User login
VIDEO: Spironolactone holds its own for treating women’s acne
WAILEA, Hawaii – While spironolactone is an old drug, it remains a safe and effective treatment option for acne in women, according to Julie Harper, MD, of the University of Alabama, Birmingham.
In a video interview, Dr. Harper said that she usually does not choose spironolactone as a first-line drug, “but more often than not this is a drug that is an add-on to other therapies” that have been tried. She tends to start with a low dose and titrates up based on side effects. The drug has been tested in men, but Dr. Harper cited a Japanese study that discontinued a male treatment arm because men developed gynecomastia.
In her opinion, it isn’t always necessary to routinely check potassium levels in patients on spironolactone. “In the vast majority of patients, I do not check labs routinely” before starting spironolactone, she said at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But she noted that some physicians feel more comfortable checking baseline labs.
Dr. Harper disclosed financial relationships with Allergan, Galderma, BioPharmX, La Roche-Posay, Promius, Valeant, and Bayer.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, Hawaii – While spironolactone is an old drug, it remains a safe and effective treatment option for acne in women, according to Julie Harper, MD, of the University of Alabama, Birmingham.
In a video interview, Dr. Harper said that she usually does not choose spironolactone as a first-line drug, “but more often than not this is a drug that is an add-on to other therapies” that have been tried. She tends to start with a low dose and titrates up based on side effects. The drug has been tested in men, but Dr. Harper cited a Japanese study that discontinued a male treatment arm because men developed gynecomastia.
In her opinion, it isn’t always necessary to routinely check potassium levels in patients on spironolactone. “In the vast majority of patients, I do not check labs routinely” before starting spironolactone, she said at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But she noted that some physicians feel more comfortable checking baseline labs.
Dr. Harper disclosed financial relationships with Allergan, Galderma, BioPharmX, La Roche-Posay, Promius, Valeant, and Bayer.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, Hawaii – While spironolactone is an old drug, it remains a safe and effective treatment option for acne in women, according to Julie Harper, MD, of the University of Alabama, Birmingham.
In a video interview, Dr. Harper said that she usually does not choose spironolactone as a first-line drug, “but more often than not this is a drug that is an add-on to other therapies” that have been tried. She tends to start with a low dose and titrates up based on side effects. The drug has been tested in men, but Dr. Harper cited a Japanese study that discontinued a male treatment arm because men developed gynecomastia.
In her opinion, it isn’t always necessary to routinely check potassium levels in patients on spironolactone. “In the vast majority of patients, I do not check labs routinely” before starting spironolactone, she said at the meeting, provided by Global Academy for Medical Education/Skin Disease Education Foundation. But she noted that some physicians feel more comfortable checking baseline labs.
Dr. Harper disclosed financial relationships with Allergan, Galderma, BioPharmX, La Roche-Posay, Promius, Valeant, and Bayer.
SDEF and this news organization are owned by the same parent organization.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR

Parents seek easily understood public reporting of cardiac outcome measures
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”

“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”
“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
HOUSTON – Parents of children with congenital heart disease cite survival statistics, surgeon-specific experience, and complication rates as the three most important congenital heart surgery outcome measures to report publicly, results from a large survey show.
“Recently, an increasing demand for the public reporting of pediatric heart surgery outcomes has led to the development of several different reporting schemes, including a hospital star rating system and procedure-specific mortality data tables for the Society of Thoracic Surgeons benchmark operations,” study investigator Mallory L. Irons, MD, said during a press briefing at the annual meeting of the Society of Thoracic Surgeons. “However, despite the availability of these reporting schemes, there remain unanswered questions about the optimal format and content of public reporting for pediatric heart surgery outcomes.”
“These procedures have been determined to represent more homogenous patient groups,” she said. “How data [are] presented may be just as important as the data itself. Noticeably absent from these frameworks is parent input regarding the information that may be necessary to make an informed choice about their child’s care.
“Failure to consider this perspective may contribute to suboptimal reporting and misunderstanding of the data presented. The goal of the current study was to identify parent preferences regarding the content of pediatric heart surgery outcomes reports, specifically with respect to the type of data that is included as well as the optimal format for presentation of this data.”
She and her associates developed a 43-question survey for 1,862 parents of children born with heart defects. The parents were invited to participate through member lists from patient advocacy groups Mended Little Hearts, the Pediatric Congenital Heart Association, and Sisters by Heart, and from a cohort of patients who underwent surgical correction for an STS benchmark procedure at the Children’s Hospital of Philadelphia after Jan. 1, 2007.
Of the 1,862 parents, 1,281 (69%) provided complete responses for inclusion in the final analysis. The mean age of respondents was 37 years, 92% were mothers of children with congenital heart disease, and 92% were white. “Most reported household incomes in excess of $65,000 per year, but lower income households were also significantly represented,” Dr. Irons added. More than half of the children (57%) were diagnosed with CHD prenatally, 63% underwent an initial repair in the neonatal period, and 60% of families were referred to a cardiac surgical center by a physician, while 23% were transferred from their birth hospital.
When the respondents were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme on a scale of 1 (most important) to 8 (least important), they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important. These preferences were stable across differences in education levels, household incomes, and race or ethnicity, Dr. Irons said.
Presented with three display formats for hospital-specific mortality rates, most parents (89%) identified a numerical procedure-based approach as the best format, and more than half (60%) identified the hospital star rating system as the worst potential format to display mortality data. These preferences also were stable across differences in education levels, household incomes, and race or ethnicity.
Dr. Irons acknowledged certain limitations of the study, including its retrospective design, and the fact that it lacked input from parents who do not have Internet access. “Similarly, the availability of the survey in English only prevents non-native English speakers from contributing,” she said. “Finally, while we have identified what types of information parents want, we must acknowledge that small case numbers limit the presentation of certain types of data, such as surgeon-specific outcomes, in a statistically meaningful way.”
In her opinion, an optimal reporting system requires a common database in which to collect and analyze data, a robust methodology for risk adjustment, and a way to compare performance across a field that is inherently heterogeneous.
“The ideal public reporting system should be valid as well as easily understood by all stakeholders,” Dr. Irons concluded. “We must recognize that just because parents want certain data, [it] does not mean that we can provide it in a meaningful, statistically valid way. Perhaps the most important takeaway from our study is the importance of involving parents and other stakeholders in the design and planning of methodologies for public reporting of congenital heart surgery outcomes. Ultimately, the optimal platform will represent a melding of what parents want, and what is statistically meaningful and valid.”
Jeffrey P. Jacobs, MD, a pediatric heart surgeon at Johns Hopkins University, Baltimore, who also chairs the STS Workforce on National Databases, characterized the study as “an extremely important paper that examines the format and structure of how it might be best to share information about cardiac surgical outcomes with patients and their families.” He said the STS “has studied multiple different strategies, and currently we use a method where we report outcomes using a categorical system of star ratings and augment that with detailed specific data with point estimates for confidence intervals. We continue to study and explore better ways to share this information with our patients and with their families.”
Dr. Irons reported having no financial disclosures.
AT THE STS ANNUAL MEETING
Key clinical point:
Major finding: When parents of children with congenital heart disease were asked to rank categories of outcome measures or other types of information to include in an optimal public reporting scheme, they identified survival statistics, surgeons’ experience with congenital heart surgery, and complication rates as the three most important
Data source: A retrospective survey of 1,862 parents of children born with heart defects.
Disclosures: Dr. Irons reported having no financial disclosures.

