User login
Perioperative statin associated with reduction in all-cause perioperative mortality in noncardiac surgery
CLINICAL QUESTION: Does perioperative statin use reduce 30-day mortality in noncardiac surgery?
BACKGROUND: Current perioperative guidelines focus on continuation of existing therapy in long-term statin users with weak recommendations of potential efficacy in reducing perioperative complications.
STUDY DESIGN: Retrospective, observational cohort analysis.
SETTING: Veterans’ Affairs Hospitals.
SYNOPSIS: Using the Veterans Affairs Surgical Quality Improvement Program database, 96,486 patients were studied who were undergoing elective or emergent noncardiac surgery (vascular, general, orthopedic, neurosurgery, otolaryngology, and urology). 96.3% were men. Patients who died the day of the surgery or the day after were excluded, as were patients with multiple surgeries during the assessment period. Statin exposure on the day of or the day after surgery was compared with no statin use. The primary outcome was 30-day mortality and the secondary outcomes were significant reduction in any other complication.
Statin exposure was associated with reduced 30-day all-cause mortality with a marginally favorable effect with longer-term statin use (6 months to 1 year before admission). For the secondary outcomes, there was significant risk reduction in cardiac, infectious, respiratory, and renal complications but no significant change in central nervous system or nonatherosclerotic thrombotic complications.
Statin exposure may be associated with adherence to medical treatment and follow-up thus causing a selection bias.
BOTTOM LINE: Perioperative statin use was associated with a reduction in 30-day mortality and other complications.
CITATIONS: London MJ, Schwartz GG, Hur K, Henderson WG. Association of perioperative statin use with mortality and morbidity after major noncardiac surgery. JAMA Intern Med. 2017 Feb 1;177(2):231-42.
Dr. Dietsche is a clinical instructor, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: Does perioperative statin use reduce 30-day mortality in noncardiac surgery?
BACKGROUND: Current perioperative guidelines focus on continuation of existing therapy in long-term statin users with weak recommendations of potential efficacy in reducing perioperative complications.
STUDY DESIGN: Retrospective, observational cohort analysis.
SETTING: Veterans’ Affairs Hospitals.
SYNOPSIS: Using the Veterans Affairs Surgical Quality Improvement Program database, 96,486 patients were studied who were undergoing elective or emergent noncardiac surgery (vascular, general, orthopedic, neurosurgery, otolaryngology, and urology). 96.3% were men. Patients who died the day of the surgery or the day after were excluded, as were patients with multiple surgeries during the assessment period. Statin exposure on the day of or the day after surgery was compared with no statin use. The primary outcome was 30-day mortality and the secondary outcomes were significant reduction in any other complication.
Statin exposure was associated with reduced 30-day all-cause mortality with a marginally favorable effect with longer-term statin use (6 months to 1 year before admission). For the secondary outcomes, there was significant risk reduction in cardiac, infectious, respiratory, and renal complications but no significant change in central nervous system or nonatherosclerotic thrombotic complications.
Statin exposure may be associated with adherence to medical treatment and follow-up thus causing a selection bias.
BOTTOM LINE: Perioperative statin use was associated with a reduction in 30-day mortality and other complications.
CITATIONS: London MJ, Schwartz GG, Hur K, Henderson WG. Association of perioperative statin use with mortality and morbidity after major noncardiac surgery. JAMA Intern Med. 2017 Feb 1;177(2):231-42.
Dr. Dietsche is a clinical instructor, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
CLINICAL QUESTION: Does perioperative statin use reduce 30-day mortality in noncardiac surgery?
BACKGROUND: Current perioperative guidelines focus on continuation of existing therapy in long-term statin users with weak recommendations of potential efficacy in reducing perioperative complications.
STUDY DESIGN: Retrospective, observational cohort analysis.
SETTING: Veterans’ Affairs Hospitals.
SYNOPSIS: Using the Veterans Affairs Surgical Quality Improvement Program database, 96,486 patients were studied who were undergoing elective or emergent noncardiac surgery (vascular, general, orthopedic, neurosurgery, otolaryngology, and urology). 96.3% were men. Patients who died the day of the surgery or the day after were excluded, as were patients with multiple surgeries during the assessment period. Statin exposure on the day of or the day after surgery was compared with no statin use. The primary outcome was 30-day mortality and the secondary outcomes were significant reduction in any other complication.
Statin exposure was associated with reduced 30-day all-cause mortality with a marginally favorable effect with longer-term statin use (6 months to 1 year before admission). For the secondary outcomes, there was significant risk reduction in cardiac, infectious, respiratory, and renal complications but no significant change in central nervous system or nonatherosclerotic thrombotic complications.
Statin exposure may be associated with adherence to medical treatment and follow-up thus causing a selection bias.
BOTTOM LINE: Perioperative statin use was associated with a reduction in 30-day mortality and other complications.
CITATIONS: London MJ, Schwartz GG, Hur K, Henderson WG. Association of perioperative statin use with mortality and morbidity after major noncardiac surgery. JAMA Intern Med. 2017 Feb 1;177(2):231-42.
Dr. Dietsche is a clinical instructor, Division of Hospital Medicine, University of Colorado School of Medicine, Aurora.
Male vs. female hospitalists, a comparison in mortality and readmission rate for Medicare patients
Clinical Question: Does physician sex affect hospitalized patient outcomes?
Background: Previous studies had suggested different practice patterns between male and female physicians in process measure of quality. No prior evaluation of patient outcomes examining those differences was studied in the past.![]()
Setting: U.S. national sample (20%) of Medicare beneficiaries aged 65 years or older, hospitalized with acute medical conditions.
Synopsis: This observational study assessed the difference in patients’ outcomes that were treated by a male or female physician. 30-days mortality rate was analyzed from 1,583,028 hospitalizations. The mortality rate of patients cared for by female physicians was lower and statistically significant: 11.07% vs. 11.49% (adjusted risk difference, –0.43%; 95% CI, –0.57% to –0.28%; P less than .001). The difference did not change after considering patient and physician characteristics as well as when looking at hospital fixed effects (that is, hospital indicators). In order to prevent one death, a female physician needs to treat 233 patients.
Also, 30-day readmission rate, after adjustment readmissions (from 1,540,797 hospitalizations) was 15.02% vs. 15.57% (adjusted risk difference, –0.55%; 95% confidence interval, –0.71% to 0.39%; P less than .001) showing that the care provided by a female physician can reduce one readmission when treating 182 patients.
Bottom line: Patients older than 65 years have lower 30-day mortality and readmission rates when receiving inpatient care from a female internist, compared with care by a male internist.
Citations: Tsugawa Y, Jena AB, Figueroa JF, et al. Comparison of hospital mortality and readmission rates for Medicare patients treated by male vs. female physicians. JAMA Intern Med. 2017 Feb;177(2):206-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
Clinical Question: Does physician sex affect hospitalized patient outcomes?
Background: Previous studies had suggested different practice patterns between male and female physicians in process measure of quality. No prior evaluation of patient outcomes examining those differences was studied in the past.![]()
Setting: U.S. national sample (20%) of Medicare beneficiaries aged 65 years or older, hospitalized with acute medical conditions.
Synopsis: This observational study assessed the difference in patients’ outcomes that were treated by a male or female physician. 30-days mortality rate was analyzed from 1,583,028 hospitalizations. The mortality rate of patients cared for by female physicians was lower and statistically significant: 11.07% vs. 11.49% (adjusted risk difference, –0.43%; 95% CI, –0.57% to –0.28%; P less than .001). The difference did not change after considering patient and physician characteristics as well as when looking at hospital fixed effects (that is, hospital indicators). In order to prevent one death, a female physician needs to treat 233 patients.
Also, 30-day readmission rate, after adjustment readmissions (from 1,540,797 hospitalizations) was 15.02% vs. 15.57% (adjusted risk difference, –0.55%; 95% confidence interval, –0.71% to 0.39%; P less than .001) showing that the care provided by a female physician can reduce one readmission when treating 182 patients.
Bottom line: Patients older than 65 years have lower 30-day mortality and readmission rates when receiving inpatient care from a female internist, compared with care by a male internist.
Citations: Tsugawa Y, Jena AB, Figueroa JF, et al. Comparison of hospital mortality and readmission rates for Medicare patients treated by male vs. female physicians. JAMA Intern Med. 2017 Feb;177(2):206-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
Clinical Question: Does physician sex affect hospitalized patient outcomes?
Background: Previous studies had suggested different practice patterns between male and female physicians in process measure of quality. No prior evaluation of patient outcomes examining those differences was studied in the past.![]()
Setting: U.S. national sample (20%) of Medicare beneficiaries aged 65 years or older, hospitalized with acute medical conditions.
Synopsis: This observational study assessed the difference in patients’ outcomes that were treated by a male or female physician. 30-days mortality rate was analyzed from 1,583,028 hospitalizations. The mortality rate of patients cared for by female physicians was lower and statistically significant: 11.07% vs. 11.49% (adjusted risk difference, –0.43%; 95% CI, –0.57% to –0.28%; P less than .001). The difference did not change after considering patient and physician characteristics as well as when looking at hospital fixed effects (that is, hospital indicators). In order to prevent one death, a female physician needs to treat 233 patients.
Also, 30-day readmission rate, after adjustment readmissions (from 1,540,797 hospitalizations) was 15.02% vs. 15.57% (adjusted risk difference, –0.55%; 95% confidence interval, –0.71% to 0.39%; P less than .001) showing that the care provided by a female physician can reduce one readmission when treating 182 patients.
Bottom line: Patients older than 65 years have lower 30-day mortality and readmission rates when receiving inpatient care from a female internist, compared with care by a male internist.
Citations: Tsugawa Y, Jena AB, Figueroa JF, et al. Comparison of hospital mortality and readmission rates for Medicare patients treated by male vs. female physicians. JAMA Intern Med. 2017 Feb;177(2):206-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
End-of-rotation resident transition in care and mortality among hospitalized patients
Clinical Question: Are hospitalized patients experiencing an increased mortality risk at the end-rotation resident transition in care and is this association related to the Accreditation Council for Graduate Medical Education (ACGME) 2011 duty-hour regulations?
Background: Prior studies of physicians’ transitions in care were associated with potential adverse patient events and outcomes. A higher mortality risk was suggested among patients with a complex hospital course or prolonged length of stay in association to house-staff transitions of care.

Setting: 10 University-affiliated U.S. Veterans Health Administration hospitals.
Synopsis: 230,701 patient discharges (mean age, 65.6 years; 95.8% male sex; median length of stay, 3 days) were included. The transition group included patients admitted at any time prior to an end-of-rotation who were either discharged or deceased within 7 days of transition. All other discharges were considered controls.
