the Embrace Watch. The investigators reviewed the detection of 55 convulsive seizures in 22 patients. They tested two classifier models, which were different combinations of electrodermal activity and heart rate changes. One classifier model had 100% sensitivity, but a moderately high rate of false alarms (1.26/day). The other classifier model had a sensitivity of 95% and a rate of 0.2 false alarms per day, which may be acceptable for a patient with uncontrolled seizures, said Dr. Krauss. A separate case study suggests that Embrace Watch accurately detects major seizures in patients with Dravet syndrome.
Brain Sentinel
The FDA is reviewing the Brain Sentinel seizure-monitoring system, which uses EMG recordings to detect convulsive seizures. The device takes advantage of a characteristic firing pattern on EMG that is associated with convulsive seizures. Research has indicated that, when used properly, the system detects seizures with near-perfect accuracy. The system’s accuracy was slightly higher in adults than in a group of adults and children. The average time between seizure onset and alarm was 5.34 seconds in adults and 7.70 seconds in adults and children. The rate of false positives per eight-hour period was 0.51 in adults and 0.48 in adults and children. Most false alarms occurred in a minority of participants. “This device is probably going to be effective for detecting convulsive seizures in patients with uncontrolled epilepsy,” said Dr. Krauss.
EpiWatch App
Dr. Krauss and Nathan Crone, MD, Professor of Neurology at Johns Hopkins University School of Medicine, are developing a seizure-detection app called EpiWatch for use on the Apple Watch. Their objective is to use the Apple Watch’s ability to monitor heart rate, movement, and position to detect seizures. Through the Apple Watch’s user interface, the app asks patients to label seizures and attempts to reduce the number of false detections. During a seizure, the app tests the user’s responsiveness by asking him or her to tap the watch. The test occurs at 20 seconds after seizure onset and at one-minute intervals thereafter. If the user is responsive, the app administers a test of working memory that involves repeating a series of random numbers. At 10 minutes after the seizure ends, the app asks the user whether he or she had had a seizure, whether he or she had had an aura, and whether he or she had lost awareness. These data are logged into a journal that can be transmitted.
Drs. Krauss and Crone are using Apple ResearchKit to study the app’s efficacy. They have enrolled approximately 700 participants in the study, and about 40% of them were able to activate the app during a seizure. The seizure types recorded so far are representative of those of the general US population of patients with epilepsy. Approximately 30% of participants had a 50% increase in heart rate during their seizure. About two-thirds of patients had a 30% increase in heart rate. A significant number of patients with complex partial seizures had decreases in heart rate during their seizure. “Heart rate alone would probably not be a sensitive screening technique for seizures, but it could be one component of an algorithm,” said Dr. Krauss.
Can These Devices Prevent SUDEP?
Many of these devices were designed with the goal of enabling interventions, particularly during severe nocturnal convulsive seizures, to prevent SUDEP. The current understanding of SUDEP provides grounds for optimism that such interventions could be achieved, said Dr. Krauss. Many patients with tonic–clonic seizures have oxygen saturation, postictal generalized EEG suppression, and autonomic alterations. If patients become immobile during a seizure and are lying face down, they may become asphyxiated. “The question is whether we can intervene at that point to prevent the subsequent cardiac arrhythmias which lead to their death,” said Dr. Krauss. A caregiver, for example, could turn a patient on his or her side and stimulate him or her to promote breathing. If the caregiver finds the patient at a later time after seizure onset, he or she could attempt resuscitation. “This is our general concept of perhaps how SUDEP intervention could be performed using mobile device detectors,” Dr. Krauss concluded.
—Erik Greb
Suggested Reading
Hoppe C, Feldmann M, Blachut B, et al. Novel techniques for automated seizure registration: Patients’ wants and needs. Epilepsy Behav. 2015;52(Pt A):1-7.
Lhatoo SD, Nei M, Raghavan M, et al. Nonseizure SUDEP: Sudden unexpected death in epilepsy without preceding epileptic seizures. Epilepsia. 2016;57(7):1161-1168.
Van de Vel A, Smets K, Wouters K, Ceulemans B. Automated non-EEG based seizure detection: Do users have a say? Epilepsy Behav. 2016;62:121-128.
Velez M, Fisher RS, Bartlett V, Le S. Tracking generalized tonic-clonic seizures with a wrist accelerometer linked to an online database. Seizure. 2016;39:13-18.

Treatment Reduces Risk of Long-Term Disability in MS
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.

Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.
Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.
Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.

New and Noteworthy Information—February 2017
Concussions may accelerate Alzheimer's disease-related brain atrophy and cognitive decline in people who are at genetic risk for the condition, according to a study published online ahead of print January 11 in Brain. A total of 160 Iraq and Afghanistan war veterans between the ages of 19 and 58, were included in this study. Among males with mild traumatic brain injury, high genetic risk for Alzheimer's disease was associated with cortical thinning as a function of time since injury. A moderated mediation analysis showed that mild traumatic brain injury and high genetic risk indirectly influenced episodic memory performance through cortical thickness. The findings highlight the importance of documenting head injuries, as they may interact with genetic risk to produce negative long-term health consequences, according to the authors.
During pregnancy, Asian women with poor sleep quality or short nocturnal sleep duration exhibit abnormal glucose regulation, according to a study published online ahead of print November 14 in Sleep. In all, 686 women with a singleton pregnancy attended a clinic visit at 26 to 28 weeks of gestation, as part of the Growing Up in Singapore Towards healthy Outcomes mother-offspring cohort study. Self-reported sleep quality and sleep duration were assessed using the Pittsburgh Sleep Quality Index. Two hundred ninety-six women had poor sleep quality, and 77 women were categorized as short sleepers. One hundred thirty-one women were diagnosed with gestational diabetes mellitus. Poor sleep quality and short nocturnal sleep duration were independently associated with increased risk of gestational diabetes mellitus.
Heightened activity in the amygdala is associated with a greater risk of heart disease and stroke, according to a study published online ahead of print January 12 in Lancet. Investigators followed 293 people age 30 or older without known cardiovascular disease or active cancer disorders, who underwent PET/CT scans between January 1, 2005, and December 31, 2008. Twenty-two people had a cardiovascular disease event during mean follow-up of 3.7 years. Amygdalar activity was associated with increased bone-marrow activity, arterial inflammation, and risk of cardiovascular disease events. In a cross-sectional study of 13 patients who underwent psychometric analysis, amygdalar activity was significantly associated with arterial inflammation, and perceived stress was associated with amygdalar activity, arterial inflammation, and C-reactive protein.
Developing hypertension at an older age may protect against dementia, according to a study published online January 16 in Alzheimer's & Dementia. The study included participants from a population-based longitudinal study of people age 90 and older (The 90+ Study) who were survivors of the Leisure World Cohort Study. Researchers estimated hypertension onset age using patient-reported information. A total of 559 participants without dementia were followed every six months for up to 10 years. Two hundred twenty-four participants developed dementia during follow-up. Compared with participants without hypertension, participants whose hypertension onset age was between 80 and 89 had a lower dementia risk, and participants with an onset age of 90 and older had the lowest risk.
Living close to heavy traffic is associated with a higher incidence of dementia, but not Parkinson's disease or multiple sclerosis, according to a study published online ahead of print January 4 in Lancet. Researchers assembled two population-based cohorts that included adults who resided in Ontario, Canada. Between 2001 and 2012, researchers identified 243,611 incident cases of dementia, 31,577 cases of Parkinson's disease, and 9,247 cases of multiple sclerosis. Dementia risk decreased as people lived farther away from a main road. Overall, there was a 7% higher risk of dementia among people living within 50 meters of a main road, a 4% higher risk at 50 to 100 meters, and a 2% higher risk at 101 to 200 meters. There was no increase in risk in those living more than 200 meters away.
The US Preventive Services Task Force (USPSTF) recommends that all women who are planning to become or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg of folic acid, according to a recommendation statement published in the January 10 issue of JAMA. In 2009, the USPSTF reviewed the effectiveness of folic acid supplementation in women of childbearing age for the prevention of neural tube defects in infants. The current review assessed new evidence on the benefits and harms of folic acid supplementation. The USPSTF evaluated one randomized clinical trial, two cohort studies, eight case-control studies, and two publications from the previous USPSTF review. The task force found no new substantial evidence about the benefits and harms of folic acid supplementation. The USPSTF reaffirmed its 2009 recommendation.
Low serum 25-hydroxyvitamin D (25[OH]D] concentration is associated with markedly higher risk of frequent headache in men, according to a study published January 3 in Scientific Reports. The study consisted of 2,601 men from the population-based Kuopio Ischaemic Heart Disease Risk Factor Study in eastern Finland. Cross-sectional associations with prevalence of self-reported frequent headache were estimated with adjusted odds ratios. Participants' average serum 25(OH)D concentration was 43.4 nmol/L. A total of 250 men reported frequent (ie, weekly or daily) headache. The average serum 25(OH)D concentration among those with frequent headache was 38.3 nmol/L and 43.9 nmol/L among those without frequent headache, after adjustment for age and year and month of blood draw. After multivariable adjustments, those in the lowest versus the highest serum 25(OH)D quartile had 113% higher odds for frequent headache.
Moderate postlunch napping is associated with better cognition in Chinese older adults, according to a cross-sectional study published online ahead of print December 20, 2016, in the Journal of the American Geriatrics Society. A total of 2,974 people age 65 and older from the China Health and Retirement Longitudinal Study were included in this study. Investigators conducted interview-based cognitive assessments of orientation and attention, episodic memory, and visuospatial abilities. Patients reported their postlunch napping habits. Postlunch napping was reported in 57.7% of participants (mean duration, 63 minutes). Cognitive function was significantly associated with napping. Moderate nappers had better overall cognition than nonnappers or extended nappers. Nonnappers also had significantly poorer cognition than short nappers.
Physical exercise may be effective in the prevention of dementia, according to a study published in the January issue of the Journal of Alzheimer's Disease. Researchers assessed the interactive relationship of APOE genotype and physical exercise on dementia risk over a five-year period in 1,646 older adults from the Canadian Study of Health and Aging who were dementia-free at baseline. Physical exercise moderated the relationship between genotype and dementia. For APOE ε4 noncarriers, the odds of developing dementia were higher in nonexercisers than in exercisers (odds ratio, 1.98). For APOE ε4 carriers, the odds of developing dementia were not significantly different between nonexercisers and exercisers. "Given that most individuals are not at genetic risk, physical exercise may be an effective prevention strategy," the researchers concluded.
Lower adherence to a Mediterranean-type diet is predictive of total brain atrophy over a three-year period, according to a study published online ahead of print January 4 in Neurology. Researchers focused on total brain volume, gray matter volume, and cortical thickness. Investigators gathered information on the eating habits of 967 Scottish people at age 70. In regression models adjusting for relevant demographic and physical health indicators, lower adherence to the Mediterranean-type diet was associated with greater three-year reduction in total brain volume. Cross-sectional associations between Mediterranean-type diet and baseline MRI measures in 562 participants were not significant. Targeted analyses of meat and fish consumption did not replicate previous associations with total brain volume or total gray matter volume.
