User login
One-third of drug postmarket studies go unpublished
More than one-third of postmarket studies following drug approval that should be published are not, according to new research.
Investigators examined a Food and Drug Administration internal database to identify all postmarket drug studies between 2009 and 2013 identified by the agency as completed, with a follow-up search to find if/where the results of the studies were published.
“As of July 2016, 183 of the 288 postmarket studies (63.5%) meeting inclusion criteria were published in either the scientific literature or on the ClinicalTrials.gov website,” Marisa Cruz, MD, medical officer in the Food and Drug Administration’s Office of Public Health Strategy and Analysis, and her colleagues wrote in a researcher letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1313).
More studies were published in journals (175) than in the agency’s clinical trial registry (87), and the 183 interventional clinical trials had a higher overall publication rate (87.4%) than the other 105 studies combined (21.9%).
Of the 69 interventional clinical trials that were focused on efficacy, 86.2% were categorized as having results that were favorable to the trial sponsor. However, the 57 interventional clinical trials with positive results were no more likely to be published than the 12 trials with negative results, Dr. Cruz and colleagues noted.
The findings are consistent with previous research, the researchers noted, with the analysis demonstrating “that postmarket study results are not consistently disseminated, either through journal publication or trial registries.”
“Despite calls for data sharing and publication of all clinical trial results, publication rates for completed postmarket studies required by the FDA remain relatively low,” the researchers wrote.
While the FDA could publish the data itself, “this approach would likely require new regulations,” the authors noted. “Alternatively, increased sponsor commitment to submitting to journals and to publish all clinical trial results on trial registries, regardless of whether publication is legally required, may serve to promote dissemination of scientific knowledge.”
The researchers reported no conflicts of interest.
More than one-third of postmarket studies following drug approval that should be published are not, according to new research.
Investigators examined a Food and Drug Administration internal database to identify all postmarket drug studies between 2009 and 2013 identified by the agency as completed, with a follow-up search to find if/where the results of the studies were published.
“As of July 2016, 183 of the 288 postmarket studies (63.5%) meeting inclusion criteria were published in either the scientific literature or on the ClinicalTrials.gov website,” Marisa Cruz, MD, medical officer in the Food and Drug Administration’s Office of Public Health Strategy and Analysis, and her colleagues wrote in a researcher letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1313).
More studies were published in journals (175) than in the agency’s clinical trial registry (87), and the 183 interventional clinical trials had a higher overall publication rate (87.4%) than the other 105 studies combined (21.9%).
Of the 69 interventional clinical trials that were focused on efficacy, 86.2% were categorized as having results that were favorable to the trial sponsor. However, the 57 interventional clinical trials with positive results were no more likely to be published than the 12 trials with negative results, Dr. Cruz and colleagues noted.
The findings are consistent with previous research, the researchers noted, with the analysis demonstrating “that postmarket study results are not consistently disseminated, either through journal publication or trial registries.”
“Despite calls for data sharing and publication of all clinical trial results, publication rates for completed postmarket studies required by the FDA remain relatively low,” the researchers wrote.
While the FDA could publish the data itself, “this approach would likely require new regulations,” the authors noted. “Alternatively, increased sponsor commitment to submitting to journals and to publish all clinical trial results on trial registries, regardless of whether publication is legally required, may serve to promote dissemination of scientific knowledge.”
The researchers reported no conflicts of interest.
More than one-third of postmarket studies following drug approval that should be published are not, according to new research.
Investigators examined a Food and Drug Administration internal database to identify all postmarket drug studies between 2009 and 2013 identified by the agency as completed, with a follow-up search to find if/where the results of the studies were published.
“As of July 2016, 183 of the 288 postmarket studies (63.5%) meeting inclusion criteria were published in either the scientific literature or on the ClinicalTrials.gov website,” Marisa Cruz, MD, medical officer in the Food and Drug Administration’s Office of Public Health Strategy and Analysis, and her colleagues wrote in a researcher letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1313).
More studies were published in journals (175) than in the agency’s clinical trial registry (87), and the 183 interventional clinical trials had a higher overall publication rate (87.4%) than the other 105 studies combined (21.9%).
Of the 69 interventional clinical trials that were focused on efficacy, 86.2% were categorized as having results that were favorable to the trial sponsor. However, the 57 interventional clinical trials with positive results were no more likely to be published than the 12 trials with negative results, Dr. Cruz and colleagues noted.
The findings are consistent with previous research, the researchers noted, with the analysis demonstrating “that postmarket study results are not consistently disseminated, either through journal publication or trial registries.”
“Despite calls for data sharing and publication of all clinical trial results, publication rates for completed postmarket studies required by the FDA remain relatively low,” the researchers wrote.
While the FDA could publish the data itself, “this approach would likely require new regulations,” the authors noted. “Alternatively, increased sponsor commitment to submitting to journals and to publish all clinical trial results on trial registries, regardless of whether publication is legally required, may serve to promote dissemination of scientific knowledge.”
The researchers reported no conflicts of interest.
Value-based care didn’t trigger spikes in patient dismissals
Fears that the transition to value-based care could lead to doctors dismissing patients from their practice who could adversely affect their reimbursement didn’t come to fruition in a recent federal value-based initiative.
“Patient dismissal could be an unintended consequence of this shift as clinicians face (or perceive they face) pressure to limit their panel to patients for whom they can readily demonstrate value in order to maximize revenue,” Ann S. O’Malley, MD, senior fellow at Mathematica Policy Research, and her colleagues wrote in a research letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1309).
“A similar portion and distribution of CPC and comparison practices reported ever dismissing patients in the past 2 years,” 89% and 92%, respectively, the researchers reported.
CPC and comparison practices “dismissed patients for similar reasons,” Dr. O’Malley and colleagues added, noting the exception that more comparison practices reported dismissing patients for violating bill payment policies than CPC practices did – 43% vs. 35%, respectively.
Other reasons for dismissing patients included patients being extremely disruptive and/or behaving inappropriately toward clinicians or staff, patients violating chronic pain/controlled substances policies, patients repeatedly missing appointments, patients not following recommended lifestyle changes, and patients making frequent emergency department visits and/or frequent self-referrals to specialists.
Practices participating in the CPC initiative were also asked if participation in the value-based payment model would make them more or less likely to dismiss patients.
“According to most CPC practices, the initiative had no effect or made them less likely to dismiss patients,” the researchers found.
The CMS Centers for Medicare & Medicaid Innovation funded the study. The study authors reported no conflicts of interest.
Fears that the transition to value-based care could lead to doctors dismissing patients from their practice who could adversely affect their reimbursement didn’t come to fruition in a recent federal value-based initiative.
“Patient dismissal could be an unintended consequence of this shift as clinicians face (or perceive they face) pressure to limit their panel to patients for whom they can readily demonstrate value in order to maximize revenue,” Ann S. O’Malley, MD, senior fellow at Mathematica Policy Research, and her colleagues wrote in a research letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1309).
“A similar portion and distribution of CPC and comparison practices reported ever dismissing patients in the past 2 years,” 89% and 92%, respectively, the researchers reported.
CPC and comparison practices “dismissed patients for similar reasons,” Dr. O’Malley and colleagues added, noting the exception that more comparison practices reported dismissing patients for violating bill payment policies than CPC practices did – 43% vs. 35%, respectively.
Other reasons for dismissing patients included patients being extremely disruptive and/or behaving inappropriately toward clinicians or staff, patients violating chronic pain/controlled substances policies, patients repeatedly missing appointments, patients not following recommended lifestyle changes, and patients making frequent emergency department visits and/or frequent self-referrals to specialists.
Practices participating in the CPC initiative were also asked if participation in the value-based payment model would make them more or less likely to dismiss patients.
“According to most CPC practices, the initiative had no effect or made them less likely to dismiss patients,” the researchers found.
The CMS Centers for Medicare & Medicaid Innovation funded the study. The study authors reported no conflicts of interest.
Fears that the transition to value-based care could lead to doctors dismissing patients from their practice who could adversely affect their reimbursement didn’t come to fruition in a recent federal value-based initiative.
“Patient dismissal could be an unintended consequence of this shift as clinicians face (or perceive they face) pressure to limit their panel to patients for whom they can readily demonstrate value in order to maximize revenue,” Ann S. O’Malley, MD, senior fellow at Mathematica Policy Research, and her colleagues wrote in a research letter published online May 15 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2017.1309).
“A similar portion and distribution of CPC and comparison practices reported ever dismissing patients in the past 2 years,” 89% and 92%, respectively, the researchers reported.
CPC and comparison practices “dismissed patients for similar reasons,” Dr. O’Malley and colleagues added, noting the exception that more comparison practices reported dismissing patients for violating bill payment policies than CPC practices did – 43% vs. 35%, respectively.
Other reasons for dismissing patients included patients being extremely disruptive and/or behaving inappropriately toward clinicians or staff, patients violating chronic pain/controlled substances policies, patients repeatedly missing appointments, patients not following recommended lifestyle changes, and patients making frequent emergency department visits and/or frequent self-referrals to specialists.
Practices participating in the CPC initiative were also asked if participation in the value-based payment model would make them more or less likely to dismiss patients.
“According to most CPC practices, the initiative had no effect or made them less likely to dismiss patients,” the researchers found.
The CMS Centers for Medicare & Medicaid Innovation funded the study. The study authors reported no conflicts of interest.
Pediatric Dermatology Consult - May 2017
BY LAWRENCE F. EICHENFIELD, MD, and JENNA BOROK
Nevus sebaceous (NS) is considered a subtype of an epidermal nevus, a benign hamartoma that includes an excess or deficiency of structural elements of the skin, such as epidermis, sebaceous, and apocrine glands.1
Nevus sebaceous, also known as nevus sebaceous of Jadassohn, was first described in 1895 by Josef Jadassohn as a nevoid growth composed predominantly of sebaceous glands.2 Sebaceous glands are found everywhere on the body where hair is found and are located adjacent to hair follicles with ducts, through which sebum flows.3
NS clinically appears as a waxy, yellowish-orange to pink, hairless plaque, ranging from 1 cm to over 10 cm in size and usually located on the scalp, face, neck, or trunk.1 When the lesions are linear, they typically follow Blaschko lines.1 The lesions change over time. An infant’s lesion will be slightly raised and can be hardly noticeable. If the lesion is located on the scalp, it will remain hairless. During later childhood, the nevus may thicken. The lesions may become thicker and verrucous during adolescence.
Histologically, NS are benign hamartomas with epidermal, follicular, sebaceous, and apocrine elements.4 The malformation is primarily within the individual folliculosebaceous units.1 An infantile lesion will deviate little from normal skin as the follicular units are so small.1 During childhood, microscopically, it is easier to see misshapen follicles and thickened epidermis.1 During adolescence, the histological pattern is similar to that of an epidermal nevi, which includes acanthosis and fibroplasia of the papillary dermis.
There are now several lines of evidence showing that nevus sebaceous is caused by genetic postzygotic mosaic mutations in the mitogen–activated protein kinase (MAPK) pathway, which specifically activate ras mutations including H ras and K ras genes.5-7 Since NS is caused by a somatic mosaicism mutation, there are a several syndromic findings associated with NS depending on the timing of the mutations during development and whether single versus multiple tissues are affected.8 Specifically, NS has been associated with Schimmelpenning-Feuerstein-Mims syndrome that includes NS, and skeletal, ocular, and neurologic abnormalities.1,7 A study found that cutaneous skeletal hypophosphatemia syndrome, manifested as NS and vitamin D–resistant rickets, has identical ras mutations in both skin and bone tissues, providing further support that these syndromic findings are a result of a multilineage somatic ras mutation.8
Diagnosis
NS is typically diagnosed clinically, based on the presence of a circumscribed, thin, yellow-orange, oval, round, or linear plaque, usually on the scalp or face. During infancy or the first stage, the lesions remain stable. In the second stage, during puberty, the lesions thicken and become verrucous or nodular because of changes in sebaceous gland activity that are driven by hormones. In the third stage of their natural course, benign and malignant epithelial neoplasms can develop, including trichoblastoma, syringocystadenoma papilliferum, sebaceous epithelioma, basal cell carcinoma, and trichilemmoma.9
The associated syndrome, nevus sebaceous syndrome, also known as Schimmelpenning syndrome, has more extensive cutaneous lesions along Blaschko lines and presents with CNS, ocular, or skeletal defects. The CNS abnormalities include mental retardation, seizures, and hemimegalencephaly.1 Therefore, a thorough neurologic and ophthalmologic examination should be performed in patients with suspected nevus sebaceous syndrome.
Aplasia cutis congenita is the absence of the skin at birth that presents with an erosion or deep ulceration to a scar or a defect that is covered with an epidermal membrane.1 Some aplasia cutis may present as a smooth, hairless surface at birth, making differentiation from nevus sebaceous difficult. The pinkish, orange to yellow hue of NS may help differentiate these entities. Juvenile xanthogranuloma is a fairly common histiocytosis and is the most common histiocytic disease of childhood.1 It is a benign proliferation of dermal dendrocytes, and it presents in infants as many red to yellow papules or a few nodules on the head and neck. Many lesions even remain undetected.1
Syringocystadenoma papilliferum is a benign neoplasm with apocrine differentiation and presents as a papule or plaque on the head and neck. It can be associated with nevus sebaceous.1
Treatment
The definitive treatment is an excision. The necessity and timing of excision of these lesions is still under debate.9 Secondary neoplasms do arise from the nevus sebaceous, although the incidence is low pre puberty.1 It has been estimated that 16% of cases develop benign tumors and that 8% of cases develop malignant tumors.9 The majority of malignant lesions are basal cell carcinomas, and a large recent study found that only 1% of patients had malignancies.10 While most of these tumors develop in adulthood, there have been reports of malignancies in children.10
An additional reason to excise NS is that, over time, they grow more verrucous, become inflamed, bleed with trauma, and may be unappealing cosmetically.1 Some experts recommend earlier excision in childhood, especially with larger lesions or facial lesions where minimizing deformity is important and with the possibility of less noticeable scarring.9 The prophylactic removal of NS remains controversial, and there is a lack of consensus among experts about the timing of excision. It is recommended that each lesion be evaluated on a case-by-case basis.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Borok is a medical student at the University of California, Los Angeles. Dr. Eichenfield and Ms. Borok said they had no relevant financial disclosures. Email them at [email protected].
References
1. “Dermatology.” 3rd ed. (St Louis, Mo: Elsevier, 2012).