The primary outcome was in-hospital mortality rate; secondary outcomes included 30-day and 90-day mortality and readmission rates. An absolute increase of 1.5% to 1.9% in a unadjusted in-hospitality risk was found. The 30-day and 90-day mortality odds ratios were 1.10 and 1.21, respectively. A possible stronger association was found among interns’ transitions in care and the in-hospital and after-discharge mortality post-ACGME 2011 duty hour regulations. The latter raises questions about the interns’ inexperience and their amount of shift-to-shift handoffs. An adjusted analysis of the readmission rates at 30-day and 90-day was not significantly different between transition vs. control patients.
Bottom line: Elevated in-hospital mortality was seen among patients admitted to the inpatient medicine service at the end-of-rotation resident transitions in care. The association was stronger after the duty-hour ACGME (2011) regulations.
Citations: Denson JL, Jensen A, Saag HS, et al. Association between end-of-rotation resident transition in care and mortality among hospitalized patients. JAMA. 2016 Dec 6;316(21):2204-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
Clinical Question: Are hospitalized patients experiencing an increased mortality risk at the end-rotation resident transition in care and is this association related to the Accreditation Council for Graduate Medical Education (ACGME) 2011 duty-hour regulations?
Background: Prior studies of physicians’ transitions in care were associated with potential adverse patient events and outcomes. A higher mortality risk was suggested among patients with a complex hospital course or prolonged length of stay in association to house-staff transitions of care.
Setting: 10 University-affiliated U.S. Veterans Health Administration hospitals.
Synopsis: 230,701 patient discharges (mean age, 65.6 years; 95.8% male sex; median length of stay, 3 days) were included. The transition group included patients admitted at any time prior to an end-of-rotation who were either discharged or deceased within 7 days of transition. All other discharges were considered controls.
The primary outcome was in-hospital mortality rate; secondary outcomes included 30-day and 90-day mortality and readmission rates. An absolute increase of 1.5% to 1.9% in a unadjusted in-hospitality risk was found. The 30-day and 90-day mortality odds ratios were 1.10 and 1.21, respectively. A possible stronger association was found among interns’ transitions in care and the in-hospital and after-discharge mortality post-ACGME 2011 duty hour regulations. The latter raises questions about the interns’ inexperience and their amount of shift-to-shift handoffs. An adjusted analysis of the readmission rates at 30-day and 90-day was not significantly different between transition vs. control patients.
Bottom line: Elevated in-hospital mortality was seen among patients admitted to the inpatient medicine service at the end-of-rotation resident transitions in care. The association was stronger after the duty-hour ACGME (2011) regulations.
Citations: Denson JL, Jensen A, Saag HS, et al. Association between end-of-rotation resident transition in care and mortality among hospitalized patients. JAMA. 2016 Dec 6;316(21):2204-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
Clinical Question: Are hospitalized patients experiencing an increased mortality risk at the end-rotation resident transition in care and is this association related to the Accreditation Council for Graduate Medical Education (ACGME) 2011 duty-hour regulations?
Background: Prior studies of physicians’ transitions in care were associated with potential adverse patient events and outcomes. A higher mortality risk was suggested among patients with a complex hospital course or prolonged length of stay in association to house-staff transitions of care.
Setting: 10 University-affiliated U.S. Veterans Health Administration hospitals.
Synopsis: 230,701 patient discharges (mean age, 65.6 years; 95.8% male sex; median length of stay, 3 days) were included. The transition group included patients admitted at any time prior to an end-of-rotation who were either discharged or deceased within 7 days of transition. All other discharges were considered controls.
The primary outcome was in-hospital mortality rate; secondary outcomes included 30-day and 90-day mortality and readmission rates. An absolute increase of 1.5% to 1.9% in a unadjusted in-hospitality risk was found. The 30-day and 90-day mortality odds ratios were 1.10 and 1.21, respectively. A possible stronger association was found among interns’ transitions in care and the in-hospital and after-discharge mortality post-ACGME 2011 duty hour regulations. The latter raises questions about the interns’ inexperience and their amount of shift-to-shift handoffs. An adjusted analysis of the readmission rates at 30-day and 90-day was not significantly different between transition vs. control patients.
Bottom line: Elevated in-hospital mortality was seen among patients admitted to the inpatient medicine service at the end-of-rotation resident transitions in care. The association was stronger after the duty-hour ACGME (2011) regulations.
Citations: Denson JL, Jensen A, Saag HS, et al. Association between end-of-rotation resident transition in care and mortality among hospitalized patients. JAMA. 2016 Dec 6;316(21):2204-13.
Dr. Orjuela is assistant professor of neurology at the University of Colorado School of Medicine, Aurora.
VIDEO: Picowave laser uses are expanding beyond tattoo removal
ORLANDO – The applications for picowavelength lasers are expanding, with emerging data on their uses for cosmetic indications other than tattoo removal, according to Anne Chapas, MD, who is in private practice in New York.
First introduced and cleared by the Food and Drug Administration for tattoo removal, “picowave devices ... are now being studied in multiple different cosmetic conditions, including their use in acne scars, fine lines and wrinkles, and melasma,” Dr. Chapas said in a video interview at the annual meeting of the American Academy of Dermatology.
The No. 1 thing dermatologists need to know is that these types of lasers are delivering energy extremely quickly,” at 1,000 times faster than nanosecond lasers, she said. Another difference between the two is that “the laser tissue interaction between the two types of devices is completely different.”
In the interview, she highlighted other important points about picowave lasers, including less downtime after treatment.
At the meeting, Dr. Chapas spoke during a session entitled “the Science Behind New Devices in Dermatology.”
Her disclosures include serving as a consultant and investigator for Syneron and Candela.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – The applications for picowavelength lasers are expanding, with emerging data on their uses for cosmetic indications other than tattoo removal, according to Anne Chapas, MD, who is in private practice in New York.
First introduced and cleared by the Food and Drug Administration for tattoo removal, “picowave devices ... are now being studied in multiple different cosmetic conditions, including their use in acne scars, fine lines and wrinkles, and melasma,” Dr. Chapas said in a video interview at the annual meeting of the American Academy of Dermatology.
The No. 1 thing dermatologists need to know is that these types of lasers are delivering energy extremely quickly,” at 1,000 times faster than nanosecond lasers, she said. Another difference between the two is that “the laser tissue interaction between the two types of devices is completely different.”
In the interview, she highlighted other important points about picowave lasers, including less downtime after treatment.
At the meeting, Dr. Chapas spoke during a session entitled “the Science Behind New Devices in Dermatology.”
Her disclosures include serving as a consultant and investigator for Syneron and Candela.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – The applications for picowavelength lasers are expanding, with emerging data on their uses for cosmetic indications other than tattoo removal, according to Anne Chapas, MD, who is in private practice in New York.
First introduced and cleared by the Food and Drug Administration for tattoo removal, “picowave devices ... are now being studied in multiple different cosmetic conditions, including their use in acne scars, fine lines and wrinkles, and melasma,” Dr. Chapas said in a video interview at the annual meeting of the American Academy of Dermatology.
The No. 1 thing dermatologists need to know is that these types of lasers are delivering energy extremely quickly,” at 1,000 times faster than nanosecond lasers, she said. Another difference between the two is that “the laser tissue interaction between the two types of devices is completely different.”
In the interview, she highlighted other important points about picowave lasers, including less downtime after treatment.
At the meeting, Dr. Chapas spoke during a session entitled “the Science Behind New Devices in Dermatology.”
Her disclosures include serving as a consultant and investigator for Syneron and Candela.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT AAD 17

VIDEO: Internet-based intervention shows antihypertensive efficacy
WASHINGTON – Patients who regularly accessed 30 minute, Internet-based behavioral counseling videos cut their systolic blood pressure, compared with baseline over 1 year by an average 4 mm Hg more than control patients in a randomized, phase II study with 264 patients.
Electronic counseling (e-counseling) “enhanced the efficacy of usual care for hypertension,” Robert P. Nolan, Ph.D., said at the annual meeting of the American College of Cardiology.
“We hope to optimize the efficacy of medical treatments with a behavioral intervention,” said Dr. Nolan, who added that the magnitude of the added benefit from the e-counseling program was “like adding an additional antihypertensive medication.”
“We know antihypertensive treatments work, but compliance is a huge challenge” for health care providers, commented E. Magnus Ohman, MBBS, a professor and cardiologist at Duke University in Durham, N.C. “Having a new way to enhance compliance would be fantastic,” he said.
The Internet-based counseling program devised by Dr. Nolan and his associates consisted of a year-long series of 28 videos, each about 30 minutes long, that participants in the active arm accessed over the Internet. During the study, participants received a series of emailed messages that sent links to the videos on a set schedule over 12 months: During the first 4 months they received an emailed link weekly, during the next 4 months they received an emailed link to a new video every other week, and during the final 4 months of the intervention participants received emailed links once a month. Patients could access each video more than once if they wished, and they were free to share the links with any family members or friends who helped the patients with lifestyle management of their hypertension.
Patients in the e-counseling intervention arm received links to videos that focused on motivational messages and teaching cognitive behavioral skills. Patients in the control arm received emails with generic messages on blood pressure management and without links to videos.
The REACH (E-Counseling Promotes Blood Pressure Reduction and Therapeutic Lifestyle Change in Hypertension) study ran at four Canadian sites. It sent invitations to participate to 609 patients with stage 1 or 2 hypertension, with a blood pressure prior to treatment of 140/90-180/110 mm Hg. Among the invited patients, 264 elected to participate; 100 patients in the e-counseling arm and 97 control patients completed the 1-year program. Participants averaged 58 years of age, their average body mass index was 31 kg/m2, and 9% smoked. Their blood pressure at entry averaged 141/87 mm Hg, their average pulse pressure was about 54 mm Hg, and their average 10-year risk for a cardiovascular disease event, measured by the Framingham Risk Score, was about 16%. At entry, patients in the study received an average of 1.5 antihypertensive drugs each.
At the end of the 1-year program, systolic blood pressure fell by an average of 6 mm Hg from baseline among patients who completed the control program, and by an average of 10.1 mm Hg among the patients who completed the e-counseling arm, a statistically significant difference for one of the study’s primary endpoints. Change in pulse pressure from baseline showed an average 1.5–mm Hg drop in the control patients and an average 4.3–mm Hg decline in the e-counseling patients, another statistically significant difference for a second primary endpoint, reported Dr. Nolan, a clinical psychologist and director of the cardiac eHealth program at the University of Toronto.
A third primary endpoint was change in the Framingham Risk Score, which fell by an average of 1.9% after 12 months in the e-counseling patients and rose by an average of 0.2% among the controls.
The final primary endpoint was the change in diastolic blood pressure from baseline, which showed a better than 4–mm Hg incremental decline in the men who received e-counseling, compared with controls, but among women in the study, the drop in diastolic blood pressure from baseline was nearly the same – about 6 mm Hg – in both the controls and e-counseling patients.
