User login
Get ready for cancer immunotherapy-induced rheumatic diseases
SNOWMASS, COLO. – Physicians can expect to encounter more and more patients with inflammatory arthritis and other rheumatic adverse events induced by immune checkpoint inhibitors as a result of anticipated exponential growth in the use of these drugs to treat an expanding list of cancers, Clifton O. Bingham III, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
These cancer immunotherapy–induced rheumatic diseases may superficially look like the classic forms of familiar autoimmune diseases, but they have highly atypical features that will affect treatment decisions.

“What we’ve seen consistently is that the normal doses of prednisone we would use to treat an inflammatory arthritis are really ineffective in most of these patients. We’ve had to use super doses – up to 120 mg/day – for initial control, and then 7.5-40 mg daily for maintenance of response,” according to Dr. Bingham, professor of medicine and director of the Johns Hopkins Arthritis Center in Baltimore.
To date, only limited data from case series are available on rheumatic IRAEs. There are no prospective patient registries logging accurate data on the incidence of these rheumatic adverse events among cancer patients treated with immune checkpoint inhibitors (ICIs). These IRAEs, which lie at the intersection of rheumatology and oncology, are of special interest to Dr. Bingham – he and his coinvestigators have published five articles on the topic over the course of a single year.
In a wide-ranging talk at the symposium, he touched on the phenotypic spectrum of rheumatologic IRAEs, his conviction that they are greatly underdiagnosed, why physicians can expect to encounter them much more frequently, rheumatologic IRAE treatment issues, and the risks of prescribing ICIs in patients with known preexisting rheumatologic disease.
Rheumatologic IRAE presentations
Inflammatory arthritis is the most common form of rheumatologic IRAE, followed by sicca syndrome. At the Johns Hopkins Arthritis Center, Dr. Bingham and his coworkers have 25 well-characterized patients with inflammatory arthritis resulting from an ICI, only 1 of whom is HLA-B27-positive.
“Also, just one is autoantibody-positive, even though they all look for all the world as though they have rheumatoid arthritis,” the rheumatologist observed.
This ICI-induced inflammatory arthritis initially presents most commonly in the midsize and large joints – knees, ankles, elbows – then expands to include small joints such as the wrists, proximal interphalangeal joints, and the metacarpophalangeal joints.
Notably, the Hopkins group also has three patients with classic reactive arthritis marked by conjunctivitis, urethritis, arthritis, and dactylitis.
“I don’t know about you, but, in our general rheumatology practice, we see maybe one case of reactive arthritis in several years, so this is something that has struck us as really quite interesting,” said Dr. Bingham, who is also director of research in the division of rheumatology at Johns Hopkins.
The arthritis center is also managing a group of patients with ICI-induced sicca syndrome, which is uniformly extremely severe and treatment resistant, as well as a couple of patients with myositis IRAE, one with polymyalgia rheumatica, and two with crystal disease that is highly inflammatory in nature, difficult to treat, and includes an inflammatory polyarthritis component not typical in patients with crystal arthritis.
Why physicians will see more rheumatologic IRAEs
ICIs have dramatically transformed the treatment of selected advanced-stage cancers. For example, whereas patients with metastatic melanoma historically had a 2-year survival rate of 5%, combination therapy with the ICIs ipilimumab (Yervoy) and nivolumab (Opdivo) resulted in a 60% rate of partial or complete remission in a landmark clinical trial.
The basis of cancer immunotherapy is the discovery that, in order for cancer cells to thrive, they emit blocking signals that downregulate the native ability of T cells to recognize and kill them. This is true for both solid tumors and hematologic malignancies. The ICIs inhibit these blocking signals, which include cytotoxic T-lymphocyte–associated protein 4 (CTLA4), programmed death-1 (PD-1), and programmed death ligand-1 (PDL-1), thereby freeing up the T cells for tumor fighting.
Because of the nonspecific mechanism of this T-cell activation, however, ICIs have, as their main toxicities, T-cell–mediated autoimmune inflammatory tissue damage, which gets lumped under the umbrella term IRAEs. It can affect almost every organ system. Skin rashes are the most common, colitis second. Other commonly encountered IRAEs include thyroiditis, hypophysitis, hepatitis, peripheral neuropathy, and pneumonitis.
In addition to the four currently approved ICIs – ipilimumab, nivolumab, pembrolizumab (Keytruda), and atezolizumab (Tecentriq) – investigational ICIs targeting CTLA4, PD-1, and/or PDL-1 are in development. Plus, new ICIs targeting other blocking signals, including lymphocyte activation gene-3, CD137, and T-cell immunoglobulin and mucin domain-3, are now in clinical trials.
Clinical trials aimed at expanding the indications of existing ICIs and using ICIs in earlier-stage cancers in an effort to improve rates of lasting remission are also underway.
All told, probably at least 400 clinical trials of ICIs are ongoing worldwide, the rheumatologist estimated.
“More people will be exposed to these drugs, and we’ll see more and more of these rheumatologic IRAEs,” Dr. Bingham predicted.
Rheumatologic IRAEs are seriously underdiagnosed
Back in the pre-ICI days, Dr. Bingham was coauthor of a major study which concluded that clinical trialists in oncology consistently downgrade the severity of rheumatologic adverse events, often by 1 or 2 grades (J Rheumatol. 2007 Jun;34[6]:1401-14).
Unpublished details of ICI clinical trials in melanoma that he obtained from Bristol-Myers Squibb suggest that the true rate of rheumatologic IRAEs is about 20%, or roughly double that reported in the studies. That’s because the adverse events–grading system used in oncology undercalls the severity of arthritis and autoimmune disorders.
Indeed, the National Cancer Institute’s Common Terminology Criteria for Adverse Events, used in oncology clinical trials, is confusing on the topic of musculoskeletal and connective tissue disorders as treatment-emergent adverse events, according to Dr. Bingham. He noted that an oncologist can code a swollen joint in three different ways – joint effusion, arthritis, or arthralgia – and it takes disabling interference with self-care in activities of daily living for that swollen joint to rise to the level of a Grade 3 adverse event. From a rheumatology trialist’s perspective, that would be a Grade 4 disability.
Plus, neither the product labeling nor the patient information guides for the approved immunotherapy drugs mention the importance of monitoring for rheumatologic IRAEs or their management.
“There is poor awareness of musculoskeletal and rheumatic IRAEs in the general oncology community,” Dr. Bingham asserted. “But, if you talk with any oncology nurses who work in a clinical trial, they will tell you they’re seeing these events with significant frequency and severity.”
Treatment and response
It’s critical to gain control of rheumatologic IRAEs quickly so that patients can get on with their cancer immunotherapy. Dr. Bingham uses intra-articular steroid injections for patients with oligoarthritis and high-dose oral prednisone for polyarticular disease. He starts methotrexate and/or leflunomide early because the conventional disease-modifying antirheumatic drugs have roughly a 2-month delay in onset of action. He has had several patients who are unable to taper steroids despite background methotrexate.
In the most severely affected patients, he has turned to biologic agents in consultation with their oncologists. Tumor necrosis factor (TNF) inhibitors are the ones he and other rheumatologists have used most often.
“Notably, we have not been able to taper down very well. We have patients who are out more than 2 years now who still require their TNF inhibitor to treat their inflammatory arthritis, and these are patients on conventional disease–modifying antirheumatic drugs as well. As soon as it’s tapered, the arthritis begins to come back,” according to Dr. Bingham.
In marked contrast, colitis as an IRAE typically clears in response to just one or two doses of a TNF inhibitor.
One audience member related that she’d encountered a roadblock in trying to get authorization for a TNF inhibitor for a patient with a rheumatologic IRAE secondary to ICI treatment for metastatic melanoma because the labeling states these agents are relatively contraindicated in melanoma patients. Dr. Bingham offered a tip: Collaborate with the patient’s oncologist.
“In most cases, oncologists can get infliximab for these patients and administer it in their infusion centers. They are able to get things authorized with very little trouble,” he said.
Besides, most of these patients with severe inflammatory arthritis meet conventional criteria for TNF inhibitor therapy, based on their number of infected joints and elevated acute phase reactants for longer than 6 weeks, Dr. Bingham noted.
“We’ve had some very interesting conversations with patients. It’s impressive to see the impact arthritis can have on people. A lot of patients have said, ‘I don’t care if I die. Get me functional right now.’ That’s pretty profound. Quality of life is still very important for people, even when dealing with life-threatening diseases,” he observed.
Oncologists are actually eager for their patients to get on steroid-sparing therapy because of concern that high doses of steroids may reduce the efficacy of cancer immunotherapy. That’s not an issue with the TNF inhibitors, the rheumatologist continued.
Turning to the utility of other classes of biologic agents, Dr. Bingham advised avoiding abatacept (Orencia) because its mechanism of action is likely to cause interference with the cancer immunotherapy. Rituximab (Rituxan) takes too long to act. Anakinra (Kineret), tofacitinib (Xeljanz), and tocilizumab (Actemra), on the other hand, are agents he is interested in using as alternatives to TNF inhibitors, although he hasn’t done so yet.
Use of ICIs in patients with preexisting autoimmune disease
The experience here is entirely anecdotal, since such patients have been excluded from ICI clinical trials, but the available evidence suggests physicians should be prepared for higher rheumatologic IRAE rates in this setting. Investigators at Vanderbilt University reported that 8 of 30 cancer patients with known preexisting autoimmune disease experienced flares of that disease when treated with ipilimumab, and 10 developed a new IRAE (Therap Adv Gastroenterol. 2016 Jul;9[4]:457-62).
The Hopkins group has three patients with preexisting rheumatoid arthritis and two with preexisting scleroderma who have received ICIs. All three rheumatoid arthritis patients flared. Rheumatologists are trying to manage these flares so the patients can continue on their ICI. One of the scleroderma patients experienced no change in that disease while on an ICI, while the other showed a definite improvement in scleroderma symptoms.
“I think the jury’s still out in terms of what you do about ICI therapy in patients with preexisting autoimmunity. The data would say that there’s maybe a 50-50 chance of the autoimmune disease becoming worse, but, if patients have an otherwise fatal cancer, I think it’s probably worth the chance,” Dr. Bingham said.
Anecdotal reports suggest that more severe IRAEs may be a favorable prognostic sign in terms of cancer eradication, but a lot more patient experience will be needed in order to be sure, the rheumatologist said.
Dr. Bingham reported serving as a consultant to Bristol-Myers Squibb.
SNOWMASS, COLO. – Physicians can expect to encounter more and more patients with inflammatory arthritis and other rheumatic adverse events induced by immune checkpoint inhibitors as a result of anticipated exponential growth in the use of these drugs to treat an expanding list of cancers, Clifton O. Bingham III, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
These cancer immunotherapy–induced rheumatic diseases may superficially look like the classic forms of familiar autoimmune diseases, but they have highly atypical features that will affect treatment decisions.
“What we’ve seen consistently is that the normal doses of prednisone we would use to treat an inflammatory arthritis are really ineffective in most of these patients. We’ve had to use super doses – up to 120 mg/day – for initial control, and then 7.5-40 mg daily for maintenance of response,” according to Dr. Bingham, professor of medicine and director of the Johns Hopkins Arthritis Center in Baltimore.
To date, only limited data from case series are available on rheumatic IRAEs. There are no prospective patient registries logging accurate data on the incidence of these rheumatic adverse events among cancer patients treated with immune checkpoint inhibitors (ICIs). These IRAEs, which lie at the intersection of rheumatology and oncology, are of special interest to Dr. Bingham – he and his coinvestigators have published five articles on the topic over the course of a single year.
In a wide-ranging talk at the symposium, he touched on the phenotypic spectrum of rheumatologic IRAEs, his conviction that they are greatly underdiagnosed, why physicians can expect to encounter them much more frequently, rheumatologic IRAE treatment issues, and the risks of prescribing ICIs in patients with known preexisting rheumatologic disease.
Rheumatologic IRAE presentations
Inflammatory arthritis is the most common form of rheumatologic IRAE, followed by sicca syndrome. At the Johns Hopkins Arthritis Center, Dr. Bingham and his coworkers have 25 well-characterized patients with inflammatory arthritis resulting from an ICI, only 1 of whom is HLA-B27-positive.
“Also, just one is autoantibody-positive, even though they all look for all the world as though they have rheumatoid arthritis,” the rheumatologist observed.
This ICI-induced inflammatory arthritis initially presents most commonly in the midsize and large joints – knees, ankles, elbows – then expands to include small joints such as the wrists, proximal interphalangeal joints, and the metacarpophalangeal joints.
Notably, the Hopkins group also has three patients with classic reactive arthritis marked by conjunctivitis, urethritis, arthritis, and dactylitis.
“I don’t know about you, but, in our general rheumatology practice, we see maybe one case of reactive arthritis in several years, so this is something that has struck us as really quite interesting,” said Dr. Bingham, who is also director of research in the division of rheumatology at Johns Hopkins.
The arthritis center is also managing a group of patients with ICI-induced sicca syndrome, which is uniformly extremely severe and treatment resistant, as well as a couple of patients with myositis IRAE, one with polymyalgia rheumatica, and two with crystal disease that is highly inflammatory in nature, difficult to treat, and includes an inflammatory polyarthritis component not typical in patients with crystal arthritis.
Why physicians will see more rheumatologic IRAEs
ICIs have dramatically transformed the treatment of selected advanced-stage cancers. For example, whereas patients with metastatic melanoma historically had a 2-year survival rate of 5%, combination therapy with the ICIs ipilimumab (Yervoy) and nivolumab (Opdivo) resulted in a 60% rate of partial or complete remission in a landmark clinical trial.
The basis of cancer immunotherapy is the discovery that, in order for cancer cells to thrive, they emit blocking signals that downregulate the native ability of T cells to recognize and kill them. This is true for both solid tumors and hematologic malignancies. The ICIs inhibit these blocking signals, which include cytotoxic T-lymphocyte–associated protein 4 (CTLA4), programmed death-1 (PD-1), and programmed death ligand-1 (PDL-1), thereby freeing up the T cells for tumor fighting.
Because of the nonspecific mechanism of this T-cell activation, however, ICIs have, as their main toxicities, T-cell–mediated autoimmune inflammatory tissue damage, which gets lumped under the umbrella term IRAEs. It can affect almost every organ system. Skin rashes are the most common, colitis second. Other commonly encountered IRAEs include thyroiditis, hypophysitis, hepatitis, peripheral neuropathy, and pneumonitis.
In addition to the four currently approved ICIs – ipilimumab, nivolumab, pembrolizumab (Keytruda), and atezolizumab (Tecentriq) – investigational ICIs targeting CTLA4, PD-1, and/or PDL-1 are in development. Plus, new ICIs targeting other blocking signals, including lymphocyte activation gene-3, CD137, and T-cell immunoglobulin and mucin domain-3, are now in clinical trials.
Clinical trials aimed at expanding the indications of existing ICIs and using ICIs in earlier-stage cancers in an effort to improve rates of lasting remission are also underway.
All told, probably at least 400 clinical trials of ICIs are ongoing worldwide, the rheumatologist estimated.
“More people will be exposed to these drugs, and we’ll see more and more of these rheumatologic IRAEs,” Dr. Bingham predicted.
Rheumatologic IRAEs are seriously underdiagnosed
Back in the pre-ICI days, Dr. Bingham was coauthor of a major study which concluded that clinical trialists in oncology consistently downgrade the severity of rheumatologic adverse events, often by 1 or 2 grades (J Rheumatol. 2007 Jun;34[6]:1401-14).
Unpublished details of ICI clinical trials in melanoma that he obtained from Bristol-Myers Squibb suggest that the true rate of rheumatologic IRAEs is about 20%, or roughly double that reported in the studies. That’s because the adverse events–grading system used in oncology undercalls the severity of arthritis and autoimmune disorders.
Indeed, the National Cancer Institute’s Common Terminology Criteria for Adverse Events, used in oncology clinical trials, is confusing on the topic of musculoskeletal and connective tissue disorders as treatment-emergent adverse events, according to Dr. Bingham. He noted that an oncologist can code a swollen joint in three different ways – joint effusion, arthritis, or arthralgia – and it takes disabling interference with self-care in activities of daily living for that swollen joint to rise to the level of a Grade 3 adverse event. From a rheumatology trialist’s perspective, that would be a Grade 4 disability.
Plus, neither the product labeling nor the patient information guides for the approved immunotherapy drugs mention the importance of monitoring for rheumatologic IRAEs or their management.
“There is poor awareness of musculoskeletal and rheumatic IRAEs in the general oncology community,” Dr. Bingham asserted. “But, if you talk with any oncology nurses who work in a clinical trial, they will tell you they’re seeing these events with significant frequency and severity.”
Treatment and response
It’s critical to gain control of rheumatologic IRAEs quickly so that patients can get on with their cancer immunotherapy. Dr. Bingham uses intra-articular steroid injections for patients with oligoarthritis and high-dose oral prednisone for polyarticular disease. He starts methotrexate and/or leflunomide early because the conventional disease-modifying antirheumatic drugs have roughly a 2-month delay in onset of action. He has had several patients who are unable to taper steroids despite background methotrexate.
In the most severely affected patients, he has turned to biologic agents in consultation with their oncologists. Tumor necrosis factor (TNF) inhibitors are the ones he and other rheumatologists have used most often.
“Notably, we have not been able to taper down very well. We have patients who are out more than 2 years now who still require their TNF inhibitor to treat their inflammatory arthritis, and these are patients on conventional disease–modifying antirheumatic drugs as well. As soon as it’s tapered, the arthritis begins to come back,” according to Dr. Bingham.
In marked contrast, colitis as an IRAE typically clears in response to just one or two doses of a TNF inhibitor.
One audience member related that she’d encountered a roadblock in trying to get authorization for a TNF inhibitor for a patient with a rheumatologic IRAE secondary to ICI treatment for metastatic melanoma because the labeling states these agents are relatively contraindicated in melanoma patients. Dr. Bingham offered a tip: Collaborate with the patient’s oncologist.
“In most cases, oncologists can get infliximab for these patients and administer it in their infusion centers. They are able to get things authorized with very little trouble,” he said.
Besides, most of these patients with severe inflammatory arthritis meet conventional criteria for TNF inhibitor therapy, based on their number of infected joints and elevated acute phase reactants for longer than 6 weeks, Dr. Bingham noted.
“We’ve had some very interesting conversations with patients. It’s impressive to see the impact arthritis can have on people. A lot of patients have said, ‘I don’t care if I die. Get me functional right now.’ That’s pretty profound. Quality of life is still very important for people, even when dealing with life-threatening diseases,” he observed.
Oncologists are actually eager for their patients to get on steroid-sparing therapy because of concern that high doses of steroids may reduce the efficacy of cancer immunotherapy. That’s not an issue with the TNF inhibitors, the rheumatologist continued.
Turning to the utility of other classes of biologic agents, Dr. Bingham advised avoiding abatacept (Orencia) because its mechanism of action is likely to cause interference with the cancer immunotherapy. Rituximab (Rituxan) takes too long to act. Anakinra (Kineret), tofacitinib (Xeljanz), and tocilizumab (Actemra), on the other hand, are agents he is interested in using as alternatives to TNF inhibitors, although he hasn’t done so yet.
Use of ICIs in patients with preexisting autoimmune disease
The experience here is entirely anecdotal, since such patients have been excluded from ICI clinical trials, but the available evidence suggests physicians should be prepared for higher rheumatologic IRAE rates in this setting. Investigators at Vanderbilt University reported that 8 of 30 cancer patients with known preexisting autoimmune disease experienced flares of that disease when treated with ipilimumab, and 10 developed a new IRAE (Therap Adv Gastroenterol. 2016 Jul;9[4]:457-62).
The Hopkins group has three patients with preexisting rheumatoid arthritis and two with preexisting scleroderma who have received ICIs. All three rheumatoid arthritis patients flared. Rheumatologists are trying to manage these flares so the patients can continue on their ICI. One of the scleroderma patients experienced no change in that disease while on an ICI, while the other showed a definite improvement in scleroderma symptoms.
“I think the jury’s still out in terms of what you do about ICI therapy in patients with preexisting autoimmunity. The data would say that there’s maybe a 50-50 chance of the autoimmune disease becoming worse, but, if patients have an otherwise fatal cancer, I think it’s probably worth the chance,” Dr. Bingham said.
Anecdotal reports suggest that more severe IRAEs may be a favorable prognostic sign in terms of cancer eradication, but a lot more patient experience will be needed in order to be sure, the rheumatologist said.
Dr. Bingham reported serving as a consultant to Bristol-Myers Squibb.
SNOWMASS, COLO. – Physicians can expect to encounter more and more patients with inflammatory arthritis and other rheumatic adverse events induced by immune checkpoint inhibitors as a result of anticipated exponential growth in the use of these drugs to treat an expanding list of cancers, Clifton O. Bingham III, MD, said at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
These cancer immunotherapy–induced rheumatic diseases may superficially look like the classic forms of familiar autoimmune diseases, but they have highly atypical features that will affect treatment decisions.
“What we’ve seen consistently is that the normal doses of prednisone we would use to treat an inflammatory arthritis are really ineffective in most of these patients. We’ve had to use super doses – up to 120 mg/day – for initial control, and then 7.5-40 mg daily for maintenance of response,” according to Dr. Bingham, professor of medicine and director of the Johns Hopkins Arthritis Center in Baltimore.
To date, only limited data from case series are available on rheumatic IRAEs. There are no prospective patient registries logging accurate data on the incidence of these rheumatic adverse events among cancer patients treated with immune checkpoint inhibitors (ICIs). These IRAEs, which lie at the intersection of rheumatology and oncology, are of special interest to Dr. Bingham – he and his coinvestigators have published five articles on the topic over the course of a single year.
In a wide-ranging talk at the symposium, he touched on the phenotypic spectrum of rheumatologic IRAEs, his conviction that they are greatly underdiagnosed, why physicians can expect to encounter them much more frequently, rheumatologic IRAE treatment issues, and the risks of prescribing ICIs in patients with known preexisting rheumatologic disease.
Rheumatologic IRAE presentations
Inflammatory arthritis is the most common form of rheumatologic IRAE, followed by sicca syndrome. At the Johns Hopkins Arthritis Center, Dr. Bingham and his coworkers have 25 well-characterized patients with inflammatory arthritis resulting from an ICI, only 1 of whom is HLA-B27-positive.
“Also, just one is autoantibody-positive, even though they all look for all the world as though they have rheumatoid arthritis,” the rheumatologist observed.
This ICI-induced inflammatory arthritis initially presents most commonly in the midsize and large joints – knees, ankles, elbows – then expands to include small joints such as the wrists, proximal interphalangeal joints, and the metacarpophalangeal joints.
Notably, the Hopkins group also has three patients with classic reactive arthritis marked by conjunctivitis, urethritis, arthritis, and dactylitis.
“I don’t know about you, but, in our general rheumatology practice, we see maybe one case of reactive arthritis in several years, so this is something that has struck us as really quite interesting,” said Dr. Bingham, who is also director of research in the division of rheumatology at Johns Hopkins.
The arthritis center is also managing a group of patients with ICI-induced sicca syndrome, which is uniformly extremely severe and treatment resistant, as well as a couple of patients with myositis IRAE, one with polymyalgia rheumatica, and two with crystal disease that is highly inflammatory in nature, difficult to treat, and includes an inflammatory polyarthritis component not typical in patients with crystal arthritis.
Why physicians will see more rheumatologic IRAEs
ICIs have dramatically transformed the treatment of selected advanced-stage cancers. For example, whereas patients with metastatic melanoma historically had a 2-year survival rate of 5%, combination therapy with the ICIs ipilimumab (Yervoy) and nivolumab (Opdivo) resulted in a 60% rate of partial or complete remission in a landmark clinical trial.
The basis of cancer immunotherapy is the discovery that, in order for cancer cells to thrive, they emit blocking signals that downregulate the native ability of T cells to recognize and kill them. This is true for both solid tumors and hematologic malignancies. The ICIs inhibit these blocking signals, which include cytotoxic T-lymphocyte–associated protein 4 (CTLA4), programmed death-1 (PD-1), and programmed death ligand-1 (PDL-1), thereby freeing up the T cells for tumor fighting.
Because of the nonspecific mechanism of this T-cell activation, however, ICIs have, as their main toxicities, T-cell–mediated autoimmune inflammatory tissue damage, which gets lumped under the umbrella term IRAEs. It can affect almost every organ system. Skin rashes are the most common, colitis second. Other commonly encountered IRAEs include thyroiditis, hypophysitis, hepatitis, peripheral neuropathy, and pneumonitis.
In addition to the four currently approved ICIs – ipilimumab, nivolumab, pembrolizumab (Keytruda), and atezolizumab (Tecentriq) – investigational ICIs targeting CTLA4, PD-1, and/or PDL-1 are in development. Plus, new ICIs targeting other blocking signals, including lymphocyte activation gene-3, CD137, and T-cell immunoglobulin and mucin domain-3, are now in clinical trials.
Clinical trials aimed at expanding the indications of existing ICIs and using ICIs in earlier-stage cancers in an effort to improve rates of lasting remission are also underway.
All told, probably at least 400 clinical trials of ICIs are ongoing worldwide, the rheumatologist estimated.
“More people will be exposed to these drugs, and we’ll see more and more of these rheumatologic IRAEs,” Dr. Bingham predicted.
Rheumatologic IRAEs are seriously underdiagnosed
Back in the pre-ICI days, Dr. Bingham was coauthor of a major study which concluded that clinical trialists in oncology consistently downgrade the severity of rheumatologic adverse events, often by 1 or 2 grades (J Rheumatol. 2007 Jun;34[6]:1401-14).
Unpublished details of ICI clinical trials in melanoma that he obtained from Bristol-Myers Squibb suggest that the true rate of rheumatologic IRAEs is about 20%, or roughly double that reported in the studies. That’s because the adverse events–grading system used in oncology undercalls the severity of arthritis and autoimmune disorders.
Indeed, the National Cancer Institute’s Common Terminology Criteria for Adverse Events, used in oncology clinical trials, is confusing on the topic of musculoskeletal and connective tissue disorders as treatment-emergent adverse events, according to Dr. Bingham. He noted that an oncologist can code a swollen joint in three different ways – joint effusion, arthritis, or arthralgia – and it takes disabling interference with self-care in activities of daily living for that swollen joint to rise to the level of a Grade 3 adverse event. From a rheumatology trialist’s perspective, that would be a Grade 4 disability.
Plus, neither the product labeling nor the patient information guides for the approved immunotherapy drugs mention the importance of monitoring for rheumatologic IRAEs or their management.
“There is poor awareness of musculoskeletal and rheumatic IRAEs in the general oncology community,” Dr. Bingham asserted. “But, if you talk with any oncology nurses who work in a clinical trial, they will tell you they’re seeing these events with significant frequency and severity.”
Treatment and response
It’s critical to gain control of rheumatologic IRAEs quickly so that patients can get on with their cancer immunotherapy. Dr. Bingham uses intra-articular steroid injections for patients with oligoarthritis and high-dose oral prednisone for polyarticular disease. He starts methotrexate and/or leflunomide early because the conventional disease-modifying antirheumatic drugs have roughly a 2-month delay in onset of action. He has had several patients who are unable to taper steroids despite background methotrexate.
In the most severely affected patients, he has turned to biologic agents in consultation with their oncologists. Tumor necrosis factor (TNF) inhibitors are the ones he and other rheumatologists have used most often.
“Notably, we have not been able to taper down very well. We have patients who are out more than 2 years now who still require their TNF inhibitor to treat their inflammatory arthritis, and these are patients on conventional disease–modifying antirheumatic drugs as well. As soon as it’s tapered, the arthritis begins to come back,” according to Dr. Bingham.
In marked contrast, colitis as an IRAE typically clears in response to just one or two doses of a TNF inhibitor.
One audience member related that she’d encountered a roadblock in trying to get authorization for a TNF inhibitor for a patient with a rheumatologic IRAE secondary to ICI treatment for metastatic melanoma because the labeling states these agents are relatively contraindicated in melanoma patients. Dr. Bingham offered a tip: Collaborate with the patient’s oncologist.
“In most cases, oncologists can get infliximab for these patients and administer it in their infusion centers. They are able to get things authorized with very little trouble,” he said.
Besides, most of these patients with severe inflammatory arthritis meet conventional criteria for TNF inhibitor therapy, based on their number of infected joints and elevated acute phase reactants for longer than 6 weeks, Dr. Bingham noted.
“We’ve had some very interesting conversations with patients. It’s impressive to see the impact arthritis can have on people. A lot of patients have said, ‘I don’t care if I die. Get me functional right now.’ That’s pretty profound. Quality of life is still very important for people, even when dealing with life-threatening diseases,” he observed.
Oncologists are actually eager for their patients to get on steroid-sparing therapy because of concern that high doses of steroids may reduce the efficacy of cancer immunotherapy. That’s not an issue with the TNF inhibitors, the rheumatologist continued.
Turning to the utility of other classes of biologic agents, Dr. Bingham advised avoiding abatacept (Orencia) because its mechanism of action is likely to cause interference with the cancer immunotherapy. Rituximab (Rituxan) takes too long to act. Anakinra (Kineret), tofacitinib (Xeljanz), and tocilizumab (Actemra), on the other hand, are agents he is interested in using as alternatives to TNF inhibitors, although he hasn’t done so yet.
Use of ICIs in patients with preexisting autoimmune disease
The experience here is entirely anecdotal, since such patients have been excluded from ICI clinical trials, but the available evidence suggests physicians should be prepared for higher rheumatologic IRAE rates in this setting. Investigators at Vanderbilt University reported that 8 of 30 cancer patients with known preexisting autoimmune disease experienced flares of that disease when treated with ipilimumab, and 10 developed a new IRAE (Therap Adv Gastroenterol. 2016 Jul;9[4]:457-62).
The Hopkins group has three patients with preexisting rheumatoid arthritis and two with preexisting scleroderma who have received ICIs. All three rheumatoid arthritis patients flared. Rheumatologists are trying to manage these flares so the patients can continue on their ICI. One of the scleroderma patients experienced no change in that disease while on an ICI, while the other showed a definite improvement in scleroderma symptoms.
“I think the jury’s still out in terms of what you do about ICI therapy in patients with preexisting autoimmunity. The data would say that there’s maybe a 50-50 chance of the autoimmune disease becoming worse, but, if patients have an otherwise fatal cancer, I think it’s probably worth the chance,” Dr. Bingham said.
Anecdotal reports suggest that more severe IRAEs may be a favorable prognostic sign in terms of cancer eradication, but a lot more patient experience will be needed in order to be sure, the rheumatologist said.
Dr. Bingham reported serving as a consultant to Bristol-Myers Squibb.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
Sacubitril/valsartan enhances glycemic control in diabetic patients with heart failure
Washington – Patients with heart failure with reduced ejection fraction and comorbid diabetes whose heart failure was treated with sacubitril/valsartan experienced significantly enhanced glycemic control in addition to reduced morbidity and mortality due to heart failure in the landmark PARADIGM-HF trial, Jelena P. Seferovic, MD, reported at the annual meeting of the American College of Cardiology.
PARADIGM-HF was a randomized, double-blind clinical trial of oral sacubitril/valsartan, an angiotensin receptor–neprilysin inhibitor, or ARNI, at 97 mg/103 mg twice daily versus enalapril at 10 mg twice daily in 8,442 patients with heart failure with reduced ejection fraction (HFrEF). The primary results, which demonstrated significant reductions in heart failure morbidity and mortality in the sacubitril/valsartan group, have been published (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The findings led to Food and Drug Administration approval of the drug, marketed as Entresto, for HFrEF, as well as a top level Class I recommendation for the drug’s use in the 2016 ACC/AHA heart failure management guidelines.

