User login
New Onset Type 1 Diabetes: "Fear Not - Easing Your Concerns"
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
![]()
OptumCare Medical Group, Orange County, Calif; Adjunct Faculty, A.T. Still University/Arizona School of Health Sciences, Mesa, Ariz
![]()
OptumCare Medical Group, Orange County, Calif; Adjunct Faculty, A.T. Still University/Arizona School of Health Sciences, Mesa, Ariz
![]()
OptumCare Medical Group, Orange County, Calif; Adjunct Faculty, A.T. Still University/Arizona School of Health Sciences, Mesa, Ariz
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EMA recommends orphan designation for cord blood product

The European Medicines Agency’s (EMA’s) Committee for Orphan Medicinal Products has recommended that NiCord® receive orphan designation as a treatment for patients who require a hematopoietic stem cell transplant.
NiCord is a stand-alone graft derived from a single umbilical cord blood unit that has been expanded in culture and enriched with stem and progenitor cells.
NiCord already has orphan designation in the European Union as a treatment for patients with acute myeloid leukemia.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days.
NiCord also has orphan designation and breakthrough designation from the US Food and Drug Administration for the treatment of hematologic malignancies.
NiCord research
Data from the pilot study of NiCord suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
And research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
NiCord is currently being studied in a phase 3 registration study as a graft for patients with hematologic malignancies who do not have a rapidly available, fully matched donor.
Gamida Cell, the company developing NiCord, announced last month that the first patient in the study had been transplanted. ![]()
The European Medicines Agency’s (EMA’s) Committee for Orphan Medicinal Products has recommended that NiCord® receive orphan designation as a treatment for patients who require a hematopoietic stem cell transplant.
NiCord is a stand-alone graft derived from a single umbilical cord blood unit that has been expanded in culture and enriched with stem and progenitor cells.
NiCord already has orphan designation in the European Union as a treatment for patients with acute myeloid leukemia.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days.
NiCord also has orphan designation and breakthrough designation from the US Food and Drug Administration for the treatment of hematologic malignancies.
NiCord research
Data from the pilot study of NiCord suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
And research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
NiCord is currently being studied in a phase 3 registration study as a graft for patients with hematologic malignancies who do not have a rapidly available, fully matched donor.
Gamida Cell, the company developing NiCord, announced last month that the first patient in the study had been transplanted. ![]()
The European Medicines Agency’s (EMA’s) Committee for Orphan Medicinal Products has recommended that NiCord® receive orphan designation as a treatment for patients who require a hematopoietic stem cell transplant.
NiCord is a stand-alone graft derived from a single umbilical cord blood unit that has been expanded in culture and enriched with stem and progenitor cells.
NiCord already has orphan designation in the European Union as a treatment for patients with acute myeloid leukemia.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval. The designation also provides incentives for companies seeking protocol assistance from the EMA during the product development phase and direct access to the centralized authorization procedure.
The EMA adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision. The European Commission typically makes a decision within 30 days.
NiCord also has orphan designation and breakthrough designation from the US Food and Drug Administration for the treatment of hematologic malignancies.
NiCord research
Data from the pilot study of NiCord suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
And research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
NiCord is currently being studied in a phase 3 registration study as a graft for patients with hematologic malignancies who do not have a rapidly available, fully matched donor.
Gamida Cell, the company developing NiCord, announced last month that the first patient in the study had been transplanted. ![]()
Sneak Peek: Journal of Hospital Medicine
BACKGROUND: Readmissions after hospitalization for pneumonia are common, but the few risk-prediction models have poor to modest predictive ability. Data routinely collected in the EHR may improve prediction.
DESIGN: Observational cohort study using backward-stepwise selection and cross validation.
SUBJECTS: Consecutive pneumonia hospitalizations from six diverse hospitals in north Texas from 2009 to 2010.
MEASURES: All-cause, nonelective, 30-day readmissions, ascertained from 75 regional hospitals.
RESULTS: Of 1,463 patients, 13.6% were readmitted. The first-day, pneumonia-specific model included sociodemographic factors, prior hospitalizations, thrombocytosis, and a modified pneumonia severity index. The full-stay model included disposition status, vital sign instabilities on discharge, and an updated pneumonia severity index calculated using values from the day of discharge as additional predictors. The full-stay, pneumonia-specific model outperformed the first-day model (C-statistic, 0.731 vs. 0.695; P = .02; net reclassification index = 0.08). Compared with a validated multicondition readmission model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores, the full-stay pneumonia-specific model had better discrimination (C-statistic, 0.604-0.681; P less than 0.01 for all comparisons), predicted a broader range of risk, and better reclassified individuals by their true risk (net reclassification index range, 0.09-0.18).
CONCLUSIONS: EHR data collected from the entire hospitalization can accurately predict readmission risk among patients hospitalized for pneumonia. This approach outperforms a first-day, pneumonia-specific model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores.
Also In JHM This Month
Evaluating automated rules for rapid response system alarm triggers in medical and surgical patients
AUTHORS: Santiago Romero-Brufau, MD; Bruce W. Morlan, MS; Matthew Johnson, MPH; Joel Hickman; Lisa L. Kirkland, MD; James M. Naessens, ScD; Jeanne Huddleston, MD, FACP, FHM
Prognosticating with the Hospital-Patient One-year Mortality Risk score using information abstracted from the medical record
AUTHORS: Genevieve Casey, MD, and Carl van Walraven, MD, FRCPC, MSc
Automating venous thromboembolism risk calculation using electronic health record data upon hospital admission: The Automated Padua Prediction Score
AUTHORS: Pierre Elias, MD; Raman Khanna, MD; Adams Dudley, MD, MBA; Jason Davies, MD, PhD; Ronald Jacolbia, MSN; Kara McArthur, BA; Andrew D. Auerbach, MD, MPH, SFHM
The value of ultrasound in cellulitis to rule out deep venous thrombosis
AUTHORS: Hyung J. Cho, MD, and Andrew S. Dunn, MD, SFHM
Hospital medicine and perioperative care: A framework for high quality, high value collaborative care
AUTHORS: Rachel E. Thompson, MD, MPH, SFHM; Kurt Pfeifer, MD, FHM; Paul Grant, MD, SFHM; Cornelia Taylor, MD; Barbara Slawski, MD, FACP, MS, SFHM; Christopher Whinney, MD, FACP, FHM; Laurence Wellikson, MD, MHM; Amir K. Jaffer, MD, MBA, SFHM
BACKGROUND: Readmissions after hospitalization for pneumonia are common, but the few risk-prediction models have poor to modest predictive ability. Data routinely collected in the EHR may improve prediction.
DESIGN: Observational cohort study using backward-stepwise selection and cross validation.
SUBJECTS: Consecutive pneumonia hospitalizations from six diverse hospitals in north Texas from 2009 to 2010.
MEASURES: All-cause, nonelective, 30-day readmissions, ascertained from 75 regional hospitals.
RESULTS: Of 1,463 patients, 13.6% were readmitted. The first-day, pneumonia-specific model included sociodemographic factors, prior hospitalizations, thrombocytosis, and a modified pneumonia severity index. The full-stay model included disposition status, vital sign instabilities on discharge, and an updated pneumonia severity index calculated using values from the day of discharge as additional predictors. The full-stay, pneumonia-specific model outperformed the first-day model (C-statistic, 0.731 vs. 0.695; P = .02; net reclassification index = 0.08). Compared with a validated multicondition readmission model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores, the full-stay pneumonia-specific model had better discrimination (C-statistic, 0.604-0.681; P less than 0.01 for all comparisons), predicted a broader range of risk, and better reclassified individuals by their true risk (net reclassification index range, 0.09-0.18).
CONCLUSIONS: EHR data collected from the entire hospitalization can accurately predict readmission risk among patients hospitalized for pneumonia. This approach outperforms a first-day, pneumonia-specific model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores.
Also In JHM This Month
Evaluating automated rules for rapid response system alarm triggers in medical and surgical patients
AUTHORS: Santiago Romero-Brufau, MD; Bruce W. Morlan, MS; Matthew Johnson, MPH; Joel Hickman; Lisa L. Kirkland, MD; James M. Naessens, ScD; Jeanne Huddleston, MD, FACP, FHM
Prognosticating with the Hospital-Patient One-year Mortality Risk score using information abstracted from the medical record
AUTHORS: Genevieve Casey, MD, and Carl van Walraven, MD, FRCPC, MSc
Automating venous thromboembolism risk calculation using electronic health record data upon hospital admission: The Automated Padua Prediction Score
AUTHORS: Pierre Elias, MD; Raman Khanna, MD; Adams Dudley, MD, MBA; Jason Davies, MD, PhD; Ronald Jacolbia, MSN; Kara McArthur, BA; Andrew D. Auerbach, MD, MPH, SFHM
The value of ultrasound in cellulitis to rule out deep venous thrombosis
AUTHORS: Hyung J. Cho, MD, and Andrew S. Dunn, MD, SFHM
Hospital medicine and perioperative care: A framework for high quality, high value collaborative care
AUTHORS: Rachel E. Thompson, MD, MPH, SFHM; Kurt Pfeifer, MD, FHM; Paul Grant, MD, SFHM; Cornelia Taylor, MD; Barbara Slawski, MD, FACP, MS, SFHM; Christopher Whinney, MD, FACP, FHM; Laurence Wellikson, MD, MHM; Amir K. Jaffer, MD, MBA, SFHM
BACKGROUND: Readmissions after hospitalization for pneumonia are common, but the few risk-prediction models have poor to modest predictive ability. Data routinely collected in the EHR may improve prediction.
DESIGN: Observational cohort study using backward-stepwise selection and cross validation.
SUBJECTS: Consecutive pneumonia hospitalizations from six diverse hospitals in north Texas from 2009 to 2010.
MEASURES: All-cause, nonelective, 30-day readmissions, ascertained from 75 regional hospitals.
RESULTS: Of 1,463 patients, 13.6% were readmitted. The first-day, pneumonia-specific model included sociodemographic factors, prior hospitalizations, thrombocytosis, and a modified pneumonia severity index. The full-stay model included disposition status, vital sign instabilities on discharge, and an updated pneumonia severity index calculated using values from the day of discharge as additional predictors. The full-stay, pneumonia-specific model outperformed the first-day model (C-statistic, 0.731 vs. 0.695; P = .02; net reclassification index = 0.08). Compared with a validated multicondition readmission model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores, the full-stay pneumonia-specific model had better discrimination (C-statistic, 0.604-0.681; P less than 0.01 for all comparisons), predicted a broader range of risk, and better reclassified individuals by their true risk (net reclassification index range, 0.09-0.18).
CONCLUSIONS: EHR data collected from the entire hospitalization can accurately predict readmission risk among patients hospitalized for pneumonia. This approach outperforms a first-day, pneumonia-specific model, the Centers for Medicare & Medicaid Services pneumonia model, and two commonly used pneumonia severity of illness scores.