“This tells us that we need to better tailor the [e-counseling] intervention to men and to women,” Dr. Nolan said in a video interview. He also envisions better tailoring of the e-counseling videos to various socioeconomic and ethnic groups. He plans to continue testing of a revised version of the e-counseling intervention in a larger, phase III study, but he also hopes that the intervention videos can soon be available at no charge for use in routine practice.
REACH received no commercial funding. Dr. Nolan had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
I love the REACH study. Hypertension is incredibly prevalent among the patients I see, and they often need three different antihypertensive drugs to control their blood pressure. Lifestyle interventions can be very effective at helping to lower blood pressure, but during the 10-minute visits I have with most of my patients, it’s hard for me to have much impact on their behavior.
What I especially like about the Internet-based counseling used in this study was its application of evidence-based approaches to change patient behavior. This was a well-designed and exciting trial.
Sandra J. Lewis, MD, chief of cardiology at Legacy Good Samaritan Hospital in Portland, Ore., made these comments during a press conference. She had no disclosures.
I love the REACH study. Hypertension is incredibly prevalent among the patients I see, and they often need three different antihypertensive drugs to control their blood pressure. Lifestyle interventions can be very effective at helping to lower blood pressure, but during the 10-minute visits I have with most of my patients, it’s hard for me to have much impact on their behavior.
What I especially like about the Internet-based counseling used in this study was its application of evidence-based approaches to change patient behavior. This was a well-designed and exciting trial.
Sandra J. Lewis, MD, chief of cardiology at Legacy Good Samaritan Hospital in Portland, Ore., made these comments during a press conference. She had no disclosures.
I love the REACH study. Hypertension is incredibly prevalent among the patients I see, and they often need three different antihypertensive drugs to control their blood pressure. Lifestyle interventions can be very effective at helping to lower blood pressure, but during the 10-minute visits I have with most of my patients, it’s hard for me to have much impact on their behavior.
What I especially like about the Internet-based counseling used in this study was its application of evidence-based approaches to change patient behavior. This was a well-designed and exciting trial.
Sandra J. Lewis, MD, chief of cardiology at Legacy Good Samaritan Hospital in Portland, Ore., made these comments during a press conference. She had no disclosures.
WASHINGTON – Patients who regularly accessed 30 minute, Internet-based behavioral counseling videos cut their systolic blood pressure, compared with baseline over 1 year by an average 4 mm Hg more than control patients in a randomized, phase II study with 264 patients.
Electronic counseling (e-counseling) “enhanced the efficacy of usual care for hypertension,” Robert P. Nolan, Ph.D., said at the annual meeting of the American College of Cardiology.
“We hope to optimize the efficacy of medical treatments with a behavioral intervention,” said Dr. Nolan, who added that the magnitude of the added benefit from the e-counseling program was “like adding an additional antihypertensive medication.”
“We know antihypertensive treatments work, but compliance is a huge challenge” for health care providers, commented E. Magnus Ohman, MBBS, a professor and cardiologist at Duke University in Durham, N.C. “Having a new way to enhance compliance would be fantastic,” he said.
The Internet-based counseling program devised by Dr. Nolan and his associates consisted of a year-long series of 28 videos, each about 30 minutes long, that participants in the active arm accessed over the Internet. During the study, participants received a series of emailed messages that sent links to the videos on a set schedule over 12 months: During the first 4 months they received an emailed link weekly, during the next 4 months they received an emailed link to a new video every other week, and during the final 4 months of the intervention participants received emailed links once a month. Patients could access each video more than once if they wished, and they were free to share the links with any family members or friends who helped the patients with lifestyle management of their hypertension.
Patients in the e-counseling intervention arm received links to videos that focused on motivational messages and teaching cognitive behavioral skills. Patients in the control arm received emails with generic messages on blood pressure management and without links to videos.
The REACH (E-Counseling Promotes Blood Pressure Reduction and Therapeutic Lifestyle Change in Hypertension) study ran at four Canadian sites. It sent invitations to participate to 609 patients with stage 1 or 2 hypertension, with a blood pressure prior to treatment of 140/90-180/110 mm Hg. Among the invited patients, 264 elected to participate; 100 patients in the e-counseling arm and 97 control patients completed the 1-year program. Participants averaged 58 years of age, their average body mass index was 31 kg/m2, and 9% smoked. Their blood pressure at entry averaged 141/87 mm Hg, their average pulse pressure was about 54 mm Hg, and their average 10-year risk for a cardiovascular disease event, measured by the Framingham Risk Score, was about 16%. At entry, patients in the study received an average of 1.5 antihypertensive drugs each.
At the end of the 1-year program, systolic blood pressure fell by an average of 6 mm Hg from baseline among patients who completed the control program, and by an average of 10.1 mm Hg among the patients who completed the e-counseling arm, a statistically significant difference for one of the study’s primary endpoints. Change in pulse pressure from baseline showed an average 1.5–mm Hg drop in the control patients and an average 4.3–mm Hg decline in the e-counseling patients, another statistically significant difference for a second primary endpoint, reported Dr. Nolan, a clinical psychologist and director of the cardiac eHealth program at the University of Toronto.
A third primary endpoint was change in the Framingham Risk Score, which fell by an average of 1.9% after 12 months in the e-counseling patients and rose by an average of 0.2% among the controls.
The final primary endpoint was the change in diastolic blood pressure from baseline, which showed a better than 4–mm Hg incremental decline in the men who received e-counseling, compared with controls, but among women in the study, the drop in diastolic blood pressure from baseline was nearly the same – about 6 mm Hg – in both the controls and e-counseling patients.
“This tells us that we need to better tailor the [e-counseling] intervention to men and to women,” Dr. Nolan said in a video interview. He also envisions better tailoring of the e-counseling videos to various socioeconomic and ethnic groups. He plans to continue testing of a revised version of the e-counseling intervention in a larger, phase III study, but he also hopes that the intervention videos can soon be available at no charge for use in routine practice.
REACH received no commercial funding. Dr. Nolan had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
WASHINGTON – Patients who regularly accessed 30 minute, Internet-based behavioral counseling videos cut their systolic blood pressure, compared with baseline over 1 year by an average 4 mm Hg more than control patients in a randomized, phase II study with 264 patients.
Electronic counseling (e-counseling) “enhanced the efficacy of usual care for hypertension,” Robert P. Nolan, Ph.D., said at the annual meeting of the American College of Cardiology.
“We hope to optimize the efficacy of medical treatments with a behavioral intervention,” said Dr. Nolan, who added that the magnitude of the added benefit from the e-counseling program was “like adding an additional antihypertensive medication.”
“We know antihypertensive treatments work, but compliance is a huge challenge” for health care providers, commented E. Magnus Ohman, MBBS, a professor and cardiologist at Duke University in Durham, N.C. “Having a new way to enhance compliance would be fantastic,” he said.
The Internet-based counseling program devised by Dr. Nolan and his associates consisted of a year-long series of 28 videos, each about 30 minutes long, that participants in the active arm accessed over the Internet. During the study, participants received a series of emailed messages that sent links to the videos on a set schedule over 12 months: During the first 4 months they received an emailed link weekly, during the next 4 months they received an emailed link to a new video every other week, and during the final 4 months of the intervention participants received emailed links once a month. Patients could access each video more than once if they wished, and they were free to share the links with any family members or friends who helped the patients with lifestyle management of their hypertension.
Patients in the e-counseling intervention arm received links to videos that focused on motivational messages and teaching cognitive behavioral skills. Patients in the control arm received emails with generic messages on blood pressure management and without links to videos.
The REACH (E-Counseling Promotes Blood Pressure Reduction and Therapeutic Lifestyle Change in Hypertension) study ran at four Canadian sites. It sent invitations to participate to 609 patients with stage 1 or 2 hypertension, with a blood pressure prior to treatment of 140/90-180/110 mm Hg. Among the invited patients, 264 elected to participate; 100 patients in the e-counseling arm and 97 control patients completed the 1-year program. Participants averaged 58 years of age, their average body mass index was 31 kg/m2, and 9% smoked. Their blood pressure at entry averaged 141/87 mm Hg, their average pulse pressure was about 54 mm Hg, and their average 10-year risk for a cardiovascular disease event, measured by the Framingham Risk Score, was about 16%. At entry, patients in the study received an average of 1.5 antihypertensive drugs each.
At the end of the 1-year program, systolic blood pressure fell by an average of 6 mm Hg from baseline among patients who completed the control program, and by an average of 10.1 mm Hg among the patients who completed the e-counseling arm, a statistically significant difference for one of the study’s primary endpoints. Change in pulse pressure from baseline showed an average 1.5–mm Hg drop in the control patients and an average 4.3–mm Hg decline in the e-counseling patients, another statistically significant difference for a second primary endpoint, reported Dr. Nolan, a clinical psychologist and director of the cardiac eHealth program at the University of Toronto.
A third primary endpoint was change in the Framingham Risk Score, which fell by an average of 1.9% after 12 months in the e-counseling patients and rose by an average of 0.2% among the controls.
The final primary endpoint was the change in diastolic blood pressure from baseline, which showed a better than 4–mm Hg incremental decline in the men who received e-counseling, compared with controls, but among women in the study, the drop in diastolic blood pressure from baseline was nearly the same – about 6 mm Hg – in both the controls and e-counseling patients.
“This tells us that we need to better tailor the [e-counseling] intervention to men and to women,” Dr. Nolan said in a video interview. He also envisions better tailoring of the e-counseling videos to various socioeconomic and ethnic groups. He plans to continue testing of a revised version of the e-counseling intervention in a larger, phase III study, but he also hopes that the intervention videos can soon be available at no charge for use in routine practice.
REACH received no commercial funding. Dr. Nolan had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
[email protected]
On Twitter @mitchelzoler
AT ACC 17
Key clinical point:
Major finding: The Internet-based program reduced systolic blood pressure from baseline by an average additional 4.1 mm Hg, compared with controls.
Data source: REACH, a multicenter, randomized trial with 264 hypertensive patients.
Disclosures: REACH received no commercial funding. Dr. Nolan had no disclosures.
VIDEO: Looking at keloids from a different perspective
ORLANDO – It may be time to start considering new options for treating keloids, according to Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C.
At the annual meeting of the American Academy of Dermatology, Dr. McMichael discussed one of the highlights of the annual symposium of the Skin of Color Society, held right before the annual meeting, a presentation by Michael Tirgan, MD, who has treated patients with keloids for about 10 years.
Dr. Tirgan, an oncologist based in New York, has a large database and registry of patients and shared some interesting data at the symposium. “What he’s found is that those who come with the supermassive and massive keloids are those who have had the most surgery on their keloid,” Dr. McMichael said in a video interview at the meeting.
His findings shed light on what she described as “a new perspective in the way that we think about keloids” and a new approach to treatment – considering keloids as tumors – not just a scar.
