User login
Rotterdam Study: High T4 levels increased the risk for atherosclerotic events, death
ORLANDO – Elevated serum levels of free T4 are associated with a greater risk of atherosclerotic events and, in some cases, death, among adults in their 60s, Arjola Bano, MD, said at a press briefing at the annual meeting of the Endocrine Society.
Earlier research has shown that high FT4 levels are associated with a greater likelihood of development of atherosclerosis. But no one has looked beyond that to see if an excess of FT4 can change the course of the disease.
The investigators used electron beam computed tomography to measure coronary artery calcification. Confounders such as age, sex, smoking, alcohol intake, body mass index, total cholesterol, triglycerides, systolic blood pressure, diabetes, and use of anti-hypertension or lipid lowering medications were controlled for using multivariable-adjusted Cox proportional and logistic regression models.
Dr. Bano reported that during a median follow-up of 8.8 years (range, 4.5-11.8 years), there were 580 ASCV deaths and 1,130 first-time hard ASCV events. The risk of ASCV mortality increased with higher FT4 levels (hazard ratio, 2.35; 95% confidence interval, 1.61-3.41 per 1 ng/dL) and lower TSH levels (HR, 0.92; 95% CI, 0.84-1.00/1 logTSH), predominantly among participants with prevalent ASCV disease (HR, 5.76; 95% CI, 2.79-11.89 for FT4; HR, 0.81; 95% CI, 0.69-0.95 for TSH).
In addition, higher FT4 levels were associated with higher risk of first-time hard ASCV event (HR, 1.87; 95% CI, 1.34-2.59). Also, FT4 levels were positively associated with having a high CAC score (OR, 2.34; 95% CI, 1.36-4.04).
It is noteworthy that results remained similar after restricting the analyses to participants with thyroid function within reference ranges, she stressed.
How to explain these findings? These data suggest that the link between thyroid function and atherosclerosis is mediated through yet unexplored cardiovascular risk factors or via alternative pathways.
Dr. Bano and her associates all report that they have no relevant financial conflicts of interest.
ORLANDO – Elevated serum levels of free T4 are associated with a greater risk of atherosclerotic events and, in some cases, death, among adults in their 60s, Arjola Bano, MD, said at a press briefing at the annual meeting of the Endocrine Society.
Earlier research has shown that high FT4 levels are associated with a greater likelihood of development of atherosclerosis. But no one has looked beyond that to see if an excess of FT4 can change the course of the disease.
The investigators used electron beam computed tomography to measure coronary artery calcification. Confounders such as age, sex, smoking, alcohol intake, body mass index, total cholesterol, triglycerides, systolic blood pressure, diabetes, and use of anti-hypertension or lipid lowering medications were controlled for using multivariable-adjusted Cox proportional and logistic regression models.
Dr. Bano reported that during a median follow-up of 8.8 years (range, 4.5-11.8 years), there were 580 ASCV deaths and 1,130 first-time hard ASCV events. The risk of ASCV mortality increased with higher FT4 levels (hazard ratio, 2.35; 95% confidence interval, 1.61-3.41 per 1 ng/dL) and lower TSH levels (HR, 0.92; 95% CI, 0.84-1.00/1 logTSH), predominantly among participants with prevalent ASCV disease (HR, 5.76; 95% CI, 2.79-11.89 for FT4; HR, 0.81; 95% CI, 0.69-0.95 for TSH).
In addition, higher FT4 levels were associated with higher risk of first-time hard ASCV event (HR, 1.87; 95% CI, 1.34-2.59). Also, FT4 levels were positively associated with having a high CAC score (OR, 2.34; 95% CI, 1.36-4.04).
It is noteworthy that results remained similar after restricting the analyses to participants with thyroid function within reference ranges, she stressed.
How to explain these findings? These data suggest that the link between thyroid function and atherosclerosis is mediated through yet unexplored cardiovascular risk factors or via alternative pathways.
Dr. Bano and her associates all report that they have no relevant financial conflicts of interest.
ORLANDO – Elevated serum levels of free T4 are associated with a greater risk of atherosclerotic events and, in some cases, death, among adults in their 60s, Arjola Bano, MD, said at a press briefing at the annual meeting of the Endocrine Society.
Earlier research has shown that high FT4 levels are associated with a greater likelihood of development of atherosclerosis. But no one has looked beyond that to see if an excess of FT4 can change the course of the disease.
The investigators used electron beam computed tomography to measure coronary artery calcification. Confounders such as age, sex, smoking, alcohol intake, body mass index, total cholesterol, triglycerides, systolic blood pressure, diabetes, and use of anti-hypertension or lipid lowering medications were controlled for using multivariable-adjusted Cox proportional and logistic regression models.
Dr. Bano reported that during a median follow-up of 8.8 years (range, 4.5-11.8 years), there were 580 ASCV deaths and 1,130 first-time hard ASCV events. The risk of ASCV mortality increased with higher FT4 levels (hazard ratio, 2.35; 95% confidence interval, 1.61-3.41 per 1 ng/dL) and lower TSH levels (HR, 0.92; 95% CI, 0.84-1.00/1 logTSH), predominantly among participants with prevalent ASCV disease (HR, 5.76; 95% CI, 2.79-11.89 for FT4; HR, 0.81; 95% CI, 0.69-0.95 for TSH).
In addition, higher FT4 levels were associated with higher risk of first-time hard ASCV event (HR, 1.87; 95% CI, 1.34-2.59). Also, FT4 levels were positively associated with having a high CAC score (OR, 2.34; 95% CI, 1.36-4.04).
It is noteworthy that results remained similar after restricting the analyses to participants with thyroid function within reference ranges, she stressed.
How to explain these findings? These data suggest that the link between thyroid function and atherosclerosis is mediated through yet unexplored cardiovascular risk factors or via alternative pathways.
Dr. Bano and her associates all report that they have no relevant financial conflicts of interest.
AT ENDO 2017
Key clinical point: Major finding: The odds of an atherosclerotic event were 2.28 times higher in adults with elevated FT4 levels than those with high TSH, even when the high levels were still within the normal range.
Data source: Prospective study of 9,231 adults followed over 8.8 years.
Disclosures: Dr. Bano and her associates all report that they have no relevant financial conflicts of interest.
Assay intended to aid PV diagnosis cleared for use in US

The US Food and Drug Administration has granted 510(k) clearance for QIAGEN’s ipsogen® JAK2 RGQ PCR Kit (ipsogen JAK2 assay), and the company has launched the assay in the US.
The ipsogen JAK2 assay is designed to detect the JAK2 V617F/G1849T allele in genomic DNA extracted from EDTA whole blood.
The assay is intended for use in conjunction with other clinicopathological factors to aid the diagnosis of polycythemia vera (PV).
The test does not detect less common mutations associated with PV, including mutations in exon 12, and is not intended for stand-alone diagnosis of PV.
The ipsogen JAK2 assay is a real-time polymerase chain reaction test performed on the QIAGEN Rotor-Gene Q MDx instrument.
Researchers evaluated the utility of the ipsogen JAK2 assay for PV diagnosis in a prospective trial enrolling more than 200 subjects.
Data from this trial have not been published. However, according to QIAGEN, the assay provided 94.6% sensitivity and 98.1% specificity, together with a 100% positive percentage agreement and a 99.4% negative percentage agreement to bi-directional sequencing.
QIAGEN said these results suggest the ipsogen JAK2 assay enables detection of PV in the majority of subjects with the disease and helps rule out PV in the majority of individuals without it.
“We are pleased to be able to offer our ipsogen JAK2 assay, which is already available in Europe and other markets, for use in the United States and make it easier for hematologists and oncologists to follow recommended diagnostic testing algorithms and international guidelines for suspected PV patients,” said Thierry Bernard, senior vice president and head of QIAGEN’s Molecular Diagnostics Business Area. ![]()
The US Food and Drug Administration has granted 510(k) clearance for QIAGEN’s ipsogen® JAK2 RGQ PCR Kit (ipsogen JAK2 assay), and the company has launched the assay in the US.