Second dose rates of meningococcal vaccines low among HIV-positive men who have sex with men
ATLANTA – HIV-positive men who have sex with men should be getting vaccinated against invasive meningococcal disease twice, but an alarming majority are only getting vaccinated once, according to a new study presented at a conference on STD prevention sponsored the Centers for Disease Control and Prevention.
“This analysis underscores the need for active patient recall in order to maximize return for second dose among HIV-infected [men who have sex with men], although [that] may be resource-intensive,” said Kelly Jamison, MPH, of New York City’s department of health and mental hygiene.
Ms. Jamison and her coinvestigators examined medical record data of HIV-infected men who have sex with men who visited New York City STD clinics between Oct. 5, 2012 and Dec. 31, 2014, looking for individuals who received their first meningococcal vaccinations during that time period. The primary endpoint was to find the rate at which individuals who received the first vaccination came back within 1 year (Dec. 31, 2015) to receive a second vaccination.
The study was prompted by the invasive meningococcal disease (IMD) outbreak that New York City experienced from 2010-2013, in which 22 cases were identified in men who have sex with men, of which 55% involved men who were HIV-infected. All IMD cases involved serotype C, with a case fatality rate that was three times what public health officials anticipated at the time.
Because of this, the city launched a meningitis vaccination campaign. Vaccination was recommended for all men who have sex with men who were residents of New York City and had high-risk sexual exposure after Sept. 1, 2012. In early October, STD clinics around the city began offering free MCV4 vaccines. By late November, the recommendations were updated to include men who have sex with men who lived in specific parts of Brooklyn and had experienced high-risk sexual exposure after Sept. 1. In March 2013, the recommendations were further updated to state that all HIV-infected men who have sex with men and all such men with high-risk sexual exposure should be vaccinated. In August 2013, after the outbreak was over, the recommendations were updated one last time to state that they were recommendations for “ongoing vaccination.”
“A single dose of MCV4 is not sufficient for HIV-infected persons, so a second dose is recommended to occur 8 weeks after the first dose, and in order to increase two-dose coverage among HIV-infected MSM, STD clinicians provided the date for person to return for their second dose on a vaccine card given to patients at time of their first dose,” Ms. Jamison explained.
In total, 1,212 individuals were included in study. Over the course of the study period, only 322 (26.6%) returned within 1 year for a second vaccination. In terms of individual years, 2012 experienced the highest rate of second vaccination returns, at 38.6% (P less than .001). Of the 322 who received the second vaccination, 144 (44.7%) came to the STD clinic specifically for the second dose, 69 (21.4%) asked for the second vaccination along with other STD services, and 109 (33.9%) were “opportunistically vaccinated while presenting for other services.”
Older men who have sex with men were more likely to return for their second vaccination, as only 63 (18%) of those who did were under the age of 30. Those aged between 30 and 39 years numbered 80 (23%), those between 40 and 49 years numbered 102 (33%), and those aged 50 years or older numbered 77 (40%), meaning that older men were two to three times more likely to get that second dose (P less than .001).
“We did see suboptimal return for second doses, but this may be an underestimate, [because] we were unable to capture second doses received at non-STD clinic providers,” Ms. Jamison noted.
Ms. Jamison did not report any financial disclosures for this study.
ATLANTA – HIV-positive men who have sex with men should be getting vaccinated against invasive meningococcal disease twice, but an alarming majority are only getting vaccinated once, according to a new study presented at a conference on STD prevention sponsored the Centers for Disease Control and Prevention.
“This analysis underscores the need for active patient recall in order to maximize return for second dose among HIV-infected [men who have sex with men], although [that] may be resource-intensive,” said Kelly Jamison, MPH, of New York City’s department of health and mental hygiene.
Ms. Jamison and her coinvestigators examined medical record data of HIV-infected men who have sex with men who visited New York City STD clinics between Oct. 5, 2012 and Dec. 31, 2014, looking for individuals who received their first meningococcal vaccinations during that time period. The primary endpoint was to find the rate at which individuals who received the first vaccination came back within 1 year (Dec. 31, 2015) to receive a second vaccination.
The study was prompted by the invasive meningococcal disease (IMD) outbreak that New York City experienced from 2010-2013, in which 22 cases were identified in men who have sex with men, of which 55% involved men who were HIV-infected. All IMD cases involved serotype C, with a case fatality rate that was three times what public health officials anticipated at the time.
Because of this, the city launched a meningitis vaccination campaign. Vaccination was recommended for all men who have sex with men who were residents of New York City and had high-risk sexual exposure after Sept. 1, 2012. In early October, STD clinics around the city began offering free MCV4 vaccines. By late November, the recommendations were updated to include men who have sex with men who lived in specific parts of Brooklyn and had experienced high-risk sexual exposure after Sept. 1. In March 2013, the recommendations were further updated to state that all HIV-infected men who have sex with men and all such men with high-risk sexual exposure should be vaccinated. In August 2013, after the outbreak was over, the recommendations were updated one last time to state that they were recommendations for “ongoing vaccination.”
“A single dose of MCV4 is not sufficient for HIV-infected persons, so a second dose is recommended to occur 8 weeks after the first dose, and in order to increase two-dose coverage among HIV-infected MSM, STD clinicians provided the date for person to return for their second dose on a vaccine card given to patients at time of their first dose,” Ms. Jamison explained.
In total, 1,212 individuals were included in study. Over the course of the study period, only 322 (26.6%) returned within 1 year for a second vaccination. In terms of individual years, 2012 experienced the highest rate of second vaccination returns, at 38.6% (P less than .001). Of the 322 who received the second vaccination, 144 (44.7%) came to the STD clinic specifically for the second dose, 69 (21.4%) asked for the second vaccination along with other STD services, and 109 (33.9%) were “opportunistically vaccinated while presenting for other services.”
Older men who have sex with men were more likely to return for their second vaccination, as only 63 (18%) of those who did were under the age of 30. Those aged between 30 and 39 years numbered 80 (23%), those between 40 and 49 years numbered 102 (33%), and those aged 50 years or older numbered 77 (40%), meaning that older men were two to three times more likely to get that second dose (P less than .001).
“We did see suboptimal return for second doses, but this may be an underestimate, [because] we were unable to capture second doses received at non-STD clinic providers,” Ms. Jamison noted.
Ms. Jamison did not report any financial disclosures for this study.
ATLANTA – HIV-positive men who have sex with men should be getting vaccinated against invasive meningococcal disease twice, but an alarming majority are only getting vaccinated once, according to a new study presented at a conference on STD prevention sponsored the Centers for Disease Control and Prevention.
“This analysis underscores the need for active patient recall in order to maximize return for second dose among HIV-infected [men who have sex with men], although [that] may be resource-intensive,” said Kelly Jamison, MPH, of New York City’s department of health and mental hygiene.
Ms. Jamison and her coinvestigators examined medical record data of HIV-infected men who have sex with men who visited New York City STD clinics between Oct. 5, 2012 and Dec. 31, 2014, looking for individuals who received their first meningococcal vaccinations during that time period. The primary endpoint was to find the rate at which individuals who received the first vaccination came back within 1 year (Dec. 31, 2015) to receive a second vaccination.
The study was prompted by the invasive meningococcal disease (IMD) outbreak that New York City experienced from 2010-2013, in which 22 cases were identified in men who have sex with men, of which 55% involved men who were HIV-infected. All IMD cases involved serotype C, with a case fatality rate that was three times what public health officials anticipated at the time.
