User login
Survey: Most doctors would pick single payer over ACA, ACHA
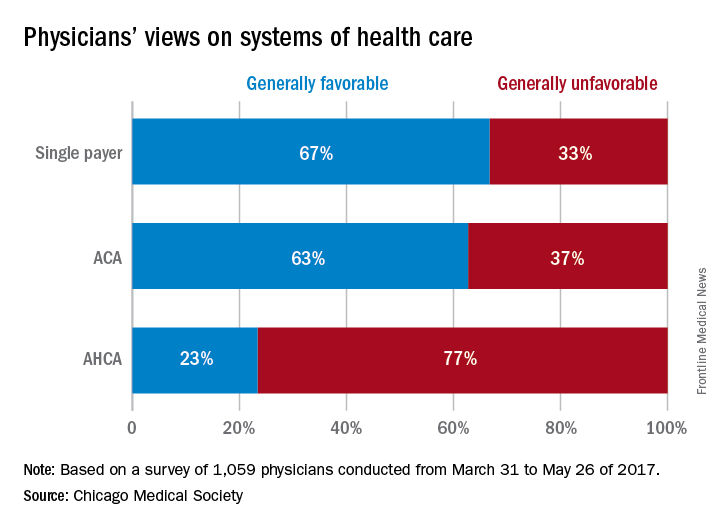
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
CHICAGO – If given the option, the majority of physicians would scrap both the Affordable Care Act and the proposed American Health Care Act (AHCA) and opt for a single payer health care system, according to a survey of 1,059 doctors by the Chicago Medical Society (CMS).
When asked their preferred health care structure, 53% of physician said they would prefer a single payer health system, while 26% preferred the Affordable Care Act, and 13% said they would like to see the ACA repealed and replaced with the AHCA. Another 8% of doctors stated they would prefer repeal of the ACA but did not offer a replacement option.
The high percentage of physicians who favored a single payer system was surprising, said A. Jay Chauhan, DO, secretary and chair of public health for the Chicago Medical Society.
“That is a shift from past surveys,” Dr. Chauhan said during an interview at a conference held by the American Bar Association. “It certainly speaks to the frustration that physicians are [feeling] and how difficult it is to practice. I think they’re trying to reach out for other alternatives because the current manner in which we’re practicing doesn’t seem to fulfill our desires to better take care of patients.”
Respondents also choose a single payer system as their top preference when asked which health care system they believed would provide “the best care to the greatest number of people for a given amount of funding.”
A primary takeaway from the survey is that physicians want to see better access to health care for their patients and more affordable insurance coverage, said Katherine M. Tynus, MD, immediate past president of the Chicago Medical Society and president-elect of the Illinois State Medical Society.
“I think what the Affordable Care Act did was raise expectations as far as access to care and people being able to afford their health care,” Dr. Tynus said in an interview at the meeting. “Since that system seems to be failing, the expectation remains. Now, we need to find an alternative solution to achieve that.”
The online survey, released at the Physicians Legal Issues Conference held by the American Bar Association, was conducted between March 2017 and May 2017 and featured questions about health reform. Survey participants were physicians primarily based in the Chicago area or within Illinois and the majority practiced in an urban area. Respondents represented a variety of political affiliations and medical specialties. The majority said they identifying as independent (43%), and the most common specialty was general medicine (19%).
[email protected]
On Twitter @legal_med
AT THE PHYSICIANS LEGAL ISSUES CONFERENCE
VIDEO: Tocilizumab tested in children with sJIA under 2 years old
MADRID – The results of the first trial of a biologic agent in children less than 2 years of age with systemic juvenile idiopathic arthritis (sJIA) suggest that tocilizumab is likely to be effective in this age group.
“sJIA is the most severe form of childhood arthritis, and as you are aware, it’s the most difficult to treat as well,” said Navita L. Mallalieu, PhD, director of clinical pharmacology at Roche Innovation Center New York, the company that funded the study.
Tocilizumab (Actemra) has been available for the treatment of sJIA, both in the United States and the European Union since 2011, she observed at the European Congress of Rheumatology, but only for children aged 2 years or older at the current time.
Because of this prior history of use in sJIA, “we have confidence in the safety profile, and so we were able to go to the next step of testing children who were even younger than 2 years of age,” Dr. Mallalieu said in a video interview.
[polldaddy:9771949]
Dr. Mallalieu presented findings from an open-label, single-arm, phase I trial that evaluated a 12 mg/kg dosing regimen of tocilizumab, which was given intravenously every 2 weeks for 12 weeks. Eleven children were studied who had a mean age of 1.3 years and active disease for at least 1 month despite treatment with glucocorticoids or nonsteroidal anti-inflammatory drugs.
The primary endpoint was the pharmacokinetics of tocilizumab in this younger patient population, and secondary endpoints were safety, pharmacodynamics, and exploring the efficacy over 12 weeks on top of stable background therapy, she explained.
Results showed that tocilizumab in children under 2 years of age could achieve pharmacokinetics similar to those seen in older children in the TENDER trial (N Engl J Med. 2012;367:2385-95), which is the trial that helped the biologic get licensed for use in the older sJIA population. Reductions in soluble interleukin-6 receptor, C-reactive protein, and the erythrocyte sedimentation rate were seen, again to a similar extent as seen in the TENDER trial. There was also an indication that similar reductions in the Juvenile Arthritis Disease Activity Score (JADAS)-71 score could be achieved, Dr. Mallalieu reported.
While the pattern and nature of adverse events were similar to those seen in the TENDER trial, there were more cases of hypersensitivity in this phase I study. Four cases of hypersensitivity were clinically confirmed, three of which were deemed serious. The three serious cases were observed at day 15, with two of the cases associated with multiple signs and symptoms that were confounded by either subclinical macrophage activation syndrome (MAS) or a faster infusion rate. One patient had urticaria and was hospitalized for observation.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MADRID – The results of the first trial of a biologic agent in children less than 2 years of age with systemic juvenile idiopathic arthritis (sJIA) suggest that tocilizumab is likely to be effective in this age group.
“sJIA is the most severe form of childhood arthritis, and as you are aware, it’s the most difficult to treat as well,” said Navita L. Mallalieu, PhD, director of clinical pharmacology at Roche Innovation Center New York, the company that funded the study.
Tocilizumab (Actemra) has been available for the treatment of sJIA, both in the United States and the European Union since 2011, she observed at the European Congress of Rheumatology, but only for children aged 2 years or older at the current time.
Because of this prior history of use in sJIA, “we have confidence in the safety profile, and so we were able to go to the next step of testing children who were even younger than 2 years of age,” Dr. Mallalieu said in a video interview.
[polldaddy:9771949]
Dr. Mallalieu presented findings from an open-label, single-arm, phase I trial that evaluated a 12 mg/kg dosing regimen of tocilizumab, which was given intravenously every 2 weeks for 12 weeks. Eleven children were studied who had a mean age of 1.3 years and active disease for at least 1 month despite treatment with glucocorticoids or nonsteroidal anti-inflammatory drugs.
The primary endpoint was the pharmacokinetics of tocilizumab in this younger patient population, and secondary endpoints were safety, pharmacodynamics, and exploring the efficacy over 12 weeks on top of stable background therapy, she explained.
Results showed that tocilizumab in children under 2 years of age could achieve pharmacokinetics similar to those seen in older children in the TENDER trial (N Engl J Med. 2012;367:2385-95), which is the trial that helped the biologic get licensed for use in the older sJIA population. Reductions in soluble interleukin-6 receptor, C-reactive protein, and the erythrocyte sedimentation rate were seen, again to a similar extent as seen in the TENDER trial. There was also an indication that similar reductions in the Juvenile Arthritis Disease Activity Score (JADAS)-71 score could be achieved, Dr. Mallalieu reported.