Dr. Seferovic presented a new post hoc secondary analysis of PARADIGM-HF focused on the 3,778 participants with HFrEF and diabetes. During the first year of study follow-up, hemoglobin A1c decreased by 0.26% from a baseline of 7.44% in the ARNI group, significantly greater than the 0.16% reduction in enalapril-treated controls. This benefit persisted during years 2 and 3.
Moreover, this effect was accompanied by a 29% reduction in new use of insulin in the ARNI group, 7% of whom began insulin therapy during follow-up compared with 10% of controls. Similarly, a 23% reduction in new use of oral antihyperglycemic drugs was seen in the ARNI group, reported Dr. Seferovic of Brigham and Women’s Hospital, Boston.
“Our post hoc study findings should be considered hypothesis-generating, but they suggest that sacubitril/valsartan, which has already been proven to reduce morbidity and mortality in heart failure, might provide additional metabolic benefits in patients with diabetes. Also, our findings suggest that diabetic patients who are treated with sacubitril/valsartan for their heart failure may require dose adjustment of their antihyperglycemic therapy,” she said.
Dr. Seferovic added that this need for dose adjustment is not just a theoretical concern. It actually occurred during the PARADIGM-HF trial.
The impetus for the post hoc analysis was driven in part by animal studies demonstrating that neprilysin inhibition improves insulin sensitivity. Although the mechanism of metabolic benefit for sacubitril/valsartan is not fully understood, it’s known that neprilysin is expressed in adipocytes, cardiac myocytes, smooth muscle cells, and endothelial cells. Neprilysin increases postprandial lipid oxidation, promotes adiponectin release, and boosts the oxidative capacity of muscle. Moreover, neprilysin is responsible for breakdown of natriuretic peptides as well as glucagon-like peptide 1.
“We hypothesize that the beneficial antihyperglycemic effect of sacubitril/valsartan revealed in this analysis is most probably due to the neprilysin inhibition and modulation of its circulating substrates,” said Dr. Seferovic.
One audience member asked Dr. Seferovic if she deemed the 0.14% greater absolute reduction in HbA1c achieved with the ARNI over the course of 3 years to be clinically meaningful. She responded with an emphatic yes.
“We believe any decrease in HbA1c is clinically important,” she declared.
Comorbid diabetes is present in up to 40% of patients with heart failure and has been shown to be a strong independent risk factor for heart failure progression.
Simultaneously with her presentation of the new PARADIGM-HF analysis at ACC 17, the study results were published online in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Gregory Giamouzis, MD, and Javed Butler, MD, cited a handful of reasons why the new findings are important and exciting. For example, polypharmacy has been linked to poor treatment adherence in heart failure, so a drug that can simultaneously improve diabetes and heart failure is attractive. Also, beta blockers and diuretics – cornerstones of heart failure therapy – have been implicated in worsening hyperglycemia.
“Thus, any heart failure therapy that is protective against incident diabetes or worsening glycemic control is a welcome addition,” according to Dr. Giamouzis of the University of Thessaly, Greece, and Dr. Butler of Stony Brook (N.Y.) University.
They added that important unresolved questions include whether sacubitril/valsartan will provide meaningful metabolic benefits in patients with heart failure and comorbid metabolic syndrome, as well as the effects of the ARNI in diabetic patients with heart failure with preserved ejection fraction. The latter issue is the focus of the ongoing major multicenter PARAGON-HF trial.
The PARADIGM-HF trial was sponsored by Novartis. Dr. Seferovic reported having no financial conflicts.
Washington – Patients with heart failure with reduced ejection fraction and comorbid diabetes whose heart failure was treated with sacubitril/valsartan experienced significantly enhanced glycemic control in addition to reduced morbidity and mortality due to heart failure in the landmark PARADIGM-HF trial, Jelena P. Seferovic, MD, reported at the annual meeting of the American College of Cardiology.
PARADIGM-HF was a randomized, double-blind clinical trial of oral sacubitril/valsartan, an angiotensin receptor–neprilysin inhibitor, or ARNI, at 97 mg/103 mg twice daily versus enalapril at 10 mg twice daily in 8,442 patients with heart failure with reduced ejection fraction (HFrEF). The primary results, which demonstrated significant reductions in heart failure morbidity and mortality in the sacubitril/valsartan group, have been published (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The findings led to Food and Drug Administration approval of the drug, marketed as Entresto, for HFrEF, as well as a top level Class I recommendation for the drug’s use in the 2016 ACC/AHA heart failure management guidelines.
Dr. Seferovic presented a new post hoc secondary analysis of PARADIGM-HF focused on the 3,778 participants with HFrEF and diabetes. During the first year of study follow-up, hemoglobin A1c decreased by 0.26% from a baseline of 7.44% in the ARNI group, significantly greater than the 0.16% reduction in enalapril-treated controls. This benefit persisted during years 2 and 3.
Moreover, this effect was accompanied by a 29% reduction in new use of insulin in the ARNI group, 7% of whom began insulin therapy during follow-up compared with 10% of controls. Similarly, a 23% reduction in new use of oral antihyperglycemic drugs was seen in the ARNI group, reported Dr. Seferovic of Brigham and Women’s Hospital, Boston.
“Our post hoc study findings should be considered hypothesis-generating, but they suggest that sacubitril/valsartan, which has already been proven to reduce morbidity and mortality in heart failure, might provide additional metabolic benefits in patients with diabetes. Also, our findings suggest that diabetic patients who are treated with sacubitril/valsartan for their heart failure may require dose adjustment of their antihyperglycemic therapy,” she said.
Dr. Seferovic added that this need for dose adjustment is not just a theoretical concern. It actually occurred during the PARADIGM-HF trial.
The impetus for the post hoc analysis was driven in part by animal studies demonstrating that neprilysin inhibition improves insulin sensitivity. Although the mechanism of metabolic benefit for sacubitril/valsartan is not fully understood, it’s known that neprilysin is expressed in adipocytes, cardiac myocytes, smooth muscle cells, and endothelial cells. Neprilysin increases postprandial lipid oxidation, promotes adiponectin release, and boosts the oxidative capacity of muscle. Moreover, neprilysin is responsible for breakdown of natriuretic peptides as well as glucagon-like peptide 1.
“We hypothesize that the beneficial antihyperglycemic effect of sacubitril/valsartan revealed in this analysis is most probably due to the neprilysin inhibition and modulation of its circulating substrates,” said Dr. Seferovic.
One audience member asked Dr. Seferovic if she deemed the 0.14% greater absolute reduction in HbA1c achieved with the ARNI over the course of 3 years to be clinically meaningful. She responded with an emphatic yes.
“We believe any decrease in HbA1c is clinically important,” she declared.
Comorbid diabetes is present in up to 40% of patients with heart failure and has been shown to be a strong independent risk factor for heart failure progression.
Simultaneously with her presentation of the new PARADIGM-HF analysis at ACC 17, the study results were published online in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Gregory Giamouzis, MD, and Javed Butler, MD, cited a handful of reasons why the new findings are important and exciting. For example, polypharmacy has been linked to poor treatment adherence in heart failure, so a drug that can simultaneously improve diabetes and heart failure is attractive. Also, beta blockers and diuretics – cornerstones of heart failure therapy – have been implicated in worsening hyperglycemia.
“Thus, any heart failure therapy that is protective against incident diabetes or worsening glycemic control is a welcome addition,” according to Dr. Giamouzis of the University of Thessaly, Greece, and Dr. Butler of Stony Brook (N.Y.) University.
They added that important unresolved questions include whether sacubitril/valsartan will provide meaningful metabolic benefits in patients with heart failure and comorbid metabolic syndrome, as well as the effects of the ARNI in diabetic patients with heart failure with preserved ejection fraction. The latter issue is the focus of the ongoing major multicenter PARAGON-HF trial.
The PARADIGM-HF trial was sponsored by Novartis. Dr. Seferovic reported having no financial conflicts.
Washington – Patients with heart failure with reduced ejection fraction and comorbid diabetes whose heart failure was treated with sacubitril/valsartan experienced significantly enhanced glycemic control in addition to reduced morbidity and mortality due to heart failure in the landmark PARADIGM-HF trial, Jelena P. Seferovic, MD, reported at the annual meeting of the American College of Cardiology.
PARADIGM-HF was a randomized, double-blind clinical trial of oral sacubitril/valsartan, an angiotensin receptor–neprilysin inhibitor, or ARNI, at 97 mg/103 mg twice daily versus enalapril at 10 mg twice daily in 8,442 patients with heart failure with reduced ejection fraction (HFrEF). The primary results, which demonstrated significant reductions in heart failure morbidity and mortality in the sacubitril/valsartan group, have been published (N Engl J Med. 2014 Sep 11;371[11]:993-1004). The findings led to Food and Drug Administration approval of the drug, marketed as Entresto, for HFrEF, as well as a top level Class I recommendation for the drug’s use in the 2016 ACC/AHA heart failure management guidelines.
Dr. Seferovic presented a new post hoc secondary analysis of PARADIGM-HF focused on the 3,778 participants with HFrEF and diabetes. During the first year of study follow-up, hemoglobin A1c decreased by 0.26% from a baseline of 7.44% in the ARNI group, significantly greater than the 0.16% reduction in enalapril-treated controls. This benefit persisted during years 2 and 3.
Moreover, this effect was accompanied by a 29% reduction in new use of insulin in the ARNI group, 7% of whom began insulin therapy during follow-up compared with 10% of controls. Similarly, a 23% reduction in new use of oral antihyperglycemic drugs was seen in the ARNI group, reported Dr. Seferovic of Brigham and Women’s Hospital, Boston.
“Our post hoc study findings should be considered hypothesis-generating, but they suggest that sacubitril/valsartan, which has already been proven to reduce morbidity and mortality in heart failure, might provide additional metabolic benefits in patients with diabetes. Also, our findings suggest that diabetic patients who are treated with sacubitril/valsartan for their heart failure may require dose adjustment of their antihyperglycemic therapy,” she said.
Dr. Seferovic added that this need for dose adjustment is not just a theoretical concern. It actually occurred during the PARADIGM-HF trial.
The impetus for the post hoc analysis was driven in part by animal studies demonstrating that neprilysin inhibition improves insulin sensitivity. Although the mechanism of metabolic benefit for sacubitril/valsartan is not fully understood, it’s known that neprilysin is expressed in adipocytes, cardiac myocytes, smooth muscle cells, and endothelial cells. Neprilysin increases postprandial lipid oxidation, promotes adiponectin release, and boosts the oxidative capacity of muscle. Moreover, neprilysin is responsible for breakdown of natriuretic peptides as well as glucagon-like peptide 1.
“We hypothesize that the beneficial antihyperglycemic effect of sacubitril/valsartan revealed in this analysis is most probably due to the neprilysin inhibition and modulation of its circulating substrates,” said Dr. Seferovic.
One audience member asked Dr. Seferovic if she deemed the 0.14% greater absolute reduction in HbA1c achieved with the ARNI over the course of 3 years to be clinically meaningful. She responded with an emphatic yes.
“We believe any decrease in HbA1c is clinically important,” she declared.
Comorbid diabetes is present in up to 40% of patients with heart failure and has been shown to be a strong independent risk factor for heart failure progression.
Simultaneously with her presentation of the new PARADIGM-HF analysis at ACC 17, the study results were published online in The Lancet Diabetes & Endocrinology.
In an accompanying editorial, Gregory Giamouzis, MD, and Javed Butler, MD, cited a handful of reasons why the new findings are important and exciting. For example, polypharmacy has been linked to poor treatment adherence in heart failure, so a drug that can simultaneously improve diabetes and heart failure is attractive. Also, beta blockers and diuretics – cornerstones of heart failure therapy – have been implicated in worsening hyperglycemia.
“Thus, any heart failure therapy that is protective against incident diabetes or worsening glycemic control is a welcome addition,” according to Dr. Giamouzis of the University of Thessaly, Greece, and Dr. Butler of Stony Brook (N.Y.) University.
They added that important unresolved questions include whether sacubitril/valsartan will provide meaningful metabolic benefits in patients with heart failure and comorbid metabolic syndrome, as well as the effects of the ARNI in diabetic patients with heart failure with preserved ejection fraction. The latter issue is the focus of the ongoing major multicenter PARAGON-HF trial.
The PARADIGM-HF trial was sponsored by Novartis. Dr. Seferovic reported having no financial conflicts.
At ACC 17
Key clinical point:
Major finding: Sacubitril/valsartan reduced the need for new use of insulin by 29% in diabetic patients with heart failure with reduced ejection fraction.
Data source: A secondary post hoc analysis of the 3,778 participants in the randomized pivotal PARADIGM-HF trial who had heart failure with reduced ejection fraction and comorbid diabetes.
Disclosures: The PARADIGM-HF trial was sponsored by Novartis. The study presenter reported having no financial conflicts.
Cardiogenic shock: From ECMO to Impella and beyond
A 43-year-old man presented to a community hospital with acute chest pain and shortness of breath and was diagnosed with anterior ST-elevation myocardial infarction. He was a smoker with a history of alcohol abuse, hypertension, and hyperlipidemia, and in the past he had undergone percutaneous coronary interventions to the right coronary artery and the first obtuse marginal artery.
Angiography showed total occlusion in the left anterior descending artery, 90% stenosis in the right coronary artery, and mild disease in the left circumflex artery. A drug-eluting stent was placed in the left anterior descending artery, resulting in good blood flow.
However, his left ventricle continued to have severe dysfunction. An intra-aortic balloon pump was inserted. Afterward, computed tomography showed subsegmental pulmonary embolism with congestion. His mean arterial pressure was 60 mm Hg (normal 70–110), central venous pressure 12 mm Hg (3–8), pulmonary artery pressure 38/26 mm Hg (15–30/4–12), pulmonary capillary wedge pressure 24 mm Hg (2–15), and cardiac index 1.4 L/min (2.5–4).
The patient was started on dobutamine and norepinephrine and transferred to Cleveland Clinic on day 2. Over the next day, he had runs of ventricular tachycardia, for which he was given amiodarone and lidocaine. His urine output was low, and his serum creatinine was elevated at 1.65 mg/dL (baseline 1.2, normal 0.5–1.5). Liver function tests were also elevated, with aspartate aminotransferase at 115 U/L(14–40) and alanine aminotransferase at 187 U/L (10–54).
Poor oxygenation was evident: his arterial partial pressure of oxygen was 64 mm Hg (normal 75–100). He was intubated and given 100% oxygen with positive end-expiratory pressure of 12 cm H2O.
Echocardiography showed a left ventricular ejection fraction of 15% (normal 55%–70%) and mild right ventricular dysfunction.
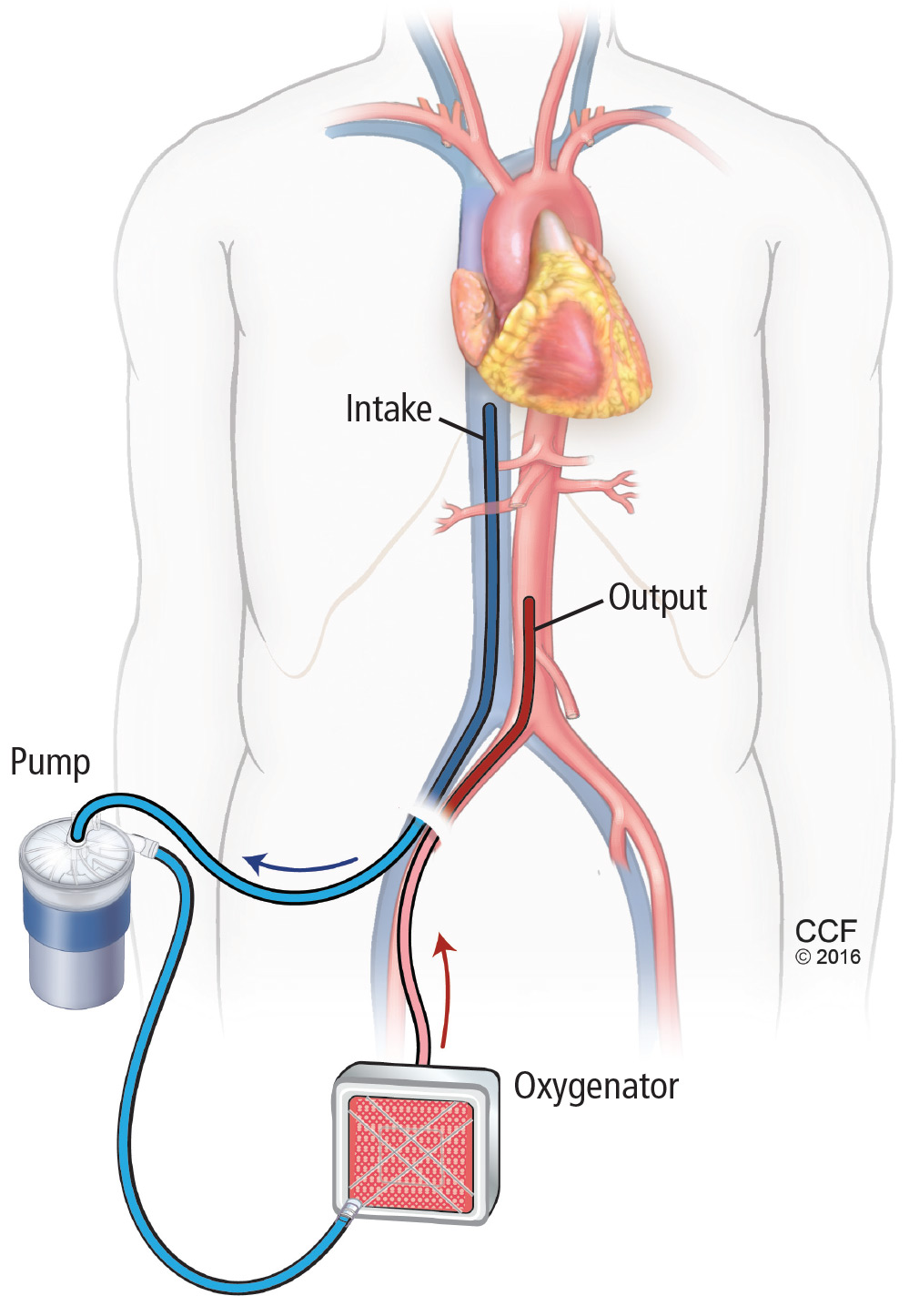
ECMO and then Impella placement
On his third hospital day, a venoarterial extracorporeal membrane oxygenation (ECMO) device was placed peripherally (Figure 1).
His hemodynamic variables stabilized, and he was weaned off dobutamine and norepinephrine. Results of liver function tests normalized, his urinary output increased, and his serum creatinine dropped to a normal 1.0 mg/dL. However, a chest radiograph showed pulmonary congestion, and echocardiography now showed severe left ventricular dysfunction.
On hospital day 5, the patient underwent surgical placement of an Impella 5.0 device (Abiomed, Danvers, MA) through the right axillary artery in an effort to improve his pulmonary edema. The ECMO device was removed. Placement of a venovenous ECMO device was deemed unnecessary when oxygenation improved with the Impella.
Three days after Impella placement, radiography showed improved edema with some remaining pleural effusion.
ACUTE CARDIOGENIC SHOCK
Cardiogenic shock remains a challenging clinical problem: patients with it are among the sickest in the hospital, and many of them die. ECMO was once the only therapy available and is still widely used. However, it is a 2-edged sword; complications such as bleeding, infection, and thrombosis are almost inevitable if it is used for long. Importantly, patients are usually kept intubated and bedridden.
In recent years, new devices have become available that are easier to place (some in the catheterization laboratory or even at the bedside) and allow safer bridging to recovery, transplant, or other therapies.
This case illustrates the natural history of cardiogenic shock and the preferred clinical approach: ie, ongoing evaluation that permits rapid response to evolving challenges.
In general, acute cardiogenic shock occurs within 24 to 48 hours after the initial insult, so even if a procedure succeeds, the patient may develop progressive hypotension and organ dysfunction. Reduced cardiac output causes a downward spiral with multiple systemic and inflammatory processes as well as increased nitric oxide synthesis, leading to progressive decline and eventual end-organ dysfunction.
Continuously evaluate
The cardiac team should continuously assess the acuity and severity of a patient’s condition, with the goals of maintaining end-organ perfusion and identifying the source of problems. Refractory cardiogenic shock, with tissue hypoperfusion despite vasoactive medications and treatment of the underlying cause, is associated with in-hospital mortality rates ranging from 30% to 50%.1,2 The rates have actually increased over the past decade, as sicker patients are being treated.
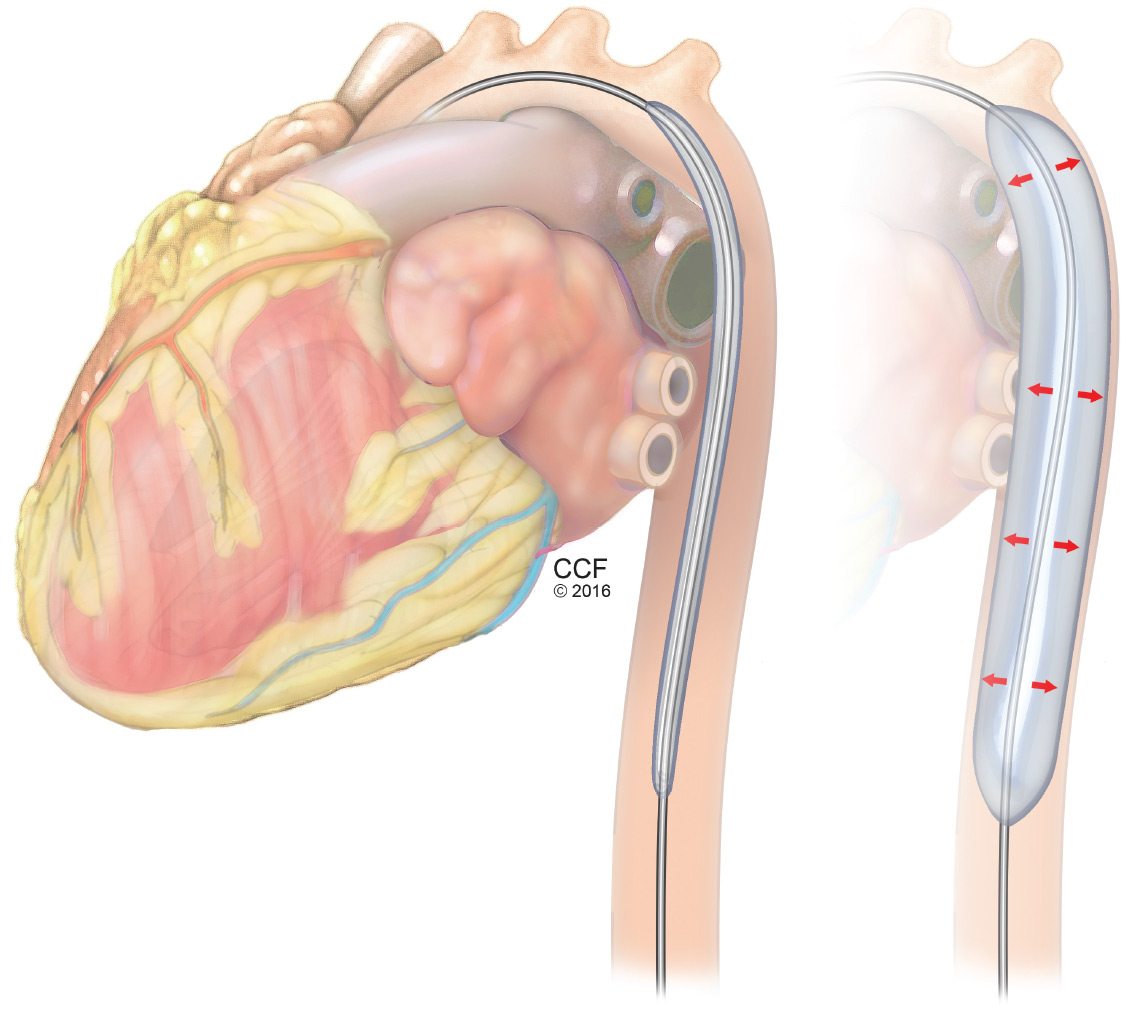
When a patient presents with cardiogenic shock, we first try a series of vasoactive drugs and usually an intra-aortic balloon pump (Figure 2). We then tailor treatment depending on etiology. For example, a patient may have viral myocarditis and may even require a biopsy.
If cardiogenic shock is refractory, mechanical circulatory support devices can be a short-term bridge to either recovery or a new decision. A multidisciplinary team should be consulted to consider transplant, a long-term device, or palliative care. Sometimes a case requires “bridging to a bridge,” with several devices used short-term in turn.
Prognostic factors in cardiogenic shock
Several tools help predict outcome in a severely ill patient. End-organ function, indicated by blood lactate levels and estimated glomerular filtration rate, is perhaps the most informative and should be monitored serially.
CardShock3 is a simple scoring system based on age, mental status at presentation, laboratory values, and medical history. Patients receive 1 point for each of the following factors:
- Age > 75
- Confusion at presentation
- Previous myocardial infarction or coronary artery bypass grafting
- Acute coronary syndrome etiology
- Left ventricular ejection fraction < 40%
- Blood lactate level between 2 and 4 mmol/L, inclusively (2 points for lactate levels > 4 mmol/L)
- Estimated glomerular filtration rate between 30 and 60 mL/min/1.73 m2, inclusively (2 points if < 30 mL/min/1.73 m2).
Thus, scores range from 0 (best) to 9 (worst). A score of 0 to 3 points was associated with a 9% risk of death in the hospital, a score of 4 or 5 with a risk of 36%, and a score of 6 through 9 with a risk of 77%.3
The Survival After Veno-arterial ECMO (SAVE) score (www.save-score.com) is a prediction tool derived from a large international ECMO registry.4 It is based on patient age, diagnosis, and indicators of end-organ dysfunction. Scores range from –35 (worst) to +7 (best).
The mortality rate associated with postcardiotomy cardiogenic shock increases with the amount of inotropic support provided. In a 1996–1999 case series of patients who underwent open-heart surgery,5 the hospital mortality rate was 40% in those who received 2 inotropes in high doses and 80% in those who received 3. A strategy of early implementation of mechanical support is critical.
Selection criteria for destination therapy
Deciding whether a patient should receive a long-term device is frequently a challenge. The decision often must be based on limited information about not only the medical indications but also psychosocial factors that influence long-term success.
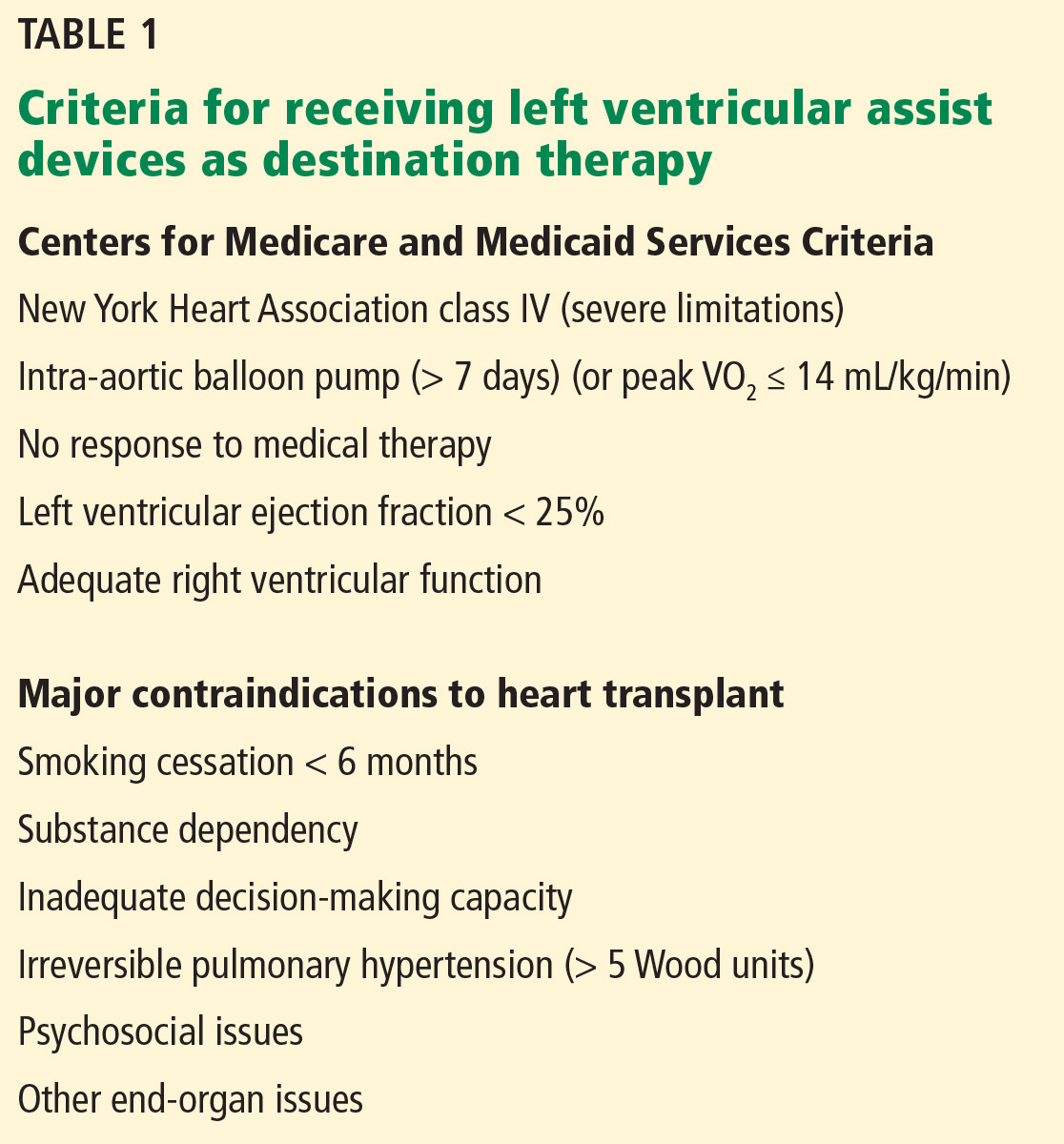
The Centers for Medicare and Medicaid Services have established criteria for candidates for left ventricular assist devices (LVADs) as destination therapy.6 Contraindications established for heart transplant should also be considered (Table 1).
CASE REVISITED
Several factors argued against LVAD placement in our patient. He had no health insurance and had been off medications. He smoked and said he consumed 3 hard liquor drinks per week. His Stanford Integrated Psychosocial Assessment for Transplantation score was 30 (minimally acceptable). He had hypoxia with subsegmental pulmonary edema, a strong contraindication to immediate transplant.
On the other hand, he had only mild right ventricular dysfunction. His CardShock score was 4 (intermediate risk, based on lactate 1.5 mmol/L and estimated glomerular filtration rate 52 mL/min/1.73 m2). His SAVE score was –9 (class IV), which overall is associated with a 30% risk of death (low enough to consider treatment).
During the patient’s time on temporary support, the team had the opportunity to better understand him and assess his family support and his ability to handle a permanent device. His surviving the acute course bolstered the team’s confidence that he could enjoy long-term survival with destination therapy.
CATHETERIZATION LABORATORY DEVICE CAPABILITIES
Although most implantation procedures are done in the operating room, they are often done in the catheterization laboratory because patients undergoing catheterization may not be stable enough for transfer, or an emergency intervention may be required during the night. Catheterization interventionists are also an important part of the team to help determine the best approach for long-term therapy.
The catheterization laboratory has multiple acute intervention options. Usually, decisions must be made quickly. In general, patients needing mechanical support are managed as follows:
- Those who need circulation support and oxygenation receive ECMO
- Those who need circulation support alone because of mechanical issues (eg, myocardial infarction) are considered for an intra-aortic balloon pump, Impella, or TandemHeart pump (Cardiac Assist, Pittsburgh, PA).
Factors that guide the selection of a temporary pump include:
- Left ventricular function
- Right ventricular function
- Aortic valve stenosis (some devices cannot be inserted through critical aortic stenosis)
- Aortic regurgitation (can affect some devices)
- Peripheral artery disease (some devices are large and must be placed percutaneously).
CHOOSING AMONG PERCUTANEOUS DEVICES
Circulatory support in cardiogenic shock improves outcomes, and devices play an important role in supporting high-risk procedures. The goal is not necessarily to use the device throughout the hospital stay. Acute stabilization is most important initially; a more considered decision about long-term therapy can be made when more is known about the patient.
Patient selection is the most important component of success. However, randomized data to support outcomes with the various devices are sparse and complicated by the critically ill state of the patient population.
SHORT-TERM CIRCULATORY SUPPORT: ECMO, IMPELLA, TANDEMHEART
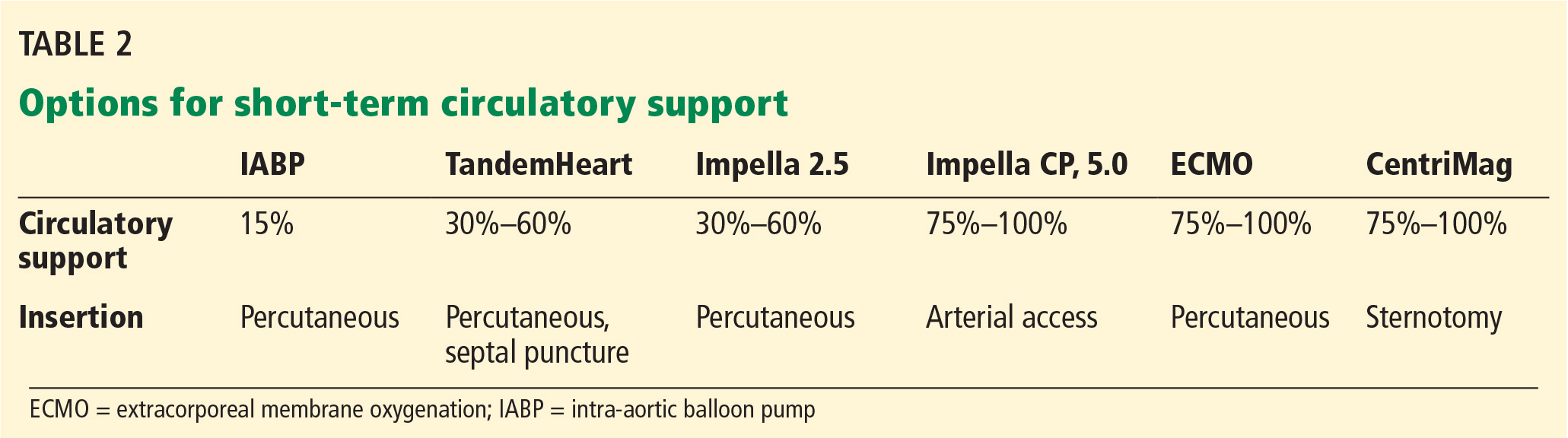
A menu of options is available for temporary mechanical support. Options differ by their degree of circulatory support and ease of insertion (Table 2).
ECMO: A fast option with many advantages
ECMO has evolved and now can be placed quickly. A remote diagnostic platform such as CardioHub permits management at the bedside, in the medical unit, or in the cardiac intensive care unit.7
ECMO has several advantages. It can be used during cardiopulmonary bypass, it provides oxygenation, it is the only option in the setting of lung injury, it can be placed peripherally (without thoracotomy), and it is the only percutaneous option for biventricular support.
ECMO also has significant disadvantages
ECMO is a good device for acute resuscitation of a patient in shock, as it offers quick placement and resuscitation. But it is falling out of favor because of significant disadvantages.
Its major drawback is that it provides no left ventricular unloading. Although in a very unstable patient ECMO can stabilize end organs and restore their function, the lack of left ventricular unloading and reduced ventricular work threaten the myocardium. It creates extremely high afterload; therefore, in a left ventricle with poor function, wall tension and myocardial oxygen demand increase. Multiple studies have shown that coronary perfusion worsens, especially if the patient is cannulated peripherally. Because relative cerebral hypoxia occurs in many situations, it is imperative to check blood saturations at multiple sites to determine if perfusion is adequate everywhere.
Ineffective left ventricular unloading with venoarterial ECMO is managed in several ways. Sometimes left ventricular distention is slight and the effects are subtle. Left ventricular distention causing pulmonary edema can be addressed with:
- Inotropes (in moderate doses)
- Anticoagulation to prevent left ventricular thrombus formation
- An intra-aortic balloon pump. Most patients on ECMO already have an intra-aortic balloon pump in place, and it should be left in to provide additional support. For those who do not have one, it should be placed via the contralateral femoral artery.
If problems persist despite these measures, apical cannulation or left ventricular septostomy can be performed.
Outcomes with ECMO have been disappointing. Studies show that whether ECMO was indicated for cardiac failure or for respiratory failure, survival is only about 25% at 5 years. Analyzing data only for arteriovenous ECMO, survival was 48% in bridged patients and 41% in patients who were weaned.
The Extracorporeal Life Support Organization Registry, in their international summary from 2010, found that 34% of cardiac patients on ECMO survived to discharge or transfer. Most of these patients had cardiogenic shock from acute myocardial infarction. Outcomes are so poor because of complications endemic to ECMO, eg, dialysis-dependent renal failure (about 40%) and neurologic complications (about 30%), often involving ischemic or hemorrhagic stroke.
Limb and pump complications were also significant in the past. These have been reduced with the new reperfusion cannula and the Quadrox oxygenator.
Complications unique to ECMO should be understood and anticipated so that they can be avoided. Better tools are available, ie, Impella and TandemHeart.
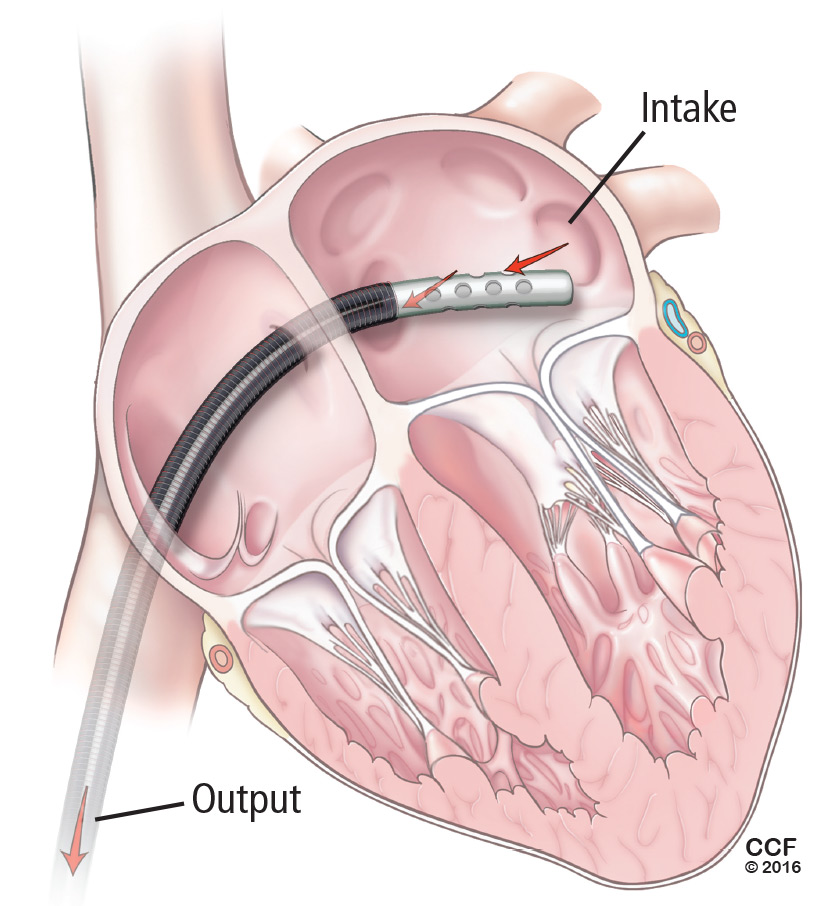
Left-sided Impella: A longer-term temporary support
ECMO is a temporary fix that is usually used only for a few days. If longer support is needed, axillary placement of an Impella should be used as a bridge to recovery, transplant, or a durable LVAD.

The Impella device (Figure 3) is a miniature rotary blood pump increasingly used to treat cardiogenic shock. It is inserted retrograde across the aortic valve to provide short-term ventricular support. Most devices are approved by the US Food and Drug Administration (FDA) for less than 7 days of use, but we have experience using them up to 30 days. They are very hemocompatible, involving minimal hemolysis. Axillary placement allows early extubation and ambulation and is more stable than groin placement.
Several models are available: the 2.5 and 3.5 L/min devices can be placed percutaneously, while the 5 L/min model must be surgically placed in the axillary or groin region. Heparin is required with their use. They can replace ECMO. A right ventricular assist device (RVAD), Impella RP, is also available.
Physiologic impact of the Impella
The Impella fully unloads the left ventricle, reducing myocardial oxygen demand and increasing myocardial blood flow. It reduces end-diastolic volume and pressure, the mechanical work of the heart, and wall tension. Microvascular resistance is reduced, allowing increased coronary flow. Cardiac output and power are increased by multiple means.8–11
The RECOVER 1 trial evaluated the 5L Impella placed after cardiac surgery. The cardiac index increased in all the patients, and the systemic vascular resistance and wedge pressure decreased.12
Unloading the ventricle is critical. Meyns and colleagues13 found a fivefold reduction in infarct size from baseline in a left anterior descending occlusion model in pigs after off-loading the ventricle.
Impella has the advantage of simple percutaneous insertion (the 2.5 and CP models). It also tests right ventricular tolerance: if the right ventricle is doing well, one can predict with high certainty that it will tolerate an LVAD (eg, HeartWare, HeartMate 2 (Pleasanton, CA), or HeartMate 3 when available).
Disadvantages include that it provides only left ventricular support, although a right ventricular device can be inserted for dual support. Placement requires fluoroscopic or echocardiographic guidance.
TandemHeart requires septal puncture
The TandemHeart is approved for short-term and biventricular use. It consists of an extracorporeal centrifugal pump that withdraws blood from the left atrium via a trans-septal cannula placed through the femoral vein (Figure 4) and returns it to one or both femoral arteries. The blood is pumped at up to 5 L/min.
It is designed to reduce the pulmonary capillary wedge pressure, ventricular work, and myocardial oxygen demand and increase cardiac output and mean arterial pressure. It has the advantages of percutaneous placement and the ability to provide biventricular support with 2 devices. It can be used for up to 3 weeks. It can easily be converted to ECMO by either splicing in an oxygenator or adding another cannula.
Although the TandemHeart provides significant support, it is no longer often used. A 21F venous cannula must be passed to the left atrium by trans-septal puncture, which requires advanced skill and must be done in the catheterization laboratory. Insertion can take too much time and cause bleeding in patients taking an anticoagulant. Insertion usually destroys the septum, and removal requires a complete patch of the entire septum. Systemic anticoagulation is required. Other disadvantages are risks of hemolysis, limb ischemia, and infection with longer support times.
The CentriMag (Levitronix LLC; Framingham, MA) is an improved device that requires only 1 cannula instead of 2 to cover both areas.
DEVICES FOR RIGHT-SIDED SUPPORT
Most early devices were designed for left-sided support. The right heart, especially in failure, has been more difficult to manage. Previously the only option for a patient with right ventricular failure was venoarterial ECMO. This is more support than needed for a patient with isolated right ventricular failure and involves the risk of multiple complications from the device.

With more options available for the right heart (Table 3), we can choose the most appropriate device according to the underlying cause of right heart failure (eg, right ventricular infarct, pulmonary hypertension), the likelihood of recovery, and the expected time to recovery.
The ideal RVAD would be easy to implant, maintain, and remove. It would allow for chest closure and patient ambulation. It would be durable and biocompatible, so that it could remain implanted for months if necessary. It would cause little blood trauma, have the capability for adding an oxygenator for pulmonary support, and be cost-effective.
Although no single system has all these qualities, each available device fulfills certain combinations of these criteria, so the best one can be selected for each patient’s needs.
ECMO Rotaflow centrifugal pump: Fast, simple, inexpensive
A recent improvement to ECMO is the Rotaflow centrifugal pump (Maquet, Wayne, NJ), which is connected by sewing an 8-mm graft onto the pulmonary artery and placing a venous cannula in the femoral vein. If the patient is not bleeding, the chest can then be closed. This creates a fast, simple, and inexpensive temporary RVAD system. When the patient is ready to be weaned, the outflow graft can be disconnected at the bedside without reopening the chest.
The disadvantage is that the Rotaflow system contains a sapphire bearing. Although it is magnetically coupled, it generates heat and is a nidus for thrombus formation, which can lead to pump failure and embolization. This system can be used for patients who are expected to need support for less than 5 to 7 days. Beyond this duration, the incidence of complications increases.
CentriMag Ventricular Assist System offers right, left, or bilateral support
The CentriMag Ventricular Assist System is a fully magnetically levitated pump containing no bearings or seals, and with the same technology as is found in many of the durable devices such as HeartMate 3. It is coupled with a reusable motor and is easy to use.
CentriMag offers versatility, allowing for right, left, or bilateral ventricular support. An oxygenator can be added for pulmonary edema and additional support. It is the most biocompatible device and is FDA-approved for use for 4 weeks, although it has been used successfully for much longer. It allows for chest closure and ambulation. It is especially important as a bridge to transplant. The main disadvantage is that insertion and removal require sternotomy.
Impella RP: One size does not fit all
The Impella RP (Figure 5) has an 11F catheter diameter, 23F pump, and a maximum flow rate of more than 4 L/minute. It has a unique 3-dimensional cannula design based on computed tomography 3-dimensional reconstructions from hundreds of patients.