Because of this, the city launched a meningitis vaccination campaign. Vaccination was recommended for all men who have sex with men who were residents of New York City and had high-risk sexual exposure after Sept. 1, 2012. In early October, STD clinics around the city began offering free MCV4 vaccines. By late November, the recommendations were updated to include men who have sex with men who lived in specific parts of Brooklyn and had experienced high-risk sexual exposure after Sept. 1. In March 2013, the recommendations were further updated to state that all HIV-infected men who have sex with men and all such men with high-risk sexual exposure should be vaccinated. In August 2013, after the outbreak was over, the recommendations were updated one last time to state that they were recommendations for “ongoing vaccination.”
“A single dose of MCV4 is not sufficient for HIV-infected persons, so a second dose is recommended to occur 8 weeks after the first dose, and in order to increase two-dose coverage among HIV-infected MSM, STD clinicians provided the date for person to return for their second dose on a vaccine card given to patients at time of their first dose,” Ms. Jamison explained.
In total, 1,212 individuals were included in study. Over the course of the study period, only 322 (26.6%) returned within 1 year for a second vaccination. In terms of individual years, 2012 experienced the highest rate of second vaccination returns, at 38.6% (P less than .001). Of the 322 who received the second vaccination, 144 (44.7%) came to the STD clinic specifically for the second dose, 69 (21.4%) asked for the second vaccination along with other STD services, and 109 (33.9%) were “opportunistically vaccinated while presenting for other services.”
Older men who have sex with men were more likely to return for their second vaccination, as only 63 (18%) of those who did were under the age of 30. Those aged between 30 and 39 years numbered 80 (23%), those between 40 and 49 years numbered 102 (33%), and those aged 50 years or older numbered 77 (40%), meaning that older men were two to three times more likely to get that second dose (P less than .001).
“We did see suboptimal return for second doses, but this may be an underestimate, [because] we were unable to capture second doses received at non-STD clinic providers,” Ms. Jamison noted.
Ms. Jamison did not report any financial disclosures for this study.
AT THE 2016 STD PREVENTION CONFERENCE
Key clinical point:
Major finding: Only 26.6% (322 of 1,212) of men who have sex with men received a second dose within a year of receiving their first, with older men who have sex with men 2-3 times more likely to get the second dose than younger men who have sex with men.
Data source: Retrospective analysis of 1,212 men who have sex with men who visited New York City STD clinics from 2012-2015.
Disclosures: Ms. Jamison did not report any financial disclosures.
Circulating DNA catches lymphoma relapse early
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: Major finding: Circulating tumor DNA was found in 73% of relapse patients a mean of 188 days before relapse was detected by standard-of-care radiologic techniques. Circulating tumor DNA was found in the plasma of 100% of patients at diagnosis, but only 37% had abnormally high serum lactate dehydrogenase, currently the most commonly used biomarker.
Data source: Analysis of 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma.
Disclosures: Roche bought the rights to CAPP-Seq from Stanford (Calif.) University in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consults. Two are employees. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
Puerperal NSAIDs show no hypertension risk
LAS VEGAS – Puerperal NSAID treatment appeared safe for women with severe preeclampsia and hypertension postpartum in a single-center, retrospective analysis with 324 women.
Given that an opioid is generally the alternative to analgesia with a nonsteroidal anti-inflammatory drug, these new data help refute a recent call to limit puerperal NSAID use, Oscar A. Viteri, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.

Given the apparent safety of NSAIDs in this new analysis, their safety for nursing women, and concerns about opiates, it makes sense to defer any recommendations about avoiding NSAIDs in women with hypertension postpartum until their harm is proven in a adequately powered randomized trial, said Dr. Viteri, a maternal fetal medicine specialist at the University of Texas, Houston. “Opiates are a public health problem,” he stressed.
His analysis used data collected from all women who delivered at Children’s Memorial Hermann Hospital in Houston during 2013-2015. In that group he identified 399 mothers with preeclampsia with severe features that had been diagnosed prior to delivery, and among them 324 mothers had hypertension (a systolic blood pressure of at least 140 mm Hg, a diastolic pressure of at least 90 mm Hg, or both) at or after 24 hours following delivery. Within this subgroup of 324 mothers, 243 (75%) received puerperal NSAID treatment and 81 women (25%) did not. Dr. Viteri highlighted that three-quarters of the women in the study subgroup had received NSAIDs “despite” the 2013 Task Force recommendation.
“Many units” continue to use puerperal NSAIDs in women with hypertension postpartum, commented Mary E. D’Alton, MD, professor and chair of ob.gyn. at Columbia University, New York.

Dr. Viteri defined persistent hypertension in these women as a systolic blood pressure of at least 150 mm Hg, a diastolic pressure of at least 100 mm Hg, or both measured after delivery at least twice at an interval of at least 4 hours. This primary endpoint occurred in 70% of the women treated with an NSAID and in 73% of those who received no NSAID, a difference that was not statistically significant after adjustment for laboratory abnormalities, gestational age, and mode of delivery, Dr. Viteri reported. The women who received NSAIDs also showed a numerically lower rate of receiving new or additional antihypertensive drugs of 20%, compared with 31% among those not on NSAIDs, a nonsignificant difference.
The analysis also showed no differences between the women on NSAIDs and those who did not take them for all the other parameters examined, including highest, average, and discharge systolic and diastolic blood pressures. In addition, among the women who received NSAIDs the results showed no differences in blood pressures regardless of whether the women also were receiving antihypertensive treatment with labetalol or nifedipine. This is the largest study yet reported to examine the effect of puerperal NSAID treatment on women with hypertension, and also the first data on the impact of NSAID treatment on blood pressure in women taking various types of antihypertensive drugs, Dr. Viteri noted.
Despite this reassuring data “it is important to be cautious” when using NSAIDs to treat the type of women enrolled in this study, Dr. D’Alton said in an interview. One concern to keep in mind is the risk for renal injury from NSAID use in women with a history of severe hypertension. Although Dr. D’Alton believed that it is not necessary to monitor renal function routinely in hypertensive women receiving puerperal NSAID treatment, the impact of this practice on the kidneys was worth further investigation, she said.
Dr. Viteri and Dr. D’Alton had no disclosures.
[email protected]
On Twitter @mitchelzoler
LAS VEGAS – Puerperal NSAID treatment appeared safe for women with severe preeclampsia and hypertension postpartum in a single-center, retrospective analysis with 324 women.
Given that an opioid is generally the alternative to analgesia with a nonsteroidal anti-inflammatory drug, these new data help refute a recent call to limit puerperal NSAID use, Oscar A. Viteri, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Given the apparent safety of NSAIDs in this new analysis, their safety for nursing women, and concerns about opiates, it makes sense to defer any recommendations about avoiding NSAIDs in women with hypertension postpartum until their harm is proven in a adequately powered randomized trial, said Dr. Viteri, a maternal fetal medicine specialist at the University of Texas, Houston. “Opiates are a public health problem,” he stressed.
His analysis used data collected from all women who delivered at Children’s Memorial Hermann Hospital in Houston during 2013-2015. In that group he identified 399 mothers with preeclampsia with severe features that had been diagnosed prior to delivery, and among them 324 mothers had hypertension (a systolic blood pressure of at least 140 mm Hg, a diastolic pressure of at least 90 mm Hg, or both) at or after 24 hours following delivery. Within this subgroup of 324 mothers, 243 (75%) received puerperal NSAID treatment and 81 women (25%) did not. Dr. Viteri highlighted that three-quarters of the women in the study subgroup had received NSAIDs “despite” the 2013 Task Force recommendation.