Also In JHM This Month
Evaluating automated rules for rapid response system alarm triggers in medical and surgical patients
AUTHORS: Santiago Romero-Brufau, MD; Bruce W. Morlan, MS; Matthew Johnson, MPH; Joel Hickman; Lisa L. Kirkland, MD; James M. Naessens, ScD; Jeanne Huddleston, MD, FACP, FHM
Prognosticating with the Hospital-Patient One-year Mortality Risk score using information abstracted from the medical record
AUTHORS: Genevieve Casey, MD, and Carl van Walraven, MD, FRCPC, MSc
Automating venous thromboembolism risk calculation using electronic health record data upon hospital admission: The Automated Padua Prediction Score
AUTHORS: Pierre Elias, MD; Raman Khanna, MD; Adams Dudley, MD, MBA; Jason Davies, MD, PhD; Ronald Jacolbia, MSN; Kara McArthur, BA; Andrew D. Auerbach, MD, MPH, SFHM
The value of ultrasound in cellulitis to rule out deep venous thrombosis
AUTHORS: Hyung J. Cho, MD, and Andrew S. Dunn, MD, SFHM
Hospital medicine and perioperative care: A framework for high quality, high value collaborative care
AUTHORS: Rachel E. Thompson, MD, MPH, SFHM; Kurt Pfeifer, MD, FHM; Paul Grant, MD, SFHM; Cornelia Taylor, MD; Barbara Slawski, MD, FACP, MS, SFHM; Christopher Whinney, MD, FACP, FHM; Laurence Wellikson, MD, MHM; Amir K. Jaffer, MD, MBA, SFHM

Dabigatran crushes warfarin for AF ablation
Washington – Uninterrupted dabigatran for periprocedural anticoagulation in patients undergoing catheter ablation for atrial fibrillation proved far superior to uninterrupted warfarin – the current standard – in the randomized multicenter RE-CIRCUIT trial, Hugh Calkins, MD, reported at the annual meeting of the American College of Cardiology.
The primary study endpoint – the incidence of major bleeding events from the time of the first femoral puncture at the procedure’s start through the subsequent 8 weeks – occurred in 1.6% of the dabigatran (Pradaxa) group and 6.9% of the warfarin group, for an absolute 5.9% reduction in risk and a 77% relative risk reduction favoring the novel anticoagulant.
“This trial will definitely affect my own practice, and I think it will quickly affect the practices of electrophysiologists around the world,” declared Dr. Calkins, professor of cardiology and medicine and director of the clinical electrophysiology laboratory and the arrhythmia service at Johns Hopkins University, Baltimore.

RE-CIRCUIT (Randomized Evaluation of Dabigatran Etexilate Compared to Warfarin in Pulmonary Vein Ablation: Assessment of an Uninterrupted Periprocedural Anticoagulation Strategy) was a multicenter, prospective, international trial conducted in 635 atrial fibrillation (AF) patients who underwent catheter ablation at 104 sites. The trial was of necessity open label because of the need for frequent adjustments of warfarin dosing; however, outcome assessment was carried out by a blinded panel of six cardiologists and three neurologists.
Standard practice among AF ablationists is to continue oral anticoagulation periprocedurally because prior studies have convincingly shown that periprocedural interruption of warfarin in an effort to reduce bleeding results in a sharply increased risk of periprocedural stroke. So participants in RE-CIRCUIT were randomized to 4-8 weeks of uninterrupted anticoagulation with either dabigatran at 150 mg b.i.d. or warfarin with a target international normalized ratio (INR) of 2.0-3.0 prior to the ablation procedure, during it, and for 8 weeks afterward, at which time an individualized decision was made as to whether to stop or continue the drug.
Major bleeding events were defined by the International Society on Thrombosis and Hemostatis criteria. Most of these bleeds occurred within the first day or two after the procedure. Pericardial tamponades and groin hematomas were significantly less common with dabigatran.
The incidence of minor bleeding events was similar, at around 18% in the two treatment arms. No strokes or systemic embolisms occurred in the study. One patient on warfarin experienced a transient ischemic attack.
Dr. Calkins elaborated on why RE-CIRCUIT will change clinical practice: “A stroke is a terrible thing during an AF procedure and cardiac tamponade is the most common cause of death from the procedure. And now we have high-quality data showing that if you perform this procedure on uninterrupted dabigatran, the risk of stroke and other systemic embolic events is extremely low, and the rate of major bleeding was 77% less.
“Plus, the logistics of warfarin are a pain,” he continued. “If the patient presents on the day of ablation with an INR that’s too high, the procedure is canceled, and if they present with an INR that’s too low and the procedure is carried out, it’s done so with an increased stroke risk.”
Dr. Calkins said he suspects the sharp reduction in major bleeding events during and after AF catheter ablation is a class effect shared by the other NOACs. Studies with those agents are ongoing. But for now, the unique availability of an immediate reversal agent in the form of idarucizumab (Praxbind) for dabigatran in the event of uncontrolled major bleeding is a source of reassurance for operators and patients alike. The antidote was never required in RE-CIRCUIT, though, the cardiologist noted.
Discussant William G. Stevenson, MD, called the trial “informative and helpful.”
“Something we’ve all been struggling with was that some concern was earlier raised that dabigatran might be associated with more thromboembolic events in this scenario. This study clearly refutes that concern,” observed Dr. Stevenson, director of the clinical cardiac electrophysiology program at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Stevenson wondered whether the outcome differences between the two study groups could be explained by differences in operator techniques and tools. That’s highly unlikely, Dr. Calkins replied. Randomization was done patient by patient, not center by center.
Then why the big difference in major bleeding complications? Dr. Stevenson asked.
“It may be that, if you poke a hole when a patient is on a more forgiving anticoagulant like dabigatran, the bleeding doesn’t persist and turn into a tamponade, whereas if you poke a hole on warfarin it turns into a bigger problem,” Dr. Calkins responded. “When you think about it, warfarin really impacts the whole coagulation cascade through factors VII, IX, and X, so multiple coagulation factors are rendered impotent, whereas dabigatran is a direct thrombin inhibitor, so you’re selectively knocking out just one component of the coagulation cascade. It provides more leeway in preventing a small hole from turning into a big effusion,” he said.

The RE-CIRCUIT trial was funded by Boehringer Ingelheim. Dr. Calkins reported receiving lecture fees from that company and from Medtronic, and serving as a consultant to Medtronic, Abbott Medical, and AtriCure.
Simultaneously with Dr. Calkins’ presentation at ACC 17, the RE-CIRCUIT study was published online (N Engl J Med. 2017 Mar 19. doi: 10.1056/NEJMoa1701005).
Washington – Uninterrupted dabigatran for periprocedural anticoagulation in patients undergoing catheter ablation for atrial fibrillation proved far superior to uninterrupted warfarin – the current standard – in the randomized multicenter RE-CIRCUIT trial, Hugh Calkins, MD, reported at the annual meeting of the American College of Cardiology.
The primary study endpoint – the incidence of major bleeding events from the time of the first femoral puncture at the procedure’s start through the subsequent 8 weeks – occurred in 1.6% of the dabigatran (Pradaxa) group and 6.9% of the warfarin group, for an absolute 5.9% reduction in risk and a 77% relative risk reduction favoring the novel anticoagulant.
“This trial will definitely affect my own practice, and I think it will quickly affect the practices of electrophysiologists around the world,” declared Dr. Calkins, professor of cardiology and medicine and director of the clinical electrophysiology laboratory and the arrhythmia service at Johns Hopkins University, Baltimore.
RE-CIRCUIT (Randomized Evaluation of Dabigatran Etexilate Compared to Warfarin in Pulmonary Vein Ablation: Assessment of an Uninterrupted Periprocedural Anticoagulation Strategy) was a multicenter, prospective, international trial conducted in 635 atrial fibrillation (AF) patients who underwent catheter ablation at 104 sites. The trial was of necessity open label because of the need for frequent adjustments of warfarin dosing; however, outcome assessment was carried out by a blinded panel of six cardiologists and three neurologists.
Standard practice among AF ablationists is to continue oral anticoagulation periprocedurally because prior studies have convincingly shown that periprocedural interruption of warfarin in an effort to reduce bleeding results in a sharply increased risk of periprocedural stroke. So participants in RE-CIRCUIT were randomized to 4-8 weeks of uninterrupted anticoagulation with either dabigatran at 150 mg b.i.d. or warfarin with a target international normalized ratio (INR) of 2.0-3.0 prior to the ablation procedure, during it, and for 8 weeks afterward, at which time an individualized decision was made as to whether to stop or continue the drug.
Major bleeding events were defined by the International Society on Thrombosis and Hemostatis criteria. Most of these bleeds occurred within the first day or two after the procedure. Pericardial tamponades and groin hematomas were significantly less common with dabigatran.
The incidence of minor bleeding events was similar, at around 18% in the two treatment arms. No strokes or systemic embolisms occurred in the study. One patient on warfarin experienced a transient ischemic attack.
Dr. Calkins elaborated on why RE-CIRCUIT will change clinical practice: “A stroke is a terrible thing during an AF procedure and cardiac tamponade is the most common cause of death from the procedure. And now we have high-quality data showing that if you perform this procedure on uninterrupted dabigatran, the risk of stroke and other systemic embolic events is extremely low, and the rate of major bleeding was 77% less.
“Plus, the logistics of warfarin are a pain,” he continued. “If the patient presents on the day of ablation with an INR that’s too high, the procedure is canceled, and if they present with an INR that’s too low and the procedure is carried out, it’s done so with an increased stroke risk.”
Dr. Calkins said he suspects the sharp reduction in major bleeding events during and after AF catheter ablation is a class effect shared by the other NOACs. Studies with those agents are ongoing. But for now, the unique availability of an immediate reversal agent in the form of idarucizumab (Praxbind) for dabigatran in the event of uncontrolled major bleeding is a source of reassurance for operators and patients alike. The antidote was never required in RE-CIRCUIT, though, the cardiologist noted.
Discussant William G. Stevenson, MD, called the trial “informative and helpful.”
“Something we’ve all been struggling with was that some concern was earlier raised that dabigatran might be associated with more thromboembolic events in this scenario. This study clearly refutes that concern,” observed Dr. Stevenson, director of the clinical cardiac electrophysiology program at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Stevenson wondered whether the outcome differences between the two study groups could be explained by differences in operator techniques and tools. That’s highly unlikely, Dr. Calkins replied. Randomization was done patient by patient, not center by center.
Then why the big difference in major bleeding complications? Dr. Stevenson asked.
“It may be that, if you poke a hole when a patient is on a more forgiving anticoagulant like dabigatran, the bleeding doesn’t persist and turn into a tamponade, whereas if you poke a hole on warfarin it turns into a bigger problem,” Dr. Calkins responded. “When you think about it, warfarin really impacts the whole coagulation cascade through factors VII, IX, and X, so multiple coagulation factors are rendered impotent, whereas dabigatran is a direct thrombin inhibitor, so you’re selectively knocking out just one component of the coagulation cascade. It provides more leeway in preventing a small hole from turning into a big effusion,” he said.
The RE-CIRCUIT trial was funded by Boehringer Ingelheim. Dr. Calkins reported receiving lecture fees from that company and from Medtronic, and serving as a consultant to Medtronic, Abbott Medical, and AtriCure.
Simultaneously with Dr. Calkins’ presentation at ACC 17, the RE-CIRCUIT study was published online (N Engl J Med. 2017 Mar 19. doi: 10.1056/NEJMoa1701005).
Washington – Uninterrupted dabigatran for periprocedural anticoagulation in patients undergoing catheter ablation for atrial fibrillation proved far superior to uninterrupted warfarin – the current standard – in the randomized multicenter RE-CIRCUIT trial, Hugh Calkins, MD, reported at the annual meeting of the American College of Cardiology.
The primary study endpoint – the incidence of major bleeding events from the time of the first femoral puncture at the procedure’s start through the subsequent 8 weeks – occurred in 1.6% of the dabigatran (Pradaxa) group and 6.9% of the warfarin group, for an absolute 5.9% reduction in risk and a 77% relative risk reduction favoring the novel anticoagulant.