2. Arch Dermatol Res. 1895. doi: 10.1007/BF01842810.
3. J Invest Dermatol. 2004 Jul;123(1):1-12.
4. J Cutan Pathol. 1984;11(5):396-414.
5. J Invest Dermatol. 2013 Mar;133(3):827-30.
6. J Invest Dermatol. 2013 Mar;133(3):597-600.
7. Nat Genet. 2012 Jun 10;44(7):783-7.
8. JAAD. 2016 Aug;75(2):420-7.
9. Pediatr Dermatol. 2012 Jan-Feb;29(1):15-23.
10. Pediatr Dermatol. 2009 Nov-Dec;26(6):676-81.
BY LAWRENCE F. EICHENFIELD, MD, and JENNA BOROK
Nevus sebaceous (NS) is considered a subtype of an epidermal nevus, a benign hamartoma that includes an excess or deficiency of structural elements of the skin, such as epidermis, sebaceous, and apocrine glands.1
Nevus sebaceous, also known as nevus sebaceous of Jadassohn, was first described in 1895 by Josef Jadassohn as a nevoid growth composed predominantly of sebaceous glands.2 Sebaceous glands are found everywhere on the body where hair is found and are located adjacent to hair follicles with ducts, through which sebum flows.3
NS clinically appears as a waxy, yellowish-orange to pink, hairless plaque, ranging from 1 cm to over 10 cm in size and usually located on the scalp, face, neck, or trunk.1 When the lesions are linear, they typically follow Blaschko lines.1 The lesions change over time. An infant’s lesion will be slightly raised and can be hardly noticeable. If the lesion is located on the scalp, it will remain hairless. During later childhood, the nevus may thicken. The lesions may become thicker and verrucous during adolescence.
Histologically, NS are benign hamartomas with epidermal, follicular, sebaceous, and apocrine elements.4 The malformation is primarily within the individual folliculosebaceous units.1 An infantile lesion will deviate little from normal skin as the follicular units are so small.1 During childhood, microscopically, it is easier to see misshapen follicles and thickened epidermis.1 During adolescence, the histological pattern is similar to that of an epidermal nevi, which includes acanthosis and fibroplasia of the papillary dermis.
There are now several lines of evidence showing that nevus sebaceous is caused by genetic postzygotic mosaic mutations in the mitogen–activated protein kinase (MAPK) pathway, which specifically activate ras mutations including H ras and K ras genes.5-7 Since NS is caused by a somatic mosaicism mutation, there are a several syndromic findings associated with NS depending on the timing of the mutations during development and whether single versus multiple tissues are affected.8 Specifically, NS has been associated with Schimmelpenning-Feuerstein-Mims syndrome that includes NS, and skeletal, ocular, and neurologic abnormalities.1,7 A study found that cutaneous skeletal hypophosphatemia syndrome, manifested as NS and vitamin D–resistant rickets, has identical ras mutations in both skin and bone tissues, providing further support that these syndromic findings are a result of a multilineage somatic ras mutation.8
Diagnosis
NS is typically diagnosed clinically, based on the presence of a circumscribed, thin, yellow-orange, oval, round, or linear plaque, usually on the scalp or face. During infancy or the first stage, the lesions remain stable. In the second stage, during puberty, the lesions thicken and become verrucous or nodular because of changes in sebaceous gland activity that are driven by hormones. In the third stage of their natural course, benign and malignant epithelial neoplasms can develop, including trichoblastoma, syringocystadenoma papilliferum, sebaceous epithelioma, basal cell carcinoma, and trichilemmoma.9
The associated syndrome, nevus sebaceous syndrome, also known as Schimmelpenning syndrome, has more extensive cutaneous lesions along Blaschko lines and presents with CNS, ocular, or skeletal defects. The CNS abnormalities include mental retardation, seizures, and hemimegalencephaly.1 Therefore, a thorough neurologic and ophthalmologic examination should be performed in patients with suspected nevus sebaceous syndrome.
Aplasia cutis congenita is the absence of the skin at birth that presents with an erosion or deep ulceration to a scar or a defect that is covered with an epidermal membrane.1 Some aplasia cutis may present as a smooth, hairless surface at birth, making differentiation from nevus sebaceous difficult. The pinkish, orange to yellow hue of NS may help differentiate these entities. Juvenile xanthogranuloma is a fairly common histiocytosis and is the most common histiocytic disease of childhood.1 It is a benign proliferation of dermal dendrocytes, and it presents in infants as many red to yellow papules or a few nodules on the head and neck. Many lesions even remain undetected.1
Syringocystadenoma papilliferum is a benign neoplasm with apocrine differentiation and presents as a papule or plaque on the head and neck. It can be associated with nevus sebaceous.1
Treatment
The definitive treatment is an excision. The necessity and timing of excision of these lesions is still under debate.9 Secondary neoplasms do arise from the nevus sebaceous, although the incidence is low pre puberty.1 It has been estimated that 16% of cases develop benign tumors and that 8% of cases develop malignant tumors.9 The majority of malignant lesions are basal cell carcinomas, and a large recent study found that only 1% of patients had malignancies.10 While most of these tumors develop in adulthood, there have been reports of malignancies in children.10
An additional reason to excise NS is that, over time, they grow more verrucous, become inflamed, bleed with trauma, and may be unappealing cosmetically.1 Some experts recommend earlier excision in childhood, especially with larger lesions or facial lesions where minimizing deformity is important and with the possibility of less noticeable scarring.9 The prophylactic removal of NS remains controversial, and there is a lack of consensus among experts about the timing of excision. It is recommended that each lesion be evaluated on a case-by-case basis.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Borok is a medical student at the University of California, Los Angeles. Dr. Eichenfield and Ms. Borok said they had no relevant financial disclosures. Email them at [email protected].
References
1. “Dermatology.” 3rd ed. (St Louis, Mo: Elsevier, 2012).
2. Arch Dermatol Res. 1895. doi: 10.1007/BF01842810.
3. J Invest Dermatol. 2004 Jul;123(1):1-12.
4. J Cutan Pathol. 1984;11(5):396-414.
5. J Invest Dermatol. 2013 Mar;133(3):827-30.
6. J Invest Dermatol. 2013 Mar;133(3):597-600.
7. Nat Genet. 2012 Jun 10;44(7):783-7.
8. JAAD. 2016 Aug;75(2):420-7.
9. Pediatr Dermatol. 2012 Jan-Feb;29(1):15-23.
10. Pediatr Dermatol. 2009 Nov-Dec;26(6):676-81.
BY LAWRENCE F. EICHENFIELD, MD, and JENNA BOROK
Nevus sebaceous (NS) is considered a subtype of an epidermal nevus, a benign hamartoma that includes an excess or deficiency of structural elements of the skin, such as epidermis, sebaceous, and apocrine glands.1
Nevus sebaceous, also known as nevus sebaceous of Jadassohn, was first described in 1895 by Josef Jadassohn as a nevoid growth composed predominantly of sebaceous glands.2 Sebaceous glands are found everywhere on the body where hair is found and are located adjacent to hair follicles with ducts, through which sebum flows.3
NS clinically appears as a waxy, yellowish-orange to pink, hairless plaque, ranging from 1 cm to over 10 cm in size and usually located on the scalp, face, neck, or trunk.1 When the lesions are linear, they typically follow Blaschko lines.1 The lesions change over time. An infant’s lesion will be slightly raised and can be hardly noticeable. If the lesion is located on the scalp, it will remain hairless. During later childhood, the nevus may thicken. The lesions may become thicker and verrucous during adolescence.
Histologically, NS are benign hamartomas with epidermal, follicular, sebaceous, and apocrine elements.4 The malformation is primarily within the individual folliculosebaceous units.1 An infantile lesion will deviate little from normal skin as the follicular units are so small.1 During childhood, microscopically, it is easier to see misshapen follicles and thickened epidermis.1 During adolescence, the histological pattern is similar to that of an epidermal nevi, which includes acanthosis and fibroplasia of the papillary dermis.
There are now several lines of evidence showing that nevus sebaceous is caused by genetic postzygotic mosaic mutations in the mitogen–activated protein kinase (MAPK) pathway, which specifically activate ras mutations including H ras and K ras genes.5-7 Since NS is caused by a somatic mosaicism mutation, there are a several syndromic findings associated with NS depending on the timing of the mutations during development and whether single versus multiple tissues are affected.8 Specifically, NS has been associated with Schimmelpenning-Feuerstein-Mims syndrome that includes NS, and skeletal, ocular, and neurologic abnormalities.1,7 A study found that cutaneous skeletal hypophosphatemia syndrome, manifested as NS and vitamin D–resistant rickets, has identical ras mutations in both skin and bone tissues, providing further support that these syndromic findings are a result of a multilineage somatic ras mutation.8
Diagnosis
NS is typically diagnosed clinically, based on the presence of a circumscribed, thin, yellow-orange, oval, round, or linear plaque, usually on the scalp or face. During infancy or the first stage, the lesions remain stable. In the second stage, during puberty, the lesions thicken and become verrucous or nodular because of changes in sebaceous gland activity that are driven by hormones. In the third stage of their natural course, benign and malignant epithelial neoplasms can develop, including trichoblastoma, syringocystadenoma papilliferum, sebaceous epithelioma, basal cell carcinoma, and trichilemmoma.9
The associated syndrome, nevus sebaceous syndrome, also known as Schimmelpenning syndrome, has more extensive cutaneous lesions along Blaschko lines and presents with CNS, ocular, or skeletal defects. The CNS abnormalities include mental retardation, seizures, and hemimegalencephaly.1 Therefore, a thorough neurologic and ophthalmologic examination should be performed in patients with suspected nevus sebaceous syndrome.
Aplasia cutis congenita is the absence of the skin at birth that presents with an erosion or deep ulceration to a scar or a defect that is covered with an epidermal membrane.1 Some aplasia cutis may present as a smooth, hairless surface at birth, making differentiation from nevus sebaceous difficult. The pinkish, orange to yellow hue of NS may help differentiate these entities. Juvenile xanthogranuloma is a fairly common histiocytosis and is the most common histiocytic disease of childhood.1 It is a benign proliferation of dermal dendrocytes, and it presents in infants as many red to yellow papules or a few nodules on the head and neck. Many lesions even remain undetected.1
Syringocystadenoma papilliferum is a benign neoplasm with apocrine differentiation and presents as a papule or plaque on the head and neck. It can be associated with nevus sebaceous.1
Treatment
The definitive treatment is an excision. The necessity and timing of excision of these lesions is still under debate.9 Secondary neoplasms do arise from the nevus sebaceous, although the incidence is low pre puberty.1 It has been estimated that 16% of cases develop benign tumors and that 8% of cases develop malignant tumors.9 The majority of malignant lesions are basal cell carcinomas, and a large recent study found that only 1% of patients had malignancies.10 While most of these tumors develop in adulthood, there have been reports of malignancies in children.10
An additional reason to excise NS is that, over time, they grow more verrucous, become inflamed, bleed with trauma, and may be unappealing cosmetically.1 Some experts recommend earlier excision in childhood, especially with larger lesions or facial lesions where minimizing deformity is important and with the possibility of less noticeable scarring.9 The prophylactic removal of NS remains controversial, and there is a lack of consensus among experts about the timing of excision. It is recommended that each lesion be evaluated on a case-by-case basis.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego and professor of dermatology and pediatrics at the University of California, San Diego. Ms. Borok is a medical student at the University of California, Los Angeles. Dr. Eichenfield and Ms. Borok said they had no relevant financial disclosures. Email them at [email protected].
References
1. “Dermatology.” 3rd ed. (St Louis, Mo: Elsevier, 2012).
2. Arch Dermatol Res. 1895. doi: 10.1007/BF01842810.
3. J Invest Dermatol. 2004 Jul;123(1):1-12.
4. J Cutan Pathol. 1984;11(5):396-414.
5. J Invest Dermatol. 2013 Mar;133(3):827-30.
6. J Invest Dermatol. 2013 Mar;133(3):597-600.
7. Nat Genet. 2012 Jun 10;44(7):783-7.
8. JAAD. 2016 Aug;75(2):420-7.
9. Pediatr Dermatol. 2012 Jan-Feb;29(1):15-23.
10. Pediatr Dermatol. 2009 Nov-Dec;26(6):676-81.
A 4-year-old boy presents with a yellow-orange lesion on his scalp. His mother states that it was present at birth and does not seem to bother him. The mother also complains that he is not growing hair over the bump area on his head. The bump has grown proportionally with the patient since birth.
He is otherwise healthy and has no other bumps like this one on his body. He was born at term with an unremarkable perinatal history.
During the physical exam, you find a yellow-orange, smooth, hairless plaque on the scalp. The plaque is 3 cm in size and is well circumscribed. The infant’s general physical, skin exam, and neurological exam are normal. He has no skeletal defects.
Mycobacteria subset plagues pulmonary patients
Nontuberculous mycobacteria accounts for an increasing percentage of pulmonary disease, and nonsurgical treatment alone has not shown effectiveness, according to data from a meta-analysis of 24 studies and 1,224 patients. The study results were published online in Chest.
Data on therapeutic successes in cases of nontuberculosis mycobacteria (NTM)–related pulmonary disease are limited, in particular for those species not related to the Mycobacterium avium complex (non-MAC), wrote Roland Diel, MD, of University Medical Hospital Schleswig-Holstein, Germany, and his colleagues.
In particular, non-MAC species Mycobacterium xenopi (MX), Mycobacterium abscessus, Mycobacterium malmoense, and Mycobacterium kansasii (MK) were addressed in the studies, which included 16 retrospective chart reviews, 5 randomized trials, and 3 prospective, nonrandomized studies (Chest 2017. doi: 10.1016/j.chest.2017.04.166).
Treatment success was measured by rates of sputum culture conversion (SCC).
Overall, the average proportion of SCC for patients with M. abscessus was 41% after subtraction for posttreatment relapses, but reached 70% for subspecies M. massiliense in macrolide-containing treatments. The average proportion of SCC was 80% for patients with M. kansasii, 32% for those with MX, and 54% for those with M. malmoense.
Treatment success ranged from 9% to 73% for M. xenopi patients, but all-cause mortality was 69%. Of note, a 100% success rate was noted in M. kansasii patients using a three-drug TB regimen of isoniazid, rifampicin, and ethambutol, or with a combination of ethambutol, rifampicin, and clarithromycin, the researchers noted.
The percentage of SCC in 55 patients with lung resection and either MX or M. abscessus was considered high at 76%.