While the pattern and nature of adverse events were similar to those seen in the TENDER trial, there were more cases of hypersensitivity in this phase I study. Four cases of hypersensitivity were clinically confirmed, three of which were deemed serious. The three serious cases were observed at day 15, with two of the cases associated with multiple signs and symptoms that were confounded by either subclinical macrophage activation syndrome (MAS) or a faster infusion rate. One patient had urticaria and was hospitalized for observation.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MADRID – The results of the first trial of a biologic agent in children less than 2 years of age with systemic juvenile idiopathic arthritis (sJIA) suggest that tocilizumab is likely to be effective in this age group.
“sJIA is the most severe form of childhood arthritis, and as you are aware, it’s the most difficult to treat as well,” said Navita L. Mallalieu, PhD, director of clinical pharmacology at Roche Innovation Center New York, the company that funded the study.
Tocilizumab (Actemra) has been available for the treatment of sJIA, both in the United States and the European Union since 2011, she observed at the European Congress of Rheumatology, but only for children aged 2 years or older at the current time.
Because of this prior history of use in sJIA, “we have confidence in the safety profile, and so we were able to go to the next step of testing children who were even younger than 2 years of age,” Dr. Mallalieu said in a video interview.
[polldaddy:9771949]
Dr. Mallalieu presented findings from an open-label, single-arm, phase I trial that evaluated a 12 mg/kg dosing regimen of tocilizumab, which was given intravenously every 2 weeks for 12 weeks. Eleven children were studied who had a mean age of 1.3 years and active disease for at least 1 month despite treatment with glucocorticoids or nonsteroidal anti-inflammatory drugs.
The primary endpoint was the pharmacokinetics of tocilizumab in this younger patient population, and secondary endpoints were safety, pharmacodynamics, and exploring the efficacy over 12 weeks on top of stable background therapy, she explained.
Results showed that tocilizumab in children under 2 years of age could achieve pharmacokinetics similar to those seen in older children in the TENDER trial (N Engl J Med. 2012;367:2385-95), which is the trial that helped the biologic get licensed for use in the older sJIA population. Reductions in soluble interleukin-6 receptor, C-reactive protein, and the erythrocyte sedimentation rate were seen, again to a similar extent as seen in the TENDER trial. There was also an indication that similar reductions in the Juvenile Arthritis Disease Activity Score (JADAS)-71 score could be achieved, Dr. Mallalieu reported.
While the pattern and nature of adverse events were similar to those seen in the TENDER trial, there were more cases of hypersensitivity in this phase I study. Four cases of hypersensitivity were clinically confirmed, three of which were deemed serious. The three serious cases were observed at day 15, with two of the cases associated with multiple signs and symptoms that were confounded by either subclinical macrophage activation syndrome (MAS) or a faster infusion rate. One patient had urticaria and was hospitalized for observation.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: Similar pharmacokinetics were observed in children under 2 years of age as those seen in a prior study of older children.
Data source: Open-label, single-arm, phase I trial that evaluated a 12-mg/kg dosing regimen of tocilizumab given intravenously every 2 weeks for 12 weeks.
Disclosures: Roche funded the study. The presenter is an employee of Roche.

Teens’ overall tobacco use falls, but e-cigs now most popular product
Twenty percent of surveyed high school students and 7% of middle school students were using some kind of tobacco product in 2016 – and e-cigarettes were the most commonly used product among those groups, according to an analysis from federal researchers.
, although combustible tobacco product use declined in both groups, said Ahmed Jamal, MD, of the Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and his associates. That was determined using data from the 2011-2016 National Youth Tobacco Surveys, which assessed tobacco use in the past 30 days by groups of middle school and high school students numbering from more than 17,000 to almost 25,000.
High school boys had higher use of any tobacco product, two or more tobacco products, cigars, smokeless tobacco, and pipe tobacco than did high school girls. The most commonly used tobacco product among non-Hispanic white (13.7%) and Hispanic high school students (10%) were e-cigarettes; cigars were the most commonly used tobacco product among non-Hispanic black high school students (9.5%).
Seven percent of middle school students had used any tobacco product within the past 30 days, and 3% had used two or more tobacco products. Similar to high school students, e-cigarettes were the most commonly used tobacco product among middle school students (4.3%), followed by cigarettes (2%), cigars (2%), smokeless tobacco (2%), hookahs (2%), pipe tobacco (0.7%), and bidis (0.3%).
Use of any tobacco product among middle school boys was 8.3%, and among middle school girls use was 6%. Hispanic middle school students reported higher use of any tobacco product, were more likely to use two or more tobacco products, and said they used hookahs more often than did non-Hispanic white middle school students.
Looking at the changes from 2011 to 2016, current use of any tobacco product did not change significantly among high school students (falling from 24% to 20%), but there was a reduction in current use of any combustible tobacco product (22%-14%) and in use of two or more tobacco products (12%-9.6%) over this time period.
By product type, there were increases in current use of e-cigarettes (from 1.5% to 11.3%) and hookahs (from 4.1% to 4.8%) among high school students, as well as decreases in current use of cigarettes (from 16% to 8%), cigars (from 12% to 8%), smokeless tobacco (from 8% to 6%), pipe tobacco (from 4% to 1%), and bidis (from 2% to 0.5%).
Among middle school students during 2011-2016, there was a rise in current use of e-cigarettes (from 0.6% to 4%), and in current use of hookahs (from 1% to 2%). There was a drop in current use of any combustible tobacco products (from 6% to 4%), cigarettes (from 4% to 2%), cigars (from 3.5% to 2.2%), and pipe tobacco (from 2% to 0.7%).
“Since February 2014, the Food and Drug Administration’s first national tobacco public education campaign, the Real Cost, has broadcasted tobacco education advertising designed for youths aged 12-17 years; the campaign was associated with an estimated 348,398 U.S. youths who did not initiate cigarette smoking during February 2014–March 2016,” the investigators said. “Continued implementation of these strategies can help prevent and further reduce the use of all forms of tobacco product among U.S. youths.”
Read more in MMWR (2017 Jun 16;66[23]:597-603).
Twenty percent of surveyed high school students and 7% of middle school students were using some kind of tobacco product in 2016 – and e-cigarettes were the most commonly used product among those groups, according to an analysis from federal researchers.
, although combustible tobacco product use declined in both groups, said Ahmed Jamal, MD, of the Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and his associates. That was determined using data from the 2011-2016 National Youth Tobacco Surveys, which assessed tobacco use in the past 30 days by groups of middle school and high school students numbering from more than 17,000 to almost 25,000.
High school boys had higher use of any tobacco product, two or more tobacco products, cigars, smokeless tobacco, and pipe tobacco than did high school girls. The most commonly used tobacco product among non-Hispanic white (13.7%) and Hispanic high school students (10%) were e-cigarettes; cigars were the most commonly used tobacco product among non-Hispanic black high school students (9.5%).
Seven percent of middle school students had used any tobacco product within the past 30 days, and 3% had used two or more tobacco products. Similar to high school students, e-cigarettes were the most commonly used tobacco product among middle school students (4.3%), followed by cigarettes (2%), cigars (2%), smokeless tobacco (2%), hookahs (2%), pipe tobacco (0.7%), and bidis (0.3%).
Use of any tobacco product among middle school boys was 8.3%, and among middle school girls use was 6%. Hispanic middle school students reported higher use of any tobacco product, were more likely to use two or more tobacco products, and said they used hookahs more often than did non-Hispanic white middle school students.
Looking at the changes from 2011 to 2016, current use of any tobacco product did not change significantly among high school students (falling from 24% to 20%), but there was a reduction in current use of any combustible tobacco product (22%-14%) and in use of two or more tobacco products (12%-9.6%) over this time period.