“This trial will definitely affect my own practice, and I think it will quickly affect the practices of electrophysiologists around the world,” declared Dr. Calkins, professor of cardiology and medicine and director of the clinical electrophysiology laboratory and the arrhythmia service at Johns Hopkins University, Baltimore.
RE-CIRCUIT (Randomized Evaluation of Dabigatran Etexilate Compared to Warfarin in Pulmonary Vein Ablation: Assessment of an Uninterrupted Periprocedural Anticoagulation Strategy) was a multicenter, prospective, international trial conducted in 635 atrial fibrillation (AF) patients who underwent catheter ablation at 104 sites. The trial was of necessity open label because of the need for frequent adjustments of warfarin dosing; however, outcome assessment was carried out by a blinded panel of six cardiologists and three neurologists.
Standard practice among AF ablationists is to continue oral anticoagulation periprocedurally because prior studies have convincingly shown that periprocedural interruption of warfarin in an effort to reduce bleeding results in a sharply increased risk of periprocedural stroke. So participants in RE-CIRCUIT were randomized to 4-8 weeks of uninterrupted anticoagulation with either dabigatran at 150 mg b.i.d. or warfarin with a target international normalized ratio (INR) of 2.0-3.0 prior to the ablation procedure, during it, and for 8 weeks afterward, at which time an individualized decision was made as to whether to stop or continue the drug.
Major bleeding events were defined by the International Society on Thrombosis and Hemostatis criteria. Most of these bleeds occurred within the first day or two after the procedure. Pericardial tamponades and groin hematomas were significantly less common with dabigatran.
The incidence of minor bleeding events was similar, at around 18% in the two treatment arms. No strokes or systemic embolisms occurred in the study. One patient on warfarin experienced a transient ischemic attack.
Dr. Calkins elaborated on why RE-CIRCUIT will change clinical practice: “A stroke is a terrible thing during an AF procedure and cardiac tamponade is the most common cause of death from the procedure. And now we have high-quality data showing that if you perform this procedure on uninterrupted dabigatran, the risk of stroke and other systemic embolic events is extremely low, and the rate of major bleeding was 77% less.
“Plus, the logistics of warfarin are a pain,” he continued. “If the patient presents on the day of ablation with an INR that’s too high, the procedure is canceled, and if they present with an INR that’s too low and the procedure is carried out, it’s done so with an increased stroke risk.”
Dr. Calkins said he suspects the sharp reduction in major bleeding events during and after AF catheter ablation is a class effect shared by the other NOACs. Studies with those agents are ongoing. But for now, the unique availability of an immediate reversal agent in the form of idarucizumab (Praxbind) for dabigatran in the event of uncontrolled major bleeding is a source of reassurance for operators and patients alike. The antidote was never required in RE-CIRCUIT, though, the cardiologist noted.
Discussant William G. Stevenson, MD, called the trial “informative and helpful.”
“Something we’ve all been struggling with was that some concern was earlier raised that dabigatran might be associated with more thromboembolic events in this scenario. This study clearly refutes that concern,” observed Dr. Stevenson, director of the clinical cardiac electrophysiology program at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, both in Boston.
Dr. Stevenson wondered whether the outcome differences between the two study groups could be explained by differences in operator techniques and tools. That’s highly unlikely, Dr. Calkins replied. Randomization was done patient by patient, not center by center.
Then why the big difference in major bleeding complications? Dr. Stevenson asked.
“It may be that, if you poke a hole when a patient is on a more forgiving anticoagulant like dabigatran, the bleeding doesn’t persist and turn into a tamponade, whereas if you poke a hole on warfarin it turns into a bigger problem,” Dr. Calkins responded. “When you think about it, warfarin really impacts the whole coagulation cascade through factors VII, IX, and X, so multiple coagulation factors are rendered impotent, whereas dabigatran is a direct thrombin inhibitor, so you’re selectively knocking out just one component of the coagulation cascade. It provides more leeway in preventing a small hole from turning into a big effusion,” he said.
The RE-CIRCUIT trial was funded by Boehringer Ingelheim. Dr. Calkins reported receiving lecture fees from that company and from Medtronic, and serving as a consultant to Medtronic, Abbott Medical, and AtriCure.
Simultaneously with Dr. Calkins’ presentation at ACC 17, the RE-CIRCUIT study was published online (N Engl J Med. 2017 Mar 19. doi: 10.1056/NEJMoa1701005).
At ACC 17
Key clinical point:
Major finding: The incidence of major bleeding events in conjunction with catheter ablation of atrial fibrillation was reduced by 77% in patients on periprocedural dabigatran compared with those on warfarin.
Data source: A randomized multicenter prospective international trial of 635 patients who underwent catheter ablation for atrial fibrillation supported by uninterrupted oral anticoagulation.
Disclosures: The RE-CIRCUIT trial was funded by Boehringer Ingelheim. Dr. Calkins reported receiving lecture fees from that company and from Medtronic, and serving as a consultant to Medtronic, Abbott Medical, and AtriCure.
Unavoidable, random DNA replication errors are the most common cancer drivers
Up to two-thirds of the mutations that drive human cancers may be due to DNA replication errors in normally dividing stem cells, not by inherited or environmentally induced mutations, according to a mathematical modeling study.
The proportion of replication error-driven mutations varied widely among 17 cancers analyzed, but the overall attributable risk of these errors was remarkably consistent among 69 countries included in the study, said Cristian Tomasetti, PhD, a coauthor of the paper and a biostatistician at Johns Hopkins University, Baltimore.
The findings should be a game-changer in the cancer field, Dr. Tomasetti said during a press briefing sponsored by the American Association for the Advancement of Science. Research dogma has long held that most cancers are related to lifestyle and environmental exposure, with a few primarily due to genetic factors.
“We have now determined that there is a third factor, and that it causes most of the mutations that drive cancer,” Dr. Tomasetti said. “We cannot ignore it and pretend it doesn’t exist. This is a complete paradigm shift in how we think of cancer and what causes it.”
The finding that 66% of cancer-driving mutations are based on unavoidable replication errors doesn’t challenge well-established epidemiology, said Dr. Tomasetti and his coauthor, Bert Vogelstein, MD. Rather, it fits perfectly with several key understandings of cancer: that about 40% of cases are preventable, that rapidly dividing tissues are more prone to develop cancers, and that cancer incidence rises exponentially as humans age.
“If we have as our starting point the assumption that 42% of cancers are preventable, we are completely consistent with that,” in finding that about 60% of cancers are unavoidable, Dr. Tomasetti said. “Those two numbers go perfectly together.”
The study also found that replication-error mutations (R) were most likely to drive cancers in tissues with rapid turnover, such as colorectal tissue. This makes intuitive sense, given that basal mutation rates hover at about three errors per cell replication cycle regardless of tissue type.
“The basal mutation rate in all cells is pretty even,” said Dr. Vogelstein, the Clayton Professor of Oncology and Pathology at John Hopkins University, Baltimore. “The difference is the number of stem cells. The more cells, the more divisions, and the more mistakes.”
R-mutations also contribute to age-related cancer incidence. As a person ages, more cell divisions accumulate, thus increasing the risk of a cancer-driving R-error. But these mutations also occur in children, who have rapid cell division in all their tissues. In fact, the colleagues suspect that R-errors are the main drivers of almost all pediatric cancers.
The new study bolsters the duo’s controversial 2015 work.
The theory sparked controversy among scholars and researchers. They challenged it on a number of technical fronts, from stem cell counts and division rates to charges that it didn’t adequately assess the interaction between R-mutations and environmental risks.
Some commentators, perceiving nihilism in the paper, expressed concern that clinicians and patients would get the idea that cancer prevention strategies were useless, since most cancers were simply a case of “bad luck.”
A pervading theme of these counter arguments was one familiar to any researcher: Correlation does not equal causation. The new study was an attempt to expand upon and strengthen the original findings, Dr. Tomasetti said.
“There are well-known environmental risk variations across the world, and there was a question of how our findings might change if we did this analysis in a different country. This paper is also the very first time that someone has ever looked at the proportions of mutations in each cancer type and assigned them to these factors.”
The new study employed a similar mathematical model, but comprised data from 423 cancer registries in 69 countries. The researchers examined the relationship between the lifetime risk of 17 cancers (including breast and prostate, which were not included in the 2015 study) and lifetime stem cell divisions for each tissue. The median correlation coefficient was 0.80; 89% of the countries examined had a correlation of greater than 0.70. This was “remarkably similar” to the correlation determined in the 2015 U.S.-only study.
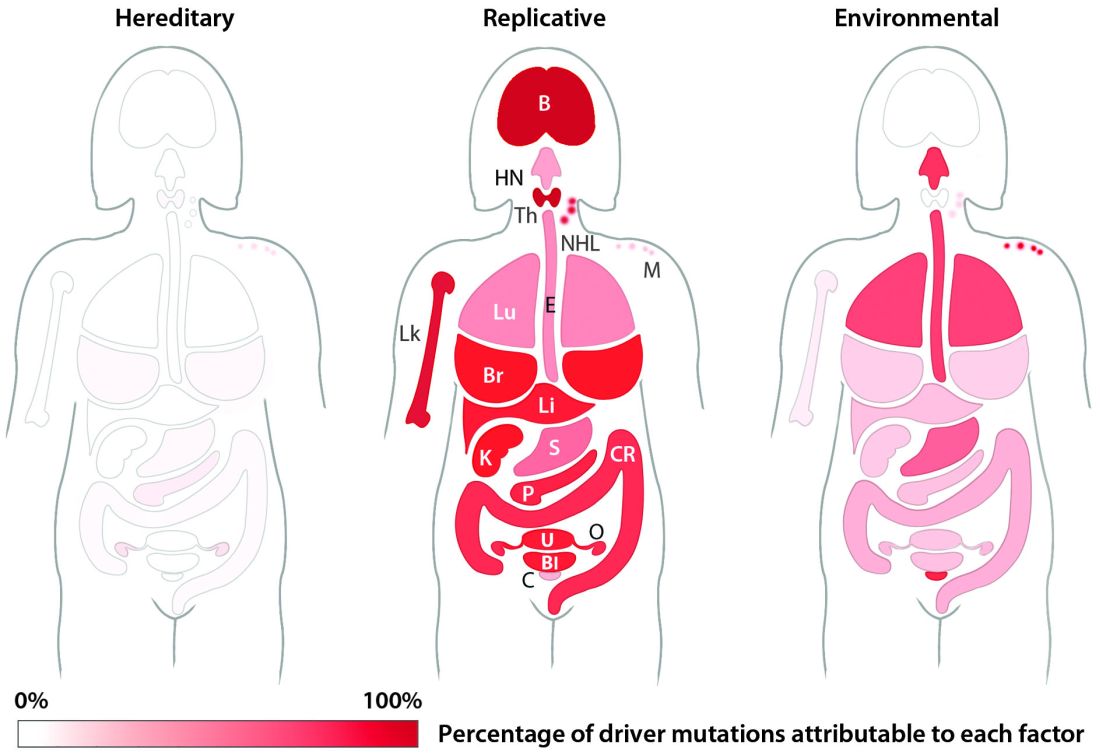
The team’s next step was to determine what fraction of cancer-driving mutations arose from R-errors, from environmental factors (E), and from hereditary factors (H). They examined these proportions in 32 different cancers in which environmental, lifestyle, and genetic factors have been thoroughly studied. Overall, 29% of the driver mutations were due to environment, 5% to heredity, and 66% to R-errors.