The study findings were limited by the diverse definitions of treatment success and by the variety of treatments and “an optimal multidrug treatment cannot be derived from the few studies and has yet to be determined,” the researchers said. In the absence of optimal drug therapy, functional and quality of life elements deserve greater consideration when evaluating outcomes in patients with non-MAC NTM pulmonary disease, they added.
Dr. Diel reported receiving lecturing and/or consulting fees from Insmed and Riemser.
Nontuberculous mycobacteria accounts for an increasing percentage of pulmonary disease, and nonsurgical treatment alone has not shown effectiveness, according to data from a meta-analysis of 24 studies and 1,224 patients. The study results were published online in Chest.
Data on therapeutic successes in cases of nontuberculosis mycobacteria (NTM)–related pulmonary disease are limited, in particular for those species not related to the Mycobacterium avium complex (non-MAC), wrote Roland Diel, MD, of University Medical Hospital Schleswig-Holstein, Germany, and his colleagues.
In particular, non-MAC species Mycobacterium xenopi (MX), Mycobacterium abscessus, Mycobacterium malmoense, and Mycobacterium kansasii (MK) were addressed in the studies, which included 16 retrospective chart reviews, 5 randomized trials, and 3 prospective, nonrandomized studies (Chest 2017. doi: 10.1016/j.chest.2017.04.166).
Treatment success was measured by rates of sputum culture conversion (SCC).
Overall, the average proportion of SCC for patients with M. abscessus was 41% after subtraction for posttreatment relapses, but reached 70% for subspecies M. massiliense in macrolide-containing treatments. The average proportion of SCC was 80% for patients with M. kansasii, 32% for those with MX, and 54% for those with M. malmoense.
Treatment success ranged from 9% to 73% for M. xenopi patients, but all-cause mortality was 69%. Of note, a 100% success rate was noted in M. kansasii patients using a three-drug TB regimen of isoniazid, rifampicin, and ethambutol, or with a combination of ethambutol, rifampicin, and clarithromycin, the researchers noted.
The percentage of SCC in 55 patients with lung resection and either MX or M. abscessus was considered high at 76%.
The study findings were limited by the diverse definitions of treatment success and by the variety of treatments and “an optimal multidrug treatment cannot be derived from the few studies and has yet to be determined,” the researchers said. In the absence of optimal drug therapy, functional and quality of life elements deserve greater consideration when evaluating outcomes in patients with non-MAC NTM pulmonary disease, they added.
Dr. Diel reported receiving lecturing and/or consulting fees from Insmed and Riemser.
Nontuberculous mycobacteria accounts for an increasing percentage of pulmonary disease, and nonsurgical treatment alone has not shown effectiveness, according to data from a meta-analysis of 24 studies and 1,224 patients. The study results were published online in Chest.
Data on therapeutic successes in cases of nontuberculosis mycobacteria (NTM)–related pulmonary disease are limited, in particular for those species not related to the Mycobacterium avium complex (non-MAC), wrote Roland Diel, MD, of University Medical Hospital Schleswig-Holstein, Germany, and his colleagues.
In particular, non-MAC species Mycobacterium xenopi (MX), Mycobacterium abscessus, Mycobacterium malmoense, and Mycobacterium kansasii (MK) were addressed in the studies, which included 16 retrospective chart reviews, 5 randomized trials, and 3 prospective, nonrandomized studies (Chest 2017. doi: 10.1016/j.chest.2017.04.166).
Treatment success was measured by rates of sputum culture conversion (SCC).
Overall, the average proportion of SCC for patients with M. abscessus was 41% after subtraction for posttreatment relapses, but reached 70% for subspecies M. massiliense in macrolide-containing treatments. The average proportion of SCC was 80% for patients with M. kansasii, 32% for those with MX, and 54% for those with M. malmoense.
Treatment success ranged from 9% to 73% for M. xenopi patients, but all-cause mortality was 69%. Of note, a 100% success rate was noted in M. kansasii patients using a three-drug TB regimen of isoniazid, rifampicin, and ethambutol, or with a combination of ethambutol, rifampicin, and clarithromycin, the researchers noted.
The percentage of SCC in 55 patients with lung resection and either MX or M. abscessus was considered high at 76%.
The study findings were limited by the diverse definitions of treatment success and by the variety of treatments and “an optimal multidrug treatment cannot be derived from the few studies and has yet to be determined,” the researchers said. In the absence of optimal drug therapy, functional and quality of life elements deserve greater consideration when evaluating outcomes in patients with non-MAC NTM pulmonary disease, they added.
Dr. Diel reported receiving lecturing and/or consulting fees from Insmed and Riemser.
FROM CHEST
Key clinical point: An optimal multidrug treatment has not yet been found for patients with nontuberculosis mycobacteria (NTM)–related pulmonary disease.
Major finding: The average proportion of sputum culture conversion (SCC) for patients with M. abscessus was 42% after subtraction for posttreatment relapses, but reached 79% for subspecies M. massiliense in macrolide-containing treatments. The average proportion of SCC was 80% for patients with M. kansasii, 32% for those with M. xenopi, and 54% for those with M. malmoense.
Data source: A meta-analysis of 24 studies and 1,224 patients.
Disclosures: Dr. Roland Diel reported receiving lecturing and/or consulting fees from Insmed and Riemser.
Digital transference: New dangers in a new world
We are in a new age of psychiatric practice caught in the wider shift from an industrial to a technology-based society. Although this transformation has been occurring over the past half-century, the last decade has seen a rapid acceleration driven by mobile phones, social networking, and the Internet.
Thomas Friedman, in his book “Thank you for Being Late: An Optimist’s Guide to Thriving in the Age of Accelerations” (New York: Farrar, Straus & Girous, 2016), cites 2007 as the year our world changed with the launching of the iPhone, the globalization of Facebook and Twitter, the release of the Kindle and Android, the founding of Airbnb, Google’s purchase of YouTube, and IBM’s creation of its AI system, Watson. Psychiatry has been gradually incorporating technology into everyday practice using mobile devices, email, videoconferencing, Internet, and electronic medical records, as well as being impacted by more rapidly evolving technologies, such as texting and social networking platforms.

Transference remains a core tenant in the psychiatric conceptualization of the psychiatrist-patient relationship. There are numerous formal definitions of this phenomenon. This article will use a broad reductionist definition of transference as the “unconscious projection of a past relationship/experience onto a current relationship” and combine the terms transference (from patient to psychiatrist) and countertransference (from psychiatrist to patient; often defined as a psychiatrist’s reaction to a patient’s transference).
How do a psychiatrist and patient dyad’s previous experiences with technology and technology-based relationships affect a current clinical relationship? How does the type of technology being used influence shared meanings and assumptions? Does technology introduce new implicit biases that go unrecognized? Does distant communication increase the risk of missing contextual clues more apparent for in-person interactions? These critical questions have largely gone unaddressed, but what is known raises concerns. The question is not whether to use these technologies, which have demonstrated utility to transform care. Rather, concerns around our lack of understanding of the technologies’ strengths, weaknesses, and influences on the doctor-patient relationship need to be explored. Below we will briefly examine each of these questions.
A relatively new paradigm has been inserting itself from the field of education into medicine that describes a patient’s previous technology experiences. “Digital immigrants” is a term for those who did not grow up with today’s technology and began using our current technologies as adults. They contrast with “digital natives,” who have grown up incorporating technology into their daily lives. Broad assumptions are that digital natives tend to be more comfortable, flexible, and adaptable with technologies, compared with digital immigrants, who are more hesitant and slower to adopt and integrate technology. However, the experience of a specific patient with technology is multifactorial and more nuanced than the digital native vs. digital immigrant classification. There are those who argue that technology use from an early age is altering on a biological level the way the human brain processes both information and emotion. Depending on their experiences and backgrounds (immigrant vs. native), a psychiatrist and patient using videoconferencing to enable remote access could have initial as well as ongoing positive or negative transferences to treatment.
The specific technology being used also sets parameters for communication that influence interpretation. Text and email communication are very different from live interactive video conferencing and involve use of language that may not be shared between the psychiatrist and patient, such as text abbreviations and emojis. Lack of visual and auditory information necessitates more interpretation by the receiver to fill in tone, meaning, and intent drawn from their past conscious and unconscious experiences and assumptions. The opportunity for misinterpretation is further compounded by implicit bias built into the technology. Although biases embedded in medical technologies have yet to be examined, there are some alarming examples from society in general.
A recent report by the Georgetown University’s Center on Privacy & Technology drew attention to inherent racial bias in facial recognition technology used by law enforcement agencies. This bias was a product of both the underlying software and programming, as well as the real world implementation of these systems. As the field of medicine increasingly turns to artificial intelligence for help with pattern recognition, data management, and population health, what implicit biases are being built into these systems? Could a web-assisted, evidence-based therapy that uses an algorithmic approach have built-in biases for certain populations of patients, affecting the therapeutic interaction?
A final issue worth considering is the power of technology to distort shared context. When a psychiatrist meets with a patient in person, they are sharing the same environmental context at the same point of time during treatment. When communicating over distance, they are occupying different environments and, with asynchronous communication (for example, email), different points in time. These disparate contexts may lend themselves to additional assumptions that get projected onto the clinical relationship. For example, a telepsychiatrist working with Northern Plains Indian Communities via videoconferencing has a new patient in a new clinic setting visually similar to other clinics they have visited in the past. If not mindful of context, the telepsychiatrist may risk making unwarranted assumptions about the patient’s environmental context based on the physician’s previous work. In a different example, a psychiatrist sees a patient for an in-person visit and then reads an email sent 12 hours prior to the visit by the patient expressing upset at psychiatrist’s structuring of treatment. This issue was not addressed in the session that just ended. What is the impact of this email to both the psychiatrist and patient, and their current feelings about the therapeutic relationship? Is this now current or past context for the patient and psychiatrist?
For many, questions about bias, context, and previous experiences with technology can be seen as “grist for the mill” for psychiatrists to understand the transferences and other processes within doctor-patient relationships. This knowledge can then be leveraged to appropriately attend to the therapeutic relationship. The danger in the age of hybrid relationships is when there are embedded issues that psychiatry as a field and individual psychiatrists are unaware of and not attending to in treatment. As the acknowledged experts in medicine in the doctor-patient relationship say, psychiatrists need to take leadership roles in better understanding the impact of technologies on clinical processes – both for those processes on the surface, as well as those that lurk beneath the digital waves.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center at the University of Colorado at Denver, Aurora. He also serves as associate professor of psychiatry at the university.
We are in a new age of psychiatric practice caught in the wider shift from an industrial to a technology-based society. Although this transformation has been occurring over the past half-century, the last decade has seen a rapid acceleration driven by mobile phones, social networking, and the Internet.
Thomas Friedman, in his book “Thank you for Being Late: An Optimist’s Guide to Thriving in the Age of Accelerations” (New York: Farrar, Straus & Girous, 2016), cites 2007 as the year our world changed with the launching of the iPhone, the globalization of Facebook and Twitter, the release of the Kindle and Android, the founding of Airbnb, Google’s purchase of YouTube, and IBM’s creation of its AI system, Watson. Psychiatry has been gradually incorporating technology into everyday practice using mobile devices, email, videoconferencing, Internet, and electronic medical records, as well as being impacted by more rapidly evolving technologies, such as texting and social networking platforms.
Transference remains a core tenant in the psychiatric conceptualization of the psychiatrist-patient relationship. There are numerous formal definitions of this phenomenon. This article will use a broad reductionist definition of transference as the “unconscious projection of a past relationship/experience onto a current relationship” and combine the terms transference (from patient to psychiatrist) and countertransference (from psychiatrist to patient; often defined as a psychiatrist’s reaction to a patient’s transference).
How do a psychiatrist and patient dyad’s previous experiences with technology and technology-based relationships affect a current clinical relationship? How does the type of technology being used influence shared meanings and assumptions? Does technology introduce new implicit biases that go unrecognized? Does distant communication increase the risk of missing contextual clues more apparent for in-person interactions? These critical questions have largely gone unaddressed, but what is known raises concerns. The question is not whether to use these technologies, which have demonstrated utility to transform care. Rather, concerns around our lack of understanding of the technologies’ strengths, weaknesses, and influences on the doctor-patient relationship need to be explored. Below we will briefly examine each of these questions.
A relatively new paradigm has been inserting itself from the field of education into medicine that describes a patient’s previous technology experiences. “Digital immigrants” is a term for those who did not grow up with today’s technology and began using our current technologies as adults. They contrast with “digital natives,” who have grown up incorporating technology into their daily lives. Broad assumptions are that digital natives tend to be more comfortable, flexible, and adaptable with technologies, compared with digital immigrants, who are more hesitant and slower to adopt and integrate technology. However, the experience of a specific patient with technology is multifactorial and more nuanced than the digital native vs. digital immigrant classification. There are those who argue that technology use from an early age is altering on a biological level the way the human brain processes both information and emotion. Depending on their experiences and backgrounds (immigrant vs. native), a psychiatrist and patient using videoconferencing to enable remote access could have initial as well as ongoing positive or negative transferences to treatment.
The specific technology being used also sets parameters for communication that influence interpretation. Text and email communication are very different from live interactive video conferencing and involve use of language that may not be shared between the psychiatrist and patient, such as text abbreviations and emojis. Lack of visual and auditory information necessitates more interpretation by the receiver to fill in tone, meaning, and intent drawn from their past conscious and unconscious experiences and assumptions. The opportunity for misinterpretation is further compounded by implicit bias built into the technology. Although biases embedded in medical technologies have yet to be examined, there are some alarming examples from society in general.
A recent report by the Georgetown University’s Center on Privacy & Technology drew attention to inherent racial bias in facial recognition technology used by law enforcement agencies. This bias was a product of both the underlying software and programming, as well as the real world implementation of these systems. As the field of medicine increasingly turns to artificial intelligence for help with pattern recognition, data management, and population health, what implicit biases are being built into these systems? Could a web-assisted, evidence-based therapy that uses an algorithmic approach have built-in biases for certain populations of patients, affecting the therapeutic interaction?