The ipsogen JAK2 assay is designed to detect the JAK2 V617F/G1849T allele in genomic DNA extracted from EDTA whole blood.
The assay is intended for use in conjunction with other clinicopathological factors to aid the diagnosis of polycythemia vera (PV).
The test does not detect less common mutations associated with PV, including mutations in exon 12, and is not intended for stand-alone diagnosis of PV.
The ipsogen JAK2 assay is a real-time polymerase chain reaction test performed on the QIAGEN Rotor-Gene Q MDx instrument.
Researchers evaluated the utility of the ipsogen JAK2 assay for PV diagnosis in a prospective trial enrolling more than 200 subjects.
Data from this trial have not been published. However, according to QIAGEN, the assay provided 94.6% sensitivity and 98.1% specificity, together with a 100% positive percentage agreement and a 99.4% negative percentage agreement to bi-directional sequencing.
QIAGEN said these results suggest the ipsogen JAK2 assay enables detection of PV in the majority of subjects with the disease and helps rule out PV in the majority of individuals without it.
“We are pleased to be able to offer our ipsogen JAK2 assay, which is already available in Europe and other markets, for use in the United States and make it easier for hematologists and oncologists to follow recommended diagnostic testing algorithms and international guidelines for suspected PV patients,” said Thierry Bernard, senior vice president and head of QIAGEN’s Molecular Diagnostics Business Area. ![]()
The US Food and Drug Administration has granted 510(k) clearance for QIAGEN’s ipsogen® JAK2 RGQ PCR Kit (ipsogen JAK2 assay), and the company has launched the assay in the US.
The ipsogen JAK2 assay is designed to detect the JAK2 V617F/G1849T allele in genomic DNA extracted from EDTA whole blood.
The assay is intended for use in conjunction with other clinicopathological factors to aid the diagnosis of polycythemia vera (PV).
The test does not detect less common mutations associated with PV, including mutations in exon 12, and is not intended for stand-alone diagnosis of PV.
The ipsogen JAK2 assay is a real-time polymerase chain reaction test performed on the QIAGEN Rotor-Gene Q MDx instrument.
Researchers evaluated the utility of the ipsogen JAK2 assay for PV diagnosis in a prospective trial enrolling more than 200 subjects.
Data from this trial have not been published. However, according to QIAGEN, the assay provided 94.6% sensitivity and 98.1% specificity, together with a 100% positive percentage agreement and a 99.4% negative percentage agreement to bi-directional sequencing.
QIAGEN said these results suggest the ipsogen JAK2 assay enables detection of PV in the majority of subjects with the disease and helps rule out PV in the majority of individuals without it.
“We are pleased to be able to offer our ipsogen JAK2 assay, which is already available in Europe and other markets, for use in the United States and make it easier for hematologists and oncologists to follow recommended diagnostic testing algorithms and international guidelines for suspected PV patients,” said Thierry Bernard, senior vice president and head of QIAGEN’s Molecular Diagnostics Business Area. ![]()
Degrees of Distinction
Thank you for stating that ARNPs “do not need physician endorsement for the advanced component” of their practice. ARNPs need to be responsible for themselves. In California, NPs are given a certificate, not a license, and operate under the rules of the state board of nursing and the board of business and professional codes. We must act in a prudent and competent manner. I think this has been demonstrated where full practice authority is in force.
The American Medical Association (AMA) and American Academy of Family Physicians (AAFP), which still want “supervision, collaboration, or participating” designations for PAs and NPs, have tripped on their own stethoscopes on this issue. In trying to suppress advanced practice providers, they have helped create a provider shortage. Many NPs will not work in a state that has practice limitations.
In Humboldt County, California, family practice doctors are so overworked due to provider shortages that they are leaving the area. Enter locum tenens to fill the gap. But at a point, there is no benefit to being in such demand. The cost of health care has risen, and patients are unhappy with the care they receive. New patients cannot see doctors in a timely manner; when they are finally seen, they have a few minutes to share their concerns with the provider, who rarely sits down or looks away from the computer screen to make eye contact with them.
We are already seeing the push for advanced education for our NPs and PAs. We have witnessed the changeover to NP programs that culminate in a doctorate (not a master’s) degree. By 2021, PA programs will be required to be master’s level; although the process has started, there are still a few holdouts. But I consider Washington State to be a front-runner in this area.
This, for me, is the area we need to address: degree designation and equivalency. Rather than give “diplomat” or similar status to someone whose base degree is an associate’s, a better idea—and one more palatable to AMA and AAFP—might be to bring everyone to at least a master’s level. For example, the Academy of Integrative Pain Management (AIPM) gives “Fellow” designation to those with master’s preparation who successfully pass AIPM’s examination, and “Diplomat” status to doctorate-prepared practitioners who have also passed the exam.
At the end of the day, many patients prefer to see a PA or NP rather than a medical doctor. Yes, patients care about credentials—but they care more about their provider being respectful, listening, remembering their history, connecting the history from their previous provider, and offering the proper treatment for the correct diagnosis.
Jan Morgan, MS, ARNP
Fellow, Academy of Integrative Pain Management
Eureka, California
Thank you for stating that ARNPs “do not need physician endorsement for the advanced component” of their practice. ARNPs need to be responsible for themselves. In California, NPs are given a certificate, not a license, and operate under the rules of the state board of nursing and the board of business and professional codes. We must act in a prudent and competent manner. I think this has been demonstrated where full practice authority is in force.
The American Medical Association (AMA) and American Academy of Family Physicians (AAFP), which still want “supervision, collaboration, or participating” designations for PAs and NPs, have tripped on their own stethoscopes on this issue. In trying to suppress advanced practice providers, they have helped create a provider shortage. Many NPs will not work in a state that has practice limitations.
In Humboldt County, California, family practice doctors are so overworked due to provider shortages that they are leaving the area. Enter locum tenens to fill the gap. But at a point, there is no benefit to being in such demand. The cost of health care has risen, and patients are unhappy with the care they receive. New patients cannot see doctors in a timely manner; when they are finally seen, they have a few minutes to share their concerns with the provider, who rarely sits down or looks away from the computer screen to make eye contact with them.
We are already seeing the push for advanced education for our NPs and PAs. We have witnessed the changeover to NP programs that culminate in a doctorate (not a master’s) degree. By 2021, PA programs will be required to be master’s level; although the process has started, there are still a few holdouts. But I consider Washington State to be a front-runner in this area.
This, for me, is the area we need to address: degree designation and equivalency. Rather than give “diplomat” or similar status to someone whose base degree is an associate’s, a better idea—and one more palatable to AMA and AAFP—might be to bring everyone to at least a master’s level. For example, the Academy of Integrative Pain Management (AIPM) gives “Fellow” designation to those with master’s preparation who successfully pass AIPM’s examination, and “Diplomat” status to doctorate-prepared practitioners who have also passed the exam.
At the end of the day, many patients prefer to see a PA or NP rather than a medical doctor. Yes, patients care about credentials—but they care more about their provider being respectful, listening, remembering their history, connecting the history from their previous provider, and offering the proper treatment for the correct diagnosis.
Jan Morgan, MS, ARNP
Fellow, Academy of Integrative Pain Management
Eureka, California
Thank you for stating that ARNPs “do not need physician endorsement for the advanced component” of their practice. ARNPs need to be responsible for themselves. In California, NPs are given a certificate, not a license, and operate under the rules of the state board of nursing and the board of business and professional codes. We must act in a prudent and competent manner. I think this has been demonstrated where full practice authority is in force.
The American Medical Association (AMA) and American Academy of Family Physicians (AAFP), which still want “supervision, collaboration, or participating” designations for PAs and NPs, have tripped on their own stethoscopes on this issue. In trying to suppress advanced practice providers, they have helped create a provider shortage. Many NPs will not work in a state that has practice limitations.