The proportions of these drivers did vary widely between the cancer types, the team noted. For example, lung and esophageal cancers and melanoma were primarily driven by environmental factors (more than 60% each). However, they wrote, “even in lung adenocarcinomas, R contributes a third of the total mutations, with tobacco smoke [including secondhand smoke], diet, radiation, and occupational exposures contributing the remainder. In cancers that are less strongly associated with environmental factors, such as those of the pancreas, brain, bone, or prostate, the majority of the mutations are attributable to R.”
During the press briefing, Dr. Tomasetti and Dr. Vogelstein stressed that most of the inevitable R-errors don’t precipitate cancer – and that even if they do increase risk, that risk may not ever trip the disease process.
“Most of the time these replicative mutations do no harm,” Dr Vogelstein said. “They occur in junk DNA genes, or in areas that are unimportant with respect to cancer. That’s the good luck. Occasionally, they occur in a cancer driver gene, and that is bad luck.”
But even a dose of bad luck isn’t enough to cause cancer. Most cancers require multiple hits to develop – which makes primary prevention strategies more important than ever, Dr. Tomasetti said.
“In the case of lung cancer, for instance, three or more mutations are needed. We showed that these mutations are caused by a combination of environment and R-errors. In theory, then, all of these cancers are preventable because if we can prevent even one of the environmentally caused mutations, then that patient won’t develop cancer.”
However, he said, some cancers do appear to be entirely driven by E-errors and, thus, appear entirely unavoidable. This is an extremely difficult area for clinicians and patients to navigate, said Dr. Vogelstein, a former pediatrician.
“We hope that understanding this will offer some comfort to the literally millions of patients who develop cancer despite having lead a near-perfect life,” in terms of managing risk factors. “Cancer develops in people who haven’t smoked, who avoided the sun and wore sunscreen, who eat perfectly healthy diets and exercise regularly. This is a particularly important concept for parents of children who have cancer, who think ‘I either transmitted a bad gene or unknowingly exposed my child to an environmental agent that caused their cancer.’ They need to understand that these cancers would have occurred no matter what they did.”
Dr. Tomasetti had no disclosures. Dr. Vogelstein is on the scientific advisory boards of Morphotek, Exelixis GP, and Sysmex Inostics, and is a founder of PapGene and Personal Genome Diagnostics.
[email protected]
On Twitter @Alz_gal
Up to two-thirds of the mutations that drive human cancers may be due to DNA replication errors in normally dividing stem cells, not by inherited or environmentally induced mutations, according to a mathematical modeling study.
The proportion of replication error-driven mutations varied widely among 17 cancers analyzed, but the overall attributable risk of these errors was remarkably consistent among 69 countries included in the study, said Cristian Tomasetti, PhD, a coauthor of the paper and a biostatistician at Johns Hopkins University, Baltimore.
The findings should be a game-changer in the cancer field, Dr. Tomasetti said during a press briefing sponsored by the American Association for the Advancement of Science. Research dogma has long held that most cancers are related to lifestyle and environmental exposure, with a few primarily due to genetic factors.
“We have now determined that there is a third factor, and that it causes most of the mutations that drive cancer,” Dr. Tomasetti said. “We cannot ignore it and pretend it doesn’t exist. This is a complete paradigm shift in how we think of cancer and what causes it.”
The finding that 66% of cancer-driving mutations are based on unavoidable replication errors doesn’t challenge well-established epidemiology, said Dr. Tomasetti and his coauthor, Bert Vogelstein, MD. Rather, it fits perfectly with several key understandings of cancer: that about 40% of cases are preventable, that rapidly dividing tissues are more prone to develop cancers, and that cancer incidence rises exponentially as humans age.
“If we have as our starting point the assumption that 42% of cancers are preventable, we are completely consistent with that,” in finding that about 60% of cancers are unavoidable, Dr. Tomasetti said. “Those two numbers go perfectly together.”
The study also found that replication-error mutations (R) were most likely to drive cancers in tissues with rapid turnover, such as colorectal tissue. This makes intuitive sense, given that basal mutation rates hover at about three errors per cell replication cycle regardless of tissue type.
“The basal mutation rate in all cells is pretty even,” said Dr. Vogelstein, the Clayton Professor of Oncology and Pathology at John Hopkins University, Baltimore. “The difference is the number of stem cells. The more cells, the more divisions, and the more mistakes.”
R-mutations also contribute to age-related cancer incidence. As a person ages, more cell divisions accumulate, thus increasing the risk of a cancer-driving R-error. But these mutations also occur in children, who have rapid cell division in all their tissues. In fact, the colleagues suspect that R-errors are the main drivers of almost all pediatric cancers.
The new study bolsters the duo’s controversial 2015 work.
The theory sparked controversy among scholars and researchers. They challenged it on a number of technical fronts, from stem cell counts and division rates to charges that it didn’t adequately assess the interaction between R-mutations and environmental risks.
Some commentators, perceiving nihilism in the paper, expressed concern that clinicians and patients would get the idea that cancer prevention strategies were useless, since most cancers were simply a case of “bad luck.”
A pervading theme of these counter arguments was one familiar to any researcher: Correlation does not equal causation. The new study was an attempt to expand upon and strengthen the original findings, Dr. Tomasetti said.
“There are well-known environmental risk variations across the world, and there was a question of how our findings might change if we did this analysis in a different country. This paper is also the very first time that someone has ever looked at the proportions of mutations in each cancer type and assigned them to these factors.”
The new study employed a similar mathematical model, but comprised data from 423 cancer registries in 69 countries. The researchers examined the relationship between the lifetime risk of 17 cancers (including breast and prostate, which were not included in the 2015 study) and lifetime stem cell divisions for each tissue. The median correlation coefficient was 0.80; 89% of the countries examined had a correlation of greater than 0.70. This was “remarkably similar” to the correlation determined in the 2015 U.S.-only study.
The team’s next step was to determine what fraction of cancer-driving mutations arose from R-errors, from environmental factors (E), and from hereditary factors (H). They examined these proportions in 32 different cancers in which environmental, lifestyle, and genetic factors have been thoroughly studied. Overall, 29% of the driver mutations were due to environment, 5% to heredity, and 66% to R-errors.
The proportions of these drivers did vary widely between the cancer types, the team noted. For example, lung and esophageal cancers and melanoma were primarily driven by environmental factors (more than 60% each). However, they wrote, “even in lung adenocarcinomas, R contributes a third of the total mutations, with tobacco smoke [including secondhand smoke], diet, radiation, and occupational exposures contributing the remainder. In cancers that are less strongly associated with environmental factors, such as those of the pancreas, brain, bone, or prostate, the majority of the mutations are attributable to R.”
During the press briefing, Dr. Tomasetti and Dr. Vogelstein stressed that most of the inevitable R-errors don’t precipitate cancer – and that even if they do increase risk, that risk may not ever trip the disease process.
“Most of the time these replicative mutations do no harm,” Dr Vogelstein said. “They occur in junk DNA genes, or in areas that are unimportant with respect to cancer. That’s the good luck. Occasionally, they occur in a cancer driver gene, and that is bad luck.”
But even a dose of bad luck isn’t enough to cause cancer. Most cancers require multiple hits to develop – which makes primary prevention strategies more important than ever, Dr. Tomasetti said.
“In the case of lung cancer, for instance, three or more mutations are needed. We showed that these mutations are caused by a combination of environment and R-errors. In theory, then, all of these cancers are preventable because if we can prevent even one of the environmentally caused mutations, then that patient won’t develop cancer.”
However, he said, some cancers do appear to be entirely driven by E-errors and, thus, appear entirely unavoidable. This is an extremely difficult area for clinicians and patients to navigate, said Dr. Vogelstein, a former pediatrician.
“We hope that understanding this will offer some comfort to the literally millions of patients who develop cancer despite having lead a near-perfect life,” in terms of managing risk factors. “Cancer develops in people who haven’t smoked, who avoided the sun and wore sunscreen, who eat perfectly healthy diets and exercise regularly. This is a particularly important concept for parents of children who have cancer, who think ‘I either transmitted a bad gene or unknowingly exposed my child to an environmental agent that caused their cancer.’ They need to understand that these cancers would have occurred no matter what they did.”
Dr. Tomasetti had no disclosures. Dr. Vogelstein is on the scientific advisory boards of Morphotek, Exelixis GP, and Sysmex Inostics, and is a founder of PapGene and Personal Genome Diagnostics.
[email protected]
On Twitter @Alz_gal
Up to two-thirds of the mutations that drive human cancers may be due to DNA replication errors in normally dividing stem cells, not by inherited or environmentally induced mutations, according to a mathematical modeling study.
The proportion of replication error-driven mutations varied widely among 17 cancers analyzed, but the overall attributable risk of these errors was remarkably consistent among 69 countries included in the study, said Cristian Tomasetti, PhD, a coauthor of the paper and a biostatistician at Johns Hopkins University, Baltimore.
The findings should be a game-changer in the cancer field, Dr. Tomasetti said during a press briefing sponsored by the American Association for the Advancement of Science. Research dogma has long held that most cancers are related to lifestyle and environmental exposure, with a few primarily due to genetic factors.
“We have now determined that there is a third factor, and that it causes most of the mutations that drive cancer,” Dr. Tomasetti said. “We cannot ignore it and pretend it doesn’t exist. This is a complete paradigm shift in how we think of cancer and what causes it.”
The finding that 66% of cancer-driving mutations are based on unavoidable replication errors doesn’t challenge well-established epidemiology, said Dr. Tomasetti and his coauthor, Bert Vogelstein, MD. Rather, it fits perfectly with several key understandings of cancer: that about 40% of cases are preventable, that rapidly dividing tissues are more prone to develop cancers, and that cancer incidence rises exponentially as humans age.
“If we have as our starting point the assumption that 42% of cancers are preventable, we are completely consistent with that,” in finding that about 60% of cancers are unavoidable, Dr. Tomasetti said. “Those two numbers go perfectly together.”
The study also found that replication-error mutations (R) were most likely to drive cancers in tissues with rapid turnover, such as colorectal tissue. This makes intuitive sense, given that basal mutation rates hover at about three errors per cell replication cycle regardless of tissue type.
“The basal mutation rate in all cells is pretty even,” said Dr. Vogelstein, the Clayton Professor of Oncology and Pathology at John Hopkins University, Baltimore. “The difference is the number of stem cells. The more cells, the more divisions, and the more mistakes.”
R-mutations also contribute to age-related cancer incidence. As a person ages, more cell divisions accumulate, thus increasing the risk of a cancer-driving R-error. But these mutations also occur in children, who have rapid cell division in all their tissues. In fact, the colleagues suspect that R-errors are the main drivers of almost all pediatric cancers.
The new study bolsters the duo’s controversial 2015 work.
The theory sparked controversy among scholars and researchers. They challenged it on a number of technical fronts, from stem cell counts and division rates to charges that it didn’t adequately assess the interaction between R-mutations and environmental risks.
Some commentators, perceiving nihilism in the paper, expressed concern that clinicians and patients would get the idea that cancer prevention strategies were useless, since most cancers were simply a case of “bad luck.”
A pervading theme of these counter arguments was one familiar to any researcher: Correlation does not equal causation. The new study was an attempt to expand upon and strengthen the original findings, Dr. Tomasetti said.
“There are well-known environmental risk variations across the world, and there was a question of how our findings might change if we did this analysis in a different country. This paper is also the very first time that someone has ever looked at the proportions of mutations in each cancer type and assigned them to these factors.”