By product type, there were increases in current use of e-cigarettes (from 1.5% to 11.3%) and hookahs (from 4.1% to 4.8%) among high school students, as well as decreases in current use of cigarettes (from 16% to 8%), cigars (from 12% to 8%), smokeless tobacco (from 8% to 6%), pipe tobacco (from 4% to 1%), and bidis (from 2% to 0.5%).
Among middle school students during 2011-2016, there was a rise in current use of e-cigarettes (from 0.6% to 4%), and in current use of hookahs (from 1% to 2%). There was a drop in current use of any combustible tobacco products (from 6% to 4%), cigarettes (from 4% to 2%), cigars (from 3.5% to 2.2%), and pipe tobacco (from 2% to 0.7%).
“Since February 2014, the Food and Drug Administration’s first national tobacco public education campaign, the Real Cost, has broadcasted tobacco education advertising designed for youths aged 12-17 years; the campaign was associated with an estimated 348,398 U.S. youths who did not initiate cigarette smoking during February 2014–March 2016,” the investigators said. “Continued implementation of these strategies can help prevent and further reduce the use of all forms of tobacco product among U.S. youths.”
Read more in MMWR (2017 Jun 16;66[23]:597-603).
Twenty percent of surveyed high school students and 7% of middle school students were using some kind of tobacco product in 2016 – and e-cigarettes were the most commonly used product among those groups, according to an analysis from federal researchers.
, although combustible tobacco product use declined in both groups, said Ahmed Jamal, MD, of the Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, and his associates. That was determined using data from the 2011-2016 National Youth Tobacco Surveys, which assessed tobacco use in the past 30 days by groups of middle school and high school students numbering from more than 17,000 to almost 25,000.
High school boys had higher use of any tobacco product, two or more tobacco products, cigars, smokeless tobacco, and pipe tobacco than did high school girls. The most commonly used tobacco product among non-Hispanic white (13.7%) and Hispanic high school students (10%) were e-cigarettes; cigars were the most commonly used tobacco product among non-Hispanic black high school students (9.5%).
Seven percent of middle school students had used any tobacco product within the past 30 days, and 3% had used two or more tobacco products. Similar to high school students, e-cigarettes were the most commonly used tobacco product among middle school students (4.3%), followed by cigarettes (2%), cigars (2%), smokeless tobacco (2%), hookahs (2%), pipe tobacco (0.7%), and bidis (0.3%).
Use of any tobacco product among middle school boys was 8.3%, and among middle school girls use was 6%. Hispanic middle school students reported higher use of any tobacco product, were more likely to use two or more tobacco products, and said they used hookahs more often than did non-Hispanic white middle school students.
Looking at the changes from 2011 to 2016, current use of any tobacco product did not change significantly among high school students (falling from 24% to 20%), but there was a reduction in current use of any combustible tobacco product (22%-14%) and in use of two or more tobacco products (12%-9.6%) over this time period.
By product type, there were increases in current use of e-cigarettes (from 1.5% to 11.3%) and hookahs (from 4.1% to 4.8%) among high school students, as well as decreases in current use of cigarettes (from 16% to 8%), cigars (from 12% to 8%), smokeless tobacco (from 8% to 6%), pipe tobacco (from 4% to 1%), and bidis (from 2% to 0.5%).
Among middle school students during 2011-2016, there was a rise in current use of e-cigarettes (from 0.6% to 4%), and in current use of hookahs (from 1% to 2%). There was a drop in current use of any combustible tobacco products (from 6% to 4%), cigarettes (from 4% to 2%), cigars (from 3.5% to 2.2%), and pipe tobacco (from 2% to 0.7%).
“Since February 2014, the Food and Drug Administration’s first national tobacco public education campaign, the Real Cost, has broadcasted tobacco education advertising designed for youths aged 12-17 years; the campaign was associated with an estimated 348,398 U.S. youths who did not initiate cigarette smoking during February 2014–March 2016,” the investigators said. “Continued implementation of these strategies can help prevent and further reduce the use of all forms of tobacco product among U.S. youths.”
Read more in MMWR (2017 Jun 16;66[23]:597-603).
FROM MMWR
The hype behind facial oils
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?

Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.

Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
Completeness of Facial Self-application of Sunscreen in Cosmetic Surgery Patients
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
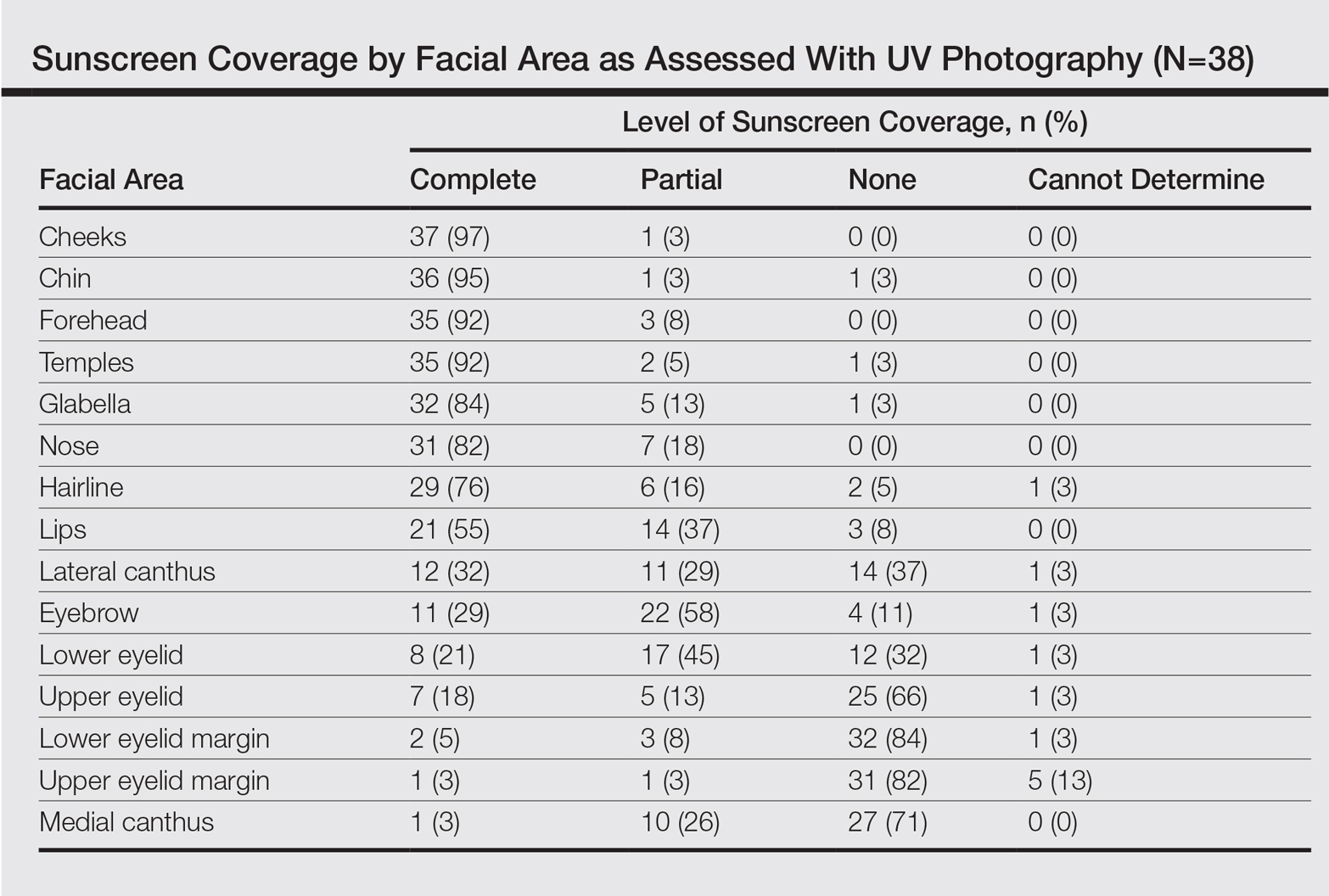
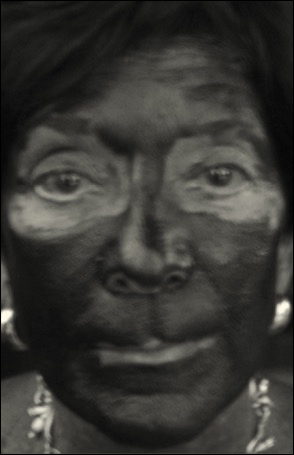
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
Resident Pearl
- Patients may benefit from their physician taking a moment to describe the importance of applying sunscreen to the eyelids while applying it to the rest of the face.