Dr. McMichael had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – It may be time to start considering new options for treating keloids, according to Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C.
At the annual meeting of the American Academy of Dermatology, Dr. McMichael discussed one of the highlights of the annual symposium of the Skin of Color Society, held right before the annual meeting, a presentation by Michael Tirgan, MD, who has treated patients with keloids for about 10 years.
Dr. Tirgan, an oncologist based in New York, has a large database and registry of patients and shared some interesting data at the symposium. “What he’s found is that those who come with the supermassive and massive keloids are those who have had the most surgery on their keloid,” Dr. McMichael said in a video interview at the meeting.
His findings shed light on what she described as “a new perspective in the way that we think about keloids” and a new approach to treatment – considering keloids as tumors – not just a scar.
Dr. McMichael had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ORLANDO – It may be time to start considering new options for treating keloids, according to Amy McMichael, MD, professor of dermatology at Wake Forest University, Winston-Salem, N.C.
At the annual meeting of the American Academy of Dermatology, Dr. McMichael discussed one of the highlights of the annual symposium of the Skin of Color Society, held right before the annual meeting, a presentation by Michael Tirgan, MD, who has treated patients with keloids for about 10 years.
Dr. Tirgan, an oncologist based in New York, has a large database and registry of patients and shared some interesting data at the symposium. “What he’s found is that those who come with the supermassive and massive keloids are those who have had the most surgery on their keloid,” Dr. McMichael said in a video interview at the meeting.
His findings shed light on what she described as “a new perspective in the way that we think about keloids” and a new approach to treatment – considering keloids as tumors – not just a scar.
Dr. McMichael had no relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT AAD 17

Rehabilitation Program Improves Symptoms of Functional Movement Disorders
RIVIERA BEACH, FL—A comprehensive, interdisciplinary rehabilitation program for functional movement disorders (FMD) is providing high rates of sustained improvement in patients with this challenging clinical problem, according to an initial analysis. In this program, which is administered during a one-week in-hospital stay, the emphasis is on relearning normal movement through physical therapy, but attention is also paid to the psychological component of the disorder.

What Is FMD?
FMD includes movement abnormalities such as tremor, gait disturbances, or dystonia that are not explained by organic lesions or diseases. FMD is common and occurs in 3% to 5% of patients presenting at movement disorder clinics, according to Dr. LaFaver. Although FMD has an important psychogenic component, Dr. LaFaver said that the symptoms can be as persistent and debilitating as those associated with organic disorders. As with organic diseases, the consequences of FMD include chronic disability.
This last point was emphasized in the demographics of a series of 32 patients with FMD presented by Dr. LaFaver. The mean duration of symptoms was seven years, and 56% of patients were on disability at the time of enrollment into the MoRe program. Consistent with other series of patients with FMD, the population was predominantly female (75%), and a substantial proportion reported posttraumatic stress disorder (53%), sexual abuse (48%), and physical abuse (41%). Mean scores on the Beck Depression Inventory (16.59) and the State-Trait Anxiety Index (40.79) indicated that mood disorders were common. This result also has been previously reported in patients with FMD.
The MoRe Program
Over the course of the inpatient MoRe program, patients begin with simple, repetitive, and structured exercises relevant to their FMD, progressing to more complex motor tasks as they improve. Positive gains with physical therapy, which is provided for five consecutive days, are reinforced with structured cognitive behavioral therapy (CBT). The motor reprogramming provided is analogous to that offered for various neurologic symptoms associated with organic diseases, such as paraplegia or hemiparesis. Importantly, participants in the MoRe program are encouraged to think of their disorder as definable and treatable, even if the psychogenic component is not concealed.
“We do set the expectation that they will be normal by the end of the week,” said Dr. LaFaver, who explains to patients that neurologic abnormalities are likely to be involved, even if they cannot be objectively demonstrated.
MoRe is run as an inpatient program to permit an adequate intensity of physical therapy and to allow patients to develop trust in their physical and psychological therapists, Dr. LaFaver said. She also suggested that the emphasis on physical therapy in the MoRe program allows patients to frame the goals of treatment in a useful way. The psychological support is essentially adjunctive.
“It can be helpful to use analogies, such as describing the movement disorder as a software [problem] rather than a hardware problem,” Dr. LaFaver explained. The emphasis is on engaging patients to participate in treatment that will reverse adverse changes in the neurologic circuitry that is driving the symptoms. Citing recent functional MRI (fMRI) studies that have shown changes in right temporoparietal junction connectivity in patients with FMD, Dr. LaFaver suggested that the premise of a change in brain function with FMD has evidential support.
Rehabilitation Yields Improvements
In the series of 32 patients treated during a two-year period starting in 2014, the predominant symptoms were abnormal gait in 31%, dystonia in 31%, tremor in 13%, chorea in 13%, myoclonus in 6%, and weakness in 6%. On video rating performed by a movement disorder specialist to compare symptom severity at baseline with that following treatment, movement symptoms improved by 59% on average from day 1 to day 5 of treatment.
The improvement in video ratings was supported by patient self-assessment. On a descending scale of 7 to 1, with 1 signifying the greatest symptom control, the mean patient-assessment score was 2.07 immediately after completing the MoRe program and 2.78 at the six-month follow-up, according to Dr. LaFaver.
Patient satisfaction with the program was high. On an ascending scale of 0 to 10, with 10 providing the best rating, patients gave physical therapy an average rating of 9.23 and psychological skills training an average rating of 8.87. For mental practice training, another aspect of the MoRe program used to reinforce motor reprogramming, the average patient rating was 8.62. Ninety-six percent of patients reported that they would participate in the program again.
Taking a Systematic Approach
Patient selection is important, according to Dr. LaFaver. Although she does not believe it is necessary to rule out all organic diseases with an exhaustive series of diagnostic studies, she did suggest that a movement disorder specialist capable of performing a detailed differential diagnosis should be engaged to confirm FMD. She also suggested that patients are more likely to respond to a program like MoRe after they have accepted a diagnosis of FMD over other potential etiologies, such as Lyme disease.
So far, patients accepted into the MoRe program have typically had significant disability, which has facilitated the justification for inpatient treatment, according to Dr. LaFaver. As a result, third-party reimbursement is usually obtained. For patients with lower symptom burden, such as isolated tremor, similar principles have been employed in an outpatient basis with encouraging rates of response, said Dr. LaFaver. These responses emphasize the value of a systematic approach to a condition that deserves greater public awareness, as well as further clinical research, she added.
Even if FMD is primarily a psychogenic disorder, “patients treated with psychotherapy alone often do not get better,” Dr. LaFaver observed. “It is our job as neurologists to try to make a difference for these patients,” she added. She believes that the principles employed in the MoRe program, many of which were borrowed from an outpatient program at the Mayo Clinic in Rochester, Minnesota (where Dr. LaFaver trained), are broadly applicable in FMD.
Dr. LaFaver reported participation in studies of Parkinson’s disease and Huntington’s disease that had been sponsored by industry and by the NIH, but had no disclosures relevant to FMD.
—Theodore Bosworth
RIVIERA BEACH, FL—A comprehensive, interdisciplinary rehabilitation program for functional movement disorders (FMD) is providing high rates of sustained improvement in patients with this challenging clinical problem, according to an initial analysis. In this program, which is administered during a one-week in-hospital stay, the emphasis is on relearning normal movement through physical therapy, but attention is also paid to the psychological component of the disorder.
What Is FMD?
FMD includes movement abnormalities such as tremor, gait disturbances, or dystonia that are not explained by organic lesions or diseases. FMD is common and occurs in 3% to 5% of patients presenting at movement disorder clinics, according to Dr. LaFaver. Although FMD has an important psychogenic component, Dr. LaFaver said that the symptoms can be as persistent and debilitating as those associated with organic disorders. As with organic diseases, the consequences of FMD include chronic disability.
This last point was emphasized in the demographics of a series of 32 patients with FMD presented by Dr. LaFaver. The mean duration of symptoms was seven years, and 56% of patients were on disability at the time of enrollment into the MoRe program. Consistent with other series of patients with FMD, the population was predominantly female (75%), and a substantial proportion reported posttraumatic stress disorder (53%), sexual abuse (48%), and physical abuse (41%). Mean scores on the Beck Depression Inventory (16.59) and the State-Trait Anxiety Index (40.79) indicated that mood disorders were common. This result also has been previously reported in patients with FMD.
The MoRe Program
Over the course of the inpatient MoRe program, patients begin with simple, repetitive, and structured exercises relevant to their FMD, progressing to more complex motor tasks as they improve. Positive gains with physical therapy, which is provided for five consecutive days, are reinforced with structured cognitive behavioral therapy (CBT). The motor reprogramming provided is analogous to that offered for various neurologic symptoms associated with organic diseases, such as paraplegia or hemiparesis. Importantly, participants in the MoRe program are encouraged to think of their disorder as definable and treatable, even if the psychogenic component is not concealed.
“We do set the expectation that they will be normal by the end of the week,” said Dr. LaFaver, who explains to patients that neurologic abnormalities are likely to be involved, even if they cannot be objectively demonstrated.
MoRe is run as an inpatient program to permit an adequate intensity of physical therapy and to allow patients to develop trust in their physical and psychological therapists, Dr. LaFaver said. She also suggested that the emphasis on physical therapy in the MoRe program allows patients to frame the goals of treatment in a useful way. The psychological support is essentially adjunctive.
“It can be helpful to use analogies, such as describing the movement disorder as a software [problem] rather than a hardware problem,” Dr. LaFaver explained. The emphasis is on engaging patients to participate in treatment that will reverse adverse changes in the neurologic circuitry that is driving the symptoms. Citing recent functional MRI (fMRI) studies that have shown changes in right temporoparietal junction connectivity in patients with FMD, Dr. LaFaver suggested that the premise of a change in brain function with FMD has evidential support.
Rehabilitation Yields Improvements
In the series of 32 patients treated during a two-year period starting in 2014, the predominant symptoms were abnormal gait in 31%, dystonia in 31%, tremor in 13%, chorea in 13%, myoclonus in 6%, and weakness in 6%. On video rating performed by a movement disorder specialist to compare symptom severity at baseline with that following treatment, movement symptoms improved by 59% on average from day 1 to day 5 of treatment.
The improvement in video ratings was supported by patient self-assessment. On a descending scale of 7 to 1, with 1 signifying the greatest symptom control, the mean patient-assessment score was 2.07 immediately after completing the MoRe program and 2.78 at the six-month follow-up, according to Dr. LaFaver.
Patient satisfaction with the program was high. On an ascending scale of 0 to 10, with 10 providing the best rating, patients gave physical therapy an average rating of 9.23 and psychological skills training an average rating of 8.87. For mental practice training, another aspect of the MoRe program used to reinforce motor reprogramming, the average patient rating was 8.62. Ninety-six percent of patients reported that they would participate in the program again.