The device is biocompatible and can be used for support for more than 7 days, although most patients require only 3 or 4 days. There is almost no priming volume, so there is no hemodilution.
The disadvantages are that it is more challenging to place than other devices, and some patients cannot use it because the cannula does not fit. It also does not provide pulmonary support. Finally, it is the most expensive of the 3 right-sided devices.
CASE REVISITED
The patient described at the beginning of this article was extubated on day 12 but was then reintubated. On day 20, a tracheotomy tube was placed. By day 24, he had improved so little that his family signed a “do-not-resuscitate–comfort-care-arrest” order (ie, if the patient’s heart or breathing stops, only comfort care is to be provided).
But slowly he got better, and the Impella was removed on day 30. Afterward, serum creatinine and liver function tests began rising again, requiring dobutamine for heart support.
On day 34, his family reversed the do-not-resuscitate order, and he was reevaluated for an LVAD as destination therapy. At this point, echocardiography showed a left ventricular ejection fraction of 10%, normal right ventricular function, with a normal heartbeat and valves. On day 47, a HeartMate II LVAD was placed.
On postoperative day 18, he was transferred out of the intensive care unit, then discharged to an acute rehabilitation facility 8 days later (hospital day 73). He was subsequently discharged.
At a recent follow-up appointment, the patient said that he was feeling “pretty good” and walked with no shortness of breath.
- Reyentovich A, Barghash MH, Hochman JS. Management of refractory cardiogenic shock. Nat Rev Cardiol 2016; 13:481–492.
- Wayangankar SA, Bangalore S, McCoy LA, et al. Temporal trends and outcomes of patients undergoing percutaneous coronary interventions for cardiogenic shock in the setting of acute myocardial infarction: a report from the CathPCI registry. JACC Cardiovasc Interv 2016; 9:341–351.
- Harjola VP, Lassus J, Sionis A, et al; CardShock Study Investigators; GREAT network. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17:501–509.
- Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J 2015; 36:2246–2256.
- Samuels LE, Kaufman MS, Thomas MP, Holmes EC, Brockman SK, Wechsler AS. Pharmacological criteria for ventricular assist device insertion following postcardiotomy shock: experience with the Abiomed BVS system. J Card Surg 1999; 14:288–293.
- Centers for Medicare & Medicaid Services. Decision memo for ventricular assist devices as destination therapy (CAG-00119R2). www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=243&ver=9&NcaName=Ventricular+Assist+Devices+as+Destination+Therapy+(2nd+Recon)&bc=BEAAAAAAEAAA&&fromdb=true. Accessed March 10, 2017.
- Kulkarni T, Sharma NS, Diaz-Guzman E. Extracorporeal membrane oxygenation in adults: a practical guide for internists. Cleve Clin J Med 2016; 83:373–384.
- Remmelink M, Sjauw KD, Henriques JP, et al. Effects of left ventricular unloading by Impella Recover LP2.5 on coronary hemodynamics. Catheter Cardiovasc Interv 2007; 70:532–537.
- Aqel RA, Hage FG, Iskandrian AE. Improvement of myocardial perfusion with a percutaneously inserted left ventricular assist device. J Nucl Cardiol 2010; 17:158–160.
- Sarnoff SJ, Braunwald E, Welch Jr GH, Case RB, Stainsby WN, Macruz R. Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension-time index. Am J Physiol 1957; 192:148–156.
- Braunwald E. 50th anniversary historical article. Myocardial oxygen consumption: the quest for its determinants and some clinical fallout. J Am Coll Cardiol 1999; 34:1365–1368.
- Griffith BP, Anderson MB, Samuels LE, Pae WE Jr, Naka Y, Frazier OH. The RECOVER I: A multicenter prospective study of Impella 5.0/LD for postcardiotomy circulatory support. J Thorac Cardiovasc Surg 2013; 145:548–554
- Meyns B, Stolinski J, Leunens V, Verbeken E, Flameng W. Left ventricular support by cathteter-mounted axial flow pump reduces infarct size. J Am Coll Cardiol 2003; 41:1087–1095.
A 43-year-old man presented to a community hospital with acute chest pain and shortness of breath and was diagnosed with anterior ST-elevation myocardial infarction. He was a smoker with a history of alcohol abuse, hypertension, and hyperlipidemia, and in the past he had undergone percutaneous coronary interventions to the right coronary artery and the first obtuse marginal artery.
Angiography showed total occlusion in the left anterior descending artery, 90% stenosis in the right coronary artery, and mild disease in the left circumflex artery. A drug-eluting stent was placed in the left anterior descending artery, resulting in good blood flow.
However, his left ventricle continued to have severe dysfunction. An intra-aortic balloon pump was inserted. Afterward, computed tomography showed subsegmental pulmonary embolism with congestion. His mean arterial pressure was 60 mm Hg (normal 70–110), central venous pressure 12 mm Hg (3–8), pulmonary artery pressure 38/26 mm Hg (15–30/4–12), pulmonary capillary wedge pressure 24 mm Hg (2–15), and cardiac index 1.4 L/min (2.5–4).
The patient was started on dobutamine and norepinephrine and transferred to Cleveland Clinic on day 2. Over the next day, he had runs of ventricular tachycardia, for which he was given amiodarone and lidocaine. His urine output was low, and his serum creatinine was elevated at 1.65 mg/dL (baseline 1.2, normal 0.5–1.5). Liver function tests were also elevated, with aspartate aminotransferase at 115 U/L(14–40) and alanine aminotransferase at 187 U/L (10–54).
Poor oxygenation was evident: his arterial partial pressure of oxygen was 64 mm Hg (normal 75–100). He was intubated and given 100% oxygen with positive end-expiratory pressure of 12 cm H2O.
Echocardiography showed a left ventricular ejection fraction of 15% (normal 55%–70%) and mild right ventricular dysfunction.
ECMO and then Impella placement
On his third hospital day, a venoarterial extracorporeal membrane oxygenation (ECMO) device was placed peripherally (Figure 1).
His hemodynamic variables stabilized, and he was weaned off dobutamine and norepinephrine. Results of liver function tests normalized, his urinary output increased, and his serum creatinine dropped to a normal 1.0 mg/dL. However, a chest radiograph showed pulmonary congestion, and echocardiography now showed severe left ventricular dysfunction.
On hospital day 5, the patient underwent surgical placement of an Impella 5.0 device (Abiomed, Danvers, MA) through the right axillary artery in an effort to improve his pulmonary edema. The ECMO device was removed. Placement of a venovenous ECMO device was deemed unnecessary when oxygenation improved with the Impella.
Three days after Impella placement, radiography showed improved edema with some remaining pleural effusion.
ACUTE CARDIOGENIC SHOCK
Cardiogenic shock remains a challenging clinical problem: patients with it are among the sickest in the hospital, and many of them die. ECMO was once the only therapy available and is still widely used. However, it is a 2-edged sword; complications such as bleeding, infection, and thrombosis are almost inevitable if it is used for long. Importantly, patients are usually kept intubated and bedridden.
In recent years, new devices have become available that are easier to place (some in the catheterization laboratory or even at the bedside) and allow safer bridging to recovery, transplant, or other therapies.
This case illustrates the natural history of cardiogenic shock and the preferred clinical approach: ie, ongoing evaluation that permits rapid response to evolving challenges.
In general, acute cardiogenic shock occurs within 24 to 48 hours after the initial insult, so even if a procedure succeeds, the patient may develop progressive hypotension and organ dysfunction. Reduced cardiac output causes a downward spiral with multiple systemic and inflammatory processes as well as increased nitric oxide synthesis, leading to progressive decline and eventual end-organ dysfunction.
Continuously evaluate
The cardiac team should continuously assess the acuity and severity of a patient’s condition, with the goals of maintaining end-organ perfusion and identifying the source of problems. Refractory cardiogenic shock, with tissue hypoperfusion despite vasoactive medications and treatment of the underlying cause, is associated with in-hospital mortality rates ranging from 30% to 50%.1,2 The rates have actually increased over the past decade, as sicker patients are being treated.
When a patient presents with cardiogenic shock, we first try a series of vasoactive drugs and usually an intra-aortic balloon pump (Figure 2). We then tailor treatment depending on etiology. For example, a patient may have viral myocarditis and may even require a biopsy.
If cardiogenic shock is refractory, mechanical circulatory support devices can be a short-term bridge to either recovery or a new decision. A multidisciplinary team should be consulted to consider transplant, a long-term device, or palliative care. Sometimes a case requires “bridging to a bridge,” with several devices used short-term in turn.
Prognostic factors in cardiogenic shock
Several tools help predict outcome in a severely ill patient. End-organ function, indicated by blood lactate levels and estimated glomerular filtration rate, is perhaps the most informative and should be monitored serially.
CardShock3 is a simple scoring system based on age, mental status at presentation, laboratory values, and medical history. Patients receive 1 point for each of the following factors:
- Age > 75
- Confusion at presentation
- Previous myocardial infarction or coronary artery bypass grafting
- Acute coronary syndrome etiology
- Left ventricular ejection fraction < 40%
- Blood lactate level between 2 and 4 mmol/L, inclusively (2 points for lactate levels > 4 mmol/L)
- Estimated glomerular filtration rate between 30 and 60 mL/min/1.73 m2, inclusively (2 points if < 30 mL/min/1.73 m2).
Thus, scores range from 0 (best) to 9 (worst). A score of 0 to 3 points was associated with a 9% risk of death in the hospital, a score of 4 or 5 with a risk of 36%, and a score of 6 through 9 with a risk of 77%.3
The Survival After Veno-arterial ECMO (SAVE) score (www.save-score.com) is a prediction tool derived from a large international ECMO registry.4 It is based on patient age, diagnosis, and indicators of end-organ dysfunction. Scores range from –35 (worst) to +7 (best).
The mortality rate associated with postcardiotomy cardiogenic shock increases with the amount of inotropic support provided. In a 1996–1999 case series of patients who underwent open-heart surgery,5 the hospital mortality rate was 40% in those who received 2 inotropes in high doses and 80% in those who received 3. A strategy of early implementation of mechanical support is critical.
Selection criteria for destination therapy
Deciding whether a patient should receive a long-term device is frequently a challenge. The decision often must be based on limited information about not only the medical indications but also psychosocial factors that influence long-term success.
The Centers for Medicare and Medicaid Services have established criteria for candidates for left ventricular assist devices (LVADs) as destination therapy.6 Contraindications established for heart transplant should also be considered (Table 1).
CASE REVISITED
Several factors argued against LVAD placement in our patient. He had no health insurance and had been off medications. He smoked and said he consumed 3 hard liquor drinks per week. His Stanford Integrated Psychosocial Assessment for Transplantation score was 30 (minimally acceptable). He had hypoxia with subsegmental pulmonary edema, a strong contraindication to immediate transplant.
On the other hand, he had only mild right ventricular dysfunction. His CardShock score was 4 (intermediate risk, based on lactate 1.5 mmol/L and estimated glomerular filtration rate 52 mL/min/1.73 m2). His SAVE score was –9 (class IV), which overall is associated with a 30% risk of death (low enough to consider treatment).
During the patient’s time on temporary support, the team had the opportunity to better understand him and assess his family support and his ability to handle a permanent device. His surviving the acute course bolstered the team’s confidence that he could enjoy long-term survival with destination therapy.
CATHETERIZATION LABORATORY DEVICE CAPABILITIES
Although most implantation procedures are done in the operating room, they are often done in the catheterization laboratory because patients undergoing catheterization may not be stable enough for transfer, or an emergency intervention may be required during the night. Catheterization interventionists are also an important part of the team to help determine the best approach for long-term therapy.
The catheterization laboratory has multiple acute intervention options. Usually, decisions must be made quickly. In general, patients needing mechanical support are managed as follows:
- Those who need circulation support and oxygenation receive ECMO
- Those who need circulation support alone because of mechanical issues (eg, myocardial infarction) are considered for an intra-aortic balloon pump, Impella, or TandemHeart pump (Cardiac Assist, Pittsburgh, PA).
Factors that guide the selection of a temporary pump include:
- Left ventricular function
- Right ventricular function
- Aortic valve stenosis (some devices cannot be inserted through critical aortic stenosis)
- Aortic regurgitation (can affect some devices)
- Peripheral artery disease (some devices are large and must be placed percutaneously).
CHOOSING AMONG PERCUTANEOUS DEVICES
Circulatory support in cardiogenic shock improves outcomes, and devices play an important role in supporting high-risk procedures. The goal is not necessarily to use the device throughout the hospital stay. Acute stabilization is most important initially; a more considered decision about long-term therapy can be made when more is known about the patient.
Patient selection is the most important component of success. However, randomized data to support outcomes with the various devices are sparse and complicated by the critically ill state of the patient population.
SHORT-TERM CIRCULATORY SUPPORT: ECMO, IMPELLA, TANDEMHEART
A menu of options is available for temporary mechanical support. Options differ by their degree of circulatory support and ease of insertion (Table 2).
ECMO: A fast option with many advantages
ECMO has evolved and now can be placed quickly. A remote diagnostic platform such as CardioHub permits management at the bedside, in the medical unit, or in the cardiac intensive care unit.7
ECMO has several advantages. It can be used during cardiopulmonary bypass, it provides oxygenation, it is the only option in the setting of lung injury, it can be placed peripherally (without thoracotomy), and it is the only percutaneous option for biventricular support.
ECMO also has significant disadvantages
ECMO is a good device for acute resuscitation of a patient in shock, as it offers quick placement and resuscitation. But it is falling out of favor because of significant disadvantages.
Its major drawback is that it provides no left ventricular unloading. Although in a very unstable patient ECMO can stabilize end organs and restore their function, the lack of left ventricular unloading and reduced ventricular work threaten the myocardium. It creates extremely high afterload; therefore, in a left ventricle with poor function, wall tension and myocardial oxygen demand increase. Multiple studies have shown that coronary perfusion worsens, especially if the patient is cannulated peripherally. Because relative cerebral hypoxia occurs in many situations, it is imperative to check blood saturations at multiple sites to determine if perfusion is adequate everywhere.
Ineffective left ventricular unloading with venoarterial ECMO is managed in several ways. Sometimes left ventricular distention is slight and the effects are subtle. Left ventricular distention causing pulmonary edema can be addressed with:
- Inotropes (in moderate doses)
- Anticoagulation to prevent left ventricular thrombus formation
- An intra-aortic balloon pump. Most patients on ECMO already have an intra-aortic balloon pump in place, and it should be left in to provide additional support. For those who do not have one, it should be placed via the contralateral femoral artery.
If problems persist despite these measures, apical cannulation or left ventricular septostomy can be performed.
Outcomes with ECMO have been disappointing. Studies show that whether ECMO was indicated for cardiac failure or for respiratory failure, survival is only about 25% at 5 years. Analyzing data only for arteriovenous ECMO, survival was 48% in bridged patients and 41% in patients who were weaned.
The Extracorporeal Life Support Organization Registry, in their international summary from 2010, found that 34% of cardiac patients on ECMO survived to discharge or transfer. Most of these patients had cardiogenic shock from acute myocardial infarction. Outcomes are so poor because of complications endemic to ECMO, eg, dialysis-dependent renal failure (about 40%) and neurologic complications (about 30%), often involving ischemic or hemorrhagic stroke.
Limb and pump complications were also significant in the past. These have been reduced with the new reperfusion cannula and the Quadrox oxygenator.
Complications unique to ECMO should be understood and anticipated so that they can be avoided. Better tools are available, ie, Impella and TandemHeart.
Left-sided Impella: A longer-term temporary support
ECMO is a temporary fix that is usually used only for a few days. If longer support is needed, axillary placement of an Impella should be used as a bridge to recovery, transplant, or a durable LVAD.
The Impella device (Figure 3) is a miniature rotary blood pump increasingly used to treat cardiogenic shock. It is inserted retrograde across the aortic valve to provide short-term ventricular support. Most devices are approved by the US Food and Drug Administration (FDA) for less than 7 days of use, but we have experience using them up to 30 days. They are very hemocompatible, involving minimal hemolysis. Axillary placement allows early extubation and ambulation and is more stable than groin placement.
Several models are available: the 2.5 and 3.5 L/min devices can be placed percutaneously, while the 5 L/min model must be surgically placed in the axillary or groin region. Heparin is required with their use. They can replace ECMO. A right ventricular assist device (RVAD), Impella RP, is also available.
Physiologic impact of the Impella
The Impella fully unloads the left ventricle, reducing myocardial oxygen demand and increasing myocardial blood flow. It reduces end-diastolic volume and pressure, the mechanical work of the heart, and wall tension. Microvascular resistance is reduced, allowing increased coronary flow. Cardiac output and power are increased by multiple means.8–11
The RECOVER 1 trial evaluated the 5L Impella placed after cardiac surgery. The cardiac index increased in all the patients, and the systemic vascular resistance and wedge pressure decreased.12
Unloading the ventricle is critical. Meyns and colleagues13 found a fivefold reduction in infarct size from baseline in a left anterior descending occlusion model in pigs after off-loading the ventricle.
Impella has the advantage of simple percutaneous insertion (the 2.5 and CP models). It also tests right ventricular tolerance: if the right ventricle is doing well, one can predict with high certainty that it will tolerate an LVAD (eg, HeartWare, HeartMate 2 (Pleasanton, CA), or HeartMate 3 when available).
Disadvantages include that it provides only left ventricular support, although a right ventricular device can be inserted for dual support. Placement requires fluoroscopic or echocardiographic guidance.
TandemHeart requires septal puncture
The TandemHeart is approved for short-term and biventricular use. It consists of an extracorporeal centrifugal pump that withdraws blood from the left atrium via a trans-septal cannula placed through the femoral vein (Figure 4) and returns it to one or both femoral arteries. The blood is pumped at up to 5 L/min.
It is designed to reduce the pulmonary capillary wedge pressure, ventricular work, and myocardial oxygen demand and increase cardiac output and mean arterial pressure. It has the advantages of percutaneous placement and the ability to provide biventricular support with 2 devices. It can be used for up to 3 weeks. It can easily be converted to ECMO by either splicing in an oxygenator or adding another cannula.
Although the TandemHeart provides significant support, it is no longer often used. A 21F venous cannula must be passed to the left atrium by trans-septal puncture, which requires advanced skill and must be done in the catheterization laboratory. Insertion can take too much time and cause bleeding in patients taking an anticoagulant. Insertion usually destroys the septum, and removal requires a complete patch of the entire septum. Systemic anticoagulation is required. Other disadvantages are risks of hemolysis, limb ischemia, and infection with longer support times.
The CentriMag (Levitronix LLC; Framingham, MA) is an improved device that requires only 1 cannula instead of 2 to cover both areas.
DEVICES FOR RIGHT-SIDED SUPPORT
Most early devices were designed for left-sided support. The right heart, especially in failure, has been more difficult to manage. Previously the only option for a patient with right ventricular failure was venoarterial ECMO. This is more support than needed for a patient with isolated right ventricular failure and involves the risk of multiple complications from the device.
With more options available for the right heart (Table 3), we can choose the most appropriate device according to the underlying cause of right heart failure (eg, right ventricular infarct, pulmonary hypertension), the likelihood of recovery, and the expected time to recovery.
The ideal RVAD would be easy to implant, maintain, and remove. It would allow for chest closure and patient ambulation. It would be durable and biocompatible, so that it could remain implanted for months if necessary. It would cause little blood trauma, have the capability for adding an oxygenator for pulmonary support, and be cost-effective.
Although no single system has all these qualities, each available device fulfills certain combinations of these criteria, so the best one can be selected for each patient’s needs.
ECMO Rotaflow centrifugal pump: Fast, simple, inexpensive
A recent improvement to ECMO is the Rotaflow centrifugal pump (Maquet, Wayne, NJ), which is connected by sewing an 8-mm graft onto the pulmonary artery and placing a venous cannula in the femoral vein. If the patient is not bleeding, the chest can then be closed. This creates a fast, simple, and inexpensive temporary RVAD system. When the patient is ready to be weaned, the outflow graft can be disconnected at the bedside without reopening the chest.
The disadvantage is that the Rotaflow system contains a sapphire bearing. Although it is magnetically coupled, it generates heat and is a nidus for thrombus formation, which can lead to pump failure and embolization. This system can be used for patients who are expected to need support for less than 5 to 7 days. Beyond this duration, the incidence of complications increases.
CentriMag Ventricular Assist System offers right, left, or bilateral support
The CentriMag Ventricular Assist System is a fully magnetically levitated pump containing no bearings or seals, and with the same technology as is found in many of the durable devices such as HeartMate 3. It is coupled with a reusable motor and is easy to use.
CentriMag offers versatility, allowing for right, left, or bilateral ventricular support. An oxygenator can be added for pulmonary edema and additional support. It is the most biocompatible device and is FDA-approved for use for 4 weeks, although it has been used successfully for much longer. It allows for chest closure and ambulation. It is especially important as a bridge to transplant. The main disadvantage is that insertion and removal require sternotomy.
Impella RP: One size does not fit all
The Impella RP (Figure 5) has an 11F catheter diameter, 23F pump, and a maximum flow rate of more than 4 L/minute. It has a unique 3-dimensional cannula design based on computed tomography 3-dimensional reconstructions from hundreds of patients.
The device is biocompatible and can be used for support for more than 7 days, although most patients require only 3 or 4 days. There is almost no priming volume, so there is no hemodilution.
The disadvantages are that it is more challenging to place than other devices, and some patients cannot use it because the cannula does not fit. It also does not provide pulmonary support. Finally, it is the most expensive of the 3 right-sided devices.
CASE REVISITED
The patient described at the beginning of this article was extubated on day 12 but was then reintubated. On day 20, a tracheotomy tube was placed. By day 24, he had improved so little that his family signed a “do-not-resuscitate–comfort-care-arrest” order (ie, if the patient’s heart or breathing stops, only comfort care is to be provided).
But slowly he got better, and the Impella was removed on day 30. Afterward, serum creatinine and liver function tests began rising again, requiring dobutamine for heart support.
On day 34, his family reversed the do-not-resuscitate order, and he was reevaluated for an LVAD as destination therapy. At this point, echocardiography showed a left ventricular ejection fraction of 10%, normal right ventricular function, with a normal heartbeat and valves. On day 47, a HeartMate II LVAD was placed.
On postoperative day 18, he was transferred out of the intensive care unit, then discharged to an acute rehabilitation facility 8 days later (hospital day 73). He was subsequently discharged.
At a recent follow-up appointment, the patient said that he was feeling “pretty good” and walked with no shortness of breath.
A 43-year-old man presented to a community hospital with acute chest pain and shortness of breath and was diagnosed with anterior ST-elevation myocardial infarction. He was a smoker with a history of alcohol abuse, hypertension, and hyperlipidemia, and in the past he had undergone percutaneous coronary interventions to the right coronary artery and the first obtuse marginal artery.
Angiography showed total occlusion in the left anterior descending artery, 90% stenosis in the right coronary artery, and mild disease in the left circumflex artery. A drug-eluting stent was placed in the left anterior descending artery, resulting in good blood flow.
However, his left ventricle continued to have severe dysfunction. An intra-aortic balloon pump was inserted. Afterward, computed tomography showed subsegmental pulmonary embolism with congestion. His mean arterial pressure was 60 mm Hg (normal 70–110), central venous pressure 12 mm Hg (3–8), pulmonary artery pressure 38/26 mm Hg (15–30/4–12), pulmonary capillary wedge pressure 24 mm Hg (2–15), and cardiac index 1.4 L/min (2.5–4).
The patient was started on dobutamine and norepinephrine and transferred to Cleveland Clinic on day 2. Over the next day, he had runs of ventricular tachycardia, for which he was given amiodarone and lidocaine. His urine output was low, and his serum creatinine was elevated at 1.65 mg/dL (baseline 1.2, normal 0.5–1.5). Liver function tests were also elevated, with aspartate aminotransferase at 115 U/L(14–40) and alanine aminotransferase at 187 U/L (10–54).
Poor oxygenation was evident: his arterial partial pressure of oxygen was 64 mm Hg (normal 75–100). He was intubated and given 100% oxygen with positive end-expiratory pressure of 12 cm H2O.
Echocardiography showed a left ventricular ejection fraction of 15% (normal 55%–70%) and mild right ventricular dysfunction.
ECMO and then Impella placement
On his third hospital day, a venoarterial extracorporeal membrane oxygenation (ECMO) device was placed peripherally (Figure 1).
His hemodynamic variables stabilized, and he was weaned off dobutamine and norepinephrine. Results of liver function tests normalized, his urinary output increased, and his serum creatinine dropped to a normal 1.0 mg/dL. However, a chest radiograph showed pulmonary congestion, and echocardiography now showed severe left ventricular dysfunction.
On hospital day 5, the patient underwent surgical placement of an Impella 5.0 device (Abiomed, Danvers, MA) through the right axillary artery in an effort to improve his pulmonary edema. The ECMO device was removed. Placement of a venovenous ECMO device was deemed unnecessary when oxygenation improved with the Impella.
Three days after Impella placement, radiography showed improved edema with some remaining pleural effusion.
ACUTE CARDIOGENIC SHOCK
Cardiogenic shock remains a challenging clinical problem: patients with it are among the sickest in the hospital, and many of them die. ECMO was once the only therapy available and is still widely used. However, it is a 2-edged sword; complications such as bleeding, infection, and thrombosis are almost inevitable if it is used for long. Importantly, patients are usually kept intubated and bedridden.
In recent years, new devices have become available that are easier to place (some in the catheterization laboratory or even at the bedside) and allow safer bridging to recovery, transplant, or other therapies.
This case illustrates the natural history of cardiogenic shock and the preferred clinical approach: ie, ongoing evaluation that permits rapid response to evolving challenges.
In general, acute cardiogenic shock occurs within 24 to 48 hours after the initial insult, so even if a procedure succeeds, the patient may develop progressive hypotension and organ dysfunction. Reduced cardiac output causes a downward spiral with multiple systemic and inflammatory processes as well as increased nitric oxide synthesis, leading to progressive decline and eventual end-organ dysfunction.
Continuously evaluate
The cardiac team should continuously assess the acuity and severity of a patient’s condition, with the goals of maintaining end-organ perfusion and identifying the source of problems. Refractory cardiogenic shock, with tissue hypoperfusion despite vasoactive medications and treatment of the underlying cause, is associated with in-hospital mortality rates ranging from 30% to 50%.1,2 The rates have actually increased over the past decade, as sicker patients are being treated.
When a patient presents with cardiogenic shock, we first try a series of vasoactive drugs and usually an intra-aortic balloon pump (Figure 2). We then tailor treatment depending on etiology. For example, a patient may have viral myocarditis and may even require a biopsy.
If cardiogenic shock is refractory, mechanical circulatory support devices can be a short-term bridge to either recovery or a new decision. A multidisciplinary team should be consulted to consider transplant, a long-term device, or palliative care. Sometimes a case requires “bridging to a bridge,” with several devices used short-term in turn.
Prognostic factors in cardiogenic shock
Several tools help predict outcome in a severely ill patient. End-organ function, indicated by blood lactate levels and estimated glomerular filtration rate, is perhaps the most informative and should be monitored serially.
CardShock3 is a simple scoring system based on age, mental status at presentation, laboratory values, and medical history. Patients receive 1 point for each of the following factors:
- Age > 75
- Confusion at presentation
- Previous myocardial infarction or coronary artery bypass grafting
- Acute coronary syndrome etiology
- Left ventricular ejection fraction < 40%
- Blood lactate level between 2 and 4 mmol/L, inclusively (2 points for lactate levels > 4 mmol/L)
- Estimated glomerular filtration rate between 30 and 60 mL/min/1.73 m2, inclusively (2 points if < 30 mL/min/1.73 m2).
Thus, scores range from 0 (best) to 9 (worst). A score of 0 to 3 points was associated with a 9% risk of death in the hospital, a score of 4 or 5 with a risk of 36%, and a score of 6 through 9 with a risk of 77%.3
The Survival After Veno-arterial ECMO (SAVE) score (www.save-score.com) is a prediction tool derived from a large international ECMO registry.4 It is based on patient age, diagnosis, and indicators of end-organ dysfunction. Scores range from –35 (worst) to +7 (best).
The mortality rate associated with postcardiotomy cardiogenic shock increases with the amount of inotropic support provided. In a 1996–1999 case series of patients who underwent open-heart surgery,5 the hospital mortality rate was 40% in those who received 2 inotropes in high doses and 80% in those who received 3. A strategy of early implementation of mechanical support is critical.
Selection criteria for destination therapy
Deciding whether a patient should receive a long-term device is frequently a challenge. The decision often must be based on limited information about not only the medical indications but also psychosocial factors that influence long-term success.
The Centers for Medicare and Medicaid Services have established criteria for candidates for left ventricular assist devices (LVADs) as destination therapy.6 Contraindications established for heart transplant should also be considered (Table 1).
CASE REVISITED
Several factors argued against LVAD placement in our patient. He had no health insurance and had been off medications. He smoked and said he consumed 3 hard liquor drinks per week. His Stanford Integrated Psychosocial Assessment for Transplantation score was 30 (minimally acceptable). He had hypoxia with subsegmental pulmonary edema, a strong contraindication to immediate transplant.
On the other hand, he had only mild right ventricular dysfunction. His CardShock score was 4 (intermediate risk, based on lactate 1.5 mmol/L and estimated glomerular filtration rate 52 mL/min/1.73 m2). His SAVE score was –9 (class IV), which overall is associated with a 30% risk of death (low enough to consider treatment).
During the patient’s time on temporary support, the team had the opportunity to better understand him and assess his family support and his ability to handle a permanent device. His surviving the acute course bolstered the team’s confidence that he could enjoy long-term survival with destination therapy.
CATHETERIZATION LABORATORY DEVICE CAPABILITIES
Although most implantation procedures are done in the operating room, they are often done in the catheterization laboratory because patients undergoing catheterization may not be stable enough for transfer, or an emergency intervention may be required during the night. Catheterization interventionists are also an important part of the team to help determine the best approach for long-term therapy.
The catheterization laboratory has multiple acute intervention options. Usually, decisions must be made quickly. In general, patients needing mechanical support are managed as follows:
- Those who need circulation support and oxygenation receive ECMO
- Those who need circulation support alone because of mechanical issues (eg, myocardial infarction) are considered for an intra-aortic balloon pump, Impella, or TandemHeart pump (Cardiac Assist, Pittsburgh, PA).
Factors that guide the selection of a temporary pump include:
- Left ventricular function
- Right ventricular function
- Aortic valve stenosis (some devices cannot be inserted through critical aortic stenosis)
- Aortic regurgitation (can affect some devices)
- Peripheral artery disease (some devices are large and must be placed percutaneously).
CHOOSING AMONG PERCUTANEOUS DEVICES
Circulatory support in cardiogenic shock improves outcomes, and devices play an important role in supporting high-risk procedures. The goal is not necessarily to use the device throughout the hospital stay. Acute stabilization is most important initially; a more considered decision about long-term therapy can be made when more is known about the patient.
Patient selection is the most important component of success. However, randomized data to support outcomes with the various devices are sparse and complicated by the critically ill state of the patient population.
SHORT-TERM CIRCULATORY SUPPORT: ECMO, IMPELLA, TANDEMHEART
A menu of options is available for temporary mechanical support. Options differ by their degree of circulatory support and ease of insertion (Table 2).
ECMO: A fast option with many advantages
ECMO has evolved and now can be placed quickly. A remote diagnostic platform such as CardioHub permits management at the bedside, in the medical unit, or in the cardiac intensive care unit.7
ECMO has several advantages. It can be used during cardiopulmonary bypass, it provides oxygenation, it is the only option in the setting of lung injury, it can be placed peripherally (without thoracotomy), and it is the only percutaneous option for biventricular support.
ECMO also has significant disadvantages
ECMO is a good device for acute resuscitation of a patient in shock, as it offers quick placement and resuscitation. But it is falling out of favor because of significant disadvantages.
Its major drawback is that it provides no left ventricular unloading. Although in a very unstable patient ECMO can stabilize end organs and restore their function, the lack of left ventricular unloading and reduced ventricular work threaten the myocardium. It creates extremely high afterload; therefore, in a left ventricle with poor function, wall tension and myocardial oxygen demand increase. Multiple studies have shown that coronary perfusion worsens, especially if the patient is cannulated peripherally. Because relative cerebral hypoxia occurs in many situations, it is imperative to check blood saturations at multiple sites to determine if perfusion is adequate everywhere.
Ineffective left ventricular unloading with venoarterial ECMO is managed in several ways. Sometimes left ventricular distention is slight and the effects are subtle. Left ventricular distention causing pulmonary edema can be addressed with:
- Inotropes (in moderate doses)
- Anticoagulation to prevent left ventricular thrombus formation
- An intra-aortic balloon pump. Most patients on ECMO already have an intra-aortic balloon pump in place, and it should be left in to provide additional support. For those who do not have one, it should be placed via the contralateral femoral artery.
If problems persist despite these measures, apical cannulation or left ventricular septostomy can be performed.
Outcomes with ECMO have been disappointing. Studies show that whether ECMO was indicated for cardiac failure or for respiratory failure, survival is only about 25% at 5 years. Analyzing data only for arteriovenous ECMO, survival was 48% in bridged patients and 41% in patients who were weaned.
The Extracorporeal Life Support Organization Registry, in their international summary from 2010, found that 34% of cardiac patients on ECMO survived to discharge or transfer. Most of these patients had cardiogenic shock from acute myocardial infarction. Outcomes are so poor because of complications endemic to ECMO, eg, dialysis-dependent renal failure (about 40%) and neurologic complications (about 30%), often involving ischemic or hemorrhagic stroke.
Limb and pump complications were also significant in the past. These have been reduced with the new reperfusion cannula and the Quadrox oxygenator.
Complications unique to ECMO should be understood and anticipated so that they can be avoided. Better tools are available, ie, Impella and TandemHeart.
Left-sided Impella: A longer-term temporary support
ECMO is a temporary fix that is usually used only for a few days. If longer support is needed, axillary placement of an Impella should be used as a bridge to recovery, transplant, or a durable LVAD.
The Impella device (Figure 3) is a miniature rotary blood pump increasingly used to treat cardiogenic shock. It is inserted retrograde across the aortic valve to provide short-term ventricular support. Most devices are approved by the US Food and Drug Administration (FDA) for less than 7 days of use, but we have experience using them up to 30 days. They are very hemocompatible, involving minimal hemolysis. Axillary placement allows early extubation and ambulation and is more stable than groin placement.
Several models are available: the 2.5 and 3.5 L/min devices can be placed percutaneously, while the 5 L/min model must be surgically placed in the axillary or groin region. Heparin is required with their use. They can replace ECMO. A right ventricular assist device (RVAD), Impella RP, is also available.
Physiologic impact of the Impella
The Impella fully unloads the left ventricle, reducing myocardial oxygen demand and increasing myocardial blood flow. It reduces end-diastolic volume and pressure, the mechanical work of the heart, and wall tension. Microvascular resistance is reduced, allowing increased coronary flow. Cardiac output and power are increased by multiple means.8–11
The RECOVER 1 trial evaluated the 5L Impella placed after cardiac surgery. The cardiac index increased in all the patients, and the systemic vascular resistance and wedge pressure decreased.12
Unloading the ventricle is critical. Meyns and colleagues13 found a fivefold reduction in infarct size from baseline in a left anterior descending occlusion model in pigs after off-loading the ventricle.
Impella has the advantage of simple percutaneous insertion (the 2.5 and CP models). It also tests right ventricular tolerance: if the right ventricle is doing well, one can predict with high certainty that it will tolerate an LVAD (eg, HeartWare, HeartMate 2 (Pleasanton, CA), or HeartMate 3 when available).
Disadvantages include that it provides only left ventricular support, although a right ventricular device can be inserted for dual support. Placement requires fluoroscopic or echocardiographic guidance.
TandemHeart requires septal puncture
The TandemHeart is approved for short-term and biventricular use. It consists of an extracorporeal centrifugal pump that withdraws blood from the left atrium via a trans-septal cannula placed through the femoral vein (Figure 4) and returns it to one or both femoral arteries. The blood is pumped at up to 5 L/min.
It is designed to reduce the pulmonary capillary wedge pressure, ventricular work, and myocardial oxygen demand and increase cardiac output and mean arterial pressure. It has the advantages of percutaneous placement and the ability to provide biventricular support with 2 devices. It can be used for up to 3 weeks. It can easily be converted to ECMO by either splicing in an oxygenator or adding another cannula.
Although the TandemHeart provides significant support, it is no longer often used. A 21F venous cannula must be passed to the left atrium by trans-septal puncture, which requires advanced skill and must be done in the catheterization laboratory. Insertion can take too much time and cause bleeding in patients taking an anticoagulant. Insertion usually destroys the septum, and removal requires a complete patch of the entire septum. Systemic anticoagulation is required. Other disadvantages are risks of hemolysis, limb ischemia, and infection with longer support times.
The CentriMag (Levitronix LLC; Framingham, MA) is an improved device that requires only 1 cannula instead of 2 to cover both areas.
DEVICES FOR RIGHT-SIDED SUPPORT
Most early devices were designed for left-sided support. The right heart, especially in failure, has been more difficult to manage. Previously the only option for a patient with right ventricular failure was venoarterial ECMO. This is more support than needed for a patient with isolated right ventricular failure and involves the risk of multiple complications from the device.
With more options available for the right heart (Table 3), we can choose the most appropriate device according to the underlying cause of right heart failure (eg, right ventricular infarct, pulmonary hypertension), the likelihood of recovery, and the expected time to recovery.
The ideal RVAD would be easy to implant, maintain, and remove. It would allow for chest closure and patient ambulation. It would be durable and biocompatible, so that it could remain implanted for months if necessary. It would cause little blood trauma, have the capability for adding an oxygenator for pulmonary support, and be cost-effective.
Although no single system has all these qualities, each available device fulfills certain combinations of these criteria, so the best one can be selected for each patient’s needs.
ECMO Rotaflow centrifugal pump: Fast, simple, inexpensive
A recent improvement to ECMO is the Rotaflow centrifugal pump (Maquet, Wayne, NJ), which is connected by sewing an 8-mm graft onto the pulmonary artery and placing a venous cannula in the femoral vein. If the patient is not bleeding, the chest can then be closed. This creates a fast, simple, and inexpensive temporary RVAD system. When the patient is ready to be weaned, the outflow graft can be disconnected at the bedside without reopening the chest.
The disadvantage is that the Rotaflow system contains a sapphire bearing. Although it is magnetically coupled, it generates heat and is a nidus for thrombus formation, which can lead to pump failure and embolization. This system can be used for patients who are expected to need support for less than 5 to 7 days. Beyond this duration, the incidence of complications increases.
CentriMag Ventricular Assist System offers right, left, or bilateral support
The CentriMag Ventricular Assist System is a fully magnetically levitated pump containing no bearings or seals, and with the same technology as is found in many of the durable devices such as HeartMate 3. It is coupled with a reusable motor and is easy to use.
CentriMag offers versatility, allowing for right, left, or bilateral ventricular support. An oxygenator can be added for pulmonary edema and additional support. It is the most biocompatible device and is FDA-approved for use for 4 weeks, although it has been used successfully for much longer. It allows for chest closure and ambulation. It is especially important as a bridge to transplant. The main disadvantage is that insertion and removal require sternotomy.
Impella RP: One size does not fit all
The Impella RP (Figure 5) has an 11F catheter diameter, 23F pump, and a maximum flow rate of more than 4 L/minute. It has a unique 3-dimensional cannula design based on computed tomography 3-dimensional reconstructions from hundreds of patients.
The device is biocompatible and can be used for support for more than 7 days, although most patients require only 3 or 4 days. There is almost no priming volume, so there is no hemodilution.
The disadvantages are that it is more challenging to place than other devices, and some patients cannot use it because the cannula does not fit. It also does not provide pulmonary support. Finally, it is the most expensive of the 3 right-sided devices.
CASE REVISITED
The patient described at the beginning of this article was extubated on day 12 but was then reintubated. On day 20, a tracheotomy tube was placed. By day 24, he had improved so little that his family signed a “do-not-resuscitate–comfort-care-arrest” order (ie, if the patient’s heart or breathing stops, only comfort care is to be provided).
But slowly he got better, and the Impella was removed on day 30. Afterward, serum creatinine and liver function tests began rising again, requiring dobutamine for heart support.
On day 34, his family reversed the do-not-resuscitate order, and he was reevaluated for an LVAD as destination therapy. At this point, echocardiography showed a left ventricular ejection fraction of 10%, normal right ventricular function, with a normal heartbeat and valves. On day 47, a HeartMate II LVAD was placed.
On postoperative day 18, he was transferred out of the intensive care unit, then discharged to an acute rehabilitation facility 8 days later (hospital day 73). He was subsequently discharged.
At a recent follow-up appointment, the patient said that he was feeling “pretty good” and walked with no shortness of breath.
- Reyentovich A, Barghash MH, Hochman JS. Management of refractory cardiogenic shock. Nat Rev Cardiol 2016; 13:481–492.
- Wayangankar SA, Bangalore S, McCoy LA, et al. Temporal trends and outcomes of patients undergoing percutaneous coronary interventions for cardiogenic shock in the setting of acute myocardial infarction: a report from the CathPCI registry. JACC Cardiovasc Interv 2016; 9:341–351.
- Harjola VP, Lassus J, Sionis A, et al; CardShock Study Investigators; GREAT network. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17:501–509.
- Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J 2015; 36:2246–2256.
- Samuels LE, Kaufman MS, Thomas MP, Holmes EC, Brockman SK, Wechsler AS. Pharmacological criteria for ventricular assist device insertion following postcardiotomy shock: experience with the Abiomed BVS system. J Card Surg 1999; 14:288–293.
- Centers for Medicare & Medicaid Services. Decision memo for ventricular assist devices as destination therapy (CAG-00119R2). www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=243&ver=9&NcaName=Ventricular+Assist+Devices+as+Destination+Therapy+(2nd+Recon)&bc=BEAAAAAAEAAA&&fromdb=true. Accessed March 10, 2017.
- Kulkarni T, Sharma NS, Diaz-Guzman E. Extracorporeal membrane oxygenation in adults: a practical guide for internists. Cleve Clin J Med 2016; 83:373–384.
- Remmelink M, Sjauw KD, Henriques JP, et al. Effects of left ventricular unloading by Impella Recover LP2.5 on coronary hemodynamics. Catheter Cardiovasc Interv 2007; 70:532–537.
- Aqel RA, Hage FG, Iskandrian AE. Improvement of myocardial perfusion with a percutaneously inserted left ventricular assist device. J Nucl Cardiol 2010; 17:158–160.
- Sarnoff SJ, Braunwald E, Welch Jr GH, Case RB, Stainsby WN, Macruz R. Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension-time index. Am J Physiol 1957; 192:148–156.
- Braunwald E. 50th anniversary historical article. Myocardial oxygen consumption: the quest for its determinants and some clinical fallout. J Am Coll Cardiol 1999; 34:1365–1368.
- Griffith BP, Anderson MB, Samuels LE, Pae WE Jr, Naka Y, Frazier OH. The RECOVER I: A multicenter prospective study of Impella 5.0/LD for postcardiotomy circulatory support. J Thorac Cardiovasc Surg 2013; 145:548–554
- Meyns B, Stolinski J, Leunens V, Verbeken E, Flameng W. Left ventricular support by cathteter-mounted axial flow pump reduces infarct size. J Am Coll Cardiol 2003; 41:1087–1095.
- Reyentovich A, Barghash MH, Hochman JS. Management of refractory cardiogenic shock. Nat Rev Cardiol 2016; 13:481–492.
- Wayangankar SA, Bangalore S, McCoy LA, et al. Temporal trends and outcomes of patients undergoing percutaneous coronary interventions for cardiogenic shock in the setting of acute myocardial infarction: a report from the CathPCI registry. JACC Cardiovasc Interv 2016; 9:341–351.
- Harjola VP, Lassus J, Sionis A, et al; CardShock Study Investigators; GREAT network. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17:501–509.
- Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J 2015; 36:2246–2256.
- Samuels LE, Kaufman MS, Thomas MP, Holmes EC, Brockman SK, Wechsler AS. Pharmacological criteria for ventricular assist device insertion following postcardiotomy shock: experience with the Abiomed BVS system. J Card Surg 1999; 14:288–293.
- Centers for Medicare & Medicaid Services. Decision memo for ventricular assist devices as destination therapy (CAG-00119R2). www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=243&ver=9&NcaName=Ventricular+Assist+Devices+as+Destination+Therapy+(2nd+Recon)&bc=BEAAAAAAEAAA&&fromdb=true. Accessed March 10, 2017.
- Kulkarni T, Sharma NS, Diaz-Guzman E. Extracorporeal membrane oxygenation in adults: a practical guide for internists. Cleve Clin J Med 2016; 83:373–384.
- Remmelink M, Sjauw KD, Henriques JP, et al. Effects of left ventricular unloading by Impella Recover LP2.5 on coronary hemodynamics. Catheter Cardiovasc Interv 2007; 70:532–537.
- Aqel RA, Hage FG, Iskandrian AE. Improvement of myocardial perfusion with a percutaneously inserted left ventricular assist device. J Nucl Cardiol 2010; 17:158–160.
- Sarnoff SJ, Braunwald E, Welch Jr GH, Case RB, Stainsby WN, Macruz R. Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension-time index. Am J Physiol 1957; 192:148–156.
- Braunwald E. 50th anniversary historical article. Myocardial oxygen consumption: the quest for its determinants and some clinical fallout. J Am Coll Cardiol 1999; 34:1365–1368.
- Griffith BP, Anderson MB, Samuels LE, Pae WE Jr, Naka Y, Frazier OH. The RECOVER I: A multicenter prospective study of Impella 5.0/LD for postcardiotomy circulatory support. J Thorac Cardiovasc Surg 2013; 145:548–554
- Meyns B, Stolinski J, Leunens V, Verbeken E, Flameng W. Left ventricular support by cathteter-mounted axial flow pump reduces infarct size. J Am Coll Cardiol 2003; 41:1087–1095.
KEY POINTS
- ECMO is the fastest way to stabilize a patient in acute cardiogenic shock and prevent end-organ failure, but it should likely be used for a short time and does not reduce the work of (“unload”) the left ventricle.
- An intra-aortic balloon pump may provide diastolic filling in a patient on ECMO.
- The TandemHeart provides significant support, but its insertion requires puncture of the atrial septum.
- The Impella fully unloads the left ventricle, critically reducing the work of the heart.
- Options for right-ventricular support include the ECMO Rotaflow circuit, CentriMag, and Impella RP.
- The CentriMag is the most versatile device, allowing right, left, or biventricular support, but placement requires sternotomy.
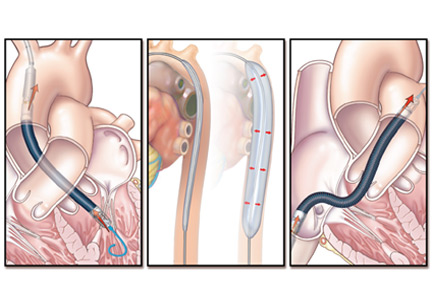
Confusion and hypercalcemia in an 80-year-old man
A retired 80-year-old man presented to the emergency department after 10 days of increasing polydipsia, polyuria, dry mouth, confusion, and slurred speech. He also reported that he had gradually and unintentionally lost 20 pounds and had loss of appetite, constipation, and chronic itching. He denied fevers, chills, night sweats, nausea, vomiting, and abdominal pain.
Medical history. He had type 2 diabetes mellitus that was well controlled by oral hypoglycemics, hypothyroidism treated with levothyroxine in stable doses, and chronic hepatitis C complicated by liver cirrhosis without focal hepatic lesions. He also had hypertension, well controlled with hydrochlorothiazide and losartan. For his long-standing pruritus he had tried prescription drugs including gabapentin and pregabalin without improvement. He had also seen a naturopathic practitioner, who had prescribed supplements that relieved the symptoms.
Examination. The patient was in no acute distress. He appeared thin, with a weight of 140 lb and a body mass index of 21 kg/m2. His temperature was 36.8°C (98.2°F), blood pressure 198/82 mm Hg, heart rate 72 beats per minute, respiratory rate 16 breaths per minute, and oxygen saturation 97%. His skin was without jaundice or rashes. The mucous membranes in the oropharynx were dry.
Neurologic examination revealed mild confusion, dysarthria, and ataxic gait. Sensation to light touch, pinprick, and vibration was intact. Generalized weakness was noted. Cranial nerves II through XII were intact. Deep tendon reflexes were symmetrically globally suppressed. Asterixis was absent. The remainder of the physical examination was unremarkable.
Laboratory values in the emergency department. We initially suspected he had symptomatic hyperglycemia, but a bedside blood glucose value of 113 mg/dL ruled this out. Other initial laboratory values:
- Blood urea nitrogen 31 mg/dL (reference range 9–24)
- Serum creatinine 1.7 mg/dL (0.73–1.22; an earlier value had been 1.0 mg/dL)
- Total serum calcium 14.4 mg/dL (8.6–10.0)
Complete blood cell counts were unremarkable. Computed tomography of the head was negative for acute pathology.

In view of the patient’s hypercalcemia, he was given aggressive intravenous fluid resuscitation (2 L of normal saline over 2 hours) and was admitted to the hospital. His laboratory values on admission are shown in Table 1. Fluid resuscitation was continued while the laboratory results were pending.
CAUSES OF HYPERCALCEMIA
1. Based on this information, which is the most likely cause of this patient’s hypercalcemia?
- Primary hyperparathyroidism
- Malignancy
- Hyperthyroidism
- Hypervitaminosis D
- Sarcoidosis
Traditionally, the workup for hypercalcemia in an outpatient starts with measuring the serum parathyroid hormone (PTH) level. Based on the results, a further evaluation of PTH-mediated vs PTH-independent causes of hypercalcemia would be initiated.
Primary hyperparathyroidism and malignancy account for 90% of all cases of hypercalcemia. The serum PTH concentration is usually high in primary hyperparathyroidism but low in malignancy, which helps distinguish the conditions from each other.1
Primary hyperparathyroidism
In primary hyperparathyroidism, there is overproduction of PTH, most commonly from a parathyroid adenoma, though parathyroid hyperplasia or, more rarely, parathyroid carcinoma can also overproduce the hormone.
PTH increases serum calcium levels through 3 primary mechanisms: increasing bone resorption, increasing intestinal absorption of calcium, and decreasing renal excretion of calcium. It also induces renal phosphorus excretion.
Typically, in primary hyperparathyroidism, the increases in serum calcium are small (with serum levels of total calcium rising to no higher than 11 mg/dL) and often intermittent.2 Our patient had extremely high serum calcium, low PTH, and high phosphorus levels—all of which are inconsistent with primary hyperparathyroidism.
Malignancy
In some solid tumors, the major mechanism of hypercalcemia is secretion of PTH-related peptide (PTHrP) through promotion of osteoclast function and also increased renal absorption of calcium.3 Hematologic malignancies (eg, multiple myeloma) produce osteoclast-activating factors such as RANK ligand, lymphotoxin, and interleukin 6. Direct tumor invasion of bone can cause osteolysis and subsequent hypercalcemia.4 These mechanisms are usually associated with a fall in PTH.
Less commonly, tumors can also increase levels of 1,25-dihydroxyvitamin D or produce PTH independently of the parathyroid gland.5 There have also been reports of severe hypercalcemia from hepatocellular carcinoma due to PTHrP production.6
Our patient is certainly at risk for malignancy, given his long-standing history of hepatitis C and cirrhosis. He also had a mildly elevated alpha fetoprotein level and suppressed PTH. However, his PTHrP level was normal, and ultrasonography done recently to screen for hepatocellular carcinoma (recommended every 6 months by the American Association for the Study of Liver Diseases in high-risk patients) was negative.7
Multiple myeloma screening involves testing with serum protein electrophoresis with immunofixation in combination with either a serum free light chain assay or 24-hour urine protein electrophoresis with immunofixation. This provides a 97% sensitivity.8 In this patient, these tests for multiple myeloma were negative.
Hyperthyroidism
As many as half of all patients with hyperthyroidism have elevated levels of ionized serum calcium.9 Increased osteoclastic activity is the likely mechanism. Hyperthyroid patients have increased levels of serum interleukin 6 and increased sensitivity of bone to this factor. This cytokine induces differentiation of monocytic cells into osteoclast precursors.10 These patients also have normal or low PTH levels.9
Our patient was receiving levothyroxine for hypothyroidism, but there was no evidence that the dosage was too high, as his thyroid-stimulating hormone level was within an acceptable range.
Hypervitaminosis D