Relatives of NAFLD patients: 12-fold higher risk
Asymptomatic first-degree relatives of patients who have nonalcoholic fatty liver disease with cirrhosis are at a 12-fold higher risk for advanced liver fibrosis compared with the general population, according to a report published online June 19 in the Journal of Clinical Investigation.
If this preliminary but robust association is confirmed in further research, it may well change clinical practice. First-degree relatives would likely require screening for advanced fibrosis, and those found to have it would likely need continued surveillance for hepatocellular carcinoma.

They noted that previous studies have suggested a familial component to NAFLD, and decided to assess the risk of advanced fibrosis in first-degree relatives of patients who had NAFLD plus cirrhosis. The investigators used noninvasive imaging techniques – MRI-PDFF (MRI proton density fat fraction) and MRE (magnetic resonance elastography) – to quantify liver fat and liver fibrosis in 26 patients who had NAFLD plus cirrhosis, 39 of their first-degree relatives who were asymptomatic, 69 community-dwelling adults who did not have NAFLD or cirrhosis, and 69 of their first-degree relatives.
The primary outcome measure, the prevalence of advanced liver fibrosis, was 18% among first-degree relatives of patients who had NAFLD plus cirrhosis. This was markedly greater than the prevalence of advanced fibrosis among first-degree relatives of unaffected adults (1.4%).
The odds ratio of having advanced fibrosis among first-degree relatives of affected patients was 14.9, compared with the control population. When the data were adjusted to account for age, sex, body mass index, and diabetes status, the OR remained statistically and clinically significant at 12.5, Dr. Caussy and her associates said (doi.org/10.1172/JCI93465).
This study was limited in that it was a single-center investigation and used advanced MRI techniques that may not be routinely available at other centers. In addition, since it was cross-sectional in design, long-term outcomes, such as the development of hepatocellular carcinoma and survival rates, could not be assessed.
“Despite these limitations, we believe that this study provides important data that require validation in larger studies to then change clinical practice guidelines to screen first-degree relatives of patients with NAFLD with cirrhosis,” the investigators added.
The National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute of Environmental Health Sciences supported the study. Dr. Caussy and her associates reported having no relevant financial disclosures.
Asymptomatic first-degree relatives of patients who have nonalcoholic fatty liver disease with cirrhosis are at a 12-fold higher risk for advanced liver fibrosis compared with the general population, according to a report published online June 19 in the Journal of Clinical Investigation.
If this preliminary but robust association is confirmed in further research, it may well change clinical practice. First-degree relatives would likely require screening for advanced fibrosis, and those found to have it would likely need continued surveillance for hepatocellular carcinoma.
They noted that previous studies have suggested a familial component to NAFLD, and decided to assess the risk of advanced fibrosis in first-degree relatives of patients who had NAFLD plus cirrhosis. The investigators used noninvasive imaging techniques – MRI-PDFF (MRI proton density fat fraction) and MRE (magnetic resonance elastography) – to quantify liver fat and liver fibrosis in 26 patients who had NAFLD plus cirrhosis, 39 of their first-degree relatives who were asymptomatic, 69 community-dwelling adults who did not have NAFLD or cirrhosis, and 69 of their first-degree relatives.
The primary outcome measure, the prevalence of advanced liver fibrosis, was 18% among first-degree relatives of patients who had NAFLD plus cirrhosis. This was markedly greater than the prevalence of advanced fibrosis among first-degree relatives of unaffected adults (1.4%).
The odds ratio of having advanced fibrosis among first-degree relatives of affected patients was 14.9, compared with the control population. When the data were adjusted to account for age, sex, body mass index, and diabetes status, the OR remained statistically and clinically significant at 12.5, Dr. Caussy and her associates said (doi.org/10.1172/JCI93465).
This study was limited in that it was a single-center investigation and used advanced MRI techniques that may not be routinely available at other centers. In addition, since it was cross-sectional in design, long-term outcomes, such as the development of hepatocellular carcinoma and survival rates, could not be assessed.
“Despite these limitations, we believe that this study provides important data that require validation in larger studies to then change clinical practice guidelines to screen first-degree relatives of patients with NAFLD with cirrhosis,” the investigators added.
The National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute of Environmental Health Sciences supported the study. Dr. Caussy and her associates reported having no relevant financial disclosures.
Asymptomatic first-degree relatives of patients who have nonalcoholic fatty liver disease with cirrhosis are at a 12-fold higher risk for advanced liver fibrosis compared with the general population, according to a report published online June 19 in the Journal of Clinical Investigation.
If this preliminary but robust association is confirmed in further research, it may well change clinical practice. First-degree relatives would likely require screening for advanced fibrosis, and those found to have it would likely need continued surveillance for hepatocellular carcinoma.
They noted that previous studies have suggested a familial component to NAFLD, and decided to assess the risk of advanced fibrosis in first-degree relatives of patients who had NAFLD plus cirrhosis. The investigators used noninvasive imaging techniques – MRI-PDFF (MRI proton density fat fraction) and MRE (magnetic resonance elastography) – to quantify liver fat and liver fibrosis in 26 patients who had NAFLD plus cirrhosis, 39 of their first-degree relatives who were asymptomatic, 69 community-dwelling adults who did not have NAFLD or cirrhosis, and 69 of their first-degree relatives.
The primary outcome measure, the prevalence of advanced liver fibrosis, was 18% among first-degree relatives of patients who had NAFLD plus cirrhosis. This was markedly greater than the prevalence of advanced fibrosis among first-degree relatives of unaffected adults (1.4%).
The odds ratio of having advanced fibrosis among first-degree relatives of affected patients was 14.9, compared with the control population. When the data were adjusted to account for age, sex, body mass index, and diabetes status, the OR remained statistically and clinically significant at 12.5, Dr. Caussy and her associates said (doi.org/10.1172/JCI93465).
This study was limited in that it was a single-center investigation and used advanced MRI techniques that may not be routinely available at other centers. In addition, since it was cross-sectional in design, long-term outcomes, such as the development of hepatocellular carcinoma and survival rates, could not be assessed.
“Despite these limitations, we believe that this study provides important data that require validation in larger studies to then change clinical practice guidelines to screen first-degree relatives of patients with NAFLD with cirrhosis,” the investigators added.
The National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute of Environmental Health Sciences supported the study. Dr. Caussy and her associates reported having no relevant financial disclosures.
FROM THE JOURNAL OF CLINICAL INVESTIGATION
Key clinical point: First-degree relatives of patients who have nonalcoholic fatty liver disease with cirrhosis are at a 12-fold higher risk of advanced liver fibrosis compared with the general population.
Major finding: The adjusted odds ratio of having advanced fibrosis among first-degree relatives of affected patients was 12.5, compared with the control population.
Data source: A cross-sectional cohort study involving 25 probands with NAFLD + cirrhosis, 39 first-degree relatives, and 69 control pairs of relatives from the general population.