“Many units” continue to use puerperal NSAIDs in women with hypertension postpartum, commented Mary E. D’Alton, MD, professor and chair of ob.gyn. at Columbia University, New York.
Dr. Viteri defined persistent hypertension in these women as a systolic blood pressure of at least 150 mm Hg, a diastolic pressure of at least 100 mm Hg, or both measured after delivery at least twice at an interval of at least 4 hours. This primary endpoint occurred in 70% of the women treated with an NSAID and in 73% of those who received no NSAID, a difference that was not statistically significant after adjustment for laboratory abnormalities, gestational age, and mode of delivery, Dr. Viteri reported. The women who received NSAIDs also showed a numerically lower rate of receiving new or additional antihypertensive drugs of 20%, compared with 31% among those not on NSAIDs, a nonsignificant difference.
The analysis also showed no differences between the women on NSAIDs and those who did not take them for all the other parameters examined, including highest, average, and discharge systolic and diastolic blood pressures. In addition, among the women who received NSAIDs the results showed no differences in blood pressures regardless of whether the women also were receiving antihypertensive treatment with labetalol or nifedipine. This is the largest study yet reported to examine the effect of puerperal NSAID treatment on women with hypertension, and also the first data on the impact of NSAID treatment on blood pressure in women taking various types of antihypertensive drugs, Dr. Viteri noted.
Despite this reassuring data “it is important to be cautious” when using NSAIDs to treat the type of women enrolled in this study, Dr. D’Alton said in an interview. One concern to keep in mind is the risk for renal injury from NSAID use in women with a history of severe hypertension. Although Dr. D’Alton believed that it is not necessary to monitor renal function routinely in hypertensive women receiving puerperal NSAID treatment, the impact of this practice on the kidneys was worth further investigation, she said.
Dr. Viteri and Dr. D’Alton had no disclosures.
[email protected]
On Twitter @mitchelzoler
LAS VEGAS – Puerperal NSAID treatment appeared safe for women with severe preeclampsia and hypertension postpartum in a single-center, retrospective analysis with 324 women.
Given that an opioid is generally the alternative to analgesia with a nonsteroidal anti-inflammatory drug, these new data help refute a recent call to limit puerperal NSAID use, Oscar A. Viteri, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Given the apparent safety of NSAIDs in this new analysis, their safety for nursing women, and concerns about opiates, it makes sense to defer any recommendations about avoiding NSAIDs in women with hypertension postpartum until their harm is proven in a adequately powered randomized trial, said Dr. Viteri, a maternal fetal medicine specialist at the University of Texas, Houston. “Opiates are a public health problem,” he stressed.
His analysis used data collected from all women who delivered at Children’s Memorial Hermann Hospital in Houston during 2013-2015. In that group he identified 399 mothers with preeclampsia with severe features that had been diagnosed prior to delivery, and among them 324 mothers had hypertension (a systolic blood pressure of at least 140 mm Hg, a diastolic pressure of at least 90 mm Hg, or both) at or after 24 hours following delivery. Within this subgroup of 324 mothers, 243 (75%) received puerperal NSAID treatment and 81 women (25%) did not. Dr. Viteri highlighted that three-quarters of the women in the study subgroup had received NSAIDs “despite” the 2013 Task Force recommendation.
“Many units” continue to use puerperal NSAIDs in women with hypertension postpartum, commented Mary E. D’Alton, MD, professor and chair of ob.gyn. at Columbia University, New York.
Dr. Viteri defined persistent hypertension in these women as a systolic blood pressure of at least 150 mm Hg, a diastolic pressure of at least 100 mm Hg, or both measured after delivery at least twice at an interval of at least 4 hours. This primary endpoint occurred in 70% of the women treated with an NSAID and in 73% of those who received no NSAID, a difference that was not statistically significant after adjustment for laboratory abnormalities, gestational age, and mode of delivery, Dr. Viteri reported. The women who received NSAIDs also showed a numerically lower rate of receiving new or additional antihypertensive drugs of 20%, compared with 31% among those not on NSAIDs, a nonsignificant difference.
The analysis also showed no differences between the women on NSAIDs and those who did not take them for all the other parameters examined, including highest, average, and discharge systolic and diastolic blood pressures. In addition, among the women who received NSAIDs the results showed no differences in blood pressures regardless of whether the women also were receiving antihypertensive treatment with labetalol or nifedipine. This is the largest study yet reported to examine the effect of puerperal NSAID treatment on women with hypertension, and also the first data on the impact of NSAID treatment on blood pressure in women taking various types of antihypertensive drugs, Dr. Viteri noted.
Despite this reassuring data “it is important to be cautious” when using NSAIDs to treat the type of women enrolled in this study, Dr. D’Alton said in an interview. One concern to keep in mind is the risk for renal injury from NSAID use in women with a history of severe hypertension. Although Dr. D’Alton believed that it is not necessary to monitor renal function routinely in hypertensive women receiving puerperal NSAID treatment, the impact of this practice on the kidneys was worth further investigation, she said.
Dr. Viteri and Dr. D’Alton had no disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE PREGNANCY MEETING
Key clinical point:
Major finding: The incidence of persistent hypertension was 70% in women who received NSAIDs and 73% in women not on NSAISDs.
Data source: Retrospective analysis of data from 324 women at a single U.S. center.
Disclosures: Dr. Viteri and Dr. D’Alton had no disclosures.
Adolescents’ moderate use of digital technology tied to positive mental well-being
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
The moderate use of digital technology is not intrinsically harmful for adolescents and may be good for their mental well-being.
Those are the results of a study of 120,115 adolescents from the United Kingdom’s Department for Education National Pupil Database who were asked to complete questionnaires about their mental well-being and digital screen time, reported Andrew K. Przybylski, PhD, of the University of Oxford (England), and Netta Weinstein, PhD, of Cardiff (Wales) University.
The researchers began the study using what they called the “digital Goldilocks hypothesis.”
At the beginning of the study, Dr. Przybylski, Dr. Weinstein, and their team asked 15-year-olds from across England to complete the Warick-Edinburgh Mental Well-Being Scale, a 14-item self-report that seeks to measure factors such as happiness, life satisfaction, and psychological and social functioning. Meanwhile, the adolescents’ screen time was assessed through four questions asking about “watching films and other media, playing games, and using computers, and smartphones.”
About 20% of the participants reported a sum of more than 12 hours of digital engagement on weekdays, and 35% of the sample reported a total of more than 12 hours on weekend days. Girls reported spending more time using smartphones, using computers, and watching videos, and the boys devoted more time to playing computer and console games. Smartphones, however, were used more often daily among both girls and boys, Dr. Przybylski and Dr. Weinstein said.
After comparing the well-being and screen time data, the reseachers found that “the relations between screen time and mental well-being were either positive (P less than or equal to .001) or flat (P greater than .183), except for a negative link in the case of weekend smartphone use,” they said.
The investigators said their findings inform current guidelines that seek to limit adolescents’ technology use. “Future research and recommendations building on the Goldilocks hypothesis would be sensitive to the various types and contexts of media use and would be based on peaks and drops in well-being as well as other meaningful outcomes identified systematically,” they wrote.
Dr. Przybylski and Dr. Weinstein reported that they had no conflicts of interest to disclose.
FROM PSYCHOLOGICAL SCIENCE
Study provides new insight into B-cell metabolism
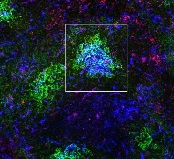
the spleen of a mouse, showing
inactivated GSK3 (magenta)
in B cells (blue) near follicular
dendritic cells (green).