Vitamin D precursors arise from the skin and from the diet. These precursors are hydroxylated in the liver and then the kidneys to biologically active 1,25-dihydroxyvitamin D (Figure 1).11 Vitamin D’s primary actions are in the intestines to increase absorption of calcium and in bone to induce osteoclast action. These actions raise the serum calcium level, which in turn lowers the PTH level through negative feedback on the parathyroid gland.
Most vitamin D supplements consist of the inactive precursor cholecalciferol (vitamin D3). To assess the degree of supplementation, 25-hydroxyvitamin D levels, which indicate the size of the body’s vitamin D reservoir, are measured.11,12
Our patient’s 25-hydroxyvitamin D level is extremely elevated, well beyond the 250-ng/mL upper limit that is considered safe.13 His low PTH level, lack of other likely causes, and history of supplement use point toward the diagnosis of hypervitaminosis D.
Sarcoidosis
Up to 10% of patients with sarcoidosis have hypercalcemia that is not mediated by PTH. Hypercalcemia in sarcoidosis has several potential mechanisms, including increased activity of the enzyme 1-alpha hydroxylase with a subsequent increase in physiologically active 1,25-dihydroxyvitamin D3 production.14
Our patient had elevated levels of 25-hydroxyvitamin D, but his biologically active 1,25-dihydroxyvitamin D level remained within the laboratory’s reference range.
LESS LIKELY CAUSES OF HYPERCALCEMIA
2. Which of the following would be least likely to cause hypercalcemia?
- Thiazide diuretics
- Over-the-counter antacid tablets
- Lithium
- Vitamin A supplementation
- Proton pump inhibitors
Thiazide diuretics
This class of drugs is well known to cause hypercalcemia. The most familiar of the mechanisms is a reduction in urinary calcium excretion. There is also an increase in intestinal absorption of dietary calcium. Evidence is increasing that most patients (as many as two-thirds) who develop hypercalcemia while using a thiazide diuretic have subclinical primary hyperparathyroidism that is uncovered with use of the diuretic.
Of importance, the hypercalcemia that thiazide diuretics cause is mild. In a series of 72 patients with thiazide-induced hypercalcemia, the average serum calcium level was 10.7 mg/dL.15
Our patient was receiving a thiazide diuretic but presented with severe hypercalcemia, which is inconsistent with thiazide-induced hypercalcemia.
Over-the-counter antacid tablets
Calcium carbonate, a popular over-the-counter antacid, can cause a milk-alkali syndrome that is defined by ingestion of excessive calcium and alkalotic substances, leading to metabolic alkalosis, hypercalcemia, and renal insufficiency. To induce this syndrome generally requires up to 4 g of calcium intake daily, but even lower levels (1.0 to 1.5 g) are known to cause it.16
Lithium
Lithium is known to cause hypercalcemia. Multiple mechanisms have been proposed, including direct action on renal tubules and the intestines leading to calcium reabsorption and stimulation of PTH release. Interestingly, parathyroid gland hyperplasia has been noted in long-term users of lithium. An often-proposed mechanism is that lithium increases the threshold at which the parathyroid glands slow their production of PTH, making them less sensitive to serum calcium levels.17
Vitamin A supplementation
Multiple case reports have linked hypercalcemia to ingestion of large doses of vitamin A. The mechanism is thought to be increased bone resorption.18.19
Although our patient reported supplement use, he denied taking vitamin A in any form.
Proton pump inhibitors
Proton pump inhibitors are not known to cause hypercalcemia. On the contrary, case reports suggest that prolonged use of proton pump inhibitors is associated with hypocalcemia and hypomagnesemia, although the mechanism is still not fully understood. A low magnesium level is known to reduce PTH secretion and also skeletal responsiveness to PTH, which can lead to profound hypocalcemia.20
CASE CONTINUED
On further questioning, the patient revealed that the supplement prescribed by his naturopathic practitioner contained vitamin D. Although he had been instructed to take 1 tablet weekly, he had begun taking it daily with his other routine medications, resulting in a daily dose in excess of 60,000 IU of cholecalciferol (vitamin D3). The recommended dose is no more than 4,000 IU/day.
The supplement was immediately discontinued. His hydrochlorothiazide was also held due to its known effect of reducing urinary calcium excretion.
INITIAL TREATMENT OF HYPERCALCEMIA
3. Which of the following treatments is not recommended as part of this patient’s initial treatment?
- Bisphosphonates
- Calcitonin
- Intravenous fluids
- Furosemide
Our patient met the criteria for the diagnosis of hypercalcemic crisis, usually defined as an albumin-corrected serum calcium level higher than 14 mg/dL associated with multiorgan dysfunction resulting from the hypercalcemia.21 The mnemonic “stones, bones, abdominal moans, and psychic groans” captures the renal, skeletal, gastrointestinal, and neurologic manifestations.1
Bisphosphonates
Bisphosphonates are analogues of pyrophosphonates, which are normally incorporated into bone. Unlike pyrophosphonates, bisphosphonates inhibit osteoclast function. They are often used to treat hypercalcemia of any cause, although they are currently approved by the US Food and Drug Administration for treating hypercalcemia of malignancy only. As intravenous monotherapy, they are superior to other forms of treatment and are among the first-line agents in management.
Two bisphosphonates shown to be effective in hypercalcemia are zoledronate and pamidronate. Pamidronate begins to lower serum calcium levels within 2 days, with a peak effect at around 6 days.22 However, in studies comparing the 2 drugs, zoledronate has been shown to be more effective in normalizing serum calcium, with the additional benefit of having a much more rapid infusion time.23 Zoledronate is contraindicated in patients with creatinine clearance less than 30 mL/min; however, pamidronate may continue to be used.24
Calcitonin
This hormone inhibits bone resorption and increases excretion of calcium in the kidneys. It is not recommended for use alone because of its short duration of action and tachyphylaxis, but it can be used in combination with other agents, particularly in hypercalcemic crisis.22 It has the most rapid onset (within 2 hours) of the available medications, and when used in combination with bisphosphonates it produces a more substantial and rapid reduction in serum calcium.25,26
In a patient such as ours, with severe hypercalcemia and evidence of neurologic consequences, calcitonin should be used for its rapid and effective action in lowering serum calcium as other interventions take effect.
Intravenous fluids
Like our patient, many patients with significant hypercalcemia have volume depletion as a result of calciuresis-induced polyuria. Many also have nephrogenic diabetes insipidus from the cytotoxic effect of calcium on renal cells, leading to further volume depletion.27
All management approaches call for fluid repletion as an initial step in hypercalcemia. However, for severe hypercalcemia, volume resuscitation alone is unlikely to completely correct the imbalance. In addition to correcting dehydration, giving fluids increases glomerular filtration, allowing for increased secretion of calcium at the distal tubule.28 The recommendation is 2.5 to 4 L of normal saline over the first 24 hours, with continued aggressive hydration until good urine output is established.21
Our patient, in addition to having acute kidney injury thought to be due to prerenal azotemia, appeared to be volume-depleted and was given aggressive intravenous hydration.
Furosemide
Furosemide inhibits calcium reabsorption at the thick ascending loop of Henle, but this effect depends on the glomerular filtration rate. While our patient would likely eventually benefit from furosemide, it should not be considered the first-line therapy, as diuretic use in the setting of volume depletion can cause circulatory collapse.29 A relative contraindication was his presentation with acute kidney injury.
LONG-TERM TREATMENT
4. In the continued management of a patient with vitamin D toxicity with severe hypercalcemia, which of the following provides prolonged benefit?
- Intravenous hydrocortisone
- Fluid repletion
- Pamidronate
- Calcium-restricted diet
Much has been postulated concerning the mechanism of vitamin D intoxication and subsequent hypercalcemia. Studies have shown it is not an increase in dietary calcium absorption that drives the hypercalcemia but rather an increase in bone resorption. As such, bisphosphonates such as pamidronate have been shown to have a dramatic and rapid effect on severe hypercalcemia from vitamin D toxicity. The duration of action varies but is typically between 1 and 2 weeks.22,30
Corticosteroids such as hydrocortisone are also indicated in situations of severe toxicity. They block the action of 1-alpha-hydroxylase, which converts inactive 25-hydroxyvitamin D to the active 1,25-dihydroxyvitamin D. Corticosteroids have also been shown to more directly reduce calcium resorption from bone and intestine in addition to increasing calciuresis.31 A small study in the United Kingdom noted that while bisphosphonates and steroids were equally effective in reducing serum calcium levels, bisphosphonates accomplished this reduction more rapidly, with a time to therapeutic effect of 9 days as opposed to 22 days.
Fluid hydration, though necessary, is unlikely to produce complete correction on its own, as previously discussed.
THE PATIENT RECOVERS
The patient was treated with intravenous fluids over 3 days and received 1 dose of pamidronate. Calcitonin was provided over the first 48 hours after presentation to more rapidly reduce his calcium levels. He was advised to avoid taking the supplements prescribed by his naturopathic practitioner.
On follow-up with an endocrinologist 1 week later, his symptoms had entirely resolved, and his calcium level was 10.5 mg/dL.
TAKE-AWAY POINTS
- A good medication history includes over-the-counter products such as vitamin D supplements, as more and more people are taking them.
- The level of 25-hydroxyvitamin D should be monitored within 3 to 4 months after initiating treatment for vitamin D deficiency.11
- Vitamin D toxicity can have profound consequences, which are usually seen when levels of 25-hydroxyvitamin D rise above 250 ng/mL.13
- The Institute of Medicine recommends that the dosage of vitamin D supplements be no more than 4,000 IU/day and that doses may need to be lowered to account for concurrent use of hypercalcemia-inducing drugs and other vitamin D-containing supplements.32
- Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician 2003; 67:1959–1966.
- al Zahrani A, Levine MA. Primary hyperparathyroidism. Lancet 1997; 349:1233–1238.
- Mundy GR, Edwards JR. PTH-related peptide (PTHrP) in hypercalcemia. J Am Soc Nephrol 2008; 19:672–675.
- Ratcliffe WA, Hutchesson AC, Bundred NJ, Ratcliffe JG. Role of assays for parathyroid-hormone-related protein in investigation of hypercalcaemia. Lancet 1992; 339:164–167.
- Hewison M, Kantorovich V, Liker HR, et al. Vitamin D-mediated hypercalcemia in lymphoma: evidence for hormone production by tumor-adjacent macrophages. J Bone Miner Res 2003; 18:579–582.
- Ghobrial MW, George J, Mannam S, Henien SR. Severe hypercalcemia as an initial presenting manifestation of hepatocellular carcinoma. Can J Gastroenterol 2002; 16:607–609.
- Zhao C, Nguyen MH. Hepatocellular carcinoma screening and surveillance: practice guidelines and real-life practice. J Clin Gastroenterol 2016; 50:120–133.
- Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc 2016; 91:101–119.
- Burman KD, Monchik JM, Earll JM, Wartofsky L. Ionized and total serum calcium and parathyroid hormone in hyperthyroidism. Ann Intern Med 1976; 84:668–671.
- Iqbal AA, Burgess EH, Gallina DL, Nanes MS, Cook CB. Hypercalcemia in hyperthyroidism: patterns of serum calcium, parathyroid hormone, and 1,25-dihydroxyvitamin D3 levels during management of thyrotoxicosis. Endocr Pract 2003; 9:517–521.
- Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357:266–281.
- Wolpowitz D, Gilchrest BA. The vitamin D questions: how much do you need and how should you get it? J Am Acad Dermatol 2006; 54:301–317.
- Jones G. Pharmacokinetics of vitamin D toxicity. Am J Clin Nutr 2008; 88:582S–586S.
- Inui N, Murayama A, Sasaki S, et al. Correlation between 25-hydroxyvitamin D3 1 alpha-hydroxylase gene expression in alveolar macrophages and the activity of sarcoidosis. Am J Med 2001; 110:687–693.
- Wermers RA, Kearns AE, Jenkins GD, Melton LJ 3rd. Incidence and clinical spectrum of thiazide-associated hypercalcemia. Am J Med 2007; 120:911.e9–e15.
- Patel AM, Goldfarb S. Got calcium? Welcome to the calcium-alkali syndrome. J Am Soc Nephrol 2010; 21:1440–1443.
- Shapiro HI, Davis KA. Hypercalcemia and “primary” hyperparathyroidism during lithium therapy. Am J Psychiatry 2015; 172:12–15.
- Farrington K, Miller P, Varghese Z, Baillod RA, Moorhead JF. Vitamin A toxicity and hypercalcaemia in chronic renal failure. Br Med J (Clin Res Ed) 1981; 282:1999–2002.
- Frame B, Jackson CE, Reynolds WA, Umphrey JE. Hypercalcemia and skeletal effects in chronic hypervitaminosis A. Ann Intern Med 1974; 80:44–48.
- Florentin M, Elisaf MS. Proton pump inhibitor-induced hypomagnesemia: a new challenge. World J Nephrol 2012; 1:151–154.
- Ahmad S, Kuraganti G, Steenkamp D. Hypercalcemic crisis: a clinical review. Am J Med 2015; 128:239–245.
- Nussbaum SR, Younger J, Vandepol CJ, et al. Single-dose intravenous therapy with pamidronate for the treatment of hypercalcemia of malignancy: comparison of 30-, 60-, and 90-mg dosages. Am J Med 1993; 95:297–304.
- Major P, Lortholary A, Hon J, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol 2001; 19:558–567.
- Perazella MA, Markowitz GS. Bisphosphonate nephrotoxicity. Kidney Int 2008; 74:1385–1393.
- Bilezikian JP. Management of acute hypercalcemia. N Engl J Med 1992; 326:1196–1203.
- Ralston SH. Medical management of hypercalcaemia. Br J Clin Pharmacol 1992; 34:11–20.
- Garofeanu CG, Weir M, Rosas-Arellano MP, Henson G, Garg AX, Clark WF. Causes of reversible nephrogenic diabetes insipidus: a systematic review. Am J Kidney Dis 2005; 45:626–637.
- Hosking DJ, Cowley A, Bucknall CA. Rehydration in the treatment of severe hypercalcaemia. Q J Med 1981; 50:473–481.
- Suki WN, Yium JJ, Von Minden M, Saller-Hebert C, Eknoyan G, Martinez-Maldonado M. Acute treatment of hypercalcemia with furosemide. N Engl J Med 1970; 283:836–840.
- Selby PL, Davies M, Marks JS, Mawer EB. Vitamin D intoxication causes hypercalcaemia by increased bone resorption which responds to pamidronate. Clin Endocrinol 1995; 43:531–536.
- Davies M, Mawer EB, Freemont AJ. The osteodystrophy of hypervitaminosis D: a metabolic study. Q J Med 1986; 61:911–919.
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al, eds. Dietary reference intakes for calcium and vitamin D. Washington, DC: National Academies Press (US); 2011.
A retired 80-year-old man presented to the emergency department after 10 days of increasing polydipsia, polyuria, dry mouth, confusion, and slurred speech. He also reported that he had gradually and unintentionally lost 20 pounds and had loss of appetite, constipation, and chronic itching. He denied fevers, chills, night sweats, nausea, vomiting, and abdominal pain.
Medical history. He had type 2 diabetes mellitus that was well controlled by oral hypoglycemics, hypothyroidism treated with levothyroxine in stable doses, and chronic hepatitis C complicated by liver cirrhosis without focal hepatic lesions. He also had hypertension, well controlled with hydrochlorothiazide and losartan. For his long-standing pruritus he had tried prescription drugs including gabapentin and pregabalin without improvement. He had also seen a naturopathic practitioner, who had prescribed supplements that relieved the symptoms.
Examination. The patient was in no acute distress. He appeared thin, with a weight of 140 lb and a body mass index of 21 kg/m2. His temperature was 36.8°C (98.2°F), blood pressure 198/82 mm Hg, heart rate 72 beats per minute, respiratory rate 16 breaths per minute, and oxygen saturation 97%. His skin was without jaundice or rashes. The mucous membranes in the oropharynx were dry.
Neurologic examination revealed mild confusion, dysarthria, and ataxic gait. Sensation to light touch, pinprick, and vibration was intact. Generalized weakness was noted. Cranial nerves II through XII were intact. Deep tendon reflexes were symmetrically globally suppressed. Asterixis was absent. The remainder of the physical examination was unremarkable.
Laboratory values in the emergency department. We initially suspected he had symptomatic hyperglycemia, but a bedside blood glucose value of 113 mg/dL ruled this out. Other initial laboratory values:
- Blood urea nitrogen 31 mg/dL (reference range 9–24)
- Serum creatinine 1.7 mg/dL (0.73–1.22; an earlier value had been 1.0 mg/dL)
- Total serum calcium 14.4 mg/dL (8.6–10.0)
Complete blood cell counts were unremarkable. Computed tomography of the head was negative for acute pathology.
In view of the patient’s hypercalcemia, he was given aggressive intravenous fluid resuscitation (2 L of normal saline over 2 hours) and was admitted to the hospital. His laboratory values on admission are shown in Table 1. Fluid resuscitation was continued while the laboratory results were pending.
CAUSES OF HYPERCALCEMIA
1. Based on this information, which is the most likely cause of this patient’s hypercalcemia?
- Primary hyperparathyroidism
- Malignancy
- Hyperthyroidism
- Hypervitaminosis D
- Sarcoidosis
Traditionally, the workup for hypercalcemia in an outpatient starts with measuring the serum parathyroid hormone (PTH) level. Based on the results, a further evaluation of PTH-mediated vs PTH-independent causes of hypercalcemia would be initiated.
Primary hyperparathyroidism and malignancy account for 90% of all cases of hypercalcemia. The serum PTH concentration is usually high in primary hyperparathyroidism but low in malignancy, which helps distinguish the conditions from each other.1
Primary hyperparathyroidism
In primary hyperparathyroidism, there is overproduction of PTH, most commonly from a parathyroid adenoma, though parathyroid hyperplasia or, more rarely, parathyroid carcinoma can also overproduce the hormone.
PTH increases serum calcium levels through 3 primary mechanisms: increasing bone resorption, increasing intestinal absorption of calcium, and decreasing renal excretion of calcium. It also induces renal phosphorus excretion.
Typically, in primary hyperparathyroidism, the increases in serum calcium are small (with serum levels of total calcium rising to no higher than 11 mg/dL) and often intermittent.2 Our patient had extremely high serum calcium, low PTH, and high phosphorus levels—all of which are inconsistent with primary hyperparathyroidism.
Malignancy
In some solid tumors, the major mechanism of hypercalcemia is secretion of PTH-related peptide (PTHrP) through promotion of osteoclast function and also increased renal absorption of calcium.3 Hematologic malignancies (eg, multiple myeloma) produce osteoclast-activating factors such as RANK ligand, lymphotoxin, and interleukin 6. Direct tumor invasion of bone can cause osteolysis and subsequent hypercalcemia.4 These mechanisms are usually associated with a fall in PTH.
Less commonly, tumors can also increase levels of 1,25-dihydroxyvitamin D or produce PTH independently of the parathyroid gland.5 There have also been reports of severe hypercalcemia from hepatocellular carcinoma due to PTHrP production.6
Our patient is certainly at risk for malignancy, given his long-standing history of hepatitis C and cirrhosis. He also had a mildly elevated alpha fetoprotein level and suppressed PTH. However, his PTHrP level was normal, and ultrasonography done recently to screen for hepatocellular carcinoma (recommended every 6 months by the American Association for the Study of Liver Diseases in high-risk patients) was negative.7
Multiple myeloma screening involves testing with serum protein electrophoresis with immunofixation in combination with either a serum free light chain assay or 24-hour urine protein electrophoresis with immunofixation. This provides a 97% sensitivity.8 In this patient, these tests for multiple myeloma were negative.
Hyperthyroidism
As many as half of all patients with hyperthyroidism have elevated levels of ionized serum calcium.9 Increased osteoclastic activity is the likely mechanism. Hyperthyroid patients have increased levels of serum interleukin 6 and increased sensitivity of bone to this factor. This cytokine induces differentiation of monocytic cells into osteoclast precursors.10 These patients also have normal or low PTH levels.9
Our patient was receiving levothyroxine for hypothyroidism, but there was no evidence that the dosage was too high, as his thyroid-stimulating hormone level was within an acceptable range.
Hypervitaminosis D
Vitamin D precursors arise from the skin and from the diet. These precursors are hydroxylated in the liver and then the kidneys to biologically active 1,25-dihydroxyvitamin D (Figure 1).11 Vitamin D’s primary actions are in the intestines to increase absorption of calcium and in bone to induce osteoclast action. These actions raise the serum calcium level, which in turn lowers the PTH level through negative feedback on the parathyroid gland.
Most vitamin D supplements consist of the inactive precursor cholecalciferol (vitamin D3). To assess the degree of supplementation, 25-hydroxyvitamin D levels, which indicate the size of the body’s vitamin D reservoir, are measured.11,12
Our patient’s 25-hydroxyvitamin D level is extremely elevated, well beyond the 250-ng/mL upper limit that is considered safe.13 His low PTH level, lack of other likely causes, and history of supplement use point toward the diagnosis of hypervitaminosis D.
Sarcoidosis
Up to 10% of patients with sarcoidosis have hypercalcemia that is not mediated by PTH. Hypercalcemia in sarcoidosis has several potential mechanisms, including increased activity of the enzyme 1-alpha hydroxylase with a subsequent increase in physiologically active 1,25-dihydroxyvitamin D3 production.14
Our patient had elevated levels of 25-hydroxyvitamin D, but his biologically active 1,25-dihydroxyvitamin D level remained within the laboratory’s reference range.
LESS LIKELY CAUSES OF HYPERCALCEMIA
2. Which of the following would be least likely to cause hypercalcemia?
- Thiazide diuretics
- Over-the-counter antacid tablets
- Lithium
- Vitamin A supplementation
- Proton pump inhibitors
Thiazide diuretics
This class of drugs is well known to cause hypercalcemia. The most familiar of the mechanisms is a reduction in urinary calcium excretion. There is also an increase in intestinal absorption of dietary calcium. Evidence is increasing that most patients (as many as two-thirds) who develop hypercalcemia while using a thiazide diuretic have subclinical primary hyperparathyroidism that is uncovered with use of the diuretic.
Of importance, the hypercalcemia that thiazide diuretics cause is mild. In a series of 72 patients with thiazide-induced hypercalcemia, the average serum calcium level was 10.7 mg/dL.15
Our patient was receiving a thiazide diuretic but presented with severe hypercalcemia, which is inconsistent with thiazide-induced hypercalcemia.
Over-the-counter antacid tablets
Calcium carbonate, a popular over-the-counter antacid, can cause a milk-alkali syndrome that is defined by ingestion of excessive calcium and alkalotic substances, leading to metabolic alkalosis, hypercalcemia, and renal insufficiency. To induce this syndrome generally requires up to 4 g of calcium intake daily, but even lower levels (1.0 to 1.5 g) are known to cause it.16
Lithium
Lithium is known to cause hypercalcemia. Multiple mechanisms have been proposed, including direct action on renal tubules and the intestines leading to calcium reabsorption and stimulation of PTH release. Interestingly, parathyroid gland hyperplasia has been noted in long-term users of lithium. An often-proposed mechanism is that lithium increases the threshold at which the parathyroid glands slow their production of PTH, making them less sensitive to serum calcium levels.17
Vitamin A supplementation
Multiple case reports have linked hypercalcemia to ingestion of large doses of vitamin A. The mechanism is thought to be increased bone resorption.18.19
Although our patient reported supplement use, he denied taking vitamin A in any form.
Proton pump inhibitors
Proton pump inhibitors are not known to cause hypercalcemia. On the contrary, case reports suggest that prolonged use of proton pump inhibitors is associated with hypocalcemia and hypomagnesemia, although the mechanism is still not fully understood. A low magnesium level is known to reduce PTH secretion and also skeletal responsiveness to PTH, which can lead to profound hypocalcemia.20
CASE CONTINUED
On further questioning, the patient revealed that the supplement prescribed by his naturopathic practitioner contained vitamin D. Although he had been instructed to take 1 tablet weekly, he had begun taking it daily with his other routine medications, resulting in a daily dose in excess of 60,000 IU of cholecalciferol (vitamin D3). The recommended dose is no more than 4,000 IU/day.
The supplement was immediately discontinued. His hydrochlorothiazide was also held due to its known effect of reducing urinary calcium excretion.
INITIAL TREATMENT OF HYPERCALCEMIA
3. Which of the following treatments is not recommended as part of this patient’s initial treatment?
- Bisphosphonates
- Calcitonin
- Intravenous fluids
- Furosemide
Our patient met the criteria for the diagnosis of hypercalcemic crisis, usually defined as an albumin-corrected serum calcium level higher than 14 mg/dL associated with multiorgan dysfunction resulting from the hypercalcemia.21 The mnemonic “stones, bones, abdominal moans, and psychic groans” captures the renal, skeletal, gastrointestinal, and neurologic manifestations.1
Bisphosphonates
Bisphosphonates are analogues of pyrophosphonates, which are normally incorporated into bone. Unlike pyrophosphonates, bisphosphonates inhibit osteoclast function. They are often used to treat hypercalcemia of any cause, although they are currently approved by the US Food and Drug Administration for treating hypercalcemia of malignancy only. As intravenous monotherapy, they are superior to other forms of treatment and are among the first-line agents in management.
Two bisphosphonates shown to be effective in hypercalcemia are zoledronate and pamidronate. Pamidronate begins to lower serum calcium levels within 2 days, with a peak effect at around 6 days.22 However, in studies comparing the 2 drugs, zoledronate has been shown to be more effective in normalizing serum calcium, with the additional benefit of having a much more rapid infusion time.23 Zoledronate is contraindicated in patients with creatinine clearance less than 30 mL/min; however, pamidronate may continue to be used.24
Calcitonin
This hormone inhibits bone resorption and increases excretion of calcium in the kidneys. It is not recommended for use alone because of its short duration of action and tachyphylaxis, but it can be used in combination with other agents, particularly in hypercalcemic crisis.22 It has the most rapid onset (within 2 hours) of the available medications, and when used in combination with bisphosphonates it produces a more substantial and rapid reduction in serum calcium.25,26
In a patient such as ours, with severe hypercalcemia and evidence of neurologic consequences, calcitonin should be used for its rapid and effective action in lowering serum calcium as other interventions take effect.
Intravenous fluids
Like our patient, many patients with significant hypercalcemia have volume depletion as a result of calciuresis-induced polyuria. Many also have nephrogenic diabetes insipidus from the cytotoxic effect of calcium on renal cells, leading to further volume depletion.27
All management approaches call for fluid repletion as an initial step in hypercalcemia. However, for severe hypercalcemia, volume resuscitation alone is unlikely to completely correct the imbalance. In addition to correcting dehydration, giving fluids increases glomerular filtration, allowing for increased secretion of calcium at the distal tubule.28 The recommendation is 2.5 to 4 L of normal saline over the first 24 hours, with continued aggressive hydration until good urine output is established.21
Our patient, in addition to having acute kidney injury thought to be due to prerenal azotemia, appeared to be volume-depleted and was given aggressive intravenous hydration.
Furosemide
Furosemide inhibits calcium reabsorption at the thick ascending loop of Henle, but this effect depends on the glomerular filtration rate. While our patient would likely eventually benefit from furosemide, it should not be considered the first-line therapy, as diuretic use in the setting of volume depletion can cause circulatory collapse.29 A relative contraindication was his presentation with acute kidney injury.
LONG-TERM TREATMENT
4. In the continued management of a patient with vitamin D toxicity with severe hypercalcemia, which of the following provides prolonged benefit?
- Intravenous hydrocortisone
- Fluid repletion
- Pamidronate
- Calcium-restricted diet
Much has been postulated concerning the mechanism of vitamin D intoxication and subsequent hypercalcemia. Studies have shown it is not an increase in dietary calcium absorption that drives the hypercalcemia but rather an increase in bone resorption. As such, bisphosphonates such as pamidronate have been shown to have a dramatic and rapid effect on severe hypercalcemia from vitamin D toxicity. The duration of action varies but is typically between 1 and 2 weeks.22,30
Corticosteroids such as hydrocortisone are also indicated in situations of severe toxicity. They block the action of 1-alpha-hydroxylase, which converts inactive 25-hydroxyvitamin D to the active 1,25-dihydroxyvitamin D. Corticosteroids have also been shown to more directly reduce calcium resorption from bone and intestine in addition to increasing calciuresis.31 A small study in the United Kingdom noted that while bisphosphonates and steroids were equally effective in reducing serum calcium levels, bisphosphonates accomplished this reduction more rapidly, with a time to therapeutic effect of 9 days as opposed to 22 days.
Fluid hydration, though necessary, is unlikely to produce complete correction on its own, as previously discussed.
THE PATIENT RECOVERS
The patient was treated with intravenous fluids over 3 days and received 1 dose of pamidronate. Calcitonin was provided over the first 48 hours after presentation to more rapidly reduce his calcium levels. He was advised to avoid taking the supplements prescribed by his naturopathic practitioner.
On follow-up with an endocrinologist 1 week later, his symptoms had entirely resolved, and his calcium level was 10.5 mg/dL.
TAKE-AWAY POINTS
- A good medication history includes over-the-counter products such as vitamin D supplements, as more and more people are taking them.
- The level of 25-hydroxyvitamin D should be monitored within 3 to 4 months after initiating treatment for vitamin D deficiency.11
- Vitamin D toxicity can have profound consequences, which are usually seen when levels of 25-hydroxyvitamin D rise above 250 ng/mL.13
- The Institute of Medicine recommends that the dosage of vitamin D supplements be no more than 4,000 IU/day and that doses may need to be lowered to account for concurrent use of hypercalcemia-inducing drugs and other vitamin D-containing supplements.32
A retired 80-year-old man presented to the emergency department after 10 days of increasing polydipsia, polyuria, dry mouth, confusion, and slurred speech. He also reported that he had gradually and unintentionally lost 20 pounds and had loss of appetite, constipation, and chronic itching. He denied fevers, chills, night sweats, nausea, vomiting, and abdominal pain.
Medical history. He had type 2 diabetes mellitus that was well controlled by oral hypoglycemics, hypothyroidism treated with levothyroxine in stable doses, and chronic hepatitis C complicated by liver cirrhosis without focal hepatic lesions. He also had hypertension, well controlled with hydrochlorothiazide and losartan. For his long-standing pruritus he had tried prescription drugs including gabapentin and pregabalin without improvement. He had also seen a naturopathic practitioner, who had prescribed supplements that relieved the symptoms.
Examination. The patient was in no acute distress. He appeared thin, with a weight of 140 lb and a body mass index of 21 kg/m2. His temperature was 36.8°C (98.2°F), blood pressure 198/82 mm Hg, heart rate 72 beats per minute, respiratory rate 16 breaths per minute, and oxygen saturation 97%. His skin was without jaundice or rashes. The mucous membranes in the oropharynx were dry.
Neurologic examination revealed mild confusion, dysarthria, and ataxic gait. Sensation to light touch, pinprick, and vibration was intact. Generalized weakness was noted. Cranial nerves II through XII were intact. Deep tendon reflexes were symmetrically globally suppressed. Asterixis was absent. The remainder of the physical examination was unremarkable.
Laboratory values in the emergency department. We initially suspected he had symptomatic hyperglycemia, but a bedside blood glucose value of 113 mg/dL ruled this out. Other initial laboratory values:
- Blood urea nitrogen 31 mg/dL (reference range 9–24)
- Serum creatinine 1.7 mg/dL (0.73–1.22; an earlier value had been 1.0 mg/dL)
- Total serum calcium 14.4 mg/dL (8.6–10.0)
Complete blood cell counts were unremarkable. Computed tomography of the head was negative for acute pathology.
In view of the patient’s hypercalcemia, he was given aggressive intravenous fluid resuscitation (2 L of normal saline over 2 hours) and was admitted to the hospital. His laboratory values on admission are shown in Table 1. Fluid resuscitation was continued while the laboratory results were pending.
CAUSES OF HYPERCALCEMIA
1. Based on this information, which is the most likely cause of this patient’s hypercalcemia?
- Primary hyperparathyroidism
- Malignancy
- Hyperthyroidism
- Hypervitaminosis D
- Sarcoidosis
Traditionally, the workup for hypercalcemia in an outpatient starts with measuring the serum parathyroid hormone (PTH) level. Based on the results, a further evaluation of PTH-mediated vs PTH-independent causes of hypercalcemia would be initiated.
Primary hyperparathyroidism and malignancy account for 90% of all cases of hypercalcemia. The serum PTH concentration is usually high in primary hyperparathyroidism but low in malignancy, which helps distinguish the conditions from each other.1
Primary hyperparathyroidism
In primary hyperparathyroidism, there is overproduction of PTH, most commonly from a parathyroid adenoma, though parathyroid hyperplasia or, more rarely, parathyroid carcinoma can also overproduce the hormone.
PTH increases serum calcium levels through 3 primary mechanisms: increasing bone resorption, increasing intestinal absorption of calcium, and decreasing renal excretion of calcium. It also induces renal phosphorus excretion.
Typically, in primary hyperparathyroidism, the increases in serum calcium are small (with serum levels of total calcium rising to no higher than 11 mg/dL) and often intermittent.2 Our patient had extremely high serum calcium, low PTH, and high phosphorus levels—all of which are inconsistent with primary hyperparathyroidism.
Malignancy
In some solid tumors, the major mechanism of hypercalcemia is secretion of PTH-related peptide (PTHrP) through promotion of osteoclast function and also increased renal absorption of calcium.3 Hematologic malignancies (eg, multiple myeloma) produce osteoclast-activating factors such as RANK ligand, lymphotoxin, and interleukin 6. Direct tumor invasion of bone can cause osteolysis and subsequent hypercalcemia.4 These mechanisms are usually associated with a fall in PTH.
Less commonly, tumors can also increase levels of 1,25-dihydroxyvitamin D or produce PTH independently of the parathyroid gland.5 There have also been reports of severe hypercalcemia from hepatocellular carcinoma due to PTHrP production.6
Our patient is certainly at risk for malignancy, given his long-standing history of hepatitis C and cirrhosis. He also had a mildly elevated alpha fetoprotein level and suppressed PTH. However, his PTHrP level was normal, and ultrasonography done recently to screen for hepatocellular carcinoma (recommended every 6 months by the American Association for the Study of Liver Diseases in high-risk patients) was negative.7
Multiple myeloma screening involves testing with serum protein electrophoresis with immunofixation in combination with either a serum free light chain assay or 24-hour urine protein electrophoresis with immunofixation. This provides a 97% sensitivity.8 In this patient, these tests for multiple myeloma were negative.
Hyperthyroidism
As many as half of all patients with hyperthyroidism have elevated levels of ionized serum calcium.9 Increased osteoclastic activity is the likely mechanism. Hyperthyroid patients have increased levels of serum interleukin 6 and increased sensitivity of bone to this factor. This cytokine induces differentiation of monocytic cells into osteoclast precursors.10 These patients also have normal or low PTH levels.9
Our patient was receiving levothyroxine for hypothyroidism, but there was no evidence that the dosage was too high, as his thyroid-stimulating hormone level was within an acceptable range.
Hypervitaminosis D
Vitamin D precursors arise from the skin and from the diet. These precursors are hydroxylated in the liver and then the kidneys to biologically active 1,25-dihydroxyvitamin D (Figure 1).11 Vitamin D’s primary actions are in the intestines to increase absorption of calcium and in bone to induce osteoclast action. These actions raise the serum calcium level, which in turn lowers the PTH level through negative feedback on the parathyroid gland.
Most vitamin D supplements consist of the inactive precursor cholecalciferol (vitamin D3). To assess the degree of supplementation, 25-hydroxyvitamin D levels, which indicate the size of the body’s vitamin D reservoir, are measured.11,12
Our patient’s 25-hydroxyvitamin D level is extremely elevated, well beyond the 250-ng/mL upper limit that is considered safe.13 His low PTH level, lack of other likely causes, and history of supplement use point toward the diagnosis of hypervitaminosis D.
Sarcoidosis
Up to 10% of patients with sarcoidosis have hypercalcemia that is not mediated by PTH. Hypercalcemia in sarcoidosis has several potential mechanisms, including increased activity of the enzyme 1-alpha hydroxylase with a subsequent increase in physiologically active 1,25-dihydroxyvitamin D3 production.14
Our patient had elevated levels of 25-hydroxyvitamin D, but his biologically active 1,25-dihydroxyvitamin D level remained within the laboratory’s reference range.
LESS LIKELY CAUSES OF HYPERCALCEMIA
2. Which of the following would be least likely to cause hypercalcemia?
- Thiazide diuretics
- Over-the-counter antacid tablets
- Lithium
- Vitamin A supplementation
- Proton pump inhibitors
Thiazide diuretics
This class of drugs is well known to cause hypercalcemia. The most familiar of the mechanisms is a reduction in urinary calcium excretion. There is also an increase in intestinal absorption of dietary calcium. Evidence is increasing that most patients (as many as two-thirds) who develop hypercalcemia while using a thiazide diuretic have subclinical primary hyperparathyroidism that is uncovered with use of the diuretic.
Of importance, the hypercalcemia that thiazide diuretics cause is mild. In a series of 72 patients with thiazide-induced hypercalcemia, the average serum calcium level was 10.7 mg/dL.15
Our patient was receiving a thiazide diuretic but presented with severe hypercalcemia, which is inconsistent with thiazide-induced hypercalcemia.
Over-the-counter antacid tablets
Calcium carbonate, a popular over-the-counter antacid, can cause a milk-alkali syndrome that is defined by ingestion of excessive calcium and alkalotic substances, leading to metabolic alkalosis, hypercalcemia, and renal insufficiency. To induce this syndrome generally requires up to 4 g of calcium intake daily, but even lower levels (1.0 to 1.5 g) are known to cause it.16
Lithium
Lithium is known to cause hypercalcemia. Multiple mechanisms have been proposed, including direct action on renal tubules and the intestines leading to calcium reabsorption and stimulation of PTH release. Interestingly, parathyroid gland hyperplasia has been noted in long-term users of lithium. An often-proposed mechanism is that lithium increases the threshold at which the parathyroid glands slow their production of PTH, making them less sensitive to serum calcium levels.17
Vitamin A supplementation
Multiple case reports have linked hypercalcemia to ingestion of large doses of vitamin A. The mechanism is thought to be increased bone resorption.18.19
Although our patient reported supplement use, he denied taking vitamin A in any form.
Proton pump inhibitors
Proton pump inhibitors are not known to cause hypercalcemia. On the contrary, case reports suggest that prolonged use of proton pump inhibitors is associated with hypocalcemia and hypomagnesemia, although the mechanism is still not fully understood. A low magnesium level is known to reduce PTH secretion and also skeletal responsiveness to PTH, which can lead to profound hypocalcemia.20
CASE CONTINUED
On further questioning, the patient revealed that the supplement prescribed by his naturopathic practitioner contained vitamin D. Although he had been instructed to take 1 tablet weekly, he had begun taking it daily with his other routine medications, resulting in a daily dose in excess of 60,000 IU of cholecalciferol (vitamin D3). The recommended dose is no more than 4,000 IU/day.
The supplement was immediately discontinued. His hydrochlorothiazide was also held due to its known effect of reducing urinary calcium excretion.
INITIAL TREATMENT OF HYPERCALCEMIA
3. Which of the following treatments is not recommended as part of this patient’s initial treatment?
- Bisphosphonates
- Calcitonin
- Intravenous fluids
- Furosemide
Our patient met the criteria for the diagnosis of hypercalcemic crisis, usually defined as an albumin-corrected serum calcium level higher than 14 mg/dL associated with multiorgan dysfunction resulting from the hypercalcemia.21 The mnemonic “stones, bones, abdominal moans, and psychic groans” captures the renal, skeletal, gastrointestinal, and neurologic manifestations.1
Bisphosphonates
Bisphosphonates are analogues of pyrophosphonates, which are normally incorporated into bone. Unlike pyrophosphonates, bisphosphonates inhibit osteoclast function. They are often used to treat hypercalcemia of any cause, although they are currently approved by the US Food and Drug Administration for treating hypercalcemia of malignancy only. As intravenous monotherapy, they are superior to other forms of treatment and are among the first-line agents in management.
Two bisphosphonates shown to be effective in hypercalcemia are zoledronate and pamidronate. Pamidronate begins to lower serum calcium levels within 2 days, with a peak effect at around 6 days.22 However, in studies comparing the 2 drugs, zoledronate has been shown to be more effective in normalizing serum calcium, with the additional benefit of having a much more rapid infusion time.23 Zoledronate is contraindicated in patients with creatinine clearance less than 30 mL/min; however, pamidronate may continue to be used.24
Calcitonin
This hormone inhibits bone resorption and increases excretion of calcium in the kidneys. It is not recommended for use alone because of its short duration of action and tachyphylaxis, but it can be used in combination with other agents, particularly in hypercalcemic crisis.22 It has the most rapid onset (within 2 hours) of the available medications, and when used in combination with bisphosphonates it produces a more substantial and rapid reduction in serum calcium.25,26
In a patient such as ours, with severe hypercalcemia and evidence of neurologic consequences, calcitonin should be used for its rapid and effective action in lowering serum calcium as other interventions take effect.
Intravenous fluids
Like our patient, many patients with significant hypercalcemia have volume depletion as a result of calciuresis-induced polyuria. Many also have nephrogenic diabetes insipidus from the cytotoxic effect of calcium on renal cells, leading to further volume depletion.27
All management approaches call for fluid repletion as an initial step in hypercalcemia. However, for severe hypercalcemia, volume resuscitation alone is unlikely to completely correct the imbalance. In addition to correcting dehydration, giving fluids increases glomerular filtration, allowing for increased secretion of calcium at the distal tubule.28 The recommendation is 2.5 to 4 L of normal saline over the first 24 hours, with continued aggressive hydration until good urine output is established.21
Our patient, in addition to having acute kidney injury thought to be due to prerenal azotemia, appeared to be volume-depleted and was given aggressive intravenous hydration.
Furosemide
Furosemide inhibits calcium reabsorption at the thick ascending loop of Henle, but this effect depends on the glomerular filtration rate. While our patient would likely eventually benefit from furosemide, it should not be considered the first-line therapy, as diuretic use in the setting of volume depletion can cause circulatory collapse.29 A relative contraindication was his presentation with acute kidney injury.
LONG-TERM TREATMENT
4. In the continued management of a patient with vitamin D toxicity with severe hypercalcemia, which of the following provides prolonged benefit?
- Intravenous hydrocortisone
- Fluid repletion
- Pamidronate
- Calcium-restricted diet
Much has been postulated concerning the mechanism of vitamin D intoxication and subsequent hypercalcemia. Studies have shown it is not an increase in dietary calcium absorption that drives the hypercalcemia but rather an increase in bone resorption. As such, bisphosphonates such as pamidronate have been shown to have a dramatic and rapid effect on severe hypercalcemia from vitamin D toxicity. The duration of action varies but is typically between 1 and 2 weeks.22,30
Corticosteroids such as hydrocortisone are also indicated in situations of severe toxicity. They block the action of 1-alpha-hydroxylase, which converts inactive 25-hydroxyvitamin D to the active 1,25-dihydroxyvitamin D. Corticosteroids have also been shown to more directly reduce calcium resorption from bone and intestine in addition to increasing calciuresis.31 A small study in the United Kingdom noted that while bisphosphonates and steroids were equally effective in reducing serum calcium levels, bisphosphonates accomplished this reduction more rapidly, with a time to therapeutic effect of 9 days as opposed to 22 days.
Fluid hydration, though necessary, is unlikely to produce complete correction on its own, as previously discussed.
THE PATIENT RECOVERS
The patient was treated with intravenous fluids over 3 days and received 1 dose of pamidronate. Calcitonin was provided over the first 48 hours after presentation to more rapidly reduce his calcium levels. He was advised to avoid taking the supplements prescribed by his naturopathic practitioner.
On follow-up with an endocrinologist 1 week later, his symptoms had entirely resolved, and his calcium level was 10.5 mg/dL.
TAKE-AWAY POINTS
- A good medication history includes over-the-counter products such as vitamin D supplements, as more and more people are taking them.
- The level of 25-hydroxyvitamin D should be monitored within 3 to 4 months after initiating treatment for vitamin D deficiency.11
- Vitamin D toxicity can have profound consequences, which are usually seen when levels of 25-hydroxyvitamin D rise above 250 ng/mL.13
- The Institute of Medicine recommends that the dosage of vitamin D supplements be no more than 4,000 IU/day and that doses may need to be lowered to account for concurrent use of hypercalcemia-inducing drugs and other vitamin D-containing supplements.32
- Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician 2003; 67:1959–1966.
- al Zahrani A, Levine MA. Primary hyperparathyroidism. Lancet 1997; 349:1233–1238.
- Mundy GR, Edwards JR. PTH-related peptide (PTHrP) in hypercalcemia. J Am Soc Nephrol 2008; 19:672–675.
- Ratcliffe WA, Hutchesson AC, Bundred NJ, Ratcliffe JG. Role of assays for parathyroid-hormone-related protein in investigation of hypercalcaemia. Lancet 1992; 339:164–167.
- Hewison M, Kantorovich V, Liker HR, et al. Vitamin D-mediated hypercalcemia in lymphoma: evidence for hormone production by tumor-adjacent macrophages. J Bone Miner Res 2003; 18:579–582.
- Ghobrial MW, George J, Mannam S, Henien SR. Severe hypercalcemia as an initial presenting manifestation of hepatocellular carcinoma. Can J Gastroenterol 2002; 16:607–609.
- Zhao C, Nguyen MH. Hepatocellular carcinoma screening and surveillance: practice guidelines and real-life practice. J Clin Gastroenterol 2016; 50:120–133.
- Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc 2016; 91:101–119.
- Burman KD, Monchik JM, Earll JM, Wartofsky L. Ionized and total serum calcium and parathyroid hormone in hyperthyroidism. Ann Intern Med 1976; 84:668–671.
- Iqbal AA, Burgess EH, Gallina DL, Nanes MS, Cook CB. Hypercalcemia in hyperthyroidism: patterns of serum calcium, parathyroid hormone, and 1,25-dihydroxyvitamin D3 levels during management of thyrotoxicosis. Endocr Pract 2003; 9:517–521.
- Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357:266–281.
- Wolpowitz D, Gilchrest BA. The vitamin D questions: how much do you need and how should you get it? J Am Acad Dermatol 2006; 54:301–317.
- Jones G. Pharmacokinetics of vitamin D toxicity. Am J Clin Nutr 2008; 88:582S–586S.
- Inui N, Murayama A, Sasaki S, et al. Correlation between 25-hydroxyvitamin D3 1 alpha-hydroxylase gene expression in alveolar macrophages and the activity of sarcoidosis. Am J Med 2001; 110:687–693.
- Wermers RA, Kearns AE, Jenkins GD, Melton LJ 3rd. Incidence and clinical spectrum of thiazide-associated hypercalcemia. Am J Med 2007; 120:911.e9–e15.
- Patel AM, Goldfarb S. Got calcium? Welcome to the calcium-alkali syndrome. J Am Soc Nephrol 2010; 21:1440–1443.
- Shapiro HI, Davis KA. Hypercalcemia and “primary” hyperparathyroidism during lithium therapy. Am J Psychiatry 2015; 172:12–15.
- Farrington K, Miller P, Varghese Z, Baillod RA, Moorhead JF. Vitamin A toxicity and hypercalcaemia in chronic renal failure. Br Med J (Clin Res Ed) 1981; 282:1999–2002.
- Frame B, Jackson CE, Reynolds WA, Umphrey JE. Hypercalcemia and skeletal effects in chronic hypervitaminosis A. Ann Intern Med 1974; 80:44–48.
- Florentin M, Elisaf MS. Proton pump inhibitor-induced hypomagnesemia: a new challenge. World J Nephrol 2012; 1:151–154.
- Ahmad S, Kuraganti G, Steenkamp D. Hypercalcemic crisis: a clinical review. Am J Med 2015; 128:239–245.
- Nussbaum SR, Younger J, Vandepol CJ, et al. Single-dose intravenous therapy with pamidronate for the treatment of hypercalcemia of malignancy: comparison of 30-, 60-, and 90-mg dosages. Am J Med 1993; 95:297–304.
- Major P, Lortholary A, Hon J, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol 2001; 19:558–567.
- Perazella MA, Markowitz GS. Bisphosphonate nephrotoxicity. Kidney Int 2008; 74:1385–1393.
- Bilezikian JP. Management of acute hypercalcemia. N Engl J Med 1992; 326:1196–1203.
- Ralston SH. Medical management of hypercalcaemia. Br J Clin Pharmacol 1992; 34:11–20.
- Garofeanu CG, Weir M, Rosas-Arellano MP, Henson G, Garg AX, Clark WF. Causes of reversible nephrogenic diabetes insipidus: a systematic review. Am J Kidney Dis 2005; 45:626–637.
- Hosking DJ, Cowley A, Bucknall CA. Rehydration in the treatment of severe hypercalcaemia. Q J Med 1981; 50:473–481.
- Suki WN, Yium JJ, Von Minden M, Saller-Hebert C, Eknoyan G, Martinez-Maldonado M. Acute treatment of hypercalcemia with furosemide. N Engl J Med 1970; 283:836–840.
- Selby PL, Davies M, Marks JS, Mawer EB. Vitamin D intoxication causes hypercalcaemia by increased bone resorption which responds to pamidronate. Clin Endocrinol 1995; 43:531–536.
- Davies M, Mawer EB, Freemont AJ. The osteodystrophy of hypervitaminosis D: a metabolic study. Q J Med 1986; 61:911–919.
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al, eds. Dietary reference intakes for calcium and vitamin D. Washington, DC: National Academies Press (US); 2011.
- Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician 2003; 67:1959–1966.
- al Zahrani A, Levine MA. Primary hyperparathyroidism. Lancet 1997; 349:1233–1238.
- Mundy GR, Edwards JR. PTH-related peptide (PTHrP) in hypercalcemia. J Am Soc Nephrol 2008; 19:672–675.
- Ratcliffe WA, Hutchesson AC, Bundred NJ, Ratcliffe JG. Role of assays for parathyroid-hormone-related protein in investigation of hypercalcaemia. Lancet 1992; 339:164–167.
- Hewison M, Kantorovich V, Liker HR, et al. Vitamin D-mediated hypercalcemia in lymphoma: evidence for hormone production by tumor-adjacent macrophages. J Bone Miner Res 2003; 18:579–582.
- Ghobrial MW, George J, Mannam S, Henien SR. Severe hypercalcemia as an initial presenting manifestation of hepatocellular carcinoma. Can J Gastroenterol 2002; 16:607–609.
- Zhao C, Nguyen MH. Hepatocellular carcinoma screening and surveillance: practice guidelines and real-life practice. J Clin Gastroenterol 2016; 50:120–133.
- Rajkumar SV, Kumar S. Multiple myeloma: diagnosis and treatment. Mayo Clin Proc 2016; 91:101–119.
- Burman KD, Monchik JM, Earll JM, Wartofsky L. Ionized and total serum calcium and parathyroid hormone in hyperthyroidism. Ann Intern Med 1976; 84:668–671.
- Iqbal AA, Burgess EH, Gallina DL, Nanes MS, Cook CB. Hypercalcemia in hyperthyroidism: patterns of serum calcium, parathyroid hormone, and 1,25-dihydroxyvitamin D3 levels during management of thyrotoxicosis. Endocr Pract 2003; 9:517–521.
- Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357:266–281.
- Wolpowitz D, Gilchrest BA. The vitamin D questions: how much do you need and how should you get it? J Am Acad Dermatol 2006; 54:301–317.
- Jones G. Pharmacokinetics of vitamin D toxicity. Am J Clin Nutr 2008; 88:582S–586S.
- Inui N, Murayama A, Sasaki S, et al. Correlation between 25-hydroxyvitamin D3 1 alpha-hydroxylase gene expression in alveolar macrophages and the activity of sarcoidosis. Am J Med 2001; 110:687–693.
- Wermers RA, Kearns AE, Jenkins GD, Melton LJ 3rd. Incidence and clinical spectrum of thiazide-associated hypercalcemia. Am J Med 2007; 120:911.e9–e15.
- Patel AM, Goldfarb S. Got calcium? Welcome to the calcium-alkali syndrome. J Am Soc Nephrol 2010; 21:1440–1443.
- Shapiro HI, Davis KA. Hypercalcemia and “primary” hyperparathyroidism during lithium therapy. Am J Psychiatry 2015; 172:12–15.
- Farrington K, Miller P, Varghese Z, Baillod RA, Moorhead JF. Vitamin A toxicity and hypercalcaemia in chronic renal failure. Br Med J (Clin Res Ed) 1981; 282:1999–2002.
- Frame B, Jackson CE, Reynolds WA, Umphrey JE. Hypercalcemia and skeletal effects in chronic hypervitaminosis A. Ann Intern Med 1974; 80:44–48.
- Florentin M, Elisaf MS. Proton pump inhibitor-induced hypomagnesemia: a new challenge. World J Nephrol 2012; 1:151–154.
- Ahmad S, Kuraganti G, Steenkamp D. Hypercalcemic crisis: a clinical review. Am J Med 2015; 128:239–245.
- Nussbaum SR, Younger J, Vandepol CJ, et al. Single-dose intravenous therapy with pamidronate for the treatment of hypercalcemia of malignancy: comparison of 30-, 60-, and 90-mg dosages. Am J Med 1993; 95:297–304.
- Major P, Lortholary A, Hon J, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. J Clin Oncol 2001; 19:558–567.
- Perazella MA, Markowitz GS. Bisphosphonate nephrotoxicity. Kidney Int 2008; 74:1385–1393.
- Bilezikian JP. Management of acute hypercalcemia. N Engl J Med 1992; 326:1196–1203.
- Ralston SH. Medical management of hypercalcaemia. Br J Clin Pharmacol 1992; 34:11–20.
- Garofeanu CG, Weir M, Rosas-Arellano MP, Henson G, Garg AX, Clark WF. Causes of reversible nephrogenic diabetes insipidus: a systematic review. Am J Kidney Dis 2005; 45:626–637.
- Hosking DJ, Cowley A, Bucknall CA. Rehydration in the treatment of severe hypercalcaemia. Q J Med 1981; 50:473–481.
- Suki WN, Yium JJ, Von Minden M, Saller-Hebert C, Eknoyan G, Martinez-Maldonado M. Acute treatment of hypercalcemia with furosemide. N Engl J Med 1970; 283:836–840.
- Selby PL, Davies M, Marks JS, Mawer EB. Vitamin D intoxication causes hypercalcaemia by increased bone resorption which responds to pamidronate. Clin Endocrinol 1995; 43:531–536.
- Davies M, Mawer EB, Freemont AJ. The osteodystrophy of hypervitaminosis D: a metabolic study. Q J Med 1986; 61:911–919.
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al, eds. Dietary reference intakes for calcium and vitamin D. Washington, DC: National Academies Press (US); 2011.