Taking a Systematic Approach
Patient selection is important, according to Dr. LaFaver. Although she does not believe it is necessary to rule out all organic diseases with an exhaustive series of diagnostic studies, she did suggest that a movement disorder specialist capable of performing a detailed differential diagnosis should be engaged to confirm FMD. She also suggested that patients are more likely to respond to a program like MoRe after they have accepted a diagnosis of FMD over other potential etiologies, such as Lyme disease.
So far, patients accepted into the MoRe program have typically had significant disability, which has facilitated the justification for inpatient treatment, according to Dr. LaFaver. As a result, third-party reimbursement is usually obtained. For patients with lower symptom burden, such as isolated tremor, similar principles have been employed in an outpatient basis with encouraging rates of response, said Dr. LaFaver. These responses emphasize the value of a systematic approach to a condition that deserves greater public awareness, as well as further clinical research, she added.
Even if FMD is primarily a psychogenic disorder, “patients treated with psychotherapy alone often do not get better,” Dr. LaFaver observed. “It is our job as neurologists to try to make a difference for these patients,” she added. She believes that the principles employed in the MoRe program, many of which were borrowed from an outpatient program at the Mayo Clinic in Rochester, Minnesota (where Dr. LaFaver trained), are broadly applicable in FMD.
Dr. LaFaver reported participation in studies of Parkinson’s disease and Huntington’s disease that had been sponsored by industry and by the NIH, but had no disclosures relevant to FMD.
—Theodore Bosworth
RIVIERA BEACH, FL—A comprehensive, interdisciplinary rehabilitation program for functional movement disorders (FMD) is providing high rates of sustained improvement in patients with this challenging clinical problem, according to an initial analysis. In this program, which is administered during a one-week in-hospital stay, the emphasis is on relearning normal movement through physical therapy, but attention is also paid to the psychological component of the disorder.
What Is FMD?
FMD includes movement abnormalities such as tremor, gait disturbances, or dystonia that are not explained by organic lesions or diseases. FMD is common and occurs in 3% to 5% of patients presenting at movement disorder clinics, according to Dr. LaFaver. Although FMD has an important psychogenic component, Dr. LaFaver said that the symptoms can be as persistent and debilitating as those associated with organic disorders. As with organic diseases, the consequences of FMD include chronic disability.
This last point was emphasized in the demographics of a series of 32 patients with FMD presented by Dr. LaFaver. The mean duration of symptoms was seven years, and 56% of patients were on disability at the time of enrollment into the MoRe program. Consistent with other series of patients with FMD, the population was predominantly female (75%), and a substantial proportion reported posttraumatic stress disorder (53%), sexual abuse (48%), and physical abuse (41%). Mean scores on the Beck Depression Inventory (16.59) and the State-Trait Anxiety Index (40.79) indicated that mood disorders were common. This result also has been previously reported in patients with FMD.
The MoRe Program
Over the course of the inpatient MoRe program, patients begin with simple, repetitive, and structured exercises relevant to their FMD, progressing to more complex motor tasks as they improve. Positive gains with physical therapy, which is provided for five consecutive days, are reinforced with structured cognitive behavioral therapy (CBT). The motor reprogramming provided is analogous to that offered for various neurologic symptoms associated with organic diseases, such as paraplegia or hemiparesis. Importantly, participants in the MoRe program are encouraged to think of their disorder as definable and treatable, even if the psychogenic component is not concealed.
“We do set the expectation that they will be normal by the end of the week,” said Dr. LaFaver, who explains to patients that neurologic abnormalities are likely to be involved, even if they cannot be objectively demonstrated.
MoRe is run as an inpatient program to permit an adequate intensity of physical therapy and to allow patients to develop trust in their physical and psychological therapists, Dr. LaFaver said. She also suggested that the emphasis on physical therapy in the MoRe program allows patients to frame the goals of treatment in a useful way. The psychological support is essentially adjunctive.
“It can be helpful to use analogies, such as describing the movement disorder as a software [problem] rather than a hardware problem,” Dr. LaFaver explained. The emphasis is on engaging patients to participate in treatment that will reverse adverse changes in the neurologic circuitry that is driving the symptoms. Citing recent functional MRI (fMRI) studies that have shown changes in right temporoparietal junction connectivity in patients with FMD, Dr. LaFaver suggested that the premise of a change in brain function with FMD has evidential support.
Rehabilitation Yields Improvements
In the series of 32 patients treated during a two-year period starting in 2014, the predominant symptoms were abnormal gait in 31%, dystonia in 31%, tremor in 13%, chorea in 13%, myoclonus in 6%, and weakness in 6%. On video rating performed by a movement disorder specialist to compare symptom severity at baseline with that following treatment, movement symptoms improved by 59% on average from day 1 to day 5 of treatment.
The improvement in video ratings was supported by patient self-assessment. On a descending scale of 7 to 1, with 1 signifying the greatest symptom control, the mean patient-assessment score was 2.07 immediately after completing the MoRe program and 2.78 at the six-month follow-up, according to Dr. LaFaver.
Patient satisfaction with the program was high. On an ascending scale of 0 to 10, with 10 providing the best rating, patients gave physical therapy an average rating of 9.23 and psychological skills training an average rating of 8.87. For mental practice training, another aspect of the MoRe program used to reinforce motor reprogramming, the average patient rating was 8.62. Ninety-six percent of patients reported that they would participate in the program again.
Taking a Systematic Approach
Patient selection is important, according to Dr. LaFaver. Although she does not believe it is necessary to rule out all organic diseases with an exhaustive series of diagnostic studies, she did suggest that a movement disorder specialist capable of performing a detailed differential diagnosis should be engaged to confirm FMD. She also suggested that patients are more likely to respond to a program like MoRe after they have accepted a diagnosis of FMD over other potential etiologies, such as Lyme disease.
So far, patients accepted into the MoRe program have typically had significant disability, which has facilitated the justification for inpatient treatment, according to Dr. LaFaver. As a result, third-party reimbursement is usually obtained. For patients with lower symptom burden, such as isolated tremor, similar principles have been employed in an outpatient basis with encouraging rates of response, said Dr. LaFaver. These responses emphasize the value of a systematic approach to a condition that deserves greater public awareness, as well as further clinical research, she added.
Even if FMD is primarily a psychogenic disorder, “patients treated with psychotherapy alone often do not get better,” Dr. LaFaver observed. “It is our job as neurologists to try to make a difference for these patients,” she added. She believes that the principles employed in the MoRe program, many of which were borrowed from an outpatient program at the Mayo Clinic in Rochester, Minnesota (where Dr. LaFaver trained), are broadly applicable in FMD.
Dr. LaFaver reported participation in studies of Parkinson’s disease and Huntington’s disease that had been sponsored by industry and by the NIH, but had no disclosures relevant to FMD.
—Theodore Bosworth
Collagenous and Elastotic Marginal Plaques of the Hands
To the Editor:
Collagenous and elastotic marginal plaques of the hands (CEMPHs) has several names including degenerative collagenous plaques of the hands, keratoelastoidosis marginalis, and digital papular calcific elastosis. This rare disorder is an acquired, slowly progressive, asymptomatic, dermal connective tissue abnormality that is underrecognized and underdiagnosed. Clinical presentation includes hyperkeratotic translucent papules arranged linearly on the radial aspect of the hands.
A 74-year-old woman described having "rough hands" of more than 20 years' duration. She presented with 4-cm wide longitudinal, erythematous, firm, depressed plaques along the lateral edge of the second finger and extending to the medial thumb in both hands (Figure 1). She had attempted multiple treatments by her primary care physician, including topical and oral medications unknown to the patient and light therapy, all without benefit over a period of several years. We have attempted salicylic acid 40%, clobetasol cream 0.05%, and emollient creams containing α-hydroxy acid. At best the condition fluctuated between a subtle raised scale at the edge to smooth and occasionally more red-pink, seemingly unrelated to any treatments.

The patient did not have plaques elsewhere on the body, and notably, the feet were clear. She did not have a history of repeated trauma to the hands and did not engage in manual labor. She denied excessive sun exposure, though she had Fitzpatrick skin type III and a history of multiple precancers and nonmelanoma skin cancers 7 years prior to presentation.
Histology of CEMPH reveals a hyperkeratotic epidermis with an avascular and acellular replacement of the superficial reticular dermis by haphazardly arranged, thickened collagen fibers (Figure 2A-2C). Collagen fibers were oriented perpendicularly to the epidermal surface. Intervening amorphous basophilic elastotic masses were present in the upper dermis with occasional calcification and degenerative elastic fibers (Figure 2D).

Collagenous and elastotic marginal plaques of the hands is a chronic, asymptomatic, sclerotic skin disorder described in a 1960 case series of 5 patients reported by Burks et al.1 Although it has many names, the most common is CEMPH. Collagenous and elastotic marginal plaques of the hands most often presents in white men aged 50 to 60 years.2 Patients typically are asymptomatic with plaques limited to the junction of the palmar and dorsal surfaces of the hands with only minimal intermittent stiffness around the flexor creases. Lesions begin as discrete yellow papules that coalesce to form hyperkeratotic linear plaques with occasional telangiectasia.3
The etiology of CEMPH is attributed to collagen and elastin degeneration by chronic actinic damage, pressure, or trauma.4,5 The 3 stages of degeneration include an initial linear padded stage, an intermediate padded plaque stage, and an advanced padded hyperkeratotic plaque stage.4 Vascular compromise is seen from the enlarged and fused thickened collagen and elastic fibers that in turn lead to ischemic changes, hyperkeratosis with epidermal atrophy, and papillary dermis telangiectasia. Absence or weak expression of keratins 14 and 10 and strong expression of keratin 16 have been reported in the epidermis of CEMPH patients.4
Collagenous and elastotic marginal plaques of the hands do not have a specific treatment, as it is a benign, slowly progressive condition. Several treatments such as laser therapy, high-potency topical corticosteroids, topical tazarotene and tretinoin, oral isotretinoin, and cryotherapy have been tried with little long-term success.4 Moisturizing may help reduce fissuring, and patients are advised to avoid the sun and repeated trauma to the hands.