Children who sustain concussions have a 35% smaller neural response to pitch on average, according to a study published online ahead of print December 22, 2016, in Scientific Reports. Researchers studied 40 children with concussion and a control group. Children with concussion exhibited a signature neural profile. Children had worse representation of the fundamental frequency and smaller, more sluggish neural responses. As the children recovered from their head injuries, their ability to process pitch returned to normal. Neural processing of sound correctly identified 90% of concussion cases and cleared 95% of control cases, suggesting this approach has practical potential as a scalable biologic marker for sports-related concussion and other mild traumatic brain injuries.
People who are homeless sleep less and are more likely to have insomnia and daytime fatigue than people in the general population, according to a study published online ahead of print December 27, 2016, in JAMA Internal Medicine. Investigators analyzed survey responses from 3,453 people who were homeless (2,068 men; mean age, 39.8) and compared them with responses from individuals in the general population. Homeless people reported significantly shorter total sleep time than the general population (6 h 31 min vs 7 h 9 min). Eight percent reported less than four hours of total sleep time over the past 24 hours, compared with 3% of the general population. Homeless women were twice as likely as men to report that they slept less than four hours. Furthermore, insomnia was reported by 41% of homeless people, compared with 19% of controls.
—Kimberly Williams
Concussions may accelerate Alzheimer's disease-related brain atrophy and cognitive decline in people who are at genetic risk for the condition, according to a study published online ahead of print January 11 in Brain. A total of 160 Iraq and Afghanistan war veterans between the ages of 19 and 58, were included in this study. Among males with mild traumatic brain injury, high genetic risk for Alzheimer's disease was associated with cortical thinning as a function of time since injury. A moderated mediation analysis showed that mild traumatic brain injury and high genetic risk indirectly influenced episodic memory performance through cortical thickness. The findings highlight the importance of documenting head injuries, as they may interact with genetic risk to produce negative long-term health consequences, according to the authors.
During pregnancy, Asian women with poor sleep quality or short nocturnal sleep duration exhibit abnormal glucose regulation, according to a study published online ahead of print November 14 in Sleep. In all, 686 women with a singleton pregnancy attended a clinic visit at 26 to 28 weeks of gestation, as part of the Growing Up in Singapore Towards healthy Outcomes mother-offspring cohort study. Self-reported sleep quality and sleep duration were assessed using the Pittsburgh Sleep Quality Index. Two hundred ninety-six women had poor sleep quality, and 77 women were categorized as short sleepers. One hundred thirty-one women were diagnosed with gestational diabetes mellitus. Poor sleep quality and short nocturnal sleep duration were independently associated with increased risk of gestational diabetes mellitus.
Heightened activity in the amygdala is associated with a greater risk of heart disease and stroke, according to a study published online ahead of print January 12 in Lancet. Investigators followed 293 people age 30 or older without known cardiovascular disease or active cancer disorders, who underwent PET/CT scans between January 1, 2005, and December 31, 2008. Twenty-two people had a cardiovascular disease event during mean follow-up of 3.7 years. Amygdalar activity was associated with increased bone-marrow activity, arterial inflammation, and risk of cardiovascular disease events. In a cross-sectional study of 13 patients who underwent psychometric analysis, amygdalar activity was significantly associated with arterial inflammation, and perceived stress was associated with amygdalar activity, arterial inflammation, and C-reactive protein.
Developing hypertension at an older age may protect against dementia, according to a study published online January 16 in Alzheimer's & Dementia. The study included participants from a population-based longitudinal study of people age 90 and older (The 90+ Study) who were survivors of the Leisure World Cohort Study. Researchers estimated hypertension onset age using patient-reported information. A total of 559 participants without dementia were followed every six months for up to 10 years. Two hundred twenty-four participants developed dementia during follow-up. Compared with participants without hypertension, participants whose hypertension onset age was between 80 and 89 had a lower dementia risk, and participants with an onset age of 90 and older had the lowest risk.
Living close to heavy traffic is associated with a higher incidence of dementia, but not Parkinson's disease or multiple sclerosis, according to a study published online ahead of print January 4 in Lancet. Researchers assembled two population-based cohorts that included adults who resided in Ontario, Canada. Between 2001 and 2012, researchers identified 243,611 incident cases of dementia, 31,577 cases of Parkinson's disease, and 9,247 cases of multiple sclerosis. Dementia risk decreased as people lived farther away from a main road. Overall, there was a 7% higher risk of dementia among people living within 50 meters of a main road, a 4% higher risk at 50 to 100 meters, and a 2% higher risk at 101 to 200 meters. There was no increase in risk in those living more than 200 meters away.
The US Preventive Services Task Force (USPSTF) recommends that all women who are planning to become or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg of folic acid, according to a recommendation statement published in the January 10 issue of JAMA. In 2009, the USPSTF reviewed the effectiveness of folic acid supplementation in women of childbearing age for the prevention of neural tube defects in infants. The current review assessed new evidence on the benefits and harms of folic acid supplementation. The USPSTF evaluated one randomized clinical trial, two cohort studies, eight case-control studies, and two publications from the previous USPSTF review. The task force found no new substantial evidence about the benefits and harms of folic acid supplementation. The USPSTF reaffirmed its 2009 recommendation.
Low serum 25-hydroxyvitamin D (25[OH]D] concentration is associated with markedly higher risk of frequent headache in men, according to a study published January 3 in Scientific Reports. The study consisted of 2,601 men from the population-based Kuopio Ischaemic Heart Disease Risk Factor Study in eastern Finland. Cross-sectional associations with prevalence of self-reported frequent headache were estimated with adjusted odds ratios. Participants' average serum 25(OH)D concentration was 43.4 nmol/L. A total of 250 men reported frequent (ie, weekly or daily) headache. The average serum 25(OH)D concentration among those with frequent headache was 38.3 nmol/L and 43.9 nmol/L among those without frequent headache, after adjustment for age and year and month of blood draw. After multivariable adjustments, those in the lowest versus the highest serum 25(OH)D quartile had 113% higher odds for frequent headache.
Moderate postlunch napping is associated with better cognition in Chinese older adults, according to a cross-sectional study published online ahead of print December 20, 2016, in the Journal of the American Geriatrics Society. A total of 2,974 people age 65 and older from the China Health and Retirement Longitudinal Study were included in this study. Investigators conducted interview-based cognitive assessments of orientation and attention, episodic memory, and visuospatial abilities. Patients reported their postlunch napping habits. Postlunch napping was reported in 57.7% of participants (mean duration, 63 minutes). Cognitive function was significantly associated with napping. Moderate nappers had better overall cognition than nonnappers or extended nappers. Nonnappers also had significantly poorer cognition than short nappers.
Physical exercise may be effective in the prevention of dementia, according to a study published in the January issue of the Journal of Alzheimer's Disease. Researchers assessed the interactive relationship of APOE genotype and physical exercise on dementia risk over a five-year period in 1,646 older adults from the Canadian Study of Health and Aging who were dementia-free at baseline. Physical exercise moderated the relationship between genotype and dementia. For APOE ε4 noncarriers, the odds of developing dementia were higher in nonexercisers than in exercisers (odds ratio, 1.98). For APOE ε4 carriers, the odds of developing dementia were not significantly different between nonexercisers and exercisers. "Given that most individuals are not at genetic risk, physical exercise may be an effective prevention strategy," the researchers concluded.
Lower adherence to a Mediterranean-type diet is predictive of total brain atrophy over a three-year period, according to a study published online ahead of print January 4 in Neurology. Researchers focused on total brain volume, gray matter volume, and cortical thickness. Investigators gathered information on the eating habits of 967 Scottish people at age 70. In regression models adjusting for relevant demographic and physical health indicators, lower adherence to the Mediterranean-type diet was associated with greater three-year reduction in total brain volume. Cross-sectional associations between Mediterranean-type diet and baseline MRI measures in 562 participants were not significant. Targeted analyses of meat and fish consumption did not replicate previous associations with total brain volume or total gray matter volume.
Children who sustain concussions have a 35% smaller neural response to pitch on average, according to a study published online ahead of print December 22, 2016, in Scientific Reports. Researchers studied 40 children with concussion and a control group. Children with concussion exhibited a signature neural profile. Children had worse representation of the fundamental frequency and smaller, more sluggish neural responses. As the children recovered from their head injuries, their ability to process pitch returned to normal. Neural processing of sound correctly identified 90% of concussion cases and cleared 95% of control cases, suggesting this approach has practical potential as a scalable biologic marker for sports-related concussion and other mild traumatic brain injuries.
People who are homeless sleep less and are more likely to have insomnia and daytime fatigue than people in the general population, according to a study published online ahead of print December 27, 2016, in JAMA Internal Medicine. Investigators analyzed survey responses from 3,453 people who were homeless (2,068 men; mean age, 39.8) and compared them with responses from individuals in the general population. Homeless people reported significantly shorter total sleep time than the general population (6 h 31 min vs 7 h 9 min). Eight percent reported less than four hours of total sleep time over the past 24 hours, compared with 3% of the general population. Homeless women were twice as likely as men to report that they slept less than four hours. Furthermore, insomnia was reported by 41% of homeless people, compared with 19% of controls.
—Kimberly Williams
Concussions may accelerate Alzheimer's disease-related brain atrophy and cognitive decline in people who are at genetic risk for the condition, according to a study published online ahead of print January 11 in Brain. A total of 160 Iraq and Afghanistan war veterans between the ages of 19 and 58, were included in this study. Among males with mild traumatic brain injury, high genetic risk for Alzheimer's disease was associated with cortical thinning as a function of time since injury. A moderated mediation analysis showed that mild traumatic brain injury and high genetic risk indirectly influenced episodic memory performance through cortical thickness. The findings highlight the importance of documenting head injuries, as they may interact with genetic risk to produce negative long-term health consequences, according to the authors.
During pregnancy, Asian women with poor sleep quality or short nocturnal sleep duration exhibit abnormal glucose regulation, according to a study published online ahead of print November 14 in Sleep. In all, 686 women with a singleton pregnancy attended a clinic visit at 26 to 28 weeks of gestation, as part of the Growing Up in Singapore Towards healthy Outcomes mother-offspring cohort study. Self-reported sleep quality and sleep duration were assessed using the Pittsburgh Sleep Quality Index. Two hundred ninety-six women had poor sleep quality, and 77 women were categorized as short sleepers. One hundred thirty-one women were diagnosed with gestational diabetes mellitus. Poor sleep quality and short nocturnal sleep duration were independently associated with increased risk of gestational diabetes mellitus.
Heightened activity in the amygdala is associated with a greater risk of heart disease and stroke, according to a study published online ahead of print January 12 in Lancet. Investigators followed 293 people age 30 or older without known cardiovascular disease or active cancer disorders, who underwent PET/CT scans between January 1, 2005, and December 31, 2008. Twenty-two people had a cardiovascular disease event during mean follow-up of 3.7 years. Amygdalar activity was associated with increased bone-marrow activity, arterial inflammation, and risk of cardiovascular disease events. In a cross-sectional study of 13 patients who underwent psychometric analysis, amygdalar activity was significantly associated with arterial inflammation, and perceived stress was associated with amygdalar activity, arterial inflammation, and C-reactive protein.