An unexpected cause of shoulder pain
A 58-year-old woman who sustained right-sided traumatic rib fractures after falling down stairs 8 months earlier presented with right shoulder pain that had been present for 6 months. She received nonsteroidal anti-inflammatory drugs at another hospital, which were partially effective. Magnetic resonance imaging of the neck and right shoulder had shown no abnormalities.

On physical examination, her right scapula was found to protrude abnormally (ie, to “wing”) during forward flexion and abduction of the right arm (Figure 1). Electromyography showed evidence of right serratus anterior paralysis and denervation of the right long thoracic nerve, leading to a diagnosis of traumatic long thoracic nerve paralysis. A course of physical therapy was initiated to improve her symptoms.
LONG THORACIC NERVE PARALYSIS
Scapular winging is caused by dysfunction of any of the 3 main muscles that attach the scapula to the posterior thoracic wall—the serratus anterior, the trapezius, and the rhomboid. The problem is most often in the serratus anterior muscle, innervated by the long thoracic nerve, a pure motor nerve that originates from the fifth, sixth, and seventh cervical nerves and descends along the lateral thoracic wall.
Long thoracic nerve paralysis can have traumatic, nontraumatic, or iatrogenic causes. Traumatic injuries result from blunt trauma to the neck, shoulder girdle, and thorax, while nontraumatic causes include viral illness, toxic exposure, apical pulmonary tumor, and C7 radiculopathy.1–3 Iatrogenic injuries may be caused by mastectomy with axillary dissection, chest tube thoracostomy, first-rib resection, or scalenotomy, or occur after general anesthesia.1,2,4
Scapular winging due to paralysis of the serratus anterior muscle is accentuated by forward elevation and—particularly—by pushing against a wall, and the entire scapula is displaced more medially and superiorly.2 The compensatory muscular activity required for shoulder stability induces secondary shoulder pain.5
The diagnosis is often delayed, as the clinical presentation may mimic the symptoms of shoulder joint or rotator cuff pathology. Although physical therapy resolves the pain and improves the function of the arm, mild endurance deficits and asymptomatic scapular winging may persist. Tendon transfer surgery is considered if adequate recovery is not achieved after a 6- to-24-month course of physical therapy.2
- Vastamäki M, Kauppila LI. Etiologic factors in isolated paralysis of the serratus anterior muscle: a report of 197 cases. J Shoulder Elbow Surg 1993; 2:240–243.
- Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med 2008; 1:1–11.
- Toshkezi G, Dejesus J, Jabre JF, Hohler A, Davies K. Long thoracic neuropathy caused by an apical pulmonary tumor. J Neurosurg 2009; 110:754–757.
- Kauppila LI, Vastamäki M. Iatrogenic serratus anterior paralysis. Long-term outcome in 26 patients. Chest 1996; 109:31–34.
- Nath RK, Lyons AB, Bietz G. Microneurolysis and decompression of long thoracic nerve injury are effective in reversing scapular winging: long-term results in 50 cases. BMC Musculoskelet Disord 2007; 8:25.
A 58-year-old woman who sustained right-sided traumatic rib fractures after falling down stairs 8 months earlier presented with right shoulder pain that had been present for 6 months. She received nonsteroidal anti-inflammatory drugs at another hospital, which were partially effective. Magnetic resonance imaging of the neck and right shoulder had shown no abnormalities.
On physical examination, her right scapula was found to protrude abnormally (ie, to “wing”) during forward flexion and abduction of the right arm (Figure 1). Electromyography showed evidence of right serratus anterior paralysis and denervation of the right long thoracic nerve, leading to a diagnosis of traumatic long thoracic nerve paralysis. A course of physical therapy was initiated to improve her symptoms.
LONG THORACIC NERVE PARALYSIS
Scapular winging is caused by dysfunction of any of the 3 main muscles that attach the scapula to the posterior thoracic wall—the serratus anterior, the trapezius, and the rhomboid. The problem is most often in the serratus anterior muscle, innervated by the long thoracic nerve, a pure motor nerve that originates from the fifth, sixth, and seventh cervical nerves and descends along the lateral thoracic wall.
Long thoracic nerve paralysis can have traumatic, nontraumatic, or iatrogenic causes. Traumatic injuries result from blunt trauma to the neck, shoulder girdle, and thorax, while nontraumatic causes include viral illness, toxic exposure, apical pulmonary tumor, and C7 radiculopathy.1–3 Iatrogenic injuries may be caused by mastectomy with axillary dissection, chest tube thoracostomy, first-rib resection, or scalenotomy, or occur after general anesthesia.1,2,4
Scapular winging due to paralysis of the serratus anterior muscle is accentuated by forward elevation and—particularly—by pushing against a wall, and the entire scapula is displaced more medially and superiorly.2 The compensatory muscular activity required for shoulder stability induces secondary shoulder pain.5
The diagnosis is often delayed, as the clinical presentation may mimic the symptoms of shoulder joint or rotator cuff pathology. Although physical therapy resolves the pain and improves the function of the arm, mild endurance deficits and asymptomatic scapular winging may persist. Tendon transfer surgery is considered if adequate recovery is not achieved after a 6- to-24-month course of physical therapy.2
A 58-year-old woman who sustained right-sided traumatic rib fractures after falling down stairs 8 months earlier presented with right shoulder pain that had been present for 6 months. She received nonsteroidal anti-inflammatory drugs at another hospital, which were partially effective. Magnetic resonance imaging of the neck and right shoulder had shown no abnormalities.
On physical examination, her right scapula was found to protrude abnormally (ie, to “wing”) during forward flexion and abduction of the right arm (Figure 1). Electromyography showed evidence of right serratus anterior paralysis and denervation of the right long thoracic nerve, leading to a diagnosis of traumatic long thoracic nerve paralysis. A course of physical therapy was initiated to improve her symptoms.
LONG THORACIC NERVE PARALYSIS
Scapular winging is caused by dysfunction of any of the 3 main muscles that attach the scapula to the posterior thoracic wall—the serratus anterior, the trapezius, and the rhomboid. The problem is most often in the serratus anterior muscle, innervated by the long thoracic nerve, a pure motor nerve that originates from the fifth, sixth, and seventh cervical nerves and descends along the lateral thoracic wall.
Long thoracic nerve paralysis can have traumatic, nontraumatic, or iatrogenic causes. Traumatic injuries result from blunt trauma to the neck, shoulder girdle, and thorax, while nontraumatic causes include viral illness, toxic exposure, apical pulmonary tumor, and C7 radiculopathy.1–3 Iatrogenic injuries may be caused by mastectomy with axillary dissection, chest tube thoracostomy, first-rib resection, or scalenotomy, or occur after general anesthesia.1,2,4
Scapular winging due to paralysis of the serratus anterior muscle is accentuated by forward elevation and—particularly—by pushing against a wall, and the entire scapula is displaced more medially and superiorly.2 The compensatory muscular activity required for shoulder stability induces secondary shoulder pain.5
The diagnosis is often delayed, as the clinical presentation may mimic the symptoms of shoulder joint or rotator cuff pathology. Although physical therapy resolves the pain and improves the function of the arm, mild endurance deficits and asymptomatic scapular winging may persist. Tendon transfer surgery is considered if adequate recovery is not achieved after a 6- to-24-month course of physical therapy.2
- Vastamäki M, Kauppila LI. Etiologic factors in isolated paralysis of the serratus anterior muscle: a report of 197 cases. J Shoulder Elbow Surg 1993; 2:240–243.
- Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med 2008; 1:1–11.
- Toshkezi G, Dejesus J, Jabre JF, Hohler A, Davies K. Long thoracic neuropathy caused by an apical pulmonary tumor. J Neurosurg 2009; 110:754–757.
- Kauppila LI, Vastamäki M. Iatrogenic serratus anterior paralysis. Long-term outcome in 26 patients. Chest 1996; 109:31–34.
- Nath RK, Lyons AB, Bietz G. Microneurolysis and decompression of long thoracic nerve injury are effective in reversing scapular winging: long-term results in 50 cases. BMC Musculoskelet Disord 2007; 8:25.
- Vastamäki M, Kauppila LI. Etiologic factors in isolated paralysis of the serratus anterior muscle: a report of 197 cases. J Shoulder Elbow Surg 1993; 2:240–243.
- Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med 2008; 1:1–11.
- Toshkezi G, Dejesus J, Jabre JF, Hohler A, Davies K. Long thoracic neuropathy caused by an apical pulmonary tumor. J Neurosurg 2009; 110:754–757.
- Kauppila LI, Vastamäki M. Iatrogenic serratus anterior paralysis. Long-term outcome in 26 patients. Chest 1996; 109:31–34.
- Nath RK, Lyons AB, Bietz G. Microneurolysis and decompression of long thoracic nerve injury are effective in reversing scapular winging: long-term results in 50 cases. BMC Musculoskelet Disord 2007; 8:25.

When the tail wags the dog: Clinical skills in the age of technology
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
- Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
- Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
- Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
- Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
- Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
- Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
- Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
- Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
- Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
- Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
- Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
- Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
- Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
- Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
- Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
- Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
- Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
- Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
- Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.

Blending classic clinical skills with new technology

Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
- Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
- Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.
Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
- Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
- Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.
- Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
- Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
- Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.