The new study employed a similar mathematical model, but comprised data from 423 cancer registries in 69 countries. The researchers examined the relationship between the lifetime risk of 17 cancers (including breast and prostate, which were not included in the 2015 study) and lifetime stem cell divisions for each tissue. The median correlation coefficient was 0.80; 89% of the countries examined had a correlation of greater than 0.70. This was “remarkably similar” to the correlation determined in the 2015 U.S.-only study.
The team’s next step was to determine what fraction of cancer-driving mutations arose from R-errors, from environmental factors (E), and from hereditary factors (H). They examined these proportions in 32 different cancers in which environmental, lifestyle, and genetic factors have been thoroughly studied. Overall, 29% of the driver mutations were due to environment, 5% to heredity, and 66% to R-errors.
The proportions of these drivers did vary widely between the cancer types, the team noted. For example, lung and esophageal cancers and melanoma were primarily driven by environmental factors (more than 60% each). However, they wrote, “even in lung adenocarcinomas, R contributes a third of the total mutations, with tobacco smoke [including secondhand smoke], diet, radiation, and occupational exposures contributing the remainder. In cancers that are less strongly associated with environmental factors, such as those of the pancreas, brain, bone, or prostate, the majority of the mutations are attributable to R.”
During the press briefing, Dr. Tomasetti and Dr. Vogelstein stressed that most of the inevitable R-errors don’t precipitate cancer – and that even if they do increase risk, that risk may not ever trip the disease process.
“Most of the time these replicative mutations do no harm,” Dr Vogelstein said. “They occur in junk DNA genes, or in areas that are unimportant with respect to cancer. That’s the good luck. Occasionally, they occur in a cancer driver gene, and that is bad luck.”
But even a dose of bad luck isn’t enough to cause cancer. Most cancers require multiple hits to develop – which makes primary prevention strategies more important than ever, Dr. Tomasetti said.
“In the case of lung cancer, for instance, three or more mutations are needed. We showed that these mutations are caused by a combination of environment and R-errors. In theory, then, all of these cancers are preventable because if we can prevent even one of the environmentally caused mutations, then that patient won’t develop cancer.”
However, he said, some cancers do appear to be entirely driven by E-errors and, thus, appear entirely unavoidable. This is an extremely difficult area for clinicians and patients to navigate, said Dr. Vogelstein, a former pediatrician.
“We hope that understanding this will offer some comfort to the literally millions of patients who develop cancer despite having lead a near-perfect life,” in terms of managing risk factors. “Cancer develops in people who haven’t smoked, who avoided the sun and wore sunscreen, who eat perfectly healthy diets and exercise regularly. This is a particularly important concept for parents of children who have cancer, who think ‘I either transmitted a bad gene or unknowingly exposed my child to an environmental agent that caused their cancer.’ They need to understand that these cancers would have occurred no matter what they did.”
Dr. Tomasetti had no disclosures. Dr. Vogelstein is on the scientific advisory boards of Morphotek, Exelixis GP, and Sysmex Inostics, and is a founder of PapGene and Personal Genome Diagnostics.
[email protected]
On Twitter @Alz_gal
Key clinical point:
Major finding: Two-thirds (66%) of cancer drivers are replication errors, 29% are environmentally induced, and 5% are hereditary.
Data source: The researchers examined cancer mutation drivers in two cohorts that spanned 69 countries.
Disclosures: Dr. Tomasetti had no disclosures. Dr. Vogelstein is on the scientific advisory boards of Morphotek, Exelixis GP, and Sysmex Inostics, and is a founder of PapGene and Personal Genome Diagnostics.
American Samoa could be a model for responding to Zika outbreaks
Syndromic and enhanced surveillance employed during a Zika outbreak in American Samoa last year is credited for bringing a quick end to ongoing transmission and could be used to predict when ongoing transmission in similarly small populations will end.
“Establishing a timeline for discontinuing screening of asymptomatic pregnant women allows ASDoH [the American Samoa Department of Health] to allocate resources appropriately toward early interventions for children and families affected by Zika virus,” W. Thane Hancock, MD, of the CDC’s Office of Public Health Preparedness and Response, and his colleagues wrote in the Morbidity and Mortality Weekly Report (2017 Mar 24;66[11]:299-301).
Laboratory-confirmed Zika cases first cropped up in American Samoa in January 2016, prompting the implementation of protocols to reduce the mosquito population, along with syndromic surveillance based on electronic health records to determine which patients may be at higher risk. Routine testing of all asymptomatic pregnant woman, along with individuals with one or more symptoms of Zika virus, also became standard procedure. Real-time, reverse transcription–polymerase chain reaction (rRT-PCR) testing was used to confirm suspected Zika virus cases.
“Early in the response, collection and testing of specimens from pregnant women was prioritized over the collection from symptomatic nonpregnant patients because of limited testing and shipping capacity,” the researchers wrote.
By May 2016, suspected cases had dropped from six per week during January and February, to just one per week, with the last laboratory-confirmed case occurring on June 19, 2016. In August, the ASDoH proposed ending routine screening of asymptomatic pregnant women by Oct. 15, 2016. Transmission data from American Samoa and the CDC were used to determine the Oct. 15 date as an estimate for when active mosquito-borne transmission would end.
To confirm that local transmission was no longer ongoing, enhanced surveillance was implemented from Aug. 31 to Oct. 15, involving free testing at local clinics. Over the course of 45 days, there were a total of 32 patients suspected of having a Zika virus infection.
Two of these subjects’ specimens were not sufficient in sample size to be tested, but the other 30 underwent rRT-PCR testing within 30 days of symptom onset, and all the results were negative. Additionally, 277 asymptomatic pregnant women were tested and 86 (31%) tested anti-Zika IgM–positive or equivocal. All 86 specimens later tested negative by rRT-PCR.
Given the possibility that Zika virus can persist in semen for 6 months, officials recommended permissive testing of asymptomatic pregnant women who conceive through April 15, 2017 “as a conservative approach.”
“The surveillance processes outlined and the timeline established for American Samoa might have implications for jurisdictions where small populations and similar population immunity following widespread Zika virus exposure can facilitate interruption of transmission,” the researchers wrote.
Syndromic and enhanced surveillance employed during a Zika outbreak in American Samoa last year is credited for bringing a quick end to ongoing transmission and could be used to predict when ongoing transmission in similarly small populations will end.
“Establishing a timeline for discontinuing screening of asymptomatic pregnant women allows ASDoH [the American Samoa Department of Health] to allocate resources appropriately toward early interventions for children and families affected by Zika virus,” W. Thane Hancock, MD, of the CDC’s Office of Public Health Preparedness and Response, and his colleagues wrote in the Morbidity and Mortality Weekly Report (2017 Mar 24;66[11]:299-301).
Laboratory-confirmed Zika cases first cropped up in American Samoa in January 2016, prompting the implementation of protocols to reduce the mosquito population, along with syndromic surveillance based on electronic health records to determine which patients may be at higher risk. Routine testing of all asymptomatic pregnant woman, along with individuals with one or more symptoms of Zika virus, also became standard procedure. Real-time, reverse transcription–polymerase chain reaction (rRT-PCR) testing was used to confirm suspected Zika virus cases.
“Early in the response, collection and testing of specimens from pregnant women was prioritized over the collection from symptomatic nonpregnant patients because of limited testing and shipping capacity,” the researchers wrote.
By May 2016, suspected cases had dropped from six per week during January and February, to just one per week, with the last laboratory-confirmed case occurring on June 19, 2016. In August, the ASDoH proposed ending routine screening of asymptomatic pregnant women by Oct. 15, 2016. Transmission data from American Samoa and the CDC were used to determine the Oct. 15 date as an estimate for when active mosquito-borne transmission would end.
To confirm that local transmission was no longer ongoing, enhanced surveillance was implemented from Aug. 31 to Oct. 15, involving free testing at local clinics. Over the course of 45 days, there were a total of 32 patients suspected of having a Zika virus infection.
Two of these subjects’ specimens were not sufficient in sample size to be tested, but the other 30 underwent rRT-PCR testing within 30 days of symptom onset, and all the results were negative. Additionally, 277 asymptomatic pregnant women were tested and 86 (31%) tested anti-Zika IgM–positive or equivocal. All 86 specimens later tested negative by rRT-PCR.
Given the possibility that Zika virus can persist in semen for 6 months, officials recommended permissive testing of asymptomatic pregnant women who conceive through April 15, 2017 “as a conservative approach.”
“The surveillance processes outlined and the timeline established for American Samoa might have implications for jurisdictions where small populations and similar population immunity following widespread Zika virus exposure can facilitate interruption of transmission,” the researchers wrote.
Syndromic and enhanced surveillance employed during a Zika outbreak in American Samoa last year is credited for bringing a quick end to ongoing transmission and could be used to predict when ongoing transmission in similarly small populations will end.
“Establishing a timeline for discontinuing screening of asymptomatic pregnant women allows ASDoH [the American Samoa Department of Health] to allocate resources appropriately toward early interventions for children and families affected by Zika virus,” W. Thane Hancock, MD, of the CDC’s Office of Public Health Preparedness and Response, and his colleagues wrote in the Morbidity and Mortality Weekly Report (2017 Mar 24;66[11]:299-301).
Laboratory-confirmed Zika cases first cropped up in American Samoa in January 2016, prompting the implementation of protocols to reduce the mosquito population, along with syndromic surveillance based on electronic health records to determine which patients may be at higher risk. Routine testing of all asymptomatic pregnant woman, along with individuals with one or more symptoms of Zika virus, also became standard procedure. Real-time, reverse transcription–polymerase chain reaction (rRT-PCR) testing was used to confirm suspected Zika virus cases.
“Early in the response, collection and testing of specimens from pregnant women was prioritized over the collection from symptomatic nonpregnant patients because of limited testing and shipping capacity,” the researchers wrote.
By May 2016, suspected cases had dropped from six per week during January and February, to just one per week, with the last laboratory-confirmed case occurring on June 19, 2016. In August, the ASDoH proposed ending routine screening of asymptomatic pregnant women by Oct. 15, 2016. Transmission data from American Samoa and the CDC were used to determine the Oct. 15 date as an estimate for when active mosquito-borne transmission would end.
To confirm that local transmission was no longer ongoing, enhanced surveillance was implemented from Aug. 31 to Oct. 15, involving free testing at local clinics. Over the course of 45 days, there were a total of 32 patients suspected of having a Zika virus infection.
Two of these subjects’ specimens were not sufficient in sample size to be tested, but the other 30 underwent rRT-PCR testing within 30 days of symptom onset, and all the results were negative. Additionally, 277 asymptomatic pregnant women were tested and 86 (31%) tested anti-Zika IgM–positive or equivocal. All 86 specimens later tested negative by rRT-PCR.
Given the possibility that Zika virus can persist in semen for 6 months, officials recommended permissive testing of asymptomatic pregnant women who conceive through April 15, 2017 “as a conservative approach.”
“The surveillance processes outlined and the timeline established for American Samoa might have implications for jurisdictions where small populations and similar population immunity following widespread Zika virus exposure can facilitate interruption of transmission,” the researchers wrote.
FROM MMWR
Wanna See My Not-Tan Lines?
A 16-year-old African-American girl is brought in by her mother for evaluation of skin changes affecting both arms: small, round, slightly scaly, 2- to 3-cm patches on the triceps, antecubitals, and deltoids. The changes manifested in early spring and worsened with the arrival of summer.