In Humboldt County, California, family practice doctors are so overworked due to provider shortages that they are leaving the area. Enter locum tenens to fill the gap. But at a point, there is no benefit to being in such demand. The cost of health care has risen, and patients are unhappy with the care they receive. New patients cannot see doctors in a timely manner; when they are finally seen, they have a few minutes to share their concerns with the provider, who rarely sits down or looks away from the computer screen to make eye contact with them.
We are already seeing the push for advanced education for our NPs and PAs. We have witnessed the changeover to NP programs that culminate in a doctorate (not a master’s) degree. By 2021, PA programs will be required to be master’s level; although the process has started, there are still a few holdouts. But I consider Washington State to be a front-runner in this area.
This, for me, is the area we need to address: degree designation and equivalency. Rather than give “diplomat” or similar status to someone whose base degree is an associate’s, a better idea—and one more palatable to AMA and AAFP—might be to bring everyone to at least a master’s level. For example, the Academy of Integrative Pain Management (AIPM) gives “Fellow” designation to those with master’s preparation who successfully pass AIPM’s examination, and “Diplomat” status to doctorate-prepared practitioners who have also passed the exam.
At the end of the day, many patients prefer to see a PA or NP rather than a medical doctor. Yes, patients care about credentials—but they care more about their provider being respectful, listening, remembering their history, connecting the history from their previous provider, and offering the proper treatment for the correct diagnosis.
Jan Morgan, MS, ARNP
Fellow, Academy of Integrative Pain Management
Eureka, California
You’re a PA? Sorry, Not Eligible for This Job
Thank you for your thoughtful commentary on the pertinent topic of full practice authority for PAs (2017;27[2]:12-14). In more than 30 years as a PA, I have rarely regretted my career choice. In 1982, when I was planning my career path, I chose to become a PA instead of an NP because I didn’t want to further my nursing training (I was already an LPN) to advance my practice, and my impression was that PAs and NPs were equivalent in the workforce. This perception held true until the past few years; I have lost job opportunities specifically because the employer didn’t want to deal with the administrative details of PA supervisory requirements here in Colorado. I find this frustrating, as well as perplexing.
Although I’ve become more comfortable with autonomy throughout my years of practice, I’ve always reserved the right to consult when necessary and appropriate, based on my own judgment and comfort level. I certainly wouldn’t mind more relaxed supervision, but I wouldn’t want to be cut entirely loose, either. On the other hand, I resent being ineligible for job opportunities simply for administrative reasons. While this is surely misguided on the part of the employers, it is a reality that practitioners encounter.
I learned recently—to my astonishment—that my NP colleagues pay about a tenth of what I do for malpractice insurance. Apparently the underwriters (and/or the plaintiffs) haven’t caught up with the nuances of responsibility and autonomy! From my perspective, PAs and NPs have more in common in the practice setting than NPs and RNs do. The fact that NPs are governed by nursing boards and insured as nurses is more an antiquated accident than a reflection of function in the workforce.
Ideally, there should be a governing body dedicated to the entire spectrum of nonphysician providers who are qualified to diagnose, treat, and prescribe. Since that is not likely to happen, it is our responsibility as PAs to match NPs in the marketplace while maintaining our integrity as providers.
Elizabeth Upper, PA-C
Denver, Colorado
Thank you for your thoughtful commentary on the pertinent topic of full practice authority for PAs (2017;27[2]:12-14). In more than 30 years as a PA, I have rarely regretted my career choice. In 1982, when I was planning my career path, I chose to become a PA instead of an NP because I didn’t want to further my nursing training (I was already an LPN) to advance my practice, and my impression was that PAs and NPs were equivalent in the workforce. This perception held true until the past few years; I have lost job opportunities specifically because the employer didn’t want to deal with the administrative details of PA supervisory requirements here in Colorado. I find this frustrating, as well as perplexing.
Although I’ve become more comfortable with autonomy throughout my years of practice, I’ve always reserved the right to consult when necessary and appropriate, based on my own judgment and comfort level. I certainly wouldn’t mind more relaxed supervision, but I wouldn’t want to be cut entirely loose, either. On the other hand, I resent being ineligible for job opportunities simply for administrative reasons. While this is surely misguided on the part of the employers, it is a reality that practitioners encounter.
I learned recently—to my astonishment—that my NP colleagues pay about a tenth of what I do for malpractice insurance. Apparently the underwriters (and/or the plaintiffs) haven’t caught up with the nuances of responsibility and autonomy! From my perspective, PAs and NPs have more in common in the practice setting than NPs and RNs do. The fact that NPs are governed by nursing boards and insured as nurses is more an antiquated accident than a reflection of function in the workforce.
Ideally, there should be a governing body dedicated to the entire spectrum of nonphysician providers who are qualified to diagnose, treat, and prescribe. Since that is not likely to happen, it is our responsibility as PAs to match NPs in the marketplace while maintaining our integrity as providers.
Elizabeth Upper, PA-C
Denver, Colorado
Thank you for your thoughtful commentary on the pertinent topic of full practice authority for PAs (2017;27[2]:12-14). In more than 30 years as a PA, I have rarely regretted my career choice. In 1982, when I was planning my career path, I chose to become a PA instead of an NP because I didn’t want to further my nursing training (I was already an LPN) to advance my practice, and my impression was that PAs and NPs were equivalent in the workforce. This perception held true until the past few years; I have lost job opportunities specifically because the employer didn’t want to deal with the administrative details of PA supervisory requirements here in Colorado. I find this frustrating, as well as perplexing.
Although I’ve become more comfortable with autonomy throughout my years of practice, I’ve always reserved the right to consult when necessary and appropriate, based on my own judgment and comfort level. I certainly wouldn’t mind more relaxed supervision, but I wouldn’t want to be cut entirely loose, either. On the other hand, I resent being ineligible for job opportunities simply for administrative reasons. While this is surely misguided on the part of the employers, it is a reality that practitioners encounter.
I learned recently—to my astonishment—that my NP colleagues pay about a tenth of what I do for malpractice insurance. Apparently the underwriters (and/or the plaintiffs) haven’t caught up with the nuances of responsibility and autonomy! From my perspective, PAs and NPs have more in common in the practice setting than NPs and RNs do. The fact that NPs are governed by nursing boards and insured as nurses is more an antiquated accident than a reflection of function in the workforce.
Ideally, there should be a governing body dedicated to the entire spectrum of nonphysician providers who are qualified to diagnose, treat, and prescribe. Since that is not likely to happen, it is our responsibility as PAs to match NPs in the marketplace while maintaining our integrity as providers.
Elizabeth Upper, PA-C
Denver, Colorado
Milk interferes with levothyroxine absorption
ORLANDO – Consuming milk and levothyroxine at the same time reduced the absorption of the thyroid hormone replacement, according to Deborah Chon, MD, speaking at a press briefing at the annual meeting of the Endocrine Society.
This finding comes from a small study of 10 healthy adults with normal TSH concentration at baseline. The study participants had a mean age of 34 years and 6 were men.
The total serum T4 absorption over 6 hours, calculated as area under the curve, was significantly lower when participants took levothyroxine and milk concurrently, compared with taking it alone (67.26 vs. 73.48; P equals .02).
The best interval between taking levothyroxine and drinking milk has yet to be established, according to Dr. Chon, who is on the faculty of the University of California, Los Angeles. Findings from earlier research showed that use of elemental calcium supplements interfere with absorption of levothyroxine.
In 2014, levothyroxine became the most commonly prescribed drug in the United States, according to a survey by the IMS Institute for Healthcare Informatics, now QuintilesIMS. Patients who need to take it because of Hashimoto’s thyroiditis or after thyroidectomy are often unhappy with how they feel. Dose adjustments are common as endocrinologists struggle to improve patients’ quality of life. It may be that a simple strategy of not taking the thyroid replacement at the same time as milk might leave patients feeling better.