Life after breast, prostate, and colon cancer: Primary care’s role
In 2015, about 1.6 million Americans received a diagnosis of cancer.1 In 2012, when 13.7 million people were living with cancer in the United States, the estimated 5-year survival rate of all cancers was 66.5%.1 Today, breast, prostate, and colon cancers have 5-year survival rates of 89.4%, 98.9%, and 64.9%, respectively.
With this rising trend in survival, primary care physicians have been steadily assuming the long-term care of these patients. The phrase “cancer survivorship” was coined by the National Comprehensive Cancer Network to describe the experience of living with, through, and beyond a cancer diagnosis.2
As cancer becomes a chronic medical condition, the primary care physician assumes a vital role in the treatment of the unique and evolving needs of this patient population.
This article discusses the specific needs of patients surviving breast, prostate, and colon cancer with special focus on surveillance guidelines for recurrence, development of concomitant malignancies, assessment of psychosocial and physical effects, and disease conditions related to the treatment of cancer itself.
FOLLOW-UP CARE AND SURVEILLANCE
Follow-up care in patients being treated for cancer is vital to survivorship. It includes promoting healthy living, managing treatment side effects, and monitoring for long-term side effects and possible recurrence.
Patients previously treated for malignancy are more susceptible to second primary cancers, for an array of reasons including the effects of prior treatment, shared environmental exposures such as smoking, and genetic susceptibility.2 Therefore, it is important for the primary care physician to recognize signs and symptoms and to screen cancer survivors appropriately. The American Society of Clinical Oncology (ASCO) has developed evidence-based recommendations for follow-up care,3 which we review here.
Breast cancer
For breast cancer patients, history and physical examinations are recommended every 3 to 6 months for the first 3 years, every 6 to 12 months in years 4 and 5, and annually thereafter.3
A repeat mammogram should be performed 1 year after the initial mammogram that led to the diagnosis. If the patient underwent radiation therapy, a repeat mammogram of the affected breast should be done 6 months after completion of radiation. Finally, a mammogram should be done every 6 to 12 months thereafter.3 It is also recommended that patients perform a monthly breast self-examination, but this does not replace the annual mammogram.3
Women who are treated with tamoxifen should have an annual gynecologic assessment if they have a uterus and should be encouraged to discuss any abnormal vaginal bleeding with their physician, given the increased risk of uterine cancer.2
ASCO does not recommend routine use of complete blood cell counts, complete metabolic panels, bone scans, chest radiography, computed tomography, ultrasonography, positron-emission tomography, or tumor markers in patients who are asymptomatic.3
Prostate cancer
ASCO’s recommendations for patients recovering from prostate cancer include regular histories and physical examinations and general health promotion. Prostate-specific antigen (PSA) testing is recommended every 6 to 12 months for the first 5 years after treatment and annually thereafter. More frequent PSA testing may be required in men at higher risk of recurrence or in patients who may undergo additional treatment, including radiation and surgery.4 Higher risk of disease recurrence is thought to depend on disease-specific factors at the time of original diagnosis including pretreatment PSA, Gleason score, and tumor stage.4 This should be discussed between the oncologist and primary care physician.
In regard to digital rectal examinations, the oncologist and primary care physician should jointly determine the frequency of examination. The frequency of digital rectal examinations remains an area of controversy due to their low sensitivity for detecting recurrences. Digital rectal examinations may be omitted in patients with undetectable levels of PSA.4
In regard to second primary malignancies, prostate cancer survivors who have undergone pelvic radiation therapy have a slightly higher risk of bladder and colorectal cancer. The lifetime incidence of bladder cancer after pelvic radiation is 5% to 6%, compared with 2.4% in the general population.1,5 A prostate cancer survivor presenting with hematuria should be referred to a urologist for cystoscopy and evaluation of the upper urinary tract to rule out cancer.4
Similarly, patients presenting with rectal bleeding should be referred to a gastroenterologist and the treating radiation oncologist for complete evaluation. The risk of rectal cancer after pelvic radiation therapy increases to about the same level as in someone who has a first-degree relative with colorectal cancer.5 Therefore, it is recommended that patients undergo screening for colorectal cancer in conjunction with existing evidence-based guidelines. There is no evidence to suggest that increased intensity of screening improves overall or disease-specific survival.4
Colon cancer
In patients with resected colorectal cancer, continued surveillance is important to evaluate for recurrent cancer as well as for metachronous neoplasms. Consensus statements indicate that surveillance colonoscopy should be continued for those who have undergone surgical resection for stage I, II, or III colon or rectal cancers, and for those patients with stage IV who have undergone surgical resection with curative intent.6
Patients who undergo curative resection of rectal or colon cancer should have a colonoscopy 1 year after resection or 1 year after the colonoscopy was performed, to clear the colon of synchronous disease. Subsequently, if the colonoscopy done at 1 year is normal, the interval before the next colonoscopy is 3 years. If that colonoscopy is normal, the next colonoscopy is in 5 years. Time intervals may be shorter if there is evidence of hereditary nonpolyposis colorectal cancer or adenoma.
Patients who underwent low anterior resection of rectal cancer should undergo periodic examination of the rectum to evaluate for local recurrence. Although effectiveness is not proven, endoscopic ultrasonography or flexible sigmoidoscopy is suggested at 3- to 6-month intervals for the first 2 to 3 years after resection. This is independent of colonoscopy.6,7
Additionally, ASCO recommends a history and physical examination and carcinoembryonic antigen testing every 3 to 6 months for the first 5 years. Computed tomography of the chest, abdomen, and pelvis should be done annually for the first 3 years after the end of treatment.7
HEALTH PROMOTION
Maintaining a healthy body weight and a nutritionally balanced diet should be encouraged in all cancer survivors. Poor diet, lack of exercise, excessive alcohol consumption, and smoking reduce quality of life and increase the risk of cancer.2
Diet
Numerous studies have looked at dietary modifications and risk reduction, and although there is no consensus on specific dietary guidelines, there is consensus that diet modification to maintain normal body weight will improve overall quality of life.8 Patients should be encouraged to consume a well-balanced diet consisting mostly of fruits, vegetables, whole grains, and beans, and to limit consumption of animal protein.8
There is little evidence to support taking vitamins or other dietary supplements to prevent or control cancer or to prevent its recurrence. The primary care physician should assess supplement use on a regular basis during office visits.2
Exercise
Rest is an important component of the initial recovery process. Too much inactivity, however, leads to loss of physical conditioning and muscle strength. This in turn may negatively affect a patient’s ability to perform activities of daily living and may worsen fatigue associated with treatment.
Accordingly, the National Comprehensive Cancer Network recommends at least 150 minutes of moderate activity and up to 75 minutes of more rigorous activity divided throughout the week.2,8 The regimen should include endurance and muscle strength training, which aid in balance, bone, health, and functional status. The intensity of exercise should be increased in a stepwise fashion, taking into account individual capabilities and limitations.2
Cancer survivors may need specific exercise recommendations and supervised programs to ensure safety and limit long-term side effects of their treatment. For example:
Patients with neuropathy should have their stability, balance, and gait assessed before starting a new program. These patients may benefit from an aerobic exercise program that includes riding a stationary bike rather than running.
Patients with poor bone health should have their fracture risk assessed.
Those with an ostomy bag should empty the bag before physical activity. They should avoid contact sports and activities that increase intra-abdominal pressure.
Patients suffering from lymphedema should wear compression garments when engaging in physical activity. They should undergo baseline and periodic reevaluation of the lymphedema and initiate strength training in the affected body part only if the lymphedema is stable (ie, no need for therapy for 3 months, no recent infections requiring antibiotics, and no change in circumference > 10%).2
Mental health
Health promotion should focus not only on the physical health of the patient, but also on his or her emotional and psychological well-being. As they make the transition from cancer patient to survivor, many individuals may develop or have worsening depression and anxiety due to fear of recurrence. These feelings of powerlessness can linger for years after the initial treatment.
Patients should be screened regularly for signs and symptoms of depression by asking about their family and social support. Referral to support groups, psychologists, and psychiatrists may be warranted.9
MITIGATING CANCER-RELATED FATIGUE
Cancer-related fatigue involves a patient’s subjective sense of physical, emotional, and cognitive exhaustion related to cancer or treatment that is disproportionate to that expected from recent daily activity.2 Fatigue is a common complaint among survivors and can occur months to years after treatment ends.10
Patients should be screened for fatigue at regular intervals. The primary care physician should focus the history to include information regarding the onset, pattern, duration, associated factors, assessment of other treatable comorbidities, medications, psychological well-being, nutritional status, and pain level of each patient who complains of fatigue.
Laboratory tests for treatable causes of fatigue include:
- A complete blood cell count to evaluate for anemia
- A comprehensive metabolic panel to evaluate electrolytes, renal function, and hepatic function
- The thyroid-stimulating hormone level to evaluate thyroid function, particularly in breast cancer patients who have received radiation therapy.2
If no organic cause is uncovered, the focus should shift to lifestyle interventions as the treatment of choice. The treatment of fatigue in this situation is increased physical activity with the goals discussed above. Psychological intervention may be required with cognitive behavioral therapy, psychological and supportive therapies, education on sleep hygiene, and possible sleep restriction.
If alternative causes of fatigue are ruled out and physical and psychological support fails to reduce symptoms, the practitioner can consider a psychostimulant such as methylphenidate, but this should be used cautiously.2
SEXUAL DYSFUNCTION
Intimate relationships and sexuality are an important part of life and are affected by a variety of factors including physical health, psychological well-being, body image perception, and overall status of relationships. As a side effect of chemotherapy, cancer survivors may complain of erectile dysfunction, penile shortening, dyspareunia, vaginal dryness, decreased libido, anorgasmy, and changes in body image. These issues are frequently unaddressed, whether due to the physician’s discomfort in discussing the topic or to the patient’s embarrassment and reluctance to discuss the matter.11
Breast cancer patients may experience sexual dysfunction both during and after treatment due to a combination of systemic effects of treatment, changes in physical appearance leading to impaired body image, strains on partner relationships, and psychological sequelae of diagnosis and treatment of cancer.12 Manipulation and radiation to the breast affect sexual functioning by altering body contour and image. Additionally, chemotherapy can lead to early menopause and hormonal alterations due to endocrine therapies, which can negatively affect sexual organs.11
Studies have shown that treatment with tamoxifen causes less sexual dysfunction than do aromatase inhibitors. In the Arimidex, Tamoxifen, Alone or in Combination trial, therapy with anastrozole was associated with more vaginal dryness, dyspareunia, and decreased libido compared with tamoxifen.12
Treatment requires a comprehensive history, a physical examination, and a discussion of relationship satisfaction with the patient.
Vaginal dryness and dyspareunia can be treated with vaginal lubricants and moisturizers. Moisturizers are effective if used multiple times per week, whereas lubricants can be used on demand. Low-dose vaginal estrogen preparations can be used in select patients with severe vaginal dryness; the goal should be discussed. Hormone replacement therapy is contraindicated in breast cancer survivors due to the risk of recurrence.11
Prostate cancer survivors. Up to 70% of men felt their quality of life and sexual function were adversely affected after the diagnosis and treatment.13,14 Erectile dysfunction following radical prostatectomy and radiation therapy remains one of the leading causes of sexual dysfunction.14–15 Erectile dysfunction is multifactorial, with both psychogenic and organic causes. Comorbidities must be considered including hypertension, diabetes, hyperlipidemia, and smoking. Early penile rehabilitation is a proposed treatment strategy.14
First-line therapy for penile rehabilitation includes introduction of daily low-dose phosphodiesterase type 5 inhibitors as early as the time of catheter removal to within the first month after surgery. The need for daily dosing vs on-demand dosing has been controversial.15 Two large multicenter, double-blind studies had conflicting outcomes. The first reported that in men receiving nightly sildenafil (50 or 100 mg) after radical prostatectomy, 27% had increased return of spontaneous erectile function vs 4% with placebo16; the second study showed no difference between nightly and on-demand dosing.17 The consensus is that a phosphodiesterase type 5 inhibitor should be initiated early.
Second-line therapy includes intracavernosal injections and vacuum erection devices. Finally, a penile prosthesis implant can be offered to patients who have responded poorly to medical therapy.13
Colorectal cancer survivors suffer from sexually related problems similar to those stated above, including erectile dysfunction, ejaculation problems, dyspareunia, vaginal dryness, and decreased enjoyment.18 These patients should be provided treatments similar to those described above. In addition, they may suffer from body image issues, particularly those with a permanent ostomy.9
Sexual dysfunction is a multifaceted problem for patients. Encouraging couples to discuss sexual intimacy frequently helps to reveal and cope with the problems, whether physical or psychological. It is the primary care physician’s role to recognize any sexual concerns and refer to the appropriate specialist.
OSTEOPOROSIS
Osteoporosis is a metabolic bone disease characterized by low bone mineral density. As a result, bones become weak and fracture more easily from minor injuries.
Risk factors for osteoporosis include female sex, family history, advanced age, low body weight, low calcium and vitamin D levels, sedentary lifestyle, smoking, and low estrogen levels.19 Cancer treatment places patients at a greater risk for osteoporosis, particularly for those patients with chemotherapy-induced ovarian failure, those treated with aromatase inhibitors, men receiving androgen-deprivation therapy, and patients on glucocorticoid therapy. The morbidity and mortality associated with bone loss can be prevented with appropriate screening, lifestyle changes, and therapy.2
According to the National Osteoporosis Foundation Guideline for Preventing and Treating Osteoporosis, all men and postmenopausal women age 50 and older should be evaluated clinically for osteoporosis risk to determine the need for bone mineral density testing.2,19 The US Preventive Services Task Force recommends bone mineral density testing in all women age 65 and older, and for women 60 to 64 who are at high risk for bone loss. ASCO agrees, and further suggests bone mineral density screening for women with breast cancer who have risk factors such as positive family history, body weight less than 70 kg, and prior nontraumatic fracture, as well as for postmenopausal women of any age receiving aromatase inhibitors and for premenopausal women with therapy-induced ovarian failure.11
Androgen deprivation therapy is a mainstay of treatment in recurrent and metastatic prostate cancer. The effect is severe hypogonadism with reductions in serum testosterone levels. Androgen deprivation therapy accelerates bone turnover, decreases bone mineral density, and contributes to fracture risk. The National Comprehensive Cancer Network additionally suggests measuring bone mineral density at baseline for all men receiving androgen deprivation therapy or other medications associated with bone loss, repeating it 1 year after androgen deprivation therapy and then every 2 years, or as clinically indicated.20
The gold standard for measuring bone mineral density is dual-energy x-ray absorptiometry. The World Health Organization FRAX tool uses bone mineral density and several clinical factors to estimate the risk of fracture in the next 10 years, which can help guide therapy. Cancer patients with elevated fracture risk should be evaluated every 2 years. Counseling should be provided to address modifiable risk factors such as smoking, alcohol consumption, physical inactivity, and low calcium and vitamin D intake. Therapy should be strongly considered in patients with a bone mineral density below a T-score of –2.0. 2,19
Treatment begins with lifestyle modifications such as weight-bearing exercises to improve balance and muscle strength and to prevent falls, and adequate intake of calcium (≥ 1,200 mg daily) and vitamin D (800–1,000 IU daily) for adults age 50 and older. Treatment with bisphosphonates may be required.2,11,20
NEUROPATHY
Many chemotherapeutic agents can lead to neuropathy and can result in long-term disability in patients. Patients treated with taxane- and platinum-based chemotherapy are at particular risk.
Paclitaxel, used in the treatment of breast, ovarian, and lung cancer, can lead to distal neuropathy. This neuropathy commonly has a stocking-and-glove distribution and is primarily sensory; however, it may have motor and autonomic components. The neuropathy typically lessens when the medication is stopped, although in some patients it can persist and lead to long-term disability.
Treatment can include massage. Medications such as gabapentin and pregabalin can also be used, but randomized controlled trials do not support them, as they predominantly treat the tingling rather than the numbness.11
BLADDER AND BOWEL DYSFUNCTION
Urinary incontinence and dysfunction are frequent complications in prostate cancer survivors. Urinary function should be discussed regularly with patients, addressing quality of the urinary stream, difficulty emptying the bladder, timing, and incontinence.4 Urinary incontinence is frequently seen in postprostatectomy patients.
The cornerstone of treating urinary incontinence is determining the cause of the incontinence, whether it is stress or urge incontinence, or both.21 For those patients with urge incontinence alone, practitioners can address the problem with a combination of behavior modification, pelvic floor exercises, and anticholinergic medications such as oxybutynin. If the problem stems from difficulty initiating or a slow stream, physicians may consider alpha-blockers.4,21 If the incontinence is persistent, bothersome, and has components of stress incontinence, the patient should be referred to a urologist for urodynamic testing, cystoscopy, and surgical evaluation for possible placement of a male urethral sling or artificial urinary sphincter.21
Colorectal cancer survivors, particularly those who received radiation therapy, are at high risk of bowel dysfunction such as chronic diarrhea and stool incontinence. Patients should be educated about this possible side effect. Symptoms of bowel dysfunction can affect body image and interfere with social functioning and overall quality of life. Patients should be provided with coping tools such as antidiarrheal medication, stool bulking agents, changes in diet, and protective underwear.
CARDIOVASCULAR DISEASE
Evidence suggests that certain types of chemotherapy and radiation therapy increase the risk of cardiovascular disease. Prostate cancer survivors treated with androgen deprivation therapy, particularly those more than 75 years old, are at increased risk of cardiovascular disease and diabetes.22
It is recommended that men be screened with fasting plasma glucose at baseline and yearly thereafter while receiving androgen deprivation therapy. Lipid panel testing should be done 1 year from initiation of androgen deprivation therapy and then, if results are normal, every 5 years or as clinically warranted. The focus should be on primary prevention with emphasis on smoking cessation, treating hypertension per guidelines, lifestyle modifications, and treatment with aspirin and statins when clinically appropriate.20
Radiation therapy, chemotherapy, and endocrine therapy have all been suggested to lead to cardiotoxicity in breast cancer patients. Anthracycline-based chemotherapies have a well-recognized association with cardiomyopathy. Factors associated with increased risk of anthracycline-induced cardiomyopathy include older age, hypertension, pre-existing coronary artery disease, and previous mediastinal radiation.
Early detection of cardiomyopathy may lead to avoidance of irreversible cardiotoxicity, but there are currently no clear guidelines for cardiac screening in breast cancer survivors. If cardiomyopathy is detected, treatment should include beta-blockers and angiotensin-converting enzyme inhibitors as well as modification of other cardiovascular risk factors.11
A SURVIVORSHIP CARE PLAN
There is life beyond the diagnosis of cancer. As patients are living longer, with an estimated 5-year survival rate of 66.5% of all cancers in the United States, there must be a transition of care from the oncologist to the primary care physician.1 While the oncologist will remain involved in the initial years of follow-up care, these visits will go from twice a year to once a year, and eventually the patient will make a full transition to care by the primary care physician. The timing of this changeover varies from physician to physician, but the primary care physician is ultimately responsible for the follow-up.
A tool to ease this transition is a survivorship care plan. The goal of a survivorship care plan is to individualize a follow-up plan while keeping in mind the necessary surveillance as outlined. These care plans are created with the patient and oncologist and then brought to the primary care physician. While there is an abundance of literature regarding the creation and initiation of survivorship care plans, the success of these plans is uncertain. Ultimately, the goal of a survivorship care plan is to create open dialogue among the oncologist, the primary care physician, and the patient. This unique patient population requires close follow-up by a multidisciplinary team with the primary care physician serving as the steward.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results Program. SEER cancer stat fact sheets. http://seer.cancer.gov/statfacts. Accessed March 6, 2017.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines Survivorship: 2015. www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf. Accessed March 6, 2017.
- Khatcheressian JL, Hurley P, Bantug E, et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology Clinical Practice Guideline update. J Clin Oncol 2013; 31:961–965.
- Resnick MJ, Lacchetti C, Bergman J, et al. Prostate cancer survivorship care guideline: American Society of Clinical Oncology Clinical Practice Guideline endorsement. J Clin Oncol 2015; 33:1078–1085.
- Sountoulides P, Koletsas N, Kikidakis D, Paschalidis K, Sofikitis N. Secondary malignancies following radiotherapy for prostate cancer. Ther Adv Urol 2010; 2:119–125.
- Rex DK, Kahi CJ, Levin B, et al. Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and US Multi-Society Task Force on Colorectal Cancer. CA Cancer J Clin 2006; 56:160–168.
- Meyerhardt JA, Mangu PB, Flynn PJ, et al; American Society of Clinical Oncology. Follow-up care, surveillance protocol, and secondary prevention measures for survivors of colorectal cancer: American Society of Clinical Oncology clinical practice guideline endorsement. J Clin Oncol 2013; 31:4465–4470.
- Davies NJ, Batehup L, Thomas R. The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: a review of the literature. Br J Cancer 2011; 105(suppl 1):S52–S73.
- Miller K, editor. Excellent Care for Cancer Survivors: A Guide to Fully Meet Their Needs in Medical Offices and in the Community (Praeger Series on Contemporary Health & Living). 1st ed. Santa Barbara, CA: Praeger; 2012.
- Stanton AL, Rowland JH, Ganz PA. Life after diagnosis and treatment of cancer in adulthood: contributions from psychosocial oncology research. Am Psychol 2015; 70:159–174.
- Stan D, Loprinzi CL, Ruddy KJ. Breast cancer survivorship issues. Hematol Oncol Clin North Am 2013; 27:805–827.
- Fallowfield L, Cella D, Cuzick J, Francis S, Locker G, Howell A. Quality of life of postmenopausal women in the Arimidex, Tamoxifen, Alone or in Combination (ATAC) Adjuvant Breast Cancer Trial. J Clin Oncol 2004; 22:426–471.
- Chung E, Gillman M. Prostate cancer survivorship: a review of erectile dysfunction and penile rehabilitation after prostate cancer therapy. Med J Aust 2014; 200:582–585.
- Sherer BA, Levine LA. Current management of erectile dysfunction in prostate cancer survivors. Curr Opin Urol 2014; 24:401–416.
- Chung E, Brock G. Sexual rehabilitation and cancer survivorship: a state of art review of current literature and management strategies in male sexual dysfunction among prostate cancer survivors. J Sex Med 2013; 10(suppl 1):102–111.
- Padma-Nathan H, McCullough AR, Levine LA, et al; Study Group. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res 2008; 20:479–486.
- Montorsi F, Brock G, Lee J, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol 2008; 54:924–931.
- Den Oudsten BL, Traa MJ, Thong MS, et al. Higher prevalence of sexual dysfunction in colon and rectal cancer survivors compared with the normative population: a population-based study. Eur J Cancer 2012; 48:3161–3170.
- National Osteoporosis Foundation (NOF). http://nof.org. Accessed March 3, 2017.
- Saylor PJ, Keating NL, Smith MR. Prostate cancer survivorship: prevention and treatment of the adverse effects of androgen deprivation therapy. J Gen Intern Med 2009; 24(suppl 2):S389–S394.
- Gupta S, Peterson AC. Stress urinary incontinence in the prostate cancer survivor. Curr Opin Urol 2014; 24:395–400.
- Morgans AK, Fan KH, Koyama T, et al. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J Urol 2015; 193:1226–1231.
In 2015, about 1.6 million Americans received a diagnosis of cancer.1 In 2012, when 13.7 million people were living with cancer in the United States, the estimated 5-year survival rate of all cancers was 66.5%.1 Today, breast, prostate, and colon cancers have 5-year survival rates of 89.4%, 98.9%, and 64.9%, respectively.
With this rising trend in survival, primary care physicians have been steadily assuming the long-term care of these patients. The phrase “cancer survivorship” was coined by the National Comprehensive Cancer Network to describe the experience of living with, through, and beyond a cancer diagnosis.2
As cancer becomes a chronic medical condition, the primary care physician assumes a vital role in the treatment of the unique and evolving needs of this patient population.
This article discusses the specific needs of patients surviving breast, prostate, and colon cancer with special focus on surveillance guidelines for recurrence, development of concomitant malignancies, assessment of psychosocial and physical effects, and disease conditions related to the treatment of cancer itself.
FOLLOW-UP CARE AND SURVEILLANCE
Follow-up care in patients being treated for cancer is vital to survivorship. It includes promoting healthy living, managing treatment side effects, and monitoring for long-term side effects and possible recurrence.
Patients previously treated for malignancy are more susceptible to second primary cancers, for an array of reasons including the effects of prior treatment, shared environmental exposures such as smoking, and genetic susceptibility.2 Therefore, it is important for the primary care physician to recognize signs and symptoms and to screen cancer survivors appropriately. The American Society of Clinical Oncology (ASCO) has developed evidence-based recommendations for follow-up care,3 which we review here.
Breast cancer
For breast cancer patients, history and physical examinations are recommended every 3 to 6 months for the first 3 years, every 6 to 12 months in years 4 and 5, and annually thereafter.3
A repeat mammogram should be performed 1 year after the initial mammogram that led to the diagnosis. If the patient underwent radiation therapy, a repeat mammogram of the affected breast should be done 6 months after completion of radiation. Finally, a mammogram should be done every 6 to 12 months thereafter.3 It is also recommended that patients perform a monthly breast self-examination, but this does not replace the annual mammogram.3
Women who are treated with tamoxifen should have an annual gynecologic assessment if they have a uterus and should be encouraged to discuss any abnormal vaginal bleeding with their physician, given the increased risk of uterine cancer.2
ASCO does not recommend routine use of complete blood cell counts, complete metabolic panels, bone scans, chest radiography, computed tomography, ultrasonography, positron-emission tomography, or tumor markers in patients who are asymptomatic.3
Prostate cancer
ASCO’s recommendations for patients recovering from prostate cancer include regular histories and physical examinations and general health promotion. Prostate-specific antigen (PSA) testing is recommended every 6 to 12 months for the first 5 years after treatment and annually thereafter. More frequent PSA testing may be required in men at higher risk of recurrence or in patients who may undergo additional treatment, including radiation and surgery.4 Higher risk of disease recurrence is thought to depend on disease-specific factors at the time of original diagnosis including pretreatment PSA, Gleason score, and tumor stage.4 This should be discussed between the oncologist and primary care physician.
In regard to digital rectal examinations, the oncologist and primary care physician should jointly determine the frequency of examination. The frequency of digital rectal examinations remains an area of controversy due to their low sensitivity for detecting recurrences. Digital rectal examinations may be omitted in patients with undetectable levels of PSA.4
In regard to second primary malignancies, prostate cancer survivors who have undergone pelvic radiation therapy have a slightly higher risk of bladder and colorectal cancer. The lifetime incidence of bladder cancer after pelvic radiation is 5% to 6%, compared with 2.4% in the general population.1,5 A prostate cancer survivor presenting with hematuria should be referred to a urologist for cystoscopy and evaluation of the upper urinary tract to rule out cancer.4
Similarly, patients presenting with rectal bleeding should be referred to a gastroenterologist and the treating radiation oncologist for complete evaluation. The risk of rectal cancer after pelvic radiation therapy increases to about the same level as in someone who has a first-degree relative with colorectal cancer.5 Therefore, it is recommended that patients undergo screening for colorectal cancer in conjunction with existing evidence-based guidelines. There is no evidence to suggest that increased intensity of screening improves overall or disease-specific survival.4
Colon cancer
In patients with resected colorectal cancer, continued surveillance is important to evaluate for recurrent cancer as well as for metachronous neoplasms. Consensus statements indicate that surveillance colonoscopy should be continued for those who have undergone surgical resection for stage I, II, or III colon or rectal cancers, and for those patients with stage IV who have undergone surgical resection with curative intent.6
Patients who undergo curative resection of rectal or colon cancer should have a colonoscopy 1 year after resection or 1 year after the colonoscopy was performed, to clear the colon of synchronous disease. Subsequently, if the colonoscopy done at 1 year is normal, the interval before the next colonoscopy is 3 years. If that colonoscopy is normal, the next colonoscopy is in 5 years. Time intervals may be shorter if there is evidence of hereditary nonpolyposis colorectal cancer or adenoma.
Patients who underwent low anterior resection of rectal cancer should undergo periodic examination of the rectum to evaluate for local recurrence. Although effectiveness is not proven, endoscopic ultrasonography or flexible sigmoidoscopy is suggested at 3- to 6-month intervals for the first 2 to 3 years after resection. This is independent of colonoscopy.6,7
Additionally, ASCO recommends a history and physical examination and carcinoembryonic antigen testing every 3 to 6 months for the first 5 years. Computed tomography of the chest, abdomen, and pelvis should be done annually for the first 3 years after the end of treatment.7
HEALTH PROMOTION
Maintaining a healthy body weight and a nutritionally balanced diet should be encouraged in all cancer survivors. Poor diet, lack of exercise, excessive alcohol consumption, and smoking reduce quality of life and increase the risk of cancer.2
Diet
Numerous studies have looked at dietary modifications and risk reduction, and although there is no consensus on specific dietary guidelines, there is consensus that diet modification to maintain normal body weight will improve overall quality of life.8 Patients should be encouraged to consume a well-balanced diet consisting mostly of fruits, vegetables, whole grains, and beans, and to limit consumption of animal protein.8
There is little evidence to support taking vitamins or other dietary supplements to prevent or control cancer or to prevent its recurrence. The primary care physician should assess supplement use on a regular basis during office visits.2
Exercise
Rest is an important component of the initial recovery process. Too much inactivity, however, leads to loss of physical conditioning and muscle strength. This in turn may negatively affect a patient’s ability to perform activities of daily living and may worsen fatigue associated with treatment.
Accordingly, the National Comprehensive Cancer Network recommends at least 150 minutes of moderate activity and up to 75 minutes of more rigorous activity divided throughout the week.2,8 The regimen should include endurance and muscle strength training, which aid in balance, bone, health, and functional status. The intensity of exercise should be increased in a stepwise fashion, taking into account individual capabilities and limitations.2
Cancer survivors may need specific exercise recommendations and supervised programs to ensure safety and limit long-term side effects of their treatment. For example:
Patients with neuropathy should have their stability, balance, and gait assessed before starting a new program. These patients may benefit from an aerobic exercise program that includes riding a stationary bike rather than running.
Patients with poor bone health should have their fracture risk assessed.
Those with an ostomy bag should empty the bag before physical activity. They should avoid contact sports and activities that increase intra-abdominal pressure.
Patients suffering from lymphedema should wear compression garments when engaging in physical activity. They should undergo baseline and periodic reevaluation of the lymphedema and initiate strength training in the affected body part only if the lymphedema is stable (ie, no need for therapy for 3 months, no recent infections requiring antibiotics, and no change in circumference > 10%).2
Mental health
Health promotion should focus not only on the physical health of the patient, but also on his or her emotional and psychological well-being. As they make the transition from cancer patient to survivor, many individuals may develop or have worsening depression and anxiety due to fear of recurrence. These feelings of powerlessness can linger for years after the initial treatment.
Patients should be screened regularly for signs and symptoms of depression by asking about their family and social support. Referral to support groups, psychologists, and psychiatrists may be warranted.9
MITIGATING CANCER-RELATED FATIGUE
Cancer-related fatigue involves a patient’s subjective sense of physical, emotional, and cognitive exhaustion related to cancer or treatment that is disproportionate to that expected from recent daily activity.2 Fatigue is a common complaint among survivors and can occur months to years after treatment ends.10
Patients should be screened for fatigue at regular intervals. The primary care physician should focus the history to include information regarding the onset, pattern, duration, associated factors, assessment of other treatable comorbidities, medications, psychological well-being, nutritional status, and pain level of each patient who complains of fatigue.
Laboratory tests for treatable causes of fatigue include:
- A complete blood cell count to evaluate for anemia
- A comprehensive metabolic panel to evaluate electrolytes, renal function, and hepatic function
- The thyroid-stimulating hormone level to evaluate thyroid function, particularly in breast cancer patients who have received radiation therapy.2
If no organic cause is uncovered, the focus should shift to lifestyle interventions as the treatment of choice. The treatment of fatigue in this situation is increased physical activity with the goals discussed above. Psychological intervention may be required with cognitive behavioral therapy, psychological and supportive therapies, education on sleep hygiene, and possible sleep restriction.
If alternative causes of fatigue are ruled out and physical and psychological support fails to reduce symptoms, the practitioner can consider a psychostimulant such as methylphenidate, but this should be used cautiously.2
SEXUAL DYSFUNCTION
Intimate relationships and sexuality are an important part of life and are affected by a variety of factors including physical health, psychological well-being, body image perception, and overall status of relationships. As a side effect of chemotherapy, cancer survivors may complain of erectile dysfunction, penile shortening, dyspareunia, vaginal dryness, decreased libido, anorgasmy, and changes in body image. These issues are frequently unaddressed, whether due to the physician’s discomfort in discussing the topic or to the patient’s embarrassment and reluctance to discuss the matter.11
Breast cancer patients may experience sexual dysfunction both during and after treatment due to a combination of systemic effects of treatment, changes in physical appearance leading to impaired body image, strains on partner relationships, and psychological sequelae of diagnosis and treatment of cancer.12 Manipulation and radiation to the breast affect sexual functioning by altering body contour and image. Additionally, chemotherapy can lead to early menopause and hormonal alterations due to endocrine therapies, which can negatively affect sexual organs.11
Studies have shown that treatment with tamoxifen causes less sexual dysfunction than do aromatase inhibitors. In the Arimidex, Tamoxifen, Alone or in Combination trial, therapy with anastrozole was associated with more vaginal dryness, dyspareunia, and decreased libido compared with tamoxifen.12
Treatment requires a comprehensive history, a physical examination, and a discussion of relationship satisfaction with the patient.
Vaginal dryness and dyspareunia can be treated with vaginal lubricants and moisturizers. Moisturizers are effective if used multiple times per week, whereas lubricants can be used on demand. Low-dose vaginal estrogen preparations can be used in select patients with severe vaginal dryness; the goal should be discussed. Hormone replacement therapy is contraindicated in breast cancer survivors due to the risk of recurrence.11
Prostate cancer survivors. Up to 70% of men felt their quality of life and sexual function were adversely affected after the diagnosis and treatment.13,14 Erectile dysfunction following radical prostatectomy and radiation therapy remains one of the leading causes of sexual dysfunction.14–15 Erectile dysfunction is multifactorial, with both psychogenic and organic causes. Comorbidities must be considered including hypertension, diabetes, hyperlipidemia, and smoking. Early penile rehabilitation is a proposed treatment strategy.14
First-line therapy for penile rehabilitation includes introduction of daily low-dose phosphodiesterase type 5 inhibitors as early as the time of catheter removal to within the first month after surgery. The need for daily dosing vs on-demand dosing has been controversial.15 Two large multicenter, double-blind studies had conflicting outcomes. The first reported that in men receiving nightly sildenafil (50 or 100 mg) after radical prostatectomy, 27% had increased return of spontaneous erectile function vs 4% with placebo16; the second study showed no difference between nightly and on-demand dosing.17 The consensus is that a phosphodiesterase type 5 inhibitor should be initiated early.
Second-line therapy includes intracavernosal injections and vacuum erection devices. Finally, a penile prosthesis implant can be offered to patients who have responded poorly to medical therapy.13
Colorectal cancer survivors suffer from sexually related problems similar to those stated above, including erectile dysfunction, ejaculation problems, dyspareunia, vaginal dryness, and decreased enjoyment.18 These patients should be provided treatments similar to those described above. In addition, they may suffer from body image issues, particularly those with a permanent ostomy.9
Sexual dysfunction is a multifaceted problem for patients. Encouraging couples to discuss sexual intimacy frequently helps to reveal and cope with the problems, whether physical or psychological. It is the primary care physician’s role to recognize any sexual concerns and refer to the appropriate specialist.
OSTEOPOROSIS
Osteoporosis is a metabolic bone disease characterized by low bone mineral density. As a result, bones become weak and fracture more easily from minor injuries.
Risk factors for osteoporosis include female sex, family history, advanced age, low body weight, low calcium and vitamin D levels, sedentary lifestyle, smoking, and low estrogen levels.19 Cancer treatment places patients at a greater risk for osteoporosis, particularly for those patients with chemotherapy-induced ovarian failure, those treated with aromatase inhibitors, men receiving androgen-deprivation therapy, and patients on glucocorticoid therapy. The morbidity and mortality associated with bone loss can be prevented with appropriate screening, lifestyle changes, and therapy.2
According to the National Osteoporosis Foundation Guideline for Preventing and Treating Osteoporosis, all men and postmenopausal women age 50 and older should be evaluated clinically for osteoporosis risk to determine the need for bone mineral density testing.2,19 The US Preventive Services Task Force recommends bone mineral density testing in all women age 65 and older, and for women 60 to 64 who are at high risk for bone loss. ASCO agrees, and further suggests bone mineral density screening for women with breast cancer who have risk factors such as positive family history, body weight less than 70 kg, and prior nontraumatic fracture, as well as for postmenopausal women of any age receiving aromatase inhibitors and for premenopausal women with therapy-induced ovarian failure.11
Androgen deprivation therapy is a mainstay of treatment in recurrent and metastatic prostate cancer. The effect is severe hypogonadism with reductions in serum testosterone levels. Androgen deprivation therapy accelerates bone turnover, decreases bone mineral density, and contributes to fracture risk. The National Comprehensive Cancer Network additionally suggests measuring bone mineral density at baseline for all men receiving androgen deprivation therapy or other medications associated with bone loss, repeating it 1 year after androgen deprivation therapy and then every 2 years, or as clinically indicated.20
The gold standard for measuring bone mineral density is dual-energy x-ray absorptiometry. The World Health Organization FRAX tool uses bone mineral density and several clinical factors to estimate the risk of fracture in the next 10 years, which can help guide therapy. Cancer patients with elevated fracture risk should be evaluated every 2 years. Counseling should be provided to address modifiable risk factors such as smoking, alcohol consumption, physical inactivity, and low calcium and vitamin D intake. Therapy should be strongly considered in patients with a bone mineral density below a T-score of –2.0. 2,19
Treatment begins with lifestyle modifications such as weight-bearing exercises to improve balance and muscle strength and to prevent falls, and adequate intake of calcium (≥ 1,200 mg daily) and vitamin D (800–1,000 IU daily) for adults age 50 and older. Treatment with bisphosphonates may be required.2,11,20
NEUROPATHY
Many chemotherapeutic agents can lead to neuropathy and can result in long-term disability in patients. Patients treated with taxane- and platinum-based chemotherapy are at particular risk.
Paclitaxel, used in the treatment of breast, ovarian, and lung cancer, can lead to distal neuropathy. This neuropathy commonly has a stocking-and-glove distribution and is primarily sensory; however, it may have motor and autonomic components. The neuropathy typically lessens when the medication is stopped, although in some patients it can persist and lead to long-term disability.
Treatment can include massage. Medications such as gabapentin and pregabalin can also be used, but randomized controlled trials do not support them, as they predominantly treat the tingling rather than the numbness.11
BLADDER AND BOWEL DYSFUNCTION
Urinary incontinence and dysfunction are frequent complications in prostate cancer survivors. Urinary function should be discussed regularly with patients, addressing quality of the urinary stream, difficulty emptying the bladder, timing, and incontinence.4 Urinary incontinence is frequently seen in postprostatectomy patients.
The cornerstone of treating urinary incontinence is determining the cause of the incontinence, whether it is stress or urge incontinence, or both.21 For those patients with urge incontinence alone, practitioners can address the problem with a combination of behavior modification, pelvic floor exercises, and anticholinergic medications such as oxybutynin. If the problem stems from difficulty initiating or a slow stream, physicians may consider alpha-blockers.4,21 If the incontinence is persistent, bothersome, and has components of stress incontinence, the patient should be referred to a urologist for urodynamic testing, cystoscopy, and surgical evaluation for possible placement of a male urethral sling or artificial urinary sphincter.21
Colorectal cancer survivors, particularly those who received radiation therapy, are at high risk of bowel dysfunction such as chronic diarrhea and stool incontinence. Patients should be educated about this possible side effect. Symptoms of bowel dysfunction can affect body image and interfere with social functioning and overall quality of life. Patients should be provided with coping tools such as antidiarrheal medication, stool bulking agents, changes in diet, and protective underwear.
CARDIOVASCULAR DISEASE
Evidence suggests that certain types of chemotherapy and radiation therapy increase the risk of cardiovascular disease. Prostate cancer survivors treated with androgen deprivation therapy, particularly those more than 75 years old, are at increased risk of cardiovascular disease and diabetes.22
It is recommended that men be screened with fasting plasma glucose at baseline and yearly thereafter while receiving androgen deprivation therapy. Lipid panel testing should be done 1 year from initiation of androgen deprivation therapy and then, if results are normal, every 5 years or as clinically warranted. The focus should be on primary prevention with emphasis on smoking cessation, treating hypertension per guidelines, lifestyle modifications, and treatment with aspirin and statins when clinically appropriate.20
Radiation therapy, chemotherapy, and endocrine therapy have all been suggested to lead to cardiotoxicity in breast cancer patients. Anthracycline-based chemotherapies have a well-recognized association with cardiomyopathy. Factors associated with increased risk of anthracycline-induced cardiomyopathy include older age, hypertension, pre-existing coronary artery disease, and previous mediastinal radiation.
Early detection of cardiomyopathy may lead to avoidance of irreversible cardiotoxicity, but there are currently no clear guidelines for cardiac screening in breast cancer survivors. If cardiomyopathy is detected, treatment should include beta-blockers and angiotensin-converting enzyme inhibitors as well as modification of other cardiovascular risk factors.11
A SURVIVORSHIP CARE PLAN
There is life beyond the diagnosis of cancer. As patients are living longer, with an estimated 5-year survival rate of 66.5% of all cancers in the United States, there must be a transition of care from the oncologist to the primary care physician.1 While the oncologist will remain involved in the initial years of follow-up care, these visits will go from twice a year to once a year, and eventually the patient will make a full transition to care by the primary care physician. The timing of this changeover varies from physician to physician, but the primary care physician is ultimately responsible for the follow-up.
A tool to ease this transition is a survivorship care plan. The goal of a survivorship care plan is to individualize a follow-up plan while keeping in mind the necessary surveillance as outlined. These care plans are created with the patient and oncologist and then brought to the primary care physician. While there is an abundance of literature regarding the creation and initiation of survivorship care plans, the success of these plans is uncertain. Ultimately, the goal of a survivorship care plan is to create open dialogue among the oncologist, the primary care physician, and the patient. This unique patient population requires close follow-up by a multidisciplinary team with the primary care physician serving as the steward.
In 2015, about 1.6 million Americans received a diagnosis of cancer.1 In 2012, when 13.7 million people were living with cancer in the United States, the estimated 5-year survival rate of all cancers was 66.5%.1 Today, breast, prostate, and colon cancers have 5-year survival rates of 89.4%, 98.9%, and 64.9%, respectively.
With this rising trend in survival, primary care physicians have been steadily assuming the long-term care of these patients. The phrase “cancer survivorship” was coined by the National Comprehensive Cancer Network to describe the experience of living with, through, and beyond a cancer diagnosis.2
As cancer becomes a chronic medical condition, the primary care physician assumes a vital role in the treatment of the unique and evolving needs of this patient population.
This article discusses the specific needs of patients surviving breast, prostate, and colon cancer with special focus on surveillance guidelines for recurrence, development of concomitant malignancies, assessment of psychosocial and physical effects, and disease conditions related to the treatment of cancer itself.
FOLLOW-UP CARE AND SURVEILLANCE
Follow-up care in patients being treated for cancer is vital to survivorship. It includes promoting healthy living, managing treatment side effects, and monitoring for long-term side effects and possible recurrence.
Patients previously treated for malignancy are more susceptible to second primary cancers, for an array of reasons including the effects of prior treatment, shared environmental exposures such as smoking, and genetic susceptibility.2 Therefore, it is important for the primary care physician to recognize signs and symptoms and to screen cancer survivors appropriately. The American Society of Clinical Oncology (ASCO) has developed evidence-based recommendations for follow-up care,3 which we review here.
Breast cancer
For breast cancer patients, history and physical examinations are recommended every 3 to 6 months for the first 3 years, every 6 to 12 months in years 4 and 5, and annually thereafter.3
A repeat mammogram should be performed 1 year after the initial mammogram that led to the diagnosis. If the patient underwent radiation therapy, a repeat mammogram of the affected breast should be done 6 months after completion of radiation. Finally, a mammogram should be done every 6 to 12 months thereafter.3 It is also recommended that patients perform a monthly breast self-examination, but this does not replace the annual mammogram.3
Women who are treated with tamoxifen should have an annual gynecologic assessment if they have a uterus and should be encouraged to discuss any abnormal vaginal bleeding with their physician, given the increased risk of uterine cancer.2
ASCO does not recommend routine use of complete blood cell counts, complete metabolic panels, bone scans, chest radiography, computed tomography, ultrasonography, positron-emission tomography, or tumor markers in patients who are asymptomatic.3
Prostate cancer
ASCO’s recommendations for patients recovering from prostate cancer include regular histories and physical examinations and general health promotion. Prostate-specific antigen (PSA) testing is recommended every 6 to 12 months for the first 5 years after treatment and annually thereafter. More frequent PSA testing may be required in men at higher risk of recurrence or in patients who may undergo additional treatment, including radiation and surgery.4 Higher risk of disease recurrence is thought to depend on disease-specific factors at the time of original diagnosis including pretreatment PSA, Gleason score, and tumor stage.4 This should be discussed between the oncologist and primary care physician.
In regard to digital rectal examinations, the oncologist and primary care physician should jointly determine the frequency of examination. The frequency of digital rectal examinations remains an area of controversy due to their low sensitivity for detecting recurrences. Digital rectal examinations may be omitted in patients with undetectable levels of PSA.4
In regard to second primary malignancies, prostate cancer survivors who have undergone pelvic radiation therapy have a slightly higher risk of bladder and colorectal cancer. The lifetime incidence of bladder cancer after pelvic radiation is 5% to 6%, compared with 2.4% in the general population.1,5 A prostate cancer survivor presenting with hematuria should be referred to a urologist for cystoscopy and evaluation of the upper urinary tract to rule out cancer.4
Similarly, patients presenting with rectal bleeding should be referred to a gastroenterologist and the treating radiation oncologist for complete evaluation. The risk of rectal cancer after pelvic radiation therapy increases to about the same level as in someone who has a first-degree relative with colorectal cancer.5 Therefore, it is recommended that patients undergo screening for colorectal cancer in conjunction with existing evidence-based guidelines. There is no evidence to suggest that increased intensity of screening improves overall or disease-specific survival.4
Colon cancer
In patients with resected colorectal cancer, continued surveillance is important to evaluate for recurrent cancer as well as for metachronous neoplasms. Consensus statements indicate that surveillance colonoscopy should be continued for those who have undergone surgical resection for stage I, II, or III colon or rectal cancers, and for those patients with stage IV who have undergone surgical resection with curative intent.6
Patients who undergo curative resection of rectal or colon cancer should have a colonoscopy 1 year after resection or 1 year after the colonoscopy was performed, to clear the colon of synchronous disease. Subsequently, if the colonoscopy done at 1 year is normal, the interval before the next colonoscopy is 3 years. If that colonoscopy is normal, the next colonoscopy is in 5 years. Time intervals may be shorter if there is evidence of hereditary nonpolyposis colorectal cancer or adenoma.
Patients who underwent low anterior resection of rectal cancer should undergo periodic examination of the rectum to evaluate for local recurrence. Although effectiveness is not proven, endoscopic ultrasonography or flexible sigmoidoscopy is suggested at 3- to 6-month intervals for the first 2 to 3 years after resection. This is independent of colonoscopy.6,7
Additionally, ASCO recommends a history and physical examination and carcinoembryonic antigen testing every 3 to 6 months for the first 5 years. Computed tomography of the chest, abdomen, and pelvis should be done annually for the first 3 years after the end of treatment.7
HEALTH PROMOTION
Maintaining a healthy body weight and a nutritionally balanced diet should be encouraged in all cancer survivors. Poor diet, lack of exercise, excessive alcohol consumption, and smoking reduce quality of life and increase the risk of cancer.2
Diet
Numerous studies have looked at dietary modifications and risk reduction, and although there is no consensus on specific dietary guidelines, there is consensus that diet modification to maintain normal body weight will improve overall quality of life.8 Patients should be encouraged to consume a well-balanced diet consisting mostly of fruits, vegetables, whole grains, and beans, and to limit consumption of animal protein.8
There is little evidence to support taking vitamins or other dietary supplements to prevent or control cancer or to prevent its recurrence. The primary care physician should assess supplement use on a regular basis during office visits.2
Exercise
Rest is an important component of the initial recovery process. Too much inactivity, however, leads to loss of physical conditioning and muscle strength. This in turn may negatively affect a patient’s ability to perform activities of daily living and may worsen fatigue associated with treatment.
Accordingly, the National Comprehensive Cancer Network recommends at least 150 minutes of moderate activity and up to 75 minutes of more rigorous activity divided throughout the week.2,8 The regimen should include endurance and muscle strength training, which aid in balance, bone, health, and functional status. The intensity of exercise should be increased in a stepwise fashion, taking into account individual capabilities and limitations.2
Cancer survivors may need specific exercise recommendations and supervised programs to ensure safety and limit long-term side effects of their treatment. For example:
Patients with neuropathy should have their stability, balance, and gait assessed before starting a new program. These patients may benefit from an aerobic exercise program that includes riding a stationary bike rather than running.
Patients with poor bone health should have their fracture risk assessed.
Those with an ostomy bag should empty the bag before physical activity. They should avoid contact sports and activities that increase intra-abdominal pressure.
Patients suffering from lymphedema should wear compression garments when engaging in physical activity. They should undergo baseline and periodic reevaluation of the lymphedema and initiate strength training in the affected body part only if the lymphedema is stable (ie, no need for therapy for 3 months, no recent infections requiring antibiotics, and no change in circumference > 10%).2
Mental health
Health promotion should focus not only on the physical health of the patient, but also on his or her emotional and psychological well-being. As they make the transition from cancer patient to survivor, many individuals may develop or have worsening depression and anxiety due to fear of recurrence. These feelings of powerlessness can linger for years after the initial treatment.
Patients should be screened regularly for signs and symptoms of depression by asking about their family and social support. Referral to support groups, psychologists, and psychiatrists may be warranted.9
MITIGATING CANCER-RELATED FATIGUE
Cancer-related fatigue involves a patient’s subjective sense of physical, emotional, and cognitive exhaustion related to cancer or treatment that is disproportionate to that expected from recent daily activity.2 Fatigue is a common complaint among survivors and can occur months to years after treatment ends.10
Patients should be screened for fatigue at regular intervals. The primary care physician should focus the history to include information regarding the onset, pattern, duration, associated factors, assessment of other treatable comorbidities, medications, psychological well-being, nutritional status, and pain level of each patient who complains of fatigue.
Laboratory tests for treatable causes of fatigue include:
- A complete blood cell count to evaluate for anemia
- A comprehensive metabolic panel to evaluate electrolytes, renal function, and hepatic function
- The thyroid-stimulating hormone level to evaluate thyroid function, particularly in breast cancer patients who have received radiation therapy.2
If no organic cause is uncovered, the focus should shift to lifestyle interventions as the treatment of choice. The treatment of fatigue in this situation is increased physical activity with the goals discussed above. Psychological intervention may be required with cognitive behavioral therapy, psychological and supportive therapies, education on sleep hygiene, and possible sleep restriction.
If alternative causes of fatigue are ruled out and physical and psychological support fails to reduce symptoms, the practitioner can consider a psychostimulant such as methylphenidate, but this should be used cautiously.2
SEXUAL DYSFUNCTION
Intimate relationships and sexuality are an important part of life and are affected by a variety of factors including physical health, psychological well-being, body image perception, and overall status of relationships. As a side effect of chemotherapy, cancer survivors may complain of erectile dysfunction, penile shortening, dyspareunia, vaginal dryness, decreased libido, anorgasmy, and changes in body image. These issues are frequently unaddressed, whether due to the physician’s discomfort in discussing the topic or to the patient’s embarrassment and reluctance to discuss the matter.11
Breast cancer patients may experience sexual dysfunction both during and after treatment due to a combination of systemic effects of treatment, changes in physical appearance leading to impaired body image, strains on partner relationships, and psychological sequelae of diagnosis and treatment of cancer.12 Manipulation and radiation to the breast affect sexual functioning by altering body contour and image. Additionally, chemotherapy can lead to early menopause and hormonal alterations due to endocrine therapies, which can negatively affect sexual organs.11
Studies have shown that treatment with tamoxifen causes less sexual dysfunction than do aromatase inhibitors. In the Arimidex, Tamoxifen, Alone or in Combination trial, therapy with anastrozole was associated with more vaginal dryness, dyspareunia, and decreased libido compared with tamoxifen.12
Treatment requires a comprehensive history, a physical examination, and a discussion of relationship satisfaction with the patient.
Vaginal dryness and dyspareunia can be treated with vaginal lubricants and moisturizers. Moisturizers are effective if used multiple times per week, whereas lubricants can be used on demand. Low-dose vaginal estrogen preparations can be used in select patients with severe vaginal dryness; the goal should be discussed. Hormone replacement therapy is contraindicated in breast cancer survivors due to the risk of recurrence.11
Prostate cancer survivors. Up to 70% of men felt their quality of life and sexual function were adversely affected after the diagnosis and treatment.13,14 Erectile dysfunction following radical prostatectomy and radiation therapy remains one of the leading causes of sexual dysfunction.14–15 Erectile dysfunction is multifactorial, with both psychogenic and organic causes. Comorbidities must be considered including hypertension, diabetes, hyperlipidemia, and smoking. Early penile rehabilitation is a proposed treatment strategy.14
First-line therapy for penile rehabilitation includes introduction of daily low-dose phosphodiesterase type 5 inhibitors as early as the time of catheter removal to within the first month after surgery. The need for daily dosing vs on-demand dosing has been controversial.15 Two large multicenter, double-blind studies had conflicting outcomes. The first reported that in men receiving nightly sildenafil (50 or 100 mg) after radical prostatectomy, 27% had increased return of spontaneous erectile function vs 4% with placebo16; the second study showed no difference between nightly and on-demand dosing.17 The consensus is that a phosphodiesterase type 5 inhibitor should be initiated early.
Second-line therapy includes intracavernosal injections and vacuum erection devices. Finally, a penile prosthesis implant can be offered to patients who have responded poorly to medical therapy.13
Colorectal cancer survivors suffer from sexually related problems similar to those stated above, including erectile dysfunction, ejaculation problems, dyspareunia, vaginal dryness, and decreased enjoyment.18 These patients should be provided treatments similar to those described above. In addition, they may suffer from body image issues, particularly those with a permanent ostomy.9
Sexual dysfunction is a multifaceted problem for patients. Encouraging couples to discuss sexual intimacy frequently helps to reveal and cope with the problems, whether physical or psychological. It is the primary care physician’s role to recognize any sexual concerns and refer to the appropriate specialist.
OSTEOPOROSIS
Osteoporosis is a metabolic bone disease characterized by low bone mineral density. As a result, bones become weak and fracture more easily from minor injuries.
Risk factors for osteoporosis include female sex, family history, advanced age, low body weight, low calcium and vitamin D levels, sedentary lifestyle, smoking, and low estrogen levels.19 Cancer treatment places patients at a greater risk for osteoporosis, particularly for those patients with chemotherapy-induced ovarian failure, those treated with aromatase inhibitors, men receiving androgen-deprivation therapy, and patients on glucocorticoid therapy. The morbidity and mortality associated with bone loss can be prevented with appropriate screening, lifestyle changes, and therapy.2
According to the National Osteoporosis Foundation Guideline for Preventing and Treating Osteoporosis, all men and postmenopausal women age 50 and older should be evaluated clinically for osteoporosis risk to determine the need for bone mineral density testing.2,19 The US Preventive Services Task Force recommends bone mineral density testing in all women age 65 and older, and for women 60 to 64 who are at high risk for bone loss. ASCO agrees, and further suggests bone mineral density screening for women with breast cancer who have risk factors such as positive family history, body weight less than 70 kg, and prior nontraumatic fracture, as well as for postmenopausal women of any age receiving aromatase inhibitors and for premenopausal women with therapy-induced ovarian failure.11
Androgen deprivation therapy is a mainstay of treatment in recurrent and metastatic prostate cancer. The effect is severe hypogonadism with reductions in serum testosterone levels. Androgen deprivation therapy accelerates bone turnover, decreases bone mineral density, and contributes to fracture risk. The National Comprehensive Cancer Network additionally suggests measuring bone mineral density at baseline for all men receiving androgen deprivation therapy or other medications associated with bone loss, repeating it 1 year after androgen deprivation therapy and then every 2 years, or as clinically indicated.20
The gold standard for measuring bone mineral density is dual-energy x-ray absorptiometry. The World Health Organization FRAX tool uses bone mineral density and several clinical factors to estimate the risk of fracture in the next 10 years, which can help guide therapy. Cancer patients with elevated fracture risk should be evaluated every 2 years. Counseling should be provided to address modifiable risk factors such as smoking, alcohol consumption, physical inactivity, and low calcium and vitamin D intake. Therapy should be strongly considered in patients with a bone mineral density below a T-score of –2.0. 2,19
Treatment begins with lifestyle modifications such as weight-bearing exercises to improve balance and muscle strength and to prevent falls, and adequate intake of calcium (≥ 1,200 mg daily) and vitamin D (800–1,000 IU daily) for adults age 50 and older. Treatment with bisphosphonates may be required.2,11,20
NEUROPATHY
Many chemotherapeutic agents can lead to neuropathy and can result in long-term disability in patients. Patients treated with taxane- and platinum-based chemotherapy are at particular risk.
Paclitaxel, used in the treatment of breast, ovarian, and lung cancer, can lead to distal neuropathy. This neuropathy commonly has a stocking-and-glove distribution and is primarily sensory; however, it may have motor and autonomic components. The neuropathy typically lessens when the medication is stopped, although in some patients it can persist and lead to long-term disability.
Treatment can include massage. Medications such as gabapentin and pregabalin can also be used, but randomized controlled trials do not support them, as they predominantly treat the tingling rather than the numbness.11
BLADDER AND BOWEL DYSFUNCTION
Urinary incontinence and dysfunction are frequent complications in prostate cancer survivors. Urinary function should be discussed regularly with patients, addressing quality of the urinary stream, difficulty emptying the bladder, timing, and incontinence.4 Urinary incontinence is frequently seen in postprostatectomy patients.
The cornerstone of treating urinary incontinence is determining the cause of the incontinence, whether it is stress or urge incontinence, or both.21 For those patients with urge incontinence alone, practitioners can address the problem with a combination of behavior modification, pelvic floor exercises, and anticholinergic medications such as oxybutynin. If the problem stems from difficulty initiating or a slow stream, physicians may consider alpha-blockers.4,21 If the incontinence is persistent, bothersome, and has components of stress incontinence, the patient should be referred to a urologist for urodynamic testing, cystoscopy, and surgical evaluation for possible placement of a male urethral sling or artificial urinary sphincter.21
Colorectal cancer survivors, particularly those who received radiation therapy, are at high risk of bowel dysfunction such as chronic diarrhea and stool incontinence. Patients should be educated about this possible side effect. Symptoms of bowel dysfunction can affect body image and interfere with social functioning and overall quality of life. Patients should be provided with coping tools such as antidiarrheal medication, stool bulking agents, changes in diet, and protective underwear.
CARDIOVASCULAR DISEASE
Evidence suggests that certain types of chemotherapy and radiation therapy increase the risk of cardiovascular disease. Prostate cancer survivors treated with androgen deprivation therapy, particularly those more than 75 years old, are at increased risk of cardiovascular disease and diabetes.22
It is recommended that men be screened with fasting plasma glucose at baseline and yearly thereafter while receiving androgen deprivation therapy. Lipid panel testing should be done 1 year from initiation of androgen deprivation therapy and then, if results are normal, every 5 years or as clinically warranted. The focus should be on primary prevention with emphasis on smoking cessation, treating hypertension per guidelines, lifestyle modifications, and treatment with aspirin and statins when clinically appropriate.20
Radiation therapy, chemotherapy, and endocrine therapy have all been suggested to lead to cardiotoxicity in breast cancer patients. Anthracycline-based chemotherapies have a well-recognized association with cardiomyopathy. Factors associated with increased risk of anthracycline-induced cardiomyopathy include older age, hypertension, pre-existing coronary artery disease, and previous mediastinal radiation.
Early detection of cardiomyopathy may lead to avoidance of irreversible cardiotoxicity, but there are currently no clear guidelines for cardiac screening in breast cancer survivors. If cardiomyopathy is detected, treatment should include beta-blockers and angiotensin-converting enzyme inhibitors as well as modification of other cardiovascular risk factors.11
A SURVIVORSHIP CARE PLAN
There is life beyond the diagnosis of cancer. As patients are living longer, with an estimated 5-year survival rate of 66.5% of all cancers in the United States, there must be a transition of care from the oncologist to the primary care physician.1 While the oncologist will remain involved in the initial years of follow-up care, these visits will go from twice a year to once a year, and eventually the patient will make a full transition to care by the primary care physician. The timing of this changeover varies from physician to physician, but the primary care physician is ultimately responsible for the follow-up.
A tool to ease this transition is a survivorship care plan. The goal of a survivorship care plan is to individualize a follow-up plan while keeping in mind the necessary surveillance as outlined. These care plans are created with the patient and oncologist and then brought to the primary care physician. While there is an abundance of literature regarding the creation and initiation of survivorship care plans, the success of these plans is uncertain. Ultimately, the goal of a survivorship care plan is to create open dialogue among the oncologist, the primary care physician, and the patient. This unique patient population requires close follow-up by a multidisciplinary team with the primary care physician serving as the steward.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results Program. SEER cancer stat fact sheets. http://seer.cancer.gov/statfacts. Accessed March 6, 2017.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines Survivorship: 2015. www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf. Accessed March 6, 2017.
- Khatcheressian JL, Hurley P, Bantug E, et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology Clinical Practice Guideline update. J Clin Oncol 2013; 31:961–965.
- Resnick MJ, Lacchetti C, Bergman J, et al. Prostate cancer survivorship care guideline: American Society of Clinical Oncology Clinical Practice Guideline endorsement. J Clin Oncol 2015; 33:1078–1085.
- Sountoulides P, Koletsas N, Kikidakis D, Paschalidis K, Sofikitis N. Secondary malignancies following radiotherapy for prostate cancer. Ther Adv Urol 2010; 2:119–125.
- Rex DK, Kahi CJ, Levin B, et al. Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and US Multi-Society Task Force on Colorectal Cancer. CA Cancer J Clin 2006; 56:160–168.
- Meyerhardt JA, Mangu PB, Flynn PJ, et al; American Society of Clinical Oncology. Follow-up care, surveillance protocol, and secondary prevention measures for survivors of colorectal cancer: American Society of Clinical Oncology clinical practice guideline endorsement. J Clin Oncol 2013; 31:4465–4470.
- Davies NJ, Batehup L, Thomas R. The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: a review of the literature. Br J Cancer 2011; 105(suppl 1):S52–S73.
- Miller K, editor. Excellent Care for Cancer Survivors: A Guide to Fully Meet Their Needs in Medical Offices and in the Community (Praeger Series on Contemporary Health & Living). 1st ed. Santa Barbara, CA: Praeger; 2012.
- Stanton AL, Rowland JH, Ganz PA. Life after diagnosis and treatment of cancer in adulthood: contributions from psychosocial oncology research. Am Psychol 2015; 70:159–174.
- Stan D, Loprinzi CL, Ruddy KJ. Breast cancer survivorship issues. Hematol Oncol Clin North Am 2013; 27:805–827.
- Fallowfield L, Cella D, Cuzick J, Francis S, Locker G, Howell A. Quality of life of postmenopausal women in the Arimidex, Tamoxifen, Alone or in Combination (ATAC) Adjuvant Breast Cancer Trial. J Clin Oncol 2004; 22:426–471.
- Chung E, Gillman M. Prostate cancer survivorship: a review of erectile dysfunction and penile rehabilitation after prostate cancer therapy. Med J Aust 2014; 200:582–585.
- Sherer BA, Levine LA. Current management of erectile dysfunction in prostate cancer survivors. Curr Opin Urol 2014; 24:401–416.
- Chung E, Brock G. Sexual rehabilitation and cancer survivorship: a state of art review of current literature and management strategies in male sexual dysfunction among prostate cancer survivors. J Sex Med 2013; 10(suppl 1):102–111.
- Padma-Nathan H, McCullough AR, Levine LA, et al; Study Group. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res 2008; 20:479–486.
- Montorsi F, Brock G, Lee J, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol 2008; 54:924–931.
- Den Oudsten BL, Traa MJ, Thong MS, et al. Higher prevalence of sexual dysfunction in colon and rectal cancer survivors compared with the normative population: a population-based study. Eur J Cancer 2012; 48:3161–3170.
- National Osteoporosis Foundation (NOF). http://nof.org. Accessed March 3, 2017.
- Saylor PJ, Keating NL, Smith MR. Prostate cancer survivorship: prevention and treatment of the adverse effects of androgen deprivation therapy. J Gen Intern Med 2009; 24(suppl 2):S389–S394.
- Gupta S, Peterson AC. Stress urinary incontinence in the prostate cancer survivor. Curr Opin Urol 2014; 24:395–400.
- Morgans AK, Fan KH, Koyama T, et al. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J Urol 2015; 193:1226–1231.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results Program. SEER cancer stat fact sheets. http://seer.cancer.gov/statfacts. Accessed March 6, 2017.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines Survivorship: 2015. www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf. Accessed March 6, 2017.
- Khatcheressian JL, Hurley P, Bantug E, et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology Clinical Practice Guideline update. J Clin Oncol 2013; 31:961–965.
- Resnick MJ, Lacchetti C, Bergman J, et al. Prostate cancer survivorship care guideline: American Society of Clinical Oncology Clinical Practice Guideline endorsement. J Clin Oncol 2015; 33:1078–1085.
- Sountoulides P, Koletsas N, Kikidakis D, Paschalidis K, Sofikitis N. Secondary malignancies following radiotherapy for prostate cancer. Ther Adv Urol 2010; 2:119–125.
- Rex DK, Kahi CJ, Levin B, et al. Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and US Multi-Society Task Force on Colorectal Cancer. CA Cancer J Clin 2006; 56:160–168.
- Meyerhardt JA, Mangu PB, Flynn PJ, et al; American Society of Clinical Oncology. Follow-up care, surveillance protocol, and secondary prevention measures for survivors of colorectal cancer: American Society of Clinical Oncology clinical practice guideline endorsement. J Clin Oncol 2013; 31:4465–4470.
- Davies NJ, Batehup L, Thomas R. The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: a review of the literature. Br J Cancer 2011; 105(suppl 1):S52–S73.
- Miller K, editor. Excellent Care for Cancer Survivors: A Guide to Fully Meet Their Needs in Medical Offices and in the Community (Praeger Series on Contemporary Health & Living). 1st ed. Santa Barbara, CA: Praeger; 2012.
- Stanton AL, Rowland JH, Ganz PA. Life after diagnosis and treatment of cancer in adulthood: contributions from psychosocial oncology research. Am Psychol 2015; 70:159–174.
- Stan D, Loprinzi CL, Ruddy KJ. Breast cancer survivorship issues. Hematol Oncol Clin North Am 2013; 27:805–827.
- Fallowfield L, Cella D, Cuzick J, Francis S, Locker G, Howell A. Quality of life of postmenopausal women in the Arimidex, Tamoxifen, Alone or in Combination (ATAC) Adjuvant Breast Cancer Trial. J Clin Oncol 2004; 22:426–471.
- Chung E, Gillman M. Prostate cancer survivorship: a review of erectile dysfunction and penile rehabilitation after prostate cancer therapy. Med J Aust 2014; 200:582–585.
- Sherer BA, Levine LA. Current management of erectile dysfunction in prostate cancer survivors. Curr Opin Urol 2014; 24:401–416.
- Chung E, Brock G. Sexual rehabilitation and cancer survivorship: a state of art review of current literature and management strategies in male sexual dysfunction among prostate cancer survivors. J Sex Med 2013; 10(suppl 1):102–111.
- Padma-Nathan H, McCullough AR, Levine LA, et al; Study Group. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res 2008; 20:479–486.
- Montorsi F, Brock G, Lee J, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol 2008; 54:924–931.
- Den Oudsten BL, Traa MJ, Thong MS, et al. Higher prevalence of sexual dysfunction in colon and rectal cancer survivors compared with the normative population: a population-based study. Eur J Cancer 2012; 48:3161–3170.
- National Osteoporosis Foundation (NOF). http://nof.org. Accessed March 3, 2017.
- Saylor PJ, Keating NL, Smith MR. Prostate cancer survivorship: prevention and treatment of the adverse effects of androgen deprivation therapy. J Gen Intern Med 2009; 24(suppl 2):S389–S394.
- Gupta S, Peterson AC. Stress urinary incontinence in the prostate cancer survivor. Curr Opin Urol 2014; 24:395–400.
- Morgans AK, Fan KH, Koyama T, et al. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J Urol 2015; 193:1226–1231.
KEY POINTS
- The American Society of Clinical Oncology has developed evidence-based recommendations for follow-up care and surveillance for new and recurrent cancer in cancer survivors. In general, this surveillance should be more frequent in the first months and years after cancer treatment but can become less so as time goes on.
- Health promotion in cancer survivors involves the same advice regarding smoking cessation, diet, exercise, and mental health that all patients require.
- Depending on the type of cancer and treatment, long-term adverse effects include fatigue, sexual dysfunction, osteoporosis, neuropathy, bladder and bowel dysfunction, and cardiovascular disease.
- A survivorship care plan can be drawn up with input from the patient, oncologist, primary care physician, and other caregivers so that everyone can be clear as to what is going on.