The condition has been previously diagnosed as vitiligo by her primary care provider and as fungal infection by an urgent care provider. Nystatin cream and clotrimazole cream have had no effect.
The patient’s history includes eczema, extensive atopy manifesting with seasonal allergies, and childhood asthma. Her siblings also had these problems.
EXAMINATION
Extensive, mottled hypopigmentation is noted on the skin of both arms, in stark contrast to the patient’s type V skin. Very little scale is seen. There are focal areas of slight erythema around the antecubital folds.

What is the diagnosis?
DISCUSSION
This phenomenon is so common in dermatology clinics that it’s a rare day when we don’t see it. This form of hypopigmentation is pityriasis alba (PA), in which areas of eczema don’t tan at all while the surrounding skin darkens with sun exposure. The lateral aspects of the arms are often affected (sparing the sun-protected medial aspects), as are the sides of the face and the posterior neck. The contrast is striking, especially on those with darker skin.
PA occurs mostly in children and young adults, becoming less frequent with age. It differs from vitiligo in that PA involves seasonal, partial pigment loss; vitiligo by contrast manifests with complete pigment loss (leaving utterly white skin) that is almost always permanent.
Treatment consists of sun protection, moisturization to prevent eczema, and use of class IV steroid creams or ointments when lesions appear. Even without treatment, PA usually clears during the winter months—when the surrounding skin loses its tan—only to recur the following spring.
TAKE-HOME LEARNING POINTS
- Pityriasis alba (PA) occurs when patches of eczema fail to tan, producing marked contrast between them and the normal surrounding skin; it is often mistaken for fungal infection.
- PA favors the antecubital, deltoid, and lateral tricep areas, as well as the lateral face.
- PA is more common in atopic individuals who are prone to eczema and appears more dramatic in those with darker skin.
- Vitiligo is a major item in the differential, but color loss with PA is only partial (rather than permanent) and almost always resolves in the winter.
- Once color is lost with PA, treatment is largely ineffective. It is then best to use preventive measures (eg, sunscreen and moisturizer), plus/minus topical steroid creams, for the eczema.
A 16-year-old African-American girl is brought in by her mother for evaluation of skin changes affecting both arms: small, round, slightly scaly, 2- to 3-cm patches on the triceps, antecubitals, and deltoids. The changes manifested in early spring and worsened with the arrival of summer.
The condition has been previously diagnosed as vitiligo by her primary care provider and as fungal infection by an urgent care provider. Nystatin cream and clotrimazole cream have had no effect.
The patient’s history includes eczema, extensive atopy manifesting with seasonal allergies, and childhood asthma. Her siblings also had these problems.
EXAMINATION
Extensive, mottled hypopigmentation is noted on the skin of both arms, in stark contrast to the patient’s type V skin. Very little scale is seen. There are focal areas of slight erythema around the antecubital folds.
What is the diagnosis?
DISCUSSION
This phenomenon is so common in dermatology clinics that it’s a rare day when we don’t see it. This form of hypopigmentation is pityriasis alba (PA), in which areas of eczema don’t tan at all while the surrounding skin darkens with sun exposure. The lateral aspects of the arms are often affected (sparing the sun-protected medial aspects), as are the sides of the face and the posterior neck. The contrast is striking, especially on those with darker skin.
PA occurs mostly in children and young adults, becoming less frequent with age. It differs from vitiligo in that PA involves seasonal, partial pigment loss; vitiligo by contrast manifests with complete pigment loss (leaving utterly white skin) that is almost always permanent.
Treatment consists of sun protection, moisturization to prevent eczema, and use of class IV steroid creams or ointments when lesions appear. Even without treatment, PA usually clears during the winter months—when the surrounding skin loses its tan—only to recur the following spring.
TAKE-HOME LEARNING POINTS
- Pityriasis alba (PA) occurs when patches of eczema fail to tan, producing marked contrast between them and the normal surrounding skin; it is often mistaken for fungal infection.
- PA favors the antecubital, deltoid, and lateral tricep areas, as well as the lateral face.
- PA is more common in atopic individuals who are prone to eczema and appears more dramatic in those with darker skin.
- Vitiligo is a major item in the differential, but color loss with PA is only partial (rather than permanent) and almost always resolves in the winter.
- Once color is lost with PA, treatment is largely ineffective. It is then best to use preventive measures (eg, sunscreen and moisturizer), plus/minus topical steroid creams, for the eczema.
A 16-year-old African-American girl is brought in by her mother for evaluation of skin changes affecting both arms: small, round, slightly scaly, 2- to 3-cm patches on the triceps, antecubitals, and deltoids. The changes manifested in early spring and worsened with the arrival of summer.
The condition has been previously diagnosed as vitiligo by her primary care provider and as fungal infection by an urgent care provider. Nystatin cream and clotrimazole cream have had no effect.
The patient’s history includes eczema, extensive atopy manifesting with seasonal allergies, and childhood asthma. Her siblings also had these problems.
EXAMINATION
Extensive, mottled hypopigmentation is noted on the skin of both arms, in stark contrast to the patient’s type V skin. Very little scale is seen. There are focal areas of slight erythema around the antecubital folds.
What is the diagnosis?
DISCUSSION
This phenomenon is so common in dermatology clinics that it’s a rare day when we don’t see it. This form of hypopigmentation is pityriasis alba (PA), in which areas of eczema don’t tan at all while the surrounding skin darkens with sun exposure. The lateral aspects of the arms are often affected (sparing the sun-protected medial aspects), as are the sides of the face and the posterior neck. The contrast is striking, especially on those with darker skin.
PA occurs mostly in children and young adults, becoming less frequent with age. It differs from vitiligo in that PA involves seasonal, partial pigment loss; vitiligo by contrast manifests with complete pigment loss (leaving utterly white skin) that is almost always permanent.
Treatment consists of sun protection, moisturization to prevent eczema, and use of class IV steroid creams or ointments when lesions appear. Even without treatment, PA usually clears during the winter months—when the surrounding skin loses its tan—only to recur the following spring.
TAKE-HOME LEARNING POINTS
- Pityriasis alba (PA) occurs when patches of eczema fail to tan, producing marked contrast between them and the normal surrounding skin; it is often mistaken for fungal infection.
- PA favors the antecubital, deltoid, and lateral tricep areas, as well as the lateral face.
- PA is more common in atopic individuals who are prone to eczema and appears more dramatic in those with darker skin.
- Vitiligo is a major item in the differential, but color loss with PA is only partial (rather than permanent) and almost always resolves in the winter.
- Once color is lost with PA, treatment is largely ineffective. It is then best to use preventive measures (eg, sunscreen and moisturizer), plus/minus topical steroid creams, for the eczema.

Novel antifungal had favorable safety, efficacy profile for onychomycosis in phase IIB study
ORLANDO – A novel orally administered antifungal showed a favorable safety and efficacy profile in the treatment of distal lateral subungual onychomycosis, in a phase IIB study presented at the annual meeting of the American Academy of Dermatology.
In the RENOVATE (Restoring Nail: An Oral VT-1161 Tablet Evaluation) study, a randomized, double-blind, placebo-controlled, dose-ranging trial, 259 adults with moderate to severe distal lateral subungual onychomycosis of the large toenail were assigned to either one of four treatment arms. They were given the antifungal, currently named VT-1161, a selective CYP51 inhibitor, at doses of 300 mg or 600 mg once weekly for 10 or 22 weeks, after receiving daily loading doses for the initial 2 weeks. The trial evaluated two dose levels of VT-1161 (300 mg and 600 mg) administered once weekly for either 10 or 22 weeks following an initial 2-week, once-daily loading dose period.
At baseline, the average involvement of the large toenail was 46%, with an average of 4.6 toenails affected. In the intent-to-treat analysis, at 48 weeks, complete cure rates in the four study drug arms ranged from 32% to 42%, compared with 0% in the placebo arm.
Amir Tavakkol, PhD, chief development officer at Viamet Pharmaceuticals, which is developing VT01161, presented the study findings during a late breaking clinical session at the meeting.
Adverse event rates and discontinuation rates were comparable to placebo through week 60, with no patients discontinuing due to any laboratory abnormalities. Nausea and muscle spasms were the most commonly reported adverse events, which Dr. Tavakkol said seemed to occur in patients given the higher doses. VT-1161 is also being studied for treatment of vulvovaginal candidiasis. In October 2016, the FDA granted the drug Qualified Infectious Disease Product and Fast Track designations for the treatment of recurrent vulvovaginal candidiasis, according to the company.
Viamet sponsored the study and Dr. Tavakkol is an employee of the company.
[email protected]
On Twitter @whitneymcknight
ORLANDO – A novel orally administered antifungal showed a favorable safety and efficacy profile in the treatment of distal lateral subungual onychomycosis, in a phase IIB study presented at the annual meeting of the American Academy of Dermatology.
In the RENOVATE (Restoring Nail: An Oral VT-1161 Tablet Evaluation) study, a randomized, double-blind, placebo-controlled, dose-ranging trial, 259 adults with moderate to severe distal lateral subungual onychomycosis of the large toenail were assigned to either one of four treatment arms. They were given the antifungal, currently named VT-1161, a selective CYP51 inhibitor, at doses of 300 mg or 600 mg once weekly for 10 or 22 weeks, after receiving daily loading doses for the initial 2 weeks. The trial evaluated two dose levels of VT-1161 (300 mg and 600 mg) administered once weekly for either 10 or 22 weeks following an initial 2-week, once-daily loading dose period.
At baseline, the average involvement of the large toenail was 46%, with an average of 4.6 toenails affected. In the intent-to-treat analysis, at 48 weeks, complete cure rates in the four study drug arms ranged from 32% to 42%, compared with 0% in the placebo arm.
Amir Tavakkol, PhD, chief development officer at Viamet Pharmaceuticals, which is developing VT01161, presented the study findings during a late breaking clinical session at the meeting.
Adverse event rates and discontinuation rates were comparable to placebo through week 60, with no patients discontinuing due to any laboratory abnormalities. Nausea and muscle spasms were the most commonly reported adverse events, which Dr. Tavakkol said seemed to occur in patients given the higher doses. VT-1161 is also being studied for treatment of vulvovaginal candidiasis. In October 2016, the FDA granted the drug Qualified Infectious Disease Product and Fast Track designations for the treatment of recurrent vulvovaginal candidiasis, according to the company.
Viamet sponsored the study and Dr. Tavakkol is an employee of the company.
[email protected]
On Twitter @whitneymcknight
ORLANDO – A novel orally administered antifungal showed a favorable safety and efficacy profile in the treatment of distal lateral subungual onychomycosis, in a phase IIB study presented at the annual meeting of the American Academy of Dermatology.
In the RENOVATE (Restoring Nail: An Oral VT-1161 Tablet Evaluation) study, a randomized, double-blind, placebo-controlled, dose-ranging trial, 259 adults with moderate to severe distal lateral subungual onychomycosis of the large toenail were assigned to either one of four treatment arms. They were given the antifungal, currently named VT-1161, a selective CYP51 inhibitor, at doses of 300 mg or 600 mg once weekly for 10 or 22 weeks, after receiving daily loading doses for the initial 2 weeks. The trial evaluated two dose levels of VT-1161 (300 mg and 600 mg) administered once weekly for either 10 or 22 weeks following an initial 2-week, once-daily loading dose period.
At baseline, the average involvement of the large toenail was 46%, with an average of 4.6 toenails affected. In the intent-to-treat analysis, at 48 weeks, complete cure rates in the four study drug arms ranged from 32% to 42%, compared with 0% in the placebo arm.