Dr. Chon reported having no relevant financial conflicts of interest.
This article was updated 4/10/17.
ORLANDO – Consuming milk and levothyroxine at the same time reduced the absorption of the thyroid hormone replacement, according to Deborah Chon, MD, speaking at a press briefing at the annual meeting of the Endocrine Society.
This finding comes from a small study of 10 healthy adults with normal TSH concentration at baseline. The study participants had a mean age of 34 years and 6 were men.
The total serum T4 absorption over 6 hours, calculated as area under the curve, was significantly lower when participants took levothyroxine and milk concurrently, compared with taking it alone (67.26 vs. 73.48; P equals .02).
The best interval between taking levothyroxine and drinking milk has yet to be established, according to Dr. Chon, who is on the faculty of the University of California, Los Angeles. Findings from earlier research showed that use of elemental calcium supplements interfere with absorption of levothyroxine.
In 2014, levothyroxine became the most commonly prescribed drug in the United States, according to a survey by the IMS Institute for Healthcare Informatics, now QuintilesIMS. Patients who need to take it because of Hashimoto’s thyroiditis or after thyroidectomy are often unhappy with how they feel. Dose adjustments are common as endocrinologists struggle to improve patients’ quality of life. It may be that a simple strategy of not taking the thyroid replacement at the same time as milk might leave patients feeling better.
Dr. Chon reported having no relevant financial conflicts of interest.
This article was updated 4/10/17.
ORLANDO – Consuming milk and levothyroxine at the same time reduced the absorption of the thyroid hormone replacement, according to Deborah Chon, MD, speaking at a press briefing at the annual meeting of the Endocrine Society.
This finding comes from a small study of 10 healthy adults with normal TSH concentration at baseline. The study participants had a mean age of 34 years and 6 were men.
The total serum T4 absorption over 6 hours, calculated as area under the curve, was significantly lower when participants took levothyroxine and milk concurrently, compared with taking it alone (67.26 vs. 73.48; P equals .02).
The best interval between taking levothyroxine and drinking milk has yet to be established, according to Dr. Chon, who is on the faculty of the University of California, Los Angeles. Findings from earlier research showed that use of elemental calcium supplements interfere with absorption of levothyroxine.
In 2014, levothyroxine became the most commonly prescribed drug in the United States, according to a survey by the IMS Institute for Healthcare Informatics, now QuintilesIMS. Patients who need to take it because of Hashimoto’s thyroiditis or after thyroidectomy are often unhappy with how they feel. Dose adjustments are common as endocrinologists struggle to improve patients’ quality of life. It may be that a simple strategy of not taking the thyroid replacement at the same time as milk might leave patients feeling better.
Dr. Chon reported having no relevant financial conflicts of interest.
This article was updated 4/10/17.
AT ENDO 2017
Key clinical point:
Major finding: Calculated as an area under the curve, simultaneous consumption of levothyroxine and milk reduced absorption of the supplement by a mean of 67.26 vs. 73.48 when taken without milk.
Data source: A pharmacokinetic study of 10 healthy subjects.
Disclosures: Dr. Chon reported having no relevant conflicts of interest.
From the Vascular Community
In memoriam: Edward B. Diethrich
Edward B. Diethrich, MD, the world-renowned cardiovascular/endovascular surgeon, inventor, and philanthropist, succumbed after a brave fight with a brain tumor on February 23, 2017, at the age of 81.
Dr. Diethrich was a pioneer in noninvasive cardiovascular and vascular disease diagnosis and innovative in surgical and endovascular therapy. He obtained his undergraduate and medical degrees at the University of Michigan and completed his surgical residency at St. Joseph’s Mercy Hospital in Ann Arbor and the Henry Ford Hospital in Detroit. He went on to complete his cardiovascular surgery training under Michael DeBakey at the Baylor College of Medicine in Houston, where he played an important role in the development of human heart transplantation.
One of his first accomplishments was the invention of the sternal saw in 1962, which is still used today for open-chest surgery. He also contributed to the development of a preservation chamber for heart transplantation and established one of the first ultrasound companies. Dr. Diethrich spent a lifetime developing new technologies, from a bubble oxygenator for open-heart surgery to developing and manufacturing stent grafts for aortic aneurysms. He remained actively involved in advancing the practice of vascular surgery and keeping it up-to-date with the changing times: He founded a company that develops and manufactures endoluminal grafts, established a Translational Research Center that is dedicated to clinical research and developing new technologies, and started a company devoted to the prevention and management of cardiovascular disease. His contributions to surgical education are also legendary. He organized an annual meeting that attracted physicians from all over the world and show-cased state-of-the-art techniques and innovations. He authored over 400 scientific articles, several textbooks, and lay publications and produced hundreds of educational videos and films. In fact, he organized the first live international telecast of open-heart surgery. Above all, Dr. Diethrich trained several hundred surgeons and other specialists in cardiovascular surgery and endovascular techniques, and traveled the world to demonstrate his techniques and teach local physicians. He recently endowed the Edward B. Diethrich Research Professorship in Biomedical Engineering and Vascular Surgery at the University of Michigan to recognize the collaboration that is required between surgeons and engineers.
Dr. Diethrich has received several honors, such as the Frederick A. Coller Award; Presidency of the Denton A. Cooley Cardiovascular Surgical Society; the Medal for Innovation in Vascular Surgery from the Society for Vascular Surgery; the Medal of Independence from King Hussein of Jordan; and an honorary fellowship from the Royal College of Surgeons, Glasgow. The Edward B. Diethrich Vascular Surgical Society was established by several hundred of his trainees. I was honored to serve as the first President of that society.
It’s ironic that Dr. Diethrich was an early supporter of ceiling-mounted radiographic equipment, which is essential to endovascular interventions. Even with the most advanced radiation protection, Dr. Diethrich paid the ultimate price for his nearly daily exposure to radiation, which led to his 4-year battle with glioma, and, ultimately, his death. But true to form, he even used this unfortunate illness to educate others by working with the Organization for Occupational Radiation Safety in Interventional Fluoroscopy to produce a documentary on the ill effects of radiation.
Dr. Diethrich recently completed his memoirs (SLED: The Serendipitous Life of Edward Diethrich), which recounts his extraordinary 50-year career, from his early days of working and training with the world’s most renowned surgeons to his legendary international success as a cardiovascular surgeon and innovator.
In summary, Dr. Diethrich was a multifaceted, passionate, and charismatic man: a sportsman, musician, scientist, inventor, author, film producer, media personality, along with many others. His confidence, dexterity, and technical expertise were evident in both the operating room and the endovascular suite. Dr. Diethrich was a world-renowned leader and pioneer in Vascular Surgery. He was an eloquent speaker, prolific innovative scholar, and dedicated teacher. His energy was endless, and his manners were impeccable. He will be sorely missed, but his legendary contributions to medicine/vascular surgery, his trainees, and the many people he influenced will live on.
Dr. Diethrich is survived by his wife of 61 years, Gloria; daughter Lynne; son Tad; son-in-law Joe Jackson; daughter-in-law Terri Diethrich, and grandchildren Danielle Diethrich-Vargas, Courtney, Reese, and Trey Diethrich; Mackenzie, Tatum, Peyton, and Zack Jackson.
A celebration of his life will be planned in the near future. Details will be posted at drteddiethrich.com.
In memoriam: Edward B. Diethrich
Edward B. Diethrich, MD, the world-renowned cardiovascular/endovascular surgeon, inventor, and philanthropist, succumbed after a brave fight with a brain tumor on February 23, 2017, at the age of 81.
Dr. Diethrich was a pioneer in noninvasive cardiovascular and vascular disease diagnosis and innovative in surgical and endovascular therapy. He obtained his undergraduate and medical degrees at the University of Michigan and completed his surgical residency at St. Joseph’s Mercy Hospital in Ann Arbor and the Henry Ford Hospital in Detroit. He went on to complete his cardiovascular surgery training under Michael DeBakey at the Baylor College of Medicine in Houston, where he played an important role in the development of human heart transplantation.