Which patients with nonalcoholic fatty liver disease should undergo liver biopsy?
Patients should undergo biopsy to guide management and prognosis if suspected of having steatohepatitis or fibrosis.
WHAT IS NAFLD?
Nonalcoholic fatty liver disease (NAFLD) is the most common form of chronic liver disease in the United States and is the second most common reason for liver transplant.1 It is thought to be the hepatic consequence of systemic insulin resistance and the metabolic syndrome characterized by obesity, dyslipidemia, and type 2 diabetes mellitus.
WHAT IS THE RELATIONSHIP BETWEEN NAFLD AND NASH?
NAFLD is defined by the accumulation of hepatic fat as evidenced by imaging or histologic study and without a coexisting cause of chronic liver disease or a secondary cause of hepatic steatosis, including significant alcohol use, medications, or an inherited or acquired metabolic state.
NAFLD has two subtypes: nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH). NAFL is characterized by steatosis, including inflammation, in at least 5% of hepatocytes. NASH is defined by a constellation of features that include steatosis, lobular and portal inflammation, and liver cell injury in the form of hepatocyte ballooning.2
Clinically, it is especially important to distinguish patients with the NASH subtype, as most NAFLD patients have steatosis without necroinflammation or fibrosis and do not require medical therapy.
CLINICAL SIGNIFICANCE OF NAFLD: NASH IS WORSE THAN NAFL
NAFL carries an excellent prognosis in terms of histologic progression of liver disease, whereas NASH can histologically progress to fibrosis and, in up to 15% of patients, to cirrhosis.3
Progression of fibrosis poses secondary risks, including complications associated with portal hypertension (ascites, variceal hemorrhage, hepatic encephalopathy), end-stage liver disease, and hepatocellular carcinoma. In Western countries, 4% to 22% of cases of hepatocellular carcinoma are attributed to NAFLD.4
In a 2015 meta-analysis, patients with NAFL and stage 0 fibrosis at baseline progressed 1 stage of fibrosis over 14.3 years, whereas patients with NASH and stage 0 fibrosis experienced an accelerated rate of progression, advancing 1 stage of fibrosis over 7.1 years.5 A systematic review of patients with NASH identified age and inflammation on initial liver biopsy as independent predictors of progression to advanced fibrosis.6
Patients with NAFLD have a higher all-cause mortality rate than patients of the same age and sex without NAFLD.7
HOW SHOULD PATIENTS WITH NAFLD BE EVALUATED?
Initial evaluation of a patient with suspected NAFLD should include a thorough serologic evaluation to exclude coexisting causes of chronic liver disease. Tests include:
- A viral hepatitis panel
- Antinuclear antibody (ANA)
- Antismooth muscle antibody (ASMA)
- Antimitochondrial antibody (AMA)
- Iron studies
- Alpha-1 antitrypsin level
- Ceruloplasmin level.
Aminotransferase levels and imaging studies (ultrasonography, computed tomography, and magnetic resonance imaging) do not reliably convey the degree of NASH and fibrosis.
Biopsy. Whereas sensitive serologic tests have been introduced to detect and diagnose many causes of liver disease, liver biopsy (transjugular or percutaneous) with histologic examination remains the only way to accurately assess the degree of steatosis and, thus, to distinguish NAFL from NASH.2
The Pathology Committee of the NASH Clinical Research Network designed and validated a NAFLD scoring system,8,9 with points allocated for degrees of:
- Steatosis (0–3)
- Lobular inflammation (0–2)
- Hepatocellular ballooning (0–2)
- Fibrosis (0–4).
A NAFLD Activity Score of less than 3 is consistent with “not NASH,” a score of 3 or 4 with borderline NASH, and a score of 5 or more with NASH.8 However, the diagnosis of NASH is not based on the NAFLD scoring system, but rather on the pathologist’s overall evaluation of the liver biopsy.9
The metabolic syndrome is an established risk factor for steatohepatitis in patients with NAFLD, and its presence in patients with persistently elevated liver biochemical tests may help identify those who would benefit from further diagnostic and prognostic evaluation, including liver biopsy.2,10 In addition, a 2008 study that used a decision-tree modeling system demonstrated that early liver biopsy could provide a survival benefit.11
NONINVASIVE TESTING
Since liver biopsy is associated with procedure-related morbidity, mortality, and cost, researchers have been developing noninvasive markers of steatohepatitis and fibrosis.12
The NAFLD fibrosis score—based on patient age, body mass index, hyperglycemia, platelet count, albumin, and ratio of aspartate aminotransferase to alanine aminotransferase—has been shown to have an area under the receiver operating curve of 0.85 for predicting advanced fibrosis, with a negative predictive value of 88% to 93% and a positive predictive value of 82% to 90%.13 The NAFLD fibrosis score can be used to identify patients who may have fibrosis or cirrhosis and can help direct the use of liver biopsy in patients who would benefit from prognostication and potential treatment.
Of note, the NAFLD fibrosis score is only slightly less accurate than the imaging techniques of magnetic resonance elastography and transient elastography, particularly when the relative costs are considered.14
INDICATIONS FOR LIVER BIOPSY
There are two clear indications for liver biopsy in NAFLD.
Before starting any pharmacologic therapy for NAFLD. Most NAFLD patients have steatosis without NASH or fibrosis and do not require medical therapy. Importantly, the available treatments have significant adverse effects—prostate cancer with vitamin E, bladder cancer and weight gain with pioglitazone, and nausea with pentoxifylline.
Diagnosis. Up to 30% of patients have elevated serum ferritin and autoantibodies, including ANA, ASMA, and AMA. Liver biopsy is often needed to exclude hemochromatosis or autoimmune hepatitis.15 Occasionally, a possible confounding drug-induced liver injury may necessitate a liver biopsy.
LIFESTYLE MODIFICATION
The first step in managing patients who have NAFLD is to treat components of the metabolic syndrome, including obesity, dyslipidemia, and type 2 diabetes.
In a randomized controlled trial in 31 obese patients with biopsy-proven NASH,16 intensive lifestyle modification (consisting of diet, behavior modification, and 200 minutes of exercise weekly for 48 weeks) was shown to improve histologic NAFLD Activity Scores, including degrees of steatosis, necrosis, and inflammation. As a result, weight loss of 7% to 9% is generally recommended for patients with NAFLD.
DRUG THERAPIES
Much research has been directed toward identifying risk factors for progression of fibrosis and toward developing new therapies for patients with NAFLD. A 2015 meta-analysis concluded that pentoxifylline and obeticholic acid improve fibrosis, while vitamin E, thiazolidinediones, and obeticholic acid improve necroinflammation associated with NASH.17
Long-term studies are needed to determine the impact of these drugs on NASH-related morbidity, mortality, and need for liver transplant.
TAKE-AWAY POINTS
- NAFLD is the leading cause of chronic liver disease in the United States and is increasing as a reason for liver transplant.
- NASH is associated with the metabolic syndrome and can progress to fibrosis, cirrhosis, and end-stage liver disease. Noninvasive markers such as the NAFLD Activity Score can be useful in identifying patients who may have advanced fibrosis and can select patients who should be directed to liver biopsy for definitive diagnosis.8,9
- Liver biopsy is the gold standard for diagnosing steatohepatitis and fibrosis and is the only diagnostic tool used in clinical trials to direct pharmacotherapy for NASH.
- Liver biopsy should be reserved for patients suspected of having NASH or fibrosis and who might benefit from therapy.
- Liver biopsy is also indicated for those NAFLD patients who have confounding laboratory findings such as an elevated ferritin level and autoantibodies including ANA, ASMA, and AMA.
- Wong RJ, Aquilar M, Cheung R, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology 2015; 148:547–555.
- Chalasani N, Younossi Z, Lavine JE, et al; American Gastroenterological Association; American Association for the Study of Liver Diseases; American College of Gastroenterology. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012; 142:1592–1609.
- Ekstedt M, Franzén LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006; 44:865–873.
- Michelotti GA, Machado MV, Diehl AM. NAFLD, NASH and liver cancer. Nat Rev Gastroenterol Hepatol 2013; 10:656–665.
- Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015; 13:643–654.
- Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH. Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis. J Hepatol 2009; 51:371–379.
- Adams LA, Lymp JF, St. Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology 2005; 129:113–121.
- Kleiner DE, Brunt EM, Van Natta M, et al; Nonalcoholic Steatohepatitis Clinical Research Network. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005; 41:1313–1321.
- Brunt EM, Kleiner DE, Wilson LA, Belt P, Neuschwander-Tetri BA; NASH Clinical Research Network (CRN). Nonalcoholic fatty liver disease (NAFLD) activity score and the histopathologic diagnosis in NAFLD: distinct clinicopathologic meanings. Hepatology 2011; 53:810–820.
- Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003; 37:917–923.
- Gaidos JK, Hillner BE, Sanyal AJ. A decision analysis study of the value of a liver biopsy in nonalcoholic steatohepatitis. Liver Int 2008; 28:650–658.
- Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med 2011; 43:617–649.
- Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007; 45:846–854.
- Imajo K, Kessoku T, Honda Y, et al. Magnetic resonance imaging more accurately classifies steatosis and fibrosis in patients with nonalcoholic fatty liver disease than transient elastography. Gastroenterology 2016; 150:626–637.e7.
- Neuschwander-Tetri BA, Clark JM, Bass NM, et al; NASH Clinical Research Network. Clinical, laboratory and histological associations in adults with nonalcoholic fatty liver disease. Hepatology 2010; 52:913–924.
- Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010; 51:121–129.
- Singh S, Khera R, Allen AM, Murad H, Loomba R. Comparative effectiveness of pharmacological interventions for nonalcoholic steatohepatitis: a systematic review and network meta-analysis. Hepatology 2015; 62:1417–1432.
Patients should undergo biopsy to guide management and prognosis if suspected of having steatohepatitis or fibrosis.
WHAT IS NAFLD?
Nonalcoholic fatty liver disease (NAFLD) is the most common form of chronic liver disease in the United States and is the second most common reason for liver transplant.1 It is thought to be the hepatic consequence of systemic insulin resistance and the metabolic syndrome characterized by obesity, dyslipidemia, and type 2 diabetes mellitus.
WHAT IS THE RELATIONSHIP BETWEEN NAFLD AND NASH?
NAFLD is defined by the accumulation of hepatic fat as evidenced by imaging or histologic study and without a coexisting cause of chronic liver disease or a secondary cause of hepatic steatosis, including significant alcohol use, medications, or an inherited or acquired metabolic state.
NAFLD has two subtypes: nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH). NAFL is characterized by steatosis, including inflammation, in at least 5% of hepatocytes. NASH is defined by a constellation of features that include steatosis, lobular and portal inflammation, and liver cell injury in the form of hepatocyte ballooning.2
Clinically, it is especially important to distinguish patients with the NASH subtype, as most NAFLD patients have steatosis without necroinflammation or fibrosis and do not require medical therapy.
CLINICAL SIGNIFICANCE OF NAFLD: NASH IS WORSE THAN NAFL
NAFL carries an excellent prognosis in terms of histologic progression of liver disease, whereas NASH can histologically progress to fibrosis and, in up to 15% of patients, to cirrhosis.3
Progression of fibrosis poses secondary risks, including complications associated with portal hypertension (ascites, variceal hemorrhage, hepatic encephalopathy), end-stage liver disease, and hepatocellular carcinoma. In Western countries, 4% to 22% of cases of hepatocellular carcinoma are attributed to NAFLD.4
In a 2015 meta-analysis, patients with NAFL and stage 0 fibrosis at baseline progressed 1 stage of fibrosis over 14.3 years, whereas patients with NASH and stage 0 fibrosis experienced an accelerated rate of progression, advancing 1 stage of fibrosis over 7.1 years.5 A systematic review of patients with NASH identified age and inflammation on initial liver biopsy as independent predictors of progression to advanced fibrosis.6
Patients with NAFLD have a higher all-cause mortality rate than patients of the same age and sex without NAFLD.7
HOW SHOULD PATIENTS WITH NAFLD BE EVALUATED?
Initial evaluation of a patient with suspected NAFLD should include a thorough serologic evaluation to exclude coexisting causes of chronic liver disease. Tests include:
- A viral hepatitis panel
- Antinuclear antibody (ANA)
- Antismooth muscle antibody (ASMA)
- Antimitochondrial antibody (AMA)
- Iron studies
- Alpha-1 antitrypsin level
- Ceruloplasmin level.
Aminotransferase levels and imaging studies (ultrasonography, computed tomography, and magnetic resonance imaging) do not reliably convey the degree of NASH and fibrosis.
Biopsy. Whereas sensitive serologic tests have been introduced to detect and diagnose many causes of liver disease, liver biopsy (transjugular or percutaneous) with histologic examination remains the only way to accurately assess the degree of steatosis and, thus, to distinguish NAFL from NASH.2
The Pathology Committee of the NASH Clinical Research Network designed and validated a NAFLD scoring system,8,9 with points allocated for degrees of:
- Steatosis (0–3)
- Lobular inflammation (0–2)
- Hepatocellular ballooning (0–2)
- Fibrosis (0–4).
A NAFLD Activity Score of less than 3 is consistent with “not NASH,” a score of 3 or 4 with borderline NASH, and a score of 5 or more with NASH.8 However, the diagnosis of NASH is not based on the NAFLD scoring system, but rather on the pathologist’s overall evaluation of the liver biopsy.9
The metabolic syndrome is an established risk factor for steatohepatitis in patients with NAFLD, and its presence in patients with persistently elevated liver biochemical tests may help identify those who would benefit from further diagnostic and prognostic evaluation, including liver biopsy.2,10 In addition, a 2008 study that used a decision-tree modeling system demonstrated that early liver biopsy could provide a survival benefit.11
NONINVASIVE TESTING
Since liver biopsy is associated with procedure-related morbidity, mortality, and cost, researchers have been developing noninvasive markers of steatohepatitis and fibrosis.12
The NAFLD fibrosis score—based on patient age, body mass index, hyperglycemia, platelet count, albumin, and ratio of aspartate aminotransferase to alanine aminotransferase—has been shown to have an area under the receiver operating curve of 0.85 for predicting advanced fibrosis, with a negative predictive value of 88% to 93% and a positive predictive value of 82% to 90%.13 The NAFLD fibrosis score can be used to identify patients who may have fibrosis or cirrhosis and can help direct the use of liver biopsy in patients who would benefit from prognostication and potential treatment.
Of note, the NAFLD fibrosis score is only slightly less accurate than the imaging techniques of magnetic resonance elastography and transient elastography, particularly when the relative costs are considered.14
INDICATIONS FOR LIVER BIOPSY
There are two clear indications for liver biopsy in NAFLD.
Before starting any pharmacologic therapy for NAFLD. Most NAFLD patients have steatosis without NASH or fibrosis and do not require medical therapy. Importantly, the available treatments have significant adverse effects—prostate cancer with vitamin E, bladder cancer and weight gain with pioglitazone, and nausea with pentoxifylline.
Diagnosis. Up to 30% of patients have elevated serum ferritin and autoantibodies, including ANA, ASMA, and AMA. Liver biopsy is often needed to exclude hemochromatosis or autoimmune hepatitis.15 Occasionally, a possible confounding drug-induced liver injury may necessitate a liver biopsy.
LIFESTYLE MODIFICATION
The first step in managing patients who have NAFLD is to treat components of the metabolic syndrome, including obesity, dyslipidemia, and type 2 diabetes.
In a randomized controlled trial in 31 obese patients with biopsy-proven NASH,16 intensive lifestyle modification (consisting of diet, behavior modification, and 200 minutes of exercise weekly for 48 weeks) was shown to improve histologic NAFLD Activity Scores, including degrees of steatosis, necrosis, and inflammation. As a result, weight loss of 7% to 9% is generally recommended for patients with NAFLD.
DRUG THERAPIES
Much research has been directed toward identifying risk factors for progression of fibrosis and toward developing new therapies for patients with NAFLD. A 2015 meta-analysis concluded that pentoxifylline and obeticholic acid improve fibrosis, while vitamin E, thiazolidinediones, and obeticholic acid improve necroinflammation associated with NASH.17
Long-term studies are needed to determine the impact of these drugs on NASH-related morbidity, mortality, and need for liver transplant.
TAKE-AWAY POINTS
- NAFLD is the leading cause of chronic liver disease in the United States and is increasing as a reason for liver transplant.
- NASH is associated with the metabolic syndrome and can progress to fibrosis, cirrhosis, and end-stage liver disease. Noninvasive markers such as the NAFLD Activity Score can be useful in identifying patients who may have advanced fibrosis and can select patients who should be directed to liver biopsy for definitive diagnosis.8,9
- Liver biopsy is the gold standard for diagnosing steatohepatitis and fibrosis and is the only diagnostic tool used in clinical trials to direct pharmacotherapy for NASH.
- Liver biopsy should be reserved for patients suspected of having NASH or fibrosis and who might benefit from therapy.
- Liver biopsy is also indicated for those NAFLD patients who have confounding laboratory findings such as an elevated ferritin level and autoantibodies including ANA, ASMA, and AMA.
Patients should undergo biopsy to guide management and prognosis if suspected of having steatohepatitis or fibrosis.
WHAT IS NAFLD?
Nonalcoholic fatty liver disease (NAFLD) is the most common form of chronic liver disease in the United States and is the second most common reason for liver transplant.1 It is thought to be the hepatic consequence of systemic insulin resistance and the metabolic syndrome characterized by obesity, dyslipidemia, and type 2 diabetes mellitus.
WHAT IS THE RELATIONSHIP BETWEEN NAFLD AND NASH?
NAFLD is defined by the accumulation of hepatic fat as evidenced by imaging or histologic study and without a coexisting cause of chronic liver disease or a secondary cause of hepatic steatosis, including significant alcohol use, medications, or an inherited or acquired metabolic state.
NAFLD has two subtypes: nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH). NAFL is characterized by steatosis, including inflammation, in at least 5% of hepatocytes. NASH is defined by a constellation of features that include steatosis, lobular and portal inflammation, and liver cell injury in the form of hepatocyte ballooning.2
Clinically, it is especially important to distinguish patients with the NASH subtype, as most NAFLD patients have steatosis without necroinflammation or fibrosis and do not require medical therapy.
CLINICAL SIGNIFICANCE OF NAFLD: NASH IS WORSE THAN NAFL
NAFL carries an excellent prognosis in terms of histologic progression of liver disease, whereas NASH can histologically progress to fibrosis and, in up to 15% of patients, to cirrhosis.3
Progression of fibrosis poses secondary risks, including complications associated with portal hypertension (ascites, variceal hemorrhage, hepatic encephalopathy), end-stage liver disease, and hepatocellular carcinoma. In Western countries, 4% to 22% of cases of hepatocellular carcinoma are attributed to NAFLD.4
In a 2015 meta-analysis, patients with NAFL and stage 0 fibrosis at baseline progressed 1 stage of fibrosis over 14.3 years, whereas patients with NASH and stage 0 fibrosis experienced an accelerated rate of progression, advancing 1 stage of fibrosis over 7.1 years.5 A systematic review of patients with NASH identified age and inflammation on initial liver biopsy as independent predictors of progression to advanced fibrosis.6
Patients with NAFLD have a higher all-cause mortality rate than patients of the same age and sex without NAFLD.7
HOW SHOULD PATIENTS WITH NAFLD BE EVALUATED?
Initial evaluation of a patient with suspected NAFLD should include a thorough serologic evaluation to exclude coexisting causes of chronic liver disease. Tests include:
- A viral hepatitis panel
- Antinuclear antibody (ANA)
- Antismooth muscle antibody (ASMA)
- Antimitochondrial antibody (AMA)
- Iron studies
- Alpha-1 antitrypsin level
- Ceruloplasmin level.
Aminotransferase levels and imaging studies (ultrasonography, computed tomography, and magnetic resonance imaging) do not reliably convey the degree of NASH and fibrosis.
Biopsy. Whereas sensitive serologic tests have been introduced to detect and diagnose many causes of liver disease, liver biopsy (transjugular or percutaneous) with histologic examination remains the only way to accurately assess the degree of steatosis and, thus, to distinguish NAFL from NASH.2
The Pathology Committee of the NASH Clinical Research Network designed and validated a NAFLD scoring system,8,9 with points allocated for degrees of:
- Steatosis (0–3)
- Lobular inflammation (0–2)
- Hepatocellular ballooning (0–2)
- Fibrosis (0–4).
A NAFLD Activity Score of less than 3 is consistent with “not NASH,” a score of 3 or 4 with borderline NASH, and a score of 5 or more with NASH.8 However, the diagnosis of NASH is not based on the NAFLD scoring system, but rather on the pathologist’s overall evaluation of the liver biopsy.9
The metabolic syndrome is an established risk factor for steatohepatitis in patients with NAFLD, and its presence in patients with persistently elevated liver biochemical tests may help identify those who would benefit from further diagnostic and prognostic evaluation, including liver biopsy.2,10 In addition, a 2008 study that used a decision-tree modeling system demonstrated that early liver biopsy could provide a survival benefit.11
NONINVASIVE TESTING
Since liver biopsy is associated with procedure-related morbidity, mortality, and cost, researchers have been developing noninvasive markers of steatohepatitis and fibrosis.12
The NAFLD fibrosis score—based on patient age, body mass index, hyperglycemia, platelet count, albumin, and ratio of aspartate aminotransferase to alanine aminotransferase—has been shown to have an area under the receiver operating curve of 0.85 for predicting advanced fibrosis, with a negative predictive value of 88% to 93% and a positive predictive value of 82% to 90%.13 The NAFLD fibrosis score can be used to identify patients who may have fibrosis or cirrhosis and can help direct the use of liver biopsy in patients who would benefit from prognostication and potential treatment.
Of note, the NAFLD fibrosis score is only slightly less accurate than the imaging techniques of magnetic resonance elastography and transient elastography, particularly when the relative costs are considered.14
INDICATIONS FOR LIVER BIOPSY
There are two clear indications for liver biopsy in NAFLD.
Before starting any pharmacologic therapy for NAFLD. Most NAFLD patients have steatosis without NASH or fibrosis and do not require medical therapy. Importantly, the available treatments have significant adverse effects—prostate cancer with vitamin E, bladder cancer and weight gain with pioglitazone, and nausea with pentoxifylline.
Diagnosis. Up to 30% of patients have elevated serum ferritin and autoantibodies, including ANA, ASMA, and AMA. Liver biopsy is often needed to exclude hemochromatosis or autoimmune hepatitis.15 Occasionally, a possible confounding drug-induced liver injury may necessitate a liver biopsy.
LIFESTYLE MODIFICATION
The first step in managing patients who have NAFLD is to treat components of the metabolic syndrome, including obesity, dyslipidemia, and type 2 diabetes.
In a randomized controlled trial in 31 obese patients with biopsy-proven NASH,16 intensive lifestyle modification (consisting of diet, behavior modification, and 200 minutes of exercise weekly for 48 weeks) was shown to improve histologic NAFLD Activity Scores, including degrees of steatosis, necrosis, and inflammation. As a result, weight loss of 7% to 9% is generally recommended for patients with NAFLD.
DRUG THERAPIES
Much research has been directed toward identifying risk factors for progression of fibrosis and toward developing new therapies for patients with NAFLD. A 2015 meta-analysis concluded that pentoxifylline and obeticholic acid improve fibrosis, while vitamin E, thiazolidinediones, and obeticholic acid improve necroinflammation associated with NASH.17
Long-term studies are needed to determine the impact of these drugs on NASH-related morbidity, mortality, and need for liver transplant.
TAKE-AWAY POINTS
- NAFLD is the leading cause of chronic liver disease in the United States and is increasing as a reason for liver transplant.
- NASH is associated with the metabolic syndrome and can progress to fibrosis, cirrhosis, and end-stage liver disease. Noninvasive markers such as the NAFLD Activity Score can be useful in identifying patients who may have advanced fibrosis and can select patients who should be directed to liver biopsy for definitive diagnosis.8,9
- Liver biopsy is the gold standard for diagnosing steatohepatitis and fibrosis and is the only diagnostic tool used in clinical trials to direct pharmacotherapy for NASH.
- Liver biopsy should be reserved for patients suspected of having NASH or fibrosis and who might benefit from therapy.
- Liver biopsy is also indicated for those NAFLD patients who have confounding laboratory findings such as an elevated ferritin level and autoantibodies including ANA, ASMA, and AMA.
- Wong RJ, Aquilar M, Cheung R, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology 2015; 148:547–555.
- Chalasani N, Younossi Z, Lavine JE, et al; American Gastroenterological Association; American Association for the Study of Liver Diseases; American College of Gastroenterology. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012; 142:1592–1609.
- Ekstedt M, Franzén LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006; 44:865–873.
- Michelotti GA, Machado MV, Diehl AM. NAFLD, NASH and liver cancer. Nat Rev Gastroenterol Hepatol 2013; 10:656–665.
- Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015; 13:643–654.
- Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH. Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis. J Hepatol 2009; 51:371–379.
- Adams LA, Lymp JF, St. Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology 2005; 129:113–121.
- Kleiner DE, Brunt EM, Van Natta M, et al; Nonalcoholic Steatohepatitis Clinical Research Network. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005; 41:1313–1321.
- Brunt EM, Kleiner DE, Wilson LA, Belt P, Neuschwander-Tetri BA; NASH Clinical Research Network (CRN). Nonalcoholic fatty liver disease (NAFLD) activity score and the histopathologic diagnosis in NAFLD: distinct clinicopathologic meanings. Hepatology 2011; 53:810–820.
- Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003; 37:917–923.
- Gaidos JK, Hillner BE, Sanyal AJ. A decision analysis study of the value of a liver biopsy in nonalcoholic steatohepatitis. Liver Int 2008; 28:650–658.
- Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med 2011; 43:617–649.
- Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007; 45:846–854.
- Imajo K, Kessoku T, Honda Y, et al. Magnetic resonance imaging more accurately classifies steatosis and fibrosis in patients with nonalcoholic fatty liver disease than transient elastography. Gastroenterology 2016; 150:626–637.e7.
- Neuschwander-Tetri BA, Clark JM, Bass NM, et al; NASH Clinical Research Network. Clinical, laboratory and histological associations in adults with nonalcoholic fatty liver disease. Hepatology 2010; 52:913–924.
- Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010; 51:121–129.
- Singh S, Khera R, Allen AM, Murad H, Loomba R. Comparative effectiveness of pharmacological interventions for nonalcoholic steatohepatitis: a systematic review and network meta-analysis. Hepatology 2015; 62:1417–1432.
- Wong RJ, Aquilar M, Cheung R, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology 2015; 148:547–555.
- Chalasani N, Younossi Z, Lavine JE, et al; American Gastroenterological Association; American Association for the Study of Liver Diseases; American College of Gastroenterology. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012; 142:1592–1609.
- Ekstedt M, Franzén LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006; 44:865–873.
- Michelotti GA, Machado MV, Diehl AM. NAFLD, NASH and liver cancer. Nat Rev Gastroenterol Hepatol 2013; 10:656–665.
- Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015; 13:643–654.
- Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH. Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis. J Hepatol 2009; 51:371–379.
- Adams LA, Lymp JF, St. Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology 2005; 129:113–121.
- Kleiner DE, Brunt EM, Van Natta M, et al; Nonalcoholic Steatohepatitis Clinical Research Network. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005; 41:1313–1321.
- Brunt EM, Kleiner DE, Wilson LA, Belt P, Neuschwander-Tetri BA; NASH Clinical Research Network (CRN). Nonalcoholic fatty liver disease (NAFLD) activity score and the histopathologic diagnosis in NAFLD: distinct clinicopathologic meanings. Hepatology 2011; 53:810–820.
- Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003; 37:917–923.
- Gaidos JK, Hillner BE, Sanyal AJ. A decision analysis study of the value of a liver biopsy in nonalcoholic steatohepatitis. Liver Int 2008; 28:650–658.
- Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity. Ann Med 2011; 43:617–649.
- Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007; 45:846–854.
- Imajo K, Kessoku T, Honda Y, et al. Magnetic resonance imaging more accurately classifies steatosis and fibrosis in patients with nonalcoholic fatty liver disease than transient elastography. Gastroenterology 2016; 150:626–637.e7.
- Neuschwander-Tetri BA, Clark JM, Bass NM, et al; NASH Clinical Research Network. Clinical, laboratory and histological associations in adults with nonalcoholic fatty liver disease. Hepatology 2010; 52:913–924.
- Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010; 51:121–129.
- Singh S, Khera R, Allen AM, Murad H, Loomba R. Comparative effectiveness of pharmacological interventions for nonalcoholic steatohepatitis: a systematic review and network meta-analysis. Hepatology 2015; 62:1417–1432.
Maternal asthma: Management strategies
The incidence of maternal asthma is rising. Based on US national health surveys, the prevalence of asthma during pregnancy is between 3.7% and 8.4%.1 It is the most common respiratory illness of pregnancy.2 Hence, clinicians need to know how asthma affects the mother and the fetus. Appropriate care of asthma during pregnancy is based on several management principles, as reviewed here, and is key to ensuring good outcomes for the mother and the baby.
EFFECT OF PREGNANCY ON ASTHMA CONTROL
Asthma control can vary in pregnancy. About a third of asthmatic women experience a worsening of asthma control with pregnancy, a third remain unchanged, and another third have improvement in asthma symptoms.3 The peak worsening of asthma tends to occur in the sixth month.4 Asthma control also tends to be better in the last month of pregnancy.3
The peak expiratory flow rate was noted to increase with each trimester in a small study of 43 women.5 The authors speculated that a rising progesterone level stimulates cyclic adenosine monophosphate to cause bronchodilation, thereby improving the expiratory flow rate and asthma control. Asthma control tends to follow the pattern experienced in the previous pregnancy: ie, if asthma worsened during the previous pregnancy, the same will be likely in the subsequent pregnancy.3
Two maternal factors that adversely affect asthma severity during pregnancy are the use of asthma medications contrary to guidelines such as those of the Global Initiative for Asthma (http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention) and inadquate control of asthma before becoming pregnant.6 Pregnancy can bring on stress, and stress is known to worsen asthma. In addition, when patients themselves were interviewed to elucidate the reasons for poor adherence to asthma medications during pregnancy, concerns about medication use, especially corticosteroids, stood out.7 A study based on prescription claims data showed that in the first trimester, there was a significant decline in asthma prescription medications (a 23% decline in inhaled corticosteroids, a 13% decline in short-acting bronchodilator agents, and a 54% decline in rescue corticosteroids).8 Lack of physician education about management of asthma in pregnancy and discomfort with prescribing to pregnant women also affect asthma control.
EFFECT OF ASTHMA ON MATERNAL AND FETAL OUTCOMES
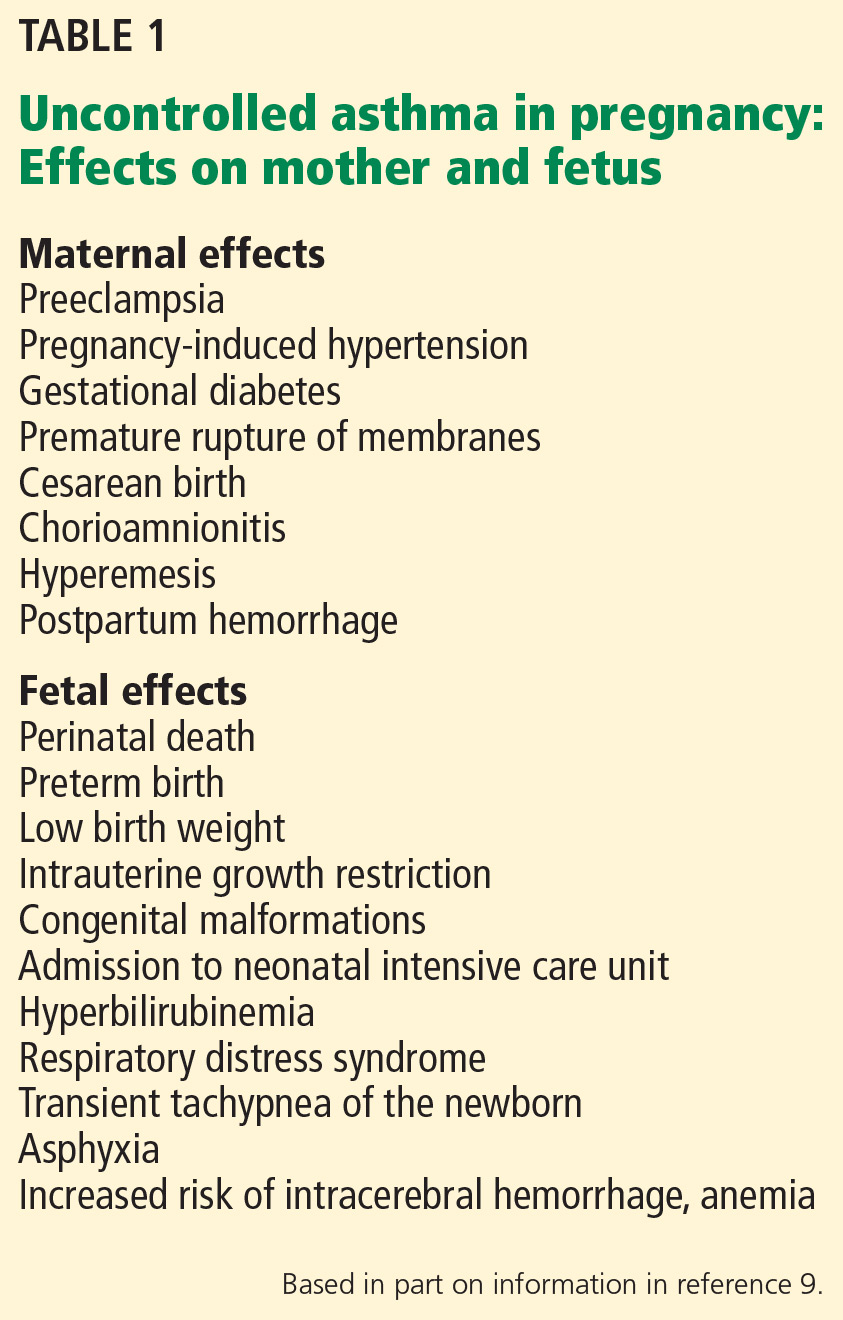
Studies of the effects of asthma on fetal and maternal outcomes have yielded mixed and conflicting results.9 Adverse outcomes that have been shown to be associated with maternal asthma are listed in Table 1. Other studies have not demonstrated an association between asthma in pregnancy and maternal or fetal adverse events.9 Such discrepant findings are due to differences in study population characteristics that make comparisons difficult. A meta-analysis involving more than 1.6 million asthmatic women showed maternal asthma was associated with a 40% greater risk of low birth weight and preterm delivery, a 50% greater risk of preeclampsia, and a 20% greater risk of the baby being small for its gestational age.10
The association of maternal asthma and preterm birth may pose short-term and long-term health risks to the child associated with prematurity.9 Short-term risks with prematurity include infection, respiratory distress syndrome, brain injury, and necrotizing enterocolitis. Long-term risks include neurodevelopmental and behavioral sequelae. Furthermore, asthma exacerbations during pregnancy are associated with a twofold higher risk of low birth weight.11 The benefits of good adherence to asthma regimens during pregnancy outweigh the risks associated with frequent symptoms and exacerbations caused by untreated asthma.12
OUTPATIENT MANAGEMENT OF MATERNAL ASTHMA
Goals
In the 2004 update of the National Asthma Education and Prevention Program (NAEPP) Working Group Report on Managing Asthma During Pregnancy, goals focused mainly on adequate asthma control for maternal health and quality of life, as well as normal fetal maturation (Table 2),12 goals similar to those in nonpregnant asthmatic women.
Assessment and monitoring
Monthly physician visits during pregnancy are recommended for assessment of symptoms and pulmonary function. If symptoms are uncontrolled, therapy must be stepped up, and any trigger for exacerbation, such as gastroesophageal reflux disease (GERD), exposure, or rhinitis, must be treated and eliminated. NAEPP guidelines recommend baseline spirometry at the time of initial assessment.12 At follow-up visits, spirometry is preferred, but measurement of the peak expiratory flow rate usually suffices. Such objective data can help differentiate dyspnea from asthma and from dyspnea that usually accompanies the physiologic changes of pregnancy. In addition, patients should be advised to monitor for adequate fetal activity. If asthma is uncontrolled or poorly controlled, serial fetal ultrasonography should be considered from 32 weeks of gestation, as well as after recovery from an asthma exacerbation. Regular monitoring of the pregnant asthmatic patient by a multidisciplinary team can improve outcomes.13
Avoiding triggers
Patients should be advised to avoid asthma triggers such as pet dander, dust mites, pollen, smoke, mold, and perfumes, as this can decrease symptoms and allow for use of lower doses of medications.12 Additionally, smoking cessation must be strongly encouraged, not only to control maternal asthma, but also to prevent harm to the fetus.
MANAGEMENT OF SPECIFIC TRIGGERS
GERD
Reflux disease often worsens during pregnancy, and it can coexist with asthma and can also exacerbate it.14 Optimal control of GERD helps maintain adequate asthma control. For mild reflux symptoms, lifestyle modifications such as elevating the head of bed, avoiding eating too close to bedtime, and avoiding foods that cause heartburn may be adequate.15,16 If medications are needed, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before using a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
Allergic rhinitis
Intranasal corticosteroids are effective against allergic rhinitis in pregnancy (Table 3).12 Montelukast, a leukotriene receptor antagonist, can be used, but data to support its use for allergic rhinitis in pregnancy are limited.
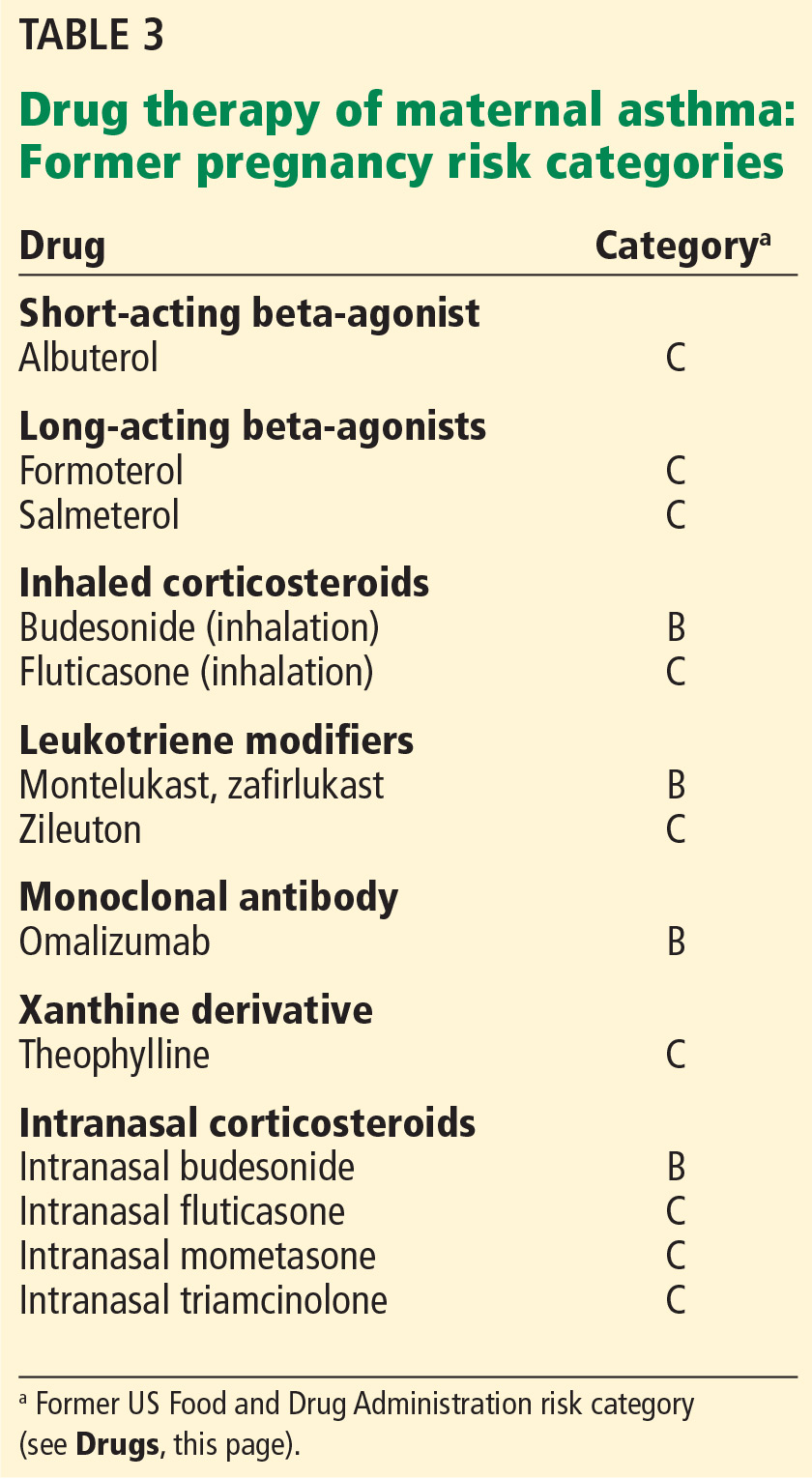
Among antihistamines, second-generation drugs such as cetirizine or loratadine can be considered.12 Oral decongestants such as pseudoephedrine in early pregnancy are associated with a rare congenital fetal abnormality called gastroschisis, caused by vascular disruption.17 Hence, if a nasal decongestant is required in early pregnancy, a local therapy such as an intranasal corticosteroid, short-term oxymetazoline, or an external nasal dilator may be considered.12 These therapies must be combined with avoidance of allergens whenever possible.
Allergies
Diagnostic allergy and skin tests during pregnancy pose a risk of anaphylaxis and thus should be avoided. Instead, the focus should be on obtaining a thorough medical history about exposures and eliminating specific asthma triggers. It is also inadvisable to start allergen immunotherapy during pregnancy because of the risk of anaphylaxis and the effect of treatment on the mother and fetus.18 However, maintenance doses of allergen immunotherapy can be continued during pregnancy.18
Patient education
Because of concern about the risks of taking medications during pregnancy, many women with asthma stop using their inhalers during pregnancy, thus compromising asthma control.8,13 The physician and multidisciplinary team must use every opportunity to emphasize the importance of good asthma control during pregnancy. Inhaler technique should also be reviewed and, if defective, corrected. Again, trigger avoidance and tobacco cessation should be addressed.
Drugs
The NAEPP recommendations state that asthma therapy should be continued during pregnancy, as it is safer both for mother and fetus to avoid exacerbations and uncontrolled asthma.12 Despite this, 25% of primary care physicians instruct their patients to decrease or discontinue their inhaled corticosteroid during pregnancy.19 As with asthma in general, treatment should involve using the lowest dose of drugs that achieves adequate control of symptoms.
In 2015, the US Food and Drug Administration (FDA) amended the labeling rule for medications used in pregnancy and lactation. The previous risk categories A (safest), B, C, D, and X (highest risk) are in the process of being removed from labels for all human prescription drugs and biologic products, to be replaced with a summary of the risks of taking the drug during pregnancy and lactation, a discussion of the data supporting the use, and relevant information to help healthcare providers make prescribing decisions and counsel women about the use of drugs during pregnancy and lactation (www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/Labeling/ucm093307.htm).
ROLES OF CONTROLLER THERAPY AND RESCUE THERAPY
Inhaled corticosteroids
Inhaled corticosteroids are the mainstay of asthma controller therapy during pregnancy. A meta-analysis of 16 studies showed no increased risk of congenital malformations, cesarean delivery, or stillbirth among mothers who used these agents during pregnancy.20 Because there are more safety data for budesonide, it is currently the preferred inhaled corticosteroid during pregnancy.9 However, if a patient’s asthma is controlled with a different corticosteroid before pregnancy, that agent may be continued during pregnancy, especially if it is thought that switching formulations could adversely affect asthma control.12 This is mainly because current data do not prove that other inhaled corticosteroids are unsafe.
Inhaled beta-agonists
Inhaled beta-agonists, both short-acting and long-acting, are used for rescue therapy. Albuterol is the preferred short-acting agent for rescue therapy in pregnant women with asthma.12 Meta-analysis has shown no increased risk of major or minor congenital malformations in pregnant patients who use bronchodilators.20 Long-acting beta-agonists typically are used as add-on therapy when asthma cannot be controlled by an inhaled corticosteroid. They should not be used without a controller medication (ie, an inhaled corticosteroid).
Guidelines for rescue therapy are similar to those for nonpregnant asthmatic patients. Although data are limited as to the gestational effects of long-acting beta-agonists (ie, formoterol, salmeterol), it can be assumed that the toxicologic and pharmacologic profiles are similar to those of the short-acting bronchodilators. Thus, the safety of albuterol can be extended potentially to the long-acting beta-agonists.12
Combining controller and rescue therapy
When asthma is not adequately controlled on inhaled corticosteroids, a long-acting beta-agonist can be added or the dose of corticosteroid can be increased. The 2004 NAEPP guidelines stated that based on available literature, there was no clear advantage of one option over the other.12 A study that compared the 2 approaches found no difference in rates of congenital malformations.21
Leukotriene receptor antagonists
There is little in the literature regarding the use of leukotriene receptor antagonists during pregnancy. However, animal safety data are reassuring,12 and human studies have not found a higher risk of major congenital malformations.22,23 Thus, they are an alternative for patients whose asthma has been well controlled on these agents before pregnancy. Montelukast and zafirlukast are in former FDA pregnancy risk factor category B (probably safe) (Table 3). However, 5-lipoxygenase inhibitors such as zileuton are contraindicated based on animal studies showing teratogenicity.24
Omalizumab
Omalizumab, a recombinant anti-immunoglobulin E antibody, can be used for allergic asthma not controlled with inhaled corticosteroids (Table 3). An analysis of the omalizumab pregnancy registry25 found no significant increase in the rate of major congenital malformations, prematurity, or babies small for gestational age in asthmatic women taking omalizumab 8 weeks before conception or during pregnancy vs pregnant asthmatic women not taking omalizumab. However, this drug carries a risk of anaphylaxis and so should not be started during pregnancy.25
Theophylline
Because of potential toxicity, use of theophylline during pregnancy requires careful monitoring to ensure the serum concentration remains between 5 and 12 µg/mL.12 Drug interactions are also common: for example, alcohol may increase the serum concentration of theophylline, and theophylline may increase the toxic effect of formoterol.
Systemic corticosteroids
Pregnant women with asthma that is not well controlled despite the therapies described above may require a daily oral corticosteroid such as prednisone to achieve adequate control. Oral steroids are also a mainstay of treatment of asthma exacerbation.
Although use of corticosteroids in the first trimester was associated with orofacial cleft in infants,12 these studies did not include many women with asthma. In 2011, a nationwide cohort study from Denmark showed no increase in the risk of orofacial cleft with the use of corticosteroids during pregnancy.26
Preeclampsia, low birth weight, and preterm delivery have been described with corticosteroid use in pregnancy. It is not known whether these problems were a result of corticosteroid use or were due to the uncontrolled nature of the underlying condition that led to the steroid use. Since the risk of uncontrolled asthma to mother and fetus outweighs the risk of systemic corticosteroids, these drugs are recommended when indicated for management of maternal asthma.12
ACUTE EXACERBATIONS REQUIRE AGGRESSIVE MANAGEMENT
Based on a systematic review, 20% of pregnant women with asthma require some intervention for an asthma exacerbation during pregnancy, and 5.8% are admitted to the hospital for an exacerbation.11 Exacerbations were associated with a higher risk of low birth weight compared with rates in women without asthma.
Exacerbations are more common late in the second trimester and are unlikely to occur during labor and delivery.2 The incidence of exacerbations increases with the severity of asthma, from 8% in mild asthma, to 47% in moderate asthma, to 65% in severe asthma.27 Risk factors for exacerbations include poor prenatal care, obesity, and lack of appropriate treatment with inhaled corticosteroids.2 The main triggers are viral respiratory infections and noncompliance with inhaled corticosteroid therapy.11