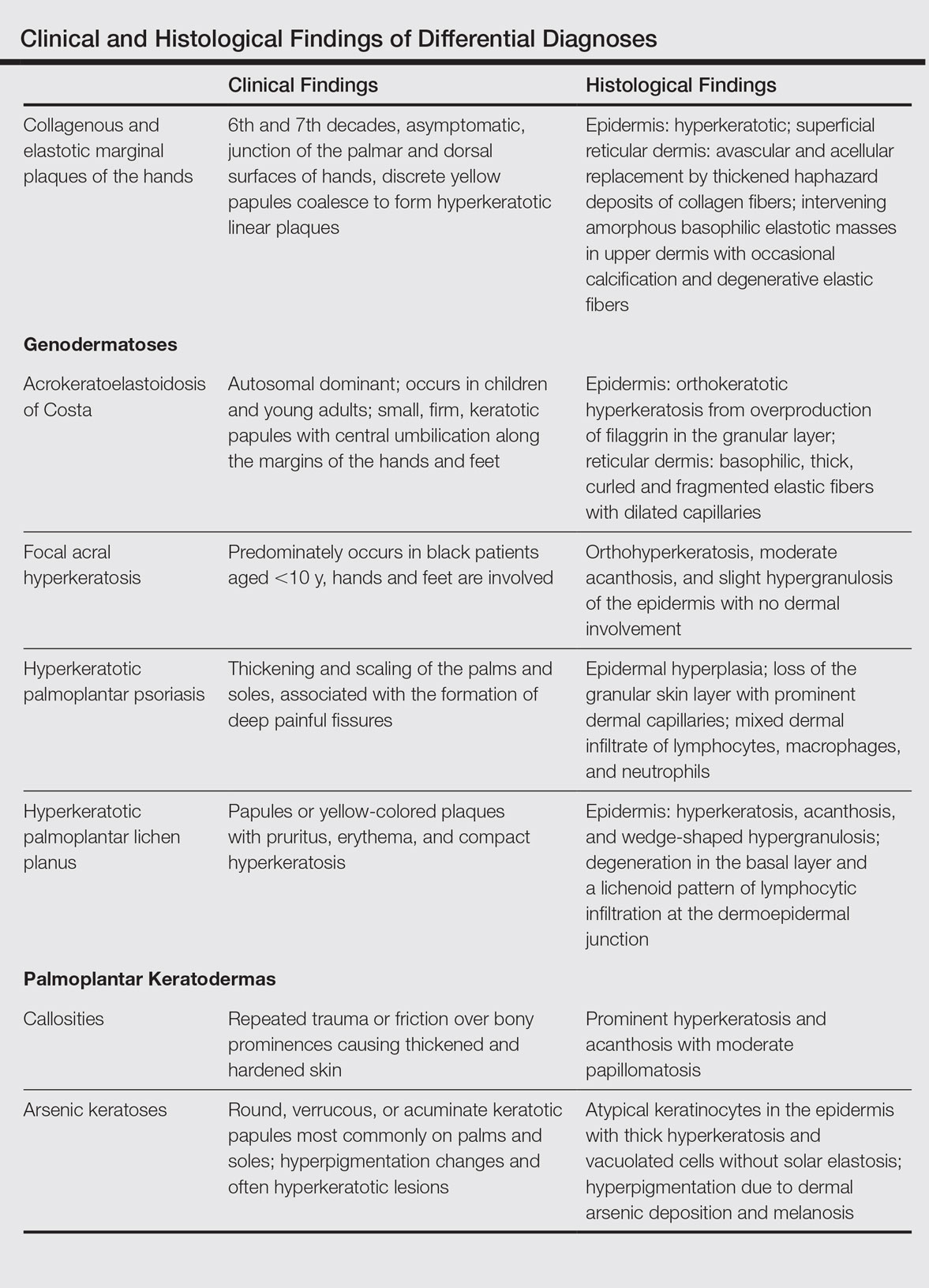
The differential diagnosis of CEMPH is summarized in the Table. Two genodermatoses—acrokeratoelastoidosis of Costa and focal acral hyperkeratosis—clinically resemble CEMPH. Acrokeratoelastoidosis of Costa is an autosomal-dominant condition that occurs without trauma in children and young adults. Histopathology shows orthokeratotic hyperkeratosis due to an overproduction of filaggrin in the granular layer of the epidermis. The reticular dermis shows basophilic, thick, curled and fragmented elastic fibers with dilated capillaries that can be seen with Weigert elastic, Verhoeff-van Gieson, or orcein stains. Focal acral hyperkeratosis occurs on the hands and feet, predominantly in black patients. On histology, the epidermis shows a characteristic orthohyperkeratosis, moderate acanthosis, and slight hypergranulosis with no dermal involvment.6
Chronic hyperkeratotic eczematous dermatitis is another common entity in the differential characterized by hyperkeratotic plaques that scale and fissure. Biopsy demonstrates a spongiotic acanthotic epidermis.7,8
Psoriasis of the hands, specifically hyperkeratotic palmoplantar psoriasis, is associated with manual labor, similar to CEMPH. Histology shows epidermal hyperplasia; regular acanthosis; loss of the granular skin layer with prominent dermal capillaries; and a mixed dermal infiltrate of lymphocytes, macrophages, and neutrophils.9 Hyperkeratotic palmoplantar lichen planus presents with pruritic papules in the third and fifth decades of life. Histologically, hyperkeratosis, acanthosis, and wedge-shaped hypergranulosis with a lichenoid lymphocytic infiltration at the dermoepidermal junction is seen.10
Palmoplantar keratodermas due to inflammatory reactive dermatoses include callosities that develop in response to repeated trauma or friction on the skin. On histology, there is prominent hyperkeratosis and acanthosis with moderate papillomatosis.11 Drug-related palmoplantar keratodermas such as those from arsenic exposure can lead to multiple, irregular, verrucous, keratotic, and pigmented lesions on the palms and soles. Histologically, atypical keratinocytes are seen in the epidermis with thick hyperkeratosis and vacuolated cells without solar elastosis.12
In conclusion, CEMPH is an underdiagnosed and underrecognized condition characterized by asymptomatic hyperkeratotic linear plaques along the medial aspect of the thumb and radial aspect of the index finger. It is important to keep CEMPH in mind when dealing with occupational cases of repeated long-term trauma or pressure to the hands as well as excessive sun exposure. It also is imperative to separate it from other diseases and avoid misdiagnosing this degenerative collagenous and elastotic disease as a malignant lesion.
- Burks JW, Wise LJ, Clark WH. Degenerative collagenous plaques of the hands. Arch Dermatol. 1960;82:362-366.
- Jordaan HF, Rossouw DJ. Digital papular calcific elastosis: a histopathological, histochemical and ultrastructural study of 20 patients. J Cutan Pathol. 1990;17:358-370.
- Mortimore RJ, Conrad RJ. Collagenous and elastotic marginal plaques of the hands. Australas J Dermatol. 2001;42:211-213.
- Tieu KD, Satter EK. Thickened plaques on the hands. Collagenous and elastotic marginal plaques of the hands (CEMPH). Arch Dermatol. 2011;147:499-504.
- Todd D, Al-Aboosi M, Hameed O, et al. The role of UV light in the pathogenesis of digital papular calcific elastosis. Arch Dermatol. 2001;137:379-381.
- Mengesha YM, Kayal JD, Swerlick RA. Keratoelastoidosis marginalis. J Cutan Med Surg. 2002;6:23-25.
- MacKee MG, Lewis MG. Keratolysis exfoliativa and the mosaic fungus. Arch Dermatol. 1931;23:445-447.
- Walling HW, Swick BL, Storrs FJ, et al. Frictional hyperkeratotic hand dermatitis responding to Grenz ray therapy. Contact Dermatitis. 2008;58:49-51.
- Farley E, Masrour S, McKey J, et al. Palmoplantar psoriasis: a phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am Acad Dermatol. 2009;60:1024-1031.
- Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.
- Unal VS, Sevin A, Dayican A. Palmar callus formation as a result of mechanical trauma during sailing. Plast Reconstr Surg. 2005;115:2161-2162.
- Cöl M, Cöl C, Soran A, et al. Arsenic-related Bowen's disease, palmar keratosis, and skin cancer. Environ Health Perspect. 1999;107:687-689.
To the Editor:
Collagenous and elastotic marginal plaques of the hands (CEMPHs) has several names including degenerative collagenous plaques of the hands, keratoelastoidosis marginalis, and digital papular calcific elastosis. This rare disorder is an acquired, slowly progressive, asymptomatic, dermal connective tissue abnormality that is underrecognized and underdiagnosed. Clinical presentation includes hyperkeratotic translucent papules arranged linearly on the radial aspect of the hands.
A 74-year-old woman described having "rough hands" of more than 20 years' duration. She presented with 4-cm wide longitudinal, erythematous, firm, depressed plaques along the lateral edge of the second finger and extending to the medial thumb in both hands (Figure 1). She had attempted multiple treatments by her primary care physician, including topical and oral medications unknown to the patient and light therapy, all without benefit over a period of several years. We have attempted salicylic acid 40%, clobetasol cream 0.05%, and emollient creams containing α-hydroxy acid. At best the condition fluctuated between a subtle raised scale at the edge to smooth and occasionally more red-pink, seemingly unrelated to any treatments.
The patient did not have plaques elsewhere on the body, and notably, the feet were clear. She did not have a history of repeated trauma to the hands and did not engage in manual labor. She denied excessive sun exposure, though she had Fitzpatrick skin type III and a history of multiple precancers and nonmelanoma skin cancers 7 years prior to presentation.
Histology of CEMPH reveals a hyperkeratotic epidermis with an avascular and acellular replacement of the superficial reticular dermis by haphazardly arranged, thickened collagen fibers (Figure 2A-2C). Collagen fibers were oriented perpendicularly to the epidermal surface. Intervening amorphous basophilic elastotic masses were present in the upper dermis with occasional calcification and degenerative elastic fibers (Figure 2D).
Collagenous and elastotic marginal plaques of the hands is a chronic, asymptomatic, sclerotic skin disorder described in a 1960 case series of 5 patients reported by Burks et al.1 Although it has many names, the most common is CEMPH. Collagenous and elastotic marginal plaques of the hands most often presents in white men aged 50 to 60 years.2 Patients typically are asymptomatic with plaques limited to the junction of the palmar and dorsal surfaces of the hands with only minimal intermittent stiffness around the flexor creases. Lesions begin as discrete yellow papules that coalesce to form hyperkeratotic linear plaques with occasional telangiectasia.3
The etiology of CEMPH is attributed to collagen and elastin degeneration by chronic actinic damage, pressure, or trauma.4,5 The 3 stages of degeneration include an initial linear padded stage, an intermediate padded plaque stage, and an advanced padded hyperkeratotic plaque stage.4 Vascular compromise is seen from the enlarged and fused thickened collagen and elastic fibers that in turn lead to ischemic changes, hyperkeratosis with epidermal atrophy, and papillary dermis telangiectasia. Absence or weak expression of keratins 14 and 10 and strong expression of keratin 16 have been reported in the epidermis of CEMPH patients.4
Collagenous and elastotic marginal plaques of the hands do not have a specific treatment, as it is a benign, slowly progressive condition. Several treatments such as laser therapy, high-potency topical corticosteroids, topical tazarotene and tretinoin, oral isotretinoin, and cryotherapy have been tried with little long-term success.4 Moisturizing may help reduce fissuring, and patients are advised to avoid the sun and repeated trauma to the hands.