A final issue worth considering is the power of technology to distort shared context. When a psychiatrist meets with a patient in person, they are sharing the same environmental context at the same point of time during treatment. When communicating over distance, they are occupying different environments and, with asynchronous communication (for example, email), different points in time. These disparate contexts may lend themselves to additional assumptions that get projected onto the clinical relationship. For example, a telepsychiatrist working with Northern Plains Indian Communities via videoconferencing has a new patient in a new clinic setting visually similar to other clinics they have visited in the past. If not mindful of context, the telepsychiatrist may risk making unwarranted assumptions about the patient’s environmental context based on the physician’s previous work. In a different example, a psychiatrist sees a patient for an in-person visit and then reads an email sent 12 hours prior to the visit by the patient expressing upset at psychiatrist’s structuring of treatment. This issue was not addressed in the session that just ended. What is the impact of this email to both the psychiatrist and patient, and their current feelings about the therapeutic relationship? Is this now current or past context for the patient and psychiatrist?
For many, questions about bias, context, and previous experiences with technology can be seen as “grist for the mill” for psychiatrists to understand the transferences and other processes within doctor-patient relationships. This knowledge can then be leveraged to appropriately attend to the therapeutic relationship. The danger in the age of hybrid relationships is when there are embedded issues that psychiatry as a field and individual psychiatrists are unaware of and not attending to in treatment. As the acknowledged experts in medicine in the doctor-patient relationship say, psychiatrists need to take leadership roles in better understanding the impact of technologies on clinical processes – both for those processes on the surface, as well as those that lurk beneath the digital waves.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center at the University of Colorado at Denver, Aurora. He also serves as associate professor of psychiatry at the university.
We are in a new age of psychiatric practice caught in the wider shift from an industrial to a technology-based society. Although this transformation has been occurring over the past half-century, the last decade has seen a rapid acceleration driven by mobile phones, social networking, and the Internet.
Thomas Friedman, in his book “Thank you for Being Late: An Optimist’s Guide to Thriving in the Age of Accelerations” (New York: Farrar, Straus & Girous, 2016), cites 2007 as the year our world changed with the launching of the iPhone, the globalization of Facebook and Twitter, the release of the Kindle and Android, the founding of Airbnb, Google’s purchase of YouTube, and IBM’s creation of its AI system, Watson. Psychiatry has been gradually incorporating technology into everyday practice using mobile devices, email, videoconferencing, Internet, and electronic medical records, as well as being impacted by more rapidly evolving technologies, such as texting and social networking platforms.
Transference remains a core tenant in the psychiatric conceptualization of the psychiatrist-patient relationship. There are numerous formal definitions of this phenomenon. This article will use a broad reductionist definition of transference as the “unconscious projection of a past relationship/experience onto a current relationship” and combine the terms transference (from patient to psychiatrist) and countertransference (from psychiatrist to patient; often defined as a psychiatrist’s reaction to a patient’s transference).
How do a psychiatrist and patient dyad’s previous experiences with technology and technology-based relationships affect a current clinical relationship? How does the type of technology being used influence shared meanings and assumptions? Does technology introduce new implicit biases that go unrecognized? Does distant communication increase the risk of missing contextual clues more apparent for in-person interactions? These critical questions have largely gone unaddressed, but what is known raises concerns. The question is not whether to use these technologies, which have demonstrated utility to transform care. Rather, concerns around our lack of understanding of the technologies’ strengths, weaknesses, and influences on the doctor-patient relationship need to be explored. Below we will briefly examine each of these questions.
A relatively new paradigm has been inserting itself from the field of education into medicine that describes a patient’s previous technology experiences. “Digital immigrants” is a term for those who did not grow up with today’s technology and began using our current technologies as adults. They contrast with “digital natives,” who have grown up incorporating technology into their daily lives. Broad assumptions are that digital natives tend to be more comfortable, flexible, and adaptable with technologies, compared with digital immigrants, who are more hesitant and slower to adopt and integrate technology. However, the experience of a specific patient with technology is multifactorial and more nuanced than the digital native vs. digital immigrant classification. There are those who argue that technology use from an early age is altering on a biological level the way the human brain processes both information and emotion. Depending on their experiences and backgrounds (immigrant vs. native), a psychiatrist and patient using videoconferencing to enable remote access could have initial as well as ongoing positive or negative transferences to treatment.
The specific technology being used also sets parameters for communication that influence interpretation. Text and email communication are very different from live interactive video conferencing and involve use of language that may not be shared between the psychiatrist and patient, such as text abbreviations and emojis. Lack of visual and auditory information necessitates more interpretation by the receiver to fill in tone, meaning, and intent drawn from their past conscious and unconscious experiences and assumptions. The opportunity for misinterpretation is further compounded by implicit bias built into the technology. Although biases embedded in medical technologies have yet to be examined, there are some alarming examples from society in general.
A recent report by the Georgetown University’s Center on Privacy & Technology drew attention to inherent racial bias in facial recognition technology used by law enforcement agencies. This bias was a product of both the underlying software and programming, as well as the real world implementation of these systems. As the field of medicine increasingly turns to artificial intelligence for help with pattern recognition, data management, and population health, what implicit biases are being built into these systems? Could a web-assisted, evidence-based therapy that uses an algorithmic approach have built-in biases for certain populations of patients, affecting the therapeutic interaction?
A final issue worth considering is the power of technology to distort shared context. When a psychiatrist meets with a patient in person, they are sharing the same environmental context at the same point of time during treatment. When communicating over distance, they are occupying different environments and, with asynchronous communication (for example, email), different points in time. These disparate contexts may lend themselves to additional assumptions that get projected onto the clinical relationship. For example, a telepsychiatrist working with Northern Plains Indian Communities via videoconferencing has a new patient in a new clinic setting visually similar to other clinics they have visited in the past. If not mindful of context, the telepsychiatrist may risk making unwarranted assumptions about the patient’s environmental context based on the physician’s previous work. In a different example, a psychiatrist sees a patient for an in-person visit and then reads an email sent 12 hours prior to the visit by the patient expressing upset at psychiatrist’s structuring of treatment. This issue was not addressed in the session that just ended. What is the impact of this email to both the psychiatrist and patient, and their current feelings about the therapeutic relationship? Is this now current or past context for the patient and psychiatrist?
For many, questions about bias, context, and previous experiences with technology can be seen as “grist for the mill” for psychiatrists to understand the transferences and other processes within doctor-patient relationships. This knowledge can then be leveraged to appropriately attend to the therapeutic relationship. The danger in the age of hybrid relationships is when there are embedded issues that psychiatry as a field and individual psychiatrists are unaware of and not attending to in treatment. As the acknowledged experts in medicine in the doctor-patient relationship say, psychiatrists need to take leadership roles in better understanding the impact of technologies on clinical processes – both for those processes on the surface, as well as those that lurk beneath the digital waves.
Dr. Shore chairs the American Psychiatric Association’s Committee on Telepsychiatry and is director of telemedicine at the Helen & Arthur E. Johnson Depression Center at the University of Colorado at Denver, Aurora. He also serves as associate professor of psychiatry at the university.
The Personal Health Inventory: Current Use, Perceived Barriers, and Benefits
To better meet the needs and values of patients, the VA has been promulgating a paradigm shift away from the disease-focused model toward a whole health, patient-centered focus.1 To achieve this goal, the VA Office of Patient Centered Care and Cultural Transformation has advocated the use of the personal health inventory (PHI). This inventory asks patients to mindfully assess why their health is important to them and to determine where they feel they are and where they want to be with respect to 8 areas of self-care (working the body, physical and emotional surroundings, personal development, food and drink, sleep, human relationships, spirituality/purpose, and awareness of relationship between mind and body).
Personal health inventory written responses are then discussed with a member of the health care team to develop a proactive, patient-driven health plan unique to that veteran’s circumstances and aspirations.2 The PHI is applicable not only to veterans, but also in primary care and other practices outside the VA to improve shared decision making and produce more effective clinician-patient partnerships.
After national PHI promotion by the VA, the authors observed that there was not widespread adoption of this practice at their institution, despite its introduction and discussion at several primary care staff meetings. The authors surveyed primary care providers (PCPs) at VA Connecticut Healthcare System (VACHS) to understand perceived barriers and benefits to the use of PHIs in clinical practice.
Methods
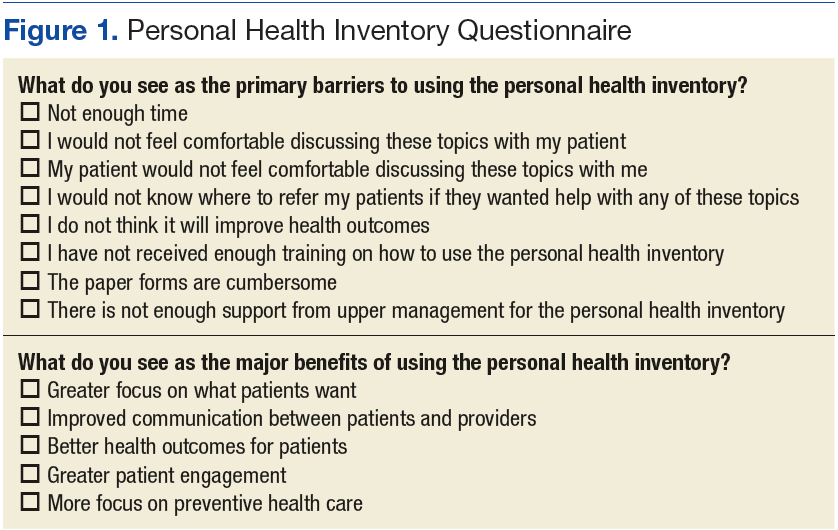
The authors surveyed PCPs at VACHS sites about their current use of the PHI as well as their perceptions of barriers and benefits for future implementation of the PHI in clinical settings. Current use of the PHI was captured in a free response question. The authors assessed comfort with the PHI using a 5-point Likert scale, asking participants how comfortable they would feel explaining the PHI to a patient and or a coworker (1 = very uncomfortable, 5 = very comfortable). Barriers and benefits of future PHI implementation were chosen from preselected lists (Figure 1). Participants also were asked how important they feel it is for VA PCPs to use the PHI (1 = very unimportant, 5 = very important).
Finally, participants were asked whether they plan to use the PHI with their patients and how often (1 = less than once a month, 5 = daily). Participants were initially asked at staff meetings to complete the survey in a paper format. Nonrespondents then were asked to complete the survey electronically. This research protocol was reviewed and approved by the institutional review board of the participating institutions.
Study Population
The survey was delivered to all PCPs in the VACHS, which consisted of 2 main facilities (West Haven and Newington campuses) and 7 community-based outpatient clinics. The VACHS provides care to Connecticut’s eligible veteran population of > 55,000 patients who are enrolled in care. Survey participants included physicians, physician assistants, and nurse practitioners. Trainees were excluded.
Statistical Analyses
Summary statistics were calculated to assess current use of the PHI, barriers to and benefits of future implementation, and other scaled responses. Chi-square tests were used to compare the responses of participants who were completing the survey online with those completing it on paper for major study outcomes. Mann-Whitney tests were conducted to assess whether responses to certain questions (eg, future plans to use the PHI) were associated with responses to other related questions (eg, importance of VACHS providers pursuing the PHI). Significance was determined as P ≤ .05.
Results
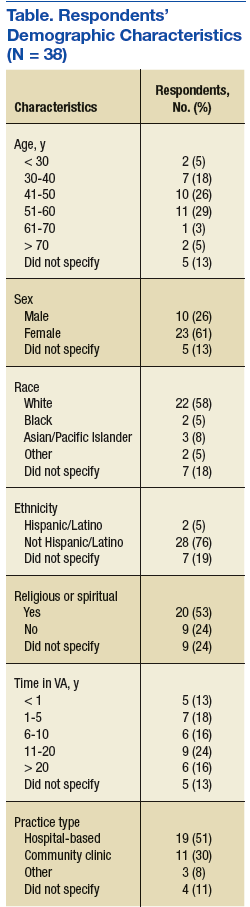
Thirty-eight (53%) of 72 PCPs completed the survey. Thirteen providers completed the survey in the online format and 25 on paper. There was no significant difference between participants who completed the survey online vs paper for each of the major outcomes assessed. Most participants were aged between 40 and 60 years (64%), female (70%), and white (76%), similar to the entire PCP population at VACHS. The majority of participants worked in a hospital-based outpatient primary care setting (58%) (Table).
Current Use of PHI
Of respondents, 84% stated that they had heard of the PHI. Of those, 68% felt very or somewhat comfortable explaining the PHI to a patient, with slightly fewer, 64%, very or somewhat comfortable explaining the PHI to a coworker. Forty-eight percent stated that they had implemented the PHI in their clinical practices. Examples of current use included “can refer to RN to complete a true PHI,” “giving blank PHI to patients to fill out and bring back/mail,” and “occasional patient who I am trying to achieve some sort of lifestyle modification or change in behavior.”
PHI Barriers and Benefits
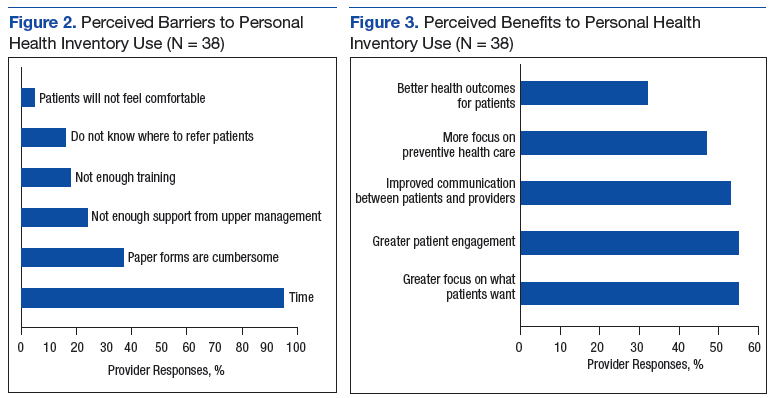
Almost all participants (95%) stated that lack of time was a barrier to using the PHI in their clinical settings (Figure 2). The next most common barriers were cumbersome paper forms (37%) and lack of support from upper management (24%). Very few participants listed discomfort as a reason for not discussing the PHI with patients (5%).
Respondents were divided evenly when identifying the benefits of the PHI. The top 3 selections were greater focus on what patients want (55%), greater patient engagement (55%), and improved patient/provider communication (53%) (Figure 3).
PHI Importance and Future Use
The majority of participants (71%) stated that it was very or somewhat important for VA PCPs to pursue the PHI. However, only 45% planned to use the PHI with their patients. Respondents who said they had implemented the PHI in the past were not more likely than others to state that pursuing the PHI was very important (P = .81). However, respondents who stated that it was very important to pursue the PHI were significantly more likely to plan to implement the PHI (P = .04). Of those planning on its use, the frequency of expected use varied from 31% planning to use the PHI daily with patients to 25% expecting to use it less than once a month.