Amir Tavakkol, PhD, chief development officer at Viamet Pharmaceuticals, which is developing VT01161, presented the study findings during a late breaking clinical session at the meeting.
Adverse event rates and discontinuation rates were comparable to placebo through week 60, with no patients discontinuing due to any laboratory abnormalities. Nausea and muscle spasms were the most commonly reported adverse events, which Dr. Tavakkol said seemed to occur in patients given the higher doses. VT-1161 is also being studied for treatment of vulvovaginal candidiasis. In October 2016, the FDA granted the drug Qualified Infectious Disease Product and Fast Track designations for the treatment of recurrent vulvovaginal candidiasis, according to the company.
Viamet sponsored the study and Dr. Tavakkol is an employee of the company.
[email protected]
On Twitter @whitneymcknight
AT AAD 17
Key clinical point:
Major finding: A new selective CYP51 inhibitor, administered orally, met the primary endpoint of complete cure rates at 48 weeks.
Data source: A phase IIB, randomized, double-blind, placebo-controlled, dose-ranging study of 259 adults with moderate-to-severe distal lateral subungual onychomycosis of the large toenail.
Disclosures: Dr. Tavakkol is the chief development officer of Viamet Pharmaceuticals, the sponsor of this trial.
Match Day: Surgery positions up, other specialties grew more
Despite a record number of applicants and slots filled for first-year residents on the 2017 Match Day, growth in all surgery positions continued to be outpaced by growth in other specialties.
“While it is encouraging to see that the number of categorical surgery positions offered has increased by 101 since 2013, representing an increase of 8.6%, over the same period, the number of positions offered in emergency medicine and family medicine positions have each increased by over 300, representing increases of 17.4% and 11.5%, respectively, and the number of internal medicine positions has increased by over 900, representing an increase of 15.2%,” Patrick Bailey, MD, FACS, medical director of advocacy for the Division of Advocacy and Health Policy at the American College of Surgeons. “The fact that over 35,969 applicants submitted program choices and only 27,688 matched into a PGY-1 position is yet another indication of the need to expand the number of graduate medical education positions available,” he added.

And while more positions may be needed, the number of categorical surgery positions that went unfilled remained low, with only 5 of 1,281 slots remaining unfilled at the conclusion of Match Day 2017, according to the data released by the National Resident Match Program (NRMP).
“This result is consistent with those since 2013 during which time the number of unfilled positions has varied between two and seven positions, e.g., 99.4%-99.8% of categorical surgery positions offered were filled,” Dr. Bailey said.
Still, the ACS is advocating for further changes to the resident matching program to help build the future workforce. “The ACS believes broad reforms in the way graduate medical education is funded and administered are necessary and overdue to ensure that our nation is able to produce the physician workforce capable of meeting the needs of the U.S. population,” he said. To that end, the ACS produced a policy paper that outlined a series of steps relative to reform for which it is advocating.
Broadly, those reforms include the collection of actionable and accurate health care workforce data, maintenance of current GME funding levels with the appropriation of temporary additional funds to modernize the system, the combination of the current GME funding streams into a single stream of funds, and the consideration of a regionalized governance system.
Overall, this is the fifth straight year the NRMP has reported growth in applicants, up 1.4% from the previous year, and applicants matched, to PGY-1 positions up 3.2% from 2016.
One factor driving the increase is the “all-in” policy that required programs registering for the Match to offer all their available positions in the Match or another national matching program. The policy, which began with the 2013 Match, has resulted in significant increases for internal medicine, family medicine, and pediatrics.
Internal medicine residency programs offered 7,233 programs, accounting for about 25% of all PGY-1 positions. This was up from 7,024 programs offered last year. U.S. seniors accounted for 44.9% of the 7,101 slots filled, a rate that was slightly lower than the 46.9% of slots filled by U.S. medical school graduates in 2016.
A record-high 18,539 allopathic medical school seniors submitted program choices and 17,480 (94.3%) were matched to first-year resident programs, a rate that has been consistent for a number of years according to NRMP data.
Of the 1,279 unfilled slots, 1,177 were offered in the Match Week Supplemental Offer and Acceptance Program, the results of which will be available in May.
One trend that stood out for NRMP President and CEO Mona Signer was the decline in both U.S.- and non–U.S.-citizen international medical school graduates (IMGs) who submitted program choices.
“I was surprised that the number of U.S.-citizen and non–U.S.-citizen IMGs declined this year, but on the other hand, the good news is their match rates went up,” Ms. Signer said in an interview.
U.S.-citizen IMGs declined by 254 to 5,069, but 54.8% were matched to first-year residency positions, the highest match rate since 2004. The number of non–U.S.-citizen IMGs declined by 176 to 7,284, but 52.4% were matched to first-year positions, the highest match rate since 2005.
Ms. Signer declined to speculate what caused the decline, noting that NRMP does not collect demographic data.
Despite a record number of applicants and slots filled for first-year residents on the 2017 Match Day, growth in all surgery positions continued to be outpaced by growth in other specialties.
“While it is encouraging to see that the number of categorical surgery positions offered has increased by 101 since 2013, representing an increase of 8.6%, over the same period, the number of positions offered in emergency medicine and family medicine positions have each increased by over 300, representing increases of 17.4% and 11.5%, respectively, and the number of internal medicine positions has increased by over 900, representing an increase of 15.2%,” Patrick Bailey, MD, FACS, medical director of advocacy for the Division of Advocacy and Health Policy at the American College of Surgeons. “The fact that over 35,969 applicants submitted program choices and only 27,688 matched into a PGY-1 position is yet another indication of the need to expand the number of graduate medical education positions available,” he added.
And while more positions may be needed, the number of categorical surgery positions that went unfilled remained low, with only 5 of 1,281 slots remaining unfilled at the conclusion of Match Day 2017, according to the data released by the National Resident Match Program (NRMP).
“This result is consistent with those since 2013 during which time the number of unfilled positions has varied between two and seven positions, e.g., 99.4%-99.8% of categorical surgery positions offered were filled,” Dr. Bailey said.
Still, the ACS is advocating for further changes to the resident matching program to help build the future workforce. “The ACS believes broad reforms in the way graduate medical education is funded and administered are necessary and overdue to ensure that our nation is able to produce the physician workforce capable of meeting the needs of the U.S. population,” he said. To that end, the ACS produced a policy paper that outlined a series of steps relative to reform for which it is advocating.
Broadly, those reforms include the collection of actionable and accurate health care workforce data, maintenance of current GME funding levels with the appropriation of temporary additional funds to modernize the system, the combination of the current GME funding streams into a single stream of funds, and the consideration of a regionalized governance system.
Overall, this is the fifth straight year the NRMP has reported growth in applicants, up 1.4% from the previous year, and applicants matched, to PGY-1 positions up 3.2% from 2016.
One factor driving the increase is the “all-in” policy that required programs registering for the Match to offer all their available positions in the Match or another national matching program. The policy, which began with the 2013 Match, has resulted in significant increases for internal medicine, family medicine, and pediatrics.
Internal medicine residency programs offered 7,233 programs, accounting for about 25% of all PGY-1 positions. This was up from 7,024 programs offered last year. U.S. seniors accounted for 44.9% of the 7,101 slots filled, a rate that was slightly lower than the 46.9% of slots filled by U.S. medical school graduates in 2016.
A record-high 18,539 allopathic medical school seniors submitted program choices and 17,480 (94.3%) were matched to first-year resident programs, a rate that has been consistent for a number of years according to NRMP data.
Of the 1,279 unfilled slots, 1,177 were offered in the Match Week Supplemental Offer and Acceptance Program, the results of which will be available in May.
One trend that stood out for NRMP President and CEO Mona Signer was the decline in both U.S.- and non–U.S.-citizen international medical school graduates (IMGs) who submitted program choices.
“I was surprised that the number of U.S.-citizen and non–U.S.-citizen IMGs declined this year, but on the other hand, the good news is their match rates went up,” Ms. Signer said in an interview.
U.S.-citizen IMGs declined by 254 to 5,069, but 54.8% were matched to first-year residency positions, the highest match rate since 2004. The number of non–U.S.-citizen IMGs declined by 176 to 7,284, but 52.4% were matched to first-year positions, the highest match rate since 2005.
Ms. Signer declined to speculate what caused the decline, noting that NRMP does not collect demographic data.
Despite a record number of applicants and slots filled for first-year residents on the 2017 Match Day, growth in all surgery positions continued to be outpaced by growth in other specialties.
“While it is encouraging to see that the number of categorical surgery positions offered has increased by 101 since 2013, representing an increase of 8.6%, over the same period, the number of positions offered in emergency medicine and family medicine positions have each increased by over 300, representing increases of 17.4% and 11.5%, respectively, and the number of internal medicine positions has increased by over 900, representing an increase of 15.2%,” Patrick Bailey, MD, FACS, medical director of advocacy for the Division of Advocacy and Health Policy at the American College of Surgeons. “The fact that over 35,969 applicants submitted program choices and only 27,688 matched into a PGY-1 position is yet another indication of the need to expand the number of graduate medical education positions available,” he added.
And while more positions may be needed, the number of categorical surgery positions that went unfilled remained low, with only 5 of 1,281 slots remaining unfilled at the conclusion of Match Day 2017, according to the data released by the National Resident Match Program (NRMP).
“This result is consistent with those since 2013 during which time the number of unfilled positions has varied between two and seven positions, e.g., 99.4%-99.8% of categorical surgery positions offered were filled,” Dr. Bailey said.
Still, the ACS is advocating for further changes to the resident matching program to help build the future workforce. “The ACS believes broad reforms in the way graduate medical education is funded and administered are necessary and overdue to ensure that our nation is able to produce the physician workforce capable of meeting the needs of the U.S. population,” he said. To that end, the ACS produced a policy paper that outlined a series of steps relative to reform for which it is advocating.
Broadly, those reforms include the collection of actionable and accurate health care workforce data, maintenance of current GME funding levels with the appropriation of temporary additional funds to modernize the system, the combination of the current GME funding streams into a single stream of funds, and the consideration of a regionalized governance system.
Overall, this is the fifth straight year the NRMP has reported growth in applicants, up 1.4% from the previous year, and applicants matched, to PGY-1 positions up 3.2% from 2016.
One factor driving the increase is the “all-in” policy that required programs registering for the Match to offer all their available positions in the Match or another national matching program. The policy, which began with the 2013 Match, has resulted in significant increases for internal medicine, family medicine, and pediatrics.
Internal medicine residency programs offered 7,233 programs, accounting for about 25% of all PGY-1 positions. This was up from 7,024 programs offered last year. U.S. seniors accounted for 44.9% of the 7,101 slots filled, a rate that was slightly lower than the 46.9% of slots filled by U.S. medical school graduates in 2016.
A record-high 18,539 allopathic medical school seniors submitted program choices and 17,480 (94.3%) were matched to first-year resident programs, a rate that has been consistent for a number of years according to NRMP data.
Of the 1,279 unfilled slots, 1,177 were offered in the Match Week Supplemental Offer and Acceptance Program, the results of which will be available in May.
One trend that stood out for NRMP President and CEO Mona Signer was the decline in both U.S.- and non–U.S.-citizen international medical school graduates (IMGs) who submitted program choices.
“I was surprised that the number of U.S.-citizen and non–U.S.-citizen IMGs declined this year, but on the other hand, the good news is their match rates went up,” Ms. Signer said in an interview.