One of his first accomplishments was the invention of the sternal saw in 1962, which is still used today for open-chest surgery. He also contributed to the development of a preservation chamber for heart transplantation and established one of the first ultrasound companies. Dr. Diethrich spent a lifetime developing new technologies, from a bubble oxygenator for open-heart surgery to developing and manufacturing stent grafts for aortic aneurysms. He remained actively involved in advancing the practice of vascular surgery and keeping it up-to-date with the changing times: He founded a company that develops and manufactures endoluminal grafts, established a Translational Research Center that is dedicated to clinical research and developing new technologies, and started a company devoted to the prevention and management of cardiovascular disease. His contributions to surgical education are also legendary. He organized an annual meeting that attracted physicians from all over the world and show-cased state-of-the-art techniques and innovations. He authored over 400 scientific articles, several textbooks, and lay publications and produced hundreds of educational videos and films. In fact, he organized the first live international telecast of open-heart surgery. Above all, Dr. Diethrich trained several hundred surgeons and other specialists in cardiovascular surgery and endovascular techniques, and traveled the world to demonstrate his techniques and teach local physicians. He recently endowed the Edward B. Diethrich Research Professorship in Biomedical Engineering and Vascular Surgery at the University of Michigan to recognize the collaboration that is required between surgeons and engineers.
Dr. Diethrich has received several honors, such as the Frederick A. Coller Award; Presidency of the Denton A. Cooley Cardiovascular Surgical Society; the Medal for Innovation in Vascular Surgery from the Society for Vascular Surgery; the Medal of Independence from King Hussein of Jordan; and an honorary fellowship from the Royal College of Surgeons, Glasgow. The Edward B. Diethrich Vascular Surgical Society was established by several hundred of his trainees. I was honored to serve as the first President of that society.
It’s ironic that Dr. Diethrich was an early supporter of ceiling-mounted radiographic equipment, which is essential to endovascular interventions. Even with the most advanced radiation protection, Dr. Diethrich paid the ultimate price for his nearly daily exposure to radiation, which led to his 4-year battle with glioma, and, ultimately, his death. But true to form, he even used this unfortunate illness to educate others by working with the Organization for Occupational Radiation Safety in Interventional Fluoroscopy to produce a documentary on the ill effects of radiation.
Dr. Diethrich recently completed his memoirs (SLED: The Serendipitous Life of Edward Diethrich), which recounts his extraordinary 50-year career, from his early days of working and training with the world’s most renowned surgeons to his legendary international success as a cardiovascular surgeon and innovator.
In summary, Dr. Diethrich was a multifaceted, passionate, and charismatic man: a sportsman, musician, scientist, inventor, author, film producer, media personality, along with many others. His confidence, dexterity, and technical expertise were evident in both the operating room and the endovascular suite. Dr. Diethrich was a world-renowned leader and pioneer in Vascular Surgery. He was an eloquent speaker, prolific innovative scholar, and dedicated teacher. His energy was endless, and his manners were impeccable. He will be sorely missed, but his legendary contributions to medicine/vascular surgery, his trainees, and the many people he influenced will live on.
Dr. Diethrich is survived by his wife of 61 years, Gloria; daughter Lynne; son Tad; son-in-law Joe Jackson; daughter-in-law Terri Diethrich, and grandchildren Danielle Diethrich-Vargas, Courtney, Reese, and Trey Diethrich; Mackenzie, Tatum, Peyton, and Zack Jackson.
A celebration of his life will be planned in the near future. Details will be posted at drteddiethrich.com.
In memoriam: Edward B. Diethrich
Edward B. Diethrich, MD, the world-renowned cardiovascular/endovascular surgeon, inventor, and philanthropist, succumbed after a brave fight with a brain tumor on February 23, 2017, at the age of 81.
Dr. Diethrich was a pioneer in noninvasive cardiovascular and vascular disease diagnosis and innovative in surgical and endovascular therapy. He obtained his undergraduate and medical degrees at the University of Michigan and completed his surgical residency at St. Joseph’s Mercy Hospital in Ann Arbor and the Henry Ford Hospital in Detroit. He went on to complete his cardiovascular surgery training under Michael DeBakey at the Baylor College of Medicine in Houston, where he played an important role in the development of human heart transplantation.
One of his first accomplishments was the invention of the sternal saw in 1962, which is still used today for open-chest surgery. He also contributed to the development of a preservation chamber for heart transplantation and established one of the first ultrasound companies. Dr. Diethrich spent a lifetime developing new technologies, from a bubble oxygenator for open-heart surgery to developing and manufacturing stent grafts for aortic aneurysms. He remained actively involved in advancing the practice of vascular surgery and keeping it up-to-date with the changing times: He founded a company that develops and manufactures endoluminal grafts, established a Translational Research Center that is dedicated to clinical research and developing new technologies, and started a company devoted to the prevention and management of cardiovascular disease. His contributions to surgical education are also legendary. He organized an annual meeting that attracted physicians from all over the world and show-cased state-of-the-art techniques and innovations. He authored over 400 scientific articles, several textbooks, and lay publications and produced hundreds of educational videos and films. In fact, he organized the first live international telecast of open-heart surgery. Above all, Dr. Diethrich trained several hundred surgeons and other specialists in cardiovascular surgery and endovascular techniques, and traveled the world to demonstrate his techniques and teach local physicians. He recently endowed the Edward B. Diethrich Research Professorship in Biomedical Engineering and Vascular Surgery at the University of Michigan to recognize the collaboration that is required between surgeons and engineers.
Dr. Diethrich has received several honors, such as the Frederick A. Coller Award; Presidency of the Denton A. Cooley Cardiovascular Surgical Society; the Medal for Innovation in Vascular Surgery from the Society for Vascular Surgery; the Medal of Independence from King Hussein of Jordan; and an honorary fellowship from the Royal College of Surgeons, Glasgow. The Edward B. Diethrich Vascular Surgical Society was established by several hundred of his trainees. I was honored to serve as the first President of that society.
It’s ironic that Dr. Diethrich was an early supporter of ceiling-mounted radiographic equipment, which is essential to endovascular interventions. Even with the most advanced radiation protection, Dr. Diethrich paid the ultimate price for his nearly daily exposure to radiation, which led to his 4-year battle with glioma, and, ultimately, his death. But true to form, he even used this unfortunate illness to educate others by working with the Organization for Occupational Radiation Safety in Interventional Fluoroscopy to produce a documentary on the ill effects of radiation.
Dr. Diethrich recently completed his memoirs (SLED: The Serendipitous Life of Edward Diethrich), which recounts his extraordinary 50-year career, from his early days of working and training with the world’s most renowned surgeons to his legendary international success as a cardiovascular surgeon and innovator.
In summary, Dr. Diethrich was a multifaceted, passionate, and charismatic man: a sportsman, musician, scientist, inventor, author, film producer, media personality, along with many others. His confidence, dexterity, and technical expertise were evident in both the operating room and the endovascular suite. Dr. Diethrich was a world-renowned leader and pioneer in Vascular Surgery. He was an eloquent speaker, prolific innovative scholar, and dedicated teacher. His energy was endless, and his manners were impeccable. He will be sorely missed, but his legendary contributions to medicine/vascular surgery, his trainees, and the many people he influenced will live on.
Dr. Diethrich is survived by his wife of 61 years, Gloria; daughter Lynne; son Tad; son-in-law Joe Jackson; daughter-in-law Terri Diethrich, and grandchildren Danielle Diethrich-Vargas, Courtney, Reese, and Trey Diethrich; Mackenzie, Tatum, Peyton, and Zack Jackson.
A celebration of his life will be planned in the near future. Details will be posted at drteddiethrich.com.