The differential diagnosis of CEMPH is summarized in the Table. Two genodermatoses—acrokeratoelastoidosis of Costa and focal acral hyperkeratosis—clinically resemble CEMPH. Acrokeratoelastoidosis of Costa is an autosomal-dominant condition that occurs without trauma in children and young adults. Histopathology shows orthokeratotic hyperkeratosis due to an overproduction of filaggrin in the granular layer of the epidermis. The reticular dermis shows basophilic, thick, curled and fragmented elastic fibers with dilated capillaries that can be seen with Weigert elastic, Verhoeff-van Gieson, or orcein stains. Focal acral hyperkeratosis occurs on the hands and feet, predominantly in black patients. On histology, the epidermis shows a characteristic orthohyperkeratosis, moderate acanthosis, and slight hypergranulosis with no dermal involvment.6
Chronic hyperkeratotic eczematous dermatitis is another common entity in the differential characterized by hyperkeratotic plaques that scale and fissure. Biopsy demonstrates a spongiotic acanthotic epidermis.7,8
Psoriasis of the hands, specifically hyperkeratotic palmoplantar psoriasis, is associated with manual labor, similar to CEMPH. Histology shows epidermal hyperplasia; regular acanthosis; loss of the granular skin layer with prominent dermal capillaries; and a mixed dermal infiltrate of lymphocytes, macrophages, and neutrophils.9 Hyperkeratotic palmoplantar lichen planus presents with pruritic papules in the third and fifth decades of life. Histologically, hyperkeratosis, acanthosis, and wedge-shaped hypergranulosis with a lichenoid lymphocytic infiltration at the dermoepidermal junction is seen.10
Palmoplantar keratodermas due to inflammatory reactive dermatoses include callosities that develop in response to repeated trauma or friction on the skin. On histology, there is prominent hyperkeratosis and acanthosis with moderate papillomatosis.11 Drug-related palmoplantar keratodermas such as those from arsenic exposure can lead to multiple, irregular, verrucous, keratotic, and pigmented lesions on the palms and soles. Histologically, atypical keratinocytes are seen in the epidermis with thick hyperkeratosis and vacuolated cells without solar elastosis.12
In conclusion, CEMPH is an underdiagnosed and underrecognized condition characterized by asymptomatic hyperkeratotic linear plaques along the medial aspect of the thumb and radial aspect of the index finger. It is important to keep CEMPH in mind when dealing with occupational cases of repeated long-term trauma or pressure to the hands as well as excessive sun exposure. It also is imperative to separate it from other diseases and avoid misdiagnosing this degenerative collagenous and elastotic disease as a malignant lesion.
To the Editor:
Collagenous and elastotic marginal plaques of the hands (CEMPHs) has several names including degenerative collagenous plaques of the hands, keratoelastoidosis marginalis, and digital papular calcific elastosis. This rare disorder is an acquired, slowly progressive, asymptomatic, dermal connective tissue abnormality that is underrecognized and underdiagnosed. Clinical presentation includes hyperkeratotic translucent papules arranged linearly on the radial aspect of the hands.
A 74-year-old woman described having "rough hands" of more than 20 years' duration. She presented with 4-cm wide longitudinal, erythematous, firm, depressed plaques along the lateral edge of the second finger and extending to the medial thumb in both hands (Figure 1). She had attempted multiple treatments by her primary care physician, including topical and oral medications unknown to the patient and light therapy, all without benefit over a period of several years. We have attempted salicylic acid 40%, clobetasol cream 0.05%, and emollient creams containing α-hydroxy acid. At best the condition fluctuated between a subtle raised scale at the edge to smooth and occasionally more red-pink, seemingly unrelated to any treatments.
The patient did not have plaques elsewhere on the body, and notably, the feet were clear. She did not have a history of repeated trauma to the hands and did not engage in manual labor. She denied excessive sun exposure, though she had Fitzpatrick skin type III and a history of multiple precancers and nonmelanoma skin cancers 7 years prior to presentation.
Histology of CEMPH reveals a hyperkeratotic epidermis with an avascular and acellular replacement of the superficial reticular dermis by haphazardly arranged, thickened collagen fibers (Figure 2A-2C). Collagen fibers were oriented perpendicularly to the epidermal surface. Intervening amorphous basophilic elastotic masses were present in the upper dermis with occasional calcification and degenerative elastic fibers (Figure 2D).
Collagenous and elastotic marginal plaques of the hands is a chronic, asymptomatic, sclerotic skin disorder described in a 1960 case series of 5 patients reported by Burks et al.1 Although it has many names, the most common is CEMPH. Collagenous and elastotic marginal plaques of the hands most often presents in white men aged 50 to 60 years.2 Patients typically are asymptomatic with plaques limited to the junction of the palmar and dorsal surfaces of the hands with only minimal intermittent stiffness around the flexor creases. Lesions begin as discrete yellow papules that coalesce to form hyperkeratotic linear plaques with occasional telangiectasia.3
The etiology of CEMPH is attributed to collagen and elastin degeneration by chronic actinic damage, pressure, or trauma.4,5 The 3 stages of degeneration include an initial linear padded stage, an intermediate padded plaque stage, and an advanced padded hyperkeratotic plaque stage.4 Vascular compromise is seen from the enlarged and fused thickened collagen and elastic fibers that in turn lead to ischemic changes, hyperkeratosis with epidermal atrophy, and papillary dermis telangiectasia. Absence or weak expression of keratins 14 and 10 and strong expression of keratin 16 have been reported in the epidermis of CEMPH patients.4
Collagenous and elastotic marginal plaques of the hands do not have a specific treatment, as it is a benign, slowly progressive condition. Several treatments such as laser therapy, high-potency topical corticosteroids, topical tazarotene and tretinoin, oral isotretinoin, and cryotherapy have been tried with little long-term success.4 Moisturizing may help reduce fissuring, and patients are advised to avoid the sun and repeated trauma to the hands.
The differential diagnosis of CEMPH is summarized in the Table. Two genodermatoses—acrokeratoelastoidosis of Costa and focal acral hyperkeratosis—clinically resemble CEMPH. Acrokeratoelastoidosis of Costa is an autosomal-dominant condition that occurs without trauma in children and young adults. Histopathology shows orthokeratotic hyperkeratosis due to an overproduction of filaggrin in the granular layer of the epidermis. The reticular dermis shows basophilic, thick, curled and fragmented elastic fibers with dilated capillaries that can be seen with Weigert elastic, Verhoeff-van Gieson, or orcein stains. Focal acral hyperkeratosis occurs on the hands and feet, predominantly in black patients. On histology, the epidermis shows a characteristic orthohyperkeratosis, moderate acanthosis, and slight hypergranulosis with no dermal involvment.6
Chronic hyperkeratotic eczematous dermatitis is another common entity in the differential characterized by hyperkeratotic plaques that scale and fissure. Biopsy demonstrates a spongiotic acanthotic epidermis.7,8
Psoriasis of the hands, specifically hyperkeratotic palmoplantar psoriasis, is associated with manual labor, similar to CEMPH. Histology shows epidermal hyperplasia; regular acanthosis; loss of the granular skin layer with prominent dermal capillaries; and a mixed dermal infiltrate of lymphocytes, macrophages, and neutrophils.9 Hyperkeratotic palmoplantar lichen planus presents with pruritic papules in the third and fifth decades of life. Histologically, hyperkeratosis, acanthosis, and wedge-shaped hypergranulosis with a lichenoid lymphocytic infiltration at the dermoepidermal junction is seen.10
Palmoplantar keratodermas due to inflammatory reactive dermatoses include callosities that develop in response to repeated trauma or friction on the skin. On histology, there is prominent hyperkeratosis and acanthosis with moderate papillomatosis.11 Drug-related palmoplantar keratodermas such as those from arsenic exposure can lead to multiple, irregular, verrucous, keratotic, and pigmented lesions on the palms and soles. Histologically, atypical keratinocytes are seen in the epidermis with thick hyperkeratosis and vacuolated cells without solar elastosis.12
In conclusion, CEMPH is an underdiagnosed and underrecognized condition characterized by asymptomatic hyperkeratotic linear plaques along the medial aspect of the thumb and radial aspect of the index finger. It is important to keep CEMPH in mind when dealing with occupational cases of repeated long-term trauma or pressure to the hands as well as excessive sun exposure. It also is imperative to separate it from other diseases and avoid misdiagnosing this degenerative collagenous and elastotic disease as a malignant lesion.
- Burks JW, Wise LJ, Clark WH. Degenerative collagenous plaques of the hands. Arch Dermatol. 1960;82:362-366.
- Jordaan HF, Rossouw DJ. Digital papular calcific elastosis: a histopathological, histochemical and ultrastructural study of 20 patients. J Cutan Pathol. 1990;17:358-370.
- Mortimore RJ, Conrad RJ. Collagenous and elastotic marginal plaques of the hands. Australas J Dermatol. 2001;42:211-213.
- Tieu KD, Satter EK. Thickened plaques on the hands. Collagenous and elastotic marginal plaques of the hands (CEMPH). Arch Dermatol. 2011;147:499-504.
- Todd D, Al-Aboosi M, Hameed O, et al. The role of UV light in the pathogenesis of digital papular calcific elastosis. Arch Dermatol. 2001;137:379-381.
- Mengesha YM, Kayal JD, Swerlick RA. Keratoelastoidosis marginalis. J Cutan Med Surg. 2002;6:23-25.
- MacKee MG, Lewis MG. Keratolysis exfoliativa and the mosaic fungus. Arch Dermatol. 1931;23:445-447.
- Walling HW, Swick BL, Storrs FJ, et al. Frictional hyperkeratotic hand dermatitis responding to Grenz ray therapy. Contact Dermatitis. 2008;58:49-51.
- Farley E, Masrour S, McKey J, et al. Palmoplantar psoriasis: a phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am Acad Dermatol. 2009;60:1024-1031.
- Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.
- Unal VS, Sevin A, Dayican A. Palmar callus formation as a result of mechanical trauma during sailing. Plast Reconstr Surg. 2005;115:2161-2162.
- Cöl M, Cöl C, Soran A, et al. Arsenic-related Bowen's disease, palmar keratosis, and skin cancer. Environ Health Perspect. 1999;107:687-689.
- Burks JW, Wise LJ, Clark WH. Degenerative collagenous plaques of the hands. Arch Dermatol. 1960;82:362-366.
- Jordaan HF, Rossouw DJ. Digital papular calcific elastosis: a histopathological, histochemical and ultrastructural study of 20 patients. J Cutan Pathol. 1990;17:358-370.