Image from the lab of
Robert Rickert, PhD
Research published in Nature Immunology helps explain how B-cell metabolism adapts to different environments.
The study suggests the protein GSK3 acts as a metabolic checkpoint regulator in B cells, promoting the survival of circulating B cells while limiting the growth and proliferation of B cells in germinal centers.
“Our research shows that the protein GSK3 plays a crucial role in helping B cells meet the energy needs of their distinct states,” said study author Robert Rickert, PhD, of Sanford Burnham Prebys Medical Discovery Institute in La Jolla, California.
“The findings are particularly relevant for certain B-cell pathologies, including lymphoma subtypes, where there is an increased demand for energy to support the hyperproliferation of cells in a microenvironment that may be limited in nutrients.”
Dr Rickert and his colleagues noted that B cells predominate in a quiescent state until they encounter an antigen, which prompts the cells to grow, proliferate, and differentiate.
The team’s new study showed that GSK3 adjusts B-cell metabolism to match the needs of these different cell states.
In circulating B cells, GSK3 limits overall metabolic activity. In proliferating B cells in germinal centers, GSK3 slows glycolysis and the production of mitochondria.
In fact, GSK3 function is essential for B-cell survival in germinal centers. To understand why, the researchers looked at how B cells in these regions generate energy.
The team found that because these B cells are so metabolically active, they consume nearly all available glucose. That switches on glycolysis.
High glycolytic activity leads to an accumulation of toxic reactive oxygen species, as does rapid manufacture of mitochondria, which tend to leak the same chemicals.
Thus, by restraining the metabolism in specific ways, GSK3 prevents cell death induced by reactive oxygen species.
“Our results were really surprising,” Dr Rickert said. “Until now, we would have thought that slowing metabolism would only be important for preventing B cells from becoming cancerous, which it indeed may be. These studies provide insight into the dynamic nature of B-cell metabolism that literally ‘fuels’ differentiation in the germinal center to produce an effective antibody response.”
“It’s not yet clear whether or how GSK3 might be a target for future therapies for B cell-related diseases, but this research opens a lot of doors for further studies. To start with, we plan to investigate how GSK3 is regulated in lymphoma and how that relates to changes in metabolism. That research could lead to new approaches to treating lymphoma.”
This research was performed in collaboration with scientists at Eli Lilly and the Lunenfeld-Tanenbaum Research Institute at the University of Toronto. Funding was provided by the National Institutes of Health, the Lilly Research Award Program, the Arthritis National Research Foundation, and the Canadian Institutes of Health Research. ![]()
the spleen of a mouse, showing
inactivated GSK3 (magenta)
in B cells (blue) near follicular
dendritic cells (green).
Image from the lab of
Robert Rickert, PhD
Research published in Nature Immunology helps explain how B-cell metabolism adapts to different environments.
The study suggests the protein GSK3 acts as a metabolic checkpoint regulator in B cells, promoting the survival of circulating B cells while limiting the growth and proliferation of B cells in germinal centers.
“Our research shows that the protein GSK3 plays a crucial role in helping B cells meet the energy needs of their distinct states,” said study author Robert Rickert, PhD, of Sanford Burnham Prebys Medical Discovery Institute in La Jolla, California.
“The findings are particularly relevant for certain B-cell pathologies, including lymphoma subtypes, where there is an increased demand for energy to support the hyperproliferation of cells in a microenvironment that may be limited in nutrients.”
Dr Rickert and his colleagues noted that B cells predominate in a quiescent state until they encounter an antigen, which prompts the cells to grow, proliferate, and differentiate.
The team’s new study showed that GSK3 adjusts B-cell metabolism to match the needs of these different cell states.
In circulating B cells, GSK3 limits overall metabolic activity. In proliferating B cells in germinal centers, GSK3 slows glycolysis and the production of mitochondria.
In fact, GSK3 function is essential for B-cell survival in germinal centers. To understand why, the researchers looked at how B cells in these regions generate energy.
The team found that because these B cells are so metabolically active, they consume nearly all available glucose. That switches on glycolysis.
High glycolytic activity leads to an accumulation of toxic reactive oxygen species, as does rapid manufacture of mitochondria, which tend to leak the same chemicals.
Thus, by restraining the metabolism in specific ways, GSK3 prevents cell death induced by reactive oxygen species.
“Our results were really surprising,” Dr Rickert said. “Until now, we would have thought that slowing metabolism would only be important for preventing B cells from becoming cancerous, which it indeed may be. These studies provide insight into the dynamic nature of B-cell metabolism that literally ‘fuels’ differentiation in the germinal center to produce an effective antibody response.”
“It’s not yet clear whether or how GSK3 might be a target for future therapies for B cell-related diseases, but this research opens a lot of doors for further studies. To start with, we plan to investigate how GSK3 is regulated in lymphoma and how that relates to changes in metabolism. That research could lead to new approaches to treating lymphoma.”
This research was performed in collaboration with scientists at Eli Lilly and the Lunenfeld-Tanenbaum Research Institute at the University of Toronto. Funding was provided by the National Institutes of Health, the Lilly Research Award Program, the Arthritis National Research Foundation, and the Canadian Institutes of Health Research. ![]()
the spleen of a mouse, showing
inactivated GSK3 (magenta)
in B cells (blue) near follicular
dendritic cells (green).
Image from the lab of
Robert Rickert, PhD
Research published in Nature Immunology helps explain how B-cell metabolism adapts to different environments.
The study suggests the protein GSK3 acts as a metabolic checkpoint regulator in B cells, promoting the survival of circulating B cells while limiting the growth and proliferation of B cells in germinal centers.
“Our research shows that the protein GSK3 plays a crucial role in helping B cells meet the energy needs of their distinct states,” said study author Robert Rickert, PhD, of Sanford Burnham Prebys Medical Discovery Institute in La Jolla, California.
“The findings are particularly relevant for certain B-cell pathologies, including lymphoma subtypes, where there is an increased demand for energy to support the hyperproliferation of cells in a microenvironment that may be limited in nutrients.”
Dr Rickert and his colleagues noted that B cells predominate in a quiescent state until they encounter an antigen, which prompts the cells to grow, proliferate, and differentiate.
The team’s new study showed that GSK3 adjusts B-cell metabolism to match the needs of these different cell states.
In circulating B cells, GSK3 limits overall metabolic activity. In proliferating B cells in germinal centers, GSK3 slows glycolysis and the production of mitochondria.
In fact, GSK3 function is essential for B-cell survival in germinal centers. To understand why, the researchers looked at how B cells in these regions generate energy.
The team found that because these B cells are so metabolically active, they consume nearly all available glucose. That switches on glycolysis.
High glycolytic activity leads to an accumulation of toxic reactive oxygen species, as does rapid manufacture of mitochondria, which tend to leak the same chemicals.
Thus, by restraining the metabolism in specific ways, GSK3 prevents cell death induced by reactive oxygen species.
“Our results were really surprising,” Dr Rickert said. “Until now, we would have thought that slowing metabolism would only be important for preventing B cells from becoming cancerous, which it indeed may be. These studies provide insight into the dynamic nature of B-cell metabolism that literally ‘fuels’ differentiation in the germinal center to produce an effective antibody response.”
“It’s not yet clear whether or how GSK3 might be a target for future therapies for B cell-related diseases, but this research opens a lot of doors for further studies. To start with, we plan to investigate how GSK3 is regulated in lymphoma and how that relates to changes in metabolism. That research could lead to new approaches to treating lymphoma.”