Asthma exacerbations during pregnancy should be managed aggressively (Table 4),12 as the risk to the fetus of hypoxia far outweighs any risk from asthma medications. Close collaboration between the primary care physician and the obstetrician allows closer monitoring of mother and fetus.
The goal oxygen saturation must be above 95%.12 Signs of acute respiratory failure in a pregnant patient include a partial pressure of arterial oxygen less than 70 mm Hg or a partial pressure of carbon dioxide greater than 35 mm Hg.
In a multicenter study comparing nonpregnant and pregnant women visiting the emergency room for asthma exacerbations,28 pregnant women were less likely to be prescribed systemic corticosteroids either in the emergency room or at the time of hospital discharge, and they were also more likely to describe an ongoing exacerbation at 2-week follow-up. However, a recent study showed a significant increase in systemic corticosteroid treatment in the emergency room (51% to 78% across the time periods, odds ratio 3.11, 95% confidence interval 1.27–7.60, P = .01). There was also an increase in steroid treatment at discharge (42% to 63%, odds ratio 2.49, 95% confidence interval 0.97–6.37, P = .054), though the increase was not statistically significant.29 Although emergency room care for pregnant asthmatic women has improved, this group concluded that further improvement is still warranted, as 1 in 3 women is discharged without corticosteroid treatment.
- Kwon HL, Belanger K, Bracken MB. Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol 2003; 13:317–324.
- Powell H, Murphy VE, Taylor DR, et al. Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomised controlled trial. Lancet 2011; 378:983–990.
- Schatz M, Harden K, Forsythe A, et al. The course of asthma during pregnancy, post partum, and with successive pregnancies: a prospective analysis. J Allergy Clin Immunol 1988; 81:509–517.
- Gluck JC, Gluck PA. The effect of pregnancy on the course of asthma. Immunol Allergy Clin North Am 2006; 26:63–80.
- Beckmann CA. Peak flow values by gestation in women with asthma. Clin Nurs Res 2008; 17:174–181.
- Belanger K, Hellenbrand ME, Holford TR, Bracken M. Effect of pregnancy on maternal asthma symptoms and medication use. Obstet Gynecol 2010; 115:559–567.
- Lim AS, Stewart K, Abramson MJ, Ryan K, George J. Asthma during pregnancy: the experiences, concerns and views of pregnant women with asthma. J Asthma 2012; 49:474–479.
- Enriquez R, Wu P, Griffin MR, et al. Cessation of asthma medication in early pregnancy. Am J Obstet Gynecol 2006; 195:149–153.
- Bain E, Pierides KL, Clifton VL, et al. Interventions for managing asthma in pregnancy. Cochrane Database Syst Rev 2014; 10:CD010660.
- Murphy VE, Namazy JA, Powell H, et al. A meta-analysis of adverse perinatal outcomes in women with asthma. BJOG 2011; 118:1314–1323.
- Murphy VE, Clifton VL, Gibson PG. Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax 2006; 61:169–176.
- National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Asthma and Pregnancy Working Group. NAEPP expert panel report. Managing asthma during pregnancy: recommendations for pharmacologic treatment—2004 update. J Allergy Clin Immunol 2005; 115:34–46.
- Lim AS, Stewart K, Abramson MJ, Walker SP, Smith CL, George J. Multidisciplinary Approach to Management of Maternal Asthma (MAMMA): a randomized controlled trial. Chest 2014; 145:1046–1054.
- Harding SM. Gastroesophageal reflux: a potential asthma trigger. Immunol Allergy Clin North Am 2005; 25:131–148.
- Ahmad S, Mokaddas E. Recent advances in the diagnosis and treatment of multidrug-resistant tuberculosis. Respir Med 2009; 103:1777–1790.
- van der Woude CJ, Metselaar HJ, Danese S. Management of gastrointestinal and liver diseases during pregnancy. Gut 2014; 63:1014–1023.
- Werler MM. Teratogen update: pseudoephedrine. Birth Defects Res A Clin Mol Teratol 2006; 76:445–452.
- Cox L, Nelson H, Lockey R, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol 2011; 127(suppl 1):S1–S55.
- Lim AS, Stewart K, Abramson MJ, George J. Management of asthma in pregnant women by general practitioners: a cross sectional survey. BMC Fam Pract 2011; 12:121.
- Murphy VE, Wang G, Namazy JA, et al. The risk of congenital malformations, perinatal mortality and neonatal hospitalisation among pregnant women with asthma: a systematic review and meta-analysis. BJOG 2013; 120:812–822.
- Eltonsy S, Forget A, Beauchesne MF, Blais L. Risk of congenital malformations for asthmatic pregnant women using a long-acting beta2-agonist and inhaled corticosteroid combination versus higher-dose inhaled corticosteroid monotherapy. J Allergy Clin Immunol 2015; 135:123–130.
- Nelsen LM, Shields KE, Cunningham ML, et al. Congenital malformations among infants born to women receiving montelukast, inhaled corticosteroids, and other asthma medications. J Allergy Clin Immunol 2012; 129:251–254.e1–e6.
- Sarkar M, Koren G, Kalra S, et al. Montelukast use during pregnancy: a multicentre, prospective, comparative study of infant outcomes. Eur J Clin Pharmacol 2009; 65:1259–1264.
- Namazy JA, Schatz M. The safety of asthma medications during pregnancy: an update for clinicians. Ther Adv Respir Dis 2014; 8:103–110.
- Namazy J, Cabana MD, Scheuerle AE, et al. The Xolair Pregnancy Registry (EXPECT): the safety of omalizumab use during pregnancy. J Allergy Clin Immunol 2015; 135:407–412.
- Hviid A, Molgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ 2011; 183:796–804.
- Murphy VE, Gibson P, Talbot PI, Clifton VL. Severe asthma exacerbations during pregnancy. Obstet Gynecol 2005; 106:1046–1054.
- Cydulka RK, Emerman CL, Schreiber D, Molander KH, Woodruff PG, Camargo CA Jr. Acute asthma among pregnant women presenting to the emergency department. Am J Respir Crit Care Med 1999; 160:887–892.
- Hasegawa K, Cydulka RK, Sullivan AF, et al. Improved management of acute asthma among pregnant women presenting to the ED. Chest 2015; 147:406–414.
The incidence of maternal asthma is rising. Based on US national health surveys, the prevalence of asthma during pregnancy is between 3.7% and 8.4%.1 It is the most common respiratory illness of pregnancy.2 Hence, clinicians need to know how asthma affects the mother and the fetus. Appropriate care of asthma during pregnancy is based on several management principles, as reviewed here, and is key to ensuring good outcomes for the mother and the baby.
EFFECT OF PREGNANCY ON ASTHMA CONTROL
Asthma control can vary in pregnancy. About a third of asthmatic women experience a worsening of asthma control with pregnancy, a third remain unchanged, and another third have improvement in asthma symptoms.3 The peak worsening of asthma tends to occur in the sixth month.4 Asthma control also tends to be better in the last month of pregnancy.3
The peak expiratory flow rate was noted to increase with each trimester in a small study of 43 women.5 The authors speculated that a rising progesterone level stimulates cyclic adenosine monophosphate to cause bronchodilation, thereby improving the expiratory flow rate and asthma control. Asthma control tends to follow the pattern experienced in the previous pregnancy: ie, if asthma worsened during the previous pregnancy, the same will be likely in the subsequent pregnancy.3
Two maternal factors that adversely affect asthma severity during pregnancy are the use of asthma medications contrary to guidelines such as those of the Global Initiative for Asthma (http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention) and inadquate control of asthma before becoming pregnant.6 Pregnancy can bring on stress, and stress is known to worsen asthma. In addition, when patients themselves were interviewed to elucidate the reasons for poor adherence to asthma medications during pregnancy, concerns about medication use, especially corticosteroids, stood out.7 A study based on prescription claims data showed that in the first trimester, there was a significant decline in asthma prescription medications (a 23% decline in inhaled corticosteroids, a 13% decline in short-acting bronchodilator agents, and a 54% decline in rescue corticosteroids).8 Lack of physician education about management of asthma in pregnancy and discomfort with prescribing to pregnant women also affect asthma control.
EFFECT OF ASTHMA ON MATERNAL AND FETAL OUTCOMES
Studies of the effects of asthma on fetal and maternal outcomes have yielded mixed and conflicting results.9 Adverse outcomes that have been shown to be associated with maternal asthma are listed in Table 1. Other studies have not demonstrated an association between asthma in pregnancy and maternal or fetal adverse events.9 Such discrepant findings are due to differences in study population characteristics that make comparisons difficult. A meta-analysis involving more than 1.6 million asthmatic women showed maternal asthma was associated with a 40% greater risk of low birth weight and preterm delivery, a 50% greater risk of preeclampsia, and a 20% greater risk of the baby being small for its gestational age.10
The association of maternal asthma and preterm birth may pose short-term and long-term health risks to the child associated with prematurity.9 Short-term risks with prematurity include infection, respiratory distress syndrome, brain injury, and necrotizing enterocolitis. Long-term risks include neurodevelopmental and behavioral sequelae. Furthermore, asthma exacerbations during pregnancy are associated with a twofold higher risk of low birth weight.11 The benefits of good adherence to asthma regimens during pregnancy outweigh the risks associated with frequent symptoms and exacerbations caused by untreated asthma.12
OUTPATIENT MANAGEMENT OF MATERNAL ASTHMA
Goals
In the 2004 update of the National Asthma Education and Prevention Program (NAEPP) Working Group Report on Managing Asthma During Pregnancy, goals focused mainly on adequate asthma control for maternal health and quality of life, as well as normal fetal maturation (Table 2),12 goals similar to those in nonpregnant asthmatic women.
Assessment and monitoring
Monthly physician visits during pregnancy are recommended for assessment of symptoms and pulmonary function. If symptoms are uncontrolled, therapy must be stepped up, and any trigger for exacerbation, such as gastroesophageal reflux disease (GERD), exposure, or rhinitis, must be treated and eliminated. NAEPP guidelines recommend baseline spirometry at the time of initial assessment.12 At follow-up visits, spirometry is preferred, but measurement of the peak expiratory flow rate usually suffices. Such objective data can help differentiate dyspnea from asthma and from dyspnea that usually accompanies the physiologic changes of pregnancy. In addition, patients should be advised to monitor for adequate fetal activity. If asthma is uncontrolled or poorly controlled, serial fetal ultrasonography should be considered from 32 weeks of gestation, as well as after recovery from an asthma exacerbation. Regular monitoring of the pregnant asthmatic patient by a multidisciplinary team can improve outcomes.13
Avoiding triggers
Patients should be advised to avoid asthma triggers such as pet dander, dust mites, pollen, smoke, mold, and perfumes, as this can decrease symptoms and allow for use of lower doses of medications.12 Additionally, smoking cessation must be strongly encouraged, not only to control maternal asthma, but also to prevent harm to the fetus.
MANAGEMENT OF SPECIFIC TRIGGERS
GERD
Reflux disease often worsens during pregnancy, and it can coexist with asthma and can also exacerbate it.14 Optimal control of GERD helps maintain adequate asthma control. For mild reflux symptoms, lifestyle modifications such as elevating the head of bed, avoiding eating too close to bedtime, and avoiding foods that cause heartburn may be adequate.15,16 If medications are needed, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before using a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
Allergic rhinitis
Intranasal corticosteroids are effective against allergic rhinitis in pregnancy (Table 3).12 Montelukast, a leukotriene receptor antagonist, can be used, but data to support its use for allergic rhinitis in pregnancy are limited.
Among antihistamines, second-generation drugs such as cetirizine or loratadine can be considered.12 Oral decongestants such as pseudoephedrine in early pregnancy are associated with a rare congenital fetal abnormality called gastroschisis, caused by vascular disruption.17 Hence, if a nasal decongestant is required in early pregnancy, a local therapy such as an intranasal corticosteroid, short-term oxymetazoline, or an external nasal dilator may be considered.12 These therapies must be combined with avoidance of allergens whenever possible.
Allergies
Diagnostic allergy and skin tests during pregnancy pose a risk of anaphylaxis and thus should be avoided. Instead, the focus should be on obtaining a thorough medical history about exposures and eliminating specific asthma triggers. It is also inadvisable to start allergen immunotherapy during pregnancy because of the risk of anaphylaxis and the effect of treatment on the mother and fetus.18 However, maintenance doses of allergen immunotherapy can be continued during pregnancy.18
Patient education
Because of concern about the risks of taking medications during pregnancy, many women with asthma stop using their inhalers during pregnancy, thus compromising asthma control.8,13 The physician and multidisciplinary team must use every opportunity to emphasize the importance of good asthma control during pregnancy. Inhaler technique should also be reviewed and, if defective, corrected. Again, trigger avoidance and tobacco cessation should be addressed.
Drugs
The NAEPP recommendations state that asthma therapy should be continued during pregnancy, as it is safer both for mother and fetus to avoid exacerbations and uncontrolled asthma.12 Despite this, 25% of primary care physicians instruct their patients to decrease or discontinue their inhaled corticosteroid during pregnancy.19 As with asthma in general, treatment should involve using the lowest dose of drugs that achieves adequate control of symptoms.
In 2015, the US Food and Drug Administration (FDA) amended the labeling rule for medications used in pregnancy and lactation. The previous risk categories A (safest), B, C, D, and X (highest risk) are in the process of being removed from labels for all human prescription drugs and biologic products, to be replaced with a summary of the risks of taking the drug during pregnancy and lactation, a discussion of the data supporting the use, and relevant information to help healthcare providers make prescribing decisions and counsel women about the use of drugs during pregnancy and lactation (www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/Labeling/ucm093307.htm).
ROLES OF CONTROLLER THERAPY AND RESCUE THERAPY
Inhaled corticosteroids
Inhaled corticosteroids are the mainstay of asthma controller therapy during pregnancy. A meta-analysis of 16 studies showed no increased risk of congenital malformations, cesarean delivery, or stillbirth among mothers who used these agents during pregnancy.20 Because there are more safety data for budesonide, it is currently the preferred inhaled corticosteroid during pregnancy.9 However, if a patient’s asthma is controlled with a different corticosteroid before pregnancy, that agent may be continued during pregnancy, especially if it is thought that switching formulations could adversely affect asthma control.12 This is mainly because current data do not prove that other inhaled corticosteroids are unsafe.
Inhaled beta-agonists
Inhaled beta-agonists, both short-acting and long-acting, are used for rescue therapy. Albuterol is the preferred short-acting agent for rescue therapy in pregnant women with asthma.12 Meta-analysis has shown no increased risk of major or minor congenital malformations in pregnant patients who use bronchodilators.20 Long-acting beta-agonists typically are used as add-on therapy when asthma cannot be controlled by an inhaled corticosteroid. They should not be used without a controller medication (ie, an inhaled corticosteroid).
Guidelines for rescue therapy are similar to those for nonpregnant asthmatic patients. Although data are limited as to the gestational effects of long-acting beta-agonists (ie, formoterol, salmeterol), it can be assumed that the toxicologic and pharmacologic profiles are similar to those of the short-acting bronchodilators. Thus, the safety of albuterol can be extended potentially to the long-acting beta-agonists.12
Combining controller and rescue therapy
When asthma is not adequately controlled on inhaled corticosteroids, a long-acting beta-agonist can be added or the dose of corticosteroid can be increased. The 2004 NAEPP guidelines stated that based on available literature, there was no clear advantage of one option over the other.12 A study that compared the 2 approaches found no difference in rates of congenital malformations.21
Leukotriene receptor antagonists
There is little in the literature regarding the use of leukotriene receptor antagonists during pregnancy. However, animal safety data are reassuring,12 and human studies have not found a higher risk of major congenital malformations.22,23 Thus, they are an alternative for patients whose asthma has been well controlled on these agents before pregnancy. Montelukast and zafirlukast are in former FDA pregnancy risk factor category B (probably safe) (Table 3). However, 5-lipoxygenase inhibitors such as zileuton are contraindicated based on animal studies showing teratogenicity.24
Omalizumab
Omalizumab, a recombinant anti-immunoglobulin E antibody, can be used for allergic asthma not controlled with inhaled corticosteroids (Table 3). An analysis of the omalizumab pregnancy registry25 found no significant increase in the rate of major congenital malformations, prematurity, or babies small for gestational age in asthmatic women taking omalizumab 8 weeks before conception or during pregnancy vs pregnant asthmatic women not taking omalizumab. However, this drug carries a risk of anaphylaxis and so should not be started during pregnancy.25
Theophylline
Because of potential toxicity, use of theophylline during pregnancy requires careful monitoring to ensure the serum concentration remains between 5 and 12 µg/mL.12 Drug interactions are also common: for example, alcohol may increase the serum concentration of theophylline, and theophylline may increase the toxic effect of formoterol.
Systemic corticosteroids
Pregnant women with asthma that is not well controlled despite the therapies described above may require a daily oral corticosteroid such as prednisone to achieve adequate control. Oral steroids are also a mainstay of treatment of asthma exacerbation.
Although use of corticosteroids in the first trimester was associated with orofacial cleft in infants,12 these studies did not include many women with asthma. In 2011, a nationwide cohort study from Denmark showed no increase in the risk of orofacial cleft with the use of corticosteroids during pregnancy.26
Preeclampsia, low birth weight, and preterm delivery have been described with corticosteroid use in pregnancy. It is not known whether these problems were a result of corticosteroid use or were due to the uncontrolled nature of the underlying condition that led to the steroid use. Since the risk of uncontrolled asthma to mother and fetus outweighs the risk of systemic corticosteroids, these drugs are recommended when indicated for management of maternal asthma.12
ACUTE EXACERBATIONS REQUIRE AGGRESSIVE MANAGEMENT
Based on a systematic review, 20% of pregnant women with asthma require some intervention for an asthma exacerbation during pregnancy, and 5.8% are admitted to the hospital for an exacerbation.11 Exacerbations were associated with a higher risk of low birth weight compared with rates in women without asthma.
Exacerbations are more common late in the second trimester and are unlikely to occur during labor and delivery.2 The incidence of exacerbations increases with the severity of asthma, from 8% in mild asthma, to 47% in moderate asthma, to 65% in severe asthma.27 Risk factors for exacerbations include poor prenatal care, obesity, and lack of appropriate treatment with inhaled corticosteroids.2 The main triggers are viral respiratory infections and noncompliance with inhaled corticosteroid therapy.11
Asthma exacerbations during pregnancy should be managed aggressively (Table 4),12 as the risk to the fetus of hypoxia far outweighs any risk from asthma medications. Close collaboration between the primary care physician and the obstetrician allows closer monitoring of mother and fetus.
The goal oxygen saturation must be above 95%.12 Signs of acute respiratory failure in a pregnant patient include a partial pressure of arterial oxygen less than 70 mm Hg or a partial pressure of carbon dioxide greater than 35 mm Hg.
In a multicenter study comparing nonpregnant and pregnant women visiting the emergency room for asthma exacerbations,28 pregnant women were less likely to be prescribed systemic corticosteroids either in the emergency room or at the time of hospital discharge, and they were also more likely to describe an ongoing exacerbation at 2-week follow-up. However, a recent study showed a significant increase in systemic corticosteroid treatment in the emergency room (51% to 78% across the time periods, odds ratio 3.11, 95% confidence interval 1.27–7.60, P = .01). There was also an increase in steroid treatment at discharge (42% to 63%, odds ratio 2.49, 95% confidence interval 0.97–6.37, P = .054), though the increase was not statistically significant.29 Although emergency room care for pregnant asthmatic women has improved, this group concluded that further improvement is still warranted, as 1 in 3 women is discharged without corticosteroid treatment.
The incidence of maternal asthma is rising. Based on US national health surveys, the prevalence of asthma during pregnancy is between 3.7% and 8.4%.1 It is the most common respiratory illness of pregnancy.2 Hence, clinicians need to know how asthma affects the mother and the fetus. Appropriate care of asthma during pregnancy is based on several management principles, as reviewed here, and is key to ensuring good outcomes for the mother and the baby.
EFFECT OF PREGNANCY ON ASTHMA CONTROL
Asthma control can vary in pregnancy. About a third of asthmatic women experience a worsening of asthma control with pregnancy, a third remain unchanged, and another third have improvement in asthma symptoms.3 The peak worsening of asthma tends to occur in the sixth month.4 Asthma control also tends to be better in the last month of pregnancy.3
The peak expiratory flow rate was noted to increase with each trimester in a small study of 43 women.5 The authors speculated that a rising progesterone level stimulates cyclic adenosine monophosphate to cause bronchodilation, thereby improving the expiratory flow rate and asthma control. Asthma control tends to follow the pattern experienced in the previous pregnancy: ie, if asthma worsened during the previous pregnancy, the same will be likely in the subsequent pregnancy.3
Two maternal factors that adversely affect asthma severity during pregnancy are the use of asthma medications contrary to guidelines such as those of the Global Initiative for Asthma (http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention) and inadquate control of asthma before becoming pregnant.6 Pregnancy can bring on stress, and stress is known to worsen asthma. In addition, when patients themselves were interviewed to elucidate the reasons for poor adherence to asthma medications during pregnancy, concerns about medication use, especially corticosteroids, stood out.7 A study based on prescription claims data showed that in the first trimester, there was a significant decline in asthma prescription medications (a 23% decline in inhaled corticosteroids, a 13% decline in short-acting bronchodilator agents, and a 54% decline in rescue corticosteroids).8 Lack of physician education about management of asthma in pregnancy and discomfort with prescribing to pregnant women also affect asthma control.
EFFECT OF ASTHMA ON MATERNAL AND FETAL OUTCOMES
Studies of the effects of asthma on fetal and maternal outcomes have yielded mixed and conflicting results.9 Adverse outcomes that have been shown to be associated with maternal asthma are listed in Table 1. Other studies have not demonstrated an association between asthma in pregnancy and maternal or fetal adverse events.9 Such discrepant findings are due to differences in study population characteristics that make comparisons difficult. A meta-analysis involving more than 1.6 million asthmatic women showed maternal asthma was associated with a 40% greater risk of low birth weight and preterm delivery, a 50% greater risk of preeclampsia, and a 20% greater risk of the baby being small for its gestational age.10
The association of maternal asthma and preterm birth may pose short-term and long-term health risks to the child associated with prematurity.9 Short-term risks with prematurity include infection, respiratory distress syndrome, brain injury, and necrotizing enterocolitis. Long-term risks include neurodevelopmental and behavioral sequelae. Furthermore, asthma exacerbations during pregnancy are associated with a twofold higher risk of low birth weight.11 The benefits of good adherence to asthma regimens during pregnancy outweigh the risks associated with frequent symptoms and exacerbations caused by untreated asthma.12
OUTPATIENT MANAGEMENT OF MATERNAL ASTHMA
Goals
In the 2004 update of the National Asthma Education and Prevention Program (NAEPP) Working Group Report on Managing Asthma During Pregnancy, goals focused mainly on adequate asthma control for maternal health and quality of life, as well as normal fetal maturation (Table 2),12 goals similar to those in nonpregnant asthmatic women.
Assessment and monitoring
Monthly physician visits during pregnancy are recommended for assessment of symptoms and pulmonary function. If symptoms are uncontrolled, therapy must be stepped up, and any trigger for exacerbation, such as gastroesophageal reflux disease (GERD), exposure, or rhinitis, must be treated and eliminated. NAEPP guidelines recommend baseline spirometry at the time of initial assessment.12 At follow-up visits, spirometry is preferred, but measurement of the peak expiratory flow rate usually suffices. Such objective data can help differentiate dyspnea from asthma and from dyspnea that usually accompanies the physiologic changes of pregnancy. In addition, patients should be advised to monitor for adequate fetal activity. If asthma is uncontrolled or poorly controlled, serial fetal ultrasonography should be considered from 32 weeks of gestation, as well as after recovery from an asthma exacerbation. Regular monitoring of the pregnant asthmatic patient by a multidisciplinary team can improve outcomes.13
Avoiding triggers
Patients should be advised to avoid asthma triggers such as pet dander, dust mites, pollen, smoke, mold, and perfumes, as this can decrease symptoms and allow for use of lower doses of medications.12 Additionally, smoking cessation must be strongly encouraged, not only to control maternal asthma, but also to prevent harm to the fetus.
MANAGEMENT OF SPECIFIC TRIGGERS
GERD
Reflux disease often worsens during pregnancy, and it can coexist with asthma and can also exacerbate it.14 Optimal control of GERD helps maintain adequate asthma control. For mild reflux symptoms, lifestyle modifications such as elevating the head of bed, avoiding eating too close to bedtime, and avoiding foods that cause heartburn may be adequate.15,16 If medications are needed, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before using a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
Allergic rhinitis
Intranasal corticosteroids are effective against allergic rhinitis in pregnancy (Table 3).12 Montelukast, a leukotriene receptor antagonist, can be used, but data to support its use for allergic rhinitis in pregnancy are limited.
Among antihistamines, second-generation drugs such as cetirizine or loratadine can be considered.12 Oral decongestants such as pseudoephedrine in early pregnancy are associated with a rare congenital fetal abnormality called gastroschisis, caused by vascular disruption.17 Hence, if a nasal decongestant is required in early pregnancy, a local therapy such as an intranasal corticosteroid, short-term oxymetazoline, or an external nasal dilator may be considered.12 These therapies must be combined with avoidance of allergens whenever possible.
Allergies
Diagnostic allergy and skin tests during pregnancy pose a risk of anaphylaxis and thus should be avoided. Instead, the focus should be on obtaining a thorough medical history about exposures and eliminating specific asthma triggers. It is also inadvisable to start allergen immunotherapy during pregnancy because of the risk of anaphylaxis and the effect of treatment on the mother and fetus.18 However, maintenance doses of allergen immunotherapy can be continued during pregnancy.18
Patient education
Because of concern about the risks of taking medications during pregnancy, many women with asthma stop using their inhalers during pregnancy, thus compromising asthma control.8,13 The physician and multidisciplinary team must use every opportunity to emphasize the importance of good asthma control during pregnancy. Inhaler technique should also be reviewed and, if defective, corrected. Again, trigger avoidance and tobacco cessation should be addressed.
Drugs
The NAEPP recommendations state that asthma therapy should be continued during pregnancy, as it is safer both for mother and fetus to avoid exacerbations and uncontrolled asthma.12 Despite this, 25% of primary care physicians instruct their patients to decrease or discontinue their inhaled corticosteroid during pregnancy.19 As with asthma in general, treatment should involve using the lowest dose of drugs that achieves adequate control of symptoms.
In 2015, the US Food and Drug Administration (FDA) amended the labeling rule for medications used in pregnancy and lactation. The previous risk categories A (safest), B, C, D, and X (highest risk) are in the process of being removed from labels for all human prescription drugs and biologic products, to be replaced with a summary of the risks of taking the drug during pregnancy and lactation, a discussion of the data supporting the use, and relevant information to help healthcare providers make prescribing decisions and counsel women about the use of drugs during pregnancy and lactation (www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/Labeling/ucm093307.htm).
ROLES OF CONTROLLER THERAPY AND RESCUE THERAPY
Inhaled corticosteroids
Inhaled corticosteroids are the mainstay of asthma controller therapy during pregnancy. A meta-analysis of 16 studies showed no increased risk of congenital malformations, cesarean delivery, or stillbirth among mothers who used these agents during pregnancy.20 Because there are more safety data for budesonide, it is currently the preferred inhaled corticosteroid during pregnancy.9 However, if a patient’s asthma is controlled with a different corticosteroid before pregnancy, that agent may be continued during pregnancy, especially if it is thought that switching formulations could adversely affect asthma control.12 This is mainly because current data do not prove that other inhaled corticosteroids are unsafe.
Inhaled beta-agonists
Inhaled beta-agonists, both short-acting and long-acting, are used for rescue therapy. Albuterol is the preferred short-acting agent for rescue therapy in pregnant women with asthma.12 Meta-analysis has shown no increased risk of major or minor congenital malformations in pregnant patients who use bronchodilators.20 Long-acting beta-agonists typically are used as add-on therapy when asthma cannot be controlled by an inhaled corticosteroid. They should not be used without a controller medication (ie, an inhaled corticosteroid).
Guidelines for rescue therapy are similar to those for nonpregnant asthmatic patients. Although data are limited as to the gestational effects of long-acting beta-agonists (ie, formoterol, salmeterol), it can be assumed that the toxicologic and pharmacologic profiles are similar to those of the short-acting bronchodilators. Thus, the safety of albuterol can be extended potentially to the long-acting beta-agonists.12
Combining controller and rescue therapy
When asthma is not adequately controlled on inhaled corticosteroids, a long-acting beta-agonist can be added or the dose of corticosteroid can be increased. The 2004 NAEPP guidelines stated that based on available literature, there was no clear advantage of one option over the other.12 A study that compared the 2 approaches found no difference in rates of congenital malformations.21
Leukotriene receptor antagonists
There is little in the literature regarding the use of leukotriene receptor antagonists during pregnancy. However, animal safety data are reassuring,12 and human studies have not found a higher risk of major congenital malformations.22,23 Thus, they are an alternative for patients whose asthma has been well controlled on these agents before pregnancy. Montelukast and zafirlukast are in former FDA pregnancy risk factor category B (probably safe) (Table 3). However, 5-lipoxygenase inhibitors such as zileuton are contraindicated based on animal studies showing teratogenicity.24
Omalizumab
Omalizumab, a recombinant anti-immunoglobulin E antibody, can be used for allergic asthma not controlled with inhaled corticosteroids (Table 3). An analysis of the omalizumab pregnancy registry25 found no significant increase in the rate of major congenital malformations, prematurity, or babies small for gestational age in asthmatic women taking omalizumab 8 weeks before conception or during pregnancy vs pregnant asthmatic women not taking omalizumab. However, this drug carries a risk of anaphylaxis and so should not be started during pregnancy.25
Theophylline
Because of potential toxicity, use of theophylline during pregnancy requires careful monitoring to ensure the serum concentration remains between 5 and 12 µg/mL.12 Drug interactions are also common: for example, alcohol may increase the serum concentration of theophylline, and theophylline may increase the toxic effect of formoterol.
Systemic corticosteroids
Pregnant women with asthma that is not well controlled despite the therapies described above may require a daily oral corticosteroid such as prednisone to achieve adequate control. Oral steroids are also a mainstay of treatment of asthma exacerbation.
Although use of corticosteroids in the first trimester was associated with orofacial cleft in infants,12 these studies did not include many women with asthma. In 2011, a nationwide cohort study from Denmark showed no increase in the risk of orofacial cleft with the use of corticosteroids during pregnancy.26
Preeclampsia, low birth weight, and preterm delivery have been described with corticosteroid use in pregnancy. It is not known whether these problems were a result of corticosteroid use or were due to the uncontrolled nature of the underlying condition that led to the steroid use. Since the risk of uncontrolled asthma to mother and fetus outweighs the risk of systemic corticosteroids, these drugs are recommended when indicated for management of maternal asthma.12
ACUTE EXACERBATIONS REQUIRE AGGRESSIVE MANAGEMENT
Based on a systematic review, 20% of pregnant women with asthma require some intervention for an asthma exacerbation during pregnancy, and 5.8% are admitted to the hospital for an exacerbation.11 Exacerbations were associated with a higher risk of low birth weight compared with rates in women without asthma.
Exacerbations are more common late in the second trimester and are unlikely to occur during labor and delivery.2 The incidence of exacerbations increases with the severity of asthma, from 8% in mild asthma, to 47% in moderate asthma, to 65% in severe asthma.27 Risk factors for exacerbations include poor prenatal care, obesity, and lack of appropriate treatment with inhaled corticosteroids.2 The main triggers are viral respiratory infections and noncompliance with inhaled corticosteroid therapy.11
Asthma exacerbations during pregnancy should be managed aggressively (Table 4),12 as the risk to the fetus of hypoxia far outweighs any risk from asthma medications. Close collaboration between the primary care physician and the obstetrician allows closer monitoring of mother and fetus.
The goal oxygen saturation must be above 95%.12 Signs of acute respiratory failure in a pregnant patient include a partial pressure of arterial oxygen less than 70 mm Hg or a partial pressure of carbon dioxide greater than 35 mm Hg.
In a multicenter study comparing nonpregnant and pregnant women visiting the emergency room for asthma exacerbations,28 pregnant women were less likely to be prescribed systemic corticosteroids either in the emergency room or at the time of hospital discharge, and they were also more likely to describe an ongoing exacerbation at 2-week follow-up. However, a recent study showed a significant increase in systemic corticosteroid treatment in the emergency room (51% to 78% across the time periods, odds ratio 3.11, 95% confidence interval 1.27–7.60, P = .01). There was also an increase in steroid treatment at discharge (42% to 63%, odds ratio 2.49, 95% confidence interval 0.97–6.37, P = .054), though the increase was not statistically significant.29 Although emergency room care for pregnant asthmatic women has improved, this group concluded that further improvement is still warranted, as 1 in 3 women is discharged without corticosteroid treatment.
- Kwon HL, Belanger K, Bracken MB. Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol 2003; 13:317–324.
- Powell H, Murphy VE, Taylor DR, et al. Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomised controlled trial. Lancet 2011; 378:983–990.
- Schatz M, Harden K, Forsythe A, et al. The course of asthma during pregnancy, post partum, and with successive pregnancies: a prospective analysis. J Allergy Clin Immunol 1988; 81:509–517.
- Gluck JC, Gluck PA. The effect of pregnancy on the course of asthma. Immunol Allergy Clin North Am 2006; 26:63–80.
- Beckmann CA. Peak flow values by gestation in women with asthma. Clin Nurs Res 2008; 17:174–181.
- Belanger K, Hellenbrand ME, Holford TR, Bracken M. Effect of pregnancy on maternal asthma symptoms and medication use. Obstet Gynecol 2010; 115:559–567.
- Lim AS, Stewart K, Abramson MJ, Ryan K, George J. Asthma during pregnancy: the experiences, concerns and views of pregnant women with asthma. J Asthma 2012; 49:474–479.
- Enriquez R, Wu P, Griffin MR, et al. Cessation of asthma medication in early pregnancy. Am J Obstet Gynecol 2006; 195:149–153.
- Bain E, Pierides KL, Clifton VL, et al. Interventions for managing asthma in pregnancy. Cochrane Database Syst Rev 2014; 10:CD010660.
- Murphy VE, Namazy JA, Powell H, et al. A meta-analysis of adverse perinatal outcomes in women with asthma. BJOG 2011; 118:1314–1323.
- Murphy VE, Clifton VL, Gibson PG. Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax 2006; 61:169–176.
- National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Asthma and Pregnancy Working Group. NAEPP expert panel report. Managing asthma during pregnancy: recommendations for pharmacologic treatment—2004 update. J Allergy Clin Immunol 2005; 115:34–46.
- Lim AS, Stewart K, Abramson MJ, Walker SP, Smith CL, George J. Multidisciplinary Approach to Management of Maternal Asthma (MAMMA): a randomized controlled trial. Chest 2014; 145:1046–1054.
- Harding SM. Gastroesophageal reflux: a potential asthma trigger. Immunol Allergy Clin North Am 2005; 25:131–148.
- Ahmad S, Mokaddas E. Recent advances in the diagnosis and treatment of multidrug-resistant tuberculosis. Respir Med 2009; 103:1777–1790.
- van der Woude CJ, Metselaar HJ, Danese S. Management of gastrointestinal and liver diseases during pregnancy. Gut 2014; 63:1014–1023.
- Werler MM. Teratogen update: pseudoephedrine. Birth Defects Res A Clin Mol Teratol 2006; 76:445–452.
- Cox L, Nelson H, Lockey R, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol 2011; 127(suppl 1):S1–S55.
- Lim AS, Stewart K, Abramson MJ, George J. Management of asthma in pregnant women by general practitioners: a cross sectional survey. BMC Fam Pract 2011; 12:121.
- Murphy VE, Wang G, Namazy JA, et al. The risk of congenital malformations, perinatal mortality and neonatal hospitalisation among pregnant women with asthma: a systematic review and meta-analysis. BJOG 2013; 120:812–822.
- Eltonsy S, Forget A, Beauchesne MF, Blais L. Risk of congenital malformations for asthmatic pregnant women using a long-acting beta2-agonist and inhaled corticosteroid combination versus higher-dose inhaled corticosteroid monotherapy. J Allergy Clin Immunol 2015; 135:123–130.
- Nelsen LM, Shields KE, Cunningham ML, et al. Congenital malformations among infants born to women receiving montelukast, inhaled corticosteroids, and other asthma medications. J Allergy Clin Immunol 2012; 129:251–254.e1–e6.
- Sarkar M, Koren G, Kalra S, et al. Montelukast use during pregnancy: a multicentre, prospective, comparative study of infant outcomes. Eur J Clin Pharmacol 2009; 65:1259–1264.
- Namazy JA, Schatz M. The safety of asthma medications during pregnancy: an update for clinicians. Ther Adv Respir Dis 2014; 8:103–110.
- Namazy J, Cabana MD, Scheuerle AE, et al. The Xolair Pregnancy Registry (EXPECT): the safety of omalizumab use during pregnancy. J Allergy Clin Immunol 2015; 135:407–412.
- Hviid A, Molgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ 2011; 183:796–804.
- Murphy VE, Gibson P, Talbot PI, Clifton VL. Severe asthma exacerbations during pregnancy. Obstet Gynecol 2005; 106:1046–1054.
- Cydulka RK, Emerman CL, Schreiber D, Molander KH, Woodruff PG, Camargo CA Jr. Acute asthma among pregnant women presenting to the emergency department. Am J Respir Crit Care Med 1999; 160:887–892.
- Hasegawa K, Cydulka RK, Sullivan AF, et al. Improved management of acute asthma among pregnant women presenting to the ED. Chest 2015; 147:406–414.
- Kwon HL, Belanger K, Bracken MB. Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol 2003; 13:317–324.
- Powell H, Murphy VE, Taylor DR, et al. Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomised controlled trial. Lancet 2011; 378:983–990.
- Schatz M, Harden K, Forsythe A, et al. The course of asthma during pregnancy, post partum, and with successive pregnancies: a prospective analysis. J Allergy Clin Immunol 1988; 81:509–517.
- Gluck JC, Gluck PA. The effect of pregnancy on the course of asthma. Immunol Allergy Clin North Am 2006; 26:63–80.
- Beckmann CA. Peak flow values by gestation in women with asthma. Clin Nurs Res 2008; 17:174–181.
- Belanger K, Hellenbrand ME, Holford TR, Bracken M. Effect of pregnancy on maternal asthma symptoms and medication use. Obstet Gynecol 2010; 115:559–567.
- Lim AS, Stewart K, Abramson MJ, Ryan K, George J. Asthma during pregnancy: the experiences, concerns and views of pregnant women with asthma. J Asthma 2012; 49:474–479.
- Enriquez R, Wu P, Griffin MR, et al. Cessation of asthma medication in early pregnancy. Am J Obstet Gynecol 2006; 195:149–153.
- Bain E, Pierides KL, Clifton VL, et al. Interventions for managing asthma in pregnancy. Cochrane Database Syst Rev 2014; 10:CD010660.
- Murphy VE, Namazy JA, Powell H, et al. A meta-analysis of adverse perinatal outcomes in women with asthma. BJOG 2011; 118:1314–1323.
- Murphy VE, Clifton VL, Gibson PG. Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax 2006; 61:169–176.
- National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program Asthma and Pregnancy Working Group. NAEPP expert panel report. Managing asthma during pregnancy: recommendations for pharmacologic treatment—2004 update. J Allergy Clin Immunol 2005; 115:34–46.
- Lim AS, Stewart K, Abramson MJ, Walker SP, Smith CL, George J. Multidisciplinary Approach to Management of Maternal Asthma (MAMMA): a randomized controlled trial. Chest 2014; 145:1046–1054.
- Harding SM. Gastroesophageal reflux: a potential asthma trigger. Immunol Allergy Clin North Am 2005; 25:131–148.
- Ahmad S, Mokaddas E. Recent advances in the diagnosis and treatment of multidrug-resistant tuberculosis. Respir Med 2009; 103:1777–1790.
- van der Woude CJ, Metselaar HJ, Danese S. Management of gastrointestinal and liver diseases during pregnancy. Gut 2014; 63:1014–1023.
- Werler MM. Teratogen update: pseudoephedrine. Birth Defects Res A Clin Mol Teratol 2006; 76:445–452.
- Cox L, Nelson H, Lockey R, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol 2011; 127(suppl 1):S1–S55.
- Lim AS, Stewart K, Abramson MJ, George J. Management of asthma in pregnant women by general practitioners: a cross sectional survey. BMC Fam Pract 2011; 12:121.
- Murphy VE, Wang G, Namazy JA, et al. The risk of congenital malformations, perinatal mortality and neonatal hospitalisation among pregnant women with asthma: a systematic review and meta-analysis. BJOG 2013; 120:812–822.
- Eltonsy S, Forget A, Beauchesne MF, Blais L. Risk of congenital malformations for asthmatic pregnant women using a long-acting beta2-agonist and inhaled corticosteroid combination versus higher-dose inhaled corticosteroid monotherapy. J Allergy Clin Immunol 2015; 135:123–130.
- Nelsen LM, Shields KE, Cunningham ML, et al. Congenital malformations among infants born to women receiving montelukast, inhaled corticosteroids, and other asthma medications. J Allergy Clin Immunol 2012; 129:251–254.e1–e6.
- Sarkar M, Koren G, Kalra S, et al. Montelukast use during pregnancy: a multicentre, prospective, comparative study of infant outcomes. Eur J Clin Pharmacol 2009; 65:1259–1264.
- Namazy JA, Schatz M. The safety of asthma medications during pregnancy: an update for clinicians. Ther Adv Respir Dis 2014; 8:103–110.
- Namazy J, Cabana MD, Scheuerle AE, et al. The Xolair Pregnancy Registry (EXPECT): the safety of omalizumab use during pregnancy. J Allergy Clin Immunol 2015; 135:407–412.
- Hviid A, Molgaard-Nielsen D. Corticosteroid use during pregnancy and risk of orofacial clefts. CMAJ 2011; 183:796–804.
- Murphy VE, Gibson P, Talbot PI, Clifton VL. Severe asthma exacerbations during pregnancy. Obstet Gynecol 2005; 106:1046–1054.
- Cydulka RK, Emerman CL, Schreiber D, Molander KH, Woodruff PG, Camargo CA Jr. Acute asthma among pregnant women presenting to the emergency department. Am J Respir Crit Care Med 1999; 160:887–892.
- Hasegawa K, Cydulka RK, Sullivan AF, et al. Improved management of acute asthma among pregnant women presenting to the ED. Chest 2015; 147:406–414.
KEY POINTS
- The benefits of good adherence to asthma regimens during pregnancy outweigh the risks associated with the medications used.
- For treatment of reflux disease in pregnant women with asthma, antacids (but not sodium bicarbonate, for fear of metabolic alkalosis) and sucralfate should be considered before a histamine 2 receptor antagonist such as ranitidine. Proton pump inhibitors should be considered only if reflux symptoms are refractory to other therapies.
- Uncontrolled maternal asthma contributes to poor maternal and fetal outcomes. Management by a multi-disciplinary team, including internist, obstetrician, pharmacist, nurse, allergist, and pulmonologist, improves care and outcomes.