Developing hypertension at an older age may protect against dementia, according to a study published online January 16 in Alzheimer's & Dementia. The study included participants from a population-based longitudinal study of people age 90 and older (The 90+ Study) who were survivors of the Leisure World Cohort Study. Researchers estimated hypertension onset age using patient-reported information. A total of 559 participants without dementia were followed every six months for up to 10 years. Two hundred twenty-four participants developed dementia during follow-up. Compared with participants without hypertension, participants whose hypertension onset age was between 80 and 89 had a lower dementia risk, and participants with an onset age of 90 and older had the lowest risk.
Living close to heavy traffic is associated with a higher incidence of dementia, but not Parkinson's disease or multiple sclerosis, according to a study published online ahead of print January 4 in Lancet. Researchers assembled two population-based cohorts that included adults who resided in Ontario, Canada. Between 2001 and 2012, researchers identified 243,611 incident cases of dementia, 31,577 cases of Parkinson's disease, and 9,247 cases of multiple sclerosis. Dementia risk decreased as people lived farther away from a main road. Overall, there was a 7% higher risk of dementia among people living within 50 meters of a main road, a 4% higher risk at 50 to 100 meters, and a 2% higher risk at 101 to 200 meters. There was no increase in risk in those living more than 200 meters away.
The US Preventive Services Task Force (USPSTF) recommends that all women who are planning to become or capable of becoming pregnant take a daily supplement containing 0.4 mg to 0.8 mg of folic acid, according to a recommendation statement published in the January 10 issue of JAMA. In 2009, the USPSTF reviewed the effectiveness of folic acid supplementation in women of childbearing age for the prevention of neural tube defects in infants. The current review assessed new evidence on the benefits and harms of folic acid supplementation. The USPSTF evaluated one randomized clinical trial, two cohort studies, eight case-control studies, and two publications from the previous USPSTF review. The task force found no new substantial evidence about the benefits and harms of folic acid supplementation. The USPSTF reaffirmed its 2009 recommendation.
Low serum 25-hydroxyvitamin D (25[OH]D] concentration is associated with markedly higher risk of frequent headache in men, according to a study published January 3 in Scientific Reports. The study consisted of 2,601 men from the population-based Kuopio Ischaemic Heart Disease Risk Factor Study in eastern Finland. Cross-sectional associations with prevalence of self-reported frequent headache were estimated with adjusted odds ratios. Participants' average serum 25(OH)D concentration was 43.4 nmol/L. A total of 250 men reported frequent (ie, weekly or daily) headache. The average serum 25(OH)D concentration among those with frequent headache was 38.3 nmol/L and 43.9 nmol/L among those without frequent headache, after adjustment for age and year and month of blood draw. After multivariable adjustments, those in the lowest versus the highest serum 25(OH)D quartile had 113% higher odds for frequent headache.
Moderate postlunch napping is associated with better cognition in Chinese older adults, according to a cross-sectional study published online ahead of print December 20, 2016, in the Journal of the American Geriatrics Society. A total of 2,974 people age 65 and older from the China Health and Retirement Longitudinal Study were included in this study. Investigators conducted interview-based cognitive assessments of orientation and attention, episodic memory, and visuospatial abilities. Patients reported their postlunch napping habits. Postlunch napping was reported in 57.7% of participants (mean duration, 63 minutes). Cognitive function was significantly associated with napping. Moderate nappers had better overall cognition than nonnappers or extended nappers. Nonnappers also had significantly poorer cognition than short nappers.
Physical exercise may be effective in the prevention of dementia, according to a study published in the January issue of the Journal of Alzheimer's Disease. Researchers assessed the interactive relationship of APOE genotype and physical exercise on dementia risk over a five-year period in 1,646 older adults from the Canadian Study of Health and Aging who were dementia-free at baseline. Physical exercise moderated the relationship between genotype and dementia. For APOE ε4 noncarriers, the odds of developing dementia were higher in nonexercisers than in exercisers (odds ratio, 1.98). For APOE ε4 carriers, the odds of developing dementia were not significantly different between nonexercisers and exercisers. "Given that most individuals are not at genetic risk, physical exercise may be an effective prevention strategy," the researchers concluded.
Lower adherence to a Mediterranean-type diet is predictive of total brain atrophy over a three-year period, according to a study published online ahead of print January 4 in Neurology. Researchers focused on total brain volume, gray matter volume, and cortical thickness. Investigators gathered information on the eating habits of 967 Scottish people at age 70. In regression models adjusting for relevant demographic and physical health indicators, lower adherence to the Mediterranean-type diet was associated with greater three-year reduction in total brain volume. Cross-sectional associations between Mediterranean-type diet and baseline MRI measures in 562 participants were not significant. Targeted analyses of meat and fish consumption did not replicate previous associations with total brain volume or total gray matter volume.
Children who sustain concussions have a 35% smaller neural response to pitch on average, according to a study published online ahead of print December 22, 2016, in Scientific Reports. Researchers studied 40 children with concussion and a control group. Children with concussion exhibited a signature neural profile. Children had worse representation of the fundamental frequency and smaller, more sluggish neural responses. As the children recovered from their head injuries, their ability to process pitch returned to normal. Neural processing of sound correctly identified 90% of concussion cases and cleared 95% of control cases, suggesting this approach has practical potential as a scalable biologic marker for sports-related concussion and other mild traumatic brain injuries.
People who are homeless sleep less and are more likely to have insomnia and daytime fatigue than people in the general population, according to a study published online ahead of print December 27, 2016, in JAMA Internal Medicine. Investigators analyzed survey responses from 3,453 people who were homeless (2,068 men; mean age, 39.8) and compared them with responses from individuals in the general population. Homeless people reported significantly shorter total sleep time than the general population (6 h 31 min vs 7 h 9 min). Eight percent reported less than four hours of total sleep time over the past 24 hours, compared with 3% of the general population. Homeless women were twice as likely as men to report that they slept less than four hours. Furthermore, insomnia was reported by 41% of homeless people, compared with 19% of controls.
—Kimberly Williams

Torsades de Pointes in Severe Alcohol Withdrawal and Cirrhosis: Implications for Risk Stratification and Management
Torsades de pointes (TdP) is a life-threatening ventricular arrhythmia that is associated with both congenital and acquired QT interval prolongation. QT interval prolongation is commonly observed in acute alcohol withdrawal and cirrhotic cardiomyopathy.1-3 In both conditions, there is a positive correlation between the degree of QT interval prolongation and disease severity.4,5 The precise mechanisms of QT interval prolongation in these conditions are not well understood. One hypothesis is that autonomic hyperexcitability results in altered ventricular repolarization and QT interval prolongation. This mechanism of QT prolongation has been found in acute alcohol withdrawal independent of electrolyte abnormalities, use of QT-prolonging medications, and cirrhosis.1,2,6
The authors report the case of a veteran who was hospitalized for acute alcohol withdrawal and decompensated cirrhosis and was found to have a newly prolonged QT interval. On hospital day 3, the patient developed TdP, which required external defibrillation. Despite correction of electrolyte abnormalities, abstinence from alcohol, avoidance of QT-prolonging medications, and exclusion of cardiac ischemia, there was significant and persistent prolongation of the QT interval—ultimately attributed to cirrhotic cardiomyopathy. Acquired QT interval prolongation is common in both acute alcohol withdrawal and cirrhosis.This case highlights the importance of close monitoring of the QT interval and TdP susceptibility in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis.
Case Report
A 66-year-old male veteran with a 35-year history of alcohol dependence presented for alcohol detoxification. He reported having drunk at least 32 ounces of vodka every day of the preceding 5 years and reported having unsuccessfully attempted self-detoxification several times. Prior detoxification efforts were unsuccessful because of intractable nausea and tremulousness. Additional presenting symptoms included lethargy, anorexia, and a fall with transient right-side hemiparesis (findings on magnetic resonance imaging of the head had been normal).
His medical history included type 2 diabetes, tobacco dependence, and macular degeneration. The only medication being taken was glargine 25 units daily. On admission, the patient was afebrile (98.1°F), normotensive (103/77 mm Hg), and oriented to person, place, and time. Examination also revealed a protuberant abdomen with caput medusae, and no shifting dullness or lower extremity edema. The neurologic examination was nonfocal.