Shelving of AHCA a win for patients, experts say
SAN DIEGO – The decision by House Republicans to withdraw the American Health Care Act on March 24, 2017 was a victory for the health care of all Americans, especially older, sicker, and poorer patients, according to Nitin S. Damle, MD.
“It was a terrible bill,” Dr. Damle, president of the American College of Physicians, said during a press briefing at the annual meeting of the ACP. “Fortunately it will not become law at this point, but the story doesn’t really end here. The Trump Administration needs to decide whether it’s going to help faithfully implement the Affordable Care Act or sabotage it, either by action or inaction. It’s also important that we turn the page and begin the hard work of engaging with the administration and Congress on a bipartisan agenda to improve American health care.”
The ACHA would have eliminated the federal requirement that insurers cover 10 categories of essential benefits including emergency care, maternity services, and hospitalization, leaving it to states to decide. It also eliminated the requirement that Medicaid cover the same essential benefits. According to Dr. Damle, the AHCA’s age-based tax credits “were too low and the deductibles were going to be too high for older people and poorer patients, because insurers would have been allowed to charge older patients up to five times more than younger patients for their coverage.” For example, the CBO found that under the bill a 64-year-old male who makes $26,500 a year would have to pay $14,600 out of pocket for insurance in the non-group market, compared to $1,700 under the existing ACA, a 750% increase.
“In my practice, I have many older and sicker patients who would have been left behind had this become law, patients with diseases like congestive heart failure, diabetes, chronic obstructive pulmonary disease from smoking who require frequent and ongoing monitoring of their medications, development of any complications from their disease, and sometimes even need home-based support,” Dr. Damle said.
Robert B. Doherty, senior vice president of governmental affairs and public policy for the ACP, described efforts to roll back the ACA as “unchartered” territory. “I have never in the past seen an administration trying to roll back coverage on millions of people,” he said. “This history of the US has been incremental expansion of coverage since the creation of Medicare and Medicaid in 1965.” He acknowledged certain shortcomings of the ACA, including uneven participation by insurers from state to state, and “deductibles may be too high, and premiums too high for some people. On the other hand, the ACA has achieved an historic reduction in the uninsured rate in the United States. More than 20 million people have gained coverage, and according to the CDC, only 8.2% of Americans are without health insurance, an historic low. It’s still too high, but we’re basically 92% of the way to universal coverage in the U.S.”
Mr. Doherty expressed concern that legislative efforts to roll back the ACA could re-emerge. “The Republicans are still talking about bringing it back,” he said. “You can’t take it for granted because Republicans have been promising repeal and replace [legislation] for seven years now, and I think they want to move forward. I think we have to remain vigilant. We have to put pressure on the [Trump] administration to make sure they faithfully execute the law, which they swore to do when they took office. Then we have to reach out and say there are problems that need to be addressed, bipartisan solutions to stabilize the [health insurance] markets and to address other issues like the crushing administrative burden on physicians. You have to start by accepting that the ACA is the law of the land. We need to build upon it and improve it, not repeal it.”
SAN DIEGO – The decision by House Republicans to withdraw the American Health Care Act on March 24, 2017 was a victory for the health care of all Americans, especially older, sicker, and poorer patients, according to Nitin S. Damle, MD.
“It was a terrible bill,” Dr. Damle, president of the American College of Physicians, said during a press briefing at the annual meeting of the ACP. “Fortunately it will not become law at this point, but the story doesn’t really end here. The Trump Administration needs to decide whether it’s going to help faithfully implement the Affordable Care Act or sabotage it, either by action or inaction. It’s also important that we turn the page and begin the hard work of engaging with the administration and Congress on a bipartisan agenda to improve American health care.”
The ACHA would have eliminated the federal requirement that insurers cover 10 categories of essential benefits including emergency care, maternity services, and hospitalization, leaving it to states to decide. It also eliminated the requirement that Medicaid cover the same essential benefits. According to Dr. Damle, the AHCA’s age-based tax credits “were too low and the deductibles were going to be too high for older people and poorer patients, because insurers would have been allowed to charge older patients up to five times more than younger patients for their coverage.” For example, the CBO found that under the bill a 64-year-old male who makes $26,500 a year would have to pay $14,600 out of pocket for insurance in the non-group market, compared to $1,700 under the existing ACA, a 750% increase.
“In my practice, I have many older and sicker patients who would have been left behind had this become law, patients with diseases like congestive heart failure, diabetes, chronic obstructive pulmonary disease from smoking who require frequent and ongoing monitoring of their medications, development of any complications from their disease, and sometimes even need home-based support,” Dr. Damle said.
Robert B. Doherty, senior vice president of governmental affairs and public policy for the ACP, described efforts to roll back the ACA as “unchartered” territory. “I have never in the past seen an administration trying to roll back coverage on millions of people,” he said. “This history of the US has been incremental expansion of coverage since the creation of Medicare and Medicaid in 1965.” He acknowledged certain shortcomings of the ACA, including uneven participation by insurers from state to state, and “deductibles may be too high, and premiums too high for some people. On the other hand, the ACA has achieved an historic reduction in the uninsured rate in the United States. More than 20 million people have gained coverage, and according to the CDC, only 8.2% of Americans are without health insurance, an historic low. It’s still too high, but we’re basically 92% of the way to universal coverage in the U.S.”
Mr. Doherty expressed concern that legislative efforts to roll back the ACA could re-emerge. “The Republicans are still talking about bringing it back,” he said. “You can’t take it for granted because Republicans have been promising repeal and replace [legislation] for seven years now, and I think they want to move forward. I think we have to remain vigilant. We have to put pressure on the [Trump] administration to make sure they faithfully execute the law, which they swore to do when they took office. Then we have to reach out and say there are problems that need to be addressed, bipartisan solutions to stabilize the [health insurance] markets and to address other issues like the crushing administrative burden on physicians. You have to start by accepting that the ACA is the law of the land. We need to build upon it and improve it, not repeal it.”
SAN DIEGO – The decision by House Republicans to withdraw the American Health Care Act on March 24, 2017 was a victory for the health care of all Americans, especially older, sicker, and poorer patients, according to Nitin S. Damle, MD.
“It was a terrible bill,” Dr. Damle, president of the American College of Physicians, said during a press briefing at the annual meeting of the ACP. “Fortunately it will not become law at this point, but the story doesn’t really end here. The Trump Administration needs to decide whether it’s going to help faithfully implement the Affordable Care Act or sabotage it, either by action or inaction. It’s also important that we turn the page and begin the hard work of engaging with the administration and Congress on a bipartisan agenda to improve American health care.”
The ACHA would have eliminated the federal requirement that insurers cover 10 categories of essential benefits including emergency care, maternity services, and hospitalization, leaving it to states to decide. It also eliminated the requirement that Medicaid cover the same essential benefits. According to Dr. Damle, the AHCA’s age-based tax credits “were too low and the deductibles were going to be too high for older people and poorer patients, because insurers would have been allowed to charge older patients up to five times more than younger patients for their coverage.” For example, the CBO found that under the bill a 64-year-old male who makes $26,500 a year would have to pay $14,600 out of pocket for insurance in the non-group market, compared to $1,700 under the existing ACA, a 750% increase.
“In my practice, I have many older and sicker patients who would have been left behind had this become law, patients with diseases like congestive heart failure, diabetes, chronic obstructive pulmonary disease from smoking who require frequent and ongoing monitoring of their medications, development of any complications from their disease, and sometimes even need home-based support,” Dr. Damle said.
Robert B. Doherty, senior vice president of governmental affairs and public policy for the ACP, described efforts to roll back the ACA as “unchartered” territory. “I have never in the past seen an administration trying to roll back coverage on millions of people,” he said. “This history of the US has been incremental expansion of coverage since the creation of Medicare and Medicaid in 1965.” He acknowledged certain shortcomings of the ACA, including uneven participation by insurers from state to state, and “deductibles may be too high, and premiums too high for some people. On the other hand, the ACA has achieved an historic reduction in the uninsured rate in the United States. More than 20 million people have gained coverage, and according to the CDC, only 8.2% of Americans are without health insurance, an historic low. It’s still too high, but we’re basically 92% of the way to universal coverage in the U.S.”