U.S.-citizen IMGs declined by 254 to 5,069, but 54.8% were matched to first-year residency positions, the highest match rate since 2004. The number of non–U.S.-citizen IMGs declined by 176 to 7,284, but 52.4% were matched to first-year positions, the highest match rate since 2005.
Ms. Signer declined to speculate what caused the decline, noting that NRMP does not collect demographic data.
No link between methylation, survival in ovarian cancer
NATIONAL HARBOR, MD. – Unlike mutation, methylation of homologous recombination DNA repair pathway genes was not linked to longer survival or platinum sensitivity in high-grade serous ovarian cancer, according to molecular and clinical analyses of 332 patients.
“Methylation may be more readily reversed than mutation, allowing more rapid development of platinum resistance and negating any impact on overall survival,” said Sarah Bernards, a second-year medical student at the University of Washington, Seattle, who presented the findings at the annual meeting of the Society of Gynecologic Oncology.

The homologous recombination (HR) DNA repair pathway is critical for repairing cross-linking and double-strand breaks, Ms. Bernards noted. Genes such as BRCA1, BRCA2, and RAD51C are important in this pathway, and inherited and sporadic mutations of these genes can lead to ovarian carcinoma. Importantly, ovarian cancers with HR gene mutations are more sensitive to platinum and radiation therapy and are associated with longer progression-free survival and overall survival compared with ovarian cancers without these mutations.
Methylation of the promoter regions of BRCA1 and RAD51C reduces expression of these genes and has been found to be associated with high-grade serous ovarian cancer, Ms. Bernards explained. One previous study found promoter methylations of BRCA1 and RAD51C in 11.5% and 3% of such tumors, respectively (Nature. 2011;474[7353]:609-15).
To further characterize HR gene methylations, Ms. Bernards and her associates used methylation-sensitive PCR to analyze ovarian carcinomas from patients who underwent primary debulking surgery and were enrolled in the University of Washington gynecologic oncology tissue bank. They also tested for damaging germline and somatic mutations in 16 HR DNA repair genes.
In all, 28% of cases had mutations in HR repair pathway genes, 7% had a BRCA1 methylation, and 3% had RAD51C methylation. BRCA1 and RAD51C methylation never overlapped with mutation (P = .001), and almost never overlapped with mutations in other HR DNA repair pathway genes, Ms. Bernards said.
Fully two-thirds of BRCA1 mutated cases were sensitive to chemotherapy, compared with 59% of BRCA1 methylated cases and 53% of wild-type BRCA1 cases (P = .03). Mutations of any HR DNA repair gene were associated with improved overall survival (hazard ratio, 0.7; 95% confidence interval, 0.5-0.9; P = .02), but methylation of RAD51C and BRCA1 was not (P = .3). Patients with HR gene mutations survived a median of 66 months after diagnosis, compared with 41 months for patients with RAD51C methylation and 43 months for patients with BRCA1 methylation.
Median age at diagnosis was 53 years for BRCA1 mutated cases (P less than .0001) and 55 years for BRCA1 methylated cases (P = .03), significantly lower than the 63-year median age for diagnosis of wild-type BRCA1 cases. High-grade histology characterized 71% of wild-type BRCA1 cases, compared with 82% of BRCA1 mutated cases (P = .001) and 91% of BRCA1 methylated cases (P = .05). Somatic TP53 mutations occurred in 67% of wild-type cases, 89% of mutated cases (P = .004), and 82% of methylated cases (P = .01).
To sum up, both methylation and mutation of BRCA1 were associated with younger age at diagnosis, high-grade histology, and TP53 mutations, but only BRCA1 mutation was tied to improved overall survival or platinum sensitivity, Ms. Bernards said.
The work was supported by a grant from the University of Washington School of Medicine Medical Student Research Training Program. Ms. Bernards conducted the work under Elizabeth Swisher, MD, a medical oncologist and head of the Swisher Lab at the University of Washington, Seattle. Ms. Bernards reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Unlike mutation, methylation of homologous recombination DNA repair pathway genes was not linked to longer survival or platinum sensitivity in high-grade serous ovarian cancer, according to molecular and clinical analyses of 332 patients.
“Methylation may be more readily reversed than mutation, allowing more rapid development of platinum resistance and negating any impact on overall survival,” said Sarah Bernards, a second-year medical student at the University of Washington, Seattle, who presented the findings at the annual meeting of the Society of Gynecologic Oncology.
The homologous recombination (HR) DNA repair pathway is critical for repairing cross-linking and double-strand breaks, Ms. Bernards noted. Genes such as BRCA1, BRCA2, and RAD51C are important in this pathway, and inherited and sporadic mutations of these genes can lead to ovarian carcinoma. Importantly, ovarian cancers with HR gene mutations are more sensitive to platinum and radiation therapy and are associated with longer progression-free survival and overall survival compared with ovarian cancers without these mutations.
Methylation of the promoter regions of BRCA1 and RAD51C reduces expression of these genes and has been found to be associated with high-grade serous ovarian cancer, Ms. Bernards explained. One previous study found promoter methylations of BRCA1 and RAD51C in 11.5% and 3% of such tumors, respectively (Nature. 2011;474[7353]:609-15).
To further characterize HR gene methylations, Ms. Bernards and her associates used methylation-sensitive PCR to analyze ovarian carcinomas from patients who underwent primary debulking surgery and were enrolled in the University of Washington gynecologic oncology tissue bank. They also tested for damaging germline and somatic mutations in 16 HR DNA repair genes.
In all, 28% of cases had mutations in HR repair pathway genes, 7% had a BRCA1 methylation, and 3% had RAD51C methylation. BRCA1 and RAD51C methylation never overlapped with mutation (P = .001), and almost never overlapped with mutations in other HR DNA repair pathway genes, Ms. Bernards said.
Fully two-thirds of BRCA1 mutated cases were sensitive to chemotherapy, compared with 59% of BRCA1 methylated cases and 53% of wild-type BRCA1 cases (P = .03). Mutations of any HR DNA repair gene were associated with improved overall survival (hazard ratio, 0.7; 95% confidence interval, 0.5-0.9; P = .02), but methylation of RAD51C and BRCA1 was not (P = .3). Patients with HR gene mutations survived a median of 66 months after diagnosis, compared with 41 months for patients with RAD51C methylation and 43 months for patients with BRCA1 methylation.
Median age at diagnosis was 53 years for BRCA1 mutated cases (P less than .0001) and 55 years for BRCA1 methylated cases (P = .03), significantly lower than the 63-year median age for diagnosis of wild-type BRCA1 cases. High-grade histology characterized 71% of wild-type BRCA1 cases, compared with 82% of BRCA1 mutated cases (P = .001) and 91% of BRCA1 methylated cases (P = .05). Somatic TP53 mutations occurred in 67% of wild-type cases, 89% of mutated cases (P = .004), and 82% of methylated cases (P = .01).
To sum up, both methylation and mutation of BRCA1 were associated with younger age at diagnosis, high-grade histology, and TP53 mutations, but only BRCA1 mutation was tied to improved overall survival or platinum sensitivity, Ms. Bernards said.
The work was supported by a grant from the University of Washington School of Medicine Medical Student Research Training Program. Ms. Bernards conducted the work under Elizabeth Swisher, MD, a medical oncologist and head of the Swisher Lab at the University of Washington, Seattle. Ms. Bernards reported having no conflicts of interest.
NATIONAL HARBOR, MD. – Unlike mutation, methylation of homologous recombination DNA repair pathway genes was not linked to longer survival or platinum sensitivity in high-grade serous ovarian cancer, according to molecular and clinical analyses of 332 patients.
“Methylation may be more readily reversed than mutation, allowing more rapid development of platinum resistance and negating any impact on overall survival,” said Sarah Bernards, a second-year medical student at the University of Washington, Seattle, who presented the findings at the annual meeting of the Society of Gynecologic Oncology.
The homologous recombination (HR) DNA repair pathway is critical for repairing cross-linking and double-strand breaks, Ms. Bernards noted. Genes such as BRCA1, BRCA2, and RAD51C are important in this pathway, and inherited and sporadic mutations of these genes can lead to ovarian carcinoma. Importantly, ovarian cancers with HR gene mutations are more sensitive to platinum and radiation therapy and are associated with longer progression-free survival and overall survival compared with ovarian cancers without these mutations.
Methylation of the promoter regions of BRCA1 and RAD51C reduces expression of these genes and has been found to be associated with high-grade serous ovarian cancer, Ms. Bernards explained. One previous study found promoter methylations of BRCA1 and RAD51C in 11.5% and 3% of such tumors, respectively (Nature. 2011;474[7353]:609-15).
To further characterize HR gene methylations, Ms. Bernards and her associates used methylation-sensitive PCR to analyze ovarian carcinomas from patients who underwent primary debulking surgery and were enrolled in the University of Washington gynecologic oncology tissue bank. They also tested for damaging germline and somatic mutations in 16 HR DNA repair genes.
In all, 28% of cases had mutations in HR repair pathway genes, 7% had a BRCA1 methylation, and 3% had RAD51C methylation. BRCA1 and RAD51C methylation never overlapped with mutation (P = .001), and almost never overlapped with mutations in other HR DNA repair pathway genes, Ms. Bernards said.
Fully two-thirds of BRCA1 mutated cases were sensitive to chemotherapy, compared with 59% of BRCA1 methylated cases and 53% of wild-type BRCA1 cases (P = .03). Mutations of any HR DNA repair gene were associated with improved overall survival (hazard ratio, 0.7; 95% confidence interval, 0.5-0.9; P = .02), but methylation of RAD51C and BRCA1 was not (P = .3). Patients with HR gene mutations survived a median of 66 months after diagnosis, compared with 41 months for patients with RAD51C methylation and 43 months for patients with BRCA1 methylation.
Median age at diagnosis was 53 years for BRCA1 mutated cases (P less than .0001) and 55 years for BRCA1 methylated cases (P = .03), significantly lower than the 63-year median age for diagnosis of wild-type BRCA1 cases. High-grade histology characterized 71% of wild-type BRCA1 cases, compared with 82% of BRCA1 mutated cases (P = .001) and 91% of BRCA1 methylated cases (P = .05). Somatic TP53 mutations occurred in 67% of wild-type cases, 89% of mutated cases (P = .004), and 82% of methylated cases (P = .01).
To sum up, both methylation and mutation of BRCA1 were associated with younger age at diagnosis, high-grade histology, and TP53 mutations, but only BRCA1 mutation was tied to improved overall survival or platinum sensitivity, Ms. Bernards said.
The work was supported by a grant from the University of Washington School of Medicine Medical Student Research Training Program. Ms. Bernards conducted the work under Elizabeth Swisher, MD, a medical oncologist and head of the Swisher Lab at the University of Washington, Seattle. Ms. Bernards reported having no conflicts of interest.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Unlike mutation, methylation of BRCA1 was not linked to longer survival or platinum sensitivity in high-grade serous ovarian cancer.
Major finding: Fully two-thirds of BRCA1 mutated cases were platinum-sensitive compared with 59% of BRCA1 methylated cases and 53% of wild-type BRCA1 cases (P = .03). Mutations of HR DNA repair genes were associated with improved overall survival (hazard ratio, 0.7; 95% confidence interval, 0.5-0.9; P = .02), but methylation of BRCA1 and RAD51C was not (P = .3).
Data source: Methylation-sensitive PCR and clinical assessment of 332 primary ovarian carcinomas.
Disclosures: The University of Washington School of Medicine Medical Student Research Training Program supported the work. Ms. Bernards reported having no conflicts of interest.