Laboratory test results on admission were significant for elevated serum alcohol level (243.8 mg/dL); elevated levels of aspartate aminotransferase (144 units/L) alanine aminotransferase (25 units/L), and total bilirubin (4.2 mg/L); hypoalbuminemia; normocalemia; hypomagnesemia; normal corrected calcium level; and normal renal function (0.84 mg/dL)(Table). The patient’s admission Child-Pugh score of 10 indicated class C liver disease. Admission electrocardiogram (EKG) revealed normal sinus rhythm, first-degree atrioventricular block, and prolongation of the QTc interval (519 ms). Six years earlier, the patient’s QTc interval had been 409 ms (Figures 1 and 2). As QT interval depends on heart rate, it is most commonly expressed as corrected QT, or QTc, where QTc = QT/(√RR). 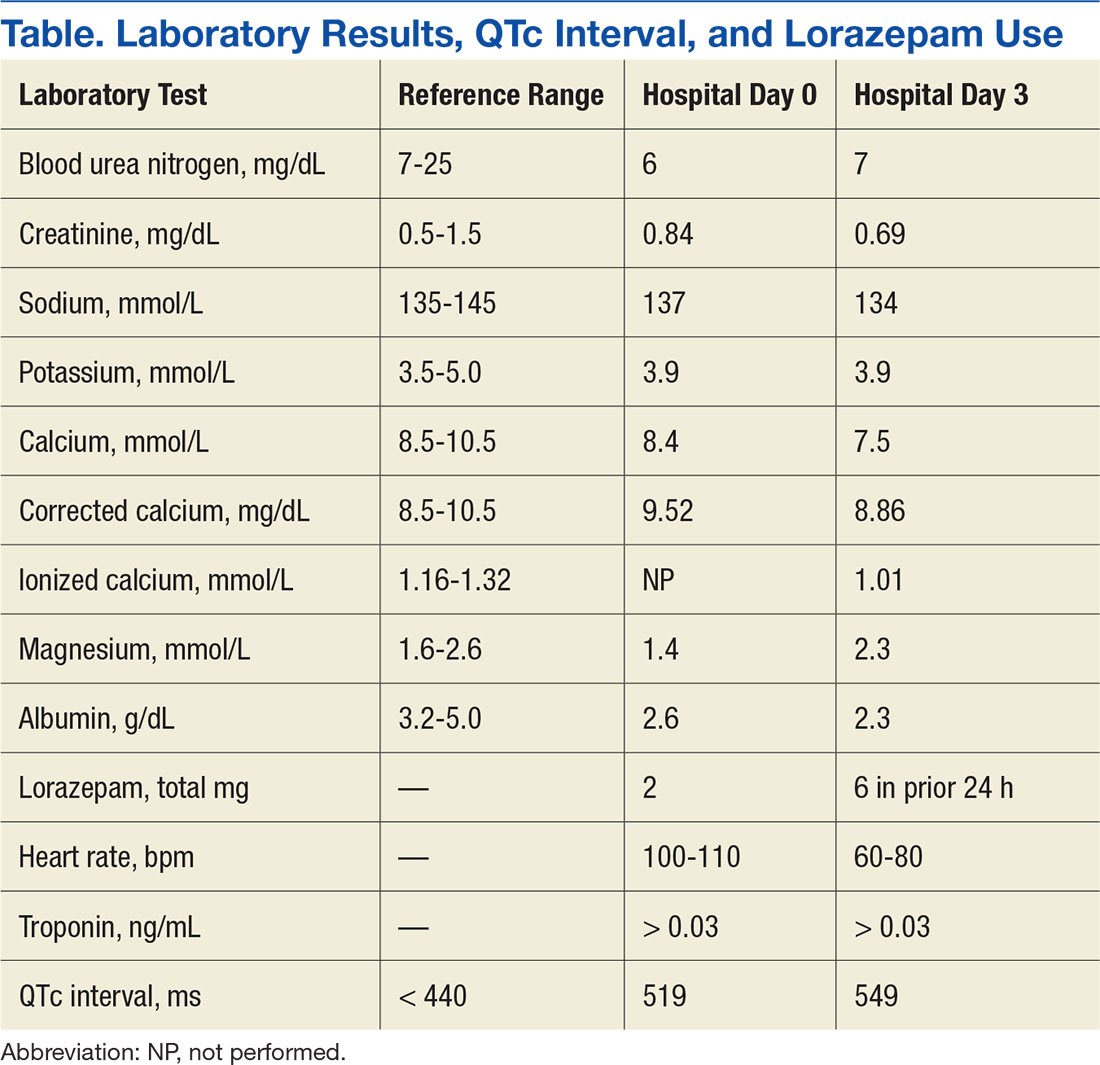
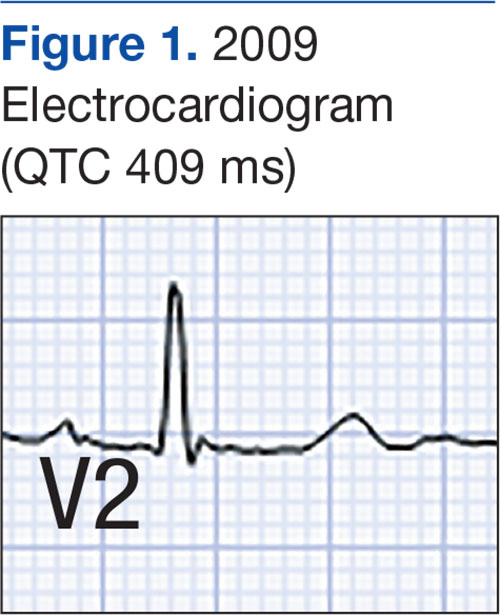
Symptom-triggered therapy for alcohol withdrawal was instituted, and the patient’s electrolyte abnormalities were corrected. Telemetry monitoring demonstrated polymorphic ventricular ectopy, including a 6.8-s run of polymorphic ventricular tachycardia and several shorter runs (4-10 beats) of nonsustained ventricular tachycardia, prompting initiation of a low-dose beta blocker. Based on elevated scores on the symptom-triggered scale for alcohol withdrawal, the Clinical Institute Withdrawal Assessement for Alcohol Withdrawal (CIWA), several doses of oral lorazepam were given for withdrawal symptoms.
The patient became increasingly confused, and new-onset nystagmus was noted. These findings raised concern for Wernicke encephalopathy, so the patient was empirically started on IV high-dose thiamine supplementation. The CIWA scores remained high, and there were frequent episodes of ventricular ectopy during the first 2 hospital days. Interval EKG revealed further prolongation of the QTc interval (549 ms) without evidence of cardiac ischemia (Figure 3). Cardiac enzymes were negative, and electrolyte levels were within normal limits.
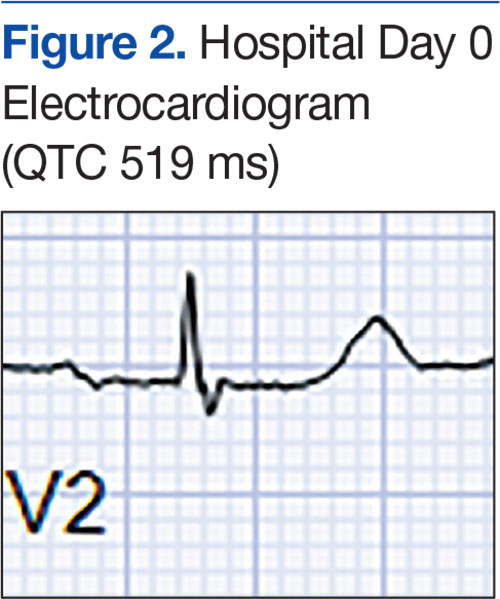
The month-long hospitalization was notable for development of significant ascites, continual electrolyte repletion in the setting of diuresis, formal diagnosis of alcoholic cirrhoisis, cognitive and physical rehabilitation. During the hospitalization, QTc interval remained prolonged (range, 460-500 ms), despite electrolyte repletion, and he was discharged with a wearable cardioverter defibrillator. A month
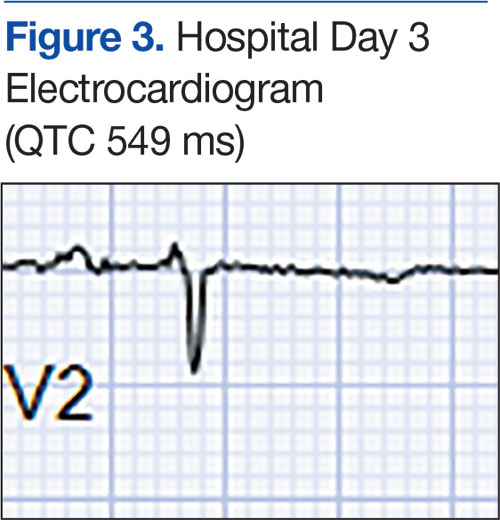
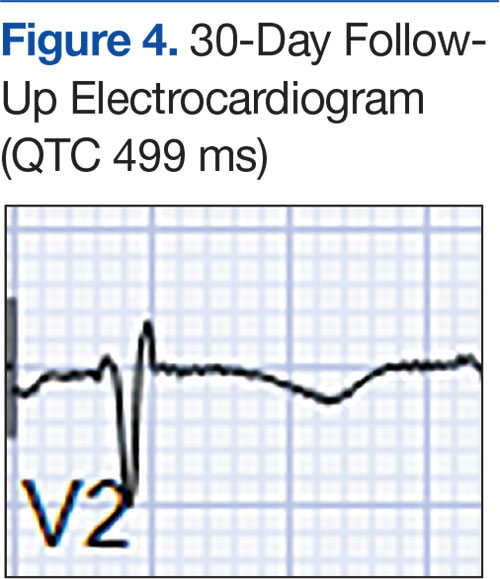
Discussion
Alcohol dependence is a common chronic and relapsing disease that often requires controlled detoxification. Investigators have found a high incidence of QT interval prolongation in alcohol withdrawal and hepatic disease.3,6 Common causes of QT interval prolongation in this setting are poor nutrition, electrolyte abnormalities (particularly hypocalcemia and hypomagnesemia), and use of certain medications.1-3,7,8 In addition, alcohol is directly toxic to the renal tubules, resulting in renal wasting of divalent cations, which may persist up to 30 days after the most recent alcohol exposure.9,10
The patient in this case report was initially thought to have hypomagnesemia-induced long QT syndrome (leading to TdP cardiac arrest), but the authors’ review of laboratory test results revealed the QT interval remained markedly prolonged, despite adequate correction of hypomagnesemia implicating the hyperadrenergic state of acute alcohol withdrawal in QT interval prolongation and TdP cardiac arrest. Interestingly, the QT interval remained prolonged 2 months after TdP arrest, despite sustained normalization of electrolyte levels and the absence of active ischemia or use of QT-prolonging medications.
Given the exclusion of other causes of QT interval prolongation, the authors hypothesized that autonomic hyperactivity of acute alcohol withdrawal and resultant QT interval prolongation were potentiated by underlying cirrhotic cardiomyopathy, a well described cause of QT interval prolongation. Cirrhotic cardiomyopathy is thought to cause QT interval prolongation by delayed repolarization of cardiomyocytes and promotion of sympatho-adrenergic hyperactivity.6 In other case series, TdP development has been associated with severe withdrawal symptoms, particularly delirium tremens.2 In cirrhosis, QT interval prolongation often is described as an early manifestation of cirrhotic cardiomyopathy, irrespective of the underlying etiology, and precedes systolic and diastolic dysfunction.6
The magnitude of QT prolongation has been associated with severity of liver disease as expressed by Child-Pugh score, with reports of QT normalization after liver transplantation.4,5 Patients with higher Child-Pugh scores should be considered to be at elevated risk for malignant ventricular arrhythmias. The authors recommend checking an EKG on admission of any patient who has liver disease or has presented for alcohol withdrawal. Patients with a prolonged QTc interval should be monitored on telemetry. The authors also recommend aggressive repletion of electrolytes, particularly potassium and magnesium, in patients who present with cirrhosis and alcohol withdrawal.
Avoidance of QT-prolonging medications is advisable for all patients with a long QT interval. Beta blockers shorten the QT interval in cirrhotic patients, but the role of beta blockers in preventing malignant arrhythmias in this group of patients is not yet clear.11 The present patient’s QT interval had been normal before he developed cirrhotic liver disease. His presentation was suggestive of acquired long QT syndrome, likely caused by cirrhotic cardiomyopathy given the exhaustive exclusion of other causes of QT interval prolongation.
Conclusion
This case highlights the importance of close monitoring of the QT interval in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis, and suggests that timely and aggressive management of withdrawal, repletion of electrolytes, and telemetry monitoring may prevent life-threatening arrhythmia.
1. Otero-Antón E, González-Quintela A, Saborido J, Torre JA, Virgós A, Barrio E. Prolongation of the QTc interval during alcohol withdrawal syndrome. Acta Cardiol. 1997;52(3):285-294.
2. Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227.
3. Mimidis K, Thomopoulos K, Tziakas D, et al. Prolongation of the QTc interval in patients with cirrhosis. Ann Gastroenterol. 2003;16(2):155-158.
4. Bernardi M, Calandra S, Colantoni A, et al. Q-T interval prolongation in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic factors. Hepatology. 1998;27(1):28-34.
5. Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease, mortality and liver transplantation. Liver Int. 2003;23(4):243-248.
6. Zardi EM, Abbate A, Zardi DM, et al. Cirrhotic cardiomyopathy. J Am Coll Cardiol. 2010;56(7):539-549.
7. Faigel DO, Metz DC, Kochman ML. Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalance. Am J Gastroenterol. 1995;90(5):822-824.