Discussion
The traditional model of care has been fraught with problems. For example, patients are frequently nonadherent to medical therapies and lifestyle recommendations.3-6 Clearly, changes need to be made. To improve health care outcomes by delivering more patient-centered care, the VA initiated the PHI.7
Although nearly three-fourths of the respondents believed that the PHI was an important tool that the VA should pursue, more than half of all respondents did not intend to use it. Of those planning on using it, a large proportion planned on using it infrequently.
The authors found that despite PCP knowledge of PHI and its acceptance as a tool to focus more on what patients want to accomplish, to enhance patient engagement, and to improve communication between patients and providers, time constraints were a universal barrier to implementation, followed by cumbersome paper forms, and not enough perceived support from local upper management.
Measures to decrease PCP time investment and involvement with paper forms, such as having the patient complete the PHI outside of an office visit with a PCP, either at home, with the assistance of a team member with less training than a PCP, or electronically could help address an identified barrier. Further, if the PHI is to be more broadly adopted, support of local upper management should be enlisted to vociferously advocate its use, thus it will be deemed more essential to enhance care and introduce an organizational system for its effective implementation.
Interestingly, only about one-third of respondents believed that the use of the PHI would lead to better health outcomes for patients. Future studies should address whether the use of the PHI improves surrogate goals, such as cholesterol levels, blood pressures, hemoglobin A1c, or medication adherence as well as harder outcomes, such as risk of cardiovascular outcomes, diabetic complications, and mortality.
Limitations
The questionnaire was used at only 1 health care system within the VA. Whether it could be generalizable to PCPs with other baseline demographic information, non-VA facilities, or even other VA facilities, is not known. Since this survey was administered to PCPs, the authors also do not know the impact of implementing the PHI in specialty settings.
Conclusion
Although the concept of the PHI is favored by the majority of PCPs within VACHS, significant barriers, the most common being time constraints, need to be overcome before it is widely adopted. Implementation of novel collaborative systems of PHI administration may be needed.
1. U.S. Department of Veterans Affairs.VA patient centered care. http://www.va.gov/patientcenteredcare/about.asp. Updated March 3, 2016. Accessed March 30, 2017.
2. U.S. Department of Veterans Affairs. MyStory: personal health inventory. http://www.va.gov/patientcenteredcare/docs/va-opcc-personal-health-inventory-final-508.pdf. Published October 7, 2013. Accessed March 30, 2017.
3. Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189-199.
4. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;(11):CD000011.
5. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35-44.
6. Viswanathan M, Golin CE, Jones CD, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann Intern Med. 2012;157(11):785-795. 7. Simmons LA, Drake CD, Gaudet TW, Snyderman R. Personalized health planning in primary care settings. Fed Pract. 2016;33(1):27-34.
To better meet the needs and values of patients, the VA has been promulgating a paradigm shift away from the disease-focused model toward a whole health, patient-centered focus.1 To achieve this goal, the VA Office of Patient Centered Care and Cultural Transformation has advocated the use of the personal health inventory (PHI). This inventory asks patients to mindfully assess why their health is important to them and to determine where they feel they are and where they want to be with respect to 8 areas of self-care (working the body, physical and emotional surroundings, personal development, food and drink, sleep, human relationships, spirituality/purpose, and awareness of relationship between mind and body).
Personal health inventory written responses are then discussed with a member of the health care team to develop a proactive, patient-driven health plan unique to that veteran’s circumstances and aspirations.2 The PHI is applicable not only to veterans, but also in primary care and other practices outside the VA to improve shared decision making and produce more effective clinician-patient partnerships.
After national PHI promotion by the VA, the authors observed that there was not widespread adoption of this practice at their institution, despite its introduction and discussion at several primary care staff meetings. The authors surveyed primary care providers (PCPs) at VA Connecticut Healthcare System (VACHS) to understand perceived barriers and benefits to the use of PHIs in clinical practice.
Methods
The authors surveyed PCPs at VACHS sites about their current use of the PHI as well as their perceptions of barriers and benefits for future implementation of the PHI in clinical settings. Current use of the PHI was captured in a free response question. The authors assessed comfort with the PHI using a 5-point Likert scale, asking participants how comfortable they would feel explaining the PHI to a patient and or a coworker (1 = very uncomfortable, 5 = very comfortable). Barriers and benefits of future PHI implementation were chosen from preselected lists (Figure 1). Participants also were asked how important they feel it is for VA PCPs to use the PHI (1 = very unimportant, 5 = very important).
Finally, participants were asked whether they plan to use the PHI with their patients and how often (1 = less than once a month, 5 = daily). Participants were initially asked at staff meetings to complete the survey in a paper format. Nonrespondents then were asked to complete the survey electronically. This research protocol was reviewed and approved by the institutional review board of the participating institutions.
Study Population
The survey was delivered to all PCPs in the VACHS, which consisted of 2 main facilities (West Haven and Newington campuses) and 7 community-based outpatient clinics. The VACHS provides care to Connecticut’s eligible veteran population of > 55,000 patients who are enrolled in care. Survey participants included physicians, physician assistants, and nurse practitioners. Trainees were excluded.
Statistical Analyses
Summary statistics were calculated to assess current use of the PHI, barriers to and benefits of future implementation, and other scaled responses. Chi-square tests were used to compare the responses of participants who were completing the survey online with those completing it on paper for major study outcomes. Mann-Whitney tests were conducted to assess whether responses to certain questions (eg, future plans to use the PHI) were associated with responses to other related questions (eg, importance of VACHS providers pursuing the PHI). Significance was determined as P ≤ .05.
Results
Thirty-eight (53%) of 72 PCPs completed the survey. Thirteen providers completed the survey in the online format and 25 on paper. There was no significant difference between participants who completed the survey online vs paper for each of the major outcomes assessed. Most participants were aged between 40 and 60 years (64%), female (70%), and white (76%), similar to the entire PCP population at VACHS. The majority of participants worked in a hospital-based outpatient primary care setting (58%) (Table).
Current Use of PHI
Of respondents, 84% stated that they had heard of the PHI. Of those, 68% felt very or somewhat comfortable explaining the PHI to a patient, with slightly fewer, 64%, very or somewhat comfortable explaining the PHI to a coworker. Forty-eight percent stated that they had implemented the PHI in their clinical practices. Examples of current use included “can refer to RN to complete a true PHI,” “giving blank PHI to patients to fill out and bring back/mail,” and “occasional patient who I am trying to achieve some sort of lifestyle modification or change in behavior.”
PHI Barriers and Benefits
Almost all participants (95%) stated that lack of time was a barrier to using the PHI in their clinical settings (Figure 2). The next most common barriers were cumbersome paper forms (37%) and lack of support from upper management (24%). Very few participants listed discomfort as a reason for not discussing the PHI with patients (5%).
Respondents were divided evenly when identifying the benefits of the PHI. The top 3 selections were greater focus on what patients want (55%), greater patient engagement (55%), and improved patient/provider communication (53%) (Figure 3).
PHI Importance and Future Use
The majority of participants (71%) stated that it was very or somewhat important for VA PCPs to pursue the PHI. However, only 45% planned to use the PHI with their patients. Respondents who said they had implemented the PHI in the past were not more likely than others to state that pursuing the PHI was very important (P = .81). However, respondents who stated that it was very important to pursue the PHI were significantly more likely to plan to implement the PHI (P = .04). Of those planning on its use, the frequency of expected use varied from 31% planning to use the PHI daily with patients to 25% expecting to use it less than once a month.
Discussion
The traditional model of care has been fraught with problems. For example, patients are frequently nonadherent to medical therapies and lifestyle recommendations.3-6 Clearly, changes need to be made. To improve health care outcomes by delivering more patient-centered care, the VA initiated the PHI.7
Although nearly three-fourths of the respondents believed that the PHI was an important tool that the VA should pursue, more than half of all respondents did not intend to use it. Of those planning on using it, a large proportion planned on using it infrequently.
The authors found that despite PCP knowledge of PHI and its acceptance as a tool to focus more on what patients want to accomplish, to enhance patient engagement, and to improve communication between patients and providers, time constraints were a universal barrier to implementation, followed by cumbersome paper forms, and not enough perceived support from local upper management.
Measures to decrease PCP time investment and involvement with paper forms, such as having the patient complete the PHI outside of an office visit with a PCP, either at home, with the assistance of a team member with less training than a PCP, or electronically could help address an identified barrier. Further, if the PHI is to be more broadly adopted, support of local upper management should be enlisted to vociferously advocate its use, thus it will be deemed more essential to enhance care and introduce an organizational system for its effective implementation.
Interestingly, only about one-third of respondents believed that the use of the PHI would lead to better health outcomes for patients. Future studies should address whether the use of the PHI improves surrogate goals, such as cholesterol levels, blood pressures, hemoglobin A1c, or medication adherence as well as harder outcomes, such as risk of cardiovascular outcomes, diabetic complications, and mortality.
Limitations
The questionnaire was used at only 1 health care system within the VA. Whether it could be generalizable to PCPs with other baseline demographic information, non-VA facilities, or even other VA facilities, is not known. Since this survey was administered to PCPs, the authors also do not know the impact of implementing the PHI in specialty settings.
Conclusion
Although the concept of the PHI is favored by the majority of PCPs within VACHS, significant barriers, the most common being time constraints, need to be overcome before it is widely adopted. Implementation of novel collaborative systems of PHI administration may be needed.
To better meet the needs and values of patients, the VA has been promulgating a paradigm shift away from the disease-focused model toward a whole health, patient-centered focus.1 To achieve this goal, the VA Office of Patient Centered Care and Cultural Transformation has advocated the use of the personal health inventory (PHI). This inventory asks patients to mindfully assess why their health is important to them and to determine where they feel they are and where they want to be with respect to 8 areas of self-care (working the body, physical and emotional surroundings, personal development, food and drink, sleep, human relationships, spirituality/purpose, and awareness of relationship between mind and body).
Personal health inventory written responses are then discussed with a member of the health care team to develop a proactive, patient-driven health plan unique to that veteran’s circumstances and aspirations.2 The PHI is applicable not only to veterans, but also in primary care and other practices outside the VA to improve shared decision making and produce more effective clinician-patient partnerships.
After national PHI promotion by the VA, the authors observed that there was not widespread adoption of this practice at their institution, despite its introduction and discussion at several primary care staff meetings. The authors surveyed primary care providers (PCPs) at VA Connecticut Healthcare System (VACHS) to understand perceived barriers and benefits to the use of PHIs in clinical practice.
Methods
The authors surveyed PCPs at VACHS sites about their current use of the PHI as well as their perceptions of barriers and benefits for future implementation of the PHI in clinical settings. Current use of the PHI was captured in a free response question. The authors assessed comfort with the PHI using a 5-point Likert scale, asking participants how comfortable they would feel explaining the PHI to a patient and or a coworker (1 = very uncomfortable, 5 = very comfortable). Barriers and benefits of future PHI implementation were chosen from preselected lists (Figure 1). Participants also were asked how important they feel it is for VA PCPs to use the PHI (1 = very unimportant, 5 = very important).
Finally, participants were asked whether they plan to use the PHI with their patients and how often (1 = less than once a month, 5 = daily). Participants were initially asked at staff meetings to complete the survey in a paper format. Nonrespondents then were asked to complete the survey electronically. This research protocol was reviewed and approved by the institutional review board of the participating institutions.
Study Population
The survey was delivered to all PCPs in the VACHS, which consisted of 2 main facilities (West Haven and Newington campuses) and 7 community-based outpatient clinics. The VACHS provides care to Connecticut’s eligible veteran population of > 55,000 patients who are enrolled in care. Survey participants included physicians, physician assistants, and nurse practitioners. Trainees were excluded.
Statistical Analyses
Summary statistics were calculated to assess current use of the PHI, barriers to and benefits of future implementation, and other scaled responses. Chi-square tests were used to compare the responses of participants who were completing the survey online with those completing it on paper for major study outcomes. Mann-Whitney tests were conducted to assess whether responses to certain questions (eg, future plans to use the PHI) were associated with responses to other related questions (eg, importance of VACHS providers pursuing the PHI). Significance was determined as P ≤ .05.
Results
Thirty-eight (53%) of 72 PCPs completed the survey. Thirteen providers completed the survey in the online format and 25 on paper. There was no significant difference between participants who completed the survey online vs paper for each of the major outcomes assessed. Most participants were aged between 40 and 60 years (64%), female (70%), and white (76%), similar to the entire PCP population at VACHS. The majority of participants worked in a hospital-based outpatient primary care setting (58%) (Table).
Current Use of PHI
Of respondents, 84% stated that they had heard of the PHI. Of those, 68% felt very or somewhat comfortable explaining the PHI to a patient, with slightly fewer, 64%, very or somewhat comfortable explaining the PHI to a coworker. Forty-eight percent stated that they had implemented the PHI in their clinical practices. Examples of current use included “can refer to RN to complete a true PHI,” “giving blank PHI to patients to fill out and bring back/mail,” and “occasional patient who I am trying to achieve some sort of lifestyle modification or change in behavior.”
PHI Barriers and Benefits
Almost all participants (95%) stated that lack of time was a barrier to using the PHI in their clinical settings (Figure 2). The next most common barriers were cumbersome paper forms (37%) and lack of support from upper management (24%). Very few participants listed discomfort as a reason for not discussing the PHI with patients (5%).
Respondents were divided evenly when identifying the benefits of the PHI. The top 3 selections were greater focus on what patients want (55%), greater patient engagement (55%), and improved patient/provider communication (53%) (Figure 3).
PHI Importance and Future Use
The majority of participants (71%) stated that it was very or somewhat important for VA PCPs to pursue the PHI. However, only 45% planned to use the PHI with their patients. Respondents who said they had implemented the PHI in the past were not more likely than others to state that pursuing the PHI was very important (P = .81). However, respondents who stated that it was very important to pursue the PHI were significantly more likely to plan to implement the PHI (P = .04). Of those planning on its use, the frequency of expected use varied from 31% planning to use the PHI daily with patients to 25% expecting to use it less than once a month.
Discussion
The traditional model of care has been fraught with problems. For example, patients are frequently nonadherent to medical therapies and lifestyle recommendations.3-6 Clearly, changes need to be made. To improve health care outcomes by delivering more patient-centered care, the VA initiated the PHI.7
Although nearly three-fourths of the respondents believed that the PHI was an important tool that the VA should pursue, more than half of all respondents did not intend to use it. Of those planning on using it, a large proportion planned on using it infrequently.