Mr. Doherty expressed concern that legislative efforts to roll back the ACA could re-emerge. “The Republicans are still talking about bringing it back,” he said. “You can’t take it for granted because Republicans have been promising repeal and replace [legislation] for seven years now, and I think they want to move forward. I think we have to remain vigilant. We have to put pressure on the [Trump] administration to make sure they faithfully execute the law, which they swore to do when they took office. Then we have to reach out and say there are problems that need to be addressed, bipartisan solutions to stabilize the [health insurance] markets and to address other issues like the crushing administrative burden on physicians. You have to start by accepting that the ACA is the law of the land. We need to build upon it and improve it, not repeal it.”
AT ACP INTERNAL MEDICINE
Clinical Challenges - April 2017 What's Your Diagnosis?
What's Your Diagnosis?
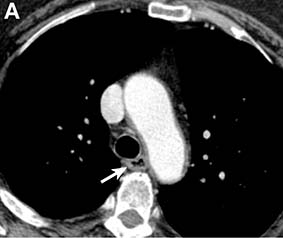
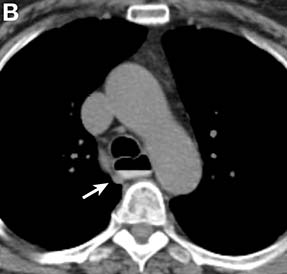
Answer to “What’s your diagnosis?” on page X: Pseudoachalasia in paraneoplastic syndrome, with radiographic documentation of onset and evolution
A barium esophagogram revealed an esophagus with characteristic features of achalasia: dilatation, retention of air and fluid, and a “bird’s beak” configuration distally (Figure E). Botulinum injection into the distal esophagus provided the patient with partial relief of her swallowing symptoms.
Evidence supporting the diagnosis of pseudoachalasia associated with paraneoplastic syndrome in this patient is 1) the development of characteristic features of achalasia in association with SCLC, the cancer that is most often associated with paraneoplastic achalasia;1 2) a serum antibody characteristic of SCLC-associated paraneoplastic syndrome; 3) peripheral neuropathy attributed to paraneoplastic syndrome; and 4) absence of an obstructive neoplasm at the gastroesophageal junction.
Pseudoachalasia associated with malignancy may occur by one of three mechanisms1-3: 1) Primary or secondary carcinoma located at or near the gastroesophageal junction, 2) neural invasion of the esophagus, or 3) as a component of the paraneoplastic syndrome. Pseudoachalasia associated with a paraneoplastic syndrome is rare (an estimated 1 in 750,000), although it may be becoming more common.1 The relatively rapid onset of dysphagia is a reported feature of pseudoachalasia, in contrast with the more gradual onset in primary achalasia. Our report documents radiographically the progression within a few months from a normal-diameter esophagus to a very dilated, poorly functioning esophagus. We know of no similar report. Botulinum toxin injection has been reported effective in a few cases.1
References
1. Katzka, D.A., Farrugia, G., Arora, A.S., et al. Achalasia secondary to neoplasia: a disease with a changing differential diagnosis. Dis Esophagus. 2012;25:331-6.
2. Liu, W., Fackler, W., Rice, T.W., et al. The pathogenesis of pseudoachalasia (A clinicopathological study of 13 cases of a rare entity). Am J Surg Pathol. 2002;26:784-8.
3. Gockel, J., Eckardt, V.F., Scmitt, T., et al. Pseudoachalasia: a case series and analysis of the literature. Scand J Gastroenterol. 2005;40:378-85.
Answer to “What’s your diagnosis?” on page X: Pseudoachalasia in paraneoplastic syndrome, with radiographic documentation of onset and evolution
A barium esophagogram revealed an esophagus with characteristic features of achalasia: dilatation, retention of air and fluid, and a “bird’s beak” configuration distally (Figure E). Botulinum injection into the distal esophagus provided the patient with partial relief of her swallowing symptoms.
Evidence supporting the diagnosis of pseudoachalasia associated with paraneoplastic syndrome in this patient is 1) the development of characteristic features of achalasia in association with SCLC, the cancer that is most often associated with paraneoplastic achalasia;1 2) a serum antibody characteristic of SCLC-associated paraneoplastic syndrome; 3) peripheral neuropathy attributed to paraneoplastic syndrome; and 4) absence of an obstructive neoplasm at the gastroesophageal junction.
Pseudoachalasia associated with malignancy may occur by one of three mechanisms1-3: 1) Primary or secondary carcinoma located at or near the gastroesophageal junction, 2) neural invasion of the esophagus, or 3) as a component of the paraneoplastic syndrome. Pseudoachalasia associated with a paraneoplastic syndrome is rare (an estimated 1 in 750,000), although it may be becoming more common.1 The relatively rapid onset of dysphagia is a reported feature of pseudoachalasia, in contrast with the more gradual onset in primary achalasia. Our report documents radiographically the progression within a few months from a normal-diameter esophagus to a very dilated, poorly functioning esophagus. We know of no similar report. Botulinum toxin injection has been reported effective in a few cases.1
References
1. Katzka, D.A., Farrugia, G., Arora, A.S., et al. Achalasia secondary to neoplasia: a disease with a changing differential diagnosis. Dis Esophagus. 2012;25:331-6.
2. Liu, W., Fackler, W., Rice, T.W., et al. The pathogenesis of pseudoachalasia (A clinicopathological study of 13 cases of a rare entity). Am J Surg Pathol. 2002;26:784-8.
3. Gockel, J., Eckardt, V.F., Scmitt, T., et al. Pseudoachalasia: a case series and analysis of the literature. Scand J Gastroenterol. 2005;40:378-85.
Answer to “What’s your diagnosis?” on page X: Pseudoachalasia in paraneoplastic syndrome, with radiographic documentation of onset and evolution
A barium esophagogram revealed an esophagus with characteristic features of achalasia: dilatation, retention of air and fluid, and a “bird’s beak” configuration distally (Figure E). Botulinum injection into the distal esophagus provided the patient with partial relief of her swallowing symptoms.
Evidence supporting the diagnosis of pseudoachalasia associated with paraneoplastic syndrome in this patient is 1) the development of characteristic features of achalasia in association with SCLC, the cancer that is most often associated with paraneoplastic achalasia;1 2) a serum antibody characteristic of SCLC-associated paraneoplastic syndrome; 3) peripheral neuropathy attributed to paraneoplastic syndrome; and 4) absence of an obstructive neoplasm at the gastroesophageal junction.
Pseudoachalasia associated with malignancy may occur by one of three mechanisms1-3: 1) Primary or secondary carcinoma located at or near the gastroesophageal junction, 2) neural invasion of the esophagus, or 3) as a component of the paraneoplastic syndrome. Pseudoachalasia associated with a paraneoplastic syndrome is rare (an estimated 1 in 750,000), although it may be becoming more common.1 The relatively rapid onset of dysphagia is a reported feature of pseudoachalasia, in contrast with the more gradual onset in primary achalasia. Our report documents radiographically the progression within a few months from a normal-diameter esophagus to a very dilated, poorly functioning esophagus. We know of no similar report. Botulinum toxin injection has been reported effective in a few cases.1
References
1. Katzka, D.A., Farrugia, G., Arora, A.S., et al. Achalasia secondary to neoplasia: a disease with a changing differential diagnosis. Dis Esophagus. 2012;25:331-6.
2. Liu, W., Fackler, W., Rice, T.W., et al. The pathogenesis of pseudoachalasia (A clinicopathological study of 13 cases of a rare entity). Am J Surg Pathol. 2002;26:784-8.