8. Kotsia AP, Dimitriadis G, Baltogiannis GG, Kolettis TM. Torsade de pointes and persistent QTc prolongation after intravenous amiodarone. Case Rep Med. 2012;2012:673019.
9. Denison H, Jern S, Jagenburg R, Wendestam C, Wallerstedt S. Influence of increased adrenergic activity and magnesium depletion on cardiac rhythm in alcohol withdrawal. Br Heart J. 1994;72(6):554-560.
10. Plaza de los Reyes M, Orozco R, Rosemblitt M, Rendic Y, Espinace M. Renal secretion of magnesium and other electrolytes under the influence of acute ingestion of alcohol, in normal subjects [in Spanish]. Rev Med Chil. 1968;96(3):138-141.
11. Bernardi M, Maggioli C, Dibra V, Zaccherini G. QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev Gastroenterol Hepatol. 2012;6(1):57-66.
Torsades de pointes (TdP) is a life-threatening ventricular arrhythmia that is associated with both congenital and acquired QT interval prolongation. QT interval prolongation is commonly observed in acute alcohol withdrawal and cirrhotic cardiomyopathy.1-3 In both conditions, there is a positive correlation between the degree of QT interval prolongation and disease severity.4,5 The precise mechanisms of QT interval prolongation in these conditions are not well understood. One hypothesis is that autonomic hyperexcitability results in altered ventricular repolarization and QT interval prolongation. This mechanism of QT prolongation has been found in acute alcohol withdrawal independent of electrolyte abnormalities, use of QT-prolonging medications, and cirrhosis.1,2,6
The authors report the case of a veteran who was hospitalized for acute alcohol withdrawal and decompensated cirrhosis and was found to have a newly prolonged QT interval. On hospital day 3, the patient developed TdP, which required external defibrillation. Despite correction of electrolyte abnormalities, abstinence from alcohol, avoidance of QT-prolonging medications, and exclusion of cardiac ischemia, there was significant and persistent prolongation of the QT interval—ultimately attributed to cirrhotic cardiomyopathy. Acquired QT interval prolongation is common in both acute alcohol withdrawal and cirrhosis.This case highlights the importance of close monitoring of the QT interval and TdP susceptibility in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis.
Case Report
A 66-year-old male veteran with a 35-year history of alcohol dependence presented for alcohol detoxification. He reported having drunk at least 32 ounces of vodka every day of the preceding 5 years and reported having unsuccessfully attempted self-detoxification several times. Prior detoxification efforts were unsuccessful because of intractable nausea and tremulousness. Additional presenting symptoms included lethargy, anorexia, and a fall with transient right-side hemiparesis (findings on magnetic resonance imaging of the head had been normal).
His medical history included type 2 diabetes, tobacco dependence, and macular degeneration. The only medication being taken was glargine 25 units daily. On admission, the patient was afebrile (98.1°F), normotensive (103/77 mm Hg), and oriented to person, place, and time. Examination also revealed a protuberant abdomen with caput medusae, and no shifting dullness or lower extremity edema. The neurologic examination was nonfocal.
Laboratory test results on admission were significant for elevated serum alcohol level (243.8 mg/dL); elevated levels of aspartate aminotransferase (144 units/L) alanine aminotransferase (25 units/L), and total bilirubin (4.2 mg/L); hypoalbuminemia; normocalemia; hypomagnesemia; normal corrected calcium level; and normal renal function (0.84 mg/dL)(Table). The patient’s admission Child-Pugh score of 10 indicated class C liver disease. Admission electrocardiogram (EKG) revealed normal sinus rhythm, first-degree atrioventricular block, and prolongation of the QTc interval (519 ms). Six years earlier, the patient’s QTc interval had been 409 ms (Figures 1 and 2). As QT interval depends on heart rate, it is most commonly expressed as corrected QT, or QTc, where QTc = QT/(√RR).
Symptom-triggered therapy for alcohol withdrawal was instituted, and the patient’s electrolyte abnormalities were corrected. Telemetry monitoring demonstrated polymorphic ventricular ectopy, including a 6.8-s run of polymorphic ventricular tachycardia and several shorter runs (4-10 beats) of nonsustained ventricular tachycardia, prompting initiation of a low-dose beta blocker. Based on elevated scores on the symptom-triggered scale for alcohol withdrawal, the Clinical Institute Withdrawal Assessement for Alcohol Withdrawal (CIWA), several doses of oral lorazepam were given for withdrawal symptoms.
The patient became increasingly confused, and new-onset nystagmus was noted. These findings raised concern for Wernicke encephalopathy, so the patient was empirically started on IV high-dose thiamine supplementation. The CIWA scores remained high, and there were frequent episodes of ventricular ectopy during the first 2 hospital days. Interval EKG revealed further prolongation of the QTc interval (549 ms) without evidence of cardiac ischemia (Figure 3). Cardiac enzymes were negative, and electrolyte levels were within normal limits.
The month-long hospitalization was notable for development of significant ascites, continual electrolyte repletion in the setting of diuresis, formal diagnosis of alcoholic cirrhoisis, cognitive and physical rehabilitation. During the hospitalization, QTc interval remained prolonged (range, 460-500 ms), despite electrolyte repletion, and he was discharged with a wearable cardioverter defibrillator. A month
Discussion
Alcohol dependence is a common chronic and relapsing disease that often requires controlled detoxification. Investigators have found a high incidence of QT interval prolongation in alcohol withdrawal and hepatic disease.3,6 Common causes of QT interval prolongation in this setting are poor nutrition, electrolyte abnormalities (particularly hypocalcemia and hypomagnesemia), and use of certain medications.1-3,7,8 In addition, alcohol is directly toxic to the renal tubules, resulting in renal wasting of divalent cations, which may persist up to 30 days after the most recent alcohol exposure.9,10
The patient in this case report was initially thought to have hypomagnesemia-induced long QT syndrome (leading to TdP cardiac arrest), but the authors’ review of laboratory test results revealed the QT interval remained markedly prolonged, despite adequate correction of hypomagnesemia implicating the hyperadrenergic state of acute alcohol withdrawal in QT interval prolongation and TdP cardiac arrest. Interestingly, the QT interval remained prolonged 2 months after TdP arrest, despite sustained normalization of electrolyte levels and the absence of active ischemia or use of QT-prolonging medications.
Given the exclusion of other causes of QT interval prolongation, the authors hypothesized that autonomic hyperactivity of acute alcohol withdrawal and resultant QT interval prolongation were potentiated by underlying cirrhotic cardiomyopathy, a well described cause of QT interval prolongation. Cirrhotic cardiomyopathy is thought to cause QT interval prolongation by delayed repolarization of cardiomyocytes and promotion of sympatho-adrenergic hyperactivity.6 In other case series, TdP development has been associated with severe withdrawal symptoms, particularly delirium tremens.2 In cirrhosis, QT interval prolongation often is described as an early manifestation of cirrhotic cardiomyopathy, irrespective of the underlying etiology, and precedes systolic and diastolic dysfunction.6
The magnitude of QT prolongation has been associated with severity of liver disease as expressed by Child-Pugh score, with reports of QT normalization after liver transplantation.4,5 Patients with higher Child-Pugh scores should be considered to be at elevated risk for malignant ventricular arrhythmias. The authors recommend checking an EKG on admission of any patient who has liver disease or has presented for alcohol withdrawal. Patients with a prolonged QTc interval should be monitored on telemetry. The authors also recommend aggressive repletion of electrolytes, particularly potassium and magnesium, in patients who present with cirrhosis and alcohol withdrawal.
Avoidance of QT-prolonging medications is advisable for all patients with a long QT interval. Beta blockers shorten the QT interval in cirrhotic patients, but the role of beta blockers in preventing malignant arrhythmias in this group of patients is not yet clear.11 The present patient’s QT interval had been normal before he developed cirrhotic liver disease. His presentation was suggestive of acquired long QT syndrome, likely caused by cirrhotic cardiomyopathy given the exhaustive exclusion of other causes of QT interval prolongation.
Conclusion
This case highlights the importance of close monitoring of the QT interval in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis, and suggests that timely and aggressive management of withdrawal, repletion of electrolytes, and telemetry monitoring may prevent life-threatening arrhythmia.
Torsades de pointes (TdP) is a life-threatening ventricular arrhythmia that is associated with both congenital and acquired QT interval prolongation. QT interval prolongation is commonly observed in acute alcohol withdrawal and cirrhotic cardiomyopathy.1-3 In both conditions, there is a positive correlation between the degree of QT interval prolongation and disease severity.4,5 The precise mechanisms of QT interval prolongation in these conditions are not well understood. One hypothesis is that autonomic hyperexcitability results in altered ventricular repolarization and QT interval prolongation. This mechanism of QT prolongation has been found in acute alcohol withdrawal independent of electrolyte abnormalities, use of QT-prolonging medications, and cirrhosis.1,2,6
The authors report the case of a veteran who was hospitalized for acute alcohol withdrawal and decompensated cirrhosis and was found to have a newly prolonged QT interval. On hospital day 3, the patient developed TdP, which required external defibrillation. Despite correction of electrolyte abnormalities, abstinence from alcohol, avoidance of QT-prolonging medications, and exclusion of cardiac ischemia, there was significant and persistent prolongation of the QT interval—ultimately attributed to cirrhotic cardiomyopathy. Acquired QT interval prolongation is common in both acute alcohol withdrawal and cirrhosis.This case highlights the importance of close monitoring of the QT interval and TdP susceptibility in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis.
Case Report
A 66-year-old male veteran with a 35-year history of alcohol dependence presented for alcohol detoxification. He reported having drunk at least 32 ounces of vodka every day of the preceding 5 years and reported having unsuccessfully attempted self-detoxification several times. Prior detoxification efforts were unsuccessful because of intractable nausea and tremulousness. Additional presenting symptoms included lethargy, anorexia, and a fall with transient right-side hemiparesis (findings on magnetic resonance imaging of the head had been normal).
His medical history included type 2 diabetes, tobacco dependence, and macular degeneration. The only medication being taken was glargine 25 units daily. On admission, the patient was afebrile (98.1°F), normotensive (103/77 mm Hg), and oriented to person, place, and time. Examination also revealed a protuberant abdomen with caput medusae, and no shifting dullness or lower extremity edema. The neurologic examination was nonfocal.
Laboratory test results on admission were significant for elevated serum alcohol level (243.8 mg/dL); elevated levels of aspartate aminotransferase (144 units/L) alanine aminotransferase (25 units/L), and total bilirubin (4.2 mg/L); hypoalbuminemia; normocalemia; hypomagnesemia; normal corrected calcium level; and normal renal function (0.84 mg/dL)(Table). The patient’s admission Child-Pugh score of 10 indicated class C liver disease. Admission electrocardiogram (EKG) revealed normal sinus rhythm, first-degree atrioventricular block, and prolongation of the QTc interval (519 ms). Six years earlier, the patient’s QTc interval had been 409 ms (Figures 1 and 2). As QT interval depends on heart rate, it is most commonly expressed as corrected QT, or QTc, where QTc = QT/(√RR).