This research was performed in collaboration with scientists at Eli Lilly and the Lunenfeld-Tanenbaum Research Institute at the University of Toronto. Funding was provided by the National Institutes of Health, the Lilly Research Award Program, the Arthritis National Research Foundation, and the Canadian Institutes of Health Research. ![]()
HAART may contribute to profound escalation in syphilis
Highly active antiretroviral therapy taken by HIV-positive men who have sex with men may be contributing to the profound escalation in syphilis infections recently observed worldwide, a recent report suggests.
After noting reports of a substantial and rapid rise in syphilis infections around the globe, which have been largely confined to HIV-positive men taking HAART, researchers constructed mathematical models to test the possibility that HAART may inadvertently alter immune responses in ways that enhance the patient’s vulnerability to Treponema pallidum.
If these findings are verified in further studies, it will be “imperative” to address this unforeseen sequela before implementing global pre-exposure prophylaxis (PrEP) programs, they noted.
The investigators devised their mathematical models to account for the possibility that either HAART itself, or the use of HAART as a surrogate marker for high-risk sex, or both factors together could influence the association with syphilis. The first model assumed that one or more components of HAART could impair the immune response to T. pallidum, and the second assumed that men taking HAART would perceive themselves as low risk and increase their number of partners, thus heightening their ability to transmit the organism.
Each model demonstrated that immunologic changes or behavioral changes could produce syphilis outbreaks similar to those reported in the literature.
“Strikingly, the peak prevalence of the syphilis outbreak produced by both behavioral and immunologic changes [acting together] is larger than the sum of the peaks of outbreaks produced independently by either type of change,” Dr. Rekart and his associates said (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052870).
In other words, HAART-associated immunologic and behavioral changes “can in principle act synergistically to increase syphilis prevalence by amounts comparable with that observed in ongoing outbreaks,” they said.
It is notable that the rates of two other STDs, gonorrhea and chlamydia, have either failed to increase as much or as rapidly as syphilis, or have actually decreased, in the same patient populations. So, the researchers also examined the biological plausibility that HAART could increase patients’ susceptibility to syphilis but not to gonorrhea and chlamydia.
The immune system’s primary clearance mechanism of T. pallidum, macrophage-mediated opsonophagocytosis, requires “unperturbed mitochondrial function to ensure peak metabolic activity within macrophages, opsonic antibody production, and ... macrophage activation.” But HIV infection reduces the quality of opsonic antibodies, and some components of HAART significantly suppress mitochondrial function, the proinflammatory response, and macrophage activation. Theoretically, the combination of these factors could impair treponemal clearance via opsonophagocytosis, Dr. Rekart and his associates said.
In contrast, gonorrhea and chlamydia are caused by pathogens that are not so reliant on opsonophagocytosis to be cleared by the immune system. So, HAART would not lead to similar surges in the rates of gonorrhea and chlamydia infection.
Further studies are needed to corroborate these findings. If they are confirmed, the use of both HAART and PrEP will require changes in patient management to mitigate this increased risk for acquiring syphilis and perhaps other disorders, the researchers noted.
“A retrospective case-control and/or a prospective cohort study comparing the prevalence and epidemiological features of infectious syphilis cases among patients who are HIV-1 positive and treated with HAART, patients who are HIV-1 positive and untreated, and patients who are HIV-1-negative ... would be enlightening,” the investigators added.
Thie study was supported by the National Institute of Allergy and Infectious Diseases. Dr. Rekart and his associates reported having no relevant financial disclosures.
The novel hypothesis proposed by Dr. Michael L. Rekart and his associates is intriguing, and warrants careful consideration.
But it is critical to emphasize that the authors are in no way suggesting that antiretroviral therapy be reconsidered for the treatment and prevention of HIV. Rather, their aim is to stimulate discussion, inform research, and address the staggering increases in syphilis rates.
The focus on HIV appears to have tempered the urgency to control other STDs. But history has shown many times over that that would be a costly mistake. This study demonstrates why screening for, diagnosing, and treating all sexually transmitted infections must be a priority.
Susan Tuddenham, MD, is in the division of infectious diseases at Johns Hopkins University, Baltimore. She and her associates reported having no relevant financial disclosures. Dr. Tuddenham and her associates made these remarks in an editorial accompanying Dr. Rekart’s study (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052940).
The novel hypothesis proposed by Dr. Michael L. Rekart and his associates is intriguing, and warrants careful consideration.
But it is critical to emphasize that the authors are in no way suggesting that antiretroviral therapy be reconsidered for the treatment and prevention of HIV. Rather, their aim is to stimulate discussion, inform research, and address the staggering increases in syphilis rates.
The focus on HIV appears to have tempered the urgency to control other STDs. But history has shown many times over that that would be a costly mistake. This study demonstrates why screening for, diagnosing, and treating all sexually transmitted infections must be a priority.
Susan Tuddenham, MD, is in the division of infectious diseases at Johns Hopkins University, Baltimore. She and her associates reported having no relevant financial disclosures. Dr. Tuddenham and her associates made these remarks in an editorial accompanying Dr. Rekart’s study (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052940).
The novel hypothesis proposed by Dr. Michael L. Rekart and his associates is intriguing, and warrants careful consideration.
But it is critical to emphasize that the authors are in no way suggesting that antiretroviral therapy be reconsidered for the treatment and prevention of HIV. Rather, their aim is to stimulate discussion, inform research, and address the staggering increases in syphilis rates.
The focus on HIV appears to have tempered the urgency to control other STDs. But history has shown many times over that that would be a costly mistake. This study demonstrates why screening for, diagnosing, and treating all sexually transmitted infections must be a priority.
Susan Tuddenham, MD, is in the division of infectious diseases at Johns Hopkins University, Baltimore. She and her associates reported having no relevant financial disclosures. Dr. Tuddenham and her associates made these remarks in an editorial accompanying Dr. Rekart’s study (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052940).
Highly active antiretroviral therapy taken by HIV-positive men who have sex with men may be contributing to the profound escalation in syphilis infections recently observed worldwide, a recent report suggests.
After noting reports of a substantial and rapid rise in syphilis infections around the globe, which have been largely confined to HIV-positive men taking HAART, researchers constructed mathematical models to test the possibility that HAART may inadvertently alter immune responses in ways that enhance the patient’s vulnerability to Treponema pallidum.
If these findings are verified in further studies, it will be “imperative” to address this unforeseen sequela before implementing global pre-exposure prophylaxis (PrEP) programs, they noted.
The investigators devised their mathematical models to account for the possibility that either HAART itself, or the use of HAART as a surrogate marker for high-risk sex, or both factors together could influence the association with syphilis. The first model assumed that one or more components of HAART could impair the immune response to T. pallidum, and the second assumed that men taking HAART would perceive themselves as low risk and increase their number of partners, thus heightening their ability to transmit the organism.
Each model demonstrated that immunologic changes or behavioral changes could produce syphilis outbreaks similar to those reported in the literature.
“Strikingly, the peak prevalence of the syphilis outbreak produced by both behavioral and immunologic changes [acting together] is larger than the sum of the peaks of outbreaks produced independently by either type of change,” Dr. Rekart and his associates said (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052870).
In other words, HAART-associated immunologic and behavioral changes “can in principle act synergistically to increase syphilis prevalence by amounts comparable with that observed in ongoing outbreaks,” they said.
It is notable that the rates of two other STDs, gonorrhea and chlamydia, have either failed to increase as much or as rapidly as syphilis, or have actually decreased, in the same patient populations. So, the researchers also examined the biological plausibility that HAART could increase patients’ susceptibility to syphilis but not to gonorrhea and chlamydia.