The authors found that despite PCP knowledge of PHI and its acceptance as a tool to focus more on what patients want to accomplish, to enhance patient engagement, and to improve communication between patients and providers, time constraints were a universal barrier to implementation, followed by cumbersome paper forms, and not enough perceived support from local upper management.
Measures to decrease PCP time investment and involvement with paper forms, such as having the patient complete the PHI outside of an office visit with a PCP, either at home, with the assistance of a team member with less training than a PCP, or electronically could help address an identified barrier. Further, if the PHI is to be more broadly adopted, support of local upper management should be enlisted to vociferously advocate its use, thus it will be deemed more essential to enhance care and introduce an organizational system for its effective implementation.
Interestingly, only about one-third of respondents believed that the use of the PHI would lead to better health outcomes for patients. Future studies should address whether the use of the PHI improves surrogate goals, such as cholesterol levels, blood pressures, hemoglobin A1c, or medication adherence as well as harder outcomes, such as risk of cardiovascular outcomes, diabetic complications, and mortality.
Limitations
The questionnaire was used at only 1 health care system within the VA. Whether it could be generalizable to PCPs with other baseline demographic information, non-VA facilities, or even other VA facilities, is not known. Since this survey was administered to PCPs, the authors also do not know the impact of implementing the PHI in specialty settings.
Conclusion
Although the concept of the PHI is favored by the majority of PCPs within VACHS, significant barriers, the most common being time constraints, need to be overcome before it is widely adopted. Implementation of novel collaborative systems of PHI administration may be needed.
1. U.S. Department of Veterans Affairs.VA patient centered care. http://www.va.gov/patientcenteredcare/about.asp. Updated March 3, 2016. Accessed March 30, 2017.
2. U.S. Department of Veterans Affairs. MyStory: personal health inventory. http://www.va.gov/patientcenteredcare/docs/va-opcc-personal-health-inventory-final-508.pdf. Published October 7, 2013. Accessed March 30, 2017.
3. Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189-199.
4. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;(11):CD000011.
5. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35-44.
6. Viswanathan M, Golin CE, Jones CD, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann Intern Med. 2012;157(11):785-795. 7. Simmons LA, Drake CD, Gaudet TW, Snyderman R. Personalized health planning in primary care settings. Fed Pract. 2016;33(1):27-34.
1. U.S. Department of Veterans Affairs.VA patient centered care. http://www.va.gov/patientcenteredcare/about.asp. Updated March 3, 2016. Accessed March 30, 2017.
2. U.S. Department of Veterans Affairs. MyStory: personal health inventory. http://www.va.gov/patientcenteredcare/docs/va-opcc-personal-health-inventory-final-508.pdf. Published October 7, 2013. Accessed March 30, 2017.
3. Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189-199.
4. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;(11):CD000011.
5. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35-44.
6. Viswanathan M, Golin CE, Jones CD, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann Intern Med. 2012;157(11):785-795. 7. Simmons LA, Drake CD, Gaudet TW, Snyderman R. Personalized health planning in primary care settings. Fed Pract. 2016;33(1):27-34.
CMV matching improves survival in HSCT recipients

Matching the cytomegalovirus (CMV) status of the donor and recipient of a hematopoietic stem cell transplant (HSCT) can significantly improve the recipient’s survival, according to a study published in Bone Marrow Transplantation.
In fact, researchers said they found evidence to suggest that CMV matching may abrogate the effect of a human leukocyte antigen (HLA) mismatch.
“This breakthrough will help us discover new and more effective ways to make sure patients in need of a transplant get the best possible match to cure blood cancer and blood disorders,” said study author Steven Marsh, PhD, of Anthony Nolan Research Institute, Royal Free Hospital in London, UK.
Dr Marsh and his colleagues studied 1271 patients who received T-cell-depleted grafts to treat a hematologic disorder, including acute or chronic leukemia, lymphoma, myeloma, myelodysplasia, and “other” disorders.
The 5-year overall survival in these patients was 40.6%.
The researchers found HSCT recipients with a 10/10 HLA-matched donor had significantly better overall survival (OS) and lower non-relapse mortality (NRM) than patients with a mismatched donor.
The 5-year OS was 43.1% for a 10/10 match, 35.6% for a 9/10 match, and 28.4% for a match less than 9/10 (P=0.001). NRM at 1 year was 20.3%, 26.0%, and 33.4%, respectively (P=0.007).
Similarly, HSCT recipients with a CMV-matched donor had significantly better OS and significantly lower NRM than recipients with a CMV-mismatched donor.
The 5-year OS was 44.1% for recipients with a CMV-matched donor and 32.2% for patients with a mismatched donor (P<0.001). NRM at 1 year was 19.1% and 30.4%, respectively (P<0.001)
Most of the associations between CMV/HLA matching and OS/NRM remained significant in multivariate analyses.
For recipients with more than 1 HLA mismatch, the relative risk (RR) of death was 1.43 (P=0.016), and the RR for NRM was 1.59 (P=0.028), when compared to patients who had received a 10/10 HLA-matched graft.
For recipients with a single mismatch, the RR for death was 1.21 (P=0.042), and the RR for NRM was 1.24 (P=0.14).
For recipients with a CMV mismatched donor, the RR for death was 1.40 (P<0.001), and the RR for NRM was 1.63 (P<0.001).
The researchers also assessed CMV and HLA status together. Compared to fully HLA-matched and CMV-matched recipients, the RRs for death were:
- 1.36 (P=0.003) for HLA matched/CMV mismatched
- 1.22 (P=0.062) for HLA mismatched/CMV matched
- 1.81 (P=0.001) for HLA and CMV mismatched.
The researchers said these results suggest it is possible to improve survival rates for patients with no HLA-matched donor by matching the CMV status of the donor and recipient.
As a result of the findings, experts at Anthony Nolan are exploring how to type donors for CMV when joining the stem cell donor register to allow CMV status to be taken into account when transplant centers are selecting potential donors for a patient.
“[B]y establishing that CMV matching has a significant impact on patient outcomes, we are making it easier for transplant centers to make informed choices about the donors they select for their patients,” Dr Marsh said. ![]()
Matching the cytomegalovirus (CMV) status of the donor and recipient of a hematopoietic stem cell transplant (HSCT) can significantly improve the recipient’s survival, according to a study published in Bone Marrow Transplantation.
In fact, researchers said they found evidence to suggest that CMV matching may abrogate the effect of a human leukocyte antigen (HLA) mismatch.
“This breakthrough will help us discover new and more effective ways to make sure patients in need of a transplant get the best possible match to cure blood cancer and blood disorders,” said study author Steven Marsh, PhD, of Anthony Nolan Research Institute, Royal Free Hospital in London, UK.
Dr Marsh and his colleagues studied 1271 patients who received T-cell-depleted grafts to treat a hematologic disorder, including acute or chronic leukemia, lymphoma, myeloma, myelodysplasia, and “other” disorders.
The 5-year overall survival in these patients was 40.6%.
The researchers found HSCT recipients with a 10/10 HLA-matched donor had significantly better overall survival (OS) and lower non-relapse mortality (NRM) than patients with a mismatched donor.
The 5-year OS was 43.1% for a 10/10 match, 35.6% for a 9/10 match, and 28.4% for a match less than 9/10 (P=0.001). NRM at 1 year was 20.3%, 26.0%, and 33.4%, respectively (P=0.007).
Similarly, HSCT recipients with a CMV-matched donor had significantly better OS and significantly lower NRM than recipients with a CMV-mismatched donor.
The 5-year OS was 44.1% for recipients with a CMV-matched donor and 32.2% for patients with a mismatched donor (P<0.001). NRM at 1 year was 19.1% and 30.4%, respectively (P<0.001)
Most of the associations between CMV/HLA matching and OS/NRM remained significant in multivariate analyses.
For recipients with more than 1 HLA mismatch, the relative risk (RR) of death was 1.43 (P=0.016), and the RR for NRM was 1.59 (P=0.028), when compared to patients who had received a 10/10 HLA-matched graft.
For recipients with a single mismatch, the RR for death was 1.21 (P=0.042), and the RR for NRM was 1.24 (P=0.14).
For recipients with a CMV mismatched donor, the RR for death was 1.40 (P<0.001), and the RR for NRM was 1.63 (P<0.001).
The researchers also assessed CMV and HLA status together. Compared to fully HLA-matched and CMV-matched recipients, the RRs for death were:
- 1.36 (P=0.003) for HLA matched/CMV mismatched
- 1.22 (P=0.062) for HLA mismatched/CMV matched
- 1.81 (P=0.001) for HLA and CMV mismatched.
The researchers said these results suggest it is possible to improve survival rates for patients with no HLA-matched donor by matching the CMV status of the donor and recipient.
As a result of the findings, experts at Anthony Nolan are exploring how to type donors for CMV when joining the stem cell donor register to allow CMV status to be taken into account when transplant centers are selecting potential donors for a patient.
“[B]y establishing that CMV matching has a significant impact on patient outcomes, we are making it easier for transplant centers to make informed choices about the donors they select for their patients,” Dr Marsh said. ![]()
Matching the cytomegalovirus (CMV) status of the donor and recipient of a hematopoietic stem cell transplant (HSCT) can significantly improve the recipient’s survival, according to a study published in Bone Marrow Transplantation.
In fact, researchers said they found evidence to suggest that CMV matching may abrogate the effect of a human leukocyte antigen (HLA) mismatch.
“This breakthrough will help us discover new and more effective ways to make sure patients in need of a transplant get the best possible match to cure blood cancer and blood disorders,” said study author Steven Marsh, PhD, of Anthony Nolan Research Institute, Royal Free Hospital in London, UK.
Dr Marsh and his colleagues studied 1271 patients who received T-cell-depleted grafts to treat a hematologic disorder, including acute or chronic leukemia, lymphoma, myeloma, myelodysplasia, and “other” disorders.
The 5-year overall survival in these patients was 40.6%.
The researchers found HSCT recipients with a 10/10 HLA-matched donor had significantly better overall survival (OS) and lower non-relapse mortality (NRM) than patients with a mismatched donor.
The 5-year OS was 43.1% for a 10/10 match, 35.6% for a 9/10 match, and 28.4% for a match less than 9/10 (P=0.001). NRM at 1 year was 20.3%, 26.0%, and 33.4%, respectively (P=0.007).
Similarly, HSCT recipients with a CMV-matched donor had significantly better OS and significantly lower NRM than recipients with a CMV-mismatched donor.
The 5-year OS was 44.1% for recipients with a CMV-matched donor and 32.2% for patients with a mismatched donor (P<0.001). NRM at 1 year was 19.1% and 30.4%, respectively (P<0.001)
Most of the associations between CMV/HLA matching and OS/NRM remained significant in multivariate analyses.
For recipients with more than 1 HLA mismatch, the relative risk (RR) of death was 1.43 (P=0.016), and the RR for NRM was 1.59 (P=0.028), when compared to patients who had received a 10/10 HLA-matched graft.
For recipients with a single mismatch, the RR for death was 1.21 (P=0.042), and the RR for NRM was 1.24 (P=0.14).
For recipients with a CMV mismatched donor, the RR for death was 1.40 (P<0.001), and the RR for NRM was 1.63 (P<0.001).
The researchers also assessed CMV and HLA status together. Compared to fully HLA-matched and CMV-matched recipients, the RRs for death were:
- 1.36 (P=0.003) for HLA matched/CMV mismatched
- 1.22 (P=0.062) for HLA mismatched/CMV matched
- 1.81 (P=0.001) for HLA and CMV mismatched.
The researchers said these results suggest it is possible to improve survival rates for patients with no HLA-matched donor by matching the CMV status of the donor and recipient.
As a result of the findings, experts at Anthony Nolan are exploring how to type donors for CMV when joining the stem cell donor register to allow CMV status to be taken into account when transplant centers are selecting potential donors for a patient.
“[B]y establishing that CMV matching has a significant impact on patient outcomes, we are making it easier for transplant centers to make informed choices about the donors they select for their patients,” Dr Marsh said. ![]()
Troublesome Foreign Bodies
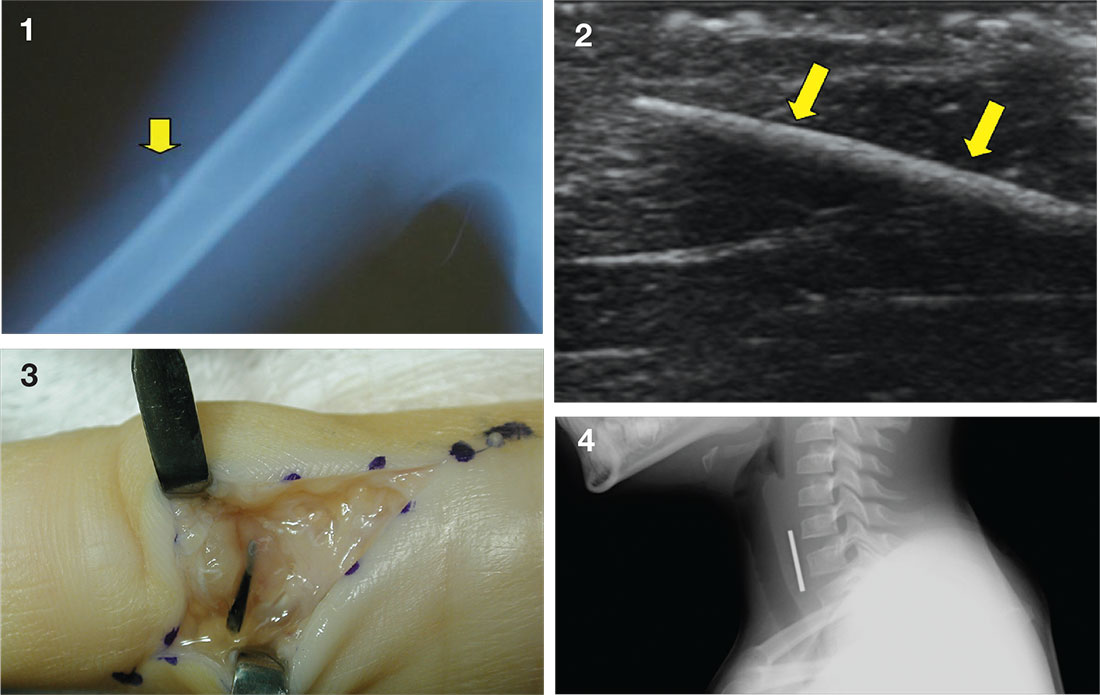
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
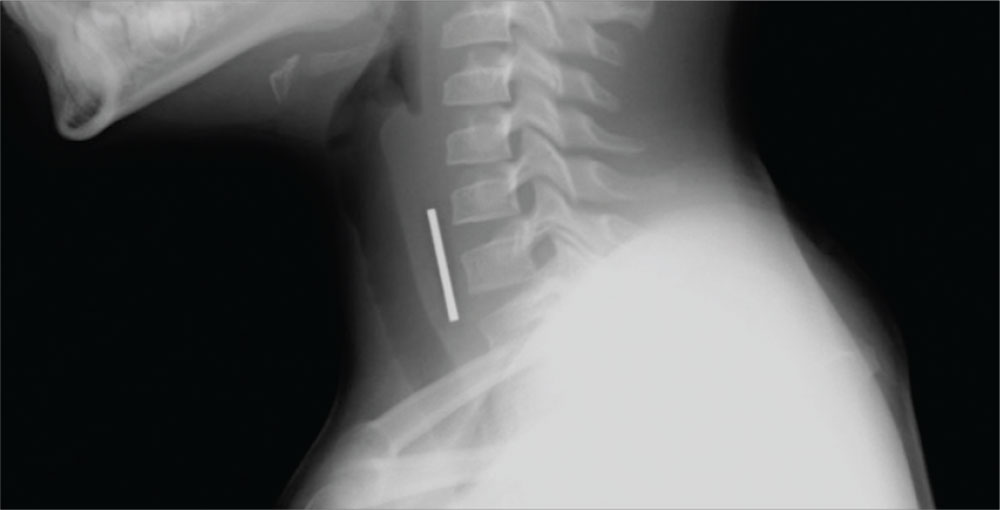
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Complete obstruction should be treated with back blows in a child aged less than 1 year and abdominal thrusts in an older child. In a more stable child, provide supplemental oxygen and consult a physician skilled in laryngoscopy and bronchoscopy for removal of the foreign body. Esophageal foreign bodies may also cause stridor. In these cases the child will often complain of dysphagia or avoid swallowing.