- Mortimore RJ, Conrad RJ. Collagenous and elastotic marginal plaques of the hands. Australas J Dermatol. 2001;42:211-213.
- Tieu KD, Satter EK. Thickened plaques on the hands. Collagenous and elastotic marginal plaques of the hands (CEMPH). Arch Dermatol. 2011;147:499-504.
- Todd D, Al-Aboosi M, Hameed O, et al. The role of UV light in the pathogenesis of digital papular calcific elastosis. Arch Dermatol. 2001;137:379-381.
- Mengesha YM, Kayal JD, Swerlick RA. Keratoelastoidosis marginalis. J Cutan Med Surg. 2002;6:23-25.
- MacKee MG, Lewis MG. Keratolysis exfoliativa and the mosaic fungus. Arch Dermatol. 1931;23:445-447.
- Walling HW, Swick BL, Storrs FJ, et al. Frictional hyperkeratotic hand dermatitis responding to Grenz ray therapy. Contact Dermatitis. 2008;58:49-51.
- Farley E, Masrour S, McKey J, et al. Palmoplantar psoriasis: a phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J Am Acad Dermatol. 2009;60:1024-1031.
- Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.
- Unal VS, Sevin A, Dayican A. Palmar callus formation as a result of mechanical trauma during sailing. Plast Reconstr Surg. 2005;115:2161-2162.
- Cöl M, Cöl C, Soran A, et al. Arsenic-related Bowen's disease, palmar keratosis, and skin cancer. Environ Health Perspect. 1999;107:687-689.
Practice Points
- The etiology of collagenous and elastotic marginal plaques of the hands (CEMPHs) is attributed to collagen and elastin degeneration by chronic actinic damage, pressure, or trauma.
- It is important to keep CEMPH in mind when dealing with occupational cases of repeated long-term trauma or pressure to the hands as well as excessive sun exposure. It should be separated from other diseases and avoid being misdiagnosed as a malignant lesion.

FDA approves first treatment for metastatic Merkel cell carcinoma
The Food and Drug Administration has granted accelerated approval to avelumab for the treatment of metastatic Merkel cell carcinoma (MCC) in adult and pediatric patients aged 12 years and older.
Avelumab, a programmed death-ligand 1 (PD-L1)–blocking human IgG1 lambda monoclonal antibody, is the first FDA-approved treatment for metastatic MCC.
Approval was based on a 33% overall response rate in a single arm trial (JAVELIN Merkel 200 trial) of 88 patients with metastatic MCC who had been previously treated with at least one prior chemotherapy regimen, the FDA said in a written statement.
The response duration among that 33% ranged from 2.8 to 23.3+ months, and 86% of responses were durable for 6 months or more. “Responses were observed in patients regardless of PD-L1 tumor expression or presence of Merkel cell polyomavirus,” the FDA said.
There were safety data in 1,738 patients, who received 10 mg/kg of avelumab every 2 weeks. Immune-mediated adverse reactions (pneumonitis, colitis, hepatitis, adrenal insufficiency, hypo- and hyperthyroidism, diabetes mellitus, and nephritis) and life-threatening infusion reactions were the most common, serious adverse events associated with avelumab. Of the 88 patients in the JAVELIN Merkel 200 trial, the most common adverse reactions were fatigue, musculoskeletal pain, diarrhea, nausea, infusion-related reaction, rash, decreased appetite, and peripheral edema. Serious adverse reactions that occurred in more than one patient in the trial were acute kidney injury, anemia, abdominal pain, ileus, asthenia, and cellulitis, the FDA said.
The recommended dose of avelumab is 10 mg/kg administered in an intravenous infusion over 60 minutes every 2 weeks. Labeling includes the recommendation that all patients should be premedicated with an antihistamine and acetaminophen before each of the first four infusions.
“As a condition of accelerated approval, an additional study is required to confirm the clinical benefit of avelumab for this indication,” according to the FDA.
The drug is being marketed as Bavencio by EMD Serono.
The Food and Drug Administration has granted accelerated approval to avelumab for the treatment of metastatic Merkel cell carcinoma (MCC) in adult and pediatric patients aged 12 years and older.
Avelumab, a programmed death-ligand 1 (PD-L1)–blocking human IgG1 lambda monoclonal antibody, is the first FDA-approved treatment for metastatic MCC.
Approval was based on a 33% overall response rate in a single arm trial (JAVELIN Merkel 200 trial) of 88 patients with metastatic MCC who had been previously treated with at least one prior chemotherapy regimen, the FDA said in a written statement.
The response duration among that 33% ranged from 2.8 to 23.3+ months, and 86% of responses were durable for 6 months or more. “Responses were observed in patients regardless of PD-L1 tumor expression or presence of Merkel cell polyomavirus,” the FDA said.
There were safety data in 1,738 patients, who received 10 mg/kg of avelumab every 2 weeks. Immune-mediated adverse reactions (pneumonitis, colitis, hepatitis, adrenal insufficiency, hypo- and hyperthyroidism, diabetes mellitus, and nephritis) and life-threatening infusion reactions were the most common, serious adverse events associated with avelumab. Of the 88 patients in the JAVELIN Merkel 200 trial, the most common adverse reactions were fatigue, musculoskeletal pain, diarrhea, nausea, infusion-related reaction, rash, decreased appetite, and peripheral edema. Serious adverse reactions that occurred in more than one patient in the trial were acute kidney injury, anemia, abdominal pain, ileus, asthenia, and cellulitis, the FDA said.
The recommended dose of avelumab is 10 mg/kg administered in an intravenous infusion over 60 minutes every 2 weeks. Labeling includes the recommendation that all patients should be premedicated with an antihistamine and acetaminophen before each of the first four infusions.
“As a condition of accelerated approval, an additional study is required to confirm the clinical benefit of avelumab for this indication,” according to the FDA.
The drug is being marketed as Bavencio by EMD Serono.
The Food and Drug Administration has granted accelerated approval to avelumab for the treatment of metastatic Merkel cell carcinoma (MCC) in adult and pediatric patients aged 12 years and older.
Avelumab, a programmed death-ligand 1 (PD-L1)–blocking human IgG1 lambda monoclonal antibody, is the first FDA-approved treatment for metastatic MCC.
Approval was based on a 33% overall response rate in a single arm trial (JAVELIN Merkel 200 trial) of 88 patients with metastatic MCC who had been previously treated with at least one prior chemotherapy regimen, the FDA said in a written statement.
The response duration among that 33% ranged from 2.8 to 23.3+ months, and 86% of responses were durable for 6 months or more. “Responses were observed in patients regardless of PD-L1 tumor expression or presence of Merkel cell polyomavirus,” the FDA said.
There were safety data in 1,738 patients, who received 10 mg/kg of avelumab every 2 weeks. Immune-mediated adverse reactions (pneumonitis, colitis, hepatitis, adrenal insufficiency, hypo- and hyperthyroidism, diabetes mellitus, and nephritis) and life-threatening infusion reactions were the most common, serious adverse events associated with avelumab. Of the 88 patients in the JAVELIN Merkel 200 trial, the most common adverse reactions were fatigue, musculoskeletal pain, diarrhea, nausea, infusion-related reaction, rash, decreased appetite, and peripheral edema. Serious adverse reactions that occurred in more than one patient in the trial were acute kidney injury, anemia, abdominal pain, ileus, asthenia, and cellulitis, the FDA said.
The recommended dose of avelumab is 10 mg/kg administered in an intravenous infusion over 60 minutes every 2 weeks. Labeling includes the recommendation that all patients should be premedicated with an antihistamine and acetaminophen before each of the first four infusions.
“As a condition of accelerated approval, an additional study is required to confirm the clinical benefit of avelumab for this indication,” according to the FDA.
The drug is being marketed as Bavencio by EMD Serono.
Grandparents aid in early diagnosis of autism
Family members other than parents can play a key role in initial recognition of problems prior to diagnosis of autism, which may lead to earlier diagnosis and potentially better outcomes, a study found.
Of 477 parents of children with autism who were surveyed online, 25% of parents reported that other individuals indicated their child might have a serious condition before they themselves suspected it. “The two most common categories of individuals are maternal grandmothers (27%) and teachers (24%),” Nachum Sicherman, PhD, of Columbia Business School, New York, and associates said. “If one adds maternal and paternal grandmothers and grandfathers together, then 59% of respondents who reported that anyone had raised concerns before they were aware that their child had a problem identified grandparents as having done so” (Autism. 2017. doi: 10.1177/1362361316679632)”
Children with no siblings were diagnosed 6-8 months earlier than children with siblings (P less than .01).Children with an older sibling were diagnosed approximately 10 months earlier, relative to those with only younger siblings. (P less than .01).
Thus, the presence of grandparents and siblings significantly affects age of diagnosis in autistic children, Dr. Sicherman and associates said.
*This article was update 3/27/2018
Family members other than parents can play a key role in initial recognition of problems prior to diagnosis of autism, which may lead to earlier diagnosis and potentially better outcomes, a study found.
Of 477 parents of children with autism who were surveyed online, 25% of parents reported that other individuals indicated their child might have a serious condition before they themselves suspected it. “The two most common categories of individuals are maternal grandmothers (27%) and teachers (24%),” Nachum Sicherman, PhD, of Columbia Business School, New York, and associates said. “If one adds maternal and paternal grandmothers and grandfathers together, then 59% of respondents who reported that anyone had raised concerns before they were aware that their child had a problem identified grandparents as having done so” (Autism. 2017. doi: 10.1177/1362361316679632)”
Children with no siblings were diagnosed 6-8 months earlier than children with siblings (P less than .01).Children with an older sibling were diagnosed approximately 10 months earlier, relative to those with only younger siblings. (P less than .01).
Thus, the presence of grandparents and siblings significantly affects age of diagnosis in autistic children, Dr. Sicherman and associates said.
*This article was update 3/27/2018
Family members other than parents can play a key role in initial recognition of problems prior to diagnosis of autism, which may lead to earlier diagnosis and potentially better outcomes, a study found.
Of 477 parents of children with autism who were surveyed online, 25% of parents reported that other individuals indicated their child might have a serious condition before they themselves suspected it. “The two most common categories of individuals are maternal grandmothers (27%) and teachers (24%),” Nachum Sicherman, PhD, of Columbia Business School, New York, and associates said. “If one adds maternal and paternal grandmothers and grandfathers together, then 59% of respondents who reported that anyone had raised concerns before they were aware that their child had a problem identified grandparents as having done so” (Autism. 2017. doi: 10.1177/1362361316679632)”
Children with no siblings were diagnosed 6-8 months earlier than children with siblings (P less than .01).Children with an older sibling were diagnosed approximately 10 months earlier, relative to those with only younger siblings. (P less than .01).
Thus, the presence of grandparents and siblings significantly affects age of diagnosis in autistic children, Dr. Sicherman and associates said.
*This article was update 3/27/2018