Disclosures: The National Institute of Diabetes and Digestive and Kidney Diseases and the National Institute of Environmental Health Sciences supported the study. Dr. Caussy and her associates reported having no relevant financial disclosures.
PROTECT: Pazopanib falls short as adjuvant therapy for high-risk RCC
CHICAGO – The antiangiogenic agent pazopanib is not efficacious when used as adjuvant therapy for resected renal cell carcinoma (RCC) with features that confer a high risk of recurrence, the PROTECT investigators reported at the annual meeting of the American Society of Clinical Oncology.
Pazopanib (Votrient) is an oral multitargeted tyrosine kinase inhibitor active against the vascular endothelial growth factor receptor (VEGFR). Adjuvant use of other agents in this class has yielded mixed results, noted lead investigator Robert J. Motzer, MD, of Memorial Sloan-Kettering Cancer Center in New York.

In PROTECT, a phase III randomized controlled trial of more than 1,500 patients who had undergone nephrectomy for high-risk locally advanced RCC, pazopanib started at 600 mg daily did not yield significantly better disease-free survival than placebo, the trial’s primary endpoint. The drug did have a significant benefit when started at 800 mg daily, but that dose had to be lowered partway through because of a high rate of discontinuation due to adverse events.
“The trial did not meet its primary endpoint,” Dr. Motzer concluded. “Pazopanib is not recommended for adjuvant therapy following resection of locally advanced RCC.”
Expert perspective
“The current landscape of RCC adjuvant therapy is really controversial,” commented invited discussant Daniel Y. C. Heng, MD, MPH, of the University of Calgary (Alta.) Tom Baker Cancer Centre.

“Are these [factors] important or not? I think a lot of this is being overshadowed by things that are going on right now,” Dr. Heng maintained. “There are newer medications, such as PD-1 and PD-L1 inhibitors that are now being studied. And there are now perioperative studies as well – should we be using these drugs before nephrectomy and after nephrectomy to prime the immune system to get better outcomes?”
At the end of the day, identification of a reliable predictive biomarker will be key to using the VEGFR tyrosine kinase inhibitors, he concluded. “I look forward to the future where we can actually use these tests to determine who will benefit most from adjuvant therapy so that we can maximize patient outcomes.”
Study details
The PROTECT trial was funded by Novartis Oncology and randomized 1,538 patients with resected pT2 (high grade), pT3, or greater nonmetastatic clear cell RCC, a highly vascular tumor typically reliant on aberrant signaling in the VEGF pathway.
The patients were assigned evenly to receive pazopanib or placebo for 1 year. The starting dose was lowered from 800 mg daily to 600 mg daily (with escalation permitted) after 403 patients had been treated.
In intention-to-treat analysis among patients started on the 600-mg dose and having a median follow-up of about 31 months, disease-free survival was better with pazopanib but not significantly so (hazard ratio, 0.86; P = .16), Dr. Motzer reported.
In secondary analyses, pazopanib did have a significant disease-free survival benefit among patients started on the 800-mg dose (hazard ratio, 0.69; P = .02) and among the entire trial population started on either dose (hazard ratio, 0.80; P = .01).
One possible explanation for the differing results seen with the two doses was the difference in follow-up, as the 800-mg group was treated earlier in the trial, he proposed. But with an additional year of blinded follow-up, the benefit in the 600-mg group actually diminished, whereas that in the 800-mg group did not.
Another possibility was the somewhat better performance of the placebo group used for comparison with the lower dose: the 3-year disease-free survival rate with placebo was 64% for the 600-mg comparison but 56% for the 800-mg comparison. “One factor that could explain differences in the outcomes of the placebo groups includes unidentified patient demographic characteristics,” Dr. Motzer noted.
Overall survival was statistically indistinguishable between the pazopanib and placebo groups, regardless of dose. However, “the results are inconclusive as the data are not yet mature,” he said, with a definitive analysis planned for 2019.
Compared with counterparts given placebo, patients started on the 600-mg dose of pazopanib had a higher rate of grade 3 or 4 adverse events overall (60% vs. 21%), driven in large part by higher rates of hypertension and increased alanine aminotransferase levels.
“Although the intent of modifying the protocol dose of pazopanib from 800 mg to 600 mg was to reduce the rate of discontinuation and improve the safety profile ... both cohorts had similar discontinuation rates and safety profiles,” Dr. Motzer noted.
A quality of life analysis for the 600-mg group using the 19-item Functional Assessment of Cancer Therapy (FACT) Kidney Symptom Index (FKSI-19) showed values were consistently lower with the drug than with placebo during treatment, with a crossing of the threshold for a minimally important difference at week 8.
Pharmacokinetic analyses from the trial, reported in a poster at the meeting (Abstract 4564), showed that in the group starting pazopanib at 600 mg, disease-free survival was longer in patients who achieved higher drug trough concentrations at week 3 or 5.
CHICAGO – The antiangiogenic agent pazopanib is not efficacious when used as adjuvant therapy for resected renal cell carcinoma (RCC) with features that confer a high risk of recurrence, the PROTECT investigators reported at the annual meeting of the American Society of Clinical Oncology.
Pazopanib (Votrient) is an oral multitargeted tyrosine kinase inhibitor active against the vascular endothelial growth factor receptor (VEGFR). Adjuvant use of other agents in this class has yielded mixed results, noted lead investigator Robert J. Motzer, MD, of Memorial Sloan-Kettering Cancer Center in New York.
In PROTECT, a phase III randomized controlled trial of more than 1,500 patients who had undergone nephrectomy for high-risk locally advanced RCC, pazopanib started at 600 mg daily did not yield significantly better disease-free survival than placebo, the trial’s primary endpoint. The drug did have a significant benefit when started at 800 mg daily, but that dose had to be lowered partway through because of a high rate of discontinuation due to adverse events.
“The trial did not meet its primary endpoint,” Dr. Motzer concluded. “Pazopanib is not recommended for adjuvant therapy following resection of locally advanced RCC.”
Expert perspective
“The current landscape of RCC adjuvant therapy is really controversial,” commented invited discussant Daniel Y. C. Heng, MD, MPH, of the University of Calgary (Alta.) Tom Baker Cancer Centre.
“Are these [factors] important or not? I think a lot of this is being overshadowed by things that are going on right now,” Dr. Heng maintained. “There are newer medications, such as PD-1 and PD-L1 inhibitors that are now being studied. And there are now perioperative studies as well – should we be using these drugs before nephrectomy and after nephrectomy to prime the immune system to get better outcomes?”
At the end of the day, identification of a reliable predictive biomarker will be key to using the VEGFR tyrosine kinase inhibitors, he concluded. “I look forward to the future where we can actually use these tests to determine who will benefit most from adjuvant therapy so that we can maximize patient outcomes.”
Study details
The PROTECT trial was funded by Novartis Oncology and randomized 1,538 patients with resected pT2 (high grade), pT3, or greater nonmetastatic clear cell RCC, a highly vascular tumor typically reliant on aberrant signaling in the VEGF pathway.
The patients were assigned evenly to receive pazopanib or placebo for 1 year. The starting dose was lowered from 800 mg daily to 600 mg daily (with escalation permitted) after 403 patients had been treated.
In intention-to-treat analysis among patients started on the 600-mg dose and having a median follow-up of about 31 months, disease-free survival was better with pazopanib but not significantly so (hazard ratio, 0.86; P = .16), Dr. Motzer reported.
In secondary analyses, pazopanib did have a significant disease-free survival benefit among patients started on the 800-mg dose (hazard ratio, 0.69; P = .02) and among the entire trial population started on either dose (hazard ratio, 0.80; P = .01).
One possible explanation for the differing results seen with the two doses was the difference in follow-up, as the 800-mg group was treated earlier in the trial, he proposed. But with an additional year of blinded follow-up, the benefit in the 600-mg group actually diminished, whereas that in the 800-mg group did not.