The immune system’s primary clearance mechanism of T. pallidum, macrophage-mediated opsonophagocytosis, requires “unperturbed mitochondrial function to ensure peak metabolic activity within macrophages, opsonic antibody production, and ... macrophage activation.” But HIV infection reduces the quality of opsonic antibodies, and some components of HAART significantly suppress mitochondrial function, the proinflammatory response, and macrophage activation. Theoretically, the combination of these factors could impair treponemal clearance via opsonophagocytosis, Dr. Rekart and his associates said.
In contrast, gonorrhea and chlamydia are caused by pathogens that are not so reliant on opsonophagocytosis to be cleared by the immune system. So, HAART would not lead to similar surges in the rates of gonorrhea and chlamydia infection.
Further studies are needed to corroborate these findings. If they are confirmed, the use of both HAART and PrEP will require changes in patient management to mitigate this increased risk for acquiring syphilis and perhaps other disorders, the researchers noted.
“A retrospective case-control and/or a prospective cohort study comparing the prevalence and epidemiological features of infectious syphilis cases among patients who are HIV-1 positive and treated with HAART, patients who are HIV-1 positive and untreated, and patients who are HIV-1-negative ... would be enlightening,” the investigators added.
Thie study was supported by the National Institute of Allergy and Infectious Diseases. Dr. Rekart and his associates reported having no relevant financial disclosures.
Highly active antiretroviral therapy taken by HIV-positive men who have sex with men may be contributing to the profound escalation in syphilis infections recently observed worldwide, a recent report suggests.
After noting reports of a substantial and rapid rise in syphilis infections around the globe, which have been largely confined to HIV-positive men taking HAART, researchers constructed mathematical models to test the possibility that HAART may inadvertently alter immune responses in ways that enhance the patient’s vulnerability to Treponema pallidum.
If these findings are verified in further studies, it will be “imperative” to address this unforeseen sequela before implementing global pre-exposure prophylaxis (PrEP) programs, they noted.
The investigators devised their mathematical models to account for the possibility that either HAART itself, or the use of HAART as a surrogate marker for high-risk sex, or both factors together could influence the association with syphilis. The first model assumed that one or more components of HAART could impair the immune response to T. pallidum, and the second assumed that men taking HAART would perceive themselves as low risk and increase their number of partners, thus heightening their ability to transmit the organism.
Each model demonstrated that immunologic changes or behavioral changes could produce syphilis outbreaks similar to those reported in the literature.
“Strikingly, the peak prevalence of the syphilis outbreak produced by both behavioral and immunologic changes [acting together] is larger than the sum of the peaks of outbreaks produced independently by either type of change,” Dr. Rekart and his associates said (Sex Transm Infect. 2017 Jan 16. doi: 10.1136/sextrans.2016.052870).
In other words, HAART-associated immunologic and behavioral changes “can in principle act synergistically to increase syphilis prevalence by amounts comparable with that observed in ongoing outbreaks,” they said.
It is notable that the rates of two other STDs, gonorrhea and chlamydia, have either failed to increase as much or as rapidly as syphilis, or have actually decreased, in the same patient populations. So, the researchers also examined the biological plausibility that HAART could increase patients’ susceptibility to syphilis but not to gonorrhea and chlamydia.
The immune system’s primary clearance mechanism of T. pallidum, macrophage-mediated opsonophagocytosis, requires “unperturbed mitochondrial function to ensure peak metabolic activity within macrophages, opsonic antibody production, and ... macrophage activation.” But HIV infection reduces the quality of opsonic antibodies, and some components of HAART significantly suppress mitochondrial function, the proinflammatory response, and macrophage activation. Theoretically, the combination of these factors could impair treponemal clearance via opsonophagocytosis, Dr. Rekart and his associates said.
In contrast, gonorrhea and chlamydia are caused by pathogens that are not so reliant on opsonophagocytosis to be cleared by the immune system. So, HAART would not lead to similar surges in the rates of gonorrhea and chlamydia infection.
Further studies are needed to corroborate these findings. If they are confirmed, the use of both HAART and PrEP will require changes in patient management to mitigate this increased risk for acquiring syphilis and perhaps other disorders, the researchers noted.
“A retrospective case-control and/or a prospective cohort study comparing the prevalence and epidemiological features of infectious syphilis cases among patients who are HIV-1 positive and treated with HAART, patients who are HIV-1 positive and untreated, and patients who are HIV-1-negative ... would be enlightening,” the investigators added.
Thie study was supported by the National Institute of Allergy and Infectious Diseases. Dr. Rekart and his associates reported having no relevant financial disclosures.
FROM SEXUALLY TRANSMITTED INFECTIONS
Key clinical point: HAART may be contributing to the profound escalation in syphilis infections worldwide, perhaps by impairing immunity to Treponema pallidum.
Major finding: HAART-associated immunologic and behavioral changes can in principle act synergistically to increase syphilis prevalence by amounts comparable with that observed in ongoing outbreaks.
Data source: Mathematical modeling studies of potential HAART-induced changes in immune function and behavior among HIV-positive men who have sex with men.
Disclosures: This study supported by the National Institute of Allergy and Infectious Diseases. Dr. Rekart and his associates reported having no relevant financial disclosures.
Carbapenem-resistant K. pneumoniae occurs in 25% of long-term acute care hospital cultures
Nearly one-quarter of Klebsiella pneumoniae cultures in a network of U.S. long-term acute care hospitals are resistant to carbapenem, according to Jennifer H. Han, MD, and her associates.
From a sample of 3,846 K. pneumoniae cultures taken from 64 long-term acute care hospitals in 16 states, 946, or 24.6%, of the cultures were carbapenem-resistant, and were taken from 821 patients. Just under 54% of CRKP isolates were taken from a respiratory source, with 37% coming from urine and the remaining 9.4% coming from blood. Nearly all CRKP isolates were resistant to fluoroquinolones, and 59.2% were resistant to amikacin.
Of the 16 states where cultures were taken from, California had the highest rate of carbapenem resistance, with 45.5% of K. pneumoniae cultures showing resistance. Other states with high rates of CRKP included South Carolina, Kentucky, and Indiana.
“Given the chronically, critically ill population, with convergence of at-risk patients from multiple facilities, future studies of optimal infection prevention strategies are urgently needed for this setting. In addition, expansion of national surveillance efforts and improved communication between [long-term acute care hospitals] and acute care hospitals will be critical for reducing the continued emergence and dissemination of CRKP across the health care continuum,” Dr. Han and her associates concluded.
Find the full study in Clinical Infectious Diseases (doi: 10.1 LTACHs 093/cid/ciw856)
Nearly one-quarter of Klebsiella pneumoniae cultures in a network of U.S. long-term acute care hospitals are resistant to carbapenem, according to Jennifer H. Han, MD, and her associates.
From a sample of 3,846 K. pneumoniae cultures taken from 64 long-term acute care hospitals in 16 states, 946, or 24.6%, of the cultures were carbapenem-resistant, and were taken from 821 patients. Just under 54% of CRKP isolates were taken from a respiratory source, with 37% coming from urine and the remaining 9.4% coming from blood. Nearly all CRKP isolates were resistant to fluoroquinolones, and 59.2% were resistant to amikacin.
Of the 16 states where cultures were taken from, California had the highest rate of carbapenem resistance, with 45.5% of K. pneumoniae cultures showing resistance. Other states with high rates of CRKP included South Carolina, Kentucky, and Indiana.