Symptom-triggered therapy for alcohol withdrawal was instituted, and the patient’s electrolyte abnormalities were corrected. Telemetry monitoring demonstrated polymorphic ventricular ectopy, including a 6.8-s run of polymorphic ventricular tachycardia and several shorter runs (4-10 beats) of nonsustained ventricular tachycardia, prompting initiation of a low-dose beta blocker. Based on elevated scores on the symptom-triggered scale for alcohol withdrawal, the Clinical Institute Withdrawal Assessement for Alcohol Withdrawal (CIWA), several doses of oral lorazepam were given for withdrawal symptoms.
The patient became increasingly confused, and new-onset nystagmus was noted. These findings raised concern for Wernicke encephalopathy, so the patient was empirically started on IV high-dose thiamine supplementation. The CIWA scores remained high, and there were frequent episodes of ventricular ectopy during the first 2 hospital days. Interval EKG revealed further prolongation of the QTc interval (549 ms) without evidence of cardiac ischemia (Figure 3). Cardiac enzymes were negative, and electrolyte levels were within normal limits.
The month-long hospitalization was notable for development of significant ascites, continual electrolyte repletion in the setting of diuresis, formal diagnosis of alcoholic cirrhoisis, cognitive and physical rehabilitation. During the hospitalization, QTc interval remained prolonged (range, 460-500 ms), despite electrolyte repletion, and he was discharged with a wearable cardioverter defibrillator. A month
Discussion
Alcohol dependence is a common chronic and relapsing disease that often requires controlled detoxification. Investigators have found a high incidence of QT interval prolongation in alcohol withdrawal and hepatic disease.3,6 Common causes of QT interval prolongation in this setting are poor nutrition, electrolyte abnormalities (particularly hypocalcemia and hypomagnesemia), and use of certain medications.1-3,7,8 In addition, alcohol is directly toxic to the renal tubules, resulting in renal wasting of divalent cations, which may persist up to 30 days after the most recent alcohol exposure.9,10
The patient in this case report was initially thought to have hypomagnesemia-induced long QT syndrome (leading to TdP cardiac arrest), but the authors’ review of laboratory test results revealed the QT interval remained markedly prolonged, despite adequate correction of hypomagnesemia implicating the hyperadrenergic state of acute alcohol withdrawal in QT interval prolongation and TdP cardiac arrest. Interestingly, the QT interval remained prolonged 2 months after TdP arrest, despite sustained normalization of electrolyte levels and the absence of active ischemia or use of QT-prolonging medications.
Given the exclusion of other causes of QT interval prolongation, the authors hypothesized that autonomic hyperactivity of acute alcohol withdrawal and resultant QT interval prolongation were potentiated by underlying cirrhotic cardiomyopathy, a well described cause of QT interval prolongation. Cirrhotic cardiomyopathy is thought to cause QT interval prolongation by delayed repolarization of cardiomyocytes and promotion of sympatho-adrenergic hyperactivity.6 In other case series, TdP development has been associated with severe withdrawal symptoms, particularly delirium tremens.2 In cirrhosis, QT interval prolongation often is described as an early manifestation of cirrhotic cardiomyopathy, irrespective of the underlying etiology, and precedes systolic and diastolic dysfunction.6
The magnitude of QT prolongation has been associated with severity of liver disease as expressed by Child-Pugh score, with reports of QT normalization after liver transplantation.4,5 Patients with higher Child-Pugh scores should be considered to be at elevated risk for malignant ventricular arrhythmias. The authors recommend checking an EKG on admission of any patient who has liver disease or has presented for alcohol withdrawal. Patients with a prolonged QTc interval should be monitored on telemetry. The authors also recommend aggressive repletion of electrolytes, particularly potassium and magnesium, in patients who present with cirrhosis and alcohol withdrawal.
Avoidance of QT-prolonging medications is advisable for all patients with a long QT interval. Beta blockers shorten the QT interval in cirrhotic patients, but the role of beta blockers in preventing malignant arrhythmias in this group of patients is not yet clear.11 The present patient’s QT interval had been normal before he developed cirrhotic liver disease. His presentation was suggestive of acquired long QT syndrome, likely caused by cirrhotic cardiomyopathy given the exhaustive exclusion of other causes of QT interval prolongation.
Conclusion
This case highlights the importance of close monitoring of the QT interval in patients being treated for acute alcohol withdrawal, particularly those with cirrhosis, and suggests that timely and aggressive management of withdrawal, repletion of electrolytes, and telemetry monitoring may prevent life-threatening arrhythmia.
1. Otero-Antón E, González-Quintela A, Saborido J, Torre JA, Virgós A, Barrio E. Prolongation of the QTc interval during alcohol withdrawal syndrome. Acta Cardiol. 1997;52(3):285-294.
2. Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227.
3. Mimidis K, Thomopoulos K, Tziakas D, et al. Prolongation of the QTc interval in patients with cirrhosis. Ann Gastroenterol. 2003;16(2):155-158.
4. Bernardi M, Calandra S, Colantoni A, et al. Q-T interval prolongation in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic factors. Hepatology. 1998;27(1):28-34.
5. Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease, mortality and liver transplantation. Liver Int. 2003;23(4):243-248.
6. Zardi EM, Abbate A, Zardi DM, et al. Cirrhotic cardiomyopathy. J Am Coll Cardiol. 2010;56(7):539-549.
7. Faigel DO, Metz DC, Kochman ML. Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalance. Am J Gastroenterol. 1995;90(5):822-824.
8. Kotsia AP, Dimitriadis G, Baltogiannis GG, Kolettis TM. Torsade de pointes and persistent QTc prolongation after intravenous amiodarone. Case Rep Med. 2012;2012:673019.
9. Denison H, Jern S, Jagenburg R, Wendestam C, Wallerstedt S. Influence of increased adrenergic activity and magnesium depletion on cardiac rhythm in alcohol withdrawal. Br Heart J. 1994;72(6):554-560.
10. Plaza de los Reyes M, Orozco R, Rosemblitt M, Rendic Y, Espinace M. Renal secretion of magnesium and other electrolytes under the influence of acute ingestion of alcohol, in normal subjects [in Spanish]. Rev Med Chil. 1968;96(3):138-141.
11. Bernardi M, Maggioli C, Dibra V, Zaccherini G. QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev Gastroenterol Hepatol. 2012;6(1):57-66.
1. Otero-Antón E, González-Quintela A, Saborido J, Torre JA, Virgós A, Barrio E. Prolongation of the QTc interval during alcohol withdrawal syndrome. Acta Cardiol. 1997;52(3):285-294.
2. Cuculi F, Kobza R, Ehmann T, Erne P. ECG changes amongst patients with alcohol withdrawal seizures and delirium tremens. Swiss Med Wkly. 2006;136(13-14):223-227.
3. Mimidis K, Thomopoulos K, Tziakas D, et al. Prolongation of the QTc interval in patients with cirrhosis. Ann Gastroenterol. 2003;16(2):155-158.
4. Bernardi M, Calandra S, Colantoni A, et al. Q-T interval prolongation in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic factors. Hepatology. 1998;27(1):28-34.
5. Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease, mortality and liver transplantation. Liver Int. 2003;23(4):243-248.
6. Zardi EM, Abbate A, Zardi DM, et al. Cirrhotic cardiomyopathy. J Am Coll Cardiol. 2010;56(7):539-549.
7. Faigel DO, Metz DC, Kochman ML. Torsade de pointes complicating the treatment of bleeding esophageal varices: association with neuroleptics, vasopressin, and electrolyte imbalance. Am J Gastroenterol. 1995;90(5):822-824.
8. Kotsia AP, Dimitriadis G, Baltogiannis GG, Kolettis TM. Torsade de pointes and persistent QTc prolongation after intravenous amiodarone. Case Rep Med. 2012;2012:673019.
9. Denison H, Jern S, Jagenburg R, Wendestam C, Wallerstedt S. Influence of increased adrenergic activity and magnesium depletion on cardiac rhythm in alcohol withdrawal. Br Heart J. 1994;72(6):554-560.
10. Plaza de los Reyes M, Orozco R, Rosemblitt M, Rendic Y, Espinace M. Renal secretion of magnesium and other electrolytes under the influence of acute ingestion of alcohol, in normal subjects [in Spanish]. Rev Med Chil. 1968;96(3):138-141.
11. Bernardi M, Maggioli C, Dibra V, Zaccherini G. QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev Gastroenterol Hepatol. 2012;6(1):57-66.
How Far Does a Cough Travel?
A single cough can propel as many as 3,000 droplets into the air at a velocity of 6 to 28 m/s. The droplets travel in what classic fluid mechanics calls a “2-stage jet”: the starting jet (when the cough starts) and interrupted jet (when the cough stops). After the original cough ends, a “leading vortex” carries particles forward, but as the momentum slows, particles fall out of the jet according to researchers from the University of Hong Kong and Shenzhen Institute of Research and Innovation, both in China, who studied cough trajectories and the implications for disease transmission in buildings.
Once the penetration velocity drops below 0.01 m/s, environmental factors, such as ventilation and human body temperature, begin to influence the flow. Beyond 1 to 2 m, the exhaled air stream dissolves into the room airflow, and the pathogen-containing droplets or droplet nuclei are dispersed according to the global airflow in the room.
When a cough doesn’t last long, the researchers say, the velocity of fine particles decays significantly after the jet is interrupted. However, even short coughs have consequences: Pathogen-containing droplets as large as ≥ 5 µm in diameter can be directly deposited on the nasal or oral mucosa of a nearby “new host.”
But coughs differ in many ways, including how far and wide they send the droplets. The researchers conducted experiments to help determine spread by discharging dyed or particle-filled water into a water tank. They examined 3 different temporal exit velocity profiles: pulsation, sinusoidal, and real-cough.
The “most striking phenomenon,” the researchers say, is that the particle clouds of all 3 sizes of particles (small [8-14 µm], medium [57-68 µm], large [96-114 µm]) penetrated almost the same distance at different time steps. In other words, large particles can travel as far as fine particles.
The cough flow’s maximum penetration distance was 53.4 to 69.7 opening diameter. That is, for a mouth opening to a diameter of 2 cm, the large particles could penetrate 1 to 1.4 m in a “real cough case,” they note. Cough duration was important in determining the spread range of particles. Their maximum travel distance was “much enhanced” in a long starting jet, especially for small particles.
Source:
Wei J, Li Y. PLoS One. 2017;12(1): e0169235.
doi: 10.1371/journal.pone.0169235.
A single cough can propel as many as 3,000 droplets into the air at a velocity of 6 to 28 m/s. The droplets travel in what classic fluid mechanics calls a “2-stage jet”: the starting jet (when the cough starts) and interrupted jet (when the cough stops). After the original cough ends, a “leading vortex” carries particles forward, but as the momentum slows, particles fall out of the jet according to researchers from the University of Hong Kong and Shenzhen Institute of Research and Innovation, both in China, who studied cough trajectories and the implications for disease transmission in buildings.