Another possibility was the somewhat better performance of the placebo group used for comparison with the lower dose: the 3-year disease-free survival rate with placebo was 64% for the 600-mg comparison but 56% for the 800-mg comparison. “One factor that could explain differences in the outcomes of the placebo groups includes unidentified patient demographic characteristics,” Dr. Motzer noted.
Overall survival was statistically indistinguishable between the pazopanib and placebo groups, regardless of dose. However, “the results are inconclusive as the data are not yet mature,” he said, with a definitive analysis planned for 2019.
Compared with counterparts given placebo, patients started on the 600-mg dose of pazopanib had a higher rate of grade 3 or 4 adverse events overall (60% vs. 21%), driven in large part by higher rates of hypertension and increased alanine aminotransferase levels.
“Although the intent of modifying the protocol dose of pazopanib from 800 mg to 600 mg was to reduce the rate of discontinuation and improve the safety profile ... both cohorts had similar discontinuation rates and safety profiles,” Dr. Motzer noted.
A quality of life analysis for the 600-mg group using the 19-item Functional Assessment of Cancer Therapy (FACT) Kidney Symptom Index (FKSI-19) showed values were consistently lower with the drug than with placebo during treatment, with a crossing of the threshold for a minimally important difference at week 8.
Pharmacokinetic analyses from the trial, reported in a poster at the meeting (Abstract 4564), showed that in the group starting pazopanib at 600 mg, disease-free survival was longer in patients who achieved higher drug trough concentrations at week 3 or 5.
CHICAGO – The antiangiogenic agent pazopanib is not efficacious when used as adjuvant therapy for resected renal cell carcinoma (RCC) with features that confer a high risk of recurrence, the PROTECT investigators reported at the annual meeting of the American Society of Clinical Oncology.
Pazopanib (Votrient) is an oral multitargeted tyrosine kinase inhibitor active against the vascular endothelial growth factor receptor (VEGFR). Adjuvant use of other agents in this class has yielded mixed results, noted lead investigator Robert J. Motzer, MD, of Memorial Sloan-Kettering Cancer Center in New York.
In PROTECT, a phase III randomized controlled trial of more than 1,500 patients who had undergone nephrectomy for high-risk locally advanced RCC, pazopanib started at 600 mg daily did not yield significantly better disease-free survival than placebo, the trial’s primary endpoint. The drug did have a significant benefit when started at 800 mg daily, but that dose had to be lowered partway through because of a high rate of discontinuation due to adverse events.
“The trial did not meet its primary endpoint,” Dr. Motzer concluded. “Pazopanib is not recommended for adjuvant therapy following resection of locally advanced RCC.”
Expert perspective
“The current landscape of RCC adjuvant therapy is really controversial,” commented invited discussant Daniel Y. C. Heng, MD, MPH, of the University of Calgary (Alta.) Tom Baker Cancer Centre.
“Are these [factors] important or not? I think a lot of this is being overshadowed by things that are going on right now,” Dr. Heng maintained. “There are newer medications, such as PD-1 and PD-L1 inhibitors that are now being studied. And there are now perioperative studies as well – should we be using these drugs before nephrectomy and after nephrectomy to prime the immune system to get better outcomes?”
At the end of the day, identification of a reliable predictive biomarker will be key to using the VEGFR tyrosine kinase inhibitors, he concluded. “I look forward to the future where we can actually use these tests to determine who will benefit most from adjuvant therapy so that we can maximize patient outcomes.”
Study details
The PROTECT trial was funded by Novartis Oncology and randomized 1,538 patients with resected pT2 (high grade), pT3, or greater nonmetastatic clear cell RCC, a highly vascular tumor typically reliant on aberrant signaling in the VEGF pathway.
The patients were assigned evenly to receive pazopanib or placebo for 1 year. The starting dose was lowered from 800 mg daily to 600 mg daily (with escalation permitted) after 403 patients had been treated.
In intention-to-treat analysis among patients started on the 600-mg dose and having a median follow-up of about 31 months, disease-free survival was better with pazopanib but not significantly so (hazard ratio, 0.86; P = .16), Dr. Motzer reported.
In secondary analyses, pazopanib did have a significant disease-free survival benefit among patients started on the 800-mg dose (hazard ratio, 0.69; P = .02) and among the entire trial population started on either dose (hazard ratio, 0.80; P = .01).
One possible explanation for the differing results seen with the two doses was the difference in follow-up, as the 800-mg group was treated earlier in the trial, he proposed. But with an additional year of blinded follow-up, the benefit in the 600-mg group actually diminished, whereas that in the 800-mg group did not.
Another possibility was the somewhat better performance of the placebo group used for comparison with the lower dose: the 3-year disease-free survival rate with placebo was 64% for the 600-mg comparison but 56% for the 800-mg comparison. “One factor that could explain differences in the outcomes of the placebo groups includes unidentified patient demographic characteristics,” Dr. Motzer noted.
Overall survival was statistically indistinguishable between the pazopanib and placebo groups, regardless of dose. However, “the results are inconclusive as the data are not yet mature,” he said, with a definitive analysis planned for 2019.
Compared with counterparts given placebo, patients started on the 600-mg dose of pazopanib had a higher rate of grade 3 or 4 adverse events overall (60% vs. 21%), driven in large part by higher rates of hypertension and increased alanine aminotransferase levels.
“Although the intent of modifying the protocol dose of pazopanib from 800 mg to 600 mg was to reduce the rate of discontinuation and improve the safety profile ... both cohorts had similar discontinuation rates and safety profiles,” Dr. Motzer noted.
A quality of life analysis for the 600-mg group using the 19-item Functional Assessment of Cancer Therapy (FACT) Kidney Symptom Index (FKSI-19) showed values were consistently lower with the drug than with placebo during treatment, with a crossing of the threshold for a minimally important difference at week 8.
Pharmacokinetic analyses from the trial, reported in a poster at the meeting (Abstract 4564), showed that in the group starting pazopanib at 600 mg, disease-free survival was longer in patients who achieved higher drug trough concentrations at week 3 or 5.
AT ASCO 2017
Key clinical point:
Major finding: Compared with placebo, pazopanib started at 600 mg daily did not significantly reduce the risk of disease-free survival events (hazard ratio, 0.86; P = .16).
Data source: A phase III randomized controlled trial among 1,538 patients who had undergone nephrectomy for high-risk locally advanced RCC (PROTECT trial).
Disclosures: Dr. Motzer disclosed that he is a consultant to Eisai, Exelixis, Merck, Novartis, and Pfizer, and that he receives research funding from Bristol-Myers Squibb (institutional), Eisai (institutional), Genentech/Roche (institutional), GlaxoSmithKline (institutional), Novartis (institutional), and Pfizer (institutional). The trial was funded by Novartis Oncology.
Most arrhythmia clinic patients have undetected OSA
BOSTON – In a study of patients without a previous diagnosis of obstructive sleep apnea (OSA), 85% of participants in outpatient arrhythmia clinics had undetected OSA.
The study, which also excluded patients who had ever been treated for OSA, was presented by Colin Shapiro, MD, of the Department of Psychiatry, Toronto Western Hospital, University of Toronto, at the annual meeting of the Associated Professional Sleep Societies.
A binary logistic regression analysis showed that only age and male gender were significant predictors of OSA.
Along with a home sleep study, researchers tested 75 nonselected consecutive patients (mean age of 64 years; 72% male) from three outpatient arrhythmia clinics for symptoms indicative of OSA using the Epworth Sleepiness Scale (ESS), the Fatigue Severity Scale (FSS), the Non-Restorative Sleep Scale (NRSS), and other questionnaires.
On the ESS, 32% of patients had a score of 8 or greater, indicating higher than normal daytime sleepiness. Almost half (47%) of patients had a high level of fatigue on the FSS, and symptoms of nonrestorative sleep were detected in 15% (NRSS score greater than or equal to 46).