While some objects, such as coins, can be visualized on plain imaging, a negative film does not rule out a foreign body and a specialist should be consulted for endoscopy. A coin in the trachea will be seen on its edge in an anteroposterior view. In the esophagus, it will generally appear as a full circle (en face) in an anteroposterior oblique view. For the lateral view, it is just the opposite, as seen in the case figure.
For more information, see “Differential Diagnosis of Stridor in Children.” Emergency Medicine. 2009 September;41(9):10-11.
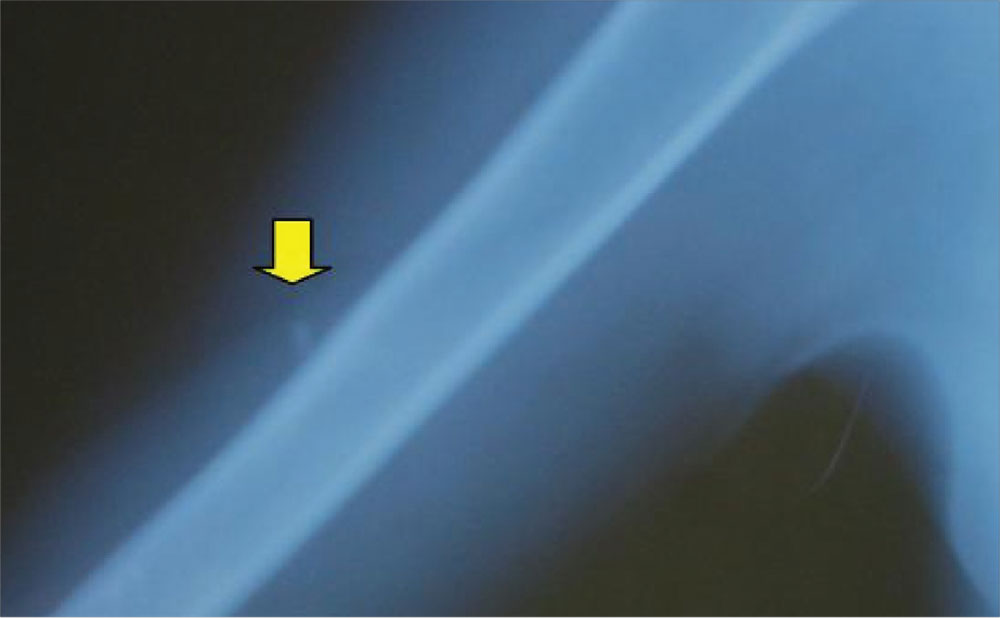
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
You anesthetize the area and begin dissection in an attempt to locate the glass fragment, which goes on for 20 minutes without success. The child and her mother are becoming anxious. You call for the portable ultrasound system, and using its high-frequency transducer, quickly locate the foreign body. After additional anesthesia is applied, the splinter is easily removed under ultrasound guidance and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
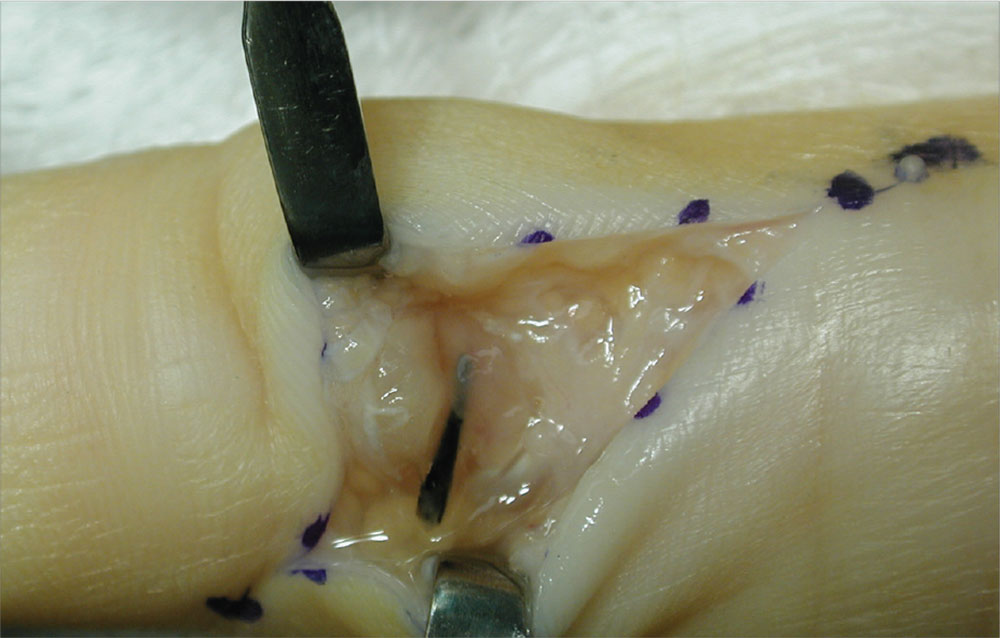
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
The palmar puncture wound site was surgically explored, and no foreign body fragments were found. In addition, the tendons, retracted and delivered through the skin incision, appeared normal.
Histopathology of a specimen intraoperatively biopsied from the flexor tendon sheath showed some refractile foreign material consistent with plant material. After surgery, swelling persisted, and the patient developed limited motion at the extremes of active flexion and extension.
After 2 months, the decision was made to re-explore the palmar puncture site and flexor tendon and obtain tissue specimens for culture, including atypical mycobacterial and fungal cultures. During the second surgery, the palmar site and flexor tendon still appeared unremarkable. As there was some swelling in the long finger, the flexor tendon sheath was explored distally through a separate incision over the middle phalanx. A transversely oriented fragment of the sago palm thorn was found within the flexor tendon sheath. Flexor tendon sheath material was cultured and subsequently found to be negative.
For more information, see “Distal Migration of a Foreign Body (Sago Palm Thorn Fragment) Within the Long-Finger Flexor Tendon Sheath.” Am J Orthop. 2008;37(4):208-209.
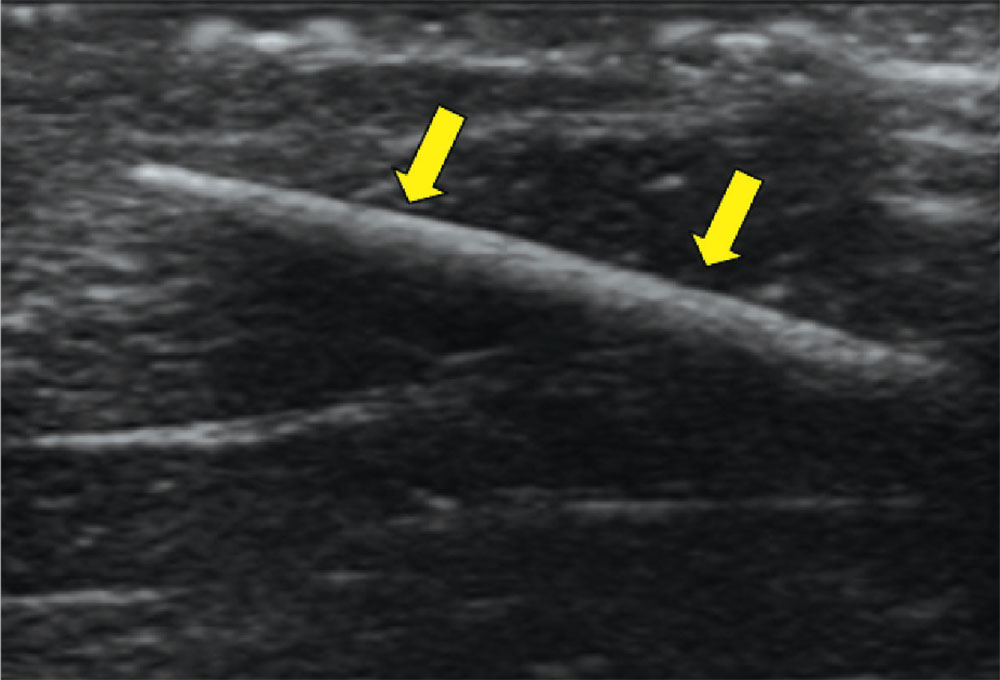
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
With local anesthesia and ultrasound guidance, the splinter is easily removed and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Complete obstruction should be treated with back blows in a child aged less than 1 year and abdominal thrusts in an older child. In a more stable child, provide supplemental oxygen and consult a physician skilled in laryngoscopy and bronchoscopy for removal of the foreign body. Esophageal foreign bodies may also cause stridor. In these cases the child will often complain of dysphagia or avoid swallowing.
While some objects, such as coins, can be visualized on plain imaging, a negative film does not rule out a foreign body and a specialist should be consulted for endoscopy. A coin in the trachea will be seen on its edge in an anteroposterior view. In the esophagus, it will generally appear as a full circle (en face) in an anteroposterior oblique view. For the lateral view, it is just the opposite, as seen in the case figure.
For more information, see “Differential Diagnosis of Stridor in Children.” Emergency Medicine. 2009 September;41(9):10-11.
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
You anesthetize the area and begin dissection in an attempt to locate the glass fragment, which goes on for 20 minutes without success. The child and her mother are becoming anxious. You call for the portable ultrasound system, and using its high-frequency transducer, quickly locate the foreign body. After additional anesthesia is applied, the splinter is easily removed under ultrasound guidance and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
The palmar puncture wound site was surgically explored, and no foreign body fragments were found. In addition, the tendons, retracted and delivered through the skin incision, appeared normal.
Histopathology of a specimen intraoperatively biopsied from the flexor tendon sheath showed some refractile foreign material consistent with plant material. After surgery, swelling persisted, and the patient developed limited motion at the extremes of active flexion and extension.
After 2 months, the decision was made to re-explore the palmar puncture site and flexor tendon and obtain tissue specimens for culture, including atypical mycobacterial and fungal cultures. During the second surgery, the palmar site and flexor tendon still appeared unremarkable. As there was some swelling in the long finger, the flexor tendon sheath was explored distally through a separate incision over the middle phalanx. A transversely oriented fragment of the sago palm thorn was found within the flexor tendon sheath. Flexor tendon sheath material was cultured and subsequently found to be negative.
For more information, see “Distal Migration of a Foreign Body (Sago Palm Thorn Fragment) Within the Long-Finger Flexor Tendon Sheath.” Am J Orthop. 2008;37(4):208-209.
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
With local anesthesia and ultrasound guidance, the splinter is easily removed and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
Case a. A 30-month-old boy, who is in obvious distress with a barking cough and croup-like symptoms but no fever, is brought by his mother for examination. History is unremarkable except for a recent choking episode. A radiograph is ordered.
Complete obstruction should be treated with back blows in a child aged less than 1 year and abdominal thrusts in an older child. In a more stable child, provide supplemental oxygen and consult a physician skilled in laryngoscopy and bronchoscopy for removal of the foreign body. Esophageal foreign bodies may also cause stridor. In these cases the child will often complain of dysphagia or avoid swallowing.
While some objects, such as coins, can be visualized on plain imaging, a negative film does not rule out a foreign body and a specialist should be consulted for endoscopy. A coin in the trachea will be seen on its edge in an anteroposterior view. In the esophagus, it will generally appear as a full circle (en face) in an anteroposterior oblique view. For the lateral view, it is just the opposite, as seen in the case figure.
For more information, see “Differential Diagnosis of Stridor in Children.” Emergency Medicine. 2009 September;41(9):10-11.
Case b. A 13-year-old girl presents to urgent care with a laceration that occurred when she fell through a glass door. You note a 2-cm linear laceration, and radiography shows what appears to be a residual piece of glass at or near the site of the laceration.
You anesthetize the area and begin dissection in an attempt to locate the glass fragment, which goes on for 20 minutes without success. The child and her mother are becoming anxious. You call for the portable ultrasound system, and using its high-frequency transducer, quickly locate the foreign body. After additional anesthesia is applied, the splinter is easily removed under ultrasound guidance and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
The palmar puncture wound site was surgically explored, and no foreign body fragments were found. In addition, the tendons, retracted and delivered through the skin incision, appeared normal.