Once the penetration velocity drops below 0.01 m/s, environmental factors, such as ventilation and human body temperature, begin to influence the flow. Beyond 1 to 2 m, the exhaled air stream dissolves into the room airflow, and the pathogen-containing droplets or droplet nuclei are dispersed according to the global airflow in the room.
When a cough doesn’t last long, the researchers say, the velocity of fine particles decays significantly after the jet is interrupted. However, even short coughs have consequences: Pathogen-containing droplets as large as ≥ 5 µm in diameter can be directly deposited on the nasal or oral mucosa of a nearby “new host.”
But coughs differ in many ways, including how far and wide they send the droplets. The researchers conducted experiments to help determine spread by discharging dyed or particle-filled water into a water tank. They examined 3 different temporal exit velocity profiles: pulsation, sinusoidal, and real-cough.
The “most striking phenomenon,” the researchers say, is that the particle clouds of all 3 sizes of particles (small [8-14 µm], medium [57-68 µm], large [96-114 µm]) penetrated almost the same distance at different time steps. In other words, large particles can travel as far as fine particles.
The cough flow’s maximum penetration distance was 53.4 to 69.7 opening diameter. That is, for a mouth opening to a diameter of 2 cm, the large particles could penetrate 1 to 1.4 m in a “real cough case,” they note. Cough duration was important in determining the spread range of particles. Their maximum travel distance was “much enhanced” in a long starting jet, especially for small particles.
Source:
Wei J, Li Y. PLoS One. 2017;12(1): e0169235.
doi: 10.1371/journal.pone.0169235.
A single cough can propel as many as 3,000 droplets into the air at a velocity of 6 to 28 m/s. The droplets travel in what classic fluid mechanics calls a “2-stage jet”: the starting jet (when the cough starts) and interrupted jet (when the cough stops). After the original cough ends, a “leading vortex” carries particles forward, but as the momentum slows, particles fall out of the jet according to researchers from the University of Hong Kong and Shenzhen Institute of Research and Innovation, both in China, who studied cough trajectories and the implications for disease transmission in buildings.
Once the penetration velocity drops below 0.01 m/s, environmental factors, such as ventilation and human body temperature, begin to influence the flow. Beyond 1 to 2 m, the exhaled air stream dissolves into the room airflow, and the pathogen-containing droplets or droplet nuclei are dispersed according to the global airflow in the room.
When a cough doesn’t last long, the researchers say, the velocity of fine particles decays significantly after the jet is interrupted. However, even short coughs have consequences: Pathogen-containing droplets as large as ≥ 5 µm in diameter can be directly deposited on the nasal or oral mucosa of a nearby “new host.”
But coughs differ in many ways, including how far and wide they send the droplets. The researchers conducted experiments to help determine spread by discharging dyed or particle-filled water into a water tank. They examined 3 different temporal exit velocity profiles: pulsation, sinusoidal, and real-cough.
The “most striking phenomenon,” the researchers say, is that the particle clouds of all 3 sizes of particles (small [8-14 µm], medium [57-68 µm], large [96-114 µm]) penetrated almost the same distance at different time steps. In other words, large particles can travel as far as fine particles.
The cough flow’s maximum penetration distance was 53.4 to 69.7 opening diameter. That is, for a mouth opening to a diameter of 2 cm, the large particles could penetrate 1 to 1.4 m in a “real cough case,” they note. Cough duration was important in determining the spread range of particles. Their maximum travel distance was “much enhanced” in a long starting jet, especially for small particles.
Source:
Wei J, Li Y. PLoS One. 2017;12(1): e0169235.
doi: 10.1371/journal.pone.0169235.
Racial disparity in cervical cancer deaths higher than previously reported
Corrected mortality rates for cervical cancer indicate a greater disparity between races, according to a report in Cancer.
Because previous estimates did not adjust for women who’d had a hysterectomy or who were otherwise not at risk for cervical cancer, investigators performed a “corrected” analysis using data from the Behavioral Risk Factor Surveillance System and from the National Center for Health Statistics and the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, for the years 2002 through 2012.
The corrected mortality rate in black women is 10.1 per 100,000 women (95% confidence interval, 9.6-10.6) and 4.7 per 100,000 in white women (95% CI, 4.6-4.8), an overall difference of 44%. The previous, uncorrected mortality rate for black women was 5.7 per 100,000 (95% CI, 5.5-6.0) and 3.2 per 100,000 (95% CI, 3.1-3.2) for white women, reported Anne F. Rositch, PhD, of Johns Hopkins Bloomberg School of Public Health, Baltimore, and her colleagues.
The corrected findings do not indicate a rise in the overall cervical cancer death rate, but do show that the disparity between the races is higher, despite declines in such deaths among black women over the years: The corrected analysis over the decade showed that the rate of decrease in cervical cancer mortality rates was 0.8% in white women and 3.6% in black women (P less than .05), Dr. Rositch and her associates reported (Cancer 2017 Jan 23 doi: 10.1002/cncr.30507). Both corrected and uncorrected rates were significantly higher in older black women, especially those 85 years and older at 18.6 per 100,000 (95% CI, 15.4-21.7) before correction, and 37.2 per 100,000 (95% CI, 31.0-43.5) after correction.
“Future research should focus on overcoming the underlying factors that contribute to this mortality gap (differential follow-up for abnormal Papanicolaou test results and barriers to care after diagnosis) and on determining why black women and older women receive different and inadequate treatment for the same disease,” wrote Dr. Rositch and her colleagues.
The elimination of mortality differences across the two races in women aged 20-29 years and those 35-39 years was “encouraging ... because these age cohorts correspond to the patients who are most likely to have been vaccinated against the human papillomavirus (HPV) virus,” Heather J. Dalton, MD, and John Farley, MD, of Creighton University School of Medicine at St. Joseph’s Hospital and Medical Center, Phoenix, Ariz., wrote in an accompanying editorial (Cancer 2017 Jan. 23 doi: 10.1002/cncr.30501).
High-risk HPV infections and lack of adequate screening are the “only factors definitely associated with the incidence of cervical cancer,” they noted.
[email protected]
On Twitter @whitneymcknight
Corrected mortality rates for cervical cancer indicate a greater disparity between races, according to a report in Cancer.
Because previous estimates did not adjust for women who’d had a hysterectomy or who were otherwise not at risk for cervical cancer, investigators performed a “corrected” analysis using data from the Behavioral Risk Factor Surveillance System and from the National Center for Health Statistics and the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, for the years 2002 through 2012.
The corrected mortality rate in black women is 10.1 per 100,000 women (95% confidence interval, 9.6-10.6) and 4.7 per 100,000 in white women (95% CI, 4.6-4.8), an overall difference of 44%. The previous, uncorrected mortality rate for black women was 5.7 per 100,000 (95% CI, 5.5-6.0) and 3.2 per 100,000 (95% CI, 3.1-3.2) for white women, reported Anne F. Rositch, PhD, of Johns Hopkins Bloomberg School of Public Health, Baltimore, and her colleagues.
The corrected findings do not indicate a rise in the overall cervical cancer death rate, but do show that the disparity between the races is higher, despite declines in such deaths among black women over the years: The corrected analysis over the decade showed that the rate of decrease in cervical cancer mortality rates was 0.8% in white women and 3.6% in black women (P less than .05), Dr. Rositch and her associates reported (Cancer 2017 Jan 23 doi: 10.1002/cncr.30507). Both corrected and uncorrected rates were significantly higher in older black women, especially those 85 years and older at 18.6 per 100,000 (95% CI, 15.4-21.7) before correction, and 37.2 per 100,000 (95% CI, 31.0-43.5) after correction.
“Future research should focus on overcoming the underlying factors that contribute to this mortality gap (differential follow-up for abnormal Papanicolaou test results and barriers to care after diagnosis) and on determining why black women and older women receive different and inadequate treatment for the same disease,” wrote Dr. Rositch and her colleagues.
The elimination of mortality differences across the two races in women aged 20-29 years and those 35-39 years was “encouraging ... because these age cohorts correspond to the patients who are most likely to have been vaccinated against the human papillomavirus (HPV) virus,” Heather J. Dalton, MD, and John Farley, MD, of Creighton University School of Medicine at St. Joseph’s Hospital and Medical Center, Phoenix, Ariz., wrote in an accompanying editorial (Cancer 2017 Jan. 23 doi: 10.1002/cncr.30501).
High-risk HPV infections and lack of adequate screening are the “only factors definitely associated with the incidence of cervical cancer,” they noted.
[email protected]
On Twitter @whitneymcknight
Corrected mortality rates for cervical cancer indicate a greater disparity between races, according to a report in Cancer.
Because previous estimates did not adjust for women who’d had a hysterectomy or who were otherwise not at risk for cervical cancer, investigators performed a “corrected” analysis using data from the Behavioral Risk Factor Surveillance System and from the National Center for Health Statistics and the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, for the years 2002 through 2012.
The corrected mortality rate in black women is 10.1 per 100,000 women (95% confidence interval, 9.6-10.6) and 4.7 per 100,000 in white women (95% CI, 4.6-4.8), an overall difference of 44%. The previous, uncorrected mortality rate for black women was 5.7 per 100,000 (95% CI, 5.5-6.0) and 3.2 per 100,000 (95% CI, 3.1-3.2) for white women, reported Anne F. Rositch, PhD, of Johns Hopkins Bloomberg School of Public Health, Baltimore, and her colleagues.
The corrected findings do not indicate a rise in the overall cervical cancer death rate, but do show that the disparity between the races is higher, despite declines in such deaths among black women over the years: The corrected analysis over the decade showed that the rate of decrease in cervical cancer mortality rates was 0.8% in white women and 3.6% in black women (P less than .05), Dr. Rositch and her associates reported (Cancer 2017 Jan 23 doi: 10.1002/cncr.30507). Both corrected and uncorrected rates were significantly higher in older black women, especially those 85 years and older at 18.6 per 100,000 (95% CI, 15.4-21.7) before correction, and 37.2 per 100,000 (95% CI, 31.0-43.5) after correction.
“Future research should focus on overcoming the underlying factors that contribute to this mortality gap (differential follow-up for abnormal Papanicolaou test results and barriers to care after diagnosis) and on determining why black women and older women receive different and inadequate treatment for the same disease,” wrote Dr. Rositch and her colleagues.
The elimination of mortality differences across the two races in women aged 20-29 years and those 35-39 years was “encouraging ... because these age cohorts correspond to the patients who are most likely to have been vaccinated against the human papillomavirus (HPV) virus,” Heather J. Dalton, MD, and John Farley, MD, of Creighton University School of Medicine at St. Joseph’s Hospital and Medical Center, Phoenix, Ariz., wrote in an accompanying editorial (Cancer 2017 Jan. 23 doi: 10.1002/cncr.30501).
High-risk HPV infections and lack of adequate screening are the “only factors definitely associated with the incidence of cervical cancer,” they noted.