Dr. Shapiro noted that “high scores suggestive of daytime sleepiness, fatigue, or insomnia did not particularly predict the presence of OSA in patients with arrhythmia.” He concluded that, “with a hit rate of 85%, just about every patient with an arrhythmia should have a sleep study.”
Dr. Shapiro informed attendees at the annual meeting of the Professional Sleep Societies that he was presenting in place of his student and the abstract’s first author, Dr. Asmaa M. Abumuamar, MD, who was denied a visa to attend the meeting. Dr. Abumuamar is from the Toronto Western Research Institute, University of Toronto.
Dr. Shapiro reported that Dr. Abumuamar has no conflicts of interest. Dr. Shapiro reported that he is an investor in the company that supplied the home sleep testing apparatus.
BOSTON – In a study of patients without a previous diagnosis of obstructive sleep apnea (OSA), 85% of participants in outpatient arrhythmia clinics had undetected OSA.
The study, which also excluded patients who had ever been treated for OSA, was presented by Colin Shapiro, MD, of the Department of Psychiatry, Toronto Western Hospital, University of Toronto, at the annual meeting of the Associated Professional Sleep Societies.
A binary logistic regression analysis showed that only age and male gender were significant predictors of OSA.
Along with a home sleep study, researchers tested 75 nonselected consecutive patients (mean age of 64 years; 72% male) from three outpatient arrhythmia clinics for symptoms indicative of OSA using the Epworth Sleepiness Scale (ESS), the Fatigue Severity Scale (FSS), the Non-Restorative Sleep Scale (NRSS), and other questionnaires.
On the ESS, 32% of patients had a score of 8 or greater, indicating higher than normal daytime sleepiness. Almost half (47%) of patients had a high level of fatigue on the FSS, and symptoms of nonrestorative sleep were detected in 15% (NRSS score greater than or equal to 46).
Dr. Shapiro noted that “high scores suggestive of daytime sleepiness, fatigue, or insomnia did not particularly predict the presence of OSA in patients with arrhythmia.” He concluded that, “with a hit rate of 85%, just about every patient with an arrhythmia should have a sleep study.”
Dr. Shapiro informed attendees at the annual meeting of the Professional Sleep Societies that he was presenting in place of his student and the abstract’s first author, Dr. Asmaa M. Abumuamar, MD, who was denied a visa to attend the meeting. Dr. Abumuamar is from the Toronto Western Research Institute, University of Toronto.
Dr. Shapiro reported that Dr. Abumuamar has no conflicts of interest. Dr. Shapiro reported that he is an investor in the company that supplied the home sleep testing apparatus.
BOSTON – In a study of patients without a previous diagnosis of obstructive sleep apnea (OSA), 85% of participants in outpatient arrhythmia clinics had undetected OSA.
The study, which also excluded patients who had ever been treated for OSA, was presented by Colin Shapiro, MD, of the Department of Psychiatry, Toronto Western Hospital, University of Toronto, at the annual meeting of the Associated Professional Sleep Societies.
A binary logistic regression analysis showed that only age and male gender were significant predictors of OSA.
Along with a home sleep study, researchers tested 75 nonselected consecutive patients (mean age of 64 years; 72% male) from three outpatient arrhythmia clinics for symptoms indicative of OSA using the Epworth Sleepiness Scale (ESS), the Fatigue Severity Scale (FSS), the Non-Restorative Sleep Scale (NRSS), and other questionnaires.
On the ESS, 32% of patients had a score of 8 or greater, indicating higher than normal daytime sleepiness. Almost half (47%) of patients had a high level of fatigue on the FSS, and symptoms of nonrestorative sleep were detected in 15% (NRSS score greater than or equal to 46).
Dr. Shapiro noted that “high scores suggestive of daytime sleepiness, fatigue, or insomnia did not particularly predict the presence of OSA in patients with arrhythmia.” He concluded that, “with a hit rate of 85%, just about every patient with an arrhythmia should have a sleep study.”
Dr. Shapiro informed attendees at the annual meeting of the Professional Sleep Societies that he was presenting in place of his student and the abstract’s first author, Dr. Asmaa M. Abumuamar, MD, who was denied a visa to attend the meeting. Dr. Abumuamar is from the Toronto Western Research Institute, University of Toronto.
Dr. Shapiro reported that Dr. Abumuamar has no conflicts of interest. Dr. Shapiro reported that he is an investor in the company that supplied the home sleep testing apparatus.
AT SLEEP 2017
Key clinical point: The majority of patients attending an outpatient arrhythmia clinic had undetected OSA.
Major finding: Of the participants, 91% of males and 71% of females with no history of OSA were found to have the disorder (85% of total).
Data source: A screening study using a randomized, unselected population drawn from outpatient arrhythmia clinics. Those with a diagnoses of OSA were excluded.
Disclosures: Dr. Shapiro reported that Dr. Abumuamar has no conflicts of interest. Dr. Shapiro reported that he is an investor in the company that supplied the home sleep testing apparatus.
KHN Exclusive: White House task force echoes Pharma proposals
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump repeatedly talks tough about reining in the pharmaceutical industry, but his administration’s efforts to lower drug prices are shrouded in secrecy.
Senior administrative officials met Friday to discuss an executive order on the cost of pharmaceuticals, a roundtable informed by Trump’s “Drug Pricing and Innovation Working Group.” Kaiser Health News examined documents that shed light on the workings of this working group.
The documents reveal behind-the-scenes discussions that are influenced by the pharmaceutical industry. Joe Grogan, associate director of health programs for the Office of Management and Budget (OMB), has led the group. Until March, Grogan served as a lobbyist for Gilead Sciences, the pharmaceutical company that priced its hepatitis C drugs at $1,000 per pill.
To solve the crisis of high drug prices, the group discussed strengthening the monopoly rights of pharmaceuticals overseas, ending discounts for low-income hospitals and accelerating drug approvals by the Food and Drug Administration. The White House declined to comment on the working group.
The group initially met May 4 in the Eisenhower Executive Office Building and has since met every two weeks. In addition to OMB, the working group includes officials from the White House National Economic Council, the Domestic Policy Council, Health and Human Services, the FDA, the Federal Trade Commission, the Department of Commerce, the Office of the U.S. Trade Representative and the Department of Justice.
According to the documents – the latest of which is dated June 1– the working group focused on the following “principles” and “talking points”:
1. Extending the patent life of drugs in foreign markets to “provide for protection and enforcement of intellectual property rights.” This will ensure “that American consumers do not unfairly subsidize research and development for people throughout the globe.” Extending monopoly protections for drugs overseas has been one of the pharmaceutical industry’s top priorities since the Trans-Pacific Partnership was defeated last year. That policy would push up global drug prices, according to Médecins Sans Frontières.
2. Promoting competition in the U.S. drug market – both by “modernizing our regulatory and reimbursement systems” and limiting “barrier to entry, including the cost of research and development,” according to the documents. The working group also discussed two broad policy ideas that have been championed by the pharmaceutical industry, according to sources familiar with the process:
3. Value-based pricing, under which pharmaceutical companies keep the list prices of drugs unchanged but offer rebates if patients don’t improve, is one option. It’s unclear who would audit the effectiveness of the drugs, what criteria they would use to evaluate them, and who would receive the rebates. Grogan invited Robert Shapiro – an adviser for Gilead and former secretary of Commerce under President Bill Clinton – to brief the working group on value-based pricing on May 18. Shapiro is the chairman and cofounder of Sonecon, a Washington, D.C., firm that consulted with Gilead, Amgen, and PhRMA, according to his curriculum vitae.