“Given the chronically, critically ill population, with convergence of at-risk patients from multiple facilities, future studies of optimal infection prevention strategies are urgently needed for this setting. In addition, expansion of national surveillance efforts and improved communication between [long-term acute care hospitals] and acute care hospitals will be critical for reducing the continued emergence and dissemination of CRKP across the health care continuum,” Dr. Han and her associates concluded.
Find the full study in Clinical Infectious Diseases (doi: 10.1 LTACHs 093/cid/ciw856)
Nearly one-quarter of Klebsiella pneumoniae cultures in a network of U.S. long-term acute care hospitals are resistant to carbapenem, according to Jennifer H. Han, MD, and her associates.
From a sample of 3,846 K. pneumoniae cultures taken from 64 long-term acute care hospitals in 16 states, 946, or 24.6%, of the cultures were carbapenem-resistant, and were taken from 821 patients. Just under 54% of CRKP isolates were taken from a respiratory source, with 37% coming from urine and the remaining 9.4% coming from blood. Nearly all CRKP isolates were resistant to fluoroquinolones, and 59.2% were resistant to amikacin.
Of the 16 states where cultures were taken from, California had the highest rate of carbapenem resistance, with 45.5% of K. pneumoniae cultures showing resistance. Other states with high rates of CRKP included South Carolina, Kentucky, and Indiana.
“Given the chronically, critically ill population, with convergence of at-risk patients from multiple facilities, future studies of optimal infection prevention strategies are urgently needed for this setting. In addition, expansion of national surveillance efforts and improved communication between [long-term acute care hospitals] and acute care hospitals will be critical for reducing the continued emergence and dissemination of CRKP across the health care continuum,” Dr. Han and her associates concluded.
Find the full study in Clinical Infectious Diseases (doi: 10.1 LTACHs 093/cid/ciw856)
FROM CLINICAL INFECTIOUS DISEASES
Asymptomatic carriage of carbapenem-resistant Enterobacteriaceae ‘considerable’
Asymptomatic carriage of carbapenem-resistant Enterobacteriaceae is “considerable,” according to genetic analyses of bacterial isolates obtained from patients at four large U.S. hospitals.
To better understand the “urgent threat” of carbapenem resistance – specifically, to obtain a “snapshot” of how the resistant enterobacteria evolve, diversify, and spread – the researchers performed genetic analyses on 122 carbapenem-resistant and 141 carbapenem-susceptible bacterial isolates from patients hospitalized during a 16-month period at three Boston and one California medical centers. The isolates were obtained from urine (44%), respiratory tract (16%), blood (11%), wound (11%), and other samples, said Gustavo C. Cerqueira, PhD, of the Broad Institute of MIT and Harvard University in Cambridge, Mass., and his associates.
They found 8 species of bacteria that exhibited carbapenem resistance, chiefly Klebsiella pneumoniae. There also was a significant degree of diversity among resistant Enterobacteria. Most importantly, the investigators found evidence of substantial asymptomatic carriage of resistant bacteria and discovered several previously unrecognized mechanisms that produced resistance. Taken together, the findings indicate “continued innovation by these organisms to thwart the action of this important class of antibiotics,” reported Dr. Cerqueira, also affiliated with Massachusetts General Hospital in Boston, and his associates (Proc Nat Acad Sci USA. 2017 Jan 16 [doi:10.1073/pnas.1616248114]).
The study findings underscore the need for “an aggressive approach to surveillance and isolation” to control this continuing threat, they added.
This work was supported by the National Institute of Allergy and Infectious Diseases. Dr. Cerqueira and his associates reported having no relevant financial disclosures.
Asymptomatic carriage of carbapenem-resistant Enterobacteriaceae is “considerable,” according to genetic analyses of bacterial isolates obtained from patients at four large U.S. hospitals.
To better understand the “urgent threat” of carbapenem resistance – specifically, to obtain a “snapshot” of how the resistant enterobacteria evolve, diversify, and spread – the researchers performed genetic analyses on 122 carbapenem-resistant and 141 carbapenem-susceptible bacterial isolates from patients hospitalized during a 16-month period at three Boston and one California medical centers. The isolates were obtained from urine (44%), respiratory tract (16%), blood (11%), wound (11%), and other samples, said Gustavo C. Cerqueira, PhD, of the Broad Institute of MIT and Harvard University in Cambridge, Mass., and his associates.
They found 8 species of bacteria that exhibited carbapenem resistance, chiefly Klebsiella pneumoniae. There also was a significant degree of diversity among resistant Enterobacteria. Most importantly, the investigators found evidence of substantial asymptomatic carriage of resistant bacteria and discovered several previously unrecognized mechanisms that produced resistance. Taken together, the findings indicate “continued innovation by these organisms to thwart the action of this important class of antibiotics,” reported Dr. Cerqueira, also affiliated with Massachusetts General Hospital in Boston, and his associates (Proc Nat Acad Sci USA. 2017 Jan 16 [doi:10.1073/pnas.1616248114]).
The study findings underscore the need for “an aggressive approach to surveillance and isolation” to control this continuing threat, they added.
This work was supported by the National Institute of Allergy and Infectious Diseases. Dr. Cerqueira and his associates reported having no relevant financial disclosures.
Asymptomatic carriage of carbapenem-resistant Enterobacteriaceae is “considerable,” according to genetic analyses of bacterial isolates obtained from patients at four large U.S. hospitals.
To better understand the “urgent threat” of carbapenem resistance – specifically, to obtain a “snapshot” of how the resistant enterobacteria evolve, diversify, and spread – the researchers performed genetic analyses on 122 carbapenem-resistant and 141 carbapenem-susceptible bacterial isolates from patients hospitalized during a 16-month period at three Boston and one California medical centers. The isolates were obtained from urine (44%), respiratory tract (16%), blood (11%), wound (11%), and other samples, said Gustavo C. Cerqueira, PhD, of the Broad Institute of MIT and Harvard University in Cambridge, Mass., and his associates.
They found 8 species of bacteria that exhibited carbapenem resistance, chiefly Klebsiella pneumoniae. There also was a significant degree of diversity among resistant Enterobacteria. Most importantly, the investigators found evidence of substantial asymptomatic carriage of resistant bacteria and discovered several previously unrecognized mechanisms that produced resistance. Taken together, the findings indicate “continued innovation by these organisms to thwart the action of this important class of antibiotics,” reported Dr. Cerqueira, also affiliated with Massachusetts General Hospital in Boston, and his associates (Proc Nat Acad Sci USA. 2017 Jan 16 [doi:10.1073/pnas.1616248114]).
The study findings underscore the need for “an aggressive approach to surveillance and isolation” to control this continuing threat, they added.
This work was supported by the National Institute of Allergy and Infectious Diseases. Dr. Cerqueira and his associates reported having no relevant financial disclosures.
FROM THE PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES
Key clinical point: Asymptomatic carriage of carbapenem-resistant Enterobacteriaceae is “considerable.”
Major finding: Researchers found eight species of bacteria that exhibited carbapenem resistance, a significant degree of diversity among resistant enterobacteria, evidence of substantial asymptomatic carriage of resistant bacteria, and several previously unrecognized mechanisms that produced resistance.
Data source: Genetic analyses of 122 carbapenem-resistant and 141 carbapenem-susceptible bacterial isolates obtained from patients at 4 large U.S. hospitals.
Disclosures: This work was supported by the National Institute of Allergy and Infectious Diseases. Dr. Cerqueira and his associates reported having no relevant financial disclosures.