[email protected]
On Twitter @whitneymcknight
FROM CANCER
Key clinical point:
Major finding: Black women die from cervical cancer at a rate of 10.1 per 100,000 women; the rate for white women is 4.7 per 100,000, a 44% disparity.
Data source: National population database study from 2002 to 2012, adjusted for women not at risk for cervical cancer.
Disclosures: Dr. Patti E. Gravitt reported support from Hologic for research not related to this study.
Does Cannabidiol Affect Seizure Severity?
HOUSTON—Pharmaceutical-grade cannabidiol (CBD) may reduce seizure severity in adults and children with medically refractory epilepsy, according to an open-label trial described at the 70th Annual Meeting of the American Epilepsy Society. A controlled trial to confirm the drug’s effect may be warranted.
Jennifer L. DeWolfe, DO, Associate Professor of Neurology at the University of Alabama at Birmingham, and colleagues conducted a state-sponsored compassionate-use study of CBD in patients with refractory epilepsy. Patients received Epidiolex (a CBD formulation developed by GW Pharmaceuticals) in addition to their antiepileptic drugs. Eligible participants were adults and children with epilepsy confirmed by video EEG. Participants were required to have failed four antiepileptic drugs and had to have had four countable seizures per month. Exclusion criteria included psychogenic nonepileptic seizures confirmed by video EEG and prior CBD use.

Measuring Seizure Severity Over Time
The investigators measured participants’ seizure frequency and used the Chalfont Seizure Severity Scale to measure seizure severity. The scale solicits information about various factors, such as whether the patient lost awareness, dropped an object, fell, or was injured. The total possible score on the scale is 178, and the score increases with seizure severity. Changes of 10 or more points were considered significant. The researchers particularly focused on participants’ most frequent seizure type, which the Chalfont Seizure Severity Scale names the Type 1 seizure.
Dr. DeWolfe and colleagues measured patients’ total seizure severity scores and severity scores for Type 1 seizures at baseline, three months, and six months. To compare the scores, the researchers calculated time-weighted average values. They also examined percent change in seizures; seizure severity in adults, children, and all patients; and severity in responders and nonresponders. Responders were defined as patients who had a reduction in seizure frequency of more than 50%. The analysis included 81 participants, approximately half of whom were children. At the time of the analysis, 57 patients had undergone evaluation at three months, and 47 patients had undergone evaluation at six months. At baseline, the majority of patients had at least two types of seizures.
Seizure Severity Was Reduced
The total change in Chalfont Seizure Severity Scale score at three months was significant for adults, children, and all patients. The change remained significant at six months. The difference in the percent change in seizure severity between responders and nonresponders was significant at three months, but not at six months.
The change in severity of Type 1 seizures was significant for adults, children, and all patients at three months and at six months. The difference between responders and nonresponders in change in severity of Type 1 seizures was significant at three months, but not at six months.
At three months, the majority of adults, the majority of all patients, the majority of responders, and the majority of nonresponders had a reduction in seizure severity of at least 10 points. Approximately one-third of children had a reduction in seizure severity of at least 10 points at three months. At six months, the majority of adults, children, all patients, responders, and nonresponders had a decrease in seizure severity of at least 10 points. Patients’ average seizure severity tended to increase at six months, compared with the three-month point, but was still significantly lower than at baseline.
“One of the things I find most exciting is [that] … even if you were considered a nonresponder, you still had improvement in seizure severity,” said Dr. DeWolfe. She and her colleagues plan to examine the data by seizure type (eg, absence or tonic-clonic), to identify which factors measured by the Chalfont Seizure Severity Scale contributed most to the reductions in seizure severity, and to examine whether the effect of CBD on levels of antiepileptic drugs contributed to the change in seizure severity. The findings of this open-label trial suggest that CBD may improve seizure severity in people with medically refractory epilepsy. Randomized placebo-controlled studies are needed to further evaluate the effects of CBD on seizure severity.
—Erik Greb
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Porter BE, Jacobson C. Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy. Epilepsy Behav. 2013;29(3):574-577.
HOUSTON—Pharmaceutical-grade cannabidiol (CBD) may reduce seizure severity in adults and children with medically refractory epilepsy, according to an open-label trial described at the 70th Annual Meeting of the American Epilepsy Society. A controlled trial to confirm the drug’s effect may be warranted.
Jennifer L. DeWolfe, DO, Associate Professor of Neurology at the University of Alabama at Birmingham, and colleagues conducted a state-sponsored compassionate-use study of CBD in patients with refractory epilepsy. Patients received Epidiolex (a CBD formulation developed by GW Pharmaceuticals) in addition to their antiepileptic drugs. Eligible participants were adults and children with epilepsy confirmed by video EEG. Participants were required to have failed four antiepileptic drugs and had to have had four countable seizures per month. Exclusion criteria included psychogenic nonepileptic seizures confirmed by video EEG and prior CBD use.
Measuring Seizure Severity Over Time
The investigators measured participants’ seizure frequency and used the Chalfont Seizure Severity Scale to measure seizure severity. The scale solicits information about various factors, such as whether the patient lost awareness, dropped an object, fell, or was injured. The total possible score on the scale is 178, and the score increases with seizure severity. Changes of 10 or more points were considered significant. The researchers particularly focused on participants’ most frequent seizure type, which the Chalfont Seizure Severity Scale names the Type 1 seizure.
Dr. DeWolfe and colleagues measured patients’ total seizure severity scores and severity scores for Type 1 seizures at baseline, three months, and six months. To compare the scores, the researchers calculated time-weighted average values. They also examined percent change in seizures; seizure severity in adults, children, and all patients; and severity in responders and nonresponders. Responders were defined as patients who had a reduction in seizure frequency of more than 50%. The analysis included 81 participants, approximately half of whom were children. At the time of the analysis, 57 patients had undergone evaluation at three months, and 47 patients had undergone evaluation at six months. At baseline, the majority of patients had at least two types of seizures.
Seizure Severity Was Reduced
The total change in Chalfont Seizure Severity Scale score at three months was significant for adults, children, and all patients. The change remained significant at six months. The difference in the percent change in seizure severity between responders and nonresponders was significant at three months, but not at six months.
The change in severity of Type 1 seizures was significant for adults, children, and all patients at three months and at six months. The difference between responders and nonresponders in change in severity of Type 1 seizures was significant at three months, but not at six months.
At three months, the majority of adults, the majority of all patients, the majority of responders, and the majority of nonresponders had a reduction in seizure severity of at least 10 points. Approximately one-third of children had a reduction in seizure severity of at least 10 points at three months. At six months, the majority of adults, children, all patients, responders, and nonresponders had a decrease in seizure severity of at least 10 points. Patients’ average seizure severity tended to increase at six months, compared with the three-month point, but was still significantly lower than at baseline.
“One of the things I find most exciting is [that] … even if you were considered a nonresponder, you still had improvement in seizure severity,” said Dr. DeWolfe. She and her colleagues plan to examine the data by seizure type (eg, absence or tonic-clonic), to identify which factors measured by the Chalfont Seizure Severity Scale contributed most to the reductions in seizure severity, and to examine whether the effect of CBD on levels of antiepileptic drugs contributed to the change in seizure severity. The findings of this open-label trial suggest that CBD may improve seizure severity in people with medically refractory epilepsy. Randomized placebo-controlled studies are needed to further evaluate the effects of CBD on seizure severity.
—Erik Greb
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Porter BE, Jacobson C. Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy. Epilepsy Behav. 2013;29(3):574-577.
HOUSTON—Pharmaceutical-grade cannabidiol (CBD) may reduce seizure severity in adults and children with medically refractory epilepsy, according to an open-label trial described at the 70th Annual Meeting of the American Epilepsy Society. A controlled trial to confirm the drug’s effect may be warranted.
Jennifer L. DeWolfe, DO, Associate Professor of Neurology at the University of Alabama at Birmingham, and colleagues conducted a state-sponsored compassionate-use study of CBD in patients with refractory epilepsy. Patients received Epidiolex (a CBD formulation developed by GW Pharmaceuticals) in addition to their antiepileptic drugs. Eligible participants were adults and children with epilepsy confirmed by video EEG. Participants were required to have failed four antiepileptic drugs and had to have had four countable seizures per month. Exclusion criteria included psychogenic nonepileptic seizures confirmed by video EEG and prior CBD use.
Measuring Seizure Severity Over Time
The investigators measured participants’ seizure frequency and used the Chalfont Seizure Severity Scale to measure seizure severity. The scale solicits information about various factors, such as whether the patient lost awareness, dropped an object, fell, or was injured. The total possible score on the scale is 178, and the score increases with seizure severity. Changes of 10 or more points were considered significant. The researchers particularly focused on participants’ most frequent seizure type, which the Chalfont Seizure Severity Scale names the Type 1 seizure.
Dr. DeWolfe and colleagues measured patients’ total seizure severity scores and severity scores for Type 1 seizures at baseline, three months, and six months. To compare the scores, the researchers calculated time-weighted average values. They also examined percent change in seizures; seizure severity in adults, children, and all patients; and severity in responders and nonresponders. Responders were defined as patients who had a reduction in seizure frequency of more than 50%. The analysis included 81 participants, approximately half of whom were children. At the time of the analysis, 57 patients had undergone evaluation at three months, and 47 patients had undergone evaluation at six months. At baseline, the majority of patients had at least two types of seizures.
Seizure Severity Was Reduced
The total change in Chalfont Seizure Severity Scale score at three months was significant for adults, children, and all patients. The change remained significant at six months. The difference in the percent change in seizure severity between responders and nonresponders was significant at three months, but not at six months.
The change in severity of Type 1 seizures was significant for adults, children, and all patients at three months and at six months. The difference between responders and nonresponders in change in severity of Type 1 seizures was significant at three months, but not at six months.
At three months, the majority of adults, the majority of all patients, the majority of responders, and the majority of nonresponders had a reduction in seizure severity of at least 10 points. Approximately one-third of children had a reduction in seizure severity of at least 10 points at three months. At six months, the majority of adults, children, all patients, responders, and nonresponders had a decrease in seizure severity of at least 10 points. Patients’ average seizure severity tended to increase at six months, compared with the three-month point, but was still significantly lower than at baseline.
“One of the things I find most exciting is [that] … even if you were considered a nonresponder, you still had improvement in seizure severity,” said Dr. DeWolfe. She and her colleagues plan to examine the data by seizure type (eg, absence or tonic-clonic), to identify which factors measured by the Chalfont Seizure Severity Scale contributed most to the reductions in seizure severity, and to examine whether the effect of CBD on levels of antiepileptic drugs contributed to the change in seizure severity. The findings of this open-label trial suggest that CBD may improve seizure severity in people with medically refractory epilepsy. Randomized placebo-controlled studies are needed to further evaluate the effects of CBD on seizure severity.
—Erik Greb
Suggested Reading
Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15(3):270-278.
Porter BE, Jacobson C. Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy. Epilepsy Behav. 2013;29(3):574-577.

CMS makes economics of primary care ACOs more appealing
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.

However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.
However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.
However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.