4. Grogan and Shapiro also discussed issuing 10-year U.S. Treasury bonds to drug manufacturers to pay for expensive hepatitis C drugs like Sovaldi and Harvoni under Medicare and Medicaid, to avoid rationing drugs to the sickest patients. The 2015 Senate investigation, for example, found that, though Medicaid spent more than $1 billion on Sovaldi, just 2.4% of Medicaid patients with hepatitis C were treated.
After the working group’s first meeting on May 4, Grogan distributed detailed policy recommendations on options for expediting generic drug approvals, creating a new tax credit “of up to 50%” for investments in generic drug manufacturing, distribution, and research and development. The documents also propose scaling back the 340B program, which requires drug manufacturers to provide some medicines at a discount to hospitals that treat low-income patients.
Most of these policies would not ease patient costs, and at least one would increase prices, said experts who reviewed the documents at the request of Kaiser Health News.
“This six-page document contains the kinds of solutions to the cost-of-drugs problem that you would get if you gathered together all the executives of pharma and asked them ‘What sort of token gestures can we do?’ ” said Vinay Prasad, MD, a professor of medicine at Oregon Health and Sciences University who studies the costs of cancer drugs.
The pharma-friendly recommendations appear to clash with earlier press reports indicating that OMB Director Mick Mulvaney was considering requiring drug makers to pay rebates to Medicare patients, a measure the pharmaceutical lobby fiercely opposes.
Brand-name drug prices – which account for 72% of drug spending – go untouched in the handouts, said Fiona Scott Morton, PhD, a Yale economics professor and former attorney with the Justice Department’s antitrust division.
“The changes to generic markets to promote competition look helpful, but there need to be some more ideas to create more competition for branded drugs or consumers aren’t really going to notice this,” Scott Morton said.
Some of the text in the document is cribbed directly from policy papers published by the pharmaceutical industry’s powerful lobby – Pharmaceutical Research and Manufacturers Association (PhRMA).
Under the subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval,” one handout proposes the FDA use less rigorous clinical trial standards to speed drug approvals.
The handout cites a PhRMA paper from March 2016 that includes an identical subtitle, “Encourage Use of 21st Century Tools for Drug Evaluation, Review, and Approval” and recommends the FDA implement less rigorous clinical trial standards.
These recommendations would not lower drug prices, experts say. Such measures “would be like a firefighter spraying gasoline on your burning garage,” Prasad said.
Another section – which recommends giving the FDA more discretion to evaluate generic copies of complex drugs – closely resembles a National Law Review article written by two lobbyists in the pharmaceutical division of Foley & Lardner, whose clients include generic drug makers.
The handouts further recommend allowing drug makers to supply data and off-label information to insurers and pharmacy benefit managers during the clinical trial period, before they secure FDA approval.
That’s a “terrible idea,” said Jerry Avorn, MD, a professor at Harvard Medical School and the chief of the Division of Pharmacoepidemiology and Pharmacoeconomics at Brigham and Women’s Hospital. “That’s why we have the whole approval process, to determine what’s actually true,” he said.
KHN’s coverage of prescription drug development, costs and pricing is supported in part by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Ear to the door: Five things being weighed in secret health bill also weigh it down
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Anyone following the debate over the “repeal and replace” of the Affordable Care Act knows that the 13 Republican senators writing the bill are meeting behind closed doors.
While Senate Majority Leader Mitch McConnell (R-Ky.) continues to push for a vote before the July 4 Senate recess, Washington’s favorite parlor game has become guessing what is, or will be, in the Senate bill.
Spoiler: No one knows what the final Senate bill will look like – not even those writing it.
“It’s an iterative process,” Senate Majority Whip John Cornyn (R-Texas) told Politico, adding that senators in the room are sending options to the Congressional Budget Office to try to figure out, in general, how much they would cost. Those conversations between senators and the CBO – common for lawmakers working on major, complex pieces of legislation – sometimes prompt members to press through and other times to change course.
Although specifics, to the extent there are any, have largely stayed secret, some of the policies under consideration have slipped out, and pressure points of the debate are fairly clear. Anything can happen, but here’s what we know so far:
1. Medicaid expansion
The Republicans are determined to roll back the expansion of Medicaid under the Affordable Care Act. The question is, How to do it? The ACA called for an expansion of the Medicaid program for those with low incomes to everyone who earns less than 133% of poverty (around $16,000 a year for an individual), with the federal government footing much of the bill. The Supreme Court ruled in 2012 that the expansion was optional for states, but 31 have done so, providing new coverage to an estimated 14 million people.
The Republican bill passed by the House on May 4 would phase out the federal funding for those made eligible by the ACA over 2 years, beginning in 2020. But, Republican moderates in the Senate want a much slower end to the additional federal aid. Several have suggested that they could accept a 7-year phaseout.
Keeping the federal expansion money flowing that long, however, would cut into the bill’s budget savings. That matters: In order to protect the Senate’s ability to pass the bill under budget rules that require only a simple majority rather than 60 votes, the bill’s savings must at least match those of the House version. Any extra money spent on Medicaid expansion would have to be cut elsewhere.
2. Medicaid caps
A related issue is whether and at what level to cap federal Medicaid spending. Medicaid currently covers more than 70 million low-income people. Medicaid covers half of all births and half of the nation’s bill for long-term care, including nursing home stays. Right now, the federal government matches whatever states spend at least 50-50 and provides more matching funds for less wealthy states.
The House bill would, for the first time, cap the amount the federal government provides to states for their Medicaid programs. The CBO estimated that the caps would put more of the financial burden for the program on states, which would respond by a combination of cutting payments to health care providers like doctors and hospitals, eliminating benefits for patients, and restricting eligibility.
The Medicaid cap may or may not be included in the Senate bill, depending on whom you ask. However, sources with direct knowledge of the negotiations say the real sticking point is not whether or not to impose a cap – they want to do that. The hurdles are how to be fair to states that get less federal money and how fast the caps should rise.
Again, if the Senate proposal is more generous than the House’s version, it will be harder to meet the bill’s required budget targets.
3. Restrictions on abortion coverage
The senators are actively considering two measures that would limit funding for abortions, though it is not clear if either would be allowed to remain in the bill according to the Senate’s rules. The Senate Parliamentarian, who must review the bill after the senators complete it but before it comes to the floor, will decide.
The House-passed bill would ban the use of federal tax credits to purchase private coverage that includes abortion as a benefit. This is a key demand for a large portion of the Republican base. However, the Senate version of the bill must abide by strict rules that limit its content to provisions that directly impact the federal budget. In the past, abortion language in budget bills has been ruled out of order.
4. Reading between the lines
A related issue is whether House language to temporarily bar Planned Parenthood from participating in the Medicaid program will be allowed in the Senate.
While the Parliamentarian allowed identical language defunding Planned Parenthood to remain in a similar budget bill in 2015, it was not clear at the time that Planned Parenthood would have been the only provider affected by the language. Planned Parenthood backers say they will argue to the Parliamentarian that the budget impact of the language is “merely incidental” to the policy aim and, therefore, should not be allowed in the Senate bill.
5. Insurance market reforms
Senators are also struggling with provisions of the House-passed bill that would allow states to waive certain insurance requirements in the Affordable Care Act, including those laying out “essential” benefits that policies must cover and those banning insurers from charging sicker people higher premiums. That language, as well as an amendment seeking to ensure more funding to help people with preexisting conditions, was instrumental in gaining enough votes for the bill to pass the House.
Eliminating insurance regulations imposed by the ACA is a top priority for conservatives. “Conservatives would like to clear the books of Obamacare’s most costly regulations and free the states to regulate their markets how they wish,” wrote Sen. Mike Lee (R-Utah), who is one of the 13 senators negotiating the details of the bill, in an op-ed in May.
However, budget experts suggest that none of the insurance market provisions is likely to clear the Parliamentarian hurdle as being primarily budget-related.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.