3. Gockel, J., Eckardt, V.F., Scmitt, T., et al. Pseudoachalasia: a case series and analysis of the literature. Scand J Gastroenterol. 2005;40:378-85.
What's Your Diagnosis?
What's Your Diagnosis?
By William R. Brown, MD, and Elizabeth K. Dee, MD.
Published previously in Gastroenterology (2013;144:34, 252).
A 67-year-old woman with neuroendocrine small-cell lung cancer (SCLC), recurrent after chemotherapy and radiation therapy, complained of recent-onset dysphagia. She noticed regurgitation of liquids and some solid-food dysphagia. She had lost 20 pounds in the past 2 months. She had no past history of gastroesophageal reflux symptoms or esophagitis. Physical examination reveals no significant abnormalities, but she had had a peripheral sensory neuropathy that improved with treatment of her SCLC. Laboratory tests are unremarkable except for a positive Hu immunoglobulin (Ig)G serum anti-neuronal nuclear antibody test – an antibody that is associated with SCLC.


April 2017 Quiz 2
Q2. Answer: C
Rationale: MALT lymphomas are associated with H. pylori infection in 80%-90% of cases. H. pylori triggers a B-cell clonal expansion leading to lymphoma. Detection of chronic H. pylori using histology is directly dependent on the number of mucosal biopsies. Negative H. pylori testing should prompt an alternative test for H. pylori (either breath or stool antigen test). Treatment of H. pylori is successful in achieving complete remission in up to 80% of cases. Surveillance after treatment of MALT lymphoma is indicated, though the exact protocol has not been established.
References
1. ASGE Standards of Practice Committee. The role of endoscopy in management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015 82(1):1-8.
2. Gisbert J.P., Calvet X. Review article: common misconceptions in the management of Helicobacter pylori-associated gastric MALT-lymphoma. Aliment Pharmacol Ther. 2011 Nov;34(9):1047-62.
Q2. Answer: C
Rationale: MALT lymphomas are associated with H. pylori infection in 80%-90% of cases. H. pylori triggers a B-cell clonal expansion leading to lymphoma. Detection of chronic H. pylori using histology is directly dependent on the number of mucosal biopsies. Negative H. pylori testing should prompt an alternative test for H. pylori (either breath or stool antigen test). Treatment of H. pylori is successful in achieving complete remission in up to 80% of cases. Surveillance after treatment of MALT lymphoma is indicated, though the exact protocol has not been established.
References
1. ASGE Standards of Practice Committee. The role of endoscopy in management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015 82(1):1-8.
2. Gisbert J.P., Calvet X. Review article: common misconceptions in the management of Helicobacter pylori-associated gastric MALT-lymphoma. Aliment Pharmacol Ther. 2011 Nov;34(9):1047-62.
Q2. Answer: C
Rationale: MALT lymphomas are associated with H. pylori infection in 80%-90% of cases. H. pylori triggers a B-cell clonal expansion leading to lymphoma. Detection of chronic H. pylori using histology is directly dependent on the number of mucosal biopsies. Negative H. pylori testing should prompt an alternative test for H. pylori (either breath or stool antigen test). Treatment of H. pylori is successful in achieving complete remission in up to 80% of cases. Surveillance after treatment of MALT lymphoma is indicated, though the exact protocol has not been established.
References
1. ASGE Standards of Practice Committee. The role of endoscopy in management of premalignant and malignant conditions of the stomach. Gastrointest Endosc. 2015 82(1):1-8.
2. Gisbert J.P., Calvet X. Review article: common misconceptions in the management of Helicobacter pylori-associated gastric MALT-lymphoma. Aliment Pharmacol Ther. 2011 Nov;34(9):1047-62.
Q2. A 56-year-old woman presents with epigastric pain and is found to have a 3-cm submucosal mass with thickened rugal folds in the gastric body. Biopsies of the mass show mucosa-associated lymphoid tissue (MALT lymphoma). There is no evidence of Helicobacter pylori infection in the biopsies.
April 2017 Quiz 1
Q1. Answer: A
While heartburn responds well to acid suppression with a proton pump inhibitor, regurgitation does not necessarily improve. It is well known that reflux persists despite acid suppression; in some patients, this manifests as troublesome postprandial regurgitation. Transient LES relaxations (TLESRs) are the prime mechanism for persisting reflex, in patients both with and without hiatal hernias.
Baclofen, a gamma amino butyric acid B (GABA-B) agonist, inhibits TLESRs and has potential to improve persisting regurgitation. Metoclopramide has been demonstrated to have no adjunctive value in treating reflux disease. Hyoscyamine and sucralfate are similarly not of particular benefit in this setting. Cholesytramine is a bile salt binding resin that has value in the management of postcholecystectomy diarrhea.
References
1. Kahrilas P.J., Jonsson A., Denison H., et al. Regurgitation is less responsive to acid suppression than heartburn in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10(6):612-9.
2. Vela M.F., Camacho-Lobato L., Srinivasan R., et al. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology. 2001 Jun;120(7):1599-606.
3. Vela M.F., Tutuian R, Katz PO, et al. Baclofen decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and pH. Aliment Pharmacol Ther. 2003 Jan;17(2):243-51.
Q1. Answer: A
While heartburn responds well to acid suppression with a proton pump inhibitor, regurgitation does not necessarily improve. It is well known that reflux persists despite acid suppression; in some patients, this manifests as troublesome postprandial regurgitation. Transient LES relaxations (TLESRs) are the prime mechanism for persisting reflex, in patients both with and without hiatal hernias.
Baclofen, a gamma amino butyric acid B (GABA-B) agonist, inhibits TLESRs and has potential to improve persisting regurgitation. Metoclopramide has been demonstrated to have no adjunctive value in treating reflux disease. Hyoscyamine and sucralfate are similarly not of particular benefit in this setting. Cholesytramine is a bile salt binding resin that has value in the management of postcholecystectomy diarrhea.
References
1. Kahrilas P.J., Jonsson A., Denison H., et al. Regurgitation is less responsive to acid suppression than heartburn in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10(6):612-9.
2. Vela M.F., Camacho-Lobato L., Srinivasan R., et al. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology. 2001 Jun;120(7):1599-606.
3. Vela M.F., Tutuian R, Katz PO, et al. Baclofen decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and pH. Aliment Pharmacol Ther. 2003 Jan;17(2):243-51.
Q1. Answer: A
While heartburn responds well to acid suppression with a proton pump inhibitor, regurgitation does not necessarily improve. It is well known that reflux persists despite acid suppression; in some patients, this manifests as troublesome postprandial regurgitation. Transient LES relaxations (TLESRs) are the prime mechanism for persisting reflex, in patients both with and without hiatal hernias.
Baclofen, a gamma amino butyric acid B (GABA-B) agonist, inhibits TLESRs and has potential to improve persisting regurgitation. Metoclopramide has been demonstrated to have no adjunctive value in treating reflux disease. Hyoscyamine and sucralfate are similarly not of particular benefit in this setting. Cholesytramine is a bile salt binding resin that has value in the management of postcholecystectomy diarrhea.
References
1. Kahrilas P.J., Jonsson A., Denison H., et al. Regurgitation is less responsive to acid suppression than heartburn in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10(6):612-9.
2. Vela M.F., Camacho-Lobato L., Srinivasan R., et al. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology. 2001 Jun;120(7):1599-606.
3. Vela M.F., Tutuian R, Katz PO, et al. Baclofen decreases acid and non-acid post-prandial gastro-oesophageal reflux measured by combined multichannel intraluminal impedance and pH. Aliment Pharmacol Ther. 2003 Jan;17(2):243-51.
Q1. A 25-year-old woman presents with postprandial regurgitation, typically after dinner. She initially had both heartburn and regurgitation. After she started esomeprazole 40 mg once a day 8 weeks ago, her heartburn completely resolved. An upper endoscopy, performed due to ongoing regurgitation symptoms, reveals a normal esophagus, and a 2-cm sliding hiatal hernia.