Histopathology of a specimen intraoperatively biopsied from the flexor tendon sheath showed some refractile foreign material consistent with plant material. After surgery, swelling persisted, and the patient developed limited motion at the extremes of active flexion and extension.
After 2 months, the decision was made to re-explore the palmar puncture site and flexor tendon and obtain tissue specimens for culture, including atypical mycobacterial and fungal cultures. During the second surgery, the palmar site and flexor tendon still appeared unremarkable. As there was some swelling in the long finger, the flexor tendon sheath was explored distally through a separate incision over the middle phalanx. A transversely oriented fragment of the sago palm thorn was found within the flexor tendon sheath. Flexor tendon sheath material was cultured and subsequently found to be negative.
For more information, see “Distal Migration of a Foreign Body (Sago Palm Thorn Fragment) Within the Long-Finger Flexor Tendon Sheath.” Am J Orthop. 2008;37(4):208-209.
Case d. A 2-year-old boy complains of pain after stepping on a toothpick. His father suspects that part of the toothpick remains embedded. Examination reveals a plantar puncture wound but no sign of a foreign body. Radiography shows no deformity. An ultrasound is ordered and reveals a toothpick segment.
With local anesthesia and ultrasound guidance, the splinter is easily removed and the patient is discharged.
For more information, see “Capturing Elusive Foreign Bodies With Ultrasound.” Emergency Medicine. 2009 June;41(6):36-42.
Study: Most oncologists don’t discuss exercise with patients

Results of a small, single-center study suggest oncologists may not provide cancer patients with adequate guidance on exercise.
A majority of the patients and oncologists surveyed for this study placed importance on exercise during cancer care, but most of the oncologists failed to give patients recommendations on exercise.
“Our results indicate that exercise is perceived as important to patients with cancer, both from a patient and physician perspective,” said study author Agnes Smaradottir, MD, of Gundersen Health System in La Crosse, Wisconsin.
“However, physicians are reluctant to consistently include [physical activity] recommendations in their patient discussions.”
Dr Smaradottir and her colleagues reported these findings in JNCCN.
The researchers surveyed 20 cancer patients and 9 oncologists for this study.
The patients’ mean age was 64. Ten patients had stage I-III non-metastatic cancer after adjuvant therapy, and 10 had stage IV metastatic disease and were undergoing palliative treatment. Most patients had solid tumor malignancies, but 1 had chronic lymphocytic leukemia.
The oncologists’ mean age was 45, 56% were male, and they had a mean of 12 years of practice. Most (89%) said they exercise on a regular basis.
Discussions
Nineteen (95%) of the patients surveyed felt they benefited from exercise during treatment, but only 3 of the patients recalled being instructed to exercise.
Exercise was felt to be an equally important part of treatment and well-being for patients with early stage cancer treated with curative intent as well as patients receiving palliative therapy.
Although all the oncologists noted that exercise can benefit cancer patients, only 1 of the 9 surveyed documented discussion of exercise in patient charts.
Preferences and concerns
More than 80% of the patients said they would prefer a home-based exercise regimen that could be performed in alignment with their personal schedules and symptoms.
Patients also noted a preference that exercise recommendations come from their oncologists, as they have an established relationship and feel their oncologists best understand the complexities of their personalized treatment plans.
The oncologists, on the other hand, wanted to refer patients to specialist care for exercise recommendations. Reasons for this included the oncologists’ mounting clinic schedules and a lack of education about appropriate physical activity recommendations for patients.
The oncologists also expressed concern about asking patients to be more physically active during chemotherapy and radiation and expressed trepidation about prescribing exercise to frail patients with limited mobility.
“We were surprised by the gap in expectations regarding exercise recommendation between patients and providers,” Dr Smaradottir said. “Many providers, ourselves included, thought patients would prefer to be referred to an exercise center, but they clearly preferred to have a home-based program recommended by their oncologist.”
“Our findings highlight the value of examining both patient and provider attitudes and behavioral intentions. While we uncovered barriers to exercise recommendations, questions remain on how to bridge the gap between patient and provider preferences.” ![]()
Results of a small, single-center study suggest oncologists may not provide cancer patients with adequate guidance on exercise.
A majority of the patients and oncologists surveyed for this study placed importance on exercise during cancer care, but most of the oncologists failed to give patients recommendations on exercise.
“Our results indicate that exercise is perceived as important to patients with cancer, both from a patient and physician perspective,” said study author Agnes Smaradottir, MD, of Gundersen Health System in La Crosse, Wisconsin.
“However, physicians are reluctant to consistently include [physical activity] recommendations in their patient discussions.”
Dr Smaradottir and her colleagues reported these findings in JNCCN.
The researchers surveyed 20 cancer patients and 9 oncologists for this study.
The patients’ mean age was 64. Ten patients had stage I-III non-metastatic cancer after adjuvant therapy, and 10 had stage IV metastatic disease and were undergoing palliative treatment. Most patients had solid tumor malignancies, but 1 had chronic lymphocytic leukemia.
The oncologists’ mean age was 45, 56% were male, and they had a mean of 12 years of practice. Most (89%) said they exercise on a regular basis.
Discussions
Nineteen (95%) of the patients surveyed felt they benefited from exercise during treatment, but only 3 of the patients recalled being instructed to exercise.
Exercise was felt to be an equally important part of treatment and well-being for patients with early stage cancer treated with curative intent as well as patients receiving palliative therapy.
Although all the oncologists noted that exercise can benefit cancer patients, only 1 of the 9 surveyed documented discussion of exercise in patient charts.
Preferences and concerns
More than 80% of the patients said they would prefer a home-based exercise regimen that could be performed in alignment with their personal schedules and symptoms.
Patients also noted a preference that exercise recommendations come from their oncologists, as they have an established relationship and feel their oncologists best understand the complexities of their personalized treatment plans.
The oncologists, on the other hand, wanted to refer patients to specialist care for exercise recommendations. Reasons for this included the oncologists’ mounting clinic schedules and a lack of education about appropriate physical activity recommendations for patients.
The oncologists also expressed concern about asking patients to be more physically active during chemotherapy and radiation and expressed trepidation about prescribing exercise to frail patients with limited mobility.
“We were surprised by the gap in expectations regarding exercise recommendation between patients and providers,” Dr Smaradottir said. “Many providers, ourselves included, thought patients would prefer to be referred to an exercise center, but they clearly preferred to have a home-based program recommended by their oncologist.”
“Our findings highlight the value of examining both patient and provider attitudes and behavioral intentions. While we uncovered barriers to exercise recommendations, questions remain on how to bridge the gap between patient and provider preferences.” ![]()
Results of a small, single-center study suggest oncologists may not provide cancer patients with adequate guidance on exercise.
A majority of the patients and oncologists surveyed for this study placed importance on exercise during cancer care, but most of the oncologists failed to give patients recommendations on exercise.
“Our results indicate that exercise is perceived as important to patients with cancer, both from a patient and physician perspective,” said study author Agnes Smaradottir, MD, of Gundersen Health System in La Crosse, Wisconsin.
“However, physicians are reluctant to consistently include [physical activity] recommendations in their patient discussions.”
Dr Smaradottir and her colleagues reported these findings in JNCCN.
The researchers surveyed 20 cancer patients and 9 oncologists for this study.
The patients’ mean age was 64. Ten patients had stage I-III non-metastatic cancer after adjuvant therapy, and 10 had stage IV metastatic disease and were undergoing palliative treatment. Most patients had solid tumor malignancies, but 1 had chronic lymphocytic leukemia.
The oncologists’ mean age was 45, 56% were male, and they had a mean of 12 years of practice. Most (89%) said they exercise on a regular basis.
Discussions
Nineteen (95%) of the patients surveyed felt they benefited from exercise during treatment, but only 3 of the patients recalled being instructed to exercise.
Exercise was felt to be an equally important part of treatment and well-being for patients with early stage cancer treated with curative intent as well as patients receiving palliative therapy.
Although all the oncologists noted that exercise can benefit cancer patients, only 1 of the 9 surveyed documented discussion of exercise in patient charts.
Preferences and concerns
More than 80% of the patients said they would prefer a home-based exercise regimen that could be performed in alignment with their personal schedules and symptoms.
Patients also noted a preference that exercise recommendations come from their oncologists, as they have an established relationship and feel their oncologists best understand the complexities of their personalized treatment plans.
The oncologists, on the other hand, wanted to refer patients to specialist care for exercise recommendations. Reasons for this included the oncologists’ mounting clinic schedules and a lack of education about appropriate physical activity recommendations for patients.
The oncologists also expressed concern about asking patients to be more physically active during chemotherapy and radiation and expressed trepidation about prescribing exercise to frail patients with limited mobility.
“We were surprised by the gap in expectations regarding exercise recommendation between patients and providers,” Dr Smaradottir said. “Many providers, ourselves included, thought patients would prefer to be referred to an exercise center, but they clearly preferred to have a home-based program recommended by their oncologist.”
“Our findings highlight the value of examining both patient and provider attitudes and behavioral intentions. While we uncovered barriers to exercise recommendations, questions remain on how to bridge the gap between patient and provider preferences.” ![]()
System monitors and maintains drug levels in the body

New technology could make it easier to ensure patients receive the correct dose of chemotherapy and other drugs, according to research published in Nature Biomedical Engineering.
Researchers developed a closed-loop system that was able to continuously regulate drug levels in rabbits and rats.
“This is the first time anyone has been able to continuously control the drug levels in the body in real time,” said study author H. Tom Soh, PhD, of Stanford University in California.
“This is a novel concept with big implications because we believe we can adapt our technology to control the levels of a wide range of drugs.”
The researchers’ system has 3 basic components: a real-time biosensor to continuously monitor drug levels in the bloodstream, a control system to calculate the right dose, and a programmable pump that delivers just enough medicine to maintain a desired dose.
The sensor contains aptamers that are specially designed to bind a drug of interest. When the drug is present in the bloodstream, the aptamer changes shape, which an electric sensor detects. The more drug, the more aptamers change shape.
That information, captured every few seconds, is routed through software that controls the pump to deliver additional drugs as needed.
Researchers tested the technology by administering the chemotherapy drug doxorubicin to rabbits and rats.
Despite physiological and metabolic differences among individual animals, the team was able to keep a constant dosage in all the animals, something not possible with current drug delivery methods.
The researchers also tested for acute drug-drug interactions and found the system was able to stabilize drug levels to moderate what might otherwise be a dangerous spike or dip.
Dr Soh and his colleagues believe this technology could be particularly useful in treating pediatric cancer patients, who are notoriously difficult to dose because a child’s metabolism is usually different from an adult’s.
The team plans to miniaturize the system so it can be implanted or worn by the patient.
At present, the technology is an external apparatus, like a smart IV drip. The biosensor is a device about the size of a microscope slide.
The current setup might be suitable for a chemotherapy drug but not for continual use.
The researchers are also adapting the system with different aptamers so it can sense and regulate the levels of other biomolecules in the body. ![]()
New technology could make it easier to ensure patients receive the correct dose of chemotherapy and other drugs, according to research published in Nature Biomedical Engineering.
Researchers developed a closed-loop system that was able to continuously regulate drug levels in rabbits and rats.
“This is the first time anyone has been able to continuously control the drug levels in the body in real time,” said study author H. Tom Soh, PhD, of Stanford University in California.
“This is a novel concept with big implications because we believe we can adapt our technology to control the levels of a wide range of drugs.”
The researchers’ system has 3 basic components: a real-time biosensor to continuously monitor drug levels in the bloodstream, a control system to calculate the right dose, and a programmable pump that delivers just enough medicine to maintain a desired dose.
The sensor contains aptamers that are specially designed to bind a drug of interest. When the drug is present in the bloodstream, the aptamer changes shape, which an electric sensor detects. The more drug, the more aptamers change shape.
That information, captured every few seconds, is routed through software that controls the pump to deliver additional drugs as needed.
Researchers tested the technology by administering the chemotherapy drug doxorubicin to rabbits and rats.
Despite physiological and metabolic differences among individual animals, the team was able to keep a constant dosage in all the animals, something not possible with current drug delivery methods.
The researchers also tested for acute drug-drug interactions and found the system was able to stabilize drug levels to moderate what might otherwise be a dangerous spike or dip.
Dr Soh and his colleagues believe this technology could be particularly useful in treating pediatric cancer patients, who are notoriously difficult to dose because a child’s metabolism is usually different from an adult’s.
The team plans to miniaturize the system so it can be implanted or worn by the patient.
At present, the technology is an external apparatus, like a smart IV drip. The biosensor is a device about the size of a microscope slide.
The current setup might be suitable for a chemotherapy drug but not for continual use.
The researchers are also adapting the system with different aptamers so it can sense and regulate the levels of other biomolecules in the body. ![]()
New technology could make it easier to ensure patients receive the correct dose of chemotherapy and other drugs, according to research published in Nature Biomedical Engineering.
Researchers developed a closed-loop system that was able to continuously regulate drug levels in rabbits and rats.
“This is the first time anyone has been able to continuously control the drug levels in the body in real time,” said study author H. Tom Soh, PhD, of Stanford University in California.
“This is a novel concept with big implications because we believe we can adapt our technology to control the levels of a wide range of drugs.”
The researchers’ system has 3 basic components: a real-time biosensor to continuously monitor drug levels in the bloodstream, a control system to calculate the right dose, and a programmable pump that delivers just enough medicine to maintain a desired dose.
The sensor contains aptamers that are specially designed to bind a drug of interest. When the drug is present in the bloodstream, the aptamer changes shape, which an electric sensor detects. The more drug, the more aptamers change shape.
That information, captured every few seconds, is routed through software that controls the pump to deliver additional drugs as needed.
Researchers tested the technology by administering the chemotherapy drug doxorubicin to rabbits and rats.
Despite physiological and metabolic differences among individual animals, the team was able to keep a constant dosage in all the animals, something not possible with current drug delivery methods.
The researchers also tested for acute drug-drug interactions and found the system was able to stabilize drug levels to moderate what might otherwise be a dangerous spike or dip.
Dr Soh and his colleagues believe this technology could be particularly useful in treating pediatric cancer patients, who are notoriously difficult to dose because a child’s metabolism is usually different from an adult’s.
The team plans to miniaturize the system so it can be implanted or worn by the patient.
At present, the technology is an external apparatus, like a smart IV drip. The biosensor is a device about the size of a microscope slide.
The current setup might be suitable for a chemotherapy drug but not for continual use.
The researchers are also adapting the system with different aptamers so it can sense and regulate the levels of other biomolecules in the body. ![]()